User login
Official Newspaper of the American College of Surgeons
Right-side mini-AVR an option for frail patients
Many patients with aortic valve disease still undergo conventional aortic valve replacement (AVR) with standard full sternotomy or seek out alternative treatments like transcatheter aortic valve insertion (TAVI). But a minimally invasive approach that uses a sutureless prostheses may reduce operation times and put AVR within reach of more frail patients.
Investigators from G. Pasquinucci Heart Hospital in Massa, Italy, reported on 593 patients who had AVR through right anterior minithoracotomy (RAMT) over 10 years at their institution (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.06.045). In 302 of the patients, the researchers used a sutureless or rapidly implantable biological prosthesis.
“More surgeons should enrich their armamentarium by RAMT AVR,” lead author Dr. Mattia Glauber and his coauthors said. “Sutureless prostheses can increase adoption of RAMT AVR.”
The authors acknowledged that minimally invasive approaches to AVR, including partial sternotomy, require longer operation times than open surgery despite reduced aortic cross-clamping and cardiopulmonary bypass times, but have resulted in better outcomes and lower death rates.
A new generation of aortic valve prostheses, including sutureless devices, have emerged in an attempt to further reduce operative times and improve outcomes, so the Italian investigators designed their study to compare early and midterm outcomes after minimally invasive AVR using sutured and sutureless repair at their institution between 2004 and 2014.
In 302 (50.9%) patients, sutureless or rapidly implantable biological prosthesis was used, 23 (3.9%) had a mechanical prosthesis, and the remainder received a conventional biological prosthesis.
The investigators determined patients were suitable for RAMT if CT scan showed specific anatomic features, including rightward positioning of the ascending aorta at the level of the main pulmonary artery. Once the sutureless prostheses became available in 2011, every patient undergoing AVR via RAMT was considered a potential candidate, although the investigators decided that patients with type 1 and 2 bicuspid aortic valves without raphe and asymmetric aortic root were not suitable for the sutureless approach.
The subgroup that underwent sutureless repair tended to be older and sicker than the overall study population and had a higher prevalence of tricuspid aortic valve and aortic stenosis, a slightly higher body mass index, and a higher propensity to be obese. The sutureless subgroup also had fewer smokers.
Cardiopulmonary bypass time averaged 88 minutes and aortic cross-clamping times 55 minutes in the sutureless subgroup vs. 107 and 74 minutes, respectively, in the overall RAMT study subgroup.
The death before discharge rate of patients who had RAMT repair was 1%, and the 30-day in-hospital death rate was 1.5%. Overall, 97% of patients who had RAMT did not require reoperation at 5 years.
Between the sutured and sutureless subgroups, hospital and intensive care unit lengths of stay were similar, as were bleeding rates and in-hospital mortality. One measure in which the two subgroups deviated was prolonged ICU stay – a rate of 11.3% in the sutureless subgroup and 6.6% in the sutured subgroup.
“To the best of our knowledge, this is the largest up-to-date single-center experience on minimally invasive AVR through RAMT,” Dr. Glauber and coauthors said. “Our data along with earlier reports confirm that minimally invasive AVR through RAMT is safe and reproducible. It is associated with low perioperative mortality and morbidity.”
Dr. Glauber and coauthor Dr. Marco Solinas disclosed a commercial/financial relationship with Sorin Group.
“Have we found the end of the road, and the future for isolated AVR is made up of RAMT with sutureless AVR?” asks Dr. Patrick M. McCarthy, chief of cardiac surgery at Northwestern University Feinberg School of Medicine in Chicago, in his invited commentary (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.07.007). “The cardiology literature serves as a reality check.”
He noted that results from the NOTION Trial of transaortic valve replacement (TAVR) vs. surgical AVR (J Am Coll Cardiol. 2015;65:2184-94) had 30-day results similar to the G. Pasquinucci Heart Hospital results. However, 34% in the TAVR group in NOTION needed pacemakers, and 16% had moderate or greater valvular regurgitation and higher rates of dyspnea.

|
Dr. Patrick M. McCarthy |
Right anterior minithoracotomy is different from other minimally invasive approaches, Dr. McCarthy said. “It’s more of a tunnel down to the aortic valve which is why patient selection based on anatomic factors determined by preoperative CT scan (which is an unnecessary expense for hemisternotomy) is so important,” he said.
The evolution of TAVR is still in the early stage, so the “flaws” involved in the approach can yet be eliminated, “but the message that TAVR outcomes today are still very different than [surgical] AVR in low-risk patients, the type that have a minimally invasive AVR, may be lost on many readers,” Dr. McCarthy said.
For isolated aortic stenosis, the era of minimally invasive procedures that involve bypass, cross-clamping and a difficult surgical approach may be fading, he said. “The handwriting is on the wall, or in the journals in this case.”
Dr. McCarthy disclosed relationships with Edwards Lifesciences and Abbott Vascular. He is the inventor of the Edwards MC3 Ring and dETlogix Ring and coinventor of the IMR ETlogix Ring.
“Have we found the end of the road, and the future for isolated AVR is made up of RAMT with sutureless AVR?” asks Dr. Patrick M. McCarthy, chief of cardiac surgery at Northwestern University Feinberg School of Medicine in Chicago, in his invited commentary (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.07.007). “The cardiology literature serves as a reality check.”
He noted that results from the NOTION Trial of transaortic valve replacement (TAVR) vs. surgical AVR (J Am Coll Cardiol. 2015;65:2184-94) had 30-day results similar to the G. Pasquinucci Heart Hospital results. However, 34% in the TAVR group in NOTION needed pacemakers, and 16% had moderate or greater valvular regurgitation and higher rates of dyspnea.
|
|
Dr. Patrick M. McCarthy |
Right anterior minithoracotomy is different from other minimally invasive approaches, Dr. McCarthy said. “It’s more of a tunnel down to the aortic valve which is why patient selection based on anatomic factors determined by preoperative CT scan (which is an unnecessary expense for hemisternotomy) is so important,” he said.
The evolution of TAVR is still in the early stage, so the “flaws” involved in the approach can yet be eliminated, “but the message that TAVR outcomes today are still very different than [surgical] AVR in low-risk patients, the type that have a minimally invasive AVR, may be lost on many readers,” Dr. McCarthy said.
For isolated aortic stenosis, the era of minimally invasive procedures that involve bypass, cross-clamping and a difficult surgical approach may be fading, he said. “The handwriting is on the wall, or in the journals in this case.”
Dr. McCarthy disclosed relationships with Edwards Lifesciences and Abbott Vascular. He is the inventor of the Edwards MC3 Ring and dETlogix Ring and coinventor of the IMR ETlogix Ring.
“Have we found the end of the road, and the future for isolated AVR is made up of RAMT with sutureless AVR?” asks Dr. Patrick M. McCarthy, chief of cardiac surgery at Northwestern University Feinberg School of Medicine in Chicago, in his invited commentary (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.07.007). “The cardiology literature serves as a reality check.”
He noted that results from the NOTION Trial of transaortic valve replacement (TAVR) vs. surgical AVR (J Am Coll Cardiol. 2015;65:2184-94) had 30-day results similar to the G. Pasquinucci Heart Hospital results. However, 34% in the TAVR group in NOTION needed pacemakers, and 16% had moderate or greater valvular regurgitation and higher rates of dyspnea.
|
|
Dr. Patrick M. McCarthy |
Right anterior minithoracotomy is different from other minimally invasive approaches, Dr. McCarthy said. “It’s more of a tunnel down to the aortic valve which is why patient selection based on anatomic factors determined by preoperative CT scan (which is an unnecessary expense for hemisternotomy) is so important,” he said.
The evolution of TAVR is still in the early stage, so the “flaws” involved in the approach can yet be eliminated, “but the message that TAVR outcomes today are still very different than [surgical] AVR in low-risk patients, the type that have a minimally invasive AVR, may be lost on many readers,” Dr. McCarthy said.
For isolated aortic stenosis, the era of minimally invasive procedures that involve bypass, cross-clamping and a difficult surgical approach may be fading, he said. “The handwriting is on the wall, or in the journals in this case.”
Dr. McCarthy disclosed relationships with Edwards Lifesciences and Abbott Vascular. He is the inventor of the Edwards MC3 Ring and dETlogix Ring and coinventor of the IMR ETlogix Ring.
Many patients with aortic valve disease still undergo conventional aortic valve replacement (AVR) with standard full sternotomy or seek out alternative treatments like transcatheter aortic valve insertion (TAVI). But a minimally invasive approach that uses a sutureless prostheses may reduce operation times and put AVR within reach of more frail patients.
Investigators from G. Pasquinucci Heart Hospital in Massa, Italy, reported on 593 patients who had AVR through right anterior minithoracotomy (RAMT) over 10 years at their institution (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.06.045). In 302 of the patients, the researchers used a sutureless or rapidly implantable biological prosthesis.
“More surgeons should enrich their armamentarium by RAMT AVR,” lead author Dr. Mattia Glauber and his coauthors said. “Sutureless prostheses can increase adoption of RAMT AVR.”
The authors acknowledged that minimally invasive approaches to AVR, including partial sternotomy, require longer operation times than open surgery despite reduced aortic cross-clamping and cardiopulmonary bypass times, but have resulted in better outcomes and lower death rates.
A new generation of aortic valve prostheses, including sutureless devices, have emerged in an attempt to further reduce operative times and improve outcomes, so the Italian investigators designed their study to compare early and midterm outcomes after minimally invasive AVR using sutured and sutureless repair at their institution between 2004 and 2014.
In 302 (50.9%) patients, sutureless or rapidly implantable biological prosthesis was used, 23 (3.9%) had a mechanical prosthesis, and the remainder received a conventional biological prosthesis.
The investigators determined patients were suitable for RAMT if CT scan showed specific anatomic features, including rightward positioning of the ascending aorta at the level of the main pulmonary artery. Once the sutureless prostheses became available in 2011, every patient undergoing AVR via RAMT was considered a potential candidate, although the investigators decided that patients with type 1 and 2 bicuspid aortic valves without raphe and asymmetric aortic root were not suitable for the sutureless approach.
The subgroup that underwent sutureless repair tended to be older and sicker than the overall study population and had a higher prevalence of tricuspid aortic valve and aortic stenosis, a slightly higher body mass index, and a higher propensity to be obese. The sutureless subgroup also had fewer smokers.
Cardiopulmonary bypass time averaged 88 minutes and aortic cross-clamping times 55 minutes in the sutureless subgroup vs. 107 and 74 minutes, respectively, in the overall RAMT study subgroup.
The death before discharge rate of patients who had RAMT repair was 1%, and the 30-day in-hospital death rate was 1.5%. Overall, 97% of patients who had RAMT did not require reoperation at 5 years.
Between the sutured and sutureless subgroups, hospital and intensive care unit lengths of stay were similar, as were bleeding rates and in-hospital mortality. One measure in which the two subgroups deviated was prolonged ICU stay – a rate of 11.3% in the sutureless subgroup and 6.6% in the sutured subgroup.
“To the best of our knowledge, this is the largest up-to-date single-center experience on minimally invasive AVR through RAMT,” Dr. Glauber and coauthors said. “Our data along with earlier reports confirm that minimally invasive AVR through RAMT is safe and reproducible. It is associated with low perioperative mortality and morbidity.”
Dr. Glauber and coauthor Dr. Marco Solinas disclosed a commercial/financial relationship with Sorin Group.
Many patients with aortic valve disease still undergo conventional aortic valve replacement (AVR) with standard full sternotomy or seek out alternative treatments like transcatheter aortic valve insertion (TAVI). But a minimally invasive approach that uses a sutureless prostheses may reduce operation times and put AVR within reach of more frail patients.
Investigators from G. Pasquinucci Heart Hospital in Massa, Italy, reported on 593 patients who had AVR through right anterior minithoracotomy (RAMT) over 10 years at their institution (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.06.045). In 302 of the patients, the researchers used a sutureless or rapidly implantable biological prosthesis.
“More surgeons should enrich their armamentarium by RAMT AVR,” lead author Dr. Mattia Glauber and his coauthors said. “Sutureless prostheses can increase adoption of RAMT AVR.”
The authors acknowledged that minimally invasive approaches to AVR, including partial sternotomy, require longer operation times than open surgery despite reduced aortic cross-clamping and cardiopulmonary bypass times, but have resulted in better outcomes and lower death rates.
A new generation of aortic valve prostheses, including sutureless devices, have emerged in an attempt to further reduce operative times and improve outcomes, so the Italian investigators designed their study to compare early and midterm outcomes after minimally invasive AVR using sutured and sutureless repair at their institution between 2004 and 2014.
In 302 (50.9%) patients, sutureless or rapidly implantable biological prosthesis was used, 23 (3.9%) had a mechanical prosthesis, and the remainder received a conventional biological prosthesis.
The investigators determined patients were suitable for RAMT if CT scan showed specific anatomic features, including rightward positioning of the ascending aorta at the level of the main pulmonary artery. Once the sutureless prostheses became available in 2011, every patient undergoing AVR via RAMT was considered a potential candidate, although the investigators decided that patients with type 1 and 2 bicuspid aortic valves without raphe and asymmetric aortic root were not suitable for the sutureless approach.
The subgroup that underwent sutureless repair tended to be older and sicker than the overall study population and had a higher prevalence of tricuspid aortic valve and aortic stenosis, a slightly higher body mass index, and a higher propensity to be obese. The sutureless subgroup also had fewer smokers.
Cardiopulmonary bypass time averaged 88 minutes and aortic cross-clamping times 55 minutes in the sutureless subgroup vs. 107 and 74 minutes, respectively, in the overall RAMT study subgroup.
The death before discharge rate of patients who had RAMT repair was 1%, and the 30-day in-hospital death rate was 1.5%. Overall, 97% of patients who had RAMT did not require reoperation at 5 years.
Between the sutured and sutureless subgroups, hospital and intensive care unit lengths of stay were similar, as were bleeding rates and in-hospital mortality. One measure in which the two subgroups deviated was prolonged ICU stay – a rate of 11.3% in the sutureless subgroup and 6.6% in the sutured subgroup.
“To the best of our knowledge, this is the largest up-to-date single-center experience on minimally invasive AVR through RAMT,” Dr. Glauber and coauthors said. “Our data along with earlier reports confirm that minimally invasive AVR through RAMT is safe and reproducible. It is associated with low perioperative mortality and morbidity.”
Dr. Glauber and coauthor Dr. Marco Solinas disclosed a commercial/financial relationship with Sorin Group.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Aortic valve replacement through right anterior minithoracotomy provides excellent outcomes. Sutureless prostheses facilitate mini-AVR.
Major finding: Study subjects had a survival rate of 95% at 31.5 months follow-up on average, and operative times were significantly shorter with sutureless prostheses, compared with sutured prostheses.
Data source: A retrospective, observational cohort study with prospective data collection on 593 patients who had right anterior minithoracotomy for AVR at a single institution over a 10-yar period.
Disclosures: Study coauthors Mattia Glauber and Marco Solinas disclosed a commercial/financial relationship with Sorin Group.

SYNTAX: Early CABG results with arterial grafts similar to venous in matched groups
While single-center studies have supported the advantages of multiple arterial grafts over venous grafts in coronary artery bypass surgery, an analysis of patients in the international and multicenter SYNTAX trial has shown that, on propensity matching, rates of cardiac events and death are actually similar between the two groups.
These findings of the SYNTAX investigators, led by Dr. Catalina Parasca of Erasmus University in Rotterdam, the Netherlands, were published online in the Journal of Thoracic and Cardiovascular Surgery (doi:10.1016/j.jtcvs.2015.05.010).
The SYNTAX trial compared percutaneous coronary intervention (PCI) with coronary artery bypass grafting (CABG) in patients with left main or three-vessel coronary artery disease (Lancet. 2013;381[9867]:629-38).
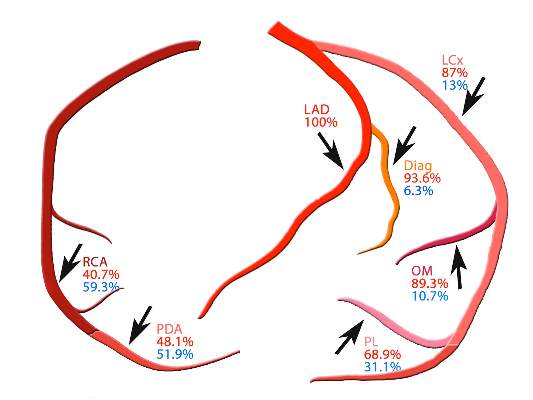
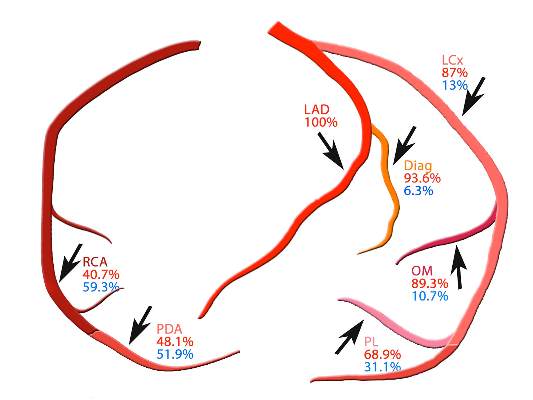
In the latest report, the SYNTAX investigators found that patients in unmatched groups who received arterial grafts in addition to an arterial graft of the left anterior descending artery (LAD) had noticeably lower rates of death and a composite endpoint of death-stroke-MI than did those who received a second venous graft. However, when the researchers applied propensity matching, the outcomes between the two groups were similar.
Because large randomized trials have yet to prove the superiority of multiarterial grafts, the adoption rate has been low, Dr. Parasca and colleagues said. “The objective of this study was to assess the effect of using a second arterial graft on 5-year outcomes in patients who underwent CABG in the SYNTAX trial and registry,” they said.
They looked at 1,322 SYNTAX trial patients who had CABG with 5-year follow-up. In unmatched groups, the safety endpoint of the death-stroke-MI composite was 13.3% in the multiarterial group vs. 18.7% in the vein graft group. Although the incidence of stroke, MI, and graft occlusion was similar between the unmatched groups, the second-graft arterial group had a higher revascularization rate at 5 years, 12.6% vs. 9.6%, mainly due to repeat PCI. The element of the composite where the two unmatched groups deviated was the all-cause death rate at 5 years: 8.9% in the second-graft arterial group and 13.1% in the venous group.
However, when the investigators applied propensity matching, the differences between the two groups were insignificant.
“The results of the present study must be seen in the light of a multicenter CABG cohort with complex coronary disease, where revascularization was performed according to surgeon’s personal experience and local practices,” Dr. Parasca and coauthors noted. “The result was a high heterogeneity of CABG techniques, which shows different understanding of the best ‘graft-target match’ across centers.”
While the SYNTAX analysis demonstrates the variation in patient selection and operator technique with regard to arterial revascularization typical of a multicenter study, “extended follow-up beyond 5 years is required to estimate its impact on long-term outcomes,” Dr. Parasca and colleagues said.
Boston Scientific supported the trial. Coauthor Keith Dawkins is employed by Boston Scientific and coauthor Ted Feldman has received consulting fees from the company. The other authors reported no disclosures.
That arterial grafts are a better long-term match in coronary bypass surgery has been a tenet in cardiac surgery, but multiple factors have prevented their more widespread acceptance, Dr. Davis C. Drinkwater Jr. said in his invited commentary (J Thorac Cardiovasc Surg. 2015.doi:10.1016/j.jtcvs.2015.06.014). Concerns about sternal wound healing, particularly in diabetic or obese patients, as well as the alternative generally good early and mid-term results in multivessel coronary artery disease using the left internal thoracic artery to LAD accompanied by saphenous vein grafts, have made surgeons hesitant to take up the approach more readily, said Dr. Drinkwater of Frist Cardiology, Tristar Centennial Medical Center, Nashville, Tenn.
The SYNTAX investigators’ main finding of no survival advantage among the matched groups at 5 years is in line with most reports comparing patency between arterial and venous grafts, “requiring between 5- and 10-year follow-up to show a divergence,” Dr. Drinkwater said.
He pointed out that the patients who had second arterial grafts in the unmatched group were younger and healthier – the average age was 62 years, and 27% of them had previous heart attacks, compared with 66 years of age and a heart attack rate of 35.6% in the venous graft group – and that may explain the higher reintervention rate in the former group. Another factor may be the younger and healthier patients had longer cardiopulmonary bypass and aortic cross clamp times despite a greater percentage having undergone the off-pump technique.
“This counterintuitive information underscores an inherent weakness of this multicenter trial that is without surgical randomization into the two arterial groups, and with potentially varied surgical experience using nonstandardized technical and management protocols,” Dr. Drinkwater said. “This is in stark contrast to the previous and well accepted single high-volume-center reports of the benefits of using multiple arterial bypass grafts.”
Because the report points out the technical challenges of achieving complete revascularization with multiple arterial grafting at “the early” interval of up to 5 years, the authors may be inappropriately discouraging centers that do not currently offer multiarterial grafting from embracing it, Dr. Drinkwater concluded.
He had no disclosures to report.
That arterial grafts are a better long-term match in coronary bypass surgery has been a tenet in cardiac surgery, but multiple factors have prevented their more widespread acceptance, Dr. Davis C. Drinkwater Jr. said in his invited commentary (J Thorac Cardiovasc Surg. 2015.doi:10.1016/j.jtcvs.2015.06.014). Concerns about sternal wound healing, particularly in diabetic or obese patients, as well as the alternative generally good early and mid-term results in multivessel coronary artery disease using the left internal thoracic artery to LAD accompanied by saphenous vein grafts, have made surgeons hesitant to take up the approach more readily, said Dr. Drinkwater of Frist Cardiology, Tristar Centennial Medical Center, Nashville, Tenn.
The SYNTAX investigators’ main finding of no survival advantage among the matched groups at 5 years is in line with most reports comparing patency between arterial and venous grafts, “requiring between 5- and 10-year follow-up to show a divergence,” Dr. Drinkwater said.
He pointed out that the patients who had second arterial grafts in the unmatched group were younger and healthier – the average age was 62 years, and 27% of them had previous heart attacks, compared with 66 years of age and a heart attack rate of 35.6% in the venous graft group – and that may explain the higher reintervention rate in the former group. Another factor may be the younger and healthier patients had longer cardiopulmonary bypass and aortic cross clamp times despite a greater percentage having undergone the off-pump technique.
“This counterintuitive information underscores an inherent weakness of this multicenter trial that is without surgical randomization into the two arterial groups, and with potentially varied surgical experience using nonstandardized technical and management protocols,” Dr. Drinkwater said. “This is in stark contrast to the previous and well accepted single high-volume-center reports of the benefits of using multiple arterial bypass grafts.”
Because the report points out the technical challenges of achieving complete revascularization with multiple arterial grafting at “the early” interval of up to 5 years, the authors may be inappropriately discouraging centers that do not currently offer multiarterial grafting from embracing it, Dr. Drinkwater concluded.
He had no disclosures to report.
That arterial grafts are a better long-term match in coronary bypass surgery has been a tenet in cardiac surgery, but multiple factors have prevented their more widespread acceptance, Dr. Davis C. Drinkwater Jr. said in his invited commentary (J Thorac Cardiovasc Surg. 2015.doi:10.1016/j.jtcvs.2015.06.014). Concerns about sternal wound healing, particularly in diabetic or obese patients, as well as the alternative generally good early and mid-term results in multivessel coronary artery disease using the left internal thoracic artery to LAD accompanied by saphenous vein grafts, have made surgeons hesitant to take up the approach more readily, said Dr. Drinkwater of Frist Cardiology, Tristar Centennial Medical Center, Nashville, Tenn.
The SYNTAX investigators’ main finding of no survival advantage among the matched groups at 5 years is in line with most reports comparing patency between arterial and venous grafts, “requiring between 5- and 10-year follow-up to show a divergence,” Dr. Drinkwater said.
He pointed out that the patients who had second arterial grafts in the unmatched group were younger and healthier – the average age was 62 years, and 27% of them had previous heart attacks, compared with 66 years of age and a heart attack rate of 35.6% in the venous graft group – and that may explain the higher reintervention rate in the former group. Another factor may be the younger and healthier patients had longer cardiopulmonary bypass and aortic cross clamp times despite a greater percentage having undergone the off-pump technique.
“This counterintuitive information underscores an inherent weakness of this multicenter trial that is without surgical randomization into the two arterial groups, and with potentially varied surgical experience using nonstandardized technical and management protocols,” Dr. Drinkwater said. “This is in stark contrast to the previous and well accepted single high-volume-center reports of the benefits of using multiple arterial bypass grafts.”
Because the report points out the technical challenges of achieving complete revascularization with multiple arterial grafting at “the early” interval of up to 5 years, the authors may be inappropriately discouraging centers that do not currently offer multiarterial grafting from embracing it, Dr. Drinkwater concluded.
He had no disclosures to report.
While single-center studies have supported the advantages of multiple arterial grafts over venous grafts in coronary artery bypass surgery, an analysis of patients in the international and multicenter SYNTAX trial has shown that, on propensity matching, rates of cardiac events and death are actually similar between the two groups.
These findings of the SYNTAX investigators, led by Dr. Catalina Parasca of Erasmus University in Rotterdam, the Netherlands, were published online in the Journal of Thoracic and Cardiovascular Surgery (doi:10.1016/j.jtcvs.2015.05.010).
The SYNTAX trial compared percutaneous coronary intervention (PCI) with coronary artery bypass grafting (CABG) in patients with left main or three-vessel coronary artery disease (Lancet. 2013;381[9867]:629-38).
In the latest report, the SYNTAX investigators found that patients in unmatched groups who received arterial grafts in addition to an arterial graft of the left anterior descending artery (LAD) had noticeably lower rates of death and a composite endpoint of death-stroke-MI than did those who received a second venous graft. However, when the researchers applied propensity matching, the outcomes between the two groups were similar.
Because large randomized trials have yet to prove the superiority of multiarterial grafts, the adoption rate has been low, Dr. Parasca and colleagues said. “The objective of this study was to assess the effect of using a second arterial graft on 5-year outcomes in patients who underwent CABG in the SYNTAX trial and registry,” they said.
They looked at 1,322 SYNTAX trial patients who had CABG with 5-year follow-up. In unmatched groups, the safety endpoint of the death-stroke-MI composite was 13.3% in the multiarterial group vs. 18.7% in the vein graft group. Although the incidence of stroke, MI, and graft occlusion was similar between the unmatched groups, the second-graft arterial group had a higher revascularization rate at 5 years, 12.6% vs. 9.6%, mainly due to repeat PCI. The element of the composite where the two unmatched groups deviated was the all-cause death rate at 5 years: 8.9% in the second-graft arterial group and 13.1% in the venous group.
However, when the investigators applied propensity matching, the differences between the two groups were insignificant.
“The results of the present study must be seen in the light of a multicenter CABG cohort with complex coronary disease, where revascularization was performed according to surgeon’s personal experience and local practices,” Dr. Parasca and coauthors noted. “The result was a high heterogeneity of CABG techniques, which shows different understanding of the best ‘graft-target match’ across centers.”
While the SYNTAX analysis demonstrates the variation in patient selection and operator technique with regard to arterial revascularization typical of a multicenter study, “extended follow-up beyond 5 years is required to estimate its impact on long-term outcomes,” Dr. Parasca and colleagues said.
Boston Scientific supported the trial. Coauthor Keith Dawkins is employed by Boston Scientific and coauthor Ted Feldman has received consulting fees from the company. The other authors reported no disclosures.
While single-center studies have supported the advantages of multiple arterial grafts over venous grafts in coronary artery bypass surgery, an analysis of patients in the international and multicenter SYNTAX trial has shown that, on propensity matching, rates of cardiac events and death are actually similar between the two groups.
These findings of the SYNTAX investigators, led by Dr. Catalina Parasca of Erasmus University in Rotterdam, the Netherlands, were published online in the Journal of Thoracic and Cardiovascular Surgery (doi:10.1016/j.jtcvs.2015.05.010).
The SYNTAX trial compared percutaneous coronary intervention (PCI) with coronary artery bypass grafting (CABG) in patients with left main or three-vessel coronary artery disease (Lancet. 2013;381[9867]:629-38).
In the latest report, the SYNTAX investigators found that patients in unmatched groups who received arterial grafts in addition to an arterial graft of the left anterior descending artery (LAD) had noticeably lower rates of death and a composite endpoint of death-stroke-MI than did those who received a second venous graft. However, when the researchers applied propensity matching, the outcomes between the two groups were similar.
Because large randomized trials have yet to prove the superiority of multiarterial grafts, the adoption rate has been low, Dr. Parasca and colleagues said. “The objective of this study was to assess the effect of using a second arterial graft on 5-year outcomes in patients who underwent CABG in the SYNTAX trial and registry,” they said.
They looked at 1,322 SYNTAX trial patients who had CABG with 5-year follow-up. In unmatched groups, the safety endpoint of the death-stroke-MI composite was 13.3% in the multiarterial group vs. 18.7% in the vein graft group. Although the incidence of stroke, MI, and graft occlusion was similar between the unmatched groups, the second-graft arterial group had a higher revascularization rate at 5 years, 12.6% vs. 9.6%, mainly due to repeat PCI. The element of the composite where the two unmatched groups deviated was the all-cause death rate at 5 years: 8.9% in the second-graft arterial group and 13.1% in the venous group.
However, when the investigators applied propensity matching, the differences between the two groups were insignificant.
“The results of the present study must be seen in the light of a multicenter CABG cohort with complex coronary disease, where revascularization was performed according to surgeon’s personal experience and local practices,” Dr. Parasca and coauthors noted. “The result was a high heterogeneity of CABG techniques, which shows different understanding of the best ‘graft-target match’ across centers.”
While the SYNTAX analysis demonstrates the variation in patient selection and operator technique with regard to arterial revascularization typical of a multicenter study, “extended follow-up beyond 5 years is required to estimate its impact on long-term outcomes,” Dr. Parasca and colleagues said.
Boston Scientific supported the trial. Coauthor Keith Dawkins is employed by Boston Scientific and coauthor Ted Feldman has received consulting fees from the company. The other authors reported no disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Surgeons should choose arterial grafts for multigraft coronary artery bypass surgery when feasible.
Major finding: Patients who received multiple arterial graft had significantly lower rates of death and other problems than did those who received venous grafts in unmatched groups, but results were similar between propensity matched groups.
Data source: Registry of 1,322 patients who had 5-year follow-up after coronary artery bypass surgery within the SYNTAX trial.
Disclosures: Boston Scientific supported the trial. Coauthor Keith Dawkins is employed by Boston Scientific and coauthor Ted Feldman has received consulting fees from the company. The other authors reported no disclosures.
Heart attack risk rises in first month after knee, hip arthroplasty
Total knee and hip arthroplasty were associated with a significantly increased risk of myocardial infarction in the first month after surgery, but not at 6 months after surgery, a cohort study showed.
The finding challenges other studies suggesting that total knee or hip arthroplasty surgery reduces the risk of serious cardiovascular events among individuals with osteoarthritis.

Analysis of data from 13,849 British patients who underwent a total knee arthroplasty, 6,063 patients who received total hip arthroplasty, and an equal number of matched controls showed a greater than eightfold increase in the risk of myocardial infarction in the first postoperative month in the knee arthroplasty group (hazard ratio, 8.75), and a fourfold increase in risk in the hip arthroplasty group (HR, 4.33), compared with controls.
However, the hazard ratio declined to insignificance after 6 months, in contrast to the risk of venous thromboembolism – a known complication of arthroplasty – according to a paper published online in the Aug. 31 edition of Arthritis & Rheumatology.
“The major difference between the previous study and ours is that cardiovascular events occurring shortly after total joint arthroplasty were excluded from the previous study,” wrote Na Lu and his colleagues from Boston University.
The study observed 306 cases of myocardial infarction among individuals who underwent total knee arthroplasty and 128 cases in those who underwent total hip arthroplasty (Arthritis Rheumatol. 2015; August 31 [doi:10.1002/art.39246]).
The study was partly support by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. There were no other conflicts of interest declared.
Total knee and hip arthroplasty were associated with a significantly increased risk of myocardial infarction in the first month after surgery, but not at 6 months after surgery, a cohort study showed.
The finding challenges other studies suggesting that total knee or hip arthroplasty surgery reduces the risk of serious cardiovascular events among individuals with osteoarthritis.
Analysis of data from 13,849 British patients who underwent a total knee arthroplasty, 6,063 patients who received total hip arthroplasty, and an equal number of matched controls showed a greater than eightfold increase in the risk of myocardial infarction in the first postoperative month in the knee arthroplasty group (hazard ratio, 8.75), and a fourfold increase in risk in the hip arthroplasty group (HR, 4.33), compared with controls.
However, the hazard ratio declined to insignificance after 6 months, in contrast to the risk of venous thromboembolism – a known complication of arthroplasty – according to a paper published online in the Aug. 31 edition of Arthritis & Rheumatology.
“The major difference between the previous study and ours is that cardiovascular events occurring shortly after total joint arthroplasty were excluded from the previous study,” wrote Na Lu and his colleagues from Boston University.
The study observed 306 cases of myocardial infarction among individuals who underwent total knee arthroplasty and 128 cases in those who underwent total hip arthroplasty (Arthritis Rheumatol. 2015; August 31 [doi:10.1002/art.39246]).
The study was partly support by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. There were no other conflicts of interest declared.
Total knee and hip arthroplasty were associated with a significantly increased risk of myocardial infarction in the first month after surgery, but not at 6 months after surgery, a cohort study showed.
The finding challenges other studies suggesting that total knee or hip arthroplasty surgery reduces the risk of serious cardiovascular events among individuals with osteoarthritis.
Analysis of data from 13,849 British patients who underwent a total knee arthroplasty, 6,063 patients who received total hip arthroplasty, and an equal number of matched controls showed a greater than eightfold increase in the risk of myocardial infarction in the first postoperative month in the knee arthroplasty group (hazard ratio, 8.75), and a fourfold increase in risk in the hip arthroplasty group (HR, 4.33), compared with controls.
However, the hazard ratio declined to insignificance after 6 months, in contrast to the risk of venous thromboembolism – a known complication of arthroplasty – according to a paper published online in the Aug. 31 edition of Arthritis & Rheumatology.
“The major difference between the previous study and ours is that cardiovascular events occurring shortly after total joint arthroplasty were excluded from the previous study,” wrote Na Lu and his colleagues from Boston University.
The study observed 306 cases of myocardial infarction among individuals who underwent total knee arthroplasty and 128 cases in those who underwent total hip arthroplasty (Arthritis Rheumatol. 2015; August 31 [doi:10.1002/art.39246]).
The study was partly support by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. There were no other conflicts of interest declared.
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point: Total knee and hip arthroplasty were associated with a significantly increased risk of myocardial infarction in the first month after surgery.
Major finding: Patients undergoing total knee arthroplasty have an eightfold increase in the risk of myocardial infarction in the month after surgery.
Data source: Cohort study of 13,849 total knee arthroplasty patients and 6,063 total hip arthroplasty patients and an equal number of matched controls.
Disclosures: The study was partly support by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. There were no conflicts of interest declared.

ESC: Lead-free pacemaker shows good safety, efficacy at 6 months
LONDON – A wireless pacemaker that is secured within the right ventricle of the heart proved both effective and safe in a prospective, nonrandomized, multicenter study.
Interim results obtained for 300 patients at 6 months’ follow-up in the LEADLESS II study showed that the primary efficacy endpoint of both an acceptable pacing threshold and an acceptable sensing amplitude was achieved in 90% of patients, and the primary safety endpoint of freedom from device-related serious adverse events was achieved in 93.3%.

Both of these findings exceeded the performance goal of 85% set in the study, said principal study investigator Dr. Vivek Reddy at the annual congress of the European Society of Cardiology.
“Regular pacemakers are very reliable devices; they’ve been around for half a century,” said Dr. Reddy, who is professor of medicine at Mount Sinai Hospital in New York. “Having said that, they are not perfect,” he observed.
Conventional pacemakers require surgical implantation in the chest, and the wires or leads that go from the device need to be embedded in the vasculature of the heart itself. While the risk of complications is low (around 4% of all implanted devices), when they do happen they usually occur around the site where the pacemaker is implanted or involve placement of the leads in veins.
In contrast, the small cylindrical Nanostim device used in the study is a fully self-contained leadless pacemaker that can be nonsurgically implanted and removed via a catheter threaded through the femoral vein and into the patient’s right ventricle. It is about the size of an AAA battery and, based on the study’s findings, has a potential battery life of 15 years. This is comparable to similar standard single-chamber ventricular pacemakers, according to the manufacturer, St. Jude Medical.
The feasibility of using the device was first shown in the LEADLESS study (Circulation 2014;129:1466-71) and are now confirmed in the LEADLESS II study, which has enrolled 526 patients to date, with successful implantation of the device in 504 patients.
The mean age of the mostly male (61.8%) study cohort was 76 years, with the primary indication for pacemaker placement being atrial fibrillation with atrioventricular block in 55.9%.
The study was performed in 56 centers in the United States, Canada, and Australia and involved 100 operators, only one of whom had prior experience with leadless pacing, Dr. Reddy observed. On average the leadless device was placed within a half hour, and the majority (70.2%) did not require repositioning of the device during the original procedure.
The rate of serious device-related adverse events, such as dislodgement warranting percutaneous retrieval or cardiac perforation, was low, at a rate of 6.7% overall and 1.7% and 1.3%, respectively, with just 1.3% of patients needing to have the device removed because of an increased pacing threshold. There were no device-related deaths, but two deaths occurred that were thought to be procedure related. This is comparable to traditional pacemakers, Dr. Reddy said, although he noted that he was referring to historical controls as this was not a randomized trial.
“The device was shown to be retrievable in a subgroup of seven patients who needed a replacement at a mean of 160 days after implantation,” he noted. Due to the relatively short duration of follow-up, however, “we really can’t talk about what happens with extended follow-up and what happens 5, 10, or 15 years down the line whether we retrieve the devices or simply abandon them and put in a second device.”
The study included patients who had an indication for a single-chamber pacemaker only. Dr. Reddy noted that one of the study limitations is that the device is not suitable for patients needing dual-chamber pacing. The observational nature of the trial also limits the conclusions that can be drawn, and the device does not provide electrocardiogram data.
The Nanostim device is one of two self-contained, miniature wireless pacemakers given marketing authorization in Europe, but both have yet to be approved by the Food and Drug Administration. The other device, Medtronic’s Micra Transcatheter Pacing System, is also placed in the right ventricle and is being studied in the Micra Transcatheter Pacing Study, with promising first-in-human results presented recently at Heart Rhythm 2015.
St. Jude Medical funded the study. Dr. Reddy has received grant support, acted as a consultant to, and received stock options in Nanostim from the company.
LONDON – A wireless pacemaker that is secured within the right ventricle of the heart proved both effective and safe in a prospective, nonrandomized, multicenter study.
Interim results obtained for 300 patients at 6 months’ follow-up in the LEADLESS II study showed that the primary efficacy endpoint of both an acceptable pacing threshold and an acceptable sensing amplitude was achieved in 90% of patients, and the primary safety endpoint of freedom from device-related serious adverse events was achieved in 93.3%.
Both of these findings exceeded the performance goal of 85% set in the study, said principal study investigator Dr. Vivek Reddy at the annual congress of the European Society of Cardiology.
“Regular pacemakers are very reliable devices; they’ve been around for half a century,” said Dr. Reddy, who is professor of medicine at Mount Sinai Hospital in New York. “Having said that, they are not perfect,” he observed.
Conventional pacemakers require surgical implantation in the chest, and the wires or leads that go from the device need to be embedded in the vasculature of the heart itself. While the risk of complications is low (around 4% of all implanted devices), when they do happen they usually occur around the site where the pacemaker is implanted or involve placement of the leads in veins.
In contrast, the small cylindrical Nanostim device used in the study is a fully self-contained leadless pacemaker that can be nonsurgically implanted and removed via a catheter threaded through the femoral vein and into the patient’s right ventricle. It is about the size of an AAA battery and, based on the study’s findings, has a potential battery life of 15 years. This is comparable to similar standard single-chamber ventricular pacemakers, according to the manufacturer, St. Jude Medical.
The feasibility of using the device was first shown in the LEADLESS study (Circulation 2014;129:1466-71) and are now confirmed in the LEADLESS II study, which has enrolled 526 patients to date, with successful implantation of the device in 504 patients.
The mean age of the mostly male (61.8%) study cohort was 76 years, with the primary indication for pacemaker placement being atrial fibrillation with atrioventricular block in 55.9%.
The study was performed in 56 centers in the United States, Canada, and Australia and involved 100 operators, only one of whom had prior experience with leadless pacing, Dr. Reddy observed. On average the leadless device was placed within a half hour, and the majority (70.2%) did not require repositioning of the device during the original procedure.
The rate of serious device-related adverse events, such as dislodgement warranting percutaneous retrieval or cardiac perforation, was low, at a rate of 6.7% overall and 1.7% and 1.3%, respectively, with just 1.3% of patients needing to have the device removed because of an increased pacing threshold. There were no device-related deaths, but two deaths occurred that were thought to be procedure related. This is comparable to traditional pacemakers, Dr. Reddy said, although he noted that he was referring to historical controls as this was not a randomized trial.
“The device was shown to be retrievable in a subgroup of seven patients who needed a replacement at a mean of 160 days after implantation,” he noted. Due to the relatively short duration of follow-up, however, “we really can’t talk about what happens with extended follow-up and what happens 5, 10, or 15 years down the line whether we retrieve the devices or simply abandon them and put in a second device.”
The study included patients who had an indication for a single-chamber pacemaker only. Dr. Reddy noted that one of the study limitations is that the device is not suitable for patients needing dual-chamber pacing. The observational nature of the trial also limits the conclusions that can be drawn, and the device does not provide electrocardiogram data.
The Nanostim device is one of two self-contained, miniature wireless pacemakers given marketing authorization in Europe, but both have yet to be approved by the Food and Drug Administration. The other device, Medtronic’s Micra Transcatheter Pacing System, is also placed in the right ventricle and is being studied in the Micra Transcatheter Pacing Study, with promising first-in-human results presented recently at Heart Rhythm 2015.
St. Jude Medical funded the study. Dr. Reddy has received grant support, acted as a consultant to, and received stock options in Nanostim from the company.
LONDON – A wireless pacemaker that is secured within the right ventricle of the heart proved both effective and safe in a prospective, nonrandomized, multicenter study.
Interim results obtained for 300 patients at 6 months’ follow-up in the LEADLESS II study showed that the primary efficacy endpoint of both an acceptable pacing threshold and an acceptable sensing amplitude was achieved in 90% of patients, and the primary safety endpoint of freedom from device-related serious adverse events was achieved in 93.3%.
Both of these findings exceeded the performance goal of 85% set in the study, said principal study investigator Dr. Vivek Reddy at the annual congress of the European Society of Cardiology.
“Regular pacemakers are very reliable devices; they’ve been around for half a century,” said Dr. Reddy, who is professor of medicine at Mount Sinai Hospital in New York. “Having said that, they are not perfect,” he observed.
Conventional pacemakers require surgical implantation in the chest, and the wires or leads that go from the device need to be embedded in the vasculature of the heart itself. While the risk of complications is low (around 4% of all implanted devices), when they do happen they usually occur around the site where the pacemaker is implanted or involve placement of the leads in veins.
In contrast, the small cylindrical Nanostim device used in the study is a fully self-contained leadless pacemaker that can be nonsurgically implanted and removed via a catheter threaded through the femoral vein and into the patient’s right ventricle. It is about the size of an AAA battery and, based on the study’s findings, has a potential battery life of 15 years. This is comparable to similar standard single-chamber ventricular pacemakers, according to the manufacturer, St. Jude Medical.
The feasibility of using the device was first shown in the LEADLESS study (Circulation 2014;129:1466-71) and are now confirmed in the LEADLESS II study, which has enrolled 526 patients to date, with successful implantation of the device in 504 patients.
The mean age of the mostly male (61.8%) study cohort was 76 years, with the primary indication for pacemaker placement being atrial fibrillation with atrioventricular block in 55.9%.
The study was performed in 56 centers in the United States, Canada, and Australia and involved 100 operators, only one of whom had prior experience with leadless pacing, Dr. Reddy observed. On average the leadless device was placed within a half hour, and the majority (70.2%) did not require repositioning of the device during the original procedure.
The rate of serious device-related adverse events, such as dislodgement warranting percutaneous retrieval or cardiac perforation, was low, at a rate of 6.7% overall and 1.7% and 1.3%, respectively, with just 1.3% of patients needing to have the device removed because of an increased pacing threshold. There were no device-related deaths, but two deaths occurred that were thought to be procedure related. This is comparable to traditional pacemakers, Dr. Reddy said, although he noted that he was referring to historical controls as this was not a randomized trial.
“The device was shown to be retrievable in a subgroup of seven patients who needed a replacement at a mean of 160 days after implantation,” he noted. Due to the relatively short duration of follow-up, however, “we really can’t talk about what happens with extended follow-up and what happens 5, 10, or 15 years down the line whether we retrieve the devices or simply abandon them and put in a second device.”
The study included patients who had an indication for a single-chamber pacemaker only. Dr. Reddy noted that one of the study limitations is that the device is not suitable for patients needing dual-chamber pacing. The observational nature of the trial also limits the conclusions that can be drawn, and the device does not provide electrocardiogram data.
The Nanostim device is one of two self-contained, miniature wireless pacemakers given marketing authorization in Europe, but both have yet to be approved by the Food and Drug Administration. The other device, Medtronic’s Micra Transcatheter Pacing System, is also placed in the right ventricle and is being studied in the Micra Transcatheter Pacing Study, with promising first-in-human results presented recently at Heart Rhythm 2015.
St. Jude Medical funded the study. Dr. Reddy has received grant support, acted as a consultant to, and received stock options in Nanostim from the company.
Key clinical point: The Nanostim leadless pacemaker showed good efficacy and safety in this observational study.
Major finding: At 6 months, the primary efficacy and safety endpoints were met in 90% and 93.5% of 300 patients, respectively.
Data source: Interim results of an ongoing, prospective, nonrandomized, multicenter study, in 565 patients in need of single-chamber ventricular pacing.
Disclosures: St. Jude Medical funded the study. Dr. Reddy has received grant support, acted as a consultant to, and received stock options in Nanostim from the company.

Less posttransplant primary biliary cirrhosis with preventive UDCA
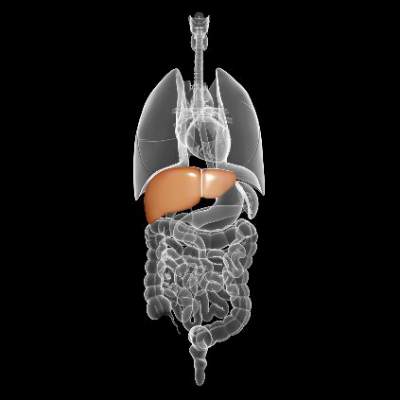
Only 21% of liver transplantation patients who received ursodeoxycholic acid (UDCA) after surgery developed recurrent primary biliary cirrhosis, compared with 62% of patients who did not receive the bile acid, researchers reported in the Journal of Hepatology.
The results provide strong evidence that routinely giving liver transplant patients UDCA can prevent or delay recurrent primary biliary cirrhosis, said Alexie Bosch at Hôpital Edouard Herriot in Lyon, France, and his associates.
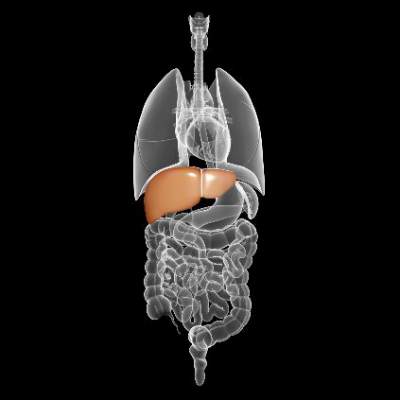
Primary biliary cirrhosis can recur after liver transplantation and increases the chances of graft dysfunction, the researchers noted. UDCA is the only approved medical treatment for primary biliary cirrhosis in the United States or Europe, but no research team has studied its potential to prevent recurrent primary biliary cirrhosis after liver transplantation, they added. Therefore, they retrospectively studied 90 patients with primary biliary cirrhosis who underwent liver transplantation at five centers in France and Switzerland between 1988 and 2010. In all, 21% of patients received oral UDCA (10-15 mg/kg per day in two divided doses) within 2 weeks after their operation, while the rest received it only if they developed biopsy-confirmed recurrent primary biliary cirrhosis. Biopsies were taken at posttransplant year 1 and every 5 years after that, or when clinically indicated, the investigators noted (J Hepatol. 2015 Aug. 14. doi: 10.1016/j.jhep.2015.07.038).
Patients who received preventive UDCA had a lower cumulative rate of recurrence throughout 15 years of postsurgical follow-up (P = .014), the researchers reported. The chances of recurrent primary biliary cirrhosis at 5, 10, and 15 years after transplantation were 11%, 21%, and 40% in the UDCA group, compared with 32%, 53%, and 70% for patients who did not receive prophylactic UDCA, they added. A multivariable analysis showed that recurrent primary biliary cirrhosis was associated with not receiving prophylactic UDCA (hazard ratio, 0.32; 95% confidence interval, 0.11, 0.91), but was not linked to donor age, Model For End-Stage Liver Disease (MELD) score, or sex mismatch between donor and recipient, the investigators said. Preventive UDCA also was tied to a 1.6-year longer median time to recurrence, although the trend did not reach statistical significance.
Although the study was retrospective and most patients who received UDCA were treated at one transplant center, all centers had similar histologic findings for recurrent primary biliary cirrhosis, said the researchers. Biopsies also were histologically similar regardless of whether they were event driven or obtained based on the study protocol, and time to recurrence did not vary based on biopsy type, they added. “In our multivariate analysis, we took care to account for all risk factors and confounders, as well as to test multilevel models in order to exclude potential misleading results and center effects,” they emphasized. “Given the extremely limited feasibility of prospective studies and the good tolerance and acceptability of long-term UDCA therapy, these results support the extended use of UDCA as prophylaxis for primary biliary cirrhosis recurrence after liver transplantation.”
The researchers declared no funding sources and reported having no conflicts of interest.
Only 21% of liver transplantation patients who received ursodeoxycholic acid (UDCA) after surgery developed recurrent primary biliary cirrhosis, compared with 62% of patients who did not receive the bile acid, researchers reported in the Journal of Hepatology.
The results provide strong evidence that routinely giving liver transplant patients UDCA can prevent or delay recurrent primary biliary cirrhosis, said Alexie Bosch at Hôpital Edouard Herriot in Lyon, France, and his associates.
Primary biliary cirrhosis can recur after liver transplantation and increases the chances of graft dysfunction, the researchers noted. UDCA is the only approved medical treatment for primary biliary cirrhosis in the United States or Europe, but no research team has studied its potential to prevent recurrent primary biliary cirrhosis after liver transplantation, they added. Therefore, they retrospectively studied 90 patients with primary biliary cirrhosis who underwent liver transplantation at five centers in France and Switzerland between 1988 and 2010. In all, 21% of patients received oral UDCA (10-15 mg/kg per day in two divided doses) within 2 weeks after their operation, while the rest received it only if they developed biopsy-confirmed recurrent primary biliary cirrhosis. Biopsies were taken at posttransplant year 1 and every 5 years after that, or when clinically indicated, the investigators noted (J Hepatol. 2015 Aug. 14. doi: 10.1016/j.jhep.2015.07.038).
Patients who received preventive UDCA had a lower cumulative rate of recurrence throughout 15 years of postsurgical follow-up (P = .014), the researchers reported. The chances of recurrent primary biliary cirrhosis at 5, 10, and 15 years after transplantation were 11%, 21%, and 40% in the UDCA group, compared with 32%, 53%, and 70% for patients who did not receive prophylactic UDCA, they added. A multivariable analysis showed that recurrent primary biliary cirrhosis was associated with not receiving prophylactic UDCA (hazard ratio, 0.32; 95% confidence interval, 0.11, 0.91), but was not linked to donor age, Model For End-Stage Liver Disease (MELD) score, or sex mismatch between donor and recipient, the investigators said. Preventive UDCA also was tied to a 1.6-year longer median time to recurrence, although the trend did not reach statistical significance.
Although the study was retrospective and most patients who received UDCA were treated at one transplant center, all centers had similar histologic findings for recurrent primary biliary cirrhosis, said the researchers. Biopsies also were histologically similar regardless of whether they were event driven or obtained based on the study protocol, and time to recurrence did not vary based on biopsy type, they added. “In our multivariate analysis, we took care to account for all risk factors and confounders, as well as to test multilevel models in order to exclude potential misleading results and center effects,” they emphasized. “Given the extremely limited feasibility of prospective studies and the good tolerance and acceptability of long-term UDCA therapy, these results support the extended use of UDCA as prophylaxis for primary biliary cirrhosis recurrence after liver transplantation.”
The researchers declared no funding sources and reported having no conflicts of interest.
Only 21% of liver transplantation patients who received ursodeoxycholic acid (UDCA) after surgery developed recurrent primary biliary cirrhosis, compared with 62% of patients who did not receive the bile acid, researchers reported in the Journal of Hepatology.
The results provide strong evidence that routinely giving liver transplant patients UDCA can prevent or delay recurrent primary biliary cirrhosis, said Alexie Bosch at Hôpital Edouard Herriot in Lyon, France, and his associates.
Primary biliary cirrhosis can recur after liver transplantation and increases the chances of graft dysfunction, the researchers noted. UDCA is the only approved medical treatment for primary biliary cirrhosis in the United States or Europe, but no research team has studied its potential to prevent recurrent primary biliary cirrhosis after liver transplantation, they added. Therefore, they retrospectively studied 90 patients with primary biliary cirrhosis who underwent liver transplantation at five centers in France and Switzerland between 1988 and 2010. In all, 21% of patients received oral UDCA (10-15 mg/kg per day in two divided doses) within 2 weeks after their operation, while the rest received it only if they developed biopsy-confirmed recurrent primary biliary cirrhosis. Biopsies were taken at posttransplant year 1 and every 5 years after that, or when clinically indicated, the investigators noted (J Hepatol. 2015 Aug. 14. doi: 10.1016/j.jhep.2015.07.038).
Patients who received preventive UDCA had a lower cumulative rate of recurrence throughout 15 years of postsurgical follow-up (P = .014), the researchers reported. The chances of recurrent primary biliary cirrhosis at 5, 10, and 15 years after transplantation were 11%, 21%, and 40% in the UDCA group, compared with 32%, 53%, and 70% for patients who did not receive prophylactic UDCA, they added. A multivariable analysis showed that recurrent primary biliary cirrhosis was associated with not receiving prophylactic UDCA (hazard ratio, 0.32; 95% confidence interval, 0.11, 0.91), but was not linked to donor age, Model For End-Stage Liver Disease (MELD) score, or sex mismatch between donor and recipient, the investigators said. Preventive UDCA also was tied to a 1.6-year longer median time to recurrence, although the trend did not reach statistical significance.
Although the study was retrospective and most patients who received UDCA were treated at one transplant center, all centers had similar histologic findings for recurrent primary biliary cirrhosis, said the researchers. Biopsies also were histologically similar regardless of whether they were event driven or obtained based on the study protocol, and time to recurrence did not vary based on biopsy type, they added. “In our multivariate analysis, we took care to account for all risk factors and confounders, as well as to test multilevel models in order to exclude potential misleading results and center effects,” they emphasized. “Given the extremely limited feasibility of prospective studies and the good tolerance and acceptability of long-term UDCA therapy, these results support the extended use of UDCA as prophylaxis for primary biliary cirrhosis recurrence after liver transplantation.”
The researchers declared no funding sources and reported having no conflicts of interest.
FROM THE JOURNAL OF HEPATOLOGY
Key clinical point: Treatment with prophylactic ursodeoxycholic acid might help prevent recurrent primary biliary cirrhosis after liver transplantation.
Major finding: Patients who received preventive UDCA had a lower cumulative rate of recurrence throughout 15 years of follow-up (P = .014).
Data source: Multicenter retrospective study of 90 patients who underwent liver transplantation for primary biliary cirrhosis.
Disclosures: The researchers declared no funding sources and reported having no conflicts of interest.
CMS: We’re ready to accept and process ICD-10 claims
The Centers for Medicare and Medicaid Services says it completed its final Medicare fee-for-service end-to-end testing of ICD-10 with positive results.
“This final end-to-end testing [that occurred July 20-24] demonstrated that CMS systems are ready to accept and process ICD-10 claims,” the agency said in an email update.

A separate report on the most recent testing noted that “no new ICD-10 related issues were identified in any of the Medicare fee-for-service claims processing systems. There were zero rejects due to front-end CMS systems issues,” and concerns from previous tests were resolved prior to the final testing week.
The final test was based on 1,200 participants, including physicians, health care providers, clearinghouses, and billing agencies. They submitted more than 29,000 test claims, including some that were intentionally erroneous to make sure a claim was rejected.
The agency reported an 87% acceptance rate, with 1.8% of test claims rejected because of invalid submission of ICD-10 diagnosis or procedure codes and 2.6% of test claims rejected due to invalid submission of ICD-9 diagnosis or procedure codes.
The acceptance rate (88%) was consistent with the previous test from April 27 to May 1 and up from the 81% acceptance rate reported during the Jan. 26–Feb. 3 testing period.
Additional rejections were generated from non-ICD-10 related errors, including incorrect NPI, health insurance claim number, or submitter ID; dates of service outside the range valid for testing; invalid HCPCS codes; and invalid place of service.
“Most rejects were the result of provider submission errors in the testing environment that would not occur when actual claims are submitted for processing,” the agency said in a report.
The ICD-10 compliance date is Oct. 1; however, CMS announced in July that during that first year using the new coding system, Medicare will not deny claims based solely on the specificity of diagnosis codes, provided they are in the appropriate family of ICD-10 codes.
The Centers for Medicare and Medicaid Services says it completed its final Medicare fee-for-service end-to-end testing of ICD-10 with positive results.
“This final end-to-end testing [that occurred July 20-24] demonstrated that CMS systems are ready to accept and process ICD-10 claims,” the agency said in an email update.
A separate report on the most recent testing noted that “no new ICD-10 related issues were identified in any of the Medicare fee-for-service claims processing systems. There were zero rejects due to front-end CMS systems issues,” and concerns from previous tests were resolved prior to the final testing week.
The final test was based on 1,200 participants, including physicians, health care providers, clearinghouses, and billing agencies. They submitted more than 29,000 test claims, including some that were intentionally erroneous to make sure a claim was rejected.
The agency reported an 87% acceptance rate, with 1.8% of test claims rejected because of invalid submission of ICD-10 diagnosis or procedure codes and 2.6% of test claims rejected due to invalid submission of ICD-9 diagnosis or procedure codes.
The acceptance rate (88%) was consistent with the previous test from April 27 to May 1 and up from the 81% acceptance rate reported during the Jan. 26–Feb. 3 testing period.
Additional rejections were generated from non-ICD-10 related errors, including incorrect NPI, health insurance claim number, or submitter ID; dates of service outside the range valid for testing; invalid HCPCS codes; and invalid place of service.
“Most rejects were the result of provider submission errors in the testing environment that would not occur when actual claims are submitted for processing,” the agency said in a report.
The ICD-10 compliance date is Oct. 1; however, CMS announced in July that during that first year using the new coding system, Medicare will not deny claims based solely on the specificity of diagnosis codes, provided they are in the appropriate family of ICD-10 codes.
The Centers for Medicare and Medicaid Services says it completed its final Medicare fee-for-service end-to-end testing of ICD-10 with positive results.
“This final end-to-end testing [that occurred July 20-24] demonstrated that CMS systems are ready to accept and process ICD-10 claims,” the agency said in an email update.
A separate report on the most recent testing noted that “no new ICD-10 related issues were identified in any of the Medicare fee-for-service claims processing systems. There were zero rejects due to front-end CMS systems issues,” and concerns from previous tests were resolved prior to the final testing week.
The final test was based on 1,200 participants, including physicians, health care providers, clearinghouses, and billing agencies. They submitted more than 29,000 test claims, including some that were intentionally erroneous to make sure a claim was rejected.
The agency reported an 87% acceptance rate, with 1.8% of test claims rejected because of invalid submission of ICD-10 diagnosis or procedure codes and 2.6% of test claims rejected due to invalid submission of ICD-9 diagnosis or procedure codes.
The acceptance rate (88%) was consistent with the previous test from April 27 to May 1 and up from the 81% acceptance rate reported during the Jan. 26–Feb. 3 testing period.
Additional rejections were generated from non-ICD-10 related errors, including incorrect NPI, health insurance claim number, or submitter ID; dates of service outside the range valid for testing; invalid HCPCS codes; and invalid place of service.
“Most rejects were the result of provider submission errors in the testing environment that would not occur when actual claims are submitted for processing,” the agency said in a report.
The ICD-10 compliance date is Oct. 1; however, CMS announced in July that during that first year using the new coding system, Medicare will not deny claims based solely on the specificity of diagnosis codes, provided they are in the appropriate family of ICD-10 codes.

ACOs generate savings, but few get bonuses
Accountable care organizations (ACOs) accounted for savings of more than $411 million in 2014, according to the Centers for Medicare & Medicaid Services.
However, of the 20 Pioneer ACO programs and the 333 ACOs participating in the Medicare shared savings program, 97 qualified for shared savings payments of more than $422 million by meeting quality standards and their saving threshold, according to a report from the CMS.

In addition to savings, provider groups also reported improvement on certain quality metrics. For those in the Pioneer ACO program, groups demonstrated improvement on 28 of 33 quality measures and experienced a 3.6% improvement across all quality measures, compared with the previous year. Top areas of improvement were medication reconciliation, screening for clinical depression and follow-up plan, and qualification for electronic health record incentive payments.
For ACOs participating in the Medicare Shared Savings program, improvement was shown in 27 of 33 quality measures, including patients’ ratings of clinicians’ communication, patients’ ratings of their doctors, screening for tobacco use and cessation, screening for high blood pressure, and EHR use.
“Accountable care organizations as a group are on the path toward transforming how care is provided,” CMS Acting Administrator Andy Slavitt said in a statement. “Many of these ACOs are demonstrating that they can deliver a higher level of coordinated care that leads to healthier people and smarter spending.”
Accountable care organizations (ACOs) accounted for savings of more than $411 million in 2014, according to the Centers for Medicare & Medicaid Services.
However, of the 20 Pioneer ACO programs and the 333 ACOs participating in the Medicare shared savings program, 97 qualified for shared savings payments of more than $422 million by meeting quality standards and their saving threshold, according to a report from the CMS.
In addition to savings, provider groups also reported improvement on certain quality metrics. For those in the Pioneer ACO program, groups demonstrated improvement on 28 of 33 quality measures and experienced a 3.6% improvement across all quality measures, compared with the previous year. Top areas of improvement were medication reconciliation, screening for clinical depression and follow-up plan, and qualification for electronic health record incentive payments.
For ACOs participating in the Medicare Shared Savings program, improvement was shown in 27 of 33 quality measures, including patients’ ratings of clinicians’ communication, patients’ ratings of their doctors, screening for tobacco use and cessation, screening for high blood pressure, and EHR use.
“Accountable care organizations as a group are on the path toward transforming how care is provided,” CMS Acting Administrator Andy Slavitt said in a statement. “Many of these ACOs are demonstrating that they can deliver a higher level of coordinated care that leads to healthier people and smarter spending.”
Accountable care organizations (ACOs) accounted for savings of more than $411 million in 2014, according to the Centers for Medicare & Medicaid Services.
However, of the 20 Pioneer ACO programs and the 333 ACOs participating in the Medicare shared savings program, 97 qualified for shared savings payments of more than $422 million by meeting quality standards and their saving threshold, according to a report from the CMS.
In addition to savings, provider groups also reported improvement on certain quality metrics. For those in the Pioneer ACO program, groups demonstrated improvement on 28 of 33 quality measures and experienced a 3.6% improvement across all quality measures, compared with the previous year. Top areas of improvement were medication reconciliation, screening for clinical depression and follow-up plan, and qualification for electronic health record incentive payments.
For ACOs participating in the Medicare Shared Savings program, improvement was shown in 27 of 33 quality measures, including patients’ ratings of clinicians’ communication, patients’ ratings of their doctors, screening for tobacco use and cessation, screening for high blood pressure, and EHR use.
“Accountable care organizations as a group are on the path toward transforming how care is provided,” CMS Acting Administrator Andy Slavitt said in a statement. “Many of these ACOs are demonstrating that they can deliver a higher level of coordinated care that leads to healthier people and smarter spending.”

Burning the midnight oil does not impact surgical outcomes
Attending physicians who work through the wee hours of the night do not have measurably different short-term outcomes for elective surgeries performed the next day, according to a population-based, matched-control study published online Aug. 26.
The primary composite outcome of death, readmission, or complications within 30 days occurred in 22.2% of patients undergoing elective daytime surgery by an attending who treated patients from midnight to 7 a.m. and in 22.4% of those undergoing the same procedure by the same attending, but after a night when no clinical work had been performed (P = .66).

There was no significant between-group difference in the primary outcome in adjusted analyses (adjusted odds ratio, 0.99; P = .65).
Secondary outcomes also were similar between the postmidnight and control groups: death within 30 days (both 1.1%), readmission within 30 days (6.6% vs. 7.1%), complications within 30 days (18.1% vs. 18.2%), median length of stay (both 3 days), and median duration of surgery (both 2.6 hours).
“These data suggest that calls for broad-based policy shifts in duty hours and practices of attending surgeons may not be necessary at this time,” wrote surgical oncologist Dr. Anand Govindarajan of Mount Sinai Hospital, Toronto, and his associates (N Engl J Med. 2015;373:845-53. doi: 10.1056/NEJMsa1415994).
The current study addresses a gap in the literature on the effects of sleep deprivation and may help inform policy discussions on this issue, the authors suggested.
Most studies of physicians suggesting that sleep deprivation may affect mood, cognition, and psycho-motor function have focused on medical trainees, but few studies have examined the effects of sleep deprivation in attending physicians and the results have been conflicting.
A 2009 single-center study prompted calls for policy-level changes regarding sleep deprivation in surgeons after showing a higher rate of complications for procedures performed by attending physicians with sleep opportunities of less than 6 hours (JAMA. 2009 Oct 14;302[14]:1565-72), but the findings have not been replicated by other groups, Dr. Govindarajan and his associates observed.
In the current study, a small but significant increase in complications was observed in the subset of patients whose physician had performed two or more procedures the night before (adjusted OR, 1.14; P = .05). Importantly, this isolated finding was from a post-hoc subgroup analysis and may be the result of random error, they suggested.
Further, three a priori analyses found no significant difference in outcomes after stratification for academic vs. nonacademic center, physician age, or type of procedure.
The current study involved 38,978 patients who underwent 1 of 12 elective daytime procedures performed by 1,448 physicians at 147 hospitals in Ontario. Patients undergoing procedures performed by a physician who had treated patients from midnight to 7 a.m. were matched in a 1:1 ratio to patients undergoing the same procedure by the same physician on a day when the physician had not treated patients after midnight.
The physicians had been in practice for a median of 20 years, and 40.6% of procedures were performed at academic institutions. Physicians who treated patients after midnight performed a mean of 1.25 procedures during that time.
The elective procedures (cholecystectomy, gastric bypass, colon resection, coronary artery bypass grafting, coronary angioplasty, knee replacement, hip replacement, hip fracture repair, hysterectomy, spinal surgery, craniotomy, and lung resection) were all performed on weekdays.
The investigators selected procedures that varied in duration and were associated with a range of complication rates because sleep studies have suggested that tasks requiring longer periods of concentration may be more affected by sleep deprivation.
“The broad scope of the study enhances its generalizability, a particularly relevant consideration if policy changes are being contemplated with respect to duty hours,” Dr. Govindarajan and his associates noted.
Other strengths of the study are the matched study groups and sufficiently sized cohorts and event rates to provide adequate power to show clinically meaningful differences.
Limitations of the study are the inability to quantify the number of hours that a physician was deprived of sleep and to determine whether there was a difference in outcomes between daytime procedures performed later in the day and those performed earlier in the day or whether procedures may have been postponed till later in the day because of substantial sleep deprivation. “However, given the constraints of operating room schedules in Ontario, it would not usually be feasible to postpone an operation until later in the day on short notice,” the investigators wrote.
Dr. Govindarajan reported grant support from the Canadian Institutes for Health Research and the University of Toronto Dean’s Fund while conducting the study.
On Twitter @pwendl
Attending physicians who work through the wee hours of the night do not have measurably different short-term outcomes for elective surgeries performed the next day, according to a population-based, matched-control study published online Aug. 26.
The primary composite outcome of death, readmission, or complications within 30 days occurred in 22.2% of patients undergoing elective daytime surgery by an attending who treated patients from midnight to 7 a.m. and in 22.4% of those undergoing the same procedure by the same attending, but after a night when no clinical work had been performed (P = .66).
There was no significant between-group difference in the primary outcome in adjusted analyses (adjusted odds ratio, 0.99; P = .65).
Secondary outcomes also were similar between the postmidnight and control groups: death within 30 days (both 1.1%), readmission within 30 days (6.6% vs. 7.1%), complications within 30 days (18.1% vs. 18.2%), median length of stay (both 3 days), and median duration of surgery (both 2.6 hours).
“These data suggest that calls for broad-based policy shifts in duty hours and practices of attending surgeons may not be necessary at this time,” wrote surgical oncologist Dr. Anand Govindarajan of Mount Sinai Hospital, Toronto, and his associates (N Engl J Med. 2015;373:845-53. doi: 10.1056/NEJMsa1415994).
The current study addresses a gap in the literature on the effects of sleep deprivation and may help inform policy discussions on this issue, the authors suggested.
Most studies of physicians suggesting that sleep deprivation may affect mood, cognition, and psycho-motor function have focused on medical trainees, but few studies have examined the effects of sleep deprivation in attending physicians and the results have been conflicting.
A 2009 single-center study prompted calls for policy-level changes regarding sleep deprivation in surgeons after showing a higher rate of complications for procedures performed by attending physicians with sleep opportunities of less than 6 hours (JAMA. 2009 Oct 14;302[14]:1565-72), but the findings have not been replicated by other groups, Dr. Govindarajan and his associates observed.
In the current study, a small but significant increase in complications was observed in the subset of patients whose physician had performed two or more procedures the night before (adjusted OR, 1.14; P = .05). Importantly, this isolated finding was from a post-hoc subgroup analysis and may be the result of random error, they suggested.
Further, three a priori analyses found no significant difference in outcomes after stratification for academic vs. nonacademic center, physician age, or type of procedure.
The current study involved 38,978 patients who underwent 1 of 12 elective daytime procedures performed by 1,448 physicians at 147 hospitals in Ontario. Patients undergoing procedures performed by a physician who had treated patients from midnight to 7 a.m. were matched in a 1:1 ratio to patients undergoing the same procedure by the same physician on a day when the physician had not treated patients after midnight.
The physicians had been in practice for a median of 20 years, and 40.6% of procedures were performed at academic institutions. Physicians who treated patients after midnight performed a mean of 1.25 procedures during that time.
The elective procedures (cholecystectomy, gastric bypass, colon resection, coronary artery bypass grafting, coronary angioplasty, knee replacement, hip replacement, hip fracture repair, hysterectomy, spinal surgery, craniotomy, and lung resection) were all performed on weekdays.
The investigators selected procedures that varied in duration and were associated with a range of complication rates because sleep studies have suggested that tasks requiring longer periods of concentration may be more affected by sleep deprivation.
“The broad scope of the study enhances its generalizability, a particularly relevant consideration if policy changes are being contemplated with respect to duty hours,” Dr. Govindarajan and his associates noted.
Other strengths of the study are the matched study groups and sufficiently sized cohorts and event rates to provide adequate power to show clinically meaningful differences.
Limitations of the study are the inability to quantify the number of hours that a physician was deprived of sleep and to determine whether there was a difference in outcomes between daytime procedures performed later in the day and those performed earlier in the day or whether procedures may have been postponed till later in the day because of substantial sleep deprivation. “However, given the constraints of operating room schedules in Ontario, it would not usually be feasible to postpone an operation until later in the day on short notice,” the investigators wrote.
Dr. Govindarajan reported grant support from the Canadian Institutes for Health Research and the University of Toronto Dean’s Fund while conducting the study.
On Twitter @pwendl
Attending physicians who work through the wee hours of the night do not have measurably different short-term outcomes for elective surgeries performed the next day, according to a population-based, matched-control study published online Aug. 26.
The primary composite outcome of death, readmission, or complications within 30 days occurred in 22.2% of patients undergoing elective daytime surgery by an attending who treated patients from midnight to 7 a.m. and in 22.4% of those undergoing the same procedure by the same attending, but after a night when no clinical work had been performed (P = .66).
There was no significant between-group difference in the primary outcome in adjusted analyses (adjusted odds ratio, 0.99; P = .65).
Secondary outcomes also were similar between the postmidnight and control groups: death within 30 days (both 1.1%), readmission within 30 days (6.6% vs. 7.1%), complications within 30 days (18.1% vs. 18.2%), median length of stay (both 3 days), and median duration of surgery (both 2.6 hours).
“These data suggest that calls for broad-based policy shifts in duty hours and practices of attending surgeons may not be necessary at this time,” wrote surgical oncologist Dr. Anand Govindarajan of Mount Sinai Hospital, Toronto, and his associates (N Engl J Med. 2015;373:845-53. doi: 10.1056/NEJMsa1415994).
The current study addresses a gap in the literature on the effects of sleep deprivation and may help inform policy discussions on this issue, the authors suggested.
Most studies of physicians suggesting that sleep deprivation may affect mood, cognition, and psycho-motor function have focused on medical trainees, but few studies have examined the effects of sleep deprivation in attending physicians and the results have been conflicting.
A 2009 single-center study prompted calls for policy-level changes regarding sleep deprivation in surgeons after showing a higher rate of complications for procedures performed by attending physicians with sleep opportunities of less than 6 hours (JAMA. 2009 Oct 14;302[14]:1565-72), but the findings have not been replicated by other groups, Dr. Govindarajan and his associates observed.
In the current study, a small but significant increase in complications was observed in the subset of patients whose physician had performed two or more procedures the night before (adjusted OR, 1.14; P = .05). Importantly, this isolated finding was from a post-hoc subgroup analysis and may be the result of random error, they suggested.
Further, three a priori analyses found no significant difference in outcomes after stratification for academic vs. nonacademic center, physician age, or type of procedure.
The current study involved 38,978 patients who underwent 1 of 12 elective daytime procedures performed by 1,448 physicians at 147 hospitals in Ontario. Patients undergoing procedures performed by a physician who had treated patients from midnight to 7 a.m. were matched in a 1:1 ratio to patients undergoing the same procedure by the same physician on a day when the physician had not treated patients after midnight.
The physicians had been in practice for a median of 20 years, and 40.6% of procedures were performed at academic institutions. Physicians who treated patients after midnight performed a mean of 1.25 procedures during that time.
The elective procedures (cholecystectomy, gastric bypass, colon resection, coronary artery bypass grafting, coronary angioplasty, knee replacement, hip replacement, hip fracture repair, hysterectomy, spinal surgery, craniotomy, and lung resection) were all performed on weekdays.
The investigators selected procedures that varied in duration and were associated with a range of complication rates because sleep studies have suggested that tasks requiring longer periods of concentration may be more affected by sleep deprivation.
“The broad scope of the study enhances its generalizability, a particularly relevant consideration if policy changes are being contemplated with respect to duty hours,” Dr. Govindarajan and his associates noted.
Other strengths of the study are the matched study groups and sufficiently sized cohorts and event rates to provide adequate power to show clinically meaningful differences.
Limitations of the study are the inability to quantify the number of hours that a physician was deprived of sleep and to determine whether there was a difference in outcomes between daytime procedures performed later in the day and those performed earlier in the day or whether procedures may have been postponed till later in the day because of substantial sleep deprivation. “However, given the constraints of operating room schedules in Ontario, it would not usually be feasible to postpone an operation until later in the day on short notice,” the investigators wrote.
Dr. Govindarajan reported grant support from the Canadian Institutes for Health Research and the University of Toronto Dean’s Fund while conducting the study.
On Twitter @pwendl
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: The risks of adverse outcomes of elective daytime surgical procedures were similar whether or not the attending physician had provided medical care the previous night.
Major finding: The primary composite endpoint was similar between the postmidnight and control groups (22.2% vs. 22.4%; P = .66).
Data source: Population-based, retrospective, matched cohort study in 38,978 patients.
Disclosures: Dr. Govindarajan reported grant support from the Canadian Institutes for Health Research and the University of Toronto Dean’s Fund while conducting the study.

Scoring tool points to postop ventilator dependence
CHICAGO – A new preoperative risk scoring tool may help identify patients at high risk for requiring mechanical ventilation for more than 48 hours in the 30 days after surgery, a study suggests.
The risk score is based on seven measures: whether patients have had a small bowel procedure, have had an esophageal procedure, are current smokers, have severe chronic obstructive pulmonary disease, have hypoalbuminemia, are older than age 60 years, or have signs of systemic inflammatory response syndrome or sepsis.
The score was validated via the American College of Surgeons (ACS)/National Surgical Quality Improvement Program (NSQIP) database to identify patients who underwent nonemergent general or vascular surgery at Thomas Jefferson University Hospital between 2006 and 2013, Dr. Adam P. Johnson, study coauthor, reported at the ACS/NSQIP National Conference.
The risk score assigned 1 point each for a small bowel procedure, current smoking, severe chronic obstructive pulmonary disease, and hypoalbuminemia (less than 3.5 mg/dL); 2 points each for age over 60 years and signs of systemic inflammatory response syndrome or sepsis; and 3 points for esophageal procedures. Total risk scores ranged from 0 to 7 points for the population.
The median score was 2 for patients who did not need a ventilator after surgery and 3 for those who did, Dr. Johnson said.
Notably, patients with a risk score of more than 3 comprised the 20%-30% of patients who experienced 60%-70% of adverse events. A cutoff value of 3 identified the top 20% of patients at highest risk for ventilator dependence, with a ventilator dependence rate of 5.4% (P less than .01).
The risk factors and scoring system are specific to Thomas Jefferson University Hospital, where many patients with advanced gastrointestinal malignancies are treated. However, other institutions should be able to use the methodology and framework to identify ventilator risk factors in their own patients, Dr. Johnson suggested.
Future steps include evaluating how the risk tool performs when compared with risk scores derived from national datasets, automating the best performing risk score, and using the score in the preadmission testing of every patient undergoing elective general surgery or vascular operations. Once identified, high-risk patients would then be entered into an aggressive pre-, intra-, and postoperative pulmonary optimization pathway.
“The pathway might be resource intensive for all patients, but we might be able to hone in and use it more effectively for patients at greatest risk,” Dr. Johnson said in a statement.
Although ventilator dependence occurs in only about 1-3% of patients, the consequences are nonetheless significant, increasing mortality and health care costs, said Dr. Scott W. Cowan, senior study author and Jefferson’s NSQIP Surgeon Champion.
CHICAGO – A new preoperative risk scoring tool may help identify patients at high risk for requiring mechanical ventilation for more than 48 hours in the 30 days after surgery, a study suggests.
The risk score is based on seven measures: whether patients have had a small bowel procedure, have had an esophageal procedure, are current smokers, have severe chronic obstructive pulmonary disease, have hypoalbuminemia, are older than age 60 years, or have signs of systemic inflammatory response syndrome or sepsis.
The score was validated via the American College of Surgeons (ACS)/National Surgical Quality Improvement Program (NSQIP) database to identify patients who underwent nonemergent general or vascular surgery at Thomas Jefferson University Hospital between 2006 and 2013, Dr. Adam P. Johnson, study coauthor, reported at the ACS/NSQIP National Conference.
The risk score assigned 1 point each for a small bowel procedure, current smoking, severe chronic obstructive pulmonary disease, and hypoalbuminemia (less than 3.5 mg/dL); 2 points each for age over 60 years and signs of systemic inflammatory response syndrome or sepsis; and 3 points for esophageal procedures. Total risk scores ranged from 0 to 7 points for the population.
The median score was 2 for patients who did not need a ventilator after surgery and 3 for those who did, Dr. Johnson said.
Notably, patients with a risk score of more than 3 comprised the 20%-30% of patients who experienced 60%-70% of adverse events. A cutoff value of 3 identified the top 20% of patients at highest risk for ventilator dependence, with a ventilator dependence rate of 5.4% (P less than .01).
The risk factors and scoring system are specific to Thomas Jefferson University Hospital, where many patients with advanced gastrointestinal malignancies are treated. However, other institutions should be able to use the methodology and framework to identify ventilator risk factors in their own patients, Dr. Johnson suggested.
Future steps include evaluating how the risk tool performs when compared with risk scores derived from national datasets, automating the best performing risk score, and using the score in the preadmission testing of every patient undergoing elective general surgery or vascular operations. Once identified, high-risk patients would then be entered into an aggressive pre-, intra-, and postoperative pulmonary optimization pathway.
“The pathway might be resource intensive for all patients, but we might be able to hone in and use it more effectively for patients at greatest risk,” Dr. Johnson said in a statement.
Although ventilator dependence occurs in only about 1-3% of patients, the consequences are nonetheless significant, increasing mortality and health care costs, said Dr. Scott W. Cowan, senior study author and Jefferson’s NSQIP Surgeon Champion.
CHICAGO – A new preoperative risk scoring tool may help identify patients at high risk for requiring mechanical ventilation for more than 48 hours in the 30 days after surgery, a study suggests.
The risk score is based on seven measures: whether patients have had a small bowel procedure, have had an esophageal procedure, are current smokers, have severe chronic obstructive pulmonary disease, have hypoalbuminemia, are older than age 60 years, or have signs of systemic inflammatory response syndrome or sepsis.
The score was validated via the American College of Surgeons (ACS)/National Surgical Quality Improvement Program (NSQIP) database to identify patients who underwent nonemergent general or vascular surgery at Thomas Jefferson University Hospital between 2006 and 2013, Dr. Adam P. Johnson, study coauthor, reported at the ACS/NSQIP National Conference.
The risk score assigned 1 point each for a small bowel procedure, current smoking, severe chronic obstructive pulmonary disease, and hypoalbuminemia (less than 3.5 mg/dL); 2 points each for age over 60 years and signs of systemic inflammatory response syndrome or sepsis; and 3 points for esophageal procedures. Total risk scores ranged from 0 to 7 points for the population.
The median score was 2 for patients who did not need a ventilator after surgery and 3 for those who did, Dr. Johnson said.
Notably, patients with a risk score of more than 3 comprised the 20%-30% of patients who experienced 60%-70% of adverse events. A cutoff value of 3 identified the top 20% of patients at highest risk for ventilator dependence, with a ventilator dependence rate of 5.4% (P less than .01).
The risk factors and scoring system are specific to Thomas Jefferson University Hospital, where many patients with advanced gastrointestinal malignancies are treated. However, other institutions should be able to use the methodology and framework to identify ventilator risk factors in their own patients, Dr. Johnson suggested.
Future steps include evaluating how the risk tool performs when compared with risk scores derived from national datasets, automating the best performing risk score, and using the score in the preadmission testing of every patient undergoing elective general surgery or vascular operations. Once identified, high-risk patients would then be entered into an aggressive pre-, intra-, and postoperative pulmonary optimization pathway.
“The pathway might be resource intensive for all patients, but we might be able to hone in and use it more effectively for patients at greatest risk,” Dr. Johnson said in a statement.
Although ventilator dependence occurs in only about 1-3% of patients, the consequences are nonetheless significant, increasing mortality and health care costs, said Dr. Scott W. Cowan, senior study author and Jefferson’s NSQIP Surgeon Champion.
AT THE ACS NSQIP NATIONAL CONFERENCE
Key clinical point: A preoperative risk score can help identify patients at highest risk for postoperative ventilator dependence.
Major finding: A risk score greater than 3 identified the top 20%-30% of patients experiencing 60%-70% of postop ventilator dependence events.
Data source: Retrospective analysis of 7,473 elective general and vascular surgical patients.
Disclosures: The authors reported having no financial disclosures.
Decision aids benefit OA patients considering joint replacement
Osteoarthritis patients who received patient decision aids (PtDA) in addition to usual educational resources had shorter wait times and fewer surgeries, and were more likely to reach good decision quality about joint replacement surgery, although the overall effect was not statistically significant, reported Dawn Stacey, Ph.D., of the University of Ottawa (Ont.) and her coauthors.

In a randomized, controlled trial of 343 patients undergoing orthopedic screening for hip or knee replacement surgery at an academic hospital or a community hospital, being given a PtDA (intervention) was associated with reduced wait times, compared with controls who received usual care (hazard ratio = 1.25; 95% CI, 0.99–1.60; P = .0653). Mean age of the patients was 66 years; about half had high school education or less and half had household incomes at or below the median income ($58,000) for couples aged 65 or older in Canada.
Surgery rates were 73.2% in the intervention group, compared with 80.5% in controls (relative risk = 0.91; 95% CI, 0.81-1.03), the investigators found. Good decision quality was reached by 56.1% of intervention patients and 44.5% of controls (RR = 1.25; 95% CI, 1.00–1.56, P = .050). However, the overall effect was not significant, Dr. Stacey and coauthors reported.
Most patients in the study had more severe osteoarthritis and were appropriate for considering surgery, but the PtDA may have had “greater effect and discrimination” when it was given to patients with earlier stages of osteoarthritis and may have helped them to consider their nonsurgical options, the investigators wrote.
Read the full study in Osteoarthritis and Cartilage.
Osteoarthritis patients who received patient decision aids (PtDA) in addition to usual educational resources had shorter wait times and fewer surgeries, and were more likely to reach good decision quality about joint replacement surgery, although the overall effect was not statistically significant, reported Dawn Stacey, Ph.D., of the University of Ottawa (Ont.) and her coauthors.
In a randomized, controlled trial of 343 patients undergoing orthopedic screening for hip or knee replacement surgery at an academic hospital or a community hospital, being given a PtDA (intervention) was associated with reduced wait times, compared with controls who received usual care (hazard ratio = 1.25; 95% CI, 0.99–1.60; P = .0653). Mean age of the patients was 66 years; about half had high school education or less and half had household incomes at or below the median income ($58,000) for couples aged 65 or older in Canada.
Surgery rates were 73.2% in the intervention group, compared with 80.5% in controls (relative risk = 0.91; 95% CI, 0.81-1.03), the investigators found. Good decision quality was reached by 56.1% of intervention patients and 44.5% of controls (RR = 1.25; 95% CI, 1.00–1.56, P = .050). However, the overall effect was not significant, Dr. Stacey and coauthors reported.
Most patients in the study had more severe osteoarthritis and were appropriate for considering surgery, but the PtDA may have had “greater effect and discrimination” when it was given to patients with earlier stages of osteoarthritis and may have helped them to consider their nonsurgical options, the investigators wrote.
Read the full study in Osteoarthritis and Cartilage.
Osteoarthritis patients who received patient decision aids (PtDA) in addition to usual educational resources had shorter wait times and fewer surgeries, and were more likely to reach good decision quality about joint replacement surgery, although the overall effect was not statistically significant, reported Dawn Stacey, Ph.D., of the University of Ottawa (Ont.) and her coauthors.
In a randomized, controlled trial of 343 patients undergoing orthopedic screening for hip or knee replacement surgery at an academic hospital or a community hospital, being given a PtDA (intervention) was associated with reduced wait times, compared with controls who received usual care (hazard ratio = 1.25; 95% CI, 0.99–1.60; P = .0653). Mean age of the patients was 66 years; about half had high school education or less and half had household incomes at or below the median income ($58,000) for couples aged 65 or older in Canada.
Surgery rates were 73.2% in the intervention group, compared with 80.5% in controls (relative risk = 0.91; 95% CI, 0.81-1.03), the investigators found. Good decision quality was reached by 56.1% of intervention patients and 44.5% of controls (RR = 1.25; 95% CI, 1.00–1.56, P = .050). However, the overall effect was not significant, Dr. Stacey and coauthors reported.
Most patients in the study had more severe osteoarthritis and were appropriate for considering surgery, but the PtDA may have had “greater effect and discrimination” when it was given to patients with earlier stages of osteoarthritis and may have helped them to consider their nonsurgical options, the investigators wrote.
Read the full study in Osteoarthritis and Cartilage.
