User login
Admission to an intensive care unit (ICU) is lifesaving for some patients, but for many, the admission carries high expectations and financial costs and fails to provide desirable outcomes. Patients who receive intensive care have a mortality rate of about 20%, and the costs of this care comprise about 4% of the U.S. health care budget.1,2 In a study of Medicare recipients, treatment intensity and expenses increased between the mid-1980s and 1999 but without any increase in survivorship; per capita ICU expenses were higher for patients who did not survive the ICU.3 Use of the ICU in patients’ final stages of life has increased in proportion since then, and the demand for critical care is likely to continue as the relative proportion of elderly patients in the population rises.2,4,5
Physicians and nurses who responded to a European survey on the inappropriateness of intensive care overwhelmingly endorsed the problems of “too much care” (89%) and “other patients would benefit more” (38%).6 Receiving terminal care in the ICU runs counter to the preferences of most patients.7 Therefore, the challenges are to define the true beneficiaries of critical care and to minimize the discomfort and unrealistic expectations of patients who will not benefit from intensive care.
For ICU patients, morbidity and mortality depend on the interaction of an acute insult (or a surgery), major comorbidities, and physiologic reserve. Aside from those with objective criteria of extreme illness, many patients have an indeterminate prognosis that is difficult to reliably predict.8,9 Several prognostic scores, including the APACHE (Acute Physiologic Assessment and Chronic Health Evaluation) and SOFA (Sequential Organ Failure Assessment) scores, have proved useful in understanding the illness burden of a population when comparing outcomes in different ICUs. Yet their use in assessing the survival of individual patients has not been advocated.10-15 The utility of such models is further challenged by the significant differences in survival between patients with similar illness scores; by the sometimes poor applicability of a model’s derivation cohort to other ICU populations (surgical in particular); by cases of huge disparities between actual and predicted mortality; and by the periodic need to recalibrate models according to advances in care.16-20
Physician intuition regarding prognosis is highly variable. In a series of medical (floor and ICU) admissions, resident physician estimates of illness severity and postdischarge status were associated with stepwise differences in mortality and APACHE scores.21,22 However, in a pure ICU population, in most cases seasoned providers could not accurately predict a patient’s chance of survival.23 Physicians are likewise poor in predicting family preferences regarding aggressive care vs alternatives, and often, survival is couched in terms of ICU survival, which for family members may not be as meaningful as long-term survival or functional recovery. Further, quality of life and patient preferences are not discussed in most cases, even those associated with poor outcomes.24 There also is a large amount of heterogeneity in the end of-life care of ICU patients. For example, cardiopulmonary resuscitation was attempted in up to 70% of dying patients in some ICUs and in as little as 4% in other ICUs.25 Thus, the limitations of predictive models, combined with misperceptions of patient preference, poor communication, and local traditions, lead to aggressive care being given to patients who might not benefit from or desire such care.
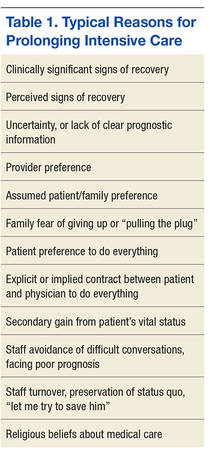
It has been stated that the trajectory of most critical illness is unclear enough so that patients should be admitted to the ICU for a trial of therapy, and that in outcome predictions, the response to intensive treatment may be more useful than laboratory and other data comprising illness severity scores.15,26 However, there is no consensus as to what constitutes a trial of intensive care therapy—vs a round of chemotherapy, a course of antibiotics, or a palliative ileostomy—yet this is the basis of many ICU admissions. Slight corrections in laboratory or physiologic findings often lead to continuation of aggressive care, often without any discussion of expected outcomes and the process of identifying and caring for patients who do not respond to therapy. Intensive care also may be prolonged because of several medical, personal, and social factors (Table 1).
At best, deciding how long to provide intensive care involves a synthesis of information about the trajectory, physiologic reserve, beliefs, values, and preferences of the patient. Any or all of these elements may not be known to the care decision-makers.
The authors conducted a study to determine whether a particular duration of care exists that represents a reasonable trial of therapy. As the VA Palo Alto Health Care System (VAPAHCS) ICU treats both medical and surgical patients, the authors were able to compare these subpopulations’ outcomes while providing the same standard of care. They analyzed the aggregate of patients as well as the medical and surgical subpopulations.
Methods
The VA Research and Development Committee and the Stanford Panel on Human Subjects approved the authors’ data collection and reporting.The study was conducted at the 15-bed mixed-medical/surgical VAPAHCS ICU. Analyzed data were drawn from all patients admitted during a 19-month period (July 14, 2008, to January 28, 2010). A serial log was used to prospectively capture basic data regarding each admission. Medical patients received care from the ICU service, and surgical patients were comanaged by the surgical and ICU teams.
A mortality database was constructed with data from the Decedent Affairs Office and from the national VistA database. The data included all deaths recorded either inside or outside the hospital or systemwide nursing facility. Mortality reported in the Computerized Patient Record System (CPRS) was queried further for patients with a length of stay (LOS) of more than 14 days.
Statistical Analysis
Calculations were based on denominators of individual patients or on number of admissions. All mortality calculations were based on a denominator of individual patients. For mortality analysis, only the last admission was included, unless a patient survived a full year between admissions. The Kruskal-Wallis test for nonnormally distributed data and the Dunn posttest for multiple comparisons were used for continuous variables (eg, age, LOS, risk scores); the Fisher exact test was used for categorical data; and the log-rank test was used to compare survival curves. For all analyses, P < .05 was considered statistically significant.
Mortality and Functional Status
Mortality risk scores on ICU admission were calculated with the Mortality Prediction Model–Admission III (MPM-III), using data from the CPRS. Specifics on this calculation are described in the eAppendix.
Current survival status of patients who were in the ICU more than 14 days was determined from the CPRS and telephone discussions with the patient or with relatives. Functional status was evaluated with the 36-Item Short Form Health Survey (SF-36), which has been used in comparable studies.27,28 Disposition at 6 months and 1 year was established by inspecting the CPRS for dates corresponding to these exact periods. For example, a patient in the hospital about 1 year after ICU discharge would be considered to be at home if discharged 1 day before the 365-day anniversary. In a few cases, progress notes indicated that the patient was receiving around-the-clock nursing care at home; in the analysis, these cases were included with those of patients known to be in traditional nursing facilities. In cases in which the CPRS lacked mortality information, the patient was presumed to be alive even if there were no records of clinic visits or other medical attention. Serial admission data from a mixed-medical/surgical ICU were collected over a 19-month period (July 14, 2008, to January 28, 2010) and analyzed.
Results
The final data set consisted of 1,113 admissions and 976 patients (one-third medical, two-thirds surgical). In this cohort, 12% of all patients studied were readmitted to the ICU at least once, and 12% of all ICU admissions were repeat admissions. The medical/surgical proportion was similar for readmitted patients. Demographics and other data are available in eTable 1.

Length of Stay
The distribution of all patients by LOS in the study period is shown in eFigure 1A. Data are skewed rightward toward longer LOS. The median LOS of 3 days for the entire population differed according to specialty, with a median of 3 days for medical patients (interquartile range, 2-7 days) and a median of 2 days for surgical patients (interquartile range, 1-5 days; P < .01 for medical vs surgical patients).

The LOS differed between ICU patients admitted for the first time and those readmitted within the 19-month study period. For both admission categories, LOS was longer for medical patients than for surgical patients. However, there were no significant differences between percentages of medical and surgical patients who were readmitted (Table 2). Despite comprising about 12% of the population, patients with more than 1 admission accounted for 23% of admissions and 25% of all bed occupancies during the study period.

Figure e1B shows ICU bed occupancy for different LOS intervals (calculated as bed days) and indicates that despite accounting for a small percentage of admissions, patients with long LOS accounted for a significant portion of total occupancy (32% for more than 1 month, 45% for more than 14 days). The medical and surgical contributions of these long-LOS patients were about equal. The figures indicate that more than half of medical ICU patient occupancy involved LOS of more than 14 days, while surgical patients tended to have shorter LOS.
Mortality
Of all the patients in this study, 5.1% died in the ICU; the mortality rate was 11% for medical patients and 2.1% for surgical patients. Thirty days after discharge, overall mortality was 10.4%, or 23.5% for medical patients and 3.9% for surgical patients. Finally, 1 year after discharge, mortality rates were 21.5% (overall), 39.4% (medical patients), and 12.5% (surgical patients) (Table 3). Survival curves demonstrated the difference between medical and surgical patients at 30 days and 1 year (Figures 1A & 1B).



Impact of LOS on Mortality
One-year mortality was 17% for patients who were in the ICU less than 14 days and 40% for those in the ICU more than 14 days (relative risk [RR] = 2.35; P < .01) (Table 4). 

Mortality also was higher in patients with more than 1 ICU admission. For the aggregate of ICU patients, readmission status was significantly associated with a 10% increase in mortality. For both single- and multiple-admission status, the mortality rate was 2.5-fold higher for medical patients than for surgical patients. The increased mortality associated with readmission status was not significantly different for either medical or surgical patients analyzed as subgroups (eAppendix Table.)
Impact of Age on Mortality
Figures 4A and 4B shows 30-day and 1-year mortality associated with age; regression analysis indicated that age is an independent predictor of ICU mortality. For 30-day mortality, increased age was positively associated with mortality in medical patients but not in surgical patients (r2 = 0.91; P < .0001). Age had a significant impact on 1-year mortality for both medical and surgical patients but less so in the latter (r2 = 0.95 and 0.65, respectively; P < .001 for both). Although increased mortality was associated with both LOS and age, there was no clear association between the latter 2 variables.
Survival of Chronic Critical Illness
As eTable 2 shows, 21.5% of all patients died either in the ICU or within the first year after ICU discharge. To evaluate the survival of chronic ICU residence, the authors performed a detailed analysis of functional status and mortality of patients with LOS of more than 14 days. Seventy-one patients fit that profile (their mean LOS was 41 days; median, 28 days). Of these patients, 11 died in the ICU, and another 17 died within 6 months (including 2 in a stepdown unit and 7 in hospice). Overall, 28 (39%) of the 71 patients died either in the ICU or within 6 months (35% aggregate, 53% of medical patients, and 27% of surgical patients in ICU > 2 weeks). Another 8 patients (11%) died between 6 and 12 months after discharge. One-year mortality among patients in the ICU more than 14 days was 40% overall, 50% for medical patients, and 29% for surgical patients—or twice that predicted by the MPM-III model, which figured mortality rates of 25% and 12% for medical and surgical patients, respectively. In this cohort, the mean MPM-III score was 18.6% for 1-year survivors and 29.3% for nonsurvivors (P = .016, Mann-Whitney U test). Mortality was associated with a trend toward higher MPM-III scores in both medical and surgical patients but did not reach statistical significance.

Of the cohort patients who lived at least 6 months after ICU discharge, 45% were still in a hospital or were in a nursing facility at 6 months. Of the patients who lived at least 1 year, 33% were still in a hospital or were in a nursing facility (Figure 5). At 1 year, mean age was 63 years for survivors and 69 years for the deceased (P < .01 by Student t test). 
Quality-of-Life Survey
The authors successfully contacted 32 of the 39 patients who lived at least 1 year after discharge after an ICU stay of more than 14 days. The subgroups’ median SF-36 scores were similar: 57 for medical patients and 51 for surgical patients. These average scores over 8 domains are similar to those reported by Graf and colleagues for 9 months after ICU discharge (53.7) and are lower than the normative data reported by those authors for the German population (mean, 66.5).29
Discussion
The goals of the present study were 2-fold—to gain a better understanding of the survival and functioning of patients after ICU residence and to define what may constitute a trial of therapy in ICU, or specifically to determine whether there is a particular ICU interval or point at which further care fails to improve survival. The study also compared medical and surgical subpopulations.
The main finding of this study was a 4-fold difference between ICU mortality and 1-year mortality. This mortality increase occurred in both medical and surgical patients, but there were large differences in magnitude between these groups. The survival rates generally were better than those of other general intensive care populations, though such a comparison should be made with caution, as survival differs by country, population, admitting practices, and a variety of other hospital characteristics.30,31 Although some findings of the present study may relate to its largely male U.S. veteran population, the authors believe they have provided a data-collection-and-analysis model that can be used by any hospital trying to understand the course and outcome of its ICU patients and recognizing the value of this knowledge in discussions on goals of care.
Mortality and LOS
As each interval of ICU residence was associated with a stepwise increase in mortality, there was no clear cutoff for diminishing return. To create a reference point, the authors analyzed the data of patients who were in an ICU more than 14 days—thinking that this duration may represent an outer limit of a reasonable trial of therapy and a measure that probably distinguishes acute from chronic critical illness.32 Use of this interval represented a conservative approach, as only 6.5% of the patients in this cohort had a LOS of more than 14 days. This small percentage of patients accounted for 45% of total bed occupancy in this study and 54% of all medical bed occupancy. In the more-than-14-days group, mortality was 37.5% for surgical patients and 46.3% for medical patients. Thus, LOS may be a dynamic measure of physiologic reserve and disease severity—reflecting variables such as response to therapy, severity of comorbidities, resistance to new problems, and rebound from chronic stress, inflammation, and catabolism. This view is supported by the nearly 2-fold higher mortality in medical patients and nearly 3-fold higher mortality in surgical patients in comparison with MPM-III predictions.
Twelve percent of all patients were admitted to ICU multiple times, and these admissions accounted for 25% of all bed occupancies. Multiple admissions indicate a high disease burden or a low physiologic reserve that prevents full recovery from critical illness. As mortality was higher in patients with multiple admissions, ICU readmission should be regarded as a marker for poor overall recovery and should prompt consideration of both initial discharge criteria and trajectory as well as goals of care.
Medical vs Surgical Patients
In this cohort, medical and surgical patients were distinguished on several grounds. Despite the similar mean age of these subpopulations, medical patients had longer LOS and higher short- and long-term mortality. These findings are not surprising, as medical patients in the ICU have high rates of end-stage disease, malignancy, and high comorbidity burden and are often admitted to have potentially life-ending conditions stabilized. Surgical patients generally are selected on their ability to withstand major systemic perturbations—palliative and emergency operations excepted—and generally have medical conditions optimized before surgery. As the expectation of postoperative survival likely biases clinician behavior toward aggressive care, some short-term survival may reflect this behavior.
In contrast, such biased behavior is not an issue in 1-year survival, which instead accurately reflects underlying health. The different slopes of medical and surgical patients on age-vs-mortality in Figures 4A & 4B indicate the different physiologic makeups of these ICU patients. With short and long LOS compared, the difference between surgical and medical patients in the ICU is striking: Sixty-one percent of all surgical bed days vs 45% of all medical bed days are for LOS less than 14 days. Nevertheless, chronic critical illness has a significant impact on both medical and surgical patients and tends to equalize some of the survival differences between these groups. These populations had similar ICU readmission rates as well as similar higher mortality rates for LOS of more than 14 days and especially for LOS of more than 1 month. With longer LOS, the survival curve of surgical patients begins to resemble that of medical patients—suggesting that the phenotype of chronic critical illness becomes the dominant force influencing survival and function (Figures 3A & 3B). Indeed, for surgical patients, the highest mortality categories were ICU readmission and LOS of more than 30 days.
The mortality rate was significantly lower for surgical patients than it was for medical patients at all intervals studied, with the largest separation in the short-term categories of ICU and 30-day mortality. The post-ICU mortality rates for medical and surgical patients are similar to those reported in several other studies, including a study of veterans.14-16,33,34 Among the present patients with LOS of more than 14 days, surviving surgical patients were significantly younger than nonsurviving surgical patients and both surviving and nonsurviving medical patients.


The few SF-36 responses collected revealed no differences between medical and surgical patients.
A Trial of Therapy
The present data are useful in describing the landscape of post-ICU survival to patients and their families. The data demonstrated a higher mortality trend that correlated with increases in age and increases in ICU duration and readmission. Within this continuum, there was no break point at which survivors and nonsurvivors clearly separated. The data therefore lack a boundary that can be used to define a trial of therapy. However, the added risks of age and recovery longer than 1 week are clear and should be included in care decisions. The generally better survival of surgical patients (nearly all of whom had elective surgery) in comparison with medical patients suggests these populations should be considered separately.
In the absence of a point distinguishing survivors from nonsurvivors, the authors performed a more detailed analysis of patients in the ICU for more than 14 days to provide some perspective on health care dependence in the subsequent year. That ICU survival does not necessarily equate to overall survival and independence long after ICU residence is an important matter for patients and families to consider when making decisions about critical care residence. The 14-day LOS data, though using a fairly arbitrary time point, suggest that patients who cannot recover from critical illness in less than 14 days should be advised of the range of short- and long-term mortality and the likelihood of high dependence on medical care within the subsequent year.
The concepts of hospital-dependent patient and persistent inflammation, immunosuppression, and catabolism syndrome have been introduced to describe the condition of progressive deterioration and inability to regain full independence after illness.32,35 These illness patterns deserve attention in prognosis discussions. The present study focused not on ICU survival but on 1-year mortality and functional independence, and it is these longer term outcomes that critical care professionals should consider. Intensive care units are successful in improving short-term survival, but a long line of successful ICU discharges may lead an intensivist to think that longer term survival is important as well and convey this impression to patients and their families.
Study Strengths
This study is one of a few to investigate the short- and long-term survival of an unselected cohort of critically ill patients and is unique in its inclusion of both medical and surgical patients receiving care in the same environment. Medical and surgical patients have different survival profiles that may necessitate separate studies of these subpopulations. However, the finding of different survival profiles under the same care highlights the intrinsic differences between these groups. Use of a 1.5-year study period allowed the authors to capture ICU patients with long LOS and to include multiple episodes of care provided by more than 10 different attending physicians. Therefore, these data likely were not influenced by any rare events or idiosyncrasies in practice styles. Further, the same teams of physicians and nurses cared for all the medical and surgical patients, and all unit-based protocols and quality improvement activities were applied to all patients.
Study Limitations
The intensive care patients come from a large catchment area; however, conditions seen in tertiary referral centers, such as bone marrow transplants, cerebrovascular, transplant surgery, and ventricular-assist devices are not represented in this population.
In this study, bed days were used as a crude measure of care burden. From a nursing perspective, however, the workload may be higher with quick-turnover beds than with long-term residents. On the other hand, long-term ICU residents are visited by multiple consultants and receive a much larger set of interventions, including weeks of ventilation and hemodialysis, line changes, and family meetings. A comparison of the costs involved for different ICU subpopulations would add valuable information to this discussion.
The authors took a conservative approach in establishing the mortality and residence of patients 1 year after their ICU stays. At 6 months, 1-year patients without evidence of hospital or nursing facility residence were assumed to be home. In reality, nearly all these patients had multiple admissions or emergency department stays, or there was other evidence of intensive care. Some patients who were assumed to be home may have left the area and become untraceable. All estimates of care dependence and mortality should therefore be considered minimums. The authors cannot envision how any of their estimates could overstate the morbidity and mortality.
The concept of hospital dependence is applicable to the majority of the ICU survivors, though the authors did not attempt to create a quantitative measure of this status.36 Another study limitation is that absence of hospitalization does not equal functional independence. A better definition of this status, and its application to a broad spectrum of LOS, would be a valuable adjunct to ICU decision making.
The convention by which the authors considered the first day of their study period a “fresh slate” did not adjust for the situation that some first admissions actually were readmissions. Assuming the validity of the finding that readmitted patients had a higher burden of morbidity and mortality, misclassification of admission status would tend to inflate the mortality of single-admission patients and minimize the magnitude of the differences found in this study. Similarly, an admission near the end of the study period may have been analyzed as a single admission, even if the patient was readmitted and died the next year. The latter situation also would tend to inflate the mortality of the single-admission category. None of these possible mathematical errors negates the fact that a second ICU admission should be regarded as a marker for poor recovery.
A more accurate estimate of short- and long-term prognosis likely can be obtained by examining laboratory studies and interventions such as vasopressors, dialysis, and ventilation at defined time points. Although the authors did not attempt it, development of such a model would be a valuable undertaking. They focused on describing the expected course of ICU patients and determining what patterns emerged from care duration. As this study found that the prognosis for long-term ICU residents remained guarded a long time after discharge, survival models of patients with 1- to 2-week ICU residences likely would be valuable in clinical decision making.
A quality-of-life survey was administered only to patients in the ICU longer than 2 weeks. This limited study was conducted to explore the feasibility of assessing outcomes other than survival and to determine the staffing requirements needed to research this further. A more meaningful analysis would come from a broader analysis of scores from 3 or 4 different ICU lengths of stay.
Clinician and family behavior can influence some of the outcomes measured in this study—particularly in cases in which an illness is poorly characterized and an evidence basis for decision making is lacking. In these situations, values and individual clinician judgment likely predominate, possibly introducing variability to care duration. Nevertheless, cumulative mortality 1 month or more after ICU residence would eliminate biased clinician behavior. The heterogeneity of care providers’ and families’ decision making, captured in this analysis, likely is a normal phenomenon that should help inform physicians’ understanding of prolonged ICU residence.


1. Halpern NA. Can the costs of critical care be controlled? Curr Opin Crit Care. 2009;15(6):591-596.
2. Angus DC, Barnato AE, Linde-Zwirble WT, et al; Robert Wood Johnson Foundation ICU End-of-Life Peer Group. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med. 2004;32(3):638-643.
3. Barnato AE, McClellan MB, Kagay CR, Garber AM. Trends in inpatient treatment intensity among Medicare beneficiaries at the end of life. Health Serv Res. 2004;39(2):363-375.
4. Teno JM, Gozalo PL, Bynum JP, et al. Change in end-of-life care for Medicare beneficiaries: site of death, place of care, and health care transitions in 2000, 2005, and 2009. JAMA. 2013;309(5):470-477.
5. Zilberberg MD, Shorr AF. Economics at the end of life: hospital and ICU perspectives. Semin Respir Crit Care Med. 2012;33(4):362-369.
6. Piers RD, Azoulay E, Ricou B, et al; APPROPRICUS Study Group of the Ethics Section of the ESICM. Perceptions of appropriateness of care among European and Israeli intensive care unit nurses and physicians. JAMA. 2011;306(24):2694-2703.
7. Higginson IJ, Sen-Gupta GJ. Place of care in advanced cancer: a qualitative systematic literature review of patient p. J Palliat Med. 2000;3(3):287-300.
8. McClish DK, Powell SH. How well can physicians estimate mortality in a medical intensive care unit? Med Decis Making. 1989;9(2):125-132.
9. Barrera R, Nygard S, Sogoloff H, Groeger J, Wilson R. Accuracy of predictions of survival at admission to the intensive care unit. J Crit Care. 2001;16(1):32-35.
10. Johnson AE, Kramer AA, Clifford GD. A new severity of illness scale using a subset of Acute Physiology and Chronic Health Evaluation data elements shows comparable predictive accuracy. Crit Care Med. 2013;41(7):1711-1718.
11. D'Hoore W, Bouckaert A, Tilquin C. Practical considerations on the use of the Charlson comorbidity index with administrative data bases. J Clin Epidemiol. 1996;49(12):1429-1433.
12. Knaus WA, Wagner DP, Zimmerman JE, Draper EA. Variations in mortality and length of stay in intensive care units. Ann Intern Med. 1993;118(10):753-761.
13. Lemeshow S, Teres D, Klar J, Avrunin JS, Gehlbach SH, Rapoport J. Mortality Probability Models (MPM II) based on an international cohort of intensive care unit patients. JAMA. 1993;270(20):2478-2486.
14. Render ML, Kim HM, Welsh DE, et al; VA ICU Project (VIP) Investigators. Automated intensive care unit risk adjustment: results from a national Veterans Affairs study. Crit Care Med. 2003;31(6):1638-1646.
15. Viviand X, Gouvernet J, Granthil C, François G. Simplification of the SAPS by selecting independent variables. Intensive Care Med. 1991;17(3):164-168.
16. Higgins TL, Teres D, Copes WS, Nathanson BH, Stark M, Kramer AA. Assessing contemporary intensive care unit outcome: an updated Mortality Probability Admission Model (MPM0-III). Crit Care Med. 2007;35(3):827-835.
17. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818-829.
18. Poses RM, McClish DK, Smith WR, et al. Results of report cards for patients with congestive heart failure depend on the method used to adjust for severity. Ann Intern Med. 2000;133(1):10-20.
19. Schuster DP. Predicting outcome after ICU admission. The art and science of assessing risk. Chest. 1992;102(6):1861-1870.
20. Teno JM, Fisher E, Hamel MB, et al. Decision-making and outcomes of prolonged ICU stays in seriously ill patients. J Am Geriatr Soc. 2000;48(suppl 5):S70-S74.
21. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245-1251.
22. Pompei P, Charlson ME, Ales K, MacKenzie CR, Norton M. Relating patient characteristics at the time of admission to outcomes of hospitalization. J Clin Epidemiol. 1991;44(10):1063-1069.
23. Meadow W, Pohlman A, Frain L, et al. Power and limitations of daily prognostications of death in the medical intensive care unit. Crit Care Med. 2011;39(3):474-479.
24. Douglas SL, Daly BJ, Lipson AR. Neglect of quality-of-life considerations in intensive care unit family meetings for long-stay intensive care unit patients. Crit Care Med. 2012;40(2):461-467.
25. Prendergast TJ, Claessens MT, Luce JM. A national survey of end-of-life care for critically ill patients. Am J Respir Crit Care Med. 1998;158(4):1163-1167.
26. Luce JM. A history of resolving conflicts over end-of-life care in intensive care units in the United States. Crit Care Med. 2010;38(8):1623-1629.
27. Bashour CA, Yared JP, Ryan TA, et al. Long-term survival and functional capacity in cardiac surgery patients after prolonged intensive care. Crit Care Med. 2000;28(12):3847-3853.
28. Eddleston JM, White P, Guthrie E. Survival, morbidity, and quality of life after discharge from intensive care. Crit Care Med. 2000;28(7):2293-2299.
29. Graf J, Koch M, Dujardin R, Kersten A, Janssens U. Health-related quality of life before, 1 month after, and 9 months after intensive care in medical cardiovascular and pulmonary patients. Crit Care Med. 2003;31(8):2163-2169.
30. Montuclard L, Garrouste-Orgeas M, Timsit JF, Misset B, De Jonghe B, Carlet J. Outcome, functional autonomy, and quality of life of elderly patients with a long-term intensive care unit stay. Crit Care Med. 2000;28(10):3389-3395.
31. Teno JM, Harrell FE Jr, Knaus W, et al. Prediction of survival for older hospitalized patients: the HELP survival model. Hospitalized Elderly Longitudinal Project. J Am Geriatr Soc. 2000;48(suppl 5):S16-S24.
32. Lamas D. Chronic critical illness. N Engl J Med. 2014;370(2):175-177.
33. Konopad E, Noseworthy TW, Johnston R, Shustack A, Grace M. Quality of life measures before and one year after admission to an intensive care unit. Crit Care Med. 1995;23(10):1653-1659.
34. Render ML, Kim HM, Deddens J, et al. Variation in outcomes in Veterans Affairs intensive care units with a computerized severity measure. Crit Care Med. 2005;33(5):930-939.
35. Gentile LF, Cuenca AG, Efron PA, et al. Persistent inflammation and immunosuppression: a common syndrome and new horizon for surgical intensive care. J Trauma Acute Care Surg. 2012;72(6):1491-1501.
36. Reuben DB, Tinetti ME. The hospital-dependent patient. N Engl J Med. 2014;370(8):694-697.
Admission to an intensive care unit (ICU) is lifesaving for some patients, but for many, the admission carries high expectations and financial costs and fails to provide desirable outcomes. Patients who receive intensive care have a mortality rate of about 20%, and the costs of this care comprise about 4% of the U.S. health care budget.1,2 In a study of Medicare recipients, treatment intensity and expenses increased between the mid-1980s and 1999 but without any increase in survivorship; per capita ICU expenses were higher for patients who did not survive the ICU.3 Use of the ICU in patients’ final stages of life has increased in proportion since then, and the demand for critical care is likely to continue as the relative proportion of elderly patients in the population rises.2,4,5
Physicians and nurses who responded to a European survey on the inappropriateness of intensive care overwhelmingly endorsed the problems of “too much care” (89%) and “other patients would benefit more” (38%).6 Receiving terminal care in the ICU runs counter to the preferences of most patients.7 Therefore, the challenges are to define the true beneficiaries of critical care and to minimize the discomfort and unrealistic expectations of patients who will not benefit from intensive care.
For ICU patients, morbidity and mortality depend on the interaction of an acute insult (or a surgery), major comorbidities, and physiologic reserve. Aside from those with objective criteria of extreme illness, many patients have an indeterminate prognosis that is difficult to reliably predict.8,9 Several prognostic scores, including the APACHE (Acute Physiologic Assessment and Chronic Health Evaluation) and SOFA (Sequential Organ Failure Assessment) scores, have proved useful in understanding the illness burden of a population when comparing outcomes in different ICUs. Yet their use in assessing the survival of individual patients has not been advocated.10-15 The utility of such models is further challenged by the significant differences in survival between patients with similar illness scores; by the sometimes poor applicability of a model’s derivation cohort to other ICU populations (surgical in particular); by cases of huge disparities between actual and predicted mortality; and by the periodic need to recalibrate models according to advances in care.16-20
Physician intuition regarding prognosis is highly variable. In a series of medical (floor and ICU) admissions, resident physician estimates of illness severity and postdischarge status were associated with stepwise differences in mortality and APACHE scores.21,22 However, in a pure ICU population, in most cases seasoned providers could not accurately predict a patient’s chance of survival.23 Physicians are likewise poor in predicting family preferences regarding aggressive care vs alternatives, and often, survival is couched in terms of ICU survival, which for family members may not be as meaningful as long-term survival or functional recovery. Further, quality of life and patient preferences are not discussed in most cases, even those associated with poor outcomes.24 There also is a large amount of heterogeneity in the end of-life care of ICU patients. For example, cardiopulmonary resuscitation was attempted in up to 70% of dying patients in some ICUs and in as little as 4% in other ICUs.25 Thus, the limitations of predictive models, combined with misperceptions of patient preference, poor communication, and local traditions, lead to aggressive care being given to patients who might not benefit from or desire such care.
It has been stated that the trajectory of most critical illness is unclear enough so that patients should be admitted to the ICU for a trial of therapy, and that in outcome predictions, the response to intensive treatment may be more useful than laboratory and other data comprising illness severity scores.15,26 However, there is no consensus as to what constitutes a trial of intensive care therapy—vs a round of chemotherapy, a course of antibiotics, or a palliative ileostomy—yet this is the basis of many ICU admissions. Slight corrections in laboratory or physiologic findings often lead to continuation of aggressive care, often without any discussion of expected outcomes and the process of identifying and caring for patients who do not respond to therapy. Intensive care also may be prolonged because of several medical, personal, and social factors (Table 1).
At best, deciding how long to provide intensive care involves a synthesis of information about the trajectory, physiologic reserve, beliefs, values, and preferences of the patient. Any or all of these elements may not be known to the care decision-makers.
The authors conducted a study to determine whether a particular duration of care exists that represents a reasonable trial of therapy. As the VA Palo Alto Health Care System (VAPAHCS) ICU treats both medical and surgical patients, the authors were able to compare these subpopulations’ outcomes while providing the same standard of care. They analyzed the aggregate of patients as well as the medical and surgical subpopulations.
Methods
The VA Research and Development Committee and the Stanford Panel on Human Subjects approved the authors’ data collection and reporting.The study was conducted at the 15-bed mixed-medical/surgical VAPAHCS ICU. Analyzed data were drawn from all patients admitted during a 19-month period (July 14, 2008, to January 28, 2010). A serial log was used to prospectively capture basic data regarding each admission. Medical patients received care from the ICU service, and surgical patients were comanaged by the surgical and ICU teams.
A mortality database was constructed with data from the Decedent Affairs Office and from the national VistA database. The data included all deaths recorded either inside or outside the hospital or systemwide nursing facility. Mortality reported in the Computerized Patient Record System (CPRS) was queried further for patients with a length of stay (LOS) of more than 14 days.
Statistical Analysis
Calculations were based on denominators of individual patients or on number of admissions. All mortality calculations were based on a denominator of individual patients. For mortality analysis, only the last admission was included, unless a patient survived a full year between admissions. The Kruskal-Wallis test for nonnormally distributed data and the Dunn posttest for multiple comparisons were used for continuous variables (eg, age, LOS, risk scores); the Fisher exact test was used for categorical data; and the log-rank test was used to compare survival curves. For all analyses, P < .05 was considered statistically significant.
Mortality and Functional Status
Mortality risk scores on ICU admission were calculated with the Mortality Prediction Model–Admission III (MPM-III), using data from the CPRS. Specifics on this calculation are described in the eAppendix.
Current survival status of patients who were in the ICU more than 14 days was determined from the CPRS and telephone discussions with the patient or with relatives. Functional status was evaluated with the 36-Item Short Form Health Survey (SF-36), which has been used in comparable studies.27,28 Disposition at 6 months and 1 year was established by inspecting the CPRS for dates corresponding to these exact periods. For example, a patient in the hospital about 1 year after ICU discharge would be considered to be at home if discharged 1 day before the 365-day anniversary. In a few cases, progress notes indicated that the patient was receiving around-the-clock nursing care at home; in the analysis, these cases were included with those of patients known to be in traditional nursing facilities. In cases in which the CPRS lacked mortality information, the patient was presumed to be alive even if there were no records of clinic visits or other medical attention. Serial admission data from a mixed-medical/surgical ICU were collected over a 19-month period (July 14, 2008, to January 28, 2010) and analyzed.
Results
The final data set consisted of 1,113 admissions and 976 patients (one-third medical, two-thirds surgical). In this cohort, 12% of all patients studied were readmitted to the ICU at least once, and 12% of all ICU admissions were repeat admissions. The medical/surgical proportion was similar for readmitted patients. Demographics and other data are available in eTable 1.
Length of Stay
The distribution of all patients by LOS in the study period is shown in eFigure 1A. Data are skewed rightward toward longer LOS. The median LOS of 3 days for the entire population differed according to specialty, with a median of 3 days for medical patients (interquartile range, 2-7 days) and a median of 2 days for surgical patients (interquartile range, 1-5 days; P < .01 for medical vs surgical patients).
The LOS differed between ICU patients admitted for the first time and those readmitted within the 19-month study period. For both admission categories, LOS was longer for medical patients than for surgical patients. However, there were no significant differences between percentages of medical and surgical patients who were readmitted (Table 2). Despite comprising about 12% of the population, patients with more than 1 admission accounted for 23% of admissions and 25% of all bed occupancies during the study period.
Figure e1B shows ICU bed occupancy for different LOS intervals (calculated as bed days) and indicates that despite accounting for a small percentage of admissions, patients with long LOS accounted for a significant portion of total occupancy (32% for more than 1 month, 45% for more than 14 days). The medical and surgical contributions of these long-LOS patients were about equal. The figures indicate that more than half of medical ICU patient occupancy involved LOS of more than 14 days, while surgical patients tended to have shorter LOS.
Mortality
Of all the patients in this study, 5.1% died in the ICU; the mortality rate was 11% for medical patients and 2.1% for surgical patients. Thirty days after discharge, overall mortality was 10.4%, or 23.5% for medical patients and 3.9% for surgical patients. Finally, 1 year after discharge, mortality rates were 21.5% (overall), 39.4% (medical patients), and 12.5% (surgical patients) (Table 3). Survival curves demonstrated the difference between medical and surgical patients at 30 days and 1 year (Figures 1A & 1B).
Impact of LOS on Mortality
One-year mortality was 17% for patients who were in the ICU less than 14 days and 40% for those in the ICU more than 14 days (relative risk [RR] = 2.35; P < .01) (Table 4).
Mortality also was higher in patients with more than 1 ICU admission. For the aggregate of ICU patients, readmission status was significantly associated with a 10% increase in mortality. For both single- and multiple-admission status, the mortality rate was 2.5-fold higher for medical patients than for surgical patients. The increased mortality associated with readmission status was not significantly different for either medical or surgical patients analyzed as subgroups (eAppendix Table.)
Impact of Age on Mortality
Figures 4A and 4B shows 30-day and 1-year mortality associated with age; regression analysis indicated that age is an independent predictor of ICU mortality. For 30-day mortality, increased age was positively associated with mortality in medical patients but not in surgical patients (r2 = 0.91; P < .0001). Age had a significant impact on 1-year mortality for both medical and surgical patients but less so in the latter (r2 = 0.95 and 0.65, respectively; P < .001 for both). Although increased mortality was associated with both LOS and age, there was no clear association between the latter 2 variables.
Survival of Chronic Critical Illness
As eTable 2 shows, 21.5% of all patients died either in the ICU or within the first year after ICU discharge. To evaluate the survival of chronic ICU residence, the authors performed a detailed analysis of functional status and mortality of patients with LOS of more than 14 days. Seventy-one patients fit that profile (their mean LOS was 41 days; median, 28 days). Of these patients, 11 died in the ICU, and another 17 died within 6 months (including 2 in a stepdown unit and 7 in hospice). Overall, 28 (39%) of the 71 patients died either in the ICU or within 6 months (35% aggregate, 53% of medical patients, and 27% of surgical patients in ICU > 2 weeks). Another 8 patients (11%) died between 6 and 12 months after discharge. One-year mortality among patients in the ICU more than 14 days was 40% overall, 50% for medical patients, and 29% for surgical patients—or twice that predicted by the MPM-III model, which figured mortality rates of 25% and 12% for medical and surgical patients, respectively. In this cohort, the mean MPM-III score was 18.6% for 1-year survivors and 29.3% for nonsurvivors (P = .016, Mann-Whitney U test). Mortality was associated with a trend toward higher MPM-III scores in both medical and surgical patients but did not reach statistical significance.
Of the cohort patients who lived at least 6 months after ICU discharge, 45% were still in a hospital or were in a nursing facility at 6 months. Of the patients who lived at least 1 year, 33% were still in a hospital or were in a nursing facility (Figure 5). At 1 year, mean age was 63 years for survivors and 69 years for the deceased (P < .01 by Student t test).
Quality-of-Life Survey
The authors successfully contacted 32 of the 39 patients who lived at least 1 year after discharge after an ICU stay of more than 14 days. The subgroups’ median SF-36 scores were similar: 57 for medical patients and 51 for surgical patients. These average scores over 8 domains are similar to those reported by Graf and colleagues for 9 months after ICU discharge (53.7) and are lower than the normative data reported by those authors for the German population (mean, 66.5).29
Discussion
The goals of the present study were 2-fold—to gain a better understanding of the survival and functioning of patients after ICU residence and to define what may constitute a trial of therapy in ICU, or specifically to determine whether there is a particular ICU interval or point at which further care fails to improve survival. The study also compared medical and surgical subpopulations.
The main finding of this study was a 4-fold difference between ICU mortality and 1-year mortality. This mortality increase occurred in both medical and surgical patients, but there were large differences in magnitude between these groups. The survival rates generally were better than those of other general intensive care populations, though such a comparison should be made with caution, as survival differs by country, population, admitting practices, and a variety of other hospital characteristics.30,31 Although some findings of the present study may relate to its largely male U.S. veteran population, the authors believe they have provided a data-collection-and-analysis model that can be used by any hospital trying to understand the course and outcome of its ICU patients and recognizing the value of this knowledge in discussions on goals of care.
Mortality and LOS
As each interval of ICU residence was associated with a stepwise increase in mortality, there was no clear cutoff for diminishing return. To create a reference point, the authors analyzed the data of patients who were in an ICU more than 14 days—thinking that this duration may represent an outer limit of a reasonable trial of therapy and a measure that probably distinguishes acute from chronic critical illness.32 Use of this interval represented a conservative approach, as only 6.5% of the patients in this cohort had a LOS of more than 14 days. This small percentage of patients accounted for 45% of total bed occupancy in this study and 54% of all medical bed occupancy. In the more-than-14-days group, mortality was 37.5% for surgical patients and 46.3% for medical patients. Thus, LOS may be a dynamic measure of physiologic reserve and disease severity—reflecting variables such as response to therapy, severity of comorbidities, resistance to new problems, and rebound from chronic stress, inflammation, and catabolism. This view is supported by the nearly 2-fold higher mortality in medical patients and nearly 3-fold higher mortality in surgical patients in comparison with MPM-III predictions.
Twelve percent of all patients were admitted to ICU multiple times, and these admissions accounted for 25% of all bed occupancies. Multiple admissions indicate a high disease burden or a low physiologic reserve that prevents full recovery from critical illness. As mortality was higher in patients with multiple admissions, ICU readmission should be regarded as a marker for poor overall recovery and should prompt consideration of both initial discharge criteria and trajectory as well as goals of care.
Medical vs Surgical Patients
In this cohort, medical and surgical patients were distinguished on several grounds. Despite the similar mean age of these subpopulations, medical patients had longer LOS and higher short- and long-term mortality. These findings are not surprising, as medical patients in the ICU have high rates of end-stage disease, malignancy, and high comorbidity burden and are often admitted to have potentially life-ending conditions stabilized. Surgical patients generally are selected on their ability to withstand major systemic perturbations—palliative and emergency operations excepted—and generally have medical conditions optimized before surgery. As the expectation of postoperative survival likely biases clinician behavior toward aggressive care, some short-term survival may reflect this behavior.
In contrast, such biased behavior is not an issue in 1-year survival, which instead accurately reflects underlying health. The different slopes of medical and surgical patients on age-vs-mortality in Figures 4A & 4B indicate the different physiologic makeups of these ICU patients. With short and long LOS compared, the difference between surgical and medical patients in the ICU is striking: Sixty-one percent of all surgical bed days vs 45% of all medical bed days are for LOS less than 14 days. Nevertheless, chronic critical illness has a significant impact on both medical and surgical patients and tends to equalize some of the survival differences between these groups. These populations had similar ICU readmission rates as well as similar higher mortality rates for LOS of more than 14 days and especially for LOS of more than 1 month. With longer LOS, the survival curve of surgical patients begins to resemble that of medical patients—suggesting that the phenotype of chronic critical illness becomes the dominant force influencing survival and function (Figures 3A & 3B). Indeed, for surgical patients, the highest mortality categories were ICU readmission and LOS of more than 30 days.
The mortality rate was significantly lower for surgical patients than it was for medical patients at all intervals studied, with the largest separation in the short-term categories of ICU and 30-day mortality. The post-ICU mortality rates for medical and surgical patients are similar to those reported in several other studies, including a study of veterans.14-16,33,34 Among the present patients with LOS of more than 14 days, surviving surgical patients were significantly younger than nonsurviving surgical patients and both surviving and nonsurviving medical patients.
The few SF-36 responses collected revealed no differences between medical and surgical patients.
A Trial of Therapy
The present data are useful in describing the landscape of post-ICU survival to patients and their families. The data demonstrated a higher mortality trend that correlated with increases in age and increases in ICU duration and readmission. Within this continuum, there was no break point at which survivors and nonsurvivors clearly separated. The data therefore lack a boundary that can be used to define a trial of therapy. However, the added risks of age and recovery longer than 1 week are clear and should be included in care decisions. The generally better survival of surgical patients (nearly all of whom had elective surgery) in comparison with medical patients suggests these populations should be considered separately.
In the absence of a point distinguishing survivors from nonsurvivors, the authors performed a more detailed analysis of patients in the ICU for more than 14 days to provide some perspective on health care dependence in the subsequent year. That ICU survival does not necessarily equate to overall survival and independence long after ICU residence is an important matter for patients and families to consider when making decisions about critical care residence. The 14-day LOS data, though using a fairly arbitrary time point, suggest that patients who cannot recover from critical illness in less than 14 days should be advised of the range of short- and long-term mortality and the likelihood of high dependence on medical care within the subsequent year.
The concepts of hospital-dependent patient and persistent inflammation, immunosuppression, and catabolism syndrome have been introduced to describe the condition of progressive deterioration and inability to regain full independence after illness.32,35 These illness patterns deserve attention in prognosis discussions. The present study focused not on ICU survival but on 1-year mortality and functional independence, and it is these longer term outcomes that critical care professionals should consider. Intensive care units are successful in improving short-term survival, but a long line of successful ICU discharges may lead an intensivist to think that longer term survival is important as well and convey this impression to patients and their families.
Study Strengths
This study is one of a few to investigate the short- and long-term survival of an unselected cohort of critically ill patients and is unique in its inclusion of both medical and surgical patients receiving care in the same environment. Medical and surgical patients have different survival profiles that may necessitate separate studies of these subpopulations. However, the finding of different survival profiles under the same care highlights the intrinsic differences between these groups. Use of a 1.5-year study period allowed the authors to capture ICU patients with long LOS and to include multiple episodes of care provided by more than 10 different attending physicians. Therefore, these data likely were not influenced by any rare events or idiosyncrasies in practice styles. Further, the same teams of physicians and nurses cared for all the medical and surgical patients, and all unit-based protocols and quality improvement activities were applied to all patients.
Study Limitations
The intensive care patients come from a large catchment area; however, conditions seen in tertiary referral centers, such as bone marrow transplants, cerebrovascular, transplant surgery, and ventricular-assist devices are not represented in this population.
In this study, bed days were used as a crude measure of care burden. From a nursing perspective, however, the workload may be higher with quick-turnover beds than with long-term residents. On the other hand, long-term ICU residents are visited by multiple consultants and receive a much larger set of interventions, including weeks of ventilation and hemodialysis, line changes, and family meetings. A comparison of the costs involved for different ICU subpopulations would add valuable information to this discussion.
The authors took a conservative approach in establishing the mortality and residence of patients 1 year after their ICU stays. At 6 months, 1-year patients without evidence of hospital or nursing facility residence were assumed to be home. In reality, nearly all these patients had multiple admissions or emergency department stays, or there was other evidence of intensive care. Some patients who were assumed to be home may have left the area and become untraceable. All estimates of care dependence and mortality should therefore be considered minimums. The authors cannot envision how any of their estimates could overstate the morbidity and mortality.
The concept of hospital dependence is applicable to the majority of the ICU survivors, though the authors did not attempt to create a quantitative measure of this status.36 Another study limitation is that absence of hospitalization does not equal functional independence. A better definition of this status, and its application to a broad spectrum of LOS, would be a valuable adjunct to ICU decision making.
The convention by which the authors considered the first day of their study period a “fresh slate” did not adjust for the situation that some first admissions actually were readmissions. Assuming the validity of the finding that readmitted patients had a higher burden of morbidity and mortality, misclassification of admission status would tend to inflate the mortality of single-admission patients and minimize the magnitude of the differences found in this study. Similarly, an admission near the end of the study period may have been analyzed as a single admission, even if the patient was readmitted and died the next year. The latter situation also would tend to inflate the mortality of the single-admission category. None of these possible mathematical errors negates the fact that a second ICU admission should be regarded as a marker for poor recovery.
A more accurate estimate of short- and long-term prognosis likely can be obtained by examining laboratory studies and interventions such as vasopressors, dialysis, and ventilation at defined time points. Although the authors did not attempt it, development of such a model would be a valuable undertaking. They focused on describing the expected course of ICU patients and determining what patterns emerged from care duration. As this study found that the prognosis for long-term ICU residents remained guarded a long time after discharge, survival models of patients with 1- to 2-week ICU residences likely would be valuable in clinical decision making.
A quality-of-life survey was administered only to patients in the ICU longer than 2 weeks. This limited study was conducted to explore the feasibility of assessing outcomes other than survival and to determine the staffing requirements needed to research this further. A more meaningful analysis would come from a broader analysis of scores from 3 or 4 different ICU lengths of stay.
Clinician and family behavior can influence some of the outcomes measured in this study—particularly in cases in which an illness is poorly characterized and an evidence basis for decision making is lacking. In these situations, values and individual clinician judgment likely predominate, possibly introducing variability to care duration. Nevertheless, cumulative mortality 1 month or more after ICU residence would eliminate biased clinician behavior. The heterogeneity of care providers’ and families’ decision making, captured in this analysis, likely is a normal phenomenon that should help inform physicians’ understanding of prolonged ICU residence.
Admission to an intensive care unit (ICU) is lifesaving for some patients, but for many, the admission carries high expectations and financial costs and fails to provide desirable outcomes. Patients who receive intensive care have a mortality rate of about 20%, and the costs of this care comprise about 4% of the U.S. health care budget.1,2 In a study of Medicare recipients, treatment intensity and expenses increased between the mid-1980s and 1999 but without any increase in survivorship; per capita ICU expenses were higher for patients who did not survive the ICU.3 Use of the ICU in patients’ final stages of life has increased in proportion since then, and the demand for critical care is likely to continue as the relative proportion of elderly patients in the population rises.2,4,5
Physicians and nurses who responded to a European survey on the inappropriateness of intensive care overwhelmingly endorsed the problems of “too much care” (89%) and “other patients would benefit more” (38%).6 Receiving terminal care in the ICU runs counter to the preferences of most patients.7 Therefore, the challenges are to define the true beneficiaries of critical care and to minimize the discomfort and unrealistic expectations of patients who will not benefit from intensive care.
For ICU patients, morbidity and mortality depend on the interaction of an acute insult (or a surgery), major comorbidities, and physiologic reserve. Aside from those with objective criteria of extreme illness, many patients have an indeterminate prognosis that is difficult to reliably predict.8,9 Several prognostic scores, including the APACHE (Acute Physiologic Assessment and Chronic Health Evaluation) and SOFA (Sequential Organ Failure Assessment) scores, have proved useful in understanding the illness burden of a population when comparing outcomes in different ICUs. Yet their use in assessing the survival of individual patients has not been advocated.10-15 The utility of such models is further challenged by the significant differences in survival between patients with similar illness scores; by the sometimes poor applicability of a model’s derivation cohort to other ICU populations (surgical in particular); by cases of huge disparities between actual and predicted mortality; and by the periodic need to recalibrate models according to advances in care.16-20
Physician intuition regarding prognosis is highly variable. In a series of medical (floor and ICU) admissions, resident physician estimates of illness severity and postdischarge status were associated with stepwise differences in mortality and APACHE scores.21,22 However, in a pure ICU population, in most cases seasoned providers could not accurately predict a patient’s chance of survival.23 Physicians are likewise poor in predicting family preferences regarding aggressive care vs alternatives, and often, survival is couched in terms of ICU survival, which for family members may not be as meaningful as long-term survival or functional recovery. Further, quality of life and patient preferences are not discussed in most cases, even those associated with poor outcomes.24 There also is a large amount of heterogeneity in the end of-life care of ICU patients. For example, cardiopulmonary resuscitation was attempted in up to 70% of dying patients in some ICUs and in as little as 4% in other ICUs.25 Thus, the limitations of predictive models, combined with misperceptions of patient preference, poor communication, and local traditions, lead to aggressive care being given to patients who might not benefit from or desire such care.
It has been stated that the trajectory of most critical illness is unclear enough so that patients should be admitted to the ICU for a trial of therapy, and that in outcome predictions, the response to intensive treatment may be more useful than laboratory and other data comprising illness severity scores.15,26 However, there is no consensus as to what constitutes a trial of intensive care therapy—vs a round of chemotherapy, a course of antibiotics, or a palliative ileostomy—yet this is the basis of many ICU admissions. Slight corrections in laboratory or physiologic findings often lead to continuation of aggressive care, often without any discussion of expected outcomes and the process of identifying and caring for patients who do not respond to therapy. Intensive care also may be prolonged because of several medical, personal, and social factors (Table 1).
At best, deciding how long to provide intensive care involves a synthesis of information about the trajectory, physiologic reserve, beliefs, values, and preferences of the patient. Any or all of these elements may not be known to the care decision-makers.
The authors conducted a study to determine whether a particular duration of care exists that represents a reasonable trial of therapy. As the VA Palo Alto Health Care System (VAPAHCS) ICU treats both medical and surgical patients, the authors were able to compare these subpopulations’ outcomes while providing the same standard of care. They analyzed the aggregate of patients as well as the medical and surgical subpopulations.
Methods
The VA Research and Development Committee and the Stanford Panel on Human Subjects approved the authors’ data collection and reporting.The study was conducted at the 15-bed mixed-medical/surgical VAPAHCS ICU. Analyzed data were drawn from all patients admitted during a 19-month period (July 14, 2008, to January 28, 2010). A serial log was used to prospectively capture basic data regarding each admission. Medical patients received care from the ICU service, and surgical patients were comanaged by the surgical and ICU teams.
A mortality database was constructed with data from the Decedent Affairs Office and from the national VistA database. The data included all deaths recorded either inside or outside the hospital or systemwide nursing facility. Mortality reported in the Computerized Patient Record System (CPRS) was queried further for patients with a length of stay (LOS) of more than 14 days.
Statistical Analysis
Calculations were based on denominators of individual patients or on number of admissions. All mortality calculations were based on a denominator of individual patients. For mortality analysis, only the last admission was included, unless a patient survived a full year between admissions. The Kruskal-Wallis test for nonnormally distributed data and the Dunn posttest for multiple comparisons were used for continuous variables (eg, age, LOS, risk scores); the Fisher exact test was used for categorical data; and the log-rank test was used to compare survival curves. For all analyses, P < .05 was considered statistically significant.
Mortality and Functional Status
Mortality risk scores on ICU admission were calculated with the Mortality Prediction Model–Admission III (MPM-III), using data from the CPRS. Specifics on this calculation are described in the eAppendix.
Current survival status of patients who were in the ICU more than 14 days was determined from the CPRS and telephone discussions with the patient or with relatives. Functional status was evaluated with the 36-Item Short Form Health Survey (SF-36), which has been used in comparable studies.27,28 Disposition at 6 months and 1 year was established by inspecting the CPRS for dates corresponding to these exact periods. For example, a patient in the hospital about 1 year after ICU discharge would be considered to be at home if discharged 1 day before the 365-day anniversary. In a few cases, progress notes indicated that the patient was receiving around-the-clock nursing care at home; in the analysis, these cases were included with those of patients known to be in traditional nursing facilities. In cases in which the CPRS lacked mortality information, the patient was presumed to be alive even if there were no records of clinic visits or other medical attention. Serial admission data from a mixed-medical/surgical ICU were collected over a 19-month period (July 14, 2008, to January 28, 2010) and analyzed.
Results
The final data set consisted of 1,113 admissions and 976 patients (one-third medical, two-thirds surgical). In this cohort, 12% of all patients studied were readmitted to the ICU at least once, and 12% of all ICU admissions were repeat admissions. The medical/surgical proportion was similar for readmitted patients. Demographics and other data are available in eTable 1.
Length of Stay
The distribution of all patients by LOS in the study period is shown in eFigure 1A. Data are skewed rightward toward longer LOS. The median LOS of 3 days for the entire population differed according to specialty, with a median of 3 days for medical patients (interquartile range, 2-7 days) and a median of 2 days for surgical patients (interquartile range, 1-5 days; P < .01 for medical vs surgical patients).
The LOS differed between ICU patients admitted for the first time and those readmitted within the 19-month study period. For both admission categories, LOS was longer for medical patients than for surgical patients. However, there were no significant differences between percentages of medical and surgical patients who were readmitted (Table 2). Despite comprising about 12% of the population, patients with more than 1 admission accounted for 23% of admissions and 25% of all bed occupancies during the study period.
Figure e1B shows ICU bed occupancy for different LOS intervals (calculated as bed days) and indicates that despite accounting for a small percentage of admissions, patients with long LOS accounted for a significant portion of total occupancy (32% for more than 1 month, 45% for more than 14 days). The medical and surgical contributions of these long-LOS patients were about equal. The figures indicate that more than half of medical ICU patient occupancy involved LOS of more than 14 days, while surgical patients tended to have shorter LOS.
Mortality
Of all the patients in this study, 5.1% died in the ICU; the mortality rate was 11% for medical patients and 2.1% for surgical patients. Thirty days after discharge, overall mortality was 10.4%, or 23.5% for medical patients and 3.9% for surgical patients. Finally, 1 year after discharge, mortality rates were 21.5% (overall), 39.4% (medical patients), and 12.5% (surgical patients) (Table 3). Survival curves demonstrated the difference between medical and surgical patients at 30 days and 1 year (Figures 1A & 1B).
Impact of LOS on Mortality
One-year mortality was 17% for patients who were in the ICU less than 14 days and 40% for those in the ICU more than 14 days (relative risk [RR] = 2.35; P < .01) (Table 4).
Mortality also was higher in patients with more than 1 ICU admission. For the aggregate of ICU patients, readmission status was significantly associated with a 10% increase in mortality. For both single- and multiple-admission status, the mortality rate was 2.5-fold higher for medical patients than for surgical patients. The increased mortality associated with readmission status was not significantly different for either medical or surgical patients analyzed as subgroups (eAppendix Table.)
Impact of Age on Mortality
Figures 4A and 4B shows 30-day and 1-year mortality associated with age; regression analysis indicated that age is an independent predictor of ICU mortality. For 30-day mortality, increased age was positively associated with mortality in medical patients but not in surgical patients (r2 = 0.91; P < .0001). Age had a significant impact on 1-year mortality for both medical and surgical patients but less so in the latter (r2 = 0.95 and 0.65, respectively; P < .001 for both). Although increased mortality was associated with both LOS and age, there was no clear association between the latter 2 variables.
Survival of Chronic Critical Illness
As eTable 2 shows, 21.5% of all patients died either in the ICU or within the first year after ICU discharge. To evaluate the survival of chronic ICU residence, the authors performed a detailed analysis of functional status and mortality of patients with LOS of more than 14 days. Seventy-one patients fit that profile (their mean LOS was 41 days; median, 28 days). Of these patients, 11 died in the ICU, and another 17 died within 6 months (including 2 in a stepdown unit and 7 in hospice). Overall, 28 (39%) of the 71 patients died either in the ICU or within 6 months (35% aggregate, 53% of medical patients, and 27% of surgical patients in ICU > 2 weeks). Another 8 patients (11%) died between 6 and 12 months after discharge. One-year mortality among patients in the ICU more than 14 days was 40% overall, 50% for medical patients, and 29% for surgical patients—or twice that predicted by the MPM-III model, which figured mortality rates of 25% and 12% for medical and surgical patients, respectively. In this cohort, the mean MPM-III score was 18.6% for 1-year survivors and 29.3% for nonsurvivors (P = .016, Mann-Whitney U test). Mortality was associated with a trend toward higher MPM-III scores in both medical and surgical patients but did not reach statistical significance.
Of the cohort patients who lived at least 6 months after ICU discharge, 45% were still in a hospital or were in a nursing facility at 6 months. Of the patients who lived at least 1 year, 33% were still in a hospital or were in a nursing facility (Figure 5). At 1 year, mean age was 63 years for survivors and 69 years for the deceased (P < .01 by Student t test).
Quality-of-Life Survey
The authors successfully contacted 32 of the 39 patients who lived at least 1 year after discharge after an ICU stay of more than 14 days. The subgroups’ median SF-36 scores were similar: 57 for medical patients and 51 for surgical patients. These average scores over 8 domains are similar to those reported by Graf and colleagues for 9 months after ICU discharge (53.7) and are lower than the normative data reported by those authors for the German population (mean, 66.5).29
Discussion
The goals of the present study were 2-fold—to gain a better understanding of the survival and functioning of patients after ICU residence and to define what may constitute a trial of therapy in ICU, or specifically to determine whether there is a particular ICU interval or point at which further care fails to improve survival. The study also compared medical and surgical subpopulations.
The main finding of this study was a 4-fold difference between ICU mortality and 1-year mortality. This mortality increase occurred in both medical and surgical patients, but there were large differences in magnitude between these groups. The survival rates generally were better than those of other general intensive care populations, though such a comparison should be made with caution, as survival differs by country, population, admitting practices, and a variety of other hospital characteristics.30,31 Although some findings of the present study may relate to its largely male U.S. veteran population, the authors believe they have provided a data-collection-and-analysis model that can be used by any hospital trying to understand the course and outcome of its ICU patients and recognizing the value of this knowledge in discussions on goals of care.
Mortality and LOS
As each interval of ICU residence was associated with a stepwise increase in mortality, there was no clear cutoff for diminishing return. To create a reference point, the authors analyzed the data of patients who were in an ICU more than 14 days—thinking that this duration may represent an outer limit of a reasonable trial of therapy and a measure that probably distinguishes acute from chronic critical illness.32 Use of this interval represented a conservative approach, as only 6.5% of the patients in this cohort had a LOS of more than 14 days. This small percentage of patients accounted for 45% of total bed occupancy in this study and 54% of all medical bed occupancy. In the more-than-14-days group, mortality was 37.5% for surgical patients and 46.3% for medical patients. Thus, LOS may be a dynamic measure of physiologic reserve and disease severity—reflecting variables such as response to therapy, severity of comorbidities, resistance to new problems, and rebound from chronic stress, inflammation, and catabolism. This view is supported by the nearly 2-fold higher mortality in medical patients and nearly 3-fold higher mortality in surgical patients in comparison with MPM-III predictions.
Twelve percent of all patients were admitted to ICU multiple times, and these admissions accounted for 25% of all bed occupancies. Multiple admissions indicate a high disease burden or a low physiologic reserve that prevents full recovery from critical illness. As mortality was higher in patients with multiple admissions, ICU readmission should be regarded as a marker for poor overall recovery and should prompt consideration of both initial discharge criteria and trajectory as well as goals of care.
Medical vs Surgical Patients
In this cohort, medical and surgical patients were distinguished on several grounds. Despite the similar mean age of these subpopulations, medical patients had longer LOS and higher short- and long-term mortality. These findings are not surprising, as medical patients in the ICU have high rates of end-stage disease, malignancy, and high comorbidity burden and are often admitted to have potentially life-ending conditions stabilized. Surgical patients generally are selected on their ability to withstand major systemic perturbations—palliative and emergency operations excepted—and generally have medical conditions optimized before surgery. As the expectation of postoperative survival likely biases clinician behavior toward aggressive care, some short-term survival may reflect this behavior.
In contrast, such biased behavior is not an issue in 1-year survival, which instead accurately reflects underlying health. The different slopes of medical and surgical patients on age-vs-mortality in Figures 4A & 4B indicate the different physiologic makeups of these ICU patients. With short and long LOS compared, the difference between surgical and medical patients in the ICU is striking: Sixty-one percent of all surgical bed days vs 45% of all medical bed days are for LOS less than 14 days. Nevertheless, chronic critical illness has a significant impact on both medical and surgical patients and tends to equalize some of the survival differences between these groups. These populations had similar ICU readmission rates as well as similar higher mortality rates for LOS of more than 14 days and especially for LOS of more than 1 month. With longer LOS, the survival curve of surgical patients begins to resemble that of medical patients—suggesting that the phenotype of chronic critical illness becomes the dominant force influencing survival and function (Figures 3A & 3B). Indeed, for surgical patients, the highest mortality categories were ICU readmission and LOS of more than 30 days.
The mortality rate was significantly lower for surgical patients than it was for medical patients at all intervals studied, with the largest separation in the short-term categories of ICU and 30-day mortality. The post-ICU mortality rates for medical and surgical patients are similar to those reported in several other studies, including a study of veterans.14-16,33,34 Among the present patients with LOS of more than 14 days, surviving surgical patients were significantly younger than nonsurviving surgical patients and both surviving and nonsurviving medical patients.
The few SF-36 responses collected revealed no differences between medical and surgical patients.
A Trial of Therapy
The present data are useful in describing the landscape of post-ICU survival to patients and their families. The data demonstrated a higher mortality trend that correlated with increases in age and increases in ICU duration and readmission. Within this continuum, there was no break point at which survivors and nonsurvivors clearly separated. The data therefore lack a boundary that can be used to define a trial of therapy. However, the added risks of age and recovery longer than 1 week are clear and should be included in care decisions. The generally better survival of surgical patients (nearly all of whom had elective surgery) in comparison with medical patients suggests these populations should be considered separately.
In the absence of a point distinguishing survivors from nonsurvivors, the authors performed a more detailed analysis of patients in the ICU for more than 14 days to provide some perspective on health care dependence in the subsequent year. That ICU survival does not necessarily equate to overall survival and independence long after ICU residence is an important matter for patients and families to consider when making decisions about critical care residence. The 14-day LOS data, though using a fairly arbitrary time point, suggest that patients who cannot recover from critical illness in less than 14 days should be advised of the range of short- and long-term mortality and the likelihood of high dependence on medical care within the subsequent year.
The concepts of hospital-dependent patient and persistent inflammation, immunosuppression, and catabolism syndrome have been introduced to describe the condition of progressive deterioration and inability to regain full independence after illness.32,35 These illness patterns deserve attention in prognosis discussions. The present study focused not on ICU survival but on 1-year mortality and functional independence, and it is these longer term outcomes that critical care professionals should consider. Intensive care units are successful in improving short-term survival, but a long line of successful ICU discharges may lead an intensivist to think that longer term survival is important as well and convey this impression to patients and their families.
Study Strengths
This study is one of a few to investigate the short- and long-term survival of an unselected cohort of critically ill patients and is unique in its inclusion of both medical and surgical patients receiving care in the same environment. Medical and surgical patients have different survival profiles that may necessitate separate studies of these subpopulations. However, the finding of different survival profiles under the same care highlights the intrinsic differences between these groups. Use of a 1.5-year study period allowed the authors to capture ICU patients with long LOS and to include multiple episodes of care provided by more than 10 different attending physicians. Therefore, these data likely were not influenced by any rare events or idiosyncrasies in practice styles. Further, the same teams of physicians and nurses cared for all the medical and surgical patients, and all unit-based protocols and quality improvement activities were applied to all patients.
Study Limitations
The intensive care patients come from a large catchment area; however, conditions seen in tertiary referral centers, such as bone marrow transplants, cerebrovascular, transplant surgery, and ventricular-assist devices are not represented in this population.
In this study, bed days were used as a crude measure of care burden. From a nursing perspective, however, the workload may be higher with quick-turnover beds than with long-term residents. On the other hand, long-term ICU residents are visited by multiple consultants and receive a much larger set of interventions, including weeks of ventilation and hemodialysis, line changes, and family meetings. A comparison of the costs involved for different ICU subpopulations would add valuable information to this discussion.
The authors took a conservative approach in establishing the mortality and residence of patients 1 year after their ICU stays. At 6 months, 1-year patients without evidence of hospital or nursing facility residence were assumed to be home. In reality, nearly all these patients had multiple admissions or emergency department stays, or there was other evidence of intensive care. Some patients who were assumed to be home may have left the area and become untraceable. All estimates of care dependence and mortality should therefore be considered minimums. The authors cannot envision how any of their estimates could overstate the morbidity and mortality.
The concept of hospital dependence is applicable to the majority of the ICU survivors, though the authors did not attempt to create a quantitative measure of this status.36 Another study limitation is that absence of hospitalization does not equal functional independence. A better definition of this status, and its application to a broad spectrum of LOS, would be a valuable adjunct to ICU decision making.
The convention by which the authors considered the first day of their study period a “fresh slate” did not adjust for the situation that some first admissions actually were readmissions. Assuming the validity of the finding that readmitted patients had a higher burden of morbidity and mortality, misclassification of admission status would tend to inflate the mortality of single-admission patients and minimize the magnitude of the differences found in this study. Similarly, an admission near the end of the study period may have been analyzed as a single admission, even if the patient was readmitted and died the next year. The latter situation also would tend to inflate the mortality of the single-admission category. None of these possible mathematical errors negates the fact that a second ICU admission should be regarded as a marker for poor recovery.
A more accurate estimate of short- and long-term prognosis likely can be obtained by examining laboratory studies and interventions such as vasopressors, dialysis, and ventilation at defined time points. Although the authors did not attempt it, development of such a model would be a valuable undertaking. They focused on describing the expected course of ICU patients and determining what patterns emerged from care duration. As this study found that the prognosis for long-term ICU residents remained guarded a long time after discharge, survival models of patients with 1- to 2-week ICU residences likely would be valuable in clinical decision making.
A quality-of-life survey was administered only to patients in the ICU longer than 2 weeks. This limited study was conducted to explore the feasibility of assessing outcomes other than survival and to determine the staffing requirements needed to research this further. A more meaningful analysis would come from a broader analysis of scores from 3 or 4 different ICU lengths of stay.
Clinician and family behavior can influence some of the outcomes measured in this study—particularly in cases in which an illness is poorly characterized and an evidence basis for decision making is lacking. In these situations, values and individual clinician judgment likely predominate, possibly introducing variability to care duration. Nevertheless, cumulative mortality 1 month or more after ICU residence would eliminate biased clinician behavior. The heterogeneity of care providers’ and families’ decision making, captured in this analysis, likely is a normal phenomenon that should help inform physicians’ understanding of prolonged ICU residence.
1. Halpern NA. Can the costs of critical care be controlled? Curr Opin Crit Care. 2009;15(6):591-596.
2. Angus DC, Barnato AE, Linde-Zwirble WT, et al; Robert Wood Johnson Foundation ICU End-of-Life Peer Group. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med. 2004;32(3):638-643.
3. Barnato AE, McClellan MB, Kagay CR, Garber AM. Trends in inpatient treatment intensity among Medicare beneficiaries at the end of life. Health Serv Res. 2004;39(2):363-375.
4. Teno JM, Gozalo PL, Bynum JP, et al. Change in end-of-life care for Medicare beneficiaries: site of death, place of care, and health care transitions in 2000, 2005, and 2009. JAMA. 2013;309(5):470-477.
5. Zilberberg MD, Shorr AF. Economics at the end of life: hospital and ICU perspectives. Semin Respir Crit Care Med. 2012;33(4):362-369.
6. Piers RD, Azoulay E, Ricou B, et al; APPROPRICUS Study Group of the Ethics Section of the ESICM. Perceptions of appropriateness of care among European and Israeli intensive care unit nurses and physicians. JAMA. 2011;306(24):2694-2703.
7. Higginson IJ, Sen-Gupta GJ. Place of care in advanced cancer: a qualitative systematic literature review of patient p. J Palliat Med. 2000;3(3):287-300.
8. McClish DK, Powell SH. How well can physicians estimate mortality in a medical intensive care unit? Med Decis Making. 1989;9(2):125-132.
9. Barrera R, Nygard S, Sogoloff H, Groeger J, Wilson R. Accuracy of predictions of survival at admission to the intensive care unit. J Crit Care. 2001;16(1):32-35.
10. Johnson AE, Kramer AA, Clifford GD. A new severity of illness scale using a subset of Acute Physiology and Chronic Health Evaluation data elements shows comparable predictive accuracy. Crit Care Med. 2013;41(7):1711-1718.
11. D'Hoore W, Bouckaert A, Tilquin C. Practical considerations on the use of the Charlson comorbidity index with administrative data bases. J Clin Epidemiol. 1996;49(12):1429-1433.
12. Knaus WA, Wagner DP, Zimmerman JE, Draper EA. Variations in mortality and length of stay in intensive care units. Ann Intern Med. 1993;118(10):753-761.
13. Lemeshow S, Teres D, Klar J, Avrunin JS, Gehlbach SH, Rapoport J. Mortality Probability Models (MPM II) based on an international cohort of intensive care unit patients. JAMA. 1993;270(20):2478-2486.
14. Render ML, Kim HM, Welsh DE, et al; VA ICU Project (VIP) Investigators. Automated intensive care unit risk adjustment: results from a national Veterans Affairs study. Crit Care Med. 2003;31(6):1638-1646.
15. Viviand X, Gouvernet J, Granthil C, François G. Simplification of the SAPS by selecting independent variables. Intensive Care Med. 1991;17(3):164-168.
16. Higgins TL, Teres D, Copes WS, Nathanson BH, Stark M, Kramer AA. Assessing contemporary intensive care unit outcome: an updated Mortality Probability Admission Model (MPM0-III). Crit Care Med. 2007;35(3):827-835.
17. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818-829.
18. Poses RM, McClish DK, Smith WR, et al. Results of report cards for patients with congestive heart failure depend on the method used to adjust for severity. Ann Intern Med. 2000;133(1):10-20.
19. Schuster DP. Predicting outcome after ICU admission. The art and science of assessing risk. Chest. 1992;102(6):1861-1870.
20. Teno JM, Fisher E, Hamel MB, et al. Decision-making and outcomes of prolonged ICU stays in seriously ill patients. J Am Geriatr Soc. 2000;48(suppl 5):S70-S74.
21. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245-1251.
22. Pompei P, Charlson ME, Ales K, MacKenzie CR, Norton M. Relating patient characteristics at the time of admission to outcomes of hospitalization. J Clin Epidemiol. 1991;44(10):1063-1069.
23. Meadow W, Pohlman A, Frain L, et al. Power and limitations of daily prognostications of death in the medical intensive care unit. Crit Care Med. 2011;39(3):474-479.
24. Douglas SL, Daly BJ, Lipson AR. Neglect of quality-of-life considerations in intensive care unit family meetings for long-stay intensive care unit patients. Crit Care Med. 2012;40(2):461-467.
25. Prendergast TJ, Claessens MT, Luce JM. A national survey of end-of-life care for critically ill patients. Am J Respir Crit Care Med. 1998;158(4):1163-1167.
26. Luce JM. A history of resolving conflicts over end-of-life care in intensive care units in the United States. Crit Care Med. 2010;38(8):1623-1629.
27. Bashour CA, Yared JP, Ryan TA, et al. Long-term survival and functional capacity in cardiac surgery patients after prolonged intensive care. Crit Care Med. 2000;28(12):3847-3853.
28. Eddleston JM, White P, Guthrie E. Survival, morbidity, and quality of life after discharge from intensive care. Crit Care Med. 2000;28(7):2293-2299.
29. Graf J, Koch M, Dujardin R, Kersten A, Janssens U. Health-related quality of life before, 1 month after, and 9 months after intensive care in medical cardiovascular and pulmonary patients. Crit Care Med. 2003;31(8):2163-2169.
30. Montuclard L, Garrouste-Orgeas M, Timsit JF, Misset B, De Jonghe B, Carlet J. Outcome, functional autonomy, and quality of life of elderly patients with a long-term intensive care unit stay. Crit Care Med. 2000;28(10):3389-3395.
31. Teno JM, Harrell FE Jr, Knaus W, et al. Prediction of survival for older hospitalized patients: the HELP survival model. Hospitalized Elderly Longitudinal Project. J Am Geriatr Soc. 2000;48(suppl 5):S16-S24.
32. Lamas D. Chronic critical illness. N Engl J Med. 2014;370(2):175-177.
33. Konopad E, Noseworthy TW, Johnston R, Shustack A, Grace M. Quality of life measures before and one year after admission to an intensive care unit. Crit Care Med. 1995;23(10):1653-1659.
34. Render ML, Kim HM, Deddens J, et al. Variation in outcomes in Veterans Affairs intensive care units with a computerized severity measure. Crit Care Med. 2005;33(5):930-939.
35. Gentile LF, Cuenca AG, Efron PA, et al. Persistent inflammation and immunosuppression: a common syndrome and new horizon for surgical intensive care. J Trauma Acute Care Surg. 2012;72(6):1491-1501.
36. Reuben DB, Tinetti ME. The hospital-dependent patient. N Engl J Med. 2014;370(8):694-697.
1. Halpern NA. Can the costs of critical care be controlled? Curr Opin Crit Care. 2009;15(6):591-596.
2. Angus DC, Barnato AE, Linde-Zwirble WT, et al; Robert Wood Johnson Foundation ICU End-of-Life Peer Group. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med. 2004;32(3):638-643.
3. Barnato AE, McClellan MB, Kagay CR, Garber AM. Trends in inpatient treatment intensity among Medicare beneficiaries at the end of life. Health Serv Res. 2004;39(2):363-375.
4. Teno JM, Gozalo PL, Bynum JP, et al. Change in end-of-life care for Medicare beneficiaries: site of death, place of care, and health care transitions in 2000, 2005, and 2009. JAMA. 2013;309(5):470-477.
5. Zilberberg MD, Shorr AF. Economics at the end of life: hospital and ICU perspectives. Semin Respir Crit Care Med. 2012;33(4):362-369.
6. Piers RD, Azoulay E, Ricou B, et al; APPROPRICUS Study Group of the Ethics Section of the ESICM. Perceptions of appropriateness of care among European and Israeli intensive care unit nurses and physicians. JAMA. 2011;306(24):2694-2703.
7. Higginson IJ, Sen-Gupta GJ. Place of care in advanced cancer: a qualitative systematic literature review of patient p. J Palliat Med. 2000;3(3):287-300.
8. McClish DK, Powell SH. How well can physicians estimate mortality in a medical intensive care unit? Med Decis Making. 1989;9(2):125-132.
9. Barrera R, Nygard S, Sogoloff H, Groeger J, Wilson R. Accuracy of predictions of survival at admission to the intensive care unit. J Crit Care. 2001;16(1):32-35.
10. Johnson AE, Kramer AA, Clifford GD. A new severity of illness scale using a subset of Acute Physiology and Chronic Health Evaluation data elements shows comparable predictive accuracy. Crit Care Med. 2013;41(7):1711-1718.
11. D'Hoore W, Bouckaert A, Tilquin C. Practical considerations on the use of the Charlson comorbidity index with administrative data bases. J Clin Epidemiol. 1996;49(12):1429-1433.
12. Knaus WA, Wagner DP, Zimmerman JE, Draper EA. Variations in mortality and length of stay in intensive care units. Ann Intern Med. 1993;118(10):753-761.
13. Lemeshow S, Teres D, Klar J, Avrunin JS, Gehlbach SH, Rapoport J. Mortality Probability Models (MPM II) based on an international cohort of intensive care unit patients. JAMA. 1993;270(20):2478-2486.
14. Render ML, Kim HM, Welsh DE, et al; VA ICU Project (VIP) Investigators. Automated intensive care unit risk adjustment: results from a national Veterans Affairs study. Crit Care Med. 2003;31(6):1638-1646.
15. Viviand X, Gouvernet J, Granthil C, François G. Simplification of the SAPS by selecting independent variables. Intensive Care Med. 1991;17(3):164-168.
16. Higgins TL, Teres D, Copes WS, Nathanson BH, Stark M, Kramer AA. Assessing contemporary intensive care unit outcome: an updated Mortality Probability Admission Model (MPM0-III). Crit Care Med. 2007;35(3):827-835.
17. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818-829.
18. Poses RM, McClish DK, Smith WR, et al. Results of report cards for patients with congestive heart failure depend on the method used to adjust for severity. Ann Intern Med. 2000;133(1):10-20.
19. Schuster DP. Predicting outcome after ICU admission. The art and science of assessing risk. Chest. 1992;102(6):1861-1870.
20. Teno JM, Fisher E, Hamel MB, et al. Decision-making and outcomes of prolonged ICU stays in seriously ill patients. J Am Geriatr Soc. 2000;48(suppl 5):S70-S74.
21. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245-1251.
22. Pompei P, Charlson ME, Ales K, MacKenzie CR, Norton M. Relating patient characteristics at the time of admission to outcomes of hospitalization. J Clin Epidemiol. 1991;44(10):1063-1069.
23. Meadow W, Pohlman A, Frain L, et al. Power and limitations of daily prognostications of death in the medical intensive care unit. Crit Care Med. 2011;39(3):474-479.
24. Douglas SL, Daly BJ, Lipson AR. Neglect of quality-of-life considerations in intensive care unit family meetings for long-stay intensive care unit patients. Crit Care Med. 2012;40(2):461-467.
25. Prendergast TJ, Claessens MT, Luce JM. A national survey of end-of-life care for critically ill patients. Am J Respir Crit Care Med. 1998;158(4):1163-1167.
26. Luce JM. A history of resolving conflicts over end-of-life care in intensive care units in the United States. Crit Care Med. 2010;38(8):1623-1629.
27. Bashour CA, Yared JP, Ryan TA, et al. Long-term survival and functional capacity in cardiac surgery patients after prolonged intensive care. Crit Care Med. 2000;28(12):3847-3853.
28. Eddleston JM, White P, Guthrie E. Survival, morbidity, and quality of life after discharge from intensive care. Crit Care Med. 2000;28(7):2293-2299.
29. Graf J, Koch M, Dujardin R, Kersten A, Janssens U. Health-related quality of life before, 1 month after, and 9 months after intensive care in medical cardiovascular and pulmonary patients. Crit Care Med. 2003;31(8):2163-2169.
30. Montuclard L, Garrouste-Orgeas M, Timsit JF, Misset B, De Jonghe B, Carlet J. Outcome, functional autonomy, and quality of life of elderly patients with a long-term intensive care unit stay. Crit Care Med. 2000;28(10):3389-3395.
31. Teno JM, Harrell FE Jr, Knaus W, et al. Prediction of survival for older hospitalized patients: the HELP survival model. Hospitalized Elderly Longitudinal Project. J Am Geriatr Soc. 2000;48(suppl 5):S16-S24.
32. Lamas D. Chronic critical illness. N Engl J Med. 2014;370(2):175-177.
33. Konopad E, Noseworthy TW, Johnston R, Shustack A, Grace M. Quality of life measures before and one year after admission to an intensive care unit. Crit Care Med. 1995;23(10):1653-1659.
34. Render ML, Kim HM, Deddens J, et al. Variation in outcomes in Veterans Affairs intensive care units with a computerized severity measure. Crit Care Med. 2005;33(5):930-939.
35. Gentile LF, Cuenca AG, Efron PA, et al. Persistent inflammation and immunosuppression: a common syndrome and new horizon for surgical intensive care. J Trauma Acute Care Surg. 2012;72(6):1491-1501.
36. Reuben DB, Tinetti ME. The hospital-dependent patient. N Engl J Med. 2014;370(8):694-697.
