User login
Transient tachypnea of newborn increases bronchiolitis risk
MADRID – A new Finnish study raises a provocative question: Is transient tachypnea of the newborn really transient?
Transient tachypnea of the newborn (TTN) has traditionally been viewed as a benign, self-limited condition involving 1-3 days of respiratory distress. But data from Finland’s comprehensive national health registries indicate that TTN in term babies is associated with significantly increased risk of subsequent bronchiolitis during infancy, Otto Helve, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“This association suggests similar pathogenic mechanisms in transient tachypnea of the newborn and bronchiolitis. We suggest that an intrinsic defect in sodium ion–driven pulmonary fluid transport may predispose to clinically significant bronchiolitis during the first year of life,” said Dr. Helve, a pediatrician at the National Institute for Health and Welfare, Helsinki, and the University of Helsinki.
Of more than 1 million term babies born in Finland during 1996-2015, 17,569 were diagnosed with TTN. During the same period, 40,338 infants were hospitalized with a diagnosis of bronchiolitis attributable to respiratory syncytial virus infection.
In a multivariate analysis adjusted for birth year, gender, delivery method, gestational age, and parity, TTN was independently associated with a 1.2-fold increased risk of bronchiolitis during the first year of life.
Dr. Helve reported having no financial conflicts of interest regarding his study.

MADRID – A new Finnish study raises a provocative question: Is transient tachypnea of the newborn really transient?
Transient tachypnea of the newborn (TTN) has traditionally been viewed as a benign, self-limited condition involving 1-3 days of respiratory distress. But data from Finland’s comprehensive national health registries indicate that TTN in term babies is associated with significantly increased risk of subsequent bronchiolitis during infancy, Otto Helve, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“This association suggests similar pathogenic mechanisms in transient tachypnea of the newborn and bronchiolitis. We suggest that an intrinsic defect in sodium ion–driven pulmonary fluid transport may predispose to clinically significant bronchiolitis during the first year of life,” said Dr. Helve, a pediatrician at the National Institute for Health and Welfare, Helsinki, and the University of Helsinki.
Of more than 1 million term babies born in Finland during 1996-2015, 17,569 were diagnosed with TTN. During the same period, 40,338 infants were hospitalized with a diagnosis of bronchiolitis attributable to respiratory syncytial virus infection.
In a multivariate analysis adjusted for birth year, gender, delivery method, gestational age, and parity, TTN was independently associated with a 1.2-fold increased risk of bronchiolitis during the first year of life.
Dr. Helve reported having no financial conflicts of interest regarding his study.
MADRID – A new Finnish study raises a provocative question: Is transient tachypnea of the newborn really transient?
Transient tachypnea of the newborn (TTN) has traditionally been viewed as a benign, self-limited condition involving 1-3 days of respiratory distress. But data from Finland’s comprehensive national health registries indicate that TTN in term babies is associated with significantly increased risk of subsequent bronchiolitis during infancy, Otto Helve, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“This association suggests similar pathogenic mechanisms in transient tachypnea of the newborn and bronchiolitis. We suggest that an intrinsic defect in sodium ion–driven pulmonary fluid transport may predispose to clinically significant bronchiolitis during the first year of life,” said Dr. Helve, a pediatrician at the National Institute for Health and Welfare, Helsinki, and the University of Helsinki.
Of more than 1 million term babies born in Finland during 1996-2015, 17,569 were diagnosed with TTN. During the same period, 40,338 infants were hospitalized with a diagnosis of bronchiolitis attributable to respiratory syncytial virus infection.
In a multivariate analysis adjusted for birth year, gender, delivery method, gestational age, and parity, TTN was independently associated with a 1.2-fold increased risk of bronchiolitis during the first year of life.
Dr. Helve reported having no financial conflicts of interest regarding his study.
AT ESPID 2017
Key clinical point:
Major finding: Transient tachypnea of the newborn was independently associated with a 1.2-fold increased risk of bronchiolitis during the first year of life of Finnish term babies.
Data source: This population-based case-control study included 17,569 Finnish term babies diagnosed with transient tachypnea of the newborn and 40,338 diagnosed with bronchiolitis.
Disclosures: Dr. Helve reported having no financial conflicts of interest.
Metabolic syndrome doesn’t cause hand osteoarthritis
LAS VEGAS – Metabolic syndrome is not causally related to hand osteoarthritis, according to data from the Framingham Offspring Study.
The new Framingham analysis, which features rigorous longitudinal follow-up, puts a serious dent in the popular hypothesis that metabolic syndrome is a risk factor for osteoarthritis through the proposed mechanism of systemic inflammation, Ida K. Haugen, MD, said at the World Congress on Osteoarthritis.

In recent years, the growing obesity epidemic and the related phenomenon of the metabolic syndrome have been posited to be the hub around which a variety of chronic diseases orbit, including type 2 diabetes, cardiovascular disease, some cancers, and osteoarthritis. Hand osteoarthritis is the phenotype of osteoarthritis best suited to investigation of whether metabolic syndrome promotes osteoarthritis by creating a systemic inflammatory state. Unlike knee, hip, or ankle osteoarthritis, the obesity that is a core feature of metabolic syndrome doesn’t cause much extra loading of the finger joints, Dr. Haugen explained at the meeting sponsored by the Osteoarthritis Research Society International.
Dr. Haugen, a rheumatologist at Diakonhjemmet Hospital in Oslo, presented an analysis of 1,089 Framingham Offspring Study participants aged 50-75 years at baseline, all free of rheumatoid arthritis and all with baseline hand radiographs. Of those patients, 41% met American Heart Association criteria for metabolic syndrome. In a cross-sectional analysis at baseline, the prevalence of metabolic syndrome in the subgroup with baseline hand osteoarthritis was no different from that in those without the disease.
The focus of the study involved the 785 patients who had both baseline hand radiographs and repeat hand x-rays at 7 years of follow-up. At baseline, 199 of these patients (25%) already had hand osteoarthritis, as defined by two or more interphalangeal joints with Kellgren-Lawrence grade 2-4 findings, and 49 patients had erosive hand osteoarthritis.
In a cross-sectional analysis at baseline, there was no association between metabolic syndrome and hand osteoarthritis. In contrast to the findings in earlier studies by other investigators, metabolic syndrome was actually associated with a significantly reduced risk of erosive hand osteoarthritis. Indeed, in a logistic regression analysis adjusted for age, sex, and body mass index, having metabolic syndrome was associated with a 58% reduction in the risk of prevalent erosive hand osteoarthritis.
During a mean follow-up of 7 years, 26% of patients who were free of hand osteoarthritis at baseline developed the condition. Of those, 8% developed incident erosive hand osteoarthritis. Metabolic syndrome was unrelated to the risk of these conditions.
Moreover, among patients with baseline hand osteoarthritis, there was no association between having metabolic syndrome and worsening Kellgren-Lawrence scores over time.
“We found no dose-response relationship between the number of metabolic syndrome components and the risk of developing hand osteoarthritis during follow-up,” according to the rheumatologist. “Those with all five components present did not have any higher risk of hand osteoarthritis, compared with those with no components.”
When she and her coinvestigators looked at the impact of the individual components of metabolic syndrome, they found a significant association between hypertension and worsening Kellgren-Lawrence scores over time. In an analysis adjusted for age, sex, and body mass index, having hypertension was associated with a 47% increased likelihood of radiographic worsening in patients with hand osteoarthritis at baseline. However, the association between hypertension and incident hand osteoarthritis was weaker and not statistically significant.
Drilling down further, the investigators found a dose-response relationship between the quartile of diastolic blood pressure and the risk of having hand osteoarthritis at baseline. This was not the case for systolic blood pressure, however. The apparent association between hypertension and hand osteoarthritis is worthy of further exploration, Dr. Haugen said.
None of the other elements of the metabolic syndrome showed any relationship with hand osteoarthritis risk.
The Framingham Offspring Study is supported by the National Heart, Lung, and Blood Institute. Dr. Haugen’s involvement was supported by Extrastiftelsen. She reported having no financial conflicts of interest.
LAS VEGAS – Metabolic syndrome is not causally related to hand osteoarthritis, according to data from the Framingham Offspring Study.
The new Framingham analysis, which features rigorous longitudinal follow-up, puts a serious dent in the popular hypothesis that metabolic syndrome is a risk factor for osteoarthritis through the proposed mechanism of systemic inflammation, Ida K. Haugen, MD, said at the World Congress on Osteoarthritis.
In recent years, the growing obesity epidemic and the related phenomenon of the metabolic syndrome have been posited to be the hub around which a variety of chronic diseases orbit, including type 2 diabetes, cardiovascular disease, some cancers, and osteoarthritis. Hand osteoarthritis is the phenotype of osteoarthritis best suited to investigation of whether metabolic syndrome promotes osteoarthritis by creating a systemic inflammatory state. Unlike knee, hip, or ankle osteoarthritis, the obesity that is a core feature of metabolic syndrome doesn’t cause much extra loading of the finger joints, Dr. Haugen explained at the meeting sponsored by the Osteoarthritis Research Society International.
Dr. Haugen, a rheumatologist at Diakonhjemmet Hospital in Oslo, presented an analysis of 1,089 Framingham Offspring Study participants aged 50-75 years at baseline, all free of rheumatoid arthritis and all with baseline hand radiographs. Of those patients, 41% met American Heart Association criteria for metabolic syndrome. In a cross-sectional analysis at baseline, the prevalence of metabolic syndrome in the subgroup with baseline hand osteoarthritis was no different from that in those without the disease.
The focus of the study involved the 785 patients who had both baseline hand radiographs and repeat hand x-rays at 7 years of follow-up. At baseline, 199 of these patients (25%) already had hand osteoarthritis, as defined by two or more interphalangeal joints with Kellgren-Lawrence grade 2-4 findings, and 49 patients had erosive hand osteoarthritis.
In a cross-sectional analysis at baseline, there was no association between metabolic syndrome and hand osteoarthritis. In contrast to the findings in earlier studies by other investigators, metabolic syndrome was actually associated with a significantly reduced risk of erosive hand osteoarthritis. Indeed, in a logistic regression analysis adjusted for age, sex, and body mass index, having metabolic syndrome was associated with a 58% reduction in the risk of prevalent erosive hand osteoarthritis.
During a mean follow-up of 7 years, 26% of patients who were free of hand osteoarthritis at baseline developed the condition. Of those, 8% developed incident erosive hand osteoarthritis. Metabolic syndrome was unrelated to the risk of these conditions.
Moreover, among patients with baseline hand osteoarthritis, there was no association between having metabolic syndrome and worsening Kellgren-Lawrence scores over time.
“We found no dose-response relationship between the number of metabolic syndrome components and the risk of developing hand osteoarthritis during follow-up,” according to the rheumatologist. “Those with all five components present did not have any higher risk of hand osteoarthritis, compared with those with no components.”
When she and her coinvestigators looked at the impact of the individual components of metabolic syndrome, they found a significant association between hypertension and worsening Kellgren-Lawrence scores over time. In an analysis adjusted for age, sex, and body mass index, having hypertension was associated with a 47% increased likelihood of radiographic worsening in patients with hand osteoarthritis at baseline. However, the association between hypertension and incident hand osteoarthritis was weaker and not statistically significant.
Drilling down further, the investigators found a dose-response relationship between the quartile of diastolic blood pressure and the risk of having hand osteoarthritis at baseline. This was not the case for systolic blood pressure, however. The apparent association between hypertension and hand osteoarthritis is worthy of further exploration, Dr. Haugen said.
None of the other elements of the metabolic syndrome showed any relationship with hand osteoarthritis risk.
The Framingham Offspring Study is supported by the National Heart, Lung, and Blood Institute. Dr. Haugen’s involvement was supported by Extrastiftelsen. She reported having no financial conflicts of interest.
LAS VEGAS – Metabolic syndrome is not causally related to hand osteoarthritis, according to data from the Framingham Offspring Study.
The new Framingham analysis, which features rigorous longitudinal follow-up, puts a serious dent in the popular hypothesis that metabolic syndrome is a risk factor for osteoarthritis through the proposed mechanism of systemic inflammation, Ida K. Haugen, MD, said at the World Congress on Osteoarthritis.
In recent years, the growing obesity epidemic and the related phenomenon of the metabolic syndrome have been posited to be the hub around which a variety of chronic diseases orbit, including type 2 diabetes, cardiovascular disease, some cancers, and osteoarthritis. Hand osteoarthritis is the phenotype of osteoarthritis best suited to investigation of whether metabolic syndrome promotes osteoarthritis by creating a systemic inflammatory state. Unlike knee, hip, or ankle osteoarthritis, the obesity that is a core feature of metabolic syndrome doesn’t cause much extra loading of the finger joints, Dr. Haugen explained at the meeting sponsored by the Osteoarthritis Research Society International.
Dr. Haugen, a rheumatologist at Diakonhjemmet Hospital in Oslo, presented an analysis of 1,089 Framingham Offspring Study participants aged 50-75 years at baseline, all free of rheumatoid arthritis and all with baseline hand radiographs. Of those patients, 41% met American Heart Association criteria for metabolic syndrome. In a cross-sectional analysis at baseline, the prevalence of metabolic syndrome in the subgroup with baseline hand osteoarthritis was no different from that in those without the disease.
The focus of the study involved the 785 patients who had both baseline hand radiographs and repeat hand x-rays at 7 years of follow-up. At baseline, 199 of these patients (25%) already had hand osteoarthritis, as defined by two or more interphalangeal joints with Kellgren-Lawrence grade 2-4 findings, and 49 patients had erosive hand osteoarthritis.
In a cross-sectional analysis at baseline, there was no association between metabolic syndrome and hand osteoarthritis. In contrast to the findings in earlier studies by other investigators, metabolic syndrome was actually associated with a significantly reduced risk of erosive hand osteoarthritis. Indeed, in a logistic regression analysis adjusted for age, sex, and body mass index, having metabolic syndrome was associated with a 58% reduction in the risk of prevalent erosive hand osteoarthritis.
During a mean follow-up of 7 years, 26% of patients who were free of hand osteoarthritis at baseline developed the condition. Of those, 8% developed incident erosive hand osteoarthritis. Metabolic syndrome was unrelated to the risk of these conditions.
Moreover, among patients with baseline hand osteoarthritis, there was no association between having metabolic syndrome and worsening Kellgren-Lawrence scores over time.
“We found no dose-response relationship between the number of metabolic syndrome components and the risk of developing hand osteoarthritis during follow-up,” according to the rheumatologist. “Those with all five components present did not have any higher risk of hand osteoarthritis, compared with those with no components.”
When she and her coinvestigators looked at the impact of the individual components of metabolic syndrome, they found a significant association between hypertension and worsening Kellgren-Lawrence scores over time. In an analysis adjusted for age, sex, and body mass index, having hypertension was associated with a 47% increased likelihood of radiographic worsening in patients with hand osteoarthritis at baseline. However, the association between hypertension and incident hand osteoarthritis was weaker and not statistically significant.
Drilling down further, the investigators found a dose-response relationship between the quartile of diastolic blood pressure and the risk of having hand osteoarthritis at baseline. This was not the case for systolic blood pressure, however. The apparent association between hypertension and hand osteoarthritis is worthy of further exploration, Dr. Haugen said.
None of the other elements of the metabolic syndrome showed any relationship with hand osteoarthritis risk.
The Framingham Offspring Study is supported by the National Heart, Lung, and Blood Institute. Dr. Haugen’s involvement was supported by Extrastiftelsen. She reported having no financial conflicts of interest.
AT OARSI 2017
Key clinical point:
Major finding: Patients with metabolic syndrome are not at increased risk of developing hand osteoarthritis, erosive hand osteoarthritis, or accelerated progression of existing hand osteoarthritis.
Data source: A prospective observational study of 785 patients with hand radiographs at baseline and 7 years’ follow-up, during which 26% developed new-onset hand osteoarthritis.
Disclosures: The Framingham Offspring Study is supported by the National Heart, Lung, and Blood Institute. Dr. Haugen’s involvement was supported by Extrastiftelsen. She reported having no financial conflicts of interest.

Knee bone density improved in osteoarthritis with load-reducing shoe
LAS VEGAS – Patients with medial compartment knee osteoarthritis who wore a patented flexible mobility shoe experienced a favorable reduction in medial tibial bone mineral density that directly correlated with their improved gait biomechanics and reduced peak knee adduction moment, Najia Shakoor, MD, reported at the World Congress on Osteoarthritis.
“Our results suggest that bone can be modified with sustained load reduction and that evaluation of tibial bone density may be an inexpensive tool for evaluating the consequences of load-reducing interventions,” said Dr. Shakoor, a rheumatologist at Rush University in Chicago.
Indeed, measuring changes in medial tibial bone density over time via serial dual x-ray absorptiometry is an attractive surrogate anatomic marker of a patient’s response to a biomechanical load-reducing intervention such as a special shoe or knee brace, Dr. Shakoor noted at the meeting sponsored by the Osteoarthritis Research Society International.
After all, she added, bone density measurement is simpler than sending a patient to a motion analysis laboratory for multicamera gait analysis using a force plate to evaluate changes in the peak external knee adduction moment (a validated marker of load distribution across the tibial plateau).
Studies suggest that bone, not cartilage, bears the bulk of the load burden across the knee joint. That’s why patients with knee osteoarthritis have increased proximal tibial bone mineral density. Dr. Shakoor presented evidence that sustained reduction in dynamic knee loading results in a proportionate reduction in medial tibial bone density over the course of 6 months.
She reported on 51 patients with mild to moderate radiographic and symptomatic medial compartment knee osteoarthritis who were randomized to wear a commercially available flexible mobility shoe or a similar-looking but nonflexible control shoe for 6 hours per day for at least 6 days per week for 6 months. At baseline and again at 6 months, the participants underwent knee bone density measurement and formal gait analysis.
Peak knee adduction moment decreased by 14% over the course of 6 months in the flexible shoe group, significantly greater than the 6% reduction in the controls. Moreover, Dr. Shakoor and her coinvestigators documented a significant reduction in medial tibial bone density in the flexible shoe group. The greater the improvement in knee adduction moment, the larger the reduction in bone density.
In contrast, medial tibial bone density didn’t change significantly in the controls.
Dr. Shakoor said that she had also expected to see a reduction in the ratio of medial to lateral tibial bone density in the flexible shoe group. However, there was no statistically significant change, although there was a trend in that direction.
Asked if reduction in knee adduction moment and/or medial tibial bone density correlated with improved knee pain scores, Dr. Shakoor replied that almost everyone in the study reported improvement in pain, suggesting a placebo effect for that endpoint. In any event, the relatively small study wasn’t powered to evaluate change in pain over time.
The Arthritis Foundation funded the study. Dr. Shakoor is coinventor of the flexible shoe used in the study. The patent, owned by Rush University, has been licensed to Dr. Comfort, which markets the shoe as the Dr. Comfort Flex-OA Mobility Shoe. A percentage of the proceeds from shoe sales is distributed to the university and the coinventors.
LAS VEGAS – Patients with medial compartment knee osteoarthritis who wore a patented flexible mobility shoe experienced a favorable reduction in medial tibial bone mineral density that directly correlated with their improved gait biomechanics and reduced peak knee adduction moment, Najia Shakoor, MD, reported at the World Congress on Osteoarthritis.
“Our results suggest that bone can be modified with sustained load reduction and that evaluation of tibial bone density may be an inexpensive tool for evaluating the consequences of load-reducing interventions,” said Dr. Shakoor, a rheumatologist at Rush University in Chicago.
Indeed, measuring changes in medial tibial bone density over time via serial dual x-ray absorptiometry is an attractive surrogate anatomic marker of a patient’s response to a biomechanical load-reducing intervention such as a special shoe or knee brace, Dr. Shakoor noted at the meeting sponsored by the Osteoarthritis Research Society International.
After all, she added, bone density measurement is simpler than sending a patient to a motion analysis laboratory for multicamera gait analysis using a force plate to evaluate changes in the peak external knee adduction moment (a validated marker of load distribution across the tibial plateau).
Studies suggest that bone, not cartilage, bears the bulk of the load burden across the knee joint. That’s why patients with knee osteoarthritis have increased proximal tibial bone mineral density. Dr. Shakoor presented evidence that sustained reduction in dynamic knee loading results in a proportionate reduction in medial tibial bone density over the course of 6 months.
She reported on 51 patients with mild to moderate radiographic and symptomatic medial compartment knee osteoarthritis who were randomized to wear a commercially available flexible mobility shoe or a similar-looking but nonflexible control shoe for 6 hours per day for at least 6 days per week for 6 months. At baseline and again at 6 months, the participants underwent knee bone density measurement and formal gait analysis.
Peak knee adduction moment decreased by 14% over the course of 6 months in the flexible shoe group, significantly greater than the 6% reduction in the controls. Moreover, Dr. Shakoor and her coinvestigators documented a significant reduction in medial tibial bone density in the flexible shoe group. The greater the improvement in knee adduction moment, the larger the reduction in bone density.
In contrast, medial tibial bone density didn’t change significantly in the controls.
Dr. Shakoor said that she had also expected to see a reduction in the ratio of medial to lateral tibial bone density in the flexible shoe group. However, there was no statistically significant change, although there was a trend in that direction.
Asked if reduction in knee adduction moment and/or medial tibial bone density correlated with improved knee pain scores, Dr. Shakoor replied that almost everyone in the study reported improvement in pain, suggesting a placebo effect for that endpoint. In any event, the relatively small study wasn’t powered to evaluate change in pain over time.
The Arthritis Foundation funded the study. Dr. Shakoor is coinventor of the flexible shoe used in the study. The patent, owned by Rush University, has been licensed to Dr. Comfort, which markets the shoe as the Dr. Comfort Flex-OA Mobility Shoe. A percentage of the proceeds from shoe sales is distributed to the university and the coinventors.
LAS VEGAS – Patients with medial compartment knee osteoarthritis who wore a patented flexible mobility shoe experienced a favorable reduction in medial tibial bone mineral density that directly correlated with their improved gait biomechanics and reduced peak knee adduction moment, Najia Shakoor, MD, reported at the World Congress on Osteoarthritis.
“Our results suggest that bone can be modified with sustained load reduction and that evaluation of tibial bone density may be an inexpensive tool for evaluating the consequences of load-reducing interventions,” said Dr. Shakoor, a rheumatologist at Rush University in Chicago.
Indeed, measuring changes in medial tibial bone density over time via serial dual x-ray absorptiometry is an attractive surrogate anatomic marker of a patient’s response to a biomechanical load-reducing intervention such as a special shoe or knee brace, Dr. Shakoor noted at the meeting sponsored by the Osteoarthritis Research Society International.
After all, she added, bone density measurement is simpler than sending a patient to a motion analysis laboratory for multicamera gait analysis using a force plate to evaluate changes in the peak external knee adduction moment (a validated marker of load distribution across the tibial plateau).
Studies suggest that bone, not cartilage, bears the bulk of the load burden across the knee joint. That’s why patients with knee osteoarthritis have increased proximal tibial bone mineral density. Dr. Shakoor presented evidence that sustained reduction in dynamic knee loading results in a proportionate reduction in medial tibial bone density over the course of 6 months.
She reported on 51 patients with mild to moderate radiographic and symptomatic medial compartment knee osteoarthritis who were randomized to wear a commercially available flexible mobility shoe or a similar-looking but nonflexible control shoe for 6 hours per day for at least 6 days per week for 6 months. At baseline and again at 6 months, the participants underwent knee bone density measurement and formal gait analysis.
Peak knee adduction moment decreased by 14% over the course of 6 months in the flexible shoe group, significantly greater than the 6% reduction in the controls. Moreover, Dr. Shakoor and her coinvestigators documented a significant reduction in medial tibial bone density in the flexible shoe group. The greater the improvement in knee adduction moment, the larger the reduction in bone density.
In contrast, medial tibial bone density didn’t change significantly in the controls.
Dr. Shakoor said that she had also expected to see a reduction in the ratio of medial to lateral tibial bone density in the flexible shoe group. However, there was no statistically significant change, although there was a trend in that direction.
Asked if reduction in knee adduction moment and/or medial tibial bone density correlated with improved knee pain scores, Dr. Shakoor replied that almost everyone in the study reported improvement in pain, suggesting a placebo effect for that endpoint. In any event, the relatively small study wasn’t powered to evaluate change in pain over time.
The Arthritis Foundation funded the study. Dr. Shakoor is coinventor of the flexible shoe used in the study. The patent, owned by Rush University, has been licensed to Dr. Comfort, which markets the shoe as the Dr. Comfort Flex-OA Mobility Shoe. A percentage of the proceeds from shoe sales is distributed to the university and the coinventors.
AT OARSI 2017
Key clinical point:
Major finding: Knee osteoarthritis patients who wore a flexible mobility shoe designed to reduce dynamic loading of the joint had a 14% reduction in peak external knee adduction moment over a 6-month period, with a parallel decrease in medial tibial bone density.
Data source: A 6-month randomized trial involving 51 patients with symptomatic radiographic medial compartment knee osteoarthritis, who were assigned to wear a shoe designed to reduce dynamic knee loading or a similar-looking control shoe.
Disclosures: The Arthritis Foundation funded the study. Dr. Shakoor is coinventor of the flexible shoe used in the study. The patent, owned by Rush University, has been licensed to Dr. Comfort, which markets the shoe as the Dr. Comfort Flex-OA Mobility Shoe. A percentage of the proceeds from shoe sales is distributed to the university and the coinventors.
CRPM may be promising predictive biomarker for knee osteoarthritis
LAS VEGAS – , Anne-Christine Bay-Jensen, PhD, said at the World Congress on Osteoarthritis.

That way, investigators maximize the likelihood of obtaining a positive outcome undiluted by giving the therapy to the wrong patients.
CRPM shows preliminary evidence of passing muster on both counts, according to Dr. Bay-Jensen, head of rheumatology at Nordic Bioscience in Herløv, Denmark.
The Danish researcher introduced herself to the Las Vegas audience by announcing, “My purpose in life is to develop biomarkers for identifying phenotypes in osteoarthritis.”
Indeed, she has been a pioneer in investigating the clinical utility of CRPM, a degradation fragment of C-reactive protein that is produced in the joint and thus reflects joint-specific tissue inflammation. Unlike C-reactive protein, which is an acute phase reactant, CRPM reflects chronic inflammation, she explained at the meeting sponsored by the Osteoarthritis Research Society International.
Her early work with CRPM explored its use as a biomarker in rheumatoid arthritis (RA) patients. She demonstrated, for example, in a secondary analysis of the phase III, double-blind, placebo-controlled LITHE trial that an 11% reduction in CRPM at week 4 of treatment with tocilizumab (Actemra) plus methotrexate was associated with a fourfold increased likelihood of a clinical response at week 16. That finding indicates that utilizing CRPM as an early predictor of tocilizumab efficacy promotes a more targeted, cost-effective, and personalized use of the biologic agent.
At OARSI 2017, Dr. Bay-Jensen presented evidence that even though the mean serum CRPM is significantly higher in patients with RA than in those with knee osteoarthritis (KOA), one-third or more of KOA patients have levels of joint tissue inflammation comparable to that seen in RA. That patient subset with a highly inflammatory KOA phenotype would be the logical focus of future clinical trials of agents having potent anti-inflammatory effects, rather than potential therapies with bone- or cartilage-modifying effects.
The data came from a biomarker study of 113 patients with early RA, as well as from two Nordic Bioscience–sponsored phase III randomized, multicenter, placebo-controlled clinical trials of oral salmon calcitonin in a total of 2,306 patients with knee osteoarthritis, both of which proved negative (Osteoarthritis Cartilage. 2015 Apr;23[4]:532-43). The mean baseline CRPM in the early RA patients was 17.1 ng/mL, compared with 8.5 ng/mL in the KOA patients. However, 31% of KOA patients in one phase III oral calcitonin trial and 41% in the other had a baseline serum CRPM greater than 9 ng/mL, a level that overlapped with 75% of the RA patients.
A related substudy of the oral calcitonin trials examined CRPM as a predictive biomarker. It included 153 knees without OA at baseline, 50 of which developed radiographic evidence of KOA, as evidenced by a Kellgren-Lawrence grade of 2 or 3 during 2 years of prospective follow-up. A serum CRPM of 9 ng/mL or more at baseline was associated with a 4.6-fold increased likelihood of incident KOA during follow-up.
Nordic Bioscience, Dr. Bay-Jensen’s employer, markets numerous proprietary biomarker assays, including one for CRPM.
LAS VEGAS – , Anne-Christine Bay-Jensen, PhD, said at the World Congress on Osteoarthritis.
That way, investigators maximize the likelihood of obtaining a positive outcome undiluted by giving the therapy to the wrong patients.
CRPM shows preliminary evidence of passing muster on both counts, according to Dr. Bay-Jensen, head of rheumatology at Nordic Bioscience in Herløv, Denmark.
The Danish researcher introduced herself to the Las Vegas audience by announcing, “My purpose in life is to develop biomarkers for identifying phenotypes in osteoarthritis.”
Indeed, she has been a pioneer in investigating the clinical utility of CRPM, a degradation fragment of C-reactive protein that is produced in the joint and thus reflects joint-specific tissue inflammation. Unlike C-reactive protein, which is an acute phase reactant, CRPM reflects chronic inflammation, she explained at the meeting sponsored by the Osteoarthritis Research Society International.
Her early work with CRPM explored its use as a biomarker in rheumatoid arthritis (RA) patients. She demonstrated, for example, in a secondary analysis of the phase III, double-blind, placebo-controlled LITHE trial that an 11% reduction in CRPM at week 4 of treatment with tocilizumab (Actemra) plus methotrexate was associated with a fourfold increased likelihood of a clinical response at week 16. That finding indicates that utilizing CRPM as an early predictor of tocilizumab efficacy promotes a more targeted, cost-effective, and personalized use of the biologic agent.
At OARSI 2017, Dr. Bay-Jensen presented evidence that even though the mean serum CRPM is significantly higher in patients with RA than in those with knee osteoarthritis (KOA), one-third or more of KOA patients have levels of joint tissue inflammation comparable to that seen in RA. That patient subset with a highly inflammatory KOA phenotype would be the logical focus of future clinical trials of agents having potent anti-inflammatory effects, rather than potential therapies with bone- or cartilage-modifying effects.
The data came from a biomarker study of 113 patients with early RA, as well as from two Nordic Bioscience–sponsored phase III randomized, multicenter, placebo-controlled clinical trials of oral salmon calcitonin in a total of 2,306 patients with knee osteoarthritis, both of which proved negative (Osteoarthritis Cartilage. 2015 Apr;23[4]:532-43). The mean baseline CRPM in the early RA patients was 17.1 ng/mL, compared with 8.5 ng/mL in the KOA patients. However, 31% of KOA patients in one phase III oral calcitonin trial and 41% in the other had a baseline serum CRPM greater than 9 ng/mL, a level that overlapped with 75% of the RA patients.
A related substudy of the oral calcitonin trials examined CRPM as a predictive biomarker. It included 153 knees without OA at baseline, 50 of which developed radiographic evidence of KOA, as evidenced by a Kellgren-Lawrence grade of 2 or 3 during 2 years of prospective follow-up. A serum CRPM of 9 ng/mL or more at baseline was associated with a 4.6-fold increased likelihood of incident KOA during follow-up.
Nordic Bioscience, Dr. Bay-Jensen’s employer, markets numerous proprietary biomarker assays, including one for CRPM.
LAS VEGAS – , Anne-Christine Bay-Jensen, PhD, said at the World Congress on Osteoarthritis.
That way, investigators maximize the likelihood of obtaining a positive outcome undiluted by giving the therapy to the wrong patients.
CRPM shows preliminary evidence of passing muster on both counts, according to Dr. Bay-Jensen, head of rheumatology at Nordic Bioscience in Herløv, Denmark.
The Danish researcher introduced herself to the Las Vegas audience by announcing, “My purpose in life is to develop biomarkers for identifying phenotypes in osteoarthritis.”
Indeed, she has been a pioneer in investigating the clinical utility of CRPM, a degradation fragment of C-reactive protein that is produced in the joint and thus reflects joint-specific tissue inflammation. Unlike C-reactive protein, which is an acute phase reactant, CRPM reflects chronic inflammation, she explained at the meeting sponsored by the Osteoarthritis Research Society International.
Her early work with CRPM explored its use as a biomarker in rheumatoid arthritis (RA) patients. She demonstrated, for example, in a secondary analysis of the phase III, double-blind, placebo-controlled LITHE trial that an 11% reduction in CRPM at week 4 of treatment with tocilizumab (Actemra) plus methotrexate was associated with a fourfold increased likelihood of a clinical response at week 16. That finding indicates that utilizing CRPM as an early predictor of tocilizumab efficacy promotes a more targeted, cost-effective, and personalized use of the biologic agent.
At OARSI 2017, Dr. Bay-Jensen presented evidence that even though the mean serum CRPM is significantly higher in patients with RA than in those with knee osteoarthritis (KOA), one-third or more of KOA patients have levels of joint tissue inflammation comparable to that seen in RA. That patient subset with a highly inflammatory KOA phenotype would be the logical focus of future clinical trials of agents having potent anti-inflammatory effects, rather than potential therapies with bone- or cartilage-modifying effects.
The data came from a biomarker study of 113 patients with early RA, as well as from two Nordic Bioscience–sponsored phase III randomized, multicenter, placebo-controlled clinical trials of oral salmon calcitonin in a total of 2,306 patients with knee osteoarthritis, both of which proved negative (Osteoarthritis Cartilage. 2015 Apr;23[4]:532-43). The mean baseline CRPM in the early RA patients was 17.1 ng/mL, compared with 8.5 ng/mL in the KOA patients. However, 31% of KOA patients in one phase III oral calcitonin trial and 41% in the other had a baseline serum CRPM greater than 9 ng/mL, a level that overlapped with 75% of the RA patients.
A related substudy of the oral calcitonin trials examined CRPM as a predictive biomarker. It included 153 knees without OA at baseline, 50 of which developed radiographic evidence of KOA, as evidenced by a Kellgren-Lawrence grade of 2 or 3 during 2 years of prospective follow-up. A serum CRPM of 9 ng/mL or more at baseline was associated with a 4.6-fold increased likelihood of incident KOA during follow-up.
Nordic Bioscience, Dr. Bay-Jensen’s employer, markets numerous proprietary biomarker assays, including one for CRPM.
EXPERT ANALYSIS FROM OARSI 2017
Novel ibuprofen formulation cuts GI side effects in patients with knee pain flares
LAS VEGAS – A novel lipid formulation of ibuprofen given at 1,200 mg/day proved noninferior to high-dose standard ibuprofen at 2,400 mg/day for management of episodic knee pain flares in a phase III randomized trial, and it accomplished this with significantly fewer gastrointestinal side effects, Sita M.A. Bierma-Zeinstra, MD, reported.
Episodic flares of knee pain are a disabling feature of knee osteoarthritis that can occur at all stages of the disease, including prior to clinical diagnosis. There is a need for a fast-acting analgesic designed for short-term use with minimal side effects to provide pain relief during these flares. This was the motivation for developing Flarin, a lipid formulation soft-gel capsule of ibuprofen that is effective at less-than-standard doses of the conventional NSAID, she explained at the World Congress on Osteoarthritis.

The primary outcome was change in the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain subscale after 5 days of treatment. The score dropped from a mean of 5.72 at baseline out of a possible maximum of 10 to 3.05 in the lipid ibuprofen group, from 5.6 to 3.26 in patients on standard ibuprofen at 1,200 mg/day, and from 5.61 to 2.82 in subjects on standard ibuprofen at 2,400 mg/day. Those between-group differences were not statistically significant, reported Dr. Bierma-Zeinstra, professor of osteoarthritis and related disorders at Erasmus University Medical Center in Rotterdam.
In contrast, the rate of gastrointestinal side effects was significantly different across the three treatment arms: 16.2% in the lipid ibuprofen group, 22.6% with conventional ibuprofen at 1,200 mg/day, and 28.3% with ibuprofen at 2,400 mg/day, she said at the congress, which was sponsored by the Osteoarthritis Research Society International.
The group on the investigational formulation of ibuprofen also showed a consistent trend for superior results on the WOMAC swelling, pain, stiffness, and function subscales after 5 days of treatment, although only the improvement in swelling achieved statistical significance, Dr. Bierma-Zeinstra continued.
Flarin is approved and marketed in the United Kingdom. Infirst Healthcare, the novel NSAID’s developer and the sponsor of the phase III randomized trial, is seeking to gain regulatory approval throughout Europe. The U.K. company also has an agreement with McNeil Consumer Pharmaceuticals to market its products in the United States, once approved.
Dr. Bierma-Zeinstra reported having received a research grant from Infirst.
LAS VEGAS – A novel lipid formulation of ibuprofen given at 1,200 mg/day proved noninferior to high-dose standard ibuprofen at 2,400 mg/day for management of episodic knee pain flares in a phase III randomized trial, and it accomplished this with significantly fewer gastrointestinal side effects, Sita M.A. Bierma-Zeinstra, MD, reported.
Episodic flares of knee pain are a disabling feature of knee osteoarthritis that can occur at all stages of the disease, including prior to clinical diagnosis. There is a need for a fast-acting analgesic designed for short-term use with minimal side effects to provide pain relief during these flares. This was the motivation for developing Flarin, a lipid formulation soft-gel capsule of ibuprofen that is effective at less-than-standard doses of the conventional NSAID, she explained at the World Congress on Osteoarthritis.
The primary outcome was change in the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain subscale after 5 days of treatment. The score dropped from a mean of 5.72 at baseline out of a possible maximum of 10 to 3.05 in the lipid ibuprofen group, from 5.6 to 3.26 in patients on standard ibuprofen at 1,200 mg/day, and from 5.61 to 2.82 in subjects on standard ibuprofen at 2,400 mg/day. Those between-group differences were not statistically significant, reported Dr. Bierma-Zeinstra, professor of osteoarthritis and related disorders at Erasmus University Medical Center in Rotterdam.
In contrast, the rate of gastrointestinal side effects was significantly different across the three treatment arms: 16.2% in the lipid ibuprofen group, 22.6% with conventional ibuprofen at 1,200 mg/day, and 28.3% with ibuprofen at 2,400 mg/day, she said at the congress, which was sponsored by the Osteoarthritis Research Society International.
The group on the investigational formulation of ibuprofen also showed a consistent trend for superior results on the WOMAC swelling, pain, stiffness, and function subscales after 5 days of treatment, although only the improvement in swelling achieved statistical significance, Dr. Bierma-Zeinstra continued.
Flarin is approved and marketed in the United Kingdom. Infirst Healthcare, the novel NSAID’s developer and the sponsor of the phase III randomized trial, is seeking to gain regulatory approval throughout Europe. The U.K. company also has an agreement with McNeil Consumer Pharmaceuticals to market its products in the United States, once approved.
Dr. Bierma-Zeinstra reported having received a research grant from Infirst.
LAS VEGAS – A novel lipid formulation of ibuprofen given at 1,200 mg/day proved noninferior to high-dose standard ibuprofen at 2,400 mg/day for management of episodic knee pain flares in a phase III randomized trial, and it accomplished this with significantly fewer gastrointestinal side effects, Sita M.A. Bierma-Zeinstra, MD, reported.
Episodic flares of knee pain are a disabling feature of knee osteoarthritis that can occur at all stages of the disease, including prior to clinical diagnosis. There is a need for a fast-acting analgesic designed for short-term use with minimal side effects to provide pain relief during these flares. This was the motivation for developing Flarin, a lipid formulation soft-gel capsule of ibuprofen that is effective at less-than-standard doses of the conventional NSAID, she explained at the World Congress on Osteoarthritis.
The primary outcome was change in the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain subscale after 5 days of treatment. The score dropped from a mean of 5.72 at baseline out of a possible maximum of 10 to 3.05 in the lipid ibuprofen group, from 5.6 to 3.26 in patients on standard ibuprofen at 1,200 mg/day, and from 5.61 to 2.82 in subjects on standard ibuprofen at 2,400 mg/day. Those between-group differences were not statistically significant, reported Dr. Bierma-Zeinstra, professor of osteoarthritis and related disorders at Erasmus University Medical Center in Rotterdam.
In contrast, the rate of gastrointestinal side effects was significantly different across the three treatment arms: 16.2% in the lipid ibuprofen group, 22.6% with conventional ibuprofen at 1,200 mg/day, and 28.3% with ibuprofen at 2,400 mg/day, she said at the congress, which was sponsored by the Osteoarthritis Research Society International.
The group on the investigational formulation of ibuprofen also showed a consistent trend for superior results on the WOMAC swelling, pain, stiffness, and function subscales after 5 days of treatment, although only the improvement in swelling achieved statistical significance, Dr. Bierma-Zeinstra continued.
Flarin is approved and marketed in the United Kingdom. Infirst Healthcare, the novel NSAID’s developer and the sponsor of the phase III randomized trial, is seeking to gain regulatory approval throughout Europe. The U.K. company also has an agreement with McNeil Consumer Pharmaceuticals to market its products in the United States, once approved.
Dr. Bierma-Zeinstra reported having received a research grant from Infirst.
AT OARSI 2017
Key clinical point:
Major finding: The incidence of GI side effects in patients being treated for an episodic knee pain flare was 16.2% after 5 days of treatment with a novel lipid formulation of ibuprofen at 1,200 mg/day, significantly lower than in patients randomized to conventional ibuprofen soft-gel capsules at 1,200 or 2,400 mg/day.
Data source: This three-arm, multicenter, international randomized trial involved 462 patients experiencing a recent-onset episodic flare of knee pain.
Disclosures: The presenter reported having received a research grant from Infirst Healthcare, which funded the study.
How to prevent secondary posttraumatic knee osteoarthritis
LAS VEGAS – A variety of evidence-based strategies are available for preventing posttraumatic knee osteoarthritis (KOA) in patients who have already sustained an anterior cruciate ligament (ACL) injury. And they’re generally ignored, according to May Arna Risberg, PhD.
“We have a lot of knowledge. We can use secondary prevention strategies. And here I think we, as physical therapists, physicians, and orthopedic surgeons, are doing a lousy job because we are sending these ACL-injured patients back to sports before they have normalized knee function and quadriceps strength,” said Dr. Risberg, professor of sports medicine at the Norwegian School of Sport Sciences in Oslo.
With no proven disease-modifying therapy for KOA available to date, secondary prevention of posttraumatic KOA is worthy of high-priority status, she said at the World Congress on Osteoarthritis. An estimated 250,00 ACL injuries occur annually in the United States, and up to one-half of affected patients, most of whom are young, active people, will experience a second ACL rupture within the first few years after undergoing their initial reconstruction. This second ACL injury greatly increases their risk of developing posttraumatic KOA within 15-20 years, while they are still relatively young, she said.
Moreover, if the second ACL injury involves meniscus surgery, the 5-year risk of posttraumatic KOA roughly triples to up to 48%.
She highlighted a few effective strategies for preventing posttraumatic KOA in patients who already have an ACL injury.
Avoid reinjury
Dr. Risberg was senior author of a recent report from the prospective Delaware-Oslo Cohort Study involving 106 athletes who underwent ACL reconstruction following injury in what she termed level I sports. These are sports that entail lots of pivoting, jumping, and hard cutting, such as basketball, soccer, and handball.
In the first 2 years after ACL repair, 30% of patients who returned to participation in a level 1 sport experienced an ACL reinjury, compared with just 8% who opted for a lower-level sport. Athletes who returned to a level 1 sport had an adjusted 4.3 times greater ACL reinjury rate than those who didn’t, Dr. Risberg noted at the congress sponsored by the Osteoarthritis Research Society International.
The good news is that this sharply increased reinjury risk was mitigated if return to a level 1 sport was delayed for at least 9 months post surgery and if the patient had regained quadriceps strength comparable to the uninjured side. For every month that return to sport was delayed out until 9 months post ACL reconstruction, the knee reinjury rate was reduced by 51% (Br J Sports Med. 2016;50:804-8).
In a meta-analysis by other investigators of 12 studies including 5,707 participants, weakness of the knee extensor muscles was independently associated with a 1.65 times increased risk of developing KOA (Osteoarthritis Cartilage. 2015 Feb;23[2]:171-7).
Attend to BMI
A discussion of the importance of maintaining a healthy body weight is an important aspect of patient education for athletes with knee injuries. In a cohort study of 988 patients who underwent primary ACL reconstruction, being overweight or obese was associated with a significantly increased risk of subsequent meniscal tears and chondral lesions (Am J Sports Med. 2015 Dec;43[12]:2966-73).
Also, it’s well established that obesity is a risk factor for knee OA, and Canadian investigators have shown that young athletes with a sports-related intra-articular knee injury were 3.75 times more likely to be overweight or obese 3-10 years post injury, compared with matched uninjured controls (Osteoarthritis Cartilage. 2015 Jul;23[7]:1122-9).
Consider prehabilitative exercise training
Dr. Risberg and coinvestigators have reported that preoperative quadriceps muscle strength deficits are predictive of impaired knee function, as measured by the Cincinnati Knee Score 2 years post surgery. She said she believes ACL reconstruction shouldn’t be done until quadriceps muscle strength is at least 80% of that in the uninjured limb (Br J Sports Med. 2009 May;43[5]:371-6). She and her coinvestigators have published the details of a 5-week progressive exercise therapy program in which they have shown results in significantly improved early postoperative knee function (J Orthop Sports Phys Ther. 2010 Nov;40[11]:705-21). They now try to have patients complete the twice-weekly, 5-week program before final decisions are reached regarding whether to have ACL reconstruction.
Test all before okaying return to sport
It’s important to know if patients who have undergone ACL reconstruction have gotten full knee function back before determining if they’re ready for full-on sports participation. In the Delaware-Oslo Cohort Study, patients who delayed their return until at least 9 months after surgery and passed the return-to-sports test had a 5.6% reinjury rate within 2 years, while those who failed the return-to-sports criteria had a 38.2% ACL reinjury rate.
The return-to-sports testing utilized in this study entailed isokinetic quadriceps strength testing, the single hop leg test, the 14-item self-rated Knee Outcome Survey–Activities of Daily Living Scale, and a self-rated Global Rating Scale of perceived function on a 0-100 scale. To be cleared for return to sports, a patient had to demonstrate having regained at least 90% of quadriceps muscle strength and hop performance along with scoring in the normative range on both of the self-rating instruments.
Surgical vs. nonsurgical treatment of ACL rupture
The evidence on this score is conflicting, according to Dr. Risberg. While most physical therapists believe ACL reconstruction doesn’t protect against later development of KOA, as reflected in a meta-analysis of published studies (J Bone Joint Surg Am. 2014 Feb 19;96[4]:292-300), a more recent retrospective comparison of 964 patients with an isolated ACL tear and an equal number of matched controls concluded that patients treated nonoperatively were six times more likely to have been diagnosed with KOA and 16.7 times more likely to have undergone total knee replacement at a mean follow-up of 13.7 years than were those treated with ACL reconstruction (Am J Sports Med. 2016 Jul;44[7]:1699-707).
Dr. Risberg’s fellow panelist Jackie Whittaker, PhD, said that, as long as quadriceps muscle strengthening is a priority, it makes sense to strengthen the hamstring as well, particularly if the ACL reconstruction utilized the hamstring tendon.
“Also, I would add that it’s important to develop a relationship with these ACL-injured people, who are often very young. Preventing a disease that they’re going to get 20 years later isn’t a priority for them. You need to develop that relationship and build it up over time. Helping them set realistic expectations is very important. And we need to do what we can to help them find some sort of competitive outlet. A lot of these kids were very competitive, and now they’ve had an injury and can’t compete. They don’t want to go back to playing just any sport. They want to be able to be competitive, and if you don’t help them find another way to express that, they sort of give up on physical activity altogether,” according to Dr. Whittaker of the University of Alberta in Edmonton.
Dr. Risberg and Dr. Whittaker reported having no financial conflicts of interest.
LAS VEGAS – A variety of evidence-based strategies are available for preventing posttraumatic knee osteoarthritis (KOA) in patients who have already sustained an anterior cruciate ligament (ACL) injury. And they’re generally ignored, according to May Arna Risberg, PhD.
“We have a lot of knowledge. We can use secondary prevention strategies. And here I think we, as physical therapists, physicians, and orthopedic surgeons, are doing a lousy job because we are sending these ACL-injured patients back to sports before they have normalized knee function and quadriceps strength,” said Dr. Risberg, professor of sports medicine at the Norwegian School of Sport Sciences in Oslo.
With no proven disease-modifying therapy for KOA available to date, secondary prevention of posttraumatic KOA is worthy of high-priority status, she said at the World Congress on Osteoarthritis. An estimated 250,00 ACL injuries occur annually in the United States, and up to one-half of affected patients, most of whom are young, active people, will experience a second ACL rupture within the first few years after undergoing their initial reconstruction. This second ACL injury greatly increases their risk of developing posttraumatic KOA within 15-20 years, while they are still relatively young, she said.
Moreover, if the second ACL injury involves meniscus surgery, the 5-year risk of posttraumatic KOA roughly triples to up to 48%.
She highlighted a few effective strategies for preventing posttraumatic KOA in patients who already have an ACL injury.
Avoid reinjury
Dr. Risberg was senior author of a recent report from the prospective Delaware-Oslo Cohort Study involving 106 athletes who underwent ACL reconstruction following injury in what she termed level I sports. These are sports that entail lots of pivoting, jumping, and hard cutting, such as basketball, soccer, and handball.
In the first 2 years after ACL repair, 30% of patients who returned to participation in a level 1 sport experienced an ACL reinjury, compared with just 8% who opted for a lower-level sport. Athletes who returned to a level 1 sport had an adjusted 4.3 times greater ACL reinjury rate than those who didn’t, Dr. Risberg noted at the congress sponsored by the Osteoarthritis Research Society International.
The good news is that this sharply increased reinjury risk was mitigated if return to a level 1 sport was delayed for at least 9 months post surgery and if the patient had regained quadriceps strength comparable to the uninjured side. For every month that return to sport was delayed out until 9 months post ACL reconstruction, the knee reinjury rate was reduced by 51% (Br J Sports Med. 2016;50:804-8).
In a meta-analysis by other investigators of 12 studies including 5,707 participants, weakness of the knee extensor muscles was independently associated with a 1.65 times increased risk of developing KOA (Osteoarthritis Cartilage. 2015 Feb;23[2]:171-7).
Attend to BMI
A discussion of the importance of maintaining a healthy body weight is an important aspect of patient education for athletes with knee injuries. In a cohort study of 988 patients who underwent primary ACL reconstruction, being overweight or obese was associated with a significantly increased risk of subsequent meniscal tears and chondral lesions (Am J Sports Med. 2015 Dec;43[12]:2966-73).
Also, it’s well established that obesity is a risk factor for knee OA, and Canadian investigators have shown that young athletes with a sports-related intra-articular knee injury were 3.75 times more likely to be overweight or obese 3-10 years post injury, compared with matched uninjured controls (Osteoarthritis Cartilage. 2015 Jul;23[7]:1122-9).
Consider prehabilitative exercise training
Dr. Risberg and coinvestigators have reported that preoperative quadriceps muscle strength deficits are predictive of impaired knee function, as measured by the Cincinnati Knee Score 2 years post surgery. She said she believes ACL reconstruction shouldn’t be done until quadriceps muscle strength is at least 80% of that in the uninjured limb (Br J Sports Med. 2009 May;43[5]:371-6). She and her coinvestigators have published the details of a 5-week progressive exercise therapy program in which they have shown results in significantly improved early postoperative knee function (J Orthop Sports Phys Ther. 2010 Nov;40[11]:705-21). They now try to have patients complete the twice-weekly, 5-week program before final decisions are reached regarding whether to have ACL reconstruction.
Test all before okaying return to sport
It’s important to know if patients who have undergone ACL reconstruction have gotten full knee function back before determining if they’re ready for full-on sports participation. In the Delaware-Oslo Cohort Study, patients who delayed their return until at least 9 months after surgery and passed the return-to-sports test had a 5.6% reinjury rate within 2 years, while those who failed the return-to-sports criteria had a 38.2% ACL reinjury rate.
The return-to-sports testing utilized in this study entailed isokinetic quadriceps strength testing, the single hop leg test, the 14-item self-rated Knee Outcome Survey–Activities of Daily Living Scale, and a self-rated Global Rating Scale of perceived function on a 0-100 scale. To be cleared for return to sports, a patient had to demonstrate having regained at least 90% of quadriceps muscle strength and hop performance along with scoring in the normative range on both of the self-rating instruments.
Surgical vs. nonsurgical treatment of ACL rupture
The evidence on this score is conflicting, according to Dr. Risberg. While most physical therapists believe ACL reconstruction doesn’t protect against later development of KOA, as reflected in a meta-analysis of published studies (J Bone Joint Surg Am. 2014 Feb 19;96[4]:292-300), a more recent retrospective comparison of 964 patients with an isolated ACL tear and an equal number of matched controls concluded that patients treated nonoperatively were six times more likely to have been diagnosed with KOA and 16.7 times more likely to have undergone total knee replacement at a mean follow-up of 13.7 years than were those treated with ACL reconstruction (Am J Sports Med. 2016 Jul;44[7]:1699-707).
Dr. Risberg’s fellow panelist Jackie Whittaker, PhD, said that, as long as quadriceps muscle strengthening is a priority, it makes sense to strengthen the hamstring as well, particularly if the ACL reconstruction utilized the hamstring tendon.
“Also, I would add that it’s important to develop a relationship with these ACL-injured people, who are often very young. Preventing a disease that they’re going to get 20 years later isn’t a priority for them. You need to develop that relationship and build it up over time. Helping them set realistic expectations is very important. And we need to do what we can to help them find some sort of competitive outlet. A lot of these kids were very competitive, and now they’ve had an injury and can’t compete. They don’t want to go back to playing just any sport. They want to be able to be competitive, and if you don’t help them find another way to express that, they sort of give up on physical activity altogether,” according to Dr. Whittaker of the University of Alberta in Edmonton.
Dr. Risberg and Dr. Whittaker reported having no financial conflicts of interest.
LAS VEGAS – A variety of evidence-based strategies are available for preventing posttraumatic knee osteoarthritis (KOA) in patients who have already sustained an anterior cruciate ligament (ACL) injury. And they’re generally ignored, according to May Arna Risberg, PhD.
“We have a lot of knowledge. We can use secondary prevention strategies. And here I think we, as physical therapists, physicians, and orthopedic surgeons, are doing a lousy job because we are sending these ACL-injured patients back to sports before they have normalized knee function and quadriceps strength,” said Dr. Risberg, professor of sports medicine at the Norwegian School of Sport Sciences in Oslo.
With no proven disease-modifying therapy for KOA available to date, secondary prevention of posttraumatic KOA is worthy of high-priority status, she said at the World Congress on Osteoarthritis. An estimated 250,00 ACL injuries occur annually in the United States, and up to one-half of affected patients, most of whom are young, active people, will experience a second ACL rupture within the first few years after undergoing their initial reconstruction. This second ACL injury greatly increases their risk of developing posttraumatic KOA within 15-20 years, while they are still relatively young, she said.
Moreover, if the second ACL injury involves meniscus surgery, the 5-year risk of posttraumatic KOA roughly triples to up to 48%.
She highlighted a few effective strategies for preventing posttraumatic KOA in patients who already have an ACL injury.
Avoid reinjury
Dr. Risberg was senior author of a recent report from the prospective Delaware-Oslo Cohort Study involving 106 athletes who underwent ACL reconstruction following injury in what she termed level I sports. These are sports that entail lots of pivoting, jumping, and hard cutting, such as basketball, soccer, and handball.
In the first 2 years after ACL repair, 30% of patients who returned to participation in a level 1 sport experienced an ACL reinjury, compared with just 8% who opted for a lower-level sport. Athletes who returned to a level 1 sport had an adjusted 4.3 times greater ACL reinjury rate than those who didn’t, Dr. Risberg noted at the congress sponsored by the Osteoarthritis Research Society International.
The good news is that this sharply increased reinjury risk was mitigated if return to a level 1 sport was delayed for at least 9 months post surgery and if the patient had regained quadriceps strength comparable to the uninjured side. For every month that return to sport was delayed out until 9 months post ACL reconstruction, the knee reinjury rate was reduced by 51% (Br J Sports Med. 2016;50:804-8).
In a meta-analysis by other investigators of 12 studies including 5,707 participants, weakness of the knee extensor muscles was independently associated with a 1.65 times increased risk of developing KOA (Osteoarthritis Cartilage. 2015 Feb;23[2]:171-7).
Attend to BMI
A discussion of the importance of maintaining a healthy body weight is an important aspect of patient education for athletes with knee injuries. In a cohort study of 988 patients who underwent primary ACL reconstruction, being overweight or obese was associated with a significantly increased risk of subsequent meniscal tears and chondral lesions (Am J Sports Med. 2015 Dec;43[12]:2966-73).
Also, it’s well established that obesity is a risk factor for knee OA, and Canadian investigators have shown that young athletes with a sports-related intra-articular knee injury were 3.75 times more likely to be overweight or obese 3-10 years post injury, compared with matched uninjured controls (Osteoarthritis Cartilage. 2015 Jul;23[7]:1122-9).
Consider prehabilitative exercise training
Dr. Risberg and coinvestigators have reported that preoperative quadriceps muscle strength deficits are predictive of impaired knee function, as measured by the Cincinnati Knee Score 2 years post surgery. She said she believes ACL reconstruction shouldn’t be done until quadriceps muscle strength is at least 80% of that in the uninjured limb (Br J Sports Med. 2009 May;43[5]:371-6). She and her coinvestigators have published the details of a 5-week progressive exercise therapy program in which they have shown results in significantly improved early postoperative knee function (J Orthop Sports Phys Ther. 2010 Nov;40[11]:705-21). They now try to have patients complete the twice-weekly, 5-week program before final decisions are reached regarding whether to have ACL reconstruction.
Test all before okaying return to sport
It’s important to know if patients who have undergone ACL reconstruction have gotten full knee function back before determining if they’re ready for full-on sports participation. In the Delaware-Oslo Cohort Study, patients who delayed their return until at least 9 months after surgery and passed the return-to-sports test had a 5.6% reinjury rate within 2 years, while those who failed the return-to-sports criteria had a 38.2% ACL reinjury rate.
The return-to-sports testing utilized in this study entailed isokinetic quadriceps strength testing, the single hop leg test, the 14-item self-rated Knee Outcome Survey–Activities of Daily Living Scale, and a self-rated Global Rating Scale of perceived function on a 0-100 scale. To be cleared for return to sports, a patient had to demonstrate having regained at least 90% of quadriceps muscle strength and hop performance along with scoring in the normative range on both of the self-rating instruments.
Surgical vs. nonsurgical treatment of ACL rupture
The evidence on this score is conflicting, according to Dr. Risberg. While most physical therapists believe ACL reconstruction doesn’t protect against later development of KOA, as reflected in a meta-analysis of published studies (J Bone Joint Surg Am. 2014 Feb 19;96[4]:292-300), a more recent retrospective comparison of 964 patients with an isolated ACL tear and an equal number of matched controls concluded that patients treated nonoperatively were six times more likely to have been diagnosed with KOA and 16.7 times more likely to have undergone total knee replacement at a mean follow-up of 13.7 years than were those treated with ACL reconstruction (Am J Sports Med. 2016 Jul;44[7]:1699-707).
Dr. Risberg’s fellow panelist Jackie Whittaker, PhD, said that, as long as quadriceps muscle strengthening is a priority, it makes sense to strengthen the hamstring as well, particularly if the ACL reconstruction utilized the hamstring tendon.
“Also, I would add that it’s important to develop a relationship with these ACL-injured people, who are often very young. Preventing a disease that they’re going to get 20 years later isn’t a priority for them. You need to develop that relationship and build it up over time. Helping them set realistic expectations is very important. And we need to do what we can to help them find some sort of competitive outlet. A lot of these kids were very competitive, and now they’ve had an injury and can’t compete. They don’t want to go back to playing just any sport. They want to be able to be competitive, and if you don’t help them find another way to express that, they sort of give up on physical activity altogether,” according to Dr. Whittaker of the University of Alberta in Edmonton.
Dr. Risberg and Dr. Whittaker reported having no financial conflicts of interest.
EXPERT ANALYSIS FROM OARSI 2017
Tipoffs that an infant hospitalized with pertussis may require ICU
MADRID – Infants hospitalized for pertussis are more likely to develop severe disease requiring pediatric ICU admission if they are experiencing apnea, are unvaccinated against pertussis, or are less than 2 months old, Maria Arranz, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“The presence of these parameters on admission should warn us of possible severe disease,” said Dr. Arranz of Gregorio Maranon Hospital in Madrid.

Dr. Arranz presented a retrospective observational study of 101 children under 1 year of age who were hospitalized for pertussis at the Madrid tertiary center prior to the hospital’s 2016 shift to a strategy of maternal immunization during pregnancy as a means of preventing pertussis in infancy. Thirteen percent of the children required admission to the pediatric ICU and thus by definition had severe disease.
Half of infants in the study were not vaccinated against pertussis. That proved to be a powerful risk factor for severe disease requiring an ICU stay. Only 8% of children with severe pertussis were vaccinated, compared with a 58% vaccination rate among those who avoided the ICU.
Apneic pauses were noted in 67% of the severe disease group, compared with 28% of the infants who didn’t need the ICU.
The pertussis patients admitted to the pediatric ICU averaged 1 month of age, compared with age 2 months in the nonsevere group.
The maximum leukocyte, lymphocyte, and neutrophil counts during the hospital stay of the severe disease group averaged 23,600 cells/mm3, 18,000/mm3, and 5,000/mm3, respectively, significantly greater than the 15,300, 10,700, and 3,900 cells/mm3 in infants who did not require the ICU. Levels of all three cells also were higher at admission in the severe pertussis group than in those who didn’t make it to the ICU, albeit not statistically significantly so.
Dr. Arranz reported having no financial conflicts of interest regarding her study.
MADRID – Infants hospitalized for pertussis are more likely to develop severe disease requiring pediatric ICU admission if they are experiencing apnea, are unvaccinated against pertussis, or are less than 2 months old, Maria Arranz, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“The presence of these parameters on admission should warn us of possible severe disease,” said Dr. Arranz of Gregorio Maranon Hospital in Madrid.
Dr. Arranz presented a retrospective observational study of 101 children under 1 year of age who were hospitalized for pertussis at the Madrid tertiary center prior to the hospital’s 2016 shift to a strategy of maternal immunization during pregnancy as a means of preventing pertussis in infancy. Thirteen percent of the children required admission to the pediatric ICU and thus by definition had severe disease.
Half of infants in the study were not vaccinated against pertussis. That proved to be a powerful risk factor for severe disease requiring an ICU stay. Only 8% of children with severe pertussis were vaccinated, compared with a 58% vaccination rate among those who avoided the ICU.
Apneic pauses were noted in 67% of the severe disease group, compared with 28% of the infants who didn’t need the ICU.
The pertussis patients admitted to the pediatric ICU averaged 1 month of age, compared with age 2 months in the nonsevere group.
The maximum leukocyte, lymphocyte, and neutrophil counts during the hospital stay of the severe disease group averaged 23,600 cells/mm3, 18,000/mm3, and 5,000/mm3, respectively, significantly greater than the 15,300, 10,700, and 3,900 cells/mm3 in infants who did not require the ICU. Levels of all three cells also were higher at admission in the severe pertussis group than in those who didn’t make it to the ICU, albeit not statistically significantly so.
Dr. Arranz reported having no financial conflicts of interest regarding her study.
MADRID – Infants hospitalized for pertussis are more likely to develop severe disease requiring pediatric ICU admission if they are experiencing apnea, are unvaccinated against pertussis, or are less than 2 months old, Maria Arranz, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“The presence of these parameters on admission should warn us of possible severe disease,” said Dr. Arranz of Gregorio Maranon Hospital in Madrid.
Dr. Arranz presented a retrospective observational study of 101 children under 1 year of age who were hospitalized for pertussis at the Madrid tertiary center prior to the hospital’s 2016 shift to a strategy of maternal immunization during pregnancy as a means of preventing pertussis in infancy. Thirteen percent of the children required admission to the pediatric ICU and thus by definition had severe disease.
Half of infants in the study were not vaccinated against pertussis. That proved to be a powerful risk factor for severe disease requiring an ICU stay. Only 8% of children with severe pertussis were vaccinated, compared with a 58% vaccination rate among those who avoided the ICU.
Apneic pauses were noted in 67% of the severe disease group, compared with 28% of the infants who didn’t need the ICU.
The pertussis patients admitted to the pediatric ICU averaged 1 month of age, compared with age 2 months in the nonsevere group.
The maximum leukocyte, lymphocyte, and neutrophil counts during the hospital stay of the severe disease group averaged 23,600 cells/mm3, 18,000/mm3, and 5,000/mm3, respectively, significantly greater than the 15,300, 10,700, and 3,900 cells/mm3 in infants who did not require the ICU. Levels of all three cells also were higher at admission in the severe pertussis group than in those who didn’t make it to the ICU, albeit not statistically significantly so.
Dr. Arranz reported having no financial conflicts of interest regarding her study.
AT ESPID 2017
Key clinical point:
Major finding: Among infants hospitalized for pertussis, apneic pauses were present in two-thirds of those with severe disease, ultimately resulting in admission to the pediatric ICU, compared with 28% of those who didn’t require an ICU stay.
Data source: This retrospective observational study sought to identify factors associated with severe pertussis requiring an ICU stay in a group of 101 Spanish infants hospitalized with the disease.
Disclosures: The presenter reported having no financial conflicts of interest regarding her study.
FFR stumbles in revascularization deferral decisions for ACS
Paris – One-year outcomes were significantly worse in patients with acute coronary syndrome whose revascularization was deferred based upon the results of fractional flow reserve than with instantaneous wave-free ratio, in the largest-ever study of patients whose revascularization decision was guided by physiologic measurements obtained via a pressure guidewire.
“The hypothesis that some authors have put forth – that in an ACS the hyperemic response of the myocardium is blunted by the ACS, and that this will affect the FFR hyperemic index – is now strengthened,” Javier Escaned, MD, said in presenting the study results at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The study was a pooled, patient-level meta-analysis of the 4,529 participants with angiographically determined intermediate-risk stenoses in the previously reported randomized DEFINE FLAIR (N Engl J Med. 2017 May 11;376[19]:1824-34) and iFR SWEDEHEART (N Engl J Med. 2017 May 11;376[19]:1813-23) studies. The primary endpoint was the composite of death, nonfatal MI, or unplanned coronary revascularization within 12 months. And while the analysis brought unwelcome news for proponents of FFR with regard to the subset of patients with ACS, such patients comprised only 17% of the total study population.

“I think that overall these results are very reassuring. The big finding is that we have dramatically improved the safety of deferral of revascularization using pressure guidewires. If you look at the MACE [major adverse cardiovascular event] rate in the deferred ACS group, it was about 6%, which is much less than the event rate at 1 year with deferral in patients with stable coronary disease in the pivotal DEFER trial [Circulation. 2001 Jun 19;103(24):2928-34], which was our former standard,” observed Dr. Escaned, an interventional cardiologist at San Carlos Hospital in Madrid and a DEFER coinvestigator.
He attributed these greatly improved outcomes of physiologically guided revascularization during the past 15 years to vastly improved stent technology and more effective optimal medical management.
Among the key findings of the combined analysis of DEFINE FLAIR and iFR SWEDEHEART:
• More patients were deferred from PCI when iFR was used for decision-making: 50%, compared with 45% in the FFR arm. Yet 1-year outcomes were as good in the deferred iFR group as in the FFR group overall, and better than with FFR in the deferred ACS patients.
• Event rates were significantly higher in deferred ACS patients overall than in deferred patients with stable coronary disease: 5.9% versus 3.6%. But the deferral tool made a difference: When iFR was utilized, the 1-year event rate was 5.4% in deferred ACS patients, not significantly different from the 3.8% rate in deferred patients with stable coronary disease. In contrast, the event rate in ACS patients with FFR-based deferral was 6.4%, significantly higher than the 3.4% rate in FFR-deferred patients with stable coronary disease.
Dr. Escaned noted that this finding is consistent with the cautionary results of several recent studies, including one, albeit tenfold smaller, in which ACS patients in whom revascularization was deferred based on FFR had a 25% rate of major adverse cardiovascular events at 3.4 years, compared with a 12% rate in patients with stable coronary disease (J Am Coll Cardiol. 2016 Sep 13;68[11]:1181-91).
Discussant Peter Jüni, MD, professor of medicine at the University of Toronto, said “the main results of your study show in a completely waterproof fashion that there is no signal of harm with the experimental strategy” of deferred revascularization based on physiologic measurements, at least in patients with stable ischemic coronary disease.
The results, however, also raise the question of whether physiology-based revascularization decision-making in ACS patients is the best strategy.
“Considering that the event rate in the deferred ACS group was nearly twice as high compared with stable patients, my question to you is: Should we ignore any functional testing in ACS patients and just say, ‘Let’s move forward with revascularization because this clinical presentation is a very good clinical characteristic for risk stratification?’ ”
Dr. Escaned rejected that option. He noted that both the European and U.S. guidelines now state that it’s inappropriate to base a revascularization decision solely on a coronary vessel’s angiographic appearance, because that has been shown to result in unnecessary treatment, which causes harm. Adoption of pressure guidewires to assist in revascularization decision making, whether by FFR or iFR, is still limited in interventional cardiology. The priority in the field now should be to encourage more widespread use of this technology, regardless of which method is selected, he argued.
“The biggest room in the world is the room for improvement,” the cardiologist mused.
“I think one of the real problems that’s impeding adoption of physiologic testing is that many physicians are still afraid of leaving a stenosis without treatment,” he continued. “It’s strange: If you perform angioplasty and it wasn’t indicated and there is a complication, physicians seem to have some type of peace of mind that they did their best and they were trying to help the patient. That’s why it’s so important to establish that deferring revascularization – not treating when it is not needed – is safe.”
The DEFINE FLAIR and iFR SWEDEHEART studies were funded by unrestricted grants from Philips Volcano. Dr. Escaned reported serving as a consultant to Abbott, AstraZeneca, Biosensors, Boston Scientific, Medtronic, OrbusNeich, and Philips Healthcare.
Paris – One-year outcomes were significantly worse in patients with acute coronary syndrome whose revascularization was deferred based upon the results of fractional flow reserve than with instantaneous wave-free ratio, in the largest-ever study of patients whose revascularization decision was guided by physiologic measurements obtained via a pressure guidewire.
“The hypothesis that some authors have put forth – that in an ACS the hyperemic response of the myocardium is blunted by the ACS, and that this will affect the FFR hyperemic index – is now strengthened,” Javier Escaned, MD, said in presenting the study results at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The study was a pooled, patient-level meta-analysis of the 4,529 participants with angiographically determined intermediate-risk stenoses in the previously reported randomized DEFINE FLAIR (N Engl J Med. 2017 May 11;376[19]:1824-34) and iFR SWEDEHEART (N Engl J Med. 2017 May 11;376[19]:1813-23) studies. The primary endpoint was the composite of death, nonfatal MI, or unplanned coronary revascularization within 12 months. And while the analysis brought unwelcome news for proponents of FFR with regard to the subset of patients with ACS, such patients comprised only 17% of the total study population.
“I think that overall these results are very reassuring. The big finding is that we have dramatically improved the safety of deferral of revascularization using pressure guidewires. If you look at the MACE [major adverse cardiovascular event] rate in the deferred ACS group, it was about 6%, which is much less than the event rate at 1 year with deferral in patients with stable coronary disease in the pivotal DEFER trial [Circulation. 2001 Jun 19;103(24):2928-34], which was our former standard,” observed Dr. Escaned, an interventional cardiologist at San Carlos Hospital in Madrid and a DEFER coinvestigator.
He attributed these greatly improved outcomes of physiologically guided revascularization during the past 15 years to vastly improved stent technology and more effective optimal medical management.
Among the key findings of the combined analysis of DEFINE FLAIR and iFR SWEDEHEART:
• More patients were deferred from PCI when iFR was used for decision-making: 50%, compared with 45% in the FFR arm. Yet 1-year outcomes were as good in the deferred iFR group as in the FFR group overall, and better than with FFR in the deferred ACS patients.
• Event rates were significantly higher in deferred ACS patients overall than in deferred patients with stable coronary disease: 5.9% versus 3.6%. But the deferral tool made a difference: When iFR was utilized, the 1-year event rate was 5.4% in deferred ACS patients, not significantly different from the 3.8% rate in deferred patients with stable coronary disease. In contrast, the event rate in ACS patients with FFR-based deferral was 6.4%, significantly higher than the 3.4% rate in FFR-deferred patients with stable coronary disease.
Dr. Escaned noted that this finding is consistent with the cautionary results of several recent studies, including one, albeit tenfold smaller, in which ACS patients in whom revascularization was deferred based on FFR had a 25% rate of major adverse cardiovascular events at 3.4 years, compared with a 12% rate in patients with stable coronary disease (J Am Coll Cardiol. 2016 Sep 13;68[11]:1181-91).
Discussant Peter Jüni, MD, professor of medicine at the University of Toronto, said “the main results of your study show in a completely waterproof fashion that there is no signal of harm with the experimental strategy” of deferred revascularization based on physiologic measurements, at least in patients with stable ischemic coronary disease.
The results, however, also raise the question of whether physiology-based revascularization decision-making in ACS patients is the best strategy.
“Considering that the event rate in the deferred ACS group was nearly twice as high compared with stable patients, my question to you is: Should we ignore any functional testing in ACS patients and just say, ‘Let’s move forward with revascularization because this clinical presentation is a very good clinical characteristic for risk stratification?’ ”
Dr. Escaned rejected that option. He noted that both the European and U.S. guidelines now state that it’s inappropriate to base a revascularization decision solely on a coronary vessel’s angiographic appearance, because that has been shown to result in unnecessary treatment, which causes harm. Adoption of pressure guidewires to assist in revascularization decision making, whether by FFR or iFR, is still limited in interventional cardiology. The priority in the field now should be to encourage more widespread use of this technology, regardless of which method is selected, he argued.
“The biggest room in the world is the room for improvement,” the cardiologist mused.
“I think one of the real problems that’s impeding adoption of physiologic testing is that many physicians are still afraid of leaving a stenosis without treatment,” he continued. “It’s strange: If you perform angioplasty and it wasn’t indicated and there is a complication, physicians seem to have some type of peace of mind that they did their best and they were trying to help the patient. That’s why it’s so important to establish that deferring revascularization – not treating when it is not needed – is safe.”
The DEFINE FLAIR and iFR SWEDEHEART studies were funded by unrestricted grants from Philips Volcano. Dr. Escaned reported serving as a consultant to Abbott, AstraZeneca, Biosensors, Boston Scientific, Medtronic, OrbusNeich, and Philips Healthcare.
Paris – One-year outcomes were significantly worse in patients with acute coronary syndrome whose revascularization was deferred based upon the results of fractional flow reserve than with instantaneous wave-free ratio, in the largest-ever study of patients whose revascularization decision was guided by physiologic measurements obtained via a pressure guidewire.
“The hypothesis that some authors have put forth – that in an ACS the hyperemic response of the myocardium is blunted by the ACS, and that this will affect the FFR hyperemic index – is now strengthened,” Javier Escaned, MD, said in presenting the study results at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The study was a pooled, patient-level meta-analysis of the 4,529 participants with angiographically determined intermediate-risk stenoses in the previously reported randomized DEFINE FLAIR (N Engl J Med. 2017 May 11;376[19]:1824-34) and iFR SWEDEHEART (N Engl J Med. 2017 May 11;376[19]:1813-23) studies. The primary endpoint was the composite of death, nonfatal MI, or unplanned coronary revascularization within 12 months. And while the analysis brought unwelcome news for proponents of FFR with regard to the subset of patients with ACS, such patients comprised only 17% of the total study population.
“I think that overall these results are very reassuring. The big finding is that we have dramatically improved the safety of deferral of revascularization using pressure guidewires. If you look at the MACE [major adverse cardiovascular event] rate in the deferred ACS group, it was about 6%, which is much less than the event rate at 1 year with deferral in patients with stable coronary disease in the pivotal DEFER trial [Circulation. 2001 Jun 19;103(24):2928-34], which was our former standard,” observed Dr. Escaned, an interventional cardiologist at San Carlos Hospital in Madrid and a DEFER coinvestigator.
He attributed these greatly improved outcomes of physiologically guided revascularization during the past 15 years to vastly improved stent technology and more effective optimal medical management.
Among the key findings of the combined analysis of DEFINE FLAIR and iFR SWEDEHEART:
• More patients were deferred from PCI when iFR was used for decision-making: 50%, compared with 45% in the FFR arm. Yet 1-year outcomes were as good in the deferred iFR group as in the FFR group overall, and better than with FFR in the deferred ACS patients.
• Event rates were significantly higher in deferred ACS patients overall than in deferred patients with stable coronary disease: 5.9% versus 3.6%. But the deferral tool made a difference: When iFR was utilized, the 1-year event rate was 5.4% in deferred ACS patients, not significantly different from the 3.8% rate in deferred patients with stable coronary disease. In contrast, the event rate in ACS patients with FFR-based deferral was 6.4%, significantly higher than the 3.4% rate in FFR-deferred patients with stable coronary disease.
Dr. Escaned noted that this finding is consistent with the cautionary results of several recent studies, including one, albeit tenfold smaller, in which ACS patients in whom revascularization was deferred based on FFR had a 25% rate of major adverse cardiovascular events at 3.4 years, compared with a 12% rate in patients with stable coronary disease (J Am Coll Cardiol. 2016 Sep 13;68[11]:1181-91).
Discussant Peter Jüni, MD, professor of medicine at the University of Toronto, said “the main results of your study show in a completely waterproof fashion that there is no signal of harm with the experimental strategy” of deferred revascularization based on physiologic measurements, at least in patients with stable ischemic coronary disease.
The results, however, also raise the question of whether physiology-based revascularization decision-making in ACS patients is the best strategy.
“Considering that the event rate in the deferred ACS group was nearly twice as high compared with stable patients, my question to you is: Should we ignore any functional testing in ACS patients and just say, ‘Let’s move forward with revascularization because this clinical presentation is a very good clinical characteristic for risk stratification?’ ”
Dr. Escaned rejected that option. He noted that both the European and U.S. guidelines now state that it’s inappropriate to base a revascularization decision solely on a coronary vessel’s angiographic appearance, because that has been shown to result in unnecessary treatment, which causes harm. Adoption of pressure guidewires to assist in revascularization decision making, whether by FFR or iFR, is still limited in interventional cardiology. The priority in the field now should be to encourage more widespread use of this technology, regardless of which method is selected, he argued.
“The biggest room in the world is the room for improvement,” the cardiologist mused.
“I think one of the real problems that’s impeding adoption of physiologic testing is that many physicians are still afraid of leaving a stenosis without treatment,” he continued. “It’s strange: If you perform angioplasty and it wasn’t indicated and there is a complication, physicians seem to have some type of peace of mind that they did their best and they were trying to help the patient. That’s why it’s so important to establish that deferring revascularization – not treating when it is not needed – is safe.”
The DEFINE FLAIR and iFR SWEDEHEART studies were funded by unrestricted grants from Philips Volcano. Dr. Escaned reported serving as a consultant to Abbott, AstraZeneca, Biosensors, Boston Scientific, Medtronic, OrbusNeich, and Philips Healthcare.
AT EUROPCR
Key clinical point:
Major finding: In patients with acute coronary syndrome, the 1-year adverse event rate in patients with FFR-based deferral was 6.4%, significantly higher than the 3.4% rate in patients with FFR-based deferral with stable coronary disease.
Data source: A pooled patient-level meta-analysis of the 4,529 participants with angiographically intermediate-risk stenoses in two previously reported randomized trials of physiologic assessment of lesions by fractional flow reserve or instantaneous wave-free ratio.
Disclosures: The DEFINE FLAIR and iFR SWEDEHEART studies were funded by unrestricted grants from Philips Volcano. The presenter reported serving as a consultant to Abbott, AstraZeneca, Biosensors, Boston Scientific, Medtronic, OrbusNeich, and Philips Healthcare.
Exercise tops NSAIDs for knee osteoarthritis
LAS VEGAS – After participating in an 8-week neuromuscular exercise therapy program, patients with mild to moderate knee osteoarthritis showed significantly greater symptomatic improvement at 12 months of follow-up than if they had been instructed to treat with analgesics and anti-inflammatory agents in the randomized EXERPHARMA trial.
“Neuromuscular exercise could be the superior choice for long-term relief of symptoms such as swelling, stiffness, and catching, while avoiding the potential side effects of analgesics and anti-inflammatory drugs,” Anders Holsgaard-Larsen, MD, said in his presentation of the 1-year study results at the World Congress on Osteoarthritis.
Ninety-three patients with mild to moderate medial knee osteoarthritis – “a group we commonly see in primary care,” he noted – were randomized to the structured 8-week neuromuscular exercise therapy program or to 8 weeks of instruction in the appropriate use of NSAIDs and acetaminophen. The exercise program entailed two hour-long, physical therapist-supervised sessions per week, which included functional, proprioceptive, strength, and endurance exercises of three or four progressive degrees of difficulty.
The initial results obtained at the conclusion of the 8-week interventions – change in knee joint load while walking – have been published (Osteoarthritis Cartilage. 2017 Apr;25[4]:470-80). There was no significant difference between the two study groups. But outcomes at the prespecified 12-month follow-up designed to capture any late improvement were a different story, Dr. Holsgaard-Larsen said at the congress sponsored by the Osteoarthritis Research Society International.
The neuromuscular exercise therapy group showed a significantly greater improvement on the Knee Injury and Osteoarthritis Scores (KOOS) symptom subscale at 12 months: a mean 10.9-point improvement from baseline, compared with a 3.3-point improvement with drug therapy.
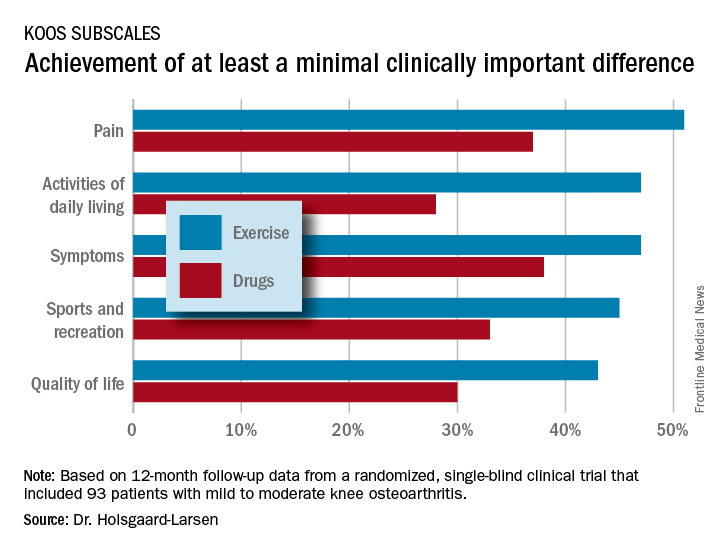
That being said, the prespecified primary endpoint at 12 months was change on the activities of daily living subscale – and this between-group difference didn’t reach statistical significance. So technically EXERPHARMA was a negative study, according to the investigator.
That comment caused audience member Theodore P. Pincus, MD, to rise in protest.
“I might argue that perhaps we’ve gotten too focused on P-values rather than looking at the whole picture. In my opinion, your hypothesis is more validated than you seem to think,” said Dr. Pincus, professor of rheumatology at Rush University in Chicago.
The EXERPHARMA trial was funded by the Danish Rheumatism Association and other noncommercial research support. Dr. Holsgaard-Larsen reported having no financial conflicts of interest.
LAS VEGAS – After participating in an 8-week neuromuscular exercise therapy program, patients with mild to moderate knee osteoarthritis showed significantly greater symptomatic improvement at 12 months of follow-up than if they had been instructed to treat with analgesics and anti-inflammatory agents in the randomized EXERPHARMA trial.
“Neuromuscular exercise could be the superior choice for long-term relief of symptoms such as swelling, stiffness, and catching, while avoiding the potential side effects of analgesics and anti-inflammatory drugs,” Anders Holsgaard-Larsen, MD, said in his presentation of the 1-year study results at the World Congress on Osteoarthritis.
Ninety-three patients with mild to moderate medial knee osteoarthritis – “a group we commonly see in primary care,” he noted – were randomized to the structured 8-week neuromuscular exercise therapy program or to 8 weeks of instruction in the appropriate use of NSAIDs and acetaminophen. The exercise program entailed two hour-long, physical therapist-supervised sessions per week, which included functional, proprioceptive, strength, and endurance exercises of three or four progressive degrees of difficulty.
The initial results obtained at the conclusion of the 8-week interventions – change in knee joint load while walking – have been published (Osteoarthritis Cartilage. 2017 Apr;25[4]:470-80). There was no significant difference between the two study groups. But outcomes at the prespecified 12-month follow-up designed to capture any late improvement were a different story, Dr. Holsgaard-Larsen said at the congress sponsored by the Osteoarthritis Research Society International.
The neuromuscular exercise therapy group showed a significantly greater improvement on the Knee Injury and Osteoarthritis Scores (KOOS) symptom subscale at 12 months: a mean 10.9-point improvement from baseline, compared with a 3.3-point improvement with drug therapy.
That being said, the prespecified primary endpoint at 12 months was change on the activities of daily living subscale – and this between-group difference didn’t reach statistical significance. So technically EXERPHARMA was a negative study, according to the investigator.
That comment caused audience member Theodore P. Pincus, MD, to rise in protest.
“I might argue that perhaps we’ve gotten too focused on P-values rather than looking at the whole picture. In my opinion, your hypothesis is more validated than you seem to think,” said Dr. Pincus, professor of rheumatology at Rush University in Chicago.
The EXERPHARMA trial was funded by the Danish Rheumatism Association and other noncommercial research support. Dr. Holsgaard-Larsen reported having no financial conflicts of interest.
LAS VEGAS – After participating in an 8-week neuromuscular exercise therapy program, patients with mild to moderate knee osteoarthritis showed significantly greater symptomatic improvement at 12 months of follow-up than if they had been instructed to treat with analgesics and anti-inflammatory agents in the randomized EXERPHARMA trial.
“Neuromuscular exercise could be the superior choice for long-term relief of symptoms such as swelling, stiffness, and catching, while avoiding the potential side effects of analgesics and anti-inflammatory drugs,” Anders Holsgaard-Larsen, MD, said in his presentation of the 1-year study results at the World Congress on Osteoarthritis.
Ninety-three patients with mild to moderate medial knee osteoarthritis – “a group we commonly see in primary care,” he noted – were randomized to the structured 8-week neuromuscular exercise therapy program or to 8 weeks of instruction in the appropriate use of NSAIDs and acetaminophen. The exercise program entailed two hour-long, physical therapist-supervised sessions per week, which included functional, proprioceptive, strength, and endurance exercises of three or four progressive degrees of difficulty.
The initial results obtained at the conclusion of the 8-week interventions – change in knee joint load while walking – have been published (Osteoarthritis Cartilage. 2017 Apr;25[4]:470-80). There was no significant difference between the two study groups. But outcomes at the prespecified 12-month follow-up designed to capture any late improvement were a different story, Dr. Holsgaard-Larsen said at the congress sponsored by the Osteoarthritis Research Society International.
The neuromuscular exercise therapy group showed a significantly greater improvement on the Knee Injury and Osteoarthritis Scores (KOOS) symptom subscale at 12 months: a mean 10.9-point improvement from baseline, compared with a 3.3-point improvement with drug therapy.
That being said, the prespecified primary endpoint at 12 months was change on the activities of daily living subscale – and this between-group difference didn’t reach statistical significance. So technically EXERPHARMA was a negative study, according to the investigator.
That comment caused audience member Theodore P. Pincus, MD, to rise in protest.
“I might argue that perhaps we’ve gotten too focused on P-values rather than looking at the whole picture. In my opinion, your hypothesis is more validated than you seem to think,” said Dr. Pincus, professor of rheumatology at Rush University in Chicago.
The EXERPHARMA trial was funded by the Danish Rheumatism Association and other noncommercial research support. Dr. Holsgaard-Larsen reported having no financial conflicts of interest.
AT OARSI 2017
Key clinical point:
Major finding: At 12 months of follow-up, patients with knee osteoarthritis who had been assigned to an 8-week structured neuromuscular exercise therapy program had a mean 10.9-point improvement on the KOOS symptom subscale, significantly better than the 3.3-point improvement in patients assigned to primary therapy with NSAIDs and acetaminophen.
Data source: This randomized, single-blind clinical trial included 93 patients with mild to moderate knee osteoarthritis.
Disclosures: The EXERPHARMA trial was funded by the Danish Rheumatism Association and other noncommercial research support. The presenter reported having no financial conflicts of interest.
HCV/HIV-coinfected teens rapidly progress to advanced liver disease
MADRID – Roughly one in four children with vertically transmitted hepatitis C virus (HCV)/HIV coinfection will progress to advanced hepatic fibrosis by age 20 years despite treatment with pegylated interferon plus ribavirin, Carolina Fernández McPhee, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
This rate was nearly five times higher than in matched children with vertically acquired HCV monoinfection in a multicenter retrospective study, according to Dr. McPhee of Hospital General Universitario Gregorio Marañón in Madrid.

She presented a multicenter retrospective study of liver disease progression in 71 HCV/HIV coinfected children and 71 age- and sex-matched HCV-monoinfected children. The coinfected children are being followed in CORISPES (the Spanish Cohort of HIV-infected Children), where they receive state-of-the-art care.
All was quiet through age 9 years, with no progression to liver fibrosis in either patient group. Among patients followed to age 20 years, however, 9 (24%) of 38 HCV/HIV-coinfected patients showed progression to advanced fibrosis, compared with just 3 (6%) of 54 patients with HCV only.
Of HCV/HIV coinfected patients, 73% were infected with the hard to treat viral genotypes 1 or 4, compared with 93% of patients with HCV-only.
In the study group, 22 patients with HCV/HIV and 52 patients with HCV-only underwent treatment with pegylated interferon and ribavirin. At the time of treatment, three coinfected patients already had cirrhosis, another eight had moderate to advanced fibrosis, and half had no or mild fibrosis. In contrast, only one patient with HCV monoinfection had cirrhosis, four had moderate to advanced fibrosis, and the rest – nearly 90% of the total group – had no or mild fibrosis.
At treatment initiation, 96% of the HCV/HIV group were on antiretroviral therapy, 86% showed suppression of HIV RNA, 44% had AIDS, and 32% had a CD4 count below 500 cells/mm3.
The sustained viral response rate was similar in the two groups of patients – 41% in the HCV/HIV group and 42% in HCV-only patients – despite the fact that the HCV monoinfected patients had a higher prevalence of the tough to treat genotypes.
Roughly 12 million people worldwide are coinfected with HCV and HIV.
Dr. McPhee reported having no relevant financial disclosures.
MADRID – Roughly one in four children with vertically transmitted hepatitis C virus (HCV)/HIV coinfection will progress to advanced hepatic fibrosis by age 20 years despite treatment with pegylated interferon plus ribavirin, Carolina Fernández McPhee, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
This rate was nearly five times higher than in matched children with vertically acquired HCV monoinfection in a multicenter retrospective study, according to Dr. McPhee of Hospital General Universitario Gregorio Marañón in Madrid.
She presented a multicenter retrospective study of liver disease progression in 71 HCV/HIV coinfected children and 71 age- and sex-matched HCV-monoinfected children. The coinfected children are being followed in CORISPES (the Spanish Cohort of HIV-infected Children), where they receive state-of-the-art care.
All was quiet through age 9 years, with no progression to liver fibrosis in either patient group. Among patients followed to age 20 years, however, 9 (24%) of 38 HCV/HIV-coinfected patients showed progression to advanced fibrosis, compared with just 3 (6%) of 54 patients with HCV only.
Of HCV/HIV coinfected patients, 73% were infected with the hard to treat viral genotypes 1 or 4, compared with 93% of patients with HCV-only.
In the study group, 22 patients with HCV/HIV and 52 patients with HCV-only underwent treatment with pegylated interferon and ribavirin. At the time of treatment, three coinfected patients already had cirrhosis, another eight had moderate to advanced fibrosis, and half had no or mild fibrosis. In contrast, only one patient with HCV monoinfection had cirrhosis, four had moderate to advanced fibrosis, and the rest – nearly 90% of the total group – had no or mild fibrosis.
At treatment initiation, 96% of the HCV/HIV group were on antiretroviral therapy, 86% showed suppression of HIV RNA, 44% had AIDS, and 32% had a CD4 count below 500 cells/mm3.
The sustained viral response rate was similar in the two groups of patients – 41% in the HCV/HIV group and 42% in HCV-only patients – despite the fact that the HCV monoinfected patients had a higher prevalence of the tough to treat genotypes.
Roughly 12 million people worldwide are coinfected with HCV and HIV.
Dr. McPhee reported having no relevant financial disclosures.
MADRID – Roughly one in four children with vertically transmitted hepatitis C virus (HCV)/HIV coinfection will progress to advanced hepatic fibrosis by age 20 years despite treatment with pegylated interferon plus ribavirin, Carolina Fernández McPhee, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
This rate was nearly five times higher than in matched children with vertically acquired HCV monoinfection in a multicenter retrospective study, according to Dr. McPhee of Hospital General Universitario Gregorio Marañón in Madrid.
She presented a multicenter retrospective study of liver disease progression in 71 HCV/HIV coinfected children and 71 age- and sex-matched HCV-monoinfected children. The coinfected children are being followed in CORISPES (the Spanish Cohort of HIV-infected Children), where they receive state-of-the-art care.
All was quiet through age 9 years, with no progression to liver fibrosis in either patient group. Among patients followed to age 20 years, however, 9 (24%) of 38 HCV/HIV-coinfected patients showed progression to advanced fibrosis, compared with just 3 (6%) of 54 patients with HCV only.
Of HCV/HIV coinfected patients, 73% were infected with the hard to treat viral genotypes 1 or 4, compared with 93% of patients with HCV-only.
In the study group, 22 patients with HCV/HIV and 52 patients with HCV-only underwent treatment with pegylated interferon and ribavirin. At the time of treatment, three coinfected patients already had cirrhosis, another eight had moderate to advanced fibrosis, and half had no or mild fibrosis. In contrast, only one patient with HCV monoinfection had cirrhosis, four had moderate to advanced fibrosis, and the rest – nearly 90% of the total group – had no or mild fibrosis.
At treatment initiation, 96% of the HCV/HIV group were on antiretroviral therapy, 86% showed suppression of HIV RNA, 44% had AIDS, and 32% had a CD4 count below 500 cells/mm3.
The sustained viral response rate was similar in the two groups of patients – 41% in the HCV/HIV group and 42% in HCV-only patients – despite the fact that the HCV monoinfected patients had a higher prevalence of the tough to treat genotypes.
Roughly 12 million people worldwide are coinfected with HCV and HIV.
Dr. McPhee reported having no relevant financial disclosures.
AT ESPID 2017
Key clinical point:
Major finding: By age 20 years, 24% of a group of patients with vertically transmitted HCV/HIV coinfection had progressed to advanced hepatic fibrosis, compared with 6% of patients with vertically transmitted HCV monoinfection.
Data source: This retrospective, multicenter, observational Spanish study included 71 children with vertically transmitted HCV/HIV coinfection and 71 with vertically transmitted HCV monoinfection.
Disclosures: Dr. McPhee reported having no relevant financial disclosures.