User login
Volume Control, Part II

Last month I began looking at ways hospitalist practices can manage unpredictable increases in patient volume, also known as surge staffing. I provided my view of a “jeopardy” system and a patient volume cap for hospitalists. While both are potentially very effective, they have a high cost and in my view are imperfect solutions. This month I’ll examine some less common strategies to provide surge staffing. Although less popular, I think these options are more valuable.
Schedule More Providers
I’ve worked with a lot of practices and am struck by how patient volume for nearly all of them falls within a reasonably predictable range. While no one can predict with certainty which days will be unusually busy or slow, nearly all practices have a range of daily encounters that is roughly half to 1 1/2 of the mean. For example, if a practice has a mean of 60 billable encounters per day, it probably ranges from about 30 to 90 encounters on any given day. (The larger the practice, the more likely they are to conform to this range. Small practices, with average daily encounters fewer than 20, have a much wider range of daily volumes as a percent of the mean.)
Despite knowing that volumes will vary unpredictably, most practices provide the same fixed “dose” of provider staffing every day—that is, the single most common model for staffing and scheduling is to provide a fixed number of day-shift doctors (“rounders”) who work a fixed number of hours. For example, with an average of 60 billable encounters a day, a hospitalist group might decide to staff with four day-shift rounders working 12-hour shifts. This equates to a fixed 48 hours of daytime staffing. This is reasonable until the busy days arrive. Those four doctors will be much busier than average when there are 90 patients to see in a day, and will probably have a hard time seeing 22 or 23 patients each during their 12-hour shift. If such a busy day occurs more than a couple of times annually, then the practice should probably make some changes.
One approach to solving this type of staffing predicament is to add a fifth day-shift rounder. In other words, when making staffing decisions, consider giving more weight to the busiest days than the average day. This sounds fine until thinking about the practice budget. It will be pretty expensive to add doctors every day just so there are enough on duty when things get really busy. But if the hospitalists are willing to accept reduced compensation, then it might be financially reasonable to go ahead and add staff. This is easiest to do when the hospitalists are paid a significant (e.g. ≥50%) portion of their income based on their productivity, which will enable the hospitalists themselves to have a lot of say about when it is time to add staff. (Being paid on a nearly fixed annual salary means that it is the finance person who usually has the say about when it is time to add staff. And you can bet he’ll be making staffing decisions based on the average daily encounters, rather than the busy days.)
My own preference would be to do just that: Accept a reduction in compensation in return for protection against really busy and stressful days. I’m not suggesting others should agree with me, and in my experience, most don’t. (My own practice partners don’t agree with me on this one.) So I’m not really recommending it as a best practice, but I want to ensure that you don’t forget it is an option. And keep in mind you could adjust staffing by degrees; some settings might add a half-time physician or a nonphysician provider to try to find the sweet spot between having enough staff on duty every day to handle surges in volume and the cost of that staffing to the employer—or the hospitalists themselves.
Of course, if I were willing to reduce my compensation and average daily workload, then I would expect to be freed from the expectation that all rounding doctors work 12-hour shifts. Let’s turn our attention to the interplay between fixed day-shift durations and surge staffing.
Fixed-Shift Schedules Inhibit Surge Capacity
I think it usually is best to avoid fixed durations for day shifts. It might be necessary to require at least one daytime rounder to stay at least until a specified time (e.g. the arrival of the night-shift doctor), but in most cases it is reasonable for some rounders to leave when their work is done. They might need to continue responding to pages until the start of the night shift, but it usually isn’t necessary to have all rounders in the hospital until a predetermined end of the shift.
The problem is that when shifts have a fixed duration, the providers will focus on the start and stop time of their shift and might be unwilling to work beyond it. If instead there are no clearly fixed start and stop times for each day shift, then the hospitalists are likely to be willing to simply work longer on busy days, as long as they can work shorter on slow days. This is probably the most effective method of surge capacity, and it fits well with staffing each day with more providers than are required for the average patient volume.
Simply having the rounding doctors work longer on busy days must be done within reason. And there is a really wide range of opinion about what is reasonable. I think it is reasonable if a hospitalist works two or three hours longer than usual for three or four consecutive busy days, as long as the hospitalist is allowed to work less on days that are not very busy. But just what is a reasonable maximum daily amount of work for even one day is a topic that can lead to passionate debate. You’ll have to decide the details of what is and isn’t acceptable in your group.
Unit-Based Assignments
Aside from fixed-duration day shifts, unit-based assignment of hospitalists is the most common practice inhibiting surge capacity. Not long ago I worked with a practice that followed very strict unit-based assignments, which significantly inhibited “load-leveling,” and thus surge capacity. On any given day the patient volume for the whole practice might be very reasonable, but because it was never distributed evenly among the rounders, there was a very good chance that at least one doctor was drowning in work. And because of the strict approach, the other doctors didn’t come to the rescue.
I think the only reasonable approach is to deviate from such a strict unit-based assignment, at least a little. One rounder could be a utility doctor who doesn’t have her own unit and instead roams throughout the hospital, having been assigned patients based on the workload of each of her unit-based colleagues. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants (www.nelsonflores.com) and codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Last month I began looking at ways hospitalist practices can manage unpredictable increases in patient volume, also known as surge staffing. I provided my view of a “jeopardy” system and a patient volume cap for hospitalists. While both are potentially very effective, they have a high cost and in my view are imperfect solutions. This month I’ll examine some less common strategies to provide surge staffing. Although less popular, I think these options are more valuable.
Schedule More Providers
I’ve worked with a lot of practices and am struck by how patient volume for nearly all of them falls within a reasonably predictable range. While no one can predict with certainty which days will be unusually busy or slow, nearly all practices have a range of daily encounters that is roughly half to 1 1/2 of the mean. For example, if a practice has a mean of 60 billable encounters per day, it probably ranges from about 30 to 90 encounters on any given day. (The larger the practice, the more likely they are to conform to this range. Small practices, with average daily encounters fewer than 20, have a much wider range of daily volumes as a percent of the mean.)
Despite knowing that volumes will vary unpredictably, most practices provide the same fixed “dose” of provider staffing every day—that is, the single most common model for staffing and scheduling is to provide a fixed number of day-shift doctors (“rounders”) who work a fixed number of hours. For example, with an average of 60 billable encounters a day, a hospitalist group might decide to staff with four day-shift rounders working 12-hour shifts. This equates to a fixed 48 hours of daytime staffing. This is reasonable until the busy days arrive. Those four doctors will be much busier than average when there are 90 patients to see in a day, and will probably have a hard time seeing 22 or 23 patients each during their 12-hour shift. If such a busy day occurs more than a couple of times annually, then the practice should probably make some changes.
One approach to solving this type of staffing predicament is to add a fifth day-shift rounder. In other words, when making staffing decisions, consider giving more weight to the busiest days than the average day. This sounds fine until thinking about the practice budget. It will be pretty expensive to add doctors every day just so there are enough on duty when things get really busy. But if the hospitalists are willing to accept reduced compensation, then it might be financially reasonable to go ahead and add staff. This is easiest to do when the hospitalists are paid a significant (e.g. ≥50%) portion of their income based on their productivity, which will enable the hospitalists themselves to have a lot of say about when it is time to add staff. (Being paid on a nearly fixed annual salary means that it is the finance person who usually has the say about when it is time to add staff. And you can bet he’ll be making staffing decisions based on the average daily encounters, rather than the busy days.)
My own preference would be to do just that: Accept a reduction in compensation in return for protection against really busy and stressful days. I’m not suggesting others should agree with me, and in my experience, most don’t. (My own practice partners don’t agree with me on this one.) So I’m not really recommending it as a best practice, but I want to ensure that you don’t forget it is an option. And keep in mind you could adjust staffing by degrees; some settings might add a half-time physician or a nonphysician provider to try to find the sweet spot between having enough staff on duty every day to handle surges in volume and the cost of that staffing to the employer—or the hospitalists themselves.
Of course, if I were willing to reduce my compensation and average daily workload, then I would expect to be freed from the expectation that all rounding doctors work 12-hour shifts. Let’s turn our attention to the interplay between fixed day-shift durations and surge staffing.
Fixed-Shift Schedules Inhibit Surge Capacity
I think it usually is best to avoid fixed durations for day shifts. It might be necessary to require at least one daytime rounder to stay at least until a specified time (e.g. the arrival of the night-shift doctor), but in most cases it is reasonable for some rounders to leave when their work is done. They might need to continue responding to pages until the start of the night shift, but it usually isn’t necessary to have all rounders in the hospital until a predetermined end of the shift.
The problem is that when shifts have a fixed duration, the providers will focus on the start and stop time of their shift and might be unwilling to work beyond it. If instead there are no clearly fixed start and stop times for each day shift, then the hospitalists are likely to be willing to simply work longer on busy days, as long as they can work shorter on slow days. This is probably the most effective method of surge capacity, and it fits well with staffing each day with more providers than are required for the average patient volume.
Simply having the rounding doctors work longer on busy days must be done within reason. And there is a really wide range of opinion about what is reasonable. I think it is reasonable if a hospitalist works two or three hours longer than usual for three or four consecutive busy days, as long as the hospitalist is allowed to work less on days that are not very busy. But just what is a reasonable maximum daily amount of work for even one day is a topic that can lead to passionate debate. You’ll have to decide the details of what is and isn’t acceptable in your group.
Unit-Based Assignments
Aside from fixed-duration day shifts, unit-based assignment of hospitalists is the most common practice inhibiting surge capacity. Not long ago I worked with a practice that followed very strict unit-based assignments, which significantly inhibited “load-leveling,” and thus surge capacity. On any given day the patient volume for the whole practice might be very reasonable, but because it was never distributed evenly among the rounders, there was a very good chance that at least one doctor was drowning in work. And because of the strict approach, the other doctors didn’t come to the rescue.
I think the only reasonable approach is to deviate from such a strict unit-based assignment, at least a little. One rounder could be a utility doctor who doesn’t have her own unit and instead roams throughout the hospital, having been assigned patients based on the workload of each of her unit-based colleagues. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants (www.nelsonflores.com) and codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Last month I began looking at ways hospitalist practices can manage unpredictable increases in patient volume, also known as surge staffing. I provided my view of a “jeopardy” system and a patient volume cap for hospitalists. While both are potentially very effective, they have a high cost and in my view are imperfect solutions. This month I’ll examine some less common strategies to provide surge staffing. Although less popular, I think these options are more valuable.
Schedule More Providers
I’ve worked with a lot of practices and am struck by how patient volume for nearly all of them falls within a reasonably predictable range. While no one can predict with certainty which days will be unusually busy or slow, nearly all practices have a range of daily encounters that is roughly half to 1 1/2 of the mean. For example, if a practice has a mean of 60 billable encounters per day, it probably ranges from about 30 to 90 encounters on any given day. (The larger the practice, the more likely they are to conform to this range. Small practices, with average daily encounters fewer than 20, have a much wider range of daily volumes as a percent of the mean.)
Despite knowing that volumes will vary unpredictably, most practices provide the same fixed “dose” of provider staffing every day—that is, the single most common model for staffing and scheduling is to provide a fixed number of day-shift doctors (“rounders”) who work a fixed number of hours. For example, with an average of 60 billable encounters a day, a hospitalist group might decide to staff with four day-shift rounders working 12-hour shifts. This equates to a fixed 48 hours of daytime staffing. This is reasonable until the busy days arrive. Those four doctors will be much busier than average when there are 90 patients to see in a day, and will probably have a hard time seeing 22 or 23 patients each during their 12-hour shift. If such a busy day occurs more than a couple of times annually, then the practice should probably make some changes.
One approach to solving this type of staffing predicament is to add a fifth day-shift rounder. In other words, when making staffing decisions, consider giving more weight to the busiest days than the average day. This sounds fine until thinking about the practice budget. It will be pretty expensive to add doctors every day just so there are enough on duty when things get really busy. But if the hospitalists are willing to accept reduced compensation, then it might be financially reasonable to go ahead and add staff. This is easiest to do when the hospitalists are paid a significant (e.g. ≥50%) portion of their income based on their productivity, which will enable the hospitalists themselves to have a lot of say about when it is time to add staff. (Being paid on a nearly fixed annual salary means that it is the finance person who usually has the say about when it is time to add staff. And you can bet he’ll be making staffing decisions based on the average daily encounters, rather than the busy days.)
My own preference would be to do just that: Accept a reduction in compensation in return for protection against really busy and stressful days. I’m not suggesting others should agree with me, and in my experience, most don’t. (My own practice partners don’t agree with me on this one.) So I’m not really recommending it as a best practice, but I want to ensure that you don’t forget it is an option. And keep in mind you could adjust staffing by degrees; some settings might add a half-time physician or a nonphysician provider to try to find the sweet spot between having enough staff on duty every day to handle surges in volume and the cost of that staffing to the employer—or the hospitalists themselves.
Of course, if I were willing to reduce my compensation and average daily workload, then I would expect to be freed from the expectation that all rounding doctors work 12-hour shifts. Let’s turn our attention to the interplay between fixed day-shift durations and surge staffing.
Fixed-Shift Schedules Inhibit Surge Capacity
I think it usually is best to avoid fixed durations for day shifts. It might be necessary to require at least one daytime rounder to stay at least until a specified time (e.g. the arrival of the night-shift doctor), but in most cases it is reasonable for some rounders to leave when their work is done. They might need to continue responding to pages until the start of the night shift, but it usually isn’t necessary to have all rounders in the hospital until a predetermined end of the shift.
The problem is that when shifts have a fixed duration, the providers will focus on the start and stop time of their shift and might be unwilling to work beyond it. If instead there are no clearly fixed start and stop times for each day shift, then the hospitalists are likely to be willing to simply work longer on busy days, as long as they can work shorter on slow days. This is probably the most effective method of surge capacity, and it fits well with staffing each day with more providers than are required for the average patient volume.
Simply having the rounding doctors work longer on busy days must be done within reason. And there is a really wide range of opinion about what is reasonable. I think it is reasonable if a hospitalist works two or three hours longer than usual for three or four consecutive busy days, as long as the hospitalist is allowed to work less on days that are not very busy. But just what is a reasonable maximum daily amount of work for even one day is a topic that can lead to passionate debate. You’ll have to decide the details of what is and isn’t acceptable in your group.
Unit-Based Assignments
Aside from fixed-duration day shifts, unit-based assignment of hospitalists is the most common practice inhibiting surge capacity. Not long ago I worked with a practice that followed very strict unit-based assignments, which significantly inhibited “load-leveling,” and thus surge capacity. On any given day the patient volume for the whole practice might be very reasonable, but because it was never distributed evenly among the rounders, there was a very good chance that at least one doctor was drowning in work. And because of the strict approach, the other doctors didn’t come to the rescue.
I think the only reasonable approach is to deviate from such a strict unit-based assignment, at least a little. One rounder could be a utility doctor who doesn’t have her own unit and instead roams throughout the hospital, having been assigned patients based on the workload of each of her unit-based colleagues. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants (www.nelsonflores.com) and codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Kids and Divorce: A Long-Term Commitment
Divorce is so common in the United States – ending about half of all marriages – that it will affect many patients and families in your practice. If your practice has about 2,000 children and adolescents from about 1,500 families, for example, hundreds of families will be dealing with predivorce marital tension, the divorce itself, or postdivorce concerns.
Start by screening for family functioning at every annual visit. Specifically, try to identify strife and stress early on, at a time when your inventions have the greatest preventive impact. Ask open-ended questions such as, “How are things going in the family?” or “Is there any tension or discord in the family or in the marriage?”
I recommend using the broader term “discord” because it will pick up a pending divorce and also identify other family stressors for the child. For example, research indicates that the years of arguing and fighting that often precede divorce may be more damaging to the child in the long term than the divorce itself.
Once you identify marital or family stress, strive for the following three long-term goals to optimize a healthy outcome for the child.
▸ First, make sure the child continues to function well in school, with peers, in activities, and in areas of self-esteem. The firr certain key signs that a child is not functioning well. Persistently lower school performance is one sign. Most children are't concentrate or perform as well at school in the year of the divorce, but it is a warning sign if the problems persist. Determine whether the child is still having difficulty adjusting to the divorce, and assess if there is ongoing discord or fighting about visitation, custody, child rearing, or finances after the divorce. Another warning sign is the child who drops an after-school activity during a divorce crisis, and fails to retume itin the next school year.
How a child relates to friends after the divorce can be important. In particular, ascertain how young or midadolescents treat members of the opposite sex. Look for patterns in their relationships that repeat some of the dysfunctional behaviors of their parents' marriage. Keep in mind that children are often unaware that they are repeating these family patterns.
For example, are girls who are adversely affected by divorce especially vulnerable to getting involved with older teenagers who might take advantage of them? Do you see any evidence of longing in the girls, or signs that they are seeking to replace something missing in their paternal relationship? This type of behavior is much less likely if the girl has had a good relationship with her father before, during, and after the divorce.
With teenage boys, consider how they treat their girlfriends. Is the boy supportive in his relationships, or does he have girlfriend after girlfriend because of a callous or insensitive attitude?
Referral for a mental health evaluation might be appropriate if you see a pattern of continuing dysfunction in a major area of the child's life or of unsatisfactory relationships as these younger teenagers enter high school, particularly if they are alienated from a parent.
▸ Second, ensure that parents are open and willing to answer the child's questions as the child tries to make sense of the divorce at each developmental stage. Help postdivorce families encourage the child to ask questions on an ongoing basis. If divorce happened when the child was a toddler, for example, they are going to have questions 5, 10, and 15 years later that they could not conceptualize until they reached the appropriate developmental point.
Parents may need your advice on how best to talk to their 5- or 8-year-old, a time when information should be concrete and straightforward. In contrast, a 14-year-old may be able to understand more conceptual and nuanced answers to their questions. For example, a younger child is unlikely to think about the divorce in terms of an extramarital affair or the impact on their college finances, but that may not be the case when the child is 14 or 15 years old. Keep in mind that many adolescents do not ask parents such difficult questions unless they are given permission in advance, and it's at a time when they feel safe and at ease.
▸ Third, counsel the family to facilitate a good relationship between the child and each parent over the long term. When families come to me and there is a lot of tension about visitation, custody, and money, I often focus them on the long-term goals. I ask, “What kind of relationship do you want with your child 10 and 15 years from now?”; “What is likely to result in a good long-term relationship with them?”; “Do you want to be able to be at their wedding?”; “Do you want to be close to your grandchildren?” Going all out for an extra few hours of visitation or not paying a bill is not likely to help achieve these long-term goals.
Again, early screening and intervention make your job easier. If a patient or family comes to you after years of negativity and a court fight over a bitter divorce, your ability to intervene effectively is already very limited.
Divorce is often an angry and divisive time. You can advise parents not to act out of anger by offering examples of divorcing parents who invested a lot of time and energy into winning short-term victories, only to see their efforts backfire later. Some parents believe that the child will be closer to them if they can make the child angry at the spouse. But children who feel they have to betray one parent to please the other often become resentful of this role over time.
In contrast, children who observe their parents working together with a sense of harmony and cooperation to make the custody, visitation, financial, and other arrangements successful are much less likely to blame themselves for the divorce. They also are much less likely to feel guilty when they connect more to one parent or the other at different points in their development.
It is important to monitor your patients for long-term effects of divorce up to and including the time you transition them to an adult care provider. Ask the older adolescent questions such as, “How do you feel about the divorce now, looking back on it [5, 10, or 15] years later?”; “How do you think it's affected you?”; and “Are there any things you'd like to change?”
If you do a review of how they integrated the divorce when they are in 10th or 11th grade, you will still have time to address any unresolved issues. If the child is distant with one parent, you can at least wonder if this is a point in time to reconnect and repair that relationship before the teenager goes to work or college and moves to being fully independent.
Pediatricians often have limited time to intervene. Some find this work very gratifying and feel comfortable with divorce-related issues. Others may choose to refer the patient to a social worker, psychologist, or child and adolescent psychiatrist, according to the severity of the situation. Some pediatric practices are fortunate to have a full- or part-time social worker.
If you want to counsel but your time is limited, consider offering a divorced-parent discussion and education group in your practice. You and/or a social worker could facilitate this forum. This resource can help parents share their experiences and strategies to ensure that children emerge as happy and healthy as possible after a divorce. In addition, this intervention can be cost-neutral if you charge parents a nominal fee.
Divorce is so common in the United States – ending about half of all marriages – that it will affect many patients and families in your practice. If your practice has about 2,000 children and adolescents from about 1,500 families, for example, hundreds of families will be dealing with predivorce marital tension, the divorce itself, or postdivorce concerns.
Start by screening for family functioning at every annual visit. Specifically, try to identify strife and stress early on, at a time when your inventions have the greatest preventive impact. Ask open-ended questions such as, “How are things going in the family?” or “Is there any tension or discord in the family or in the marriage?”
I recommend using the broader term “discord” because it will pick up a pending divorce and also identify other family stressors for the child. For example, research indicates that the years of arguing and fighting that often precede divorce may be more damaging to the child in the long term than the divorce itself.
Once you identify marital or family stress, strive for the following three long-term goals to optimize a healthy outcome for the child.
▸ First, make sure the child continues to function well in school, with peers, in activities, and in areas of self-esteem. The firr certain key signs that a child is not functioning well. Persistently lower school performance is one sign. Most children are't concentrate or perform as well at school in the year of the divorce, but it is a warning sign if the problems persist. Determine whether the child is still having difficulty adjusting to the divorce, and assess if there is ongoing discord or fighting about visitation, custody, child rearing, or finances after the divorce. Another warning sign is the child who drops an after-school activity during a divorce crisis, and fails to retume itin the next school year.
How a child relates to friends after the divorce can be important. In particular, ascertain how young or midadolescents treat members of the opposite sex. Look for patterns in their relationships that repeat some of the dysfunctional behaviors of their parents' marriage. Keep in mind that children are often unaware that they are repeating these family patterns.
For example, are girls who are adversely affected by divorce especially vulnerable to getting involved with older teenagers who might take advantage of them? Do you see any evidence of longing in the girls, or signs that they are seeking to replace something missing in their paternal relationship? This type of behavior is much less likely if the girl has had a good relationship with her father before, during, and after the divorce.
With teenage boys, consider how they treat their girlfriends. Is the boy supportive in his relationships, or does he have girlfriend after girlfriend because of a callous or insensitive attitude?
Referral for a mental health evaluation might be appropriate if you see a pattern of continuing dysfunction in a major area of the child's life or of unsatisfactory relationships as these younger teenagers enter high school, particularly if they are alienated from a parent.
▸ Second, ensure that parents are open and willing to answer the child's questions as the child tries to make sense of the divorce at each developmental stage. Help postdivorce families encourage the child to ask questions on an ongoing basis. If divorce happened when the child was a toddler, for example, they are going to have questions 5, 10, and 15 years later that they could not conceptualize until they reached the appropriate developmental point.
Parents may need your advice on how best to talk to their 5- or 8-year-old, a time when information should be concrete and straightforward. In contrast, a 14-year-old may be able to understand more conceptual and nuanced answers to their questions. For example, a younger child is unlikely to think about the divorce in terms of an extramarital affair or the impact on their college finances, but that may not be the case when the child is 14 or 15 years old. Keep in mind that many adolescents do not ask parents such difficult questions unless they are given permission in advance, and it's at a time when they feel safe and at ease.
▸ Third, counsel the family to facilitate a good relationship between the child and each parent over the long term. When families come to me and there is a lot of tension about visitation, custody, and money, I often focus them on the long-term goals. I ask, “What kind of relationship do you want with your child 10 and 15 years from now?”; “What is likely to result in a good long-term relationship with them?”; “Do you want to be able to be at their wedding?”; “Do you want to be close to your grandchildren?” Going all out for an extra few hours of visitation or not paying a bill is not likely to help achieve these long-term goals.
Again, early screening and intervention make your job easier. If a patient or family comes to you after years of negativity and a court fight over a bitter divorce, your ability to intervene effectively is already very limited.
Divorce is often an angry and divisive time. You can advise parents not to act out of anger by offering examples of divorcing parents who invested a lot of time and energy into winning short-term victories, only to see their efforts backfire later. Some parents believe that the child will be closer to them if they can make the child angry at the spouse. But children who feel they have to betray one parent to please the other often become resentful of this role over time.
In contrast, children who observe their parents working together with a sense of harmony and cooperation to make the custody, visitation, financial, and other arrangements successful are much less likely to blame themselves for the divorce. They also are much less likely to feel guilty when they connect more to one parent or the other at different points in their development.
It is important to monitor your patients for long-term effects of divorce up to and including the time you transition them to an adult care provider. Ask the older adolescent questions such as, “How do you feel about the divorce now, looking back on it [5, 10, or 15] years later?”; “How do you think it's affected you?”; and “Are there any things you'd like to change?”
If you do a review of how they integrated the divorce when they are in 10th or 11th grade, you will still have time to address any unresolved issues. If the child is distant with one parent, you can at least wonder if this is a point in time to reconnect and repair that relationship before the teenager goes to work or college and moves to being fully independent.
Pediatricians often have limited time to intervene. Some find this work very gratifying and feel comfortable with divorce-related issues. Others may choose to refer the patient to a social worker, psychologist, or child and adolescent psychiatrist, according to the severity of the situation. Some pediatric practices are fortunate to have a full- or part-time social worker.
If you want to counsel but your time is limited, consider offering a divorced-parent discussion and education group in your practice. You and/or a social worker could facilitate this forum. This resource can help parents share their experiences and strategies to ensure that children emerge as happy and healthy as possible after a divorce. In addition, this intervention can be cost-neutral if you charge parents a nominal fee.
Divorce is so common in the United States – ending about half of all marriages – that it will affect many patients and families in your practice. If your practice has about 2,000 children and adolescents from about 1,500 families, for example, hundreds of families will be dealing with predivorce marital tension, the divorce itself, or postdivorce concerns.
Start by screening for family functioning at every annual visit. Specifically, try to identify strife and stress early on, at a time when your inventions have the greatest preventive impact. Ask open-ended questions such as, “How are things going in the family?” or “Is there any tension or discord in the family or in the marriage?”
I recommend using the broader term “discord” because it will pick up a pending divorce and also identify other family stressors for the child. For example, research indicates that the years of arguing and fighting that often precede divorce may be more damaging to the child in the long term than the divorce itself.
Once you identify marital or family stress, strive for the following three long-term goals to optimize a healthy outcome for the child.
▸ First, make sure the child continues to function well in school, with peers, in activities, and in areas of self-esteem. The firr certain key signs that a child is not functioning well. Persistently lower school performance is one sign. Most children are't concentrate or perform as well at school in the year of the divorce, but it is a warning sign if the problems persist. Determine whether the child is still having difficulty adjusting to the divorce, and assess if there is ongoing discord or fighting about visitation, custody, child rearing, or finances after the divorce. Another warning sign is the child who drops an after-school activity during a divorce crisis, and fails to retume itin the next school year.
How a child relates to friends after the divorce can be important. In particular, ascertain how young or midadolescents treat members of the opposite sex. Look for patterns in their relationships that repeat some of the dysfunctional behaviors of their parents' marriage. Keep in mind that children are often unaware that they are repeating these family patterns.
For example, are girls who are adversely affected by divorce especially vulnerable to getting involved with older teenagers who might take advantage of them? Do you see any evidence of longing in the girls, or signs that they are seeking to replace something missing in their paternal relationship? This type of behavior is much less likely if the girl has had a good relationship with her father before, during, and after the divorce.
With teenage boys, consider how they treat their girlfriends. Is the boy supportive in his relationships, or does he have girlfriend after girlfriend because of a callous or insensitive attitude?
Referral for a mental health evaluation might be appropriate if you see a pattern of continuing dysfunction in a major area of the child's life or of unsatisfactory relationships as these younger teenagers enter high school, particularly if they are alienated from a parent.
▸ Second, ensure that parents are open and willing to answer the child's questions as the child tries to make sense of the divorce at each developmental stage. Help postdivorce families encourage the child to ask questions on an ongoing basis. If divorce happened when the child was a toddler, for example, they are going to have questions 5, 10, and 15 years later that they could not conceptualize until they reached the appropriate developmental point.
Parents may need your advice on how best to talk to their 5- or 8-year-old, a time when information should be concrete and straightforward. In contrast, a 14-year-old may be able to understand more conceptual and nuanced answers to their questions. For example, a younger child is unlikely to think about the divorce in terms of an extramarital affair or the impact on their college finances, but that may not be the case when the child is 14 or 15 years old. Keep in mind that many adolescents do not ask parents such difficult questions unless they are given permission in advance, and it's at a time when they feel safe and at ease.
▸ Third, counsel the family to facilitate a good relationship between the child and each parent over the long term. When families come to me and there is a lot of tension about visitation, custody, and money, I often focus them on the long-term goals. I ask, “What kind of relationship do you want with your child 10 and 15 years from now?”; “What is likely to result in a good long-term relationship with them?”; “Do you want to be able to be at their wedding?”; “Do you want to be close to your grandchildren?” Going all out for an extra few hours of visitation or not paying a bill is not likely to help achieve these long-term goals.
Again, early screening and intervention make your job easier. If a patient or family comes to you after years of negativity and a court fight over a bitter divorce, your ability to intervene effectively is already very limited.
Divorce is often an angry and divisive time. You can advise parents not to act out of anger by offering examples of divorcing parents who invested a lot of time and energy into winning short-term victories, only to see their efforts backfire later. Some parents believe that the child will be closer to them if they can make the child angry at the spouse. But children who feel they have to betray one parent to please the other often become resentful of this role over time.
In contrast, children who observe their parents working together with a sense of harmony and cooperation to make the custody, visitation, financial, and other arrangements successful are much less likely to blame themselves for the divorce. They also are much less likely to feel guilty when they connect more to one parent or the other at different points in their development.
It is important to monitor your patients for long-term effects of divorce up to and including the time you transition them to an adult care provider. Ask the older adolescent questions such as, “How do you feel about the divorce now, looking back on it [5, 10, or 15] years later?”; “How do you think it's affected you?”; and “Are there any things you'd like to change?”
If you do a review of how they integrated the divorce when they are in 10th or 11th grade, you will still have time to address any unresolved issues. If the child is distant with one parent, you can at least wonder if this is a point in time to reconnect and repair that relationship before the teenager goes to work or college and moves to being fully independent.
Pediatricians often have limited time to intervene. Some find this work very gratifying and feel comfortable with divorce-related issues. Others may choose to refer the patient to a social worker, psychologist, or child and adolescent psychiatrist, according to the severity of the situation. Some pediatric practices are fortunate to have a full- or part-time social worker.
If you want to counsel but your time is limited, consider offering a divorced-parent discussion and education group in your practice. You and/or a social worker could facilitate this forum. This resource can help parents share their experiences and strategies to ensure that children emerge as happy and healthy as possible after a divorce. In addition, this intervention can be cost-neutral if you charge parents a nominal fee.
Surge Protection

Unpredictable workloads and frequent interruptions are the things I regard as the most stressful components of work as a hospitalist. Your list might be very different, but I bet unpredictable workloads ranks at least in the top five of every hospitalist’s list.
I’ve discussed interruptions previously (see “Really, It’s Switch-Tasking,” p. 68, November 2008; “Technological Advance or Workplace Setback?” p. 69, December 2008), but this month and next will turn to unpredictable workloads. In other words, what are the strategies available to a hospitalist practice to provide surge capacity in response to such unpredictable increases in patient volume as an uptick in census or daily admissions 50% to 100% above normal? I’ll leave to others the topic of how hospitals respond to such disasters as terrorist attacks, earthquakes, etc.
The Bottom Line
Sadly, there is no magic bullet for the “surge” problem, and no way to protect on-duty hospitalists from the need to work harder when it gets busy. But we needn’t feel too sorry for ourselves; doctors in most other specialties who practice in the hospital face the same problem and tend to rely heavily on simply working harder and longer when it is unusually busy. Sometimes they couple the “work harder” mantra with other strategies, such as calling another doctor in to help.
Hospitalists have a duty to ensure high patient volume doesn’t lead to deterioration in the quality of patient care, but occasionally working longer days than average probably poses a low risk, and might be less risky than the additional handoffs usually associated with having a doctor on “jeopardy” to be called in when it’s busy. Routinely or frequently working unreasonably long days is another story.
The trick for HM programs is to build some surge capacity into the routine daily staffing 1) without exceeding a reasonable budget, while 2) ensuring that the hospitalists don’t simply become accustomed to light workloads as the only reasonable norm, which could lead to them becoming unwilling to accept higher, but still reasonable, workloads when needed. (More on these issues later.) First, I’ll go through what I see as the pros and cons of several approaches to addressing surges in patient volume. All are in use with variable frequency around the country.
“Jeopardy” System
In its most common form, a jeopardy system has an unscheduled doctor each day who must remain available on short notice by pager. When patient volume surges, the unscheduled doctor is paged to come in and help. In most cases, this doctor focuses primarily—or exclusively—on admitting patients for a few hours. So it is most common for this doctor to be called in late in the afternoon or early in the evening. The jeopardy doctor usually turns over all admitted patients to another hospitalist in the group for all subsequent care. In addition to providing surge capacity, the jeopardy doctor almost always is used to cover unexpected absences of scheduled doctors, including illness-related absences.
Sometimes this doctor is paid extra for each day or week spent being “available” on jeopardy duty (not to be confused with jury duty, though it can be equally difficult to get exempted from). Then again, it is not uncommon to have jeopardy duty included in base compensation. However, once a jeopardy doctor is actually called in to work, most practices pay additional compensation, often based on an hourly rate that usually is higher than the average compensation generated per hour for nonjeopardy work.
There are a number of reasonable ways to compensate the jeopardy doctor. You probably can get some good ideas by talking with others in your hospital who function in a similar capacity, such as cath-lab technicians who get called in on nights and weekends.
No definitive data are available to show how common the jeopardy system is, but my experience is that 30% to 50% of HM groups use some form of it. Its popularity is proof that it is a reasonable system, but I’m not convinced. I think it is in use by a lot of groups not because it is an optimal way to ensure surge capacity, but because it is easy to conceptualize and put in place, and because many hospitalists came from residency programs in which the system was standard.
The gaps between theoretical and realized benefits become evident once a practice implements a jeopardy system. For example, it might be really busy today, but Dr. Stravinsky doesn’t call in Dr. Copeland, who is on jeopardy, because next week their roles will be reversed and Dr. Stravinsky sure hopes he won’t be called in. No one wants to be the weak doctor who calls in the jeopardy doctor and spoils what was otherwise a day off.
I’ve worked with a lot of practices who say they have a jeopardy system in place, but when I ask for the last time the jeopardy doctor was called in, they say it has been more than a year, or in some cases never. So even if the policy manual says they have a jeopardy system, the doctors never activate it, so it provides no benefit.
Practices that do utilize the jeopardy doctor have their own problems, such as assigning that doctor’s admissions the next day. The jeopardy doctor might provide some relief today, but they essentially just delay the work of having to get to know all of those new patients until the morning, when everyone is very busy with rounds. So while there might be significant benefit in activating the jeopardy system today, it could just delay the problem of high workload until the next morning, which isn’t much of a net benefit for the practice.
A small number of practices call in the jeopardy doctor frequently, and sometimes have that doctor continue to round on admitted patients for the next few days. This usage might get the most value out of the system, but the practice should consider if it is more cost-effective, and less stressful for the doctors, if the system were reversed. For example, instead of having the doctor on jeopardy and called in as necessary, the doctor would report to work and be given the day off or let go early when it isn’t busy.
Despite my reservations, if you are convinced the jeopardy system is valuable and cost-effective, keep it in place. However, if your group is thinking about options to handle surge capacity, don’t be too quick to adopt a jeopardy system. It usually falls far short of a perfect solution.
Patient Volume Cap
Another way to address the problem of unpredictable increases in patient volume is to establish a patient volume (e.g., total census) cap for the whole hospitalist practice. Like the jeopardy system, this is an appealingly uncomplicated idea, and hospitalists who have finished residency within the last few years all worked with a cap.
Except for the rarest of exceptions, this is a poor idea and should be avoided if at all possible. I’ll leave for another time a discussion of all the political and financial costs of a cap system, but trust me on this one. It is best to avoid a cap.
Stay Tuned …
Next month, I’ll examine other strategies to provide surge capacity. I think they’re more valuable than the two I’ve mentioned here, but I need to warn you that they aren’t perfect and are more complicated to operationalize. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Unpredictable workloads and frequent interruptions are the things I regard as the most stressful components of work as a hospitalist. Your list might be very different, but I bet unpredictable workloads ranks at least in the top five of every hospitalist’s list.
I’ve discussed interruptions previously (see “Really, It’s Switch-Tasking,” p. 68, November 2008; “Technological Advance or Workplace Setback?” p. 69, December 2008), but this month and next will turn to unpredictable workloads. In other words, what are the strategies available to a hospitalist practice to provide surge capacity in response to such unpredictable increases in patient volume as an uptick in census or daily admissions 50% to 100% above normal? I’ll leave to others the topic of how hospitals respond to such disasters as terrorist attacks, earthquakes, etc.
The Bottom Line
Sadly, there is no magic bullet for the “surge” problem, and no way to protect on-duty hospitalists from the need to work harder when it gets busy. But we needn’t feel too sorry for ourselves; doctors in most other specialties who practice in the hospital face the same problem and tend to rely heavily on simply working harder and longer when it is unusually busy. Sometimes they couple the “work harder” mantra with other strategies, such as calling another doctor in to help.
Hospitalists have a duty to ensure high patient volume doesn’t lead to deterioration in the quality of patient care, but occasionally working longer days than average probably poses a low risk, and might be less risky than the additional handoffs usually associated with having a doctor on “jeopardy” to be called in when it’s busy. Routinely or frequently working unreasonably long days is another story.
The trick for HM programs is to build some surge capacity into the routine daily staffing 1) without exceeding a reasonable budget, while 2) ensuring that the hospitalists don’t simply become accustomed to light workloads as the only reasonable norm, which could lead to them becoming unwilling to accept higher, but still reasonable, workloads when needed. (More on these issues later.) First, I’ll go through what I see as the pros and cons of several approaches to addressing surges in patient volume. All are in use with variable frequency around the country.
“Jeopardy” System
In its most common form, a jeopardy system has an unscheduled doctor each day who must remain available on short notice by pager. When patient volume surges, the unscheduled doctor is paged to come in and help. In most cases, this doctor focuses primarily—or exclusively—on admitting patients for a few hours. So it is most common for this doctor to be called in late in the afternoon or early in the evening. The jeopardy doctor usually turns over all admitted patients to another hospitalist in the group for all subsequent care. In addition to providing surge capacity, the jeopardy doctor almost always is used to cover unexpected absences of scheduled doctors, including illness-related absences.
Sometimes this doctor is paid extra for each day or week spent being “available” on jeopardy duty (not to be confused with jury duty, though it can be equally difficult to get exempted from). Then again, it is not uncommon to have jeopardy duty included in base compensation. However, once a jeopardy doctor is actually called in to work, most practices pay additional compensation, often based on an hourly rate that usually is higher than the average compensation generated per hour for nonjeopardy work.
There are a number of reasonable ways to compensate the jeopardy doctor. You probably can get some good ideas by talking with others in your hospital who function in a similar capacity, such as cath-lab technicians who get called in on nights and weekends.
No definitive data are available to show how common the jeopardy system is, but my experience is that 30% to 50% of HM groups use some form of it. Its popularity is proof that it is a reasonable system, but I’m not convinced. I think it is in use by a lot of groups not because it is an optimal way to ensure surge capacity, but because it is easy to conceptualize and put in place, and because many hospitalists came from residency programs in which the system was standard.
The gaps between theoretical and realized benefits become evident once a practice implements a jeopardy system. For example, it might be really busy today, but Dr. Stravinsky doesn’t call in Dr. Copeland, who is on jeopardy, because next week their roles will be reversed and Dr. Stravinsky sure hopes he won’t be called in. No one wants to be the weak doctor who calls in the jeopardy doctor and spoils what was otherwise a day off.
I’ve worked with a lot of practices who say they have a jeopardy system in place, but when I ask for the last time the jeopardy doctor was called in, they say it has been more than a year, or in some cases never. So even if the policy manual says they have a jeopardy system, the doctors never activate it, so it provides no benefit.
Practices that do utilize the jeopardy doctor have their own problems, such as assigning that doctor’s admissions the next day. The jeopardy doctor might provide some relief today, but they essentially just delay the work of having to get to know all of those new patients until the morning, when everyone is very busy with rounds. So while there might be significant benefit in activating the jeopardy system today, it could just delay the problem of high workload until the next morning, which isn’t much of a net benefit for the practice.
A small number of practices call in the jeopardy doctor frequently, and sometimes have that doctor continue to round on admitted patients for the next few days. This usage might get the most value out of the system, but the practice should consider if it is more cost-effective, and less stressful for the doctors, if the system were reversed. For example, instead of having the doctor on jeopardy and called in as necessary, the doctor would report to work and be given the day off or let go early when it isn’t busy.
Despite my reservations, if you are convinced the jeopardy system is valuable and cost-effective, keep it in place. However, if your group is thinking about options to handle surge capacity, don’t be too quick to adopt a jeopardy system. It usually falls far short of a perfect solution.
Patient Volume Cap
Another way to address the problem of unpredictable increases in patient volume is to establish a patient volume (e.g., total census) cap for the whole hospitalist practice. Like the jeopardy system, this is an appealingly uncomplicated idea, and hospitalists who have finished residency within the last few years all worked with a cap.
Except for the rarest of exceptions, this is a poor idea and should be avoided if at all possible. I’ll leave for another time a discussion of all the political and financial costs of a cap system, but trust me on this one. It is best to avoid a cap.
Stay Tuned …
Next month, I’ll examine other strategies to provide surge capacity. I think they’re more valuable than the two I’ve mentioned here, but I need to warn you that they aren’t perfect and are more complicated to operationalize. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Unpredictable workloads and frequent interruptions are the things I regard as the most stressful components of work as a hospitalist. Your list might be very different, but I bet unpredictable workloads ranks at least in the top five of every hospitalist’s list.
I’ve discussed interruptions previously (see “Really, It’s Switch-Tasking,” p. 68, November 2008; “Technological Advance or Workplace Setback?” p. 69, December 2008), but this month and next will turn to unpredictable workloads. In other words, what are the strategies available to a hospitalist practice to provide surge capacity in response to such unpredictable increases in patient volume as an uptick in census or daily admissions 50% to 100% above normal? I’ll leave to others the topic of how hospitals respond to such disasters as terrorist attacks, earthquakes, etc.
The Bottom Line
Sadly, there is no magic bullet for the “surge” problem, and no way to protect on-duty hospitalists from the need to work harder when it gets busy. But we needn’t feel too sorry for ourselves; doctors in most other specialties who practice in the hospital face the same problem and tend to rely heavily on simply working harder and longer when it is unusually busy. Sometimes they couple the “work harder” mantra with other strategies, such as calling another doctor in to help.
Hospitalists have a duty to ensure high patient volume doesn’t lead to deterioration in the quality of patient care, but occasionally working longer days than average probably poses a low risk, and might be less risky than the additional handoffs usually associated with having a doctor on “jeopardy” to be called in when it’s busy. Routinely or frequently working unreasonably long days is another story.
The trick for HM programs is to build some surge capacity into the routine daily staffing 1) without exceeding a reasonable budget, while 2) ensuring that the hospitalists don’t simply become accustomed to light workloads as the only reasonable norm, which could lead to them becoming unwilling to accept higher, but still reasonable, workloads when needed. (More on these issues later.) First, I’ll go through what I see as the pros and cons of several approaches to addressing surges in patient volume. All are in use with variable frequency around the country.
“Jeopardy” System
In its most common form, a jeopardy system has an unscheduled doctor each day who must remain available on short notice by pager. When patient volume surges, the unscheduled doctor is paged to come in and help. In most cases, this doctor focuses primarily—or exclusively—on admitting patients for a few hours. So it is most common for this doctor to be called in late in the afternoon or early in the evening. The jeopardy doctor usually turns over all admitted patients to another hospitalist in the group for all subsequent care. In addition to providing surge capacity, the jeopardy doctor almost always is used to cover unexpected absences of scheduled doctors, including illness-related absences.
Sometimes this doctor is paid extra for each day or week spent being “available” on jeopardy duty (not to be confused with jury duty, though it can be equally difficult to get exempted from). Then again, it is not uncommon to have jeopardy duty included in base compensation. However, once a jeopardy doctor is actually called in to work, most practices pay additional compensation, often based on an hourly rate that usually is higher than the average compensation generated per hour for nonjeopardy work.
There are a number of reasonable ways to compensate the jeopardy doctor. You probably can get some good ideas by talking with others in your hospital who function in a similar capacity, such as cath-lab technicians who get called in on nights and weekends.
No definitive data are available to show how common the jeopardy system is, but my experience is that 30% to 50% of HM groups use some form of it. Its popularity is proof that it is a reasonable system, but I’m not convinced. I think it is in use by a lot of groups not because it is an optimal way to ensure surge capacity, but because it is easy to conceptualize and put in place, and because many hospitalists came from residency programs in which the system was standard.
The gaps between theoretical and realized benefits become evident once a practice implements a jeopardy system. For example, it might be really busy today, but Dr. Stravinsky doesn’t call in Dr. Copeland, who is on jeopardy, because next week their roles will be reversed and Dr. Stravinsky sure hopes he won’t be called in. No one wants to be the weak doctor who calls in the jeopardy doctor and spoils what was otherwise a day off.
I’ve worked with a lot of practices who say they have a jeopardy system in place, but when I ask for the last time the jeopardy doctor was called in, they say it has been more than a year, or in some cases never. So even if the policy manual says they have a jeopardy system, the doctors never activate it, so it provides no benefit.
Practices that do utilize the jeopardy doctor have their own problems, such as assigning that doctor’s admissions the next day. The jeopardy doctor might provide some relief today, but they essentially just delay the work of having to get to know all of those new patients until the morning, when everyone is very busy with rounds. So while there might be significant benefit in activating the jeopardy system today, it could just delay the problem of high workload until the next morning, which isn’t much of a net benefit for the practice.
A small number of practices call in the jeopardy doctor frequently, and sometimes have that doctor continue to round on admitted patients for the next few days. This usage might get the most value out of the system, but the practice should consider if it is more cost-effective, and less stressful for the doctors, if the system were reversed. For example, instead of having the doctor on jeopardy and called in as necessary, the doctor would report to work and be given the day off or let go early when it isn’t busy.
Despite my reservations, if you are convinced the jeopardy system is valuable and cost-effective, keep it in place. However, if your group is thinking about options to handle surge capacity, don’t be too quick to adopt a jeopardy system. It usually falls far short of a perfect solution.
Patient Volume Cap
Another way to address the problem of unpredictable increases in patient volume is to establish a patient volume (e.g., total census) cap for the whole hospitalist practice. Like the jeopardy system, this is an appealingly uncomplicated idea, and hospitalists who have finished residency within the last few years all worked with a cap.
Except for the rarest of exceptions, this is a poor idea and should be avoided if at all possible. I’ll leave for another time a discussion of all the political and financial costs of a cap system, but trust me on this one. It is best to avoid a cap.
Stay Tuned …
Next month, I’ll examine other strategies to provide surge capacity. I think they’re more valuable than the two I’ve mentioned here, but I need to warn you that they aren’t perfect and are more complicated to operationalize. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Help Parents Change Style for Raising Teens
www.CHADIS.compdnews@elsevier.com
Adolescents are often the most intimidating of our patients. Let's face it: Most of us chose pediatrics because we like little kids. If a 15-minute office visit with a sullen teenager can be so difficult, imagine living with one 24/7. Actually, many of us won't have to imagine—we ourselves are the parents of adolescents, and we know just how challenging that can be.
Despite our own feelings of inadequacy, we can help parents make the transition from raising the innocent younger child to guiding the testy teen into adulthood. A failure to make that transition in parenting style can contribute greatly to a suboptimal outcome.
But your guidance needs to start early. When a parent comes into the office demanding that you administer a drug test or a pregnancy test, you have probably missed the window for effective action. The horse is well out of the barn.
The time to start is earlier—much earlier. All of parenting involves the balancing act between supporting dependency and promoting independence. When people first become parents, they are consumed with accepting the huge dependency of their baby. As the child gets older, parents must allow the child more independence for things to go smoothly.
But adolescence is a time when that balancing act requires truly skilled acrobatics. Teens and their parents need to negotiate the “Four I's” of adolescent development: Initiative, Individuation, Independence, and Intimacy.
Adolescents clearly need to take the initiative in their activities, including when they do their chores and how they manage homework. If parents get in the way and try to structure all of that, they're going to get a lot of pushback.
In terms of individuation—discovering who they are—teenagers are highly sensitive to the standards of peers. They're more interested in what their peers think they should do than what their parents think they should do. On one level, this includes how many ear piercings they have and how they dress. But on a broader level, they need to think their parents are wrong about most things in order to feel “like their own person.” Offering an opinion can be beneficial in giving the adolescent something to counter, but ideally save consequences for more substantial failings. In terms of independence, teenagers are better educated by learning from the consequences of their own actions when those actions are not harmful to their futures.
And in terms of intimacy, teens want and need privacy for their budding relationships. Parents need to learn how to be available to talk about relationships, but not ask too many questions.
Different teens move through these changes at different times. And on top of that, the transition may not always go in one direction. A teen may want to be very independent in choosing her clothes. But the same teen may want a lot of parental help on getting her homework done and on handling peer situations. That's part of what makes parenting adolescents so difficult.
Parents need to gradually release control and let their teens exert more independence. But the key word in that sentence is “gradually,” and parents need to be alert for signs that the child is not ready or has not yet earned that freedom.
Let's say the parents have allowed their 13-year-old to have a cell phone. Let's say that a few weeks later, the child hurls the phone against the wall in anger, shattering it beyond repair. Some parents might be tempted to say: “That's it. I'm not buying you another cell phone until you're in college,” but that is unlikely to be the most educational solution. The time frame should be measured in days or weeks, not in months or years. If consequences are too severe, kids tend to write their parents off completely and feel they have been written off.
Instead, the parents should give the teen a clear path to re-earning the privilege, negotiating the terms. Maybe he has to contribute 80% of his allowance and do some extra chores until the phone is paid for. Showing that they're reasonable and willing to negotiate is a model of adult behavior, and it's also their key to success.
The older the child, the more important it is to negotiate what the rules are to be, and also what exceptions there might be. It's fine if there's a general rule that they can't stay out after 11 o'clock. But if a special event comes along that starts at 10 o'clock and won't end until 2 a.m., it's best to be flexible about the curfew this one time. When teens and parents negotiate one-time exceptions as needed, there is structure but rebellion or sneaking is not brought out.
Negotiation is important. A 30-year longitudinal study from the University of California, Berkeley, demonstrated that parents who managed to negotiate the rules with their children had more harmonious relationships with them later (New Dir. Child Adolesc. Dev. 2005;108:61–9). Often a dynamic arises in families where the parents are so generally annoyed with their teen that they reflexively answer, “No!” to any request. That can be really counterproductive when it comes to parenting adolescents. The first response should be: “Yes, if at all possible. Let's talk about it.”
I recommend that parents explicitly discuss the request using the following six points in deciding with the adolescent on their request. Posting these on the refrigerator and making discussing them a routine lets the teen know they are being taken seriously, slows the reflex to say “no,” and may help install them as a mantra in the teen's brain for future decision making:
Six Guides for Decision Making
1. Is it safe?
2. Is it legal?
3. Does it conflict with responsibilities?
4. Does it meet a developmental need?
5. Does it interfere with others?
6. Could it harm his/her development?
Anyone who's read “The Catcher in the Rye” (New York: Little, Brown and Co., 1951) by J.D. Salinger knows that teenagers are especially sensitive to hypocrisy. Parents often talk about the importance of being a moral person, but the teen is aware that they're cheating on their income taxes. They will reject their parents' moral code if they see them being hypocritical.
Clearly, the best way for the parent to encourage their offspring to uphold good moral standards is to actually live those standards 24/7. But almost everyone fails to live up to those standards from time to time, and if they're parents of an adolescent, the teen is sure to be right there when they do. Adolescents appreciate and learn from honesty when that happens. The parent could admit, “Yes, I know I said that you should never curse another driver, but I was so angry that I forgot my own rule.”
In these days of one- and two-child families, where parents often depend on their own children for friendship and companionship, it can be especially devastating to hear a teen say: “I hate you. You're the worst parents ever.” When that happens—and it's almost certain to happen, since it's the rare child who never utters such a sentiment—the parent's best response is not to rise to the bait of an angry teenager. They don't really mean it. And if the parent shows too much visible distress, or starts to punish them for saying those things, there won't be as much opportunity to recover. A simple “I am sorry you feel that way right now. I can see that you are really angry about [my decision, your curfew, what I said].”
And when the teen notices that the parent has not reacted to such provocation, that in itself is a valuable life lesson. The next time a street tough tosses off an insult, he'll be more likely to simply shrug his shoulders and walk away. For additional information on dealing with adolescents, the American Academy of Pediatrics maintains a particularly good collection of resources for parents at www.healthychildren.org
www.CHADIS.compdnews@elsevier.com
Adolescents are often the most intimidating of our patients. Let's face it: Most of us chose pediatrics because we like little kids. If a 15-minute office visit with a sullen teenager can be so difficult, imagine living with one 24/7. Actually, many of us won't have to imagine—we ourselves are the parents of adolescents, and we know just how challenging that can be.
Despite our own feelings of inadequacy, we can help parents make the transition from raising the innocent younger child to guiding the testy teen into adulthood. A failure to make that transition in parenting style can contribute greatly to a suboptimal outcome.
But your guidance needs to start early. When a parent comes into the office demanding that you administer a drug test or a pregnancy test, you have probably missed the window for effective action. The horse is well out of the barn.
The time to start is earlier—much earlier. All of parenting involves the balancing act between supporting dependency and promoting independence. When people first become parents, they are consumed with accepting the huge dependency of their baby. As the child gets older, parents must allow the child more independence for things to go smoothly.
But adolescence is a time when that balancing act requires truly skilled acrobatics. Teens and their parents need to negotiate the “Four I's” of adolescent development: Initiative, Individuation, Independence, and Intimacy.
Adolescents clearly need to take the initiative in their activities, including when they do their chores and how they manage homework. If parents get in the way and try to structure all of that, they're going to get a lot of pushback.
In terms of individuation—discovering who they are—teenagers are highly sensitive to the standards of peers. They're more interested in what their peers think they should do than what their parents think they should do. On one level, this includes how many ear piercings they have and how they dress. But on a broader level, they need to think their parents are wrong about most things in order to feel “like their own person.” Offering an opinion can be beneficial in giving the adolescent something to counter, but ideally save consequences for more substantial failings. In terms of independence, teenagers are better educated by learning from the consequences of their own actions when those actions are not harmful to their futures.
And in terms of intimacy, teens want and need privacy for their budding relationships. Parents need to learn how to be available to talk about relationships, but not ask too many questions.
Different teens move through these changes at different times. And on top of that, the transition may not always go in one direction. A teen may want to be very independent in choosing her clothes. But the same teen may want a lot of parental help on getting her homework done and on handling peer situations. That's part of what makes parenting adolescents so difficult.
Parents need to gradually release control and let their teens exert more independence. But the key word in that sentence is “gradually,” and parents need to be alert for signs that the child is not ready or has not yet earned that freedom.
Let's say the parents have allowed their 13-year-old to have a cell phone. Let's say that a few weeks later, the child hurls the phone against the wall in anger, shattering it beyond repair. Some parents might be tempted to say: “That's it. I'm not buying you another cell phone until you're in college,” but that is unlikely to be the most educational solution. The time frame should be measured in days or weeks, not in months or years. If consequences are too severe, kids tend to write their parents off completely and feel they have been written off.
Instead, the parents should give the teen a clear path to re-earning the privilege, negotiating the terms. Maybe he has to contribute 80% of his allowance and do some extra chores until the phone is paid for. Showing that they're reasonable and willing to negotiate is a model of adult behavior, and it's also their key to success.
The older the child, the more important it is to negotiate what the rules are to be, and also what exceptions there might be. It's fine if there's a general rule that they can't stay out after 11 o'clock. But if a special event comes along that starts at 10 o'clock and won't end until 2 a.m., it's best to be flexible about the curfew this one time. When teens and parents negotiate one-time exceptions as needed, there is structure but rebellion or sneaking is not brought out.
Negotiation is important. A 30-year longitudinal study from the University of California, Berkeley, demonstrated that parents who managed to negotiate the rules with their children had more harmonious relationships with them later (New Dir. Child Adolesc. Dev. 2005;108:61–9). Often a dynamic arises in families where the parents are so generally annoyed with their teen that they reflexively answer, “No!” to any request. That can be really counterproductive when it comes to parenting adolescents. The first response should be: “Yes, if at all possible. Let's talk about it.”
I recommend that parents explicitly discuss the request using the following six points in deciding with the adolescent on their request. Posting these on the refrigerator and making discussing them a routine lets the teen know they are being taken seriously, slows the reflex to say “no,” and may help install them as a mantra in the teen's brain for future decision making:
Six Guides for Decision Making
1. Is it safe?
2. Is it legal?
3. Does it conflict with responsibilities?
4. Does it meet a developmental need?
5. Does it interfere with others?
6. Could it harm his/her development?
Anyone who's read “The Catcher in the Rye” (New York: Little, Brown and Co., 1951) by J.D. Salinger knows that teenagers are especially sensitive to hypocrisy. Parents often talk about the importance of being a moral person, but the teen is aware that they're cheating on their income taxes. They will reject their parents' moral code if they see them being hypocritical.
Clearly, the best way for the parent to encourage their offspring to uphold good moral standards is to actually live those standards 24/7. But almost everyone fails to live up to those standards from time to time, and if they're parents of an adolescent, the teen is sure to be right there when they do. Adolescents appreciate and learn from honesty when that happens. The parent could admit, “Yes, I know I said that you should never curse another driver, but I was so angry that I forgot my own rule.”
In these days of one- and two-child families, where parents often depend on their own children for friendship and companionship, it can be especially devastating to hear a teen say: “I hate you. You're the worst parents ever.” When that happens—and it's almost certain to happen, since it's the rare child who never utters such a sentiment—the parent's best response is not to rise to the bait of an angry teenager. They don't really mean it. And if the parent shows too much visible distress, or starts to punish them for saying those things, there won't be as much opportunity to recover. A simple “I am sorry you feel that way right now. I can see that you are really angry about [my decision, your curfew, what I said].”
And when the teen notices that the parent has not reacted to such provocation, that in itself is a valuable life lesson. The next time a street tough tosses off an insult, he'll be more likely to simply shrug his shoulders and walk away. For additional information on dealing with adolescents, the American Academy of Pediatrics maintains a particularly good collection of resources for parents at www.healthychildren.org
www.CHADIS.compdnews@elsevier.com
Adolescents are often the most intimidating of our patients. Let's face it: Most of us chose pediatrics because we like little kids. If a 15-minute office visit with a sullen teenager can be so difficult, imagine living with one 24/7. Actually, many of us won't have to imagine—we ourselves are the parents of adolescents, and we know just how challenging that can be.
Despite our own feelings of inadequacy, we can help parents make the transition from raising the innocent younger child to guiding the testy teen into adulthood. A failure to make that transition in parenting style can contribute greatly to a suboptimal outcome.
But your guidance needs to start early. When a parent comes into the office demanding that you administer a drug test or a pregnancy test, you have probably missed the window for effective action. The horse is well out of the barn.
The time to start is earlier—much earlier. All of parenting involves the balancing act between supporting dependency and promoting independence. When people first become parents, they are consumed with accepting the huge dependency of their baby. As the child gets older, parents must allow the child more independence for things to go smoothly.
But adolescence is a time when that balancing act requires truly skilled acrobatics. Teens and their parents need to negotiate the “Four I's” of adolescent development: Initiative, Individuation, Independence, and Intimacy.
Adolescents clearly need to take the initiative in their activities, including when they do their chores and how they manage homework. If parents get in the way and try to structure all of that, they're going to get a lot of pushback.
In terms of individuation—discovering who they are—teenagers are highly sensitive to the standards of peers. They're more interested in what their peers think they should do than what their parents think they should do. On one level, this includes how many ear piercings they have and how they dress. But on a broader level, they need to think their parents are wrong about most things in order to feel “like their own person.” Offering an opinion can be beneficial in giving the adolescent something to counter, but ideally save consequences for more substantial failings. In terms of independence, teenagers are better educated by learning from the consequences of their own actions when those actions are not harmful to their futures.
And in terms of intimacy, teens want and need privacy for their budding relationships. Parents need to learn how to be available to talk about relationships, but not ask too many questions.
Different teens move through these changes at different times. And on top of that, the transition may not always go in one direction. A teen may want to be very independent in choosing her clothes. But the same teen may want a lot of parental help on getting her homework done and on handling peer situations. That's part of what makes parenting adolescents so difficult.
Parents need to gradually release control and let their teens exert more independence. But the key word in that sentence is “gradually,” and parents need to be alert for signs that the child is not ready or has not yet earned that freedom.
Let's say the parents have allowed their 13-year-old to have a cell phone. Let's say that a few weeks later, the child hurls the phone against the wall in anger, shattering it beyond repair. Some parents might be tempted to say: “That's it. I'm not buying you another cell phone until you're in college,” but that is unlikely to be the most educational solution. The time frame should be measured in days or weeks, not in months or years. If consequences are too severe, kids tend to write their parents off completely and feel they have been written off.
Instead, the parents should give the teen a clear path to re-earning the privilege, negotiating the terms. Maybe he has to contribute 80% of his allowance and do some extra chores until the phone is paid for. Showing that they're reasonable and willing to negotiate is a model of adult behavior, and it's also their key to success.
The older the child, the more important it is to negotiate what the rules are to be, and also what exceptions there might be. It's fine if there's a general rule that they can't stay out after 11 o'clock. But if a special event comes along that starts at 10 o'clock and won't end until 2 a.m., it's best to be flexible about the curfew this one time. When teens and parents negotiate one-time exceptions as needed, there is structure but rebellion or sneaking is not brought out.
Negotiation is important. A 30-year longitudinal study from the University of California, Berkeley, demonstrated that parents who managed to negotiate the rules with their children had more harmonious relationships with them later (New Dir. Child Adolesc. Dev. 2005;108:61–9). Often a dynamic arises in families where the parents are so generally annoyed with their teen that they reflexively answer, “No!” to any request. That can be really counterproductive when it comes to parenting adolescents. The first response should be: “Yes, if at all possible. Let's talk about it.”
I recommend that parents explicitly discuss the request using the following six points in deciding with the adolescent on their request. Posting these on the refrigerator and making discussing them a routine lets the teen know they are being taken seriously, slows the reflex to say “no,” and may help install them as a mantra in the teen's brain for future decision making:
Six Guides for Decision Making
1. Is it safe?
2. Is it legal?
3. Does it conflict with responsibilities?
4. Does it meet a developmental need?
5. Does it interfere with others?
6. Could it harm his/her development?
Anyone who's read “The Catcher in the Rye” (New York: Little, Brown and Co., 1951) by J.D. Salinger knows that teenagers are especially sensitive to hypocrisy. Parents often talk about the importance of being a moral person, but the teen is aware that they're cheating on their income taxes. They will reject their parents' moral code if they see them being hypocritical.
Clearly, the best way for the parent to encourage their offspring to uphold good moral standards is to actually live those standards 24/7. But almost everyone fails to live up to those standards from time to time, and if they're parents of an adolescent, the teen is sure to be right there when they do. Adolescents appreciate and learn from honesty when that happens. The parent could admit, “Yes, I know I said that you should never curse another driver, but I was so angry that I forgot my own rule.”
In these days of one- and two-child families, where parents often depend on their own children for friendship and companionship, it can be especially devastating to hear a teen say: “I hate you. You're the worst parents ever.” When that happens—and it's almost certain to happen, since it's the rare child who never utters such a sentiment—the parent's best response is not to rise to the bait of an angry teenager. They don't really mean it. And if the parent shows too much visible distress, or starts to punish them for saying those things, there won't be as much opportunity to recover. A simple “I am sorry you feel that way right now. I can see that you are really angry about [my decision, your curfew, what I said].”
And when the teen notices that the parent has not reacted to such provocation, that in itself is a valuable life lesson. The next time a street tough tosses off an insult, he'll be more likely to simply shrug his shoulders and walk away. For additional information on dealing with adolescents, the American Academy of Pediatrics maintains a particularly good collection of resources for parents at www.healthychildren.org
Financial Risk

When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Be Alert to Red Flags Heralding Families at Risk
Stress is nothing new to American families, who—over the generations—have endured wars, epidemics, natural disasters, and numerous economic downturns.
Today's dismal economic climate with continuing unemployment poses real challenges for families.
You should be especially attuned to warning signs that more children in your practice may be at risk for hunger, displacement from their homes and schools, and poverty-associated trauma, both physical and psychological.
The statistics are sobering.
In June 2010, unemployment stood at 14.6 million people, or 9.5% of the working-age population nationwide. Even more people are jobless in some unfortunate states and cities—more than 14% in Nevada, for instance; 14.5% in Las Vegas, Nev.; and 27.6% in tiny El Centro, Calif.
Homelessness among American families is growing, with 170,000 families seeking shelter in 2009, up from 159,000 the year before, according to the U.S. Department of Housing and Urban Development.
Every 3 months, another 250,000 families' homes enter foreclosure, putting one child in every classroom at risk of losing his or her home, according to the Mortgage Bankers Association. That statistic is so stunning—home foreclosures impacting one child in every classroom—that it bears repeating as it indicates every pediatric practice has more red flags in terms of psychosocial stressors then at any time in most pediatrician's career.
Families, as always, face crises unrelated to the economy as well: illness, marital discord, substance abuse, and intergenerational pressures, but economic downturns increase the prevalence of almost all of the crises on this list.
Poverty is the elephant in the room, exposing children to a host of contributors to an unstable environment that sets the stage for poor academic performance, increased mental health disorders, conduct problems, substance abuse, and difficulties in relationships.
The first red flag raised by a family in economic trouble probably isn't even seen in the examining room, but in your billing department, where reimbursements are likely down and delinquent accounts are likely up.
A family may be unable to produce a copay for a visit, or may have lost health insurance along with mom or dad's job. They may report multiple changes in their address. Mail from your office may be returned as undeliverable.
This is, of course, an economic problem for you and your practice, but it likely heralds medical and psychosocial problems as well. A child whose family cannot pay for your services may be twice as likely as a financially secure child to have depression, anxiety, and learning problems at school.
Your office staff may want to alert you to financial red flags not only as they appear on the office balance sheet, but as they relate to your care of the child as well.
Moving, for example, has many implications for a child's development and well-being.
A new address may mean changes in a child's school and after-school activities, the loss of friends and close access to extended family members, and a shattering of the security of familiar places and routines. If the move was involuntary, say, a forced exit from a foreclosed home, parents may be so distracted and emotionally spent, they may not have devoted time to calmly explaining to the child what will change and what will stay the same.
I always think it's a good idea, but especially so in hard times, for you to ask one screening question of every family during routine office visits.
That bushel basket question is, “Are there any ongoing tensions affecting the family?”
Answers can potentially cover a lot of ground, and may open the door to a family sharing financial concerns, as well as any other issues that may be troubling them: a recent move, concern about a family member, or signs of domestic strife.
Red flags may appear during your examination as well. Immunizations may not be up to date, problems are suddenly arising at school, or a there may be a change in trajectory of the child's weight curve due to a lack of nutritious food.
Fatigue and stress associated with family troubles may be cloaked in somatic diagnoses: headaches, stomachaches, chest pain, weakness, or dizziness in a child who never had such complaints before or where these symptoms previously have signaled stress.
Take a good look at the parent accompanying your patient as well. Does the mother or father seem more withdrawn, sadder, or more anxious than expected?
Often, you have an internal red flag, a vaguely unsettled feeling that something is not right. Do not underestimate the value of this clinical sixth sense. Listen to it. It may not be anything specific that you can put your finger on or diagnose, but if you're getting that signal from within, sit down and take the pulse of the family in these troubling times.
Stress is nothing new to American families, who—over the generations—have endured wars, epidemics, natural disasters, and numerous economic downturns.
Today's dismal economic climate with continuing unemployment poses real challenges for families.
You should be especially attuned to warning signs that more children in your practice may be at risk for hunger, displacement from their homes and schools, and poverty-associated trauma, both physical and psychological.
The statistics are sobering.
In June 2010, unemployment stood at 14.6 million people, or 9.5% of the working-age population nationwide. Even more people are jobless in some unfortunate states and cities—more than 14% in Nevada, for instance; 14.5% in Las Vegas, Nev.; and 27.6% in tiny El Centro, Calif.
Homelessness among American families is growing, with 170,000 families seeking shelter in 2009, up from 159,000 the year before, according to the U.S. Department of Housing and Urban Development.
Every 3 months, another 250,000 families' homes enter foreclosure, putting one child in every classroom at risk of losing his or her home, according to the Mortgage Bankers Association. That statistic is so stunning—home foreclosures impacting one child in every classroom—that it bears repeating as it indicates every pediatric practice has more red flags in terms of psychosocial stressors then at any time in most pediatrician's career.
Families, as always, face crises unrelated to the economy as well: illness, marital discord, substance abuse, and intergenerational pressures, but economic downturns increase the prevalence of almost all of the crises on this list.
Poverty is the elephant in the room, exposing children to a host of contributors to an unstable environment that sets the stage for poor academic performance, increased mental health disorders, conduct problems, substance abuse, and difficulties in relationships.
The first red flag raised by a family in economic trouble probably isn't even seen in the examining room, but in your billing department, where reimbursements are likely down and delinquent accounts are likely up.
A family may be unable to produce a copay for a visit, or may have lost health insurance along with mom or dad's job. They may report multiple changes in their address. Mail from your office may be returned as undeliverable.
This is, of course, an economic problem for you and your practice, but it likely heralds medical and psychosocial problems as well. A child whose family cannot pay for your services may be twice as likely as a financially secure child to have depression, anxiety, and learning problems at school.
Your office staff may want to alert you to financial red flags not only as they appear on the office balance sheet, but as they relate to your care of the child as well.
Moving, for example, has many implications for a child's development and well-being.
A new address may mean changes in a child's school and after-school activities, the loss of friends and close access to extended family members, and a shattering of the security of familiar places and routines. If the move was involuntary, say, a forced exit from a foreclosed home, parents may be so distracted and emotionally spent, they may not have devoted time to calmly explaining to the child what will change and what will stay the same.
I always think it's a good idea, but especially so in hard times, for you to ask one screening question of every family during routine office visits.
That bushel basket question is, “Are there any ongoing tensions affecting the family?”
Answers can potentially cover a lot of ground, and may open the door to a family sharing financial concerns, as well as any other issues that may be troubling them: a recent move, concern about a family member, or signs of domestic strife.
Red flags may appear during your examination as well. Immunizations may not be up to date, problems are suddenly arising at school, or a there may be a change in trajectory of the child's weight curve due to a lack of nutritious food.
Fatigue and stress associated with family troubles may be cloaked in somatic diagnoses: headaches, stomachaches, chest pain, weakness, or dizziness in a child who never had such complaints before or where these symptoms previously have signaled stress.
Take a good look at the parent accompanying your patient as well. Does the mother or father seem more withdrawn, sadder, or more anxious than expected?
Often, you have an internal red flag, a vaguely unsettled feeling that something is not right. Do not underestimate the value of this clinical sixth sense. Listen to it. It may not be anything specific that you can put your finger on or diagnose, but if you're getting that signal from within, sit down and take the pulse of the family in these troubling times.
Stress is nothing new to American families, who—over the generations—have endured wars, epidemics, natural disasters, and numerous economic downturns.
Today's dismal economic climate with continuing unemployment poses real challenges for families.
You should be especially attuned to warning signs that more children in your practice may be at risk for hunger, displacement from their homes and schools, and poverty-associated trauma, both physical and psychological.
The statistics are sobering.
In June 2010, unemployment stood at 14.6 million people, or 9.5% of the working-age population nationwide. Even more people are jobless in some unfortunate states and cities—more than 14% in Nevada, for instance; 14.5% in Las Vegas, Nev.; and 27.6% in tiny El Centro, Calif.
Homelessness among American families is growing, with 170,000 families seeking shelter in 2009, up from 159,000 the year before, according to the U.S. Department of Housing and Urban Development.
Every 3 months, another 250,000 families' homes enter foreclosure, putting one child in every classroom at risk of losing his or her home, according to the Mortgage Bankers Association. That statistic is so stunning—home foreclosures impacting one child in every classroom—that it bears repeating as it indicates every pediatric practice has more red flags in terms of psychosocial stressors then at any time in most pediatrician's career.
Families, as always, face crises unrelated to the economy as well: illness, marital discord, substance abuse, and intergenerational pressures, but economic downturns increase the prevalence of almost all of the crises on this list.
Poverty is the elephant in the room, exposing children to a host of contributors to an unstable environment that sets the stage for poor academic performance, increased mental health disorders, conduct problems, substance abuse, and difficulties in relationships.
The first red flag raised by a family in economic trouble probably isn't even seen in the examining room, but in your billing department, where reimbursements are likely down and delinquent accounts are likely up.
A family may be unable to produce a copay for a visit, or may have lost health insurance along with mom or dad's job. They may report multiple changes in their address. Mail from your office may be returned as undeliverable.
This is, of course, an economic problem for you and your practice, but it likely heralds medical and psychosocial problems as well. A child whose family cannot pay for your services may be twice as likely as a financially secure child to have depression, anxiety, and learning problems at school.
Your office staff may want to alert you to financial red flags not only as they appear on the office balance sheet, but as they relate to your care of the child as well.
Moving, for example, has many implications for a child's development and well-being.
A new address may mean changes in a child's school and after-school activities, the loss of friends and close access to extended family members, and a shattering of the security of familiar places and routines. If the move was involuntary, say, a forced exit from a foreclosed home, parents may be so distracted and emotionally spent, they may not have devoted time to calmly explaining to the child what will change and what will stay the same.
I always think it's a good idea, but especially so in hard times, for you to ask one screening question of every family during routine office visits.
That bushel basket question is, “Are there any ongoing tensions affecting the family?”
Answers can potentially cover a lot of ground, and may open the door to a family sharing financial concerns, as well as any other issues that may be troubling them: a recent move, concern about a family member, or signs of domestic strife.
Red flags may appear during your examination as well. Immunizations may not be up to date, problems are suddenly arising at school, or a there may be a change in trajectory of the child's weight curve due to a lack of nutritious food.
Fatigue and stress associated with family troubles may be cloaked in somatic diagnoses: headaches, stomachaches, chest pain, weakness, or dizziness in a child who never had such complaints before or where these symptoms previously have signaled stress.
Take a good look at the parent accompanying your patient as well. Does the mother or father seem more withdrawn, sadder, or more anxious than expected?
Often, you have an internal red flag, a vaguely unsettled feeling that something is not right. Do not underestimate the value of this clinical sixth sense. Listen to it. It may not be anything specific that you can put your finger on or diagnose, but if you're getting that signal from within, sit down and take the pulse of the family in these troubling times.
Hospitalist Salary Spike

In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
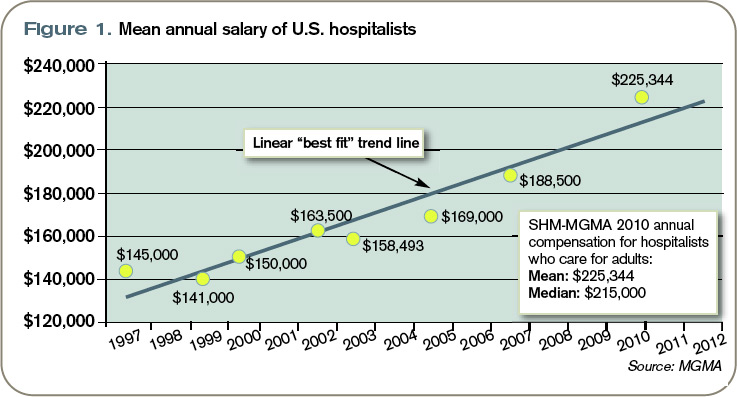
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Urge Parents to React Calmly to Sibling Rivalry
www.CHADIS.compdnews@elsevier.com
From Cane and Abel to Linus and Lucy, Wally and the Beaver to Bart and Lisa Simpson, sibling rivalry is the stuff of legend and comedy. But when it presents as a source of serious concern for parents during pediatric office visits, it's usually no laughing matter for them.
Research suggests that 64% of school-age siblings fight “sometimes or often”—a figure likely matched in magnitude if not muscle by younger siblings as well.
Sibling rivalry is so common, in fact, that we may tend to think back to our own sibling spats, or those of our kids, roll our eyes and offer the “they'll grow out of it” platitude.
But in truth, sibling wars can have consequences. While injuries are rare in most sibling disputes, in 25% of child abuse cases a sibling has been involved in victimization (usually in concert with adults).
Serious sibling conflict tremendously compromises quality of life for children, and for their parents as well. We know that marriages suffer in households with high levels of sibling discord, with the issue a common flashpoint for disagreements between parents about how to respond. Children exposed to serious sibling conflict in middle childhood appear to suffer higher levels of anxiety, depression, and delinquent behavior in early adolescence. Down the road, people carry the grudges of sibling difficulties for decades, undermining bonds that might otherwise be a significant source of support in our increasingly fragmented society.
So sibling struggles are worthy of our time and thoughtfulness, and addressing them productively will build trust in your relationship with parents and perhaps bring some semblance of peace to their households.
The first response to a parent's frustration over sibling quarrels should be to listen with respect. Their pain is often significant as they describe the battles unfolding among children they hold precious. Patiently listening to the details of sibling encounters also can help you sort out whether the issues they're describing fall into the normal range or may signify more serious individual or relational issues that deserve attention.
Assuming it's the former, I think it helps to remind parents of how common sibling rivalry is, and more importantly, why it occurs. Annoying as they may be, fracases actually serve a number of important biological functions. Watch any nature documentary featuring lions lounging under a tree on the savannah, and what are the cubs doing? Attacking, defending, tumbling, and biting, growling all the while.
In kids, like cubs, important social skills arise from the sibling relationship, even when the dust flies. Siblings teach each other to giggle and laugh, bait and switch, sneak and chase, parry and defend. From each other, they learn which jokes fly and which land with a thud, how to toss out an insult and absorb one tossed their way.
Siblings also learn how to pull their punches, practicing evolutionarily useful conflict skills while stopping short of inflicting serious harm.
The question remains, how does a family foster productive resilience-building sibling interactions while preserving affectionate connections and at least a modicum of household calm?
Like so many things in life, household chaos is associated with unhealthy levels of sibling conflict, according to research by psychologist Judy Dunn, the author of “Sisters and Brothers” (Cambridge: Harvard University Press, 1985), “Separate Lives: Why Siblings Are So Different” (New York: Basic Books, 1992), and “From One Child to Two” (New York: Ballantine Books, 1995).
Corporal punishment in the family makes rivalry worse as well.
Individual temperaments, the presence of a child with special needs, and family structure (children of opposite sexes) also have been found to play roles in sibling relationships, but spacing of children makes less of a difference than most people think. In general, children spaced more than 4 years apart have less conflict, but they also spend less time together and have less of an integrated relationship than closely spaced siblings do.
When looking at underlying dynamics, research points to the perception of favoritism by the parents as the main contributing factor. Importantly, the children's impressions of favoritism are not always accurate, but they are such an important driver of sibling conflict that they deserve consideration.
I suggest to parents that they make a special effort to provide roughly equal “alone” time with each child. When one child's needs really do require inordinate attention—as in the case of homework time for a child with learning disabilities—they need to be up front about that reality, and say, “If you need something special, I will be there for you, too.” Remind the child who feels slighted about exceptional times when all the focus was on them: during assembly of the science fair project, or when they learned to ride a bike, for example.
Acknowledge jealousy as a real and understandable emotion, but one that must be handled within limits and household rules.
Parents will do well to practice prevention with siblings, reinforcing cooperation in general and any specific examples of good deeds performed on behalf of each other with acknowledgment or even rewards if the rivalry is serious.
Advise parents to be sensitive to situations, like boredom, that lend themselves to sibling disputes, and to intervene with distractions. Promote cooperative projects and noncompetitive games: building a fort or puzzle, playing in the sprinkler, or making breakfast as a family, instead of games with winners and losers.
When board games are necessarily competitive, make it a practice to turn the board around every fourth move to minimize age-related inequities. Even out the teams in driveway basketball as well.
Once children are old enough to participate, family meetings are an excellent forum in which to air grievances. Again, ground rules apply; everyone gets to be heard. No interrupting. Solutions can be brainstormed and tried out, to be reviewed at the next regularly scheduled session.
A stepwise approach to dealing with actual sibling disputes also helps bring order to the chaos that feeds sibling wars. Parents may want to read the popular if optimistically titled book by Adele Faber and Irene Mazlish, “Siblings Without Rivalry” (New York: HarperCollins Publishing, 2004).
Essentially, their basic plan is to teach parents to ignore whatever can be ignored, thus avoiding a self-feeding loop of inadvertent reinforcement of the conflicts.
Situations that are a bit too much to ignore should be handled dispassionately. The parent may want to ask, “Is this a real fight or a play fight?” If it's a play fight but noisy, they might want to suggest a new venue—in the basement or outdoors.
If it's a real fight, encourage parents to simply describe the situation they see. “It looks like you both want to play with the truck, and it's hard to decide how to work it out.” Follow this with an affirming statement like, “I'm sure you can figure out a solution.”
If things are even more volatile—maybe someone has hit or pinched—parents should intervene, but in an unbiased manner and with the least amount of punishment that makes sense. They need to emphasize that hitting is never acceptable, but not take sides. A useful mantra for parents: “Don't try to judge who started it. You can never tell.”
Depending on the situation, both children may need to be sent to a room away from the toy to make a plan for resolution. The toy may need to be put in time out. Both kids may need to be put in time out for the same amount of time, with duration based on the younger child's age. Each child may need to take on an individual chore card, or even chores requiring the effort of both kids.
Whatever the solution, it should be brief.
Counsel parents that rivalry is part of sibling interaction: a challenge best met through prevention, structured responses, and reliance on family rules.
Remind them of the fleeting nature of sibling spats—don't they hear the kids giggling 15 minutes later?—and the permanence of warm, mutually respectful, sibling bonds through a lifetime.
www.CHADIS.compdnews@elsevier.com
From Cane and Abel to Linus and Lucy, Wally and the Beaver to Bart and Lisa Simpson, sibling rivalry is the stuff of legend and comedy. But when it presents as a source of serious concern for parents during pediatric office visits, it's usually no laughing matter for them.
Research suggests that 64% of school-age siblings fight “sometimes or often”—a figure likely matched in magnitude if not muscle by younger siblings as well.
Sibling rivalry is so common, in fact, that we may tend to think back to our own sibling spats, or those of our kids, roll our eyes and offer the “they'll grow out of it” platitude.
But in truth, sibling wars can have consequences. While injuries are rare in most sibling disputes, in 25% of child abuse cases a sibling has been involved in victimization (usually in concert with adults).
Serious sibling conflict tremendously compromises quality of life for children, and for their parents as well. We know that marriages suffer in households with high levels of sibling discord, with the issue a common flashpoint for disagreements between parents about how to respond. Children exposed to serious sibling conflict in middle childhood appear to suffer higher levels of anxiety, depression, and delinquent behavior in early adolescence. Down the road, people carry the grudges of sibling difficulties for decades, undermining bonds that might otherwise be a significant source of support in our increasingly fragmented society.
So sibling struggles are worthy of our time and thoughtfulness, and addressing them productively will build trust in your relationship with parents and perhaps bring some semblance of peace to their households.
The first response to a parent's frustration over sibling quarrels should be to listen with respect. Their pain is often significant as they describe the battles unfolding among children they hold precious. Patiently listening to the details of sibling encounters also can help you sort out whether the issues they're describing fall into the normal range or may signify more serious individual or relational issues that deserve attention.
Assuming it's the former, I think it helps to remind parents of how common sibling rivalry is, and more importantly, why it occurs. Annoying as they may be, fracases actually serve a number of important biological functions. Watch any nature documentary featuring lions lounging under a tree on the savannah, and what are the cubs doing? Attacking, defending, tumbling, and biting, growling all the while.
In kids, like cubs, important social skills arise from the sibling relationship, even when the dust flies. Siblings teach each other to giggle and laugh, bait and switch, sneak and chase, parry and defend. From each other, they learn which jokes fly and which land with a thud, how to toss out an insult and absorb one tossed their way.
Siblings also learn how to pull their punches, practicing evolutionarily useful conflict skills while stopping short of inflicting serious harm.
The question remains, how does a family foster productive resilience-building sibling interactions while preserving affectionate connections and at least a modicum of household calm?
Like so many things in life, household chaos is associated with unhealthy levels of sibling conflict, according to research by psychologist Judy Dunn, the author of “Sisters and Brothers” (Cambridge: Harvard University Press, 1985), “Separate Lives: Why Siblings Are So Different” (New York: Basic Books, 1992), and “From One Child to Two” (New York: Ballantine Books, 1995).
Corporal punishment in the family makes rivalry worse as well.
Individual temperaments, the presence of a child with special needs, and family structure (children of opposite sexes) also have been found to play roles in sibling relationships, but spacing of children makes less of a difference than most people think. In general, children spaced more than 4 years apart have less conflict, but they also spend less time together and have less of an integrated relationship than closely spaced siblings do.
When looking at underlying dynamics, research points to the perception of favoritism by the parents as the main contributing factor. Importantly, the children's impressions of favoritism are not always accurate, but they are such an important driver of sibling conflict that they deserve consideration.
I suggest to parents that they make a special effort to provide roughly equal “alone” time with each child. When one child's needs really do require inordinate attention—as in the case of homework time for a child with learning disabilities—they need to be up front about that reality, and say, “If you need something special, I will be there for you, too.” Remind the child who feels slighted about exceptional times when all the focus was on them: during assembly of the science fair project, or when they learned to ride a bike, for example.
Acknowledge jealousy as a real and understandable emotion, but one that must be handled within limits and household rules.
Parents will do well to practice prevention with siblings, reinforcing cooperation in general and any specific examples of good deeds performed on behalf of each other with acknowledgment or even rewards if the rivalry is serious.
Advise parents to be sensitive to situations, like boredom, that lend themselves to sibling disputes, and to intervene with distractions. Promote cooperative projects and noncompetitive games: building a fort or puzzle, playing in the sprinkler, or making breakfast as a family, instead of games with winners and losers.
When board games are necessarily competitive, make it a practice to turn the board around every fourth move to minimize age-related inequities. Even out the teams in driveway basketball as well.
Once children are old enough to participate, family meetings are an excellent forum in which to air grievances. Again, ground rules apply; everyone gets to be heard. No interrupting. Solutions can be brainstormed and tried out, to be reviewed at the next regularly scheduled session.
A stepwise approach to dealing with actual sibling disputes also helps bring order to the chaos that feeds sibling wars. Parents may want to read the popular if optimistically titled book by Adele Faber and Irene Mazlish, “Siblings Without Rivalry” (New York: HarperCollins Publishing, 2004).
Essentially, their basic plan is to teach parents to ignore whatever can be ignored, thus avoiding a self-feeding loop of inadvertent reinforcement of the conflicts.
Situations that are a bit too much to ignore should be handled dispassionately. The parent may want to ask, “Is this a real fight or a play fight?” If it's a play fight but noisy, they might want to suggest a new venue—in the basement or outdoors.
If it's a real fight, encourage parents to simply describe the situation they see. “It looks like you both want to play with the truck, and it's hard to decide how to work it out.” Follow this with an affirming statement like, “I'm sure you can figure out a solution.”
If things are even more volatile—maybe someone has hit or pinched—parents should intervene, but in an unbiased manner and with the least amount of punishment that makes sense. They need to emphasize that hitting is never acceptable, but not take sides. A useful mantra for parents: “Don't try to judge who started it. You can never tell.”
Depending on the situation, both children may need to be sent to a room away from the toy to make a plan for resolution. The toy may need to be put in time out. Both kids may need to be put in time out for the same amount of time, with duration based on the younger child's age. Each child may need to take on an individual chore card, or even chores requiring the effort of both kids.
Whatever the solution, it should be brief.
Counsel parents that rivalry is part of sibling interaction: a challenge best met through prevention, structured responses, and reliance on family rules.
Remind them of the fleeting nature of sibling spats—don't they hear the kids giggling 15 minutes later?—and the permanence of warm, mutually respectful, sibling bonds through a lifetime.
www.CHADIS.compdnews@elsevier.com
From Cane and Abel to Linus and Lucy, Wally and the Beaver to Bart and Lisa Simpson, sibling rivalry is the stuff of legend and comedy. But when it presents as a source of serious concern for parents during pediatric office visits, it's usually no laughing matter for them.
Research suggests that 64% of school-age siblings fight “sometimes or often”—a figure likely matched in magnitude if not muscle by younger siblings as well.
Sibling rivalry is so common, in fact, that we may tend to think back to our own sibling spats, or those of our kids, roll our eyes and offer the “they'll grow out of it” platitude.
But in truth, sibling wars can have consequences. While injuries are rare in most sibling disputes, in 25% of child abuse cases a sibling has been involved in victimization (usually in concert with adults).
Serious sibling conflict tremendously compromises quality of life for children, and for their parents as well. We know that marriages suffer in households with high levels of sibling discord, with the issue a common flashpoint for disagreements between parents about how to respond. Children exposed to serious sibling conflict in middle childhood appear to suffer higher levels of anxiety, depression, and delinquent behavior in early adolescence. Down the road, people carry the grudges of sibling difficulties for decades, undermining bonds that might otherwise be a significant source of support in our increasingly fragmented society.
So sibling struggles are worthy of our time and thoughtfulness, and addressing them productively will build trust in your relationship with parents and perhaps bring some semblance of peace to their households.
The first response to a parent's frustration over sibling quarrels should be to listen with respect. Their pain is often significant as they describe the battles unfolding among children they hold precious. Patiently listening to the details of sibling encounters also can help you sort out whether the issues they're describing fall into the normal range or may signify more serious individual or relational issues that deserve attention.
Assuming it's the former, I think it helps to remind parents of how common sibling rivalry is, and more importantly, why it occurs. Annoying as they may be, fracases actually serve a number of important biological functions. Watch any nature documentary featuring lions lounging under a tree on the savannah, and what are the cubs doing? Attacking, defending, tumbling, and biting, growling all the while.
In kids, like cubs, important social skills arise from the sibling relationship, even when the dust flies. Siblings teach each other to giggle and laugh, bait and switch, sneak and chase, parry and defend. From each other, they learn which jokes fly and which land with a thud, how to toss out an insult and absorb one tossed their way.
Siblings also learn how to pull their punches, practicing evolutionarily useful conflict skills while stopping short of inflicting serious harm.
The question remains, how does a family foster productive resilience-building sibling interactions while preserving affectionate connections and at least a modicum of household calm?
Like so many things in life, household chaos is associated with unhealthy levels of sibling conflict, according to research by psychologist Judy Dunn, the author of “Sisters and Brothers” (Cambridge: Harvard University Press, 1985), “Separate Lives: Why Siblings Are So Different” (New York: Basic Books, 1992), and “From One Child to Two” (New York: Ballantine Books, 1995).
Corporal punishment in the family makes rivalry worse as well.
Individual temperaments, the presence of a child with special needs, and family structure (children of opposite sexes) also have been found to play roles in sibling relationships, but spacing of children makes less of a difference than most people think. In general, children spaced more than 4 years apart have less conflict, but they also spend less time together and have less of an integrated relationship than closely spaced siblings do.
When looking at underlying dynamics, research points to the perception of favoritism by the parents as the main contributing factor. Importantly, the children's impressions of favoritism are not always accurate, but they are such an important driver of sibling conflict that they deserve consideration.
I suggest to parents that they make a special effort to provide roughly equal “alone” time with each child. When one child's needs really do require inordinate attention—as in the case of homework time for a child with learning disabilities—they need to be up front about that reality, and say, “If you need something special, I will be there for you, too.” Remind the child who feels slighted about exceptional times when all the focus was on them: during assembly of the science fair project, or when they learned to ride a bike, for example.
Acknowledge jealousy as a real and understandable emotion, but one that must be handled within limits and household rules.
Parents will do well to practice prevention with siblings, reinforcing cooperation in general and any specific examples of good deeds performed on behalf of each other with acknowledgment or even rewards if the rivalry is serious.
Advise parents to be sensitive to situations, like boredom, that lend themselves to sibling disputes, and to intervene with distractions. Promote cooperative projects and noncompetitive games: building a fort or puzzle, playing in the sprinkler, or making breakfast as a family, instead of games with winners and losers.
When board games are necessarily competitive, make it a practice to turn the board around every fourth move to minimize age-related inequities. Even out the teams in driveway basketball as well.
Once children are old enough to participate, family meetings are an excellent forum in which to air grievances. Again, ground rules apply; everyone gets to be heard. No interrupting. Solutions can be brainstormed and tried out, to be reviewed at the next regularly scheduled session.
A stepwise approach to dealing with actual sibling disputes also helps bring order to the chaos that feeds sibling wars. Parents may want to read the popular if optimistically titled book by Adele Faber and Irene Mazlish, “Siblings Without Rivalry” (New York: HarperCollins Publishing, 2004).
Essentially, their basic plan is to teach parents to ignore whatever can be ignored, thus avoiding a self-feeding loop of inadvertent reinforcement of the conflicts.
Situations that are a bit too much to ignore should be handled dispassionately. The parent may want to ask, “Is this a real fight or a play fight?” If it's a play fight but noisy, they might want to suggest a new venue—in the basement or outdoors.
If it's a real fight, encourage parents to simply describe the situation they see. “It looks like you both want to play with the truck, and it's hard to decide how to work it out.” Follow this with an affirming statement like, “I'm sure you can figure out a solution.”
If things are even more volatile—maybe someone has hit or pinched—parents should intervene, but in an unbiased manner and with the least amount of punishment that makes sense. They need to emphasize that hitting is never acceptable, but not take sides. A useful mantra for parents: “Don't try to judge who started it. You can never tell.”
Depending on the situation, both children may need to be sent to a room away from the toy to make a plan for resolution. The toy may need to be put in time out. Both kids may need to be put in time out for the same amount of time, with duration based on the younger child's age. Each child may need to take on an individual chore card, or even chores requiring the effort of both kids.
Whatever the solution, it should be brief.
Counsel parents that rivalry is part of sibling interaction: a challenge best met through prevention, structured responses, and reliance on family rules.
Remind them of the fleeting nature of sibling spats—don't they hear the kids giggling 15 minutes later?—and the permanence of warm, mutually respectful, sibling bonds through a lifetime.
Square Peg, Square Hole

I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
The Earlier, the Better

Most hospitals work hard to increase the portion of discharges that occur early in the workday and decrease the number that occur in the afternoon or evening. In every case, hospitalists have an important role in making this happen.
In my April 2009 column (“Top O’ the Morning,” p. 53), I wrote about why this is important to hospitals and which strategies hospitalists could adopt. But this is still such a big issue for hospitalists that I thought I would elaborate on a few of the really simple ideas. Your HM group could implement most of the following strategies beginning next week, and you wouldn’t need months of meetings with other hospital departments.
But before I get to the ideas, I want to mention a couple of other things. First, I can’t resist pointing out that giving hospitalists a financial incentive for writing the majority of discharge orders by a certain time in the morning has met with mixed results, despite the fact that some institutions believe this approach is valuable. In the absence of computerized physician order entry (CPOE), it can be really difficult to track exactly when the doctor wrote the discharge order. And, more importantly, a financial incentive might discourage a hospitalist from discharging a patient this afternoon, and they might instead wait to discharge tomorrow morning—adding to length of stay and defeating the goal of the incentive.
It turns out that a lot has been written about throughput; just do an Internet search and pair “throughput” with terms like “hospital,” “hospitalist,” “ED,” etc. Remarkably, I haven’t been able to dig up much material that specifically addresses early-morning discharges, which is an important component of throughput.
Let’s turn our attention to some specific recommendations for increasing morning discharges. Remember, I’ve selected these because they’re easy to implement and won’t require HM groups to negotiate with others at the hospital.
Write “Probable Discharge Tomorrow” Orders
Letting other staff know the anticipated discharge date via an order in the chart typically is more effective than writing the same information in the progress note section of the chart. Although a hospitalist should verbally communicate the anticipated discharge date with the patient’s nurse and discharge planner, it still is worthwhile to write an order, because it increases the chance all, or nearly all, staff (e.g., night nurses) will be aware of the plan and communicate the same message to the family.
Your group could establish a rule or financial incentive, such that all charts will be reviewed after discharge, and a certain portion (e.g., 85%) must have such an order written sometime prior to discharge. It doesn’t always need to be written on the day prior to discharge; instead, an order written on Monday could say “likely discharge on Wednesday or Thursday.” And, of course, there shouldn’t be a requirement that the patient actually be discharged on the day that was forecast.
Prepare the Day Prior
Typically, hospitalized-patient discharges are very time-consuming. Most discharges are complicated by last-minute medical or social loose ends that require attention. Routinely trying to uncover and address these on the evening prior to discharge will ensure that a larger percentage of patients will be discharged—and vacate their room—earlier the next day. Here is what this might look like:
On Tuesday, Dr. Guaraldi is wrapping up most work for the day. He stops by to see his patient, Mr. Schultz, to see if he is improving as expected. Indeed, Mr. Schultz is looking better and probably will be ready for discharge Wednesday morning. So, Dr. Guaraldi talks with Mr. Schultz and calls the patient’s daughter to answer any questions and concerns, ensuring no surprises by the Wednesday-morning discharge. When the daughter asks (as nearly all family members do) what time she should plan to pick up her dad, Dr. Guaraldi can suggest a time based on when he will be able to round in the morning. He also can arrange to have the discharge planning staff alerted if there are more complicated issues (e.g., arranging for professional transport home).
Dr. Guaraldi then dictates the discharge summary, addresses the discharge medicine reconciliation, and writes the prescriptions. In doing so, he might uncover some loose ends and might end up ordering a lab or imaging test to be done in the evening so the results will be available early Wednesday morning and won’t delay the routine discharge.
On Wednesday morning, Dr. Guaraldi rounds on Mr. Schultz early, finds the patient is improving as expected, and writes the discharge order. The whole visit takes only a few minutes, as most of the time-consuming work was completed the prior evening. In fact, because it is a relatively short visit, it is a lot easier for Dr. Guaraldi to arrange to round on Mr. Schultz early in the day (e.g., even on the way to see ICU patients), as the hospital’s chief medical officer is always asking him to do.
I hope this scenario doesn’t sound too difficult. (Another benefit of dictating discharge summaries the evening before discharge is that the typed document should be available the next morning, so the patient can have a copy to take with him at discharge.) Of course, it won’t apply to all patients, such as those patients whose discharges can’t be predicted.
Many hospitalists think arranging for discharge the evening before is impossible because “I’m just too spent at the end of a long day to stay late getting patients ready for discharge tomorrow!” But realize you won’t be doing any more work; you’re rearranging when you do the work. The time you spend arranging for discharge in advance will save you time and stress tomorrow. My own experience is that it is much easier to do all the discharge work the evening before than in the morning when I’m so busy and am being pulled in 10 different directions. Most morning discharge visits are relatively quick and painless, which is really valuable for increasing the efficiency and decreasing the stress of morning rounds.
The alert reader already has figured out there is a pretty big cost to doing the discharge work the evening before. Some patients won’t be able to discharge as planned (e.g., they have a fever overnight) and the preparations will have been in vain. My experience is that such “failed” discharges are reasonably common, but even when they occur, it is usually reasonable to use most of the original prescriptions and discharge summary, with an addendum as required. For example, Dr. Guaraldi could dictate an addendum stating:
“The patient originally was planned for discharge on Wednesday but had a temperature of 38.6 degrees Celsius the night before, so stayed in the hospital for two more days for … ”
Start Rounds Earlier
This strategy might be the most difficult for you and your HM group to arrange, but I propose it because you could do it without having to negotiate with a lot of other departments in the hospital. If your group currently has a day shift that starts at 8 a.m. with a team conference, you could instead start at 7 a.m. Your group could try to shorten the duration of the morning team conference, or eliminate it. Whether the need to get patients discharged early in the day is worth the complexity of rearranging your schedule will depend on the circumstances of your hospital and your group. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Most hospitals work hard to increase the portion of discharges that occur early in the workday and decrease the number that occur in the afternoon or evening. In every case, hospitalists have an important role in making this happen.
In my April 2009 column (“Top O’ the Morning,” p. 53), I wrote about why this is important to hospitals and which strategies hospitalists could adopt. But this is still such a big issue for hospitalists that I thought I would elaborate on a few of the really simple ideas. Your HM group could implement most of the following strategies beginning next week, and you wouldn’t need months of meetings with other hospital departments.
But before I get to the ideas, I want to mention a couple of other things. First, I can’t resist pointing out that giving hospitalists a financial incentive for writing the majority of discharge orders by a certain time in the morning has met with mixed results, despite the fact that some institutions believe this approach is valuable. In the absence of computerized physician order entry (CPOE), it can be really difficult to track exactly when the doctor wrote the discharge order. And, more importantly, a financial incentive might discourage a hospitalist from discharging a patient this afternoon, and they might instead wait to discharge tomorrow morning—adding to length of stay and defeating the goal of the incentive.
It turns out that a lot has been written about throughput; just do an Internet search and pair “throughput” with terms like “hospital,” “hospitalist,” “ED,” etc. Remarkably, I haven’t been able to dig up much material that specifically addresses early-morning discharges, which is an important component of throughput.
Let’s turn our attention to some specific recommendations for increasing morning discharges. Remember, I’ve selected these because they’re easy to implement and won’t require HM groups to negotiate with others at the hospital.
Write “Probable Discharge Tomorrow” Orders
Letting other staff know the anticipated discharge date via an order in the chart typically is more effective than writing the same information in the progress note section of the chart. Although a hospitalist should verbally communicate the anticipated discharge date with the patient’s nurse and discharge planner, it still is worthwhile to write an order, because it increases the chance all, or nearly all, staff (e.g., night nurses) will be aware of the plan and communicate the same message to the family.
Your group could establish a rule or financial incentive, such that all charts will be reviewed after discharge, and a certain portion (e.g., 85%) must have such an order written sometime prior to discharge. It doesn’t always need to be written on the day prior to discharge; instead, an order written on Monday could say “likely discharge on Wednesday or Thursday.” And, of course, there shouldn’t be a requirement that the patient actually be discharged on the day that was forecast.
Prepare the Day Prior
Typically, hospitalized-patient discharges are very time-consuming. Most discharges are complicated by last-minute medical or social loose ends that require attention. Routinely trying to uncover and address these on the evening prior to discharge will ensure that a larger percentage of patients will be discharged—and vacate their room—earlier the next day. Here is what this might look like:
On Tuesday, Dr. Guaraldi is wrapping up most work for the day. He stops by to see his patient, Mr. Schultz, to see if he is improving as expected. Indeed, Mr. Schultz is looking better and probably will be ready for discharge Wednesday morning. So, Dr. Guaraldi talks with Mr. Schultz and calls the patient’s daughter to answer any questions and concerns, ensuring no surprises by the Wednesday-morning discharge. When the daughter asks (as nearly all family members do) what time she should plan to pick up her dad, Dr. Guaraldi can suggest a time based on when he will be able to round in the morning. He also can arrange to have the discharge planning staff alerted if there are more complicated issues (e.g., arranging for professional transport home).
Dr. Guaraldi then dictates the discharge summary, addresses the discharge medicine reconciliation, and writes the prescriptions. In doing so, he might uncover some loose ends and might end up ordering a lab or imaging test to be done in the evening so the results will be available early Wednesday morning and won’t delay the routine discharge.
On Wednesday morning, Dr. Guaraldi rounds on Mr. Schultz early, finds the patient is improving as expected, and writes the discharge order. The whole visit takes only a few minutes, as most of the time-consuming work was completed the prior evening. In fact, because it is a relatively short visit, it is a lot easier for Dr. Guaraldi to arrange to round on Mr. Schultz early in the day (e.g., even on the way to see ICU patients), as the hospital’s chief medical officer is always asking him to do.
I hope this scenario doesn’t sound too difficult. (Another benefit of dictating discharge summaries the evening before discharge is that the typed document should be available the next morning, so the patient can have a copy to take with him at discharge.) Of course, it won’t apply to all patients, such as those patients whose discharges can’t be predicted.
Many hospitalists think arranging for discharge the evening before is impossible because “I’m just too spent at the end of a long day to stay late getting patients ready for discharge tomorrow!” But realize you won’t be doing any more work; you’re rearranging when you do the work. The time you spend arranging for discharge in advance will save you time and stress tomorrow. My own experience is that it is much easier to do all the discharge work the evening before than in the morning when I’m so busy and am being pulled in 10 different directions. Most morning discharge visits are relatively quick and painless, which is really valuable for increasing the efficiency and decreasing the stress of morning rounds.
The alert reader already has figured out there is a pretty big cost to doing the discharge work the evening before. Some patients won’t be able to discharge as planned (e.g., they have a fever overnight) and the preparations will have been in vain. My experience is that such “failed” discharges are reasonably common, but even when they occur, it is usually reasonable to use most of the original prescriptions and discharge summary, with an addendum as required. For example, Dr. Guaraldi could dictate an addendum stating:
“The patient originally was planned for discharge on Wednesday but had a temperature of 38.6 degrees Celsius the night before, so stayed in the hospital for two more days for … ”
Start Rounds Earlier
This strategy might be the most difficult for you and your HM group to arrange, but I propose it because you could do it without having to negotiate with a lot of other departments in the hospital. If your group currently has a day shift that starts at 8 a.m. with a team conference, you could instead start at 7 a.m. Your group could try to shorten the duration of the morning team conference, or eliminate it. Whether the need to get patients discharged early in the day is worth the complexity of rearranging your schedule will depend on the circumstances of your hospital and your group. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Most hospitals work hard to increase the portion of discharges that occur early in the workday and decrease the number that occur in the afternoon or evening. In every case, hospitalists have an important role in making this happen.
In my April 2009 column (“Top O’ the Morning,” p. 53), I wrote about why this is important to hospitals and which strategies hospitalists could adopt. But this is still such a big issue for hospitalists that I thought I would elaborate on a few of the really simple ideas. Your HM group could implement most of the following strategies beginning next week, and you wouldn’t need months of meetings with other hospital departments.
But before I get to the ideas, I want to mention a couple of other things. First, I can’t resist pointing out that giving hospitalists a financial incentive for writing the majority of discharge orders by a certain time in the morning has met with mixed results, despite the fact that some institutions believe this approach is valuable. In the absence of computerized physician order entry (CPOE), it can be really difficult to track exactly when the doctor wrote the discharge order. And, more importantly, a financial incentive might discourage a hospitalist from discharging a patient this afternoon, and they might instead wait to discharge tomorrow morning—adding to length of stay and defeating the goal of the incentive.
It turns out that a lot has been written about throughput; just do an Internet search and pair “throughput” with terms like “hospital,” “hospitalist,” “ED,” etc. Remarkably, I haven’t been able to dig up much material that specifically addresses early-morning discharges, which is an important component of throughput.
Let’s turn our attention to some specific recommendations for increasing morning discharges. Remember, I’ve selected these because they’re easy to implement and won’t require HM groups to negotiate with others at the hospital.
Write “Probable Discharge Tomorrow” Orders
Letting other staff know the anticipated discharge date via an order in the chart typically is more effective than writing the same information in the progress note section of the chart. Although a hospitalist should verbally communicate the anticipated discharge date with the patient’s nurse and discharge planner, it still is worthwhile to write an order, because it increases the chance all, or nearly all, staff (e.g., night nurses) will be aware of the plan and communicate the same message to the family.
Your group could establish a rule or financial incentive, such that all charts will be reviewed after discharge, and a certain portion (e.g., 85%) must have such an order written sometime prior to discharge. It doesn’t always need to be written on the day prior to discharge; instead, an order written on Monday could say “likely discharge on Wednesday or Thursday.” And, of course, there shouldn’t be a requirement that the patient actually be discharged on the day that was forecast.
Prepare the Day Prior
Typically, hospitalized-patient discharges are very time-consuming. Most discharges are complicated by last-minute medical or social loose ends that require attention. Routinely trying to uncover and address these on the evening prior to discharge will ensure that a larger percentage of patients will be discharged—and vacate their room—earlier the next day. Here is what this might look like:
On Tuesday, Dr. Guaraldi is wrapping up most work for the day. He stops by to see his patient, Mr. Schultz, to see if he is improving as expected. Indeed, Mr. Schultz is looking better and probably will be ready for discharge Wednesday morning. So, Dr. Guaraldi talks with Mr. Schultz and calls the patient’s daughter to answer any questions and concerns, ensuring no surprises by the Wednesday-morning discharge. When the daughter asks (as nearly all family members do) what time she should plan to pick up her dad, Dr. Guaraldi can suggest a time based on when he will be able to round in the morning. He also can arrange to have the discharge planning staff alerted if there are more complicated issues (e.g., arranging for professional transport home).
Dr. Guaraldi then dictates the discharge summary, addresses the discharge medicine reconciliation, and writes the prescriptions. In doing so, he might uncover some loose ends and might end up ordering a lab or imaging test to be done in the evening so the results will be available early Wednesday morning and won’t delay the routine discharge.
On Wednesday morning, Dr. Guaraldi rounds on Mr. Schultz early, finds the patient is improving as expected, and writes the discharge order. The whole visit takes only a few minutes, as most of the time-consuming work was completed the prior evening. In fact, because it is a relatively short visit, it is a lot easier for Dr. Guaraldi to arrange to round on Mr. Schultz early in the day (e.g., even on the way to see ICU patients), as the hospital’s chief medical officer is always asking him to do.
I hope this scenario doesn’t sound too difficult. (Another benefit of dictating discharge summaries the evening before discharge is that the typed document should be available the next morning, so the patient can have a copy to take with him at discharge.) Of course, it won’t apply to all patients, such as those patients whose discharges can’t be predicted.
Many hospitalists think arranging for discharge the evening before is impossible because “I’m just too spent at the end of a long day to stay late getting patients ready for discharge tomorrow!” But realize you won’t be doing any more work; you’re rearranging when you do the work. The time you spend arranging for discharge in advance will save you time and stress tomorrow. My own experience is that it is much easier to do all the discharge work the evening before than in the morning when I’m so busy and am being pulled in 10 different directions. Most morning discharge visits are relatively quick and painless, which is really valuable for increasing the efficiency and decreasing the stress of morning rounds.
The alert reader already has figured out there is a pretty big cost to doing the discharge work the evening before. Some patients won’t be able to discharge as planned (e.g., they have a fever overnight) and the preparations will have been in vain. My experience is that such “failed” discharges are reasonably common, but even when they occur, it is usually reasonable to use most of the original prescriptions and discharge summary, with an addendum as required. For example, Dr. Guaraldi could dictate an addendum stating:
“The patient originally was planned for discharge on Wednesday but had a temperature of 38.6 degrees Celsius the night before, so stayed in the hospital for two more days for … ”
Start Rounds Earlier
This strategy might be the most difficult for you and your HM group to arrange, but I propose it because you could do it without having to negotiate with a lot of other departments in the hospital. If your group currently has a day shift that starts at 8 a.m. with a team conference, you could instead start at 7 a.m. Your group could try to shorten the duration of the morning team conference, or eliminate it. Whether the need to get patients discharged early in the day is worth the complexity of rearranging your schedule will depend on the circumstances of your hospital and your group. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.