User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
New melanoma treatments linked to mortality decline
Recent advances in treatment appear to have reversed the course of melanoma mortality since 2013, according to data published in the American Journal of Public Health.
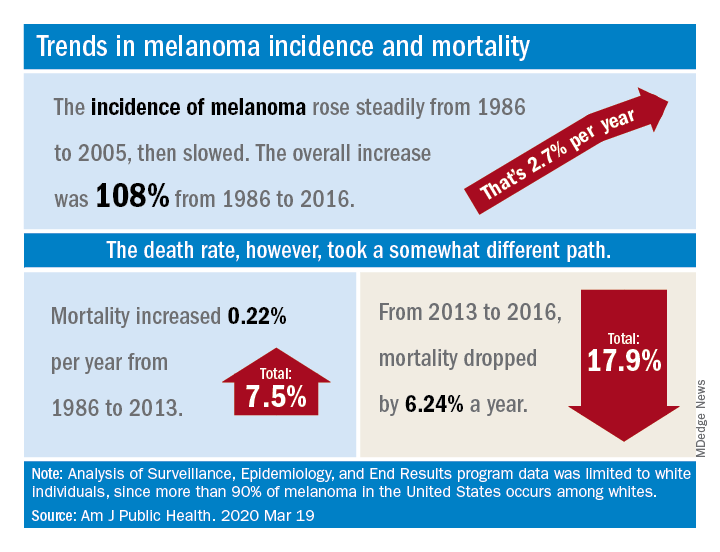
The U.S. death rate for melanoma, which had been rising at a rate of 0.22% a year for more than 2 decades, dropped by 17.9%, or 6.24% per year, during 2013-2016. That decline “coincides with the introduction of multiple new and efficacious treatments for metastatic melanoma,” such as BRAF inhibitors and immune checkpoint inhibitors, study author Juliana Berk-Krauss, MD, of the State University of New York Downstate Medical Center in Brooklyn and colleagues wrote.
The other possible explanation for the decline in deaths, “education and early detection resulting in migration toward earlier stage melanomas with a greater chance of surgical cure,” is unlikely, according to the investigators. That’s because the small decrease in median tumor thickness that occurred during 1989-2009 “is not associated with changes in prognosis.”
The investigators’ analysis encompassed data from the Surveillance, Epidemiology, and End Results registry recorded during 1986-2016. Nine registry areas were included (Atlanta, Connecticut, Detroit, Hawaii, Iowa, New Mexico, San Francisco-Oakland, Seattle-Puget Sound, and Utah), which covered about 9.4% of the U.S. population. The analysis was limited to the white population, which accounts for more than 90% of melanoma cases in the United States.
The data showed a slight decline in annual percent change in melanoma incidence, from 3.24% for 1986-2005 to 1.72% for 2006-2016. However, over the whole period studied (1986-2016), melanoma incidence increased by 108%, or about 2.7% per year.
“Given the increased incidence of melanoma throughout this period and the lack of stage migration, these data strongly suggest that the mortality decline is due to the extended survival associated with these [newer] treatments,” the investigators wrote.
This study was funded by NYU Langone. Two investigators disclosed potential conflicts of interest, including relationships with Bio-Rad Laboratories, Novartis, Merck, and several other companies.
SOURCE: Berk-Krauss J et al. Am J Public Health. 2020 Mar 19. doi: 10.2105/AJPH.2020.305567.
Recent advances in treatment appear to have reversed the course of melanoma mortality since 2013, according to data published in the American Journal of Public Health.
The U.S. death rate for melanoma, which had been rising at a rate of 0.22% a year for more than 2 decades, dropped by 17.9%, or 6.24% per year, during 2013-2016. That decline “coincides with the introduction of multiple new and efficacious treatments for metastatic melanoma,” such as BRAF inhibitors and immune checkpoint inhibitors, study author Juliana Berk-Krauss, MD, of the State University of New York Downstate Medical Center in Brooklyn and colleagues wrote.
The other possible explanation for the decline in deaths, “education and early detection resulting in migration toward earlier stage melanomas with a greater chance of surgical cure,” is unlikely, according to the investigators. That’s because the small decrease in median tumor thickness that occurred during 1989-2009 “is not associated with changes in prognosis.”
The investigators’ analysis encompassed data from the Surveillance, Epidemiology, and End Results registry recorded during 1986-2016. Nine registry areas were included (Atlanta, Connecticut, Detroit, Hawaii, Iowa, New Mexico, San Francisco-Oakland, Seattle-Puget Sound, and Utah), which covered about 9.4% of the U.S. population. The analysis was limited to the white population, which accounts for more than 90% of melanoma cases in the United States.
The data showed a slight decline in annual percent change in melanoma incidence, from 3.24% for 1986-2005 to 1.72% for 2006-2016. However, over the whole period studied (1986-2016), melanoma incidence increased by 108%, or about 2.7% per year.
“Given the increased incidence of melanoma throughout this period and the lack of stage migration, these data strongly suggest that the mortality decline is due to the extended survival associated with these [newer] treatments,” the investigators wrote.
This study was funded by NYU Langone. Two investigators disclosed potential conflicts of interest, including relationships with Bio-Rad Laboratories, Novartis, Merck, and several other companies.
SOURCE: Berk-Krauss J et al. Am J Public Health. 2020 Mar 19. doi: 10.2105/AJPH.2020.305567.
Recent advances in treatment appear to have reversed the course of melanoma mortality since 2013, according to data published in the American Journal of Public Health.
The U.S. death rate for melanoma, which had been rising at a rate of 0.22% a year for more than 2 decades, dropped by 17.9%, or 6.24% per year, during 2013-2016. That decline “coincides with the introduction of multiple new and efficacious treatments for metastatic melanoma,” such as BRAF inhibitors and immune checkpoint inhibitors, study author Juliana Berk-Krauss, MD, of the State University of New York Downstate Medical Center in Brooklyn and colleagues wrote.
The other possible explanation for the decline in deaths, “education and early detection resulting in migration toward earlier stage melanomas with a greater chance of surgical cure,” is unlikely, according to the investigators. That’s because the small decrease in median tumor thickness that occurred during 1989-2009 “is not associated with changes in prognosis.”
The investigators’ analysis encompassed data from the Surveillance, Epidemiology, and End Results registry recorded during 1986-2016. Nine registry areas were included (Atlanta, Connecticut, Detroit, Hawaii, Iowa, New Mexico, San Francisco-Oakland, Seattle-Puget Sound, and Utah), which covered about 9.4% of the U.S. population. The analysis was limited to the white population, which accounts for more than 90% of melanoma cases in the United States.
The data showed a slight decline in annual percent change in melanoma incidence, from 3.24% for 1986-2005 to 1.72% for 2006-2016. However, over the whole period studied (1986-2016), melanoma incidence increased by 108%, or about 2.7% per year.
“Given the increased incidence of melanoma throughout this period and the lack of stage migration, these data strongly suggest that the mortality decline is due to the extended survival associated with these [newer] treatments,” the investigators wrote.
This study was funded by NYU Langone. Two investigators disclosed potential conflicts of interest, including relationships with Bio-Rad Laboratories, Novartis, Merck, and several other companies.
SOURCE: Berk-Krauss J et al. Am J Public Health. 2020 Mar 19. doi: 10.2105/AJPH.2020.305567.
FROM THE AMERICAN JOURNAL OF PUBLIC HEALTH
Doublet may be beneficial in wild-type, advanced NSCLC
Combination apatinib and vinorelbine “may have potential” for treating patients with wild-type, advanced non–small cell lung cancer (NSCLC) who failed at least two prior lines of chemotherapy, according to researchers.
In a phase 2 trial, apatinib plus vinorelbine produced an overall response rate of 36.7% and a disease control rate of 76.7%. Nearly half of patients required dose reductions, and 17% discontinued treatment due to adverse events.
Xiangyu Zhang, MD, of Hunan Cancer Hospital in Changsha, China, and colleagues conducted this trial (NCT03652857) and detailed the results in JAMA Network Open.
The researchers noted that there is no standard treatment strategy for patients who have advanced NSCLC without actionable mutations and have failed two or more lines of chemotherapy. So the team tested apatinib plus vinorelbine in 30 such patients.
The patients’ median age was 63 years (range, 34-78 years), 60% were men, and 90% had stage IV disease. They had received a median of 2 (range, 2-5) prior lines of chemotherapy.
In this study, patients received apatinib at 500 mg once daily and vinorelbine at 60 mg/m2 once weekly. The dose of apatinib could be interrupted or reduced to manage adverse events. Patients could receive 250 mg or 500 mg on alternate days or 250 mg once daily. Patients were treated until they progressed, withdrew, or had unacceptable adverse events.
Results
Patients were treated for a median of 4 months (range, 1-22 months), and the median follow-up was 11 months (range, 4.5-14.1 months). Most patients (n = 25) continued treatment until they progressed, 17 were able to remain on the 500-mg dose of apatinib, 13 received the 250-mg dose of apatinib, and 5 patients discontinued treatment due to adverse events.
The overall response rate was 36.7%, and the disease control rate, defined as the proportion of patients with complete response, partial response, and stable disease, was 76.7%. There were no complete responses, 11 partial responses, 12 patients with stable disease, and 7 patients who progressed. Rates of response, disease control, and progression were similar whether patients received the 500-mg dose of apatinib or the 250-mg dose.
The median progression-free survival was 4.5 months, and the median overall survival was 10 months.
Hand-foot syndrome was the most common adverse event, with grade 1-2 hand-foot syndrome occurring in 13 patients (43%), grade 3 occurring in 5 patients (17%), and grade 4 occurring in 1 patient (3%).
The adverse events that led to treatment discontinuation were grade 3 weakness (n = 1), pleural effusion (n = 1), fungal infection (n = 1), and grade 3 hand-foot syndrome (n = 2). There were no fatal adverse events.
“” the researchers concluded. “Further evaluation of this combination in phase 3 trials is warranted.”
The current study was funded by grants from the National Natural Science Foundation of China and the Hunan Natural Science Foundation. The researchers disclosed no conflicts of interest.
SOURCE: Zhang X et al. JAMA Netw Open. 2020;3(3):e201226. doi: 10.1001/jamanetworkopen.2020.12.
Combination apatinib and vinorelbine “may have potential” for treating patients with wild-type, advanced non–small cell lung cancer (NSCLC) who failed at least two prior lines of chemotherapy, according to researchers.
In a phase 2 trial, apatinib plus vinorelbine produced an overall response rate of 36.7% and a disease control rate of 76.7%. Nearly half of patients required dose reductions, and 17% discontinued treatment due to adverse events.
Xiangyu Zhang, MD, of Hunan Cancer Hospital in Changsha, China, and colleagues conducted this trial (NCT03652857) and detailed the results in JAMA Network Open.
The researchers noted that there is no standard treatment strategy for patients who have advanced NSCLC without actionable mutations and have failed two or more lines of chemotherapy. So the team tested apatinib plus vinorelbine in 30 such patients.
The patients’ median age was 63 years (range, 34-78 years), 60% were men, and 90% had stage IV disease. They had received a median of 2 (range, 2-5) prior lines of chemotherapy.
In this study, patients received apatinib at 500 mg once daily and vinorelbine at 60 mg/m2 once weekly. The dose of apatinib could be interrupted or reduced to manage adverse events. Patients could receive 250 mg or 500 mg on alternate days or 250 mg once daily. Patients were treated until they progressed, withdrew, or had unacceptable adverse events.
Results
Patients were treated for a median of 4 months (range, 1-22 months), and the median follow-up was 11 months (range, 4.5-14.1 months). Most patients (n = 25) continued treatment until they progressed, 17 were able to remain on the 500-mg dose of apatinib, 13 received the 250-mg dose of apatinib, and 5 patients discontinued treatment due to adverse events.
The overall response rate was 36.7%, and the disease control rate, defined as the proportion of patients with complete response, partial response, and stable disease, was 76.7%. There were no complete responses, 11 partial responses, 12 patients with stable disease, and 7 patients who progressed. Rates of response, disease control, and progression were similar whether patients received the 500-mg dose of apatinib or the 250-mg dose.
The median progression-free survival was 4.5 months, and the median overall survival was 10 months.
Hand-foot syndrome was the most common adverse event, with grade 1-2 hand-foot syndrome occurring in 13 patients (43%), grade 3 occurring in 5 patients (17%), and grade 4 occurring in 1 patient (3%).
The adverse events that led to treatment discontinuation were grade 3 weakness (n = 1), pleural effusion (n = 1), fungal infection (n = 1), and grade 3 hand-foot syndrome (n = 2). There were no fatal adverse events.
“” the researchers concluded. “Further evaluation of this combination in phase 3 trials is warranted.”
The current study was funded by grants from the National Natural Science Foundation of China and the Hunan Natural Science Foundation. The researchers disclosed no conflicts of interest.
SOURCE: Zhang X et al. JAMA Netw Open. 2020;3(3):e201226. doi: 10.1001/jamanetworkopen.2020.12.
Combination apatinib and vinorelbine “may have potential” for treating patients with wild-type, advanced non–small cell lung cancer (NSCLC) who failed at least two prior lines of chemotherapy, according to researchers.
In a phase 2 trial, apatinib plus vinorelbine produced an overall response rate of 36.7% and a disease control rate of 76.7%. Nearly half of patients required dose reductions, and 17% discontinued treatment due to adverse events.
Xiangyu Zhang, MD, of Hunan Cancer Hospital in Changsha, China, and colleagues conducted this trial (NCT03652857) and detailed the results in JAMA Network Open.
The researchers noted that there is no standard treatment strategy for patients who have advanced NSCLC without actionable mutations and have failed two or more lines of chemotherapy. So the team tested apatinib plus vinorelbine in 30 such patients.
The patients’ median age was 63 years (range, 34-78 years), 60% were men, and 90% had stage IV disease. They had received a median of 2 (range, 2-5) prior lines of chemotherapy.
In this study, patients received apatinib at 500 mg once daily and vinorelbine at 60 mg/m2 once weekly. The dose of apatinib could be interrupted or reduced to manage adverse events. Patients could receive 250 mg or 500 mg on alternate days or 250 mg once daily. Patients were treated until they progressed, withdrew, or had unacceptable adverse events.
Results
Patients were treated for a median of 4 months (range, 1-22 months), and the median follow-up was 11 months (range, 4.5-14.1 months). Most patients (n = 25) continued treatment until they progressed, 17 were able to remain on the 500-mg dose of apatinib, 13 received the 250-mg dose of apatinib, and 5 patients discontinued treatment due to adverse events.
The overall response rate was 36.7%, and the disease control rate, defined as the proportion of patients with complete response, partial response, and stable disease, was 76.7%. There were no complete responses, 11 partial responses, 12 patients with stable disease, and 7 patients who progressed. Rates of response, disease control, and progression were similar whether patients received the 500-mg dose of apatinib or the 250-mg dose.
The median progression-free survival was 4.5 months, and the median overall survival was 10 months.
Hand-foot syndrome was the most common adverse event, with grade 1-2 hand-foot syndrome occurring in 13 patients (43%), grade 3 occurring in 5 patients (17%), and grade 4 occurring in 1 patient (3%).
The adverse events that led to treatment discontinuation were grade 3 weakness (n = 1), pleural effusion (n = 1), fungal infection (n = 1), and grade 3 hand-foot syndrome (n = 2). There were no fatal adverse events.
“” the researchers concluded. “Further evaluation of this combination in phase 3 trials is warranted.”
The current study was funded by grants from the National Natural Science Foundation of China and the Hunan Natural Science Foundation. The researchers disclosed no conflicts of interest.
SOURCE: Zhang X et al. JAMA Netw Open. 2020;3(3):e201226. doi: 10.1001/jamanetworkopen.2020.12.
FROM JAMA NETWORK OPEN
‘Like a coin flip’: Assay denies some cancer patients new drug
In December, at a major breast cancer conference, some attendees couldn’t find a seat and were told to leave an overcrowded session on immunotherapy for metastatic triple-negative breast cancer (TNBC). They refused, and pushed in to hear what was being said.
The crowd might have been surprised to learn that the main draw of the event, a successful new drug, was not all it might have been for women with the disease, being handicapped by a test that determines who is eligible for it.
“That room was overpacked ― there were five people deep against the wall. ... It was amazing,” said Janice Cowden of Bradenton, Florida. She attended the meeting, the San Antonio Breast Cancer Symposium, as a patient advocate.
Cowden lives with metastatic TNBC, which is known for poor prognoses, aggressiveness, and a lack of targeted treatment options. “Stage IV is a state of desperation. We just want something to work,” she said.
That’s why the conference room was packed – the session was focused on something that had been found to work – the immunotherapy atezolizumab (Tecentriq, Genentech/Roche).
Atezolizumab had recently been conditionally approved for first-line use in advanced TNBC, having been shown to significantly slow disease progression and, in some patients, to possibly improve survival. A pair of medical oncologists reviewed the clinical trial data during the session.
One important point from the trial data was that the benefit was greater in patients whose tumors had the biomarker PD-L1, and so the Food and Drug Administration approval of the drug specified that it should be used only in those patients.
The drug approval was accompanied by approval of a companion diagnostic test used to identify this PD-L1-positive subgroup of patients, the Ventana SP142 Assay (Roche Diagnostics).
At the meeting, pathologist David Rimm, MD, of Yale University, New Haven, Connecticut, discussed the biomarker PD-L1 and the test. Rimm had a subtle but unsettling message about the crucial test: that the SP142 diagnostic assay, when used by increasing numbers of pathologists, resulted in increasing rates of PD-L1 scores that were not concordant.
A related meeting poster, presented the next day with Rimm as senior author, was more explicit and concluded that “more than half of the pathologists in real-world situations may mis- assign” patient scores with SP142 (and another Roche assay) because of wide variability in readouts.
“They’ve made a test that is inadequate – it just doesn’t work. It’s like flipping a coin,” he told Medscape Medical News about Roche’s SP142 assay in everyday practice.
The general problem is not a new one – for some years there have been problems with the use of PD-L1 as a biomarker for immunotherapy and with assays for that biomarker, with many groups questioning both accuracy and reproducibility. But the problems with SP142 are “the most egregious,” said Rimm, who has served as a paid consultant to Roche Diagnostics in the past.
In clinical practice, Rimm’s overall message is that because of the difficulty of reading SP142 assay results, some TNBC patients who were PD-L1-positive would not get the drug, and some who were not positive would get the drug.
Patient advocate Cowden was not worried about overtreatment. She was concerned about patients who “might die without receiving a potentially life-extending treatment.”
In an essay in the Pathologist, Rimm echoed that sentiment about undertreatment (as well as overtreatment) with atezolizumab for breast cancer: “In all cases, the patients are the potential victims, but this appears to be completely under the radar of the hype surrounding this new drug.”
Roche Disputes Problems With Assay
Roche, manufacturer of both atezolizumab and the companion diagnostic test, disputes that there is a problem.
The FDA and multiple health authorities worldwide have approved atezolizumab and the companion diagnostic SP142 assay for use in TNBC, points out Eslie Dennis, MD, vice president of medical affairs at Roche Tissue Diagnostics.
“The role of a companion diagnostic assay is to discriminate between responders and non-responders for a specific therapeutic product in a specific indication, with a cut-off based on clinical outcomes,” she wrote in an email to Medscape Medical News.
Data from the pivotal IMpassion130 trial show that the assay was effective at that task. Among the 369 patients in the 902-patient trial whose tumors were ≥1% positive for PD-L1, those treated with atezolizumab (and nab-paclitaxel; n = 185) had a median progression-free survival (PFS) of 7.4 months, vs. 4.8 months among those treated with placebo (and nab-paclitaxel; n = 184) (P < .0001).
“Exploratory analysis showed no [PFS] benefit in PD-L1-negative patients as tested by the SP142 assay [in IMpassion130],” Dennis and three other physicians write in a reply to Rimm in a letter published in July 2019 in the Pathologist.
The same held true for overall survival in exploratory analysis – there was no benefit with atezolizumab among the PD-L1-negative patients, they write.
Notably, overall survival benefit for patients who were PD-L1 positive was about 10 months (at the first interim analysis; at the second analysis, the benefit dropped to 7 months and was not statistically significant).
But Rimm points out that the pivotal trial used only one pathologist in a central lab to determine PD-L1 status, who was undoubtedly an expert with the SP142 assay.
Further, Rimm observes that additional data submitted to the FDA to show that SP142 test results are reproducible outside of the pivotal trial setting were performed with only three pathologists and thus unsurprisingly yielded high rates of agreement – all above 90%.
The data from both of these circumstances are problematic, Rimm said, because in the real world, hundreds of pathologists will score the SP142 assay – all in the context of a busy day reading a variety of other tests for other diseases.
It’s one thing to get an FDA approval for an assay, and it’s another thing to be a reliable, well-functioning assay in the real world, he summarized.
Last year, Roberto Salgado, MD, PhD, a pathologist at the Université Libre de Bruxelles, Belgium, commented that “a positive phase III trial should not be taken as a guarantee that the assay used in the trial can be implemented in daily practice” in an opinion piece in the Pathologist.
SP142 Identifies the “Fewest Possible Patients”
The SP142 assay has been shown in multiple studies to have lower sensitivity for PD-L1 than other competing PD-L1 assays, said Rimm, citing examples such as a 2017 study and a 2018 study.
Angela DeMichele, MD, a medical oncologist at the University of Pennsylvania in Philadelphia, agreed and explained what that meant in practical terms for women whose tumors are tested with SP142. “It means that the test is going to identify the fewest possible PD-L1-positive patients [relative to the other available assays],” she said. “It [the SP142 assay] is far from a perfect test for this situation,” added DeMichele, an expert on biomarkers in breast cancer clinical trials.
She said that biomarker tests, like many products of science, tend to become dated with the passage of time, as more is learned about the target and new assays are developed. “Unfortunately, you can’t change assays midstream,” said DeMichele. She has received a grant from Roche and Stand Up to Cancer to study atezolizumab and another drug in a clinical trial among patients with metastatic TNBC who have minimal residual disease.
DeMichele also said that “David Rimm is one of the most knowledgeable people in the world about this issue.”
But DeMichelle also points out the practical: “We’re stuck as clinicians” because regulatory bodies and insurance companies only pay for atezolizumab when the SP142 assay indicates PD-L1 positivity. That’s not the case in Europe, where health authorities do not specify which PD-L1 assay is to be used with atezolizumab for breast cancer, pointed out Belgium’s Salgado last year.
Another Level of Complexity
At the immunotherapy session in San Antonio, Rimm discussed the results of a study of 68 TNBC archived cases in which specimens were stained with the SP142 assay at Yale and were distributed via electronic images to 19 pathologists at 14 institutions across the United States for PD-L1 scoring.
The study, coauthored by academics from Iowa, Texas A&M, UC San Diego, Mayo Clinic, Memorial Sloan Kettering, and others, used a novel method to determine the minimum number of evaluators needed to estimate “concordance” or agreement about a test result among large numbers of readers. The consensus/agreement was as high as 80% when eight or fewer pathologists’ scores were compared, but was as low as 40% when results from more than eight pathologists were included, said Rimm.
These are some of the data that led him to declare that using the assay is no better than flipping a coin.
Yes, PD-L1 testing is a challenge, and it has “introduced another level of complexity” for pathologists in reading assays, write experts Emina Torlakovic, MD, University of Saskatchewan, Canada, and Allen Gown, MD, PhenoPath Laboratories, Seattle, in response to Rimm last year.
But there is “poor” consensus among pathologists, they point out, “for many scoring systems that are still clinically applied (such as Gleason grading).” Consensus “improves with education and training,” the pair add. To that end, Roche has initiated a global training program for pathologists using the SP142 assay for TNBC. At San Antonio, Roche’s Dennis reported that among 432 pathologists from 58 countries, there was overall agreement of 98.2% in scoring assays.
Rimm commented that such high agreement would not be a surprise if testing took place soon after any such training program.
In an email to Medscape Medical News, Torlakovic encouraged pathologists who wish to practice their skill in interpreting assays, including SP142, to visit CBQAReadout.ca, a testing site. The site, which was founded by Torlakovic and may be one of a kind, offers CME credits and is sponsored by independent pathology organizations, such as CAP-ACP and the Saskatchewan Health Authority, as well as pharmaceutical companies, including Roche.
No Clue
Patient advocate Cowden believes the controversy about PD-L1 testing for atezolizumab is largely unknown among breast cancer patients. She learned about SP142 assay ambiguities in San Antonio, when the Florida Breast Cancer Foundation funded her trip to the meeting and the Alamo Breast Cancer Foundation asked her to write a report on Rimm’s presentation.
Cowden is a member of a Facebook group for stage IV TNBC, which has about 1500 members. She estimates that 75%-80% would be willing to try atezolizumab “no matter what,” meaning they don’t care about PD-L1 positivity being associated with efficacy.
The Facebook group members “know there is a test and if you are positive, there is an immunotherapy for their breast cancer,” said Cowden.
None know that women may be excluded from treatment because of shortcomings with the SP142 test. “They have no clue,” she said.
Rimm and DeMichele have financial ties to Roche and other companies. Dennis is an employee of Roche. Torlakovic has ties to multiple companies, including Roche, for whom she has acted as a paid consultant, grant recipient, and paid lecturer. Gown did not respond to a request for financial disclosures. Cowden reports no relevant financial relationships.
This article first appeared on Medscape.com.
In December, at a major breast cancer conference, some attendees couldn’t find a seat and were told to leave an overcrowded session on immunotherapy for metastatic triple-negative breast cancer (TNBC). They refused, and pushed in to hear what was being said.
The crowd might have been surprised to learn that the main draw of the event, a successful new drug, was not all it might have been for women with the disease, being handicapped by a test that determines who is eligible for it.
“That room was overpacked ― there were five people deep against the wall. ... It was amazing,” said Janice Cowden of Bradenton, Florida. She attended the meeting, the San Antonio Breast Cancer Symposium, as a patient advocate.
Cowden lives with metastatic TNBC, which is known for poor prognoses, aggressiveness, and a lack of targeted treatment options. “Stage IV is a state of desperation. We just want something to work,” she said.
That’s why the conference room was packed – the session was focused on something that had been found to work – the immunotherapy atezolizumab (Tecentriq, Genentech/Roche).
Atezolizumab had recently been conditionally approved for first-line use in advanced TNBC, having been shown to significantly slow disease progression and, in some patients, to possibly improve survival. A pair of medical oncologists reviewed the clinical trial data during the session.
One important point from the trial data was that the benefit was greater in patients whose tumors had the biomarker PD-L1, and so the Food and Drug Administration approval of the drug specified that it should be used only in those patients.
The drug approval was accompanied by approval of a companion diagnostic test used to identify this PD-L1-positive subgroup of patients, the Ventana SP142 Assay (Roche Diagnostics).
At the meeting, pathologist David Rimm, MD, of Yale University, New Haven, Connecticut, discussed the biomarker PD-L1 and the test. Rimm had a subtle but unsettling message about the crucial test: that the SP142 diagnostic assay, when used by increasing numbers of pathologists, resulted in increasing rates of PD-L1 scores that were not concordant.
A related meeting poster, presented the next day with Rimm as senior author, was more explicit and concluded that “more than half of the pathologists in real-world situations may mis- assign” patient scores with SP142 (and another Roche assay) because of wide variability in readouts.
“They’ve made a test that is inadequate – it just doesn’t work. It’s like flipping a coin,” he told Medscape Medical News about Roche’s SP142 assay in everyday practice.
The general problem is not a new one – for some years there have been problems with the use of PD-L1 as a biomarker for immunotherapy and with assays for that biomarker, with many groups questioning both accuracy and reproducibility. But the problems with SP142 are “the most egregious,” said Rimm, who has served as a paid consultant to Roche Diagnostics in the past.
In clinical practice, Rimm’s overall message is that because of the difficulty of reading SP142 assay results, some TNBC patients who were PD-L1-positive would not get the drug, and some who were not positive would get the drug.
Patient advocate Cowden was not worried about overtreatment. She was concerned about patients who “might die without receiving a potentially life-extending treatment.”
In an essay in the Pathologist, Rimm echoed that sentiment about undertreatment (as well as overtreatment) with atezolizumab for breast cancer: “In all cases, the patients are the potential victims, but this appears to be completely under the radar of the hype surrounding this new drug.”
Roche Disputes Problems With Assay
Roche, manufacturer of both atezolizumab and the companion diagnostic test, disputes that there is a problem.
The FDA and multiple health authorities worldwide have approved atezolizumab and the companion diagnostic SP142 assay for use in TNBC, points out Eslie Dennis, MD, vice president of medical affairs at Roche Tissue Diagnostics.
“The role of a companion diagnostic assay is to discriminate between responders and non-responders for a specific therapeutic product in a specific indication, with a cut-off based on clinical outcomes,” she wrote in an email to Medscape Medical News.
Data from the pivotal IMpassion130 trial show that the assay was effective at that task. Among the 369 patients in the 902-patient trial whose tumors were ≥1% positive for PD-L1, those treated with atezolizumab (and nab-paclitaxel; n = 185) had a median progression-free survival (PFS) of 7.4 months, vs. 4.8 months among those treated with placebo (and nab-paclitaxel; n = 184) (P < .0001).
“Exploratory analysis showed no [PFS] benefit in PD-L1-negative patients as tested by the SP142 assay [in IMpassion130],” Dennis and three other physicians write in a reply to Rimm in a letter published in July 2019 in the Pathologist.
The same held true for overall survival in exploratory analysis – there was no benefit with atezolizumab among the PD-L1-negative patients, they write.
Notably, overall survival benefit for patients who were PD-L1 positive was about 10 months (at the first interim analysis; at the second analysis, the benefit dropped to 7 months and was not statistically significant).
But Rimm points out that the pivotal trial used only one pathologist in a central lab to determine PD-L1 status, who was undoubtedly an expert with the SP142 assay.
Further, Rimm observes that additional data submitted to the FDA to show that SP142 test results are reproducible outside of the pivotal trial setting were performed with only three pathologists and thus unsurprisingly yielded high rates of agreement – all above 90%.
The data from both of these circumstances are problematic, Rimm said, because in the real world, hundreds of pathologists will score the SP142 assay – all in the context of a busy day reading a variety of other tests for other diseases.
It’s one thing to get an FDA approval for an assay, and it’s another thing to be a reliable, well-functioning assay in the real world, he summarized.
Last year, Roberto Salgado, MD, PhD, a pathologist at the Université Libre de Bruxelles, Belgium, commented that “a positive phase III trial should not be taken as a guarantee that the assay used in the trial can be implemented in daily practice” in an opinion piece in the Pathologist.
SP142 Identifies the “Fewest Possible Patients”
The SP142 assay has been shown in multiple studies to have lower sensitivity for PD-L1 than other competing PD-L1 assays, said Rimm, citing examples such as a 2017 study and a 2018 study.
Angela DeMichele, MD, a medical oncologist at the University of Pennsylvania in Philadelphia, agreed and explained what that meant in practical terms for women whose tumors are tested with SP142. “It means that the test is going to identify the fewest possible PD-L1-positive patients [relative to the other available assays],” she said. “It [the SP142 assay] is far from a perfect test for this situation,” added DeMichele, an expert on biomarkers in breast cancer clinical trials.
She said that biomarker tests, like many products of science, tend to become dated with the passage of time, as more is learned about the target and new assays are developed. “Unfortunately, you can’t change assays midstream,” said DeMichele. She has received a grant from Roche and Stand Up to Cancer to study atezolizumab and another drug in a clinical trial among patients with metastatic TNBC who have minimal residual disease.
DeMichele also said that “David Rimm is one of the most knowledgeable people in the world about this issue.”
But DeMichelle also points out the practical: “We’re stuck as clinicians” because regulatory bodies and insurance companies only pay for atezolizumab when the SP142 assay indicates PD-L1 positivity. That’s not the case in Europe, where health authorities do not specify which PD-L1 assay is to be used with atezolizumab for breast cancer, pointed out Belgium’s Salgado last year.
Another Level of Complexity
At the immunotherapy session in San Antonio, Rimm discussed the results of a study of 68 TNBC archived cases in which specimens were stained with the SP142 assay at Yale and were distributed via electronic images to 19 pathologists at 14 institutions across the United States for PD-L1 scoring.
The study, coauthored by academics from Iowa, Texas A&M, UC San Diego, Mayo Clinic, Memorial Sloan Kettering, and others, used a novel method to determine the minimum number of evaluators needed to estimate “concordance” or agreement about a test result among large numbers of readers. The consensus/agreement was as high as 80% when eight or fewer pathologists’ scores were compared, but was as low as 40% when results from more than eight pathologists were included, said Rimm.
These are some of the data that led him to declare that using the assay is no better than flipping a coin.
Yes, PD-L1 testing is a challenge, and it has “introduced another level of complexity” for pathologists in reading assays, write experts Emina Torlakovic, MD, University of Saskatchewan, Canada, and Allen Gown, MD, PhenoPath Laboratories, Seattle, in response to Rimm last year.
But there is “poor” consensus among pathologists, they point out, “for many scoring systems that are still clinically applied (such as Gleason grading).” Consensus “improves with education and training,” the pair add. To that end, Roche has initiated a global training program for pathologists using the SP142 assay for TNBC. At San Antonio, Roche’s Dennis reported that among 432 pathologists from 58 countries, there was overall agreement of 98.2% in scoring assays.
Rimm commented that such high agreement would not be a surprise if testing took place soon after any such training program.
In an email to Medscape Medical News, Torlakovic encouraged pathologists who wish to practice their skill in interpreting assays, including SP142, to visit CBQAReadout.ca, a testing site. The site, which was founded by Torlakovic and may be one of a kind, offers CME credits and is sponsored by independent pathology organizations, such as CAP-ACP and the Saskatchewan Health Authority, as well as pharmaceutical companies, including Roche.
No Clue
Patient advocate Cowden believes the controversy about PD-L1 testing for atezolizumab is largely unknown among breast cancer patients. She learned about SP142 assay ambiguities in San Antonio, when the Florida Breast Cancer Foundation funded her trip to the meeting and the Alamo Breast Cancer Foundation asked her to write a report on Rimm’s presentation.
Cowden is a member of a Facebook group for stage IV TNBC, which has about 1500 members. She estimates that 75%-80% would be willing to try atezolizumab “no matter what,” meaning they don’t care about PD-L1 positivity being associated with efficacy.
The Facebook group members “know there is a test and if you are positive, there is an immunotherapy for their breast cancer,” said Cowden.
None know that women may be excluded from treatment because of shortcomings with the SP142 test. “They have no clue,” she said.
Rimm and DeMichele have financial ties to Roche and other companies. Dennis is an employee of Roche. Torlakovic has ties to multiple companies, including Roche, for whom she has acted as a paid consultant, grant recipient, and paid lecturer. Gown did not respond to a request for financial disclosures. Cowden reports no relevant financial relationships.
This article first appeared on Medscape.com.
In December, at a major breast cancer conference, some attendees couldn’t find a seat and were told to leave an overcrowded session on immunotherapy for metastatic triple-negative breast cancer (TNBC). They refused, and pushed in to hear what was being said.
The crowd might have been surprised to learn that the main draw of the event, a successful new drug, was not all it might have been for women with the disease, being handicapped by a test that determines who is eligible for it.
“That room was overpacked ― there were five people deep against the wall. ... It was amazing,” said Janice Cowden of Bradenton, Florida. She attended the meeting, the San Antonio Breast Cancer Symposium, as a patient advocate.
Cowden lives with metastatic TNBC, which is known for poor prognoses, aggressiveness, and a lack of targeted treatment options. “Stage IV is a state of desperation. We just want something to work,” she said.
That’s why the conference room was packed – the session was focused on something that had been found to work – the immunotherapy atezolizumab (Tecentriq, Genentech/Roche).
Atezolizumab had recently been conditionally approved for first-line use in advanced TNBC, having been shown to significantly slow disease progression and, in some patients, to possibly improve survival. A pair of medical oncologists reviewed the clinical trial data during the session.
One important point from the trial data was that the benefit was greater in patients whose tumors had the biomarker PD-L1, and so the Food and Drug Administration approval of the drug specified that it should be used only in those patients.
The drug approval was accompanied by approval of a companion diagnostic test used to identify this PD-L1-positive subgroup of patients, the Ventana SP142 Assay (Roche Diagnostics).
At the meeting, pathologist David Rimm, MD, of Yale University, New Haven, Connecticut, discussed the biomarker PD-L1 and the test. Rimm had a subtle but unsettling message about the crucial test: that the SP142 diagnostic assay, when used by increasing numbers of pathologists, resulted in increasing rates of PD-L1 scores that were not concordant.
A related meeting poster, presented the next day with Rimm as senior author, was more explicit and concluded that “more than half of the pathologists in real-world situations may mis- assign” patient scores with SP142 (and another Roche assay) because of wide variability in readouts.
“They’ve made a test that is inadequate – it just doesn’t work. It’s like flipping a coin,” he told Medscape Medical News about Roche’s SP142 assay in everyday practice.
The general problem is not a new one – for some years there have been problems with the use of PD-L1 as a biomarker for immunotherapy and with assays for that biomarker, with many groups questioning both accuracy and reproducibility. But the problems with SP142 are “the most egregious,” said Rimm, who has served as a paid consultant to Roche Diagnostics in the past.
In clinical practice, Rimm’s overall message is that because of the difficulty of reading SP142 assay results, some TNBC patients who were PD-L1-positive would not get the drug, and some who were not positive would get the drug.
Patient advocate Cowden was not worried about overtreatment. She was concerned about patients who “might die without receiving a potentially life-extending treatment.”
In an essay in the Pathologist, Rimm echoed that sentiment about undertreatment (as well as overtreatment) with atezolizumab for breast cancer: “In all cases, the patients are the potential victims, but this appears to be completely under the radar of the hype surrounding this new drug.”
Roche Disputes Problems With Assay
Roche, manufacturer of both atezolizumab and the companion diagnostic test, disputes that there is a problem.
The FDA and multiple health authorities worldwide have approved atezolizumab and the companion diagnostic SP142 assay for use in TNBC, points out Eslie Dennis, MD, vice president of medical affairs at Roche Tissue Diagnostics.
“The role of a companion diagnostic assay is to discriminate between responders and non-responders for a specific therapeutic product in a specific indication, with a cut-off based on clinical outcomes,” she wrote in an email to Medscape Medical News.
Data from the pivotal IMpassion130 trial show that the assay was effective at that task. Among the 369 patients in the 902-patient trial whose tumors were ≥1% positive for PD-L1, those treated with atezolizumab (and nab-paclitaxel; n = 185) had a median progression-free survival (PFS) of 7.4 months, vs. 4.8 months among those treated with placebo (and nab-paclitaxel; n = 184) (P < .0001).
“Exploratory analysis showed no [PFS] benefit in PD-L1-negative patients as tested by the SP142 assay [in IMpassion130],” Dennis and three other physicians write in a reply to Rimm in a letter published in July 2019 in the Pathologist.
The same held true for overall survival in exploratory analysis – there was no benefit with atezolizumab among the PD-L1-negative patients, they write.
Notably, overall survival benefit for patients who were PD-L1 positive was about 10 months (at the first interim analysis; at the second analysis, the benefit dropped to 7 months and was not statistically significant).
But Rimm points out that the pivotal trial used only one pathologist in a central lab to determine PD-L1 status, who was undoubtedly an expert with the SP142 assay.
Further, Rimm observes that additional data submitted to the FDA to show that SP142 test results are reproducible outside of the pivotal trial setting were performed with only three pathologists and thus unsurprisingly yielded high rates of agreement – all above 90%.
The data from both of these circumstances are problematic, Rimm said, because in the real world, hundreds of pathologists will score the SP142 assay – all in the context of a busy day reading a variety of other tests for other diseases.
It’s one thing to get an FDA approval for an assay, and it’s another thing to be a reliable, well-functioning assay in the real world, he summarized.
Last year, Roberto Salgado, MD, PhD, a pathologist at the Université Libre de Bruxelles, Belgium, commented that “a positive phase III trial should not be taken as a guarantee that the assay used in the trial can be implemented in daily practice” in an opinion piece in the Pathologist.
SP142 Identifies the “Fewest Possible Patients”
The SP142 assay has been shown in multiple studies to have lower sensitivity for PD-L1 than other competing PD-L1 assays, said Rimm, citing examples such as a 2017 study and a 2018 study.
Angela DeMichele, MD, a medical oncologist at the University of Pennsylvania in Philadelphia, agreed and explained what that meant in practical terms for women whose tumors are tested with SP142. “It means that the test is going to identify the fewest possible PD-L1-positive patients [relative to the other available assays],” she said. “It [the SP142 assay] is far from a perfect test for this situation,” added DeMichele, an expert on biomarkers in breast cancer clinical trials.
She said that biomarker tests, like many products of science, tend to become dated with the passage of time, as more is learned about the target and new assays are developed. “Unfortunately, you can’t change assays midstream,” said DeMichele. She has received a grant from Roche and Stand Up to Cancer to study atezolizumab and another drug in a clinical trial among patients with metastatic TNBC who have minimal residual disease.
DeMichele also said that “David Rimm is one of the most knowledgeable people in the world about this issue.”
But DeMichelle also points out the practical: “We’re stuck as clinicians” because regulatory bodies and insurance companies only pay for atezolizumab when the SP142 assay indicates PD-L1 positivity. That’s not the case in Europe, where health authorities do not specify which PD-L1 assay is to be used with atezolizumab for breast cancer, pointed out Belgium’s Salgado last year.
Another Level of Complexity
At the immunotherapy session in San Antonio, Rimm discussed the results of a study of 68 TNBC archived cases in which specimens were stained with the SP142 assay at Yale and were distributed via electronic images to 19 pathologists at 14 institutions across the United States for PD-L1 scoring.
The study, coauthored by academics from Iowa, Texas A&M, UC San Diego, Mayo Clinic, Memorial Sloan Kettering, and others, used a novel method to determine the minimum number of evaluators needed to estimate “concordance” or agreement about a test result among large numbers of readers. The consensus/agreement was as high as 80% when eight or fewer pathologists’ scores were compared, but was as low as 40% when results from more than eight pathologists were included, said Rimm.
These are some of the data that led him to declare that using the assay is no better than flipping a coin.
Yes, PD-L1 testing is a challenge, and it has “introduced another level of complexity” for pathologists in reading assays, write experts Emina Torlakovic, MD, University of Saskatchewan, Canada, and Allen Gown, MD, PhenoPath Laboratories, Seattle, in response to Rimm last year.
But there is “poor” consensus among pathologists, they point out, “for many scoring systems that are still clinically applied (such as Gleason grading).” Consensus “improves with education and training,” the pair add. To that end, Roche has initiated a global training program for pathologists using the SP142 assay for TNBC. At San Antonio, Roche’s Dennis reported that among 432 pathologists from 58 countries, there was overall agreement of 98.2% in scoring assays.
Rimm commented that such high agreement would not be a surprise if testing took place soon after any such training program.
In an email to Medscape Medical News, Torlakovic encouraged pathologists who wish to practice their skill in interpreting assays, including SP142, to visit CBQAReadout.ca, a testing site. The site, which was founded by Torlakovic and may be one of a kind, offers CME credits and is sponsored by independent pathology organizations, such as CAP-ACP and the Saskatchewan Health Authority, as well as pharmaceutical companies, including Roche.
No Clue
Patient advocate Cowden believes the controversy about PD-L1 testing for atezolizumab is largely unknown among breast cancer patients. She learned about SP142 assay ambiguities in San Antonio, when the Florida Breast Cancer Foundation funded her trip to the meeting and the Alamo Breast Cancer Foundation asked her to write a report on Rimm’s presentation.
Cowden is a member of a Facebook group for stage IV TNBC, which has about 1500 members. She estimates that 75%-80% would be willing to try atezolizumab “no matter what,” meaning they don’t care about PD-L1 positivity being associated with efficacy.
The Facebook group members “know there is a test and if you are positive, there is an immunotherapy for their breast cancer,” said Cowden.
None know that women may be excluded from treatment because of shortcomings with the SP142 test. “They have no clue,” she said.
Rimm and DeMichele have financial ties to Roche and other companies. Dennis is an employee of Roche. Torlakovic has ties to multiple companies, including Roche, for whom she has acted as a paid consultant, grant recipient, and paid lecturer. Gown did not respond to a request for financial disclosures. Cowden reports no relevant financial relationships.
This article first appeared on Medscape.com.
ASCO guidelines take global view of late-stage colorectal cancer
Ideally, all cases of colorectal cancer would be detected at an early and curable stage, but, as new guidelines for late-stage colorectal cancer suggest, the world is far from perfect.
“Different regions of the world, both among and within countries, differ with respect to access to early detection,” the guideline authors wrote in JCO Global Oncology. “Many regions do not have mass or even opportunistic screening, and even within regions with mass screening, subpopulations may not have access to screening.”
The guidelines were developed by the American Society of Clinical Oncology’s Resource-Stratified Guidelines Advisory Group. Based on and adapted from existing guidelines developed by four international agencies, the ASCO guidelines take into account economic and social realities and offer recommendations for diagnosis, staging, and treatment by resource level: basic, limited, enhanced, or maximal.
“We made these guidelines to apply to countries or regions that have basic resources,” lead author E. Gabriela Chiorean, MD, of the University of Washington, Seattle, and the Seattle Cancer Care Alliance, said in an interview.
“We decided what should be the most basic resources – diagnostics, imaging, and treatment – that should be available to patients, and we make recommendations for the use of limited resources and supplies,” she added.
The guidelines pose and answer seven questions about optimal initial symptom management, diagnosis, and staging; optimal first and later lines of therapy; liver-directed therapy options for patients with late-stage colorectal cancer and liver metastases; and optimal on-treatment surveillance and follow-up strategies for patients treated for metastatic colorectal cancer.
For each question, the document offers guidance based on the availability of resources. As defined by the authors, the recommendations are stratified according to the following categories:
- Basic resources – “Core resources or fundamental services that are absolutely necessary for any cancer health care system to function.”
- Limited resources – “Second-tier resources or services that are intended to produce major improvements in outcome, such as increased survival and cost effectiveness, and are attainable with limited financial means and modest infrastructure.”
- Enhanced resources – “Third-tier resources or services that are optional but important; enhanced-level resources should produce further improvements in outcome and increase the number and quality of options and patient choice.”
- Maximal resources – “High-level/state-of-the art resources or services that may be used/available in some high-resource regions and/or may be recommended by high-resource setting guidelines that do not adapt to resource constraints but that nonetheless should be considered a lower priority than those resources or services listed in the other categories on the basis of extreme cost and/or impracticality for broad use in a resource-limited environment.”
The guidelines address common elements of symptom management for patients with acute disease, such as diagnosis involving the primary tumor, endoscopy when possible, and staging to include digital rectal exam and/or imaging when possible. The guidelines also include information tailored to resource level about chemotherapy and surgical resection.
“If, for example, a patient presents with bleeding and you suspect it to be of colorectal origin, we make recommendations that if the patient has symptoms of obstruction and bleeding and is resectable, they should undergo surgery, which should be available in countries of all resource levels,” Dr. Chiorean said.
The guidelines also recommend following the ASCO palliative care guidelines (J Clin Oncol. 2017 Jan;35[1]:96-112) for those patients who present with clinically unstable disease because of bowel obstruction, uncontrolled bleeding, or uncontrolled pain. Patients with clinically stable disease and ongoing bleeding from the primary tumor site are recommended to undergo transfusion and primary-site resection if only basic resources are available or transfusion plus multidisciplinary specialized evaluation when higher-level resources are available.
The ASCO guidelines are adapted from guidelines developed by Cancer Council Australia; the European Society for Medical Oncology; the National Institute for Health and Care Excellence, including separate recommendation for therapy combinations (https://www.nice.org.uk/guidance/ta212, https://www.nice.org.uk/guidance/ta439); and the National Comprehensive Cancer Network. Some of these guidelines have been updated since the creation of the ASCO guidelines.
ASCO funds the guideline development process. Dr. Chiorean and other authors disclosed relationships with multiple companies.
SOURCE: Chiorean EG et al. JCO Glob Oncol. 2020 Mar;6:414-38.
Ideally, all cases of colorectal cancer would be detected at an early and curable stage, but, as new guidelines for late-stage colorectal cancer suggest, the world is far from perfect.
“Different regions of the world, both among and within countries, differ with respect to access to early detection,” the guideline authors wrote in JCO Global Oncology. “Many regions do not have mass or even opportunistic screening, and even within regions with mass screening, subpopulations may not have access to screening.”
The guidelines were developed by the American Society of Clinical Oncology’s Resource-Stratified Guidelines Advisory Group. Based on and adapted from existing guidelines developed by four international agencies, the ASCO guidelines take into account economic and social realities and offer recommendations for diagnosis, staging, and treatment by resource level: basic, limited, enhanced, or maximal.
“We made these guidelines to apply to countries or regions that have basic resources,” lead author E. Gabriela Chiorean, MD, of the University of Washington, Seattle, and the Seattle Cancer Care Alliance, said in an interview.
“We decided what should be the most basic resources – diagnostics, imaging, and treatment – that should be available to patients, and we make recommendations for the use of limited resources and supplies,” she added.
The guidelines pose and answer seven questions about optimal initial symptom management, diagnosis, and staging; optimal first and later lines of therapy; liver-directed therapy options for patients with late-stage colorectal cancer and liver metastases; and optimal on-treatment surveillance and follow-up strategies for patients treated for metastatic colorectal cancer.
For each question, the document offers guidance based on the availability of resources. As defined by the authors, the recommendations are stratified according to the following categories:
- Basic resources – “Core resources or fundamental services that are absolutely necessary for any cancer health care system to function.”
- Limited resources – “Second-tier resources or services that are intended to produce major improvements in outcome, such as increased survival and cost effectiveness, and are attainable with limited financial means and modest infrastructure.”
- Enhanced resources – “Third-tier resources or services that are optional but important; enhanced-level resources should produce further improvements in outcome and increase the number and quality of options and patient choice.”
- Maximal resources – “High-level/state-of-the art resources or services that may be used/available in some high-resource regions and/or may be recommended by high-resource setting guidelines that do not adapt to resource constraints but that nonetheless should be considered a lower priority than those resources or services listed in the other categories on the basis of extreme cost and/or impracticality for broad use in a resource-limited environment.”
The guidelines address common elements of symptom management for patients with acute disease, such as diagnosis involving the primary tumor, endoscopy when possible, and staging to include digital rectal exam and/or imaging when possible. The guidelines also include information tailored to resource level about chemotherapy and surgical resection.
“If, for example, a patient presents with bleeding and you suspect it to be of colorectal origin, we make recommendations that if the patient has symptoms of obstruction and bleeding and is resectable, they should undergo surgery, which should be available in countries of all resource levels,” Dr. Chiorean said.
The guidelines also recommend following the ASCO palliative care guidelines (J Clin Oncol. 2017 Jan;35[1]:96-112) for those patients who present with clinically unstable disease because of bowel obstruction, uncontrolled bleeding, or uncontrolled pain. Patients with clinically stable disease and ongoing bleeding from the primary tumor site are recommended to undergo transfusion and primary-site resection if only basic resources are available or transfusion plus multidisciplinary specialized evaluation when higher-level resources are available.
The ASCO guidelines are adapted from guidelines developed by Cancer Council Australia; the European Society for Medical Oncology; the National Institute for Health and Care Excellence, including separate recommendation for therapy combinations (https://www.nice.org.uk/guidance/ta212, https://www.nice.org.uk/guidance/ta439); and the National Comprehensive Cancer Network. Some of these guidelines have been updated since the creation of the ASCO guidelines.
ASCO funds the guideline development process. Dr. Chiorean and other authors disclosed relationships with multiple companies.
SOURCE: Chiorean EG et al. JCO Glob Oncol. 2020 Mar;6:414-38.
Ideally, all cases of colorectal cancer would be detected at an early and curable stage, but, as new guidelines for late-stage colorectal cancer suggest, the world is far from perfect.
“Different regions of the world, both among and within countries, differ with respect to access to early detection,” the guideline authors wrote in JCO Global Oncology. “Many regions do not have mass or even opportunistic screening, and even within regions with mass screening, subpopulations may not have access to screening.”
The guidelines were developed by the American Society of Clinical Oncology’s Resource-Stratified Guidelines Advisory Group. Based on and adapted from existing guidelines developed by four international agencies, the ASCO guidelines take into account economic and social realities and offer recommendations for diagnosis, staging, and treatment by resource level: basic, limited, enhanced, or maximal.
“We made these guidelines to apply to countries or regions that have basic resources,” lead author E. Gabriela Chiorean, MD, of the University of Washington, Seattle, and the Seattle Cancer Care Alliance, said in an interview.
“We decided what should be the most basic resources – diagnostics, imaging, and treatment – that should be available to patients, and we make recommendations for the use of limited resources and supplies,” she added.
The guidelines pose and answer seven questions about optimal initial symptom management, diagnosis, and staging; optimal first and later lines of therapy; liver-directed therapy options for patients with late-stage colorectal cancer and liver metastases; and optimal on-treatment surveillance and follow-up strategies for patients treated for metastatic colorectal cancer.
For each question, the document offers guidance based on the availability of resources. As defined by the authors, the recommendations are stratified according to the following categories:
- Basic resources – “Core resources or fundamental services that are absolutely necessary for any cancer health care system to function.”
- Limited resources – “Second-tier resources or services that are intended to produce major improvements in outcome, such as increased survival and cost effectiveness, and are attainable with limited financial means and modest infrastructure.”
- Enhanced resources – “Third-tier resources or services that are optional but important; enhanced-level resources should produce further improvements in outcome and increase the number and quality of options and patient choice.”
- Maximal resources – “High-level/state-of-the art resources or services that may be used/available in some high-resource regions and/or may be recommended by high-resource setting guidelines that do not adapt to resource constraints but that nonetheless should be considered a lower priority than those resources or services listed in the other categories on the basis of extreme cost and/or impracticality for broad use in a resource-limited environment.”
The guidelines address common elements of symptom management for patients with acute disease, such as diagnosis involving the primary tumor, endoscopy when possible, and staging to include digital rectal exam and/or imaging when possible. The guidelines also include information tailored to resource level about chemotherapy and surgical resection.
“If, for example, a patient presents with bleeding and you suspect it to be of colorectal origin, we make recommendations that if the patient has symptoms of obstruction and bleeding and is resectable, they should undergo surgery, which should be available in countries of all resource levels,” Dr. Chiorean said.
The guidelines also recommend following the ASCO palliative care guidelines (J Clin Oncol. 2017 Jan;35[1]:96-112) for those patients who present with clinically unstable disease because of bowel obstruction, uncontrolled bleeding, or uncontrolled pain. Patients with clinically stable disease and ongoing bleeding from the primary tumor site are recommended to undergo transfusion and primary-site resection if only basic resources are available or transfusion plus multidisciplinary specialized evaluation when higher-level resources are available.
The ASCO guidelines are adapted from guidelines developed by Cancer Council Australia; the European Society for Medical Oncology; the National Institute for Health and Care Excellence, including separate recommendation for therapy combinations (https://www.nice.org.uk/guidance/ta212, https://www.nice.org.uk/guidance/ta439); and the National Comprehensive Cancer Network. Some of these guidelines have been updated since the creation of the ASCO guidelines.
ASCO funds the guideline development process. Dr. Chiorean and other authors disclosed relationships with multiple companies.
SOURCE: Chiorean EG et al. JCO Glob Oncol. 2020 Mar;6:414-38.
FROM JCO GLOBAL ONCOLOGY
COVID-19: Older patients with cancer especially vulnerable
For oncologists and other clinicians caring for patients with cancer, the COVID-19 pandemic represents a dynamic clinical challenge that is changing daily and that can feel overwhelming at times, say experts.
“Oncology clinicians are well versed in caring for immunosuppressed patients with cancer, of all ages,” Merry-Jennifer Markham, MD, interim chief of the Division of Hematology and Oncology at the University of Florida Health, Gainesville, told Medscape Medical News.
However, she emphasized that, during this COVID-19 outbreak, “we must be especially diligent about screening for symptoms and exposure, and we must recognize that our older patients with cancer may be especially vulnerable.”
Patients with cancer who are in active treatment are immunosuppressed and are more susceptible to infection and to complications from infection, Markham pointed out. “While we don’t yet have much data on how COVID-19 impacts patients with cancer, I have to suspect that patients undergoing active cancer treatment may be especially vulnerable to the more severe illness associated with COVID-19,” she said.
Indeed, a recent report from China that was published in the Lancet Oncology supports this. The authors suggest that patients with cancer are at higher risk for COVID-19 and have a worse prognosis if they become infected than do those without cancer.
Commonsense rules
Commonsense rules apply for all patients with cancer, regardless of age, said Markham. Measures include thorough handwashing, staying home when sick, and avoiding sick contacts.
Markham, who acts as an expert spokesperson for the American Society of Clinical Oncology, provides information on what patients with cancer need to know about COVID-19 at Cancer.net, the society’s website for patients with cancer.
“Unfortunately, this outbreak of COVID-19 is happening rapidly and in real time,” Markham noted. “The entire medical community is learning as we go, rather than having the luxury of years of evidence-based literature to guide us.”
Another expert agrees. “Unfortunately, there are not a lot of data on how COVID-19 affects cancer patients,” Cardinale Smith, MD, PhD, director of Quality for Cancer Services in the Mount Sinai Health System, New York City, said in an interview.
“We need to minimize the risk for patients and minimize our own exposure by treating this situation like we would a really bad flu season,” Smith told Medscape Medical News. “Some patients have had a bad outcome, but the vast majority do not. The best we can do is stay calm and focused.”
At Mount Sinai, for patients with cancer, routine, nonurgent appointments are being rescheduled for May, Smith said. Those in active treatment are screened by telephone 24 to 48 hours before arrival, after which they undergo a full risk assessment in an isolation room. Those with a respiratory infection are given a mask.
“Patients are very anxious and worried about COVID-19,” said Smith, who has young children and an elderly parent at home. “We don’t have all the answers, and this can heighten anxiety.”
To help allay fears, social workers are asking patients with cancer who express anxiety to discuss their concerns and provide information. A one-page handout on both flu and COVID-10 is available in the waiting room.
The Web portal MyChart gives patients access to updated information on COVID-19 precautions and provides links to the hospital website and to the US Centers for Disease Control and Prevention. Patients who are not feeling well can speak to someone or get answers if they have additional questions.
When counseling patients, Smith advises them to use “an abundance of caution” and to be creative in efforts to minimize risk. “My suggestion is to use FaceTime and Skype to connect and communicate with your community,” she said.
Some churches are conducting services via teleconferencing to minimize risk, and seniors’ centers that offer yoga and other classes are also beginning to provide services virtually, she pointed out.
Data from China
A report published February 14 in the Lancet Oncology appears to be the first analysis in the literature to focus on COVID-19 in patients with cancer.
“Patients with cancer are more susceptible to infection than individuals without cancer because of their systemic immunosuppressive state caused by the malignancy and anticancer treatments, such as chemotherapy or surgery,” write the authors, led by Wenhua Liang, MD, of Guangzhou Medical University. However, in correspondence published in the Lancet Oncology, other experts in China question some of Liang’s and colleagues’ findings.
The report by Liang and colleagues concerns a prospective cohort of 1590 patients with COVID-19.
There were 2007 laboratory-confirmed cases of COVID-19 among patients admitted to 575 hospitals throughout China as of January 31. Of those cases, 417 were excluded from the analysis because of insufficient information regarding disease history.
The team reports that of 18 patients with cancer and COVID-19, 39% were at significantly higher risk for “severe events.” By comparison, of 1572 patients with COVID-19 who did not have cancer, 8% were at significantly higher risk (P = .0003). These events included rapid clinical deterioration that required admission to intensive care; invasive ventilation; or death.
Patients with cancer experienced a much more rapid deterioration in clinical status than did those without cancer. The median time to severe events was 13 days, vs 43 days (hazard ratio [HR] adjusted for age, 3.56; P < .0001).
The analysis also shows that patients who underwent chemotherapy or surgery in the past month had a 75% risk of experiencing clinically severe events, compared with a 43% risk for those who had not received recent treatment.
After adjusting for other risk factors, including age and smoking history, older age was the only risk factor for severe events (odds ratio [OR], 1.43; 95% confidence interval [CI], 0.97 – 2.12; P = .072), the study authors say.
Patients with lung cancer did not have a higher probability of severe events compared with patients with other cancer types (20% vs 62%, respectively; P = .294).
Liang and colleagues conclude that these findings provide “a timely reminder to physicians that more intensive attention should be paid to patients with cancer, in case of rapid deterioration.”
The team also proposes three strategies for managing patients with cancer who are at risk for COVID-19 or any other severe infectious disease. They recommend that intentional postponement of adjuvant chemotherapy or elective surgery be considered for patients with stable cancer who live in areas where disease is endemic. Stronger “personal protection provisions” could also be made for patients with cancer or for cancer survivors. Lastly, for patients with cancer who have COVID-19, especially those who are older or who have comorbidities, more intensive surveillance or treatment should be considered.
However, in comments in the Lancet Oncology, other authors in China say these findings should be interpreted with caution.
One group suggests that the increased susceptibility to COVID-19 in patients with cancer could be the result of higher rates of smoking compared with patients who did not have cancer. “Overall, current evidence remains insufficient to explain a conclusive association between cancer and COVID-19,” say Huahao Shen, PhD, of Zhejiang University School of Medicine, Hangzhou, Zhejiang, and colleagues.
Another group suggests that the significantly higher median age of patients with cancer compared with noncancer patients (63 years vs 49 years) may have contributed to poor prognosis.
These authors, led by Li Zhang, MD, PhD, and Hanping Wang, MD, of Peking Union Medical College and the Chinese Academy of Medical Sciences, Beijing, emphasize that patients with cancer need online medical counseling and that critical cases need to be identified and treated.
“In endemic areas outside Wuhan, decisions on whether or not to postpone cancer treatment need to made on a patient-by-patient basis and according to the risk to the patient and the prevailing situation because delays could lead to tumor progression and ultimately poorer outcomes,” they write.
The study was funded by the China National Science Foundation and the Key Project of Guangzhou Scientific Research Project. Liang and coauthors, Shen and coauthors, Zhang, Wang, and Smith have disclosed no relevant financial relationships. Markham has relationships with Aduro Biotech, Lilly, Tesaro, Novartis, and VBL Therapeutics.
This article first appeared on Medscape.com.
For oncologists and other clinicians caring for patients with cancer, the COVID-19 pandemic represents a dynamic clinical challenge that is changing daily and that can feel overwhelming at times, say experts.
“Oncology clinicians are well versed in caring for immunosuppressed patients with cancer, of all ages,” Merry-Jennifer Markham, MD, interim chief of the Division of Hematology and Oncology at the University of Florida Health, Gainesville, told Medscape Medical News.
However, she emphasized that, during this COVID-19 outbreak, “we must be especially diligent about screening for symptoms and exposure, and we must recognize that our older patients with cancer may be especially vulnerable.”
Patients with cancer who are in active treatment are immunosuppressed and are more susceptible to infection and to complications from infection, Markham pointed out. “While we don’t yet have much data on how COVID-19 impacts patients with cancer, I have to suspect that patients undergoing active cancer treatment may be especially vulnerable to the more severe illness associated with COVID-19,” she said.
Indeed, a recent report from China that was published in the Lancet Oncology supports this. The authors suggest that patients with cancer are at higher risk for COVID-19 and have a worse prognosis if they become infected than do those without cancer.
Commonsense rules
Commonsense rules apply for all patients with cancer, regardless of age, said Markham. Measures include thorough handwashing, staying home when sick, and avoiding sick contacts.
Markham, who acts as an expert spokesperson for the American Society of Clinical Oncology, provides information on what patients with cancer need to know about COVID-19 at Cancer.net, the society’s website for patients with cancer.
“Unfortunately, this outbreak of COVID-19 is happening rapidly and in real time,” Markham noted. “The entire medical community is learning as we go, rather than having the luxury of years of evidence-based literature to guide us.”
Another expert agrees. “Unfortunately, there are not a lot of data on how COVID-19 affects cancer patients,” Cardinale Smith, MD, PhD, director of Quality for Cancer Services in the Mount Sinai Health System, New York City, said in an interview.
“We need to minimize the risk for patients and minimize our own exposure by treating this situation like we would a really bad flu season,” Smith told Medscape Medical News. “Some patients have had a bad outcome, but the vast majority do not. The best we can do is stay calm and focused.”
At Mount Sinai, for patients with cancer, routine, nonurgent appointments are being rescheduled for May, Smith said. Those in active treatment are screened by telephone 24 to 48 hours before arrival, after which they undergo a full risk assessment in an isolation room. Those with a respiratory infection are given a mask.
“Patients are very anxious and worried about COVID-19,” said Smith, who has young children and an elderly parent at home. “We don’t have all the answers, and this can heighten anxiety.”
To help allay fears, social workers are asking patients with cancer who express anxiety to discuss their concerns and provide information. A one-page handout on both flu and COVID-10 is available in the waiting room.
The Web portal MyChart gives patients access to updated information on COVID-19 precautions and provides links to the hospital website and to the US Centers for Disease Control and Prevention. Patients who are not feeling well can speak to someone or get answers if they have additional questions.
When counseling patients, Smith advises them to use “an abundance of caution” and to be creative in efforts to minimize risk. “My suggestion is to use FaceTime and Skype to connect and communicate with your community,” she said.
Some churches are conducting services via teleconferencing to minimize risk, and seniors’ centers that offer yoga and other classes are also beginning to provide services virtually, she pointed out.
Data from China
A report published February 14 in the Lancet Oncology appears to be the first analysis in the literature to focus on COVID-19 in patients with cancer.
“Patients with cancer are more susceptible to infection than individuals without cancer because of their systemic immunosuppressive state caused by the malignancy and anticancer treatments, such as chemotherapy or surgery,” write the authors, led by Wenhua Liang, MD, of Guangzhou Medical University. However, in correspondence published in the Lancet Oncology, other experts in China question some of Liang’s and colleagues’ findings.
The report by Liang and colleagues concerns a prospective cohort of 1590 patients with COVID-19.
There were 2007 laboratory-confirmed cases of COVID-19 among patients admitted to 575 hospitals throughout China as of January 31. Of those cases, 417 were excluded from the analysis because of insufficient information regarding disease history.
The team reports that of 18 patients with cancer and COVID-19, 39% were at significantly higher risk for “severe events.” By comparison, of 1572 patients with COVID-19 who did not have cancer, 8% were at significantly higher risk (P = .0003). These events included rapid clinical deterioration that required admission to intensive care; invasive ventilation; or death.
Patients with cancer experienced a much more rapid deterioration in clinical status than did those without cancer. The median time to severe events was 13 days, vs 43 days (hazard ratio [HR] adjusted for age, 3.56; P < .0001).
The analysis also shows that patients who underwent chemotherapy or surgery in the past month had a 75% risk of experiencing clinically severe events, compared with a 43% risk for those who had not received recent treatment.
After adjusting for other risk factors, including age and smoking history, older age was the only risk factor for severe events (odds ratio [OR], 1.43; 95% confidence interval [CI], 0.97 – 2.12; P = .072), the study authors say.
Patients with lung cancer did not have a higher probability of severe events compared with patients with other cancer types (20% vs 62%, respectively; P = .294).
Liang and colleagues conclude that these findings provide “a timely reminder to physicians that more intensive attention should be paid to patients with cancer, in case of rapid deterioration.”
The team also proposes three strategies for managing patients with cancer who are at risk for COVID-19 or any other severe infectious disease. They recommend that intentional postponement of adjuvant chemotherapy or elective surgery be considered for patients with stable cancer who live in areas where disease is endemic. Stronger “personal protection provisions” could also be made for patients with cancer or for cancer survivors. Lastly, for patients with cancer who have COVID-19, especially those who are older or who have comorbidities, more intensive surveillance or treatment should be considered.
However, in comments in the Lancet Oncology, other authors in China say these findings should be interpreted with caution.
One group suggests that the increased susceptibility to COVID-19 in patients with cancer could be the result of higher rates of smoking compared with patients who did not have cancer. “Overall, current evidence remains insufficient to explain a conclusive association between cancer and COVID-19,” say Huahao Shen, PhD, of Zhejiang University School of Medicine, Hangzhou, Zhejiang, and colleagues.
Another group suggests that the significantly higher median age of patients with cancer compared with noncancer patients (63 years vs 49 years) may have contributed to poor prognosis.
These authors, led by Li Zhang, MD, PhD, and Hanping Wang, MD, of Peking Union Medical College and the Chinese Academy of Medical Sciences, Beijing, emphasize that patients with cancer need online medical counseling and that critical cases need to be identified and treated.
“In endemic areas outside Wuhan, decisions on whether or not to postpone cancer treatment need to made on a patient-by-patient basis and according to the risk to the patient and the prevailing situation because delays could lead to tumor progression and ultimately poorer outcomes,” they write.
The study was funded by the China National Science Foundation and the Key Project of Guangzhou Scientific Research Project. Liang and coauthors, Shen and coauthors, Zhang, Wang, and Smith have disclosed no relevant financial relationships. Markham has relationships with Aduro Biotech, Lilly, Tesaro, Novartis, and VBL Therapeutics.
This article first appeared on Medscape.com.
For oncologists and other clinicians caring for patients with cancer, the COVID-19 pandemic represents a dynamic clinical challenge that is changing daily and that can feel overwhelming at times, say experts.
“Oncology clinicians are well versed in caring for immunosuppressed patients with cancer, of all ages,” Merry-Jennifer Markham, MD, interim chief of the Division of Hematology and Oncology at the University of Florida Health, Gainesville, told Medscape Medical News.
However, she emphasized that, during this COVID-19 outbreak, “we must be especially diligent about screening for symptoms and exposure, and we must recognize that our older patients with cancer may be especially vulnerable.”
Patients with cancer who are in active treatment are immunosuppressed and are more susceptible to infection and to complications from infection, Markham pointed out. “While we don’t yet have much data on how COVID-19 impacts patients with cancer, I have to suspect that patients undergoing active cancer treatment may be especially vulnerable to the more severe illness associated with COVID-19,” she said.
Indeed, a recent report from China that was published in the Lancet Oncology supports this. The authors suggest that patients with cancer are at higher risk for COVID-19 and have a worse prognosis if they become infected than do those without cancer.
Commonsense rules
Commonsense rules apply for all patients with cancer, regardless of age, said Markham. Measures include thorough handwashing, staying home when sick, and avoiding sick contacts.
Markham, who acts as an expert spokesperson for the American Society of Clinical Oncology, provides information on what patients with cancer need to know about COVID-19 at Cancer.net, the society’s website for patients with cancer.
“Unfortunately, this outbreak of COVID-19 is happening rapidly and in real time,” Markham noted. “The entire medical community is learning as we go, rather than having the luxury of years of evidence-based literature to guide us.”
Another expert agrees. “Unfortunately, there are not a lot of data on how COVID-19 affects cancer patients,” Cardinale Smith, MD, PhD, director of Quality for Cancer Services in the Mount Sinai Health System, New York City, said in an interview.
“We need to minimize the risk for patients and minimize our own exposure by treating this situation like we would a really bad flu season,” Smith told Medscape Medical News. “Some patients have had a bad outcome, but the vast majority do not. The best we can do is stay calm and focused.”
At Mount Sinai, for patients with cancer, routine, nonurgent appointments are being rescheduled for May, Smith said. Those in active treatment are screened by telephone 24 to 48 hours before arrival, after which they undergo a full risk assessment in an isolation room. Those with a respiratory infection are given a mask.
“Patients are very anxious and worried about COVID-19,” said Smith, who has young children and an elderly parent at home. “We don’t have all the answers, and this can heighten anxiety.”
To help allay fears, social workers are asking patients with cancer who express anxiety to discuss their concerns and provide information. A one-page handout on both flu and COVID-10 is available in the waiting room.
The Web portal MyChart gives patients access to updated information on COVID-19 precautions and provides links to the hospital website and to the US Centers for Disease Control and Prevention. Patients who are not feeling well can speak to someone or get answers if they have additional questions.
When counseling patients, Smith advises them to use “an abundance of caution” and to be creative in efforts to minimize risk. “My suggestion is to use FaceTime and Skype to connect and communicate with your community,” she said.
Some churches are conducting services via teleconferencing to minimize risk, and seniors’ centers that offer yoga and other classes are also beginning to provide services virtually, she pointed out.
Data from China
A report published February 14 in the Lancet Oncology appears to be the first analysis in the literature to focus on COVID-19 in patients with cancer.
“Patients with cancer are more susceptible to infection than individuals without cancer because of their systemic immunosuppressive state caused by the malignancy and anticancer treatments, such as chemotherapy or surgery,” write the authors, led by Wenhua Liang, MD, of Guangzhou Medical University. However, in correspondence published in the Lancet Oncology, other experts in China question some of Liang’s and colleagues’ findings.
The report by Liang and colleagues concerns a prospective cohort of 1590 patients with COVID-19.
There were 2007 laboratory-confirmed cases of COVID-19 among patients admitted to 575 hospitals throughout China as of January 31. Of those cases, 417 were excluded from the analysis because of insufficient information regarding disease history.
The team reports that of 18 patients with cancer and COVID-19, 39% were at significantly higher risk for “severe events.” By comparison, of 1572 patients with COVID-19 who did not have cancer, 8% were at significantly higher risk (P = .0003). These events included rapid clinical deterioration that required admission to intensive care; invasive ventilation; or death.
Patients with cancer experienced a much more rapid deterioration in clinical status than did those without cancer. The median time to severe events was 13 days, vs 43 days (hazard ratio [HR] adjusted for age, 3.56; P < .0001).
The analysis also shows that patients who underwent chemotherapy or surgery in the past month had a 75% risk of experiencing clinically severe events, compared with a 43% risk for those who had not received recent treatment.
After adjusting for other risk factors, including age and smoking history, older age was the only risk factor for severe events (odds ratio [OR], 1.43; 95% confidence interval [CI], 0.97 – 2.12; P = .072), the study authors say.
Patients with lung cancer did not have a higher probability of severe events compared with patients with other cancer types (20% vs 62%, respectively; P = .294).
Liang and colleagues conclude that these findings provide “a timely reminder to physicians that more intensive attention should be paid to patients with cancer, in case of rapid deterioration.”
The team also proposes three strategies for managing patients with cancer who are at risk for COVID-19 or any other severe infectious disease. They recommend that intentional postponement of adjuvant chemotherapy or elective surgery be considered for patients with stable cancer who live in areas where disease is endemic. Stronger “personal protection provisions” could also be made for patients with cancer or for cancer survivors. Lastly, for patients with cancer who have COVID-19, especially those who are older or who have comorbidities, more intensive surveillance or treatment should be considered.
However, in comments in the Lancet Oncology, other authors in China say these findings should be interpreted with caution.
One group suggests that the increased susceptibility to COVID-19 in patients with cancer could be the result of higher rates of smoking compared with patients who did not have cancer. “Overall, current evidence remains insufficient to explain a conclusive association between cancer and COVID-19,” say Huahao Shen, PhD, of Zhejiang University School of Medicine, Hangzhou, Zhejiang, and colleagues.
Another group suggests that the significantly higher median age of patients with cancer compared with noncancer patients (63 years vs 49 years) may have contributed to poor prognosis.
These authors, led by Li Zhang, MD, PhD, and Hanping Wang, MD, of Peking Union Medical College and the Chinese Academy of Medical Sciences, Beijing, emphasize that patients with cancer need online medical counseling and that critical cases need to be identified and treated.
“In endemic areas outside Wuhan, decisions on whether or not to postpone cancer treatment need to made on a patient-by-patient basis and according to the risk to the patient and the prevailing situation because delays could lead to tumor progression and ultimately poorer outcomes,” they write.
The study was funded by the China National Science Foundation and the Key Project of Guangzhou Scientific Research Project. Liang and coauthors, Shen and coauthors, Zhang, Wang, and Smith have disclosed no relevant financial relationships. Markham has relationships with Aduro Biotech, Lilly, Tesaro, Novartis, and VBL Therapeutics.
This article first appeared on Medscape.com.
Patients accept artificial intelligence in skin cancer screening
In a small survey, 75% of dermatology patients said they would recommend the use of artificial intelligence (AI) for skin cancer screening to friends and family members, but 94% emphasized the need for symbiosis between doctors, patients, and AI.
AI under investigation in dermatology includes both direct-to-patient and clinician decision-support AI tools for skin cancer screening, but patients’ perceptions of AI in health care remains unclear, Caroline A. Nelson, MD, of Yale University in New Haven, Conn., and colleagues wrote in JAMA Dermatology.
“We sought to elucidate perceived benefits and risks, strengths and weaknesses, implementation, response to conflict between human and AI clinical decision making, and recommendation for or against AI,” the researchers wrote.
They identified 48 patients seen from May 6, 2019, to July 8, 2019, at general dermatology clinics and melanoma clinics. This included 16 patients with a history of melanoma, 16 with a history of nonmelanoma skin cancer, and 16 with no history of skin cancer. The average age of the patients was 53.3 years, 54% were women, and 94% were white.
The researchers interviewed 24 patients about a direct-to-patient AI tool and 24 patients about a clinician decision-support AI tool.
Overall, 36 patients (75%) said they would recommend the AI tool to family and friends, with 17 patients (71%) saying they would recommend the direct-to-patient tool and 19 (79%) saying they would recommend the clinician decision-support tool. Another nine patients (19%) were ambivalent about the AI tools, and three patients (6%) said they would not recommend the tools.
Diagnostic speed and health care access were the most common perceived benefits of AI (by 60% of patients for each), and increased patient anxiety was the most common perceived risk (by 40% of patients). In addition, 69% of patients perceived more accurate diagnosis to be the greatest strength of an AI tool, and 85% perceived less accurate diagnosis to be the greatest weakness.
The study findings were limited by several factors, including the small sample size, qualitative design, use of a hypothetical rather than real-world situation, and a homogeneous study population, the researchers noted. However, the results merit more studies to obtain perspectives from diverse populations, they said.
“This expansion is particularly important in light of concerns raised that AI tools may exacerbate health care disparities in dermatology,” the researchers wrote.
From the patient perspective, the use of AI “may improve health care quality but should be implemented in a manner that preserves the integrity of the human physician-patient relationship,” the authors concluded.
“Although AI technology has not been widely implemented in dermatology yet, it is the pivotal time to assess patients’ views on the subject to understand their knowledge base, as well as values, preferences, and concerns regarding AI,” wrote Carrie L. Kovarik, MD, of the University of Pennsylvania in Philadelphia, in an accompanying editorial.
“Vulnerable patients, including racial and ethnic minorities, the underinsured or uninsured, economically disadvantaged, and those with chronic health conditions, may be at risk for improper consent for or use of AI,” she wrote.
Dr. Kovarik cited the position statement on augmented intelligence from the American Academy of Dermatology, which states that, for both patients and clinicians, “there should be transparency and choice on how their medical information is gathered, utilized, and stored and when, what, and how augmented intelligence technologies are utilized in their care process. There should be clarity in the symbiotic and synergistic roles of augmented intelligence and human judgment so that it is clear to the patient and provider when and how this technology is utilized to augment human judgment and interpretation.”
Clinicians will need to understand the perspectives on AI from patients of a range of backgrounds to achieve this goal, Dr. Kovarik said.
Dr. Nelson had no financial conflicts to disclose, but her colleagues disclosed relationships with pharmaceutical companies, government agencies, and nonprofit organizations. Dr. Kovarik disclosed serving on the artificial intelligence task force for the American Academy of Dermatology.
SOURCES: Nelson CA et al. JAMA Dermatol. 2020 Mar 11. doi: 10.1001/jamadermatol.2019.5014; Kovarik CL. JAMA Dermatol. 2020 Mar 11. doi: 10.1001/jamadermatol.2019.5013.
In a small survey, 75% of dermatology patients said they would recommend the use of artificial intelligence (AI) for skin cancer screening to friends and family members, but 94% emphasized the need for symbiosis between doctors, patients, and AI.
AI under investigation in dermatology includes both direct-to-patient and clinician decision-support AI tools for skin cancer screening, but patients’ perceptions of AI in health care remains unclear, Caroline A. Nelson, MD, of Yale University in New Haven, Conn., and colleagues wrote in JAMA Dermatology.
“We sought to elucidate perceived benefits and risks, strengths and weaknesses, implementation, response to conflict between human and AI clinical decision making, and recommendation for or against AI,” the researchers wrote.
They identified 48 patients seen from May 6, 2019, to July 8, 2019, at general dermatology clinics and melanoma clinics. This included 16 patients with a history of melanoma, 16 with a history of nonmelanoma skin cancer, and 16 with no history of skin cancer. The average age of the patients was 53.3 years, 54% were women, and 94% were white.
The researchers interviewed 24 patients about a direct-to-patient AI tool and 24 patients about a clinician decision-support AI tool.
Overall, 36 patients (75%) said they would recommend the AI tool to family and friends, with 17 patients (71%) saying they would recommend the direct-to-patient tool and 19 (79%) saying they would recommend the clinician decision-support tool. Another nine patients (19%) were ambivalent about the AI tools, and three patients (6%) said they would not recommend the tools.
Diagnostic speed and health care access were the most common perceived benefits of AI (by 60% of patients for each), and increased patient anxiety was the most common perceived risk (by 40% of patients). In addition, 69% of patients perceived more accurate diagnosis to be the greatest strength of an AI tool, and 85% perceived less accurate diagnosis to be the greatest weakness.
The study findings were limited by several factors, including the small sample size, qualitative design, use of a hypothetical rather than real-world situation, and a homogeneous study population, the researchers noted. However, the results merit more studies to obtain perspectives from diverse populations, they said.
“This expansion is particularly important in light of concerns raised that AI tools may exacerbate health care disparities in dermatology,” the researchers wrote.
From the patient perspective, the use of AI “may improve health care quality but should be implemented in a manner that preserves the integrity of the human physician-patient relationship,” the authors concluded.
“Although AI technology has not been widely implemented in dermatology yet, it is the pivotal time to assess patients’ views on the subject to understand their knowledge base, as well as values, preferences, and concerns regarding AI,” wrote Carrie L. Kovarik, MD, of the University of Pennsylvania in Philadelphia, in an accompanying editorial.
“Vulnerable patients, including racial and ethnic minorities, the underinsured or uninsured, economically disadvantaged, and those with chronic health conditions, may be at risk for improper consent for or use of AI,” she wrote.
Dr. Kovarik cited the position statement on augmented intelligence from the American Academy of Dermatology, which states that, for both patients and clinicians, “there should be transparency and choice on how their medical information is gathered, utilized, and stored and when, what, and how augmented intelligence technologies are utilized in their care process. There should be clarity in the symbiotic and synergistic roles of augmented intelligence and human judgment so that it is clear to the patient and provider when and how this technology is utilized to augment human judgment and interpretation.”
Clinicians will need to understand the perspectives on AI from patients of a range of backgrounds to achieve this goal, Dr. Kovarik said.
Dr. Nelson had no financial conflicts to disclose, but her colleagues disclosed relationships with pharmaceutical companies, government agencies, and nonprofit organizations. Dr. Kovarik disclosed serving on the artificial intelligence task force for the American Academy of Dermatology.
SOURCES: Nelson CA et al. JAMA Dermatol. 2020 Mar 11. doi: 10.1001/jamadermatol.2019.5014; Kovarik CL. JAMA Dermatol. 2020 Mar 11. doi: 10.1001/jamadermatol.2019.5013.
In a small survey, 75% of dermatology patients said they would recommend the use of artificial intelligence (AI) for skin cancer screening to friends and family members, but 94% emphasized the need for symbiosis between doctors, patients, and AI.
AI under investigation in dermatology includes both direct-to-patient and clinician decision-support AI tools for skin cancer screening, but patients’ perceptions of AI in health care remains unclear, Caroline A. Nelson, MD, of Yale University in New Haven, Conn., and colleagues wrote in JAMA Dermatology.
“We sought to elucidate perceived benefits and risks, strengths and weaknesses, implementation, response to conflict between human and AI clinical decision making, and recommendation for or against AI,” the researchers wrote.
They identified 48 patients seen from May 6, 2019, to July 8, 2019, at general dermatology clinics and melanoma clinics. This included 16 patients with a history of melanoma, 16 with a history of nonmelanoma skin cancer, and 16 with no history of skin cancer. The average age of the patients was 53.3 years, 54% were women, and 94% were white.
The researchers interviewed 24 patients about a direct-to-patient AI tool and 24 patients about a clinician decision-support AI tool.
Overall, 36 patients (75%) said they would recommend the AI tool to family and friends, with 17 patients (71%) saying they would recommend the direct-to-patient tool and 19 (79%) saying they would recommend the clinician decision-support tool. Another nine patients (19%) were ambivalent about the AI tools, and three patients (6%) said they would not recommend the tools.
Diagnostic speed and health care access were the most common perceived benefits of AI (by 60% of patients for each), and increased patient anxiety was the most common perceived risk (by 40% of patients). In addition, 69% of patients perceived more accurate diagnosis to be the greatest strength of an AI tool, and 85% perceived less accurate diagnosis to be the greatest weakness.
The study findings were limited by several factors, including the small sample size, qualitative design, use of a hypothetical rather than real-world situation, and a homogeneous study population, the researchers noted. However, the results merit more studies to obtain perspectives from diverse populations, they said.
“This expansion is particularly important in light of concerns raised that AI tools may exacerbate health care disparities in dermatology,” the researchers wrote.
From the patient perspective, the use of AI “may improve health care quality but should be implemented in a manner that preserves the integrity of the human physician-patient relationship,” the authors concluded.
“Although AI technology has not been widely implemented in dermatology yet, it is the pivotal time to assess patients’ views on the subject to understand their knowledge base, as well as values, preferences, and concerns regarding AI,” wrote Carrie L. Kovarik, MD, of the University of Pennsylvania in Philadelphia, in an accompanying editorial.
“Vulnerable patients, including racial and ethnic minorities, the underinsured or uninsured, economically disadvantaged, and those with chronic health conditions, may be at risk for improper consent for or use of AI,” she wrote.
Dr. Kovarik cited the position statement on augmented intelligence from the American Academy of Dermatology, which states that, for both patients and clinicians, “there should be transparency and choice on how their medical information is gathered, utilized, and stored and when, what, and how augmented intelligence technologies are utilized in their care process. There should be clarity in the symbiotic and synergistic roles of augmented intelligence and human judgment so that it is clear to the patient and provider when and how this technology is utilized to augment human judgment and interpretation.”
Clinicians will need to understand the perspectives on AI from patients of a range of backgrounds to achieve this goal, Dr. Kovarik said.
Dr. Nelson had no financial conflicts to disclose, but her colleagues disclosed relationships with pharmaceutical companies, government agencies, and nonprofit organizations. Dr. Kovarik disclosed serving on the artificial intelligence task force for the American Academy of Dermatology.
SOURCES: Nelson CA et al. JAMA Dermatol. 2020 Mar 11. doi: 10.1001/jamadermatol.2019.5014; Kovarik CL. JAMA Dermatol. 2020 Mar 11. doi: 10.1001/jamadermatol.2019.5013.
FROM JAMA DERMATOLOGY
Bariatric surgery may curtail colorectal cancer risk
Bariatric surgery was associated with a significant reduction in the risk of colorectal cancer among obese adults in a retrospective study of more than 1 million individuals.
Although some studies have suggested that bariatric surgery may reduce the risk of obesity-associated cancers, such as colorectal cancer, other studies have shown an increased colorectal cancer risk after surgery, according to Laurent Bailly, MD, of Université Côte d’Azur in Nice, France, and colleagues.
In a study published in JAMA Surgery, Dr. Bailly and colleagues compared the incidence of colorectal cancer in obese patients who underwent bariatric surgery with the incidence in obese patients who did not have surgery and the incidence in the general population.
Using the French National Health Insurance Information System database, the researchers identified 1,045,348 obese adults aged 50-75 years who had no colorectal cancer at baseline. Of these patients, 74,131 underwent bariatric surgery and 971,217 did not. The mean age was 57.3 years in the surgery group and 63.4 years in the nonsurgery group.
The mean follow-up period was 6.2 years for patients who underwent adjustable gastric banding, 5.5 years for those with sleeve gastrectomy, 5.7 years for those who underwent gastric bypass, and 5.3 years for the nonsurgery group.
Results
Overall, the colorectal cancer rate was 0.6% in the surgery group and 1.3% in the nonsurgery group (P < .001).
The researchers calculated standardized incidence ratios (SIRs) to compare the risk of colorectal cancer in the study population with the risk among the French general population; in other words, the number of observed colorectal cancer cases divided by the number of expected cases.
In the surgery group, 423 cases of colorectal cancer were observed and 428 cases were expected, which leads to an SIR of 1.0. In the nonsurgery group, 12,629 cases were observed and 9,417 cases were expected, leading to an SIR of 1.34.
These results suggest patients in the nonsurgery group had a 34% higher risk of colorectal cancer compared with the general population, whereas the risk in the surgery group was similar to that in the general population.
Patients who underwent either gastric bypass or sleeve gastrectomy had fewer new colorectal cancer diagnoses (0.5% for both) compared with patients who had adjustable gastric banding (0.7%).
The researchers noted that this study was limited by several factors, including the retrospective, observational design and potential selection bias among surgery patients. However, the results were strengthened by the large study population and long-term follow-up.
Putting results into context
The authors of an invited commentary noted that this study is supported by results from a retrospective, U.S.-based study, which indicated that bariatric surgery has a “protective effect” against colorectal cancer (Ann Surg. 2019 Jan;269[1]:95-101).
However, these results conflict with other retrospective studies. A study of Nordic patients suggested that bariatric surgery is associated with an increased risk of colon cancer but perhaps not rectal cancer (Int J Cancer. 2019. doi: 10.1002/ijc.32770).
And a study of English patients showed an increased risk of colorectal cancer in patients who underwent gastric bypass but not in those who underwent gastric banding or sleeve gastrectomy (Br J Surg. 2018;105(12):1650-7).
These conflicting results “imply that the jury is still out on whether bariatric surgery increases or decreases” the risk of colorectal cancer, the commentators wrote. They added that future studies “must account for differences in study population (i.e., race/ethnicity and national origin), mechanistic variation in bariatric surgical type, and length of follow-up, while also distinguishing between rectal and colon cancer before the case is settled.”
This study had no outside sponsorship, and the researchers and commentators had no financial conflicts to disclose.
SOURCE: Bailly L et al. JAMA Surg. 2020 Mar 11. doi:10.1001/jamasurg.2020.0089; Davidson LE et al. JAMA Surg. 2020 Mar. 11. doi:10.1001/jamasurg.2020.0090.
Bariatric surgery was associated with a significant reduction in the risk of colorectal cancer among obese adults in a retrospective study of more than 1 million individuals.
Although some studies have suggested that bariatric surgery may reduce the risk of obesity-associated cancers, such as colorectal cancer, other studies have shown an increased colorectal cancer risk after surgery, according to Laurent Bailly, MD, of Université Côte d’Azur in Nice, France, and colleagues.
In a study published in JAMA Surgery, Dr. Bailly and colleagues compared the incidence of colorectal cancer in obese patients who underwent bariatric surgery with the incidence in obese patients who did not have surgery and the incidence in the general population.
Using the French National Health Insurance Information System database, the researchers identified 1,045,348 obese adults aged 50-75 years who had no colorectal cancer at baseline. Of these patients, 74,131 underwent bariatric surgery and 971,217 did not. The mean age was 57.3 years in the surgery group and 63.4 years in the nonsurgery group.
The mean follow-up period was 6.2 years for patients who underwent adjustable gastric banding, 5.5 years for those with sleeve gastrectomy, 5.7 years for those who underwent gastric bypass, and 5.3 years for the nonsurgery group.
Results
Overall, the colorectal cancer rate was 0.6% in the surgery group and 1.3% in the nonsurgery group (P < .001).
The researchers calculated standardized incidence ratios (SIRs) to compare the risk of colorectal cancer in the study population with the risk among the French general population; in other words, the number of observed colorectal cancer cases divided by the number of expected cases.
In the surgery group, 423 cases of colorectal cancer were observed and 428 cases were expected, which leads to an SIR of 1.0. In the nonsurgery group, 12,629 cases were observed and 9,417 cases were expected, leading to an SIR of 1.34.
These results suggest patients in the nonsurgery group had a 34% higher risk of colorectal cancer compared with the general population, whereas the risk in the surgery group was similar to that in the general population.
Patients who underwent either gastric bypass or sleeve gastrectomy had fewer new colorectal cancer diagnoses (0.5% for both) compared with patients who had adjustable gastric banding (0.7%).
The researchers noted that this study was limited by several factors, including the retrospective, observational design and potential selection bias among surgery patients. However, the results were strengthened by the large study population and long-term follow-up.
Putting results into context
The authors of an invited commentary noted that this study is supported by results from a retrospective, U.S.-based study, which indicated that bariatric surgery has a “protective effect” against colorectal cancer (Ann Surg. 2019 Jan;269[1]:95-101).
However, these results conflict with other retrospective studies. A study of Nordic patients suggested that bariatric surgery is associated with an increased risk of colon cancer but perhaps not rectal cancer (Int J Cancer. 2019. doi: 10.1002/ijc.32770).
And a study of English patients showed an increased risk of colorectal cancer in patients who underwent gastric bypass but not in those who underwent gastric banding or sleeve gastrectomy (Br J Surg. 2018;105(12):1650-7).
These conflicting results “imply that the jury is still out on whether bariatric surgery increases or decreases” the risk of colorectal cancer, the commentators wrote. They added that future studies “must account for differences in study population (i.e., race/ethnicity and national origin), mechanistic variation in bariatric surgical type, and length of follow-up, while also distinguishing between rectal and colon cancer before the case is settled.”
This study had no outside sponsorship, and the researchers and commentators had no financial conflicts to disclose.
SOURCE: Bailly L et al. JAMA Surg. 2020 Mar 11. doi:10.1001/jamasurg.2020.0089; Davidson LE et al. JAMA Surg. 2020 Mar. 11. doi:10.1001/jamasurg.2020.0090.
Bariatric surgery was associated with a significant reduction in the risk of colorectal cancer among obese adults in a retrospective study of more than 1 million individuals.
Although some studies have suggested that bariatric surgery may reduce the risk of obesity-associated cancers, such as colorectal cancer, other studies have shown an increased colorectal cancer risk after surgery, according to Laurent Bailly, MD, of Université Côte d’Azur in Nice, France, and colleagues.
In a study published in JAMA Surgery, Dr. Bailly and colleagues compared the incidence of colorectal cancer in obese patients who underwent bariatric surgery with the incidence in obese patients who did not have surgery and the incidence in the general population.
Using the French National Health Insurance Information System database, the researchers identified 1,045,348 obese adults aged 50-75 years who had no colorectal cancer at baseline. Of these patients, 74,131 underwent bariatric surgery and 971,217 did not. The mean age was 57.3 years in the surgery group and 63.4 years in the nonsurgery group.
The mean follow-up period was 6.2 years for patients who underwent adjustable gastric banding, 5.5 years for those with sleeve gastrectomy, 5.7 years for those who underwent gastric bypass, and 5.3 years for the nonsurgery group.
Results
Overall, the colorectal cancer rate was 0.6% in the surgery group and 1.3% in the nonsurgery group (P < .001).
The researchers calculated standardized incidence ratios (SIRs) to compare the risk of colorectal cancer in the study population with the risk among the French general population; in other words, the number of observed colorectal cancer cases divided by the number of expected cases.
In the surgery group, 423 cases of colorectal cancer were observed and 428 cases were expected, which leads to an SIR of 1.0. In the nonsurgery group, 12,629 cases were observed and 9,417 cases were expected, leading to an SIR of 1.34.
These results suggest patients in the nonsurgery group had a 34% higher risk of colorectal cancer compared with the general population, whereas the risk in the surgery group was similar to that in the general population.
Patients who underwent either gastric bypass or sleeve gastrectomy had fewer new colorectal cancer diagnoses (0.5% for both) compared with patients who had adjustable gastric banding (0.7%).
The researchers noted that this study was limited by several factors, including the retrospective, observational design and potential selection bias among surgery patients. However, the results were strengthened by the large study population and long-term follow-up.
Putting results into context
The authors of an invited commentary noted that this study is supported by results from a retrospective, U.S.-based study, which indicated that bariatric surgery has a “protective effect” against colorectal cancer (Ann Surg. 2019 Jan;269[1]:95-101).
However, these results conflict with other retrospective studies. A study of Nordic patients suggested that bariatric surgery is associated with an increased risk of colon cancer but perhaps not rectal cancer (Int J Cancer. 2019. doi: 10.1002/ijc.32770).
And a study of English patients showed an increased risk of colorectal cancer in patients who underwent gastric bypass but not in those who underwent gastric banding or sleeve gastrectomy (Br J Surg. 2018;105(12):1650-7).
These conflicting results “imply that the jury is still out on whether bariatric surgery increases or decreases” the risk of colorectal cancer, the commentators wrote. They added that future studies “must account for differences in study population (i.e., race/ethnicity and national origin), mechanistic variation in bariatric surgical type, and length of follow-up, while also distinguishing between rectal and colon cancer before the case is settled.”
This study had no outside sponsorship, and the researchers and commentators had no financial conflicts to disclose.
SOURCE: Bailly L et al. JAMA Surg. 2020 Mar 11. doi:10.1001/jamasurg.2020.0089; Davidson LE et al. JAMA Surg. 2020 Mar. 11. doi:10.1001/jamasurg.2020.0090.
FROM JAMA SURGERY
Colorectal cancer burden rises in younger age groups
Current trends in the incidence and mortality of colorectal cancer (CRC) in the United States suggest CRC will become a disease that largely affects young and middle-aged adults, according to a report published in CA: A Cancer Journal for Clinicians.
As the second leading cause of cancer-related death in the United States, and with modifiable risk factors accounting for over 50% of cases and deaths, CRC is largely a preventable disease, explained study author Rebecca L. Siegel, of the American Cancer Society, and colleagues.
According to the investigators, CRC incidence dropped by 3.3% per year from 2011 through 2016 among individuals aged 65 years or older, but the opposite was observed for those aged 50-64 years, with rates increasing by 1% per year. The increase was even greater for those younger than 50 years, with an increase of 2.2% per year.
The CRC incidence from 2012 through 2016 was highest among Alaska Natives (89 cases per 100,000 persons) and lowest among Asian/Pacific Islanders (30 cases per 100,000 persons).
“CRC has been the most commonly diagnosed cancer in Alaska Natives since the early 1970s for reasons that are unknown but may include a higher prevalence of risk factors,” the investigators wrote.
The risk of developing CRC is related to several factors, including obesity, vitamin D deficiency, diabetes, smoking, and other dietary factors, the team further explained.
Among those aged 65 years or older, CRC death rates decreased by 3% per year from 2008 through 2017. For those aged 50-64 years, death rates dropped by 0.6% per year. In contrast, death rates rose by 1.3% per year for those younger than 50 years.
“The uptick in young adults, which is most rapid among non-Hispanic whites (2% per year), began around 2004 and was preceded by declines of 1% to 2% per year since at least 1975,” the investigators wrote.
The reduction in incidence and mortality among older adults is partially attributable to higher uptake of CRC screening. According to recent data, CRC screening rates were lower for those aged 50-64 years compared with individuals aged 65 years and older.
Based on current recommendations from the American Cancer Society, CRC screening should begin at age 45, with some higher-risk patients starting at age 40.
“Progress against CRC can be accelerated by increasing access to guideline-recommended screening and high quality treatment, particularly among Alaska Natives, and elucidating causes for rising incidence in young and middle-aged adults,” the investigators concluded.
The authors disclosed financial affiliations with the American Cancer Society, which funded the study, as well as Array Biopharma, Bayer, RGenix, Tesaro, and Seattle Genetics.
SOURCE: Siegel RL et al. CA Cancer J Clin. 2020 Mar 5. doi: 10.3322/caac.21601.
Current trends in the incidence and mortality of colorectal cancer (CRC) in the United States suggest CRC will become a disease that largely affects young and middle-aged adults, according to a report published in CA: A Cancer Journal for Clinicians.
As the second leading cause of cancer-related death in the United States, and with modifiable risk factors accounting for over 50% of cases and deaths, CRC is largely a preventable disease, explained study author Rebecca L. Siegel, of the American Cancer Society, and colleagues.
According to the investigators, CRC incidence dropped by 3.3% per year from 2011 through 2016 among individuals aged 65 years or older, but the opposite was observed for those aged 50-64 years, with rates increasing by 1% per year. The increase was even greater for those younger than 50 years, with an increase of 2.2% per year.
The CRC incidence from 2012 through 2016 was highest among Alaska Natives (89 cases per 100,000 persons) and lowest among Asian/Pacific Islanders (30 cases per 100,000 persons).
“CRC has been the most commonly diagnosed cancer in Alaska Natives since the early 1970s for reasons that are unknown but may include a higher prevalence of risk factors,” the investigators wrote.
The risk of developing CRC is related to several factors, including obesity, vitamin D deficiency, diabetes, smoking, and other dietary factors, the team further explained.
Among those aged 65 years or older, CRC death rates decreased by 3% per year from 2008 through 2017. For those aged 50-64 years, death rates dropped by 0.6% per year. In contrast, death rates rose by 1.3% per year for those younger than 50 years.
“The uptick in young adults, which is most rapid among non-Hispanic whites (2% per year), began around 2004 and was preceded by declines of 1% to 2% per year since at least 1975,” the investigators wrote.
The reduction in incidence and mortality among older adults is partially attributable to higher uptake of CRC screening. According to recent data, CRC screening rates were lower for those aged 50-64 years compared with individuals aged 65 years and older.
Based on current recommendations from the American Cancer Society, CRC screening should begin at age 45, with some higher-risk patients starting at age 40.
“Progress against CRC can be accelerated by increasing access to guideline-recommended screening and high quality treatment, particularly among Alaska Natives, and elucidating causes for rising incidence in young and middle-aged adults,” the investigators concluded.
The authors disclosed financial affiliations with the American Cancer Society, which funded the study, as well as Array Biopharma, Bayer, RGenix, Tesaro, and Seattle Genetics.
SOURCE: Siegel RL et al. CA Cancer J Clin. 2020 Mar 5. doi: 10.3322/caac.21601.
Current trends in the incidence and mortality of colorectal cancer (CRC) in the United States suggest CRC will become a disease that largely affects young and middle-aged adults, according to a report published in CA: A Cancer Journal for Clinicians.
As the second leading cause of cancer-related death in the United States, and with modifiable risk factors accounting for over 50% of cases and deaths, CRC is largely a preventable disease, explained study author Rebecca L. Siegel, of the American Cancer Society, and colleagues.
According to the investigators, CRC incidence dropped by 3.3% per year from 2011 through 2016 among individuals aged 65 years or older, but the opposite was observed for those aged 50-64 years, with rates increasing by 1% per year. The increase was even greater for those younger than 50 years, with an increase of 2.2% per year.
The CRC incidence from 2012 through 2016 was highest among Alaska Natives (89 cases per 100,000 persons) and lowest among Asian/Pacific Islanders (30 cases per 100,000 persons).
“CRC has been the most commonly diagnosed cancer in Alaska Natives since the early 1970s for reasons that are unknown but may include a higher prevalence of risk factors,” the investigators wrote.
The risk of developing CRC is related to several factors, including obesity, vitamin D deficiency, diabetes, smoking, and other dietary factors, the team further explained.
Among those aged 65 years or older, CRC death rates decreased by 3% per year from 2008 through 2017. For those aged 50-64 years, death rates dropped by 0.6% per year. In contrast, death rates rose by 1.3% per year for those younger than 50 years.
“The uptick in young adults, which is most rapid among non-Hispanic whites (2% per year), began around 2004 and was preceded by declines of 1% to 2% per year since at least 1975,” the investigators wrote.
The reduction in incidence and mortality among older adults is partially attributable to higher uptake of CRC screening. According to recent data, CRC screening rates were lower for those aged 50-64 years compared with individuals aged 65 years and older.
Based on current recommendations from the American Cancer Society, CRC screening should begin at age 45, with some higher-risk patients starting at age 40.
“Progress against CRC can be accelerated by increasing access to guideline-recommended screening and high quality treatment, particularly among Alaska Natives, and elucidating causes for rising incidence in young and middle-aged adults,” the investigators concluded.
The authors disclosed financial affiliations with the American Cancer Society, which funded the study, as well as Array Biopharma, Bayer, RGenix, Tesaro, and Seattle Genetics.
SOURCE: Siegel RL et al. CA Cancer J Clin. 2020 Mar 5. doi: 10.3322/caac.21601.
FROM CA: A CANCER JOURNAL FOR CLINICIANS
Best definition of malnutrition varies by cancer type
For patients undergoing major oncologic surgery, the best definition of malnutrition used to assess postoperative risk varies by cancer type, results of a retrospective study suggest.

The current, one-size-fits-all approach to nutritional status leads to both undertreatment and overtreatment of malnutrition, as well as inaccurate estimations of postoperative risk, reported lead study author Nicholas P. McKenna, MD, of the Mayo Clinic in Rochester, Minn., and colleagues.
“Assessing nutritional status is important because it impacts preoperative planning, particularly with respect to the use of prehabilitation,” the investigators wrote. Their report is in the Journal of the American College of Surgeons. They noted that while prehabilitation has been shown to reduce postoperative risk among those who need it, identification of these patients is an area that needs improvement.
With this in mind, Dr. McKenna and colleagues analyzed 205,840 major oncologic operations, with data drawn from the American College of Surgeons National Surgical Quality Improvement (NSQIP) database.
The researchers evaluated patients’ nutritional status using three techniques: the NSQIP method, the European Society for Clinical Nutrition and Metabolism (ESPEN) definitions, and the World Health Organization body mass index (BMI) classification system.
Combining these three assessments led to seven hierarchical nutritional status categories:
- Severe malnutrition – BMI less than 18.5 kg/m2 and greater than 10% weight loss
- ESPEN 1 – BMI 18.5-20 kg/m2 (if younger than 70 years) or less than 22 kg/m2 (if 70 years or older) plus greater than 10% weight loss
- ESPEN 2 – BMI less than 18.5 kg/m2
- NSQIP – BMI greater than 20 kg/m2 (if younger than 70 years) or 22 kg/m2 (if 70 years or older) plus greater than 10% weight loss
- Mild malnutrition – BMI 18.5-20 kg/m2 (if younger than 70 years) or less than 22 kg/m2 (if 70 years or older)
- Obese – BMI at least 30 kg/m2
- No malnutrition.
The study’s primary outcomes were 30-day mortality and 30-day morbidity. The latter included a variety of complications, such as deep incisional surgical site infection, septic shock, and acute renal failure. Demographic and clinical factors were included in multivariate analyses.
Results
Most of the operations involved patients with colorectal cancer (74%), followed by pancreatic (10%), lung (9%), gastric (3%), esophageal (3%), and liver (2%) cancer.
Across all patients, 16% fell into one of five malnutrition categories: mild malnutrition (6%), NSQIP (6%), ESPEN 2 (2%), ESPEN 1 (1%), or severe malnutrition (0.6%). The remainder of patients were either obese (31%) or had normal nutritional status (54%).
Malnutrition was most common among patients with pancreatic cancer (28%) and least common among those with colorectal cancer (14%).
Aligning with previous research, this study showed that nutritional status was associated with postoperative risk. Mortality risk was highest among patients with severe malnutrition, and morbidity was most common in the severe and ESPEN 1 groups (P less than .0001 for both).
While the spectrum of classifications appeared accurate across the population, multivariable models for mortality and morbidity revealed an interaction between cancer type and malnutrition definition (P less than .0001 for both), which suggested the most accurate definition of malnutrition differed from one type of cancer to another.
Specifically, a classification of severe malnutrition was most predictive of mortality among patients with esophageal or colorectal cancer. ESPEN 1 was most predictive of mortality for patients with gastric or lung cancer, and NSQIP was most predictive for those with liver cancer.
For predicting morbidity, severe malnutrition was most accurate among patients with colorectal cancer, whereas ESPEN 1 was better suited for gastric and lung cancer.
Interpreting and applying the results
“The biggest takeaway is that the optimal definition of malnutrition varies by cancer type,” Dr. McKenna said in an interview.
He went on to explain that weight loss is a particularly important indicator of malnutrition for patients with esophageal or gastric cancer. “These are the cancers that more commonly undergo neoadjuvant chemotherapy,” he noted.
The other major finding, Dr. McKenna said, offers some perspective on short-term versus long-term risk.
“Most people consider obesity a negative prognostic factor,” he said. “But in terms of operative risk, it’s kind of a neutral effect. It doesn’t really affect the short-term outcomes of an operation.”
Still, Dr. McKenna warned that a visual assessment of patient body condition is not enough to predict postoperative risk. Instead, he recommended accurate height and weight measurements during annual and preoperative exams. He also noted that more patients are at risk than clinicians may suspect.
“Even definitions that didn’t previously exist, such as mild malnutrition, had a somewhat negative effect within colorectal cancer and esophageal cancer,” Dr. McKenna said. “So these are patients who previously probably would be considered pretty healthy, but there is probably some room to improve their nutritional status.”
While the study revealed that different types of cancer should have unique tools for measuring nutritional status, development of these systems will require more research concerning prehabilitation outcomes, according to Dr. McKenna. In the meantime, he highlighted a point of action in the clinic.
“We think, overall, especially with the rise of neoadjuvant chemotherapy upfront, before surgery, that identifying patients at risk before they start neoadjuvant chemotherapy is going to be important,” he said. “They are the ones who really need to be targeted.”
There was no external funding for this study, and the investigators reported no conflicts of interest.
SOURCE: McKenna NP et al. J Am Coll Surg. 2020 Feb 26. doi: 10.1016/j.jamcollsurg.2019.12.034.
For patients undergoing major oncologic surgery, the best definition of malnutrition used to assess postoperative risk varies by cancer type, results of a retrospective study suggest.
The current, one-size-fits-all approach to nutritional status leads to both undertreatment and overtreatment of malnutrition, as well as inaccurate estimations of postoperative risk, reported lead study author Nicholas P. McKenna, MD, of the Mayo Clinic in Rochester, Minn., and colleagues.
“Assessing nutritional status is important because it impacts preoperative planning, particularly with respect to the use of prehabilitation,” the investigators wrote. Their report is in the Journal of the American College of Surgeons. They noted that while prehabilitation has been shown to reduce postoperative risk among those who need it, identification of these patients is an area that needs improvement.
With this in mind, Dr. McKenna and colleagues analyzed 205,840 major oncologic operations, with data drawn from the American College of Surgeons National Surgical Quality Improvement (NSQIP) database.
The researchers evaluated patients’ nutritional status using three techniques: the NSQIP method, the European Society for Clinical Nutrition and Metabolism (ESPEN) definitions, and the World Health Organization body mass index (BMI) classification system.
Combining these three assessments led to seven hierarchical nutritional status categories:
- Severe malnutrition – BMI less than 18.5 kg/m2 and greater than 10% weight loss
- ESPEN 1 – BMI 18.5-20 kg/m2 (if younger than 70 years) or less than 22 kg/m2 (if 70 years or older) plus greater than 10% weight loss
- ESPEN 2 – BMI less than 18.5 kg/m2
- NSQIP – BMI greater than 20 kg/m2 (if younger than 70 years) or 22 kg/m2 (if 70 years or older) plus greater than 10% weight loss
- Mild malnutrition – BMI 18.5-20 kg/m2 (if younger than 70 years) or less than 22 kg/m2 (if 70 years or older)
- Obese – BMI at least 30 kg/m2
- No malnutrition.
The study’s primary outcomes were 30-day mortality and 30-day morbidity. The latter included a variety of complications, such as deep incisional surgical site infection, septic shock, and acute renal failure. Demographic and clinical factors were included in multivariate analyses.
Results
Most of the operations involved patients with colorectal cancer (74%), followed by pancreatic (10%), lung (9%), gastric (3%), esophageal (3%), and liver (2%) cancer.
Across all patients, 16% fell into one of five malnutrition categories: mild malnutrition (6%), NSQIP (6%), ESPEN 2 (2%), ESPEN 1 (1%), or severe malnutrition (0.6%). The remainder of patients were either obese (31%) or had normal nutritional status (54%).
Malnutrition was most common among patients with pancreatic cancer (28%) and least common among those with colorectal cancer (14%).
Aligning with previous research, this study showed that nutritional status was associated with postoperative risk. Mortality risk was highest among patients with severe malnutrition, and morbidity was most common in the severe and ESPEN 1 groups (P less than .0001 for both).
While the spectrum of classifications appeared accurate across the population, multivariable models for mortality and morbidity revealed an interaction between cancer type and malnutrition definition (P less than .0001 for both), which suggested the most accurate definition of malnutrition differed from one type of cancer to another.
Specifically, a classification of severe malnutrition was most predictive of mortality among patients with esophageal or colorectal cancer. ESPEN 1 was most predictive of mortality for patients with gastric or lung cancer, and NSQIP was most predictive for those with liver cancer.
For predicting morbidity, severe malnutrition was most accurate among patients with colorectal cancer, whereas ESPEN 1 was better suited for gastric and lung cancer.
Interpreting and applying the results
“The biggest takeaway is that the optimal definition of malnutrition varies by cancer type,” Dr. McKenna said in an interview.
He went on to explain that weight loss is a particularly important indicator of malnutrition for patients with esophageal or gastric cancer. “These are the cancers that more commonly undergo neoadjuvant chemotherapy,” he noted.
The other major finding, Dr. McKenna said, offers some perspective on short-term versus long-term risk.
“Most people consider obesity a negative prognostic factor,” he said. “But in terms of operative risk, it’s kind of a neutral effect. It doesn’t really affect the short-term outcomes of an operation.”
Still, Dr. McKenna warned that a visual assessment of patient body condition is not enough to predict postoperative risk. Instead, he recommended accurate height and weight measurements during annual and preoperative exams. He also noted that more patients are at risk than clinicians may suspect.
“Even definitions that didn’t previously exist, such as mild malnutrition, had a somewhat negative effect within colorectal cancer and esophageal cancer,” Dr. McKenna said. “So these are patients who previously probably would be considered pretty healthy, but there is probably some room to improve their nutritional status.”
While the study revealed that different types of cancer should have unique tools for measuring nutritional status, development of these systems will require more research concerning prehabilitation outcomes, according to Dr. McKenna. In the meantime, he highlighted a point of action in the clinic.
“We think, overall, especially with the rise of neoadjuvant chemotherapy upfront, before surgery, that identifying patients at risk before they start neoadjuvant chemotherapy is going to be important,” he said. “They are the ones who really need to be targeted.”
There was no external funding for this study, and the investigators reported no conflicts of interest.
SOURCE: McKenna NP et al. J Am Coll Surg. 2020 Feb 26. doi: 10.1016/j.jamcollsurg.2019.12.034.
For patients undergoing major oncologic surgery, the best definition of malnutrition used to assess postoperative risk varies by cancer type, results of a retrospective study suggest.
The current, one-size-fits-all approach to nutritional status leads to both undertreatment and overtreatment of malnutrition, as well as inaccurate estimations of postoperative risk, reported lead study author Nicholas P. McKenna, MD, of the Mayo Clinic in Rochester, Minn., and colleagues.
“Assessing nutritional status is important because it impacts preoperative planning, particularly with respect to the use of prehabilitation,” the investigators wrote. Their report is in the Journal of the American College of Surgeons. They noted that while prehabilitation has been shown to reduce postoperative risk among those who need it, identification of these patients is an area that needs improvement.
With this in mind, Dr. McKenna and colleagues analyzed 205,840 major oncologic operations, with data drawn from the American College of Surgeons National Surgical Quality Improvement (NSQIP) database.
The researchers evaluated patients’ nutritional status using three techniques: the NSQIP method, the European Society for Clinical Nutrition and Metabolism (ESPEN) definitions, and the World Health Organization body mass index (BMI) classification system.
Combining these three assessments led to seven hierarchical nutritional status categories:
- Severe malnutrition – BMI less than 18.5 kg/m2 and greater than 10% weight loss
- ESPEN 1 – BMI 18.5-20 kg/m2 (if younger than 70 years) or less than 22 kg/m2 (if 70 years or older) plus greater than 10% weight loss
- ESPEN 2 – BMI less than 18.5 kg/m2
- NSQIP – BMI greater than 20 kg/m2 (if younger than 70 years) or 22 kg/m2 (if 70 years or older) plus greater than 10% weight loss
- Mild malnutrition – BMI 18.5-20 kg/m2 (if younger than 70 years) or less than 22 kg/m2 (if 70 years or older)
- Obese – BMI at least 30 kg/m2
- No malnutrition.
The study’s primary outcomes were 30-day mortality and 30-day morbidity. The latter included a variety of complications, such as deep incisional surgical site infection, septic shock, and acute renal failure. Demographic and clinical factors were included in multivariate analyses.
Results
Most of the operations involved patients with colorectal cancer (74%), followed by pancreatic (10%), lung (9%), gastric (3%), esophageal (3%), and liver (2%) cancer.
Across all patients, 16% fell into one of five malnutrition categories: mild malnutrition (6%), NSQIP (6%), ESPEN 2 (2%), ESPEN 1 (1%), or severe malnutrition (0.6%). The remainder of patients were either obese (31%) or had normal nutritional status (54%).
Malnutrition was most common among patients with pancreatic cancer (28%) and least common among those with colorectal cancer (14%).
Aligning with previous research, this study showed that nutritional status was associated with postoperative risk. Mortality risk was highest among patients with severe malnutrition, and morbidity was most common in the severe and ESPEN 1 groups (P less than .0001 for both).
While the spectrum of classifications appeared accurate across the population, multivariable models for mortality and morbidity revealed an interaction between cancer type and malnutrition definition (P less than .0001 for both), which suggested the most accurate definition of malnutrition differed from one type of cancer to another.
Specifically, a classification of severe malnutrition was most predictive of mortality among patients with esophageal or colorectal cancer. ESPEN 1 was most predictive of mortality for patients with gastric or lung cancer, and NSQIP was most predictive for those with liver cancer.
For predicting morbidity, severe malnutrition was most accurate among patients with colorectal cancer, whereas ESPEN 1 was better suited for gastric and lung cancer.
Interpreting and applying the results
“The biggest takeaway is that the optimal definition of malnutrition varies by cancer type,” Dr. McKenna said in an interview.
He went on to explain that weight loss is a particularly important indicator of malnutrition for patients with esophageal or gastric cancer. “These are the cancers that more commonly undergo neoadjuvant chemotherapy,” he noted.
The other major finding, Dr. McKenna said, offers some perspective on short-term versus long-term risk.
“Most people consider obesity a negative prognostic factor,” he said. “But in terms of operative risk, it’s kind of a neutral effect. It doesn’t really affect the short-term outcomes of an operation.”
Still, Dr. McKenna warned that a visual assessment of patient body condition is not enough to predict postoperative risk. Instead, he recommended accurate height and weight measurements during annual and preoperative exams. He also noted that more patients are at risk than clinicians may suspect.
“Even definitions that didn’t previously exist, such as mild malnutrition, had a somewhat negative effect within colorectal cancer and esophageal cancer,” Dr. McKenna said. “So these are patients who previously probably would be considered pretty healthy, but there is probably some room to improve their nutritional status.”
While the study revealed that different types of cancer should have unique tools for measuring nutritional status, development of these systems will require more research concerning prehabilitation outcomes, according to Dr. McKenna. In the meantime, he highlighted a point of action in the clinic.
“We think, overall, especially with the rise of neoadjuvant chemotherapy upfront, before surgery, that identifying patients at risk before they start neoadjuvant chemotherapy is going to be important,” he said. “They are the ones who really need to be targeted.”
There was no external funding for this study, and the investigators reported no conflicts of interest.
SOURCE: McKenna NP et al. J Am Coll Surg. 2020 Feb 26. doi: 10.1016/j.jamcollsurg.2019.12.034.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF SURGEONS
Stored CD34 cells for multiple myeloma patients largely unused
ORLANDO – Collecting and storing extra stem cells on the off chance that a patient with multiple myeloma will need a salvage autologous stem cell transplant may not be worth the money or effort, investigators say.

Among patients with multiple myeloma who had adequate collection of mobilized and stored cells, only 3 of 146 eligible patients were given the stored cells in a second autologous stem cell transplant (ASCT), reported Nausheen Ahmed, MD, from the Case Western Reserve Cancer Center and University Hospitals Seidman Cancer Center, both in Cleveland.
“We found overall low utilization of salvage transplants and storage stem cells at our institution, which may not justify the strategy of early collection for all patients fit for transplant,” she said at the Transplantation and Cellular Therapy Meetings.
But Sergio Giralt, MD, a transplant specialist from Memorial Sloan Kettering Cancer Center, New York, who was not involved in the study, warned against changing practice “for the wrong reason, because it’s just a financial reason.”
Get them while they’re fresh
The rationale for collecting and storing extra cells is the risk that mobilization will fail in the future following prolonged maintenance with immunomodulatory agents such as lenalidomide (Revlimid), and the risk for genetic or epigenetic damage to cells from high-dose melphalan used in transplant-conditioning regimens, Dr. Ahmed noted at the meeting held by the American Society for Blood and Marrow Transplantation and the Center for International Blood and Marrow Transplant Research.
“However, there are potential issues with early mobilization and storage, including cost, resources, apheresis scheduling, uncertainty of cell viability, and liability. There’s also risk of side effects with filgrastim and plerixafor use [for mobilization],” she said.
Dr. Ahmed and colleagues conducted a study to determine how stored stem cells for second ASCT were used, describe how second ASCTs are used in patients who meet the Mayo Consensus Stratification for Myeloma & Risk-Adapted Therapy (mSMART) criteria, and the costs of mobilizing and storing stem cells for a second ASCT.
They took a retrospective look at all adults aged 18 years and older with a diagnosis of multiple myeloma who received a first ASCT at their institution from 2009 to 2017. They excluded patients who had amyloidosis without myeloma or POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal plasma proliferative disorder, skin changes) syndrome.
Patients were considered eligible for a second ASCT based on mSMART recommendations if they had a relapse either 18 or more months without maintenance therapy or after at least 36 months on maintenance. The investigators defined an extra day of collection as an additional day of apheresis to obtain 2 million or more CD34 cells/kg for storage only.
They estimated costs from the institution’s charge master as the sum of cell processing, leukapheresis costs, additional plerixafor costs, and storage costs, and calculated the total duration of storage as months from the date of collection until the last follow-up.
The median age of the total study population of 179 patients was 61 years, with a majority of male and white patients. Of this group, 98% had an Eastern Cooperative Oncology Group performance score of 0-1. In all, 63.7% of the patients had standard-risk cytogenetics, 22.4% had high-risk disease, and the remainder had unknown cytogenetic risk.
At a median follow-up of 56.5 months, 95 patients (53.1%) had experienced a relapse after transplant with a median time to progression of 47.5 months. The majority of patients (166; 92.7%) had received a single transplant, 10 (5.6%) had received tandem transplants, and only 3 (1.6%) had a second transplant at relapse.
Looking at the use of second transplant in patients who met the criteria for salvage transplant based on mSMART (excluding patients who had undergone tandem transplant) and whose maintenance status was known, they identified 61 patients on maintenance therapy and 24 with no maintenance. A total of 31 patients (18 in the maintenance group and 13 in the no-maintenance group) met mSMART criteria for salvage ASCT.
Dr. Ahmed and colleagues next looked at the 146 patients who had at least 2 million stored cells/kg, and found that the stored cells were used for only three patients. Of the 146 patients, 66 had 1 extra collection day, 17 had 2 extra days, and 4 had 3 extra days, for an average additional cost per patient of $16,859.
‘Woefully underutilized’
Discussing the study, Dr. Giralt asked: “How valid are the SMART criteria of 36 months? And the answer is there is no data to support it, and if we actually go back to our oncology, any patient who has had more than 18 months without exposure to a drug can continue to have sensitivity to that drug, and that’s why if we used the ASBMT criteria of greater than 18 months you’d have a larger population” of patients eligible for salvage transplant.
He stated that, “we know these patients exist, we know they have cells in the freezer, but we’re not using those cells. Second transplant is woefully underutilized in myeloma patients,” and he added that stored cells could also be used to support those patients who develop cytopenias following chimeric antigen receptor (CAR) T-cell therapy.
Yago Nieto, MD, from the University of Texas MD Anderson Cancer Center, Houston, who comoderated the session where the data were presented, agreed with Dr. Giralt that stored stem cells are underutilized in the treatment of patients with multiple myeloma.
“I don’t think that the experience from Case Western, where the percentage of patients who are eligible for salvage transplant and actually got it was less than 10%, can be extrapolated to many other centers. I think that in most centers the actual percentage is higher than that,” he said in an interview.
“There are going to be therapies like CAR T that will compete with salvage transplants, but I think more patients should be considered for this salvage procedure,” he added.
No funding source for the story was disclosed. Dr. Ahmed reported no financial disclosures. Dr. Giralt reported consulting/advisory activities and receiving research funding from multiple companies. Dr. Nieto disclosed research funding from, and consultancy for, several companies.
SOURCE: Ahmed N et al. TCT 2020, Abstract 28.
ORLANDO – Collecting and storing extra stem cells on the off chance that a patient with multiple myeloma will need a salvage autologous stem cell transplant may not be worth the money or effort, investigators say.
Among patients with multiple myeloma who had adequate collection of mobilized and stored cells, only 3 of 146 eligible patients were given the stored cells in a second autologous stem cell transplant (ASCT), reported Nausheen Ahmed, MD, from the Case Western Reserve Cancer Center and University Hospitals Seidman Cancer Center, both in Cleveland.
“We found overall low utilization of salvage transplants and storage stem cells at our institution, which may not justify the strategy of early collection for all patients fit for transplant,” she said at the Transplantation and Cellular Therapy Meetings.
But Sergio Giralt, MD, a transplant specialist from Memorial Sloan Kettering Cancer Center, New York, who was not involved in the study, warned against changing practice “for the wrong reason, because it’s just a financial reason.”
Get them while they’re fresh
The rationale for collecting and storing extra cells is the risk that mobilization will fail in the future following prolonged maintenance with immunomodulatory agents such as lenalidomide (Revlimid), and the risk for genetic or epigenetic damage to cells from high-dose melphalan used in transplant-conditioning regimens, Dr. Ahmed noted at the meeting held by the American Society for Blood and Marrow Transplantation and the Center for International Blood and Marrow Transplant Research.
“However, there are potential issues with early mobilization and storage, including cost, resources, apheresis scheduling, uncertainty of cell viability, and liability. There’s also risk of side effects with filgrastim and plerixafor use [for mobilization],” she said.
Dr. Ahmed and colleagues conducted a study to determine how stored stem cells for second ASCT were used, describe how second ASCTs are used in patients who meet the Mayo Consensus Stratification for Myeloma & Risk-Adapted Therapy (mSMART) criteria, and the costs of mobilizing and storing stem cells for a second ASCT.
They took a retrospective look at all adults aged 18 years and older with a diagnosis of multiple myeloma who received a first ASCT at their institution from 2009 to 2017. They excluded patients who had amyloidosis without myeloma or POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal plasma proliferative disorder, skin changes) syndrome.
Patients were considered eligible for a second ASCT based on mSMART recommendations if they had a relapse either 18 or more months without maintenance therapy or after at least 36 months on maintenance. The investigators defined an extra day of collection as an additional day of apheresis to obtain 2 million or more CD34 cells/kg for storage only.
They estimated costs from the institution’s charge master as the sum of cell processing, leukapheresis costs, additional plerixafor costs, and storage costs, and calculated the total duration of storage as months from the date of collection until the last follow-up.
The median age of the total study population of 179 patients was 61 years, with a majority of male and white patients. Of this group, 98% had an Eastern Cooperative Oncology Group performance score of 0-1. In all, 63.7% of the patients had standard-risk cytogenetics, 22.4% had high-risk disease, and the remainder had unknown cytogenetic risk.
At a median follow-up of 56.5 months, 95 patients (53.1%) had experienced a relapse after transplant with a median time to progression of 47.5 months. The majority of patients (166; 92.7%) had received a single transplant, 10 (5.6%) had received tandem transplants, and only 3 (1.6%) had a second transplant at relapse.
Looking at the use of second transplant in patients who met the criteria for salvage transplant based on mSMART (excluding patients who had undergone tandem transplant) and whose maintenance status was known, they identified 61 patients on maintenance therapy and 24 with no maintenance. A total of 31 patients (18 in the maintenance group and 13 in the no-maintenance group) met mSMART criteria for salvage ASCT.
Dr. Ahmed and colleagues next looked at the 146 patients who had at least 2 million stored cells/kg, and found that the stored cells were used for only three patients. Of the 146 patients, 66 had 1 extra collection day, 17 had 2 extra days, and 4 had 3 extra days, for an average additional cost per patient of $16,859.
‘Woefully underutilized’
Discussing the study, Dr. Giralt asked: “How valid are the SMART criteria of 36 months? And the answer is there is no data to support it, and if we actually go back to our oncology, any patient who has had more than 18 months without exposure to a drug can continue to have sensitivity to that drug, and that’s why if we used the ASBMT criteria of greater than 18 months you’d have a larger population” of patients eligible for salvage transplant.
He stated that, “we know these patients exist, we know they have cells in the freezer, but we’re not using those cells. Second transplant is woefully underutilized in myeloma patients,” and he added that stored cells could also be used to support those patients who develop cytopenias following chimeric antigen receptor (CAR) T-cell therapy.
Yago Nieto, MD, from the University of Texas MD Anderson Cancer Center, Houston, who comoderated the session where the data were presented, agreed with Dr. Giralt that stored stem cells are underutilized in the treatment of patients with multiple myeloma.
“I don’t think that the experience from Case Western, where the percentage of patients who are eligible for salvage transplant and actually got it was less than 10%, can be extrapolated to many other centers. I think that in most centers the actual percentage is higher than that,” he said in an interview.
“There are going to be therapies like CAR T that will compete with salvage transplants, but I think more patients should be considered for this salvage procedure,” he added.
No funding source for the story was disclosed. Dr. Ahmed reported no financial disclosures. Dr. Giralt reported consulting/advisory activities and receiving research funding from multiple companies. Dr. Nieto disclosed research funding from, and consultancy for, several companies.
SOURCE: Ahmed N et al. TCT 2020, Abstract 28.
ORLANDO – Collecting and storing extra stem cells on the off chance that a patient with multiple myeloma will need a salvage autologous stem cell transplant may not be worth the money or effort, investigators say.
Among patients with multiple myeloma who had adequate collection of mobilized and stored cells, only 3 of 146 eligible patients were given the stored cells in a second autologous stem cell transplant (ASCT), reported Nausheen Ahmed, MD, from the Case Western Reserve Cancer Center and University Hospitals Seidman Cancer Center, both in Cleveland.
“We found overall low utilization of salvage transplants and storage stem cells at our institution, which may not justify the strategy of early collection for all patients fit for transplant,” she said at the Transplantation and Cellular Therapy Meetings.
But Sergio Giralt, MD, a transplant specialist from Memorial Sloan Kettering Cancer Center, New York, who was not involved in the study, warned against changing practice “for the wrong reason, because it’s just a financial reason.”
Get them while they’re fresh
The rationale for collecting and storing extra cells is the risk that mobilization will fail in the future following prolonged maintenance with immunomodulatory agents such as lenalidomide (Revlimid), and the risk for genetic or epigenetic damage to cells from high-dose melphalan used in transplant-conditioning regimens, Dr. Ahmed noted at the meeting held by the American Society for Blood and Marrow Transplantation and the Center for International Blood and Marrow Transplant Research.
“However, there are potential issues with early mobilization and storage, including cost, resources, apheresis scheduling, uncertainty of cell viability, and liability. There’s also risk of side effects with filgrastim and plerixafor use [for mobilization],” she said.
Dr. Ahmed and colleagues conducted a study to determine how stored stem cells for second ASCT were used, describe how second ASCTs are used in patients who meet the Mayo Consensus Stratification for Myeloma & Risk-Adapted Therapy (mSMART) criteria, and the costs of mobilizing and storing stem cells for a second ASCT.
They took a retrospective look at all adults aged 18 years and older with a diagnosis of multiple myeloma who received a first ASCT at their institution from 2009 to 2017. They excluded patients who had amyloidosis without myeloma or POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal plasma proliferative disorder, skin changes) syndrome.
Patients were considered eligible for a second ASCT based on mSMART recommendations if they had a relapse either 18 or more months without maintenance therapy or after at least 36 months on maintenance. The investigators defined an extra day of collection as an additional day of apheresis to obtain 2 million or more CD34 cells/kg for storage only.
They estimated costs from the institution’s charge master as the sum of cell processing, leukapheresis costs, additional plerixafor costs, and storage costs, and calculated the total duration of storage as months from the date of collection until the last follow-up.
The median age of the total study population of 179 patients was 61 years, with a majority of male and white patients. Of this group, 98% had an Eastern Cooperative Oncology Group performance score of 0-1. In all, 63.7% of the patients had standard-risk cytogenetics, 22.4% had high-risk disease, and the remainder had unknown cytogenetic risk.
At a median follow-up of 56.5 months, 95 patients (53.1%) had experienced a relapse after transplant with a median time to progression of 47.5 months. The majority of patients (166; 92.7%) had received a single transplant, 10 (5.6%) had received tandem transplants, and only 3 (1.6%) had a second transplant at relapse.
Looking at the use of second transplant in patients who met the criteria for salvage transplant based on mSMART (excluding patients who had undergone tandem transplant) and whose maintenance status was known, they identified 61 patients on maintenance therapy and 24 with no maintenance. A total of 31 patients (18 in the maintenance group and 13 in the no-maintenance group) met mSMART criteria for salvage ASCT.
Dr. Ahmed and colleagues next looked at the 146 patients who had at least 2 million stored cells/kg, and found that the stored cells were used for only three patients. Of the 146 patients, 66 had 1 extra collection day, 17 had 2 extra days, and 4 had 3 extra days, for an average additional cost per patient of $16,859.
‘Woefully underutilized’
Discussing the study, Dr. Giralt asked: “How valid are the SMART criteria of 36 months? And the answer is there is no data to support it, and if we actually go back to our oncology, any patient who has had more than 18 months without exposure to a drug can continue to have sensitivity to that drug, and that’s why if we used the ASBMT criteria of greater than 18 months you’d have a larger population” of patients eligible for salvage transplant.
He stated that, “we know these patients exist, we know they have cells in the freezer, but we’re not using those cells. Second transplant is woefully underutilized in myeloma patients,” and he added that stored cells could also be used to support those patients who develop cytopenias following chimeric antigen receptor (CAR) T-cell therapy.
Yago Nieto, MD, from the University of Texas MD Anderson Cancer Center, Houston, who comoderated the session where the data were presented, agreed with Dr. Giralt that stored stem cells are underutilized in the treatment of patients with multiple myeloma.
“I don’t think that the experience from Case Western, where the percentage of patients who are eligible for salvage transplant and actually got it was less than 10%, can be extrapolated to many other centers. I think that in most centers the actual percentage is higher than that,” he said in an interview.
“There are going to be therapies like CAR T that will compete with salvage transplants, but I think more patients should be considered for this salvage procedure,” he added.
No funding source for the story was disclosed. Dr. Ahmed reported no financial disclosures. Dr. Giralt reported consulting/advisory activities and receiving research funding from multiple companies. Dr. Nieto disclosed research funding from, and consultancy for, several companies.
SOURCE: Ahmed N et al. TCT 2020, Abstract 28.
REPORTING FROM TCT 2020