User login

In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
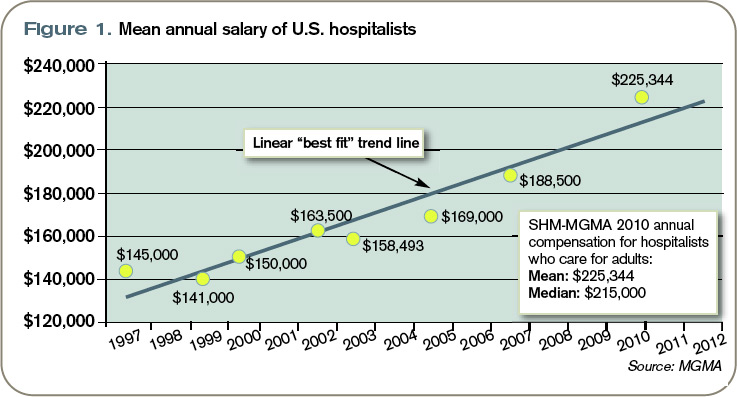
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.