User login
Fast-tracking psilocybin for refractory depression makes sense
A significant proportion of patients with major depressive disorder (MDD) either do not respond or have partial responses to the currently available Food and Drug Administration–approved antidepressants.

In controlled clinical trials, there is about a 40%-60% symptom remission rate with a 20%-40% remission rate in community-based treatment settings. Not only do those medications lack efficacy in treating MDD, but there are currently no cures for this debilitating illness. As a result, many patients with MDD continue to suffer.

In response to those poor outcomes, researchers and clinicians have developed algorithms aimed at diagnosing the condition of treatment-resistant depression (TRD),1 which enable opportunities for various treatment methods.2 Several studies underway across the United States are testing what some might consider medically invasive procedures, such as electroconvulsive therapy (ECT), deep brain stimulation (DBS), and vagus nerve stimulation (VNS). ECT often is considered the gold standard of treatment response, but it requires anesthesia, induces a convulsion, and needs a willing patient and clinician. DBS has been used more widely in neurological treatment of movement disorders. Pioneering neurosurgical treatment for TRD reported recently in the American Journal of Psychiatry found that DBS of an area in the brain called the subcallosal cingulate produces clear and apparently sustained antidepressant effects.3 VNS4 remains an experimental treatment for MDD. TMS is safe, noninvasive, and approved by the FDA for depression, but responses appear similar to those with usual antidepressants.
It is not surprising, given those outcomes, that ketamine was fast-tracked in 2016. The enthusiasm related to ketamine’s effect on MDD and TRD has grown over time as more research findings reach the public. While it is unknown how ketamine affects the biological neural network, a single intravenous dose of ketamine (0.5 mg/kg) in patients diagnosed with TRD can lead to improved depression symptoms outcomes within a few hours – and those effects were sustained in 65%-70% of patients at 24 hours. Antidepressants take many weeks to show effects. Ketamine’s exciting findings also offered hope to clinicians and patients trying to manage suicidal thoughts and plans. Ketamine was quickly approved by the FDA as a nasal spray medication.
Now, in another encouraging development, the FDA has granted the Usona Institute Breakthrough Therapy designation for psilocybin for the treatment of MDD. The medical benefits of psilocybin, or “magic mushrooms,” has a long empirical history in our literature. Most recently, psilocybin was featured on “60 Minutes,”5 and in his book, “How to Change Your Mind,”6Michael Pollan details how psychedelic drugs where used to investigate and treat psychiatric disorders until the 1960s, when street use and unsupervised administration led to restrictions on their research and clinical use.
With protocol-driven specific trials, they might become critical medications for a wide range of psychiatric disorders, such as depression, PTSD, anxiety, and addictions. Exciting findings are coming from Roland R. Griffiths, PhD, and his team at Johns Hopkins University’s Center for Psychedelic and Consciousness Research. In a recent study8 with cancer patients suffering from depression and anxiety, carefully administered, specific and supervised high doses of psilocybin produced decreases in depression and anxiety, and increases in quality of life and life meaning attitudes. Those improved attitudes, behavior, and responses were sustained by 80% of the sample 6 months post treatment.
Dr. Griffiths’ center is collaborating with Usona, and this collaboration should result in specific guidelines for dose, safety, and protection against abuse and diversion,9 as the study and FDA trials for ketamine have as well.10 It is very encouraging that psychedelic drugs are receiving fast-track designations, and this development reflects a shift in the risk-benefit considerations taking place in our society. Changing attitudes about depression and other psychiatric diseases are encouraging new approaches and new treatments. Psychiatric suffering and pain are being prioritized in research and appreciated by the general public as devastating. Serious, random assignment placebo-controlled and double- blind research studies will define just how valuable these medications might be, what is the safe dose and duration, and for whom they might prove more effective than existing treatments.
The process will take some time. And it is worth remembering that, although research has been promising,11 the number of patients studied, research design, and outcomes are not yet proven for psilosybin.12 The FDA fast-track makes sense, and the agency should continue supporting these efforts for psychedelics. In fact, we think the FDA also should support the promising trials of nitrous oxide13 (laughing gas), and other safe and novel approaches to successfully treat refractory depression. While we wait for personalized psychiatric medicines to be developed and validated through the long process of FDA approval, we will at least have a larger suite of treatment options to match patients with, along with some new algorithms that treat MDD,* TRD, and other disorders just are around the corner.
Dr. Patterson Silver Wolf is an associate professor at Washington University in St. Louis’s Brown School of Social Work. He is a training faculty member for two National Institutes of Health–funded (T32) training programs and serves as the director of the Community Academic Partnership on Addiction (CAPA). He’s chief research officer at the new CAPA Clinic, a teaching addiction treatment facility that is incorporating and testing various performance-based practice technology tools to respond to the opioid crisis and improve addiction treatment outcomes. Dr. Gold is professor of psychiatry (adjunct) at Washington University, St. Louis. He is the 17th Distinguished Alumni Professor at the University of Florida, Gainesville. For more than 40 years, Dr. Gold has worked on developing models for understanding the effects of opioid, tobacco, cocaine, and other drugs, as well as food, on the brain and behavior. He has written several books and published more than 1,000 peer-reviewed scientific articles, texts, and practice guidelines.
References
1. Sackeim HA et al. J Psychiatr Res. 2019 Jun;113:125-36.
2. Conway CR et al. J Clin Psychiatry. 25 Nov;76(11):1569-70.
3. Crowell AL et al. Am J Psychiatry. 2019 Oct 4. doi: 10.1176.appi.ajp.2019.18121427.
4. Kumar A et al. Neuropsychiatr Dis Treat. 2019 Feb 13;15:457-68.
5. Psilocybin sessions: Psychedelics could help people with addiction and anxiety. “60 Minutes” CBS News. 2019 Oct 13.
6. Pollan M. How to Change Your Mind: What the New Science of Psychedelics Teaches Us About Consciousness, Dying, Addiction, Depression, and Transcendence (Penguin Random House, 2018).
7. Nutt D. Dialogues Clin Neurosci. 2019;21(2):139-47.
8. Griffiths RR et al. J Psychopharmacol 2016 Dec;30(12):1181-97.
9. Johnson MW et al. Neuropsychopharmacology. 2018 Nov;142:143-66.
10. Schwenk ES et al. Reg Anesth Pain Med. 2018 Jul;43(5):456-66.
11. Johnson MW et al. Neurotherapeutics. 2017 Jul;14(3):734-40.
12. Mutonni S et al. J Affect Disord. 2019 Nov.1;258:11-24.
13. Nagele P et al. J Clin Psychopharmacol. 2018 Apr;38(2):144-8.
*Correction, 1/9/2020: An earlier version of this story misidentified the intended disease state.
A significant proportion of patients with major depressive disorder (MDD) either do not respond or have partial responses to the currently available Food and Drug Administration–approved antidepressants.
In controlled clinical trials, there is about a 40%-60% symptom remission rate with a 20%-40% remission rate in community-based treatment settings. Not only do those medications lack efficacy in treating MDD, but there are currently no cures for this debilitating illness. As a result, many patients with MDD continue to suffer.
In response to those poor outcomes, researchers and clinicians have developed algorithms aimed at diagnosing the condition of treatment-resistant depression (TRD),1 which enable opportunities for various treatment methods.2 Several studies underway across the United States are testing what some might consider medically invasive procedures, such as electroconvulsive therapy (ECT), deep brain stimulation (DBS), and vagus nerve stimulation (VNS). ECT often is considered the gold standard of treatment response, but it requires anesthesia, induces a convulsion, and needs a willing patient and clinician. DBS has been used more widely in neurological treatment of movement disorders. Pioneering neurosurgical treatment for TRD reported recently in the American Journal of Psychiatry found that DBS of an area in the brain called the subcallosal cingulate produces clear and apparently sustained antidepressant effects.3 VNS4 remains an experimental treatment for MDD. TMS is safe, noninvasive, and approved by the FDA for depression, but responses appear similar to those with usual antidepressants.
It is not surprising, given those outcomes, that ketamine was fast-tracked in 2016. The enthusiasm related to ketamine’s effect on MDD and TRD has grown over time as more research findings reach the public. While it is unknown how ketamine affects the biological neural network, a single intravenous dose of ketamine (0.5 mg/kg) in patients diagnosed with TRD can lead to improved depression symptoms outcomes within a few hours – and those effects were sustained in 65%-70% of patients at 24 hours. Antidepressants take many weeks to show effects. Ketamine’s exciting findings also offered hope to clinicians and patients trying to manage suicidal thoughts and plans. Ketamine was quickly approved by the FDA as a nasal spray medication.
Now, in another encouraging development, the FDA has granted the Usona Institute Breakthrough Therapy designation for psilocybin for the treatment of MDD. The medical benefits of psilocybin, or “magic mushrooms,” has a long empirical history in our literature. Most recently, psilocybin was featured on “60 Minutes,”5 and in his book, “How to Change Your Mind,”6Michael Pollan details how psychedelic drugs where used to investigate and treat psychiatric disorders until the 1960s, when street use and unsupervised administration led to restrictions on their research and clinical use.
With protocol-driven specific trials, they might become critical medications for a wide range of psychiatric disorders, such as depression, PTSD, anxiety, and addictions. Exciting findings are coming from Roland R. Griffiths, PhD, and his team at Johns Hopkins University’s Center for Psychedelic and Consciousness Research. In a recent study8 with cancer patients suffering from depression and anxiety, carefully administered, specific and supervised high doses of psilocybin produced decreases in depression and anxiety, and increases in quality of life and life meaning attitudes. Those improved attitudes, behavior, and responses were sustained by 80% of the sample 6 months post treatment.
Dr. Griffiths’ center is collaborating with Usona, and this collaboration should result in specific guidelines for dose, safety, and protection against abuse and diversion,9 as the study and FDA trials for ketamine have as well.10 It is very encouraging that psychedelic drugs are receiving fast-track designations, and this development reflects a shift in the risk-benefit considerations taking place in our society. Changing attitudes about depression and other psychiatric diseases are encouraging new approaches and new treatments. Psychiatric suffering and pain are being prioritized in research and appreciated by the general public as devastating. Serious, random assignment placebo-controlled and double- blind research studies will define just how valuable these medications might be, what is the safe dose and duration, and for whom they might prove more effective than existing treatments.
The process will take some time. And it is worth remembering that, although research has been promising,11 the number of patients studied, research design, and outcomes are not yet proven for psilosybin.12 The FDA fast-track makes sense, and the agency should continue supporting these efforts for psychedelics. In fact, we think the FDA also should support the promising trials of nitrous oxide13 (laughing gas), and other safe and novel approaches to successfully treat refractory depression. While we wait for personalized psychiatric medicines to be developed and validated through the long process of FDA approval, we will at least have a larger suite of treatment options to match patients with, along with some new algorithms that treat MDD,* TRD, and other disorders just are around the corner.
Dr. Patterson Silver Wolf is an associate professor at Washington University in St. Louis’s Brown School of Social Work. He is a training faculty member for two National Institutes of Health–funded (T32) training programs and serves as the director of the Community Academic Partnership on Addiction (CAPA). He’s chief research officer at the new CAPA Clinic, a teaching addiction treatment facility that is incorporating and testing various performance-based practice technology tools to respond to the opioid crisis and improve addiction treatment outcomes. Dr. Gold is professor of psychiatry (adjunct) at Washington University, St. Louis. He is the 17th Distinguished Alumni Professor at the University of Florida, Gainesville. For more than 40 years, Dr. Gold has worked on developing models for understanding the effects of opioid, tobacco, cocaine, and other drugs, as well as food, on the brain and behavior. He has written several books and published more than 1,000 peer-reviewed scientific articles, texts, and practice guidelines.
References
1. Sackeim HA et al. J Psychiatr Res. 2019 Jun;113:125-36.
2. Conway CR et al. J Clin Psychiatry. 25 Nov;76(11):1569-70.
3. Crowell AL et al. Am J Psychiatry. 2019 Oct 4. doi: 10.1176.appi.ajp.2019.18121427.
4. Kumar A et al. Neuropsychiatr Dis Treat. 2019 Feb 13;15:457-68.
5. Psilocybin sessions: Psychedelics could help people with addiction and anxiety. “60 Minutes” CBS News. 2019 Oct 13.
6. Pollan M. How to Change Your Mind: What the New Science of Psychedelics Teaches Us About Consciousness, Dying, Addiction, Depression, and Transcendence (Penguin Random House, 2018).
7. Nutt D. Dialogues Clin Neurosci. 2019;21(2):139-47.
8. Griffiths RR et al. J Psychopharmacol 2016 Dec;30(12):1181-97.
9. Johnson MW et al. Neuropsychopharmacology. 2018 Nov;142:143-66.
10. Schwenk ES et al. Reg Anesth Pain Med. 2018 Jul;43(5):456-66.
11. Johnson MW et al. Neurotherapeutics. 2017 Jul;14(3):734-40.
12. Mutonni S et al. J Affect Disord. 2019 Nov.1;258:11-24.
13. Nagele P et al. J Clin Psychopharmacol. 2018 Apr;38(2):144-8.
*Correction, 1/9/2020: An earlier version of this story misidentified the intended disease state.
A significant proportion of patients with major depressive disorder (MDD) either do not respond or have partial responses to the currently available Food and Drug Administration–approved antidepressants.
In controlled clinical trials, there is about a 40%-60% symptom remission rate with a 20%-40% remission rate in community-based treatment settings. Not only do those medications lack efficacy in treating MDD, but there are currently no cures for this debilitating illness. As a result, many patients with MDD continue to suffer.
In response to those poor outcomes, researchers and clinicians have developed algorithms aimed at diagnosing the condition of treatment-resistant depression (TRD),1 which enable opportunities for various treatment methods.2 Several studies underway across the United States are testing what some might consider medically invasive procedures, such as electroconvulsive therapy (ECT), deep brain stimulation (DBS), and vagus nerve stimulation (VNS). ECT often is considered the gold standard of treatment response, but it requires anesthesia, induces a convulsion, and needs a willing patient and clinician. DBS has been used more widely in neurological treatment of movement disorders. Pioneering neurosurgical treatment for TRD reported recently in the American Journal of Psychiatry found that DBS of an area in the brain called the subcallosal cingulate produces clear and apparently sustained antidepressant effects.3 VNS4 remains an experimental treatment for MDD. TMS is safe, noninvasive, and approved by the FDA for depression, but responses appear similar to those with usual antidepressants.
It is not surprising, given those outcomes, that ketamine was fast-tracked in 2016. The enthusiasm related to ketamine’s effect on MDD and TRD has grown over time as more research findings reach the public. While it is unknown how ketamine affects the biological neural network, a single intravenous dose of ketamine (0.5 mg/kg) in patients diagnosed with TRD can lead to improved depression symptoms outcomes within a few hours – and those effects were sustained in 65%-70% of patients at 24 hours. Antidepressants take many weeks to show effects. Ketamine’s exciting findings also offered hope to clinicians and patients trying to manage suicidal thoughts and plans. Ketamine was quickly approved by the FDA as a nasal spray medication.
Now, in another encouraging development, the FDA has granted the Usona Institute Breakthrough Therapy designation for psilocybin for the treatment of MDD. The medical benefits of psilocybin, or “magic mushrooms,” has a long empirical history in our literature. Most recently, psilocybin was featured on “60 Minutes,”5 and in his book, “How to Change Your Mind,”6Michael Pollan details how psychedelic drugs where used to investigate and treat psychiatric disorders until the 1960s, when street use and unsupervised administration led to restrictions on their research and clinical use.
With protocol-driven specific trials, they might become critical medications for a wide range of psychiatric disorders, such as depression, PTSD, anxiety, and addictions. Exciting findings are coming from Roland R. Griffiths, PhD, and his team at Johns Hopkins University’s Center for Psychedelic and Consciousness Research. In a recent study8 with cancer patients suffering from depression and anxiety, carefully administered, specific and supervised high doses of psilocybin produced decreases in depression and anxiety, and increases in quality of life and life meaning attitudes. Those improved attitudes, behavior, and responses were sustained by 80% of the sample 6 months post treatment.
Dr. Griffiths’ center is collaborating with Usona, and this collaboration should result in specific guidelines for dose, safety, and protection against abuse and diversion,9 as the study and FDA trials for ketamine have as well.10 It is very encouraging that psychedelic drugs are receiving fast-track designations, and this development reflects a shift in the risk-benefit considerations taking place in our society. Changing attitudes about depression and other psychiatric diseases are encouraging new approaches and new treatments. Psychiatric suffering and pain are being prioritized in research and appreciated by the general public as devastating. Serious, random assignment placebo-controlled and double- blind research studies will define just how valuable these medications might be, what is the safe dose and duration, and for whom they might prove more effective than existing treatments.
The process will take some time. And it is worth remembering that, although research has been promising,11 the number of patients studied, research design, and outcomes are not yet proven for psilosybin.12 The FDA fast-track makes sense, and the agency should continue supporting these efforts for psychedelics. In fact, we think the FDA also should support the promising trials of nitrous oxide13 (laughing gas), and other safe and novel approaches to successfully treat refractory depression. While we wait for personalized psychiatric medicines to be developed and validated through the long process of FDA approval, we will at least have a larger suite of treatment options to match patients with, along with some new algorithms that treat MDD,* TRD, and other disorders just are around the corner.
Dr. Patterson Silver Wolf is an associate professor at Washington University in St. Louis’s Brown School of Social Work. He is a training faculty member for two National Institutes of Health–funded (T32) training programs and serves as the director of the Community Academic Partnership on Addiction (CAPA). He’s chief research officer at the new CAPA Clinic, a teaching addiction treatment facility that is incorporating and testing various performance-based practice technology tools to respond to the opioid crisis and improve addiction treatment outcomes. Dr. Gold is professor of psychiatry (adjunct) at Washington University, St. Louis. He is the 17th Distinguished Alumni Professor at the University of Florida, Gainesville. For more than 40 years, Dr. Gold has worked on developing models for understanding the effects of opioid, tobacco, cocaine, and other drugs, as well as food, on the brain and behavior. He has written several books and published more than 1,000 peer-reviewed scientific articles, texts, and practice guidelines.
References
1. Sackeim HA et al. J Psychiatr Res. 2019 Jun;113:125-36.
2. Conway CR et al. J Clin Psychiatry. 25 Nov;76(11):1569-70.
3. Crowell AL et al. Am J Psychiatry. 2019 Oct 4. doi: 10.1176.appi.ajp.2019.18121427.
4. Kumar A et al. Neuropsychiatr Dis Treat. 2019 Feb 13;15:457-68.
5. Psilocybin sessions: Psychedelics could help people with addiction and anxiety. “60 Minutes” CBS News. 2019 Oct 13.
6. Pollan M. How to Change Your Mind: What the New Science of Psychedelics Teaches Us About Consciousness, Dying, Addiction, Depression, and Transcendence (Penguin Random House, 2018).
7. Nutt D. Dialogues Clin Neurosci. 2019;21(2):139-47.
8. Griffiths RR et al. J Psychopharmacol 2016 Dec;30(12):1181-97.
9. Johnson MW et al. Neuropsychopharmacology. 2018 Nov;142:143-66.
10. Schwenk ES et al. Reg Anesth Pain Med. 2018 Jul;43(5):456-66.
11. Johnson MW et al. Neurotherapeutics. 2017 Jul;14(3):734-40.
12. Mutonni S et al. J Affect Disord. 2019 Nov.1;258:11-24.
13. Nagele P et al. J Clin Psychopharmacol. 2018 Apr;38(2):144-8.
*Correction, 1/9/2020: An earlier version of this story misidentified the intended disease state.
Negligent use of steroids
Question: Mr. M, a car mechanic, was treated with long-term ACTH and Kenalog after he developed severe contact dermatitis from daily exposure to petroleum-based solvents. His subsequent course was complicated by cataracts and osteoporosis. Which of the following is true in case he files a malpractice action?
A. Treatment with steroids was medically indicated for Mr. Mechanic’s dermatologic condition, so the doctor could not have breached the standard of care.
B. Under the “Learned Intermediary” doctrine, both the manufacturer and the prescribing doctor are jointly liable.
C. Corticosteroids are a known cause of osteoporosis and other complications, but not of cataracts, so that part of the malpractice action should be thrown out.
D. The plaintiff would prevail even if he could not find an expert witnesses to testify as to standard of care, since it is “common knowledge” that steroids cause osteoporosis.
E. Lack of informed consent may be his best legal theory of liability, as many jurisdictions now use the patient-centered standard, which does not require expert testimony.
Answer: E. The above hypothetical was modified from an old Montana case1 in which the patient failed in his negligence lawsuit because he did not have expert witnesses to testify as to standard of care and to adequacy of warning label. However, in some jurisdictions under today’s case law, informed consent relies on a subjective, i.e., patient-oriented standard, and expert testimony is unnecessary to prove breach of duty, although still needed to prove causation.
Steroid-related litigation
Steroid-related malpractice litigation is quite prevalent. In a retrospective study of a tertiary medical center from 1996 to 2008, Nash and coworkers identified 83 such cases.2 Steroids were prescribed for pain (23%), asthma or another pulmonary condition (20%), a dermatologic condition (18%), an autoimmune condition (17%), or allergies (6%).

Learned intermediary
“Drug reps” have a responsibility to inform doctors of both benefits and risks of their medications, a process termed “fair balance.” Generally speaking, if a doctor fails to warn the patient of a medication risk, and injury results, the patient may have a claim against the doctor but not the drug manufacturer. This is termed the “learned intermediary” doctrine, which is also applicable to medical devices such as dialysis equipment, breast implants, and blood products.
The justification is that manufacturers can reasonably rely on the treating doctor to warn of adverse effects, which are disclosed to the profession through their sales reps and in the package insert and PDR. The treating doctor, in turn, is expected to use his or her professional judgment to adequately warn the patient. It is simply not feasible for the manufacturer to directly warn every patient without usurping the doctor-patient relationship. However, where known complications were undisclosed to the FDA and the profession, then plaintiff attorneys can file class action lawsuits directed at the manufacturer.
Complications
Complications arising out of the use of steroids are typical examples of medical products liability. This may be on the basis of the doctor having prescribed the medication without a proper indication or where contraindicated, or may have prescribed “the wrong dose for the wrong patient by the wrong route.” In addition, there may have been a lack of informed consent, i.e., failure to explain the underlying condition and the material risks associated with using the drug. Other acts of negligence, e.g., vicarious liability, may also apply.
Corticosteroids such as Prednisone, Decadron, Kenalog, etc., are widely prescribed, and can cause serious complications, especially when used in high doses for extended periods. Examples include suppression of the immune system with supervening infections, steroid osteoporosis and fractures,3 aseptic necrosis, steroid diabetes, hypertension, emotional changes, weight gain, cataracts, neurological complications, and many others. As in all malpractice actions, the plaintiff bears the burden of proof covering the four requisite tort elements, i.e., duty, breach of duty, causation, and damages. Expert testimony is almost always needed in a professional negligence lawsuit.
Aseptic necrosis is a feared complication of steroid therapy.
A recent report4 featured a nurse in her 40s who developed aseptic necrosis of the right shoulder and both hips after taking high dose prednisone for 6 months. She was being treated for idiopathic thrombocytopenic purpura by a hematologist as well as sarcoidosis by a pulmonologist. The plaintiff claimed that both defendants negligently prescribed the medication for an extended period of time without proper monitoring, which caused her severe bone complications requiring a hip and shoulder replacement. The defendants maintained that the steroid medication was necessary to treat the life-threatening conditions from which the plaintiff suffered and that the dosage was carefully monitored and was not excessive. However, in a jury trial, the defendant hematologist and pulmonologist were each found 50% negligent, and the patient was awarded $4.1 million in damages.
In a case5 of steroid-related neurological sequelae, a Colorado jury awarded $14.9 million to a couple against an outpatient surgery center for negligently administering an epidural dose of Kenalog that rendered the patient paraplegic, and for failure to obtain informed consent. The jury awarded the woman, age 57, approximately $1.7 million in past and future medical expenses; $3.2 million in unspecified economic damages; and $6.5 million in past and future noneconomic damages such as pain and suffering. Her husband will receive $3.5 million in past and future noneconomic damages for loss of consortium, according to the verdict. Two years before the injection date of 2013, the drug maker had announced that Kenalog should not be used for epidural procedures because of cord complications including infarction and paraplegia.
Contributory role
The putative offending drug does not have to be the sole cause of injury; if it played a contributory role, the court may find the presence of liability. For example, a Kansas appeals court6 upheld a jury award of $2.88 million in the case of a 40-year-old man who took his life after neurologic complications followed an epidural injection. During one of patient’s visits for chronic low back pain, the defendant-anesthesiologist administered an epidural steroid injection into an area left swollen from a previous injection.
The patient developed neurologic symptoms, and lumbar puncture yielded green pus caused by methicillin-resistant Staphylococcus aureus. He went on to develop arachnoiditis, which left him with impotence, incontinence, and excruciating pain. His lawsuit contended the injection needle had passed through an infected edematous area, causing meningitis and arachnoiditis. Before the case went to trial, the patient took his life because of unremitting pain.
In March 2014, a Johnson County jury found the doctor 75% at fault and the clinic 25% at fault and awarded damages, which were reduced to $1.67 million because Kansas caps noneconomic damages at $250,000. The court rejected the defendants’ argument that the trial judge improperly instructed the jury it could find liability only if negligence “caused” rather than merely “contributed to” the patient’s death, holding that “... one who contributes to a wrongful death is a cause of that death as contemplated by the wrongful death statute.”
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at siang@hawaii.edu .
References
1. Hill v. Squibb Sons, E.R, 592 P.2d 1383 (Mont. 1979).
2. Nash JJ et al, Medical malpractice and corticosteroid use. Otolaryngol Head Neck Surg. 2011; 144:10-5.
3. Buckley L. et al, Glucocorticoid-Induced Osteoporosis. N Engl J Med 2018; 379:2547-56.
4. Zarin’s Jury Verdict: Review and Analysis. Article ID 40229, Philadelphia County.
5. Robbin Smith et al. v. The Surgery Center at Lone Tree, 2015-CV-30922, Douglas County District Court, Colo. Verdict for plaintiff, March 23, 2017.
6. Burnette v. Kimber L. Eubanks, M.D., & Paincare, P.A., 379 P.3d 372 (Kan. Ct. App. 2016).
Question: Mr. M, a car mechanic, was treated with long-term ACTH and Kenalog after he developed severe contact dermatitis from daily exposure to petroleum-based solvents. His subsequent course was complicated by cataracts and osteoporosis. Which of the following is true in case he files a malpractice action?
A. Treatment with steroids was medically indicated for Mr. Mechanic’s dermatologic condition, so the doctor could not have breached the standard of care.
B. Under the “Learned Intermediary” doctrine, both the manufacturer and the prescribing doctor are jointly liable.
C. Corticosteroids are a known cause of osteoporosis and other complications, but not of cataracts, so that part of the malpractice action should be thrown out.
D. The plaintiff would prevail even if he could not find an expert witnesses to testify as to standard of care, since it is “common knowledge” that steroids cause osteoporosis.
E. Lack of informed consent may be his best legal theory of liability, as many jurisdictions now use the patient-centered standard, which does not require expert testimony.
Answer: E. The above hypothetical was modified from an old Montana case1 in which the patient failed in his negligence lawsuit because he did not have expert witnesses to testify as to standard of care and to adequacy of warning label. However, in some jurisdictions under today’s case law, informed consent relies on a subjective, i.e., patient-oriented standard, and expert testimony is unnecessary to prove breach of duty, although still needed to prove causation.
Steroid-related litigation
Steroid-related malpractice litigation is quite prevalent. In a retrospective study of a tertiary medical center from 1996 to 2008, Nash and coworkers identified 83 such cases.2 Steroids were prescribed for pain (23%), asthma or another pulmonary condition (20%), a dermatologic condition (18%), an autoimmune condition (17%), or allergies (6%).
Learned intermediary
“Drug reps” have a responsibility to inform doctors of both benefits and risks of their medications, a process termed “fair balance.” Generally speaking, if a doctor fails to warn the patient of a medication risk, and injury results, the patient may have a claim against the doctor but not the drug manufacturer. This is termed the “learned intermediary” doctrine, which is also applicable to medical devices such as dialysis equipment, breast implants, and blood products.
The justification is that manufacturers can reasonably rely on the treating doctor to warn of adverse effects, which are disclosed to the profession through their sales reps and in the package insert and PDR. The treating doctor, in turn, is expected to use his or her professional judgment to adequately warn the patient. It is simply not feasible for the manufacturer to directly warn every patient without usurping the doctor-patient relationship. However, where known complications were undisclosed to the FDA and the profession, then plaintiff attorneys can file class action lawsuits directed at the manufacturer.
Complications
Complications arising out of the use of steroids are typical examples of medical products liability. This may be on the basis of the doctor having prescribed the medication without a proper indication or where contraindicated, or may have prescribed “the wrong dose for the wrong patient by the wrong route.” In addition, there may have been a lack of informed consent, i.e., failure to explain the underlying condition and the material risks associated with using the drug. Other acts of negligence, e.g., vicarious liability, may also apply.
Corticosteroids such as Prednisone, Decadron, Kenalog, etc., are widely prescribed, and can cause serious complications, especially when used in high doses for extended periods. Examples include suppression of the immune system with supervening infections, steroid osteoporosis and fractures,3 aseptic necrosis, steroid diabetes, hypertension, emotional changes, weight gain, cataracts, neurological complications, and many others. As in all malpractice actions, the plaintiff bears the burden of proof covering the four requisite tort elements, i.e., duty, breach of duty, causation, and damages. Expert testimony is almost always needed in a professional negligence lawsuit.
Aseptic necrosis is a feared complication of steroid therapy.
A recent report4 featured a nurse in her 40s who developed aseptic necrosis of the right shoulder and both hips after taking high dose prednisone for 6 months. She was being treated for idiopathic thrombocytopenic purpura by a hematologist as well as sarcoidosis by a pulmonologist. The plaintiff claimed that both defendants negligently prescribed the medication for an extended period of time without proper monitoring, which caused her severe bone complications requiring a hip and shoulder replacement. The defendants maintained that the steroid medication was necessary to treat the life-threatening conditions from which the plaintiff suffered and that the dosage was carefully monitored and was not excessive. However, in a jury trial, the defendant hematologist and pulmonologist were each found 50% negligent, and the patient was awarded $4.1 million in damages.
In a case5 of steroid-related neurological sequelae, a Colorado jury awarded $14.9 million to a couple against an outpatient surgery center for negligently administering an epidural dose of Kenalog that rendered the patient paraplegic, and for failure to obtain informed consent. The jury awarded the woman, age 57, approximately $1.7 million in past and future medical expenses; $3.2 million in unspecified economic damages; and $6.5 million in past and future noneconomic damages such as pain and suffering. Her husband will receive $3.5 million in past and future noneconomic damages for loss of consortium, according to the verdict. Two years before the injection date of 2013, the drug maker had announced that Kenalog should not be used for epidural procedures because of cord complications including infarction and paraplegia.
Contributory role
The putative offending drug does not have to be the sole cause of injury; if it played a contributory role, the court may find the presence of liability. For example, a Kansas appeals court6 upheld a jury award of $2.88 million in the case of a 40-year-old man who took his life after neurologic complications followed an epidural injection. During one of patient’s visits for chronic low back pain, the defendant-anesthesiologist administered an epidural steroid injection into an area left swollen from a previous injection.
The patient developed neurologic symptoms, and lumbar puncture yielded green pus caused by methicillin-resistant Staphylococcus aureus. He went on to develop arachnoiditis, which left him with impotence, incontinence, and excruciating pain. His lawsuit contended the injection needle had passed through an infected edematous area, causing meningitis and arachnoiditis. Before the case went to trial, the patient took his life because of unremitting pain.
In March 2014, a Johnson County jury found the doctor 75% at fault and the clinic 25% at fault and awarded damages, which were reduced to $1.67 million because Kansas caps noneconomic damages at $250,000. The court rejected the defendants’ argument that the trial judge improperly instructed the jury it could find liability only if negligence “caused” rather than merely “contributed to” the patient’s death, holding that “... one who contributes to a wrongful death is a cause of that death as contemplated by the wrongful death statute.”
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at siang@hawaii.edu .
References
1. Hill v. Squibb Sons, E.R, 592 P.2d 1383 (Mont. 1979).
2. Nash JJ et al, Medical malpractice and corticosteroid use. Otolaryngol Head Neck Surg. 2011; 144:10-5.
3. Buckley L. et al, Glucocorticoid-Induced Osteoporosis. N Engl J Med 2018; 379:2547-56.
4. Zarin’s Jury Verdict: Review and Analysis. Article ID 40229, Philadelphia County.
5. Robbin Smith et al. v. The Surgery Center at Lone Tree, 2015-CV-30922, Douglas County District Court, Colo. Verdict for plaintiff, March 23, 2017.
6. Burnette v. Kimber L. Eubanks, M.D., & Paincare, P.A., 379 P.3d 372 (Kan. Ct. App. 2016).
Question: Mr. M, a car mechanic, was treated with long-term ACTH and Kenalog after he developed severe contact dermatitis from daily exposure to petroleum-based solvents. His subsequent course was complicated by cataracts and osteoporosis. Which of the following is true in case he files a malpractice action?
A. Treatment with steroids was medically indicated for Mr. Mechanic’s dermatologic condition, so the doctor could not have breached the standard of care.
B. Under the “Learned Intermediary” doctrine, both the manufacturer and the prescribing doctor are jointly liable.
C. Corticosteroids are a known cause of osteoporosis and other complications, but not of cataracts, so that part of the malpractice action should be thrown out.
D. The plaintiff would prevail even if he could not find an expert witnesses to testify as to standard of care, since it is “common knowledge” that steroids cause osteoporosis.
E. Lack of informed consent may be his best legal theory of liability, as many jurisdictions now use the patient-centered standard, which does not require expert testimony.
Answer: E. The above hypothetical was modified from an old Montana case1 in which the patient failed in his negligence lawsuit because he did not have expert witnesses to testify as to standard of care and to adequacy of warning label. However, in some jurisdictions under today’s case law, informed consent relies on a subjective, i.e., patient-oriented standard, and expert testimony is unnecessary to prove breach of duty, although still needed to prove causation.
Steroid-related litigation
Steroid-related malpractice litigation is quite prevalent. In a retrospective study of a tertiary medical center from 1996 to 2008, Nash and coworkers identified 83 such cases.2 Steroids were prescribed for pain (23%), asthma or another pulmonary condition (20%), a dermatologic condition (18%), an autoimmune condition (17%), or allergies (6%).
Learned intermediary
“Drug reps” have a responsibility to inform doctors of both benefits and risks of their medications, a process termed “fair balance.” Generally speaking, if a doctor fails to warn the patient of a medication risk, and injury results, the patient may have a claim against the doctor but not the drug manufacturer. This is termed the “learned intermediary” doctrine, which is also applicable to medical devices such as dialysis equipment, breast implants, and blood products.
The justification is that manufacturers can reasonably rely on the treating doctor to warn of adverse effects, which are disclosed to the profession through their sales reps and in the package insert and PDR. The treating doctor, in turn, is expected to use his or her professional judgment to adequately warn the patient. It is simply not feasible for the manufacturer to directly warn every patient without usurping the doctor-patient relationship. However, where known complications were undisclosed to the FDA and the profession, then plaintiff attorneys can file class action lawsuits directed at the manufacturer.
Complications
Complications arising out of the use of steroids are typical examples of medical products liability. This may be on the basis of the doctor having prescribed the medication without a proper indication or where contraindicated, or may have prescribed “the wrong dose for the wrong patient by the wrong route.” In addition, there may have been a lack of informed consent, i.e., failure to explain the underlying condition and the material risks associated with using the drug. Other acts of negligence, e.g., vicarious liability, may also apply.
Corticosteroids such as Prednisone, Decadron, Kenalog, etc., are widely prescribed, and can cause serious complications, especially when used in high doses for extended periods. Examples include suppression of the immune system with supervening infections, steroid osteoporosis and fractures,3 aseptic necrosis, steroid diabetes, hypertension, emotional changes, weight gain, cataracts, neurological complications, and many others. As in all malpractice actions, the plaintiff bears the burden of proof covering the four requisite tort elements, i.e., duty, breach of duty, causation, and damages. Expert testimony is almost always needed in a professional negligence lawsuit.
Aseptic necrosis is a feared complication of steroid therapy.
A recent report4 featured a nurse in her 40s who developed aseptic necrosis of the right shoulder and both hips after taking high dose prednisone for 6 months. She was being treated for idiopathic thrombocytopenic purpura by a hematologist as well as sarcoidosis by a pulmonologist. The plaintiff claimed that both defendants negligently prescribed the medication for an extended period of time without proper monitoring, which caused her severe bone complications requiring a hip and shoulder replacement. The defendants maintained that the steroid medication was necessary to treat the life-threatening conditions from which the plaintiff suffered and that the dosage was carefully monitored and was not excessive. However, in a jury trial, the defendant hematologist and pulmonologist were each found 50% negligent, and the patient was awarded $4.1 million in damages.
In a case5 of steroid-related neurological sequelae, a Colorado jury awarded $14.9 million to a couple against an outpatient surgery center for negligently administering an epidural dose of Kenalog that rendered the patient paraplegic, and for failure to obtain informed consent. The jury awarded the woman, age 57, approximately $1.7 million in past and future medical expenses; $3.2 million in unspecified economic damages; and $6.5 million in past and future noneconomic damages such as pain and suffering. Her husband will receive $3.5 million in past and future noneconomic damages for loss of consortium, according to the verdict. Two years before the injection date of 2013, the drug maker had announced that Kenalog should not be used for epidural procedures because of cord complications including infarction and paraplegia.
Contributory role
The putative offending drug does not have to be the sole cause of injury; if it played a contributory role, the court may find the presence of liability. For example, a Kansas appeals court6 upheld a jury award of $2.88 million in the case of a 40-year-old man who took his life after neurologic complications followed an epidural injection. During one of patient’s visits for chronic low back pain, the defendant-anesthesiologist administered an epidural steroid injection into an area left swollen from a previous injection.
The patient developed neurologic symptoms, and lumbar puncture yielded green pus caused by methicillin-resistant Staphylococcus aureus. He went on to develop arachnoiditis, which left him with impotence, incontinence, and excruciating pain. His lawsuit contended the injection needle had passed through an infected edematous area, causing meningitis and arachnoiditis. Before the case went to trial, the patient took his life because of unremitting pain.
In March 2014, a Johnson County jury found the doctor 75% at fault and the clinic 25% at fault and awarded damages, which were reduced to $1.67 million because Kansas caps noneconomic damages at $250,000. The court rejected the defendants’ argument that the trial judge improperly instructed the jury it could find liability only if negligence “caused” rather than merely “contributed to” the patient’s death, holding that “... one who contributes to a wrongful death is a cause of that death as contemplated by the wrongful death statute.”
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at siang@hawaii.edu .
References
1. Hill v. Squibb Sons, E.R, 592 P.2d 1383 (Mont. 1979).
2. Nash JJ et al, Medical malpractice and corticosteroid use. Otolaryngol Head Neck Surg. 2011; 144:10-5.
3. Buckley L. et al, Glucocorticoid-Induced Osteoporosis. N Engl J Med 2018; 379:2547-56.
4. Zarin’s Jury Verdict: Review and Analysis. Article ID 40229, Philadelphia County.
5. Robbin Smith et al. v. The Surgery Center at Lone Tree, 2015-CV-30922, Douglas County District Court, Colo. Verdict for plaintiff, March 23, 2017.
6. Burnette v. Kimber L. Eubanks, M.D., & Paincare, P.A., 379 P.3d 372 (Kan. Ct. App. 2016).
Evidence grows for early axSpA treatment, uveitis flare prevention
The findings from the C-axSpAnd study that Jonathan Kay, MD, and colleagues reported at the annual meeting of the American College of Rheumatology are not surprising. Earlier studies in patients with ankylosing spondylitis showed that short symptom duration is one of the best predictors of good treatment response to TNFi therapy. The highest response rates were obtained in studies conducted in axSpA patients with symptom duration of less than 5 years or even less than 3 years. Since nonradiographic axial spondyloarthritis (nr-axSpA) and r-axSpA are considered as two stages of one disease, it is logical that the same effect is also observed in studies in nr-axSpA. Indeed, in the first study of a tumor necrosis factor inhibitor (TNFi) in nr-axSpA (ABILITY-1), patients with symptom duration less than 5 years responded much better to the TNFi adalimumab than did those with longer symptom duration, and the delta of the response between adalimumab and placebo was much greater. All these results together indicate that early disease stage associated with favorable treatment response in axSpA is better defined by symptom duration than by the presence or absence of structural damage in the sacroiliac joints. Furthermore, these data stress the importance of the early diagnosis in axSpA.
We also know from observational studies and subanalyses from clinical trials that treatment with monoclonal antibodies against TNF is associated with reduction of uveitis flares in axSpA. However, no prospective clinical studies had been conducted with acute anterior uveitis flares as the primary outcome until the C-VIEW study, which was presented by Irene E. van der Horst-Bruinsma, MD, PhD, at ACR 2019. The results of C-VIEW are therefore the first to prospectively address the question of reduction of uveitis flares under TNFi. The main limitation of the study is the lack of a control group, which makes interpretation of the results difficult because it is not clear to what extent the natural course of the disease – which might involve very long flare-free periods lasting from months to years – contributed to the reduction of flares. A randomized, controlled study aimed at label extension is highly desired for patients with acute anterior uveitis, especially for those with a frequently relapsing course resistant to local treatment.

Denis Poddubnyy, MD , is head of the rheumatology department at Charite-Universitätsmedizin Berlin. He disclosed receiving research grants from AbbVie, Lilly, Merck, Novartis, and Pfizer, as well as receiving consultancy or speaker fees from AbbVie, Bristol-Myers Squibb, Celgene, Janssen, Lilly, Merck, Novartis, Pfizer, Roche, and UCB.
The findings from the C-axSpAnd study that Jonathan Kay, MD, and colleagues reported at the annual meeting of the American College of Rheumatology are not surprising. Earlier studies in patients with ankylosing spondylitis showed that short symptom duration is one of the best predictors of good treatment response to TNFi therapy. The highest response rates were obtained in studies conducted in axSpA patients with symptom duration of less than 5 years or even less than 3 years. Since nonradiographic axial spondyloarthritis (nr-axSpA) and r-axSpA are considered as two stages of one disease, it is logical that the same effect is also observed in studies in nr-axSpA. Indeed, in the first study of a tumor necrosis factor inhibitor (TNFi) in nr-axSpA (ABILITY-1), patients with symptom duration less than 5 years responded much better to the TNFi adalimumab than did those with longer symptom duration, and the delta of the response between adalimumab and placebo was much greater. All these results together indicate that early disease stage associated with favorable treatment response in axSpA is better defined by symptom duration than by the presence or absence of structural damage in the sacroiliac joints. Furthermore, these data stress the importance of the early diagnosis in axSpA.
We also know from observational studies and subanalyses from clinical trials that treatment with monoclonal antibodies against TNF is associated with reduction of uveitis flares in axSpA. However, no prospective clinical studies had been conducted with acute anterior uveitis flares as the primary outcome until the C-VIEW study, which was presented by Irene E. van der Horst-Bruinsma, MD, PhD, at ACR 2019. The results of C-VIEW are therefore the first to prospectively address the question of reduction of uveitis flares under TNFi. The main limitation of the study is the lack of a control group, which makes interpretation of the results difficult because it is not clear to what extent the natural course of the disease – which might involve very long flare-free periods lasting from months to years – contributed to the reduction of flares. A randomized, controlled study aimed at label extension is highly desired for patients with acute anterior uveitis, especially for those with a frequently relapsing course resistant to local treatment.
Denis Poddubnyy, MD , is head of the rheumatology department at Charite-Universitätsmedizin Berlin. He disclosed receiving research grants from AbbVie, Lilly, Merck, Novartis, and Pfizer, as well as receiving consultancy or speaker fees from AbbVie, Bristol-Myers Squibb, Celgene, Janssen, Lilly, Merck, Novartis, Pfizer, Roche, and UCB.
The findings from the C-axSpAnd study that Jonathan Kay, MD, and colleagues reported at the annual meeting of the American College of Rheumatology are not surprising. Earlier studies in patients with ankylosing spondylitis showed that short symptom duration is one of the best predictors of good treatment response to TNFi therapy. The highest response rates were obtained in studies conducted in axSpA patients with symptom duration of less than 5 years or even less than 3 years. Since nonradiographic axial spondyloarthritis (nr-axSpA) and r-axSpA are considered as two stages of one disease, it is logical that the same effect is also observed in studies in nr-axSpA. Indeed, in the first study of a tumor necrosis factor inhibitor (TNFi) in nr-axSpA (ABILITY-1), patients with symptom duration less than 5 years responded much better to the TNFi adalimumab than did those with longer symptom duration, and the delta of the response between adalimumab and placebo was much greater. All these results together indicate that early disease stage associated with favorable treatment response in axSpA is better defined by symptom duration than by the presence or absence of structural damage in the sacroiliac joints. Furthermore, these data stress the importance of the early diagnosis in axSpA.
We also know from observational studies and subanalyses from clinical trials that treatment with monoclonal antibodies against TNF is associated with reduction of uveitis flares in axSpA. However, no prospective clinical studies had been conducted with acute anterior uveitis flares as the primary outcome until the C-VIEW study, which was presented by Irene E. van der Horst-Bruinsma, MD, PhD, at ACR 2019. The results of C-VIEW are therefore the first to prospectively address the question of reduction of uveitis flares under TNFi. The main limitation of the study is the lack of a control group, which makes interpretation of the results difficult because it is not clear to what extent the natural course of the disease – which might involve very long flare-free periods lasting from months to years – contributed to the reduction of flares. A randomized, controlled study aimed at label extension is highly desired for patients with acute anterior uveitis, especially for those with a frequently relapsing course resistant to local treatment.
Denis Poddubnyy, MD , is head of the rheumatology department at Charite-Universitätsmedizin Berlin. He disclosed receiving research grants from AbbVie, Lilly, Merck, Novartis, and Pfizer, as well as receiving consultancy or speaker fees from AbbVie, Bristol-Myers Squibb, Celgene, Janssen, Lilly, Merck, Novartis, Pfizer, Roche, and UCB.
The clinical impact of new approvals in sickle cell, MCL
In this edition of “How I Will Treat My Next Patient,” I highlight two recent drug approvals by the Food and Drug Administration – crizanlizumab for sickle cell patients with painful crises and zanubrutinib for mantle cell lymphoma (MCL) patients in relapse.

Crizanlizumab
P-selectin is an adhesion molecule expressed on activated vascular endothelial cells and platelets. It is a key molecule in the initiation of leukocyte rolling on vessel walls and promotes firm attachment and extravasation to underlying tissues during inflammation. Up-regulation of P-selectin on endothelial cells and platelets contributes to the cell-cell interactions involved in the pathogenesis of sickle cell pain crises.
The SUSTAIN study was a multisite, placebo-controlled, randomized phase 2 trial of two different dosage levels of intravenous crizanlizumab (2.5 mg/kg or 5 mg/kg for 52 weeks), a humanized anti–P-selectin antibody, examining its effect on pain crises in patients with sickle cell disease. The primary endpoint was the annual rate of sickle cell pain crises, with a variety of clinically relevant secondary endpoints. The target population had 2-10 pain crises in the 12 months before enrollment. Patients on a stable dose of hydroxyurea for at least the most recent 3 months were allowed to enter, but if patients were not receiving hydroxyurea, it could not be initiated during the trial. Patients who were undergoing chronic red-cell transfusion therapy were excluded.
Among 198 enrolled patients, 35% did not complete the 52 weeks of treatment. Discontinuations were equally balanced among patients assigned to the high-dose, low-dose, and placebo cohorts. Adverse events associated with crizanlizumab included back pain, nausea, pyrexia, and arthralgia. Serious adverse events occurred in 55 patients, with 5 deaths, all of which were unrelated to treatment. Crizanlizumab did not augment hemolysis or bacterial infections.
In the efficacy analysis, patients receiving high-dose crizanlizumab had a median annual rate of 1.63 health care visits for sickle cell pain crises, compared with 2.98 visits for placebo patients (P = .01). In comparison with placebo, high-dose crizanlizumab also delayed the first pain crisis after starting treatment (4.1 months vs. 1.4 months), delayed the median time to a second pain crisis, and decreased the median number of pain crises annually.
More than twice as many high-dose crizanlizumab patients had no pain crisis episodes, compared with placebo patients. In general, differences were more striking in patients who were not taking hydroxyurea and who had non–hemoglobin SS disease. Differences in the primary endpoint between low-dose crizanlizumab and placebo were numerically, but not statistically, different.
How these results influence practice
It has been over 20 years since a new agent (hydroxyurea) was approved for sickle cell patients and, despite its use, sickle cell pain crises remain a frequent problem. Pain crises are associated with worse quality of life and increased risk of death. A promising advance is badly needed, especially in an era in which sensitivity to providers’ role in the opioid addiction crisis is highly scrutinized and may contribute to future undertreatment of pain episodes. This is especially true for patients from areas with high levels of opioid misuse.
The SUSTAIN trial was international, multi-institutional, placebo-controlled, and inclusive. These attributes enhance the likelihood that crizanlizumab will enhance patient care in routine practice. As an intravenous agent, monitoring adherence and toxicity are less challenging than with hydroxyurea. Despite these factors, however, there are some concerns. Crizanlizumab was not free of toxicity, quality of life via the Brief Pain Inventory used in the trial was not improved, and changes in the pain-severity and pain-interference domains were small. Treatment in SUSTAIN ensued for 52 weeks, so the emergence of late neutralizing antibodies and late toxicities with longer-term therapy will require careful postmarketing assessment.
These concerns notwithstanding, anyone who has cared for sickle cell patients would be excited about the potential benefits crizanlizumab could bring to patient care.
Zanubrutinib
The FDA has approved zanubrutinib for the treatment of MCL in adult patients who have received at least one prior therapy. The approval is based on the results of two studies in which overall response rate was the primary endpoint.
BGB-3111-206 (NCT03206970) was a phase 2, open-label, multicenter, single-arm trial of 86 patients with MCL who received at least one prior therapy. Zanubrutinib was given orally at 160 mg twice daily until disease progression or unacceptable toxicity. BGB-3111-AU-003 (NCT 02343120) was a phase 1/2, open-label, dose-escalation trial of B-cell malignancies, including 32 previously treated MCL patients treated with zanubrutinib at 160 mg twice daily or 320 mg once daily.
In the phase 2 trial, 18fluorodeoxyglucose (FDG)–PET scans were required and the ORR was 84% (95% confidence interval, 74%-91%), with a complete response rate of 59% (95% CI, 48%-70%) and a median response duration of 19.5 months (95% CI, 16.6% to not estimable). In the phase 1/2 dose-escalation trial, FDG-PET scans were not required and the ORR was 84% (95% CI, 67%-95%), with a complete response rate of 22% (95% CI, 9%-40%) and a median response duration of 18.5 months (95% CI, 12.6% to not estimable). In both trials, median follow-up on study was about 18 months.
The most common adverse reactions were cytopenias, upper respiratory tract infection, rash, bruising, diarrhea, and cough. The most common serious adverse reactions were pneumonia in 11% and hemorrhage in 5% of patients. Of 118 MCL patients, 8 stopped therapy because of an adverse event, most frequently pneumonia (3.4%).
How these results influence practice
Unfortunately, the therapy of recurrent MCL is noncurative, because of the rapid development of treatment resistance. There are multiple single-and multiagent chemotherapy regimens that may be tried, many incorporating immunotherapy options such as anti-CD20- or Bruton tyrosine kinase (BTK)–targeted agents. Given the limited efficacy of these agents, temporary nature of remissions, and paucity of data comparing these various treatment options, participation in clinical trials is encouraged whenever possible.
Outside of a clinical trial, zanubrutinib joins ibrutinib and acalabrutinib as approved single-agent BTK inhibitors for adult MCL patients in relapse. The impressive ORR and response duration reported for zanubrutinib are similar to the results achieved with the other agents, but the toxicity pattern may be slightly different.
As in the treatment of hormonally sensitive breast cancer, clinicians and patients benefit when they have multiple similar, equally efficacious oral agents with slightly different toxicity patterns so that quality of life can be improved and treatment duration maximized before treatment resistance develops and a more toxic and/or inconvenient therapy needs to be employed.
Whether zanubrutinib has benefits beyond those for MCL patients in relapse will depend on the results of confirmatory trials and patient-reported outcome data.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
In this edition of “How I Will Treat My Next Patient,” I highlight two recent drug approvals by the Food and Drug Administration – crizanlizumab for sickle cell patients with painful crises and zanubrutinib for mantle cell lymphoma (MCL) patients in relapse.
Crizanlizumab
P-selectin is an adhesion molecule expressed on activated vascular endothelial cells and platelets. It is a key molecule in the initiation of leukocyte rolling on vessel walls and promotes firm attachment and extravasation to underlying tissues during inflammation. Up-regulation of P-selectin on endothelial cells and platelets contributes to the cell-cell interactions involved in the pathogenesis of sickle cell pain crises.
The SUSTAIN study was a multisite, placebo-controlled, randomized phase 2 trial of two different dosage levels of intravenous crizanlizumab (2.5 mg/kg or 5 mg/kg for 52 weeks), a humanized anti–P-selectin antibody, examining its effect on pain crises in patients with sickle cell disease. The primary endpoint was the annual rate of sickle cell pain crises, with a variety of clinically relevant secondary endpoints. The target population had 2-10 pain crises in the 12 months before enrollment. Patients on a stable dose of hydroxyurea for at least the most recent 3 months were allowed to enter, but if patients were not receiving hydroxyurea, it could not be initiated during the trial. Patients who were undergoing chronic red-cell transfusion therapy were excluded.
Among 198 enrolled patients, 35% did not complete the 52 weeks of treatment. Discontinuations were equally balanced among patients assigned to the high-dose, low-dose, and placebo cohorts. Adverse events associated with crizanlizumab included back pain, nausea, pyrexia, and arthralgia. Serious adverse events occurred in 55 patients, with 5 deaths, all of which were unrelated to treatment. Crizanlizumab did not augment hemolysis or bacterial infections.
In the efficacy analysis, patients receiving high-dose crizanlizumab had a median annual rate of 1.63 health care visits for sickle cell pain crises, compared with 2.98 visits for placebo patients (P = .01). In comparison with placebo, high-dose crizanlizumab also delayed the first pain crisis after starting treatment (4.1 months vs. 1.4 months), delayed the median time to a second pain crisis, and decreased the median number of pain crises annually.
More than twice as many high-dose crizanlizumab patients had no pain crisis episodes, compared with placebo patients. In general, differences were more striking in patients who were not taking hydroxyurea and who had non–hemoglobin SS disease. Differences in the primary endpoint between low-dose crizanlizumab and placebo were numerically, but not statistically, different.
How these results influence practice
It has been over 20 years since a new agent (hydroxyurea) was approved for sickle cell patients and, despite its use, sickle cell pain crises remain a frequent problem. Pain crises are associated with worse quality of life and increased risk of death. A promising advance is badly needed, especially in an era in which sensitivity to providers’ role in the opioid addiction crisis is highly scrutinized and may contribute to future undertreatment of pain episodes. This is especially true for patients from areas with high levels of opioid misuse.
The SUSTAIN trial was international, multi-institutional, placebo-controlled, and inclusive. These attributes enhance the likelihood that crizanlizumab will enhance patient care in routine practice. As an intravenous agent, monitoring adherence and toxicity are less challenging than with hydroxyurea. Despite these factors, however, there are some concerns. Crizanlizumab was not free of toxicity, quality of life via the Brief Pain Inventory used in the trial was not improved, and changes in the pain-severity and pain-interference domains were small. Treatment in SUSTAIN ensued for 52 weeks, so the emergence of late neutralizing antibodies and late toxicities with longer-term therapy will require careful postmarketing assessment.
These concerns notwithstanding, anyone who has cared for sickle cell patients would be excited about the potential benefits crizanlizumab could bring to patient care.
Zanubrutinib
The FDA has approved zanubrutinib for the treatment of MCL in adult patients who have received at least one prior therapy. The approval is based on the results of two studies in which overall response rate was the primary endpoint.
BGB-3111-206 (NCT03206970) was a phase 2, open-label, multicenter, single-arm trial of 86 patients with MCL who received at least one prior therapy. Zanubrutinib was given orally at 160 mg twice daily until disease progression or unacceptable toxicity. BGB-3111-AU-003 (NCT 02343120) was a phase 1/2, open-label, dose-escalation trial of B-cell malignancies, including 32 previously treated MCL patients treated with zanubrutinib at 160 mg twice daily or 320 mg once daily.
In the phase 2 trial, 18fluorodeoxyglucose (FDG)–PET scans were required and the ORR was 84% (95% confidence interval, 74%-91%), with a complete response rate of 59% (95% CI, 48%-70%) and a median response duration of 19.5 months (95% CI, 16.6% to not estimable). In the phase 1/2 dose-escalation trial, FDG-PET scans were not required and the ORR was 84% (95% CI, 67%-95%), with a complete response rate of 22% (95% CI, 9%-40%) and a median response duration of 18.5 months (95% CI, 12.6% to not estimable). In both trials, median follow-up on study was about 18 months.
The most common adverse reactions were cytopenias, upper respiratory tract infection, rash, bruising, diarrhea, and cough. The most common serious adverse reactions were pneumonia in 11% and hemorrhage in 5% of patients. Of 118 MCL patients, 8 stopped therapy because of an adverse event, most frequently pneumonia (3.4%).
How these results influence practice
Unfortunately, the therapy of recurrent MCL is noncurative, because of the rapid development of treatment resistance. There are multiple single-and multiagent chemotherapy regimens that may be tried, many incorporating immunotherapy options such as anti-CD20- or Bruton tyrosine kinase (BTK)–targeted agents. Given the limited efficacy of these agents, temporary nature of remissions, and paucity of data comparing these various treatment options, participation in clinical trials is encouraged whenever possible.
Outside of a clinical trial, zanubrutinib joins ibrutinib and acalabrutinib as approved single-agent BTK inhibitors for adult MCL patients in relapse. The impressive ORR and response duration reported for zanubrutinib are similar to the results achieved with the other agents, but the toxicity pattern may be slightly different.
As in the treatment of hormonally sensitive breast cancer, clinicians and patients benefit when they have multiple similar, equally efficacious oral agents with slightly different toxicity patterns so that quality of life can be improved and treatment duration maximized before treatment resistance develops and a more toxic and/or inconvenient therapy needs to be employed.
Whether zanubrutinib has benefits beyond those for MCL patients in relapse will depend on the results of confirmatory trials and patient-reported outcome data.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
In this edition of “How I Will Treat My Next Patient,” I highlight two recent drug approvals by the Food and Drug Administration – crizanlizumab for sickle cell patients with painful crises and zanubrutinib for mantle cell lymphoma (MCL) patients in relapse.
Crizanlizumab
P-selectin is an adhesion molecule expressed on activated vascular endothelial cells and platelets. It is a key molecule in the initiation of leukocyte rolling on vessel walls and promotes firm attachment and extravasation to underlying tissues during inflammation. Up-regulation of P-selectin on endothelial cells and platelets contributes to the cell-cell interactions involved in the pathogenesis of sickle cell pain crises.
The SUSTAIN study was a multisite, placebo-controlled, randomized phase 2 trial of two different dosage levels of intravenous crizanlizumab (2.5 mg/kg or 5 mg/kg for 52 weeks), a humanized anti–P-selectin antibody, examining its effect on pain crises in patients with sickle cell disease. The primary endpoint was the annual rate of sickle cell pain crises, with a variety of clinically relevant secondary endpoints. The target population had 2-10 pain crises in the 12 months before enrollment. Patients on a stable dose of hydroxyurea for at least the most recent 3 months were allowed to enter, but if patients were not receiving hydroxyurea, it could not be initiated during the trial. Patients who were undergoing chronic red-cell transfusion therapy were excluded.
Among 198 enrolled patients, 35% did not complete the 52 weeks of treatment. Discontinuations were equally balanced among patients assigned to the high-dose, low-dose, and placebo cohorts. Adverse events associated with crizanlizumab included back pain, nausea, pyrexia, and arthralgia. Serious adverse events occurred in 55 patients, with 5 deaths, all of which were unrelated to treatment. Crizanlizumab did not augment hemolysis or bacterial infections.
In the efficacy analysis, patients receiving high-dose crizanlizumab had a median annual rate of 1.63 health care visits for sickle cell pain crises, compared with 2.98 visits for placebo patients (P = .01). In comparison with placebo, high-dose crizanlizumab also delayed the first pain crisis after starting treatment (4.1 months vs. 1.4 months), delayed the median time to a second pain crisis, and decreased the median number of pain crises annually.
More than twice as many high-dose crizanlizumab patients had no pain crisis episodes, compared with placebo patients. In general, differences were more striking in patients who were not taking hydroxyurea and who had non–hemoglobin SS disease. Differences in the primary endpoint between low-dose crizanlizumab and placebo were numerically, but not statistically, different.
How these results influence practice
It has been over 20 years since a new agent (hydroxyurea) was approved for sickle cell patients and, despite its use, sickle cell pain crises remain a frequent problem. Pain crises are associated with worse quality of life and increased risk of death. A promising advance is badly needed, especially in an era in which sensitivity to providers’ role in the opioid addiction crisis is highly scrutinized and may contribute to future undertreatment of pain episodes. This is especially true for patients from areas with high levels of opioid misuse.
The SUSTAIN trial was international, multi-institutional, placebo-controlled, and inclusive. These attributes enhance the likelihood that crizanlizumab will enhance patient care in routine practice. As an intravenous agent, monitoring adherence and toxicity are less challenging than with hydroxyurea. Despite these factors, however, there are some concerns. Crizanlizumab was not free of toxicity, quality of life via the Brief Pain Inventory used in the trial was not improved, and changes in the pain-severity and pain-interference domains were small. Treatment in SUSTAIN ensued for 52 weeks, so the emergence of late neutralizing antibodies and late toxicities with longer-term therapy will require careful postmarketing assessment.
These concerns notwithstanding, anyone who has cared for sickle cell patients would be excited about the potential benefits crizanlizumab could bring to patient care.
Zanubrutinib
The FDA has approved zanubrutinib for the treatment of MCL in adult patients who have received at least one prior therapy. The approval is based on the results of two studies in which overall response rate was the primary endpoint.
BGB-3111-206 (NCT03206970) was a phase 2, open-label, multicenter, single-arm trial of 86 patients with MCL who received at least one prior therapy. Zanubrutinib was given orally at 160 mg twice daily until disease progression or unacceptable toxicity. BGB-3111-AU-003 (NCT 02343120) was a phase 1/2, open-label, dose-escalation trial of B-cell malignancies, including 32 previously treated MCL patients treated with zanubrutinib at 160 mg twice daily or 320 mg once daily.
In the phase 2 trial, 18fluorodeoxyglucose (FDG)–PET scans were required and the ORR was 84% (95% confidence interval, 74%-91%), with a complete response rate of 59% (95% CI, 48%-70%) and a median response duration of 19.5 months (95% CI, 16.6% to not estimable). In the phase 1/2 dose-escalation trial, FDG-PET scans were not required and the ORR was 84% (95% CI, 67%-95%), with a complete response rate of 22% (95% CI, 9%-40%) and a median response duration of 18.5 months (95% CI, 12.6% to not estimable). In both trials, median follow-up on study was about 18 months.
The most common adverse reactions were cytopenias, upper respiratory tract infection, rash, bruising, diarrhea, and cough. The most common serious adverse reactions were pneumonia in 11% and hemorrhage in 5% of patients. Of 118 MCL patients, 8 stopped therapy because of an adverse event, most frequently pneumonia (3.4%).
How these results influence practice
Unfortunately, the therapy of recurrent MCL is noncurative, because of the rapid development of treatment resistance. There are multiple single-and multiagent chemotherapy regimens that may be tried, many incorporating immunotherapy options such as anti-CD20- or Bruton tyrosine kinase (BTK)–targeted agents. Given the limited efficacy of these agents, temporary nature of remissions, and paucity of data comparing these various treatment options, participation in clinical trials is encouraged whenever possible.
Outside of a clinical trial, zanubrutinib joins ibrutinib and acalabrutinib as approved single-agent BTK inhibitors for adult MCL patients in relapse. The impressive ORR and response duration reported for zanubrutinib are similar to the results achieved with the other agents, but the toxicity pattern may be slightly different.
As in the treatment of hormonally sensitive breast cancer, clinicians and patients benefit when they have multiple similar, equally efficacious oral agents with slightly different toxicity patterns so that quality of life can be improved and treatment duration maximized before treatment resistance develops and a more toxic and/or inconvenient therapy needs to be employed.
Whether zanubrutinib has benefits beyond those for MCL patients in relapse will depend on the results of confirmatory trials and patient-reported outcome data.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
Progressive, pruritic eruption of firm, skin-colored papules
Scleromyxedema, or generalized lichen myxedematosus, is a primary cutaneous mucinosis with unknown pathogenesis characterized by generalized firm, skin-colored papules and is commonly associated with an underlying monoclonal gammopathy (usually Ig-gamma paraproteinemia).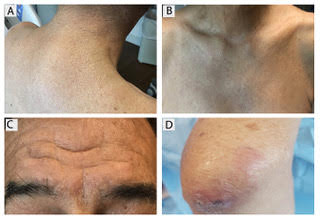
Scleromyxedema may have associated internal involvement, including neurologic, gastrointestinal, pulmonary, renal, cardiovascular, ophthalmological, or musculoskeletal. Histopathology demonstrates mucin in the dermis seen with Alcian blue staining, proliferation of fibroblasts, and increased collagen deposition.
The condition is chronic and progressive. Intravenous immunoglobulin is considered first-line treatment. Thalidomide and corticosteroids have been reported to also be efficacious.
It is associated with hematologic disorders, including IgA monoclonal gammopathy, as well as myeloproliferative disorders, leukemia, infections, and inflammatory bowel disease. Although its pathophysiology is not well understood, vascular immune complex deposition, repetitive inflammation, and subsequent fibrosis may play a role. On histology, there is leukocytoclastic vasculitis with polymorphonuclear cell infiltrate and fibrin deposition in the superficial and mid-dermis and onion-skin fibrosis.
EED often self-resolves within 5-10 years, although it can become chronic and recurrent. Dapsone, niacinamide, antimalarials, NSAIDs, tetracyclines, corticosteroids, colchicine, and plasmapheresis are reported treatments. This patient’s EED was recalcitrant to prednisone and responded to colchicine.
Scleromyxedema and EED are both rare, distinct cutaneous entities associated with different underlying paraproteinemias and to the best of our knowledge, have not been previously reported to coexist in a single patient.

This case and the photos were submitted by Rachel Fayne, BA; Yumeng Li, MD, MS; Fabrizio Galimberti, MD, PhD; and Brian Morrison, MD, of the department of dermatology and cutaneous surgery at the University of Miami.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
Scleromyxedema, or generalized lichen myxedematosus, is a primary cutaneous mucinosis with unknown pathogenesis characterized by generalized firm, skin-colored papules and is commonly associated with an underlying monoclonal gammopathy (usually Ig-gamma paraproteinemia).
Scleromyxedema may have associated internal involvement, including neurologic, gastrointestinal, pulmonary, renal, cardiovascular, ophthalmological, or musculoskeletal. Histopathology demonstrates mucin in the dermis seen with Alcian blue staining, proliferation of fibroblasts, and increased collagen deposition.
The condition is chronic and progressive. Intravenous immunoglobulin is considered first-line treatment. Thalidomide and corticosteroids have been reported to also be efficacious.
It is associated with hematologic disorders, including IgA monoclonal gammopathy, as well as myeloproliferative disorders, leukemia, infections, and inflammatory bowel disease. Although its pathophysiology is not well understood, vascular immune complex deposition, repetitive inflammation, and subsequent fibrosis may play a role. On histology, there is leukocytoclastic vasculitis with polymorphonuclear cell infiltrate and fibrin deposition in the superficial and mid-dermis and onion-skin fibrosis.
EED often self-resolves within 5-10 years, although it can become chronic and recurrent. Dapsone, niacinamide, antimalarials, NSAIDs, tetracyclines, corticosteroids, colchicine, and plasmapheresis are reported treatments. This patient’s EED was recalcitrant to prednisone and responded to colchicine.
Scleromyxedema and EED are both rare, distinct cutaneous entities associated with different underlying paraproteinemias and to the best of our knowledge, have not been previously reported to coexist in a single patient.
This case and the photos were submitted by Rachel Fayne, BA; Yumeng Li, MD, MS; Fabrizio Galimberti, MD, PhD; and Brian Morrison, MD, of the department of dermatology and cutaneous surgery at the University of Miami.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
Scleromyxedema, or generalized lichen myxedematosus, is a primary cutaneous mucinosis with unknown pathogenesis characterized by generalized firm, skin-colored papules and is commonly associated with an underlying monoclonal gammopathy (usually Ig-gamma paraproteinemia).
Scleromyxedema may have associated internal involvement, including neurologic, gastrointestinal, pulmonary, renal, cardiovascular, ophthalmological, or musculoskeletal. Histopathology demonstrates mucin in the dermis seen with Alcian blue staining, proliferation of fibroblasts, and increased collagen deposition.
The condition is chronic and progressive. Intravenous immunoglobulin is considered first-line treatment. Thalidomide and corticosteroids have been reported to also be efficacious.
It is associated with hematologic disorders, including IgA monoclonal gammopathy, as well as myeloproliferative disorders, leukemia, infections, and inflammatory bowel disease. Although its pathophysiology is not well understood, vascular immune complex deposition, repetitive inflammation, and subsequent fibrosis may play a role. On histology, there is leukocytoclastic vasculitis with polymorphonuclear cell infiltrate and fibrin deposition in the superficial and mid-dermis and onion-skin fibrosis.
EED often self-resolves within 5-10 years, although it can become chronic and recurrent. Dapsone, niacinamide, antimalarials, NSAIDs, tetracyclines, corticosteroids, colchicine, and plasmapheresis are reported treatments. This patient’s EED was recalcitrant to prednisone and responded to colchicine.
Scleromyxedema and EED are both rare, distinct cutaneous entities associated with different underlying paraproteinemias and to the best of our knowledge, have not been previously reported to coexist in a single patient.
This case and the photos were submitted by Rachel Fayne, BA; Yumeng Li, MD, MS; Fabrizio Galimberti, MD, PhD; and Brian Morrison, MD, of the department of dermatology and cutaneous surgery at the University of Miami.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.

Bariatric surgery should be considered in individuals with class 1 obesity
Mitchel L. Zoler’s article on Abstract A105, presented at Obesity Week 2019, addresses an important health concern and is timely.
Over the past 4 decades we have seen a rise in the prevalence of obesity and associated health complications, not just in the United States but across the world. The incidence of obesity (having a BMI greater than 30) was 35% for women and 31% for men in the United States, and associated deaths and disability were primarily attributed to diabetes and cardiovascular disease resulting from obesity.

This article references the benefits of bariatric/metabolic surgery in individuals with class 1 obesity. In the United States, more than half of those who meet the criteria for obesity come under the class 1 category (BMI, 30-34.9). Those in this class of obesity are at increased risk of developing diabetes, hypertension, hyperlipidemia, coronary artery disease, cerebrovascular disease, obstructive sleep apnea, polycystic ovarian syndrome, and bone and joint disorders.
There are several studies that document the significant reduction in incidence of the above cardiometabolic risks with sustained weight loss. Nonsurgical interventions in individuals with class 1 obesity through lifestyle modifications and pharmacotherapy have not demonstrated success in providing persistent weight loss or metabolic benefits. The data presented in this article are of great significance to patients and physicians alike as they highlight the long-term benefits and reversal of metabolic disorders.
Current guidelines for bariatric surgery for individuals with a BMI greater than 35 were published in 1991. Since then several safe surgical options including laparoscopic procedures, sleeve gastrectomy, and adjustable gastric banding have been developed with decreased surgical risks, morbidity, and mortality.
The International Federation for the Surgery of Obesity and Metabolic Disorders, the International Diabetes Federation, and the National Institute for Health and Care Excellence of the United Kingdom, have supported the option of bariatric surgery in class 1 obese individuals with metabolic disorders.
While lifestyle modifications with medications should be the first-line treatment for class 1 obesity, as a primary care physician I believe that, given the major changes in the surgical options, the proven long-term benefits, and the rising incidences of obesity and metabolic syndrome, it is time for the health care community, insurers, patients, and all other stakeholders to consider bariatric surgery in class 1 obese individuals as a potential and viable option.
Noel N. Deep, MD, is a general internist in a multispecialty group practice with Aspirus Antigo (Wis.) Clinic and the chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo. He is also assistant clinical professor at the Medical College of Wisconsin, Central Wisconsin Campus, Wausau, and the governor of the Wisconsin chapter of the American College of Physicians. Dr. Deep serves on the editorial advisory board of Internal Medicine News.
He made these comments in response to questions from MDedge and had no relevant disclosures.
Mitchel L. Zoler’s article on Abstract A105, presented at Obesity Week 2019, addresses an important health concern and is timely.
Over the past 4 decades we have seen a rise in the prevalence of obesity and associated health complications, not just in the United States but across the world. The incidence of obesity (having a BMI greater than 30) was 35% for women and 31% for men in the United States, and associated deaths and disability were primarily attributed to diabetes and cardiovascular disease resulting from obesity.
This article references the benefits of bariatric/metabolic surgery in individuals with class 1 obesity. In the United States, more than half of those who meet the criteria for obesity come under the class 1 category (BMI, 30-34.9). Those in this class of obesity are at increased risk of developing diabetes, hypertension, hyperlipidemia, coronary artery disease, cerebrovascular disease, obstructive sleep apnea, polycystic ovarian syndrome, and bone and joint disorders.
There are several studies that document the significant reduction in incidence of the above cardiometabolic risks with sustained weight loss. Nonsurgical interventions in individuals with class 1 obesity through lifestyle modifications and pharmacotherapy have not demonstrated success in providing persistent weight loss or metabolic benefits. The data presented in this article are of great significance to patients and physicians alike as they highlight the long-term benefits and reversal of metabolic disorders.
Current guidelines for bariatric surgery for individuals with a BMI greater than 35 were published in 1991. Since then several safe surgical options including laparoscopic procedures, sleeve gastrectomy, and adjustable gastric banding have been developed with decreased surgical risks, morbidity, and mortality.
The International Federation for the Surgery of Obesity and Metabolic Disorders, the International Diabetes Federation, and the National Institute for Health and Care Excellence of the United Kingdom, have supported the option of bariatric surgery in class 1 obese individuals with metabolic disorders.
While lifestyle modifications with medications should be the first-line treatment for class 1 obesity, as a primary care physician I believe that, given the major changes in the surgical options, the proven long-term benefits, and the rising incidences of obesity and metabolic syndrome, it is time for the health care community, insurers, patients, and all other stakeholders to consider bariatric surgery in class 1 obese individuals as a potential and viable option.
Noel N. Deep, MD, is a general internist in a multispecialty group practice with Aspirus Antigo (Wis.) Clinic and the chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo. He is also assistant clinical professor at the Medical College of Wisconsin, Central Wisconsin Campus, Wausau, and the governor of the Wisconsin chapter of the American College of Physicians. Dr. Deep serves on the editorial advisory board of Internal Medicine News.
He made these comments in response to questions from MDedge and had no relevant disclosures.
Mitchel L. Zoler’s article on Abstract A105, presented at Obesity Week 2019, addresses an important health concern and is timely.
Over the past 4 decades we have seen a rise in the prevalence of obesity and associated health complications, not just in the United States but across the world. The incidence of obesity (having a BMI greater than 30) was 35% for women and 31% for men in the United States, and associated deaths and disability were primarily attributed to diabetes and cardiovascular disease resulting from obesity.
This article references the benefits of bariatric/metabolic surgery in individuals with class 1 obesity. In the United States, more than half of those who meet the criteria for obesity come under the class 1 category (BMI, 30-34.9). Those in this class of obesity are at increased risk of developing diabetes, hypertension, hyperlipidemia, coronary artery disease, cerebrovascular disease, obstructive sleep apnea, polycystic ovarian syndrome, and bone and joint disorders.
There are several studies that document the significant reduction in incidence of the above cardiometabolic risks with sustained weight loss. Nonsurgical interventions in individuals with class 1 obesity through lifestyle modifications and pharmacotherapy have not demonstrated success in providing persistent weight loss or metabolic benefits. The data presented in this article are of great significance to patients and physicians alike as they highlight the long-term benefits and reversal of metabolic disorders.
Current guidelines for bariatric surgery for individuals with a BMI greater than 35 were published in 1991. Since then several safe surgical options including laparoscopic procedures, sleeve gastrectomy, and adjustable gastric banding have been developed with decreased surgical risks, morbidity, and mortality.
The International Federation for the Surgery of Obesity and Metabolic Disorders, the International Diabetes Federation, and the National Institute for Health and Care Excellence of the United Kingdom, have supported the option of bariatric surgery in class 1 obese individuals with metabolic disorders.
While lifestyle modifications with medications should be the first-line treatment for class 1 obesity, as a primary care physician I believe that, given the major changes in the surgical options, the proven long-term benefits, and the rising incidences of obesity and metabolic syndrome, it is time for the health care community, insurers, patients, and all other stakeholders to consider bariatric surgery in class 1 obese individuals as a potential and viable option.
Noel N. Deep, MD, is a general internist in a multispecialty group practice with Aspirus Antigo (Wis.) Clinic and the chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo. He is also assistant clinical professor at the Medical College of Wisconsin, Central Wisconsin Campus, Wausau, and the governor of the Wisconsin chapter of the American College of Physicians. Dr. Deep serves on the editorial advisory board of Internal Medicine News.
He made these comments in response to questions from MDedge and had no relevant disclosures.
Is it time for neurologists to manage high blood pressure?
In the Nov. 1, 2019, issue of JAMA Neurology, an editorial argues that it’s time for neurologists to start managing high blood pressure.

It makes some very valid points: that targeting a systolic blood pressure of less than 120 mm Hg results in lower rates of cardiovascular events and all causes of mortality, that poorly controlled hypertension leads to debilitating neurologic conditions, and that high blood pressure is the most common modifiable risk factor for stroke.
All are strong points. I agree with them and definitely believe that more can and should be done to control hypertension.
The editorial then goes on to say that “first and foremost we are charging neurologists with actively diagnosing hypertension and prescribing medications when appropriate.”
Uh, no. I’m not going to be the one managing hypertension, nor should any outpatient neurologist.
Outpatient hypertension treatment has historically been, and should remain, the province of general practitioners, cardiologists, and nephrologists. Too many cooks, as they say, spoils the broth. I don’t want to be in a situation where two (or more) doctors are simultaneously trying to treat the same condition. On that path lies danger.
This doesn’t mean I ignore blood pressure. On the contrary, I take it (myself) at every patient visit, and put it in my note. In most cases I do nothing further, as nothing further needs to be done. On occasion, though, if it’s concerningly high, I’ll write it down for the patient and direct them to call the physician handling it. I also fax a note about it to that office, and if it’s dangerously high will call the doctor myself.
But try to manage it? No. Elevated readings definitely overlap with my world, but treating them shouldn’t.
The article says that, for some chronic patients, neurologists are their de facto internist. Perhaps for a few, but when a patient calls with concerns about a respiratory ailment, gastrointestinal problem, or other nonneurologic issue, I tell them to call their general practitioner. If they don’t have one I’m happy to give them the names and phone numbers of colleagues who practice that field, or even urgent care and emergency department information if needed. Just because I see them for their neurologic problems doesn’t qualify me to practice another branch of medicine.

Beyond the dangers of having more than one doctor involved, as a specialist it’s not practical for me to know the antihypertensive medications – possibly the largest group of agents on the market, – in detail, with their mechanisms of action, side effects, and contraindications. Yes, I do keep a handful in mind, since they’re needed off label for migraines and tremors, but not in the kind of detail a cardiologist would. I have to keep track of enough medications in my specialty as it is.
I wouldn’t try to handle blood pressure any more than I’d expect a nephrologist to treat epilepsy. It’s just looking for trouble.
Even when covering the hospital, I’ll stay out of that arena. This doesn’t mean I ignore blood pressure in such serious conditions as stroke or posterior reversible encephalopathy syndrome. I’m more than happy to provide guidelines and parameters. But as far as choosing the medications and doses? No.
Like driving, we all have to share the road. We may even be focused on the same journey (or patient). But part of practicing medicine and handling traffic is knowing when to stay in your lane.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
In the Nov. 1, 2019, issue of JAMA Neurology, an editorial argues that it’s time for neurologists to start managing high blood pressure.
It makes some very valid points: that targeting a systolic blood pressure of less than 120 mm Hg results in lower rates of cardiovascular events and all causes of mortality, that poorly controlled hypertension leads to debilitating neurologic conditions, and that high blood pressure is the most common modifiable risk factor for stroke.
All are strong points. I agree with them and definitely believe that more can and should be done to control hypertension.
The editorial then goes on to say that “first and foremost we are charging neurologists with actively diagnosing hypertension and prescribing medications when appropriate.”
Uh, no. I’m not going to be the one managing hypertension, nor should any outpatient neurologist.
Outpatient hypertension treatment has historically been, and should remain, the province of general practitioners, cardiologists, and nephrologists. Too many cooks, as they say, spoils the broth. I don’t want to be in a situation where two (or more) doctors are simultaneously trying to treat the same condition. On that path lies danger.
This doesn’t mean I ignore blood pressure. On the contrary, I take it (myself) at every patient visit, and put it in my note. In most cases I do nothing further, as nothing further needs to be done. On occasion, though, if it’s concerningly high, I’ll write it down for the patient and direct them to call the physician handling it. I also fax a note about it to that office, and if it’s dangerously high will call the doctor myself.
But try to manage it? No. Elevated readings definitely overlap with my world, but treating them shouldn’t.
The article says that, for some chronic patients, neurologists are their de facto internist. Perhaps for a few, but when a patient calls with concerns about a respiratory ailment, gastrointestinal problem, or other nonneurologic issue, I tell them to call their general practitioner. If they don’t have one I’m happy to give them the names and phone numbers of colleagues who practice that field, or even urgent care and emergency department information if needed. Just because I see them for their neurologic problems doesn’t qualify me to practice another branch of medicine.
Beyond the dangers of having more than one doctor involved, as a specialist it’s not practical for me to know the antihypertensive medications – possibly the largest group of agents on the market, – in detail, with their mechanisms of action, side effects, and contraindications. Yes, I do keep a handful in mind, since they’re needed off label for migraines and tremors, but not in the kind of detail a cardiologist would. I have to keep track of enough medications in my specialty as it is.
I wouldn’t try to handle blood pressure any more than I’d expect a nephrologist to treat epilepsy. It’s just looking for trouble.
Even when covering the hospital, I’ll stay out of that arena. This doesn’t mean I ignore blood pressure in such serious conditions as stroke or posterior reversible encephalopathy syndrome. I’m more than happy to provide guidelines and parameters. But as far as choosing the medications and doses? No.
Like driving, we all have to share the road. We may even be focused on the same journey (or patient). But part of practicing medicine and handling traffic is knowing when to stay in your lane.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
In the Nov. 1, 2019, issue of JAMA Neurology, an editorial argues that it’s time for neurologists to start managing high blood pressure.
It makes some very valid points: that targeting a systolic blood pressure of less than 120 mm Hg results in lower rates of cardiovascular events and all causes of mortality, that poorly controlled hypertension leads to debilitating neurologic conditions, and that high blood pressure is the most common modifiable risk factor for stroke.
All are strong points. I agree with them and definitely believe that more can and should be done to control hypertension.
The editorial then goes on to say that “first and foremost we are charging neurologists with actively diagnosing hypertension and prescribing medications when appropriate.”
Uh, no. I’m not going to be the one managing hypertension, nor should any outpatient neurologist.
Outpatient hypertension treatment has historically been, and should remain, the province of general practitioners, cardiologists, and nephrologists. Too many cooks, as they say, spoils the broth. I don’t want to be in a situation where two (or more) doctors are simultaneously trying to treat the same condition. On that path lies danger.
This doesn’t mean I ignore blood pressure. On the contrary, I take it (myself) at every patient visit, and put it in my note. In most cases I do nothing further, as nothing further needs to be done. On occasion, though, if it’s concerningly high, I’ll write it down for the patient and direct them to call the physician handling it. I also fax a note about it to that office, and if it’s dangerously high will call the doctor myself.
But try to manage it? No. Elevated readings definitely overlap with my world, but treating them shouldn’t.
The article says that, for some chronic patients, neurologists are their de facto internist. Perhaps for a few, but when a patient calls with concerns about a respiratory ailment, gastrointestinal problem, or other nonneurologic issue, I tell them to call their general practitioner. If they don’t have one I’m happy to give them the names and phone numbers of colleagues who practice that field, or even urgent care and emergency department information if needed. Just because I see them for their neurologic problems doesn’t qualify me to practice another branch of medicine.
Beyond the dangers of having more than one doctor involved, as a specialist it’s not practical for me to know the antihypertensive medications – possibly the largest group of agents on the market, – in detail, with their mechanisms of action, side effects, and contraindications. Yes, I do keep a handful in mind, since they’re needed off label for migraines and tremors, but not in the kind of detail a cardiologist would. I have to keep track of enough medications in my specialty as it is.
I wouldn’t try to handle blood pressure any more than I’d expect a nephrologist to treat epilepsy. It’s just looking for trouble.
Even when covering the hospital, I’ll stay out of that arena. This doesn’t mean I ignore blood pressure in such serious conditions as stroke or posterior reversible encephalopathy syndrome. I’m more than happy to provide guidelines and parameters. But as far as choosing the medications and doses? No.
Like driving, we all have to share the road. We may even be focused on the same journey (or patient). But part of practicing medicine and handling traffic is knowing when to stay in your lane.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Presence
The plan was in motion before I got on the plane.

When your leukemia came back suddenly 3 years after your stem cell transplant, it was devastating. But we had a plan. Your cancer developed a new mutation we could target with a chemotherapy drug. If we got you into a second remission, we could consolidate it by infusing more of your donor’s stem cells.
We met in the hospital, but I was adamant to “keep” you as my patient when you got to the clinic. I made swaps to see you, to get the continuity I value so much but often lose as a fellow, rotating from clinic to hospital to clinic.
I was grateful to see how well you dealt with the chemotherapy. Typically it’s a tough regimen, but you hardly had side effects. Between visits, I would check your blood counts on my phone, watching your blast count fall and your normal blood cells rise. Watching the cancer disappear.
Your lumbar punctures were negative, negative, negative – my favorite word, I told you. I was involved in long email threads coordinating the timing of your stem cell infusion with the remission we were achieving.
We were on our way.
One day, your lumbar puncture came back with a few “atypical” cells. I called the pathologist, and upon further review they were convinced the cells were reactive, not cancer. The next lumbar puncture was normal, but it was hard to ignore.
“Are you worried?” I asked my attending in clinic.
“I’m always worried,” she said. Neither of us truly believed the leukemia was back, but with the odds against us, we pored over every detail, always on the alert for a clue to an outcome we feared.
By now, the stem cell infusion was all set up. The donor was ready; so was the medical team; so were you. It was exciting. I thought of how a different attending described his interest in leukemia: There’s a subset you get to cure. Yes, you were going to be one of them.
Your big day coincided with a vacation I had scheduled months before. I was sorry I would be missing the actual moment, but happy I would come back to good news.
I left my coat and badge at the hospital, packed my bags, and got on the plane. I refrained from immediately checking your blood counts on my phone as soon as we landed. That night, jet lagged, I let myself look before I go to sleep. Relief. Your numbers still looked good.
Every day, I explored. My Internet was spotty during my travels, and when I would I finally get service I would peek at your latest blood tests.
Day 1. Cooled lava canyons. Black sand beaches. Circulating blast count: 0%.
Day 2: Glacier tour. A national park. Geysers. Blast count: 2%.
Day 3: We drive along the shore to see a famous waterfall, where you can climb a set of winding stairs to the top.
I check my phone before we start the climb. No service.
And so we begin. The wind cuts as I count steps. 403, 404, 405 … and 406. We are there. The air is thin, the world quiet. My nose is running from the cold.
We hike a bit, and I glance down again. Still no signal. It’s probably for the best. The scenery is spectacular.
Two miles later, I get service. I open the blood work first. Circulating blast count: 5%. But the other counts are okay. It could still be reactive, I say to myself, though on a deeper level I think of my attending’s words: I’m always worried. The stem cell infusion is scheduled for tomorrow.
I hear the rush of the water hitting the rocks below. Icicles form to our left. Sheep graze on our right. I appreciate the feeling of my muscles aching as we climb, higher and higher, a reminder of where I am and my place in it.
At the very top, we pause to take photos. And I get a signal again. I open the bone marrow biopsy report and skim the pathologist’s words. My eyes glue on the summary: 80% blasts, compatible with relapsed leukemia.
I let out an audible gasp.
Do you know? How will they tell you? I am painfully aware of the distance between us, in so many ways.
I want to be present. And soon I will be back, and I will be visiting in the hospital, and we will be having hard conversations and thinking about hard decisions.

But I’m not there right now. Someone else is. Here, now, I realize what I cannot do. The best way I can be present for you later is to be present where I am now.
I stuff my phone in my backpack and zip it closed. I step carefully forward on the rocks, slippery from the rain. My nose is running again, but not from the cold.
“What do you think?” my partner asks.
“The views are incredible,” I say.
Minor details of this story were changed to protect privacy.
Dr. Yurkiewicz is a fellow in hematology and oncology at Stanford (Calif.) University. Follow her on Twitter @ilanayurkiewicz and listen to her each week on the Blood & Cancer podcast.
The plan was in motion before I got on the plane.
When your leukemia came back suddenly 3 years after your stem cell transplant, it was devastating. But we had a plan. Your cancer developed a new mutation we could target with a chemotherapy drug. If we got you into a second remission, we could consolidate it by infusing more of your donor’s stem cells.
We met in the hospital, but I was adamant to “keep” you as my patient when you got to the clinic. I made swaps to see you, to get the continuity I value so much but often lose as a fellow, rotating from clinic to hospital to clinic.
I was grateful to see how well you dealt with the chemotherapy. Typically it’s a tough regimen, but you hardly had side effects. Between visits, I would check your blood counts on my phone, watching your blast count fall and your normal blood cells rise. Watching the cancer disappear.
Your lumbar punctures were negative, negative, negative – my favorite word, I told you. I was involved in long email threads coordinating the timing of your stem cell infusion with the remission we were achieving.
We were on our way.
One day, your lumbar puncture came back with a few “atypical” cells. I called the pathologist, and upon further review they were convinced the cells were reactive, not cancer. The next lumbar puncture was normal, but it was hard to ignore.
“Are you worried?” I asked my attending in clinic.
“I’m always worried,” she said. Neither of us truly believed the leukemia was back, but with the odds against us, we pored over every detail, always on the alert for a clue to an outcome we feared.
By now, the stem cell infusion was all set up. The donor was ready; so was the medical team; so were you. It was exciting. I thought of how a different attending described his interest in leukemia: There’s a subset you get to cure. Yes, you were going to be one of them.
Your big day coincided with a vacation I had scheduled months before. I was sorry I would be missing the actual moment, but happy I would come back to good news.
I left my coat and badge at the hospital, packed my bags, and got on the plane. I refrained from immediately checking your blood counts on my phone as soon as we landed. That night, jet lagged, I let myself look before I go to sleep. Relief. Your numbers still looked good.
Every day, I explored. My Internet was spotty during my travels, and when I would I finally get service I would peek at your latest blood tests.
Day 1. Cooled lava canyons. Black sand beaches. Circulating blast count: 0%.
Day 2: Glacier tour. A national park. Geysers. Blast count: 2%.
Day 3: We drive along the shore to see a famous waterfall, where you can climb a set of winding stairs to the top.
I check my phone before we start the climb. No service.
And so we begin. The wind cuts as I count steps. 403, 404, 405 … and 406. We are there. The air is thin, the world quiet. My nose is running from the cold.
We hike a bit, and I glance down again. Still no signal. It’s probably for the best. The scenery is spectacular.
Two miles later, I get service. I open the blood work first. Circulating blast count: 5%. But the other counts are okay. It could still be reactive, I say to myself, though on a deeper level I think of my attending’s words: I’m always worried. The stem cell infusion is scheduled for tomorrow.
I hear the rush of the water hitting the rocks below. Icicles form to our left. Sheep graze on our right. I appreciate the feeling of my muscles aching as we climb, higher and higher, a reminder of where I am and my place in it.
At the very top, we pause to take photos. And I get a signal again. I open the bone marrow biopsy report and skim the pathologist’s words. My eyes glue on the summary: 80% blasts, compatible with relapsed leukemia.
I let out an audible gasp.
Do you know? How will they tell you? I am painfully aware of the distance between us, in so many ways.
I want to be present. And soon I will be back, and I will be visiting in the hospital, and we will be having hard conversations and thinking about hard decisions.
But I’m not there right now. Someone else is. Here, now, I realize what I cannot do. The best way I can be present for you later is to be present where I am now.
I stuff my phone in my backpack and zip it closed. I step carefully forward on the rocks, slippery from the rain. My nose is running again, but not from the cold.
“What do you think?” my partner asks.
“The views are incredible,” I say.
Minor details of this story were changed to protect privacy.
Dr. Yurkiewicz is a fellow in hematology and oncology at Stanford (Calif.) University. Follow her on Twitter @ilanayurkiewicz and listen to her each week on the Blood & Cancer podcast.
The plan was in motion before I got on the plane.
When your leukemia came back suddenly 3 years after your stem cell transplant, it was devastating. But we had a plan. Your cancer developed a new mutation we could target with a chemotherapy drug. If we got you into a second remission, we could consolidate it by infusing more of your donor’s stem cells.
We met in the hospital, but I was adamant to “keep” you as my patient when you got to the clinic. I made swaps to see you, to get the continuity I value so much but often lose as a fellow, rotating from clinic to hospital to clinic.
I was grateful to see how well you dealt with the chemotherapy. Typically it’s a tough regimen, but you hardly had side effects. Between visits, I would check your blood counts on my phone, watching your blast count fall and your normal blood cells rise. Watching the cancer disappear.
Your lumbar punctures were negative, negative, negative – my favorite word, I told you. I was involved in long email threads coordinating the timing of your stem cell infusion with the remission we were achieving.
We were on our way.
One day, your lumbar puncture came back with a few “atypical” cells. I called the pathologist, and upon further review they were convinced the cells were reactive, not cancer. The next lumbar puncture was normal, but it was hard to ignore.
“Are you worried?” I asked my attending in clinic.
“I’m always worried,” she said. Neither of us truly believed the leukemia was back, but with the odds against us, we pored over every detail, always on the alert for a clue to an outcome we feared.
By now, the stem cell infusion was all set up. The donor was ready; so was the medical team; so were you. It was exciting. I thought of how a different attending described his interest in leukemia: There’s a subset you get to cure. Yes, you were going to be one of them.
Your big day coincided with a vacation I had scheduled months before. I was sorry I would be missing the actual moment, but happy I would come back to good news.
I left my coat and badge at the hospital, packed my bags, and got on the plane. I refrained from immediately checking your blood counts on my phone as soon as we landed. That night, jet lagged, I let myself look before I go to sleep. Relief. Your numbers still looked good.
Every day, I explored. My Internet was spotty during my travels, and when I would I finally get service I would peek at your latest blood tests.
Day 1. Cooled lava canyons. Black sand beaches. Circulating blast count: 0%.
Day 2: Glacier tour. A national park. Geysers. Blast count: 2%.
Day 3: We drive along the shore to see a famous waterfall, where you can climb a set of winding stairs to the top.
I check my phone before we start the climb. No service.
And so we begin. The wind cuts as I count steps. 403, 404, 405 … and 406. We are there. The air is thin, the world quiet. My nose is running from the cold.
We hike a bit, and I glance down again. Still no signal. It’s probably for the best. The scenery is spectacular.
Two miles later, I get service. I open the blood work first. Circulating blast count: 5%. But the other counts are okay. It could still be reactive, I say to myself, though on a deeper level I think of my attending’s words: I’m always worried. The stem cell infusion is scheduled for tomorrow.
I hear the rush of the water hitting the rocks below. Icicles form to our left. Sheep graze on our right. I appreciate the feeling of my muscles aching as we climb, higher and higher, a reminder of where I am and my place in it.
At the very top, we pause to take photos. And I get a signal again. I open the bone marrow biopsy report and skim the pathologist’s words. My eyes glue on the summary: 80% blasts, compatible with relapsed leukemia.
I let out an audible gasp.
Do you know? How will they tell you? I am painfully aware of the distance between us, in so many ways.
I want to be present. And soon I will be back, and I will be visiting in the hospital, and we will be having hard conversations and thinking about hard decisions.
But I’m not there right now. Someone else is. Here, now, I realize what I cannot do. The best way I can be present for you later is to be present where I am now.
I stuff my phone in my backpack and zip it closed. I step carefully forward on the rocks, slippery from the rain. My nose is running again, but not from the cold.
“What do you think?” my partner asks.
“The views are incredible,” I say.
Minor details of this story were changed to protect privacy.
Dr. Yurkiewicz is a fellow in hematology and oncology at Stanford (Calif.) University. Follow her on Twitter @ilanayurkiewicz and listen to her each week on the Blood & Cancer podcast.
Resignation
Along with resigning as chairman of the department of hematology and medical oncology at the Cleveland Clinic (Reunion), I am also resigning as editor in chief of Hematology News. In contrast to the drawn out process of choosing the next department chairman, however, I was in the enviable position of being able to hand pick my successor as editor in chief. I am proud to announce that Ifeyinwa (Ify) Osunkwo, MD, MPH, will be the new editor in chief of Hematology News. Dr. Osunkwo’s new perspective and energy will guide the further development of Hematology News for the benefit of our readers.

As editor in chief, I have had the opportunity to write essays for Hematology News that reflect my experience as a leader in an academic medical department. By doing so, I was trying to summarize some of what I learned along my career path. In my final essay, I want to direct some of these nuggets of wisdom directly to aspiring leaders who are closer to the beginning of their career journey than I am.
My junior colleagues are very interested in developing their careers to maximize opportunities in leadership, and I have coached many to try to understand that the path to leadership is not always straight, may be difficult, and does not always end comfortably. While the goal may seem to be in one direction, the path may lead to another. That is what has happened to me.
I did not seek to be Chairman. The opportunity came to me while I was busy doing other things. As I expressed in an earlier editorial (Seeking the chair), those who are diligent about their work without actively trying to rise through the leadership hierarchy are the ones who seem to rise more often.
Ambition is overrated. The ambitious find it harder to accept failure, and some degree of failure is likely. In his book “Falling Upward: A Spirituality for the Two Halves of Life,” Father Richard Rohr suggests that failure is required in order to mature from someone whose life centers on self to someone whose self centers on life.
Junior faculty tend to focus on self. They try to excel at whatever they attempt as they always have. Whether that is teaching, performing research, or treating patients, they try to be the absolute best teacher, researcher, or practitioner they can be. Many try to do all three well. Rare are those who can perfectly balance all three endeavors. Tension results, both at work and at home. Here is where failure often happens. The student disappoints, the paper is rejected, the grant isn’t funded, the patient relapses, and the family wishes you were home more. This confluence of difficulties challenges our concept of self. Maybe we aren’t perfect after all. Perhaps for the first time, failure looms.
In my experience, the usual solution to the possibility of failure is a desire to reduce patient care responsibilities. Academic faculty cherish their protected time and usually look for ways to increase it rather than to balance it (Professional time). Academic careers require thick CVs, not satisfied patients. A talk on leukemia at a major conference is more valued than talking to a patient about their leukemia. The cognitive dissonance between what we think is important and what is actually important challenges our personal sense of identity. The resulting burnout represents the necessary failure required to then mature spiritually and reprioritize our ambitions.
On some level, then, the path most of us are on is the time-honored – but painful – journey that must be traveled in order to attain peace.
I also recommend planning a career path with quality work, not a future title, as the goal. Quality work implies measurable objectives. For teachers, work could be measured by teaching scores and student accomplishments. For researchers, work could be measured by published papers, grants received, and invited lectures. For practitioners, work could be measured by outcomes, particularly patient-reported outcomes. Once work is measured, continuous improvements can be made and tracked. Highly reliable teachers, researchers, and practitioners who value quality work will be rewarded both personally and professionally (Defining high reliability).
There is a difference, however, between trying to be the best and trying to improve. The former implies competition with someone else, while the latter involves only one person. Competition can be motivating, but can also undermine interpersonal relationships while causing unhealthy behaviors like overworking and sleep deprivation. If the position sought requires selfish and destructive behaviors, it is not a position worth seeking (Rat race).
By doing quality work – not just more work – leadership positions will inevitably follow. Once a position is obtained, the work increases because a leader is now responsible for others. There are some easy-to-learn tools that can help with that responsibility. I find them very useful for helping colleagues work through interpersonal struggles and resource issues (Leadership hacks: The drama triangle; Leadership hacks: Structural tension).
Success as a leader is harder to measure, but many institutions employ engagement surveys similar to job satisfaction surveys. Leadership scores are generally accurate reflections of leader effectiveness, as are 360-degree surveys of those who work with you. Of course, being a leader also means holding those in your charge accountable for their behaviors (The white wall; Full disclosure). Leadership is no place for someone unwilling to hold crucial and difficult conversations with colleagues.
Success, of course, begets success and additional leadership roles are offered to successful leaders. Meanwhile, the work you started in order to get to the leadership position will probably need to be scaled back as excellence in teaching, research, patient care, and leadership is daunting, difficult to manage, and threatens work-life balance. The ability to say “no” is a valuable skill to learn as leadership roles increase.
Even though none of us work alone, academic medicine generally rewards only the individual. Yet, the camaraderie developed over time working together helps balance work and life roles. To advance as a leader, learning to work in a team is a critical ability. There is a science behind teamwork and aspiring leaders should acquaint themselves with it (Successful teams). While you may be rewarded as an individual, your success will be dependent on your ability to work on a team.
Finally, at least for clinicians, our obligation to our patients largely supersedes all our other commitments. Knowing the most, or being the most technically gifted, is not what patients value. They value empathy and relationships. We need to develop care designed for them, not us (Timed perfectly). We need to communicate with them on their terms, not ours (Pathologic superstition). We must walk with patients on their path, not ours. A patient-centered approach to care and career can take you far. Good luck on your journey.
Dr. Kalaycio is the outgoing editor in chief of Hematology News. He is a hematologist-oncologist at the Cleveland Clinic Taussig Cancer Institute. Contact him at kalaycm@ccf.org.
Along with resigning as chairman of the department of hematology and medical oncology at the Cleveland Clinic (Reunion), I am also resigning as editor in chief of Hematology News. In contrast to the drawn out process of choosing the next department chairman, however, I was in the enviable position of being able to hand pick my successor as editor in chief. I am proud to announce that Ifeyinwa (Ify) Osunkwo, MD, MPH, will be the new editor in chief of Hematology News. Dr. Osunkwo’s new perspective and energy will guide the further development of Hematology News for the benefit of our readers.
As editor in chief, I have had the opportunity to write essays for Hematology News that reflect my experience as a leader in an academic medical department. By doing so, I was trying to summarize some of what I learned along my career path. In my final essay, I want to direct some of these nuggets of wisdom directly to aspiring leaders who are closer to the beginning of their career journey than I am.
My junior colleagues are very interested in developing their careers to maximize opportunities in leadership, and I have coached many to try to understand that the path to leadership is not always straight, may be difficult, and does not always end comfortably. While the goal may seem to be in one direction, the path may lead to another. That is what has happened to me.
I did not seek to be Chairman. The opportunity came to me while I was busy doing other things. As I expressed in an earlier editorial (Seeking the chair), those who are diligent about their work without actively trying to rise through the leadership hierarchy are the ones who seem to rise more often.
Ambition is overrated. The ambitious find it harder to accept failure, and some degree of failure is likely. In his book “Falling Upward: A Spirituality for the Two Halves of Life,” Father Richard Rohr suggests that failure is required in order to mature from someone whose life centers on self to someone whose self centers on life.
Junior faculty tend to focus on self. They try to excel at whatever they attempt as they always have. Whether that is teaching, performing research, or treating patients, they try to be the absolute best teacher, researcher, or practitioner they can be. Many try to do all three well. Rare are those who can perfectly balance all three endeavors. Tension results, both at work and at home. Here is where failure often happens. The student disappoints, the paper is rejected, the grant isn’t funded, the patient relapses, and the family wishes you were home more. This confluence of difficulties challenges our concept of self. Maybe we aren’t perfect after all. Perhaps for the first time, failure looms.
In my experience, the usual solution to the possibility of failure is a desire to reduce patient care responsibilities. Academic faculty cherish their protected time and usually look for ways to increase it rather than to balance it (Professional time). Academic careers require thick CVs, not satisfied patients. A talk on leukemia at a major conference is more valued than talking to a patient about their leukemia. The cognitive dissonance between what we think is important and what is actually important challenges our personal sense of identity. The resulting burnout represents the necessary failure required to then mature spiritually and reprioritize our ambitions.
On some level, then, the path most of us are on is the time-honored – but painful – journey that must be traveled in order to attain peace.
I also recommend planning a career path with quality work, not a future title, as the goal. Quality work implies measurable objectives. For teachers, work could be measured by teaching scores and student accomplishments. For researchers, work could be measured by published papers, grants received, and invited lectures. For practitioners, work could be measured by outcomes, particularly patient-reported outcomes. Once work is measured, continuous improvements can be made and tracked. Highly reliable teachers, researchers, and practitioners who value quality work will be rewarded both personally and professionally (Defining high reliability).
There is a difference, however, between trying to be the best and trying to improve. The former implies competition with someone else, while the latter involves only one person. Competition can be motivating, but can also undermine interpersonal relationships while causing unhealthy behaviors like overworking and sleep deprivation. If the position sought requires selfish and destructive behaviors, it is not a position worth seeking (Rat race).
By doing quality work – not just more work – leadership positions will inevitably follow. Once a position is obtained, the work increases because a leader is now responsible for others. There are some easy-to-learn tools that can help with that responsibility. I find them very useful for helping colleagues work through interpersonal struggles and resource issues (Leadership hacks: The drama triangle; Leadership hacks: Structural tension).
Success as a leader is harder to measure, but many institutions employ engagement surveys similar to job satisfaction surveys. Leadership scores are generally accurate reflections of leader effectiveness, as are 360-degree surveys of those who work with you. Of course, being a leader also means holding those in your charge accountable for their behaviors (The white wall; Full disclosure). Leadership is no place for someone unwilling to hold crucial and difficult conversations with colleagues.
Success, of course, begets success and additional leadership roles are offered to successful leaders. Meanwhile, the work you started in order to get to the leadership position will probably need to be scaled back as excellence in teaching, research, patient care, and leadership is daunting, difficult to manage, and threatens work-life balance. The ability to say “no” is a valuable skill to learn as leadership roles increase.
Even though none of us work alone, academic medicine generally rewards only the individual. Yet, the camaraderie developed over time working together helps balance work and life roles. To advance as a leader, learning to work in a team is a critical ability. There is a science behind teamwork and aspiring leaders should acquaint themselves with it (Successful teams). While you may be rewarded as an individual, your success will be dependent on your ability to work on a team.
Finally, at least for clinicians, our obligation to our patients largely supersedes all our other commitments. Knowing the most, or being the most technically gifted, is not what patients value. They value empathy and relationships. We need to develop care designed for them, not us (Timed perfectly). We need to communicate with them on their terms, not ours (Pathologic superstition). We must walk with patients on their path, not ours. A patient-centered approach to care and career can take you far. Good luck on your journey.
Dr. Kalaycio is the outgoing editor in chief of Hematology News. He is a hematologist-oncologist at the Cleveland Clinic Taussig Cancer Institute. Contact him at kalaycm@ccf.org.
Along with resigning as chairman of the department of hematology and medical oncology at the Cleveland Clinic (Reunion), I am also resigning as editor in chief of Hematology News. In contrast to the drawn out process of choosing the next department chairman, however, I was in the enviable position of being able to hand pick my successor as editor in chief. I am proud to announce that Ifeyinwa (Ify) Osunkwo, MD, MPH, will be the new editor in chief of Hematology News. Dr. Osunkwo’s new perspective and energy will guide the further development of Hematology News for the benefit of our readers.
As editor in chief, I have had the opportunity to write essays for Hematology News that reflect my experience as a leader in an academic medical department. By doing so, I was trying to summarize some of what I learned along my career path. In my final essay, I want to direct some of these nuggets of wisdom directly to aspiring leaders who are closer to the beginning of their career journey than I am.
My junior colleagues are very interested in developing their careers to maximize opportunities in leadership, and I have coached many to try to understand that the path to leadership is not always straight, may be difficult, and does not always end comfortably. While the goal may seem to be in one direction, the path may lead to another. That is what has happened to me.
I did not seek to be Chairman. The opportunity came to me while I was busy doing other things. As I expressed in an earlier editorial (Seeking the chair), those who are diligent about their work without actively trying to rise through the leadership hierarchy are the ones who seem to rise more often.
Ambition is overrated. The ambitious find it harder to accept failure, and some degree of failure is likely. In his book “Falling Upward: A Spirituality for the Two Halves of Life,” Father Richard Rohr suggests that failure is required in order to mature from someone whose life centers on self to someone whose self centers on life.
Junior faculty tend to focus on self. They try to excel at whatever they attempt as they always have. Whether that is teaching, performing research, or treating patients, they try to be the absolute best teacher, researcher, or practitioner they can be. Many try to do all three well. Rare are those who can perfectly balance all three endeavors. Tension results, both at work and at home. Here is where failure often happens. The student disappoints, the paper is rejected, the grant isn’t funded, the patient relapses, and the family wishes you were home more. This confluence of difficulties challenges our concept of self. Maybe we aren’t perfect after all. Perhaps for the first time, failure looms.
In my experience, the usual solution to the possibility of failure is a desire to reduce patient care responsibilities. Academic faculty cherish their protected time and usually look for ways to increase it rather than to balance it (Professional time). Academic careers require thick CVs, not satisfied patients. A talk on leukemia at a major conference is more valued than talking to a patient about their leukemia. The cognitive dissonance between what we think is important and what is actually important challenges our personal sense of identity. The resulting burnout represents the necessary failure required to then mature spiritually and reprioritize our ambitions.
On some level, then, the path most of us are on is the time-honored – but painful – journey that must be traveled in order to attain peace.
I also recommend planning a career path with quality work, not a future title, as the goal. Quality work implies measurable objectives. For teachers, work could be measured by teaching scores and student accomplishments. For researchers, work could be measured by published papers, grants received, and invited lectures. For practitioners, work could be measured by outcomes, particularly patient-reported outcomes. Once work is measured, continuous improvements can be made and tracked. Highly reliable teachers, researchers, and practitioners who value quality work will be rewarded both personally and professionally (Defining high reliability).
There is a difference, however, between trying to be the best and trying to improve. The former implies competition with someone else, while the latter involves only one person. Competition can be motivating, but can also undermine interpersonal relationships while causing unhealthy behaviors like overworking and sleep deprivation. If the position sought requires selfish and destructive behaviors, it is not a position worth seeking (Rat race).
By doing quality work – not just more work – leadership positions will inevitably follow. Once a position is obtained, the work increases because a leader is now responsible for others. There are some easy-to-learn tools that can help with that responsibility. I find them very useful for helping colleagues work through interpersonal struggles and resource issues (Leadership hacks: The drama triangle; Leadership hacks: Structural tension).
Success as a leader is harder to measure, but many institutions employ engagement surveys similar to job satisfaction surveys. Leadership scores are generally accurate reflections of leader effectiveness, as are 360-degree surveys of those who work with you. Of course, being a leader also means holding those in your charge accountable for their behaviors (The white wall; Full disclosure). Leadership is no place for someone unwilling to hold crucial and difficult conversations with colleagues.
Success, of course, begets success and additional leadership roles are offered to successful leaders. Meanwhile, the work you started in order to get to the leadership position will probably need to be scaled back as excellence in teaching, research, patient care, and leadership is daunting, difficult to manage, and threatens work-life balance. The ability to say “no” is a valuable skill to learn as leadership roles increase.
Even though none of us work alone, academic medicine generally rewards only the individual. Yet, the camaraderie developed over time working together helps balance work and life roles. To advance as a leader, learning to work in a team is a critical ability. There is a science behind teamwork and aspiring leaders should acquaint themselves with it (Successful teams). While you may be rewarded as an individual, your success will be dependent on your ability to work on a team.
Finally, at least for clinicians, our obligation to our patients largely supersedes all our other commitments. Knowing the most, or being the most technically gifted, is not what patients value. They value empathy and relationships. We need to develop care designed for them, not us (Timed perfectly). We need to communicate with them on their terms, not ours (Pathologic superstition). We must walk with patients on their path, not ours. A patient-centered approach to care and career can take you far. Good luck on your journey.
Dr. Kalaycio is the outgoing editor in chief of Hematology News. He is a hematologist-oncologist at the Cleveland Clinic Taussig Cancer Institute. Contact him at kalaycm@ccf.org.
Inner demons
Julia Brennan sings about inner demons. They just won’t go away and they don’t play fair with angels. We have marveled at the miracles of fecal microbiome transplants (FMT), but this month we read about an inner demon. Two patients developed bacteremia from extended-spectrum beta-lactamase (ESBL)–producing Escherichia coli transmitted during FMT from stool derived from a single donor. One patient, with cirrhosis, who received FMT as part of a trial to treat hepatic encephalopathy, recovered. A second patient with myelodysplastic syndrome underwent allogeneic hematopoietic stem cell transplantation and received FMT as part of a phase 2 trial. This severely immunocompromised patient succumbed to sepsis related to the E. coli bacteremia. Both organisms were genetically traced to the donor stool. The AGA has NIH funding to develop and maintain an FMT registry (see https://www.gastrojournal.org/article/S0016-5085(17)30088-4/pdf) so we can understand long-term risks and benefits.

These rare experiences will lead to increased scrutiny and likely further FDA regulations. Gastroenterologists should be careful about choosing patients for FMT.
This month, we again feature an article about incorporating telehealth into your practice – this month’s article highlights the potential for private practices to incorporate this emerging technology. There are interesting articles about treatment of eosinophilic esophagitis, acute liver failure, and postcolonoscopy interval cancers. Finally, we are cautioned about the vulnerability of our biosimilar market. This market may wither despite the great potential to reduce therapeutic costs.
Last week, I taught an undergraduate course about health care economics. After recounting current challenges, one student said, “I am a first-year medical student, what should I do?” I was caught off guard. The future is too overwhelming. As we enter the 12-month countdown to a national election, I would suggest that we continue to advocate for our patients and educate our political leaders about verifiable root causes of our major problems. Despite current antipathy to science and data, we are scientists and eventually truth will prevail. “The arc of the moral universe is long, but it bends towards justice” (Dr. Martin Luther King, Jr.).
John I. Allen, MD, MBA, AGAF
Editor in Chief
Julia Brennan sings about inner demons. They just won’t go away and they don’t play fair with angels. We have marveled at the miracles of fecal microbiome transplants (FMT), but this month we read about an inner demon. Two patients developed bacteremia from extended-spectrum beta-lactamase (ESBL)–producing Escherichia coli transmitted during FMT from stool derived from a single donor. One patient, with cirrhosis, who received FMT as part of a trial to treat hepatic encephalopathy, recovered. A second patient with myelodysplastic syndrome underwent allogeneic hematopoietic stem cell transplantation and received FMT as part of a phase 2 trial. This severely immunocompromised patient succumbed to sepsis related to the E. coli bacteremia. Both organisms were genetically traced to the donor stool. The AGA has NIH funding to develop and maintain an FMT registry (see https://www.gastrojournal.org/article/S0016-5085(17)30088-4/pdf) so we can understand long-term risks and benefits.
These rare experiences will lead to increased scrutiny and likely further FDA regulations. Gastroenterologists should be careful about choosing patients for FMT.
This month, we again feature an article about incorporating telehealth into your practice – this month’s article highlights the potential for private practices to incorporate this emerging technology. There are interesting articles about treatment of eosinophilic esophagitis, acute liver failure, and postcolonoscopy interval cancers. Finally, we are cautioned about the vulnerability of our biosimilar market. This market may wither despite the great potential to reduce therapeutic costs.
Last week, I taught an undergraduate course about health care economics. After recounting current challenges, one student said, “I am a first-year medical student, what should I do?” I was caught off guard. The future is too overwhelming. As we enter the 12-month countdown to a national election, I would suggest that we continue to advocate for our patients and educate our political leaders about verifiable root causes of our major problems. Despite current antipathy to science and data, we are scientists and eventually truth will prevail. “The arc of the moral universe is long, but it bends towards justice” (Dr. Martin Luther King, Jr.).
John I. Allen, MD, MBA, AGAF
Editor in Chief
Julia Brennan sings about inner demons. They just won’t go away and they don’t play fair with angels. We have marveled at the miracles of fecal microbiome transplants (FMT), but this month we read about an inner demon. Two patients developed bacteremia from extended-spectrum beta-lactamase (ESBL)–producing Escherichia coli transmitted during FMT from stool derived from a single donor. One patient, with cirrhosis, who received FMT as part of a trial to treat hepatic encephalopathy, recovered. A second patient with myelodysplastic syndrome underwent allogeneic hematopoietic stem cell transplantation and received FMT as part of a phase 2 trial. This severely immunocompromised patient succumbed to sepsis related to the E. coli bacteremia. Both organisms were genetically traced to the donor stool. The AGA has NIH funding to develop and maintain an FMT registry (see https://www.gastrojournal.org/article/S0016-5085(17)30088-4/pdf) so we can understand long-term risks and benefits.
These rare experiences will lead to increased scrutiny and likely further FDA regulations. Gastroenterologists should be careful about choosing patients for FMT.
This month, we again feature an article about incorporating telehealth into your practice – this month’s article highlights the potential for private practices to incorporate this emerging technology. There are interesting articles about treatment of eosinophilic esophagitis, acute liver failure, and postcolonoscopy interval cancers. Finally, we are cautioned about the vulnerability of our biosimilar market. This market may wither despite the great potential to reduce therapeutic costs.
Last week, I taught an undergraduate course about health care economics. After recounting current challenges, one student said, “I am a first-year medical student, what should I do?” I was caught off guard. The future is too overwhelming. As we enter the 12-month countdown to a national election, I would suggest that we continue to advocate for our patients and educate our political leaders about verifiable root causes of our major problems. Despite current antipathy to science and data, we are scientists and eventually truth will prevail. “The arc of the moral universe is long, but it bends towards justice” (Dr. Martin Luther King, Jr.).
John I. Allen, MD, MBA, AGAF
Editor in Chief
