User login
Official Newspaper of the American College of Surgeons
Postop delirium heightens risk of other dangerous complications
Delirium is not only the most common major complication of elective surgery in older adults, it also markedly raises the risk of all adverse outcomes, including prolonged length of stay, discharge to an institution rather than home, and readmission within 30 days, according to a report published online Sept. 9 in JAMA Surgery.
“Given its high prevalence and negative effect, delirium should be considered as the leading postoperative complication contributing to adverse outcomes” in this patient population, wrote Dr. Lauren J. Gleason of the department of medicine at Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, and her associates.

Delirium is typically considered a less serious event than other major postoperative complications, even though its association with higher in-hospital mortality, 6-month mortality, functional decline, and higher health care costs has been well documented. To assess whether delirium should be considered equivalent to other major life-altering or life-threatening complications, the investigators studied 566 patients aged 70 years and older who underwent elective orthopedic, general, or vascular procedures at Beth Israel Deaconess or Brigham and Women’s Hospital in a 3-year period. The data were collected for the Successful Aging after Elective Surgery (SAGES) study.
Operations included total hip or knee replacement, lumbar or cervical laminectomy, lower-extremity bypass, open abdominal aortic aneurysm repair, open colectomyt, and laparoscopic colectomy. In general, these patients were highly functional and highly educated. The mean age was 76.7 years, and 93% of the study participants were white.
Delirium developed in 135 patients (24%) – much more frequently than all other major complications combined (47 patients, or 8%). This is comparable with rates of delirium reported in other studies of elective noncardiac surgeries, Dr. Gleason and her associates noted. Other major complications included unstable arrhythmias, respiratory failure, abscess requiring incision and drainage, abdominal compartment syndrome, anastomotic leak, deep surgical site infection, and hernia repair.
Compared with patients who didn’t develop delirium, those who did had a twofold higher risk of prolonged length of stay, a 50% higher risk of discharge to an institution, and more than double the risk of 30-day readmission, the investigators reported (JAMA Surg. 2015 Sept 9. doi: 10.1001/jamasurg.2015.2606).
Since delirium is often preventable, clinicians should try harder to implement preventive strategies before surgery and continue them afterward. The Hospital Elder Life Program, proactive geriatric consultation, and comanagement services all have proved effective in this regard, they added.
This study was supported by the National Institute on Aging, the Health and Resources Services Administration, and the John A. Hartford Foundation. The authors reported no relevant disclosures.
Delirium is not only the most common major complication of elective surgery in older adults, it also markedly raises the risk of all adverse outcomes, including prolonged length of stay, discharge to an institution rather than home, and readmission within 30 days, according to a report published online Sept. 9 in JAMA Surgery.
“Given its high prevalence and negative effect, delirium should be considered as the leading postoperative complication contributing to adverse outcomes” in this patient population, wrote Dr. Lauren J. Gleason of the department of medicine at Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, and her associates.
Delirium is typically considered a less serious event than other major postoperative complications, even though its association with higher in-hospital mortality, 6-month mortality, functional decline, and higher health care costs has been well documented. To assess whether delirium should be considered equivalent to other major life-altering or life-threatening complications, the investigators studied 566 patients aged 70 years and older who underwent elective orthopedic, general, or vascular procedures at Beth Israel Deaconess or Brigham and Women’s Hospital in a 3-year period. The data were collected for the Successful Aging after Elective Surgery (SAGES) study.
Operations included total hip or knee replacement, lumbar or cervical laminectomy, lower-extremity bypass, open abdominal aortic aneurysm repair, open colectomyt, and laparoscopic colectomy. In general, these patients were highly functional and highly educated. The mean age was 76.7 years, and 93% of the study participants were white.
Delirium developed in 135 patients (24%) – much more frequently than all other major complications combined (47 patients, or 8%). This is comparable with rates of delirium reported in other studies of elective noncardiac surgeries, Dr. Gleason and her associates noted. Other major complications included unstable arrhythmias, respiratory failure, abscess requiring incision and drainage, abdominal compartment syndrome, anastomotic leak, deep surgical site infection, and hernia repair.
Compared with patients who didn’t develop delirium, those who did had a twofold higher risk of prolonged length of stay, a 50% higher risk of discharge to an institution, and more than double the risk of 30-day readmission, the investigators reported (JAMA Surg. 2015 Sept 9. doi: 10.1001/jamasurg.2015.2606).
Since delirium is often preventable, clinicians should try harder to implement preventive strategies before surgery and continue them afterward. The Hospital Elder Life Program, proactive geriatric consultation, and comanagement services all have proved effective in this regard, they added.
This study was supported by the National Institute on Aging, the Health and Resources Services Administration, and the John A. Hartford Foundation. The authors reported no relevant disclosures.
Delirium is not only the most common major complication of elective surgery in older adults, it also markedly raises the risk of all adverse outcomes, including prolonged length of stay, discharge to an institution rather than home, and readmission within 30 days, according to a report published online Sept. 9 in JAMA Surgery.
“Given its high prevalence and negative effect, delirium should be considered as the leading postoperative complication contributing to adverse outcomes” in this patient population, wrote Dr. Lauren J. Gleason of the department of medicine at Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, and her associates.
Delirium is typically considered a less serious event than other major postoperative complications, even though its association with higher in-hospital mortality, 6-month mortality, functional decline, and higher health care costs has been well documented. To assess whether delirium should be considered equivalent to other major life-altering or life-threatening complications, the investigators studied 566 patients aged 70 years and older who underwent elective orthopedic, general, or vascular procedures at Beth Israel Deaconess or Brigham and Women’s Hospital in a 3-year period. The data were collected for the Successful Aging after Elective Surgery (SAGES) study.
Operations included total hip or knee replacement, lumbar or cervical laminectomy, lower-extremity bypass, open abdominal aortic aneurysm repair, open colectomyt, and laparoscopic colectomy. In general, these patients were highly functional and highly educated. The mean age was 76.7 years, and 93% of the study participants were white.
Delirium developed in 135 patients (24%) – much more frequently than all other major complications combined (47 patients, or 8%). This is comparable with rates of delirium reported in other studies of elective noncardiac surgeries, Dr. Gleason and her associates noted. Other major complications included unstable arrhythmias, respiratory failure, abscess requiring incision and drainage, abdominal compartment syndrome, anastomotic leak, deep surgical site infection, and hernia repair.
Compared with patients who didn’t develop delirium, those who did had a twofold higher risk of prolonged length of stay, a 50% higher risk of discharge to an institution, and more than double the risk of 30-day readmission, the investigators reported (JAMA Surg. 2015 Sept 9. doi: 10.1001/jamasurg.2015.2606).
Since delirium is often preventable, clinicians should try harder to implement preventive strategies before surgery and continue them afterward. The Hospital Elder Life Program, proactive geriatric consultation, and comanagement services all have proved effective in this regard, they added.
This study was supported by the National Institute on Aging, the Health and Resources Services Administration, and the John A. Hartford Foundation. The authors reported no relevant disclosures.
FROM JAMA SURGERY
Key clinical point: Delirium is the most common and among the most harmful of complications of elective surgery in older adults.
Major finding: Elderly patients who developed delirium had a twofold higher risk of prolonged length of stay, a 50% higher risk of discharge to an institution, and more than double the risk of 30-day readmission.
Data source: A prospective cohort study involving 566 older adults undergoing elective surgery at two hospitals in a 3-year period.
Disclosures: This study was supported by the National Institute on Aging, the Health and Resources Services Administration, and the John A. Hartford Foundation.

ESC: CERTITUDE casts doubt on defibrillator benefit in CRT
LONDON – Heart failure patients who are candidates for cardiac resynchronization therapy in a routine clinical practice setting will likely not benefit from the addition of a defibrillator to a pacemaker, according to results of the CERTITUDE cohort study.
In CERTITUDE, most of the deaths in patients fitted with a cardiac resynchronization therapy–pacemaker (CRT-P) device were predominantly from causes other than sudden cardiac death (SCD), which is the main rationale for using a CRT-defibrillator (CRT-D) device, said lead investigator Jean-Yves Le Heuzey at the annual congress of the European Society of Cardiology.

“Our results should not be interpreted as a general lack of benefit from CRT-D vs. CRT-P or vice versa. Rather we demonstrate that given currently selected CRT-P patients in the French population, addition of a defibrillator may not significantly add to survival.” Therefore, patients who may be eligible for CRT should not “automatically” be considered as requiring a CRT-D, suggested Dr. Le Heuzey and his coinvestigators in an article that was published online at the time of the study’s presentation (Eur Heart J. 2015 Sep 1. doi: 10.1093/eurheartj/ehv455).
Current ESC guidelines on cardiac pacing and cardiac resynchronization therapy “leave flexibility for the physician” on the use of CRT-P and CRT-D” because there was no evidence of a superior effect of the latter over CRT alone, said Dr. Le Heuzey of René Descartes University in Paris at the meeting. A randomized, controlled trial would be the only way to determine this, but such a trial is unlikely to ever be conducted, he noted.
Despite the lack of evidence, however, CRT-D is widely used, more so in the United States than in Europe, Dr. Le Heuzey observed, where more than 90% of patients needing CRT would likely have a CRT-D rather than a CRT-P device implanted.
The aims of the CERTITUDE cohort study were to look at the extent to which CRT-P patients differ from CRT-D patients in a real-life setting, and to also see if there were patients in the CRT-P group that might have benefited from CRT-D.
The prospective, observational study involved 1,705 patients who were recruited at 41 centers throughout France over a 2-year period starting in January 2008. Of these, 31% were fitted with a CRT-P device and 69% with a CRT-D.
Results showed that patients who had a CRT-P versus a CRT-D implanted were significantly older, more often female, and more symptomatic. They were also significantly less likely to have coronary artery disease, more likely to have wider QRS intervals and to have atrial fibrillation, and more often had at least two comorbidities.
Analysis of the causes of death was performed at 2 years’ follow-up, which Dr. Le Heuzey conceded was a short period of time. At this point, 267 of 1,611 patients with complete follow-up data had died, giving an overall mortality rate of 8.4% per 100 patient-years for the entire cohort.
The crude mortality rate was found to be higher among CRT-P than CRT-D patients, at 13.1% versus 6.5% per 100 patient-years (relative risk, 2.01; 95% confidence interval, 1.56-2.58; P less than .0001). But when the cause of death was examined more closely, there was no significant difference in the number of SCDs between the groups (RR, 1.57; 95% CI, 0.71-3.46; P = .42) and no significant difference when a specific cause of death analysis was performed.
The main reasons for the almost doubled risk of death in the CRT-P group was an increase in non-SCD cardiovascular mortality, mainly progressive heart failure (RR, 0.27; 95% CI, 1.62-3.18) and other cardiovascular causes (RR, 4.4; 95% CI, 1.29-15.03), Dr. Le Heuzey and associates noted in the article.
“Overall, 95% of the excess mortality among CRT-P recipients was not related to SCD,” they wrote, noting that this “suggests that the presence of a back-up defibrillator would probably not have been beneficial in terms of improving survival for these patients.”
So where does this leave clinicians? Dr. Le Heuzey referred to Table 17 in the European guidelines (Eur Heart J. 2013;34:2281-2329) with guidance on factors favoring CRT-P or CRT-D. For instance, CRT-P might be favorable in a patient with advanced heart failure or one with severe renal insufficiency or on dialysis. Other major comorbidities or frailty or cachexia might veer a decision towards CRT without a defibrillator. On the other hand, factors favoring CRT-D include a life expectancy of more than 1 year; stable, moderate (New York Heart Association class II) disease; or low to moderate–risk ischemic heart disease, with a lack of comorbidities.
CERTITUDE was funded by grants from the French Institute of Health and Medical Research (INSERM) and from the French Cardiology Society. The latter received specific grants from Biotronik, Boston Scientific, Medtronic, Saint Jude Medical, and Sorin in order to perform the study. Dr. Le Heuzey disclosed receiving fees for participation in advisory boards and conferences from AstraZeneca, Bayer, Boehringer-Ingelheim, Bristol Myers Squibb/Pfizer, Correvio, Daiichi-Sankyo, Meda, Sanofi, and Servier.
LONDON – Heart failure patients who are candidates for cardiac resynchronization therapy in a routine clinical practice setting will likely not benefit from the addition of a defibrillator to a pacemaker, according to results of the CERTITUDE cohort study.
In CERTITUDE, most of the deaths in patients fitted with a cardiac resynchronization therapy–pacemaker (CRT-P) device were predominantly from causes other than sudden cardiac death (SCD), which is the main rationale for using a CRT-defibrillator (CRT-D) device, said lead investigator Jean-Yves Le Heuzey at the annual congress of the European Society of Cardiology.
“Our results should not be interpreted as a general lack of benefit from CRT-D vs. CRT-P or vice versa. Rather we demonstrate that given currently selected CRT-P patients in the French population, addition of a defibrillator may not significantly add to survival.” Therefore, patients who may be eligible for CRT should not “automatically” be considered as requiring a CRT-D, suggested Dr. Le Heuzey and his coinvestigators in an article that was published online at the time of the study’s presentation (Eur Heart J. 2015 Sep 1. doi: 10.1093/eurheartj/ehv455).
Current ESC guidelines on cardiac pacing and cardiac resynchronization therapy “leave flexibility for the physician” on the use of CRT-P and CRT-D” because there was no evidence of a superior effect of the latter over CRT alone, said Dr. Le Heuzey of René Descartes University in Paris at the meeting. A randomized, controlled trial would be the only way to determine this, but such a trial is unlikely to ever be conducted, he noted.
Despite the lack of evidence, however, CRT-D is widely used, more so in the United States than in Europe, Dr. Le Heuzey observed, where more than 90% of patients needing CRT would likely have a CRT-D rather than a CRT-P device implanted.
The aims of the CERTITUDE cohort study were to look at the extent to which CRT-P patients differ from CRT-D patients in a real-life setting, and to also see if there were patients in the CRT-P group that might have benefited from CRT-D.
The prospective, observational study involved 1,705 patients who were recruited at 41 centers throughout France over a 2-year period starting in January 2008. Of these, 31% were fitted with a CRT-P device and 69% with a CRT-D.
Results showed that patients who had a CRT-P versus a CRT-D implanted were significantly older, more often female, and more symptomatic. They were also significantly less likely to have coronary artery disease, more likely to have wider QRS intervals and to have atrial fibrillation, and more often had at least two comorbidities.
Analysis of the causes of death was performed at 2 years’ follow-up, which Dr. Le Heuzey conceded was a short period of time. At this point, 267 of 1,611 patients with complete follow-up data had died, giving an overall mortality rate of 8.4% per 100 patient-years for the entire cohort.
The crude mortality rate was found to be higher among CRT-P than CRT-D patients, at 13.1% versus 6.5% per 100 patient-years (relative risk, 2.01; 95% confidence interval, 1.56-2.58; P less than .0001). But when the cause of death was examined more closely, there was no significant difference in the number of SCDs between the groups (RR, 1.57; 95% CI, 0.71-3.46; P = .42) and no significant difference when a specific cause of death analysis was performed.
The main reasons for the almost doubled risk of death in the CRT-P group was an increase in non-SCD cardiovascular mortality, mainly progressive heart failure (RR, 0.27; 95% CI, 1.62-3.18) and other cardiovascular causes (RR, 4.4; 95% CI, 1.29-15.03), Dr. Le Heuzey and associates noted in the article.
“Overall, 95% of the excess mortality among CRT-P recipients was not related to SCD,” they wrote, noting that this “suggests that the presence of a back-up defibrillator would probably not have been beneficial in terms of improving survival for these patients.”
So where does this leave clinicians? Dr. Le Heuzey referred to Table 17 in the European guidelines (Eur Heart J. 2013;34:2281-2329) with guidance on factors favoring CRT-P or CRT-D. For instance, CRT-P might be favorable in a patient with advanced heart failure or one with severe renal insufficiency or on dialysis. Other major comorbidities or frailty or cachexia might veer a decision towards CRT without a defibrillator. On the other hand, factors favoring CRT-D include a life expectancy of more than 1 year; stable, moderate (New York Heart Association class II) disease; or low to moderate–risk ischemic heart disease, with a lack of comorbidities.
CERTITUDE was funded by grants from the French Institute of Health and Medical Research (INSERM) and from the French Cardiology Society. The latter received specific grants from Biotronik, Boston Scientific, Medtronic, Saint Jude Medical, and Sorin in order to perform the study. Dr. Le Heuzey disclosed receiving fees for participation in advisory boards and conferences from AstraZeneca, Bayer, Boehringer-Ingelheim, Bristol Myers Squibb/Pfizer, Correvio, Daiichi-Sankyo, Meda, Sanofi, and Servier.
LONDON – Heart failure patients who are candidates for cardiac resynchronization therapy in a routine clinical practice setting will likely not benefit from the addition of a defibrillator to a pacemaker, according to results of the CERTITUDE cohort study.
In CERTITUDE, most of the deaths in patients fitted with a cardiac resynchronization therapy–pacemaker (CRT-P) device were predominantly from causes other than sudden cardiac death (SCD), which is the main rationale for using a CRT-defibrillator (CRT-D) device, said lead investigator Jean-Yves Le Heuzey at the annual congress of the European Society of Cardiology.
“Our results should not be interpreted as a general lack of benefit from CRT-D vs. CRT-P or vice versa. Rather we demonstrate that given currently selected CRT-P patients in the French population, addition of a defibrillator may not significantly add to survival.” Therefore, patients who may be eligible for CRT should not “automatically” be considered as requiring a CRT-D, suggested Dr. Le Heuzey and his coinvestigators in an article that was published online at the time of the study’s presentation (Eur Heart J. 2015 Sep 1. doi: 10.1093/eurheartj/ehv455).
Current ESC guidelines on cardiac pacing and cardiac resynchronization therapy “leave flexibility for the physician” on the use of CRT-P and CRT-D” because there was no evidence of a superior effect of the latter over CRT alone, said Dr. Le Heuzey of René Descartes University in Paris at the meeting. A randomized, controlled trial would be the only way to determine this, but such a trial is unlikely to ever be conducted, he noted.
Despite the lack of evidence, however, CRT-D is widely used, more so in the United States than in Europe, Dr. Le Heuzey observed, where more than 90% of patients needing CRT would likely have a CRT-D rather than a CRT-P device implanted.
The aims of the CERTITUDE cohort study were to look at the extent to which CRT-P patients differ from CRT-D patients in a real-life setting, and to also see if there were patients in the CRT-P group that might have benefited from CRT-D.
The prospective, observational study involved 1,705 patients who were recruited at 41 centers throughout France over a 2-year period starting in January 2008. Of these, 31% were fitted with a CRT-P device and 69% with a CRT-D.
Results showed that patients who had a CRT-P versus a CRT-D implanted were significantly older, more often female, and more symptomatic. They were also significantly less likely to have coronary artery disease, more likely to have wider QRS intervals and to have atrial fibrillation, and more often had at least two comorbidities.
Analysis of the causes of death was performed at 2 years’ follow-up, which Dr. Le Heuzey conceded was a short period of time. At this point, 267 of 1,611 patients with complete follow-up data had died, giving an overall mortality rate of 8.4% per 100 patient-years for the entire cohort.
The crude mortality rate was found to be higher among CRT-P than CRT-D patients, at 13.1% versus 6.5% per 100 patient-years (relative risk, 2.01; 95% confidence interval, 1.56-2.58; P less than .0001). But when the cause of death was examined more closely, there was no significant difference in the number of SCDs between the groups (RR, 1.57; 95% CI, 0.71-3.46; P = .42) and no significant difference when a specific cause of death analysis was performed.
The main reasons for the almost doubled risk of death in the CRT-P group was an increase in non-SCD cardiovascular mortality, mainly progressive heart failure (RR, 0.27; 95% CI, 1.62-3.18) and other cardiovascular causes (RR, 4.4; 95% CI, 1.29-15.03), Dr. Le Heuzey and associates noted in the article.
“Overall, 95% of the excess mortality among CRT-P recipients was not related to SCD,” they wrote, noting that this “suggests that the presence of a back-up defibrillator would probably not have been beneficial in terms of improving survival for these patients.”
So where does this leave clinicians? Dr. Le Heuzey referred to Table 17 in the European guidelines (Eur Heart J. 2013;34:2281-2329) with guidance on factors favoring CRT-P or CRT-D. For instance, CRT-P might be favorable in a patient with advanced heart failure or one with severe renal insufficiency or on dialysis. Other major comorbidities or frailty or cachexia might veer a decision towards CRT without a defibrillator. On the other hand, factors favoring CRT-D include a life expectancy of more than 1 year; stable, moderate (New York Heart Association class II) disease; or low to moderate–risk ischemic heart disease, with a lack of comorbidities.
CERTITUDE was funded by grants from the French Institute of Health and Medical Research (INSERM) and from the French Cardiology Society. The latter received specific grants from Biotronik, Boston Scientific, Medtronic, Saint Jude Medical, and Sorin in order to perform the study. Dr. Le Heuzey disclosed receiving fees for participation in advisory boards and conferences from AstraZeneca, Bayer, Boehringer-Ingelheim, Bristol Myers Squibb/Pfizer, Correvio, Daiichi-Sankyo, Meda, Sanofi, and Servier.
AT THE ESC CONGRESS 2015
Key clinical point:There appears to be no survival benefit of cardiac resynchronization therapy with a defibrillator CRT-D over a pacemaker (CRT-P).
Major finding: Although there was a higher death rate among CRT-P recipients, 95% of the excess mortality, compared with CRT-D recipients, was not related to sudden cardiac death.
Data source: The prospective, observational CERTITUDE cohort study in 1,705 French patients fitted with a CRT-P or CRT-D.
Disclosures: CERTITUDE was funded by grants from the French Institute of Health and Medical Research (INSERM) and from the French Cardiology Society. The latter received specific grants from Biotronik, Boston Scientific, Medtronic, St. Jude Medical, and Sorin in order to perform the study. Dr. Le Heuzey disclosed receiving fees for participation in advisory boards and conferences from AstraZeneca, Bayer, Boehringer-Ingelheim, Bristol Myers Squibb/Pfizer, Correvio, Daiichi-Sankyo, Meda, Sanofi, and Servier.

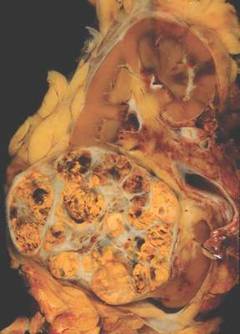
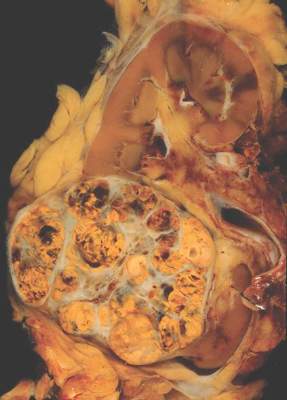
Individualized approach improves surveillance after renal cell carcinoma resection
A novel approach to oncologic surveillance after surgical resection for renal cell carcinoma (RCC) that incorporates patient age, Charlson comorbidity index, pathologic tumor stage, and relapse location–specific data, may provide better recommendations for surveillance duration than current guidelines, researchers reported.
“By providing more individualized recommendations and by eliminating oversimplified time thresholds for surveillance, this strategy, we believe, represents an improvement over current guidelines,” wrote Dr. Suzanne Stewart-Merrill of the department of urology, Mayo Clinic, Rochester, Minn., and colleagues (J Clin Oncol. 2015 Sep 7. doi: 10.1200/JCO.2015.61.8009).
Guidelines suggest surveillance durations based on cumulative incidence of recurrences, but do not account for individual patient risk factors. Adherence to the guidelines could miss up to one-third of all recurrences, the authors noted. The longest surveillance duration advocated by the National Comprehensive Cancer Network or the American Urological Association is 5 years.
Researchers used Weibull models for risk of recurrence, stratified by stage and relapse location, combined with risk estimates for non-RCC death, to estimate the optimum surveillance duration. For example, for patients aged 50-59 years with pT1Nx-0 disease and a Charlson comorbidity index of less than or equal to 1, risk of non-RCC death exceeded the risk of abdominal recurrence at 7 years, marking the recommended surveillance duration for that subgroup. The recommended surveillance duration for patients with similar characteristics aged 60-69 years is 2.5 years, and for patients aged 70-79 years it is 1.5 years.
When taking into account individual risk factors, the method produced a wide range of surveillance durations. For patients under 50 years old with pT1Nx-0 disease and a Charlson comorbidity index less than or equal to 1, the risk of non-RCC death did not exceed the risk of abdominal recurrence for more than 20 years. By contrast, patients with pT1Nx-0 disease and Charlson comorbidity index greater than or equal to 2, had a higher risk of non-RCC death than risk of abdominal recurrence at 30 days after surgery.
The retrospective study of 2,511 patients who underwent surgical resection for M0 sporadic RCC between 1990 and 2008 had a median follow up of 9.0 years (interquartile range 6.4-12.7 years).
The researchers noted that recurrences beyond 5 years are fairly common, with up to 15% of patients, by one study’s estimate, experiencing recurrence during the decade following surgery. Cumulative incidence of recurrence does not capture how a patient’s risk of recurrence changes with time or how comorbid conditions influence risk.
The proposed surveillance method results in shorter surveillance durations for some patients and longer surveillance durations than currently recommended for others. This diversity in stopping points “better reflects the range of disease courses appreciated in patients with RCC on the basis of the interplay that occurs between the risk of recurrence and other competing health factors,” Dr. Stewart-Merrill and associates explained.
Dr. Stewart-Merrill reported having no disclosures.
A novel approach to oncologic surveillance after surgical resection for renal cell carcinoma (RCC) that incorporates patient age, Charlson comorbidity index, pathologic tumor stage, and relapse location–specific data, may provide better recommendations for surveillance duration than current guidelines, researchers reported.
“By providing more individualized recommendations and by eliminating oversimplified time thresholds for surveillance, this strategy, we believe, represents an improvement over current guidelines,” wrote Dr. Suzanne Stewart-Merrill of the department of urology, Mayo Clinic, Rochester, Minn., and colleagues (J Clin Oncol. 2015 Sep 7. doi: 10.1200/JCO.2015.61.8009).
Guidelines suggest surveillance durations based on cumulative incidence of recurrences, but do not account for individual patient risk factors. Adherence to the guidelines could miss up to one-third of all recurrences, the authors noted. The longest surveillance duration advocated by the National Comprehensive Cancer Network or the American Urological Association is 5 years.
Researchers used Weibull models for risk of recurrence, stratified by stage and relapse location, combined with risk estimates for non-RCC death, to estimate the optimum surveillance duration. For example, for patients aged 50-59 years with pT1Nx-0 disease and a Charlson comorbidity index of less than or equal to 1, risk of non-RCC death exceeded the risk of abdominal recurrence at 7 years, marking the recommended surveillance duration for that subgroup. The recommended surveillance duration for patients with similar characteristics aged 60-69 years is 2.5 years, and for patients aged 70-79 years it is 1.5 years.
When taking into account individual risk factors, the method produced a wide range of surveillance durations. For patients under 50 years old with pT1Nx-0 disease and a Charlson comorbidity index less than or equal to 1, the risk of non-RCC death did not exceed the risk of abdominal recurrence for more than 20 years. By contrast, patients with pT1Nx-0 disease and Charlson comorbidity index greater than or equal to 2, had a higher risk of non-RCC death than risk of abdominal recurrence at 30 days after surgery.
The retrospective study of 2,511 patients who underwent surgical resection for M0 sporadic RCC between 1990 and 2008 had a median follow up of 9.0 years (interquartile range 6.4-12.7 years).
The researchers noted that recurrences beyond 5 years are fairly common, with up to 15% of patients, by one study’s estimate, experiencing recurrence during the decade following surgery. Cumulative incidence of recurrence does not capture how a patient’s risk of recurrence changes with time or how comorbid conditions influence risk.
The proposed surveillance method results in shorter surveillance durations for some patients and longer surveillance durations than currently recommended for others. This diversity in stopping points “better reflects the range of disease courses appreciated in patients with RCC on the basis of the interplay that occurs between the risk of recurrence and other competing health factors,” Dr. Stewart-Merrill and associates explained.
Dr. Stewart-Merrill reported having no disclosures.
A novel approach to oncologic surveillance after surgical resection for renal cell carcinoma (RCC) that incorporates patient age, Charlson comorbidity index, pathologic tumor stage, and relapse location–specific data, may provide better recommendations for surveillance duration than current guidelines, researchers reported.
“By providing more individualized recommendations and by eliminating oversimplified time thresholds for surveillance, this strategy, we believe, represents an improvement over current guidelines,” wrote Dr. Suzanne Stewart-Merrill of the department of urology, Mayo Clinic, Rochester, Minn., and colleagues (J Clin Oncol. 2015 Sep 7. doi: 10.1200/JCO.2015.61.8009).
Guidelines suggest surveillance durations based on cumulative incidence of recurrences, but do not account for individual patient risk factors. Adherence to the guidelines could miss up to one-third of all recurrences, the authors noted. The longest surveillance duration advocated by the National Comprehensive Cancer Network or the American Urological Association is 5 years.
Researchers used Weibull models for risk of recurrence, stratified by stage and relapse location, combined with risk estimates for non-RCC death, to estimate the optimum surveillance duration. For example, for patients aged 50-59 years with pT1Nx-0 disease and a Charlson comorbidity index of less than or equal to 1, risk of non-RCC death exceeded the risk of abdominal recurrence at 7 years, marking the recommended surveillance duration for that subgroup. The recommended surveillance duration for patients with similar characteristics aged 60-69 years is 2.5 years, and for patients aged 70-79 years it is 1.5 years.
When taking into account individual risk factors, the method produced a wide range of surveillance durations. For patients under 50 years old with pT1Nx-0 disease and a Charlson comorbidity index less than or equal to 1, the risk of non-RCC death did not exceed the risk of abdominal recurrence for more than 20 years. By contrast, patients with pT1Nx-0 disease and Charlson comorbidity index greater than or equal to 2, had a higher risk of non-RCC death than risk of abdominal recurrence at 30 days after surgery.
The retrospective study of 2,511 patients who underwent surgical resection for M0 sporadic RCC between 1990 and 2008 had a median follow up of 9.0 years (interquartile range 6.4-12.7 years).
The researchers noted that recurrences beyond 5 years are fairly common, with up to 15% of patients, by one study’s estimate, experiencing recurrence during the decade following surgery. Cumulative incidence of recurrence does not capture how a patient’s risk of recurrence changes with time or how comorbid conditions influence risk.
The proposed surveillance method results in shorter surveillance durations for some patients and longer surveillance durations than currently recommended for others. This diversity in stopping points “better reflects the range of disease courses appreciated in patients with RCC on the basis of the interplay that occurs between the risk of recurrence and other competing health factors,” Dr. Stewart-Merrill and associates explained.
Dr. Stewart-Merrill reported having no disclosures.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: An individualized approach to surveillance after surgical resection in patients with renal cell carcinoma may provide better patient benefit and resource allocation.
Major finding: Weibull models for risk of recurrence, stratified by stage and relapse location, combined with risk estimates for non-RCC death, provided the basis for recommendations on surveillance duration.
Data source: Retrospective study of 2,511 patients who underwent surgical resection for M0 sporadic RCC between 1990 and 2008, with a median follow up of 9.0 years (interquartile range 6.4-12.7 years).
Disclosures: Dr. Stewart-Merrill reported having no disclosures.
VIDEO: Consistency is key to monitoring patients on opioids
ORLANDO – Take a consistent approach with all patients on opioid therapy, regardless of a patient’s perceived potential for abuse, Dr. Melissa B. Weimer advised.
“This is an area of medicine where I feel we need to apply universal precautions to all patients,” noted Dr. Weimer, assistant professor of medicine, Oregon Health and Science University, Portland. “We’re treating all patients as at some level of potential harm from this medication.”
In an interview at a meeting held by the American Pain Society and Global Academy for Medical Education, Dr. Weimer outlined a strategy that employs the same protocol to monitor therapy, even when the abuse potential is considered to be low.
Global Academy and this news organization are owned by the same company. Dr. Weimer reported no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ORLANDO – Take a consistent approach with all patients on opioid therapy, regardless of a patient’s perceived potential for abuse, Dr. Melissa B. Weimer advised.
“This is an area of medicine where I feel we need to apply universal precautions to all patients,” noted Dr. Weimer, assistant professor of medicine, Oregon Health and Science University, Portland. “We’re treating all patients as at some level of potential harm from this medication.”
In an interview at a meeting held by the American Pain Society and Global Academy for Medical Education, Dr. Weimer outlined a strategy that employs the same protocol to monitor therapy, even when the abuse potential is considered to be low.
Global Academy and this news organization are owned by the same company. Dr. Weimer reported no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ORLANDO – Take a consistent approach with all patients on opioid therapy, regardless of a patient’s perceived potential for abuse, Dr. Melissa B. Weimer advised.
“This is an area of medicine where I feel we need to apply universal precautions to all patients,” noted Dr. Weimer, assistant professor of medicine, Oregon Health and Science University, Portland. “We’re treating all patients as at some level of potential harm from this medication.”
In an interview at a meeting held by the American Pain Society and Global Academy for Medical Education, Dr. Weimer outlined a strategy that employs the same protocol to monitor therapy, even when the abuse potential is considered to be low.
Global Academy and this news organization are owned by the same company. Dr. Weimer reported no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM PAIN CARE FOR PRIMARY CARE

Prescription opioid overdoses targeted in new CDC program
The Centers for Disease Control and Prevention has launched a program aimed at helping states combat and prevent opioid drug overdoses.
The Prescription Drug Overdose: Prevention for States program will be launching in 16 states chosen in a competitive application process. The CDC is committing $20 million in fiscal year 2015, and each state will receive $750,000 to $1 million each year for the next 4 years to advance prevention in several areas, such as enhancing prescription drug–monitoring programs, putting prevention into action in communities nationwide, and investigating the connection between prescription opioid abuse and heroin use, the CDC said in a press release.
In 2013, 16,000 people died from prescription opioid overdoses, four times more than in 1999, with prescription of opioids increasing at the same rate over the same time. Despite more opioids being prescribed, the amount of pain Americans report has not changed. In addition, heroin deaths also have spiked, with the 8,000 heroin overdose deaths nearly three times as many as in 2010.
“The prescription drug overdose epidemic requires a multifaceted approach, and states are key partners in our efforts on the front lines to prevent overdose deaths. With this funding, states can improve their ability to track the problem, work with insurers to help providers make informed prescribing decisions, and take action to combat this epidemic,” U.S. Department of Health & Human Services Secretary Sylvia M. Burwell said in the release.
Find the full CDC press release here.
The Centers for Disease Control and Prevention has launched a program aimed at helping states combat and prevent opioid drug overdoses.
The Prescription Drug Overdose: Prevention for States program will be launching in 16 states chosen in a competitive application process. The CDC is committing $20 million in fiscal year 2015, and each state will receive $750,000 to $1 million each year for the next 4 years to advance prevention in several areas, such as enhancing prescription drug–monitoring programs, putting prevention into action in communities nationwide, and investigating the connection between prescription opioid abuse and heroin use, the CDC said in a press release.
In 2013, 16,000 people died from prescription opioid overdoses, four times more than in 1999, with prescription of opioids increasing at the same rate over the same time. Despite more opioids being prescribed, the amount of pain Americans report has not changed. In addition, heroin deaths also have spiked, with the 8,000 heroin overdose deaths nearly three times as many as in 2010.
“The prescription drug overdose epidemic requires a multifaceted approach, and states are key partners in our efforts on the front lines to prevent overdose deaths. With this funding, states can improve their ability to track the problem, work with insurers to help providers make informed prescribing decisions, and take action to combat this epidemic,” U.S. Department of Health & Human Services Secretary Sylvia M. Burwell said in the release.
Find the full CDC press release here.
The Centers for Disease Control and Prevention has launched a program aimed at helping states combat and prevent opioid drug overdoses.
The Prescription Drug Overdose: Prevention for States program will be launching in 16 states chosen in a competitive application process. The CDC is committing $20 million in fiscal year 2015, and each state will receive $750,000 to $1 million each year for the next 4 years to advance prevention in several areas, such as enhancing prescription drug–monitoring programs, putting prevention into action in communities nationwide, and investigating the connection between prescription opioid abuse and heroin use, the CDC said in a press release.
In 2013, 16,000 people died from prescription opioid overdoses, four times more than in 1999, with prescription of opioids increasing at the same rate over the same time. Despite more opioids being prescribed, the amount of pain Americans report has not changed. In addition, heroin deaths also have spiked, with the 8,000 heroin overdose deaths nearly three times as many as in 2010.
“The prescription drug overdose epidemic requires a multifaceted approach, and states are key partners in our efforts on the front lines to prevent overdose deaths. With this funding, states can improve their ability to track the problem, work with insurers to help providers make informed prescribing decisions, and take action to combat this epidemic,” U.S. Department of Health & Human Services Secretary Sylvia M. Burwell said in the release.
Find the full CDC press release here.
ESC: Statins reduce postoperative noncardiac surgery event rates
LONDON – Statin therapy, given the week before a host of noncardiac surgical procedures, reduced the postoperative risk for death and cardiac complications at 30 days by 17% when compared with no statin use in a large, international observational study.
Results of the prospective VISION (Vascular Events in Noncardiac Surgery Patients Cohort Evaluation) study showed that the primary composite endpoint of all-cause mortality, myocardial injury after noncardiac surgery (MINS), or stroke at 30 days was 11.8% in a propensity-matched cohort of patients, 2,845 of whom were treated with a statin and 4,492 who were not. The relative risk (RR) for this composite endpoint was 0.83 favoring the use of preoperative statins, with a 95% confidence interval (CI) of 0.73-0.95 and a P value of .007.

Perioperative statin vs. no statin use also cut all-cause mortality by 42% (RR, 0.58; 95% CI, 0.40-0.83; P = .003), cardiovascular mortality by 58% (RR, 0.42; 95% CI, 0.23-0.76; P = .004), and MINS by 14% (RR, 0.86; 95% CI, 0.73-0.98; P = .002).
“These study results are hypothesis generating at most,” emphasized Dr. Otavio Berwanger, who presented the findings at the annual congress of the European Society of Cardiology while they were simultaneously published online (Eur Heart J. 2015 Sept. 1. doi: 10.1093/eurheartj/ehv456).
“It is true that, in this large representative cohort of contemporary patients, statins were associated with lower event rates,” added Dr. Berwanger of Hospital do Coração in São Paulo, Brazil, and “together with the previous body of evidence, statins appear to be an interesting and attractive intervention to reduce postoperative events.” A large-scale, randomized trial is needed, however, to answer the question of whether statins should be used preoperatively to prevent postoperative events in noncardiac surgery patients.
Over a 4-year period that started in August 2007, more than 15,000 individuals aged 45 years or older who were undergoing a variety of noncardiac surgical procedures that required regional or a general anesthetic and at least an overnight stay in the hospital were recruited at 12 centers in eight countries in North and South America, Africa, Asia, Australia, and Europe.
One of the objectives of the study was to examine the use of perioperative statins on cardiovascular events at 30 days, and to do this, the VISION investigators identified the patients who had received a statin in the 7 days prior to surgery and then used propensity matching to form a control group of patients that had not received a statin in the week before surgery.
Just under half of the propensity-matched population was male, with an average age of nearly 69 years. Around 70% of the population had hypertension, 9%-10% had a prior stroke, and 13% had active cancer. Surgeries were urgent in about 2% and emergent in 8%. Around a quarter had undergone orthopedic procedures, and 4% were vascular surgeries. Overall, 36% of surgeries were classified as low risk and 39% as other.
One of the limitations of the study, however, is that, despite the propensity matching, there were some variables that remained different between the two groups, with higher rates of coronary artery disease (20% vs. 14%), peripheral vascular disease (8% vs. 5%), diabetes (30% vs. 25%), and preoperative use of aspirin (25% vs. 19%) and angiotensin-converting enzyme inhibitors or angiotensin receptor blockers (53% vs. 48%) in the statin- versus nonstatin-treated patients.
Other limitations are that these data are observational and the use of statins could be just a surrogate for unmeasured confounders that relate to prognosis. Information on the type and dosing of statins also was not obtained, and there was no information collected on potential liver or muscle function side effects.
Nevertheless, the VISION investigators noted in the published paper that the results are consistent with those from other observational studies and prior small-scale, randomized trials and so do add important information. They noted that these data were collected prospectively in a broader range of patients and types of surgeries than has been reported previously. In addition, patients were recruited from several countries and were actively monitored for outcomes and events were centrally adjudicated. VISION is also the only study to report on the effects of statins on MINS.
“Another message from our results is that the use of long-term statins is sub-optimal in high cardiovascular risk patients, who should be on long-term lipid-lowering therapy independently of surgery,” the VISION investigators wrote in their report.
The study was funded by Hamilton Health Sciences Corp. at McMaster University. Dr. Berwanger disclosed receiving research contracts from AstraZeneca, Bayer Healthcare, Amgen, Boehringer-Ingelheim, Pfizer, and Roche Diagnostics.
LONDON – Statin therapy, given the week before a host of noncardiac surgical procedures, reduced the postoperative risk for death and cardiac complications at 30 days by 17% when compared with no statin use in a large, international observational study.
Results of the prospective VISION (Vascular Events in Noncardiac Surgery Patients Cohort Evaluation) study showed that the primary composite endpoint of all-cause mortality, myocardial injury after noncardiac surgery (MINS), or stroke at 30 days was 11.8% in a propensity-matched cohort of patients, 2,845 of whom were treated with a statin and 4,492 who were not. The relative risk (RR) for this composite endpoint was 0.83 favoring the use of preoperative statins, with a 95% confidence interval (CI) of 0.73-0.95 and a P value of .007.
Perioperative statin vs. no statin use also cut all-cause mortality by 42% (RR, 0.58; 95% CI, 0.40-0.83; P = .003), cardiovascular mortality by 58% (RR, 0.42; 95% CI, 0.23-0.76; P = .004), and MINS by 14% (RR, 0.86; 95% CI, 0.73-0.98; P = .002).
“These study results are hypothesis generating at most,” emphasized Dr. Otavio Berwanger, who presented the findings at the annual congress of the European Society of Cardiology while they were simultaneously published online (Eur Heart J. 2015 Sept. 1. doi: 10.1093/eurheartj/ehv456).
“It is true that, in this large representative cohort of contemporary patients, statins were associated with lower event rates,” added Dr. Berwanger of Hospital do Coração in São Paulo, Brazil, and “together with the previous body of evidence, statins appear to be an interesting and attractive intervention to reduce postoperative events.” A large-scale, randomized trial is needed, however, to answer the question of whether statins should be used preoperatively to prevent postoperative events in noncardiac surgery patients.
Over a 4-year period that started in August 2007, more than 15,000 individuals aged 45 years or older who were undergoing a variety of noncardiac surgical procedures that required regional or a general anesthetic and at least an overnight stay in the hospital were recruited at 12 centers in eight countries in North and South America, Africa, Asia, Australia, and Europe.
One of the objectives of the study was to examine the use of perioperative statins on cardiovascular events at 30 days, and to do this, the VISION investigators identified the patients who had received a statin in the 7 days prior to surgery and then used propensity matching to form a control group of patients that had not received a statin in the week before surgery.
Just under half of the propensity-matched population was male, with an average age of nearly 69 years. Around 70% of the population had hypertension, 9%-10% had a prior stroke, and 13% had active cancer. Surgeries were urgent in about 2% and emergent in 8%. Around a quarter had undergone orthopedic procedures, and 4% were vascular surgeries. Overall, 36% of surgeries were classified as low risk and 39% as other.
One of the limitations of the study, however, is that, despite the propensity matching, there were some variables that remained different between the two groups, with higher rates of coronary artery disease (20% vs. 14%), peripheral vascular disease (8% vs. 5%), diabetes (30% vs. 25%), and preoperative use of aspirin (25% vs. 19%) and angiotensin-converting enzyme inhibitors or angiotensin receptor blockers (53% vs. 48%) in the statin- versus nonstatin-treated patients.
Other limitations are that these data are observational and the use of statins could be just a surrogate for unmeasured confounders that relate to prognosis. Information on the type and dosing of statins also was not obtained, and there was no information collected on potential liver or muscle function side effects.
Nevertheless, the VISION investigators noted in the published paper that the results are consistent with those from other observational studies and prior small-scale, randomized trials and so do add important information. They noted that these data were collected prospectively in a broader range of patients and types of surgeries than has been reported previously. In addition, patients were recruited from several countries and were actively monitored for outcomes and events were centrally adjudicated. VISION is also the only study to report on the effects of statins on MINS.
“Another message from our results is that the use of long-term statins is sub-optimal in high cardiovascular risk patients, who should be on long-term lipid-lowering therapy independently of surgery,” the VISION investigators wrote in their report.
The study was funded by Hamilton Health Sciences Corp. at McMaster University. Dr. Berwanger disclosed receiving research contracts from AstraZeneca, Bayer Healthcare, Amgen, Boehringer-Ingelheim, Pfizer, and Roche Diagnostics.
LONDON – Statin therapy, given the week before a host of noncardiac surgical procedures, reduced the postoperative risk for death and cardiac complications at 30 days by 17% when compared with no statin use in a large, international observational study.
Results of the prospective VISION (Vascular Events in Noncardiac Surgery Patients Cohort Evaluation) study showed that the primary composite endpoint of all-cause mortality, myocardial injury after noncardiac surgery (MINS), or stroke at 30 days was 11.8% in a propensity-matched cohort of patients, 2,845 of whom were treated with a statin and 4,492 who were not. The relative risk (RR) for this composite endpoint was 0.83 favoring the use of preoperative statins, with a 95% confidence interval (CI) of 0.73-0.95 and a P value of .007.
Perioperative statin vs. no statin use also cut all-cause mortality by 42% (RR, 0.58; 95% CI, 0.40-0.83; P = .003), cardiovascular mortality by 58% (RR, 0.42; 95% CI, 0.23-0.76; P = .004), and MINS by 14% (RR, 0.86; 95% CI, 0.73-0.98; P = .002).
“These study results are hypothesis generating at most,” emphasized Dr. Otavio Berwanger, who presented the findings at the annual congress of the European Society of Cardiology while they were simultaneously published online (Eur Heart J. 2015 Sept. 1. doi: 10.1093/eurheartj/ehv456).
“It is true that, in this large representative cohort of contemporary patients, statins were associated with lower event rates,” added Dr. Berwanger of Hospital do Coração in São Paulo, Brazil, and “together with the previous body of evidence, statins appear to be an interesting and attractive intervention to reduce postoperative events.” A large-scale, randomized trial is needed, however, to answer the question of whether statins should be used preoperatively to prevent postoperative events in noncardiac surgery patients.
Over a 4-year period that started in August 2007, more than 15,000 individuals aged 45 years or older who were undergoing a variety of noncardiac surgical procedures that required regional or a general anesthetic and at least an overnight stay in the hospital were recruited at 12 centers in eight countries in North and South America, Africa, Asia, Australia, and Europe.
One of the objectives of the study was to examine the use of perioperative statins on cardiovascular events at 30 days, and to do this, the VISION investigators identified the patients who had received a statin in the 7 days prior to surgery and then used propensity matching to form a control group of patients that had not received a statin in the week before surgery.
Just under half of the propensity-matched population was male, with an average age of nearly 69 years. Around 70% of the population had hypertension, 9%-10% had a prior stroke, and 13% had active cancer. Surgeries were urgent in about 2% and emergent in 8%. Around a quarter had undergone orthopedic procedures, and 4% were vascular surgeries. Overall, 36% of surgeries were classified as low risk and 39% as other.
One of the limitations of the study, however, is that, despite the propensity matching, there were some variables that remained different between the two groups, with higher rates of coronary artery disease (20% vs. 14%), peripheral vascular disease (8% vs. 5%), diabetes (30% vs. 25%), and preoperative use of aspirin (25% vs. 19%) and angiotensin-converting enzyme inhibitors or angiotensin receptor blockers (53% vs. 48%) in the statin- versus nonstatin-treated patients.
Other limitations are that these data are observational and the use of statins could be just a surrogate for unmeasured confounders that relate to prognosis. Information on the type and dosing of statins also was not obtained, and there was no information collected on potential liver or muscle function side effects.
Nevertheless, the VISION investigators noted in the published paper that the results are consistent with those from other observational studies and prior small-scale, randomized trials and so do add important information. They noted that these data were collected prospectively in a broader range of patients and types of surgeries than has been reported previously. In addition, patients were recruited from several countries and were actively monitored for outcomes and events were centrally adjudicated. VISION is also the only study to report on the effects of statins on MINS.
“Another message from our results is that the use of long-term statins is sub-optimal in high cardiovascular risk patients, who should be on long-term lipid-lowering therapy independently of surgery,” the VISION investigators wrote in their report.
The study was funded by Hamilton Health Sciences Corp. at McMaster University. Dr. Berwanger disclosed receiving research contracts from AstraZeneca, Bayer Healthcare, Amgen, Boehringer-Ingelheim, Pfizer, and Roche Diagnostics.
AT THE ESC CONGRESS 2015
Key clinical point: Statin therapy, given the week before a host of noncardiac surgical procedures, reduced the postoperative risk for death and cardiac complications at 30 days, but the findings are hypothesis generating and need validation in a randomized controlled clinical trial.
Major finding: The primary composite outcome (all-cause mortality, myocardial injury after noncardiac surgery, or stroke at 30 days) was 11.8% overall in the propensity-matched cohort, with a 17% relative risk reduction favoring the use of statin versus no statin (P = .007).
Data source: The VISION study is an international, prospective, observational study of more than 15,000 patients who underwent noncardiac surgery between 2007 and 2011.
Disclosures: The study was funded by Hamilton Health Sciences Corp. at McMaster University. Dr. Berwanger disclosed receiving research contracts from AstraZeneca, Bayer Healthcare, Amgen, Boehringer-Ingelheim, Pfizer, and Roche Diagnostics.

HHS: Expand antidiscrimination protections to transgender patients
Transgender patients who receive health care via government programs or funding must receive equal access to treatments and insurance coverage, according to a proposed rule issued Sept. 3 by the Health and Human Services department. The rule would extend antidiscrimination policies under the Affordable Care Act to include gender identity.
The rule would apply to health providers who accept patients covered by Medicare and Medicaid as well as insurance purchased via the health insurance marketplaces.

“The proposed rule clarifies and harmonizes existing well-established federal civil rights laws and clarifies the standards that HHS and in particular, the Office of Civil Rights, will apply in implementing [ACA] Section 1557,” Jocelyn Samuels, OCR director, said in a press conference. “Prior laws enforced by the Office of Civil Rights barred discrimination based only on race, color, national origin, age, or disability. All of the protections against sex discrimination that will be incorporated into the rule are new in this space.”
Section 1557 of the ACA extends civil rights protections to ban sex discrimination in federal health care programs and activities. The new proposed rule establishes that the prohibition on sex discrimination includes discrimination based on gender identity. The rule also includes requirements for effective communication for patients with disabilities and enhanced language assistance for patients with limited English proficiency.
Specifics of the proposed rule include:
• Patients must be treated equally and consistent with their gender identity by health providers. Insurers must provide fair access to coverage regardless of gender identity. For example, some insurers have historically excluded coverage of all care related to gender transition. Such categorical exclusions are prohibited under the proposed rule.
• Women must be treated equally with men in the health care they receive, not only in the health coverage they obtain but in the services they seek from providers.
• For patients with disabilities, the rule contains requirements for the provision of auxiliary aids and services, including alternative formats and sign language interpreters and the accessibility of programs offered through electronic and information technology.
• The rule bolsters language assistance for people with limited English proficiency so that patients are able to more effectively communicate with their providers to describe their symptoms and understand treatment.
During the press conference, Ms. Samuels clarified that the rule does not mean that health insurers must cover any specific treatments or procedures, rather they must apply nondiscriminatory criteria when assessing coverage requests.
The proposed extension of protections is, in part, driven by ongoing cases of sex and identity discrimination by some health providers. In one case, a hospital denied a transgender patient a room assignment consistent with her gender identity. In another, a male domestic violence victim was denied services at a hospital because he did not fit the traditional profile of a domestic violence victim, Ms. Samuels said. In another case, a health provider required that a husband be the guarantor for his wife’s medical bills but did not require the same for male patients and their spouses.
“There continue to be serious problems of discrimination in the health care arena,” she said. “This proposed rule provides very valuable tools for us to be able to appropriately address them.”
HHS is requesting comments on whether Section 1557 should include exemptions for religious organizations and, if so, to what extent. The administration notes that nothing in the proposed rule would affect the application of existing protections for religious beliefs and practices, such as provider conscience laws and regulations under the ACA involving preventive health services.
Comments on the rule will be accepted at www.regulations.gov until Nov. 6.
On Twitter @legal_med
Transgender patients who receive health care via government programs or funding must receive equal access to treatments and insurance coverage, according to a proposed rule issued Sept. 3 by the Health and Human Services department. The rule would extend antidiscrimination policies under the Affordable Care Act to include gender identity.
The rule would apply to health providers who accept patients covered by Medicare and Medicaid as well as insurance purchased via the health insurance marketplaces.
“The proposed rule clarifies and harmonizes existing well-established federal civil rights laws and clarifies the standards that HHS and in particular, the Office of Civil Rights, will apply in implementing [ACA] Section 1557,” Jocelyn Samuels, OCR director, said in a press conference. “Prior laws enforced by the Office of Civil Rights barred discrimination based only on race, color, national origin, age, or disability. All of the protections against sex discrimination that will be incorporated into the rule are new in this space.”
Section 1557 of the ACA extends civil rights protections to ban sex discrimination in federal health care programs and activities. The new proposed rule establishes that the prohibition on sex discrimination includes discrimination based on gender identity. The rule also includes requirements for effective communication for patients with disabilities and enhanced language assistance for patients with limited English proficiency.
Specifics of the proposed rule include:
• Patients must be treated equally and consistent with their gender identity by health providers. Insurers must provide fair access to coverage regardless of gender identity. For example, some insurers have historically excluded coverage of all care related to gender transition. Such categorical exclusions are prohibited under the proposed rule.
• Women must be treated equally with men in the health care they receive, not only in the health coverage they obtain but in the services they seek from providers.
• For patients with disabilities, the rule contains requirements for the provision of auxiliary aids and services, including alternative formats and sign language interpreters and the accessibility of programs offered through electronic and information technology.
• The rule bolsters language assistance for people with limited English proficiency so that patients are able to more effectively communicate with their providers to describe their symptoms and understand treatment.
During the press conference, Ms. Samuels clarified that the rule does not mean that health insurers must cover any specific treatments or procedures, rather they must apply nondiscriminatory criteria when assessing coverage requests.
The proposed extension of protections is, in part, driven by ongoing cases of sex and identity discrimination by some health providers. In one case, a hospital denied a transgender patient a room assignment consistent with her gender identity. In another, a male domestic violence victim was denied services at a hospital because he did not fit the traditional profile of a domestic violence victim, Ms. Samuels said. In another case, a health provider required that a husband be the guarantor for his wife’s medical bills but did not require the same for male patients and their spouses.
“There continue to be serious problems of discrimination in the health care arena,” she said. “This proposed rule provides very valuable tools for us to be able to appropriately address them.”
HHS is requesting comments on whether Section 1557 should include exemptions for religious organizations and, if so, to what extent. The administration notes that nothing in the proposed rule would affect the application of existing protections for religious beliefs and practices, such as provider conscience laws and regulations under the ACA involving preventive health services.
Comments on the rule will be accepted at www.regulations.gov until Nov. 6.
On Twitter @legal_med
Transgender patients who receive health care via government programs or funding must receive equal access to treatments and insurance coverage, according to a proposed rule issued Sept. 3 by the Health and Human Services department. The rule would extend antidiscrimination policies under the Affordable Care Act to include gender identity.
The rule would apply to health providers who accept patients covered by Medicare and Medicaid as well as insurance purchased via the health insurance marketplaces.
“The proposed rule clarifies and harmonizes existing well-established federal civil rights laws and clarifies the standards that HHS and in particular, the Office of Civil Rights, will apply in implementing [ACA] Section 1557,” Jocelyn Samuels, OCR director, said in a press conference. “Prior laws enforced by the Office of Civil Rights barred discrimination based only on race, color, national origin, age, or disability. All of the protections against sex discrimination that will be incorporated into the rule are new in this space.”
Section 1557 of the ACA extends civil rights protections to ban sex discrimination in federal health care programs and activities. The new proposed rule establishes that the prohibition on sex discrimination includes discrimination based on gender identity. The rule also includes requirements for effective communication for patients with disabilities and enhanced language assistance for patients with limited English proficiency.
Specifics of the proposed rule include:
• Patients must be treated equally and consistent with their gender identity by health providers. Insurers must provide fair access to coverage regardless of gender identity. For example, some insurers have historically excluded coverage of all care related to gender transition. Such categorical exclusions are prohibited under the proposed rule.
• Women must be treated equally with men in the health care they receive, not only in the health coverage they obtain but in the services they seek from providers.
• For patients with disabilities, the rule contains requirements for the provision of auxiliary aids and services, including alternative formats and sign language interpreters and the accessibility of programs offered through electronic and information technology.
• The rule bolsters language assistance for people with limited English proficiency so that patients are able to more effectively communicate with their providers to describe their symptoms and understand treatment.
During the press conference, Ms. Samuels clarified that the rule does not mean that health insurers must cover any specific treatments or procedures, rather they must apply nondiscriminatory criteria when assessing coverage requests.
The proposed extension of protections is, in part, driven by ongoing cases of sex and identity discrimination by some health providers. In one case, a hospital denied a transgender patient a room assignment consistent with her gender identity. In another, a male domestic violence victim was denied services at a hospital because he did not fit the traditional profile of a domestic violence victim, Ms. Samuels said. In another case, a health provider required that a husband be the guarantor for his wife’s medical bills but did not require the same for male patients and their spouses.
“There continue to be serious problems of discrimination in the health care arena,” she said. “This proposed rule provides very valuable tools for us to be able to appropriately address them.”
HHS is requesting comments on whether Section 1557 should include exemptions for religious organizations and, if so, to what extent. The administration notes that nothing in the proposed rule would affect the application of existing protections for religious beliefs and practices, such as provider conscience laws and regulations under the ACA involving preventive health services.
Comments on the rule will be accepted at www.regulations.gov until Nov. 6.
On Twitter @legal_med

Melanoma regression a positive prognostic indicator
Histologic regression in melanoma is associated with a significantly lower risk of sentinel lymph node positivity and may serve as a prognostic factor when deciding whether to perform a sentinel lymph node biopsy, according to a study published online Sept. 2 in JAMA Dermatology.
Researchers conducted a meta-analysis of 14 studies in 10,098 patients who showed histologic regression of a primary melanoma and whose sentinel lymph node status was available. In the 14 studies combined, the analysis showed patients with histologic regression had a 44% lower likelihood of having a positive sentinel lymph node than patients without regression, reported Dr. Simone Ribero of the University of Turin (Italy), and coauthors (JAMA Dermatol. 2015 Sep 2. doi: 10.1001/jamadermatol.2015.2235).
This figure was even lower for patients enrolled in high-quality studies, compared with lower-quality studies, they said. In the nine studies considered high quality, patients with regression had a 52% lower likelihood of having a positive sentinel lymph node, while those enrolled in the five studies considered low quality had a 27% lower likelihood of having a positive sentinel lymph node.
The prognostic significance of regression in primary melanoma has been confounded by the fact that disappearance of part of the tumor can result in an underestimation of the original Breslow thickness. Some previous studies have found an increase in sentinel lymph node positivity associated with regression, while other studies suggested that regression was in fact a protective factor against sentinel lymph node metastasis.
Although the studies used different definitions of histologic regression and all were observational (counted among the limitations of the studies), the authors concluded that regression was prognostically favorable. “The results of this meta-analysis may be useful when deciding to offer SLNB [sentinel lymph node biopsy] to patients with regressions of melanomas,” they wrote, adding: “It may help clinicians make a final selection of the most appropriate patients for this procedure.”
The authors had no conflicts of interest to declare.
The finding that patients with histologic regression have half the risk for micrometastases in sentinel lymph node biopsy, compared with patients without regression gives a clear answer to the question of whether patients with thin melanoma and regression should undergo SLNB, and that answer is “No.”

|
Dr. Claus Garbe |
These findings underline that fact that prognosis of patients with melanoma does not depend only on the characteristics of the tumor itself, such as tumor thickness, ulceration, and mitosis, but also on the immune response of the host.
Dr. Claus Garbe is from the Department of Dermatology, University Hospital Tübingen (Germany). These comments are taken from an accompanying editorial (JAMA Dermatol. 2015 Sep 2. doi: 10.1001/jamadermatol.2015.2235). No conflicts of interest were declared.
The finding that patients with histologic regression have half the risk for micrometastases in sentinel lymph node biopsy, compared with patients without regression gives a clear answer to the question of whether patients with thin melanoma and regression should undergo SLNB, and that answer is “No.”
|
|
Dr. Claus Garbe |
These findings underline that fact that prognosis of patients with melanoma does not depend only on the characteristics of the tumor itself, such as tumor thickness, ulceration, and mitosis, but also on the immune response of the host.
Dr. Claus Garbe is from the Department of Dermatology, University Hospital Tübingen (Germany). These comments are taken from an accompanying editorial (JAMA Dermatol. 2015 Sep 2. doi: 10.1001/jamadermatol.2015.2235). No conflicts of interest were declared.
The finding that patients with histologic regression have half the risk for micrometastases in sentinel lymph node biopsy, compared with patients without regression gives a clear answer to the question of whether patients with thin melanoma and regression should undergo SLNB, and that answer is “No.”
|
|
Dr. Claus Garbe |
These findings underline that fact that prognosis of patients with melanoma does not depend only on the characteristics of the tumor itself, such as tumor thickness, ulceration, and mitosis, but also on the immune response of the host.
Dr. Claus Garbe is from the Department of Dermatology, University Hospital Tübingen (Germany). These comments are taken from an accompanying editorial (JAMA Dermatol. 2015 Sep 2. doi: 10.1001/jamadermatol.2015.2235). No conflicts of interest were declared.
Histologic regression in melanoma is associated with a significantly lower risk of sentinel lymph node positivity and may serve as a prognostic factor when deciding whether to perform a sentinel lymph node biopsy, according to a study published online Sept. 2 in JAMA Dermatology.
Researchers conducted a meta-analysis of 14 studies in 10,098 patients who showed histologic regression of a primary melanoma and whose sentinel lymph node status was available. In the 14 studies combined, the analysis showed patients with histologic regression had a 44% lower likelihood of having a positive sentinel lymph node than patients without regression, reported Dr. Simone Ribero of the University of Turin (Italy), and coauthors (JAMA Dermatol. 2015 Sep 2. doi: 10.1001/jamadermatol.2015.2235).
This figure was even lower for patients enrolled in high-quality studies, compared with lower-quality studies, they said. In the nine studies considered high quality, patients with regression had a 52% lower likelihood of having a positive sentinel lymph node, while those enrolled in the five studies considered low quality had a 27% lower likelihood of having a positive sentinel lymph node.
The prognostic significance of regression in primary melanoma has been confounded by the fact that disappearance of part of the tumor can result in an underestimation of the original Breslow thickness. Some previous studies have found an increase in sentinel lymph node positivity associated with regression, while other studies suggested that regression was in fact a protective factor against sentinel lymph node metastasis.
Although the studies used different definitions of histologic regression and all were observational (counted among the limitations of the studies), the authors concluded that regression was prognostically favorable. “The results of this meta-analysis may be useful when deciding to offer SLNB [sentinel lymph node biopsy] to patients with regressions of melanomas,” they wrote, adding: “It may help clinicians make a final selection of the most appropriate patients for this procedure.”
The authors had no conflicts of interest to declare.
Histologic regression in melanoma is associated with a significantly lower risk of sentinel lymph node positivity and may serve as a prognostic factor when deciding whether to perform a sentinel lymph node biopsy, according to a study published online Sept. 2 in JAMA Dermatology.
Researchers conducted a meta-analysis of 14 studies in 10,098 patients who showed histologic regression of a primary melanoma and whose sentinel lymph node status was available. In the 14 studies combined, the analysis showed patients with histologic regression had a 44% lower likelihood of having a positive sentinel lymph node than patients without regression, reported Dr. Simone Ribero of the University of Turin (Italy), and coauthors (JAMA Dermatol. 2015 Sep 2. doi: 10.1001/jamadermatol.2015.2235).
This figure was even lower for patients enrolled in high-quality studies, compared with lower-quality studies, they said. In the nine studies considered high quality, patients with regression had a 52% lower likelihood of having a positive sentinel lymph node, while those enrolled in the five studies considered low quality had a 27% lower likelihood of having a positive sentinel lymph node.
The prognostic significance of regression in primary melanoma has been confounded by the fact that disappearance of part of the tumor can result in an underestimation of the original Breslow thickness. Some previous studies have found an increase in sentinel lymph node positivity associated with regression, while other studies suggested that regression was in fact a protective factor against sentinel lymph node metastasis.
Although the studies used different definitions of histologic regression and all were observational (counted among the limitations of the studies), the authors concluded that regression was prognostically favorable. “The results of this meta-analysis may be useful when deciding to offer SLNB [sentinel lymph node biopsy] to patients with regressions of melanomas,” they wrote, adding: “It may help clinicians make a final selection of the most appropriate patients for this procedure.”
The authors had no conflicts of interest to declare.
FROM JAMA DERMATOLOGY
Key clinical point: Histologic regression in melanoma is associated with a significantly lower risk of sentinel lymph node positivity.
Major finding: Individuals with histologic regression in melanoma had a 44% lower likelihood of having a positive sentinel lymph node than patients without regression.
Data source: A meta-analysis evaluated 14 studies in 10,098 patients.
Disclosures: None of the authors had conflicts of interest to disclose.

Patients rate specialists on timeliness of care
When it comes to giving patients timely care, hematology/oncology practices have an edge over other specialties, the Agency for Healthcare Research and Quality reported.
In a composite of five survey questions asking if physicians provided timely appointments, care, and information, 69% of hematology/oncology patients said that their physicians always provided such care, compared with 66% of cardiology and surgery patients and 65% of pulmonology patients. None of the other specialties included in the report had an always rate higher than 63%, according to data from the Consumer Assessment of Healthcare Providers and Systems (CAHPS) Clinician & Group Survey.
When specialists of the non–primary care variety were considered as a group, 64% of respondents said that they always received timely care, compared with 59% for primary care physicians (not including pediatricians). Overall, 62% of respondents said that physician offices always provided timely care, the survey data show.
The CAHPS database includes a total of 798,967 patient responses submitted in 2014 and early 2015 by 3,962 medical practices.
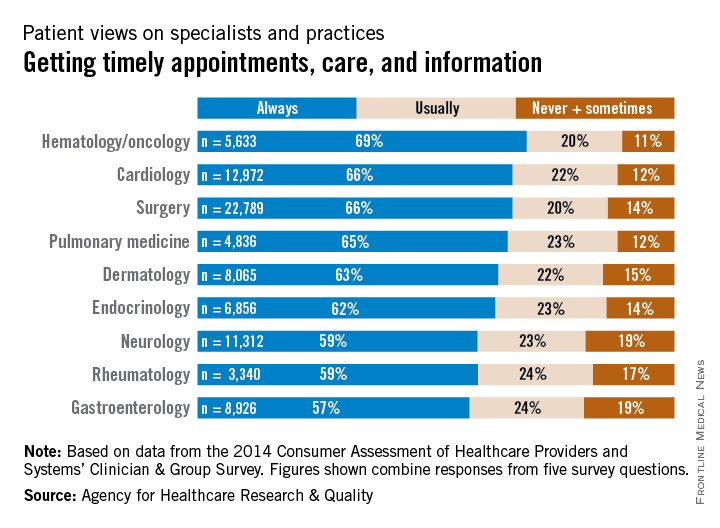
When it comes to giving patients timely care, hematology/oncology practices have an edge over other specialties, the Agency for Healthcare Research and Quality reported.
In a composite of five survey questions asking if physicians provided timely appointments, care, and information, 69% of hematology/oncology patients said that their physicians always provided such care, compared with 66% of cardiology and surgery patients and 65% of pulmonology patients. None of the other specialties included in the report had an always rate higher than 63%, according to data from the Consumer Assessment of Healthcare Providers and Systems (CAHPS) Clinician & Group Survey.
When specialists of the non–primary care variety were considered as a group, 64% of respondents said that they always received timely care, compared with 59% for primary care physicians (not including pediatricians). Overall, 62% of respondents said that physician offices always provided timely care, the survey data show.
The CAHPS database includes a total of 798,967 patient responses submitted in 2014 and early 2015 by 3,962 medical practices.
When it comes to giving patients timely care, hematology/oncology practices have an edge over other specialties, the Agency for Healthcare Research and Quality reported.
In a composite of five survey questions asking if physicians provided timely appointments, care, and information, 69% of hematology/oncology patients said that their physicians always provided such care, compared with 66% of cardiology and surgery patients and 65% of pulmonology patients. None of the other specialties included in the report had an always rate higher than 63%, according to data from the Consumer Assessment of Healthcare Providers and Systems (CAHPS) Clinician & Group Survey.
When specialists of the non–primary care variety were considered as a group, 64% of respondents said that they always received timely care, compared with 59% for primary care physicians (not including pediatricians). Overall, 62% of respondents said that physician offices always provided timely care, the survey data show.
The CAHPS database includes a total of 798,967 patient responses submitted in 2014 and early 2015 by 3,962 medical practices.
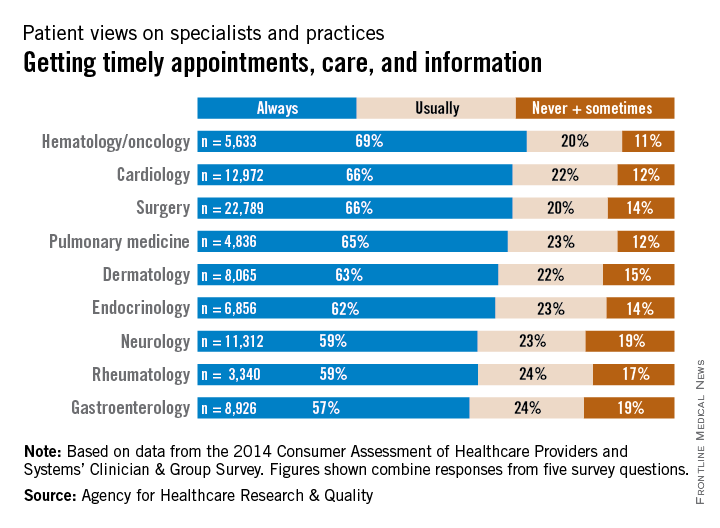
Circulating tumor DNA marked progressive liver cancer
A personalized PCR test for circulating tumor DNA identified cases of progressive hepatocellular carcinoma, investigators reported in the September issue of Cellular and Molecular Gastroenterology and Hepatology.
Patients with liver cancer who underwent resection or transplantation and were positive for ctDNA had significantly higher rates of recurrence (P <.0102) and metastasis (P <.0386), reported Dr. Atsushi Ono of Hiroshima (Japan) University and the RIKEN Center for Integrative Medical Sciences and associates. The study also found that transcatheter arterial chemoembolization [TACE] increased levels of ctDNA, compared with total cell-free DNA, making the marker easier to detect.

“Analyzing cell-free DNA after TACE in unresectable and recurrent cases as a liquid biopsy to establish cancer genome profiles might … guide selection of an individualized therapeutic regimen without requiring percutaneous biopsy,” they added.
Assays for ctDNA have shown promise for diagnosing other cancers and targeting their treatments, but HCC diagnosis relies primarily on imaging, and HCC ctDNA has not been well characterized, noted the investigators. They performed massively parallel whole-genome sequencing of DNA extracted from resected HCCs from 46 patients. They serially measured plasma ctDNA levels before and after surgery using personalized quantitative PCR assays that targeted somatic rearrangements. They also used chemiluminescent immunoassays to test for two conventional tumor markers, alpha-fetoprotein and des-gamma-carboxy prothrombin (Cell Mol Gastroenterol Hepatol. 2015 Jul 2 [doi: 10.1016/j.jcmgh.2015.06.009]).
In all, 25 somatic mutations were present in both primary tumor tissue and in cell-free DNA samples, and 83% of mutations in the primary tumor were detectable in cell-free DNA. Among seven patients who tested positive for ctDNA before surgery, six developed recurrent disease and four developed extrahepatic metastases, Dr. Ono and associates said.
Levels of ctDNA increased as disease progressed and dropped in response to treatment, and one case remained positive for ctDNA even after alpha-fetoprotein and des-gamma-carboxy prothrombin became negative or dropped below threshold after resection. “This suggests that, in some patients, ctDNA might be a better and more sensitive biomarker for HCC than the conventional tumor markers,” they said.
The assay analyzed plasma instead of serum because serum was likely to have more normal cell-free nucleic acids, which would make it harder to detect mutant alleles, the investigators noted. Testing for ctDNA could help address the problem of tumor heterogeneity because ctDNA contains the entire tumor genome, including variants from independent tumors, but the assay will need further validation, especially because its lower limits varied by primer sets, which reduced its sensitivity and meant that some cases went undetected, they added.
The study was funded by the government of Japan, the RIKEN President’s Fund, the Princess Takamatsu Cancer Research Fund, and the Takeda Science Foundation. The investigators declared no competing interests.
As the oncology field advances toward implementation of personalized medicine programs, molecular and genomic analysis of circulating tumor DNA (ctDNA) represents a promising approach for diagnosis, prognosis, therapy selection, and minimal residual disease monitoring of a wide array of malignancies.

|
| Dr. Larissa Furtado |
With the purpose of assessing the utility of extracellular tumor DNA as a potential biomarker for hepatocellular carcinoma (HCC), Dr. Ono and colleagues analyzed serum ctDNA from 46 HCC patients using quantitative PCR assays for somatic rearrangements uncovered by whole-genome sequencing of their primary tumors.
For the seven patients with detectable ctDNA in preoperative serum, the incidence of recurrence and extrahepatic metastasis within 2 years following hepatectomy were significantly worse than in the ctDNA-negative group, although no significant difference in the cumulative survival rate was observed between these patients. The ctDNA positivity also was found to be an independent predictor of microscopic vascular invasion of the portal vein, and it correlated with larger tumor size and higher alpha-fetoprotein and des-gamma-carboxy prothrombin levels.
In addition, the investigators demonstrated that transcatheter arterial chemoembolization (TACE) enriched ctDNA levels in cell-free DNA in blood, and that serum ctDNA levels were increased with disease progression and reflected response to treatments.

|
| Dr. Jeremy Segal |
The diagnosis of HCC is currently based on imaging and/or biopsies. Even though there are no well-established biomarkers for early detection and monitoring of HCC at present, the data presented here indicate the potential utility of personalized ctDNA testing for individualized management of hepatocellular carcinoma patients.
Dr. Larissa V. Furtado and Dr. Jeremy P. Segal are both assistant professors and assistant directors of the division of genomic and molecular pathology in the department of pathology at the University of Chicago Medical Center. Neither has conflicts of interest.
As the oncology field advances toward implementation of personalized medicine programs, molecular and genomic analysis of circulating tumor DNA (ctDNA) represents a promising approach for diagnosis, prognosis, therapy selection, and minimal residual disease monitoring of a wide array of malignancies.
|
|
| Dr. Larissa Furtado |
With the purpose of assessing the utility of extracellular tumor DNA as a potential biomarker for hepatocellular carcinoma (HCC), Dr. Ono and colleagues analyzed serum ctDNA from 46 HCC patients using quantitative PCR assays for somatic rearrangements uncovered by whole-genome sequencing of their primary tumors.
For the seven patients with detectable ctDNA in preoperative serum, the incidence of recurrence and extrahepatic metastasis within 2 years following hepatectomy were significantly worse than in the ctDNA-negative group, although no significant difference in the cumulative survival rate was observed between these patients. The ctDNA positivity also was found to be an independent predictor of microscopic vascular invasion of the portal vein, and it correlated with larger tumor size and higher alpha-fetoprotein and des-gamma-carboxy prothrombin levels.
In addition, the investigators demonstrated that transcatheter arterial chemoembolization (TACE) enriched ctDNA levels in cell-free DNA in blood, and that serum ctDNA levels were increased with disease progression and reflected response to treatments.
|
|
| Dr. Jeremy Segal |
The diagnosis of HCC is currently based on imaging and/or biopsies. Even though there are no well-established biomarkers for early detection and monitoring of HCC at present, the data presented here indicate the potential utility of personalized ctDNA testing for individualized management of hepatocellular carcinoma patients.
Dr. Larissa V. Furtado and Dr. Jeremy P. Segal are both assistant professors and assistant directors of the division of genomic and molecular pathology in the department of pathology at the University of Chicago Medical Center. Neither has conflicts of interest.
As the oncology field advances toward implementation of personalized medicine programs, molecular and genomic analysis of circulating tumor DNA (ctDNA) represents a promising approach for diagnosis, prognosis, therapy selection, and minimal residual disease monitoring of a wide array of malignancies.
|
|
| Dr. Larissa Furtado |
With the purpose of assessing the utility of extracellular tumor DNA as a potential biomarker for hepatocellular carcinoma (HCC), Dr. Ono and colleagues analyzed serum ctDNA from 46 HCC patients using quantitative PCR assays for somatic rearrangements uncovered by whole-genome sequencing of their primary tumors.
For the seven patients with detectable ctDNA in preoperative serum, the incidence of recurrence and extrahepatic metastasis within 2 years following hepatectomy were significantly worse than in the ctDNA-negative group, although no significant difference in the cumulative survival rate was observed between these patients. The ctDNA positivity also was found to be an independent predictor of microscopic vascular invasion of the portal vein, and it correlated with larger tumor size and higher alpha-fetoprotein and des-gamma-carboxy prothrombin levels.
In addition, the investigators demonstrated that transcatheter arterial chemoembolization (TACE) enriched ctDNA levels in cell-free DNA in blood, and that serum ctDNA levels were increased with disease progression and reflected response to treatments.
|
|
| Dr. Jeremy Segal |
The diagnosis of HCC is currently based on imaging and/or biopsies. Even though there are no well-established biomarkers for early detection and monitoring of HCC at present, the data presented here indicate the potential utility of personalized ctDNA testing for individualized management of hepatocellular carcinoma patients.
Dr. Larissa V. Furtado and Dr. Jeremy P. Segal are both assistant professors and assistant directors of the division of genomic and molecular pathology in the department of pathology at the University of Chicago Medical Center. Neither has conflicts of interest.
A personalized PCR test for circulating tumor DNA identified cases of progressive hepatocellular carcinoma, investigators reported in the September issue of Cellular and Molecular Gastroenterology and Hepatology.
Patients with liver cancer who underwent resection or transplantation and were positive for ctDNA had significantly higher rates of recurrence (P <.0102) and metastasis (P <.0386), reported Dr. Atsushi Ono of Hiroshima (Japan) University and the RIKEN Center for Integrative Medical Sciences and associates. The study also found that transcatheter arterial chemoembolization [TACE] increased levels of ctDNA, compared with total cell-free DNA, making the marker easier to detect.
“Analyzing cell-free DNA after TACE in unresectable and recurrent cases as a liquid biopsy to establish cancer genome profiles might … guide selection of an individualized therapeutic regimen without requiring percutaneous biopsy,” they added.
Assays for ctDNA have shown promise for diagnosing other cancers and targeting their treatments, but HCC diagnosis relies primarily on imaging, and HCC ctDNA has not been well characterized, noted the investigators. They performed massively parallel whole-genome sequencing of DNA extracted from resected HCCs from 46 patients. They serially measured plasma ctDNA levels before and after surgery using personalized quantitative PCR assays that targeted somatic rearrangements. They also used chemiluminescent immunoassays to test for two conventional tumor markers, alpha-fetoprotein and des-gamma-carboxy prothrombin (Cell Mol Gastroenterol Hepatol. 2015 Jul 2 [doi: 10.1016/j.jcmgh.2015.06.009]).
In all, 25 somatic mutations were present in both primary tumor tissue and in cell-free DNA samples, and 83% of mutations in the primary tumor were detectable in cell-free DNA. Among seven patients who tested positive for ctDNA before surgery, six developed recurrent disease and four developed extrahepatic metastases, Dr. Ono and associates said.
Levels of ctDNA increased as disease progressed and dropped in response to treatment, and one case remained positive for ctDNA even after alpha-fetoprotein and des-gamma-carboxy prothrombin became negative or dropped below threshold after resection. “This suggests that, in some patients, ctDNA might be a better and more sensitive biomarker for HCC than the conventional tumor markers,” they said.
The assay analyzed plasma instead of serum because serum was likely to have more normal cell-free nucleic acids, which would make it harder to detect mutant alleles, the investigators noted. Testing for ctDNA could help address the problem of tumor heterogeneity because ctDNA contains the entire tumor genome, including variants from independent tumors, but the assay will need further validation, especially because its lower limits varied by primer sets, which reduced its sensitivity and meant that some cases went undetected, they added.
The study was funded by the government of Japan, the RIKEN President’s Fund, the Princess Takamatsu Cancer Research Fund, and the Takeda Science Foundation. The investigators declared no competing interests.
A personalized PCR test for circulating tumor DNA identified cases of progressive hepatocellular carcinoma, investigators reported in the September issue of Cellular and Molecular Gastroenterology and Hepatology.
Patients with liver cancer who underwent resection or transplantation and were positive for ctDNA had significantly higher rates of recurrence (P <.0102) and metastasis (P <.0386), reported Dr. Atsushi Ono of Hiroshima (Japan) University and the RIKEN Center for Integrative Medical Sciences and associates. The study also found that transcatheter arterial chemoembolization [TACE] increased levels of ctDNA, compared with total cell-free DNA, making the marker easier to detect.
“Analyzing cell-free DNA after TACE in unresectable and recurrent cases as a liquid biopsy to establish cancer genome profiles might … guide selection of an individualized therapeutic regimen without requiring percutaneous biopsy,” they added.
Assays for ctDNA have shown promise for diagnosing other cancers and targeting their treatments, but HCC diagnosis relies primarily on imaging, and HCC ctDNA has not been well characterized, noted the investigators. They performed massively parallel whole-genome sequencing of DNA extracted from resected HCCs from 46 patients. They serially measured plasma ctDNA levels before and after surgery using personalized quantitative PCR assays that targeted somatic rearrangements. They also used chemiluminescent immunoassays to test for two conventional tumor markers, alpha-fetoprotein and des-gamma-carboxy prothrombin (Cell Mol Gastroenterol Hepatol. 2015 Jul 2 [doi: 10.1016/j.jcmgh.2015.06.009]).
In all, 25 somatic mutations were present in both primary tumor tissue and in cell-free DNA samples, and 83% of mutations in the primary tumor were detectable in cell-free DNA. Among seven patients who tested positive for ctDNA before surgery, six developed recurrent disease and four developed extrahepatic metastases, Dr. Ono and associates said.
Levels of ctDNA increased as disease progressed and dropped in response to treatment, and one case remained positive for ctDNA even after alpha-fetoprotein and des-gamma-carboxy prothrombin became negative or dropped below threshold after resection. “This suggests that, in some patients, ctDNA might be a better and more sensitive biomarker for HCC than the conventional tumor markers,” they said.
The assay analyzed plasma instead of serum because serum was likely to have more normal cell-free nucleic acids, which would make it harder to detect mutant alleles, the investigators noted. Testing for ctDNA could help address the problem of tumor heterogeneity because ctDNA contains the entire tumor genome, including variants from independent tumors, but the assay will need further validation, especially because its lower limits varied by primer sets, which reduced its sensitivity and meant that some cases went undetected, they added.
The study was funded by the government of Japan, the RIKEN President’s Fund, the Princess Takamatsu Cancer Research Fund, and the Takeda Science Foundation. The investigators declared no competing interests.
FROM CELLULAR AND MOLECULAR GASTROENTEROLOGY AND HEPATOLOGY
Key clinical point: The presence of circulating tumor (ct) DNA indicated progression of hepatocellular carcinoma.
Major finding: Among seven patients who tested positive for ctDNA before undergoing surgical resection, six developed recurrent HCC and four developed extrahepatic metastases.
Data source: Real-time quantitative PCR analysis of serum samples from 46 patients with HCC who underwent hepatectomy or liver transplantation.
Disclosures: The study was funded by the government of Japan, the RIKEN President’s Fund, the Princess Takamatsu Cancer Research Fund, and the Takeda Science Foundation. The investigators declared no competing interests.