User login
ONLINE EXCLUSIVE: The Pros and Cons of a Super-Commuter Lifestyle
How Hospitalists Can Team with Nursing to Improve Patient Care
Establishing mutual respect and trust between hospitalists and nurses is an important part of ensuring patient safety, whether you’re on your first job or your 20th, says Angela Beck, RN, director of critical-care services at Nebraska Medical Center in Omaha.
“Nurses are important coordinators of care,” she says. “Recognizing and valuing nurses for that is truly the most important thing for the patient, and can also help hospitalists build relationships.”
Key Partners
Forming a collaborative relationship with the nursing service might depend on where you start. At Northwestern Memorial Hospital in Chicago, the nursing service enjoys a “close and collaborative relationship” with hospitalists, according to Kristin Ramsey, RN, MSN, MPPM, NE-BC, associate chief nurse and executive director of operations. New hospitalists are oriented to the care-delivery models on the inpatient care units. In addition, hospitalists are acculturated into the hospital’s coleadership model.
—Kristin Ramsey, RN, MSN, MPPM, NE-BC, associate chief nurse and executive director of operations, Northwestern Memorial Hospital, Chicago
“We have partnered with our hospitalists to create a model in which the physician and nurse leader collaboratively lead the development of multidisciplinary, subspecialty teams to ensure quality outcomes,” Ramsey says. “The model is so successful with the hospitalists that we are now extending it to other areas in the organization.”
Round Sharing
Absent a formalized training protocol for partnering with nursing, hospitalists still can learn a great deal by listening to and communicating with the nursing staff, says Connie Ogden, RN, MSN, NEA-BC, executive director of adult acute services at Nebraska Medical Center. “Nurses are there around the clock caring for patients and may have a different insight” about patients’ evolving conditions, she says.
Care for the patient improves if everyone is on the same page, Ogden adds. That’s why it makes sense, she says, to include nurses during rounds. Beck agrees: “If nurses aren’t there to hear how the plan of care comes about, there is no reason to believe they can effectively describe it once the physician turns around and walks away to see another patient.”
In critical-care units, according to Beck, nurses can function as a bridge between patients and physicians. For example, they can help patients define and express their goals. Some of these goals can be incremental, she notes, such as “I really want to get out of bed this afternoon,” or “I really want my family here to listen to this message.”
Different Role, Same Goal
As director of adult acute services, Ogden often receives complaints from physicians about calls they receive from nurses. Often, these calls emanate from a concern for the patient (e.g. a 2 a.m. call for a Tylenol order to address a headache) or from the requirement that nurses follow policy and clarify orders. If hospitalists understand the back story of the call, their perception of its purpose can change.
Although there have been strides toward better nurse-physician collaboration, “we still have a lot of opportunities for improvement,” Beck asserts.
Establishing mutual respect and trust is not an overnight accomplishment. As Ogden explains, physicians and nurses have different roles, but they share the same goal: quality outcomes in patient care.
Gretchen Henkel is a freelance writer based in southern California.
► For more career-related articles, visit the SHM Career Center.
BEST WAYS TO IMPROVE HOSPITALIST-NURSING COLLABORATION
“A good portion of nurses are relationship builders,” says Beck, director of critical-care services at Nebraska Medical Center. She urges hospitalists on a new job to just “be physically present, in the beginning, on inpatient units” whenever possible. “Acting like you care is really important, and nurses will respond to that,” she says. “You can create an environment in which nurses’ feedback is valued.”
She also recommends, especially for new hospitalists, Dr. Peter J. Pronovost’s three-part talk “The Science of Safety,” delivered to incoming residents at Johns Hopkins University Medical Center in Baltimore, where Dr. Provonost is medical director of the quality and safety research group.—GH
Establishing mutual respect and trust between hospitalists and nurses is an important part of ensuring patient safety, whether you’re on your first job or your 20th, says Angela Beck, RN, director of critical-care services at Nebraska Medical Center in Omaha.
“Nurses are important coordinators of care,” she says. “Recognizing and valuing nurses for that is truly the most important thing for the patient, and can also help hospitalists build relationships.”
Key Partners
Forming a collaborative relationship with the nursing service might depend on where you start. At Northwestern Memorial Hospital in Chicago, the nursing service enjoys a “close and collaborative relationship” with hospitalists, according to Kristin Ramsey, RN, MSN, MPPM, NE-BC, associate chief nurse and executive director of operations. New hospitalists are oriented to the care-delivery models on the inpatient care units. In addition, hospitalists are acculturated into the hospital’s coleadership model.
—Kristin Ramsey, RN, MSN, MPPM, NE-BC, associate chief nurse and executive director of operations, Northwestern Memorial Hospital, Chicago
“We have partnered with our hospitalists to create a model in which the physician and nurse leader collaboratively lead the development of multidisciplinary, subspecialty teams to ensure quality outcomes,” Ramsey says. “The model is so successful with the hospitalists that we are now extending it to other areas in the organization.”
Round Sharing
Absent a formalized training protocol for partnering with nursing, hospitalists still can learn a great deal by listening to and communicating with the nursing staff, says Connie Ogden, RN, MSN, NEA-BC, executive director of adult acute services at Nebraska Medical Center. “Nurses are there around the clock caring for patients and may have a different insight” about patients’ evolving conditions, she says.
Care for the patient improves if everyone is on the same page, Ogden adds. That’s why it makes sense, she says, to include nurses during rounds. Beck agrees: “If nurses aren’t there to hear how the plan of care comes about, there is no reason to believe they can effectively describe it once the physician turns around and walks away to see another patient.”
In critical-care units, according to Beck, nurses can function as a bridge between patients and physicians. For example, they can help patients define and express their goals. Some of these goals can be incremental, she notes, such as “I really want to get out of bed this afternoon,” or “I really want my family here to listen to this message.”
Different Role, Same Goal
As director of adult acute services, Ogden often receives complaints from physicians about calls they receive from nurses. Often, these calls emanate from a concern for the patient (e.g. a 2 a.m. call for a Tylenol order to address a headache) or from the requirement that nurses follow policy and clarify orders. If hospitalists understand the back story of the call, their perception of its purpose can change.
Although there have been strides toward better nurse-physician collaboration, “we still have a lot of opportunities for improvement,” Beck asserts.
Establishing mutual respect and trust is not an overnight accomplishment. As Ogden explains, physicians and nurses have different roles, but they share the same goal: quality outcomes in patient care.
Gretchen Henkel is a freelance writer based in southern California.
► For more career-related articles, visit the SHM Career Center.
BEST WAYS TO IMPROVE HOSPITALIST-NURSING COLLABORATION
“A good portion of nurses are relationship builders,” says Beck, director of critical-care services at Nebraska Medical Center. She urges hospitalists on a new job to just “be physically present, in the beginning, on inpatient units” whenever possible. “Acting like you care is really important, and nurses will respond to that,” she says. “You can create an environment in which nurses’ feedback is valued.”
She also recommends, especially for new hospitalists, Dr. Peter J. Pronovost’s three-part talk “The Science of Safety,” delivered to incoming residents at Johns Hopkins University Medical Center in Baltimore, where Dr. Provonost is medical director of the quality and safety research group.—GH
Establishing mutual respect and trust between hospitalists and nurses is an important part of ensuring patient safety, whether you’re on your first job or your 20th, says Angela Beck, RN, director of critical-care services at Nebraska Medical Center in Omaha.
“Nurses are important coordinators of care,” she says. “Recognizing and valuing nurses for that is truly the most important thing for the patient, and can also help hospitalists build relationships.”
Key Partners
Forming a collaborative relationship with the nursing service might depend on where you start. At Northwestern Memorial Hospital in Chicago, the nursing service enjoys a “close and collaborative relationship” with hospitalists, according to Kristin Ramsey, RN, MSN, MPPM, NE-BC, associate chief nurse and executive director of operations. New hospitalists are oriented to the care-delivery models on the inpatient care units. In addition, hospitalists are acculturated into the hospital’s coleadership model.
—Kristin Ramsey, RN, MSN, MPPM, NE-BC, associate chief nurse and executive director of operations, Northwestern Memorial Hospital, Chicago
“We have partnered with our hospitalists to create a model in which the physician and nurse leader collaboratively lead the development of multidisciplinary, subspecialty teams to ensure quality outcomes,” Ramsey says. “The model is so successful with the hospitalists that we are now extending it to other areas in the organization.”
Round Sharing
Absent a formalized training protocol for partnering with nursing, hospitalists still can learn a great deal by listening to and communicating with the nursing staff, says Connie Ogden, RN, MSN, NEA-BC, executive director of adult acute services at Nebraska Medical Center. “Nurses are there around the clock caring for patients and may have a different insight” about patients’ evolving conditions, she says.
Care for the patient improves if everyone is on the same page, Ogden adds. That’s why it makes sense, she says, to include nurses during rounds. Beck agrees: “If nurses aren’t there to hear how the plan of care comes about, there is no reason to believe they can effectively describe it once the physician turns around and walks away to see another patient.”
In critical-care units, according to Beck, nurses can function as a bridge between patients and physicians. For example, they can help patients define and express their goals. Some of these goals can be incremental, she notes, such as “I really want to get out of bed this afternoon,” or “I really want my family here to listen to this message.”
Different Role, Same Goal
As director of adult acute services, Ogden often receives complaints from physicians about calls they receive from nurses. Often, these calls emanate from a concern for the patient (e.g. a 2 a.m. call for a Tylenol order to address a headache) or from the requirement that nurses follow policy and clarify orders. If hospitalists understand the back story of the call, their perception of its purpose can change.
Although there have been strides toward better nurse-physician collaboration, “we still have a lot of opportunities for improvement,” Beck asserts.
Establishing mutual respect and trust is not an overnight accomplishment. As Ogden explains, physicians and nurses have different roles, but they share the same goal: quality outcomes in patient care.
Gretchen Henkel is a freelance writer based in southern California.
► For more career-related articles, visit the SHM Career Center.
BEST WAYS TO IMPROVE HOSPITALIST-NURSING COLLABORATION
“A good portion of nurses are relationship builders,” says Beck, director of critical-care services at Nebraska Medical Center. She urges hospitalists on a new job to just “be physically present, in the beginning, on inpatient units” whenever possible. “Acting like you care is really important, and nurses will respond to that,” she says. “You can create an environment in which nurses’ feedback is valued.”
She also recommends, especially for new hospitalists, Dr. Peter J. Pronovost’s three-part talk “The Science of Safety,” delivered to incoming residents at Johns Hopkins University Medical Center in Baltimore, where Dr. Provonost is medical director of the quality and safety research group.—GH
Mount Sinai Team Reduces LOS, Costs with Mobile ACE Approach

With our aging population, the challenges of meeting the unique needs of frail elderly patients will continue to mount. In the current issue of the Journal of Hospital Medicine, authors from Mount Sinai Medical Center in New York City report on their adaptation of the acute care for the elderly, or ACE, approach.1 They found that by bringing geriatrics-focused, team-based care to the patient (instead of locating the patient only in the ACE unit), they were able to reduce costs by an average of $4,943 per patient.
And, beginning in year two of the study, when the team incorporated hospitalists into their model, the ACE team decreased length of stay (LOS) by 1.6 days per patient.
From ACE to MACE
Since the mid-1990s, studies have shown that the ACE unit model can be effective in meeting the unique needs of frail, elderly patients. But even at institutions where these geriatric-focused units have been established, hospitals might not have enough dedicated beds for every elderly patient.
“A geographically based unit is difficult to accomplish when you have high occupancy rates in the hospital,” says lead author Jeffrey Farber, MD, assistant professor of geriatrics and palliative medicine and director of the Mobile ACE Service at Mount Sinai.
Dr. Farber and his colleagues began their mobile ACE (MACE) approach in 2007. Their retrospective cohort study compared outcomes of 8,094 hospitalized elderly patients cared for in the traditional ACE, the general medical service, or the MACE over a three-year period. To compare ACE and MACE patient outcomes, they limited their study sample to patients who already had been seen as part of their outpatient geriatrics service. Besides the shorter LOS, the MACE model also realized a net savings of $2,081 in direct hospital costs, $9,37 in nursing costs, and $223 in pharmacy costs in year two.
The MACE team, comprised of a geriatrician-hospitalist, geriatric medicine fellow, social worker, and nurse coordinator, met daily or twice a day. The nurse coordinator identified and resolved complex family and living situations, and daily check-ins with the patients’ caregivers or family members ensured that care plans and discharge plans were clearly understood before the patient left the hospital, Dr. Farber explains.

—Jeffrey Farber, MD, assistant professor of geriatrics and palliative medicine, director, Mobile ACE Service, Mount Sinai Medical Center, New York City
Gathering pre-hospitalization history is facilitated by the linkage of the hospital’s electronic health record with that of the Mount Sinai outpatient geriatrics practice and the hospital’s affiliated nursing home. Dr. Farber admits the integrated system confers an advantage to the geriatrics service. But community-based hospitalists can increase their odds of having accurate pre-hospitalization information by concerted outreach to referral sources in their community, he says.
Commenting on the study’s results, Heidi Wald, MD, MSPH, associate professor of medicine in the division of healthcare policy research at the University of Colorado Denver School of Medicine, notes that “hospitalists are great at providing efficient care, and geriatricians are good at preserving function and mitigating harm, so it was only logical that hybrids of the two models might achieve both sets of aims.”
One model that she and her UC Denver colleagues have studied utilizes “geriatricized” hospitalists (through focused geriatrics and CME programs), which allows the physicians to feel comfortable managing the unique needs of these patients. She says that functional outcomes warrant attention in the next generation of studies in this area.
Dr. Farber’s colleague, William Hung, MD, is analyzing the data of a prospective, longitudinal study focusing on functional status and post-hospitalization follow-up.
Gretchen Henkel is a freelance writer based in southern California.
Reference
1. Farber JI, Korc-Grodzicki B, Du Q, Leipzig, RM, Siu, AL. Operational and quality outcomes of a mobile acute care for the elderly service. J Hosp Med. 2011;6(6):358-363.
With our aging population, the challenges of meeting the unique needs of frail elderly patients will continue to mount. In the current issue of the Journal of Hospital Medicine, authors from Mount Sinai Medical Center in New York City report on their adaptation of the acute care for the elderly, or ACE, approach.1 They found that by bringing geriatrics-focused, team-based care to the patient (instead of locating the patient only in the ACE unit), they were able to reduce costs by an average of $4,943 per patient.
And, beginning in year two of the study, when the team incorporated hospitalists into their model, the ACE team decreased length of stay (LOS) by 1.6 days per patient.
From ACE to MACE
Since the mid-1990s, studies have shown that the ACE unit model can be effective in meeting the unique needs of frail, elderly patients. But even at institutions where these geriatric-focused units have been established, hospitals might not have enough dedicated beds for every elderly patient.
“A geographically based unit is difficult to accomplish when you have high occupancy rates in the hospital,” says lead author Jeffrey Farber, MD, assistant professor of geriatrics and palliative medicine and director of the Mobile ACE Service at Mount Sinai.
Dr. Farber and his colleagues began their mobile ACE (MACE) approach in 2007. Their retrospective cohort study compared outcomes of 8,094 hospitalized elderly patients cared for in the traditional ACE, the general medical service, or the MACE over a three-year period. To compare ACE and MACE patient outcomes, they limited their study sample to patients who already had been seen as part of their outpatient geriatrics service. Besides the shorter LOS, the MACE model also realized a net savings of $2,081 in direct hospital costs, $9,37 in nursing costs, and $223 in pharmacy costs in year two.
The MACE team, comprised of a geriatrician-hospitalist, geriatric medicine fellow, social worker, and nurse coordinator, met daily or twice a day. The nurse coordinator identified and resolved complex family and living situations, and daily check-ins with the patients’ caregivers or family members ensured that care plans and discharge plans were clearly understood before the patient left the hospital, Dr. Farber explains.
—Jeffrey Farber, MD, assistant professor of geriatrics and palliative medicine, director, Mobile ACE Service, Mount Sinai Medical Center, New York City
Gathering pre-hospitalization history is facilitated by the linkage of the hospital’s electronic health record with that of the Mount Sinai outpatient geriatrics practice and the hospital’s affiliated nursing home. Dr. Farber admits the integrated system confers an advantage to the geriatrics service. But community-based hospitalists can increase their odds of having accurate pre-hospitalization information by concerted outreach to referral sources in their community, he says.
Commenting on the study’s results, Heidi Wald, MD, MSPH, associate professor of medicine in the division of healthcare policy research at the University of Colorado Denver School of Medicine, notes that “hospitalists are great at providing efficient care, and geriatricians are good at preserving function and mitigating harm, so it was only logical that hybrids of the two models might achieve both sets of aims.”
One model that she and her UC Denver colleagues have studied utilizes “geriatricized” hospitalists (through focused geriatrics and CME programs), which allows the physicians to feel comfortable managing the unique needs of these patients. She says that functional outcomes warrant attention in the next generation of studies in this area.
Dr. Farber’s colleague, William Hung, MD, is analyzing the data of a prospective, longitudinal study focusing on functional status and post-hospitalization follow-up.
Gretchen Henkel is a freelance writer based in southern California.
Reference
1. Farber JI, Korc-Grodzicki B, Du Q, Leipzig, RM, Siu, AL. Operational and quality outcomes of a mobile acute care for the elderly service. J Hosp Med. 2011;6(6):358-363.
With our aging population, the challenges of meeting the unique needs of frail elderly patients will continue to mount. In the current issue of the Journal of Hospital Medicine, authors from Mount Sinai Medical Center in New York City report on their adaptation of the acute care for the elderly, or ACE, approach.1 They found that by bringing geriatrics-focused, team-based care to the patient (instead of locating the patient only in the ACE unit), they were able to reduce costs by an average of $4,943 per patient.
And, beginning in year two of the study, when the team incorporated hospitalists into their model, the ACE team decreased length of stay (LOS) by 1.6 days per patient.
From ACE to MACE
Since the mid-1990s, studies have shown that the ACE unit model can be effective in meeting the unique needs of frail, elderly patients. But even at institutions where these geriatric-focused units have been established, hospitals might not have enough dedicated beds for every elderly patient.
“A geographically based unit is difficult to accomplish when you have high occupancy rates in the hospital,” says lead author Jeffrey Farber, MD, assistant professor of geriatrics and palliative medicine and director of the Mobile ACE Service at Mount Sinai.
Dr. Farber and his colleagues began their mobile ACE (MACE) approach in 2007. Their retrospective cohort study compared outcomes of 8,094 hospitalized elderly patients cared for in the traditional ACE, the general medical service, or the MACE over a three-year period. To compare ACE and MACE patient outcomes, they limited their study sample to patients who already had been seen as part of their outpatient geriatrics service. Besides the shorter LOS, the MACE model also realized a net savings of $2,081 in direct hospital costs, $9,37 in nursing costs, and $223 in pharmacy costs in year two.
The MACE team, comprised of a geriatrician-hospitalist, geriatric medicine fellow, social worker, and nurse coordinator, met daily or twice a day. The nurse coordinator identified and resolved complex family and living situations, and daily check-ins with the patients’ caregivers or family members ensured that care plans and discharge plans were clearly understood before the patient left the hospital, Dr. Farber explains.
—Jeffrey Farber, MD, assistant professor of geriatrics and palliative medicine, director, Mobile ACE Service, Mount Sinai Medical Center, New York City
Gathering pre-hospitalization history is facilitated by the linkage of the hospital’s electronic health record with that of the Mount Sinai outpatient geriatrics practice and the hospital’s affiliated nursing home. Dr. Farber admits the integrated system confers an advantage to the geriatrics service. But community-based hospitalists can increase their odds of having accurate pre-hospitalization information by concerted outreach to referral sources in their community, he says.
Commenting on the study’s results, Heidi Wald, MD, MSPH, associate professor of medicine in the division of healthcare policy research at the University of Colorado Denver School of Medicine, notes that “hospitalists are great at providing efficient care, and geriatricians are good at preserving function and mitigating harm, so it was only logical that hybrids of the two models might achieve both sets of aims.”
One model that she and her UC Denver colleagues have studied utilizes “geriatricized” hospitalists (through focused geriatrics and CME programs), which allows the physicians to feel comfortable managing the unique needs of these patients. She says that functional outcomes warrant attention in the next generation of studies in this area.
Dr. Farber’s colleague, William Hung, MD, is analyzing the data of a prospective, longitudinal study focusing on functional status and post-hospitalization follow-up.
Gretchen Henkel is a freelance writer based in southern California.
Reference
1. Farber JI, Korc-Grodzicki B, Du Q, Leipzig, RM, Siu, AL. Operational and quality outcomes of a mobile acute care for the elderly service. J Hosp Med. 2011;6(6):358-363.
Investment Strategies for Early Career Hospitalists
There are no hard and fast rules for crafting an investment strategy, especially early in your career. As with so many domains, the devil’s in the details, according to two top financial advisors.
Disability Coverage Checkup
Protecting your income is job one when creating a sound investment strategy. “Your biggest asset is your earning power,” says Bob Wacker, CFP, president of R.E. Wacker Associates Inc. in San Luis Obispo, Calif. That’s why you need to examine your disability coverage as soon as you start working.
Joel Greenwald, MD, CFP, partner at Sterling Retirement Resources in St. Louis Park, Minn., who often presents financial workshops to groups of residents at the University of Minnesota Medical School, agrees. Many physicians assume that group disability coverage offered through the hospital or physicians group is adequate. But it might not be.
Group insurance policies differ from individual policies in key ways. For example, group carriers might supply disability benefits for two to five years, based on one definition of your occupation, and then, according to their definition of “reasonable” occupation, stop paying if you do not take work in a related capacity.
What you want, says Dr. Greenwald, is a policy—often an individual one—that ties the definition of disability to the performance of activities specific to your specialty. A financial advisor or an insurance agent who specializes in disability insurance can review your coverage and help tailor it to your needs.
For more on this issue, visit http://issuu.com/metrodoctors/docs/julyaugust2010.
Analyze and Prioritize Debt
One of the first questions high-income earners have to ask themselves is: Should I pay off my debt right away or start saving? “There is no right answer,” Dr. Greenwald says.
High-interest credit card debt is bad, so physicians should eliminate it as soon as possible.
School loans? The experts suggest paying off the higher-interest loans first. But if you can, you should resist the urge to pay down low-interest loans. The interest on your debt, Wacker explains, might be tax-deductible. Look for a financial planner who has a “robust” tax background to help you weigh the tax consequences of debt payoff versus savings.
Investment Literacy
When you choose a financial planner (see “Finding an Advisor”), expect to examine your disability and debt portfolios, as well as create an estate plan. Make sure you fully fund your retirement plan at work. A 401(k) allows you to contribute $16,500 per year, and most plans match your contributions at 25%, 50%, or 100%, which automatically boosts your balance sheet. It’s also a good idea to establish 529 plans for your children’s education.
Remember that a financial plan is not static; it will require revisiting on a regular basis. And that will entail learning about a whole new body of knowledge. Choose your guides wisely.
Gretchen Henkel is a freelance writer based in California.
There are no hard and fast rules for crafting an investment strategy, especially early in your career. As with so many domains, the devil’s in the details, according to two top financial advisors.
Disability Coverage Checkup
Protecting your income is job one when creating a sound investment strategy. “Your biggest asset is your earning power,” says Bob Wacker, CFP, president of R.E. Wacker Associates Inc. in San Luis Obispo, Calif. That’s why you need to examine your disability coverage as soon as you start working.
Joel Greenwald, MD, CFP, partner at Sterling Retirement Resources in St. Louis Park, Minn., who often presents financial workshops to groups of residents at the University of Minnesota Medical School, agrees. Many physicians assume that group disability coverage offered through the hospital or physicians group is adequate. But it might not be.
Group insurance policies differ from individual policies in key ways. For example, group carriers might supply disability benefits for two to five years, based on one definition of your occupation, and then, according to their definition of “reasonable” occupation, stop paying if you do not take work in a related capacity.
What you want, says Dr. Greenwald, is a policy—often an individual one—that ties the definition of disability to the performance of activities specific to your specialty. A financial advisor or an insurance agent who specializes in disability insurance can review your coverage and help tailor it to your needs.
For more on this issue, visit http://issuu.com/metrodoctors/docs/julyaugust2010.
Analyze and Prioritize Debt
One of the first questions high-income earners have to ask themselves is: Should I pay off my debt right away or start saving? “There is no right answer,” Dr. Greenwald says.
High-interest credit card debt is bad, so physicians should eliminate it as soon as possible.
School loans? The experts suggest paying off the higher-interest loans first. But if you can, you should resist the urge to pay down low-interest loans. The interest on your debt, Wacker explains, might be tax-deductible. Look for a financial planner who has a “robust” tax background to help you weigh the tax consequences of debt payoff versus savings.
Investment Literacy
When you choose a financial planner (see “Finding an Advisor”), expect to examine your disability and debt portfolios, as well as create an estate plan. Make sure you fully fund your retirement plan at work. A 401(k) allows you to contribute $16,500 per year, and most plans match your contributions at 25%, 50%, or 100%, which automatically boosts your balance sheet. It’s also a good idea to establish 529 plans for your children’s education.
Remember that a financial plan is not static; it will require revisiting on a regular basis. And that will entail learning about a whole new body of knowledge. Choose your guides wisely.
Gretchen Henkel is a freelance writer based in California.
There are no hard and fast rules for crafting an investment strategy, especially early in your career. As with so many domains, the devil’s in the details, according to two top financial advisors.
Disability Coverage Checkup
Protecting your income is job one when creating a sound investment strategy. “Your biggest asset is your earning power,” says Bob Wacker, CFP, president of R.E. Wacker Associates Inc. in San Luis Obispo, Calif. That’s why you need to examine your disability coverage as soon as you start working.
Joel Greenwald, MD, CFP, partner at Sterling Retirement Resources in St. Louis Park, Minn., who often presents financial workshops to groups of residents at the University of Minnesota Medical School, agrees. Many physicians assume that group disability coverage offered through the hospital or physicians group is adequate. But it might not be.
Group insurance policies differ from individual policies in key ways. For example, group carriers might supply disability benefits for two to five years, based on one definition of your occupation, and then, according to their definition of “reasonable” occupation, stop paying if you do not take work in a related capacity.
What you want, says Dr. Greenwald, is a policy—often an individual one—that ties the definition of disability to the performance of activities specific to your specialty. A financial advisor or an insurance agent who specializes in disability insurance can review your coverage and help tailor it to your needs.
For more on this issue, visit http://issuu.com/metrodoctors/docs/julyaugust2010.
Analyze and Prioritize Debt
One of the first questions high-income earners have to ask themselves is: Should I pay off my debt right away or start saving? “There is no right answer,” Dr. Greenwald says.
High-interest credit card debt is bad, so physicians should eliminate it as soon as possible.
School loans? The experts suggest paying off the higher-interest loans first. But if you can, you should resist the urge to pay down low-interest loans. The interest on your debt, Wacker explains, might be tax-deductible. Look for a financial planner who has a “robust” tax background to help you weigh the tax consequences of debt payoff versus savings.
Investment Literacy
When you choose a financial planner (see “Finding an Advisor”), expect to examine your disability and debt portfolios, as well as create an estate plan. Make sure you fully fund your retirement plan at work. A 401(k) allows you to contribute $16,500 per year, and most plans match your contributions at 25%, 50%, or 100%, which automatically boosts your balance sheet. It’s also a good idea to establish 529 plans for your children’s education.
Remember that a financial plan is not static; it will require revisiting on a regular basis. And that will entail learning about a whole new body of knowledge. Choose your guides wisely.
Gretchen Henkel is a freelance writer based in California.
Power Through Afternoon Energy Slumps

Late-afternoon slowdowns are natural, explains Susan Swadener, PhD, RD, dietetic internship director and lecturer in the Food Science and Nutrition Department at California State University San Luis Obispo. "Your enzyme levels go down, which is part of your diurnal pattern to slow down the body's processes to get ready for the evening and sleep," she says.
Common-Sense Nutrition
To fight afternoon fatigue, adopt good nutritional habits throughout your day. It's essential to have a healthy breakfast in the morning, advises Dr. Swadener, who's also a registered dietitian in private practice. Make sure you eat lunch, too, with a balance of protein, carbohydrates, and fats.
Afternoon snacks are a good idea, especially if they incorporate some protein. Foods high in protein can increase norepinephrine and epinephrine production, which helps you stay alert. Some examples of quick and nutritious snacks: string cheese and an apple; sliced cheese or peanut butter on whole-wheat crackers; yogurt; a handful of almonds or walnuts; or trail mix.
And don't forget one of the most common directives to your patients: "Push the fluids." Have a glass of water or nonfat milk with your lunch, and make sure you keep your water bottle handy at your desk.
As for coffee, "you don't want to be drinking it constantly to keep your energy level up, because you'll just crash afterwards," Dr. Swadener says. If you don't abuse caffeine, one cup of coffee in the morning and one in the afternoon is found to be most effective in increasing your alertness.
Change It Up
Desk tasks can make you drowsy. Daniel Markovitz is president of TimeBack Management, which specializes in applying Lean manufacturing principles to increase personal productivity for healthcare workers. He's found—and research such as a 2003 study in Ergonomics and a 2007 National Institute for Occupational Safety and Health study in the American Journal of Industrial Medicine supports these conclusions—that taking mini-breaks and then returning to the task at hand can refresh you and make you more productive.
You also get energy by using it, so a brisk walk around the hospital or walking up and down a couple of flights of stairs can increase circulation and blood flow to the brain. "You don't even have to get up from your desk," Markovitz says. "Just by changing the nature of the work you're doing, it's refreshing to your brain." That might mean switching from dictation to administrative work, or from scheduling to research.
And remember the value of play, Markovitz advises. "We tend to discourage going on Facebook or playing a video game at work. But if you take a 15-minute break to do something that's pleasurable, that causes your brain to fire in different ways, that can be another helpful adaptation."
Gretchen Henkel is a freelance writer based in California.
Interactions are Engaging
You've just finished a brain-numbing administrative report, and you've got 10 minutes before your next task. Don't just fill that time with checking your email.
Corporate consultant Daniel Markovitz advises another tack: Walk down the hall to touch base with colleagues. "You don't have to get into an involved conversation about their QI project. Just ask them how it's going for them," he advises.
Breaking up a busy day with exercise or a social call can get you over the doldrums hump, he says, because "you're getting up and interacting with someone. At the same time, you're doing something that's really important for the hospital: You're strengthening those bonds and interrelationships with people.—GH
Late-afternoon slowdowns are natural, explains Susan Swadener, PhD, RD, dietetic internship director and lecturer in the Food Science and Nutrition Department at California State University San Luis Obispo. "Your enzyme levels go down, which is part of your diurnal pattern to slow down the body's processes to get ready for the evening and sleep," she says.
Common-Sense Nutrition
To fight afternoon fatigue, adopt good nutritional habits throughout your day. It's essential to have a healthy breakfast in the morning, advises Dr. Swadener, who's also a registered dietitian in private practice. Make sure you eat lunch, too, with a balance of protein, carbohydrates, and fats.
Afternoon snacks are a good idea, especially if they incorporate some protein. Foods high in protein can increase norepinephrine and epinephrine production, which helps you stay alert. Some examples of quick and nutritious snacks: string cheese and an apple; sliced cheese or peanut butter on whole-wheat crackers; yogurt; a handful of almonds or walnuts; or trail mix.
And don't forget one of the most common directives to your patients: "Push the fluids." Have a glass of water or nonfat milk with your lunch, and make sure you keep your water bottle handy at your desk.
As for coffee, "you don't want to be drinking it constantly to keep your energy level up, because you'll just crash afterwards," Dr. Swadener says. If you don't abuse caffeine, one cup of coffee in the morning and one in the afternoon is found to be most effective in increasing your alertness.
Change It Up
Desk tasks can make you drowsy. Daniel Markovitz is president of TimeBack Management, which specializes in applying Lean manufacturing principles to increase personal productivity for healthcare workers. He's found—and research such as a 2003 study in Ergonomics and a 2007 National Institute for Occupational Safety and Health study in the American Journal of Industrial Medicine supports these conclusions—that taking mini-breaks and then returning to the task at hand can refresh you and make you more productive.
You also get energy by using it, so a brisk walk around the hospital or walking up and down a couple of flights of stairs can increase circulation and blood flow to the brain. "You don't even have to get up from your desk," Markovitz says. "Just by changing the nature of the work you're doing, it's refreshing to your brain." That might mean switching from dictation to administrative work, or from scheduling to research.
And remember the value of play, Markovitz advises. "We tend to discourage going on Facebook or playing a video game at work. But if you take a 15-minute break to do something that's pleasurable, that causes your brain to fire in different ways, that can be another helpful adaptation."
Gretchen Henkel is a freelance writer based in California.
Interactions are Engaging
You've just finished a brain-numbing administrative report, and you've got 10 minutes before your next task. Don't just fill that time with checking your email.
Corporate consultant Daniel Markovitz advises another tack: Walk down the hall to touch base with colleagues. "You don't have to get into an involved conversation about their QI project. Just ask them how it's going for them," he advises.
Breaking up a busy day with exercise or a social call can get you over the doldrums hump, he says, because "you're getting up and interacting with someone. At the same time, you're doing something that's really important for the hospital: You're strengthening those bonds and interrelationships with people.—GH
Late-afternoon slowdowns are natural, explains Susan Swadener, PhD, RD, dietetic internship director and lecturer in the Food Science and Nutrition Department at California State University San Luis Obispo. "Your enzyme levels go down, which is part of your diurnal pattern to slow down the body's processes to get ready for the evening and sleep," she says.
Common-Sense Nutrition
To fight afternoon fatigue, adopt good nutritional habits throughout your day. It's essential to have a healthy breakfast in the morning, advises Dr. Swadener, who's also a registered dietitian in private practice. Make sure you eat lunch, too, with a balance of protein, carbohydrates, and fats.
Afternoon snacks are a good idea, especially if they incorporate some protein. Foods high in protein can increase norepinephrine and epinephrine production, which helps you stay alert. Some examples of quick and nutritious snacks: string cheese and an apple; sliced cheese or peanut butter on whole-wheat crackers; yogurt; a handful of almonds or walnuts; or trail mix.
And don't forget one of the most common directives to your patients: "Push the fluids." Have a glass of water or nonfat milk with your lunch, and make sure you keep your water bottle handy at your desk.
As for coffee, "you don't want to be drinking it constantly to keep your energy level up, because you'll just crash afterwards," Dr. Swadener says. If you don't abuse caffeine, one cup of coffee in the morning and one in the afternoon is found to be most effective in increasing your alertness.
Change It Up
Desk tasks can make you drowsy. Daniel Markovitz is president of TimeBack Management, which specializes in applying Lean manufacturing principles to increase personal productivity for healthcare workers. He's found—and research such as a 2003 study in Ergonomics and a 2007 National Institute for Occupational Safety and Health study in the American Journal of Industrial Medicine supports these conclusions—that taking mini-breaks and then returning to the task at hand can refresh you and make you more productive.
You also get energy by using it, so a brisk walk around the hospital or walking up and down a couple of flights of stairs can increase circulation and blood flow to the brain. "You don't even have to get up from your desk," Markovitz says. "Just by changing the nature of the work you're doing, it's refreshing to your brain." That might mean switching from dictation to administrative work, or from scheduling to research.
And remember the value of play, Markovitz advises. "We tend to discourage going on Facebook or playing a video game at work. But if you take a 15-minute break to do something that's pleasurable, that causes your brain to fire in different ways, that can be another helpful adaptation."
Gretchen Henkel is a freelance writer based in California.
Interactions are Engaging
You've just finished a brain-numbing administrative report, and you've got 10 minutes before your next task. Don't just fill that time with checking your email.
Corporate consultant Daniel Markovitz advises another tack: Walk down the hall to touch base with colleagues. "You don't have to get into an involved conversation about their QI project. Just ask them how it's going for them," he advises.
Breaking up a busy day with exercise or a social call can get you over the doldrums hump, he says, because "you're getting up and interacting with someone. At the same time, you're doing something that's really important for the hospital: You're strengthening those bonds and interrelationships with people.—GH
ONLINE EXCLUSIVE: Scheduling Rules of Thumb
John Krisa, MD, medical director of the hospitalist group at Albany Memorial Hospital in New York, pictures his HM group as an organic whole when he draws up the schedule. He tries to avoid a strict 50-50 parceling out of night and day shifts. The hospitalist group makes liberal use of per-diem hospitalists and moonlighters, and has a few nocturnists.
“The vast majority of the work at night is processing new admissions, so these tend to be single encounters. You want your full-time people there multiple consecutive days for continuity and to represent the face of your program,” he says.
But for the required, ’round-the-clock coverage, he and other group members are expected to pull their share of nights as well. “I was always more of a nighttime person, in terms of my body clock,” Dr. Krisa says, “but now that I have more daytime nonclinical duties [as regional site director for Cogent HMG], it’s been more of a challenge to juggle home responsibilities, night shifts, and multiple administrative meetings.”
There are some basic principles of sleep hygiene and lessons learned from industrial settings that are good to keep in mind, says Christopher P. Landrigan, MD, SFHM, MPH, associate professor of medicine and pediatrics at Harvard Medical School and director of the Sleep and Patient Safety Program at Brigham and Women’s Hospital in Boston. “It’s really incumbent upon hospitalist group leaders to recognize the hazards of scheduling people for too many nights in a row, which conveys a risk both to the patients and to the hospitalists themselves,” Dr. Landrigan says. “We know that if hospitalists are driving home after night shifts, particularly multiple night shifts, that they’re at risk for motor vehicle crashes and at risk of sticking themselves with needles and scalpels toward the tail end of their shifts. None of us want that.”
Dr. Landrigan advises hospitalist groups to be cognizant of the hazards and think about the schedule “proactively.”
John Krisa, MD, medical director of the hospitalist group at Albany Memorial Hospital in New York, pictures his HM group as an organic whole when he draws up the schedule. He tries to avoid a strict 50-50 parceling out of night and day shifts. The hospitalist group makes liberal use of per-diem hospitalists and moonlighters, and has a few nocturnists.
“The vast majority of the work at night is processing new admissions, so these tend to be single encounters. You want your full-time people there multiple consecutive days for continuity and to represent the face of your program,” he says.
But for the required, ’round-the-clock coverage, he and other group members are expected to pull their share of nights as well. “I was always more of a nighttime person, in terms of my body clock,” Dr. Krisa says, “but now that I have more daytime nonclinical duties [as regional site director for Cogent HMG], it’s been more of a challenge to juggle home responsibilities, night shifts, and multiple administrative meetings.”
There are some basic principles of sleep hygiene and lessons learned from industrial settings that are good to keep in mind, says Christopher P. Landrigan, MD, SFHM, MPH, associate professor of medicine and pediatrics at Harvard Medical School and director of the Sleep and Patient Safety Program at Brigham and Women’s Hospital in Boston. “It’s really incumbent upon hospitalist group leaders to recognize the hazards of scheduling people for too many nights in a row, which conveys a risk both to the patients and to the hospitalists themselves,” Dr. Landrigan says. “We know that if hospitalists are driving home after night shifts, particularly multiple night shifts, that they’re at risk for motor vehicle crashes and at risk of sticking themselves with needles and scalpels toward the tail end of their shifts. None of us want that.”
Dr. Landrigan advises hospitalist groups to be cognizant of the hazards and think about the schedule “proactively.”
John Krisa, MD, medical director of the hospitalist group at Albany Memorial Hospital in New York, pictures his HM group as an organic whole when he draws up the schedule. He tries to avoid a strict 50-50 parceling out of night and day shifts. The hospitalist group makes liberal use of per-diem hospitalists and moonlighters, and has a few nocturnists.
“The vast majority of the work at night is processing new admissions, so these tend to be single encounters. You want your full-time people there multiple consecutive days for continuity and to represent the face of your program,” he says.
But for the required, ’round-the-clock coverage, he and other group members are expected to pull their share of nights as well. “I was always more of a nighttime person, in terms of my body clock,” Dr. Krisa says, “but now that I have more daytime nonclinical duties [as regional site director for Cogent HMG], it’s been more of a challenge to juggle home responsibilities, night shifts, and multiple administrative meetings.”
There are some basic principles of sleep hygiene and lessons learned from industrial settings that are good to keep in mind, says Christopher P. Landrigan, MD, SFHM, MPH, associate professor of medicine and pediatrics at Harvard Medical School and director of the Sleep and Patient Safety Program at Brigham and Women’s Hospital in Boston. “It’s really incumbent upon hospitalist group leaders to recognize the hazards of scheduling people for too many nights in a row, which conveys a risk both to the patients and to the hospitalists themselves,” Dr. Landrigan says. “We know that if hospitalists are driving home after night shifts, particularly multiple night shifts, that they’re at risk for motor vehicle crashes and at risk of sticking themselves with needles and scalpels toward the tail end of their shifts. None of us want that.”
Dr. Landrigan advises hospitalist groups to be cognizant of the hazards and think about the schedule “proactively.”
No Easy Task
In college, while most of her fellow students were staying up late and sleeping in, Alice Marshbanks, MD, FHM, was an early riser. Now she regularly works from 4 p.m. to 2 a.m., and she sleeps in most mornings. "I’m sleeping later and living more of a teenage lifestyle," she jokes. "I’m actually getting younger."
Dr. Marshbanks might be an anomaly among established hospitalists. A physician since 1989 and a hospitalist since 1995, she actually prefers working the swing shift, and she says she’s the only one in her group at WakeMed Hospital in Raleigh, N.C., who does. Although Dr. Marshbanks is not a true nocturnist—she doesn’t work the typical 7 p.m. to 7 a.m. graveyard shift—her contracted position provides valuable transition coverage for night admissions, which have increased as the HM program at WakeMed has grown.
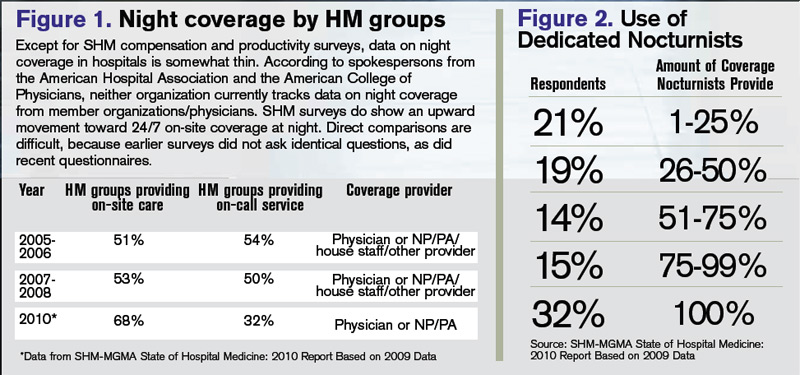
Surveys indicate that HM groups continue to move toward in-house coverage models to provide 24/7 hospitalist responsiveness. In the 2011 SHM-MGMA State of Hospital Medicine report, which will be released next month, 81% of responding nonteaching hospitalist practices reported providing on-site care at night. That’s up from 68% of responding HM practices that reported furnishing that service in the 2010 report. Only 53% of HM groups reported providing on-site night hospitalists in the 2007-2008 State of Hospital Medicine survey, which was produced solely by SHM.
Kenneth R. Epstein, MD, MBA, FACP, FHM, chief medical officer for Hospitalist Consultants Inc., headquartered in Traverse City, Mich., has observed this trend first-hand. In academic hospitals, due to new Accreditation Council for Graduate Medical Education (ACGME) and Resident Review Committee (RRC) regulations, "the only safety valve to handle admissions after the house staff numbers are capped is the hospitalist."
The need for such a safety valve will increase again this summer, as new ACGME duty-hour regulations on resident hours and supervision kick in.
Nonteaching hospitals are not exempt from these pressures. To deal with increasing demands for night coverage, HM groups across the country are using a variety of practice models, such as hiring dedicated nocturnists or moonlighters to cover nights, rotating shifts among team members, or using midlevel providers (physician assistants or nurse practitioners) as night staffers. On-call or in-house coverage models are determined by a variety of factors, including the size of the HM group, patient volume and acuity, and staff availability. Sustainability continues to be a challenge for most groups; however, the in-house coverage model seems to increase nursing and ED satisfaction, most experts say, and is an added value for hospital administration, although financial returns vary.
Continuity of care is at the heart of the night-coverage issue. Some experts worry that patient outcomes will suffer if there isn’t an in-house presence, but studies looking at this issue have been inconclusive, asserts Patti VanDort, RN, MSN, NEA-BC, vice president of nursing and chief nursing officer at Holland Hospital in southwestern Michigan.
"You’ve got to have the same level and quality of care during nights and weekends that you have during the weekdays," she says. "It’s got to be the same for all."
That said, some hospitals don’t have the volume to justify in-house night staffing. Hospitalists and program directors have described the ways in which they handle night staffing, balancing demand, program size, and physician satisfaction.
Tailored to Fit
"Hospitalist programs have different scale and scope depending on the needs of the institution," says Michael R. Humphrey, MD, vice president and chief clinical officer for Emergency and Ambulatory Services at St. Rita’s Medical Center in Lima, Ohio. A 365-bed community hospital, St. Rita’s employs nocturnists as part of its 24-hour hospitalist program. Dr. Humphrey still works as an ED physician and reports that the hospitalists are invaluable for admitting, providing cross-cover, covering the ICU, and handling code blue and rapid responses. "As a Level II trauma center, we can’t have ED physicians leave the department to run upstairs and do codes," he says. "They typically don’t get back within five minutes."
Holland Hospital, a 213-bed facility, provides around-the-clock hospitalist coverage in its eight-bed ICU, according to VanDort. That change was precipitated by the nursing staff’s decision to pursue Magnet Status, which was awarded in 2007 by the American Nurses Credentialing Center (ANCC). For inpatient coverage, the hospital-owned HM group Lakeshore Health Partners, headed by Bart D. Sak, MD, MA, FHM, maintains six FTE hospitalists on a rotating block schedule. Each night, one physician works from 4 p.m. until midnight, overlapping with a nonphysician provider (NPP), a member of the hospitalist group, who works a 7 p.m. to 7 a.m. shift.
"We have two providers in-house when admissions from the ED are heating up, and then we have an NPP in-house to cover the one to three additional admissions that may come in after midnight and to field floor calls," Dr. Sak says.
The physician who worked until midnight is on call for backup support and might come back to the hospital if things get too intense in the pre-dawn hours. "This arrangement works quite well for a program of our size," Dr. Sak says. "It takes a team-oriented approach and experienced NPPs who can work independently."
The Holland approach simply wouldn’t work at Kaiser Permanente’s East Bay site in Oakland, Calif., where Tom Baudendistel, MD, FACP, is part of a 50-member hospitalist group and director of the internal-medicine residency program. "Between codes, cross-cover, ICU, and floor admissions, there is simply too much acuity and volume," he says.
The peak hours for East Bay admissions are mid-afternoon to midnight. Two overnight hospitalist shifts (one from 8 a.m. to 8 p.m., another from 7 a.m. to 7 p.m.) are supplemented with two swing shifts (one from 2 to 10 p.m., another from 4 p.m. to midnight). Four full-time nocturnists cover 10 of the 14 overnight shifts per week, which allows for vacation and some protected administrative time. The balance of the overnight shifts are covered by the rest of the hospitalist group, which has 50 members.
The contracted nocturnists are incentivized with additional compensation at the end of the year, when the chief of hospitalists allocates bonuses. They also work fewer shifts a month than the other members of the group. "One thing our group agrees on is that the night docs should get a little more," Dr. Baudendistel says. "It’s a very fair tradeoff for everyone."
A Mile in Their Shoes
Medical directors must balance a variety of factors when scheduling around-the-clock coverage. From day one, the hospitalist program at Albany Memorial Hospital in New York, where John Krisa, MD, is medical director, has been an in-house 24/7 program. Dr. Krisa’s group uses per diem physicians or fellows on their days off to cover most of the nights. The other hospitalists on the team do not escape occasional night duty, and they cover what is left after plugging in the moonlighters. This leaves from zero to five nights per month for each full-time hospitalist. Even the medical director covers night shifts, something Dr. Krisa thinks is valuable to his leadership.
"You, as the leader, still have to walk a mile in that other person’s shoes," he says. "There are different challenges associated with both day and night shifts, so you have to appreciate what your colleagues are going through on the other shifts."
Hospitalist Consultants’ Dr. Epstein agrees with that concept.
"Whenever medical directors have personal experience of how the system is working, they are better able to recommend and make changes," he says.
It’s also valuable, Dr. Krisa explains, for the group leader to interact with ED staff and hear their concerns. Working night shifts helps avoid the night team versus day team schisms, which can lead to group disunity, he says.
Different Skill Set, Different Mindset?
The fact of the matter, though, is that pulling night shifts does not appeal to most established hospitalists. Sleep researchers have found that humans’ body clocks prefer office hours. Even if night-shift hours are consistent, those who work nights never really catch up on the sleep they need during the daytime.
Even so, some physicians embrace the graveyard shift. Working the night swing shift agrees with Dr. Marshbanks’ schedule. The hours are consistent, she works fewer shifts to qualify for FTE pay, and her shift is time-limited, as opposed to work-limited. She’s also filling a niche that others in her group eschew. "It’s a shift that most people with children don’t like because the hours are very disruptive to family life," she says.
The workload at night is different. Instead of the routine rounding typical in day shifts, her work is more urgent. She does more admissions because she works the busiest ED hours, covers acute-stroke codes, and provides cross-cover. And, she says, night staff tends to be "a solid group, so we interact more on a regular basis, since there are fewer of us."
The nocturnists at St. Rita’s Hospital are not held to the same meeting schedule as their daytime hospitalist colleagues, but they’re expected to read meeting minutes and to be responsible for any changes in guidelines or operational information, Dr. Humphrey says. Also stipulated in their hospitalist contracts is the requirement that they maintain competency in procedures, such as central-line placement and airway management.
What’s Better for Patients?
Experts have raised concerns that patient care can be compromised during off-hours, when staffing levels are reduced.1 The Leapfrog Group’s ICU Physician Safety (IPS) Standard argues for high-intensity ICU staffing to reduce patient mortality.2 A number of investigators have tried to determine whether patients admitted off-hours (weekends, nights, holidays) fare worse than those admitted during weekdays. Peter Cram, MD, MBA, acting director of the division of general internal medicine and associate professor of medicine at the Carver College of Medicine at the University of Iowa in Iowa City, found in a 2004 study that patients admitted to hospitals on weekends experienced slightly higher risk-adjusted mortality than did patients admitted on weekdays.3
But here’s the problem with studies such as this, says Dr. Cram: "Patients admitted on evenings and weekends are not the same as those admitted 9 to 5 on weekdays."
During weekdays, admissions combine patients with emergent issues and those scheduled for elective procedures. On weekends, "you get only emergencies—you don’t have low-risk patients," he points out. "So, even with optimal 24/7 staffing, you would still expect those patients coming in at night, and on holidays, to have worse outcomes because they are coming in with more acute problems. It remains an open question whether 24/7 staffing will improve off-hours outcomes." More research, Dr. Cram adds, is needed to establish whether full in-house staffing is the best solution.
Dr. Epstein has compared on-call versus in-house night staffing. In a 2007 study, he found no difference when using indicators such as length of stay, readmission rates, and patient satisfaction.4 However, he noticed positives from in-house coverage. "Although there are no data supporting the value of hospitalists on these parameters, having a nocturnist in-house increases nursing satisfaction, because they are responsive to pages when there is a question about a patient," he says. "It’s also a service to hospital medical staff, because they can handle rapid responses and codes."
There is some evidence that working nights can be deleterious to physicians’ and nurses’ health. One study found that interns were more likely to be involved in collisions after leaving extended night shifts; another found an increased risk of needle-stick injury at the end of a long night shift; and data from the long-running Nurses’ Health Study indicate that long-term night work can result in increased risk of colorectal and breast cancers.5,6,7,8 The increased risks of cancer could be related to lack of exposure to light at night and the body’s decreased production of melatonin, although this remains a topic of ongoing research.
"No Easy Answers"
VanDort, the nursing director, is "passionate" about having 24/7 coverage and reports that her nursing staff is happy with the hybrid model currently used at Holland Hospital. "I do envision a day when we’ll have physicians here around the clock," she says. "Patients are sick during the middle of the night, so you can’t staff your system one way during the daytime hours and your nighttime differently. It’s not fair to those patients."
Dr. Cram, who is a hospitalist, outcomes researcher, and division director, says that in an ideal world, it would make more business sense to have the hospital operating at full capacity around the clock, seven days a week. "But we don’t live in that world," he admits. "It is hard to find ways to achieve ’round-the-clock staffing at the levels we’d like."
He also concludes that there are "no easy answers" to the night-coverage conundrum. "But it might be prudent to think about incentives," he says. "Perhaps we should pay more for staffing weekends, evenings, and holidays, or we could reduce the annual number of shifts we expect our nocturnists to do, relative to those physicians who staff days."
Dr. Krisa says he, too, is biased toward an in-house coverage model, especially when programs reach a critical volume. "There is no substitute for the immediate ability to evaluate a sick patient," he explains. "My feeling is that an in-house, 24/7 presence will become the standard." TH
Gretchen Henkel is a freelance writer based in California.
References
- Wong HJ, Morra D. Excellent hospital care for all: open and operating 24/7. J Gen Intern Med. 2011.
- Pronovost PJ, Angus DC, Dorman T, Robinson KA, Dremsizov TT, Young TL. Physician staffing patterns and clinical outcomes in critically ill patients: a systemic review. JAMA. 2002;288(17):2151-2162.
- Cram P, Hillis SL, Barnett M, Rosenthal GE. Effects of weekend admission and hospital teaching status on in-hospital mortality. Am J Med. 2004;117(3):151-157.
- Epstein KR, Juarez E, Loya K, Gorman MJ, Singer A. The effect of 24-7 hospitalist coverage on clinical metrics. Presented May 2007, annual meeting, Society of Hospital Medicine, Dallas.
- Barger LK, Cade BE, Ayas NT, et al. Extended work shifts and the risk of motor vehicle crashes among interns. N Engl J Med. 2005;352:125-134.
- Ayas NT, Barger LK, Cade BE, et al. Extended work duration and the risk of self-reported percutaneous injuries in interns. JAMA. 2006;296(9):1055-1062.
- Schernhammer ES, Laden F, Speizer FE, et al. Night-shift work and risk of colorectal cancer in the nurses’ health study. J Natl Cancer Inst. 2003;95(11):825-828.
- Schernhammer ES, Laden F, Speizer FE, et al. Rotating night shifts and risk of breast cancer in women partici-pating in the nurses’ health study. J Natl Cancer Inst. 2001;93(20):1563-1568.
In college, while most of her fellow students were staying up late and sleeping in, Alice Marshbanks, MD, FHM, was an early riser. Now she regularly works from 4 p.m. to 2 a.m., and she sleeps in most mornings. "I’m sleeping later and living more of a teenage lifestyle," she jokes. "I’m actually getting younger."
Dr. Marshbanks might be an anomaly among established hospitalists. A physician since 1989 and a hospitalist since 1995, she actually prefers working the swing shift, and she says she’s the only one in her group at WakeMed Hospital in Raleigh, N.C., who does. Although Dr. Marshbanks is not a true nocturnist—she doesn’t work the typical 7 p.m. to 7 a.m. graveyard shift—her contracted position provides valuable transition coverage for night admissions, which have increased as the HM program at WakeMed has grown.
Surveys indicate that HM groups continue to move toward in-house coverage models to provide 24/7 hospitalist responsiveness. In the 2011 SHM-MGMA State of Hospital Medicine report, which will be released next month, 81% of responding nonteaching hospitalist practices reported providing on-site care at night. That’s up from 68% of responding HM practices that reported furnishing that service in the 2010 report. Only 53% of HM groups reported providing on-site night hospitalists in the 2007-2008 State of Hospital Medicine survey, which was produced solely by SHM.
Kenneth R. Epstein, MD, MBA, FACP, FHM, chief medical officer for Hospitalist Consultants Inc., headquartered in Traverse City, Mich., has observed this trend first-hand. In academic hospitals, due to new Accreditation Council for Graduate Medical Education (ACGME) and Resident Review Committee (RRC) regulations, "the only safety valve to handle admissions after the house staff numbers are capped is the hospitalist."
The need for such a safety valve will increase again this summer, as new ACGME duty-hour regulations on resident hours and supervision kick in.
Nonteaching hospitals are not exempt from these pressures. To deal with increasing demands for night coverage, HM groups across the country are using a variety of practice models, such as hiring dedicated nocturnists or moonlighters to cover nights, rotating shifts among team members, or using midlevel providers (physician assistants or nurse practitioners) as night staffers. On-call or in-house coverage models are determined by a variety of factors, including the size of the HM group, patient volume and acuity, and staff availability. Sustainability continues to be a challenge for most groups; however, the in-house coverage model seems to increase nursing and ED satisfaction, most experts say, and is an added value for hospital administration, although financial returns vary.
Continuity of care is at the heart of the night-coverage issue. Some experts worry that patient outcomes will suffer if there isn’t an in-house presence, but studies looking at this issue have been inconclusive, asserts Patti VanDort, RN, MSN, NEA-BC, vice president of nursing and chief nursing officer at Holland Hospital in southwestern Michigan.
"You’ve got to have the same level and quality of care during nights and weekends that you have during the weekdays," she says. "It’s got to be the same for all."
That said, some hospitals don’t have the volume to justify in-house night staffing. Hospitalists and program directors have described the ways in which they handle night staffing, balancing demand, program size, and physician satisfaction.
Tailored to Fit
"Hospitalist programs have different scale and scope depending on the needs of the institution," says Michael R. Humphrey, MD, vice president and chief clinical officer for Emergency and Ambulatory Services at St. Rita’s Medical Center in Lima, Ohio. A 365-bed community hospital, St. Rita’s employs nocturnists as part of its 24-hour hospitalist program. Dr. Humphrey still works as an ED physician and reports that the hospitalists are invaluable for admitting, providing cross-cover, covering the ICU, and handling code blue and rapid responses. "As a Level II trauma center, we can’t have ED physicians leave the department to run upstairs and do codes," he says. "They typically don’t get back within five minutes."
Holland Hospital, a 213-bed facility, provides around-the-clock hospitalist coverage in its eight-bed ICU, according to VanDort. That change was precipitated by the nursing staff’s decision to pursue Magnet Status, which was awarded in 2007 by the American Nurses Credentialing Center (ANCC). For inpatient coverage, the hospital-owned HM group Lakeshore Health Partners, headed by Bart D. Sak, MD, MA, FHM, maintains six FTE hospitalists on a rotating block schedule. Each night, one physician works from 4 p.m. until midnight, overlapping with a nonphysician provider (NPP), a member of the hospitalist group, who works a 7 p.m. to 7 a.m. shift.
"We have two providers in-house when admissions from the ED are heating up, and then we have an NPP in-house to cover the one to three additional admissions that may come in after midnight and to field floor calls," Dr. Sak says.
The physician who worked until midnight is on call for backup support and might come back to the hospital if things get too intense in the pre-dawn hours. "This arrangement works quite well for a program of our size," Dr. Sak says. "It takes a team-oriented approach and experienced NPPs who can work independently."
The Holland approach simply wouldn’t work at Kaiser Permanente’s East Bay site in Oakland, Calif., where Tom Baudendistel, MD, FACP, is part of a 50-member hospitalist group and director of the internal-medicine residency program. "Between codes, cross-cover, ICU, and floor admissions, there is simply too much acuity and volume," he says.
The peak hours for East Bay admissions are mid-afternoon to midnight. Two overnight hospitalist shifts (one from 8 a.m. to 8 p.m., another from 7 a.m. to 7 p.m.) are supplemented with two swing shifts (one from 2 to 10 p.m., another from 4 p.m. to midnight). Four full-time nocturnists cover 10 of the 14 overnight shifts per week, which allows for vacation and some protected administrative time. The balance of the overnight shifts are covered by the rest of the hospitalist group, which has 50 members.
The contracted nocturnists are incentivized with additional compensation at the end of the year, when the chief of hospitalists allocates bonuses. They also work fewer shifts a month than the other members of the group. "One thing our group agrees on is that the night docs should get a little more," Dr. Baudendistel says. "It’s a very fair tradeoff for everyone."
A Mile in Their Shoes
Medical directors must balance a variety of factors when scheduling around-the-clock coverage. From day one, the hospitalist program at Albany Memorial Hospital in New York, where John Krisa, MD, is medical director, has been an in-house 24/7 program. Dr. Krisa’s group uses per diem physicians or fellows on their days off to cover most of the nights. The other hospitalists on the team do not escape occasional night duty, and they cover what is left after plugging in the moonlighters. This leaves from zero to five nights per month for each full-time hospitalist. Even the medical director covers night shifts, something Dr. Krisa thinks is valuable to his leadership.
"You, as the leader, still have to walk a mile in that other person’s shoes," he says. "There are different challenges associated with both day and night shifts, so you have to appreciate what your colleagues are going through on the other shifts."
Hospitalist Consultants’ Dr. Epstein agrees with that concept.
"Whenever medical directors have personal experience of how the system is working, they are better able to recommend and make changes," he says.
It’s also valuable, Dr. Krisa explains, for the group leader to interact with ED staff and hear their concerns. Working night shifts helps avoid the night team versus day team schisms, which can lead to group disunity, he says.
Different Skill Set, Different Mindset?
The fact of the matter, though, is that pulling night shifts does not appeal to most established hospitalists. Sleep researchers have found that humans’ body clocks prefer office hours. Even if night-shift hours are consistent, those who work nights never really catch up on the sleep they need during the daytime.
Even so, some physicians embrace the graveyard shift. Working the night swing shift agrees with Dr. Marshbanks’ schedule. The hours are consistent, she works fewer shifts to qualify for FTE pay, and her shift is time-limited, as opposed to work-limited. She’s also filling a niche that others in her group eschew. "It’s a shift that most people with children don’t like because the hours are very disruptive to family life," she says.
The workload at night is different. Instead of the routine rounding typical in day shifts, her work is more urgent. She does more admissions because she works the busiest ED hours, covers acute-stroke codes, and provides cross-cover. And, she says, night staff tends to be "a solid group, so we interact more on a regular basis, since there are fewer of us."
The nocturnists at St. Rita’s Hospital are not held to the same meeting schedule as their daytime hospitalist colleagues, but they’re expected to read meeting minutes and to be responsible for any changes in guidelines or operational information, Dr. Humphrey says. Also stipulated in their hospitalist contracts is the requirement that they maintain competency in procedures, such as central-line placement and airway management.
What’s Better for Patients?
Experts have raised concerns that patient care can be compromised during off-hours, when staffing levels are reduced.1 The Leapfrog Group’s ICU Physician Safety (IPS) Standard argues for high-intensity ICU staffing to reduce patient mortality.2 A number of investigators have tried to determine whether patients admitted off-hours (weekends, nights, holidays) fare worse than those admitted during weekdays. Peter Cram, MD, MBA, acting director of the division of general internal medicine and associate professor of medicine at the Carver College of Medicine at the University of Iowa in Iowa City, found in a 2004 study that patients admitted to hospitals on weekends experienced slightly higher risk-adjusted mortality than did patients admitted on weekdays.3
But here’s the problem with studies such as this, says Dr. Cram: "Patients admitted on evenings and weekends are not the same as those admitted 9 to 5 on weekdays."
During weekdays, admissions combine patients with emergent issues and those scheduled for elective procedures. On weekends, "you get only emergencies—you don’t have low-risk patients," he points out. "So, even with optimal 24/7 staffing, you would still expect those patients coming in at night, and on holidays, to have worse outcomes because they are coming in with more acute problems. It remains an open question whether 24/7 staffing will improve off-hours outcomes." More research, Dr. Cram adds, is needed to establish whether full in-house staffing is the best solution.
Dr. Epstein has compared on-call versus in-house night staffing. In a 2007 study, he found no difference when using indicators such as length of stay, readmission rates, and patient satisfaction.4 However, he noticed positives from in-house coverage. "Although there are no data supporting the value of hospitalists on these parameters, having a nocturnist in-house increases nursing satisfaction, because they are responsive to pages when there is a question about a patient," he says. "It’s also a service to hospital medical staff, because they can handle rapid responses and codes."
There is some evidence that working nights can be deleterious to physicians’ and nurses’ health. One study found that interns were more likely to be involved in collisions after leaving extended night shifts; another found an increased risk of needle-stick injury at the end of a long night shift; and data from the long-running Nurses’ Health Study indicate that long-term night work can result in increased risk of colorectal and breast cancers.5,6,7,8 The increased risks of cancer could be related to lack of exposure to light at night and the body’s decreased production of melatonin, although this remains a topic of ongoing research.
"No Easy Answers"
VanDort, the nursing director, is "passionate" about having 24/7 coverage and reports that her nursing staff is happy with the hybrid model currently used at Holland Hospital. "I do envision a day when we’ll have physicians here around the clock," she says. "Patients are sick during the middle of the night, so you can’t staff your system one way during the daytime hours and your nighttime differently. It’s not fair to those patients."
Dr. Cram, who is a hospitalist, outcomes researcher, and division director, says that in an ideal world, it would make more business sense to have the hospital operating at full capacity around the clock, seven days a week. "But we don’t live in that world," he admits. "It is hard to find ways to achieve ’round-the-clock staffing at the levels we’d like."
He also concludes that there are "no easy answers" to the night-coverage conundrum. "But it might be prudent to think about incentives," he says. "Perhaps we should pay more for staffing weekends, evenings, and holidays, or we could reduce the annual number of shifts we expect our nocturnists to do, relative to those physicians who staff days."
Dr. Krisa says he, too, is biased toward an in-house coverage model, especially when programs reach a critical volume. "There is no substitute for the immediate ability to evaluate a sick patient," he explains. "My feeling is that an in-house, 24/7 presence will become the standard." TH
Gretchen Henkel is a freelance writer based in California.
References
- Wong HJ, Morra D. Excellent hospital care for all: open and operating 24/7. J Gen Intern Med. 2011.
- Pronovost PJ, Angus DC, Dorman T, Robinson KA, Dremsizov TT, Young TL. Physician staffing patterns and clinical outcomes in critically ill patients: a systemic review. JAMA. 2002;288(17):2151-2162.
- Cram P, Hillis SL, Barnett M, Rosenthal GE. Effects of weekend admission and hospital teaching status on in-hospital mortality. Am J Med. 2004;117(3):151-157.
- Epstein KR, Juarez E, Loya K, Gorman MJ, Singer A. The effect of 24-7 hospitalist coverage on clinical metrics. Presented May 2007, annual meeting, Society of Hospital Medicine, Dallas.
- Barger LK, Cade BE, Ayas NT, et al. Extended work shifts and the risk of motor vehicle crashes among interns. N Engl J Med. 2005;352:125-134.
- Ayas NT, Barger LK, Cade BE, et al. Extended work duration and the risk of self-reported percutaneous injuries in interns. JAMA. 2006;296(9):1055-1062.
- Schernhammer ES, Laden F, Speizer FE, et al. Night-shift work and risk of colorectal cancer in the nurses’ health study. J Natl Cancer Inst. 2003;95(11):825-828.
- Schernhammer ES, Laden F, Speizer FE, et al. Rotating night shifts and risk of breast cancer in women partici-pating in the nurses’ health study. J Natl Cancer Inst. 2001;93(20):1563-1568.
In college, while most of her fellow students were staying up late and sleeping in, Alice Marshbanks, MD, FHM, was an early riser. Now she regularly works from 4 p.m. to 2 a.m., and she sleeps in most mornings. "I’m sleeping later and living more of a teenage lifestyle," she jokes. "I’m actually getting younger."
Dr. Marshbanks might be an anomaly among established hospitalists. A physician since 1989 and a hospitalist since 1995, she actually prefers working the swing shift, and she says she’s the only one in her group at WakeMed Hospital in Raleigh, N.C., who does. Although Dr. Marshbanks is not a true nocturnist—she doesn’t work the typical 7 p.m. to 7 a.m. graveyard shift—her contracted position provides valuable transition coverage for night admissions, which have increased as the HM program at WakeMed has grown.
Surveys indicate that HM groups continue to move toward in-house coverage models to provide 24/7 hospitalist responsiveness. In the 2011 SHM-MGMA State of Hospital Medicine report, which will be released next month, 81% of responding nonteaching hospitalist practices reported providing on-site care at night. That’s up from 68% of responding HM practices that reported furnishing that service in the 2010 report. Only 53% of HM groups reported providing on-site night hospitalists in the 2007-2008 State of Hospital Medicine survey, which was produced solely by SHM.
Kenneth R. Epstein, MD, MBA, FACP, FHM, chief medical officer for Hospitalist Consultants Inc., headquartered in Traverse City, Mich., has observed this trend first-hand. In academic hospitals, due to new Accreditation Council for Graduate Medical Education (ACGME) and Resident Review Committee (RRC) regulations, "the only safety valve to handle admissions after the house staff numbers are capped is the hospitalist."
The need for such a safety valve will increase again this summer, as new ACGME duty-hour regulations on resident hours and supervision kick in.
Nonteaching hospitals are not exempt from these pressures. To deal with increasing demands for night coverage, HM groups across the country are using a variety of practice models, such as hiring dedicated nocturnists or moonlighters to cover nights, rotating shifts among team members, or using midlevel providers (physician assistants or nurse practitioners) as night staffers. On-call or in-house coverage models are determined by a variety of factors, including the size of the HM group, patient volume and acuity, and staff availability. Sustainability continues to be a challenge for most groups; however, the in-house coverage model seems to increase nursing and ED satisfaction, most experts say, and is an added value for hospital administration, although financial returns vary.
Continuity of care is at the heart of the night-coverage issue. Some experts worry that patient outcomes will suffer if there isn’t an in-house presence, but studies looking at this issue have been inconclusive, asserts Patti VanDort, RN, MSN, NEA-BC, vice president of nursing and chief nursing officer at Holland Hospital in southwestern Michigan.
"You’ve got to have the same level and quality of care during nights and weekends that you have during the weekdays," she says. "It’s got to be the same for all."
That said, some hospitals don’t have the volume to justify in-house night staffing. Hospitalists and program directors have described the ways in which they handle night staffing, balancing demand, program size, and physician satisfaction.
Tailored to Fit
"Hospitalist programs have different scale and scope depending on the needs of the institution," says Michael R. Humphrey, MD, vice president and chief clinical officer for Emergency and Ambulatory Services at St. Rita’s Medical Center in Lima, Ohio. A 365-bed community hospital, St. Rita’s employs nocturnists as part of its 24-hour hospitalist program. Dr. Humphrey still works as an ED physician and reports that the hospitalists are invaluable for admitting, providing cross-cover, covering the ICU, and handling code blue and rapid responses. "As a Level II trauma center, we can’t have ED physicians leave the department to run upstairs and do codes," he says. "They typically don’t get back within five minutes."
Holland Hospital, a 213-bed facility, provides around-the-clock hospitalist coverage in its eight-bed ICU, according to VanDort. That change was precipitated by the nursing staff’s decision to pursue Magnet Status, which was awarded in 2007 by the American Nurses Credentialing Center (ANCC). For inpatient coverage, the hospital-owned HM group Lakeshore Health Partners, headed by Bart D. Sak, MD, MA, FHM, maintains six FTE hospitalists on a rotating block schedule. Each night, one physician works from 4 p.m. until midnight, overlapping with a nonphysician provider (NPP), a member of the hospitalist group, who works a 7 p.m. to 7 a.m. shift.
"We have two providers in-house when admissions from the ED are heating up, and then we have an NPP in-house to cover the one to three additional admissions that may come in after midnight and to field floor calls," Dr. Sak says.
The physician who worked until midnight is on call for backup support and might come back to the hospital if things get too intense in the pre-dawn hours. "This arrangement works quite well for a program of our size," Dr. Sak says. "It takes a team-oriented approach and experienced NPPs who can work independently."
The Holland approach simply wouldn’t work at Kaiser Permanente’s East Bay site in Oakland, Calif., where Tom Baudendistel, MD, FACP, is part of a 50-member hospitalist group and director of the internal-medicine residency program. "Between codes, cross-cover, ICU, and floor admissions, there is simply too much acuity and volume," he says.
The peak hours for East Bay admissions are mid-afternoon to midnight. Two overnight hospitalist shifts (one from 8 a.m. to 8 p.m., another from 7 a.m. to 7 p.m.) are supplemented with two swing shifts (one from 2 to 10 p.m., another from 4 p.m. to midnight). Four full-time nocturnists cover 10 of the 14 overnight shifts per week, which allows for vacation and some protected administrative time. The balance of the overnight shifts are covered by the rest of the hospitalist group, which has 50 members.
The contracted nocturnists are incentivized with additional compensation at the end of the year, when the chief of hospitalists allocates bonuses. They also work fewer shifts a month than the other members of the group. "One thing our group agrees on is that the night docs should get a little more," Dr. Baudendistel says. "It’s a very fair tradeoff for everyone."
A Mile in Their Shoes
Medical directors must balance a variety of factors when scheduling around-the-clock coverage. From day one, the hospitalist program at Albany Memorial Hospital in New York, where John Krisa, MD, is medical director, has been an in-house 24/7 program. Dr. Krisa’s group uses per diem physicians or fellows on their days off to cover most of the nights. The other hospitalists on the team do not escape occasional night duty, and they cover what is left after plugging in the moonlighters. This leaves from zero to five nights per month for each full-time hospitalist. Even the medical director covers night shifts, something Dr. Krisa thinks is valuable to his leadership.
"You, as the leader, still have to walk a mile in that other person’s shoes," he says. "There are different challenges associated with both day and night shifts, so you have to appreciate what your colleagues are going through on the other shifts."
Hospitalist Consultants’ Dr. Epstein agrees with that concept.
"Whenever medical directors have personal experience of how the system is working, they are better able to recommend and make changes," he says.
It’s also valuable, Dr. Krisa explains, for the group leader to interact with ED staff and hear their concerns. Working night shifts helps avoid the night team versus day team schisms, which can lead to group disunity, he says.
Different Skill Set, Different Mindset?
The fact of the matter, though, is that pulling night shifts does not appeal to most established hospitalists. Sleep researchers have found that humans’ body clocks prefer office hours. Even if night-shift hours are consistent, those who work nights never really catch up on the sleep they need during the daytime.
Even so, some physicians embrace the graveyard shift. Working the night swing shift agrees with Dr. Marshbanks’ schedule. The hours are consistent, she works fewer shifts to qualify for FTE pay, and her shift is time-limited, as opposed to work-limited. She’s also filling a niche that others in her group eschew. "It’s a shift that most people with children don’t like because the hours are very disruptive to family life," she says.
The workload at night is different. Instead of the routine rounding typical in day shifts, her work is more urgent. She does more admissions because she works the busiest ED hours, covers acute-stroke codes, and provides cross-cover. And, she says, night staff tends to be "a solid group, so we interact more on a regular basis, since there are fewer of us."
The nocturnists at St. Rita’s Hospital are not held to the same meeting schedule as their daytime hospitalist colleagues, but they’re expected to read meeting minutes and to be responsible for any changes in guidelines or operational information, Dr. Humphrey says. Also stipulated in their hospitalist contracts is the requirement that they maintain competency in procedures, such as central-line placement and airway management.
What’s Better for Patients?
Experts have raised concerns that patient care can be compromised during off-hours, when staffing levels are reduced.1 The Leapfrog Group’s ICU Physician Safety (IPS) Standard argues for high-intensity ICU staffing to reduce patient mortality.2 A number of investigators have tried to determine whether patients admitted off-hours (weekends, nights, holidays) fare worse than those admitted during weekdays. Peter Cram, MD, MBA, acting director of the division of general internal medicine and associate professor of medicine at the Carver College of Medicine at the University of Iowa in Iowa City, found in a 2004 study that patients admitted to hospitals on weekends experienced slightly higher risk-adjusted mortality than did patients admitted on weekdays.3
But here’s the problem with studies such as this, says Dr. Cram: "Patients admitted on evenings and weekends are not the same as those admitted 9 to 5 on weekdays."
During weekdays, admissions combine patients with emergent issues and those scheduled for elective procedures. On weekends, "you get only emergencies—you don’t have low-risk patients," he points out. "So, even with optimal 24/7 staffing, you would still expect those patients coming in at night, and on holidays, to have worse outcomes because they are coming in with more acute problems. It remains an open question whether 24/7 staffing will improve off-hours outcomes." More research, Dr. Cram adds, is needed to establish whether full in-house staffing is the best solution.
Dr. Epstein has compared on-call versus in-house night staffing. In a 2007 study, he found no difference when using indicators such as length of stay, readmission rates, and patient satisfaction.4 However, he noticed positives from in-house coverage. "Although there are no data supporting the value of hospitalists on these parameters, having a nocturnist in-house increases nursing satisfaction, because they are responsive to pages when there is a question about a patient," he says. "It’s also a service to hospital medical staff, because they can handle rapid responses and codes."
There is some evidence that working nights can be deleterious to physicians’ and nurses’ health. One study found that interns were more likely to be involved in collisions after leaving extended night shifts; another found an increased risk of needle-stick injury at the end of a long night shift; and data from the long-running Nurses’ Health Study indicate that long-term night work can result in increased risk of colorectal and breast cancers.5,6,7,8 The increased risks of cancer could be related to lack of exposure to light at night and the body’s decreased production of melatonin, although this remains a topic of ongoing research.
"No Easy Answers"
VanDort, the nursing director, is "passionate" about having 24/7 coverage and reports that her nursing staff is happy with the hybrid model currently used at Holland Hospital. "I do envision a day when we’ll have physicians here around the clock," she says. "Patients are sick during the middle of the night, so you can’t staff your system one way during the daytime hours and your nighttime differently. It’s not fair to those patients."
Dr. Cram, who is a hospitalist, outcomes researcher, and division director, says that in an ideal world, it would make more business sense to have the hospital operating at full capacity around the clock, seven days a week. "But we don’t live in that world," he admits. "It is hard to find ways to achieve ’round-the-clock staffing at the levels we’d like."
He also concludes that there are "no easy answers" to the night-coverage conundrum. "But it might be prudent to think about incentives," he says. "Perhaps we should pay more for staffing weekends, evenings, and holidays, or we could reduce the annual number of shifts we expect our nocturnists to do, relative to those physicians who staff days."
Dr. Krisa says he, too, is biased toward an in-house coverage model, especially when programs reach a critical volume. "There is no substitute for the immediate ability to evaluate a sick patient," he explains. "My feeling is that an in-house, 24/7 presence will become the standard." TH
Gretchen Henkel is a freelance writer based in California.
References
- Wong HJ, Morra D. Excellent hospital care for all: open and operating 24/7. J Gen Intern Med. 2011.
- Pronovost PJ, Angus DC, Dorman T, Robinson KA, Dremsizov TT, Young TL. Physician staffing patterns and clinical outcomes in critically ill patients: a systemic review. JAMA. 2002;288(17):2151-2162.
- Cram P, Hillis SL, Barnett M, Rosenthal GE. Effects of weekend admission and hospital teaching status on in-hospital mortality. Am J Med. 2004;117(3):151-157.
- Epstein KR, Juarez E, Loya K, Gorman MJ, Singer A. The effect of 24-7 hospitalist coverage on clinical metrics. Presented May 2007, annual meeting, Society of Hospital Medicine, Dallas.
- Barger LK, Cade BE, Ayas NT, et al. Extended work shifts and the risk of motor vehicle crashes among interns. N Engl J Med. 2005;352:125-134.
- Ayas NT, Barger LK, Cade BE, et al. Extended work duration and the risk of self-reported percutaneous injuries in interns. JAMA. 2006;296(9):1055-1062.
- Schernhammer ES, Laden F, Speizer FE, et al. Night-shift work and risk of colorectal cancer in the nurses’ health study. J Natl Cancer Inst. 2003;95(11):825-828.
- Schernhammer ES, Laden F, Speizer FE, et al. Rotating night shifts and risk of breast cancer in women partici-pating in the nurses’ health study. J Natl Cancer Inst. 2001;93(20):1563-1568.
ONLINE EXCLUSIVE: How to minimize the adverse affects of working night shifts
Click here to listen to Dr. Landrigan
Click here to listen to Dr. Landrigan
Click here to listen to Dr. Landrigan
Hospitalists Can Be Champions of Clinical Documentation
To improve your hospital’s reimbursements and key indicators, including observed and expected (O/E) mortality ratios, personalize your collaboration with clinical documentation specialists (CDSs). That’s what has worked at two medical centers where hospitalists teamed up with CDSs to improve their hospitals’ claims processes.
At Northwestern Memorial Hospital in Chicago, the hematology/oncology service was selected for a pilot program to focus on improving expected mortality rates. The specialists needed to ensure that coded data sent to state- and hospital-associated databases (as well as payor claims, such as those submitted to Medicare) accurately represented the severity of patients’ conditions upon admission. To do that, they needed buy-in from hospitalists to make their notes as complete as possible.
Hospitalists usually encounter CDSs anonymously, through an electronic query in the electronic health record (EHR). Kristine Green, RN, a CDS, quality leader, and interim manager at Northwestern’s clinical documentation program, approached hospitalist Charlotta Weaver, MD, medical director of the oncology HM service and a clinical instructor at Northwestern University’s Feinberg School of Medicine. Green suggested she shadow Dr. Weaver on rounds.
“We had implemented this technique in a couple of our other service lines, with good results,” Green says. She compared her notes on patient visits with Dr. Weaver’s notes and was able to catch conditions that were being undercoded. They generated a list, now posted in the work room, disseminated via email, and included in the orientation binder, of frequently missed coding diagnoses.
For example, Dr. Weaver explains, “instead of writing ‘AKI-obstructive,’ we now write ‘AKI due to ureteral obstruction from peritoneal carcinomatosis from metastatic gastric cancer.’ ”
Such specificity in physicians’ notes translates to a more accurate level of billing for the hospital and a more accurate reflection of patients’ acuity in comparative databases. With Dr. Weaver paving the way, Green has forged “a nice rapport” with the other hospitalists in the oncology medicine service.
Audiences for Your Notes
CDS and hospitalists might initially view notes differently. Most physicians train in programs where the “primary intent of a note” is to communicate to the rest of the medical team what’s happening with the patient, Dr. Weaver says.

“When we train, we’re always thinking about communicating with each other,” says Theodore (Ted) Tsomides, MD, PhD, an attending physician on the hospital medicine service at WakeMed Hospital and assistant professor of medicine at the University of North Carolina’s School of Medicine in Raleigh. “But as we get into the system, we realize that there are a lot of eyes on those documents. And whether we think about it or not, those are all our different audiences.”
Once hospitalists develop confidence and comfort on the job, Dr. Tsomides says, they can move on to aligning themselves with the hospital’s interests. Dr. Weaver thinks hospitalists are uniquely positioned to help champion the CDI efforts. “We’re here to improve the mission of the hospital,” she says.
As physician liaison for quality programs, Dr. Tsomides began working on clinical documentation improvement. He became a resource for the department, and then worked to achieve a financial incentive plan for hospital physicians when their documentation improved. He’s also been pushing his institution to make the documentation process easier by using electronic queries, and by introducing residents to the “real world” of clinical documentation in their curriculum. (Click here to listen to more of Dr. Tsomides’ ideas to improve clinical documentation.)
He advises hospitalists meet their clinical documentation specialists face to face. “Once you know there are people who are doing their part, and have a relationship with them, you approach the whole problem differently,” Dr. Tsomides says, “as opposed to [viewing them] as anonymous reviewers breathing down your neck and giving you yet another thing to worry about.”
Gretchen Henkel is a freelance writer based in California.
To improve your hospital’s reimbursements and key indicators, including observed and expected (O/E) mortality ratios, personalize your collaboration with clinical documentation specialists (CDSs). That’s what has worked at two medical centers where hospitalists teamed up with CDSs to improve their hospitals’ claims processes.
At Northwestern Memorial Hospital in Chicago, the hematology/oncology service was selected for a pilot program to focus on improving expected mortality rates. The specialists needed to ensure that coded data sent to state- and hospital-associated databases (as well as payor claims, such as those submitted to Medicare) accurately represented the severity of patients’ conditions upon admission. To do that, they needed buy-in from hospitalists to make their notes as complete as possible.
Hospitalists usually encounter CDSs anonymously, through an electronic query in the electronic health record (EHR). Kristine Green, RN, a CDS, quality leader, and interim manager at Northwestern’s clinical documentation program, approached hospitalist Charlotta Weaver, MD, medical director of the oncology HM service and a clinical instructor at Northwestern University’s Feinberg School of Medicine. Green suggested she shadow Dr. Weaver on rounds.
“We had implemented this technique in a couple of our other service lines, with good results,” Green says. She compared her notes on patient visits with Dr. Weaver’s notes and was able to catch conditions that were being undercoded. They generated a list, now posted in the work room, disseminated via email, and included in the orientation binder, of frequently missed coding diagnoses.
For example, Dr. Weaver explains, “instead of writing ‘AKI-obstructive,’ we now write ‘AKI due to ureteral obstruction from peritoneal carcinomatosis from metastatic gastric cancer.’ ”
Such specificity in physicians’ notes translates to a more accurate level of billing for the hospital and a more accurate reflection of patients’ acuity in comparative databases. With Dr. Weaver paving the way, Green has forged “a nice rapport” with the other hospitalists in the oncology medicine service.
Audiences for Your Notes
CDS and hospitalists might initially view notes differently. Most physicians train in programs where the “primary intent of a note” is to communicate to the rest of the medical team what’s happening with the patient, Dr. Weaver says.
“When we train, we’re always thinking about communicating with each other,” says Theodore (Ted) Tsomides, MD, PhD, an attending physician on the hospital medicine service at WakeMed Hospital and assistant professor of medicine at the University of North Carolina’s School of Medicine in Raleigh. “But as we get into the system, we realize that there are a lot of eyes on those documents. And whether we think about it or not, those are all our different audiences.”
Once hospitalists develop confidence and comfort on the job, Dr. Tsomides says, they can move on to aligning themselves with the hospital’s interests. Dr. Weaver thinks hospitalists are uniquely positioned to help champion the CDI efforts. “We’re here to improve the mission of the hospital,” she says.
As physician liaison for quality programs, Dr. Tsomides began working on clinical documentation improvement. He became a resource for the department, and then worked to achieve a financial incentive plan for hospital physicians when their documentation improved. He’s also been pushing his institution to make the documentation process easier by using electronic queries, and by introducing residents to the “real world” of clinical documentation in their curriculum. (Click here to listen to more of Dr. Tsomides’ ideas to improve clinical documentation.)
He advises hospitalists meet their clinical documentation specialists face to face. “Once you know there are people who are doing their part, and have a relationship with them, you approach the whole problem differently,” Dr. Tsomides says, “as opposed to [viewing them] as anonymous reviewers breathing down your neck and giving you yet another thing to worry about.”
Gretchen Henkel is a freelance writer based in California.
To improve your hospital’s reimbursements and key indicators, including observed and expected (O/E) mortality ratios, personalize your collaboration with clinical documentation specialists (CDSs). That’s what has worked at two medical centers where hospitalists teamed up with CDSs to improve their hospitals’ claims processes.
At Northwestern Memorial Hospital in Chicago, the hematology/oncology service was selected for a pilot program to focus on improving expected mortality rates. The specialists needed to ensure that coded data sent to state- and hospital-associated databases (as well as payor claims, such as those submitted to Medicare) accurately represented the severity of patients’ conditions upon admission. To do that, they needed buy-in from hospitalists to make their notes as complete as possible.
Hospitalists usually encounter CDSs anonymously, through an electronic query in the electronic health record (EHR). Kristine Green, RN, a CDS, quality leader, and interim manager at Northwestern’s clinical documentation program, approached hospitalist Charlotta Weaver, MD, medical director of the oncology HM service and a clinical instructor at Northwestern University’s Feinberg School of Medicine. Green suggested she shadow Dr. Weaver on rounds.
“We had implemented this technique in a couple of our other service lines, with good results,” Green says. She compared her notes on patient visits with Dr. Weaver’s notes and was able to catch conditions that were being undercoded. They generated a list, now posted in the work room, disseminated via email, and included in the orientation binder, of frequently missed coding diagnoses.
For example, Dr. Weaver explains, “instead of writing ‘AKI-obstructive,’ we now write ‘AKI due to ureteral obstruction from peritoneal carcinomatosis from metastatic gastric cancer.’ ”
Such specificity in physicians’ notes translates to a more accurate level of billing for the hospital and a more accurate reflection of patients’ acuity in comparative databases. With Dr. Weaver paving the way, Green has forged “a nice rapport” with the other hospitalists in the oncology medicine service.
Audiences for Your Notes
CDS and hospitalists might initially view notes differently. Most physicians train in programs where the “primary intent of a note” is to communicate to the rest of the medical team what’s happening with the patient, Dr. Weaver says.
“When we train, we’re always thinking about communicating with each other,” says Theodore (Ted) Tsomides, MD, PhD, an attending physician on the hospital medicine service at WakeMed Hospital and assistant professor of medicine at the University of North Carolina’s School of Medicine in Raleigh. “But as we get into the system, we realize that there are a lot of eyes on those documents. And whether we think about it or not, those are all our different audiences.”
Once hospitalists develop confidence and comfort on the job, Dr. Tsomides says, they can move on to aligning themselves with the hospital’s interests. Dr. Weaver thinks hospitalists are uniquely positioned to help champion the CDI efforts. “We’re here to improve the mission of the hospital,” she says.
As physician liaison for quality programs, Dr. Tsomides began working on clinical documentation improvement. He became a resource for the department, and then worked to achieve a financial incentive plan for hospital physicians when their documentation improved. He’s also been pushing his institution to make the documentation process easier by using electronic queries, and by introducing residents to the “real world” of clinical documentation in their curriculum. (Click here to listen to more of Dr. Tsomides’ ideas to improve clinical documentation.)
He advises hospitalists meet their clinical documentation specialists face to face. “Once you know there are people who are doing their part, and have a relationship with them, you approach the whole problem differently,” Dr. Tsomides says, “as opposed to [viewing them] as anonymous reviewers breathing down your neck and giving you yet another thing to worry about.”
Gretchen Henkel is a freelance writer based in California.
The Billing & Coding Bandwagon

It’s no secret that documenting and coding one’s work is not the average hospitalist’s favorite thing to do. It’s probably not even in the top 10 or 20. In fact, many consider the whole documentation process a “thorn in the side.”
“When I first started working, I couldn’t believe that I could get audited and fined just because I didn’t add ‘10-point’ or ‘12-point’ to my note of ‘review of systems: negative,’ ” says hospitalist Amaka Nweke, MD, assistant director with Hospitalists Management Group (HMG) at Kenosha Medical Center in Kenosha, Wis. “I had a lot of frustration, because I had to repackage and re-present my notes in a manner that makes sense to Medicare but makes no sense to physicians.”
Like it or not, healthcare providers live in a highly regulated world, says Richard D. Pinson, MD, FACP, CCS, who became a certified coding specialist and formed his own consulting company, Houston-based HCQ Consulting, to help hospitals and physicians achieve diagnostic accuracy for inpatient care. Documentation and coding have become a serious, high-stakes word game, he says. “Perfectly good clinical documentation, especially with some important diagnoses, may not correspond at all to what is required by the strict coding rules that govern code assignments,” he says.
A hospitalist’s documentation is at the heart of accurate coding, whether it’s for the hospital’s DRG reimbursement, quality and performance scores, or for assigning current procedural terminology (CPT) and evaluation and management (E/M) codes for billing for their own professional services. And if hospitalists don’t buy into the coding mindset, they risk decreased reimbursement for their services, monetary losses for the hospital, Medicare audits, compromised quality scores for both the hospital and themselves, and noncompliance.
“If your documentation is not up to par, then the hospital may get fined and lose money, and you can’t prove your worth as a hospitalist,” Dr. Nweke says.
What’s at Stake?

Inadequate documentation results in “undercoding” a patient’s condition and underpayment to your hospital (see Table 1, right). Undercoding also can result in inadequate representation of the severity of a patient’s illness, complexity, and cost of care. If a patient gets worse in the hospital, then that initial lower severity of illness might show up in poor performance scores on outcome measures. If a patient’s severity of illness is miscoded, Medicare might question the medical necessity for inpatient admission and deny payment.
On the other hand, if overcoding occurs because the clinical criteria for a specific diagnosis have not been met, Medicare will take action to recover the overpayment, leveling penalties and sanctions. (For more information on Medicare’s Recovery Audit Contractor program, dubbed “Medicare’s repo men” by Dr. Pinson, see “Take Proactive Approach to Recovery Audit Contractors,” p. 28.)
Lack of specificity also hampers reimbursement for professional fees, says Barb Pierce, CCS-P, ACS-EM, president of Barb Pierce Coding and Consulting Inc. of West Des Moines, Iowa. “Unfortunately,” she observes, “the code isn’t just based on decision-making, which is why physicians went to school for all those years. The guidelines [Documentation Guidelines for Evaluation and Management Services] mandate that if you forget one little bullet in history or examination, even if you’ve got the riskiest, highest-level, decision-making patient in front of you, that could pull down the whole code selection.”1
How costly might such small mistakes be for an HM group? According to the State of Hospital Medicine: 2010 Report Based on 2009 Data survey, internal-medicine hospitalists generate a median of 1.86 work relative value units (wRVUs) per encounter, and collect $45.57 per wRVU.2 If a hospitalist has 2,200 encounters per year and averages only 1.65 wRVUs per encounter, improving documentation and coding performance could add an additional 0.21 wRVUs, meeting the national average. Multiplying those 2,200 encounters by the national average of 1.86, the hospitalist could potentially add an additional 462 wRVUs for the year. Such documentation improvement—up to the national average—would equate to $21,053 in additional billed revenue without increasing the physician’s overall workload.
Dr. Pinson explains that physicians often perceive their time constraints as so severe that they’d be hard pressed to find the time to learn about documentation and coding. But he maintains that even short seminars yield “a huge amount of information that would astound [hospitalists], in terms of usefulness for their own clinical practices.”
Barriers to the Coding Mindset

Most hospitalists receive little or no training in documentation and coding during medical school or residency. The lack of education is further complicated because there are several coding sets healthcare providers must master, each with different rules governing assignment of diagnoses and levels of care (see “Coding Sets: Separate but Overlapping,” above).
Inexperience with coding guidelines can lead to mismatches. Nelly Leon-Chisen, RHIA, director of coding and classification for the American Hospital Association (AHA), gives one example: The ICD-9-CM Official Coding Guideline stipulates that coders cannot assign diagnosis codes based on lab results.3 So although it might appear intuitive to a physician that repeated blood sugars and monitoring of insulin levels indicate a patient has diabetes, the coder cannot assign the diagnosis unless it’s explicitly stated in the record.
Some physicians could simply be using outmoded terminology, such as “renal insufficiency” instead of “acute renal failure,” Dr. Pinson notes. If hospitalists learn to focus on evidence-based clinical criteria to support the codes, it leads to more effective care, he says.
The nature of hospitalist programs might not lend itself to efficient revenue-cycle processes for their own professional billing, says Jeri Leong, RN, CPC, CPC-H, president and CEO of Honolulu-based Healthcare Coding Consultants of Hawaii. If the HM group contracts with several hospitals, the hospitalists will be together rarely as a group, “so they don’t have the luxury of sitting down together with their billers to get important feedback and coding updates,” she says.
Leong’s company identifies missed charges, for instance, when charge tags from different shifts do not get married together (Hospitalist A might round on the patient in the morning and turn in a charge tag; Hospitalist B might do a procedure in the afternoon, but the two tags do not get combined). Examples such as these, she says, “can be an issue from a compliance perspective, and can leave money on the table.”
One of the problems Kathy DeVault, RHIA, CCS, CCS-P, manager of professional practice resources for the American Health Information Management Association (AHIMA), sees is a lack of continuity between initial admitting diagnosis and discharge summaries. For example, a hospitalist might admit a patient for acute renal failure—the correct diagnosis—and be able to reverse the condition fairly quickly, especially if the failure is due to dehydration.
The patient, whose issue is resolved, could be discharged by an attending physician who does not note the acute diagnosis in the summary. “That acute condition disappears, and the RAC auditor may then challenge the claim for payment,” DeVault says.
The Remedies
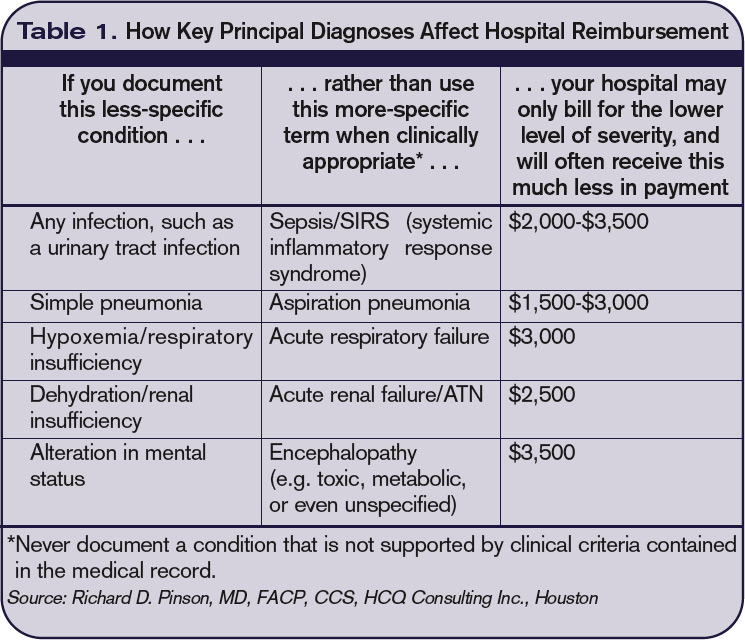
While physicians might think that they don’t have the time to acquire coding education, there could be other incentives coming down the pike. Dr. Pinson has noticed that hospitals are beginning to incorporate documentation accuracy into their contractual reimbursement formulas.
Documentation fixes vary according to domain. A hospital’s clinical documentation specialists can query physicians for clarity and detail in their notes; for instance, a diagnosis of congestive heart failure (CHF) must be accompanied by additional documentation stating whether the CHF is acute or chronic, and whether it is systolic or diastolic.
Many hospitals have instituted clinical documentation improvement (CDI) programs, sometimes called clinical documentation integrity programs, to address documentation discrepancies. CDI programs are essential to hospitals’ financial survival, Dr. Pinson says, and hospitalists are ideally positioned to join those efforts.
“[The hospitalists] are the most important people to the hospital in all of this,” he says. “They’re at the center of this whirlpool. If you have these skills, your value to the hospital and to your group is greatly enhanced.” (Visit the-hospitalist.org to listen to Dr. Pinson discuss HM’s role in documentation improvement.)
Leon-Chisen also says that the relationship between coders and physicians should be collaborative. “If it’s adversarial, nobody wins,” she points out, adding that CDI programs present an opportunity for mutual education.
Conducting audits of the practice’s documentation and coding can identify coding strengths and weaknesses, says Pierce, who is faculty for SHM’s billing and coding pre-course and regularly consults with hospitalist groups. Audits are helpful, she says, not just for increasing group revenue, but for compliance reasons as well. “You need to know what you’re doing well, and what you’re not doing quite so well, and get it fixed internally before an entity like Medicare discovers it,” she says.
It’s no doubt difficult for a busy HM group to stay on top of annual coding updates and changes to guidelines for reporting their services, Leong notes. Her company has worked with many hospitalist groups over the years, offering coding workshops, “back end” audits, and real-time feedback of E/M and CPT coding choices. If all of the hospitalists in a group cannot convene simultaneously, Leong provides the feedback (in the form of a scorecard) to the group’s physician champion, who becomes the lead contact to help those physicians who struggle more with their coding. (Leong talks more about real-time feedback and capturing CPT and E/M codes at the-hospitalist.org.)
In lieu of hiring professional coders, some HM groups use electronic coding devices. The software could be a standalone product, or it could interface with other products, such as electronic medical records (EMRs). These programs assist with a variety of coding-related activities, such as CPT or ICD-9 lookups, or calculation of E/M key components with assignment of an appropriate level of billing. Leong, however, cautions too much reliance on technology.
“While these devices can be accurate, compact, and convenient, it’s important to maintain a current [software] subscription to keep abreast of updates to the code sets, which occur sometimes as often as quarterly,” she says.
Pierce adds that coding tools should be double-checked against an audit tool. She has sometimes found discrepancies when auditing against an EMR product that assigns the E/M level.

Attitude Adjustment
Coding experts emphasize that physicians need not worry about mastering coding manuals, but they should forge relationships with both their hospital’s billers and the coders for their practice.
Dr. Nweke took advantage of coding and billing workshops offered by her group, HMG, and through the seminars began to understand what a DRG meant not just for her hospital but for her own evaluations and the expansion of her HM group, too. “Now, when I get questions from billers and coders, I try to answer them quickly,” she says. “I don’t look upon them as the enemy, but rather as people who are helping me document appropriately, so I don’t get audited by Medicare. I think the way you view the coders and billers definitely affects your willingness to learn.”
Dr. Nweke also takes a broader view of her role as a hospitalist. “You are there to take care of patients and assist with transitioning them in and out of the hospital, but you’re also there to ensure that the hospital remains afloat financially,” she says. “Your documentation plays a huge role in that. We have a huge contribution to make.”
The patient gains, too, says Leon-Chisen, who explains that documentation should be as accurate as possible “because someone else—the patient’s primary physician—will be taking over care of that patient and needs to understand what happened in the hospital.”
“The bottom line,” Dr. Pinson says, “is that we need accurate documentation that can be correctly coded to reflect the true complexity of care and severity of illness. If we do that, good things will follow.” TH
Gretchen Henkel is a freelance writer based in California.
References
- 1997 Documentation Guidelines for Evaluation and Management Services. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed April 11, 2011.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Society of Hospital Medicine and Medical Group Management Association; Philadelphia and Englewood, Colo.; 2010.
- ICD-9-CM Official Coding Guidelines. CMS and National Center for Health Statistics; Washington, D.C.; 2008. Available at: www.ama-assn.org/resources/doc/cpt/icd9cm_coding_guidelines_08_09_full.pdf. Accessed April 10, 2011.
Take Proactive Approach to Recovery Audit Contractors
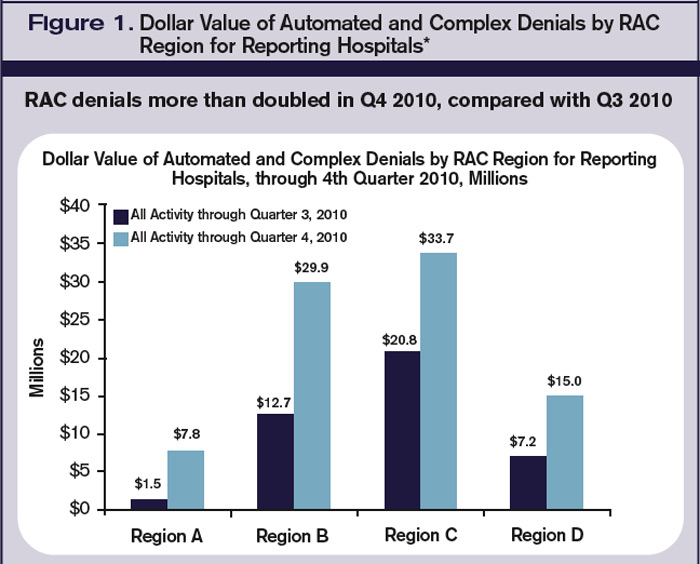
The congressionally authorized Medicare Recovery Audit Contractor (RAC) program began with a three-year demonstration pilot project in 2005. In August 2010, the program expanded to the entire country. The RAC’s main objective is to identify improper Medicare payments, both overpayments and underpayments, to providers. CMS, which administrates Medicare and the RAC program, has agreements with contractors who are authorized to audit and review claims that are up to three years old.
According to Elizabeth Baskett, senior associate director of policy at the AHA, medical necessity review was a big focus of the RAC demonstration project and now is “under way in the permanent RAC program. We are bracing ourselves for a significant amount of denials.”
The AHA has created a free, Web-based survey called RAC Trac (www.aha.org/aha/issues/RAC/ractrac.html) to assess the nationwide impact the RAC program has on U.S. hospitals. In a report released Feb. 24, the RAC Trac survey shows that $82 million in denials were reported, more than double the dollar amount of denials reported in the third quarter of 2010 (see Figure 1, below). It also shows 57% of the more than 1,850 participating hospitals cited “medically unnecessary” as a reason for a denial of a claim.
Nearly 80% of the participating hospitals reported RAC activity in 2010, with general medical and surgical hospitals reporting the most activity. Fifty percent of reporting hospitals noted that their administrative burden—in the form of hiring consultants, copying medical records, hiring legal counsel, and the like—had increased as a result of RAC activity.
Most importantly, the report shows the average dollar value of automated denials was $399. But when a complex review—one involving a human review of requested records—was conducted, the average value of the denial was $5,281. Additionally, inpatient facilities were most likely to experience complex denials, which account for 90% of the value of denied claims.
Leong says RAC audits are just one area of “exposure to review for hospitals and providers. Other third-party payers, including individual commercial insurance companies,” she says, “also do routine post-payment review and recoupment, several years after payment.”—GH
It’s no secret that documenting and coding one’s work is not the average hospitalist’s favorite thing to do. It’s probably not even in the top 10 or 20. In fact, many consider the whole documentation process a “thorn in the side.”
“When I first started working, I couldn’t believe that I could get audited and fined just because I didn’t add ‘10-point’ or ‘12-point’ to my note of ‘review of systems: negative,’ ” says hospitalist Amaka Nweke, MD, assistant director with Hospitalists Management Group (HMG) at Kenosha Medical Center in Kenosha, Wis. “I had a lot of frustration, because I had to repackage and re-present my notes in a manner that makes sense to Medicare but makes no sense to physicians.”
Like it or not, healthcare providers live in a highly regulated world, says Richard D. Pinson, MD, FACP, CCS, who became a certified coding specialist and formed his own consulting company, Houston-based HCQ Consulting, to help hospitals and physicians achieve diagnostic accuracy for inpatient care. Documentation and coding have become a serious, high-stakes word game, he says. “Perfectly good clinical documentation, especially with some important diagnoses, may not correspond at all to what is required by the strict coding rules that govern code assignments,” he says.
A hospitalist’s documentation is at the heart of accurate coding, whether it’s for the hospital’s DRG reimbursement, quality and performance scores, or for assigning current procedural terminology (CPT) and evaluation and management (E/M) codes for billing for their own professional services. And if hospitalists don’t buy into the coding mindset, they risk decreased reimbursement for their services, monetary losses for the hospital, Medicare audits, compromised quality scores for both the hospital and themselves, and noncompliance.
“If your documentation is not up to par, then the hospital may get fined and lose money, and you can’t prove your worth as a hospitalist,” Dr. Nweke says.
What’s at Stake?
Inadequate documentation results in “undercoding” a patient’s condition and underpayment to your hospital (see Table 1, right). Undercoding also can result in inadequate representation of the severity of a patient’s illness, complexity, and cost of care. If a patient gets worse in the hospital, then that initial lower severity of illness might show up in poor performance scores on outcome measures. If a patient’s severity of illness is miscoded, Medicare might question the medical necessity for inpatient admission and deny payment.
On the other hand, if overcoding occurs because the clinical criteria for a specific diagnosis have not been met, Medicare will take action to recover the overpayment, leveling penalties and sanctions. (For more information on Medicare’s Recovery Audit Contractor program, dubbed “Medicare’s repo men” by Dr. Pinson, see “Take Proactive Approach to Recovery Audit Contractors,” p. 28.)
Lack of specificity also hampers reimbursement for professional fees, says Barb Pierce, CCS-P, ACS-EM, president of Barb Pierce Coding and Consulting Inc. of West Des Moines, Iowa. “Unfortunately,” she observes, “the code isn’t just based on decision-making, which is why physicians went to school for all those years. The guidelines [Documentation Guidelines for Evaluation and Management Services] mandate that if you forget one little bullet in history or examination, even if you’ve got the riskiest, highest-level, decision-making patient in front of you, that could pull down the whole code selection.”1
How costly might such small mistakes be for an HM group? According to the State of Hospital Medicine: 2010 Report Based on 2009 Data survey, internal-medicine hospitalists generate a median of 1.86 work relative value units (wRVUs) per encounter, and collect $45.57 per wRVU.2 If a hospitalist has 2,200 encounters per year and averages only 1.65 wRVUs per encounter, improving documentation and coding performance could add an additional 0.21 wRVUs, meeting the national average. Multiplying those 2,200 encounters by the national average of 1.86, the hospitalist could potentially add an additional 462 wRVUs for the year. Such documentation improvement—up to the national average—would equate to $21,053 in additional billed revenue without increasing the physician’s overall workload.
Dr. Pinson explains that physicians often perceive their time constraints as so severe that they’d be hard pressed to find the time to learn about documentation and coding. But he maintains that even short seminars yield “a huge amount of information that would astound [hospitalists], in terms of usefulness for their own clinical practices.”
Barriers to the Coding Mindset
Most hospitalists receive little or no training in documentation and coding during medical school or residency. The lack of education is further complicated because there are several coding sets healthcare providers must master, each with different rules governing assignment of diagnoses and levels of care (see “Coding Sets: Separate but Overlapping,” above).
Inexperience with coding guidelines can lead to mismatches. Nelly Leon-Chisen, RHIA, director of coding and classification for the American Hospital Association (AHA), gives one example: The ICD-9-CM Official Coding Guideline stipulates that coders cannot assign diagnosis codes based on lab results.3 So although it might appear intuitive to a physician that repeated blood sugars and monitoring of insulin levels indicate a patient has diabetes, the coder cannot assign the diagnosis unless it’s explicitly stated in the record.
Some physicians could simply be using outmoded terminology, such as “renal insufficiency” instead of “acute renal failure,” Dr. Pinson notes. If hospitalists learn to focus on evidence-based clinical criteria to support the codes, it leads to more effective care, he says.
The nature of hospitalist programs might not lend itself to efficient revenue-cycle processes for their own professional billing, says Jeri Leong, RN, CPC, CPC-H, president and CEO of Honolulu-based Healthcare Coding Consultants of Hawaii. If the HM group contracts with several hospitals, the hospitalists will be together rarely as a group, “so they don’t have the luxury of sitting down together with their billers to get important feedback and coding updates,” she says.
Leong’s company identifies missed charges, for instance, when charge tags from different shifts do not get married together (Hospitalist A might round on the patient in the morning and turn in a charge tag; Hospitalist B might do a procedure in the afternoon, but the two tags do not get combined). Examples such as these, she says, “can be an issue from a compliance perspective, and can leave money on the table.”
One of the problems Kathy DeVault, RHIA, CCS, CCS-P, manager of professional practice resources for the American Health Information Management Association (AHIMA), sees is a lack of continuity between initial admitting diagnosis and discharge summaries. For example, a hospitalist might admit a patient for acute renal failure—the correct diagnosis—and be able to reverse the condition fairly quickly, especially if the failure is due to dehydration.
The patient, whose issue is resolved, could be discharged by an attending physician who does not note the acute diagnosis in the summary. “That acute condition disappears, and the RAC auditor may then challenge the claim for payment,” DeVault says.
The Remedies
While physicians might think that they don’t have the time to acquire coding education, there could be other incentives coming down the pike. Dr. Pinson has noticed that hospitals are beginning to incorporate documentation accuracy into their contractual reimbursement formulas.
Documentation fixes vary according to domain. A hospital’s clinical documentation specialists can query physicians for clarity and detail in their notes; for instance, a diagnosis of congestive heart failure (CHF) must be accompanied by additional documentation stating whether the CHF is acute or chronic, and whether it is systolic or diastolic.
Many hospitals have instituted clinical documentation improvement (CDI) programs, sometimes called clinical documentation integrity programs, to address documentation discrepancies. CDI programs are essential to hospitals’ financial survival, Dr. Pinson says, and hospitalists are ideally positioned to join those efforts.
“[The hospitalists] are the most important people to the hospital in all of this,” he says. “They’re at the center of this whirlpool. If you have these skills, your value to the hospital and to your group is greatly enhanced.” (Visit the-hospitalist.org to listen to Dr. Pinson discuss HM’s role in documentation improvement.)
Leon-Chisen also says that the relationship between coders and physicians should be collaborative. “If it’s adversarial, nobody wins,” she points out, adding that CDI programs present an opportunity for mutual education.
Conducting audits of the practice’s documentation and coding can identify coding strengths and weaknesses, says Pierce, who is faculty for SHM’s billing and coding pre-course and regularly consults with hospitalist groups. Audits are helpful, she says, not just for increasing group revenue, but for compliance reasons as well. “You need to know what you’re doing well, and what you’re not doing quite so well, and get it fixed internally before an entity like Medicare discovers it,” she says.
It’s no doubt difficult for a busy HM group to stay on top of annual coding updates and changes to guidelines for reporting their services, Leong notes. Her company has worked with many hospitalist groups over the years, offering coding workshops, “back end” audits, and real-time feedback of E/M and CPT coding choices. If all of the hospitalists in a group cannot convene simultaneously, Leong provides the feedback (in the form of a scorecard) to the group’s physician champion, who becomes the lead contact to help those physicians who struggle more with their coding. (Leong talks more about real-time feedback and capturing CPT and E/M codes at the-hospitalist.org.)
In lieu of hiring professional coders, some HM groups use electronic coding devices. The software could be a standalone product, or it could interface with other products, such as electronic medical records (EMRs). These programs assist with a variety of coding-related activities, such as CPT or ICD-9 lookups, or calculation of E/M key components with assignment of an appropriate level of billing. Leong, however, cautions too much reliance on technology.
“While these devices can be accurate, compact, and convenient, it’s important to maintain a current [software] subscription to keep abreast of updates to the code sets, which occur sometimes as often as quarterly,” she says.
Pierce adds that coding tools should be double-checked against an audit tool. She has sometimes found discrepancies when auditing against an EMR product that assigns the E/M level.
Attitude Adjustment
Coding experts emphasize that physicians need not worry about mastering coding manuals, but they should forge relationships with both their hospital’s billers and the coders for their practice.
Dr. Nweke took advantage of coding and billing workshops offered by her group, HMG, and through the seminars began to understand what a DRG meant not just for her hospital but for her own evaluations and the expansion of her HM group, too. “Now, when I get questions from billers and coders, I try to answer them quickly,” she says. “I don’t look upon them as the enemy, but rather as people who are helping me document appropriately, so I don’t get audited by Medicare. I think the way you view the coders and billers definitely affects your willingness to learn.”
Dr. Nweke also takes a broader view of her role as a hospitalist. “You are there to take care of patients and assist with transitioning them in and out of the hospital, but you’re also there to ensure that the hospital remains afloat financially,” she says. “Your documentation plays a huge role in that. We have a huge contribution to make.”
The patient gains, too, says Leon-Chisen, who explains that documentation should be as accurate as possible “because someone else—the patient’s primary physician—will be taking over care of that patient and needs to understand what happened in the hospital.”
“The bottom line,” Dr. Pinson says, “is that we need accurate documentation that can be correctly coded to reflect the true complexity of care and severity of illness. If we do that, good things will follow.” TH
Gretchen Henkel is a freelance writer based in California.
References
- 1997 Documentation Guidelines for Evaluation and Management Services. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed April 11, 2011.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Society of Hospital Medicine and Medical Group Management Association; Philadelphia and Englewood, Colo.; 2010.
- ICD-9-CM Official Coding Guidelines. CMS and National Center for Health Statistics; Washington, D.C.; 2008. Available at: www.ama-assn.org/resources/doc/cpt/icd9cm_coding_guidelines_08_09_full.pdf. Accessed April 10, 2011.
Take Proactive Approach to Recovery Audit Contractors
The congressionally authorized Medicare Recovery Audit Contractor (RAC) program began with a three-year demonstration pilot project in 2005. In August 2010, the program expanded to the entire country. The RAC’s main objective is to identify improper Medicare payments, both overpayments and underpayments, to providers. CMS, which administrates Medicare and the RAC program, has agreements with contractors who are authorized to audit and review claims that are up to three years old.
According to Elizabeth Baskett, senior associate director of policy at the AHA, medical necessity review was a big focus of the RAC demonstration project and now is “under way in the permanent RAC program. We are bracing ourselves for a significant amount of denials.”
The AHA has created a free, Web-based survey called RAC Trac (www.aha.org/aha/issues/RAC/ractrac.html) to assess the nationwide impact the RAC program has on U.S. hospitals. In a report released Feb. 24, the RAC Trac survey shows that $82 million in denials were reported, more than double the dollar amount of denials reported in the third quarter of 2010 (see Figure 1, below). It also shows 57% of the more than 1,850 participating hospitals cited “medically unnecessary” as a reason for a denial of a claim.
Nearly 80% of the participating hospitals reported RAC activity in 2010, with general medical and surgical hospitals reporting the most activity. Fifty percent of reporting hospitals noted that their administrative burden—in the form of hiring consultants, copying medical records, hiring legal counsel, and the like—had increased as a result of RAC activity.
Most importantly, the report shows the average dollar value of automated denials was $399. But when a complex review—one involving a human review of requested records—was conducted, the average value of the denial was $5,281. Additionally, inpatient facilities were most likely to experience complex denials, which account for 90% of the value of denied claims.
Leong says RAC audits are just one area of “exposure to review for hospitals and providers. Other third-party payers, including individual commercial insurance companies,” she says, “also do routine post-payment review and recoupment, several years after payment.”—GH
It’s no secret that documenting and coding one’s work is not the average hospitalist’s favorite thing to do. It’s probably not even in the top 10 or 20. In fact, many consider the whole documentation process a “thorn in the side.”
“When I first started working, I couldn’t believe that I could get audited and fined just because I didn’t add ‘10-point’ or ‘12-point’ to my note of ‘review of systems: negative,’ ” says hospitalist Amaka Nweke, MD, assistant director with Hospitalists Management Group (HMG) at Kenosha Medical Center in Kenosha, Wis. “I had a lot of frustration, because I had to repackage and re-present my notes in a manner that makes sense to Medicare but makes no sense to physicians.”
Like it or not, healthcare providers live in a highly regulated world, says Richard D. Pinson, MD, FACP, CCS, who became a certified coding specialist and formed his own consulting company, Houston-based HCQ Consulting, to help hospitals and physicians achieve diagnostic accuracy for inpatient care. Documentation and coding have become a serious, high-stakes word game, he says. “Perfectly good clinical documentation, especially with some important diagnoses, may not correspond at all to what is required by the strict coding rules that govern code assignments,” he says.
A hospitalist’s documentation is at the heart of accurate coding, whether it’s for the hospital’s DRG reimbursement, quality and performance scores, or for assigning current procedural terminology (CPT) and evaluation and management (E/M) codes for billing for their own professional services. And if hospitalists don’t buy into the coding mindset, they risk decreased reimbursement for their services, monetary losses for the hospital, Medicare audits, compromised quality scores for both the hospital and themselves, and noncompliance.
“If your documentation is not up to par, then the hospital may get fined and lose money, and you can’t prove your worth as a hospitalist,” Dr. Nweke says.
What’s at Stake?
Inadequate documentation results in “undercoding” a patient’s condition and underpayment to your hospital (see Table 1, right). Undercoding also can result in inadequate representation of the severity of a patient’s illness, complexity, and cost of care. If a patient gets worse in the hospital, then that initial lower severity of illness might show up in poor performance scores on outcome measures. If a patient’s severity of illness is miscoded, Medicare might question the medical necessity for inpatient admission and deny payment.
On the other hand, if overcoding occurs because the clinical criteria for a specific diagnosis have not been met, Medicare will take action to recover the overpayment, leveling penalties and sanctions. (For more information on Medicare’s Recovery Audit Contractor program, dubbed “Medicare’s repo men” by Dr. Pinson, see “Take Proactive Approach to Recovery Audit Contractors,” p. 28.)
Lack of specificity also hampers reimbursement for professional fees, says Barb Pierce, CCS-P, ACS-EM, president of Barb Pierce Coding and Consulting Inc. of West Des Moines, Iowa. “Unfortunately,” she observes, “the code isn’t just based on decision-making, which is why physicians went to school for all those years. The guidelines [Documentation Guidelines for Evaluation and Management Services] mandate that if you forget one little bullet in history or examination, even if you’ve got the riskiest, highest-level, decision-making patient in front of you, that could pull down the whole code selection.”1
How costly might such small mistakes be for an HM group? According to the State of Hospital Medicine: 2010 Report Based on 2009 Data survey, internal-medicine hospitalists generate a median of 1.86 work relative value units (wRVUs) per encounter, and collect $45.57 per wRVU.2 If a hospitalist has 2,200 encounters per year and averages only 1.65 wRVUs per encounter, improving documentation and coding performance could add an additional 0.21 wRVUs, meeting the national average. Multiplying those 2,200 encounters by the national average of 1.86, the hospitalist could potentially add an additional 462 wRVUs for the year. Such documentation improvement—up to the national average—would equate to $21,053 in additional billed revenue without increasing the physician’s overall workload.
Dr. Pinson explains that physicians often perceive their time constraints as so severe that they’d be hard pressed to find the time to learn about documentation and coding. But he maintains that even short seminars yield “a huge amount of information that would astound [hospitalists], in terms of usefulness for their own clinical practices.”
Barriers to the Coding Mindset
Most hospitalists receive little or no training in documentation and coding during medical school or residency. The lack of education is further complicated because there are several coding sets healthcare providers must master, each with different rules governing assignment of diagnoses and levels of care (see “Coding Sets: Separate but Overlapping,” above).
Inexperience with coding guidelines can lead to mismatches. Nelly Leon-Chisen, RHIA, director of coding and classification for the American Hospital Association (AHA), gives one example: The ICD-9-CM Official Coding Guideline stipulates that coders cannot assign diagnosis codes based on lab results.3 So although it might appear intuitive to a physician that repeated blood sugars and monitoring of insulin levels indicate a patient has diabetes, the coder cannot assign the diagnosis unless it’s explicitly stated in the record.
Some physicians could simply be using outmoded terminology, such as “renal insufficiency” instead of “acute renal failure,” Dr. Pinson notes. If hospitalists learn to focus on evidence-based clinical criteria to support the codes, it leads to more effective care, he says.
The nature of hospitalist programs might not lend itself to efficient revenue-cycle processes for their own professional billing, says Jeri Leong, RN, CPC, CPC-H, president and CEO of Honolulu-based Healthcare Coding Consultants of Hawaii. If the HM group contracts with several hospitals, the hospitalists will be together rarely as a group, “so they don’t have the luxury of sitting down together with their billers to get important feedback and coding updates,” she says.
Leong’s company identifies missed charges, for instance, when charge tags from different shifts do not get married together (Hospitalist A might round on the patient in the morning and turn in a charge tag; Hospitalist B might do a procedure in the afternoon, but the two tags do not get combined). Examples such as these, she says, “can be an issue from a compliance perspective, and can leave money on the table.”
One of the problems Kathy DeVault, RHIA, CCS, CCS-P, manager of professional practice resources for the American Health Information Management Association (AHIMA), sees is a lack of continuity between initial admitting diagnosis and discharge summaries. For example, a hospitalist might admit a patient for acute renal failure—the correct diagnosis—and be able to reverse the condition fairly quickly, especially if the failure is due to dehydration.
The patient, whose issue is resolved, could be discharged by an attending physician who does not note the acute diagnosis in the summary. “That acute condition disappears, and the RAC auditor may then challenge the claim for payment,” DeVault says.
The Remedies
While physicians might think that they don’t have the time to acquire coding education, there could be other incentives coming down the pike. Dr. Pinson has noticed that hospitals are beginning to incorporate documentation accuracy into their contractual reimbursement formulas.
Documentation fixes vary according to domain. A hospital’s clinical documentation specialists can query physicians for clarity and detail in their notes; for instance, a diagnosis of congestive heart failure (CHF) must be accompanied by additional documentation stating whether the CHF is acute or chronic, and whether it is systolic or diastolic.
Many hospitals have instituted clinical documentation improvement (CDI) programs, sometimes called clinical documentation integrity programs, to address documentation discrepancies. CDI programs are essential to hospitals’ financial survival, Dr. Pinson says, and hospitalists are ideally positioned to join those efforts.
“[The hospitalists] are the most important people to the hospital in all of this,” he says. “They’re at the center of this whirlpool. If you have these skills, your value to the hospital and to your group is greatly enhanced.” (Visit the-hospitalist.org to listen to Dr. Pinson discuss HM’s role in documentation improvement.)
Leon-Chisen also says that the relationship between coders and physicians should be collaborative. “If it’s adversarial, nobody wins,” she points out, adding that CDI programs present an opportunity for mutual education.
Conducting audits of the practice’s documentation and coding can identify coding strengths and weaknesses, says Pierce, who is faculty for SHM’s billing and coding pre-course and regularly consults with hospitalist groups. Audits are helpful, she says, not just for increasing group revenue, but for compliance reasons as well. “You need to know what you’re doing well, and what you’re not doing quite so well, and get it fixed internally before an entity like Medicare discovers it,” she says.
It’s no doubt difficult for a busy HM group to stay on top of annual coding updates and changes to guidelines for reporting their services, Leong notes. Her company has worked with many hospitalist groups over the years, offering coding workshops, “back end” audits, and real-time feedback of E/M and CPT coding choices. If all of the hospitalists in a group cannot convene simultaneously, Leong provides the feedback (in the form of a scorecard) to the group’s physician champion, who becomes the lead contact to help those physicians who struggle more with their coding. (Leong talks more about real-time feedback and capturing CPT and E/M codes at the-hospitalist.org.)
In lieu of hiring professional coders, some HM groups use electronic coding devices. The software could be a standalone product, or it could interface with other products, such as electronic medical records (EMRs). These programs assist with a variety of coding-related activities, such as CPT or ICD-9 lookups, or calculation of E/M key components with assignment of an appropriate level of billing. Leong, however, cautions too much reliance on technology.
“While these devices can be accurate, compact, and convenient, it’s important to maintain a current [software] subscription to keep abreast of updates to the code sets, which occur sometimes as often as quarterly,” she says.
Pierce adds that coding tools should be double-checked against an audit tool. She has sometimes found discrepancies when auditing against an EMR product that assigns the E/M level.
Attitude Adjustment
Coding experts emphasize that physicians need not worry about mastering coding manuals, but they should forge relationships with both their hospital’s billers and the coders for their practice.
Dr. Nweke took advantage of coding and billing workshops offered by her group, HMG, and through the seminars began to understand what a DRG meant not just for her hospital but for her own evaluations and the expansion of her HM group, too. “Now, when I get questions from billers and coders, I try to answer them quickly,” she says. “I don’t look upon them as the enemy, but rather as people who are helping me document appropriately, so I don’t get audited by Medicare. I think the way you view the coders and billers definitely affects your willingness to learn.”
Dr. Nweke also takes a broader view of her role as a hospitalist. “You are there to take care of patients and assist with transitioning them in and out of the hospital, but you’re also there to ensure that the hospital remains afloat financially,” she says. “Your documentation plays a huge role in that. We have a huge contribution to make.”
The patient gains, too, says Leon-Chisen, who explains that documentation should be as accurate as possible “because someone else—the patient’s primary physician—will be taking over care of that patient and needs to understand what happened in the hospital.”
“The bottom line,” Dr. Pinson says, “is that we need accurate documentation that can be correctly coded to reflect the true complexity of care and severity of illness. If we do that, good things will follow.” TH
Gretchen Henkel is a freelance writer based in California.
References
- 1997 Documentation Guidelines for Evaluation and Management Services. Centers for Medicare & Medicaid Services website. Available at: www.cms.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed April 11, 2011.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Society of Hospital Medicine and Medical Group Management Association; Philadelphia and Englewood, Colo.; 2010.
- ICD-9-CM Official Coding Guidelines. CMS and National Center for Health Statistics; Washington, D.C.; 2008. Available at: www.ama-assn.org/resources/doc/cpt/icd9cm_coding_guidelines_08_09_full.pdf. Accessed April 10, 2011.
Take Proactive Approach to Recovery Audit Contractors
The congressionally authorized Medicare Recovery Audit Contractor (RAC) program began with a three-year demonstration pilot project in 2005. In August 2010, the program expanded to the entire country. The RAC’s main objective is to identify improper Medicare payments, both overpayments and underpayments, to providers. CMS, which administrates Medicare and the RAC program, has agreements with contractors who are authorized to audit and review claims that are up to three years old.
According to Elizabeth Baskett, senior associate director of policy at the AHA, medical necessity review was a big focus of the RAC demonstration project and now is “under way in the permanent RAC program. We are bracing ourselves for a significant amount of denials.”
The AHA has created a free, Web-based survey called RAC Trac (www.aha.org/aha/issues/RAC/ractrac.html) to assess the nationwide impact the RAC program has on U.S. hospitals. In a report released Feb. 24, the RAC Trac survey shows that $82 million in denials were reported, more than double the dollar amount of denials reported in the third quarter of 2010 (see Figure 1, below). It also shows 57% of the more than 1,850 participating hospitals cited “medically unnecessary” as a reason for a denial of a claim.
Nearly 80% of the participating hospitals reported RAC activity in 2010, with general medical and surgical hospitals reporting the most activity. Fifty percent of reporting hospitals noted that their administrative burden—in the form of hiring consultants, copying medical records, hiring legal counsel, and the like—had increased as a result of RAC activity.
Most importantly, the report shows the average dollar value of automated denials was $399. But when a complex review—one involving a human review of requested records—was conducted, the average value of the denial was $5,281. Additionally, inpatient facilities were most likely to experience complex denials, which account for 90% of the value of denied claims.
Leong says RAC audits are just one area of “exposure to review for hospitals and providers. Other third-party payers, including individual commercial insurance companies,” she says, “also do routine post-payment review and recoupment, several years after payment.”—GH