User login
Direct peritoneal resuscitation beneficial after damage control surgery
SCOTTSDALE, ARIZ. – Direct peritoneal resuscitation with 2.5% Delflex solution significantly reduced abdominal closure time and operative complications in patients with hemorrhagic shock undergoing damage control surgery, a prospective case-control study showed.
The time to definitive wound closure fell from 5.7 days with standard resuscitation to 3.6 days with the addition of direct peritoneal resuscitation (DPR) with 2.5% Delflex solution (P = .006).

In addition, the control group was 3.2 times more likely to develop an intra-abdominal complication than was the DPR group (odds ratio, 3.2; P = .03), Dr. Jason W. Smith reported at the annual scientific assembly of the Eastern Association for the Surgery of Trauma..
"DPR is a safe, simple, and inexpensive method of managing an open abdomen following damage control surgery," he said. "DPR may attenuate persistent hepatic injury following hemorrhagic shock."
Dr. Smith and his colleagues at the University of Louisville (Ky.) have been strong proponents of the technique, and previously reported that DPR with Delflex shortened abdominal closure by 2.7 days in a retrospective proof-of-concept study in 19 trauma patients (J. Am. Coll. Surg. 2010;210:658-67).
Vasodilators and heparin can be used to augment microvascular circulation and prevent blood clots, but in patients with hemorrhagic shock, this generally leads to bad results. Activated drotrecogin alfa (Xigris), which was pulled from the market in October 2011, was initially used, but the sepsis drug treats only the symptoms, Dr. Smith explained.
"We selected Delflex because of its ability to have an effect on microvascular permeability as well as microvascular blood flow," he said. "So really this is a new take on what is a very old medicine."
Between 2008 and 2011, the investigators prospectively enrolled 42 patients who underwent damage control surgery and conventional resuscitation plus DPR consisting of peritoneal lavage with an 800-mL bolus of 2.5% Delflex for the first hour and a 400-mL/hr infusion thereafter. A 19 Fr drain was placed along the root of the mesentery into the pelvis, and suction dressing was applied to drain fluid. The infusion was stopped when the abdomen was closed definitively either by primary closure or by the use of an absorbable or a biologic mesh.
The patients (average age, 30.6 years) were propensity matched against 42 case controls (average age, 29.1 years) who had undergone conventional resuscitation at the discretion of the treating surgeon after damage control surgery. All patients underwent blood product resuscitation in the first 24-48 hours of treatment.
The average Injury Severity Score was 19 among patients and 21 among controls. The hepatic Abbreviated Injury Scale (AIS) score was 3.4 in both groups, and roughly 40% of patients underwent a liver operation.
Control patients had significantly elevated alanine transaminase levels at 48 (731 vs. 507 U/L) and 72 hours (791 vs. 501 U/L) post resuscitation, compared with DPR patients, and this difference continued up to 14 days after the initial injury (all P less than .01), Dr. Smith said.
International normalized ratio (INR) levels were persistently higher in the control group, reaching statistical significance at 72 hours (1.3 vs. 1.8; P = .03). Time to INR normalization was no different whether the red blood cell to fresh frozen plasma (FFP) ratio was 1:1 or 1:2, he said.
Controls achieved a slightly better transfusion ratio (1.57 vs. 1.76; P = .52), although DPR patients had significantly lower FFP requirements after 48 hours (P = .04), and received significantly fewer transfusions at 72 hours post admission (31 vs. 41; P = .007).
As observed in the pilot study, the primary fascial closure rate was significantly higher with DPR than conventional resuscitation alone (88% vs. 66%; P = .01), and mortality was similar (10% vs. 17%; P = .25), Dr. Smith said. There were no complications with DPR administration.

In a multivariate analysis, the two strongest predictors of persistent hepatic injury following hemorrhagic shock were hepatic AIS greater than 3 (OR, 3.18), followed by nonutilization of DPR (OR, 0.63).
Invited discussant Dr. Greta Piper of Yale University, New Haven, Conn., asked whether the results would have been even better with a higher infusion rate or concentration of Delflex since one effect of the infusion is continuous dialysis, with a potential reduction in total body salt and water content.
Dr. Smith replied that they have tried DPR with other agents such as mannitol and Delflex 1.5% and 4.25%, but said the 2.5% concentration "is kind of a Goldilocks dose," as 1.5% is too weak to do anything and 4.25% desiccates the intravascular space.
"The 2.5% doesn’t desiccate the intravascular space, but you still get all the benefits of microvascular augmentation," he added.
Dr. Smith noted that DPR with 2.5% Delflex has produced similar results in patients undergoing emergency surgery as well as in those with intestinal obstruction and significant bowel edema. The researchers are currently enrolling adult trauma patients into a prospective randomized trial that will evaluate changes in hepatic blood flow as well as the effect of DPR on the inflammatory process following hemorrhagic shock.
The National Institute of General Medicine Sciences supported this research. Dr. Smith and his coauthors reported no relevant financial disclosures.
SCOTTSDALE, ARIZ. – Direct peritoneal resuscitation with 2.5% Delflex solution significantly reduced abdominal closure time and operative complications in patients with hemorrhagic shock undergoing damage control surgery, a prospective case-control study showed.
The time to definitive wound closure fell from 5.7 days with standard resuscitation to 3.6 days with the addition of direct peritoneal resuscitation (DPR) with 2.5% Delflex solution (P = .006).
In addition, the control group was 3.2 times more likely to develop an intra-abdominal complication than was the DPR group (odds ratio, 3.2; P = .03), Dr. Jason W. Smith reported at the annual scientific assembly of the Eastern Association for the Surgery of Trauma..
"DPR is a safe, simple, and inexpensive method of managing an open abdomen following damage control surgery," he said. "DPR may attenuate persistent hepatic injury following hemorrhagic shock."
Dr. Smith and his colleagues at the University of Louisville (Ky.) have been strong proponents of the technique, and previously reported that DPR with Delflex shortened abdominal closure by 2.7 days in a retrospective proof-of-concept study in 19 trauma patients (J. Am. Coll. Surg. 2010;210:658-67).
Vasodilators and heparin can be used to augment microvascular circulation and prevent blood clots, but in patients with hemorrhagic shock, this generally leads to bad results. Activated drotrecogin alfa (Xigris), which was pulled from the market in October 2011, was initially used, but the sepsis drug treats only the symptoms, Dr. Smith explained.
"We selected Delflex because of its ability to have an effect on microvascular permeability as well as microvascular blood flow," he said. "So really this is a new take on what is a very old medicine."
Between 2008 and 2011, the investigators prospectively enrolled 42 patients who underwent damage control surgery and conventional resuscitation plus DPR consisting of peritoneal lavage with an 800-mL bolus of 2.5% Delflex for the first hour and a 400-mL/hr infusion thereafter. A 19 Fr drain was placed along the root of the mesentery into the pelvis, and suction dressing was applied to drain fluid. The infusion was stopped when the abdomen was closed definitively either by primary closure or by the use of an absorbable or a biologic mesh.
The patients (average age, 30.6 years) were propensity matched against 42 case controls (average age, 29.1 years) who had undergone conventional resuscitation at the discretion of the treating surgeon after damage control surgery. All patients underwent blood product resuscitation in the first 24-48 hours of treatment.
The average Injury Severity Score was 19 among patients and 21 among controls. The hepatic Abbreviated Injury Scale (AIS) score was 3.4 in both groups, and roughly 40% of patients underwent a liver operation.
Control patients had significantly elevated alanine transaminase levels at 48 (731 vs. 507 U/L) and 72 hours (791 vs. 501 U/L) post resuscitation, compared with DPR patients, and this difference continued up to 14 days after the initial injury (all P less than .01), Dr. Smith said.
International normalized ratio (INR) levels were persistently higher in the control group, reaching statistical significance at 72 hours (1.3 vs. 1.8; P = .03). Time to INR normalization was no different whether the red blood cell to fresh frozen plasma (FFP) ratio was 1:1 or 1:2, he said.
Controls achieved a slightly better transfusion ratio (1.57 vs. 1.76; P = .52), although DPR patients had significantly lower FFP requirements after 48 hours (P = .04), and received significantly fewer transfusions at 72 hours post admission (31 vs. 41; P = .007).
As observed in the pilot study, the primary fascial closure rate was significantly higher with DPR than conventional resuscitation alone (88% vs. 66%; P = .01), and mortality was similar (10% vs. 17%; P = .25), Dr. Smith said. There were no complications with DPR administration.
In a multivariate analysis, the two strongest predictors of persistent hepatic injury following hemorrhagic shock were hepatic AIS greater than 3 (OR, 3.18), followed by nonutilization of DPR (OR, 0.63).
Invited discussant Dr. Greta Piper of Yale University, New Haven, Conn., asked whether the results would have been even better with a higher infusion rate or concentration of Delflex since one effect of the infusion is continuous dialysis, with a potential reduction in total body salt and water content.
Dr. Smith replied that they have tried DPR with other agents such as mannitol and Delflex 1.5% and 4.25%, but said the 2.5% concentration "is kind of a Goldilocks dose," as 1.5% is too weak to do anything and 4.25% desiccates the intravascular space.
"The 2.5% doesn’t desiccate the intravascular space, but you still get all the benefits of microvascular augmentation," he added.
Dr. Smith noted that DPR with 2.5% Delflex has produced similar results in patients undergoing emergency surgery as well as in those with intestinal obstruction and significant bowel edema. The researchers are currently enrolling adult trauma patients into a prospective randomized trial that will evaluate changes in hepatic blood flow as well as the effect of DPR on the inflammatory process following hemorrhagic shock.
The National Institute of General Medicine Sciences supported this research. Dr. Smith and his coauthors reported no relevant financial disclosures.
SCOTTSDALE, ARIZ. – Direct peritoneal resuscitation with 2.5% Delflex solution significantly reduced abdominal closure time and operative complications in patients with hemorrhagic shock undergoing damage control surgery, a prospective case-control study showed.
The time to definitive wound closure fell from 5.7 days with standard resuscitation to 3.6 days with the addition of direct peritoneal resuscitation (DPR) with 2.5% Delflex solution (P = .006).
In addition, the control group was 3.2 times more likely to develop an intra-abdominal complication than was the DPR group (odds ratio, 3.2; P = .03), Dr. Jason W. Smith reported at the annual scientific assembly of the Eastern Association for the Surgery of Trauma..
"DPR is a safe, simple, and inexpensive method of managing an open abdomen following damage control surgery," he said. "DPR may attenuate persistent hepatic injury following hemorrhagic shock."
Dr. Smith and his colleagues at the University of Louisville (Ky.) have been strong proponents of the technique, and previously reported that DPR with Delflex shortened abdominal closure by 2.7 days in a retrospective proof-of-concept study in 19 trauma patients (J. Am. Coll. Surg. 2010;210:658-67).
Vasodilators and heparin can be used to augment microvascular circulation and prevent blood clots, but in patients with hemorrhagic shock, this generally leads to bad results. Activated drotrecogin alfa (Xigris), which was pulled from the market in October 2011, was initially used, but the sepsis drug treats only the symptoms, Dr. Smith explained.
"We selected Delflex because of its ability to have an effect on microvascular permeability as well as microvascular blood flow," he said. "So really this is a new take on what is a very old medicine."
Between 2008 and 2011, the investigators prospectively enrolled 42 patients who underwent damage control surgery and conventional resuscitation plus DPR consisting of peritoneal lavage with an 800-mL bolus of 2.5% Delflex for the first hour and a 400-mL/hr infusion thereafter. A 19 Fr drain was placed along the root of the mesentery into the pelvis, and suction dressing was applied to drain fluid. The infusion was stopped when the abdomen was closed definitively either by primary closure or by the use of an absorbable or a biologic mesh.
The patients (average age, 30.6 years) were propensity matched against 42 case controls (average age, 29.1 years) who had undergone conventional resuscitation at the discretion of the treating surgeon after damage control surgery. All patients underwent blood product resuscitation in the first 24-48 hours of treatment.
The average Injury Severity Score was 19 among patients and 21 among controls. The hepatic Abbreviated Injury Scale (AIS) score was 3.4 in both groups, and roughly 40% of patients underwent a liver operation.
Control patients had significantly elevated alanine transaminase levels at 48 (731 vs. 507 U/L) and 72 hours (791 vs. 501 U/L) post resuscitation, compared with DPR patients, and this difference continued up to 14 days after the initial injury (all P less than .01), Dr. Smith said.
International normalized ratio (INR) levels were persistently higher in the control group, reaching statistical significance at 72 hours (1.3 vs. 1.8; P = .03). Time to INR normalization was no different whether the red blood cell to fresh frozen plasma (FFP) ratio was 1:1 or 1:2, he said.
Controls achieved a slightly better transfusion ratio (1.57 vs. 1.76; P = .52), although DPR patients had significantly lower FFP requirements after 48 hours (P = .04), and received significantly fewer transfusions at 72 hours post admission (31 vs. 41; P = .007).
As observed in the pilot study, the primary fascial closure rate was significantly higher with DPR than conventional resuscitation alone (88% vs. 66%; P = .01), and mortality was similar (10% vs. 17%; P = .25), Dr. Smith said. There were no complications with DPR administration.
In a multivariate analysis, the two strongest predictors of persistent hepatic injury following hemorrhagic shock were hepatic AIS greater than 3 (OR, 3.18), followed by nonutilization of DPR (OR, 0.63).
Invited discussant Dr. Greta Piper of Yale University, New Haven, Conn., asked whether the results would have been even better with a higher infusion rate or concentration of Delflex since one effect of the infusion is continuous dialysis, with a potential reduction in total body salt and water content.
Dr. Smith replied that they have tried DPR with other agents such as mannitol and Delflex 1.5% and 4.25%, but said the 2.5% concentration "is kind of a Goldilocks dose," as 1.5% is too weak to do anything and 4.25% desiccates the intravascular space.
"The 2.5% doesn’t desiccate the intravascular space, but you still get all the benefits of microvascular augmentation," he added.
Dr. Smith noted that DPR with 2.5% Delflex has produced similar results in patients undergoing emergency surgery as well as in those with intestinal obstruction and significant bowel edema. The researchers are currently enrolling adult trauma patients into a prospective randomized trial that will evaluate changes in hepatic blood flow as well as the effect of DPR on the inflammatory process following hemorrhagic shock.
The National Institute of General Medicine Sciences supported this research. Dr. Smith and his coauthors reported no relevant financial disclosures.
AT THE EAST SCIENTIFIC ASSEMBLY
Major Finding: Time to definitive wound closure was 5.7 days with standard resuscitation vs. 3.6 days with the addition of direct peritoneal resuscitation with 2.5% Delflex (P = .006).
Data Source: Prospective, case-control study in 84 patients with hemorrhagic shock undergoing damage control surgery.
Disclosures: The National Institute of General Medicine Sciences supported this research. Dr. Smith and his coauthors reported no relevant financial disclosures.

Embolectomy for ischemic stroke remains unproven
Patients with large-vessel, anterior circulation ischemic stroke who underwent pretreatment neuroimaging to identify favorable penumbral patterns had similar clinical outcomes after treatment with either embolectomy or standard medical care regardless of the imaging results in the MR RESCUE trial.
"MR RESCUE underscores the importance of confirming hypotheses in randomized, controlled trials prior to implementing treatment approaches in clinical practice," co-primary investigator Dr. Chelsea Kidwell said during a late-breaking plenary session at the International Stroke Conference.

Possible reasons for the results are low recanalization rates with less-effective, first-generation devices (Merci Retriever or Penumbra System), the introduction of two imaging modalities, and the potential for favorable outcomes in penumbral patients regardless of treatment due to sufficient perfusion through collateral vessels. Another possibility is that the penumbral imaging selection hypothesis is flawed as currently conceived, she said.
The MR RESCUE (Mechanical Retrieval and Recanalization of Stroke Clots Using Embolectomy) investigators hypothesized that CT or MRI would identify patients with a favorable penumbral pattern – defined as a predicted infarct core of 90 mL or less and 70% or less of the predicted infarct tissue within the at-risk region – who would differentially benefit from embolectomy. Patients were treated within 8 hours of onset of large-vessel, anterior circulation strokes. Embolectomy is particularly attractive in these cases as intravenous tissue plasminogen activator (TPA) often is not effective on these large, frequently disabling clots.
There was no significant interaction, however, between treatment assignment and penumbral pattern by shift analysis of the 90-day modified Rankin Scale (mRS) score, reported Dr. Kidwell, professor of neurology at Georgetown University Medical Center in Washington. The mean mRS scores in patients with a favorable penumbral pattern were 3.9 with embolectomy and 3.4 with standard care, and 4.0 and 4.4, respectively, among patients without a favorable penumbral pattern (P = .14).
"As such, the trial failed to demonstrate that penumbral imaging identifies patients who will differentially benefit from endovascular therapy for acute ischemic stroke," she said.
Among all patients, mean modified Rankin scores at 90 days were similar between embolectomy and standard care (3.9 vs. 3.9; P = .99).
"Further randomized, controlled trials of new-generation devices are needed to test the full spectrum of the penumbral imaging selection hypothesis and the clinical efficacy of new-generation stent-retriever devices," she said.
That may be easier said than done, despite the lack of randomized, controlled trial data proving the benefit of penumbral imaging selection or recanalization with embolectomy.
In an editorial (N. Engl. J. Med. 2013 [doi:10.1056/NEJMe1215730]) published online with the MR RESCUE results (N. Engl. J. Med. 2013 [doi:10.1056/NEJMoa1212793]), Dr. Marc Chimowitz with the neurosciences department at Medical University of South Carolina, Charleston, points out that recruitment to the IMS (Interventional Management of Stroke) III and MR RESCUE trials was difficult "because once the Food and Drug Administration approved the devices and Medicare provided reimbursement for these procedures, endovascular treatment became widespread and many physicians who were treating patients with acute stroke felt that the ‘answer was in.’ Therefore, treatment equipoise was lost."
In all, 127 patients were enrolled between 2004 and 2011, of which 118 were fully eligible. Their mean age was 65.5 years and median National Institutes of Health Stroke Scale score was 17. Overall, 37% received intravenous TPA, and 80% underwent imaging with MRI.
Symptomatic hemorrhage occurred in 4% and 21% died, Dr. Kidwell said. The mean time to groin puncture was 6.2 hours.

"All of this means that we still need to put more and more patients in research protocols to better figure out who will benefit the most from endovascular therapy," American Heart Association past-president Dr. Ralph Sacco, chair of neurology at the University of Miami, said in an interview. "It has been shown now, including the subanalysis from IMS III, that the earlier you recanalize the better, and so we need to be still thinking about time windows. Just like with IV [intravenous] TPA, the earlier we treat, the better. Well, with endovascular therapy that may be true as well and you have to remember that sometimes penumbral imaging adds time."
Although embolectomy proponents and device manufacturers may see the results as a setback, another take was expressed by an audience member, who described the results as good news.
"The vast majority of people in the United States and the world probably have better access to primary care facilities rather than having access to academic centers, so to my patient population and to people I think in the vast majority, when we see that IV TPA is perhaps equivalent to more aggressive treatments that require more expansive techniques and depth of expertise, it’s kind of good news," she said to a round of applause.
Dr. Kidwell thanked her for the comment, but added, "I think there still are those among us who do believe that advanced neuroimaging, as well as endovascular therapy, will have a role down the line. I think we just need further trials with the new stent retriever devices to really sort this out."
MR RESCUE was funded by the National Institute of Neurological Disorders and Stroke. Concentric Medical Inc. provided study catheters and devices for part of the trial, with costs thereafter covered by study funds or third-party payers. Seven of the coauthors are employees of the University of California, which holds a patent on Merci Retriever devices. Dr. Chimowitz disclosed research support from the National Institutes of Health. Dr. Sacco reported no disclosures.
Patients with large-vessel, anterior circulation ischemic stroke who underwent pretreatment neuroimaging to identify favorable penumbral patterns had similar clinical outcomes after treatment with either embolectomy or standard medical care regardless of the imaging results in the MR RESCUE trial.
"MR RESCUE underscores the importance of confirming hypotheses in randomized, controlled trials prior to implementing treatment approaches in clinical practice," co-primary investigator Dr. Chelsea Kidwell said during a late-breaking plenary session at the International Stroke Conference.
Possible reasons for the results are low recanalization rates with less-effective, first-generation devices (Merci Retriever or Penumbra System), the introduction of two imaging modalities, and the potential for favorable outcomes in penumbral patients regardless of treatment due to sufficient perfusion through collateral vessels. Another possibility is that the penumbral imaging selection hypothesis is flawed as currently conceived, she said.
The MR RESCUE (Mechanical Retrieval and Recanalization of Stroke Clots Using Embolectomy) investigators hypothesized that CT or MRI would identify patients with a favorable penumbral pattern – defined as a predicted infarct core of 90 mL or less and 70% or less of the predicted infarct tissue within the at-risk region – who would differentially benefit from embolectomy. Patients were treated within 8 hours of onset of large-vessel, anterior circulation strokes. Embolectomy is particularly attractive in these cases as intravenous tissue plasminogen activator (TPA) often is not effective on these large, frequently disabling clots.
There was no significant interaction, however, between treatment assignment and penumbral pattern by shift analysis of the 90-day modified Rankin Scale (mRS) score, reported Dr. Kidwell, professor of neurology at Georgetown University Medical Center in Washington. The mean mRS scores in patients with a favorable penumbral pattern were 3.9 with embolectomy and 3.4 with standard care, and 4.0 and 4.4, respectively, among patients without a favorable penumbral pattern (P = .14).
"As such, the trial failed to demonstrate that penumbral imaging identifies patients who will differentially benefit from endovascular therapy for acute ischemic stroke," she said.
Among all patients, mean modified Rankin scores at 90 days were similar between embolectomy and standard care (3.9 vs. 3.9; P = .99).
"Further randomized, controlled trials of new-generation devices are needed to test the full spectrum of the penumbral imaging selection hypothesis and the clinical efficacy of new-generation stent-retriever devices," she said.
That may be easier said than done, despite the lack of randomized, controlled trial data proving the benefit of penumbral imaging selection or recanalization with embolectomy.
In an editorial (N. Engl. J. Med. 2013 [doi:10.1056/NEJMe1215730]) published online with the MR RESCUE results (N. Engl. J. Med. 2013 [doi:10.1056/NEJMoa1212793]), Dr. Marc Chimowitz with the neurosciences department at Medical University of South Carolina, Charleston, points out that recruitment to the IMS (Interventional Management of Stroke) III and MR RESCUE trials was difficult "because once the Food and Drug Administration approved the devices and Medicare provided reimbursement for these procedures, endovascular treatment became widespread and many physicians who were treating patients with acute stroke felt that the ‘answer was in.’ Therefore, treatment equipoise was lost."
In all, 127 patients were enrolled between 2004 and 2011, of which 118 were fully eligible. Their mean age was 65.5 years and median National Institutes of Health Stroke Scale score was 17. Overall, 37% received intravenous TPA, and 80% underwent imaging with MRI.
Symptomatic hemorrhage occurred in 4% and 21% died, Dr. Kidwell said. The mean time to groin puncture was 6.2 hours.
"All of this means that we still need to put more and more patients in research protocols to better figure out who will benefit the most from endovascular therapy," American Heart Association past-president Dr. Ralph Sacco, chair of neurology at the University of Miami, said in an interview. "It has been shown now, including the subanalysis from IMS III, that the earlier you recanalize the better, and so we need to be still thinking about time windows. Just like with IV [intravenous] TPA, the earlier we treat, the better. Well, with endovascular therapy that may be true as well and you have to remember that sometimes penumbral imaging adds time."
Although embolectomy proponents and device manufacturers may see the results as a setback, another take was expressed by an audience member, who described the results as good news.
"The vast majority of people in the United States and the world probably have better access to primary care facilities rather than having access to academic centers, so to my patient population and to people I think in the vast majority, when we see that IV TPA is perhaps equivalent to more aggressive treatments that require more expansive techniques and depth of expertise, it’s kind of good news," she said to a round of applause.
Dr. Kidwell thanked her for the comment, but added, "I think there still are those among us who do believe that advanced neuroimaging, as well as endovascular therapy, will have a role down the line. I think we just need further trials with the new stent retriever devices to really sort this out."
MR RESCUE was funded by the National Institute of Neurological Disorders and Stroke. Concentric Medical Inc. provided study catheters and devices for part of the trial, with costs thereafter covered by study funds or third-party payers. Seven of the coauthors are employees of the University of California, which holds a patent on Merci Retriever devices. Dr. Chimowitz disclosed research support from the National Institutes of Health. Dr. Sacco reported no disclosures.
Patients with large-vessel, anterior circulation ischemic stroke who underwent pretreatment neuroimaging to identify favorable penumbral patterns had similar clinical outcomes after treatment with either embolectomy or standard medical care regardless of the imaging results in the MR RESCUE trial.
"MR RESCUE underscores the importance of confirming hypotheses in randomized, controlled trials prior to implementing treatment approaches in clinical practice," co-primary investigator Dr. Chelsea Kidwell said during a late-breaking plenary session at the International Stroke Conference.
Possible reasons for the results are low recanalization rates with less-effective, first-generation devices (Merci Retriever or Penumbra System), the introduction of two imaging modalities, and the potential for favorable outcomes in penumbral patients regardless of treatment due to sufficient perfusion through collateral vessels. Another possibility is that the penumbral imaging selection hypothesis is flawed as currently conceived, she said.
The MR RESCUE (Mechanical Retrieval and Recanalization of Stroke Clots Using Embolectomy) investigators hypothesized that CT or MRI would identify patients with a favorable penumbral pattern – defined as a predicted infarct core of 90 mL or less and 70% or less of the predicted infarct tissue within the at-risk region – who would differentially benefit from embolectomy. Patients were treated within 8 hours of onset of large-vessel, anterior circulation strokes. Embolectomy is particularly attractive in these cases as intravenous tissue plasminogen activator (TPA) often is not effective on these large, frequently disabling clots.
There was no significant interaction, however, between treatment assignment and penumbral pattern by shift analysis of the 90-day modified Rankin Scale (mRS) score, reported Dr. Kidwell, professor of neurology at Georgetown University Medical Center in Washington. The mean mRS scores in patients with a favorable penumbral pattern were 3.9 with embolectomy and 3.4 with standard care, and 4.0 and 4.4, respectively, among patients without a favorable penumbral pattern (P = .14).
"As such, the trial failed to demonstrate that penumbral imaging identifies patients who will differentially benefit from endovascular therapy for acute ischemic stroke," she said.
Among all patients, mean modified Rankin scores at 90 days were similar between embolectomy and standard care (3.9 vs. 3.9; P = .99).
"Further randomized, controlled trials of new-generation devices are needed to test the full spectrum of the penumbral imaging selection hypothesis and the clinical efficacy of new-generation stent-retriever devices," she said.
That may be easier said than done, despite the lack of randomized, controlled trial data proving the benefit of penumbral imaging selection or recanalization with embolectomy.
In an editorial (N. Engl. J. Med. 2013 [doi:10.1056/NEJMe1215730]) published online with the MR RESCUE results (N. Engl. J. Med. 2013 [doi:10.1056/NEJMoa1212793]), Dr. Marc Chimowitz with the neurosciences department at Medical University of South Carolina, Charleston, points out that recruitment to the IMS (Interventional Management of Stroke) III and MR RESCUE trials was difficult "because once the Food and Drug Administration approved the devices and Medicare provided reimbursement for these procedures, endovascular treatment became widespread and many physicians who were treating patients with acute stroke felt that the ‘answer was in.’ Therefore, treatment equipoise was lost."
In all, 127 patients were enrolled between 2004 and 2011, of which 118 were fully eligible. Their mean age was 65.5 years and median National Institutes of Health Stroke Scale score was 17. Overall, 37% received intravenous TPA, and 80% underwent imaging with MRI.
Symptomatic hemorrhage occurred in 4% and 21% died, Dr. Kidwell said. The mean time to groin puncture was 6.2 hours.
"All of this means that we still need to put more and more patients in research protocols to better figure out who will benefit the most from endovascular therapy," American Heart Association past-president Dr. Ralph Sacco, chair of neurology at the University of Miami, said in an interview. "It has been shown now, including the subanalysis from IMS III, that the earlier you recanalize the better, and so we need to be still thinking about time windows. Just like with IV [intravenous] TPA, the earlier we treat, the better. Well, with endovascular therapy that may be true as well and you have to remember that sometimes penumbral imaging adds time."
Although embolectomy proponents and device manufacturers may see the results as a setback, another take was expressed by an audience member, who described the results as good news.
"The vast majority of people in the United States and the world probably have better access to primary care facilities rather than having access to academic centers, so to my patient population and to people I think in the vast majority, when we see that IV TPA is perhaps equivalent to more aggressive treatments that require more expansive techniques and depth of expertise, it’s kind of good news," she said to a round of applause.
Dr. Kidwell thanked her for the comment, but added, "I think there still are those among us who do believe that advanced neuroimaging, as well as endovascular therapy, will have a role down the line. I think we just need further trials with the new stent retriever devices to really sort this out."
MR RESCUE was funded by the National Institute of Neurological Disorders and Stroke. Concentric Medical Inc. provided study catheters and devices for part of the trial, with costs thereafter covered by study funds or third-party payers. Seven of the coauthors are employees of the University of California, which holds a patent on Merci Retriever devices. Dr. Chimowitz disclosed research support from the National Institutes of Health. Dr. Sacco reported no disclosures.
AT THE INTERNATIONAL STROKE CONFERENCE
Major Finding: Among all patients, mean modified Rankin scores at 90 days were similar between embolectomy and standard care (3.9 vs. 3.9; P = .99).
Data Source: Phase IIb study in 118 patients with ischemic stroke.
Disclosures: MR RESCUE was funded by the National Institute of Neurological Disorders and Stroke. Concentric Medical Inc. provided study catheters and devices for part of the trial, with costs thereafter covered by study funds or third-party payers. Seven of the co-authors are employees of the University of California, which holds a patent on Merci Retriever devices. Dr. Chimowitz disclosed research support from the National Institutes of Health. Dr. Sacco reported no disclosures.

DP-b99 dead in the water as stroke therapy
HONOLULU – The investigational agent DP-b99 provides no more neuroprotection than placebo for patients with acute ischemic stroke, according to the results of the phase III Membrane-Activated Chelator Stroke Intervention trial.
"There is no evidence that this drug offers any clinical benefit when administered within 9 hours of symptom onset," lead investigator Dr. Kennedy Lees said in a late-breaking abstract session at the International Stroke Conference.

DP-b99 is a first-in-class, membrane-activated ion chelator of zinc, which has been associated with cell signaling and, if overloaded, can be a precursor for cell death and subsequent brain degeneration following a stroke.
"The theory is that if you chelate the signaling within the membrane, you could improve the outcome and reduce the damage," said Dr. Lees, who is with the University of Glasgow, Scotland.
DP-b99 produced promising results in animal models and two phase II studies at a daily dose of 1 mg/kg for 4 days. In one of those trials, a 4-day course of DP-b99 failed to significantly alter the primary endpoint of change in National Institutes of Health Stroke Scale (NIHSS) score at 90 days, but significantly improved recovery at 90 days, as measured by modified Rankin Scale scores. In addition, patients with moderate stroke severity (NIHSS score of 10-16) appeared to gain a particular advantage from DP-b99 therapy, experiencing a significant change in NIHSS scores by day 90 (Stroke 2008;39:1774-8).
Based on these intriguing findings, the double-blind, multicenter phase III MACSI (Membrane-Activated Chelator Stroke Intervention) trial was restricted to patients within 9 hours of acute ischemic stroke onset who had a baseline NIHSS score of 10-16, were not treated with the recombinant TPA drug alteplase (Activase), and had cortical stroke findings. At the time of a preplanned futility analysis, 446 patients had been randomly assigned to intravenous DP-b99 for 4 consecutive days or placebo.
The 218 Dp-b99 patients and 219 controls with at least one outcome in the intent-to-treat analysis were reasonably balanced, with the exception of controls being slightly younger (69.7 years vs. 73 years) and less likely to have had a previous stroke (17% vs. 22%), noted Dr. Lees, professor of cerebrovascular medicine at the University of Glasgow, Scotland. Median NIHSS scores were 13 and 12.5, respectively.
The study’s primary endpoint, ordinal modified Rankin score distributions at 90 days, were not significantly different between the placebo and DP-b99 groups (P = .105), even when adjusted for baseline age and NIHSS score (P = .21).
Moreover, fewer patients treated with DP-b99 than placebo achieved a modified Rankin score of 0 or 1 (odds ratio, 0.64) or a NIHSS score of 0 or 1 (OR, 0.69), and both groups had similar time at home within the first 90 days (OR, 1.28) and mortality (OR, 0.90).
The trial was stopped due to futility, although the authors reluctantly went on to perform subgroup analyses at the behest of Stroke, which simultaneously published the results online (Stroke 2013 Feb. 7 [doi: 10.1161/strokeaha.111.000013]).
"The bottom line: no effect there," regardless of whether the data were cut by gender, history of prior stroke, premorbid modified Rankin Score 0 or deficit, onset to treatment time, or age, Dr. Lees said at the conference, sponsored by the American Heart Association.
D-Pharm sponsored the trial. The authors received fees and expenses for their role on the MACSI trial steering committee. Dr. Lees and his coauthors reported relationships with drug and device companies, but none directly related to MACSI.
HONOLULU – The investigational agent DP-b99 provides no more neuroprotection than placebo for patients with acute ischemic stroke, according to the results of the phase III Membrane-Activated Chelator Stroke Intervention trial.
"There is no evidence that this drug offers any clinical benefit when administered within 9 hours of symptom onset," lead investigator Dr. Kennedy Lees said in a late-breaking abstract session at the International Stroke Conference.
DP-b99 is a first-in-class, membrane-activated ion chelator of zinc, which has been associated with cell signaling and, if overloaded, can be a precursor for cell death and subsequent brain degeneration following a stroke.
"The theory is that if you chelate the signaling within the membrane, you could improve the outcome and reduce the damage," said Dr. Lees, who is with the University of Glasgow, Scotland.
DP-b99 produced promising results in animal models and two phase II studies at a daily dose of 1 mg/kg for 4 days. In one of those trials, a 4-day course of DP-b99 failed to significantly alter the primary endpoint of change in National Institutes of Health Stroke Scale (NIHSS) score at 90 days, but significantly improved recovery at 90 days, as measured by modified Rankin Scale scores. In addition, patients with moderate stroke severity (NIHSS score of 10-16) appeared to gain a particular advantage from DP-b99 therapy, experiencing a significant change in NIHSS scores by day 90 (Stroke 2008;39:1774-8).
Based on these intriguing findings, the double-blind, multicenter phase III MACSI (Membrane-Activated Chelator Stroke Intervention) trial was restricted to patients within 9 hours of acute ischemic stroke onset who had a baseline NIHSS score of 10-16, were not treated with the recombinant TPA drug alteplase (Activase), and had cortical stroke findings. At the time of a preplanned futility analysis, 446 patients had been randomly assigned to intravenous DP-b99 for 4 consecutive days or placebo.
The 218 Dp-b99 patients and 219 controls with at least one outcome in the intent-to-treat analysis were reasonably balanced, with the exception of controls being slightly younger (69.7 years vs. 73 years) and less likely to have had a previous stroke (17% vs. 22%), noted Dr. Lees, professor of cerebrovascular medicine at the University of Glasgow, Scotland. Median NIHSS scores were 13 and 12.5, respectively.
The study’s primary endpoint, ordinal modified Rankin score distributions at 90 days, were not significantly different between the placebo and DP-b99 groups (P = .105), even when adjusted for baseline age and NIHSS score (P = .21).
Moreover, fewer patients treated with DP-b99 than placebo achieved a modified Rankin score of 0 or 1 (odds ratio, 0.64) or a NIHSS score of 0 or 1 (OR, 0.69), and both groups had similar time at home within the first 90 days (OR, 1.28) and mortality (OR, 0.90).
The trial was stopped due to futility, although the authors reluctantly went on to perform subgroup analyses at the behest of Stroke, which simultaneously published the results online (Stroke 2013 Feb. 7 [doi: 10.1161/strokeaha.111.000013]).
"The bottom line: no effect there," regardless of whether the data were cut by gender, history of prior stroke, premorbid modified Rankin Score 0 or deficit, onset to treatment time, or age, Dr. Lees said at the conference, sponsored by the American Heart Association.
D-Pharm sponsored the trial. The authors received fees and expenses for their role on the MACSI trial steering committee. Dr. Lees and his coauthors reported relationships with drug and device companies, but none directly related to MACSI.
HONOLULU – The investigational agent DP-b99 provides no more neuroprotection than placebo for patients with acute ischemic stroke, according to the results of the phase III Membrane-Activated Chelator Stroke Intervention trial.
"There is no evidence that this drug offers any clinical benefit when administered within 9 hours of symptom onset," lead investigator Dr. Kennedy Lees said in a late-breaking abstract session at the International Stroke Conference.
DP-b99 is a first-in-class, membrane-activated ion chelator of zinc, which has been associated with cell signaling and, if overloaded, can be a precursor for cell death and subsequent brain degeneration following a stroke.
"The theory is that if you chelate the signaling within the membrane, you could improve the outcome and reduce the damage," said Dr. Lees, who is with the University of Glasgow, Scotland.
DP-b99 produced promising results in animal models and two phase II studies at a daily dose of 1 mg/kg for 4 days. In one of those trials, a 4-day course of DP-b99 failed to significantly alter the primary endpoint of change in National Institutes of Health Stroke Scale (NIHSS) score at 90 days, but significantly improved recovery at 90 days, as measured by modified Rankin Scale scores. In addition, patients with moderate stroke severity (NIHSS score of 10-16) appeared to gain a particular advantage from DP-b99 therapy, experiencing a significant change in NIHSS scores by day 90 (Stroke 2008;39:1774-8).
Based on these intriguing findings, the double-blind, multicenter phase III MACSI (Membrane-Activated Chelator Stroke Intervention) trial was restricted to patients within 9 hours of acute ischemic stroke onset who had a baseline NIHSS score of 10-16, were not treated with the recombinant TPA drug alteplase (Activase), and had cortical stroke findings. At the time of a preplanned futility analysis, 446 patients had been randomly assigned to intravenous DP-b99 for 4 consecutive days or placebo.
The 218 Dp-b99 patients and 219 controls with at least one outcome in the intent-to-treat analysis were reasonably balanced, with the exception of controls being slightly younger (69.7 years vs. 73 years) and less likely to have had a previous stroke (17% vs. 22%), noted Dr. Lees, professor of cerebrovascular medicine at the University of Glasgow, Scotland. Median NIHSS scores were 13 and 12.5, respectively.
The study’s primary endpoint, ordinal modified Rankin score distributions at 90 days, were not significantly different between the placebo and DP-b99 groups (P = .105), even when adjusted for baseline age and NIHSS score (P = .21).
Moreover, fewer patients treated with DP-b99 than placebo achieved a modified Rankin score of 0 or 1 (odds ratio, 0.64) or a NIHSS score of 0 or 1 (OR, 0.69), and both groups had similar time at home within the first 90 days (OR, 1.28) and mortality (OR, 0.90).
The trial was stopped due to futility, although the authors reluctantly went on to perform subgroup analyses at the behest of Stroke, which simultaneously published the results online (Stroke 2013 Feb. 7 [doi: 10.1161/strokeaha.111.000013]).
"The bottom line: no effect there," regardless of whether the data were cut by gender, history of prior stroke, premorbid modified Rankin Score 0 or deficit, onset to treatment time, or age, Dr. Lees said at the conference, sponsored by the American Heart Association.
D-Pharm sponsored the trial. The authors received fees and expenses for their role on the MACSI trial steering committee. Dr. Lees and his coauthors reported relationships with drug and device companies, but none directly related to MACSI.
AT THE INTERNATIONAL STROKE CONFERENCE
Major Finding: Ordinal modified Rankin score distributions at 90 days were not significantly different between the placebo and DP-b99 groups (P = .105), even when adjusted for baseline age and NIHSS score (P = .21).
Data Source: Double-blind, multicenter phase III trial in 437 patients with acute ischemic stroke.
Disclosures: D-Pharm sponsored the trial. The authors received fees and expenses for their role on the MACSI trial steering committee. Dr. Lees and his coauthors reported relationships with drug and device companies, but none directly related to MACSI.

Massachusetts ED docs reporting impaired drivers to the state
Boston emergency department physicians are now reporting impaired motorists for possible driver’s license revocation.
Over a 16-month period, 31% of admitted drivers were impaired. Of these, 17 were considered medically unqualified to drive, and 86 needed further medical evaluation.

"The vast majority of patients believe they’ll be reported [to authorities] if they arrive at the hospital impaired or under the influence, but that is not the case in Massachusetts, or in most other states from what we’ve found," according to trauma surgeon Eric Mahoney, who helped develop the reporting protocol.
Many health care personnel resist such reporting because they fear a lawsuit or retaliation. The Massachusetts Safe Driving Law of 2010 has changed the landscape by expanding the ability of health care providers and law enforcement to report drivers whom the health care providers believe are unfit to drive because of cognitive or functional impairment. The reports are sent to the Registry of Motor Vehicles (RMV), not the police.
"This has never been meant to be punitive," noted Dr. Mahoney of the department of trauma and emergency services at Boston Medical Center.
The intent has always been to get impaired drivers to visit their physicians to adjust their medication if needed, reevaluate their medical condition, or, if impairment results from substance abuse, counsel them. It’s been shown that the more contact patients have with health care, the more successful they will be at managing their health problems, he said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
The protocol may also reduce motor vehicle crashes by having recidivists held accountable for their actions.

"In our state, the acquittal rate is close to 90% for first-time DUI offenders, so we know the current system in place really isn’t working," according to study coauthor Lisa Allee, Boston Medical Center’s injury prevention coordinator. "So our goal is to reduce recidivism and get people the help they need," she said.
Dr. Mahoney and his colleagues used the Massachusetts RMV definition of impaired driving and vetted HIPPA compliance through the hospital’s legal department. A physician can request that the RMV medical advisory board seek medical evaluation of a driver when the physician has a good faith belief of impairment based on personal observation, physical examinations, or laboratory studies. The request cannot be based on driver age or previous diagnosis.
When the accident involves substance abuse, reporting is limited to instances of a "violent/high risk" to the public such as driving in the wrong direction of traffic, speed exceeding 55 mph, having a child or loaded firearm in the car, or fleeing from police
In the 16-month study period, 363 motor vehicle–crash drivers were admitted to the ED, of which 114 (31%) were impaired and 90% met the "dangerousness" requirement, Dr. Mahoney reported. Their average age was 42 years, 60% were white, 23% were black, 8% were Hispanic, and 41% had private commercial insurance.
Of those reported as being impaired, 18% were incapacitated by a medical condition, 78% were impaired because of substance use, and 3% were incapacitated by both.
Syncope and seizure were the most common medical conditions causing impairment (50% and 25%), followed by about 5% each of narcolepsy, brain lesion, respiratory failure, dizziness, dementia, normal pressure hydrocephalus, and cerebrovascular accident.
Alcohol was the most common substance causing impairment, present in more than 80% of cases, followed by a benzodiazepine, cocaine, and other prescriptions, he said.
"Impairment is common in drivers admitted to the trauma center, and 90% are violent, dangerous to the public," Dr. Mahoney said. "We need to encourage and empower others to report."

The topic of impaired drivers was on the radar of other EAST investigators. Dr. Felicia Ivascu of the Beaumont Health System in Royal Oak, Mich., reported that 11% of the 541 crash victims treated from 2008 to 2010 at their level I trauma center were legally intoxicated. Moreover, data available on 52 of these drivers revealed these patients cost the hospital $5.2 million in total charges, which accounts for 12% of all charges for drivers.
Michigan is one of 12 states to have no-fault automobile insurance, and the only one that provides unlimited medical benefits. Because of the high costs, House Bill 5588 was recently introduced to remove no-fault benefits if a person is found driving while intoxicated or impaired at the time of the accident, regardless of responsibility.
The dilemma, however, is that passage of the bill would reduce net revenue, and "this will lead to a large financial burden for hospitals that treat intoxicated drivers, requiring them to either absorb this cost or pass it on to Medicaid," the authors wrote.
Dr. Mahoney, Dr. Ivascu, and their coauthors reported no relevant financial disclosures.
Boston emergency department physicians are now reporting impaired motorists for possible driver’s license revocation.
Over a 16-month period, 31% of admitted drivers were impaired. Of these, 17 were considered medically unqualified to drive, and 86 needed further medical evaluation.
"The vast majority of patients believe they’ll be reported [to authorities] if they arrive at the hospital impaired or under the influence, but that is not the case in Massachusetts, or in most other states from what we’ve found," according to trauma surgeon Eric Mahoney, who helped develop the reporting protocol.
Many health care personnel resist such reporting because they fear a lawsuit or retaliation. The Massachusetts Safe Driving Law of 2010 has changed the landscape by expanding the ability of health care providers and law enforcement to report drivers whom the health care providers believe are unfit to drive because of cognitive or functional impairment. The reports are sent to the Registry of Motor Vehicles (RMV), not the police.
"This has never been meant to be punitive," noted Dr. Mahoney of the department of trauma and emergency services at Boston Medical Center.
The intent has always been to get impaired drivers to visit their physicians to adjust their medication if needed, reevaluate their medical condition, or, if impairment results from substance abuse, counsel them. It’s been shown that the more contact patients have with health care, the more successful they will be at managing their health problems, he said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
The protocol may also reduce motor vehicle crashes by having recidivists held accountable for their actions.
"In our state, the acquittal rate is close to 90% for first-time DUI offenders, so we know the current system in place really isn’t working," according to study coauthor Lisa Allee, Boston Medical Center’s injury prevention coordinator. "So our goal is to reduce recidivism and get people the help they need," she said.
Dr. Mahoney and his colleagues used the Massachusetts RMV definition of impaired driving and vetted HIPPA compliance through the hospital’s legal department. A physician can request that the RMV medical advisory board seek medical evaluation of a driver when the physician has a good faith belief of impairment based on personal observation, physical examinations, or laboratory studies. The request cannot be based on driver age or previous diagnosis.
When the accident involves substance abuse, reporting is limited to instances of a "violent/high risk" to the public such as driving in the wrong direction of traffic, speed exceeding 55 mph, having a child or loaded firearm in the car, or fleeing from police
In the 16-month study period, 363 motor vehicle–crash drivers were admitted to the ED, of which 114 (31%) were impaired and 90% met the "dangerousness" requirement, Dr. Mahoney reported. Their average age was 42 years, 60% were white, 23% were black, 8% were Hispanic, and 41% had private commercial insurance.
Of those reported as being impaired, 18% were incapacitated by a medical condition, 78% were impaired because of substance use, and 3% were incapacitated by both.
Syncope and seizure were the most common medical conditions causing impairment (50% and 25%), followed by about 5% each of narcolepsy, brain lesion, respiratory failure, dizziness, dementia, normal pressure hydrocephalus, and cerebrovascular accident.
Alcohol was the most common substance causing impairment, present in more than 80% of cases, followed by a benzodiazepine, cocaine, and other prescriptions, he said.
"Impairment is common in drivers admitted to the trauma center, and 90% are violent, dangerous to the public," Dr. Mahoney said. "We need to encourage and empower others to report."
The topic of impaired drivers was on the radar of other EAST investigators. Dr. Felicia Ivascu of the Beaumont Health System in Royal Oak, Mich., reported that 11% of the 541 crash victims treated from 2008 to 2010 at their level I trauma center were legally intoxicated. Moreover, data available on 52 of these drivers revealed these patients cost the hospital $5.2 million in total charges, which accounts for 12% of all charges for drivers.
Michigan is one of 12 states to have no-fault automobile insurance, and the only one that provides unlimited medical benefits. Because of the high costs, House Bill 5588 was recently introduced to remove no-fault benefits if a person is found driving while intoxicated or impaired at the time of the accident, regardless of responsibility.
The dilemma, however, is that passage of the bill would reduce net revenue, and "this will lead to a large financial burden for hospitals that treat intoxicated drivers, requiring them to either absorb this cost or pass it on to Medicaid," the authors wrote.
Dr. Mahoney, Dr. Ivascu, and their coauthors reported no relevant financial disclosures.
Boston emergency department physicians are now reporting impaired motorists for possible driver’s license revocation.
Over a 16-month period, 31% of admitted drivers were impaired. Of these, 17 were considered medically unqualified to drive, and 86 needed further medical evaluation.
"The vast majority of patients believe they’ll be reported [to authorities] if they arrive at the hospital impaired or under the influence, but that is not the case in Massachusetts, or in most other states from what we’ve found," according to trauma surgeon Eric Mahoney, who helped develop the reporting protocol.
Many health care personnel resist such reporting because they fear a lawsuit or retaliation. The Massachusetts Safe Driving Law of 2010 has changed the landscape by expanding the ability of health care providers and law enforcement to report drivers whom the health care providers believe are unfit to drive because of cognitive or functional impairment. The reports are sent to the Registry of Motor Vehicles (RMV), not the police.
"This has never been meant to be punitive," noted Dr. Mahoney of the department of trauma and emergency services at Boston Medical Center.
The intent has always been to get impaired drivers to visit their physicians to adjust their medication if needed, reevaluate their medical condition, or, if impairment results from substance abuse, counsel them. It’s been shown that the more contact patients have with health care, the more successful they will be at managing their health problems, he said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
The protocol may also reduce motor vehicle crashes by having recidivists held accountable for their actions.
"In our state, the acquittal rate is close to 90% for first-time DUI offenders, so we know the current system in place really isn’t working," according to study coauthor Lisa Allee, Boston Medical Center’s injury prevention coordinator. "So our goal is to reduce recidivism and get people the help they need," she said.
Dr. Mahoney and his colleagues used the Massachusetts RMV definition of impaired driving and vetted HIPPA compliance through the hospital’s legal department. A physician can request that the RMV medical advisory board seek medical evaluation of a driver when the physician has a good faith belief of impairment based on personal observation, physical examinations, or laboratory studies. The request cannot be based on driver age or previous diagnosis.
When the accident involves substance abuse, reporting is limited to instances of a "violent/high risk" to the public such as driving in the wrong direction of traffic, speed exceeding 55 mph, having a child or loaded firearm in the car, or fleeing from police
In the 16-month study period, 363 motor vehicle–crash drivers were admitted to the ED, of which 114 (31%) were impaired and 90% met the "dangerousness" requirement, Dr. Mahoney reported. Their average age was 42 years, 60% were white, 23% were black, 8% were Hispanic, and 41% had private commercial insurance.
Of those reported as being impaired, 18% were incapacitated by a medical condition, 78% were impaired because of substance use, and 3% were incapacitated by both.
Syncope and seizure were the most common medical conditions causing impairment (50% and 25%), followed by about 5% each of narcolepsy, brain lesion, respiratory failure, dizziness, dementia, normal pressure hydrocephalus, and cerebrovascular accident.
Alcohol was the most common substance causing impairment, present in more than 80% of cases, followed by a benzodiazepine, cocaine, and other prescriptions, he said.
"Impairment is common in drivers admitted to the trauma center, and 90% are violent, dangerous to the public," Dr. Mahoney said. "We need to encourage and empower others to report."
The topic of impaired drivers was on the radar of other EAST investigators. Dr. Felicia Ivascu of the Beaumont Health System in Royal Oak, Mich., reported that 11% of the 541 crash victims treated from 2008 to 2010 at their level I trauma center were legally intoxicated. Moreover, data available on 52 of these drivers revealed these patients cost the hospital $5.2 million in total charges, which accounts for 12% of all charges for drivers.
Michigan is one of 12 states to have no-fault automobile insurance, and the only one that provides unlimited medical benefits. Because of the high costs, House Bill 5588 was recently introduced to remove no-fault benefits if a person is found driving while intoxicated or impaired at the time of the accident, regardless of responsibility.
The dilemma, however, is that passage of the bill would reduce net revenue, and "this will lead to a large financial burden for hospitals that treat intoxicated drivers, requiring them to either absorb this cost or pass it on to Medicaid," the authors wrote.
Dr. Mahoney, Dr. Ivascu, and their coauthors reported no relevant financial disclosures.
AT THE EAST SCIENTIFIC ASSEMBLY
Major Finding: Over a 16-month period, 31% of drivers were impaired because of a medical condition or substance abuse.
Data Source: Retrospective analysis of a prospective impaired driver reporting protocol.
Disclosures: Dr. Mahoney, Dr. Ivascu, and their coauthors reported no relevant financial disclosures.

Survey: Most support transfusing to increase organ donation
SCOTTSDALE, ARIZ. – The majority of trauma surgeons would aggressively manage patients with a lethal brain injury for the purposes of organ donation.
Consensus on how best to transfuse these patients to protect their organs appears to be another matter, a survey of Eastern Association for the Surgery of Trauma (EAST) members reveals.

"Further investigation is needed to determine what the transfusion triggers and limits should be in order to maximize our donor conversion rates," said Dr. Stancie Rhodes and her colleagues at Robert Wood Johnson University Hospital, New Brunswick, N.J.
Many institutions have set up aggressive donor management protocols to help address the worldwide shortage of transplantable organs. At press time, 117,090 candidates were on the U.S. Department of Health and Human Services’ Organ Procurement and Transplantation Network waiting list, with just 25,785 transplants performed between January and November 2012.
Aggressive donor management (ADM) protocols typically include guidelines for invasive monitoring and correction of metabolic disturbances that follow brain death, but many continue to lack guidelines on when and in what quantity to transfuse potential organ donors, explained Dr. Rhodes, a trauma surgeon at Robert Wood Johnson.
To further develop these guidelines, the investigators electronically surveyed all trauma surgeons in EAST regarding their transfusion practices in patients with nonsurvivable brain injury. In all, 285 members responded (24.5%). Among these respondents, 53.5% currently transfuse these patients.
Almost three-fourths, 72.5%, of respondents agreed with aggressive medical management of patients with lethal brain injury in the hope they could donate organs, while 9.4% strongly disagreed, Dr. Rhodes reported in a poster at the EAST’s annual meeting.
Trauma surgeons practicing in a suburban setting were significantly more likely to agree with transfusion than were those in rural or urban settings (77% vs. 52% vs. 55%; P less than .04).
Before deciding to aggressively manage a potential organ donor, respondents were divided on whether the testing for declaration of brain death must already be underway (111 strongly agree/26 strongly disagree), the patient must be declared brain dead (11 strongly agree/84 strongly disagree), or consent for donation of organs must have been obtained (6 strongly agree/114 strongly disagree, Dr. Rhodes reported.
"I think the important piece is that respondents overwhelmingly agreed that they would not wait for declaration of brain death to begin to aggressively manage these patients," she said in an interview. "This is important, as these patients succumb to hypoperfusion, coagulopathy, and acidosis if their ongoing hemorrhage is uncontrolled early in their course."
The majority of respondents (75%) agreed that they have a limit to the amount of product they would administer.
If the potential donor was in hemorrhagic shock, 6 respondents strongly agreed and 12 agreed they would consider transfusing blood products, while 114 disagreed and 119 strongly disagreed with the practice.
Respondents were more likely to consider transfusing, however, if the potential donor was having coagulopathic bleeding. In all, 47 strongly agreed and 106 agreed with transfusing in this setting, while 30 disagreed and 15 strongly disagreed.
If either hemorrhagic shock or coagulopathic bleeding were present, most respondents would limit packed red blood cells and fresh frozen plasma to no more than 5-8 units, and platelets to no more than 1-4 units, the authors reported.
Of those surgeons surveyed, 42% were between the ages of 40 and 49 years, 10.2% practiced primarily in a rural setting, 15.1% practiced in an suburban setting – defined as a population less than 500,000 – and 45.6% were in an urban setting, defined by a population in excess of 500,000 residents.
Dr. Rhodes and her coauthors have nothing to disclose.
transfuse, survey, Eastern Association for the Surgery of Trauma, EAST, Dr. Stancie Rhodes, aggressive donor management protocols, worldwide shortage of transplantable organs, U.S. Department of Health and Human Services’ Organ Procurement and Transplantation Network waiting list,
SCOTTSDALE, ARIZ. – The majority of trauma surgeons would aggressively manage patients with a lethal brain injury for the purposes of organ donation.
Consensus on how best to transfuse these patients to protect their organs appears to be another matter, a survey of Eastern Association for the Surgery of Trauma (EAST) members reveals.
"Further investigation is needed to determine what the transfusion triggers and limits should be in order to maximize our donor conversion rates," said Dr. Stancie Rhodes and her colleagues at Robert Wood Johnson University Hospital, New Brunswick, N.J.
Many institutions have set up aggressive donor management protocols to help address the worldwide shortage of transplantable organs. At press time, 117,090 candidates were on the U.S. Department of Health and Human Services’ Organ Procurement and Transplantation Network waiting list, with just 25,785 transplants performed between January and November 2012.
Aggressive donor management (ADM) protocols typically include guidelines for invasive monitoring and correction of metabolic disturbances that follow brain death, but many continue to lack guidelines on when and in what quantity to transfuse potential organ donors, explained Dr. Rhodes, a trauma surgeon at Robert Wood Johnson.
To further develop these guidelines, the investigators electronically surveyed all trauma surgeons in EAST regarding their transfusion practices in patients with nonsurvivable brain injury. In all, 285 members responded (24.5%). Among these respondents, 53.5% currently transfuse these patients.
Almost three-fourths, 72.5%, of respondents agreed with aggressive medical management of patients with lethal brain injury in the hope they could donate organs, while 9.4% strongly disagreed, Dr. Rhodes reported in a poster at the EAST’s annual meeting.
Trauma surgeons practicing in a suburban setting were significantly more likely to agree with transfusion than were those in rural or urban settings (77% vs. 52% vs. 55%; P less than .04).
Before deciding to aggressively manage a potential organ donor, respondents were divided on whether the testing for declaration of brain death must already be underway (111 strongly agree/26 strongly disagree), the patient must be declared brain dead (11 strongly agree/84 strongly disagree), or consent for donation of organs must have been obtained (6 strongly agree/114 strongly disagree, Dr. Rhodes reported.
"I think the important piece is that respondents overwhelmingly agreed that they would not wait for declaration of brain death to begin to aggressively manage these patients," she said in an interview. "This is important, as these patients succumb to hypoperfusion, coagulopathy, and acidosis if their ongoing hemorrhage is uncontrolled early in their course."
The majority of respondents (75%) agreed that they have a limit to the amount of product they would administer.
If the potential donor was in hemorrhagic shock, 6 respondents strongly agreed and 12 agreed they would consider transfusing blood products, while 114 disagreed and 119 strongly disagreed with the practice.
Respondents were more likely to consider transfusing, however, if the potential donor was having coagulopathic bleeding. In all, 47 strongly agreed and 106 agreed with transfusing in this setting, while 30 disagreed and 15 strongly disagreed.
If either hemorrhagic shock or coagulopathic bleeding were present, most respondents would limit packed red blood cells and fresh frozen plasma to no more than 5-8 units, and platelets to no more than 1-4 units, the authors reported.
Of those surgeons surveyed, 42% were between the ages of 40 and 49 years, 10.2% practiced primarily in a rural setting, 15.1% practiced in an suburban setting – defined as a population less than 500,000 – and 45.6% were in an urban setting, defined by a population in excess of 500,000 residents.
Dr. Rhodes and her coauthors have nothing to disclose.
SCOTTSDALE, ARIZ. – The majority of trauma surgeons would aggressively manage patients with a lethal brain injury for the purposes of organ donation.
Consensus on how best to transfuse these patients to protect their organs appears to be another matter, a survey of Eastern Association for the Surgery of Trauma (EAST) members reveals.
"Further investigation is needed to determine what the transfusion triggers and limits should be in order to maximize our donor conversion rates," said Dr. Stancie Rhodes and her colleagues at Robert Wood Johnson University Hospital, New Brunswick, N.J.
Many institutions have set up aggressive donor management protocols to help address the worldwide shortage of transplantable organs. At press time, 117,090 candidates were on the U.S. Department of Health and Human Services’ Organ Procurement and Transplantation Network waiting list, with just 25,785 transplants performed between January and November 2012.
Aggressive donor management (ADM) protocols typically include guidelines for invasive monitoring and correction of metabolic disturbances that follow brain death, but many continue to lack guidelines on when and in what quantity to transfuse potential organ donors, explained Dr. Rhodes, a trauma surgeon at Robert Wood Johnson.
To further develop these guidelines, the investigators electronically surveyed all trauma surgeons in EAST regarding their transfusion practices in patients with nonsurvivable brain injury. In all, 285 members responded (24.5%). Among these respondents, 53.5% currently transfuse these patients.
Almost three-fourths, 72.5%, of respondents agreed with aggressive medical management of patients with lethal brain injury in the hope they could donate organs, while 9.4% strongly disagreed, Dr. Rhodes reported in a poster at the EAST’s annual meeting.
Trauma surgeons practicing in a suburban setting were significantly more likely to agree with transfusion than were those in rural or urban settings (77% vs. 52% vs. 55%; P less than .04).
Before deciding to aggressively manage a potential organ donor, respondents were divided on whether the testing for declaration of brain death must already be underway (111 strongly agree/26 strongly disagree), the patient must be declared brain dead (11 strongly agree/84 strongly disagree), or consent for donation of organs must have been obtained (6 strongly agree/114 strongly disagree, Dr. Rhodes reported.
"I think the important piece is that respondents overwhelmingly agreed that they would not wait for declaration of brain death to begin to aggressively manage these patients," she said in an interview. "This is important, as these patients succumb to hypoperfusion, coagulopathy, and acidosis if their ongoing hemorrhage is uncontrolled early in their course."
The majority of respondents (75%) agreed that they have a limit to the amount of product they would administer.
If the potential donor was in hemorrhagic shock, 6 respondents strongly agreed and 12 agreed they would consider transfusing blood products, while 114 disagreed and 119 strongly disagreed with the practice.
Respondents were more likely to consider transfusing, however, if the potential donor was having coagulopathic bleeding. In all, 47 strongly agreed and 106 agreed with transfusing in this setting, while 30 disagreed and 15 strongly disagreed.
If either hemorrhagic shock or coagulopathic bleeding were present, most respondents would limit packed red blood cells and fresh frozen plasma to no more than 5-8 units, and platelets to no more than 1-4 units, the authors reported.
Of those surgeons surveyed, 42% were between the ages of 40 and 49 years, 10.2% practiced primarily in a rural setting, 15.1% practiced in an suburban setting – defined as a population less than 500,000 – and 45.6% were in an urban setting, defined by a population in excess of 500,000 residents.
Dr. Rhodes and her coauthors have nothing to disclose.
transfuse, survey, Eastern Association for the Surgery of Trauma, EAST, Dr. Stancie Rhodes, aggressive donor management protocols, worldwide shortage of transplantable organs, U.S. Department of Health and Human Services’ Organ Procurement and Transplantation Network waiting list,
transfuse, survey, Eastern Association for the Surgery of Trauma, EAST, Dr. Stancie Rhodes, aggressive donor management protocols, worldwide shortage of transplantable organs, U.S. Department of Health and Human Services’ Organ Procurement and Transplantation Network waiting list,
EXPERT ANALYSIS FROM THE EAST ANNUAL MEETING
Major Finding: Among respondents, 72.5% agreed with aggressive medical management of patients with lethal brain injury for the sake of organ donation, but there was less consensus on when and how to manage these patients.
Data Source: Electronic survey of 285 trauma surgeons in the Eastern Association for the Surgery of Trauma.
Disclosures: Dr. Rhodes and her coauthors have nothing to disclose.

Aggressive BP lowering after lacunar stroke may reduce recurrence
HONOLULU – In patients with recent lacunar strokes, aggressive lowering of systolic blood pressure safely reduced the risk of recurrent stroke by about 20% in the BP intervention arm of the Secondary Prevention of Small Subcortical Strokes trial.
The primary endpoint of recurrent ischemic and hemorrhagic stroke was 2.3% per year in patients with a target systolic blood pressure of less than 130 mm Hg and 2.8% among those randomized to a target of 130-149 mm Hg (hazard ratio, 0.81; P = .08). Annual ischemic stroke rates also trended lower (2.0 vs. 2.4%; HR, 0.84; P = .19).

The lower blood pressure target, however, significantly reduced intracerebral hemorrhage by nearly two-thirds (0.11% vs. 0.29%; HR, 0.37; P = .03), Dr. Oscar R. Benavente reported on behalf of the Secondary Prevention of Small Subcortical Strokes (SPS3) investigators during a late-breaking plenary session at the International Stroke Conference.
The results are consistent with previous randomized controlled trials of BP lowering in stroke, but do not answer how low blood pressure should go or what the optimal target is, he said at a press briefing.
At 1-year follow-up, the average systolic BPs were 138 mm Hg and 127 mm Hg in the higher- and lower-target groups, having fallen from an average of 145 mm Hg and 144 mm Hg, respectively, at baseline.
Despite the lack of statistical significance for the primary endpoint, plenary session comoderator Dr. Steven Greenberg, professor of neurology at Harvard Medical School and director of hemorrhagic stroke research at Massachusetts General Hospital, both in Boston, told reporters, "as a clinician in practice, I would take these results very seriously."
He observed that clinicians often make decisions without a P value at the .05 level of certainty, and said the reduction in hemorrhagic stroke was a "very powerful finding" since studies have shown that the outcome from hemorrhagic stroke is even worse than that from ischemic stroke.
"This very much reinforces the impression that many of us already have – but now that the data are stronger – that we should aim for a lower blood pressure target in our patients," he said at the press briefing.

While the hemorrhagic stroke finding is important, the problem is that ischemic strokes make up the vast majority of recurrent strokes, commented Dr. Philip Gorelick, professor of translation science and molecular medicine, Michigan State University, and medical director of the Hauenstein Neuroscience Center, both in Grand Rapids, Mich.
"There wasn’t a clear-cut significance there, and so we’re still wrestling with this issue of where to drop that blood pressure point [to]," he said in an interview.
The intervention was well tolerated, however, "so you are not trading strokes for major safety events," pointed out Dr. Benavente of the brain research center, University of British Columbia, Vancouver.
As previously reported, the dual-therapy arm of SPS3 was stopped early because treatment with clopidogrel plus aspirin not only failed to significantly reduce the risk of recurrent stroke, but significantly increased the risk of all-cause mortality and major hemorrhage, compared with aspirin alone.
In the BP intervention arm, the higher- and lower-target groups had similar rates of serious complications of hypotension (15 events vs. 23 events; HR, 1.53; P = .20), including orthostatic syncope (5 events vs. 11 events; HR, 2.18; P = .14), stroke (1 event vs. 2 events; HR, 2.00; P = .57), myocardial infarction (0 events in both groups), and fall with injury (0 events vs. 3 events; HR and P not available).

Serious complications related to BP medications were limited to one case of bradycardia requiring hospitalization in the lower-target group, Dr. Benavente said at the conference, sponsored by the American Heart Association.
He also noted that there was no interaction between the BP intervention and diabetes, which was present in a little more than one-third of patients in both groups.
This finding is important since the American Diabetes Association recently raised its BP treatment goal from less than 130 mm Hg to less than 140 mm Hg to reflect clinical trial data showing limited benefit to more-intensive BP treatment in patients with diabetes, Dr. Gorelick observed. In the PROGRESS trial in which Dr. Gorelick served on the steering committee, he noted that it took at least 6 months for the curves to begin to separate for stroke recurrence.
"I think that blood pressures in the 130-139 [mm Hg] range is where you want to be, because you’re not going to know who’s going to have a hemorrhage; you’re not going to know who’s going to have a heart attack necessarily or a stroke; so I think we need to be reasonable here," he said.
Dr. Benavente told reporters that while BP lowering is recommended for stroke patients in other guidelines, there are no set BP targets.
Patients in SPS3 had an imaging-verified lacunar stroke within 180 days of study entry and were followed for a mean of 3.7 years. There were 1,519 patients in the higher-target group and 1,501 in the lower-target group. Their baseline diastolic BPs were 80 mm Hg and 78 mm Hg. They were on an average of 1.4 and 1.2 BP medications at study entry, and 1.4 and 1.3 at 1 year. Blood pressure medications were not specified by protocol.
Antihypertensives were not discontinued at study entry. At last visit, 60% of the higher-target group and 78% of the lower-target group were on an angiotensin-converting enzyme inhibitor or angiotensin II receptor blocker, 39% vs. 43% on a calcium channel blocker, and 38% vs. 54% on thiazides.
At the last observed visit, the average systolic BP difference between groups was 11 mm Hg. Major vascular events, defined as stroke, MI, and vascular deaths, occurred in 3.4% of the higher-target group (188 events) vs. 3.0% of the lower-target group (160 events) (HR,0.84; P = .10), Dr. Benavente said.
SPS3 is sponsored by the National Institute of Neurological Disorders and Stroke (NINDS). Sanofi-Aventis and Bristol-Myers Squibb donated the study drugs. Dr. Benavente has received research support from NINDS. Dr. Greenberg reported receiving research grants from the National Institutes of Health and serving as a consultant/advisory board member for Hoffman-La Roche. Dr. Gorelick reported having no relevant financial disclosures.
HONOLULU – In patients with recent lacunar strokes, aggressive lowering of systolic blood pressure safely reduced the risk of recurrent stroke by about 20% in the BP intervention arm of the Secondary Prevention of Small Subcortical Strokes trial.
The primary endpoint of recurrent ischemic and hemorrhagic stroke was 2.3% per year in patients with a target systolic blood pressure of less than 130 mm Hg and 2.8% among those randomized to a target of 130-149 mm Hg (hazard ratio, 0.81; P = .08). Annual ischemic stroke rates also trended lower (2.0 vs. 2.4%; HR, 0.84; P = .19).
The lower blood pressure target, however, significantly reduced intracerebral hemorrhage by nearly two-thirds (0.11% vs. 0.29%; HR, 0.37; P = .03), Dr. Oscar R. Benavente reported on behalf of the Secondary Prevention of Small Subcortical Strokes (SPS3) investigators during a late-breaking plenary session at the International Stroke Conference.
The results are consistent with previous randomized controlled trials of BP lowering in stroke, but do not answer how low blood pressure should go or what the optimal target is, he said at a press briefing.
At 1-year follow-up, the average systolic BPs were 138 mm Hg and 127 mm Hg in the higher- and lower-target groups, having fallen from an average of 145 mm Hg and 144 mm Hg, respectively, at baseline.
Despite the lack of statistical significance for the primary endpoint, plenary session comoderator Dr. Steven Greenberg, professor of neurology at Harvard Medical School and director of hemorrhagic stroke research at Massachusetts General Hospital, both in Boston, told reporters, "as a clinician in practice, I would take these results very seriously."
He observed that clinicians often make decisions without a P value at the .05 level of certainty, and said the reduction in hemorrhagic stroke was a "very powerful finding" since studies have shown that the outcome from hemorrhagic stroke is even worse than that from ischemic stroke.
"This very much reinforces the impression that many of us already have – but now that the data are stronger – that we should aim for a lower blood pressure target in our patients," he said at the press briefing.
While the hemorrhagic stroke finding is important, the problem is that ischemic strokes make up the vast majority of recurrent strokes, commented Dr. Philip Gorelick, professor of translation science and molecular medicine, Michigan State University, and medical director of the Hauenstein Neuroscience Center, both in Grand Rapids, Mich.
"There wasn’t a clear-cut significance there, and so we’re still wrestling with this issue of where to drop that blood pressure point [to]," he said in an interview.
The intervention was well tolerated, however, "so you are not trading strokes for major safety events," pointed out Dr. Benavente of the brain research center, University of British Columbia, Vancouver.
As previously reported, the dual-therapy arm of SPS3 was stopped early because treatment with clopidogrel plus aspirin not only failed to significantly reduce the risk of recurrent stroke, but significantly increased the risk of all-cause mortality and major hemorrhage, compared with aspirin alone.
In the BP intervention arm, the higher- and lower-target groups had similar rates of serious complications of hypotension (15 events vs. 23 events; HR, 1.53; P = .20), including orthostatic syncope (5 events vs. 11 events; HR, 2.18; P = .14), stroke (1 event vs. 2 events; HR, 2.00; P = .57), myocardial infarction (0 events in both groups), and fall with injury (0 events vs. 3 events; HR and P not available).
Serious complications related to BP medications were limited to one case of bradycardia requiring hospitalization in the lower-target group, Dr. Benavente said at the conference, sponsored by the American Heart Association.
He also noted that there was no interaction between the BP intervention and diabetes, which was present in a little more than one-third of patients in both groups.
This finding is important since the American Diabetes Association recently raised its BP treatment goal from less than 130 mm Hg to less than 140 mm Hg to reflect clinical trial data showing limited benefit to more-intensive BP treatment in patients with diabetes, Dr. Gorelick observed. In the PROGRESS trial in which Dr. Gorelick served on the steering committee, he noted that it took at least 6 months for the curves to begin to separate for stroke recurrence.
"I think that blood pressures in the 130-139 [mm Hg] range is where you want to be, because you’re not going to know who’s going to have a hemorrhage; you’re not going to know who’s going to have a heart attack necessarily or a stroke; so I think we need to be reasonable here," he said.
Dr. Benavente told reporters that while BP lowering is recommended for stroke patients in other guidelines, there are no set BP targets.
Patients in SPS3 had an imaging-verified lacunar stroke within 180 days of study entry and were followed for a mean of 3.7 years. There were 1,519 patients in the higher-target group and 1,501 in the lower-target group. Their baseline diastolic BPs were 80 mm Hg and 78 mm Hg. They were on an average of 1.4 and 1.2 BP medications at study entry, and 1.4 and 1.3 at 1 year. Blood pressure medications were not specified by protocol.
Antihypertensives were not discontinued at study entry. At last visit, 60% of the higher-target group and 78% of the lower-target group were on an angiotensin-converting enzyme inhibitor or angiotensin II receptor blocker, 39% vs. 43% on a calcium channel blocker, and 38% vs. 54% on thiazides.
At the last observed visit, the average systolic BP difference between groups was 11 mm Hg. Major vascular events, defined as stroke, MI, and vascular deaths, occurred in 3.4% of the higher-target group (188 events) vs. 3.0% of the lower-target group (160 events) (HR,0.84; P = .10), Dr. Benavente said.
SPS3 is sponsored by the National Institute of Neurological Disorders and Stroke (NINDS). Sanofi-Aventis and Bristol-Myers Squibb donated the study drugs. Dr. Benavente has received research support from NINDS. Dr. Greenberg reported receiving research grants from the National Institutes of Health and serving as a consultant/advisory board member for Hoffman-La Roche. Dr. Gorelick reported having no relevant financial disclosures.
HONOLULU – In patients with recent lacunar strokes, aggressive lowering of systolic blood pressure safely reduced the risk of recurrent stroke by about 20% in the BP intervention arm of the Secondary Prevention of Small Subcortical Strokes trial.
The primary endpoint of recurrent ischemic and hemorrhagic stroke was 2.3% per year in patients with a target systolic blood pressure of less than 130 mm Hg and 2.8% among those randomized to a target of 130-149 mm Hg (hazard ratio, 0.81; P = .08). Annual ischemic stroke rates also trended lower (2.0 vs. 2.4%; HR, 0.84; P = .19).
The lower blood pressure target, however, significantly reduced intracerebral hemorrhage by nearly two-thirds (0.11% vs. 0.29%; HR, 0.37; P = .03), Dr. Oscar R. Benavente reported on behalf of the Secondary Prevention of Small Subcortical Strokes (SPS3) investigators during a late-breaking plenary session at the International Stroke Conference.
The results are consistent with previous randomized controlled trials of BP lowering in stroke, but do not answer how low blood pressure should go or what the optimal target is, he said at a press briefing.
At 1-year follow-up, the average systolic BPs were 138 mm Hg and 127 mm Hg in the higher- and lower-target groups, having fallen from an average of 145 mm Hg and 144 mm Hg, respectively, at baseline.
Despite the lack of statistical significance for the primary endpoint, plenary session comoderator Dr. Steven Greenberg, professor of neurology at Harvard Medical School and director of hemorrhagic stroke research at Massachusetts General Hospital, both in Boston, told reporters, "as a clinician in practice, I would take these results very seriously."
He observed that clinicians often make decisions without a P value at the .05 level of certainty, and said the reduction in hemorrhagic stroke was a "very powerful finding" since studies have shown that the outcome from hemorrhagic stroke is even worse than that from ischemic stroke.
"This very much reinforces the impression that many of us already have – but now that the data are stronger – that we should aim for a lower blood pressure target in our patients," he said at the press briefing.
While the hemorrhagic stroke finding is important, the problem is that ischemic strokes make up the vast majority of recurrent strokes, commented Dr. Philip Gorelick, professor of translation science and molecular medicine, Michigan State University, and medical director of the Hauenstein Neuroscience Center, both in Grand Rapids, Mich.
"There wasn’t a clear-cut significance there, and so we’re still wrestling with this issue of where to drop that blood pressure point [to]," he said in an interview.
The intervention was well tolerated, however, "so you are not trading strokes for major safety events," pointed out Dr. Benavente of the brain research center, University of British Columbia, Vancouver.
As previously reported, the dual-therapy arm of SPS3 was stopped early because treatment with clopidogrel plus aspirin not only failed to significantly reduce the risk of recurrent stroke, but significantly increased the risk of all-cause mortality and major hemorrhage, compared with aspirin alone.
In the BP intervention arm, the higher- and lower-target groups had similar rates of serious complications of hypotension (15 events vs. 23 events; HR, 1.53; P = .20), including orthostatic syncope (5 events vs. 11 events; HR, 2.18; P = .14), stroke (1 event vs. 2 events; HR, 2.00; P = .57), myocardial infarction (0 events in both groups), and fall with injury (0 events vs. 3 events; HR and P not available).
Serious complications related to BP medications were limited to one case of bradycardia requiring hospitalization in the lower-target group, Dr. Benavente said at the conference, sponsored by the American Heart Association.
He also noted that there was no interaction between the BP intervention and diabetes, which was present in a little more than one-third of patients in both groups.
This finding is important since the American Diabetes Association recently raised its BP treatment goal from less than 130 mm Hg to less than 140 mm Hg to reflect clinical trial data showing limited benefit to more-intensive BP treatment in patients with diabetes, Dr. Gorelick observed. In the PROGRESS trial in which Dr. Gorelick served on the steering committee, he noted that it took at least 6 months for the curves to begin to separate for stroke recurrence.
"I think that blood pressures in the 130-139 [mm Hg] range is where you want to be, because you’re not going to know who’s going to have a hemorrhage; you’re not going to know who’s going to have a heart attack necessarily or a stroke; so I think we need to be reasonable here," he said.
Dr. Benavente told reporters that while BP lowering is recommended for stroke patients in other guidelines, there are no set BP targets.
Patients in SPS3 had an imaging-verified lacunar stroke within 180 days of study entry and were followed for a mean of 3.7 years. There were 1,519 patients in the higher-target group and 1,501 in the lower-target group. Their baseline diastolic BPs were 80 mm Hg and 78 mm Hg. They were on an average of 1.4 and 1.2 BP medications at study entry, and 1.4 and 1.3 at 1 year. Blood pressure medications were not specified by protocol.
Antihypertensives were not discontinued at study entry. At last visit, 60% of the higher-target group and 78% of the lower-target group were on an angiotensin-converting enzyme inhibitor or angiotensin II receptor blocker, 39% vs. 43% on a calcium channel blocker, and 38% vs. 54% on thiazides.
At the last observed visit, the average systolic BP difference between groups was 11 mm Hg. Major vascular events, defined as stroke, MI, and vascular deaths, occurred in 3.4% of the higher-target group (188 events) vs. 3.0% of the lower-target group (160 events) (HR,0.84; P = .10), Dr. Benavente said.
SPS3 is sponsored by the National Institute of Neurological Disorders and Stroke (NINDS). Sanofi-Aventis and Bristol-Myers Squibb donated the study drugs. Dr. Benavente has received research support from NINDS. Dr. Greenberg reported receiving research grants from the National Institutes of Health and serving as a consultant/advisory board member for Hoffman-La Roche. Dr. Gorelick reported having no relevant financial disclosures.
AT THE INTERNATIONAL STROKE CONFERENCE
Major Finding: Annual rates of recurrent ischemic and hemorrhagic stroke were 2.3% in patients with a target systolic BP of less than 130 mm Hg and 2.8% in those with a target of 130-149 mm Hg (HR, 0.81; P = .08).
Data Source: Randomized, multicenter, international trial in 3,020 patients with lacunar strokes.
Disclosures: The SPS3 trial is sponsored by the National Institute of Neurological Disorders and Stroke. Sanofi-Aventis and Bristol-Myers Squibb donated the study drugs. Dr. Benavente has received research support from NINDS. Dr. Greenberg reported receiving research grants from the National Institutes of Health and serving as a consultant/advisory board member for Hoffman-La Roche. Dr. Gorelick reported having no relevant financial disclosures.

Eptifibatide combo passes phase II hurdle
HONOLULU – Eptifibatide plus medium-dose tissue plasminogen activator was safe in a phase IIb study, and a larger, phase III trial is now needed to determine whether the combination can improve ischemic stroke outcomes.
Symptomatic intracerebral hemorrhage (ICH) within 36 hours, the primary safety end point of the trial, occurred in 2% of patients randomized to the combination and in 12% given standard intravenous recombinant tissue plasminogen activator (rt-PA) alone.

A modified Rankin Scale score of 0 or 1 or return to baseline mRS at 90 days, the primary efficacy outcome, was achieved by 36% on rt-PA alone and by 49.5% on the combination. The outcome values far exceeded the 33% prespecified "no-go" criterion set for phase III evaluation, Dr. Opeolu Adeoye said on behalf of the CLEAR-ER (Combined Approach to Lysis Utilizing Eptifibatide and rt-PA in Acute Ischemic Stroke- Enhanced Regimen) trial investigators at the International Stroke Conference.
Dr. Adeoye acknowledged that "unexpected imbalances," however, existed between groups. The combination therapy group tended to be younger than the rt-PA only group (mean, 68.9 years vs. 70.9 years), had less severe strokes based on NIHSS scores (median 12 vs. 17), and had a slightly higher proportion of patients with a baseline mRS of 0 or 1 (84.2% vs. 72%).
The unadjusted odds ratio for the primary efficacy end point was 1.74, and the odds ratio was 1.38 after adjustment for age, baseline NIHSS (National Institutes of Health Stroke Scale) score, time to rt-PA, and baseline mRS. After adjustment for all but baseline mRS, the relative risk was 1.16.
"Obviously, this is a phase II study and was not designed to assess efficacy, but after adjusting for these imbalances, what we think is a clinically meaningful treatment effect persisted between groups," said Dr. Adeoye, of the University of Cincinnati Neuroscience Institute.
He noted that no obvious efficacy signal was observed in the dose-escalation, safety CLEAR Stroke trial, which was stopped early due to safety concerns about dosing rt-PA at 0.45 mg/kg over 60 minutes with a 75-mcg/kg bolus of eptifibatide followed by a 2-hour infusion at 0.75 mcg/kg/min (Stroke 2008;39:3268-76).
Among patients with myocardial infarction, combining the glycoprotein IIb/IIIa receptor inhibitor plus unfractionated heparin offered no added benefit and significantly increased the rate of bleeding in the ASSIST trial.
In CLEAR-ER, 126 ischemic stroke patients, aged 18-85 years, with an NIHSS score of more than 5 were randomized 5:1 to rt-PA 0.6 mg/kg over 40 minutes plus eptifibatide 135 mcg/kg bolus followed by a 2-hour infusion at 0.75 mcg/kg/min or standard-dose rt-PA 0.9 mg/kg. Treatment was initiated within 3 hours of symptom onset.
At day 7, symptomatic ICH rates held constant in the combination and rt-PA only groups at 2% and 12%, respectively (OR, 0.15), while asymptomatic ICH was seen in 15.8% and 12% (OR, 1.38).
At 90 days, at least one serious adverse event was reported in 26% of the combination group and 28% of the rt-PA only group. All-cause mortality rates were 20% vs. 16%, respectively, and were 15% vs. 16% for stroke-related death.
Dr. Andrei Alexandrov, director of the division of cerebrovascular disease at the University of Alabama, Birmingham, who moderated the late-breaking abstract session, questioned whether a phase III trial may be premature given that vascular imaging was not used in the current trial to determine whether vessel occlusions were present.
Dr. Adeoye responded that at the time the trial was designed, the standard of care was variable at the nine participating sites. Moreover, the data were stratified using an NIHSS score of more than or less than 12, and showed that "the bulk of the treatment effect actually appeared to be in the patients with a higher stroke scale. Not having imaging, I can’t speak to whether or not that definitely means those strokes were open; but clinically, I would venture to suggest that is what’s going on."
The conference was sponsored by the American Heart Association.
The National Heart, Lung and Blood Institute funded the study. Genentech and Merck supplied the study drugs. Dr. Adeoye reported serving as a speaker for Genentech; his coauthors reported no disclosures.
HONOLULU – Eptifibatide plus medium-dose tissue plasminogen activator was safe in a phase IIb study, and a larger, phase III trial is now needed to determine whether the combination can improve ischemic stroke outcomes.
Symptomatic intracerebral hemorrhage (ICH) within 36 hours, the primary safety end point of the trial, occurred in 2% of patients randomized to the combination and in 12% given standard intravenous recombinant tissue plasminogen activator (rt-PA) alone.
A modified Rankin Scale score of 0 or 1 or return to baseline mRS at 90 days, the primary efficacy outcome, was achieved by 36% on rt-PA alone and by 49.5% on the combination. The outcome values far exceeded the 33% prespecified "no-go" criterion set for phase III evaluation, Dr. Opeolu Adeoye said on behalf of the CLEAR-ER (Combined Approach to Lysis Utilizing Eptifibatide and rt-PA in Acute Ischemic Stroke- Enhanced Regimen) trial investigators at the International Stroke Conference.
Dr. Adeoye acknowledged that "unexpected imbalances," however, existed between groups. The combination therapy group tended to be younger than the rt-PA only group (mean, 68.9 years vs. 70.9 years), had less severe strokes based on NIHSS scores (median 12 vs. 17), and had a slightly higher proportion of patients with a baseline mRS of 0 or 1 (84.2% vs. 72%).
The unadjusted odds ratio for the primary efficacy end point was 1.74, and the odds ratio was 1.38 after adjustment for age, baseline NIHSS (National Institutes of Health Stroke Scale) score, time to rt-PA, and baseline mRS. After adjustment for all but baseline mRS, the relative risk was 1.16.
"Obviously, this is a phase II study and was not designed to assess efficacy, but after adjusting for these imbalances, what we think is a clinically meaningful treatment effect persisted between groups," said Dr. Adeoye, of the University of Cincinnati Neuroscience Institute.
He noted that no obvious efficacy signal was observed in the dose-escalation, safety CLEAR Stroke trial, which was stopped early due to safety concerns about dosing rt-PA at 0.45 mg/kg over 60 minutes with a 75-mcg/kg bolus of eptifibatide followed by a 2-hour infusion at 0.75 mcg/kg/min (Stroke 2008;39:3268-76).
Among patients with myocardial infarction, combining the glycoprotein IIb/IIIa receptor inhibitor plus unfractionated heparin offered no added benefit and significantly increased the rate of bleeding in the ASSIST trial.
In CLEAR-ER, 126 ischemic stroke patients, aged 18-85 years, with an NIHSS score of more than 5 were randomized 5:1 to rt-PA 0.6 mg/kg over 40 minutes plus eptifibatide 135 mcg/kg bolus followed by a 2-hour infusion at 0.75 mcg/kg/min or standard-dose rt-PA 0.9 mg/kg. Treatment was initiated within 3 hours of symptom onset.
At day 7, symptomatic ICH rates held constant in the combination and rt-PA only groups at 2% and 12%, respectively (OR, 0.15), while asymptomatic ICH was seen in 15.8% and 12% (OR, 1.38).
At 90 days, at least one serious adverse event was reported in 26% of the combination group and 28% of the rt-PA only group. All-cause mortality rates were 20% vs. 16%, respectively, and were 15% vs. 16% for stroke-related death.
Dr. Andrei Alexandrov, director of the division of cerebrovascular disease at the University of Alabama, Birmingham, who moderated the late-breaking abstract session, questioned whether a phase III trial may be premature given that vascular imaging was not used in the current trial to determine whether vessel occlusions were present.
Dr. Adeoye responded that at the time the trial was designed, the standard of care was variable at the nine participating sites. Moreover, the data were stratified using an NIHSS score of more than or less than 12, and showed that "the bulk of the treatment effect actually appeared to be in the patients with a higher stroke scale. Not having imaging, I can’t speak to whether or not that definitely means those strokes were open; but clinically, I would venture to suggest that is what’s going on."
The conference was sponsored by the American Heart Association.
The National Heart, Lung and Blood Institute funded the study. Genentech and Merck supplied the study drugs. Dr. Adeoye reported serving as a speaker for Genentech; his coauthors reported no disclosures.
HONOLULU – Eptifibatide plus medium-dose tissue plasminogen activator was safe in a phase IIb study, and a larger, phase III trial is now needed to determine whether the combination can improve ischemic stroke outcomes.
Symptomatic intracerebral hemorrhage (ICH) within 36 hours, the primary safety end point of the trial, occurred in 2% of patients randomized to the combination and in 12% given standard intravenous recombinant tissue plasminogen activator (rt-PA) alone.
A modified Rankin Scale score of 0 or 1 or return to baseline mRS at 90 days, the primary efficacy outcome, was achieved by 36% on rt-PA alone and by 49.5% on the combination. The outcome values far exceeded the 33% prespecified "no-go" criterion set for phase III evaluation, Dr. Opeolu Adeoye said on behalf of the CLEAR-ER (Combined Approach to Lysis Utilizing Eptifibatide and rt-PA in Acute Ischemic Stroke- Enhanced Regimen) trial investigators at the International Stroke Conference.
Dr. Adeoye acknowledged that "unexpected imbalances," however, existed between groups. The combination therapy group tended to be younger than the rt-PA only group (mean, 68.9 years vs. 70.9 years), had less severe strokes based on NIHSS scores (median 12 vs. 17), and had a slightly higher proportion of patients with a baseline mRS of 0 or 1 (84.2% vs. 72%).
The unadjusted odds ratio for the primary efficacy end point was 1.74, and the odds ratio was 1.38 after adjustment for age, baseline NIHSS (National Institutes of Health Stroke Scale) score, time to rt-PA, and baseline mRS. After adjustment for all but baseline mRS, the relative risk was 1.16.
"Obviously, this is a phase II study and was not designed to assess efficacy, but after adjusting for these imbalances, what we think is a clinically meaningful treatment effect persisted between groups," said Dr. Adeoye, of the University of Cincinnati Neuroscience Institute.
He noted that no obvious efficacy signal was observed in the dose-escalation, safety CLEAR Stroke trial, which was stopped early due to safety concerns about dosing rt-PA at 0.45 mg/kg over 60 minutes with a 75-mcg/kg bolus of eptifibatide followed by a 2-hour infusion at 0.75 mcg/kg/min (Stroke 2008;39:3268-76).
Among patients with myocardial infarction, combining the glycoprotein IIb/IIIa receptor inhibitor plus unfractionated heparin offered no added benefit and significantly increased the rate of bleeding in the ASSIST trial.
In CLEAR-ER, 126 ischemic stroke patients, aged 18-85 years, with an NIHSS score of more than 5 were randomized 5:1 to rt-PA 0.6 mg/kg over 40 minutes plus eptifibatide 135 mcg/kg bolus followed by a 2-hour infusion at 0.75 mcg/kg/min or standard-dose rt-PA 0.9 mg/kg. Treatment was initiated within 3 hours of symptom onset.
At day 7, symptomatic ICH rates held constant in the combination and rt-PA only groups at 2% and 12%, respectively (OR, 0.15), while asymptomatic ICH was seen in 15.8% and 12% (OR, 1.38).
At 90 days, at least one serious adverse event was reported in 26% of the combination group and 28% of the rt-PA only group. All-cause mortality rates were 20% vs. 16%, respectively, and were 15% vs. 16% for stroke-related death.
Dr. Andrei Alexandrov, director of the division of cerebrovascular disease at the University of Alabama, Birmingham, who moderated the late-breaking abstract session, questioned whether a phase III trial may be premature given that vascular imaging was not used in the current trial to determine whether vessel occlusions were present.
Dr. Adeoye responded that at the time the trial was designed, the standard of care was variable at the nine participating sites. Moreover, the data were stratified using an NIHSS score of more than or less than 12, and showed that "the bulk of the treatment effect actually appeared to be in the patients with a higher stroke scale. Not having imaging, I can’t speak to whether or not that definitely means those strokes were open; but clinically, I would venture to suggest that is what’s going on."
The conference was sponsored by the American Heart Association.
The National Heart, Lung and Blood Institute funded the study. Genentech and Merck supplied the study drugs. Dr. Adeoye reported serving as a speaker for Genentech; his coauthors reported no disclosures.
AT THE INTERNATIONAL STROKE CONFERENCE
Major finding: Symptomatic intracerebral hemorrhage within 36 hours occurred in 2% of patients on medium-dose rt-PA plus eptifibatide and in 12% of those on standard rt-PA alone (OR, 0.15).
Data source: Prospective, multicenter, double-blind phase IIb study of 126 patients with acute ischemic stroke.
Disclosures: The National Heart, Lung and Blood Institute funded the study. Genentech and Merck supplied the study drugs. Dr. Adeoye reported serving as a speaker for Genentech; his coauthors reported no disclosures.

Hemodynamic complications commonly found in veterans after TBI
HONOLULU – Cerebral vasospasm and intracranial hypertension may be frequent secondary insults following wartime traumatic brain injury, according to a retrospective study of 122 consecutive veterans.
Transcranial Doppler (TCD) ultrasonography signs of mild, moderate, and severe vasospasm involving anterior circulation vessels were observed in 71%, 42%, and 16% of the veterans with traumatic brain injury (TBI), respectively.
TCD signs involving posterior circulation vessels were observed in 57%, 32%, and 14%, respectively.
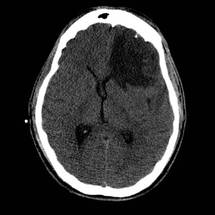
Intracranial hypertension was recorded in 43% of patients, lead author Alexander Razumovsky, Ph.D., reported at the International Stroke Conference.
"Cerebral blood flow velocity measurements permit detection of early signs of cerebral vasospasm and allow physicians to better define management strategies," he said.
TCD monitoring is routinely used by the U.S. Army, but it has not been fully embraced elsewhere because many physicians are unaware of how it can be used within the continuum of TBI care to help reverse outcomes, said study coauthor Col. Rocco Armonda, MC, USA.
"There’s this lack of drive to change outcomes because people haven’t seen how you can take someone who is in a comatose state and eventually gain functional independence," said Dr. Armonda, who is the director of cerebrovascular surgery and interventional neuroradiology at the National Naval Medical Center in Bethesda, Md.
A recent study from Walter Reed National Military Medical Center (J. Trauma Acute Care Surg. 2012;73:1525-30), however, reported that 63% of veterans with a penetrating TBI and a mean discharge Glasgow Coma Scale (GCS) score of 6-8 progressed to functional independence – a number twice as high as would be expected, Dr. Armonda remarked.

Dr. Razumovsky said that simple, noninvasive TCD monitoring should be performed in the daily management of hospitalized TBI patients to complement other monitoring strategies, and it can be used alone in emergency situations when intracranial pressure monitoring is contraindicated or not readily available.
TCD monitoring is not necessary during outpatient follow-up of patients with TBI, with the exception of the subset who’ve undergone hemicraniectomy, Dr. Armonda said.
"In those patients who’ve had hemicraniectomy, some of them suffer prolonged duration from atmospheric pressure of the cranial defect, and TCD has actually been helpful to look at the cerebral blood flow dynamics," he said at a press briefing on the study.
The results confirm earlier data that TBI is associated with a high incidence of cerebral vasospasm, particularly in patients with severe TBI, and are applicable to civilian TBI patients because a significant number will experience post-traumatic bleeding that will lead to vasospasm and intracranial hypertension, said Dr. Razumovsky, director of Sentient NeuroCare Services in Hunt Valley, Md., which provides services to the National Naval Medical Hospital.

In the current study, patients were admitted to Walter Reed a mean of 6.7 days after injury from Oct. 1, 2008, to Nov. 30, 2012. Mean cerebral blood flow velocity (CBFV) of 100-139 cm/s was used to define mild vasospasm, 140-199 cm/s moderate vasospasm, and more than 200 cm/s severe vasospasm.
In all, 88 patients had penetrating head injury, of whom 45 (51%) had a secondary diagnosis of blast injury; and 34 patients had a closed head injury, of whom 15 (44%) had a secondary diagnosis of blast injury. Their mean age was 26 years.
In the mild vasospasm group, the mean anterior circulation CBFV was 122.5 cm/s and mean posterior CBFV was 61 cm/s. Their average GCS score changed from 8 at baseline to 6.1 at discharge, Dr. Razumovsky said.
In the moderate vasospasm group, the mean anterior circulation CBFV was 156.6 cm/s and mean posterior CBFV was 77.5 cm/s. Their average GCS score changed from 5.9 at baseline to 5.3 at discharge.
Patients with severe vasospasm had an average anterior circulation CBFV of 241.9 cm/s and a mean posterior CBFV of 101.8 cm/s. Their average GCS score was 4.8 at both time periods.
Eight patients (7%) underwent transluminal angioplasty for post-traumatic symptomatic vasospasm, he said at the meeting, sponsored by the American Heart Association.
Dr. Larry Goldstein, director of the Duke Stroke Center in Durham, N.C., said in an interview that the detection of vasospasm by TCD was potentially important because there is an increased risk of vasospasm after subarachnoid hemorrhage that can lead to delayed ischemic neurological deficits. Although it was unclear from the data how many patients had traumatic subarachnoid hemorrhage associated with their brain injury, he noted that the risk of vasospasm seems to be similar for traumatic and nontraumatic subarachnoid hemorrhage.
"In many centers, both groups of patients are routinely monitored with transcranial Dopplers over the first couple of weeks or so, which is when the peak period of vasospasm develops," Dr. Goldstein said. "Showing that monitoring leads to interventions that then change outcome, that’s not so straightforward."
The study was supported in part by the U.S. Army Medical Research and Materiel Command’s Telemedicine and Advanced Technology Research Center. Dr. Razumovsky and two of his coauthors reported financial remuneration from private practice.
posterior circulation vessels, Alexander Razumovsky, Ph.D., the International Stroke Conference, Cerebral blood flow velocity, U.S. Army, Col. Rocco Armonda, MC, USA,
HONOLULU – Cerebral vasospasm and intracranial hypertension may be frequent secondary insults following wartime traumatic brain injury, according to a retrospective study of 122 consecutive veterans.
Transcranial Doppler (TCD) ultrasonography signs of mild, moderate, and severe vasospasm involving anterior circulation vessels were observed in 71%, 42%, and 16% of the veterans with traumatic brain injury (TBI), respectively.
TCD signs involving posterior circulation vessels were observed in 57%, 32%, and 14%, respectively.
Intracranial hypertension was recorded in 43% of patients, lead author Alexander Razumovsky, Ph.D., reported at the International Stroke Conference.
"Cerebral blood flow velocity measurements permit detection of early signs of cerebral vasospasm and allow physicians to better define management strategies," he said.
TCD monitoring is routinely used by the U.S. Army, but it has not been fully embraced elsewhere because many physicians are unaware of how it can be used within the continuum of TBI care to help reverse outcomes, said study coauthor Col. Rocco Armonda, MC, USA.
"There’s this lack of drive to change outcomes because people haven’t seen how you can take someone who is in a comatose state and eventually gain functional independence," said Dr. Armonda, who is the director of cerebrovascular surgery and interventional neuroradiology at the National Naval Medical Center in Bethesda, Md.
A recent study from Walter Reed National Military Medical Center (J. Trauma Acute Care Surg. 2012;73:1525-30), however, reported that 63% of veterans with a penetrating TBI and a mean discharge Glasgow Coma Scale (GCS) score of 6-8 progressed to functional independence – a number twice as high as would be expected, Dr. Armonda remarked.
Dr. Razumovsky said that simple, noninvasive TCD monitoring should be performed in the daily management of hospitalized TBI patients to complement other monitoring strategies, and it can be used alone in emergency situations when intracranial pressure monitoring is contraindicated or not readily available.
TCD monitoring is not necessary during outpatient follow-up of patients with TBI, with the exception of the subset who’ve undergone hemicraniectomy, Dr. Armonda said.
"In those patients who’ve had hemicraniectomy, some of them suffer prolonged duration from atmospheric pressure of the cranial defect, and TCD has actually been helpful to look at the cerebral blood flow dynamics," he said at a press briefing on the study.
The results confirm earlier data that TBI is associated with a high incidence of cerebral vasospasm, particularly in patients with severe TBI, and are applicable to civilian TBI patients because a significant number will experience post-traumatic bleeding that will lead to vasospasm and intracranial hypertension, said Dr. Razumovsky, director of Sentient NeuroCare Services in Hunt Valley, Md., which provides services to the National Naval Medical Hospital.
In the current study, patients were admitted to Walter Reed a mean of 6.7 days after injury from Oct. 1, 2008, to Nov. 30, 2012. Mean cerebral blood flow velocity (CBFV) of 100-139 cm/s was used to define mild vasospasm, 140-199 cm/s moderate vasospasm, and more than 200 cm/s severe vasospasm.
In all, 88 patients had penetrating head injury, of whom 45 (51%) had a secondary diagnosis of blast injury; and 34 patients had a closed head injury, of whom 15 (44%) had a secondary diagnosis of blast injury. Their mean age was 26 years.
In the mild vasospasm group, the mean anterior circulation CBFV was 122.5 cm/s and mean posterior CBFV was 61 cm/s. Their average GCS score changed from 8 at baseline to 6.1 at discharge, Dr. Razumovsky said.
In the moderate vasospasm group, the mean anterior circulation CBFV was 156.6 cm/s and mean posterior CBFV was 77.5 cm/s. Their average GCS score changed from 5.9 at baseline to 5.3 at discharge.
Patients with severe vasospasm had an average anterior circulation CBFV of 241.9 cm/s and a mean posterior CBFV of 101.8 cm/s. Their average GCS score was 4.8 at both time periods.
Eight patients (7%) underwent transluminal angioplasty for post-traumatic symptomatic vasospasm, he said at the meeting, sponsored by the American Heart Association.
Dr. Larry Goldstein, director of the Duke Stroke Center in Durham, N.C., said in an interview that the detection of vasospasm by TCD was potentially important because there is an increased risk of vasospasm after subarachnoid hemorrhage that can lead to delayed ischemic neurological deficits. Although it was unclear from the data how many patients had traumatic subarachnoid hemorrhage associated with their brain injury, he noted that the risk of vasospasm seems to be similar for traumatic and nontraumatic subarachnoid hemorrhage.
"In many centers, both groups of patients are routinely monitored with transcranial Dopplers over the first couple of weeks or so, which is when the peak period of vasospasm develops," Dr. Goldstein said. "Showing that monitoring leads to interventions that then change outcome, that’s not so straightforward."
The study was supported in part by the U.S. Army Medical Research and Materiel Command’s Telemedicine and Advanced Technology Research Center. Dr. Razumovsky and two of his coauthors reported financial remuneration from private practice.
HONOLULU – Cerebral vasospasm and intracranial hypertension may be frequent secondary insults following wartime traumatic brain injury, according to a retrospective study of 122 consecutive veterans.
Transcranial Doppler (TCD) ultrasonography signs of mild, moderate, and severe vasospasm involving anterior circulation vessels were observed in 71%, 42%, and 16% of the veterans with traumatic brain injury (TBI), respectively.
TCD signs involving posterior circulation vessels were observed in 57%, 32%, and 14%, respectively.
Intracranial hypertension was recorded in 43% of patients, lead author Alexander Razumovsky, Ph.D., reported at the International Stroke Conference.
"Cerebral blood flow velocity measurements permit detection of early signs of cerebral vasospasm and allow physicians to better define management strategies," he said.
TCD monitoring is routinely used by the U.S. Army, but it has not been fully embraced elsewhere because many physicians are unaware of how it can be used within the continuum of TBI care to help reverse outcomes, said study coauthor Col. Rocco Armonda, MC, USA.
"There’s this lack of drive to change outcomes because people haven’t seen how you can take someone who is in a comatose state and eventually gain functional independence," said Dr. Armonda, who is the director of cerebrovascular surgery and interventional neuroradiology at the National Naval Medical Center in Bethesda, Md.
A recent study from Walter Reed National Military Medical Center (J. Trauma Acute Care Surg. 2012;73:1525-30), however, reported that 63% of veterans with a penetrating TBI and a mean discharge Glasgow Coma Scale (GCS) score of 6-8 progressed to functional independence – a number twice as high as would be expected, Dr. Armonda remarked.
Dr. Razumovsky said that simple, noninvasive TCD monitoring should be performed in the daily management of hospitalized TBI patients to complement other monitoring strategies, and it can be used alone in emergency situations when intracranial pressure monitoring is contraindicated or not readily available.
TCD monitoring is not necessary during outpatient follow-up of patients with TBI, with the exception of the subset who’ve undergone hemicraniectomy, Dr. Armonda said.
"In those patients who’ve had hemicraniectomy, some of them suffer prolonged duration from atmospheric pressure of the cranial defect, and TCD has actually been helpful to look at the cerebral blood flow dynamics," he said at a press briefing on the study.
The results confirm earlier data that TBI is associated with a high incidence of cerebral vasospasm, particularly in patients with severe TBI, and are applicable to civilian TBI patients because a significant number will experience post-traumatic bleeding that will lead to vasospasm and intracranial hypertension, said Dr. Razumovsky, director of Sentient NeuroCare Services in Hunt Valley, Md., which provides services to the National Naval Medical Hospital.
In the current study, patients were admitted to Walter Reed a mean of 6.7 days after injury from Oct. 1, 2008, to Nov. 30, 2012. Mean cerebral blood flow velocity (CBFV) of 100-139 cm/s was used to define mild vasospasm, 140-199 cm/s moderate vasospasm, and more than 200 cm/s severe vasospasm.
In all, 88 patients had penetrating head injury, of whom 45 (51%) had a secondary diagnosis of blast injury; and 34 patients had a closed head injury, of whom 15 (44%) had a secondary diagnosis of blast injury. Their mean age was 26 years.
In the mild vasospasm group, the mean anterior circulation CBFV was 122.5 cm/s and mean posterior CBFV was 61 cm/s. Their average GCS score changed from 8 at baseline to 6.1 at discharge, Dr. Razumovsky said.
In the moderate vasospasm group, the mean anterior circulation CBFV was 156.6 cm/s and mean posterior CBFV was 77.5 cm/s. Their average GCS score changed from 5.9 at baseline to 5.3 at discharge.
Patients with severe vasospasm had an average anterior circulation CBFV of 241.9 cm/s and a mean posterior CBFV of 101.8 cm/s. Their average GCS score was 4.8 at both time periods.
Eight patients (7%) underwent transluminal angioplasty for post-traumatic symptomatic vasospasm, he said at the meeting, sponsored by the American Heart Association.
Dr. Larry Goldstein, director of the Duke Stroke Center in Durham, N.C., said in an interview that the detection of vasospasm by TCD was potentially important because there is an increased risk of vasospasm after subarachnoid hemorrhage that can lead to delayed ischemic neurological deficits. Although it was unclear from the data how many patients had traumatic subarachnoid hemorrhage associated with their brain injury, he noted that the risk of vasospasm seems to be similar for traumatic and nontraumatic subarachnoid hemorrhage.
"In many centers, both groups of patients are routinely monitored with transcranial Dopplers over the first couple of weeks or so, which is when the peak period of vasospasm develops," Dr. Goldstein said. "Showing that monitoring leads to interventions that then change outcome, that’s not so straightforward."
The study was supported in part by the U.S. Army Medical Research and Materiel Command’s Telemedicine and Advanced Technology Research Center. Dr. Razumovsky and two of his coauthors reported financial remuneration from private practice.
posterior circulation vessels, Alexander Razumovsky, Ph.D., the International Stroke Conference, Cerebral blood flow velocity, U.S. Army, Col. Rocco Armonda, MC, USA,
posterior circulation vessels, Alexander Razumovsky, Ph.D., the International Stroke Conference, Cerebral blood flow velocity, U.S. Army, Col. Rocco Armonda, MC, USA,
AT THE INTERNATIONAL STROKE CONFERENCE
Major finding: Transcranial Doppler ultrasonography revealed signs of mild, moderate, and severe vasospasm involving anterior circulation vessels in 71%, 42%, and 16% of patients, respectively, but slightly less often in posterior circulation vessels (57%, 32%, and 14%).
Data source: A retrospective study of 122 consecutive patients with combat-related traumatic brain injury.
Disclosures: The study was supported in part by the U.S. Army Medical Research and Materiel Command’s Telemedicine and Advanced Technology Research Center. Dr. Razumovsky and two of his coauthors reported financial remuneration from private practice.
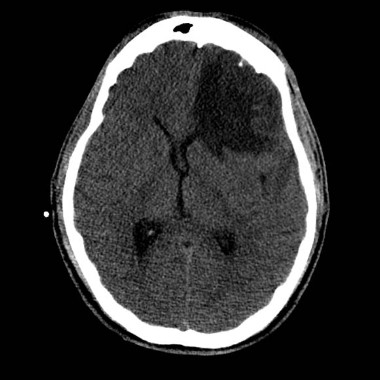
VIDEO: Marijuana may raise stroke risk
Dr. Alan Barber of the University of Auckland discusses the surprising potential link between cannabis use and stroke revealed by a new case-control study of stroke patients. And he outlines the potential implications for physicians prescribing medical marijuana to their patients.
Dr. Alan Barber of the University of Auckland discusses the surprising potential link between cannabis use and stroke revealed by a new case-control study of stroke patients. And he outlines the potential implications for physicians prescribing medical marijuana to their patients.
Dr. Alan Barber of the University of Auckland discusses the surprising potential link between cannabis use and stroke revealed by a new case-control study of stroke patients. And he outlines the potential implications for physicians prescribing medical marijuana to their patients.

Hybrid CFV endovenectomy promising, but not for the faint at heart
CHICAGO – Common femoral endovenectomy with endoluminal iliac recanalization should be considered in patients with chronic post-thrombotic iliofemoral venous obstruction.
The procedure substantially reduces post-thrombotic syndrome morbidity and improves quality of life, although it "is not a procedure for the faint of heart," acknowledged Dr. Anthony Comerota, director of the Jobst Vascular Center at ProMedica Toledo (Ohio) Hospital.

Postthrombotic syndrome occurs in 30%-40% of all patients with a lower-extremity deep vein thrombosis (DVT) at 2 years, despite the use of anticoagulation. Postthrombotic syndrome can be particularly debilitating following an iliofemoral DVT if the common femoral vein (CFV) is badly obstructed or occluded, resulting in such poor quality of life that Dr. Comerota compared it with angina, cancer, and congestive heart failure.
Stenting and angioplasty are often successful in treating postthrombotic iliac vein occlusion, although the risk of stent occlusion is at least 3.8-fold higher in postthrombotic limbs if the stent is extended below the inguinal ligament, he noted.
Relative obstruction of the CFV also can persist after percutaneous intervention and compromise drainage from the profunda femoris vein. This mitigates the benefits of iliac vein recanalization and can actually worsen the patient’s post-thrombotic symptoms, Dr. Comerota said at a symposium on vascular surgery sponsored by Northwestern University.
"It is crucial to open up the orifice of the profunda," he said. "One of the problems we’ve seen in patients referred to us is that, when the common femoral was stented and the stent takes that fibrous tissue and plasters it up against the orifice of the profunda, if there was any minimal drainage from the profunda, it will obliterate it and those patients got worse."
Having previously detailed the technical aspects of the procedure (J. Vasc. Surg. 2012;55:129-35), Dr. Comerota highlighted outcomes of 14 patients and 16 limbs treated to date for severe post-thrombotic, iliofemoral/caval venous obstruction with CEAP (clinical severity, etiology, anatomy, pathophysiology) classification of C3-C6. The median duration of obstruction was nearly 7 years (range, 7 months to 25 years) and median follow-up 3 years (range, 5 months to 6 years). Two patients were lost to follow-up.
To date, one death occurred in a 52-year-old woman with multiple cardiovascular risk factors 9 days after discharge because of an acute myocardial infarction, Dr. Comerota said.
Three patients required surgical evacuation of wound hematomas and three developed early postoperative thrombosis treated with lysis in two cases and thrombectomy in one. All three patients were discharged with patency restored.
One segmental occlusion of the CFV has occurred, and a recent patient with longstanding sickle cell disease developed significant acute lymphedema "that we are still at a loss to explain," he said.
At 6 months, significant improvements were observed in preoperative scores on the Villalta scale (mean, 14 vs. 6; P = .002), Venous Clinical Severity Score (mean, 17 vs. 10; P = .02), CEAP (mean, 4.8 vs. 3.8; P less than .05) and Venous Insufficiency Epidemiological and Economic Study-Quality of Life/Sym questionnaire (data not provided; P = .01).
In some patients, the turnaround was quite dramatic, observed Dr. Comerota, who described a patient who suffered severe trauma and was unable to be anticoagulated. He subsequently had chronic iliofemoral and caval obstruction causing a swollen limb and a painful ulcer for 4 years. The day after surgery, there was remarkable change in the color of the ulcer and leg, and within 3 months the ulcer was completely healed, most of the edema was controlled, and his legs were no longer painful to compression, he said. The patient is back to full activity and has lost 30 pounds.
As a result of inactivity, many of the patients had gained a significant amount of weight, thereby requiring a large incision.
"It is a big procedure," said Dr. Comerota, adding that "it is certainly a procedure in evolution."
Some of the issues requiring further study include the risk/benefit of combined preoperative platelet inhibition and the optimal postoperative anticoagulation; location of an arteriovenous (AV) fistula; and size of the wound drain, currently a 7F closed suction drain.
Three days prior to the procedure, patients receive platelet inhibition with aspirin 81 mg/day and clopidogrel 75 mg/day and twice-daily chlorhexidine showers.
On the day of surgery, patients are fully anticoagulated with 100 IU/kg of unfractionated heparin. It is not reversed with protamine after the surgery is complete, but rather followed with a standard intravenous therapeutic heparin infusion, he said. To reduce the need for supratherapeutic systemic anticoagulation in some patients, a silastic intravenous catheter was placed in a dorsal foot vein to infuse the postoperative heparin.
A small AV fistula of 3.5-4 mm has been required in about half of procedures after continuous wave Doppler failed to identify robust venous velocity signals. The goal of the AV fistula is to increase velocity but not venous pressure, and it has typically been constructed with a wrap around the greater saphenous vein to ensure that it will not enlarge over time, Dr. Comerota said.
"I’ve never been sorry I did an AV fistula. I certainly have been sorry that I have not, so now it’s a routine part of the procedure," he added.
If an iliac venous stenosis or occlusion needs to be stented, Dr. Comerota said that he prefers Wallstents.
"I’m not sure if radial strength is the best term, but Wallstents have the best compression to pressure," he explained. "We’ve used Nitinol [stents] earlier on in our experience, but we had to go back in and reline 50% to 60% of them because they just didn’t hold up the vein properly."
Initially, the team also attempted to keep the stents above the inguinal ligament, but it now takes the approach that the iliac venous occlusion can be stented into the endovenectomized portion of the external iliac vein or CFV, with the caveat that the distal end of the stent must stay above the saphenofemoral junction to preserve profunda femoris venous drainage. Stenting avoids skip lesions that might lead to recurrent thrombosis or continued functional compromise, Dr. Comerota noted.
During a discussion of the procedure, he said that symptomatic presentation and degree of disability are used to determine whether patients should undergo the rigorous procedure.
Surgeons at the Mayo Clinic reported far less promising results in 12 patients who underwent CFV endovenectomy, patch angioplasty, and stenting for chronic iliofemoral venous obstruction, with a 30% 2-year patency and 50% of ulcers with patent grafts recurring (J. Vasc. Surg. 2011;53:383-93).
Dr. Comerata presents an aggressive approach to venous obstructive disease, with operative resection of the fibrotic tissue within the common femoral vein, coupled with endovascular stenting of the iliac segment. He reports relatively good results for these complex patients with a large operative procedure. Other groups have yet to replicate his results and the study population is still relatively small. Certainly, this technique is worth further prospective assessment, as this patient population does experience fairly debilitating symptoms. Whether open surgical treatment coupled with endovascular intervention is the best option remains to be seen.
Dr. Linda Harris is chief of the division of vascular surgery at the State University of New York, Buffalo. Dr. Harris stated that she had no disclosures.
Dr. Comerata presents an aggressive approach to venous obstructive disease, with operative resection of the fibrotic tissue within the common femoral vein, coupled with endovascular stenting of the iliac segment. He reports relatively good results for these complex patients with a large operative procedure. Other groups have yet to replicate his results and the study population is still relatively small. Certainly, this technique is worth further prospective assessment, as this patient population does experience fairly debilitating symptoms. Whether open surgical treatment coupled with endovascular intervention is the best option remains to be seen.
Dr. Linda Harris is chief of the division of vascular surgery at the State University of New York, Buffalo. Dr. Harris stated that she had no disclosures.
Dr. Comerata presents an aggressive approach to venous obstructive disease, with operative resection of the fibrotic tissue within the common femoral vein, coupled with endovascular stenting of the iliac segment. He reports relatively good results for these complex patients with a large operative procedure. Other groups have yet to replicate his results and the study population is still relatively small. Certainly, this technique is worth further prospective assessment, as this patient population does experience fairly debilitating symptoms. Whether open surgical treatment coupled with endovascular intervention is the best option remains to be seen.
Dr. Linda Harris is chief of the division of vascular surgery at the State University of New York, Buffalo. Dr. Harris stated that she had no disclosures.
CHICAGO – Common femoral endovenectomy with endoluminal iliac recanalization should be considered in patients with chronic post-thrombotic iliofemoral venous obstruction.
The procedure substantially reduces post-thrombotic syndrome morbidity and improves quality of life, although it "is not a procedure for the faint of heart," acknowledged Dr. Anthony Comerota, director of the Jobst Vascular Center at ProMedica Toledo (Ohio) Hospital.
Postthrombotic syndrome occurs in 30%-40% of all patients with a lower-extremity deep vein thrombosis (DVT) at 2 years, despite the use of anticoagulation. Postthrombotic syndrome can be particularly debilitating following an iliofemoral DVT if the common femoral vein (CFV) is badly obstructed or occluded, resulting in such poor quality of life that Dr. Comerota compared it with angina, cancer, and congestive heart failure.
Stenting and angioplasty are often successful in treating postthrombotic iliac vein occlusion, although the risk of stent occlusion is at least 3.8-fold higher in postthrombotic limbs if the stent is extended below the inguinal ligament, he noted.
Relative obstruction of the CFV also can persist after percutaneous intervention and compromise drainage from the profunda femoris vein. This mitigates the benefits of iliac vein recanalization and can actually worsen the patient’s post-thrombotic symptoms, Dr. Comerota said at a symposium on vascular surgery sponsored by Northwestern University.
"It is crucial to open up the orifice of the profunda," he said. "One of the problems we’ve seen in patients referred to us is that, when the common femoral was stented and the stent takes that fibrous tissue and plasters it up against the orifice of the profunda, if there was any minimal drainage from the profunda, it will obliterate it and those patients got worse."
Having previously detailed the technical aspects of the procedure (J. Vasc. Surg. 2012;55:129-35), Dr. Comerota highlighted outcomes of 14 patients and 16 limbs treated to date for severe post-thrombotic, iliofemoral/caval venous obstruction with CEAP (clinical severity, etiology, anatomy, pathophysiology) classification of C3-C6. The median duration of obstruction was nearly 7 years (range, 7 months to 25 years) and median follow-up 3 years (range, 5 months to 6 years). Two patients were lost to follow-up.
To date, one death occurred in a 52-year-old woman with multiple cardiovascular risk factors 9 days after discharge because of an acute myocardial infarction, Dr. Comerota said.
Three patients required surgical evacuation of wound hematomas and three developed early postoperative thrombosis treated with lysis in two cases and thrombectomy in one. All three patients were discharged with patency restored.
One segmental occlusion of the CFV has occurred, and a recent patient with longstanding sickle cell disease developed significant acute lymphedema "that we are still at a loss to explain," he said.
At 6 months, significant improvements were observed in preoperative scores on the Villalta scale (mean, 14 vs. 6; P = .002), Venous Clinical Severity Score (mean, 17 vs. 10; P = .02), CEAP (mean, 4.8 vs. 3.8; P less than .05) and Venous Insufficiency Epidemiological and Economic Study-Quality of Life/Sym questionnaire (data not provided; P = .01).
In some patients, the turnaround was quite dramatic, observed Dr. Comerota, who described a patient who suffered severe trauma and was unable to be anticoagulated. He subsequently had chronic iliofemoral and caval obstruction causing a swollen limb and a painful ulcer for 4 years. The day after surgery, there was remarkable change in the color of the ulcer and leg, and within 3 months the ulcer was completely healed, most of the edema was controlled, and his legs were no longer painful to compression, he said. The patient is back to full activity and has lost 30 pounds.
As a result of inactivity, many of the patients had gained a significant amount of weight, thereby requiring a large incision.
"It is a big procedure," said Dr. Comerota, adding that "it is certainly a procedure in evolution."
Some of the issues requiring further study include the risk/benefit of combined preoperative platelet inhibition and the optimal postoperative anticoagulation; location of an arteriovenous (AV) fistula; and size of the wound drain, currently a 7F closed suction drain.
Three days prior to the procedure, patients receive platelet inhibition with aspirin 81 mg/day and clopidogrel 75 mg/day and twice-daily chlorhexidine showers.
On the day of surgery, patients are fully anticoagulated with 100 IU/kg of unfractionated heparin. It is not reversed with protamine after the surgery is complete, but rather followed with a standard intravenous therapeutic heparin infusion, he said. To reduce the need for supratherapeutic systemic anticoagulation in some patients, a silastic intravenous catheter was placed in a dorsal foot vein to infuse the postoperative heparin.
A small AV fistula of 3.5-4 mm has been required in about half of procedures after continuous wave Doppler failed to identify robust venous velocity signals. The goal of the AV fistula is to increase velocity but not venous pressure, and it has typically been constructed with a wrap around the greater saphenous vein to ensure that it will not enlarge over time, Dr. Comerota said.
"I’ve never been sorry I did an AV fistula. I certainly have been sorry that I have not, so now it’s a routine part of the procedure," he added.
If an iliac venous stenosis or occlusion needs to be stented, Dr. Comerota said that he prefers Wallstents.
"I’m not sure if radial strength is the best term, but Wallstents have the best compression to pressure," he explained. "We’ve used Nitinol [stents] earlier on in our experience, but we had to go back in and reline 50% to 60% of them because they just didn’t hold up the vein properly."
Initially, the team also attempted to keep the stents above the inguinal ligament, but it now takes the approach that the iliac venous occlusion can be stented into the endovenectomized portion of the external iliac vein or CFV, with the caveat that the distal end of the stent must stay above the saphenofemoral junction to preserve profunda femoris venous drainage. Stenting avoids skip lesions that might lead to recurrent thrombosis or continued functional compromise, Dr. Comerota noted.
During a discussion of the procedure, he said that symptomatic presentation and degree of disability are used to determine whether patients should undergo the rigorous procedure.
Surgeons at the Mayo Clinic reported far less promising results in 12 patients who underwent CFV endovenectomy, patch angioplasty, and stenting for chronic iliofemoral venous obstruction, with a 30% 2-year patency and 50% of ulcers with patent grafts recurring (J. Vasc. Surg. 2011;53:383-93).
CHICAGO – Common femoral endovenectomy with endoluminal iliac recanalization should be considered in patients with chronic post-thrombotic iliofemoral venous obstruction.
The procedure substantially reduces post-thrombotic syndrome morbidity and improves quality of life, although it "is not a procedure for the faint of heart," acknowledged Dr. Anthony Comerota, director of the Jobst Vascular Center at ProMedica Toledo (Ohio) Hospital.
Postthrombotic syndrome occurs in 30%-40% of all patients with a lower-extremity deep vein thrombosis (DVT) at 2 years, despite the use of anticoagulation. Postthrombotic syndrome can be particularly debilitating following an iliofemoral DVT if the common femoral vein (CFV) is badly obstructed or occluded, resulting in such poor quality of life that Dr. Comerota compared it with angina, cancer, and congestive heart failure.
Stenting and angioplasty are often successful in treating postthrombotic iliac vein occlusion, although the risk of stent occlusion is at least 3.8-fold higher in postthrombotic limbs if the stent is extended below the inguinal ligament, he noted.
Relative obstruction of the CFV also can persist after percutaneous intervention and compromise drainage from the profunda femoris vein. This mitigates the benefits of iliac vein recanalization and can actually worsen the patient’s post-thrombotic symptoms, Dr. Comerota said at a symposium on vascular surgery sponsored by Northwestern University.
"It is crucial to open up the orifice of the profunda," he said. "One of the problems we’ve seen in patients referred to us is that, when the common femoral was stented and the stent takes that fibrous tissue and plasters it up against the orifice of the profunda, if there was any minimal drainage from the profunda, it will obliterate it and those patients got worse."
Having previously detailed the technical aspects of the procedure (J. Vasc. Surg. 2012;55:129-35), Dr. Comerota highlighted outcomes of 14 patients and 16 limbs treated to date for severe post-thrombotic, iliofemoral/caval venous obstruction with CEAP (clinical severity, etiology, anatomy, pathophysiology) classification of C3-C6. The median duration of obstruction was nearly 7 years (range, 7 months to 25 years) and median follow-up 3 years (range, 5 months to 6 years). Two patients were lost to follow-up.
To date, one death occurred in a 52-year-old woman with multiple cardiovascular risk factors 9 days after discharge because of an acute myocardial infarction, Dr. Comerota said.
Three patients required surgical evacuation of wound hematomas and three developed early postoperative thrombosis treated with lysis in two cases and thrombectomy in one. All three patients were discharged with patency restored.
One segmental occlusion of the CFV has occurred, and a recent patient with longstanding sickle cell disease developed significant acute lymphedema "that we are still at a loss to explain," he said.
At 6 months, significant improvements were observed in preoperative scores on the Villalta scale (mean, 14 vs. 6; P = .002), Venous Clinical Severity Score (mean, 17 vs. 10; P = .02), CEAP (mean, 4.8 vs. 3.8; P less than .05) and Venous Insufficiency Epidemiological and Economic Study-Quality of Life/Sym questionnaire (data not provided; P = .01).
In some patients, the turnaround was quite dramatic, observed Dr. Comerota, who described a patient who suffered severe trauma and was unable to be anticoagulated. He subsequently had chronic iliofemoral and caval obstruction causing a swollen limb and a painful ulcer for 4 years. The day after surgery, there was remarkable change in the color of the ulcer and leg, and within 3 months the ulcer was completely healed, most of the edema was controlled, and his legs were no longer painful to compression, he said. The patient is back to full activity and has lost 30 pounds.
As a result of inactivity, many of the patients had gained a significant amount of weight, thereby requiring a large incision.
"It is a big procedure," said Dr. Comerota, adding that "it is certainly a procedure in evolution."
Some of the issues requiring further study include the risk/benefit of combined preoperative platelet inhibition and the optimal postoperative anticoagulation; location of an arteriovenous (AV) fistula; and size of the wound drain, currently a 7F closed suction drain.
Three days prior to the procedure, patients receive platelet inhibition with aspirin 81 mg/day and clopidogrel 75 mg/day and twice-daily chlorhexidine showers.
On the day of surgery, patients are fully anticoagulated with 100 IU/kg of unfractionated heparin. It is not reversed with protamine after the surgery is complete, but rather followed with a standard intravenous therapeutic heparin infusion, he said. To reduce the need for supratherapeutic systemic anticoagulation in some patients, a silastic intravenous catheter was placed in a dorsal foot vein to infuse the postoperative heparin.
A small AV fistula of 3.5-4 mm has been required in about half of procedures after continuous wave Doppler failed to identify robust venous velocity signals. The goal of the AV fistula is to increase velocity but not venous pressure, and it has typically been constructed with a wrap around the greater saphenous vein to ensure that it will not enlarge over time, Dr. Comerota said.
"I’ve never been sorry I did an AV fistula. I certainly have been sorry that I have not, so now it’s a routine part of the procedure," he added.
If an iliac venous stenosis or occlusion needs to be stented, Dr. Comerota said that he prefers Wallstents.
"I’m not sure if radial strength is the best term, but Wallstents have the best compression to pressure," he explained. "We’ve used Nitinol [stents] earlier on in our experience, but we had to go back in and reline 50% to 60% of them because they just didn’t hold up the vein properly."
Initially, the team also attempted to keep the stents above the inguinal ligament, but it now takes the approach that the iliac venous occlusion can be stented into the endovenectomized portion of the external iliac vein or CFV, with the caveat that the distal end of the stent must stay above the saphenofemoral junction to preserve profunda femoris venous drainage. Stenting avoids skip lesions that might lead to recurrent thrombosis or continued functional compromise, Dr. Comerota noted.
During a discussion of the procedure, he said that symptomatic presentation and degree of disability are used to determine whether patients should undergo the rigorous procedure.
Surgeons at the Mayo Clinic reported far less promising results in 12 patients who underwent CFV endovenectomy, patch angioplasty, and stenting for chronic iliofemoral venous obstruction, with a 30% 2-year patency and 50% of ulcers with patent grafts recurring (J. Vasc. Surg. 2011;53:383-93).
AT A SYMPOSIUM ON VASCULAR SURGERY SPONSORED BY NORTHWESTERN UNIVERSITY
Major Finding: At 6 months, significant improvements were observed in preoperative scores on the Villalta scale (mean 14 vs. 6; P = .002), Venous Clinical Severity Score (mean 17 vs. 10; P = .02), and CEAP (mean 4.8 vs. 3.8; P less than .05).
Data Source: Outcomes of 14 patients and 16 limbs treated to date for severe post-thrombotic, iliofemoral/caval venous obstruction with CEAP classification of C3-C6.
Disclosures: Dr. Comerota reported no relevant conflicts of interest.