User login
Bacterial epidemiology shifting nationally in febrile infants
NEW ORLEANS – Escherichia coli has replaced Group B Streptococcus as the most common cause of bacteremia in febrile infants in a nationally representative, retrospective study.
Among the 183 positive blood cultures drawn from 179 febrile but otherwise healthy-appearing infants, 76 were E. coli (42%), 41 Streptococcus agalactiae (22%), 10 S. pneumoniae (5%), and 10 S. aureus (5%). Roughly half of the cultures were gram negative.
Notably, no cases of Listeria bacteremia were identified, Dr. Rianna Evans said during the plenary session at the Pediatric Hospital Medicine 2013 meeting.
"There has been a definite rise in ampicillin-resistant gram-negative pathogens, which is going to be affecting our cephalosporin resistance," she said. "There is not a national database yet on this that we know of, but we identified ampicillin-resistance patterns at several of our sites, and it’s been noted in other cities as well."
Results from the current study, conducted at six sites across the United States, are supported by prior regional studies indicating a shift in bacterial epidemiology from Group B strep toward gram-negative pathogens in young infants. A change in the types of pathogens being seen is expected given the introduction of universal Group B strep prophylaxis in pregnant mothers and several new vaccines in the past decade, said Dr. Evans, a hospitalist at Children’s Hospital of The King’s Daughters, Norfolk, Va.
The investigators analyzed positive blood cultures from infants, age up to 90 days, drawn from January 2006 through December 2012 at six sites: Illinois; Rochester and Albany, N.Y.; Virginia; Minneapolis; and Los Angeles. Cultures were excluded if they were drawn in the intensive care unit, from indwelling vascular catheters, or from infants with a history of major surgery.
In all, 79% of the infants were classified as non–low risk according to Modified Rochester Criteria, 71% were febrile at the time the culture was drawn, 49% had a concurrent urinary tract infection, and 13% had concurrent meningitis. Their average age was 39 days.
Infants with E. coli were significantly more likely to be non–low risk than low risk (P = .001), while 56% of those with S. aureus bacteremia had evidence of a skin and soft tissue infection, Dr. Evans said.
She recommended single coverage with third-generation cephalosporin in febrile, non–toxic infants and that clinicians consider S. aureus and Enterococcus spp. coverage in ill-appearing infants with evidence of skin and soft-tissue infections.
During a discussion of the results, an audience member said it was dangerous to propose practice change based on a retrospective study, even if it was multicentered. Dr. Evans agreed and said there was a lot of discussion about their recommendations.
"It’s a bold statement, and I know it’s not going to be taken universally, which is why we need a prospective study identifying this," she said. "But with our work and all of the other studies that have been done on a regional level, I think there’s good enough data to at least suggest this and take it forward with a prospective study to see if there are true differences."
Dr. Evans said they could expand the retrospective analysis to bring in other sites, possibly through coauthor Dr. Eric Biondi’s ongoing study evaluating the time to blood culture positivity.
As a result of increasing antibiotic resistance to several types of gram-negative bacilli, the Centers for Disease Control and Prevention has also set up the Multi-Site Resistant Gram-Negative Bacilli Surveillance Initiative (MuGSI) to track infections due to carbapenem-resistant organisms including E. coli, Enterobacter cloacae, Enterobacter aerogenes, Klebsiella pneumoniae, K. oxytoca, and multidrug-resistant Acinetobacter baumannii. Data from the initiative are expected this year.
In one of the regional studies from Kaiser Permanente Northern California, E. coli was identified in 56% of positive samples collected from 2005 to 2009, and again there were no cases of Listeria bacteremia (Pediatrics 2012;129:e590-6).
Clinicians should consider Listeria if the maternal history or cerebrospinal fluid is suggestive of meningitis, but may want to revise their thinking when teaching residents about the bacterial causes of serious bacterial infections, Dr. Evans suggested.
Finally, another audience member expressed concern about whether cephalosporin alone would be a safe choice, particularly by residents, given that there was a fair amount of enterococcus in the sample and residents often miss this and forget about ampicillin. Dr. Evans observed that this has been the most provocative point when discussing the results with other institutions, but she said enterococcus was present in just 4% of the study’s positive samples and prior studies have shown that only 2% of well-appearing children presenting with fever are expected to have bacteremia. "It’s still a fairly low number, and you’re seeing a higher number of kids with ampicillin-resistant gram-negative rods," she added.
The meeting was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association. Dr. Evans and her coauthors reported having no financial disclosures.

|
| Dr. Michelle M. Marks |
Even though this study is retrospective in nature, it points out that the epidemiology of serious bacterial infection in young infants is changing. This is an important first step in understanding the change as well as the desire for further prospective study.
While Dr. Evans and other study participants make a bold statement for change in initial antibiotic coverage in these infants, it has invited national debate and thus puts a spotlight on the subject.
Michelle M. Marks, D.O., is the interim chair of the department of pediatric hospital medicine at the Cleveland Clinic Children's Hospital. She is also medical director of inpatient pediatrics for the Children's Hospital.
|
|
| Dr. Michelle M. Marks |
Even though this study is retrospective in nature, it points out that the epidemiology of serious bacterial infection in young infants is changing. This is an important first step in understanding the change as well as the desire for further prospective study.
While Dr. Evans and other study participants make a bold statement for change in initial antibiotic coverage in these infants, it has invited national debate and thus puts a spotlight on the subject.
Michelle M. Marks, D.O., is the interim chair of the department of pediatric hospital medicine at the Cleveland Clinic Children's Hospital. She is also medical director of inpatient pediatrics for the Children's Hospital.
|
|
| Dr. Michelle M. Marks |
Even though this study is retrospective in nature, it points out that the epidemiology of serious bacterial infection in young infants is changing. This is an important first step in understanding the change as well as the desire for further prospective study.
While Dr. Evans and other study participants make a bold statement for change in initial antibiotic coverage in these infants, it has invited national debate and thus puts a spotlight on the subject.
Michelle M. Marks, D.O., is the interim chair of the department of pediatric hospital medicine at the Cleveland Clinic Children's Hospital. She is also medical director of inpatient pediatrics for the Children's Hospital.
NEW ORLEANS – Escherichia coli has replaced Group B Streptococcus as the most common cause of bacteremia in febrile infants in a nationally representative, retrospective study.
Among the 183 positive blood cultures drawn from 179 febrile but otherwise healthy-appearing infants, 76 were E. coli (42%), 41 Streptococcus agalactiae (22%), 10 S. pneumoniae (5%), and 10 S. aureus (5%). Roughly half of the cultures were gram negative.
Notably, no cases of Listeria bacteremia were identified, Dr. Rianna Evans said during the plenary session at the Pediatric Hospital Medicine 2013 meeting.
"There has been a definite rise in ampicillin-resistant gram-negative pathogens, which is going to be affecting our cephalosporin resistance," she said. "There is not a national database yet on this that we know of, but we identified ampicillin-resistance patterns at several of our sites, and it’s been noted in other cities as well."
Results from the current study, conducted at six sites across the United States, are supported by prior regional studies indicating a shift in bacterial epidemiology from Group B strep toward gram-negative pathogens in young infants. A change in the types of pathogens being seen is expected given the introduction of universal Group B strep prophylaxis in pregnant mothers and several new vaccines in the past decade, said Dr. Evans, a hospitalist at Children’s Hospital of The King’s Daughters, Norfolk, Va.
The investigators analyzed positive blood cultures from infants, age up to 90 days, drawn from January 2006 through December 2012 at six sites: Illinois; Rochester and Albany, N.Y.; Virginia; Minneapolis; and Los Angeles. Cultures were excluded if they were drawn in the intensive care unit, from indwelling vascular catheters, or from infants with a history of major surgery.
In all, 79% of the infants were classified as non–low risk according to Modified Rochester Criteria, 71% were febrile at the time the culture was drawn, 49% had a concurrent urinary tract infection, and 13% had concurrent meningitis. Their average age was 39 days.
Infants with E. coli were significantly more likely to be non–low risk than low risk (P = .001), while 56% of those with S. aureus bacteremia had evidence of a skin and soft tissue infection, Dr. Evans said.
She recommended single coverage with third-generation cephalosporin in febrile, non–toxic infants and that clinicians consider S. aureus and Enterococcus spp. coverage in ill-appearing infants with evidence of skin and soft-tissue infections.
During a discussion of the results, an audience member said it was dangerous to propose practice change based on a retrospective study, even if it was multicentered. Dr. Evans agreed and said there was a lot of discussion about their recommendations.
"It’s a bold statement, and I know it’s not going to be taken universally, which is why we need a prospective study identifying this," she said. "But with our work and all of the other studies that have been done on a regional level, I think there’s good enough data to at least suggest this and take it forward with a prospective study to see if there are true differences."
Dr. Evans said they could expand the retrospective analysis to bring in other sites, possibly through coauthor Dr. Eric Biondi’s ongoing study evaluating the time to blood culture positivity.
As a result of increasing antibiotic resistance to several types of gram-negative bacilli, the Centers for Disease Control and Prevention has also set up the Multi-Site Resistant Gram-Negative Bacilli Surveillance Initiative (MuGSI) to track infections due to carbapenem-resistant organisms including E. coli, Enterobacter cloacae, Enterobacter aerogenes, Klebsiella pneumoniae, K. oxytoca, and multidrug-resistant Acinetobacter baumannii. Data from the initiative are expected this year.
In one of the regional studies from Kaiser Permanente Northern California, E. coli was identified in 56% of positive samples collected from 2005 to 2009, and again there were no cases of Listeria bacteremia (Pediatrics 2012;129:e590-6).
Clinicians should consider Listeria if the maternal history or cerebrospinal fluid is suggestive of meningitis, but may want to revise their thinking when teaching residents about the bacterial causes of serious bacterial infections, Dr. Evans suggested.
Finally, another audience member expressed concern about whether cephalosporin alone would be a safe choice, particularly by residents, given that there was a fair amount of enterococcus in the sample and residents often miss this and forget about ampicillin. Dr. Evans observed that this has been the most provocative point when discussing the results with other institutions, but she said enterococcus was present in just 4% of the study’s positive samples and prior studies have shown that only 2% of well-appearing children presenting with fever are expected to have bacteremia. "It’s still a fairly low number, and you’re seeing a higher number of kids with ampicillin-resistant gram-negative rods," she added.
The meeting was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association. Dr. Evans and her coauthors reported having no financial disclosures.
NEW ORLEANS – Escherichia coli has replaced Group B Streptococcus as the most common cause of bacteremia in febrile infants in a nationally representative, retrospective study.
Among the 183 positive blood cultures drawn from 179 febrile but otherwise healthy-appearing infants, 76 were E. coli (42%), 41 Streptococcus agalactiae (22%), 10 S. pneumoniae (5%), and 10 S. aureus (5%). Roughly half of the cultures were gram negative.
Notably, no cases of Listeria bacteremia were identified, Dr. Rianna Evans said during the plenary session at the Pediatric Hospital Medicine 2013 meeting.
"There has been a definite rise in ampicillin-resistant gram-negative pathogens, which is going to be affecting our cephalosporin resistance," she said. "There is not a national database yet on this that we know of, but we identified ampicillin-resistance patterns at several of our sites, and it’s been noted in other cities as well."
Results from the current study, conducted at six sites across the United States, are supported by prior regional studies indicating a shift in bacterial epidemiology from Group B strep toward gram-negative pathogens in young infants. A change in the types of pathogens being seen is expected given the introduction of universal Group B strep prophylaxis in pregnant mothers and several new vaccines in the past decade, said Dr. Evans, a hospitalist at Children’s Hospital of The King’s Daughters, Norfolk, Va.
The investigators analyzed positive blood cultures from infants, age up to 90 days, drawn from January 2006 through December 2012 at six sites: Illinois; Rochester and Albany, N.Y.; Virginia; Minneapolis; and Los Angeles. Cultures were excluded if they were drawn in the intensive care unit, from indwelling vascular catheters, or from infants with a history of major surgery.
In all, 79% of the infants were classified as non–low risk according to Modified Rochester Criteria, 71% were febrile at the time the culture was drawn, 49% had a concurrent urinary tract infection, and 13% had concurrent meningitis. Their average age was 39 days.
Infants with E. coli were significantly more likely to be non–low risk than low risk (P = .001), while 56% of those with S. aureus bacteremia had evidence of a skin and soft tissue infection, Dr. Evans said.
She recommended single coverage with third-generation cephalosporin in febrile, non–toxic infants and that clinicians consider S. aureus and Enterococcus spp. coverage in ill-appearing infants with evidence of skin and soft-tissue infections.
During a discussion of the results, an audience member said it was dangerous to propose practice change based on a retrospective study, even if it was multicentered. Dr. Evans agreed and said there was a lot of discussion about their recommendations.
"It’s a bold statement, and I know it’s not going to be taken universally, which is why we need a prospective study identifying this," she said. "But with our work and all of the other studies that have been done on a regional level, I think there’s good enough data to at least suggest this and take it forward with a prospective study to see if there are true differences."
Dr. Evans said they could expand the retrospective analysis to bring in other sites, possibly through coauthor Dr. Eric Biondi’s ongoing study evaluating the time to blood culture positivity.
As a result of increasing antibiotic resistance to several types of gram-negative bacilli, the Centers for Disease Control and Prevention has also set up the Multi-Site Resistant Gram-Negative Bacilli Surveillance Initiative (MuGSI) to track infections due to carbapenem-resistant organisms including E. coli, Enterobacter cloacae, Enterobacter aerogenes, Klebsiella pneumoniae, K. oxytoca, and multidrug-resistant Acinetobacter baumannii. Data from the initiative are expected this year.
In one of the regional studies from Kaiser Permanente Northern California, E. coli was identified in 56% of positive samples collected from 2005 to 2009, and again there were no cases of Listeria bacteremia (Pediatrics 2012;129:e590-6).
Clinicians should consider Listeria if the maternal history or cerebrospinal fluid is suggestive of meningitis, but may want to revise their thinking when teaching residents about the bacterial causes of serious bacterial infections, Dr. Evans suggested.
Finally, another audience member expressed concern about whether cephalosporin alone would be a safe choice, particularly by residents, given that there was a fair amount of enterococcus in the sample and residents often miss this and forget about ampicillin. Dr. Evans observed that this has been the most provocative point when discussing the results with other institutions, but she said enterococcus was present in just 4% of the study’s positive samples and prior studies have shown that only 2% of well-appearing children presenting with fever are expected to have bacteremia. "It’s still a fairly low number, and you’re seeing a higher number of kids with ampicillin-resistant gram-negative rods," she added.
The meeting was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association. Dr. Evans and her coauthors reported having no financial disclosures.
AT PEDIATRIC HOSPITAL MEDICINE 2013

Bacterial epidemiology shifting nationally in febrile infants
NEW ORLEANS – Escherichia coli has replaced Group B Streptococcus as the most common cause of bacteremia in febrile infants in a nationally representative, retrospective study.
Among the 183 positive blood cultures drawn from 179 febrile but otherwise healthy-appearing infants, 76 were E. coli (42%), 41 Streptococcus agalactiae (22%), 10 S. pneumoniae (5%), and 10 S. aureus (5%). Roughly half of the cultures were gram negative.

Notably, no cases of Listeria bacteremia were identified, Dr. Rianna Evans said during the plenary session at the Pediatric Hospital Medicine 2013 meeting.
"There has been a definite rise in ampicillin-resistant gram-negative pathogens, which is going to be affecting our cephalosporin resistance," she said. "There is not a national database yet on this that we know of, but we identified ampicillin-resistance patterns at several of our sites, and it’s been noted in other cities as well."
Results from the current study, conducted at six sites across the United States, are supported by prior regional studies indicating a shift in bacterial epidemiology from Group B strep toward gram-negative pathogens in young infants. A change in the types of pathogens being seen is expected given the introduction of universal Group B strep prophylaxis in pregnant mothers and several new vaccines in the past decade, said Dr. Evans, a hospitalist at Children’s Hospital of The King’s Daughters, Norfolk, Va.
The investigators analyzed positive blood cultures from infants, age up to 90 days, drawn from January 2006 through December 2012 at six sites: Illinois; Rochester and Albany, N.Y.; Virginia; Minneapolis; and Los Angeles. Cultures were excluded if they were drawn in the intensive care unit, from indwelling vascular catheters, or from infants with a history of major surgery.
In all, 79% of the infants were classified as non–low risk according to Modified Rochester Criteria, 71% were febrile at the time the culture was drawn, 49% had a concurrent urinary tract infection, and 13% had concurrent meningitis. Their average age was 39 days.
Infants with E. coli were significantly more likely to be non–low risk than low risk (P = .001), while 56% of those with S. aureus bacteremia had evidence of a skin and soft tissue infection, Dr. Evans said.
She recommended single coverage with third-generation cephalosporin in febrile, non–toxic infants and that clinicians consider S. aureus and Enterococcus spp. coverage in ill-appearing infants with evidence of skin and soft-tissue infections.
During a discussion of the results, an audience member said it was dangerous to propose practice change based on a retrospective study, even if it was multicentered. Dr. Evans agreed and said there was a lot of discussion about their recommendations.
"It’s a bold statement, and I know it’s not going to be taken universally, which is why we need a prospective study identifying this," she said. "But with our work and all of the other studies that have been done on a regional level, I think there’s good enough data to at least suggest this and take it forward with a prospective study to see if there are true differences."
Dr. Evans said they could expand the retrospective analysis to bring in other sites, possibly through coauthor Dr. Eric Biondi’s ongoing study evaluating the time to blood culture positivity.
As a result of increasing antibiotic resistance to several types of gram-negative bacilli, the Centers for Disease Control and Prevention has also set up the Multi-Site Resistant Gram-Negative Bacilli Surveillance Initiative (MuGSI) to track infections due to carbapenem-resistant organisms including E. coli, Enterobacter cloacae, Enterobacter aerogenes, Klebsiella pneumoniae, K. oxytoca, and multidrug-resistant Acinetobacter baumannii. Data from the initiative are expected this year.
In one of the regional studies from Kaiser Permanente Northern California, E. coli was identified in 56% of positive samples collected from 2005 to 2009, and again there were no cases of Listeria bacteremia (Pediatrics 2012;129:e590-6).
Clinicians should consider Listeria if the maternal history or cerebrospinal fluid is suggestive of meningitis, but may want to revise their thinking when teaching residents about the bacterial causes of serious bacterial infections, Dr. Evans suggested.
Finally, another audience member expressed concern about whether cephalosporin alone would be a safe choice, particularly by residents, given that there was a fair amount of enterococcus in the sample and residents often miss this and forget about ampicillin. Dr. Evans observed that this has been the most provocative point when discussing the results with other institutions, but she said enterococcus was present in just 4% of the study’s positive samples and prior studies have shown that only 2% of well-appearing children presenting with fever are expected to have bacteremia. "It’s still a fairly low number, and you’re seeing a higher number of kids with ampicillin-resistant gram-negative rods," she added.
The meeting was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association. Dr. Evans and her coauthors reported having no financial disclosures.
|
|
| Dr. Michelle M. Marks |
Even though this study is retrospective in nature, it points out that the epidemiology of serious bacterial infection in young infants is changing. This is an important first step in understanding the change as well as the desire for further prospective study.
While Dr. Evans and other study participants make a bold statement for change in initial antibiotic coverage in these infants, it has invited national debate and thus puts a spotlight on the subject.
Michelle M. Marks, D.O., is the interim chair of the department of pediatric hospital medicine at the Cleveland Clinic Children's Hospital. She is also medical director of inpatient pediatrics for the Children's Hospital.
|
|
| Dr. Michelle M. Marks |
Even though this study is retrospective in nature, it points out that the epidemiology of serious bacterial infection in young infants is changing. This is an important first step in understanding the change as well as the desire for further prospective study.
While Dr. Evans and other study participants make a bold statement for change in initial antibiotic coverage in these infants, it has invited national debate and thus puts a spotlight on the subject.
Michelle M. Marks, D.O., is the interim chair of the department of pediatric hospital medicine at the Cleveland Clinic Children's Hospital. She is also medical director of inpatient pediatrics for the Children's Hospital.
|
|
| Dr. Michelle M. Marks |
Even though this study is retrospective in nature, it points out that the epidemiology of serious bacterial infection in young infants is changing. This is an important first step in understanding the change as well as the desire for further prospective study.
While Dr. Evans and other study participants make a bold statement for change in initial antibiotic coverage in these infants, it has invited national debate and thus puts a spotlight on the subject.
Michelle M. Marks, D.O., is the interim chair of the department of pediatric hospital medicine at the Cleveland Clinic Children's Hospital. She is also medical director of inpatient pediatrics for the Children's Hospital.
NEW ORLEANS – Escherichia coli has replaced Group B Streptococcus as the most common cause of bacteremia in febrile infants in a nationally representative, retrospective study.
Among the 183 positive blood cultures drawn from 179 febrile but otherwise healthy-appearing infants, 76 were E. coli (42%), 41 Streptococcus agalactiae (22%), 10 S. pneumoniae (5%), and 10 S. aureus (5%). Roughly half of the cultures were gram negative.
Notably, no cases of Listeria bacteremia were identified, Dr. Rianna Evans said during the plenary session at the Pediatric Hospital Medicine 2013 meeting.
"There has been a definite rise in ampicillin-resistant gram-negative pathogens, which is going to be affecting our cephalosporin resistance," she said. "There is not a national database yet on this that we know of, but we identified ampicillin-resistance patterns at several of our sites, and it’s been noted in other cities as well."
Results from the current study, conducted at six sites across the United States, are supported by prior regional studies indicating a shift in bacterial epidemiology from Group B strep toward gram-negative pathogens in young infants. A change in the types of pathogens being seen is expected given the introduction of universal Group B strep prophylaxis in pregnant mothers and several new vaccines in the past decade, said Dr. Evans, a hospitalist at Children’s Hospital of The King’s Daughters, Norfolk, Va.
The investigators analyzed positive blood cultures from infants, age up to 90 days, drawn from January 2006 through December 2012 at six sites: Illinois; Rochester and Albany, N.Y.; Virginia; Minneapolis; and Los Angeles. Cultures were excluded if they were drawn in the intensive care unit, from indwelling vascular catheters, or from infants with a history of major surgery.
In all, 79% of the infants were classified as non–low risk according to Modified Rochester Criteria, 71% were febrile at the time the culture was drawn, 49% had a concurrent urinary tract infection, and 13% had concurrent meningitis. Their average age was 39 days.
Infants with E. coli were significantly more likely to be non–low risk than low risk (P = .001), while 56% of those with S. aureus bacteremia had evidence of a skin and soft tissue infection, Dr. Evans said.
She recommended single coverage with third-generation cephalosporin in febrile, non–toxic infants and that clinicians consider S. aureus and Enterococcus spp. coverage in ill-appearing infants with evidence of skin and soft-tissue infections.
During a discussion of the results, an audience member said it was dangerous to propose practice change based on a retrospective study, even if it was multicentered. Dr. Evans agreed and said there was a lot of discussion about their recommendations.
"It’s a bold statement, and I know it’s not going to be taken universally, which is why we need a prospective study identifying this," she said. "But with our work and all of the other studies that have been done on a regional level, I think there’s good enough data to at least suggest this and take it forward with a prospective study to see if there are true differences."
Dr. Evans said they could expand the retrospective analysis to bring in other sites, possibly through coauthor Dr. Eric Biondi’s ongoing study evaluating the time to blood culture positivity.
As a result of increasing antibiotic resistance to several types of gram-negative bacilli, the Centers for Disease Control and Prevention has also set up the Multi-Site Resistant Gram-Negative Bacilli Surveillance Initiative (MuGSI) to track infections due to carbapenem-resistant organisms including E. coli, Enterobacter cloacae, Enterobacter aerogenes, Klebsiella pneumoniae, K. oxytoca, and multidrug-resistant Acinetobacter baumannii. Data from the initiative are expected this year.
In one of the regional studies from Kaiser Permanente Northern California, E. coli was identified in 56% of positive samples collected from 2005 to 2009, and again there were no cases of Listeria bacteremia (Pediatrics 2012;129:e590-6).
Clinicians should consider Listeria if the maternal history or cerebrospinal fluid is suggestive of meningitis, but may want to revise their thinking when teaching residents about the bacterial causes of serious bacterial infections, Dr. Evans suggested.
Finally, another audience member expressed concern about whether cephalosporin alone would be a safe choice, particularly by residents, given that there was a fair amount of enterococcus in the sample and residents often miss this and forget about ampicillin. Dr. Evans observed that this has been the most provocative point when discussing the results with other institutions, but she said enterococcus was present in just 4% of the study’s positive samples and prior studies have shown that only 2% of well-appearing children presenting with fever are expected to have bacteremia. "It’s still a fairly low number, and you’re seeing a higher number of kids with ampicillin-resistant gram-negative rods," she added.
The meeting was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association. Dr. Evans and her coauthors reported having no financial disclosures.
NEW ORLEANS – Escherichia coli has replaced Group B Streptococcus as the most common cause of bacteremia in febrile infants in a nationally representative, retrospective study.
Among the 183 positive blood cultures drawn from 179 febrile but otherwise healthy-appearing infants, 76 were E. coli (42%), 41 Streptococcus agalactiae (22%), 10 S. pneumoniae (5%), and 10 S. aureus (5%). Roughly half of the cultures were gram negative.
Notably, no cases of Listeria bacteremia were identified, Dr. Rianna Evans said during the plenary session at the Pediatric Hospital Medicine 2013 meeting.
"There has been a definite rise in ampicillin-resistant gram-negative pathogens, which is going to be affecting our cephalosporin resistance," she said. "There is not a national database yet on this that we know of, but we identified ampicillin-resistance patterns at several of our sites, and it’s been noted in other cities as well."
Results from the current study, conducted at six sites across the United States, are supported by prior regional studies indicating a shift in bacterial epidemiology from Group B strep toward gram-negative pathogens in young infants. A change in the types of pathogens being seen is expected given the introduction of universal Group B strep prophylaxis in pregnant mothers and several new vaccines in the past decade, said Dr. Evans, a hospitalist at Children’s Hospital of The King’s Daughters, Norfolk, Va.
The investigators analyzed positive blood cultures from infants, age up to 90 days, drawn from January 2006 through December 2012 at six sites: Illinois; Rochester and Albany, N.Y.; Virginia; Minneapolis; and Los Angeles. Cultures were excluded if they were drawn in the intensive care unit, from indwelling vascular catheters, or from infants with a history of major surgery.
In all, 79% of the infants were classified as non–low risk according to Modified Rochester Criteria, 71% were febrile at the time the culture was drawn, 49% had a concurrent urinary tract infection, and 13% had concurrent meningitis. Their average age was 39 days.
Infants with E. coli were significantly more likely to be non–low risk than low risk (P = .001), while 56% of those with S. aureus bacteremia had evidence of a skin and soft tissue infection, Dr. Evans said.
She recommended single coverage with third-generation cephalosporin in febrile, non–toxic infants and that clinicians consider S. aureus and Enterococcus spp. coverage in ill-appearing infants with evidence of skin and soft-tissue infections.
During a discussion of the results, an audience member said it was dangerous to propose practice change based on a retrospective study, even if it was multicentered. Dr. Evans agreed and said there was a lot of discussion about their recommendations.
"It’s a bold statement, and I know it’s not going to be taken universally, which is why we need a prospective study identifying this," she said. "But with our work and all of the other studies that have been done on a regional level, I think there’s good enough data to at least suggest this and take it forward with a prospective study to see if there are true differences."
Dr. Evans said they could expand the retrospective analysis to bring in other sites, possibly through coauthor Dr. Eric Biondi’s ongoing study evaluating the time to blood culture positivity.
As a result of increasing antibiotic resistance to several types of gram-negative bacilli, the Centers for Disease Control and Prevention has also set up the Multi-Site Resistant Gram-Negative Bacilli Surveillance Initiative (MuGSI) to track infections due to carbapenem-resistant organisms including E. coli, Enterobacter cloacae, Enterobacter aerogenes, Klebsiella pneumoniae, K. oxytoca, and multidrug-resistant Acinetobacter baumannii. Data from the initiative are expected this year.
In one of the regional studies from Kaiser Permanente Northern California, E. coli was identified in 56% of positive samples collected from 2005 to 2009, and again there were no cases of Listeria bacteremia (Pediatrics 2012;129:e590-6).
Clinicians should consider Listeria if the maternal history or cerebrospinal fluid is suggestive of meningitis, but may want to revise their thinking when teaching residents about the bacterial causes of serious bacterial infections, Dr. Evans suggested.
Finally, another audience member expressed concern about whether cephalosporin alone would be a safe choice, particularly by residents, given that there was a fair amount of enterococcus in the sample and residents often miss this and forget about ampicillin. Dr. Evans observed that this has been the most provocative point when discussing the results with other institutions, but she said enterococcus was present in just 4% of the study’s positive samples and prior studies have shown that only 2% of well-appearing children presenting with fever are expected to have bacteremia. "It’s still a fairly low number, and you’re seeing a higher number of kids with ampicillin-resistant gram-negative rods," she added.
The meeting was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association. Dr. Evans and her coauthors reported having no financial disclosures.
AT PEDIATRIC HOSPITAL MEDICINE 2013
Major finding: E. coli was the most common cause (42%) of bacteremia seen in positive blood cultures.
Data source: Retrospective chart study of 183 positive blood cultures from 179 febrile infants.
Disclosures: Dr. Evans and her coauthors reported having no financial disclosures.

Pulsed dye laser targets keratosis pilaris rubra
MILWAUKEE – Pulsed dye laser therapy reduced the redness associated with chronic keratosis pilaris rubra in as little as one session in a case series of seven adolescents.
The problem, however, is convincing insurers to pay for the procedure.

"That’s part of why we brought this to a forum like this meeting," Dr. Jennifer J. Schoch said at the annual meeting of the Society for Pediatric Dermatology. "These kids are so significantly affected by this and embarrassed [by the condition], that if we can do something in just one treatment and have a good response, it makes sense. But these kids required a lot of letters to the insurance companies, and a lot of them paid out of pocket."
Several attendees at the meeting echoed these comments, and some observed that pulse dye laser (PDL) therapy is not as effective in patients with higher Fitzpatrick skin types or that it was out of reach for their patients at a price tag of $200 or more per session.
"It seems to make a lot of sense, but I don’t think it would be worth the cost for my patients," Dr. Aimee Smidt, University of New Mexico, Albuquerque, said in an interview.
Keratosis pilaris rubra is often viewed as a benign condition, but one patient found it so socially disturbing that he flew from Alabama to Minnesota for treatment, said Dr. Schoch, a dermatologist at the Mayo Clinic in Rochester, Minn.

Dr. Schoch noted that there are few data in the literature on PDL treatment of keratosis pilaris rubra, and the current series is occurring over a 13-year-period at the clinic. In this series, adolescents aged 14-17 years received one to four sessions of PDL at a wavelength of 585 nm or 595 nm, for erythema and hyperkeratotic follicular papules on both cheeks. Two patients also received treatment to the chin, forehead and/or neck.
All patients had Fitzpatrick skin type I or II, five were male, and two also had ulerythema ophryogenes. Some patients had been misdiagnosed with severe acne, and all had failed a range of treatments including emollients, lactic acid, topical retinoids, urea, sulfacetamide lotion, and weak topical corticosteroids, as well as laser therapy with intense pulsed light, Fraxel, and Nd:YAG lasers, she said.
PDL treatment was physician-dependent. Starting fluences ranged from 4-9 J/cm2, with the goal of achieving a mild, bruiselike response. The spot size was predominantly 7 mm, and pulse duration was 1.5, 3, or 10 msec.
"I hypothesize that people are probably undertreating because it’s a benign condition, and you don’t want to cause problems, but to be effective, it seems you have to go for a little more aggressive response," Dr. Schoch said in an interview.
All patients experienced significant improvement after one to four treatments, based on patient report or provider assessment. Bruising resolved in 1-2 weeks. Resolution of erythema was observed, but not specifically measured. Patients also experienced some transient purpura, which was not well documented, said Dr. Schoch.

After 1-19 months follow-up, most patients remained satisfied with the results, although some flushing returned in two patients, she said. Blanching has not been a significant problem, and overlapping the treated areas reduced the risk of a honeycomb pattern developing on the skin.
The investigators are considering a prospective study to more objectively monitor responses. Treatment parameters will depend on patient’s response to test spots, Dr. Schoch said.
Dr. Schoch and her coauthors reported having no financial disclosures.
MILWAUKEE – Pulsed dye laser therapy reduced the redness associated with chronic keratosis pilaris rubra in as little as one session in a case series of seven adolescents.
The problem, however, is convincing insurers to pay for the procedure.
"That’s part of why we brought this to a forum like this meeting," Dr. Jennifer J. Schoch said at the annual meeting of the Society for Pediatric Dermatology. "These kids are so significantly affected by this and embarrassed [by the condition], that if we can do something in just one treatment and have a good response, it makes sense. But these kids required a lot of letters to the insurance companies, and a lot of them paid out of pocket."
Several attendees at the meeting echoed these comments, and some observed that pulse dye laser (PDL) therapy is not as effective in patients with higher Fitzpatrick skin types or that it was out of reach for their patients at a price tag of $200 or more per session.
"It seems to make a lot of sense, but I don’t think it would be worth the cost for my patients," Dr. Aimee Smidt, University of New Mexico, Albuquerque, said in an interview.
Keratosis pilaris rubra is often viewed as a benign condition, but one patient found it so socially disturbing that he flew from Alabama to Minnesota for treatment, said Dr. Schoch, a dermatologist at the Mayo Clinic in Rochester, Minn.
Dr. Schoch noted that there are few data in the literature on PDL treatment of keratosis pilaris rubra, and the current series is occurring over a 13-year-period at the clinic. In this series, adolescents aged 14-17 years received one to four sessions of PDL at a wavelength of 585 nm or 595 nm, for erythema and hyperkeratotic follicular papules on both cheeks. Two patients also received treatment to the chin, forehead and/or neck.
All patients had Fitzpatrick skin type I or II, five were male, and two also had ulerythema ophryogenes. Some patients had been misdiagnosed with severe acne, and all had failed a range of treatments including emollients, lactic acid, topical retinoids, urea, sulfacetamide lotion, and weak topical corticosteroids, as well as laser therapy with intense pulsed light, Fraxel, and Nd:YAG lasers, she said.
PDL treatment was physician-dependent. Starting fluences ranged from 4-9 J/cm2, with the goal of achieving a mild, bruiselike response. The spot size was predominantly 7 mm, and pulse duration was 1.5, 3, or 10 msec.
"I hypothesize that people are probably undertreating because it’s a benign condition, and you don’t want to cause problems, but to be effective, it seems you have to go for a little more aggressive response," Dr. Schoch said in an interview.
All patients experienced significant improvement after one to four treatments, based on patient report or provider assessment. Bruising resolved in 1-2 weeks. Resolution of erythema was observed, but not specifically measured. Patients also experienced some transient purpura, which was not well documented, said Dr. Schoch.
After 1-19 months follow-up, most patients remained satisfied with the results, although some flushing returned in two patients, she said. Blanching has not been a significant problem, and overlapping the treated areas reduced the risk of a honeycomb pattern developing on the skin.
The investigators are considering a prospective study to more objectively monitor responses. Treatment parameters will depend on patient’s response to test spots, Dr. Schoch said.
Dr. Schoch and her coauthors reported having no financial disclosures.
MILWAUKEE – Pulsed dye laser therapy reduced the redness associated with chronic keratosis pilaris rubra in as little as one session in a case series of seven adolescents.
The problem, however, is convincing insurers to pay for the procedure.
"That’s part of why we brought this to a forum like this meeting," Dr. Jennifer J. Schoch said at the annual meeting of the Society for Pediatric Dermatology. "These kids are so significantly affected by this and embarrassed [by the condition], that if we can do something in just one treatment and have a good response, it makes sense. But these kids required a lot of letters to the insurance companies, and a lot of them paid out of pocket."
Several attendees at the meeting echoed these comments, and some observed that pulse dye laser (PDL) therapy is not as effective in patients with higher Fitzpatrick skin types or that it was out of reach for their patients at a price tag of $200 or more per session.
"It seems to make a lot of sense, but I don’t think it would be worth the cost for my patients," Dr. Aimee Smidt, University of New Mexico, Albuquerque, said in an interview.
Keratosis pilaris rubra is often viewed as a benign condition, but one patient found it so socially disturbing that he flew from Alabama to Minnesota for treatment, said Dr. Schoch, a dermatologist at the Mayo Clinic in Rochester, Minn.
Dr. Schoch noted that there are few data in the literature on PDL treatment of keratosis pilaris rubra, and the current series is occurring over a 13-year-period at the clinic. In this series, adolescents aged 14-17 years received one to four sessions of PDL at a wavelength of 585 nm or 595 nm, for erythema and hyperkeratotic follicular papules on both cheeks. Two patients also received treatment to the chin, forehead and/or neck.
All patients had Fitzpatrick skin type I or II, five were male, and two also had ulerythema ophryogenes. Some patients had been misdiagnosed with severe acne, and all had failed a range of treatments including emollients, lactic acid, topical retinoids, urea, sulfacetamide lotion, and weak topical corticosteroids, as well as laser therapy with intense pulsed light, Fraxel, and Nd:YAG lasers, she said.
PDL treatment was physician-dependent. Starting fluences ranged from 4-9 J/cm2, with the goal of achieving a mild, bruiselike response. The spot size was predominantly 7 mm, and pulse duration was 1.5, 3, or 10 msec.
"I hypothesize that people are probably undertreating because it’s a benign condition, and you don’t want to cause problems, but to be effective, it seems you have to go for a little more aggressive response," Dr. Schoch said in an interview.
All patients experienced significant improvement after one to four treatments, based on patient report or provider assessment. Bruising resolved in 1-2 weeks. Resolution of erythema was observed, but not specifically measured. Patients also experienced some transient purpura, which was not well documented, said Dr. Schoch.
After 1-19 months follow-up, most patients remained satisfied with the results, although some flushing returned in two patients, she said. Blanching has not been a significant problem, and overlapping the treated areas reduced the risk of a honeycomb pattern developing on the skin.
The investigators are considering a prospective study to more objectively monitor responses. Treatment parameters will depend on patient’s response to test spots, Dr. Schoch said.
Dr. Schoch and her coauthors reported having no financial disclosures.
AT THE SPD ANNUAL MEETING

Aortic valve-sparing surgery shows durability
MINNEAPOLIS – Despite the complexity of aortic valve–sparing techniques, early outcomes and 1-year survival were similar to those achieved with valve replacing during root replacement surgery in patients with Marfan syndrome in a prospective registry study.
Major adverse valve-related events (MAVREs) at 1 year were also comparable, although there was an increase, of course, in aortic valve regurgitation with valve sparing (7% vs. 0%), Dr. Joseph S. Coselli said at the annual meeting of the American Association for Thoracic Surgery.
"Follow-up is needed for this particular incident because we don’t know exactly what’s going to happen to these 2-plus aortic regurgitations," he said. "It’s quite possible they may remain stable over a long period of time and don’t represent a failure of the concept."

In an initial report from the international registry, valve-sparing techniques were the most common, and provided comparable 30-day outcomes in 151 patients (J. Thorac. Cardiovasc. Surg. 2009;137:1124-32).
The current analysis involved 316 patients, aged 4-70 years, who underwent aortic valve–sparing (AVS) (N = 239) or aortic valve–replacing (AVR) (N = 63 mechanical and 14 tissue) root replacement surgery at 19 centers between March 2005 and November 2010. The type of operation was determined by clinical factors, and by surgeon and patient preference. AVR surgery was considered the only option in 17% of patients. At 1 year, clinical follow-up was complete in 98% and imaging follow-up in 93%.
"Interestingly, when we started out this particular collection of patients, over 30% were receiving aortic valve replacement, but toward the end of this observational study, late 2010, virtually almost all patients were receiving aortic valve sparing," said Dr. Coselli, chief of adult cardiac surgery at Baylor College of Medicine, Texas Heart Institute, Houston.
AVS patients were younger (33 vs. 39 years); had smaller sinuses of Valsalva (49 vs. 53 mm); and had less acute dissection (3% vs. 9%), chronic dissection (3% vs. 12%), and previous cardiovascular surgery (5% vs. 14%).
Aortic-sparing techniques required significantly longer cardiopulmonary bypass time (195 vs. 152 minutes) and aortic clamp time (156 vs. 115 minutes), but cut ICU time from 46 hours with AVR surgery to 26 hours, ventilator support time from 12 to 8 hours, and hospital length of stay from 7 to 6 days, Dr. Coselli reported.
At 30 days, MAVREs were reported in 6 patients in the AVR group and 15 in the AVS group (P = .4), with no differences in nonstructural dysfunction (1 vs. 7), embolism (1 vs. 3), or bleeding (2 vs. 3 events).
Two AVS patients required early reoperation: One required same-day reintervention because of coronary artery kinking after a Florida sleeve procedure, and the second needed reintervention because of a coronary pseudoaneurysm 6 days after a David-V procedure, he said. Two early deaths occurred, one in each group, but neither was valve related.
One-year survival rates were 98% after AVS surgery and 97% after AVR surgery (4 vs. 2 deaths; P = .06).
At 1 year, MAVREs occurred in 8 AVR and 35 AVS patients (P = .5). There was no significant difference between AVR and AVS in freedom from valve-related death (1 vs. 2), embolism (2 vs. 4 events), reintervention (0 vs. 1), endocarditis (1 vs. 0), valve thrombosis (0 both), or valve-related morbidity (7 vs. 28), Dr. Coselli said.
The AVS group had significantly more nonstructural dysfunction/structural valve deterioration (23 events vs. 1 event; P = .04), but significantly less bleeding (3 vs. 5 events; P = .01).
In a Cox regression analysis at 1 year, the type of surgery was not associated with overall survival, MAVREs, or any other valve-related outcome, he said.
Dr. Coselli reported research support from St. Jude Medical; an educational grant, consultancy, and royalties from Vascutek Terumo; and research support, speaking for, and steering committee membership with Medtronic. Two coauthors reported consultant/advisory board participation with Medtronic or Edwards Lifesciences.
MINNEAPOLIS – Despite the complexity of aortic valve–sparing techniques, early outcomes and 1-year survival were similar to those achieved with valve replacing during root replacement surgery in patients with Marfan syndrome in a prospective registry study.
Major adverse valve-related events (MAVREs) at 1 year were also comparable, although there was an increase, of course, in aortic valve regurgitation with valve sparing (7% vs. 0%), Dr. Joseph S. Coselli said at the annual meeting of the American Association for Thoracic Surgery.
"Follow-up is needed for this particular incident because we don’t know exactly what’s going to happen to these 2-plus aortic regurgitations," he said. "It’s quite possible they may remain stable over a long period of time and don’t represent a failure of the concept."
In an initial report from the international registry, valve-sparing techniques were the most common, and provided comparable 30-day outcomes in 151 patients (J. Thorac. Cardiovasc. Surg. 2009;137:1124-32).
The current analysis involved 316 patients, aged 4-70 years, who underwent aortic valve–sparing (AVS) (N = 239) or aortic valve–replacing (AVR) (N = 63 mechanical and 14 tissue) root replacement surgery at 19 centers between March 2005 and November 2010. The type of operation was determined by clinical factors, and by surgeon and patient preference. AVR surgery was considered the only option in 17% of patients. At 1 year, clinical follow-up was complete in 98% and imaging follow-up in 93%.
"Interestingly, when we started out this particular collection of patients, over 30% were receiving aortic valve replacement, but toward the end of this observational study, late 2010, virtually almost all patients were receiving aortic valve sparing," said Dr. Coselli, chief of adult cardiac surgery at Baylor College of Medicine, Texas Heart Institute, Houston.
AVS patients were younger (33 vs. 39 years); had smaller sinuses of Valsalva (49 vs. 53 mm); and had less acute dissection (3% vs. 9%), chronic dissection (3% vs. 12%), and previous cardiovascular surgery (5% vs. 14%).
Aortic-sparing techniques required significantly longer cardiopulmonary bypass time (195 vs. 152 minutes) and aortic clamp time (156 vs. 115 minutes), but cut ICU time from 46 hours with AVR surgery to 26 hours, ventilator support time from 12 to 8 hours, and hospital length of stay from 7 to 6 days, Dr. Coselli reported.
At 30 days, MAVREs were reported in 6 patients in the AVR group and 15 in the AVS group (P = .4), with no differences in nonstructural dysfunction (1 vs. 7), embolism (1 vs. 3), or bleeding (2 vs. 3 events).
Two AVS patients required early reoperation: One required same-day reintervention because of coronary artery kinking after a Florida sleeve procedure, and the second needed reintervention because of a coronary pseudoaneurysm 6 days after a David-V procedure, he said. Two early deaths occurred, one in each group, but neither was valve related.
One-year survival rates were 98% after AVS surgery and 97% after AVR surgery (4 vs. 2 deaths; P = .06).
At 1 year, MAVREs occurred in 8 AVR and 35 AVS patients (P = .5). There was no significant difference between AVR and AVS in freedom from valve-related death (1 vs. 2), embolism (2 vs. 4 events), reintervention (0 vs. 1), endocarditis (1 vs. 0), valve thrombosis (0 both), or valve-related morbidity (7 vs. 28), Dr. Coselli said.
The AVS group had significantly more nonstructural dysfunction/structural valve deterioration (23 events vs. 1 event; P = .04), but significantly less bleeding (3 vs. 5 events; P = .01).
In a Cox regression analysis at 1 year, the type of surgery was not associated with overall survival, MAVREs, or any other valve-related outcome, he said.
Dr. Coselli reported research support from St. Jude Medical; an educational grant, consultancy, and royalties from Vascutek Terumo; and research support, speaking for, and steering committee membership with Medtronic. Two coauthors reported consultant/advisory board participation with Medtronic or Edwards Lifesciences.
MINNEAPOLIS – Despite the complexity of aortic valve–sparing techniques, early outcomes and 1-year survival were similar to those achieved with valve replacing during root replacement surgery in patients with Marfan syndrome in a prospective registry study.
Major adverse valve-related events (MAVREs) at 1 year were also comparable, although there was an increase, of course, in aortic valve regurgitation with valve sparing (7% vs. 0%), Dr. Joseph S. Coselli said at the annual meeting of the American Association for Thoracic Surgery.
"Follow-up is needed for this particular incident because we don’t know exactly what’s going to happen to these 2-plus aortic regurgitations," he said. "It’s quite possible they may remain stable over a long period of time and don’t represent a failure of the concept."
In an initial report from the international registry, valve-sparing techniques were the most common, and provided comparable 30-day outcomes in 151 patients (J. Thorac. Cardiovasc. Surg. 2009;137:1124-32).
The current analysis involved 316 patients, aged 4-70 years, who underwent aortic valve–sparing (AVS) (N = 239) or aortic valve–replacing (AVR) (N = 63 mechanical and 14 tissue) root replacement surgery at 19 centers between March 2005 and November 2010. The type of operation was determined by clinical factors, and by surgeon and patient preference. AVR surgery was considered the only option in 17% of patients. At 1 year, clinical follow-up was complete in 98% and imaging follow-up in 93%.
"Interestingly, when we started out this particular collection of patients, over 30% were receiving aortic valve replacement, but toward the end of this observational study, late 2010, virtually almost all patients were receiving aortic valve sparing," said Dr. Coselli, chief of adult cardiac surgery at Baylor College of Medicine, Texas Heart Institute, Houston.
AVS patients were younger (33 vs. 39 years); had smaller sinuses of Valsalva (49 vs. 53 mm); and had less acute dissection (3% vs. 9%), chronic dissection (3% vs. 12%), and previous cardiovascular surgery (5% vs. 14%).
Aortic-sparing techniques required significantly longer cardiopulmonary bypass time (195 vs. 152 minutes) and aortic clamp time (156 vs. 115 minutes), but cut ICU time from 46 hours with AVR surgery to 26 hours, ventilator support time from 12 to 8 hours, and hospital length of stay from 7 to 6 days, Dr. Coselli reported.
At 30 days, MAVREs were reported in 6 patients in the AVR group and 15 in the AVS group (P = .4), with no differences in nonstructural dysfunction (1 vs. 7), embolism (1 vs. 3), or bleeding (2 vs. 3 events).
Two AVS patients required early reoperation: One required same-day reintervention because of coronary artery kinking after a Florida sleeve procedure, and the second needed reintervention because of a coronary pseudoaneurysm 6 days after a David-V procedure, he said. Two early deaths occurred, one in each group, but neither was valve related.
One-year survival rates were 98% after AVS surgery and 97% after AVR surgery (4 vs. 2 deaths; P = .06).
At 1 year, MAVREs occurred in 8 AVR and 35 AVS patients (P = .5). There was no significant difference between AVR and AVS in freedom from valve-related death (1 vs. 2), embolism (2 vs. 4 events), reintervention (0 vs. 1), endocarditis (1 vs. 0), valve thrombosis (0 both), or valve-related morbidity (7 vs. 28), Dr. Coselli said.
The AVS group had significantly more nonstructural dysfunction/structural valve deterioration (23 events vs. 1 event; P = .04), but significantly less bleeding (3 vs. 5 events; P = .01).
In a Cox regression analysis at 1 year, the type of surgery was not associated with overall survival, MAVREs, or any other valve-related outcome, he said.
Dr. Coselli reported research support from St. Jude Medical; an educational grant, consultancy, and royalties from Vascutek Terumo; and research support, speaking for, and steering committee membership with Medtronic. Two coauthors reported consultant/advisory board participation with Medtronic or Edwards Lifesciences.
AT THE AATS ANNUAL MEETING
Epidermolysis bullosa patients rate itching worse than pain
MILWAUKEE – Itching is more problematic than is pain for patients with epidermolysis bullosa, according to an online survey of 146 patients.
Symptoms reported in conjunction with itching included pain, stinging, burning, and a sensation of ants crawling on the skin, as well as a feeling that the itch was too deep to scratch, Christina Danial and her associates reported at the annual meeting of the Society for Pediatric Dermatology.
Although data from a prior study of 11 children with epidermolysis bullosa (EB) hinted that pruritus is more bothersome than pain is (Acta. Derm. Venereol. 2008;88:143-50), the results are nonetheless startling given that EB is a mutilating disease of the skin and mucosa, Ms. Danial said. Patients with this rare condition cope with blistering of the skin and/or epithelial lining of the organs, GI complications, anemia, and shortened survival due to infection or cancer.
In this study, 216 EB patients and/or caregivers registered in the Epidermolysis Bullosa Clinical Research Consortium received a 42-item online questionnaire, and 146 completed the survey. Responses were based on a 5-point Likert scale in which 1 was "never" and 5 was "always."
Itchiness was rated the most bothersome item (mean 3.3), followed by acute pain (mean 2.9), chronic pain (mean 2.7), problems eating (mean 2.7), stomach problems (mean 2.6), dental problems (mean 2.6), movement (2.5), and surgical procedures (mean 2.4), reported Ms. Danial, a medical student at Stanford (Calif.) University.
Patients with the more severe recessive dystrophic EB subtype had significantly more pruritus than did those with EB simplex (mean 3.9 vs. 3.1; P = .01).
The frequency of itching increased as the day progressed, with bedtime having the highest frequency (mean 3.8). Not surprisingly, itching was found to interfere with sleep (mean 3.1), she noted.
Sweating (mean 3.9) and stress (mean 4.0) increased itching, as did dryness (mean 4.0), heat (mean 3.8), and humidity (mean 3.5).
The 146 respondents comprised 90 patients, 36 caregivers, and 20 patient/caregivers. The average age of the respondents was 22 years; 73 were male and 73 were female.
EB patients reported that pruritus makes them feel frustrated, agitated, and as if they cannot control the itch, although activity was noted to relieve the itching, Ms. Danial reported.
Ms. Danial suggested that further investigation is necessary to determine which treatments are most effective against itching in EB, but recommended that patients avoid dryness, heat, and humidity, and consider nighttime treatment. Treatments to control pain also may help alleviate pruritus, since patients may experience pain while itching, she added.
In all, 66% of patients had dystrophic EB, 21% had EB simplex, 10% had junctional EB, and the EB subtype of 3% was unknown. Severe disease was reported in 38% of those with recessive dystrophic EB, 14% with dominant dystrophic EB, 17% with unknown dystrophic subtype, 3% with EB simplex, 36% with junctional EB, and none with unknown EB.
Ms. Danial and her coauthors reported having no financial disclosures.
MILWAUKEE – Itching is more problematic than is pain for patients with epidermolysis bullosa, according to an online survey of 146 patients.
Symptoms reported in conjunction with itching included pain, stinging, burning, and a sensation of ants crawling on the skin, as well as a feeling that the itch was too deep to scratch, Christina Danial and her associates reported at the annual meeting of the Society for Pediatric Dermatology.
Although data from a prior study of 11 children with epidermolysis bullosa (EB) hinted that pruritus is more bothersome than pain is (Acta. Derm. Venereol. 2008;88:143-50), the results are nonetheless startling given that EB is a mutilating disease of the skin and mucosa, Ms. Danial said. Patients with this rare condition cope with blistering of the skin and/or epithelial lining of the organs, GI complications, anemia, and shortened survival due to infection or cancer.
In this study, 216 EB patients and/or caregivers registered in the Epidermolysis Bullosa Clinical Research Consortium received a 42-item online questionnaire, and 146 completed the survey. Responses were based on a 5-point Likert scale in which 1 was "never" and 5 was "always."
Itchiness was rated the most bothersome item (mean 3.3), followed by acute pain (mean 2.9), chronic pain (mean 2.7), problems eating (mean 2.7), stomach problems (mean 2.6), dental problems (mean 2.6), movement (2.5), and surgical procedures (mean 2.4), reported Ms. Danial, a medical student at Stanford (Calif.) University.
Patients with the more severe recessive dystrophic EB subtype had significantly more pruritus than did those with EB simplex (mean 3.9 vs. 3.1; P = .01).
The frequency of itching increased as the day progressed, with bedtime having the highest frequency (mean 3.8). Not surprisingly, itching was found to interfere with sleep (mean 3.1), she noted.
Sweating (mean 3.9) and stress (mean 4.0) increased itching, as did dryness (mean 4.0), heat (mean 3.8), and humidity (mean 3.5).
The 146 respondents comprised 90 patients, 36 caregivers, and 20 patient/caregivers. The average age of the respondents was 22 years; 73 were male and 73 were female.
EB patients reported that pruritus makes them feel frustrated, agitated, and as if they cannot control the itch, although activity was noted to relieve the itching, Ms. Danial reported.
Ms. Danial suggested that further investigation is necessary to determine which treatments are most effective against itching in EB, but recommended that patients avoid dryness, heat, and humidity, and consider nighttime treatment. Treatments to control pain also may help alleviate pruritus, since patients may experience pain while itching, she added.
In all, 66% of patients had dystrophic EB, 21% had EB simplex, 10% had junctional EB, and the EB subtype of 3% was unknown. Severe disease was reported in 38% of those with recessive dystrophic EB, 14% with dominant dystrophic EB, 17% with unknown dystrophic subtype, 3% with EB simplex, 36% with junctional EB, and none with unknown EB.
Ms. Danial and her coauthors reported having no financial disclosures.
MILWAUKEE – Itching is more problematic than is pain for patients with epidermolysis bullosa, according to an online survey of 146 patients.
Symptoms reported in conjunction with itching included pain, stinging, burning, and a sensation of ants crawling on the skin, as well as a feeling that the itch was too deep to scratch, Christina Danial and her associates reported at the annual meeting of the Society for Pediatric Dermatology.
Although data from a prior study of 11 children with epidermolysis bullosa (EB) hinted that pruritus is more bothersome than pain is (Acta. Derm. Venereol. 2008;88:143-50), the results are nonetheless startling given that EB is a mutilating disease of the skin and mucosa, Ms. Danial said. Patients with this rare condition cope with blistering of the skin and/or epithelial lining of the organs, GI complications, anemia, and shortened survival due to infection or cancer.
In this study, 216 EB patients and/or caregivers registered in the Epidermolysis Bullosa Clinical Research Consortium received a 42-item online questionnaire, and 146 completed the survey. Responses were based on a 5-point Likert scale in which 1 was "never" and 5 was "always."
Itchiness was rated the most bothersome item (mean 3.3), followed by acute pain (mean 2.9), chronic pain (mean 2.7), problems eating (mean 2.7), stomach problems (mean 2.6), dental problems (mean 2.6), movement (2.5), and surgical procedures (mean 2.4), reported Ms. Danial, a medical student at Stanford (Calif.) University.
Patients with the more severe recessive dystrophic EB subtype had significantly more pruritus than did those with EB simplex (mean 3.9 vs. 3.1; P = .01).
The frequency of itching increased as the day progressed, with bedtime having the highest frequency (mean 3.8). Not surprisingly, itching was found to interfere with sleep (mean 3.1), she noted.
Sweating (mean 3.9) and stress (mean 4.0) increased itching, as did dryness (mean 4.0), heat (mean 3.8), and humidity (mean 3.5).
The 146 respondents comprised 90 patients, 36 caregivers, and 20 patient/caregivers. The average age of the respondents was 22 years; 73 were male and 73 were female.
EB patients reported that pruritus makes them feel frustrated, agitated, and as if they cannot control the itch, although activity was noted to relieve the itching, Ms. Danial reported.
Ms. Danial suggested that further investigation is necessary to determine which treatments are most effective against itching in EB, but recommended that patients avoid dryness, heat, and humidity, and consider nighttime treatment. Treatments to control pain also may help alleviate pruritus, since patients may experience pain while itching, she added.
In all, 66% of patients had dystrophic EB, 21% had EB simplex, 10% had junctional EB, and the EB subtype of 3% was unknown. Severe disease was reported in 38% of those with recessive dystrophic EB, 14% with dominant dystrophic EB, 17% with unknown dystrophic subtype, 3% with EB simplex, 36% with junctional EB, and none with unknown EB.
Ms. Danial and her coauthors reported having no financial disclosures.
AT THE SPD ANNUAL MEETING
Major finding: Itchiness was rated the most bothersome symptom (mean 3.3 on a 5-point scale), followed by acute pain (mean 2.9), chronic pain (mean 2.7), and problems eating (mean 2.7).
Data source: Online survey of 146 patients with epidermolysis bullosa and/or their caregivers.
Disclosures: Ms. Danial and her coauthors reported having no financial disclosures.
The chicken or the egg: Obesity or psoriasis?
Earn 0.25 hours AMA PRA Category 1 credit: Read this article, and click the link at the end to take the post-test.
MILWAUKEE – Excess adiposity occurred prior to psoriasis in 93% of 29 overweight and obese psoriatic children, in a chart review examining the relationship between psoriasis and obesity.
Further, 78% of patients were obese before developing psoriasis, Dr. Lauren Becker reported at the annual meeting of the Society for Pediatric Dermatology.
Although the authors anticipated that most of the children would show increased adiposity before psoriasis based on clinical observations, "none of us predicted that it would be 27 of 29," she said in an interview. "It really was incredible, and even the ones who were normal weight became overweight or obese within a year of their psoriasis."
The review was sparked by a recent international study, led by senior author Dr. Amy Paller of Northwestern University in Chicago, in which 38% of psoriatic children had excess central adiposity (high waist-to-height ratio) compared with 21% of controls. The odds of obesity were also several times higher than those reported for adults with psoriasis, jumping 4.29-fold overall in psoriatic children versus controls, 4.92-fold in those with severe versus mild psoriasis, and 7.6-fold in the United States. (JAMA Dermatol. 2013;149:166-76).
Although other studies in children support an association between obesity and psoriasis, the international study was the first to measure central adiposity, a more sensitive indicator of cardiovascular risk in children than BMI, Dr. Kelly Cordoro remarked in a separate lecture on the comorbidities of pediatric psoriasis at the meeting.
"Adiposity, hypertension, hyperlipidemia, and diabetes are increased in prevalence among pediatric psoriasis patients, but the obesity association is the strongest," she said. "It’s global, and the effect is most pronounced in the United States, where in particular, central obesity is highest and has the accompanying higher cardiovascular risk."
Previous research has shown that obesity is strongly correlated with psoriasis in adults. A recent meta-analysis showed that psoriatic adults were more likely to be obese than those without psoriasis (pooled odds ratio, 1.66), and that the odds were even higher in patients with severe versus mild psoriasis (OR, 2.23, vs. OR, 1.46) (Nutr. Diabetes 2012 ;2:e54).
Both clinicians observed that psoriasis and obesity are chronic inflammatory states, marked by overexpression of circulating proinflammatory cytokines derived from Th1 and Th17 lymphocyte subsets, as well as tumor necrosis factor–alpha and adipokines. In addition, a fat cell is a microenvironment of inflammation, with adipose tissue releasing proinflammatory cytokines such as interleukin-6 and TNF-alpha.
The two diseases drive one another, but the exact relationship remains unclear, said Dr. Becker, a pediatrician and dermatology fellow at Northwestern at the time of the study. In addition, the impact on quality of life and social interactions of being both obese or overweight and having psoriasis may predispose patients to mental and physical health problems.
"Children with excess adiposity or with the highly visible lesions of psoriasis are more often teased or bullied, which may contribute to the tendency to become socially isolated, decrease physical activity, and increase eating," she said. "It really is a vicious circle."
Although the data are clear that psoriasis and obesity are associated, the current chart review suggesting that obesity precedes psoriasis is too small to definitively answer the question, Dr. Cordoro, a pediatric dermatologist at the University of California, San Francisco, said in an interview.
Dr. Becker said obesity clearly came before psoriasis in their study cohort, but agreed that further study is needed to confirm the results. She also stressed the need for biomarker analyses to identify overweight/obese children who are at risk for psoriasis, and studies to address whether weight loss can reverse the severity of pediatric psoriasis.
For example, data from a study of overweight psoriatic adults showed that eating a low-calorie diet improved psoriasis severity and quality of life after 4 months (JAMA Dermatol. 2013;149:795-801).
However, in the absence of adequate data, clinicians should consider metabolic testing to determine whether their overweight pediatric patients are on the path to the metabolic syndrome, Dr. Becker and Dr. Cordoro suggested. Metabolic testing was not performed on any of the 29 children in the chart review, although 48% had a family history of hyperlipidemia and 45% had a family history of obesity.
The average age of the children was 12.6 years; the average age of onset of obesity was 4 years (range, 2-12 years), and the average age of onset of psoriasis was 9 years (range, 2-14 years).
Two obese patients were able to reduce their BMIs from obese to overweight status 1 year after being diagnosed with psoriasis; however, both have remained in the 85th-95th BMI percentile for more than 2 years, Dr. Becker said. Both of the children who had a normal BMI prior to their psoriasis had a BMI in the overweight or obese range within 1 year after diagnosis, Dr. Becker noted.
Dr. Cordoro also made an impassioned plea for clinicians to address the significant psychosocial comorbidity present in psoriatic children.
"You can think about obesity, psoriasis, and depression as being reciprocal exacerbating factors, such that each triggers the other and represents an insult to self-esteem and the overall well-being of these patients," she said. "They end up having high stress levels and really dismal quality of life. These issues are as important in the management of the child as the medical considerations."
Dr. Becker, her coauthors, and Dr. Cordoro reported having no relevant financial disclosures.
To earn 0.25 hours AMA PRA Category 1 credit after reading this article, take the post-test here.
Earn 0.25 hours AMA PRA Category 1 credit: Read this article, and click the link at the end to take the post-test.
MILWAUKEE – Excess adiposity occurred prior to psoriasis in 93% of 29 overweight and obese psoriatic children, in a chart review examining the relationship between psoriasis and obesity.
Further, 78% of patients were obese before developing psoriasis, Dr. Lauren Becker reported at the annual meeting of the Society for Pediatric Dermatology.
Although the authors anticipated that most of the children would show increased adiposity before psoriasis based on clinical observations, "none of us predicted that it would be 27 of 29," she said in an interview. "It really was incredible, and even the ones who were normal weight became overweight or obese within a year of their psoriasis."
The review was sparked by a recent international study, led by senior author Dr. Amy Paller of Northwestern University in Chicago, in which 38% of psoriatic children had excess central adiposity (high waist-to-height ratio) compared with 21% of controls. The odds of obesity were also several times higher than those reported for adults with psoriasis, jumping 4.29-fold overall in psoriatic children versus controls, 4.92-fold in those with severe versus mild psoriasis, and 7.6-fold in the United States. (JAMA Dermatol. 2013;149:166-76).
Although other studies in children support an association between obesity and psoriasis, the international study was the first to measure central adiposity, a more sensitive indicator of cardiovascular risk in children than BMI, Dr. Kelly Cordoro remarked in a separate lecture on the comorbidities of pediatric psoriasis at the meeting.
"Adiposity, hypertension, hyperlipidemia, and diabetes are increased in prevalence among pediatric psoriasis patients, but the obesity association is the strongest," she said. "It’s global, and the effect is most pronounced in the United States, where in particular, central obesity is highest and has the accompanying higher cardiovascular risk."
Previous research has shown that obesity is strongly correlated with psoriasis in adults. A recent meta-analysis showed that psoriatic adults were more likely to be obese than those without psoriasis (pooled odds ratio, 1.66), and that the odds were even higher in patients with severe versus mild psoriasis (OR, 2.23, vs. OR, 1.46) (Nutr. Diabetes 2012 ;2:e54).
Both clinicians observed that psoriasis and obesity are chronic inflammatory states, marked by overexpression of circulating proinflammatory cytokines derived from Th1 and Th17 lymphocyte subsets, as well as tumor necrosis factor–alpha and adipokines. In addition, a fat cell is a microenvironment of inflammation, with adipose tissue releasing proinflammatory cytokines such as interleukin-6 and TNF-alpha.
The two diseases drive one another, but the exact relationship remains unclear, said Dr. Becker, a pediatrician and dermatology fellow at Northwestern at the time of the study. In addition, the impact on quality of life and social interactions of being both obese or overweight and having psoriasis may predispose patients to mental and physical health problems.
"Children with excess adiposity or with the highly visible lesions of psoriasis are more often teased or bullied, which may contribute to the tendency to become socially isolated, decrease physical activity, and increase eating," she said. "It really is a vicious circle."
Although the data are clear that psoriasis and obesity are associated, the current chart review suggesting that obesity precedes psoriasis is too small to definitively answer the question, Dr. Cordoro, a pediatric dermatologist at the University of California, San Francisco, said in an interview.
Dr. Becker said obesity clearly came before psoriasis in their study cohort, but agreed that further study is needed to confirm the results. She also stressed the need for biomarker analyses to identify overweight/obese children who are at risk for psoriasis, and studies to address whether weight loss can reverse the severity of pediatric psoriasis.
For example, data from a study of overweight psoriatic adults showed that eating a low-calorie diet improved psoriasis severity and quality of life after 4 months (JAMA Dermatol. 2013;149:795-801).
However, in the absence of adequate data, clinicians should consider metabolic testing to determine whether their overweight pediatric patients are on the path to the metabolic syndrome, Dr. Becker and Dr. Cordoro suggested. Metabolic testing was not performed on any of the 29 children in the chart review, although 48% had a family history of hyperlipidemia and 45% had a family history of obesity.
The average age of the children was 12.6 years; the average age of onset of obesity was 4 years (range, 2-12 years), and the average age of onset of psoriasis was 9 years (range, 2-14 years).
Two obese patients were able to reduce their BMIs from obese to overweight status 1 year after being diagnosed with psoriasis; however, both have remained in the 85th-95th BMI percentile for more than 2 years, Dr. Becker said. Both of the children who had a normal BMI prior to their psoriasis had a BMI in the overweight or obese range within 1 year after diagnosis, Dr. Becker noted.
Dr. Cordoro also made an impassioned plea for clinicians to address the significant psychosocial comorbidity present in psoriatic children.
"You can think about obesity, psoriasis, and depression as being reciprocal exacerbating factors, such that each triggers the other and represents an insult to self-esteem and the overall well-being of these patients," she said. "They end up having high stress levels and really dismal quality of life. These issues are as important in the management of the child as the medical considerations."
Dr. Becker, her coauthors, and Dr. Cordoro reported having no relevant financial disclosures.
To earn 0.25 hours AMA PRA Category 1 credit after reading this article, take the post-test here.
Earn 0.25 hours AMA PRA Category 1 credit: Read this article, and click the link at the end to take the post-test.
MILWAUKEE – Excess adiposity occurred prior to psoriasis in 93% of 29 overweight and obese psoriatic children, in a chart review examining the relationship between psoriasis and obesity.
Further, 78% of patients were obese before developing psoriasis, Dr. Lauren Becker reported at the annual meeting of the Society for Pediatric Dermatology.
Although the authors anticipated that most of the children would show increased adiposity before psoriasis based on clinical observations, "none of us predicted that it would be 27 of 29," she said in an interview. "It really was incredible, and even the ones who were normal weight became overweight or obese within a year of their psoriasis."
The review was sparked by a recent international study, led by senior author Dr. Amy Paller of Northwestern University in Chicago, in which 38% of psoriatic children had excess central adiposity (high waist-to-height ratio) compared with 21% of controls. The odds of obesity were also several times higher than those reported for adults with psoriasis, jumping 4.29-fold overall in psoriatic children versus controls, 4.92-fold in those with severe versus mild psoriasis, and 7.6-fold in the United States. (JAMA Dermatol. 2013;149:166-76).
Although other studies in children support an association between obesity and psoriasis, the international study was the first to measure central adiposity, a more sensitive indicator of cardiovascular risk in children than BMI, Dr. Kelly Cordoro remarked in a separate lecture on the comorbidities of pediatric psoriasis at the meeting.
"Adiposity, hypertension, hyperlipidemia, and diabetes are increased in prevalence among pediatric psoriasis patients, but the obesity association is the strongest," she said. "It’s global, and the effect is most pronounced in the United States, where in particular, central obesity is highest and has the accompanying higher cardiovascular risk."
Previous research has shown that obesity is strongly correlated with psoriasis in adults. A recent meta-analysis showed that psoriatic adults were more likely to be obese than those without psoriasis (pooled odds ratio, 1.66), and that the odds were even higher in patients with severe versus mild psoriasis (OR, 2.23, vs. OR, 1.46) (Nutr. Diabetes 2012 ;2:e54).
Both clinicians observed that psoriasis and obesity are chronic inflammatory states, marked by overexpression of circulating proinflammatory cytokines derived from Th1 and Th17 lymphocyte subsets, as well as tumor necrosis factor–alpha and adipokines. In addition, a fat cell is a microenvironment of inflammation, with adipose tissue releasing proinflammatory cytokines such as interleukin-6 and TNF-alpha.
The two diseases drive one another, but the exact relationship remains unclear, said Dr. Becker, a pediatrician and dermatology fellow at Northwestern at the time of the study. In addition, the impact on quality of life and social interactions of being both obese or overweight and having psoriasis may predispose patients to mental and physical health problems.
"Children with excess adiposity or with the highly visible lesions of psoriasis are more often teased or bullied, which may contribute to the tendency to become socially isolated, decrease physical activity, and increase eating," she said. "It really is a vicious circle."
Although the data are clear that psoriasis and obesity are associated, the current chart review suggesting that obesity precedes psoriasis is too small to definitively answer the question, Dr. Cordoro, a pediatric dermatologist at the University of California, San Francisco, said in an interview.
Dr. Becker said obesity clearly came before psoriasis in their study cohort, but agreed that further study is needed to confirm the results. She also stressed the need for biomarker analyses to identify overweight/obese children who are at risk for psoriasis, and studies to address whether weight loss can reverse the severity of pediatric psoriasis.
For example, data from a study of overweight psoriatic adults showed that eating a low-calorie diet improved psoriasis severity and quality of life after 4 months (JAMA Dermatol. 2013;149:795-801).
However, in the absence of adequate data, clinicians should consider metabolic testing to determine whether their overweight pediatric patients are on the path to the metabolic syndrome, Dr. Becker and Dr. Cordoro suggested. Metabolic testing was not performed on any of the 29 children in the chart review, although 48% had a family history of hyperlipidemia and 45% had a family history of obesity.
The average age of the children was 12.6 years; the average age of onset of obesity was 4 years (range, 2-12 years), and the average age of onset of psoriasis was 9 years (range, 2-14 years).
Two obese patients were able to reduce their BMIs from obese to overweight status 1 year after being diagnosed with psoriasis; however, both have remained in the 85th-95th BMI percentile for more than 2 years, Dr. Becker said. Both of the children who had a normal BMI prior to their psoriasis had a BMI in the overweight or obese range within 1 year after diagnosis, Dr. Becker noted.
Dr. Cordoro also made an impassioned plea for clinicians to address the significant psychosocial comorbidity present in psoriatic children.
"You can think about obesity, psoriasis, and depression as being reciprocal exacerbating factors, such that each triggers the other and represents an insult to self-esteem and the overall well-being of these patients," she said. "They end up having high stress levels and really dismal quality of life. These issues are as important in the management of the child as the medical considerations."
Dr. Becker, her coauthors, and Dr. Cordoro reported having no relevant financial disclosures.
To earn 0.25 hours AMA PRA Category 1 credit after reading this article, take the post-test here.
AT THE SPD ANNUAL MEETING
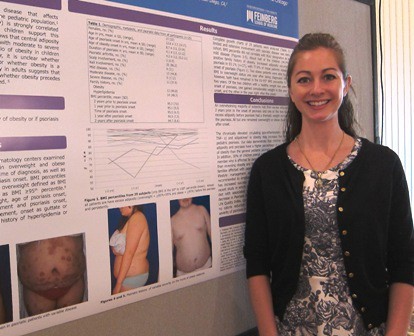
The chicken or the egg: Obesity or psoriasis?
MILWAUKEE – Excess adiposity occurred prior to psoriasis in 93% of 29 overweight and obese psoriatic children, in a chart review examining the relationship between psoriasis and obesity.
Further, 78% of patients were obese before developing psoriasis, Dr. Lauren Becker reported at the annual meeting of the Society for Pediatric Dermatology.
Although the authors anticipated that most of the children would show increased adiposity before psoriasis based on clinical observations, "none of us predicted that it would be 27 of 29," she said in an interview. "It really was incredible, and even the ones who were normal weight became overweight or obese within a year of their psoriasis."
The review was sparked by a recent international study, led by senior author Dr. Amy Paller of Northwestern University in Chicago, in which 38% of psoriatic children had excess central adiposity (high waist-to-height ratio) compared with 21% of controls. The odds of obesity were also several times higher than those reported for adults with psoriasis, jumping 4.29-fold overall in psoriatic children versus controls, 4.92-fold in those with severe versus mild psoriasis, and 7.6-fold in the United States. (JAMA Dermatol. 2013;149:166-76).
Although other studies in children support an association between obesity and psoriasis, the international study was the first to measure central adiposity, a more sensitive indicator of cardiovascular risk in children than BMI, Dr. Kelly Cordoro remarked in a separate lecture on the comorbidities of pediatric psoriasis at the meeting.
"Adiposity, hypertension, hyperlipidemia, and diabetes are increased in prevalence among pediatric psoriasis patients, but the obesity association is the strongest," she said. "It’s global, and the effect is most pronounced in the United States, where in particular, central obesity is highest and has the accompanying higher cardiovascular risk."
Previous research has shown that obesity is strongly correlated with psoriasis in adults. A recent meta-analysis showed that psoriatic adults were more likely to be obese than those without psoriasis (pooled odds ratio, 1.66), and that the odds were even higher in patients with severe versus mild psoriasis (OR, 2.23, vs. OR, 1.46) (Nutr. Diabetes 2012 ;2:e54).

Both clinicians observed that psoriasis and obesity are chronic inflammatory states, marked by overexpression of circulating proinflammatory cytokines derived from Th1 and Th17 lymphocyte subsets, as well as tumor necrosis factor–alpha and adipokines. In addition, a fat cell is a microenvironment of inflammation, with adipose tissue releasing proinflammatory cytokines such as interleukin-6 and TNF-alpha.
The two diseases drive one another, but the exact relationship remains unclear, said Dr. Becker, a pediatrician and dermatology fellow at Northwestern at the time of the study. In addition, the impact on quality of life and social interactions of being both obese or overweight and having psoriasis may predispose patients to mental and physical health problems.
"Children with excess adiposity or with the highly visible lesions of psoriasis are more often teased or bullied, which may contribute to the tendency to become socially isolated, decrease physical activity, and increase eating," she said. "It really is a vicious circle."
Although the data are clear that psoriasis and obesity are associated, the current chart review suggesting that obesity precedes psoriasis is too small to definitively answer the question, Dr. Cordoro, a pediatric dermatologist at the University of California, San Francisco, said in an interview.
Dr. Becker said obesity clearly came before psoriasis in their study cohort, but agreed that further study is needed to confirm the results. She also stressed the need for biomarker analyses to identify overweight/obese children who are at risk for psoriasis, and studies to address whether weight loss can reverse the severity of pediatric psoriasis.
For example, data from a study of overweight psoriatic adults showed that eating a low-calorie diet improved psoriasis severity and quality of life after 4 months (JAMA Dermatol. 2013;149:795-801).
However, in the absence of adequate data, clinicians should consider metabolic testing to determine whether their overweight pediatric patients are on the path to the metabolic syndrome, Dr. Becker and Dr. Cordoro suggested. Metabolic testing was not performed on any of the 29 children in the chart review, although 48% had a family history of hyperlipidemia and 45% had a family history of obesity.
The average age of the children was 12.6 years; the average age of onset of obesity was 4 years (range, 2-12 years), and the average age of onset of psoriasis was 9 years (range, 2-14 years).
Two obese patients were able to reduce their BMIs from obese to overweight status 1 year after being diagnosed with psoriasis; however, both have remained in the 85th-95th BMI percentile for more than 2 years, Dr. Becker said. Both of the children who had a normal BMI prior to their psoriasis had a BMI in the overweight or obese range within 1 year after diagnosis, Dr. Becker noted.
Dr. Cordoro also made an impassioned plea for clinicians to address the significant psychosocial comorbidity present in psoriatic children.
"You can think about obesity, psoriasis, and depression as being reciprocal exacerbating factors, such that each triggers the other and represents an insult to self-esteem and the overall well-being of these patients," she said. "They end up having high stress levels and really dismal quality of life. These issues are as important in the management of the child as the medical considerations."
Dr. Becker, her coauthors, and Dr. Cordoro reported having no relevant financial disclosures.
MILWAUKEE – Excess adiposity occurred prior to psoriasis in 93% of 29 overweight and obese psoriatic children, in a chart review examining the relationship between psoriasis and obesity.
Further, 78% of patients were obese before developing psoriasis, Dr. Lauren Becker reported at the annual meeting of the Society for Pediatric Dermatology.
Although the authors anticipated that most of the children would show increased adiposity before psoriasis based on clinical observations, "none of us predicted that it would be 27 of 29," she said in an interview. "It really was incredible, and even the ones who were normal weight became overweight or obese within a year of their psoriasis."
The review was sparked by a recent international study, led by senior author Dr. Amy Paller of Northwestern University in Chicago, in which 38% of psoriatic children had excess central adiposity (high waist-to-height ratio) compared with 21% of controls. The odds of obesity were also several times higher than those reported for adults with psoriasis, jumping 4.29-fold overall in psoriatic children versus controls, 4.92-fold in those with severe versus mild psoriasis, and 7.6-fold in the United States. (JAMA Dermatol. 2013;149:166-76).
Although other studies in children support an association between obesity and psoriasis, the international study was the first to measure central adiposity, a more sensitive indicator of cardiovascular risk in children than BMI, Dr. Kelly Cordoro remarked in a separate lecture on the comorbidities of pediatric psoriasis at the meeting.
"Adiposity, hypertension, hyperlipidemia, and diabetes are increased in prevalence among pediatric psoriasis patients, but the obesity association is the strongest," she said. "It’s global, and the effect is most pronounced in the United States, where in particular, central obesity is highest and has the accompanying higher cardiovascular risk."
Previous research has shown that obesity is strongly correlated with psoriasis in adults. A recent meta-analysis showed that psoriatic adults were more likely to be obese than those without psoriasis (pooled odds ratio, 1.66), and that the odds were even higher in patients with severe versus mild psoriasis (OR, 2.23, vs. OR, 1.46) (Nutr. Diabetes 2012 ;2:e54).
Both clinicians observed that psoriasis and obesity are chronic inflammatory states, marked by overexpression of circulating proinflammatory cytokines derived from Th1 and Th17 lymphocyte subsets, as well as tumor necrosis factor–alpha and adipokines. In addition, a fat cell is a microenvironment of inflammation, with adipose tissue releasing proinflammatory cytokines such as interleukin-6 and TNF-alpha.
The two diseases drive one another, but the exact relationship remains unclear, said Dr. Becker, a pediatrician and dermatology fellow at Northwestern at the time of the study. In addition, the impact on quality of life and social interactions of being both obese or overweight and having psoriasis may predispose patients to mental and physical health problems.
"Children with excess adiposity or with the highly visible lesions of psoriasis are more often teased or bullied, which may contribute to the tendency to become socially isolated, decrease physical activity, and increase eating," she said. "It really is a vicious circle."
Although the data are clear that psoriasis and obesity are associated, the current chart review suggesting that obesity precedes psoriasis is too small to definitively answer the question, Dr. Cordoro, a pediatric dermatologist at the University of California, San Francisco, said in an interview.
Dr. Becker said obesity clearly came before psoriasis in their study cohort, but agreed that further study is needed to confirm the results. She also stressed the need for biomarker analyses to identify overweight/obese children who are at risk for psoriasis, and studies to address whether weight loss can reverse the severity of pediatric psoriasis.
For example, data from a study of overweight psoriatic adults showed that eating a low-calorie diet improved psoriasis severity and quality of life after 4 months (JAMA Dermatol. 2013;149:795-801).
However, in the absence of adequate data, clinicians should consider metabolic testing to determine whether their overweight pediatric patients are on the path to the metabolic syndrome, Dr. Becker and Dr. Cordoro suggested. Metabolic testing was not performed on any of the 29 children in the chart review, although 48% had a family history of hyperlipidemia and 45% had a family history of obesity.
The average age of the children was 12.6 years; the average age of onset of obesity was 4 years (range, 2-12 years), and the average age of onset of psoriasis was 9 years (range, 2-14 years).
Two obese patients were able to reduce their BMIs from obese to overweight status 1 year after being diagnosed with psoriasis; however, both have remained in the 85th-95th BMI percentile for more than 2 years, Dr. Becker said. Both of the children who had a normal BMI prior to their psoriasis had a BMI in the overweight or obese range within 1 year after diagnosis, Dr. Becker noted.
Dr. Cordoro also made an impassioned plea for clinicians to address the significant psychosocial comorbidity present in psoriatic children.
"You can think about obesity, psoriasis, and depression as being reciprocal exacerbating factors, such that each triggers the other and represents an insult to self-esteem and the overall well-being of these patients," she said. "They end up having high stress levels and really dismal quality of life. These issues are as important in the management of the child as the medical considerations."
Dr. Becker, her coauthors, and Dr. Cordoro reported having no relevant financial disclosures.
MILWAUKEE – Excess adiposity occurred prior to psoriasis in 93% of 29 overweight and obese psoriatic children, in a chart review examining the relationship between psoriasis and obesity.
Further, 78% of patients were obese before developing psoriasis, Dr. Lauren Becker reported at the annual meeting of the Society for Pediatric Dermatology.
Although the authors anticipated that most of the children would show increased adiposity before psoriasis based on clinical observations, "none of us predicted that it would be 27 of 29," she said in an interview. "It really was incredible, and even the ones who were normal weight became overweight or obese within a year of their psoriasis."
The review was sparked by a recent international study, led by senior author Dr. Amy Paller of Northwestern University in Chicago, in which 38% of psoriatic children had excess central adiposity (high waist-to-height ratio) compared with 21% of controls. The odds of obesity were also several times higher than those reported for adults with psoriasis, jumping 4.29-fold overall in psoriatic children versus controls, 4.92-fold in those with severe versus mild psoriasis, and 7.6-fold in the United States. (JAMA Dermatol. 2013;149:166-76).
Although other studies in children support an association between obesity and psoriasis, the international study was the first to measure central adiposity, a more sensitive indicator of cardiovascular risk in children than BMI, Dr. Kelly Cordoro remarked in a separate lecture on the comorbidities of pediatric psoriasis at the meeting.
"Adiposity, hypertension, hyperlipidemia, and diabetes are increased in prevalence among pediatric psoriasis patients, but the obesity association is the strongest," she said. "It’s global, and the effect is most pronounced in the United States, where in particular, central obesity is highest and has the accompanying higher cardiovascular risk."
Previous research has shown that obesity is strongly correlated with psoriasis in adults. A recent meta-analysis showed that psoriatic adults were more likely to be obese than those without psoriasis (pooled odds ratio, 1.66), and that the odds were even higher in patients with severe versus mild psoriasis (OR, 2.23, vs. OR, 1.46) (Nutr. Diabetes 2012 ;2:e54).
Both clinicians observed that psoriasis and obesity are chronic inflammatory states, marked by overexpression of circulating proinflammatory cytokines derived from Th1 and Th17 lymphocyte subsets, as well as tumor necrosis factor–alpha and adipokines. In addition, a fat cell is a microenvironment of inflammation, with adipose tissue releasing proinflammatory cytokines such as interleukin-6 and TNF-alpha.
The two diseases drive one another, but the exact relationship remains unclear, said Dr. Becker, a pediatrician and dermatology fellow at Northwestern at the time of the study. In addition, the impact on quality of life and social interactions of being both obese or overweight and having psoriasis may predispose patients to mental and physical health problems.
"Children with excess adiposity or with the highly visible lesions of psoriasis are more often teased or bullied, which may contribute to the tendency to become socially isolated, decrease physical activity, and increase eating," she said. "It really is a vicious circle."
Although the data are clear that psoriasis and obesity are associated, the current chart review suggesting that obesity precedes psoriasis is too small to definitively answer the question, Dr. Cordoro, a pediatric dermatologist at the University of California, San Francisco, said in an interview.
Dr. Becker said obesity clearly came before psoriasis in their study cohort, but agreed that further study is needed to confirm the results. She also stressed the need for biomarker analyses to identify overweight/obese children who are at risk for psoriasis, and studies to address whether weight loss can reverse the severity of pediatric psoriasis.
For example, data from a study of overweight psoriatic adults showed that eating a low-calorie diet improved psoriasis severity and quality of life after 4 months (JAMA Dermatol. 2013;149:795-801).
However, in the absence of adequate data, clinicians should consider metabolic testing to determine whether their overweight pediatric patients are on the path to the metabolic syndrome, Dr. Becker and Dr. Cordoro suggested. Metabolic testing was not performed on any of the 29 children in the chart review, although 48% had a family history of hyperlipidemia and 45% had a family history of obesity.
The average age of the children was 12.6 years; the average age of onset of obesity was 4 years (range, 2-12 years), and the average age of onset of psoriasis was 9 years (range, 2-14 years).
Two obese patients were able to reduce their BMIs from obese to overweight status 1 year after being diagnosed with psoriasis; however, both have remained in the 85th-95th BMI percentile for more than 2 years, Dr. Becker said. Both of the children who had a normal BMI prior to their psoriasis had a BMI in the overweight or obese range within 1 year after diagnosis, Dr. Becker noted.
Dr. Cordoro also made an impassioned plea for clinicians to address the significant psychosocial comorbidity present in psoriatic children.
"You can think about obesity, psoriasis, and depression as being reciprocal exacerbating factors, such that each triggers the other and represents an insult to self-esteem and the overall well-being of these patients," she said. "They end up having high stress levels and really dismal quality of life. These issues are as important in the management of the child as the medical considerations."
Dr. Becker, her coauthors, and Dr. Cordoro reported having no relevant financial disclosures.
AT THE SPD ANNUAL MEETING
Major finding: Among 29 children, 93% met criteria for excess adiposity prior to developing psoriasis, and 78% of these were obese before their psoriasis.
Data source: A growth chart review of 29 obese/overweight children with psoriasis.
Disclosures: Dr. Becker, her coauthors, and Dr. Cordoro reported having no relevant financial disclosures.
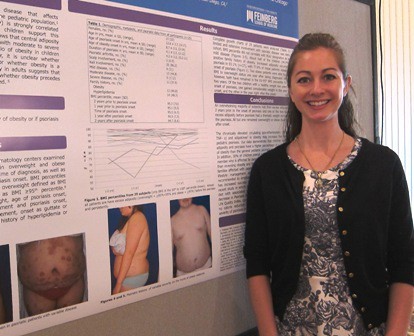
Tune in to hearing problems in ichthyosis
MILWAUKEE – More than two-thirds of patients with ichthyosis reported hearing problems, based on data from a survey of 135 patients ranging in age from 5 months to 80 years.
Overall, 80% of the survey respondents had ear pruritus, 66% had trouble hearing, 29% reported frequent ear pain, 28% had abnormal hearing test results, and 16% had used hearing aids.
Notably, of the 88 patients who reported trouble hearing, 27% had never seen a hearing specialist, Dr. Jennifer T. Huang reported at the annual meeting of the Society for Pediatric Dermatology.
"Early diagnosis and intervention, by both pediatric dermatologists and pediatricians, may improve quality of life," she said.
She also recommended that "regular ear canal debridement and hearing tests should become routine care for patients reporting ear symptoms."
Ichthyosis includes a heterogeneous array of skin disorders characterized by dry, scaling skin, and otologic issues may be attributed to abnormal keratinization of the external ear canals and tympanic membranes and/or accumulation of emollients within the ear canals, said Dr. Huang of Boston Children’s Hospital, Mass. Sufficient build-up causes the ear canals to become plugged, resulting in conductive (though not permanent) hearing loss. While ear structures can be affected, ear-related symptoms have never been investigated in patients with ichthyosis, according to the authors of the award-winning research poster.
The pilot survey was posted on the Foundation for Ichthyosis & Related Skin Types (FIRST) website for 6 months, and Dr. Huang and her colleagues analyzed the data for 135 of 148 respondents. Patients with keratitis ichthyosis deafness (KID) syndrome and surveys with fewer than two completed items were excluded from the analysis.
Lamellar ichthyosis was the most common type of ichthyosis (30%), followed by unknown (17%), vulgaris (13%), X-linked (12%), congenital ichthyosiform erythroderma (10%), and epidermolytic hyperkeratosis (10%). The patients ranged in age from 5 months to 80 years, with an average age of 27 years; 43% were younger than 18 years.
Adult patients, defined as those 18 years and older, were significantly more likely than pediatric patients to report trouble hearing (74% vs. 53%), Dr. Huang reported.
There were no significant differences, however, between older and younger patients in the reported frequency of rubbing/scratching (79% vs. 74%), ear pain (22% vs. 38%), abnormal hearing test results (30% vs. 26), and use of hearing aids (17% vs. 14%).
However, parents who completed the survey for their infant or child may not have been able to fully report the child’s hearing difficulties, she noted.
Of the 75 patients who had a previous hearing test, half (51%) were found to have hearing deficits. Half of those patients who had abnormal results also reported using hearing aids. Two-thirds of patients reported previous ear cleaning (66%).
Finally, the frequency of trouble hearing, ear pruritus, and ear pain was not significantly different among types of ichthyosis.
"Patients with all forms of ichthyosis, across all age groups, are affected," noted Dr. Huang, who called for further studies using objective tools to measure hearing loss and intervention assessments.
Dr. Huang reported having no financial disclosures, but acknowledged the assistance of the Foundation for Ichthyosis & Related Skin Types in the execution of the survey.
MILWAUKEE – More than two-thirds of patients with ichthyosis reported hearing problems, based on data from a survey of 135 patients ranging in age from 5 months to 80 years.
Overall, 80% of the survey respondents had ear pruritus, 66% had trouble hearing, 29% reported frequent ear pain, 28% had abnormal hearing test results, and 16% had used hearing aids.
Notably, of the 88 patients who reported trouble hearing, 27% had never seen a hearing specialist, Dr. Jennifer T. Huang reported at the annual meeting of the Society for Pediatric Dermatology.
"Early diagnosis and intervention, by both pediatric dermatologists and pediatricians, may improve quality of life," she said.
She also recommended that "regular ear canal debridement and hearing tests should become routine care for patients reporting ear symptoms."
Ichthyosis includes a heterogeneous array of skin disorders characterized by dry, scaling skin, and otologic issues may be attributed to abnormal keratinization of the external ear canals and tympanic membranes and/or accumulation of emollients within the ear canals, said Dr. Huang of Boston Children’s Hospital, Mass. Sufficient build-up causes the ear canals to become plugged, resulting in conductive (though not permanent) hearing loss. While ear structures can be affected, ear-related symptoms have never been investigated in patients with ichthyosis, according to the authors of the award-winning research poster.
The pilot survey was posted on the Foundation for Ichthyosis & Related Skin Types (FIRST) website for 6 months, and Dr. Huang and her colleagues analyzed the data for 135 of 148 respondents. Patients with keratitis ichthyosis deafness (KID) syndrome and surveys with fewer than two completed items were excluded from the analysis.
Lamellar ichthyosis was the most common type of ichthyosis (30%), followed by unknown (17%), vulgaris (13%), X-linked (12%), congenital ichthyosiform erythroderma (10%), and epidermolytic hyperkeratosis (10%). The patients ranged in age from 5 months to 80 years, with an average age of 27 years; 43% were younger than 18 years.
Adult patients, defined as those 18 years and older, were significantly more likely than pediatric patients to report trouble hearing (74% vs. 53%), Dr. Huang reported.
There were no significant differences, however, between older and younger patients in the reported frequency of rubbing/scratching (79% vs. 74%), ear pain (22% vs. 38%), abnormal hearing test results (30% vs. 26), and use of hearing aids (17% vs. 14%).
However, parents who completed the survey for their infant or child may not have been able to fully report the child’s hearing difficulties, she noted.
Of the 75 patients who had a previous hearing test, half (51%) were found to have hearing deficits. Half of those patients who had abnormal results also reported using hearing aids. Two-thirds of patients reported previous ear cleaning (66%).
Finally, the frequency of trouble hearing, ear pruritus, and ear pain was not significantly different among types of ichthyosis.
"Patients with all forms of ichthyosis, across all age groups, are affected," noted Dr. Huang, who called for further studies using objective tools to measure hearing loss and intervention assessments.
Dr. Huang reported having no financial disclosures, but acknowledged the assistance of the Foundation for Ichthyosis & Related Skin Types in the execution of the survey.
MILWAUKEE – More than two-thirds of patients with ichthyosis reported hearing problems, based on data from a survey of 135 patients ranging in age from 5 months to 80 years.
Overall, 80% of the survey respondents had ear pruritus, 66% had trouble hearing, 29% reported frequent ear pain, 28% had abnormal hearing test results, and 16% had used hearing aids.
Notably, of the 88 patients who reported trouble hearing, 27% had never seen a hearing specialist, Dr. Jennifer T. Huang reported at the annual meeting of the Society for Pediatric Dermatology.
"Early diagnosis and intervention, by both pediatric dermatologists and pediatricians, may improve quality of life," she said.
She also recommended that "regular ear canal debridement and hearing tests should become routine care for patients reporting ear symptoms."
Ichthyosis includes a heterogeneous array of skin disorders characterized by dry, scaling skin, and otologic issues may be attributed to abnormal keratinization of the external ear canals and tympanic membranes and/or accumulation of emollients within the ear canals, said Dr. Huang of Boston Children’s Hospital, Mass. Sufficient build-up causes the ear canals to become plugged, resulting in conductive (though not permanent) hearing loss. While ear structures can be affected, ear-related symptoms have never been investigated in patients with ichthyosis, according to the authors of the award-winning research poster.
The pilot survey was posted on the Foundation for Ichthyosis & Related Skin Types (FIRST) website for 6 months, and Dr. Huang and her colleagues analyzed the data for 135 of 148 respondents. Patients with keratitis ichthyosis deafness (KID) syndrome and surveys with fewer than two completed items were excluded from the analysis.
Lamellar ichthyosis was the most common type of ichthyosis (30%), followed by unknown (17%), vulgaris (13%), X-linked (12%), congenital ichthyosiform erythroderma (10%), and epidermolytic hyperkeratosis (10%). The patients ranged in age from 5 months to 80 years, with an average age of 27 years; 43% were younger than 18 years.
Adult patients, defined as those 18 years and older, were significantly more likely than pediatric patients to report trouble hearing (74% vs. 53%), Dr. Huang reported.
There were no significant differences, however, between older and younger patients in the reported frequency of rubbing/scratching (79% vs. 74%), ear pain (22% vs. 38%), abnormal hearing test results (30% vs. 26), and use of hearing aids (17% vs. 14%).
However, parents who completed the survey for their infant or child may not have been able to fully report the child’s hearing difficulties, she noted.
Of the 75 patients who had a previous hearing test, half (51%) were found to have hearing deficits. Half of those patients who had abnormal results also reported using hearing aids. Two-thirds of patients reported previous ear cleaning (66%).
Finally, the frequency of trouble hearing, ear pruritus, and ear pain was not significantly different among types of ichthyosis.
"Patients with all forms of ichthyosis, across all age groups, are affected," noted Dr. Huang, who called for further studies using objective tools to measure hearing loss and intervention assessments.
Dr. Huang reported having no financial disclosures, but acknowledged the assistance of the Foundation for Ichthyosis & Related Skin Types in the execution of the survey.
AT THE ANNUAL MEETING OF THE SOCIETY FOR PEDIATRIC DERMATOLOGY
Major finding: Among 135 respondents, 80% reported ear pruritus, 66% trouble hearing, 29% frequent ear pain, 28% abnormal hearing test results, and 16% had used hearing aids.
Data source: Pilot survey study involving 135 respondents with ichthyosis.
Disclosures: Dr. Huang reported having no financial disclosures, but acknowledged the assistance of the Foundation for Ichthyosis and Related Skin Types in conducting the survey.
High-dose isotretinoin restrains acne relapse
MILWAUKEE– Boosting cumulative isotretinoin doses above 220 mg/kg significantly reduced the risk of relapse without dramatically increasing side effects in patients with severe, treatment-resistant nodulocystic acne in a prospective, observational study.
During the 12-month study, 27% of patients who received more than 220 mg/kg and 47% of those who received less than 220 mg/kg had a relapse, defined as treatment with another prescription acne medicine (P = .029).
The number of patients needing retreatment with isotretinoin was similar in both groups (2 vs. 0; P = .31), Mr. Christopher Stamey reported at the annual meeting of the Society for Pediatric Dermatology.
He acknowledged that the dosing regimen in this study was considerably higher than in previous studies of isotretinoin, which support a cumulative dose of 120-150 mg/kg over conventional dosing of less than 100 mg/kg to decrease the risk of relapse/retrial.

Low-dose regimens also have minimal rates of many side effects, but clinicians are becoming more comfortable giving higher doses, explained Mr. Stamey, a fourth-year medical student* and research fellow in dermatology at the University of North Carolina at Chapel Hill (UNC).
A study from a tertiary care center in the New York reported a 100% cure rate and significantly improved quality of life among 80 patients with nodulocystic acne, who were maintained on a cumulative dose of 290 mg/kg (average daily dose, 1.6 mg/kg per day) for an average of 178 days (Int. J. Dermatol. 2012;51:1123-30).
In the current 116-patient study, the average cumulative dose was 309.8 mg/kg in the high-dose group and 170.8 mg/kg in the low-dose group (P less than .000). The daily dose varied by patient and provider, but averaged 120-160 mg/day in the high-dose group, Mr. Stamey said.
Patients were started on 40 mg/day for the first month and then increased to greater than 1 mg/kg per day to avoid any kind of fulminant acne reaction that can occur with isotretinoin. Eventually, the dose was titrated and the patients in the high-dose group were maintained on 1.5-2 mg/kg per day.
In the low-dose group, treated at a cumulative dose less than 220 mg/kg, patients were given 30 mg twice per day.
Treatment duration was significantly longer in the high-dose group compared with the low-dose group (6.5 vs. 5.8 months).
During a discussion of the study at the meeting, concerns were raised about the dosing and the ability to maintain children who are highly inflammatory on such a high daily dose. By initiating the medication at a dose less than 1 mg/kg per day for the first month, brisk inflammatory reactions were avoided, Mr. Stamey said. No patient in the high-dose group had to discontinue isotretinoin for an inflammatory reaction, although two low-dose patients discontinued treatment for 1 month and 1 week, respectively, because of elevated triglycerides.
"The initiation of dosing was the most important aspect with regard to avoiding inflammatory reactions," Mr. Stamey said in an interview. "This is a general practice when using isotretinoin at UNC dermatology clinics."
Overall, the side effects were similar between the groups. Mr. Stamey said. Only retinoid dermatitis was significantly more common during high-dose treatment than lower-dose treatment (54% vs. 32%).
Laboratory abnormalities were slightly, but not significantly higher in the high-dose group. These values included aspartate aminotransferase greater than 90 U/L (6.41% vs. 0%), alanine aminotransferase greater than 105 U/L (1.3% vs. 0%), a total cholesterol level greater than 300 mg/dL (1.3% vs. 0%), and triglycerides greater than 300 mg/dL (11.5% vs. 5.3%).
No differences were observed in itching, muscle or joint aches, mood, or suicidal ideation, although 13.8% of all patients had nail changes, including paronychia in 7.8%, Mr. Stamey noted.
Three-fourths of the patient cohort were white, approximately half were female, and the average age in the high- and low-dose groups was 21 years and 18 years, respectively.
Mr. Stamey reported having no relevant financial disclosures.
*Correction, 7/26/2013: A previous version of this story misstated Mr. Stamey's position as resident. He is a medical student.
MILWAUKEE– Boosting cumulative isotretinoin doses above 220 mg/kg significantly reduced the risk of relapse without dramatically increasing side effects in patients with severe, treatment-resistant nodulocystic acne in a prospective, observational study.
During the 12-month study, 27% of patients who received more than 220 mg/kg and 47% of those who received less than 220 mg/kg had a relapse, defined as treatment with another prescription acne medicine (P = .029).
The number of patients needing retreatment with isotretinoin was similar in both groups (2 vs. 0; P = .31), Mr. Christopher Stamey reported at the annual meeting of the Society for Pediatric Dermatology.
He acknowledged that the dosing regimen in this study was considerably higher than in previous studies of isotretinoin, which support a cumulative dose of 120-150 mg/kg over conventional dosing of less than 100 mg/kg to decrease the risk of relapse/retrial.
Low-dose regimens also have minimal rates of many side effects, but clinicians are becoming more comfortable giving higher doses, explained Mr. Stamey, a fourth-year medical student* and research fellow in dermatology at the University of North Carolina at Chapel Hill (UNC).
A study from a tertiary care center in the New York reported a 100% cure rate and significantly improved quality of life among 80 patients with nodulocystic acne, who were maintained on a cumulative dose of 290 mg/kg (average daily dose, 1.6 mg/kg per day) for an average of 178 days (Int. J. Dermatol. 2012;51:1123-30).
In the current 116-patient study, the average cumulative dose was 309.8 mg/kg in the high-dose group and 170.8 mg/kg in the low-dose group (P less than .000). The daily dose varied by patient and provider, but averaged 120-160 mg/day in the high-dose group, Mr. Stamey said.
Patients were started on 40 mg/day for the first month and then increased to greater than 1 mg/kg per day to avoid any kind of fulminant acne reaction that can occur with isotretinoin. Eventually, the dose was titrated and the patients in the high-dose group were maintained on 1.5-2 mg/kg per day.
In the low-dose group, treated at a cumulative dose less than 220 mg/kg, patients were given 30 mg twice per day.
Treatment duration was significantly longer in the high-dose group compared with the low-dose group (6.5 vs. 5.8 months).
During a discussion of the study at the meeting, concerns were raised about the dosing and the ability to maintain children who are highly inflammatory on such a high daily dose. By initiating the medication at a dose less than 1 mg/kg per day for the first month, brisk inflammatory reactions were avoided, Mr. Stamey said. No patient in the high-dose group had to discontinue isotretinoin for an inflammatory reaction, although two low-dose patients discontinued treatment for 1 month and 1 week, respectively, because of elevated triglycerides.
"The initiation of dosing was the most important aspect with regard to avoiding inflammatory reactions," Mr. Stamey said in an interview. "This is a general practice when using isotretinoin at UNC dermatology clinics."
Overall, the side effects were similar between the groups. Mr. Stamey said. Only retinoid dermatitis was significantly more common during high-dose treatment than lower-dose treatment (54% vs. 32%).
Laboratory abnormalities were slightly, but not significantly higher in the high-dose group. These values included aspartate aminotransferase greater than 90 U/L (6.41% vs. 0%), alanine aminotransferase greater than 105 U/L (1.3% vs. 0%), a total cholesterol level greater than 300 mg/dL (1.3% vs. 0%), and triglycerides greater than 300 mg/dL (11.5% vs. 5.3%).
No differences were observed in itching, muscle or joint aches, mood, or suicidal ideation, although 13.8% of all patients had nail changes, including paronychia in 7.8%, Mr. Stamey noted.
Three-fourths of the patient cohort were white, approximately half were female, and the average age in the high- and low-dose groups was 21 years and 18 years, respectively.
Mr. Stamey reported having no relevant financial disclosures.
*Correction, 7/26/2013: A previous version of this story misstated Mr. Stamey's position as resident. He is a medical student.
MILWAUKEE– Boosting cumulative isotretinoin doses above 220 mg/kg significantly reduced the risk of relapse without dramatically increasing side effects in patients with severe, treatment-resistant nodulocystic acne in a prospective, observational study.
During the 12-month study, 27% of patients who received more than 220 mg/kg and 47% of those who received less than 220 mg/kg had a relapse, defined as treatment with another prescription acne medicine (P = .029).
The number of patients needing retreatment with isotretinoin was similar in both groups (2 vs. 0; P = .31), Mr. Christopher Stamey reported at the annual meeting of the Society for Pediatric Dermatology.
He acknowledged that the dosing regimen in this study was considerably higher than in previous studies of isotretinoin, which support a cumulative dose of 120-150 mg/kg over conventional dosing of less than 100 mg/kg to decrease the risk of relapse/retrial.
Low-dose regimens also have minimal rates of many side effects, but clinicians are becoming more comfortable giving higher doses, explained Mr. Stamey, a fourth-year medical student* and research fellow in dermatology at the University of North Carolina at Chapel Hill (UNC).
A study from a tertiary care center in the New York reported a 100% cure rate and significantly improved quality of life among 80 patients with nodulocystic acne, who were maintained on a cumulative dose of 290 mg/kg (average daily dose, 1.6 mg/kg per day) for an average of 178 days (Int. J. Dermatol. 2012;51:1123-30).
In the current 116-patient study, the average cumulative dose was 309.8 mg/kg in the high-dose group and 170.8 mg/kg in the low-dose group (P less than .000). The daily dose varied by patient and provider, but averaged 120-160 mg/day in the high-dose group, Mr. Stamey said.
Patients were started on 40 mg/day for the first month and then increased to greater than 1 mg/kg per day to avoid any kind of fulminant acne reaction that can occur with isotretinoin. Eventually, the dose was titrated and the patients in the high-dose group were maintained on 1.5-2 mg/kg per day.
In the low-dose group, treated at a cumulative dose less than 220 mg/kg, patients were given 30 mg twice per day.
Treatment duration was significantly longer in the high-dose group compared with the low-dose group (6.5 vs. 5.8 months).
During a discussion of the study at the meeting, concerns were raised about the dosing and the ability to maintain children who are highly inflammatory on such a high daily dose. By initiating the medication at a dose less than 1 mg/kg per day for the first month, brisk inflammatory reactions were avoided, Mr. Stamey said. No patient in the high-dose group had to discontinue isotretinoin for an inflammatory reaction, although two low-dose patients discontinued treatment for 1 month and 1 week, respectively, because of elevated triglycerides.
"The initiation of dosing was the most important aspect with regard to avoiding inflammatory reactions," Mr. Stamey said in an interview. "This is a general practice when using isotretinoin at UNC dermatology clinics."
Overall, the side effects were similar between the groups. Mr. Stamey said. Only retinoid dermatitis was significantly more common during high-dose treatment than lower-dose treatment (54% vs. 32%).
Laboratory abnormalities were slightly, but not significantly higher in the high-dose group. These values included aspartate aminotransferase greater than 90 U/L (6.41% vs. 0%), alanine aminotransferase greater than 105 U/L (1.3% vs. 0%), a total cholesterol level greater than 300 mg/dL (1.3% vs. 0%), and triglycerides greater than 300 mg/dL (11.5% vs. 5.3%).
No differences were observed in itching, muscle or joint aches, mood, or suicidal ideation, although 13.8% of all patients had nail changes, including paronychia in 7.8%, Mr. Stamey noted.
Three-fourths of the patient cohort were white, approximately half were female, and the average age in the high- and low-dose groups was 21 years and 18 years, respectively.
Mr. Stamey reported having no relevant financial disclosures.
*Correction, 7/26/2013: A previous version of this story misstated Mr. Stamey's position as resident. He is a medical student.
AT THE SPD ANNUAL MEETING
Major finding: The rate of relapse was 27% in patients whose cumulative dose of isotretinoin exceeded 220 mg/kg and 47% in patients with a cumulative dose below 220 mg/kg (P = .029).
Data source: A prospective, observational intervention study of 116 patients with treatment-resistant nodulocystic acne.
Disclosures: Dr. Stamey reported having no relevant financial disclosures.

Osteoprotegerin ups risk of vascular events in type 1 diabetes
CHICAGO – Serum osteoprotegerin is an independent predictor of both cardiovascular complications and peripheral vascular disease in type 1 diabetes, according to an analysis of a large prospective Finnish cohort.
Previous studies have suggested that high levels of the glycoprotein are associated with cardiovascular mortality in patients with diabetes, but the Finnish Diabetic Nephropathy (FinnDiane) study is the first to show an independent link between osteoprotegerin (OPG) and incident peripheral vascular disease. The findings come from a retrospective analysis of 1,939 patients with type 1 diabetes in the FinnDiane database.

Baseline serum OPG levels were significantly higher in the 80 patients who underwent amputation or peripheral revascularization than in those who did not (2.0 vs. 1.6 mg/L).
Increased OPG was a significant, independent risk marker for amputation or peripheral revascularization in multivariate analysis after adjustment for other associated factors (hazard ratio, 1.46), Dr. Daniel Gordin reported at the annual scientific sessions of the American Diabetes Association.
Baseline OPG levels were also significantly elevated in the 166 patients who suffered a first-ever cardiovascular event, compared with those with no event (2.2 vs. 1.6 mg/L). This association remained significant after adjustment for factors associated with cardiovascular disease and OPG concentrations.
Osteoprotegerin, a member of the inflammatory tumor necrosis factor superfamily, is increased in patients with coronary artery disease and is associated with the degree of arterial stiffness, explained Dr. Gordin of the division of nephrology, Helsinki (Finland) University Central Hospital.
A recent study reported that a high OPG level was an independent risk marker of all-cause mortality in hemodialysis patients and cardiovascular disease (Clin. Nephrol. 2013 Apr 2 [Epub ahead of print]).
In the current study, serum OPG levels were elevated only in patients with macroalbuminuria and/or moderate to severe renal disease. Patients with end-stage disease were excluded from the analysis.
Patients with established cardiovascular disease also had higher OPG concentrations, but this was attributable to an excess of patients with chronic kidney disease and eliminated after adjustment for renal function.
OPG remained independently correlated, however, after adjustment for renal function, with high C-reactive protein, a marker of systemic inflammation, and with hemoglobin A1c, according to study data simultaneously published online (Diabetes Care 2013;36:1827-33).
The investigators followed patients for an average of 10.4 years, and verified events and mortality from hospital discharge registries and the Finnish National Death Registry.
To no surprise, patients with macroalbuminuria and high levels of OPG at baseline were at the highest risk for cardiovascular disease events, while those with normoalbuminuria and low OPG levels were at lowest risk, Dr. Gordin said.
"However, patients with a normal urinary albumin excretion rate and high OPG concentrations, and microalbuminuric patients with high OPG concentrations, were at a similar risk for cardiovascular disease events, suggesting a predictive role of OPG on top of the associated covariates," he added.
Although patients with incident coronary heart disease and stroke had elevated baseline OPG levels, the association with OPG was not significant after correction for associated covariates.
Finally, OPG concentrations were significantly higher in the 566 patients who died during follow-up than in those who stayed alive (2.0 vs. 1.6 mg/L, but, again, the association between OPG and all-cause mortality lost statistical significance after adjustment.
Dr. Gordin observed that experimental data support a causal link between OPG and the development of cardiovascular complications. Thus, it’s possible that blocking the actions of OPG slows the development and progression of vascular disease in diabetes. In mice, however, complete blockage of OPG causes early onset of osteoporosis and arterial calcification, suggesting that a better target for prevention may be to augment its ligands, RANKL (receptor activator of nuclear factor-kappa B ligand) and TRAIL (tumor necrosis factor-alpha–related apoptosis-inducing ligand). Indeed, studies using TRAIL in apolipoprotein E knockout mice with type 1 diabetes have already reported promising reductions in atherogenesis, the authors noted.
Session moderator Dr. William Cefalu, chief and professor of endocrinology, diabetes, and metabolism at Louisiana State University, New Orleans, said in an interview that the results are interesting but that more information is needed, particularly on the impact of glucose control on OPG levels over time.
"HbA1c is going to vary day to day, so when you talk about one measure that predicts something over 7-10 years, what’s going to be the yearly variation because of glycemic control? That’s my question," he said.
The study was supported by grants from several Finnish foundations, Helsinki University Central Hospital, the Finnish Medical Society, and the Diabetes Research Foundation. Dr. Gordin reported having no financial disclosures.
CHICAGO – Serum osteoprotegerin is an independent predictor of both cardiovascular complications and peripheral vascular disease in type 1 diabetes, according to an analysis of a large prospective Finnish cohort.
Previous studies have suggested that high levels of the glycoprotein are associated with cardiovascular mortality in patients with diabetes, but the Finnish Diabetic Nephropathy (FinnDiane) study is the first to show an independent link between osteoprotegerin (OPG) and incident peripheral vascular disease. The findings come from a retrospective analysis of 1,939 patients with type 1 diabetes in the FinnDiane database.
Baseline serum OPG levels were significantly higher in the 80 patients who underwent amputation or peripheral revascularization than in those who did not (2.0 vs. 1.6 mg/L).
Increased OPG was a significant, independent risk marker for amputation or peripheral revascularization in multivariate analysis after adjustment for other associated factors (hazard ratio, 1.46), Dr. Daniel Gordin reported at the annual scientific sessions of the American Diabetes Association.
Baseline OPG levels were also significantly elevated in the 166 patients who suffered a first-ever cardiovascular event, compared with those with no event (2.2 vs. 1.6 mg/L). This association remained significant after adjustment for factors associated with cardiovascular disease and OPG concentrations.
Osteoprotegerin, a member of the inflammatory tumor necrosis factor superfamily, is increased in patients with coronary artery disease and is associated with the degree of arterial stiffness, explained Dr. Gordin of the division of nephrology, Helsinki (Finland) University Central Hospital.
A recent study reported that a high OPG level was an independent risk marker of all-cause mortality in hemodialysis patients and cardiovascular disease (Clin. Nephrol. 2013 Apr 2 [Epub ahead of print]).
In the current study, serum OPG levels were elevated only in patients with macroalbuminuria and/or moderate to severe renal disease. Patients with end-stage disease were excluded from the analysis.
Patients with established cardiovascular disease also had higher OPG concentrations, but this was attributable to an excess of patients with chronic kidney disease and eliminated after adjustment for renal function.
OPG remained independently correlated, however, after adjustment for renal function, with high C-reactive protein, a marker of systemic inflammation, and with hemoglobin A1c, according to study data simultaneously published online (Diabetes Care 2013;36:1827-33).
The investigators followed patients for an average of 10.4 years, and verified events and mortality from hospital discharge registries and the Finnish National Death Registry.
To no surprise, patients with macroalbuminuria and high levels of OPG at baseline were at the highest risk for cardiovascular disease events, while those with normoalbuminuria and low OPG levels were at lowest risk, Dr. Gordin said.
"However, patients with a normal urinary albumin excretion rate and high OPG concentrations, and microalbuminuric patients with high OPG concentrations, were at a similar risk for cardiovascular disease events, suggesting a predictive role of OPG on top of the associated covariates," he added.
Although patients with incident coronary heart disease and stroke had elevated baseline OPG levels, the association with OPG was not significant after correction for associated covariates.
Finally, OPG concentrations were significantly higher in the 566 patients who died during follow-up than in those who stayed alive (2.0 vs. 1.6 mg/L, but, again, the association between OPG and all-cause mortality lost statistical significance after adjustment.
Dr. Gordin observed that experimental data support a causal link between OPG and the development of cardiovascular complications. Thus, it’s possible that blocking the actions of OPG slows the development and progression of vascular disease in diabetes. In mice, however, complete blockage of OPG causes early onset of osteoporosis and arterial calcification, suggesting that a better target for prevention may be to augment its ligands, RANKL (receptor activator of nuclear factor-kappa B ligand) and TRAIL (tumor necrosis factor-alpha–related apoptosis-inducing ligand). Indeed, studies using TRAIL in apolipoprotein E knockout mice with type 1 diabetes have already reported promising reductions in atherogenesis, the authors noted.
Session moderator Dr. William Cefalu, chief and professor of endocrinology, diabetes, and metabolism at Louisiana State University, New Orleans, said in an interview that the results are interesting but that more information is needed, particularly on the impact of glucose control on OPG levels over time.
"HbA1c is going to vary day to day, so when you talk about one measure that predicts something over 7-10 years, what’s going to be the yearly variation because of glycemic control? That’s my question," he said.
The study was supported by grants from several Finnish foundations, Helsinki University Central Hospital, the Finnish Medical Society, and the Diabetes Research Foundation. Dr. Gordin reported having no financial disclosures.
CHICAGO – Serum osteoprotegerin is an independent predictor of both cardiovascular complications and peripheral vascular disease in type 1 diabetes, according to an analysis of a large prospective Finnish cohort.
Previous studies have suggested that high levels of the glycoprotein are associated with cardiovascular mortality in patients with diabetes, but the Finnish Diabetic Nephropathy (FinnDiane) study is the first to show an independent link between osteoprotegerin (OPG) and incident peripheral vascular disease. The findings come from a retrospective analysis of 1,939 patients with type 1 diabetes in the FinnDiane database.
Baseline serum OPG levels were significantly higher in the 80 patients who underwent amputation or peripheral revascularization than in those who did not (2.0 vs. 1.6 mg/L).
Increased OPG was a significant, independent risk marker for amputation or peripheral revascularization in multivariate analysis after adjustment for other associated factors (hazard ratio, 1.46), Dr. Daniel Gordin reported at the annual scientific sessions of the American Diabetes Association.
Baseline OPG levels were also significantly elevated in the 166 patients who suffered a first-ever cardiovascular event, compared with those with no event (2.2 vs. 1.6 mg/L). This association remained significant after adjustment for factors associated with cardiovascular disease and OPG concentrations.
Osteoprotegerin, a member of the inflammatory tumor necrosis factor superfamily, is increased in patients with coronary artery disease and is associated with the degree of arterial stiffness, explained Dr. Gordin of the division of nephrology, Helsinki (Finland) University Central Hospital.
A recent study reported that a high OPG level was an independent risk marker of all-cause mortality in hemodialysis patients and cardiovascular disease (Clin. Nephrol. 2013 Apr 2 [Epub ahead of print]).
In the current study, serum OPG levels were elevated only in patients with macroalbuminuria and/or moderate to severe renal disease. Patients with end-stage disease were excluded from the analysis.
Patients with established cardiovascular disease also had higher OPG concentrations, but this was attributable to an excess of patients with chronic kidney disease and eliminated after adjustment for renal function.
OPG remained independently correlated, however, after adjustment for renal function, with high C-reactive protein, a marker of systemic inflammation, and with hemoglobin A1c, according to study data simultaneously published online (Diabetes Care 2013;36:1827-33).
The investigators followed patients for an average of 10.4 years, and verified events and mortality from hospital discharge registries and the Finnish National Death Registry.
To no surprise, patients with macroalbuminuria and high levels of OPG at baseline were at the highest risk for cardiovascular disease events, while those with normoalbuminuria and low OPG levels were at lowest risk, Dr. Gordin said.
"However, patients with a normal urinary albumin excretion rate and high OPG concentrations, and microalbuminuric patients with high OPG concentrations, were at a similar risk for cardiovascular disease events, suggesting a predictive role of OPG on top of the associated covariates," he added.
Although patients with incident coronary heart disease and stroke had elevated baseline OPG levels, the association with OPG was not significant after correction for associated covariates.
Finally, OPG concentrations were significantly higher in the 566 patients who died during follow-up than in those who stayed alive (2.0 vs. 1.6 mg/L, but, again, the association between OPG and all-cause mortality lost statistical significance after adjustment.
Dr. Gordin observed that experimental data support a causal link between OPG and the development of cardiovascular complications. Thus, it’s possible that blocking the actions of OPG slows the development and progression of vascular disease in diabetes. In mice, however, complete blockage of OPG causes early onset of osteoporosis and arterial calcification, suggesting that a better target for prevention may be to augment its ligands, RANKL (receptor activator of nuclear factor-kappa B ligand) and TRAIL (tumor necrosis factor-alpha–related apoptosis-inducing ligand). Indeed, studies using TRAIL in apolipoprotein E knockout mice with type 1 diabetes have already reported promising reductions in atherogenesis, the authors noted.
Session moderator Dr. William Cefalu, chief and professor of endocrinology, diabetes, and metabolism at Louisiana State University, New Orleans, said in an interview that the results are interesting but that more information is needed, particularly on the impact of glucose control on OPG levels over time.
"HbA1c is going to vary day to day, so when you talk about one measure that predicts something over 7-10 years, what’s going to be the yearly variation because of glycemic control? That’s my question," he said.
The study was supported by grants from several Finnish foundations, Helsinki University Central Hospital, the Finnish Medical Society, and the Diabetes Research Foundation. Dr. Gordin reported having no financial disclosures.
AT THE ANNUAL ADA SCIENTIFIC SESSIONS
Major finding: Elevated osteoprotegerin levels were a significant independent risk marker for incident cardiovascular events (hazard ratio, 1.21) and amputation or peripheral revascularization (HR, 1.46).
Data source: Retrospective analysis of 1,939 patients with type 1 diabetes in the prospective nationwide Finnish Diabetic Nephropathy study.
Disclosures: The study was supported by grants from several Finnish foundations, Helsinki University Central Hospital, the Finnish Medical Society, and the Diabetes Research Foundation. Dr. Gordin reported having no financial disclosures.
