User login
Market Watch
New Drugs, Devices, Indications, and Approvals
- Alglucosidase alfa (Lumizyme) has been approved by the FDA for the treatment of patients older than 8 with late (noninfantile) onset Pompe disease (GAA deficiency) who do not have evidence of cardiac hypertrophy.1
- Dutasteride and tamsulosin (Jalyn) has been approved by the FDA in a fixed-dose combination product for treating symptomatic benign prostatic hypertrophy.2
- Gatifloxacin ophthalmic solution 0.5% (Zymaxid) has been approved by the FDA to treat bacterial conjunctivitis caused by susceptible bacterial strains.3 It has the highest concentration of gatifloxacin ophthalmic on the U.S. market.
- Memantine hydrochloride (Namenda XR) has been approved by the FDA as an extended-release product to treat moderate to severe dementia of the Alzheimer's type.4 It is available as a 28 mg, once-daily dosage form. The immediate-release product is dosed twice daily.
- Mesenchymal stem cells for intravenous infusion (MSCs, Prochymal) formulated into Prochymal has been granted orphan drug status to treat Type 1 diabetes mellitus (T1DM).5 This agent is in Phase 2 clinical trials in a collaboration with the Juvenile Diabetes Research Foundation as a treatment for patients with newly diagnosed T1DM.
- Mometasone furoate/formoterol fumarate (Dulera) has been approved by the FDA as a combination treatment for asthmatics aged 12 and older.6
- Naproxen/esomeprazole (Vimovo) has been approved by the FDA as a fixed combination for patients with arthritis who are at risk for developing gastric ulcers.7
- Pioglitazone/metformin (ACTOplus met XR) has been approved by the FDA in an extended-release fixed combination for treating Type 2 diabetes mellitus (T2DM) as an adjunct to diet and exercise.8
- Ranibizumab (Lucentis) has received a new indication from the FDA for treating retinal vein occlusion.9 The original approval of ranibizumab was for wet age-related macular degeneration.
- Tramadol HCl, orally disintegrating tablets (Rybix ODT), have been approved by the FDA for treating moderate to moderately severe pain in patients 16 years of age and older.10
Pipeline
- Dronedarone (Multaq) is being investigated as to whether it can reduce major cardiovascular events in patients being treated with the agent for atrial fibrillation.11 Study endpoints will include a reduction in a major cardiovascular event such as stroke or myocardial infarction, or a reduction in cardiovascular hospitalization or death.
- The combination product ibuprofen and famotidine (to be known as Duexa) has been filed as a new drug application (NDA) for reducing the risk of developing upper gastrointestinal (GI) ulcers in patients with pain and arthritis.12 Two Phase 3 trials showed about a 50% reduction in GI ulcers in combination treatment compared with ibuprofen alone.
- Rifaximin (Xifaxan) has been submitted to the FDA at its higher dose (550 mg) for treatment of nonconstipation irritable bowel syndrome (Non-C-IBS) and IBS-related bloating.13 Rifaximin already has approval from the FDA for hepatic encephalopathy and diarrhea.
- TC-5214 has begun Phase 3 clinical trials.14 It is a nicotinic channel blocker for the adjunctive treatment of major depressive disorder in adults who have had an inadequate response to selective serotonin reuptake inhibitors (SSRIs) or serotonin/norepinephrine reuptake inhibitors (SNRIs). A Phase 2 study evaluating TC-5214 as a second-line (“switch”) monotherapy is planned for this year.
- An NDA for vilazodone has been filed for treating major depressive disorder.15 It is a dual-acting potent and selective serotonin reuptake inhibitor and a 5-HT1A receptor partial agonist.
Safety, Warnings, and Label Changes
- Tramadol and tramadol/acetaminophen have undergone a label change related to strengthened warnings of the risk of suicide for patients who are addiction-prone, taking tranquilizers, drinking alcohol, or taking other central-nervous-system-active drugs.16 Addictive effects might occur when tramadol is combined with alcohol, other opioids, or illicit drugs that have central-nervous-system-depressive effects. Serious potential consequences of overdosage are CNS and/or respiratory depression, and death.
- Earlier this year, the FDA once again updated the warning related to severe liver injury related to the use of propylthiouracil (PTU).17 This time, PTU has garnered a boxed warning, which includes reports of severe hepatotoxicity and acute liver failure in both adults and children. Some of these reactions were fatal. Use of PTU should be reserved for patients who do not tolerate other treatments for hyperthyroidism, such as methimazole, radioactive iodine, or are not surgery candidates. PTU might be preferred over methimazole just before and/or during the first trimester of pregnancy due to the occurrence of birth defects with methimazole during this timeframe. A medication guide has been developed and is to be given to patients when they fill PTU prescriptions. The guide alerts patients to the signs and symptoms of hepatotoxicity. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Genzyme receives FDA approval for lumizyme for Pompe disease. Business Wire website. Available at: www.businesswire.com/portal/site/home/email/alert/?ndmViewId=news_view&newsLang=en&newsId=20100525006514. Accessed June 30, 2010.
- Dennis M. FDA approves GlaxoSmithKline’s combination BPH drug Jalyn. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=B5F703CADB0347DF970A7B7542D99982&logRowId=369156. Accessed June 30, 2010.
- Allergan receives FDA approval for Zymaxid ophthalmic solution. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/189397.php. Accessed June 29, 2010.
- Forest and Merz announce FDA approval of Namenda XR for the treatment of moderate to severe dementia of the Alzheimer’s type. Forest Laboratories website. Available at: http://www.frx.com/news/PressRelease.aspx?ID=1440385. Accessed June 30, 2010.
- Osiris Therapeutics receives FDA orphan drug designation for stem cell treatment for Type 1 diabetes. Osiris Therapeutics website. Available at: http://osiris.com/pdf/2010-05-04%20T1D%20Orphan%20Drug%20Designation.pdf. Accessed June 30, 2010.
- FDA approves Merck’s new lung drug Dulera. The Economic Times website. Available at: http://economictimes.indiatimes.com/articleshow/6087079.cms. Accessed June 30, 2010.
- Dane L. FDA approves AstraZeneca, Pozen’s Vimovo. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=0C2915EE4D2D47D287D41D90DFE4240D. Accessed June 30, 2010.
- ACTOplus met XR available for diabetes. Monthly Prescribing Reference website. Available at: http://www.empr.com/actoplus-met-xr-available-for-diabetes/article/172985/. Accessed June 30, 2010.
- Dennis M. Roche’s Lucentis garners expanded FDA approval for macular oedema. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=5146664F5A4C48108209D15EA744A614&logRowId=370643. Accessed June 30, 2010.
- Rybix ODT launched for moderate to moderately severe pain. Monthly Prescribing Reference website. Available at: http://www.empr.com/rybix-odt-launched-for-moderate-to-moderately-severe-pain/article/172743/. Accessed June 30, 3010.
- Dennis M. Sanofi-Aventis begins late-stage study of Multaq in patients with permanent AF. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=E43104A2DB604649A812E69C58F89304&logRowId=364228. Accessed July 7, 2010.
- FDA accepts NDA for Duexa for ulcer risk reduction in arthritis patients. Monthly Prescribing Reference website. Available at: http://www.empr.com/fda-accepts-nda-for-duexa-for-ulcer-risk-reduction-in-arthritis-patients/article/171054/. Accessed July 7, 2010.
- Salix Pharmaceuticals announces NDA submission for Xifaxan550 for treatment of non-constipation irritable bowel syndrome. Salix Pharmaceuticals website. Available at: http://salix.com/news/stories/20100608.aspx. Accessed June 9, 2010.
- AstraZeneca and Targacept initiate Phase 3 clinical development of TC-5214 as an adjunct treatment for major depressive disorder. Targacept website. Available at: http://www.targacept.com/wt/page/pr_1277240993. Accessed June 29, 2010.
- Clinical Data, Inc. announces FDA acceptance of new drug application for Vilazodone for the treatment of major depressive disorder. Clinical Data Inc. website. Available at: http://clda.com/uploads/CLDA%20NDA%20acceptance%20FINAL.pdf. Accessed July 7, 2010.
- Ultram (tramadol hydrochloride), Ultracet (tramadol hydrochloride/acetaminophen): Label change. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm213264.htm. Accessed July 8, 2010.
- FDA Drug Safety Communication: New boxed warning on severe liver injury with propylthiouracil. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm209023.htm. Accessed July 8, 2010.
New Drugs, Devices, Indications, and Approvals
- Alglucosidase alfa (Lumizyme) has been approved by the FDA for the treatment of patients older than 8 with late (noninfantile) onset Pompe disease (GAA deficiency) who do not have evidence of cardiac hypertrophy.1
- Dutasteride and tamsulosin (Jalyn) has been approved by the FDA in a fixed-dose combination product for treating symptomatic benign prostatic hypertrophy.2
- Gatifloxacin ophthalmic solution 0.5% (Zymaxid) has been approved by the FDA to treat bacterial conjunctivitis caused by susceptible bacterial strains.3 It has the highest concentration of gatifloxacin ophthalmic on the U.S. market.
- Memantine hydrochloride (Namenda XR) has been approved by the FDA as an extended-release product to treat moderate to severe dementia of the Alzheimer's type.4 It is available as a 28 mg, once-daily dosage form. The immediate-release product is dosed twice daily.
- Mesenchymal stem cells for intravenous infusion (MSCs, Prochymal) formulated into Prochymal has been granted orphan drug status to treat Type 1 diabetes mellitus (T1DM).5 This agent is in Phase 2 clinical trials in a collaboration with the Juvenile Diabetes Research Foundation as a treatment for patients with newly diagnosed T1DM.
- Mometasone furoate/formoterol fumarate (Dulera) has been approved by the FDA as a combination treatment for asthmatics aged 12 and older.6
- Naproxen/esomeprazole (Vimovo) has been approved by the FDA as a fixed combination for patients with arthritis who are at risk for developing gastric ulcers.7
- Pioglitazone/metformin (ACTOplus met XR) has been approved by the FDA in an extended-release fixed combination for treating Type 2 diabetes mellitus (T2DM) as an adjunct to diet and exercise.8
- Ranibizumab (Lucentis) has received a new indication from the FDA for treating retinal vein occlusion.9 The original approval of ranibizumab was for wet age-related macular degeneration.
- Tramadol HCl, orally disintegrating tablets (Rybix ODT), have been approved by the FDA for treating moderate to moderately severe pain in patients 16 years of age and older.10
Pipeline
- Dronedarone (Multaq) is being investigated as to whether it can reduce major cardiovascular events in patients being treated with the agent for atrial fibrillation.11 Study endpoints will include a reduction in a major cardiovascular event such as stroke or myocardial infarction, or a reduction in cardiovascular hospitalization or death.
- The combination product ibuprofen and famotidine (to be known as Duexa) has been filed as a new drug application (NDA) for reducing the risk of developing upper gastrointestinal (GI) ulcers in patients with pain and arthritis.12 Two Phase 3 trials showed about a 50% reduction in GI ulcers in combination treatment compared with ibuprofen alone.
- Rifaximin (Xifaxan) has been submitted to the FDA at its higher dose (550 mg) for treatment of nonconstipation irritable bowel syndrome (Non-C-IBS) and IBS-related bloating.13 Rifaximin already has approval from the FDA for hepatic encephalopathy and diarrhea.
- TC-5214 has begun Phase 3 clinical trials.14 It is a nicotinic channel blocker for the adjunctive treatment of major depressive disorder in adults who have had an inadequate response to selective serotonin reuptake inhibitors (SSRIs) or serotonin/norepinephrine reuptake inhibitors (SNRIs). A Phase 2 study evaluating TC-5214 as a second-line (“switch”) monotherapy is planned for this year.
- An NDA for vilazodone has been filed for treating major depressive disorder.15 It is a dual-acting potent and selective serotonin reuptake inhibitor and a 5-HT1A receptor partial agonist.
Safety, Warnings, and Label Changes
- Tramadol and tramadol/acetaminophen have undergone a label change related to strengthened warnings of the risk of suicide for patients who are addiction-prone, taking tranquilizers, drinking alcohol, or taking other central-nervous-system-active drugs.16 Addictive effects might occur when tramadol is combined with alcohol, other opioids, or illicit drugs that have central-nervous-system-depressive effects. Serious potential consequences of overdosage are CNS and/or respiratory depression, and death.
- Earlier this year, the FDA once again updated the warning related to severe liver injury related to the use of propylthiouracil (PTU).17 This time, PTU has garnered a boxed warning, which includes reports of severe hepatotoxicity and acute liver failure in both adults and children. Some of these reactions were fatal. Use of PTU should be reserved for patients who do not tolerate other treatments for hyperthyroidism, such as methimazole, radioactive iodine, or are not surgery candidates. PTU might be preferred over methimazole just before and/or during the first trimester of pregnancy due to the occurrence of birth defects with methimazole during this timeframe. A medication guide has been developed and is to be given to patients when they fill PTU prescriptions. The guide alerts patients to the signs and symptoms of hepatotoxicity. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Genzyme receives FDA approval for lumizyme for Pompe disease. Business Wire website. Available at: www.businesswire.com/portal/site/home/email/alert/?ndmViewId=news_view&newsLang=en&newsId=20100525006514. Accessed June 30, 2010.
- Dennis M. FDA approves GlaxoSmithKline’s combination BPH drug Jalyn. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=B5F703CADB0347DF970A7B7542D99982&logRowId=369156. Accessed June 30, 2010.
- Allergan receives FDA approval for Zymaxid ophthalmic solution. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/189397.php. Accessed June 29, 2010.
- Forest and Merz announce FDA approval of Namenda XR for the treatment of moderate to severe dementia of the Alzheimer’s type. Forest Laboratories website. Available at: http://www.frx.com/news/PressRelease.aspx?ID=1440385. Accessed June 30, 2010.
- Osiris Therapeutics receives FDA orphan drug designation for stem cell treatment for Type 1 diabetes. Osiris Therapeutics website. Available at: http://osiris.com/pdf/2010-05-04%20T1D%20Orphan%20Drug%20Designation.pdf. Accessed June 30, 2010.
- FDA approves Merck’s new lung drug Dulera. The Economic Times website. Available at: http://economictimes.indiatimes.com/articleshow/6087079.cms. Accessed June 30, 2010.
- Dane L. FDA approves AstraZeneca, Pozen’s Vimovo. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=0C2915EE4D2D47D287D41D90DFE4240D. Accessed June 30, 2010.
- ACTOplus met XR available for diabetes. Monthly Prescribing Reference website. Available at: http://www.empr.com/actoplus-met-xr-available-for-diabetes/article/172985/. Accessed June 30, 2010.
- Dennis M. Roche’s Lucentis garners expanded FDA approval for macular oedema. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=5146664F5A4C48108209D15EA744A614&logRowId=370643. Accessed June 30, 2010.
- Rybix ODT launched for moderate to moderately severe pain. Monthly Prescribing Reference website. Available at: http://www.empr.com/rybix-odt-launched-for-moderate-to-moderately-severe-pain/article/172743/. Accessed June 30, 3010.
- Dennis M. Sanofi-Aventis begins late-stage study of Multaq in patients with permanent AF. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=E43104A2DB604649A812E69C58F89304&logRowId=364228. Accessed July 7, 2010.
- FDA accepts NDA for Duexa for ulcer risk reduction in arthritis patients. Monthly Prescribing Reference website. Available at: http://www.empr.com/fda-accepts-nda-for-duexa-for-ulcer-risk-reduction-in-arthritis-patients/article/171054/. Accessed July 7, 2010.
- Salix Pharmaceuticals announces NDA submission for Xifaxan550 for treatment of non-constipation irritable bowel syndrome. Salix Pharmaceuticals website. Available at: http://salix.com/news/stories/20100608.aspx. Accessed June 9, 2010.
- AstraZeneca and Targacept initiate Phase 3 clinical development of TC-5214 as an adjunct treatment for major depressive disorder. Targacept website. Available at: http://www.targacept.com/wt/page/pr_1277240993. Accessed June 29, 2010.
- Clinical Data, Inc. announces FDA acceptance of new drug application for Vilazodone for the treatment of major depressive disorder. Clinical Data Inc. website. Available at: http://clda.com/uploads/CLDA%20NDA%20acceptance%20FINAL.pdf. Accessed July 7, 2010.
- Ultram (tramadol hydrochloride), Ultracet (tramadol hydrochloride/acetaminophen): Label change. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm213264.htm. Accessed July 8, 2010.
- FDA Drug Safety Communication: New boxed warning on severe liver injury with propylthiouracil. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm209023.htm. Accessed July 8, 2010.
New Drugs, Devices, Indications, and Approvals
- Alglucosidase alfa (Lumizyme) has been approved by the FDA for the treatment of patients older than 8 with late (noninfantile) onset Pompe disease (GAA deficiency) who do not have evidence of cardiac hypertrophy.1
- Dutasteride and tamsulosin (Jalyn) has been approved by the FDA in a fixed-dose combination product for treating symptomatic benign prostatic hypertrophy.2
- Gatifloxacin ophthalmic solution 0.5% (Zymaxid) has been approved by the FDA to treat bacterial conjunctivitis caused by susceptible bacterial strains.3 It has the highest concentration of gatifloxacin ophthalmic on the U.S. market.
- Memantine hydrochloride (Namenda XR) has been approved by the FDA as an extended-release product to treat moderate to severe dementia of the Alzheimer's type.4 It is available as a 28 mg, once-daily dosage form. The immediate-release product is dosed twice daily.
- Mesenchymal stem cells for intravenous infusion (MSCs, Prochymal) formulated into Prochymal has been granted orphan drug status to treat Type 1 diabetes mellitus (T1DM).5 This agent is in Phase 2 clinical trials in a collaboration with the Juvenile Diabetes Research Foundation as a treatment for patients with newly diagnosed T1DM.
- Mometasone furoate/formoterol fumarate (Dulera) has been approved by the FDA as a combination treatment for asthmatics aged 12 and older.6
- Naproxen/esomeprazole (Vimovo) has been approved by the FDA as a fixed combination for patients with arthritis who are at risk for developing gastric ulcers.7
- Pioglitazone/metformin (ACTOplus met XR) has been approved by the FDA in an extended-release fixed combination for treating Type 2 diabetes mellitus (T2DM) as an adjunct to diet and exercise.8
- Ranibizumab (Lucentis) has received a new indication from the FDA for treating retinal vein occlusion.9 The original approval of ranibizumab was for wet age-related macular degeneration.
- Tramadol HCl, orally disintegrating tablets (Rybix ODT), have been approved by the FDA for treating moderate to moderately severe pain in patients 16 years of age and older.10
Pipeline
- Dronedarone (Multaq) is being investigated as to whether it can reduce major cardiovascular events in patients being treated with the agent for atrial fibrillation.11 Study endpoints will include a reduction in a major cardiovascular event such as stroke or myocardial infarction, or a reduction in cardiovascular hospitalization or death.
- The combination product ibuprofen and famotidine (to be known as Duexa) has been filed as a new drug application (NDA) for reducing the risk of developing upper gastrointestinal (GI) ulcers in patients with pain and arthritis.12 Two Phase 3 trials showed about a 50% reduction in GI ulcers in combination treatment compared with ibuprofen alone.
- Rifaximin (Xifaxan) has been submitted to the FDA at its higher dose (550 mg) for treatment of nonconstipation irritable bowel syndrome (Non-C-IBS) and IBS-related bloating.13 Rifaximin already has approval from the FDA for hepatic encephalopathy and diarrhea.
- TC-5214 has begun Phase 3 clinical trials.14 It is a nicotinic channel blocker for the adjunctive treatment of major depressive disorder in adults who have had an inadequate response to selective serotonin reuptake inhibitors (SSRIs) or serotonin/norepinephrine reuptake inhibitors (SNRIs). A Phase 2 study evaluating TC-5214 as a second-line (“switch”) monotherapy is planned for this year.
- An NDA for vilazodone has been filed for treating major depressive disorder.15 It is a dual-acting potent and selective serotonin reuptake inhibitor and a 5-HT1A receptor partial agonist.
Safety, Warnings, and Label Changes
- Tramadol and tramadol/acetaminophen have undergone a label change related to strengthened warnings of the risk of suicide for patients who are addiction-prone, taking tranquilizers, drinking alcohol, or taking other central-nervous-system-active drugs.16 Addictive effects might occur when tramadol is combined with alcohol, other opioids, or illicit drugs that have central-nervous-system-depressive effects. Serious potential consequences of overdosage are CNS and/or respiratory depression, and death.
- Earlier this year, the FDA once again updated the warning related to severe liver injury related to the use of propylthiouracil (PTU).17 This time, PTU has garnered a boxed warning, which includes reports of severe hepatotoxicity and acute liver failure in both adults and children. Some of these reactions were fatal. Use of PTU should be reserved for patients who do not tolerate other treatments for hyperthyroidism, such as methimazole, radioactive iodine, or are not surgery candidates. PTU might be preferred over methimazole just before and/or during the first trimester of pregnancy due to the occurrence of birth defects with methimazole during this timeframe. A medication guide has been developed and is to be given to patients when they fill PTU prescriptions. The guide alerts patients to the signs and symptoms of hepatotoxicity. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Genzyme receives FDA approval for lumizyme for Pompe disease. Business Wire website. Available at: www.businesswire.com/portal/site/home/email/alert/?ndmViewId=news_view&newsLang=en&newsId=20100525006514. Accessed June 30, 2010.
- Dennis M. FDA approves GlaxoSmithKline’s combination BPH drug Jalyn. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=B5F703CADB0347DF970A7B7542D99982&logRowId=369156. Accessed June 30, 2010.
- Allergan receives FDA approval for Zymaxid ophthalmic solution. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/189397.php. Accessed June 29, 2010.
- Forest and Merz announce FDA approval of Namenda XR for the treatment of moderate to severe dementia of the Alzheimer’s type. Forest Laboratories website. Available at: http://www.frx.com/news/PressRelease.aspx?ID=1440385. Accessed June 30, 2010.
- Osiris Therapeutics receives FDA orphan drug designation for stem cell treatment for Type 1 diabetes. Osiris Therapeutics website. Available at: http://osiris.com/pdf/2010-05-04%20T1D%20Orphan%20Drug%20Designation.pdf. Accessed June 30, 2010.
- FDA approves Merck’s new lung drug Dulera. The Economic Times website. Available at: http://economictimes.indiatimes.com/articleshow/6087079.cms. Accessed June 30, 2010.
- Dane L. FDA approves AstraZeneca, Pozen’s Vimovo. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=0C2915EE4D2D47D287D41D90DFE4240D. Accessed June 30, 2010.
- ACTOplus met XR available for diabetes. Monthly Prescribing Reference website. Available at: http://www.empr.com/actoplus-met-xr-available-for-diabetes/article/172985/. Accessed June 30, 2010.
- Dennis M. Roche’s Lucentis garners expanded FDA approval for macular oedema. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=5146664F5A4C48108209D15EA744A614&logRowId=370643. Accessed June 30, 2010.
- Rybix ODT launched for moderate to moderately severe pain. Monthly Prescribing Reference website. Available at: http://www.empr.com/rybix-odt-launched-for-moderate-to-moderately-severe-pain/article/172743/. Accessed June 30, 3010.
- Dennis M. Sanofi-Aventis begins late-stage study of Multaq in patients with permanent AF. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=E43104A2DB604649A812E69C58F89304&logRowId=364228. Accessed July 7, 2010.
- FDA accepts NDA for Duexa for ulcer risk reduction in arthritis patients. Monthly Prescribing Reference website. Available at: http://www.empr.com/fda-accepts-nda-for-duexa-for-ulcer-risk-reduction-in-arthritis-patients/article/171054/. Accessed July 7, 2010.
- Salix Pharmaceuticals announces NDA submission for Xifaxan550 for treatment of non-constipation irritable bowel syndrome. Salix Pharmaceuticals website. Available at: http://salix.com/news/stories/20100608.aspx. Accessed June 9, 2010.
- AstraZeneca and Targacept initiate Phase 3 clinical development of TC-5214 as an adjunct treatment for major depressive disorder. Targacept website. Available at: http://www.targacept.com/wt/page/pr_1277240993. Accessed June 29, 2010.
- Clinical Data, Inc. announces FDA acceptance of new drug application for Vilazodone for the treatment of major depressive disorder. Clinical Data Inc. website. Available at: http://clda.com/uploads/CLDA%20NDA%20acceptance%20FINAL.pdf. Accessed July 7, 2010.
- Ultram (tramadol hydrochloride), Ultracet (tramadol hydrochloride/acetaminophen): Label change. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm213264.htm. Accessed July 8, 2010.
- FDA Drug Safety Communication: New boxed warning on severe liver injury with propylthiouracil. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm209023.htm. Accessed July 8, 2010.
Market Watch
New Generics
- Anastrazole tablets (generic Arimidex)1
- Azelastine hydrochloride ophthalmic solution 0.05% (generic Optivar)2
- Aztreonam for injection in single-dose vials of 1 g/20 mL and 2 g/30 mL (generic Azactam)3
- Bupropion hydrochloride extended-release 150-mg tablets (generic Zyban)4
- Meropenem injection, USP, IV, 500-mg and 1-g vials (generic Merrem IV)5
- Levetiracetam injection in 100 mg/1 mL and 500 mg/5 mL single-use vials (generic Keppra injection)6
- Tacrolimus 5-mg capsules (generic Prograf)7
- Trandolapril/verapamil tablets (generic Tarka)8
- Valacyclovir hydrochloride tablets, USP (generic Valtrex)9
- Venlafaxine extended-release capsules (generic Effexor XR)10
New Drugs, Indications, Approval Recommendations
- The Alair Bronchial Thermoplasty System is the first device to be FDA-approved for treating severe and persistent asthma.11 It is to be used by adults who are still symptomatic despite treatment with high-dose inhaled corticosteroids (ICS) and long-acting beta-agonists (LABAs). Radiofrequency signals are converted into heat that warms the lining of targeted airways via bronchoscope. There are a number of contraindications and warnings for this device. Treatment is delivered using a standard bronchoscope under moderate sedation.
- Buprenorphine Transdermal System (Butrans) is FDA-approved to treat moderate to severe chronic pain in patients requiring continuous, around-the-clock opioid analgesia for an extended period of time.12 It is a Schedule III controlled substance and will be available in early 2011 in 5 mcg/hour, 10 mcg/hour, and 20 mcg/hour dosage strengths. Patches continuously release the drug over seven days.
- Denosumab injection (Prolia) has been approved by the FDA for treating postmenopausal women with osteoporosis at high risk for fractures.13
- Fingolimod (FTY720), an oral sphingosine 1-phosphate receptor (S1PR) modulator and disease-modifying treatment for relapsing-remitting multiple sclerosis (RRMS), has received a positive review by an FDA Advisory Committee.14 The committee voted 25-0, stating that in clinical trials to date that FTY720 has demonstrated substantial evidence of effectiveness in patients with RRMS, reducing the frequency of clinical exacerbations. This agent works by retaining lymphocytes in the lymph nodes, preventing them from entering the central nervous system to cause damage. This lymphocyte retention is reversible, allowing circulating lymphocytes to regain normal levels if treatment is stopped.
- Ketorolac tromethamine intranasal (Sprix) is FDA-approved for treating acute moderate to moderately severe pain requiring opioid-level analgesia for up to five days.15 Even though it is administered intranasally, gastrointestinal hemorrhage, bleeding, and cardiovascular risks are included in the labeling as adverse events.
- HCV Rapid Antibody Test (OraQuick) has been approved by the FDA for use in patients 15 and older to identify hepatitis C virus (HCV) antibodies.16 Available as a test strip, it identifies HCV antibodies within 20 minutes, which allows patients to more quickly present for evaluation and treatment.
- Lopinavir/ritonavir (Kaletra) has been approved by the FDA for once-daily dosing for treatment-experienced HIV patients.17 The agent had been approved for once-daily treatment for therapy-naive patients.
Pipeline
- HPV vaccine (Gardasil) is being evaluated by the FDA in order to potentially expand its indication to include women 27 to 45 years old.18 A decision is expected by the end of the year.
- Roflumilast is a phosphodiesterase 4 (PDE4) enzyme inhibitor that targets underlying inflammation in COPD patients.19 The FDA has issued a complete response letter for Roflumilast, which was filed as a potential treatment to reduce COPD exacerbations associated with chronic bronchitis in patients at risk for exacerbations. No new clinical trials have been requested.
Product Discontinuation
- Estradiol vaginal tablets 10 mcg (Vagifem) will replace estradiol vaginal tablets 25 mcg to treat the symptoms of atrophic vaginitis due to menopause.20 Sales of the 25-mcg formulation were discontinued July 31.
Medication Safety
GlaxoSmithKline has received reports of dispensing errors related to rosiglitazone (Avandia), glimepiride (Amaryl), rosiglitazone/metformin (Avandamet), candesartan (Atacand), and warfarin (Coumadin). In some instances, the patient received the wrong medication (one severe case led to impaired mental status). Errors likely occurred due to illegible written prescriptions and/or incorrectly interpreted, labeled, and filled prescriptions. Some of these products have similar dosage strengths and also look alike, leading to the errors.21
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Teva gets FDA approval for generic cancer drug. Forbes.com website. Available at: http://www.forbes.com/feeds/ap/2010/06/28/business-health-care-us-teva-pharmaceutical-industries-fda_7726375.html. Accessed June 29, 2010.
- Sun Pharma bags FDA approval for generic Optivar. Pharmaceutical Business Review website. Available at: http://regulatoryaffairs.pharmaceutical-business-review.com/news/sun_pharma_bags_fda_approval_for_generic_optivar_100622/. Accessed June 25, 2010.
- APP Pharmaceuticals Inc receives FDA approval for generic Aztreonam for injection, USP. TradingMarkets.com website. Available at: http://www.tradingmarkets.com/news/stock-alert/appx_apcvz_app-pharmaceuticals-inc-receives-fda-approval-for-generic-aztreonam-for-injection-usp-995249.html. Accessed June 24, 2010.
- Mylan gets FDA approval for generic Zyban. Forbes.com website. Available at: http://www.forbes.com/feeds/prnewswire/2010/05/04/prnewswire201005040700PR_NEWS_USPR_____NE98210.html. Accessed June 25, 2010.
- Hospira receives FDA approval for Meropenem for injection, USP (I.V.) Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192733.php. Accessed June 24, 2010.
- Sun Pharma announces USFDA approval for generic Keppra injection. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192275.php. Accessed June 24, 2010.
- Watson’s generic Prograf 5 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1443895. Accessed July 7, 2010.
- Glenmark arm gets US FDA nod for Tarka generic; stk up. Money Control website. Available at: http://www.moneycontrol.com/news/buzzing-stocks/glenmark-gets-us-fda-nod-for-tarka-generic-stk-up_460856.html. Accessed June 25, 2010.
- Watson’s generic Valtrex 500 mg and 1000 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1430538&highlight=. Accessed June 25, 2010.
- Walsh S. FDA approves first generic Effexor extended release capsules to treat major depressive disorder. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217624.htm Accessed June 29, 2010.
- Waknine Y. FDA approves first non-drug treatment for severe, persistent asthma. Medscape website. Available at: www.medscape.com/viewarticle/720922. Accessed June 30, 2010.
- Butrans transdermal system approved for chronic pain. Monthly Prescribing Reference website. Available at: www.empr.com/butrans-transdermal-system-approved-for-chronic-pain/article/173803/. Accessed July 7, 2010.
- Amgen’s Prolia garners FDA approval. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=BDE45B4D9F3F4C4A9326074859FF661F&logRowId=366890. Accessed June 30, 2010.
- FDA advisory committee unanimously recommends approval of Novartis investigational treatment FTY720 to treat relapsing remitting MS. Novartis Pharmaceuticals Corporation website. Available at: www.pharma.us.novartis.com/newsroom/press-release.jsp?PRID=2284. Accessed June 29, 2010.
- Roxro announces FDA approval of Sprix. Sprix website. Available at: www.sprix.com/docs/SPRIX-approval-press-release.pdf. Accessed June 29, 2010.
- FDA approves rapid test for antibodies to hepatitis C virus. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217318. Accessed July 7, 2010.
- Abbott receives FDA approval for once-daily dosing of Kaletra (lopinavir/ritonavir) for treatment-experienced patients. Abbott website. Available at: www.abbott.com/global/url/pressRelease/en_US/60.5:5/Press_Release_0849.htm. Accessed June 30, 2010.
- Dane L. FDA extends review of Merck & Co.’s Gardasil for use in older women. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=2843FE3BFE2B44C5B463DBA787F213ED&logRowId=369474. Accessed July 7, 2010.
- Forest Laboratories and Nycomed receive complete response letter for Roflumilast. Forest Laboratories website. Available at: www.frx.com/news/PressRelease.aspx?ID=1428047. Accessed July 25, 2010.
- Vagifem 10 mcg to replace Vagifem 25 mcg formulation for atrophic vaginitis due to menopause. Novo Nordisk website. Available at: http://press.novonordisk-us.com/index.php?s=43&item=252. Accessed June 29, 2010.
- Dear Pharmacist Letter, June 2010. Important Drug Warnings: Medication Dispensing Errors; GlaxoSmithKline.
- New Jersey State Board of Pharmacy News, April 2010;24:2-3.
New Generics
- Anastrazole tablets (generic Arimidex)1
- Azelastine hydrochloride ophthalmic solution 0.05% (generic Optivar)2
- Aztreonam for injection in single-dose vials of 1 g/20 mL and 2 g/30 mL (generic Azactam)3
- Bupropion hydrochloride extended-release 150-mg tablets (generic Zyban)4
- Meropenem injection, USP, IV, 500-mg and 1-g vials (generic Merrem IV)5
- Levetiracetam injection in 100 mg/1 mL and 500 mg/5 mL single-use vials (generic Keppra injection)6
- Tacrolimus 5-mg capsules (generic Prograf)7
- Trandolapril/verapamil tablets (generic Tarka)8
- Valacyclovir hydrochloride tablets, USP (generic Valtrex)9
- Venlafaxine extended-release capsules (generic Effexor XR)10
New Drugs, Indications, Approval Recommendations
- The Alair Bronchial Thermoplasty System is the first device to be FDA-approved for treating severe and persistent asthma.11 It is to be used by adults who are still symptomatic despite treatment with high-dose inhaled corticosteroids (ICS) and long-acting beta-agonists (LABAs). Radiofrequency signals are converted into heat that warms the lining of targeted airways via bronchoscope. There are a number of contraindications and warnings for this device. Treatment is delivered using a standard bronchoscope under moderate sedation.
- Buprenorphine Transdermal System (Butrans) is FDA-approved to treat moderate to severe chronic pain in patients requiring continuous, around-the-clock opioid analgesia for an extended period of time.12 It is a Schedule III controlled substance and will be available in early 2011 in 5 mcg/hour, 10 mcg/hour, and 20 mcg/hour dosage strengths. Patches continuously release the drug over seven days.
- Denosumab injection (Prolia) has been approved by the FDA for treating postmenopausal women with osteoporosis at high risk for fractures.13
- Fingolimod (FTY720), an oral sphingosine 1-phosphate receptor (S1PR) modulator and disease-modifying treatment for relapsing-remitting multiple sclerosis (RRMS), has received a positive review by an FDA Advisory Committee.14 The committee voted 25-0, stating that in clinical trials to date that FTY720 has demonstrated substantial evidence of effectiveness in patients with RRMS, reducing the frequency of clinical exacerbations. This agent works by retaining lymphocytes in the lymph nodes, preventing them from entering the central nervous system to cause damage. This lymphocyte retention is reversible, allowing circulating lymphocytes to regain normal levels if treatment is stopped.
- Ketorolac tromethamine intranasal (Sprix) is FDA-approved for treating acute moderate to moderately severe pain requiring opioid-level analgesia for up to five days.15 Even though it is administered intranasally, gastrointestinal hemorrhage, bleeding, and cardiovascular risks are included in the labeling as adverse events.
- HCV Rapid Antibody Test (OraQuick) has been approved by the FDA for use in patients 15 and older to identify hepatitis C virus (HCV) antibodies.16 Available as a test strip, it identifies HCV antibodies within 20 minutes, which allows patients to more quickly present for evaluation and treatment.
- Lopinavir/ritonavir (Kaletra) has been approved by the FDA for once-daily dosing for treatment-experienced HIV patients.17 The agent had been approved for once-daily treatment for therapy-naive patients.
Pipeline
- HPV vaccine (Gardasil) is being evaluated by the FDA in order to potentially expand its indication to include women 27 to 45 years old.18 A decision is expected by the end of the year.
- Roflumilast is a phosphodiesterase 4 (PDE4) enzyme inhibitor that targets underlying inflammation in COPD patients.19 The FDA has issued a complete response letter for Roflumilast, which was filed as a potential treatment to reduce COPD exacerbations associated with chronic bronchitis in patients at risk for exacerbations. No new clinical trials have been requested.
Product Discontinuation
- Estradiol vaginal tablets 10 mcg (Vagifem) will replace estradiol vaginal tablets 25 mcg to treat the symptoms of atrophic vaginitis due to menopause.20 Sales of the 25-mcg formulation were discontinued July 31.
Medication Safety
GlaxoSmithKline has received reports of dispensing errors related to rosiglitazone (Avandia), glimepiride (Amaryl), rosiglitazone/metformin (Avandamet), candesartan (Atacand), and warfarin (Coumadin). In some instances, the patient received the wrong medication (one severe case led to impaired mental status). Errors likely occurred due to illegible written prescriptions and/or incorrectly interpreted, labeled, and filled prescriptions. Some of these products have similar dosage strengths and also look alike, leading to the errors.21
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Teva gets FDA approval for generic cancer drug. Forbes.com website. Available at: http://www.forbes.com/feeds/ap/2010/06/28/business-health-care-us-teva-pharmaceutical-industries-fda_7726375.html. Accessed June 29, 2010.
- Sun Pharma bags FDA approval for generic Optivar. Pharmaceutical Business Review website. Available at: http://regulatoryaffairs.pharmaceutical-business-review.com/news/sun_pharma_bags_fda_approval_for_generic_optivar_100622/. Accessed June 25, 2010.
- APP Pharmaceuticals Inc receives FDA approval for generic Aztreonam for injection, USP. TradingMarkets.com website. Available at: http://www.tradingmarkets.com/news/stock-alert/appx_apcvz_app-pharmaceuticals-inc-receives-fda-approval-for-generic-aztreonam-for-injection-usp-995249.html. Accessed June 24, 2010.
- Mylan gets FDA approval for generic Zyban. Forbes.com website. Available at: http://www.forbes.com/feeds/prnewswire/2010/05/04/prnewswire201005040700PR_NEWS_USPR_____NE98210.html. Accessed June 25, 2010.
- Hospira receives FDA approval for Meropenem for injection, USP (I.V.) Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192733.php. Accessed June 24, 2010.
- Sun Pharma announces USFDA approval for generic Keppra injection. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192275.php. Accessed June 24, 2010.
- Watson’s generic Prograf 5 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1443895. Accessed July 7, 2010.
- Glenmark arm gets US FDA nod for Tarka generic; stk up. Money Control website. Available at: http://www.moneycontrol.com/news/buzzing-stocks/glenmark-gets-us-fda-nod-for-tarka-generic-stk-up_460856.html. Accessed June 25, 2010.
- Watson’s generic Valtrex 500 mg and 1000 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1430538&highlight=. Accessed June 25, 2010.
- Walsh S. FDA approves first generic Effexor extended release capsules to treat major depressive disorder. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217624.htm Accessed June 29, 2010.
- Waknine Y. FDA approves first non-drug treatment for severe, persistent asthma. Medscape website. Available at: www.medscape.com/viewarticle/720922. Accessed June 30, 2010.
- Butrans transdermal system approved for chronic pain. Monthly Prescribing Reference website. Available at: www.empr.com/butrans-transdermal-system-approved-for-chronic-pain/article/173803/. Accessed July 7, 2010.
- Amgen’s Prolia garners FDA approval. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=BDE45B4D9F3F4C4A9326074859FF661F&logRowId=366890. Accessed June 30, 2010.
- FDA advisory committee unanimously recommends approval of Novartis investigational treatment FTY720 to treat relapsing remitting MS. Novartis Pharmaceuticals Corporation website. Available at: www.pharma.us.novartis.com/newsroom/press-release.jsp?PRID=2284. Accessed June 29, 2010.
- Roxro announces FDA approval of Sprix. Sprix website. Available at: www.sprix.com/docs/SPRIX-approval-press-release.pdf. Accessed June 29, 2010.
- FDA approves rapid test for antibodies to hepatitis C virus. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217318. Accessed July 7, 2010.
- Abbott receives FDA approval for once-daily dosing of Kaletra (lopinavir/ritonavir) for treatment-experienced patients. Abbott website. Available at: www.abbott.com/global/url/pressRelease/en_US/60.5:5/Press_Release_0849.htm. Accessed June 30, 2010.
- Dane L. FDA extends review of Merck & Co.’s Gardasil for use in older women. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=2843FE3BFE2B44C5B463DBA787F213ED&logRowId=369474. Accessed July 7, 2010.
- Forest Laboratories and Nycomed receive complete response letter for Roflumilast. Forest Laboratories website. Available at: www.frx.com/news/PressRelease.aspx?ID=1428047. Accessed July 25, 2010.
- Vagifem 10 mcg to replace Vagifem 25 mcg formulation for atrophic vaginitis due to menopause. Novo Nordisk website. Available at: http://press.novonordisk-us.com/index.php?s=43&item=252. Accessed June 29, 2010.
- Dear Pharmacist Letter, June 2010. Important Drug Warnings: Medication Dispensing Errors; GlaxoSmithKline.
- New Jersey State Board of Pharmacy News, April 2010;24:2-3.
New Generics
- Anastrazole tablets (generic Arimidex)1
- Azelastine hydrochloride ophthalmic solution 0.05% (generic Optivar)2
- Aztreonam for injection in single-dose vials of 1 g/20 mL and 2 g/30 mL (generic Azactam)3
- Bupropion hydrochloride extended-release 150-mg tablets (generic Zyban)4
- Meropenem injection, USP, IV, 500-mg and 1-g vials (generic Merrem IV)5
- Levetiracetam injection in 100 mg/1 mL and 500 mg/5 mL single-use vials (generic Keppra injection)6
- Tacrolimus 5-mg capsules (generic Prograf)7
- Trandolapril/verapamil tablets (generic Tarka)8
- Valacyclovir hydrochloride tablets, USP (generic Valtrex)9
- Venlafaxine extended-release capsules (generic Effexor XR)10
New Drugs, Indications, Approval Recommendations
- The Alair Bronchial Thermoplasty System is the first device to be FDA-approved for treating severe and persistent asthma.11 It is to be used by adults who are still symptomatic despite treatment with high-dose inhaled corticosteroids (ICS) and long-acting beta-agonists (LABAs). Radiofrequency signals are converted into heat that warms the lining of targeted airways via bronchoscope. There are a number of contraindications and warnings for this device. Treatment is delivered using a standard bronchoscope under moderate sedation.
- Buprenorphine Transdermal System (Butrans) is FDA-approved to treat moderate to severe chronic pain in patients requiring continuous, around-the-clock opioid analgesia for an extended period of time.12 It is a Schedule III controlled substance and will be available in early 2011 in 5 mcg/hour, 10 mcg/hour, and 20 mcg/hour dosage strengths. Patches continuously release the drug over seven days.
- Denosumab injection (Prolia) has been approved by the FDA for treating postmenopausal women with osteoporosis at high risk for fractures.13
- Fingolimod (FTY720), an oral sphingosine 1-phosphate receptor (S1PR) modulator and disease-modifying treatment for relapsing-remitting multiple sclerosis (RRMS), has received a positive review by an FDA Advisory Committee.14 The committee voted 25-0, stating that in clinical trials to date that FTY720 has demonstrated substantial evidence of effectiveness in patients with RRMS, reducing the frequency of clinical exacerbations. This agent works by retaining lymphocytes in the lymph nodes, preventing them from entering the central nervous system to cause damage. This lymphocyte retention is reversible, allowing circulating lymphocytes to regain normal levels if treatment is stopped.
- Ketorolac tromethamine intranasal (Sprix) is FDA-approved for treating acute moderate to moderately severe pain requiring opioid-level analgesia for up to five days.15 Even though it is administered intranasally, gastrointestinal hemorrhage, bleeding, and cardiovascular risks are included in the labeling as adverse events.
- HCV Rapid Antibody Test (OraQuick) has been approved by the FDA for use in patients 15 and older to identify hepatitis C virus (HCV) antibodies.16 Available as a test strip, it identifies HCV antibodies within 20 minutes, which allows patients to more quickly present for evaluation and treatment.
- Lopinavir/ritonavir (Kaletra) has been approved by the FDA for once-daily dosing for treatment-experienced HIV patients.17 The agent had been approved for once-daily treatment for therapy-naive patients.
Pipeline
- HPV vaccine (Gardasil) is being evaluated by the FDA in order to potentially expand its indication to include women 27 to 45 years old.18 A decision is expected by the end of the year.
- Roflumilast is a phosphodiesterase 4 (PDE4) enzyme inhibitor that targets underlying inflammation in COPD patients.19 The FDA has issued a complete response letter for Roflumilast, which was filed as a potential treatment to reduce COPD exacerbations associated with chronic bronchitis in patients at risk for exacerbations. No new clinical trials have been requested.
Product Discontinuation
- Estradiol vaginal tablets 10 mcg (Vagifem) will replace estradiol vaginal tablets 25 mcg to treat the symptoms of atrophic vaginitis due to menopause.20 Sales of the 25-mcg formulation were discontinued July 31.
Medication Safety
GlaxoSmithKline has received reports of dispensing errors related to rosiglitazone (Avandia), glimepiride (Amaryl), rosiglitazone/metformin (Avandamet), candesartan (Atacand), and warfarin (Coumadin). In some instances, the patient received the wrong medication (one severe case led to impaired mental status). Errors likely occurred due to illegible written prescriptions and/or incorrectly interpreted, labeled, and filled prescriptions. Some of these products have similar dosage strengths and also look alike, leading to the errors.21
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Teva gets FDA approval for generic cancer drug. Forbes.com website. Available at: http://www.forbes.com/feeds/ap/2010/06/28/business-health-care-us-teva-pharmaceutical-industries-fda_7726375.html. Accessed June 29, 2010.
- Sun Pharma bags FDA approval for generic Optivar. Pharmaceutical Business Review website. Available at: http://regulatoryaffairs.pharmaceutical-business-review.com/news/sun_pharma_bags_fda_approval_for_generic_optivar_100622/. Accessed June 25, 2010.
- APP Pharmaceuticals Inc receives FDA approval for generic Aztreonam for injection, USP. TradingMarkets.com website. Available at: http://www.tradingmarkets.com/news/stock-alert/appx_apcvz_app-pharmaceuticals-inc-receives-fda-approval-for-generic-aztreonam-for-injection-usp-995249.html. Accessed June 24, 2010.
- Mylan gets FDA approval for generic Zyban. Forbes.com website. Available at: http://www.forbes.com/feeds/prnewswire/2010/05/04/prnewswire201005040700PR_NEWS_USPR_____NE98210.html. Accessed June 25, 2010.
- Hospira receives FDA approval for Meropenem for injection, USP (I.V.) Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192733.php. Accessed June 24, 2010.
- Sun Pharma announces USFDA approval for generic Keppra injection. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/192275.php. Accessed June 24, 2010.
- Watson’s generic Prograf 5 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1443895. Accessed July 7, 2010.
- Glenmark arm gets US FDA nod for Tarka generic; stk up. Money Control website. Available at: http://www.moneycontrol.com/news/buzzing-stocks/glenmark-gets-us-fda-nod-for-tarka-generic-stk-up_460856.html. Accessed June 25, 2010.
- Watson’s generic Valtrex 500 mg and 1000 mg receives FDA approval. Watson website. Available at: http://ir.watson.com/phoenix.zhtml?c=65778&p=irol-newsArticle&ID=1430538&highlight=. Accessed June 25, 2010.
- Walsh S. FDA approves first generic Effexor extended release capsules to treat major depressive disorder. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217624.htm Accessed June 29, 2010.
- Waknine Y. FDA approves first non-drug treatment for severe, persistent asthma. Medscape website. Available at: www.medscape.com/viewarticle/720922. Accessed June 30, 2010.
- Butrans transdermal system approved for chronic pain. Monthly Prescribing Reference website. Available at: www.empr.com/butrans-transdermal-system-approved-for-chronic-pain/article/173803/. Accessed July 7, 2010.
- Amgen’s Prolia garners FDA approval. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=BDE45B4D9F3F4C4A9326074859FF661F&logRowId=366890. Accessed June 30, 2010.
- FDA advisory committee unanimously recommends approval of Novartis investigational treatment FTY720 to treat relapsing remitting MS. Novartis Pharmaceuticals Corporation website. Available at: www.pharma.us.novartis.com/newsroom/press-release.jsp?PRID=2284. Accessed June 29, 2010.
- Roxro announces FDA approval of Sprix. Sprix website. Available at: www.sprix.com/docs/SPRIX-approval-press-release.pdf. Accessed June 29, 2010.
- FDA approves rapid test for antibodies to hepatitis C virus. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm217318. Accessed July 7, 2010.
- Abbott receives FDA approval for once-daily dosing of Kaletra (lopinavir/ritonavir) for treatment-experienced patients. Abbott website. Available at: www.abbott.com/global/url/pressRelease/en_US/60.5:5/Press_Release_0849.htm. Accessed June 30, 2010.
- Dane L. FDA extends review of Merck & Co.’s Gardasil for use in older women. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=2843FE3BFE2B44C5B463DBA787F213ED&logRowId=369474. Accessed July 7, 2010.
- Forest Laboratories and Nycomed receive complete response letter for Roflumilast. Forest Laboratories website. Available at: www.frx.com/news/PressRelease.aspx?ID=1428047. Accessed July 25, 2010.
- Vagifem 10 mcg to replace Vagifem 25 mcg formulation for atrophic vaginitis due to menopause. Novo Nordisk website. Available at: http://press.novonordisk-us.com/index.php?s=43&item=252. Accessed June 29, 2010.
- Dear Pharmacist Letter, June 2010. Important Drug Warnings: Medication Dispensing Errors; GlaxoSmithKline.
- New Jersey State Board of Pharmacy News, April 2010;24:2-3.
Market Watch
New Drugs, Indications, Dosage Forms, and Approvals
- Hydromorphone extended-release tablets (Exalgo) have been approved by the FDA as a once-daily treatment for managing moderate to severe pain in opioid-tolerant patients needing continuous opioid analgesia for an extended period of time.1 This formulation uses the OROS osmotic delivery system to control the release rate. It is a CII controlled substance and is accompanied by a comprehensive Risk Evaluation and Mitigation Strategy (REMS) to ensure that the medication’s benefits outweigh its risks.
- IMGN910 has received orphan drug status for treating Merkel cell carcinoma, a skin cancer that usually occurs on the head or neck.2 It is in early-stage clinical trials.
- Immune globulin subcutaneous (human) 20% liquid (Hizentra) has been approved by the FDA as a once-weekly immunoglobulin replacement therapy for patients with primary immunodeficiency.3 It’s the first 20% subcutaneous immunoglobulin to receive FDA approval. This high-concentration product is stabilized with L-proline, a naturally occurring amino acid, which allows it to be stored at room temperature (up to 25°C [77°F]). Some adverse reactions include injection site bruising, pain, cysts, eczema, irritation, headache, cough, diarrhea, and fatigue.4
- Velaglucerase alfa for injection (VPRIV) has been approved by the FDA to treat adults and children with the rare genetic disorder Gaucher disease.5 Patients with Gaucher disease have a deficiency of the glucocerebrosidase enzyme. This enzyme prevents lipids from building up in the liver, spleen, bone marrow, and nervous system, which prevents them from working properly. VPRIV, a long-term replacement therapy, is approved for Type 1 Gaucher disease, the most common form, and is an alternative to imiglucerase (Cerezyme), which is in short supply. The most common reactions seen in clinical trials were allergic reactions, headache, dizziness, abdominal and back pain, nausea, fatigue/weakness, fever, and prolonged activated partial thromboplastin time.
Pipeline
- Betrixaban is a once-daily oral anticoagulant in Phase 2 clinical studies.6 Compared with warfarin in the EXPLORE-Xa study, betrixaban decreased the bleeding incidence in patients with nonvalvular atrial fibrillation or atrial flutter who had at least one stroke risk factor. The major and clinically relevant nonmajor bleeding episodes occurred less frequently in betrixaban-treated patients.
- Dabigatran etexilate is an oral anticoagulant in Phase 3 clinical trials.7 At the recent American College of Cardiology meeting in Ingelheim, Germany, dabigatran demonstrated consistent stroke prevention in patients with atrial fibrillation. It also reduced the number of strokes in patients with atrial fibrillation, compared with warfarin therapy. Additionally, dabigatran etexilate 110 mg and 150 mg twice daily was associated with a lower rate of major bleeding compared with warfarin in atrial fibrillation patients at low risk of stroke.
- Fentanyl sublingual spray (SL Spray) is in Phase 3 clinical trials to treat breakthrough pain in cancer patients. Sublingual administration of this product showed rapid, effective pain relief within five minutes.8
- Ketamine intranasal (Ereska) is a nonopioid NMDA receptor antagonist analgesic, which is undergoing Phase 3 clinical trials for managing moderate to severe acute pain.9 Studies have shown rapid, statistically significant relief of moderate to severe acute postoperative pain following dental surgery, following a variety of major orthopedic surgical procedures, and in cancer breakthrough pain.
- Lu AA21004 and Lu AA24530 are undergoing Phase 3 clinical trials for treating major depressive disorder (MDD).10 Lu AA21004 is a 5-HT3, 5-HT7 and 5-HT1B receptor antagonist, 5HT1A receptor agonist, and 5-HT transporter inhibitor. To date, it has shown a low propensity for drug-drug interactions and is extensively metabolized in the liver. Lu AA24530 has shown activity as a multimodal enhancer with reuptake inhibition at monoamine transporters, and having 5-HT3 and 5-HT2c receptor antagonist activity.
- Lurasidone is an atypical antipsychotic with high affinity and antagonist effects at the dopamine D2, serotonin 5-HT2, and serotonin 5-HT7 receptors.11 It is a partial agonist at serotonin 5HT1A receptor. The NDA was filed for this agent Dec. 30, 2009.
- Mipomersen, an apo-B synthesis inhibitor, is in Phase 3 clinical trials for treating patients with homozygous familial hypercholesterolemia (HoFM).12 This agent is proposed to reduce LDL-C by preventing the development of atherogenic lipids. In a study published in Lancet, mipomersen reduced LDL-C levels by an average of more than 100 mg/dL in HoFM patients.13
- Oxycodone/niacin (Acurox), an abuse deterrent formulation for this popular opioid, has been rejected by the FDA.14 According to the FDA and its review committee, the rejection was due to the “flushing” from the niacin, which was deemed ineffective as an abuse deterrent. In addition, the FDA said the “flushing” could be overcome by food intake or administration with over-the-counter pain relievers.
- Vilanterol/fluticasone is a combination of the inhaled corticosteroid fluticasone and the long-acting beta-agonist (LABA) vilanterol.15 It is in Phase 3 clinical trials for treating asthma. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- FDA approves Exaglo (hydromorphone HCl) extended-release tablets. Drugs.com website. Available at: www.drugs.com/newdrugs/fda-approves-exaglo-hydromorphone-hcl-extended-release-2033.html?printable=1. Accessed April 27, 2010.
- ImmunoGen’s skin cancer drug gets orphan drug status. Reuters website. Available at: www.reuters.com/article/idUSSGE6270L720100308. Accessed April 27, 2010.
- CSL Behring receives FDA approval of Hizentra, first 20 percent subcutaneous immunoglobulin therapy. Drugs.com website. Available at: www.drugs.com/newdrugs/csl-behring-receives-fda-approval-hizentra-first-20-percent-subcutaneous-immunoglobulin-therapy-2037.html. Accessed April 27, 2010.
- Petrochko C. FDA okays 20% skin-injection immunodeficiency treatment. MedPage Today website. Available at: www.medpagetoday.com/tbprint.cfm?tbid=18858. Accessed April 27, 2010.
- Gansz Bobo E. FDA approves therapy to treat Gaucher disease. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm202288.htm. Accessed April 27, 2010.
- Portola Pharmaceuticals and Merck announce that Phase 2 study showed investigational factor Xa inhibitor, betrixaban, reduced incidence of bleeding compared to warfarin in patients with atrial fibrillation. Merck website. Available at: www.merck.com/newsroom/news-release-archive/research-and-development/2010_0315.html. Accessed April 27, 2010.
- Dabigatran etexilate shows greater reductions than warfarin in stroke in patients with atrial fibrillation across all stroke risk groups. Beohringer Ingelheim website. Available at: www.boehringer-ingelheim.com/news/news_releases/press_releases/2010/15_march_2010.html. Accessed April 27, 2010.
- INSYS Therapeutics, Inc. Announces Positive Phase III Efficacy Trial Results for Fentanyl Sublingual Spray. INSYS Therapeutics website. Available at: www.insysrx.com/news.htm. Accessed April 27, 2010.
- Third party reexamination of Javelin Pharmaceuticals’ Phase III trial data for Ereska (intranasal ketamine) yields statistically significant primary endpoint. Javelin website. Available at: ir.javelinpharmaceuticals.com/releasedetail.cfm?ReleaseID=444353. Accessed April 27, 2010.
- Lundbeck and Takeda finalise plans to initiate phase III pivotal clinical trials with Lu AA21004 and Lu AA24530. Takeda Pharmaceutical Company Limited website. Available at: www.takeda.com/press/article_35859.html. Accessed April 27, 2010.
- Dainippon Sumitomo Pharma America announces FDA acceptance of lurasidone new drug application for treatment of schizophrenia. PR Newswire website. Available at: www.prnewswire.com/news-releases/dainippon-sumitomo-pharma-america-announces-fda-acceptance-of-lurasidone-new-drug-application-for-treatment-of-schizophrenia-87265597.html. Accessed April 27, 2010.
- Mipomersen Phase 3 study in HoFH featured in The Lancet. Business Wire website. Available at: www.businesswire.com/portal/site/home/email/alert/?ndmViewId=news_view&newsLang=en&newsId=20100315005928. Accessed April 27, 2010.
- Raal FJ, Santos RD, Blom DJ, et al. Mipomersen, an apolipoprotein B synthesis inhibitor, for lowering of LDL cholesterol concentrations in patients with homozygous familial hypercholesterolaemia: a randomised, double-blind, placebo-controlled trial. Lancet. 2010;375(9719):998-1006.
- US FDA panel rejects King, Acura painkiller. Reuters website. Available at: www.reuters.com/assets/print?aid=USN2223552220100422. Accessed April 27, 2010.
- Dennis M. GlaxoSmithKline begins late-stage clinical programme for asthma drug Relovair. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=E256469FBD8F4A2F80C5DD3E844CC1E1&logRowId=356423. Accessed April 27, 2010.
New Drugs, Indications, Dosage Forms, and Approvals
- Hydromorphone extended-release tablets (Exalgo) have been approved by the FDA as a once-daily treatment for managing moderate to severe pain in opioid-tolerant patients needing continuous opioid analgesia for an extended period of time.1 This formulation uses the OROS osmotic delivery system to control the release rate. It is a CII controlled substance and is accompanied by a comprehensive Risk Evaluation and Mitigation Strategy (REMS) to ensure that the medication’s benefits outweigh its risks.
- IMGN910 has received orphan drug status for treating Merkel cell carcinoma, a skin cancer that usually occurs on the head or neck.2 It is in early-stage clinical trials.
- Immune globulin subcutaneous (human) 20% liquid (Hizentra) has been approved by the FDA as a once-weekly immunoglobulin replacement therapy for patients with primary immunodeficiency.3 It’s the first 20% subcutaneous immunoglobulin to receive FDA approval. This high-concentration product is stabilized with L-proline, a naturally occurring amino acid, which allows it to be stored at room temperature (up to 25°C [77°F]). Some adverse reactions include injection site bruising, pain, cysts, eczema, irritation, headache, cough, diarrhea, and fatigue.4
- Velaglucerase alfa for injection (VPRIV) has been approved by the FDA to treat adults and children with the rare genetic disorder Gaucher disease.5 Patients with Gaucher disease have a deficiency of the glucocerebrosidase enzyme. This enzyme prevents lipids from building up in the liver, spleen, bone marrow, and nervous system, which prevents them from working properly. VPRIV, a long-term replacement therapy, is approved for Type 1 Gaucher disease, the most common form, and is an alternative to imiglucerase (Cerezyme), which is in short supply. The most common reactions seen in clinical trials were allergic reactions, headache, dizziness, abdominal and back pain, nausea, fatigue/weakness, fever, and prolonged activated partial thromboplastin time.
Pipeline
- Betrixaban is a once-daily oral anticoagulant in Phase 2 clinical studies.6 Compared with warfarin in the EXPLORE-Xa study, betrixaban decreased the bleeding incidence in patients with nonvalvular atrial fibrillation or atrial flutter who had at least one stroke risk factor. The major and clinically relevant nonmajor bleeding episodes occurred less frequently in betrixaban-treated patients.
- Dabigatran etexilate is an oral anticoagulant in Phase 3 clinical trials.7 At the recent American College of Cardiology meeting in Ingelheim, Germany, dabigatran demonstrated consistent stroke prevention in patients with atrial fibrillation. It also reduced the number of strokes in patients with atrial fibrillation, compared with warfarin therapy. Additionally, dabigatran etexilate 110 mg and 150 mg twice daily was associated with a lower rate of major bleeding compared with warfarin in atrial fibrillation patients at low risk of stroke.
- Fentanyl sublingual spray (SL Spray) is in Phase 3 clinical trials to treat breakthrough pain in cancer patients. Sublingual administration of this product showed rapid, effective pain relief within five minutes.8
- Ketamine intranasal (Ereska) is a nonopioid NMDA receptor antagonist analgesic, which is undergoing Phase 3 clinical trials for managing moderate to severe acute pain.9 Studies have shown rapid, statistically significant relief of moderate to severe acute postoperative pain following dental surgery, following a variety of major orthopedic surgical procedures, and in cancer breakthrough pain.
- Lu AA21004 and Lu AA24530 are undergoing Phase 3 clinical trials for treating major depressive disorder (MDD).10 Lu AA21004 is a 5-HT3, 5-HT7 and 5-HT1B receptor antagonist, 5HT1A receptor agonist, and 5-HT transporter inhibitor. To date, it has shown a low propensity for drug-drug interactions and is extensively metabolized in the liver. Lu AA24530 has shown activity as a multimodal enhancer with reuptake inhibition at monoamine transporters, and having 5-HT3 and 5-HT2c receptor antagonist activity.
- Lurasidone is an atypical antipsychotic with high affinity and antagonist effects at the dopamine D2, serotonin 5-HT2, and serotonin 5-HT7 receptors.11 It is a partial agonist at serotonin 5HT1A receptor. The NDA was filed for this agent Dec. 30, 2009.
- Mipomersen, an apo-B synthesis inhibitor, is in Phase 3 clinical trials for treating patients with homozygous familial hypercholesterolemia (HoFM).12 This agent is proposed to reduce LDL-C by preventing the development of atherogenic lipids. In a study published in Lancet, mipomersen reduced LDL-C levels by an average of more than 100 mg/dL in HoFM patients.13
- Oxycodone/niacin (Acurox), an abuse deterrent formulation for this popular opioid, has been rejected by the FDA.14 According to the FDA and its review committee, the rejection was due to the “flushing” from the niacin, which was deemed ineffective as an abuse deterrent. In addition, the FDA said the “flushing” could be overcome by food intake or administration with over-the-counter pain relievers.
- Vilanterol/fluticasone is a combination of the inhaled corticosteroid fluticasone and the long-acting beta-agonist (LABA) vilanterol.15 It is in Phase 3 clinical trials for treating asthma. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- FDA approves Exaglo (hydromorphone HCl) extended-release tablets. Drugs.com website. Available at: www.drugs.com/newdrugs/fda-approves-exaglo-hydromorphone-hcl-extended-release-2033.html?printable=1. Accessed April 27, 2010.
- ImmunoGen’s skin cancer drug gets orphan drug status. Reuters website. Available at: www.reuters.com/article/idUSSGE6270L720100308. Accessed April 27, 2010.
- CSL Behring receives FDA approval of Hizentra, first 20 percent subcutaneous immunoglobulin therapy. Drugs.com website. Available at: www.drugs.com/newdrugs/csl-behring-receives-fda-approval-hizentra-first-20-percent-subcutaneous-immunoglobulin-therapy-2037.html. Accessed April 27, 2010.
- Petrochko C. FDA okays 20% skin-injection immunodeficiency treatment. MedPage Today website. Available at: www.medpagetoday.com/tbprint.cfm?tbid=18858. Accessed April 27, 2010.
- Gansz Bobo E. FDA approves therapy to treat Gaucher disease. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm202288.htm. Accessed April 27, 2010.
- Portola Pharmaceuticals and Merck announce that Phase 2 study showed investigational factor Xa inhibitor, betrixaban, reduced incidence of bleeding compared to warfarin in patients with atrial fibrillation. Merck website. Available at: www.merck.com/newsroom/news-release-archive/research-and-development/2010_0315.html. Accessed April 27, 2010.
- Dabigatran etexilate shows greater reductions than warfarin in stroke in patients with atrial fibrillation across all stroke risk groups. Beohringer Ingelheim website. Available at: www.boehringer-ingelheim.com/news/news_releases/press_releases/2010/15_march_2010.html. Accessed April 27, 2010.
- INSYS Therapeutics, Inc. Announces Positive Phase III Efficacy Trial Results for Fentanyl Sublingual Spray. INSYS Therapeutics website. Available at: www.insysrx.com/news.htm. Accessed April 27, 2010.
- Third party reexamination of Javelin Pharmaceuticals’ Phase III trial data for Ereska (intranasal ketamine) yields statistically significant primary endpoint. Javelin website. Available at: ir.javelinpharmaceuticals.com/releasedetail.cfm?ReleaseID=444353. Accessed April 27, 2010.
- Lundbeck and Takeda finalise plans to initiate phase III pivotal clinical trials with Lu AA21004 and Lu AA24530. Takeda Pharmaceutical Company Limited website. Available at: www.takeda.com/press/article_35859.html. Accessed April 27, 2010.
- Dainippon Sumitomo Pharma America announces FDA acceptance of lurasidone new drug application for treatment of schizophrenia. PR Newswire website. Available at: www.prnewswire.com/news-releases/dainippon-sumitomo-pharma-america-announces-fda-acceptance-of-lurasidone-new-drug-application-for-treatment-of-schizophrenia-87265597.html. Accessed April 27, 2010.
- Mipomersen Phase 3 study in HoFH featured in The Lancet. Business Wire website. Available at: www.businesswire.com/portal/site/home/email/alert/?ndmViewId=news_view&newsLang=en&newsId=20100315005928. Accessed April 27, 2010.
- Raal FJ, Santos RD, Blom DJ, et al. Mipomersen, an apolipoprotein B synthesis inhibitor, for lowering of LDL cholesterol concentrations in patients with homozygous familial hypercholesterolaemia: a randomised, double-blind, placebo-controlled trial. Lancet. 2010;375(9719):998-1006.
- US FDA panel rejects King, Acura painkiller. Reuters website. Available at: www.reuters.com/assets/print?aid=USN2223552220100422. Accessed April 27, 2010.
- Dennis M. GlaxoSmithKline begins late-stage clinical programme for asthma drug Relovair. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=E256469FBD8F4A2F80C5DD3E844CC1E1&logRowId=356423. Accessed April 27, 2010.
New Drugs, Indications, Dosage Forms, and Approvals
- Hydromorphone extended-release tablets (Exalgo) have been approved by the FDA as a once-daily treatment for managing moderate to severe pain in opioid-tolerant patients needing continuous opioid analgesia for an extended period of time.1 This formulation uses the OROS osmotic delivery system to control the release rate. It is a CII controlled substance and is accompanied by a comprehensive Risk Evaluation and Mitigation Strategy (REMS) to ensure that the medication’s benefits outweigh its risks.
- IMGN910 has received orphan drug status for treating Merkel cell carcinoma, a skin cancer that usually occurs on the head or neck.2 It is in early-stage clinical trials.
- Immune globulin subcutaneous (human) 20% liquid (Hizentra) has been approved by the FDA as a once-weekly immunoglobulin replacement therapy for patients with primary immunodeficiency.3 It’s the first 20% subcutaneous immunoglobulin to receive FDA approval. This high-concentration product is stabilized with L-proline, a naturally occurring amino acid, which allows it to be stored at room temperature (up to 25°C [77°F]). Some adverse reactions include injection site bruising, pain, cysts, eczema, irritation, headache, cough, diarrhea, and fatigue.4
- Velaglucerase alfa for injection (VPRIV) has been approved by the FDA to treat adults and children with the rare genetic disorder Gaucher disease.5 Patients with Gaucher disease have a deficiency of the glucocerebrosidase enzyme. This enzyme prevents lipids from building up in the liver, spleen, bone marrow, and nervous system, which prevents them from working properly. VPRIV, a long-term replacement therapy, is approved for Type 1 Gaucher disease, the most common form, and is an alternative to imiglucerase (Cerezyme), which is in short supply. The most common reactions seen in clinical trials were allergic reactions, headache, dizziness, abdominal and back pain, nausea, fatigue/weakness, fever, and prolonged activated partial thromboplastin time.
Pipeline
- Betrixaban is a once-daily oral anticoagulant in Phase 2 clinical studies.6 Compared with warfarin in the EXPLORE-Xa study, betrixaban decreased the bleeding incidence in patients with nonvalvular atrial fibrillation or atrial flutter who had at least one stroke risk factor. The major and clinically relevant nonmajor bleeding episodes occurred less frequently in betrixaban-treated patients.
- Dabigatran etexilate is an oral anticoagulant in Phase 3 clinical trials.7 At the recent American College of Cardiology meeting in Ingelheim, Germany, dabigatran demonstrated consistent stroke prevention in patients with atrial fibrillation. It also reduced the number of strokes in patients with atrial fibrillation, compared with warfarin therapy. Additionally, dabigatran etexilate 110 mg and 150 mg twice daily was associated with a lower rate of major bleeding compared with warfarin in atrial fibrillation patients at low risk of stroke.
- Fentanyl sublingual spray (SL Spray) is in Phase 3 clinical trials to treat breakthrough pain in cancer patients. Sublingual administration of this product showed rapid, effective pain relief within five minutes.8
- Ketamine intranasal (Ereska) is a nonopioid NMDA receptor antagonist analgesic, which is undergoing Phase 3 clinical trials for managing moderate to severe acute pain.9 Studies have shown rapid, statistically significant relief of moderate to severe acute postoperative pain following dental surgery, following a variety of major orthopedic surgical procedures, and in cancer breakthrough pain.
- Lu AA21004 and Lu AA24530 are undergoing Phase 3 clinical trials for treating major depressive disorder (MDD).10 Lu AA21004 is a 5-HT3, 5-HT7 and 5-HT1B receptor antagonist, 5HT1A receptor agonist, and 5-HT transporter inhibitor. To date, it has shown a low propensity for drug-drug interactions and is extensively metabolized in the liver. Lu AA24530 has shown activity as a multimodal enhancer with reuptake inhibition at monoamine transporters, and having 5-HT3 and 5-HT2c receptor antagonist activity.
- Lurasidone is an atypical antipsychotic with high affinity and antagonist effects at the dopamine D2, serotonin 5-HT2, and serotonin 5-HT7 receptors.11 It is a partial agonist at serotonin 5HT1A receptor. The NDA was filed for this agent Dec. 30, 2009.
- Mipomersen, an apo-B synthesis inhibitor, is in Phase 3 clinical trials for treating patients with homozygous familial hypercholesterolemia (HoFM).12 This agent is proposed to reduce LDL-C by preventing the development of atherogenic lipids. In a study published in Lancet, mipomersen reduced LDL-C levels by an average of more than 100 mg/dL in HoFM patients.13
- Oxycodone/niacin (Acurox), an abuse deterrent formulation for this popular opioid, has been rejected by the FDA.14 According to the FDA and its review committee, the rejection was due to the “flushing” from the niacin, which was deemed ineffective as an abuse deterrent. In addition, the FDA said the “flushing” could be overcome by food intake or administration with over-the-counter pain relievers.
- Vilanterol/fluticasone is a combination of the inhaled corticosteroid fluticasone and the long-acting beta-agonist (LABA) vilanterol.15 It is in Phase 3 clinical trials for treating asthma. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- FDA approves Exaglo (hydromorphone HCl) extended-release tablets. Drugs.com website. Available at: www.drugs.com/newdrugs/fda-approves-exaglo-hydromorphone-hcl-extended-release-2033.html?printable=1. Accessed April 27, 2010.
- ImmunoGen’s skin cancer drug gets orphan drug status. Reuters website. Available at: www.reuters.com/article/idUSSGE6270L720100308. Accessed April 27, 2010.
- CSL Behring receives FDA approval of Hizentra, first 20 percent subcutaneous immunoglobulin therapy. Drugs.com website. Available at: www.drugs.com/newdrugs/csl-behring-receives-fda-approval-hizentra-first-20-percent-subcutaneous-immunoglobulin-therapy-2037.html. Accessed April 27, 2010.
- Petrochko C. FDA okays 20% skin-injection immunodeficiency treatment. MedPage Today website. Available at: www.medpagetoday.com/tbprint.cfm?tbid=18858. Accessed April 27, 2010.
- Gansz Bobo E. FDA approves therapy to treat Gaucher disease. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm202288.htm. Accessed April 27, 2010.
- Portola Pharmaceuticals and Merck announce that Phase 2 study showed investigational factor Xa inhibitor, betrixaban, reduced incidence of bleeding compared to warfarin in patients with atrial fibrillation. Merck website. Available at: www.merck.com/newsroom/news-release-archive/research-and-development/2010_0315.html. Accessed April 27, 2010.
- Dabigatran etexilate shows greater reductions than warfarin in stroke in patients with atrial fibrillation across all stroke risk groups. Beohringer Ingelheim website. Available at: www.boehringer-ingelheim.com/news/news_releases/press_releases/2010/15_march_2010.html. Accessed April 27, 2010.
- INSYS Therapeutics, Inc. Announces Positive Phase III Efficacy Trial Results for Fentanyl Sublingual Spray. INSYS Therapeutics website. Available at: www.insysrx.com/news.htm. Accessed April 27, 2010.
- Third party reexamination of Javelin Pharmaceuticals’ Phase III trial data for Ereska (intranasal ketamine) yields statistically significant primary endpoint. Javelin website. Available at: ir.javelinpharmaceuticals.com/releasedetail.cfm?ReleaseID=444353. Accessed April 27, 2010.
- Lundbeck and Takeda finalise plans to initiate phase III pivotal clinical trials with Lu AA21004 and Lu AA24530. Takeda Pharmaceutical Company Limited website. Available at: www.takeda.com/press/article_35859.html. Accessed April 27, 2010.
- Dainippon Sumitomo Pharma America announces FDA acceptance of lurasidone new drug application for treatment of schizophrenia. PR Newswire website. Available at: www.prnewswire.com/news-releases/dainippon-sumitomo-pharma-america-announces-fda-acceptance-of-lurasidone-new-drug-application-for-treatment-of-schizophrenia-87265597.html. Accessed April 27, 2010.
- Mipomersen Phase 3 study in HoFH featured in The Lancet. Business Wire website. Available at: www.businesswire.com/portal/site/home/email/alert/?ndmViewId=news_view&newsLang=en&newsId=20100315005928. Accessed April 27, 2010.
- Raal FJ, Santos RD, Blom DJ, et al. Mipomersen, an apolipoprotein B synthesis inhibitor, for lowering of LDL cholesterol concentrations in patients with homozygous familial hypercholesterolaemia: a randomised, double-blind, placebo-controlled trial. Lancet. 2010;375(9719):998-1006.
- US FDA panel rejects King, Acura painkiller. Reuters website. Available at: www.reuters.com/assets/print?aid=USN2223552220100422. Accessed April 27, 2010.
- Dennis M. GlaxoSmithKline begins late-stage clinical programme for asthma drug Relovair. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=E256469FBD8F4A2F80C5DD3E844CC1E1&logRowId=356423. Accessed April 27, 2010.
Market Watch
Pipeline Drugs
- Phentermine/topiramate (Qnexa) is an investigational drug for the treatment of obesity. This includes weight loss and weight-loss maintenance in patients who are obese or overweight with such comorbidities as hypertension, Type 2 diabetes, dyslipidemia, or central adiposity. A new drug application (NDA) was filed with the FDA for this agent late in 2009.1 Qnexa is a once-daily, oral, controlled-release formulation comprised of low-dose phentermine and topiramate, which works on both patient satiety and appetite. Clinical trials show the drug has led to significant weight loss, glycemic control, and improved cardiovascular risk factors. Common side effects in clinical trials were dry mouth, tingling, and constipation.
- Pirfenidone, a potential treatment for idiopathic pulmonary fibrosis (IPF), has been granted a priority review by the FDA.2 Idiopathic pulmonary fibrosis is a disabling and fatal disease characterized by lung inflammation and scarring. The median survival time from diagnosis is two to five years, with an approximate five-year survival rate of 20%. Patients usually are diagnosed between the ages of 20 and 70, with a median of 63 years. It affects slightly more men than women. There are no medications approved to treat this fatal disease. Pirfenidone has been shown to have both antifibrotic and anti-inflammatory properties. The most common side effects are photosensitivity rash and gastrointestinal symptoms.3 The FDA’s action date is expected to be May 4.
- FDA approval was requested for retigabine, a potential new adjunctive epilepsy treatment, on Dec. 30, 2009.4 Retigabine is a neuronal potassium channel opener for use in adults with partial-onset seizures. In Phase 3 clinical trials, common adverse effects (occurring in more than 5% of patients) were dizziness, fatigue, confused state, vertigo, tremor, abnormal coordination, diplopia, attention disturbance, asthenia, and visual blurring.
Safety Information
- Desipramine (Norpramin), a tricyclic antidepressant approved by the FDA for treating major depression in adults, has undergone a label change to reflect new safety information. The “Warnings” and “Overdosage” sections of the product label now include information stating that extreme caution needs to be used when desipramine is administered to patients with a family history of sudden death, cardiac dysrhythmias, and cardiac conduction disturbances. The information also states that seizures might precede cardiac dysrhythmias and death in some patients.5 In a related “Dear Healthcare Professional” letter, information related to this warning was included with regard to identifying patients who present with a desipramine overdose, managing gastrointestinal decontamination with activated charcoal, managing cardiovascular effects, and deletion of measuring plasma-concentration desipramine as a guide to patient monitoring.5
- Diclofenac gel (Voltaren gel), a topical NSAID indicated for the relief of osteoarthritis pain of joints amenable to topical treatment (e.g., knees and hands), has undergone a label change related to its hepatic effects section. The label has revised warnings and precautions about the potential for liver function test elevations while receiving treatment with all diclofenac-containing products.6 There have been post-marketing reports of drug-induced hepatotoxicity within the first month of treatment with this topical agent. However, this reaction can occur at any time during diclofenac treatment. Severe hepatic reactions have been reported, including liver necrosis, jaundice, fulminant hepatitis with and without jaundice, and liver failure. Some of these cases resulted in fatalities or liver transplantation. Oral diclofenac also is hepatotoxic; it’s one of the most hepatotoxic NSAIDs available. To monitor patients receiving topical diclofenac, you should, after obtaining baseline transaminases, periodically measure transaminases in patients receiving long-term therapy. The optimum times for measurement are unknown. Based on available data from clinical trials and other cases, transaminases should be monitored within four to eight weeks after initiating diclofenac treatment.
- Fosamprenavir (Lexiva) has undergone a label change in the “Warnings” and “Precautions” sections, which is related to a potential association between the agent and the occurrence of myocardial infarction and dyslipidemia in adults with HIV.7 The updated label notes that patient cholesterol levels might increase if treated with fosamprenavir, and that lipid monitoring prior to and after initiating the agent should occur.
- Valproate sodium, valproic acid, and divalproex sodium have been associated with an increased risk of neural tube defects and other major birth defects (e.g., craniofacial defects and cardiovascular malformations) in babies exposed to these agents during pregnancy.8 Healthcare providers need to inform women of childbearing potential about these risks and consider alternative therapies, especially if the use of valproate is considered to treat migraines or other conditions that are not considered life-threatening. Women who are not actively planning a pregnancy and require use of valproate for medical conditions should use contraception, as birth-defect risks are high during the first trimester of pregnancy. Pregnant women using valproate should be encouraged to enroll in the North American Antiepileptic Drug Pregnancy Registry (888-233-2334 or www.aedpregnancyregistry.org). A medication guide explaining the risk and benefits of such treatment is required to be distributed with each dispensed valproate prescription.9 TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- NDA submitted for Qnexa. Drugs.com Web site. Available at: http://www.drugs.com/nda/qnexa_091229.html. Accessed Jan. 7, 2010.
- Todoruk M. InterMune’s pulmonary drug pirfenidone granted priority review by FDA. FirstWord Web site. Available at: http://www.firstwordplus.com/Fws.do?articleid=5C01296C0574469B9A67F3574353FB1E&logRowId=343385. Accessed Jan. 7, 2010.
- FDA grants priority review of pirfenidone NDA for the treatment of patients with IPF. InterMune Web site. Available at: http://phx.corporate-ir.net/phoenix.zhtml?c=100067&p=irol-newsArticle&ID=1370133&highlight=. Accessed Jan. 7, 2010.
- FDA accepts NDA filing for retigabine. Drugs.com Web site. Available at: http://www.drugs.com/nda/retigabine_091230.html. Accessed Jan. 7, 2010.
- Norpramin (desipramine hydrochloride)—Dear Healthcare Professional letter. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm192655.htm. Accessed Jan. 7, 2010.
- Voltaren gel (diclofenac sodium topical gel) 1%—hepatic effects labeling changes. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm193047.htm. Accessed Jan. 7, 2009.
- Lexiva (fosamprenavir calcium)—Dear Healthcare Professional letter. Food and Drug Administration Web site. Available at http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm192699.htm. Accessed Jan. 7, 2010.
- FDA warns of birth defects with valproate sodium, valproic acid, and divalproex sodium. Monthly Prescribing Reference Web site. Available at: http://www.empr.com/fda-warns-of-birth-defects-with-valproate-sodium-valproic-acid-and-divalproex-sodium/article/159034/. Accessed Jan. 7, 2010.
- Valproate sodium and related products (valproic acid and divalproex sodium): risk of birth defects. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm192788.htm. Accessed Jan. 7, 2009.
Pipeline Drugs
- Phentermine/topiramate (Qnexa) is an investigational drug for the treatment of obesity. This includes weight loss and weight-loss maintenance in patients who are obese or overweight with such comorbidities as hypertension, Type 2 diabetes, dyslipidemia, or central adiposity. A new drug application (NDA) was filed with the FDA for this agent late in 2009.1 Qnexa is a once-daily, oral, controlled-release formulation comprised of low-dose phentermine and topiramate, which works on both patient satiety and appetite. Clinical trials show the drug has led to significant weight loss, glycemic control, and improved cardiovascular risk factors. Common side effects in clinical trials were dry mouth, tingling, and constipation.
- Pirfenidone, a potential treatment for idiopathic pulmonary fibrosis (IPF), has been granted a priority review by the FDA.2 Idiopathic pulmonary fibrosis is a disabling and fatal disease characterized by lung inflammation and scarring. The median survival time from diagnosis is two to five years, with an approximate five-year survival rate of 20%. Patients usually are diagnosed between the ages of 20 and 70, with a median of 63 years. It affects slightly more men than women. There are no medications approved to treat this fatal disease. Pirfenidone has been shown to have both antifibrotic and anti-inflammatory properties. The most common side effects are photosensitivity rash and gastrointestinal symptoms.3 The FDA’s action date is expected to be May 4.
- FDA approval was requested for retigabine, a potential new adjunctive epilepsy treatment, on Dec. 30, 2009.4 Retigabine is a neuronal potassium channel opener for use in adults with partial-onset seizures. In Phase 3 clinical trials, common adverse effects (occurring in more than 5% of patients) were dizziness, fatigue, confused state, vertigo, tremor, abnormal coordination, diplopia, attention disturbance, asthenia, and visual blurring.
Safety Information
- Desipramine (Norpramin), a tricyclic antidepressant approved by the FDA for treating major depression in adults, has undergone a label change to reflect new safety information. The “Warnings” and “Overdosage” sections of the product label now include information stating that extreme caution needs to be used when desipramine is administered to patients with a family history of sudden death, cardiac dysrhythmias, and cardiac conduction disturbances. The information also states that seizures might precede cardiac dysrhythmias and death in some patients.5 In a related “Dear Healthcare Professional” letter, information related to this warning was included with regard to identifying patients who present with a desipramine overdose, managing gastrointestinal decontamination with activated charcoal, managing cardiovascular effects, and deletion of measuring plasma-concentration desipramine as a guide to patient monitoring.5
- Diclofenac gel (Voltaren gel), a topical NSAID indicated for the relief of osteoarthritis pain of joints amenable to topical treatment (e.g., knees and hands), has undergone a label change related to its hepatic effects section. The label has revised warnings and precautions about the potential for liver function test elevations while receiving treatment with all diclofenac-containing products.6 There have been post-marketing reports of drug-induced hepatotoxicity within the first month of treatment with this topical agent. However, this reaction can occur at any time during diclofenac treatment. Severe hepatic reactions have been reported, including liver necrosis, jaundice, fulminant hepatitis with and without jaundice, and liver failure. Some of these cases resulted in fatalities or liver transplantation. Oral diclofenac also is hepatotoxic; it’s one of the most hepatotoxic NSAIDs available. To monitor patients receiving topical diclofenac, you should, after obtaining baseline transaminases, periodically measure transaminases in patients receiving long-term therapy. The optimum times for measurement are unknown. Based on available data from clinical trials and other cases, transaminases should be monitored within four to eight weeks after initiating diclofenac treatment.
- Fosamprenavir (Lexiva) has undergone a label change in the “Warnings” and “Precautions” sections, which is related to a potential association between the agent and the occurrence of myocardial infarction and dyslipidemia in adults with HIV.7 The updated label notes that patient cholesterol levels might increase if treated with fosamprenavir, and that lipid monitoring prior to and after initiating the agent should occur.
- Valproate sodium, valproic acid, and divalproex sodium have been associated with an increased risk of neural tube defects and other major birth defects (e.g., craniofacial defects and cardiovascular malformations) in babies exposed to these agents during pregnancy.8 Healthcare providers need to inform women of childbearing potential about these risks and consider alternative therapies, especially if the use of valproate is considered to treat migraines or other conditions that are not considered life-threatening. Women who are not actively planning a pregnancy and require use of valproate for medical conditions should use contraception, as birth-defect risks are high during the first trimester of pregnancy. Pregnant women using valproate should be encouraged to enroll in the North American Antiepileptic Drug Pregnancy Registry (888-233-2334 or www.aedpregnancyregistry.org). A medication guide explaining the risk and benefits of such treatment is required to be distributed with each dispensed valproate prescription.9 TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- NDA submitted for Qnexa. Drugs.com Web site. Available at: http://www.drugs.com/nda/qnexa_091229.html. Accessed Jan. 7, 2010.
- Todoruk M. InterMune’s pulmonary drug pirfenidone granted priority review by FDA. FirstWord Web site. Available at: http://www.firstwordplus.com/Fws.do?articleid=5C01296C0574469B9A67F3574353FB1E&logRowId=343385. Accessed Jan. 7, 2010.
- FDA grants priority review of pirfenidone NDA for the treatment of patients with IPF. InterMune Web site. Available at: http://phx.corporate-ir.net/phoenix.zhtml?c=100067&p=irol-newsArticle&ID=1370133&highlight=. Accessed Jan. 7, 2010.
- FDA accepts NDA filing for retigabine. Drugs.com Web site. Available at: http://www.drugs.com/nda/retigabine_091230.html. Accessed Jan. 7, 2010.
- Norpramin (desipramine hydrochloride)—Dear Healthcare Professional letter. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm192655.htm. Accessed Jan. 7, 2010.
- Voltaren gel (diclofenac sodium topical gel) 1%—hepatic effects labeling changes. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm193047.htm. Accessed Jan. 7, 2009.
- Lexiva (fosamprenavir calcium)—Dear Healthcare Professional letter. Food and Drug Administration Web site. Available at http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm192699.htm. Accessed Jan. 7, 2010.
- FDA warns of birth defects with valproate sodium, valproic acid, and divalproex sodium. Monthly Prescribing Reference Web site. Available at: http://www.empr.com/fda-warns-of-birth-defects-with-valproate-sodium-valproic-acid-and-divalproex-sodium/article/159034/. Accessed Jan. 7, 2010.
- Valproate sodium and related products (valproic acid and divalproex sodium): risk of birth defects. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm192788.htm. Accessed Jan. 7, 2009.
Pipeline Drugs
- Phentermine/topiramate (Qnexa) is an investigational drug for the treatment of obesity. This includes weight loss and weight-loss maintenance in patients who are obese or overweight with such comorbidities as hypertension, Type 2 diabetes, dyslipidemia, or central adiposity. A new drug application (NDA) was filed with the FDA for this agent late in 2009.1 Qnexa is a once-daily, oral, controlled-release formulation comprised of low-dose phentermine and topiramate, which works on both patient satiety and appetite. Clinical trials show the drug has led to significant weight loss, glycemic control, and improved cardiovascular risk factors. Common side effects in clinical trials were dry mouth, tingling, and constipation.
- Pirfenidone, a potential treatment for idiopathic pulmonary fibrosis (IPF), has been granted a priority review by the FDA.2 Idiopathic pulmonary fibrosis is a disabling and fatal disease characterized by lung inflammation and scarring. The median survival time from diagnosis is two to five years, with an approximate five-year survival rate of 20%. Patients usually are diagnosed between the ages of 20 and 70, with a median of 63 years. It affects slightly more men than women. There are no medications approved to treat this fatal disease. Pirfenidone has been shown to have both antifibrotic and anti-inflammatory properties. The most common side effects are photosensitivity rash and gastrointestinal symptoms.3 The FDA’s action date is expected to be May 4.
- FDA approval was requested for retigabine, a potential new adjunctive epilepsy treatment, on Dec. 30, 2009.4 Retigabine is a neuronal potassium channel opener for use in adults with partial-onset seizures. In Phase 3 clinical trials, common adverse effects (occurring in more than 5% of patients) were dizziness, fatigue, confused state, vertigo, tremor, abnormal coordination, diplopia, attention disturbance, asthenia, and visual blurring.
Safety Information
- Desipramine (Norpramin), a tricyclic antidepressant approved by the FDA for treating major depression in adults, has undergone a label change to reflect new safety information. The “Warnings” and “Overdosage” sections of the product label now include information stating that extreme caution needs to be used when desipramine is administered to patients with a family history of sudden death, cardiac dysrhythmias, and cardiac conduction disturbances. The information also states that seizures might precede cardiac dysrhythmias and death in some patients.5 In a related “Dear Healthcare Professional” letter, information related to this warning was included with regard to identifying patients who present with a desipramine overdose, managing gastrointestinal decontamination with activated charcoal, managing cardiovascular effects, and deletion of measuring plasma-concentration desipramine as a guide to patient monitoring.5
- Diclofenac gel (Voltaren gel), a topical NSAID indicated for the relief of osteoarthritis pain of joints amenable to topical treatment (e.g., knees and hands), has undergone a label change related to its hepatic effects section. The label has revised warnings and precautions about the potential for liver function test elevations while receiving treatment with all diclofenac-containing products.6 There have been post-marketing reports of drug-induced hepatotoxicity within the first month of treatment with this topical agent. However, this reaction can occur at any time during diclofenac treatment. Severe hepatic reactions have been reported, including liver necrosis, jaundice, fulminant hepatitis with and without jaundice, and liver failure. Some of these cases resulted in fatalities or liver transplantation. Oral diclofenac also is hepatotoxic; it’s one of the most hepatotoxic NSAIDs available. To monitor patients receiving topical diclofenac, you should, after obtaining baseline transaminases, periodically measure transaminases in patients receiving long-term therapy. The optimum times for measurement are unknown. Based on available data from clinical trials and other cases, transaminases should be monitored within four to eight weeks after initiating diclofenac treatment.
- Fosamprenavir (Lexiva) has undergone a label change in the “Warnings” and “Precautions” sections, which is related to a potential association between the agent and the occurrence of myocardial infarction and dyslipidemia in adults with HIV.7 The updated label notes that patient cholesterol levels might increase if treated with fosamprenavir, and that lipid monitoring prior to and after initiating the agent should occur.
- Valproate sodium, valproic acid, and divalproex sodium have been associated with an increased risk of neural tube defects and other major birth defects (e.g., craniofacial defects and cardiovascular malformations) in babies exposed to these agents during pregnancy.8 Healthcare providers need to inform women of childbearing potential about these risks and consider alternative therapies, especially if the use of valproate is considered to treat migraines or other conditions that are not considered life-threatening. Women who are not actively planning a pregnancy and require use of valproate for medical conditions should use contraception, as birth-defect risks are high during the first trimester of pregnancy. Pregnant women using valproate should be encouraged to enroll in the North American Antiepileptic Drug Pregnancy Registry (888-233-2334 or www.aedpregnancyregistry.org). A medication guide explaining the risk and benefits of such treatment is required to be distributed with each dispensed valproate prescription.9 TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- NDA submitted for Qnexa. Drugs.com Web site. Available at: http://www.drugs.com/nda/qnexa_091229.html. Accessed Jan. 7, 2010.
- Todoruk M. InterMune’s pulmonary drug pirfenidone granted priority review by FDA. FirstWord Web site. Available at: http://www.firstwordplus.com/Fws.do?articleid=5C01296C0574469B9A67F3574353FB1E&logRowId=343385. Accessed Jan. 7, 2010.
- FDA grants priority review of pirfenidone NDA for the treatment of patients with IPF. InterMune Web site. Available at: http://phx.corporate-ir.net/phoenix.zhtml?c=100067&p=irol-newsArticle&ID=1370133&highlight=. Accessed Jan. 7, 2010.
- FDA accepts NDA filing for retigabine. Drugs.com Web site. Available at: http://www.drugs.com/nda/retigabine_091230.html. Accessed Jan. 7, 2010.
- Norpramin (desipramine hydrochloride)—Dear Healthcare Professional letter. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm192655.htm. Accessed Jan. 7, 2010.
- Voltaren gel (diclofenac sodium topical gel) 1%—hepatic effects labeling changes. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm193047.htm. Accessed Jan. 7, 2009.
- Lexiva (fosamprenavir calcium)—Dear Healthcare Professional letter. Food and Drug Administration Web site. Available at http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm192699.htm. Accessed Jan. 7, 2010.
- FDA warns of birth defects with valproate sodium, valproic acid, and divalproex sodium. Monthly Prescribing Reference Web site. Available at: http://www.empr.com/fda-warns-of-birth-defects-with-valproate-sodium-valproic-acid-and-divalproex-sodium/article/159034/. Accessed Jan. 7, 2010.
- Valproate sodium and related products (valproic acid and divalproex sodium): risk of birth defects. Food and Drug Administration Web site. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm192788.htm. Accessed Jan. 7, 2009.
When Should an IVC Filter Be Used to Treat a DVT?
Case
A 67-year-old man with a history of hypertension presents with a swollen right lower extremity. An ultrasound reveals a DVT, and he is commenced on low-molecular-weight heparin and warfarin. Two days later, he develops slurred speech and right-sided weakness. A head CT reveals an intracranial hemorrhage. When should an inferior vena cava (IVC) filter be utilized for treatment of DVT?
Overview
It is estimated that 350,000 to 600,000 Americans develop a VTE each year.1 Patients with a DVT are at high risk of developing a pulmonary embolism (PE). In a multicenter study, nearly 40% of patients admitted with a DVT had evidence of a PE on ventilation perfusion scan.2 Treatment of a DVT is aimed at preventing the extension of the DVT and embolization.3 The American College of Chest Physicians (ACCP) recommends anticoagulation as the primary DVT treatment (Grade 1A).4 However, IVC filters might be considered when anticoagulation is contraindicated.
In 1868, Trousseau created the conceptual model of surgical interruption of the IVC to prevent PE. However, it wasn’t until 1959 by Bottini that the surgical interruption was successfully performed.5 The Mobin-Uddin filter was introduced in 1967 as the first mechanical IVC filter.6 IVC filters mechanically trap the DVT, preventing emboli from traveling into the pulmonary vasculature.7
There are two classes of IVC filters: permanent filters and removable filters. Removable filters include both temporary filters and retrievable filters. Temporary filters are attached to a catheter that exits the skin and therefore must be removed due to the risk of infection and embolization.7 Retrievable filters are similar in design to permanent filters but are designed to be removed. However, this must be done with caution, as neointimal hyperplasia can prevent removal or cause vessel wall damage upon removal.8
IVC filters are inserted into the vena cava percutaneously via the femoral or jugular approach under fluoroscopy or ultrasound guidance (see Figure 1, p. 16). The filters typically are placed infrarenally, unless there is an indication for a suprarenal filter (e.g., renal vein thrombosis or IVC thrombus extending above the renal veins).7 Complete IVC thrombosis is an absolute contraindication to IVC filter placement, and the relative contraindications include significant coagulopathy and bacteremia.9
The incidence of complications related to IVC filter placement is 4% to 11%. Complications include:
- Insertion-site thrombosis;
- IVC thrombosis;
- Recurrent DVT postphlebitic syndrome;
- Filter migration;
- Erosion of the filter through the vessel wall; and
- Vena caval obstruction.10
A review of the National Hospital Discharge Survey database for trends in IVC filter use in the U.S. found a dramatic increase in the use of IVC filters from 1979 to 1999—to 49,000 patients from 2,000 patients with IVC filters in place. The indications for IVC filter use vary such that it is imperative there are well-designed trials and guidelines to guide appropriate use.11

The Evidence
The 2008 ACCP guidelines on VTE management follow a grading system that classifies recommendations as Grade 1 (strong) or Grade 2 (weak), and classifies the quality of evidence as A (high), B (moderate), or C (low).12 The ACCP guidelines’ recommended first-line treatment for a confirmed DVT is anticoagulation with subcutaneous low-molecular-weight heparin, intravenous unfractionated heparin, monitored subcutaneous heparin, fixed-dose subcutaneous unfractionated heparin, or subcutaneous fondaparinux (all Grade 1A recommendations). The ACCP recommends against the routine use of an IVC filter in addition to anticoagulants (Grade 1A). However, for patients with acute proximal DVT, if anticoagulant therapy is not possible because of the risk of bleeding, IVC filter placement is recommended (Grade 1C). If a patient requires an IVC filter for treatment of an acute DVT as an alternative to anticoagulation, it is recommended to start anticoagulant therapy once the risk of bleeding resolves (Grade 1C).4
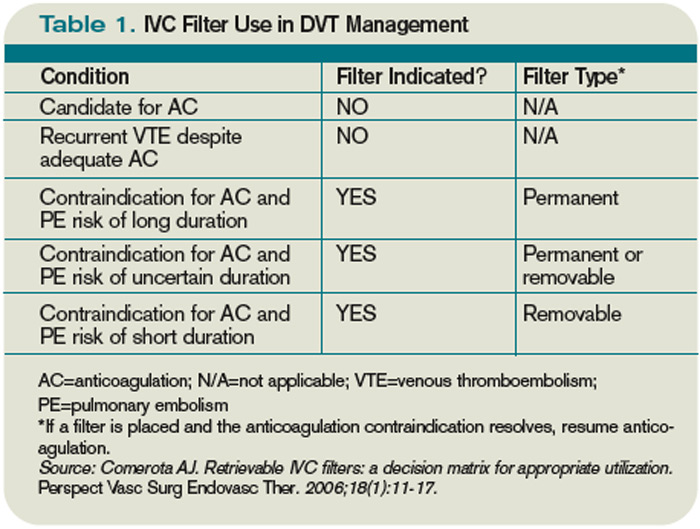
The 2008 ACCP guidelines for IVC filter use have a few important changes from the 2004 version. First, the IVC filter placement recommendation for patients with contraindications to anticoagulation was strengthened from Grade 2C to Grade 1C. Second, the 2008 guidelines omitted the early recommendation of IVC filter use for recurrent VTE, despite adequate anticoagulation (Grade 2C).13
Only one randomized study has evaluated the efficacy of IVC filters. All other studies of IVC filters are retrospective or prospective case series.
The PREPIC study randomized 400 patients with proximal DVT considered to be at high risk for PE to receive either an IVC filter or no IVC filter. Additionally, patients were randomized to receive enoxaparin or unfractionated heparin as a bridge to warfarin therapy, which was continued for at least three months. The primary endpoints were recurrent DVT, PE, major bleeding, or death. The patients were followed up at day 12, two years, and then annually up to eight years following randomization.14 At day 12, there were fewer PEs in the group that received filters (OR 0.22, 95% CI, 0.05-0.90). However, at year two, there was no significant difference in PE development in the filter group compared with the no-filter group (OR 0.50, 95% CI, 0.19-1.33).
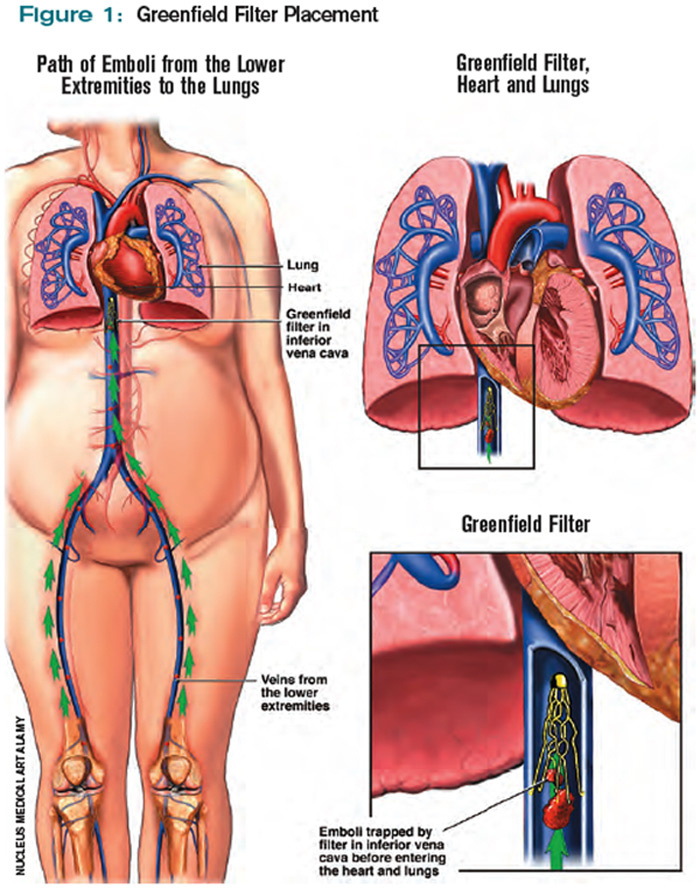
Additionally, at year two, the filter group was more likely to develop recurrent DVT (OR 1.87, 95% CI, 1.10-3.20). At year eight, there was a significant reduction in the number of PEs in the filter group versus the no-filter group (6.2% vs.15.1%, P=0.008). However, at eight-year followup, IVC filter use was associated with increased DVT (35.7% vs. 27.5%, P=0.042). There was no difference in mortality between the two groups.
In summary, the use of IVC filters was associated with decreased incidence of PE at eight years, offset by higher rates of recurrent DVT and no overall mortality benefit.14,15 Importantly, the indications for IVC filter use in this study differ from the current ACCP guidelines; all patients were given concomitant anticoagulation for at least three months, which might not be possible in patients for whom the ACCP recommends IVC filters.
There are no randomized studies to compare the efficacy of permanent IVC filters and retrievable filters for PE prevention. A retrospective study comparing the clinical effectiveness of the two filter types reported no difference in the rates of symptomatic PE (permanent filter 4% vs. retrievable filter 4.7%, P=0.67) or DVT (11.3% vs. 12.6%, P=0.59). In addition, the frequency of symptomatic IVC thrombosis was similar (1.1% vs. 0.5%, p=0.39).16 A paper reviewing the efficacy of IVC filters reported that permanent filters were associated with a 0%-6.2% rate of PE versus a 0%-1.9% rate with retrievable filters.7 Notably, these studies were not randomized controlled trials—rather, case series—and the indications for IVC filters were not necessarily those currently recommended by the ACCP.
Due to the long-term complications of permanent IVC filters, it is suggested that a retrievable IVC filter be used for patients with temporary contraindications to anticoagulation.17 Comerata et al created a clinical decision-making tool for picking the type of filter to employ. If the duration of contraindication to anticoagulation is short or uncertain, a retrievable filter is recommended.18 Table 1 (p. 15) outlines the recommendations for IVC filter placement.
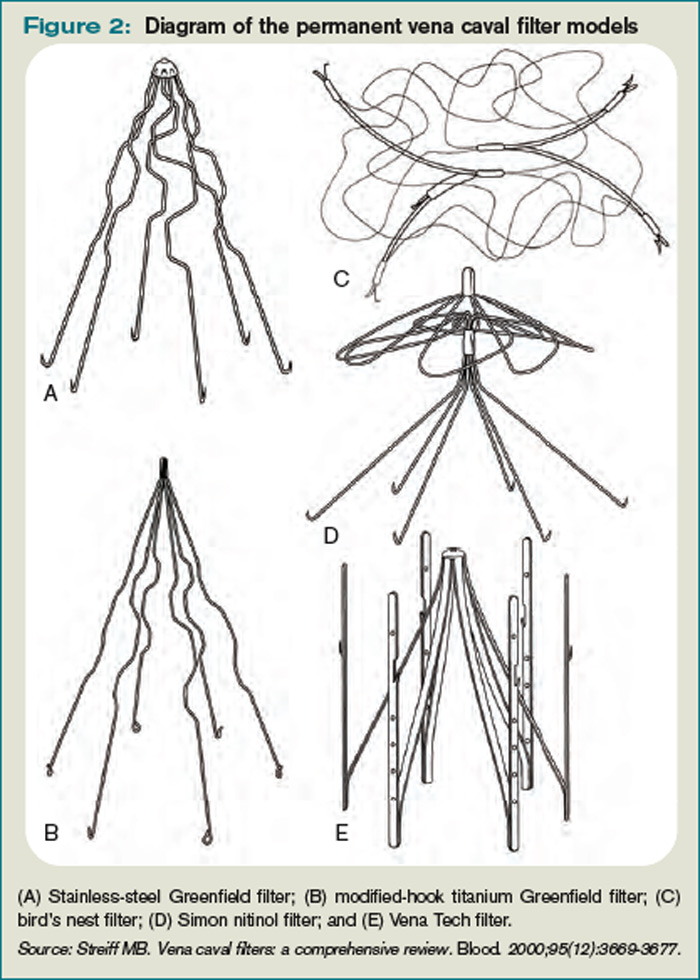
There are no randomized controlled trials to guide the use of concomitant anticoagulation after filter insertion, although this intervention may be beneficial to prevent DVT propagation, recurrence, or IVC filter thrombosis.5 A meta-analysis of 14 studies evaluating the rates of VTE after IVC filter placement demonstrated a non-statistically significant trend toward fewer VTE events in the patients with an IVC filter and concomitant anticoagulation in comparison with those who solely had an IVC filter (OR 0.64, 95% CI, 0.35-1.2). The duration and degree of anticoagulation was not presented in all of the studies in the meta-analysis, therefore limiting the analysis.19
In addition to the ACCP guidelines, there have been other proposed indications for IVC filter use, including recurrent VTE despite anticoagulation, chronic recurrent PE with pulmonary hypertension, extensive free-floating iliofemoral thrombus, and thrombolysis of ilio-caval thrombus.20 The ACCP guidelines do not specifically address these individual indications, and at this time there are no randomized controlled trials to guide IVC filter use in these cases.
Back to the Case
Our patient developed a significant complication from anticoagulation. Current ACCP guidelines recommend an IVC filter if anticoagulant therapy is contraindicated (Grade 1C). The anticoagulation was discontinued and a retrievable IVC filter was placed. Once a patient no longer has a contraindication for anticoagulation, the ACCP recommends restarting a conventional course of anticoagulation. Thus, once the patient can tolerate anticoagulation, consideration will be given to removal of the retrievable filter.
Bottom Line
An IVC filter should be considered in patients with a DVT who have a contraindication to anticoagulation. Other indications for IVC filter use are not supported by the current literature. TH
Drs. Bhogal and Eid are hospitalist fellows and instructors at Johns Hopkins Bayview Medical Center in Baltimore. Dr. Kantsiper is a hospitalist and assistant professor at Bayview Medical Center.
References
- The Surgeon General’s Call to Action to Prevent Deep Vein Thrombosis and Pulmonary Embolism. U.S. Department of Health & Human Services Web site. Available at: www.surgeongeneral.gov/topics/deepvein/. Accessed Jan. 25, 2010.
- Moser KM, Fedullo PR, LitteJohn JK, Crawford R. Frequent asymptomatic pulmonary embolism in patients with deep venous thrombosis. JAMA. 1994;271(3):223-225.
- Bates SM, Ginsberg JS. Treatment of deep vein thrombosis. N Engl J Med. 2004;351:268-277.
- Kearon C, Kahn SR, Agnelli G, Goldhaber S, Raskob GE, Comerota AJ, American College of Chest Physicians. Antithrombotic therapy for venous theomboembolic disease: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):454S-545S.
- Becker DM, Philbrick JT, Selby JB. Inferior vena cava filters. Indications, safety, effectiveness. Arch Intern Med. 1992;152(10):1985-1994.
- Streiff MB. Vena caval filters: a comprehensive review. Blood. 2000;95(12):3669-3677.
- Chung J, Owen RJ. Using inferior vena cava filters to prevent pulmonary embolism. Can Fam Physician. 2008;54(1):49-55.
- Ku GH. Billett HH. Long lives, short indications. The case for removable inferior cava filters. Thromb Haemost. 2005;93(1):17-22.
- Stavropoulos WS. Inferior vena cava filters. Tech Vasc Interv Radiol. 2004;7(2):91-95.
- Crowther MA. Inferior vena cava filters in the management of venous thromboembolism. Am J Med. 2007;120(10 Suppl 2):S13–S17.
- Stein PD, Kayali F, Olson RE. Twenty-one-year trends in the use of inferior vena cava filters. Arch Intern Med. 2004;164(14):1541-1545.
- Guyatt G, Gutterman D, Baumann MH, et al. Grading strength of recommendations and quality of evidence in clinical guidelines: report from an American College of Chest Physicians task force. Chest. 2006;129(1):174-181.
- Büller HR, Agnelli G, Hull RD, Hyers TM, Prins MH, Raskob GE. Antithrombotic therapy for venous thromboembolic disease: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(3 Suppl):401S-428S.
- Decousus H, Leizorovicz A, Parent F, et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. Prévention du Risque d’Embolie Pulmonaire par Interruption Cave Study Group. N Engl J Med. 1998;338(7):409-415.
- Decousus H, Barral F, Buchmuller-Cordier A, et al. Participating centers eight-year follow-up of patients with permanent vena cava filters in the prevention of pulmonary embolism: the PREPIC randomization croup. Circulation. 2005;112:416-422.
- Kim HS, Young MJ, Narayan AK, Liddell RP, Streiff MB. A comparison of clinical outcomes with retrievable and permanent inferior vena cava filters. J Vasc Interv Radiol. 2008:19(3):393-399.
- Houman Fekrazad M, Lopes RD, Stashenko GJ, Alexander JH, Garcia D. Treatment of venous thromboembolism: guidelines translated for the clinician. J Thromb Thrombolysis. 2009; 28(3):270–275.
- Comerota AJ. Retrievable IVC filters: a decision matrix for appropriate utilization. Perspect Vasc Surg Endovasc Ther. 2006;18(1):11-17.
- Ray CE Jr, Prochazka A. The need for anticoagulation following inferior vena cava filter placement: systematic review. Cardiovasc Intervent Radiol. 2008; 31(2):316-324.
- Hajduk B, Tomkowski WZ, Malek G, Davidson BL. Vena cava filter occlusion and venous thromboembolism risk in persistently anticoagulated patients: A prospective, observational cohort study. Chest. 2009.
Case
A 67-year-old man with a history of hypertension presents with a swollen right lower extremity. An ultrasound reveals a DVT, and he is commenced on low-molecular-weight heparin and warfarin. Two days later, he develops slurred speech and right-sided weakness. A head CT reveals an intracranial hemorrhage. When should an inferior vena cava (IVC) filter be utilized for treatment of DVT?
Overview
It is estimated that 350,000 to 600,000 Americans develop a VTE each year.1 Patients with a DVT are at high risk of developing a pulmonary embolism (PE). In a multicenter study, nearly 40% of patients admitted with a DVT had evidence of a PE on ventilation perfusion scan.2 Treatment of a DVT is aimed at preventing the extension of the DVT and embolization.3 The American College of Chest Physicians (ACCP) recommends anticoagulation as the primary DVT treatment (Grade 1A).4 However, IVC filters might be considered when anticoagulation is contraindicated.
In 1868, Trousseau created the conceptual model of surgical interruption of the IVC to prevent PE. However, it wasn’t until 1959 by Bottini that the surgical interruption was successfully performed.5 The Mobin-Uddin filter was introduced in 1967 as the first mechanical IVC filter.6 IVC filters mechanically trap the DVT, preventing emboli from traveling into the pulmonary vasculature.7
There are two classes of IVC filters: permanent filters and removable filters. Removable filters include both temporary filters and retrievable filters. Temporary filters are attached to a catheter that exits the skin and therefore must be removed due to the risk of infection and embolization.7 Retrievable filters are similar in design to permanent filters but are designed to be removed. However, this must be done with caution, as neointimal hyperplasia can prevent removal or cause vessel wall damage upon removal.8
IVC filters are inserted into the vena cava percutaneously via the femoral or jugular approach under fluoroscopy or ultrasound guidance (see Figure 1, p. 16). The filters typically are placed infrarenally, unless there is an indication for a suprarenal filter (e.g., renal vein thrombosis or IVC thrombus extending above the renal veins).7 Complete IVC thrombosis is an absolute contraindication to IVC filter placement, and the relative contraindications include significant coagulopathy and bacteremia.9
The incidence of complications related to IVC filter placement is 4% to 11%. Complications include:
- Insertion-site thrombosis;
- IVC thrombosis;
- Recurrent DVT postphlebitic syndrome;
- Filter migration;
- Erosion of the filter through the vessel wall; and
- Vena caval obstruction.10
A review of the National Hospital Discharge Survey database for trends in IVC filter use in the U.S. found a dramatic increase in the use of IVC filters from 1979 to 1999—to 49,000 patients from 2,000 patients with IVC filters in place. The indications for IVC filter use vary such that it is imperative there are well-designed trials and guidelines to guide appropriate use.11
The Evidence
The 2008 ACCP guidelines on VTE management follow a grading system that classifies recommendations as Grade 1 (strong) or Grade 2 (weak), and classifies the quality of evidence as A (high), B (moderate), or C (low).12 The ACCP guidelines’ recommended first-line treatment for a confirmed DVT is anticoagulation with subcutaneous low-molecular-weight heparin, intravenous unfractionated heparin, monitored subcutaneous heparin, fixed-dose subcutaneous unfractionated heparin, or subcutaneous fondaparinux (all Grade 1A recommendations). The ACCP recommends against the routine use of an IVC filter in addition to anticoagulants (Grade 1A). However, for patients with acute proximal DVT, if anticoagulant therapy is not possible because of the risk of bleeding, IVC filter placement is recommended (Grade 1C). If a patient requires an IVC filter for treatment of an acute DVT as an alternative to anticoagulation, it is recommended to start anticoagulant therapy once the risk of bleeding resolves (Grade 1C).4
The 2008 ACCP guidelines for IVC filter use have a few important changes from the 2004 version. First, the IVC filter placement recommendation for patients with contraindications to anticoagulation was strengthened from Grade 2C to Grade 1C. Second, the 2008 guidelines omitted the early recommendation of IVC filter use for recurrent VTE, despite adequate anticoagulation (Grade 2C).13
Only one randomized study has evaluated the efficacy of IVC filters. All other studies of IVC filters are retrospective or prospective case series.
The PREPIC study randomized 400 patients with proximal DVT considered to be at high risk for PE to receive either an IVC filter or no IVC filter. Additionally, patients were randomized to receive enoxaparin or unfractionated heparin as a bridge to warfarin therapy, which was continued for at least three months. The primary endpoints were recurrent DVT, PE, major bleeding, or death. The patients were followed up at day 12, two years, and then annually up to eight years following randomization.14 At day 12, there were fewer PEs in the group that received filters (OR 0.22, 95% CI, 0.05-0.90). However, at year two, there was no significant difference in PE development in the filter group compared with the no-filter group (OR 0.50, 95% CI, 0.19-1.33).
Additionally, at year two, the filter group was more likely to develop recurrent DVT (OR 1.87, 95% CI, 1.10-3.20). At year eight, there was a significant reduction in the number of PEs in the filter group versus the no-filter group (6.2% vs.15.1%, P=0.008). However, at eight-year followup, IVC filter use was associated with increased DVT (35.7% vs. 27.5%, P=0.042). There was no difference in mortality between the two groups.
In summary, the use of IVC filters was associated with decreased incidence of PE at eight years, offset by higher rates of recurrent DVT and no overall mortality benefit.14,15 Importantly, the indications for IVC filter use in this study differ from the current ACCP guidelines; all patients were given concomitant anticoagulation for at least three months, which might not be possible in patients for whom the ACCP recommends IVC filters.
There are no randomized studies to compare the efficacy of permanent IVC filters and retrievable filters for PE prevention. A retrospective study comparing the clinical effectiveness of the two filter types reported no difference in the rates of symptomatic PE (permanent filter 4% vs. retrievable filter 4.7%, P=0.67) or DVT (11.3% vs. 12.6%, P=0.59). In addition, the frequency of symptomatic IVC thrombosis was similar (1.1% vs. 0.5%, p=0.39).16 A paper reviewing the efficacy of IVC filters reported that permanent filters were associated with a 0%-6.2% rate of PE versus a 0%-1.9% rate with retrievable filters.7 Notably, these studies were not randomized controlled trials—rather, case series—and the indications for IVC filters were not necessarily those currently recommended by the ACCP.
Due to the long-term complications of permanent IVC filters, it is suggested that a retrievable IVC filter be used for patients with temporary contraindications to anticoagulation.17 Comerata et al created a clinical decision-making tool for picking the type of filter to employ. If the duration of contraindication to anticoagulation is short or uncertain, a retrievable filter is recommended.18 Table 1 (p. 15) outlines the recommendations for IVC filter placement.
There are no randomized controlled trials to guide the use of concomitant anticoagulation after filter insertion, although this intervention may be beneficial to prevent DVT propagation, recurrence, or IVC filter thrombosis.5 A meta-analysis of 14 studies evaluating the rates of VTE after IVC filter placement demonstrated a non-statistically significant trend toward fewer VTE events in the patients with an IVC filter and concomitant anticoagulation in comparison with those who solely had an IVC filter (OR 0.64, 95% CI, 0.35-1.2). The duration and degree of anticoagulation was not presented in all of the studies in the meta-analysis, therefore limiting the analysis.19
In addition to the ACCP guidelines, there have been other proposed indications for IVC filter use, including recurrent VTE despite anticoagulation, chronic recurrent PE with pulmonary hypertension, extensive free-floating iliofemoral thrombus, and thrombolysis of ilio-caval thrombus.20 The ACCP guidelines do not specifically address these individual indications, and at this time there are no randomized controlled trials to guide IVC filter use in these cases.
Back to the Case
Our patient developed a significant complication from anticoagulation. Current ACCP guidelines recommend an IVC filter if anticoagulant therapy is contraindicated (Grade 1C). The anticoagulation was discontinued and a retrievable IVC filter was placed. Once a patient no longer has a contraindication for anticoagulation, the ACCP recommends restarting a conventional course of anticoagulation. Thus, once the patient can tolerate anticoagulation, consideration will be given to removal of the retrievable filter.
Bottom Line
An IVC filter should be considered in patients with a DVT who have a contraindication to anticoagulation. Other indications for IVC filter use are not supported by the current literature. TH
Drs. Bhogal and Eid are hospitalist fellows and instructors at Johns Hopkins Bayview Medical Center in Baltimore. Dr. Kantsiper is a hospitalist and assistant professor at Bayview Medical Center.
References
- The Surgeon General’s Call to Action to Prevent Deep Vein Thrombosis and Pulmonary Embolism. U.S. Department of Health & Human Services Web site. Available at: www.surgeongeneral.gov/topics/deepvein/. Accessed Jan. 25, 2010.
- Moser KM, Fedullo PR, LitteJohn JK, Crawford R. Frequent asymptomatic pulmonary embolism in patients with deep venous thrombosis. JAMA. 1994;271(3):223-225.
- Bates SM, Ginsberg JS. Treatment of deep vein thrombosis. N Engl J Med. 2004;351:268-277.
- Kearon C, Kahn SR, Agnelli G, Goldhaber S, Raskob GE, Comerota AJ, American College of Chest Physicians. Antithrombotic therapy for venous theomboembolic disease: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):454S-545S.
- Becker DM, Philbrick JT, Selby JB. Inferior vena cava filters. Indications, safety, effectiveness. Arch Intern Med. 1992;152(10):1985-1994.
- Streiff MB. Vena caval filters: a comprehensive review. Blood. 2000;95(12):3669-3677.
- Chung J, Owen RJ. Using inferior vena cava filters to prevent pulmonary embolism. Can Fam Physician. 2008;54(1):49-55.
- Ku GH. Billett HH. Long lives, short indications. The case for removable inferior cava filters. Thromb Haemost. 2005;93(1):17-22.
- Stavropoulos WS. Inferior vena cava filters. Tech Vasc Interv Radiol. 2004;7(2):91-95.
- Crowther MA. Inferior vena cava filters in the management of venous thromboembolism. Am J Med. 2007;120(10 Suppl 2):S13–S17.
- Stein PD, Kayali F, Olson RE. Twenty-one-year trends in the use of inferior vena cava filters. Arch Intern Med. 2004;164(14):1541-1545.
- Guyatt G, Gutterman D, Baumann MH, et al. Grading strength of recommendations and quality of evidence in clinical guidelines: report from an American College of Chest Physicians task force. Chest. 2006;129(1):174-181.
- Büller HR, Agnelli G, Hull RD, Hyers TM, Prins MH, Raskob GE. Antithrombotic therapy for venous thromboembolic disease: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(3 Suppl):401S-428S.
- Decousus H, Leizorovicz A, Parent F, et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. Prévention du Risque d’Embolie Pulmonaire par Interruption Cave Study Group. N Engl J Med. 1998;338(7):409-415.
- Decousus H, Barral F, Buchmuller-Cordier A, et al. Participating centers eight-year follow-up of patients with permanent vena cava filters in the prevention of pulmonary embolism: the PREPIC randomization croup. Circulation. 2005;112:416-422.
- Kim HS, Young MJ, Narayan AK, Liddell RP, Streiff MB. A comparison of clinical outcomes with retrievable and permanent inferior vena cava filters. J Vasc Interv Radiol. 2008:19(3):393-399.
- Houman Fekrazad M, Lopes RD, Stashenko GJ, Alexander JH, Garcia D. Treatment of venous thromboembolism: guidelines translated for the clinician. J Thromb Thrombolysis. 2009; 28(3):270–275.
- Comerota AJ. Retrievable IVC filters: a decision matrix for appropriate utilization. Perspect Vasc Surg Endovasc Ther. 2006;18(1):11-17.
- Ray CE Jr, Prochazka A. The need for anticoagulation following inferior vena cava filter placement: systematic review. Cardiovasc Intervent Radiol. 2008; 31(2):316-324.
- Hajduk B, Tomkowski WZ, Malek G, Davidson BL. Vena cava filter occlusion and venous thromboembolism risk in persistently anticoagulated patients: A prospective, observational cohort study. Chest. 2009.
Case
A 67-year-old man with a history of hypertension presents with a swollen right lower extremity. An ultrasound reveals a DVT, and he is commenced on low-molecular-weight heparin and warfarin. Two days later, he develops slurred speech and right-sided weakness. A head CT reveals an intracranial hemorrhage. When should an inferior vena cava (IVC) filter be utilized for treatment of DVT?
Overview
It is estimated that 350,000 to 600,000 Americans develop a VTE each year.1 Patients with a DVT are at high risk of developing a pulmonary embolism (PE). In a multicenter study, nearly 40% of patients admitted with a DVT had evidence of a PE on ventilation perfusion scan.2 Treatment of a DVT is aimed at preventing the extension of the DVT and embolization.3 The American College of Chest Physicians (ACCP) recommends anticoagulation as the primary DVT treatment (Grade 1A).4 However, IVC filters might be considered when anticoagulation is contraindicated.
In 1868, Trousseau created the conceptual model of surgical interruption of the IVC to prevent PE. However, it wasn’t until 1959 by Bottini that the surgical interruption was successfully performed.5 The Mobin-Uddin filter was introduced in 1967 as the first mechanical IVC filter.6 IVC filters mechanically trap the DVT, preventing emboli from traveling into the pulmonary vasculature.7
There are two classes of IVC filters: permanent filters and removable filters. Removable filters include both temporary filters and retrievable filters. Temporary filters are attached to a catheter that exits the skin and therefore must be removed due to the risk of infection and embolization.7 Retrievable filters are similar in design to permanent filters but are designed to be removed. However, this must be done with caution, as neointimal hyperplasia can prevent removal or cause vessel wall damage upon removal.8
IVC filters are inserted into the vena cava percutaneously via the femoral or jugular approach under fluoroscopy or ultrasound guidance (see Figure 1, p. 16). The filters typically are placed infrarenally, unless there is an indication for a suprarenal filter (e.g., renal vein thrombosis or IVC thrombus extending above the renal veins).7 Complete IVC thrombosis is an absolute contraindication to IVC filter placement, and the relative contraindications include significant coagulopathy and bacteremia.9
The incidence of complications related to IVC filter placement is 4% to 11%. Complications include:
- Insertion-site thrombosis;
- IVC thrombosis;
- Recurrent DVT postphlebitic syndrome;
- Filter migration;
- Erosion of the filter through the vessel wall; and
- Vena caval obstruction.10
A review of the National Hospital Discharge Survey database for trends in IVC filter use in the U.S. found a dramatic increase in the use of IVC filters from 1979 to 1999—to 49,000 patients from 2,000 patients with IVC filters in place. The indications for IVC filter use vary such that it is imperative there are well-designed trials and guidelines to guide appropriate use.11
The Evidence
The 2008 ACCP guidelines on VTE management follow a grading system that classifies recommendations as Grade 1 (strong) or Grade 2 (weak), and classifies the quality of evidence as A (high), B (moderate), or C (low).12 The ACCP guidelines’ recommended first-line treatment for a confirmed DVT is anticoagulation with subcutaneous low-molecular-weight heparin, intravenous unfractionated heparin, monitored subcutaneous heparin, fixed-dose subcutaneous unfractionated heparin, or subcutaneous fondaparinux (all Grade 1A recommendations). The ACCP recommends against the routine use of an IVC filter in addition to anticoagulants (Grade 1A). However, for patients with acute proximal DVT, if anticoagulant therapy is not possible because of the risk of bleeding, IVC filter placement is recommended (Grade 1C). If a patient requires an IVC filter for treatment of an acute DVT as an alternative to anticoagulation, it is recommended to start anticoagulant therapy once the risk of bleeding resolves (Grade 1C).4
The 2008 ACCP guidelines for IVC filter use have a few important changes from the 2004 version. First, the IVC filter placement recommendation for patients with contraindications to anticoagulation was strengthened from Grade 2C to Grade 1C. Second, the 2008 guidelines omitted the early recommendation of IVC filter use for recurrent VTE, despite adequate anticoagulation (Grade 2C).13
Only one randomized study has evaluated the efficacy of IVC filters. All other studies of IVC filters are retrospective or prospective case series.
The PREPIC study randomized 400 patients with proximal DVT considered to be at high risk for PE to receive either an IVC filter or no IVC filter. Additionally, patients were randomized to receive enoxaparin or unfractionated heparin as a bridge to warfarin therapy, which was continued for at least three months. The primary endpoints were recurrent DVT, PE, major bleeding, or death. The patients were followed up at day 12, two years, and then annually up to eight years following randomization.14 At day 12, there were fewer PEs in the group that received filters (OR 0.22, 95% CI, 0.05-0.90). However, at year two, there was no significant difference in PE development in the filter group compared with the no-filter group (OR 0.50, 95% CI, 0.19-1.33).
Additionally, at year two, the filter group was more likely to develop recurrent DVT (OR 1.87, 95% CI, 1.10-3.20). At year eight, there was a significant reduction in the number of PEs in the filter group versus the no-filter group (6.2% vs.15.1%, P=0.008). However, at eight-year followup, IVC filter use was associated with increased DVT (35.7% vs. 27.5%, P=0.042). There was no difference in mortality between the two groups.
In summary, the use of IVC filters was associated with decreased incidence of PE at eight years, offset by higher rates of recurrent DVT and no overall mortality benefit.14,15 Importantly, the indications for IVC filter use in this study differ from the current ACCP guidelines; all patients were given concomitant anticoagulation for at least three months, which might not be possible in patients for whom the ACCP recommends IVC filters.
There are no randomized studies to compare the efficacy of permanent IVC filters and retrievable filters for PE prevention. A retrospective study comparing the clinical effectiveness of the two filter types reported no difference in the rates of symptomatic PE (permanent filter 4% vs. retrievable filter 4.7%, P=0.67) or DVT (11.3% vs. 12.6%, P=0.59). In addition, the frequency of symptomatic IVC thrombosis was similar (1.1% vs. 0.5%, p=0.39).16 A paper reviewing the efficacy of IVC filters reported that permanent filters were associated with a 0%-6.2% rate of PE versus a 0%-1.9% rate with retrievable filters.7 Notably, these studies were not randomized controlled trials—rather, case series—and the indications for IVC filters were not necessarily those currently recommended by the ACCP.
Due to the long-term complications of permanent IVC filters, it is suggested that a retrievable IVC filter be used for patients with temporary contraindications to anticoagulation.17 Comerata et al created a clinical decision-making tool for picking the type of filter to employ. If the duration of contraindication to anticoagulation is short or uncertain, a retrievable filter is recommended.18 Table 1 (p. 15) outlines the recommendations for IVC filter placement.
There are no randomized controlled trials to guide the use of concomitant anticoagulation after filter insertion, although this intervention may be beneficial to prevent DVT propagation, recurrence, or IVC filter thrombosis.5 A meta-analysis of 14 studies evaluating the rates of VTE after IVC filter placement demonstrated a non-statistically significant trend toward fewer VTE events in the patients with an IVC filter and concomitant anticoagulation in comparison with those who solely had an IVC filter (OR 0.64, 95% CI, 0.35-1.2). The duration and degree of anticoagulation was not presented in all of the studies in the meta-analysis, therefore limiting the analysis.19
In addition to the ACCP guidelines, there have been other proposed indications for IVC filter use, including recurrent VTE despite anticoagulation, chronic recurrent PE with pulmonary hypertension, extensive free-floating iliofemoral thrombus, and thrombolysis of ilio-caval thrombus.20 The ACCP guidelines do not specifically address these individual indications, and at this time there are no randomized controlled trials to guide IVC filter use in these cases.
Back to the Case
Our patient developed a significant complication from anticoagulation. Current ACCP guidelines recommend an IVC filter if anticoagulant therapy is contraindicated (Grade 1C). The anticoagulation was discontinued and a retrievable IVC filter was placed. Once a patient no longer has a contraindication for anticoagulation, the ACCP recommends restarting a conventional course of anticoagulation. Thus, once the patient can tolerate anticoagulation, consideration will be given to removal of the retrievable filter.
Bottom Line
An IVC filter should be considered in patients with a DVT who have a contraindication to anticoagulation. Other indications for IVC filter use are not supported by the current literature. TH
Drs. Bhogal and Eid are hospitalist fellows and instructors at Johns Hopkins Bayview Medical Center in Baltimore. Dr. Kantsiper is a hospitalist and assistant professor at Bayview Medical Center.
References
- The Surgeon General’s Call to Action to Prevent Deep Vein Thrombosis and Pulmonary Embolism. U.S. Department of Health & Human Services Web site. Available at: www.surgeongeneral.gov/topics/deepvein/. Accessed Jan. 25, 2010.
- Moser KM, Fedullo PR, LitteJohn JK, Crawford R. Frequent asymptomatic pulmonary embolism in patients with deep venous thrombosis. JAMA. 1994;271(3):223-225.
- Bates SM, Ginsberg JS. Treatment of deep vein thrombosis. N Engl J Med. 2004;351:268-277.
- Kearon C, Kahn SR, Agnelli G, Goldhaber S, Raskob GE, Comerota AJ, American College of Chest Physicians. Antithrombotic therapy for venous theomboembolic disease: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):454S-545S.
- Becker DM, Philbrick JT, Selby JB. Inferior vena cava filters. Indications, safety, effectiveness. Arch Intern Med. 1992;152(10):1985-1994.
- Streiff MB. Vena caval filters: a comprehensive review. Blood. 2000;95(12):3669-3677.
- Chung J, Owen RJ. Using inferior vena cava filters to prevent pulmonary embolism. Can Fam Physician. 2008;54(1):49-55.
- Ku GH. Billett HH. Long lives, short indications. The case for removable inferior cava filters. Thromb Haemost. 2005;93(1):17-22.
- Stavropoulos WS. Inferior vena cava filters. Tech Vasc Interv Radiol. 2004;7(2):91-95.
- Crowther MA. Inferior vena cava filters in the management of venous thromboembolism. Am J Med. 2007;120(10 Suppl 2):S13–S17.
- Stein PD, Kayali F, Olson RE. Twenty-one-year trends in the use of inferior vena cava filters. Arch Intern Med. 2004;164(14):1541-1545.
- Guyatt G, Gutterman D, Baumann MH, et al. Grading strength of recommendations and quality of evidence in clinical guidelines: report from an American College of Chest Physicians task force. Chest. 2006;129(1):174-181.
- Büller HR, Agnelli G, Hull RD, Hyers TM, Prins MH, Raskob GE. Antithrombotic therapy for venous thromboembolic disease: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(3 Suppl):401S-428S.
- Decousus H, Leizorovicz A, Parent F, et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. Prévention du Risque d’Embolie Pulmonaire par Interruption Cave Study Group. N Engl J Med. 1998;338(7):409-415.
- Decousus H, Barral F, Buchmuller-Cordier A, et al. Participating centers eight-year follow-up of patients with permanent vena cava filters in the prevention of pulmonary embolism: the PREPIC randomization croup. Circulation. 2005;112:416-422.
- Kim HS, Young MJ, Narayan AK, Liddell RP, Streiff MB. A comparison of clinical outcomes with retrievable and permanent inferior vena cava filters. J Vasc Interv Radiol. 2008:19(3):393-399.
- Houman Fekrazad M, Lopes RD, Stashenko GJ, Alexander JH, Garcia D. Treatment of venous thromboembolism: guidelines translated for the clinician. J Thromb Thrombolysis. 2009; 28(3):270–275.
- Comerota AJ. Retrievable IVC filters: a decision matrix for appropriate utilization. Perspect Vasc Surg Endovasc Ther. 2006;18(1):11-17.
- Ray CE Jr, Prochazka A. The need for anticoagulation following inferior vena cava filter placement: systematic review. Cardiovasc Intervent Radiol. 2008; 31(2):316-324.
- Hajduk B, Tomkowski WZ, Malek G, Davidson BL. Vena cava filter occlusion and venous thromboembolism risk in persistently anticoagulated patients: A prospective, observational cohort study. Chest. 2009.
Market Watch
New Generics
- Donepezil orally disintegrating tablets (generic Aricept ODT)1
- Nizatadine oral solution (generic Axid oral solution), 15mg/mL.2 It is available in peppermint flavor.
New Drugs, Indications, and Dosage Forms
- Clonidine ER tablets and suspension (Clonidine ER suspension and Clonidine ER tablets) have been approved by the FDA.3
- Estradiol 10 mcg vaginal (Vagifem) low-dose tablets have been approved by the FDA for treating atrophic vaginitis due to menopause.4
- Olanzapine (Zyprexa) has been approved by the FDA to treat schizophrenia and manic or mixed episodes associated with bipolar I disorder in patients aged 13 to 17 years old.5 Prescribers must consider the potential for weight gain and hyperlipidemia, as well as other long-term risks that might occur in adolescents compared with adult patients.
- Olanzapine injection (Zyprexa Relprevv) has been approved by the FDA for treating schizophrenia in adults.6 A risk-evaluation and mitigation strategy (REMS) will be implemented with this agent. It is a long-acting, intramuscular depot injection given every two to four weeks, depending on the dose.7
- Quetiapine extended-release (Zyprexa) has been approved by the FDA as add-on therapy to antidepressants in managing adults with major depressive disorder.8 AstraZeneca, the drug manufacturer, also is seeking approval for a monotherapy indication to manage depression in the acute and maintenance phases.
- Sildenafil intravenous (Revatio IV) has been approved by the FDA for treating pulmonary arterial hypertension for patients who are temporarily unable to take the oral medication.9 The injection is administered as a single-dose of 10 mg up to three times daily. According to the manufacturer, this is bioequivalent to 20 mg three times a day for the oral formulation.
- Tiotropium bromide inhalation powder (Spiriva HandiHaler) has been approved by the FDA for reducing exacerbations in patients with chronic obstructive pulmonary disease (COPD).10
Pipeline
- Approval is pending for Aztreonam lysine inhaled (Cayston) for the treatment of Pseudomonas aeruginosa infections in patients with cystic fibrosis.11 The FDA’s Anti-Infectives Drugs Advisory Committee voted 15-2 in favor of the drug’s safety and effectiveness, and 17-0 in favor of a regimen of 75 mg three times a day. The FDA usually approves drugs recommended by its panels.
- Darapladib, a selective and orally active LpPLA2 inhibitor, has begun Phase 3 clinical trials in the management of acute coronary syndrome (ACS).12 The study will include 11,500 male and female patients from 40 countries. It is a double-blind, randomized, placebo-controlled clinical efficacy trial of the long-term use of darapladib when added to standard of care. The study will test whether darapladib affects the chances of having a cardiovascular event, such as a myocardial infarction or a stroke, when treatment is started within 30 days after an ACS.
- Denosumab has received a positive opinion from the European Union for treating osteoporosis in postmenopausal women at increased risk of fractures, and also for treating bone loss in men with prostate cancer who are at increased risk of fractures.13 In the U.S., approval by the FDA is pending for management of osteoporosis in postmenopausal women.14 The FDA’s reproductive health advisory committee, which evaluated the agent, voted 12-1 to require the drug to carry a REMS.
- Ocrelizumab, a Phase 3 humanized anti-CD20 monoclonal antibody for treating rheumatoid arthritis (RA), recently reported positive results when given in combination with methotrexate (MTX) in an international, randomized, multicenter, double-blind trial.15 Ocrelizumab or placebo administered by intravenous infusion on days one and 15 met the primary endpoint of improving the signs and symptoms of RA in patients with an inadequate response to MTX.
- A response to an FDA complete response letter dated May 2009 was expected for rivaroxaban, an oral, direct Factor Xa inhibitor for preventing DVT and pulmonary embolism in patients undergoing hip or knee surgery. Complete review of rivaroxaban data was deferred by its manufacturers until February.16,17
- The FDA is considering a new indication for rosuvastatin (Crestor), following recommendations of the Endocrinologic and Metabolic Drugs Advisory Committee on Dec. 15, 2009.18
Safety Information
Pay attention to two agents manufactured by AstraZeneca: Dexlansoprazole (Kapidex), a new formulation of the proton-pump inhibitor lansoprazole, and bicalutamide (Casodex), which is used in combination with a hormone treatment for prostate cancer, have had medication mixups. The agent names look alike and sound alike when written and verbalized. Both written and verbal prescriptions have been dispensed in error. Bicalutamide is available as 50-mg tablets; dexlansoprazole is available as 30-mg and 60-mg capsules. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Walsh S. FDA Approves Generic Aricept to Treat Dementia Related to Alzheimer’s Disease. U.S. Food and Drug Administration Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm194173.htm. Accessed Dec. 28, 2009.
- Amenal Receives FDA Approval For Nizatidine Oral Solution, the First Oral Solution for Axid in the Market. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/173591.php. Accessed Dec. 28, 2009.
- Clonidine ER Suspension and Clonidine ER Tablets approved. Monthly Prescribing Reference Web site. Available at: www.empr.com/clonidine-er-suspension-and-clonidine-er-tablets-approved/article/159148/. Accessed Dec. 28, 2009.
- FDA Approves Mcg Dose of Vagifem For the Treatment of Atrophic Vaginitis Due to Menopause. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/172804.php. Accessed Dec. 28, 2009.
- Todoruk M. Eli Lilly’s Zyprexa approved in US for adolescents. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=B5699B38AADB46AF85E7B34F508DB943&logRowId=340534. Accessed Dec. 28, 2009.
- Dennis M. FDA approves Eli Lilly’s long-acting Zyprexa injection. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=30C504823E42425FA0C3B9BB8490D5AA&logRowId=341775. Accessed Dec. 28, 2009.
- Gever J. FDA Approves Long-Acting Olanzapine. MedPage Today Web site. Available at: www.medpagetoday.com/ProductAlert/Prescriptions/17539. Accessed Dec. 28, 2009.
- Dennis M. FDA approves AstraZeneca’s Seroquel XR as add-on therapy; requires more data as monotherapy. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=0530A906ABCB44B5A32EC05E148E0220&logRowId=340531. Accessed Dec. 28, 2009.
- Petrochko C. FDA Approves IV Sildenafil for Hypertension. MedPage Today Web site. Available at: www.medpagetoday.com/ProductAlert/Prescriptions/17296. Accessed Dec. 28, 2009.
- FDA Approves Spiriva HandiHaler for the Reduction of COPD Exacerbations. Pfizer Web site. Available at: mediaroom.pfizer.com/portal/site/pfizer/?ndmViewId=news_view&newsId=20091217006384&newsLang=en. Accessed Dec. 28, 2009.
- Leuty R. Gilead wins panel OK for cystic fibrosis drug. San Francisco Business Times Web site. Available at: sanfrancisco.bizjournals.com/sanfrancisco/stories/2009/12/07/daily59.html?surround=etf&ana=e_article. Accessed Dec. 28, 2009.
- GSK initiates second pivotal Phase III trial for investigational cardiovascular medication Darapladib. GlaxoSmithKline Web site. Available at: www.gsk.com/media/pressreleases/2009/2009_pressrelease_10141.htm. Accessed Dec. 29, 2009.
- Todoruk M. EU panel issues positive opinion for Amgen’s Prolia. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=A9F30DD044A14893899DF7D880FB8AB0&logRowId=342650. Accessed Dec. 29, 2009.
- Walker EP. FDA Panel Backs Denosumab for Osteoporosis, But Not Osteopenia. MedPage Web site. Available at: www.medpagetoday.com/Endocrinology/Osteoporosis/15530. Accessed Dec. 29, 2009.
- Phase 3 study of ocrelizumab for rheumatoid arthritis (RA). Monthly Prescribing Reference Web site. Available at: www.empr.com/phase-3-study-of-ocrelizumab-for-rheumatoid-arthritis-ra/article/159474/. Accessed Dec. 29, 2009.
- Phase III EINSTEIN-Extension Study of Bayer’s Rivaroxaban Shows Significant Benefit in the Prevention of Secondary Symptomatic VTE. Bayer Web site. Available at: www.bayer.com/en/News-Detail.aspx?id=12554. Accessed Dec. 20, 2009.
- Todoruk M. Bayer, Johnson & Johnson provide update on Xarelto complete response to FDA. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=8F8AEC62E7DB46C3809C1E77A8384F30&logRowId=340535. Accessed Dec. 29, 2009.
- O’Riordan M. FDA advisory panel votes in favor of broadened rosuvastatin indication. TheHeart.org Web site. Available at: www.theheart.org/article/1035155/print.do. Accessed Dec. 29, 2009.
- Kapidex-Casodex confusion. Institute for Safe Medication Practices Web site. Available at: www.ismp.org/newsletters/ambulatory/archives/200907_1.asp. Accessed Dec. 28, 2009.
New Generics
- Donepezil orally disintegrating tablets (generic Aricept ODT)1
- Nizatadine oral solution (generic Axid oral solution), 15mg/mL.2 It is available in peppermint flavor.
New Drugs, Indications, and Dosage Forms
- Clonidine ER tablets and suspension (Clonidine ER suspension and Clonidine ER tablets) have been approved by the FDA.3
- Estradiol 10 mcg vaginal (Vagifem) low-dose tablets have been approved by the FDA for treating atrophic vaginitis due to menopause.4
- Olanzapine (Zyprexa) has been approved by the FDA to treat schizophrenia and manic or mixed episodes associated with bipolar I disorder in patients aged 13 to 17 years old.5 Prescribers must consider the potential for weight gain and hyperlipidemia, as well as other long-term risks that might occur in adolescents compared with adult patients.
- Olanzapine injection (Zyprexa Relprevv) has been approved by the FDA for treating schizophrenia in adults.6 A risk-evaluation and mitigation strategy (REMS) will be implemented with this agent. It is a long-acting, intramuscular depot injection given every two to four weeks, depending on the dose.7
- Quetiapine extended-release (Zyprexa) has been approved by the FDA as add-on therapy to antidepressants in managing adults with major depressive disorder.8 AstraZeneca, the drug manufacturer, also is seeking approval for a monotherapy indication to manage depression in the acute and maintenance phases.
- Sildenafil intravenous (Revatio IV) has been approved by the FDA for treating pulmonary arterial hypertension for patients who are temporarily unable to take the oral medication.9 The injection is administered as a single-dose of 10 mg up to three times daily. According to the manufacturer, this is bioequivalent to 20 mg three times a day for the oral formulation.
- Tiotropium bromide inhalation powder (Spiriva HandiHaler) has been approved by the FDA for reducing exacerbations in patients with chronic obstructive pulmonary disease (COPD).10
Pipeline
- Approval is pending for Aztreonam lysine inhaled (Cayston) for the treatment of Pseudomonas aeruginosa infections in patients with cystic fibrosis.11 The FDA’s Anti-Infectives Drugs Advisory Committee voted 15-2 in favor of the drug’s safety and effectiveness, and 17-0 in favor of a regimen of 75 mg three times a day. The FDA usually approves drugs recommended by its panels.
- Darapladib, a selective and orally active LpPLA2 inhibitor, has begun Phase 3 clinical trials in the management of acute coronary syndrome (ACS).12 The study will include 11,500 male and female patients from 40 countries. It is a double-blind, randomized, placebo-controlled clinical efficacy trial of the long-term use of darapladib when added to standard of care. The study will test whether darapladib affects the chances of having a cardiovascular event, such as a myocardial infarction or a stroke, when treatment is started within 30 days after an ACS.
- Denosumab has received a positive opinion from the European Union for treating osteoporosis in postmenopausal women at increased risk of fractures, and also for treating bone loss in men with prostate cancer who are at increased risk of fractures.13 In the U.S., approval by the FDA is pending for management of osteoporosis in postmenopausal women.14 The FDA’s reproductive health advisory committee, which evaluated the agent, voted 12-1 to require the drug to carry a REMS.
- Ocrelizumab, a Phase 3 humanized anti-CD20 monoclonal antibody for treating rheumatoid arthritis (RA), recently reported positive results when given in combination with methotrexate (MTX) in an international, randomized, multicenter, double-blind trial.15 Ocrelizumab or placebo administered by intravenous infusion on days one and 15 met the primary endpoint of improving the signs and symptoms of RA in patients with an inadequate response to MTX.
- A response to an FDA complete response letter dated May 2009 was expected for rivaroxaban, an oral, direct Factor Xa inhibitor for preventing DVT and pulmonary embolism in patients undergoing hip or knee surgery. Complete review of rivaroxaban data was deferred by its manufacturers until February.16,17
- The FDA is considering a new indication for rosuvastatin (Crestor), following recommendations of the Endocrinologic and Metabolic Drugs Advisory Committee on Dec. 15, 2009.18
Safety Information
Pay attention to two agents manufactured by AstraZeneca: Dexlansoprazole (Kapidex), a new formulation of the proton-pump inhibitor lansoprazole, and bicalutamide (Casodex), which is used in combination with a hormone treatment for prostate cancer, have had medication mixups. The agent names look alike and sound alike when written and verbalized. Both written and verbal prescriptions have been dispensed in error. Bicalutamide is available as 50-mg tablets; dexlansoprazole is available as 30-mg and 60-mg capsules. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Walsh S. FDA Approves Generic Aricept to Treat Dementia Related to Alzheimer’s Disease. U.S. Food and Drug Administration Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm194173.htm. Accessed Dec. 28, 2009.
- Amenal Receives FDA Approval For Nizatidine Oral Solution, the First Oral Solution for Axid in the Market. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/173591.php. Accessed Dec. 28, 2009.
- Clonidine ER Suspension and Clonidine ER Tablets approved. Monthly Prescribing Reference Web site. Available at: www.empr.com/clonidine-er-suspension-and-clonidine-er-tablets-approved/article/159148/. Accessed Dec. 28, 2009.
- FDA Approves Mcg Dose of Vagifem For the Treatment of Atrophic Vaginitis Due to Menopause. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/172804.php. Accessed Dec. 28, 2009.
- Todoruk M. Eli Lilly’s Zyprexa approved in US for adolescents. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=B5699B38AADB46AF85E7B34F508DB943&logRowId=340534. Accessed Dec. 28, 2009.
- Dennis M. FDA approves Eli Lilly’s long-acting Zyprexa injection. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=30C504823E42425FA0C3B9BB8490D5AA&logRowId=341775. Accessed Dec. 28, 2009.
- Gever J. FDA Approves Long-Acting Olanzapine. MedPage Today Web site. Available at: www.medpagetoday.com/ProductAlert/Prescriptions/17539. Accessed Dec. 28, 2009.
- Dennis M. FDA approves AstraZeneca’s Seroquel XR as add-on therapy; requires more data as monotherapy. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=0530A906ABCB44B5A32EC05E148E0220&logRowId=340531. Accessed Dec. 28, 2009.
- Petrochko C. FDA Approves IV Sildenafil for Hypertension. MedPage Today Web site. Available at: www.medpagetoday.com/ProductAlert/Prescriptions/17296. Accessed Dec. 28, 2009.
- FDA Approves Spiriva HandiHaler for the Reduction of COPD Exacerbations. Pfizer Web site. Available at: mediaroom.pfizer.com/portal/site/pfizer/?ndmViewId=news_view&newsId=20091217006384&newsLang=en. Accessed Dec. 28, 2009.
- Leuty R. Gilead wins panel OK for cystic fibrosis drug. San Francisco Business Times Web site. Available at: sanfrancisco.bizjournals.com/sanfrancisco/stories/2009/12/07/daily59.html?surround=etf&ana=e_article. Accessed Dec. 28, 2009.
- GSK initiates second pivotal Phase III trial for investigational cardiovascular medication Darapladib. GlaxoSmithKline Web site. Available at: www.gsk.com/media/pressreleases/2009/2009_pressrelease_10141.htm. Accessed Dec. 29, 2009.
- Todoruk M. EU panel issues positive opinion for Amgen’s Prolia. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=A9F30DD044A14893899DF7D880FB8AB0&logRowId=342650. Accessed Dec. 29, 2009.
- Walker EP. FDA Panel Backs Denosumab for Osteoporosis, But Not Osteopenia. MedPage Web site. Available at: www.medpagetoday.com/Endocrinology/Osteoporosis/15530. Accessed Dec. 29, 2009.
- Phase 3 study of ocrelizumab for rheumatoid arthritis (RA). Monthly Prescribing Reference Web site. Available at: www.empr.com/phase-3-study-of-ocrelizumab-for-rheumatoid-arthritis-ra/article/159474/. Accessed Dec. 29, 2009.
- Phase III EINSTEIN-Extension Study of Bayer’s Rivaroxaban Shows Significant Benefit in the Prevention of Secondary Symptomatic VTE. Bayer Web site. Available at: www.bayer.com/en/News-Detail.aspx?id=12554. Accessed Dec. 20, 2009.
- Todoruk M. Bayer, Johnson & Johnson provide update on Xarelto complete response to FDA. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=8F8AEC62E7DB46C3809C1E77A8384F30&logRowId=340535. Accessed Dec. 29, 2009.
- O’Riordan M. FDA advisory panel votes in favor of broadened rosuvastatin indication. TheHeart.org Web site. Available at: www.theheart.org/article/1035155/print.do. Accessed Dec. 29, 2009.
- Kapidex-Casodex confusion. Institute for Safe Medication Practices Web site. Available at: www.ismp.org/newsletters/ambulatory/archives/200907_1.asp. Accessed Dec. 28, 2009.
New Generics
- Donepezil orally disintegrating tablets (generic Aricept ODT)1
- Nizatadine oral solution (generic Axid oral solution), 15mg/mL.2 It is available in peppermint flavor.
New Drugs, Indications, and Dosage Forms
- Clonidine ER tablets and suspension (Clonidine ER suspension and Clonidine ER tablets) have been approved by the FDA.3
- Estradiol 10 mcg vaginal (Vagifem) low-dose tablets have been approved by the FDA for treating atrophic vaginitis due to menopause.4
- Olanzapine (Zyprexa) has been approved by the FDA to treat schizophrenia and manic or mixed episodes associated with bipolar I disorder in patients aged 13 to 17 years old.5 Prescribers must consider the potential for weight gain and hyperlipidemia, as well as other long-term risks that might occur in adolescents compared with adult patients.
- Olanzapine injection (Zyprexa Relprevv) has been approved by the FDA for treating schizophrenia in adults.6 A risk-evaluation and mitigation strategy (REMS) will be implemented with this agent. It is a long-acting, intramuscular depot injection given every two to four weeks, depending on the dose.7
- Quetiapine extended-release (Zyprexa) has been approved by the FDA as add-on therapy to antidepressants in managing adults with major depressive disorder.8 AstraZeneca, the drug manufacturer, also is seeking approval for a monotherapy indication to manage depression in the acute and maintenance phases.
- Sildenafil intravenous (Revatio IV) has been approved by the FDA for treating pulmonary arterial hypertension for patients who are temporarily unable to take the oral medication.9 The injection is administered as a single-dose of 10 mg up to three times daily. According to the manufacturer, this is bioequivalent to 20 mg three times a day for the oral formulation.
- Tiotropium bromide inhalation powder (Spiriva HandiHaler) has been approved by the FDA for reducing exacerbations in patients with chronic obstructive pulmonary disease (COPD).10
Pipeline
- Approval is pending for Aztreonam lysine inhaled (Cayston) for the treatment of Pseudomonas aeruginosa infections in patients with cystic fibrosis.11 The FDA’s Anti-Infectives Drugs Advisory Committee voted 15-2 in favor of the drug’s safety and effectiveness, and 17-0 in favor of a regimen of 75 mg three times a day. The FDA usually approves drugs recommended by its panels.
- Darapladib, a selective and orally active LpPLA2 inhibitor, has begun Phase 3 clinical trials in the management of acute coronary syndrome (ACS).12 The study will include 11,500 male and female patients from 40 countries. It is a double-blind, randomized, placebo-controlled clinical efficacy trial of the long-term use of darapladib when added to standard of care. The study will test whether darapladib affects the chances of having a cardiovascular event, such as a myocardial infarction or a stroke, when treatment is started within 30 days after an ACS.
- Denosumab has received a positive opinion from the European Union for treating osteoporosis in postmenopausal women at increased risk of fractures, and also for treating bone loss in men with prostate cancer who are at increased risk of fractures.13 In the U.S., approval by the FDA is pending for management of osteoporosis in postmenopausal women.14 The FDA’s reproductive health advisory committee, which evaluated the agent, voted 12-1 to require the drug to carry a REMS.
- Ocrelizumab, a Phase 3 humanized anti-CD20 monoclonal antibody for treating rheumatoid arthritis (RA), recently reported positive results when given in combination with methotrexate (MTX) in an international, randomized, multicenter, double-blind trial.15 Ocrelizumab or placebo administered by intravenous infusion on days one and 15 met the primary endpoint of improving the signs and symptoms of RA in patients with an inadequate response to MTX.
- A response to an FDA complete response letter dated May 2009 was expected for rivaroxaban, an oral, direct Factor Xa inhibitor for preventing DVT and pulmonary embolism in patients undergoing hip or knee surgery. Complete review of rivaroxaban data was deferred by its manufacturers until February.16,17
- The FDA is considering a new indication for rosuvastatin (Crestor), following recommendations of the Endocrinologic and Metabolic Drugs Advisory Committee on Dec. 15, 2009.18
Safety Information
Pay attention to two agents manufactured by AstraZeneca: Dexlansoprazole (Kapidex), a new formulation of the proton-pump inhibitor lansoprazole, and bicalutamide (Casodex), which is used in combination with a hormone treatment for prostate cancer, have had medication mixups. The agent names look alike and sound alike when written and verbalized. Both written and verbal prescriptions have been dispensed in error. Bicalutamide is available as 50-mg tablets; dexlansoprazole is available as 30-mg and 60-mg capsules. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Walsh S. FDA Approves Generic Aricept to Treat Dementia Related to Alzheimer’s Disease. U.S. Food and Drug Administration Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm194173.htm. Accessed Dec. 28, 2009.
- Amenal Receives FDA Approval For Nizatidine Oral Solution, the First Oral Solution for Axid in the Market. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/173591.php. Accessed Dec. 28, 2009.
- Clonidine ER Suspension and Clonidine ER Tablets approved. Monthly Prescribing Reference Web site. Available at: www.empr.com/clonidine-er-suspension-and-clonidine-er-tablets-approved/article/159148/. Accessed Dec. 28, 2009.
- FDA Approves Mcg Dose of Vagifem For the Treatment of Atrophic Vaginitis Due to Menopause. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/172804.php. Accessed Dec. 28, 2009.
- Todoruk M. Eli Lilly’s Zyprexa approved in US for adolescents. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=B5699B38AADB46AF85E7B34F508DB943&logRowId=340534. Accessed Dec. 28, 2009.
- Dennis M. FDA approves Eli Lilly’s long-acting Zyprexa injection. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=30C504823E42425FA0C3B9BB8490D5AA&logRowId=341775. Accessed Dec. 28, 2009.
- Gever J. FDA Approves Long-Acting Olanzapine. MedPage Today Web site. Available at: www.medpagetoday.com/ProductAlert/Prescriptions/17539. Accessed Dec. 28, 2009.
- Dennis M. FDA approves AstraZeneca’s Seroquel XR as add-on therapy; requires more data as monotherapy. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=0530A906ABCB44B5A32EC05E148E0220&logRowId=340531. Accessed Dec. 28, 2009.
- Petrochko C. FDA Approves IV Sildenafil for Hypertension. MedPage Today Web site. Available at: www.medpagetoday.com/ProductAlert/Prescriptions/17296. Accessed Dec. 28, 2009.
- FDA Approves Spiriva HandiHaler for the Reduction of COPD Exacerbations. Pfizer Web site. Available at: mediaroom.pfizer.com/portal/site/pfizer/?ndmViewId=news_view&newsId=20091217006384&newsLang=en. Accessed Dec. 28, 2009.
- Leuty R. Gilead wins panel OK for cystic fibrosis drug. San Francisco Business Times Web site. Available at: sanfrancisco.bizjournals.com/sanfrancisco/stories/2009/12/07/daily59.html?surround=etf&ana=e_article. Accessed Dec. 28, 2009.
- GSK initiates second pivotal Phase III trial for investigational cardiovascular medication Darapladib. GlaxoSmithKline Web site. Available at: www.gsk.com/media/pressreleases/2009/2009_pressrelease_10141.htm. Accessed Dec. 29, 2009.
- Todoruk M. EU panel issues positive opinion for Amgen’s Prolia. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=A9F30DD044A14893899DF7D880FB8AB0&logRowId=342650. Accessed Dec. 29, 2009.
- Walker EP. FDA Panel Backs Denosumab for Osteoporosis, But Not Osteopenia. MedPage Web site. Available at: www.medpagetoday.com/Endocrinology/Osteoporosis/15530. Accessed Dec. 29, 2009.
- Phase 3 study of ocrelizumab for rheumatoid arthritis (RA). Monthly Prescribing Reference Web site. Available at: www.empr.com/phase-3-study-of-ocrelizumab-for-rheumatoid-arthritis-ra/article/159474/. Accessed Dec. 29, 2009.
- Phase III EINSTEIN-Extension Study of Bayer’s Rivaroxaban Shows Significant Benefit in the Prevention of Secondary Symptomatic VTE. Bayer Web site. Available at: www.bayer.com/en/News-Detail.aspx?id=12554. Accessed Dec. 20, 2009.
- Todoruk M. Bayer, Johnson & Johnson provide update on Xarelto complete response to FDA. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=8F8AEC62E7DB46C3809C1E77A8384F30&logRowId=340535. Accessed Dec. 29, 2009.
- O’Riordan M. FDA advisory panel votes in favor of broadened rosuvastatin indication. TheHeart.org Web site. Available at: www.theheart.org/article/1035155/print.do. Accessed Dec. 29, 2009.
- Kapidex-Casodex confusion. Institute for Safe Medication Practices Web site. Available at: www.ismp.org/newsletters/ambulatory/archives/200907_1.asp. Accessed Dec. 28, 2009.
Market Watch
New Generics
- Fentanyl citrate troche/lozenge (generic Actiq) transmucosal lollipop1,2
- Perindopril erbumine (generic Aceon) tablets3
New Drugs, Indications, Label Changes, and Dosage Forms
- Capsaicin 8% patch (Qutenza) has been approved by the U.S. Food and Drug Administration (FDA) as a prescription medication to treat pain associated with post-herpetic neuralgia.4 The patch is a higher concentration than over-the-counter (OTC) products. The most common side effects in clinical trials were pain, swelling, itching, redness, and bumps at the application site, as well as blood pressure increases.5 Patch placement requires the use of a topical anesthetic and additional pain relief (ice or opioid pain relievers). Therefore, patch placement must be performed by a healthcare professional. Once the patch is applied, the patient must be observed for at least an hour, as there could be a significant increase in blood pressure.
- Diclofenac sodium topical (Pennsaid) has been approved by the FDA as a topical treatment to manage knee osteoarthritis.6 The transdermal carrier dimethylsulfoxide (DMSO) is utilized to deliver active diclofenac sodium through the skin to the pain site.7
- Exenatide injection (Byetta) has been approved by the FDA as monotherapy for treating patients with Type 2 diabetes mellitus, along with diet and exercise.8
- Human papilloma virus (HPV) vaccine (Gardasil) has been approved by the FDA for preventing condyloma acuminata due to HPV types 6 and 11 in males ages 9 to 26.9 The makers hope that this vaccine will decrease the need to treat genital warts. Clinical studies showed that in males not infected with HPV at the beginning of the study, the vaccine was close to 90% effective in preventing genital warts caused by infection of HPV types 6 and 11. The manufacturer plans to obtain additional safety and effectiveness information in this patient population.
- Lansoprazole 24HR (Prevacid OTC) 15-mg delayed-release capsules are available for treating frequent heartburn.10 The capsules will be available by prescription in both the 15-mg and 30-mg dosage strengths.
- Metoclopramide HCl orally disintegrating tablet (Metozolv ODT) has been approved by the FDA for treating both acute and recurrent diabetic gastroparesis and for the short-term management (four to 12 weeks) of adults with documented symptomatic gastroesophageal reflux disease who do not respond to conventional therapy.11
- Peramivir intravenous will be made available by the Centers for Disease Control (CDC) as an emergency treatment for children and adult patients who develop H1N1 influenza and are nonresponsive to oral or inhaled antiviral therapies.12
- Rosuvastatin (Crestor) has been approved by the FDA for treating heterozygous familial cholesterolemia in children ages 10-17.13
- Telmisartan 80-mg tablets (Micardis) have been approved by the FDA for risk reduction of myocardial infarction, stroke, or death from cardiovascular causes in patients 55 years and older who are at high risk for major cardiovascular events, or who are not able to take angiotensin-converting enzyme inhibitors.14
- Telmisartan/amlodipine tablets (Twynsta) have been approved by the FDA as a new combination for treating hypertension, either alone or in combination with other antihypertensive agents. This combination is not indicated for cardiovascular risk reduction. The tablets are available in the following strengths of telmisartan/amlodipine, respectively: 40 mg/5 mg, 40 mg/10 mg, 80 mg/5 mg, and 80 mg/10 mg.
- Tranexamic acid (Lysteda) has been approved by the FDA for the treatment of menorrhagia.15 This is the first nonhormonal, oral therapeutic agent approved to treat this condition.16
Pipeline
- Indacaterol is being investigated as a once-daily bronchodilator for treating adults with chronic obstructive pulmonary disease (COPD).17 Novartis has received a complete response letter from the FDA requesting additional data on the dosing of the agent. The company is working with the FDA to resolve these issues.
- Rituximab injection (Rituxan) is approved for treating moderate to severe rheumatoid arthritis after patients have been treated with methotrexate, as well as non-Hodgkin’s lymphoma.18 Genentech/Biogen is attempting to expand rituximab use to treat patients earlier in the course of their disease. The FDA recently rejected this application, citing the rare but serious safety risk of developing progressive multifocal leukoencephalopathy.
Safety Information
Use of omeprazole and clopidogrel combination therapy should be avoided, according to new data from the FDA.18 Current data suggest that clopidogrel’s antiplatelet effect may be hindered by 50% with concomitant omeprazole therapy. Omeprazole blocks the conversion of clopidogrel to its active, antiplatelet form, thus significantly decreasing its effectiveness. It is not known if other proton-pump inhibitors interfere with clopidogrel’s effectiveness. Other drugs that should not be used with clopidogrel include esomeprazole (Nexium), cimetidine (Tagamet and Tagamet HB), fluconazole (Diflucan), ketoconazole (Nizoral), voriconazole (VFEND), etravirine (Intelence), felbamate (Felbatol), fluoxetine (Prozac, Sarafem, and Symbyax), fluvoxamine (Luvox), and ticlopidine (Ticlid). TH
Michele B. Kaufman is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/docs/obdetail.cfm?Appl_No=077312&TABLE1=OB_Rx. Accessed Nov. 19, 2009.
- Covidien gets approval of generic pain drug. Forbes.com Web site. Available at: http://www.forbes.com/feeds/ap/2009/10/30/business-health-care-us-covidien-actiq_7069457.html. Accessed Nov. 19, 2009.
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/default.cfm Accessed Nov. 19, 2009.
- Riley K. FDA Approves New Drug Treatment for Long-Term Pain Relief after Shingles Attacks. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191003.htm. Accessed Nov. 19, 2009.
- Qutenza Approved for Post-Shingles Nerve Pain. U.S. News and World Report Web site. Available at: health.usnews.com/articles/health/healthday/2009/11/17/qutenza-approved-for-post-shingles-nerve-pain.html. Accessed Nov. 19, 2009.
- Nuvo shares surge on FDA pain cream approval. Reuters Web site. Available at: www.reuters.com/article/email/idUSN0543459820091105. Accessed Nov. 19, 2009.
- Pennsaid. Nuvo Web site. Available at: www.nuvoresearch.com/pipeline/pennsaid.asp. Accessed Nov. 19, 2009.
- BYETTA Approved For Expanded Use As First-Line Treatment For Type 2 Diabetes. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/169396.php. Accessed Nov. 19, 2009.
- Burgess S. FDA Approves New Indication for Gardasil to Prevent Genital Warts in Men and Boys. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm187003.htm Accessed Nov. 19, 2009.
- Prevacid 24hr available over-the-counter. Monthly Prescribing Reference Web site. Available at: www.empr.com/prevacid-24hr-available-over-the-counter/article/157592/. Accessed Nov. 19, 2009.
- FDA Approves New Salix Product Exclusively in Catalent’s Zydis Fast Dissolve Technology. Catalent Web site. Available at: www.catalent.com/about-us/news/45. Accessed Nov. 19, 2009.
- Peramivir to be Used for Special Swine Flu Cases. Pharmaceutical-Technology.com Web site. Available at: www.pharmaceutical-technology.com/News/News68102.html. Accessed Nov. 19, 2009.
- Dennis M. AstraZeneca’s Crestor approved in US for paediatric use; Vimovo filed in Europe. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=41E54BF434C54C8E903A9EB4EF0839AA&logRowId=332380. Accessed Nov. 19, 2009.
- FDA Approves New Use for Micardis in Cardiovascular Risk Reduction and Twynsta as New Combination Treatment for High Blood Pressure. Boehringer Ingelheim Web site. Available at: us.boehringer-ingelheim.com/newsroom/2009/files/micardis_twynsta_approve_10-19-09.pdf. Accessed Nov. 19, 2009.
- Todoruk M. FDA approves Xanodyne’s Lysteda for menorrhaegia. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=8FCB424A8E7147A08CEC9BFCD8A450D2&logRowId=337054. Accessed Nov. 19, 2009.
- Xanodyne announces FDA approval of Lysteda for treatment of women with heavy menstrual bleeding. Xanodyne Web site. Available at: www.xanodyne.com/newsroom_details.asp?NewsId=61. Accessed Nov. 19, 2009.
- Todoruk M. FDA requests additional data for Novartis’ COPD drug indacaterol. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=B426F5ED30AB43A89338DAD0124168A7&logRowId=332718. Accessed Nov. 19, 2009.
- Genentech and Biogen Idec Receive a Complete Response from FDA for Earlier Use of Rituxan for Rheumatoid Arthritis. Genentech Web site. Available at: www.gene.com/gene/news/press-releases/display.do?method=detail&id=12407. Accessed Nov. 19, 2009.
- Walsh S. FDA Announces New Warning on Plavix: Avoid Use with Prilosec/Prilosec OTC. FDA Web site. Available at www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191169.htm. Accessed Nov. 19, 2009.
New Generics
- Fentanyl citrate troche/lozenge (generic Actiq) transmucosal lollipop1,2
- Perindopril erbumine (generic Aceon) tablets3
New Drugs, Indications, Label Changes, and Dosage Forms
- Capsaicin 8% patch (Qutenza) has been approved by the U.S. Food and Drug Administration (FDA) as a prescription medication to treat pain associated with post-herpetic neuralgia.4 The patch is a higher concentration than over-the-counter (OTC) products. The most common side effects in clinical trials were pain, swelling, itching, redness, and bumps at the application site, as well as blood pressure increases.5 Patch placement requires the use of a topical anesthetic and additional pain relief (ice or opioid pain relievers). Therefore, patch placement must be performed by a healthcare professional. Once the patch is applied, the patient must be observed for at least an hour, as there could be a significant increase in blood pressure.
- Diclofenac sodium topical (Pennsaid) has been approved by the FDA as a topical treatment to manage knee osteoarthritis.6 The transdermal carrier dimethylsulfoxide (DMSO) is utilized to deliver active diclofenac sodium through the skin to the pain site.7
- Exenatide injection (Byetta) has been approved by the FDA as monotherapy for treating patients with Type 2 diabetes mellitus, along with diet and exercise.8
- Human papilloma virus (HPV) vaccine (Gardasil) has been approved by the FDA for preventing condyloma acuminata due to HPV types 6 and 11 in males ages 9 to 26.9 The makers hope that this vaccine will decrease the need to treat genital warts. Clinical studies showed that in males not infected with HPV at the beginning of the study, the vaccine was close to 90% effective in preventing genital warts caused by infection of HPV types 6 and 11. The manufacturer plans to obtain additional safety and effectiveness information in this patient population.
- Lansoprazole 24HR (Prevacid OTC) 15-mg delayed-release capsules are available for treating frequent heartburn.10 The capsules will be available by prescription in both the 15-mg and 30-mg dosage strengths.
- Metoclopramide HCl orally disintegrating tablet (Metozolv ODT) has been approved by the FDA for treating both acute and recurrent diabetic gastroparesis and for the short-term management (four to 12 weeks) of adults with documented symptomatic gastroesophageal reflux disease who do not respond to conventional therapy.11
- Peramivir intravenous will be made available by the Centers for Disease Control (CDC) as an emergency treatment for children and adult patients who develop H1N1 influenza and are nonresponsive to oral or inhaled antiviral therapies.12
- Rosuvastatin (Crestor) has been approved by the FDA for treating heterozygous familial cholesterolemia in children ages 10-17.13
- Telmisartan 80-mg tablets (Micardis) have been approved by the FDA for risk reduction of myocardial infarction, stroke, or death from cardiovascular causes in patients 55 years and older who are at high risk for major cardiovascular events, or who are not able to take angiotensin-converting enzyme inhibitors.14
- Telmisartan/amlodipine tablets (Twynsta) have been approved by the FDA as a new combination for treating hypertension, either alone or in combination with other antihypertensive agents. This combination is not indicated for cardiovascular risk reduction. The tablets are available in the following strengths of telmisartan/amlodipine, respectively: 40 mg/5 mg, 40 mg/10 mg, 80 mg/5 mg, and 80 mg/10 mg.
- Tranexamic acid (Lysteda) has been approved by the FDA for the treatment of menorrhagia.15 This is the first nonhormonal, oral therapeutic agent approved to treat this condition.16
Pipeline
- Indacaterol is being investigated as a once-daily bronchodilator for treating adults with chronic obstructive pulmonary disease (COPD).17 Novartis has received a complete response letter from the FDA requesting additional data on the dosing of the agent. The company is working with the FDA to resolve these issues.
- Rituximab injection (Rituxan) is approved for treating moderate to severe rheumatoid arthritis after patients have been treated with methotrexate, as well as non-Hodgkin’s lymphoma.18 Genentech/Biogen is attempting to expand rituximab use to treat patients earlier in the course of their disease. The FDA recently rejected this application, citing the rare but serious safety risk of developing progressive multifocal leukoencephalopathy.
Safety Information
Use of omeprazole and clopidogrel combination therapy should be avoided, according to new data from the FDA.18 Current data suggest that clopidogrel’s antiplatelet effect may be hindered by 50% with concomitant omeprazole therapy. Omeprazole blocks the conversion of clopidogrel to its active, antiplatelet form, thus significantly decreasing its effectiveness. It is not known if other proton-pump inhibitors interfere with clopidogrel’s effectiveness. Other drugs that should not be used with clopidogrel include esomeprazole (Nexium), cimetidine (Tagamet and Tagamet HB), fluconazole (Diflucan), ketoconazole (Nizoral), voriconazole (VFEND), etravirine (Intelence), felbamate (Felbatol), fluoxetine (Prozac, Sarafem, and Symbyax), fluvoxamine (Luvox), and ticlopidine (Ticlid). TH
Michele B. Kaufman is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/docs/obdetail.cfm?Appl_No=077312&TABLE1=OB_Rx. Accessed Nov. 19, 2009.
- Covidien gets approval of generic pain drug. Forbes.com Web site. Available at: http://www.forbes.com/feeds/ap/2009/10/30/business-health-care-us-covidien-actiq_7069457.html. Accessed Nov. 19, 2009.
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/default.cfm Accessed Nov. 19, 2009.
- Riley K. FDA Approves New Drug Treatment for Long-Term Pain Relief after Shingles Attacks. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191003.htm. Accessed Nov. 19, 2009.
- Qutenza Approved for Post-Shingles Nerve Pain. U.S. News and World Report Web site. Available at: health.usnews.com/articles/health/healthday/2009/11/17/qutenza-approved-for-post-shingles-nerve-pain.html. Accessed Nov. 19, 2009.
- Nuvo shares surge on FDA pain cream approval. Reuters Web site. Available at: www.reuters.com/article/email/idUSN0543459820091105. Accessed Nov. 19, 2009.
- Pennsaid. Nuvo Web site. Available at: www.nuvoresearch.com/pipeline/pennsaid.asp. Accessed Nov. 19, 2009.
- BYETTA Approved For Expanded Use As First-Line Treatment For Type 2 Diabetes. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/169396.php. Accessed Nov. 19, 2009.
- Burgess S. FDA Approves New Indication for Gardasil to Prevent Genital Warts in Men and Boys. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm187003.htm Accessed Nov. 19, 2009.
- Prevacid 24hr available over-the-counter. Monthly Prescribing Reference Web site. Available at: www.empr.com/prevacid-24hr-available-over-the-counter/article/157592/. Accessed Nov. 19, 2009.
- FDA Approves New Salix Product Exclusively in Catalent’s Zydis Fast Dissolve Technology. Catalent Web site. Available at: www.catalent.com/about-us/news/45. Accessed Nov. 19, 2009.
- Peramivir to be Used for Special Swine Flu Cases. Pharmaceutical-Technology.com Web site. Available at: www.pharmaceutical-technology.com/News/News68102.html. Accessed Nov. 19, 2009.
- Dennis M. AstraZeneca’s Crestor approved in US for paediatric use; Vimovo filed in Europe. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=41E54BF434C54C8E903A9EB4EF0839AA&logRowId=332380. Accessed Nov. 19, 2009.
- FDA Approves New Use for Micardis in Cardiovascular Risk Reduction and Twynsta as New Combination Treatment for High Blood Pressure. Boehringer Ingelheim Web site. Available at: us.boehringer-ingelheim.com/newsroom/2009/files/micardis_twynsta_approve_10-19-09.pdf. Accessed Nov. 19, 2009.
- Todoruk M. FDA approves Xanodyne’s Lysteda for menorrhaegia. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=8FCB424A8E7147A08CEC9BFCD8A450D2&logRowId=337054. Accessed Nov. 19, 2009.
- Xanodyne announces FDA approval of Lysteda for treatment of women with heavy menstrual bleeding. Xanodyne Web site. Available at: www.xanodyne.com/newsroom_details.asp?NewsId=61. Accessed Nov. 19, 2009.
- Todoruk M. FDA requests additional data for Novartis’ COPD drug indacaterol. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=B426F5ED30AB43A89338DAD0124168A7&logRowId=332718. Accessed Nov. 19, 2009.
- Genentech and Biogen Idec Receive a Complete Response from FDA for Earlier Use of Rituxan for Rheumatoid Arthritis. Genentech Web site. Available at: www.gene.com/gene/news/press-releases/display.do?method=detail&id=12407. Accessed Nov. 19, 2009.
- Walsh S. FDA Announces New Warning on Plavix: Avoid Use with Prilosec/Prilosec OTC. FDA Web site. Available at www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191169.htm. Accessed Nov. 19, 2009.
New Generics
- Fentanyl citrate troche/lozenge (generic Actiq) transmucosal lollipop1,2
- Perindopril erbumine (generic Aceon) tablets3
New Drugs, Indications, Label Changes, and Dosage Forms
- Capsaicin 8% patch (Qutenza) has been approved by the U.S. Food and Drug Administration (FDA) as a prescription medication to treat pain associated with post-herpetic neuralgia.4 The patch is a higher concentration than over-the-counter (OTC) products. The most common side effects in clinical trials were pain, swelling, itching, redness, and bumps at the application site, as well as blood pressure increases.5 Patch placement requires the use of a topical anesthetic and additional pain relief (ice or opioid pain relievers). Therefore, patch placement must be performed by a healthcare professional. Once the patch is applied, the patient must be observed for at least an hour, as there could be a significant increase in blood pressure.
- Diclofenac sodium topical (Pennsaid) has been approved by the FDA as a topical treatment to manage knee osteoarthritis.6 The transdermal carrier dimethylsulfoxide (DMSO) is utilized to deliver active diclofenac sodium through the skin to the pain site.7
- Exenatide injection (Byetta) has been approved by the FDA as monotherapy for treating patients with Type 2 diabetes mellitus, along with diet and exercise.8
- Human papilloma virus (HPV) vaccine (Gardasil) has been approved by the FDA for preventing condyloma acuminata due to HPV types 6 and 11 in males ages 9 to 26.9 The makers hope that this vaccine will decrease the need to treat genital warts. Clinical studies showed that in males not infected with HPV at the beginning of the study, the vaccine was close to 90% effective in preventing genital warts caused by infection of HPV types 6 and 11. The manufacturer plans to obtain additional safety and effectiveness information in this patient population.
- Lansoprazole 24HR (Prevacid OTC) 15-mg delayed-release capsules are available for treating frequent heartburn.10 The capsules will be available by prescription in both the 15-mg and 30-mg dosage strengths.
- Metoclopramide HCl orally disintegrating tablet (Metozolv ODT) has been approved by the FDA for treating both acute and recurrent diabetic gastroparesis and for the short-term management (four to 12 weeks) of adults with documented symptomatic gastroesophageal reflux disease who do not respond to conventional therapy.11
- Peramivir intravenous will be made available by the Centers for Disease Control (CDC) as an emergency treatment for children and adult patients who develop H1N1 influenza and are nonresponsive to oral or inhaled antiviral therapies.12
- Rosuvastatin (Crestor) has been approved by the FDA for treating heterozygous familial cholesterolemia in children ages 10-17.13
- Telmisartan 80-mg tablets (Micardis) have been approved by the FDA for risk reduction of myocardial infarction, stroke, or death from cardiovascular causes in patients 55 years and older who are at high risk for major cardiovascular events, or who are not able to take angiotensin-converting enzyme inhibitors.14
- Telmisartan/amlodipine tablets (Twynsta) have been approved by the FDA as a new combination for treating hypertension, either alone or in combination with other antihypertensive agents. This combination is not indicated for cardiovascular risk reduction. The tablets are available in the following strengths of telmisartan/amlodipine, respectively: 40 mg/5 mg, 40 mg/10 mg, 80 mg/5 mg, and 80 mg/10 mg.
- Tranexamic acid (Lysteda) has been approved by the FDA for the treatment of menorrhagia.15 This is the first nonhormonal, oral therapeutic agent approved to treat this condition.16
Pipeline
- Indacaterol is being investigated as a once-daily bronchodilator for treating adults with chronic obstructive pulmonary disease (COPD).17 Novartis has received a complete response letter from the FDA requesting additional data on the dosing of the agent. The company is working with the FDA to resolve these issues.
- Rituximab injection (Rituxan) is approved for treating moderate to severe rheumatoid arthritis after patients have been treated with methotrexate, as well as non-Hodgkin’s lymphoma.18 Genentech/Biogen is attempting to expand rituximab use to treat patients earlier in the course of their disease. The FDA recently rejected this application, citing the rare but serious safety risk of developing progressive multifocal leukoencephalopathy.
Safety Information
Use of omeprazole and clopidogrel combination therapy should be avoided, according to new data from the FDA.18 Current data suggest that clopidogrel’s antiplatelet effect may be hindered by 50% with concomitant omeprazole therapy. Omeprazole blocks the conversion of clopidogrel to its active, antiplatelet form, thus significantly decreasing its effectiveness. It is not known if other proton-pump inhibitors interfere with clopidogrel’s effectiveness. Other drugs that should not be used with clopidogrel include esomeprazole (Nexium), cimetidine (Tagamet and Tagamet HB), fluconazole (Diflucan), ketoconazole (Nizoral), voriconazole (VFEND), etravirine (Intelence), felbamate (Felbatol), fluoxetine (Prozac, Sarafem, and Symbyax), fluvoxamine (Luvox), and ticlopidine (Ticlid). TH
Michele B. Kaufman is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/docs/obdetail.cfm?Appl_No=077312&TABLE1=OB_Rx. Accessed Nov. 19, 2009.
- Covidien gets approval of generic pain drug. Forbes.com Web site. Available at: http://www.forbes.com/feeds/ap/2009/10/30/business-health-care-us-covidien-actiq_7069457.html. Accessed Nov. 19, 2009.
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/default.cfm Accessed Nov. 19, 2009.
- Riley K. FDA Approves New Drug Treatment for Long-Term Pain Relief after Shingles Attacks. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191003.htm. Accessed Nov. 19, 2009.
- Qutenza Approved for Post-Shingles Nerve Pain. U.S. News and World Report Web site. Available at: health.usnews.com/articles/health/healthday/2009/11/17/qutenza-approved-for-post-shingles-nerve-pain.html. Accessed Nov. 19, 2009.
- Nuvo shares surge on FDA pain cream approval. Reuters Web site. Available at: www.reuters.com/article/email/idUSN0543459820091105. Accessed Nov. 19, 2009.
- Pennsaid. Nuvo Web site. Available at: www.nuvoresearch.com/pipeline/pennsaid.asp. Accessed Nov. 19, 2009.
- BYETTA Approved For Expanded Use As First-Line Treatment For Type 2 Diabetes. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/169396.php. Accessed Nov. 19, 2009.
- Burgess S. FDA Approves New Indication for Gardasil to Prevent Genital Warts in Men and Boys. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm187003.htm Accessed Nov. 19, 2009.
- Prevacid 24hr available over-the-counter. Monthly Prescribing Reference Web site. Available at: www.empr.com/prevacid-24hr-available-over-the-counter/article/157592/. Accessed Nov. 19, 2009.
- FDA Approves New Salix Product Exclusively in Catalent’s Zydis Fast Dissolve Technology. Catalent Web site. Available at: www.catalent.com/about-us/news/45. Accessed Nov. 19, 2009.
- Peramivir to be Used for Special Swine Flu Cases. Pharmaceutical-Technology.com Web site. Available at: www.pharmaceutical-technology.com/News/News68102.html. Accessed Nov. 19, 2009.
- Dennis M. AstraZeneca’s Crestor approved in US for paediatric use; Vimovo filed in Europe. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=41E54BF434C54C8E903A9EB4EF0839AA&logRowId=332380. Accessed Nov. 19, 2009.
- FDA Approves New Use for Micardis in Cardiovascular Risk Reduction and Twynsta as New Combination Treatment for High Blood Pressure. Boehringer Ingelheim Web site. Available at: us.boehringer-ingelheim.com/newsroom/2009/files/micardis_twynsta_approve_10-19-09.pdf. Accessed Nov. 19, 2009.
- Todoruk M. FDA approves Xanodyne’s Lysteda for menorrhaegia. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=8FCB424A8E7147A08CEC9BFCD8A450D2&logRowId=337054. Accessed Nov. 19, 2009.
- Xanodyne announces FDA approval of Lysteda for treatment of women with heavy menstrual bleeding. Xanodyne Web site. Available at: www.xanodyne.com/newsroom_details.asp?NewsId=61. Accessed Nov. 19, 2009.
- Todoruk M. FDA requests additional data for Novartis’ COPD drug indacaterol. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=B426F5ED30AB43A89338DAD0124168A7&logRowId=332718. Accessed Nov. 19, 2009.
- Genentech and Biogen Idec Receive a Complete Response from FDA for Earlier Use of Rituxan for Rheumatoid Arthritis. Genentech Web site. Available at: www.gene.com/gene/news/press-releases/display.do?method=detail&id=12407. Accessed Nov. 19, 2009.
- Walsh S. FDA Announces New Warning on Plavix: Avoid Use with Prilosec/Prilosec OTC. FDA Web site. Available at www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191169.htm. Accessed Nov. 19, 2009.
Growth Spurt
Despite intravenous medication, a young boy in status epilepticus had the pediatric ICU team at the University of Wisconsin School of Medicine and Public Health in Madison stumped. The team called for a consult with the Integrative Medicine Program, which works with licensed acupuncturists and has been affiliated with the department of family medicine since 2001. Acupuncture’s efficacy in this setting has not been validated, but it has been shown to ease chemotherapy-induced nausea and vomiting, as well as radiation-induced xerostomia.1,2
Following several treatments by a licensed acupuncturist and continued conventional care, the boy’s seizures subsided and he was transitioned to the medical floor. Did the acupuncture contribute to bringing the seizures under control? “I can’t say that it was the acupuncture—it was probably a function of all the therapies working together,” says David P. Rakel, MD, assistant professor and director of UW’s Integrative Medicine Program.
The UW case illustrates both current trends and the constant conundrum that surrounds hospital-based complementary medicine: Complementary and alternative medicine’s use is increasing in some U.S. hospitals, yet the existing research evidence for the efficacy of its multiple modalities is decidedly mixed.
Even if your hospital does not offer complementary and alternative medicine (CAM), your patients are using CAM at ever-increasing rates. In 1993, 34% of Americans reported using some type of CAM (e.g., supplements, massage therapy, prayer, and so on). That number has almost doubled to 62%.3 Americans spend $47 billion a year—of their own money—for CAM therapies, chiropractors, acupuncturists, and massage therapists. And older patients with chronic conditions—the kind of patient hospitalists are most familiar with—tend to try CAM more than younger patients.4
These trends can directly affect hospitalists’ treatment decisions, but they also play a part in how you establish communication and trust with your patients, and how you keep your patients safe from adverse drug interactions. According to the National Academy of Sciences, in order to effectively counsel patients and ensure high-quality comprehensive care, conventional professionals need more CAM-related education.5
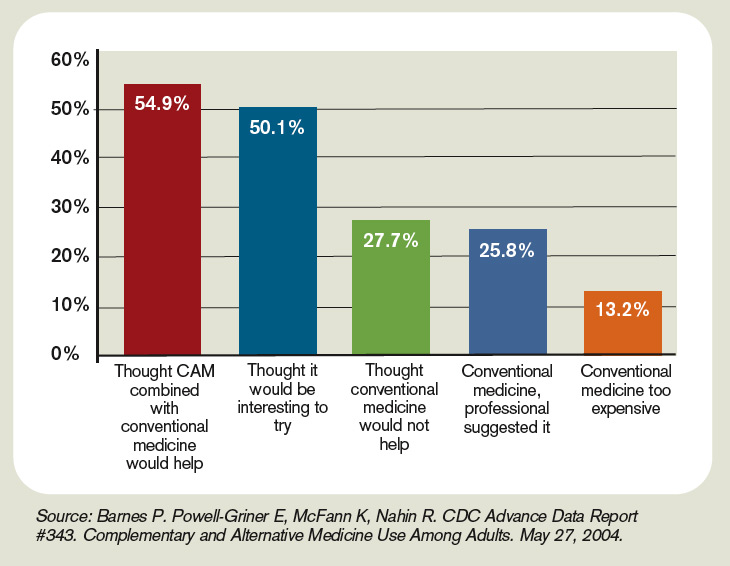

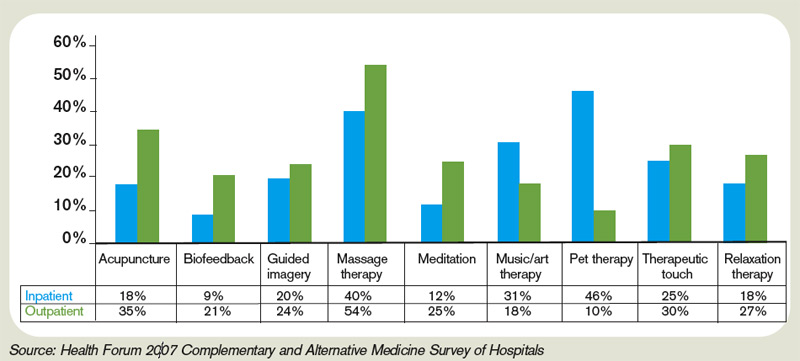
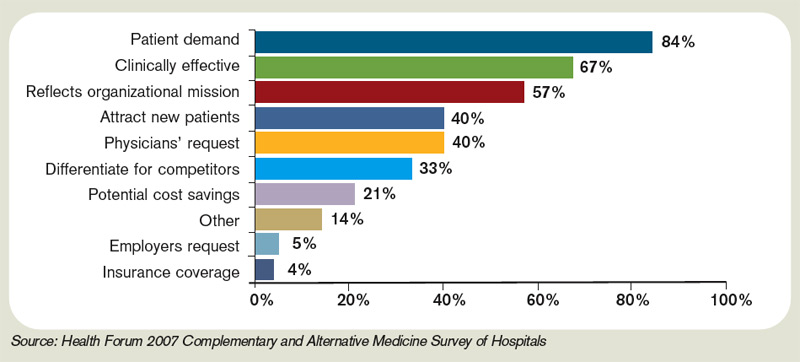
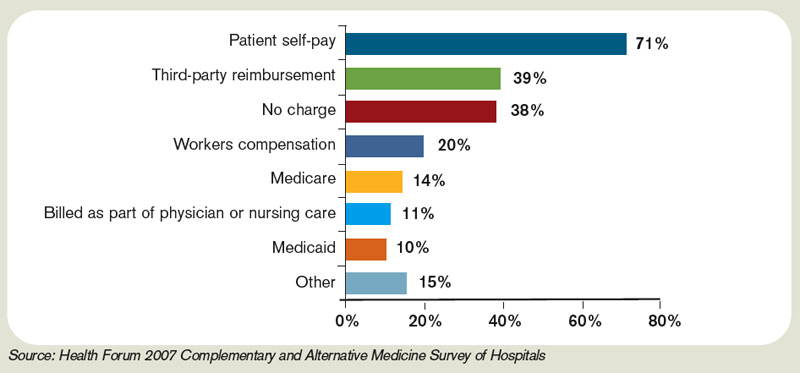

—Suzanne Bertisch, MD, MPH, fellow, Harvard Medical School’s Osher Research Center
Complementary Medicine: Online Resources

- National Center for Complementary and Alternative Medicine: http://nccam.nih.gov
- Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center’s About Herbs: www.mskcc.org/mskcc/html/11570.cfm
- Natural Standard: www.naturalstandard.com
- The M.D. Anderson Cancer Center’s Complementary/Integrative Medicine Education Resources: www.mdanderson.org/departments/CIMER
What Trends Show
In 2007, according to the American Hospital Association, 20.8% of community hospitals offered some type of care or treatment not based on traditional Western allopathic medicine. That’s up from 8.6% of reporting hospitals that offered those services in 1998.
The 1990s saw rapid growth of integrative medicine centers at major research institutions, and the majority of U.S. cancer centers now offer some form of complementary therapy, says Barrie R. Cassileth, MS, PhD, the Laurance S. Rockefeller Chair in Integrative Medicine and chief of the Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center in New York City.
The 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals reported that complementary programs are more common in urban rather than rural hospitals; services vary by hospital size (see Figure 2, above); and the top six modalities offered on an inpatient basis are pet therapy, massage therapy, music/art therapy, guided imagery, acupuncture, and reiki (see “Glossary of Complementary Terms,” above). Eighty-four percent of hospitals offer complementary services due to patient demand, the survey showed.
Joseph Ming-Wah Li, MD, FHM, SHM board member and assistant professor of medicine at Harvard Medical School and director of the hospital medicine program and associate chief of the division of general medicine and primary care at Beth Israel Deaconess Medical Center in Boston, doesn’t see a problem with modalities that can make his patients feel better. Patients at his hospital have access to pet therapy, massage, and acupuncture. “I don’t think these modalities hurt our patients, and there is very little downside, except for potential cost,” says Dr. Li, an SHM board member. “What’s not clear is whether these therapies work or not.”
What’s in a Name?
Numerous therapies and modalities crowd under the CAM umbrella, but most experts classify “complementary” modalities as those used in conjunction with conventional medicine to mitigate symptoms of disease or treatment, whereas “alternative” connotes therapies claiming to treat or cure the underlying disease. Some harmful, dangerous, and dishonest practices fall into the “alternative” category, such as Hulda Clark’s “Zapper” device, which was promoted as a cure for liver flukes, something she says cause everything from diabetes to heart disease. (For more on questionable practices, visit www.quackwatch.com or the National Council Against Health Fraud’s Web site at www.ncahf.org.)
The National Institutes of Health’s National Center for Complementary and Alternative Medicine (NCCAM) defines CAM as a group of “diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine.” Dr. Cassileth says the conflation of “complementary and alternative” into one neat acronym—CAM—causes confusion among patients and medical professionals. NCCAM will be changing its name soon, she says, to the National Center for Integrative Medicine, emphasizing the use of adjunctive modalities along with conventional medical treatments.
Hospitalist Suzanne Bertisch, MD, MPH, recently completed a research fellowship at Harvard Medical School’s Osher Research Center. She explains that integrative medicine uses a macro model of health, claiming a middle ground between the traditional, allopathic model of treating disease.
All Kinds of Evidence
Twenty years of complementary medicine research has yielded some information about safety—namely, what works and what doesn’t. For example, saw palmetto has not panned out as an effective treatment for benign prostatic hyperplasia; St. John’s wort, useful for mild depression, interferes with many medications, including cyclosporine and warfarin, and should be avoided at least five days prior to surgery.7,8
Since NCCAM’s inception in October 1998, its research portfolio has stirred debate in the scientific community. Part of the disagreement stems from the difficulty of fitting multidimensional interventions, some of which are provider-dependent (e.g., massage or acupuncture), into the gold standard of the randomized, double-blind, placebo-controlled trial, explains Darshan Mehta, MD, MPH, associate director of medical education at the Benson-Henry Institute for Mind Body Medicine at Massachusetts General Hospital in Boston. The manner in which the effectiveness of integrative techniques is assessed requires a higher sophistication of systems research, Dr. Mehta says.
“The way we construe evidence needs to change,” she adds.
Likely to Expand
Most private health plans do not cover complementary services, although Medicare and numerous insurance plans will reimburse treatment in conjunction with physical therapy (e.g., massage) in the outpatient setting. Twenty-three states cover chiropractic care under Medicaid, and Medicare has begun to assess the cost-effectiveness of including acupuncture—especially for postoperative and chemotherapy-associated nausea and vomiting—in its benefits package.9 Other modalities, ranging from aromatherapy to guided imagery training, are paid for largely out-of-pocket.10
Dr. Rakel notes that the delivery of integrative medicine services at UW entails conversations with patients about out-of-pocket payments. “It can pose a barrier to the clinician-patient relationship if you give them acupuncture to help with their chemotherapy-induced nausea and then ask for their credit card,” he says.
Hospitalist Preparation
Most complementary therapies are currently offered on an outpatient basis. Because of this trend, and because they deal with acute conditions, hospitalists are less likely to be involved with complementary or integrative medicine services, says Beth Israel Deaconess Medical Center hospitalist Andrew C. Ahn, MD, MPH. But that’s not to say complementary medicine is something hospitalists should ignore; patients arrive at the hospital with CAM regimens in tow. It’s the No. 1 reason, Dr. Ahn says, hospitalists should be knowledgeable and exposed to CAM therapies.
Physicians must understand patient patterns and preferences regarding allopathic and complementary medicine, says Sita Ananth, MHA, director of knowledge services and optimal healing environments at the Samueli Institute in Alexandria, Va., and author of the 2007 AHA report. She points to a 2006 survey conducted by AARP and NCCAM that found almost 70% of respondents did not tell their physicians about their complementary medicine approaches. These patients are within the age range most likely to be cared for by hospitalists, and failure to communicate about complementary treatment, such as supplemental vitamin use, could lead to safety issues. Moreover, without complete disclosure, the patient-physician relationship might not be as open as possible, Dr. Ananth says.
Many acute-care hospitalists do not have formal dietary supplement policies, and less than half of U.S. children’s hospitals require documentation of a check for drug or dietary supplement interaction.11,12 As a safety issue, it is always incumbent on hospitalists, says Dr. Li, to ask about any supplements or therapies patients are trying on their own as part of the history and physical examination. The policy at Memorial Sloan-Kettering Cancer Center, Dr. Cassileth says, is that patients on chemotherapy or who are undergoing radiation or facing surgery must avoid herbal dietary supplements.
Beyond Safety
Dr. Bertisch advises hospitalists to pose questions about complementary therapies in an open manner, avoiding antagonistic discussions. “Even when I disagree, I try to guide them to issues about safety and nonsafety, and coax in my concerns,” she says. “The most challenging part about complementary medicine is that patients’ beliefs in these therapies may be so strong that even if the doctor says it won’t work, that will not necessarily change that belief.” A 2001 study in the Archives of Internal Medicine revealed that 70% of respondents would continue to take supplements even if a major study or their physician told them they didn’t work.13
The attraction to complementary medicine often reflects patients’ preferences for a holistic approach to health, says Dr. Ahn, or it may emanate from traditions carried with them from their country of origin. “Once you do understand their reasons for using CAM, then the patient-physician relationship can be significantly strengthened,” he says. With nearly two-thirds of Americans using some form of CAM, hospitalists need to engage in this dialogue.
Dr. Rakel agrees understanding patient culture is vital to uncovering useful information. “Most clinicians would agree that if we can match a therapy to the patient culture and belief system, we are more likely to get buy-in from the patient,” he says.
Dr. Mehta also is a clinical instructor of medicine at Harvard Medical School. He teaches his residents to educate themselves about credentialing, certification, and licensure of complementary providers. He also asks them to maintain an open mind. He says the most important preparation for hospitalists right now is to help educate their patients to be more proactive in their own healthcare. “An engaged patient,” he says, “is better than a disengaged patient.” TH
Gretchen Henkel is a freelance writer based in California.
References
- Deng G, Cassileth BR, Yeung KS. Complementary therapies for cancer-related symptoms. J Support Oncol. 2004;2(5):419-426.
- Kahn ST, Johnstone PA. Management of xerostomia related to radiotherapy for head and neck cancer. Oncology. 2005;19(14):1827-1832.
- Barnes PM, Powell-Griner E, McFann K, Nahin RL. Complementary and alternative medicine use among adults: United States, 2002. Adv Data. 2004;27(343):1-19.
- Eisenberg DM, Davis RB, Ettner SL, et al. Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. JAMA. 1998;280(18):1569-1575.
- Committee on the Use of Complementary and Alternative Medicine by the American Public. Complementary and Alternative Medicine in the United States. Washington, D.C: National Academies Press; 2005.
- Ananth S. 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals. Health Forum LLC. 2008.
- Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354(6):557-566.
- Bauer BA. The herbal hospitalist. The Hospitalist. 2006;10(2);16-17.
- Ananth S. Applying integrative healthcare. Explore. 2009;5(2):119-120.
- Eisenberg DM, Kessler RC, Foster C, Norlock FE, Calkins DR, Delbanco TL. Unconventional medicine in the United States. Prevalence, costs, and patterns of use. N Engl J Med. 1993;328:246-52
- Bassie KL, Witmer DR, Pinto B, Bush C, Clark J, Deffenbaugh J Jr. National survey of dietary supplement policies in acute care facilities. Am J Health Syst Pharm. 2006;63(1):65-70.
- Gardiner P, Phillips RS, Kemper KJ, Legedza A, Henlon S, Woolf AD. Dietary supplements: inpatient policies in US children’s hospitals. Pediatrics. 2008;121(4):e775-781.
- Blendon RJ, DesRoches CM, Benson JM, Brodie M, Altman DE. Americans’ views on the use and regulation of dietary supplements. Arch Intern Med. 2001;161(6):805-810.
Top Image Source: TETRA IMAGES
Despite intravenous medication, a young boy in status epilepticus had the pediatric ICU team at the University of Wisconsin School of Medicine and Public Health in Madison stumped. The team called for a consult with the Integrative Medicine Program, which works with licensed acupuncturists and has been affiliated with the department of family medicine since 2001. Acupuncture’s efficacy in this setting has not been validated, but it has been shown to ease chemotherapy-induced nausea and vomiting, as well as radiation-induced xerostomia.1,2
Following several treatments by a licensed acupuncturist and continued conventional care, the boy’s seizures subsided and he was transitioned to the medical floor. Did the acupuncture contribute to bringing the seizures under control? “I can’t say that it was the acupuncture—it was probably a function of all the therapies working together,” says David P. Rakel, MD, assistant professor and director of UW’s Integrative Medicine Program.
The UW case illustrates both current trends and the constant conundrum that surrounds hospital-based complementary medicine: Complementary and alternative medicine’s use is increasing in some U.S. hospitals, yet the existing research evidence for the efficacy of its multiple modalities is decidedly mixed.
Even if your hospital does not offer complementary and alternative medicine (CAM), your patients are using CAM at ever-increasing rates. In 1993, 34% of Americans reported using some type of CAM (e.g., supplements, massage therapy, prayer, and so on). That number has almost doubled to 62%.3 Americans spend $47 billion a year—of their own money—for CAM therapies, chiropractors, acupuncturists, and massage therapists. And older patients with chronic conditions—the kind of patient hospitalists are most familiar with—tend to try CAM more than younger patients.4
These trends can directly affect hospitalists’ treatment decisions, but they also play a part in how you establish communication and trust with your patients, and how you keep your patients safe from adverse drug interactions. According to the National Academy of Sciences, in order to effectively counsel patients and ensure high-quality comprehensive care, conventional professionals need more CAM-related education.5
—Suzanne Bertisch, MD, MPH, fellow, Harvard Medical School’s Osher Research Center
Complementary Medicine: Online Resources
- National Center for Complementary and Alternative Medicine: http://nccam.nih.gov
- Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center’s About Herbs: www.mskcc.org/mskcc/html/11570.cfm
- Natural Standard: www.naturalstandard.com
- The M.D. Anderson Cancer Center’s Complementary/Integrative Medicine Education Resources: www.mdanderson.org/departments/CIMER
What Trends Show
In 2007, according to the American Hospital Association, 20.8% of community hospitals offered some type of care or treatment not based on traditional Western allopathic medicine. That’s up from 8.6% of reporting hospitals that offered those services in 1998.
The 1990s saw rapid growth of integrative medicine centers at major research institutions, and the majority of U.S. cancer centers now offer some form of complementary therapy, says Barrie R. Cassileth, MS, PhD, the Laurance S. Rockefeller Chair in Integrative Medicine and chief of the Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center in New York City.
The 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals reported that complementary programs are more common in urban rather than rural hospitals; services vary by hospital size (see Figure 2, above); and the top six modalities offered on an inpatient basis are pet therapy, massage therapy, music/art therapy, guided imagery, acupuncture, and reiki (see “Glossary of Complementary Terms,” above). Eighty-four percent of hospitals offer complementary services due to patient demand, the survey showed.
Joseph Ming-Wah Li, MD, FHM, SHM board member and assistant professor of medicine at Harvard Medical School and director of the hospital medicine program and associate chief of the division of general medicine and primary care at Beth Israel Deaconess Medical Center in Boston, doesn’t see a problem with modalities that can make his patients feel better. Patients at his hospital have access to pet therapy, massage, and acupuncture. “I don’t think these modalities hurt our patients, and there is very little downside, except for potential cost,” says Dr. Li, an SHM board member. “What’s not clear is whether these therapies work or not.”
What’s in a Name?
Numerous therapies and modalities crowd under the CAM umbrella, but most experts classify “complementary” modalities as those used in conjunction with conventional medicine to mitigate symptoms of disease or treatment, whereas “alternative” connotes therapies claiming to treat or cure the underlying disease. Some harmful, dangerous, and dishonest practices fall into the “alternative” category, such as Hulda Clark’s “Zapper” device, which was promoted as a cure for liver flukes, something she says cause everything from diabetes to heart disease. (For more on questionable practices, visit www.quackwatch.com or the National Council Against Health Fraud’s Web site at www.ncahf.org.)
The National Institutes of Health’s National Center for Complementary and Alternative Medicine (NCCAM) defines CAM as a group of “diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine.” Dr. Cassileth says the conflation of “complementary and alternative” into one neat acronym—CAM—causes confusion among patients and medical professionals. NCCAM will be changing its name soon, she says, to the National Center for Integrative Medicine, emphasizing the use of adjunctive modalities along with conventional medical treatments.
Hospitalist Suzanne Bertisch, MD, MPH, recently completed a research fellowship at Harvard Medical School’s Osher Research Center. She explains that integrative medicine uses a macro model of health, claiming a middle ground between the traditional, allopathic model of treating disease.
All Kinds of Evidence
Twenty years of complementary medicine research has yielded some information about safety—namely, what works and what doesn’t. For example, saw palmetto has not panned out as an effective treatment for benign prostatic hyperplasia; St. John’s wort, useful for mild depression, interferes with many medications, including cyclosporine and warfarin, and should be avoided at least five days prior to surgery.7,8
Since NCCAM’s inception in October 1998, its research portfolio has stirred debate in the scientific community. Part of the disagreement stems from the difficulty of fitting multidimensional interventions, some of which are provider-dependent (e.g., massage or acupuncture), into the gold standard of the randomized, double-blind, placebo-controlled trial, explains Darshan Mehta, MD, MPH, associate director of medical education at the Benson-Henry Institute for Mind Body Medicine at Massachusetts General Hospital in Boston. The manner in which the effectiveness of integrative techniques is assessed requires a higher sophistication of systems research, Dr. Mehta says.
“The way we construe evidence needs to change,” she adds.
Likely to Expand
Most private health plans do not cover complementary services, although Medicare and numerous insurance plans will reimburse treatment in conjunction with physical therapy (e.g., massage) in the outpatient setting. Twenty-three states cover chiropractic care under Medicaid, and Medicare has begun to assess the cost-effectiveness of including acupuncture—especially for postoperative and chemotherapy-associated nausea and vomiting—in its benefits package.9 Other modalities, ranging from aromatherapy to guided imagery training, are paid for largely out-of-pocket.10
Dr. Rakel notes that the delivery of integrative medicine services at UW entails conversations with patients about out-of-pocket payments. “It can pose a barrier to the clinician-patient relationship if you give them acupuncture to help with their chemotherapy-induced nausea and then ask for their credit card,” he says.
Hospitalist Preparation
Most complementary therapies are currently offered on an outpatient basis. Because of this trend, and because they deal with acute conditions, hospitalists are less likely to be involved with complementary or integrative medicine services, says Beth Israel Deaconess Medical Center hospitalist Andrew C. Ahn, MD, MPH. But that’s not to say complementary medicine is something hospitalists should ignore; patients arrive at the hospital with CAM regimens in tow. It’s the No. 1 reason, Dr. Ahn says, hospitalists should be knowledgeable and exposed to CAM therapies.
Physicians must understand patient patterns and preferences regarding allopathic and complementary medicine, says Sita Ananth, MHA, director of knowledge services and optimal healing environments at the Samueli Institute in Alexandria, Va., and author of the 2007 AHA report. She points to a 2006 survey conducted by AARP and NCCAM that found almost 70% of respondents did not tell their physicians about their complementary medicine approaches. These patients are within the age range most likely to be cared for by hospitalists, and failure to communicate about complementary treatment, such as supplemental vitamin use, could lead to safety issues. Moreover, without complete disclosure, the patient-physician relationship might not be as open as possible, Dr. Ananth says.
Many acute-care hospitalists do not have formal dietary supplement policies, and less than half of U.S. children’s hospitals require documentation of a check for drug or dietary supplement interaction.11,12 As a safety issue, it is always incumbent on hospitalists, says Dr. Li, to ask about any supplements or therapies patients are trying on their own as part of the history and physical examination. The policy at Memorial Sloan-Kettering Cancer Center, Dr. Cassileth says, is that patients on chemotherapy or who are undergoing radiation or facing surgery must avoid herbal dietary supplements.
Beyond Safety
Dr. Bertisch advises hospitalists to pose questions about complementary therapies in an open manner, avoiding antagonistic discussions. “Even when I disagree, I try to guide them to issues about safety and nonsafety, and coax in my concerns,” she says. “The most challenging part about complementary medicine is that patients’ beliefs in these therapies may be so strong that even if the doctor says it won’t work, that will not necessarily change that belief.” A 2001 study in the Archives of Internal Medicine revealed that 70% of respondents would continue to take supplements even if a major study or their physician told them they didn’t work.13
The attraction to complementary medicine often reflects patients’ preferences for a holistic approach to health, says Dr. Ahn, or it may emanate from traditions carried with them from their country of origin. “Once you do understand their reasons for using CAM, then the patient-physician relationship can be significantly strengthened,” he says. With nearly two-thirds of Americans using some form of CAM, hospitalists need to engage in this dialogue.
Dr. Rakel agrees understanding patient culture is vital to uncovering useful information. “Most clinicians would agree that if we can match a therapy to the patient culture and belief system, we are more likely to get buy-in from the patient,” he says.
Dr. Mehta also is a clinical instructor of medicine at Harvard Medical School. He teaches his residents to educate themselves about credentialing, certification, and licensure of complementary providers. He also asks them to maintain an open mind. He says the most important preparation for hospitalists right now is to help educate their patients to be more proactive in their own healthcare. “An engaged patient,” he says, “is better than a disengaged patient.” TH
Gretchen Henkel is a freelance writer based in California.
References
- Deng G, Cassileth BR, Yeung KS. Complementary therapies for cancer-related symptoms. J Support Oncol. 2004;2(5):419-426.
- Kahn ST, Johnstone PA. Management of xerostomia related to radiotherapy for head and neck cancer. Oncology. 2005;19(14):1827-1832.
- Barnes PM, Powell-Griner E, McFann K, Nahin RL. Complementary and alternative medicine use among adults: United States, 2002. Adv Data. 2004;27(343):1-19.
- Eisenberg DM, Davis RB, Ettner SL, et al. Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. JAMA. 1998;280(18):1569-1575.
- Committee on the Use of Complementary and Alternative Medicine by the American Public. Complementary and Alternative Medicine in the United States. Washington, D.C: National Academies Press; 2005.
- Ananth S. 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals. Health Forum LLC. 2008.
- Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354(6):557-566.
- Bauer BA. The herbal hospitalist. The Hospitalist. 2006;10(2);16-17.
- Ananth S. Applying integrative healthcare. Explore. 2009;5(2):119-120.
- Eisenberg DM, Kessler RC, Foster C, Norlock FE, Calkins DR, Delbanco TL. Unconventional medicine in the United States. Prevalence, costs, and patterns of use. N Engl J Med. 1993;328:246-52
- Bassie KL, Witmer DR, Pinto B, Bush C, Clark J, Deffenbaugh J Jr. National survey of dietary supplement policies in acute care facilities. Am J Health Syst Pharm. 2006;63(1):65-70.
- Gardiner P, Phillips RS, Kemper KJ, Legedza A, Henlon S, Woolf AD. Dietary supplements: inpatient policies in US children’s hospitals. Pediatrics. 2008;121(4):e775-781.
- Blendon RJ, DesRoches CM, Benson JM, Brodie M, Altman DE. Americans’ views on the use and regulation of dietary supplements. Arch Intern Med. 2001;161(6):805-810.
Top Image Source: TETRA IMAGES
Despite intravenous medication, a young boy in status epilepticus had the pediatric ICU team at the University of Wisconsin School of Medicine and Public Health in Madison stumped. The team called for a consult with the Integrative Medicine Program, which works with licensed acupuncturists and has been affiliated with the department of family medicine since 2001. Acupuncture’s efficacy in this setting has not been validated, but it has been shown to ease chemotherapy-induced nausea and vomiting, as well as radiation-induced xerostomia.1,2
Following several treatments by a licensed acupuncturist and continued conventional care, the boy’s seizures subsided and he was transitioned to the medical floor. Did the acupuncture contribute to bringing the seizures under control? “I can’t say that it was the acupuncture—it was probably a function of all the therapies working together,” says David P. Rakel, MD, assistant professor and director of UW’s Integrative Medicine Program.
The UW case illustrates both current trends and the constant conundrum that surrounds hospital-based complementary medicine: Complementary and alternative medicine’s use is increasing in some U.S. hospitals, yet the existing research evidence for the efficacy of its multiple modalities is decidedly mixed.
Even if your hospital does not offer complementary and alternative medicine (CAM), your patients are using CAM at ever-increasing rates. In 1993, 34% of Americans reported using some type of CAM (e.g., supplements, massage therapy, prayer, and so on). That number has almost doubled to 62%.3 Americans spend $47 billion a year—of their own money—for CAM therapies, chiropractors, acupuncturists, and massage therapists. And older patients with chronic conditions—the kind of patient hospitalists are most familiar with—tend to try CAM more than younger patients.4
These trends can directly affect hospitalists’ treatment decisions, but they also play a part in how you establish communication and trust with your patients, and how you keep your patients safe from adverse drug interactions. According to the National Academy of Sciences, in order to effectively counsel patients and ensure high-quality comprehensive care, conventional professionals need more CAM-related education.5
—Suzanne Bertisch, MD, MPH, fellow, Harvard Medical School’s Osher Research Center
Complementary Medicine: Online Resources
- National Center for Complementary and Alternative Medicine: http://nccam.nih.gov
- Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center’s About Herbs: www.mskcc.org/mskcc/html/11570.cfm
- Natural Standard: www.naturalstandard.com
- The M.D. Anderson Cancer Center’s Complementary/Integrative Medicine Education Resources: www.mdanderson.org/departments/CIMER
What Trends Show
In 2007, according to the American Hospital Association, 20.8% of community hospitals offered some type of care or treatment not based on traditional Western allopathic medicine. That’s up from 8.6% of reporting hospitals that offered those services in 1998.
The 1990s saw rapid growth of integrative medicine centers at major research institutions, and the majority of U.S. cancer centers now offer some form of complementary therapy, says Barrie R. Cassileth, MS, PhD, the Laurance S. Rockefeller Chair in Integrative Medicine and chief of the Integrative Medicine Service at Memorial Sloan-Kettering Cancer Center in New York City.
The 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals reported that complementary programs are more common in urban rather than rural hospitals; services vary by hospital size (see Figure 2, above); and the top six modalities offered on an inpatient basis are pet therapy, massage therapy, music/art therapy, guided imagery, acupuncture, and reiki (see “Glossary of Complementary Terms,” above). Eighty-four percent of hospitals offer complementary services due to patient demand, the survey showed.
Joseph Ming-Wah Li, MD, FHM, SHM board member and assistant professor of medicine at Harvard Medical School and director of the hospital medicine program and associate chief of the division of general medicine and primary care at Beth Israel Deaconess Medical Center in Boston, doesn’t see a problem with modalities that can make his patients feel better. Patients at his hospital have access to pet therapy, massage, and acupuncture. “I don’t think these modalities hurt our patients, and there is very little downside, except for potential cost,” says Dr. Li, an SHM board member. “What’s not clear is whether these therapies work or not.”
What’s in a Name?
Numerous therapies and modalities crowd under the CAM umbrella, but most experts classify “complementary” modalities as those used in conjunction with conventional medicine to mitigate symptoms of disease or treatment, whereas “alternative” connotes therapies claiming to treat or cure the underlying disease. Some harmful, dangerous, and dishonest practices fall into the “alternative” category, such as Hulda Clark’s “Zapper” device, which was promoted as a cure for liver flukes, something she says cause everything from diabetes to heart disease. (For more on questionable practices, visit www.quackwatch.com or the National Council Against Health Fraud’s Web site at www.ncahf.org.)
The National Institutes of Health’s National Center for Complementary and Alternative Medicine (NCCAM) defines CAM as a group of “diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine.” Dr. Cassileth says the conflation of “complementary and alternative” into one neat acronym—CAM—causes confusion among patients and medical professionals. NCCAM will be changing its name soon, she says, to the National Center for Integrative Medicine, emphasizing the use of adjunctive modalities along with conventional medical treatments.
Hospitalist Suzanne Bertisch, MD, MPH, recently completed a research fellowship at Harvard Medical School’s Osher Research Center. She explains that integrative medicine uses a macro model of health, claiming a middle ground between the traditional, allopathic model of treating disease.
All Kinds of Evidence
Twenty years of complementary medicine research has yielded some information about safety—namely, what works and what doesn’t. For example, saw palmetto has not panned out as an effective treatment for benign prostatic hyperplasia; St. John’s wort, useful for mild depression, interferes with many medications, including cyclosporine and warfarin, and should be avoided at least five days prior to surgery.7,8
Since NCCAM’s inception in October 1998, its research portfolio has stirred debate in the scientific community. Part of the disagreement stems from the difficulty of fitting multidimensional interventions, some of which are provider-dependent (e.g., massage or acupuncture), into the gold standard of the randomized, double-blind, placebo-controlled trial, explains Darshan Mehta, MD, MPH, associate director of medical education at the Benson-Henry Institute for Mind Body Medicine at Massachusetts General Hospital in Boston. The manner in which the effectiveness of integrative techniques is assessed requires a higher sophistication of systems research, Dr. Mehta says.
“The way we construe evidence needs to change,” she adds.
Likely to Expand
Most private health plans do not cover complementary services, although Medicare and numerous insurance plans will reimburse treatment in conjunction with physical therapy (e.g., massage) in the outpatient setting. Twenty-three states cover chiropractic care under Medicaid, and Medicare has begun to assess the cost-effectiveness of including acupuncture—especially for postoperative and chemotherapy-associated nausea and vomiting—in its benefits package.9 Other modalities, ranging from aromatherapy to guided imagery training, are paid for largely out-of-pocket.10
Dr. Rakel notes that the delivery of integrative medicine services at UW entails conversations with patients about out-of-pocket payments. “It can pose a barrier to the clinician-patient relationship if you give them acupuncture to help with their chemotherapy-induced nausea and then ask for their credit card,” he says.
Hospitalist Preparation
Most complementary therapies are currently offered on an outpatient basis. Because of this trend, and because they deal with acute conditions, hospitalists are less likely to be involved with complementary or integrative medicine services, says Beth Israel Deaconess Medical Center hospitalist Andrew C. Ahn, MD, MPH. But that’s not to say complementary medicine is something hospitalists should ignore; patients arrive at the hospital with CAM regimens in tow. It’s the No. 1 reason, Dr. Ahn says, hospitalists should be knowledgeable and exposed to CAM therapies.
Physicians must understand patient patterns and preferences regarding allopathic and complementary medicine, says Sita Ananth, MHA, director of knowledge services and optimal healing environments at the Samueli Institute in Alexandria, Va., and author of the 2007 AHA report. She points to a 2006 survey conducted by AARP and NCCAM that found almost 70% of respondents did not tell their physicians about their complementary medicine approaches. These patients are within the age range most likely to be cared for by hospitalists, and failure to communicate about complementary treatment, such as supplemental vitamin use, could lead to safety issues. Moreover, without complete disclosure, the patient-physician relationship might not be as open as possible, Dr. Ananth says.
Many acute-care hospitalists do not have formal dietary supplement policies, and less than half of U.S. children’s hospitals require documentation of a check for drug or dietary supplement interaction.11,12 As a safety issue, it is always incumbent on hospitalists, says Dr. Li, to ask about any supplements or therapies patients are trying on their own as part of the history and physical examination. The policy at Memorial Sloan-Kettering Cancer Center, Dr. Cassileth says, is that patients on chemotherapy or who are undergoing radiation or facing surgery must avoid herbal dietary supplements.
Beyond Safety
Dr. Bertisch advises hospitalists to pose questions about complementary therapies in an open manner, avoiding antagonistic discussions. “Even when I disagree, I try to guide them to issues about safety and nonsafety, and coax in my concerns,” she says. “The most challenging part about complementary medicine is that patients’ beliefs in these therapies may be so strong that even if the doctor says it won’t work, that will not necessarily change that belief.” A 2001 study in the Archives of Internal Medicine revealed that 70% of respondents would continue to take supplements even if a major study or their physician told them they didn’t work.13
The attraction to complementary medicine often reflects patients’ preferences for a holistic approach to health, says Dr. Ahn, or it may emanate from traditions carried with them from their country of origin. “Once you do understand their reasons for using CAM, then the patient-physician relationship can be significantly strengthened,” he says. With nearly two-thirds of Americans using some form of CAM, hospitalists need to engage in this dialogue.
Dr. Rakel agrees understanding patient culture is vital to uncovering useful information. “Most clinicians would agree that if we can match a therapy to the patient culture and belief system, we are more likely to get buy-in from the patient,” he says.
Dr. Mehta also is a clinical instructor of medicine at Harvard Medical School. He teaches his residents to educate themselves about credentialing, certification, and licensure of complementary providers. He also asks them to maintain an open mind. He says the most important preparation for hospitalists right now is to help educate their patients to be more proactive in their own healthcare. “An engaged patient,” he says, “is better than a disengaged patient.” TH
Gretchen Henkel is a freelance writer based in California.
References
- Deng G, Cassileth BR, Yeung KS. Complementary therapies for cancer-related symptoms. J Support Oncol. 2004;2(5):419-426.
- Kahn ST, Johnstone PA. Management of xerostomia related to radiotherapy for head and neck cancer. Oncology. 2005;19(14):1827-1832.
- Barnes PM, Powell-Griner E, McFann K, Nahin RL. Complementary and alternative medicine use among adults: United States, 2002. Adv Data. 2004;27(343):1-19.
- Eisenberg DM, Davis RB, Ettner SL, et al. Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. JAMA. 1998;280(18):1569-1575.
- Committee on the Use of Complementary and Alternative Medicine by the American Public. Complementary and Alternative Medicine in the United States. Washington, D.C: National Academies Press; 2005.
- Ananth S. 2007 Health Forum/AHA Complementary and Alternative Medicine Survey of Hospitals. Health Forum LLC. 2008.
- Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354(6):557-566.
- Bauer BA. The herbal hospitalist. The Hospitalist. 2006;10(2);16-17.
- Ananth S. Applying integrative healthcare. Explore. 2009;5(2):119-120.
- Eisenberg DM, Kessler RC, Foster C, Norlock FE, Calkins DR, Delbanco TL. Unconventional medicine in the United States. Prevalence, costs, and patterns of use. N Engl J Med. 1993;328:246-52
- Bassie KL, Witmer DR, Pinto B, Bush C, Clark J, Deffenbaugh J Jr. National survey of dietary supplement policies in acute care facilities. Am J Health Syst Pharm. 2006;63(1):65-70.
- Gardiner P, Phillips RS, Kemper KJ, Legedza A, Henlon S, Woolf AD. Dietary supplements: inpatient policies in US children’s hospitals. Pediatrics. 2008;121(4):e775-781.
- Blendon RJ, DesRoches CM, Benson JM, Brodie M, Altman DE. Americans’ views on the use and regulation of dietary supplements. Arch Intern Med. 2001;161(6):805-810.
Top Image Source: TETRA IMAGES