User login
Psychodiagnostic testing services: The elusive quest for clinicians
Assessment psychologists should be colocated in specialty practices
Imagine the clinical care consequences if patients seen in specialty or primary care practices did not have ready access to laboratory, other medical tests, and/or consultative services deemed critical to quickly establishing diagnostic status and the development of an appropriate treatment plan. For instance, what would be the implications if a dentistry practice did not employ a dental hygienist; an otolaryngology group was not staffed with an audiologist; or a gastroenterology practice had no one available for digestive/nutritional consultation support.

Consider a neurologist who suspects that a patient has a potentially life-threatening brain condition, but the patient has to wait months for brain imaging or – even worse – is tasked to find their own provider for this diagnostic test only to be told that the neuroimaging service does not take their insurance and/or there are no available appointments for several months.
Situations of this kind would not be – and should not be – tolerated by medical professionals or their patients.
A common “real-world” scenario: After evaluation, a psychiatrist needs clarification regarding a possible subtle psychotic process, or, in another instance, suspects that there is an early degenerative cognitive change underlying recent changes in mood and personality. However, the psychiatrist has no dependable access to an assessment psychologist to assist in cases of this kind.
Patients are frequently told by psychiatrists and other physicians that they should have psychodiagnostic testing to arrive at a clearer picture of their clinical status and treatment needs. However, most medical practices, in particular, psychiatry, pediatrics, neurology, and neurosurgery, who see substantial numbers of patients who could benefit from testing, do not employ psychologists. When they do, many do not possess the requisite assessment skills to address the reason(s) for referral.
If the patient needing testing services is fortunate enough, he/she is referred to a well-trained psychologist within commuting distance who takes the patient’s insurance and is able to set up a timely appointment – an unlikely set of circumstances in today’s health care environment.
Some state psychological associations allow for a “matching service” of sorts in the form of announcements in the organization’s listserv, which reviews the referral and includes a back channel for psychologists to contact the patient regarding their availability for testing.
Over the past 2 decades, significant advancements have been made in the integration of primary and mental health care. Those need to continue to include colocating assessment psychologists in medical specialty practices, such as psychiatry, which make frequent referrals for psychodiagnostic testing or would like to but have no place to turn.
Dr. Pollak is affiliated with the Seacoast Mental Health Center in Portsmouth, N.H.
Assessment psychologists should be colocated in specialty practices
Assessment psychologists should be colocated in specialty practices
Imagine the clinical care consequences if patients seen in specialty or primary care practices did not have ready access to laboratory, other medical tests, and/or consultative services deemed critical to quickly establishing diagnostic status and the development of an appropriate treatment plan. For instance, what would be the implications if a dentistry practice did not employ a dental hygienist; an otolaryngology group was not staffed with an audiologist; or a gastroenterology practice had no one available for digestive/nutritional consultation support.
Consider a neurologist who suspects that a patient has a potentially life-threatening brain condition, but the patient has to wait months for brain imaging or – even worse – is tasked to find their own provider for this diagnostic test only to be told that the neuroimaging service does not take their insurance and/or there are no available appointments for several months.
Situations of this kind would not be – and should not be – tolerated by medical professionals or their patients.
A common “real-world” scenario: After evaluation, a psychiatrist needs clarification regarding a possible subtle psychotic process, or, in another instance, suspects that there is an early degenerative cognitive change underlying recent changes in mood and personality. However, the psychiatrist has no dependable access to an assessment psychologist to assist in cases of this kind.
Patients are frequently told by psychiatrists and other physicians that they should have psychodiagnostic testing to arrive at a clearer picture of their clinical status and treatment needs. However, most medical practices, in particular, psychiatry, pediatrics, neurology, and neurosurgery, who see substantial numbers of patients who could benefit from testing, do not employ psychologists. When they do, many do not possess the requisite assessment skills to address the reason(s) for referral.
If the patient needing testing services is fortunate enough, he/she is referred to a well-trained psychologist within commuting distance who takes the patient’s insurance and is able to set up a timely appointment – an unlikely set of circumstances in today’s health care environment.
Some state psychological associations allow for a “matching service” of sorts in the form of announcements in the organization’s listserv, which reviews the referral and includes a back channel for psychologists to contact the patient regarding their availability for testing.
Over the past 2 decades, significant advancements have been made in the integration of primary and mental health care. Those need to continue to include colocating assessment psychologists in medical specialty practices, such as psychiatry, which make frequent referrals for psychodiagnostic testing or would like to but have no place to turn.
Dr. Pollak is affiliated with the Seacoast Mental Health Center in Portsmouth, N.H.
Imagine the clinical care consequences if patients seen in specialty or primary care practices did not have ready access to laboratory, other medical tests, and/or consultative services deemed critical to quickly establishing diagnostic status and the development of an appropriate treatment plan. For instance, what would be the implications if a dentistry practice did not employ a dental hygienist; an otolaryngology group was not staffed with an audiologist; or a gastroenterology practice had no one available for digestive/nutritional consultation support.
Consider a neurologist who suspects that a patient has a potentially life-threatening brain condition, but the patient has to wait months for brain imaging or – even worse – is tasked to find their own provider for this diagnostic test only to be told that the neuroimaging service does not take their insurance and/or there are no available appointments for several months.
Situations of this kind would not be – and should not be – tolerated by medical professionals or their patients.
A common “real-world” scenario: After evaluation, a psychiatrist needs clarification regarding a possible subtle psychotic process, or, in another instance, suspects that there is an early degenerative cognitive change underlying recent changes in mood and personality. However, the psychiatrist has no dependable access to an assessment psychologist to assist in cases of this kind.
Patients are frequently told by psychiatrists and other physicians that they should have psychodiagnostic testing to arrive at a clearer picture of their clinical status and treatment needs. However, most medical practices, in particular, psychiatry, pediatrics, neurology, and neurosurgery, who see substantial numbers of patients who could benefit from testing, do not employ psychologists. When they do, many do not possess the requisite assessment skills to address the reason(s) for referral.
If the patient needing testing services is fortunate enough, he/she is referred to a well-trained psychologist within commuting distance who takes the patient’s insurance and is able to set up a timely appointment – an unlikely set of circumstances in today’s health care environment.
Some state psychological associations allow for a “matching service” of sorts in the form of announcements in the organization’s listserv, which reviews the referral and includes a back channel for psychologists to contact the patient regarding their availability for testing.
Over the past 2 decades, significant advancements have been made in the integration of primary and mental health care. Those need to continue to include colocating assessment psychologists in medical specialty practices, such as psychiatry, which make frequent referrals for psychodiagnostic testing or would like to but have no place to turn.
Dr. Pollak is affiliated with the Seacoast Mental Health Center in Portsmouth, N.H.
Primary CNS lymphoma: R-CHOP hits back
Primary central nervous system lymphoma (PCNSL) is a rare and aggressive form of non-Hodgkin lymphoma solely confined to the CNS. The majority of PCNSL histologically presents as diffuse large B-cell lymphoma (DLBCL). However, outcomes in these patients are notably inferior, compared with nodal or other extranodal DLBCL. In order to achieve long-term progression-free survival, high-dose methotrexate (HD-MTX)–based chemotherapy followed by consolidation is needed. However, this treatment is associated with high toxicity burden and it is restricted to a select patient population – the young and fit – and requires administration at specialized hematological centers.

In the 1990s, the conventional DLBCL treatment regimen with CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) was tested in PCNSL patients. The results were rather disappointing. The addition of CHOP to whole brain radiation or HD-MTX could not improve survival.1-3 The reason for CHOP failure was poor CNS penetration of doxorubicin and cyclophosphamide because of their high molecular weight. Consequently, it was concluded that there is no role for CHOP-like chemotherapy in the treatment of PCNSL.4
But is this really the case? Twenty years later, this traditional view has been challenged by Andres J.M. Ferreri, MD, and colleagues in the INGRID trial.5 Dr. Ferreri presented findings from the trial at the International Conference on Malignant Lymphoma in Lugano, Switzerland, which was greeted with much excitement.6
INGRID is a phase 2 trial conducted on patients with refractory/relapsed PCNSL. It consisted of a CHOP plus rituximab (R-CHOP) regimen, which was upgraded by engineered tumor necrosis factor–alpha (TNF-alpha). The idea was to enhance the blood-brain barrier (BBB) permeability and consequently improve the efficacy of R-CHOP in PCNSL. The use of human TNF-alpha is limited by relevant toxicities. In order to avoid that, a fusion of human TNF-alpha and CNGRCG peptide (called NGR-TNF) was developed.
CNGRCG peptide is a ligand of CD13, an aminopeptidase that is expressed almost exclusively on tumor blood vessels. Preclinical data showed that binding of CNGRCG to CD13 results in targeted – local, not systemic – delivery of TNF-alpha to the tumor blood vessels. Consequently, TNF-alpha led to increased vascular permeability in tumor tissue and enabled higher penetration of chemotherapeutic agents.7,8

Altogether, 12 heavily pretreated PCNSL patients were included in the INGRID trial. Seven patients had two or more previous treatment regimens. Within this trial, patients received R-CHOP with NGR-TNF (0.8 mcg/m2) applied 2 hours prior to R-CHOP. The great majority of grade 3/4 adverse events were hematological toxicities. Importantly, no neurological side effects of any grade occurred.
The primary aim of this study was to investigate the CD13 expression on tumor tissue and provide a proof of concept for the use of NGR-TNF/R-CHOP. Indeed, CD13 expression was observed on tumor vessels in all patients. Consequently, increased BBB permeability in tumor tissue after NGR-TNF infusion was observed using dynamic contrast-enhanced MRI and by brain scintigraphy (SPECT). This was assessed 1 day after NGR-TNF/R-CHOP treatment. More importantly, this effect on BBB seems to be sustained because it was also observed after the last cycle of NGR-TNF/R-CHOP. The fact that there was no change of drug concentrations of R-CHOP components in plasma or cerebrospinal fluid suggests that the effect of NGR-TNF is restricted to tumor vessels.
The authors also reported preliminary results regarding response rates to NGR-TNF/R-CHOP. The overall response rate was 75%. Of note, six patients achieved complete remission and one patient achieved a partial remission. The median duration of response was 10 months (range, 7-14 months), and nine patients were able to proceed to consolidation treatment.
These preliminary results are encouraging and open a new window for the treatment strategies in PCNSL patients. NGR-TNF/R-CHOP treatment induced responses in 75% of these heavily pretreated patients. The low toxicity profile and feasibility of this regimen could allow clinicians to carry out this treatment approach in outpatient settings, as well as in older and comorbid patients. Extensive supportive therapy – such as intensive hydration or leucovorin-rescue by HD-MTX – is not needed.
These results will need to be confirmed through testing in a larger patient population. Dr. Ferreri and colleagues are currently conducting the extended phase of this study and aim to recruit 28 patients. If they report positive results from that study, evaluation of NGR-TNF/R-CHOP as a first-line treatment of PCNSL seems to be the next reasonable step.
Dr. Zeremski and Dr. Fischer are both in the department of hematology/oncology and affiliated with the Health Campus Immunology, Infectiology and Inflammation at Otto-von-Guericke University Magdeburg (Germany). Dr. Fischer is a member of the editorial advisory board of Hematology News. The authors reported having no conflicts of interest.
References
1. J Clin Oncol. 1996;14:556-64.
2. Cancer. 2000;89:1359-70.
3. J Neurooncol. 1996;30:257-65.
4. Guidelines on the diagnosis and management of adult patients with primary CNS lymphoma (PCNSL) and primary intra-ocular lymphoma (PIOL). British Society for Haematology/British Committee for Standards in Haematology; HO/016, 2009.
5. Blood. 2019;134:252-62.
6. Hematol Oncol. 2019; 37:159.
7. BioDrugs. 2013;27:591-603.
8. J Clin Invest. 2002;110:475-82.
Primary central nervous system lymphoma (PCNSL) is a rare and aggressive form of non-Hodgkin lymphoma solely confined to the CNS. The majority of PCNSL histologically presents as diffuse large B-cell lymphoma (DLBCL). However, outcomes in these patients are notably inferior, compared with nodal or other extranodal DLBCL. In order to achieve long-term progression-free survival, high-dose methotrexate (HD-MTX)–based chemotherapy followed by consolidation is needed. However, this treatment is associated with high toxicity burden and it is restricted to a select patient population – the young and fit – and requires administration at specialized hematological centers.
In the 1990s, the conventional DLBCL treatment regimen with CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) was tested in PCNSL patients. The results were rather disappointing. The addition of CHOP to whole brain radiation or HD-MTX could not improve survival.1-3 The reason for CHOP failure was poor CNS penetration of doxorubicin and cyclophosphamide because of their high molecular weight. Consequently, it was concluded that there is no role for CHOP-like chemotherapy in the treatment of PCNSL.4
But is this really the case? Twenty years later, this traditional view has been challenged by Andres J.M. Ferreri, MD, and colleagues in the INGRID trial.5 Dr. Ferreri presented findings from the trial at the International Conference on Malignant Lymphoma in Lugano, Switzerland, which was greeted with much excitement.6
INGRID is a phase 2 trial conducted on patients with refractory/relapsed PCNSL. It consisted of a CHOP plus rituximab (R-CHOP) regimen, which was upgraded by engineered tumor necrosis factor–alpha (TNF-alpha). The idea was to enhance the blood-brain barrier (BBB) permeability and consequently improve the efficacy of R-CHOP in PCNSL. The use of human TNF-alpha is limited by relevant toxicities. In order to avoid that, a fusion of human TNF-alpha and CNGRCG peptide (called NGR-TNF) was developed.
CNGRCG peptide is a ligand of CD13, an aminopeptidase that is expressed almost exclusively on tumor blood vessels. Preclinical data showed that binding of CNGRCG to CD13 results in targeted – local, not systemic – delivery of TNF-alpha to the tumor blood vessels. Consequently, TNF-alpha led to increased vascular permeability in tumor tissue and enabled higher penetration of chemotherapeutic agents.7,8
Altogether, 12 heavily pretreated PCNSL patients were included in the INGRID trial. Seven patients had two or more previous treatment regimens. Within this trial, patients received R-CHOP with NGR-TNF (0.8 mcg/m2) applied 2 hours prior to R-CHOP. The great majority of grade 3/4 adverse events were hematological toxicities. Importantly, no neurological side effects of any grade occurred.
The primary aim of this study was to investigate the CD13 expression on tumor tissue and provide a proof of concept for the use of NGR-TNF/R-CHOP. Indeed, CD13 expression was observed on tumor vessels in all patients. Consequently, increased BBB permeability in tumor tissue after NGR-TNF infusion was observed using dynamic contrast-enhanced MRI and by brain scintigraphy (SPECT). This was assessed 1 day after NGR-TNF/R-CHOP treatment. More importantly, this effect on BBB seems to be sustained because it was also observed after the last cycle of NGR-TNF/R-CHOP. The fact that there was no change of drug concentrations of R-CHOP components in plasma or cerebrospinal fluid suggests that the effect of NGR-TNF is restricted to tumor vessels.
The authors also reported preliminary results regarding response rates to NGR-TNF/R-CHOP. The overall response rate was 75%. Of note, six patients achieved complete remission and one patient achieved a partial remission. The median duration of response was 10 months (range, 7-14 months), and nine patients were able to proceed to consolidation treatment.
These preliminary results are encouraging and open a new window for the treatment strategies in PCNSL patients. NGR-TNF/R-CHOP treatment induced responses in 75% of these heavily pretreated patients. The low toxicity profile and feasibility of this regimen could allow clinicians to carry out this treatment approach in outpatient settings, as well as in older and comorbid patients. Extensive supportive therapy – such as intensive hydration or leucovorin-rescue by HD-MTX – is not needed.
These results will need to be confirmed through testing in a larger patient population. Dr. Ferreri and colleagues are currently conducting the extended phase of this study and aim to recruit 28 patients. If they report positive results from that study, evaluation of NGR-TNF/R-CHOP as a first-line treatment of PCNSL seems to be the next reasonable step.
Dr. Zeremski and Dr. Fischer are both in the department of hematology/oncology and affiliated with the Health Campus Immunology, Infectiology and Inflammation at Otto-von-Guericke University Magdeburg (Germany). Dr. Fischer is a member of the editorial advisory board of Hematology News. The authors reported having no conflicts of interest.
References
1. J Clin Oncol. 1996;14:556-64.
2. Cancer. 2000;89:1359-70.
3. J Neurooncol. 1996;30:257-65.
4. Guidelines on the diagnosis and management of adult patients with primary CNS lymphoma (PCNSL) and primary intra-ocular lymphoma (PIOL). British Society for Haematology/British Committee for Standards in Haematology; HO/016, 2009.
5. Blood. 2019;134:252-62.
6. Hematol Oncol. 2019; 37:159.
7. BioDrugs. 2013;27:591-603.
8. J Clin Invest. 2002;110:475-82.
Primary central nervous system lymphoma (PCNSL) is a rare and aggressive form of non-Hodgkin lymphoma solely confined to the CNS. The majority of PCNSL histologically presents as diffuse large B-cell lymphoma (DLBCL). However, outcomes in these patients are notably inferior, compared with nodal or other extranodal DLBCL. In order to achieve long-term progression-free survival, high-dose methotrexate (HD-MTX)–based chemotherapy followed by consolidation is needed. However, this treatment is associated with high toxicity burden and it is restricted to a select patient population – the young and fit – and requires administration at specialized hematological centers.
In the 1990s, the conventional DLBCL treatment regimen with CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) was tested in PCNSL patients. The results were rather disappointing. The addition of CHOP to whole brain radiation or HD-MTX could not improve survival.1-3 The reason for CHOP failure was poor CNS penetration of doxorubicin and cyclophosphamide because of their high molecular weight. Consequently, it was concluded that there is no role for CHOP-like chemotherapy in the treatment of PCNSL.4
But is this really the case? Twenty years later, this traditional view has been challenged by Andres J.M. Ferreri, MD, and colleagues in the INGRID trial.5 Dr. Ferreri presented findings from the trial at the International Conference on Malignant Lymphoma in Lugano, Switzerland, which was greeted with much excitement.6
INGRID is a phase 2 trial conducted on patients with refractory/relapsed PCNSL. It consisted of a CHOP plus rituximab (R-CHOP) regimen, which was upgraded by engineered tumor necrosis factor–alpha (TNF-alpha). The idea was to enhance the blood-brain barrier (BBB) permeability and consequently improve the efficacy of R-CHOP in PCNSL. The use of human TNF-alpha is limited by relevant toxicities. In order to avoid that, a fusion of human TNF-alpha and CNGRCG peptide (called NGR-TNF) was developed.
CNGRCG peptide is a ligand of CD13, an aminopeptidase that is expressed almost exclusively on tumor blood vessels. Preclinical data showed that binding of CNGRCG to CD13 results in targeted – local, not systemic – delivery of TNF-alpha to the tumor blood vessels. Consequently, TNF-alpha led to increased vascular permeability in tumor tissue and enabled higher penetration of chemotherapeutic agents.7,8
Altogether, 12 heavily pretreated PCNSL patients were included in the INGRID trial. Seven patients had two or more previous treatment regimens. Within this trial, patients received R-CHOP with NGR-TNF (0.8 mcg/m2) applied 2 hours prior to R-CHOP. The great majority of grade 3/4 adverse events were hematological toxicities. Importantly, no neurological side effects of any grade occurred.
The primary aim of this study was to investigate the CD13 expression on tumor tissue and provide a proof of concept for the use of NGR-TNF/R-CHOP. Indeed, CD13 expression was observed on tumor vessels in all patients. Consequently, increased BBB permeability in tumor tissue after NGR-TNF infusion was observed using dynamic contrast-enhanced MRI and by brain scintigraphy (SPECT). This was assessed 1 day after NGR-TNF/R-CHOP treatment. More importantly, this effect on BBB seems to be sustained because it was also observed after the last cycle of NGR-TNF/R-CHOP. The fact that there was no change of drug concentrations of R-CHOP components in plasma or cerebrospinal fluid suggests that the effect of NGR-TNF is restricted to tumor vessels.
The authors also reported preliminary results regarding response rates to NGR-TNF/R-CHOP. The overall response rate was 75%. Of note, six patients achieved complete remission and one patient achieved a partial remission. The median duration of response was 10 months (range, 7-14 months), and nine patients were able to proceed to consolidation treatment.
These preliminary results are encouraging and open a new window for the treatment strategies in PCNSL patients. NGR-TNF/R-CHOP treatment induced responses in 75% of these heavily pretreated patients. The low toxicity profile and feasibility of this regimen could allow clinicians to carry out this treatment approach in outpatient settings, as well as in older and comorbid patients. Extensive supportive therapy – such as intensive hydration or leucovorin-rescue by HD-MTX – is not needed.
These results will need to be confirmed through testing in a larger patient population. Dr. Ferreri and colleagues are currently conducting the extended phase of this study and aim to recruit 28 patients. If they report positive results from that study, evaluation of NGR-TNF/R-CHOP as a first-line treatment of PCNSL seems to be the next reasonable step.
Dr. Zeremski and Dr. Fischer are both in the department of hematology/oncology and affiliated with the Health Campus Immunology, Infectiology and Inflammation at Otto-von-Guericke University Magdeburg (Germany). Dr. Fischer is a member of the editorial advisory board of Hematology News. The authors reported having no conflicts of interest.
References
1. J Clin Oncol. 1996;14:556-64.
2. Cancer. 2000;89:1359-70.
3. J Neurooncol. 1996;30:257-65.
4. Guidelines on the diagnosis and management of adult patients with primary CNS lymphoma (PCNSL) and primary intra-ocular lymphoma (PIOL). British Society for Haematology/British Committee for Standards in Haematology; HO/016, 2009.
5. Blood. 2019;134:252-62.
6. Hematol Oncol. 2019; 37:159.
7. BioDrugs. 2013;27:591-603.
8. J Clin Invest. 2002;110:475-82.
‘Clean’ and ‘natural’ beauty products
Clean beauty products have taken over the skin care market. A wave of new indie brands has entered the skin care market, some of which have garnered fame from bloggers and celebrities and via social media. There has also been a shift towards larger, more-established brands developing and marketing cleaner alternatives to their established skin care lines.

As consumers, physicians, and parents, we all want nontoxic products. However, as highlighted in a recent editorial by Bruce Brod, MD, and Courtney Blair Rubin, MD, of the department of dermatology at the University of Pennsylvania, Philadelphia, the Food and Drug Administration has “failed to define clean and natural, leaving these labels open to interpretation by nondermatologist retailers, bloggers, and celebrities who have set out to define clean beauty for themselves” (JAMA Dermatol. 2019 Sep 25. doi: 10.1001/jamadermatol.2019.2724). This vague interpretation has given rise to a billion-dollar industry of products that is unregulated and may, in fact, not be safer than other products.
For the last decade, to skin care products have also been on the rise. Some of the ingredients deemed toxic include petrolatum and parabens, which have good safety profiles and clinically, are among the least allergenic ingredients in skin products, particularly among patients with the most sensitive skin. In contrast, botanical oils, essential oils, and plant-based natural fragrances are chronic culprits of contact sensitivities and severe skin allergies.

I encourage all dermatologists to read this viewpoint as this topic will inevitably be a point of discussion with many patients. Large studies and expert consensus of safety profiles of chemicals – particularly those deemed carcinogenic, endocrine disruptors, and environmental hazards – are often lacking, leading to confusion for consumers. Our professional organizations and industry should be leading the efforts to establish standardized definitions and FDA regulations of skin care products deemed clean and natural so that the differentiation between marketing taglines and true, substantiated FDA-supported claims are clearer for consumers.

Dr. Talakoub and Dr. Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at dermnews@mdedge.com. They had no relevant disclosures.
Clean beauty products have taken over the skin care market. A wave of new indie brands has entered the skin care market, some of which have garnered fame from bloggers and celebrities and via social media. There has also been a shift towards larger, more-established brands developing and marketing cleaner alternatives to their established skin care lines.
As consumers, physicians, and parents, we all want nontoxic products. However, as highlighted in a recent editorial by Bruce Brod, MD, and Courtney Blair Rubin, MD, of the department of dermatology at the University of Pennsylvania, Philadelphia, the Food and Drug Administration has “failed to define clean and natural, leaving these labels open to interpretation by nondermatologist retailers, bloggers, and celebrities who have set out to define clean beauty for themselves” (JAMA Dermatol. 2019 Sep 25. doi: 10.1001/jamadermatol.2019.2724). This vague interpretation has given rise to a billion-dollar industry of products that is unregulated and may, in fact, not be safer than other products.
For the last decade, to skin care products have also been on the rise. Some of the ingredients deemed toxic include petrolatum and parabens, which have good safety profiles and clinically, are among the least allergenic ingredients in skin products, particularly among patients with the most sensitive skin. In contrast, botanical oils, essential oils, and plant-based natural fragrances are chronic culprits of contact sensitivities and severe skin allergies.
I encourage all dermatologists to read this viewpoint as this topic will inevitably be a point of discussion with many patients. Large studies and expert consensus of safety profiles of chemicals – particularly those deemed carcinogenic, endocrine disruptors, and environmental hazards – are often lacking, leading to confusion for consumers. Our professional organizations and industry should be leading the efforts to establish standardized definitions and FDA regulations of skin care products deemed clean and natural so that the differentiation between marketing taglines and true, substantiated FDA-supported claims are clearer for consumers.
Dr. Talakoub and Dr. Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at dermnews@mdedge.com. They had no relevant disclosures.
Clean beauty products have taken over the skin care market. A wave of new indie brands has entered the skin care market, some of which have garnered fame from bloggers and celebrities and via social media. There has also been a shift towards larger, more-established brands developing and marketing cleaner alternatives to their established skin care lines.
As consumers, physicians, and parents, we all want nontoxic products. However, as highlighted in a recent editorial by Bruce Brod, MD, and Courtney Blair Rubin, MD, of the department of dermatology at the University of Pennsylvania, Philadelphia, the Food and Drug Administration has “failed to define clean and natural, leaving these labels open to interpretation by nondermatologist retailers, bloggers, and celebrities who have set out to define clean beauty for themselves” (JAMA Dermatol. 2019 Sep 25. doi: 10.1001/jamadermatol.2019.2724). This vague interpretation has given rise to a billion-dollar industry of products that is unregulated and may, in fact, not be safer than other products.
For the last decade, to skin care products have also been on the rise. Some of the ingredients deemed toxic include petrolatum and parabens, which have good safety profiles and clinically, are among the least allergenic ingredients in skin products, particularly among patients with the most sensitive skin. In contrast, botanical oils, essential oils, and plant-based natural fragrances are chronic culprits of contact sensitivities and severe skin allergies.
I encourage all dermatologists to read this viewpoint as this topic will inevitably be a point of discussion with many patients. Large studies and expert consensus of safety profiles of chemicals – particularly those deemed carcinogenic, endocrine disruptors, and environmental hazards – are often lacking, leading to confusion for consumers. Our professional organizations and industry should be leading the efforts to establish standardized definitions and FDA regulations of skin care products deemed clean and natural so that the differentiation between marketing taglines and true, substantiated FDA-supported claims are clearer for consumers.
Dr. Talakoub and Dr. Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at dermnews@mdedge.com. They had no relevant disclosures.
Violaceous papules on calf & foot
that usually presents on the distal lower extremities or feet as red to violaceous papules, patches, and plaques.
Clinically, lesions may look similar to Kaposi sarcoma (KS). It is considered to be a variant of stasis dermatitis or severe chronic venous stasis with a more exuberant vascular proliferation of preexisting vasculature. Although the exact etiology is unknown, it is thought that chronic edema, increased venous pressure, and tissue hypoxia may induce fibroblast and vascular proliferation.
It has also been described in association with vascular anomalies, such as Klippel-Trenaunay syndrome, Stewart-Bluefarb syndrome, and Prader-Labhart-Willi syndrome, and is caused by arteriovenous fistulae. Paralysis of lower extremities and amputation stumps are predisposing factors.
KS has four clinical variants: classic KS, African endemic KS, KS in immunocompromised patients, and AIDS-related epidemic KS. All types are caused by the human herpesvirus-8 (HHV-8). Violaceous lesions generally begin as macules and may progress to nodules or tumors.
Punch biopsies were performed in our patient. Histologically, thin-walled, dilated, capillary-like structures were present with a thin layer of surrounding pericytes with reactive fibrosis, hemorrhage, hemosiderin, and a scant chronic inflammatory cell infiltrate. The endothelial cells did not show atypia or mitotic activity. Endothelial cells were positive for CD31, CD34, and CD99. Pericytes and some of the endothelial cells were positive for actin and negative for D2-40, desmin, and HHV-8. In KS, vessels appear like slitlike or jagged spaces lined by spindled endothelial cells. Mild cytologic atypia is usually present. Endothelial cells are characteristically plump. A distinguishing feature in KS is the “promontory sign,” in which new vessels protrude into the vascular space. CD34 is usually negative and HHV-8 is positive.

Acroangiodermatitis of Mali may improve when the underlying venous insufficiency is addressed with compression stockings, pumps, or vascular intervention. Laser ablation of individual lesions has been described in the literature. Dapsone, oral erythromycin, and topical corticosteroids have been reported as helpful in some patients.
This case and these photos were submitted by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
that usually presents on the distal lower extremities or feet as red to violaceous papules, patches, and plaques.
Clinically, lesions may look similar to Kaposi sarcoma (KS). It is considered to be a variant of stasis dermatitis or severe chronic venous stasis with a more exuberant vascular proliferation of preexisting vasculature. Although the exact etiology is unknown, it is thought that chronic edema, increased venous pressure, and tissue hypoxia may induce fibroblast and vascular proliferation.
It has also been described in association with vascular anomalies, such as Klippel-Trenaunay syndrome, Stewart-Bluefarb syndrome, and Prader-Labhart-Willi syndrome, and is caused by arteriovenous fistulae. Paralysis of lower extremities and amputation stumps are predisposing factors.
KS has four clinical variants: classic KS, African endemic KS, KS in immunocompromised patients, and AIDS-related epidemic KS. All types are caused by the human herpesvirus-8 (HHV-8). Violaceous lesions generally begin as macules and may progress to nodules or tumors.
Punch biopsies were performed in our patient. Histologically, thin-walled, dilated, capillary-like structures were present with a thin layer of surrounding pericytes with reactive fibrosis, hemorrhage, hemosiderin, and a scant chronic inflammatory cell infiltrate. The endothelial cells did not show atypia or mitotic activity. Endothelial cells were positive for CD31, CD34, and CD99. Pericytes and some of the endothelial cells were positive for actin and negative for D2-40, desmin, and HHV-8. In KS, vessels appear like slitlike or jagged spaces lined by spindled endothelial cells. Mild cytologic atypia is usually present. Endothelial cells are characteristically plump. A distinguishing feature in KS is the “promontory sign,” in which new vessels protrude into the vascular space. CD34 is usually negative and HHV-8 is positive.
Acroangiodermatitis of Mali may improve when the underlying venous insufficiency is addressed with compression stockings, pumps, or vascular intervention. Laser ablation of individual lesions has been described in the literature. Dapsone, oral erythromycin, and topical corticosteroids have been reported as helpful in some patients.
This case and these photos were submitted by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
that usually presents on the distal lower extremities or feet as red to violaceous papules, patches, and plaques.
Clinically, lesions may look similar to Kaposi sarcoma (KS). It is considered to be a variant of stasis dermatitis or severe chronic venous stasis with a more exuberant vascular proliferation of preexisting vasculature. Although the exact etiology is unknown, it is thought that chronic edema, increased venous pressure, and tissue hypoxia may induce fibroblast and vascular proliferation.
It has also been described in association with vascular anomalies, such as Klippel-Trenaunay syndrome, Stewart-Bluefarb syndrome, and Prader-Labhart-Willi syndrome, and is caused by arteriovenous fistulae. Paralysis of lower extremities and amputation stumps are predisposing factors.
KS has four clinical variants: classic KS, African endemic KS, KS in immunocompromised patients, and AIDS-related epidemic KS. All types are caused by the human herpesvirus-8 (HHV-8). Violaceous lesions generally begin as macules and may progress to nodules or tumors.
Punch biopsies were performed in our patient. Histologically, thin-walled, dilated, capillary-like structures were present with a thin layer of surrounding pericytes with reactive fibrosis, hemorrhage, hemosiderin, and a scant chronic inflammatory cell infiltrate. The endothelial cells did not show atypia or mitotic activity. Endothelial cells were positive for CD31, CD34, and CD99. Pericytes and some of the endothelial cells were positive for actin and negative for D2-40, desmin, and HHV-8. In KS, vessels appear like slitlike or jagged spaces lined by spindled endothelial cells. Mild cytologic atypia is usually present. Endothelial cells are characteristically plump. A distinguishing feature in KS is the “promontory sign,” in which new vessels protrude into the vascular space. CD34 is usually negative and HHV-8 is positive.
Acroangiodermatitis of Mali may improve when the underlying venous insufficiency is addressed with compression stockings, pumps, or vascular intervention. Laser ablation of individual lesions has been described in the literature. Dapsone, oral erythromycin, and topical corticosteroids have been reported as helpful in some patients.
This case and these photos were submitted by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.

Psilocybin research at Johns Hopkins
A new center opens to study novel treatment uses for psychedelics
Psychiatry Grand Rounds started on Monday, Oct. 7, 2019, as they do every Monday at Johns Hopkins, with the department chair interviewing a patient.

The patient told James Potash, MD, that he had suffered with depression for many years and that medications were only a partial fix. His participation in a psilocybin trial at Johns Hopkins in Baltimore was different, and 3 months after the second, and final, treatment, he felt remarkably better. The treatment had quieted the self-deprecating script that had looped through his thoughts for years. “It was nothing like what I was expecting,” the patient said. “I didn’t feel out of control. And now I’m not fighting with myself all day.”
Grand Rounds at Hopkins are different from those at other institutions in that the rounds are given by departments’ full-time faculty members; psychiatrists from other institutions are invited to come speak at other times during the week. But Grand Rounds are reserved for the faculty to present their own research. The patient interview was followed by a lecture by Roland Griffiths, PhD, on “Psilocybin: A potentially promising treatment for depression.” Dr. Griffiths has been studying the effects of psychedelic drugs for the past 40 years; he’s been at Hopkins since 1972. The Grand Rounds presentation came just weeks after it was announced that Dr. Griffiths would be heading the Johns Hopkins Center for Psychedelic & Consciousness Research, funded with $17 million in private donations.
Dr. Griffiths began by talking about the history of psychedelic drug research and the fact that research had been dormant for several decades. “There was – and still is – concern about potential adverse reactions, including panic reactions and the possibility of precipitating psychosis,” he said.
Originally, he conducted several studies in healthy volunteers with no history of psychedelic use. Participants had one or more day-long sessions with staff members who would then serve as monitors when psilocybin was administered; these preliminary meetings were designed to build trust and rapport with the team and to decrease the risk of adverse reactions. On session days when psilocybin was administered, participants were told to eat a low-fat breakfast and then were given a high dose of psilocybin in a capsule. The next 6 hours were spent with the volunteer lying on a couch with an eye mask, headphones with soft music, and two monitors in the room. “The room is decorated like a living room. We created a container for people to explore their inner experience.”
Dr. Griffiths talked about the experiences people reported.
“There were large increases in personally meaningful and insight-type experiences. People reported a sense of unity and interconnectedness of all things, accompanied by a sense of preciousness or reverence, and by the sense that ... the experience was more real or true than everyday waking consciousness. Although the acute effects of psilocybin resolved by the end of the session day, the memories remain and people reported enduring changes in mood, attitude, and behavior.”
The data were remarkable. One month after these high-dose psilocybin sessions, 78% of the volunteers rated the experience as among the top five most personally meaningful experiences of their lives, 94% said they had an increased sense of well-being with improved life satisfaction, and nearly 90% endorsed positive behavior change. Six months after the last session, participants still endorsed having more positive relationships, feeling more love, tolerance, empathy and compassion, friends, family members, and others. Family members and work colleagues who were interviewed noted these positive changes as well.
At this point in Grand Rounds, I was ready to volunteer. My best estimate (tongue in cheek, with no corroboration) is that about half of the audience was waiting on free psilocybin samples, while the other half was remembering Timothy Leary, PhD, bad trips, and psychosis. “We’ve been down this road before,” the gentleman next to me commented.
Dr. Griffiths went on to talk about trials of psilocybin in clinical populations. In one study, the effects of psilocybin were examined in cancer patients with depression and anxiety. Of the 51 cancer patients, half previously had been treated with psychotropic medications before coming to the study. This randomized, double-blind crossover study compared high-dose psilocybin with an extremely low dose of psilocybin used as the placebo.
Another study looked at patients with major depression who, like the patient interviewed, had not had full resolution of symptoms with conventional antidepressants. Of the 24 participants in that group, 69% reported clinically significant improvement 12 weeks after the treatment. Just over half of participants reported a full remission to normal.
Dr. Griffiths ended by concluding that the positive experiences people have with psilocybin are associated with “enduring positive trait changes in attitudes, mood and behavior, spirituality, and altruism ... and that such experiences are now amenable to systematic prospective scientific study.”
J. Raymond DePaulo, MD, chair of the National Network of Depression Centers and former chair of psychiatry at Johns Hopkins, noted that he used to be skeptical. He has been impressed that Dr. Griffiths has listened to criticism and addressed concerns others have raised. “When it was suggested that this was the result of delirium, he started giving people cognitive tests while they were using psilocybin and he showed it wasn’t the case.”
“I have always objected to words like ‘psychedelic’ and ‘hallucinogen,’ ” said Dr. DePaulo. “They are confusing and inaccurate. No one takes these medications because they want to hallucinate. They take them to change their mood. That said, I am thrilled that we are on the precipice of being able to use this to treat depression.”
Since 1999, the Johns Hopkins Psilocybin Research Project has conducted more than 700 sessions with 369 participants. When might psilocybin be available to patients outside of a research protocol? Two companies have obtained approval from the Food and Drug Administration to initiate registration in trials for treatment of depression. Dr. Griffiths estimates that it could be another 5 years before psilocybin will be available for medical use.

The new center with its generous funding will allow for more studies with more patient populations. The center’s projects will look at using psilocybin as a treatment for opioid use disorder, comorbid depression and alcohol use disorder, anorexia nervosa, depression in Alzheimer’s disease, posttreatment Lyme disease syndrome, and PTSD.
Scott Aaronson, MD, is a mood disorder expert and director of clinical research at the Sheppard Pratt Health System in Towson/Baltimore. Dr. Aaronson, who also studies psilocybin as a treatment for depression, noted: “The problem with the development of psychedelics is that we are not really prepared to capture the improvement we see with their use, as the main changes are not in the classic markers of depression like the Montgomery-Åsberg or the Hamilton Depression rating scales, but [rather] in the patient’s perception of who they are, how they fit in with the world, and what is most important. We need to develop ways to capture those critical changes and work with the FDA to develop an entirely new vision of what constitutes improvement in psychiatric illness. My overall take is that it is a terrific time to specialize in treatment-resistant mood disorders!”
Dr. Miller is coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore.
A new center opens to study novel treatment uses for psychedelics
A new center opens to study novel treatment uses for psychedelics
Psychiatry Grand Rounds started on Monday, Oct. 7, 2019, as they do every Monday at Johns Hopkins, with the department chair interviewing a patient.
The patient told James Potash, MD, that he had suffered with depression for many years and that medications were only a partial fix. His participation in a psilocybin trial at Johns Hopkins in Baltimore was different, and 3 months after the second, and final, treatment, he felt remarkably better. The treatment had quieted the self-deprecating script that had looped through his thoughts for years. “It was nothing like what I was expecting,” the patient said. “I didn’t feel out of control. And now I’m not fighting with myself all day.”
Grand Rounds at Hopkins are different from those at other institutions in that the rounds are given by departments’ full-time faculty members; psychiatrists from other institutions are invited to come speak at other times during the week. But Grand Rounds are reserved for the faculty to present their own research. The patient interview was followed by a lecture by Roland Griffiths, PhD, on “Psilocybin: A potentially promising treatment for depression.” Dr. Griffiths has been studying the effects of psychedelic drugs for the past 40 years; he’s been at Hopkins since 1972. The Grand Rounds presentation came just weeks after it was announced that Dr. Griffiths would be heading the Johns Hopkins Center for Psychedelic & Consciousness Research, funded with $17 million in private donations.
Dr. Griffiths began by talking about the history of psychedelic drug research and the fact that research had been dormant for several decades. “There was – and still is – concern about potential adverse reactions, including panic reactions and the possibility of precipitating psychosis,” he said.
Originally, he conducted several studies in healthy volunteers with no history of psychedelic use. Participants had one or more day-long sessions with staff members who would then serve as monitors when psilocybin was administered; these preliminary meetings were designed to build trust and rapport with the team and to decrease the risk of adverse reactions. On session days when psilocybin was administered, participants were told to eat a low-fat breakfast and then were given a high dose of psilocybin in a capsule. The next 6 hours were spent with the volunteer lying on a couch with an eye mask, headphones with soft music, and two monitors in the room. “The room is decorated like a living room. We created a container for people to explore their inner experience.”
Dr. Griffiths talked about the experiences people reported.
“There were large increases in personally meaningful and insight-type experiences. People reported a sense of unity and interconnectedness of all things, accompanied by a sense of preciousness or reverence, and by the sense that ... the experience was more real or true than everyday waking consciousness. Although the acute effects of psilocybin resolved by the end of the session day, the memories remain and people reported enduring changes in mood, attitude, and behavior.”
The data were remarkable. One month after these high-dose psilocybin sessions, 78% of the volunteers rated the experience as among the top five most personally meaningful experiences of their lives, 94% said they had an increased sense of well-being with improved life satisfaction, and nearly 90% endorsed positive behavior change. Six months after the last session, participants still endorsed having more positive relationships, feeling more love, tolerance, empathy and compassion, friends, family members, and others. Family members and work colleagues who were interviewed noted these positive changes as well.
At this point in Grand Rounds, I was ready to volunteer. My best estimate (tongue in cheek, with no corroboration) is that about half of the audience was waiting on free psilocybin samples, while the other half was remembering Timothy Leary, PhD, bad trips, and psychosis. “We’ve been down this road before,” the gentleman next to me commented.
Dr. Griffiths went on to talk about trials of psilocybin in clinical populations. In one study, the effects of psilocybin were examined in cancer patients with depression and anxiety. Of the 51 cancer patients, half previously had been treated with psychotropic medications before coming to the study. This randomized, double-blind crossover study compared high-dose psilocybin with an extremely low dose of psilocybin used as the placebo.
Another study looked at patients with major depression who, like the patient interviewed, had not had full resolution of symptoms with conventional antidepressants. Of the 24 participants in that group, 69% reported clinically significant improvement 12 weeks after the treatment. Just over half of participants reported a full remission to normal.
Dr. Griffiths ended by concluding that the positive experiences people have with psilocybin are associated with “enduring positive trait changes in attitudes, mood and behavior, spirituality, and altruism ... and that such experiences are now amenable to systematic prospective scientific study.”
J. Raymond DePaulo, MD, chair of the National Network of Depression Centers and former chair of psychiatry at Johns Hopkins, noted that he used to be skeptical. He has been impressed that Dr. Griffiths has listened to criticism and addressed concerns others have raised. “When it was suggested that this was the result of delirium, he started giving people cognitive tests while they were using psilocybin and he showed it wasn’t the case.”
“I have always objected to words like ‘psychedelic’ and ‘hallucinogen,’ ” said Dr. DePaulo. “They are confusing and inaccurate. No one takes these medications because they want to hallucinate. They take them to change their mood. That said, I am thrilled that we are on the precipice of being able to use this to treat depression.”
Since 1999, the Johns Hopkins Psilocybin Research Project has conducted more than 700 sessions with 369 participants. When might psilocybin be available to patients outside of a research protocol? Two companies have obtained approval from the Food and Drug Administration to initiate registration in trials for treatment of depression. Dr. Griffiths estimates that it could be another 5 years before psilocybin will be available for medical use.
The new center with its generous funding will allow for more studies with more patient populations. The center’s projects will look at using psilocybin as a treatment for opioid use disorder, comorbid depression and alcohol use disorder, anorexia nervosa, depression in Alzheimer’s disease, posttreatment Lyme disease syndrome, and PTSD.
Scott Aaronson, MD, is a mood disorder expert and director of clinical research at the Sheppard Pratt Health System in Towson/Baltimore. Dr. Aaronson, who also studies psilocybin as a treatment for depression, noted: “The problem with the development of psychedelics is that we are not really prepared to capture the improvement we see with their use, as the main changes are not in the classic markers of depression like the Montgomery-Åsberg or the Hamilton Depression rating scales, but [rather] in the patient’s perception of who they are, how they fit in with the world, and what is most important. We need to develop ways to capture those critical changes and work with the FDA to develop an entirely new vision of what constitutes improvement in psychiatric illness. My overall take is that it is a terrific time to specialize in treatment-resistant mood disorders!”
Dr. Miller is coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore.
Psychiatry Grand Rounds started on Monday, Oct. 7, 2019, as they do every Monday at Johns Hopkins, with the department chair interviewing a patient.
The patient told James Potash, MD, that he had suffered with depression for many years and that medications were only a partial fix. His participation in a psilocybin trial at Johns Hopkins in Baltimore was different, and 3 months after the second, and final, treatment, he felt remarkably better. The treatment had quieted the self-deprecating script that had looped through his thoughts for years. “It was nothing like what I was expecting,” the patient said. “I didn’t feel out of control. And now I’m not fighting with myself all day.”
Grand Rounds at Hopkins are different from those at other institutions in that the rounds are given by departments’ full-time faculty members; psychiatrists from other institutions are invited to come speak at other times during the week. But Grand Rounds are reserved for the faculty to present their own research. The patient interview was followed by a lecture by Roland Griffiths, PhD, on “Psilocybin: A potentially promising treatment for depression.” Dr. Griffiths has been studying the effects of psychedelic drugs for the past 40 years; he’s been at Hopkins since 1972. The Grand Rounds presentation came just weeks after it was announced that Dr. Griffiths would be heading the Johns Hopkins Center for Psychedelic & Consciousness Research, funded with $17 million in private donations.
Dr. Griffiths began by talking about the history of psychedelic drug research and the fact that research had been dormant for several decades. “There was – and still is – concern about potential adverse reactions, including panic reactions and the possibility of precipitating psychosis,” he said.
Originally, he conducted several studies in healthy volunteers with no history of psychedelic use. Participants had one or more day-long sessions with staff members who would then serve as monitors when psilocybin was administered; these preliminary meetings were designed to build trust and rapport with the team and to decrease the risk of adverse reactions. On session days when psilocybin was administered, participants were told to eat a low-fat breakfast and then were given a high dose of psilocybin in a capsule. The next 6 hours were spent with the volunteer lying on a couch with an eye mask, headphones with soft music, and two monitors in the room. “The room is decorated like a living room. We created a container for people to explore their inner experience.”
Dr. Griffiths talked about the experiences people reported.
“There were large increases in personally meaningful and insight-type experiences. People reported a sense of unity and interconnectedness of all things, accompanied by a sense of preciousness or reverence, and by the sense that ... the experience was more real or true than everyday waking consciousness. Although the acute effects of psilocybin resolved by the end of the session day, the memories remain and people reported enduring changes in mood, attitude, and behavior.”
The data were remarkable. One month after these high-dose psilocybin sessions, 78% of the volunteers rated the experience as among the top five most personally meaningful experiences of their lives, 94% said they had an increased sense of well-being with improved life satisfaction, and nearly 90% endorsed positive behavior change. Six months after the last session, participants still endorsed having more positive relationships, feeling more love, tolerance, empathy and compassion, friends, family members, and others. Family members and work colleagues who were interviewed noted these positive changes as well.
At this point in Grand Rounds, I was ready to volunteer. My best estimate (tongue in cheek, with no corroboration) is that about half of the audience was waiting on free psilocybin samples, while the other half was remembering Timothy Leary, PhD, bad trips, and psychosis. “We’ve been down this road before,” the gentleman next to me commented.
Dr. Griffiths went on to talk about trials of psilocybin in clinical populations. In one study, the effects of psilocybin were examined in cancer patients with depression and anxiety. Of the 51 cancer patients, half previously had been treated with psychotropic medications before coming to the study. This randomized, double-blind crossover study compared high-dose psilocybin with an extremely low dose of psilocybin used as the placebo.
Another study looked at patients with major depression who, like the patient interviewed, had not had full resolution of symptoms with conventional antidepressants. Of the 24 participants in that group, 69% reported clinically significant improvement 12 weeks after the treatment. Just over half of participants reported a full remission to normal.
Dr. Griffiths ended by concluding that the positive experiences people have with psilocybin are associated with “enduring positive trait changes in attitudes, mood and behavior, spirituality, and altruism ... and that such experiences are now amenable to systematic prospective scientific study.”
J. Raymond DePaulo, MD, chair of the National Network of Depression Centers and former chair of psychiatry at Johns Hopkins, noted that he used to be skeptical. He has been impressed that Dr. Griffiths has listened to criticism and addressed concerns others have raised. “When it was suggested that this was the result of delirium, he started giving people cognitive tests while they were using psilocybin and he showed it wasn’t the case.”
“I have always objected to words like ‘psychedelic’ and ‘hallucinogen,’ ” said Dr. DePaulo. “They are confusing and inaccurate. No one takes these medications because they want to hallucinate. They take them to change their mood. That said, I am thrilled that we are on the precipice of being able to use this to treat depression.”
Since 1999, the Johns Hopkins Psilocybin Research Project has conducted more than 700 sessions with 369 participants. When might psilocybin be available to patients outside of a research protocol? Two companies have obtained approval from the Food and Drug Administration to initiate registration in trials for treatment of depression. Dr. Griffiths estimates that it could be another 5 years before psilocybin will be available for medical use.
The new center with its generous funding will allow for more studies with more patient populations. The center’s projects will look at using psilocybin as a treatment for opioid use disorder, comorbid depression and alcohol use disorder, anorexia nervosa, depression in Alzheimer’s disease, posttreatment Lyme disease syndrome, and PTSD.
Scott Aaronson, MD, is a mood disorder expert and director of clinical research at the Sheppard Pratt Health System in Towson/Baltimore. Dr. Aaronson, who also studies psilocybin as a treatment for depression, noted: “The problem with the development of psychedelics is that we are not really prepared to capture the improvement we see with their use, as the main changes are not in the classic markers of depression like the Montgomery-Åsberg or the Hamilton Depression rating scales, but [rather] in the patient’s perception of who they are, how they fit in with the world, and what is most important. We need to develop ways to capture those critical changes and work with the FDA to develop an entirely new vision of what constitutes improvement in psychiatric illness. My overall take is that it is a terrific time to specialize in treatment-resistant mood disorders!”
Dr. Miller is coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins, both in Baltimore.

Yoga life lessons
I love empty storefronts. The realtor headshot in the window is a sign of hope. What was here is no more. What is coming will be better.

I’ve waited a year for one such sign to come down and scaffolding to go up. Just one block from my condo, my curiosity has been slaked: a yoga studio! At first, disappointment; so many potentials unrealized: a coffee shop, cleaners, speakeasy! Yet, I decided to make the best of it. I bought Rainbow sandals, a Lululemon mat, and a pack of 10 classes. As it turns out, yoga can transform your life.
I didn’t realize how beautifully yoga combines physical exertion, meditation, and spirituality. It is both a model for understanding and a ritualistic training for life. Take resting pigeon for example. (Yogis reading this will forgive my imperfect explanation.) This moderately difficult pose opens your hip and stretches your glutes. Imagine doing a split but with your front knee bent and your forehead and arms resting on the floor in front of you. Done correctly, it puts a stretch deep into the hip of the forward leg. It is uncomfortable. Holding it for a minute or 2 is hard. But rather than just focusing on releasing, with each breath you find yourself deepening the stretch. Sweat streams down your arms and the discomfort builds as you hold. All you can think about is your breath. Then, it’s over. You feel freer, lighter than you were before. The deeper the discomfort, the deeper the delight that arises afterward. You are wise, yogis would say, to have chosen “the good over the pleasant.”

We have many opportunities for resting pigeon in everyday life. The patient to be added to your Monday morning clinic – which already had added patients. The Friday afternoon Mohs case that went to periosteum and still needs a flap to close. The “yet another” GI bleed patient that needs to be scoped tonight. These are all deep stretches, uncomfortable hip openings. Rather, when you must be uncomfortable, breathe and lean into it. Choosing the good sometimes means choosing suffering, but it isn’t the pain that makes it hard to bear. It is a lack of significance for that difficulty. By choosing what is good, you answer the question: “Who am I?” I am the one able and willing to endure inconvenience or disquiet to help others. This is my job, what I’m here to do. The pose, the call, the case will be over quickly. The freedom you feel after, along with the satisfaction you have served your purpose, will sustain you.
There are many poses and endless lessons from yoga. In fact, doing yoga is called “practicing.” Each time you learn and try. Each time you are imperfect and uncomfortable and reemerge sweaty and satisfied, just a little better human than you were before.
Dr. Benabio is director of health care transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
I love empty storefronts. The realtor headshot in the window is a sign of hope. What was here is no more. What is coming will be better.
I’ve waited a year for one such sign to come down and scaffolding to go up. Just one block from my condo, my curiosity has been slaked: a yoga studio! At first, disappointment; so many potentials unrealized: a coffee shop, cleaners, speakeasy! Yet, I decided to make the best of it. I bought Rainbow sandals, a Lululemon mat, and a pack of 10 classes. As it turns out, yoga can transform your life.
I didn’t realize how beautifully yoga combines physical exertion, meditation, and spirituality. It is both a model for understanding and a ritualistic training for life. Take resting pigeon for example. (Yogis reading this will forgive my imperfect explanation.) This moderately difficult pose opens your hip and stretches your glutes. Imagine doing a split but with your front knee bent and your forehead and arms resting on the floor in front of you. Done correctly, it puts a stretch deep into the hip of the forward leg. It is uncomfortable. Holding it for a minute or 2 is hard. But rather than just focusing on releasing, with each breath you find yourself deepening the stretch. Sweat streams down your arms and the discomfort builds as you hold. All you can think about is your breath. Then, it’s over. You feel freer, lighter than you were before. The deeper the discomfort, the deeper the delight that arises afterward. You are wise, yogis would say, to have chosen “the good over the pleasant.”
We have many opportunities for resting pigeon in everyday life. The patient to be added to your Monday morning clinic – which already had added patients. The Friday afternoon Mohs case that went to periosteum and still needs a flap to close. The “yet another” GI bleed patient that needs to be scoped tonight. These are all deep stretches, uncomfortable hip openings. Rather, when you must be uncomfortable, breathe and lean into it. Choosing the good sometimes means choosing suffering, but it isn’t the pain that makes it hard to bear. It is a lack of significance for that difficulty. By choosing what is good, you answer the question: “Who am I?” I am the one able and willing to endure inconvenience or disquiet to help others. This is my job, what I’m here to do. The pose, the call, the case will be over quickly. The freedom you feel after, along with the satisfaction you have served your purpose, will sustain you.
There are many poses and endless lessons from yoga. In fact, doing yoga is called “practicing.” Each time you learn and try. Each time you are imperfect and uncomfortable and reemerge sweaty and satisfied, just a little better human than you were before.
Dr. Benabio is director of health care transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
I love empty storefronts. The realtor headshot in the window is a sign of hope. What was here is no more. What is coming will be better.
I’ve waited a year for one such sign to come down and scaffolding to go up. Just one block from my condo, my curiosity has been slaked: a yoga studio! At first, disappointment; so many potentials unrealized: a coffee shop, cleaners, speakeasy! Yet, I decided to make the best of it. I bought Rainbow sandals, a Lululemon mat, and a pack of 10 classes. As it turns out, yoga can transform your life.
I didn’t realize how beautifully yoga combines physical exertion, meditation, and spirituality. It is both a model for understanding and a ritualistic training for life. Take resting pigeon for example. (Yogis reading this will forgive my imperfect explanation.) This moderately difficult pose opens your hip and stretches your glutes. Imagine doing a split but with your front knee bent and your forehead and arms resting on the floor in front of you. Done correctly, it puts a stretch deep into the hip of the forward leg. It is uncomfortable. Holding it for a minute or 2 is hard. But rather than just focusing on releasing, with each breath you find yourself deepening the stretch. Sweat streams down your arms and the discomfort builds as you hold. All you can think about is your breath. Then, it’s over. You feel freer, lighter than you were before. The deeper the discomfort, the deeper the delight that arises afterward. You are wise, yogis would say, to have chosen “the good over the pleasant.”
We have many opportunities for resting pigeon in everyday life. The patient to be added to your Monday morning clinic – which already had added patients. The Friday afternoon Mohs case that went to periosteum and still needs a flap to close. The “yet another” GI bleed patient that needs to be scoped tonight. These are all deep stretches, uncomfortable hip openings. Rather, when you must be uncomfortable, breathe and lean into it. Choosing the good sometimes means choosing suffering, but it isn’t the pain that makes it hard to bear. It is a lack of significance for that difficulty. By choosing what is good, you answer the question: “Who am I?” I am the one able and willing to endure inconvenience or disquiet to help others. This is my job, what I’m here to do. The pose, the call, the case will be over quickly. The freedom you feel after, along with the satisfaction you have served your purpose, will sustain you.
There are many poses and endless lessons from yoga. In fact, doing yoga is called “practicing.” Each time you learn and try. Each time you are imperfect and uncomfortable and reemerge sweaty and satisfied, just a little better human than you were before.
Dr. Benabio is director of health care transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
Making and using guidelines
Modern medicine increasingly relies on the adoption and use of guidelines.

Forty years ago, medicine was like free-form, rhythmic gymnastics in which physicians would develop an artisanal treatment plan for each patient. Now, medicine frequently involves recognizing when we need to do a triple-twisting, double-back somersault (the Biles II) and then performing it. The belief is that better outcomes flow from reduced variability in diagnostic and treatment plans, based on guidelines developed from evidence-based medicine from large meta-analyses. This dogma, still unproven in real life, probably works best for 95% of patients. The physician must not omit a step of deciding whether their particular patient is one of the 5% of patients to whom the guideline does not apply.
To be useful, the guidelines must be based on accurate science, produce a significantly positive cost-benefit-risk analysis, be wisely constructed, and be clearly written.
Alas, many guidelines fall far short of this ideal, and when they fail, they impugn all of medical care, they lower the credibility of the organizations that issue them, and they lower the public’s trust in medicine, which thereby impedes improving the public health. Don’t sweat the small stuff for public health guidelines.
The science matters. Nutritional guidelines have been particularly rickety, as John P.A. Ioannidis, MD, wrote in a JAMA op-ed 1 year ago.1 For instance, previous dietary recommendations to reduce cholesterol by avoiding eggs have since been shown to be wrong. The recommendation for reducing salt intake has been heavily criticized. Now the decades-long condemnation of red meat has been challenged. New “guidelines,” suggested by one group (let’s view it as a minority report that contradicts many official guidelines) in the October 1, 2019, issue of Annals of Internal Medicine, say that red meat and processed meats aren’t the boogeyman.2 The authors of the accompanying editorial are from the Center for Pediatric and Adolescent Comparative Effectiveness Research at Indiana University, Indianapolis.3 The editorial supports the new study, criticizing past recommendations because “the field of nutritional epidemiology is plagued by observational studies that have conducted inappropriate analyses, accompanied by likely erroneous conclusions.”
Clarity also matters. One factor in the current opiate epidemic was guidance in the mid-1990s making pain the “fifth vital sign.” This certainly was not the only factor nor was it necessarily the primary one. Most disasters, like most codes on the ward, proceed from multiple smaller failures and missteps. An emphasis on assessing pain in hospitalized patients did not intend to be interpreted as requiring that all pain be eliminated with strong medication, but that was the practical consequence. In response to the epidemic of overdose deaths, guidelines were promulgated in 2016 recommending reducing doses used for chronic opiate regimens. Some patients with chronic pain feared, and soon experienced, the consequences of those changes. In October 2019, those guidelines were revised telling physicians to go slower.4 In explaining the revision, one government official is quoted as saying: “Clearly we believe that there has been misinterpretation of the guidelines, which were very clear.”5 F. Scott Fitzgerald once wrote that “the test of a first-rate intelligence is the ability to hold two opposed ideas in mind at the same time and still retain the ability to function.” I reread that governmental doublespeak three times and my brain broke.
Clinical practice guidelines are an important part of modern medicine. But we need to be wiser about their creation. The science needs to be rigorous. The committees need to contain skeptics rather than just research scientists and clinicians with a vested interest in the field. The purported benefits of the guideline must be weighed against costs, risks, and unintended consequences. Humility is important. All physicians are taught the principle: “First, do no harm.” In explaining medical ethics to students, I rephrase that principle as: “Be cautious and humble. You are not as smart as you think you are.” Consider this food for thought the next time you read or create a guideline.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
References
1. JAMA. 2018;320(10):969-70.
2. Ann Intern Med. 2019 Oct 1. doi: 10.7326/M19-1621.
3. Ann Intern Med. 2019 Oct 1. doi: 10.7326/M19-2620.
4. U.S. Department of Health & Human Services. HHS guide for clinicians on the appropriate dosage reduction or discontinuation of opioid analgesics. https://www.hhs.gov/opioids/sites/default/files/2019-10/Dosage_Reduction_Discontinuation.pdf.
5. “New guidelines on opioid tapering tell doctors to go slow.” Washington Post. 2019 Oct 10.
Modern medicine increasingly relies on the adoption and use of guidelines.
Forty years ago, medicine was like free-form, rhythmic gymnastics in which physicians would develop an artisanal treatment plan for each patient. Now, medicine frequently involves recognizing when we need to do a triple-twisting, double-back somersault (the Biles II) and then performing it. The belief is that better outcomes flow from reduced variability in diagnostic and treatment plans, based on guidelines developed from evidence-based medicine from large meta-analyses. This dogma, still unproven in real life, probably works best for 95% of patients. The physician must not omit a step of deciding whether their particular patient is one of the 5% of patients to whom the guideline does not apply.
To be useful, the guidelines must be based on accurate science, produce a significantly positive cost-benefit-risk analysis, be wisely constructed, and be clearly written.
Alas, many guidelines fall far short of this ideal, and when they fail, they impugn all of medical care, they lower the credibility of the organizations that issue them, and they lower the public’s trust in medicine, which thereby impedes improving the public health. Don’t sweat the small stuff for public health guidelines.
The science matters. Nutritional guidelines have been particularly rickety, as John P.A. Ioannidis, MD, wrote in a JAMA op-ed 1 year ago.1 For instance, previous dietary recommendations to reduce cholesterol by avoiding eggs have since been shown to be wrong. The recommendation for reducing salt intake has been heavily criticized. Now the decades-long condemnation of red meat has been challenged. New “guidelines,” suggested by one group (let’s view it as a minority report that contradicts many official guidelines) in the October 1, 2019, issue of Annals of Internal Medicine, say that red meat and processed meats aren’t the boogeyman.2 The authors of the accompanying editorial are from the Center for Pediatric and Adolescent Comparative Effectiveness Research at Indiana University, Indianapolis.3 The editorial supports the new study, criticizing past recommendations because “the field of nutritional epidemiology is plagued by observational studies that have conducted inappropriate analyses, accompanied by likely erroneous conclusions.”
Clarity also matters. One factor in the current opiate epidemic was guidance in the mid-1990s making pain the “fifth vital sign.” This certainly was not the only factor nor was it necessarily the primary one. Most disasters, like most codes on the ward, proceed from multiple smaller failures and missteps. An emphasis on assessing pain in hospitalized patients did not intend to be interpreted as requiring that all pain be eliminated with strong medication, but that was the practical consequence. In response to the epidemic of overdose deaths, guidelines were promulgated in 2016 recommending reducing doses used for chronic opiate regimens. Some patients with chronic pain feared, and soon experienced, the consequences of those changes. In October 2019, those guidelines were revised telling physicians to go slower.4 In explaining the revision, one government official is quoted as saying: “Clearly we believe that there has been misinterpretation of the guidelines, which were very clear.”5 F. Scott Fitzgerald once wrote that “the test of a first-rate intelligence is the ability to hold two opposed ideas in mind at the same time and still retain the ability to function.” I reread that governmental doublespeak three times and my brain broke.
Clinical practice guidelines are an important part of modern medicine. But we need to be wiser about their creation. The science needs to be rigorous. The committees need to contain skeptics rather than just research scientists and clinicians with a vested interest in the field. The purported benefits of the guideline must be weighed against costs, risks, and unintended consequences. Humility is important. All physicians are taught the principle: “First, do no harm.” In explaining medical ethics to students, I rephrase that principle as: “Be cautious and humble. You are not as smart as you think you are.” Consider this food for thought the next time you read or create a guideline.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
References
1. JAMA. 2018;320(10):969-70.
2. Ann Intern Med. 2019 Oct 1. doi: 10.7326/M19-1621.
3. Ann Intern Med. 2019 Oct 1. doi: 10.7326/M19-2620.
4. U.S. Department of Health & Human Services. HHS guide for clinicians on the appropriate dosage reduction or discontinuation of opioid analgesics. https://www.hhs.gov/opioids/sites/default/files/2019-10/Dosage_Reduction_Discontinuation.pdf.
5. “New guidelines on opioid tapering tell doctors to go slow.” Washington Post. 2019 Oct 10.
Modern medicine increasingly relies on the adoption and use of guidelines.
Forty years ago, medicine was like free-form, rhythmic gymnastics in which physicians would develop an artisanal treatment plan for each patient. Now, medicine frequently involves recognizing when we need to do a triple-twisting, double-back somersault (the Biles II) and then performing it. The belief is that better outcomes flow from reduced variability in diagnostic and treatment plans, based on guidelines developed from evidence-based medicine from large meta-analyses. This dogma, still unproven in real life, probably works best for 95% of patients. The physician must not omit a step of deciding whether their particular patient is one of the 5% of patients to whom the guideline does not apply.
To be useful, the guidelines must be based on accurate science, produce a significantly positive cost-benefit-risk analysis, be wisely constructed, and be clearly written.
Alas, many guidelines fall far short of this ideal, and when they fail, they impugn all of medical care, they lower the credibility of the organizations that issue them, and they lower the public’s trust in medicine, which thereby impedes improving the public health. Don’t sweat the small stuff for public health guidelines.
The science matters. Nutritional guidelines have been particularly rickety, as John P.A. Ioannidis, MD, wrote in a JAMA op-ed 1 year ago.1 For instance, previous dietary recommendations to reduce cholesterol by avoiding eggs have since been shown to be wrong. The recommendation for reducing salt intake has been heavily criticized. Now the decades-long condemnation of red meat has been challenged. New “guidelines,” suggested by one group (let’s view it as a minority report that contradicts many official guidelines) in the October 1, 2019, issue of Annals of Internal Medicine, say that red meat and processed meats aren’t the boogeyman.2 The authors of the accompanying editorial are from the Center for Pediatric and Adolescent Comparative Effectiveness Research at Indiana University, Indianapolis.3 The editorial supports the new study, criticizing past recommendations because “the field of nutritional epidemiology is plagued by observational studies that have conducted inappropriate analyses, accompanied by likely erroneous conclusions.”
Clarity also matters. One factor in the current opiate epidemic was guidance in the mid-1990s making pain the “fifth vital sign.” This certainly was not the only factor nor was it necessarily the primary one. Most disasters, like most codes on the ward, proceed from multiple smaller failures and missteps. An emphasis on assessing pain in hospitalized patients did not intend to be interpreted as requiring that all pain be eliminated with strong medication, but that was the practical consequence. In response to the epidemic of overdose deaths, guidelines were promulgated in 2016 recommending reducing doses used for chronic opiate regimens. Some patients with chronic pain feared, and soon experienced, the consequences of those changes. In October 2019, those guidelines were revised telling physicians to go slower.4 In explaining the revision, one government official is quoted as saying: “Clearly we believe that there has been misinterpretation of the guidelines, which were very clear.”5 F. Scott Fitzgerald once wrote that “the test of a first-rate intelligence is the ability to hold two opposed ideas in mind at the same time and still retain the ability to function.” I reread that governmental doublespeak three times and my brain broke.
Clinical practice guidelines are an important part of modern medicine. But we need to be wiser about their creation. The science needs to be rigorous. The committees need to contain skeptics rather than just research scientists and clinicians with a vested interest in the field. The purported benefits of the guideline must be weighed against costs, risks, and unintended consequences. Humility is important. All physicians are taught the principle: “First, do no harm.” In explaining medical ethics to students, I rephrase that principle as: “Be cautious and humble. You are not as smart as you think you are.” Consider this food for thought the next time you read or create a guideline.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
References
1. JAMA. 2018;320(10):969-70.
2. Ann Intern Med. 2019 Oct 1. doi: 10.7326/M19-1621.
3. Ann Intern Med. 2019 Oct 1. doi: 10.7326/M19-2620.
4. U.S. Department of Health & Human Services. HHS guide for clinicians on the appropriate dosage reduction or discontinuation of opioid analgesics. https://www.hhs.gov/opioids/sites/default/files/2019-10/Dosage_Reduction_Discontinuation.pdf.
5. “New guidelines on opioid tapering tell doctors to go slow.” Washington Post. 2019 Oct 10.
Help wanted
In a Pediatrics article, Hsuan-hsiu Annie Chen, MD, offers a very personal and candid narrative of her struggle with depression during medical school and residency (Pediatrics. 2019 Sep 1. doi: 10.1542/peds.2019-1210). Dr. Chen knows from personal experience that she was not alone in her cohort as she faced the challenges of sleep deprivation and emotional trauma that continue to be a part of a physician’s education and training. In her discussion of how future medical trainees might be spared some of the long hours she endured, Dr. Chen suggests that this country consider expanding its physician workforce by “increasing the number of medical schools and recruiting foreign medical graduates” as some European countries have done. Dr. Chen now works in the pediatric residency office at Children’s Hospital, Los Angeles.

Ironically, or maybe it was intentionally, the editors of Pediatrics chose to open the same issue in which Dr. Chen’s personal story appears with a Pediatrics Perspective commentary that looks into the murky waters of physician workforce research (Pediatrics. 2019 Sep 1. doi: 10.1542/peds.2019-0469). Gary L. Freed, MD, MPH, at the Child Health Evaluation and Research Center at the University of Michigan, Ann Arbor, claims that, in general, the data currently being generated by workforce research must be interpreted with caution because many of the studies are flawed by one or more biases.
You may have survived the gauntlet of medical school and residency relatively unscathed. But Is part of the problem that your clinic is seeing too many patients with too few physicians? Do your colleagues share your opinion? Is the administration actively recruiting more physicians, but failing to find interested and qualified doctors? Is this a strictly local phenomenon limited to your community, or is it a regional shortage? Do you think your situation reflects a national trend that deserves attention?
Like Dr. Chen, do you think that more medical schools and active recruitment of foreign medical students would allow you to work less hours? Obviously, even if you were a teenager when you entered your residency, opening more medical schools is not going to allow you to shorten your workday. But are more medical schools the best solution for this country’s overworked physicians even in the long term? Dr. Freed’s observations should make you hesitant to even venture a guess.

You, I, and Dr. Chen only can report on how we perceive our own work environment. Your local physician shortage may be in part because the school system in your community has a poor reputation and young physicians don’t want to move there. It may be that the hospital that owns your practice is struggling and can’t afford to offer a competitive salary. Producing more physicians may not be the answer to the physician shortage in communities like yours, even in the long run.
This is a very large country with relatively porous boundaries between the states for physicians. Physician supply and demand seldom dictates where physicians choose to practice. In fact, a medically needy community is probably the least likely place a physician just finishing her training will choose to settle.
Although adding another physician to your practice may decrease your workload, can your personal finances handle the hit that might occur as you see less patients? Particularly, if the new hire turns out to be a rock star who siphons off more of your patients than you anticipated. On the other hand, there is always the chance that, despite careful vetting, your group hires a lemon who ends up creating more trouble than he is worth.
As Dr. Freed suggests, trying to determine just how many and what kind of physicians we need is complicated. It may be just a roll of the dice at best.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
In a Pediatrics article, Hsuan-hsiu Annie Chen, MD, offers a very personal and candid narrative of her struggle with depression during medical school and residency (Pediatrics. 2019 Sep 1. doi: 10.1542/peds.2019-1210). Dr. Chen knows from personal experience that she was not alone in her cohort as she faced the challenges of sleep deprivation and emotional trauma that continue to be a part of a physician’s education and training. In her discussion of how future medical trainees might be spared some of the long hours she endured, Dr. Chen suggests that this country consider expanding its physician workforce by “increasing the number of medical schools and recruiting foreign medical graduates” as some European countries have done. Dr. Chen now works in the pediatric residency office at Children’s Hospital, Los Angeles.
Ironically, or maybe it was intentionally, the editors of Pediatrics chose to open the same issue in which Dr. Chen’s personal story appears with a Pediatrics Perspective commentary that looks into the murky waters of physician workforce research (Pediatrics. 2019 Sep 1. doi: 10.1542/peds.2019-0469). Gary L. Freed, MD, MPH, at the Child Health Evaluation and Research Center at the University of Michigan, Ann Arbor, claims that, in general, the data currently being generated by workforce research must be interpreted with caution because many of the studies are flawed by one or more biases.
You may have survived the gauntlet of medical school and residency relatively unscathed. But Is part of the problem that your clinic is seeing too many patients with too few physicians? Do your colleagues share your opinion? Is the administration actively recruiting more physicians, but failing to find interested and qualified doctors? Is this a strictly local phenomenon limited to your community, or is it a regional shortage? Do you think your situation reflects a national trend that deserves attention?
Like Dr. Chen, do you think that more medical schools and active recruitment of foreign medical students would allow you to work less hours? Obviously, even if you were a teenager when you entered your residency, opening more medical schools is not going to allow you to shorten your workday. But are more medical schools the best solution for this country’s overworked physicians even in the long term? Dr. Freed’s observations should make you hesitant to even venture a guess.
You, I, and Dr. Chen only can report on how we perceive our own work environment. Your local physician shortage may be in part because the school system in your community has a poor reputation and young physicians don’t want to move there. It may be that the hospital that owns your practice is struggling and can’t afford to offer a competitive salary. Producing more physicians may not be the answer to the physician shortage in communities like yours, even in the long run.
This is a very large country with relatively porous boundaries between the states for physicians. Physician supply and demand seldom dictates where physicians choose to practice. In fact, a medically needy community is probably the least likely place a physician just finishing her training will choose to settle.
Although adding another physician to your practice may decrease your workload, can your personal finances handle the hit that might occur as you see less patients? Particularly, if the new hire turns out to be a rock star who siphons off more of your patients than you anticipated. On the other hand, there is always the chance that, despite careful vetting, your group hires a lemon who ends up creating more trouble than he is worth.
As Dr. Freed suggests, trying to determine just how many and what kind of physicians we need is complicated. It may be just a roll of the dice at best.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
In a Pediatrics article, Hsuan-hsiu Annie Chen, MD, offers a very personal and candid narrative of her struggle with depression during medical school and residency (Pediatrics. 2019 Sep 1. doi: 10.1542/peds.2019-1210). Dr. Chen knows from personal experience that she was not alone in her cohort as she faced the challenges of sleep deprivation and emotional trauma that continue to be a part of a physician’s education and training. In her discussion of how future medical trainees might be spared some of the long hours she endured, Dr. Chen suggests that this country consider expanding its physician workforce by “increasing the number of medical schools and recruiting foreign medical graduates” as some European countries have done. Dr. Chen now works in the pediatric residency office at Children’s Hospital, Los Angeles.
Ironically, or maybe it was intentionally, the editors of Pediatrics chose to open the same issue in which Dr. Chen’s personal story appears with a Pediatrics Perspective commentary that looks into the murky waters of physician workforce research (Pediatrics. 2019 Sep 1. doi: 10.1542/peds.2019-0469). Gary L. Freed, MD, MPH, at the Child Health Evaluation and Research Center at the University of Michigan, Ann Arbor, claims that, in general, the data currently being generated by workforce research must be interpreted with caution because many of the studies are flawed by one or more biases.
You may have survived the gauntlet of medical school and residency relatively unscathed. But Is part of the problem that your clinic is seeing too many patients with too few physicians? Do your colleagues share your opinion? Is the administration actively recruiting more physicians, but failing to find interested and qualified doctors? Is this a strictly local phenomenon limited to your community, or is it a regional shortage? Do you think your situation reflects a national trend that deserves attention?
Like Dr. Chen, do you think that more medical schools and active recruitment of foreign medical students would allow you to work less hours? Obviously, even if you were a teenager when you entered your residency, opening more medical schools is not going to allow you to shorten your workday. But are more medical schools the best solution for this country’s overworked physicians even in the long term? Dr. Freed’s observations should make you hesitant to even venture a guess.
You, I, and Dr. Chen only can report on how we perceive our own work environment. Your local physician shortage may be in part because the school system in your community has a poor reputation and young physicians don’t want to move there. It may be that the hospital that owns your practice is struggling and can’t afford to offer a competitive salary. Producing more physicians may not be the answer to the physician shortage in communities like yours, even in the long run.
This is a very large country with relatively porous boundaries between the states for physicians. Physician supply and demand seldom dictates where physicians choose to practice. In fact, a medically needy community is probably the least likely place a physician just finishing her training will choose to settle.
Although adding another physician to your practice may decrease your workload, can your personal finances handle the hit that might occur as you see less patients? Particularly, if the new hire turns out to be a rock star who siphons off more of your patients than you anticipated. On the other hand, there is always the chance that, despite careful vetting, your group hires a lemon who ends up creating more trouble than he is worth.
As Dr. Freed suggests, trying to determine just how many and what kind of physicians we need is complicated. It may be just a roll of the dice at best.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
It’s all in the timing
It is often fun and sometimes exhausting watching the speed with which children run around or switch from one game to another. A lot of us were attracted to pediatrics to share the quick joy of children and also the speed of their physical recovery. We get to see premature infants gain an ounce a day, and see wounds heal in less than a week. We give advice on sleep and see success in a month. We and the families get used to quick fixes.

Parents and children are forewarned and reassured by our knowledge about how long things typically take: Respiratory syncytial virus (RSV) peaks in 5 days, colic lessens in 3 months, changing sleep patterns takes 3 weeks, habit formation 6 weeks, menses come 2 years after breast development, and so on. But the timing of daily parenting is rarely as predictable. Sometimes a child’s clock is running fast, making waiting even seconds for a snack or a bathroom difficult; other times are slow, as when walking down the sidewalk noticing every leaf. The child’s clock is independent of the adult’s – and complicated by clocks of siblings.
Parent pace also is determined by many factors unrelated to the child: work demands, deadlines, train schedules, something in the oven, needs of siblings, and so on. To those can be added intrinsic factors affecting parent’s tolerance to shifting pace to the child’s such as temperament, fatigue, illness, pain, or even adult ADHD. And don’t forget caffeine (or other drugs) affecting the internal metronome. When impatience with the child is a complaint, it is useful to ask, “What makes waiting for your child difficult for you?”
When discussing time, I find it important to discuss the poison “s-word” of parenting – “should.” This trickster often comes from time illusions in childrearing. After seeing so many behaviors change quickly, parents expect all change to be equally fast. She should be able to sleep through the night by now! He should be able to dress and get to the table in 5 minutes. And sometimes it is the parent’s s-word that creates pain – I should love pushing for as long as she wants to swing, if I am a good parent. The problem with thinking “should” is that it implies willful or moral behavior, and it may prompt a judgmental or punitive parental response.
Otherwise well intentioned, cooperative children who take longer to shift their attention from homework to shower can be seen as oppositional. Worse yet, if the example used is from playing video games (something fun) to getting to the bus stop (an undesirable shift), you may hear parents critically say, “He only wants to do what he wants to do.” When examining examples (always key to helping with behavior), pointing out that all kinds of transitions are difficult for this child may be educational and allow for a more reasoned response. And specifically being on electronics puts adults as well as children in a time warp which is hard to escape.
There are many kinds of thwarted expectations, but expectations about how long things take are pretty universal. Frustration generates anger and even can lead to violence, such as road rage. Children – who all step to the beat of a different drummer, especially those with different “clocks” such as in ADHD – may experience frustration most of the day. This can manifest as irritability for them and sometimes as an irritable response back from the parent.
The first step in adapting to differences in parent and child pace is to realize that time is the problem. Naming it, saying “we are on toddler time,” can be a “signal to self” to slow down. Generations of children loved Mr. Rogers because he always conveyed having all the time in the world for the person he was with. It actually does not take as long as it feels at first to do this. Listening while keeping eye contact, breathing deeply, and waiting until two breaths after the child goes silent before speaking or moving conveys your interest and respect. For some behaviors, such as tantrums, such quiet attention may be all that is needed to resolve the issue. We adults can practice this, but even infants can be helped to develop patience by reinforcement with brief attention from their caregivers for tiny increments of waiting.

I sometimes suggest that parents time behaviors to develop perspective, reset expectations, practice waiting, and perhaps even distract themselves from intervening and making things worse by lending attention to negative behaviors. Timing as observation can be helpful for tantrums, breath holding spells, whining, and sibling squabbles; maximum times for baths and video games; minimum times for meals, sitting to poop, and special time. Timers are not just for Time Out! “Visual timers” that show green then yellow then red and sometimes flashing lights as warnings of an upcoming stopping point are helpful for children preschool and older. These timers help them to develop a better sense of time and begin managing their own transitions. A game of guessing how long things take can build timing skills and patience. I think every child past preschool benefits from a wristwatch, first to build time sense, and second to avoid looking at a smartphone to see the hour, then being distracted by content! Diaries of behaviors over time are a staple of behavior change plans, with the added benefit of lending perspective on actually how often and how long a troublesome behavior occurs. Practicing mindfulness – nonjudgmental watching of our thoughts and feelings, often with deep breathing and relaxation – also can help both children and adults build time tolerance.
Children have little control over their daily schedule. Surrendering when you can for them to do things at their own pace can reduce their frustration, build the parent-child relationship, and promote positive behaviors. Plus family life is more enjoyable lived slower. You even can remind parents that “the days are long but the years are short” before their children will be grown and gone.
Dr. Howard is an assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS. She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. Email her at pdnews@mdedge.com.
It is often fun and sometimes exhausting watching the speed with which children run around or switch from one game to another. A lot of us were attracted to pediatrics to share the quick joy of children and also the speed of their physical recovery. We get to see premature infants gain an ounce a day, and see wounds heal in less than a week. We give advice on sleep and see success in a month. We and the families get used to quick fixes.
Parents and children are forewarned and reassured by our knowledge about how long things typically take: Respiratory syncytial virus (RSV) peaks in 5 days, colic lessens in 3 months, changing sleep patterns takes 3 weeks, habit formation 6 weeks, menses come 2 years after breast development, and so on. But the timing of daily parenting is rarely as predictable. Sometimes a child’s clock is running fast, making waiting even seconds for a snack or a bathroom difficult; other times are slow, as when walking down the sidewalk noticing every leaf. The child’s clock is independent of the adult’s – and complicated by clocks of siblings.
Parent pace also is determined by many factors unrelated to the child: work demands, deadlines, train schedules, something in the oven, needs of siblings, and so on. To those can be added intrinsic factors affecting parent’s tolerance to shifting pace to the child’s such as temperament, fatigue, illness, pain, or even adult ADHD. And don’t forget caffeine (or other drugs) affecting the internal metronome. When impatience with the child is a complaint, it is useful to ask, “What makes waiting for your child difficult for you?”
When discussing time, I find it important to discuss the poison “s-word” of parenting – “should.” This trickster often comes from time illusions in childrearing. After seeing so many behaviors change quickly, parents expect all change to be equally fast. She should be able to sleep through the night by now! He should be able to dress and get to the table in 5 minutes. And sometimes it is the parent’s s-word that creates pain – I should love pushing for as long as she wants to swing, if I am a good parent. The problem with thinking “should” is that it implies willful or moral behavior, and it may prompt a judgmental or punitive parental response.
Otherwise well intentioned, cooperative children who take longer to shift their attention from homework to shower can be seen as oppositional. Worse yet, if the example used is from playing video games (something fun) to getting to the bus stop (an undesirable shift), you may hear parents critically say, “He only wants to do what he wants to do.” When examining examples (always key to helping with behavior), pointing out that all kinds of transitions are difficult for this child may be educational and allow for a more reasoned response. And specifically being on electronics puts adults as well as children in a time warp which is hard to escape.
There are many kinds of thwarted expectations, but expectations about how long things take are pretty universal. Frustration generates anger and even can lead to violence, such as road rage. Children – who all step to the beat of a different drummer, especially those with different “clocks” such as in ADHD – may experience frustration most of the day. This can manifest as irritability for them and sometimes as an irritable response back from the parent.
The first step in adapting to differences in parent and child pace is to realize that time is the problem. Naming it, saying “we are on toddler time,” can be a “signal to self” to slow down. Generations of children loved Mr. Rogers because he always conveyed having all the time in the world for the person he was with. It actually does not take as long as it feels at first to do this. Listening while keeping eye contact, breathing deeply, and waiting until two breaths after the child goes silent before speaking or moving conveys your interest and respect. For some behaviors, such as tantrums, such quiet attention may be all that is needed to resolve the issue. We adults can practice this, but even infants can be helped to develop patience by reinforcement with brief attention from their caregivers for tiny increments of waiting.
I sometimes suggest that parents time behaviors to develop perspective, reset expectations, practice waiting, and perhaps even distract themselves from intervening and making things worse by lending attention to negative behaviors. Timing as observation can be helpful for tantrums, breath holding spells, whining, and sibling squabbles; maximum times for baths and video games; minimum times for meals, sitting to poop, and special time. Timers are not just for Time Out! “Visual timers” that show green then yellow then red and sometimes flashing lights as warnings of an upcoming stopping point are helpful for children preschool and older. These timers help them to develop a better sense of time and begin managing their own transitions. A game of guessing how long things take can build timing skills and patience. I think every child past preschool benefits from a wristwatch, first to build time sense, and second to avoid looking at a smartphone to see the hour, then being distracted by content! Diaries of behaviors over time are a staple of behavior change plans, with the added benefit of lending perspective on actually how often and how long a troublesome behavior occurs. Practicing mindfulness – nonjudgmental watching of our thoughts and feelings, often with deep breathing and relaxation – also can help both children and adults build time tolerance.
Children have little control over their daily schedule. Surrendering when you can for them to do things at their own pace can reduce their frustration, build the parent-child relationship, and promote positive behaviors. Plus family life is more enjoyable lived slower. You even can remind parents that “the days are long but the years are short” before their children will be grown and gone.
Dr. Howard is an assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS. She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. Email her at pdnews@mdedge.com.
It is often fun and sometimes exhausting watching the speed with which children run around or switch from one game to another. A lot of us were attracted to pediatrics to share the quick joy of children and also the speed of their physical recovery. We get to see premature infants gain an ounce a day, and see wounds heal in less than a week. We give advice on sleep and see success in a month. We and the families get used to quick fixes.
Parents and children are forewarned and reassured by our knowledge about how long things typically take: Respiratory syncytial virus (RSV) peaks in 5 days, colic lessens in 3 months, changing sleep patterns takes 3 weeks, habit formation 6 weeks, menses come 2 years after breast development, and so on. But the timing of daily parenting is rarely as predictable. Sometimes a child’s clock is running fast, making waiting even seconds for a snack or a bathroom difficult; other times are slow, as when walking down the sidewalk noticing every leaf. The child’s clock is independent of the adult’s – and complicated by clocks of siblings.
Parent pace also is determined by many factors unrelated to the child: work demands, deadlines, train schedules, something in the oven, needs of siblings, and so on. To those can be added intrinsic factors affecting parent’s tolerance to shifting pace to the child’s such as temperament, fatigue, illness, pain, or even adult ADHD. And don’t forget caffeine (or other drugs) affecting the internal metronome. When impatience with the child is a complaint, it is useful to ask, “What makes waiting for your child difficult for you?”
When discussing time, I find it important to discuss the poison “s-word” of parenting – “should.” This trickster often comes from time illusions in childrearing. After seeing so many behaviors change quickly, parents expect all change to be equally fast. She should be able to sleep through the night by now! He should be able to dress and get to the table in 5 minutes. And sometimes it is the parent’s s-word that creates pain – I should love pushing for as long as she wants to swing, if I am a good parent. The problem with thinking “should” is that it implies willful or moral behavior, and it may prompt a judgmental or punitive parental response.
Otherwise well intentioned, cooperative children who take longer to shift their attention from homework to shower can be seen as oppositional. Worse yet, if the example used is from playing video games (something fun) to getting to the bus stop (an undesirable shift), you may hear parents critically say, “He only wants to do what he wants to do.” When examining examples (always key to helping with behavior), pointing out that all kinds of transitions are difficult for this child may be educational and allow for a more reasoned response. And specifically being on electronics puts adults as well as children in a time warp which is hard to escape.
There are many kinds of thwarted expectations, but expectations about how long things take are pretty universal. Frustration generates anger and even can lead to violence, such as road rage. Children – who all step to the beat of a different drummer, especially those with different “clocks” such as in ADHD – may experience frustration most of the day. This can manifest as irritability for them and sometimes as an irritable response back from the parent.
The first step in adapting to differences in parent and child pace is to realize that time is the problem. Naming it, saying “we are on toddler time,” can be a “signal to self” to slow down. Generations of children loved Mr. Rogers because he always conveyed having all the time in the world for the person he was with. It actually does not take as long as it feels at first to do this. Listening while keeping eye contact, breathing deeply, and waiting until two breaths after the child goes silent before speaking or moving conveys your interest and respect. For some behaviors, such as tantrums, such quiet attention may be all that is needed to resolve the issue. We adults can practice this, but even infants can be helped to develop patience by reinforcement with brief attention from their caregivers for tiny increments of waiting.
I sometimes suggest that parents time behaviors to develop perspective, reset expectations, practice waiting, and perhaps even distract themselves from intervening and making things worse by lending attention to negative behaviors. Timing as observation can be helpful for tantrums, breath holding spells, whining, and sibling squabbles; maximum times for baths and video games; minimum times for meals, sitting to poop, and special time. Timers are not just for Time Out! “Visual timers” that show green then yellow then red and sometimes flashing lights as warnings of an upcoming stopping point are helpful for children preschool and older. These timers help them to develop a better sense of time and begin managing their own transitions. A game of guessing how long things take can build timing skills and patience. I think every child past preschool benefits from a wristwatch, first to build time sense, and second to avoid looking at a smartphone to see the hour, then being distracted by content! Diaries of behaviors over time are a staple of behavior change plans, with the added benefit of lending perspective on actually how often and how long a troublesome behavior occurs. Practicing mindfulness – nonjudgmental watching of our thoughts and feelings, often with deep breathing and relaxation – also can help both children and adults build time tolerance.
Children have little control over their daily schedule. Surrendering when you can for them to do things at their own pace can reduce their frustration, build the parent-child relationship, and promote positive behaviors. Plus family life is more enjoyable lived slower. You even can remind parents that “the days are long but the years are short” before their children will be grown and gone.
Dr. Howard is an assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS. She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. Email her at pdnews@mdedge.com.
What repair is best for juxtarenal aneurysm?
CHICAGO – Outcomes with fenestrated endografts and endograft anchors to repair abdominal aortic aneurysms (AAAs) in the region of the renal artery have improved as the techniques have gained popularity in recent years, but open repair may still achieve better overall results, vascular surgeons on opposite sides of the controversy contended during a debate at the annual meeting of the Midwestern Vascular Surgery Society.
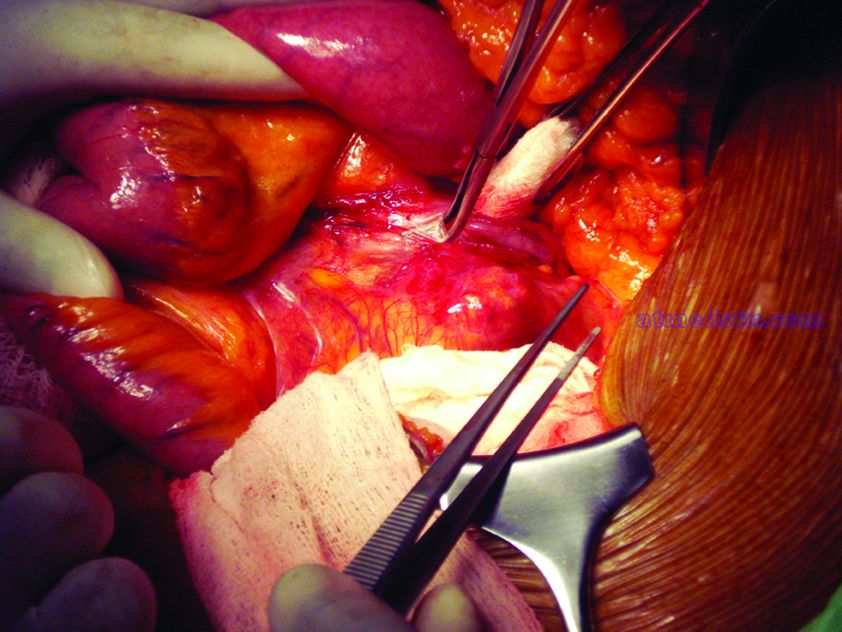
Fenestrated endovascular aortic repair (FEVAR) “is as safe as open surgery to treat complex aneurysm,” said Carlos Bechara, MD, of Loyola University Medical Center in Chicago. “EndoAnchors [Medtronic] do provide an excellent off-the-shelf solution to treat short, hostile necks with promising short-term results.”
Arguing for open repair was Paul DiMusto, MD, of the University of Wisconsin–Madison. “Open repair has an equal perioperative mortality to FEVAR,” Dr. DiMusto said, adding that the open approach also has a higher long-term branch patency rate, lower secondary-intervention rate, a lower incidence of long-term renal failure, and higher long-term survival. “So putting that all together, open repair is best,” he said.
They staked out their positions by citing a host of published trials.
“The presence of a short neck can create a challenging clinical scenario for an endovascular repair of abdominal aortic aneurysm,” Dr. Bechara said. However, he noted he was discussing complex aneurysm in which the aortic clamp is placed above the renal arteries, differentiating it from infrarenal AAA in which the clamp is below the renal arteries with no renal ischemia time. He noted a 2011 study that determined a short neck was a predictor of Type 1A endoleak after AAA repair, but that compliance with best practices at the time was poor; more than 44% of EVARs did not follow the manufacturer’s instruction (Circulation. 2011;123:2848-55).
But FEVAR was approved by the Food and Drug Administration in 2012, with an indication for an infrarenal neck length of 4-14 mm, Dr. Bechara noted. Since then, several studies have reported excellent outcomes with the technique. An early small study of 67 patients reported a 100% technical success rate with one patient having a Type 1 endoleak at 3 years (J Vasc Surg. 2014;60:1420-8).
This year, a larger study evaluated 6,825 patients in the American College of Surgeons National Surgical Quality Improvement Program who had FEVAR, open AAA repair or standard infrarenal endovascular repair during 2012-2016. “Actually, the fenestrated approach had fewer complications than open repair and the outcomes were comparable to standard EVAR,” Dr. Bechara noted. The trial reported FEVAR had lower rates of perioperative mortality (1.8% vs. 8.8%; P = .001), postoperative renal dysfunction (1.4% vs. 7.7%; P = .002), and overall complications (11% vs. 33%; P less than.001) than did open repair (J Vasc Surg. 2019;69:1670-78).
In regard to the use of endograft anchors for treatment of endoleaks, migrating grafts, and high-risk seal zones, Dr. Bechara noted they are a good “off-the-shelf” choice for complex AAA repair. He cited current results of a cohort of 70 patients with short-neck AAA (J Vasc Surg. 2019;70:732-40). “This study showed a procedural success rate at 97% and a technical success rate at 88.6%,” he said. “They had no stent migration, no increase in sac size or AAA rupture or open conversion.”
He also pointed to just-published results from a randomized trial of 881 patients with up to 14 years of follow-up that found comparable rates of death/secondary procedures, as well as durability, between patients who had endovascular and open repairs (77.7% and 75.5%, respectively, N Engl J Med. 2019;380:2126-35). Also, he noted that hospital volume is an important predictor of success with open repair, with high-volume centers reporting lower mortality (3.9%) than low-volume centers (9%; Ann Surg. 2018 Nov 29. doi: 10.1097/SLA.0000000000002873). “So not many centers are doing high-volume open aortic surgery,” he said.
To make his case that open surgery for juxtarenal AAAs is superior, Dr. DiMusto cited a number of recent studies, including a three-center trial of 200 patients who had open and FEVAR procedures (J Endovasc Ther. 2019;26:105-12). “There was no difference in perioperative mortality [2.2% for FEVAR, 1.9% in open repair], ” Dr. DiMusto said “There was a higher freedom from reintervention in the open group [96% vs. 78%], and there was higher long-term vessel patency in the open group” (97.5% having target patency for open vs. 93.3% for FEVAR).
He also pointed to a meta-analysis of 2,326 patients that found similar outcomes for mortality and postoperative renal insufficiency between FEVAR and open repair, around 4.1%, but showed significantly higher rates of renal failure in FEVAR, at 19.7% versus 7.7% (J Vasc Surg. 2015;61:242-55). This study also reported significantly more secondary interventions with FEVAR, 12.7% vs. 4.9%, Dr. DiMusto said.
Another study of 3,253 complex AAA repairs, including 887 FEVAR and 2,125 open procedures, showed that FEVAR had a technical success rate of 97%, with no appreciable difference in perioperative mortality between the two procedures (Ann Surg. 2019 Feb 1. doi: 10.1097/SLA.0000000000003094).
However, Dr. DiMusto said, adjusted 3-year mortality in this study was higher with FEVAR, and further analysis yielded outcomes that favored open repair. “After excluding perioperative deaths, differences remained, with 9% mortality for FEVAR and 5% for open repair [P = .02],” he said. “This corresponded to a 66% higher risk for overall mortality following FEVAR.”
What’s more, Dr. DiMusto said, draft guidelines from the National Institute for Health and Care Excellence in the United Kingdom advise against offering complex EVAR to people with an unruptured AAA under two scenarios: if open surgery is an option; and even if they’re unable to have surgery because of anesthetic or medical issues. The final guidelines have yet to be released.
Dr. Bechara disclosed financial relationships with Gore Medical and Cook Medical and equity interest in MOKITA Medical. Dr. DiMusto has no relevant financial disclosures.
CHICAGO – Outcomes with fenestrated endografts and endograft anchors to repair abdominal aortic aneurysms (AAAs) in the region of the renal artery have improved as the techniques have gained popularity in recent years, but open repair may still achieve better overall results, vascular surgeons on opposite sides of the controversy contended during a debate at the annual meeting of the Midwestern Vascular Surgery Society.
Fenestrated endovascular aortic repair (FEVAR) “is as safe as open surgery to treat complex aneurysm,” said Carlos Bechara, MD, of Loyola University Medical Center in Chicago. “EndoAnchors [Medtronic] do provide an excellent off-the-shelf solution to treat short, hostile necks with promising short-term results.”
Arguing for open repair was Paul DiMusto, MD, of the University of Wisconsin–Madison. “Open repair has an equal perioperative mortality to FEVAR,” Dr. DiMusto said, adding that the open approach also has a higher long-term branch patency rate, lower secondary-intervention rate, a lower incidence of long-term renal failure, and higher long-term survival. “So putting that all together, open repair is best,” he said.
They staked out their positions by citing a host of published trials.
“The presence of a short neck can create a challenging clinical scenario for an endovascular repair of abdominal aortic aneurysm,” Dr. Bechara said. However, he noted he was discussing complex aneurysm in which the aortic clamp is placed above the renal arteries, differentiating it from infrarenal AAA in which the clamp is below the renal arteries with no renal ischemia time. He noted a 2011 study that determined a short neck was a predictor of Type 1A endoleak after AAA repair, but that compliance with best practices at the time was poor; more than 44% of EVARs did not follow the manufacturer’s instruction (Circulation. 2011;123:2848-55).
But FEVAR was approved by the Food and Drug Administration in 2012, with an indication for an infrarenal neck length of 4-14 mm, Dr. Bechara noted. Since then, several studies have reported excellent outcomes with the technique. An early small study of 67 patients reported a 100% technical success rate with one patient having a Type 1 endoleak at 3 years (J Vasc Surg. 2014;60:1420-8).
This year, a larger study evaluated 6,825 patients in the American College of Surgeons National Surgical Quality Improvement Program who had FEVAR, open AAA repair or standard infrarenal endovascular repair during 2012-2016. “Actually, the fenestrated approach had fewer complications than open repair and the outcomes were comparable to standard EVAR,” Dr. Bechara noted. The trial reported FEVAR had lower rates of perioperative mortality (1.8% vs. 8.8%; P = .001), postoperative renal dysfunction (1.4% vs. 7.7%; P = .002), and overall complications (11% vs. 33%; P less than.001) than did open repair (J Vasc Surg. 2019;69:1670-78).
In regard to the use of endograft anchors for treatment of endoleaks, migrating grafts, and high-risk seal zones, Dr. Bechara noted they are a good “off-the-shelf” choice for complex AAA repair. He cited current results of a cohort of 70 patients with short-neck AAA (J Vasc Surg. 2019;70:732-40). “This study showed a procedural success rate at 97% and a technical success rate at 88.6%,” he said. “They had no stent migration, no increase in sac size or AAA rupture or open conversion.”
He also pointed to just-published results from a randomized trial of 881 patients with up to 14 years of follow-up that found comparable rates of death/secondary procedures, as well as durability, between patients who had endovascular and open repairs (77.7% and 75.5%, respectively, N Engl J Med. 2019;380:2126-35). Also, he noted that hospital volume is an important predictor of success with open repair, with high-volume centers reporting lower mortality (3.9%) than low-volume centers (9%; Ann Surg. 2018 Nov 29. doi: 10.1097/SLA.0000000000002873). “So not many centers are doing high-volume open aortic surgery,” he said.
To make his case that open surgery for juxtarenal AAAs is superior, Dr. DiMusto cited a number of recent studies, including a three-center trial of 200 patients who had open and FEVAR procedures (J Endovasc Ther. 2019;26:105-12). “There was no difference in perioperative mortality [2.2% for FEVAR, 1.9% in open repair], ” Dr. DiMusto said “There was a higher freedom from reintervention in the open group [96% vs. 78%], and there was higher long-term vessel patency in the open group” (97.5% having target patency for open vs. 93.3% for FEVAR).
He also pointed to a meta-analysis of 2,326 patients that found similar outcomes for mortality and postoperative renal insufficiency between FEVAR and open repair, around 4.1%, but showed significantly higher rates of renal failure in FEVAR, at 19.7% versus 7.7% (J Vasc Surg. 2015;61:242-55). This study also reported significantly more secondary interventions with FEVAR, 12.7% vs. 4.9%, Dr. DiMusto said.
Another study of 3,253 complex AAA repairs, including 887 FEVAR and 2,125 open procedures, showed that FEVAR had a technical success rate of 97%, with no appreciable difference in perioperative mortality between the two procedures (Ann Surg. 2019 Feb 1. doi: 10.1097/SLA.0000000000003094).
However, Dr. DiMusto said, adjusted 3-year mortality in this study was higher with FEVAR, and further analysis yielded outcomes that favored open repair. “After excluding perioperative deaths, differences remained, with 9% mortality for FEVAR and 5% for open repair [P = .02],” he said. “This corresponded to a 66% higher risk for overall mortality following FEVAR.”
What’s more, Dr. DiMusto said, draft guidelines from the National Institute for Health and Care Excellence in the United Kingdom advise against offering complex EVAR to people with an unruptured AAA under two scenarios: if open surgery is an option; and even if they’re unable to have surgery because of anesthetic or medical issues. The final guidelines have yet to be released.
Dr. Bechara disclosed financial relationships with Gore Medical and Cook Medical and equity interest in MOKITA Medical. Dr. DiMusto has no relevant financial disclosures.
CHICAGO – Outcomes with fenestrated endografts and endograft anchors to repair abdominal aortic aneurysms (AAAs) in the region of the renal artery have improved as the techniques have gained popularity in recent years, but open repair may still achieve better overall results, vascular surgeons on opposite sides of the controversy contended during a debate at the annual meeting of the Midwestern Vascular Surgery Society.
Fenestrated endovascular aortic repair (FEVAR) “is as safe as open surgery to treat complex aneurysm,” said Carlos Bechara, MD, of Loyola University Medical Center in Chicago. “EndoAnchors [Medtronic] do provide an excellent off-the-shelf solution to treat short, hostile necks with promising short-term results.”
Arguing for open repair was Paul DiMusto, MD, of the University of Wisconsin–Madison. “Open repair has an equal perioperative mortality to FEVAR,” Dr. DiMusto said, adding that the open approach also has a higher long-term branch patency rate, lower secondary-intervention rate, a lower incidence of long-term renal failure, and higher long-term survival. “So putting that all together, open repair is best,” he said.
They staked out their positions by citing a host of published trials.
“The presence of a short neck can create a challenging clinical scenario for an endovascular repair of abdominal aortic aneurysm,” Dr. Bechara said. However, he noted he was discussing complex aneurysm in which the aortic clamp is placed above the renal arteries, differentiating it from infrarenal AAA in which the clamp is below the renal arteries with no renal ischemia time. He noted a 2011 study that determined a short neck was a predictor of Type 1A endoleak after AAA repair, but that compliance with best practices at the time was poor; more than 44% of EVARs did not follow the manufacturer’s instruction (Circulation. 2011;123:2848-55).
But FEVAR was approved by the Food and Drug Administration in 2012, with an indication for an infrarenal neck length of 4-14 mm, Dr. Bechara noted. Since then, several studies have reported excellent outcomes with the technique. An early small study of 67 patients reported a 100% technical success rate with one patient having a Type 1 endoleak at 3 years (J Vasc Surg. 2014;60:1420-8).
This year, a larger study evaluated 6,825 patients in the American College of Surgeons National Surgical Quality Improvement Program who had FEVAR, open AAA repair or standard infrarenal endovascular repair during 2012-2016. “Actually, the fenestrated approach had fewer complications than open repair and the outcomes were comparable to standard EVAR,” Dr. Bechara noted. The trial reported FEVAR had lower rates of perioperative mortality (1.8% vs. 8.8%; P = .001), postoperative renal dysfunction (1.4% vs. 7.7%; P = .002), and overall complications (11% vs. 33%; P less than.001) than did open repair (J Vasc Surg. 2019;69:1670-78).
In regard to the use of endograft anchors for treatment of endoleaks, migrating grafts, and high-risk seal zones, Dr. Bechara noted they are a good “off-the-shelf” choice for complex AAA repair. He cited current results of a cohort of 70 patients with short-neck AAA (J Vasc Surg. 2019;70:732-40). “This study showed a procedural success rate at 97% and a technical success rate at 88.6%,” he said. “They had no stent migration, no increase in sac size or AAA rupture or open conversion.”
He also pointed to just-published results from a randomized trial of 881 patients with up to 14 years of follow-up that found comparable rates of death/secondary procedures, as well as durability, between patients who had endovascular and open repairs (77.7% and 75.5%, respectively, N Engl J Med. 2019;380:2126-35). Also, he noted that hospital volume is an important predictor of success with open repair, with high-volume centers reporting lower mortality (3.9%) than low-volume centers (9%; Ann Surg. 2018 Nov 29. doi: 10.1097/SLA.0000000000002873). “So not many centers are doing high-volume open aortic surgery,” he said.
To make his case that open surgery for juxtarenal AAAs is superior, Dr. DiMusto cited a number of recent studies, including a three-center trial of 200 patients who had open and FEVAR procedures (J Endovasc Ther. 2019;26:105-12). “There was no difference in perioperative mortality [2.2% for FEVAR, 1.9% in open repair], ” Dr. DiMusto said “There was a higher freedom from reintervention in the open group [96% vs. 78%], and there was higher long-term vessel patency in the open group” (97.5% having target patency for open vs. 93.3% for FEVAR).
He also pointed to a meta-analysis of 2,326 patients that found similar outcomes for mortality and postoperative renal insufficiency between FEVAR and open repair, around 4.1%, but showed significantly higher rates of renal failure in FEVAR, at 19.7% versus 7.7% (J Vasc Surg. 2015;61:242-55). This study also reported significantly more secondary interventions with FEVAR, 12.7% vs. 4.9%, Dr. DiMusto said.
Another study of 3,253 complex AAA repairs, including 887 FEVAR and 2,125 open procedures, showed that FEVAR had a technical success rate of 97%, with no appreciable difference in perioperative mortality between the two procedures (Ann Surg. 2019 Feb 1. doi: 10.1097/SLA.0000000000003094).
However, Dr. DiMusto said, adjusted 3-year mortality in this study was higher with FEVAR, and further analysis yielded outcomes that favored open repair. “After excluding perioperative deaths, differences remained, with 9% mortality for FEVAR and 5% for open repair [P = .02],” he said. “This corresponded to a 66% higher risk for overall mortality following FEVAR.”
What’s more, Dr. DiMusto said, draft guidelines from the National Institute for Health and Care Excellence in the United Kingdom advise against offering complex EVAR to people with an unruptured AAA under two scenarios: if open surgery is an option; and even if they’re unable to have surgery because of anesthetic or medical issues. The final guidelines have yet to be released.
Dr. Bechara disclosed financial relationships with Gore Medical and Cook Medical and equity interest in MOKITA Medical. Dr. DiMusto has no relevant financial disclosures.
EXPERT ANALYSIS FROM MIDWESTERN VASCULAR 2019