User login
Sharon Worcester is an award-winning medical journalist for MDedge News. She has been with the company since 1996, first as the Southeast Bureau Chief (1996-2009) when the company was known as International Medical News Group, then as a freelance writer (2010-2015) before returning as a reporter in 2015. She previously worked as a daily newspaper reporter covering health and local government. Sharon currently reports primarily on oncology and hematology. She has a BA from Eckerd College and an MA in Mass Communication/Print Journalism from the University of Florida. Connect with her via LinkedIn and follow her on twitter @SW_MedReporter.
Secondary CNS lymphoma regimen linked to 41% survival at 5 years
Treatment with high doses of antimetabolites followed by rituximab plus high-dose sequential chemoimmunotherapy and autologous stem-cell transplantation was feasible and effective in a multicenter phase II study of 38 patients with aggressive B-cell lymphoma and secondary central nervous system involvement.
The patients, aged 18 to 70 years with Eastern Cooperative Oncology Group performance status of 3 or less at enrollment, were treated with high doses of methotrexate and cytarabine, followed by rituximab plus high-dose sequential chemoimmunotherapy (R-HDS) consisting of cylcophosphamide, cytarabine, and etoposide supported by autologous stem-cell transplantation in eligible patients.
Toxicity was typically manageable, but 30 treatment courses were complicated by grade 3 or 4 febrile neutropenia and/or infections; 4 patients died because of toxicity, Dr. Andres J. M. Ferreri of San Raffaele Scientific Institute, Milan, Italy and colleagues reported online Aug. 17 in the Journal of Clinical Oncology.
The complete response rate was 63% (24 patients), and 17 patients remained relapse free at a median follow-up of 48 months, with a 2-year event-free survival rate of 50%, and a 5-year survival rate of 41%, the investigators said (J Clin Oncol. 2015 Aug 17. doi: 10.1200/JCO.2015.61.1236).
This novel radiotherapy-free regimen, developed based on encouraging outcomes with antimetabolites in patients with primary CNS lymphoma and with R-HDS in relapsed aggressive lymphoma, appears safe and effective in the setting of secondary CNS lymphoma (SCNSL).
“We propose this strategy as the standard of care for patients with SCNSL and as a comparison control regimen for future trials,” they concluded.
Dr. Ferreri reported having no disclosures. One co-author, Dr. Federico Caligaris-Cappio, reported serving in a consulting or advisory role for Janssen and Pharmacyclics.
The findings of Ferreri et al highlight the significant progress that has been made toward finding a cure for aggressive B-cell lymphoma with concomitant or subsequent CNS involvement.
Just a few years ago, this condition was fatal in nearly all cases, but in light of these and other recent findings, needed improvements in treatment seem possible.
Among other strategies, complete elimination of non-[blood-brain barrier]-crossing agents and administration of more than two cycles of induction chemotherapy might prove to be of value. In addition, oral targeted therapies with small molecules, most of which easily cross the BBB, hold promise.
Dr. Norbert Schmitz and Huei-Shan Wuthey are with Asklepios Hospital St. Georg, Hamburg, Germany. They made their remarks in an editorial(J Clin Oncol. 2015 Aug 17. doi: 10.1200/JCO.2015.63.1143) that accompanied the study. Dr. Schmitz reported serving in a consulting or advisory role for Roche and receiving research funding from Roche. Huei-Shan Wu reported having no disclosures.
The findings of Ferreri et al highlight the significant progress that has been made toward finding a cure for aggressive B-cell lymphoma with concomitant or subsequent CNS involvement.
Just a few years ago, this condition was fatal in nearly all cases, but in light of these and other recent findings, needed improvements in treatment seem possible.
Among other strategies, complete elimination of non-[blood-brain barrier]-crossing agents and administration of more than two cycles of induction chemotherapy might prove to be of value. In addition, oral targeted therapies with small molecules, most of which easily cross the BBB, hold promise.
Dr. Norbert Schmitz and Huei-Shan Wuthey are with Asklepios Hospital St. Georg, Hamburg, Germany. They made their remarks in an editorial(J Clin Oncol. 2015 Aug 17. doi: 10.1200/JCO.2015.63.1143) that accompanied the study. Dr. Schmitz reported serving in a consulting or advisory role for Roche and receiving research funding from Roche. Huei-Shan Wu reported having no disclosures.
The findings of Ferreri et al highlight the significant progress that has been made toward finding a cure for aggressive B-cell lymphoma with concomitant or subsequent CNS involvement.
Just a few years ago, this condition was fatal in nearly all cases, but in light of these and other recent findings, needed improvements in treatment seem possible.
Among other strategies, complete elimination of non-[blood-brain barrier]-crossing agents and administration of more than two cycles of induction chemotherapy might prove to be of value. In addition, oral targeted therapies with small molecules, most of which easily cross the BBB, hold promise.
Dr. Norbert Schmitz and Huei-Shan Wuthey are with Asklepios Hospital St. Georg, Hamburg, Germany. They made their remarks in an editorial(J Clin Oncol. 2015 Aug 17. doi: 10.1200/JCO.2015.63.1143) that accompanied the study. Dr. Schmitz reported serving in a consulting or advisory role for Roche and receiving research funding from Roche. Huei-Shan Wu reported having no disclosures.
Treatment with high doses of antimetabolites followed by rituximab plus high-dose sequential chemoimmunotherapy and autologous stem-cell transplantation was feasible and effective in a multicenter phase II study of 38 patients with aggressive B-cell lymphoma and secondary central nervous system involvement.
The patients, aged 18 to 70 years with Eastern Cooperative Oncology Group performance status of 3 or less at enrollment, were treated with high doses of methotrexate and cytarabine, followed by rituximab plus high-dose sequential chemoimmunotherapy (R-HDS) consisting of cylcophosphamide, cytarabine, and etoposide supported by autologous stem-cell transplantation in eligible patients.
Toxicity was typically manageable, but 30 treatment courses were complicated by grade 3 or 4 febrile neutropenia and/or infections; 4 patients died because of toxicity, Dr. Andres J. M. Ferreri of San Raffaele Scientific Institute, Milan, Italy and colleagues reported online Aug. 17 in the Journal of Clinical Oncology.
The complete response rate was 63% (24 patients), and 17 patients remained relapse free at a median follow-up of 48 months, with a 2-year event-free survival rate of 50%, and a 5-year survival rate of 41%, the investigators said (J Clin Oncol. 2015 Aug 17. doi: 10.1200/JCO.2015.61.1236).
This novel radiotherapy-free regimen, developed based on encouraging outcomes with antimetabolites in patients with primary CNS lymphoma and with R-HDS in relapsed aggressive lymphoma, appears safe and effective in the setting of secondary CNS lymphoma (SCNSL).
“We propose this strategy as the standard of care for patients with SCNSL and as a comparison control regimen for future trials,” they concluded.
Dr. Ferreri reported having no disclosures. One co-author, Dr. Federico Caligaris-Cappio, reported serving in a consulting or advisory role for Janssen and Pharmacyclics.
Treatment with high doses of antimetabolites followed by rituximab plus high-dose sequential chemoimmunotherapy and autologous stem-cell transplantation was feasible and effective in a multicenter phase II study of 38 patients with aggressive B-cell lymphoma and secondary central nervous system involvement.
The patients, aged 18 to 70 years with Eastern Cooperative Oncology Group performance status of 3 or less at enrollment, were treated with high doses of methotrexate and cytarabine, followed by rituximab plus high-dose sequential chemoimmunotherapy (R-HDS) consisting of cylcophosphamide, cytarabine, and etoposide supported by autologous stem-cell transplantation in eligible patients.
Toxicity was typically manageable, but 30 treatment courses were complicated by grade 3 or 4 febrile neutropenia and/or infections; 4 patients died because of toxicity, Dr. Andres J. M. Ferreri of San Raffaele Scientific Institute, Milan, Italy and colleagues reported online Aug. 17 in the Journal of Clinical Oncology.
The complete response rate was 63% (24 patients), and 17 patients remained relapse free at a median follow-up of 48 months, with a 2-year event-free survival rate of 50%, and a 5-year survival rate of 41%, the investigators said (J Clin Oncol. 2015 Aug 17. doi: 10.1200/JCO.2015.61.1236).
This novel radiotherapy-free regimen, developed based on encouraging outcomes with antimetabolites in patients with primary CNS lymphoma and with R-HDS in relapsed aggressive lymphoma, appears safe and effective in the setting of secondary CNS lymphoma (SCNSL).
“We propose this strategy as the standard of care for patients with SCNSL and as a comparison control regimen for future trials,” they concluded.
Dr. Ferreri reported having no disclosures. One co-author, Dr. Federico Caligaris-Cappio, reported serving in a consulting or advisory role for Janssen and Pharmacyclics.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: High doses of antimetabolites followed by R-HDS and autologous stem-cell transplantation was feasible and effective in 38 patients with aggressive B-cell lymphoma and secondary central nervous system involvement.
Major finding: The 2-year event-free survival rate was 50%, and the 5-year survival rate was 41%
Data source: A multicenter phase II study of 38 adults.
Disclosures: Dr. Ferreri reported having no disclosures. One co-author, Dr. Federico Caligaris-Cappio, reported serving in a consulting or advisory role for Janssen and Pharmacyclics.
Cervical cancer screening guidelines slow to gain traction
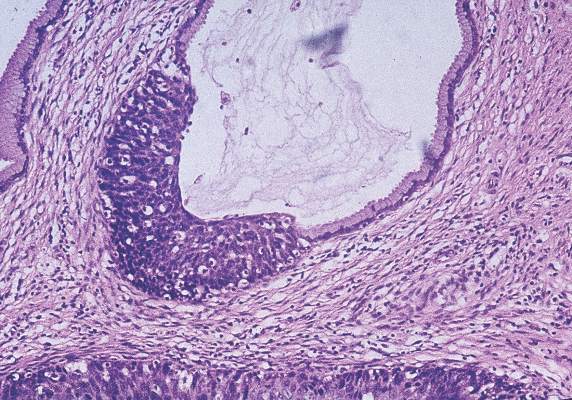
More than 3 years after the release of new cervical cancer screening guidelines, patients remain largely unaware of substantial changes in screening, and many physicians remain confused about or resistant to those changes.
The confusion is a matter of education, said Dr. Owen Montgomery, chairman of the department of obstetrics and gynecology at Drexel University, Philadelphia. As for the resistance, that’s less a reflection of concern about the science and more about the emotional and sociological processes involved in change, he said.
“It’s really good science,” Dr. Montgomery said of the data that formed the basis for the guidelines. “I was on the executive board of the [American College of Obstetricians and Gynecologists] when we signed off on the new recommendations. The science is valid.”
Two sets of guidelines were released in 2012, one by the U.S. Preventive Services Task Force (USPSTF) and one by the American Cancer Society (ACS) in conjunction with the American Society for Clinical Pathology (ASCP) and the American Society for Colposcopy and Cervical Pathology (ASCCP). Although the two guidelines differ in some respects, both recommend against a longstanding tradition: routine yearly Pap testing. The guidelines now call for screening intervals of 3-5 years depending on patient age and other factors, and recommend against screening those under age 21 years and over age 65 years in the absence of risk factors.
Knowledge gaps
Despite the widespread organizational support for the guidelines, data suggest that knowledge of them may be lacking among both patients and physicians. For instance, about 85% of 249 adult women who participated in a recent survey answered incorrectly when asked how often low-risk women aged 21-29 should be screened, and nearly 95% answered incorrectly when asked about the recommended frequency of screening in low-risk women over age 30 years.
According to Dr. Katherine O’Flynn O’Brien and her colleagues at George Washington University, Washington, who presented the results earlier this year at the American College of Obstetricians and Gynecologists annual scientific meeting, the findings suggest “that providers should focus more on educating women about changes to screening practices.”
But another survey presented at the same ACOG meeting showed that many providers may be unaware of the guideline changes or hesitant about embracing those changes.
Using a convenience sample of 165 medical and osteopathic physicians, physician assistants, and nurse practitioners, the investigators found that, in contrast with the current guidelines, about half do not perform cotesting in women aged 30-65 years every 5 years, and nearly 57% do not screen women aged 21-29 years with cytology alone every 3 years. More than 40% reported that they do not perform cytology screening in women aged 30-65 years every 3 years.
Addressing the ‘what ifs’
Confusion about the guidelines, and hesitation about implementing them, is not surprising as the changes – particularly the 3- to 5-year screening interval changes – are some of the most dramatic in recent memory, according to Dr. Constance Bohon, an ob.gyn. in Washington, D.C., and assistant clinical professor of ob.gyn. at George Washington University.

Certainly the guidelines have evolved with the science over the years, and some changes, such as screening only those over age 21 years, have been embraced, she said.
“But some changes are easier to accept than others,” she added, noting that “doing a Pap with cotesting in women after age 30 and repeating it again in 5 years is very difficult for many clinicians to accept ... part of the issue is that fine line in medicine between using the data and relying on clinical sense, clinical expertise.”
There is concern about the exceptions and the “what ifs,” she said.
What if a patient has a new partner? What if she develops an illness that results in a shift in immunity?
These concerns are valid, agreed Dr. Jill Rabin, professor of obstetrics and gynecology and cochief of the division of ambulatory care, Women’s Health Programs–PCAP Services at North Shore–Long Island Jewish Health System, New Hyde Park, N.Y.
But she stressed in an interview that the guidelines are just that – guidelines. “They aren’t written in stone,” she said, adding that the recommendations are based on good science, and that a careful reading shows there is plenty of room for clinical judgment.

“Guidelines evolve and we have to keep an open mind and make sure that we don’t use a one-size-fits-all model. That doesn’t really help our patients,” said Dr. Rabin, who also is head of the urogynecology department at Long Island Jewish Medical Center.
Patient expectations
Another hurdle to embracing the guidelines is that of patient expectations. One of the big misunderstandings among patients of all ages is that they will skip all visits for 3 years because of the interval in Pap testing, Dr. Montgomery said. It is important to stress that “the Pap is just one of the services done during the visit, and a relatively small one when you look at all the other things that are part of a comprehensive well woman visit,” he said.
He further noted that both patient and physician age may be an important factor in acceptance of the guidelines and the changes in screening frequency.
As a physician with a large population of patients in their postreproductive years, and as one who trains young residents, he has noticed a generational difference: Younger patients and physicians are more accepting of the changes, but women who have spent 30 or 40 years coming in for an annual Pap smear equate that with health; they feel that they have done their part in staying healthy, and they have a greater sense of the value of the visit, he said.
Dr. Bohon predicted that both the advancing science and the concerns of patients and physicians will be considered when new guidelines are developed.
“My hope is that we have a realistic view of what the Pap can do,” Dr. Bohon said, adding that she expects that human papillomavirus (HPV) testing will get more and more reliable, and that clinicians will gain experience with following the HPV test and using that as a determining factor in patient care.
Guidelines at a glance
The USPSTF guidelines recommend screening with cytology every 3 years in women aged 21-29 years, and either screening with cytology every 3 years or cotesting using cytology and HPV testing every 5 years in those aged 30-65.
They also recommend against screening after hysterectomy with removal of the cervix in women with no history of high-grade precancer or cervical cancer, and against screening with HPV testing in women younger than age 30, either alone or with cytology.
The ACS/ASCP/ASCCP guidelines recommend a Pap test every 3 years in women aged 21-29 years, with HPV testing only if needed after an abnormal Pap test result. Those aged 30-65 years should have both a Pap test and an HPV test every 5 years, although a Pap test alone every 3 years is also acceptable. Women over age 65 years who have been screened regularly with normal results do not require screening, but those over age 65 years who are diagnosed with cervical precancer should continue to be screened, the guidelines say.
In April, the American College of Physicians in April released its own set of guidelines for screening average-risk women; these guidelines adhere closely to the USPSTF guidelines, and have been endorsed by the American Congress of Obstetricians and Gynecologists and the ASCP (Ann Intern Med. 2015;162[12]:851-9).
More than 3 years after the release of new cervical cancer screening guidelines, patients remain largely unaware of substantial changes in screening, and many physicians remain confused about or resistant to those changes.
The confusion is a matter of education, said Dr. Owen Montgomery, chairman of the department of obstetrics and gynecology at Drexel University, Philadelphia. As for the resistance, that’s less a reflection of concern about the science and more about the emotional and sociological processes involved in change, he said.
“It’s really good science,” Dr. Montgomery said of the data that formed the basis for the guidelines. “I was on the executive board of the [American College of Obstetricians and Gynecologists] when we signed off on the new recommendations. The science is valid.”
Two sets of guidelines were released in 2012, one by the U.S. Preventive Services Task Force (USPSTF) and one by the American Cancer Society (ACS) in conjunction with the American Society for Clinical Pathology (ASCP) and the American Society for Colposcopy and Cervical Pathology (ASCCP). Although the two guidelines differ in some respects, both recommend against a longstanding tradition: routine yearly Pap testing. The guidelines now call for screening intervals of 3-5 years depending on patient age and other factors, and recommend against screening those under age 21 years and over age 65 years in the absence of risk factors.
Knowledge gaps
Despite the widespread organizational support for the guidelines, data suggest that knowledge of them may be lacking among both patients and physicians. For instance, about 85% of 249 adult women who participated in a recent survey answered incorrectly when asked how often low-risk women aged 21-29 should be screened, and nearly 95% answered incorrectly when asked about the recommended frequency of screening in low-risk women over age 30 years.
According to Dr. Katherine O’Flynn O’Brien and her colleagues at George Washington University, Washington, who presented the results earlier this year at the American College of Obstetricians and Gynecologists annual scientific meeting, the findings suggest “that providers should focus more on educating women about changes to screening practices.”
But another survey presented at the same ACOG meeting showed that many providers may be unaware of the guideline changes or hesitant about embracing those changes.
Using a convenience sample of 165 medical and osteopathic physicians, physician assistants, and nurse practitioners, the investigators found that, in contrast with the current guidelines, about half do not perform cotesting in women aged 30-65 years every 5 years, and nearly 57% do not screen women aged 21-29 years with cytology alone every 3 years. More than 40% reported that they do not perform cytology screening in women aged 30-65 years every 3 years.
Addressing the ‘what ifs’
Confusion about the guidelines, and hesitation about implementing them, is not surprising as the changes – particularly the 3- to 5-year screening interval changes – are some of the most dramatic in recent memory, according to Dr. Constance Bohon, an ob.gyn. in Washington, D.C., and assistant clinical professor of ob.gyn. at George Washington University.
Certainly the guidelines have evolved with the science over the years, and some changes, such as screening only those over age 21 years, have been embraced, she said.
“But some changes are easier to accept than others,” she added, noting that “doing a Pap with cotesting in women after age 30 and repeating it again in 5 years is very difficult for many clinicians to accept ... part of the issue is that fine line in medicine between using the data and relying on clinical sense, clinical expertise.”
There is concern about the exceptions and the “what ifs,” she said.
What if a patient has a new partner? What if she develops an illness that results in a shift in immunity?
These concerns are valid, agreed Dr. Jill Rabin, professor of obstetrics and gynecology and cochief of the division of ambulatory care, Women’s Health Programs–PCAP Services at North Shore–Long Island Jewish Health System, New Hyde Park, N.Y.
But she stressed in an interview that the guidelines are just that – guidelines. “They aren’t written in stone,” she said, adding that the recommendations are based on good science, and that a careful reading shows there is plenty of room for clinical judgment.
“Guidelines evolve and we have to keep an open mind and make sure that we don’t use a one-size-fits-all model. That doesn’t really help our patients,” said Dr. Rabin, who also is head of the urogynecology department at Long Island Jewish Medical Center.
Patient expectations
Another hurdle to embracing the guidelines is that of patient expectations. One of the big misunderstandings among patients of all ages is that they will skip all visits for 3 years because of the interval in Pap testing, Dr. Montgomery said. It is important to stress that “the Pap is just one of the services done during the visit, and a relatively small one when you look at all the other things that are part of a comprehensive well woman visit,” he said.
He further noted that both patient and physician age may be an important factor in acceptance of the guidelines and the changes in screening frequency.
As a physician with a large population of patients in their postreproductive years, and as one who trains young residents, he has noticed a generational difference: Younger patients and physicians are more accepting of the changes, but women who have spent 30 or 40 years coming in for an annual Pap smear equate that with health; they feel that they have done their part in staying healthy, and they have a greater sense of the value of the visit, he said.
Dr. Bohon predicted that both the advancing science and the concerns of patients and physicians will be considered when new guidelines are developed.
“My hope is that we have a realistic view of what the Pap can do,” Dr. Bohon said, adding that she expects that human papillomavirus (HPV) testing will get more and more reliable, and that clinicians will gain experience with following the HPV test and using that as a determining factor in patient care.
Guidelines at a glance
The USPSTF guidelines recommend screening with cytology every 3 years in women aged 21-29 years, and either screening with cytology every 3 years or cotesting using cytology and HPV testing every 5 years in those aged 30-65.
They also recommend against screening after hysterectomy with removal of the cervix in women with no history of high-grade precancer or cervical cancer, and against screening with HPV testing in women younger than age 30, either alone or with cytology.
The ACS/ASCP/ASCCP guidelines recommend a Pap test every 3 years in women aged 21-29 years, with HPV testing only if needed after an abnormal Pap test result. Those aged 30-65 years should have both a Pap test and an HPV test every 5 years, although a Pap test alone every 3 years is also acceptable. Women over age 65 years who have been screened regularly with normal results do not require screening, but those over age 65 years who are diagnosed with cervical precancer should continue to be screened, the guidelines say.
In April, the American College of Physicians in April released its own set of guidelines for screening average-risk women; these guidelines adhere closely to the USPSTF guidelines, and have been endorsed by the American Congress of Obstetricians and Gynecologists and the ASCP (Ann Intern Med. 2015;162[12]:851-9).
More than 3 years after the release of new cervical cancer screening guidelines, patients remain largely unaware of substantial changes in screening, and many physicians remain confused about or resistant to those changes.
The confusion is a matter of education, said Dr. Owen Montgomery, chairman of the department of obstetrics and gynecology at Drexel University, Philadelphia. As for the resistance, that’s less a reflection of concern about the science and more about the emotional and sociological processes involved in change, he said.
“It’s really good science,” Dr. Montgomery said of the data that formed the basis for the guidelines. “I was on the executive board of the [American College of Obstetricians and Gynecologists] when we signed off on the new recommendations. The science is valid.”
Two sets of guidelines were released in 2012, one by the U.S. Preventive Services Task Force (USPSTF) and one by the American Cancer Society (ACS) in conjunction with the American Society for Clinical Pathology (ASCP) and the American Society for Colposcopy and Cervical Pathology (ASCCP). Although the two guidelines differ in some respects, both recommend against a longstanding tradition: routine yearly Pap testing. The guidelines now call for screening intervals of 3-5 years depending on patient age and other factors, and recommend against screening those under age 21 years and over age 65 years in the absence of risk factors.
Knowledge gaps
Despite the widespread organizational support for the guidelines, data suggest that knowledge of them may be lacking among both patients and physicians. For instance, about 85% of 249 adult women who participated in a recent survey answered incorrectly when asked how often low-risk women aged 21-29 should be screened, and nearly 95% answered incorrectly when asked about the recommended frequency of screening in low-risk women over age 30 years.
According to Dr. Katherine O’Flynn O’Brien and her colleagues at George Washington University, Washington, who presented the results earlier this year at the American College of Obstetricians and Gynecologists annual scientific meeting, the findings suggest “that providers should focus more on educating women about changes to screening practices.”
But another survey presented at the same ACOG meeting showed that many providers may be unaware of the guideline changes or hesitant about embracing those changes.
Using a convenience sample of 165 medical and osteopathic physicians, physician assistants, and nurse practitioners, the investigators found that, in contrast with the current guidelines, about half do not perform cotesting in women aged 30-65 years every 5 years, and nearly 57% do not screen women aged 21-29 years with cytology alone every 3 years. More than 40% reported that they do not perform cytology screening in women aged 30-65 years every 3 years.
Addressing the ‘what ifs’
Confusion about the guidelines, and hesitation about implementing them, is not surprising as the changes – particularly the 3- to 5-year screening interval changes – are some of the most dramatic in recent memory, according to Dr. Constance Bohon, an ob.gyn. in Washington, D.C., and assistant clinical professor of ob.gyn. at George Washington University.
Certainly the guidelines have evolved with the science over the years, and some changes, such as screening only those over age 21 years, have been embraced, she said.
“But some changes are easier to accept than others,” she added, noting that “doing a Pap with cotesting in women after age 30 and repeating it again in 5 years is very difficult for many clinicians to accept ... part of the issue is that fine line in medicine between using the data and relying on clinical sense, clinical expertise.”
There is concern about the exceptions and the “what ifs,” she said.
What if a patient has a new partner? What if she develops an illness that results in a shift in immunity?
These concerns are valid, agreed Dr. Jill Rabin, professor of obstetrics and gynecology and cochief of the division of ambulatory care, Women’s Health Programs–PCAP Services at North Shore–Long Island Jewish Health System, New Hyde Park, N.Y.
But she stressed in an interview that the guidelines are just that – guidelines. “They aren’t written in stone,” she said, adding that the recommendations are based on good science, and that a careful reading shows there is plenty of room for clinical judgment.
“Guidelines evolve and we have to keep an open mind and make sure that we don’t use a one-size-fits-all model. That doesn’t really help our patients,” said Dr. Rabin, who also is head of the urogynecology department at Long Island Jewish Medical Center.
Patient expectations
Another hurdle to embracing the guidelines is that of patient expectations. One of the big misunderstandings among patients of all ages is that they will skip all visits for 3 years because of the interval in Pap testing, Dr. Montgomery said. It is important to stress that “the Pap is just one of the services done during the visit, and a relatively small one when you look at all the other things that are part of a comprehensive well woman visit,” he said.
He further noted that both patient and physician age may be an important factor in acceptance of the guidelines and the changes in screening frequency.
As a physician with a large population of patients in their postreproductive years, and as one who trains young residents, he has noticed a generational difference: Younger patients and physicians are more accepting of the changes, but women who have spent 30 or 40 years coming in for an annual Pap smear equate that with health; they feel that they have done their part in staying healthy, and they have a greater sense of the value of the visit, he said.
Dr. Bohon predicted that both the advancing science and the concerns of patients and physicians will be considered when new guidelines are developed.
“My hope is that we have a realistic view of what the Pap can do,” Dr. Bohon said, adding that she expects that human papillomavirus (HPV) testing will get more and more reliable, and that clinicians will gain experience with following the HPV test and using that as a determining factor in patient care.
Guidelines at a glance
The USPSTF guidelines recommend screening with cytology every 3 years in women aged 21-29 years, and either screening with cytology every 3 years or cotesting using cytology and HPV testing every 5 years in those aged 30-65.
They also recommend against screening after hysterectomy with removal of the cervix in women with no history of high-grade precancer or cervical cancer, and against screening with HPV testing in women younger than age 30, either alone or with cytology.
The ACS/ASCP/ASCCP guidelines recommend a Pap test every 3 years in women aged 21-29 years, with HPV testing only if needed after an abnormal Pap test result. Those aged 30-65 years should have both a Pap test and an HPV test every 5 years, although a Pap test alone every 3 years is also acceptable. Women over age 65 years who have been screened regularly with normal results do not require screening, but those over age 65 years who are diagnosed with cervical precancer should continue to be screened, the guidelines say.
In April, the American College of Physicians in April released its own set of guidelines for screening average-risk women; these guidelines adhere closely to the USPSTF guidelines, and have been endorsed by the American Congress of Obstetricians and Gynecologists and the ASCP (Ann Intern Med. 2015;162[12]:851-9).
ESTIMABL trial: Current rhTSH cost outweighs benefits
The thyroid ablation rate with recombinant human thyroid stimulating hormone injections, or rhTSH, was shown in the randomized phase III Etude Stimulation Ablation trial to be similar to that with thyroid hormone withdrawal when used with either 1.1 or 3.7 GBq iodine-131 in patients with thyroid cancer, but a new analysis of data from the trial shows that the use of rhTSH would not be cost effective.
While rhTSH was associated with stable health-related quality of life and was more effective than thyroid hormone withdrawal (THW) with respect to quality-adjusted life-years (mean increase of 0.013 vs. THW), it is far more expensive, and a cost-effectiveness analysis showed that at a willingness-to-pay threshold of $53,300 per QALY, the probability that rhTSH would be cost effective was 47% when direct costs were considered. This increased to 70% when the cost of rhTSH was lowered by 30%, Isabelle Borget, Pharm.D., Ph.D., of Gustave Roussy, Villejuif, France, and her colleagues reported online in the Journal of Clinical Oncology.
Using 1.1 rather than 3.7 GBq of iodine-131 decreased efficacy slightly (mean decrease of 0.007 QALY), but also reduced costs by $1,018, and the probability of cost-effectiveness at the lower iodine-131 level was 65%, the investigators said (J Clin Oncol. 2015 Aug 3. doi: 10.1200/JCO.2015.61.6722).
Although rhTSH was not associated with the transient deterioration in health-related quality of life seen with thyroid hormone withdrawal in the first few months of treatment, it was cost effective only when the price was reduced by 30%; lower iodine-131 activity also reduced overall costs, they concluded.
Dr. Borget reported receiving honoraria from Roche and Janssen-Cilag, and travel, accommodations, and expenses from Janssen-Cilag. Several coauthors reported relationships with Genzyme, Sanofi, Novartis, and/or GE Healthcare, including receiving research support, honoraria, travel/accommodations/expenses, and/or serving as a consultant or advisor.
The thyroid ablation rate with recombinant human thyroid stimulating hormone injections, or rhTSH, was shown in the randomized phase III Etude Stimulation Ablation trial to be similar to that with thyroid hormone withdrawal when used with either 1.1 or 3.7 GBq iodine-131 in patients with thyroid cancer, but a new analysis of data from the trial shows that the use of rhTSH would not be cost effective.
While rhTSH was associated with stable health-related quality of life and was more effective than thyroid hormone withdrawal (THW) with respect to quality-adjusted life-years (mean increase of 0.013 vs. THW), it is far more expensive, and a cost-effectiveness analysis showed that at a willingness-to-pay threshold of $53,300 per QALY, the probability that rhTSH would be cost effective was 47% when direct costs were considered. This increased to 70% when the cost of rhTSH was lowered by 30%, Isabelle Borget, Pharm.D., Ph.D., of Gustave Roussy, Villejuif, France, and her colleagues reported online in the Journal of Clinical Oncology.
Using 1.1 rather than 3.7 GBq of iodine-131 decreased efficacy slightly (mean decrease of 0.007 QALY), but also reduced costs by $1,018, and the probability of cost-effectiveness at the lower iodine-131 level was 65%, the investigators said (J Clin Oncol. 2015 Aug 3. doi: 10.1200/JCO.2015.61.6722).
Although rhTSH was not associated with the transient deterioration in health-related quality of life seen with thyroid hormone withdrawal in the first few months of treatment, it was cost effective only when the price was reduced by 30%; lower iodine-131 activity also reduced overall costs, they concluded.
Dr. Borget reported receiving honoraria from Roche and Janssen-Cilag, and travel, accommodations, and expenses from Janssen-Cilag. Several coauthors reported relationships with Genzyme, Sanofi, Novartis, and/or GE Healthcare, including receiving research support, honoraria, travel/accommodations/expenses, and/or serving as a consultant or advisor.
The thyroid ablation rate with recombinant human thyroid stimulating hormone injections, or rhTSH, was shown in the randomized phase III Etude Stimulation Ablation trial to be similar to that with thyroid hormone withdrawal when used with either 1.1 or 3.7 GBq iodine-131 in patients with thyroid cancer, but a new analysis of data from the trial shows that the use of rhTSH would not be cost effective.
While rhTSH was associated with stable health-related quality of life and was more effective than thyroid hormone withdrawal (THW) with respect to quality-adjusted life-years (mean increase of 0.013 vs. THW), it is far more expensive, and a cost-effectiveness analysis showed that at a willingness-to-pay threshold of $53,300 per QALY, the probability that rhTSH would be cost effective was 47% when direct costs were considered. This increased to 70% when the cost of rhTSH was lowered by 30%, Isabelle Borget, Pharm.D., Ph.D., of Gustave Roussy, Villejuif, France, and her colleagues reported online in the Journal of Clinical Oncology.
Using 1.1 rather than 3.7 GBq of iodine-131 decreased efficacy slightly (mean decrease of 0.007 QALY), but also reduced costs by $1,018, and the probability of cost-effectiveness at the lower iodine-131 level was 65%, the investigators said (J Clin Oncol. 2015 Aug 3. doi: 10.1200/JCO.2015.61.6722).
Although rhTSH was not associated with the transient deterioration in health-related quality of life seen with thyroid hormone withdrawal in the first few months of treatment, it was cost effective only when the price was reduced by 30%; lower iodine-131 activity also reduced overall costs, they concluded.
Dr. Borget reported receiving honoraria from Roche and Janssen-Cilag, and travel, accommodations, and expenses from Janssen-Cilag. Several coauthors reported relationships with Genzyme, Sanofi, Novartis, and/or GE Healthcare, including receiving research support, honoraria, travel/accommodations/expenses, and/or serving as a consultant or advisor.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Recombinant human thyroid-stimulating hormone injections are as effective as thyroid hormone withdrawal for thyroid ablation, but are not cost-effective, according to a new analysis of data from the Etude Stimulation Ablation (ESTIMABL) trial.
Major finding: At a willingness-to-pay threshold of $53,300 per QALY, the probability of rhTSH cost-effectiveness was 47%.
Data source: The randomized phase III ESTIMABL Trial involving 752 patients.
Disclosures: Dr. Borget reported receiving honoraria from Roche and Janssen-Cilag, and travel, accommodations, and expenses from Janssen-Cilag. Several coauthors reported relationships with Genzyme, Sanofi, Novartis, and/or GE Healthcare, including receiving research support, honoraria, travel/accommodations/expenses, and/or serving as a consultant or advisor.
In psoriasis, low cholesterol efflux capacity may predict heart risk
Low cholesterol efflux capacity may be an important biomarker for subclinical coronary atherosclerosis in patients with psoriasis, based on findings from a prospective cohort study.
High-density lipoprotein cholesterol efflux capacity (CEC) was inversely correlated with the noncalcified burden (NCB) of coronary atherosclerosis in baseline data from the first 101 patients enrolled in the 4-year study, Dr. Taufiq Salahuddin of the National Heart, Lung, and Blood Institute and colleagues reported online in the European Heart Journal.
The relationship between CEC and NCB “suggests that higher CEC may promote reverse cholesterol transport from earlier, more lipid-rich plaques. … Others have found this noncalcified plaque to be the culprit lesion in acute coronary syndromes. Therefore, in the context of our study, there is strong biological plausibility for observing a relationship between CEC and NCB; psoriasis is associated with both increased future cardiovascular events and impaired HDL function, and our findings suggest that this may be due to predisposition toward formation of noncalcified plaque,” the researchers wrote.
The relationship between CEC (quantified using a cell-based ex vivo assay), and NCB plaque indexes (assessed by quantitative coronary computed tomography angiography) persisted after adjustment for cardiovascular risk factors, high-density lipoprotein cholesterol levels, and apolipoprotein A1 levels.
Of note, the relationship between CEC and NCB was stronger in women than in men, with a statistically significant gender interaction, the investigators found (Eur Heart J. 2015 Jul 18. doi.org/10.1093/eurheartj/ehv339).
Cholesterol efflux capacity has been shown in prior studies to predict future cardiovascular events, and since psoriasis both increases cardiovascular risk and impairs CEC, the investigators sought to assess the cross-sectional relationship between coronary plaque burden and CEC.
Study subjects were adults over age 18 years with moderate skin disease severity (median psoriasis area severity index [PASI] score, 6.2), and a low 10-year pooled cohort equation risk score (median, 2.7%). Traditional lipid profiles were within normal limits, and the median CEC was 0.94.
In addition to the inverse correlation between CEC and NCB at baseline, significant relationships were seen between CEC and PASI score, body surface area affected by psoriasis, and HDL cholesterol level, and between noncalcified burden and CEC, psoriasis severity, body surface area affected by psoriasis, and HDL cholesterol.
“Stratified by the sample’s median CEC value, patients with low CEC had greater total burden of coronary plaque and greater NCB than did patients with high CEC (0.0131 and 0.0127 mm2 in low CEC vs. 0.0106 and 0.0103 mm2 with high CEC),” they wrote.
No differences were seen based on psoriasis treatment status or statin use, although systemic/biologic therapy was associated with a reduction in noncalcified burden.
The findings with respect to gender differences may suggest that greater CEC is more protective against noncalcified plaque in women than it is in men, the investigators added, concluding that “ongoing follow-up of these patients will inform whether aggressive treatment of psoriasis and lifestyle measures improve CEC and ultimately noncalcified burden within the coronary arteries in psoriasis.”
This study was supported by a National Institutes of Health intramural grant, and the NIH Medical Research Scholars Program. The investigators reported having no relevant financial disclosures.
Low cholesterol efflux capacity may be an important biomarker for subclinical coronary atherosclerosis in patients with psoriasis, based on findings from a prospective cohort study.
High-density lipoprotein cholesterol efflux capacity (CEC) was inversely correlated with the noncalcified burden (NCB) of coronary atherosclerosis in baseline data from the first 101 patients enrolled in the 4-year study, Dr. Taufiq Salahuddin of the National Heart, Lung, and Blood Institute and colleagues reported online in the European Heart Journal.
The relationship between CEC and NCB “suggests that higher CEC may promote reverse cholesterol transport from earlier, more lipid-rich plaques. … Others have found this noncalcified plaque to be the culprit lesion in acute coronary syndromes. Therefore, in the context of our study, there is strong biological plausibility for observing a relationship between CEC and NCB; psoriasis is associated with both increased future cardiovascular events and impaired HDL function, and our findings suggest that this may be due to predisposition toward formation of noncalcified plaque,” the researchers wrote.
The relationship between CEC (quantified using a cell-based ex vivo assay), and NCB plaque indexes (assessed by quantitative coronary computed tomography angiography) persisted after adjustment for cardiovascular risk factors, high-density lipoprotein cholesterol levels, and apolipoprotein A1 levels.
Of note, the relationship between CEC and NCB was stronger in women than in men, with a statistically significant gender interaction, the investigators found (Eur Heart J. 2015 Jul 18. doi.org/10.1093/eurheartj/ehv339).
Cholesterol efflux capacity has been shown in prior studies to predict future cardiovascular events, and since psoriasis both increases cardiovascular risk and impairs CEC, the investigators sought to assess the cross-sectional relationship between coronary plaque burden and CEC.
Study subjects were adults over age 18 years with moderate skin disease severity (median psoriasis area severity index [PASI] score, 6.2), and a low 10-year pooled cohort equation risk score (median, 2.7%). Traditional lipid profiles were within normal limits, and the median CEC was 0.94.
In addition to the inverse correlation between CEC and NCB at baseline, significant relationships were seen between CEC and PASI score, body surface area affected by psoriasis, and HDL cholesterol level, and between noncalcified burden and CEC, psoriasis severity, body surface area affected by psoriasis, and HDL cholesterol.
“Stratified by the sample’s median CEC value, patients with low CEC had greater total burden of coronary plaque and greater NCB than did patients with high CEC (0.0131 and 0.0127 mm2 in low CEC vs. 0.0106 and 0.0103 mm2 with high CEC),” they wrote.
No differences were seen based on psoriasis treatment status or statin use, although systemic/biologic therapy was associated with a reduction in noncalcified burden.
The findings with respect to gender differences may suggest that greater CEC is more protective against noncalcified plaque in women than it is in men, the investigators added, concluding that “ongoing follow-up of these patients will inform whether aggressive treatment of psoriasis and lifestyle measures improve CEC and ultimately noncalcified burden within the coronary arteries in psoriasis.”
This study was supported by a National Institutes of Health intramural grant, and the NIH Medical Research Scholars Program. The investigators reported having no relevant financial disclosures.
Low cholesterol efflux capacity may be an important biomarker for subclinical coronary atherosclerosis in patients with psoriasis, based on findings from a prospective cohort study.
High-density lipoprotein cholesterol efflux capacity (CEC) was inversely correlated with the noncalcified burden (NCB) of coronary atherosclerosis in baseline data from the first 101 patients enrolled in the 4-year study, Dr. Taufiq Salahuddin of the National Heart, Lung, and Blood Institute and colleagues reported online in the European Heart Journal.
The relationship between CEC and NCB “suggests that higher CEC may promote reverse cholesterol transport from earlier, more lipid-rich plaques. … Others have found this noncalcified plaque to be the culprit lesion in acute coronary syndromes. Therefore, in the context of our study, there is strong biological plausibility for observing a relationship between CEC and NCB; psoriasis is associated with both increased future cardiovascular events and impaired HDL function, and our findings suggest that this may be due to predisposition toward formation of noncalcified plaque,” the researchers wrote.
The relationship between CEC (quantified using a cell-based ex vivo assay), and NCB plaque indexes (assessed by quantitative coronary computed tomography angiography) persisted after adjustment for cardiovascular risk factors, high-density lipoprotein cholesterol levels, and apolipoprotein A1 levels.
Of note, the relationship between CEC and NCB was stronger in women than in men, with a statistically significant gender interaction, the investigators found (Eur Heart J. 2015 Jul 18. doi.org/10.1093/eurheartj/ehv339).
Cholesterol efflux capacity has been shown in prior studies to predict future cardiovascular events, and since psoriasis both increases cardiovascular risk and impairs CEC, the investigators sought to assess the cross-sectional relationship between coronary plaque burden and CEC.
Study subjects were adults over age 18 years with moderate skin disease severity (median psoriasis area severity index [PASI] score, 6.2), and a low 10-year pooled cohort equation risk score (median, 2.7%). Traditional lipid profiles were within normal limits, and the median CEC was 0.94.
In addition to the inverse correlation between CEC and NCB at baseline, significant relationships were seen between CEC and PASI score, body surface area affected by psoriasis, and HDL cholesterol level, and between noncalcified burden and CEC, psoriasis severity, body surface area affected by psoriasis, and HDL cholesterol.
“Stratified by the sample’s median CEC value, patients with low CEC had greater total burden of coronary plaque and greater NCB than did patients with high CEC (0.0131 and 0.0127 mm2 in low CEC vs. 0.0106 and 0.0103 mm2 with high CEC),” they wrote.
No differences were seen based on psoriasis treatment status or statin use, although systemic/biologic therapy was associated with a reduction in noncalcified burden.
The findings with respect to gender differences may suggest that greater CEC is more protective against noncalcified plaque in women than it is in men, the investigators added, concluding that “ongoing follow-up of these patients will inform whether aggressive treatment of psoriasis and lifestyle measures improve CEC and ultimately noncalcified burden within the coronary arteries in psoriasis.”
This study was supported by a National Institutes of Health intramural grant, and the NIH Medical Research Scholars Program. The investigators reported having no relevant financial disclosures.
FROM THE EUROPEAN HEART JOURNAL
Key clinical point: Low cholesterol efflux capacity may be an important biomarker for subclinical coronary atherosclerosis in patients with psoriasis, according to findings from a prospective cohort study.
Major finding: Baseline data showed an inverse correlation between HDL cholesterol efflux capacity and noncalcified burden of coronary atherosclerosis (unadjusted beta-coefficient, –0.33).
Data source: The first 101 patients in a 4-year prospective cohort study.
Disclosures: This study was supported by a National Institutes of Health intramural grant, and the NIH Medical Research Scholars Program. The investigators reported having no relevant financial disclosures.
Short-term CVD Risk Rises With Testicular Cancer Chemotherapy
Patients with testicular nonseminoma who undergo chemotherapy experience a nearly fivefold increase in the risk of cardiovascular disease mortality in the year following diagnosis, according to findings from a large population-based study.
The standardized mortality ratio (SMR), after accounting for the effects of age, treatment, extent of disease, and other factors on CVD mortality, was 1.36 among 6,909 patients with testicular nonseminoma who underwent chemotherapy and who were included in the Surveillance, Epidemiology, and End Results (SEER) program from 1980 to 2010. Significant excess deaths following chemotherapy occurred only in the first year after testicular cancer (TC) diagnosis (SMR, 5.31; absolute excess risk [AER], 13.90), and included deaths from cerebrovascular disease (SMR, 21.72; AER, 7.43), and heart disease (SMR, 3.45; AER, 6.64), Dr. Chunkit Fung of the University of Rochester (N.Y.) and colleagues, reported online Aug. 3 in the Journal of Clinical Oncology.

No increase was seen in CVD mortality after surgery among 8,097 patients (SMR, 0.81).
Multivariable analyses also showed that the risk of CVD mortality occurred only during the first year after diagnosis (hazard ratio, 4.86), and that distant nonseminoma (HR, 1.91) and older age at diagnosis (HR, 3.47, 8.97, and 34.26 for ages 30-39 years, 40-49 years, and 50 years or older) were independent risk factors, the investigators said (J Clin Onc. 2015 Aug 3. doi: 10.1200/JCO.2014.60.3654.).
The findings “remain to be confirmed in analytic studies that also identify patients with TC at the highest risk of thromboembolic events to formulate comprehensive, evidence-based approaches for risk stratification and reduction,” they concluded, noting that in the interim, effective TC chemotherapy should be administered when clinically indicated, and that clinicians should continue to apply existing clinical practice guidelines for VTE prophylaxis and treatment.
Dr. Fung reported owning GlaxoSmithKline stock; consulting or serving in an advisory role for Janssen Scientific Affairs, Dendreon, and Bayer; and receiving research funding from Astellas Pharma. Coauthor Michael T. Milano received honoraria from Accuray. The remaining authors reported having no disclosures.
Patients with testicular nonseminoma who undergo chemotherapy experience a nearly fivefold increase in the risk of cardiovascular disease mortality in the year following diagnosis, according to findings from a large population-based study.
The standardized mortality ratio (SMR), after accounting for the effects of age, treatment, extent of disease, and other factors on CVD mortality, was 1.36 among 6,909 patients with testicular nonseminoma who underwent chemotherapy and who were included in the Surveillance, Epidemiology, and End Results (SEER) program from 1980 to 2010. Significant excess deaths following chemotherapy occurred only in the first year after testicular cancer (TC) diagnosis (SMR, 5.31; absolute excess risk [AER], 13.90), and included deaths from cerebrovascular disease (SMR, 21.72; AER, 7.43), and heart disease (SMR, 3.45; AER, 6.64), Dr. Chunkit Fung of the University of Rochester (N.Y.) and colleagues, reported online Aug. 3 in the Journal of Clinical Oncology.
No increase was seen in CVD mortality after surgery among 8,097 patients (SMR, 0.81).
Multivariable analyses also showed that the risk of CVD mortality occurred only during the first year after diagnosis (hazard ratio, 4.86), and that distant nonseminoma (HR, 1.91) and older age at diagnosis (HR, 3.47, 8.97, and 34.26 for ages 30-39 years, 40-49 years, and 50 years or older) were independent risk factors, the investigators said (J Clin Onc. 2015 Aug 3. doi: 10.1200/JCO.2014.60.3654.).
The findings “remain to be confirmed in analytic studies that also identify patients with TC at the highest risk of thromboembolic events to formulate comprehensive, evidence-based approaches for risk stratification and reduction,” they concluded, noting that in the interim, effective TC chemotherapy should be administered when clinically indicated, and that clinicians should continue to apply existing clinical practice guidelines for VTE prophylaxis and treatment.
Dr. Fung reported owning GlaxoSmithKline stock; consulting or serving in an advisory role for Janssen Scientific Affairs, Dendreon, and Bayer; and receiving research funding from Astellas Pharma. Coauthor Michael T. Milano received honoraria from Accuray. The remaining authors reported having no disclosures.
Patients with testicular nonseminoma who undergo chemotherapy experience a nearly fivefold increase in the risk of cardiovascular disease mortality in the year following diagnosis, according to findings from a large population-based study.
The standardized mortality ratio (SMR), after accounting for the effects of age, treatment, extent of disease, and other factors on CVD mortality, was 1.36 among 6,909 patients with testicular nonseminoma who underwent chemotherapy and who were included in the Surveillance, Epidemiology, and End Results (SEER) program from 1980 to 2010. Significant excess deaths following chemotherapy occurred only in the first year after testicular cancer (TC) diagnosis (SMR, 5.31; absolute excess risk [AER], 13.90), and included deaths from cerebrovascular disease (SMR, 21.72; AER, 7.43), and heart disease (SMR, 3.45; AER, 6.64), Dr. Chunkit Fung of the University of Rochester (N.Y.) and colleagues, reported online Aug. 3 in the Journal of Clinical Oncology.
No increase was seen in CVD mortality after surgery among 8,097 patients (SMR, 0.81).
Multivariable analyses also showed that the risk of CVD mortality occurred only during the first year after diagnosis (hazard ratio, 4.86), and that distant nonseminoma (HR, 1.91) and older age at diagnosis (HR, 3.47, 8.97, and 34.26 for ages 30-39 years, 40-49 years, and 50 years or older) were independent risk factors, the investigators said (J Clin Onc. 2015 Aug 3. doi: 10.1200/JCO.2014.60.3654.).
The findings “remain to be confirmed in analytic studies that also identify patients with TC at the highest risk of thromboembolic events to formulate comprehensive, evidence-based approaches for risk stratification and reduction,” they concluded, noting that in the interim, effective TC chemotherapy should be administered when clinically indicated, and that clinicians should continue to apply existing clinical practice guidelines for VTE prophylaxis and treatment.
Dr. Fung reported owning GlaxoSmithKline stock; consulting or serving in an advisory role for Janssen Scientific Affairs, Dendreon, and Bayer; and receiving research funding from Astellas Pharma. Coauthor Michael T. Milano received honoraria from Accuray. The remaining authors reported having no disclosures.
FROM THE JOURNAL OF CLINICAL ONCOLOGY

Short-term CVD risk rises with testicular cancer chemotherapy
Patients with testicular nonseminoma who undergo chemotherapy experience a nearly fivefold increase in the risk of cardiovascular disease mortality in the year following diagnosis, according to findings from a large population-based study.
The standardized mortality ratio (SMR), after accounting for the effects of age, treatment, extent of disease, and other factors on CVD mortality, was 1.36 among 6,909 patients with testicular nonseminoma who underwent chemotherapy and who were included in the Surveillance, Epidemiology, and End Results (SEER) program from 1980 to 2010. Significant excess deaths following chemotherapy occurred only in the first year after testicular cancer (TC) diagnosis (SMR, 5.31; absolute excess risk [AER], 13.90), and included deaths from cerebrovascular disease (SMR, 21.72; AER, 7.43), and heart disease (SMR, 3.45; AER, 6.64), Dr. Chunkit Fung of the University of Rochester (N.Y.) and colleagues, reported online Aug. 3 in the Journal of Clinical Oncology.
No increase was seen in CVD mortality after surgery among 8,097 patients (SMR, 0.81).
Multivariable analyses also showed that the risk of CVD mortality occurred only during the first year after diagnosis (hazard ratio, 4.86), and that distant nonseminoma (HR, 1.91) and older age at diagnosis (HR, 3.47, 8.97, and 34.26 for ages 30-39 years, 40-49 years, and 50 years or older) were independent risk factors, the investigators said (J Clin Onc. 2015 Aug 3. doi: 10.1200/JCO.2014.60.3654.).
The findings “remain to be confirmed in analytic studies that also identify patients with TC at the highest risk of thromboembolic events to formulate comprehensive, evidence-based approaches for risk stratification and reduction,” they concluded, noting that in the interim, effective TC chemotherapy should be administered when clinically indicated, and that clinicians should continue to apply existing clinical practice guidelines for VTE prophylaxis and treatment.
Dr. Fung reported owning GlaxoSmithKline stock; consulting or serving in an advisory role for Janssen Scientific Affairs, Dendreon, and Bayer; and receiving research funding from Astellas Pharma. Coauthor Michael T. Milano received honoraria from Accuray. The remaining authors reported having no disclosures.
Patients with testicular nonseminoma who undergo chemotherapy experience a nearly fivefold increase in the risk of cardiovascular disease mortality in the year following diagnosis, according to findings from a large population-based study.
The standardized mortality ratio (SMR), after accounting for the effects of age, treatment, extent of disease, and other factors on CVD mortality, was 1.36 among 6,909 patients with testicular nonseminoma who underwent chemotherapy and who were included in the Surveillance, Epidemiology, and End Results (SEER) program from 1980 to 2010. Significant excess deaths following chemotherapy occurred only in the first year after testicular cancer (TC) diagnosis (SMR, 5.31; absolute excess risk [AER], 13.90), and included deaths from cerebrovascular disease (SMR, 21.72; AER, 7.43), and heart disease (SMR, 3.45; AER, 6.64), Dr. Chunkit Fung of the University of Rochester (N.Y.) and colleagues, reported online Aug. 3 in the Journal of Clinical Oncology.
No increase was seen in CVD mortality after surgery among 8,097 patients (SMR, 0.81).
Multivariable analyses also showed that the risk of CVD mortality occurred only during the first year after diagnosis (hazard ratio, 4.86), and that distant nonseminoma (HR, 1.91) and older age at diagnosis (HR, 3.47, 8.97, and 34.26 for ages 30-39 years, 40-49 years, and 50 years or older) were independent risk factors, the investigators said (J Clin Onc. 2015 Aug 3. doi: 10.1200/JCO.2014.60.3654.).
The findings “remain to be confirmed in analytic studies that also identify patients with TC at the highest risk of thromboembolic events to formulate comprehensive, evidence-based approaches for risk stratification and reduction,” they concluded, noting that in the interim, effective TC chemotherapy should be administered when clinically indicated, and that clinicians should continue to apply existing clinical practice guidelines for VTE prophylaxis and treatment.
Dr. Fung reported owning GlaxoSmithKline stock; consulting or serving in an advisory role for Janssen Scientific Affairs, Dendreon, and Bayer; and receiving research funding from Astellas Pharma. Coauthor Michael T. Milano received honoraria from Accuray. The remaining authors reported having no disclosures.
Patients with testicular nonseminoma who undergo chemotherapy experience a nearly fivefold increase in the risk of cardiovascular disease mortality in the year following diagnosis, according to findings from a large population-based study.
The standardized mortality ratio (SMR), after accounting for the effects of age, treatment, extent of disease, and other factors on CVD mortality, was 1.36 among 6,909 patients with testicular nonseminoma who underwent chemotherapy and who were included in the Surveillance, Epidemiology, and End Results (SEER) program from 1980 to 2010. Significant excess deaths following chemotherapy occurred only in the first year after testicular cancer (TC) diagnosis (SMR, 5.31; absolute excess risk [AER], 13.90), and included deaths from cerebrovascular disease (SMR, 21.72; AER, 7.43), and heart disease (SMR, 3.45; AER, 6.64), Dr. Chunkit Fung of the University of Rochester (N.Y.) and colleagues, reported online Aug. 3 in the Journal of Clinical Oncology.
No increase was seen in CVD mortality after surgery among 8,097 patients (SMR, 0.81).
Multivariable analyses also showed that the risk of CVD mortality occurred only during the first year after diagnosis (hazard ratio, 4.86), and that distant nonseminoma (HR, 1.91) and older age at diagnosis (HR, 3.47, 8.97, and 34.26 for ages 30-39 years, 40-49 years, and 50 years or older) were independent risk factors, the investigators said (J Clin Onc. 2015 Aug 3. doi: 10.1200/JCO.2014.60.3654.).
The findings “remain to be confirmed in analytic studies that also identify patients with TC at the highest risk of thromboembolic events to formulate comprehensive, evidence-based approaches for risk stratification and reduction,” they concluded, noting that in the interim, effective TC chemotherapy should be administered when clinically indicated, and that clinicians should continue to apply existing clinical practice guidelines for VTE prophylaxis and treatment.
Dr. Fung reported owning GlaxoSmithKline stock; consulting or serving in an advisory role for Janssen Scientific Affairs, Dendreon, and Bayer; and receiving research funding from Astellas Pharma. Coauthor Michael T. Milano received honoraria from Accuray. The remaining authors reported having no disclosures.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Patients with testicular nonseminoma who undergo chemotherapy experience a nearly fivefold increase in the risk of cardiovascular disease mortality in the year following diagnosis.
Major finding: The risk of CVD mortality among TC patients receiving chemotherapy was increased during the first year after diagnosis (HR, 4.86).
Data source: An analysis of SEER data for 15,006 patients.
Disclosures: Dr. Fung reported owning GlaxoSmithKline stock; consulting or serving in an advisory role for Janssen Scientific Affairs, Dendreon, and Bayer; and receiving research funding from Astellas Pharma. Coauthor Dr. Michael T. Milano received honoraria from Accuray. The remaining authors reported having no disclosures.
Potential Parkinson’s disease drug target: PPAR gamma pathways
A current prescription for an antidiabetic glitazone drug was associated with a reduced incidence of Parkinson’s disease among diabetic patients in a large retrospective cohort study, suggesting that peroxisome proliferation–activated receptor (PPAR) gamma pathways are a promising Parkinson’s disease drug target.
The incidence rate for Parkinson’s disease among 44,597 antidiabetic glitazone drug users included in the study, which used primary care data from the United Kingdom Clinical Practice Research Datalink, was 6.4 per 10,000 patients, compared with 8.8 per 10,000 among 120,373 other antidiabetic drug users (incidence rate ratio, 0.72), Ruth Brauer, Ph.D., of the London School of Hygiene & Tropical Medicine and her colleagues reported online July 21 in PLoS Medicine.
After adjusting for potential confounding variables such as smoking, other medications, head injury, and disease severity, the incidence rate ratio changed only slightly to 0.75. However, the incidence was reduced among only those with current glitazone prescriptions (incidence rate ratios of 0.59 vs. 0.85 for those with a current vs. past prescription), the investigators said, noting that it is unclear whether glitazone drugs prevent or slow progression of Parkinson’s disease, as only patients without a Parkinson’s disease diagnosis at the time they were prescribed a glitazone drug were included in the study (PLoS Med. 2015;12:e1001854 [doi:10.1371/journal.pmed.1001854]).
The “strong evidence for a protective association” of glitazone exposure with respect to the clinical presentation of Parkinson’s disease in humans is consistent with previously reported findings in animal and in vitro studies, they said.
This study was funded by a research grant from the Michael J. Fox Foundation for Parkinson’s Research, and by a Medical Research Council methodology research fellowship, a National Institute for Health Research postdoctoral fellowship, and a Wellcome Trust Senior Research Fellowship in Clinical Science grant, each awarded to individual authors. Dr. Bauer reported having no disclosures; two coauthors reported receiving research funding from GSK or consulting for and holding stock in GSK.
A current prescription for an antidiabetic glitazone drug was associated with a reduced incidence of Parkinson’s disease among diabetic patients in a large retrospective cohort study, suggesting that peroxisome proliferation–activated receptor (PPAR) gamma pathways are a promising Parkinson’s disease drug target.
The incidence rate for Parkinson’s disease among 44,597 antidiabetic glitazone drug users included in the study, which used primary care data from the United Kingdom Clinical Practice Research Datalink, was 6.4 per 10,000 patients, compared with 8.8 per 10,000 among 120,373 other antidiabetic drug users (incidence rate ratio, 0.72), Ruth Brauer, Ph.D., of the London School of Hygiene & Tropical Medicine and her colleagues reported online July 21 in PLoS Medicine.
After adjusting for potential confounding variables such as smoking, other medications, head injury, and disease severity, the incidence rate ratio changed only slightly to 0.75. However, the incidence was reduced among only those with current glitazone prescriptions (incidence rate ratios of 0.59 vs. 0.85 for those with a current vs. past prescription), the investigators said, noting that it is unclear whether glitazone drugs prevent or slow progression of Parkinson’s disease, as only patients without a Parkinson’s disease diagnosis at the time they were prescribed a glitazone drug were included in the study (PLoS Med. 2015;12:e1001854 [doi:10.1371/journal.pmed.1001854]).
The “strong evidence for a protective association” of glitazone exposure with respect to the clinical presentation of Parkinson’s disease in humans is consistent with previously reported findings in animal and in vitro studies, they said.
This study was funded by a research grant from the Michael J. Fox Foundation for Parkinson’s Research, and by a Medical Research Council methodology research fellowship, a National Institute for Health Research postdoctoral fellowship, and a Wellcome Trust Senior Research Fellowship in Clinical Science grant, each awarded to individual authors. Dr. Bauer reported having no disclosures; two coauthors reported receiving research funding from GSK or consulting for and holding stock in GSK.
A current prescription for an antidiabetic glitazone drug was associated with a reduced incidence of Parkinson’s disease among diabetic patients in a large retrospective cohort study, suggesting that peroxisome proliferation–activated receptor (PPAR) gamma pathways are a promising Parkinson’s disease drug target.
The incidence rate for Parkinson’s disease among 44,597 antidiabetic glitazone drug users included in the study, which used primary care data from the United Kingdom Clinical Practice Research Datalink, was 6.4 per 10,000 patients, compared with 8.8 per 10,000 among 120,373 other antidiabetic drug users (incidence rate ratio, 0.72), Ruth Brauer, Ph.D., of the London School of Hygiene & Tropical Medicine and her colleagues reported online July 21 in PLoS Medicine.
After adjusting for potential confounding variables such as smoking, other medications, head injury, and disease severity, the incidence rate ratio changed only slightly to 0.75. However, the incidence was reduced among only those with current glitazone prescriptions (incidence rate ratios of 0.59 vs. 0.85 for those with a current vs. past prescription), the investigators said, noting that it is unclear whether glitazone drugs prevent or slow progression of Parkinson’s disease, as only patients without a Parkinson’s disease diagnosis at the time they were prescribed a glitazone drug were included in the study (PLoS Med. 2015;12:e1001854 [doi:10.1371/journal.pmed.1001854]).
The “strong evidence for a protective association” of glitazone exposure with respect to the clinical presentation of Parkinson’s disease in humans is consistent with previously reported findings in animal and in vitro studies, they said.
This study was funded by a research grant from the Michael J. Fox Foundation for Parkinson’s Research, and by a Medical Research Council methodology research fellowship, a National Institute for Health Research postdoctoral fellowship, and a Wellcome Trust Senior Research Fellowship in Clinical Science grant, each awarded to individual authors. Dr. Bauer reported having no disclosures; two coauthors reported receiving research funding from GSK or consulting for and holding stock in GSK.
FROM PLOS MEDICINE
Key clinical point: A current prescription for an antidiabetic glitazone drug was associated with a reduced incidence of Parkinson’s disease among diabetic patients in a large retrospective cohort study.
Major finding: The Parkinson’s disease incidence rate was 6.4 per 10,000 antidiabetic glitazone drug users vs. 8.8 per 10,000 other antidiabetic drug users (incidence rate ratio, 0.72).
Data source: A retrospective cohort study of 164,970 diabetic patients.
Disclosures: This study was funded by a research grant from the Michael J. Fox Foundation for Parkinson’s Research, a Medical Research Council methodology research fellowship, a National Institute for Health Research postdoctoral fellowship, and a Wellcome Trust Senior Research Fellowship in Clinical Science grant, each awarded to individual authors. Dr. Bauer reported having no disclosures; two coauthors reported receiving research funding from GSK or consulting for and holding stock in GSK.
Extreme weight states may activate the HPA axis
Cortisol measures in women vary across the weight spectrum, with the lowest levels occurring in overweight-class 1 obese women, and the highest levels occurring in those with anorexia nervosa, according to findings from a cross-sectional study.
Cortisol levels rise with more significant obesity – but not to levels as high as those seen in women with anorexia nervosa, suggesting that extreme underweight and overweight states may activate the hypothalamic-pituitary-adrenal (HPA) axis and that hypercortisolemia may contribute to increased adiposity in those with caloric excess, Dr. Melanie Schorr and her colleagues at Massachusetts General Hospital and Harvard Medical School, Boston, reported online in the Journal of Clinical Endocrinology & Metabolism.

Among the 60 women, aged 18-45 years, who were included in the study, 21 were overweight/obese, 18 had anorexia nervosa, and 21 were of normal weight. A U-shaped relationship was seen between cortisol measures and body mass index (most notably between urinary free cortisol/creatinine clearance [UFC/CrCl] and BMI and between mean overnight serum cortisol and BMI, r = 0.55 and 0.66, respectively), and between cortisol measures and visceral adipose tissue and total fat mass (for example, r = 0.50 for UFC/CrCl and adipose tissue, and 0.61 for UFC/CrCl and total fat mass), and either no relationship or a weak negative linear relationship was observed between lean mass and cortisol measures (for example, r = –0.34 for UFC/CrCL and lean mass). The latter “may be because it is the adipose component that is associated with cortisol measures or because hypercortisolemia contributes to muscle wasting,” the investigators wrote (J. Clin. Endocrinol. Metab. 2015 July [doi:10.1210/JC.2015-2078]).
They also noted that cortisol measures were negatively associated with bone mineral density across the weight spectrum between urinary free cortisol/creatinine clearance and lean body mass, suggesting that “relative hypercortisolemia may contribute to bone loss in the setting of both caloric restriction and excess.”
“Given the fact that obesity has reached epidemic proportions and significantly increases the risk of the metabolic syndrome and cardiovascular disease among other comorbidities, insight into the factors that contribute to obesity and/or its complications may have important therapeutic implications,” they concluded.
The authors reported having no disclosures.
Cortisol measures in women vary across the weight spectrum, with the lowest levels occurring in overweight-class 1 obese women, and the highest levels occurring in those with anorexia nervosa, according to findings from a cross-sectional study.
Cortisol levels rise with more significant obesity – but not to levels as high as those seen in women with anorexia nervosa, suggesting that extreme underweight and overweight states may activate the hypothalamic-pituitary-adrenal (HPA) axis and that hypercortisolemia may contribute to increased adiposity in those with caloric excess, Dr. Melanie Schorr and her colleagues at Massachusetts General Hospital and Harvard Medical School, Boston, reported online in the Journal of Clinical Endocrinology & Metabolism.
Among the 60 women, aged 18-45 years, who were included in the study, 21 were overweight/obese, 18 had anorexia nervosa, and 21 were of normal weight. A U-shaped relationship was seen between cortisol measures and body mass index (most notably between urinary free cortisol/creatinine clearance [UFC/CrCl] and BMI and between mean overnight serum cortisol and BMI, r = 0.55 and 0.66, respectively), and between cortisol measures and visceral adipose tissue and total fat mass (for example, r = 0.50 for UFC/CrCl and adipose tissue, and 0.61 for UFC/CrCl and total fat mass), and either no relationship or a weak negative linear relationship was observed between lean mass and cortisol measures (for example, r = –0.34 for UFC/CrCL and lean mass). The latter “may be because it is the adipose component that is associated with cortisol measures or because hypercortisolemia contributes to muscle wasting,” the investigators wrote (J. Clin. Endocrinol. Metab. 2015 July [doi:10.1210/JC.2015-2078]).
They also noted that cortisol measures were negatively associated with bone mineral density across the weight spectrum between urinary free cortisol/creatinine clearance and lean body mass, suggesting that “relative hypercortisolemia may contribute to bone loss in the setting of both caloric restriction and excess.”
“Given the fact that obesity has reached epidemic proportions and significantly increases the risk of the metabolic syndrome and cardiovascular disease among other comorbidities, insight into the factors that contribute to obesity and/or its complications may have important therapeutic implications,” they concluded.
The authors reported having no disclosures.
Cortisol measures in women vary across the weight spectrum, with the lowest levels occurring in overweight-class 1 obese women, and the highest levels occurring in those with anorexia nervosa, according to findings from a cross-sectional study.
Cortisol levels rise with more significant obesity – but not to levels as high as those seen in women with anorexia nervosa, suggesting that extreme underweight and overweight states may activate the hypothalamic-pituitary-adrenal (HPA) axis and that hypercortisolemia may contribute to increased adiposity in those with caloric excess, Dr. Melanie Schorr and her colleagues at Massachusetts General Hospital and Harvard Medical School, Boston, reported online in the Journal of Clinical Endocrinology & Metabolism.
Among the 60 women, aged 18-45 years, who were included in the study, 21 were overweight/obese, 18 had anorexia nervosa, and 21 were of normal weight. A U-shaped relationship was seen between cortisol measures and body mass index (most notably between urinary free cortisol/creatinine clearance [UFC/CrCl] and BMI and between mean overnight serum cortisol and BMI, r = 0.55 and 0.66, respectively), and between cortisol measures and visceral adipose tissue and total fat mass (for example, r = 0.50 for UFC/CrCl and adipose tissue, and 0.61 for UFC/CrCl and total fat mass), and either no relationship or a weak negative linear relationship was observed between lean mass and cortisol measures (for example, r = –0.34 for UFC/CrCL and lean mass). The latter “may be because it is the adipose component that is associated with cortisol measures or because hypercortisolemia contributes to muscle wasting,” the investigators wrote (J. Clin. Endocrinol. Metab. 2015 July [doi:10.1210/JC.2015-2078]).
They also noted that cortisol measures were negatively associated with bone mineral density across the weight spectrum between urinary free cortisol/creatinine clearance and lean body mass, suggesting that “relative hypercortisolemia may contribute to bone loss in the setting of both caloric restriction and excess.”
“Given the fact that obesity has reached epidemic proportions and significantly increases the risk of the metabolic syndrome and cardiovascular disease among other comorbidities, insight into the factors that contribute to obesity and/or its complications may have important therapeutic implications,” they concluded.
The authors reported having no disclosures.
FROM THE JOURNAL OF CLINICAL ENDOCRINOLOGY & METABOLISM
Key clinical point: The variation in cortisol measures suggest that extreme underweight and overweight states may activate the hypothalamic-pituitary-adrenal axis.
Major finding: A U-shaped relationship was seen between cortisol measures and BMI (most notably between urinary free cortisol/creatinine clearance [UFC/CrCl] and BMI, and between mean overnight serum cortisol and BMI, R = 0.55 and 0.66, respectively).
Data source: A cross-sectional study of 60 women.
Disclosures: The authors reported having no disclosures.

New Guidelines Focus on Pediatric Thyroid Nodules and Cancer
The evaluation and treatment of thyroid nodules in children should differ from evaluation and treatment in adults in that ultrasound characteristics and clinical context should be used rather than size alone to identify nodules that warrant fine-needle aspiration, according to new pediatric-specific guidelines from the American Thyroid Association.
The Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer – the first-ever guidelines for the evaluation and management of thyroid nodules and cancer in children – also note that fine-needle aspiration (FNA) in children should be performed under ultrasound guidance, that preoperative FNA of a hyperfunctioning nodule in a child is not warranted as long as the lesion is removed, that a diffusely infiltrative form of papillary thyroid cancer may occur in children and should be considered in a clinically suspicious gland, and that surgery (lobectomy plus isthmusectomy) is favored over repeat FNA for most nodules with indeterminate cytology, Dr. Gary L. Francis of Virginia Commonwealth University and Children’s Hospital of Richmond, Va., and his colleagues from the American Thyroid Association Guidelines Task Force on Pediatric Thyroid Cancer determined based on an extensive literature search.
Together this guidance with respect to thyroid nodules represents just one of 34 recommendations contained in the guidelines, which, according to the authors, represent “the current optimal care for children and adolescents with these conditions.”
The guidelines were published in the July issue of Thyroid (2015;25:716-59).
Previous guidelines were geared toward adults, but thyroid neoplasms in children differ from those in adults with respect to pathophysiology, clinical presentation, and long-term outcomes. Further, therapy that may be appropriate in adults may not be appropriate for children at low risk for death but higher risk of long-term harm from certain treatments, they said.
For example, recent studies with long-term follow-up revealed an increase in all-cause mortality for survivors of childhood differentiated thyroid cancer (DTC), primarily caused by second malignancies in children treated with radiation.
“These observations, coupled with a better understanding of the excellent prognosis associated with pediatric DTC, have now prompted the American Thyroid Association to specifically address treatment of children with benign and malignant thyroid tumors,” they wrote.
While the task force acknowledged a paucity of randomized, double-blind, controlled clinical trials involving children with DTC, they note that “retrospective analysis of therapeutic options has led to a reconsideration of the former concept that all children with DTC should be similarly treated and has provided the opportunity ... to broaden the scope of acceptable therapy in an attempt to provide aggressive therapy when warranted and to limit overtreatment to those children who are unlikely to benefit.”
In addition to addressing the evaluation and management of thyroid nodules, the guidelines also address DTC, including preoperative staging, surgical management, postoperative staging, the role of radioactive iodine therapy, and goals for thyrotropin suppression. Management algorithms are proposed, and separate recommendations for papillary and follicular thyroid cancers are provided.
The authors note that since DTC recurrence has been reported as long as 40 years after initial therapy, children with DTC should be “followed for life, albeit with decreasing intensity for those with no evidence for disease.”
The guidelines are timely, as Surveillance, Epidemiology and End Results (SEER) program data indicate that new cases of thyroid cancer in persons under the age of 20 years represent 1.8% of all thyroid malignancies diagnosed in the United States, and that the incidence appears to be increasing.
Among 15- to 19-year old adolescents, thyroid cancer is the eighth most frequently diagnosed cancer, and it is the second most common cancer among girls, the authors said, noting that adolescents have a 10-fold greater incidence than do younger children, and that there is a female to male preponderance.
The development of pediatric-specific guidelines was critical, according to guidelines coauthor, Dr. Peter Angelos, professor of surgery and surgical ethics and chief of endocrine surgery at the University of Chicago Medicine and Biological Sciences.
“As they say, ‘children are not just small adults,’ ” he said in an interview.
In addition to the guidance provided on which types of nodules should be evaluated in children (since size alone should not be used to dictate who undergoes biopsy), a highlight of the guidelines is a recommendation that children with thyroid cancer be treated by multidisciplinary teams of physician in high-volume centers, he said.
“Thyroid cancer in children is different than in adults in that children have much higher rates of involved lymph nodes, but their overall prognosis is excellent despite the frequency of involved nodes. This confluence of findings pushes surgeons to do more aggressive operations to clear lymph nodes. This is a good thing, but unfortunately, can lead to higher complication rates (things such as permanently low calcium levels in the blood),” he said, adding that “the implications of finding a high-volume thyroid cancer surgeon with experience in thyroid cancer surgery on children are very significant and the guidelines make some recommendations about how many operations are necessary to constitute high volume.”
The push to limit the use of radioactive iodine in children further underscores the need for an experienced surgeon, he said.
“In an effort to avoid exposing children to radiation, surgeons are further pushed to be more aggressive in the operating room. Thus, it becomes even more important to see an experienced surgeon so that complications can be minimized. Even a seemingly ‘mild’ complication can be devastating for a child who will likely have to live with that complication for decades to come since the prognosis for thyroid cancer is so good,” he said.
An important potential benefit of treatment at centers with multidisciplinary interest and expertise is facilitation of additional research, particularly in areas of uncertainty, including the proper use of 131I, the interpretation of thyroglobulin (Tg) and TgAb (antibody) levels, the role of prospective ultrasound monitoring in presymptomatic children at risk for thyroid neoplasia, the use of novel targeted therapies for advanced disease that fails to respond to 131I, and the long-term psychosocial impacts of the disease on children and their families, the guideline authors said.
“These areas require well-designed long-term, multicenter studies that will be difficult to perform because of the rarity of pediatric DTC and the prolonged follow-up required to reach meaningful endpoints. Further research should be facilitated by ensuring that children with DTC are treated when possible at centers with multidisciplinary interest and expertise in this disease,” they concluded.
The guidelines were funded by the American Thyroid Association and ThyCa: Thyroid Cancer Survivors’ Association. Dr. Francis reported serving as an adviser to ThyCa and receiving research support from Grifols, Novo Nordisk, and the Juvenile Diabetes Research Foundation. Other authors reported relationships (consulting, receiving research support, and/or serving as a speaker) with Akrimax, IBSA Institut Biochimique, Pfizer, Novo Nordisk, Eli Lilly, AstraZeneca, Bayer Healthcare, Genzyme, Sobi, Henning, and Merck, and ThyCa.
The evaluation and treatment of thyroid nodules in children should differ from evaluation and treatment in adults in that ultrasound characteristics and clinical context should be used rather than size alone to identify nodules that warrant fine-needle aspiration, according to new pediatric-specific guidelines from the American Thyroid Association.
The Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer – the first-ever guidelines for the evaluation and management of thyroid nodules and cancer in children – also note that fine-needle aspiration (FNA) in children should be performed under ultrasound guidance, that preoperative FNA of a hyperfunctioning nodule in a child is not warranted as long as the lesion is removed, that a diffusely infiltrative form of papillary thyroid cancer may occur in children and should be considered in a clinically suspicious gland, and that surgery (lobectomy plus isthmusectomy) is favored over repeat FNA for most nodules with indeterminate cytology, Dr. Gary L. Francis of Virginia Commonwealth University and Children’s Hospital of Richmond, Va., and his colleagues from the American Thyroid Association Guidelines Task Force on Pediatric Thyroid Cancer determined based on an extensive literature search.
Together this guidance with respect to thyroid nodules represents just one of 34 recommendations contained in the guidelines, which, according to the authors, represent “the current optimal care for children and adolescents with these conditions.”
The guidelines were published in the July issue of Thyroid (2015;25:716-59).
Previous guidelines were geared toward adults, but thyroid neoplasms in children differ from those in adults with respect to pathophysiology, clinical presentation, and long-term outcomes. Further, therapy that may be appropriate in adults may not be appropriate for children at low risk for death but higher risk of long-term harm from certain treatments, they said.
For example, recent studies with long-term follow-up revealed an increase in all-cause mortality for survivors of childhood differentiated thyroid cancer (DTC), primarily caused by second malignancies in children treated with radiation.
“These observations, coupled with a better understanding of the excellent prognosis associated with pediatric DTC, have now prompted the American Thyroid Association to specifically address treatment of children with benign and malignant thyroid tumors,” they wrote.
While the task force acknowledged a paucity of randomized, double-blind, controlled clinical trials involving children with DTC, they note that “retrospective analysis of therapeutic options has led to a reconsideration of the former concept that all children with DTC should be similarly treated and has provided the opportunity ... to broaden the scope of acceptable therapy in an attempt to provide aggressive therapy when warranted and to limit overtreatment to those children who are unlikely to benefit.”
In addition to addressing the evaluation and management of thyroid nodules, the guidelines also address DTC, including preoperative staging, surgical management, postoperative staging, the role of radioactive iodine therapy, and goals for thyrotropin suppression. Management algorithms are proposed, and separate recommendations for papillary and follicular thyroid cancers are provided.
The authors note that since DTC recurrence has been reported as long as 40 years after initial therapy, children with DTC should be “followed for life, albeit with decreasing intensity for those with no evidence for disease.”
The guidelines are timely, as Surveillance, Epidemiology and End Results (SEER) program data indicate that new cases of thyroid cancer in persons under the age of 20 years represent 1.8% of all thyroid malignancies diagnosed in the United States, and that the incidence appears to be increasing.
Among 15- to 19-year old adolescents, thyroid cancer is the eighth most frequently diagnosed cancer, and it is the second most common cancer among girls, the authors said, noting that adolescents have a 10-fold greater incidence than do younger children, and that there is a female to male preponderance.
The development of pediatric-specific guidelines was critical, according to guidelines coauthor, Dr. Peter Angelos, professor of surgery and surgical ethics and chief of endocrine surgery at the University of Chicago Medicine and Biological Sciences.
“As they say, ‘children are not just small adults,’ ” he said in an interview.
In addition to the guidance provided on which types of nodules should be evaluated in children (since size alone should not be used to dictate who undergoes biopsy), a highlight of the guidelines is a recommendation that children with thyroid cancer be treated by multidisciplinary teams of physician in high-volume centers, he said.
“Thyroid cancer in children is different than in adults in that children have much higher rates of involved lymph nodes, but their overall prognosis is excellent despite the frequency of involved nodes. This confluence of findings pushes surgeons to do more aggressive operations to clear lymph nodes. This is a good thing, but unfortunately, can lead to higher complication rates (things such as permanently low calcium levels in the blood),” he said, adding that “the implications of finding a high-volume thyroid cancer surgeon with experience in thyroid cancer surgery on children are very significant and the guidelines make some recommendations about how many operations are necessary to constitute high volume.”
The push to limit the use of radioactive iodine in children further underscores the need for an experienced surgeon, he said.
“In an effort to avoid exposing children to radiation, surgeons are further pushed to be more aggressive in the operating room. Thus, it becomes even more important to see an experienced surgeon so that complications can be minimized. Even a seemingly ‘mild’ complication can be devastating for a child who will likely have to live with that complication for decades to come since the prognosis for thyroid cancer is so good,” he said.
An important potential benefit of treatment at centers with multidisciplinary interest and expertise is facilitation of additional research, particularly in areas of uncertainty, including the proper use of 131I, the interpretation of thyroglobulin (Tg) and TgAb (antibody) levels, the role of prospective ultrasound monitoring in presymptomatic children at risk for thyroid neoplasia, the use of novel targeted therapies for advanced disease that fails to respond to 131I, and the long-term psychosocial impacts of the disease on children and their families, the guideline authors said.
“These areas require well-designed long-term, multicenter studies that will be difficult to perform because of the rarity of pediatric DTC and the prolonged follow-up required to reach meaningful endpoints. Further research should be facilitated by ensuring that children with DTC are treated when possible at centers with multidisciplinary interest and expertise in this disease,” they concluded.
The guidelines were funded by the American Thyroid Association and ThyCa: Thyroid Cancer Survivors’ Association. Dr. Francis reported serving as an adviser to ThyCa and receiving research support from Grifols, Novo Nordisk, and the Juvenile Diabetes Research Foundation. Other authors reported relationships (consulting, receiving research support, and/or serving as a speaker) with Akrimax, IBSA Institut Biochimique, Pfizer, Novo Nordisk, Eli Lilly, AstraZeneca, Bayer Healthcare, Genzyme, Sobi, Henning, and Merck, and ThyCa.
The evaluation and treatment of thyroid nodules in children should differ from evaluation and treatment in adults in that ultrasound characteristics and clinical context should be used rather than size alone to identify nodules that warrant fine-needle aspiration, according to new pediatric-specific guidelines from the American Thyroid Association.
The Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer – the first-ever guidelines for the evaluation and management of thyroid nodules and cancer in children – also note that fine-needle aspiration (FNA) in children should be performed under ultrasound guidance, that preoperative FNA of a hyperfunctioning nodule in a child is not warranted as long as the lesion is removed, that a diffusely infiltrative form of papillary thyroid cancer may occur in children and should be considered in a clinically suspicious gland, and that surgery (lobectomy plus isthmusectomy) is favored over repeat FNA for most nodules with indeterminate cytology, Dr. Gary L. Francis of Virginia Commonwealth University and Children’s Hospital of Richmond, Va., and his colleagues from the American Thyroid Association Guidelines Task Force on Pediatric Thyroid Cancer determined based on an extensive literature search.
Together this guidance with respect to thyroid nodules represents just one of 34 recommendations contained in the guidelines, which, according to the authors, represent “the current optimal care for children and adolescents with these conditions.”
The guidelines were published in the July issue of Thyroid (2015;25:716-59).
Previous guidelines were geared toward adults, but thyroid neoplasms in children differ from those in adults with respect to pathophysiology, clinical presentation, and long-term outcomes. Further, therapy that may be appropriate in adults may not be appropriate for children at low risk for death but higher risk of long-term harm from certain treatments, they said.
For example, recent studies with long-term follow-up revealed an increase in all-cause mortality for survivors of childhood differentiated thyroid cancer (DTC), primarily caused by second malignancies in children treated with radiation.
“These observations, coupled with a better understanding of the excellent prognosis associated with pediatric DTC, have now prompted the American Thyroid Association to specifically address treatment of children with benign and malignant thyroid tumors,” they wrote.
While the task force acknowledged a paucity of randomized, double-blind, controlled clinical trials involving children with DTC, they note that “retrospective analysis of therapeutic options has led to a reconsideration of the former concept that all children with DTC should be similarly treated and has provided the opportunity ... to broaden the scope of acceptable therapy in an attempt to provide aggressive therapy when warranted and to limit overtreatment to those children who are unlikely to benefit.”
In addition to addressing the evaluation and management of thyroid nodules, the guidelines also address DTC, including preoperative staging, surgical management, postoperative staging, the role of radioactive iodine therapy, and goals for thyrotropin suppression. Management algorithms are proposed, and separate recommendations for papillary and follicular thyroid cancers are provided.
The authors note that since DTC recurrence has been reported as long as 40 years after initial therapy, children with DTC should be “followed for life, albeit with decreasing intensity for those with no evidence for disease.”
The guidelines are timely, as Surveillance, Epidemiology and End Results (SEER) program data indicate that new cases of thyroid cancer in persons under the age of 20 years represent 1.8% of all thyroid malignancies diagnosed in the United States, and that the incidence appears to be increasing.
Among 15- to 19-year old adolescents, thyroid cancer is the eighth most frequently diagnosed cancer, and it is the second most common cancer among girls, the authors said, noting that adolescents have a 10-fold greater incidence than do younger children, and that there is a female to male preponderance.
The development of pediatric-specific guidelines was critical, according to guidelines coauthor, Dr. Peter Angelos, professor of surgery and surgical ethics and chief of endocrine surgery at the University of Chicago Medicine and Biological Sciences.
“As they say, ‘children are not just small adults,’ ” he said in an interview.
In addition to the guidance provided on which types of nodules should be evaluated in children (since size alone should not be used to dictate who undergoes biopsy), a highlight of the guidelines is a recommendation that children with thyroid cancer be treated by multidisciplinary teams of physician in high-volume centers, he said.
“Thyroid cancer in children is different than in adults in that children have much higher rates of involved lymph nodes, but their overall prognosis is excellent despite the frequency of involved nodes. This confluence of findings pushes surgeons to do more aggressive operations to clear lymph nodes. This is a good thing, but unfortunately, can lead to higher complication rates (things such as permanently low calcium levels in the blood),” he said, adding that “the implications of finding a high-volume thyroid cancer surgeon with experience in thyroid cancer surgery on children are very significant and the guidelines make some recommendations about how many operations are necessary to constitute high volume.”
The push to limit the use of radioactive iodine in children further underscores the need for an experienced surgeon, he said.
“In an effort to avoid exposing children to radiation, surgeons are further pushed to be more aggressive in the operating room. Thus, it becomes even more important to see an experienced surgeon so that complications can be minimized. Even a seemingly ‘mild’ complication can be devastating for a child who will likely have to live with that complication for decades to come since the prognosis for thyroid cancer is so good,” he said.
An important potential benefit of treatment at centers with multidisciplinary interest and expertise is facilitation of additional research, particularly in areas of uncertainty, including the proper use of 131I, the interpretation of thyroglobulin (Tg) and TgAb (antibody) levels, the role of prospective ultrasound monitoring in presymptomatic children at risk for thyroid neoplasia, the use of novel targeted therapies for advanced disease that fails to respond to 131I, and the long-term psychosocial impacts of the disease on children and their families, the guideline authors said.
“These areas require well-designed long-term, multicenter studies that will be difficult to perform because of the rarity of pediatric DTC and the prolonged follow-up required to reach meaningful endpoints. Further research should be facilitated by ensuring that children with DTC are treated when possible at centers with multidisciplinary interest and expertise in this disease,” they concluded.
The guidelines were funded by the American Thyroid Association and ThyCa: Thyroid Cancer Survivors’ Association. Dr. Francis reported serving as an adviser to ThyCa and receiving research support from Grifols, Novo Nordisk, and the Juvenile Diabetes Research Foundation. Other authors reported relationships (consulting, receiving research support, and/or serving as a speaker) with Akrimax, IBSA Institut Biochimique, Pfizer, Novo Nordisk, Eli Lilly, AstraZeneca, Bayer Healthcare, Genzyme, Sobi, Henning, and Merck, and ThyCa.
FROM THYROID
New guidelines focus on pediatric thyroid nodules and cancer
The evaluation and treatment of thyroid nodules in children should differ from evaluation and treatment in adults in that ultrasound characteristics and clinical context should be used rather than size alone to identify nodules that warrant fine-needle aspiration, according to new pediatric-specific guidelines from the American Thyroid Association.
The Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer – the first-ever guidelines for the evaluation and management of thyroid nodules and cancer in children – also note that fine-needle aspiration (FNA) in children should be performed under ultrasound guidance, that preoperative FNA of a hyperfunctioning nodule in a child is not warranted as long as the lesion is removed, that a diffusely infiltrative form of papillary thyroid cancer may occur in children and should be considered in a clinically suspicious gland, and that surgery (lobectomy plus isthmusectomy) is favored over repeat FNA for most nodules with indeterminate cytology, Dr. Gary L. Francis of Virginia Commonwealth University and Children’s Hospital of Richmond, Va., and his colleagues from the American Thyroid Association Guidelines Task Force on Pediatric Thyroid Cancer determined based on an extensive literature search.
Together this guidance with respect to thyroid nodules represents just one of 34 recommendations contained in the guidelines, which, according to the authors, represent “the current optimal care for children and adolescents with these conditions.”
The guidelines were published in the July issue of Thyroid (2015;25:716-59).
Previous guidelines were geared toward adults, but thyroid neoplasms in children differ from those in adults with respect to pathophysiology, clinical presentation, and long-term outcomes. Further, therapy that may be appropriate in adults may not be appropriate for children at low risk for death but higher risk of long-term harm from certain treatments, they said.
For example, recent studies with long-term follow-up revealed an increase in all-cause mortality for survivors of childhood differentiated thyroid cancer (DTC), primarily caused by second malignancies in children treated with radiation.
“These observations, coupled with a better understanding of the excellent prognosis associated with pediatric DTC, have now prompted the American Thyroid Association to specifically address treatment of children with benign and malignant thyroid tumors,” they wrote.
While the task force acknowledged a paucity of randomized, double-blind, controlled clinical trials involving children with DTC, they note that “retrospective analysis of therapeutic options has led to a reconsideration of the former concept that all children with DTC should be similarly treated and has provided the opportunity ... to broaden the scope of acceptable therapy in an attempt to provide aggressive therapy when warranted and to limit overtreatment to those children who are unlikely to benefit.”
In addition to addressing the evaluation and management of thyroid nodules, the guidelines also address DTC, including preoperative staging, surgical management, postoperative staging, the role of radioactive iodine therapy, and goals for thyrotropin suppression. Management algorithms are proposed, and separate recommendations for papillary and follicular thyroid cancers are provided.
The authors note that since DTC recurrence has been reported as long as 40 years after initial therapy, children with DTC should be “followed for life, albeit with decreasing intensity for those with no evidence for disease.”
The guidelines are timely, as Surveillance, Epidemiology and End Results (SEER) program data indicate that new cases of thyroid cancer in persons under the age of 20 years represent 1.8% of all thyroid malignancies diagnosed in the United States, and that the incidence appears to be increasing.
Among 15- to 19-year old adolescents, thyroid cancer is the eighth most frequently diagnosed cancer, and it is the second most common cancer among girls, the authors said, noting that adolescents have a 10-fold greater incidence than do younger children, and that there is a female to male preponderance.
The development of pediatric-specific guidelines was critical, according to guidelines coauthor, Dr. Peter Angelos, professor of surgery and surgical ethics and chief of endocrine surgery at the University of Chicago Medicine and Biological Sciences.
“As they say, ‘children are not just small adults,’ ” he said in an interview.
In addition to the guidance provided on which types of nodules should be evaluated in children (since size alone should not be used to dictate who undergoes biopsy), a highlight of the guidelines is a recommendation that children with thyroid cancer be treated by multidisciplinary teams of physician in high-volume centers, he said.
“Thyroid cancer in children is different than in adults in that children have much higher rates of involved lymph nodes, but their overall prognosis is excellent despite the frequency of involved nodes. This confluence of findings pushes surgeons to do more aggressive operations to clear lymph nodes. This is a good thing, but unfortunately, can lead to higher complication rates (things such as permanently low calcium levels in the blood),” he said, adding that “the implications of finding a high-volume thyroid cancer surgeon with experience in thyroid cancer surgery on children are very significant and the guidelines make some recommendations about how many operations are necessary to constitute high volume.”
The push to limit the use of radioactive iodine in children further underscores the need for an experienced surgeon, he said.
“In an effort to avoid exposing children to radiation, surgeons are further pushed to be more aggressive in the operating room. Thus, it becomes even more important to see an experienced surgeon so that complications can be minimized. Even a seemingly ‘mild’ complication can be devastating for a child who will likely have to live with that complication for decades to come since the prognosis for thyroid cancer is so good,” he said.
An important potential benefit of treatment at centers with multidisciplinary interest and expertise is facilitation of additional research, particularly in areas of uncertainty, including the proper use of 131I, the interpretation of thyroglobulin (Tg) and TgAb (antibody) levels, the role of prospective ultrasound monitoring in presymptomatic children at risk for thyroid neoplasia, the use of novel targeted therapies for advanced disease that fails to respond to 131I, and the long-term psychosocial impacts of the disease on children and their families, the guideline authors said.
“These areas require well-designed long-term, multicenter studies that will be difficult to perform because of the rarity of pediatric DTC and the prolonged follow-up required to reach meaningful endpoints. Further research should be facilitated by ensuring that children with DTC are treated when possible at centers with multidisciplinary interest and expertise in this disease,” they concluded.
The guidelines were funded by the American Thyroid Association and ThyCa: Thyroid Cancer Survivors’ Association. Dr. Francis reported serving as an adviser to ThyCa and receiving research support from Grifols, Novo Nordisk, and the Juvenile Diabetes Research Foundation. Other authors reported relationships (consulting, receiving research support, and/or serving as a speaker) with Akrimax, IBSA Institut Biochimique, Pfizer, Novo Nordisk, Eli Lilly, AstraZeneca, Bayer Healthcare, Genzyme, Sobi, Henning, and Merck, and ThyCa.
The evaluation and treatment of thyroid nodules in children should differ from evaluation and treatment in adults in that ultrasound characteristics and clinical context should be used rather than size alone to identify nodules that warrant fine-needle aspiration, according to new pediatric-specific guidelines from the American Thyroid Association.
The Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer – the first-ever guidelines for the evaluation and management of thyroid nodules and cancer in children – also note that fine-needle aspiration (FNA) in children should be performed under ultrasound guidance, that preoperative FNA of a hyperfunctioning nodule in a child is not warranted as long as the lesion is removed, that a diffusely infiltrative form of papillary thyroid cancer may occur in children and should be considered in a clinically suspicious gland, and that surgery (lobectomy plus isthmusectomy) is favored over repeat FNA for most nodules with indeterminate cytology, Dr. Gary L. Francis of Virginia Commonwealth University and Children’s Hospital of Richmond, Va., and his colleagues from the American Thyroid Association Guidelines Task Force on Pediatric Thyroid Cancer determined based on an extensive literature search.
Together this guidance with respect to thyroid nodules represents just one of 34 recommendations contained in the guidelines, which, according to the authors, represent “the current optimal care for children and adolescents with these conditions.”
The guidelines were published in the July issue of Thyroid (2015;25:716-59).
Previous guidelines were geared toward adults, but thyroid neoplasms in children differ from those in adults with respect to pathophysiology, clinical presentation, and long-term outcomes. Further, therapy that may be appropriate in adults may not be appropriate for children at low risk for death but higher risk of long-term harm from certain treatments, they said.
For example, recent studies with long-term follow-up revealed an increase in all-cause mortality for survivors of childhood differentiated thyroid cancer (DTC), primarily caused by second malignancies in children treated with radiation.
“These observations, coupled with a better understanding of the excellent prognosis associated with pediatric DTC, have now prompted the American Thyroid Association to specifically address treatment of children with benign and malignant thyroid tumors,” they wrote.
While the task force acknowledged a paucity of randomized, double-blind, controlled clinical trials involving children with DTC, they note that “retrospective analysis of therapeutic options has led to a reconsideration of the former concept that all children with DTC should be similarly treated and has provided the opportunity ... to broaden the scope of acceptable therapy in an attempt to provide aggressive therapy when warranted and to limit overtreatment to those children who are unlikely to benefit.”
In addition to addressing the evaluation and management of thyroid nodules, the guidelines also address DTC, including preoperative staging, surgical management, postoperative staging, the role of radioactive iodine therapy, and goals for thyrotropin suppression. Management algorithms are proposed, and separate recommendations for papillary and follicular thyroid cancers are provided.
The authors note that since DTC recurrence has been reported as long as 40 years after initial therapy, children with DTC should be “followed for life, albeit with decreasing intensity for those with no evidence for disease.”
The guidelines are timely, as Surveillance, Epidemiology and End Results (SEER) program data indicate that new cases of thyroid cancer in persons under the age of 20 years represent 1.8% of all thyroid malignancies diagnosed in the United States, and that the incidence appears to be increasing.
Among 15- to 19-year old adolescents, thyroid cancer is the eighth most frequently diagnosed cancer, and it is the second most common cancer among girls, the authors said, noting that adolescents have a 10-fold greater incidence than do younger children, and that there is a female to male preponderance.
The development of pediatric-specific guidelines was critical, according to guidelines coauthor, Dr. Peter Angelos, professor of surgery and surgical ethics and chief of endocrine surgery at the University of Chicago Medicine and Biological Sciences.
“As they say, ‘children are not just small adults,’ ” he said in an interview.
In addition to the guidance provided on which types of nodules should be evaluated in children (since size alone should not be used to dictate who undergoes biopsy), a highlight of the guidelines is a recommendation that children with thyroid cancer be treated by multidisciplinary teams of physician in high-volume centers, he said.
“Thyroid cancer in children is different than in adults in that children have much higher rates of involved lymph nodes, but their overall prognosis is excellent despite the frequency of involved nodes. This confluence of findings pushes surgeons to do more aggressive operations to clear lymph nodes. This is a good thing, but unfortunately, can lead to higher complication rates (things such as permanently low calcium levels in the blood),” he said, adding that “the implications of finding a high-volume thyroid cancer surgeon with experience in thyroid cancer surgery on children are very significant and the guidelines make some recommendations about how many operations are necessary to constitute high volume.”
The push to limit the use of radioactive iodine in children further underscores the need for an experienced surgeon, he said.
“In an effort to avoid exposing children to radiation, surgeons are further pushed to be more aggressive in the operating room. Thus, it becomes even more important to see an experienced surgeon so that complications can be minimized. Even a seemingly ‘mild’ complication can be devastating for a child who will likely have to live with that complication for decades to come since the prognosis for thyroid cancer is so good,” he said.
An important potential benefit of treatment at centers with multidisciplinary interest and expertise is facilitation of additional research, particularly in areas of uncertainty, including the proper use of 131I, the interpretation of thyroglobulin (Tg) and TgAb (antibody) levels, the role of prospective ultrasound monitoring in presymptomatic children at risk for thyroid neoplasia, the use of novel targeted therapies for advanced disease that fails to respond to 131I, and the long-term psychosocial impacts of the disease on children and their families, the guideline authors said.
“These areas require well-designed long-term, multicenter studies that will be difficult to perform because of the rarity of pediatric DTC and the prolonged follow-up required to reach meaningful endpoints. Further research should be facilitated by ensuring that children with DTC are treated when possible at centers with multidisciplinary interest and expertise in this disease,” they concluded.
The guidelines were funded by the American Thyroid Association and ThyCa: Thyroid Cancer Survivors’ Association. Dr. Francis reported serving as an adviser to ThyCa and receiving research support from Grifols, Novo Nordisk, and the Juvenile Diabetes Research Foundation. Other authors reported relationships (consulting, receiving research support, and/or serving as a speaker) with Akrimax, IBSA Institut Biochimique, Pfizer, Novo Nordisk, Eli Lilly, AstraZeneca, Bayer Healthcare, Genzyme, Sobi, Henning, and Merck, and ThyCa.
The evaluation and treatment of thyroid nodules in children should differ from evaluation and treatment in adults in that ultrasound characteristics and clinical context should be used rather than size alone to identify nodules that warrant fine-needle aspiration, according to new pediatric-specific guidelines from the American Thyroid Association.
The Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer – the first-ever guidelines for the evaluation and management of thyroid nodules and cancer in children – also note that fine-needle aspiration (FNA) in children should be performed under ultrasound guidance, that preoperative FNA of a hyperfunctioning nodule in a child is not warranted as long as the lesion is removed, that a diffusely infiltrative form of papillary thyroid cancer may occur in children and should be considered in a clinically suspicious gland, and that surgery (lobectomy plus isthmusectomy) is favored over repeat FNA for most nodules with indeterminate cytology, Dr. Gary L. Francis of Virginia Commonwealth University and Children’s Hospital of Richmond, Va., and his colleagues from the American Thyroid Association Guidelines Task Force on Pediatric Thyroid Cancer determined based on an extensive literature search.
Together this guidance with respect to thyroid nodules represents just one of 34 recommendations contained in the guidelines, which, according to the authors, represent “the current optimal care for children and adolescents with these conditions.”
The guidelines were published in the July issue of Thyroid (2015;25:716-59).
Previous guidelines were geared toward adults, but thyroid neoplasms in children differ from those in adults with respect to pathophysiology, clinical presentation, and long-term outcomes. Further, therapy that may be appropriate in adults may not be appropriate for children at low risk for death but higher risk of long-term harm from certain treatments, they said.
For example, recent studies with long-term follow-up revealed an increase in all-cause mortality for survivors of childhood differentiated thyroid cancer (DTC), primarily caused by second malignancies in children treated with radiation.
“These observations, coupled with a better understanding of the excellent prognosis associated with pediatric DTC, have now prompted the American Thyroid Association to specifically address treatment of children with benign and malignant thyroid tumors,” they wrote.
While the task force acknowledged a paucity of randomized, double-blind, controlled clinical trials involving children with DTC, they note that “retrospective analysis of therapeutic options has led to a reconsideration of the former concept that all children with DTC should be similarly treated and has provided the opportunity ... to broaden the scope of acceptable therapy in an attempt to provide aggressive therapy when warranted and to limit overtreatment to those children who are unlikely to benefit.”
In addition to addressing the evaluation and management of thyroid nodules, the guidelines also address DTC, including preoperative staging, surgical management, postoperative staging, the role of radioactive iodine therapy, and goals for thyrotropin suppression. Management algorithms are proposed, and separate recommendations for papillary and follicular thyroid cancers are provided.
The authors note that since DTC recurrence has been reported as long as 40 years after initial therapy, children with DTC should be “followed for life, albeit with decreasing intensity for those with no evidence for disease.”
The guidelines are timely, as Surveillance, Epidemiology and End Results (SEER) program data indicate that new cases of thyroid cancer in persons under the age of 20 years represent 1.8% of all thyroid malignancies diagnosed in the United States, and that the incidence appears to be increasing.
Among 15- to 19-year old adolescents, thyroid cancer is the eighth most frequently diagnosed cancer, and it is the second most common cancer among girls, the authors said, noting that adolescents have a 10-fold greater incidence than do younger children, and that there is a female to male preponderance.
The development of pediatric-specific guidelines was critical, according to guidelines coauthor, Dr. Peter Angelos, professor of surgery and surgical ethics and chief of endocrine surgery at the University of Chicago Medicine and Biological Sciences.
“As they say, ‘children are not just small adults,’ ” he said in an interview.
In addition to the guidance provided on which types of nodules should be evaluated in children (since size alone should not be used to dictate who undergoes biopsy), a highlight of the guidelines is a recommendation that children with thyroid cancer be treated by multidisciplinary teams of physician in high-volume centers, he said.
“Thyroid cancer in children is different than in adults in that children have much higher rates of involved lymph nodes, but their overall prognosis is excellent despite the frequency of involved nodes. This confluence of findings pushes surgeons to do more aggressive operations to clear lymph nodes. This is a good thing, but unfortunately, can lead to higher complication rates (things such as permanently low calcium levels in the blood),” he said, adding that “the implications of finding a high-volume thyroid cancer surgeon with experience in thyroid cancer surgery on children are very significant and the guidelines make some recommendations about how many operations are necessary to constitute high volume.”
The push to limit the use of radioactive iodine in children further underscores the need for an experienced surgeon, he said.
“In an effort to avoid exposing children to radiation, surgeons are further pushed to be more aggressive in the operating room. Thus, it becomes even more important to see an experienced surgeon so that complications can be minimized. Even a seemingly ‘mild’ complication can be devastating for a child who will likely have to live with that complication for decades to come since the prognosis for thyroid cancer is so good,” he said.
An important potential benefit of treatment at centers with multidisciplinary interest and expertise is facilitation of additional research, particularly in areas of uncertainty, including the proper use of 131I, the interpretation of thyroglobulin (Tg) and TgAb (antibody) levels, the role of prospective ultrasound monitoring in presymptomatic children at risk for thyroid neoplasia, the use of novel targeted therapies for advanced disease that fails to respond to 131I, and the long-term psychosocial impacts of the disease on children and their families, the guideline authors said.
“These areas require well-designed long-term, multicenter studies that will be difficult to perform because of the rarity of pediatric DTC and the prolonged follow-up required to reach meaningful endpoints. Further research should be facilitated by ensuring that children with DTC are treated when possible at centers with multidisciplinary interest and expertise in this disease,” they concluded.
The guidelines were funded by the American Thyroid Association and ThyCa: Thyroid Cancer Survivors’ Association. Dr. Francis reported serving as an adviser to ThyCa and receiving research support from Grifols, Novo Nordisk, and the Juvenile Diabetes Research Foundation. Other authors reported relationships (consulting, receiving research support, and/or serving as a speaker) with Akrimax, IBSA Institut Biochimique, Pfizer, Novo Nordisk, Eli Lilly, AstraZeneca, Bayer Healthcare, Genzyme, Sobi, Henning, and Merck, and ThyCa.
FROM THYROID