User login
Official Newspaper of the American College of Surgeons
VIDEO: Sometimes, comfort care is best for ruptured AAAs
CHICAGO – Four preoperative variables predict whether or not patients will survive ruptured abdominal aortic aneurysm repairs, according to investigators from Harborview Medical Center in Seattle.
It’s an important finding because until now, it’s been hard to know how they’ll do. Previous risk scores also rely on intraoperative variables, or haven’t been validated for endovascular repair.
Investigator Dr. Ty Garland, chief vascular surgery resident at the University of Washington, explained in a video interview what the four variables are at a meeting hosted by the Society for Vascular Surgery, and why it was so important for a level 1 trauma center like Harborview to identify them.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – Four preoperative variables predict whether or not patients will survive ruptured abdominal aortic aneurysm repairs, according to investigators from Harborview Medical Center in Seattle.
It’s an important finding because until now, it’s been hard to know how they’ll do. Previous risk scores also rely on intraoperative variables, or haven’t been validated for endovascular repair.
Investigator Dr. Ty Garland, chief vascular surgery resident at the University of Washington, explained in a video interview what the four variables are at a meeting hosted by the Society for Vascular Surgery, and why it was so important for a level 1 trauma center like Harborview to identify them.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – Four preoperative variables predict whether or not patients will survive ruptured abdominal aortic aneurysm repairs, according to investigators from Harborview Medical Center in Seattle.
It’s an important finding because until now, it’s been hard to know how they’ll do. Previous risk scores also rely on intraoperative variables, or haven’t been validated for endovascular repair.
Investigator Dr. Ty Garland, chief vascular surgery resident at the University of Washington, explained in a video interview what the four variables are at a meeting hosted by the Society for Vascular Surgery, and why it was so important for a level 1 trauma center like Harborview to identify them.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE 2015 VASCULAR ANNUAL MEETING

Vermont leads the way in marketplace enrollment
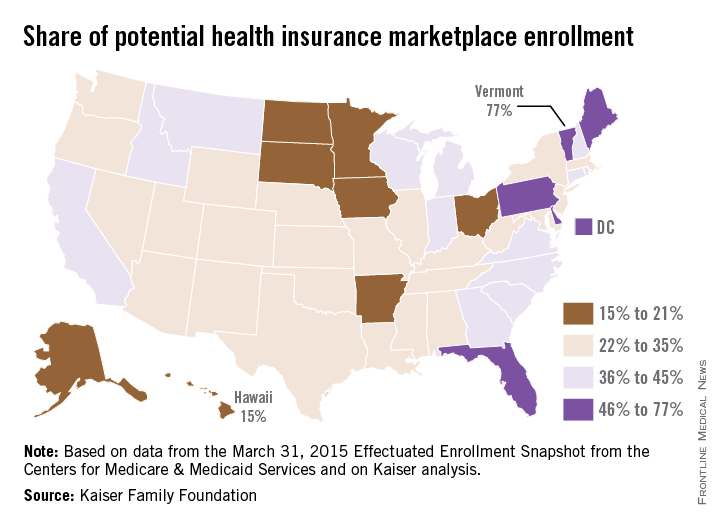
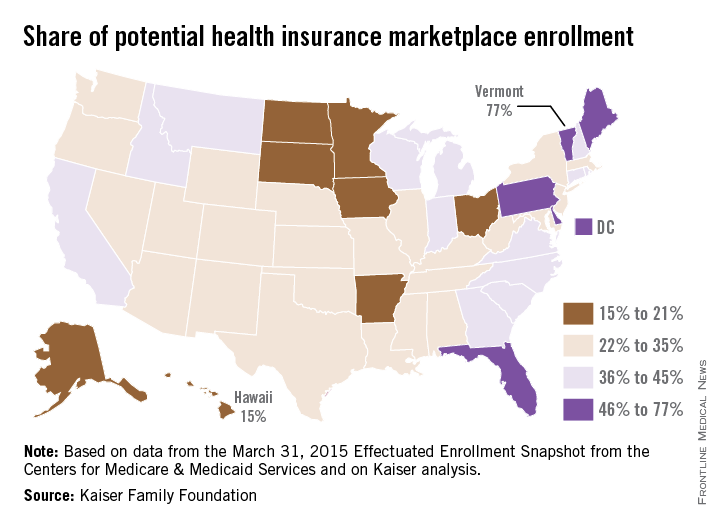
Vermont enrolled the highest percentage of potential enrollees for the Health Insurance Marketplace in 2015, while Hawaii enrolled the lowest percentage, according to an analysis from the Kaiser Family Foundation.
Enrollment in Vermont’s state-based marketplace as of March 31 was 34,923 – which works out to 77% of the estimated potential population of 45,000. The state with the next-highest enrollment was Florida, with 57% of the potential population, then Maine at 55%, Pennsylvania at 48%, and Delaware at 47%, Kaiser reported.
Hawaii had a marketplace enrollment of 8,200 out of an estimated potential population of 55,000, or 15%, as of March 31. Just ahead of Hawaii were Iowa (17%), Minnesota (19%), South Dakota (19%), and Ohio (20%).
Vermont, Hawaii, and Minnesota have state-based marketplaces, while those in Florida, Maine, Pennsylvania, South Dakota, and Ohio are federally facilitated. Delaware and Iowa have state-partnership marketplaces.
Number-crunching reveals that the 14 state-based marketplaces have the highest average enrollment at 35.6%, followed by the 27 federally facilitated marketplaces at 34.1%, the 7 state partnerships at 33%, and the 3 states with federally supported marketplaces at 28.3%, according to the Kaiser data, which come from the March 31, 2015 Effectuated Enrollment Snapshot from the Centers for Medicare & Medicaid Services and analysis based on 2014 Medicaid eligibility levels and the 2014 Current Population Survey.
Vermont enrolled the highest percentage of potential enrollees for the Health Insurance Marketplace in 2015, while Hawaii enrolled the lowest percentage, according to an analysis from the Kaiser Family Foundation.
Enrollment in Vermont’s state-based marketplace as of March 31 was 34,923 – which works out to 77% of the estimated potential population of 45,000. The state with the next-highest enrollment was Florida, with 57% of the potential population, then Maine at 55%, Pennsylvania at 48%, and Delaware at 47%, Kaiser reported.
Hawaii had a marketplace enrollment of 8,200 out of an estimated potential population of 55,000, or 15%, as of March 31. Just ahead of Hawaii were Iowa (17%), Minnesota (19%), South Dakota (19%), and Ohio (20%).
Vermont, Hawaii, and Minnesota have state-based marketplaces, while those in Florida, Maine, Pennsylvania, South Dakota, and Ohio are federally facilitated. Delaware and Iowa have state-partnership marketplaces.
Number-crunching reveals that the 14 state-based marketplaces have the highest average enrollment at 35.6%, followed by the 27 federally facilitated marketplaces at 34.1%, the 7 state partnerships at 33%, and the 3 states with federally supported marketplaces at 28.3%, according to the Kaiser data, which come from the March 31, 2015 Effectuated Enrollment Snapshot from the Centers for Medicare & Medicaid Services and analysis based on 2014 Medicaid eligibility levels and the 2014 Current Population Survey.
Vermont enrolled the highest percentage of potential enrollees for the Health Insurance Marketplace in 2015, while Hawaii enrolled the lowest percentage, according to an analysis from the Kaiser Family Foundation.
Enrollment in Vermont’s state-based marketplace as of March 31 was 34,923 – which works out to 77% of the estimated potential population of 45,000. The state with the next-highest enrollment was Florida, with 57% of the potential population, then Maine at 55%, Pennsylvania at 48%, and Delaware at 47%, Kaiser reported.
Hawaii had a marketplace enrollment of 8,200 out of an estimated potential population of 55,000, or 15%, as of March 31. Just ahead of Hawaii were Iowa (17%), Minnesota (19%), South Dakota (19%), and Ohio (20%).
Vermont, Hawaii, and Minnesota have state-based marketplaces, while those in Florida, Maine, Pennsylvania, South Dakota, and Ohio are federally facilitated. Delaware and Iowa have state-partnership marketplaces.
Number-crunching reveals that the 14 state-based marketplaces have the highest average enrollment at 35.6%, followed by the 27 federally facilitated marketplaces at 34.1%, the 7 state partnerships at 33%, and the 3 states with federally supported marketplaces at 28.3%, according to the Kaiser data, which come from the March 31, 2015 Effectuated Enrollment Snapshot from the Centers for Medicare & Medicaid Services and analysis based on 2014 Medicaid eligibility levels and the 2014 Current Population Survey.
Sonothrombolysis equivalent to endovascular therapy in some large-vessel stroke patients
VIENNA – Sonothrombolysis proved to be an effective alternative to endovascular treatment in patients with large intracranial occlusions, but clot removal via a retrievable stent appeared to have the edge when it came to achieving a good functional outcome, according to data presented at the annual European Stroke Conference.
In the first head-to-head comparison of the two strategies, there was no difference in the primary end point of the final modified Rankin Scale (mRS) score at the end of neurorehabilitation or death within 90 days. The mean final mRS was 3.78 with endovascular treatment and 3.95 with sonothrombolysis, with a nonsignificant (P = .12) odds ratio of 1.70 favoring the noninvasive procedure.
However, patients who underwent endovascular therapy were 3.89 times more likely than were those who had sonothrombolysis to achieve the secondary end point of a good functional outcome defined as a final mRS of 0-2 (24.7% vs. 13.6%; P = .02). Early recanalization was also possible in more patients with endovascular therapy than with sonothrombolysis (82.2% vs. 32.2%; OR, 15.77; P < .001).
“At the moment, everything veers toward using stent retrieval with thrombectomy, which requires very high costs at present and cannot be performed in every center,” noted study investigator Matthias Reinhard of the University Medical Center Freiburg (Germany) in an interview. On the other hand, Dr. Reinhard said, “sonothrombolysis is much less invasive and does not need specific interventionists, and it can be done with normal ultrasound devices, which are already available in every stroke unit.”
Sonothrombolysis enhances the thrombolytic activity of recombinant tissue plasminogen activator (rTPA) near to the clot, he explained, and has been shown in a Cochrane review to double the odds for functional independence, as well as upping the chances for recanalization around threefold (Cochrane Database Syst. Rev. 2012;10:CD008348). This is on a par with the results obtained with endovascular treatment in recent trials.
Since the two methods for enhancing thrombolysis with rTPA had not been directly compared before, Dr. Reinhard and his associates decided to look back at the medical records of patients with acute anterior circulation stroke with M1 or carotid T occlusion who were treated at two adjacent medical centers that used one or other of the methods as a standard treatment. After thrombolysis with rTPA, patients at one center underwent endovascular treatment with stent retrieval while patients at the other center had sonothrombolysis.
A total of 132 patients were assessed: 73 underwent endovascular treatment and 59 had sonothrombolysis. The median age in each group was 71 and 75 years, respectively, with around half the participants in each group being male. The groups had similar mean National Institutes of Health Stroke Scale scores (15 and 13). The majority of patients in each group had M1 vessel occlusions (60% and 69%) with the remainder (40% and 31%) having carotid T vessel occlusions. The mean onset to rTPA was 117 minutes and 105 minutes, respectively.
Subgroup analysis showed a significant benefit for endovascular treatment over sonothrombolysis in patients with carotid T occlusions, with an adjusted OR of 5.61 (P = .008). However, the two methods were comparable (OR, 1.07; P = .880) in patients with M1 occlusions.
“The main finding was that sonothrombolysis might perhaps be as equally effective as endovascular treatment in moderate-size occlusions such as middle cerebral artery occlusions but not in the very proximal occlusions of the carotid T,” Dr. Reinhard said. “So, one strategy might be to first apply sonothrombolysis and if this does not work, then to move the patient to the endovascular treatment,” he suggested, noting that this might be a better strategy to test in a future clinical trial than directly comparing the methods in a larger number of patients.
In terms of safety, there was no significant advantage of using one procedure over the other, despite three (4.1%) patients in the endovascular group and none in the sonothrombolysis group experiencing symptomatic intracranial hemorrhage (P = .25). Type 1 parenchymal hematomas were more common in patients who had sonothrombolysis than in those who had endovascular therapy (15.3% vs. 5.5%, P = .09). Mortality at 90 days was around 20% in both groups.
Dr. Reinhard had no disclosures.
VIENNA – Sonothrombolysis proved to be an effective alternative to endovascular treatment in patients with large intracranial occlusions, but clot removal via a retrievable stent appeared to have the edge when it came to achieving a good functional outcome, according to data presented at the annual European Stroke Conference.
In the first head-to-head comparison of the two strategies, there was no difference in the primary end point of the final modified Rankin Scale (mRS) score at the end of neurorehabilitation or death within 90 days. The mean final mRS was 3.78 with endovascular treatment and 3.95 with sonothrombolysis, with a nonsignificant (P = .12) odds ratio of 1.70 favoring the noninvasive procedure.
However, patients who underwent endovascular therapy were 3.89 times more likely than were those who had sonothrombolysis to achieve the secondary end point of a good functional outcome defined as a final mRS of 0-2 (24.7% vs. 13.6%; P = .02). Early recanalization was also possible in more patients with endovascular therapy than with sonothrombolysis (82.2% vs. 32.2%; OR, 15.77; P < .001).
“At the moment, everything veers toward using stent retrieval with thrombectomy, which requires very high costs at present and cannot be performed in every center,” noted study investigator Matthias Reinhard of the University Medical Center Freiburg (Germany) in an interview. On the other hand, Dr. Reinhard said, “sonothrombolysis is much less invasive and does not need specific interventionists, and it can be done with normal ultrasound devices, which are already available in every stroke unit.”
Sonothrombolysis enhances the thrombolytic activity of recombinant tissue plasminogen activator (rTPA) near to the clot, he explained, and has been shown in a Cochrane review to double the odds for functional independence, as well as upping the chances for recanalization around threefold (Cochrane Database Syst. Rev. 2012;10:CD008348). This is on a par with the results obtained with endovascular treatment in recent trials.
Since the two methods for enhancing thrombolysis with rTPA had not been directly compared before, Dr. Reinhard and his associates decided to look back at the medical records of patients with acute anterior circulation stroke with M1 or carotid T occlusion who were treated at two adjacent medical centers that used one or other of the methods as a standard treatment. After thrombolysis with rTPA, patients at one center underwent endovascular treatment with stent retrieval while patients at the other center had sonothrombolysis.
A total of 132 patients were assessed: 73 underwent endovascular treatment and 59 had sonothrombolysis. The median age in each group was 71 and 75 years, respectively, with around half the participants in each group being male. The groups had similar mean National Institutes of Health Stroke Scale scores (15 and 13). The majority of patients in each group had M1 vessel occlusions (60% and 69%) with the remainder (40% and 31%) having carotid T vessel occlusions. The mean onset to rTPA was 117 minutes and 105 minutes, respectively.
Subgroup analysis showed a significant benefit for endovascular treatment over sonothrombolysis in patients with carotid T occlusions, with an adjusted OR of 5.61 (P = .008). However, the two methods were comparable (OR, 1.07; P = .880) in patients with M1 occlusions.
“The main finding was that sonothrombolysis might perhaps be as equally effective as endovascular treatment in moderate-size occlusions such as middle cerebral artery occlusions but not in the very proximal occlusions of the carotid T,” Dr. Reinhard said. “So, one strategy might be to first apply sonothrombolysis and if this does not work, then to move the patient to the endovascular treatment,” he suggested, noting that this might be a better strategy to test in a future clinical trial than directly comparing the methods in a larger number of patients.
In terms of safety, there was no significant advantage of using one procedure over the other, despite three (4.1%) patients in the endovascular group and none in the sonothrombolysis group experiencing symptomatic intracranial hemorrhage (P = .25). Type 1 parenchymal hematomas were more common in patients who had sonothrombolysis than in those who had endovascular therapy (15.3% vs. 5.5%, P = .09). Mortality at 90 days was around 20% in both groups.
Dr. Reinhard had no disclosures.
VIENNA – Sonothrombolysis proved to be an effective alternative to endovascular treatment in patients with large intracranial occlusions, but clot removal via a retrievable stent appeared to have the edge when it came to achieving a good functional outcome, according to data presented at the annual European Stroke Conference.
In the first head-to-head comparison of the two strategies, there was no difference in the primary end point of the final modified Rankin Scale (mRS) score at the end of neurorehabilitation or death within 90 days. The mean final mRS was 3.78 with endovascular treatment and 3.95 with sonothrombolysis, with a nonsignificant (P = .12) odds ratio of 1.70 favoring the noninvasive procedure.
However, patients who underwent endovascular therapy were 3.89 times more likely than were those who had sonothrombolysis to achieve the secondary end point of a good functional outcome defined as a final mRS of 0-2 (24.7% vs. 13.6%; P = .02). Early recanalization was also possible in more patients with endovascular therapy than with sonothrombolysis (82.2% vs. 32.2%; OR, 15.77; P < .001).
“At the moment, everything veers toward using stent retrieval with thrombectomy, which requires very high costs at present and cannot be performed in every center,” noted study investigator Matthias Reinhard of the University Medical Center Freiburg (Germany) in an interview. On the other hand, Dr. Reinhard said, “sonothrombolysis is much less invasive and does not need specific interventionists, and it can be done with normal ultrasound devices, which are already available in every stroke unit.”
Sonothrombolysis enhances the thrombolytic activity of recombinant tissue plasminogen activator (rTPA) near to the clot, he explained, and has been shown in a Cochrane review to double the odds for functional independence, as well as upping the chances for recanalization around threefold (Cochrane Database Syst. Rev. 2012;10:CD008348). This is on a par with the results obtained with endovascular treatment in recent trials.
Since the two methods for enhancing thrombolysis with rTPA had not been directly compared before, Dr. Reinhard and his associates decided to look back at the medical records of patients with acute anterior circulation stroke with M1 or carotid T occlusion who were treated at two adjacent medical centers that used one or other of the methods as a standard treatment. After thrombolysis with rTPA, patients at one center underwent endovascular treatment with stent retrieval while patients at the other center had sonothrombolysis.
A total of 132 patients were assessed: 73 underwent endovascular treatment and 59 had sonothrombolysis. The median age in each group was 71 and 75 years, respectively, with around half the participants in each group being male. The groups had similar mean National Institutes of Health Stroke Scale scores (15 and 13). The majority of patients in each group had M1 vessel occlusions (60% and 69%) with the remainder (40% and 31%) having carotid T vessel occlusions. The mean onset to rTPA was 117 minutes and 105 minutes, respectively.
Subgroup analysis showed a significant benefit for endovascular treatment over sonothrombolysis in patients with carotid T occlusions, with an adjusted OR of 5.61 (P = .008). However, the two methods were comparable (OR, 1.07; P = .880) in patients with M1 occlusions.
“The main finding was that sonothrombolysis might perhaps be as equally effective as endovascular treatment in moderate-size occlusions such as middle cerebral artery occlusions but not in the very proximal occlusions of the carotid T,” Dr. Reinhard said. “So, one strategy might be to first apply sonothrombolysis and if this does not work, then to move the patient to the endovascular treatment,” he suggested, noting that this might be a better strategy to test in a future clinical trial than directly comparing the methods in a larger number of patients.
In terms of safety, there was no significant advantage of using one procedure over the other, despite three (4.1%) patients in the endovascular group and none in the sonothrombolysis group experiencing symptomatic intracranial hemorrhage (P = .25). Type 1 parenchymal hematomas were more common in patients who had sonothrombolysis than in those who had endovascular therapy (15.3% vs. 5.5%, P = .09). Mortality at 90 days was around 20% in both groups.
Dr. Reinhard had no disclosures.
AT THE EUROPEAN STROKE CONFERENCE
Key clinical point: In patients with middle cerebral artery occlusions, sonothrombolysis might be a suitable alternative to endovascular treatment.
Major finding: There was no difference in the primary end point of final mRS comparing endovascular treatment with sonothrombolysis (OR, 1.70, P = .12).
Data source: Retrospective, observational analysis of 134 patients with acute anterior circulation stroke with M1 or carotid T occlusion who underwent endovascular stent retrieval or sonothrombolysis.
Disclosures: Dr. Reinhard had no disclosures.
Older MI patients missing out on ICDs
Fewer than one in 10 elderly patients with a low ejection fraction after myocardial infarction who are eligible to receive an implantable cardioverter-defibrillator actually receive one within a year of their myocardial infarction, a study has found.
The retrospective observational study of 10,318 patients aged over 65 years who had experienced a myocardial infarction and had an ejection fraction of 35% or less showed only 8.1% received an implantable cardioverter-defibrillator (ICD) within a year of their MI, even though implantation within a year was associated with a 36% reduction in mortality at 2 years.
Those patients who did receive an ICD were more likely to have had a prior coronary artery bypass graft, had higher peak troponin levels, experienced in-hospital cardiogenic shock, or had a cardiology follow-up within 2 weeks of discharge, according to the paper published June 23 in JAMA.
“Individualized shared decision making, taking into context the patient’s quality of life, treatment goals, and preferences, is critical, because ICD therapy may shift death from a sudden event to a more gradual comorbid process,” wrote Dr. Sean D. Pokorney, of Duke University Medical Center, Durham, N.C., and co-authors (JAMA 2015;313:2433-40 [doi: 10.1001/jama.2015.6409]).
The study was supported by the Agency for Healthcare Research& Quality, and Boston Scientific. Some authors declared research grants, honoraria, advisory board positions, and consultancies with private industry.
It is concerning that so few potentially ICD-eligible elderly patients are undergoing implantation, especially considering that ICDs significantly improve survival.
A possible scenario is that many of these patients did not receive an appropriate ICD simply because they fell into a crevasse of the fragmented health system in which overly burdened primary care physicians are expected to connect all the clinical and diagnostic information without the essential tools and necessary facts.
Dr. Robert G. Hauser is affiliated with the Minneapolis Heart Institute at the Abbott Northwestern Hospital. These comments are taken from an accompanying editorial (JAMA 2015;313:2429-31 [doi:10.1001/jama.2015.6408]). No conflicts of interest were declared.
It is concerning that so few potentially ICD-eligible elderly patients are undergoing implantation, especially considering that ICDs significantly improve survival.
A possible scenario is that many of these patients did not receive an appropriate ICD simply because they fell into a crevasse of the fragmented health system in which overly burdened primary care physicians are expected to connect all the clinical and diagnostic information without the essential tools and necessary facts.
Dr. Robert G. Hauser is affiliated with the Minneapolis Heart Institute at the Abbott Northwestern Hospital. These comments are taken from an accompanying editorial (JAMA 2015;313:2429-31 [doi:10.1001/jama.2015.6408]). No conflicts of interest were declared.
It is concerning that so few potentially ICD-eligible elderly patients are undergoing implantation, especially considering that ICDs significantly improve survival.
A possible scenario is that many of these patients did not receive an appropriate ICD simply because they fell into a crevasse of the fragmented health system in which overly burdened primary care physicians are expected to connect all the clinical and diagnostic information without the essential tools and necessary facts.
Dr. Robert G. Hauser is affiliated with the Minneapolis Heart Institute at the Abbott Northwestern Hospital. These comments are taken from an accompanying editorial (JAMA 2015;313:2429-31 [doi:10.1001/jama.2015.6408]). No conflicts of interest were declared.
Fewer than one in 10 elderly patients with a low ejection fraction after myocardial infarction who are eligible to receive an implantable cardioverter-defibrillator actually receive one within a year of their myocardial infarction, a study has found.
The retrospective observational study of 10,318 patients aged over 65 years who had experienced a myocardial infarction and had an ejection fraction of 35% or less showed only 8.1% received an implantable cardioverter-defibrillator (ICD) within a year of their MI, even though implantation within a year was associated with a 36% reduction in mortality at 2 years.
Those patients who did receive an ICD were more likely to have had a prior coronary artery bypass graft, had higher peak troponin levels, experienced in-hospital cardiogenic shock, or had a cardiology follow-up within 2 weeks of discharge, according to the paper published June 23 in JAMA.
“Individualized shared decision making, taking into context the patient’s quality of life, treatment goals, and preferences, is critical, because ICD therapy may shift death from a sudden event to a more gradual comorbid process,” wrote Dr. Sean D. Pokorney, of Duke University Medical Center, Durham, N.C., and co-authors (JAMA 2015;313:2433-40 [doi: 10.1001/jama.2015.6409]).
The study was supported by the Agency for Healthcare Research& Quality, and Boston Scientific. Some authors declared research grants, honoraria, advisory board positions, and consultancies with private industry.
Fewer than one in 10 elderly patients with a low ejection fraction after myocardial infarction who are eligible to receive an implantable cardioverter-defibrillator actually receive one within a year of their myocardial infarction, a study has found.
The retrospective observational study of 10,318 patients aged over 65 years who had experienced a myocardial infarction and had an ejection fraction of 35% or less showed only 8.1% received an implantable cardioverter-defibrillator (ICD) within a year of their MI, even though implantation within a year was associated with a 36% reduction in mortality at 2 years.
Those patients who did receive an ICD were more likely to have had a prior coronary artery bypass graft, had higher peak troponin levels, experienced in-hospital cardiogenic shock, or had a cardiology follow-up within 2 weeks of discharge, according to the paper published June 23 in JAMA.
“Individualized shared decision making, taking into context the patient’s quality of life, treatment goals, and preferences, is critical, because ICD therapy may shift death from a sudden event to a more gradual comorbid process,” wrote Dr. Sean D. Pokorney, of Duke University Medical Center, Durham, N.C., and co-authors (JAMA 2015;313:2433-40 [doi: 10.1001/jama.2015.6409]).
The study was supported by the Agency for Healthcare Research& Quality, and Boston Scientific. Some authors declared research grants, honoraria, advisory board positions, and consultancies with private industry.
FROM JAMA
Key clinical point: Many elderly patients who are eligible for an implantable cardioverter-defibrillator after a myocardial infarction are not receiving them.
Major finding: Only 8.1% of older patients with an ejection fraction of less than 35% after a myocardial infarction receive an implantable cardioverter-defibrillator.
Data source: Retrospective observational study of 10,318 patients aged over 65 years.
Disclosures: The study was supported by the Agency for Healthcare Research & Quality, and Boston Scientific. Some authors declared research grants, honoraria, advisory board positions, and consultancies with private industry.
An Update on Acute Care Surgery, Part 2
In continuing with the series, An Update in Acute Care Surgery, the following section highlights the evolution of the training process for the Acute Care Surgery fellowship.
Grace S. Rozycki, MD, FACS
The Willis D. Gatch Professor of Surgery
Associate Chair, Department of Surgery, Indiana University
Chief of Surgery, IUH-Methodist Hospital, Indianapolis
Acute Care Surgery: The Training Paradigm
BY CLAY COTHREN BURLEW, MD, FACS, AND GREGORY J. JURKOVICH, MD., FACS
The acute care surgery fellowships are designed to follow core training in general surgery (J. Trauma 2007;62:553-6). Currently, this means the acute care surgery fellowship follows the completion of an Accreditation Council for Graduate Medical Education general surgery residency program and is in alignment with the core competencies of the general surgery residency. The 2-year curriculum was defined by the AAST, and incorporates the requirements of an ACGME-approved surgical critical care fellowship.
Although there are mandatory components of this fellowship, a certain amount of latitude and creativity are encouraged so to capitalize on the strength of the individual program as well as to meet the individual needs of the fellow.
The basic principles of the training paradigm include the followi
1. The program is 2 years in length.
2. The acute care surgery fellowship programs must have the ACGME approved surgical critical care residency.
3.The fellowship must include specific surgical technical training in hepatobiliary disorders, thoracic surgery, and vascular surgery.
4. Trainees should participate in acute care surgery call for at least 12 months and 52 nights of acute care surgery call (trauma and emergency general surgery).
5. Flexibility in the rotations should be used to optimize the fellow’s training.
6. The rationale for out-of-system rotations and the structure of the 24-month training should be used to optimize the fellow’s training.
7. Participation in elective surgery, both to supplement general surgery training and experience and to serve in a supervisory role to residents, is an essential component of this fellowship training.
8. An academic environment is necessary and the fellows should be trained to teach others and conduct research in acute care surgery.
The rationale for the rotations of Thoracic Surgery, Transplant/Hepatobiliary/ Pancreatic, and Vascular (including vascular interventional) is twofold: 1) Many complex operative cases in these areas are infrequently encountered in modern trauma centers; and, 2) experts in these areas can provide mentorship and operative expertise and teaching for the fellow who obtains a focused, quality operative experience in these areas. Further, these rotations have specific competency related goals so that the fellow has specific requirements to meet. The AAST is currently revising its method of confirming this training expertise by examining specific components of operative technique and exposure as well as length of time on specific rotations (see below).
Program Application and Approval
The required background and expectations for the acute care surgery fellowship include the following: 1) Fellows must have successfully completed the core training requirements of an RRC-approved residency in General Surgery; and 2) the acute care surgery fellowship programs must provide the necessary education to qualify the fellow as an acute care surgical specialist in clinical, education, and research areas. Each program must have support from its parent institution, including administrative personnel, the chairman of the department of surgery, division chief, and participating acute care surgery faculty. The program should have all of the necessary resources to fulfill the training requirements and create an environment of inquiry and scholarship while allowing for progressive responsibility throughout the training period.
The process of becoming an approved acute care surgery fellowship program can be divided into the following steps:
1. The Program Director completes the Program Information Form (PIF) form (downloaded from the AAST website, http://www.aast.org).
2. The PIF is reviewed by three members of the AAST Acute Care Surgery Committee to determine whether it is complete and if it meets the essential requirements. If the initial review is successful, then a site visit of the program is scheduled.
3. The site visit is conducted by two members of AAST Acute Care Surgery Committee. The site visit consists of an evening business dinner meeting with the following personnel: the program director for the acute care surgery fellowship, the program director for the general surgery residency program, select administrators, and division chiefs. Current fellows in the program are also invited to participate. The following day, the site visitors tour the institution, and conduct one-on-one interviews with the personnel who were present at the site visit dinner. A chart review is conducted to assess the operative case load and the involvement of the faculty, residents, and fellows in the care of the patients. At the conclusion of the day, a summation interview is conducted with the acute care surgery fellowship program director.
4. Following the site visit, a written assessment of the program is performed, which covers an overview/program description, strengths/weaknesses, major deficiencies, and a summary with recommendations.
5. If no major deficiencies are noted, the senior site visitor presents the highlights of the program to the members of the AAST Acute Care Surgery Committee and, if approved subsequently to the AAST Board of Managers for final approval.
Acute Care Surgery Committee and Curriculum
BY CLAY COTHREN BURLEW, MD

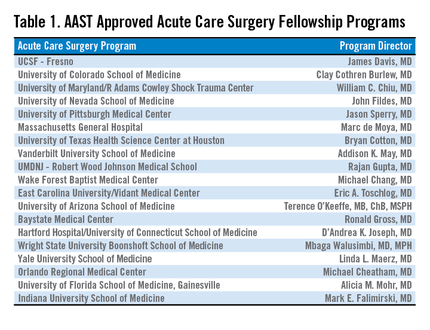
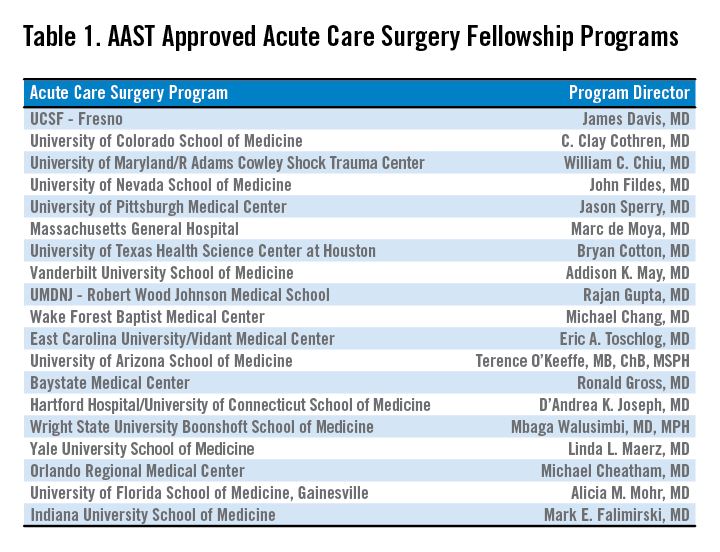
With the development of a fellowship-based training paradigm in acute care surgery, the AAST also developed an oversight committee. This committee, aptly named the Acute Care Surgery Committee, is comprised of 25 appointed AAST members. The committee represents a varied group of stakeholders including members of the senior leadership of the AAST and fellowship program directors. The Acute Care Surgery Committee’s role has evolved over the past decade. Initially the members of the Committee formulated and implemented the training paradigm for the fellowship, including the requirements enumerated above. Following the certification of several successful training fellowships in 2008-2009, the Committee encouraged additional institutions to initiate training fellows by assisting with educational development. This led to the expansion of acute care surgery training in 19 accredited programs. (see Table).
Throughout this decade of growth, the Acute Care Surgery committee has also been dedicated to the oversight and continual evaluation of the training process. Two specific measures were implemented in this regard.
First, each fellowship graduate must take not only the American Board of Surgery examination for certification in Surgical Critical Care, but also the examination in acute care surgery written by the AAST. The Acute Care Surgery Committee formed a subcommittee that has spent innumerable hours researching and writing test questions for this examination. That subcommittee is now reviewing each of the questions from the originally produced examination and reformatting the test. New questions are being created by the subcommittee, and the examination will become electronically administered.
Second, acute care surgery fellows must track their operative experience through the AAST-supported on-line case log system. Although fellows have been provided with a list of essential and desired operative cases, the case log system permits specific delineation of each fellow’s experience. Using the case log system, the Acute Care Surgery Committee was able to analyze the fellows’ experience, identify gaps in operative training, and refine the curriculum as indicated. The Committee has performed two such analyses and, based on the findings of those reports, modification of the curriculum is now underway. (J. Trauma Acute Care Surg. 2014;76:329-39.; J. Trauma Acute Care Surg. 2015;78:259-64).
One of the current initiatives of the Acute Care Surgery Committee is the revision of the acute care surgery fellowship curriculum. In revising the curriculum, several key points were considered. One observation, derived from the case log review, was that the original case list captured only a portion of the operative experience of acute care surgery fellows. Additionally, it was apparent that operative trauma cases alone do not provide adequate exposure to some of the more complex cases thought to be essential components of this specialty. Therefore, the Committee determined that incorporating specific surgical approaches or anatomic exposures performed during elective and urgent cases are valuable experiences for the fellow. The totality of training in advanced operative techniques over the breadth of anatomic locations remains the unique feature of our specialty.(J. Trauma Acute Care Surg. 2015; 78:192-196).
Based upon these observations, the new curriculum is now organized by anatomic subsections (Head/Neck, Thoracic, Abdominal, Vascular), as well as organ-based management. Each section of the curriculum now lists specific case numbers required for surgical approaches or exposures, and also addresses organ-based management. For example, within the thoracic section of the curriculum, required case numbers now exist for thoracotomy, thoracoscopy, sternotomy, and pericardotomy (exposures) as well as lung, diaphragm, heart, esophagus, and intrathoracic great vessels. In each anatomic subsection, simulation may be used to satisfy a requirement.
Opportunities to accomplish these requirements may be through the American College of Surgeons Advanced Trauma Operative Management or the Advanced Surgical Skills for Exposure in Trauma courses. Organ harvest exposures may also be used for less common surgical exposures. Fellows can choose both the exposure and the organ-based procedure code for each operative case performed when logging their cases.(J. Trauma Acute Care Surg. 2014;76:329-39). Identification of a minimum number of operative cases needed in specific body regions reflects the defined case volumes in general surgery as required by the Accreditation Council for Graduate Medical Education.
The Acute Care Surgery Committee considered that the implementation of the required case volumes would serve two purposes: First, the list would provide guidance to the fellows as to the types of cases they should actively identify and in which they should participate; and, second, it would provide guidance to program directors and subspecialty colleagues as to the cases deemed important for fellowship training. Ongoing review of the fellows’ case logs with implementation of the new curriculum will remain a focus of the Acute Care Surgery Committee as it transitions to a new case log system soon.
An earlier version of the graphic misstated the name of Clay Cothren Burlew.
In continuing with the series, An Update in Acute Care Surgery, the following section highlights the evolution of the training process for the Acute Care Surgery fellowship.
Grace S. Rozycki, MD, FACS
The Willis D. Gatch Professor of Surgery
Associate Chair, Department of Surgery, Indiana University
Chief of Surgery, IUH-Methodist Hospital, Indianapolis
Acute Care Surgery: The Training Paradigm
BY CLAY COTHREN BURLEW, MD, FACS, AND GREGORY J. JURKOVICH, MD., FACS
The acute care surgery fellowships are designed to follow core training in general surgery (J. Trauma 2007;62:553-6). Currently, this means the acute care surgery fellowship follows the completion of an Accreditation Council for Graduate Medical Education general surgery residency program and is in alignment with the core competencies of the general surgery residency. The 2-year curriculum was defined by the AAST, and incorporates the requirements of an ACGME-approved surgical critical care fellowship.
Although there are mandatory components of this fellowship, a certain amount of latitude and creativity are encouraged so to capitalize on the strength of the individual program as well as to meet the individual needs of the fellow.
The basic principles of the training paradigm include the followi
1. The program is 2 years in length.
2. The acute care surgery fellowship programs must have the ACGME approved surgical critical care residency.
3.The fellowship must include specific surgical technical training in hepatobiliary disorders, thoracic surgery, and vascular surgery.
4. Trainees should participate in acute care surgery call for at least 12 months and 52 nights of acute care surgery call (trauma and emergency general surgery).
5. Flexibility in the rotations should be used to optimize the fellow’s training.
6. The rationale for out-of-system rotations and the structure of the 24-month training should be used to optimize the fellow’s training.
7. Participation in elective surgery, both to supplement general surgery training and experience and to serve in a supervisory role to residents, is an essential component of this fellowship training.
8. An academic environment is necessary and the fellows should be trained to teach others and conduct research in acute care surgery.
The rationale for the rotations of Thoracic Surgery, Transplant/Hepatobiliary/ Pancreatic, and Vascular (including vascular interventional) is twofold: 1) Many complex operative cases in these areas are infrequently encountered in modern trauma centers; and, 2) experts in these areas can provide mentorship and operative expertise and teaching for the fellow who obtains a focused, quality operative experience in these areas. Further, these rotations have specific competency related goals so that the fellow has specific requirements to meet. The AAST is currently revising its method of confirming this training expertise by examining specific components of operative technique and exposure as well as length of time on specific rotations (see below).
Program Application and Approval
The required background and expectations for the acute care surgery fellowship include the following: 1) Fellows must have successfully completed the core training requirements of an RRC-approved residency in General Surgery; and 2) the acute care surgery fellowship programs must provide the necessary education to qualify the fellow as an acute care surgical specialist in clinical, education, and research areas. Each program must have support from its parent institution, including administrative personnel, the chairman of the department of surgery, division chief, and participating acute care surgery faculty. The program should have all of the necessary resources to fulfill the training requirements and create an environment of inquiry and scholarship while allowing for progressive responsibility throughout the training period.
The process of becoming an approved acute care surgery fellowship program can be divided into the following steps:
1. The Program Director completes the Program Information Form (PIF) form (downloaded from the AAST website, http://www.aast.org).
2. The PIF is reviewed by three members of the AAST Acute Care Surgery Committee to determine whether it is complete and if it meets the essential requirements. If the initial review is successful, then a site visit of the program is scheduled.
3. The site visit is conducted by two members of AAST Acute Care Surgery Committee. The site visit consists of an evening business dinner meeting with the following personnel: the program director for the acute care surgery fellowship, the program director for the general surgery residency program, select administrators, and division chiefs. Current fellows in the program are also invited to participate. The following day, the site visitors tour the institution, and conduct one-on-one interviews with the personnel who were present at the site visit dinner. A chart review is conducted to assess the operative case load and the involvement of the faculty, residents, and fellows in the care of the patients. At the conclusion of the day, a summation interview is conducted with the acute care surgery fellowship program director.
4. Following the site visit, a written assessment of the program is performed, which covers an overview/program description, strengths/weaknesses, major deficiencies, and a summary with recommendations.
5. If no major deficiencies are noted, the senior site visitor presents the highlights of the program to the members of the AAST Acute Care Surgery Committee and, if approved subsequently to the AAST Board of Managers for final approval.
Acute Care Surgery Committee and Curriculum
BY CLAY COTHREN BURLEW, MD
With the development of a fellowship-based training paradigm in acute care surgery, the AAST also developed an oversight committee. This committee, aptly named the Acute Care Surgery Committee, is comprised of 25 appointed AAST members. The committee represents a varied group of stakeholders including members of the senior leadership of the AAST and fellowship program directors. The Acute Care Surgery Committee’s role has evolved over the past decade. Initially the members of the Committee formulated and implemented the training paradigm for the fellowship, including the requirements enumerated above. Following the certification of several successful training fellowships in 2008-2009, the Committee encouraged additional institutions to initiate training fellows by assisting with educational development. This led to the expansion of acute care surgery training in 19 accredited programs. (see Table).
Throughout this decade of growth, the Acute Care Surgery committee has also been dedicated to the oversight and continual evaluation of the training process. Two specific measures were implemented in this regard.
First, each fellowship graduate must take not only the American Board of Surgery examination for certification in Surgical Critical Care, but also the examination in acute care surgery written by the AAST. The Acute Care Surgery Committee formed a subcommittee that has spent innumerable hours researching and writing test questions for this examination. That subcommittee is now reviewing each of the questions from the originally produced examination and reformatting the test. New questions are being created by the subcommittee, and the examination will become electronically administered.
Second, acute care surgery fellows must track their operative experience through the AAST-supported on-line case log system. Although fellows have been provided with a list of essential and desired operative cases, the case log system permits specific delineation of each fellow’s experience. Using the case log system, the Acute Care Surgery Committee was able to analyze the fellows’ experience, identify gaps in operative training, and refine the curriculum as indicated. The Committee has performed two such analyses and, based on the findings of those reports, modification of the curriculum is now underway. (J. Trauma Acute Care Surg. 2014;76:329-39.; J. Trauma Acute Care Surg. 2015;78:259-64).
One of the current initiatives of the Acute Care Surgery Committee is the revision of the acute care surgery fellowship curriculum. In revising the curriculum, several key points were considered. One observation, derived from the case log review, was that the original case list captured only a portion of the operative experience of acute care surgery fellows. Additionally, it was apparent that operative trauma cases alone do not provide adequate exposure to some of the more complex cases thought to be essential components of this specialty. Therefore, the Committee determined that incorporating specific surgical approaches or anatomic exposures performed during elective and urgent cases are valuable experiences for the fellow. The totality of training in advanced operative techniques over the breadth of anatomic locations remains the unique feature of our specialty.(J. Trauma Acute Care Surg. 2015; 78:192-196).
Based upon these observations, the new curriculum is now organized by anatomic subsections (Head/Neck, Thoracic, Abdominal, Vascular), as well as organ-based management. Each section of the curriculum now lists specific case numbers required for surgical approaches or exposures, and also addresses organ-based management. For example, within the thoracic section of the curriculum, required case numbers now exist for thoracotomy, thoracoscopy, sternotomy, and pericardotomy (exposures) as well as lung, diaphragm, heart, esophagus, and intrathoracic great vessels. In each anatomic subsection, simulation may be used to satisfy a requirement.
Opportunities to accomplish these requirements may be through the American College of Surgeons Advanced Trauma Operative Management or the Advanced Surgical Skills for Exposure in Trauma courses. Organ harvest exposures may also be used for less common surgical exposures. Fellows can choose both the exposure and the organ-based procedure code for each operative case performed when logging their cases.(J. Trauma Acute Care Surg. 2014;76:329-39). Identification of a minimum number of operative cases needed in specific body regions reflects the defined case volumes in general surgery as required by the Accreditation Council for Graduate Medical Education.
The Acute Care Surgery Committee considered that the implementation of the required case volumes would serve two purposes: First, the list would provide guidance to the fellows as to the types of cases they should actively identify and in which they should participate; and, second, it would provide guidance to program directors and subspecialty colleagues as to the cases deemed important for fellowship training. Ongoing review of the fellows’ case logs with implementation of the new curriculum will remain a focus of the Acute Care Surgery Committee as it transitions to a new case log system soon.
An earlier version of the graphic misstated the name of Clay Cothren Burlew.
In continuing with the series, An Update in Acute Care Surgery, the following section highlights the evolution of the training process for the Acute Care Surgery fellowship.
Grace S. Rozycki, MD, FACS
The Willis D. Gatch Professor of Surgery
Associate Chair, Department of Surgery, Indiana University
Chief of Surgery, IUH-Methodist Hospital, Indianapolis
Acute Care Surgery: The Training Paradigm
BY CLAY COTHREN BURLEW, MD, FACS, AND GREGORY J. JURKOVICH, MD., FACS
The acute care surgery fellowships are designed to follow core training in general surgery (J. Trauma 2007;62:553-6). Currently, this means the acute care surgery fellowship follows the completion of an Accreditation Council for Graduate Medical Education general surgery residency program and is in alignment with the core competencies of the general surgery residency. The 2-year curriculum was defined by the AAST, and incorporates the requirements of an ACGME-approved surgical critical care fellowship.
Although there are mandatory components of this fellowship, a certain amount of latitude and creativity are encouraged so to capitalize on the strength of the individual program as well as to meet the individual needs of the fellow.
The basic principles of the training paradigm include the followi
1. The program is 2 years in length.
2. The acute care surgery fellowship programs must have the ACGME approved surgical critical care residency.
3.The fellowship must include specific surgical technical training in hepatobiliary disorders, thoracic surgery, and vascular surgery.
4. Trainees should participate in acute care surgery call for at least 12 months and 52 nights of acute care surgery call (trauma and emergency general surgery).
5. Flexibility in the rotations should be used to optimize the fellow’s training.
6. The rationale for out-of-system rotations and the structure of the 24-month training should be used to optimize the fellow’s training.
7. Participation in elective surgery, both to supplement general surgery training and experience and to serve in a supervisory role to residents, is an essential component of this fellowship training.
8. An academic environment is necessary and the fellows should be trained to teach others and conduct research in acute care surgery.
The rationale for the rotations of Thoracic Surgery, Transplant/Hepatobiliary/ Pancreatic, and Vascular (including vascular interventional) is twofold: 1) Many complex operative cases in these areas are infrequently encountered in modern trauma centers; and, 2) experts in these areas can provide mentorship and operative expertise and teaching for the fellow who obtains a focused, quality operative experience in these areas. Further, these rotations have specific competency related goals so that the fellow has specific requirements to meet. The AAST is currently revising its method of confirming this training expertise by examining specific components of operative technique and exposure as well as length of time on specific rotations (see below).
Program Application and Approval
The required background and expectations for the acute care surgery fellowship include the following: 1) Fellows must have successfully completed the core training requirements of an RRC-approved residency in General Surgery; and 2) the acute care surgery fellowship programs must provide the necessary education to qualify the fellow as an acute care surgical specialist in clinical, education, and research areas. Each program must have support from its parent institution, including administrative personnel, the chairman of the department of surgery, division chief, and participating acute care surgery faculty. The program should have all of the necessary resources to fulfill the training requirements and create an environment of inquiry and scholarship while allowing for progressive responsibility throughout the training period.
The process of becoming an approved acute care surgery fellowship program can be divided into the following steps:
1. The Program Director completes the Program Information Form (PIF) form (downloaded from the AAST website, http://www.aast.org).
2. The PIF is reviewed by three members of the AAST Acute Care Surgery Committee to determine whether it is complete and if it meets the essential requirements. If the initial review is successful, then a site visit of the program is scheduled.
3. The site visit is conducted by two members of AAST Acute Care Surgery Committee. The site visit consists of an evening business dinner meeting with the following personnel: the program director for the acute care surgery fellowship, the program director for the general surgery residency program, select administrators, and division chiefs. Current fellows in the program are also invited to participate. The following day, the site visitors tour the institution, and conduct one-on-one interviews with the personnel who were present at the site visit dinner. A chart review is conducted to assess the operative case load and the involvement of the faculty, residents, and fellows in the care of the patients. At the conclusion of the day, a summation interview is conducted with the acute care surgery fellowship program director.
4. Following the site visit, a written assessment of the program is performed, which covers an overview/program description, strengths/weaknesses, major deficiencies, and a summary with recommendations.
5. If no major deficiencies are noted, the senior site visitor presents the highlights of the program to the members of the AAST Acute Care Surgery Committee and, if approved subsequently to the AAST Board of Managers for final approval.
Acute Care Surgery Committee and Curriculum
BY CLAY COTHREN BURLEW, MD
With the development of a fellowship-based training paradigm in acute care surgery, the AAST also developed an oversight committee. This committee, aptly named the Acute Care Surgery Committee, is comprised of 25 appointed AAST members. The committee represents a varied group of stakeholders including members of the senior leadership of the AAST and fellowship program directors. The Acute Care Surgery Committee’s role has evolved over the past decade. Initially the members of the Committee formulated and implemented the training paradigm for the fellowship, including the requirements enumerated above. Following the certification of several successful training fellowships in 2008-2009, the Committee encouraged additional institutions to initiate training fellows by assisting with educational development. This led to the expansion of acute care surgery training in 19 accredited programs. (see Table).
Throughout this decade of growth, the Acute Care Surgery committee has also been dedicated to the oversight and continual evaluation of the training process. Two specific measures were implemented in this regard.
First, each fellowship graduate must take not only the American Board of Surgery examination for certification in Surgical Critical Care, but also the examination in acute care surgery written by the AAST. The Acute Care Surgery Committee formed a subcommittee that has spent innumerable hours researching and writing test questions for this examination. That subcommittee is now reviewing each of the questions from the originally produced examination and reformatting the test. New questions are being created by the subcommittee, and the examination will become electronically administered.
Second, acute care surgery fellows must track their operative experience through the AAST-supported on-line case log system. Although fellows have been provided with a list of essential and desired operative cases, the case log system permits specific delineation of each fellow’s experience. Using the case log system, the Acute Care Surgery Committee was able to analyze the fellows’ experience, identify gaps in operative training, and refine the curriculum as indicated. The Committee has performed two such analyses and, based on the findings of those reports, modification of the curriculum is now underway. (J. Trauma Acute Care Surg. 2014;76:329-39.; J. Trauma Acute Care Surg. 2015;78:259-64).
One of the current initiatives of the Acute Care Surgery Committee is the revision of the acute care surgery fellowship curriculum. In revising the curriculum, several key points were considered. One observation, derived from the case log review, was that the original case list captured only a portion of the operative experience of acute care surgery fellows. Additionally, it was apparent that operative trauma cases alone do not provide adequate exposure to some of the more complex cases thought to be essential components of this specialty. Therefore, the Committee determined that incorporating specific surgical approaches or anatomic exposures performed during elective and urgent cases are valuable experiences for the fellow. The totality of training in advanced operative techniques over the breadth of anatomic locations remains the unique feature of our specialty.(J. Trauma Acute Care Surg. 2015; 78:192-196).
Based upon these observations, the new curriculum is now organized by anatomic subsections (Head/Neck, Thoracic, Abdominal, Vascular), as well as organ-based management. Each section of the curriculum now lists specific case numbers required for surgical approaches or exposures, and also addresses organ-based management. For example, within the thoracic section of the curriculum, required case numbers now exist for thoracotomy, thoracoscopy, sternotomy, and pericardotomy (exposures) as well as lung, diaphragm, heart, esophagus, and intrathoracic great vessels. In each anatomic subsection, simulation may be used to satisfy a requirement.
Opportunities to accomplish these requirements may be through the American College of Surgeons Advanced Trauma Operative Management or the Advanced Surgical Skills for Exposure in Trauma courses. Organ harvest exposures may also be used for less common surgical exposures. Fellows can choose both the exposure and the organ-based procedure code for each operative case performed when logging their cases.(J. Trauma Acute Care Surg. 2014;76:329-39). Identification of a minimum number of operative cases needed in specific body regions reflects the defined case volumes in general surgery as required by the Accreditation Council for Graduate Medical Education.
The Acute Care Surgery Committee considered that the implementation of the required case volumes would serve two purposes: First, the list would provide guidance to the fellows as to the types of cases they should actively identify and in which they should participate; and, second, it would provide guidance to program directors and subspecialty colleagues as to the cases deemed important for fellowship training. Ongoing review of the fellows’ case logs with implementation of the new curriculum will remain a focus of the Acute Care Surgery Committee as it transitions to a new case log system soon.
An earlier version of the graphic misstated the name of Clay Cothren Burlew.
Earlier start to plasma transfusions for persistent postpartum hemorrhage does not improve maternal outcomes
TORONTO – For women with persistent postpartum hemorrhage, correction of coagulopathy by administering plasma is often an inevitable treatment decision. There are little clinical data, however, on whether an early or a late start for plasma transfusion leads to more positive maternal outcomes.
Data presented on Wednesday at the ISTH 2015 Congress by Dr. Dacia Henriquez of the department of obstetrics and gynecology at Leiden (the Netherlands) University Medical Center, may help answer that question.
“Our findings do not support the notion that plasma transfusion within 60 minutes after diagnosing persistent postpartum hemorrhage contributes to the reduction of the risk of adverse maternal outcomes,” Dr. Henriquez said in an interview.

The TeMpOh-1 (Transfusion Strategies in Women with Major Obstetric Hemorrhage) study included 1,217 women with postpartum hemorrhage (PPH) that was refractory to first-line obstetric interventions. The women were treated at 61 Dutch hospitals in 2011 and 2012.
“With this selection, our study results can be easily translated to daily clinical practice because of this clearly identifiable turning-point in treatment,” she said.
All women included in the study received either at least four units of red blood cells or a multicomponent transfusion within 24 hours after delivery (≥ 1000 mL). Median bleeding rate at baseline was 1.1 L at 1 hour, and median total blood loss was 3.0 L. Marginal structural models with inverse probability of treatment weighting were constructed to quantify the difference in maternal outcomes – including arterial embolism, hysterectomy, and maternal mortality – between an early (within 60 minutes) and a late (after 60 minutes) start of plasma transfusion (163 women vs. 1,054 women, respectively).
After adjustment for baseline parameters, bleeding severity, and changes over time, no significant differences were seen between the groups (odds ratios, 1.1 and 0.8, respectively).
“It seemed that after adjustment for patient and bleeding characteristics, plasma transfusion within 60 minutes after diagnosis of persistent PPH was not associated with a reduction in adverse maternal outcomes,” she said, noting that analyses are ongoing, and efforts are underway to determine whether time-dependent confounding was handled properly in the study.
Plans are also in place to perform subgroup analyses to assess whether treatment effect will differ between those with the most severe bleeding and those with initially milder hemorrhage, she said.
“With the TeMpOH-1 data, we were also able to demonstrate that dilutional coagulopathy due to volume resuscitation with crystalloids and colloids was associated with greater total blood loss and more adverse maternal outcomes when the clear fluids volume exceeded 4 L,” Dr. Henriquez said.
“A treatment strategy aiming at prevention rather than correction of coagulopathy in women with persistent PPH in daily clinical practice seems justified, because correction of coagulopathy by administering plasma appears to be of limited value in reducing adverse maternal outcomes,” Dr. Henriquez said.
Dr. Henriquez declared no disclosures.
TORONTO – For women with persistent postpartum hemorrhage, correction of coagulopathy by administering plasma is often an inevitable treatment decision. There are little clinical data, however, on whether an early or a late start for plasma transfusion leads to more positive maternal outcomes.
Data presented on Wednesday at the ISTH 2015 Congress by Dr. Dacia Henriquez of the department of obstetrics and gynecology at Leiden (the Netherlands) University Medical Center, may help answer that question.
“Our findings do not support the notion that plasma transfusion within 60 minutes after diagnosing persistent postpartum hemorrhage contributes to the reduction of the risk of adverse maternal outcomes,” Dr. Henriquez said in an interview.
The TeMpOh-1 (Transfusion Strategies in Women with Major Obstetric Hemorrhage) study included 1,217 women with postpartum hemorrhage (PPH) that was refractory to first-line obstetric interventions. The women were treated at 61 Dutch hospitals in 2011 and 2012.
“With this selection, our study results can be easily translated to daily clinical practice because of this clearly identifiable turning-point in treatment,” she said.
All women included in the study received either at least four units of red blood cells or a multicomponent transfusion within 24 hours after delivery (≥ 1000 mL). Median bleeding rate at baseline was 1.1 L at 1 hour, and median total blood loss was 3.0 L. Marginal structural models with inverse probability of treatment weighting were constructed to quantify the difference in maternal outcomes – including arterial embolism, hysterectomy, and maternal mortality – between an early (within 60 minutes) and a late (after 60 minutes) start of plasma transfusion (163 women vs. 1,054 women, respectively).
After adjustment for baseline parameters, bleeding severity, and changes over time, no significant differences were seen between the groups (odds ratios, 1.1 and 0.8, respectively).
“It seemed that after adjustment for patient and bleeding characteristics, plasma transfusion within 60 minutes after diagnosis of persistent PPH was not associated with a reduction in adverse maternal outcomes,” she said, noting that analyses are ongoing, and efforts are underway to determine whether time-dependent confounding was handled properly in the study.
Plans are also in place to perform subgroup analyses to assess whether treatment effect will differ between those with the most severe bleeding and those with initially milder hemorrhage, she said.
“With the TeMpOH-1 data, we were also able to demonstrate that dilutional coagulopathy due to volume resuscitation with crystalloids and colloids was associated with greater total blood loss and more adverse maternal outcomes when the clear fluids volume exceeded 4 L,” Dr. Henriquez said.
“A treatment strategy aiming at prevention rather than correction of coagulopathy in women with persistent PPH in daily clinical practice seems justified, because correction of coagulopathy by administering plasma appears to be of limited value in reducing adverse maternal outcomes,” Dr. Henriquez said.
Dr. Henriquez declared no disclosures.
TORONTO – For women with persistent postpartum hemorrhage, correction of coagulopathy by administering plasma is often an inevitable treatment decision. There are little clinical data, however, on whether an early or a late start for plasma transfusion leads to more positive maternal outcomes.
Data presented on Wednesday at the ISTH 2015 Congress by Dr. Dacia Henriquez of the department of obstetrics and gynecology at Leiden (the Netherlands) University Medical Center, may help answer that question.
“Our findings do not support the notion that plasma transfusion within 60 minutes after diagnosing persistent postpartum hemorrhage contributes to the reduction of the risk of adverse maternal outcomes,” Dr. Henriquez said in an interview.
The TeMpOh-1 (Transfusion Strategies in Women with Major Obstetric Hemorrhage) study included 1,217 women with postpartum hemorrhage (PPH) that was refractory to first-line obstetric interventions. The women were treated at 61 Dutch hospitals in 2011 and 2012.
“With this selection, our study results can be easily translated to daily clinical practice because of this clearly identifiable turning-point in treatment,” she said.
All women included in the study received either at least four units of red blood cells or a multicomponent transfusion within 24 hours after delivery (≥ 1000 mL). Median bleeding rate at baseline was 1.1 L at 1 hour, and median total blood loss was 3.0 L. Marginal structural models with inverse probability of treatment weighting were constructed to quantify the difference in maternal outcomes – including arterial embolism, hysterectomy, and maternal mortality – between an early (within 60 minutes) and a late (after 60 minutes) start of plasma transfusion (163 women vs. 1,054 women, respectively).
After adjustment for baseline parameters, bleeding severity, and changes over time, no significant differences were seen between the groups (odds ratios, 1.1 and 0.8, respectively).
“It seemed that after adjustment for patient and bleeding characteristics, plasma transfusion within 60 minutes after diagnosis of persistent PPH was not associated with a reduction in adverse maternal outcomes,” she said, noting that analyses are ongoing, and efforts are underway to determine whether time-dependent confounding was handled properly in the study.
Plans are also in place to perform subgroup analyses to assess whether treatment effect will differ between those with the most severe bleeding and those with initially milder hemorrhage, she said.
“With the TeMpOH-1 data, we were also able to demonstrate that dilutional coagulopathy due to volume resuscitation with crystalloids and colloids was associated with greater total blood loss and more adverse maternal outcomes when the clear fluids volume exceeded 4 L,” Dr. Henriquez said.
“A treatment strategy aiming at prevention rather than correction of coagulopathy in women with persistent PPH in daily clinical practice seems justified, because correction of coagulopathy by administering plasma appears to be of limited value in reducing adverse maternal outcomes,” Dr. Henriquez said.
Dr. Henriquez declared no disclosures.
AT 2015 ISTH
Key clinical point: Plasma transfusion within 60 minutes after diagnosis of persistent PPH was not associated with a reduction in adverse maternal outcomes.
Major finding: No significant differences were seen in maternal outcomes (ncluding arterial embolism, hysterectomy and maternal mortality) between the patients treated with plasma transfusions early (within 60 minutes) and late (after 60 minutes) (odds ratios, 1.1 and 0.8, respectively).
Data source: 1,217 women with postpartum hemorrhage (PPH) that was refractory to first-line obstetric interventions I.
Disclosures: Dr. Henriquez declared no disclosures.

Optical imaging has bright future for cancer surgery
For cancer patients and the surgeons who treat them, tumor margins matter. The amount of malignant tissue left behind after cancer surgery can make a profound difference in overall survival, but sparing healthy tissue while removing as much tumor as possible is limited by the surgeon’s ability to differentiate one from the other.
Now, new optical imaging techniques that deliver fluorescing molecules specifically to tumor targets show promise to allow both surgeons and pathologists to optimize cancer surgery. These intraoperative techniques use fluorescent molecules tagged to a ligand that binds to a target site on malignant cells. Thus, uptake occurs only in the malignant cells, highlighting them for the surgeon and for pathologists assessing margin adequacy.
Dr. Sunil Singhal of the University of Pennsylvania, Philadelphia, has coined the term “optical biopsy” to describe what’s happening during optical imaging-guided surgery. “For so long, we as surgeons have just had our eyes and our hands – and our intuition – to guide us. This technology allows us to really focus our attention where it needs to be in surgery.”
Optical imaging in surgery uses a variety of fluorescing molecules, some of which were originally derived from sources as diverse as scorpions and fireflies. Some of these glow in the visible spectrum, but increasingly, optical imaging techniques are employing molecules that fluoresce when excited by light in the near-infrared spectrum.
Using the near-infrared spectrum, said Dr. Eben Rosenthal, the Anne and John Doerr Medical Director of the Stanford (Calif.) Cancer Center, does two things: it allows for visualization deeper into tissues – up to 1 or 2 cm – and it improves the signal-to-noise ratio that can be a problem in the visual spectrum, where tissue autofluorescence occurs.
Cameras, endoscopes, and surgical microscopes can all be equipped to display the fluorescence and coregister the image with the white-light view the surgeon or pathologist normally sees. Surgeons using optical imaging techniques can usually continue to use the same tools and the same interface they are accustomed to.
Ligands can be small molecules, such as folate, or complex glycoproteins, such as monoclonal antibodies: all will bind selectively to sites on tumor cells. Patients are infused with the fluorescence-tagged ligand complexes before surgery, with timing appropriate to the half-lives of the agents, so infusions may happen the day before or the day of surgery.
For Dr. Rosenthal, using monoclonal antibodies to target tumors for optical imaging techniques affords several advantages. The antibodies are approved by the Food and Drug Administration, with known safety and side effect profiles. The antibodies can be tagged with an FDA-approved fluorescing molecule, allowing an easier approval process for the compound agent. Finally, the epidermal growth factor receptor (EGFR) target of these monoclonal antibodies is well expressed in many target tumor cells, including melanoma, breast, glioma, and colorectal cancers.
Dr. Singhal’s group has been working with fluorescein-tagged folate to identify pulmonary adenocarcinomas and is exploring use of other agents as well. “We like small molecules,” he said. “We can avoid lots of problems with biotoxicity.”
Annexin A2 (ANXA2) is a molecule expressed on the surface of cancer cells but found intracellularly in healthy cells, and it is the target of the chlorotoxin conjugate used by Dr. Jim Olson of Seattle’s Fred Hutchinson Cancer Research Center. Target malignancies may include glioblastoma, medullablastoma, sarcoma, and prostate and intestinal cancers.
Regardless of the target, however, optical imaging techniques may be particularly well suited for tumors occurring in areas where a generous dissection can have potentially devastating consequences, as in the head and neck, and for brain tumors. By giving the surgeon a clear delineation of malignant tissue, optical imaging can help the surgeon strike a balance to achieve the most conservative dissection that still achieves a complete gross dissection of the malignancy.
Achieving gross total dissection during cancer surgery is an important goal, said Dr. Olson. Citing devastating childhood brain tumors such as medulloblastomas and gliomablastomas, he noted that optical imaging can help surgeons avoid leaving behind any bulk areas of tumor, where hypoxic regions and therapy-resistant changes in tumor physiology may reduce the chance for cure. “Surgery is one of the most important elements of curing cancer,” he said. He pointed out that, in children with medulloblastomas, if nearly all tumor tissue is removed, less radiation is needed and survival is improved, even with less radiation – even if very small amounts of cancer remain.
Limitations of these technologies depend, to some extent, on the tissue targets, on substrates used to deliver the fluorescing molecules, and on the fluorescent agents themselves. Even with the enhanced tissue penetration of near-infrared light, the surgeon can really only see a centimeter or two beneath the surface of a solid organ. Said Dr. Singhal, “The basic limitation is that we’re talking about light.” However, if presurgery imaging identifies an area of concern, the surgeon can direct his or her dissection more carefully when the malignant tissue glows during surgery.
Dr. Rosenthal noted that pathologists also are making use of optical imaging to guide their processes. Since only about 5% of most tumor margins are sampled, there is an inevitable chance of sampling error with the resulting potential for a false-negative pathology result. “This technique augments the pathologist’s role and allows for improved biopsy results,” he said. Using image-guided pathology offers a way to test the margins immediately, helping the pathologist ascertain where the surgeon’s attention should be focused. Optical imaging, he said, “will in many ways change and enhance the experience for everybody.”
Dr. Olson, looking forward, asked, “If we can deliver the ability to light up, why can’t we deliver chemotherapy?” He sees an optical imaging future that will make flexible use of ligands to delineate tumors and test drug delivery.
There are many ways optical imaging can improve the practice of cancer surgery, Dr. Rosenthal said. “Historically, surgery has been a hard area to study because it’s so variable.” Following results from optical imaging–guided precision surgery, he said, will allow surgeons to identify and achieve “the right margin for the right cancer.”
Looking to the future, Dr. Singhal said, “it won’t be an either/or scenario. I think there will be multiple targets, multiple agents for this technology. We, as surgeons, have an obligation to our profession to move ahead with this.”
On Twitter @karioakes
For cancer patients and the surgeons who treat them, tumor margins matter. The amount of malignant tissue left behind after cancer surgery can make a profound difference in overall survival, but sparing healthy tissue while removing as much tumor as possible is limited by the surgeon’s ability to differentiate one from the other.
Now, new optical imaging techniques that deliver fluorescing molecules specifically to tumor targets show promise to allow both surgeons and pathologists to optimize cancer surgery. These intraoperative techniques use fluorescent molecules tagged to a ligand that binds to a target site on malignant cells. Thus, uptake occurs only in the malignant cells, highlighting them for the surgeon and for pathologists assessing margin adequacy.
Dr. Sunil Singhal of the University of Pennsylvania, Philadelphia, has coined the term “optical biopsy” to describe what’s happening during optical imaging-guided surgery. “For so long, we as surgeons have just had our eyes and our hands – and our intuition – to guide us. This technology allows us to really focus our attention where it needs to be in surgery.”
Optical imaging in surgery uses a variety of fluorescing molecules, some of which were originally derived from sources as diverse as scorpions and fireflies. Some of these glow in the visible spectrum, but increasingly, optical imaging techniques are employing molecules that fluoresce when excited by light in the near-infrared spectrum.
Using the near-infrared spectrum, said Dr. Eben Rosenthal, the Anne and John Doerr Medical Director of the Stanford (Calif.) Cancer Center, does two things: it allows for visualization deeper into tissues – up to 1 or 2 cm – and it improves the signal-to-noise ratio that can be a problem in the visual spectrum, where tissue autofluorescence occurs.
Cameras, endoscopes, and surgical microscopes can all be equipped to display the fluorescence and coregister the image with the white-light view the surgeon or pathologist normally sees. Surgeons using optical imaging techniques can usually continue to use the same tools and the same interface they are accustomed to.
Ligands can be small molecules, such as folate, or complex glycoproteins, such as monoclonal antibodies: all will bind selectively to sites on tumor cells. Patients are infused with the fluorescence-tagged ligand complexes before surgery, with timing appropriate to the half-lives of the agents, so infusions may happen the day before or the day of surgery.
For Dr. Rosenthal, using monoclonal antibodies to target tumors for optical imaging techniques affords several advantages. The antibodies are approved by the Food and Drug Administration, with known safety and side effect profiles. The antibodies can be tagged with an FDA-approved fluorescing molecule, allowing an easier approval process for the compound agent. Finally, the epidermal growth factor receptor (EGFR) target of these monoclonal antibodies is well expressed in many target tumor cells, including melanoma, breast, glioma, and colorectal cancers.
Dr. Singhal’s group has been working with fluorescein-tagged folate to identify pulmonary adenocarcinomas and is exploring use of other agents as well. “We like small molecules,” he said. “We can avoid lots of problems with biotoxicity.”
Annexin A2 (ANXA2) is a molecule expressed on the surface of cancer cells but found intracellularly in healthy cells, and it is the target of the chlorotoxin conjugate used by Dr. Jim Olson of Seattle’s Fred Hutchinson Cancer Research Center. Target malignancies may include glioblastoma, medullablastoma, sarcoma, and prostate and intestinal cancers.
Regardless of the target, however, optical imaging techniques may be particularly well suited for tumors occurring in areas where a generous dissection can have potentially devastating consequences, as in the head and neck, and for brain tumors. By giving the surgeon a clear delineation of malignant tissue, optical imaging can help the surgeon strike a balance to achieve the most conservative dissection that still achieves a complete gross dissection of the malignancy.
Achieving gross total dissection during cancer surgery is an important goal, said Dr. Olson. Citing devastating childhood brain tumors such as medulloblastomas and gliomablastomas, he noted that optical imaging can help surgeons avoid leaving behind any bulk areas of tumor, where hypoxic regions and therapy-resistant changes in tumor physiology may reduce the chance for cure. “Surgery is one of the most important elements of curing cancer,” he said. He pointed out that, in children with medulloblastomas, if nearly all tumor tissue is removed, less radiation is needed and survival is improved, even with less radiation – even if very small amounts of cancer remain.
Limitations of these technologies depend, to some extent, on the tissue targets, on substrates used to deliver the fluorescing molecules, and on the fluorescent agents themselves. Even with the enhanced tissue penetration of near-infrared light, the surgeon can really only see a centimeter or two beneath the surface of a solid organ. Said Dr. Singhal, “The basic limitation is that we’re talking about light.” However, if presurgery imaging identifies an area of concern, the surgeon can direct his or her dissection more carefully when the malignant tissue glows during surgery.
Dr. Rosenthal noted that pathologists also are making use of optical imaging to guide their processes. Since only about 5% of most tumor margins are sampled, there is an inevitable chance of sampling error with the resulting potential for a false-negative pathology result. “This technique augments the pathologist’s role and allows for improved biopsy results,” he said. Using image-guided pathology offers a way to test the margins immediately, helping the pathologist ascertain where the surgeon’s attention should be focused. Optical imaging, he said, “will in many ways change and enhance the experience for everybody.”
Dr. Olson, looking forward, asked, “If we can deliver the ability to light up, why can’t we deliver chemotherapy?” He sees an optical imaging future that will make flexible use of ligands to delineate tumors and test drug delivery.
There are many ways optical imaging can improve the practice of cancer surgery, Dr. Rosenthal said. “Historically, surgery has been a hard area to study because it’s so variable.” Following results from optical imaging–guided precision surgery, he said, will allow surgeons to identify and achieve “the right margin for the right cancer.”
Looking to the future, Dr. Singhal said, “it won’t be an either/or scenario. I think there will be multiple targets, multiple agents for this technology. We, as surgeons, have an obligation to our profession to move ahead with this.”
On Twitter @karioakes
For cancer patients and the surgeons who treat them, tumor margins matter. The amount of malignant tissue left behind after cancer surgery can make a profound difference in overall survival, but sparing healthy tissue while removing as much tumor as possible is limited by the surgeon’s ability to differentiate one from the other.
Now, new optical imaging techniques that deliver fluorescing molecules specifically to tumor targets show promise to allow both surgeons and pathologists to optimize cancer surgery. These intraoperative techniques use fluorescent molecules tagged to a ligand that binds to a target site on malignant cells. Thus, uptake occurs only in the malignant cells, highlighting them for the surgeon and for pathologists assessing margin adequacy.
Dr. Sunil Singhal of the University of Pennsylvania, Philadelphia, has coined the term “optical biopsy” to describe what’s happening during optical imaging-guided surgery. “For so long, we as surgeons have just had our eyes and our hands – and our intuition – to guide us. This technology allows us to really focus our attention where it needs to be in surgery.”
Optical imaging in surgery uses a variety of fluorescing molecules, some of which were originally derived from sources as diverse as scorpions and fireflies. Some of these glow in the visible spectrum, but increasingly, optical imaging techniques are employing molecules that fluoresce when excited by light in the near-infrared spectrum.
Using the near-infrared spectrum, said Dr. Eben Rosenthal, the Anne and John Doerr Medical Director of the Stanford (Calif.) Cancer Center, does two things: it allows for visualization deeper into tissues – up to 1 or 2 cm – and it improves the signal-to-noise ratio that can be a problem in the visual spectrum, where tissue autofluorescence occurs.
Cameras, endoscopes, and surgical microscopes can all be equipped to display the fluorescence and coregister the image with the white-light view the surgeon or pathologist normally sees. Surgeons using optical imaging techniques can usually continue to use the same tools and the same interface they are accustomed to.
Ligands can be small molecules, such as folate, or complex glycoproteins, such as monoclonal antibodies: all will bind selectively to sites on tumor cells. Patients are infused with the fluorescence-tagged ligand complexes before surgery, with timing appropriate to the half-lives of the agents, so infusions may happen the day before or the day of surgery.
For Dr. Rosenthal, using monoclonal antibodies to target tumors for optical imaging techniques affords several advantages. The antibodies are approved by the Food and Drug Administration, with known safety and side effect profiles. The antibodies can be tagged with an FDA-approved fluorescing molecule, allowing an easier approval process for the compound agent. Finally, the epidermal growth factor receptor (EGFR) target of these monoclonal antibodies is well expressed in many target tumor cells, including melanoma, breast, glioma, and colorectal cancers.
Dr. Singhal’s group has been working with fluorescein-tagged folate to identify pulmonary adenocarcinomas and is exploring use of other agents as well. “We like small molecules,” he said. “We can avoid lots of problems with biotoxicity.”
Annexin A2 (ANXA2) is a molecule expressed on the surface of cancer cells but found intracellularly in healthy cells, and it is the target of the chlorotoxin conjugate used by Dr. Jim Olson of Seattle’s Fred Hutchinson Cancer Research Center. Target malignancies may include glioblastoma, medullablastoma, sarcoma, and prostate and intestinal cancers.
Regardless of the target, however, optical imaging techniques may be particularly well suited for tumors occurring in areas where a generous dissection can have potentially devastating consequences, as in the head and neck, and for brain tumors. By giving the surgeon a clear delineation of malignant tissue, optical imaging can help the surgeon strike a balance to achieve the most conservative dissection that still achieves a complete gross dissection of the malignancy.
Achieving gross total dissection during cancer surgery is an important goal, said Dr. Olson. Citing devastating childhood brain tumors such as medulloblastomas and gliomablastomas, he noted that optical imaging can help surgeons avoid leaving behind any bulk areas of tumor, where hypoxic regions and therapy-resistant changes in tumor physiology may reduce the chance for cure. “Surgery is one of the most important elements of curing cancer,” he said. He pointed out that, in children with medulloblastomas, if nearly all tumor tissue is removed, less radiation is needed and survival is improved, even with less radiation – even if very small amounts of cancer remain.
Limitations of these technologies depend, to some extent, on the tissue targets, on substrates used to deliver the fluorescing molecules, and on the fluorescent agents themselves. Even with the enhanced tissue penetration of near-infrared light, the surgeon can really only see a centimeter or two beneath the surface of a solid organ. Said Dr. Singhal, “The basic limitation is that we’re talking about light.” However, if presurgery imaging identifies an area of concern, the surgeon can direct his or her dissection more carefully when the malignant tissue glows during surgery.
Dr. Rosenthal noted that pathologists also are making use of optical imaging to guide their processes. Since only about 5% of most tumor margins are sampled, there is an inevitable chance of sampling error with the resulting potential for a false-negative pathology result. “This technique augments the pathologist’s role and allows for improved biopsy results,” he said. Using image-guided pathology offers a way to test the margins immediately, helping the pathologist ascertain where the surgeon’s attention should be focused. Optical imaging, he said, “will in many ways change and enhance the experience for everybody.”
Dr. Olson, looking forward, asked, “If we can deliver the ability to light up, why can’t we deliver chemotherapy?” He sees an optical imaging future that will make flexible use of ligands to delineate tumors and test drug delivery.
There are many ways optical imaging can improve the practice of cancer surgery, Dr. Rosenthal said. “Historically, surgery has been a hard area to study because it’s so variable.” Following results from optical imaging–guided precision surgery, he said, will allow surgeons to identify and achieve “the right margin for the right cancer.”
Looking to the future, Dr. Singhal said, “it won’t be an either/or scenario. I think there will be multiple targets, multiple agents for this technology. We, as surgeons, have an obligation to our profession to move ahead with this.”
On Twitter @karioakes

Surgical bleeding risk ‘remarkable’ with platelet disorders
VIENNA – Inherited platelet function disorders are associated with a significant bleeding risk during surgery, a retrospective, multicenter study shows.
“The frequency of excessive bleeding assessed by one of three criteria at surgery is pretty remarkable because we had rates ranging from 13% to about 19% depending on the assessment criteria,” Dr. Paolo Gresele said at the annual congress of the European Hematology Association.

Any excessive bleeding by any criteria took place in about 23% of patients.
Although conventionally considered rare, inherited platelet function disorders (IPFD) are more frequent than previously thought, and recent advances in their diagnosis have expanded the forms and number of reported patients.
Only a handful of case reports or small case series have evaluated the bleeding risk associated with surgery in patients with IPFD. As a result, the exact bleeding risk and most appropriate management options in IPFD are not known, Dr. Gresele of University of Perugia (Italy) said.
He reported on a retrospective study involving patients with IPFD enrolled at 42 centers from 16 countries. The median age of the 205 patients was 35 years, and 56% were women; 89 had Glanzmann thrombasthenia, 46 had primary secretion defect, 14 had combined alpha-delta granule deficiency, 11 had Hermansky-Pudlak syndrome, 9 had gray platelet syndrome, and 36 had other forms of IPFD.
Data were collected from 389 procedures, of which 54.5% were surgeries, 30% were dental procedures, and 15.5% were invasive procedures. The most frequent surgeries were otolaryngologic, abdominal, orthopedic, gynecologic, urologic, and dermatologic.
The frequency of excessive bleeding at surgery was about 19.7% by the Bleeding Academic Research Consortium (BARC) bleeding classification, 17% by subjective evaluation by the surgeon or patient, and 13% based on duration of bleeding at surgery of at least 6 or more hours, Dr. Gresele said.
The World Health Organization (WHO) bleeding scale before surgery was quite predictive of excessive bleeding at surgery, with patients at grade 3 and 4 having an odds ratio for excessive bleeding of 9.22 and 28, respectively, compared with patients at grade 0, he said.
Somewhat unexpectedly, the most serious bleeders based on a BARC of at least 2 or more at surgery were patients with Hermansky-Pudlak syndrome, Glanzmann thrombasthenia, and gray platelet syndrome. Those with primary secretion defect and combined alpha-delta granule deficiency had a relatively low risk of bleeding at surgery, he said.
The procedures associated with more excessive bleeding were urologic surgery, gynecologic surgery, and abdominal surgery.
Preparation for surgery was made in 82% of procedures and included prophylactic platelet transfusions in 38.5%, desmopressin (DDAVP) in about 19%, antifibrinolytic agents in about 12%, factor VIIa in less than 10%, and other interventions such as cryoprecipitate, fibrinogen, fresh frozen plasma, intravenous immunoglobulin, suture, and local hemostatic agent in less than 5%.
Generally all measures had a good ability to prevent excessive bleeding, bringing rates down to about 20% or less, Dr. Gresele said. The two exceptions were no prophylaxis and “other” interventions, where the bleeding rate reached a high of about 45% for the latter. In contrast, bleeding risk was significantly reduced when any prophylaxis (odds ratio, 0.38) or DDAVP (OR, 0.24) were used.
In 87 cases, however, emergency treatment for excessive bleeding was required, he said. Platelet transfusions were the most common treatment, given in roughly half of patients, followed by antifibrinolytic agents. The success rate was about 80% for all measures, except for “other” interventions, which had a success rate of about 65%.
“Treatment of excessive bleeding is made mostly with platelet transfusions or antifibrinolytic agents and is able to stop bleeding in many, but not all cases,” Dr. Gresele concluded.
On Twitter @pwendl
VIENNA – Inherited platelet function disorders are associated with a significant bleeding risk during surgery, a retrospective, multicenter study shows.
“The frequency of excessive bleeding assessed by one of three criteria at surgery is pretty remarkable because we had rates ranging from 13% to about 19% depending on the assessment criteria,” Dr. Paolo Gresele said at the annual congress of the European Hematology Association.
Any excessive bleeding by any criteria took place in about 23% of patients.
Although conventionally considered rare, inherited platelet function disorders (IPFD) are more frequent than previously thought, and recent advances in their diagnosis have expanded the forms and number of reported patients.
Only a handful of case reports or small case series have evaluated the bleeding risk associated with surgery in patients with IPFD. As a result, the exact bleeding risk and most appropriate management options in IPFD are not known, Dr. Gresele of University of Perugia (Italy) said.
He reported on a retrospective study involving patients with IPFD enrolled at 42 centers from 16 countries. The median age of the 205 patients was 35 years, and 56% were women; 89 had Glanzmann thrombasthenia, 46 had primary secretion defect, 14 had combined alpha-delta granule deficiency, 11 had Hermansky-Pudlak syndrome, 9 had gray platelet syndrome, and 36 had other forms of IPFD.
Data were collected from 389 procedures, of which 54.5% were surgeries, 30% were dental procedures, and 15.5% were invasive procedures. The most frequent surgeries were otolaryngologic, abdominal, orthopedic, gynecologic, urologic, and dermatologic.
The frequency of excessive bleeding at surgery was about 19.7% by the Bleeding Academic Research Consortium (BARC) bleeding classification, 17% by subjective evaluation by the surgeon or patient, and 13% based on duration of bleeding at surgery of at least 6 or more hours, Dr. Gresele said.
The World Health Organization (WHO) bleeding scale before surgery was quite predictive of excessive bleeding at surgery, with patients at grade 3 and 4 having an odds ratio for excessive bleeding of 9.22 and 28, respectively, compared with patients at grade 0, he said.
Somewhat unexpectedly, the most serious bleeders based on a BARC of at least 2 or more at surgery were patients with Hermansky-Pudlak syndrome, Glanzmann thrombasthenia, and gray platelet syndrome. Those with primary secretion defect and combined alpha-delta granule deficiency had a relatively low risk of bleeding at surgery, he said.
The procedures associated with more excessive bleeding were urologic surgery, gynecologic surgery, and abdominal surgery.
Preparation for surgery was made in 82% of procedures and included prophylactic platelet transfusions in 38.5%, desmopressin (DDAVP) in about 19%, antifibrinolytic agents in about 12%, factor VIIa in less than 10%, and other interventions such as cryoprecipitate, fibrinogen, fresh frozen plasma, intravenous immunoglobulin, suture, and local hemostatic agent in less than 5%.
Generally all measures had a good ability to prevent excessive bleeding, bringing rates down to about 20% or less, Dr. Gresele said. The two exceptions were no prophylaxis and “other” interventions, where the bleeding rate reached a high of about 45% for the latter. In contrast, bleeding risk was significantly reduced when any prophylaxis (odds ratio, 0.38) or DDAVP (OR, 0.24) were used.
In 87 cases, however, emergency treatment for excessive bleeding was required, he said. Platelet transfusions were the most common treatment, given in roughly half of patients, followed by antifibrinolytic agents. The success rate was about 80% for all measures, except for “other” interventions, which had a success rate of about 65%.
“Treatment of excessive bleeding is made mostly with platelet transfusions or antifibrinolytic agents and is able to stop bleeding in many, but not all cases,” Dr. Gresele concluded.
On Twitter @pwendl
VIENNA – Inherited platelet function disorders are associated with a significant bleeding risk during surgery, a retrospective, multicenter study shows.
“The frequency of excessive bleeding assessed by one of three criteria at surgery is pretty remarkable because we had rates ranging from 13% to about 19% depending on the assessment criteria,” Dr. Paolo Gresele said at the annual congress of the European Hematology Association.
Any excessive bleeding by any criteria took place in about 23% of patients.
Although conventionally considered rare, inherited platelet function disorders (IPFD) are more frequent than previously thought, and recent advances in their diagnosis have expanded the forms and number of reported patients.
Only a handful of case reports or small case series have evaluated the bleeding risk associated with surgery in patients with IPFD. As a result, the exact bleeding risk and most appropriate management options in IPFD are not known, Dr. Gresele of University of Perugia (Italy) said.
He reported on a retrospective study involving patients with IPFD enrolled at 42 centers from 16 countries. The median age of the 205 patients was 35 years, and 56% were women; 89 had Glanzmann thrombasthenia, 46 had primary secretion defect, 14 had combined alpha-delta granule deficiency, 11 had Hermansky-Pudlak syndrome, 9 had gray platelet syndrome, and 36 had other forms of IPFD.
Data were collected from 389 procedures, of which 54.5% were surgeries, 30% were dental procedures, and 15.5% were invasive procedures. The most frequent surgeries were otolaryngologic, abdominal, orthopedic, gynecologic, urologic, and dermatologic.
The frequency of excessive bleeding at surgery was about 19.7% by the Bleeding Academic Research Consortium (BARC) bleeding classification, 17% by subjective evaluation by the surgeon or patient, and 13% based on duration of bleeding at surgery of at least 6 or more hours, Dr. Gresele said.
The World Health Organization (WHO) bleeding scale before surgery was quite predictive of excessive bleeding at surgery, with patients at grade 3 and 4 having an odds ratio for excessive bleeding of 9.22 and 28, respectively, compared with patients at grade 0, he said.
Somewhat unexpectedly, the most serious bleeders based on a BARC of at least 2 or more at surgery were patients with Hermansky-Pudlak syndrome, Glanzmann thrombasthenia, and gray platelet syndrome. Those with primary secretion defect and combined alpha-delta granule deficiency had a relatively low risk of bleeding at surgery, he said.
The procedures associated with more excessive bleeding were urologic surgery, gynecologic surgery, and abdominal surgery.
Preparation for surgery was made in 82% of procedures and included prophylactic platelet transfusions in 38.5%, desmopressin (DDAVP) in about 19%, antifibrinolytic agents in about 12%, factor VIIa in less than 10%, and other interventions such as cryoprecipitate, fibrinogen, fresh frozen plasma, intravenous immunoglobulin, suture, and local hemostatic agent in less than 5%.
Generally all measures had a good ability to prevent excessive bleeding, bringing rates down to about 20% or less, Dr. Gresele said. The two exceptions were no prophylaxis and “other” interventions, where the bleeding rate reached a high of about 45% for the latter. In contrast, bleeding risk was significantly reduced when any prophylaxis (odds ratio, 0.38) or DDAVP (OR, 0.24) were used.
In 87 cases, however, emergency treatment for excessive bleeding was required, he said. Platelet transfusions were the most common treatment, given in roughly half of patients, followed by antifibrinolytic agents. The success rate was about 80% for all measures, except for “other” interventions, which had a success rate of about 65%.
“Treatment of excessive bleeding is made mostly with platelet transfusions or antifibrinolytic agents and is able to stop bleeding in many, but not all cases,” Dr. Gresele concluded.
On Twitter @pwendl
AT THE EHA CONGRESS
Key clinical point: Inherited platelet function disorders are associated with a significant surgical bleeding risk.
Major finding: The frequency of excessive bleeding ranged from about 13% to about 19%.
Data source: Retrospective, multicenter study in 205 patients with inherited platelet function disorders and 389 procedures.
Disclosures: Dr. Gesele reported no financial disclosures.

AATS: Metformin linked to better progression-free survival in early-stage NSCLC
SEATTLE – Metformin use before surgery for stage I and II non–small cell lung cancer (NSCLC) was associated with improved progression-free survival at 5 years in a retrospective database study of 138 patients who also had type 2 diabetes.
The patients were treated for stage I and II NSCLC at Rush University Medical Center, Chicago. They also had type 2 diabetes; 81 (59%) were on metformin in the 6 months before pulmonary resection, and 57 (41%) were not, reported Rush medical student Robert Medairos, who is one of the study researchers.

At 5 years follow-up, progression-free survival was 60% in the metformin group, but about 35% in the no-metformin group (P = .01). Overall survival was about 90% at 5 years in both study arms.
A larger study or longer follow-up may show overall survival benefits for metformin users, Mr. Medairos said at the annual meeting of the American Association for Thoracic Surgery.
Patients were about 70 years old on average in both groups, with 35 pack-year smoking histories, and an average body mass index of about 30 kg/m2. Both study arms had slightly more men than women, and were otherwise balanced for ethnicity and comorbidities.
About 12% of patients in the metformin group and 40% in the no-metformin group, were on insulin prior to surgery. Mean preoperative creatinine was 1 mg/dL in the metformin group, and 1.7 mg/dL in the no-metformin group. There were trends towards higher-stage disease and more lymph node involvement in the no-metformin group. About half the patients in both arms had adenocarcinomas, but a greater proportion of patients in the no-metformin group had squamous cell carcinomas.
The Rush study might be the first to look into metformin for early NSCLC, but there have been several studies in advanced disease. A recent retrospective analysis of 750 diabetes patients with stage IV NSCLC found a median survival of 5 months for the 61% on metformin at diagnosis, but 3 months for those who were not (Am. J. Respir. Crit. Care. Med. 2015;191:448-54).
Currently, there are about a dozen ongoing trials of the drug for lung cancer, and scores more for prostate, breast, brain, uterine, colorectal, thyroid, and other cancers.
Metformin’s metabolic effects might reduce the ability of cancers to grow and metabolize, or the drug might somehow boost the antineoplastic effects of chemotherapeutics. “Our next step is to look at histological and tissues samples to see if metformin changes gene transcription in lung cancer cells,” Mr. Medairos said.
Mr. Medairos has no disclosures.
SEATTLE – Metformin use before surgery for stage I and II non–small cell lung cancer (NSCLC) was associated with improved progression-free survival at 5 years in a retrospective database study of 138 patients who also had type 2 diabetes.
The patients were treated for stage I and II NSCLC at Rush University Medical Center, Chicago. They also had type 2 diabetes; 81 (59%) were on metformin in the 6 months before pulmonary resection, and 57 (41%) were not, reported Rush medical student Robert Medairos, who is one of the study researchers.
At 5 years follow-up, progression-free survival was 60% in the metformin group, but about 35% in the no-metformin group (P = .01). Overall survival was about 90% at 5 years in both study arms.
A larger study or longer follow-up may show overall survival benefits for metformin users, Mr. Medairos said at the annual meeting of the American Association for Thoracic Surgery.
Patients were about 70 years old on average in both groups, with 35 pack-year smoking histories, and an average body mass index of about 30 kg/m2. Both study arms had slightly more men than women, and were otherwise balanced for ethnicity and comorbidities.
About 12% of patients in the metformin group and 40% in the no-metformin group, were on insulin prior to surgery. Mean preoperative creatinine was 1 mg/dL in the metformin group, and 1.7 mg/dL in the no-metformin group. There were trends towards higher-stage disease and more lymph node involvement in the no-metformin group. About half the patients in both arms had adenocarcinomas, but a greater proportion of patients in the no-metformin group had squamous cell carcinomas.
The Rush study might be the first to look into metformin for early NSCLC, but there have been several studies in advanced disease. A recent retrospective analysis of 750 diabetes patients with stage IV NSCLC found a median survival of 5 months for the 61% on metformin at diagnosis, but 3 months for those who were not (Am. J. Respir. Crit. Care. Med. 2015;191:448-54).
Currently, there are about a dozen ongoing trials of the drug for lung cancer, and scores more for prostate, breast, brain, uterine, colorectal, thyroid, and other cancers.
Metformin’s metabolic effects might reduce the ability of cancers to grow and metabolize, or the drug might somehow boost the antineoplastic effects of chemotherapeutics. “Our next step is to look at histological and tissues samples to see if metformin changes gene transcription in lung cancer cells,” Mr. Medairos said.
Mr. Medairos has no disclosures.
SEATTLE – Metformin use before surgery for stage I and II non–small cell lung cancer (NSCLC) was associated with improved progression-free survival at 5 years in a retrospective database study of 138 patients who also had type 2 diabetes.
The patients were treated for stage I and II NSCLC at Rush University Medical Center, Chicago. They also had type 2 diabetes; 81 (59%) were on metformin in the 6 months before pulmonary resection, and 57 (41%) were not, reported Rush medical student Robert Medairos, who is one of the study researchers.
At 5 years follow-up, progression-free survival was 60% in the metformin group, but about 35% in the no-metformin group (P = .01). Overall survival was about 90% at 5 years in both study arms.
A larger study or longer follow-up may show overall survival benefits for metformin users, Mr. Medairos said at the annual meeting of the American Association for Thoracic Surgery.
Patients were about 70 years old on average in both groups, with 35 pack-year smoking histories, and an average body mass index of about 30 kg/m2. Both study arms had slightly more men than women, and were otherwise balanced for ethnicity and comorbidities.
About 12% of patients in the metformin group and 40% in the no-metformin group, were on insulin prior to surgery. Mean preoperative creatinine was 1 mg/dL in the metformin group, and 1.7 mg/dL in the no-metformin group. There were trends towards higher-stage disease and more lymph node involvement in the no-metformin group. About half the patients in both arms had adenocarcinomas, but a greater proportion of patients in the no-metformin group had squamous cell carcinomas.
The Rush study might be the first to look into metformin for early NSCLC, but there have been several studies in advanced disease. A recent retrospective analysis of 750 diabetes patients with stage IV NSCLC found a median survival of 5 months for the 61% on metformin at diagnosis, but 3 months for those who were not (Am. J. Respir. Crit. Care. Med. 2015;191:448-54).
Currently, there are about a dozen ongoing trials of the drug for lung cancer, and scores more for prostate, breast, brain, uterine, colorectal, thyroid, and other cancers.
Metformin’s metabolic effects might reduce the ability of cancers to grow and metabolize, or the drug might somehow boost the antineoplastic effects of chemotherapeutics. “Our next step is to look at histological and tissues samples to see if metformin changes gene transcription in lung cancer cells,” Mr. Medairos said.
Mr. Medairos has no disclosures.
AT THE AATS ANNUAL MEETING
Key clinical point: Metformin might one day be part of routine lung cancer care.
Major finding: Five years after pulmonary resection for non–small cell lung cancer, progression-free survival was 60% in patients who were on metformin before surgery, but 35% in patients who were not (P = .01).
Data source: Retrospective study of 138 patients with type 2 diabetes and stage I and II non–small cell lung cancer.
Disclosures: The lead investigator has no relevant disclosures.

Invasive approaches ‘overused’ for evaluating pulmonary nodules
One in four intermediate-sized (8-20 mm) pulmonary nodules were found to be malignant, based on results from a retrospective study of 377 patients seen in 18 community pulmonology practices.
Malignant nodules were more likely to be found in current or former smokers and to be larger than the benign nodules.
Further, despite guideline recommendations for surveillance of pulmonary nodules with less than a 5% pretest probability of malignancy, 44% of 36 patients with low-risk pulmonary nodules underwent at least one invasive procedure.
“To our knowledge, this is the first study that documents the prevalence of cancer (25%) in patients with intermediate-sized nodules referred to community-based pulmonologists,” wrote Dr. Nichole T. Tanner of the Medical University of South Carolina, Charleston, and her coauthors in the study published online (Chest 2015 June 18 [doi:10.1378/chest.15-0630]). “This finding has implications for managing pulmonary nodules in the community; because the risk of cancer is substantial, patients should be managed based on their individualized risk for malignancy.”

Biopsy – either by transthoracic needle aspiration or bronchoscopy – was performed in 33% (125) of patients, of whom 35% were found to have a malignancy and 57% had a specific benign diagnosis; biopsies in 8% were nondiagnostic and those patients were followed for 2 years.
Referrals for surgery were given to 20% (77) of patients; 19 had previously undergone a biopsy, with 11 having a nondiagnostic biopsy and eight having a received a benign result. Of patients who underwent surgery, 65% were diagnosed with a malignancy, and 35% had benign disease. However, the rate of surgical resection was similar regardless of patients’ pretest probability of malignancy.
PET scanning, performed in 37% of patients, was more likely in those who had a biopsy or surgery. The overall accuracy of PET was 74%, and the false-negative rate decreased slightly as the size of the nodule increased.
“Guidelines recommend surgery if the pretest probability of cancer is high (pCA > 65%) because a negative biopsy would not dissuade the clinician from pursuing a definitive diagnosis and a positive biopsy would lead to surgery anyway.”
The researchers pointed out that there are a range of noninvasive options now available to determine the likelihood that a nodule is malignant, such as CT scanning with the use of volumetric software to measure diameter and volume-doubling time of a nodule in between scans.
The study was supported by Integrated Diagnostics. All but one study author declared consulting fees, grant funding, stock options, or employment with Integrated Diagnostics.
One in four intermediate-sized (8-20 mm) pulmonary nodules were found to be malignant, based on results from a retrospective study of 377 patients seen in 18 community pulmonology practices.
Malignant nodules were more likely to be found in current or former smokers and to be larger than the benign nodules.
Further, despite guideline recommendations for surveillance of pulmonary nodules with less than a 5% pretest probability of malignancy, 44% of 36 patients with low-risk pulmonary nodules underwent at least one invasive procedure.
“To our knowledge, this is the first study that documents the prevalence of cancer (25%) in patients with intermediate-sized nodules referred to community-based pulmonologists,” wrote Dr. Nichole T. Tanner of the Medical University of South Carolina, Charleston, and her coauthors in the study published online (Chest 2015 June 18 [doi:10.1378/chest.15-0630]). “This finding has implications for managing pulmonary nodules in the community; because the risk of cancer is substantial, patients should be managed based on their individualized risk for malignancy.”
Biopsy – either by transthoracic needle aspiration or bronchoscopy – was performed in 33% (125) of patients, of whom 35% were found to have a malignancy and 57% had a specific benign diagnosis; biopsies in 8% were nondiagnostic and those patients were followed for 2 years.
Referrals for surgery were given to 20% (77) of patients; 19 had previously undergone a biopsy, with 11 having a nondiagnostic biopsy and eight having a received a benign result. Of patients who underwent surgery, 65% were diagnosed with a malignancy, and 35% had benign disease. However, the rate of surgical resection was similar regardless of patients’ pretest probability of malignancy.
PET scanning, performed in 37% of patients, was more likely in those who had a biopsy or surgery. The overall accuracy of PET was 74%, and the false-negative rate decreased slightly as the size of the nodule increased.
“Guidelines recommend surgery if the pretest probability of cancer is high (pCA > 65%) because a negative biopsy would not dissuade the clinician from pursuing a definitive diagnosis and a positive biopsy would lead to surgery anyway.”
The researchers pointed out that there are a range of noninvasive options now available to determine the likelihood that a nodule is malignant, such as CT scanning with the use of volumetric software to measure diameter and volume-doubling time of a nodule in between scans.
The study was supported by Integrated Diagnostics. All but one study author declared consulting fees, grant funding, stock options, or employment with Integrated Diagnostics.
One in four intermediate-sized (8-20 mm) pulmonary nodules were found to be malignant, based on results from a retrospective study of 377 patients seen in 18 community pulmonology practices.
Malignant nodules were more likely to be found in current or former smokers and to be larger than the benign nodules.
Further, despite guideline recommendations for surveillance of pulmonary nodules with less than a 5% pretest probability of malignancy, 44% of 36 patients with low-risk pulmonary nodules underwent at least one invasive procedure.
“To our knowledge, this is the first study that documents the prevalence of cancer (25%) in patients with intermediate-sized nodules referred to community-based pulmonologists,” wrote Dr. Nichole T. Tanner of the Medical University of South Carolina, Charleston, and her coauthors in the study published online (Chest 2015 June 18 [doi:10.1378/chest.15-0630]). “This finding has implications for managing pulmonary nodules in the community; because the risk of cancer is substantial, patients should be managed based on their individualized risk for malignancy.”
Biopsy – either by transthoracic needle aspiration or bronchoscopy – was performed in 33% (125) of patients, of whom 35% were found to have a malignancy and 57% had a specific benign diagnosis; biopsies in 8% were nondiagnostic and those patients were followed for 2 years.
Referrals for surgery were given to 20% (77) of patients; 19 had previously undergone a biopsy, with 11 having a nondiagnostic biopsy and eight having a received a benign result. Of patients who underwent surgery, 65% were diagnosed with a malignancy, and 35% had benign disease. However, the rate of surgical resection was similar regardless of patients’ pretest probability of malignancy.
PET scanning, performed in 37% of patients, was more likely in those who had a biopsy or surgery. The overall accuracy of PET was 74%, and the false-negative rate decreased slightly as the size of the nodule increased.
“Guidelines recommend surgery if the pretest probability of cancer is high (pCA > 65%) because a negative biopsy would not dissuade the clinician from pursuing a definitive diagnosis and a positive biopsy would lead to surgery anyway.”
The researchers pointed out that there are a range of noninvasive options now available to determine the likelihood that a nodule is malignant, such as CT scanning with the use of volumetric software to measure diameter and volume-doubling time of a nodule in between scans.
The study was supported by Integrated Diagnostics. All but one study author declared consulting fees, grant funding, stock options, or employment with Integrated Diagnostics.
FROM CHEST
Key clinical point: One in four pulmonary nodules 8-20 mm in size are malignant, and invasive tests are being overused in low-risk patients in community settings.
Major finding: Despite guidelines recommending pulmonary nodes with a less than 5% pretest probability of malignancy be managed with surveillance only, 44% of low-risk patients in the study underwent at least one invasive procedure for what proved to be a benign nodule.
Data source: A multicenter, retrospective study in 377 patients.
Disclosures: The study was supported by Integrated Diagnostics. All but one author declared consulting fees, grant funding, stock options, or employment with Integrated Diagnostics.
