User login
Study IDs microbial signature of celiac disease in children
Eleven operational taxonomic units (OTUs) of fecal bacteria were less abundant in children with celiac disease than in healthy children, according to the findings of a study published in Gastroenterology.

This microbial signature correctly identified approximately four out of five cases of celiac disease, regardless of whether children were newly diagnosed or had already modified their diet, reported Konstantina Zafeiropoulou and Ben Nichols, PhD, of the Glasgow Royal Infirmary. “It is not clear whether the microbes identified [in this study] contribute to the pathogenesis of celiac disease or are the result of it. Future research should explore the role of the disease-specific species identified here,” the researchers wrote in Gastroenterology.
Celiac disease is multifactorial. While up to 40% of people are genetically predisposed, only a small proportion develop it, suggesting that environmental factors are key to pathogenesis. Recent studies have linked celiac disease with alterations in the gut microbiome, but it is unclear whether dysbiosis is pathogenic or a secondary effect of disease processes such as nutrient malabsorption, or whether dysbiosis is present at disease onset or results from a gluten-free diet.
For the study, the researchers performed gas chromatography and 16S ribosomal RNA sequencing of fecal samples from 141 children, including 20 with newly biopsy-confirmed, previously untreated celiac disease, 45 who were previously diagnosed and on a gluten-free diet, 19 unaffected siblings, and 57 healthy children who were not on regular medications and had no history of chronic gastrointestinal symptoms. A single fecal sample was tested for all but the previously untreated children, who were tested at baseline and then after 6 and 12 months on a gluten-free diet.
Children with new-onset celiac disease showed no evidence of dysbiosis, while a gluten-free diet explained up to 2.8% of variation in microbiota between patients and controls. Microbial alpha diversity, a measure of species-level diversity, was generally similar among groups, but between 3% and 5% of all taxa differed. Irrespective of treatment, the decreased abundance of the 11 OTUs was diagnostic for celiac disease with an error rate of 21.5% (P < .001 vs. random classification). Notably, most of these 11 discrepant OTUs were associated with nutrient or food group intake and with biomarkers of gluten ingestion, the researchers said. Gas chromatography showed that, after patients started a gluten-free diet, fecal levels of butyrate and ammonia decreased.
“Even though we identified differences in the abundance of a few species between patients with untreated celiac disease and healthy controls, the profound microbial dysbiosis noted in Crohn’s disease was not observed, at least using crude diversity indices,” the investigators commented. “Although several alterations in the intestinal microbiota of children with established celiac disease appear to be effects of a gluten-free diet, there are specific bacteria that are distinct biomarkers of celiac disease.”
Future research might involve performing in vitro tests of “candidate” bacteria, coculturing these bacteria with human immune cells, and studying whether dietary interventions alter the relative abundance of these bacteria in the gut microbiome, the researchers said.
Nutricia Research Foundation, the Biotechnology and Biological Sciences Research Council, and The Catherine McEwan Foundation provided funding. Three coinvestigators disclosed ties to Nutricia, 4D Pharma, AbbVie, Celltrion, Janssen, Takeda, and several other pharmaceutical companies. One coinvestigator reported chairing the working group for ISLI Europe. The remaining investigators reported having no conflicts of interest.
SOURCE: Zafeiropoulou K et al. Gastroenterology. 2020 Aug 10;S0016-5085(20)35023-X. doi: 10.1053/j.gastro.2020.08.007.
It is well known that gluten ingestion in genetically susceptible individuals does not guarantee celiac disease, and research over the past decade has searched for environmental triggers. Gut microbiota play a role in activation of innate immunity, which leads to the adaptive immune response and the small bowel damage that is characteristic of celiac disease. The authors of this study sought to identify whether there is a distinct microbial pattern among celiac disease patients, both those with treated and untreated disease, in comparison with healthy controls and healthy siblings.

A significantly different microbial profile and metabolites were identified in subjects on gluten-free diets. The consequences of the gluten-free diet are an important consideration when committing a patient to this life-long therapy. The microbiome changes may play a role in persistent symptoms and the increased health conditions we see in treated celiac disease. Those on a gluten-free diet have other micronutrient deficiencies in addition to microbiome changes and the health sequelae of this are not fully understood. A gluten-free diet focused on restoring the normal gut flora through probiotic or gluten-free prebiotic or fiber supplementation in celiac disease patients could prove beneficial.
Dawn Wiese Adams, MD, MS, is assistant professor and medical director, Center for Human Nutrition, department of gastroenterology, hepatology, and nutrition, Vanderbilt University Medical Center, Nashville, Tenn. She has no conflicts of interest.
It is well known that gluten ingestion in genetically susceptible individuals does not guarantee celiac disease, and research over the past decade has searched for environmental triggers. Gut microbiota play a role in activation of innate immunity, which leads to the adaptive immune response and the small bowel damage that is characteristic of celiac disease. The authors of this study sought to identify whether there is a distinct microbial pattern among celiac disease patients, both those with treated and untreated disease, in comparison with healthy controls and healthy siblings.
A significantly different microbial profile and metabolites were identified in subjects on gluten-free diets. The consequences of the gluten-free diet are an important consideration when committing a patient to this life-long therapy. The microbiome changes may play a role in persistent symptoms and the increased health conditions we see in treated celiac disease. Those on a gluten-free diet have other micronutrient deficiencies in addition to microbiome changes and the health sequelae of this are not fully understood. A gluten-free diet focused on restoring the normal gut flora through probiotic or gluten-free prebiotic or fiber supplementation in celiac disease patients could prove beneficial.
Dawn Wiese Adams, MD, MS, is assistant professor and medical director, Center for Human Nutrition, department of gastroenterology, hepatology, and nutrition, Vanderbilt University Medical Center, Nashville, Tenn. She has no conflicts of interest.
It is well known that gluten ingestion in genetically susceptible individuals does not guarantee celiac disease, and research over the past decade has searched for environmental triggers. Gut microbiota play a role in activation of innate immunity, which leads to the adaptive immune response and the small bowel damage that is characteristic of celiac disease. The authors of this study sought to identify whether there is a distinct microbial pattern among celiac disease patients, both those with treated and untreated disease, in comparison with healthy controls and healthy siblings.
A significantly different microbial profile and metabolites were identified in subjects on gluten-free diets. The consequences of the gluten-free diet are an important consideration when committing a patient to this life-long therapy. The microbiome changes may play a role in persistent symptoms and the increased health conditions we see in treated celiac disease. Those on a gluten-free diet have other micronutrient deficiencies in addition to microbiome changes and the health sequelae of this are not fully understood. A gluten-free diet focused on restoring the normal gut flora through probiotic or gluten-free prebiotic or fiber supplementation in celiac disease patients could prove beneficial.
Dawn Wiese Adams, MD, MS, is assistant professor and medical director, Center for Human Nutrition, department of gastroenterology, hepatology, and nutrition, Vanderbilt University Medical Center, Nashville, Tenn. She has no conflicts of interest.
Eleven operational taxonomic units (OTUs) of fecal bacteria were less abundant in children with celiac disease than in healthy children, according to the findings of a study published in Gastroenterology.
This microbial signature correctly identified approximately four out of five cases of celiac disease, regardless of whether children were newly diagnosed or had already modified their diet, reported Konstantina Zafeiropoulou and Ben Nichols, PhD, of the Glasgow Royal Infirmary. “It is not clear whether the microbes identified [in this study] contribute to the pathogenesis of celiac disease or are the result of it. Future research should explore the role of the disease-specific species identified here,” the researchers wrote in Gastroenterology.
Celiac disease is multifactorial. While up to 40% of people are genetically predisposed, only a small proportion develop it, suggesting that environmental factors are key to pathogenesis. Recent studies have linked celiac disease with alterations in the gut microbiome, but it is unclear whether dysbiosis is pathogenic or a secondary effect of disease processes such as nutrient malabsorption, or whether dysbiosis is present at disease onset or results from a gluten-free diet.
For the study, the researchers performed gas chromatography and 16S ribosomal RNA sequencing of fecal samples from 141 children, including 20 with newly biopsy-confirmed, previously untreated celiac disease, 45 who were previously diagnosed and on a gluten-free diet, 19 unaffected siblings, and 57 healthy children who were not on regular medications and had no history of chronic gastrointestinal symptoms. A single fecal sample was tested for all but the previously untreated children, who were tested at baseline and then after 6 and 12 months on a gluten-free diet.
Children with new-onset celiac disease showed no evidence of dysbiosis, while a gluten-free diet explained up to 2.8% of variation in microbiota between patients and controls. Microbial alpha diversity, a measure of species-level diversity, was generally similar among groups, but between 3% and 5% of all taxa differed. Irrespective of treatment, the decreased abundance of the 11 OTUs was diagnostic for celiac disease with an error rate of 21.5% (P < .001 vs. random classification). Notably, most of these 11 discrepant OTUs were associated with nutrient or food group intake and with biomarkers of gluten ingestion, the researchers said. Gas chromatography showed that, after patients started a gluten-free diet, fecal levels of butyrate and ammonia decreased.
“Even though we identified differences in the abundance of a few species between patients with untreated celiac disease and healthy controls, the profound microbial dysbiosis noted in Crohn’s disease was not observed, at least using crude diversity indices,” the investigators commented. “Although several alterations in the intestinal microbiota of children with established celiac disease appear to be effects of a gluten-free diet, there are specific bacteria that are distinct biomarkers of celiac disease.”
Future research might involve performing in vitro tests of “candidate” bacteria, coculturing these bacteria with human immune cells, and studying whether dietary interventions alter the relative abundance of these bacteria in the gut microbiome, the researchers said.
Nutricia Research Foundation, the Biotechnology and Biological Sciences Research Council, and The Catherine McEwan Foundation provided funding. Three coinvestigators disclosed ties to Nutricia, 4D Pharma, AbbVie, Celltrion, Janssen, Takeda, and several other pharmaceutical companies. One coinvestigator reported chairing the working group for ISLI Europe. The remaining investigators reported having no conflicts of interest.
SOURCE: Zafeiropoulou K et al. Gastroenterology. 2020 Aug 10;S0016-5085(20)35023-X. doi: 10.1053/j.gastro.2020.08.007.
Eleven operational taxonomic units (OTUs) of fecal bacteria were less abundant in children with celiac disease than in healthy children, according to the findings of a study published in Gastroenterology.
This microbial signature correctly identified approximately four out of five cases of celiac disease, regardless of whether children were newly diagnosed or had already modified their diet, reported Konstantina Zafeiropoulou and Ben Nichols, PhD, of the Glasgow Royal Infirmary. “It is not clear whether the microbes identified [in this study] contribute to the pathogenesis of celiac disease or are the result of it. Future research should explore the role of the disease-specific species identified here,” the researchers wrote in Gastroenterology.
Celiac disease is multifactorial. While up to 40% of people are genetically predisposed, only a small proportion develop it, suggesting that environmental factors are key to pathogenesis. Recent studies have linked celiac disease with alterations in the gut microbiome, but it is unclear whether dysbiosis is pathogenic or a secondary effect of disease processes such as nutrient malabsorption, or whether dysbiosis is present at disease onset or results from a gluten-free diet.
For the study, the researchers performed gas chromatography and 16S ribosomal RNA sequencing of fecal samples from 141 children, including 20 with newly biopsy-confirmed, previously untreated celiac disease, 45 who were previously diagnosed and on a gluten-free diet, 19 unaffected siblings, and 57 healthy children who were not on regular medications and had no history of chronic gastrointestinal symptoms. A single fecal sample was tested for all but the previously untreated children, who were tested at baseline and then after 6 and 12 months on a gluten-free diet.
Children with new-onset celiac disease showed no evidence of dysbiosis, while a gluten-free diet explained up to 2.8% of variation in microbiota between patients and controls. Microbial alpha diversity, a measure of species-level diversity, was generally similar among groups, but between 3% and 5% of all taxa differed. Irrespective of treatment, the decreased abundance of the 11 OTUs was diagnostic for celiac disease with an error rate of 21.5% (P < .001 vs. random classification). Notably, most of these 11 discrepant OTUs were associated with nutrient or food group intake and with biomarkers of gluten ingestion, the researchers said. Gas chromatography showed that, after patients started a gluten-free diet, fecal levels of butyrate and ammonia decreased.
“Even though we identified differences in the abundance of a few species between patients with untreated celiac disease and healthy controls, the profound microbial dysbiosis noted in Crohn’s disease was not observed, at least using crude diversity indices,” the investigators commented. “Although several alterations in the intestinal microbiota of children with established celiac disease appear to be effects of a gluten-free diet, there are specific bacteria that are distinct biomarkers of celiac disease.”
Future research might involve performing in vitro tests of “candidate” bacteria, coculturing these bacteria with human immune cells, and studying whether dietary interventions alter the relative abundance of these bacteria in the gut microbiome, the researchers said.
Nutricia Research Foundation, the Biotechnology and Biological Sciences Research Council, and The Catherine McEwan Foundation provided funding. Three coinvestigators disclosed ties to Nutricia, 4D Pharma, AbbVie, Celltrion, Janssen, Takeda, and several other pharmaceutical companies. One coinvestigator reported chairing the working group for ISLI Europe. The remaining investigators reported having no conflicts of interest.
SOURCE: Zafeiropoulou K et al. Gastroenterology. 2020 Aug 10;S0016-5085(20)35023-X. doi: 10.1053/j.gastro.2020.08.007.
FROM GASTROENTEROLOGY
Key clinical point: A novel microbial signature distinguished children with celiac disease from healthy controls.
Major finding: Eleven operational taxonomic units (OTUs) were less abundant in fecal samples from children with treated and untreated celiac disease than in healthy controls. The microbial signature was diagnostic for celiac disease with an error rate of 21.5% (P < .001 compared with random classification).
Study details: Gas chromatography and 16S ribosomal RNA sequencing of fecal samples from 141 children: 20 with new-onset celiac disease, 45 with an established diagnosis who were on a gluten-free diet, 19 unaffected siblings, and 57 healthy children. Also, a prospective study of fecal samples from 13 newly diagnosed children after 6 and 12 months on a gluten-free diet.
Disclosures: Nutricia Research Foundation, the Biotechnology and Biological Sciences Research Council, and The Catherine McEwan Foundation provided funding. Three coinvestigators disclosed ties to Nutricia, 4D Pharma, Abbvie, Janssen, Takeda, Celltrion, and several other pharmaceutical companies. One coinvestigator reported chairing the working group for ISLI Europe. The remaining investigators reported having no conflicts of interest.
Source: Zafeiropoulou K et al. Gastroenterology. 2020 Aug 10;S0016-5085(20)35023-X. doi: 10.1053/j.gastro.2020.08.007.

Black patients less likely to receive H. pylori eradication testing
Black patients may be significantly less likely to receive eradication testing after treatment for Helicobacter pylori infection than patients of other races/ethnic groups, based on a retrospective analysis of more than 1,700 individuals.

This disparity may exacerbate the already increased burden of H. pylori infection and gastric cancer among Black individuals, according to principal author David A. Leiman, MD, MSHP, of Duke University Medical Center in Durham, N.C.
“H. pylori infection disproportionately affects racial/ethnic minorities and those of lower socioeconomic status,” Dr. Leiman, coauthor Julius Wilder, MD, PhD, of Duke University in Durham, and colleagues wrote in their abstract presented at the annual meeting of the American College of Gastroenterology. “ACG guidelines recommend treatment for H. pylori infection followed by confirmation of cure. Adherence to these recommendations varies and its impact on practice patterns is unclear. This study characterizes the management of H. pylori infection and predictors of guideline adherence.”
The investigators analyzed electronic medical records from 1,711 patients diagnosed with H. pylori infection through the Duke University Health System between June 2016 and June 2018, most often (71%) via serum antibody test. Approximately two-thirds of those diagnosed were non-White (66%) and female (63%). Out of 1,711 patients, 622 (36%) underwent eradication testing, of whom 559 (90%) were cured.
Despite publication of the ACG H. pylori guideline midway through the study (February 2017), testing rates dropped significantly from 43.1% in 2016 to 35.9% in 2017, and finally 25.5% in 2018 (P < .0001).
“These findings are consistent with other work that has shown low rates of testing to confirm cure in patients treated for H. pylori,” Dr. Leiman said. “There remains a disappointingly low number of patients who are tested for cure.”
Across the entire study period, patients were significantly more likely to undergo eradication testing if they were treated in the gastroenterology department (52.4%), compared with rates ranging from 33% to 34.6% for internal medicine, family medicine, and other departments (P < .001).
Across all departments, Black patients underwent eradication testing significantly less often than patients of other races/ethnicities, at a rate of 30.5% versus 32.2% for White patients, 35.1% for Asian patients, and 36.7% for patients who were of other backgrounds (P < .001). Compared with White patients, Black patients were 38% less likely to undergo eradication testing (odds ratio, 0.62; 95% confidence interval, 0.48-0.79).
Dr. Leiman noted that these findings contrast with a study by Dr. Shria Kumar and colleagues from earlier this year, which found no racial disparity in eradication testing within a Veterans Health Affairs cohort.
“Black patients are significantly less likely to undergo testing for eradication than [patients of other races/ethnicities],” Dr. Leiman said. “More work is needed to understand the mechanisms driving this disparity.” He suggested a number of possible contributing factors, including provider knowledge gaps, fragmented care, and social determinants of health.
“It is clear that a greater emphasis on characterizing and addressing the social determinants of health, including poverty, education, and location, are needed,” Dr. Leiman said. “Although health systems are not solely responsible for the known and ongoing observations of disparities in care, interventions must be identified and implemented to mitigate these issues.” Such interventions would likely require broad participation, he said, including policy makers, health systems, and individual practitioners.
“We plan to perform a prospective mixed methods study to contextualize which social determinants are associated with a decreased likelihood of receiving appropriate eradication testing by exploring barriers at patient, practitioner, and health-system levels,” Dr. Leiman said. “Ultimately, we aim to leverage these findings to develop an evidence-based intervention to circumnavigate those identified barriers, thereby eliminating the observed disparities in H. pylori care.”
According to Gregory L. Hall, MD, of Northeast Ohio Medical University, Rootstown, and Case Western Reserve University, Cleveland, and codirector of the Partnership for Urban Health Research, Atlanta, the higher rate of H. pylori infection in Black individuals may stem partly from genetic factors.
“Studies have shown that African Americans with a higher proportion of African ancestry have higher rates of H. pylori, suggesting a genetic component to this increased risk,” he said.
Still, Dr. Hall, who is the author of the book Patient-Centered Clinical Care for African Americans, went on to emphasize appropriate H. pylori management and recognition of racial disparities in medicine.
“The ability to test for, treat, and confirm eradication of H. pylori infections represents a great opportunity to improve quality of life through decreased gastritis, gastric ulcers, and gastric cancer,” he said. “[The present findings] show yet another disparity in our clinical care of African Americans that needs increased awareness among providers to these communities.”
Rotonya Carr, MD, of the Hospital of the University of Pennsylvania, Philadelphia, and lead author of a recent publication addressing racism and health disparities in gastroenterology, said the findings of the present study add weight to a known equity gap.
“These data are concerning in view of the twofold higher prevalence of H. pylori seropositivity and twofold higher incidence of gastric cancer in Black patients, compared with White patients,” Dr. Carr said. “These and other data support a comprehensive approach to reduce GI disparities that includes targeted education of both GI specialists and referring providers.”
According to Dr. Leiman, individual practitioners may work toward more equitable outcomes through a comprehensive clinical approach, regardless of patient race or ethnicity.
“Clinicians should consider H. pylori therapy an episode of care that spans diagnosis, treatment, and confirmation of cure,” he said. “Closing the loop in that episode by ensuring eradication is vital to conforming with best practices, and to reduce patients’ long-term risks.”The investigators disclosed relationships with Exact Sciences, Guardant Health, and Phathom Pharmaceuticals. Dr. Hall and Dr. Carr reported no relevant conflicts of interest.
SOURCE: Reichstein J et al. ACG 2020. Abstract S1332.
Black patients may be significantly less likely to receive eradication testing after treatment for Helicobacter pylori infection than patients of other races/ethnic groups, based on a retrospective analysis of more than 1,700 individuals.
This disparity may exacerbate the already increased burden of H. pylori infection and gastric cancer among Black individuals, according to principal author David A. Leiman, MD, MSHP, of Duke University Medical Center in Durham, N.C.
“H. pylori infection disproportionately affects racial/ethnic minorities and those of lower socioeconomic status,” Dr. Leiman, coauthor Julius Wilder, MD, PhD, of Duke University in Durham, and colleagues wrote in their abstract presented at the annual meeting of the American College of Gastroenterology. “ACG guidelines recommend treatment for H. pylori infection followed by confirmation of cure. Adherence to these recommendations varies and its impact on practice patterns is unclear. This study characterizes the management of H. pylori infection and predictors of guideline adherence.”
The investigators analyzed electronic medical records from 1,711 patients diagnosed with H. pylori infection through the Duke University Health System between June 2016 and June 2018, most often (71%) via serum antibody test. Approximately two-thirds of those diagnosed were non-White (66%) and female (63%). Out of 1,711 patients, 622 (36%) underwent eradication testing, of whom 559 (90%) were cured.
Despite publication of the ACG H. pylori guideline midway through the study (February 2017), testing rates dropped significantly from 43.1% in 2016 to 35.9% in 2017, and finally 25.5% in 2018 (P < .0001).
“These findings are consistent with other work that has shown low rates of testing to confirm cure in patients treated for H. pylori,” Dr. Leiman said. “There remains a disappointingly low number of patients who are tested for cure.”
Across the entire study period, patients were significantly more likely to undergo eradication testing if they were treated in the gastroenterology department (52.4%), compared with rates ranging from 33% to 34.6% for internal medicine, family medicine, and other departments (P < .001).
Across all departments, Black patients underwent eradication testing significantly less often than patients of other races/ethnicities, at a rate of 30.5% versus 32.2% for White patients, 35.1% for Asian patients, and 36.7% for patients who were of other backgrounds (P < .001). Compared with White patients, Black patients were 38% less likely to undergo eradication testing (odds ratio, 0.62; 95% confidence interval, 0.48-0.79).
Dr. Leiman noted that these findings contrast with a study by Dr. Shria Kumar and colleagues from earlier this year, which found no racial disparity in eradication testing within a Veterans Health Affairs cohort.
“Black patients are significantly less likely to undergo testing for eradication than [patients of other races/ethnicities],” Dr. Leiman said. “More work is needed to understand the mechanisms driving this disparity.” He suggested a number of possible contributing factors, including provider knowledge gaps, fragmented care, and social determinants of health.
“It is clear that a greater emphasis on characterizing and addressing the social determinants of health, including poverty, education, and location, are needed,” Dr. Leiman said. “Although health systems are not solely responsible for the known and ongoing observations of disparities in care, interventions must be identified and implemented to mitigate these issues.” Such interventions would likely require broad participation, he said, including policy makers, health systems, and individual practitioners.
“We plan to perform a prospective mixed methods study to contextualize which social determinants are associated with a decreased likelihood of receiving appropriate eradication testing by exploring barriers at patient, practitioner, and health-system levels,” Dr. Leiman said. “Ultimately, we aim to leverage these findings to develop an evidence-based intervention to circumnavigate those identified barriers, thereby eliminating the observed disparities in H. pylori care.”
According to Gregory L. Hall, MD, of Northeast Ohio Medical University, Rootstown, and Case Western Reserve University, Cleveland, and codirector of the Partnership for Urban Health Research, Atlanta, the higher rate of H. pylori infection in Black individuals may stem partly from genetic factors.
“Studies have shown that African Americans with a higher proportion of African ancestry have higher rates of H. pylori, suggesting a genetic component to this increased risk,” he said.
Still, Dr. Hall, who is the author of the book Patient-Centered Clinical Care for African Americans, went on to emphasize appropriate H. pylori management and recognition of racial disparities in medicine.
“The ability to test for, treat, and confirm eradication of H. pylori infections represents a great opportunity to improve quality of life through decreased gastritis, gastric ulcers, and gastric cancer,” he said. “[The present findings] show yet another disparity in our clinical care of African Americans that needs increased awareness among providers to these communities.”
Rotonya Carr, MD, of the Hospital of the University of Pennsylvania, Philadelphia, and lead author of a recent publication addressing racism and health disparities in gastroenterology, said the findings of the present study add weight to a known equity gap.
“These data are concerning in view of the twofold higher prevalence of H. pylori seropositivity and twofold higher incidence of gastric cancer in Black patients, compared with White patients,” Dr. Carr said. “These and other data support a comprehensive approach to reduce GI disparities that includes targeted education of both GI specialists and referring providers.”
According to Dr. Leiman, individual practitioners may work toward more equitable outcomes through a comprehensive clinical approach, regardless of patient race or ethnicity.
“Clinicians should consider H. pylori therapy an episode of care that spans diagnosis, treatment, and confirmation of cure,” he said. “Closing the loop in that episode by ensuring eradication is vital to conforming with best practices, and to reduce patients’ long-term risks.”The investigators disclosed relationships with Exact Sciences, Guardant Health, and Phathom Pharmaceuticals. Dr. Hall and Dr. Carr reported no relevant conflicts of interest.
SOURCE: Reichstein J et al. ACG 2020. Abstract S1332.
Black patients may be significantly less likely to receive eradication testing after treatment for Helicobacter pylori infection than patients of other races/ethnic groups, based on a retrospective analysis of more than 1,700 individuals.
This disparity may exacerbate the already increased burden of H. pylori infection and gastric cancer among Black individuals, according to principal author David A. Leiman, MD, MSHP, of Duke University Medical Center in Durham, N.C.
“H. pylori infection disproportionately affects racial/ethnic minorities and those of lower socioeconomic status,” Dr. Leiman, coauthor Julius Wilder, MD, PhD, of Duke University in Durham, and colleagues wrote in their abstract presented at the annual meeting of the American College of Gastroenterology. “ACG guidelines recommend treatment for H. pylori infection followed by confirmation of cure. Adherence to these recommendations varies and its impact on practice patterns is unclear. This study characterizes the management of H. pylori infection and predictors of guideline adherence.”
The investigators analyzed electronic medical records from 1,711 patients diagnosed with H. pylori infection through the Duke University Health System between June 2016 and June 2018, most often (71%) via serum antibody test. Approximately two-thirds of those diagnosed were non-White (66%) and female (63%). Out of 1,711 patients, 622 (36%) underwent eradication testing, of whom 559 (90%) were cured.
Despite publication of the ACG H. pylori guideline midway through the study (February 2017), testing rates dropped significantly from 43.1% in 2016 to 35.9% in 2017, and finally 25.5% in 2018 (P < .0001).
“These findings are consistent with other work that has shown low rates of testing to confirm cure in patients treated for H. pylori,” Dr. Leiman said. “There remains a disappointingly low number of patients who are tested for cure.”
Across the entire study period, patients were significantly more likely to undergo eradication testing if they were treated in the gastroenterology department (52.4%), compared with rates ranging from 33% to 34.6% for internal medicine, family medicine, and other departments (P < .001).
Across all departments, Black patients underwent eradication testing significantly less often than patients of other races/ethnicities, at a rate of 30.5% versus 32.2% for White patients, 35.1% for Asian patients, and 36.7% for patients who were of other backgrounds (P < .001). Compared with White patients, Black patients were 38% less likely to undergo eradication testing (odds ratio, 0.62; 95% confidence interval, 0.48-0.79).
Dr. Leiman noted that these findings contrast with a study by Dr. Shria Kumar and colleagues from earlier this year, which found no racial disparity in eradication testing within a Veterans Health Affairs cohort.
“Black patients are significantly less likely to undergo testing for eradication than [patients of other races/ethnicities],” Dr. Leiman said. “More work is needed to understand the mechanisms driving this disparity.” He suggested a number of possible contributing factors, including provider knowledge gaps, fragmented care, and social determinants of health.
“It is clear that a greater emphasis on characterizing and addressing the social determinants of health, including poverty, education, and location, are needed,” Dr. Leiman said. “Although health systems are not solely responsible for the known and ongoing observations of disparities in care, interventions must be identified and implemented to mitigate these issues.” Such interventions would likely require broad participation, he said, including policy makers, health systems, and individual practitioners.
“We plan to perform a prospective mixed methods study to contextualize which social determinants are associated with a decreased likelihood of receiving appropriate eradication testing by exploring barriers at patient, practitioner, and health-system levels,” Dr. Leiman said. “Ultimately, we aim to leverage these findings to develop an evidence-based intervention to circumnavigate those identified barriers, thereby eliminating the observed disparities in H. pylori care.”
According to Gregory L. Hall, MD, of Northeast Ohio Medical University, Rootstown, and Case Western Reserve University, Cleveland, and codirector of the Partnership for Urban Health Research, Atlanta, the higher rate of H. pylori infection in Black individuals may stem partly from genetic factors.
“Studies have shown that African Americans with a higher proportion of African ancestry have higher rates of H. pylori, suggesting a genetic component to this increased risk,” he said.
Still, Dr. Hall, who is the author of the book Patient-Centered Clinical Care for African Americans, went on to emphasize appropriate H. pylori management and recognition of racial disparities in medicine.
“The ability to test for, treat, and confirm eradication of H. pylori infections represents a great opportunity to improve quality of life through decreased gastritis, gastric ulcers, and gastric cancer,” he said. “[The present findings] show yet another disparity in our clinical care of African Americans that needs increased awareness among providers to these communities.”
Rotonya Carr, MD, of the Hospital of the University of Pennsylvania, Philadelphia, and lead author of a recent publication addressing racism and health disparities in gastroenterology, said the findings of the present study add weight to a known equity gap.
“These data are concerning in view of the twofold higher prevalence of H. pylori seropositivity and twofold higher incidence of gastric cancer in Black patients, compared with White patients,” Dr. Carr said. “These and other data support a comprehensive approach to reduce GI disparities that includes targeted education of both GI specialists and referring providers.”
According to Dr. Leiman, individual practitioners may work toward more equitable outcomes through a comprehensive clinical approach, regardless of patient race or ethnicity.
“Clinicians should consider H. pylori therapy an episode of care that spans diagnosis, treatment, and confirmation of cure,” he said. “Closing the loop in that episode by ensuring eradication is vital to conforming with best practices, and to reduce patients’ long-term risks.”The investigators disclosed relationships with Exact Sciences, Guardant Health, and Phathom Pharmaceuticals. Dr. Hall and Dr. Carr reported no relevant conflicts of interest.
SOURCE: Reichstein J et al. ACG 2020. Abstract S1332.
FROM ACG 2020
Antibiotics fail to improve colon ischemia outcomes
Antibiotics may not significantly improve clinical outcomes in patients with colon ischemia (CI), regardless of severity level, based on a retrospective study involving more than 800 patients.
Given these findings, clinicians “should consider not giving antibiotics to patients with CI,” reported lead author Paul Feuerstadt, MD, of Yale University, New Haven , Conn., and colleagues.
“CI is the most common ischemic injury to the GI tract,” the investigators wrote in their abstract, which was presented at the annual meeting of the American College of Gastroenterology. “The clinical utility of antibiotic treatment in CI is unclear and the literature is limited.”
Dr. Feuerstadt and colleagues analyzed data from 838 patients with biopsy-proven CI who were hospitalized between 2005 and 2017, of whom 413 and 425 had moderate and severe disease, respectively.
Across all patients, 67.7% received antibiotics. While there were no significant intergroup differences in age, Charlson Comorbidity Index, or sex, patients who received antibiotics were more likely to have severe CI (54.4% vs. 42.2%; P = .001), small-bowel involvement (12.0% vs. 5.7%; P = .04), and peritonitis (11.3% vs. 4.5%; P = 002), as well as require intensive care (26.1% vs. 19.9%; P = .04).
After adjusting for severity of CI, small-bowel involvement, and comorbidities, analysis revealed no significant associations between antibiotic use and 30-day mortality, 90-day mortality, 30-day colectomy, 90-day recurrence, 90-day readmission, or length of stay. The primary outcome, 30-day mortality, remained insignificant in subgroup analyses based on CI severity and age.
Patients were most frequently prescribed ciprofloxacin-metronidazole (57.1%), followed by piperacillin-tazobactam (13.2%), ceftriaxone-metronidazole (11.1%), and other antibiotics (18.5%).
When each of these antimicrobials was compared with no antibiotic usage, only piperacillin-tazobactam correlated with a higher rate of 30-day mortality, based on an adjusted odds ratio of 3.4 (95% CI, 1.5-8.0; P = .0003). But most patients who received piperacillin-tazobactam underwent colectomy, which prompted independent analyses of patients who underwent colectomy and those who did not undergo colectomy. These findings showed no difference in 30-day mortality based on the type of antibiotic used.
During an oral presentation at the meeting, coauthor Karthik Gnanapandithan, MD, of the Mayo Clinic in Jacksonville, Fla, said, “In practice, it is reasonable to still use antibiotics in patients with small bowel ischemia and those with severe CI with a high risk of poor outcomes pending prospective studies.”
According to John F. Valentine, MD, of the University of Utah, Salt Lake City, the present study “adds to the literature that questions the role of antibiotics in CI.”
Dr. Valentine noted that, even among patients with CI who have severe inflammation, “sepsis rarely occurs without frank perforation.”
Still, like Dr. Gnanapandithan, Dr. Valentine concluded that antibiotics are still a reasonable treatment option for certain patients with CI.
“The risks and potential benefits of antibiotics must be considered,” he said. “Until prospective studies are available, use of antibiotics in colon ischemia is reasonable in the setting of severe disease with peritoneal signs, signs of sepsis, pneumatosis, or portal venous gas.”
Dr. Feuerstadt disclosed relationships with Ferring/Rebiotix, Merck, and Roche. Dr. Valentine reported no relevant conflicts of interest.
Antibiotics may not significantly improve clinical outcomes in patients with colon ischemia (CI), regardless of severity level, based on a retrospective study involving more than 800 patients.
Given these findings, clinicians “should consider not giving antibiotics to patients with CI,” reported lead author Paul Feuerstadt, MD, of Yale University, New Haven , Conn., and colleagues.
“CI is the most common ischemic injury to the GI tract,” the investigators wrote in their abstract, which was presented at the annual meeting of the American College of Gastroenterology. “The clinical utility of antibiotic treatment in CI is unclear and the literature is limited.”
Dr. Feuerstadt and colleagues analyzed data from 838 patients with biopsy-proven CI who were hospitalized between 2005 and 2017, of whom 413 and 425 had moderate and severe disease, respectively.
Across all patients, 67.7% received antibiotics. While there were no significant intergroup differences in age, Charlson Comorbidity Index, or sex, patients who received antibiotics were more likely to have severe CI (54.4% vs. 42.2%; P = .001), small-bowel involvement (12.0% vs. 5.7%; P = .04), and peritonitis (11.3% vs. 4.5%; P = 002), as well as require intensive care (26.1% vs. 19.9%; P = .04).
After adjusting for severity of CI, small-bowel involvement, and comorbidities, analysis revealed no significant associations between antibiotic use and 30-day mortality, 90-day mortality, 30-day colectomy, 90-day recurrence, 90-day readmission, or length of stay. The primary outcome, 30-day mortality, remained insignificant in subgroup analyses based on CI severity and age.
Patients were most frequently prescribed ciprofloxacin-metronidazole (57.1%), followed by piperacillin-tazobactam (13.2%), ceftriaxone-metronidazole (11.1%), and other antibiotics (18.5%).
When each of these antimicrobials was compared with no antibiotic usage, only piperacillin-tazobactam correlated with a higher rate of 30-day mortality, based on an adjusted odds ratio of 3.4 (95% CI, 1.5-8.0; P = .0003). But most patients who received piperacillin-tazobactam underwent colectomy, which prompted independent analyses of patients who underwent colectomy and those who did not undergo colectomy. These findings showed no difference in 30-day mortality based on the type of antibiotic used.
During an oral presentation at the meeting, coauthor Karthik Gnanapandithan, MD, of the Mayo Clinic in Jacksonville, Fla, said, “In practice, it is reasonable to still use antibiotics in patients with small bowel ischemia and those with severe CI with a high risk of poor outcomes pending prospective studies.”
According to John F. Valentine, MD, of the University of Utah, Salt Lake City, the present study “adds to the literature that questions the role of antibiotics in CI.”
Dr. Valentine noted that, even among patients with CI who have severe inflammation, “sepsis rarely occurs without frank perforation.”
Still, like Dr. Gnanapandithan, Dr. Valentine concluded that antibiotics are still a reasonable treatment option for certain patients with CI.
“The risks and potential benefits of antibiotics must be considered,” he said. “Until prospective studies are available, use of antibiotics in colon ischemia is reasonable in the setting of severe disease with peritoneal signs, signs of sepsis, pneumatosis, or portal venous gas.”
Dr. Feuerstadt disclosed relationships with Ferring/Rebiotix, Merck, and Roche. Dr. Valentine reported no relevant conflicts of interest.
Antibiotics may not significantly improve clinical outcomes in patients with colon ischemia (CI), regardless of severity level, based on a retrospective study involving more than 800 patients.
Given these findings, clinicians “should consider not giving antibiotics to patients with CI,” reported lead author Paul Feuerstadt, MD, of Yale University, New Haven , Conn., and colleagues.
“CI is the most common ischemic injury to the GI tract,” the investigators wrote in their abstract, which was presented at the annual meeting of the American College of Gastroenterology. “The clinical utility of antibiotic treatment in CI is unclear and the literature is limited.”
Dr. Feuerstadt and colleagues analyzed data from 838 patients with biopsy-proven CI who were hospitalized between 2005 and 2017, of whom 413 and 425 had moderate and severe disease, respectively.
Across all patients, 67.7% received antibiotics. While there were no significant intergroup differences in age, Charlson Comorbidity Index, or sex, patients who received antibiotics were more likely to have severe CI (54.4% vs. 42.2%; P = .001), small-bowel involvement (12.0% vs. 5.7%; P = .04), and peritonitis (11.3% vs. 4.5%; P = 002), as well as require intensive care (26.1% vs. 19.9%; P = .04).
After adjusting for severity of CI, small-bowel involvement, and comorbidities, analysis revealed no significant associations between antibiotic use and 30-day mortality, 90-day mortality, 30-day colectomy, 90-day recurrence, 90-day readmission, or length of stay. The primary outcome, 30-day mortality, remained insignificant in subgroup analyses based on CI severity and age.
Patients were most frequently prescribed ciprofloxacin-metronidazole (57.1%), followed by piperacillin-tazobactam (13.2%), ceftriaxone-metronidazole (11.1%), and other antibiotics (18.5%).
When each of these antimicrobials was compared with no antibiotic usage, only piperacillin-tazobactam correlated with a higher rate of 30-day mortality, based on an adjusted odds ratio of 3.4 (95% CI, 1.5-8.0; P = .0003). But most patients who received piperacillin-tazobactam underwent colectomy, which prompted independent analyses of patients who underwent colectomy and those who did not undergo colectomy. These findings showed no difference in 30-day mortality based on the type of antibiotic used.
During an oral presentation at the meeting, coauthor Karthik Gnanapandithan, MD, of the Mayo Clinic in Jacksonville, Fla, said, “In practice, it is reasonable to still use antibiotics in patients with small bowel ischemia and those with severe CI with a high risk of poor outcomes pending prospective studies.”
According to John F. Valentine, MD, of the University of Utah, Salt Lake City, the present study “adds to the literature that questions the role of antibiotics in CI.”
Dr. Valentine noted that, even among patients with CI who have severe inflammation, “sepsis rarely occurs without frank perforation.”
Still, like Dr. Gnanapandithan, Dr. Valentine concluded that antibiotics are still a reasonable treatment option for certain patients with CI.
“The risks and potential benefits of antibiotics must be considered,” he said. “Until prospective studies are available, use of antibiotics in colon ischemia is reasonable in the setting of severe disease with peritoneal signs, signs of sepsis, pneumatosis, or portal venous gas.”
Dr. Feuerstadt disclosed relationships with Ferring/Rebiotix, Merck, and Roche. Dr. Valentine reported no relevant conflicts of interest.
FROM ACG 2020
Fulminant C. diff debate: Fecal transplants or antibiotics?
Two experts at IDWeek 2020 debated the best treatment for patients with the most severe type of Clostridioides difficile infection – fulminant C. diff. The discussion pitted fecal microbiota transplants (FMT) from the stool of healthy donors against traditional antibiotics.
Fulminant C. diff infection (CDI) represents about 8% of all CDI cases and is often fatal. Patients frequently don’t respond to maximum antibiotic therapy.
Should these patients be treated with FMT before surgery is considered?
“Unequivocally, yes,” said Jessica R. Allegretti, MD, MPH, associate director of the Crohn’s and Colitis Center at Brigham and Women’s Hospital in Boston.
Patients face full colectomy
Fulminant infection, she says, typically requires a total abdominal colectomy with end ileostomy.
“Patients have a quite high perioperative and intraoperative mortality because this is typically an older population with significant comorbidities,” she said.
Often the patients are poor candidates for surgery, she added.
She pointed to the efficacy of FMT in studies such as one published in Gut Microbes in 2017. The study, by Monika Fischer, MD, of Indiana University, Indianapolis, and colleagues showed a 91% cure rate at 1 month in severe patients with an average of 1.5 fecal transplants, noting that was “quite remarkable” in this very sick population.
Though FMT is not approved by the US Food and Drug Administration for fulminant CDI, Dr. Allegretti said, the FDA does allow treatment under “enforcement discretion,” which means no investigational new drug license is needed specifically if treating CDI patients who haven’t responded to standard therapy, as long as proper consent has been obtained.
“This is a patient population that is likely going to die,” she said. “If you were the one in the ICU with fulminant C. diff and you’ve been on maximum therapy for 3-5 days and you’re not getting better, wouldn’t you want somebody to offer you a fecal transplant and give you the chance to recover and leave the hospital with your colon intact? The data suggest that is possible, with a high likelihood and a good safety profile.”
She said the most recent guidelines have supported FMT, and emerging guidelines coming within months “will support this as well.”
Unknowns with FMT
Taking the other side of the debate, Kevin Garey, PharmD, chair of the department of pharmacy practice and translational research at University of Houston College of Pharmacy, warned against trading traditional antibiotics, such as vancomycin and fidaxomicin, for the novelty of FMT.
“With the science of the microbiome and the novelty of fecal microbiota transplantation in expanding use, I think people have somewhat forgotten pharmacotherapy,” he said.
He pointed out safety concerns with FMT reported in June 2019, after which the FDA issued an alert. Two immunocompromised patients who received FMT, both from the same donor, developed invasive infections caused by extended-spectrum beta-lactamase (ESBL)–producing Escherichia coli. One died.
The FDA explained that the donated FMT samples the patients received were not tested for ESBL-producing gram-negative organisms before use.
Dr. Allegretti agreed antibiotics play a role in treatment with FMT, but she argued that the safety profile of FMT remains strong and that the safety issues came from isolated incidents at a single center.
Dr. Garey countered that there are just too many unknowns with FMT.
“We will never know what the next superbug that’s going to land in an FMT is until we’ve identified that superbug in somebody – the next Candida auris, the next CRE [carbapenem-resistant Enterobacteriaceae], the next thing that’s going to show up in FMT – until we get rid of the ‘F,’ “ Dr. Garey said.
“[Until] we get microbial therapy that’s generated without the need for healthy donors, I think we’re always going to be in this problem.”
He said although FMT “has an amazing ability to alter a microbiome” it “pales in comparison” to vancomycin’s ability to do so.
Disruption of the microbiome is, without a doubt, a hallmark of C. diff, but we don’t have to run to FMT,” Dr. Garey said. “We can think about prophylaxis strategies, we can think about new drug development that spares the microbiota. The need for FMT might be a consequence of poor pharmacotherapy management, not a part of pharmacotherapy management.”
Moderator Sam Aitken, PharmD, MPH, a clinical pharmacy specialist in infectious disease at MD Anderson Cancer Center in Houston, said in an interview the speakers found some common ground.
“I think there was a general consensus between both Dr. Allegretti and Dr. Garey that both traditional therapeutics and fecal microbiota transplantation have a role to play in these patients, although there is still quite a bit of discussion around where those might be best positioned,” Dr. Aitken said.
He added, “There’s also a general consensus that there is not likely to be one right answer for all patients with multiple recurrent CDI.”
Dr. Allegretti, Dr. Garey, and Dr. Aitken have disclosed no relevant financial relationships.
The AGA Fecal Microbiota Transplantation (FMT) National Registry will assess short- and long-term patient outcomes associated with FMT. Learn more and register to participate at www.gastro.org/fmtregistry.
A version of this article originally appeared on Medscape.com.
Two experts at IDWeek 2020 debated the best treatment for patients with the most severe type of Clostridioides difficile infection – fulminant C. diff. The discussion pitted fecal microbiota transplants (FMT) from the stool of healthy donors against traditional antibiotics.
Fulminant C. diff infection (CDI) represents about 8% of all CDI cases and is often fatal. Patients frequently don’t respond to maximum antibiotic therapy.
Should these patients be treated with FMT before surgery is considered?
“Unequivocally, yes,” said Jessica R. Allegretti, MD, MPH, associate director of the Crohn’s and Colitis Center at Brigham and Women’s Hospital in Boston.
Patients face full colectomy
Fulminant infection, she says, typically requires a total abdominal colectomy with end ileostomy.
“Patients have a quite high perioperative and intraoperative mortality because this is typically an older population with significant comorbidities,” she said.
Often the patients are poor candidates for surgery, she added.
She pointed to the efficacy of FMT in studies such as one published in Gut Microbes in 2017. The study, by Monika Fischer, MD, of Indiana University, Indianapolis, and colleagues showed a 91% cure rate at 1 month in severe patients with an average of 1.5 fecal transplants, noting that was “quite remarkable” in this very sick population.
Though FMT is not approved by the US Food and Drug Administration for fulminant CDI, Dr. Allegretti said, the FDA does allow treatment under “enforcement discretion,” which means no investigational new drug license is needed specifically if treating CDI patients who haven’t responded to standard therapy, as long as proper consent has been obtained.
“This is a patient population that is likely going to die,” she said. “If you were the one in the ICU with fulminant C. diff and you’ve been on maximum therapy for 3-5 days and you’re not getting better, wouldn’t you want somebody to offer you a fecal transplant and give you the chance to recover and leave the hospital with your colon intact? The data suggest that is possible, with a high likelihood and a good safety profile.”
She said the most recent guidelines have supported FMT, and emerging guidelines coming within months “will support this as well.”
Unknowns with FMT
Taking the other side of the debate, Kevin Garey, PharmD, chair of the department of pharmacy practice and translational research at University of Houston College of Pharmacy, warned against trading traditional antibiotics, such as vancomycin and fidaxomicin, for the novelty of FMT.
“With the science of the microbiome and the novelty of fecal microbiota transplantation in expanding use, I think people have somewhat forgotten pharmacotherapy,” he said.
He pointed out safety concerns with FMT reported in June 2019, after which the FDA issued an alert. Two immunocompromised patients who received FMT, both from the same donor, developed invasive infections caused by extended-spectrum beta-lactamase (ESBL)–producing Escherichia coli. One died.
The FDA explained that the donated FMT samples the patients received were not tested for ESBL-producing gram-negative organisms before use.
Dr. Allegretti agreed antibiotics play a role in treatment with FMT, but she argued that the safety profile of FMT remains strong and that the safety issues came from isolated incidents at a single center.
Dr. Garey countered that there are just too many unknowns with FMT.
“We will never know what the next superbug that’s going to land in an FMT is until we’ve identified that superbug in somebody – the next Candida auris, the next CRE [carbapenem-resistant Enterobacteriaceae], the next thing that’s going to show up in FMT – until we get rid of the ‘F,’ “ Dr. Garey said.
“[Until] we get microbial therapy that’s generated without the need for healthy donors, I think we’re always going to be in this problem.”
He said although FMT “has an amazing ability to alter a microbiome” it “pales in comparison” to vancomycin’s ability to do so.
Disruption of the microbiome is, without a doubt, a hallmark of C. diff, but we don’t have to run to FMT,” Dr. Garey said. “We can think about prophylaxis strategies, we can think about new drug development that spares the microbiota. The need for FMT might be a consequence of poor pharmacotherapy management, not a part of pharmacotherapy management.”
Moderator Sam Aitken, PharmD, MPH, a clinical pharmacy specialist in infectious disease at MD Anderson Cancer Center in Houston, said in an interview the speakers found some common ground.
“I think there was a general consensus between both Dr. Allegretti and Dr. Garey that both traditional therapeutics and fecal microbiota transplantation have a role to play in these patients, although there is still quite a bit of discussion around where those might be best positioned,” Dr. Aitken said.
He added, “There’s also a general consensus that there is not likely to be one right answer for all patients with multiple recurrent CDI.”
Dr. Allegretti, Dr. Garey, and Dr. Aitken have disclosed no relevant financial relationships.
The AGA Fecal Microbiota Transplantation (FMT) National Registry will assess short- and long-term patient outcomes associated with FMT. Learn more and register to participate at www.gastro.org/fmtregistry.
A version of this article originally appeared on Medscape.com.
Two experts at IDWeek 2020 debated the best treatment for patients with the most severe type of Clostridioides difficile infection – fulminant C. diff. The discussion pitted fecal microbiota transplants (FMT) from the stool of healthy donors against traditional antibiotics.
Fulminant C. diff infection (CDI) represents about 8% of all CDI cases and is often fatal. Patients frequently don’t respond to maximum antibiotic therapy.
Should these patients be treated with FMT before surgery is considered?
“Unequivocally, yes,” said Jessica R. Allegretti, MD, MPH, associate director of the Crohn’s and Colitis Center at Brigham and Women’s Hospital in Boston.
Patients face full colectomy
Fulminant infection, she says, typically requires a total abdominal colectomy with end ileostomy.
“Patients have a quite high perioperative and intraoperative mortality because this is typically an older population with significant comorbidities,” she said.
Often the patients are poor candidates for surgery, she added.
She pointed to the efficacy of FMT in studies such as one published in Gut Microbes in 2017. The study, by Monika Fischer, MD, of Indiana University, Indianapolis, and colleagues showed a 91% cure rate at 1 month in severe patients with an average of 1.5 fecal transplants, noting that was “quite remarkable” in this very sick population.
Though FMT is not approved by the US Food and Drug Administration for fulminant CDI, Dr. Allegretti said, the FDA does allow treatment under “enforcement discretion,” which means no investigational new drug license is needed specifically if treating CDI patients who haven’t responded to standard therapy, as long as proper consent has been obtained.
“This is a patient population that is likely going to die,” she said. “If you were the one in the ICU with fulminant C. diff and you’ve been on maximum therapy for 3-5 days and you’re not getting better, wouldn’t you want somebody to offer you a fecal transplant and give you the chance to recover and leave the hospital with your colon intact? The data suggest that is possible, with a high likelihood and a good safety profile.”
She said the most recent guidelines have supported FMT, and emerging guidelines coming within months “will support this as well.”
Unknowns with FMT
Taking the other side of the debate, Kevin Garey, PharmD, chair of the department of pharmacy practice and translational research at University of Houston College of Pharmacy, warned against trading traditional antibiotics, such as vancomycin and fidaxomicin, for the novelty of FMT.
“With the science of the microbiome and the novelty of fecal microbiota transplantation in expanding use, I think people have somewhat forgotten pharmacotherapy,” he said.
He pointed out safety concerns with FMT reported in June 2019, after which the FDA issued an alert. Two immunocompromised patients who received FMT, both from the same donor, developed invasive infections caused by extended-spectrum beta-lactamase (ESBL)–producing Escherichia coli. One died.
The FDA explained that the donated FMT samples the patients received were not tested for ESBL-producing gram-negative organisms before use.
Dr. Allegretti agreed antibiotics play a role in treatment with FMT, but she argued that the safety profile of FMT remains strong and that the safety issues came from isolated incidents at a single center.
Dr. Garey countered that there are just too many unknowns with FMT.
“We will never know what the next superbug that’s going to land in an FMT is until we’ve identified that superbug in somebody – the next Candida auris, the next CRE [carbapenem-resistant Enterobacteriaceae], the next thing that’s going to show up in FMT – until we get rid of the ‘F,’ “ Dr. Garey said.
“[Until] we get microbial therapy that’s generated without the need for healthy donors, I think we’re always going to be in this problem.”
He said although FMT “has an amazing ability to alter a microbiome” it “pales in comparison” to vancomycin’s ability to do so.
Disruption of the microbiome is, without a doubt, a hallmark of C. diff, but we don’t have to run to FMT,” Dr. Garey said. “We can think about prophylaxis strategies, we can think about new drug development that spares the microbiota. The need for FMT might be a consequence of poor pharmacotherapy management, not a part of pharmacotherapy management.”
Moderator Sam Aitken, PharmD, MPH, a clinical pharmacy specialist in infectious disease at MD Anderson Cancer Center in Houston, said in an interview the speakers found some common ground.
“I think there was a general consensus between both Dr. Allegretti and Dr. Garey that both traditional therapeutics and fecal microbiota transplantation have a role to play in these patients, although there is still quite a bit of discussion around where those might be best positioned,” Dr. Aitken said.
He added, “There’s also a general consensus that there is not likely to be one right answer for all patients with multiple recurrent CDI.”
Dr. Allegretti, Dr. Garey, and Dr. Aitken have disclosed no relevant financial relationships.
The AGA Fecal Microbiota Transplantation (FMT) National Registry will assess short- and long-term patient outcomes associated with FMT. Learn more and register to participate at www.gastro.org/fmtregistry.
A version of this article originally appeared on Medscape.com.
Tofacitinib retreatment effective for ulcerative colitis
Retreatment with tofacitinib after a period of treatment interruption was well tolerated and effective in patients with ulcerative colitis who had shown a previous response to tofacitinib induction, according to an analysis of data from the OCTAVE extension trial.
“Clinical response was recaptured in most patients by month 2, and about half of patients by month 36, irrespective of prior anti–[tumor necrosis factor] status,” said lead researcher Edward V. Loftus Jr, MD, from the Mayo Medical School, Rochester, Minn.
A temporary suspension of treatment with the oral, small-molecule Janus kinase (JAK) inhibitor might be necessary for a number of reasons, such as if a patient has to undergo surgery, experiences adverse events, or becomes pregnant.
For their study, Dr. Loftus and colleagues set out to assess the safety and efficacy of retreatment after a period of interruption.
“The population we’re interested in are patients who received tofacitinib during induction and placebo during maintenance” in the original OCTAVE trials, said Dr. Loftus. “They then either completed the trial or flared and rolled over to the open-label extension.”
The researchers looked at the 100 patients who had achieved a clinical response after 8 weeks of treatment with tofacitinib 10 mg twice-daily in the OCTAVE Induction 1 and OCTAVE Induction 2 trials and then received placebo in the OCTAVE Sustain trial and experienced treatment failure between week 8 and week 52. These patients went on to receive tofacitinib 10 mg twice daily as part of the ongoing, open-label, long-term extension OCTAVE Open trial.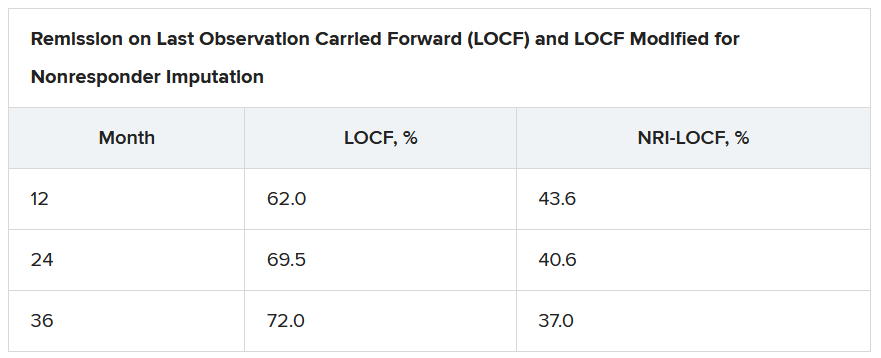
Treatment failure was defined as an increase of at least 3 points from the baseline total Mayo score achieved in OCTAVE Sustain, plus an increase of at least 1 point in rectal bleeding and endoscopic subscores and an absolute endoscopic subscore of at least 2 points after at least 8 weeks of treatment. Efficacy was evaluated for up to 36 months in the open-label extension; adverse events were assessed throughout the study period.
The median time to treatment failure was 135 days, Dr. Loftus reported during his award-winning presentation at the virtual annual meeting of the American College of Gastroenterology.
On last observation carried forward (LOCF) analysis, or observed data, 85.2% of the patients had recaptured clinical response by month 2. That rate fell to 74.3% when the analysis was modified for nonresponder imputation (NRI).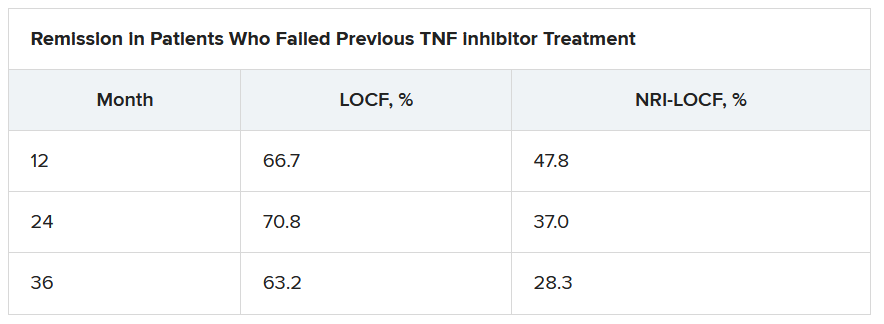
“The truth lies somewhere in between,” Dr. Loftus said.
Of interest, a clinical response to tofacitinib retreatment at month 2 was achieved by 92.5% (observed data) and 80.4% (NRI-LOCF) of patients who experienced treatment failure after tumor necrosis factor inhibitor therapy.
“Many patients were able to regain response with tofacitinib and then maintain that over time,” said Dr. Loftus.
Study supports retreatment, which is good news for patients
Incidence rates of adverse events were comparable in the retreatment population and in the overall extension cohort. “There are no signals jumping out, saying that safety events were higher or more frequent in this retreatment population, which is reassuring,” Dr. Loftus added.
Findings such as these are to be expected given the mechanism of action and pharmacologic features of tofacitinib, said Gionata Fiorino, MD, from Humanitas University in Milan, who was not involved in the study.
“I think this is important for patients who need to stop therapy for several reasons – pregnancy, adverse events that do not require permanent withdrawal of the drug, or surgical interventions – and experience a flare after drug withdrawal,” he said in an interview.
“There are several other therapeutic options for these patients, but I have experienced many patients who do not respond to other mechanisms of action apart from JAK [inhibitors],” he added. “And, in the case of a patient who has stopped the drug after having achieved remission, this study clearly supports retreatment, which is good news, especially for patients.”
This study was funded by Pfizer. Dr. Loftus reported financial relationships with AbbVie, Allergan, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Celltrion, Eli Lilly, Exact Sciences, Genentech, Gilead, Janssen, Pfizer, Robarts Clinical Trials, Takeda, and UCB. Dr. Fiorino reports financial relationships with MSD, Takeda, AbbVie, Janssen, Pfizer, Celltrion, Sandoz, AlfaSigma, Samsung, Amgen, Roche, and Ferring.
A version of this article originally appeared on Medscape.com.
Retreatment with tofacitinib after a period of treatment interruption was well tolerated and effective in patients with ulcerative colitis who had shown a previous response to tofacitinib induction, according to an analysis of data from the OCTAVE extension trial.
“Clinical response was recaptured in most patients by month 2, and about half of patients by month 36, irrespective of prior anti–[tumor necrosis factor] status,” said lead researcher Edward V. Loftus Jr, MD, from the Mayo Medical School, Rochester, Minn.
A temporary suspension of treatment with the oral, small-molecule Janus kinase (JAK) inhibitor might be necessary for a number of reasons, such as if a patient has to undergo surgery, experiences adverse events, or becomes pregnant.
For their study, Dr. Loftus and colleagues set out to assess the safety and efficacy of retreatment after a period of interruption.
“The population we’re interested in are patients who received tofacitinib during induction and placebo during maintenance” in the original OCTAVE trials, said Dr. Loftus. “They then either completed the trial or flared and rolled over to the open-label extension.”
The researchers looked at the 100 patients who had achieved a clinical response after 8 weeks of treatment with tofacitinib 10 mg twice-daily in the OCTAVE Induction 1 and OCTAVE Induction 2 trials and then received placebo in the OCTAVE Sustain trial and experienced treatment failure between week 8 and week 52. These patients went on to receive tofacitinib 10 mg twice daily as part of the ongoing, open-label, long-term extension OCTAVE Open trial.
Treatment failure was defined as an increase of at least 3 points from the baseline total Mayo score achieved in OCTAVE Sustain, plus an increase of at least 1 point in rectal bleeding and endoscopic subscores and an absolute endoscopic subscore of at least 2 points after at least 8 weeks of treatment. Efficacy was evaluated for up to 36 months in the open-label extension; adverse events were assessed throughout the study period.
The median time to treatment failure was 135 days, Dr. Loftus reported during his award-winning presentation at the virtual annual meeting of the American College of Gastroenterology.
On last observation carried forward (LOCF) analysis, or observed data, 85.2% of the patients had recaptured clinical response by month 2. That rate fell to 74.3% when the analysis was modified for nonresponder imputation (NRI).
“The truth lies somewhere in between,” Dr. Loftus said.
Of interest, a clinical response to tofacitinib retreatment at month 2 was achieved by 92.5% (observed data) and 80.4% (NRI-LOCF) of patients who experienced treatment failure after tumor necrosis factor inhibitor therapy.
“Many patients were able to regain response with tofacitinib and then maintain that over time,” said Dr. Loftus.
Study supports retreatment, which is good news for patients
Incidence rates of adverse events were comparable in the retreatment population and in the overall extension cohort. “There are no signals jumping out, saying that safety events were higher or more frequent in this retreatment population, which is reassuring,” Dr. Loftus added.
Findings such as these are to be expected given the mechanism of action and pharmacologic features of tofacitinib, said Gionata Fiorino, MD, from Humanitas University in Milan, who was not involved in the study.
“I think this is important for patients who need to stop therapy for several reasons – pregnancy, adverse events that do not require permanent withdrawal of the drug, or surgical interventions – and experience a flare after drug withdrawal,” he said in an interview.
“There are several other therapeutic options for these patients, but I have experienced many patients who do not respond to other mechanisms of action apart from JAK [inhibitors],” he added. “And, in the case of a patient who has stopped the drug after having achieved remission, this study clearly supports retreatment, which is good news, especially for patients.”
This study was funded by Pfizer. Dr. Loftus reported financial relationships with AbbVie, Allergan, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Celltrion, Eli Lilly, Exact Sciences, Genentech, Gilead, Janssen, Pfizer, Robarts Clinical Trials, Takeda, and UCB. Dr. Fiorino reports financial relationships with MSD, Takeda, AbbVie, Janssen, Pfizer, Celltrion, Sandoz, AlfaSigma, Samsung, Amgen, Roche, and Ferring.
A version of this article originally appeared on Medscape.com.
Retreatment with tofacitinib after a period of treatment interruption was well tolerated and effective in patients with ulcerative colitis who had shown a previous response to tofacitinib induction, according to an analysis of data from the OCTAVE extension trial.
“Clinical response was recaptured in most patients by month 2, and about half of patients by month 36, irrespective of prior anti–[tumor necrosis factor] status,” said lead researcher Edward V. Loftus Jr, MD, from the Mayo Medical School, Rochester, Minn.
A temporary suspension of treatment with the oral, small-molecule Janus kinase (JAK) inhibitor might be necessary for a number of reasons, such as if a patient has to undergo surgery, experiences adverse events, or becomes pregnant.
For their study, Dr. Loftus and colleagues set out to assess the safety and efficacy of retreatment after a period of interruption.
“The population we’re interested in are patients who received tofacitinib during induction and placebo during maintenance” in the original OCTAVE trials, said Dr. Loftus. “They then either completed the trial or flared and rolled over to the open-label extension.”
The researchers looked at the 100 patients who had achieved a clinical response after 8 weeks of treatment with tofacitinib 10 mg twice-daily in the OCTAVE Induction 1 and OCTAVE Induction 2 trials and then received placebo in the OCTAVE Sustain trial and experienced treatment failure between week 8 and week 52. These patients went on to receive tofacitinib 10 mg twice daily as part of the ongoing, open-label, long-term extension OCTAVE Open trial.
Treatment failure was defined as an increase of at least 3 points from the baseline total Mayo score achieved in OCTAVE Sustain, plus an increase of at least 1 point in rectal bleeding and endoscopic subscores and an absolute endoscopic subscore of at least 2 points after at least 8 weeks of treatment. Efficacy was evaluated for up to 36 months in the open-label extension; adverse events were assessed throughout the study period.
The median time to treatment failure was 135 days, Dr. Loftus reported during his award-winning presentation at the virtual annual meeting of the American College of Gastroenterology.
On last observation carried forward (LOCF) analysis, or observed data, 85.2% of the patients had recaptured clinical response by month 2. That rate fell to 74.3% when the analysis was modified for nonresponder imputation (NRI).
“The truth lies somewhere in between,” Dr. Loftus said.
Of interest, a clinical response to tofacitinib retreatment at month 2 was achieved by 92.5% (observed data) and 80.4% (NRI-LOCF) of patients who experienced treatment failure after tumor necrosis factor inhibitor therapy.
“Many patients were able to regain response with tofacitinib and then maintain that over time,” said Dr. Loftus.
Study supports retreatment, which is good news for patients
Incidence rates of adverse events were comparable in the retreatment population and in the overall extension cohort. “There are no signals jumping out, saying that safety events were higher or more frequent in this retreatment population, which is reassuring,” Dr. Loftus added.
Findings such as these are to be expected given the mechanism of action and pharmacologic features of tofacitinib, said Gionata Fiorino, MD, from Humanitas University in Milan, who was not involved in the study.
“I think this is important for patients who need to stop therapy for several reasons – pregnancy, adverse events that do not require permanent withdrawal of the drug, or surgical interventions – and experience a flare after drug withdrawal,” he said in an interview.
“There are several other therapeutic options for these patients, but I have experienced many patients who do not respond to other mechanisms of action apart from JAK [inhibitors],” he added. “And, in the case of a patient who has stopped the drug after having achieved remission, this study clearly supports retreatment, which is good news, especially for patients.”
This study was funded by Pfizer. Dr. Loftus reported financial relationships with AbbVie, Allergan, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Celltrion, Eli Lilly, Exact Sciences, Genentech, Gilead, Janssen, Pfizer, Robarts Clinical Trials, Takeda, and UCB. Dr. Fiorino reports financial relationships with MSD, Takeda, AbbVie, Janssen, Pfizer, Celltrion, Sandoz, AlfaSigma, Samsung, Amgen, Roche, and Ferring.
A version of this article originally appeared on Medscape.com.
IBD can be treated with diet alone
Dear colleagues and friends,

Thank you for your continued interest and support of the Perspectives debates. In this edition, Dr. Ashwin Ananthakrishnan and Dr. Laura Raffals explore the controversial topic of diet-based therapy in inflammatory bowel disease, highlights of the rationales for and against, and the current state of the evidence. All gastroenterologists frequently face questions pertaining to diet and its purported effects on digestive health. I found the discussion relevant to my own general practice, and I hope you will enjoy reading it as much as I did. As always, I welcome your comments and suggestions for future topics at ginews@gastro.org.
Charles Kahi, MD, MS, AGAF, professor of medicine, Indiana University, Indianapolis. He is also an associate editor for GI & Hepatology News.
IBD can be treated with diet alone
Inflammatory bowel diseases (IBD), comprising Crohn’s disease and ulcerative colitis, have emerged as global diseases. The past 3 decades have seen a rising incidence of these diseases not just in the Western hemisphere, where their prevalence has been well recognized, but also in regions of the world such as Asia and South America where they were previously rare. Whereas several possible factors have been proposed to explain this rising incidence and globalization of disease with varying degrees of supportive evidence, one of the most likely factors is a changing diet. Over the same period that the disease incidence and prevalence have risen, diets worldwide have converged with several common trends observed across countries and continents. These include reductions in dietary fiber, fruits, and vegetables, and increased intake of processed food, animal protein, fats, and sugary drinks, all of which have been linked epidemiologically to Crohn’s disease.

Treatment of Crohn’s disease and ulcerative colitis over the past 2 decades has focused on the immunologic dysfunction observed in these patients. Successful treatment has relied on suppressing immune responses either broadly or through targeted suppression of specific immunologic pathways. By and large, whereas these approaches have enabled us to make significant progress in reducing disease-related morbidity, success has been moderate at best, with fewer than half of patients in any clinical trial achieving remission at the end of a year. Thus, this approach alone may not be sufficient for most patients with IBD.
Treatment of IBD with diet was long considered out of the mainstream and confined to the realm of anecdotes and message boards. Despite most patients believing that diet played a role in development of IBD and onset of flares and that dietary modification was helpful in relieving symptoms, physicians – who for the most part were not trained in these approaches – were not believers, and probably rightly so in the absence of any supporting data.1 However, the parallel emergence of three bodies of literature has now brought diet back into the mainstream of IBD care (such that not a single IBD conference goes by without at least a session or two on diet). First, large prospective cohorts from Europe and North America provided robust evidence linking long-term adult dietary patterns to disease incidence in adult-onset IBD, which supports many important case-control observations made over the past 2 decades.2 Second, and perhaps most important, we began understanding the role of the microbiome in the development of these diseases and recognizing its centrality to bowel inflammation. One of the key determinants of the microbiome is diet, exerting both short-term and long-term influences on the microbial structure. While microbial changes are by no means the only mechanism through which diet can influence intestinal inflammation, they are among the most important, with broad effects across many dietary components. These findings provided a robust scientific basis for investigating the role of diet. Third, while still far from the high-quality (and expensive) set-up of investigational trials of pharmacologic therapies, dietary therapy studies have also evolved to randomized controlled trial designs and investigation of mechanism-driven dietary combinations. Together, I think these three recent advances, in addition to the wealth of existing literature and anecdotal experience, have been important in moving diet (back) into the IBD mainstream.
So what evidence is there that diet is effective in the treatment of IBD? Randomized controlled trials published more than a decade ago demonstrated that exclusive enteral nutrition, wherein all table foods are eliminated from a diet and the patient relies on an elemental diet alone for nutrition, was effective in not just inducing clinical remission but also improving inflammatory biomarkers.3 With results replicated in several trials, exclusive enteral nutrition is, in many parts of the world, one of the first-line treatments for pediatric Crohn’s disease. That this has not been translated to longer-term maintenance therapy is not necessarily an indicator of lack of durable efficacy, but reflects the challenges of maintaining such a restrictive diet long term while living an active, normal life. However, more recent rigorous studies have demonstrated that the effects of exclusive enteral nutrition can be mimicked either by a selected, less-restrictive diet (such as CD-TREAT4), which is more sustainable, or by combining partial enteral nutrition with an elimination diet that is quite diverse (such as CDED5). The latter two are considerably more promising as longer-term dietary treatments for Crohn’s disease with durable efficacy in open-label studies and randomized trials.
What are my final arguments for diet being used as a treatment for IBD? With the exception of very restrictive ones, diets are generally safe. Of course, patients on restricted diets need monitoring for nutritional deficiencies, but this monitoring is likely less intense than that needed for many of our immunosuppressive therapies. Dietary therapies are not associated with an increase in risk of infections or malignancy (unlike our traditional immunosuppressive therapies), and consequently are much more likely to be accepted by our patients than what we are currently offering. In addition, the existing treatments are expensive and consequently difficult to sustain globally with the increasing burden of these diseases. On the other hand, as eating and dietary choices are a routine part of day-to-day life, dietary therapies are not likely to be associated with any excess costs.
Therefore, treating IBD with diet alone is supported by epidemiologic, mechanistic, and clinical evidence and is a safe, effective, and inexpensive alternative for our patients.
References
1. Zallot C et al. Inflamm Bowel Dis. 2013 Jan;19(1):66-72.
2. Sasson AN et al. Clin Gastroenterol Hepatol. 2019 Dec 5;S1542-3565(19)31394-1.
3. Wall CL et al. World J Gastroenterol. 2013;19:7652-60.
4. Svolos V et al. Gastroenterology. 2019;156:1354-67.e6.
5. Levine A et al. Gastroenterology. 2019;157:440-50.e8.
Dr. Ananthakrishnan is a gastroenterologist in the division of gastroenterology, Crohn’s and Colitis Center, Massachusetts General Hospital and Harvard Medical School, Boston. He is supported by funding from the Crohn’s and Colitis Foundation and the Chleck Family Foundation.
IBD can be treated with diet alone – No, it cannot!
The cause of IBD is not completely understood, but we believe something in our environment triggers a dysregulated immune response in individuals with a genetic predisposition to IBD. Among the environmental triggers commonly recognized, diet is considered an important trigger through its ability to affect the composition and health of the gut microbiome and host barrier function. Epidemiologic data support this assumption. Westernization of diet has been associated with the increasing incidence of IBD across the globe and in immigrants who move from developing countries to an industrialized country. Observational studies have shown diets higher in meat and polyunsaturated fatty acids and omega-6 fatty acids are associated with a higher risk for IBD, whereas diets high in fruits, vegetables, and other sources of dietary fiber have a lower risk of IBD.

A growing body of evidence supports the impact food can have on gut health, specifically in mouse IBD models, but it is challenging to translate findings from animal studies into dietary interventions for IBD patients. Mouse studies help us understand the mechanistic basis of how diet may affect IBD, but randomized clinical trials establishing their role in IBD are lacking. This is not surprising as dietary studies are challenging, particularly if done in a robust manner, given the difficulties of ensuring and measuring dietary compliance.
Exclusive enteral nutrition (EEN) has been studied the most rigorously of all diets in IBD and has demonstrated the greatest benefit, compared with other diet studies in IBD. EEN requires the intake of elemental, semi-elemental, or polymeric formulas to meet all nutritional requirements without additional intake of food for 6-8 weeks. Studies have been performed mostly in pediatric populations and have shown effectiveness in induction of remission with reduction in inflammatory markers, including C-reactive protein, erythrocyte sedimentation rate, and fecal calprotectin, and even mucosal healing. EEN has not worked out as well for adult populations, because of the poor tolerability of exclusive intake of enteral formulas. Because of this limitation, studies of partial enteral nutrition have been performed that generally allow some food intake in addition to the enteral nutrition. When compared with EEN or anti–tumor necrosis factor–alpha therapy, partial enteral nutrition is a less-effective treatment of Crohn’s disease; however, partial enteral nutrition does appear to improve clinical symptoms.
Beyond EEN, there are many diets that have been considered for the treatment of IBD, including the specific carbohydrate diet (SCD), Crohn’s disease exclusion diet, autoimmune diet, low FODMAP (fermentable oligo-, di-, mono-saccharides and polyols), Paleolithic diet, Mediterranean diet, and the semi-vegetarian diet, to name a few. Of these, only the SCD and Crohn’s disease exclusion diets have shown improvement in clinical remission and reduction in inflammatory markers.
The SCD diet is based on the theory that malabsorption of disaccharide and polysaccharide carbohydrates leads to bacterial overgrowth and host barrier dysfunction. This diet eliminates grains, dairy, processed meats, and certain vegetables such as potatoes, yams, and legumes. Small uncontrolled studies have shown improvement in symptoms and endoscopy findings. However, this restrictive diet is nearly impossible to follow long term. The Crohn’s disease exclusion diet is a whole foods diet avoiding all processed foods, animal fats, dairy, and gluten. Small studies of this diet have also shown improvement in clinical symptoms and inflammatory markers.
The plethora of studies and reports of the therapeutic effect of diet on IBD provide some promise of the benefit dietary modifications can bring to our IBD patients. However, most dietary studies are underpowered, lack a control arm, and do not include endoscopic endpoints. The current body of evidence remains insufficient to support the use of diet alone for the treatment of IBD. We need randomized clinical controlled trials that are held to the same rigor as those of our approved medical treatments for IBD. Although such trials are challenging, we’ve seen groups rise to the task to carry out more robust dietary studies in the IBD population, and we await the results of several ongoing trials.
IBD is a challenging disease to live with and often leaves our patients feeling out of control. Dietary choices provide an avenue for patients to have some control of their health. However, current evidence does not support the prescription of dietary interventions alone to treat IBD, particularly when we have known, effective therapies. While I am not ready to prescribe diet as a stand-alone treatment for IBD, I make a point to discuss the role diet may play in helping our patients achieve optimal health. As health care providers, it is our responsibility to provide holistic care to our patients, which includes promotion of a healthy diet, absent processed foods and added sugars. Healthy lifestyle choices combined with effective medical and surgical treatments offer our patients the best shot at sustained disease control.
References
1. Hou JK et al. Am J Gastroenterol. 2011;106(4):563-73.
2. Zachos M et al. Cochrane Database Syst Rev. 2007(1):CD000542.
3. Lee D et al. Inflamm Bowel Dis. 2015;21(8):1786-93.
4. Obih C et al. Nutrition. 2016;32(4):418-25.
5. Sigall Boneh R et al. J Crohns Colitis. 2017;11(10):1205-12.
Dr. Raffals is a gastroenterologist in the division of gastroenterology and hepatology, Mayo Clinic, Rochester, Minn. She has no financial conflicts of interest relevant to this paper.
Dear colleagues and friends,
Thank you for your continued interest and support of the Perspectives debates. In this edition, Dr. Ashwin Ananthakrishnan and Dr. Laura Raffals explore the controversial topic of diet-based therapy in inflammatory bowel disease, highlights of the rationales for and against, and the current state of the evidence. All gastroenterologists frequently face questions pertaining to diet and its purported effects on digestive health. I found the discussion relevant to my own general practice, and I hope you will enjoy reading it as much as I did. As always, I welcome your comments and suggestions for future topics at ginews@gastro.org.
Charles Kahi, MD, MS, AGAF, professor of medicine, Indiana University, Indianapolis. He is also an associate editor for GI & Hepatology News.
IBD can be treated with diet alone
Inflammatory bowel diseases (IBD), comprising Crohn’s disease and ulcerative colitis, have emerged as global diseases. The past 3 decades have seen a rising incidence of these diseases not just in the Western hemisphere, where their prevalence has been well recognized, but also in regions of the world such as Asia and South America where they were previously rare. Whereas several possible factors have been proposed to explain this rising incidence and globalization of disease with varying degrees of supportive evidence, one of the most likely factors is a changing diet. Over the same period that the disease incidence and prevalence have risen, diets worldwide have converged with several common trends observed across countries and continents. These include reductions in dietary fiber, fruits, and vegetables, and increased intake of processed food, animal protein, fats, and sugary drinks, all of which have been linked epidemiologically to Crohn’s disease.
Treatment of Crohn’s disease and ulcerative colitis over the past 2 decades has focused on the immunologic dysfunction observed in these patients. Successful treatment has relied on suppressing immune responses either broadly or through targeted suppression of specific immunologic pathways. By and large, whereas these approaches have enabled us to make significant progress in reducing disease-related morbidity, success has been moderate at best, with fewer than half of patients in any clinical trial achieving remission at the end of a year. Thus, this approach alone may not be sufficient for most patients with IBD.
Treatment of IBD with diet was long considered out of the mainstream and confined to the realm of anecdotes and message boards. Despite most patients believing that diet played a role in development of IBD and onset of flares and that dietary modification was helpful in relieving symptoms, physicians – who for the most part were not trained in these approaches – were not believers, and probably rightly so in the absence of any supporting data.1 However, the parallel emergence of three bodies of literature has now brought diet back into the mainstream of IBD care (such that not a single IBD conference goes by without at least a session or two on diet). First, large prospective cohorts from Europe and North America provided robust evidence linking long-term adult dietary patterns to disease incidence in adult-onset IBD, which supports many important case-control observations made over the past 2 decades.2 Second, and perhaps most important, we began understanding the role of the microbiome in the development of these diseases and recognizing its centrality to bowel inflammation. One of the key determinants of the microbiome is diet, exerting both short-term and long-term influences on the microbial structure. While microbial changes are by no means the only mechanism through which diet can influence intestinal inflammation, they are among the most important, with broad effects across many dietary components. These findings provided a robust scientific basis for investigating the role of diet. Third, while still far from the high-quality (and expensive) set-up of investigational trials of pharmacologic therapies, dietary therapy studies have also evolved to randomized controlled trial designs and investigation of mechanism-driven dietary combinations. Together, I think these three recent advances, in addition to the wealth of existing literature and anecdotal experience, have been important in moving diet (back) into the IBD mainstream.
So what evidence is there that diet is effective in the treatment of IBD? Randomized controlled trials published more than a decade ago demonstrated that exclusive enteral nutrition, wherein all table foods are eliminated from a diet and the patient relies on an elemental diet alone for nutrition, was effective in not just inducing clinical remission but also improving inflammatory biomarkers.3 With results replicated in several trials, exclusive enteral nutrition is, in many parts of the world, one of the first-line treatments for pediatric Crohn’s disease. That this has not been translated to longer-term maintenance therapy is not necessarily an indicator of lack of durable efficacy, but reflects the challenges of maintaining such a restrictive diet long term while living an active, normal life. However, more recent rigorous studies have demonstrated that the effects of exclusive enteral nutrition can be mimicked either by a selected, less-restrictive diet (such as CD-TREAT4), which is more sustainable, or by combining partial enteral nutrition with an elimination diet that is quite diverse (such as CDED5). The latter two are considerably more promising as longer-term dietary treatments for Crohn’s disease with durable efficacy in open-label studies and randomized trials.
What are my final arguments for diet being used as a treatment for IBD? With the exception of very restrictive ones, diets are generally safe. Of course, patients on restricted diets need monitoring for nutritional deficiencies, but this monitoring is likely less intense than that needed for many of our immunosuppressive therapies. Dietary therapies are not associated with an increase in risk of infections or malignancy (unlike our traditional immunosuppressive therapies), and consequently are much more likely to be accepted by our patients than what we are currently offering. In addition, the existing treatments are expensive and consequently difficult to sustain globally with the increasing burden of these diseases. On the other hand, as eating and dietary choices are a routine part of day-to-day life, dietary therapies are not likely to be associated with any excess costs.
Therefore, treating IBD with diet alone is supported by epidemiologic, mechanistic, and clinical evidence and is a safe, effective, and inexpensive alternative for our patients.
References
1. Zallot C et al. Inflamm Bowel Dis. 2013 Jan;19(1):66-72.
2. Sasson AN et al. Clin Gastroenterol Hepatol. 2019 Dec 5;S1542-3565(19)31394-1.
3. Wall CL et al. World J Gastroenterol. 2013;19:7652-60.
4. Svolos V et al. Gastroenterology. 2019;156:1354-67.e6.
5. Levine A et al. Gastroenterology. 2019;157:440-50.e8.
Dr. Ananthakrishnan is a gastroenterologist in the division of gastroenterology, Crohn’s and Colitis Center, Massachusetts General Hospital and Harvard Medical School, Boston. He is supported by funding from the Crohn’s and Colitis Foundation and the Chleck Family Foundation.
IBD can be treated with diet alone – No, it cannot!
The cause of IBD is not completely understood, but we believe something in our environment triggers a dysregulated immune response in individuals with a genetic predisposition to IBD. Among the environmental triggers commonly recognized, diet is considered an important trigger through its ability to affect the composition and health of the gut microbiome and host barrier function. Epidemiologic data support this assumption. Westernization of diet has been associated with the increasing incidence of IBD across the globe and in immigrants who move from developing countries to an industrialized country. Observational studies have shown diets higher in meat and polyunsaturated fatty acids and omega-6 fatty acids are associated with a higher risk for IBD, whereas diets high in fruits, vegetables, and other sources of dietary fiber have a lower risk of IBD.
A growing body of evidence supports the impact food can have on gut health, specifically in mouse IBD models, but it is challenging to translate findings from animal studies into dietary interventions for IBD patients. Mouse studies help us understand the mechanistic basis of how diet may affect IBD, but randomized clinical trials establishing their role in IBD are lacking. This is not surprising as dietary studies are challenging, particularly if done in a robust manner, given the difficulties of ensuring and measuring dietary compliance.
Exclusive enteral nutrition (EEN) has been studied the most rigorously of all diets in IBD and has demonstrated the greatest benefit, compared with other diet studies in IBD. EEN requires the intake of elemental, semi-elemental, or polymeric formulas to meet all nutritional requirements without additional intake of food for 6-8 weeks. Studies have been performed mostly in pediatric populations and have shown effectiveness in induction of remission with reduction in inflammatory markers, including C-reactive protein, erythrocyte sedimentation rate, and fecal calprotectin, and even mucosal healing. EEN has not worked out as well for adult populations, because of the poor tolerability of exclusive intake of enteral formulas. Because of this limitation, studies of partial enteral nutrition have been performed that generally allow some food intake in addition to the enteral nutrition. When compared with EEN or anti–tumor necrosis factor–alpha therapy, partial enteral nutrition is a less-effective treatment of Crohn’s disease; however, partial enteral nutrition does appear to improve clinical symptoms.
Beyond EEN, there are many diets that have been considered for the treatment of IBD, including the specific carbohydrate diet (SCD), Crohn’s disease exclusion diet, autoimmune diet, low FODMAP (fermentable oligo-, di-, mono-saccharides and polyols), Paleolithic diet, Mediterranean diet, and the semi-vegetarian diet, to name a few. Of these, only the SCD and Crohn’s disease exclusion diets have shown improvement in clinical remission and reduction in inflammatory markers.
The SCD diet is based on the theory that malabsorption of disaccharide and polysaccharide carbohydrates leads to bacterial overgrowth and host barrier dysfunction. This diet eliminates grains, dairy, processed meats, and certain vegetables such as potatoes, yams, and legumes. Small uncontrolled studies have shown improvement in symptoms and endoscopy findings. However, this restrictive diet is nearly impossible to follow long term. The Crohn’s disease exclusion diet is a whole foods diet avoiding all processed foods, animal fats, dairy, and gluten. Small studies of this diet have also shown improvement in clinical symptoms and inflammatory markers.
The plethora of studies and reports of the therapeutic effect of diet on IBD provide some promise of the benefit dietary modifications can bring to our IBD patients. However, most dietary studies are underpowered, lack a control arm, and do not include endoscopic endpoints. The current body of evidence remains insufficient to support the use of diet alone for the treatment of IBD. We need randomized clinical controlled trials that are held to the same rigor as those of our approved medical treatments for IBD. Although such trials are challenging, we’ve seen groups rise to the task to carry out more robust dietary studies in the IBD population, and we await the results of several ongoing trials.
IBD is a challenging disease to live with and often leaves our patients feeling out of control. Dietary choices provide an avenue for patients to have some control of their health. However, current evidence does not support the prescription of dietary interventions alone to treat IBD, particularly when we have known, effective therapies. While I am not ready to prescribe diet as a stand-alone treatment for IBD, I make a point to discuss the role diet may play in helping our patients achieve optimal health. As health care providers, it is our responsibility to provide holistic care to our patients, which includes promotion of a healthy diet, absent processed foods and added sugars. Healthy lifestyle choices combined with effective medical and surgical treatments offer our patients the best shot at sustained disease control.
References
1. Hou JK et al. Am J Gastroenterol. 2011;106(4):563-73.
2. Zachos M et al. Cochrane Database Syst Rev. 2007(1):CD000542.
3. Lee D et al. Inflamm Bowel Dis. 2015;21(8):1786-93.
4. Obih C et al. Nutrition. 2016;32(4):418-25.
5. Sigall Boneh R et al. J Crohns Colitis. 2017;11(10):1205-12.
Dr. Raffals is a gastroenterologist in the division of gastroenterology and hepatology, Mayo Clinic, Rochester, Minn. She has no financial conflicts of interest relevant to this paper.
Dear colleagues and friends,
Thank you for your continued interest and support of the Perspectives debates. In this edition, Dr. Ashwin Ananthakrishnan and Dr. Laura Raffals explore the controversial topic of diet-based therapy in inflammatory bowel disease, highlights of the rationales for and against, and the current state of the evidence. All gastroenterologists frequently face questions pertaining to diet and its purported effects on digestive health. I found the discussion relevant to my own general practice, and I hope you will enjoy reading it as much as I did. As always, I welcome your comments and suggestions for future topics at ginews@gastro.org.
Charles Kahi, MD, MS, AGAF, professor of medicine, Indiana University, Indianapolis. He is also an associate editor for GI & Hepatology News.
IBD can be treated with diet alone
Inflammatory bowel diseases (IBD), comprising Crohn’s disease and ulcerative colitis, have emerged as global diseases. The past 3 decades have seen a rising incidence of these diseases not just in the Western hemisphere, where their prevalence has been well recognized, but also in regions of the world such as Asia and South America where they were previously rare. Whereas several possible factors have been proposed to explain this rising incidence and globalization of disease with varying degrees of supportive evidence, one of the most likely factors is a changing diet. Over the same period that the disease incidence and prevalence have risen, diets worldwide have converged with several common trends observed across countries and continents. These include reductions in dietary fiber, fruits, and vegetables, and increased intake of processed food, animal protein, fats, and sugary drinks, all of which have been linked epidemiologically to Crohn’s disease.
Treatment of Crohn’s disease and ulcerative colitis over the past 2 decades has focused on the immunologic dysfunction observed in these patients. Successful treatment has relied on suppressing immune responses either broadly or through targeted suppression of specific immunologic pathways. By and large, whereas these approaches have enabled us to make significant progress in reducing disease-related morbidity, success has been moderate at best, with fewer than half of patients in any clinical trial achieving remission at the end of a year. Thus, this approach alone may not be sufficient for most patients with IBD.
Treatment of IBD with diet was long considered out of the mainstream and confined to the realm of anecdotes and message boards. Despite most patients believing that diet played a role in development of IBD and onset of flares and that dietary modification was helpful in relieving symptoms, physicians – who for the most part were not trained in these approaches – were not believers, and probably rightly so in the absence of any supporting data.1 However, the parallel emergence of three bodies of literature has now brought diet back into the mainstream of IBD care (such that not a single IBD conference goes by without at least a session or two on diet). First, large prospective cohorts from Europe and North America provided robust evidence linking long-term adult dietary patterns to disease incidence in adult-onset IBD, which supports many important case-control observations made over the past 2 decades.2 Second, and perhaps most important, we began understanding the role of the microbiome in the development of these diseases and recognizing its centrality to bowel inflammation. One of the key determinants of the microbiome is diet, exerting both short-term and long-term influences on the microbial structure. While microbial changes are by no means the only mechanism through which diet can influence intestinal inflammation, they are among the most important, with broad effects across many dietary components. These findings provided a robust scientific basis for investigating the role of diet. Third, while still far from the high-quality (and expensive) set-up of investigational trials of pharmacologic therapies, dietary therapy studies have also evolved to randomized controlled trial designs and investigation of mechanism-driven dietary combinations. Together, I think these three recent advances, in addition to the wealth of existing literature and anecdotal experience, have been important in moving diet (back) into the IBD mainstream.
So what evidence is there that diet is effective in the treatment of IBD? Randomized controlled trials published more than a decade ago demonstrated that exclusive enteral nutrition, wherein all table foods are eliminated from a diet and the patient relies on an elemental diet alone for nutrition, was effective in not just inducing clinical remission but also improving inflammatory biomarkers.3 With results replicated in several trials, exclusive enteral nutrition is, in many parts of the world, one of the first-line treatments for pediatric Crohn’s disease. That this has not been translated to longer-term maintenance therapy is not necessarily an indicator of lack of durable efficacy, but reflects the challenges of maintaining such a restrictive diet long term while living an active, normal life. However, more recent rigorous studies have demonstrated that the effects of exclusive enteral nutrition can be mimicked either by a selected, less-restrictive diet (such as CD-TREAT4), which is more sustainable, or by combining partial enteral nutrition with an elimination diet that is quite diverse (such as CDED5). The latter two are considerably more promising as longer-term dietary treatments for Crohn’s disease with durable efficacy in open-label studies and randomized trials.
What are my final arguments for diet being used as a treatment for IBD? With the exception of very restrictive ones, diets are generally safe. Of course, patients on restricted diets need monitoring for nutritional deficiencies, but this monitoring is likely less intense than that needed for many of our immunosuppressive therapies. Dietary therapies are not associated with an increase in risk of infections or malignancy (unlike our traditional immunosuppressive therapies), and consequently are much more likely to be accepted by our patients than what we are currently offering. In addition, the existing treatments are expensive and consequently difficult to sustain globally with the increasing burden of these diseases. On the other hand, as eating and dietary choices are a routine part of day-to-day life, dietary therapies are not likely to be associated with any excess costs.
Therefore, treating IBD with diet alone is supported by epidemiologic, mechanistic, and clinical evidence and is a safe, effective, and inexpensive alternative for our patients.
References
1. Zallot C et al. Inflamm Bowel Dis. 2013 Jan;19(1):66-72.
2. Sasson AN et al. Clin Gastroenterol Hepatol. 2019 Dec 5;S1542-3565(19)31394-1.
3. Wall CL et al. World J Gastroenterol. 2013;19:7652-60.
4. Svolos V et al. Gastroenterology. 2019;156:1354-67.e6.
5. Levine A et al. Gastroenterology. 2019;157:440-50.e8.
Dr. Ananthakrishnan is a gastroenterologist in the division of gastroenterology, Crohn’s and Colitis Center, Massachusetts General Hospital and Harvard Medical School, Boston. He is supported by funding from the Crohn’s and Colitis Foundation and the Chleck Family Foundation.
IBD can be treated with diet alone – No, it cannot!
The cause of IBD is not completely understood, but we believe something in our environment triggers a dysregulated immune response in individuals with a genetic predisposition to IBD. Among the environmental triggers commonly recognized, diet is considered an important trigger through its ability to affect the composition and health of the gut microbiome and host barrier function. Epidemiologic data support this assumption. Westernization of diet has been associated with the increasing incidence of IBD across the globe and in immigrants who move from developing countries to an industrialized country. Observational studies have shown diets higher in meat and polyunsaturated fatty acids and omega-6 fatty acids are associated with a higher risk for IBD, whereas diets high in fruits, vegetables, and other sources of dietary fiber have a lower risk of IBD.
A growing body of evidence supports the impact food can have on gut health, specifically in mouse IBD models, but it is challenging to translate findings from animal studies into dietary interventions for IBD patients. Mouse studies help us understand the mechanistic basis of how diet may affect IBD, but randomized clinical trials establishing their role in IBD are lacking. This is not surprising as dietary studies are challenging, particularly if done in a robust manner, given the difficulties of ensuring and measuring dietary compliance.
Exclusive enteral nutrition (EEN) has been studied the most rigorously of all diets in IBD and has demonstrated the greatest benefit, compared with other diet studies in IBD. EEN requires the intake of elemental, semi-elemental, or polymeric formulas to meet all nutritional requirements without additional intake of food for 6-8 weeks. Studies have been performed mostly in pediatric populations and have shown effectiveness in induction of remission with reduction in inflammatory markers, including C-reactive protein, erythrocyte sedimentation rate, and fecal calprotectin, and even mucosal healing. EEN has not worked out as well for adult populations, because of the poor tolerability of exclusive intake of enteral formulas. Because of this limitation, studies of partial enteral nutrition have been performed that generally allow some food intake in addition to the enteral nutrition. When compared with EEN or anti–tumor necrosis factor–alpha therapy, partial enteral nutrition is a less-effective treatment of Crohn’s disease; however, partial enteral nutrition does appear to improve clinical symptoms.
Beyond EEN, there are many diets that have been considered for the treatment of IBD, including the specific carbohydrate diet (SCD), Crohn’s disease exclusion diet, autoimmune diet, low FODMAP (fermentable oligo-, di-, mono-saccharides and polyols), Paleolithic diet, Mediterranean diet, and the semi-vegetarian diet, to name a few. Of these, only the SCD and Crohn’s disease exclusion diets have shown improvement in clinical remission and reduction in inflammatory markers.
The SCD diet is based on the theory that malabsorption of disaccharide and polysaccharide carbohydrates leads to bacterial overgrowth and host barrier dysfunction. This diet eliminates grains, dairy, processed meats, and certain vegetables such as potatoes, yams, and legumes. Small uncontrolled studies have shown improvement in symptoms and endoscopy findings. However, this restrictive diet is nearly impossible to follow long term. The Crohn’s disease exclusion diet is a whole foods diet avoiding all processed foods, animal fats, dairy, and gluten. Small studies of this diet have also shown improvement in clinical symptoms and inflammatory markers.
The plethora of studies and reports of the therapeutic effect of diet on IBD provide some promise of the benefit dietary modifications can bring to our IBD patients. However, most dietary studies are underpowered, lack a control arm, and do not include endoscopic endpoints. The current body of evidence remains insufficient to support the use of diet alone for the treatment of IBD. We need randomized clinical controlled trials that are held to the same rigor as those of our approved medical treatments for IBD. Although such trials are challenging, we’ve seen groups rise to the task to carry out more robust dietary studies in the IBD population, and we await the results of several ongoing trials.
IBD is a challenging disease to live with and often leaves our patients feeling out of control. Dietary choices provide an avenue for patients to have some control of their health. However, current evidence does not support the prescription of dietary interventions alone to treat IBD, particularly when we have known, effective therapies. While I am not ready to prescribe diet as a stand-alone treatment for IBD, I make a point to discuss the role diet may play in helping our patients achieve optimal health. As health care providers, it is our responsibility to provide holistic care to our patients, which includes promotion of a healthy diet, absent processed foods and added sugars. Healthy lifestyle choices combined with effective medical and surgical treatments offer our patients the best shot at sustained disease control.
References
1. Hou JK et al. Am J Gastroenterol. 2011;106(4):563-73.
2. Zachos M et al. Cochrane Database Syst Rev. 2007(1):CD000542.
3. Lee D et al. Inflamm Bowel Dis. 2015;21(8):1786-93.
4. Obih C et al. Nutrition. 2016;32(4):418-25.
5. Sigall Boneh R et al. J Crohns Colitis. 2017;11(10):1205-12.
Dr. Raffals is a gastroenterologist in the division of gastroenterology and hepatology, Mayo Clinic, Rochester, Minn. She has no financial conflicts of interest relevant to this paper.
IL-23 plays key roles in antimicrobial macrophage activity
Interleukin-23 optimizes antimicrobial macrophage activity, which is reduced among persons harboring an IL-23 receptor variant that helps protect against inflammatory bowel disease (IBD), recent research has found.
“These [findings] highlight that the susceptibility to infections with therapeutic blockade of the IL-23/IL-12 pathways may be owing in part to the essential role for IL-23 in mediating antimicrobial functions in macrophages. They further highlight that carriers of the IL-23R–Q381 variant, who are relatively protected from IBD and other immune-mediated diseases, may be at increased risk for bacterial infection,” Rui Sun and Clara Abraham, MD, of Yale University, New Haven, Conn., wrote in Cellular and Molecular Gastroenterology and Hepatology.
IL-23 is key to the pathogenesis of IBD and is being studied as a therapeutic target, both alone and in combination with IL-12 blocking. Although human macrophages express low levels of IL-23 receptor, recent research reveals that IL-23R is up-regulated “within minutes of exposure to IL-23,” which promotes signaling and cytokine secretion, the investigators wrote. However, the extent to which IL-23 supports macrophage antimicrobial activity was unknown. To characterize protein expression, signaling, and bacterial uptake and clearance of bacteria by human macrophages derived from monocytes, the investigators tested these cells with Western blot, flow cytometry, and gentamicin protection, which involved coculturing human macrophages with bacteria, adding gentamicin solution, and then lysing and plating the cells onto agar to assess the extent to which the macrophages had taken up the bacteria.
After 48 hours of exposure to IL-23 or IL-12, macrophages increased their intracellular clearance of clinically relevant bacteria, including Enterococcus faecalis, adherent invasive Escherichia coli, and Salmonella typhimurium. Notably, this did not occur when the investigators reduced (“knocked down”) macrophage expression of either IL-23R or IL-12 receptor alpha 2. Additional investigations showed that in macrophages, IL-23 promotes bacterial uptake, clearance, and autophagy by inducing a pyruvate dehydrogenase kinase 1 (PDK1)–dependent pathway mediated by Janus kinase 2/tyrosine kinase 2 and by inducing reactive oxygen species (ROS) and reactive nitrogen species (RNS) pathways. IL-23 also activates two key proteins involved in autophagy (ATG5 and ATG16L1), the researchers reported. “ROS, RNS, and autophagy cooperate to mediate IL-23-induced bacterial clearance. Reduction of each ROS, RNS, and autophagy pathway partially reversed the enhanced bacterial clearance observed with chronic IL-23 treatment.”
Further tests found that IL-23 mediates antimicrobial pathways through the Janus kinase 2, tyrosine kinase 2, and STAT3 pathways, which “cooperate to mediate optimal IL-23-induced intracellular bacterial clearance in human macrophages.” Importantly, human macrophages showed less antimicrobial activity when transfected with the IL-23R–Q381 variant than with IL-23R–R381. The IL-23R-Q381 variant, which reduces susceptibility to IBD, “decreased IL-23-induced and NOD2-induced antimicrobial pathways and intracellular bacterial clearance in monocyte-derived macrophages,” the researchers explained. Evaluating actual carriers of these variants showed the same results – macrophages harboring IBD-protective IL-23R–R381/Q381 exhibited lower antimicrobial activity and less intracellular bacterial clearance compared with macrophages from carriers of IL-23R–R381/R381.
“Taken together, IL-23 promotes increased bacterial uptake and then induces a more rapid and effective clearance of these intracellular bacteria in human monocyte-derived macrophages,” the researchers wrote. “The reduced inflammatory responses observed in IL-23R Q381 carriers are associated with protection from multiple immune-mediated diseases. This would imply that loss-of-function observed with the common IL-23R–R381Q variant may lead to a disadvantage in select infectious diseases, including through [this variant’s] now identified role in promoting antimicrobial pathways in macrophages.”
The National Institutes of Health provided funding. The investigators reported having no conflicts of interest.
SOURCE: Sun R, Abraham C. Cell Molec Gastro Hepatol. 2020 May 28. doi.: 10.1016/j.jcmgh.2020.05.007.
Both genetic studies in humans and functional studies in mice have pinpointed interleukin-23 and its receptor as a key pathway in the pathogenesis of inflammatory bowel disease (IBD). IL-23 is released from myeloid cells in response to sensing of invading pathogens or danger-associated molecular patterns, where it drives induction of Th17, innate lymphoid cell responses, and inflammation.

Alison Simmons, FRCP, PhD, is professor of gastroenterology, honorary consultant gastroenterologist, MRC human immunology unit, Weatherall Institute of Molecular Medicine, University of Oxford (England), and translational gastroenterology unit, Oxford University Hospitals NHS Trust. She has consultancies from AbbVie, Bristol-Myers Squibb, and Janssen, and is a cofounder and equity holder in TRexBio.
Both genetic studies in humans and functional studies in mice have pinpointed interleukin-23 and its receptor as a key pathway in the pathogenesis of inflammatory bowel disease (IBD). IL-23 is released from myeloid cells in response to sensing of invading pathogens or danger-associated molecular patterns, where it drives induction of Th17, innate lymphoid cell responses, and inflammation.
Alison Simmons, FRCP, PhD, is professor of gastroenterology, honorary consultant gastroenterologist, MRC human immunology unit, Weatherall Institute of Molecular Medicine, University of Oxford (England), and translational gastroenterology unit, Oxford University Hospitals NHS Trust. She has consultancies from AbbVie, Bristol-Myers Squibb, and Janssen, and is a cofounder and equity holder in TRexBio.
Both genetic studies in humans and functional studies in mice have pinpointed interleukin-23 and its receptor as a key pathway in the pathogenesis of inflammatory bowel disease (IBD). IL-23 is released from myeloid cells in response to sensing of invading pathogens or danger-associated molecular patterns, where it drives induction of Th17, innate lymphoid cell responses, and inflammation.
Alison Simmons, FRCP, PhD, is professor of gastroenterology, honorary consultant gastroenterologist, MRC human immunology unit, Weatherall Institute of Molecular Medicine, University of Oxford (England), and translational gastroenterology unit, Oxford University Hospitals NHS Trust. She has consultancies from AbbVie, Bristol-Myers Squibb, and Janssen, and is a cofounder and equity holder in TRexBio.
Interleukin-23 optimizes antimicrobial macrophage activity, which is reduced among persons harboring an IL-23 receptor variant that helps protect against inflammatory bowel disease (IBD), recent research has found.
“These [findings] highlight that the susceptibility to infections with therapeutic blockade of the IL-23/IL-12 pathways may be owing in part to the essential role for IL-23 in mediating antimicrobial functions in macrophages. They further highlight that carriers of the IL-23R–Q381 variant, who are relatively protected from IBD and other immune-mediated diseases, may be at increased risk for bacterial infection,” Rui Sun and Clara Abraham, MD, of Yale University, New Haven, Conn., wrote in Cellular and Molecular Gastroenterology and Hepatology.
IL-23 is key to the pathogenesis of IBD and is being studied as a therapeutic target, both alone and in combination with IL-12 blocking. Although human macrophages express low levels of IL-23 receptor, recent research reveals that IL-23R is up-regulated “within minutes of exposure to IL-23,” which promotes signaling and cytokine secretion, the investigators wrote. However, the extent to which IL-23 supports macrophage antimicrobial activity was unknown. To characterize protein expression, signaling, and bacterial uptake and clearance of bacteria by human macrophages derived from monocytes, the investigators tested these cells with Western blot, flow cytometry, and gentamicin protection, which involved coculturing human macrophages with bacteria, adding gentamicin solution, and then lysing and plating the cells onto agar to assess the extent to which the macrophages had taken up the bacteria.
After 48 hours of exposure to IL-23 or IL-12, macrophages increased their intracellular clearance of clinically relevant bacteria, including Enterococcus faecalis, adherent invasive Escherichia coli, and Salmonella typhimurium. Notably, this did not occur when the investigators reduced (“knocked down”) macrophage expression of either IL-23R or IL-12 receptor alpha 2. Additional investigations showed that in macrophages, IL-23 promotes bacterial uptake, clearance, and autophagy by inducing a pyruvate dehydrogenase kinase 1 (PDK1)–dependent pathway mediated by Janus kinase 2/tyrosine kinase 2 and by inducing reactive oxygen species (ROS) and reactive nitrogen species (RNS) pathways. IL-23 also activates two key proteins involved in autophagy (ATG5 and ATG16L1), the researchers reported. “ROS, RNS, and autophagy cooperate to mediate IL-23-induced bacterial clearance. Reduction of each ROS, RNS, and autophagy pathway partially reversed the enhanced bacterial clearance observed with chronic IL-23 treatment.”
Further tests found that IL-23 mediates antimicrobial pathways through the Janus kinase 2, tyrosine kinase 2, and STAT3 pathways, which “cooperate to mediate optimal IL-23-induced intracellular bacterial clearance in human macrophages.” Importantly, human macrophages showed less antimicrobial activity when transfected with the IL-23R–Q381 variant than with IL-23R–R381. The IL-23R-Q381 variant, which reduces susceptibility to IBD, “decreased IL-23-induced and NOD2-induced antimicrobial pathways and intracellular bacterial clearance in monocyte-derived macrophages,” the researchers explained. Evaluating actual carriers of these variants showed the same results – macrophages harboring IBD-protective IL-23R–R381/Q381 exhibited lower antimicrobial activity and less intracellular bacterial clearance compared with macrophages from carriers of IL-23R–R381/R381.
“Taken together, IL-23 promotes increased bacterial uptake and then induces a more rapid and effective clearance of these intracellular bacteria in human monocyte-derived macrophages,” the researchers wrote. “The reduced inflammatory responses observed in IL-23R Q381 carriers are associated with protection from multiple immune-mediated diseases. This would imply that loss-of-function observed with the common IL-23R–R381Q variant may lead to a disadvantage in select infectious diseases, including through [this variant’s] now identified role in promoting antimicrobial pathways in macrophages.”
The National Institutes of Health provided funding. The investigators reported having no conflicts of interest.
SOURCE: Sun R, Abraham C. Cell Molec Gastro Hepatol. 2020 May 28. doi.: 10.1016/j.jcmgh.2020.05.007.
Interleukin-23 optimizes antimicrobial macrophage activity, which is reduced among persons harboring an IL-23 receptor variant that helps protect against inflammatory bowel disease (IBD), recent research has found.
“These [findings] highlight that the susceptibility to infections with therapeutic blockade of the IL-23/IL-12 pathways may be owing in part to the essential role for IL-23 in mediating antimicrobial functions in macrophages. They further highlight that carriers of the IL-23R–Q381 variant, who are relatively protected from IBD and other immune-mediated diseases, may be at increased risk for bacterial infection,” Rui Sun and Clara Abraham, MD, of Yale University, New Haven, Conn., wrote in Cellular and Molecular Gastroenterology and Hepatology.
IL-23 is key to the pathogenesis of IBD and is being studied as a therapeutic target, both alone and in combination with IL-12 blocking. Although human macrophages express low levels of IL-23 receptor, recent research reveals that IL-23R is up-regulated “within minutes of exposure to IL-23,” which promotes signaling and cytokine secretion, the investigators wrote. However, the extent to which IL-23 supports macrophage antimicrobial activity was unknown. To characterize protein expression, signaling, and bacterial uptake and clearance of bacteria by human macrophages derived from monocytes, the investigators tested these cells with Western blot, flow cytometry, and gentamicin protection, which involved coculturing human macrophages with bacteria, adding gentamicin solution, and then lysing and plating the cells onto agar to assess the extent to which the macrophages had taken up the bacteria.
After 48 hours of exposure to IL-23 or IL-12, macrophages increased their intracellular clearance of clinically relevant bacteria, including Enterococcus faecalis, adherent invasive Escherichia coli, and Salmonella typhimurium. Notably, this did not occur when the investigators reduced (“knocked down”) macrophage expression of either IL-23R or IL-12 receptor alpha 2. Additional investigations showed that in macrophages, IL-23 promotes bacterial uptake, clearance, and autophagy by inducing a pyruvate dehydrogenase kinase 1 (PDK1)–dependent pathway mediated by Janus kinase 2/tyrosine kinase 2 and by inducing reactive oxygen species (ROS) and reactive nitrogen species (RNS) pathways. IL-23 also activates two key proteins involved in autophagy (ATG5 and ATG16L1), the researchers reported. “ROS, RNS, and autophagy cooperate to mediate IL-23-induced bacterial clearance. Reduction of each ROS, RNS, and autophagy pathway partially reversed the enhanced bacterial clearance observed with chronic IL-23 treatment.”
Further tests found that IL-23 mediates antimicrobial pathways through the Janus kinase 2, tyrosine kinase 2, and STAT3 pathways, which “cooperate to mediate optimal IL-23-induced intracellular bacterial clearance in human macrophages.” Importantly, human macrophages showed less antimicrobial activity when transfected with the IL-23R–Q381 variant than with IL-23R–R381. The IL-23R-Q381 variant, which reduces susceptibility to IBD, “decreased IL-23-induced and NOD2-induced antimicrobial pathways and intracellular bacterial clearance in monocyte-derived macrophages,” the researchers explained. Evaluating actual carriers of these variants showed the same results – macrophages harboring IBD-protective IL-23R–R381/Q381 exhibited lower antimicrobial activity and less intracellular bacterial clearance compared with macrophages from carriers of IL-23R–R381/R381.
“Taken together, IL-23 promotes increased bacterial uptake and then induces a more rapid and effective clearance of these intracellular bacteria in human monocyte-derived macrophages,” the researchers wrote. “The reduced inflammatory responses observed in IL-23R Q381 carriers are associated with protection from multiple immune-mediated diseases. This would imply that loss-of-function observed with the common IL-23R–R381Q variant may lead to a disadvantage in select infectious diseases, including through [this variant’s] now identified role in promoting antimicrobial pathways in macrophages.”
The National Institutes of Health provided funding. The investigators reported having no conflicts of interest.
SOURCE: Sun R, Abraham C. Cell Molec Gastro Hepatol. 2020 May 28. doi.: 10.1016/j.jcmgh.2020.05.007.
FROM CELLULAR AND MOLECULAR GASTROENTEROLOGY AND HEPATOLOGY
Diarrhea prevalent among COVID-19 patients with IBD
Diarrhea affected one in every five patients with inflammatory bowel disease (IBD) and COVID-19, compared with only 7%-10% of all patients with COVID-19 in prior studies, researchers reported in Clinical Gastroenterology and Hepatology.
In a systematic review and meta-analysis of 23 studies incorporating data from 449 patients with IBD and COVID-19, their most common symptoms were fever (affecting 48.3% of patients), cough (46.5%), and diarrhea (20.5%), and diarrhea was approximately twice as prevalent as dyspnea, nausea, abdominal pain, and fatigue, wrote Ferdinando D’Amico of Humanitas University in Milan and his associates. “[S]ymptoms experienced by IBD patients with COVID-19 are similar to those occurring in the general population, except for a higher percentage of diarrhea,” they wrote. This increased prevalence might result from IBD itself or from inflammatory effects of viral gut tropism, they noted. “Currently, the diagnostic–therapeutic approach does not differ between IBD and non-IBD patients, but further studies are needed to evaluate whether fecal research of viral RNA and treatment with IBD drugs may play a role in the management of COVID-19 patients.”
To characterize the clinical presentation and course of patients with IBD and COVID-19, the researchers searched PubMed, Embase, Web of Science, and MedRxiv through July 29, 2020, for keywords related to COVID-19, Crohn’s disease, ulcerative colitis, and IBD. They identified 23 studies presenting clinical data from adults or children with a confirmed IBD diagnosis and least one case of COVID-19. Among 243,760 patients with IBD, 1,028 patients had COVID-19 infection, including 509 patients with Crohn’s disease, 428 patients with ulcerative colitis, 49 patients with indeterminate colitis, and 42 patients for whom the IBD subtype was not recorded.
In all, 0.4% of patients with IBD had COVID-19. Nearly all had been diagnosed by polymerase chain reaction of nasopharyngeal swabs, and approximately 40% also had received chest CT scans. Most were male (56.5%), and 43.5% were older than 65 years. Patients were receiving a wide range of IBD therapies, most commonly anti–tumor necrosis factor (TNF) agents, mesalamine, thiopurine (alone or in combination with biologics), vedolizumab, ustekinumab, steroids, methotrexate, and tofacitinib. Results from six studies indicated that patients with IBD were significantly more likely to be diagnosed with COVID-19 if they were older than 66 years (odds ratio, 21.3) or had other comorbidities (OR, 1.24). The most commonly used drugs for managing COVID-19 were hydroxychloroquine, lopinavir/ritonavir, steroids, antibiotics, chloroquine, tofacitinib, and infliximab.
A total of 30.6% of patients with IBD and COVID-19 were hospitalized, 11.4% stayed in the ICU, 3.7% required mechanical ventilation, and 3.8% died from COVID-19. Significant risk factors for death from COVID-19 included older age, active IBD, and a Charlson Comorbidity Index score above 1. Similarly, risk factors for severe COVID-19 included older age, having two or more comorbidities, receiving systemic steroids, and receiving mesalamine/sulfasalazine. In one study, a recent (3-month) history of corticosteroid treatment was associated with a 60% increase in the risk for severe COVID-19. Other immune-mediated therapies did not show this association. Patients with ulcerative colitis were significantly more likely to be seen in the ED or hospitalized, compared with patients with other forms of IBD (adjusted OR, 12.7).
No funding sources were disclosed. Dr. D’Amico reported having no conflicts of interest. Two coinvestigators disclosed ties to AbbVie, MSD, Schering-Plough, UCB Pharma, and several other pharmaceutical companies.
SOURCE: D’Amico F et al. Clin Gastroenterol Hepatol. 2020 Aug 7. doi: 10.1016/j.cgh.2020.08.003.
Diarrhea is one of the hallmark features in inflammatory bowel disease (IBD). The systematic review and meta-analysis by D’Amico and colleagues highlights an increased prevalence of diarrhea in IBD patients with COVID-19. We have learned that SARS-CoV-2 enters the gastrointestinal tract through angiotensin converting enzyme 2, which has been found in absorptive enterocytes of the ileum and colon. The subsequent invasion can cause a change in intestinal microbiota (dysbiosis) and trigger diarrhea. Prior studies also reported SARS-CoV-2 being isolated in the duodenum and rectum while showing RNA shedding in approximately 40% of patients. Clinicians may now face the diagnostic challenge of distinguishing the cause of diarrhea as an exacerbation from underlying IBD versus viral superinfection. The authors astutely hypothesized that having access to fecal polymerase chain reaction tests may be particularly useful to guiding clinical treatment decisions.

Lukasz Kwapisz, MD, FRCPC, is assistant professor of medicine and gastroenterology at Baylor College of Medicine, Houston. He has no conflicts of interest.
Diarrhea is one of the hallmark features in inflammatory bowel disease (IBD). The systematic review and meta-analysis by D’Amico and colleagues highlights an increased prevalence of diarrhea in IBD patients with COVID-19. We have learned that SARS-CoV-2 enters the gastrointestinal tract through angiotensin converting enzyme 2, which has been found in absorptive enterocytes of the ileum and colon. The subsequent invasion can cause a change in intestinal microbiota (dysbiosis) and trigger diarrhea. Prior studies also reported SARS-CoV-2 being isolated in the duodenum and rectum while showing RNA shedding in approximately 40% of patients. Clinicians may now face the diagnostic challenge of distinguishing the cause of diarrhea as an exacerbation from underlying IBD versus viral superinfection. The authors astutely hypothesized that having access to fecal polymerase chain reaction tests may be particularly useful to guiding clinical treatment decisions.
Lukasz Kwapisz, MD, FRCPC, is assistant professor of medicine and gastroenterology at Baylor College of Medicine, Houston. He has no conflicts of interest.
Diarrhea is one of the hallmark features in inflammatory bowel disease (IBD). The systematic review and meta-analysis by D’Amico and colleagues highlights an increased prevalence of diarrhea in IBD patients with COVID-19. We have learned that SARS-CoV-2 enters the gastrointestinal tract through angiotensin converting enzyme 2, which has been found in absorptive enterocytes of the ileum and colon. The subsequent invasion can cause a change in intestinal microbiota (dysbiosis) and trigger diarrhea. Prior studies also reported SARS-CoV-2 being isolated in the duodenum and rectum while showing RNA shedding in approximately 40% of patients. Clinicians may now face the diagnostic challenge of distinguishing the cause of diarrhea as an exacerbation from underlying IBD versus viral superinfection. The authors astutely hypothesized that having access to fecal polymerase chain reaction tests may be particularly useful to guiding clinical treatment decisions.
Lukasz Kwapisz, MD, FRCPC, is assistant professor of medicine and gastroenterology at Baylor College of Medicine, Houston. He has no conflicts of interest.
Diarrhea affected one in every five patients with inflammatory bowel disease (IBD) and COVID-19, compared with only 7%-10% of all patients with COVID-19 in prior studies, researchers reported in Clinical Gastroenterology and Hepatology.
In a systematic review and meta-analysis of 23 studies incorporating data from 449 patients with IBD and COVID-19, their most common symptoms were fever (affecting 48.3% of patients), cough (46.5%), and diarrhea (20.5%), and diarrhea was approximately twice as prevalent as dyspnea, nausea, abdominal pain, and fatigue, wrote Ferdinando D’Amico of Humanitas University in Milan and his associates. “[S]ymptoms experienced by IBD patients with COVID-19 are similar to those occurring in the general population, except for a higher percentage of diarrhea,” they wrote. This increased prevalence might result from IBD itself or from inflammatory effects of viral gut tropism, they noted. “Currently, the diagnostic–therapeutic approach does not differ between IBD and non-IBD patients, but further studies are needed to evaluate whether fecal research of viral RNA and treatment with IBD drugs may play a role in the management of COVID-19 patients.”
To characterize the clinical presentation and course of patients with IBD and COVID-19, the researchers searched PubMed, Embase, Web of Science, and MedRxiv through July 29, 2020, for keywords related to COVID-19, Crohn’s disease, ulcerative colitis, and IBD. They identified 23 studies presenting clinical data from adults or children with a confirmed IBD diagnosis and least one case of COVID-19. Among 243,760 patients with IBD, 1,028 patients had COVID-19 infection, including 509 patients with Crohn’s disease, 428 patients with ulcerative colitis, 49 patients with indeterminate colitis, and 42 patients for whom the IBD subtype was not recorded.
In all, 0.4% of patients with IBD had COVID-19. Nearly all had been diagnosed by polymerase chain reaction of nasopharyngeal swabs, and approximately 40% also had received chest CT scans. Most were male (56.5%), and 43.5% were older than 65 years. Patients were receiving a wide range of IBD therapies, most commonly anti–tumor necrosis factor (TNF) agents, mesalamine, thiopurine (alone or in combination with biologics), vedolizumab, ustekinumab, steroids, methotrexate, and tofacitinib. Results from six studies indicated that patients with IBD were significantly more likely to be diagnosed with COVID-19 if they were older than 66 years (odds ratio, 21.3) or had other comorbidities (OR, 1.24). The most commonly used drugs for managing COVID-19 were hydroxychloroquine, lopinavir/ritonavir, steroids, antibiotics, chloroquine, tofacitinib, and infliximab.
A total of 30.6% of patients with IBD and COVID-19 were hospitalized, 11.4% stayed in the ICU, 3.7% required mechanical ventilation, and 3.8% died from COVID-19. Significant risk factors for death from COVID-19 included older age, active IBD, and a Charlson Comorbidity Index score above 1. Similarly, risk factors for severe COVID-19 included older age, having two or more comorbidities, receiving systemic steroids, and receiving mesalamine/sulfasalazine. In one study, a recent (3-month) history of corticosteroid treatment was associated with a 60% increase in the risk for severe COVID-19. Other immune-mediated therapies did not show this association. Patients with ulcerative colitis were significantly more likely to be seen in the ED or hospitalized, compared with patients with other forms of IBD (adjusted OR, 12.7).
No funding sources were disclosed. Dr. D’Amico reported having no conflicts of interest. Two coinvestigators disclosed ties to AbbVie, MSD, Schering-Plough, UCB Pharma, and several other pharmaceutical companies.
SOURCE: D’Amico F et al. Clin Gastroenterol Hepatol. 2020 Aug 7. doi: 10.1016/j.cgh.2020.08.003.
Diarrhea affected one in every five patients with inflammatory bowel disease (IBD) and COVID-19, compared with only 7%-10% of all patients with COVID-19 in prior studies, researchers reported in Clinical Gastroenterology and Hepatology.
In a systematic review and meta-analysis of 23 studies incorporating data from 449 patients with IBD and COVID-19, their most common symptoms were fever (affecting 48.3% of patients), cough (46.5%), and diarrhea (20.5%), and diarrhea was approximately twice as prevalent as dyspnea, nausea, abdominal pain, and fatigue, wrote Ferdinando D’Amico of Humanitas University in Milan and his associates. “[S]ymptoms experienced by IBD patients with COVID-19 are similar to those occurring in the general population, except for a higher percentage of diarrhea,” they wrote. This increased prevalence might result from IBD itself or from inflammatory effects of viral gut tropism, they noted. “Currently, the diagnostic–therapeutic approach does not differ between IBD and non-IBD patients, but further studies are needed to evaluate whether fecal research of viral RNA and treatment with IBD drugs may play a role in the management of COVID-19 patients.”
To characterize the clinical presentation and course of patients with IBD and COVID-19, the researchers searched PubMed, Embase, Web of Science, and MedRxiv through July 29, 2020, for keywords related to COVID-19, Crohn’s disease, ulcerative colitis, and IBD. They identified 23 studies presenting clinical data from adults or children with a confirmed IBD diagnosis and least one case of COVID-19. Among 243,760 patients with IBD, 1,028 patients had COVID-19 infection, including 509 patients with Crohn’s disease, 428 patients with ulcerative colitis, 49 patients with indeterminate colitis, and 42 patients for whom the IBD subtype was not recorded.
In all, 0.4% of patients with IBD had COVID-19. Nearly all had been diagnosed by polymerase chain reaction of nasopharyngeal swabs, and approximately 40% also had received chest CT scans. Most were male (56.5%), and 43.5% were older than 65 years. Patients were receiving a wide range of IBD therapies, most commonly anti–tumor necrosis factor (TNF) agents, mesalamine, thiopurine (alone or in combination with biologics), vedolizumab, ustekinumab, steroids, methotrexate, and tofacitinib. Results from six studies indicated that patients with IBD were significantly more likely to be diagnosed with COVID-19 if they were older than 66 years (odds ratio, 21.3) or had other comorbidities (OR, 1.24). The most commonly used drugs for managing COVID-19 were hydroxychloroquine, lopinavir/ritonavir, steroids, antibiotics, chloroquine, tofacitinib, and infliximab.
A total of 30.6% of patients with IBD and COVID-19 were hospitalized, 11.4% stayed in the ICU, 3.7% required mechanical ventilation, and 3.8% died from COVID-19. Significant risk factors for death from COVID-19 included older age, active IBD, and a Charlson Comorbidity Index score above 1. Similarly, risk factors for severe COVID-19 included older age, having two or more comorbidities, receiving systemic steroids, and receiving mesalamine/sulfasalazine. In one study, a recent (3-month) history of corticosteroid treatment was associated with a 60% increase in the risk for severe COVID-19. Other immune-mediated therapies did not show this association. Patients with ulcerative colitis were significantly more likely to be seen in the ED or hospitalized, compared with patients with other forms of IBD (adjusted OR, 12.7).
No funding sources were disclosed. Dr. D’Amico reported having no conflicts of interest. Two coinvestigators disclosed ties to AbbVie, MSD, Schering-Plough, UCB Pharma, and several other pharmaceutical companies.
SOURCE: D’Amico F et al. Clin Gastroenterol Hepatol. 2020 Aug 7. doi: 10.1016/j.cgh.2020.08.003.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
C. difficile linked to surgery risk in pediatric Crohn’s
In pediatric Crohn’s disease, a Clostridioides difficile infection detected within the first year after diagnosis is associated with a shorter time to first bowel resection surgery, according to a study that included both a retrospective and prospective analysis. The researchers also found evidence that changes in methionine biosynthesis and depletion of beneficial bacteria may contribute to risk of surgery.
C. difficile infection (CDI) disproportionately affects individuals with inflammatory bowel disease (IBD). Pediatric IBD patients have a 34% risk of recurrent CDI infection, compared with 7.5% in the general population. Previous research found that adults with ulcerative colitis and CDI are at more risk of colectomy, but the finding has not been replicated in children.
In a study published in Inflammatory Bowel Diseases, researchers led by Jennifer Hellmann and Lee Denson of the University of Cincinnati conducted a single-center retrospective analysis of 75 pediatric Crohn’s disease patients. They also conducted a prospective study of 70 pediatric Crohn’s disease patients, using shotgun metagenome sequencing to examine the relationship between microbiota composition and C. difficile carriage or surgery history.
Nineteen percent of patients tested positive for C. difficile. Use of antibiotics was associated with C. difficile (odds ratio, 7.9; P = .02). Of patients who underwent C. difficile testing in the first year, 23 went on to have surgery: 21% who were C. difficile negative required surgery, compared with 67% of those who were positive (hazard ratio, 4.4; P = .0003). The mean time to surgery was 527 days for C. difficile–positive patients and 1,268 days for those who were negative.
A multivariate regression analysis on 54 patients with complete data sets showed that the presence of C. difficile was associated with increased risk of surgery (OR, 16.2; P = .0006). When the analysis was run on all 73 patients, using null value for missing data, the results were similar (OR, 9.17; P = .008).
Shotgun sequencing found that 47 of 114 bacterial species that were associated with the presence of C. difficile were also associated with prior surgery for Crohn’s disease. Species included some that may play a role in mucosal homeostasis, such as Bifidobacterium breve and several Alistipes and Ruminococcus species. That suggests that a reduction in the numbers of these taxa may be associated with C. difficile presence and surgical risk.
The researchers also found that methionine synthesis pathways were depressed in C. difficile–positive and surgery patients. Methionine may bolster antioxidant capacity and improve villus morphology. IBD patients with dysbiosis and those experiencing Crohn’s disease exacerbations have been shown to have decreased methionine pathway activity, suggesting methionine biosynthesis changes have clinical relevance.
The study was funded by the National Institutes of Health.
SOURCE: Hellmann J et al. Inflamm Bowel Dis. 2020. doi: 10.1093/ibd/izz263.
In pediatric Crohn’s disease, a Clostridioides difficile infection detected within the first year after diagnosis is associated with a shorter time to first bowel resection surgery, according to a study that included both a retrospective and prospective analysis. The researchers also found evidence that changes in methionine biosynthesis and depletion of beneficial bacteria may contribute to risk of surgery.
C. difficile infection (CDI) disproportionately affects individuals with inflammatory bowel disease (IBD). Pediatric IBD patients have a 34% risk of recurrent CDI infection, compared with 7.5% in the general population. Previous research found that adults with ulcerative colitis and CDI are at more risk of colectomy, but the finding has not been replicated in children.
In a study published in Inflammatory Bowel Diseases, researchers led by Jennifer Hellmann and Lee Denson of the University of Cincinnati conducted a single-center retrospective analysis of 75 pediatric Crohn’s disease patients. They also conducted a prospective study of 70 pediatric Crohn’s disease patients, using shotgun metagenome sequencing to examine the relationship between microbiota composition and C. difficile carriage or surgery history.
Nineteen percent of patients tested positive for C. difficile. Use of antibiotics was associated with C. difficile (odds ratio, 7.9; P = .02). Of patients who underwent C. difficile testing in the first year, 23 went on to have surgery: 21% who were C. difficile negative required surgery, compared with 67% of those who were positive (hazard ratio, 4.4; P = .0003). The mean time to surgery was 527 days for C. difficile–positive patients and 1,268 days for those who were negative.
A multivariate regression analysis on 54 patients with complete data sets showed that the presence of C. difficile was associated with increased risk of surgery (OR, 16.2; P = .0006). When the analysis was run on all 73 patients, using null value for missing data, the results were similar (OR, 9.17; P = .008).
Shotgun sequencing found that 47 of 114 bacterial species that were associated with the presence of C. difficile were also associated with prior surgery for Crohn’s disease. Species included some that may play a role in mucosal homeostasis, such as Bifidobacterium breve and several Alistipes and Ruminococcus species. That suggests that a reduction in the numbers of these taxa may be associated with C. difficile presence and surgical risk.
The researchers also found that methionine synthesis pathways were depressed in C. difficile–positive and surgery patients. Methionine may bolster antioxidant capacity and improve villus morphology. IBD patients with dysbiosis and those experiencing Crohn’s disease exacerbations have been shown to have decreased methionine pathway activity, suggesting methionine biosynthesis changes have clinical relevance.
The study was funded by the National Institutes of Health.
SOURCE: Hellmann J et al. Inflamm Bowel Dis. 2020. doi: 10.1093/ibd/izz263.
In pediatric Crohn’s disease, a Clostridioides difficile infection detected within the first year after diagnosis is associated with a shorter time to first bowel resection surgery, according to a study that included both a retrospective and prospective analysis. The researchers also found evidence that changes in methionine biosynthesis and depletion of beneficial bacteria may contribute to risk of surgery.
C. difficile infection (CDI) disproportionately affects individuals with inflammatory bowel disease (IBD). Pediatric IBD patients have a 34% risk of recurrent CDI infection, compared with 7.5% in the general population. Previous research found that adults with ulcerative colitis and CDI are at more risk of colectomy, but the finding has not been replicated in children.
In a study published in Inflammatory Bowel Diseases, researchers led by Jennifer Hellmann and Lee Denson of the University of Cincinnati conducted a single-center retrospective analysis of 75 pediatric Crohn’s disease patients. They also conducted a prospective study of 70 pediatric Crohn’s disease patients, using shotgun metagenome sequencing to examine the relationship between microbiota composition and C. difficile carriage or surgery history.
Nineteen percent of patients tested positive for C. difficile. Use of antibiotics was associated with C. difficile (odds ratio, 7.9; P = .02). Of patients who underwent C. difficile testing in the first year, 23 went on to have surgery: 21% who were C. difficile negative required surgery, compared with 67% of those who were positive (hazard ratio, 4.4; P = .0003). The mean time to surgery was 527 days for C. difficile–positive patients and 1,268 days for those who were negative.
A multivariate regression analysis on 54 patients with complete data sets showed that the presence of C. difficile was associated with increased risk of surgery (OR, 16.2; P = .0006). When the analysis was run on all 73 patients, using null value for missing data, the results were similar (OR, 9.17; P = .008).
Shotgun sequencing found that 47 of 114 bacterial species that were associated with the presence of C. difficile were also associated with prior surgery for Crohn’s disease. Species included some that may play a role in mucosal homeostasis, such as Bifidobacterium breve and several Alistipes and Ruminococcus species. That suggests that a reduction in the numbers of these taxa may be associated with C. difficile presence and surgical risk.
The researchers also found that methionine synthesis pathways were depressed in C. difficile–positive and surgery patients. Methionine may bolster antioxidant capacity and improve villus morphology. IBD patients with dysbiosis and those experiencing Crohn’s disease exacerbations have been shown to have decreased methionine pathway activity, suggesting methionine biosynthesis changes have clinical relevance.
The study was funded by the National Institutes of Health.
SOURCE: Hellmann J et al. Inflamm Bowel Dis. 2020. doi: 10.1093/ibd/izz263.
Fecal transplant linked to reduced C. difficile mortality
Vancomycin followed by fecal microbiota transplant (FMT) was associated with reduced Clostridioides difficile (C. diff)-related mortality in patients hospitalized with refractory severe or fulminant C. diff infection (CDI) at a single center. The improvements came after Indiana University implemented an FMT option in 2013.
About 8% of C. diff patients develop severe or fulminant CDI (SFCDI), which can lead to toxic colon and multiorgan failure. Surgery is the current recommended treatment for these patients if they are refractory to vancomycin, but 30-day mortality is above 40%. FMT is recommended for recurrent CDI, and it achieves cure rates greater than 80%, along with fewer relapses compared with anti-CDI antibiotic therapy.
FMT has been shown to be effective for SFCDI, with a 91% cure rate for serious CDI and 66% for fulminant CDI.
In the study published in the September issue of Clinical Gastroenterology and Hepatology, researchers led by Yao-Wen Cheng, MD, and Monika Fischer, MD, of Indiana University, assessed the effect of FMT on SFCDI after their institution adopted it as a treatment protocol for SFCDI. Patients could receive FMT if there was evidence that their SFCDI was refractory, or if they had two or more CDI recurrences. The treatment includes oral vancomycin and pseudomembrane-driven sequential FMT.
Two hundred five patients were admitted before FMT implementation, 225 after. Fifty patients received FMT because of refractory SFCDI. A median of two FMTs was conducted per patient. 21 other patients received FMT for nonrefractory SFCDI or other conditions, including 18 patients with multiple recurrent CDI.
Thirty-day CDI-related mortality dropped after FMT implementation (4.4% versus 10.2%; P =.02). This was true in both the fulminant subset (9.1% versus 21.3%; P =.015) and the refractory group (12.1% versus 43.2%; P < .001).
The researchers used segmented logistic regression to determine if the improved outcomes could be due to nontreatment factors that varied over time, and found that the difference in CDI-related mortality was eliminated except for refractory SFCDI patients (odds of mortality after FMT implementation, 0.09; P =.023). There was no significant difference between those receiving non-CDI antibiotics (4.8%) and those who did not (6.9%; P =.75).
FMT was associated with lower frequency of CDI-related colectomy overall (2.7% versus 6.8%; P =.041), as well as in the fulminant (5.5% versus 15.7%; P =.017) and refractory subgroups (7.6% versus 31.8%; P =.001).
The findings follow another study that showed improved 3-month mortality for FMT among patients hospitalized with severe CDI (12.1% versus 42.2%; P < .003).
The results underscore the utility of FMT for SFCDI, and suggest it might have the most benefit in refractory SFCDI. The authors believe that FMT should be an alternative to colectomy when first-line anti-CDI antibiotics are partially or completely ineffective. In the absence of FMT, patients who go on to fail vancomycin or fidaxomicin will likely continue to be managed medically, with up to 80% mortality, or through salvage colectomy, with postsurgical morality rates of 30-40%.
Although a randomized trial could answer the question of FMT efficacy more definitively, it is unlikely to be conducted for ethical reasons.
“Further investigation is required to clearly define FMT’s role and timing in the clinical course of severe and fulminant CDI. However, our study suggests that FMT should be offered to patients with severe and fulminant CDI who do not respond to a 5-day course of anti-CDI antibiotics and may be considered in lieu of or before colectomy,” the researchers wrote.
No source of funding was disclosed.
SOURCE: Cheng YW et al. Clin Gastroenterol Hepatol. 2020;18:2234-43. doi: 10.1016/j.cgh.2019.12.029.
Vancomycin followed by fecal microbiota transplant (FMT) was associated with reduced Clostridioides difficile (C. diff)-related mortality in patients hospitalized with refractory severe or fulminant C. diff infection (CDI) at a single center. The improvements came after Indiana University implemented an FMT option in 2013.
About 8% of C. diff patients develop severe or fulminant CDI (SFCDI), which can lead to toxic colon and multiorgan failure. Surgery is the current recommended treatment for these patients if they are refractory to vancomycin, but 30-day mortality is above 40%. FMT is recommended for recurrent CDI, and it achieves cure rates greater than 80%, along with fewer relapses compared with anti-CDI antibiotic therapy.
FMT has been shown to be effective for SFCDI, with a 91% cure rate for serious CDI and 66% for fulminant CDI.
In the study published in the September issue of Clinical Gastroenterology and Hepatology, researchers led by Yao-Wen Cheng, MD, and Monika Fischer, MD, of Indiana University, assessed the effect of FMT on SFCDI after their institution adopted it as a treatment protocol for SFCDI. Patients could receive FMT if there was evidence that their SFCDI was refractory, or if they had two or more CDI recurrences. The treatment includes oral vancomycin and pseudomembrane-driven sequential FMT.
Two hundred five patients were admitted before FMT implementation, 225 after. Fifty patients received FMT because of refractory SFCDI. A median of two FMTs was conducted per patient. 21 other patients received FMT for nonrefractory SFCDI or other conditions, including 18 patients with multiple recurrent CDI.
Thirty-day CDI-related mortality dropped after FMT implementation (4.4% versus 10.2%; P =.02). This was true in both the fulminant subset (9.1% versus 21.3%; P =.015) and the refractory group (12.1% versus 43.2%; P < .001).
The researchers used segmented logistic regression to determine if the improved outcomes could be due to nontreatment factors that varied over time, and found that the difference in CDI-related mortality was eliminated except for refractory SFCDI patients (odds of mortality after FMT implementation, 0.09; P =.023). There was no significant difference between those receiving non-CDI antibiotics (4.8%) and those who did not (6.9%; P =.75).
FMT was associated with lower frequency of CDI-related colectomy overall (2.7% versus 6.8%; P =.041), as well as in the fulminant (5.5% versus 15.7%; P =.017) and refractory subgroups (7.6% versus 31.8%; P =.001).
The findings follow another study that showed improved 3-month mortality for FMT among patients hospitalized with severe CDI (12.1% versus 42.2%; P < .003).
The results underscore the utility of FMT for SFCDI, and suggest it might have the most benefit in refractory SFCDI. The authors believe that FMT should be an alternative to colectomy when first-line anti-CDI antibiotics are partially or completely ineffective. In the absence of FMT, patients who go on to fail vancomycin or fidaxomicin will likely continue to be managed medically, with up to 80% mortality, or through salvage colectomy, with postsurgical morality rates of 30-40%.
Although a randomized trial could answer the question of FMT efficacy more definitively, it is unlikely to be conducted for ethical reasons.
“Further investigation is required to clearly define FMT’s role and timing in the clinical course of severe and fulminant CDI. However, our study suggests that FMT should be offered to patients with severe and fulminant CDI who do not respond to a 5-day course of anti-CDI antibiotics and may be considered in lieu of or before colectomy,” the researchers wrote.
No source of funding was disclosed.
SOURCE: Cheng YW et al. Clin Gastroenterol Hepatol. 2020;18:2234-43. doi: 10.1016/j.cgh.2019.12.029.
Vancomycin followed by fecal microbiota transplant (FMT) was associated with reduced Clostridioides difficile (C. diff)-related mortality in patients hospitalized with refractory severe or fulminant C. diff infection (CDI) at a single center. The improvements came after Indiana University implemented an FMT option in 2013.
About 8% of C. diff patients develop severe or fulminant CDI (SFCDI), which can lead to toxic colon and multiorgan failure. Surgery is the current recommended treatment for these patients if they are refractory to vancomycin, but 30-day mortality is above 40%. FMT is recommended for recurrent CDI, and it achieves cure rates greater than 80%, along with fewer relapses compared with anti-CDI antibiotic therapy.
FMT has been shown to be effective for SFCDI, with a 91% cure rate for serious CDI and 66% for fulminant CDI.
In the study published in the September issue of Clinical Gastroenterology and Hepatology, researchers led by Yao-Wen Cheng, MD, and Monika Fischer, MD, of Indiana University, assessed the effect of FMT on SFCDI after their institution adopted it as a treatment protocol for SFCDI. Patients could receive FMT if there was evidence that their SFCDI was refractory, or if they had two or more CDI recurrences. The treatment includes oral vancomycin and pseudomembrane-driven sequential FMT.
Two hundred five patients were admitted before FMT implementation, 225 after. Fifty patients received FMT because of refractory SFCDI. A median of two FMTs was conducted per patient. 21 other patients received FMT for nonrefractory SFCDI or other conditions, including 18 patients with multiple recurrent CDI.
Thirty-day CDI-related mortality dropped after FMT implementation (4.4% versus 10.2%; P =.02). This was true in both the fulminant subset (9.1% versus 21.3%; P =.015) and the refractory group (12.1% versus 43.2%; P < .001).
The researchers used segmented logistic regression to determine if the improved outcomes could be due to nontreatment factors that varied over time, and found that the difference in CDI-related mortality was eliminated except for refractory SFCDI patients (odds of mortality after FMT implementation, 0.09; P =.023). There was no significant difference between those receiving non-CDI antibiotics (4.8%) and those who did not (6.9%; P =.75).
FMT was associated with lower frequency of CDI-related colectomy overall (2.7% versus 6.8%; P =.041), as well as in the fulminant (5.5% versus 15.7%; P =.017) and refractory subgroups (7.6% versus 31.8%; P =.001).
The findings follow another study that showed improved 3-month mortality for FMT among patients hospitalized with severe CDI (12.1% versus 42.2%; P < .003).
The results underscore the utility of FMT for SFCDI, and suggest it might have the most benefit in refractory SFCDI. The authors believe that FMT should be an alternative to colectomy when first-line anti-CDI antibiotics are partially or completely ineffective. In the absence of FMT, patients who go on to fail vancomycin or fidaxomicin will likely continue to be managed medically, with up to 80% mortality, or through salvage colectomy, with postsurgical morality rates of 30-40%.
Although a randomized trial could answer the question of FMT efficacy more definitively, it is unlikely to be conducted for ethical reasons.
“Further investigation is required to clearly define FMT’s role and timing in the clinical course of severe and fulminant CDI. However, our study suggests that FMT should be offered to patients with severe and fulminant CDI who do not respond to a 5-day course of anti-CDI antibiotics and may be considered in lieu of or before colectomy,” the researchers wrote.
No source of funding was disclosed.
SOURCE: Cheng YW et al. Clin Gastroenterol Hepatol. 2020;18:2234-43. doi: 10.1016/j.cgh.2019.12.029.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY