User login
Official Newspaper of the American College of Surgeons
VIDEO: Elective neck dissection during primary surgery improves oral cancer survival
CHICAGO – Patients who had elective neck dissection at the time of primary surgery for oral cancers had a 12.5% better overall survival rate than did patients who had therapeutic neck dissections at the time of recurrence.
The risk of death was reduced by 36% among patients randomized in a phase III trial to neck lymph node dissection at the time of primary surgery, and the risk of recurrences was reduced by 55%, reported Dr. Anil D’Cruz of the head and neck service of Tata Memorial Centre, Mumbai, India.
“Elective neck dissection should be the standard of care for early oral, node-negative squamous cell cancers, based on the findings of our study,” he said at the annual meeting of the American Society of Clinical Oncology.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – Patients who had elective neck dissection at the time of primary surgery for oral cancers had a 12.5% better overall survival rate than did patients who had therapeutic neck dissections at the time of recurrence.
The risk of death was reduced by 36% among patients randomized in a phase III trial to neck lymph node dissection at the time of primary surgery, and the risk of recurrences was reduced by 55%, reported Dr. Anil D’Cruz of the head and neck service of Tata Memorial Centre, Mumbai, India.
“Elective neck dissection should be the standard of care for early oral, node-negative squamous cell cancers, based on the findings of our study,” he said at the annual meeting of the American Society of Clinical Oncology.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – Patients who had elective neck dissection at the time of primary surgery for oral cancers had a 12.5% better overall survival rate than did patients who had therapeutic neck dissections at the time of recurrence.
The risk of death was reduced by 36% among patients randomized in a phase III trial to neck lymph node dissection at the time of primary surgery, and the risk of recurrences was reduced by 55%, reported Dr. Anil D’Cruz of the head and neck service of Tata Memorial Centre, Mumbai, India.
“Elective neck dissection should be the standard of care for early oral, node-negative squamous cell cancers, based on the findings of our study,” he said at the annual meeting of the American Society of Clinical Oncology.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE 2015 ASCO ANNUAL MEETING

GAO questions CMS reliance on RUC to set Medicare pay rates
A government watchdog report suggests that the Centers for Medicare & Medicaid Services may be setting Medicare payment rates inaccurately based on biased recommendations from its panel of physician experts.
The Government Accountability Office (GAO) questions the transparency of the CMS’ rate calculation process and suggests that members of the American Medical Association/Specialty Society Relative Value Scale Update Committee (RUC) have conflicts of interest that affect their ability to fairly value physician services, according to a report published May 21.

The GAO report recommends that the CMS better document its process for establishing relative values and develop a process to inform the public of potentially misvalued services identified by the RUC. The CMS also should develop a plan for using funds appropriated for the collection and use of information on physicians’ services in the determination of relative values, the report stated.
In response, the American Medical Association defended the expertise and objectivity of the RUC, stressing that there is no substitute for input from experienced physicians regarding the time and resources that go into medical services.
“The RUC’s valuable expertise is balanced with the oversight of government officials who have the final say,” an AMA spokesperson said in an interview. “When CMS’ initial efforts to identify potentially misvalued services were unable to obtain reliable data from government contractors, physicians on the RUC took on this important task. When gauging how much time and resources go into one medical service compared with another, no one knows more about what is involved in providing services to Medicare patients than the physicians who care for them.”
Dr. Robert L. Wergin, president of the American Academy of Family Physicians (AAFP) said the GAO report findings are consistent with previous concerns raised by the AAFP about the RUC.
“We have advocated for more transparency” in the past, Dr. Wergin said in an interview. “We have requested that the RUC expose the survey process, and we’ve also given input that we improve it [and] make it more accurate. Adding transparency to the process might be a way to improve it.”
In its review, the GAO – a nonpartisan investigational agency of Congress – cited several weaknesses in the data collected by the RUC, including that some RUC survey data had low response rates, a low total number of responses, and large ranges in responses.
For example, the GAO found that the median number of responses to surveys for payment year 2015 was 52 but the median response rate was only 2%, and that 23 of the 231 surveys had under 30 respondents.
The report also questions the transparency of the CMS process for establishing relative values. Although the CMS states that it complies with statutory requirements to review all Medicare services every 5 years, the agency does not maintain a database to track when a service was last valued or have a documented standardized process for prioritizing its reviews, according to the GAO report.
The CMS also does not publish the potentially misvalued services identified by the RUC, so stakeholders are unaware that these services will be reviewed and payment rates for these services may change.
The report found that the CMS provides some information about its process in its rule-making but does not document the methods used to review specific RUC recommendations. For example, the CMS does not document which resources were considered during its review of RUC recommendations for specific services. The GAO report said the CMS relies too heavily on RUC recommendations when establishing relative values.
“GAO found that, in the majority of cases, CMS accepts the RUC’s recommendations, and participation by other stakeholders is limited,” the report authors said. “Given the process- and data-related weaknesses associated with the RUC’s recommendations, such heavy reliance on the RUC could result in inaccurate Medicare payment rates.”
The AMA argued that the GAO report should have better acknowledged the difficulty in obtaining data on services that are infrequently performed. For example, 80% of services paid with work valuation on the Medicare physician payment schedule have fewer than 10,000 Medicare claims per year, the association noted.
“A service performed 10,000 times per year, is done, on average, less than once per day in any state,” the AMA spokesperson said. “It would be nearly impossible to do accurate direct observation or time/motion studies to collect time data on these low volume services. The survey methodology, followed by rigorous cross-specialty RUC review, is the best way to accomplish this data collection.”
The current GAO report is far from the first to criticize the RUC. The AAFP has long argued that the RUC should include more family physicians, health plans, consumers, employers, and health care economists on its panel. In 2012, the committee added another seat for geriatric medicine and another rotating primary care seat.
In an interview, Dr. Wergin said these additions helped, but that the AAFP would like to see at least one more primary care slot, as well as slots for other stakeholders. In a January 2014 letter, the AAFP called on the CMS to correct what the AAFP referred to as “a disturbing trend seen in the recommendations of RUC.” Specifically, the AAFP urged the CMS to address undervalued services, such as office-based evaluation and management (E/M) codes.
The Medicare Payment Advisory Commission (MedPAC), an independent advisory commission to Congress, has also issued several reports questioning the effectiveness of the RUC, including a 2011 white paper that expressed skepticism about the way in which data is collected by the panel. In 2013, MedPAC executive director Mark E. Miller, in testimony before the Senate Finance Committee, criticized how the RUC operated.
In the last Congress, Rep. Jim McDermott (D-Wash.), ranking member of the Ways and Means Committee’s Subcommittee on Health, introduced the Accuracy in Medicare Physician Payment Act of 2013, which would supplement the work of RUC by establishing an expert panel within Medicare to oversee the valuation of physician services and to help correct distortions in the physician fee schedule. The bill was not considered by the House.
On Twitter @legal_med
A government watchdog report suggests that the Centers for Medicare & Medicaid Services may be setting Medicare payment rates inaccurately based on biased recommendations from its panel of physician experts.
The Government Accountability Office (GAO) questions the transparency of the CMS’ rate calculation process and suggests that members of the American Medical Association/Specialty Society Relative Value Scale Update Committee (RUC) have conflicts of interest that affect their ability to fairly value physician services, according to a report published May 21.
The GAO report recommends that the CMS better document its process for establishing relative values and develop a process to inform the public of potentially misvalued services identified by the RUC. The CMS also should develop a plan for using funds appropriated for the collection and use of information on physicians’ services in the determination of relative values, the report stated.
In response, the American Medical Association defended the expertise and objectivity of the RUC, stressing that there is no substitute for input from experienced physicians regarding the time and resources that go into medical services.
“The RUC’s valuable expertise is balanced with the oversight of government officials who have the final say,” an AMA spokesperson said in an interview. “When CMS’ initial efforts to identify potentially misvalued services were unable to obtain reliable data from government contractors, physicians on the RUC took on this important task. When gauging how much time and resources go into one medical service compared with another, no one knows more about what is involved in providing services to Medicare patients than the physicians who care for them.”
Dr. Robert L. Wergin, president of the American Academy of Family Physicians (AAFP) said the GAO report findings are consistent with previous concerns raised by the AAFP about the RUC.
“We have advocated for more transparency” in the past, Dr. Wergin said in an interview. “We have requested that the RUC expose the survey process, and we’ve also given input that we improve it [and] make it more accurate. Adding transparency to the process might be a way to improve it.”
In its review, the GAO – a nonpartisan investigational agency of Congress – cited several weaknesses in the data collected by the RUC, including that some RUC survey data had low response rates, a low total number of responses, and large ranges in responses.
For example, the GAO found that the median number of responses to surveys for payment year 2015 was 52 but the median response rate was only 2%, and that 23 of the 231 surveys had under 30 respondents.
The report also questions the transparency of the CMS process for establishing relative values. Although the CMS states that it complies with statutory requirements to review all Medicare services every 5 years, the agency does not maintain a database to track when a service was last valued or have a documented standardized process for prioritizing its reviews, according to the GAO report.
The CMS also does not publish the potentially misvalued services identified by the RUC, so stakeholders are unaware that these services will be reviewed and payment rates for these services may change.
The report found that the CMS provides some information about its process in its rule-making but does not document the methods used to review specific RUC recommendations. For example, the CMS does not document which resources were considered during its review of RUC recommendations for specific services. The GAO report said the CMS relies too heavily on RUC recommendations when establishing relative values.
“GAO found that, in the majority of cases, CMS accepts the RUC’s recommendations, and participation by other stakeholders is limited,” the report authors said. “Given the process- and data-related weaknesses associated with the RUC’s recommendations, such heavy reliance on the RUC could result in inaccurate Medicare payment rates.”
The AMA argued that the GAO report should have better acknowledged the difficulty in obtaining data on services that are infrequently performed. For example, 80% of services paid with work valuation on the Medicare physician payment schedule have fewer than 10,000 Medicare claims per year, the association noted.
“A service performed 10,000 times per year, is done, on average, less than once per day in any state,” the AMA spokesperson said. “It would be nearly impossible to do accurate direct observation or time/motion studies to collect time data on these low volume services. The survey methodology, followed by rigorous cross-specialty RUC review, is the best way to accomplish this data collection.”
The current GAO report is far from the first to criticize the RUC. The AAFP has long argued that the RUC should include more family physicians, health plans, consumers, employers, and health care economists on its panel. In 2012, the committee added another seat for geriatric medicine and another rotating primary care seat.
In an interview, Dr. Wergin said these additions helped, but that the AAFP would like to see at least one more primary care slot, as well as slots for other stakeholders. In a January 2014 letter, the AAFP called on the CMS to correct what the AAFP referred to as “a disturbing trend seen in the recommendations of RUC.” Specifically, the AAFP urged the CMS to address undervalued services, such as office-based evaluation and management (E/M) codes.
The Medicare Payment Advisory Commission (MedPAC), an independent advisory commission to Congress, has also issued several reports questioning the effectiveness of the RUC, including a 2011 white paper that expressed skepticism about the way in which data is collected by the panel. In 2013, MedPAC executive director Mark E. Miller, in testimony before the Senate Finance Committee, criticized how the RUC operated.
In the last Congress, Rep. Jim McDermott (D-Wash.), ranking member of the Ways and Means Committee’s Subcommittee on Health, introduced the Accuracy in Medicare Physician Payment Act of 2013, which would supplement the work of RUC by establishing an expert panel within Medicare to oversee the valuation of physician services and to help correct distortions in the physician fee schedule. The bill was not considered by the House.
On Twitter @legal_med
A government watchdog report suggests that the Centers for Medicare & Medicaid Services may be setting Medicare payment rates inaccurately based on biased recommendations from its panel of physician experts.
The Government Accountability Office (GAO) questions the transparency of the CMS’ rate calculation process and suggests that members of the American Medical Association/Specialty Society Relative Value Scale Update Committee (RUC) have conflicts of interest that affect their ability to fairly value physician services, according to a report published May 21.
The GAO report recommends that the CMS better document its process for establishing relative values and develop a process to inform the public of potentially misvalued services identified by the RUC. The CMS also should develop a plan for using funds appropriated for the collection and use of information on physicians’ services in the determination of relative values, the report stated.
In response, the American Medical Association defended the expertise and objectivity of the RUC, stressing that there is no substitute for input from experienced physicians regarding the time and resources that go into medical services.
“The RUC’s valuable expertise is balanced with the oversight of government officials who have the final say,” an AMA spokesperson said in an interview. “When CMS’ initial efforts to identify potentially misvalued services were unable to obtain reliable data from government contractors, physicians on the RUC took on this important task. When gauging how much time and resources go into one medical service compared with another, no one knows more about what is involved in providing services to Medicare patients than the physicians who care for them.”
Dr. Robert L. Wergin, president of the American Academy of Family Physicians (AAFP) said the GAO report findings are consistent with previous concerns raised by the AAFP about the RUC.
“We have advocated for more transparency” in the past, Dr. Wergin said in an interview. “We have requested that the RUC expose the survey process, and we’ve also given input that we improve it [and] make it more accurate. Adding transparency to the process might be a way to improve it.”
In its review, the GAO – a nonpartisan investigational agency of Congress – cited several weaknesses in the data collected by the RUC, including that some RUC survey data had low response rates, a low total number of responses, and large ranges in responses.
For example, the GAO found that the median number of responses to surveys for payment year 2015 was 52 but the median response rate was only 2%, and that 23 of the 231 surveys had under 30 respondents.
The report also questions the transparency of the CMS process for establishing relative values. Although the CMS states that it complies with statutory requirements to review all Medicare services every 5 years, the agency does not maintain a database to track when a service was last valued or have a documented standardized process for prioritizing its reviews, according to the GAO report.
The CMS also does not publish the potentially misvalued services identified by the RUC, so stakeholders are unaware that these services will be reviewed and payment rates for these services may change.
The report found that the CMS provides some information about its process in its rule-making but does not document the methods used to review specific RUC recommendations. For example, the CMS does not document which resources were considered during its review of RUC recommendations for specific services. The GAO report said the CMS relies too heavily on RUC recommendations when establishing relative values.
“GAO found that, in the majority of cases, CMS accepts the RUC’s recommendations, and participation by other stakeholders is limited,” the report authors said. “Given the process- and data-related weaknesses associated with the RUC’s recommendations, such heavy reliance on the RUC could result in inaccurate Medicare payment rates.”
The AMA argued that the GAO report should have better acknowledged the difficulty in obtaining data on services that are infrequently performed. For example, 80% of services paid with work valuation on the Medicare physician payment schedule have fewer than 10,000 Medicare claims per year, the association noted.
“A service performed 10,000 times per year, is done, on average, less than once per day in any state,” the AMA spokesperson said. “It would be nearly impossible to do accurate direct observation or time/motion studies to collect time data on these low volume services. The survey methodology, followed by rigorous cross-specialty RUC review, is the best way to accomplish this data collection.”
The current GAO report is far from the first to criticize the RUC. The AAFP has long argued that the RUC should include more family physicians, health plans, consumers, employers, and health care economists on its panel. In 2012, the committee added another seat for geriatric medicine and another rotating primary care seat.
In an interview, Dr. Wergin said these additions helped, but that the AAFP would like to see at least one more primary care slot, as well as slots for other stakeholders. In a January 2014 letter, the AAFP called on the CMS to correct what the AAFP referred to as “a disturbing trend seen in the recommendations of RUC.” Specifically, the AAFP urged the CMS to address undervalued services, such as office-based evaluation and management (E/M) codes.
The Medicare Payment Advisory Commission (MedPAC), an independent advisory commission to Congress, has also issued several reports questioning the effectiveness of the RUC, including a 2011 white paper that expressed skepticism about the way in which data is collected by the panel. In 2013, MedPAC executive director Mark E. Miller, in testimony before the Senate Finance Committee, criticized how the RUC operated.
In the last Congress, Rep. Jim McDermott (D-Wash.), ranking member of the Ways and Means Committee’s Subcommittee on Health, introduced the Accuracy in Medicare Physician Payment Act of 2013, which would supplement the work of RUC by establishing an expert panel within Medicare to oversee the valuation of physician services and to help correct distortions in the physician fee schedule. The bill was not considered by the House.
On Twitter @legal_med

AATS: Spare the aortic valve when possible during aortic root replacements
SEATTLE – Aortic valve–sparing procedures have better outcomes than Bentall procedures with biologic or mechanical valves, according to a review of 1,187 aortic root cases at the University of Toronto.
“If the aortic valve can be spared, AVS [aortic valve–sparing] procedures should be considered for patients undergoing aortic root replacement,” concluded the investigators, led by Dr. Maral Ouzounian, a cardiovascular surgeon at the university.

The team reviewed surgical outcomes there from 1990 to 2010; 282 patients had AVS procedures, 562 had Bentall procedures with biologic valve replacements (b-Bentall); and 343 had Bentalls with mechanical valve replacements (m-Bentall). About 7.5% of AVS patients had bicuspid aortic valves, versus 67.6% in the b-Bentall group and 51.7% in the m-Bentall group.
To control for confounders, patients were matched into 185 triads based on age, year of surgery, and stage of heart failure. The surgeries were all elective; patients with endocarditis or aortic dissections were excluded from the analysis.
Early postoperative outcomes and overall long-term survival were similar between the groups, with about 80% of patients in all three alive at 15-year follow-up.
However, AVS procedures had better long-term freedom from cardiac death (95% at 15 years versus 93% in the b-Bentall and 90% in the m-Bentall groups). Also, AVS patients had lower rates of anticoagulant-related hemorrhages, compared with m-Bentall patients (3.2% versus 17.8%), and lower rates of structural valve deterioration (0% versus 6.5%) and reoperations (6.5% versus 13.5%) than b-Bentall patients. The differences were statistically significant.
About 5% of AVS patients had previous cardiac surgery, versus 12.4% in the b-Bentall and 36.2% in the m-Bentall groups. AVS patients were more likely to have Marfan syndrome, and about 8% of AVS patients had preoperative ejection fractions below 40%, versus 9.3% in the b-Bentall and 13% in the m-Bentall groups. There were no between-group differences in the rates of concomitant coronary bypass or mitral valve surgery. Patients were about 50 years old on average, and about 80% were men.
“In Toronto, we are quite aggressive with valve-sparing operations. We believe in this operation, so whenever we can spare the valve, we do.” Although valve-sparing procedures have become more common in large, high-volume surgery centers over the past 20 years, “community surgeons in small-volume centers are still much more likely to do a Bentall because of the complexity of AVS operations and the art it takes to get it right,” Dr. Ouzounian said at the annual meeting of the American Association for Thoracic Surgery.
Previous investigations have found benefits for AVS procedures, as well. One concluded that “there is no significant difference in terms of re-operation between patients, who presented with [bicuspid or tricuspid aortic valves]. Re-operation rates are higher for patients who presented with severe [aortic regurgitation], but these rates do not reach statistical significance. Hence, root replacement with aortic valve sparing should be offered even in the presence of a” bicuspid aortic valve or severe aortic regurgitation (Eur. J. Cardiothorac. Surg. 2010;38:515-22).
Dr. Ouzounian said she has no disclosures.
SEATTLE – Aortic valve–sparing procedures have better outcomes than Bentall procedures with biologic or mechanical valves, according to a review of 1,187 aortic root cases at the University of Toronto.
“If the aortic valve can be spared, AVS [aortic valve–sparing] procedures should be considered for patients undergoing aortic root replacement,” concluded the investigators, led by Dr. Maral Ouzounian, a cardiovascular surgeon at the university.
The team reviewed surgical outcomes there from 1990 to 2010; 282 patients had AVS procedures, 562 had Bentall procedures with biologic valve replacements (b-Bentall); and 343 had Bentalls with mechanical valve replacements (m-Bentall). About 7.5% of AVS patients had bicuspid aortic valves, versus 67.6% in the b-Bentall group and 51.7% in the m-Bentall group.
To control for confounders, patients were matched into 185 triads based on age, year of surgery, and stage of heart failure. The surgeries were all elective; patients with endocarditis or aortic dissections were excluded from the analysis.
Early postoperative outcomes and overall long-term survival were similar between the groups, with about 80% of patients in all three alive at 15-year follow-up.
However, AVS procedures had better long-term freedom from cardiac death (95% at 15 years versus 93% in the b-Bentall and 90% in the m-Bentall groups). Also, AVS patients had lower rates of anticoagulant-related hemorrhages, compared with m-Bentall patients (3.2% versus 17.8%), and lower rates of structural valve deterioration (0% versus 6.5%) and reoperations (6.5% versus 13.5%) than b-Bentall patients. The differences were statistically significant.
About 5% of AVS patients had previous cardiac surgery, versus 12.4% in the b-Bentall and 36.2% in the m-Bentall groups. AVS patients were more likely to have Marfan syndrome, and about 8% of AVS patients had preoperative ejection fractions below 40%, versus 9.3% in the b-Bentall and 13% in the m-Bentall groups. There were no between-group differences in the rates of concomitant coronary bypass or mitral valve surgery. Patients were about 50 years old on average, and about 80% were men.
“In Toronto, we are quite aggressive with valve-sparing operations. We believe in this operation, so whenever we can spare the valve, we do.” Although valve-sparing procedures have become more common in large, high-volume surgery centers over the past 20 years, “community surgeons in small-volume centers are still much more likely to do a Bentall because of the complexity of AVS operations and the art it takes to get it right,” Dr. Ouzounian said at the annual meeting of the American Association for Thoracic Surgery.
Previous investigations have found benefits for AVS procedures, as well. One concluded that “there is no significant difference in terms of re-operation between patients, who presented with [bicuspid or tricuspid aortic valves]. Re-operation rates are higher for patients who presented with severe [aortic regurgitation], but these rates do not reach statistical significance. Hence, root replacement with aortic valve sparing should be offered even in the presence of a” bicuspid aortic valve or severe aortic regurgitation (Eur. J. Cardiothorac. Surg. 2010;38:515-22).
Dr. Ouzounian said she has no disclosures.
SEATTLE – Aortic valve–sparing procedures have better outcomes than Bentall procedures with biologic or mechanical valves, according to a review of 1,187 aortic root cases at the University of Toronto.
“If the aortic valve can be spared, AVS [aortic valve–sparing] procedures should be considered for patients undergoing aortic root replacement,” concluded the investigators, led by Dr. Maral Ouzounian, a cardiovascular surgeon at the university.
The team reviewed surgical outcomes there from 1990 to 2010; 282 patients had AVS procedures, 562 had Bentall procedures with biologic valve replacements (b-Bentall); and 343 had Bentalls with mechanical valve replacements (m-Bentall). About 7.5% of AVS patients had bicuspid aortic valves, versus 67.6% in the b-Bentall group and 51.7% in the m-Bentall group.
To control for confounders, patients were matched into 185 triads based on age, year of surgery, and stage of heart failure. The surgeries were all elective; patients with endocarditis or aortic dissections were excluded from the analysis.
Early postoperative outcomes and overall long-term survival were similar between the groups, with about 80% of patients in all three alive at 15-year follow-up.
However, AVS procedures had better long-term freedom from cardiac death (95% at 15 years versus 93% in the b-Bentall and 90% in the m-Bentall groups). Also, AVS patients had lower rates of anticoagulant-related hemorrhages, compared with m-Bentall patients (3.2% versus 17.8%), and lower rates of structural valve deterioration (0% versus 6.5%) and reoperations (6.5% versus 13.5%) than b-Bentall patients. The differences were statistically significant.
About 5% of AVS patients had previous cardiac surgery, versus 12.4% in the b-Bentall and 36.2% in the m-Bentall groups. AVS patients were more likely to have Marfan syndrome, and about 8% of AVS patients had preoperative ejection fractions below 40%, versus 9.3% in the b-Bentall and 13% in the m-Bentall groups. There were no between-group differences in the rates of concomitant coronary bypass or mitral valve surgery. Patients were about 50 years old on average, and about 80% were men.
“In Toronto, we are quite aggressive with valve-sparing operations. We believe in this operation, so whenever we can spare the valve, we do.” Although valve-sparing procedures have become more common in large, high-volume surgery centers over the past 20 years, “community surgeons in small-volume centers are still much more likely to do a Bentall because of the complexity of AVS operations and the art it takes to get it right,” Dr. Ouzounian said at the annual meeting of the American Association for Thoracic Surgery.
Previous investigations have found benefits for AVS procedures, as well. One concluded that “there is no significant difference in terms of re-operation between patients, who presented with [bicuspid or tricuspid aortic valves]. Re-operation rates are higher for patients who presented with severe [aortic regurgitation], but these rates do not reach statistical significance. Hence, root replacement with aortic valve sparing should be offered even in the presence of a” bicuspid aortic valve or severe aortic regurgitation (Eur. J. Cardiothorac. Surg. 2010;38:515-22).
Dr. Ouzounian said she has no disclosures.
AT THE AATS ANNUAL MEETING
Key clinical point: Your patients will do better with aortic valve–sparing procedures.
Major finding: Aortic valve–sparing procedures are associated with improved long-term freedom from cardiac death (95% at 15 years) when compared with Bentall procedures with biologic valves (93% freedom from cardiac death at 15 years) or mechanical valves (90% freedom at 15 years).
Data source: Review of 1,187 aortic root replacements at the University of Toronto.
Disclosures: The lead investigator has no disclosures.

AATS: No postpneumonectomy survival benefit in adding radiation to chemotherapy for NSCLC
SEATTLE – Adding radiotherapy to neoadjuvant chemotherapy does not improve long-term survival after pneumonectomy for non–small cell lung cancer, according to a Turkish investigation of 140 patients.
In the study, 100 (71.4%) patients had two to six cycles of platinum-based chemotherapy at least 3 weeks before surgery; 40 (28.6%) others underwent the same regimen with the addition of radiotherapy dosed at 45-66 Gy 6-8 weeks before surgery.

Five-year survival was 48% in the chemotherapy group and 50% in the chemoradiation group, an insignificant difference (P = .7).
“Chemotherapy before surgery is definitely beneficial, but I think we will get rid of the radiotherapy” in patients with operable tumors, said lead investigator Dr. Cengiz Gebitekin, professor and head of thoracic surgery at Uludag University in Bursa, Turkey.
“It does not provide any survival benefit,” and it might cause harm, he noted, adding that “the benefit of neoadjuvant treatment comes from the chemotherapy.”
The chemoradiation group showed a tendency toward tumor down-staging and higher complete response rates, but also a trend toward more radiation-induced tissue damage. The rate of bronchopleural fistula was 3% in the chemotherapy group and 5% in the chemoradiation group, although the difference was not significant. Even so, “some of these patients had pneumonectomies because of lung damage from the radiotherapy,” Dr. Gebitekin said at the annual meeting of the American Association for Thoracic Surgery.
It’s uncertain why radiation didn’t improve survival. The investigators excluded patients with known metastases or other malignancies, but it’s possible that some patients had occult metastases that had spread beyond the field of their localized neoadjuvant radiation, he said.
The patients were treated between 2000 and 2013 at Uludag University, Istanbul University, and Zurich University Hospital. They were 55 years old on average, and 84% were men.
About 40% of patients in both the chemotherapy and chemoradiation groups had right pneumonectomies; the rest had left pneumonectomies. Bronchopleural fistulas and other comorbidities were more common after right pneumonectomies, but not significantly so.
Seven patients (5%) in the chemotherapy group but none in the chemoradiation group died within 90 days of surgery.
About 32% of chemotherapy patients and 28% of chemoradiation patients (P = .6) developed major morbidities following surgery, including arrhythmias, pneumonia, empyema, and other problems.
Staples were used to close the bronchus in almost all patients, with the stump covered with live tissue in about 70%.
The majority of patients had stage IIb or IIIa disease on postop staging; postop staging was the only factor predictive of long-term survival, with higher-stage patients doing worse.
Dr. Gebitekin said that he had no relevant disclosures.
SEATTLE – Adding radiotherapy to neoadjuvant chemotherapy does not improve long-term survival after pneumonectomy for non–small cell lung cancer, according to a Turkish investigation of 140 patients.
In the study, 100 (71.4%) patients had two to six cycles of platinum-based chemotherapy at least 3 weeks before surgery; 40 (28.6%) others underwent the same regimen with the addition of radiotherapy dosed at 45-66 Gy 6-8 weeks before surgery.
Five-year survival was 48% in the chemotherapy group and 50% in the chemoradiation group, an insignificant difference (P = .7).
“Chemotherapy before surgery is definitely beneficial, but I think we will get rid of the radiotherapy” in patients with operable tumors, said lead investigator Dr. Cengiz Gebitekin, professor and head of thoracic surgery at Uludag University in Bursa, Turkey.
“It does not provide any survival benefit,” and it might cause harm, he noted, adding that “the benefit of neoadjuvant treatment comes from the chemotherapy.”
The chemoradiation group showed a tendency toward tumor down-staging and higher complete response rates, but also a trend toward more radiation-induced tissue damage. The rate of bronchopleural fistula was 3% in the chemotherapy group and 5% in the chemoradiation group, although the difference was not significant. Even so, “some of these patients had pneumonectomies because of lung damage from the radiotherapy,” Dr. Gebitekin said at the annual meeting of the American Association for Thoracic Surgery.
It’s uncertain why radiation didn’t improve survival. The investigators excluded patients with known metastases or other malignancies, but it’s possible that some patients had occult metastases that had spread beyond the field of their localized neoadjuvant radiation, he said.
The patients were treated between 2000 and 2013 at Uludag University, Istanbul University, and Zurich University Hospital. They were 55 years old on average, and 84% were men.
About 40% of patients in both the chemotherapy and chemoradiation groups had right pneumonectomies; the rest had left pneumonectomies. Bronchopleural fistulas and other comorbidities were more common after right pneumonectomies, but not significantly so.
Seven patients (5%) in the chemotherapy group but none in the chemoradiation group died within 90 days of surgery.
About 32% of chemotherapy patients and 28% of chemoradiation patients (P = .6) developed major morbidities following surgery, including arrhythmias, pneumonia, empyema, and other problems.
Staples were used to close the bronchus in almost all patients, with the stump covered with live tissue in about 70%.
The majority of patients had stage IIb or IIIa disease on postop staging; postop staging was the only factor predictive of long-term survival, with higher-stage patients doing worse.
Dr. Gebitekin said that he had no relevant disclosures.
SEATTLE – Adding radiotherapy to neoadjuvant chemotherapy does not improve long-term survival after pneumonectomy for non–small cell lung cancer, according to a Turkish investigation of 140 patients.
In the study, 100 (71.4%) patients had two to six cycles of platinum-based chemotherapy at least 3 weeks before surgery; 40 (28.6%) others underwent the same regimen with the addition of radiotherapy dosed at 45-66 Gy 6-8 weeks before surgery.
Five-year survival was 48% in the chemotherapy group and 50% in the chemoradiation group, an insignificant difference (P = .7).
“Chemotherapy before surgery is definitely beneficial, but I think we will get rid of the radiotherapy” in patients with operable tumors, said lead investigator Dr. Cengiz Gebitekin, professor and head of thoracic surgery at Uludag University in Bursa, Turkey.
“It does not provide any survival benefit,” and it might cause harm, he noted, adding that “the benefit of neoadjuvant treatment comes from the chemotherapy.”
The chemoradiation group showed a tendency toward tumor down-staging and higher complete response rates, but also a trend toward more radiation-induced tissue damage. The rate of bronchopleural fistula was 3% in the chemotherapy group and 5% in the chemoradiation group, although the difference was not significant. Even so, “some of these patients had pneumonectomies because of lung damage from the radiotherapy,” Dr. Gebitekin said at the annual meeting of the American Association for Thoracic Surgery.
It’s uncertain why radiation didn’t improve survival. The investigators excluded patients with known metastases or other malignancies, but it’s possible that some patients had occult metastases that had spread beyond the field of their localized neoadjuvant radiation, he said.
The patients were treated between 2000 and 2013 at Uludag University, Istanbul University, and Zurich University Hospital. They were 55 years old on average, and 84% were men.
About 40% of patients in both the chemotherapy and chemoradiation groups had right pneumonectomies; the rest had left pneumonectomies. Bronchopleural fistulas and other comorbidities were more common after right pneumonectomies, but not significantly so.
Seven patients (5%) in the chemotherapy group but none in the chemoradiation group died within 90 days of surgery.
About 32% of chemotherapy patients and 28% of chemoradiation patients (P = .6) developed major morbidities following surgery, including arrhythmias, pneumonia, empyema, and other problems.
Staples were used to close the bronchus in almost all patients, with the stump covered with live tissue in about 70%.
The majority of patients had stage IIb or IIIa disease on postop staging; postop staging was the only factor predictive of long-term survival, with higher-stage patients doing worse.
Dr. Gebitekin said that he had no relevant disclosures.
AT THE AATS ANNUAL MEETING
Key clinical point: Limit neoadjuvant treatment to chemotherapy for non–small cell lung cancer patients.
Major finding: About half of patients were alive 5 years after pneumonectomies for lung cancer, whether they had neoadjuvant chemotherapy or chemoradiation.
Data source: Retrospective study of 140 pneumonectomy patients.
Disclosures: Dr. Gebitekin had no disclosures.

AATS: Avoid mass ligation of the thoracic duct during esophagectomy
SEATTLE – Thoracic duct ligation did not seem to prevent chylothorax in a review of 827 esophagectomy cases at Brigham and Women’s Hospital in Boston.
In fact, chylothorax was most likely in patients who had mass ligation of the duct and its surrounding soft tissue, instead of ligation of simply the duct itself.
The results are surprising because ligation is actually meant to prevent chylothorax, but “it didn’t serve that purpose,” said lead investigator Dr. Yifan Zheng, a clinical research fellow at the hospital.
Results have been mixed in previous studies of ligation, with some finding benefit for preventing chylothorax but others not. With contradictory evidence, some surgeons – including some in the Brigham and Women’s review, which covered 11 years of data – opt for routine ligation, while others don’t, Dr. Zheng said at the annual meeting of the American Association for Thoracic Surgery.
At this point, “if you see the thoracic duct and you have concerns about ductal injury, your best bet is to ligate the duct directly. We observed in our series that there is a significantly higher incidence of chylothorax” with mass ligation, she said.
Of the 827 esophagectomies, 635 were performed without thoracic duct ligation; 33 (5.2%) cases developed postop chylothorax. Among the 56 cases with explicit identification and ligation of the thoracic duct alone, chylothorax developed in four (7.1%). There were 136 esophagectomies with mass ligation; 27 (19.9%) developed chylothorax (P = .0314).
The majority of the ligations were performed during open procedures. Mass ligations were mostly done with surgical sutures, while clips were used for direct ductal ligations. It’s likely that surgeons opted for direct ligation when they could see the duct and mass ligation when they could not.
Esophagectomy patients in the study were largely the same, so it’s unclear why some were ligated but others were not. About 75% in both groups had adenocarcinomas, most of which were in the distal esophagus or gastroesophageal junction. About half of the ligated group had preop chemoradiation, versus about 60% in the nonligated group.
Patients who developed postop chyle leaks were also similar, whether or not they were ligated. Most had adenocarcinomas in the distal esophagus or gastroesophageal junction, and the majority had received neoadjuvant therapy. “It’s unlikely that operative approach influenced the development of chylothorax,” Dr. Zheng said.
Both ligated and nonligated patients responded well to chylothorax management. Of the 64 total cases, 28 were successfully treated by thoracic duct embolization and 20 were successfully treated by operative thoracic duct ligation. In 10 cases, thoracic duct embolization was attempted but unsuccessful and all were successfully treated with operative ligation. Six cases were managed with chest tube drainage and total parenteral nutrition. It is possible that patients were ligated because they appeared during surgery to be at risk for postop chylothorax, which would help explain the findings.
It also is possible, however, that ligation itself – especially mass ligation – increases the risk. “The thoracic duct is a high-pressure system, so [blocking it] could create a pressure buildup and a potential leak,” Dr. Zheng said. That might be especially true with mass ligation, when both the thoracic duct and its tributaries are tied off.
Dr. Zheng said that she had no relevant disclosures.
SEATTLE – Thoracic duct ligation did not seem to prevent chylothorax in a review of 827 esophagectomy cases at Brigham and Women’s Hospital in Boston.
In fact, chylothorax was most likely in patients who had mass ligation of the duct and its surrounding soft tissue, instead of ligation of simply the duct itself.
The results are surprising because ligation is actually meant to prevent chylothorax, but “it didn’t serve that purpose,” said lead investigator Dr. Yifan Zheng, a clinical research fellow at the hospital.
Results have been mixed in previous studies of ligation, with some finding benefit for preventing chylothorax but others not. With contradictory evidence, some surgeons – including some in the Brigham and Women’s review, which covered 11 years of data – opt for routine ligation, while others don’t, Dr. Zheng said at the annual meeting of the American Association for Thoracic Surgery.
At this point, “if you see the thoracic duct and you have concerns about ductal injury, your best bet is to ligate the duct directly. We observed in our series that there is a significantly higher incidence of chylothorax” with mass ligation, she said.
Of the 827 esophagectomies, 635 were performed without thoracic duct ligation; 33 (5.2%) cases developed postop chylothorax. Among the 56 cases with explicit identification and ligation of the thoracic duct alone, chylothorax developed in four (7.1%). There were 136 esophagectomies with mass ligation; 27 (19.9%) developed chylothorax (P = .0314).
The majority of the ligations were performed during open procedures. Mass ligations were mostly done with surgical sutures, while clips were used for direct ductal ligations. It’s likely that surgeons opted for direct ligation when they could see the duct and mass ligation when they could not.
Esophagectomy patients in the study were largely the same, so it’s unclear why some were ligated but others were not. About 75% in both groups had adenocarcinomas, most of which were in the distal esophagus or gastroesophageal junction. About half of the ligated group had preop chemoradiation, versus about 60% in the nonligated group.
Patients who developed postop chyle leaks were also similar, whether or not they were ligated. Most had adenocarcinomas in the distal esophagus or gastroesophageal junction, and the majority had received neoadjuvant therapy. “It’s unlikely that operative approach influenced the development of chylothorax,” Dr. Zheng said.
Both ligated and nonligated patients responded well to chylothorax management. Of the 64 total cases, 28 were successfully treated by thoracic duct embolization and 20 were successfully treated by operative thoracic duct ligation. In 10 cases, thoracic duct embolization was attempted but unsuccessful and all were successfully treated with operative ligation. Six cases were managed with chest tube drainage and total parenteral nutrition. It is possible that patients were ligated because they appeared during surgery to be at risk for postop chylothorax, which would help explain the findings.
It also is possible, however, that ligation itself – especially mass ligation – increases the risk. “The thoracic duct is a high-pressure system, so [blocking it] could create a pressure buildup and a potential leak,” Dr. Zheng said. That might be especially true with mass ligation, when both the thoracic duct and its tributaries are tied off.
Dr. Zheng said that she had no relevant disclosures.
SEATTLE – Thoracic duct ligation did not seem to prevent chylothorax in a review of 827 esophagectomy cases at Brigham and Women’s Hospital in Boston.
In fact, chylothorax was most likely in patients who had mass ligation of the duct and its surrounding soft tissue, instead of ligation of simply the duct itself.
The results are surprising because ligation is actually meant to prevent chylothorax, but “it didn’t serve that purpose,” said lead investigator Dr. Yifan Zheng, a clinical research fellow at the hospital.
Results have been mixed in previous studies of ligation, with some finding benefit for preventing chylothorax but others not. With contradictory evidence, some surgeons – including some in the Brigham and Women’s review, which covered 11 years of data – opt for routine ligation, while others don’t, Dr. Zheng said at the annual meeting of the American Association for Thoracic Surgery.
At this point, “if you see the thoracic duct and you have concerns about ductal injury, your best bet is to ligate the duct directly. We observed in our series that there is a significantly higher incidence of chylothorax” with mass ligation, she said.
Of the 827 esophagectomies, 635 were performed without thoracic duct ligation; 33 (5.2%) cases developed postop chylothorax. Among the 56 cases with explicit identification and ligation of the thoracic duct alone, chylothorax developed in four (7.1%). There were 136 esophagectomies with mass ligation; 27 (19.9%) developed chylothorax (P = .0314).
The majority of the ligations were performed during open procedures. Mass ligations were mostly done with surgical sutures, while clips were used for direct ductal ligations. It’s likely that surgeons opted for direct ligation when they could see the duct and mass ligation when they could not.
Esophagectomy patients in the study were largely the same, so it’s unclear why some were ligated but others were not. About 75% in both groups had adenocarcinomas, most of which were in the distal esophagus or gastroesophageal junction. About half of the ligated group had preop chemoradiation, versus about 60% in the nonligated group.
Patients who developed postop chyle leaks were also similar, whether or not they were ligated. Most had adenocarcinomas in the distal esophagus or gastroesophageal junction, and the majority had received neoadjuvant therapy. “It’s unlikely that operative approach influenced the development of chylothorax,” Dr. Zheng said.
Both ligated and nonligated patients responded well to chylothorax management. Of the 64 total cases, 28 were successfully treated by thoracic duct embolization and 20 were successfully treated by operative thoracic duct ligation. In 10 cases, thoracic duct embolization was attempted but unsuccessful and all were successfully treated with operative ligation. Six cases were managed with chest tube drainage and total parenteral nutrition. It is possible that patients were ligated because they appeared during surgery to be at risk for postop chylothorax, which would help explain the findings.
It also is possible, however, that ligation itself – especially mass ligation – increases the risk. “The thoracic duct is a high-pressure system, so [blocking it] could create a pressure buildup and a potential leak,” Dr. Zheng said. That might be especially true with mass ligation, when both the thoracic duct and its tributaries are tied off.
Dr. Zheng said that she had no relevant disclosures.
AT THE AATS ANNUAL MEETING
Key clinical point: Mass thoracic duct ligation increases the risk of postop chylothorax.
Major finding: Of 827 esophagectomies, 635 were performed without thoracic duct ligation; 33 (5.2%) cases developed postop chylothorax. Among 56 cases with explicit identification and ligation of the thoracic duct alone, four (7.1%) developed chylothorax. There were 136 esophagectomies with mass ligation; 27 (19.9%) developed chylothorax (P = .0314).
Data source: Review of 827 esophagectomy cases at Brigham and Women’s Hospital in Boston.
Disclosures: The lead investigator had no disclosures.
Oral device reduced obstructive sleep apnea, not sleepiness
An oral appliance that advances a patient’s lower jaw reduced episodes of obstructive sleep apnea, snoring, and restless legs symptoms, according to a report published online June 1 in JAMA Internal Medicine.
The device, however, failed to improve daytime sleepiness or quality of life in a Swedish study of adults who had daytime sleepiness and either snoring or mild to moderate sleep apnea, said Marie Marklund, Ph.D., D.D.S., of the department of odontology at Umeå (Sweden) University and her associates (JAMA Intern. Med. 2015 June 1 [doi:10.1001/jamainternmed.2015.2051]).
Previous studies of oral appliances have focused on patients with more severe sleep apnea and have yielded conflicting results, particularly regarding daytime sleepiness.
A total of 91 patients who were randomly assigned to receive either a placebo device (46 patients) or an oral appliance individually made by a dental technician using separate plaster casts of the upper and lower teeth (45 participants) completed the study. The device’s elastomer pieces fitted over the teeth and were connected with a screw that allowed continuous gradual advancement of the lower jaw by 6-7 mm. Holding the lower mandible forward improves breathing during sleep.
After 4 months of follow-up, at-home overnight polysomnography showed “a clear, significant treatment effect”: the mean apnea-hypopnea index (AHI) was 6.7 in the active-treatment group, compared with 16.7 in the placebo group. A total of 49% of the patients receiving active treatment had an AHI lower than 5, compared with only 11% of those using the placebo device, for an odds ratio of 7.8 and a number needed to treat of 3.
Snoring and symptoms of restless legs also were significantly less frequent with the active treatment, Dr. Marklund and her associates said.
In addition, 73% of patients who used oral appliances said that their expectations of treatment were either “totally” or “sufficiently” fulfilled, compared with only 11% of those who used placebo devices. And 89% of patients who used oral appliances said they would continue the treatment after completing the study, compared with only 52% of those who used the sham device.
However, daytime sleepiness, measured subjectively using the Epworth Sleepiness Scale and the Karolinska Sleepiness Scale and measured objectively using the Oxford Sleep Resistance test, did not differ significantly between the two study groups. The number of days with headaches, the intensity of headaches, the presence of nasal congestion, difficulty falling asleep, nighttime awakenings, nightmares, and reaction times also were not significantly different, nor were scores on a quality of life measure.
The study was supported by grants from the Swedish Research Council, the Swedish Heart and Lung Foundation, and the County Council of Vasterbotten. Dr. Marklund and her associates reported no conflicts of interest.
It appears that patients generally prefer these devices to continuous positive airway pressure (CPAP) therapy. Better adherence to an oral appliance may outweigh the fact that it is not as effective as CPAP. Long-term studies comparing the two approaches are warranted.
The benefits of the mandibular advancement devices used in this study cannot be translated automatically to other devices, because there is a huge variety of these appliances on the market.
The extent of the protrusion of the lower jaw, the stability of the material, and the structural design of the devices vary widely. Several experts currently recommend avoiding the less sophisticated appliances that are not tailored to the individual’s jaw and oral cavity and instead using only customized adjustable appliances made by a trained specialist.
Dr. Winfried J. Randerath is with the pneumonology clinic and the Allergology Center for Sleep Medicine and Respiratory Care at Bethanien Hospital in Solingen, Germany. He reported having no relevant financial disclosures. He has, however, received speaking fees and research funds from companies that produce positive airway pressure devices: Heinen und Lowenstein, Resmed, Respironics, and Weinmann. Dr. Randerath made these remarks in an invited commentary (JAMA Intern. Med. 2015 June 1 [doi:10.1001/jamainternmed.2015.2059]).
It appears that patients generally prefer these devices to continuous positive airway pressure (CPAP) therapy. Better adherence to an oral appliance may outweigh the fact that it is not as effective as CPAP. Long-term studies comparing the two approaches are warranted.
The benefits of the mandibular advancement devices used in this study cannot be translated automatically to other devices, because there is a huge variety of these appliances on the market.
The extent of the protrusion of the lower jaw, the stability of the material, and the structural design of the devices vary widely. Several experts currently recommend avoiding the less sophisticated appliances that are not tailored to the individual’s jaw and oral cavity and instead using only customized adjustable appliances made by a trained specialist.
Dr. Winfried J. Randerath is with the pneumonology clinic and the Allergology Center for Sleep Medicine and Respiratory Care at Bethanien Hospital in Solingen, Germany. He reported having no relevant financial disclosures. He has, however, received speaking fees and research funds from companies that produce positive airway pressure devices: Heinen und Lowenstein, Resmed, Respironics, and Weinmann. Dr. Randerath made these remarks in an invited commentary (JAMA Intern. Med. 2015 June 1 [doi:10.1001/jamainternmed.2015.2059]).
It appears that patients generally prefer these devices to continuous positive airway pressure (CPAP) therapy. Better adherence to an oral appliance may outweigh the fact that it is not as effective as CPAP. Long-term studies comparing the two approaches are warranted.
The benefits of the mandibular advancement devices used in this study cannot be translated automatically to other devices, because there is a huge variety of these appliances on the market.
The extent of the protrusion of the lower jaw, the stability of the material, and the structural design of the devices vary widely. Several experts currently recommend avoiding the less sophisticated appliances that are not tailored to the individual’s jaw and oral cavity and instead using only customized adjustable appliances made by a trained specialist.
Dr. Winfried J. Randerath is with the pneumonology clinic and the Allergology Center for Sleep Medicine and Respiratory Care at Bethanien Hospital in Solingen, Germany. He reported having no relevant financial disclosures. He has, however, received speaking fees and research funds from companies that produce positive airway pressure devices: Heinen und Lowenstein, Resmed, Respironics, and Weinmann. Dr. Randerath made these remarks in an invited commentary (JAMA Intern. Med. 2015 June 1 [doi:10.1001/jamainternmed.2015.2059]).
An oral appliance that advances a patient’s lower jaw reduced episodes of obstructive sleep apnea, snoring, and restless legs symptoms, according to a report published online June 1 in JAMA Internal Medicine.
The device, however, failed to improve daytime sleepiness or quality of life in a Swedish study of adults who had daytime sleepiness and either snoring or mild to moderate sleep apnea, said Marie Marklund, Ph.D., D.D.S., of the department of odontology at Umeå (Sweden) University and her associates (JAMA Intern. Med. 2015 June 1 [doi:10.1001/jamainternmed.2015.2051]).
Previous studies of oral appliances have focused on patients with more severe sleep apnea and have yielded conflicting results, particularly regarding daytime sleepiness.
A total of 91 patients who were randomly assigned to receive either a placebo device (46 patients) or an oral appliance individually made by a dental technician using separate plaster casts of the upper and lower teeth (45 participants) completed the study. The device’s elastomer pieces fitted over the teeth and were connected with a screw that allowed continuous gradual advancement of the lower jaw by 6-7 mm. Holding the lower mandible forward improves breathing during sleep.
After 4 months of follow-up, at-home overnight polysomnography showed “a clear, significant treatment effect”: the mean apnea-hypopnea index (AHI) was 6.7 in the active-treatment group, compared with 16.7 in the placebo group. A total of 49% of the patients receiving active treatment had an AHI lower than 5, compared with only 11% of those using the placebo device, for an odds ratio of 7.8 and a number needed to treat of 3.
Snoring and symptoms of restless legs also were significantly less frequent with the active treatment, Dr. Marklund and her associates said.
In addition, 73% of patients who used oral appliances said that their expectations of treatment were either “totally” or “sufficiently” fulfilled, compared with only 11% of those who used placebo devices. And 89% of patients who used oral appliances said they would continue the treatment after completing the study, compared with only 52% of those who used the sham device.
However, daytime sleepiness, measured subjectively using the Epworth Sleepiness Scale and the Karolinska Sleepiness Scale and measured objectively using the Oxford Sleep Resistance test, did not differ significantly between the two study groups. The number of days with headaches, the intensity of headaches, the presence of nasal congestion, difficulty falling asleep, nighttime awakenings, nightmares, and reaction times also were not significantly different, nor were scores on a quality of life measure.
The study was supported by grants from the Swedish Research Council, the Swedish Heart and Lung Foundation, and the County Council of Vasterbotten. Dr. Marklund and her associates reported no conflicts of interest.
An oral appliance that advances a patient’s lower jaw reduced episodes of obstructive sleep apnea, snoring, and restless legs symptoms, according to a report published online June 1 in JAMA Internal Medicine.
The device, however, failed to improve daytime sleepiness or quality of life in a Swedish study of adults who had daytime sleepiness and either snoring or mild to moderate sleep apnea, said Marie Marklund, Ph.D., D.D.S., of the department of odontology at Umeå (Sweden) University and her associates (JAMA Intern. Med. 2015 June 1 [doi:10.1001/jamainternmed.2015.2051]).
Previous studies of oral appliances have focused on patients with more severe sleep apnea and have yielded conflicting results, particularly regarding daytime sleepiness.
A total of 91 patients who were randomly assigned to receive either a placebo device (46 patients) or an oral appliance individually made by a dental technician using separate plaster casts of the upper and lower teeth (45 participants) completed the study. The device’s elastomer pieces fitted over the teeth and were connected with a screw that allowed continuous gradual advancement of the lower jaw by 6-7 mm. Holding the lower mandible forward improves breathing during sleep.
After 4 months of follow-up, at-home overnight polysomnography showed “a clear, significant treatment effect”: the mean apnea-hypopnea index (AHI) was 6.7 in the active-treatment group, compared with 16.7 in the placebo group. A total of 49% of the patients receiving active treatment had an AHI lower than 5, compared with only 11% of those using the placebo device, for an odds ratio of 7.8 and a number needed to treat of 3.
Snoring and symptoms of restless legs also were significantly less frequent with the active treatment, Dr. Marklund and her associates said.
In addition, 73% of patients who used oral appliances said that their expectations of treatment were either “totally” or “sufficiently” fulfilled, compared with only 11% of those who used placebo devices. And 89% of patients who used oral appliances said they would continue the treatment after completing the study, compared with only 52% of those who used the sham device.
However, daytime sleepiness, measured subjectively using the Epworth Sleepiness Scale and the Karolinska Sleepiness Scale and measured objectively using the Oxford Sleep Resistance test, did not differ significantly between the two study groups. The number of days with headaches, the intensity of headaches, the presence of nasal congestion, difficulty falling asleep, nighttime awakenings, nightmares, and reaction times also were not significantly different, nor were scores on a quality of life measure.
The study was supported by grants from the Swedish Research Council, the Swedish Heart and Lung Foundation, and the County Council of Vasterbotten. Dr. Marklund and her associates reported no conflicts of interest.
FROM JAMA INTERNAL MEDICINE
Key clinical point: An oral appliance to advance the lower jaw reduced apneic episodes, snoring, and restless legs symptoms.
Major finding: Half of the patients receiving active treatment had an apnea-hypopnea index lower than 5, compared with only 11% of those using the placebo device, for an odds ratio of 7.8 and a number-needed-to-treat of 3.
Data source: A randomized, single-blind trial comparing a customized oral appliance against a placebo device in 96 adults with daytime sleepiness and either snoring or mild to moderate obstructive sleep apnea.
Disclosures: This study was supported by grants from the Swedish Research Council, the Swedish Heart and Lung Foundation, and the County Council of Vasterbotten. Dr. Marklund and her associates reported no conflicts of interest.
Medicare at 50: Physicians brace for transition to value-based payment
As Medicare celebrates its 50th anniversary, federal officials are beginning one of the most significant shifts in the program’s history – paying physicians based on quality and efficiency rather than for the volume of services they provide. The shift to so-called value-based payment will be phased in, but it is coming soon.
Earlier this year, federal officials announced their goal to tie 85% of all Medicare fee-for-service payments to quality or value by 2016 and 90% by 2018, relying heavily on the use of alternative payment models such as Accountable Care Organizations (ACOs) and bundled payments. The shift also is being driven by the recent repeal of Medicare’s Sustainable Growth Rate formula. The law that removed the SGR from physicians’ lives also created alternative payment pathways that tie payments to performance on certain quality metrics or successful participation as part of an ACO.
How will these changes affect how physicians deliver care in the future? We invited physicians in various practice settings to offer their perspectives on how the new payment paradigm will drive practice changes.
‘Value’ payment system is arbitrary
BY JOSEPH S. EASTERN, M.D.
While much has been written about the Centers for Medicare & Medicaid Services’ plan to shift its payment system away from fee-for-service and toward a “value-based” structure, most physicians in small and solo private settings have given little if any thought to its potential impact on their practices. That is about to change.
The principal vehicle for the CMS’s plan is something called the value-based payment modifier (VBPM), a component of the Affordable Care Act. The VBPM has not been on the radar of smaller private practices because up until now it has only applied to groups with more than 10 providers. Beginning this year, it applies to everyone. If you accept Medicare patients, regardless of the size of your practice, VBPM will become part of your life – because your 2017 Medicare payments will be adjusted based on your 2015 VBPM “score.”

It will adjust your reimbursements based on quality of care as defined by the CMS and cost, compared to other physicians. Your “score” will have a quality component and a cost component, and will be calculated based on measures reported through the Physician Quality Reporting System (PQRS). And the ACA requires that the program be budget neutral, which means that all rewards to physicians who pull the highest scores must be offset by penalties, or “negative adjustments,” to those who don’t score as well. In essence, the VBPM establishes arbitrary practice standards and spending ceilings; physicians who have the temerity to practice medicine as they see fit, or spend too much relative to their peers, will be punished.
Beyond the obvious and very real possibility of significant financial hardship, there are serious potential consequences inherent in this unprecedented new system. Health care is already among the most regulated industries in the country; the VBPM creates new incentives to practice “cookbook” medicine, and new disincentives to order tests, consults, or medications, even when doing so would clearly be in a patient’s best interest. The inevitable result will be compromised care and further limitation of patient access.
The VBPM’s potential effects on physician-patient relations and legal liability are additional serious concerns. Many patients will object to their physicians’ new reluctance to recommend appropriate interventions for fear of generating excessive costs; and should a less-than-thorough work-up lead to a missed diagnosis, the ACA offers no protection at all from any resulting malpractice litigation.
The already strained relationship between physicians and their hospitals will likely deteriorate as well. Hospital administrators will be scrutinizing each medical decision from admission to discharge, particularly in those institutions already in financial trouble, as is all too often the case. The constant necessity of justifying every significant order and consult will not be in anyone’s best interest, least of all that of patients.
For all the talk that the transition from fee-for-service to value-based reimbursement would result in better care at a lower cost, there is little evidence that care is improving, and even less that costs are decreasing. Conversely, there are plenty of warning signs that physicians in small private practices who can’t meet the new performance standards may face a significant financial burden because of the resulting penalties and lower reimbursements.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News.
Staying independent may prove costly
BY PETER M.G. DEANE, M.D.
The changes announced for Medicare and Medicaid, to be implemented over the next few years, are breathtaking in scope and ambition. A system based on payment for services is to become a system based on payment for individual health and population health outcomes. This will require enormous changes in the way health care is delivered, and this is an intended effect. Private payers will certainly desire the same results and savings.
I am a partner in a multiphysician, single-specialty private group practice. We have two hospital systems locally. Both of these are now health systems, in that they either employ or closely interact with many physicians.

Just a few years ago, our practice could comfortably make decisions about how we went about delivering care without much consideration of the plans of larger local institutions. Then came the rise of our local accountable care networks. These were created by the local health care systems to provide the overall organizational infrastructure to move from the current payment model to the coming one. We delayed for awhile but have now signed up with both. It can only be a matter of months before each of them pursues a meaningful degree of clinical integration. In other words, they will be analyzing data from our electronic medical record about our individual practice patterns and results, and giving us the results along with feedback on how to improve care.
For this to happen, our EMR system needs to be up to the task. We are unsure it will be. It has been difficult for some of us to adapt to electronic records systems. Now we need to see if our existing system can interoperate effectively. If not, we may be paying quite a bit for another one soon.
Our physicians are not accustomed to seeing report cards about their practice patterns. It will be a shock to see comparisons and rankings. But patients will be enrolled in and referred to us by the networks, and it will not be possible to ignore the reports we get.
Likely this radical change in the practice of medicine will drive some to retire, affecting the size of our group. We intend to remain in private practice, but independence may prove increasingly costly.
Already, patients see that their physicians make less eye contact with them and more time documenting care. This will likely get worse. We worry that if increased expenses cause staff cuts, the personal service we provide will suffer.
Redesigning medical practice will be a serious challenge for us. But our goal has always been to provide the best care, and in a value-based system, that should be what sustains us all.
Dr. Deane specializes in allergy, immunology, and rheumatology and is a partner in a private group practice with eight physicians and five offices in greater Rochester, N.Y. He is also the chief of allergy, immunology, and rheumatology at Unity Hospital in Rochester.
Value shift brings irreparable change to private practice
BY ROBERT SHOR, M.D.
The simple truth is that we are in transition. The current health system, for the most part, rewards “making widgets” (volume). That is, being paid for units of work actually being done. The more patients you see, the more procedures you do, the more you are compensated. We are moving from “volume” to “value” as we try to move away from “widgets” to management of population health. How do we get there? What can we as physicians and providers do?
I am part of a 40-person, single-specialty private cardiology practice in the Washington, D.C., suburbs. In the coming years, the CMS will reward (the euphemism for payment) practices that meet their definitions for quality and penalize those that don’t meet those metrics.

We have participated in PQRS/PQRI, Meaningful Use (MU), and other Medicare programs for which we are compensated. But how do you truly determine what are quality metrics and what is truly meaningful use of health system resources? How do we impact health on an individual and population view?
For us to be compliant with the Medicare rules and get paid, we have had to heavily invest in not only EHRs (we were an early adopter around 2000), but personnel costs to make sure all of the paperwork is completed appropriately for submission and for the audit that precedes the CMS payment for MU.
So how do we proceed going forward? In my opinion, what is clear is that private practice has been irreparably changed. The notion of an individual physician or a small practice surviving without some arrangement with a health system, an ACO, or a Clinical Integrated Network (CIN) is rapidly dwindling.
I have seen a variety of actions taken as providers try to survive and jockey for position to their advantage and we have explored a wide range of options. For an ACO to succeed in the shared risk model, it usually is part of a larger health care system. Thus many practices – primary care and subspecialty – have integrated with these health systems. Indeed, about 70% of the cardiology community is now integrated. To manage costs, you need to know your costs and most of the cost remains in the hospital care.
What do you do if you want to stay independent or do not feel you have a reliable health system with which you can integrate? Many practices may merge in a formal or looser network of practices to create a CIN where EHR access to patient records within the network is streamlined and care can be more effectively given. This has benefits, but also limitations. I believe that any future in which cost is contained on a larger scale will require close collaboration with hospitals given the disproportionate cost incurred during hospital care. Some practices have decided to form Physician Service Agreements with hospital systems to help manage product lines within the health system and to establish more meaningful relationships in an effort to coordinate care more effectively. This provides an opportunity to impact inpatient care, to contribute to programs that reduce hospital readmissions, and to reach the holy grail of preventing disease by better outpatient care. This would truly help with population health care management.
Some of the challenges, at least in large metropolitan areas, are that practices may work at several hospitals with different health systems. They may want to continue providing care at all of the hospitals in their community, but may be forced to choose. This does not appear to me to be in the best interest of our patients, many of whom we have cared for many years. However, the choice may be forced upon them as the health systems force the issue and make the decision for us.
The future holds much uncertainty, but also opportunity. Will our practice survive in its current form in 5 years? For now we are trying to read the tea leaves, like so many others, to make the best decisions on behalf of our patients to allow us to be able to continue to provide care in our community.
We are still reading the tea leaves.
Dr. Shor is vice president of Virginia Heart, which has nine offices in the northern Virginia region. He is the chair of the board of governors of the American College of Cardiology.
Leaving behind fee-for-service battles
BY ROBERT FIELDS, M.D.
Many of us in health care received with a mix of excitement and fear the recent news from the CMS regarding the transition to 90% value-based payments by 2018. For me, an employed family medicine physician and medical director of a new ACO in western North Carolina, I applaud the ambitious goal and understand the sentiment behind it. But, I also worry about the ability of most providers to adapt to this change in such a short time span.

The rationale behind value-based payments couldn’t be clearer – we spend too much on health care. Way too much. So much, that if we continue on this track our country will break under the financial pressures of providing care in a fee-for-service system. In addition, U.S. medical outcomes lag behind most other industrialized nations, which leads to the conclusion that the system at large is not providing the value it should.
As I put on my rose-colored glasses, I hope this restructuring encourages the system at large to coordinate care better, to improve our information systems to share relevant clinical data, and to encourage quality improvement at the practice level so that we move toward improved outcomes for our patient populations.
When talking to providers about our ACO and adding value in health care, they think we are saying that THEY are not delivering high value care. I keep reiterating, and will continue to do so, that value-based payments are not a criticism of our individual abilities as physicians or a comment on our interactions with our patients, but acknowledgment that how we communicate with and manage our populations as a network of hospitals, providers, and agencies lacks the efficiencies and coordination of services that patients deserve.
Ultimately, we are moving toward a patient-centered health care system that requires a fundamental transformation in how we pay for and deliver care. Measurement and quality improvement, although new to health care, has existed in every other industry for years.
In the end, I hope patients feel they are getting more efficient, coordinated care and that providers can start to see improvements in outcomes without the daily battle of the fee-for-service world.
Dr. Fields is a family physician and the medical director of Mission Health Partners, a physician led ACO in Asheville, N.C.
As Medicare celebrates its 50th anniversary, federal officials are beginning one of the most significant shifts in the program’s history – paying physicians based on quality and efficiency rather than for the volume of services they provide. The shift to so-called value-based payment will be phased in, but it is coming soon.
Earlier this year, federal officials announced their goal to tie 85% of all Medicare fee-for-service payments to quality or value by 2016 and 90% by 2018, relying heavily on the use of alternative payment models such as Accountable Care Organizations (ACOs) and bundled payments. The shift also is being driven by the recent repeal of Medicare’s Sustainable Growth Rate formula. The law that removed the SGR from physicians’ lives also created alternative payment pathways that tie payments to performance on certain quality metrics or successful participation as part of an ACO.
How will these changes affect how physicians deliver care in the future? We invited physicians in various practice settings to offer their perspectives on how the new payment paradigm will drive practice changes.
‘Value’ payment system is arbitrary
BY JOSEPH S. EASTERN, M.D.
While much has been written about the Centers for Medicare & Medicaid Services’ plan to shift its payment system away from fee-for-service and toward a “value-based” structure, most physicians in small and solo private settings have given little if any thought to its potential impact on their practices. That is about to change.
The principal vehicle for the CMS’s plan is something called the value-based payment modifier (VBPM), a component of the Affordable Care Act. The VBPM has not been on the radar of smaller private practices because up until now it has only applied to groups with more than 10 providers. Beginning this year, it applies to everyone. If you accept Medicare patients, regardless of the size of your practice, VBPM will become part of your life – because your 2017 Medicare payments will be adjusted based on your 2015 VBPM “score.”
It will adjust your reimbursements based on quality of care as defined by the CMS and cost, compared to other physicians. Your “score” will have a quality component and a cost component, and will be calculated based on measures reported through the Physician Quality Reporting System (PQRS). And the ACA requires that the program be budget neutral, which means that all rewards to physicians who pull the highest scores must be offset by penalties, or “negative adjustments,” to those who don’t score as well. In essence, the VBPM establishes arbitrary practice standards and spending ceilings; physicians who have the temerity to practice medicine as they see fit, or spend too much relative to their peers, will be punished.
Beyond the obvious and very real possibility of significant financial hardship, there are serious potential consequences inherent in this unprecedented new system. Health care is already among the most regulated industries in the country; the VBPM creates new incentives to practice “cookbook” medicine, and new disincentives to order tests, consults, or medications, even when doing so would clearly be in a patient’s best interest. The inevitable result will be compromised care and further limitation of patient access.
The VBPM’s potential effects on physician-patient relations and legal liability are additional serious concerns. Many patients will object to their physicians’ new reluctance to recommend appropriate interventions for fear of generating excessive costs; and should a less-than-thorough work-up lead to a missed diagnosis, the ACA offers no protection at all from any resulting malpractice litigation.
The already strained relationship between physicians and their hospitals will likely deteriorate as well. Hospital administrators will be scrutinizing each medical decision from admission to discharge, particularly in those institutions already in financial trouble, as is all too often the case. The constant necessity of justifying every significant order and consult will not be in anyone’s best interest, least of all that of patients.
For all the talk that the transition from fee-for-service to value-based reimbursement would result in better care at a lower cost, there is little evidence that care is improving, and even less that costs are decreasing. Conversely, there are plenty of warning signs that physicians in small private practices who can’t meet the new performance standards may face a significant financial burden because of the resulting penalties and lower reimbursements.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News.
Staying independent may prove costly
BY PETER M.G. DEANE, M.D.
The changes announced for Medicare and Medicaid, to be implemented over the next few years, are breathtaking in scope and ambition. A system based on payment for services is to become a system based on payment for individual health and population health outcomes. This will require enormous changes in the way health care is delivered, and this is an intended effect. Private payers will certainly desire the same results and savings.
I am a partner in a multiphysician, single-specialty private group practice. We have two hospital systems locally. Both of these are now health systems, in that they either employ or closely interact with many physicians.
Just a few years ago, our practice could comfortably make decisions about how we went about delivering care without much consideration of the plans of larger local institutions. Then came the rise of our local accountable care networks. These were created by the local health care systems to provide the overall organizational infrastructure to move from the current payment model to the coming one. We delayed for awhile but have now signed up with both. It can only be a matter of months before each of them pursues a meaningful degree of clinical integration. In other words, they will be analyzing data from our electronic medical record about our individual practice patterns and results, and giving us the results along with feedback on how to improve care.
For this to happen, our EMR system needs to be up to the task. We are unsure it will be. It has been difficult for some of us to adapt to electronic records systems. Now we need to see if our existing system can interoperate effectively. If not, we may be paying quite a bit for another one soon.
Our physicians are not accustomed to seeing report cards about their practice patterns. It will be a shock to see comparisons and rankings. But patients will be enrolled in and referred to us by the networks, and it will not be possible to ignore the reports we get.
Likely this radical change in the practice of medicine will drive some to retire, affecting the size of our group. We intend to remain in private practice, but independence may prove increasingly costly.
Already, patients see that their physicians make less eye contact with them and more time documenting care. This will likely get worse. We worry that if increased expenses cause staff cuts, the personal service we provide will suffer.
Redesigning medical practice will be a serious challenge for us. But our goal has always been to provide the best care, and in a value-based system, that should be what sustains us all.
Dr. Deane specializes in allergy, immunology, and rheumatology and is a partner in a private group practice with eight physicians and five offices in greater Rochester, N.Y. He is also the chief of allergy, immunology, and rheumatology at Unity Hospital in Rochester.
Value shift brings irreparable change to private practice
BY ROBERT SHOR, M.D.
The simple truth is that we are in transition. The current health system, for the most part, rewards “making widgets” (volume). That is, being paid for units of work actually being done. The more patients you see, the more procedures you do, the more you are compensated. We are moving from “volume” to “value” as we try to move away from “widgets” to management of population health. How do we get there? What can we as physicians and providers do?
I am part of a 40-person, single-specialty private cardiology practice in the Washington, D.C., suburbs. In the coming years, the CMS will reward (the euphemism for payment) practices that meet their definitions for quality and penalize those that don’t meet those metrics.
We have participated in PQRS/PQRI, Meaningful Use (MU), and other Medicare programs for which we are compensated. But how do you truly determine what are quality metrics and what is truly meaningful use of health system resources? How do we impact health on an individual and population view?
For us to be compliant with the Medicare rules and get paid, we have had to heavily invest in not only EHRs (we were an early adopter around 2000), but personnel costs to make sure all of the paperwork is completed appropriately for submission and for the audit that precedes the CMS payment for MU.
So how do we proceed going forward? In my opinion, what is clear is that private practice has been irreparably changed. The notion of an individual physician or a small practice surviving without some arrangement with a health system, an ACO, or a Clinical Integrated Network (CIN) is rapidly dwindling.
I have seen a variety of actions taken as providers try to survive and jockey for position to their advantage and we have explored a wide range of options. For an ACO to succeed in the shared risk model, it usually is part of a larger health care system. Thus many practices – primary care and subspecialty – have integrated with these health systems. Indeed, about 70% of the cardiology community is now integrated. To manage costs, you need to know your costs and most of the cost remains in the hospital care.
What do you do if you want to stay independent or do not feel you have a reliable health system with which you can integrate? Many practices may merge in a formal or looser network of practices to create a CIN where EHR access to patient records within the network is streamlined and care can be more effectively given. This has benefits, but also limitations. I believe that any future in which cost is contained on a larger scale will require close collaboration with hospitals given the disproportionate cost incurred during hospital care. Some practices have decided to form Physician Service Agreements with hospital systems to help manage product lines within the health system and to establish more meaningful relationships in an effort to coordinate care more effectively. This provides an opportunity to impact inpatient care, to contribute to programs that reduce hospital readmissions, and to reach the holy grail of preventing disease by better outpatient care. This would truly help with population health care management.
Some of the challenges, at least in large metropolitan areas, are that practices may work at several hospitals with different health systems. They may want to continue providing care at all of the hospitals in their community, but may be forced to choose. This does not appear to me to be in the best interest of our patients, many of whom we have cared for many years. However, the choice may be forced upon them as the health systems force the issue and make the decision for us.
The future holds much uncertainty, but also opportunity. Will our practice survive in its current form in 5 years? For now we are trying to read the tea leaves, like so many others, to make the best decisions on behalf of our patients to allow us to be able to continue to provide care in our community.
We are still reading the tea leaves.
Dr. Shor is vice president of Virginia Heart, which has nine offices in the northern Virginia region. He is the chair of the board of governors of the American College of Cardiology.
Leaving behind fee-for-service battles
BY ROBERT FIELDS, M.D.
Many of us in health care received with a mix of excitement and fear the recent news from the CMS regarding the transition to 90% value-based payments by 2018. For me, an employed family medicine physician and medical director of a new ACO in western North Carolina, I applaud the ambitious goal and understand the sentiment behind it. But, I also worry about the ability of most providers to adapt to this change in such a short time span.
The rationale behind value-based payments couldn’t be clearer – we spend too much on health care. Way too much. So much, that if we continue on this track our country will break under the financial pressures of providing care in a fee-for-service system. In addition, U.S. medical outcomes lag behind most other industrialized nations, which leads to the conclusion that the system at large is not providing the value it should.
As I put on my rose-colored glasses, I hope this restructuring encourages the system at large to coordinate care better, to improve our information systems to share relevant clinical data, and to encourage quality improvement at the practice level so that we move toward improved outcomes for our patient populations.
When talking to providers about our ACO and adding value in health care, they think we are saying that THEY are not delivering high value care. I keep reiterating, and will continue to do so, that value-based payments are not a criticism of our individual abilities as physicians or a comment on our interactions with our patients, but acknowledgment that how we communicate with and manage our populations as a network of hospitals, providers, and agencies lacks the efficiencies and coordination of services that patients deserve.
Ultimately, we are moving toward a patient-centered health care system that requires a fundamental transformation in how we pay for and deliver care. Measurement and quality improvement, although new to health care, has existed in every other industry for years.
In the end, I hope patients feel they are getting more efficient, coordinated care and that providers can start to see improvements in outcomes without the daily battle of the fee-for-service world.
Dr. Fields is a family physician and the medical director of Mission Health Partners, a physician led ACO in Asheville, N.C.
As Medicare celebrates its 50th anniversary, federal officials are beginning one of the most significant shifts in the program’s history – paying physicians based on quality and efficiency rather than for the volume of services they provide. The shift to so-called value-based payment will be phased in, but it is coming soon.
Earlier this year, federal officials announced their goal to tie 85% of all Medicare fee-for-service payments to quality or value by 2016 and 90% by 2018, relying heavily on the use of alternative payment models such as Accountable Care Organizations (ACOs) and bundled payments. The shift also is being driven by the recent repeal of Medicare’s Sustainable Growth Rate formula. The law that removed the SGR from physicians’ lives also created alternative payment pathways that tie payments to performance on certain quality metrics or successful participation as part of an ACO.
How will these changes affect how physicians deliver care in the future? We invited physicians in various practice settings to offer their perspectives on how the new payment paradigm will drive practice changes.
‘Value’ payment system is arbitrary
BY JOSEPH S. EASTERN, M.D.
While much has been written about the Centers for Medicare & Medicaid Services’ plan to shift its payment system away from fee-for-service and toward a “value-based” structure, most physicians in small and solo private settings have given little if any thought to its potential impact on their practices. That is about to change.
The principal vehicle for the CMS’s plan is something called the value-based payment modifier (VBPM), a component of the Affordable Care Act. The VBPM has not been on the radar of smaller private practices because up until now it has only applied to groups with more than 10 providers. Beginning this year, it applies to everyone. If you accept Medicare patients, regardless of the size of your practice, VBPM will become part of your life – because your 2017 Medicare payments will be adjusted based on your 2015 VBPM “score.”
It will adjust your reimbursements based on quality of care as defined by the CMS and cost, compared to other physicians. Your “score” will have a quality component and a cost component, and will be calculated based on measures reported through the Physician Quality Reporting System (PQRS). And the ACA requires that the program be budget neutral, which means that all rewards to physicians who pull the highest scores must be offset by penalties, or “negative adjustments,” to those who don’t score as well. In essence, the VBPM establishes arbitrary practice standards and spending ceilings; physicians who have the temerity to practice medicine as they see fit, or spend too much relative to their peers, will be punished.
Beyond the obvious and very real possibility of significant financial hardship, there are serious potential consequences inherent in this unprecedented new system. Health care is already among the most regulated industries in the country; the VBPM creates new incentives to practice “cookbook” medicine, and new disincentives to order tests, consults, or medications, even when doing so would clearly be in a patient’s best interest. The inevitable result will be compromised care and further limitation of patient access.
The VBPM’s potential effects on physician-patient relations and legal liability are additional serious concerns. Many patients will object to their physicians’ new reluctance to recommend appropriate interventions for fear of generating excessive costs; and should a less-than-thorough work-up lead to a missed diagnosis, the ACA offers no protection at all from any resulting malpractice litigation.
The already strained relationship between physicians and their hospitals will likely deteriorate as well. Hospital administrators will be scrutinizing each medical decision from admission to discharge, particularly in those institutions already in financial trouble, as is all too often the case. The constant necessity of justifying every significant order and consult will not be in anyone’s best interest, least of all that of patients.
For all the talk that the transition from fee-for-service to value-based reimbursement would result in better care at a lower cost, there is little evidence that care is improving, and even less that costs are decreasing. Conversely, there are plenty of warning signs that physicians in small private practices who can’t meet the new performance standards may face a significant financial burden because of the resulting penalties and lower reimbursements.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News.
Staying independent may prove costly
BY PETER M.G. DEANE, M.D.
The changes announced for Medicare and Medicaid, to be implemented over the next few years, are breathtaking in scope and ambition. A system based on payment for services is to become a system based on payment for individual health and population health outcomes. This will require enormous changes in the way health care is delivered, and this is an intended effect. Private payers will certainly desire the same results and savings.
I am a partner in a multiphysician, single-specialty private group practice. We have two hospital systems locally. Both of these are now health systems, in that they either employ or closely interact with many physicians.
Just a few years ago, our practice could comfortably make decisions about how we went about delivering care without much consideration of the plans of larger local institutions. Then came the rise of our local accountable care networks. These were created by the local health care systems to provide the overall organizational infrastructure to move from the current payment model to the coming one. We delayed for awhile but have now signed up with both. It can only be a matter of months before each of them pursues a meaningful degree of clinical integration. In other words, they will be analyzing data from our electronic medical record about our individual practice patterns and results, and giving us the results along with feedback on how to improve care.
For this to happen, our EMR system needs to be up to the task. We are unsure it will be. It has been difficult for some of us to adapt to electronic records systems. Now we need to see if our existing system can interoperate effectively. If not, we may be paying quite a bit for another one soon.
Our physicians are not accustomed to seeing report cards about their practice patterns. It will be a shock to see comparisons and rankings. But patients will be enrolled in and referred to us by the networks, and it will not be possible to ignore the reports we get.
Likely this radical change in the practice of medicine will drive some to retire, affecting the size of our group. We intend to remain in private practice, but independence may prove increasingly costly.
Already, patients see that their physicians make less eye contact with them and more time documenting care. This will likely get worse. We worry that if increased expenses cause staff cuts, the personal service we provide will suffer.
Redesigning medical practice will be a serious challenge for us. But our goal has always been to provide the best care, and in a value-based system, that should be what sustains us all.
Dr. Deane specializes in allergy, immunology, and rheumatology and is a partner in a private group practice with eight physicians and five offices in greater Rochester, N.Y. He is also the chief of allergy, immunology, and rheumatology at Unity Hospital in Rochester.
Value shift brings irreparable change to private practice
BY ROBERT SHOR, M.D.
The simple truth is that we are in transition. The current health system, for the most part, rewards “making widgets” (volume). That is, being paid for units of work actually being done. The more patients you see, the more procedures you do, the more you are compensated. We are moving from “volume” to “value” as we try to move away from “widgets” to management of population health. How do we get there? What can we as physicians and providers do?
I am part of a 40-person, single-specialty private cardiology practice in the Washington, D.C., suburbs. In the coming years, the CMS will reward (the euphemism for payment) practices that meet their definitions for quality and penalize those that don’t meet those metrics.
We have participated in PQRS/PQRI, Meaningful Use (MU), and other Medicare programs for which we are compensated. But how do you truly determine what are quality metrics and what is truly meaningful use of health system resources? How do we impact health on an individual and population view?
For us to be compliant with the Medicare rules and get paid, we have had to heavily invest in not only EHRs (we were an early adopter around 2000), but personnel costs to make sure all of the paperwork is completed appropriately for submission and for the audit that precedes the CMS payment for MU.
So how do we proceed going forward? In my opinion, what is clear is that private practice has been irreparably changed. The notion of an individual physician or a small practice surviving without some arrangement with a health system, an ACO, or a Clinical Integrated Network (CIN) is rapidly dwindling.
I have seen a variety of actions taken as providers try to survive and jockey for position to their advantage and we have explored a wide range of options. For an ACO to succeed in the shared risk model, it usually is part of a larger health care system. Thus many practices – primary care and subspecialty – have integrated with these health systems. Indeed, about 70% of the cardiology community is now integrated. To manage costs, you need to know your costs and most of the cost remains in the hospital care.
What do you do if you want to stay independent or do not feel you have a reliable health system with which you can integrate? Many practices may merge in a formal or looser network of practices to create a CIN where EHR access to patient records within the network is streamlined and care can be more effectively given. This has benefits, but also limitations. I believe that any future in which cost is contained on a larger scale will require close collaboration with hospitals given the disproportionate cost incurred during hospital care. Some practices have decided to form Physician Service Agreements with hospital systems to help manage product lines within the health system and to establish more meaningful relationships in an effort to coordinate care more effectively. This provides an opportunity to impact inpatient care, to contribute to programs that reduce hospital readmissions, and to reach the holy grail of preventing disease by better outpatient care. This would truly help with population health care management.
Some of the challenges, at least in large metropolitan areas, are that practices may work at several hospitals with different health systems. They may want to continue providing care at all of the hospitals in their community, but may be forced to choose. This does not appear to me to be in the best interest of our patients, many of whom we have cared for many years. However, the choice may be forced upon them as the health systems force the issue and make the decision for us.
The future holds much uncertainty, but also opportunity. Will our practice survive in its current form in 5 years? For now we are trying to read the tea leaves, like so many others, to make the best decisions on behalf of our patients to allow us to be able to continue to provide care in our community.
We are still reading the tea leaves.
Dr. Shor is vice president of Virginia Heart, which has nine offices in the northern Virginia region. He is the chair of the board of governors of the American College of Cardiology.
Leaving behind fee-for-service battles
BY ROBERT FIELDS, M.D.
Many of us in health care received with a mix of excitement and fear the recent news from the CMS regarding the transition to 90% value-based payments by 2018. For me, an employed family medicine physician and medical director of a new ACO in western North Carolina, I applaud the ambitious goal and understand the sentiment behind it. But, I also worry about the ability of most providers to adapt to this change in such a short time span.
The rationale behind value-based payments couldn’t be clearer – we spend too much on health care. Way too much. So much, that if we continue on this track our country will break under the financial pressures of providing care in a fee-for-service system. In addition, U.S. medical outcomes lag behind most other industrialized nations, which leads to the conclusion that the system at large is not providing the value it should.
As I put on my rose-colored glasses, I hope this restructuring encourages the system at large to coordinate care better, to improve our information systems to share relevant clinical data, and to encourage quality improvement at the practice level so that we move toward improved outcomes for our patient populations.
When talking to providers about our ACO and adding value in health care, they think we are saying that THEY are not delivering high value care. I keep reiterating, and will continue to do so, that value-based payments are not a criticism of our individual abilities as physicians or a comment on our interactions with our patients, but acknowledgment that how we communicate with and manage our populations as a network of hospitals, providers, and agencies lacks the efficiencies and coordination of services that patients deserve.
Ultimately, we are moving toward a patient-centered health care system that requires a fundamental transformation in how we pay for and deliver care. Measurement and quality improvement, although new to health care, has existed in every other industry for years.
In the end, I hope patients feel they are getting more efficient, coordinated care and that providers can start to see improvements in outcomes without the daily battle of the fee-for-service world.
Dr. Fields is a family physician and the medical director of Mission Health Partners, a physician led ACO in Asheville, N.C.

Cardiac surgeons defy guidelines for severe disease
Although expert committees spend hours developing guidelines for best practices, clinicians on the front line of care can be somewhat hesitant to adopt them, as a recent study evaluating the use of guidelines for treatment of heart attack patients at three major cardiothoracic centers in London revealed.
The study, published in the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2014.10.110]) , found that surgeons more often than not flaunted the Joint European Society of Cardiology and European Association for Cardiothoracic Surgery (ESC/EACTS) guidelines that call for a multidisciplinary “Heart Team” to discuss each case of severe coronary artery disease before treatment.
The investigators looked at January-to-June periods in 2010 (before the guidelines) and 2012 (after the guidelines had been in place for 18 months) and found identical 17% rates of multidisciplinary team discussions before treatment. Both samples involved patients who had percutaneous coronary interventions (PCI). The 621 cases in the 2010 sample and 686 cases in the 2012 group comprise “a significant proportion of the coronary revascularization workload” of the National Health Service (NHS) hospitals in London, Dr. Martin T. Yates of St. George’s Hospital, University of London, and coauthors reported. The other participating centers were Barts Health NHS Trust and King College Hospital.
The ESC/EACTS guidelines (Eur. Heart J. 2010;31:2501-55) determined that PCI at the same catheterization session as the diagnostic angiogram and elective PCI are inappropriate for patients with severe coronary artery disease, defined as proximal left-anterior descending, left-main stem or three-vessel disease. The guidelines state that these patients should be considered for surgery first.
In a previous single-center study a year after the guidelines were adopted, Dr. Yates and his colleagues reported that almost a third of all elective PCI (29%) were carried out on patients who may have benefited more from coronary artery bypass grafting (CABG) (J. Thorac. Cardiovasc. Surg. 2014;147:606-10). Of those cases, the multidisciplinary team again discussed only 17% of cases before PCI.
Dr. Yates and his colleagues intimated that the rush to PCI might be circumventing in-depth discussions about more appropriate CABG for patients with severe coronary artery disease. “Furthermore, despite the guidelines suggesting that ad hoc PCI is inappropriate in the elective setting, this practice continues,” they said. “Although this is convenient for the patient and more cost effective, it does not allow time for Heart Team discussions prior to intervention.”
In the current study, the 2010 group included 187 patients with severe coronary artery disease who had treatment without a multidisciplinary team consultation, and less than half (44%) achieved complete revascularization. The 2012 group included 225 patients with severe heart disease, and precisely half achieved complete revascularization.
In both groups, a considerable majority of patients with three-vessel disease had PCI without the multidisciplinary team discussion: 76% in 2010 and 64% in 2012.
Dr. Yates and his associates noted that this is not a problem specific to London cardiac centers. They cited variations in the use of PCI and CABG in a large study of the New York State Registry, which showed that only 53% of patients suitable for CABG, according to the American College of Cardiology/American Heart Association guidelines, actually had the procedure (Circulation 2010;121:267-75). They cited similar results in a Canadian study (CMAJ 2012;184;179-86).
One way to get cardiac surgeons to adhere to guidelines is to tie payment to treatment – an approach that may work better in the United States than in Canada or the United Kingdom. “This may be easier to implement in countries with payment linked to insurance systems as opposed to those with a nationalized service,” Dr. Yates and his associates wrote.
The authors reported no financial disclosures.
Gathering evidence over recent years has shown that multidisciplinary teams can improve overall outcomes in many clinical scenarios, Dr. M. Sertac Cicek said in his commentary (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2014.12.008]). He cited a 2012 study that showed an 18% lower mortality at 5 years when multidisciplinary teams got involved in the treatment of breast cancer, compared with cases that did not involve team consultation (BMJ 2012;344:e2718).

|
Dr. M. Sertac Cicek |
Cardiovascular disease is a specialty that demands teamwork, but controversy still surrounds the role of surgery vs. PCI for patients with severe coronary disease, despite the evidence supporting CABG as the “gold standard,” Dr. Cicek said. The data presented by Dr. Yates and his colleagues, Dr. Cicek said, “simply confirm once again how far we are away from providing the optimal care to our patients, raising the question: ‘Are guidelines there to be disrespected?’ ”
A key factor in implementing the multidisciplinary approach involves educating patients and accepting them as members of the heart team during decision-making, Dr. Cicek noted. “It seems increasingly evident that multidisciplinary teams clearly strengthen our ability to provide higher quality and more efficient care; so much so that it may not come as surprise to anyone in the practice if in the very near future practicing ‘medicine without teamwork’ were declared and added to the Seven [Social] Sins of Mahatma Gandhi as the eighth [social] sin,” Dr. Cicek wrote.
Dr. Cicek is professor of cardiovascular surgery at the Anadolu Medical Center in Kocaeli, Turkey.
Gathering evidence over recent years has shown that multidisciplinary teams can improve overall outcomes in many clinical scenarios, Dr. M. Sertac Cicek said in his commentary (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2014.12.008]). He cited a 2012 study that showed an 18% lower mortality at 5 years when multidisciplinary teams got involved in the treatment of breast cancer, compared with cases that did not involve team consultation (BMJ 2012;344:e2718).
|
|
Dr. M. Sertac Cicek |
Cardiovascular disease is a specialty that demands teamwork, but controversy still surrounds the role of surgery vs. PCI for patients with severe coronary disease, despite the evidence supporting CABG as the “gold standard,” Dr. Cicek said. The data presented by Dr. Yates and his colleagues, Dr. Cicek said, “simply confirm once again how far we are away from providing the optimal care to our patients, raising the question: ‘Are guidelines there to be disrespected?’ ”
A key factor in implementing the multidisciplinary approach involves educating patients and accepting them as members of the heart team during decision-making, Dr. Cicek noted. “It seems increasingly evident that multidisciplinary teams clearly strengthen our ability to provide higher quality and more efficient care; so much so that it may not come as surprise to anyone in the practice if in the very near future practicing ‘medicine without teamwork’ were declared and added to the Seven [Social] Sins of Mahatma Gandhi as the eighth [social] sin,” Dr. Cicek wrote.
Dr. Cicek is professor of cardiovascular surgery at the Anadolu Medical Center in Kocaeli, Turkey.
Gathering evidence over recent years has shown that multidisciplinary teams can improve overall outcomes in many clinical scenarios, Dr. M. Sertac Cicek said in his commentary (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2014.12.008]). He cited a 2012 study that showed an 18% lower mortality at 5 years when multidisciplinary teams got involved in the treatment of breast cancer, compared with cases that did not involve team consultation (BMJ 2012;344:e2718).
|
|
Dr. M. Sertac Cicek |
Cardiovascular disease is a specialty that demands teamwork, but controversy still surrounds the role of surgery vs. PCI for patients with severe coronary disease, despite the evidence supporting CABG as the “gold standard,” Dr. Cicek said. The data presented by Dr. Yates and his colleagues, Dr. Cicek said, “simply confirm once again how far we are away from providing the optimal care to our patients, raising the question: ‘Are guidelines there to be disrespected?’ ”
A key factor in implementing the multidisciplinary approach involves educating patients and accepting them as members of the heart team during decision-making, Dr. Cicek noted. “It seems increasingly evident that multidisciplinary teams clearly strengthen our ability to provide higher quality and more efficient care; so much so that it may not come as surprise to anyone in the practice if in the very near future practicing ‘medicine without teamwork’ were declared and added to the Seven [Social] Sins of Mahatma Gandhi as the eighth [social] sin,” Dr. Cicek wrote.
Dr. Cicek is professor of cardiovascular surgery at the Anadolu Medical Center in Kocaeli, Turkey.
Although expert committees spend hours developing guidelines for best practices, clinicians on the front line of care can be somewhat hesitant to adopt them, as a recent study evaluating the use of guidelines for treatment of heart attack patients at three major cardiothoracic centers in London revealed.
The study, published in the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2014.10.110]) , found that surgeons more often than not flaunted the Joint European Society of Cardiology and European Association for Cardiothoracic Surgery (ESC/EACTS) guidelines that call for a multidisciplinary “Heart Team” to discuss each case of severe coronary artery disease before treatment.
The investigators looked at January-to-June periods in 2010 (before the guidelines) and 2012 (after the guidelines had been in place for 18 months) and found identical 17% rates of multidisciplinary team discussions before treatment. Both samples involved patients who had percutaneous coronary interventions (PCI). The 621 cases in the 2010 sample and 686 cases in the 2012 group comprise “a significant proportion of the coronary revascularization workload” of the National Health Service (NHS) hospitals in London, Dr. Martin T. Yates of St. George’s Hospital, University of London, and coauthors reported. The other participating centers were Barts Health NHS Trust and King College Hospital.
The ESC/EACTS guidelines (Eur. Heart J. 2010;31:2501-55) determined that PCI at the same catheterization session as the diagnostic angiogram and elective PCI are inappropriate for patients with severe coronary artery disease, defined as proximal left-anterior descending, left-main stem or three-vessel disease. The guidelines state that these patients should be considered for surgery first.
In a previous single-center study a year after the guidelines were adopted, Dr. Yates and his colleagues reported that almost a third of all elective PCI (29%) were carried out on patients who may have benefited more from coronary artery bypass grafting (CABG) (J. Thorac. Cardiovasc. Surg. 2014;147:606-10). Of those cases, the multidisciplinary team again discussed only 17% of cases before PCI.
Dr. Yates and his colleagues intimated that the rush to PCI might be circumventing in-depth discussions about more appropriate CABG for patients with severe coronary artery disease. “Furthermore, despite the guidelines suggesting that ad hoc PCI is inappropriate in the elective setting, this practice continues,” they said. “Although this is convenient for the patient and more cost effective, it does not allow time for Heart Team discussions prior to intervention.”
In the current study, the 2010 group included 187 patients with severe coronary artery disease who had treatment without a multidisciplinary team consultation, and less than half (44%) achieved complete revascularization. The 2012 group included 225 patients with severe heart disease, and precisely half achieved complete revascularization.
In both groups, a considerable majority of patients with three-vessel disease had PCI without the multidisciplinary team discussion: 76% in 2010 and 64% in 2012.
Dr. Yates and his associates noted that this is not a problem specific to London cardiac centers. They cited variations in the use of PCI and CABG in a large study of the New York State Registry, which showed that only 53% of patients suitable for CABG, according to the American College of Cardiology/American Heart Association guidelines, actually had the procedure (Circulation 2010;121:267-75). They cited similar results in a Canadian study (CMAJ 2012;184;179-86).
One way to get cardiac surgeons to adhere to guidelines is to tie payment to treatment – an approach that may work better in the United States than in Canada or the United Kingdom. “This may be easier to implement in countries with payment linked to insurance systems as opposed to those with a nationalized service,” Dr. Yates and his associates wrote.
The authors reported no financial disclosures.
Although expert committees spend hours developing guidelines for best practices, clinicians on the front line of care can be somewhat hesitant to adopt them, as a recent study evaluating the use of guidelines for treatment of heart attack patients at three major cardiothoracic centers in London revealed.
The study, published in the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2014.10.110]) , found that surgeons more often than not flaunted the Joint European Society of Cardiology and European Association for Cardiothoracic Surgery (ESC/EACTS) guidelines that call for a multidisciplinary “Heart Team” to discuss each case of severe coronary artery disease before treatment.
The investigators looked at January-to-June periods in 2010 (before the guidelines) and 2012 (after the guidelines had been in place for 18 months) and found identical 17% rates of multidisciplinary team discussions before treatment. Both samples involved patients who had percutaneous coronary interventions (PCI). The 621 cases in the 2010 sample and 686 cases in the 2012 group comprise “a significant proportion of the coronary revascularization workload” of the National Health Service (NHS) hospitals in London, Dr. Martin T. Yates of St. George’s Hospital, University of London, and coauthors reported. The other participating centers were Barts Health NHS Trust and King College Hospital.
The ESC/EACTS guidelines (Eur. Heart J. 2010;31:2501-55) determined that PCI at the same catheterization session as the diagnostic angiogram and elective PCI are inappropriate for patients with severe coronary artery disease, defined as proximal left-anterior descending, left-main stem or three-vessel disease. The guidelines state that these patients should be considered for surgery first.
In a previous single-center study a year after the guidelines were adopted, Dr. Yates and his colleagues reported that almost a third of all elective PCI (29%) were carried out on patients who may have benefited more from coronary artery bypass grafting (CABG) (J. Thorac. Cardiovasc. Surg. 2014;147:606-10). Of those cases, the multidisciplinary team again discussed only 17% of cases before PCI.
Dr. Yates and his colleagues intimated that the rush to PCI might be circumventing in-depth discussions about more appropriate CABG for patients with severe coronary artery disease. “Furthermore, despite the guidelines suggesting that ad hoc PCI is inappropriate in the elective setting, this practice continues,” they said. “Although this is convenient for the patient and more cost effective, it does not allow time for Heart Team discussions prior to intervention.”
In the current study, the 2010 group included 187 patients with severe coronary artery disease who had treatment without a multidisciplinary team consultation, and less than half (44%) achieved complete revascularization. The 2012 group included 225 patients with severe heart disease, and precisely half achieved complete revascularization.
In both groups, a considerable majority of patients with three-vessel disease had PCI without the multidisciplinary team discussion: 76% in 2010 and 64% in 2012.
Dr. Yates and his associates noted that this is not a problem specific to London cardiac centers. They cited variations in the use of PCI and CABG in a large study of the New York State Registry, which showed that only 53% of patients suitable for CABG, according to the American College of Cardiology/American Heart Association guidelines, actually had the procedure (Circulation 2010;121:267-75). They cited similar results in a Canadian study (CMAJ 2012;184;179-86).
One way to get cardiac surgeons to adhere to guidelines is to tie payment to treatment – an approach that may work better in the United States than in Canada or the United Kingdom. “This may be easier to implement in countries with payment linked to insurance systems as opposed to those with a nationalized service,” Dr. Yates and his associates wrote.
The authors reported no financial disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Cardiac surgeons at three London hospitals complied poorly with clinical guidelines for managing patients with severe coronary artery disease.
Major finding: Only 17% of patients with severe coronary artery disease were subjects of multidisciplinary discussions before treatment in periods before and after treatment guidelines, and most were likely to have percutaneous coronary intervention rather than the recommended surgical revascularization.
Data source: Surgical patients were from the Central Cardiac Audit Database; PCI patients were from the British Cardiovascular Intervention Society database.
Disclosures: The authors reported no financial disclosures.

ASCO: German trial argues against complete nodal dissection for SLN-positive melanoma
CHICAGO – The case against performing a complete lymph node dissection in patients with melanoma who have micrometastases in their sentinel lymph node just got stronger in light of findings from a randomized, phase III clinical trial conducted by the German Dermatologic Cooperative Oncology Group (DeCOG).
With 483 patients studied and a median follow-up approaching 3 years, the rate of distant metastasis–free survival did not differ significantly between those who had a complete lymph node dissection and those who had simple watchful waiting, with just 0.3% separating the groups, the investigators reported at the annual meeting of the American Society of Clinical Oncology. Most other key outcomes were likewise statistically indistinguishable between groups.

“This is the first study which tested the general recommendation of complete lymphadenectomy in patients with positive nodes,” senior investigator Dr. Claus Garbe, a professor of dermatology at the University of Tübingen (Germany), said in a press briefing. “We cannot confirm this recommendation, and we expect that the surgical [practice] will change.”
However, Dr. Lynn Schuchter, an ASCO expert, as well as chief of hematology oncology and the C. Willard Robinson Professor of Hematology-Oncology at Penn Medicine in Philadelphia, took a more cautious view, saying that the findings require confirmation before being widely adopted into clinical practice.
“I would say this is a really important study. However, it’s a relatively small study, and I don’t think we would make a complete change in our recommendations yet based upon this study,” she commented.
The ongoing international Multicenter Selective Lymphadenectomy Trial II (MSLT-II), which has a target enrollment of about 1,900 patients and is designed to detect a smaller difference between groups, will provide further information on this issue, according to Dr. Schuchter. “So I think we’ll wait in terms of making definitive changes in our management, for the results of another, larger study with longer follow-up,” she said. “But [the German study] gives us, in that patient who is very concerned about lymphedema ... pertinent information to feel comfortable considering more of a watch-and-wait approach, in terms of monitoring somebody and not doing that surgery.”

Dr. Garbe and colleagues enrolled in their trial patients who underwent resection of a primary cutaneous melanoma of the trunk or extremities at least 1.00 mm in thickness and were determined to have stage III disease with a positive sentinel node containing individual tumor cells or micrometastases. They were randomly assigned to observation only or complete lymph node dissection. Both groups had a lymph node ultrasound exam every 3 months and CT/MRI or PET scans every 6 months.
With a median follow-up of 35 months, patients who had the complete lymph node dissection were about half as likely to develop regional metastases as peers who had watchful waiting (8.3% vs. 14.6%). But the groups did not differ significantly with respect to 3- and 5-year rates of recurrence-free survival, distant metastasis–free survival (the trial’s primary endpoint), and melanoma-specific survival.
The investigators plan to repeat their analysis in 3 years but do not expect the findings will change, according to Dr. Garbe, as the large majority of melanoma recurrences happen in the first 3 years after initial diagnosis.
Dr. Garbe disclosed ties to Amgen, Bristol-Myers Squibb, GlaxoSmithKline, Merck, Novartis, and Roche Pharma AG. The trial was funded by German Cancer Aid.
CHICAGO – The case against performing a complete lymph node dissection in patients with melanoma who have micrometastases in their sentinel lymph node just got stronger in light of findings from a randomized, phase III clinical trial conducted by the German Dermatologic Cooperative Oncology Group (DeCOG).
With 483 patients studied and a median follow-up approaching 3 years, the rate of distant metastasis–free survival did not differ significantly between those who had a complete lymph node dissection and those who had simple watchful waiting, with just 0.3% separating the groups, the investigators reported at the annual meeting of the American Society of Clinical Oncology. Most other key outcomes were likewise statistically indistinguishable between groups.
“This is the first study which tested the general recommendation of complete lymphadenectomy in patients with positive nodes,” senior investigator Dr. Claus Garbe, a professor of dermatology at the University of Tübingen (Germany), said in a press briefing. “We cannot confirm this recommendation, and we expect that the surgical [practice] will change.”
However, Dr. Lynn Schuchter, an ASCO expert, as well as chief of hematology oncology and the C. Willard Robinson Professor of Hematology-Oncology at Penn Medicine in Philadelphia, took a more cautious view, saying that the findings require confirmation before being widely adopted into clinical practice.
“I would say this is a really important study. However, it’s a relatively small study, and I don’t think we would make a complete change in our recommendations yet based upon this study,” she commented.
The ongoing international Multicenter Selective Lymphadenectomy Trial II (MSLT-II), which has a target enrollment of about 1,900 patients and is designed to detect a smaller difference between groups, will provide further information on this issue, according to Dr. Schuchter. “So I think we’ll wait in terms of making definitive changes in our management, for the results of another, larger study with longer follow-up,” she said. “But [the German study] gives us, in that patient who is very concerned about lymphedema ... pertinent information to feel comfortable considering more of a watch-and-wait approach, in terms of monitoring somebody and not doing that surgery.”
Dr. Garbe and colleagues enrolled in their trial patients who underwent resection of a primary cutaneous melanoma of the trunk or extremities at least 1.00 mm in thickness and were determined to have stage III disease with a positive sentinel node containing individual tumor cells or micrometastases. They were randomly assigned to observation only or complete lymph node dissection. Both groups had a lymph node ultrasound exam every 3 months and CT/MRI or PET scans every 6 months.
With a median follow-up of 35 months, patients who had the complete lymph node dissection were about half as likely to develop regional metastases as peers who had watchful waiting (8.3% vs. 14.6%). But the groups did not differ significantly with respect to 3- and 5-year rates of recurrence-free survival, distant metastasis–free survival (the trial’s primary endpoint), and melanoma-specific survival.
The investigators plan to repeat their analysis in 3 years but do not expect the findings will change, according to Dr. Garbe, as the large majority of melanoma recurrences happen in the first 3 years after initial diagnosis.
Dr. Garbe disclosed ties to Amgen, Bristol-Myers Squibb, GlaxoSmithKline, Merck, Novartis, and Roche Pharma AG. The trial was funded by German Cancer Aid.
CHICAGO – The case against performing a complete lymph node dissection in patients with melanoma who have micrometastases in their sentinel lymph node just got stronger in light of findings from a randomized, phase III clinical trial conducted by the German Dermatologic Cooperative Oncology Group (DeCOG).
With 483 patients studied and a median follow-up approaching 3 years, the rate of distant metastasis–free survival did not differ significantly between those who had a complete lymph node dissection and those who had simple watchful waiting, with just 0.3% separating the groups, the investigators reported at the annual meeting of the American Society of Clinical Oncology. Most other key outcomes were likewise statistically indistinguishable between groups.
“This is the first study which tested the general recommendation of complete lymphadenectomy in patients with positive nodes,” senior investigator Dr. Claus Garbe, a professor of dermatology at the University of Tübingen (Germany), said in a press briefing. “We cannot confirm this recommendation, and we expect that the surgical [practice] will change.”
However, Dr. Lynn Schuchter, an ASCO expert, as well as chief of hematology oncology and the C. Willard Robinson Professor of Hematology-Oncology at Penn Medicine in Philadelphia, took a more cautious view, saying that the findings require confirmation before being widely adopted into clinical practice.
“I would say this is a really important study. However, it’s a relatively small study, and I don’t think we would make a complete change in our recommendations yet based upon this study,” she commented.
The ongoing international Multicenter Selective Lymphadenectomy Trial II (MSLT-II), which has a target enrollment of about 1,900 patients and is designed to detect a smaller difference between groups, will provide further information on this issue, according to Dr. Schuchter. “So I think we’ll wait in terms of making definitive changes in our management, for the results of another, larger study with longer follow-up,” she said. “But [the German study] gives us, in that patient who is very concerned about lymphedema ... pertinent information to feel comfortable considering more of a watch-and-wait approach, in terms of monitoring somebody and not doing that surgery.”
Dr. Garbe and colleagues enrolled in their trial patients who underwent resection of a primary cutaneous melanoma of the trunk or extremities at least 1.00 mm in thickness and were determined to have stage III disease with a positive sentinel node containing individual tumor cells or micrometastases. They were randomly assigned to observation only or complete lymph node dissection. Both groups had a lymph node ultrasound exam every 3 months and CT/MRI or PET scans every 6 months.
With a median follow-up of 35 months, patients who had the complete lymph node dissection were about half as likely to develop regional metastases as peers who had watchful waiting (8.3% vs. 14.6%). But the groups did not differ significantly with respect to 3- and 5-year rates of recurrence-free survival, distant metastasis–free survival (the trial’s primary endpoint), and melanoma-specific survival.
The investigators plan to repeat their analysis in 3 years but do not expect the findings will change, according to Dr. Garbe, as the large majority of melanoma recurrences happen in the first 3 years after initial diagnosis.
Dr. Garbe disclosed ties to Amgen, Bristol-Myers Squibb, GlaxoSmithKline, Merck, Novartis, and Roche Pharma AG. The trial was funded by German Cancer Aid.
AT ASCO 2015
Key clinical point: Complete nodal dissection fails to reduce distant metastasis in patients with melanoma who have micrometastases in sentinel nodes.
Major finding: Patients who did and did not undergo complete lymph node dissection were statistically indistinguishable with respect to distant metastases–free survival, recurrence-free survival, and melanoma-specific survival.
Data source: A randomized, phase III trial in 483 patients with stage III melanoma and micrometastases in their sentinel nodes.
Disclosures: Dr. Garbe disclosed ties to Amgen, Bristol-Myers Squibb, GlaxoSmithKline, Merck, Novartis, and Roche Pharma AG. The trial was funded by German Cancer Aid.

NOTION: TAVI has edge in patients at low surgical risk
PARIS – The writing is on the wall: 2-year results of the NOTION* trial suggest that transcatheter aortic valve replacement is the future – and already in selected cases, the present – preferred therapy for aortic stenosis in patients at low surgical risk.
NOTION was a multicenter, prospective, nonblinded, randomized trial, the first-ever study to compare less-invasive transcatheter aortic valve implantation (TAVI, also called transcatheter aortic valve replacement, or TAVR) and traditional surgical aortic valve replacement (SAVR) in a truly low-surgical-risk population. The 280 participants had a median Society of Thoracic Surgeons score of 3 and no major comorbid conditions.

At 2 years’ follow-up, the TAVI group had significantly larger valve orifice areas and lower gradients, along with lower rates of life-threatening bleeding, cardiogenic stroke, and severe kidney injury than did the SAVR group. Moreover, the TAVI group showed a strong favorable trend in terms of the primary composite endpoint comprising all-cause mortality, MI, or stroke, although the advantage didn’t achieve statistical significance because of the relatively small study size, Dr. Lars Søndergaard said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“Longer-term data on durability and more randomized controlled trials are needed before we adopt routine use of TAVI in low-risk patients, but I think it’s reasonable to offer TAVI in selected low-risk patients today,” concluded Dr. Søndergaard of the University of Copenhagen.
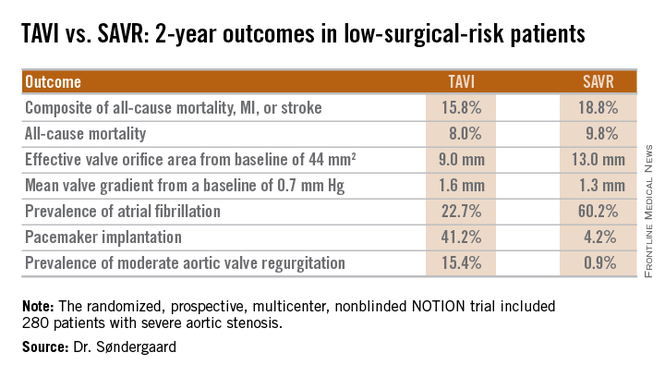
Session cochair Dr. William Wijns noted that NOTION, which utilized Medtronics’ self-expanding CoreValve for TAVI, began in 2009 and thus used an early iteration of the device. One might reasonably expect that the study results would be substantially more strongly in favor of TAVI had the contemporary version of the CoreValve been employed, observed Dr. Wijns, codirector of the cardiovascular center in Aalst, Belgium.
Dr. Søndergaard concurred. While the prevalence of moderate aortic regurgitation at 2 years in the TAVI arm of NOTION was 15.4%, in part because the valves were routinely placed under echocardiographic guidance, current-generation TAVI valves placed under CT guidance have a 1%-5% rate of moderate regurgitation. And while 41% of the TAVI group in NOTION had a pacemaker at 2 years, other studies show the rate drops to roughly 10% with the newest version of the CoreValve.
Dr. Søndergaard and coinvestigators plan to follow the NOTION participants for 10 years, issuing periodic updates. That’s a welcome development because patients at low surgical risk constitute the largest portion of those with significant aortic stenosis. Many of them are young enough that they should have a substantial remaining lifespan after aortic valve replacement, so it will be important to establish TAVI’s long-term durability.
The NOTION trial was funded by the Danish Heart Foundation. Dr. Søndergaard reported having no financial conflicts.
*Correction, 6/1/2015: An earlier version of this article misstated the name of the NOTION trial.
PARIS – The writing is on the wall: 2-year results of the NOTION* trial suggest that transcatheter aortic valve replacement is the future – and already in selected cases, the present – preferred therapy for aortic stenosis in patients at low surgical risk.
NOTION was a multicenter, prospective, nonblinded, randomized trial, the first-ever study to compare less-invasive transcatheter aortic valve implantation (TAVI, also called transcatheter aortic valve replacement, or TAVR) and traditional surgical aortic valve replacement (SAVR) in a truly low-surgical-risk population. The 280 participants had a median Society of Thoracic Surgeons score of 3 and no major comorbid conditions.
At 2 years’ follow-up, the TAVI group had significantly larger valve orifice areas and lower gradients, along with lower rates of life-threatening bleeding, cardiogenic stroke, and severe kidney injury than did the SAVR group. Moreover, the TAVI group showed a strong favorable trend in terms of the primary composite endpoint comprising all-cause mortality, MI, or stroke, although the advantage didn’t achieve statistical significance because of the relatively small study size, Dr. Lars Søndergaard said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“Longer-term data on durability and more randomized controlled trials are needed before we adopt routine use of TAVI in low-risk patients, but I think it’s reasonable to offer TAVI in selected low-risk patients today,” concluded Dr. Søndergaard of the University of Copenhagen.
Session cochair Dr. William Wijns noted that NOTION, which utilized Medtronics’ self-expanding CoreValve for TAVI, began in 2009 and thus used an early iteration of the device. One might reasonably expect that the study results would be substantially more strongly in favor of TAVI had the contemporary version of the CoreValve been employed, observed Dr. Wijns, codirector of the cardiovascular center in Aalst, Belgium.
Dr. Søndergaard concurred. While the prevalence of moderate aortic regurgitation at 2 years in the TAVI arm of NOTION was 15.4%, in part because the valves were routinely placed under echocardiographic guidance, current-generation TAVI valves placed under CT guidance have a 1%-5% rate of moderate regurgitation. And while 41% of the TAVI group in NOTION had a pacemaker at 2 years, other studies show the rate drops to roughly 10% with the newest version of the CoreValve.
Dr. Søndergaard and coinvestigators plan to follow the NOTION participants for 10 years, issuing periodic updates. That’s a welcome development because patients at low surgical risk constitute the largest portion of those with significant aortic stenosis. Many of them are young enough that they should have a substantial remaining lifespan after aortic valve replacement, so it will be important to establish TAVI’s long-term durability.
The NOTION trial was funded by the Danish Heart Foundation. Dr. Søndergaard reported having no financial conflicts.
*Correction, 6/1/2015: An earlier version of this article misstated the name of the NOTION trial.
PARIS – The writing is on the wall: 2-year results of the NOTION* trial suggest that transcatheter aortic valve replacement is the future – and already in selected cases, the present – preferred therapy for aortic stenosis in patients at low surgical risk.
NOTION was a multicenter, prospective, nonblinded, randomized trial, the first-ever study to compare less-invasive transcatheter aortic valve implantation (TAVI, also called transcatheter aortic valve replacement, or TAVR) and traditional surgical aortic valve replacement (SAVR) in a truly low-surgical-risk population. The 280 participants had a median Society of Thoracic Surgeons score of 3 and no major comorbid conditions.
At 2 years’ follow-up, the TAVI group had significantly larger valve orifice areas and lower gradients, along with lower rates of life-threatening bleeding, cardiogenic stroke, and severe kidney injury than did the SAVR group. Moreover, the TAVI group showed a strong favorable trend in terms of the primary composite endpoint comprising all-cause mortality, MI, or stroke, although the advantage didn’t achieve statistical significance because of the relatively small study size, Dr. Lars Søndergaard said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“Longer-term data on durability and more randomized controlled trials are needed before we adopt routine use of TAVI in low-risk patients, but I think it’s reasonable to offer TAVI in selected low-risk patients today,” concluded Dr. Søndergaard of the University of Copenhagen.
Session cochair Dr. William Wijns noted that NOTION, which utilized Medtronics’ self-expanding CoreValve for TAVI, began in 2009 and thus used an early iteration of the device. One might reasonably expect that the study results would be substantially more strongly in favor of TAVI had the contemporary version of the CoreValve been employed, observed Dr. Wijns, codirector of the cardiovascular center in Aalst, Belgium.
Dr. Søndergaard concurred. While the prevalence of moderate aortic regurgitation at 2 years in the TAVI arm of NOTION was 15.4%, in part because the valves were routinely placed under echocardiographic guidance, current-generation TAVI valves placed under CT guidance have a 1%-5% rate of moderate regurgitation. And while 41% of the TAVI group in NOTION had a pacemaker at 2 years, other studies show the rate drops to roughly 10% with the newest version of the CoreValve.
Dr. Søndergaard and coinvestigators plan to follow the NOTION participants for 10 years, issuing periodic updates. That’s a welcome development because patients at low surgical risk constitute the largest portion of those with significant aortic stenosis. Many of them are young enough that they should have a substantial remaining lifespan after aortic valve replacement, so it will be important to establish TAVI’s long-term durability.
The NOTION trial was funded by the Danish Heart Foundation. Dr. Søndergaard reported having no financial conflicts.
*Correction, 6/1/2015: An earlier version of this article misstated the name of the NOTION trial.
AT EUROPCR
Key clinical point: At 2 years, outcomes of TAVI look as good as and in some domains better than outcomes of surgical aortic valve replacement in low-surgical-risk patients.
Major finding: The 2-year composite outcome of all-cause mortality, MI, or stroke occurred in 15.8% of the TAVI group compared with 18.8% of surgically treated patients.
Data source: The randomized, prospective, multicenter, nonblinded NOTION trial includes 280 low-surgical-risk patients with severe aortic stenosis.
Disclosures: The NOTION trial was sponsored by the Danish Heart Foundation. The presenter reported having no financial conflicts.
