User login
Sharon Worcester is an award-winning medical journalist for MDedge News. She has been with the company since 1996, first as the Southeast Bureau Chief (1996-2009) when the company was known as International Medical News Group, then as a freelance writer (2010-2015) before returning as a reporter in 2015. She previously worked as a daily newspaper reporter covering health and local government. Sharon currently reports primarily on oncology and hematology. She has a BA from Eckerd College and an MA in Mass Communication/Print Journalism from the University of Florida. Connect with her via LinkedIn and follow her on twitter @SW_MedReporter.
ICEID: TCAD regimen shows promise against H3N2 flu variant
ATLANTA – Triple combination antiviral drug therapy offers a broad-spectrum treatment option for H3N2 variant influenza virus, according to findings from an in vitro study.
The finding suggest that the combination could play an important role in the event of an influenza pandemic, Carrie Sitz reported in a poster at the International Conference on Emerging Infectious Diseases.
After a human infection with the novel A/H3N2 variant was reported in 2011, and trivalent inactivated influenza vaccine was found to be of limited use, as it provided protection against H3N2 but not the H3N2 variant (H3N2v) in ferrets and elicited cross-protection against H3N2 in young adults but not older adults or children, a triple combination antiviral therapy (TCAD) regimen was considered.
Amantadine, oseltamivir carboxylate, and ribavirin each were tested alone and in double and triple combinations against the novel H3N2 variant virus carrying genes from avian, swine, and human origins. Triple therapy achieved a therapeutic effect with lower doses of component drugs, compared with monotherapies of antivirals as single agents, said Ms. Sitz, a microbiology research assistant at the Naval Health Research Center, San Diego.
The agents, which each have different mechanisms of action and which function at distinct points in the virus life cycle, were tested using the various combinations in 96-well plates seeded with Madin-Darby Canine Kidney (MDCK) epithelial cells. They were found to produce synergistic antiviral activity, she noted.
A control experiment in the absence of the drugs also was performed.
Of note, amantadine had no activity as a single agent against H3N2v, even at 100 mcg/mL, the highest dose tested. However, amantadine did contribute to the synergy of the TCAD regimen. This effect was concentration dependent; the potential synergy volume increased steadily and significantly from about 300 to about 450, to about 575, and to about 600 as the amantadine concentration increased from +0.32, to +1.0, to +3.2, to +10, Ms. Sitz noted, adding that this may indicate that amantadine, which is known to have widespread resistance, can still play a therapeutic role in the setting of the TCAD regimen.
Vaccines are usually an effective safeguard against seasonal influenza but may be inadequate in seasons when a novel influenza emerges, resulting in compromised standard of care for treating the emergent viruses, she said, noting that this is especially true in immunocompromised patients.
“These issues point to the likelihood that we may be unprepared for a novel influenza virus displaying both virulence and transmissibility,” she added.
The current findings suggest that TCAD, which has previously been shown to be effective against seasonal and H5 influenza strains, is a broad-spectrum treatment option that could potentially play a role in pandemic preparedness. The mechanism by which oseltamivir carboxylate and ribavirin potentiate amantadine in combination therapy is unknown, and further testing is needed for evaluation, she concluded.
This study was sponsored by the Armed Forces Health Surveillance Center. The authors reported having no conflicts of interest.
ATLANTA – Triple combination antiviral drug therapy offers a broad-spectrum treatment option for H3N2 variant influenza virus, according to findings from an in vitro study.
The finding suggest that the combination could play an important role in the event of an influenza pandemic, Carrie Sitz reported in a poster at the International Conference on Emerging Infectious Diseases.
After a human infection with the novel A/H3N2 variant was reported in 2011, and trivalent inactivated influenza vaccine was found to be of limited use, as it provided protection against H3N2 but not the H3N2 variant (H3N2v) in ferrets and elicited cross-protection against H3N2 in young adults but not older adults or children, a triple combination antiviral therapy (TCAD) regimen was considered.
Amantadine, oseltamivir carboxylate, and ribavirin each were tested alone and in double and triple combinations against the novel H3N2 variant virus carrying genes from avian, swine, and human origins. Triple therapy achieved a therapeutic effect with lower doses of component drugs, compared with monotherapies of antivirals as single agents, said Ms. Sitz, a microbiology research assistant at the Naval Health Research Center, San Diego.
The agents, which each have different mechanisms of action and which function at distinct points in the virus life cycle, were tested using the various combinations in 96-well plates seeded with Madin-Darby Canine Kidney (MDCK) epithelial cells. They were found to produce synergistic antiviral activity, she noted.
A control experiment in the absence of the drugs also was performed.
Of note, amantadine had no activity as a single agent against H3N2v, even at 100 mcg/mL, the highest dose tested. However, amantadine did contribute to the synergy of the TCAD regimen. This effect was concentration dependent; the potential synergy volume increased steadily and significantly from about 300 to about 450, to about 575, and to about 600 as the amantadine concentration increased from +0.32, to +1.0, to +3.2, to +10, Ms. Sitz noted, adding that this may indicate that amantadine, which is known to have widespread resistance, can still play a therapeutic role in the setting of the TCAD regimen.
Vaccines are usually an effective safeguard against seasonal influenza but may be inadequate in seasons when a novel influenza emerges, resulting in compromised standard of care for treating the emergent viruses, she said, noting that this is especially true in immunocompromised patients.
“These issues point to the likelihood that we may be unprepared for a novel influenza virus displaying both virulence and transmissibility,” she added.
The current findings suggest that TCAD, which has previously been shown to be effective against seasonal and H5 influenza strains, is a broad-spectrum treatment option that could potentially play a role in pandemic preparedness. The mechanism by which oseltamivir carboxylate and ribavirin potentiate amantadine in combination therapy is unknown, and further testing is needed for evaluation, she concluded.
This study was sponsored by the Armed Forces Health Surveillance Center. The authors reported having no conflicts of interest.
ATLANTA – Triple combination antiviral drug therapy offers a broad-spectrum treatment option for H3N2 variant influenza virus, according to findings from an in vitro study.
The finding suggest that the combination could play an important role in the event of an influenza pandemic, Carrie Sitz reported in a poster at the International Conference on Emerging Infectious Diseases.
After a human infection with the novel A/H3N2 variant was reported in 2011, and trivalent inactivated influenza vaccine was found to be of limited use, as it provided protection against H3N2 but not the H3N2 variant (H3N2v) in ferrets and elicited cross-protection against H3N2 in young adults but not older adults or children, a triple combination antiviral therapy (TCAD) regimen was considered.
Amantadine, oseltamivir carboxylate, and ribavirin each were tested alone and in double and triple combinations against the novel H3N2 variant virus carrying genes from avian, swine, and human origins. Triple therapy achieved a therapeutic effect with lower doses of component drugs, compared with monotherapies of antivirals as single agents, said Ms. Sitz, a microbiology research assistant at the Naval Health Research Center, San Diego.
The agents, which each have different mechanisms of action and which function at distinct points in the virus life cycle, were tested using the various combinations in 96-well plates seeded with Madin-Darby Canine Kidney (MDCK) epithelial cells. They were found to produce synergistic antiviral activity, she noted.
A control experiment in the absence of the drugs also was performed.
Of note, amantadine had no activity as a single agent against H3N2v, even at 100 mcg/mL, the highest dose tested. However, amantadine did contribute to the synergy of the TCAD regimen. This effect was concentration dependent; the potential synergy volume increased steadily and significantly from about 300 to about 450, to about 575, and to about 600 as the amantadine concentration increased from +0.32, to +1.0, to +3.2, to +10, Ms. Sitz noted, adding that this may indicate that amantadine, which is known to have widespread resistance, can still play a therapeutic role in the setting of the TCAD regimen.
Vaccines are usually an effective safeguard against seasonal influenza but may be inadequate in seasons when a novel influenza emerges, resulting in compromised standard of care for treating the emergent viruses, she said, noting that this is especially true in immunocompromised patients.
“These issues point to the likelihood that we may be unprepared for a novel influenza virus displaying both virulence and transmissibility,” she added.
The current findings suggest that TCAD, which has previously been shown to be effective against seasonal and H5 influenza strains, is a broad-spectrum treatment option that could potentially play a role in pandemic preparedness. The mechanism by which oseltamivir carboxylate and ribavirin potentiate amantadine in combination therapy is unknown, and further testing is needed for evaluation, she concluded.
This study was sponsored by the Armed Forces Health Surveillance Center. The authors reported having no conflicts of interest.
AT ICEID 2015
Key clinical point: Triple combination antiviral drug therapy, or TCAD, offers a broad-spectrum treatment option for H3N2 variant influenza virus.
Major finding: Triple therapy achieved a therapeutic effect with lower doses of component drugs, compared with monotherapies of antivirals as single agents.
Data source: An in vitro study of TCAD for H3N2v.
Disclosures: This study was sponsored by the Armed Forces Health Surveillance Center. The authors reported having no conflicts of interest.
ICEID: Data highlight biofilm role in waterborne illness
ATLANTA – Emerging biofilm-associated pathogens are overtaking those transmitted by the fecal-oral route as the most-common cause of death from waterborne illness in the United States, according to findings from a review of administrative and disease-specific surveillance data.
Between 2003 and 2009, a mean of 2,516 deaths occurred per year as a result of exposure to 1 of more of 14 different waterborne germs or diseases, including campylobacteriosis, cryptosporidiosis, Escherichia coli infections, free-living amoeba, giardiasis, hemolytic uremic syndrome, hepatitis A, Legionnaires’ disease, nontuberculous Mycobacterium, otitis externa, Pseudomonas, salmonellosis, shigellosis, and vibriosis, Julia Gargano, Ph.D., reported in a poster at the International Conference on Emerging Infectious Diseases.
The most commonly documented causes of death, accounting for 88% of deaths, were Pseudomonas pneumonia or P. septicemia, nontuberculosis Mycobacterium, and Legionnaires’ disease – all biofilm pathogens. For those illnesses potentially linked to ingestion of contaminated water – as opposed to those associated with inhalation and contact – the most-commonly documented causes of death were hepatitis A, hemolytic uremic syndrome, and vibriosis, noted Dr. Gargano of the Center for Disease Control and Prevention’s National Center for Emerging and Zoonotic Infectious Diseases, Atlanta.
The findings were obtained from U.S. death certificates, the Nationwide Inpatient Sample, and disease-specific surveillance.
Although surveillance data consistently show that transmission of waterborne diarrheal diseases continue, such diseases are rarely fatal in the United States. Further, advances in water treatment and sanitation have reduced the burden of such diseases.
The findings of this study demonstrate that the burden of mortality has shifted.
“This is the first time the annual number of deaths due to potentially waterborne disease has been calculated, and [the findings] highlight the emerging trend in biofilm-related illness,” she wrote.
Dr. Gargano reported having no financial disclosures.
ATLANTA – Emerging biofilm-associated pathogens are overtaking those transmitted by the fecal-oral route as the most-common cause of death from waterborne illness in the United States, according to findings from a review of administrative and disease-specific surveillance data.
Between 2003 and 2009, a mean of 2,516 deaths occurred per year as a result of exposure to 1 of more of 14 different waterborne germs or diseases, including campylobacteriosis, cryptosporidiosis, Escherichia coli infections, free-living amoeba, giardiasis, hemolytic uremic syndrome, hepatitis A, Legionnaires’ disease, nontuberculous Mycobacterium, otitis externa, Pseudomonas, salmonellosis, shigellosis, and vibriosis, Julia Gargano, Ph.D., reported in a poster at the International Conference on Emerging Infectious Diseases.
The most commonly documented causes of death, accounting for 88% of deaths, were Pseudomonas pneumonia or P. septicemia, nontuberculosis Mycobacterium, and Legionnaires’ disease – all biofilm pathogens. For those illnesses potentially linked to ingestion of contaminated water – as opposed to those associated with inhalation and contact – the most-commonly documented causes of death were hepatitis A, hemolytic uremic syndrome, and vibriosis, noted Dr. Gargano of the Center for Disease Control and Prevention’s National Center for Emerging and Zoonotic Infectious Diseases, Atlanta.
The findings were obtained from U.S. death certificates, the Nationwide Inpatient Sample, and disease-specific surveillance.
Although surveillance data consistently show that transmission of waterborne diarrheal diseases continue, such diseases are rarely fatal in the United States. Further, advances in water treatment and sanitation have reduced the burden of such diseases.
The findings of this study demonstrate that the burden of mortality has shifted.
“This is the first time the annual number of deaths due to potentially waterborne disease has been calculated, and [the findings] highlight the emerging trend in biofilm-related illness,” she wrote.
Dr. Gargano reported having no financial disclosures.
ATLANTA – Emerging biofilm-associated pathogens are overtaking those transmitted by the fecal-oral route as the most-common cause of death from waterborne illness in the United States, according to findings from a review of administrative and disease-specific surveillance data.
Between 2003 and 2009, a mean of 2,516 deaths occurred per year as a result of exposure to 1 of more of 14 different waterborne germs or diseases, including campylobacteriosis, cryptosporidiosis, Escherichia coli infections, free-living amoeba, giardiasis, hemolytic uremic syndrome, hepatitis A, Legionnaires’ disease, nontuberculous Mycobacterium, otitis externa, Pseudomonas, salmonellosis, shigellosis, and vibriosis, Julia Gargano, Ph.D., reported in a poster at the International Conference on Emerging Infectious Diseases.
The most commonly documented causes of death, accounting for 88% of deaths, were Pseudomonas pneumonia or P. septicemia, nontuberculosis Mycobacterium, and Legionnaires’ disease – all biofilm pathogens. For those illnesses potentially linked to ingestion of contaminated water – as opposed to those associated with inhalation and contact – the most-commonly documented causes of death were hepatitis A, hemolytic uremic syndrome, and vibriosis, noted Dr. Gargano of the Center for Disease Control and Prevention’s National Center for Emerging and Zoonotic Infectious Diseases, Atlanta.
The findings were obtained from U.S. death certificates, the Nationwide Inpatient Sample, and disease-specific surveillance.
Although surveillance data consistently show that transmission of waterborne diarrheal diseases continue, such diseases are rarely fatal in the United States. Further, advances in water treatment and sanitation have reduced the burden of such diseases.
The findings of this study demonstrate that the burden of mortality has shifted.
“This is the first time the annual number of deaths due to potentially waterborne disease has been calculated, and [the findings] highlight the emerging trend in biofilm-related illness,” she wrote.
Dr. Gargano reported having no financial disclosures.
AT ICEID 2015
Key clinical point: Emerging biofilm-associated pathogens are overtaking those transmitted by the fecal-oral route as the most-common cause of death from waterborne illness in the United States.
Major finding: 88% of deaths resulted from Pseudomonas pneumonia or P. septicemia, nontuberculosis Mycobacterium, and Legionnaires’ disease – all biofilm pathogens.
Data source: A review of administrative and disease-specific surveillance data.
Disclosures: Dr. Gargano reported having no financial disclosures.
HIT risk rises with obesity
LAS VEGAS – High body mass index is strongly associated with increased rates of heparin-induced thrombocytopenia, based on findings from a review of prospectively collected data from surgical and cardiac intensive care unit patients presumed to have the condition.
Of 304 patients included in the review, 36 (12%) were positive for heparin-induced thrombocytopenia (HIT). The rates increased in tandem with BMI. For example, the rate was 0% among 9 underweight individuals (BMI less than 18.5 kg/m2), 8% among 119 normal-weight individuals (BMI of 18.5-24.9 kg/m2), 11% among 98 overweight individuals (BMI of 25-29.9 kg/m2), 18% among 67 obese individuals (BMI of 30-39.9 kg/m2), and 36% among 11 morbidly obese individuals (BMI of 40 kg/m2 or greater), Dr. Matthew B. Bloom reported at the annual meeting of the American Association for the Surgery of Trauma.
The odds of HIT were 170% greater among obese patients, compared with normal-weight patients (odds ratio, 2.67), and 600% greater among morbidly obese patients, compared with normal-weight patient (odds ratio, 6.98), said Dr. Bloom of Cedars-Sinai Medical Center, Los Angeles.
Logistic regression showed that each 1 unit increase in BMI was associated with a 7.7% increase in the odds of developing HIT, he noted.
Additionally, an anti-heparin/PF4 (platelet factor 4) antibody OD (optical density) value of 2.0 or greater, but not of 0.4 or greater or 0.8 or greater, was also significantly increased with BMI, and in-hospital mortality increased significantly with BMI above normal, he said.
Warkentin 4T scores used to differentiate HIT from other types of thrombocytopenia were not found to correlate with changes in BMI in this study, nor were deep vein thrombosis, pulmonary embolism, or stroke.
The increase in PF4 with increasing BMI may be a marker for overall increasing levels of circulating antibodies in the obese ICU population, but more biochemical studies are needed to tease this out, he said.
Patients included in the review were all those admitted to the surgical and cardiac ICUs at Cedars-Sinai over a more than 7 year period. They had a mean age of 62.1 years, 59% were men, and their mean BMI was 27 kg/m2.
The findings are among the first to show a strong association between BMI and HIT in ICU patients, Dr. Bloom said, noting that several other studies have shown that obesity is linked with increased incidence and increased severity of immune-mediated diseases, including rheumatoid arthritis, systemic lupus erythematosus, and inflammatory bowel disease.
“And HIT is an immune-mediated disease,” he added.
“BMI may be an important new clinical variable for estimating the pre-test probability of HIT, and perhaps, in the future, patient ‘thickness’ could be considered a new ‘T’ in the 4T score, he concluded.
Dr. Bloom reported having no disclosures.
LAS VEGAS – High body mass index is strongly associated with increased rates of heparin-induced thrombocytopenia, based on findings from a review of prospectively collected data from surgical and cardiac intensive care unit patients presumed to have the condition.
Of 304 patients included in the review, 36 (12%) were positive for heparin-induced thrombocytopenia (HIT). The rates increased in tandem with BMI. For example, the rate was 0% among 9 underweight individuals (BMI less than 18.5 kg/m2), 8% among 119 normal-weight individuals (BMI of 18.5-24.9 kg/m2), 11% among 98 overweight individuals (BMI of 25-29.9 kg/m2), 18% among 67 obese individuals (BMI of 30-39.9 kg/m2), and 36% among 11 morbidly obese individuals (BMI of 40 kg/m2 or greater), Dr. Matthew B. Bloom reported at the annual meeting of the American Association for the Surgery of Trauma.
The odds of HIT were 170% greater among obese patients, compared with normal-weight patients (odds ratio, 2.67), and 600% greater among morbidly obese patients, compared with normal-weight patient (odds ratio, 6.98), said Dr. Bloom of Cedars-Sinai Medical Center, Los Angeles.
Logistic regression showed that each 1 unit increase in BMI was associated with a 7.7% increase in the odds of developing HIT, he noted.
Additionally, an anti-heparin/PF4 (platelet factor 4) antibody OD (optical density) value of 2.0 or greater, but not of 0.4 or greater or 0.8 or greater, was also significantly increased with BMI, and in-hospital mortality increased significantly with BMI above normal, he said.
Warkentin 4T scores used to differentiate HIT from other types of thrombocytopenia were not found to correlate with changes in BMI in this study, nor were deep vein thrombosis, pulmonary embolism, or stroke.
The increase in PF4 with increasing BMI may be a marker for overall increasing levels of circulating antibodies in the obese ICU population, but more biochemical studies are needed to tease this out, he said.
Patients included in the review were all those admitted to the surgical and cardiac ICUs at Cedars-Sinai over a more than 7 year period. They had a mean age of 62.1 years, 59% were men, and their mean BMI was 27 kg/m2.
The findings are among the first to show a strong association between BMI and HIT in ICU patients, Dr. Bloom said, noting that several other studies have shown that obesity is linked with increased incidence and increased severity of immune-mediated diseases, including rheumatoid arthritis, systemic lupus erythematosus, and inflammatory bowel disease.
“And HIT is an immune-mediated disease,” he added.
“BMI may be an important new clinical variable for estimating the pre-test probability of HIT, and perhaps, in the future, patient ‘thickness’ could be considered a new ‘T’ in the 4T score, he concluded.
Dr. Bloom reported having no disclosures.
LAS VEGAS – High body mass index is strongly associated with increased rates of heparin-induced thrombocytopenia, based on findings from a review of prospectively collected data from surgical and cardiac intensive care unit patients presumed to have the condition.
Of 304 patients included in the review, 36 (12%) were positive for heparin-induced thrombocytopenia (HIT). The rates increased in tandem with BMI. For example, the rate was 0% among 9 underweight individuals (BMI less than 18.5 kg/m2), 8% among 119 normal-weight individuals (BMI of 18.5-24.9 kg/m2), 11% among 98 overweight individuals (BMI of 25-29.9 kg/m2), 18% among 67 obese individuals (BMI of 30-39.9 kg/m2), and 36% among 11 morbidly obese individuals (BMI of 40 kg/m2 or greater), Dr. Matthew B. Bloom reported at the annual meeting of the American Association for the Surgery of Trauma.
The odds of HIT were 170% greater among obese patients, compared with normal-weight patients (odds ratio, 2.67), and 600% greater among morbidly obese patients, compared with normal-weight patient (odds ratio, 6.98), said Dr. Bloom of Cedars-Sinai Medical Center, Los Angeles.
Logistic regression showed that each 1 unit increase in BMI was associated with a 7.7% increase in the odds of developing HIT, he noted.
Additionally, an anti-heparin/PF4 (platelet factor 4) antibody OD (optical density) value of 2.0 or greater, but not of 0.4 or greater or 0.8 or greater, was also significantly increased with BMI, and in-hospital mortality increased significantly with BMI above normal, he said.
Warkentin 4T scores used to differentiate HIT from other types of thrombocytopenia were not found to correlate with changes in BMI in this study, nor were deep vein thrombosis, pulmonary embolism, or stroke.
The increase in PF4 with increasing BMI may be a marker for overall increasing levels of circulating antibodies in the obese ICU population, but more biochemical studies are needed to tease this out, he said.
Patients included in the review were all those admitted to the surgical and cardiac ICUs at Cedars-Sinai over a more than 7 year period. They had a mean age of 62.1 years, 59% were men, and their mean BMI was 27 kg/m2.
The findings are among the first to show a strong association between BMI and HIT in ICU patients, Dr. Bloom said, noting that several other studies have shown that obesity is linked with increased incidence and increased severity of immune-mediated diseases, including rheumatoid arthritis, systemic lupus erythematosus, and inflammatory bowel disease.
“And HIT is an immune-mediated disease,” he added.
“BMI may be an important new clinical variable for estimating the pre-test probability of HIT, and perhaps, in the future, patient ‘thickness’ could be considered a new ‘T’ in the 4T score, he concluded.
Dr. Bloom reported having no disclosures.
AT THE AAST ANNUAL MEETING
Key clinical point: Higher body mass index is strongly associated with increased rates of heparin-induced thrombocytopenia.
Major finding: The HIT rate was 0%, 8%, 11%, 18,%, and 36% among underweight, normal-weight, overweight, obese, and morbidly obese individuals, respectively.
Data source: A review of prospectively collected data for 304 patients.
Disclosures: Dr. Bloom reported having no disclosures.
Noninvasive prenatal test misuse spurs education campaign
Early findings regarding cell-free DNA screening for the detection of fetal aneuploidy in high-risk populations generated a great deal of buzz, but more recent research on the lower positive predictive value in the general population has tempered that excitement.
Further, reports that women are basing decisions about whether to continue their pregnancies solely on the results of the noninvasive prenatal tests has spurred some health organizations to try to better educate physicians and the public about the limitations of this new technology.
Education and tracking
The Perinatal Quality Foundation (PQF) has launched an educational initiative to promote more clinically appropriate use of noninvasive prenatal screening methods. The national campaign is designed to “improve understanding of the advantages, limitations, and clinically appropriate interpretation of results of noninvasive prenatal screening and other diagnostic tests for pregnant women and their health care providers,” according to a press release.
The “comprehensive education and quality-tracking program” will also involve development of an online patient registry for the purpose of collecting data. The initiative is supported by a grant from Quest Diagnostics, as well as by funding from a growing number of other supportive laboratories that provide prenatal tests.

Dr. Mary Norton, PQF president, stressed the value of cell-free DNA tests for screening, particularly for Down syndrome, but she added that many of the caveats with respect to testing were not publicized by labs eager to market their products.
The fact that most lab reports based on the testing will state either that aneuploidy is present or is not present contributed to the sense that the testing was diagnostic, and therefore to misinterpretation of results, said Dr. Norton, who is also professor of obstetrics, gynecology, and reproductive sciences at the University of California, San Francisco. Dr Norton reported receiving institutional research funding from Ariosa Diagnostics and Natera.
Inappropriate use
“Cell-free DNA screening as a screening technology became clinically available only a few years ago. It has been surrounded by immense interest since its introduction,” said Dr. Joseph R. Biggio Jr., professor of obstetrics and gynecology and director of the division of maternal-fetal medicine at the University of Alabama at Birmingham.
That interest, based largely on findings in “the select population of women at highest risk,” coupled with extensive marketing to both physicians and consumers, contributed to rapid uptake into clinical practice, he said. And despite a 2012 committee opinion from the American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine endorsing the testing only in women at higher risk for aneuploidy, many obstetricians began offering the testing regardless of risk status, he added.
In the general population, the prevalence of aneuploidy is lower, thus the positive predictive value is lower than was initially associated with the testing.
Consequently, ACOG and SMFM updated that earlier committee opinion, stressing the limits of cell-free DNA testing for aneuploidy and the importance of conventional prenatal screening methods for most pregnant women.

The updated opinion, published online in June, emphasizes the need for confirmation of any cell-free DNA screen-positive result, because false-positive results do occur, said Dr. Biggio, chair of the SMFM Committee on Genetics, which coauthored the opinion. Dr. Biggio reported serving as a site investigator at the University of Alabama for noninvasive prenatal testing (NIPT) studies supported by Sequenom and Natera.
“The committee opinion emphasizes that this technology is a screening test – not a diagnostic test – and it is associated with limitations,” he said.
A particularly concerning issue demonstrated by several recent studies is an increased risk for fetal aneuploidy among patients in whom cell-free DNA screening fails or is uninterpretable, he said.
In one study presented in February at the annual SMFM meeting, the rate of chromosomal abnormalities was 13.8% in 65 patients with no final results on cell-free DNA screening, compared with 2.4% in the overall cohort of 4,446 patients.
Such patients should receive further genetic counseling and be offered further evaluation, Dr. Biggio said, adding that “many obstetric providers have been unaware of the magnitude of this risk, and this has been associated with delays in diagnosis or failure to make a diagnosis.
“The committee opinion emphasizes this issue and the need for further follow-up for these patients,” he said.
A role for genetic counseling
Another important part of the process is genetic counseling, according to Dr. R. Curtis Rogers, senior clinical geneticist at Greenwood Genetic Center, Greenville, S.C., who prefers the term noninvasive perinatal screening (NIPS) over NIPT because of the confusion surrounding the diagnostic ability of the technology.

The genetic counselors he supervises at Greenwood Genetic Center see about 1,000 patients each year, but countless others are never seen by a counselor.
Too often, time-pressed primary care physicians are offering the testing without allotting the necessary time for in-depth counseling, he said.
“Yes, it is an exciting test and a good test, but it certainly is not a perfect test ... and I am hesitant for families to make decisions about pregnancy management based solely on NIPS unless there were obvious birth defects detected on prenatal ultrasound that were consistent with the NIPS findings,” he said.
For example, if an ultrasound shows holoprosencephaly, and NIPS shows trisomy 13, the likelihood of trisomy 13 is greater than 95%, he explained, adding that other scenarios, such as detecting partial deletions or duplications, is much less clear.
“Most patients who receive this screening should receive genetic counseling from a certified genetic counselor prior to having the test,” he said. “When we’re talking about very significant diagnoses that may alter the management of pregnancy, I think we need to be 100% correct. Yes, there is high specificity and sensitivity, and for most of the disorders – especially the trisomies – it has good positive predictive value. But it is not perfect, and I think we need to go into that with our eyes open, and families need to go in with their eyes open.”
Jennifer Stallworth, one of the genetic counselors at Greenwood Genetic Center, explained that her role is to counsel patients who may be considering the test, including informing them about the risk for chromosomal conditions in their pregnancies, and discussing the pros and cons of NIPT, compared with other screening and diagnostic testing options.
“I also counsel patients who have already had the test completed, and whether the results are normal or abnormal, I try to help them understand how that result has changed our understanding of the risk for a chromosome disorder in the pregnancy,” she said.
She, too, noted that the excitement about these tests stems largely from a desire to improve upon existing screening methods.
“I think everyone would like to have a risk-free alternative to amniocentesis and [chorionic villi sampling], but we are not yet to that point with NIPT,” Ms. Stallworth said. “I would continue to advise doctors and patients that these tests are a good way to screen for major chromosome conditions, but it is still important to consider all of a patient’s risk factors and to remember that invasive diagnostic testing offers the most complete information at this time.”
Early findings regarding cell-free DNA screening for the detection of fetal aneuploidy in high-risk populations generated a great deal of buzz, but more recent research on the lower positive predictive value in the general population has tempered that excitement.
Further, reports that women are basing decisions about whether to continue their pregnancies solely on the results of the noninvasive prenatal tests has spurred some health organizations to try to better educate physicians and the public about the limitations of this new technology.
Education and tracking
The Perinatal Quality Foundation (PQF) has launched an educational initiative to promote more clinically appropriate use of noninvasive prenatal screening methods. The national campaign is designed to “improve understanding of the advantages, limitations, and clinically appropriate interpretation of results of noninvasive prenatal screening and other diagnostic tests for pregnant women and their health care providers,” according to a press release.
The “comprehensive education and quality-tracking program” will also involve development of an online patient registry for the purpose of collecting data. The initiative is supported by a grant from Quest Diagnostics, as well as by funding from a growing number of other supportive laboratories that provide prenatal tests.
Dr. Mary Norton, PQF president, stressed the value of cell-free DNA tests for screening, particularly for Down syndrome, but she added that many of the caveats with respect to testing were not publicized by labs eager to market their products.
The fact that most lab reports based on the testing will state either that aneuploidy is present or is not present contributed to the sense that the testing was diagnostic, and therefore to misinterpretation of results, said Dr. Norton, who is also professor of obstetrics, gynecology, and reproductive sciences at the University of California, San Francisco. Dr Norton reported receiving institutional research funding from Ariosa Diagnostics and Natera.
Inappropriate use
“Cell-free DNA screening as a screening technology became clinically available only a few years ago. It has been surrounded by immense interest since its introduction,” said Dr. Joseph R. Biggio Jr., professor of obstetrics and gynecology and director of the division of maternal-fetal medicine at the University of Alabama at Birmingham.
That interest, based largely on findings in “the select population of women at highest risk,” coupled with extensive marketing to both physicians and consumers, contributed to rapid uptake into clinical practice, he said. And despite a 2012 committee opinion from the American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine endorsing the testing only in women at higher risk for aneuploidy, many obstetricians began offering the testing regardless of risk status, he added.
In the general population, the prevalence of aneuploidy is lower, thus the positive predictive value is lower than was initially associated with the testing.
Consequently, ACOG and SMFM updated that earlier committee opinion, stressing the limits of cell-free DNA testing for aneuploidy and the importance of conventional prenatal screening methods for most pregnant women.
The updated opinion, published online in June, emphasizes the need for confirmation of any cell-free DNA screen-positive result, because false-positive results do occur, said Dr. Biggio, chair of the SMFM Committee on Genetics, which coauthored the opinion. Dr. Biggio reported serving as a site investigator at the University of Alabama for noninvasive prenatal testing (NIPT) studies supported by Sequenom and Natera.
“The committee opinion emphasizes that this technology is a screening test – not a diagnostic test – and it is associated with limitations,” he said.
A particularly concerning issue demonstrated by several recent studies is an increased risk for fetal aneuploidy among patients in whom cell-free DNA screening fails or is uninterpretable, he said.
In one study presented in February at the annual SMFM meeting, the rate of chromosomal abnormalities was 13.8% in 65 patients with no final results on cell-free DNA screening, compared with 2.4% in the overall cohort of 4,446 patients.
Such patients should receive further genetic counseling and be offered further evaluation, Dr. Biggio said, adding that “many obstetric providers have been unaware of the magnitude of this risk, and this has been associated with delays in diagnosis or failure to make a diagnosis.
“The committee opinion emphasizes this issue and the need for further follow-up for these patients,” he said.
A role for genetic counseling
Another important part of the process is genetic counseling, according to Dr. R. Curtis Rogers, senior clinical geneticist at Greenwood Genetic Center, Greenville, S.C., who prefers the term noninvasive perinatal screening (NIPS) over NIPT because of the confusion surrounding the diagnostic ability of the technology.
The genetic counselors he supervises at Greenwood Genetic Center see about 1,000 patients each year, but countless others are never seen by a counselor.
Too often, time-pressed primary care physicians are offering the testing without allotting the necessary time for in-depth counseling, he said.
“Yes, it is an exciting test and a good test, but it certainly is not a perfect test ... and I am hesitant for families to make decisions about pregnancy management based solely on NIPS unless there were obvious birth defects detected on prenatal ultrasound that were consistent with the NIPS findings,” he said.
For example, if an ultrasound shows holoprosencephaly, and NIPS shows trisomy 13, the likelihood of trisomy 13 is greater than 95%, he explained, adding that other scenarios, such as detecting partial deletions or duplications, is much less clear.
“Most patients who receive this screening should receive genetic counseling from a certified genetic counselor prior to having the test,” he said. “When we’re talking about very significant diagnoses that may alter the management of pregnancy, I think we need to be 100% correct. Yes, there is high specificity and sensitivity, and for most of the disorders – especially the trisomies – it has good positive predictive value. But it is not perfect, and I think we need to go into that with our eyes open, and families need to go in with their eyes open.”
Jennifer Stallworth, one of the genetic counselors at Greenwood Genetic Center, explained that her role is to counsel patients who may be considering the test, including informing them about the risk for chromosomal conditions in their pregnancies, and discussing the pros and cons of NIPT, compared with other screening and diagnostic testing options.
“I also counsel patients who have already had the test completed, and whether the results are normal or abnormal, I try to help them understand how that result has changed our understanding of the risk for a chromosome disorder in the pregnancy,” she said.
She, too, noted that the excitement about these tests stems largely from a desire to improve upon existing screening methods.
“I think everyone would like to have a risk-free alternative to amniocentesis and [chorionic villi sampling], but we are not yet to that point with NIPT,” Ms. Stallworth said. “I would continue to advise doctors and patients that these tests are a good way to screen for major chromosome conditions, but it is still important to consider all of a patient’s risk factors and to remember that invasive diagnostic testing offers the most complete information at this time.”
Early findings regarding cell-free DNA screening for the detection of fetal aneuploidy in high-risk populations generated a great deal of buzz, but more recent research on the lower positive predictive value in the general population has tempered that excitement.
Further, reports that women are basing decisions about whether to continue their pregnancies solely on the results of the noninvasive prenatal tests has spurred some health organizations to try to better educate physicians and the public about the limitations of this new technology.
Education and tracking
The Perinatal Quality Foundation (PQF) has launched an educational initiative to promote more clinically appropriate use of noninvasive prenatal screening methods. The national campaign is designed to “improve understanding of the advantages, limitations, and clinically appropriate interpretation of results of noninvasive prenatal screening and other diagnostic tests for pregnant women and their health care providers,” according to a press release.
The “comprehensive education and quality-tracking program” will also involve development of an online patient registry for the purpose of collecting data. The initiative is supported by a grant from Quest Diagnostics, as well as by funding from a growing number of other supportive laboratories that provide prenatal tests.
Dr. Mary Norton, PQF president, stressed the value of cell-free DNA tests for screening, particularly for Down syndrome, but she added that many of the caveats with respect to testing were not publicized by labs eager to market their products.
The fact that most lab reports based on the testing will state either that aneuploidy is present or is not present contributed to the sense that the testing was diagnostic, and therefore to misinterpretation of results, said Dr. Norton, who is also professor of obstetrics, gynecology, and reproductive sciences at the University of California, San Francisco. Dr Norton reported receiving institutional research funding from Ariosa Diagnostics and Natera.
Inappropriate use
“Cell-free DNA screening as a screening technology became clinically available only a few years ago. It has been surrounded by immense interest since its introduction,” said Dr. Joseph R. Biggio Jr., professor of obstetrics and gynecology and director of the division of maternal-fetal medicine at the University of Alabama at Birmingham.
That interest, based largely on findings in “the select population of women at highest risk,” coupled with extensive marketing to both physicians and consumers, contributed to rapid uptake into clinical practice, he said. And despite a 2012 committee opinion from the American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine endorsing the testing only in women at higher risk for aneuploidy, many obstetricians began offering the testing regardless of risk status, he added.
In the general population, the prevalence of aneuploidy is lower, thus the positive predictive value is lower than was initially associated with the testing.
Consequently, ACOG and SMFM updated that earlier committee opinion, stressing the limits of cell-free DNA testing for aneuploidy and the importance of conventional prenatal screening methods for most pregnant women.
The updated opinion, published online in June, emphasizes the need for confirmation of any cell-free DNA screen-positive result, because false-positive results do occur, said Dr. Biggio, chair of the SMFM Committee on Genetics, which coauthored the opinion. Dr. Biggio reported serving as a site investigator at the University of Alabama for noninvasive prenatal testing (NIPT) studies supported by Sequenom and Natera.
“The committee opinion emphasizes that this technology is a screening test – not a diagnostic test – and it is associated with limitations,” he said.
A particularly concerning issue demonstrated by several recent studies is an increased risk for fetal aneuploidy among patients in whom cell-free DNA screening fails or is uninterpretable, he said.
In one study presented in February at the annual SMFM meeting, the rate of chromosomal abnormalities was 13.8% in 65 patients with no final results on cell-free DNA screening, compared with 2.4% in the overall cohort of 4,446 patients.
Such patients should receive further genetic counseling and be offered further evaluation, Dr. Biggio said, adding that “many obstetric providers have been unaware of the magnitude of this risk, and this has been associated with delays in diagnosis or failure to make a diagnosis.
“The committee opinion emphasizes this issue and the need for further follow-up for these patients,” he said.
A role for genetic counseling
Another important part of the process is genetic counseling, according to Dr. R. Curtis Rogers, senior clinical geneticist at Greenwood Genetic Center, Greenville, S.C., who prefers the term noninvasive perinatal screening (NIPS) over NIPT because of the confusion surrounding the diagnostic ability of the technology.
The genetic counselors he supervises at Greenwood Genetic Center see about 1,000 patients each year, but countless others are never seen by a counselor.
Too often, time-pressed primary care physicians are offering the testing without allotting the necessary time for in-depth counseling, he said.
“Yes, it is an exciting test and a good test, but it certainly is not a perfect test ... and I am hesitant for families to make decisions about pregnancy management based solely on NIPS unless there were obvious birth defects detected on prenatal ultrasound that were consistent with the NIPS findings,” he said.
For example, if an ultrasound shows holoprosencephaly, and NIPS shows trisomy 13, the likelihood of trisomy 13 is greater than 95%, he explained, adding that other scenarios, such as detecting partial deletions or duplications, is much less clear.
“Most patients who receive this screening should receive genetic counseling from a certified genetic counselor prior to having the test,” he said. “When we’re talking about very significant diagnoses that may alter the management of pregnancy, I think we need to be 100% correct. Yes, there is high specificity and sensitivity, and for most of the disorders – especially the trisomies – it has good positive predictive value. But it is not perfect, and I think we need to go into that with our eyes open, and families need to go in with their eyes open.”
Jennifer Stallworth, one of the genetic counselors at Greenwood Genetic Center, explained that her role is to counsel patients who may be considering the test, including informing them about the risk for chromosomal conditions in their pregnancies, and discussing the pros and cons of NIPT, compared with other screening and diagnostic testing options.
“I also counsel patients who have already had the test completed, and whether the results are normal or abnormal, I try to help them understand how that result has changed our understanding of the risk for a chromosome disorder in the pregnancy,” she said.
She, too, noted that the excitement about these tests stems largely from a desire to improve upon existing screening methods.
“I think everyone would like to have a risk-free alternative to amniocentesis and [chorionic villi sampling], but we are not yet to that point with NIPT,” Ms. Stallworth said. “I would continue to advise doctors and patients that these tests are a good way to screen for major chromosome conditions, but it is still important to consider all of a patient’s risk factors and to remember that invasive diagnostic testing offers the most complete information at this time.”

Jamestown Canyon virus detected in humans in Minnesota
ATLANTA – A mosquito-borne illness that has been mainly limited to white-tailed deer throughout North America is emerging as a more frequent cause of human disease, according to a report from the Minnesota Department of Health.
The Jamestown Canyon virus (JCV), a member of the California serogroup of bunyaviruses likely transmitted to humans through the bite of an infected Aedes-species mosquito, was first detected in a human in Minnesota in 2013. Due to suspicion that cases were being missed by an assay in use at the time in Minnesota, which had relatively poor sensitivity for detecting Jamestown Canyon virus, an enzyme immunoassay specific to JCV was put into use in 2014 to test serum and cerebrospinal fluid specimens submitted for other arboviral testing. Subsequently, an additional six cases were identified, Elizabeth Schiffman reported at the International Conference on Emerging Infectious Diseases.

Between May and October of 2014, 141 serum or cerebrospinal fluid samples from 107 unique patients were tested. Of these, 20 samples from 17 patients initially tested positive for JCV; further testing at the Centers for Disease Control and Prevention in Atlanta confirmed the findings in 7 specimens from 6 patients, said Ms. Schiffman, an epidemiologist at the Minnesota Department of Health, St. Paul.
Findings from other specimens were pending at the time of her presentation.
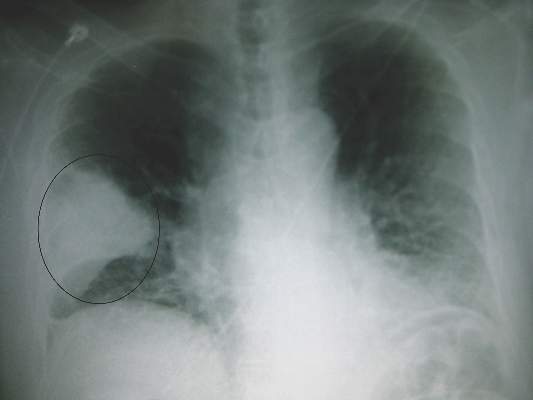
The initial patient was a 49-year-old man who had generalized symptoms, including myalgia, fatigue, and nausea for about week, who then was hospitalized after experiencing sudden onset of fever, disorientation, and aphasia. Viral encephalitis was suspected, and specimens sent to the Minnesota Department of Health, then to the CDC, were positive for JCV. The other patients with confirmed JCV ranged in age from 11 to 77 years (median, 56).
Illness onset was between late May and early September, and patients presented with symptoms typical of mosquito-borne illnesses, including fever, fatigue, myalgia/arthralgia, and/or headache, although clinical syndromes varied among individuals.
“Three patients were classified as having meningoencephalitis, three had fever without neurological involvement, and one patient developed acute flaccid paralysis,” Ms. Schiffman said, adding that six of the seven patients were hospitalized with duration ranging from 4 to 20 days (median, 7 days), and three were discharged to acute rehabilitation facilities for further care.
Although only three patients were classified as having neuroinvasive disease, five of the seven reported symptoms suggestive of some neurologic involvement, ranging from mild confusion and altered mental status, to aphasia, ataxia, and seizure, she said.
An additional case from 2002 was retrospectively identified, she noted.
Although JCV has been known to cause disease in humans since the 1970s and has been nationally notifiable since 2004, it is rarely reported. In fact, only 31 human cases were reported in the United States from 2000 to 2015, she said, adding that the disease is likely underrecognized, particularly in more mild forms.
“It is expected that continued testing and increased awareness among health care providers of JCV as a possible cause of human disease – particularly viral encephalitis – will likely aid in the identification of additional cases in the future,” she said.
This work was funded by the Epidemiology and Laboratory Capacity Cooperative Agreement with the CDC.
ATLANTA – A mosquito-borne illness that has been mainly limited to white-tailed deer throughout North America is emerging as a more frequent cause of human disease, according to a report from the Minnesota Department of Health.
The Jamestown Canyon virus (JCV), a member of the California serogroup of bunyaviruses likely transmitted to humans through the bite of an infected Aedes-species mosquito, was first detected in a human in Minnesota in 2013. Due to suspicion that cases were being missed by an assay in use at the time in Minnesota, which had relatively poor sensitivity for detecting Jamestown Canyon virus, an enzyme immunoassay specific to JCV was put into use in 2014 to test serum and cerebrospinal fluid specimens submitted for other arboviral testing. Subsequently, an additional six cases were identified, Elizabeth Schiffman reported at the International Conference on Emerging Infectious Diseases.
Between May and October of 2014, 141 serum or cerebrospinal fluid samples from 107 unique patients were tested. Of these, 20 samples from 17 patients initially tested positive for JCV; further testing at the Centers for Disease Control and Prevention in Atlanta confirmed the findings in 7 specimens from 6 patients, said Ms. Schiffman, an epidemiologist at the Minnesota Department of Health, St. Paul.
Findings from other specimens were pending at the time of her presentation.
The initial patient was a 49-year-old man who had generalized symptoms, including myalgia, fatigue, and nausea for about week, who then was hospitalized after experiencing sudden onset of fever, disorientation, and aphasia. Viral encephalitis was suspected, and specimens sent to the Minnesota Department of Health, then to the CDC, were positive for JCV. The other patients with confirmed JCV ranged in age from 11 to 77 years (median, 56).
Illness onset was between late May and early September, and patients presented with symptoms typical of mosquito-borne illnesses, including fever, fatigue, myalgia/arthralgia, and/or headache, although clinical syndromes varied among individuals.
“Three patients were classified as having meningoencephalitis, three had fever without neurological involvement, and one patient developed acute flaccid paralysis,” Ms. Schiffman said, adding that six of the seven patients were hospitalized with duration ranging from 4 to 20 days (median, 7 days), and three were discharged to acute rehabilitation facilities for further care.
Although only three patients were classified as having neuroinvasive disease, five of the seven reported symptoms suggestive of some neurologic involvement, ranging from mild confusion and altered mental status, to aphasia, ataxia, and seizure, she said.
An additional case from 2002 was retrospectively identified, she noted.
Although JCV has been known to cause disease in humans since the 1970s and has been nationally notifiable since 2004, it is rarely reported. In fact, only 31 human cases were reported in the United States from 2000 to 2015, she said, adding that the disease is likely underrecognized, particularly in more mild forms.
“It is expected that continued testing and increased awareness among health care providers of JCV as a possible cause of human disease – particularly viral encephalitis – will likely aid in the identification of additional cases in the future,” she said.
This work was funded by the Epidemiology and Laboratory Capacity Cooperative Agreement with the CDC.
ATLANTA – A mosquito-borne illness that has been mainly limited to white-tailed deer throughout North America is emerging as a more frequent cause of human disease, according to a report from the Minnesota Department of Health.
The Jamestown Canyon virus (JCV), a member of the California serogroup of bunyaviruses likely transmitted to humans through the bite of an infected Aedes-species mosquito, was first detected in a human in Minnesota in 2013. Due to suspicion that cases were being missed by an assay in use at the time in Minnesota, which had relatively poor sensitivity for detecting Jamestown Canyon virus, an enzyme immunoassay specific to JCV was put into use in 2014 to test serum and cerebrospinal fluid specimens submitted for other arboviral testing. Subsequently, an additional six cases were identified, Elizabeth Schiffman reported at the International Conference on Emerging Infectious Diseases.
Between May and October of 2014, 141 serum or cerebrospinal fluid samples from 107 unique patients were tested. Of these, 20 samples from 17 patients initially tested positive for JCV; further testing at the Centers for Disease Control and Prevention in Atlanta confirmed the findings in 7 specimens from 6 patients, said Ms. Schiffman, an epidemiologist at the Minnesota Department of Health, St. Paul.
Findings from other specimens were pending at the time of her presentation.
The initial patient was a 49-year-old man who had generalized symptoms, including myalgia, fatigue, and nausea for about week, who then was hospitalized after experiencing sudden onset of fever, disorientation, and aphasia. Viral encephalitis was suspected, and specimens sent to the Minnesota Department of Health, then to the CDC, were positive for JCV. The other patients with confirmed JCV ranged in age from 11 to 77 years (median, 56).
Illness onset was between late May and early September, and patients presented with symptoms typical of mosquito-borne illnesses, including fever, fatigue, myalgia/arthralgia, and/or headache, although clinical syndromes varied among individuals.
“Three patients were classified as having meningoencephalitis, three had fever without neurological involvement, and one patient developed acute flaccid paralysis,” Ms. Schiffman said, adding that six of the seven patients were hospitalized with duration ranging from 4 to 20 days (median, 7 days), and three were discharged to acute rehabilitation facilities for further care.
Although only three patients were classified as having neuroinvasive disease, five of the seven reported symptoms suggestive of some neurologic involvement, ranging from mild confusion and altered mental status, to aphasia, ataxia, and seizure, she said.
An additional case from 2002 was retrospectively identified, she noted.
Although JCV has been known to cause disease in humans since the 1970s and has been nationally notifiable since 2004, it is rarely reported. In fact, only 31 human cases were reported in the United States from 2000 to 2015, she said, adding that the disease is likely underrecognized, particularly in more mild forms.
“It is expected that continued testing and increased awareness among health care providers of JCV as a possible cause of human disease – particularly viral encephalitis – will likely aid in the identification of additional cases in the future,” she said.
This work was funded by the Epidemiology and Laboratory Capacity Cooperative Agreement with the CDC.
AT ICEID 2015
Key clinical point: A mosquito-borne illness that has been mainly limited to white-tailed deer throughout North America is emerging as a more frequent cause of human disease, according to a report from the Minnesota Department of Health.
Major finding: Seven specimens from six patients were confirmed as positive for JCV.
Data source: Laboratory testing of 141 serum or cerebrospinal fluid samples from 107 unique patients.
Disclosures: This work was funded by the Epidemiology and Laboratory Capacity Cooperative Agreement with the Centers for Disease Control and Prevention.

ICEID: Population-level data support ACIP flu vaccine recommendations
ATLANTA – Expanded influenza vaccination coverage among children between 2002 and 2012 appears to have provided direct benefit with respect to influenza-related hospitalizations among vaccinated children, according to an analysis of vaccination and hospitalization data.
Additionally, the coverage among children appears to have provided indirect benefits in adults, Cecile Viboud, Ph.D. of the National Institutes of Health, Bethesda, Md., reported at the International Conference on Emerging Infectious Diseases.

Between 2006-2007 and 2010-2011, the U.S. Advisory Committee on Immunization Practices (ACIP) broadened vaccination recommendations to include not only children aged 6-23 months, but also those aged 24-59 months, then those aged 5-18 years, and eventually all those over age 6 months. Consequently, the vaccine coverage rate increased from less than 5% in 2002 to about 52% in 2012 (and to about 70% in those under age 5 years). Modeling of weekly influenza-related hospitalization outcomes (pneumonia and influenza outcomes and respiratory and circulatory outcomes) provided solid evidence of a direct and significant protective effect of vaccination both in children under age 5 years and in those aged 5-19 years. This finding was consistent across disease outcomes, and remained significant in those under age 5 after adjusting for state, but the association was weaker with stratification by season, Dr. Viboud noted.
Further, hospitalization rates among working-age adults and seniors aged 65-74 years declined with increasing pediatric vaccine coverage, suggesting an indirect protective effect in that population, she said, noting that the vaccination rate among older adults remained stable across the study period.
No evidence was seen for an indirect protective effect among adults over age 74 years, she said.
Dr. Viboud and her colleagues used age-specific annual vaccination rates derived from the National Immunization Survey and the Behavioral Risk Factor Surveillance System. Age-specific rates of influenza-associated hospitalizations were estimated for each season during 1989-2012 by modeling weekly pneumonia and influenza outcomes plus respiratory and circulatory outcomes from the State Inpatient Databases of the Agency for Healthcare Research & Quality.
“In a nutshell, we see strong statistical evidence for the direct protective effects of the influenza vaccination program in children on the basis of analyses of population-level hospitalization data, which supports the expansion of the ACIP flu vaccine recommendations in the past decade,” Dr. Viboud said in an interview. “We also find weak evidence of herd immunity effects, whereby hospitalization rates are reduced in adults. That the evidence is weak is perhaps not surprising given that vaccine uptake in children remains moderate (60% in most highly vaccinated states) and vaccine effectiveness is modest at 40%-60% depending on the season. Independent information from mathematical transmission models confirms that herd immunity benefits are expected to be low given these levels of vaccine coverage.”
The indirect effects may become clearer with increasing vaccine uptake, she added.
Dr. Viboud reported having no disclosures.
ATLANTA – Expanded influenza vaccination coverage among children between 2002 and 2012 appears to have provided direct benefit with respect to influenza-related hospitalizations among vaccinated children, according to an analysis of vaccination and hospitalization data.
Additionally, the coverage among children appears to have provided indirect benefits in adults, Cecile Viboud, Ph.D. of the National Institutes of Health, Bethesda, Md., reported at the International Conference on Emerging Infectious Diseases.
Between 2006-2007 and 2010-2011, the U.S. Advisory Committee on Immunization Practices (ACIP) broadened vaccination recommendations to include not only children aged 6-23 months, but also those aged 24-59 months, then those aged 5-18 years, and eventually all those over age 6 months. Consequently, the vaccine coverage rate increased from less than 5% in 2002 to about 52% in 2012 (and to about 70% in those under age 5 years). Modeling of weekly influenza-related hospitalization outcomes (pneumonia and influenza outcomes and respiratory and circulatory outcomes) provided solid evidence of a direct and significant protective effect of vaccination both in children under age 5 years and in those aged 5-19 years. This finding was consistent across disease outcomes, and remained significant in those under age 5 after adjusting for state, but the association was weaker with stratification by season, Dr. Viboud noted.
Further, hospitalization rates among working-age adults and seniors aged 65-74 years declined with increasing pediatric vaccine coverage, suggesting an indirect protective effect in that population, she said, noting that the vaccination rate among older adults remained stable across the study period.
No evidence was seen for an indirect protective effect among adults over age 74 years, she said.
Dr. Viboud and her colleagues used age-specific annual vaccination rates derived from the National Immunization Survey and the Behavioral Risk Factor Surveillance System. Age-specific rates of influenza-associated hospitalizations were estimated for each season during 1989-2012 by modeling weekly pneumonia and influenza outcomes plus respiratory and circulatory outcomes from the State Inpatient Databases of the Agency for Healthcare Research & Quality.
“In a nutshell, we see strong statistical evidence for the direct protective effects of the influenza vaccination program in children on the basis of analyses of population-level hospitalization data, which supports the expansion of the ACIP flu vaccine recommendations in the past decade,” Dr. Viboud said in an interview. “We also find weak evidence of herd immunity effects, whereby hospitalization rates are reduced in adults. That the evidence is weak is perhaps not surprising given that vaccine uptake in children remains moderate (60% in most highly vaccinated states) and vaccine effectiveness is modest at 40%-60% depending on the season. Independent information from mathematical transmission models confirms that herd immunity benefits are expected to be low given these levels of vaccine coverage.”
The indirect effects may become clearer with increasing vaccine uptake, she added.
Dr. Viboud reported having no disclosures.
ATLANTA – Expanded influenza vaccination coverage among children between 2002 and 2012 appears to have provided direct benefit with respect to influenza-related hospitalizations among vaccinated children, according to an analysis of vaccination and hospitalization data.
Additionally, the coverage among children appears to have provided indirect benefits in adults, Cecile Viboud, Ph.D. of the National Institutes of Health, Bethesda, Md., reported at the International Conference on Emerging Infectious Diseases.
Between 2006-2007 and 2010-2011, the U.S. Advisory Committee on Immunization Practices (ACIP) broadened vaccination recommendations to include not only children aged 6-23 months, but also those aged 24-59 months, then those aged 5-18 years, and eventually all those over age 6 months. Consequently, the vaccine coverage rate increased from less than 5% in 2002 to about 52% in 2012 (and to about 70% in those under age 5 years). Modeling of weekly influenza-related hospitalization outcomes (pneumonia and influenza outcomes and respiratory and circulatory outcomes) provided solid evidence of a direct and significant protective effect of vaccination both in children under age 5 years and in those aged 5-19 years. This finding was consistent across disease outcomes, and remained significant in those under age 5 after adjusting for state, but the association was weaker with stratification by season, Dr. Viboud noted.
Further, hospitalization rates among working-age adults and seniors aged 65-74 years declined with increasing pediatric vaccine coverage, suggesting an indirect protective effect in that population, she said, noting that the vaccination rate among older adults remained stable across the study period.
No evidence was seen for an indirect protective effect among adults over age 74 years, she said.
Dr. Viboud and her colleagues used age-specific annual vaccination rates derived from the National Immunization Survey and the Behavioral Risk Factor Surveillance System. Age-specific rates of influenza-associated hospitalizations were estimated for each season during 1989-2012 by modeling weekly pneumonia and influenza outcomes plus respiratory and circulatory outcomes from the State Inpatient Databases of the Agency for Healthcare Research & Quality.
“In a nutshell, we see strong statistical evidence for the direct protective effects of the influenza vaccination program in children on the basis of analyses of population-level hospitalization data, which supports the expansion of the ACIP flu vaccine recommendations in the past decade,” Dr. Viboud said in an interview. “We also find weak evidence of herd immunity effects, whereby hospitalization rates are reduced in adults. That the evidence is weak is perhaps not surprising given that vaccine uptake in children remains moderate (60% in most highly vaccinated states) and vaccine effectiveness is modest at 40%-60% depending on the season. Independent information from mathematical transmission models confirms that herd immunity benefits are expected to be low given these levels of vaccine coverage.”
The indirect effects may become clearer with increasing vaccine uptake, she added.
Dr. Viboud reported having no disclosures.
AT ICEID 2015
Key clinical point: Expanded influenza vaccination coverage in children provided direct benefits with respect to hospitalizations.
Major finding: Vaccine coverage rate increased from less than 5% in 2002 to about 52% in 2012 .
Data source: An analysis of vaccination and hospitalization data.
Disclosures: Dr. Viboud reported having no disclosures.

ICEID: Pertussis vaccination reduces disease severity
ATLANTA – Pertussis vaccination does not eliminate the risk of disease, but it does appear to reduce disease severity, according to findings from a study of more than 10,000 cases.
In fact, despite high acellular pertussis vaccine coverage in the United States, 48,277 cases were reported in 2012, and many of these were among vaccinated individuals – a result of waning protection over time following childhood pertussis vaccination, Lucy A. McNamara, Ph.D., of the Centers for Disease Control and Prevention in Atlanta reported at the International Conference on Emerging Infectious Diseases.

To assess whether severe symptoms or complications are more common in those who are not fully vaccinated, Dr. McNamara and her colleagues identified a total of 10,092 pertussis case patients from the Enhanced Pertussis Surveillance/Emerging Infections Program network in 2010-2012 and collected case information through vaccine registries and interviews with physicians and patients at six network sites. Of those aged 3 months to 19 years, 81% were up to date for pertussis vaccinations for their age, and of adults, 45% had received Tdap.
Up-to-date status was protective against severe disease, defined as disease involving seizures, encephalopathy, pneumonia, or hospitalization, in children aged 7 months to 6 years, who had about a 60% reduction in risk, compared with those who were not up to date. Up-to-date status also reduced the risk of posttussive vomiting, which sometimes accompanies severe coughing fits, by about 25% in those aged 19 months to 64 years, she said, adding that the risk of vomiting after coughing was about 38% lower in this age group when patients received antibiotic treatment within 1 week of the start of the illness.
The effect on posttussive vomiting was independent of antibiotic treatment timing, which further underscores the value of both rapid treatment and completion of the pertussis vaccination schedule, she said.
Dr. McNamara reported having no disclosures.
ATLANTA – Pertussis vaccination does not eliminate the risk of disease, but it does appear to reduce disease severity, according to findings from a study of more than 10,000 cases.
In fact, despite high acellular pertussis vaccine coverage in the United States, 48,277 cases were reported in 2012, and many of these were among vaccinated individuals – a result of waning protection over time following childhood pertussis vaccination, Lucy A. McNamara, Ph.D., of the Centers for Disease Control and Prevention in Atlanta reported at the International Conference on Emerging Infectious Diseases.
To assess whether severe symptoms or complications are more common in those who are not fully vaccinated, Dr. McNamara and her colleagues identified a total of 10,092 pertussis case patients from the Enhanced Pertussis Surveillance/Emerging Infections Program network in 2010-2012 and collected case information through vaccine registries and interviews with physicians and patients at six network sites. Of those aged 3 months to 19 years, 81% were up to date for pertussis vaccinations for their age, and of adults, 45% had received Tdap.
Up-to-date status was protective against severe disease, defined as disease involving seizures, encephalopathy, pneumonia, or hospitalization, in children aged 7 months to 6 years, who had about a 60% reduction in risk, compared with those who were not up to date. Up-to-date status also reduced the risk of posttussive vomiting, which sometimes accompanies severe coughing fits, by about 25% in those aged 19 months to 64 years, she said, adding that the risk of vomiting after coughing was about 38% lower in this age group when patients received antibiotic treatment within 1 week of the start of the illness.
The effect on posttussive vomiting was independent of antibiotic treatment timing, which further underscores the value of both rapid treatment and completion of the pertussis vaccination schedule, she said.
Dr. McNamara reported having no disclosures.
ATLANTA – Pertussis vaccination does not eliminate the risk of disease, but it does appear to reduce disease severity, according to findings from a study of more than 10,000 cases.
In fact, despite high acellular pertussis vaccine coverage in the United States, 48,277 cases were reported in 2012, and many of these were among vaccinated individuals – a result of waning protection over time following childhood pertussis vaccination, Lucy A. McNamara, Ph.D., of the Centers for Disease Control and Prevention in Atlanta reported at the International Conference on Emerging Infectious Diseases.
To assess whether severe symptoms or complications are more common in those who are not fully vaccinated, Dr. McNamara and her colleagues identified a total of 10,092 pertussis case patients from the Enhanced Pertussis Surveillance/Emerging Infections Program network in 2010-2012 and collected case information through vaccine registries and interviews with physicians and patients at six network sites. Of those aged 3 months to 19 years, 81% were up to date for pertussis vaccinations for their age, and of adults, 45% had received Tdap.
Up-to-date status was protective against severe disease, defined as disease involving seizures, encephalopathy, pneumonia, or hospitalization, in children aged 7 months to 6 years, who had about a 60% reduction in risk, compared with those who were not up to date. Up-to-date status also reduced the risk of posttussive vomiting, which sometimes accompanies severe coughing fits, by about 25% in those aged 19 months to 64 years, she said, adding that the risk of vomiting after coughing was about 38% lower in this age group when patients received antibiotic treatment within 1 week of the start of the illness.
The effect on posttussive vomiting was independent of antibiotic treatment timing, which further underscores the value of both rapid treatment and completion of the pertussis vaccination schedule, she said.
Dr. McNamara reported having no disclosures.
AT ICEID 2015
Key clinical point: Pertussis vaccination does not eliminate the risk of disease, but it does reduce disease severity, according to findings from a study of more than 10,000 cases.
Major finding: The risk of severe disease in children aged 7 months to 6 years was about 60% lower in children with up-to-date status, compared with those who were not up to date on their pertussis vaccinations.
Data source: Surveillance data on 10,092 patients.
Disclosures: Dr. McNamara reported having no disclosures.

Surveillance data support early flu vaccination
ATLANTA – Influenza vaccine effectiveness during the 2010-2011 through 2013-2014 flu seasons was moderate for up to 6 months post vaccination – about the duration of the average flu season, according to surveillance data.
Vaccine effectiveness in 1,720 non–active duty U.S. Department of Defense beneficiaries ranged from 40% to 69% across the flu seasons, and after adjusting for age group, calendar season, and flu season, significant and fairly consistent protection was provided for up to 180 days, Dr. Jennifer M. Radin and her colleagues at the Naval Health Research Center, San Diego, reported in a poster at the International Conference on Emerging Infectious Diseases.

The adjusted vaccine effectiveness was 61% during the first 2 weeks after vaccination, 62% from days 15 through 90, and 60% during days 91 through 180. After that, the effectiveness dropped to –11%, the investigators said.
Vaccine effectiveness in this study was assessed using outpatient febrile respiratory illness surveillance among a convenience sample of individuals of all ages, 75% of whom were under age 25 years, who presented with fever, cough, or sore throat at outpatient facilities in California and Illinois. Case patients were those who tested polymerase chain reaction–positive for influenza; those who were PCR negative for influenza served as controls.
“Previous studies have found that protection from contracting influenza declines over time following influenza vaccination due to decreasing antibody levels. However, we found ... moderate, sustained protection up to 6 months post vaccination,” Dr. Radin said in a press statement, explaining that at this level of effectiveness, vaccination reduces the risk of a doctor’s visit by 50%-70%.
The findings suggest that vaccine administration close to the start of flu season is associated with slightly increased vaccine effectiveness, but the start of flu season varies each year, thus optimal timing is hard to predict.
“Consequently, early flu vaccination may still offer the best overall protection,” Dr. Radin and her colleagues wrote.
The finding of a dramatic drop in effectiveness after 6 months also underscores the importance of yearly vaccination, they noted.
The investigators reported having no disclosures.
ATLANTA – Influenza vaccine effectiveness during the 2010-2011 through 2013-2014 flu seasons was moderate for up to 6 months post vaccination – about the duration of the average flu season, according to surveillance data.
Vaccine effectiveness in 1,720 non–active duty U.S. Department of Defense beneficiaries ranged from 40% to 69% across the flu seasons, and after adjusting for age group, calendar season, and flu season, significant and fairly consistent protection was provided for up to 180 days, Dr. Jennifer M. Radin and her colleagues at the Naval Health Research Center, San Diego, reported in a poster at the International Conference on Emerging Infectious Diseases.
The adjusted vaccine effectiveness was 61% during the first 2 weeks after vaccination, 62% from days 15 through 90, and 60% during days 91 through 180. After that, the effectiveness dropped to –11%, the investigators said.
Vaccine effectiveness in this study was assessed using outpatient febrile respiratory illness surveillance among a convenience sample of individuals of all ages, 75% of whom were under age 25 years, who presented with fever, cough, or sore throat at outpatient facilities in California and Illinois. Case patients were those who tested polymerase chain reaction–positive for influenza; those who were PCR negative for influenza served as controls.
“Previous studies have found that protection from contracting influenza declines over time following influenza vaccination due to decreasing antibody levels. However, we found ... moderate, sustained protection up to 6 months post vaccination,” Dr. Radin said in a press statement, explaining that at this level of effectiveness, vaccination reduces the risk of a doctor’s visit by 50%-70%.
The findings suggest that vaccine administration close to the start of flu season is associated with slightly increased vaccine effectiveness, but the start of flu season varies each year, thus optimal timing is hard to predict.
“Consequently, early flu vaccination may still offer the best overall protection,” Dr. Radin and her colleagues wrote.
The finding of a dramatic drop in effectiveness after 6 months also underscores the importance of yearly vaccination, they noted.
The investigators reported having no disclosures.
ATLANTA – Influenza vaccine effectiveness during the 2010-2011 through 2013-2014 flu seasons was moderate for up to 6 months post vaccination – about the duration of the average flu season, according to surveillance data.
Vaccine effectiveness in 1,720 non–active duty U.S. Department of Defense beneficiaries ranged from 40% to 69% across the flu seasons, and after adjusting for age group, calendar season, and flu season, significant and fairly consistent protection was provided for up to 180 days, Dr. Jennifer M. Radin and her colleagues at the Naval Health Research Center, San Diego, reported in a poster at the International Conference on Emerging Infectious Diseases.
The adjusted vaccine effectiveness was 61% during the first 2 weeks after vaccination, 62% from days 15 through 90, and 60% during days 91 through 180. After that, the effectiveness dropped to –11%, the investigators said.
Vaccine effectiveness in this study was assessed using outpatient febrile respiratory illness surveillance among a convenience sample of individuals of all ages, 75% of whom were under age 25 years, who presented with fever, cough, or sore throat at outpatient facilities in California and Illinois. Case patients were those who tested polymerase chain reaction–positive for influenza; those who were PCR negative for influenza served as controls.
“Previous studies have found that protection from contracting influenza declines over time following influenza vaccination due to decreasing antibody levels. However, we found ... moderate, sustained protection up to 6 months post vaccination,” Dr. Radin said in a press statement, explaining that at this level of effectiveness, vaccination reduces the risk of a doctor’s visit by 50%-70%.
The findings suggest that vaccine administration close to the start of flu season is associated with slightly increased vaccine effectiveness, but the start of flu season varies each year, thus optimal timing is hard to predict.
“Consequently, early flu vaccination may still offer the best overall protection,” Dr. Radin and her colleagues wrote.
The finding of a dramatic drop in effectiveness after 6 months also underscores the importance of yearly vaccination, they noted.
The investigators reported having no disclosures.
AT ICEID 2015
Key clinical point: The flu vaccine offered about 6 months’ protection during the 2010-2011 through 2013-2014 flu seasons – about the duration of the average flu season.
Major finding: Adjusted vaccine effectiveness remained about 60% in the 6 months after vaccination during the 2010-2011 through 2013-2014 flu seasons.
Data source: A surveillance study involving 1,720 patients.
Disclosures: The investigators reported having no disclosures.

ICEID: Clothing may transmit respiratory syncytial virus in NICU
ATLANTA – Clothing worn by caregivers and visitors may be an important vehicle for the transmission of respiratory syncytial virus in the neonatal intensive care unit setting, according to findings from a prospective study conducted in an Australian hospital.
In an effort to identify potential sources of RSV transmission and to facilitate development of infection control strategies, the investigators swabbed all health personnel, every third neonate and their visitors, and any child clinically suspected of having an RSV infection. They detected RSV in one of 81 nasal specimens collected from 55 neonates and in 4% of 80 visitors’ clothing swabs, Nusrat Homaira, Ph.D., of the University of New South Wales, Sydney, and her colleagues reported in a poster at the International Conference on Emerging Infectious Diseases.
RSV also was detected in 1% of nose swabs from the visitors and in 1% of nose swabs from 84 health care workers.
No RSV was detected on the clothing of health care workers or on the hands of visitors or health care workers, which may be explained by the presence of alcohol-based hand rub at the point of care and by prevalent hand hygiene practices within the neonatal intensive care unit (NICU), the investigators noted.
The investigators also collected environmental swabs and detected RSV on 9% of high-touch areas, including bed rails; chairs; bed surfaces; countertops; and nurse’s and doctor’s station tables, computers, and chairs.
Samples were collected once each week for 8 weeks during May and June of 2014.
RSV is a major cause of morbidity in very young children, and premature infants have a 10-fold increase in the risk of acquiring RSV infection. Hospital-acquired cases are an important cause of prolonged hospitalization, Dr. Homaira and her associates noted.
The findings suggest that personal clothing may be one of the modes of virus transmission, they said.
“Though the detection rate is low, personal clothing of caregivers/visitors do get contaminated with RSV,” Dr. Homaira said in a written statement, noting that caregivers and visitors are not required to change clothing when they walk into the NICU.
“There is a need for further research to evaluate how long the virus remains infectious on personal clothing, which will have policy implications in terms of need for use of separate gowns by the visitors while they are in the NICU,” Dr. Homaira added, concluding that frequent cleaning of high-touch areas and periodic screening of visitors for RSV as they enter the NICU during seasonal epidemics also may help limit disease transmission.
The investigators reported having no disclosures.
ATLANTA – Clothing worn by caregivers and visitors may be an important vehicle for the transmission of respiratory syncytial virus in the neonatal intensive care unit setting, according to findings from a prospective study conducted in an Australian hospital.
In an effort to identify potential sources of RSV transmission and to facilitate development of infection control strategies, the investigators swabbed all health personnel, every third neonate and their visitors, and any child clinically suspected of having an RSV infection. They detected RSV in one of 81 nasal specimens collected from 55 neonates and in 4% of 80 visitors’ clothing swabs, Nusrat Homaira, Ph.D., of the University of New South Wales, Sydney, and her colleagues reported in a poster at the International Conference on Emerging Infectious Diseases.
RSV also was detected in 1% of nose swabs from the visitors and in 1% of nose swabs from 84 health care workers.
No RSV was detected on the clothing of health care workers or on the hands of visitors or health care workers, which may be explained by the presence of alcohol-based hand rub at the point of care and by prevalent hand hygiene practices within the neonatal intensive care unit (NICU), the investigators noted.
The investigators also collected environmental swabs and detected RSV on 9% of high-touch areas, including bed rails; chairs; bed surfaces; countertops; and nurse’s and doctor’s station tables, computers, and chairs.
Samples were collected once each week for 8 weeks during May and June of 2014.
RSV is a major cause of morbidity in very young children, and premature infants have a 10-fold increase in the risk of acquiring RSV infection. Hospital-acquired cases are an important cause of prolonged hospitalization, Dr. Homaira and her associates noted.
The findings suggest that personal clothing may be one of the modes of virus transmission, they said.
“Though the detection rate is low, personal clothing of caregivers/visitors do get contaminated with RSV,” Dr. Homaira said in a written statement, noting that caregivers and visitors are not required to change clothing when they walk into the NICU.
“There is a need for further research to evaluate how long the virus remains infectious on personal clothing, which will have policy implications in terms of need for use of separate gowns by the visitors while they are in the NICU,” Dr. Homaira added, concluding that frequent cleaning of high-touch areas and periodic screening of visitors for RSV as they enter the NICU during seasonal epidemics also may help limit disease transmission.
The investigators reported having no disclosures.
ATLANTA – Clothing worn by caregivers and visitors may be an important vehicle for the transmission of respiratory syncytial virus in the neonatal intensive care unit setting, according to findings from a prospective study conducted in an Australian hospital.
In an effort to identify potential sources of RSV transmission and to facilitate development of infection control strategies, the investigators swabbed all health personnel, every third neonate and their visitors, and any child clinically suspected of having an RSV infection. They detected RSV in one of 81 nasal specimens collected from 55 neonates and in 4% of 80 visitors’ clothing swabs, Nusrat Homaira, Ph.D., of the University of New South Wales, Sydney, and her colleagues reported in a poster at the International Conference on Emerging Infectious Diseases.
RSV also was detected in 1% of nose swabs from the visitors and in 1% of nose swabs from 84 health care workers.
No RSV was detected on the clothing of health care workers or on the hands of visitors or health care workers, which may be explained by the presence of alcohol-based hand rub at the point of care and by prevalent hand hygiene practices within the neonatal intensive care unit (NICU), the investigators noted.
The investigators also collected environmental swabs and detected RSV on 9% of high-touch areas, including bed rails; chairs; bed surfaces; countertops; and nurse’s and doctor’s station tables, computers, and chairs.
Samples were collected once each week for 8 weeks during May and June of 2014.
RSV is a major cause of morbidity in very young children, and premature infants have a 10-fold increase in the risk of acquiring RSV infection. Hospital-acquired cases are an important cause of prolonged hospitalization, Dr. Homaira and her associates noted.
The findings suggest that personal clothing may be one of the modes of virus transmission, they said.
“Though the detection rate is low, personal clothing of caregivers/visitors do get contaminated with RSV,” Dr. Homaira said in a written statement, noting that caregivers and visitors are not required to change clothing when they walk into the NICU.
“There is a need for further research to evaluate how long the virus remains infectious on personal clothing, which will have policy implications in terms of need for use of separate gowns by the visitors while they are in the NICU,” Dr. Homaira added, concluding that frequent cleaning of high-touch areas and periodic screening of visitors for RSV as they enter the NICU during seasonal epidemics also may help limit disease transmission.
The investigators reported having no disclosures.
AT ICEID 2015
Key clinical point: Clothing worn by caregivers and visitors may be an important vehicle for the transmission of respiratory syncytial virus in the neonatal intensive care unit setting.
Major finding: RSV was detected in 4% of 80 visitors’ clothing swabs.
Data source: A prospective study of 55 neonates, 80 visitors, and 85 health care workers.
Disclosures: The investigators reported having no disclosures.
Most pediatric norovirus cases occur from 6 to 23 months
ATLANTA – Norovirus vaccines currently in development should be administered before age 6 months to provide the most benefit, according to the findings of a global age distribution study.
The meta-analysis of data from 35 papers representing children from 23 countries showed that completion of the vaccination schedule by age 6 months could prevent about 85% of pediatric cases, compared with only about 50% of cases with delivery by age 12 months, Kayoko Shioda, D.V.M., of the National Center for Immunization and Respiratory Diseases at the Centers for Disease Control and Prevention, Atlanta, reported in a poster at the International Conference on Emerging Infectious Diseases.

For the study, Dr. Shioda and her colleagues at the CDC looked at studies involving norovirus cases among children under age 5 years. After weighting by the number of pediatric cases in each study, they found that 13% of cases occurred in those aged 0-5 months, 33% occurred among those aged 6-11 months, 36% occurred in those aged 12-23 months, and 18% were in those aged 24-59 months.
The age distribution was younger in developing countries vs. developed countries, in low income vs. high income countries, and in inpatient vs. outpatient and community settings, she said in an interview.
Also, the age distribution of severe cases was younger than for mild cases, she noted.
The findings suggest that early vaccination is particularly important in low-income settings, which had a younger age distribution that might be attributable to poorer hygiene and sanitation and/or higher levels of contact between individuals, she said, noting that the cumulative proportion of cases by 12 months was reduced by 4.1% for every $10,000 increase in per capita gross domestic product after controlling for study settings.
"Early vaccination is even more critical in low income countries, given the fact that more children get infected earlier," she added.
The findings were published earlier this summer (Vaccine. 2015, June doi: 10.1016/j.vaccine.2015.05.051).
Norovirus is increasingly recognized as a main cause of acute gastroenteritis, which occurs most often in young children. No vaccine is currently available, but one developed by Takeda is currently entering phase III trials, Dr. Shioda said.
This study was supported by the Oak Ridge (Tenn.) Institute for Science and Technology. Dr. Shioda reported having no other relevant disclosures.
ATLANTA – Norovirus vaccines currently in development should be administered before age 6 months to provide the most benefit, according to the findings of a global age distribution study.
The meta-analysis of data from 35 papers representing children from 23 countries showed that completion of the vaccination schedule by age 6 months could prevent about 85% of pediatric cases, compared with only about 50% of cases with delivery by age 12 months, Kayoko Shioda, D.V.M., of the National Center for Immunization and Respiratory Diseases at the Centers for Disease Control and Prevention, Atlanta, reported in a poster at the International Conference on Emerging Infectious Diseases.
For the study, Dr. Shioda and her colleagues at the CDC looked at studies involving norovirus cases among children under age 5 years. After weighting by the number of pediatric cases in each study, they found that 13% of cases occurred in those aged 0-5 months, 33% occurred among those aged 6-11 months, 36% occurred in those aged 12-23 months, and 18% were in those aged 24-59 months.
The age distribution was younger in developing countries vs. developed countries, in low income vs. high income countries, and in inpatient vs. outpatient and community settings, she said in an interview.
Also, the age distribution of severe cases was younger than for mild cases, she noted.
The findings suggest that early vaccination is particularly important in low-income settings, which had a younger age distribution that might be attributable to poorer hygiene and sanitation and/or higher levels of contact between individuals, she said, noting that the cumulative proportion of cases by 12 months was reduced by 4.1% for every $10,000 increase in per capita gross domestic product after controlling for study settings.
"Early vaccination is even more critical in low income countries, given the fact that more children get infected earlier," she added.
The findings were published earlier this summer (Vaccine. 2015, June doi: 10.1016/j.vaccine.2015.05.051).
Norovirus is increasingly recognized as a main cause of acute gastroenteritis, which occurs most often in young children. No vaccine is currently available, but one developed by Takeda is currently entering phase III trials, Dr. Shioda said.
This study was supported by the Oak Ridge (Tenn.) Institute for Science and Technology. Dr. Shioda reported having no other relevant disclosures.
ATLANTA – Norovirus vaccines currently in development should be administered before age 6 months to provide the most benefit, according to the findings of a global age distribution study.
The meta-analysis of data from 35 papers representing children from 23 countries showed that completion of the vaccination schedule by age 6 months could prevent about 85% of pediatric cases, compared with only about 50% of cases with delivery by age 12 months, Kayoko Shioda, D.V.M., of the National Center for Immunization and Respiratory Diseases at the Centers for Disease Control and Prevention, Atlanta, reported in a poster at the International Conference on Emerging Infectious Diseases.
For the study, Dr. Shioda and her colleagues at the CDC looked at studies involving norovirus cases among children under age 5 years. After weighting by the number of pediatric cases in each study, they found that 13% of cases occurred in those aged 0-5 months, 33% occurred among those aged 6-11 months, 36% occurred in those aged 12-23 months, and 18% were in those aged 24-59 months.
The age distribution was younger in developing countries vs. developed countries, in low income vs. high income countries, and in inpatient vs. outpatient and community settings, she said in an interview.
Also, the age distribution of severe cases was younger than for mild cases, she noted.
The findings suggest that early vaccination is particularly important in low-income settings, which had a younger age distribution that might be attributable to poorer hygiene and sanitation and/or higher levels of contact between individuals, she said, noting that the cumulative proportion of cases by 12 months was reduced by 4.1% for every $10,000 increase in per capita gross domestic product after controlling for study settings.
"Early vaccination is even more critical in low income countries, given the fact that more children get infected earlier," she added.
The findings were published earlier this summer (Vaccine. 2015, June doi: 10.1016/j.vaccine.2015.05.051).
Norovirus is increasingly recognized as a main cause of acute gastroenteritis, which occurs most often in young children. No vaccine is currently available, but one developed by Takeda is currently entering phase III trials, Dr. Shioda said.
This study was supported by the Oak Ridge (Tenn.) Institute for Science and Technology. Dr. Shioda reported having no other relevant disclosures.
AT ICEID 2015
Key clinical point: Should norovirus vaccines currently in development gain approval, immunization should be completed before age 6 months to provide the most benefit, according to the findings of a global age distribution study.
Major finding: Completion of a norovirus vaccination schedule by age 6 months could prevent about 85% of pediatric cases.
Data source: A meta-analysis of 35 studies.
Disclosures: This study was supported by the Oak Ridge (Tenn.) Institute for Science and Technology. Dr. Shioda reported having no other relevant disclosures.