User login
Official Newspaper of the American College of Surgeons
Oral cancer survival lower with positive margins, public insurance
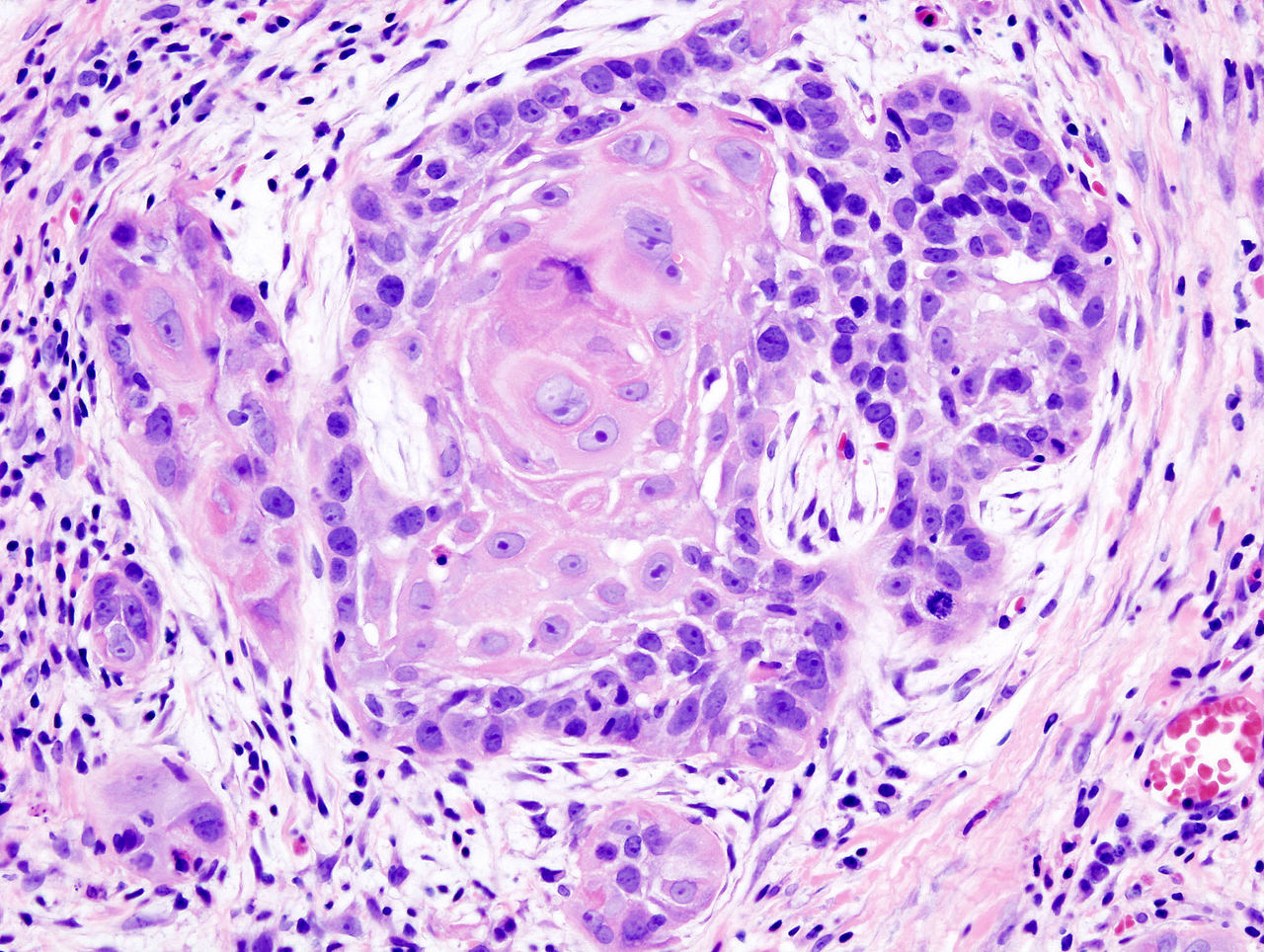
In patients who underwent surgical treatment for stage I or II oral cavity squamous cell cancer, positive tumor margin, the use of radiation or chemotherapy, treatment in a nonacademic facility, and having public health insurance were significantly associated with lower 5-year survival rates, according to a retrospective analysis published online in the JAMA Otolaryngology–Head & Neck Surgery.
The findings suggest that some factors associated with lower 5-year survival rates “may be targets for quality improvement efforts,” wrote Alexander L. Luryi of Yale University, New Haven, Conn., and colleagues.
Seventy percent of 6,830 patients who underwent surgery for stage I or II oral cavity squamous cell cancer (OCSCC) from 2003 to 2006 survived 5 years, according to information from the National Cancer Data Base.
Multivariate analysis showed higher survival rates were significantly associated with neck dissection (hazard ratio, 0.85; P = .003). Lower survival rates were significantly associated with radiation therapy (HR, 1.31; P < .001), chemotherapy (HR, 1.34; P = .03), nonprivate insurance (HR Medicaid, 1.96; HR Medicare, 1.45; P < .001), and nonacademic treatment facility (HR, 1.13; P = .03).
Care at academic centers compared with nonacademic centers was associated with improved survival, possibly due to health care provider expertise, the study authors noted (JAMA Otolaryngol. Head Neck Surg. 2015 May 14 [doi:10.1001/jamaoto.2015.0719]).
Survival rates were lower in patients treated at nonacademic cancer centers, but multivariate analysis showed no association between facility-based case volume and survival. Patients insured through Medicaid and Medicare had significantly lower 5-year survival rates (P < .001 for both). That finding may be the result of inconsistent treatment and follow-up, the investigators said, or worse baseline health among that patient population.
Controversy exists over the relationship between positive margins and outcomes, and the implications for aggressiveness of surgery. The study found positive margins were significantly associated with poorer outcomes, the researchers noted, which supports the use of aggressive surgery in early OCSCC to achieve negative margins.
Radiation and chemotherapy were linked to worse outcomes, and those therapies were possibly indicators of less aggressive resection in localized disease. The analysis could not adjust for potential confounding effects of perineural and lymphovascular invasion, because the information was not recorded in the National Cancer Data Base.
The study indicated a positive impact by neck dissection on survival. Patients with occult neck disease who underwent neck dissection likely would have been restaged to stage III or higher and removed from the early stage sample, the authors explained, which would account for higher survival rates for those remaining. Prospective trials are needed to determine the role of elective neck dissection in early OCSCC, the researchers added.
The William U. Gardner Memorial Research Fund at Yale University supported the study. Dr. Luryi and coauthors reported having no disclosures.
In patients who underwent surgical treatment for stage I or II oral cavity squamous cell cancer, positive tumor margin, the use of radiation or chemotherapy, treatment in a nonacademic facility, and having public health insurance were significantly associated with lower 5-year survival rates, according to a retrospective analysis published online in the JAMA Otolaryngology–Head & Neck Surgery.
The findings suggest that some factors associated with lower 5-year survival rates “may be targets for quality improvement efforts,” wrote Alexander L. Luryi of Yale University, New Haven, Conn., and colleagues.
Seventy percent of 6,830 patients who underwent surgery for stage I or II oral cavity squamous cell cancer (OCSCC) from 2003 to 2006 survived 5 years, according to information from the National Cancer Data Base.
Multivariate analysis showed higher survival rates were significantly associated with neck dissection (hazard ratio, 0.85; P = .003). Lower survival rates were significantly associated with radiation therapy (HR, 1.31; P < .001), chemotherapy (HR, 1.34; P = .03), nonprivate insurance (HR Medicaid, 1.96; HR Medicare, 1.45; P < .001), and nonacademic treatment facility (HR, 1.13; P = .03).
Care at academic centers compared with nonacademic centers was associated with improved survival, possibly due to health care provider expertise, the study authors noted (JAMA Otolaryngol. Head Neck Surg. 2015 May 14 [doi:10.1001/jamaoto.2015.0719]).
Survival rates were lower in patients treated at nonacademic cancer centers, but multivariate analysis showed no association between facility-based case volume and survival. Patients insured through Medicaid and Medicare had significantly lower 5-year survival rates (P < .001 for both). That finding may be the result of inconsistent treatment and follow-up, the investigators said, or worse baseline health among that patient population.
Controversy exists over the relationship between positive margins and outcomes, and the implications for aggressiveness of surgery. The study found positive margins were significantly associated with poorer outcomes, the researchers noted, which supports the use of aggressive surgery in early OCSCC to achieve negative margins.
Radiation and chemotherapy were linked to worse outcomes, and those therapies were possibly indicators of less aggressive resection in localized disease. The analysis could not adjust for potential confounding effects of perineural and lymphovascular invasion, because the information was not recorded in the National Cancer Data Base.
The study indicated a positive impact by neck dissection on survival. Patients with occult neck disease who underwent neck dissection likely would have been restaged to stage III or higher and removed from the early stage sample, the authors explained, which would account for higher survival rates for those remaining. Prospective trials are needed to determine the role of elective neck dissection in early OCSCC, the researchers added.
The William U. Gardner Memorial Research Fund at Yale University supported the study. Dr. Luryi and coauthors reported having no disclosures.
In patients who underwent surgical treatment for stage I or II oral cavity squamous cell cancer, positive tumor margin, the use of radiation or chemotherapy, treatment in a nonacademic facility, and having public health insurance were significantly associated with lower 5-year survival rates, according to a retrospective analysis published online in the JAMA Otolaryngology–Head & Neck Surgery.
The findings suggest that some factors associated with lower 5-year survival rates “may be targets for quality improvement efforts,” wrote Alexander L. Luryi of Yale University, New Haven, Conn., and colleagues.
Seventy percent of 6,830 patients who underwent surgery for stage I or II oral cavity squamous cell cancer (OCSCC) from 2003 to 2006 survived 5 years, according to information from the National Cancer Data Base.
Multivariate analysis showed higher survival rates were significantly associated with neck dissection (hazard ratio, 0.85; P = .003). Lower survival rates were significantly associated with radiation therapy (HR, 1.31; P < .001), chemotherapy (HR, 1.34; P = .03), nonprivate insurance (HR Medicaid, 1.96; HR Medicare, 1.45; P < .001), and nonacademic treatment facility (HR, 1.13; P = .03).
Care at academic centers compared with nonacademic centers was associated with improved survival, possibly due to health care provider expertise, the study authors noted (JAMA Otolaryngol. Head Neck Surg. 2015 May 14 [doi:10.1001/jamaoto.2015.0719]).
Survival rates were lower in patients treated at nonacademic cancer centers, but multivariate analysis showed no association between facility-based case volume and survival. Patients insured through Medicaid and Medicare had significantly lower 5-year survival rates (P < .001 for both). That finding may be the result of inconsistent treatment and follow-up, the investigators said, or worse baseline health among that patient population.
Controversy exists over the relationship between positive margins and outcomes, and the implications for aggressiveness of surgery. The study found positive margins were significantly associated with poorer outcomes, the researchers noted, which supports the use of aggressive surgery in early OCSCC to achieve negative margins.
Radiation and chemotherapy were linked to worse outcomes, and those therapies were possibly indicators of less aggressive resection in localized disease. The analysis could not adjust for potential confounding effects of perineural and lymphovascular invasion, because the information was not recorded in the National Cancer Data Base.
The study indicated a positive impact by neck dissection on survival. Patients with occult neck disease who underwent neck dissection likely would have been restaged to stage III or higher and removed from the early stage sample, the authors explained, which would account for higher survival rates for those remaining. Prospective trials are needed to determine the role of elective neck dissection in early OCSCC, the researchers added.
The William U. Gardner Memorial Research Fund at Yale University supported the study. Dr. Luryi and coauthors reported having no disclosures.
FROM JAMA OTOLARYNGOLOGY–HEAD & NECK SURGERY
Key clinical point: Treatment factors such as neck dissection, tumor margins, type of insurance, and health care facility impact 5-year survival after surgery for early stage oral cavity cancer.
Major finding: Radiation, chemotherapy, positive tumor margin, nonacademic facility, and nonprivate insurance were significantly associated with lower 5-year survival.
Data source: Retrospective study of 6,830 patients in National Cancer Data Base who underwent surgery to treat stage I or II oral cavity squamous cell cancer.
Disclosures: The William U. Gardner Memorial Research Fund at Yale University supported the study. Dr. Luryi and coauthors reported having no disclosures.
Copeptin levels predicted diabetes insipidus after pituitary surgery
Copeptin levels of less than 2.5 pmol/L reliably identified diabetes insipidus after pituitary surgery, while levels of more than 30 pmol/L ruled out the condition, investigators reported online in the Journal of Clinical Endocrinology and Metabolism.
“Copeptin represents a new, early, and reliable single marker for postoperative diabetes insipidus in the post–pituitary surgery setting, where no such marker currently is known,” said Dr. Bettina Winzeler at University Hospital of Basel (Switzerland) and her associates. Postoperative measures of copeptin levels might help clinicians to differentiate patients who need closer postsurgical inpatient observation from those who can safely be discharged.
About 16%-34% of patients who undergo surgery in the sellar region develop central diabetes insipidus, which, without prompt rehydration, can cause severe hypernatremia, Dr. Winzeler and her associates noted. Risk factors for postoperative diabetes insipidus are not useful markers; however, copeptin, a surrogate of arginine vasopressin, is stable and can be measured quickly and reliably.
The researchers hypothesized that patients with postoperative diabetes insipidus would not have the markedly elevated copeptin levels that surgical stress normally triggers when posterior pituitary function is adequate. To test that theory, they measured daily postoperative copeptin levels for 205 consecutive patients who underwent surgeries for sellar lesions or tumors near the hypothalamus or pituitary gland (J. Clin. Endocrinol. Metab. 2015 Apr. 29 [doi:10.1210/jc.2014-4527]).
One day after surgery, 22 (81.5%) of the 27 patients whose copeptin levels were less than 2.5 pmol/L had diabetes insipidus (positive predictive value, 81%; specificity, 97%), said the researchers. In contrast, one of 40 (2.5%) patients with copeptin levels greater than 30 pmol/L had diabetes insipidus (negative predictive value 95%; sensitivity, 94%). Patients with diabetes insipidus also had significantly lower median and interquartile (25th-75th percentile) copeptin levels, compared with other patients (median for patients with diabetes insipidus, 2.9 pmol/L; interquartile range, 1.9-7.9 pmol/L; median for other patients, 10.8 pmol/L; IQR, 5.2-30.4 pmol/L; P less than .001). In the multivariate analysis, low postoperative copeptin levels remained associated with diabetes insipidus after adjusting for age, gender, body-mass index, tumor size and type of surgery, history of surgery or radiotherapy, cerebrospinal fluid leakage, and serum sodium concentration, the investigators reported (odds ratio, 1.62; 95% confidence interval, 1.25-2.10; P less than .001).
The study did not use standardized diagnostic criteria for diabetes insipidus, and postoperative blood samples were obtained as part of daily care and not at fixed time points, Dr. Winzeler and her associates noted. “Absence of standardized sampling for copeptin measurement at a defined early time point presumably decreased copeptin accuracy in this study, rendering our findings conservative,” they cautioned.
The Swiss National Foundation partially funded the research. Three coauthors reported having received speaker honoraria from Thermo Scientific Biomarkers, which develops and makes the copeptin assay.
Copeptin levels of less than 2.5 pmol/L reliably identified diabetes insipidus after pituitary surgery, while levels of more than 30 pmol/L ruled out the condition, investigators reported online in the Journal of Clinical Endocrinology and Metabolism.
“Copeptin represents a new, early, and reliable single marker for postoperative diabetes insipidus in the post–pituitary surgery setting, where no such marker currently is known,” said Dr. Bettina Winzeler at University Hospital of Basel (Switzerland) and her associates. Postoperative measures of copeptin levels might help clinicians to differentiate patients who need closer postsurgical inpatient observation from those who can safely be discharged.
About 16%-34% of patients who undergo surgery in the sellar region develop central diabetes insipidus, which, without prompt rehydration, can cause severe hypernatremia, Dr. Winzeler and her associates noted. Risk factors for postoperative diabetes insipidus are not useful markers; however, copeptin, a surrogate of arginine vasopressin, is stable and can be measured quickly and reliably.
The researchers hypothesized that patients with postoperative diabetes insipidus would not have the markedly elevated copeptin levels that surgical stress normally triggers when posterior pituitary function is adequate. To test that theory, they measured daily postoperative copeptin levels for 205 consecutive patients who underwent surgeries for sellar lesions or tumors near the hypothalamus or pituitary gland (J. Clin. Endocrinol. Metab. 2015 Apr. 29 [doi:10.1210/jc.2014-4527]).
One day after surgery, 22 (81.5%) of the 27 patients whose copeptin levels were less than 2.5 pmol/L had diabetes insipidus (positive predictive value, 81%; specificity, 97%), said the researchers. In contrast, one of 40 (2.5%) patients with copeptin levels greater than 30 pmol/L had diabetes insipidus (negative predictive value 95%; sensitivity, 94%). Patients with diabetes insipidus also had significantly lower median and interquartile (25th-75th percentile) copeptin levels, compared with other patients (median for patients with diabetes insipidus, 2.9 pmol/L; interquartile range, 1.9-7.9 pmol/L; median for other patients, 10.8 pmol/L; IQR, 5.2-30.4 pmol/L; P less than .001). In the multivariate analysis, low postoperative copeptin levels remained associated with diabetes insipidus after adjusting for age, gender, body-mass index, tumor size and type of surgery, history of surgery or radiotherapy, cerebrospinal fluid leakage, and serum sodium concentration, the investigators reported (odds ratio, 1.62; 95% confidence interval, 1.25-2.10; P less than .001).
The study did not use standardized diagnostic criteria for diabetes insipidus, and postoperative blood samples were obtained as part of daily care and not at fixed time points, Dr. Winzeler and her associates noted. “Absence of standardized sampling for copeptin measurement at a defined early time point presumably decreased copeptin accuracy in this study, rendering our findings conservative,” they cautioned.
The Swiss National Foundation partially funded the research. Three coauthors reported having received speaker honoraria from Thermo Scientific Biomarkers, which develops and makes the copeptin assay.
Copeptin levels of less than 2.5 pmol/L reliably identified diabetes insipidus after pituitary surgery, while levels of more than 30 pmol/L ruled out the condition, investigators reported online in the Journal of Clinical Endocrinology and Metabolism.
“Copeptin represents a new, early, and reliable single marker for postoperative diabetes insipidus in the post–pituitary surgery setting, where no such marker currently is known,” said Dr. Bettina Winzeler at University Hospital of Basel (Switzerland) and her associates. Postoperative measures of copeptin levels might help clinicians to differentiate patients who need closer postsurgical inpatient observation from those who can safely be discharged.
About 16%-34% of patients who undergo surgery in the sellar region develop central diabetes insipidus, which, without prompt rehydration, can cause severe hypernatremia, Dr. Winzeler and her associates noted. Risk factors for postoperative diabetes insipidus are not useful markers; however, copeptin, a surrogate of arginine vasopressin, is stable and can be measured quickly and reliably.
The researchers hypothesized that patients with postoperative diabetes insipidus would not have the markedly elevated copeptin levels that surgical stress normally triggers when posterior pituitary function is adequate. To test that theory, they measured daily postoperative copeptin levels for 205 consecutive patients who underwent surgeries for sellar lesions or tumors near the hypothalamus or pituitary gland (J. Clin. Endocrinol. Metab. 2015 Apr. 29 [doi:10.1210/jc.2014-4527]).
One day after surgery, 22 (81.5%) of the 27 patients whose copeptin levels were less than 2.5 pmol/L had diabetes insipidus (positive predictive value, 81%; specificity, 97%), said the researchers. In contrast, one of 40 (2.5%) patients with copeptin levels greater than 30 pmol/L had diabetes insipidus (negative predictive value 95%; sensitivity, 94%). Patients with diabetes insipidus also had significantly lower median and interquartile (25th-75th percentile) copeptin levels, compared with other patients (median for patients with diabetes insipidus, 2.9 pmol/L; interquartile range, 1.9-7.9 pmol/L; median for other patients, 10.8 pmol/L; IQR, 5.2-30.4 pmol/L; P less than .001). In the multivariate analysis, low postoperative copeptin levels remained associated with diabetes insipidus after adjusting for age, gender, body-mass index, tumor size and type of surgery, history of surgery or radiotherapy, cerebrospinal fluid leakage, and serum sodium concentration, the investigators reported (odds ratio, 1.62; 95% confidence interval, 1.25-2.10; P less than .001).
The study did not use standardized diagnostic criteria for diabetes insipidus, and postoperative blood samples were obtained as part of daily care and not at fixed time points, Dr. Winzeler and her associates noted. “Absence of standardized sampling for copeptin measurement at a defined early time point presumably decreased copeptin accuracy in this study, rendering our findings conservative,” they cautioned.
The Swiss National Foundation partially funded the research. Three coauthors reported having received speaker honoraria from Thermo Scientific Biomarkers, which develops and makes the copeptin assay.
Key clinical point: Low copeptin levels reliably predicted diabetes insipidus after pituitary surgery.
Major finding: A day after surgery, 81.5% of patients with copeptin levels less than 2.5 pmol/L had diabetes insipidus, compared with 2.5% of patients with levels greater than 30 pmol/L.
Data source: Multicenter, prospective, observational cohort study of 205 consecutive pituitary surgery patients.
Disclosures: The Swiss National Foundation partially funded the research. Three coauthors reported having received speaker honoraria from Thermo Scientific Biomarkers, which develops and makes the copeptin assay.
Asymptomatic carotid stenosis and central sleep apnea linked
More than two-thirds of patients with asymptomatic carotid stenosis are likely have sleep apnea, according to an observational study.
The polysomnography results of 96 patients with asymptomatic extracranial carotid stenosis revealed that 69% had sleep apnea. Obstructive sleep apnea was present in 42% of patients and central sleep apnea in 27%.
Stenosis severity was significantly associated with central sleep apnea, but not with obstructive sleep apnea. Researchers found that central sleep apnea, but not obstructive sleep apnea, was associated with arterial hypertension and diabetes mellitus in those patients with asymptomatic carotid stenosis (CHEST 2015;147:1029-1036 [doi:10.1378/chest.14-1655]).
The patients ranged in age from 39 to 86 years (mean age, 70 years); 64 were men. Of the 96 patients, 21 had mild/moderate stenosis and 75 had severe carotid stenosis. Patients with severe stenosis were older, average age 67 years, than were those with mild/moderate stenosis, average age 61 years. The frequency of arterial hypertension and diabetes mellitus was higher in the severe stenosis group than in the mild/moderate stenosis group.
The prevalence of sleep apnea was 76% in patients with severe stenosis compared with 29% in those with mild/moderate carotid stenosis. Total apnea-hypopnea index was higher in the severe stenosis group compared with the mild/moderate stenosis group (P less than or equal to .009). Increase in sleep apnea severity was based on an increase in central apnea-hypopnea index (P less than or equal to .001) but not in obstructive apnea-hypopnea index, reflecting an augmentation of central sleep apnea and not of obstructive sleep apnea in patients with severe compared with mild/moderate carotid stenosis.
“This vascular risk constellation seems to be more strongly connected with CSA [central sleep apnea] than with OSA [obstructive sleep apnea], possibly attributable to carotid chemoreceptor dysfunction,” wrote Dr. Jens Ehrhardt and colleagues at Jena University Hospital, Germany.
No conflicts of interest were declared.
More than two-thirds of patients with asymptomatic carotid stenosis are likely have sleep apnea, according to an observational study.
The polysomnography results of 96 patients with asymptomatic extracranial carotid stenosis revealed that 69% had sleep apnea. Obstructive sleep apnea was present in 42% of patients and central sleep apnea in 27%.
Stenosis severity was significantly associated with central sleep apnea, but not with obstructive sleep apnea. Researchers found that central sleep apnea, but not obstructive sleep apnea, was associated with arterial hypertension and diabetes mellitus in those patients with asymptomatic carotid stenosis (CHEST 2015;147:1029-1036 [doi:10.1378/chest.14-1655]).
The patients ranged in age from 39 to 86 years (mean age, 70 years); 64 were men. Of the 96 patients, 21 had mild/moderate stenosis and 75 had severe carotid stenosis. Patients with severe stenosis were older, average age 67 years, than were those with mild/moderate stenosis, average age 61 years. The frequency of arterial hypertension and diabetes mellitus was higher in the severe stenosis group than in the mild/moderate stenosis group.
The prevalence of sleep apnea was 76% in patients with severe stenosis compared with 29% in those with mild/moderate carotid stenosis. Total apnea-hypopnea index was higher in the severe stenosis group compared with the mild/moderate stenosis group (P less than or equal to .009). Increase in sleep apnea severity was based on an increase in central apnea-hypopnea index (P less than or equal to .001) but not in obstructive apnea-hypopnea index, reflecting an augmentation of central sleep apnea and not of obstructive sleep apnea in patients with severe compared with mild/moderate carotid stenosis.
“This vascular risk constellation seems to be more strongly connected with CSA [central sleep apnea] than with OSA [obstructive sleep apnea], possibly attributable to carotid chemoreceptor dysfunction,” wrote Dr. Jens Ehrhardt and colleagues at Jena University Hospital, Germany.
No conflicts of interest were declared.
More than two-thirds of patients with asymptomatic carotid stenosis are likely have sleep apnea, according to an observational study.
The polysomnography results of 96 patients with asymptomatic extracranial carotid stenosis revealed that 69% had sleep apnea. Obstructive sleep apnea was present in 42% of patients and central sleep apnea in 27%.
Stenosis severity was significantly associated with central sleep apnea, but not with obstructive sleep apnea. Researchers found that central sleep apnea, but not obstructive sleep apnea, was associated with arterial hypertension and diabetes mellitus in those patients with asymptomatic carotid stenosis (CHEST 2015;147:1029-1036 [doi:10.1378/chest.14-1655]).
The patients ranged in age from 39 to 86 years (mean age, 70 years); 64 were men. Of the 96 patients, 21 had mild/moderate stenosis and 75 had severe carotid stenosis. Patients with severe stenosis were older, average age 67 years, than were those with mild/moderate stenosis, average age 61 years. The frequency of arterial hypertension and diabetes mellitus was higher in the severe stenosis group than in the mild/moderate stenosis group.
The prevalence of sleep apnea was 76% in patients with severe stenosis compared with 29% in those with mild/moderate carotid stenosis. Total apnea-hypopnea index was higher in the severe stenosis group compared with the mild/moderate stenosis group (P less than or equal to .009). Increase in sleep apnea severity was based on an increase in central apnea-hypopnea index (P less than or equal to .001) but not in obstructive apnea-hypopnea index, reflecting an augmentation of central sleep apnea and not of obstructive sleep apnea in patients with severe compared with mild/moderate carotid stenosis.
“This vascular risk constellation seems to be more strongly connected with CSA [central sleep apnea] than with OSA [obstructive sleep apnea], possibly attributable to carotid chemoreceptor dysfunction,” wrote Dr. Jens Ehrhardt and colleagues at Jena University Hospital, Germany.
No conflicts of interest were declared.
FROM CHEST
Key clinical point: More than two-thirds of patients with asymptomatic carotid stenosis are likely to have sleep apnea.
Major finding: The prevalence of sleep apnea was 76% in patients with severe stenosis compared with 29% in those with mild/moderate carotid stenosis.
Data source: Study of 96 patients with asymptomatic extracranial carotid stenosis.
Disclosures: No conflicts of interest were declared.
Weekend surgery safer with more nurses, EMR use
SAN DIEGO – More nurses, robust ancillary services, and an electronic medical record (EMR) helped reduce hospital length of stay when an urgent general surgery procedure was performed on the weekend. When these surgeon-independent resources were present, hospitals were able to overcome the weekend effect.
When a patient needs urgent surgery over the weekend, the result can be increased length of stay, higher charges, increased major and minor complications, and even increased mortality. Overall, patients admitted on the weekend have worse outcomes than do those admitted on a weekday. Factors contributing to the weekend effect for hospitals in one state were explored in a presentation at the American Surgical Association annual meeting.

“Not all hospitals are created equal in their ability to avoid the weekend effect,” noted presenter Matthew Zapf, a second-year medical student at Stritch School of Medicine, Loyola University Chicago. The work of Mr. Zapf and his colleagues at the university showed that hospitals with full electronic medical records, increased nurse-to-bed ratios, pain and wound management services, and home health programs were more likely to overcome the weekend effect, as defined by length of stay for specific urgent and emergent surgical procedures.
The study used Florida’s Healthcare Cost and Utilization Project State Inpatient Dataset (HCUP-SID), an all-payer dataset, and linked that information to Florida’s American Hospital Association annual survey database, which assesses hospital characteristics. Outcomes were assessed for cholecystectomy, hernia repair for obstructed or gangrenous hernias, and appendectomy for 126,666 people aged 18-90 years. To ensure that the study captured just urgent or emergency procedures, only procedures performed within 2 days of hospital admission were included.
By assessing whether length of stay was longer for weekend vs. weekday admissions for these procedures, the researchers identified which hospitals demonstrated the weekend effect. Of the 197 acute care hospitals identified, 117 performed more than 10 emergent cases per year and were included in the analysis. The presence or absence of a weekend effect was recorded for each hospital for each year of the study. Hospital characteristics were assessed for association with the weekend effect for a given facility in a given year.
None of the 117 hospitals were free of the weekend effect – an outcome that had not been anticipated by the study authors. “I was shocked by the fact that nobody was immune to the weekend effect,” Dr. Anai Kothari said in an interview. Dr. Kothari, also of Loyola University Chicago and first author of the study, said that 41 of the hospitals had a persistent weekend effect through all years of the study. Seventeen hospitals overcame the weekend effect during the time period studied, while 21 others developed the weekend effect during this time. Most hospitals (n = 87) oscillated between states, exhibiting a weekend effect only in some years.
Institutions with an EMR in place during the study period had an odds ratio (OR) of nearly 5 of being able to overcome the weekend effect (P = .010). The EMR, said Dr. Kothari, is especially helpful in effecting safe care transitions. “We are going to see a strong effect, especially in situations where there’s a care transition” as institutions learn how to make full use of the EMR, he said.
Inpatient resources linked with overcoming the weekend effect included a higher ratio of registered nurses to beds (P = .0036), a physical rehabilitation program (P = .017), and a pain management program (P = .001). After-care resources in the form of home health (P = .001) and wound management (P = .043) also contributed significantly to being able to overcome the weekend effect.
Discussant Dr. Lena Napolitano of the University of Michigan commented on the “incredibly robust statistical analysis” performed by the study investigators.
How, she asked, did investigators select median length of stay as the marker for outcomes, when an extended stay over the weekend may just represent poor discharge planning, and not really represent increased adverse outcomes? Senior author Dr. Paul Kuo of Loyola University Chicago replied: “We put a lot of thought into this. We found that length of stay was predictive of each outcome during modeling.”
Study limitations included the fact that data were administrative and were drawn from a single state. It was not possible, for example, to differentiate weekend vs. weekday distribution of resources at a given institution. The next steps will include searching for richer data sources to explore the full set of hospital resources that contribute to patient outcomes for urgent surgeries, said Dr. Kothari.
The authors reported no disclosures.
The complete manuscript of this study and its presentation at the American Surgical Association’s 135th Annual Meeting, April 2015, in San Diego, California, are anticipated to be published in the Annals of Surgery pending editorial review.
SAN DIEGO – More nurses, robust ancillary services, and an electronic medical record (EMR) helped reduce hospital length of stay when an urgent general surgery procedure was performed on the weekend. When these surgeon-independent resources were present, hospitals were able to overcome the weekend effect.
When a patient needs urgent surgery over the weekend, the result can be increased length of stay, higher charges, increased major and minor complications, and even increased mortality. Overall, patients admitted on the weekend have worse outcomes than do those admitted on a weekday. Factors contributing to the weekend effect for hospitals in one state were explored in a presentation at the American Surgical Association annual meeting.
“Not all hospitals are created equal in their ability to avoid the weekend effect,” noted presenter Matthew Zapf, a second-year medical student at Stritch School of Medicine, Loyola University Chicago. The work of Mr. Zapf and his colleagues at the university showed that hospitals with full electronic medical records, increased nurse-to-bed ratios, pain and wound management services, and home health programs were more likely to overcome the weekend effect, as defined by length of stay for specific urgent and emergent surgical procedures.
The study used Florida’s Healthcare Cost and Utilization Project State Inpatient Dataset (HCUP-SID), an all-payer dataset, and linked that information to Florida’s American Hospital Association annual survey database, which assesses hospital characteristics. Outcomes were assessed for cholecystectomy, hernia repair for obstructed or gangrenous hernias, and appendectomy for 126,666 people aged 18-90 years. To ensure that the study captured just urgent or emergency procedures, only procedures performed within 2 days of hospital admission were included.
By assessing whether length of stay was longer for weekend vs. weekday admissions for these procedures, the researchers identified which hospitals demonstrated the weekend effect. Of the 197 acute care hospitals identified, 117 performed more than 10 emergent cases per year and were included in the analysis. The presence or absence of a weekend effect was recorded for each hospital for each year of the study. Hospital characteristics were assessed for association with the weekend effect for a given facility in a given year.
None of the 117 hospitals were free of the weekend effect – an outcome that had not been anticipated by the study authors. “I was shocked by the fact that nobody was immune to the weekend effect,” Dr. Anai Kothari said in an interview. Dr. Kothari, also of Loyola University Chicago and first author of the study, said that 41 of the hospitals had a persistent weekend effect through all years of the study. Seventeen hospitals overcame the weekend effect during the time period studied, while 21 others developed the weekend effect during this time. Most hospitals (n = 87) oscillated between states, exhibiting a weekend effect only in some years.
Institutions with an EMR in place during the study period had an odds ratio (OR) of nearly 5 of being able to overcome the weekend effect (P = .010). The EMR, said Dr. Kothari, is especially helpful in effecting safe care transitions. “We are going to see a strong effect, especially in situations where there’s a care transition” as institutions learn how to make full use of the EMR, he said.
Inpatient resources linked with overcoming the weekend effect included a higher ratio of registered nurses to beds (P = .0036), a physical rehabilitation program (P = .017), and a pain management program (P = .001). After-care resources in the form of home health (P = .001) and wound management (P = .043) also contributed significantly to being able to overcome the weekend effect.
Discussant Dr. Lena Napolitano of the University of Michigan commented on the “incredibly robust statistical analysis” performed by the study investigators.
How, she asked, did investigators select median length of stay as the marker for outcomes, when an extended stay over the weekend may just represent poor discharge planning, and not really represent increased adverse outcomes? Senior author Dr. Paul Kuo of Loyola University Chicago replied: “We put a lot of thought into this. We found that length of stay was predictive of each outcome during modeling.”
Study limitations included the fact that data were administrative and were drawn from a single state. It was not possible, for example, to differentiate weekend vs. weekday distribution of resources at a given institution. The next steps will include searching for richer data sources to explore the full set of hospital resources that contribute to patient outcomes for urgent surgeries, said Dr. Kothari.
The authors reported no disclosures.
The complete manuscript of this study and its presentation at the American Surgical Association’s 135th Annual Meeting, April 2015, in San Diego, California, are anticipated to be published in the Annals of Surgery pending editorial review.
SAN DIEGO – More nurses, robust ancillary services, and an electronic medical record (EMR) helped reduce hospital length of stay when an urgent general surgery procedure was performed on the weekend. When these surgeon-independent resources were present, hospitals were able to overcome the weekend effect.
When a patient needs urgent surgery over the weekend, the result can be increased length of stay, higher charges, increased major and minor complications, and even increased mortality. Overall, patients admitted on the weekend have worse outcomes than do those admitted on a weekday. Factors contributing to the weekend effect for hospitals in one state were explored in a presentation at the American Surgical Association annual meeting.
“Not all hospitals are created equal in their ability to avoid the weekend effect,” noted presenter Matthew Zapf, a second-year medical student at Stritch School of Medicine, Loyola University Chicago. The work of Mr. Zapf and his colleagues at the university showed that hospitals with full electronic medical records, increased nurse-to-bed ratios, pain and wound management services, and home health programs were more likely to overcome the weekend effect, as defined by length of stay for specific urgent and emergent surgical procedures.
The study used Florida’s Healthcare Cost and Utilization Project State Inpatient Dataset (HCUP-SID), an all-payer dataset, and linked that information to Florida’s American Hospital Association annual survey database, which assesses hospital characteristics. Outcomes were assessed for cholecystectomy, hernia repair for obstructed or gangrenous hernias, and appendectomy for 126,666 people aged 18-90 years. To ensure that the study captured just urgent or emergency procedures, only procedures performed within 2 days of hospital admission were included.
By assessing whether length of stay was longer for weekend vs. weekday admissions for these procedures, the researchers identified which hospitals demonstrated the weekend effect. Of the 197 acute care hospitals identified, 117 performed more than 10 emergent cases per year and were included in the analysis. The presence or absence of a weekend effect was recorded for each hospital for each year of the study. Hospital characteristics were assessed for association with the weekend effect for a given facility in a given year.
None of the 117 hospitals were free of the weekend effect – an outcome that had not been anticipated by the study authors. “I was shocked by the fact that nobody was immune to the weekend effect,” Dr. Anai Kothari said in an interview. Dr. Kothari, also of Loyola University Chicago and first author of the study, said that 41 of the hospitals had a persistent weekend effect through all years of the study. Seventeen hospitals overcame the weekend effect during the time period studied, while 21 others developed the weekend effect during this time. Most hospitals (n = 87) oscillated between states, exhibiting a weekend effect only in some years.
Institutions with an EMR in place during the study period had an odds ratio (OR) of nearly 5 of being able to overcome the weekend effect (P = .010). The EMR, said Dr. Kothari, is especially helpful in effecting safe care transitions. “We are going to see a strong effect, especially in situations where there’s a care transition” as institutions learn how to make full use of the EMR, he said.
Inpatient resources linked with overcoming the weekend effect included a higher ratio of registered nurses to beds (P = .0036), a physical rehabilitation program (P = .017), and a pain management program (P = .001). After-care resources in the form of home health (P = .001) and wound management (P = .043) also contributed significantly to being able to overcome the weekend effect.
Discussant Dr. Lena Napolitano of the University of Michigan commented on the “incredibly robust statistical analysis” performed by the study investigators.
How, she asked, did investigators select median length of stay as the marker for outcomes, when an extended stay over the weekend may just represent poor discharge planning, and not really represent increased adverse outcomes? Senior author Dr. Paul Kuo of Loyola University Chicago replied: “We put a lot of thought into this. We found that length of stay was predictive of each outcome during modeling.”
Study limitations included the fact that data were administrative and were drawn from a single state. It was not possible, for example, to differentiate weekend vs. weekday distribution of resources at a given institution. The next steps will include searching for richer data sources to explore the full set of hospital resources that contribute to patient outcomes for urgent surgeries, said Dr. Kothari.
The authors reported no disclosures.
The complete manuscript of this study and its presentation at the American Surgical Association’s 135th Annual Meeting, April 2015, in San Diego, California, are anticipated to be published in the Annals of Surgery pending editorial review.
AT THE ASA ANNUAL MEETING
Key clinical point: Surgeon-independent factors impacted patient outcomes for urgent surgical procedures.
Major finding: Facilities with an electronic medical record, higher nurse-to-bed ratios, and strong ancillary services were significantly less likely to exhibit the weekend effect for urgent surgical procedures, as measured by patient length of stay.
Data source: Healthcare Cost and Utilization Project State Inpatient Dataset and American Hospital Association Annual Survey database for the state of Florida for 2007-2011.
Disclosures: The authors reported no disclosures.

ASA: Bowel prep, oral antibiotics cut postop colorectal complications
SAN DIEGO – A combination of bowel cleansing and oral antibiotics nearly halved the risk of common and troublesome complications in colorectal surgery. Infections, leaks, and postsurgical ileus were all significantly less likely with the combined regime, according to a study reported at the annual meeting of the American Surgical Association.
Patients preparing for colorectal surgery routinely received mechanical bowel preparation in combination with oral antibiotics in the 1970s. However, since then, the availability of IV antibiotics combined with concerns about complications from bowel preparation have contributed to a decline in use of the regime. Consensus is lacking about best practices for preparation for colorectal surgery.

Dr. P. Ravi Kiran, chief and program director of Columbia University Medical Center’s division of colorectal surgery, presented findings from a large retrospective study that addressed whether oral antibiotics and mechanical bowel preparation reduced the risk of complications from colorectal surgery. Drawing from targeted colectomy data, available from 2012 onward through the large American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database, Dr. Kiran and associates compared three groups of patients undergoing elective colectomy. Of the total 8,644 patients, 2,498 (28.9%) received no preparation, 3,822 (44.2%) received mechanical bowel preparation alone, and 2,324 (26.9%) received both oral antibiotics and mechanical bowel preparation.
Primary outcome measures included the presence of anastomotic leak from the surgery, surgical site infections, ileus, and all-cause mortality. The patients were well matched by age and gender, and surgery type; case complexity and degree of resident physician involvement in the surgical procedures were also similar between arms.
On multivariable analysis, patients who received mechanical bowel preparation and oral antibiotics were significantly less likely to have surgical site infections (odds ratio, 0.43), to sustain ileus (OR, 0.71), or to have anastomotic leak (OR, 0.56). Postoperatively, those who had received no bowel preparation were also significantly more likely to have pneumonia, to require reintubation, and to fail to wean from the ventilator. They also were more likely to have deep vein thrombosis and sepsis. All-cause 30-day mortality was also significantly less likely in the group receiving both bowel preparation and oral antibiotics.
Dr. Kiran noted that investigators were not able to determine the type of mechanical bowel preparation patients received, and likely could not control for all confounders.
Discussant Dr. Heidi Nelson of the Mayo Clinic, Rochester, Minn., noted that despite the study’s strengths, including its large size and the real-world nature of the investigation, she doubts that the study will be considered definitive. Limitations that critics might point out, she noted, are the retrospective nature of the study and the possibility that the three groups studied were not really comparable because of subtle selection biases on the part of the treating surgeons. Dr. Kiran conceded that though multivariable analysis attempted to account and control for as many between-group differences as they could identify, differences probably did persist.
Dr. Hiram Polk of the University of Louisville (Ky.) commented that studies such as these using massive databases, though they may show what is true, may not always point to what is clinically relevant. Overall, it’s been shown that about one in four patients given systemic antibiotics are given the wrong drug, he said; further, “the only place you can truly sterilize a colon is in an autoclave.” Dr. Kiran did note that the combined oral preparation regime was successful in reducing the incidence of the most common complications by about 50%.
Following with more real-world observations, Dr. Mary Otterson of the Medical College of Wisconsin, Milwaukee, commented that the effective dose of preoperative erythromycin is very close to doses that cause significant nausea and vomiting. In her experience, “If we went any higher, they vomited. We also had unplanned admits with electrolyte abnormalities.” The best-tolerated and most effective regime, she said, should be identified by a prospective, randomized, controlled trial.
The authors reported no conflicts of interest.
The complete manuscript of this study and its presentation at the American Surgical Association’s 135th Annual Meeting, April 2015, in San Diego, California, are anticipated to be published in the Annals of Surgery pending editorial review.
SAN DIEGO – A combination of bowel cleansing and oral antibiotics nearly halved the risk of common and troublesome complications in colorectal surgery. Infections, leaks, and postsurgical ileus were all significantly less likely with the combined regime, according to a study reported at the annual meeting of the American Surgical Association.
Patients preparing for colorectal surgery routinely received mechanical bowel preparation in combination with oral antibiotics in the 1970s. However, since then, the availability of IV antibiotics combined with concerns about complications from bowel preparation have contributed to a decline in use of the regime. Consensus is lacking about best practices for preparation for colorectal surgery.
Dr. P. Ravi Kiran, chief and program director of Columbia University Medical Center’s division of colorectal surgery, presented findings from a large retrospective study that addressed whether oral antibiotics and mechanical bowel preparation reduced the risk of complications from colorectal surgery. Drawing from targeted colectomy data, available from 2012 onward through the large American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database, Dr. Kiran and associates compared three groups of patients undergoing elective colectomy. Of the total 8,644 patients, 2,498 (28.9%) received no preparation, 3,822 (44.2%) received mechanical bowel preparation alone, and 2,324 (26.9%) received both oral antibiotics and mechanical bowel preparation.
Primary outcome measures included the presence of anastomotic leak from the surgery, surgical site infections, ileus, and all-cause mortality. The patients were well matched by age and gender, and surgery type; case complexity and degree of resident physician involvement in the surgical procedures were also similar between arms.
On multivariable analysis, patients who received mechanical bowel preparation and oral antibiotics were significantly less likely to have surgical site infections (odds ratio, 0.43), to sustain ileus (OR, 0.71), or to have anastomotic leak (OR, 0.56). Postoperatively, those who had received no bowel preparation were also significantly more likely to have pneumonia, to require reintubation, and to fail to wean from the ventilator. They also were more likely to have deep vein thrombosis and sepsis. All-cause 30-day mortality was also significantly less likely in the group receiving both bowel preparation and oral antibiotics.
Dr. Kiran noted that investigators were not able to determine the type of mechanical bowel preparation patients received, and likely could not control for all confounders.
Discussant Dr. Heidi Nelson of the Mayo Clinic, Rochester, Minn., noted that despite the study’s strengths, including its large size and the real-world nature of the investigation, she doubts that the study will be considered definitive. Limitations that critics might point out, she noted, are the retrospective nature of the study and the possibility that the three groups studied were not really comparable because of subtle selection biases on the part of the treating surgeons. Dr. Kiran conceded that though multivariable analysis attempted to account and control for as many between-group differences as they could identify, differences probably did persist.
Dr. Hiram Polk of the University of Louisville (Ky.) commented that studies such as these using massive databases, though they may show what is true, may not always point to what is clinically relevant. Overall, it’s been shown that about one in four patients given systemic antibiotics are given the wrong drug, he said; further, “the only place you can truly sterilize a colon is in an autoclave.” Dr. Kiran did note that the combined oral preparation regime was successful in reducing the incidence of the most common complications by about 50%.
Following with more real-world observations, Dr. Mary Otterson of the Medical College of Wisconsin, Milwaukee, commented that the effective dose of preoperative erythromycin is very close to doses that cause significant nausea and vomiting. In her experience, “If we went any higher, they vomited. We also had unplanned admits with electrolyte abnormalities.” The best-tolerated and most effective regime, she said, should be identified by a prospective, randomized, controlled trial.
The authors reported no conflicts of interest.
The complete manuscript of this study and its presentation at the American Surgical Association’s 135th Annual Meeting, April 2015, in San Diego, California, are anticipated to be published in the Annals of Surgery pending editorial review.
SAN DIEGO – A combination of bowel cleansing and oral antibiotics nearly halved the risk of common and troublesome complications in colorectal surgery. Infections, leaks, and postsurgical ileus were all significantly less likely with the combined regime, according to a study reported at the annual meeting of the American Surgical Association.
Patients preparing for colorectal surgery routinely received mechanical bowel preparation in combination with oral antibiotics in the 1970s. However, since then, the availability of IV antibiotics combined with concerns about complications from bowel preparation have contributed to a decline in use of the regime. Consensus is lacking about best practices for preparation for colorectal surgery.
Dr. P. Ravi Kiran, chief and program director of Columbia University Medical Center’s division of colorectal surgery, presented findings from a large retrospective study that addressed whether oral antibiotics and mechanical bowel preparation reduced the risk of complications from colorectal surgery. Drawing from targeted colectomy data, available from 2012 onward through the large American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database, Dr. Kiran and associates compared three groups of patients undergoing elective colectomy. Of the total 8,644 patients, 2,498 (28.9%) received no preparation, 3,822 (44.2%) received mechanical bowel preparation alone, and 2,324 (26.9%) received both oral antibiotics and mechanical bowel preparation.
Primary outcome measures included the presence of anastomotic leak from the surgery, surgical site infections, ileus, and all-cause mortality. The patients were well matched by age and gender, and surgery type; case complexity and degree of resident physician involvement in the surgical procedures were also similar between arms.
On multivariable analysis, patients who received mechanical bowel preparation and oral antibiotics were significantly less likely to have surgical site infections (odds ratio, 0.43), to sustain ileus (OR, 0.71), or to have anastomotic leak (OR, 0.56). Postoperatively, those who had received no bowel preparation were also significantly more likely to have pneumonia, to require reintubation, and to fail to wean from the ventilator. They also were more likely to have deep vein thrombosis and sepsis. All-cause 30-day mortality was also significantly less likely in the group receiving both bowel preparation and oral antibiotics.
Dr. Kiran noted that investigators were not able to determine the type of mechanical bowel preparation patients received, and likely could not control for all confounders.
Discussant Dr. Heidi Nelson of the Mayo Clinic, Rochester, Minn., noted that despite the study’s strengths, including its large size and the real-world nature of the investigation, she doubts that the study will be considered definitive. Limitations that critics might point out, she noted, are the retrospective nature of the study and the possibility that the three groups studied were not really comparable because of subtle selection biases on the part of the treating surgeons. Dr. Kiran conceded that though multivariable analysis attempted to account and control for as many between-group differences as they could identify, differences probably did persist.
Dr. Hiram Polk of the University of Louisville (Ky.) commented that studies such as these using massive databases, though they may show what is true, may not always point to what is clinically relevant. Overall, it’s been shown that about one in four patients given systemic antibiotics are given the wrong drug, he said; further, “the only place you can truly sterilize a colon is in an autoclave.” Dr. Kiran did note that the combined oral preparation regime was successful in reducing the incidence of the most common complications by about 50%.
Following with more real-world observations, Dr. Mary Otterson of the Medical College of Wisconsin, Milwaukee, commented that the effective dose of preoperative erythromycin is very close to doses that cause significant nausea and vomiting. In her experience, “If we went any higher, they vomited. We also had unplanned admits with electrolyte abnormalities.” The best-tolerated and most effective regime, she said, should be identified by a prospective, randomized, controlled trial.
The authors reported no conflicts of interest.
The complete manuscript of this study and its presentation at the American Surgical Association’s 135th Annual Meeting, April 2015, in San Diego, California, are anticipated to be published in the Annals of Surgery pending editorial review.
AT THE ASA ANNUAL MEETING
Key clinical point: A combination of mechanical cleansing and oral antibiotics reduced major colorectal surgery complications by nearly one-half.
Major findings: Mechanical bowel preparation combined with oral antibiotics resulted in reduced colorectal surgery complications, with odds ratios of 0.43 for surgical site infections, 0.71 for ileus, and 0.56 for anastomotic leak; overall mortality was also reduced.
Data source: Retrospective multivariable analysis of data for 8,644 surgical patients undergoing elective colorectal resection in 2012; targeted colectomy data drawn from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database.
Disclosures: The authors reported no conflicts of interest.

Neoadjuvant chemotherapy for triple negative breast cancer improves conservation
SAN DIEGO – More women with triple negative breast cancer are able to have breast-conserving therapy (BCT) when they receive neoadjuvant systemic chemotherapy.
In a recent trial, 42% of women who were considered ineligible for BCT became eligible for the tissue-sparing surgery after their course of neoadjuvant chemotherapy (NACT) was administered. However, surgeons and patients must work together to decide on the best course of action, according to Dr. David Ollila of the University of North Carolina, Chapel Hill.

The relationship between NACT and the option to have breast-sparing surgery had not been well understood previously, especially for women with aggressive triple negative breast cancer, Dr. Ollila said at the annual meeting of the American Surgical Association.
What has been known is that women with breast cancer who receive NACT show overall improved pathological complete response (Lancet 2014;384:164-72), which is associated with better event-free and overall survival.
The current study, conducted within the larger CALGB 40603 randomized phase II clinical trial, captured the number of patients who converted from BCT-ineligible to BCT-eligible after NACT and before surgery. Investigators also tracked pathological complete response, defined as tumor-free margins on pathologic examination, for those receiving each type of surgery. Dr. Ollila presented his findings on behalf of his coinvestigators in the Alliance for Clinical Trials in Oncology.
The study used a 2x2 factorial design to compare paclitaxel with and without carboplatin followed by doxorubicin plus cyclophosphamide with and without bevacizumab. Before NACT, the surgeon determined whether or not the patient was a candidate for BCT and if not, why not. The process was repeated after NACT, with the surgeon again documenting his or her reasoning for the choice.
Complete data were available for 404 women, distributed evenly across chemotherapy treatment arms. Before NACT, 219 (54%) were judged by their surgeons to be BCT candidates, and 197 (90%) were still deemed eligible for BCT after NACT. Of the 185 (46%) judged ineligible for BCT before chemotherapy, 72 (42%) became eligible for tissue sparing surgery after NACT. “We achieved a very high conversion rate ... from BCT ineligible to eligible,” Dr. Ollila noted.
Overall, just over two-thirds of the 404 women (n = 275, 68%) became candidates for BCT before surgery, and of those, about two-thirds (n = 191, 69%) went on to have an attempted BCT surgery. Surgery was successful for 178 of these women. “Neoadjuvant chemotherapy led to BCT in 93% of selected triple negative patients,”said Dr. Ollila.
Pathological complete response did not differ significantly among the women who received BCT or mastectomy, whether the decision was made before or after chemotherapy.
Discussant Dr. Lisa Newman of the University of Michigan observed that NACT allows some breathing space for the patient and her surgeon to weigh choices, and when indicated, to receive genetic testing.
“We know from numerous population-based and institutional studies that many are opting for bilateral mastectomy, even if a lumpectomy would be optimal,”said Dr. Newman.
She asked whether patient decision making was tracked for this study. Dr. Ollila replied, “We did not include patient factors. We do not have prospective data on what the patient was thinking because we focused on the surgeon.” However, he said, plans are underway to quantify the patient perspective during the decision-making process.
The takeaway message, said Dr. Ollila, is that “We are letting people think that mastectomy is the best option; I think that sequential surgery is all right. I think we just need to try breast conserving therapy more often than we are.”
The study was partially sponsored by the Breast Cancer Research Foundation. The authors reported no conflicts of interest.
The complete manuscript of this study and its presentation at the American Surgical Association’s 135th Annual Meeting, April 2015, in San Diego, California, are anticipated to be published in the Annals of Surgery pending editorial review.
SAN DIEGO – More women with triple negative breast cancer are able to have breast-conserving therapy (BCT) when they receive neoadjuvant systemic chemotherapy.
In a recent trial, 42% of women who were considered ineligible for BCT became eligible for the tissue-sparing surgery after their course of neoadjuvant chemotherapy (NACT) was administered. However, surgeons and patients must work together to decide on the best course of action, according to Dr. David Ollila of the University of North Carolina, Chapel Hill.
The relationship between NACT and the option to have breast-sparing surgery had not been well understood previously, especially for women with aggressive triple negative breast cancer, Dr. Ollila said at the annual meeting of the American Surgical Association.
What has been known is that women with breast cancer who receive NACT show overall improved pathological complete response (Lancet 2014;384:164-72), which is associated with better event-free and overall survival.
The current study, conducted within the larger CALGB 40603 randomized phase II clinical trial, captured the number of patients who converted from BCT-ineligible to BCT-eligible after NACT and before surgery. Investigators also tracked pathological complete response, defined as tumor-free margins on pathologic examination, for those receiving each type of surgery. Dr. Ollila presented his findings on behalf of his coinvestigators in the Alliance for Clinical Trials in Oncology.
The study used a 2x2 factorial design to compare paclitaxel with and without carboplatin followed by doxorubicin plus cyclophosphamide with and without bevacizumab. Before NACT, the surgeon determined whether or not the patient was a candidate for BCT and if not, why not. The process was repeated after NACT, with the surgeon again documenting his or her reasoning for the choice.
Complete data were available for 404 women, distributed evenly across chemotherapy treatment arms. Before NACT, 219 (54%) were judged by their surgeons to be BCT candidates, and 197 (90%) were still deemed eligible for BCT after NACT. Of the 185 (46%) judged ineligible for BCT before chemotherapy, 72 (42%) became eligible for tissue sparing surgery after NACT. “We achieved a very high conversion rate ... from BCT ineligible to eligible,” Dr. Ollila noted.
Overall, just over two-thirds of the 404 women (n = 275, 68%) became candidates for BCT before surgery, and of those, about two-thirds (n = 191, 69%) went on to have an attempted BCT surgery. Surgery was successful for 178 of these women. “Neoadjuvant chemotherapy led to BCT in 93% of selected triple negative patients,”said Dr. Ollila.
Pathological complete response did not differ significantly among the women who received BCT or mastectomy, whether the decision was made before or after chemotherapy.
Discussant Dr. Lisa Newman of the University of Michigan observed that NACT allows some breathing space for the patient and her surgeon to weigh choices, and when indicated, to receive genetic testing.
“We know from numerous population-based and institutional studies that many are opting for bilateral mastectomy, even if a lumpectomy would be optimal,”said Dr. Newman.
She asked whether patient decision making was tracked for this study. Dr. Ollila replied, “We did not include patient factors. We do not have prospective data on what the patient was thinking because we focused on the surgeon.” However, he said, plans are underway to quantify the patient perspective during the decision-making process.
The takeaway message, said Dr. Ollila, is that “We are letting people think that mastectomy is the best option; I think that sequential surgery is all right. I think we just need to try breast conserving therapy more often than we are.”
The study was partially sponsored by the Breast Cancer Research Foundation. The authors reported no conflicts of interest.
The complete manuscript of this study and its presentation at the American Surgical Association’s 135th Annual Meeting, April 2015, in San Diego, California, are anticipated to be published in the Annals of Surgery pending editorial review.
SAN DIEGO – More women with triple negative breast cancer are able to have breast-conserving therapy (BCT) when they receive neoadjuvant systemic chemotherapy.
In a recent trial, 42% of women who were considered ineligible for BCT became eligible for the tissue-sparing surgery after their course of neoadjuvant chemotherapy (NACT) was administered. However, surgeons and patients must work together to decide on the best course of action, according to Dr. David Ollila of the University of North Carolina, Chapel Hill.
The relationship between NACT and the option to have breast-sparing surgery had not been well understood previously, especially for women with aggressive triple negative breast cancer, Dr. Ollila said at the annual meeting of the American Surgical Association.
What has been known is that women with breast cancer who receive NACT show overall improved pathological complete response (Lancet 2014;384:164-72), which is associated with better event-free and overall survival.
The current study, conducted within the larger CALGB 40603 randomized phase II clinical trial, captured the number of patients who converted from BCT-ineligible to BCT-eligible after NACT and before surgery. Investigators also tracked pathological complete response, defined as tumor-free margins on pathologic examination, for those receiving each type of surgery. Dr. Ollila presented his findings on behalf of his coinvestigators in the Alliance for Clinical Trials in Oncology.
The study used a 2x2 factorial design to compare paclitaxel with and without carboplatin followed by doxorubicin plus cyclophosphamide with and without bevacizumab. Before NACT, the surgeon determined whether or not the patient was a candidate for BCT and if not, why not. The process was repeated after NACT, with the surgeon again documenting his or her reasoning for the choice.
Complete data were available for 404 women, distributed evenly across chemotherapy treatment arms. Before NACT, 219 (54%) were judged by their surgeons to be BCT candidates, and 197 (90%) were still deemed eligible for BCT after NACT. Of the 185 (46%) judged ineligible for BCT before chemotherapy, 72 (42%) became eligible for tissue sparing surgery after NACT. “We achieved a very high conversion rate ... from BCT ineligible to eligible,” Dr. Ollila noted.
Overall, just over two-thirds of the 404 women (n = 275, 68%) became candidates for BCT before surgery, and of those, about two-thirds (n = 191, 69%) went on to have an attempted BCT surgery. Surgery was successful for 178 of these women. “Neoadjuvant chemotherapy led to BCT in 93% of selected triple negative patients,”said Dr. Ollila.
Pathological complete response did not differ significantly among the women who received BCT or mastectomy, whether the decision was made before or after chemotherapy.
Discussant Dr. Lisa Newman of the University of Michigan observed that NACT allows some breathing space for the patient and her surgeon to weigh choices, and when indicated, to receive genetic testing.
“We know from numerous population-based and institutional studies that many are opting for bilateral mastectomy, even if a lumpectomy would be optimal,”said Dr. Newman.
She asked whether patient decision making was tracked for this study. Dr. Ollila replied, “We did not include patient factors. We do not have prospective data on what the patient was thinking because we focused on the surgeon.” However, he said, plans are underway to quantify the patient perspective during the decision-making process.
The takeaway message, said Dr. Ollila, is that “We are letting people think that mastectomy is the best option; I think that sequential surgery is all right. I think we just need to try breast conserving therapy more often than we are.”
The study was partially sponsored by the Breast Cancer Research Foundation. The authors reported no conflicts of interest.
The complete manuscript of this study and its presentation at the American Surgical Association’s 135th Annual Meeting, April 2015, in San Diego, California, are anticipated to be published in the Annals of Surgery pending editorial review.
AT THE ASA ANNUAL MEETING
Key clinical point: Neoadjuvant chemotherapy (NACT) for triple negative breast cancer resulted in increased eligibility for breast-conserving therapy (BCT).
Major finding: NACT allowed 42% of women with triple negative breast cancer previously ineligible for BCT to become BCT candidates.
Data source: CALGB 40603, a prospective, randomized controlled trial for women with stage II-III triple negative breast cancer.
Disclosures: The study was partially sponsored by the Breast Cancer Research Foundation. The authors reported no conflicts of interest.

VIDEO: Patient-generated health tests pose challenges, opportunities for doctors
CHICAGO – Technology advances are giving patients direct access to myriad health tests and their own health data, but what role do physicians have in responding to such patient-generated assessments?
Dr. Marc Triola of New York University in New York says that the growing reach of health care technology presents both challenges and opportunities for the physician-patient relationship. Dr. Triola spoke at the annual meeting of the American Medical Women’s Association about how physicians can embrace technology and use advancements to improve quality of care.
In this video interview, Dr. Triola speaks about the new ways in which patients can assess their own health data and how doctors should address the test results. He also discusses barriers posed by new technology and how physicians can help shape the changing delivery of health care.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @legal_med
CHICAGO – Technology advances are giving patients direct access to myriad health tests and their own health data, but what role do physicians have in responding to such patient-generated assessments?
Dr. Marc Triola of New York University in New York says that the growing reach of health care technology presents both challenges and opportunities for the physician-patient relationship. Dr. Triola spoke at the annual meeting of the American Medical Women’s Association about how physicians can embrace technology and use advancements to improve quality of care.
In this video interview, Dr. Triola speaks about the new ways in which patients can assess their own health data and how doctors should address the test results. He also discusses barriers posed by new technology and how physicians can help shape the changing delivery of health care.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @legal_med
CHICAGO – Technology advances are giving patients direct access to myriad health tests and their own health data, but what role do physicians have in responding to such patient-generated assessments?
Dr. Marc Triola of New York University in New York says that the growing reach of health care technology presents both challenges and opportunities for the physician-patient relationship. Dr. Triola spoke at the annual meeting of the American Medical Women’s Association about how physicians can embrace technology and use advancements to improve quality of care.
In this video interview, Dr. Triola speaks about the new ways in which patients can assess their own health data and how doctors should address the test results. He also discusses barriers posed by new technology and how physicians can help shape the changing delivery of health care.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @legal_med
AT THE AMWA ANNUAL MEETING

OARSI: Predictors of crossover to surgery identified in patients with meniscal tears and OA
SEATTLE – Certain clinical factors help predict which patients with knee meniscal tears and osteoarthritis will abandon physical therapy (PT) for surgery, according to a study reported at the World Congress on Osteoarthritis.
Investigators led by Dr. Jeffrey N. Katz performed a secondary analysis of the randomized, controlled MeTeOR (Meniscal Tear in Osteoarthritis Research) trial, which compared PT with arthroscopic partial meniscectomy among 351 patients.

Results showed that patients assigned to PT had a 6%-8% higher risk of crossing over to surgery if they had greater pain, a shorter symptom duration, or weaker hamstrings. But four-fifths of patients obtained pain relief from surgery, regardless of whether they were initially assigned to it or crossed over to it.
“Patients with the most painful and acute presentations and those with hamstring weakness were most likely to cross over from PT to arthroscopic partial meniscectomy in this trial,” commented Dr. Katz, who is a professor of rheumatology at Harvard Medical School and codirector of the Brigham Spine Center at Brigham and Women’s Hospital, Boston. However, “the risk ratios were very modest, suggesting we have limited capacity to predict crossovers.”
“From a research standpoint, crossovers compromise trial interpretation, so targeting patients most likely to cross over with efforts to try to retain them in their original treatment arm would enhance the value of trials,” he added. “From a clinical standpoint, there appears to be no disadvantage in delaying surgery until a trial of physical therapy has been undertaken, and that conclusion underscores the advice from many of these trials suggesting that PT be offered as first-line therapy for patients with degenerative meniscal tears.”

In an interview, Dr. Rolando Espinosa Morales, session comoderator and chief of the rheumatology service at the National Institute of Rehabilitation, Mexico City, said, “The study shows us there are no perfect predictors [of crossover] in these patients,” and careful evaluation is needed to discern which patients really need surgery and which will fare well with PT alone.
“It’s a hot topic right now in the world,” he commented. “We really don’t want to use surgery in all patients; we need to use it in a [restricted] number of patients.”
During a question and answer period, session attendee Ewa M. Roos, Ph.D., University of Southern Denmark in Odense, said, “You showed a lot of patient-related factors that could potentially explain crossover, but what is the role of the surgeon? … Is there a fact that if you can, you will cross over?”
“I agree with what I think is your implicit suggestion that there probably is a large role for the surgeon. We looked at heterogeneity in crossovers among surgeons in the trial, and there is some variability. There are probably cultural differences as well,” Dr. Katz replied. “I think … the question is, how fully are patients consented to not receiving surgery?”
Participants in MeTeOR were aged 45 years or older and had a meniscal tear on magnetic resonance imaging with degenerative cartilage changes and at least one meniscal symptom. They were randomized evenly to a standardized PT regimen emphasizing strength and range of motion, or to arthroscopic partial meniscectomy accompanied by standardized PT.
Overall, 27% of patients in the PT arm crossed over to surgery within about 5 months, Dr. Katz reported at the meeting sponsored by the Osteoarthritis Research Society International.
Multivariate analyses showed that patients initially assigned to PT were more likely to cross over to surgery if they had greater pain, scoring 40 or higher on the 100-point Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain scale (relative risk, 1.08); had experienced symptoms for less than a year (1.07); or had hamstring strength of less than 30 pounds (1.06).
However, the rate of treatment success, defined as an improvement of at least 10 points on the 100-point Knee Injury and Osteoarthritis Outcome Score (KOOS) at 6 months, was similarly high for the patients who were randomized to and received surgery (80%) and the patients who were randomized to PT but crossed over to surgery (81%).
The trial had several limitations, according to Dr. Katz. “From the standpoint of external validity, trial samples are not necessarily generalizable as we know. And with respect to internal validity, our comparison of immediate and delayed arthroscopic partial meniscectomy was post randomization, and the groups are not necessarily balanced,” he said.
Dr. Katz disclosed no relevant conflicts of interest.
SEATTLE – Certain clinical factors help predict which patients with knee meniscal tears and osteoarthritis will abandon physical therapy (PT) for surgery, according to a study reported at the World Congress on Osteoarthritis.
Investigators led by Dr. Jeffrey N. Katz performed a secondary analysis of the randomized, controlled MeTeOR (Meniscal Tear in Osteoarthritis Research) trial, which compared PT with arthroscopic partial meniscectomy among 351 patients.
Results showed that patients assigned to PT had a 6%-8% higher risk of crossing over to surgery if they had greater pain, a shorter symptom duration, or weaker hamstrings. But four-fifths of patients obtained pain relief from surgery, regardless of whether they were initially assigned to it or crossed over to it.
“Patients with the most painful and acute presentations and those with hamstring weakness were most likely to cross over from PT to arthroscopic partial meniscectomy in this trial,” commented Dr. Katz, who is a professor of rheumatology at Harvard Medical School and codirector of the Brigham Spine Center at Brigham and Women’s Hospital, Boston. However, “the risk ratios were very modest, suggesting we have limited capacity to predict crossovers.”
“From a research standpoint, crossovers compromise trial interpretation, so targeting patients most likely to cross over with efforts to try to retain them in their original treatment arm would enhance the value of trials,” he added. “From a clinical standpoint, there appears to be no disadvantage in delaying surgery until a trial of physical therapy has been undertaken, and that conclusion underscores the advice from many of these trials suggesting that PT be offered as first-line therapy for patients with degenerative meniscal tears.”
In an interview, Dr. Rolando Espinosa Morales, session comoderator and chief of the rheumatology service at the National Institute of Rehabilitation, Mexico City, said, “The study shows us there are no perfect predictors [of crossover] in these patients,” and careful evaluation is needed to discern which patients really need surgery and which will fare well with PT alone.
“It’s a hot topic right now in the world,” he commented. “We really don’t want to use surgery in all patients; we need to use it in a [restricted] number of patients.”
During a question and answer period, session attendee Ewa M. Roos, Ph.D., University of Southern Denmark in Odense, said, “You showed a lot of patient-related factors that could potentially explain crossover, but what is the role of the surgeon? … Is there a fact that if you can, you will cross over?”
“I agree with what I think is your implicit suggestion that there probably is a large role for the surgeon. We looked at heterogeneity in crossovers among surgeons in the trial, and there is some variability. There are probably cultural differences as well,” Dr. Katz replied. “I think … the question is, how fully are patients consented to not receiving surgery?”
Participants in MeTeOR were aged 45 years or older and had a meniscal tear on magnetic resonance imaging with degenerative cartilage changes and at least one meniscal symptom. They were randomized evenly to a standardized PT regimen emphasizing strength and range of motion, or to arthroscopic partial meniscectomy accompanied by standardized PT.
Overall, 27% of patients in the PT arm crossed over to surgery within about 5 months, Dr. Katz reported at the meeting sponsored by the Osteoarthritis Research Society International.
Multivariate analyses showed that patients initially assigned to PT were more likely to cross over to surgery if they had greater pain, scoring 40 or higher on the 100-point Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain scale (relative risk, 1.08); had experienced symptoms for less than a year (1.07); or had hamstring strength of less than 30 pounds (1.06).
However, the rate of treatment success, defined as an improvement of at least 10 points on the 100-point Knee Injury and Osteoarthritis Outcome Score (KOOS) at 6 months, was similarly high for the patients who were randomized to and received surgery (80%) and the patients who were randomized to PT but crossed over to surgery (81%).
The trial had several limitations, according to Dr. Katz. “From the standpoint of external validity, trial samples are not necessarily generalizable as we know. And with respect to internal validity, our comparison of immediate and delayed arthroscopic partial meniscectomy was post randomization, and the groups are not necessarily balanced,” he said.
Dr. Katz disclosed no relevant conflicts of interest.
SEATTLE – Certain clinical factors help predict which patients with knee meniscal tears and osteoarthritis will abandon physical therapy (PT) for surgery, according to a study reported at the World Congress on Osteoarthritis.
Investigators led by Dr. Jeffrey N. Katz performed a secondary analysis of the randomized, controlled MeTeOR (Meniscal Tear in Osteoarthritis Research) trial, which compared PT with arthroscopic partial meniscectomy among 351 patients.
Results showed that patients assigned to PT had a 6%-8% higher risk of crossing over to surgery if they had greater pain, a shorter symptom duration, or weaker hamstrings. But four-fifths of patients obtained pain relief from surgery, regardless of whether they were initially assigned to it or crossed over to it.
“Patients with the most painful and acute presentations and those with hamstring weakness were most likely to cross over from PT to arthroscopic partial meniscectomy in this trial,” commented Dr. Katz, who is a professor of rheumatology at Harvard Medical School and codirector of the Brigham Spine Center at Brigham and Women’s Hospital, Boston. However, “the risk ratios were very modest, suggesting we have limited capacity to predict crossovers.”
“From a research standpoint, crossovers compromise trial interpretation, so targeting patients most likely to cross over with efforts to try to retain them in their original treatment arm would enhance the value of trials,” he added. “From a clinical standpoint, there appears to be no disadvantage in delaying surgery until a trial of physical therapy has been undertaken, and that conclusion underscores the advice from many of these trials suggesting that PT be offered as first-line therapy for patients with degenerative meniscal tears.”
In an interview, Dr. Rolando Espinosa Morales, session comoderator and chief of the rheumatology service at the National Institute of Rehabilitation, Mexico City, said, “The study shows us there are no perfect predictors [of crossover] in these patients,” and careful evaluation is needed to discern which patients really need surgery and which will fare well with PT alone.
“It’s a hot topic right now in the world,” he commented. “We really don’t want to use surgery in all patients; we need to use it in a [restricted] number of patients.”
During a question and answer period, session attendee Ewa M. Roos, Ph.D., University of Southern Denmark in Odense, said, “You showed a lot of patient-related factors that could potentially explain crossover, but what is the role of the surgeon? … Is there a fact that if you can, you will cross over?”
“I agree with what I think is your implicit suggestion that there probably is a large role for the surgeon. We looked at heterogeneity in crossovers among surgeons in the trial, and there is some variability. There are probably cultural differences as well,” Dr. Katz replied. “I think … the question is, how fully are patients consented to not receiving surgery?”
Participants in MeTeOR were aged 45 years or older and had a meniscal tear on magnetic resonance imaging with degenerative cartilage changes and at least one meniscal symptom. They were randomized evenly to a standardized PT regimen emphasizing strength and range of motion, or to arthroscopic partial meniscectomy accompanied by standardized PT.
Overall, 27% of patients in the PT arm crossed over to surgery within about 5 months, Dr. Katz reported at the meeting sponsored by the Osteoarthritis Research Society International.
Multivariate analyses showed that patients initially assigned to PT were more likely to cross over to surgery if they had greater pain, scoring 40 or higher on the 100-point Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain scale (relative risk, 1.08); had experienced symptoms for less than a year (1.07); or had hamstring strength of less than 30 pounds (1.06).
However, the rate of treatment success, defined as an improvement of at least 10 points on the 100-point Knee Injury and Osteoarthritis Outcome Score (KOOS) at 6 months, was similarly high for the patients who were randomized to and received surgery (80%) and the patients who were randomized to PT but crossed over to surgery (81%).
The trial had several limitations, according to Dr. Katz. “From the standpoint of external validity, trial samples are not necessarily generalizable as we know. And with respect to internal validity, our comparison of immediate and delayed arthroscopic partial meniscectomy was post randomization, and the groups are not necessarily balanced,” he said.
Dr. Katz disclosed no relevant conflicts of interest.
AT OARSI 2015
Key clinical point: Clinical factors can help identify patients with knee meniscal tears and osteoarthritis who will eventually opt for arthroscopic partial meniscectomy.
Major finding: The risk of crossing over from PT to surgery was 6%-8% higher for patients who had greater pain, shorter symptom duration, or hamstring weakness.
Data source: An analysis of 351 patients with knee meniscal tears and osteoarthritis in a randomized trial of surgery vs. PT.
Disclosures: Dr. Katz disclosed no relevant conflicts of interest.

Ileal pouch re-dos successful in most patients
SAN DIEGO – Patients hoping to avoid a permanent stoma by having a salvage surgery to repair or replace a failing ileal pouch–anal anastomosis (IPAA) achieved good functional outcomes and quality of life in one institution’s long-term experience.
A large case series drawn from IPAA re-dos at the Cleveland Clinic over a 20-year span showed that the procedure was successful for four in five patients, and more than 90% were satisfied with their quality of life, despite some functional limitations. Dr. Feza Remzi, chairman of the department of colorectal surgery at the Cleveland Clinic, presented findings from 500 patients undergoing IPAA re-dos via the transabdominal approach. In this group, 80% (401) of transabdominally revised IPAAs were successful.

IPAA is a procedure indicated for patients with Crohn’s disease, ulcerative or indeterminate colitis, or familial adenomatous polyposis. The surgery preserves the capacity for anal defecation with intestinal continuity after proctocolectomy by fashioning a reservoir for stool from the small intestine. However, up to 15% of patients will have pouch failure, necessitating a permanent stoma unless the pouch is surgically revised, he said at the annual meeting of the American Surgical Association.
To determine outcomes for patients having a re-do of a failed IPAA, Dr. Remzi and colleagues assessed 502 IPAA re-do patients (215, male; median age, 38 years) who received their procedure at the Cleveland Clinic from 1983 to 2014. Crohn’s disease was the primary diagnosis for 419 patients (84%); just over half (n = 263) had anastomotic leak or fistula as the cause of first pouch failure, followed by pouch-vaginal fistula in 85 women (17%) and obstruction in 116 patients (23%).
The primary endpoints of the study were surgery morbidity, how many patients had a functioning pouch after re-do, pouch function, and quality of life.
Surgeon discretion dictated whether the pouch was revised, as it was in 295 patients (59%), or whether a new pouch was created. Overall, just over half of patients (n = 270) had postoperative complications, though there were no short-term deaths. Ileus and pelvic sepsis were the most common short-term complications, occurring in 81 (16%) and 50 (10%) patients, respectively. All of the other complications occurred in less than 10% of patients. Patients stayed in the hospital a median of 7 days, and 63 (13%) were readmitted.
Over the duration of the study, 101 patients (20%) had failure of their redone IPAA pouches, and pelvis sepsis and anastomotic stricture each occurred in more than 10% of patients. Short-term postoperative morbidity and occurrence of pelvic sepsis at any point after re-do surgery were associated with failure of the redone IPAA based on a Cox regression model (P = .035 and P < .0001, respectively).
Patients were overall very satisfied with their quality of life after IPAA re-do surgery; 92% of the 261 respondents said they would undergo the surgery again, and 93% would recommend the surgery. This was true although patients reported a mean of six daytime bowel movements, about half of patients reported having stool seepage or requiring pad use, and a third of patients reported dietary restrictions related to their bowel function.
Study limitations included the lack of information regarding patients in whom the re-do attempt was abandoned, or for those referred for surgery who did not have an IPAA re-do. Another limitation was the relatively low number of patients who completed all items on the function and quality of life questionnaires; investigators decided that the most robust analysis would flow from including only data for those who had completed all forms.
Discussion focused on the real-world and technical aspects of lessons learned from this large single-institution data set. Dr. David Rothenberger, Jay Phillips Professor and Chair of the department of surgery at the University of Minnesota, Minneapolis, asked whether patients had been carefully selected for this salvage procedure. In his experience, he said, obese patients or those with a heavily muscled pelvis, as well as those with a significant history of prior pelvic infections, would not necessarily be good candidates for a re-do. He suggested that an intention-to-treat analysis might give a truer denominator, and might even change the conclusion that the salvage surgery has a high likelihood of success. Dr. Remzi agreed that obesity or a high body mass index in a patient “is a very good reason not to do the surgery.”
Dr. Neil Hyman, codirector of the digestive diseases center at the University of Chicago Medicine, asked whether Dr. Remzi preferred to do an S pouch rather than a J pouch. In response, Dr. Remzi said, “We have to think about what the patient will give us. Throughout the years, I’ve learned that I like to divert the patient for 6 months before surgery. This gets them and their family engaged in the process. … It also elongates the mesentery to give you that reach. But I don’t necessarily do an intentional S pouch if the J pouch gives me what I need for the health of that patient.”
The authors reported no relevant financial disclosures.
SAN DIEGO – Patients hoping to avoid a permanent stoma by having a salvage surgery to repair or replace a failing ileal pouch–anal anastomosis (IPAA) achieved good functional outcomes and quality of life in one institution’s long-term experience.
A large case series drawn from IPAA re-dos at the Cleveland Clinic over a 20-year span showed that the procedure was successful for four in five patients, and more than 90% were satisfied with their quality of life, despite some functional limitations. Dr. Feza Remzi, chairman of the department of colorectal surgery at the Cleveland Clinic, presented findings from 500 patients undergoing IPAA re-dos via the transabdominal approach. In this group, 80% (401) of transabdominally revised IPAAs were successful.
IPAA is a procedure indicated for patients with Crohn’s disease, ulcerative or indeterminate colitis, or familial adenomatous polyposis. The surgery preserves the capacity for anal defecation with intestinal continuity after proctocolectomy by fashioning a reservoir for stool from the small intestine. However, up to 15% of patients will have pouch failure, necessitating a permanent stoma unless the pouch is surgically revised, he said at the annual meeting of the American Surgical Association.
To determine outcomes for patients having a re-do of a failed IPAA, Dr. Remzi and colleagues assessed 502 IPAA re-do patients (215, male; median age, 38 years) who received their procedure at the Cleveland Clinic from 1983 to 2014. Crohn’s disease was the primary diagnosis for 419 patients (84%); just over half (n = 263) had anastomotic leak or fistula as the cause of first pouch failure, followed by pouch-vaginal fistula in 85 women (17%) and obstruction in 116 patients (23%).
The primary endpoints of the study were surgery morbidity, how many patients had a functioning pouch after re-do, pouch function, and quality of life.
Surgeon discretion dictated whether the pouch was revised, as it was in 295 patients (59%), or whether a new pouch was created. Overall, just over half of patients (n = 270) had postoperative complications, though there were no short-term deaths. Ileus and pelvic sepsis were the most common short-term complications, occurring in 81 (16%) and 50 (10%) patients, respectively. All of the other complications occurred in less than 10% of patients. Patients stayed in the hospital a median of 7 days, and 63 (13%) were readmitted.
Over the duration of the study, 101 patients (20%) had failure of their redone IPAA pouches, and pelvis sepsis and anastomotic stricture each occurred in more than 10% of patients. Short-term postoperative morbidity and occurrence of pelvic sepsis at any point after re-do surgery were associated with failure of the redone IPAA based on a Cox regression model (P = .035 and P < .0001, respectively).
Patients were overall very satisfied with their quality of life after IPAA re-do surgery; 92% of the 261 respondents said they would undergo the surgery again, and 93% would recommend the surgery. This was true although patients reported a mean of six daytime bowel movements, about half of patients reported having stool seepage or requiring pad use, and a third of patients reported dietary restrictions related to their bowel function.
Study limitations included the lack of information regarding patients in whom the re-do attempt was abandoned, or for those referred for surgery who did not have an IPAA re-do. Another limitation was the relatively low number of patients who completed all items on the function and quality of life questionnaires; investigators decided that the most robust analysis would flow from including only data for those who had completed all forms.
Discussion focused on the real-world and technical aspects of lessons learned from this large single-institution data set. Dr. David Rothenberger, Jay Phillips Professor and Chair of the department of surgery at the University of Minnesota, Minneapolis, asked whether patients had been carefully selected for this salvage procedure. In his experience, he said, obese patients or those with a heavily muscled pelvis, as well as those with a significant history of prior pelvic infections, would not necessarily be good candidates for a re-do. He suggested that an intention-to-treat analysis might give a truer denominator, and might even change the conclusion that the salvage surgery has a high likelihood of success. Dr. Remzi agreed that obesity or a high body mass index in a patient “is a very good reason not to do the surgery.”
Dr. Neil Hyman, codirector of the digestive diseases center at the University of Chicago Medicine, asked whether Dr. Remzi preferred to do an S pouch rather than a J pouch. In response, Dr. Remzi said, “We have to think about what the patient will give us. Throughout the years, I’ve learned that I like to divert the patient for 6 months before surgery. This gets them and their family engaged in the process. … It also elongates the mesentery to give you that reach. But I don’t necessarily do an intentional S pouch if the J pouch gives me what I need for the health of that patient.”
The authors reported no relevant financial disclosures.
SAN DIEGO – Patients hoping to avoid a permanent stoma by having a salvage surgery to repair or replace a failing ileal pouch–anal anastomosis (IPAA) achieved good functional outcomes and quality of life in one institution’s long-term experience.
A large case series drawn from IPAA re-dos at the Cleveland Clinic over a 20-year span showed that the procedure was successful for four in five patients, and more than 90% were satisfied with their quality of life, despite some functional limitations. Dr. Feza Remzi, chairman of the department of colorectal surgery at the Cleveland Clinic, presented findings from 500 patients undergoing IPAA re-dos via the transabdominal approach. In this group, 80% (401) of transabdominally revised IPAAs were successful.
IPAA is a procedure indicated for patients with Crohn’s disease, ulcerative or indeterminate colitis, or familial adenomatous polyposis. The surgery preserves the capacity for anal defecation with intestinal continuity after proctocolectomy by fashioning a reservoir for stool from the small intestine. However, up to 15% of patients will have pouch failure, necessitating a permanent stoma unless the pouch is surgically revised, he said at the annual meeting of the American Surgical Association.
To determine outcomes for patients having a re-do of a failed IPAA, Dr. Remzi and colleagues assessed 502 IPAA re-do patients (215, male; median age, 38 years) who received their procedure at the Cleveland Clinic from 1983 to 2014. Crohn’s disease was the primary diagnosis for 419 patients (84%); just over half (n = 263) had anastomotic leak or fistula as the cause of first pouch failure, followed by pouch-vaginal fistula in 85 women (17%) and obstruction in 116 patients (23%).
The primary endpoints of the study were surgery morbidity, how many patients had a functioning pouch after re-do, pouch function, and quality of life.
Surgeon discretion dictated whether the pouch was revised, as it was in 295 patients (59%), or whether a new pouch was created. Overall, just over half of patients (n = 270) had postoperative complications, though there were no short-term deaths. Ileus and pelvic sepsis were the most common short-term complications, occurring in 81 (16%) and 50 (10%) patients, respectively. All of the other complications occurred in less than 10% of patients. Patients stayed in the hospital a median of 7 days, and 63 (13%) were readmitted.
Over the duration of the study, 101 patients (20%) had failure of their redone IPAA pouches, and pelvis sepsis and anastomotic stricture each occurred in more than 10% of patients. Short-term postoperative morbidity and occurrence of pelvic sepsis at any point after re-do surgery were associated with failure of the redone IPAA based on a Cox regression model (P = .035 and P < .0001, respectively).
Patients were overall very satisfied with their quality of life after IPAA re-do surgery; 92% of the 261 respondents said they would undergo the surgery again, and 93% would recommend the surgery. This was true although patients reported a mean of six daytime bowel movements, about half of patients reported having stool seepage or requiring pad use, and a third of patients reported dietary restrictions related to their bowel function.
Study limitations included the lack of information regarding patients in whom the re-do attempt was abandoned, or for those referred for surgery who did not have an IPAA re-do. Another limitation was the relatively low number of patients who completed all items on the function and quality of life questionnaires; investigators decided that the most robust analysis would flow from including only data for those who had completed all forms.
Discussion focused on the real-world and technical aspects of lessons learned from this large single-institution data set. Dr. David Rothenberger, Jay Phillips Professor and Chair of the department of surgery at the University of Minnesota, Minneapolis, asked whether patients had been carefully selected for this salvage procedure. In his experience, he said, obese patients or those with a heavily muscled pelvis, as well as those with a significant history of prior pelvic infections, would not necessarily be good candidates for a re-do. He suggested that an intention-to-treat analysis might give a truer denominator, and might even change the conclusion that the salvage surgery has a high likelihood of success. Dr. Remzi agreed that obesity or a high body mass index in a patient “is a very good reason not to do the surgery.”
Dr. Neil Hyman, codirector of the digestive diseases center at the University of Chicago Medicine, asked whether Dr. Remzi preferred to do an S pouch rather than a J pouch. In response, Dr. Remzi said, “We have to think about what the patient will give us. Throughout the years, I’ve learned that I like to divert the patient for 6 months before surgery. This gets them and their family engaged in the process. … It also elongates the mesentery to give you that reach. But I don’t necessarily do an intentional S pouch if the J pouch gives me what I need for the health of that patient.”
The authors reported no relevant financial disclosures.
AT THE ASA ANNUAL MEETING
Key clinical point: Eighty percent of transabdominal revisions of failed ileal pouch–anal anastomosis surgeries were successful; patients were overall content with the results.
Major findings: 80% (401) of transabdominally revised IPAAs were successful, and patients were overall satisfied with their quality of life, with 92% affirming that they would undergo the procedure again and 93% recommending the procedure to similarly situated patients.
Data source: A retrospective analysis of a prospectively enrolled single-center registry of patients having transabdominal re-do surgeries for failed ileal pouch–anal anastomosis between 1983 and 2014.
Disclosures: The authors reported no relevant financial disclosures.

FDA proposes 1-year blood donor deferral for gay and bisexual men
Men who have sex with men, and women who have sexual relations with them, will be permitted to donate blood if a year has elapsed between the last such sexual encounter and the time of donation, the Food and Drug Administration has recommended.
The agency’s draft guidance follows that of the federal Advisory Committee on Blood and Tissue Safety and Availability. In November 2014, the group voted 16-2 to support a 1-year deferral policy for these populations. Any deferral decision made at a donor site would be based on donor self-identification and self-report, the draft guidance noted. Clinicians should “use their own discretion” with regard to deferring a donation from a person who self-identifies as transgender.
The document would supplant prior guidance, issued in 1985, which recommended permanent deferral for men who have sex with men (MSM) and women who had sex with them.
Should it be adopted, the new policy “will better align the deferral period with that of other men and women at increased risk for HIV infection,” then FDA Commissioner Dr. Margaret A. Hamburg said in a press statement last December. Safety and blood surveillance measures already in place will be enough to detect any HIV-contaminated blood that might enter the donor pool, she said.
The national blood surveillance system will help the agency monitor the effect of any policy change and further ensure the continued safety of the blood supply. This, along with a donor education program, has reduced the risk of an HIV infection from donated blood to about 1/1.47 million transfusions, according to the draft document.
The proposal was based on the committee’s evidence review, during which data from a similar change in deferral status in Australia weighed in favor of the recommendations. During the 5 years before and after a change from lifetime deferral to the 1-year deferral for MSM, there was no change in the risk of HIV-contaminated blood entering the donor pool or the proportion of HIV-positive donors.
Despite being “a step in the right direction,” the proposed 1-year deferral still discriminates against MSM, according to David Stacy, government affairs director for the Human Rights Campaign, the nation’s largest lesbian, gay, bisexual, and transgender civil rights organization.
“This policy prevents men from donating life-saving blood based solely on their sexual orientation rather than actual risk to the blood supply,” he said in a press statement. “It simply cannot be justified in light of current scientific research and updated blood screening technology.”
The draft guidance is not binding. It will be published on the Federal Register, which at that time will announce the deadline for comment.
On Twitter @alz_gal
Men who have sex with men, and women who have sexual relations with them, will be permitted to donate blood if a year has elapsed between the last such sexual encounter and the time of donation, the Food and Drug Administration has recommended.
The agency’s draft guidance follows that of the federal Advisory Committee on Blood and Tissue Safety and Availability. In November 2014, the group voted 16-2 to support a 1-year deferral policy for these populations. Any deferral decision made at a donor site would be based on donor self-identification and self-report, the draft guidance noted. Clinicians should “use their own discretion” with regard to deferring a donation from a person who self-identifies as transgender.
The document would supplant prior guidance, issued in 1985, which recommended permanent deferral for men who have sex with men (MSM) and women who had sex with them.
Should it be adopted, the new policy “will better align the deferral period with that of other men and women at increased risk for HIV infection,” then FDA Commissioner Dr. Margaret A. Hamburg said in a press statement last December. Safety and blood surveillance measures already in place will be enough to detect any HIV-contaminated blood that might enter the donor pool, she said.
The national blood surveillance system will help the agency monitor the effect of any policy change and further ensure the continued safety of the blood supply. This, along with a donor education program, has reduced the risk of an HIV infection from donated blood to about 1/1.47 million transfusions, according to the draft document.
The proposal was based on the committee’s evidence review, during which data from a similar change in deferral status in Australia weighed in favor of the recommendations. During the 5 years before and after a change from lifetime deferral to the 1-year deferral for MSM, there was no change in the risk of HIV-contaminated blood entering the donor pool or the proportion of HIV-positive donors.
Despite being “a step in the right direction,” the proposed 1-year deferral still discriminates against MSM, according to David Stacy, government affairs director for the Human Rights Campaign, the nation’s largest lesbian, gay, bisexual, and transgender civil rights organization.
“This policy prevents men from donating life-saving blood based solely on their sexual orientation rather than actual risk to the blood supply,” he said in a press statement. “It simply cannot be justified in light of current scientific research and updated blood screening technology.”
The draft guidance is not binding. It will be published on the Federal Register, which at that time will announce the deadline for comment.
On Twitter @alz_gal
Men who have sex with men, and women who have sexual relations with them, will be permitted to donate blood if a year has elapsed between the last such sexual encounter and the time of donation, the Food and Drug Administration has recommended.
The agency’s draft guidance follows that of the federal Advisory Committee on Blood and Tissue Safety and Availability. In November 2014, the group voted 16-2 to support a 1-year deferral policy for these populations. Any deferral decision made at a donor site would be based on donor self-identification and self-report, the draft guidance noted. Clinicians should “use their own discretion” with regard to deferring a donation from a person who self-identifies as transgender.
The document would supplant prior guidance, issued in 1985, which recommended permanent deferral for men who have sex with men (MSM) and women who had sex with them.
Should it be adopted, the new policy “will better align the deferral period with that of other men and women at increased risk for HIV infection,” then FDA Commissioner Dr. Margaret A. Hamburg said in a press statement last December. Safety and blood surveillance measures already in place will be enough to detect any HIV-contaminated blood that might enter the donor pool, she said.
The national blood surveillance system will help the agency monitor the effect of any policy change and further ensure the continued safety of the blood supply. This, along with a donor education program, has reduced the risk of an HIV infection from donated blood to about 1/1.47 million transfusions, according to the draft document.
The proposal was based on the committee’s evidence review, during which data from a similar change in deferral status in Australia weighed in favor of the recommendations. During the 5 years before and after a change from lifetime deferral to the 1-year deferral for MSM, there was no change in the risk of HIV-contaminated blood entering the donor pool or the proportion of HIV-positive donors.
Despite being “a step in the right direction,” the proposed 1-year deferral still discriminates against MSM, according to David Stacy, government affairs director for the Human Rights Campaign, the nation’s largest lesbian, gay, bisexual, and transgender civil rights organization.
“This policy prevents men from donating life-saving blood based solely on their sexual orientation rather than actual risk to the blood supply,” he said in a press statement. “It simply cannot be justified in light of current scientific research and updated blood screening technology.”
The draft guidance is not binding. It will be published on the Federal Register, which at that time will announce the deadline for comment.
On Twitter @alz_gal