User login
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at john.nelson@nelsonflores.com.
Par Excellence

I’m often asked about the attributes associated with high-functioning practices, so I thought I’d offer a list of them in this column. I’ve written entire columns about some of them in prior issues of The Hospitalist, so I will provide only brief commentary about each of them here.
I think this list can serve as a valuable frame of reference for any hospitalist practice, though it is geared more toward nonacademic settings. It is based on my own career as a hospitalist, which spans more than 20 years, and 15 years’ work as a consultant with nearly 300 institutions around the country. While I think my experience has given me a valuable perspective, others might reasonably omit some attributes listed here or add others.
I believe the single most important measure of a practice is excellent outcomes for its patients. That said, all of the attributes I describe here have more to do with excellent operational, or business, performance. It is possible for a practice to have all of these attributes and still provide disappointing clinical quality for its patients, but that seems really unlikely to me. And even a practice that provides superior clinical care probably won’t be able to do so for long without high-functioning business operations.
I think each of these attributes might be a cause of a practice’s excellent performance, but it is possible that some are a result of it. They are listed in no particular order.
A culture of practice ownership. The most important attribute associated with a high-functioning practice is that the providers in the group maintain a mindset of practice ownership. Even if you are employees of a hospital or other organization, you should think of yourselves as owners of the practice’s performance. When problems arise, you shouldn’t simply assume it is up to the practice leader alone, or an administrator outside of the practice to solve it. Instead, each doctor should always be thinking about how to improve the practice and taking action to make it happen. For more, see “Foster Ownership Culture” in the August 2008 issue, or visit my website and take a quiz (http://nelsonflores.com/html/quiz.html) to assess your ownership culture.
An effective group leader. All groups need a leader who takes the role seriously and doesn’t just view the job description as making the work schedule and attending more meetings than the other hospitalists. (Unfortunately, my experience is that this is precisely what a lot of leaders think.) Of the many markers that effective leaders display, one that seems pretty reliable to me is whether the group has routinely scheduled meetings, with an agenda provided in advance and minutes circulated a few days later. I wrote about effective group leaders in a June 2008 column titled “Follow the Money.”
Autonomy in making decisions. Even when you are an employee of a larger entity, the practice should be structured so that hospitalists have as much autonomy in decision-making as possible. For example, you should always be able to adjust the group’s work schedule (e.g. when shifts start and stop). You also should have a lot of say about your staffing and workload. The latter typically requires that the group is connected to the financial consequences of its choices, which usually means a compensation system based, to a significant degree, on productivity.
While still common for hospitalists, when the largest salary component is fixed, it will always follow that someone outside the group (e.g. an administrator at the hospital) will end up deciding how hard you will have to work to justify the promised salary. And the hospitalists will almost always find fault with that person’s decision—a recipe for constant frustration that inhibits the development of an ownership culture, among other things.
Each doctor sees the job as more than just providing care to patients. In addition to providing quality care for your patients, each hospitalist in the group must work to improve the performance of the hospital. This means work on clinical protocols, medical staff functions (e.g. credentials committee), documentation and coding for both CPT and DRG billing, etc.
Strong social connections. Every high-performing practice I’ve worked with is notable for the social connections between the hospitalists themselves, as well as between hospitalists and other physicians, nursing staff, and administrators. This shouldn’t be taken lightly. Social connections matter—a lot. And while the hospitalists in most groups feel reasonably connected with one another, too often they feel isolated from the other doctors and administrators at the hospital. I wrote some more thoughts about this in a June 2010 column, “Square Peg, Square Hole.”
Hospitalists actively involved in recruiting for their practice. The hospitalists themselves—at a minimum, the group leader—should be very involved in recruiting new members for the group. Professional recruiters are very valuable but can be a lot more effective if the hospitalists themselves participate in the process. The group will land better candidates that way. For more, see “We’re Hiring,” from July 2008.
Hospitalists know data about their performance. Too many practices fail to provide routine data about each provider’s clinical and financial performance. Make sure your group isn’t in this category. Develop a routine report of key metrics for your practice. Usually it is fine, and best, to provide to the whole group unblinded performance data about each individual hospitalist. For more information, check out “Measuring Hospitalist Performance: Metrics, Reports, and Dashboards” on the SHM website.
Don’t rely solely on consensus-based decision-making. Relying on consensus is reasonable for most decisions, if a group has about eight to 10 members. Larger groups need to decide how they’ll make decisions if consensus can’t be reached easily. And they need to have the discipline to stick to their agreed upon process, usually a vote. For more on this subject, see “Play by the Rules” in the December 2007 issue. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
I’m often asked about the attributes associated with high-functioning practices, so I thought I’d offer a list of them in this column. I’ve written entire columns about some of them in prior issues of The Hospitalist, so I will provide only brief commentary about each of them here.
I think this list can serve as a valuable frame of reference for any hospitalist practice, though it is geared more toward nonacademic settings. It is based on my own career as a hospitalist, which spans more than 20 years, and 15 years’ work as a consultant with nearly 300 institutions around the country. While I think my experience has given me a valuable perspective, others might reasonably omit some attributes listed here or add others.
I believe the single most important measure of a practice is excellent outcomes for its patients. That said, all of the attributes I describe here have more to do with excellent operational, or business, performance. It is possible for a practice to have all of these attributes and still provide disappointing clinical quality for its patients, but that seems really unlikely to me. And even a practice that provides superior clinical care probably won’t be able to do so for long without high-functioning business operations.
I think each of these attributes might be a cause of a practice’s excellent performance, but it is possible that some are a result of it. They are listed in no particular order.
A culture of practice ownership. The most important attribute associated with a high-functioning practice is that the providers in the group maintain a mindset of practice ownership. Even if you are employees of a hospital or other organization, you should think of yourselves as owners of the practice’s performance. When problems arise, you shouldn’t simply assume it is up to the practice leader alone, or an administrator outside of the practice to solve it. Instead, each doctor should always be thinking about how to improve the practice and taking action to make it happen. For more, see “Foster Ownership Culture” in the August 2008 issue, or visit my website and take a quiz (http://nelsonflores.com/html/quiz.html) to assess your ownership culture.
An effective group leader. All groups need a leader who takes the role seriously and doesn’t just view the job description as making the work schedule and attending more meetings than the other hospitalists. (Unfortunately, my experience is that this is precisely what a lot of leaders think.) Of the many markers that effective leaders display, one that seems pretty reliable to me is whether the group has routinely scheduled meetings, with an agenda provided in advance and minutes circulated a few days later. I wrote about effective group leaders in a June 2008 column titled “Follow the Money.”
Autonomy in making decisions. Even when you are an employee of a larger entity, the practice should be structured so that hospitalists have as much autonomy in decision-making as possible. For example, you should always be able to adjust the group’s work schedule (e.g. when shifts start and stop). You also should have a lot of say about your staffing and workload. The latter typically requires that the group is connected to the financial consequences of its choices, which usually means a compensation system based, to a significant degree, on productivity.
While still common for hospitalists, when the largest salary component is fixed, it will always follow that someone outside the group (e.g. an administrator at the hospital) will end up deciding how hard you will have to work to justify the promised salary. And the hospitalists will almost always find fault with that person’s decision—a recipe for constant frustration that inhibits the development of an ownership culture, among other things.
Each doctor sees the job as more than just providing care to patients. In addition to providing quality care for your patients, each hospitalist in the group must work to improve the performance of the hospital. This means work on clinical protocols, medical staff functions (e.g. credentials committee), documentation and coding for both CPT and DRG billing, etc.
Strong social connections. Every high-performing practice I’ve worked with is notable for the social connections between the hospitalists themselves, as well as between hospitalists and other physicians, nursing staff, and administrators. This shouldn’t be taken lightly. Social connections matter—a lot. And while the hospitalists in most groups feel reasonably connected with one another, too often they feel isolated from the other doctors and administrators at the hospital. I wrote some more thoughts about this in a June 2010 column, “Square Peg, Square Hole.”
Hospitalists actively involved in recruiting for their practice. The hospitalists themselves—at a minimum, the group leader—should be very involved in recruiting new members for the group. Professional recruiters are very valuable but can be a lot more effective if the hospitalists themselves participate in the process. The group will land better candidates that way. For more, see “We’re Hiring,” from July 2008.
Hospitalists know data about their performance. Too many practices fail to provide routine data about each provider’s clinical and financial performance. Make sure your group isn’t in this category. Develop a routine report of key metrics for your practice. Usually it is fine, and best, to provide to the whole group unblinded performance data about each individual hospitalist. For more information, check out “Measuring Hospitalist Performance: Metrics, Reports, and Dashboards” on the SHM website.
Don’t rely solely on consensus-based decision-making. Relying on consensus is reasonable for most decisions, if a group has about eight to 10 members. Larger groups need to decide how they’ll make decisions if consensus can’t be reached easily. And they need to have the discipline to stick to their agreed upon process, usually a vote. For more on this subject, see “Play by the Rules” in the December 2007 issue. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
I’m often asked about the attributes associated with high-functioning practices, so I thought I’d offer a list of them in this column. I’ve written entire columns about some of them in prior issues of The Hospitalist, so I will provide only brief commentary about each of them here.
I think this list can serve as a valuable frame of reference for any hospitalist practice, though it is geared more toward nonacademic settings. It is based on my own career as a hospitalist, which spans more than 20 years, and 15 years’ work as a consultant with nearly 300 institutions around the country. While I think my experience has given me a valuable perspective, others might reasonably omit some attributes listed here or add others.
I believe the single most important measure of a practice is excellent outcomes for its patients. That said, all of the attributes I describe here have more to do with excellent operational, or business, performance. It is possible for a practice to have all of these attributes and still provide disappointing clinical quality for its patients, but that seems really unlikely to me. And even a practice that provides superior clinical care probably won’t be able to do so for long without high-functioning business operations.
I think each of these attributes might be a cause of a practice’s excellent performance, but it is possible that some are a result of it. They are listed in no particular order.
A culture of practice ownership. The most important attribute associated with a high-functioning practice is that the providers in the group maintain a mindset of practice ownership. Even if you are employees of a hospital or other organization, you should think of yourselves as owners of the practice’s performance. When problems arise, you shouldn’t simply assume it is up to the practice leader alone, or an administrator outside of the practice to solve it. Instead, each doctor should always be thinking about how to improve the practice and taking action to make it happen. For more, see “Foster Ownership Culture” in the August 2008 issue, or visit my website and take a quiz (http://nelsonflores.com/html/quiz.html) to assess your ownership culture.
An effective group leader. All groups need a leader who takes the role seriously and doesn’t just view the job description as making the work schedule and attending more meetings than the other hospitalists. (Unfortunately, my experience is that this is precisely what a lot of leaders think.) Of the many markers that effective leaders display, one that seems pretty reliable to me is whether the group has routinely scheduled meetings, with an agenda provided in advance and minutes circulated a few days later. I wrote about effective group leaders in a June 2008 column titled “Follow the Money.”
Autonomy in making decisions. Even when you are an employee of a larger entity, the practice should be structured so that hospitalists have as much autonomy in decision-making as possible. For example, you should always be able to adjust the group’s work schedule (e.g. when shifts start and stop). You also should have a lot of say about your staffing and workload. The latter typically requires that the group is connected to the financial consequences of its choices, which usually means a compensation system based, to a significant degree, on productivity.
While still common for hospitalists, when the largest salary component is fixed, it will always follow that someone outside the group (e.g. an administrator at the hospital) will end up deciding how hard you will have to work to justify the promised salary. And the hospitalists will almost always find fault with that person’s decision—a recipe for constant frustration that inhibits the development of an ownership culture, among other things.
Each doctor sees the job as more than just providing care to patients. In addition to providing quality care for your patients, each hospitalist in the group must work to improve the performance of the hospital. This means work on clinical protocols, medical staff functions (e.g. credentials committee), documentation and coding for both CPT and DRG billing, etc.
Strong social connections. Every high-performing practice I’ve worked with is notable for the social connections between the hospitalists themselves, as well as between hospitalists and other physicians, nursing staff, and administrators. This shouldn’t be taken lightly. Social connections matter—a lot. And while the hospitalists in most groups feel reasonably connected with one another, too often they feel isolated from the other doctors and administrators at the hospital. I wrote some more thoughts about this in a June 2010 column, “Square Peg, Square Hole.”
Hospitalists actively involved in recruiting for their practice. The hospitalists themselves—at a minimum, the group leader—should be very involved in recruiting new members for the group. Professional recruiters are very valuable but can be a lot more effective if the hospitalists themselves participate in the process. The group will land better candidates that way. For more, see “We’re Hiring,” from July 2008.
Hospitalists know data about their performance. Too many practices fail to provide routine data about each provider’s clinical and financial performance. Make sure your group isn’t in this category. Develop a routine report of key metrics for your practice. Usually it is fine, and best, to provide to the whole group unblinded performance data about each individual hospitalist. For more information, check out “Measuring Hospitalist Performance: Metrics, Reports, and Dashboards” on the SHM website.
Don’t rely solely on consensus-based decision-making. Relying on consensus is reasonable for most decisions, if a group has about eight to 10 members. Larger groups need to decide how they’ll make decisions if consensus can’t be reached easily. And they need to have the discipline to stick to their agreed upon process, usually a vote. For more on this subject, see “Play by the Rules” in the December 2007 issue. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Referral Lists

I like to ask laypeople what they think “hospitalist” means. For years, I was confident that they had never heard the term, but now my question is more often met with an accurate response.
A hotel desk clerk in 1998 actually made one of the cleverest guesses I’ve ever heard. For the whole day, she and her colleagues had in front of them a sign that read “Hospitalist Meeting in the Ballroom,” which got them talking about what in the world a hospitalist is. Seeing from my badge that I was attending that meeting, she asked me what the term meant, but she first gamely provided her best guess: “Someone who makes lists of hospitals.”
There seems to be no end to the number of healthcare-related nouns and verbs to which someone attaches the suffix “ist.” Some days I request so many consults that I’m just a “referralist” (one who refers patients; surely this is a term we can do without). But don’t let the headline of this column confuse you: I really am addressing the lists used to determine which doctor to refer patients to.
Hospitalist Referrals
The first of two common referral lists for hospitalists is a directory of primary-care physicians (PCPs) and clinics, as well as some other providers that refer patients to the hospitalist. Nearly all hospitalist groups maintain such a list, and they might apply a variety of terms such as “subscriber” (which refers to hospitalists) and “nonsubscriber” physicians.
Because most HM groups care for patients who come from all or nearly all of the PCPs in an area, it is often simpler to just create a short list of those providers who don’t refer to the hospitalists. In many hospitals, there are just four or five providers on that list. ED providers are the ones who most often access this list. When visiting other hospitals, I often see a paper copy of the list taped up at the provider workstations in the ED.
Consult Who?
The other, and much less common, type of referral list governs which doctors the hospitalists are to consult. There are two strategies that come up when thinking about this kind of list.
Do what the ED doctors do. ED physicians typically are constrained by the list of on-call physicians for each specialty, and are to always consult that doctor rather than another. For example, the ED doctor is required to consult Dr. Taylor for any patient in need of a general surgeon and doesn’t have a prior relationship with one. Tomorrow, the ED doctor is required to consult Dr. Simon. Dr. Taylor and Dr. Simon are to be contacted because they are the ones on call for the ED those days. Even if the ED doctor would rather consult Dr. Simon today (maybe she is more able, affable, and available than Dr. Taylor), that isn’t an option, because it is Dr. Taylor’s name on the ED on-call roster today.
Each PCP creates a referral list for hospitalists to follow. New hospitalist practices often agree to follow the consulting patterns of each referring PCP. This can increase PCP acceptance of the HM model, and after all, the GI doctor consulted by the hospitalist during the few days in the hospital is the same one who will be working with the PCP when the patient has outpatient issues requiring GI specialty care. This usually means that the hospitalist carries a list of each PCP, and which GI doctor, orthopedist, etc., that particular PCP likes to consult. When the hospitalist needs an ortho consult, she first verifies the PCP this patient sees, then pulls out the list to see the orthopedist(s) that PCP prefers.
In most settings, either form of a mandated referral list is a poor system for hospitalists and is best avoided. Instead, the hospitalists should be free to deviate from the ED call list as they see fit. And while they should be attentive to the consulting preferences of each PCP, it is best not to promise the PCPs that their preference will always be followed. Providing the hospitalists this latitude means they can tailor the choice of consultant to the patient’s needs and the level of service (i.e. able, affable, available) each provides. And, at least in theory, when there are competing providers in a given specialty, they will have an incentive to provide better service to the hospitalist as a way of ensuring future referrals.
Practical Considerations
Even though I think it is optimal for hospitalists to have a lot of latitude in which doctors they consult, there are some practical considerations to keep in mind. For example, if the patient’s PCP is in a group that also has surgeons, it will be best to call one of them, and not a competing surgeon, when the patient has surgical needs. And the hospitalists as a group should usually make some effort to avoid never consulting a particular provider or group, as that could lead the “blackballed” doctor or group to complain enough that the medical staff or hospital leadership might force the hospitalists to follow the ED call roster when choosing referrals.
The number of physicians seeking hospital employment, which is steadily increasing these days, will in many settings increase sensitivities around referral patterns. For example, if your hospital has had three competing general surgery groups and one chooses to become hospital-employed, then the other two groups are likely to worry a lot that the hospitalists might be directed by the hospital to preferentially refer to the newly employed surgeons. Even if your hospitalist group has never had any sort of encouragement to do this, it could be very hard to convince the non-hospital-employed surgeons of this. This could become such a sensitive issue that it might be necessary to carefully track the number of referrals to each surgical group.
And to prevent arguments like “You just consult us on the bad or uninsured patients,” you might also need to track the nature of the patient’s problem and insurance status, and whether the referral led to a procedure. The best approach will be to try to prevent these sorts of things from coming up by maintaining good communication and relations with other physician groups and thinking deliberately about your referral patterns. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
I like to ask laypeople what they think “hospitalist” means. For years, I was confident that they had never heard the term, but now my question is more often met with an accurate response.
A hotel desk clerk in 1998 actually made one of the cleverest guesses I’ve ever heard. For the whole day, she and her colleagues had in front of them a sign that read “Hospitalist Meeting in the Ballroom,” which got them talking about what in the world a hospitalist is. Seeing from my badge that I was attending that meeting, she asked me what the term meant, but she first gamely provided her best guess: “Someone who makes lists of hospitals.”
There seems to be no end to the number of healthcare-related nouns and verbs to which someone attaches the suffix “ist.” Some days I request so many consults that I’m just a “referralist” (one who refers patients; surely this is a term we can do without). But don’t let the headline of this column confuse you: I really am addressing the lists used to determine which doctor to refer patients to.
Hospitalist Referrals
The first of two common referral lists for hospitalists is a directory of primary-care physicians (PCPs) and clinics, as well as some other providers that refer patients to the hospitalist. Nearly all hospitalist groups maintain such a list, and they might apply a variety of terms such as “subscriber” (which refers to hospitalists) and “nonsubscriber” physicians.
Because most HM groups care for patients who come from all or nearly all of the PCPs in an area, it is often simpler to just create a short list of those providers who don’t refer to the hospitalists. In many hospitals, there are just four or five providers on that list. ED providers are the ones who most often access this list. When visiting other hospitals, I often see a paper copy of the list taped up at the provider workstations in the ED.
Consult Who?
The other, and much less common, type of referral list governs which doctors the hospitalists are to consult. There are two strategies that come up when thinking about this kind of list.
Do what the ED doctors do. ED physicians typically are constrained by the list of on-call physicians for each specialty, and are to always consult that doctor rather than another. For example, the ED doctor is required to consult Dr. Taylor for any patient in need of a general surgeon and doesn’t have a prior relationship with one. Tomorrow, the ED doctor is required to consult Dr. Simon. Dr. Taylor and Dr. Simon are to be contacted because they are the ones on call for the ED those days. Even if the ED doctor would rather consult Dr. Simon today (maybe she is more able, affable, and available than Dr. Taylor), that isn’t an option, because it is Dr. Taylor’s name on the ED on-call roster today.
Each PCP creates a referral list for hospitalists to follow. New hospitalist practices often agree to follow the consulting patterns of each referring PCP. This can increase PCP acceptance of the HM model, and after all, the GI doctor consulted by the hospitalist during the few days in the hospital is the same one who will be working with the PCP when the patient has outpatient issues requiring GI specialty care. This usually means that the hospitalist carries a list of each PCP, and which GI doctor, orthopedist, etc., that particular PCP likes to consult. When the hospitalist needs an ortho consult, she first verifies the PCP this patient sees, then pulls out the list to see the orthopedist(s) that PCP prefers.
In most settings, either form of a mandated referral list is a poor system for hospitalists and is best avoided. Instead, the hospitalists should be free to deviate from the ED call list as they see fit. And while they should be attentive to the consulting preferences of each PCP, it is best not to promise the PCPs that their preference will always be followed. Providing the hospitalists this latitude means they can tailor the choice of consultant to the patient’s needs and the level of service (i.e. able, affable, available) each provides. And, at least in theory, when there are competing providers in a given specialty, they will have an incentive to provide better service to the hospitalist as a way of ensuring future referrals.
Practical Considerations
Even though I think it is optimal for hospitalists to have a lot of latitude in which doctors they consult, there are some practical considerations to keep in mind. For example, if the patient’s PCP is in a group that also has surgeons, it will be best to call one of them, and not a competing surgeon, when the patient has surgical needs. And the hospitalists as a group should usually make some effort to avoid never consulting a particular provider or group, as that could lead the “blackballed” doctor or group to complain enough that the medical staff or hospital leadership might force the hospitalists to follow the ED call roster when choosing referrals.
The number of physicians seeking hospital employment, which is steadily increasing these days, will in many settings increase sensitivities around referral patterns. For example, if your hospital has had three competing general surgery groups and one chooses to become hospital-employed, then the other two groups are likely to worry a lot that the hospitalists might be directed by the hospital to preferentially refer to the newly employed surgeons. Even if your hospitalist group has never had any sort of encouragement to do this, it could be very hard to convince the non-hospital-employed surgeons of this. This could become such a sensitive issue that it might be necessary to carefully track the number of referrals to each surgical group.
And to prevent arguments like “You just consult us on the bad or uninsured patients,” you might also need to track the nature of the patient’s problem and insurance status, and whether the referral led to a procedure. The best approach will be to try to prevent these sorts of things from coming up by maintaining good communication and relations with other physician groups and thinking deliberately about your referral patterns. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
I like to ask laypeople what they think “hospitalist” means. For years, I was confident that they had never heard the term, but now my question is more often met with an accurate response.
A hotel desk clerk in 1998 actually made one of the cleverest guesses I’ve ever heard. For the whole day, she and her colleagues had in front of them a sign that read “Hospitalist Meeting in the Ballroom,” which got them talking about what in the world a hospitalist is. Seeing from my badge that I was attending that meeting, she asked me what the term meant, but she first gamely provided her best guess: “Someone who makes lists of hospitals.”
There seems to be no end to the number of healthcare-related nouns and verbs to which someone attaches the suffix “ist.” Some days I request so many consults that I’m just a “referralist” (one who refers patients; surely this is a term we can do without). But don’t let the headline of this column confuse you: I really am addressing the lists used to determine which doctor to refer patients to.
Hospitalist Referrals
The first of two common referral lists for hospitalists is a directory of primary-care physicians (PCPs) and clinics, as well as some other providers that refer patients to the hospitalist. Nearly all hospitalist groups maintain such a list, and they might apply a variety of terms such as “subscriber” (which refers to hospitalists) and “nonsubscriber” physicians.
Because most HM groups care for patients who come from all or nearly all of the PCPs in an area, it is often simpler to just create a short list of those providers who don’t refer to the hospitalists. In many hospitals, there are just four or five providers on that list. ED providers are the ones who most often access this list. When visiting other hospitals, I often see a paper copy of the list taped up at the provider workstations in the ED.
Consult Who?
The other, and much less common, type of referral list governs which doctors the hospitalists are to consult. There are two strategies that come up when thinking about this kind of list.
Do what the ED doctors do. ED physicians typically are constrained by the list of on-call physicians for each specialty, and are to always consult that doctor rather than another. For example, the ED doctor is required to consult Dr. Taylor for any patient in need of a general surgeon and doesn’t have a prior relationship with one. Tomorrow, the ED doctor is required to consult Dr. Simon. Dr. Taylor and Dr. Simon are to be contacted because they are the ones on call for the ED those days. Even if the ED doctor would rather consult Dr. Simon today (maybe she is more able, affable, and available than Dr. Taylor), that isn’t an option, because it is Dr. Taylor’s name on the ED on-call roster today.
Each PCP creates a referral list for hospitalists to follow. New hospitalist practices often agree to follow the consulting patterns of each referring PCP. This can increase PCP acceptance of the HM model, and after all, the GI doctor consulted by the hospitalist during the few days in the hospital is the same one who will be working with the PCP when the patient has outpatient issues requiring GI specialty care. This usually means that the hospitalist carries a list of each PCP, and which GI doctor, orthopedist, etc., that particular PCP likes to consult. When the hospitalist needs an ortho consult, she first verifies the PCP this patient sees, then pulls out the list to see the orthopedist(s) that PCP prefers.
In most settings, either form of a mandated referral list is a poor system for hospitalists and is best avoided. Instead, the hospitalists should be free to deviate from the ED call list as they see fit. And while they should be attentive to the consulting preferences of each PCP, it is best not to promise the PCPs that their preference will always be followed. Providing the hospitalists this latitude means they can tailor the choice of consultant to the patient’s needs and the level of service (i.e. able, affable, available) each provides. And, at least in theory, when there are competing providers in a given specialty, they will have an incentive to provide better service to the hospitalist as a way of ensuring future referrals.
Practical Considerations
Even though I think it is optimal for hospitalists to have a lot of latitude in which doctors they consult, there are some practical considerations to keep in mind. For example, if the patient’s PCP is in a group that also has surgeons, it will be best to call one of them, and not a competing surgeon, when the patient has surgical needs. And the hospitalists as a group should usually make some effort to avoid never consulting a particular provider or group, as that could lead the “blackballed” doctor or group to complain enough that the medical staff or hospital leadership might force the hospitalists to follow the ED call roster when choosing referrals.
The number of physicians seeking hospital employment, which is steadily increasing these days, will in many settings increase sensitivities around referral patterns. For example, if your hospital has had three competing general surgery groups and one chooses to become hospital-employed, then the other two groups are likely to worry a lot that the hospitalists might be directed by the hospital to preferentially refer to the newly employed surgeons. Even if your hospitalist group has never had any sort of encouragement to do this, it could be very hard to convince the non-hospital-employed surgeons of this. This could become such a sensitive issue that it might be necessary to carefully track the number of referrals to each surgical group.
And to prevent arguments like “You just consult us on the bad or uninsured patients,” you might also need to track the nature of the patient’s problem and insurance status, and whether the referral led to a procedure. The best approach will be to try to prevent these sorts of things from coming up by maintaining good communication and relations with other physician groups and thinking deliberately about your referral patterns. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
Health IT Hurdles

I rent cars regularly, and only occasionally do I get the same model twice. I’m ready to roll after spending a couple of minutes becoming familiar with a car that is new to me. I adjust the seat and climate control, etc. I resist fiddling with the radio until later. This seems OK to me.
The last time I started clinical practice in a new hospital, I did almost the same thing: I jumped right in and started seeing patients. Other than being provided with my password to the computer system and a dictation code, I had no orientation at all, not even to the hospital floor plan. This, too, seemed reasonable to me at the time. Now I see it differently.
Levels of Complexity
Years ago, learning a new hospital might not have been a lot more difficult than familiarizing yourself with a new rental car, so there didn’t seem to be much need for a detailed orientation. I’m generalizing here, but if you go back far enough in time, the general idea was that it was almost entirely up to the hospital and its staff to get to know the new doctor and how he or she practiced, rather than the doctor adapting to the hospital’s way of doing things.
While at one time hospitals and their systems might have been as similar to one another as a four-door Chevy is to a four-door Ford, today’s hospitals are far more complex. The appropriate transportation analogy might be one type of airplane to another.
The basics of what keeps a two-seat Cessna and a huge 747 flying are the same, but there are so many critical differences that specific training and certification are required for each. Even an accomplished professional pilot who is an ace in a 747 isn’t automatically certified to pilot a smaller 737. In fact, few professional pilots are certified to fly more than one type of commercial airplane at a time. One way to look at this is that the orientation to the plane is so complex that one person can’t be expected to maintain a high level of familiarity with the systems and operation of more than one at a time.
EHR: A Tipping Point
The complexity and unique attributes of hospitals have been increasing steadily for decades, but it seems to me that electronic health records (EHR) represent a huge increase in complexity. No longer can a doctor simply arrive at the hospital confident in her ability to fly this new plane. She will require a reasonably detailed introduction to the hospital’s EHR as part of an orientation that should ideally take place prior to seeing patients.
I worry that it will be increasingly difficult, and potentially unwise, for a doctor in any specialty to practice at more than one or two hospitals that don’t share the same EHR. If a doctor is not proficient in the use of the EHR at a particular site, two things are likely to happen: First, and most alarmingly, the new doctor would probably unintentionally miss important information in the EHR, or might not have time to contemplate the series of buttons to click to check all potentially relevant information. For example, he might not realize the patient already had a series of blood tests, because accessing them requires some unfamiliar clicks of the mouse.
The other thing that might happen if a doctor is not proficient in the use of the hospital’s EHR is that he might be inclined to consult the hospitalist “just to cover all the bases.” In this case, that might be the same as asking the hospitalist to be involved as an EHR expert, rather than for medical expertise that the patient needs.
I practice at a hospital that recently installed a new information system, and some doctors have joked that if they can’t figure out how to use it, they will just consult a hospitalist to look up historical data, etc. I’m not aware of any study looking at this issue, but I suspect “soft” hospitalist consults increase when a hospital installs a new information system.
Rethink New Employee Orientation
I’m convinced that new doctors in all specialties that anticipate having a hospital patient volume above a predetermined threshold should be required to have a formal orientation to the hospital, especially for its information system. This is really important for hospitalists. Every practice should think carefully about a meaningful process of orientation to the hospital and the hospitalist practice itself. The latter would include things like scheduling issues, training in CPT coding, group governance and culture, etc.
My experience is that multistate hospitalist companies have pretty detailed orientation programs; for one thing, they can use this as a differentiator when marketing their services. But private hospitalist practices and groups employed by a single hospital usually have a pretty loose orientation process. It is tricky to find the sweet spot between valuable orientation activities and so much detail that the new doctor is overwhelmed or bored, and unlikely to remember much of what is presented.
And there certainly is a role for waiting to learn some things as the new doctor begins seeing patients. For example, my feeling is that a general orientation to the floor plan is sufficient and the new hire can best learn the details independently during the course of patient care. However, all hospitalists should have some reasonable level of proficiency in the EHR before seeing their first patients.
Hospital-Certified?
If you accept my premise that hospitals were once reasonably similar, like one rental car to another, but have now become as complex and different as jumbo jets, then we’re led to another question: Will we one day decide that a doctor must be certified to practice in a particular hospital by demonstrating knowledge and competence in that particular hospital’s systems and procedures?
Nearly all present-day credentialing and privileging related to a doctor’s work in a hospital focus on that doctor’s prior training and experience. In the case of pilots, there is a requirement to demonstrate proficiency when making a transition to a new airplane.
Maybe an analogous system of certification for a doctor to “fly” each hospital would be valuable for our patients. If training might not make sense for all doctors, then perhaps limit it to those, such as hospitalists, who will have a really high patient volume at the facility.
It would be dizzyingly complex to create and referee such a certification system, so I’m not sure anything like this will happen in my career. And the last thing I want is another set of bureaucratic hurdles.
But it might be worth thinking about how to ensure doctors at a particular hospital are expert enough in that hospital’s unique systems and operations. Start with your group’s orientation process. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
I rent cars regularly, and only occasionally do I get the same model twice. I’m ready to roll after spending a couple of minutes becoming familiar with a car that is new to me. I adjust the seat and climate control, etc. I resist fiddling with the radio until later. This seems OK to me.
The last time I started clinical practice in a new hospital, I did almost the same thing: I jumped right in and started seeing patients. Other than being provided with my password to the computer system and a dictation code, I had no orientation at all, not even to the hospital floor plan. This, too, seemed reasonable to me at the time. Now I see it differently.
Levels of Complexity
Years ago, learning a new hospital might not have been a lot more difficult than familiarizing yourself with a new rental car, so there didn’t seem to be much need for a detailed orientation. I’m generalizing here, but if you go back far enough in time, the general idea was that it was almost entirely up to the hospital and its staff to get to know the new doctor and how he or she practiced, rather than the doctor adapting to the hospital’s way of doing things.
While at one time hospitals and their systems might have been as similar to one another as a four-door Chevy is to a four-door Ford, today’s hospitals are far more complex. The appropriate transportation analogy might be one type of airplane to another.
The basics of what keeps a two-seat Cessna and a huge 747 flying are the same, but there are so many critical differences that specific training and certification are required for each. Even an accomplished professional pilot who is an ace in a 747 isn’t automatically certified to pilot a smaller 737. In fact, few professional pilots are certified to fly more than one type of commercial airplane at a time. One way to look at this is that the orientation to the plane is so complex that one person can’t be expected to maintain a high level of familiarity with the systems and operation of more than one at a time.
EHR: A Tipping Point
The complexity and unique attributes of hospitals have been increasing steadily for decades, but it seems to me that electronic health records (EHR) represent a huge increase in complexity. No longer can a doctor simply arrive at the hospital confident in her ability to fly this new plane. She will require a reasonably detailed introduction to the hospital’s EHR as part of an orientation that should ideally take place prior to seeing patients.
I worry that it will be increasingly difficult, and potentially unwise, for a doctor in any specialty to practice at more than one or two hospitals that don’t share the same EHR. If a doctor is not proficient in the use of the EHR at a particular site, two things are likely to happen: First, and most alarmingly, the new doctor would probably unintentionally miss important information in the EHR, or might not have time to contemplate the series of buttons to click to check all potentially relevant information. For example, he might not realize the patient already had a series of blood tests, because accessing them requires some unfamiliar clicks of the mouse.
The other thing that might happen if a doctor is not proficient in the use of the hospital’s EHR is that he might be inclined to consult the hospitalist “just to cover all the bases.” In this case, that might be the same as asking the hospitalist to be involved as an EHR expert, rather than for medical expertise that the patient needs.
I practice at a hospital that recently installed a new information system, and some doctors have joked that if they can’t figure out how to use it, they will just consult a hospitalist to look up historical data, etc. I’m not aware of any study looking at this issue, but I suspect “soft” hospitalist consults increase when a hospital installs a new information system.
Rethink New Employee Orientation
I’m convinced that new doctors in all specialties that anticipate having a hospital patient volume above a predetermined threshold should be required to have a formal orientation to the hospital, especially for its information system. This is really important for hospitalists. Every practice should think carefully about a meaningful process of orientation to the hospital and the hospitalist practice itself. The latter would include things like scheduling issues, training in CPT coding, group governance and culture, etc.
My experience is that multistate hospitalist companies have pretty detailed orientation programs; for one thing, they can use this as a differentiator when marketing their services. But private hospitalist practices and groups employed by a single hospital usually have a pretty loose orientation process. It is tricky to find the sweet spot between valuable orientation activities and so much detail that the new doctor is overwhelmed or bored, and unlikely to remember much of what is presented.
And there certainly is a role for waiting to learn some things as the new doctor begins seeing patients. For example, my feeling is that a general orientation to the floor plan is sufficient and the new hire can best learn the details independently during the course of patient care. However, all hospitalists should have some reasonable level of proficiency in the EHR before seeing their first patients.
Hospital-Certified?
If you accept my premise that hospitals were once reasonably similar, like one rental car to another, but have now become as complex and different as jumbo jets, then we’re led to another question: Will we one day decide that a doctor must be certified to practice in a particular hospital by demonstrating knowledge and competence in that particular hospital’s systems and procedures?
Nearly all present-day credentialing and privileging related to a doctor’s work in a hospital focus on that doctor’s prior training and experience. In the case of pilots, there is a requirement to demonstrate proficiency when making a transition to a new airplane.
Maybe an analogous system of certification for a doctor to “fly” each hospital would be valuable for our patients. If training might not make sense for all doctors, then perhaps limit it to those, such as hospitalists, who will have a really high patient volume at the facility.
It would be dizzyingly complex to create and referee such a certification system, so I’m not sure anything like this will happen in my career. And the last thing I want is another set of bureaucratic hurdles.
But it might be worth thinking about how to ensure doctors at a particular hospital are expert enough in that hospital’s unique systems and operations. Start with your group’s orientation process. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
I rent cars regularly, and only occasionally do I get the same model twice. I’m ready to roll after spending a couple of minutes becoming familiar with a car that is new to me. I adjust the seat and climate control, etc. I resist fiddling with the radio until later. This seems OK to me.
The last time I started clinical practice in a new hospital, I did almost the same thing: I jumped right in and started seeing patients. Other than being provided with my password to the computer system and a dictation code, I had no orientation at all, not even to the hospital floor plan. This, too, seemed reasonable to me at the time. Now I see it differently.
Levels of Complexity
Years ago, learning a new hospital might not have been a lot more difficult than familiarizing yourself with a new rental car, so there didn’t seem to be much need for a detailed orientation. I’m generalizing here, but if you go back far enough in time, the general idea was that it was almost entirely up to the hospital and its staff to get to know the new doctor and how he or she practiced, rather than the doctor adapting to the hospital’s way of doing things.
While at one time hospitals and their systems might have been as similar to one another as a four-door Chevy is to a four-door Ford, today’s hospitals are far more complex. The appropriate transportation analogy might be one type of airplane to another.
The basics of what keeps a two-seat Cessna and a huge 747 flying are the same, but there are so many critical differences that specific training and certification are required for each. Even an accomplished professional pilot who is an ace in a 747 isn’t automatically certified to pilot a smaller 737. In fact, few professional pilots are certified to fly more than one type of commercial airplane at a time. One way to look at this is that the orientation to the plane is so complex that one person can’t be expected to maintain a high level of familiarity with the systems and operation of more than one at a time.
EHR: A Tipping Point
The complexity and unique attributes of hospitals have been increasing steadily for decades, but it seems to me that electronic health records (EHR) represent a huge increase in complexity. No longer can a doctor simply arrive at the hospital confident in her ability to fly this new plane. She will require a reasonably detailed introduction to the hospital’s EHR as part of an orientation that should ideally take place prior to seeing patients.
I worry that it will be increasingly difficult, and potentially unwise, for a doctor in any specialty to practice at more than one or two hospitals that don’t share the same EHR. If a doctor is not proficient in the use of the EHR at a particular site, two things are likely to happen: First, and most alarmingly, the new doctor would probably unintentionally miss important information in the EHR, or might not have time to contemplate the series of buttons to click to check all potentially relevant information. For example, he might not realize the patient already had a series of blood tests, because accessing them requires some unfamiliar clicks of the mouse.
The other thing that might happen if a doctor is not proficient in the use of the hospital’s EHR is that he might be inclined to consult the hospitalist “just to cover all the bases.” In this case, that might be the same as asking the hospitalist to be involved as an EHR expert, rather than for medical expertise that the patient needs.
I practice at a hospital that recently installed a new information system, and some doctors have joked that if they can’t figure out how to use it, they will just consult a hospitalist to look up historical data, etc. I’m not aware of any study looking at this issue, but I suspect “soft” hospitalist consults increase when a hospital installs a new information system.
Rethink New Employee Orientation
I’m convinced that new doctors in all specialties that anticipate having a hospital patient volume above a predetermined threshold should be required to have a formal orientation to the hospital, especially for its information system. This is really important for hospitalists. Every practice should think carefully about a meaningful process of orientation to the hospital and the hospitalist practice itself. The latter would include things like scheduling issues, training in CPT coding, group governance and culture, etc.
My experience is that multistate hospitalist companies have pretty detailed orientation programs; for one thing, they can use this as a differentiator when marketing their services. But private hospitalist practices and groups employed by a single hospital usually have a pretty loose orientation process. It is tricky to find the sweet spot between valuable orientation activities and so much detail that the new doctor is overwhelmed or bored, and unlikely to remember much of what is presented.
And there certainly is a role for waiting to learn some things as the new doctor begins seeing patients. For example, my feeling is that a general orientation to the floor plan is sufficient and the new hire can best learn the details independently during the course of patient care. However, all hospitalists should have some reasonable level of proficiency in the EHR before seeing their first patients.
Hospital-Certified?
If you accept my premise that hospitals were once reasonably similar, like one rental car to another, but have now become as complex and different as jumbo jets, then we’re led to another question: Will we one day decide that a doctor must be certified to practice in a particular hospital by demonstrating knowledge and competence in that particular hospital’s systems and procedures?
Nearly all present-day credentialing and privileging related to a doctor’s work in a hospital focus on that doctor’s prior training and experience. In the case of pilots, there is a requirement to demonstrate proficiency when making a transition to a new airplane.
Maybe an analogous system of certification for a doctor to “fly” each hospital would be valuable for our patients. If training might not make sense for all doctors, then perhaps limit it to those, such as hospitalists, who will have a really high patient volume at the facility.
It would be dizzyingly complex to create and referee such a certification system, so I’m not sure anything like this will happen in my career. And the last thing I want is another set of bureaucratic hurdles.
But it might be worth thinking about how to ensure doctors at a particular hospital are expert enough in that hospital’s unique systems and operations. Start with your group’s orientation process. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Real Doctoring

Despite never advancing his musical tastes beyond the arena bands of the 1970s and ’80s (think Def Leppard), Mark Williams, MD, FACP, FHM, editor-in-chief of the Journal of Hospital Medicine, has done a great job in securing informative and meaningful research and opinion for the journal. Did you see read the July/August 2010 issue of JHM? It is a great example of content uniquely relevant to hospitalists: several original research articles documenting how hospitalists spend their time. Anyone thinking about the best way to organize and operate a hospitalist practice should read through these studies, along with one published by Kevin O’Leary, MD, and colleagues in the March/April 2006 issue.1 But as a service, I’ll provide a CliffsNotes version of them, along with some comments here.
Time-Motion Studies
What all the studies demonstrate is that academic hospitalists spend only about 15% to 20% of their time in direct patient care, generally defined as time spent taking a patient’s history and examination, meeting with families, etc. Indirect patient care, such as time spent reviewing records, documenting, and communicating with consultants and other patient care staff, consumes about 60% to 70% of their time. The remainder of time is spent in transit (around 7% of each day) and in personal activities.
Remember, all these studies reported on academic hospitalists in large academic medical centers. As noted in the discussion sections, the results in nonteaching community hospitals might be different. My guess is that community hospitalists spend about the same portion of time in the broad categories above, but the individual activities within each category might differ. So I’m willing to believe that these studies tell us something about the majority of hospitalists who practice outside of academia.
90 Minutes of Doctoring?
While the JHM studies assess hospitalist time in a number of different categories, I think it makes the most sense to divide our time into just two categories: “real doctoring” and other. We’ll probably never see a study that divides hospitalists’ time that way, as there would be endless debate about what is and isn’t real doctoring. But it is worth thinking about your work this way.
A lot of what the studies generally defined as indirect patient care is still “real doctoring.” Things like reviewing old records are critically important and typically can’t be done adequately by a nonclinician. But the 10 minutes you spent to get the CD of outside X-rays to show up on your computer, and rearranging the faxed pages so they’re all oriented the same way and in order, are not a good use of your time; a clerical person could do it.
I periodically have an experience that makes me think I spend too much time on patients’ social issues (e.g. long conversations about why Medicare won’t pay for a patient’s skilled nursing facility stay) and too little on “real doctoring.” One such experience is when I have a patient with an unusual pulmonary infiltrate and the radiologist is able to generate a much more comprehensive differential diagnosis than I can. This is embarrassing. Maybe the radiologist is just smarter than I am, but I think it could be because, compared to me, he spends more of his time every day thinking about “real medicine,” such as pulmonary diseases, and less time dealing with nonclinical issues.
Even though we’re paid for a full day’s work, I suspect many hospitalists might spend only about 90 minutes a day immersed in thought about “real medicine,” while doctors in most other specialties probably spend a lot more. If I’m right, then it shouldn’t be a surprise that after practicing for many years, the radiologist who spends several hours a day exercising his fund of medical knowledge probably has more command of some clinical things than a hospitalist who does so only 90 minutes a day. Actively practicing as a hospitalist might not be as effective a method of maintaining proficiency as it is in other specialties. More than many other specialties, we need to rely on self-study and continuing education courses to prevent erosion of our knowledge base.
I’ve just made up this 90-minute figure. I have no idea how accurate it might be, and, the JHM studies don’t offer a lot of insight either. Clearly, it varies a lot by individual doctor and practice setting. How much of your day do you think you spend on “real doctoring” vs. other activities?
What really matters is whether we’ve ended up with too much work that isn’t “real doctoring.” Sure, all of the work needs to be done, but the system isn’t served best when paying a doctor to do work a less expensive person could do.
Max “Doctoring” Time
I think most hospitalists, including me, are stuck spending too much time on activities that don’t add value. For example, while complete and informative documentation is essential, most of us probably spend too much time on it, in part because we’re trying to immunize against lawsuits and ensure our documentation matches the relevant coding regulations.
I think hospitalists have a communication burden that is higher than that of most other specialties. The JHM article by Tipping and colleagues notes that a time-motion study of ED doctors (Ann Emerg Med. 1998:31(1):87-91) found that they spent 13% of their time communicating with other providers and staff, compared with their finding that hospitalists spent 26% of their time communicating.2 Only a portion of this communication is real doctoring. Discussing patient management with a surgeon is, but spending 20 minutes figuring out which surgeon is on call and how to reach her isn’t.
Tipping’s study also found that when patient census was above average, hospitalists spent less time communicating and documenting in the electronic record, even though the total time spent working on those days increased. Of course, it is possible that when the patient census is below average, we just work more slowly and let work fill the time available, and the reduced time spent documenting and communicating when busy simply reflects working more efficiently. But I suspect that when our patient census climbs above a certain point, or we’re made less efficient by things like implementing a new technology, we compensate in part by relying on consultants more to do the real doctoring we would otherwise be doing and communicating with them less.
All of us should be thinking about ways to make communication as efficient as possible so that we can spend less time doing it. I’m hopeful that we will figure out new ways to communicate (e-mail, text, IM, etc.) that are quicker and just as effective in certain situations.
Coda
I try to write most of my columns in a way that minimizes the editorializing and maximizes the practical advice. This month is an exception; it’s all editorializing. But I do have some advice for Dr. Williams: Investigate music options other than the arena bands of the 1980s. Try something like Alison Krauss’ live album or Puccini’s opera Gianni Schicchi, which has the beautiful aria O mio babbino caro.
Or do what I do: Ask former SHM board member Brad Flansbaum, MD, SFHM, for advice. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
References
- O’Leary KJ, Liebovitz DM, Baker DW. How hospitalists spend their time: insights on efficiency and safety. J Hosp Med. 2006;1(2):88-93.
- Tipping MD, Forth VE, O’Leary KJ, et al. Where did the day go? A time-motion study of hospitalists. J Hosp Med. 2010;5(6):323-328.
Despite never advancing his musical tastes beyond the arena bands of the 1970s and ’80s (think Def Leppard), Mark Williams, MD, FACP, FHM, editor-in-chief of the Journal of Hospital Medicine, has done a great job in securing informative and meaningful research and opinion for the journal. Did you see read the July/August 2010 issue of JHM? It is a great example of content uniquely relevant to hospitalists: several original research articles documenting how hospitalists spend their time. Anyone thinking about the best way to organize and operate a hospitalist practice should read through these studies, along with one published by Kevin O’Leary, MD, and colleagues in the March/April 2006 issue.1 But as a service, I’ll provide a CliffsNotes version of them, along with some comments here.
Time-Motion Studies
What all the studies demonstrate is that academic hospitalists spend only about 15% to 20% of their time in direct patient care, generally defined as time spent taking a patient’s history and examination, meeting with families, etc. Indirect patient care, such as time spent reviewing records, documenting, and communicating with consultants and other patient care staff, consumes about 60% to 70% of their time. The remainder of time is spent in transit (around 7% of each day) and in personal activities.
Remember, all these studies reported on academic hospitalists in large academic medical centers. As noted in the discussion sections, the results in nonteaching community hospitals might be different. My guess is that community hospitalists spend about the same portion of time in the broad categories above, but the individual activities within each category might differ. So I’m willing to believe that these studies tell us something about the majority of hospitalists who practice outside of academia.
90 Minutes of Doctoring?
While the JHM studies assess hospitalist time in a number of different categories, I think it makes the most sense to divide our time into just two categories: “real doctoring” and other. We’ll probably never see a study that divides hospitalists’ time that way, as there would be endless debate about what is and isn’t real doctoring. But it is worth thinking about your work this way.
A lot of what the studies generally defined as indirect patient care is still “real doctoring.” Things like reviewing old records are critically important and typically can’t be done adequately by a nonclinician. But the 10 minutes you spent to get the CD of outside X-rays to show up on your computer, and rearranging the faxed pages so they’re all oriented the same way and in order, are not a good use of your time; a clerical person could do it.
I periodically have an experience that makes me think I spend too much time on patients’ social issues (e.g. long conversations about why Medicare won’t pay for a patient’s skilled nursing facility stay) and too little on “real doctoring.” One such experience is when I have a patient with an unusual pulmonary infiltrate and the radiologist is able to generate a much more comprehensive differential diagnosis than I can. This is embarrassing. Maybe the radiologist is just smarter than I am, but I think it could be because, compared to me, he spends more of his time every day thinking about “real medicine,” such as pulmonary diseases, and less time dealing with nonclinical issues.
Even though we’re paid for a full day’s work, I suspect many hospitalists might spend only about 90 minutes a day immersed in thought about “real medicine,” while doctors in most other specialties probably spend a lot more. If I’m right, then it shouldn’t be a surprise that after practicing for many years, the radiologist who spends several hours a day exercising his fund of medical knowledge probably has more command of some clinical things than a hospitalist who does so only 90 minutes a day. Actively practicing as a hospitalist might not be as effective a method of maintaining proficiency as it is in other specialties. More than many other specialties, we need to rely on self-study and continuing education courses to prevent erosion of our knowledge base.
I’ve just made up this 90-minute figure. I have no idea how accurate it might be, and, the JHM studies don’t offer a lot of insight either. Clearly, it varies a lot by individual doctor and practice setting. How much of your day do you think you spend on “real doctoring” vs. other activities?
What really matters is whether we’ve ended up with too much work that isn’t “real doctoring.” Sure, all of the work needs to be done, but the system isn’t served best when paying a doctor to do work a less expensive person could do.
Max “Doctoring” Time
I think most hospitalists, including me, are stuck spending too much time on activities that don’t add value. For example, while complete and informative documentation is essential, most of us probably spend too much time on it, in part because we’re trying to immunize against lawsuits and ensure our documentation matches the relevant coding regulations.
I think hospitalists have a communication burden that is higher than that of most other specialties. The JHM article by Tipping and colleagues notes that a time-motion study of ED doctors (Ann Emerg Med. 1998:31(1):87-91) found that they spent 13% of their time communicating with other providers and staff, compared with their finding that hospitalists spent 26% of their time communicating.2 Only a portion of this communication is real doctoring. Discussing patient management with a surgeon is, but spending 20 minutes figuring out which surgeon is on call and how to reach her isn’t.
Tipping’s study also found that when patient census was above average, hospitalists spent less time communicating and documenting in the electronic record, even though the total time spent working on those days increased. Of course, it is possible that when the patient census is below average, we just work more slowly and let work fill the time available, and the reduced time spent documenting and communicating when busy simply reflects working more efficiently. But I suspect that when our patient census climbs above a certain point, or we’re made less efficient by things like implementing a new technology, we compensate in part by relying on consultants more to do the real doctoring we would otherwise be doing and communicating with them less.
All of us should be thinking about ways to make communication as efficient as possible so that we can spend less time doing it. I’m hopeful that we will figure out new ways to communicate (e-mail, text, IM, etc.) that are quicker and just as effective in certain situations.
Coda
I try to write most of my columns in a way that minimizes the editorializing and maximizes the practical advice. This month is an exception; it’s all editorializing. But I do have some advice for Dr. Williams: Investigate music options other than the arena bands of the 1980s. Try something like Alison Krauss’ live album or Puccini’s opera Gianni Schicchi, which has the beautiful aria O mio babbino caro.
Or do what I do: Ask former SHM board member Brad Flansbaum, MD, SFHM, for advice. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
References
- O’Leary KJ, Liebovitz DM, Baker DW. How hospitalists spend their time: insights on efficiency and safety. J Hosp Med. 2006;1(2):88-93.
- Tipping MD, Forth VE, O’Leary KJ, et al. Where did the day go? A time-motion study of hospitalists. J Hosp Med. 2010;5(6):323-328.
Despite never advancing his musical tastes beyond the arena bands of the 1970s and ’80s (think Def Leppard), Mark Williams, MD, FACP, FHM, editor-in-chief of the Journal of Hospital Medicine, has done a great job in securing informative and meaningful research and opinion for the journal. Did you see read the July/August 2010 issue of JHM? It is a great example of content uniquely relevant to hospitalists: several original research articles documenting how hospitalists spend their time. Anyone thinking about the best way to organize and operate a hospitalist practice should read through these studies, along with one published by Kevin O’Leary, MD, and colleagues in the March/April 2006 issue.1 But as a service, I’ll provide a CliffsNotes version of them, along with some comments here.
Time-Motion Studies
What all the studies demonstrate is that academic hospitalists spend only about 15% to 20% of their time in direct patient care, generally defined as time spent taking a patient’s history and examination, meeting with families, etc. Indirect patient care, such as time spent reviewing records, documenting, and communicating with consultants and other patient care staff, consumes about 60% to 70% of their time. The remainder of time is spent in transit (around 7% of each day) and in personal activities.
Remember, all these studies reported on academic hospitalists in large academic medical centers. As noted in the discussion sections, the results in nonteaching community hospitals might be different. My guess is that community hospitalists spend about the same portion of time in the broad categories above, but the individual activities within each category might differ. So I’m willing to believe that these studies tell us something about the majority of hospitalists who practice outside of academia.
90 Minutes of Doctoring?
While the JHM studies assess hospitalist time in a number of different categories, I think it makes the most sense to divide our time into just two categories: “real doctoring” and other. We’ll probably never see a study that divides hospitalists’ time that way, as there would be endless debate about what is and isn’t real doctoring. But it is worth thinking about your work this way.
A lot of what the studies generally defined as indirect patient care is still “real doctoring.” Things like reviewing old records are critically important and typically can’t be done adequately by a nonclinician. But the 10 minutes you spent to get the CD of outside X-rays to show up on your computer, and rearranging the faxed pages so they’re all oriented the same way and in order, are not a good use of your time; a clerical person could do it.
I periodically have an experience that makes me think I spend too much time on patients’ social issues (e.g. long conversations about why Medicare won’t pay for a patient’s skilled nursing facility stay) and too little on “real doctoring.” One such experience is when I have a patient with an unusual pulmonary infiltrate and the radiologist is able to generate a much more comprehensive differential diagnosis than I can. This is embarrassing. Maybe the radiologist is just smarter than I am, but I think it could be because, compared to me, he spends more of his time every day thinking about “real medicine,” such as pulmonary diseases, and less time dealing with nonclinical issues.
Even though we’re paid for a full day’s work, I suspect many hospitalists might spend only about 90 minutes a day immersed in thought about “real medicine,” while doctors in most other specialties probably spend a lot more. If I’m right, then it shouldn’t be a surprise that after practicing for many years, the radiologist who spends several hours a day exercising his fund of medical knowledge probably has more command of some clinical things than a hospitalist who does so only 90 minutes a day. Actively practicing as a hospitalist might not be as effective a method of maintaining proficiency as it is in other specialties. More than many other specialties, we need to rely on self-study and continuing education courses to prevent erosion of our knowledge base.
I’ve just made up this 90-minute figure. I have no idea how accurate it might be, and, the JHM studies don’t offer a lot of insight either. Clearly, it varies a lot by individual doctor and practice setting. How much of your day do you think you spend on “real doctoring” vs. other activities?
What really matters is whether we’ve ended up with too much work that isn’t “real doctoring.” Sure, all of the work needs to be done, but the system isn’t served best when paying a doctor to do work a less expensive person could do.
Max “Doctoring” Time
I think most hospitalists, including me, are stuck spending too much time on activities that don’t add value. For example, while complete and informative documentation is essential, most of us probably spend too much time on it, in part because we’re trying to immunize against lawsuits and ensure our documentation matches the relevant coding regulations.
I think hospitalists have a communication burden that is higher than that of most other specialties. The JHM article by Tipping and colleagues notes that a time-motion study of ED doctors (Ann Emerg Med. 1998:31(1):87-91) found that they spent 13% of their time communicating with other providers and staff, compared with their finding that hospitalists spent 26% of their time communicating.2 Only a portion of this communication is real doctoring. Discussing patient management with a surgeon is, but spending 20 minutes figuring out which surgeon is on call and how to reach her isn’t.
Tipping’s study also found that when patient census was above average, hospitalists spent less time communicating and documenting in the electronic record, even though the total time spent working on those days increased. Of course, it is possible that when the patient census is below average, we just work more slowly and let work fill the time available, and the reduced time spent documenting and communicating when busy simply reflects working more efficiently. But I suspect that when our patient census climbs above a certain point, or we’re made less efficient by things like implementing a new technology, we compensate in part by relying on consultants more to do the real doctoring we would otherwise be doing and communicating with them less.
All of us should be thinking about ways to make communication as efficient as possible so that we can spend less time doing it. I’m hopeful that we will figure out new ways to communicate (e-mail, text, IM, etc.) that are quicker and just as effective in certain situations.
Coda
I try to write most of my columns in a way that minimizes the editorializing and maximizes the practical advice. This month is an exception; it’s all editorializing. But I do have some advice for Dr. Williams: Investigate music options other than the arena bands of the 1980s. Try something like Alison Krauss’ live album or Puccini’s opera Gianni Schicchi, which has the beautiful aria O mio babbino caro.
Or do what I do: Ask former SHM board member Brad Flansbaum, MD, SFHM, for advice. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
References
- O’Leary KJ, Liebovitz DM, Baker DW. How hospitalists spend their time: insights on efficiency and safety. J Hosp Med. 2006;1(2):88-93.
- Tipping MD, Forth VE, O’Leary KJ, et al. Where did the day go? A time-motion study of hospitalists. J Hosp Med. 2010;5(6):323-328.
Toxic Employees

The providers in every hospitalist practice should be a good fit for the practice’s culture. They should have reasonable relationships with their colleagues in the practice, patients and families, and other staff at the hospital.
I can’t imagine anyone arguing with this point of view. But in my work with hundreds of hospitalist practices over the past 15 years, I’ve found that many practices seem to have a hard time ensuring their providers meet that standard. I can think of lots of reasons for this. The first that comes to mind is the difficult HM recruiting environment. Almost all hospitalist practices needed to grow quickly, and many lowered the bar in the qualifications and the fit of the candidates they hired to make sure they filled all of their positions.
Even if it later becomes clear a provider isn’t a good fit for the group culture, or worse still lacks the knowledge base and judgment to perform well, many practices are reluctant to replace the hospitalist because it might be difficult to find a replacement—and there is no guarantee the new person will perform any better. Because of this, a number of practices have ended up with providers who in many cases have a negative influence on others in the practice, and both the practice and the problem provider would be better off if the provider went elsewhere.
The Problem Physician
To their credit, most practices do act when a provider simply lacks the skill and judgment to perform adequately. This can mean close proctoring/mentoring for an extended period, or requiring specific CME course work to correct a skill that is lacking. But it also means reassigning the person to a different job, or termination.
But in the case of someone with a toxic personality, practices often are more reluctant to act. I’ll often hear the leadership of a practice say something like, “We knew Alice wasn’t a good fit for our practice within a few weeks of her start date.” The start date was several years ago and nothing has been done about this. Not surprisingly, Alice still performs poorly.
I’m not talking about someone who has occasional problems. I’m talking about people who cause problems almost every time they show up to work. Here are some real anecdotes, with fictitious names to ensure anonymity for the person and institution:
- Dr. Lee routinely disappears for several hours, during which he doesn’t answer pages. This even happens when he is the only doctor covering the practice.
- Dr. Lifeson, while generally getting along well with his fellow hospitalists and the nursing staff, can be counted on to complain bitterly about all levels of the hospital administration and leadership. He never misses an opportunity to try to convince other hospitalists that the leadership is not only inept, but also clearly has a malicious intent toward hospitalists.
- Dr. Peart complains incessantly about even tiny inequities in the work schedule or patient load. Others in the group have found that it is easier to ensure he always has the best schedule and lightest patient load, hoping they won’t have to hear his constant complaining. But even that hasn’t stemmed the steady downpour of negativity from him.
In all three of these cases, it seemed clear that the doctor should be terminated. And while the practice leadership agreed with me, they offered several excuses for why they hadn’t taken this step.
- “Who knows if we can find a replacement who will be any better?”
- “But he’s actually a decent doctor and doesn’t get a lot of complaints from patients.”
- “He’s such an angry guy, we worry about litigation if we fire him.”
I can’t offer any clear rule about when a practice should stop trying to improve a provider’s behavior and recognize that it is time to terminate the provider. But it is worth remembering that waiting too long has many costs, including the satisfaction of others in the group. Everyone will think less of the practice they are part of if poor behavior is tolerated.
Assess the Situation, Then Take Action
Most doctors who serve as the lead physician for their group have little or no experience dealing with problem behavior, let alone experience ensuring that necessary steps are followed prior to disciplining or terminating someone. But every hospital has someone who is very knowledgeable about these things; they should be engaged for advice, and, in the case of hospital-employed groups, should participate in the process of counseling and/or termination. It is important to take advantage of the expertise that is available.
Of course, the best approach is to prevent such problems from coming up. The best way to do this is to be very careful when hiring new providers. Checking references carefully is probably the best way to get an idea about whether someone might have behavior or personality problems. There are “job fit” survey instruments that you can use, but I’m not sure how effective they are, or how much value they add for a hospitalist practice beyond other means of assessing the candidate. And in the process of hiring someone, be sure to set behavior expectations very clearly. A new candidate should know that you will not tolerate not living up to behavioral expectations.
When dealing with bad behavior, make sure that you follow a careful and well-documented process. If someone still makes it through the hiring process only to be revealed as a troublemaker soon after their start date, don’t wait to sit that person down for very clear counseling; insist that their behavior change. Take notes of each meeting, and consider having the problem doctor sign and date the notes. While it might be easier to just wait and see if the first instance of bad behavior was an anomaly, that usually is a bad idea.
You should consider bringing the problem provider into the tent. The root of some bad behavior (i.e. criticism of leadership) is a person’s insecurity and lack of a feeling of ownership or control of their role in the practice. In that case, it might be reasonable to invite such a person into a role of greater responsibility in the practice so that they feel more in control. For example, a doctor who constantly complains about the work schedule might be invited to join the group’s executive committee or take on some other formal leadership role in the practice. This could backfire, so it should be tried only in carefully selected cases, and with the problem doctor’s clear understanding that they are being given a chance to have a bigger role in the practice but must improve their behavior or face serious consequences that could include termination.
I have seen this work beautifully in some cases, curing the problem behavior and turning the doctor into a valuable asset. I only wish there were a reliable way to know when to try this strategy. Sadly, it just requires judgment and intuition. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
The providers in every hospitalist practice should be a good fit for the practice’s culture. They should have reasonable relationships with their colleagues in the practice, patients and families, and other staff at the hospital.
I can’t imagine anyone arguing with this point of view. But in my work with hundreds of hospitalist practices over the past 15 years, I’ve found that many practices seem to have a hard time ensuring their providers meet that standard. I can think of lots of reasons for this. The first that comes to mind is the difficult HM recruiting environment. Almost all hospitalist practices needed to grow quickly, and many lowered the bar in the qualifications and the fit of the candidates they hired to make sure they filled all of their positions.
Even if it later becomes clear a provider isn’t a good fit for the group culture, or worse still lacks the knowledge base and judgment to perform well, many practices are reluctant to replace the hospitalist because it might be difficult to find a replacement—and there is no guarantee the new person will perform any better. Because of this, a number of practices have ended up with providers who in many cases have a negative influence on others in the practice, and both the practice and the problem provider would be better off if the provider went elsewhere.
The Problem Physician
To their credit, most practices do act when a provider simply lacks the skill and judgment to perform adequately. This can mean close proctoring/mentoring for an extended period, or requiring specific CME course work to correct a skill that is lacking. But it also means reassigning the person to a different job, or termination.
But in the case of someone with a toxic personality, practices often are more reluctant to act. I’ll often hear the leadership of a practice say something like, “We knew Alice wasn’t a good fit for our practice within a few weeks of her start date.” The start date was several years ago and nothing has been done about this. Not surprisingly, Alice still performs poorly.
I’m not talking about someone who has occasional problems. I’m talking about people who cause problems almost every time they show up to work. Here are some real anecdotes, with fictitious names to ensure anonymity for the person and institution:
- Dr. Lee routinely disappears for several hours, during which he doesn’t answer pages. This even happens when he is the only doctor covering the practice.
- Dr. Lifeson, while generally getting along well with his fellow hospitalists and the nursing staff, can be counted on to complain bitterly about all levels of the hospital administration and leadership. He never misses an opportunity to try to convince other hospitalists that the leadership is not only inept, but also clearly has a malicious intent toward hospitalists.
- Dr. Peart complains incessantly about even tiny inequities in the work schedule or patient load. Others in the group have found that it is easier to ensure he always has the best schedule and lightest patient load, hoping they won’t have to hear his constant complaining. But even that hasn’t stemmed the steady downpour of negativity from him.
In all three of these cases, it seemed clear that the doctor should be terminated. And while the practice leadership agreed with me, they offered several excuses for why they hadn’t taken this step.
- “Who knows if we can find a replacement who will be any better?”
- “But he’s actually a decent doctor and doesn’t get a lot of complaints from patients.”
- “He’s such an angry guy, we worry about litigation if we fire him.”
I can’t offer any clear rule about when a practice should stop trying to improve a provider’s behavior and recognize that it is time to terminate the provider. But it is worth remembering that waiting too long has many costs, including the satisfaction of others in the group. Everyone will think less of the practice they are part of if poor behavior is tolerated.
Assess the Situation, Then Take Action
Most doctors who serve as the lead physician for their group have little or no experience dealing with problem behavior, let alone experience ensuring that necessary steps are followed prior to disciplining or terminating someone. But every hospital has someone who is very knowledgeable about these things; they should be engaged for advice, and, in the case of hospital-employed groups, should participate in the process of counseling and/or termination. It is important to take advantage of the expertise that is available.
Of course, the best approach is to prevent such problems from coming up. The best way to do this is to be very careful when hiring new providers. Checking references carefully is probably the best way to get an idea about whether someone might have behavior or personality problems. There are “job fit” survey instruments that you can use, but I’m not sure how effective they are, or how much value they add for a hospitalist practice beyond other means of assessing the candidate. And in the process of hiring someone, be sure to set behavior expectations very clearly. A new candidate should know that you will not tolerate not living up to behavioral expectations.
When dealing with bad behavior, make sure that you follow a careful and well-documented process. If someone still makes it through the hiring process only to be revealed as a troublemaker soon after their start date, don’t wait to sit that person down for very clear counseling; insist that their behavior change. Take notes of each meeting, and consider having the problem doctor sign and date the notes. While it might be easier to just wait and see if the first instance of bad behavior was an anomaly, that usually is a bad idea.
You should consider bringing the problem provider into the tent. The root of some bad behavior (i.e. criticism of leadership) is a person’s insecurity and lack of a feeling of ownership or control of their role in the practice. In that case, it might be reasonable to invite such a person into a role of greater responsibility in the practice so that they feel more in control. For example, a doctor who constantly complains about the work schedule might be invited to join the group’s executive committee or take on some other formal leadership role in the practice. This could backfire, so it should be tried only in carefully selected cases, and with the problem doctor’s clear understanding that they are being given a chance to have a bigger role in the practice but must improve their behavior or face serious consequences that could include termination.
I have seen this work beautifully in some cases, curing the problem behavior and turning the doctor into a valuable asset. I only wish there were a reliable way to know when to try this strategy. Sadly, it just requires judgment and intuition. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
The providers in every hospitalist practice should be a good fit for the practice’s culture. They should have reasonable relationships with their colleagues in the practice, patients and families, and other staff at the hospital.
I can’t imagine anyone arguing with this point of view. But in my work with hundreds of hospitalist practices over the past 15 years, I’ve found that many practices seem to have a hard time ensuring their providers meet that standard. I can think of lots of reasons for this. The first that comes to mind is the difficult HM recruiting environment. Almost all hospitalist practices needed to grow quickly, and many lowered the bar in the qualifications and the fit of the candidates they hired to make sure they filled all of their positions.
Even if it later becomes clear a provider isn’t a good fit for the group culture, or worse still lacks the knowledge base and judgment to perform well, many practices are reluctant to replace the hospitalist because it might be difficult to find a replacement—and there is no guarantee the new person will perform any better. Because of this, a number of practices have ended up with providers who in many cases have a negative influence on others in the practice, and both the practice and the problem provider would be better off if the provider went elsewhere.
The Problem Physician
To their credit, most practices do act when a provider simply lacks the skill and judgment to perform adequately. This can mean close proctoring/mentoring for an extended period, or requiring specific CME course work to correct a skill that is lacking. But it also means reassigning the person to a different job, or termination.
But in the case of someone with a toxic personality, practices often are more reluctant to act. I’ll often hear the leadership of a practice say something like, “We knew Alice wasn’t a good fit for our practice within a few weeks of her start date.” The start date was several years ago and nothing has been done about this. Not surprisingly, Alice still performs poorly.
I’m not talking about someone who has occasional problems. I’m talking about people who cause problems almost every time they show up to work. Here are some real anecdotes, with fictitious names to ensure anonymity for the person and institution:
- Dr. Lee routinely disappears for several hours, during which he doesn’t answer pages. This even happens when he is the only doctor covering the practice.
- Dr. Lifeson, while generally getting along well with his fellow hospitalists and the nursing staff, can be counted on to complain bitterly about all levels of the hospital administration and leadership. He never misses an opportunity to try to convince other hospitalists that the leadership is not only inept, but also clearly has a malicious intent toward hospitalists.
- Dr. Peart complains incessantly about even tiny inequities in the work schedule or patient load. Others in the group have found that it is easier to ensure he always has the best schedule and lightest patient load, hoping they won’t have to hear his constant complaining. But even that hasn’t stemmed the steady downpour of negativity from him.
In all three of these cases, it seemed clear that the doctor should be terminated. And while the practice leadership agreed with me, they offered several excuses for why they hadn’t taken this step.
- “Who knows if we can find a replacement who will be any better?”
- “But he’s actually a decent doctor and doesn’t get a lot of complaints from patients.”
- “He’s such an angry guy, we worry about litigation if we fire him.”
I can’t offer any clear rule about when a practice should stop trying to improve a provider’s behavior and recognize that it is time to terminate the provider. But it is worth remembering that waiting too long has many costs, including the satisfaction of others in the group. Everyone will think less of the practice they are part of if poor behavior is tolerated.
Assess the Situation, Then Take Action
Most doctors who serve as the lead physician for their group have little or no experience dealing with problem behavior, let alone experience ensuring that necessary steps are followed prior to disciplining or terminating someone. But every hospital has someone who is very knowledgeable about these things; they should be engaged for advice, and, in the case of hospital-employed groups, should participate in the process of counseling and/or termination. It is important to take advantage of the expertise that is available.
Of course, the best approach is to prevent such problems from coming up. The best way to do this is to be very careful when hiring new providers. Checking references carefully is probably the best way to get an idea about whether someone might have behavior or personality problems. There are “job fit” survey instruments that you can use, but I’m not sure how effective they are, or how much value they add for a hospitalist practice beyond other means of assessing the candidate. And in the process of hiring someone, be sure to set behavior expectations very clearly. A new candidate should know that you will not tolerate not living up to behavioral expectations.
When dealing with bad behavior, make sure that you follow a careful and well-documented process. If someone still makes it through the hiring process only to be revealed as a troublemaker soon after their start date, don’t wait to sit that person down for very clear counseling; insist that their behavior change. Take notes of each meeting, and consider having the problem doctor sign and date the notes. While it might be easier to just wait and see if the first instance of bad behavior was an anomaly, that usually is a bad idea.
You should consider bringing the problem provider into the tent. The root of some bad behavior (i.e. criticism of leadership) is a person’s insecurity and lack of a feeling of ownership or control of their role in the practice. In that case, it might be reasonable to invite such a person into a role of greater responsibility in the practice so that they feel more in control. For example, a doctor who constantly complains about the work schedule might be invited to join the group’s executive committee or take on some other formal leadership role in the practice. This could backfire, so it should be tried only in carefully selected cases, and with the problem doctor’s clear understanding that they are being given a chance to have a bigger role in the practice but must improve their behavior or face serious consequences that could include termination.
I have seen this work beautifully in some cases, curing the problem behavior and turning the doctor into a valuable asset. I only wish there were a reliable way to know when to try this strategy. Sadly, it just requires judgment and intuition. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
Volume Control, Part II

Last month I began looking at ways hospitalist practices can manage unpredictable increases in patient volume, also known as surge staffing. I provided my view of a “jeopardy” system and a patient volume cap for hospitalists. While both are potentially very effective, they have a high cost and in my view are imperfect solutions. This month I’ll examine some less common strategies to provide surge staffing. Although less popular, I think these options are more valuable.
Schedule More Providers
I’ve worked with a lot of practices and am struck by how patient volume for nearly all of them falls within a reasonably predictable range. While no one can predict with certainty which days will be unusually busy or slow, nearly all practices have a range of daily encounters that is roughly half to 1 1/2 of the mean. For example, if a practice has a mean of 60 billable encounters per day, it probably ranges from about 30 to 90 encounters on any given day. (The larger the practice, the more likely they are to conform to this range. Small practices, with average daily encounters fewer than 20, have a much wider range of daily volumes as a percent of the mean.)
Despite knowing that volumes will vary unpredictably, most practices provide the same fixed “dose” of provider staffing every day—that is, the single most common model for staffing and scheduling is to provide a fixed number of day-shift doctors (“rounders”) who work a fixed number of hours. For example, with an average of 60 billable encounters a day, a hospitalist group might decide to staff with four day-shift rounders working 12-hour shifts. This equates to a fixed 48 hours of daytime staffing. This is reasonable until the busy days arrive. Those four doctors will be much busier than average when there are 90 patients to see in a day, and will probably have a hard time seeing 22 or 23 patients each during their 12-hour shift. If such a busy day occurs more than a couple of times annually, then the practice should probably make some changes.
One approach to solving this type of staffing predicament is to add a fifth day-shift rounder. In other words, when making staffing decisions, consider giving more weight to the busiest days than the average day. This sounds fine until thinking about the practice budget. It will be pretty expensive to add doctors every day just so there are enough on duty when things get really busy. But if the hospitalists are willing to accept reduced compensation, then it might be financially reasonable to go ahead and add staff. This is easiest to do when the hospitalists are paid a significant (e.g. ≥50%) portion of their income based on their productivity, which will enable the hospitalists themselves to have a lot of say about when it is time to add staff. (Being paid on a nearly fixed annual salary means that it is the finance person who usually has the say about when it is time to add staff. And you can bet he’ll be making staffing decisions based on the average daily encounters, rather than the busy days.)
My own preference would be to do just that: Accept a reduction in compensation in return for protection against really busy and stressful days. I’m not suggesting others should agree with me, and in my experience, most don’t. (My own practice partners don’t agree with me on this one.) So I’m not really recommending it as a best practice, but I want to ensure that you don’t forget it is an option. And keep in mind you could adjust staffing by degrees; some settings might add a half-time physician or a nonphysician provider to try to find the sweet spot between having enough staff on duty every day to handle surges in volume and the cost of that staffing to the employer—or the hospitalists themselves.
Of course, if I were willing to reduce my compensation and average daily workload, then I would expect to be freed from the expectation that all rounding doctors work 12-hour shifts. Let’s turn our attention to the interplay between fixed day-shift durations and surge staffing.
Fixed-Shift Schedules Inhibit Surge Capacity
I think it usually is best to avoid fixed durations for day shifts. It might be necessary to require at least one daytime rounder to stay at least until a specified time (e.g. the arrival of the night-shift doctor), but in most cases it is reasonable for some rounders to leave when their work is done. They might need to continue responding to pages until the start of the night shift, but it usually isn’t necessary to have all rounders in the hospital until a predetermined end of the shift.
The problem is that when shifts have a fixed duration, the providers will focus on the start and stop time of their shift and might be unwilling to work beyond it. If instead there are no clearly fixed start and stop times for each day shift, then the hospitalists are likely to be willing to simply work longer on busy days, as long as they can work shorter on slow days. This is probably the most effective method of surge capacity, and it fits well with staffing each day with more providers than are required for the average patient volume.
Simply having the rounding doctors work longer on busy days must be done within reason. And there is a really wide range of opinion about what is reasonable. I think it is reasonable if a hospitalist works two or three hours longer than usual for three or four consecutive busy days, as long as the hospitalist is allowed to work less on days that are not very busy. But just what is a reasonable maximum daily amount of work for even one day is a topic that can lead to passionate debate. You’ll have to decide the details of what is and isn’t acceptable in your group.
Unit-Based Assignments
Aside from fixed-duration day shifts, unit-based assignment of hospitalists is the most common practice inhibiting surge capacity. Not long ago I worked with a practice that followed very strict unit-based assignments, which significantly inhibited “load-leveling,” and thus surge capacity. On any given day the patient volume for the whole practice might be very reasonable, but because it was never distributed evenly among the rounders, there was a very good chance that at least one doctor was drowning in work. And because of the strict approach, the other doctors didn’t come to the rescue.
I think the only reasonable approach is to deviate from such a strict unit-based assignment, at least a little. One rounder could be a utility doctor who doesn’t have her own unit and instead roams throughout the hospital, having been assigned patients based on the workload of each of her unit-based colleagues. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants (www.nelsonflores.com) and codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Last month I began looking at ways hospitalist practices can manage unpredictable increases in patient volume, also known as surge staffing. I provided my view of a “jeopardy” system and a patient volume cap for hospitalists. While both are potentially very effective, they have a high cost and in my view are imperfect solutions. This month I’ll examine some less common strategies to provide surge staffing. Although less popular, I think these options are more valuable.
Schedule More Providers
I’ve worked with a lot of practices and am struck by how patient volume for nearly all of them falls within a reasonably predictable range. While no one can predict with certainty which days will be unusually busy or slow, nearly all practices have a range of daily encounters that is roughly half to 1 1/2 of the mean. For example, if a practice has a mean of 60 billable encounters per day, it probably ranges from about 30 to 90 encounters on any given day. (The larger the practice, the more likely they are to conform to this range. Small practices, with average daily encounters fewer than 20, have a much wider range of daily volumes as a percent of the mean.)
Despite knowing that volumes will vary unpredictably, most practices provide the same fixed “dose” of provider staffing every day—that is, the single most common model for staffing and scheduling is to provide a fixed number of day-shift doctors (“rounders”) who work a fixed number of hours. For example, with an average of 60 billable encounters a day, a hospitalist group might decide to staff with four day-shift rounders working 12-hour shifts. This equates to a fixed 48 hours of daytime staffing. This is reasonable until the busy days arrive. Those four doctors will be much busier than average when there are 90 patients to see in a day, and will probably have a hard time seeing 22 or 23 patients each during their 12-hour shift. If such a busy day occurs more than a couple of times annually, then the practice should probably make some changes.
One approach to solving this type of staffing predicament is to add a fifth day-shift rounder. In other words, when making staffing decisions, consider giving more weight to the busiest days than the average day. This sounds fine until thinking about the practice budget. It will be pretty expensive to add doctors every day just so there are enough on duty when things get really busy. But if the hospitalists are willing to accept reduced compensation, then it might be financially reasonable to go ahead and add staff. This is easiest to do when the hospitalists are paid a significant (e.g. ≥50%) portion of their income based on their productivity, which will enable the hospitalists themselves to have a lot of say about when it is time to add staff. (Being paid on a nearly fixed annual salary means that it is the finance person who usually has the say about when it is time to add staff. And you can bet he’ll be making staffing decisions based on the average daily encounters, rather than the busy days.)
My own preference would be to do just that: Accept a reduction in compensation in return for protection against really busy and stressful days. I’m not suggesting others should agree with me, and in my experience, most don’t. (My own practice partners don’t agree with me on this one.) So I’m not really recommending it as a best practice, but I want to ensure that you don’t forget it is an option. And keep in mind you could adjust staffing by degrees; some settings might add a half-time physician or a nonphysician provider to try to find the sweet spot between having enough staff on duty every day to handle surges in volume and the cost of that staffing to the employer—or the hospitalists themselves.
Of course, if I were willing to reduce my compensation and average daily workload, then I would expect to be freed from the expectation that all rounding doctors work 12-hour shifts. Let’s turn our attention to the interplay between fixed day-shift durations and surge staffing.
Fixed-Shift Schedules Inhibit Surge Capacity
I think it usually is best to avoid fixed durations for day shifts. It might be necessary to require at least one daytime rounder to stay at least until a specified time (e.g. the arrival of the night-shift doctor), but in most cases it is reasonable for some rounders to leave when their work is done. They might need to continue responding to pages until the start of the night shift, but it usually isn’t necessary to have all rounders in the hospital until a predetermined end of the shift.
The problem is that when shifts have a fixed duration, the providers will focus on the start and stop time of their shift and might be unwilling to work beyond it. If instead there are no clearly fixed start and stop times for each day shift, then the hospitalists are likely to be willing to simply work longer on busy days, as long as they can work shorter on slow days. This is probably the most effective method of surge capacity, and it fits well with staffing each day with more providers than are required for the average patient volume.
Simply having the rounding doctors work longer on busy days must be done within reason. And there is a really wide range of opinion about what is reasonable. I think it is reasonable if a hospitalist works two or three hours longer than usual for three or four consecutive busy days, as long as the hospitalist is allowed to work less on days that are not very busy. But just what is a reasonable maximum daily amount of work for even one day is a topic that can lead to passionate debate. You’ll have to decide the details of what is and isn’t acceptable in your group.
Unit-Based Assignments
Aside from fixed-duration day shifts, unit-based assignment of hospitalists is the most common practice inhibiting surge capacity. Not long ago I worked with a practice that followed very strict unit-based assignments, which significantly inhibited “load-leveling,” and thus surge capacity. On any given day the patient volume for the whole practice might be very reasonable, but because it was never distributed evenly among the rounders, there was a very good chance that at least one doctor was drowning in work. And because of the strict approach, the other doctors didn’t come to the rescue.
I think the only reasonable approach is to deviate from such a strict unit-based assignment, at least a little. One rounder could be a utility doctor who doesn’t have her own unit and instead roams throughout the hospital, having been assigned patients based on the workload of each of her unit-based colleagues. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants (www.nelsonflores.com) and codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Last month I began looking at ways hospitalist practices can manage unpredictable increases in patient volume, also known as surge staffing. I provided my view of a “jeopardy” system and a patient volume cap for hospitalists. While both are potentially very effective, they have a high cost and in my view are imperfect solutions. This month I’ll examine some less common strategies to provide surge staffing. Although less popular, I think these options are more valuable.
Schedule More Providers
I’ve worked with a lot of practices and am struck by how patient volume for nearly all of them falls within a reasonably predictable range. While no one can predict with certainty which days will be unusually busy or slow, nearly all practices have a range of daily encounters that is roughly half to 1 1/2 of the mean. For example, if a practice has a mean of 60 billable encounters per day, it probably ranges from about 30 to 90 encounters on any given day. (The larger the practice, the more likely they are to conform to this range. Small practices, with average daily encounters fewer than 20, have a much wider range of daily volumes as a percent of the mean.)
Despite knowing that volumes will vary unpredictably, most practices provide the same fixed “dose” of provider staffing every day—that is, the single most common model for staffing and scheduling is to provide a fixed number of day-shift doctors (“rounders”) who work a fixed number of hours. For example, with an average of 60 billable encounters a day, a hospitalist group might decide to staff with four day-shift rounders working 12-hour shifts. This equates to a fixed 48 hours of daytime staffing. This is reasonable until the busy days arrive. Those four doctors will be much busier than average when there are 90 patients to see in a day, and will probably have a hard time seeing 22 or 23 patients each during their 12-hour shift. If such a busy day occurs more than a couple of times annually, then the practice should probably make some changes.
One approach to solving this type of staffing predicament is to add a fifth day-shift rounder. In other words, when making staffing decisions, consider giving more weight to the busiest days than the average day. This sounds fine until thinking about the practice budget. It will be pretty expensive to add doctors every day just so there are enough on duty when things get really busy. But if the hospitalists are willing to accept reduced compensation, then it might be financially reasonable to go ahead and add staff. This is easiest to do when the hospitalists are paid a significant (e.g. ≥50%) portion of their income based on their productivity, which will enable the hospitalists themselves to have a lot of say about when it is time to add staff. (Being paid on a nearly fixed annual salary means that it is the finance person who usually has the say about when it is time to add staff. And you can bet he’ll be making staffing decisions based on the average daily encounters, rather than the busy days.)
My own preference would be to do just that: Accept a reduction in compensation in return for protection against really busy and stressful days. I’m not suggesting others should agree with me, and in my experience, most don’t. (My own practice partners don’t agree with me on this one.) So I’m not really recommending it as a best practice, but I want to ensure that you don’t forget it is an option. And keep in mind you could adjust staffing by degrees; some settings might add a half-time physician or a nonphysician provider to try to find the sweet spot between having enough staff on duty every day to handle surges in volume and the cost of that staffing to the employer—or the hospitalists themselves.
Of course, if I were willing to reduce my compensation and average daily workload, then I would expect to be freed from the expectation that all rounding doctors work 12-hour shifts. Let’s turn our attention to the interplay between fixed day-shift durations and surge staffing.
Fixed-Shift Schedules Inhibit Surge Capacity
I think it usually is best to avoid fixed durations for day shifts. It might be necessary to require at least one daytime rounder to stay at least until a specified time (e.g. the arrival of the night-shift doctor), but in most cases it is reasonable for some rounders to leave when their work is done. They might need to continue responding to pages until the start of the night shift, but it usually isn’t necessary to have all rounders in the hospital until a predetermined end of the shift.
The problem is that when shifts have a fixed duration, the providers will focus on the start and stop time of their shift and might be unwilling to work beyond it. If instead there are no clearly fixed start and stop times for each day shift, then the hospitalists are likely to be willing to simply work longer on busy days, as long as they can work shorter on slow days. This is probably the most effective method of surge capacity, and it fits well with staffing each day with more providers than are required for the average patient volume.
Simply having the rounding doctors work longer on busy days must be done within reason. And there is a really wide range of opinion about what is reasonable. I think it is reasonable if a hospitalist works two or three hours longer than usual for three or four consecutive busy days, as long as the hospitalist is allowed to work less on days that are not very busy. But just what is a reasonable maximum daily amount of work for even one day is a topic that can lead to passionate debate. You’ll have to decide the details of what is and isn’t acceptable in your group.
Unit-Based Assignments
Aside from fixed-duration day shifts, unit-based assignment of hospitalists is the most common practice inhibiting surge capacity. Not long ago I worked with a practice that followed very strict unit-based assignments, which significantly inhibited “load-leveling,” and thus surge capacity. On any given day the patient volume for the whole practice might be very reasonable, but because it was never distributed evenly among the rounders, there was a very good chance that at least one doctor was drowning in work. And because of the strict approach, the other doctors didn’t come to the rescue.
I think the only reasonable approach is to deviate from such a strict unit-based assignment, at least a little. One rounder could be a utility doctor who doesn’t have her own unit and instead roams throughout the hospital, having been assigned patients based on the workload of each of her unit-based colleagues. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants (www.nelsonflores.com) and codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Surge Protection

Unpredictable workloads and frequent interruptions are the things I regard as the most stressful components of work as a hospitalist. Your list might be very different, but I bet unpredictable workloads ranks at least in the top five of every hospitalist’s list.
I’ve discussed interruptions previously (see “Really, It’s Switch-Tasking,” p. 68, November 2008; “Technological Advance or Workplace Setback?” p. 69, December 2008), but this month and next will turn to unpredictable workloads. In other words, what are the strategies available to a hospitalist practice to provide surge capacity in response to such unpredictable increases in patient volume as an uptick in census or daily admissions 50% to 100% above normal? I’ll leave to others the topic of how hospitals respond to such disasters as terrorist attacks, earthquakes, etc.
The Bottom Line
Sadly, there is no magic bullet for the “surge” problem, and no way to protect on-duty hospitalists from the need to work harder when it gets busy. But we needn’t feel too sorry for ourselves; doctors in most other specialties who practice in the hospital face the same problem and tend to rely heavily on simply working harder and longer when it is unusually busy. Sometimes they couple the “work harder” mantra with other strategies, such as calling another doctor in to help.
Hospitalists have a duty to ensure high patient volume doesn’t lead to deterioration in the quality of patient care, but occasionally working longer days than average probably poses a low risk, and might be less risky than the additional handoffs usually associated with having a doctor on “jeopardy” to be called in when it’s busy. Routinely or frequently working unreasonably long days is another story.
The trick for HM programs is to build some surge capacity into the routine daily staffing 1) without exceeding a reasonable budget, while 2) ensuring that the hospitalists don’t simply become accustomed to light workloads as the only reasonable norm, which could lead to them becoming unwilling to accept higher, but still reasonable, workloads when needed. (More on these issues later.) First, I’ll go through what I see as the pros and cons of several approaches to addressing surges in patient volume. All are in use with variable frequency around the country.
“Jeopardy” System
In its most common form, a jeopardy system has an unscheduled doctor each day who must remain available on short notice by pager. When patient volume surges, the unscheduled doctor is paged to come in and help. In most cases, this doctor focuses primarily—or exclusively—on admitting patients for a few hours. So it is most common for this doctor to be called in late in the afternoon or early in the evening. The jeopardy doctor usually turns over all admitted patients to another hospitalist in the group for all subsequent care. In addition to providing surge capacity, the jeopardy doctor almost always is used to cover unexpected absences of scheduled doctors, including illness-related absences.
Sometimes this doctor is paid extra for each day or week spent being “available” on jeopardy duty (not to be confused with jury duty, though it can be equally difficult to get exempted from). Then again, it is not uncommon to have jeopardy duty included in base compensation. However, once a jeopardy doctor is actually called in to work, most practices pay additional compensation, often based on an hourly rate that usually is higher than the average compensation generated per hour for nonjeopardy work.
There are a number of reasonable ways to compensate the jeopardy doctor. You probably can get some good ideas by talking with others in your hospital who function in a similar capacity, such as cath-lab technicians who get called in on nights and weekends.
No definitive data are available to show how common the jeopardy system is, but my experience is that 30% to 50% of HM groups use some form of it. Its popularity is proof that it is a reasonable system, but I’m not convinced. I think it is in use by a lot of groups not because it is an optimal way to ensure surge capacity, but because it is easy to conceptualize and put in place, and because many hospitalists came from residency programs in which the system was standard.
The gaps between theoretical and realized benefits become evident once a practice implements a jeopardy system. For example, it might be really busy today, but Dr. Stravinsky doesn’t call in Dr. Copeland, who is on jeopardy, because next week their roles will be reversed and Dr. Stravinsky sure hopes he won’t be called in. No one wants to be the weak doctor who calls in the jeopardy doctor and spoils what was otherwise a day off.
I’ve worked with a lot of practices who say they have a jeopardy system in place, but when I ask for the last time the jeopardy doctor was called in, they say it has been more than a year, or in some cases never. So even if the policy manual says they have a jeopardy system, the doctors never activate it, so it provides no benefit.
Practices that do utilize the jeopardy doctor have their own problems, such as assigning that doctor’s admissions the next day. The jeopardy doctor might provide some relief today, but they essentially just delay the work of having to get to know all of those new patients until the morning, when everyone is very busy with rounds. So while there might be significant benefit in activating the jeopardy system today, it could just delay the problem of high workload until the next morning, which isn’t much of a net benefit for the practice.
A small number of practices call in the jeopardy doctor frequently, and sometimes have that doctor continue to round on admitted patients for the next few days. This usage might get the most value out of the system, but the practice should consider if it is more cost-effective, and less stressful for the doctors, if the system were reversed. For example, instead of having the doctor on jeopardy and called in as necessary, the doctor would report to work and be given the day off or let go early when it isn’t busy.
Despite my reservations, if you are convinced the jeopardy system is valuable and cost-effective, keep it in place. However, if your group is thinking about options to handle surge capacity, don’t be too quick to adopt a jeopardy system. It usually falls far short of a perfect solution.
Patient Volume Cap
Another way to address the problem of unpredictable increases in patient volume is to establish a patient volume (e.g., total census) cap for the whole hospitalist practice. Like the jeopardy system, this is an appealingly uncomplicated idea, and hospitalists who have finished residency within the last few years all worked with a cap.
Except for the rarest of exceptions, this is a poor idea and should be avoided if at all possible. I’ll leave for another time a discussion of all the political and financial costs of a cap system, but trust me on this one. It is best to avoid a cap.
Stay Tuned …
Next month, I’ll examine other strategies to provide surge capacity. I think they’re more valuable than the two I’ve mentioned here, but I need to warn you that they aren’t perfect and are more complicated to operationalize. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Unpredictable workloads and frequent interruptions are the things I regard as the most stressful components of work as a hospitalist. Your list might be very different, but I bet unpredictable workloads ranks at least in the top five of every hospitalist’s list.
I’ve discussed interruptions previously (see “Really, It’s Switch-Tasking,” p. 68, November 2008; “Technological Advance or Workplace Setback?” p. 69, December 2008), but this month and next will turn to unpredictable workloads. In other words, what are the strategies available to a hospitalist practice to provide surge capacity in response to such unpredictable increases in patient volume as an uptick in census or daily admissions 50% to 100% above normal? I’ll leave to others the topic of how hospitals respond to such disasters as terrorist attacks, earthquakes, etc.
The Bottom Line
Sadly, there is no magic bullet for the “surge” problem, and no way to protect on-duty hospitalists from the need to work harder when it gets busy. But we needn’t feel too sorry for ourselves; doctors in most other specialties who practice in the hospital face the same problem and tend to rely heavily on simply working harder and longer when it is unusually busy. Sometimes they couple the “work harder” mantra with other strategies, such as calling another doctor in to help.
Hospitalists have a duty to ensure high patient volume doesn’t lead to deterioration in the quality of patient care, but occasionally working longer days than average probably poses a low risk, and might be less risky than the additional handoffs usually associated with having a doctor on “jeopardy” to be called in when it’s busy. Routinely or frequently working unreasonably long days is another story.
The trick for HM programs is to build some surge capacity into the routine daily staffing 1) without exceeding a reasonable budget, while 2) ensuring that the hospitalists don’t simply become accustomed to light workloads as the only reasonable norm, which could lead to them becoming unwilling to accept higher, but still reasonable, workloads when needed. (More on these issues later.) First, I’ll go through what I see as the pros and cons of several approaches to addressing surges in patient volume. All are in use with variable frequency around the country.
“Jeopardy” System
In its most common form, a jeopardy system has an unscheduled doctor each day who must remain available on short notice by pager. When patient volume surges, the unscheduled doctor is paged to come in and help. In most cases, this doctor focuses primarily—or exclusively—on admitting patients for a few hours. So it is most common for this doctor to be called in late in the afternoon or early in the evening. The jeopardy doctor usually turns over all admitted patients to another hospitalist in the group for all subsequent care. In addition to providing surge capacity, the jeopardy doctor almost always is used to cover unexpected absences of scheduled doctors, including illness-related absences.
Sometimes this doctor is paid extra for each day or week spent being “available” on jeopardy duty (not to be confused with jury duty, though it can be equally difficult to get exempted from). Then again, it is not uncommon to have jeopardy duty included in base compensation. However, once a jeopardy doctor is actually called in to work, most practices pay additional compensation, often based on an hourly rate that usually is higher than the average compensation generated per hour for nonjeopardy work.
There are a number of reasonable ways to compensate the jeopardy doctor. You probably can get some good ideas by talking with others in your hospital who function in a similar capacity, such as cath-lab technicians who get called in on nights and weekends.
No definitive data are available to show how common the jeopardy system is, but my experience is that 30% to 50% of HM groups use some form of it. Its popularity is proof that it is a reasonable system, but I’m not convinced. I think it is in use by a lot of groups not because it is an optimal way to ensure surge capacity, but because it is easy to conceptualize and put in place, and because many hospitalists came from residency programs in which the system was standard.
The gaps between theoretical and realized benefits become evident once a practice implements a jeopardy system. For example, it might be really busy today, but Dr. Stravinsky doesn’t call in Dr. Copeland, who is on jeopardy, because next week their roles will be reversed and Dr. Stravinsky sure hopes he won’t be called in. No one wants to be the weak doctor who calls in the jeopardy doctor and spoils what was otherwise a day off.
I’ve worked with a lot of practices who say they have a jeopardy system in place, but when I ask for the last time the jeopardy doctor was called in, they say it has been more than a year, or in some cases never. So even if the policy manual says they have a jeopardy system, the doctors never activate it, so it provides no benefit.
Practices that do utilize the jeopardy doctor have their own problems, such as assigning that doctor’s admissions the next day. The jeopardy doctor might provide some relief today, but they essentially just delay the work of having to get to know all of those new patients until the morning, when everyone is very busy with rounds. So while there might be significant benefit in activating the jeopardy system today, it could just delay the problem of high workload until the next morning, which isn’t much of a net benefit for the practice.
A small number of practices call in the jeopardy doctor frequently, and sometimes have that doctor continue to round on admitted patients for the next few days. This usage might get the most value out of the system, but the practice should consider if it is more cost-effective, and less stressful for the doctors, if the system were reversed. For example, instead of having the doctor on jeopardy and called in as necessary, the doctor would report to work and be given the day off or let go early when it isn’t busy.
Despite my reservations, if you are convinced the jeopardy system is valuable and cost-effective, keep it in place. However, if your group is thinking about options to handle surge capacity, don’t be too quick to adopt a jeopardy system. It usually falls far short of a perfect solution.
Patient Volume Cap
Another way to address the problem of unpredictable increases in patient volume is to establish a patient volume (e.g., total census) cap for the whole hospitalist practice. Like the jeopardy system, this is an appealingly uncomplicated idea, and hospitalists who have finished residency within the last few years all worked with a cap.
Except for the rarest of exceptions, this is a poor idea and should be avoided if at all possible. I’ll leave for another time a discussion of all the political and financial costs of a cap system, but trust me on this one. It is best to avoid a cap.
Stay Tuned …
Next month, I’ll examine other strategies to provide surge capacity. I think they’re more valuable than the two I’ve mentioned here, but I need to warn you that they aren’t perfect and are more complicated to operationalize. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Unpredictable workloads and frequent interruptions are the things I regard as the most stressful components of work as a hospitalist. Your list might be very different, but I bet unpredictable workloads ranks at least in the top five of every hospitalist’s list.
I’ve discussed interruptions previously (see “Really, It’s Switch-Tasking,” p. 68, November 2008; “Technological Advance or Workplace Setback?” p. 69, December 2008), but this month and next will turn to unpredictable workloads. In other words, what are the strategies available to a hospitalist practice to provide surge capacity in response to such unpredictable increases in patient volume as an uptick in census or daily admissions 50% to 100% above normal? I’ll leave to others the topic of how hospitals respond to such disasters as terrorist attacks, earthquakes, etc.
The Bottom Line
Sadly, there is no magic bullet for the “surge” problem, and no way to protect on-duty hospitalists from the need to work harder when it gets busy. But we needn’t feel too sorry for ourselves; doctors in most other specialties who practice in the hospital face the same problem and tend to rely heavily on simply working harder and longer when it is unusually busy. Sometimes they couple the “work harder” mantra with other strategies, such as calling another doctor in to help.
Hospitalists have a duty to ensure high patient volume doesn’t lead to deterioration in the quality of patient care, but occasionally working longer days than average probably poses a low risk, and might be less risky than the additional handoffs usually associated with having a doctor on “jeopardy” to be called in when it’s busy. Routinely or frequently working unreasonably long days is another story.
The trick for HM programs is to build some surge capacity into the routine daily staffing 1) without exceeding a reasonable budget, while 2) ensuring that the hospitalists don’t simply become accustomed to light workloads as the only reasonable norm, which could lead to them becoming unwilling to accept higher, but still reasonable, workloads when needed. (More on these issues later.) First, I’ll go through what I see as the pros and cons of several approaches to addressing surges in patient volume. All are in use with variable frequency around the country.
“Jeopardy” System
In its most common form, a jeopardy system has an unscheduled doctor each day who must remain available on short notice by pager. When patient volume surges, the unscheduled doctor is paged to come in and help. In most cases, this doctor focuses primarily—or exclusively—on admitting patients for a few hours. So it is most common for this doctor to be called in late in the afternoon or early in the evening. The jeopardy doctor usually turns over all admitted patients to another hospitalist in the group for all subsequent care. In addition to providing surge capacity, the jeopardy doctor almost always is used to cover unexpected absences of scheduled doctors, including illness-related absences.
Sometimes this doctor is paid extra for each day or week spent being “available” on jeopardy duty (not to be confused with jury duty, though it can be equally difficult to get exempted from). Then again, it is not uncommon to have jeopardy duty included in base compensation. However, once a jeopardy doctor is actually called in to work, most practices pay additional compensation, often based on an hourly rate that usually is higher than the average compensation generated per hour for nonjeopardy work.
There are a number of reasonable ways to compensate the jeopardy doctor. You probably can get some good ideas by talking with others in your hospital who function in a similar capacity, such as cath-lab technicians who get called in on nights and weekends.
No definitive data are available to show how common the jeopardy system is, but my experience is that 30% to 50% of HM groups use some form of it. Its popularity is proof that it is a reasonable system, but I’m not convinced. I think it is in use by a lot of groups not because it is an optimal way to ensure surge capacity, but because it is easy to conceptualize and put in place, and because many hospitalists came from residency programs in which the system was standard.
The gaps between theoretical and realized benefits become evident once a practice implements a jeopardy system. For example, it might be really busy today, but Dr. Stravinsky doesn’t call in Dr. Copeland, who is on jeopardy, because next week their roles will be reversed and Dr. Stravinsky sure hopes he won’t be called in. No one wants to be the weak doctor who calls in the jeopardy doctor and spoils what was otherwise a day off.
I’ve worked with a lot of practices who say they have a jeopardy system in place, but when I ask for the last time the jeopardy doctor was called in, they say it has been more than a year, or in some cases never. So even if the policy manual says they have a jeopardy system, the doctors never activate it, so it provides no benefit.
Practices that do utilize the jeopardy doctor have their own problems, such as assigning that doctor’s admissions the next day. The jeopardy doctor might provide some relief today, but they essentially just delay the work of having to get to know all of those new patients until the morning, when everyone is very busy with rounds. So while there might be significant benefit in activating the jeopardy system today, it could just delay the problem of high workload until the next morning, which isn’t much of a net benefit for the practice.
A small number of practices call in the jeopardy doctor frequently, and sometimes have that doctor continue to round on admitted patients for the next few days. This usage might get the most value out of the system, but the practice should consider if it is more cost-effective, and less stressful for the doctors, if the system were reversed. For example, instead of having the doctor on jeopardy and called in as necessary, the doctor would report to work and be given the day off or let go early when it isn’t busy.
Despite my reservations, if you are convinced the jeopardy system is valuable and cost-effective, keep it in place. However, if your group is thinking about options to handle surge capacity, don’t be too quick to adopt a jeopardy system. It usually falls far short of a perfect solution.
Patient Volume Cap
Another way to address the problem of unpredictable increases in patient volume is to establish a patient volume (e.g., total census) cap for the whole hospitalist practice. Like the jeopardy system, this is an appealingly uncomplicated idea, and hospitalists who have finished residency within the last few years all worked with a cap.
Except for the rarest of exceptions, this is a poor idea and should be avoided if at all possible. I’ll leave for another time a discussion of all the political and financial costs of a cap system, but trust me on this one. It is best to avoid a cap.
Stay Tuned …
Next month, I’ll examine other strategies to provide surge capacity. I think they’re more valuable than the two I’ve mentioned here, but I need to warn you that they aren’t perfect and are more complicated to operationalize. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Financial Risk

When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Hospitalist Salary Spike

In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
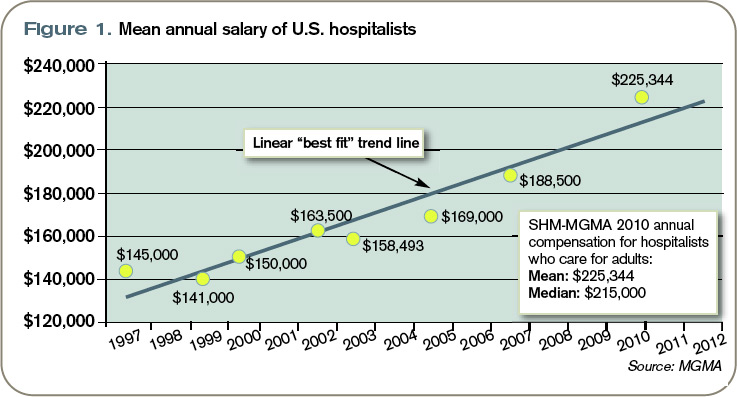
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Square Peg, Square Hole

I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.