User login
Pre–bariatric surgery weight loss improves outcomes
Preoperative weight loss improves bariatric surgery outcomes, according to findings from a single-institution retrospective analysis. The weight loss came from following a 4-week low-calorie diet (LCD) and was of greatest benefit to patients who lost 8% or more of their excess weight. These patients had a greater loss of excess weight in the 12 months following surgery, as well as shorter average hospital length of stay.

Preliminary studies indicated that short-term weight loss before surgery might reduce surgical complexity by reducing the size of the liver and intra-abdominal fat mass, but it remained uncertain what effect weight loss might have on long-term outcomes.
The LCD included 1,200 kcal/day (45% carbohydrates, 35% protein, 20% fat), which were consumed through five meal-replacement products and one food-based meal. Liquids included at least 80 ounces of calorie-free, caffeine-free, carbonation-free beverages per day. Patients were also instructed to conduct 30 minutes of moderate to vigorous activity per day.
Deborah A. Hutcheon, DCN, and her fellow researchers analyzed data from their own institution, where a presurgical 4-week LCD with a target loss of 8% or more of excess weight had been standard policy already. The population included 355 patients who underwent sleeve gastrectomy (n = 167) or Roux-en-Y gastric bypass (n = 188) between January 2014 and January 2016.
Almost two-thirds (63.3%) of patients achieved the target weight loss before surgery. There were some differences between the two groups. The group that achieved the target contained a greater proportion of men than did the other group (25.5% vs. 13.7%, respectively; P = .013), a higher proportion of white patients (84.8% vs. 74.1%; P = .011), and a higher proportion of patients taking antihypertensive medications (68.3% vs. 57.3%; P = .048). The two groups had similar rates of preoperative comorbidities and surgery types.
Those who achieved the target weight loss had a shorter hospital length of stay (1.8 days vs. 2.1 days; P = .006). They also had a higher percentage loss of excess weight at 3 months (42.3% vs. 36.1%; P less than .001), 6 months (56.0% vs. 47.5%; P less than .001), and at 12 months (65.1% vs. 55.7%; P = .003).
After controlling for patient characteristics, insurance status, 12-month diet compliance, and surgery type, successful presurgery weight loss was associated with greater weight loss at 12 months.
acssurgerynews@frontlinemedcom.com
SOURCE: Hutcheon DA et al. J Am Coll Surgeons. 2018 Jan 31. doi: 10.1016/j.jamcollsurg.2017.12.032.
Preoperative weight loss improves bariatric surgery outcomes, according to findings from a single-institution retrospective analysis. The weight loss came from following a 4-week low-calorie diet (LCD) and was of greatest benefit to patients who lost 8% or more of their excess weight. These patients had a greater loss of excess weight in the 12 months following surgery, as well as shorter average hospital length of stay.
Preliminary studies indicated that short-term weight loss before surgery might reduce surgical complexity by reducing the size of the liver and intra-abdominal fat mass, but it remained uncertain what effect weight loss might have on long-term outcomes.
The LCD included 1,200 kcal/day (45% carbohydrates, 35% protein, 20% fat), which were consumed through five meal-replacement products and one food-based meal. Liquids included at least 80 ounces of calorie-free, caffeine-free, carbonation-free beverages per day. Patients were also instructed to conduct 30 minutes of moderate to vigorous activity per day.
Deborah A. Hutcheon, DCN, and her fellow researchers analyzed data from their own institution, where a presurgical 4-week LCD with a target loss of 8% or more of excess weight had been standard policy already. The population included 355 patients who underwent sleeve gastrectomy (n = 167) or Roux-en-Y gastric bypass (n = 188) between January 2014 and January 2016.
Almost two-thirds (63.3%) of patients achieved the target weight loss before surgery. There were some differences between the two groups. The group that achieved the target contained a greater proportion of men than did the other group (25.5% vs. 13.7%, respectively; P = .013), a higher proportion of white patients (84.8% vs. 74.1%; P = .011), and a higher proportion of patients taking antihypertensive medications (68.3% vs. 57.3%; P = .048). The two groups had similar rates of preoperative comorbidities and surgery types.
Those who achieved the target weight loss had a shorter hospital length of stay (1.8 days vs. 2.1 days; P = .006). They also had a higher percentage loss of excess weight at 3 months (42.3% vs. 36.1%; P less than .001), 6 months (56.0% vs. 47.5%; P less than .001), and at 12 months (65.1% vs. 55.7%; P = .003).
After controlling for patient characteristics, insurance status, 12-month diet compliance, and surgery type, successful presurgery weight loss was associated with greater weight loss at 12 months.
acssurgerynews@frontlinemedcom.com
SOURCE: Hutcheon DA et al. J Am Coll Surgeons. 2018 Jan 31. doi: 10.1016/j.jamcollsurg.2017.12.032.
Preoperative weight loss improves bariatric surgery outcomes, according to findings from a single-institution retrospective analysis. The weight loss came from following a 4-week low-calorie diet (LCD) and was of greatest benefit to patients who lost 8% or more of their excess weight. These patients had a greater loss of excess weight in the 12 months following surgery, as well as shorter average hospital length of stay.
Preliminary studies indicated that short-term weight loss before surgery might reduce surgical complexity by reducing the size of the liver and intra-abdominal fat mass, but it remained uncertain what effect weight loss might have on long-term outcomes.
The LCD included 1,200 kcal/day (45% carbohydrates, 35% protein, 20% fat), which were consumed through five meal-replacement products and one food-based meal. Liquids included at least 80 ounces of calorie-free, caffeine-free, carbonation-free beverages per day. Patients were also instructed to conduct 30 minutes of moderate to vigorous activity per day.
Deborah A. Hutcheon, DCN, and her fellow researchers analyzed data from their own institution, where a presurgical 4-week LCD with a target loss of 8% or more of excess weight had been standard policy already. The population included 355 patients who underwent sleeve gastrectomy (n = 167) or Roux-en-Y gastric bypass (n = 188) between January 2014 and January 2016.
Almost two-thirds (63.3%) of patients achieved the target weight loss before surgery. There were some differences between the two groups. The group that achieved the target contained a greater proportion of men than did the other group (25.5% vs. 13.7%, respectively; P = .013), a higher proportion of white patients (84.8% vs. 74.1%; P = .011), and a higher proportion of patients taking antihypertensive medications (68.3% vs. 57.3%; P = .048). The two groups had similar rates of preoperative comorbidities and surgery types.
Those who achieved the target weight loss had a shorter hospital length of stay (1.8 days vs. 2.1 days; P = .006). They also had a higher percentage loss of excess weight at 3 months (42.3% vs. 36.1%; P less than .001), 6 months (56.0% vs. 47.5%; P less than .001), and at 12 months (65.1% vs. 55.7%; P = .003).
After controlling for patient characteristics, insurance status, 12-month diet compliance, and surgery type, successful presurgery weight loss was associated with greater weight loss at 12 months.
acssurgerynews@frontlinemedcom.com
SOURCE: Hutcheon DA et al. J Am Coll Surgeons. 2018 Jan 31. doi: 10.1016/j.jamcollsurg.2017.12.032.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF SURGEONS
Key clinical point: Weight loss before bariatric surgery boosts results.
Major finding: Patients who lost at least 8% of excess body weight had an average of 65.1% loss of excess weight at 12 months, compared with the 55.7% seen in those who did not.
Data source: Retrospective, single-center analysis (n = 355).
Disclosures: No source of funding was disclosed.
Source: Hutcheon DA et al. J Am Coll Surgeons. 2018 Jan 31. doi: 10.1016/j.jamcollsurg.2017.12.032.
RF-positive polyarticular JIA looks like adult RA
New evidence suggests the rheumatoid factor–positive polyarticular subtype of juvenile idiopathic arthritis bears a close genetic resemblance to adult rheumatoid arthritis, lending support to the growing suspicion that in arthritis, biological underpinnings are more important than age of onset when it comes to characterizing and, potentially, choosing treatments.
Previous work had shown that rheumatoid factor (RF)–negative patients have genetic risks similar to those of adults with RF-negative disease. “If the RF-negative patients in adult and childhood are similar, then maybe the RF-positive patients are similar in their genetic background as well. That’s what this study was testing,” study coauthor Anne M. Stevens, MD, PhD, division chief of rheumatology at the University of Washington, Seattle, said in an interview. The study was published online Feb. 9 in Arthritis & Rheumatology.

There are seven recognized categories of juvenile idiopathic arthritis (JIA), and all are believed to have genetic risk factors. Previously, the researchers used the Immunochip custom microarray to map 186 autoimmune disease-associated loci from 11 autoimmune phenotypes, including adult rheumatoid arthritis (RA). In the current work, the researchers analyzed 340 RF-positive polyarticular JIA cases (292 females) and 14,412 controls (8,002 females) from the United States, United Kingdom, Germany, Canada, and Norway. RF-positive polyarticular disease accounts for about 5% of JIA cases, and its symptoms and presentations resemble adult RA.
The researchers found associations in the human leukocyte antigen (HLA) region. The most significant was found at rs3129769, near HLA-DRB1 (P = 5.51 x 10-31). This single nucleotide polymorphism (SNP) was in strong linkage disequilibrium (LD, r2 = 0.88) with the rs660895 HLA-DRB1 SNP that has been reported in adult RA (P = 2.14 x 10-29).
The researchers examined links between RF-positive polyarticular JIA and the 27 SNPs that had been identified in the previous study of oligoarticular/RF-negative polyarticular JIA. Just 6 of those 27 SNPs were significantly associated with RF-positive polyarticular JIA (P less than .05). On the other hand, of 44 SNPs most strongly associated with RA, 19 were associated with RF-positive polyarticular JIA (P less than .05).
That suggests that RF-positive polyarticular JIA cases are different from other JIA cases. “They’re more like adult patients than they’re like child patients,” said Dr. Stevens.
The researchers also compared the weighted genetic risk scores (wGRS) produced from the top RA loci to wGRS produced from the top oligoarticular/RF-negative polyarticular JIA loci. The wGRS from the top RA loci was a better predictor of RF-positive polyarticular JIA cases (area under the curve [AUC] = 0.71 versus AUC = 0.58; P = 8.26 x 10-33).
The wGRS from RA had similar success in predicting RF-positive polyarticular JIA and early-onset RA cases (AUC = 0.75; P = .25), but it fared worse in predicting late-onset RA (at 70 years or older, AUC = 0.62), compared with the wGRS from RF-positive polyarticular JIA (P = 1.65 x 10-5).
Those results suggest that RF-positive polyarticular JIA more closely resembles younger RA cases than older RA cases.
“If you consider early-onset RA patients, less than 29 years old when they develop RA, they look like JIA patients. But older RA patients, who are over 70 when they develop RA, they look like they totally have a different genetic background,” Dr. Stevens said.
The study could have clinical implications. The lead author, Anne Hinks, PhD, is a research fellow at the University of Manchester (England) and has led the charge to characterize JIA. The wGRS score she developed has the potential to help physicians diagnose classify and treat JIA patients. Currently, they must rely on the International League of Associations for Rheumatology criteria, which can take months to work through and may lead to misclassification diagnoses.
And in any case, the emerging genetic research suggests that the underlying genetics of JIA may be a better way to classify patients. “There’s a lot of overlap and risk of misclassifying patients with the current system. This weighted genetic risk score that Dr. Hinks developed could be used to classify patients with one DNA sample. This is the kind of clinical test we need,” Dr. Stevens said.
The study received funding from a range of government and private sources. Dr. Stevens has a patent licensed to Quest Diagnostics, is conducting research collaborations with Seattle Genetics and Kineta, and has received fellowship support from Pfizer.
SOURCE: Hinks A et al. Arthritis Rheumatol. 2018 Feb 9. doi: 10.1002/art.40443
New evidence suggests the rheumatoid factor–positive polyarticular subtype of juvenile idiopathic arthritis bears a close genetic resemblance to adult rheumatoid arthritis, lending support to the growing suspicion that in arthritis, biological underpinnings are more important than age of onset when it comes to characterizing and, potentially, choosing treatments.
Previous work had shown that rheumatoid factor (RF)–negative patients have genetic risks similar to those of adults with RF-negative disease. “If the RF-negative patients in adult and childhood are similar, then maybe the RF-positive patients are similar in their genetic background as well. That’s what this study was testing,” study coauthor Anne M. Stevens, MD, PhD, division chief of rheumatology at the University of Washington, Seattle, said in an interview. The study was published online Feb. 9 in Arthritis & Rheumatology.
There are seven recognized categories of juvenile idiopathic arthritis (JIA), and all are believed to have genetic risk factors. Previously, the researchers used the Immunochip custom microarray to map 186 autoimmune disease-associated loci from 11 autoimmune phenotypes, including adult rheumatoid arthritis (RA). In the current work, the researchers analyzed 340 RF-positive polyarticular JIA cases (292 females) and 14,412 controls (8,002 females) from the United States, United Kingdom, Germany, Canada, and Norway. RF-positive polyarticular disease accounts for about 5% of JIA cases, and its symptoms and presentations resemble adult RA.
The researchers found associations in the human leukocyte antigen (HLA) region. The most significant was found at rs3129769, near HLA-DRB1 (P = 5.51 x 10-31). This single nucleotide polymorphism (SNP) was in strong linkage disequilibrium (LD, r2 = 0.88) with the rs660895 HLA-DRB1 SNP that has been reported in adult RA (P = 2.14 x 10-29).
The researchers examined links between RF-positive polyarticular JIA and the 27 SNPs that had been identified in the previous study of oligoarticular/RF-negative polyarticular JIA. Just 6 of those 27 SNPs were significantly associated with RF-positive polyarticular JIA (P less than .05). On the other hand, of 44 SNPs most strongly associated with RA, 19 were associated with RF-positive polyarticular JIA (P less than .05).
That suggests that RF-positive polyarticular JIA cases are different from other JIA cases. “They’re more like adult patients than they’re like child patients,” said Dr. Stevens.
The researchers also compared the weighted genetic risk scores (wGRS) produced from the top RA loci to wGRS produced from the top oligoarticular/RF-negative polyarticular JIA loci. The wGRS from the top RA loci was a better predictor of RF-positive polyarticular JIA cases (area under the curve [AUC] = 0.71 versus AUC = 0.58; P = 8.26 x 10-33).
The wGRS from RA had similar success in predicting RF-positive polyarticular JIA and early-onset RA cases (AUC = 0.75; P = .25), but it fared worse in predicting late-onset RA (at 70 years or older, AUC = 0.62), compared with the wGRS from RF-positive polyarticular JIA (P = 1.65 x 10-5).
Those results suggest that RF-positive polyarticular JIA more closely resembles younger RA cases than older RA cases.
“If you consider early-onset RA patients, less than 29 years old when they develop RA, they look like JIA patients. But older RA patients, who are over 70 when they develop RA, they look like they totally have a different genetic background,” Dr. Stevens said.
The study could have clinical implications. The lead author, Anne Hinks, PhD, is a research fellow at the University of Manchester (England) and has led the charge to characterize JIA. The wGRS score she developed has the potential to help physicians diagnose classify and treat JIA patients. Currently, they must rely on the International League of Associations for Rheumatology criteria, which can take months to work through and may lead to misclassification diagnoses.
And in any case, the emerging genetic research suggests that the underlying genetics of JIA may be a better way to classify patients. “There’s a lot of overlap and risk of misclassifying patients with the current system. This weighted genetic risk score that Dr. Hinks developed could be used to classify patients with one DNA sample. This is the kind of clinical test we need,” Dr. Stevens said.
The study received funding from a range of government and private sources. Dr. Stevens has a patent licensed to Quest Diagnostics, is conducting research collaborations with Seattle Genetics and Kineta, and has received fellowship support from Pfizer.
SOURCE: Hinks A et al. Arthritis Rheumatol. 2018 Feb 9. doi: 10.1002/art.40443
New evidence suggests the rheumatoid factor–positive polyarticular subtype of juvenile idiopathic arthritis bears a close genetic resemblance to adult rheumatoid arthritis, lending support to the growing suspicion that in arthritis, biological underpinnings are more important than age of onset when it comes to characterizing and, potentially, choosing treatments.
Previous work had shown that rheumatoid factor (RF)–negative patients have genetic risks similar to those of adults with RF-negative disease. “If the RF-negative patients in adult and childhood are similar, then maybe the RF-positive patients are similar in their genetic background as well. That’s what this study was testing,” study coauthor Anne M. Stevens, MD, PhD, division chief of rheumatology at the University of Washington, Seattle, said in an interview. The study was published online Feb. 9 in Arthritis & Rheumatology.
There are seven recognized categories of juvenile idiopathic arthritis (JIA), and all are believed to have genetic risk factors. Previously, the researchers used the Immunochip custom microarray to map 186 autoimmune disease-associated loci from 11 autoimmune phenotypes, including adult rheumatoid arthritis (RA). In the current work, the researchers analyzed 340 RF-positive polyarticular JIA cases (292 females) and 14,412 controls (8,002 females) from the United States, United Kingdom, Germany, Canada, and Norway. RF-positive polyarticular disease accounts for about 5% of JIA cases, and its symptoms and presentations resemble adult RA.
The researchers found associations in the human leukocyte antigen (HLA) region. The most significant was found at rs3129769, near HLA-DRB1 (P = 5.51 x 10-31). This single nucleotide polymorphism (SNP) was in strong linkage disequilibrium (LD, r2 = 0.88) with the rs660895 HLA-DRB1 SNP that has been reported in adult RA (P = 2.14 x 10-29).
The researchers examined links between RF-positive polyarticular JIA and the 27 SNPs that had been identified in the previous study of oligoarticular/RF-negative polyarticular JIA. Just 6 of those 27 SNPs were significantly associated with RF-positive polyarticular JIA (P less than .05). On the other hand, of 44 SNPs most strongly associated with RA, 19 were associated with RF-positive polyarticular JIA (P less than .05).
That suggests that RF-positive polyarticular JIA cases are different from other JIA cases. “They’re more like adult patients than they’re like child patients,” said Dr. Stevens.
The researchers also compared the weighted genetic risk scores (wGRS) produced from the top RA loci to wGRS produced from the top oligoarticular/RF-negative polyarticular JIA loci. The wGRS from the top RA loci was a better predictor of RF-positive polyarticular JIA cases (area under the curve [AUC] = 0.71 versus AUC = 0.58; P = 8.26 x 10-33).
The wGRS from RA had similar success in predicting RF-positive polyarticular JIA and early-onset RA cases (AUC = 0.75; P = .25), but it fared worse in predicting late-onset RA (at 70 years or older, AUC = 0.62), compared with the wGRS from RF-positive polyarticular JIA (P = 1.65 x 10-5).
Those results suggest that RF-positive polyarticular JIA more closely resembles younger RA cases than older RA cases.
“If you consider early-onset RA patients, less than 29 years old when they develop RA, they look like JIA patients. But older RA patients, who are over 70 when they develop RA, they look like they totally have a different genetic background,” Dr. Stevens said.
The study could have clinical implications. The lead author, Anne Hinks, PhD, is a research fellow at the University of Manchester (England) and has led the charge to characterize JIA. The wGRS score she developed has the potential to help physicians diagnose classify and treat JIA patients. Currently, they must rely on the International League of Associations for Rheumatology criteria, which can take months to work through and may lead to misclassification diagnoses.
And in any case, the emerging genetic research suggests that the underlying genetics of JIA may be a better way to classify patients. “There’s a lot of overlap and risk of misclassifying patients with the current system. This weighted genetic risk score that Dr. Hinks developed could be used to classify patients with one DNA sample. This is the kind of clinical test we need,” Dr. Stevens said.
The study received funding from a range of government and private sources. Dr. Stevens has a patent licensed to Quest Diagnostics, is conducting research collaborations with Seattle Genetics and Kineta, and has received fellowship support from Pfizer.
SOURCE: Hinks A et al. Arthritis Rheumatol. 2018 Feb 9. doi: 10.1002/art.40443
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point: Genetics underlying arthritis may be more important than age of onset.
Major finding: The weighted genetic risk scores produced from the top RA loci was a better predictor of RF-positive polyarticular JIA than that generated from the top oligoarticular/RF-negative polyarticular JIA loci.
Data source: Case-control analysis of 340 cases and 14,412 controls.
Disclosures: The study received funding from a range of government and private sources. Dr. Stevens has a patent licensed to Quest Diagnostics, is conducting research collaborations with Seattle Genetics and Kineta, and has received fellowship support from Pfizer.
Source: Hinks A et al. Arthritis Rheumatol. 2018 Feb 9. doi: 10.1002/art.40443.
EMS stroke field triage improves outcomes
LOS ANGELES – An emergency medical services protocol to identify large vessel occlusions and deliver patients to a comprehensive stroke center if it is within 30 minutes of travel time reduced the time to recanalization when compared against a separate protocol that optimized transfer of such patients from primary to comprehensive stroke centers.
The findings, which come from a sequential study conducted in an urban Rhode Island region, offer evidence to resolve the controversy over whether field triage in emergency medical services (EMS) units will improve outcomes, because field stroke severity scores won’t always be accurate, and longer travel to a comprehensive stroke center (CSC) could delay treatment to a patient who doesn’t need thrombectomy.

The region where the study was carried out has one CSC and eight primary stroke centers (PSCs). The large vessel occlusions transfer protocol instructed PSCs to contact the CSC when a patient scored 4 or 5 on the Los Angeles Motor Scale (LAMS), followed by CT and CT angiography. They then shared the resulting images with the CSC, which could make a decision whether to transfer the patient.
The field-based protocol relied on a LAMS score assessment by EMS personnel. Patients scoring 4 or 5 would then be delivered to the CSC if it was within 30 minutes from their current location. Patients scoring less than 4 would be brought to the nearest facility. In cases when the field LAMS score was 4 or greater and the nearest CSC was more than 30 miles away, EMS personnel were instructed to travel to the closest PSC, but immediately send word of an inbound patient that might need a transfer to a CSC. In those cases, the PSC’s goal was to get images to the CSC for review within 45 minutes. The protocol was executed out to 24 hours after the patient was last known well.
Even in patients who were closer to a PSC than a CSC, process outcomes were better with the field triage protocol. “Despite 8 additional minutes of transport time, IV TPA was given 17 minutes earlier, and recanalization occurred almost an hour earlier,” said Dr. McTaggart. “That would indicate that perhaps even a 30-minute window is too conservative of a protocol, because the number needed to treat for mechanical thrombectomy is 2 or 3, so you have this tremendously powerful treatment effect for these patients. If you can get it to them an hour earlier, it’s a no-brainer to me that they need to go to the right place the first time,” he said.
Instituting the changes was no picnic. Dr. McTaggart spent thousands of hours working with EMS personnel and emergency department physicians at PSCs. “It’s a lot of work, but the downstream gains are huge, not only from a disability standpoint for patients but for the economics of the health care system. We’re potentially saving patients from disability health care costs,” he said.
The study population included consecutive stroke patients in the region whose first contact was with EMS personnel during three time periods: before either change was made: (pre PSC-CSC transfer optimization, pre field triage, July 2015 to January 2016), after PSC optimization but only voluntary field triage (January 2016 to January 2017), and when both PSC optimization and field triage were mandatory (January 2017 to January 2018).
The patients had an anterior large vessel occlusion and mild to moderate early ischemic change. Outcomes included time from hospital arrival (PSC or CSC) to alteplase treatment, arterial puncture, and recanalization. Clinical measures included favorable outcomes (modified Rankin scale score 0-2) at 90 days, or discharge with a National Institutes of Health Stroke Scale score of 4 or less, in cases where 90-day follow-up did not occur.
A total of 38 patients were seen before any change, 100 after PSC optimization, and 94 after both PSC optimization and field triage were implemented. A Google Maps analysis showed that the median additional time required to travel to a CSC instead of a PSC was 8 minutes (interquartile range 4-12).
The time to first use of IV alteplase dropped from 54 minutes before any change to 49 minutes after PSC optimization, and 36 minutes after both PSC optimization and field triage. Similar drops were seen in time to arterial puncture (105 minutes, 101 minutes, 88 minutes) and time to recanalization (156 minutes, 132 minutes, 116 minutes). These differences did not reach statistical significance.
The clinical outcomes also became more favorable: 58% had a favorable outcome at 90 days with both protocols in place, compared with 51% with only PSC optimization and 31% before any changes (P = .049 for 31% to 58% comparison).
The researchers conducted a subanalysis of 150 patients for whom the PSC was closest. Of these, 94 went to a CSC and 56 went to a PSC. The elapsed time between EMS leaving the scene with the patient aboard and IV TPA treatment was an average of 51 minutes in patients taken to the CSC, compared with 68 minutes in patients taken to PSCs (P = .012). The time to arterial puncture was also shorter (98 minutes versus 155 minutes; P less than .001), as was time to recanalization (131 minutes versus 174 minutes; P less than .001).
CSC patients were more likely to have a favorable outcome (65% versus 42%; P = .01).
The study received no external funding. Dr. McTaggart reported having no financial disclosures.
SOURCE: Jayaraman M et al. ISC 2018 Abstract 95 (Stroke. 2018 Jan;49[Suppl 1]:A95)
LOS ANGELES – An emergency medical services protocol to identify large vessel occlusions and deliver patients to a comprehensive stroke center if it is within 30 minutes of travel time reduced the time to recanalization when compared against a separate protocol that optimized transfer of such patients from primary to comprehensive stroke centers.
The findings, which come from a sequential study conducted in an urban Rhode Island region, offer evidence to resolve the controversy over whether field triage in emergency medical services (EMS) units will improve outcomes, because field stroke severity scores won’t always be accurate, and longer travel to a comprehensive stroke center (CSC) could delay treatment to a patient who doesn’t need thrombectomy.
The region where the study was carried out has one CSC and eight primary stroke centers (PSCs). The large vessel occlusions transfer protocol instructed PSCs to contact the CSC when a patient scored 4 or 5 on the Los Angeles Motor Scale (LAMS), followed by CT and CT angiography. They then shared the resulting images with the CSC, which could make a decision whether to transfer the patient.
The field-based protocol relied on a LAMS score assessment by EMS personnel. Patients scoring 4 or 5 would then be delivered to the CSC if it was within 30 minutes from their current location. Patients scoring less than 4 would be brought to the nearest facility. In cases when the field LAMS score was 4 or greater and the nearest CSC was more than 30 miles away, EMS personnel were instructed to travel to the closest PSC, but immediately send word of an inbound patient that might need a transfer to a CSC. In those cases, the PSC’s goal was to get images to the CSC for review within 45 minutes. The protocol was executed out to 24 hours after the patient was last known well.
Even in patients who were closer to a PSC than a CSC, process outcomes were better with the field triage protocol. “Despite 8 additional minutes of transport time, IV TPA was given 17 minutes earlier, and recanalization occurred almost an hour earlier,” said Dr. McTaggart. “That would indicate that perhaps even a 30-minute window is too conservative of a protocol, because the number needed to treat for mechanical thrombectomy is 2 or 3, so you have this tremendously powerful treatment effect for these patients. If you can get it to them an hour earlier, it’s a no-brainer to me that they need to go to the right place the first time,” he said.
Instituting the changes was no picnic. Dr. McTaggart spent thousands of hours working with EMS personnel and emergency department physicians at PSCs. “It’s a lot of work, but the downstream gains are huge, not only from a disability standpoint for patients but for the economics of the health care system. We’re potentially saving patients from disability health care costs,” he said.
The study population included consecutive stroke patients in the region whose first contact was with EMS personnel during three time periods: before either change was made: (pre PSC-CSC transfer optimization, pre field triage, July 2015 to January 2016), after PSC optimization but only voluntary field triage (January 2016 to January 2017), and when both PSC optimization and field triage were mandatory (January 2017 to January 2018).
The patients had an anterior large vessel occlusion and mild to moderate early ischemic change. Outcomes included time from hospital arrival (PSC or CSC) to alteplase treatment, arterial puncture, and recanalization. Clinical measures included favorable outcomes (modified Rankin scale score 0-2) at 90 days, or discharge with a National Institutes of Health Stroke Scale score of 4 or less, in cases where 90-day follow-up did not occur.
A total of 38 patients were seen before any change, 100 after PSC optimization, and 94 after both PSC optimization and field triage were implemented. A Google Maps analysis showed that the median additional time required to travel to a CSC instead of a PSC was 8 minutes (interquartile range 4-12).
The time to first use of IV alteplase dropped from 54 minutes before any change to 49 minutes after PSC optimization, and 36 minutes after both PSC optimization and field triage. Similar drops were seen in time to arterial puncture (105 minutes, 101 minutes, 88 minutes) and time to recanalization (156 minutes, 132 minutes, 116 minutes). These differences did not reach statistical significance.
The clinical outcomes also became more favorable: 58% had a favorable outcome at 90 days with both protocols in place, compared with 51% with only PSC optimization and 31% before any changes (P = .049 for 31% to 58% comparison).
The researchers conducted a subanalysis of 150 patients for whom the PSC was closest. Of these, 94 went to a CSC and 56 went to a PSC. The elapsed time between EMS leaving the scene with the patient aboard and IV TPA treatment was an average of 51 minutes in patients taken to the CSC, compared with 68 minutes in patients taken to PSCs (P = .012). The time to arterial puncture was also shorter (98 minutes versus 155 minutes; P less than .001), as was time to recanalization (131 minutes versus 174 minutes; P less than .001).
CSC patients were more likely to have a favorable outcome (65% versus 42%; P = .01).
The study received no external funding. Dr. McTaggart reported having no financial disclosures.
SOURCE: Jayaraman M et al. ISC 2018 Abstract 95 (Stroke. 2018 Jan;49[Suppl 1]:A95)
LOS ANGELES – An emergency medical services protocol to identify large vessel occlusions and deliver patients to a comprehensive stroke center if it is within 30 minutes of travel time reduced the time to recanalization when compared against a separate protocol that optimized transfer of such patients from primary to comprehensive stroke centers.
The findings, which come from a sequential study conducted in an urban Rhode Island region, offer evidence to resolve the controversy over whether field triage in emergency medical services (EMS) units will improve outcomes, because field stroke severity scores won’t always be accurate, and longer travel to a comprehensive stroke center (CSC) could delay treatment to a patient who doesn’t need thrombectomy.
The region where the study was carried out has one CSC and eight primary stroke centers (PSCs). The large vessel occlusions transfer protocol instructed PSCs to contact the CSC when a patient scored 4 or 5 on the Los Angeles Motor Scale (LAMS), followed by CT and CT angiography. They then shared the resulting images with the CSC, which could make a decision whether to transfer the patient.
The field-based protocol relied on a LAMS score assessment by EMS personnel. Patients scoring 4 or 5 would then be delivered to the CSC if it was within 30 minutes from their current location. Patients scoring less than 4 would be brought to the nearest facility. In cases when the field LAMS score was 4 or greater and the nearest CSC was more than 30 miles away, EMS personnel were instructed to travel to the closest PSC, but immediately send word of an inbound patient that might need a transfer to a CSC. In those cases, the PSC’s goal was to get images to the CSC for review within 45 minutes. The protocol was executed out to 24 hours after the patient was last known well.
Even in patients who were closer to a PSC than a CSC, process outcomes were better with the field triage protocol. “Despite 8 additional minutes of transport time, IV TPA was given 17 minutes earlier, and recanalization occurred almost an hour earlier,” said Dr. McTaggart. “That would indicate that perhaps even a 30-minute window is too conservative of a protocol, because the number needed to treat for mechanical thrombectomy is 2 or 3, so you have this tremendously powerful treatment effect for these patients. If you can get it to them an hour earlier, it’s a no-brainer to me that they need to go to the right place the first time,” he said.
Instituting the changes was no picnic. Dr. McTaggart spent thousands of hours working with EMS personnel and emergency department physicians at PSCs. “It’s a lot of work, but the downstream gains are huge, not only from a disability standpoint for patients but for the economics of the health care system. We’re potentially saving patients from disability health care costs,” he said.
The study population included consecutive stroke patients in the region whose first contact was with EMS personnel during three time periods: before either change was made: (pre PSC-CSC transfer optimization, pre field triage, July 2015 to January 2016), after PSC optimization but only voluntary field triage (January 2016 to January 2017), and when both PSC optimization and field triage were mandatory (January 2017 to January 2018).
The patients had an anterior large vessel occlusion and mild to moderate early ischemic change. Outcomes included time from hospital arrival (PSC or CSC) to alteplase treatment, arterial puncture, and recanalization. Clinical measures included favorable outcomes (modified Rankin scale score 0-2) at 90 days, or discharge with a National Institutes of Health Stroke Scale score of 4 or less, in cases where 90-day follow-up did not occur.
A total of 38 patients were seen before any change, 100 after PSC optimization, and 94 after both PSC optimization and field triage were implemented. A Google Maps analysis showed that the median additional time required to travel to a CSC instead of a PSC was 8 minutes (interquartile range 4-12).
The time to first use of IV alteplase dropped from 54 minutes before any change to 49 minutes after PSC optimization, and 36 minutes after both PSC optimization and field triage. Similar drops were seen in time to arterial puncture (105 minutes, 101 minutes, 88 minutes) and time to recanalization (156 minutes, 132 minutes, 116 minutes). These differences did not reach statistical significance.
The clinical outcomes also became more favorable: 58% had a favorable outcome at 90 days with both protocols in place, compared with 51% with only PSC optimization and 31% before any changes (P = .049 for 31% to 58% comparison).
The researchers conducted a subanalysis of 150 patients for whom the PSC was closest. Of these, 94 went to a CSC and 56 went to a PSC. The elapsed time between EMS leaving the scene with the patient aboard and IV TPA treatment was an average of 51 minutes in patients taken to the CSC, compared with 68 minutes in patients taken to PSCs (P = .012). The time to arterial puncture was also shorter (98 minutes versus 155 minutes; P less than .001), as was time to recanalization (131 minutes versus 174 minutes; P less than .001).
CSC patients were more likely to have a favorable outcome (65% versus 42%; P = .01).
The study received no external funding. Dr. McTaggart reported having no financial disclosures.
SOURCE: Jayaraman M et al. ISC 2018 Abstract 95 (Stroke. 2018 Jan;49[Suppl 1]:A95)
REPORTING FROM ISC 2018
Key clinical point: EMS field triage may improve stroke patient management.
Major finding: Even when a primary stroke center was closer, the time to recanalization was shortened by 43 minutes when patients were taken to a comprehensive stroke center instead.
Data source: Prospective study of 232 consecutive stroke patients.
Disclosures: The study received no external funding. Dr. McTaggart reported having no financial disclosures.
Source: Jayaraman M et al. ISC 2018 Abstract 95 (Stroke. 2018 Jan;49[Suppl 1]:A95)
Survey highlights challenges in Asian American stroke patients
LOS ANGELES – A large survey of Asian Americans suggests that the group experiences more severe ischemic strokes and is less likely to receive intravenous tissue plasminogen activator (tPA) than do white patients, among other discrepancies. The research found that whites had declining stroke severity between 2004 and 2016, but there was no change in Asian Americans.
The research encompasses all self-identified Asian Americans in the Get-with-the-Guidelines stroke database, which is a voluntary stroke quality improvement program begun by the American Heart Association in 2003. The analysis included 64,337 Asian Americans and 1,707,962 white Americans at 2,171 hospitals nationwide that participated in the program during 2004-2016.
“I think the most important finding is that they’re not getting as much tPA and having more tPA complications, such as bleeding more. I think it gives it an urgency that maybe was lacking, an urgency that we really need to address this issue by finding innovative ways to reach Asian Americans, to educate them about stroke. We need to find culturally appropriate ways to reach out to Asian populations,” said Dr. Song, who is a vascular neurologist at Rush Medical College, Chicago.
Dr. Song is working on small-scale interventions that are culturally tailored for Asian populations. “I think the way to approach any insular community is to work from within, so that’s my goal,” Dr. Song said.
One particular finding suggested a need for better education among Asian American communities. Asian Americans were less likely than whites to report a clinical history of having heightened levels of low-density lipoproteins. “They didn’t know that they had high cholesterol, but they had a higher LDL [cholesterol levels] than Caucasians on average,” said Dr. Song. The mean LDL cholesterol value was 101 mg/dL in Asian Americans, compared with 95 mg/dL in whites, which was statistically significant.
White patients had higher rates of atrial fibrillation (21.2% vs. 16.0%), coronary artery disease (27.8% vs. 17.5%), and stenosis (4.7% vs. 2.0%), while Asian Americans were more prone to diabetes (38.0% vs. 29.2%).
Severe strokes (National Institutes of Health stroke score of 16 or greater) were more common among Asian Americans (odds ratio, 1.35; P less than .0001). After adjustment for stroke severity, the researchers found that Asian Americans were less likely to receive tPA (OR, 0.90; P less than .0001) and more likely to experience symptomatic intracerebral hemorrhage within 36 hours of receiving tPA (OR, 1.23; P = .003). “I think that may have something to do with the pathophysiology of Asian stroke that we don’t quite understand yet, but we can see there is a problem,” Dr. Song said.
Although in-hospital mortality was initially higher among Asian Americans, this trend switched after researchers corrected for stroke severity, leading to a better outcome for Asian Americans (OR, 0.95; P = .008). Some quality of care measures also favored Asian Americans, including receipt of stroke education (OR, 1.08; P = .02), receipt of IV tPA within 60 minutes of arrival (OR, 1.14; P = .0006), LDL cholesterol documentation (OR, 1.19; P less than .0001), and receipt of intensive statin therapy (OR, 1.15; P less than .0001). However, Asian Americans were less likely to receive a CT scan within 25 minutes of arrival (OR, 0.92; P less than .0001).
Between 2004 and 2016, both groups benefited from similar improvements, but there were differences. In 2016, a stroke in a white patient was less likely to be severe than in 2004 (OR, 0.97; P less than .0001), while there was no change in Asian Americans (OR, 1.00; P = .95).
The study is limited by the fact that the database is voluntary, which could lead to selection bias, and all Asian Americans are combined into one group. “One can argue that South Asian stroke is not the same as Japanese stroke or stroke in the Philippines,” Dr. Song said. Still, the findings suggest problems that need to be addressed. “I think it highlights the problem that Asian ischemic stroke patients don’t do as well, they bleed more, and they receive less tPA. I think that’s a big deal.”
The study received no specific funding. Dr. Song reported having no financial disclosures.
SOURCE: Song S et al. ISC 2018, Abstract TMP75.
LOS ANGELES – A large survey of Asian Americans suggests that the group experiences more severe ischemic strokes and is less likely to receive intravenous tissue plasminogen activator (tPA) than do white patients, among other discrepancies. The research found that whites had declining stroke severity between 2004 and 2016, but there was no change in Asian Americans.
The research encompasses all self-identified Asian Americans in the Get-with-the-Guidelines stroke database, which is a voluntary stroke quality improvement program begun by the American Heart Association in 2003. The analysis included 64,337 Asian Americans and 1,707,962 white Americans at 2,171 hospitals nationwide that participated in the program during 2004-2016.
“I think the most important finding is that they’re not getting as much tPA and having more tPA complications, such as bleeding more. I think it gives it an urgency that maybe was lacking, an urgency that we really need to address this issue by finding innovative ways to reach Asian Americans, to educate them about stroke. We need to find culturally appropriate ways to reach out to Asian populations,” said Dr. Song, who is a vascular neurologist at Rush Medical College, Chicago.
Dr. Song is working on small-scale interventions that are culturally tailored for Asian populations. “I think the way to approach any insular community is to work from within, so that’s my goal,” Dr. Song said.
One particular finding suggested a need for better education among Asian American communities. Asian Americans were less likely than whites to report a clinical history of having heightened levels of low-density lipoproteins. “They didn’t know that they had high cholesterol, but they had a higher LDL [cholesterol levels] than Caucasians on average,” said Dr. Song. The mean LDL cholesterol value was 101 mg/dL in Asian Americans, compared with 95 mg/dL in whites, which was statistically significant.
White patients had higher rates of atrial fibrillation (21.2% vs. 16.0%), coronary artery disease (27.8% vs. 17.5%), and stenosis (4.7% vs. 2.0%), while Asian Americans were more prone to diabetes (38.0% vs. 29.2%).
Severe strokes (National Institutes of Health stroke score of 16 or greater) were more common among Asian Americans (odds ratio, 1.35; P less than .0001). After adjustment for stroke severity, the researchers found that Asian Americans were less likely to receive tPA (OR, 0.90; P less than .0001) and more likely to experience symptomatic intracerebral hemorrhage within 36 hours of receiving tPA (OR, 1.23; P = .003). “I think that may have something to do with the pathophysiology of Asian stroke that we don’t quite understand yet, but we can see there is a problem,” Dr. Song said.
Although in-hospital mortality was initially higher among Asian Americans, this trend switched after researchers corrected for stroke severity, leading to a better outcome for Asian Americans (OR, 0.95; P = .008). Some quality of care measures also favored Asian Americans, including receipt of stroke education (OR, 1.08; P = .02), receipt of IV tPA within 60 minutes of arrival (OR, 1.14; P = .0006), LDL cholesterol documentation (OR, 1.19; P less than .0001), and receipt of intensive statin therapy (OR, 1.15; P less than .0001). However, Asian Americans were less likely to receive a CT scan within 25 minutes of arrival (OR, 0.92; P less than .0001).
Between 2004 and 2016, both groups benefited from similar improvements, but there were differences. In 2016, a stroke in a white patient was less likely to be severe than in 2004 (OR, 0.97; P less than .0001), while there was no change in Asian Americans (OR, 1.00; P = .95).
The study is limited by the fact that the database is voluntary, which could lead to selection bias, and all Asian Americans are combined into one group. “One can argue that South Asian stroke is not the same as Japanese stroke or stroke in the Philippines,” Dr. Song said. Still, the findings suggest problems that need to be addressed. “I think it highlights the problem that Asian ischemic stroke patients don’t do as well, they bleed more, and they receive less tPA. I think that’s a big deal.”
The study received no specific funding. Dr. Song reported having no financial disclosures.
SOURCE: Song S et al. ISC 2018, Abstract TMP75.
LOS ANGELES – A large survey of Asian Americans suggests that the group experiences more severe ischemic strokes and is less likely to receive intravenous tissue plasminogen activator (tPA) than do white patients, among other discrepancies. The research found that whites had declining stroke severity between 2004 and 2016, but there was no change in Asian Americans.
The research encompasses all self-identified Asian Americans in the Get-with-the-Guidelines stroke database, which is a voluntary stroke quality improvement program begun by the American Heart Association in 2003. The analysis included 64,337 Asian Americans and 1,707,962 white Americans at 2,171 hospitals nationwide that participated in the program during 2004-2016.
“I think the most important finding is that they’re not getting as much tPA and having more tPA complications, such as bleeding more. I think it gives it an urgency that maybe was lacking, an urgency that we really need to address this issue by finding innovative ways to reach Asian Americans, to educate them about stroke. We need to find culturally appropriate ways to reach out to Asian populations,” said Dr. Song, who is a vascular neurologist at Rush Medical College, Chicago.
Dr. Song is working on small-scale interventions that are culturally tailored for Asian populations. “I think the way to approach any insular community is to work from within, so that’s my goal,” Dr. Song said.
One particular finding suggested a need for better education among Asian American communities. Asian Americans were less likely than whites to report a clinical history of having heightened levels of low-density lipoproteins. “They didn’t know that they had high cholesterol, but they had a higher LDL [cholesterol levels] than Caucasians on average,” said Dr. Song. The mean LDL cholesterol value was 101 mg/dL in Asian Americans, compared with 95 mg/dL in whites, which was statistically significant.
White patients had higher rates of atrial fibrillation (21.2% vs. 16.0%), coronary artery disease (27.8% vs. 17.5%), and stenosis (4.7% vs. 2.0%), while Asian Americans were more prone to diabetes (38.0% vs. 29.2%).
Severe strokes (National Institutes of Health stroke score of 16 or greater) were more common among Asian Americans (odds ratio, 1.35; P less than .0001). After adjustment for stroke severity, the researchers found that Asian Americans were less likely to receive tPA (OR, 0.90; P less than .0001) and more likely to experience symptomatic intracerebral hemorrhage within 36 hours of receiving tPA (OR, 1.23; P = .003). “I think that may have something to do with the pathophysiology of Asian stroke that we don’t quite understand yet, but we can see there is a problem,” Dr. Song said.
Although in-hospital mortality was initially higher among Asian Americans, this trend switched after researchers corrected for stroke severity, leading to a better outcome for Asian Americans (OR, 0.95; P = .008). Some quality of care measures also favored Asian Americans, including receipt of stroke education (OR, 1.08; P = .02), receipt of IV tPA within 60 minutes of arrival (OR, 1.14; P = .0006), LDL cholesterol documentation (OR, 1.19; P less than .0001), and receipt of intensive statin therapy (OR, 1.15; P less than .0001). However, Asian Americans were less likely to receive a CT scan within 25 minutes of arrival (OR, 0.92; P less than .0001).
Between 2004 and 2016, both groups benefited from similar improvements, but there were differences. In 2016, a stroke in a white patient was less likely to be severe than in 2004 (OR, 0.97; P less than .0001), while there was no change in Asian Americans (OR, 1.00; P = .95).
The study is limited by the fact that the database is voluntary, which could lead to selection bias, and all Asian Americans are combined into one group. “One can argue that South Asian stroke is not the same as Japanese stroke or stroke in the Philippines,” Dr. Song said. Still, the findings suggest problems that need to be addressed. “I think it highlights the problem that Asian ischemic stroke patients don’t do as well, they bleed more, and they receive less tPA. I think that’s a big deal.”
The study received no specific funding. Dr. Song reported having no financial disclosures.
SOURCE: Song S et al. ISC 2018, Abstract TMP75.
REPORTING FROM ISC 2018
Key clinical point: Asian stroke patients don’t do as well as whites on some outcomes and quality measures.
Major finding: Asian Americans had a 35% higher frequency of severe stroke.
Data source: Retrospective analysis (n = 1,772,299).
Disclosures: The study received no specific funding. Dr. Song reported having no financial disclosures.
Source: Song S et al. ISC 2018, Abstract TMP75.
On-label stent use looks safe in intracranial atherosclerotic disease
LOS ANGELES – A postmarketing study of the Wingspan stent shows that the safety of the device in the treatment of intracranial atherosclerotic disease (ICAD) is good enough to be a reasonable alternative to medical management in these patients, but only if the device is used on label.
The results may reassure some interventionalists who were alarmed by results from the Stenting versus Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS) trial (N Engl J Med. 2011;365:993-1003), which showed a 30-day rate of stroke or death of 14.7%. The new study showed a frequency of 2.6%, so long as the device was used on label. Off-label use yielded a frequency of 23.9%.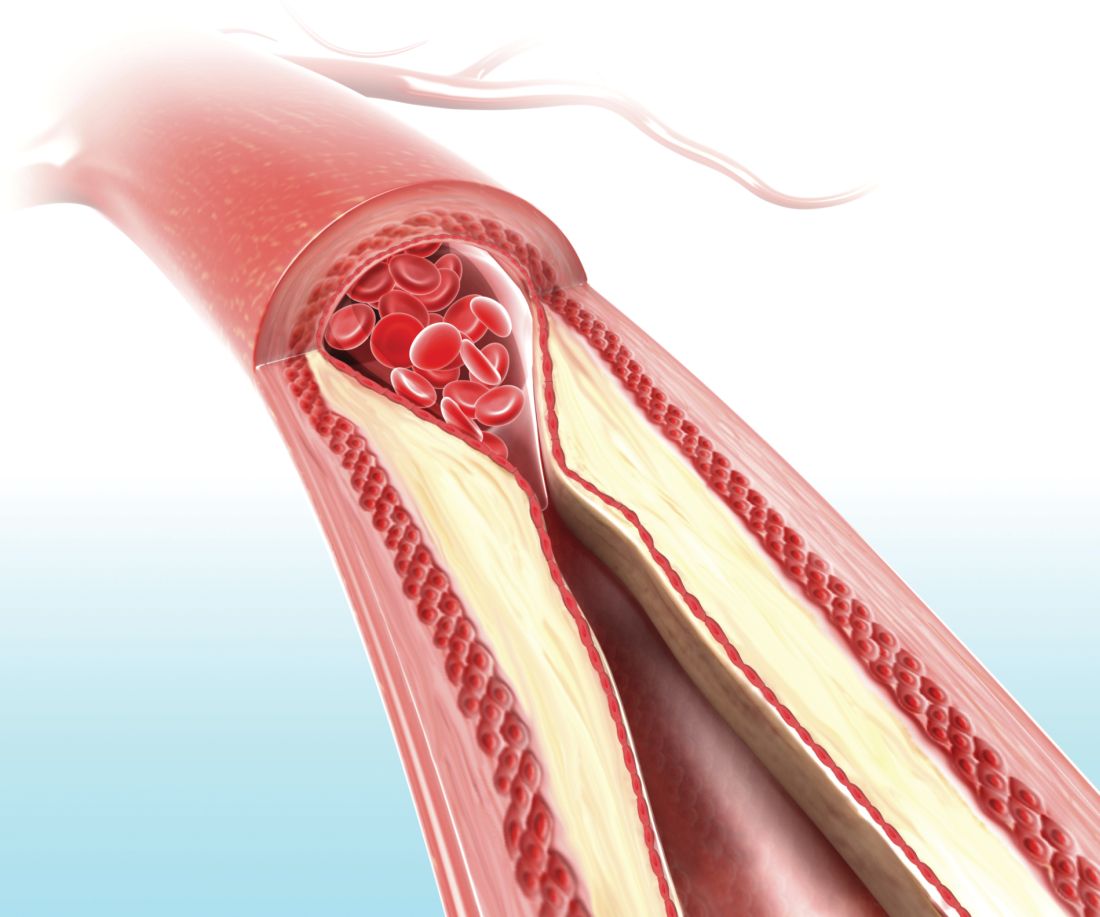
Up to 10% of strokes in the United States result from ICAD, and in China the rate is an estimated 20%-46%. The condition can also be treated medically. Early trials of the Wingspan device showed initial success with complication rates of 4.5%-6.2%, but the SAMMPRIS trial, which directly compared stenting to aggressive medical management, showed superior outcomes with medical treatment. The 30-day rate of stroke or death of 14.7% was too high to compete with medical therapy, which included aspirin 325 mg per day, clopidogrel 75 mg per day for 90 days after enrollment, and management of primary and secondary risk factors.
Dr. Alexander believes that the SAMMPRIS trial did not employ favorable patient selection. “ICAD is variable. Some patients present with hemodynamic compromise, where stenting is probably beneficial. Some present with embolic stroke, and some present with small-vessel perforator strokes that are unlikely to be responsive to stenting and better treated with medical therapy. All these patients were grouped together” in SAMMPRIS, said Dr. Alexander, who is director of the Neurovascular Center and endovascular surgery at Cedars-Sinai in Los Angeles.
The SAMMPRIS findings put a damper on stenting, and use of the procedure has dropped at many U.S. hospitals. But studies conducted prior to SAMMPRIS had shown much lower periprocedural morbidity, and those studies looked at on-label use of stenting. SAMMPRIS was off label.
Now the WEAVE study, which was an Food and Drug Administration–mandated, postmarketing surveillance study of Stryker’s Wingspan stent, suggests that the off-label use of the system in the SAMMPRIS trial may explain the poor results. SAMMPRIS had attempted to extend the approved boundaries of stenting by treating patients who presented with transient ischemic attacks only, patients who had failed medical therapy, and patients who had experienced a stroke in the past 7 days. In fact, about half of the patients were treated within 7 days of the previous event, sometimes within 24 hours.
Previous studies had shown that risk factors for poor outcomes included stenting within 10 days of the last event, stenting a posterior circulation target lesion, stenting presentations other than stroke, and sites with a low patient volume for stenting. Patient selection is vital to success, according to Dr. Alexander. Patients with hemodynamic compromise are good candidates for stenting, while those with perforator stroke alone are better off with medical therapy. Embolic stroke patients are candidates for either approach.
WEAVE looked at 152 consecutive patients treated on label at 24 institutions. The primary analysis group consisted of patients with a 70%-99% stenotic intracranial atherosclerotic lesion who were refractory to medical treatment, 22-80 years of age, and had a modified Rankin Scale (mRS) score of 3 or less at baseline. The treatment was performed at least 7 days after the last stroke. Finally, patients had to have experienced two or more strokes. This last requirement presented a problem for recruitment, according to Dr. Alexander. “That was never a criterion for any of the [previous] trials, so it’s not clear why FDA added that. That made it very difficult to enroll for this trial – to have patients who had two or more strokes and still had a functional mRS score,” he said.
The study protocol aimed for a frequency of 6.6% for periprocedural morbidity, defined as a stroke or death within 72 hours.
An interim analysis at 100 patients showed that the periprocedural morbidity frequency was below 4%, which met the agency’s requirement and allowed the trial to be halted once the trial enrolled 150 on-label patients. The total number of on-label patients reached 152, and the researchers analyzed the results from another 46 patients who were treated with stenting despite not meeting the study’s inclusion criteria, and these patients were considered to be off-label use. The final analysis showed that the on-label group had a periprocedural morbidity of 2.6%, compared with 23.9% in the off-label group (P = .0001).
The most glaring difference in the patient populations was that half of the off-label group received the stent within 7 days of experiencing a stroke. What might be the reason for worse outcomes when stenting is performed within 7 days? “There’s speculation that the plaques might be hot, and those patients might have a higher thrombotic risk with putting a foreign body in the vessel, or there’s capillary instability, so reperfusing a vessel that has a 99% stenosis has a higher risk for reperfusion hemorrhage,” Dr. Alexander said.
Experience may also be a factor. Interventionalists participating in the WEAVE trial had performed a stent using Wingspan an average of 37 times before the study began, compared with a mean of 10 cases for physicians in the SAMMPRIS trial. Those who had performed over 50 procedures had no periprocedural morbidity outcomes at all.
The study was funded by Stryker Neurovascular. Dr. Alexander has consulted for Stryker.
SOURCE: Alexander M et al. ISC 2018 Abstract LB13.
LOS ANGELES – A postmarketing study of the Wingspan stent shows that the safety of the device in the treatment of intracranial atherosclerotic disease (ICAD) is good enough to be a reasonable alternative to medical management in these patients, but only if the device is used on label.
The results may reassure some interventionalists who were alarmed by results from the Stenting versus Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS) trial (N Engl J Med. 2011;365:993-1003), which showed a 30-day rate of stroke or death of 14.7%. The new study showed a frequency of 2.6%, so long as the device was used on label. Off-label use yielded a frequency of 23.9%.
Up to 10% of strokes in the United States result from ICAD, and in China the rate is an estimated 20%-46%. The condition can also be treated medically. Early trials of the Wingspan device showed initial success with complication rates of 4.5%-6.2%, but the SAMMPRIS trial, which directly compared stenting to aggressive medical management, showed superior outcomes with medical treatment. The 30-day rate of stroke or death of 14.7% was too high to compete with medical therapy, which included aspirin 325 mg per day, clopidogrel 75 mg per day for 90 days after enrollment, and management of primary and secondary risk factors.
Dr. Alexander believes that the SAMMPRIS trial did not employ favorable patient selection. “ICAD is variable. Some patients present with hemodynamic compromise, where stenting is probably beneficial. Some present with embolic stroke, and some present with small-vessel perforator strokes that are unlikely to be responsive to stenting and better treated with medical therapy. All these patients were grouped together” in SAMMPRIS, said Dr. Alexander, who is director of the Neurovascular Center and endovascular surgery at Cedars-Sinai in Los Angeles.
The SAMMPRIS findings put a damper on stenting, and use of the procedure has dropped at many U.S. hospitals. But studies conducted prior to SAMMPRIS had shown much lower periprocedural morbidity, and those studies looked at on-label use of stenting. SAMMPRIS was off label.
Now the WEAVE study, which was an Food and Drug Administration–mandated, postmarketing surveillance study of Stryker’s Wingspan stent, suggests that the off-label use of the system in the SAMMPRIS trial may explain the poor results. SAMMPRIS had attempted to extend the approved boundaries of stenting by treating patients who presented with transient ischemic attacks only, patients who had failed medical therapy, and patients who had experienced a stroke in the past 7 days. In fact, about half of the patients were treated within 7 days of the previous event, sometimes within 24 hours.
Previous studies had shown that risk factors for poor outcomes included stenting within 10 days of the last event, stenting a posterior circulation target lesion, stenting presentations other than stroke, and sites with a low patient volume for stenting. Patient selection is vital to success, according to Dr. Alexander. Patients with hemodynamic compromise are good candidates for stenting, while those with perforator stroke alone are better off with medical therapy. Embolic stroke patients are candidates for either approach.
WEAVE looked at 152 consecutive patients treated on label at 24 institutions. The primary analysis group consisted of patients with a 70%-99% stenotic intracranial atherosclerotic lesion who were refractory to medical treatment, 22-80 years of age, and had a modified Rankin Scale (mRS) score of 3 or less at baseline. The treatment was performed at least 7 days after the last stroke. Finally, patients had to have experienced two or more strokes. This last requirement presented a problem for recruitment, according to Dr. Alexander. “That was never a criterion for any of the [previous] trials, so it’s not clear why FDA added that. That made it very difficult to enroll for this trial – to have patients who had two or more strokes and still had a functional mRS score,” he said.
The study protocol aimed for a frequency of 6.6% for periprocedural morbidity, defined as a stroke or death within 72 hours.
An interim analysis at 100 patients showed that the periprocedural morbidity frequency was below 4%, which met the agency’s requirement and allowed the trial to be halted once the trial enrolled 150 on-label patients. The total number of on-label patients reached 152, and the researchers analyzed the results from another 46 patients who were treated with stenting despite not meeting the study’s inclusion criteria, and these patients were considered to be off-label use. The final analysis showed that the on-label group had a periprocedural morbidity of 2.6%, compared with 23.9% in the off-label group (P = .0001).
The most glaring difference in the patient populations was that half of the off-label group received the stent within 7 days of experiencing a stroke. What might be the reason for worse outcomes when stenting is performed within 7 days? “There’s speculation that the plaques might be hot, and those patients might have a higher thrombotic risk with putting a foreign body in the vessel, or there’s capillary instability, so reperfusing a vessel that has a 99% stenosis has a higher risk for reperfusion hemorrhage,” Dr. Alexander said.
Experience may also be a factor. Interventionalists participating in the WEAVE trial had performed a stent using Wingspan an average of 37 times before the study began, compared with a mean of 10 cases for physicians in the SAMMPRIS trial. Those who had performed over 50 procedures had no periprocedural morbidity outcomes at all.
The study was funded by Stryker Neurovascular. Dr. Alexander has consulted for Stryker.
SOURCE: Alexander M et al. ISC 2018 Abstract LB13.
LOS ANGELES – A postmarketing study of the Wingspan stent shows that the safety of the device in the treatment of intracranial atherosclerotic disease (ICAD) is good enough to be a reasonable alternative to medical management in these patients, but only if the device is used on label.
The results may reassure some interventionalists who were alarmed by results from the Stenting versus Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS) trial (N Engl J Med. 2011;365:993-1003), which showed a 30-day rate of stroke or death of 14.7%. The new study showed a frequency of 2.6%, so long as the device was used on label. Off-label use yielded a frequency of 23.9%.
Up to 10% of strokes in the United States result from ICAD, and in China the rate is an estimated 20%-46%. The condition can also be treated medically. Early trials of the Wingspan device showed initial success with complication rates of 4.5%-6.2%, but the SAMMPRIS trial, which directly compared stenting to aggressive medical management, showed superior outcomes with medical treatment. The 30-day rate of stroke or death of 14.7% was too high to compete with medical therapy, which included aspirin 325 mg per day, clopidogrel 75 mg per day for 90 days after enrollment, and management of primary and secondary risk factors.
Dr. Alexander believes that the SAMMPRIS trial did not employ favorable patient selection. “ICAD is variable. Some patients present with hemodynamic compromise, where stenting is probably beneficial. Some present with embolic stroke, and some present with small-vessel perforator strokes that are unlikely to be responsive to stenting and better treated with medical therapy. All these patients were grouped together” in SAMMPRIS, said Dr. Alexander, who is director of the Neurovascular Center and endovascular surgery at Cedars-Sinai in Los Angeles.
The SAMMPRIS findings put a damper on stenting, and use of the procedure has dropped at many U.S. hospitals. But studies conducted prior to SAMMPRIS had shown much lower periprocedural morbidity, and those studies looked at on-label use of stenting. SAMMPRIS was off label.
Now the WEAVE study, which was an Food and Drug Administration–mandated, postmarketing surveillance study of Stryker’s Wingspan stent, suggests that the off-label use of the system in the SAMMPRIS trial may explain the poor results. SAMMPRIS had attempted to extend the approved boundaries of stenting by treating patients who presented with transient ischemic attacks only, patients who had failed medical therapy, and patients who had experienced a stroke in the past 7 days. In fact, about half of the patients were treated within 7 days of the previous event, sometimes within 24 hours.
Previous studies had shown that risk factors for poor outcomes included stenting within 10 days of the last event, stenting a posterior circulation target lesion, stenting presentations other than stroke, and sites with a low patient volume for stenting. Patient selection is vital to success, according to Dr. Alexander. Patients with hemodynamic compromise are good candidates for stenting, while those with perforator stroke alone are better off with medical therapy. Embolic stroke patients are candidates for either approach.
WEAVE looked at 152 consecutive patients treated on label at 24 institutions. The primary analysis group consisted of patients with a 70%-99% stenotic intracranial atherosclerotic lesion who were refractory to medical treatment, 22-80 years of age, and had a modified Rankin Scale (mRS) score of 3 or less at baseline. The treatment was performed at least 7 days after the last stroke. Finally, patients had to have experienced two or more strokes. This last requirement presented a problem for recruitment, according to Dr. Alexander. “That was never a criterion for any of the [previous] trials, so it’s not clear why FDA added that. That made it very difficult to enroll for this trial – to have patients who had two or more strokes and still had a functional mRS score,” he said.
The study protocol aimed for a frequency of 6.6% for periprocedural morbidity, defined as a stroke or death within 72 hours.
An interim analysis at 100 patients showed that the periprocedural morbidity frequency was below 4%, which met the agency’s requirement and allowed the trial to be halted once the trial enrolled 150 on-label patients. The total number of on-label patients reached 152, and the researchers analyzed the results from another 46 patients who were treated with stenting despite not meeting the study’s inclusion criteria, and these patients were considered to be off-label use. The final analysis showed that the on-label group had a periprocedural morbidity of 2.6%, compared with 23.9% in the off-label group (P = .0001).
The most glaring difference in the patient populations was that half of the off-label group received the stent within 7 days of experiencing a stroke. What might be the reason for worse outcomes when stenting is performed within 7 days? “There’s speculation that the plaques might be hot, and those patients might have a higher thrombotic risk with putting a foreign body in the vessel, or there’s capillary instability, so reperfusing a vessel that has a 99% stenosis has a higher risk for reperfusion hemorrhage,” Dr. Alexander said.
Experience may also be a factor. Interventionalists participating in the WEAVE trial had performed a stent using Wingspan an average of 37 times before the study began, compared with a mean of 10 cases for physicians in the SAMMPRIS trial. Those who had performed over 50 procedures had no periprocedural morbidity outcomes at all.
The study was funded by Stryker Neurovascular. Dr. Alexander has consulted for Stryker.
SOURCE: Alexander M et al. ISC 2018 Abstract LB13.
REPORTING FROM ISC 2018
Key clinical point:
Major finding: On-label 72-hour death and stroke rate was 2.6%, compared with 23.9% off label.
Data source: Postmarketing analysis of 198 consecutive patients.
Disclosures: The study was funded by Stryker Neurovascular. Dr. Alexander has consulted for Stryker.
Source: Alexander M et al. ISC 2018 Abstract LB13.
Imaging methods for stroke thrombectomy eligibility yield similar results
LOS ANGELES – The benefits of mechanical thrombectomy observed in the DAWN trial for patients with acute ischemic stroke and a mismatch between core imaging and clinical presentation out to 24 hours appear to apply regardless of whether their eligibility is determined by CT perfusion or diffusion-weighted magnetic resonance imaging, according to a subanalysis of the trial data.
Diffusion-weighted magnetic resonance imaging (DW-MRI) is considered the gold standard, but it is not as widely available as CT perfusion (CTP) and previous studies have shown that MR is associated with longer times between stroke onset and treatment randomization. “Though MR was originally preferred in DAWN, it was pretty clear that CT perfusion was going to need to be employed in the trial as well,” Cathy Sila, MD, said during her presentation of the results of the subanalysis at the International Stroke Conference 2018, sponsored by the American Heart Association.
The research sought to determine if the two imaging methods perform similarly. CTP is more readily available, but it has some issues. In patients with severe heart failure, a severe proximal stenosis, or a contralateral severe stenosis, the technique may struggle to accurately image the core infarct, which has led some to wonder if the outcomes would be as good using CTP as selection criteria. “In our institution, we’ve had this conversation very frequently,” said Dr. Sila, who is a vascular neurologist and the director of the University Hospitals Systems stroke program in Cleveland.
To be eligible for DAWN, the core infarct had to correspond to at least a 30% decrease in regional blood flow in the CTP map, or an apparent diffusion coefficient of less than 620 on DW-MRI.
The researchers included all 206 patients in the DAWN study (N Engl J Med. 2018;378:11-21), separating them into DW-MRI or CTP groups based on which imaging method was used to randomize them during the trial. There were no statistically significant differences in any of the baseline characteristics between the two imaging groups.
The 26 sites participating in DAWN had clear differences in their preferences for imaging techniques; 19 exclusively used CTP, 4 used only DW-MRI, and 3 sites used a combination of both imaging methods.
There were no statistically significant differences between the two groups in any of the measured clinical outcomes, including neurologic deterioration in hospital (22.8% with CTP vs. 15.7% with DW-MRII, P = .286), symptomatic intracranial hemorrhage (4.1% with CTP vs. 4.8% with DW-MRI, P = 1.000), or death related to stroke (19.5% with CTP vs. 13.3% with DW-MRI, P = .263). Outcomes at 90 days proved to be similar between CTP and DW-MRI for achieving functional independence (29.3% vs. 34.9%, respectively; P = .445) and utility-weighted modified Rankin Scale scores (4.2 vs. 4.9, respectively; P = .172).
Multivariate analyses showed that 90-day functional independence was predicted by thrombectomy treatment, age, blood glucose level, baseline National Institutes of Health Stroke Scale score, and core lab ASPECTS (Alberta Stroke Program Early CT Score), but not the method of imaging.
“The efficacy and safety of mechanical thrombectomy for patients meeting those clinical mismatch criteria at 6-24 hours were comparable whether the small core infarcts were measured by diffusion imaging or cerebral blood flow imaging. I believe that future clinical trials aiming to extend the eligibility outside of this prespecified population should include both imaging modalities to determine whether these results are generalizable,” Dr. Sila said.
The DAWN study was funded by Stryker Neurovascular. Dr. Sila has reported receiving honoraria from Medtronic.
SOURCE: Sila C et al. ISC 2018, abstract LB11.
LOS ANGELES – The benefits of mechanical thrombectomy observed in the DAWN trial for patients with acute ischemic stroke and a mismatch between core imaging and clinical presentation out to 24 hours appear to apply regardless of whether their eligibility is determined by CT perfusion or diffusion-weighted magnetic resonance imaging, according to a subanalysis of the trial data.
Diffusion-weighted magnetic resonance imaging (DW-MRI) is considered the gold standard, but it is not as widely available as CT perfusion (CTP) and previous studies have shown that MR is associated with longer times between stroke onset and treatment randomization. “Though MR was originally preferred in DAWN, it was pretty clear that CT perfusion was going to need to be employed in the trial as well,” Cathy Sila, MD, said during her presentation of the results of the subanalysis at the International Stroke Conference 2018, sponsored by the American Heart Association.
The research sought to determine if the two imaging methods perform similarly. CTP is more readily available, but it has some issues. In patients with severe heart failure, a severe proximal stenosis, or a contralateral severe stenosis, the technique may struggle to accurately image the core infarct, which has led some to wonder if the outcomes would be as good using CTP as selection criteria. “In our institution, we’ve had this conversation very frequently,” said Dr. Sila, who is a vascular neurologist and the director of the University Hospitals Systems stroke program in Cleveland.
To be eligible for DAWN, the core infarct had to correspond to at least a 30% decrease in regional blood flow in the CTP map, or an apparent diffusion coefficient of less than 620 on DW-MRI.
The researchers included all 206 patients in the DAWN study (N Engl J Med. 2018;378:11-21), separating them into DW-MRI or CTP groups based on which imaging method was used to randomize them during the trial. There were no statistically significant differences in any of the baseline characteristics between the two imaging groups.
The 26 sites participating in DAWN had clear differences in their preferences for imaging techniques; 19 exclusively used CTP, 4 used only DW-MRI, and 3 sites used a combination of both imaging methods.
There were no statistically significant differences between the two groups in any of the measured clinical outcomes, including neurologic deterioration in hospital (22.8% with CTP vs. 15.7% with DW-MRII, P = .286), symptomatic intracranial hemorrhage (4.1% with CTP vs. 4.8% with DW-MRI, P = 1.000), or death related to stroke (19.5% with CTP vs. 13.3% with DW-MRI, P = .263). Outcomes at 90 days proved to be similar between CTP and DW-MRI for achieving functional independence (29.3% vs. 34.9%, respectively; P = .445) and utility-weighted modified Rankin Scale scores (4.2 vs. 4.9, respectively; P = .172).
Multivariate analyses showed that 90-day functional independence was predicted by thrombectomy treatment, age, blood glucose level, baseline National Institutes of Health Stroke Scale score, and core lab ASPECTS (Alberta Stroke Program Early CT Score), but not the method of imaging.
“The efficacy and safety of mechanical thrombectomy for patients meeting those clinical mismatch criteria at 6-24 hours were comparable whether the small core infarcts were measured by diffusion imaging or cerebral blood flow imaging. I believe that future clinical trials aiming to extend the eligibility outside of this prespecified population should include both imaging modalities to determine whether these results are generalizable,” Dr. Sila said.
The DAWN study was funded by Stryker Neurovascular. Dr. Sila has reported receiving honoraria from Medtronic.
SOURCE: Sila C et al. ISC 2018, abstract LB11.
LOS ANGELES – The benefits of mechanical thrombectomy observed in the DAWN trial for patients with acute ischemic stroke and a mismatch between core imaging and clinical presentation out to 24 hours appear to apply regardless of whether their eligibility is determined by CT perfusion or diffusion-weighted magnetic resonance imaging, according to a subanalysis of the trial data.
Diffusion-weighted magnetic resonance imaging (DW-MRI) is considered the gold standard, but it is not as widely available as CT perfusion (CTP) and previous studies have shown that MR is associated with longer times between stroke onset and treatment randomization. “Though MR was originally preferred in DAWN, it was pretty clear that CT perfusion was going to need to be employed in the trial as well,” Cathy Sila, MD, said during her presentation of the results of the subanalysis at the International Stroke Conference 2018, sponsored by the American Heart Association.
The research sought to determine if the two imaging methods perform similarly. CTP is more readily available, but it has some issues. In patients with severe heart failure, a severe proximal stenosis, or a contralateral severe stenosis, the technique may struggle to accurately image the core infarct, which has led some to wonder if the outcomes would be as good using CTP as selection criteria. “In our institution, we’ve had this conversation very frequently,” said Dr. Sila, who is a vascular neurologist and the director of the University Hospitals Systems stroke program in Cleveland.
To be eligible for DAWN, the core infarct had to correspond to at least a 30% decrease in regional blood flow in the CTP map, or an apparent diffusion coefficient of less than 620 on DW-MRI.
The researchers included all 206 patients in the DAWN study (N Engl J Med. 2018;378:11-21), separating them into DW-MRI or CTP groups based on which imaging method was used to randomize them during the trial. There were no statistically significant differences in any of the baseline characteristics between the two imaging groups.
The 26 sites participating in DAWN had clear differences in their preferences for imaging techniques; 19 exclusively used CTP, 4 used only DW-MRI, and 3 sites used a combination of both imaging methods.
There were no statistically significant differences between the two groups in any of the measured clinical outcomes, including neurologic deterioration in hospital (22.8% with CTP vs. 15.7% with DW-MRII, P = .286), symptomatic intracranial hemorrhage (4.1% with CTP vs. 4.8% with DW-MRI, P = 1.000), or death related to stroke (19.5% with CTP vs. 13.3% with DW-MRI, P = .263). Outcomes at 90 days proved to be similar between CTP and DW-MRI for achieving functional independence (29.3% vs. 34.9%, respectively; P = .445) and utility-weighted modified Rankin Scale scores (4.2 vs. 4.9, respectively; P = .172).
Multivariate analyses showed that 90-day functional independence was predicted by thrombectomy treatment, age, blood glucose level, baseline National Institutes of Health Stroke Scale score, and core lab ASPECTS (Alberta Stroke Program Early CT Score), but not the method of imaging.
“The efficacy and safety of mechanical thrombectomy for patients meeting those clinical mismatch criteria at 6-24 hours were comparable whether the small core infarcts were measured by diffusion imaging or cerebral blood flow imaging. I believe that future clinical trials aiming to extend the eligibility outside of this prespecified population should include both imaging modalities to determine whether these results are generalizable,” Dr. Sila said.
The DAWN study was funded by Stryker Neurovascular. Dr. Sila has reported receiving honoraria from Medtronic.
SOURCE: Sila C et al. ISC 2018, abstract LB11.
REPORTING FROM ISC 2018
Key clinical point: DW-MRI is the gold standard for imaging, but CTP is more widely available.
Major finding: Rates of neurologic deterioration in hospital, symptomatic intracranial hemorrhage, and death related to stroke were similar regardless of whether CT or MR imaging was used to assess patients’ infarcts.
Data source: A subanalysis of the DAWN randomized, controlled trial (n = 206).
Disclosures: The DAWN study was funded by Stryker Neurovascular. Dr. Sila reported receiving honoraria from Medtronic.
Source: Sila C et al. ISC 2018, abstract LB11.
Ticagrelor may be superior to clopidogrel in poor metabolizers
LOS ANGELES – In patients who had experienced a minor stroke or a transient ischemic attack with a moderate to high risk of stroke, the combination of ticagrelor and aspirin reduced the 90-day incidence of high on-treatment platelet reactivity, according to results from the PRINCE trial.
Although the combination outperformed clopidogrel (Plavix) plus aspirin, ticagrelor (Brilinta) was associated with higher bleeding risk.
The researchers also saw a trend toward a reduction in strokes that did not reach statistical significance, but the trial was halted following an interim analysis showing that the high on-treatment platelet reactivity (HOPR) endpoint, defined as P2Y12 reaction unit (PRU) greater than 208, showed a statistically significant difference. “To prove the clinical benefit, we will need a larger sample size,” study first author and presenter Yilong Wang, MD, PhD, of Beijing Tiantan Hospital, Capital Medical University, said in an interview at the International Stroke Conference, sponsored by the American Heart Association.

Previously, the SOCRATES trial found no advantage to treatment with ticagrelor over aspirin, but a prespecified exploratory analysis focusing on Asian patients (Stroke. 2017;48:167-73) found a trend toward reducing vascular events in the ticagrelor group, compared with patients taking aspirin.
In the Platelet Reactivity in Acute Stroke or Transient Ischemic Attack (PRINCE) trial, the researchers sought to examine the safety and efficacy of ticagrelor when compared with clopidogrel in 675 Asian patients (mean age 61 years, one-quarter of whom were female) from 26 centers in China and randomized them to ticagrelor plus aspirin (Tica) or clopidogrel plus aspirin (Clop). Within 24 hours of symptom onset, patients received 180 mg ticagrelor or 300 mg clopidogrel plus 100-300 mg aspirin. During days 1-21, they received 90 mg ticagrelor twice per day or 75 mg clopidogrel once per day. Both groups received 100 mg aspirin once per day. From day 21 to day 90, they received 90 mg ticagrelor twice per day or 75 mg clopidogrel once per day, with no aspirin.
At 90 days, the mean PRU value was 175.44 in the Clop group, compared with 69.24 in the Tica group. Overall, 27.7% of the Clop group experienced HOPR in the first 7 days, compared with 3.9% of the Tica group. At 90 days, 29.7% of the Clop group had experienced HOPR, compared with 12.5% of the Tica group (odds ratio, 0.33; 95% confidence interval, 0.21-0.51; P less than .001).
Ticagrelor was associated with greater benefit among those with impaired ability to metabolize clopidogrel. Among poor metabolizers, HOPR occurred in 10.5% in the Tica group and 42.4% of the Clop group (OR, 0.16; 95% CI, 0.05-0.56; P = .004). A similar favorable effect was seen in intermediate metabolizers in the Tica group (OR, 0.24; 95% CI, 0.12-0.49; P less than .001).
The 90-day stroke rate was no different between the Tica and Clop groups (6.3% vs. 8.8%, respectively; P = .20).
Minimal bleeding was higher in the Tica group (19.0% vs. 10.6%; hazard ratio, 1.86; P = .003), as was any bleeding (22.3% vs. 14.2%; HR, 1.65; P = .007). There were three deaths in the Tica group and two in the Clop group.
Dyspnea was the most common cause of drug discontinuation, and occurred in 4.2% of patients taking ticagrelor but none of the patients taking clopidogrel (P = .0001).
The researchers hope to demonstrate the clinical benefits of the combination in the upcoming PRINCE 2 trial. The results will have an important impact because CYP2C19 loss of function alleles are more common in Asian population. “It’s a very big problem for us,” Dr. Wang said.
The study was funded by the National Natural Science Foundation of China, the Beijing Institute for Brain, and the Beijing Municipal Science & Technology Commission of Cerebral Vascular Disease. AstraZeneca provided study drugs. Dr. Wang reported having no financial disclosures.
SOURCE: Wang Y et al. ISC 2018, abstract LB8
LOS ANGELES – In patients who had experienced a minor stroke or a transient ischemic attack with a moderate to high risk of stroke, the combination of ticagrelor and aspirin reduced the 90-day incidence of high on-treatment platelet reactivity, according to results from the PRINCE trial.
Although the combination outperformed clopidogrel (Plavix) plus aspirin, ticagrelor (Brilinta) was associated with higher bleeding risk.
The researchers also saw a trend toward a reduction in strokes that did not reach statistical significance, but the trial was halted following an interim analysis showing that the high on-treatment platelet reactivity (HOPR) endpoint, defined as P2Y12 reaction unit (PRU) greater than 208, showed a statistically significant difference. “To prove the clinical benefit, we will need a larger sample size,” study first author and presenter Yilong Wang, MD, PhD, of Beijing Tiantan Hospital, Capital Medical University, said in an interview at the International Stroke Conference, sponsored by the American Heart Association.
Previously, the SOCRATES trial found no advantage to treatment with ticagrelor over aspirin, but a prespecified exploratory analysis focusing on Asian patients (Stroke. 2017;48:167-73) found a trend toward reducing vascular events in the ticagrelor group, compared with patients taking aspirin.
In the Platelet Reactivity in Acute Stroke or Transient Ischemic Attack (PRINCE) trial, the researchers sought to examine the safety and efficacy of ticagrelor when compared with clopidogrel in 675 Asian patients (mean age 61 years, one-quarter of whom were female) from 26 centers in China and randomized them to ticagrelor plus aspirin (Tica) or clopidogrel plus aspirin (Clop). Within 24 hours of symptom onset, patients received 180 mg ticagrelor or 300 mg clopidogrel plus 100-300 mg aspirin. During days 1-21, they received 90 mg ticagrelor twice per day or 75 mg clopidogrel once per day. Both groups received 100 mg aspirin once per day. From day 21 to day 90, they received 90 mg ticagrelor twice per day or 75 mg clopidogrel once per day, with no aspirin.
At 90 days, the mean PRU value was 175.44 in the Clop group, compared with 69.24 in the Tica group. Overall, 27.7% of the Clop group experienced HOPR in the first 7 days, compared with 3.9% of the Tica group. At 90 days, 29.7% of the Clop group had experienced HOPR, compared with 12.5% of the Tica group (odds ratio, 0.33; 95% confidence interval, 0.21-0.51; P less than .001).
Ticagrelor was associated with greater benefit among those with impaired ability to metabolize clopidogrel. Among poor metabolizers, HOPR occurred in 10.5% in the Tica group and 42.4% of the Clop group (OR, 0.16; 95% CI, 0.05-0.56; P = .004). A similar favorable effect was seen in intermediate metabolizers in the Tica group (OR, 0.24; 95% CI, 0.12-0.49; P less than .001).
The 90-day stroke rate was no different between the Tica and Clop groups (6.3% vs. 8.8%, respectively; P = .20).
Minimal bleeding was higher in the Tica group (19.0% vs. 10.6%; hazard ratio, 1.86; P = .003), as was any bleeding (22.3% vs. 14.2%; HR, 1.65; P = .007). There were three deaths in the Tica group and two in the Clop group.
Dyspnea was the most common cause of drug discontinuation, and occurred in 4.2% of patients taking ticagrelor but none of the patients taking clopidogrel (P = .0001).
The researchers hope to demonstrate the clinical benefits of the combination in the upcoming PRINCE 2 trial. The results will have an important impact because CYP2C19 loss of function alleles are more common in Asian population. “It’s a very big problem for us,” Dr. Wang said.
The study was funded by the National Natural Science Foundation of China, the Beijing Institute for Brain, and the Beijing Municipal Science & Technology Commission of Cerebral Vascular Disease. AstraZeneca provided study drugs. Dr. Wang reported having no financial disclosures.
SOURCE: Wang Y et al. ISC 2018, abstract LB8
LOS ANGELES – In patients who had experienced a minor stroke or a transient ischemic attack with a moderate to high risk of stroke, the combination of ticagrelor and aspirin reduced the 90-day incidence of high on-treatment platelet reactivity, according to results from the PRINCE trial.
Although the combination outperformed clopidogrel (Plavix) plus aspirin, ticagrelor (Brilinta) was associated with higher bleeding risk.
The researchers also saw a trend toward a reduction in strokes that did not reach statistical significance, but the trial was halted following an interim analysis showing that the high on-treatment platelet reactivity (HOPR) endpoint, defined as P2Y12 reaction unit (PRU) greater than 208, showed a statistically significant difference. “To prove the clinical benefit, we will need a larger sample size,” study first author and presenter Yilong Wang, MD, PhD, of Beijing Tiantan Hospital, Capital Medical University, said in an interview at the International Stroke Conference, sponsored by the American Heart Association.
Previously, the SOCRATES trial found no advantage to treatment with ticagrelor over aspirin, but a prespecified exploratory analysis focusing on Asian patients (Stroke. 2017;48:167-73) found a trend toward reducing vascular events in the ticagrelor group, compared with patients taking aspirin.
In the Platelet Reactivity in Acute Stroke or Transient Ischemic Attack (PRINCE) trial, the researchers sought to examine the safety and efficacy of ticagrelor when compared with clopidogrel in 675 Asian patients (mean age 61 years, one-quarter of whom were female) from 26 centers in China and randomized them to ticagrelor plus aspirin (Tica) or clopidogrel plus aspirin (Clop). Within 24 hours of symptom onset, patients received 180 mg ticagrelor or 300 mg clopidogrel plus 100-300 mg aspirin. During days 1-21, they received 90 mg ticagrelor twice per day or 75 mg clopidogrel once per day. Both groups received 100 mg aspirin once per day. From day 21 to day 90, they received 90 mg ticagrelor twice per day or 75 mg clopidogrel once per day, with no aspirin.
At 90 days, the mean PRU value was 175.44 in the Clop group, compared with 69.24 in the Tica group. Overall, 27.7% of the Clop group experienced HOPR in the first 7 days, compared with 3.9% of the Tica group. At 90 days, 29.7% of the Clop group had experienced HOPR, compared with 12.5% of the Tica group (odds ratio, 0.33; 95% confidence interval, 0.21-0.51; P less than .001).
Ticagrelor was associated with greater benefit among those with impaired ability to metabolize clopidogrel. Among poor metabolizers, HOPR occurred in 10.5% in the Tica group and 42.4% of the Clop group (OR, 0.16; 95% CI, 0.05-0.56; P = .004). A similar favorable effect was seen in intermediate metabolizers in the Tica group (OR, 0.24; 95% CI, 0.12-0.49; P less than .001).
The 90-day stroke rate was no different between the Tica and Clop groups (6.3% vs. 8.8%, respectively; P = .20).
Minimal bleeding was higher in the Tica group (19.0% vs. 10.6%; hazard ratio, 1.86; P = .003), as was any bleeding (22.3% vs. 14.2%; HR, 1.65; P = .007). There were three deaths in the Tica group and two in the Clop group.
Dyspnea was the most common cause of drug discontinuation, and occurred in 4.2% of patients taking ticagrelor but none of the patients taking clopidogrel (P = .0001).
The researchers hope to demonstrate the clinical benefits of the combination in the upcoming PRINCE 2 trial. The results will have an important impact because CYP2C19 loss of function alleles are more common in Asian population. “It’s a very big problem for us,” Dr. Wang said.
The study was funded by the National Natural Science Foundation of China, the Beijing Institute for Brain, and the Beijing Municipal Science & Technology Commission of Cerebral Vascular Disease. AstraZeneca provided study drugs. Dr. Wang reported having no financial disclosures.
SOURCE: Wang Y et al. ISC 2018, abstract LB8
REPORTING FROM ISC 2018
Key clinical point: Ticagrelor may be a better option than clopidogrel in patients with loss-of-function CYP2C19 alleles.
Major finding: Patients on ticagrelor had a lower 90-day risk of high on-treatment platelet reactivity (OR, 0.33).
Data source: Randomized, open-label trial with blinded assessments (n = 675).
Disclosures: The study was funded by the National Natural Science Foundation of China, the Beijing Institute for Brain, and the Beijing Municipal Science & Technology Commission of Cerebral Vascular Disease. AstraZeneca provided study drugs. Dr. Wang reported having no financial disclosures.
Source: Wang Y et al. ISC 2018, abstract LB8
Late thrombectomy for stroke has low number needed to treat for benefit
LOS ANGELES – The number of ischemic stroke patients with a clinical core mismatch showing salvageable tissue who need to be treated with thrombectomy to obtain a significant benefit on functional outcomes is just 2 when the time frame from last known well extends out to 24 hours, according a subanalysis of results from the DAWN trial.
The Jan. 4, 2018, publication of the DAWN trial revealed that patients with ischemic strokes can benefit from thrombectomy long after the time window generally thought to afford benefits had closed (N Engl J Med. 2018;378:11-21). The procedure yielded significant benefits in functional outcomes at 90 days in patients with a clinical core mismatch showing salvageable tissue.

The results are important because health care systems must now make decisions about allocating resources for the treatment of these patients, which will include installing imaging techniques and expertise at various centers. “It will be practical in some primary stroke centers and not in others. We’re going to see a lot of interesting research about what frontline hospitals should do. There are lots of options at that screening step, and we’re going to need experience to see what’s best. It won’t be the same answer for everyone,” Jeffrey Saver, MD, said during a press conference announcing the results at the meeting, which was sponsored by the American Heart Association. Dr. Saver is director of the stroke unit at the University of California, Los Angeles, and professor of clinical neurology at the university.
The DAWN trial randomized 206 patients to thrombectomy plus standard care or standard care alone. The study was halted at an enrollment of 206 patients because of overwhelming efficacy. To be eligible, the patients had to have a mismatch between the severity of clinical deficit and the infarct volume as measured via automated analysis (RAPID software, SchemaView) of diffusion-weighted MRI or perfusion CT. They had to have substantial clinical deficits, but limited infarct size, with specific criteria varying with age, National Institutes of Health Stroke Scale score, and infarct size.
The NNT for an mRS score of 0 (asymptomatic) was 19. For freedom from disability (mRS, 0-1), the NNT was 4. For functional independence (mRS, 0-2), it was 3. To achieve ambulatory status (mRS, 0-3), it was 3. To avoid a requirement for constant care (mRS, 0-4), the NNT was 9.
To achieve any reduction in disability at all, the NNT was 2. This value was identical when looking at patients in the 6- to 12-hour window and those in the 12- to 24-hour window. However, the nature of the benefit was different. “In the late window (12-24 hours), outcomes went from really bad to pretty good. In the early window, it was somewhat bad to very good. So it’s still better to be treated early,” Dr. Saver said.
In short, for every 100 patients treated, 50 would gain an improvement in disability-related quality of life, and 36 would gain functional independence. In the 6- to 12-hour group, 45 of every 100 patients would experience lower disability as a result of treatment, as would 56 of every 100 treated patients in the 12- to 24-hour group.
Stryker Neurovascular funded the study. Dr. Saver has consulted for Stryker and received travel reimbursement.
LOS ANGELES – The number of ischemic stroke patients with a clinical core mismatch showing salvageable tissue who need to be treated with thrombectomy to obtain a significant benefit on functional outcomes is just 2 when the time frame from last known well extends out to 24 hours, according a subanalysis of results from the DAWN trial.
The Jan. 4, 2018, publication of the DAWN trial revealed that patients with ischemic strokes can benefit from thrombectomy long after the time window generally thought to afford benefits had closed (N Engl J Med. 2018;378:11-21). The procedure yielded significant benefits in functional outcomes at 90 days in patients with a clinical core mismatch showing salvageable tissue.
The results are important because health care systems must now make decisions about allocating resources for the treatment of these patients, which will include installing imaging techniques and expertise at various centers. “It will be practical in some primary stroke centers and not in others. We’re going to see a lot of interesting research about what frontline hospitals should do. There are lots of options at that screening step, and we’re going to need experience to see what’s best. It won’t be the same answer for everyone,” Jeffrey Saver, MD, said during a press conference announcing the results at the meeting, which was sponsored by the American Heart Association. Dr. Saver is director of the stroke unit at the University of California, Los Angeles, and professor of clinical neurology at the university.
The DAWN trial randomized 206 patients to thrombectomy plus standard care or standard care alone. The study was halted at an enrollment of 206 patients because of overwhelming efficacy. To be eligible, the patients had to have a mismatch between the severity of clinical deficit and the infarct volume as measured via automated analysis (RAPID software, SchemaView) of diffusion-weighted MRI or perfusion CT. They had to have substantial clinical deficits, but limited infarct size, with specific criteria varying with age, National Institutes of Health Stroke Scale score, and infarct size.
The NNT for an mRS score of 0 (asymptomatic) was 19. For freedom from disability (mRS, 0-1), the NNT was 4. For functional independence (mRS, 0-2), it was 3. To achieve ambulatory status (mRS, 0-3), it was 3. To avoid a requirement for constant care (mRS, 0-4), the NNT was 9.
To achieve any reduction in disability at all, the NNT was 2. This value was identical when looking at patients in the 6- to 12-hour window and those in the 12- to 24-hour window. However, the nature of the benefit was different. “In the late window (12-24 hours), outcomes went from really bad to pretty good. In the early window, it was somewhat bad to very good. So it’s still better to be treated early,” Dr. Saver said.
In short, for every 100 patients treated, 50 would gain an improvement in disability-related quality of life, and 36 would gain functional independence. In the 6- to 12-hour group, 45 of every 100 patients would experience lower disability as a result of treatment, as would 56 of every 100 treated patients in the 12- to 24-hour group.
Stryker Neurovascular funded the study. Dr. Saver has consulted for Stryker and received travel reimbursement.
LOS ANGELES – The number of ischemic stroke patients with a clinical core mismatch showing salvageable tissue who need to be treated with thrombectomy to obtain a significant benefit on functional outcomes is just 2 when the time frame from last known well extends out to 24 hours, according a subanalysis of results from the DAWN trial.
The Jan. 4, 2018, publication of the DAWN trial revealed that patients with ischemic strokes can benefit from thrombectomy long after the time window generally thought to afford benefits had closed (N Engl J Med. 2018;378:11-21). The procedure yielded significant benefits in functional outcomes at 90 days in patients with a clinical core mismatch showing salvageable tissue.
The results are important because health care systems must now make decisions about allocating resources for the treatment of these patients, which will include installing imaging techniques and expertise at various centers. “It will be practical in some primary stroke centers and not in others. We’re going to see a lot of interesting research about what frontline hospitals should do. There are lots of options at that screening step, and we’re going to need experience to see what’s best. It won’t be the same answer for everyone,” Jeffrey Saver, MD, said during a press conference announcing the results at the meeting, which was sponsored by the American Heart Association. Dr. Saver is director of the stroke unit at the University of California, Los Angeles, and professor of clinical neurology at the university.
The DAWN trial randomized 206 patients to thrombectomy plus standard care or standard care alone. The study was halted at an enrollment of 206 patients because of overwhelming efficacy. To be eligible, the patients had to have a mismatch between the severity of clinical deficit and the infarct volume as measured via automated analysis (RAPID software, SchemaView) of diffusion-weighted MRI or perfusion CT. They had to have substantial clinical deficits, but limited infarct size, with specific criteria varying with age, National Institutes of Health Stroke Scale score, and infarct size.
The NNT for an mRS score of 0 (asymptomatic) was 19. For freedom from disability (mRS, 0-1), the NNT was 4. For functional independence (mRS, 0-2), it was 3. To achieve ambulatory status (mRS, 0-3), it was 3. To avoid a requirement for constant care (mRS, 0-4), the NNT was 9.
To achieve any reduction in disability at all, the NNT was 2. This value was identical when looking at patients in the 6- to 12-hour window and those in the 12- to 24-hour window. However, the nature of the benefit was different. “In the late window (12-24 hours), outcomes went from really bad to pretty good. In the early window, it was somewhat bad to very good. So it’s still better to be treated early,” Dr. Saver said.
In short, for every 100 patients treated, 50 would gain an improvement in disability-related quality of life, and 36 would gain functional independence. In the 6- to 12-hour group, 45 of every 100 patients would experience lower disability as a result of treatment, as would 56 of every 100 treated patients in the 12- to 24-hour group.
Stryker Neurovascular funded the study. Dr. Saver has consulted for Stryker and received travel reimbursement.
REPORTING FROM ISC 2018
Key clinical point:
Major finding: To achieve a functional improvement at 90 days, the number needed to treat was 2.
Data source: Subanalysis of the randomized, controlled DAWN trial (n = 206).
Disclosures: Stryker Neurovascular funded the study. Dr. Saver has consulted for Stryker and received travel reimbursement.
Source: Saver J et al. ISC 2018 abstract LB3
Cerebrospinal tract may help decide mild stroke treatment
LOS ANGELES – In acute ischemic stroke patients with small perfusion lesions of less than 15 mL, involvement of the corticospinal tract (CST) may help guide the decision whether to treat with alteplase.
Specifically, patients with hypoperfusion in the CST, but without CST infarction, were more likely to have a modified Rankin Scale score (mRS) of 0-2 at 90 days after treatment with alteplase. Patients with no CST involvement, or with a CST infarct, had worse outcomes with treatment.
The better outcomes “might indicate that hypoperfused CST tissue at baseline could be salvaged by timely reperfusion,” said Min Lou, MD, PhD, vice chair of neurology at Zhejiang University, Hangzhou, China, during her presentation of the study at the International Stroke Conference sponsored by the American Heart Association.
Previous studies have left physicians uncertain what to do with patients presenting with mild stroke, especially strokes that are judged to be potentially disabling despite a low National Institutes of Health Stroke Scale (NIHSS) score. These patients have a lower risk of hemorrhagic conversion, estimated at 0%-2%.
A meta-analysis showed that alteplase treatment in patients with a baseline NIHSS score of 0-4 was associated with a 48% increase in the chance of an excellent outcome. But another study showed that, among patients with a perfusion lesion smaller than 15 mL, treatment with alteplase was less likely than no treatment at all to confer an excellent outcome.
“The challenge is to identify what kind of minor stroke patient would benefit from thrombolysis therapy,” said Dr. Lou.
The researchers analyzed data from the International Stroke Perfusion Imaging Registry (INSPIRE) database, selecting 412 patients with an acute perfusion lesion less than 15 mL who had undergone computed tomography perfusion or magnetic resonance perfusion imaging within 4.5 hours of symptom onset, had had the scan repeated at 24 hours, and who were followed up at 90 days.
Among the patients, 248 were treated with alteplase, and 164 were not. The alteplase-treated group had a mean NIHSS score of 5.0, compared with 4.0 in the untreated group (P = .001). CST hypoperfusion was more common in the treated group (32.3% versus 15.9%, P less than .001), as was CST infarction (14.9% versus 5.5%, P = .004) and 24-hour intracerebral hemorrhage (ICH) (9.3% versus 0.6%, P less than .001).
The researchers divided subjects into three groups: no CST lesion (306 patients), CST hypoperfusion with no CST infarct (60), and CST infarct (46). The 24-hour ICH frequency varied between the groups, with the highest frequency in the CST infarct group (15.2%), followed by the CST hypoperfusion with no infarct group (10.0%), and the no CST lesion group (3.6%, P = .002).
At 90 days, higher frequency of an mRS score of 0-1 was only associated with alteplase treatment in the CST hypoperfusion with no infarct group (76.7% versus 47.1%, P = .035).
The reverse was true in the other groups: No treatment was associated with better odds of an mRS score of 0-1 in the group with no CST lesion (87.7% versus 79.8%, P = .067) and particularly in the group with CST infarct (88.9% versus 32.4%, P = .006).
The study is limited by the fact that it is a retrospective analysis, the investigators cautioned.
The National Natural Science Foundation of China funded the study. Dr. Lou reported having no financial disclosures.
LOS ANGELES – In acute ischemic stroke patients with small perfusion lesions of less than 15 mL, involvement of the corticospinal tract (CST) may help guide the decision whether to treat with alteplase.
Specifically, patients with hypoperfusion in the CST, but without CST infarction, were more likely to have a modified Rankin Scale score (mRS) of 0-2 at 90 days after treatment with alteplase. Patients with no CST involvement, or with a CST infarct, had worse outcomes with treatment.
The better outcomes “might indicate that hypoperfused CST tissue at baseline could be salvaged by timely reperfusion,” said Min Lou, MD, PhD, vice chair of neurology at Zhejiang University, Hangzhou, China, during her presentation of the study at the International Stroke Conference sponsored by the American Heart Association.
Previous studies have left physicians uncertain what to do with patients presenting with mild stroke, especially strokes that are judged to be potentially disabling despite a low National Institutes of Health Stroke Scale (NIHSS) score. These patients have a lower risk of hemorrhagic conversion, estimated at 0%-2%.
A meta-analysis showed that alteplase treatment in patients with a baseline NIHSS score of 0-4 was associated with a 48% increase in the chance of an excellent outcome. But another study showed that, among patients with a perfusion lesion smaller than 15 mL, treatment with alteplase was less likely than no treatment at all to confer an excellent outcome.
“The challenge is to identify what kind of minor stroke patient would benefit from thrombolysis therapy,” said Dr. Lou.
The researchers analyzed data from the International Stroke Perfusion Imaging Registry (INSPIRE) database, selecting 412 patients with an acute perfusion lesion less than 15 mL who had undergone computed tomography perfusion or magnetic resonance perfusion imaging within 4.5 hours of symptom onset, had had the scan repeated at 24 hours, and who were followed up at 90 days.
Among the patients, 248 were treated with alteplase, and 164 were not. The alteplase-treated group had a mean NIHSS score of 5.0, compared with 4.0 in the untreated group (P = .001). CST hypoperfusion was more common in the treated group (32.3% versus 15.9%, P less than .001), as was CST infarction (14.9% versus 5.5%, P = .004) and 24-hour intracerebral hemorrhage (ICH) (9.3% versus 0.6%, P less than .001).
The researchers divided subjects into three groups: no CST lesion (306 patients), CST hypoperfusion with no CST infarct (60), and CST infarct (46). The 24-hour ICH frequency varied between the groups, with the highest frequency in the CST infarct group (15.2%), followed by the CST hypoperfusion with no infarct group (10.0%), and the no CST lesion group (3.6%, P = .002).
At 90 days, higher frequency of an mRS score of 0-1 was only associated with alteplase treatment in the CST hypoperfusion with no infarct group (76.7% versus 47.1%, P = .035).
The reverse was true in the other groups: No treatment was associated with better odds of an mRS score of 0-1 in the group with no CST lesion (87.7% versus 79.8%, P = .067) and particularly in the group with CST infarct (88.9% versus 32.4%, P = .006).
The study is limited by the fact that it is a retrospective analysis, the investigators cautioned.
The National Natural Science Foundation of China funded the study. Dr. Lou reported having no financial disclosures.
LOS ANGELES – In acute ischemic stroke patients with small perfusion lesions of less than 15 mL, involvement of the corticospinal tract (CST) may help guide the decision whether to treat with alteplase.
Specifically, patients with hypoperfusion in the CST, but without CST infarction, were more likely to have a modified Rankin Scale score (mRS) of 0-2 at 90 days after treatment with alteplase. Patients with no CST involvement, or with a CST infarct, had worse outcomes with treatment.
The better outcomes “might indicate that hypoperfused CST tissue at baseline could be salvaged by timely reperfusion,” said Min Lou, MD, PhD, vice chair of neurology at Zhejiang University, Hangzhou, China, during her presentation of the study at the International Stroke Conference sponsored by the American Heart Association.
Previous studies have left physicians uncertain what to do with patients presenting with mild stroke, especially strokes that are judged to be potentially disabling despite a low National Institutes of Health Stroke Scale (NIHSS) score. These patients have a lower risk of hemorrhagic conversion, estimated at 0%-2%.
A meta-analysis showed that alteplase treatment in patients with a baseline NIHSS score of 0-4 was associated with a 48% increase in the chance of an excellent outcome. But another study showed that, among patients with a perfusion lesion smaller than 15 mL, treatment with alteplase was less likely than no treatment at all to confer an excellent outcome.
“The challenge is to identify what kind of minor stroke patient would benefit from thrombolysis therapy,” said Dr. Lou.
The researchers analyzed data from the International Stroke Perfusion Imaging Registry (INSPIRE) database, selecting 412 patients with an acute perfusion lesion less than 15 mL who had undergone computed tomography perfusion or magnetic resonance perfusion imaging within 4.5 hours of symptom onset, had had the scan repeated at 24 hours, and who were followed up at 90 days.
Among the patients, 248 were treated with alteplase, and 164 were not. The alteplase-treated group had a mean NIHSS score of 5.0, compared with 4.0 in the untreated group (P = .001). CST hypoperfusion was more common in the treated group (32.3% versus 15.9%, P less than .001), as was CST infarction (14.9% versus 5.5%, P = .004) and 24-hour intracerebral hemorrhage (ICH) (9.3% versus 0.6%, P less than .001).
The researchers divided subjects into three groups: no CST lesion (306 patients), CST hypoperfusion with no CST infarct (60), and CST infarct (46). The 24-hour ICH frequency varied between the groups, with the highest frequency in the CST infarct group (15.2%), followed by the CST hypoperfusion with no infarct group (10.0%), and the no CST lesion group (3.6%, P = .002).
At 90 days, higher frequency of an mRS score of 0-1 was only associated with alteplase treatment in the CST hypoperfusion with no infarct group (76.7% versus 47.1%, P = .035).
The reverse was true in the other groups: No treatment was associated with better odds of an mRS score of 0-1 in the group with no CST lesion (87.7% versus 79.8%, P = .067) and particularly in the group with CST infarct (88.9% versus 32.4%, P = .006).
The study is limited by the fact that it is a retrospective analysis, the investigators cautioned.
The National Natural Science Foundation of China funded the study. Dr. Lou reported having no financial disclosures.
AT ISC 2018
Key clinical point:
Major finding: 76.7% of patients with cerebrospinal tract hypoperfusion but no infarct achieved a modified Rankin Scale score of 0-1, compared with 47.1% of untreated patients.
Data source: A retrospective analysis of 412 patients drawn from the International Stroke Perfusion Imaging Registry.
Disclosures: The National Natural Science Foundation of China funded the study. Dr. Lou reported having no financial disclosures.
Modeling data suggest how to increase access to endovascular therapy
LOS ANGELES – , according to modeling of geomapping data.
The model showed that installing endovascular therapy (EVT) capability at 50 key hospitals could improve the proportion of Americans within 60 minutes of access to EVT from 63% to 71%, benefiting 22 million.
But another option could provide a stronger boost at a much lower cost. Emergency medical personnel could bypass nearby stroke centers that do not have EVT capability in favor of locations that do, even if they are a bit further away. That’s an option if the patient is clinically stable, and if they can successfully diagnose the patient with a large vessel occlusion, according to Amrou Sarraj, MD, director of the vascular neurology fellowship program at the University of Texas, Houston, who presented the study at the International Stroke Conference sponsored by the American Heart Association.
In fact, taking patients to a hospital that does not conduct EVT can lead to delays. By the time the hospital admits the patient, determines that EVT therapy is appropriate, and transfers the patient to another facility, 3 hours can easily pass, he said. “That’s just an estimation from our experience. But if the other hospital is 15 miles away, that can be driven in a few minutes.”
To estimate time to access EVT centers, the researchers identified 1,645 U.S. stroke centers and stratified them into EVT (n = 577) or non-EVT (n = 1,068), based on whether they had reported at least one thrombectomy code for acute ischemic stroke in 2016 to the Centers for Medicare & Medicaid Services or if they had been designated as a comprehensive stroke center. The researchers broke down geographical units into areas with census tracts encompassing 2,500-8,000 people, and then calculated ground and air transportation times to EVT centers.
They used a ‘greedy’ algorithm to maximize the number of people with 60-minute access. This iterative approach yields the highest incremental increases in patient access and eliminates overlap. They conducted a similar optimization for 30-minute travel time.
The researchers found that 137 million Americans (44%) live within 30 minutes of an EVT center, 195 million (63%) live within 60 minutes, and 234 million (76%) within 90 minutes. By air, 172 million (56%) live within 30 minutes of an EVT center, 268 million (87%) within 60 minutes, and 296 million (96%) within 90 minutes.
“Flipping” the top 50 non-EVT centers to EVT centers would increase the number of Americans living within 60 minutes of an EVT center by 22 million, upping the percentage from 63% to 71%. The proportion within 30 minutes would increase by 15 million, from 44% to 49%.
In fact, the number of EVT-capable centers is rapidly expanding, having grown from 577 to 797 since 2016. But this is an expensive proposition, requiring the hiring of interventionists and other changes.
Another option is the “bypass” approach, in which emergency responders transport a patient with a large vessel occlusion to the nearest EVT-capable facility, if the distance isn’t too great. In Houston, the researchers calculated the impact of 15-, 30-, 45-, and 60-minute bypass limits. A total of 45% of the city’s population lives closest to a stroke center that performs EVT. If emergency responders were granted an additional 15 minutes to reach an EVT facility, 82% could go directly to a stroke center. That proportion rose to 91% for a 15- to 30-minute bypass, 94% for a 30- to 45-minute bypass, and 95% for a bypass up to 60 minutes.
In Texas overall, flipping the top five non-EVT centers would place an additional 1.8 million people (+7.0%) within 30 minutes of an EVT center, while a 30-minute bypass would add 11.3 million (+45%).
The study did not receive outside funding. Dr. Sarraj reported receiving a research grant from Stryker and serving as a consultant to or on the advisory board of the company.
SOURCE: Sarraj A et al. ISC 2018 abstract 92.
LOS ANGELES – , according to modeling of geomapping data.
The model showed that installing endovascular therapy (EVT) capability at 50 key hospitals could improve the proportion of Americans within 60 minutes of access to EVT from 63% to 71%, benefiting 22 million.
But another option could provide a stronger boost at a much lower cost. Emergency medical personnel could bypass nearby stroke centers that do not have EVT capability in favor of locations that do, even if they are a bit further away. That’s an option if the patient is clinically stable, and if they can successfully diagnose the patient with a large vessel occlusion, according to Amrou Sarraj, MD, director of the vascular neurology fellowship program at the University of Texas, Houston, who presented the study at the International Stroke Conference sponsored by the American Heart Association.
In fact, taking patients to a hospital that does not conduct EVT can lead to delays. By the time the hospital admits the patient, determines that EVT therapy is appropriate, and transfers the patient to another facility, 3 hours can easily pass, he said. “That’s just an estimation from our experience. But if the other hospital is 15 miles away, that can be driven in a few minutes.”
To estimate time to access EVT centers, the researchers identified 1,645 U.S. stroke centers and stratified them into EVT (n = 577) or non-EVT (n = 1,068), based on whether they had reported at least one thrombectomy code for acute ischemic stroke in 2016 to the Centers for Medicare & Medicaid Services or if they had been designated as a comprehensive stroke center. The researchers broke down geographical units into areas with census tracts encompassing 2,500-8,000 people, and then calculated ground and air transportation times to EVT centers.
They used a ‘greedy’ algorithm to maximize the number of people with 60-minute access. This iterative approach yields the highest incremental increases in patient access and eliminates overlap. They conducted a similar optimization for 30-minute travel time.
The researchers found that 137 million Americans (44%) live within 30 minutes of an EVT center, 195 million (63%) live within 60 minutes, and 234 million (76%) within 90 minutes. By air, 172 million (56%) live within 30 minutes of an EVT center, 268 million (87%) within 60 minutes, and 296 million (96%) within 90 minutes.
“Flipping” the top 50 non-EVT centers to EVT centers would increase the number of Americans living within 60 minutes of an EVT center by 22 million, upping the percentage from 63% to 71%. The proportion within 30 minutes would increase by 15 million, from 44% to 49%.
In fact, the number of EVT-capable centers is rapidly expanding, having grown from 577 to 797 since 2016. But this is an expensive proposition, requiring the hiring of interventionists and other changes.
Another option is the “bypass” approach, in which emergency responders transport a patient with a large vessel occlusion to the nearest EVT-capable facility, if the distance isn’t too great. In Houston, the researchers calculated the impact of 15-, 30-, 45-, and 60-minute bypass limits. A total of 45% of the city’s population lives closest to a stroke center that performs EVT. If emergency responders were granted an additional 15 minutes to reach an EVT facility, 82% could go directly to a stroke center. That proportion rose to 91% for a 15- to 30-minute bypass, 94% for a 30- to 45-minute bypass, and 95% for a bypass up to 60 minutes.
In Texas overall, flipping the top five non-EVT centers would place an additional 1.8 million people (+7.0%) within 30 minutes of an EVT center, while a 30-minute bypass would add 11.3 million (+45%).
The study did not receive outside funding. Dr. Sarraj reported receiving a research grant from Stryker and serving as a consultant to or on the advisory board of the company.
SOURCE: Sarraj A et al. ISC 2018 abstract 92.
LOS ANGELES – , according to modeling of geomapping data.
The model showed that installing endovascular therapy (EVT) capability at 50 key hospitals could improve the proportion of Americans within 60 minutes of access to EVT from 63% to 71%, benefiting 22 million.
But another option could provide a stronger boost at a much lower cost. Emergency medical personnel could bypass nearby stroke centers that do not have EVT capability in favor of locations that do, even if they are a bit further away. That’s an option if the patient is clinically stable, and if they can successfully diagnose the patient with a large vessel occlusion, according to Amrou Sarraj, MD, director of the vascular neurology fellowship program at the University of Texas, Houston, who presented the study at the International Stroke Conference sponsored by the American Heart Association.
In fact, taking patients to a hospital that does not conduct EVT can lead to delays. By the time the hospital admits the patient, determines that EVT therapy is appropriate, and transfers the patient to another facility, 3 hours can easily pass, he said. “That’s just an estimation from our experience. But if the other hospital is 15 miles away, that can be driven in a few minutes.”
To estimate time to access EVT centers, the researchers identified 1,645 U.S. stroke centers and stratified them into EVT (n = 577) or non-EVT (n = 1,068), based on whether they had reported at least one thrombectomy code for acute ischemic stroke in 2016 to the Centers for Medicare & Medicaid Services or if they had been designated as a comprehensive stroke center. The researchers broke down geographical units into areas with census tracts encompassing 2,500-8,000 people, and then calculated ground and air transportation times to EVT centers.
They used a ‘greedy’ algorithm to maximize the number of people with 60-minute access. This iterative approach yields the highest incremental increases in patient access and eliminates overlap. They conducted a similar optimization for 30-minute travel time.
The researchers found that 137 million Americans (44%) live within 30 minutes of an EVT center, 195 million (63%) live within 60 minutes, and 234 million (76%) within 90 minutes. By air, 172 million (56%) live within 30 minutes of an EVT center, 268 million (87%) within 60 minutes, and 296 million (96%) within 90 minutes.
“Flipping” the top 50 non-EVT centers to EVT centers would increase the number of Americans living within 60 minutes of an EVT center by 22 million, upping the percentage from 63% to 71%. The proportion within 30 minutes would increase by 15 million, from 44% to 49%.
In fact, the number of EVT-capable centers is rapidly expanding, having grown from 577 to 797 since 2016. But this is an expensive proposition, requiring the hiring of interventionists and other changes.
Another option is the “bypass” approach, in which emergency responders transport a patient with a large vessel occlusion to the nearest EVT-capable facility, if the distance isn’t too great. In Houston, the researchers calculated the impact of 15-, 30-, 45-, and 60-minute bypass limits. A total of 45% of the city’s population lives closest to a stroke center that performs EVT. If emergency responders were granted an additional 15 minutes to reach an EVT facility, 82% could go directly to a stroke center. That proportion rose to 91% for a 15- to 30-minute bypass, 94% for a 30- to 45-minute bypass, and 95% for a bypass up to 60 minutes.
In Texas overall, flipping the top five non-EVT centers would place an additional 1.8 million people (+7.0%) within 30 minutes of an EVT center, while a 30-minute bypass would add 11.3 million (+45%).
The study did not receive outside funding. Dr. Sarraj reported receiving a research grant from Stryker and serving as a consultant to or on the advisory board of the company.
SOURCE: Sarraj A et al. ISC 2018 abstract 92.
REPORTING FROM ISC 2018
Key clinical point: Several options are available to increase access to endovascular therapy for many Americans.
Major finding: Just 63% of Americans live within 60 minutes of a stroke center that provides endovascular therapy.
Data source: A geomapping study of the availability of endovascular therapy across the United States.
Disclosures: The study did not receive outside funding. Dr. Sarraj reported receiving a research grant from Stryker and serving as a consultant to or on the advisory board of the company.
Source: Sarraj A et al. ISC 2018 abstract 92.