User login
Mitchel is a reporter for MDedge based in the Philadelphia area. He started with the company in 1992, when it was International Medical News Group (IMNG), and has since covered a range of medical specialties. Mitchel trained as a virologist at Roswell Park Memorial Institute in Buffalo, and then worked briefly as a researcher at Boston Children's Hospital before pivoting to journalism as a AAAS Mass Media Fellow in 1980. His first reporting job was with Science Digest magazine, and from the mid-1980s to early-1990s he was a reporter with Medical World News. @mitchelzoler
FDA makes dabigatran contraindicated for mechanical valves
The FDA has declared the anticoagulant dabigatran contraindicated for patients with a mechanical heart valve, following anecdotal reports of blood clots forming on mechanical prosthetic valves and the abrupt stoppage of a phase II trial that had been testing dabigatran in this patient population.
"The U.S. Food and Drug Administration is informing health care professionals and the public that the blood thinner Pradaxa [dabigatran etexilate mesylate] should not be used to prevent stroke or blood clots in patients with mechanical heart valves," the agency said in a Drug Safety Communication.
"Health care professionals should promptly transition any patient with a mechanical heart valve who is taking Pradaxa to another medication," the agency added.
The statement also noted that the European-based, randomized phase II study to evaluate the safety and pharmacokinetics of oral dabigatran versus warfarin in patients after heart valve replacement (RE-ALIGN) (Am. Heart J. 2012;163:931-7) had been halted earlier in December by Boehringer Ingelheim, the company that markets Pradaxa, because the dabigatran-treated patients had shown an excess of strokes, myocardial infarctions, and blood clots that formed on the valves. Patients on dabigatran also had more episodes of bleeding after valve surgery than did patients on warfarin.
Although Boehringer Ingelheim and the researchers who ran the RE-ALIGN trial have not yet released the details of exactly what happened in the study, a report appeared in October from a group of cardiac surgeons at the Ottawa (Ont.) Heart Institute on their experience with two patients with mechanical heart valves who developed a thrombus on their valves and significant symptoms within 2 or 3 months of being switched from warfarin to dabigatran by their primary care physicians (J. Am. Coll. Cardiol. 2012;60:1710-1). These switches, which occurred even though dabigatran treatment in patients with mechanical prosthetic valves is an off-label use, probably represent the tip of the iceberg, said Dr. Munir Boodhwani, a cardiac surgeon at the Heart Institute and lead author of the two case reports.
"I suspect [this off-label use] is more common than we know. We see the problems, but we don’t know the denominator," he said in an interview. "In Ottawa, we routinely evaluate heart valve recipients every 6-12 months, and we have seen a few patients who had been switched from warfarin to dabigatran or another new oral anticoagulant. It has not been just one or two isolated cases. When we see these patients, we switch them back, and we send a message to their physician who made the switch that maybe this was not a good idea."
One of the cases he and his associates reported was a 51-year-old woman with a mechanical aortic valve who had been on warfarin for 8 years without complications and then was switched to 150 mg dabigatran twice daily by her general practitioner. Within 2 months, she developed crackles and a systolic murmur, and an echocardiogram revealed severe prosthetic aortic valve stenosis and a probable mass on the prosthesis. She arrived at the Heart Institute in cardiogenic shock and had cardiac arrest in the operating room. Surgery revealed an extensive thrombus on the valve, which was replaced. After surgery she had a complete recovery.
The second reported case was a 59-year-old woman with a mechanical mitral valve who had been on warfarin treatment without complications for about 4 years before being switched by her family physicians to 150 mg dabigatran twice daily. She developed progressive dyspnea, and an echocardiogram revealed a large thrombus on the valve. She underwent valve replacement and had an uneventful recovery.
Although phase III trial results showed dabigatran safe and effective for preventing blood clots and strokes in patients with nonvalvular atrial fibrillation, "atrial fibrillation is very different in a patient with a mechanical heart valve," Dr. Boodhwani said. "You cannot translate efficacy for one population to another. For atrial fibrillation, dosages of 110 mg b.i.d. and 150 mg b.i.d were effective [in the RE-LY trial; N. Engl. J. Med. 2009;361:1139-51], but in RE-ALIGN, dabigatran seems to have not been effective even at a dosage of 300 mg b.i.d. I think that Boehringer Ingelheim and the other companies that make the new anticoagulants need to go back to the drawing board and do more preclinical studies to determine what is a safe and effective dosage for anticoagulating patients with mechanical heart valves. It will likely need a higher dose, and then the question will be, What is the bleeding risk?"
The safety and efficacy results from nonvalvular atrial fibrillation patients in RE-LY are impossible to extrapolate to patients with mechanical valves, agreed Dr. Michael D. Ezekowitz, who was a coprincipal investigator for RE-LY but had no involvement in RE-ALIGN.
"It may be that a direct thrombin inhibitor [such as dabigatran] is not the drug of choice for preventing clots from forming on the surface of valves," Dr. Ezekowtiz said in an interview. "We have nearly 50 years of experience using warfarin for patients with mechanical heart valves, and that is clearly the drug of choice. This [RE-ALIGN] was probably a high-risk trial" in terms of trying to show that a new drug was at least as safe and effective as warfarin for heart valve patients.
Dr. Ezekowitz stressed that he has not been privy to any details of the RE-ALIGN results, but he suggested that it is hard to imagine that higher dabigatran dosages than the 300 mg b.i.d tested in RE-ALIGN could be used safely. "I was principal investigator for a phase II dabigatran study in atrial fibrillation, the PETRO [Prevention of Embolic and Thrombotic Events in Patients With Persistent AF] study (Am. J. Cardiol. 2007;100:1419-26). We tested up to 300 mg b.i.d., and in older atrial fibrillation patients this caused an excess of gastrointestinal bleeds and we decided to abandon that dosage in further testing. From a purely practical standpoint, I doubt whether a dabigatran dosage of more than 150 mg b.i.d would be tolerable," said Dr. Ezekowitz, professor of medicine at Jefferson Medical College in Philadelphia and director of atrial fibrillation research and education at the Cardiovascular Research Foundation in New York.
Some community physicians seem to have been mistakenly lured into prescribing dabigatran or other new anticoagulants to mechanical heart valve patients, perhaps because these physicians equated the newer drugs with better performance, Dr. Boodhwani said. But extrapolating the atrial fibrillation experience to heart-valve patients is premature, he warned.
"There is the potential for patients to die on these drugs. The off-label use can potentially be quite dangerous."
The FDA’s action and termination of the RE-ALIGN trial should send physicians a strong warning, he said. "This doesn’t close the door to future use of these drugs for mechanical valve patients, but physicians and industry need to be more cautious. The problems with warfarin need solutions, but only in a step-by-step way."
Dr. Boodhwani said he had no relevant financial disclosures. Dr. Ezekowitz said he has been a consultant to, has received honoraria as a lecturer on behalf of, and has received research funding from Boehringer Ingelheim, as well as from other drug companies that market antithrombotic drugs.
On Twitter @mitchelzoler
The FDA has declared the anticoagulant dabigatran contraindicated for patients with a mechanical heart valve, following anecdotal reports of blood clots forming on mechanical prosthetic valves and the abrupt stoppage of a phase II trial that had been testing dabigatran in this patient population.
"The U.S. Food and Drug Administration is informing health care professionals and the public that the blood thinner Pradaxa [dabigatran etexilate mesylate] should not be used to prevent stroke or blood clots in patients with mechanical heart valves," the agency said in a Drug Safety Communication.
"Health care professionals should promptly transition any patient with a mechanical heart valve who is taking Pradaxa to another medication," the agency added.
The statement also noted that the European-based, randomized phase II study to evaluate the safety and pharmacokinetics of oral dabigatran versus warfarin in patients after heart valve replacement (RE-ALIGN) (Am. Heart J. 2012;163:931-7) had been halted earlier in December by Boehringer Ingelheim, the company that markets Pradaxa, because the dabigatran-treated patients had shown an excess of strokes, myocardial infarctions, and blood clots that formed on the valves. Patients on dabigatran also had more episodes of bleeding after valve surgery than did patients on warfarin.
Although Boehringer Ingelheim and the researchers who ran the RE-ALIGN trial have not yet released the details of exactly what happened in the study, a report appeared in October from a group of cardiac surgeons at the Ottawa (Ont.) Heart Institute on their experience with two patients with mechanical heart valves who developed a thrombus on their valves and significant symptoms within 2 or 3 months of being switched from warfarin to dabigatran by their primary care physicians (J. Am. Coll. Cardiol. 2012;60:1710-1). These switches, which occurred even though dabigatran treatment in patients with mechanical prosthetic valves is an off-label use, probably represent the tip of the iceberg, said Dr. Munir Boodhwani, a cardiac surgeon at the Heart Institute and lead author of the two case reports.
"I suspect [this off-label use] is more common than we know. We see the problems, but we don’t know the denominator," he said in an interview. "In Ottawa, we routinely evaluate heart valve recipients every 6-12 months, and we have seen a few patients who had been switched from warfarin to dabigatran or another new oral anticoagulant. It has not been just one or two isolated cases. When we see these patients, we switch them back, and we send a message to their physician who made the switch that maybe this was not a good idea."
One of the cases he and his associates reported was a 51-year-old woman with a mechanical aortic valve who had been on warfarin for 8 years without complications and then was switched to 150 mg dabigatran twice daily by her general practitioner. Within 2 months, she developed crackles and a systolic murmur, and an echocardiogram revealed severe prosthetic aortic valve stenosis and a probable mass on the prosthesis. She arrived at the Heart Institute in cardiogenic shock and had cardiac arrest in the operating room. Surgery revealed an extensive thrombus on the valve, which was replaced. After surgery she had a complete recovery.
The second reported case was a 59-year-old woman with a mechanical mitral valve who had been on warfarin treatment without complications for about 4 years before being switched by her family physicians to 150 mg dabigatran twice daily. She developed progressive dyspnea, and an echocardiogram revealed a large thrombus on the valve. She underwent valve replacement and had an uneventful recovery.
Although phase III trial results showed dabigatran safe and effective for preventing blood clots and strokes in patients with nonvalvular atrial fibrillation, "atrial fibrillation is very different in a patient with a mechanical heart valve," Dr. Boodhwani said. "You cannot translate efficacy for one population to another. For atrial fibrillation, dosages of 110 mg b.i.d. and 150 mg b.i.d were effective [in the RE-LY trial; N. Engl. J. Med. 2009;361:1139-51], but in RE-ALIGN, dabigatran seems to have not been effective even at a dosage of 300 mg b.i.d. I think that Boehringer Ingelheim and the other companies that make the new anticoagulants need to go back to the drawing board and do more preclinical studies to determine what is a safe and effective dosage for anticoagulating patients with mechanical heart valves. It will likely need a higher dose, and then the question will be, What is the bleeding risk?"
The safety and efficacy results from nonvalvular atrial fibrillation patients in RE-LY are impossible to extrapolate to patients with mechanical valves, agreed Dr. Michael D. Ezekowitz, who was a coprincipal investigator for RE-LY but had no involvement in RE-ALIGN.
"It may be that a direct thrombin inhibitor [such as dabigatran] is not the drug of choice for preventing clots from forming on the surface of valves," Dr. Ezekowtiz said in an interview. "We have nearly 50 years of experience using warfarin for patients with mechanical heart valves, and that is clearly the drug of choice. This [RE-ALIGN] was probably a high-risk trial" in terms of trying to show that a new drug was at least as safe and effective as warfarin for heart valve patients.
Dr. Ezekowitz stressed that he has not been privy to any details of the RE-ALIGN results, but he suggested that it is hard to imagine that higher dabigatran dosages than the 300 mg b.i.d tested in RE-ALIGN could be used safely. "I was principal investigator for a phase II dabigatran study in atrial fibrillation, the PETRO [Prevention of Embolic and Thrombotic Events in Patients With Persistent AF] study (Am. J. Cardiol. 2007;100:1419-26). We tested up to 300 mg b.i.d., and in older atrial fibrillation patients this caused an excess of gastrointestinal bleeds and we decided to abandon that dosage in further testing. From a purely practical standpoint, I doubt whether a dabigatran dosage of more than 150 mg b.i.d would be tolerable," said Dr. Ezekowitz, professor of medicine at Jefferson Medical College in Philadelphia and director of atrial fibrillation research and education at the Cardiovascular Research Foundation in New York.
Some community physicians seem to have been mistakenly lured into prescribing dabigatran or other new anticoagulants to mechanical heart valve patients, perhaps because these physicians equated the newer drugs with better performance, Dr. Boodhwani said. But extrapolating the atrial fibrillation experience to heart-valve patients is premature, he warned.
"There is the potential for patients to die on these drugs. The off-label use can potentially be quite dangerous."
The FDA’s action and termination of the RE-ALIGN trial should send physicians a strong warning, he said. "This doesn’t close the door to future use of these drugs for mechanical valve patients, but physicians and industry need to be more cautious. The problems with warfarin need solutions, but only in a step-by-step way."
Dr. Boodhwani said he had no relevant financial disclosures. Dr. Ezekowitz said he has been a consultant to, has received honoraria as a lecturer on behalf of, and has received research funding from Boehringer Ingelheim, as well as from other drug companies that market antithrombotic drugs.
On Twitter @mitchelzoler
The FDA has declared the anticoagulant dabigatran contraindicated for patients with a mechanical heart valve, following anecdotal reports of blood clots forming on mechanical prosthetic valves and the abrupt stoppage of a phase II trial that had been testing dabigatran in this patient population.
"The U.S. Food and Drug Administration is informing health care professionals and the public that the blood thinner Pradaxa [dabigatran etexilate mesylate] should not be used to prevent stroke or blood clots in patients with mechanical heart valves," the agency said in a Drug Safety Communication.
"Health care professionals should promptly transition any patient with a mechanical heart valve who is taking Pradaxa to another medication," the agency added.
The statement also noted that the European-based, randomized phase II study to evaluate the safety and pharmacokinetics of oral dabigatran versus warfarin in patients after heart valve replacement (RE-ALIGN) (Am. Heart J. 2012;163:931-7) had been halted earlier in December by Boehringer Ingelheim, the company that markets Pradaxa, because the dabigatran-treated patients had shown an excess of strokes, myocardial infarctions, and blood clots that formed on the valves. Patients on dabigatran also had more episodes of bleeding after valve surgery than did patients on warfarin.
Although Boehringer Ingelheim and the researchers who ran the RE-ALIGN trial have not yet released the details of exactly what happened in the study, a report appeared in October from a group of cardiac surgeons at the Ottawa (Ont.) Heart Institute on their experience with two patients with mechanical heart valves who developed a thrombus on their valves and significant symptoms within 2 or 3 months of being switched from warfarin to dabigatran by their primary care physicians (J. Am. Coll. Cardiol. 2012;60:1710-1). These switches, which occurred even though dabigatran treatment in patients with mechanical prosthetic valves is an off-label use, probably represent the tip of the iceberg, said Dr. Munir Boodhwani, a cardiac surgeon at the Heart Institute and lead author of the two case reports.
"I suspect [this off-label use] is more common than we know. We see the problems, but we don’t know the denominator," he said in an interview. "In Ottawa, we routinely evaluate heart valve recipients every 6-12 months, and we have seen a few patients who had been switched from warfarin to dabigatran or another new oral anticoagulant. It has not been just one or two isolated cases. When we see these patients, we switch them back, and we send a message to their physician who made the switch that maybe this was not a good idea."
One of the cases he and his associates reported was a 51-year-old woman with a mechanical aortic valve who had been on warfarin for 8 years without complications and then was switched to 150 mg dabigatran twice daily by her general practitioner. Within 2 months, she developed crackles and a systolic murmur, and an echocardiogram revealed severe prosthetic aortic valve stenosis and a probable mass on the prosthesis. She arrived at the Heart Institute in cardiogenic shock and had cardiac arrest in the operating room. Surgery revealed an extensive thrombus on the valve, which was replaced. After surgery she had a complete recovery.
The second reported case was a 59-year-old woman with a mechanical mitral valve who had been on warfarin treatment without complications for about 4 years before being switched by her family physicians to 150 mg dabigatran twice daily. She developed progressive dyspnea, and an echocardiogram revealed a large thrombus on the valve. She underwent valve replacement and had an uneventful recovery.
Although phase III trial results showed dabigatran safe and effective for preventing blood clots and strokes in patients with nonvalvular atrial fibrillation, "atrial fibrillation is very different in a patient with a mechanical heart valve," Dr. Boodhwani said. "You cannot translate efficacy for one population to another. For atrial fibrillation, dosages of 110 mg b.i.d. and 150 mg b.i.d were effective [in the RE-LY trial; N. Engl. J. Med. 2009;361:1139-51], but in RE-ALIGN, dabigatran seems to have not been effective even at a dosage of 300 mg b.i.d. I think that Boehringer Ingelheim and the other companies that make the new anticoagulants need to go back to the drawing board and do more preclinical studies to determine what is a safe and effective dosage for anticoagulating patients with mechanical heart valves. It will likely need a higher dose, and then the question will be, What is the bleeding risk?"
The safety and efficacy results from nonvalvular atrial fibrillation patients in RE-LY are impossible to extrapolate to patients with mechanical valves, agreed Dr. Michael D. Ezekowitz, who was a coprincipal investigator for RE-LY but had no involvement in RE-ALIGN.
"It may be that a direct thrombin inhibitor [such as dabigatran] is not the drug of choice for preventing clots from forming on the surface of valves," Dr. Ezekowtiz said in an interview. "We have nearly 50 years of experience using warfarin for patients with mechanical heart valves, and that is clearly the drug of choice. This [RE-ALIGN] was probably a high-risk trial" in terms of trying to show that a new drug was at least as safe and effective as warfarin for heart valve patients.
Dr. Ezekowitz stressed that he has not been privy to any details of the RE-ALIGN results, but he suggested that it is hard to imagine that higher dabigatran dosages than the 300 mg b.i.d tested in RE-ALIGN could be used safely. "I was principal investigator for a phase II dabigatran study in atrial fibrillation, the PETRO [Prevention of Embolic and Thrombotic Events in Patients With Persistent AF] study (Am. J. Cardiol. 2007;100:1419-26). We tested up to 300 mg b.i.d., and in older atrial fibrillation patients this caused an excess of gastrointestinal bleeds and we decided to abandon that dosage in further testing. From a purely practical standpoint, I doubt whether a dabigatran dosage of more than 150 mg b.i.d would be tolerable," said Dr. Ezekowitz, professor of medicine at Jefferson Medical College in Philadelphia and director of atrial fibrillation research and education at the Cardiovascular Research Foundation in New York.
Some community physicians seem to have been mistakenly lured into prescribing dabigatran or other new anticoagulants to mechanical heart valve patients, perhaps because these physicians equated the newer drugs with better performance, Dr. Boodhwani said. But extrapolating the atrial fibrillation experience to heart-valve patients is premature, he warned.
"There is the potential for patients to die on these drugs. The off-label use can potentially be quite dangerous."
The FDA’s action and termination of the RE-ALIGN trial should send physicians a strong warning, he said. "This doesn’t close the door to future use of these drugs for mechanical valve patients, but physicians and industry need to be more cautious. The problems with warfarin need solutions, but only in a step-by-step way."
Dr. Boodhwani said he had no relevant financial disclosures. Dr. Ezekowitz said he has been a consultant to, has received honoraria as a lecturer on behalf of, and has received research funding from Boehringer Ingelheim, as well as from other drug companies that market antithrombotic drugs.
On Twitter @mitchelzoler
Minority of surgical ICU patients drive costs
PALM BEACH, FLA. – Only a small percent of all trauma and acute care surgery patients require more than 10 days in the ICU, but the ones who do rack up an enormous chunk of ICU costs, a single-center study with more than 6,000 U.S. patients has shown.
A more detailed look at what contributes to these very prolonged ICU stays and their costs may provide new opportunities for hospital cost controls, Dr. Samir M. Fakhry, FACS, said at the annual meeting of the Southern Surgical Association.
"I think we need a paradigm shift in how these patients are managed," such as a step-down protocol that allows them to exit the ICU and wean off their ventilator, said Dr. Fakhry, professor and chief of general surgery at the Medical University of South Carolina in Charleston.
But trauma and acute care surgery patients who need less than a day in the ICU can’t be ignored either. Although their per-patient cost is relatively small, their aggregate cost is high, because many patients fall into this group.
"You need two approaches" for trying to save on surgical ICU costs, one for patients who need prolonged intensive care and a second approach for patients who require only a day, he said. "For patients with short lengths of stay and lower costs, small things like one or two fewer doses of an antibiotic or fewer tests would make a difference" when multiplied by thousands of patients, Dr. Fahkry said. Further insight into ICU costs and cost-saving approaches could come from expanding his analysis to a larger number of U.S. surgical ICUs, he added.
His analysis of data collected by the surgical ICU at the Medical University of South Carolina, a level 1 trauma center, during 2007-2011 also highlighted that the number of patients admitted to the unit jumped by 26%, rising from 1,084 patients in fiscal year 2007 to 1,364 in FY 2011. The rise was especially pronounced among nontrauma patients, increasing from 319 in 2007 to 502 in 2011, a 57% rise.
Dr. Fahkry and his associates analyzed data from a total of 6,008 patients admitted to his hospital’s surgical ICU during the 5-year period studied. Costs for this care rose from $17,243 per patient in 2007 to $26,468 in 2011, a 53% increase.
A total of 423 of these patients, 7%, stayed in the ICU for more than 10 days. This group consisted primarily of trauma patients, 320 (76%) of the 423 patients. The average length of stay among the prolonged-stay patients was about 17 days, with an overall duration of hospitalization of 31 days. About three-quarters of these patients had at least three comorbidities. Mortality was also high in this subgroup, especially in the nontrauma patients, who had a 40% death rate; in-hospital mortality among the trauma patients with prolonged ICU stays was 10%.
Although accounting for just 7% of all surgical ICU patients, this subgroup racked up 41% of total ICU costs during the 5 years studied. In contrast, 4,236 surgical ICU patients who remained in the unit for less than a full day, 71% of all patients in the analysis, were responsible for 30% of total surgical ICU costs.
The analysis also identified another marker of substantially increased ICU costs: patients who ultimately died during their index hospitalization. Among nontrauma patients who died while hospitalized, the average costs were nearly $60,000 per patient, almost eightfold higher than for the nontrauma patients who survived hospitalization. Among the trauma patients, those who died ran up more than $31,000 in costs, nearly threefold higher than the trauma patients who survived.
Dr. Fahkry said he had no relevant financial disclosures.
On Twitter @mitchelzoler
PALM BEACH, FLA. – Only a small percent of all trauma and acute care surgery patients require more than 10 days in the ICU, but the ones who do rack up an enormous chunk of ICU costs, a single-center study with more than 6,000 U.S. patients has shown.
A more detailed look at what contributes to these very prolonged ICU stays and their costs may provide new opportunities for hospital cost controls, Dr. Samir M. Fakhry, FACS, said at the annual meeting of the Southern Surgical Association.
"I think we need a paradigm shift in how these patients are managed," such as a step-down protocol that allows them to exit the ICU and wean off their ventilator, said Dr. Fakhry, professor and chief of general surgery at the Medical University of South Carolina in Charleston.
But trauma and acute care surgery patients who need less than a day in the ICU can’t be ignored either. Although their per-patient cost is relatively small, their aggregate cost is high, because many patients fall into this group.
"You need two approaches" for trying to save on surgical ICU costs, one for patients who need prolonged intensive care and a second approach for patients who require only a day, he said. "For patients with short lengths of stay and lower costs, small things like one or two fewer doses of an antibiotic or fewer tests would make a difference" when multiplied by thousands of patients, Dr. Fahkry said. Further insight into ICU costs and cost-saving approaches could come from expanding his analysis to a larger number of U.S. surgical ICUs, he added.
His analysis of data collected by the surgical ICU at the Medical University of South Carolina, a level 1 trauma center, during 2007-2011 also highlighted that the number of patients admitted to the unit jumped by 26%, rising from 1,084 patients in fiscal year 2007 to 1,364 in FY 2011. The rise was especially pronounced among nontrauma patients, increasing from 319 in 2007 to 502 in 2011, a 57% rise.
Dr. Fahkry and his associates analyzed data from a total of 6,008 patients admitted to his hospital’s surgical ICU during the 5-year period studied. Costs for this care rose from $17,243 per patient in 2007 to $26,468 in 2011, a 53% increase.
A total of 423 of these patients, 7%, stayed in the ICU for more than 10 days. This group consisted primarily of trauma patients, 320 (76%) of the 423 patients. The average length of stay among the prolonged-stay patients was about 17 days, with an overall duration of hospitalization of 31 days. About three-quarters of these patients had at least three comorbidities. Mortality was also high in this subgroup, especially in the nontrauma patients, who had a 40% death rate; in-hospital mortality among the trauma patients with prolonged ICU stays was 10%.
Although accounting for just 7% of all surgical ICU patients, this subgroup racked up 41% of total ICU costs during the 5 years studied. In contrast, 4,236 surgical ICU patients who remained in the unit for less than a full day, 71% of all patients in the analysis, were responsible for 30% of total surgical ICU costs.
The analysis also identified another marker of substantially increased ICU costs: patients who ultimately died during their index hospitalization. Among nontrauma patients who died while hospitalized, the average costs were nearly $60,000 per patient, almost eightfold higher than for the nontrauma patients who survived hospitalization. Among the trauma patients, those who died ran up more than $31,000 in costs, nearly threefold higher than the trauma patients who survived.
Dr. Fahkry said he had no relevant financial disclosures.
On Twitter @mitchelzoler
PALM BEACH, FLA. – Only a small percent of all trauma and acute care surgery patients require more than 10 days in the ICU, but the ones who do rack up an enormous chunk of ICU costs, a single-center study with more than 6,000 U.S. patients has shown.
A more detailed look at what contributes to these very prolonged ICU stays and their costs may provide new opportunities for hospital cost controls, Dr. Samir M. Fakhry, FACS, said at the annual meeting of the Southern Surgical Association.
"I think we need a paradigm shift in how these patients are managed," such as a step-down protocol that allows them to exit the ICU and wean off their ventilator, said Dr. Fakhry, professor and chief of general surgery at the Medical University of South Carolina in Charleston.
But trauma and acute care surgery patients who need less than a day in the ICU can’t be ignored either. Although their per-patient cost is relatively small, their aggregate cost is high, because many patients fall into this group.
"You need two approaches" for trying to save on surgical ICU costs, one for patients who need prolonged intensive care and a second approach for patients who require only a day, he said. "For patients with short lengths of stay and lower costs, small things like one or two fewer doses of an antibiotic or fewer tests would make a difference" when multiplied by thousands of patients, Dr. Fahkry said. Further insight into ICU costs and cost-saving approaches could come from expanding his analysis to a larger number of U.S. surgical ICUs, he added.
His analysis of data collected by the surgical ICU at the Medical University of South Carolina, a level 1 trauma center, during 2007-2011 also highlighted that the number of patients admitted to the unit jumped by 26%, rising from 1,084 patients in fiscal year 2007 to 1,364 in FY 2011. The rise was especially pronounced among nontrauma patients, increasing from 319 in 2007 to 502 in 2011, a 57% rise.
Dr. Fahkry and his associates analyzed data from a total of 6,008 patients admitted to his hospital’s surgical ICU during the 5-year period studied. Costs for this care rose from $17,243 per patient in 2007 to $26,468 in 2011, a 53% increase.
A total of 423 of these patients, 7%, stayed in the ICU for more than 10 days. This group consisted primarily of trauma patients, 320 (76%) of the 423 patients. The average length of stay among the prolonged-stay patients was about 17 days, with an overall duration of hospitalization of 31 days. About three-quarters of these patients had at least three comorbidities. Mortality was also high in this subgroup, especially in the nontrauma patients, who had a 40% death rate; in-hospital mortality among the trauma patients with prolonged ICU stays was 10%.
Although accounting for just 7% of all surgical ICU patients, this subgroup racked up 41% of total ICU costs during the 5 years studied. In contrast, 4,236 surgical ICU patients who remained in the unit for less than a full day, 71% of all patients in the analysis, were responsible for 30% of total surgical ICU costs.
The analysis also identified another marker of substantially increased ICU costs: patients who ultimately died during their index hospitalization. Among nontrauma patients who died while hospitalized, the average costs were nearly $60,000 per patient, almost eightfold higher than for the nontrauma patients who survived hospitalization. Among the trauma patients, those who died ran up more than $31,000 in costs, nearly threefold higher than the trauma patients who survived.
Dr. Fahkry said he had no relevant financial disclosures.
On Twitter @mitchelzoler
AT THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: Seven percent of surgical ICU patients stayed for more than 10 days but accounted for 41% of the costs.
Data Source: A review of 6,008 postsurgery patients admitted to the ICU of a single U.S. center during 2007-2011.
Disclosures: Dr. Fahkry said he had no relevant financial disclosures.
Florida's trauma program succeeds at patient triage
PALM BEACH, FLA. – Florida’s statewide trauma triage system, one of America’s oldest and best organized state systems, did an increasingly better job over time from 1996 through 2010 funneling severely injured children and adults to one the state’s 22 designated trauma centers, according to data collected by the state government.
Florida’s program has had less clear-cut success triaging the elderly population with severe, acute trauma injuries to designated trauma centers, but the raw data may be misleading, Dr. David J. Ciesla, FACS, said at the annual meeting of the Southern Surgical Association.

Data collected by Florida’s Agency for Health Care Administration showed that during 2010, 41% of severely injured patients older than 65 years were discharged from a designated trauma center (DTC), compared with an 85% rate among adults 16-65 years old, and a 93% rate among children under age 16, said Dr. Ciesla, medical director of the Regional Trauma Program at Tampa General Hospital.
But the strikingly lower rate of elderly patient referral to a DTC may be an artifact of how Dr. Ciesla and his associates defined severe injury in their analysis. Their definition relied on survival. Using the ICD-9 Injury Severity Score (ICISS) to rate a patient’s need for DTC referral, they rated patients with ICISS of less than 0.85 (a less than 85% survival rate) as severely injured and candidates for DTC triage. But this criterion starts to break down for older patients, he explained.
"We defined injury severity as the risk of death, but that can be age related as well as injury related. It could be that older patients are more elderly than they are injured," he said.
Many of the elderly patients who were hospitalized for trauma "may be injured, but were they severely injured, or did they have high mortality because of their age or their comorbidities?" Dr. Ciesla said in an interview.
"I think the Florida system works well. We have shown [in these data] that the system can identify severely injured children and adults and get them to designated trauma centers. The elderly patients we’re calling ‘severely injured’ may just be elderly who can be appropriately treated in community hospitals," he said.

This interpretation received support from several surgeons who heard the talk at the meeting.
"The distribution of trauma centers on the basis of need is a critical issue in the 21st century health care paradigm. While we must assure equitable access to care delivered at the highest standard, and matched to the patient’s needs, we must assure that this is accomplished in a fiscally responsible way which avoids unnecessary duplication of resources and services. The work presented here today begins to probe this highly complex challenge," commented Dr. Michael F. Rotondo, FACS, professor and chairman of surgery at East Carolina University in Greenville, N.C.*
"Does Florida have enough trauma centers? These data basically say yes, we have enough," said Dr. Joseph J. Tepas III, FACS, professor and chief of pediatric surgery at the University of Florida in Jacksonville and a coauthor of the study. "Ninety percent of the patients were direct transfers" to a DTC, indicating that "paramedic triage discretion seems to work quite well" in routing injured patients to the appropriate hospital, he said.
The study run by Dr. Ciesla, Dr. Tepas, and their associates reviewed all patients discharged from Florida hospitals during 1996-2010 using data collected by the state agency. The researchers identified injured patients by their diagnostic codes, and analyzed them by their discharge hospital and by their home zip codes. The analysis showed that the percent of severely injured patients discharged from a DTC rose from fewer than half of the state’s patients in this category in 1996 to 63% in 2010.
Among 225 severely injured children, 210 (93%) were discharged from a DTC, with only 15 children who did not receive DTC treatment. The 2010 database also included 7,469 severely injured adults, with 85% discharged from a DTC, and 7,825 elderly patients, with 41% discharged from a DTC.
The analysis of DTC discharges of severely injured patients by their home zip codes identified an area of the Florida panhandle, near Panama City, where several adult patients failed to receive care at a DTC, suggesting that residents in this area of the state might be better served by opening another, nearby DTC, said Dr. Ciesla, who is also director of acute care surgery at the University of South Florida in Tampa.
"You need enough centers to cover everyone geographically, but not so many that you dilute" patient volume at individual centers, he said. The researchers have not yet analyzed the best DTC volume to produce optimal patient outcomes, he added.
Dr. Ciesla said that he and Dr. Tepas and their associates had no disclosures. Dr. Rotondo had no disclosures.
*CORRECTION: This story originally misquoted Dr. Michael F. Rotondo. His quote should have read: "The distribution of Trauma Centers on the basis of need is a critical issue in the 21st century health care paradigm. While we must assure equitable access to care delivered at the highest standard, and matched to the patient’s needs, we must assure that this is accomplished in a fiscally responsible way which avoids unnecessary duplication of resources and services. The work presented here today begins to probe this highly complex challenge."
PALM BEACH, FLA. – Florida’s statewide trauma triage system, one of America’s oldest and best organized state systems, did an increasingly better job over time from 1996 through 2010 funneling severely injured children and adults to one the state’s 22 designated trauma centers, according to data collected by the state government.
Florida’s program has had less clear-cut success triaging the elderly population with severe, acute trauma injuries to designated trauma centers, but the raw data may be misleading, Dr. David J. Ciesla, FACS, said at the annual meeting of the Southern Surgical Association.
Data collected by Florida’s Agency for Health Care Administration showed that during 2010, 41% of severely injured patients older than 65 years were discharged from a designated trauma center (DTC), compared with an 85% rate among adults 16-65 years old, and a 93% rate among children under age 16, said Dr. Ciesla, medical director of the Regional Trauma Program at Tampa General Hospital.
But the strikingly lower rate of elderly patient referral to a DTC may be an artifact of how Dr. Ciesla and his associates defined severe injury in their analysis. Their definition relied on survival. Using the ICD-9 Injury Severity Score (ICISS) to rate a patient’s need for DTC referral, they rated patients with ICISS of less than 0.85 (a less than 85% survival rate) as severely injured and candidates for DTC triage. But this criterion starts to break down for older patients, he explained.
"We defined injury severity as the risk of death, but that can be age related as well as injury related. It could be that older patients are more elderly than they are injured," he said.
Many of the elderly patients who were hospitalized for trauma "may be injured, but were they severely injured, or did they have high mortality because of their age or their comorbidities?" Dr. Ciesla said in an interview.
"I think the Florida system works well. We have shown [in these data] that the system can identify severely injured children and adults and get them to designated trauma centers. The elderly patients we’re calling ‘severely injured’ may just be elderly who can be appropriately treated in community hospitals," he said.
This interpretation received support from several surgeons who heard the talk at the meeting.
"The distribution of trauma centers on the basis of need is a critical issue in the 21st century health care paradigm. While we must assure equitable access to care delivered at the highest standard, and matched to the patient’s needs, we must assure that this is accomplished in a fiscally responsible way which avoids unnecessary duplication of resources and services. The work presented here today begins to probe this highly complex challenge," commented Dr. Michael F. Rotondo, FACS, professor and chairman of surgery at East Carolina University in Greenville, N.C.*
"Does Florida have enough trauma centers? These data basically say yes, we have enough," said Dr. Joseph J. Tepas III, FACS, professor and chief of pediatric surgery at the University of Florida in Jacksonville and a coauthor of the study. "Ninety percent of the patients were direct transfers" to a DTC, indicating that "paramedic triage discretion seems to work quite well" in routing injured patients to the appropriate hospital, he said.
The study run by Dr. Ciesla, Dr. Tepas, and their associates reviewed all patients discharged from Florida hospitals during 1996-2010 using data collected by the state agency. The researchers identified injured patients by their diagnostic codes, and analyzed them by their discharge hospital and by their home zip codes. The analysis showed that the percent of severely injured patients discharged from a DTC rose from fewer than half of the state’s patients in this category in 1996 to 63% in 2010.
Among 225 severely injured children, 210 (93%) were discharged from a DTC, with only 15 children who did not receive DTC treatment. The 2010 database also included 7,469 severely injured adults, with 85% discharged from a DTC, and 7,825 elderly patients, with 41% discharged from a DTC.
The analysis of DTC discharges of severely injured patients by their home zip codes identified an area of the Florida panhandle, near Panama City, where several adult patients failed to receive care at a DTC, suggesting that residents in this area of the state might be better served by opening another, nearby DTC, said Dr. Ciesla, who is also director of acute care surgery at the University of South Florida in Tampa.
"You need enough centers to cover everyone geographically, but not so many that you dilute" patient volume at individual centers, he said. The researchers have not yet analyzed the best DTC volume to produce optimal patient outcomes, he added.
Dr. Ciesla said that he and Dr. Tepas and their associates had no disclosures. Dr. Rotondo had no disclosures.
*CORRECTION: This story originally misquoted Dr. Michael F. Rotondo. His quote should have read: "The distribution of Trauma Centers on the basis of need is a critical issue in the 21st century health care paradigm. While we must assure equitable access to care delivered at the highest standard, and matched to the patient’s needs, we must assure that this is accomplished in a fiscally responsible way which avoids unnecessary duplication of resources and services. The work presented here today begins to probe this highly complex challenge."
PALM BEACH, FLA. – Florida’s statewide trauma triage system, one of America’s oldest and best organized state systems, did an increasingly better job over time from 1996 through 2010 funneling severely injured children and adults to one the state’s 22 designated trauma centers, according to data collected by the state government.
Florida’s program has had less clear-cut success triaging the elderly population with severe, acute trauma injuries to designated trauma centers, but the raw data may be misleading, Dr. David J. Ciesla, FACS, said at the annual meeting of the Southern Surgical Association.
Data collected by Florida’s Agency for Health Care Administration showed that during 2010, 41% of severely injured patients older than 65 years were discharged from a designated trauma center (DTC), compared with an 85% rate among adults 16-65 years old, and a 93% rate among children under age 16, said Dr. Ciesla, medical director of the Regional Trauma Program at Tampa General Hospital.
But the strikingly lower rate of elderly patient referral to a DTC may be an artifact of how Dr. Ciesla and his associates defined severe injury in their analysis. Their definition relied on survival. Using the ICD-9 Injury Severity Score (ICISS) to rate a patient’s need for DTC referral, they rated patients with ICISS of less than 0.85 (a less than 85% survival rate) as severely injured and candidates for DTC triage. But this criterion starts to break down for older patients, he explained.
"We defined injury severity as the risk of death, but that can be age related as well as injury related. It could be that older patients are more elderly than they are injured," he said.
Many of the elderly patients who were hospitalized for trauma "may be injured, but were they severely injured, or did they have high mortality because of their age or their comorbidities?" Dr. Ciesla said in an interview.
"I think the Florida system works well. We have shown [in these data] that the system can identify severely injured children and adults and get them to designated trauma centers. The elderly patients we’re calling ‘severely injured’ may just be elderly who can be appropriately treated in community hospitals," he said.
This interpretation received support from several surgeons who heard the talk at the meeting.
"The distribution of trauma centers on the basis of need is a critical issue in the 21st century health care paradigm. While we must assure equitable access to care delivered at the highest standard, and matched to the patient’s needs, we must assure that this is accomplished in a fiscally responsible way which avoids unnecessary duplication of resources and services. The work presented here today begins to probe this highly complex challenge," commented Dr. Michael F. Rotondo, FACS, professor and chairman of surgery at East Carolina University in Greenville, N.C.*
"Does Florida have enough trauma centers? These data basically say yes, we have enough," said Dr. Joseph J. Tepas III, FACS, professor and chief of pediatric surgery at the University of Florida in Jacksonville and a coauthor of the study. "Ninety percent of the patients were direct transfers" to a DTC, indicating that "paramedic triage discretion seems to work quite well" in routing injured patients to the appropriate hospital, he said.
The study run by Dr. Ciesla, Dr. Tepas, and their associates reviewed all patients discharged from Florida hospitals during 1996-2010 using data collected by the state agency. The researchers identified injured patients by their diagnostic codes, and analyzed them by their discharge hospital and by their home zip codes. The analysis showed that the percent of severely injured patients discharged from a DTC rose from fewer than half of the state’s patients in this category in 1996 to 63% in 2010.
Among 225 severely injured children, 210 (93%) were discharged from a DTC, with only 15 children who did not receive DTC treatment. The 2010 database also included 7,469 severely injured adults, with 85% discharged from a DTC, and 7,825 elderly patients, with 41% discharged from a DTC.
The analysis of DTC discharges of severely injured patients by their home zip codes identified an area of the Florida panhandle, near Panama City, where several adult patients failed to receive care at a DTC, suggesting that residents in this area of the state might be better served by opening another, nearby DTC, said Dr. Ciesla, who is also director of acute care surgery at the University of South Florida in Tampa.
"You need enough centers to cover everyone geographically, but not so many that you dilute" patient volume at individual centers, he said. The researchers have not yet analyzed the best DTC volume to produce optimal patient outcomes, he added.
Dr. Ciesla said that he and Dr. Tepas and their associates had no disclosures. Dr. Rotondo had no disclosures.
*CORRECTION: This story originally misquoted Dr. Michael F. Rotondo. His quote should have read: "The distribution of Trauma Centers on the basis of need is a critical issue in the 21st century health care paradigm. While we must assure equitable access to care delivered at the highest standard, and matched to the patient’s needs, we must assure that this is accomplished in a fiscally responsible way which avoids unnecessary duplication of resources and services. The work presented here today begins to probe this highly complex challenge."
AT THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: Among Florida’s severely injured patients in 2010, 93% of children, 85% of adults, and 41% of elderly went to trauma centers.
Data Source: Florida’s Agency for Health Care Administration data on injured patients discharged from hospitals during 1996-2010.
Disclosures: Dr. Ciesla said that he and Dr. Tepas and their associates had no disclosures. Dr. Rotondo had no disclosures.

Laparoscopic diverticulitis surgery linked to fewer complications
PALM BEACH, FLA.– Using laparoscopic surgery for colectomy with primary anastomosis in patients with complicated diverticulitis linked with significantly fewer major complications compared with open surgical management in a review of more than 10,000 patients from a nationwide database.
However, the inherent biases at play when surgeons decide whether to manage a diverticulitis patient by a laparoscopic or open approach make it difficult to draw definitive conclusions from the findings, Dr. Edward E. Cornwell III said at the annual meeting of the Southern Surgical Association.

"If a surgeon did an operation laparoscopically, that by itself is an indicator of how sick the patient was. The surgeon selects an open operation for sicker patients, and laparoscopy for the less sick patients," he said in an interview. "Have we accounted for that difference [in the analysis]? That’s an open question," said Dr. Cornwell, professor and chairman of surgery at Howard University in Washington.
"Patients whom the surgeon deem well enough physiologically to sustain colectomy with primary anastomosis deserve strong consideration for the laparoscopic approach because those patients had the greatest difference in complications" compared with open surgery, he said.
The data Dr. Cornwell and his associates reviewed also showed a marked skewing in how surgeons used laparoscopy. Among the 10,085 patients included in the analysis, 7,562 (75%) underwent colectomy with primary anastomosis, and in this subgroup, 5,105 patients (68%) had their surgery done laparoscopically, while the remaining 2,457 (32%) were done with open surgery. In contrast, the 2,523 other patients in the series underwent a colectomy with colostomy, and within this subgroup, 2,286 patients (91%) had open surgery, with only 237 (9%) having laparoscopic surgery.
The overwhelming use of open surgery for the colostomy patients makes sense as it is a more complex operation, Dr. Cornwell said.
He and his associates used data collected during 2005-2009 at 237 U.S. hospitals by the National Surgical Quality Improvement Program of the American College of Surgeons on patients who underwent surgical management of complicated diverticulitis. The average age of the patients was 58 years, and overall 30-day mortality was 2%, while the overall postoperative complication rate during the 30 days following surgery was 23%.
Among the patients who underwent a primary anastomosis, the incidence of major complications during 30 days of follow-up was 13% in the open surgery patients and 6% in the laparoscopy patients, a statistically significant difference. Major complications included surgical site infections, dehiscence, transfusion, respiratory failure, sepsis, myocardial infarction, pulmonary embolism, stroke, renal failure or need for rehospitalization.
In a multivariate analysis that controlled for demographic parameters, body mass index, comorbidities, and functional status, patients who underwent laparoscopy had about half the number of total complications and major complications compared with patients who underwent open surgery – statistically significant differences. The laparoscopically-treated patients also had roughly half the rate of several individual major complications – wound infections, respiratory complications, and sepsis – compared with the open surgery patients, all statistically significant differences.
Thirty-day mortality was about 50% lower with laparoscopy compared with open surgery among patients who underwent a primary anastomosis, but this difference fell short of statistical significance.
The advantage of laparoscopy over open surgery was not nearly so clear among patients who underwent colectomy with colostomy. The data showed no significant difference between laparoscopy and open surgery in the rate of all major complications, although the number of major complications with laparoscopy was about 20% lower. The only individual complications significantly reduced in the laparoscopy group were wound infections, reduced by about 40% in the adjusted analysis, and respiratory complications, cut by about 50% by laparoscopy. The two surgical subgroups showed virtually no difference in 30-day mortality among patients who underwent a colectomy.
The results suggest that because of the broad reduction of major complications with laparoscopy, this approach "should be considered when primary anastomosis is deemed appropriate," Dr. Cornwell concluded.
Dr. Cornwell said that he had no disclosures.
This work falls somewhat short of actually comparing the efficacy of the laparoscopic approach and open surgery in patients with complicated diverticulitis. Without an adequate standardized description of the disease process itself, the patients’ comorbidities, and their physiologic perturbation at the time of presentation, it is exceedingly difficult to measure outcomes and the efficacy of therapeutic interventions.
I’m afraid the authors have not satisfactorily controlled for or analyzed the confounding factors so that plausible conclusions can be reached. The results are striking that mortality and complications were higher for patients treated with open surgery. I have watched the evolution of laparoscopic surgery over the past 25 years, and I am convinced that patients greatly benefit from this technology.
While the laparoscopic approach for treating diverticulitis resonates with my sensibility, the data do not support a clear recommendation. I urge surgeons to focus on this emergency, general-surgery population so that we can do important comparative effectiveness research and address some of these questions.
Dr. Michael F. Rotondo is professor and chairman of surgery at East Carolina University in Greenville, N.C. He had no disclosures. He made these comments as a designated discussant of the report.
This work falls somewhat short of actually comparing the efficacy of the laparoscopic approach and open surgery in patients with complicated diverticulitis. Without an adequate standardized description of the disease process itself, the patients’ comorbidities, and their physiologic perturbation at the time of presentation, it is exceedingly difficult to measure outcomes and the efficacy of therapeutic interventions.
I’m afraid the authors have not satisfactorily controlled for or analyzed the confounding factors so that plausible conclusions can be reached. The results are striking that mortality and complications were higher for patients treated with open surgery. I have watched the evolution of laparoscopic surgery over the past 25 years, and I am convinced that patients greatly benefit from this technology.
While the laparoscopic approach for treating diverticulitis resonates with my sensibility, the data do not support a clear recommendation. I urge surgeons to focus on this emergency, general-surgery population so that we can do important comparative effectiveness research and address some of these questions.
Dr. Michael F. Rotondo is professor and chairman of surgery at East Carolina University in Greenville, N.C. He had no disclosures. He made these comments as a designated discussant of the report.
This work falls somewhat short of actually comparing the efficacy of the laparoscopic approach and open surgery in patients with complicated diverticulitis. Without an adequate standardized description of the disease process itself, the patients’ comorbidities, and their physiologic perturbation at the time of presentation, it is exceedingly difficult to measure outcomes and the efficacy of therapeutic interventions.
I’m afraid the authors have not satisfactorily controlled for or analyzed the confounding factors so that plausible conclusions can be reached. The results are striking that mortality and complications were higher for patients treated with open surgery. I have watched the evolution of laparoscopic surgery over the past 25 years, and I am convinced that patients greatly benefit from this technology.
While the laparoscopic approach for treating diverticulitis resonates with my sensibility, the data do not support a clear recommendation. I urge surgeons to focus on this emergency, general-surgery population so that we can do important comparative effectiveness research and address some of these questions.
Dr. Michael F. Rotondo is professor and chairman of surgery at East Carolina University in Greenville, N.C. He had no disclosures. He made these comments as a designated discussant of the report.
PALM BEACH, FLA.– Using laparoscopic surgery for colectomy with primary anastomosis in patients with complicated diverticulitis linked with significantly fewer major complications compared with open surgical management in a review of more than 10,000 patients from a nationwide database.
However, the inherent biases at play when surgeons decide whether to manage a diverticulitis patient by a laparoscopic or open approach make it difficult to draw definitive conclusions from the findings, Dr. Edward E. Cornwell III said at the annual meeting of the Southern Surgical Association.
"If a surgeon did an operation laparoscopically, that by itself is an indicator of how sick the patient was. The surgeon selects an open operation for sicker patients, and laparoscopy for the less sick patients," he said in an interview. "Have we accounted for that difference [in the analysis]? That’s an open question," said Dr. Cornwell, professor and chairman of surgery at Howard University in Washington.
"Patients whom the surgeon deem well enough physiologically to sustain colectomy with primary anastomosis deserve strong consideration for the laparoscopic approach because those patients had the greatest difference in complications" compared with open surgery, he said.
The data Dr. Cornwell and his associates reviewed also showed a marked skewing in how surgeons used laparoscopy. Among the 10,085 patients included in the analysis, 7,562 (75%) underwent colectomy with primary anastomosis, and in this subgroup, 5,105 patients (68%) had their surgery done laparoscopically, while the remaining 2,457 (32%) were done with open surgery. In contrast, the 2,523 other patients in the series underwent a colectomy with colostomy, and within this subgroup, 2,286 patients (91%) had open surgery, with only 237 (9%) having laparoscopic surgery.
The overwhelming use of open surgery for the colostomy patients makes sense as it is a more complex operation, Dr. Cornwell said.
He and his associates used data collected during 2005-2009 at 237 U.S. hospitals by the National Surgical Quality Improvement Program of the American College of Surgeons on patients who underwent surgical management of complicated diverticulitis. The average age of the patients was 58 years, and overall 30-day mortality was 2%, while the overall postoperative complication rate during the 30 days following surgery was 23%.
Among the patients who underwent a primary anastomosis, the incidence of major complications during 30 days of follow-up was 13% in the open surgery patients and 6% in the laparoscopy patients, a statistically significant difference. Major complications included surgical site infections, dehiscence, transfusion, respiratory failure, sepsis, myocardial infarction, pulmonary embolism, stroke, renal failure or need for rehospitalization.
In a multivariate analysis that controlled for demographic parameters, body mass index, comorbidities, and functional status, patients who underwent laparoscopy had about half the number of total complications and major complications compared with patients who underwent open surgery – statistically significant differences. The laparoscopically-treated patients also had roughly half the rate of several individual major complications – wound infections, respiratory complications, and sepsis – compared with the open surgery patients, all statistically significant differences.
Thirty-day mortality was about 50% lower with laparoscopy compared with open surgery among patients who underwent a primary anastomosis, but this difference fell short of statistical significance.
The advantage of laparoscopy over open surgery was not nearly so clear among patients who underwent colectomy with colostomy. The data showed no significant difference between laparoscopy and open surgery in the rate of all major complications, although the number of major complications with laparoscopy was about 20% lower. The only individual complications significantly reduced in the laparoscopy group were wound infections, reduced by about 40% in the adjusted analysis, and respiratory complications, cut by about 50% by laparoscopy. The two surgical subgroups showed virtually no difference in 30-day mortality among patients who underwent a colectomy.
The results suggest that because of the broad reduction of major complications with laparoscopy, this approach "should be considered when primary anastomosis is deemed appropriate," Dr. Cornwell concluded.
Dr. Cornwell said that he had no disclosures.
PALM BEACH, FLA.– Using laparoscopic surgery for colectomy with primary anastomosis in patients with complicated diverticulitis linked with significantly fewer major complications compared with open surgical management in a review of more than 10,000 patients from a nationwide database.
However, the inherent biases at play when surgeons decide whether to manage a diverticulitis patient by a laparoscopic or open approach make it difficult to draw definitive conclusions from the findings, Dr. Edward E. Cornwell III said at the annual meeting of the Southern Surgical Association.
"If a surgeon did an operation laparoscopically, that by itself is an indicator of how sick the patient was. The surgeon selects an open operation for sicker patients, and laparoscopy for the less sick patients," he said in an interview. "Have we accounted for that difference [in the analysis]? That’s an open question," said Dr. Cornwell, professor and chairman of surgery at Howard University in Washington.
"Patients whom the surgeon deem well enough physiologically to sustain colectomy with primary anastomosis deserve strong consideration for the laparoscopic approach because those patients had the greatest difference in complications" compared with open surgery, he said.
The data Dr. Cornwell and his associates reviewed also showed a marked skewing in how surgeons used laparoscopy. Among the 10,085 patients included in the analysis, 7,562 (75%) underwent colectomy with primary anastomosis, and in this subgroup, 5,105 patients (68%) had their surgery done laparoscopically, while the remaining 2,457 (32%) were done with open surgery. In contrast, the 2,523 other patients in the series underwent a colectomy with colostomy, and within this subgroup, 2,286 patients (91%) had open surgery, with only 237 (9%) having laparoscopic surgery.
The overwhelming use of open surgery for the colostomy patients makes sense as it is a more complex operation, Dr. Cornwell said.
He and his associates used data collected during 2005-2009 at 237 U.S. hospitals by the National Surgical Quality Improvement Program of the American College of Surgeons on patients who underwent surgical management of complicated diverticulitis. The average age of the patients was 58 years, and overall 30-day mortality was 2%, while the overall postoperative complication rate during the 30 days following surgery was 23%.
Among the patients who underwent a primary anastomosis, the incidence of major complications during 30 days of follow-up was 13% in the open surgery patients and 6% in the laparoscopy patients, a statistically significant difference. Major complications included surgical site infections, dehiscence, transfusion, respiratory failure, sepsis, myocardial infarction, pulmonary embolism, stroke, renal failure or need for rehospitalization.
In a multivariate analysis that controlled for demographic parameters, body mass index, comorbidities, and functional status, patients who underwent laparoscopy had about half the number of total complications and major complications compared with patients who underwent open surgery – statistically significant differences. The laparoscopically-treated patients also had roughly half the rate of several individual major complications – wound infections, respiratory complications, and sepsis – compared with the open surgery patients, all statistically significant differences.
Thirty-day mortality was about 50% lower with laparoscopy compared with open surgery among patients who underwent a primary anastomosis, but this difference fell short of statistical significance.
The advantage of laparoscopy over open surgery was not nearly so clear among patients who underwent colectomy with colostomy. The data showed no significant difference between laparoscopy and open surgery in the rate of all major complications, although the number of major complications with laparoscopy was about 20% lower. The only individual complications significantly reduced in the laparoscopy group were wound infections, reduced by about 40% in the adjusted analysis, and respiratory complications, cut by about 50% by laparoscopy. The two surgical subgroups showed virtually no difference in 30-day mortality among patients who underwent a colectomy.
The results suggest that because of the broad reduction of major complications with laparoscopy, this approach "should be considered when primary anastomosis is deemed appropriate," Dr. Cornwell concluded.
Dr. Cornwell said that he had no disclosures.
AT THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: Among patients who underwent a primary anastomosis, the incidence of major complications during 30 days of follow-up was 13% in the open surgery patients and 6% in the laparoscopy patients.
Data Source: From 10,085 U.S. patients who had surgery for acute management of complicated diverticulitis during 2005-2009.
Disclosures: Dr. Cornwell said he had no disclosures.
Pediatric influenza triage tool shows poor specificity
A Web-based tool designed to help parents and caregivers decide whether their children are sick enough with an influenzalike illness to warrant a trip to the emergency department showed woeful specificity in a pilot test of 294 adults.
"Our findings present a cautionary tale regarding the potential effects of self-triage tools," wrote Rebecca Anhang Price, Ph.D. and her associates in an article published online on Dec. 12.
"Safety was the chief concern" of the working group set up by the Centers for Disease Control and Prevention and the American Academy of Pediatrics that developed the Web-based triage tool in 2009 for parents and caregivers to use at home during that season’s novel influenza A (H1N1) pandemic. But the results of the current pilot study, which the CDC and AAP decided was necessary before making the triage tool available, showed an "unintended consequence" of the cautious approach taken by the working group: "Had it been made available to the public in its current form, it might have led more, rather than fewer, parents to bring their children to an ED [emergency department]," the authors wrote.
"Our goal was to reduce a massive surge of anxious parents" bringing children with flu-like illness to the ED, said Dr. Arthur L. Kellermann, senior investigator on the study. The web-based triage tool would ideally "help people who would otherwise opt to go to the ED recognize that their child was not at high risk and could instead be seen by a primary-care physician or walk-in clinic. We know that a number of kids who are brought to the ED don’t need to be there," he said in an interview.
The challenge is to devise a triage tool simple enough for most parents to use that will wind up directing essentially all critically ill children with influenza to an ED while maximizing the number who are not in immediate danger away from emergency services. "The goal is to provide help that enables that to happen more consistently," said Dr. Kellermann, an emergency medicine physician, senior policy analyst, and director of RAND Health in Arlington, Va.
The results of the triage tool’s pilot test showed how hard a goal that is. The study involved parents and caregivers aged 18 year or older who had brought a child aged 18 years or younger with a flu-like presentation during Feb.-April 2012 to either of two EDs, at Children’s National Medical Center in Washington at Inova Fairfax Hospital in Virginia. Parents worked through a Web-based questionnaire, called Strategy for Off-Site Rapid Triage (SORT) for Kids, in an average of just over 4 minutes. The tool used questions that included: Is it hard for the child to breath or is she breathing fast? Is she confused? Or having trouble staying awake?
To assess the accuracy of the triage tool’s decisions, the researchers matched the SORT for Kids recommendations against the actual outcomes of each case using electronic health records available for 286 children brought in by the 294 participants (Arch. Pediatr. Adolesc. Med. 2012 [doi:10.1001/jamapediatrics.2013.1573]).
Based on the health records, 15 of the ED visits (5%) were deemed clinically necessary. In addition, 8 of 165 parents (5%) reached for follow-up information reported bringing their child back to the ED for flu-like symptoms within a week of the index visit. None of these visits involved children whose cases had initially been classified as "necessary" according to explicit clinical criteria.
Of the 15 children who met explicit criteria for initial clinical necessity, 14 were flagged as high risk by SORT for Kids, a sensitivity of 93%. The one false negative was a 4-year old described by a parent as having a cough but not fever; the child subsequently needed intravenous fluids for dehydration and was discharged with a prescription for antibiotics and chest radiograph–confirmed diagnosis of pneumonia.
Among the 271 visits initially judged by clinical criteria as not medical emergencies, SORT for Kids identified 28 as low risk and 7 as intermediate risk, for a specificity of 13%. "The main reasons the algorithm classified so many of these children as high risk were that survey reports that the child had not urinated in the last 8 hours, was ‘fussy or cranky,’ was ‘much sleepier or more tired than usual,’ or was confused," the researchers said.
Sort for Kids initially flagged all eight children who required a return ED visit as high risk, a sensitivity of 100%. Of the 157 children with follow-up data who did not need later ED care, SORT for Kids had identified 13 as low risk and 4 as intermediate risk, a sensitivity of 11%.
The findings also showed that parents and caregivers were very comfortable using SORT for Kids. Ninety percent of users said the survey was "very easy" to understand, and another 8% called it "somewhat easy."
The next step will be larger-scale assessment of the existing SORT for Kids tool as well as testing of additional potential questions using about 2,000 children, at multiple U.S. sites in collaboration with the Pediatric Emergency Care Applied Research Network The results will "hopefully help us develop a more refined instrument," Dr. Kellermann said.
Dr. Price, Dr. Kellermann, and their coauthors said that they had no disclosures. Support for this pilot study was provided by a grant from the de Beaumont Foundation.
A Web-based tool designed to help parents and caregivers decide whether their children are sick enough with an influenzalike illness to warrant a trip to the emergency department showed woeful specificity in a pilot test of 294 adults.
"Our findings present a cautionary tale regarding the potential effects of self-triage tools," wrote Rebecca Anhang Price, Ph.D. and her associates in an article published online on Dec. 12.
"Safety was the chief concern" of the working group set up by the Centers for Disease Control and Prevention and the American Academy of Pediatrics that developed the Web-based triage tool in 2009 for parents and caregivers to use at home during that season’s novel influenza A (H1N1) pandemic. But the results of the current pilot study, which the CDC and AAP decided was necessary before making the triage tool available, showed an "unintended consequence" of the cautious approach taken by the working group: "Had it been made available to the public in its current form, it might have led more, rather than fewer, parents to bring their children to an ED [emergency department]," the authors wrote.
"Our goal was to reduce a massive surge of anxious parents" bringing children with flu-like illness to the ED, said Dr. Arthur L. Kellermann, senior investigator on the study. The web-based triage tool would ideally "help people who would otherwise opt to go to the ED recognize that their child was not at high risk and could instead be seen by a primary-care physician or walk-in clinic. We know that a number of kids who are brought to the ED don’t need to be there," he said in an interview.
The challenge is to devise a triage tool simple enough for most parents to use that will wind up directing essentially all critically ill children with influenza to an ED while maximizing the number who are not in immediate danger away from emergency services. "The goal is to provide help that enables that to happen more consistently," said Dr. Kellermann, an emergency medicine physician, senior policy analyst, and director of RAND Health in Arlington, Va.
The results of the triage tool’s pilot test showed how hard a goal that is. The study involved parents and caregivers aged 18 year or older who had brought a child aged 18 years or younger with a flu-like presentation during Feb.-April 2012 to either of two EDs, at Children’s National Medical Center in Washington at Inova Fairfax Hospital in Virginia. Parents worked through a Web-based questionnaire, called Strategy for Off-Site Rapid Triage (SORT) for Kids, in an average of just over 4 minutes. The tool used questions that included: Is it hard for the child to breath or is she breathing fast? Is she confused? Or having trouble staying awake?
To assess the accuracy of the triage tool’s decisions, the researchers matched the SORT for Kids recommendations against the actual outcomes of each case using electronic health records available for 286 children brought in by the 294 participants (Arch. Pediatr. Adolesc. Med. 2012 [doi:10.1001/jamapediatrics.2013.1573]).
Based on the health records, 15 of the ED visits (5%) were deemed clinically necessary. In addition, 8 of 165 parents (5%) reached for follow-up information reported bringing their child back to the ED for flu-like symptoms within a week of the index visit. None of these visits involved children whose cases had initially been classified as "necessary" according to explicit clinical criteria.
Of the 15 children who met explicit criteria for initial clinical necessity, 14 were flagged as high risk by SORT for Kids, a sensitivity of 93%. The one false negative was a 4-year old described by a parent as having a cough but not fever; the child subsequently needed intravenous fluids for dehydration and was discharged with a prescription for antibiotics and chest radiograph–confirmed diagnosis of pneumonia.
Among the 271 visits initially judged by clinical criteria as not medical emergencies, SORT for Kids identified 28 as low risk and 7 as intermediate risk, for a specificity of 13%. "The main reasons the algorithm classified so many of these children as high risk were that survey reports that the child had not urinated in the last 8 hours, was ‘fussy or cranky,’ was ‘much sleepier or more tired than usual,’ or was confused," the researchers said.
Sort for Kids initially flagged all eight children who required a return ED visit as high risk, a sensitivity of 100%. Of the 157 children with follow-up data who did not need later ED care, SORT for Kids had identified 13 as low risk and 4 as intermediate risk, a sensitivity of 11%.
The findings also showed that parents and caregivers were very comfortable using SORT for Kids. Ninety percent of users said the survey was "very easy" to understand, and another 8% called it "somewhat easy."
The next step will be larger-scale assessment of the existing SORT for Kids tool as well as testing of additional potential questions using about 2,000 children, at multiple U.S. sites in collaboration with the Pediatric Emergency Care Applied Research Network The results will "hopefully help us develop a more refined instrument," Dr. Kellermann said.
Dr. Price, Dr. Kellermann, and their coauthors said that they had no disclosures. Support for this pilot study was provided by a grant from the de Beaumont Foundation.
A Web-based tool designed to help parents and caregivers decide whether their children are sick enough with an influenzalike illness to warrant a trip to the emergency department showed woeful specificity in a pilot test of 294 adults.
"Our findings present a cautionary tale regarding the potential effects of self-triage tools," wrote Rebecca Anhang Price, Ph.D. and her associates in an article published online on Dec. 12.
"Safety was the chief concern" of the working group set up by the Centers for Disease Control and Prevention and the American Academy of Pediatrics that developed the Web-based triage tool in 2009 for parents and caregivers to use at home during that season’s novel influenza A (H1N1) pandemic. But the results of the current pilot study, which the CDC and AAP decided was necessary before making the triage tool available, showed an "unintended consequence" of the cautious approach taken by the working group: "Had it been made available to the public in its current form, it might have led more, rather than fewer, parents to bring their children to an ED [emergency department]," the authors wrote.
"Our goal was to reduce a massive surge of anxious parents" bringing children with flu-like illness to the ED, said Dr. Arthur L. Kellermann, senior investigator on the study. The web-based triage tool would ideally "help people who would otherwise opt to go to the ED recognize that their child was not at high risk and could instead be seen by a primary-care physician or walk-in clinic. We know that a number of kids who are brought to the ED don’t need to be there," he said in an interview.
The challenge is to devise a triage tool simple enough for most parents to use that will wind up directing essentially all critically ill children with influenza to an ED while maximizing the number who are not in immediate danger away from emergency services. "The goal is to provide help that enables that to happen more consistently," said Dr. Kellermann, an emergency medicine physician, senior policy analyst, and director of RAND Health in Arlington, Va.
The results of the triage tool’s pilot test showed how hard a goal that is. The study involved parents and caregivers aged 18 year or older who had brought a child aged 18 years or younger with a flu-like presentation during Feb.-April 2012 to either of two EDs, at Children’s National Medical Center in Washington at Inova Fairfax Hospital in Virginia. Parents worked through a Web-based questionnaire, called Strategy for Off-Site Rapid Triage (SORT) for Kids, in an average of just over 4 minutes. The tool used questions that included: Is it hard for the child to breath or is she breathing fast? Is she confused? Or having trouble staying awake?
To assess the accuracy of the triage tool’s decisions, the researchers matched the SORT for Kids recommendations against the actual outcomes of each case using electronic health records available for 286 children brought in by the 294 participants (Arch. Pediatr. Adolesc. Med. 2012 [doi:10.1001/jamapediatrics.2013.1573]).
Based on the health records, 15 of the ED visits (5%) were deemed clinically necessary. In addition, 8 of 165 parents (5%) reached for follow-up information reported bringing their child back to the ED for flu-like symptoms within a week of the index visit. None of these visits involved children whose cases had initially been classified as "necessary" according to explicit clinical criteria.
Of the 15 children who met explicit criteria for initial clinical necessity, 14 were flagged as high risk by SORT for Kids, a sensitivity of 93%. The one false negative was a 4-year old described by a parent as having a cough but not fever; the child subsequently needed intravenous fluids for dehydration and was discharged with a prescription for antibiotics and chest radiograph–confirmed diagnosis of pneumonia.
Among the 271 visits initially judged by clinical criteria as not medical emergencies, SORT for Kids identified 28 as low risk and 7 as intermediate risk, for a specificity of 13%. "The main reasons the algorithm classified so many of these children as high risk were that survey reports that the child had not urinated in the last 8 hours, was ‘fussy or cranky,’ was ‘much sleepier or more tired than usual,’ or was confused," the researchers said.
Sort for Kids initially flagged all eight children who required a return ED visit as high risk, a sensitivity of 100%. Of the 157 children with follow-up data who did not need later ED care, SORT for Kids had identified 13 as low risk and 4 as intermediate risk, a sensitivity of 11%.
The findings also showed that parents and caregivers were very comfortable using SORT for Kids. Ninety percent of users said the survey was "very easy" to understand, and another 8% called it "somewhat easy."
The next step will be larger-scale assessment of the existing SORT for Kids tool as well as testing of additional potential questions using about 2,000 children, at multiple U.S. sites in collaboration with the Pediatric Emergency Care Applied Research Network The results will "hopefully help us develop a more refined instrument," Dr. Kellermann said.
Dr. Price, Dr. Kellermann, and their coauthors said that they had no disclosures. Support for this pilot study was provided by a grant from the de Beaumont Foundation.
FROM ARCHIVES OF PEDIATRIC AND ADOLESCENT MEDICINE
Major Finding: The triage tool had sensitivity of 93%-100%, but its specificity for identifying low- or intermediate-risk children was 11%-13%.
Data Source: A pilot test of a web-based triage tool, SORT for Kids, by 294 parents or caregivers who had brought a child for evaluation of flu-like symptoms at any of three U.S. emergency departments.
Disclosures: Dr. Price, Dr. Kellermann, and their coauthors said that they had no disclosures. Support for this pilot study was provided by a grant from the de Beaumont Foundation.
Ruptured AAA triage to EVAR centers proposed
PALM BEACH, FLA. – The number of U.S. patients with ruptured abdominal aortic aneurysms who were managed with endovascular aneurysm repair more than doubled during 2005-2009, suggesting that it’s time to develop a national triage system in order to perform emergency endovascular repairs around the clock, according to Dr. John J. Ricotta.
"A strategy that promotes development of EVAR [endovascular aneurysm repair] centers with triage of stable, EVAR-suitable patients may be the best approach," said Dr. Ricotta, a vascular surgeon and chairman of surgery at MedStar Washington (D.C.) Hospital Center.
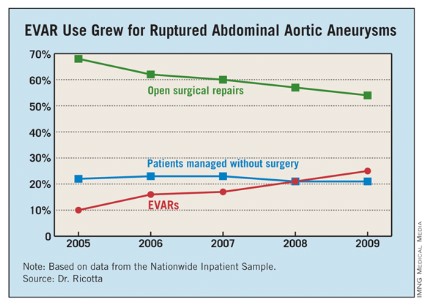
"Regionalization of EVAR services may be practical, along with a triage system to rapidly diagnose and transfer patients with RAAA [ruptured abdominal aortic aneurysm]," Dr. Ricotta said at the annual meeting of the Southern Surgical Association.
Because the time from the onset of symptoms to the start of successful EVAR repair is often more than 10 hours, stable RAAA patients could be transferred.
"The focus should be on older patients, who are more likely to survive if you do EVAR, and stable patients. Patients who are hemodynamically stable and have good anatomy [for performing EVAR] should go to an EVAR center."
Dr. Ricotta and his associates analyzed data collected from the U.S. Nationwide Inpatient Sample for all patients aged 60 years or older treated for RAAA during 2005-2009. During the 5-year period, a total of 21,218 patients in the sample underwent treatment for RAAA; 60% of the patients underwent open surgical repair, 22% had no operative repair, and 18% had EVAR.
Use of EVAR rose from 10% of RAAA patients in 2005 to 25% in 2009 (see table). Among the subset of patients who had surgical management, EVAR use rose from 13% of patients in 2005 to 32% in 2009.
EVAR was performed primarily at urban teaching hospitals and in patients under 90. Throughout the 5-year period, EVAR use at urban teaching hospitals included 25% of RAAA patients, compared with 12% of these patients managed at urban nonteaching hospitals and 7% of RAAA patients managed at rural hospitals. About 19% of RAAA patients 60-89 years old underwent EVAR, compared with 12% of those aged 90 or older.
EVAR effectively reduced mortality. Throughout the period studied, the rate of in-hospital mortality was 41% in patients managed with open surgery and 28% in those managed with EVAR, a significant difference, Dr. Ricotta said.
Furthermore, EVAR produced a mortality benefit compared with open surgery across the spectrum of patients, regardless of age. For example, among patients who were at least 90 years old, in-hospital mortality following EVAR was 36%, compared with 77% among patients who had open repair. In a multivariate analysis, EVAR was the only demographic or clinical variable associated with a significant reduction in postoperative in-hospital death, cutting mortality by 47%.
Despite EVAR’s success, use of the technique is limited by the anatomic and physiologic presentation of RAAA patients. "With current technology, EVAR is generally thought to be applicable to 30%-50% of RAAA patients," Dr. Ricotta said. "Experienced centers report the use of EVAR for about 50% of RAAA patients."
Dr. Ricotta called for regionalization and a triage and transfer model, because "widespread adoption of EVAR for RAAA is not practical," he said. "It is an expensive and evolving technology that needs a dedicated staff and a high volume of procedures." An EVAR-first program requires ready CT access and suitable imaging facilities in the operating room, a suitable stock of endografts, and an EVAR team that’s available 24/7, he said.
"Patients who are transferred might do better than patients who are not transferred," agreed Dr. Spence M. Taylor, a vascular surgeon and professor of surgery at the University of South Carolina in Greenville. But he added that patient selection may also play a role. "EVAR does better than open surgical repair in patients who can be stabilized and have this intervention compared with patients who can’t."
Dr. Ricotta and Dr. Taylor had no disclosures.
PALM BEACH, FLA. – The number of U.S. patients with ruptured abdominal aortic aneurysms who were managed with endovascular aneurysm repair more than doubled during 2005-2009, suggesting that it’s time to develop a national triage system in order to perform emergency endovascular repairs around the clock, according to Dr. John J. Ricotta.
"A strategy that promotes development of EVAR [endovascular aneurysm repair] centers with triage of stable, EVAR-suitable patients may be the best approach," said Dr. Ricotta, a vascular surgeon and chairman of surgery at MedStar Washington (D.C.) Hospital Center.
"Regionalization of EVAR services may be practical, along with a triage system to rapidly diagnose and transfer patients with RAAA [ruptured abdominal aortic aneurysm]," Dr. Ricotta said at the annual meeting of the Southern Surgical Association.
Because the time from the onset of symptoms to the start of successful EVAR repair is often more than 10 hours, stable RAAA patients could be transferred.
"The focus should be on older patients, who are more likely to survive if you do EVAR, and stable patients. Patients who are hemodynamically stable and have good anatomy [for performing EVAR] should go to an EVAR center."
Dr. Ricotta and his associates analyzed data collected from the U.S. Nationwide Inpatient Sample for all patients aged 60 years or older treated for RAAA during 2005-2009. During the 5-year period, a total of 21,218 patients in the sample underwent treatment for RAAA; 60% of the patients underwent open surgical repair, 22% had no operative repair, and 18% had EVAR.
Use of EVAR rose from 10% of RAAA patients in 2005 to 25% in 2009 (see table). Among the subset of patients who had surgical management, EVAR use rose from 13% of patients in 2005 to 32% in 2009.
EVAR was performed primarily at urban teaching hospitals and in patients under 90. Throughout the 5-year period, EVAR use at urban teaching hospitals included 25% of RAAA patients, compared with 12% of these patients managed at urban nonteaching hospitals and 7% of RAAA patients managed at rural hospitals. About 19% of RAAA patients 60-89 years old underwent EVAR, compared with 12% of those aged 90 or older.
EVAR effectively reduced mortality. Throughout the period studied, the rate of in-hospital mortality was 41% in patients managed with open surgery and 28% in those managed with EVAR, a significant difference, Dr. Ricotta said.
Furthermore, EVAR produced a mortality benefit compared with open surgery across the spectrum of patients, regardless of age. For example, among patients who were at least 90 years old, in-hospital mortality following EVAR was 36%, compared with 77% among patients who had open repair. In a multivariate analysis, EVAR was the only demographic or clinical variable associated with a significant reduction in postoperative in-hospital death, cutting mortality by 47%.
Despite EVAR’s success, use of the technique is limited by the anatomic and physiologic presentation of RAAA patients. "With current technology, EVAR is generally thought to be applicable to 30%-50% of RAAA patients," Dr. Ricotta said. "Experienced centers report the use of EVAR for about 50% of RAAA patients."
Dr. Ricotta called for regionalization and a triage and transfer model, because "widespread adoption of EVAR for RAAA is not practical," he said. "It is an expensive and evolving technology that needs a dedicated staff and a high volume of procedures." An EVAR-first program requires ready CT access and suitable imaging facilities in the operating room, a suitable stock of endografts, and an EVAR team that’s available 24/7, he said.
"Patients who are transferred might do better than patients who are not transferred," agreed Dr. Spence M. Taylor, a vascular surgeon and professor of surgery at the University of South Carolina in Greenville. But he added that patient selection may also play a role. "EVAR does better than open surgical repair in patients who can be stabilized and have this intervention compared with patients who can’t."
Dr. Ricotta and Dr. Taylor had no disclosures.
PALM BEACH, FLA. – The number of U.S. patients with ruptured abdominal aortic aneurysms who were managed with endovascular aneurysm repair more than doubled during 2005-2009, suggesting that it’s time to develop a national triage system in order to perform emergency endovascular repairs around the clock, according to Dr. John J. Ricotta.
"A strategy that promotes development of EVAR [endovascular aneurysm repair] centers with triage of stable, EVAR-suitable patients may be the best approach," said Dr. Ricotta, a vascular surgeon and chairman of surgery at MedStar Washington (D.C.) Hospital Center.
"Regionalization of EVAR services may be practical, along with a triage system to rapidly diagnose and transfer patients with RAAA [ruptured abdominal aortic aneurysm]," Dr. Ricotta said at the annual meeting of the Southern Surgical Association.
Because the time from the onset of symptoms to the start of successful EVAR repair is often more than 10 hours, stable RAAA patients could be transferred.
"The focus should be on older patients, who are more likely to survive if you do EVAR, and stable patients. Patients who are hemodynamically stable and have good anatomy [for performing EVAR] should go to an EVAR center."
Dr. Ricotta and his associates analyzed data collected from the U.S. Nationwide Inpatient Sample for all patients aged 60 years or older treated for RAAA during 2005-2009. During the 5-year period, a total of 21,218 patients in the sample underwent treatment for RAAA; 60% of the patients underwent open surgical repair, 22% had no operative repair, and 18% had EVAR.
Use of EVAR rose from 10% of RAAA patients in 2005 to 25% in 2009 (see table). Among the subset of patients who had surgical management, EVAR use rose from 13% of patients in 2005 to 32% in 2009.
EVAR was performed primarily at urban teaching hospitals and in patients under 90. Throughout the 5-year period, EVAR use at urban teaching hospitals included 25% of RAAA patients, compared with 12% of these patients managed at urban nonteaching hospitals and 7% of RAAA patients managed at rural hospitals. About 19% of RAAA patients 60-89 years old underwent EVAR, compared with 12% of those aged 90 or older.
EVAR effectively reduced mortality. Throughout the period studied, the rate of in-hospital mortality was 41% in patients managed with open surgery and 28% in those managed with EVAR, a significant difference, Dr. Ricotta said.
Furthermore, EVAR produced a mortality benefit compared with open surgery across the spectrum of patients, regardless of age. For example, among patients who were at least 90 years old, in-hospital mortality following EVAR was 36%, compared with 77% among patients who had open repair. In a multivariate analysis, EVAR was the only demographic or clinical variable associated with a significant reduction in postoperative in-hospital death, cutting mortality by 47%.
Despite EVAR’s success, use of the technique is limited by the anatomic and physiologic presentation of RAAA patients. "With current technology, EVAR is generally thought to be applicable to 30%-50% of RAAA patients," Dr. Ricotta said. "Experienced centers report the use of EVAR for about 50% of RAAA patients."
Dr. Ricotta called for regionalization and a triage and transfer model, because "widespread adoption of EVAR for RAAA is not practical," he said. "It is an expensive and evolving technology that needs a dedicated staff and a high volume of procedures." An EVAR-first program requires ready CT access and suitable imaging facilities in the operating room, a suitable stock of endografts, and an EVAR team that’s available 24/7, he said.
"Patients who are transferred might do better than patients who are not transferred," agreed Dr. Spence M. Taylor, a vascular surgeon and professor of surgery at the University of South Carolina in Greenville. But he added that patient selection may also play a role. "EVAR does better than open surgical repair in patients who can be stabilized and have this intervention compared with patients who can’t."
Dr. Ricotta and Dr. Taylor had no disclosures.
AT THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: From 2005 to 2009, the percentage of hospitalized U.S. patients with a ruptured AAA who underwent EVAR grew from 10% to 25%.
Data Source: The data came from an analysis of 21,218 U.S. patients hospitalized for a ruptured abdominal aortic aneurysm during 2005-2009 and included in the Nationwide Inpatient Sample.
Disclosures: Dr. Ricotta and Dr. Taylor had no disclosures.
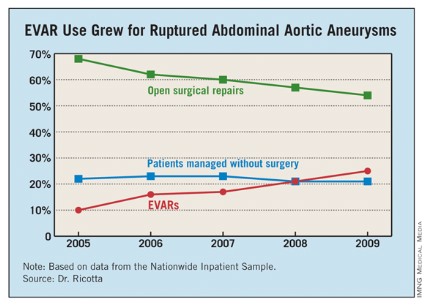
Antibiotic prophylaxis reduces colorectal surgery readmissions
PALM BEACH, FLA. – Administering a brief oral antibiotic regimen preoperatively to colorectal surgery patients cut the average postoperative hospitalization by more than a day and reduced 30-day readmissions by about 3% compared with no presurgical bowel preparation, a review of more than 8,000 patients found.
The primary driver of these beneficial effects was a reduced rate of surgical site infections, Dr. Mary T. Hawn said at the annual meeting of the Southern Surgical Association.
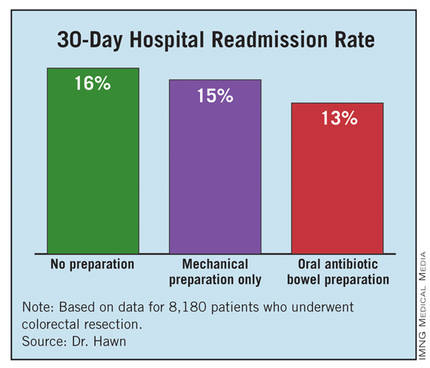
"Efforts to improve adherence with the use of oral antibiotic preparation may improve the efficiency of care for colorectal surgery," said Dr. Hawn, chief of gastrointestinal surgery at the University of Alabama, Birmingham. "Further research is needed to determine the best protocol for bowel prep prior to colorectal surgery, and to prospectively monitor the rate of Clostridium difficile infection."
The findings by Dr. Hawn’s group also showed that oral antibiotic bowel preparation (OABP) led to a small but statistically significant increase in the rate of hospital readmissions among patients with a principal diagnostic code of colitis caused by C. difficile infection. The OABP patients had a 0.5% readmission rate, compared with a 0.1% rate among patients who received no presurgical bowel preparation.
The value of OABP as shown in this study is particularly important because the use of OABP before colorectal surgery has declined in the United States over the past 20 years, Dr. Hawn added.
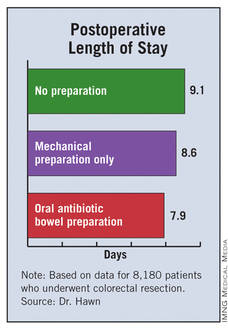
Using data collected as part of the VA Surgical Quality Improvement Program, Dr. Hawn and her colleagues analyzed results for 8,180 patients who underwent elective colorectal resection at any of 112 participating VA hospitals during 2005-2009. Patients who had a partial or total colectomy, a rectal resection, or an ostomy were included. Patients were excluded if they had a preoperative stay of more than 2 days, a postoperative stay of more than 30 days, or an American Surgical Association 5 classification, or if they died before hospital discharge.
Most of the patients (83%) underwent surgery for neoplasms; the next most common reason for surgery was diverticulitis, in 6%. OABP was the most common form of presurgical preparation, used on 44% of patients; mechanical preparation only was used on 39%, and no preparation was done in 17%. Ninety percent of the OABP patients also underwent mechanical preparation, while the other 10% had OABP only.
The average postoperative length of stay was 9.1 days among those who received no preparation, 8.6 days for those who got mechanical preparation only, and 7.9 days for those who had OABP – a statistically significant advantage for OABP. In a multivariate regression analysis that controlled for indication, age, and wound class, OABP cut length of stay by an average of 12% compared with no preparation, a statistically significant reduction. In the same analysis, mechanical preparation cut length of stay by only 4% compared with no preparation, also a significant effect.
The hospital readmission rate was 16% with no preparation, 15% with mechanical preparation only, and 13% with OABP. In the multivariate regression analysis with adjustment for procedure, age, and wound class, OABP cut the readmission rate by 19% compared with no preparation, a statistically significant reduction. Mechanical preparation only did not have a statistically significant effect.

Further analyses showed that the most common reason for readmission among all patients studied was postoperative infection, in 18%, followed by digestive-system complications, in 10%. C. difficile infection caused 3% of readmissions.
In addition, infections were responsible for readmissions among 6% of patients who underwent no presurgical preparation and in 4% of those who underwent OABP, a statistically significant difference. In contrast, use of OABP produced no statistically significant decline in noninfectious causes of readmission. This rate ran 10% among patients with no preparation, and 9% in patients who underwent OABP.
Dr. Hawn said that she had no disclosures.
Surgical site infections (SSIs) remain a vexing problem despite the significant efforts by hospitals to increase compliance with measures of the Surgical Care Improvement Project. These efforts have so far failed to translate into improved outcomes. We need to identify additional processes that can be changed to improve surgical outcomes.
Elizabeth C. Wick |

At Johns Hopkins, we addressed SSIs by implementing the Comprehensive Unit-Based Safety Program for patients undergoing colorectal surgery. Interventions included standardization of skin preparation, administration of preoperative chlorhexidine showers, selective elimination of mechanical bowel preparation, warming of patients in the preanesthesia area, adoption of enhanced sterile techniques for skin and fascial closure, and addressing previously unrecognized lapses in antibiotic prophylaxis. The program was modeled on ICU processes designed to prevent central line bloodstream infections.
Our program improved the operating room culture by engaging and empowering front-line staff to address deficits and improve processes. A recent review of the rate of SSIs during the 12 months prior to and the 12 months after implementation of this program found that infection rates fell from 27% before implementation to 18% afterward – a 33% relative decrease (J. Am. Coll. Surg. 2012;215:193-200).
We are expanding this program to colon surgery programs at more than 100 U.S. hospitals. Hospitals want to institute new processes proven to improve patient outcomes. The report by Dr. Hawn and her associates is an important step toward identifying a new approach that might further reduce SSIs.
Dr. Elizabeth C. Wick is a colorectal surgeon at Johns Hopkins Hospital in Baltimore. She had no disclosures. She made these comments as a designated discussant for Dr. Hawn’s report.
Surgical site infections (SSIs) remain a vexing problem despite the significant efforts by hospitals to increase compliance with measures of the Surgical Care Improvement Project. These efforts have so far failed to translate into improved outcomes. We need to identify additional processes that can be changed to improve surgical outcomes.
Elizabeth C. Wick |
At Johns Hopkins, we addressed SSIs by implementing the Comprehensive Unit-Based Safety Program for patients undergoing colorectal surgery. Interventions included standardization of skin preparation, administration of preoperative chlorhexidine showers, selective elimination of mechanical bowel preparation, warming of patients in the preanesthesia area, adoption of enhanced sterile techniques for skin and fascial closure, and addressing previously unrecognized lapses in antibiotic prophylaxis. The program was modeled on ICU processes designed to prevent central line bloodstream infections.
Our program improved the operating room culture by engaging and empowering front-line staff to address deficits and improve processes. A recent review of the rate of SSIs during the 12 months prior to and the 12 months after implementation of this program found that infection rates fell from 27% before implementation to 18% afterward – a 33% relative decrease (J. Am. Coll. Surg. 2012;215:193-200).
We are expanding this program to colon surgery programs at more than 100 U.S. hospitals. Hospitals want to institute new processes proven to improve patient outcomes. The report by Dr. Hawn and her associates is an important step toward identifying a new approach that might further reduce SSIs.
Dr. Elizabeth C. Wick is a colorectal surgeon at Johns Hopkins Hospital in Baltimore. She had no disclosures. She made these comments as a designated discussant for Dr. Hawn’s report.
Surgical site infections (SSIs) remain a vexing problem despite the significant efforts by hospitals to increase compliance with measures of the Surgical Care Improvement Project. These efforts have so far failed to translate into improved outcomes. We need to identify additional processes that can be changed to improve surgical outcomes.
Elizabeth C. Wick |
At Johns Hopkins, we addressed SSIs by implementing the Comprehensive Unit-Based Safety Program for patients undergoing colorectal surgery. Interventions included standardization of skin preparation, administration of preoperative chlorhexidine showers, selective elimination of mechanical bowel preparation, warming of patients in the preanesthesia area, adoption of enhanced sterile techniques for skin and fascial closure, and addressing previously unrecognized lapses in antibiotic prophylaxis. The program was modeled on ICU processes designed to prevent central line bloodstream infections.
Our program improved the operating room culture by engaging and empowering front-line staff to address deficits and improve processes. A recent review of the rate of SSIs during the 12 months prior to and the 12 months after implementation of this program found that infection rates fell from 27% before implementation to 18% afterward – a 33% relative decrease (J. Am. Coll. Surg. 2012;215:193-200).
We are expanding this program to colon surgery programs at more than 100 U.S. hospitals. Hospitals want to institute new processes proven to improve patient outcomes. The report by Dr. Hawn and her associates is an important step toward identifying a new approach that might further reduce SSIs.
Dr. Elizabeth C. Wick is a colorectal surgeon at Johns Hopkins Hospital in Baltimore. She had no disclosures. She made these comments as a designated discussant for Dr. Hawn’s report.
PALM BEACH, FLA. – Administering a brief oral antibiotic regimen preoperatively to colorectal surgery patients cut the average postoperative hospitalization by more than a day and reduced 30-day readmissions by about 3% compared with no presurgical bowel preparation, a review of more than 8,000 patients found.
The primary driver of these beneficial effects was a reduced rate of surgical site infections, Dr. Mary T. Hawn said at the annual meeting of the Southern Surgical Association.
"Efforts to improve adherence with the use of oral antibiotic preparation may improve the efficiency of care for colorectal surgery," said Dr. Hawn, chief of gastrointestinal surgery at the University of Alabama, Birmingham. "Further research is needed to determine the best protocol for bowel prep prior to colorectal surgery, and to prospectively monitor the rate of Clostridium difficile infection."
The findings by Dr. Hawn’s group also showed that oral antibiotic bowel preparation (OABP) led to a small but statistically significant increase in the rate of hospital readmissions among patients with a principal diagnostic code of colitis caused by C. difficile infection. The OABP patients had a 0.5% readmission rate, compared with a 0.1% rate among patients who received no presurgical bowel preparation.
The value of OABP as shown in this study is particularly important because the use of OABP before colorectal surgery has declined in the United States over the past 20 years, Dr. Hawn added.
Using data collected as part of the VA Surgical Quality Improvement Program, Dr. Hawn and her colleagues analyzed results for 8,180 patients who underwent elective colorectal resection at any of 112 participating VA hospitals during 2005-2009. Patients who had a partial or total colectomy, a rectal resection, or an ostomy were included. Patients were excluded if they had a preoperative stay of more than 2 days, a postoperative stay of more than 30 days, or an American Surgical Association 5 classification, or if they died before hospital discharge.
Most of the patients (83%) underwent surgery for neoplasms; the next most common reason for surgery was diverticulitis, in 6%. OABP was the most common form of presurgical preparation, used on 44% of patients; mechanical preparation only was used on 39%, and no preparation was done in 17%. Ninety percent of the OABP patients also underwent mechanical preparation, while the other 10% had OABP only.
The average postoperative length of stay was 9.1 days among those who received no preparation, 8.6 days for those who got mechanical preparation only, and 7.9 days for those who had OABP – a statistically significant advantage for OABP. In a multivariate regression analysis that controlled for indication, age, and wound class, OABP cut length of stay by an average of 12% compared with no preparation, a statistically significant reduction. In the same analysis, mechanical preparation cut length of stay by only 4% compared with no preparation, also a significant effect.
The hospital readmission rate was 16% with no preparation, 15% with mechanical preparation only, and 13% with OABP. In the multivariate regression analysis with adjustment for procedure, age, and wound class, OABP cut the readmission rate by 19% compared with no preparation, a statistically significant reduction. Mechanical preparation only did not have a statistically significant effect.
Further analyses showed that the most common reason for readmission among all patients studied was postoperative infection, in 18%, followed by digestive-system complications, in 10%. C. difficile infection caused 3% of readmissions.
In addition, infections were responsible for readmissions among 6% of patients who underwent no presurgical preparation and in 4% of those who underwent OABP, a statistically significant difference. In contrast, use of OABP produced no statistically significant decline in noninfectious causes of readmission. This rate ran 10% among patients with no preparation, and 9% in patients who underwent OABP.
Dr. Hawn said that she had no disclosures.
PALM BEACH, FLA. – Administering a brief oral antibiotic regimen preoperatively to colorectal surgery patients cut the average postoperative hospitalization by more than a day and reduced 30-day readmissions by about 3% compared with no presurgical bowel preparation, a review of more than 8,000 patients found.
The primary driver of these beneficial effects was a reduced rate of surgical site infections, Dr. Mary T. Hawn said at the annual meeting of the Southern Surgical Association.
"Efforts to improve adherence with the use of oral antibiotic preparation may improve the efficiency of care for colorectal surgery," said Dr. Hawn, chief of gastrointestinal surgery at the University of Alabama, Birmingham. "Further research is needed to determine the best protocol for bowel prep prior to colorectal surgery, and to prospectively monitor the rate of Clostridium difficile infection."
The findings by Dr. Hawn’s group also showed that oral antibiotic bowel preparation (OABP) led to a small but statistically significant increase in the rate of hospital readmissions among patients with a principal diagnostic code of colitis caused by C. difficile infection. The OABP patients had a 0.5% readmission rate, compared with a 0.1% rate among patients who received no presurgical bowel preparation.
The value of OABP as shown in this study is particularly important because the use of OABP before colorectal surgery has declined in the United States over the past 20 years, Dr. Hawn added.
Using data collected as part of the VA Surgical Quality Improvement Program, Dr. Hawn and her colleagues analyzed results for 8,180 patients who underwent elective colorectal resection at any of 112 participating VA hospitals during 2005-2009. Patients who had a partial or total colectomy, a rectal resection, or an ostomy were included. Patients were excluded if they had a preoperative stay of more than 2 days, a postoperative stay of more than 30 days, or an American Surgical Association 5 classification, or if they died before hospital discharge.
Most of the patients (83%) underwent surgery for neoplasms; the next most common reason for surgery was diverticulitis, in 6%. OABP was the most common form of presurgical preparation, used on 44% of patients; mechanical preparation only was used on 39%, and no preparation was done in 17%. Ninety percent of the OABP patients also underwent mechanical preparation, while the other 10% had OABP only.
The average postoperative length of stay was 9.1 days among those who received no preparation, 8.6 days for those who got mechanical preparation only, and 7.9 days for those who had OABP – a statistically significant advantage for OABP. In a multivariate regression analysis that controlled for indication, age, and wound class, OABP cut length of stay by an average of 12% compared with no preparation, a statistically significant reduction. In the same analysis, mechanical preparation cut length of stay by only 4% compared with no preparation, also a significant effect.
The hospital readmission rate was 16% with no preparation, 15% with mechanical preparation only, and 13% with OABP. In the multivariate regression analysis with adjustment for procedure, age, and wound class, OABP cut the readmission rate by 19% compared with no preparation, a statistically significant reduction. Mechanical preparation only did not have a statistically significant effect.
Further analyses showed that the most common reason for readmission among all patients studied was postoperative infection, in 18%, followed by digestive-system complications, in 10%. C. difficile infection caused 3% of readmissions.
In addition, infections were responsible for readmissions among 6% of patients who underwent no presurgical preparation and in 4% of those who underwent OABP, a statistically significant difference. In contrast, use of OABP produced no statistically significant decline in noninfectious causes of readmission. This rate ran 10% among patients with no preparation, and 9% in patients who underwent OABP.
Dr. Hawn said that she had no disclosures.
AT THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: Oral antibiotic preparation before colorectal surgery cut hospital readmissions by 19% compared with no preparation.
Data Source: A review of 8,180 U.S. patients who underwent colorectal surgery during 2005-2009 at 112 VA hospitals.
Disclosures: Dr. Hawn said that she had no disclosures.

Bariatric surgery cut vascular events in diabetes
PALM BEACH, FLA. – Add another notch to the evidence base for bariatric surgery as effective treatment for type 2 diabetes in obese patients.
Patients with type 2 diabetes who underwent any type of bariatric surgery had a 61%-78% relative risk reduction in their rate of macrovascular, microvascular, or vascular events during an average 20-month follow-up in a review of more than 15,000 cases in South Carolina.

"We are trying to get primary care physicians to spread the word [to patients] that bariatric surgery has come a long way over the past 30 or 40 years; the risk-to-reward ratio is much more beneficial to patients," Dr. John D. Scott said at the annual meeting of the Southern Surgical Association.
The new finding "adds to the extensive list of papers that show bariatric surgery mitigates the long-term effects of type 2 diabetes," Dr. Scott added in an interview. "Some front-line medical providers still see bariatric surgery as a procedure of last resort, but findings like ours show that a discussion [with patients on whether they should consider bariatric surgery] should happen a lot sooner."
Dr. Scott, a surgeon at University Medical Center in Greenville, S.C., recommended that patients with a body mass index of at least 35 kg/m2 and two or more comorbidities be told that they have the option of undergoing bariatric surgery and reducing their risk.
"We have an epidemic [of obesity and type 2 diabetes], and for the first time since tuberculosis, this is an epidemic where surgery has a real opportunity to positively intervene," commented Dr. Josef E. Fischer, a professor of surgery at Harvard Medical School in Boston.
The study used hospital billing data collected by the South Carolina Office of Research and Statistics as well as state vital records data for 1995-2009. The analysis included 2,580 obese patients who underwent any type of bariatric surgery and 13,371 obese patients who did not have surgery. The researchers extracted the data from records of nearly 34,000 obese patients, but excluded patients with type 1 diabetes, patients with incomplete data, and patients with advanced cardiovascular or microvascular disease at the time of their surgery or entry into the state records during this period.
During a median follow-up of about 20 months, the rate of new-onset macro- or microvascular events was 2% in the bariatric surgery patients and 11% in the patients who did not undergo surgery. The rate of an incident vascular disease event was 2% in the patients who had surgery and 13% in those who did not. Macrovascular events included myocardial infarction, stroke, and all-cause death. Microvascular events included blindness in at least one eye, laser eye surgery, nontraumatic amputation, or placement of access for dialysis. Other vascular events included new-onset heart failure or angina, or revascularization of a coronary, carotid, or peripheral artery.
In a multivariate-adjusted analysis, patients who underwent bariatric surgery had a 61% reduction in macrovascular events, a 78% reduction in microvascular events, a 75% reduction in vascular events, and a 64% reduction in combined macro- and microvascular events, compared with patients who did not have this surgery – all statistically significant differences, reported Dr. Spence M. Taylor, a coinvestigator with Dr. Scott on the study. A propensity-score matched analysis that compared the bariatric surgery patients and matched nonsurgical patients showed very similar reductions in all three event categories.
"Bariatric surgery has a substantial and lasting mitigating association on major complications associated with type 2 diabetes in the obese population," concluded Dr. Taylor, chairman of surgery at the University Medical Center in Greenville.
Dr. Scott, Dr. Fischer, and Dr. Taylor had no relevant disclosures.
PALM BEACH, FLA. – Add another notch to the evidence base for bariatric surgery as effective treatment for type 2 diabetes in obese patients.
Patients with type 2 diabetes who underwent any type of bariatric surgery had a 61%-78% relative risk reduction in their rate of macrovascular, microvascular, or vascular events during an average 20-month follow-up in a review of more than 15,000 cases in South Carolina.
"We are trying to get primary care physicians to spread the word [to patients] that bariatric surgery has come a long way over the past 30 or 40 years; the risk-to-reward ratio is much more beneficial to patients," Dr. John D. Scott said at the annual meeting of the Southern Surgical Association.
The new finding "adds to the extensive list of papers that show bariatric surgery mitigates the long-term effects of type 2 diabetes," Dr. Scott added in an interview. "Some front-line medical providers still see bariatric surgery as a procedure of last resort, but findings like ours show that a discussion [with patients on whether they should consider bariatric surgery] should happen a lot sooner."
Dr. Scott, a surgeon at University Medical Center in Greenville, S.C., recommended that patients with a body mass index of at least 35 kg/m2 and two or more comorbidities be told that they have the option of undergoing bariatric surgery and reducing their risk.
"We have an epidemic [of obesity and type 2 diabetes], and for the first time since tuberculosis, this is an epidemic where surgery has a real opportunity to positively intervene," commented Dr. Josef E. Fischer, a professor of surgery at Harvard Medical School in Boston.
The study used hospital billing data collected by the South Carolina Office of Research and Statistics as well as state vital records data for 1995-2009. The analysis included 2,580 obese patients who underwent any type of bariatric surgery and 13,371 obese patients who did not have surgery. The researchers extracted the data from records of nearly 34,000 obese patients, but excluded patients with type 1 diabetes, patients with incomplete data, and patients with advanced cardiovascular or microvascular disease at the time of their surgery or entry into the state records during this period.
During a median follow-up of about 20 months, the rate of new-onset macro- or microvascular events was 2% in the bariatric surgery patients and 11% in the patients who did not undergo surgery. The rate of an incident vascular disease event was 2% in the patients who had surgery and 13% in those who did not. Macrovascular events included myocardial infarction, stroke, and all-cause death. Microvascular events included blindness in at least one eye, laser eye surgery, nontraumatic amputation, or placement of access for dialysis. Other vascular events included new-onset heart failure or angina, or revascularization of a coronary, carotid, or peripheral artery.
In a multivariate-adjusted analysis, patients who underwent bariatric surgery had a 61% reduction in macrovascular events, a 78% reduction in microvascular events, a 75% reduction in vascular events, and a 64% reduction in combined macro- and microvascular events, compared with patients who did not have this surgery – all statistically significant differences, reported Dr. Spence M. Taylor, a coinvestigator with Dr. Scott on the study. A propensity-score matched analysis that compared the bariatric surgery patients and matched nonsurgical patients showed very similar reductions in all three event categories.
"Bariatric surgery has a substantial and lasting mitigating association on major complications associated with type 2 diabetes in the obese population," concluded Dr. Taylor, chairman of surgery at the University Medical Center in Greenville.
Dr. Scott, Dr. Fischer, and Dr. Taylor had no relevant disclosures.
PALM BEACH, FLA. – Add another notch to the evidence base for bariatric surgery as effective treatment for type 2 diabetes in obese patients.
Patients with type 2 diabetes who underwent any type of bariatric surgery had a 61%-78% relative risk reduction in their rate of macrovascular, microvascular, or vascular events during an average 20-month follow-up in a review of more than 15,000 cases in South Carolina.
"We are trying to get primary care physicians to spread the word [to patients] that bariatric surgery has come a long way over the past 30 or 40 years; the risk-to-reward ratio is much more beneficial to patients," Dr. John D. Scott said at the annual meeting of the Southern Surgical Association.
The new finding "adds to the extensive list of papers that show bariatric surgery mitigates the long-term effects of type 2 diabetes," Dr. Scott added in an interview. "Some front-line medical providers still see bariatric surgery as a procedure of last resort, but findings like ours show that a discussion [with patients on whether they should consider bariatric surgery] should happen a lot sooner."
Dr. Scott, a surgeon at University Medical Center in Greenville, S.C., recommended that patients with a body mass index of at least 35 kg/m2 and two or more comorbidities be told that they have the option of undergoing bariatric surgery and reducing their risk.
"We have an epidemic [of obesity and type 2 diabetes], and for the first time since tuberculosis, this is an epidemic where surgery has a real opportunity to positively intervene," commented Dr. Josef E. Fischer, a professor of surgery at Harvard Medical School in Boston.
The study used hospital billing data collected by the South Carolina Office of Research and Statistics as well as state vital records data for 1995-2009. The analysis included 2,580 obese patients who underwent any type of bariatric surgery and 13,371 obese patients who did not have surgery. The researchers extracted the data from records of nearly 34,000 obese patients, but excluded patients with type 1 diabetes, patients with incomplete data, and patients with advanced cardiovascular or microvascular disease at the time of their surgery or entry into the state records during this period.
During a median follow-up of about 20 months, the rate of new-onset macro- or microvascular events was 2% in the bariatric surgery patients and 11% in the patients who did not undergo surgery. The rate of an incident vascular disease event was 2% in the patients who had surgery and 13% in those who did not. Macrovascular events included myocardial infarction, stroke, and all-cause death. Microvascular events included blindness in at least one eye, laser eye surgery, nontraumatic amputation, or placement of access for dialysis. Other vascular events included new-onset heart failure or angina, or revascularization of a coronary, carotid, or peripheral artery.
In a multivariate-adjusted analysis, patients who underwent bariatric surgery had a 61% reduction in macrovascular events, a 78% reduction in microvascular events, a 75% reduction in vascular events, and a 64% reduction in combined macro- and microvascular events, compared with patients who did not have this surgery – all statistically significant differences, reported Dr. Spence M. Taylor, a coinvestigator with Dr. Scott on the study. A propensity-score matched analysis that compared the bariatric surgery patients and matched nonsurgical patients showed very similar reductions in all three event categories.
"Bariatric surgery has a substantial and lasting mitigating association on major complications associated with type 2 diabetes in the obese population," concluded Dr. Taylor, chairman of surgery at the University Medical Center in Greenville.
Dr. Scott, Dr. Fischer, and Dr. Taylor had no relevant disclosures.
AT THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: Bariatric surgery was linked to a 64% decrease in macro- and microvascular events compared with no surgery in obese type 2 diabetes patients.
Data Source: Billing information collected on 15,951 obese patients in South Carolina during 1995-2009.
Disclosures: Dr. Scott, Dr. Fischer, and Dr. Taylor had no relevant disclosures.

Prasugrel's use grows, but often off label
LOS ANGELES – Use of the antiplatelet drug prasugrel has jumped impressively in the United States since the Food and Drug Administration approved the drug in July 2009 – but not always for the right patients.
From the first quarter of 2010 to the last quarter of 2011, prasugrel prescriptions more than doubled for patients who underwent a percutaneous coronary intervention, from 8% of patients discharged following a PCI during the first 3 months of 2010 to 22% of discharged post-PCI patients during the final 3 months of 2011, according to data collected on 55,821 patients from 44 Michigan hospitals.
But several prasugrel (Effient) prescriptions fell outside of labeled indications in two important ways. First, throughout the 2-year period, 28% of the patients who underwent PCI and received prasugrel did not have an acute coronary syndrome event immediately before their procedure, Dr. Amneet Sandhu and his associates said in a poster at the annual scientific sessions of the American Heart Association. Prasugrel’s U.S. labeling specifies that it should be used following PCI only in patients who have recently had unstable angina or a myocardial infarction.
The second egregious prasugrel use was in patients with labeled contraindications for the drug: a prior history of cerebrovascular disease, weight of 60 kg or less, and age of 75 years or older. According to the reviewed records, 5%-10% of post-PCI patients who were prescribed prasugrel in Michigan had one or more of these contraindications, reported Dr. Sandhu, an internal medicine physician at the University of Michigan, Ann Arbor, and his associates. The most common contraindication in prasugrel recipients was a history of stroke or transient ischemic attack, in just over half of the patients with a contraindication. The next most common was age of 75 or older, which applied to 35% of the prasugrel recipients with a contraindication.
"Prasugrel use in patients with known contraindications is not uncommon, and may be a suitable target for focused quality-improvements efforts," noted the researchers, who used data collected by the Blue Cross Blue Shield of Michigan Cardiovascular Consortium.
Dr. Sandhu said he had no disclosures. Two of his associates received research support from Blue Cross Blue Shield of Michigan, and one associate was an employee of the company.
LOS ANGELES – Use of the antiplatelet drug prasugrel has jumped impressively in the United States since the Food and Drug Administration approved the drug in July 2009 – but not always for the right patients.
From the first quarter of 2010 to the last quarter of 2011, prasugrel prescriptions more than doubled for patients who underwent a percutaneous coronary intervention, from 8% of patients discharged following a PCI during the first 3 months of 2010 to 22% of discharged post-PCI patients during the final 3 months of 2011, according to data collected on 55,821 patients from 44 Michigan hospitals.
But several prasugrel (Effient) prescriptions fell outside of labeled indications in two important ways. First, throughout the 2-year period, 28% of the patients who underwent PCI and received prasugrel did not have an acute coronary syndrome event immediately before their procedure, Dr. Amneet Sandhu and his associates said in a poster at the annual scientific sessions of the American Heart Association. Prasugrel’s U.S. labeling specifies that it should be used following PCI only in patients who have recently had unstable angina or a myocardial infarction.
The second egregious prasugrel use was in patients with labeled contraindications for the drug: a prior history of cerebrovascular disease, weight of 60 kg or less, and age of 75 years or older. According to the reviewed records, 5%-10% of post-PCI patients who were prescribed prasugrel in Michigan had one or more of these contraindications, reported Dr. Sandhu, an internal medicine physician at the University of Michigan, Ann Arbor, and his associates. The most common contraindication in prasugrel recipients was a history of stroke or transient ischemic attack, in just over half of the patients with a contraindication. The next most common was age of 75 or older, which applied to 35% of the prasugrel recipients with a contraindication.
"Prasugrel use in patients with known contraindications is not uncommon, and may be a suitable target for focused quality-improvements efforts," noted the researchers, who used data collected by the Blue Cross Blue Shield of Michigan Cardiovascular Consortium.
Dr. Sandhu said he had no disclosures. Two of his associates received research support from Blue Cross Blue Shield of Michigan, and one associate was an employee of the company.
LOS ANGELES – Use of the antiplatelet drug prasugrel has jumped impressively in the United States since the Food and Drug Administration approved the drug in July 2009 – but not always for the right patients.
From the first quarter of 2010 to the last quarter of 2011, prasugrel prescriptions more than doubled for patients who underwent a percutaneous coronary intervention, from 8% of patients discharged following a PCI during the first 3 months of 2010 to 22% of discharged post-PCI patients during the final 3 months of 2011, according to data collected on 55,821 patients from 44 Michigan hospitals.
But several prasugrel (Effient) prescriptions fell outside of labeled indications in two important ways. First, throughout the 2-year period, 28% of the patients who underwent PCI and received prasugrel did not have an acute coronary syndrome event immediately before their procedure, Dr. Amneet Sandhu and his associates said in a poster at the annual scientific sessions of the American Heart Association. Prasugrel’s U.S. labeling specifies that it should be used following PCI only in patients who have recently had unstable angina or a myocardial infarction.
The second egregious prasugrel use was in patients with labeled contraindications for the drug: a prior history of cerebrovascular disease, weight of 60 kg or less, and age of 75 years or older. According to the reviewed records, 5%-10% of post-PCI patients who were prescribed prasugrel in Michigan had one or more of these contraindications, reported Dr. Sandhu, an internal medicine physician at the University of Michigan, Ann Arbor, and his associates. The most common contraindication in prasugrel recipients was a history of stroke or transient ischemic attack, in just over half of the patients with a contraindication. The next most common was age of 75 or older, which applied to 35% of the prasugrel recipients with a contraindication.
"Prasugrel use in patients with known contraindications is not uncommon, and may be a suitable target for focused quality-improvements efforts," noted the researchers, who used data collected by the Blue Cross Blue Shield of Michigan Cardiovascular Consortium.
Dr. Sandhu said he had no disclosures. Two of his associates received research support from Blue Cross Blue Shield of Michigan, and one associate was an employee of the company.
AT THE ANNUAL SCIENTIFIC SESSIONS OF THE AMERICAN HEART ASSOCIATION
Major Finding: Prasugrel use post PCI in Michigan grew from 8% of patients to 22% from early 2010 to late 2011.
Data Source: A review of 55,821 patients who underwent PCI in Michigan during 2010-2011.
Disclosures: Dr. Sandhu said he had no disclosures. Two of his associates received research support from Blue Cross Blue Shield of Michigan, and one associate was an employee of the company.
LBBB Poses Biggest Intraventricular Conduction-Block Risk
LOS ANGELES – The most common intraventricular conduction block following a myocardial infarction is a right bundle branch block, but it is also the least deadly and pathogenic. Left bundle branch blocks produced the most morbidity and mortality in a review of more than 25,000 myocardial infarction survivors from throughout New Jersey during 1994-2009.
The findings also showed that left anterior hemiblocks (LAHB) put post-MI patients in nearly as much jeopardy as did left bundle branch blocks (LBBB), Dr. John S. Pantazopoulos and his associates reported in a poster at the annual scientific sessions of the American Heart Association.
The researchers reviewed 16-year follow-up data from 25,026 patients enrolled in the Myocardial Infarction Data Acquisition System (MIDAS) run by the Cardiovascular Institute of New Jersey in New Brunswick. They excluded post-MI patients with congenital heart disease, a history of mitral regurgitation, atrial fibrillation, heart failure, a pacemaker, coronary bypass surgery, or a percutaneous coronary intervention prior to the first appearance of their intraventricular conduction block.
The most common conduction abnormality was a right bundle branch block (RBBB), in 13,454 patients (54%). LBBB occurred in 27%, 15% had LAHB, and 4% had LAHB plus RBBB. Dr. Pantazopoulos and his associates performed multivariate analyses to determine the morbidity and mortality risk faced by LBBB, LAHB, and LAHB plus RBBB patients compared with patients who only had RBBB. Their analysis controlled for several demographic and clinical confounders, including hypertension, diabetes, and renal failure.
The analysis showed that compared with patients with RBBB, those with LBBB had a 2.7-fold increased risk of cardiovascular death and a 48% increased rate of all-cause death, reported Dr. Pantazopoulos, a cardiologist at the Cardiovascular Institute of the University of Medicine and Dentistry of New Jersey in New Brunswick. Patients with LAHB had a 2.6-fold increased risk of cardiovascular death and 59% increased rate of all-cause death compared with RBBB patients, and those with LAHB plus RBBB had a 2.6-fold higher cardiovascular death rate and a 62% increased all-cause death rate. All these increases were statistically significant.
Patients with LBBB also had a 3.8-fold increased rate of developing heart failure during follow-up, a 68% increased rate of incident mitral regurgitation, and a 34% increased rate of atrial fibrillation compared with patients with RBBB. Patients with LAHB had a 2.6-fold increased rate of new-onset heart failure and a 15% higher rate of atrial fibrillation, and patients with both LAHB and RBBB had a 2.4-fold increased rate of heart failure. All of these increased rates were statistically significant.
Dr. Pantazopoulos said that he had no disclosures. The senior researcher on the study, Dr. John B. Kostis, has been a speaker for Merck, has received honoraria from Sanofi, and has received a research grant from Novartis.
LOS ANGELES – The most common intraventricular conduction block following a myocardial infarction is a right bundle branch block, but it is also the least deadly and pathogenic. Left bundle branch blocks produced the most morbidity and mortality in a review of more than 25,000 myocardial infarction survivors from throughout New Jersey during 1994-2009.
The findings also showed that left anterior hemiblocks (LAHB) put post-MI patients in nearly as much jeopardy as did left bundle branch blocks (LBBB), Dr. John S. Pantazopoulos and his associates reported in a poster at the annual scientific sessions of the American Heart Association.
The researchers reviewed 16-year follow-up data from 25,026 patients enrolled in the Myocardial Infarction Data Acquisition System (MIDAS) run by the Cardiovascular Institute of New Jersey in New Brunswick. They excluded post-MI patients with congenital heart disease, a history of mitral regurgitation, atrial fibrillation, heart failure, a pacemaker, coronary bypass surgery, or a percutaneous coronary intervention prior to the first appearance of their intraventricular conduction block.
The most common conduction abnormality was a right bundle branch block (RBBB), in 13,454 patients (54%). LBBB occurred in 27%, 15% had LAHB, and 4% had LAHB plus RBBB. Dr. Pantazopoulos and his associates performed multivariate analyses to determine the morbidity and mortality risk faced by LBBB, LAHB, and LAHB plus RBBB patients compared with patients who only had RBBB. Their analysis controlled for several demographic and clinical confounders, including hypertension, diabetes, and renal failure.
The analysis showed that compared with patients with RBBB, those with LBBB had a 2.7-fold increased risk of cardiovascular death and a 48% increased rate of all-cause death, reported Dr. Pantazopoulos, a cardiologist at the Cardiovascular Institute of the University of Medicine and Dentistry of New Jersey in New Brunswick. Patients with LAHB had a 2.6-fold increased risk of cardiovascular death and 59% increased rate of all-cause death compared with RBBB patients, and those with LAHB plus RBBB had a 2.6-fold higher cardiovascular death rate and a 62% increased all-cause death rate. All these increases were statistically significant.
Patients with LBBB also had a 3.8-fold increased rate of developing heart failure during follow-up, a 68% increased rate of incident mitral regurgitation, and a 34% increased rate of atrial fibrillation compared with patients with RBBB. Patients with LAHB had a 2.6-fold increased rate of new-onset heart failure and a 15% higher rate of atrial fibrillation, and patients with both LAHB and RBBB had a 2.4-fold increased rate of heart failure. All of these increased rates were statistically significant.
Dr. Pantazopoulos said that he had no disclosures. The senior researcher on the study, Dr. John B. Kostis, has been a speaker for Merck, has received honoraria from Sanofi, and has received a research grant from Novartis.
LOS ANGELES – The most common intraventricular conduction block following a myocardial infarction is a right bundle branch block, but it is also the least deadly and pathogenic. Left bundle branch blocks produced the most morbidity and mortality in a review of more than 25,000 myocardial infarction survivors from throughout New Jersey during 1994-2009.
The findings also showed that left anterior hemiblocks (LAHB) put post-MI patients in nearly as much jeopardy as did left bundle branch blocks (LBBB), Dr. John S. Pantazopoulos and his associates reported in a poster at the annual scientific sessions of the American Heart Association.
The researchers reviewed 16-year follow-up data from 25,026 patients enrolled in the Myocardial Infarction Data Acquisition System (MIDAS) run by the Cardiovascular Institute of New Jersey in New Brunswick. They excluded post-MI patients with congenital heart disease, a history of mitral regurgitation, atrial fibrillation, heart failure, a pacemaker, coronary bypass surgery, or a percutaneous coronary intervention prior to the first appearance of their intraventricular conduction block.
The most common conduction abnormality was a right bundle branch block (RBBB), in 13,454 patients (54%). LBBB occurred in 27%, 15% had LAHB, and 4% had LAHB plus RBBB. Dr. Pantazopoulos and his associates performed multivariate analyses to determine the morbidity and mortality risk faced by LBBB, LAHB, and LAHB plus RBBB patients compared with patients who only had RBBB. Their analysis controlled for several demographic and clinical confounders, including hypertension, diabetes, and renal failure.
The analysis showed that compared with patients with RBBB, those with LBBB had a 2.7-fold increased risk of cardiovascular death and a 48% increased rate of all-cause death, reported Dr. Pantazopoulos, a cardiologist at the Cardiovascular Institute of the University of Medicine and Dentistry of New Jersey in New Brunswick. Patients with LAHB had a 2.6-fold increased risk of cardiovascular death and 59% increased rate of all-cause death compared with RBBB patients, and those with LAHB plus RBBB had a 2.6-fold higher cardiovascular death rate and a 62% increased all-cause death rate. All these increases were statistically significant.
Patients with LBBB also had a 3.8-fold increased rate of developing heart failure during follow-up, a 68% increased rate of incident mitral regurgitation, and a 34% increased rate of atrial fibrillation compared with patients with RBBB. Patients with LAHB had a 2.6-fold increased rate of new-onset heart failure and a 15% higher rate of atrial fibrillation, and patients with both LAHB and RBBB had a 2.4-fold increased rate of heart failure. All of these increased rates were statistically significant.
Dr. Pantazopoulos said that he had no disclosures. The senior researcher on the study, Dr. John B. Kostis, has been a speaker for Merck, has received honoraria from Sanofi, and has received a research grant from Novartis.
AT THE ANNUAL SCIENTIFIC SESSIONS OF THE AMERICAN HEART ASSOCIATION
Major Finding: Left bundle branch block post MI was linked to a 2.7-fold increased cardiovascular death rate, compared with right bundle branch block.
Data Source: A review of 25,056 post–myocardial infarction patients enrolled in a New Jersey registry during 1994-2009.
Disclosures: Dr. Pantazopoulos had no disclosures. The senior researcher on the study, Dr. John B. Kostis, has been a speaker for Merck, has received honoraria from Sanofi, and has received a research grant from Novartis.