User login
Lucas Franki is an associate editor for MDedge News, and has been with the company since 2014. He has a BA in English from Penn State University and is an Eagle Scout.
Bipolar patients can be identified using ‘rule of three’
Dr. Hagop S. Akiskal’s “rule of three” conceptualization, which identified behavioral markers tied to bipolarity, proved effective in evaluating and differentiating patients with bipolar disorder from those with unipolar depression, according to Dr. Diogo R. Lara and his associates.
A univariate analysis of more than 70,000 samples found 29 behavioral markers significantly differentiated bipolar patients from patients with unipolar depression. Of these 29, 10 markers had odds ratios greater than 4 for bipolarity.
In a multivariate analysis, 11 markers differentiating bipolar from unipolar depression were confirmed, including reversed circadian rhythms and high debts for both genders; 3 or more provoked car accidents and talent for poetry in men; frequent book reading; 3 or more religion changes; 60 or more sexual partners; experiencing pathological love 2 or more times; heavy cursing; and extravagant dressing styles in women; found Dr. Lara of the Pontifíícia Universidade Católica do Rio Grande do Sul in Porto Alegre, Brazil, and his associates.
“Most behaviors were expressed in a minority of patients (usually 5%-30%) and usually the ‘rule of three’ was the best numerical marker to distinguish those with bipolarity,” the investigators noted.
Find the full study here: J Affect Disord. 2015 Sept 1;183:195-204. doi: 10.1016/j.jad.2015.04.046).
Dr. Hagop S. Akiskal’s “rule of three” conceptualization, which identified behavioral markers tied to bipolarity, proved effective in evaluating and differentiating patients with bipolar disorder from those with unipolar depression, according to Dr. Diogo R. Lara and his associates.
A univariate analysis of more than 70,000 samples found 29 behavioral markers significantly differentiated bipolar patients from patients with unipolar depression. Of these 29, 10 markers had odds ratios greater than 4 for bipolarity.
In a multivariate analysis, 11 markers differentiating bipolar from unipolar depression were confirmed, including reversed circadian rhythms and high debts for both genders; 3 or more provoked car accidents and talent for poetry in men; frequent book reading; 3 or more religion changes; 60 or more sexual partners; experiencing pathological love 2 or more times; heavy cursing; and extravagant dressing styles in women; found Dr. Lara of the Pontifíícia Universidade Católica do Rio Grande do Sul in Porto Alegre, Brazil, and his associates.
“Most behaviors were expressed in a minority of patients (usually 5%-30%) and usually the ‘rule of three’ was the best numerical marker to distinguish those with bipolarity,” the investigators noted.
Find the full study here: J Affect Disord. 2015 Sept 1;183:195-204. doi: 10.1016/j.jad.2015.04.046).
Dr. Hagop S. Akiskal’s “rule of three” conceptualization, which identified behavioral markers tied to bipolarity, proved effective in evaluating and differentiating patients with bipolar disorder from those with unipolar depression, according to Dr. Diogo R. Lara and his associates.
A univariate analysis of more than 70,000 samples found 29 behavioral markers significantly differentiated bipolar patients from patients with unipolar depression. Of these 29, 10 markers had odds ratios greater than 4 for bipolarity.
In a multivariate analysis, 11 markers differentiating bipolar from unipolar depression were confirmed, including reversed circadian rhythms and high debts for both genders; 3 or more provoked car accidents and talent for poetry in men; frequent book reading; 3 or more religion changes; 60 or more sexual partners; experiencing pathological love 2 or more times; heavy cursing; and extravagant dressing styles in women; found Dr. Lara of the Pontifíícia Universidade Católica do Rio Grande do Sul in Porto Alegre, Brazil, and his associates.
“Most behaviors were expressed in a minority of patients (usually 5%-30%) and usually the ‘rule of three’ was the best numerical marker to distinguish those with bipolarity,” the investigators noted.
Find the full study here: J Affect Disord. 2015 Sept 1;183:195-204. doi: 10.1016/j.jad.2015.04.046).
FROM THE JOURNAL OF AFFECTIVE DISORDERS
Lower GABA levels mean greater physical disability for MS patients
Physical disabilities in patients with progressive multiple sclerosis may be correlated with lowered gamma-aminobutyric acid (GABA) concentrations, according to Dr. Niamh Cawley of Queen Square Multiple Sclerosis Centre, University College London Institute of Neurology.
In the patient group of 30 individuals with secondary progressive MS, GABA concentrations were 0.403 mmol lower in the hippocampus than in the control group, and were 0.385 mmol lower in the sensorimotor cortex. There was no significant difference in prefrontal cortex GABA levels between the patient group and the control group (Brain. 2015 Sep;138[pt 9]:2584-95. doi: 10.1093/brain/awv209).

A decreased GABA concentration in the sensorimotor cortex was associated with diminished motor function in right upper and lower limbs, and the patient group scored worse than did the control group on all motor and sensory tests performed. Grip strength dropped by nearly 11 (kg force) for each GABA-unit decrease, and muscle strength in the right upper and lower limbs decreased by nearly 9.
“These findings raise the possibility that altered GABA neurotransmission may be a marker of neurodegeneration, but it may also suggest that GABA is a mechanism of neurodegeneration in progressive multiple sclerosis patients. If we put these findings together with the evidence that GABA may mediate neuroprotection, targeting GABA may be a productive strategy that should be further explored in multiple sclerosis,” wrote Dr. Cawley and her associates.
The work was funded by the Multiple Sclerosis Society of Great Britain and Northern Ireland, Philips Healthcare, and the U.K. National Institute for Health Research.
Read the full study in Brain.
Physical disabilities in patients with progressive multiple sclerosis may be correlated with lowered gamma-aminobutyric acid (GABA) concentrations, according to Dr. Niamh Cawley of Queen Square Multiple Sclerosis Centre, University College London Institute of Neurology.
In the patient group of 30 individuals with secondary progressive MS, GABA concentrations were 0.403 mmol lower in the hippocampus than in the control group, and were 0.385 mmol lower in the sensorimotor cortex. There was no significant difference in prefrontal cortex GABA levels between the patient group and the control group (Brain. 2015 Sep;138[pt 9]:2584-95. doi: 10.1093/brain/awv209).
A decreased GABA concentration in the sensorimotor cortex was associated with diminished motor function in right upper and lower limbs, and the patient group scored worse than did the control group on all motor and sensory tests performed. Grip strength dropped by nearly 11 (kg force) for each GABA-unit decrease, and muscle strength in the right upper and lower limbs decreased by nearly 9.
“These findings raise the possibility that altered GABA neurotransmission may be a marker of neurodegeneration, but it may also suggest that GABA is a mechanism of neurodegeneration in progressive multiple sclerosis patients. If we put these findings together with the evidence that GABA may mediate neuroprotection, targeting GABA may be a productive strategy that should be further explored in multiple sclerosis,” wrote Dr. Cawley and her associates.
The work was funded by the Multiple Sclerosis Society of Great Britain and Northern Ireland, Philips Healthcare, and the U.K. National Institute for Health Research.
Read the full study in Brain.
Physical disabilities in patients with progressive multiple sclerosis may be correlated with lowered gamma-aminobutyric acid (GABA) concentrations, according to Dr. Niamh Cawley of Queen Square Multiple Sclerosis Centre, University College London Institute of Neurology.
In the patient group of 30 individuals with secondary progressive MS, GABA concentrations were 0.403 mmol lower in the hippocampus than in the control group, and were 0.385 mmol lower in the sensorimotor cortex. There was no significant difference in prefrontal cortex GABA levels between the patient group and the control group (Brain. 2015 Sep;138[pt 9]:2584-95. doi: 10.1093/brain/awv209).
A decreased GABA concentration in the sensorimotor cortex was associated with diminished motor function in right upper and lower limbs, and the patient group scored worse than did the control group on all motor and sensory tests performed. Grip strength dropped by nearly 11 (kg force) for each GABA-unit decrease, and muscle strength in the right upper and lower limbs decreased by nearly 9.
“These findings raise the possibility that altered GABA neurotransmission may be a marker of neurodegeneration, but it may also suggest that GABA is a mechanism of neurodegeneration in progressive multiple sclerosis patients. If we put these findings together with the evidence that GABA may mediate neuroprotection, targeting GABA may be a productive strategy that should be further explored in multiple sclerosis,” wrote Dr. Cawley and her associates.
The work was funded by the Multiple Sclerosis Society of Great Britain and Northern Ireland, Philips Healthcare, and the U.K. National Institute for Health Research.
Read the full study in Brain.

NIH study aims for better understanding of RSV
A new study will expose adults to respiratory syncytial virus (RSV), so researchers can understand how it develops, with the goal of developing better RSV antivirals and vaccines in the future, according to a National Institutes of Health press release.
While RSV causes cold-like symptoms and is not much of an issue for adults, the disease can cause much more severe symptoms in very young children, in anyone with a weakened immune system, and in the elderly. Around 55,000 children are hospitalized for RSV annually, mostly infants younger than 6 months. In addition, RSV causes about 14,000 deaths per year in people older than 65, according to the NIH.
The study, conducted by the NIH’s National Institute of Allergy and Infectious Diseases, will involve up to 60 adults – men and nonpregnant women – aged 18-50 years. They will be given two droplets containing a laboratory-developed strain of RSV, called RSV A2, commonly used in medical research, and they will be closely monitored for up to 2 weeks in isolation.
“We do not anticipate that the healthy, carefully screened adult volunteers in this study will become severely sick from the RSV challenge virus because, in general, healthy adults are repeatedly exposed to RSV in their lives and either remain asymptomatic or develop a mild to moderate cold,” said Dr. Lesia K. Dropulic of NIAID’s Laboratory of Infectious Diseases.
A new study will expose adults to respiratory syncytial virus (RSV), so researchers can understand how it develops, with the goal of developing better RSV antivirals and vaccines in the future, according to a National Institutes of Health press release.
While RSV causes cold-like symptoms and is not much of an issue for adults, the disease can cause much more severe symptoms in very young children, in anyone with a weakened immune system, and in the elderly. Around 55,000 children are hospitalized for RSV annually, mostly infants younger than 6 months. In addition, RSV causes about 14,000 deaths per year in people older than 65, according to the NIH.
The study, conducted by the NIH’s National Institute of Allergy and Infectious Diseases, will involve up to 60 adults – men and nonpregnant women – aged 18-50 years. They will be given two droplets containing a laboratory-developed strain of RSV, called RSV A2, commonly used in medical research, and they will be closely monitored for up to 2 weeks in isolation.
“We do not anticipate that the healthy, carefully screened adult volunteers in this study will become severely sick from the RSV challenge virus because, in general, healthy adults are repeatedly exposed to RSV in their lives and either remain asymptomatic or develop a mild to moderate cold,” said Dr. Lesia K. Dropulic of NIAID’s Laboratory of Infectious Diseases.
A new study will expose adults to respiratory syncytial virus (RSV), so researchers can understand how it develops, with the goal of developing better RSV antivirals and vaccines in the future, according to a National Institutes of Health press release.
While RSV causes cold-like symptoms and is not much of an issue for adults, the disease can cause much more severe symptoms in very young children, in anyone with a weakened immune system, and in the elderly. Around 55,000 children are hospitalized for RSV annually, mostly infants younger than 6 months. In addition, RSV causes about 14,000 deaths per year in people older than 65, according to the NIH.
The study, conducted by the NIH’s National Institute of Allergy and Infectious Diseases, will involve up to 60 adults – men and nonpregnant women – aged 18-50 years. They will be given two droplets containing a laboratory-developed strain of RSV, called RSV A2, commonly used in medical research, and they will be closely monitored for up to 2 weeks in isolation.
“We do not anticipate that the healthy, carefully screened adult volunteers in this study will become severely sick from the RSV challenge virus because, in general, healthy adults are repeatedly exposed to RSV in their lives and either remain asymptomatic or develop a mild to moderate cold,” said Dr. Lesia K. Dropulic of NIAID’s Laboratory of Infectious Diseases.
Unusual spike in U.S. plague cases in 2015
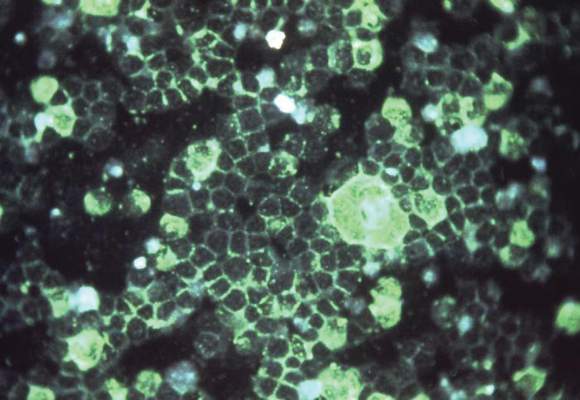
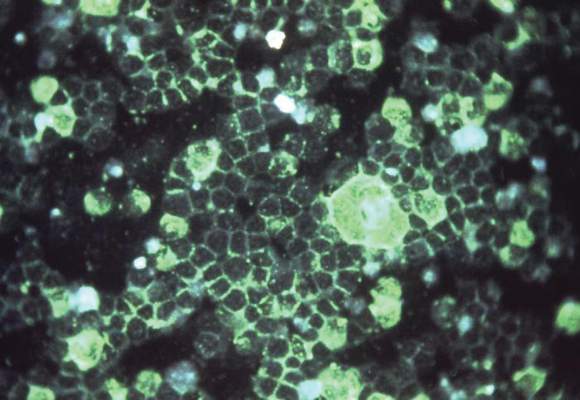
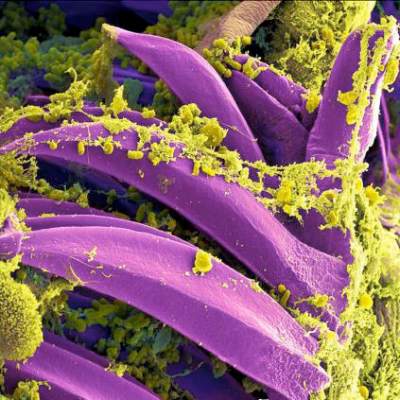
The incidence of human plague in the United States in 2015 has been higher than usual, according to the Centers for Disease Control and Prevention.
Since April 1, 2015, there have been 11 cases of plague in six states: Oregon (1), Arizona (2), California (1), Georgia (1), Colorado (4), and New Mexico (2). From 2001-2012, the annual incidence of plague has ranged from 1 to 17, with a median of 3 cases yearly. The cases in Georgia and in California were linked to exposure in or around Yosemite National Park in California. Of the 11 cases, there were 3 deaths.
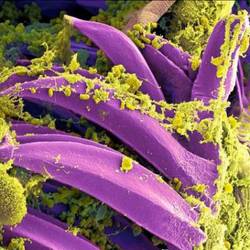
Plague is carried by fleas living on wild rodents in the western United States. Transmission can occur through flea bite, direct contact with infected tissue or body fluids, or inhaling respiratory droplets from infected animals or people. Traditional mortality ranges from 66% to 93% without antibiotics, but treatment using antimicrobials, such as aminoglycosides, fluoroquinolones, or doxycycline, reduced mortality to about 16%.
It is unclear why the incidence of human plague is significantly higher in 2015 than in previous years, the CDC said.
“Persons engaging in outdoor activities in areas where plague is endemic should wear long pants when possible and use insect repellent on clothing and skin. Persons also should avoid direct contact with ill or dead animals and never feed squirrels, chipmunks, or other rodents. In addition, pet owners should regularly use flea control products on their pets and consult a veterinarian if their pet is ill,” the CDC investigators recommended.
Find the full study here: (MMWR 2015 Aug 25;64 [early release];1-2).
The incidence of human plague in the United States in 2015 has been higher than usual, according to the Centers for Disease Control and Prevention.
Since April 1, 2015, there have been 11 cases of plague in six states: Oregon (1), Arizona (2), California (1), Georgia (1), Colorado (4), and New Mexico (2). From 2001-2012, the annual incidence of plague has ranged from 1 to 17, with a median of 3 cases yearly. The cases in Georgia and in California were linked to exposure in or around Yosemite National Park in California. Of the 11 cases, there were 3 deaths.
Plague is carried by fleas living on wild rodents in the western United States. Transmission can occur through flea bite, direct contact with infected tissue or body fluids, or inhaling respiratory droplets from infected animals or people. Traditional mortality ranges from 66% to 93% without antibiotics, but treatment using antimicrobials, such as aminoglycosides, fluoroquinolones, or doxycycline, reduced mortality to about 16%.
It is unclear why the incidence of human plague is significantly higher in 2015 than in previous years, the CDC said.
“Persons engaging in outdoor activities in areas where plague is endemic should wear long pants when possible and use insect repellent on clothing and skin. Persons also should avoid direct contact with ill or dead animals and never feed squirrels, chipmunks, or other rodents. In addition, pet owners should regularly use flea control products on their pets and consult a veterinarian if their pet is ill,” the CDC investigators recommended.
Find the full study here: (MMWR 2015 Aug 25;64 [early release];1-2).
The incidence of human plague in the United States in 2015 has been higher than usual, according to the Centers for Disease Control and Prevention.
Since April 1, 2015, there have been 11 cases of plague in six states: Oregon (1), Arizona (2), California (1), Georgia (1), Colorado (4), and New Mexico (2). From 2001-2012, the annual incidence of plague has ranged from 1 to 17, with a median of 3 cases yearly. The cases in Georgia and in California were linked to exposure in or around Yosemite National Park in California. Of the 11 cases, there were 3 deaths.
Plague is carried by fleas living on wild rodents in the western United States. Transmission can occur through flea bite, direct contact with infected tissue or body fluids, or inhaling respiratory droplets from infected animals or people. Traditional mortality ranges from 66% to 93% without antibiotics, but treatment using antimicrobials, such as aminoglycosides, fluoroquinolones, or doxycycline, reduced mortality to about 16%.
It is unclear why the incidence of human plague is significantly higher in 2015 than in previous years, the CDC said.
“Persons engaging in outdoor activities in areas where plague is endemic should wear long pants when possible and use insect repellent on clothing and skin. Persons also should avoid direct contact with ill or dead animals and never feed squirrels, chipmunks, or other rodents. In addition, pet owners should regularly use flea control products on their pets and consult a veterinarian if their pet is ill,” the CDC investigators recommended.
Find the full study here: (MMWR 2015 Aug 25;64 [early release];1-2).
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
Postexposure Prophylaxis May Prevent Ebola Disease Development
A small group of health care workers at intermediate or high risk of developing Ebola virus disease after exposure to the virus did not develop the disease after being treated with postexposure prophylaxis, according to Dr. Michael Jacobs and his associates.
Of eight health care workers evacuated to the United Kingdom between January and March 2015 and assessed using an Ebola risk calculator, four were deemed to be at intermediate or high risk for developing Ebola virus disease (EVD) and were started on postexposure prophylaxis (PEP) using oral favipiravir over 10 days. In addition, two of the four also were treated with monoclonal antibodies to Ebola glycoproteins. The favipiravir, administered in high dosages, was tolerated well by the four patients, the investigators reported in Lancet Infectious Diseases.
The second half of the eight-person study group had a low risk of EVD after assessment, and patients in this group were watched carefully, receiving no other form of treatment. No EVD developed in this low-risk group.
It cannot be known “whether or not PEP prevented the onset of Ebola virus disease in any of these individuals. However, two individuals had very high risk of Ebola virus transmission, and these are the first reported cases of transcutaneous, hollow-bore needlestick injuries contaminated with fresh blood that have not resulted in Ebola virus transmission,” noted Dr. Jacobs of the department of infection at Royal Free London NHS Foundation Trust and his associates.
In a related comment, Dr. Mark J. Mulligan and Dr. Paul N. Siebert said, “A needed next step is the development of a consensus risk determination algorithm devised by an expert panel, drawing on all available evidence, endorsed by health organizations, and disseminated to the field. The algorithm could be accompanied by a chart abstraction and case report form to standardize and organize data gathering.”
Dr. Mulligan and Dr. Siebert of the division of infectious diseases at Emory University in Atlanta added, “These data for recognized exposures in health care workers could be collated and analyzed in an international registry.”
Find the full study here: Lancet Infect Dis. 2015 Aug 26. doi: 10.1016/S1473-3099(15)00228-5.
A small group of health care workers at intermediate or high risk of developing Ebola virus disease after exposure to the virus did not develop the disease after being treated with postexposure prophylaxis, according to Dr. Michael Jacobs and his associates.
Of eight health care workers evacuated to the United Kingdom between January and March 2015 and assessed using an Ebola risk calculator, four were deemed to be at intermediate or high risk for developing Ebola virus disease (EVD) and were started on postexposure prophylaxis (PEP) using oral favipiravir over 10 days. In addition, two of the four also were treated with monoclonal antibodies to Ebola glycoproteins. The favipiravir, administered in high dosages, was tolerated well by the four patients, the investigators reported in Lancet Infectious Diseases.
The second half of the eight-person study group had a low risk of EVD after assessment, and patients in this group were watched carefully, receiving no other form of treatment. No EVD developed in this low-risk group.
It cannot be known “whether or not PEP prevented the onset of Ebola virus disease in any of these individuals. However, two individuals had very high risk of Ebola virus transmission, and these are the first reported cases of transcutaneous, hollow-bore needlestick injuries contaminated with fresh blood that have not resulted in Ebola virus transmission,” noted Dr. Jacobs of the department of infection at Royal Free London NHS Foundation Trust and his associates.
In a related comment, Dr. Mark J. Mulligan and Dr. Paul N. Siebert said, “A needed next step is the development of a consensus risk determination algorithm devised by an expert panel, drawing on all available evidence, endorsed by health organizations, and disseminated to the field. The algorithm could be accompanied by a chart abstraction and case report form to standardize and organize data gathering.”
Dr. Mulligan and Dr. Siebert of the division of infectious diseases at Emory University in Atlanta added, “These data for recognized exposures in health care workers could be collated and analyzed in an international registry.”
Find the full study here: Lancet Infect Dis. 2015 Aug 26. doi: 10.1016/S1473-3099(15)00228-5.
A small group of health care workers at intermediate or high risk of developing Ebola virus disease after exposure to the virus did not develop the disease after being treated with postexposure prophylaxis, according to Dr. Michael Jacobs and his associates.
Of eight health care workers evacuated to the United Kingdom between January and March 2015 and assessed using an Ebola risk calculator, four were deemed to be at intermediate or high risk for developing Ebola virus disease (EVD) and were started on postexposure prophylaxis (PEP) using oral favipiravir over 10 days. In addition, two of the four also were treated with monoclonal antibodies to Ebola glycoproteins. The favipiravir, administered in high dosages, was tolerated well by the four patients, the investigators reported in Lancet Infectious Diseases.
The second half of the eight-person study group had a low risk of EVD after assessment, and patients in this group were watched carefully, receiving no other form of treatment. No EVD developed in this low-risk group.
It cannot be known “whether or not PEP prevented the onset of Ebola virus disease in any of these individuals. However, two individuals had very high risk of Ebola virus transmission, and these are the first reported cases of transcutaneous, hollow-bore needlestick injuries contaminated with fresh blood that have not resulted in Ebola virus transmission,” noted Dr. Jacobs of the department of infection at Royal Free London NHS Foundation Trust and his associates.
In a related comment, Dr. Mark J. Mulligan and Dr. Paul N. Siebert said, “A needed next step is the development of a consensus risk determination algorithm devised by an expert panel, drawing on all available evidence, endorsed by health organizations, and disseminated to the field. The algorithm could be accompanied by a chart abstraction and case report form to standardize and organize data gathering.”
Dr. Mulligan and Dr. Siebert of the division of infectious diseases at Emory University in Atlanta added, “These data for recognized exposures in health care workers could be collated and analyzed in an international registry.”
Find the full study here: Lancet Infect Dis. 2015 Aug 26. doi: 10.1016/S1473-3099(15)00228-5.
Postexposure prophylaxis may prevent Ebola disease development
A small group of health care workers at intermediate or high risk of developing Ebola virus disease after exposure to the virus did not develop the disease after being treated with postexposure prophylaxis, according to Dr. Michael Jacobs and his associates.
Of eight health care workers evacuated to the United Kingdom between January and March 2015 and assessed using an Ebola risk calculator, four were deemed to be at intermediate or high risk for developing Ebola virus disease (EVD) and were started on postexposure prophylaxis (PEP) using oral favipiravir over 10 days. In addition, two of the four also were treated with monoclonal antibodies to Ebola glycoproteins. The favipiravir, administered in high dosages, was tolerated well by the four patients, the investigators reported in Lancet Infectious Diseases.
The second half of the eight-person study group had a low risk of EVD after assessment, and patients in this group were watched carefully, receiving no other form of treatment. No EVD developed in this low-risk group.
It cannot be known “whether or not PEP prevented the onset of Ebola virus disease in any of these individuals. However, two individuals had very high risk of Ebola virus transmission, and these are the first reported cases of transcutaneous, hollow-bore needlestick injuries contaminated with fresh blood that have not resulted in Ebola virus transmission,” noted Dr. Jacobs of the department of infection at Royal Free London NHS Foundation Trust and his associates.
In a related comment, Dr. Mark J. Mulligan and Dr. Paul N. Siebert said, “A needed next step is the development of a consensus risk determination algorithm devised by an expert panel, drawing on all available evidence, endorsed by health organizations, and disseminated to the field. The algorithm could be accompanied by a chart abstraction and case report form to standardize and organize data gathering.”
Dr. Mulligan and Dr. Siebert of the division of infectious diseases at Emory University in Atlanta added, “These data for recognized exposures in health care workers could be collated and analyzed in an international registry.”
Find the full study here: Lancet Infect Dis. 2015 Aug 26. doi: 10.1016/S1473-3099(15)00228-5.
A small group of health care workers at intermediate or high risk of developing Ebola virus disease after exposure to the virus did not develop the disease after being treated with postexposure prophylaxis, according to Dr. Michael Jacobs and his associates.
Of eight health care workers evacuated to the United Kingdom between January and March 2015 and assessed using an Ebola risk calculator, four were deemed to be at intermediate or high risk for developing Ebola virus disease (EVD) and were started on postexposure prophylaxis (PEP) using oral favipiravir over 10 days. In addition, two of the four also were treated with monoclonal antibodies to Ebola glycoproteins. The favipiravir, administered in high dosages, was tolerated well by the four patients, the investigators reported in Lancet Infectious Diseases.
The second half of the eight-person study group had a low risk of EVD after assessment, and patients in this group were watched carefully, receiving no other form of treatment. No EVD developed in this low-risk group.
It cannot be known “whether or not PEP prevented the onset of Ebola virus disease in any of these individuals. However, two individuals had very high risk of Ebola virus transmission, and these are the first reported cases of transcutaneous, hollow-bore needlestick injuries contaminated with fresh blood that have not resulted in Ebola virus transmission,” noted Dr. Jacobs of the department of infection at Royal Free London NHS Foundation Trust and his associates.
In a related comment, Dr. Mark J. Mulligan and Dr. Paul N. Siebert said, “A needed next step is the development of a consensus risk determination algorithm devised by an expert panel, drawing on all available evidence, endorsed by health organizations, and disseminated to the field. The algorithm could be accompanied by a chart abstraction and case report form to standardize and organize data gathering.”
Dr. Mulligan and Dr. Siebert of the division of infectious diseases at Emory University in Atlanta added, “These data for recognized exposures in health care workers could be collated and analyzed in an international registry.”
Find the full study here: Lancet Infect Dis. 2015 Aug 26. doi: 10.1016/S1473-3099(15)00228-5.
A small group of health care workers at intermediate or high risk of developing Ebola virus disease after exposure to the virus did not develop the disease after being treated with postexposure prophylaxis, according to Dr. Michael Jacobs and his associates.
Of eight health care workers evacuated to the United Kingdom between January and March 2015 and assessed using an Ebola risk calculator, four were deemed to be at intermediate or high risk for developing Ebola virus disease (EVD) and were started on postexposure prophylaxis (PEP) using oral favipiravir over 10 days. In addition, two of the four also were treated with monoclonal antibodies to Ebola glycoproteins. The favipiravir, administered in high dosages, was tolerated well by the four patients, the investigators reported in Lancet Infectious Diseases.
The second half of the eight-person study group had a low risk of EVD after assessment, and patients in this group were watched carefully, receiving no other form of treatment. No EVD developed in this low-risk group.
It cannot be known “whether or not PEP prevented the onset of Ebola virus disease in any of these individuals. However, two individuals had very high risk of Ebola virus transmission, and these are the first reported cases of transcutaneous, hollow-bore needlestick injuries contaminated with fresh blood that have not resulted in Ebola virus transmission,” noted Dr. Jacobs of the department of infection at Royal Free London NHS Foundation Trust and his associates.
In a related comment, Dr. Mark J. Mulligan and Dr. Paul N. Siebert said, “A needed next step is the development of a consensus risk determination algorithm devised by an expert panel, drawing on all available evidence, endorsed by health organizations, and disseminated to the field. The algorithm could be accompanied by a chart abstraction and case report form to standardize and organize data gathering.”
Dr. Mulligan and Dr. Siebert of the division of infectious diseases at Emory University in Atlanta added, “These data for recognized exposures in health care workers could be collated and analyzed in an international registry.”
Find the full study here: Lancet Infect Dis. 2015 Aug 26. doi: 10.1016/S1473-3099(15)00228-5.
Dual ACL, tibial osteotomy surgery helped knee OA patients
Gait biomechanics in patients with medial knee osteoarthritis were significantly improved 5 years after concomitant high tibial osteotomy and anterior cruciate ligament reconstruction, according to a prospective cohort study conducted by Kendal Marriott and associates.
In the 33 patients who underwent the dual surgeries, three-dimensional gait analysis showed that the peak knee adduction moment had decreased significantly in the surgical limb 5 years after surgery, compared with a nonsignificant increase in the nonsurgical limb. A significant decrease in the peak knee flexion moment was seen in both the surgical and nonsurgical limbs. Progress plateaued 2-5 years post surgery, but improvements gained were maintained at the 5-year postsurgery mark.
As concomitant high tibial osteotomy and anterior cruciate ligament reconstruction is relatively rare, “longer term follow-up and comparisons with other treatment strategies are both warranted and required to better evaluate the clinical effect of this seemingly biomechanically efficacious procedure,” the investigators concluded.
Find the full study in the American Journal of Sports Medicine (doi: 10.1177/0363546515591995).
Gait biomechanics in patients with medial knee osteoarthritis were significantly improved 5 years after concomitant high tibial osteotomy and anterior cruciate ligament reconstruction, according to a prospective cohort study conducted by Kendal Marriott and associates.
In the 33 patients who underwent the dual surgeries, three-dimensional gait analysis showed that the peak knee adduction moment had decreased significantly in the surgical limb 5 years after surgery, compared with a nonsignificant increase in the nonsurgical limb. A significant decrease in the peak knee flexion moment was seen in both the surgical and nonsurgical limbs. Progress plateaued 2-5 years post surgery, but improvements gained were maintained at the 5-year postsurgery mark.
As concomitant high tibial osteotomy and anterior cruciate ligament reconstruction is relatively rare, “longer term follow-up and comparisons with other treatment strategies are both warranted and required to better evaluate the clinical effect of this seemingly biomechanically efficacious procedure,” the investigators concluded.
Find the full study in the American Journal of Sports Medicine (doi: 10.1177/0363546515591995).
Gait biomechanics in patients with medial knee osteoarthritis were significantly improved 5 years after concomitant high tibial osteotomy and anterior cruciate ligament reconstruction, according to a prospective cohort study conducted by Kendal Marriott and associates.
In the 33 patients who underwent the dual surgeries, three-dimensional gait analysis showed that the peak knee adduction moment had decreased significantly in the surgical limb 5 years after surgery, compared with a nonsignificant increase in the nonsurgical limb. A significant decrease in the peak knee flexion moment was seen in both the surgical and nonsurgical limbs. Progress plateaued 2-5 years post surgery, but improvements gained were maintained at the 5-year postsurgery mark.
As concomitant high tibial osteotomy and anterior cruciate ligament reconstruction is relatively rare, “longer term follow-up and comparisons with other treatment strategies are both warranted and required to better evaluate the clinical effect of this seemingly biomechanically efficacious procedure,” the investigators concluded.
Find the full study in the American Journal of Sports Medicine (doi: 10.1177/0363546515591995).
Nonselective beta-blockers boost ovarian cancer survival
Overall survival in patients with epithelial ovarian cancer was improved by using a nonselective beta-blocker, according to a retrospective analysis of patient records.
Jack Watkins, Pharm.D., and his associates analyzed the 2000-2010 medical records of 1,425 women who were treated at several different medical centers for ovarian cancer and found that 193 of the women were taking beta1-adrenergic receptor selective agents and 76 were receiving nonselective beta antagonists. The median survival time of the 269 patients who received any beta-blocker was 47.8 months and 42 months for nonusers. However, patients who received the beta1-adrenergic selective beta-blocker had a shorter median survival time at 38 months. Patients who received a nonselective beta-blocker had a median survival rate more than twice as long as the control group at nearly 95 months.
Hypertension did significantly decrease overall survival, but patients taking the nonselective beta-blocker still had an overall survival much higher than nonusers, with median survival times of 90 months and 38.2 months, respectively. Patients in the nonselective beta-blocker group also tended to have a higher body mass index and disease stage, and were more likely to be hypertensive.
“Beta-blockers could then be used as an adjuvant therapy during surgical recovery and chemotherapy to decrease tumor angiogenesis, tumor growth, delays in wound healing, and metastasis. Beta-blockers also may reduce cancer-related psychological distress in patients newly diagnosed with cancer,” the investigators noted.
Find the full study in Cancer (doi: 10.1002/cncr.29392).
Overall survival in patients with epithelial ovarian cancer was improved by using a nonselective beta-blocker, according to a retrospective analysis of patient records.
Jack Watkins, Pharm.D., and his associates analyzed the 2000-2010 medical records of 1,425 women who were treated at several different medical centers for ovarian cancer and found that 193 of the women were taking beta1-adrenergic receptor selective agents and 76 were receiving nonselective beta antagonists. The median survival time of the 269 patients who received any beta-blocker was 47.8 months and 42 months for nonusers. However, patients who received the beta1-adrenergic selective beta-blocker had a shorter median survival time at 38 months. Patients who received a nonselective beta-blocker had a median survival rate more than twice as long as the control group at nearly 95 months.
Hypertension did significantly decrease overall survival, but patients taking the nonselective beta-blocker still had an overall survival much higher than nonusers, with median survival times of 90 months and 38.2 months, respectively. Patients in the nonselective beta-blocker group also tended to have a higher body mass index and disease stage, and were more likely to be hypertensive.
“Beta-blockers could then be used as an adjuvant therapy during surgical recovery and chemotherapy to decrease tumor angiogenesis, tumor growth, delays in wound healing, and metastasis. Beta-blockers also may reduce cancer-related psychological distress in patients newly diagnosed with cancer,” the investigators noted.
Find the full study in Cancer (doi: 10.1002/cncr.29392).
Overall survival in patients with epithelial ovarian cancer was improved by using a nonselective beta-blocker, according to a retrospective analysis of patient records.
Jack Watkins, Pharm.D., and his associates analyzed the 2000-2010 medical records of 1,425 women who were treated at several different medical centers for ovarian cancer and found that 193 of the women were taking beta1-adrenergic receptor selective agents and 76 were receiving nonselective beta antagonists. The median survival time of the 269 patients who received any beta-blocker was 47.8 months and 42 months for nonusers. However, patients who received the beta1-adrenergic selective beta-blocker had a shorter median survival time at 38 months. Patients who received a nonselective beta-blocker had a median survival rate more than twice as long as the control group at nearly 95 months.
Hypertension did significantly decrease overall survival, but patients taking the nonselective beta-blocker still had an overall survival much higher than nonusers, with median survival times of 90 months and 38.2 months, respectively. Patients in the nonselective beta-blocker group also tended to have a higher body mass index and disease stage, and were more likely to be hypertensive.
“Beta-blockers could then be used as an adjuvant therapy during surgical recovery and chemotherapy to decrease tumor angiogenesis, tumor growth, delays in wound healing, and metastasis. Beta-blockers also may reduce cancer-related psychological distress in patients newly diagnosed with cancer,” the investigators noted.
Find the full study in Cancer (doi: 10.1002/cncr.29392).
Separating heart disease myths from facts
There’s a lot of information out there about heart disease and how to prevent it, but there’s a lot of misinformation out there as well, and it’s important to get the facts straight when it comes to your heart, according to a Harvard Heart Letter report.
While it may seem logical to limit physical activity if you have a heart problem, in nearly all cases, a person with heart disease can benefit from regular, moderate amounts of exercise. And while it may also make sense to eat a very-low-fat diet, it is really only saturated fat that is harmful to the heart. A diet rich in unsaturated fat from foods such as fish, olive oil, and low-fat dairy products actually reduces the risk of heart disease.

Cholesterol-lowering drugs reduce cholesterol produced by the liver; they do not reduce cholesterol you get from food, so taking such a drug is not a free pass to continue eating fatty food. Along those lines, even if you take a drug to manage diabetes, the disease still can cause heart disease.
While it is true that women under the age of 60 years are significantly less likely to get heart disease than are men, this disparity disappears over the age of 60, and by age 80 years, women are slightly more likely to have heart disease. It is also true that quitting smoking has immediate benefits, even if you’ve been smoking for years. Heart attack risk drops by 50% after 1 year being tobacco free, and the increased risk disappears entirely after 10 years.
A small heart attack may not do much damage – it may be barely noticeable. But any heart attack is indicative of a big problem. While surgical procedures such as stenting or bypasses do a lot for managing symptoms, they do not fix the problem, and life changes are still recommended.
For more information about heart disease myths, visit the Harvard Medical School website.
There’s a lot of information out there about heart disease and how to prevent it, but there’s a lot of misinformation out there as well, and it’s important to get the facts straight when it comes to your heart, according to a Harvard Heart Letter report.
While it may seem logical to limit physical activity if you have a heart problem, in nearly all cases, a person with heart disease can benefit from regular, moderate amounts of exercise. And while it may also make sense to eat a very-low-fat diet, it is really only saturated fat that is harmful to the heart. A diet rich in unsaturated fat from foods such as fish, olive oil, and low-fat dairy products actually reduces the risk of heart disease.
Cholesterol-lowering drugs reduce cholesterol produced by the liver; they do not reduce cholesterol you get from food, so taking such a drug is not a free pass to continue eating fatty food. Along those lines, even if you take a drug to manage diabetes, the disease still can cause heart disease.
While it is true that women under the age of 60 years are significantly less likely to get heart disease than are men, this disparity disappears over the age of 60, and by age 80 years, women are slightly more likely to have heart disease. It is also true that quitting smoking has immediate benefits, even if you’ve been smoking for years. Heart attack risk drops by 50% after 1 year being tobacco free, and the increased risk disappears entirely after 10 years.
A small heart attack may not do much damage – it may be barely noticeable. But any heart attack is indicative of a big problem. While surgical procedures such as stenting or bypasses do a lot for managing symptoms, they do not fix the problem, and life changes are still recommended.
For more information about heart disease myths, visit the Harvard Medical School website.
There’s a lot of information out there about heart disease and how to prevent it, but there’s a lot of misinformation out there as well, and it’s important to get the facts straight when it comes to your heart, according to a Harvard Heart Letter report.
While it may seem logical to limit physical activity if you have a heart problem, in nearly all cases, a person with heart disease can benefit from regular, moderate amounts of exercise. And while it may also make sense to eat a very-low-fat diet, it is really only saturated fat that is harmful to the heart. A diet rich in unsaturated fat from foods such as fish, olive oil, and low-fat dairy products actually reduces the risk of heart disease.
Cholesterol-lowering drugs reduce cholesterol produced by the liver; they do not reduce cholesterol you get from food, so taking such a drug is not a free pass to continue eating fatty food. Along those lines, even if you take a drug to manage diabetes, the disease still can cause heart disease.
While it is true that women under the age of 60 years are significantly less likely to get heart disease than are men, this disparity disappears over the age of 60, and by age 80 years, women are slightly more likely to have heart disease. It is also true that quitting smoking has immediate benefits, even if you’ve been smoking for years. Heart attack risk drops by 50% after 1 year being tobacco free, and the increased risk disappears entirely after 10 years.
A small heart attack may not do much damage – it may be barely noticeable. But any heart attack is indicative of a big problem. While surgical procedures such as stenting or bypasses do a lot for managing symptoms, they do not fix the problem, and life changes are still recommended.
For more information about heart disease myths, visit the Harvard Medical School website.

Tofacitinib proves effective in RA when biologics don’t work
The oral Janus kinase inhibitor tofacitinib was effective at treating rheumatoid arthritis in patients who had never before taken or had an inadequate response to biological disease-modifying antirheumatic drugs, according to a combined analysis of results from four phase II and five phase III trials conducted by Dr. Christina Charles-Schoeman and her associates.
Each of the two main study groups, consisting of 2,812 patients naive to biological disease-modifying antirheumatic drugs (bDMARDs) and 705 bDMARD patients with an inadequate response (IR), was further split into three subgroups: a placebo group, a group receiving 5 mg tofacitinib twice daily, and a group receiving 10 mg tofacitinib twice daily. All subgroups receiving medication had a significantly improved clinical response over the placebo group, although tofacitinib had greater efficacy in the bDMARD-naive group.
The rate of adverse events was similar in all groups receiving tofacitinib, though the numerical amount of both adverse events and clinical responses was somewhat higher in the 10-mg twice-daily group. In addition, a subpopulation of patients who also were receiving glucocorticoids tended to have more serious adverse events and discontinuations as a result of serious infections and herpes zoster.
Although bDMARD-IR patients did not respond as well to tofacitinib, “bDMARD-IR patients had longer disease duration and slightly greater disease activity at baseline compared with bDMARD-naive patients, which could have influenced these results,” the investigators noted.
Find the full study in Annals of the Rheumatic Diseases (doi: 10.1136/annrheumdis-2014-207178).
The oral Janus kinase inhibitor tofacitinib was effective at treating rheumatoid arthritis in patients who had never before taken or had an inadequate response to biological disease-modifying antirheumatic drugs, according to a combined analysis of results from four phase II and five phase III trials conducted by Dr. Christina Charles-Schoeman and her associates.
Each of the two main study groups, consisting of 2,812 patients naive to biological disease-modifying antirheumatic drugs (bDMARDs) and 705 bDMARD patients with an inadequate response (IR), was further split into three subgroups: a placebo group, a group receiving 5 mg tofacitinib twice daily, and a group receiving 10 mg tofacitinib twice daily. All subgroups receiving medication had a significantly improved clinical response over the placebo group, although tofacitinib had greater efficacy in the bDMARD-naive group.
The rate of adverse events was similar in all groups receiving tofacitinib, though the numerical amount of both adverse events and clinical responses was somewhat higher in the 10-mg twice-daily group. In addition, a subpopulation of patients who also were receiving glucocorticoids tended to have more serious adverse events and discontinuations as a result of serious infections and herpes zoster.
Although bDMARD-IR patients did not respond as well to tofacitinib, “bDMARD-IR patients had longer disease duration and slightly greater disease activity at baseline compared with bDMARD-naive patients, which could have influenced these results,” the investigators noted.
Find the full study in Annals of the Rheumatic Diseases (doi: 10.1136/annrheumdis-2014-207178).
The oral Janus kinase inhibitor tofacitinib was effective at treating rheumatoid arthritis in patients who had never before taken or had an inadequate response to biological disease-modifying antirheumatic drugs, according to a combined analysis of results from four phase II and five phase III trials conducted by Dr. Christina Charles-Schoeman and her associates.
Each of the two main study groups, consisting of 2,812 patients naive to biological disease-modifying antirheumatic drugs (bDMARDs) and 705 bDMARD patients with an inadequate response (IR), was further split into three subgroups: a placebo group, a group receiving 5 mg tofacitinib twice daily, and a group receiving 10 mg tofacitinib twice daily. All subgroups receiving medication had a significantly improved clinical response over the placebo group, although tofacitinib had greater efficacy in the bDMARD-naive group.
The rate of adverse events was similar in all groups receiving tofacitinib, though the numerical amount of both adverse events and clinical responses was somewhat higher in the 10-mg twice-daily group. In addition, a subpopulation of patients who also were receiving glucocorticoids tended to have more serious adverse events and discontinuations as a result of serious infections and herpes zoster.
Although bDMARD-IR patients did not respond as well to tofacitinib, “bDMARD-IR patients had longer disease duration and slightly greater disease activity at baseline compared with bDMARD-naive patients, which could have influenced these results,” the investigators noted.
Find the full study in Annals of the Rheumatic Diseases (doi: 10.1136/annrheumdis-2014-207178).