User login
Selecting therapies in moderate to severe inflammatory bowel disease: Key factors in decision making
Despite new advances in treatment, head to head clinical trials, which are considered the gold standard when comparing therapies, remain limited. Other comparative effectiveness studies and network meta-analyses are the currently available substitutes to guide decision making.1
While efficacy is often considered first when choosing a drug, other critical factors play a role in tailoring a treatment plan. This article focuses on key considerations to help guide clinical decision making when treating patients with moderate to severe IBD (Figure 1).
Disease activity versus severity
Both disease activity and disease severity should be considered when evaluating a patient for treatment. Disease activity is a cross-sectional view of one’s signs and symptoms which can vary visit to visit. Standardized indices measure disease activity in both Crohn’s disease (CD) and ulcerative colitis (UC).2,3 Disease severity encompasses the overall prognosis of disease over time and includes factors such as the presence or absence of high risk features, prior medication exposure, history of surgery, hospitalizations and the impact on quality of life.4

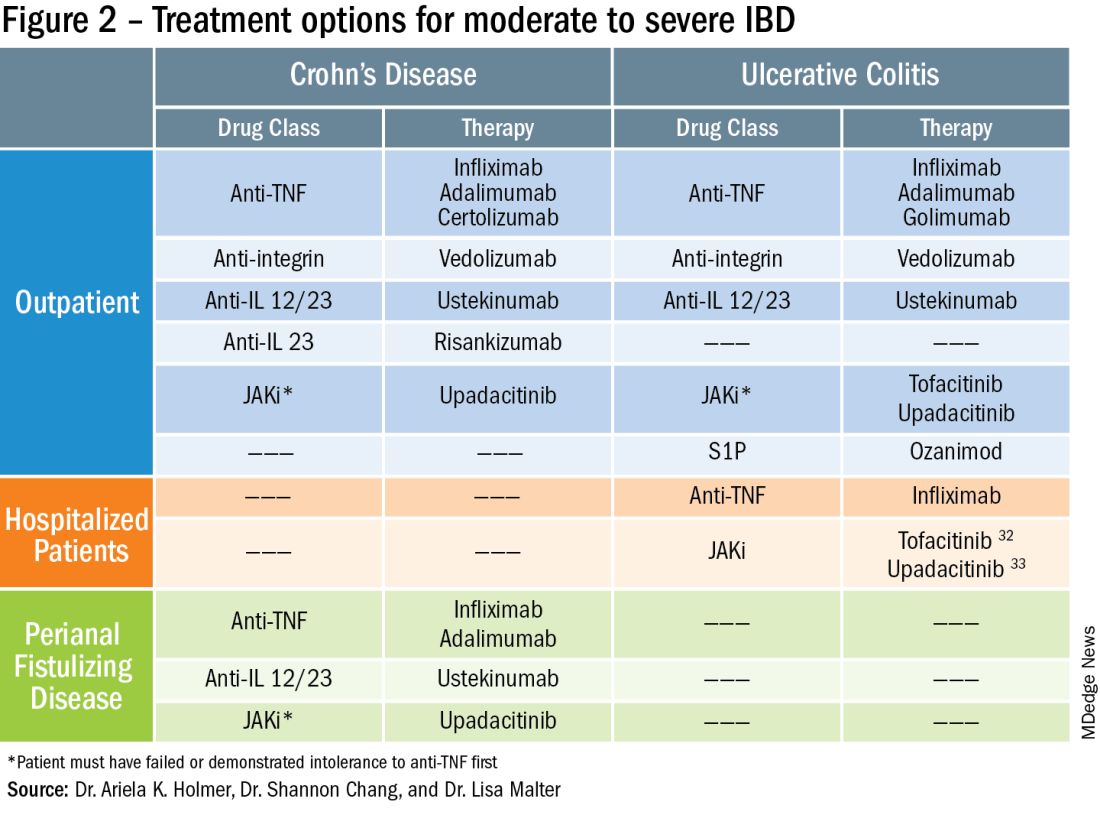
To prevent disease complications, the goals of treatment should be aimed at both reducing active symptoms (disease activity) but also healing mucosal inflammation, preventing disease progression (disease severity) and downstream sequelae including cancer, hospitalization or surgery.5 Determining the best treatment option takes disease activity and severity into account, in addition to the other key factors listed below (Figure 2).
Extraintestinal manifestations
Inflammation of organs outside of the gastrointestinal tract is common and can occur in up to 50% of patients with IBD.6 The most prevalent extraintestinal manifestations (EIMs) involve the skin and joints, which will be the primary focus in this article. We will also focus on treatment options with the most evidence supporting their use. Peripheral arthritis is often associated with intestinal inflammation, and treatment of underlying IBD can simultaneously improve joint symptoms. Conversely, axial spondyloarthritis does not commonly parallel intestinal inflammation. Anti–tumor necrosis factor (TNF) agents including infliximab and adalimumab are effective for the treatment of both peripheral and axial disease.6
Ustekinumab, an interleukin (IL)-12/23 inhibitor, may be effective for peripheral arthritis, however is ineffective for the treatment of axial spondyloarthritis.6 Janus kinase (JAK) inhibitors which include tofacitinib and upadacitinib are oral small molecules used to treat peripheral and axial spondyloarthritis and have more recently been approved for moderate to severe IBD.6,7
Erythema nodosum (EN) and pyoderma gangrenosum (PG) are skin manifestations seen in patients with IBD. EN appears as subcutaneous nodules and parallels intestinal inflammation, while PG consists of violaceous, ulcerated plaques, and presents with more significant pain. Anti-TNFs are effective for both EN and PG, with infliximab being the only biologic studied in a randomized control trial of patients with PG.8 In addition, small case reports have described some benefit from ustekinumab and upadacitinib in the treatment of PG.9,10
Safety
The safety of IBD therapies is a key consideration and often the most important factor to patients when choosing a treatment option. It is important to note that untreated disease is associated with significant morbidity, and should be weighed when discussing risks of medications with patients. In general, anti-TNFs and JAK inhibitors may be associated with an increased risk of infection and malignancy, while ustekinumab, vedolizumab, risankizumab and ozanimod offer a more favorable safety profile.11 In large registries and observational studies, infliximab was associated with up to a two times greater risk of serious infection as compared to nonbiologic medications, with the most common infections being pneumonia, sepsis and herpes zoster.12 JAK inhibitors are associated with an increased risk of herpes zoster infection, with a dose dependent effect seen in the maintenance clinical trials with tofacitinib.7
Ozanimod may be associated with atrioventricular conduction delays and bradycardia, however long-term safety data has reported a low incidence of serious cardiac related adverse events.13 Overall, though risks of infection may vary with different therapies, other consistent risk factors associated with greater rates of serious infection include prolonged corticosteroid use, combination therapy with thiopurines, and disease severity. Anti-TNFs have also been associated with a somewhat increased risk of lymphoma, increased when used in combination with thiopurines. Reassuringly, however, in patients with a prior history of cancer, anti-TNFs and non-TNF biologics have not been found to increase the risk of new or recurrent cancer.14

Ultimately, in patients with a prior history of cancer, the choice of biologic or small molecule should be made in collaboration with a patient’s oncologist.
Anti-TNF exposure
Anti-TNFs were the first available biologics for the treatment of IBD. After the approval of vedolizumab in 2014, the first non-TNF biologic, many patients enrolled in clinical trials thereafter had already tried and failed anti-TNFs. In general, exposure to anti-TNFs may reduce the efficacy of a future biologic. In patients treated with vedolizumab, endoscopic and clinical outcomes were negatively impacted by prior anti-TNF exposure.15 However, in VARSITY, a head-to-head clinical trial where 20% of patients with UC were previously exposed to anti-TNFs other than adalimumab, vedolizumab had significantly higher rates of clinical remission and endoscopic improvement compared to adalimumab.16 Clinical remission rates with tofacitinib were not impacted by exposure to anti-TNF treatment, and similar findings were observed with ustekinumab.7,17 Risankizumab, a newly approved selective anti-IL23, also does not appear to be impacted by prior anti-TNF exposure by demonstrating similar rates of clinical remission regardless of biologic exposure status.18 Therefore, in patients with prior history of anti-TNF use, consideration of ustekinumab, risankizumab or JAK inhibitors as second line agents may be more favorable as compared to vedolizumab.
Perianal fistulizing disease
Perianal fistulizing disease can affect up to one-third of patients with CD and significantly impact a patient’s quality of life.19 The most robust data for the treatment of perianal fistulizing disease includes the use of infliximab with up to one-third of patients on maintenance therapy achieving complete resolution of fistula drainage. While no head-to-head trials compare combination therapy with infliximab plus immunomodulators versus infliximab alone for this indication specifically, one observational study demonstrated higher rates of fistula closure with combination therapy as compared to infliximab mono-therapy.19 In a post hoc analysis, higher infliximab concentrations at week 14 were associated with greater fistula response and remission rates.20 In patients with perianal disease, ustekinumab and vedolizumab may also be an effective treatment option by promoting resolution of fistula drainage.21
More recently, emerging data demonstrate that upadacitinib may be an excellent option as a second-line treatment for perianal disease in patients who have failed anti-TNF therapy. Use of upadacitinib was associated with greater rates of complete resolution of fistula drainage and higher rates of external fistula closure (Figure 2).22 Lastly, as an alternative to medical therapy, mesenchymal stem cell therapy has also shown to improve fistula drainage and improve external fistula openings in patients with CD.23 Stem cell therapy is only available through clinical trials at this time.
Patient preferences
Overall, data are lacking for evaluating patient preferences in treatment options for IBD especially with the recent increase in therapeutic options. One survey demonstrated that patient preferences were most impacted by the possibility of improving abdominal pain, with patients accepting additional risk of treatment side effects in order to reduce their abdominal pain.24 An oral route of administration and improving fatigue and bowel urgency were similarly important to patients. Patient preferences can also be highly variable with some valuing avoidance of corticosteroid use while others valuing avoidance of symptoms or risks of medication side effects and surgery. It is important to tailor the discussion on treatment strategies to each individual patient and inquire about the patient’s lifestyle, medical history, and value system, which may impact their treatment preferences utilizing shared decision making.
Access to treatment including the role of social determinants of health
The expanded therapeutic armamentarium has the potential to help patients achieve the current goals of care in IBD. However, these medications are not available to all patients due to numerous barriers including step therapy payer policies, prohibitive costs, insurance prior authorizations, and the role of social determinants of health and proximity to IBD expertise.25 While clinicians work with patients to determine the best treatment option, more often than not, the decision lies with the insurance payer. Step therapy is the protocol used by insurance companies that requires patients to try a lower-cost medication and fail to respond before they approve the originally requested treatment. This can lead to treatment delays, progression of disease, and disease complications. The option to incorporate the use of biosimilars, currently available for anti-TNFs, and other biologics in the near future, will reduce cost and potentially increase access.26 Additionally, working with a clinical pharmacist to navigate access and utilize patient assistance programs may help overcome cost related barriers to treatment and prevent delays in care.
Socioeconomic status has been shown to impact IBD disease outcomes, and compliance rates in treatment vary depending on race and ethnicity.27 Certain racial and ethnic groups remain vulnerable and may require additional support to achieve treatment goals. For example, disparities in health literacy in patients with IBD have been demonstrated with older black men at risk.28 Additionally, the patient’s proximity to their health care facility may impact treatment options. Most IBD centers are located in metropolitan areas and numerous “IBD deserts” exist, potentially limiting therapies for patients from more remote/rural settings.29 Access to treatment and the interplay of social determinants of health can have a large role in therapy selection.
Special considerations: Pregnancy and older adults
Certain patient populations warrant special consideration when approaching treatment strategies. Pregnancy in IBD will not be addressed in full depth in this article, however a key takeaway is that planning is critical and providers should emphasize the importance of steroid-free clinical remission for at least 3 months before conception.30 Additionally, biologic use during pregnancy has not been shown to increase adverse fetal outcomes, thus should be continued to minimize disease flare. Newer novel small molecules are generally avoided during pregnancy due to limited available safety data.
Older adults are the largest growing patient population with IBD. Frailty, or a state of decreased reserve, is more commonly observed in older patients and has been shown to increase adverse events including hospitalization and mortaility.31 Ultimately reducing polypharmacy, ensuring adequate nutrition, minimizing corticosteroid exposure and avoiding undertreatment of active IBD are all key in optimizing outcomes in an older patient with IBD.
Conclusion
When discussing treatment options with patients with IBD, it is important to individualize care and share the decision-making process with patients. Goals include improving symptoms and quality of life while working to achieve the goal of healing intestinal inflammation. In summary, this article can serve as a guide to clinicians for key factors in decision making when selecting therapies in moderate to severe IBD.
Dr. Holmer is a gastroenterologist with NYU Langone Health specializing in inflammatory bowel disease. Dr. Chang is director of clinical operations for the NYU Langone Health Inflammatory Bowel Disease Center. Dr. Malter is director of education for the Inflammatory Bowel Disease Center at NYU Langone Health and director of the inflammatory bowel disease program at Bellevue Hospital Center. Follow Dr. Holmer on X (formerly Twitter) at @HolmerMd and Dr. Chang @shannonchangmd. Dr. Holmer disclosed affiliations with Pfizer, Bristol Myers Squibb, and AvevoRx. Dr. Chang disclosed affiliations with Pfizer and Bristol Myers Squibb. Dr. Malter disclosed receiving educational grants form Abbvie, Janssen, Pfizer and Takeda, and serving on the advisory boards of AbbVie, Bristol Myers Squibb, Celltrion, Janssen, Merck, and Takeda.
References
1. Chang S et al. Am J Gastroenterol. 2023 Aug 24. doi: 10.14309/ajg.0000000000002485.
2. Harvey RF et al. The Lancet. 1980;1:514.
3. Lewis JD et al. Inflammatory Bowel Diseases. 2008;14:1660-1666.
4. Siegel CA et al. Gut. 2018;67(2):244-54.
5. Peyrin-Biroulet L et al. Am J Gastroenterol. 2015;110:1324-38
6. Rogler G et al. Gastroenterology. 2021;161:1118-32.
7. Sandborn WJ et al. N Engl J Med. 2017;376:1723-36.
8. Brooklyn TN et al. Gut. 2006;55:505-9.
9. Fahmy M et al. Am J Gastroenterol. 2012;107:794-5.
10. Van Eycken L et al. JAAD Case Rep. 2023;37:89-91.
11. Lasa JS et al. Lancet Gastroenterol Hepatol. 2022;7:161-70.
12. Lichtenstein GR et al. Inflamm Bowel Dis. 2018;24:490-501.
13. Long MD et al. Gastroenterology. 2022;162:S-5-S-6.
14. Holmer AK et al. Clin Gastroenterol Hepatol.2023;21:1598-1606.e5.
15. Sands BE et al. Gastroenterology. 2014;147:618-27.e3.
16. Sands BE et al. N Engl J Med. 2019;381:1215-26.
17. Sands BE et al. N Engl J Med. 2019;381:1201-14.
18. D’Haens G et al. Lancet. 2022;399:2015-30.
19. Bouguen G et al. Clin Gastroenterol Hepatol. 2013;11:975-81.e1-4.
20. Papamichael K et al. Am J Gastroenterol. 2021;116:1007-14.
21. Shehab M et al. Inflamm Bowel Dis. 2023;29:367-75.
22. Colombel JF et al. J Crohns Colitis. 2023;17:i620-i623.
23. Garcia-Olmo D et al. Dis Colon Rectum. 2022;65:713-20.
24. Louis E et al. J Crohns Colitis. 2023;17:231-9.
25. Rubin DT et al. Inflamm Bowel Dis. 2017;23:224-32.
26. Gulacsi L et al. Curr Med Chem. 2019;26:259-69.
27. Cai Q et al. BMC Gastroenterol. 2022;22:545.
28. Dos Santos Marques IC et al. Crohns Colitis 360. 2020 Oct;2(4):otaa076.
29. Deepak P et al. Gastroenterology. 2023;165:11-15.
30. Mahadevan U et al. Gastroenterology. 2019;156:1508-24.
31. Faye AS et al. Inflamm Bowel Dis. 2022;28:126-32.
32. Berinstein JA et al. Clin Gastroenterol Hepatol. 2021;19:2112-20.e1.
33. Levine J et al. Gastroenterology. 2023;164:S103-S104.
Despite new advances in treatment, head to head clinical trials, which are considered the gold standard when comparing therapies, remain limited. Other comparative effectiveness studies and network meta-analyses are the currently available substitutes to guide decision making.1
While efficacy is often considered first when choosing a drug, other critical factors play a role in tailoring a treatment plan. This article focuses on key considerations to help guide clinical decision making when treating patients with moderate to severe IBD (Figure 1).
Disease activity versus severity
Both disease activity and disease severity should be considered when evaluating a patient for treatment. Disease activity is a cross-sectional view of one’s signs and symptoms which can vary visit to visit. Standardized indices measure disease activity in both Crohn’s disease (CD) and ulcerative colitis (UC).2,3 Disease severity encompasses the overall prognosis of disease over time and includes factors such as the presence or absence of high risk features, prior medication exposure, history of surgery, hospitalizations and the impact on quality of life.4
To prevent disease complications, the goals of treatment should be aimed at both reducing active symptoms (disease activity) but also healing mucosal inflammation, preventing disease progression (disease severity) and downstream sequelae including cancer, hospitalization or surgery.5 Determining the best treatment option takes disease activity and severity into account, in addition to the other key factors listed below (Figure 2).
Extraintestinal manifestations
Inflammation of organs outside of the gastrointestinal tract is common and can occur in up to 50% of patients with IBD.6 The most prevalent extraintestinal manifestations (EIMs) involve the skin and joints, which will be the primary focus in this article. We will also focus on treatment options with the most evidence supporting their use. Peripheral arthritis is often associated with intestinal inflammation, and treatment of underlying IBD can simultaneously improve joint symptoms. Conversely, axial spondyloarthritis does not commonly parallel intestinal inflammation. Anti–tumor necrosis factor (TNF) agents including infliximab and adalimumab are effective for the treatment of both peripheral and axial disease.6
Ustekinumab, an interleukin (IL)-12/23 inhibitor, may be effective for peripheral arthritis, however is ineffective for the treatment of axial spondyloarthritis.6 Janus kinase (JAK) inhibitors which include tofacitinib and upadacitinib are oral small molecules used to treat peripheral and axial spondyloarthritis and have more recently been approved for moderate to severe IBD.6,7
Erythema nodosum (EN) and pyoderma gangrenosum (PG) are skin manifestations seen in patients with IBD. EN appears as subcutaneous nodules and parallels intestinal inflammation, while PG consists of violaceous, ulcerated plaques, and presents with more significant pain. Anti-TNFs are effective for both EN and PG, with infliximab being the only biologic studied in a randomized control trial of patients with PG.8 In addition, small case reports have described some benefit from ustekinumab and upadacitinib in the treatment of PG.9,10
Safety
The safety of IBD therapies is a key consideration and often the most important factor to patients when choosing a treatment option. It is important to note that untreated disease is associated with significant morbidity, and should be weighed when discussing risks of medications with patients. In general, anti-TNFs and JAK inhibitors may be associated with an increased risk of infection and malignancy, while ustekinumab, vedolizumab, risankizumab and ozanimod offer a more favorable safety profile.11 In large registries and observational studies, infliximab was associated with up to a two times greater risk of serious infection as compared to nonbiologic medications, with the most common infections being pneumonia, sepsis and herpes zoster.12 JAK inhibitors are associated with an increased risk of herpes zoster infection, with a dose dependent effect seen in the maintenance clinical trials with tofacitinib.7
Ozanimod may be associated with atrioventricular conduction delays and bradycardia, however long-term safety data has reported a low incidence of serious cardiac related adverse events.13 Overall, though risks of infection may vary with different therapies, other consistent risk factors associated with greater rates of serious infection include prolonged corticosteroid use, combination therapy with thiopurines, and disease severity. Anti-TNFs have also been associated with a somewhat increased risk of lymphoma, increased when used in combination with thiopurines. Reassuringly, however, in patients with a prior history of cancer, anti-TNFs and non-TNF biologics have not been found to increase the risk of new or recurrent cancer.14
Ultimately, in patients with a prior history of cancer, the choice of biologic or small molecule should be made in collaboration with a patient’s oncologist.
Anti-TNF exposure
Anti-TNFs were the first available biologics for the treatment of IBD. After the approval of vedolizumab in 2014, the first non-TNF biologic, many patients enrolled in clinical trials thereafter had already tried and failed anti-TNFs. In general, exposure to anti-TNFs may reduce the efficacy of a future biologic. In patients treated with vedolizumab, endoscopic and clinical outcomes were negatively impacted by prior anti-TNF exposure.15 However, in VARSITY, a head-to-head clinical trial where 20% of patients with UC were previously exposed to anti-TNFs other than adalimumab, vedolizumab had significantly higher rates of clinical remission and endoscopic improvement compared to adalimumab.16 Clinical remission rates with tofacitinib were not impacted by exposure to anti-TNF treatment, and similar findings were observed with ustekinumab.7,17 Risankizumab, a newly approved selective anti-IL23, also does not appear to be impacted by prior anti-TNF exposure by demonstrating similar rates of clinical remission regardless of biologic exposure status.18 Therefore, in patients with prior history of anti-TNF use, consideration of ustekinumab, risankizumab or JAK inhibitors as second line agents may be more favorable as compared to vedolizumab.
Perianal fistulizing disease
Perianal fistulizing disease can affect up to one-third of patients with CD and significantly impact a patient’s quality of life.19 The most robust data for the treatment of perianal fistulizing disease includes the use of infliximab with up to one-third of patients on maintenance therapy achieving complete resolution of fistula drainage. While no head-to-head trials compare combination therapy with infliximab plus immunomodulators versus infliximab alone for this indication specifically, one observational study demonstrated higher rates of fistula closure with combination therapy as compared to infliximab mono-therapy.19 In a post hoc analysis, higher infliximab concentrations at week 14 were associated with greater fistula response and remission rates.20 In patients with perianal disease, ustekinumab and vedolizumab may also be an effective treatment option by promoting resolution of fistula drainage.21
More recently, emerging data demonstrate that upadacitinib may be an excellent option as a second-line treatment for perianal disease in patients who have failed anti-TNF therapy. Use of upadacitinib was associated with greater rates of complete resolution of fistula drainage and higher rates of external fistula closure (Figure 2).22 Lastly, as an alternative to medical therapy, mesenchymal stem cell therapy has also shown to improve fistula drainage and improve external fistula openings in patients with CD.23 Stem cell therapy is only available through clinical trials at this time.
Patient preferences
Overall, data are lacking for evaluating patient preferences in treatment options for IBD especially with the recent increase in therapeutic options. One survey demonstrated that patient preferences were most impacted by the possibility of improving abdominal pain, with patients accepting additional risk of treatment side effects in order to reduce their abdominal pain.24 An oral route of administration and improving fatigue and bowel urgency were similarly important to patients. Patient preferences can also be highly variable with some valuing avoidance of corticosteroid use while others valuing avoidance of symptoms or risks of medication side effects and surgery. It is important to tailor the discussion on treatment strategies to each individual patient and inquire about the patient’s lifestyle, medical history, and value system, which may impact their treatment preferences utilizing shared decision making.
Access to treatment including the role of social determinants of health
The expanded therapeutic armamentarium has the potential to help patients achieve the current goals of care in IBD. However, these medications are not available to all patients due to numerous barriers including step therapy payer policies, prohibitive costs, insurance prior authorizations, and the role of social determinants of health and proximity to IBD expertise.25 While clinicians work with patients to determine the best treatment option, more often than not, the decision lies with the insurance payer. Step therapy is the protocol used by insurance companies that requires patients to try a lower-cost medication and fail to respond before they approve the originally requested treatment. This can lead to treatment delays, progression of disease, and disease complications. The option to incorporate the use of biosimilars, currently available for anti-TNFs, and other biologics in the near future, will reduce cost and potentially increase access.26 Additionally, working with a clinical pharmacist to navigate access and utilize patient assistance programs may help overcome cost related barriers to treatment and prevent delays in care.
Socioeconomic status has been shown to impact IBD disease outcomes, and compliance rates in treatment vary depending on race and ethnicity.27 Certain racial and ethnic groups remain vulnerable and may require additional support to achieve treatment goals. For example, disparities in health literacy in patients with IBD have been demonstrated with older black men at risk.28 Additionally, the patient’s proximity to their health care facility may impact treatment options. Most IBD centers are located in metropolitan areas and numerous “IBD deserts” exist, potentially limiting therapies for patients from more remote/rural settings.29 Access to treatment and the interplay of social determinants of health can have a large role in therapy selection.
Special considerations: Pregnancy and older adults
Certain patient populations warrant special consideration when approaching treatment strategies. Pregnancy in IBD will not be addressed in full depth in this article, however a key takeaway is that planning is critical and providers should emphasize the importance of steroid-free clinical remission for at least 3 months before conception.30 Additionally, biologic use during pregnancy has not been shown to increase adverse fetal outcomes, thus should be continued to minimize disease flare. Newer novel small molecules are generally avoided during pregnancy due to limited available safety data.
Older adults are the largest growing patient population with IBD. Frailty, or a state of decreased reserve, is more commonly observed in older patients and has been shown to increase adverse events including hospitalization and mortaility.31 Ultimately reducing polypharmacy, ensuring adequate nutrition, minimizing corticosteroid exposure and avoiding undertreatment of active IBD are all key in optimizing outcomes in an older patient with IBD.
Conclusion
When discussing treatment options with patients with IBD, it is important to individualize care and share the decision-making process with patients. Goals include improving symptoms and quality of life while working to achieve the goal of healing intestinal inflammation. In summary, this article can serve as a guide to clinicians for key factors in decision making when selecting therapies in moderate to severe IBD.
Dr. Holmer is a gastroenterologist with NYU Langone Health specializing in inflammatory bowel disease. Dr. Chang is director of clinical operations for the NYU Langone Health Inflammatory Bowel Disease Center. Dr. Malter is director of education for the Inflammatory Bowel Disease Center at NYU Langone Health and director of the inflammatory bowel disease program at Bellevue Hospital Center. Follow Dr. Holmer on X (formerly Twitter) at @HolmerMd and Dr. Chang @shannonchangmd. Dr. Holmer disclosed affiliations with Pfizer, Bristol Myers Squibb, and AvevoRx. Dr. Chang disclosed affiliations with Pfizer and Bristol Myers Squibb. Dr. Malter disclosed receiving educational grants form Abbvie, Janssen, Pfizer and Takeda, and serving on the advisory boards of AbbVie, Bristol Myers Squibb, Celltrion, Janssen, Merck, and Takeda.
References
1. Chang S et al. Am J Gastroenterol. 2023 Aug 24. doi: 10.14309/ajg.0000000000002485.
2. Harvey RF et al. The Lancet. 1980;1:514.
3. Lewis JD et al. Inflammatory Bowel Diseases. 2008;14:1660-1666.
4. Siegel CA et al. Gut. 2018;67(2):244-54.
5. Peyrin-Biroulet L et al. Am J Gastroenterol. 2015;110:1324-38
6. Rogler G et al. Gastroenterology. 2021;161:1118-32.
7. Sandborn WJ et al. N Engl J Med. 2017;376:1723-36.
8. Brooklyn TN et al. Gut. 2006;55:505-9.
9. Fahmy M et al. Am J Gastroenterol. 2012;107:794-5.
10. Van Eycken L et al. JAAD Case Rep. 2023;37:89-91.
11. Lasa JS et al. Lancet Gastroenterol Hepatol. 2022;7:161-70.
12. Lichtenstein GR et al. Inflamm Bowel Dis. 2018;24:490-501.
13. Long MD et al. Gastroenterology. 2022;162:S-5-S-6.
14. Holmer AK et al. Clin Gastroenterol Hepatol.2023;21:1598-1606.e5.
15. Sands BE et al. Gastroenterology. 2014;147:618-27.e3.
16. Sands BE et al. N Engl J Med. 2019;381:1215-26.
17. Sands BE et al. N Engl J Med. 2019;381:1201-14.
18. D’Haens G et al. Lancet. 2022;399:2015-30.
19. Bouguen G et al. Clin Gastroenterol Hepatol. 2013;11:975-81.e1-4.
20. Papamichael K et al. Am J Gastroenterol. 2021;116:1007-14.
21. Shehab M et al. Inflamm Bowel Dis. 2023;29:367-75.
22. Colombel JF et al. J Crohns Colitis. 2023;17:i620-i623.
23. Garcia-Olmo D et al. Dis Colon Rectum. 2022;65:713-20.
24. Louis E et al. J Crohns Colitis. 2023;17:231-9.
25. Rubin DT et al. Inflamm Bowel Dis. 2017;23:224-32.
26. Gulacsi L et al. Curr Med Chem. 2019;26:259-69.
27. Cai Q et al. BMC Gastroenterol. 2022;22:545.
28. Dos Santos Marques IC et al. Crohns Colitis 360. 2020 Oct;2(4):otaa076.
29. Deepak P et al. Gastroenterology. 2023;165:11-15.
30. Mahadevan U et al. Gastroenterology. 2019;156:1508-24.
31. Faye AS et al. Inflamm Bowel Dis. 2022;28:126-32.
32. Berinstein JA et al. Clin Gastroenterol Hepatol. 2021;19:2112-20.e1.
33. Levine J et al. Gastroenterology. 2023;164:S103-S104.
Despite new advances in treatment, head to head clinical trials, which are considered the gold standard when comparing therapies, remain limited. Other comparative effectiveness studies and network meta-analyses are the currently available substitutes to guide decision making.1
While efficacy is often considered first when choosing a drug, other critical factors play a role in tailoring a treatment plan. This article focuses on key considerations to help guide clinical decision making when treating patients with moderate to severe IBD (Figure 1).
Disease activity versus severity
Both disease activity and disease severity should be considered when evaluating a patient for treatment. Disease activity is a cross-sectional view of one’s signs and symptoms which can vary visit to visit. Standardized indices measure disease activity in both Crohn’s disease (CD) and ulcerative colitis (UC).2,3 Disease severity encompasses the overall prognosis of disease over time and includes factors such as the presence or absence of high risk features, prior medication exposure, history of surgery, hospitalizations and the impact on quality of life.4
To prevent disease complications, the goals of treatment should be aimed at both reducing active symptoms (disease activity) but also healing mucosal inflammation, preventing disease progression (disease severity) and downstream sequelae including cancer, hospitalization or surgery.5 Determining the best treatment option takes disease activity and severity into account, in addition to the other key factors listed below (Figure 2).
Extraintestinal manifestations
Inflammation of organs outside of the gastrointestinal tract is common and can occur in up to 50% of patients with IBD.6 The most prevalent extraintestinal manifestations (EIMs) involve the skin and joints, which will be the primary focus in this article. We will also focus on treatment options with the most evidence supporting their use. Peripheral arthritis is often associated with intestinal inflammation, and treatment of underlying IBD can simultaneously improve joint symptoms. Conversely, axial spondyloarthritis does not commonly parallel intestinal inflammation. Anti–tumor necrosis factor (TNF) agents including infliximab and adalimumab are effective for the treatment of both peripheral and axial disease.6
Ustekinumab, an interleukin (IL)-12/23 inhibitor, may be effective for peripheral arthritis, however is ineffective for the treatment of axial spondyloarthritis.6 Janus kinase (JAK) inhibitors which include tofacitinib and upadacitinib are oral small molecules used to treat peripheral and axial spondyloarthritis and have more recently been approved for moderate to severe IBD.6,7
Erythema nodosum (EN) and pyoderma gangrenosum (PG) are skin manifestations seen in patients with IBD. EN appears as subcutaneous nodules and parallels intestinal inflammation, while PG consists of violaceous, ulcerated plaques, and presents with more significant pain. Anti-TNFs are effective for both EN and PG, with infliximab being the only biologic studied in a randomized control trial of patients with PG.8 In addition, small case reports have described some benefit from ustekinumab and upadacitinib in the treatment of PG.9,10
Safety
The safety of IBD therapies is a key consideration and often the most important factor to patients when choosing a treatment option. It is important to note that untreated disease is associated with significant morbidity, and should be weighed when discussing risks of medications with patients. In general, anti-TNFs and JAK inhibitors may be associated with an increased risk of infection and malignancy, while ustekinumab, vedolizumab, risankizumab and ozanimod offer a more favorable safety profile.11 In large registries and observational studies, infliximab was associated with up to a two times greater risk of serious infection as compared to nonbiologic medications, with the most common infections being pneumonia, sepsis and herpes zoster.12 JAK inhibitors are associated with an increased risk of herpes zoster infection, with a dose dependent effect seen in the maintenance clinical trials with tofacitinib.7
Ozanimod may be associated with atrioventricular conduction delays and bradycardia, however long-term safety data has reported a low incidence of serious cardiac related adverse events.13 Overall, though risks of infection may vary with different therapies, other consistent risk factors associated with greater rates of serious infection include prolonged corticosteroid use, combination therapy with thiopurines, and disease severity. Anti-TNFs have also been associated with a somewhat increased risk of lymphoma, increased when used in combination with thiopurines. Reassuringly, however, in patients with a prior history of cancer, anti-TNFs and non-TNF biologics have not been found to increase the risk of new or recurrent cancer.14
Ultimately, in patients with a prior history of cancer, the choice of biologic or small molecule should be made in collaboration with a patient’s oncologist.
Anti-TNF exposure
Anti-TNFs were the first available biologics for the treatment of IBD. After the approval of vedolizumab in 2014, the first non-TNF biologic, many patients enrolled in clinical trials thereafter had already tried and failed anti-TNFs. In general, exposure to anti-TNFs may reduce the efficacy of a future biologic. In patients treated with vedolizumab, endoscopic and clinical outcomes were negatively impacted by prior anti-TNF exposure.15 However, in VARSITY, a head-to-head clinical trial where 20% of patients with UC were previously exposed to anti-TNFs other than adalimumab, vedolizumab had significantly higher rates of clinical remission and endoscopic improvement compared to adalimumab.16 Clinical remission rates with tofacitinib were not impacted by exposure to anti-TNF treatment, and similar findings were observed with ustekinumab.7,17 Risankizumab, a newly approved selective anti-IL23, also does not appear to be impacted by prior anti-TNF exposure by demonstrating similar rates of clinical remission regardless of biologic exposure status.18 Therefore, in patients with prior history of anti-TNF use, consideration of ustekinumab, risankizumab or JAK inhibitors as second line agents may be more favorable as compared to vedolizumab.
Perianal fistulizing disease
Perianal fistulizing disease can affect up to one-third of patients with CD and significantly impact a patient’s quality of life.19 The most robust data for the treatment of perianal fistulizing disease includes the use of infliximab with up to one-third of patients on maintenance therapy achieving complete resolution of fistula drainage. While no head-to-head trials compare combination therapy with infliximab plus immunomodulators versus infliximab alone for this indication specifically, one observational study demonstrated higher rates of fistula closure with combination therapy as compared to infliximab mono-therapy.19 In a post hoc analysis, higher infliximab concentrations at week 14 were associated with greater fistula response and remission rates.20 In patients with perianal disease, ustekinumab and vedolizumab may also be an effective treatment option by promoting resolution of fistula drainage.21
More recently, emerging data demonstrate that upadacitinib may be an excellent option as a second-line treatment for perianal disease in patients who have failed anti-TNF therapy. Use of upadacitinib was associated with greater rates of complete resolution of fistula drainage and higher rates of external fistula closure (Figure 2).22 Lastly, as an alternative to medical therapy, mesenchymal stem cell therapy has also shown to improve fistula drainage and improve external fistula openings in patients with CD.23 Stem cell therapy is only available through clinical trials at this time.
Patient preferences
Overall, data are lacking for evaluating patient preferences in treatment options for IBD especially with the recent increase in therapeutic options. One survey demonstrated that patient preferences were most impacted by the possibility of improving abdominal pain, with patients accepting additional risk of treatment side effects in order to reduce their abdominal pain.24 An oral route of administration and improving fatigue and bowel urgency were similarly important to patients. Patient preferences can also be highly variable with some valuing avoidance of corticosteroid use while others valuing avoidance of symptoms or risks of medication side effects and surgery. It is important to tailor the discussion on treatment strategies to each individual patient and inquire about the patient’s lifestyle, medical history, and value system, which may impact their treatment preferences utilizing shared decision making.
Access to treatment including the role of social determinants of health
The expanded therapeutic armamentarium has the potential to help patients achieve the current goals of care in IBD. However, these medications are not available to all patients due to numerous barriers including step therapy payer policies, prohibitive costs, insurance prior authorizations, and the role of social determinants of health and proximity to IBD expertise.25 While clinicians work with patients to determine the best treatment option, more often than not, the decision lies with the insurance payer. Step therapy is the protocol used by insurance companies that requires patients to try a lower-cost medication and fail to respond before they approve the originally requested treatment. This can lead to treatment delays, progression of disease, and disease complications. The option to incorporate the use of biosimilars, currently available for anti-TNFs, and other biologics in the near future, will reduce cost and potentially increase access.26 Additionally, working with a clinical pharmacist to navigate access and utilize patient assistance programs may help overcome cost related barriers to treatment and prevent delays in care.
Socioeconomic status has been shown to impact IBD disease outcomes, and compliance rates in treatment vary depending on race and ethnicity.27 Certain racial and ethnic groups remain vulnerable and may require additional support to achieve treatment goals. For example, disparities in health literacy in patients with IBD have been demonstrated with older black men at risk.28 Additionally, the patient’s proximity to their health care facility may impact treatment options. Most IBD centers are located in metropolitan areas and numerous “IBD deserts” exist, potentially limiting therapies for patients from more remote/rural settings.29 Access to treatment and the interplay of social determinants of health can have a large role in therapy selection.
Special considerations: Pregnancy and older adults
Certain patient populations warrant special consideration when approaching treatment strategies. Pregnancy in IBD will not be addressed in full depth in this article, however a key takeaway is that planning is critical and providers should emphasize the importance of steroid-free clinical remission for at least 3 months before conception.30 Additionally, biologic use during pregnancy has not been shown to increase adverse fetal outcomes, thus should be continued to minimize disease flare. Newer novel small molecules are generally avoided during pregnancy due to limited available safety data.
Older adults are the largest growing patient population with IBD. Frailty, or a state of decreased reserve, is more commonly observed in older patients and has been shown to increase adverse events including hospitalization and mortaility.31 Ultimately reducing polypharmacy, ensuring adequate nutrition, minimizing corticosteroid exposure and avoiding undertreatment of active IBD are all key in optimizing outcomes in an older patient with IBD.
Conclusion
When discussing treatment options with patients with IBD, it is important to individualize care and share the decision-making process with patients. Goals include improving symptoms and quality of life while working to achieve the goal of healing intestinal inflammation. In summary, this article can serve as a guide to clinicians for key factors in decision making when selecting therapies in moderate to severe IBD.
Dr. Holmer is a gastroenterologist with NYU Langone Health specializing in inflammatory bowel disease. Dr. Chang is director of clinical operations for the NYU Langone Health Inflammatory Bowel Disease Center. Dr. Malter is director of education for the Inflammatory Bowel Disease Center at NYU Langone Health and director of the inflammatory bowel disease program at Bellevue Hospital Center. Follow Dr. Holmer on X (formerly Twitter) at @HolmerMd and Dr. Chang @shannonchangmd. Dr. Holmer disclosed affiliations with Pfizer, Bristol Myers Squibb, and AvevoRx. Dr. Chang disclosed affiliations with Pfizer and Bristol Myers Squibb. Dr. Malter disclosed receiving educational grants form Abbvie, Janssen, Pfizer and Takeda, and serving on the advisory boards of AbbVie, Bristol Myers Squibb, Celltrion, Janssen, Merck, and Takeda.
References
1. Chang S et al. Am J Gastroenterol. 2023 Aug 24. doi: 10.14309/ajg.0000000000002485.
2. Harvey RF et al. The Lancet. 1980;1:514.
3. Lewis JD et al. Inflammatory Bowel Diseases. 2008;14:1660-1666.
4. Siegel CA et al. Gut. 2018;67(2):244-54.
5. Peyrin-Biroulet L et al. Am J Gastroenterol. 2015;110:1324-38
6. Rogler G et al. Gastroenterology. 2021;161:1118-32.
7. Sandborn WJ et al. N Engl J Med. 2017;376:1723-36.
8. Brooklyn TN et al. Gut. 2006;55:505-9.
9. Fahmy M et al. Am J Gastroenterol. 2012;107:794-5.
10. Van Eycken L et al. JAAD Case Rep. 2023;37:89-91.
11. Lasa JS et al. Lancet Gastroenterol Hepatol. 2022;7:161-70.
12. Lichtenstein GR et al. Inflamm Bowel Dis. 2018;24:490-501.
13. Long MD et al. Gastroenterology. 2022;162:S-5-S-6.
14. Holmer AK et al. Clin Gastroenterol Hepatol.2023;21:1598-1606.e5.
15. Sands BE et al. Gastroenterology. 2014;147:618-27.e3.
16. Sands BE et al. N Engl J Med. 2019;381:1215-26.
17. Sands BE et al. N Engl J Med. 2019;381:1201-14.
18. D’Haens G et al. Lancet. 2022;399:2015-30.
19. Bouguen G et al. Clin Gastroenterol Hepatol. 2013;11:975-81.e1-4.
20. Papamichael K et al. Am J Gastroenterol. 2021;116:1007-14.
21. Shehab M et al. Inflamm Bowel Dis. 2023;29:367-75.
22. Colombel JF et al. J Crohns Colitis. 2023;17:i620-i623.
23. Garcia-Olmo D et al. Dis Colon Rectum. 2022;65:713-20.
24. Louis E et al. J Crohns Colitis. 2023;17:231-9.
25. Rubin DT et al. Inflamm Bowel Dis. 2017;23:224-32.
26. Gulacsi L et al. Curr Med Chem. 2019;26:259-69.
27. Cai Q et al. BMC Gastroenterol. 2022;22:545.
28. Dos Santos Marques IC et al. Crohns Colitis 360. 2020 Oct;2(4):otaa076.
29. Deepak P et al. Gastroenterology. 2023;165:11-15.
30. Mahadevan U et al. Gastroenterology. 2019;156:1508-24.
31. Faye AS et al. Inflamm Bowel Dis. 2022;28:126-32.
32. Berinstein JA et al. Clin Gastroenterol Hepatol. 2021;19:2112-20.e1.
33. Levine J et al. Gastroenterology. 2023;164:S103-S104.
Advancing personalized medicine in IBD
Gastroenterologists have more treatments at their disposal today than ever before, particularly in the last decade. “We have had tremendous advances in many areas of understanding contributors to disease,” said Dr. Melia, an assistant professor of medicine at Johns Hopkins Medicine in Baltimore who specializes in inflammatory bowel disease (IBD). But the hurdle is in translating the science to clinical care that is individualized to each patient based on condition and stage of the condition.

“That still remains a bit of a dream,” she said. Much of her career has been devoted to chasing down a particular genetic variant that contributes to IBD, with the goal of reaching more precise treatments for patients.
In an interview, she shared how she entered this line of work, and what her research has revealed about Crohn’s disease, manganese, and a common genetic variant known as ZIP8.
Q: Your expertise is in inflammatory bowel disease and manganese deficiency. Why did you choose these two areas as your focus in GI?
Dr. Melia: In talking to many patients with IBD, I was always struck by the questions around nutritional factors related to disease. As a fellow, I was embedded in a lab that focused on genetics of IBD. A micronutrient transporter, ZIP8, has a mutation in it that increases the risk of Crohn’s disease.
I’ve dedicated the last 8 years to understanding how this mutation can increase risk. It initially started out as a project focused on zinc, because that’s what the transporter was thought to regulate. However, it’s evolved as we’ve learned more about it, underscoring the importance of manganese, another micronutrient that we derive from food.
We have established that having this mutation changes how the body handles manganese and affects downstream processes that involve manganese. What I’m doing now is trying to connect those dots on why those processes are important in Crohn’s disease and whether we can target them for treatment.
Q: How does manganese deficiency lead to chronic IBD?
Dr. Melia: In individuals with this mutation, their blood manganese levels are lower than people who don’t have this mutation. When we talk about manganese deficiency or insufficiency, what we’re really talking about is lower blood levels. But it’s more complicated than that at the tissue level.
What we and other groups are working on right now is trying to understand if the manganese levels change in the gut and what happens in inflammation. The gut is a particularly interesting area for manganese, in that much of the manganese that we eat is excreted. We only absorb a small amount of it. And so, manganese levels within the gut lumen may actually be quite high – and may be even higher in inflammation. But there are things we don’t understand about that and how it relates to mucosal levels of manganese and Crohn’s disease. The ileum, the site of the Crohn’s disease that’s specifically associated with this mutation, might be particularly sensitive to changes in the manganese levels or the downstream processes that changing manganese availability affects.
One of those processes is glycosylation. Manganese is important to properly glycosylate your proteins. Many enzymes help cells put sugars on proteins, and many of those enzymes need manganese to do it. Glycosylation of proteins is important so cells know where those proteins should go, and the sugars help them stay where they need to be. When you change protein glycosylation, you can stress the cells. We know individuals who carry this mutation have changes in the glycosylation of their proteins. What we’re working on right now is understanding which key proteins might change when that happens, and why that’s a potential problem, especially in the ileum.
Q: How might your research inform clinical practice?
Dr. Melia: We’ve seen significant progress in new medications and new pathways that have emerged. We still have this fundamental problem that our immune-targeting medicines are only helping about 50% of the patients.
It’s critical that we begin to identify new pathways. And my hope is that in studying genes like the ZIP8 (SLC39A8), which is associated with the dysregulated processing of manganese, we can understand different pathways and mechanisms to target.
As an example, if we could help correct the glycosylation problem, that would help to boost the barrier function of the gut and perhaps decrease the activation of those immune cells, because you’re just reinforcing the barrier integrity of the gut.
We want to target that glycosylation problem as we would treat patients with congenital disorders of glycosylation by giving supplemental sugars. We think this problem of glycosylation extends beyond patients with the ZIP8 mutation, but it is also really important for patients with the mutation. So, the goal would be to use ZIP8 genetics to help prioritize patients for therapy targeting this problem.
Q: You’re involved in the American Gastroenterological Association Future Leaders Program. What is your role in this program? Why is it important?
Dr. Melia: I was very grateful for the opportunity to participate in the AGA’s Future Leaders Program. I think it was exceedingly valuable for two main reasons. One, it really offered an insight into the role of the AGA and the important role that the AGA plays in the careers of gastroenterologists. Two, it was such a unique opportunity to work with colleagues nationwide and to build a network of individuals who are all at a similar stage in their careers. It was a very inspiring group to meet and to have the opportunity to work with as part of that program, and I thank the AGA for supporting such an initiative.
Q: What teacher or mentor had the greatest impact on you?
Dr. Melia: I have been blessed by many clinical and research mentors through my career. I was inspired to do science at the lab of Ramnik Xavier, MD, at Massachusetts General Hospital. At Johns Hopkins, I credit Cindy Sears, MD, and Anne Marie O’Broin Lennon, MBBCh, PhD, as two physician scientists who have really shaped how I have tried to integrate my clinical and research career.
LIGHTNING ROUND
Do you prefer texting or talking?
Texting
If you weren’t a gastroenterologist, what would you be?
Teacher
What was the last movie you watched?
Great Bear Rainforest
What is your most favorite city in the U.S.?
Surry, Maine
What song do you absolutely have to sing along with when you hear it?
Any song by Whitney Houston.
Are you an introvert or extrovert?
Introvert
How many cups of coffee do you drink per day?
One
Gastroenterologists have more treatments at their disposal today than ever before, particularly in the last decade. “We have had tremendous advances in many areas of understanding contributors to disease,” said Dr. Melia, an assistant professor of medicine at Johns Hopkins Medicine in Baltimore who specializes in inflammatory bowel disease (IBD). But the hurdle is in translating the science to clinical care that is individualized to each patient based on condition and stage of the condition.
“That still remains a bit of a dream,” she said. Much of her career has been devoted to chasing down a particular genetic variant that contributes to IBD, with the goal of reaching more precise treatments for patients.
In an interview, she shared how she entered this line of work, and what her research has revealed about Crohn’s disease, manganese, and a common genetic variant known as ZIP8.
Q: Your expertise is in inflammatory bowel disease and manganese deficiency. Why did you choose these two areas as your focus in GI?
Dr. Melia: In talking to many patients with IBD, I was always struck by the questions around nutritional factors related to disease. As a fellow, I was embedded in a lab that focused on genetics of IBD. A micronutrient transporter, ZIP8, has a mutation in it that increases the risk of Crohn’s disease.
I’ve dedicated the last 8 years to understanding how this mutation can increase risk. It initially started out as a project focused on zinc, because that’s what the transporter was thought to regulate. However, it’s evolved as we’ve learned more about it, underscoring the importance of manganese, another micronutrient that we derive from food.
We have established that having this mutation changes how the body handles manganese and affects downstream processes that involve manganese. What I’m doing now is trying to connect those dots on why those processes are important in Crohn’s disease and whether we can target them for treatment.
Q: How does manganese deficiency lead to chronic IBD?
Dr. Melia: In individuals with this mutation, their blood manganese levels are lower than people who don’t have this mutation. When we talk about manganese deficiency or insufficiency, what we’re really talking about is lower blood levels. But it’s more complicated than that at the tissue level.
What we and other groups are working on right now is trying to understand if the manganese levels change in the gut and what happens in inflammation. The gut is a particularly interesting area for manganese, in that much of the manganese that we eat is excreted. We only absorb a small amount of it. And so, manganese levels within the gut lumen may actually be quite high – and may be even higher in inflammation. But there are things we don’t understand about that and how it relates to mucosal levels of manganese and Crohn’s disease. The ileum, the site of the Crohn’s disease that’s specifically associated with this mutation, might be particularly sensitive to changes in the manganese levels or the downstream processes that changing manganese availability affects.
One of those processes is glycosylation. Manganese is important to properly glycosylate your proteins. Many enzymes help cells put sugars on proteins, and many of those enzymes need manganese to do it. Glycosylation of proteins is important so cells know where those proteins should go, and the sugars help them stay where they need to be. When you change protein glycosylation, you can stress the cells. We know individuals who carry this mutation have changes in the glycosylation of their proteins. What we’re working on right now is understanding which key proteins might change when that happens, and why that’s a potential problem, especially in the ileum.
Q: How might your research inform clinical practice?
Dr. Melia: We’ve seen significant progress in new medications and new pathways that have emerged. We still have this fundamental problem that our immune-targeting medicines are only helping about 50% of the patients.
It’s critical that we begin to identify new pathways. And my hope is that in studying genes like the ZIP8 (SLC39A8), which is associated with the dysregulated processing of manganese, we can understand different pathways and mechanisms to target.
As an example, if we could help correct the glycosylation problem, that would help to boost the barrier function of the gut and perhaps decrease the activation of those immune cells, because you’re just reinforcing the barrier integrity of the gut.
We want to target that glycosylation problem as we would treat patients with congenital disorders of glycosylation by giving supplemental sugars. We think this problem of glycosylation extends beyond patients with the ZIP8 mutation, but it is also really important for patients with the mutation. So, the goal would be to use ZIP8 genetics to help prioritize patients for therapy targeting this problem.
Q: You’re involved in the American Gastroenterological Association Future Leaders Program. What is your role in this program? Why is it important?
Dr. Melia: I was very grateful for the opportunity to participate in the AGA’s Future Leaders Program. I think it was exceedingly valuable for two main reasons. One, it really offered an insight into the role of the AGA and the important role that the AGA plays in the careers of gastroenterologists. Two, it was such a unique opportunity to work with colleagues nationwide and to build a network of individuals who are all at a similar stage in their careers. It was a very inspiring group to meet and to have the opportunity to work with as part of that program, and I thank the AGA for supporting such an initiative.
Q: What teacher or mentor had the greatest impact on you?
Dr. Melia: I have been blessed by many clinical and research mentors through my career. I was inspired to do science at the lab of Ramnik Xavier, MD, at Massachusetts General Hospital. At Johns Hopkins, I credit Cindy Sears, MD, and Anne Marie O’Broin Lennon, MBBCh, PhD, as two physician scientists who have really shaped how I have tried to integrate my clinical and research career.
LIGHTNING ROUND
Do you prefer texting or talking?
Texting
If you weren’t a gastroenterologist, what would you be?
Teacher
What was the last movie you watched?
Great Bear Rainforest
What is your most favorite city in the U.S.?
Surry, Maine
What song do you absolutely have to sing along with when you hear it?
Any song by Whitney Houston.
Are you an introvert or extrovert?
Introvert
How many cups of coffee do you drink per day?
One
Gastroenterologists have more treatments at their disposal today than ever before, particularly in the last decade. “We have had tremendous advances in many areas of understanding contributors to disease,” said Dr. Melia, an assistant professor of medicine at Johns Hopkins Medicine in Baltimore who specializes in inflammatory bowel disease (IBD). But the hurdle is in translating the science to clinical care that is individualized to each patient based on condition and stage of the condition.
“That still remains a bit of a dream,” she said. Much of her career has been devoted to chasing down a particular genetic variant that contributes to IBD, with the goal of reaching more precise treatments for patients.
In an interview, she shared how she entered this line of work, and what her research has revealed about Crohn’s disease, manganese, and a common genetic variant known as ZIP8.
Q: Your expertise is in inflammatory bowel disease and manganese deficiency. Why did you choose these two areas as your focus in GI?
Dr. Melia: In talking to many patients with IBD, I was always struck by the questions around nutritional factors related to disease. As a fellow, I was embedded in a lab that focused on genetics of IBD. A micronutrient transporter, ZIP8, has a mutation in it that increases the risk of Crohn’s disease.
I’ve dedicated the last 8 years to understanding how this mutation can increase risk. It initially started out as a project focused on zinc, because that’s what the transporter was thought to regulate. However, it’s evolved as we’ve learned more about it, underscoring the importance of manganese, another micronutrient that we derive from food.
We have established that having this mutation changes how the body handles manganese and affects downstream processes that involve manganese. What I’m doing now is trying to connect those dots on why those processes are important in Crohn’s disease and whether we can target them for treatment.
Q: How does manganese deficiency lead to chronic IBD?
Dr. Melia: In individuals with this mutation, their blood manganese levels are lower than people who don’t have this mutation. When we talk about manganese deficiency or insufficiency, what we’re really talking about is lower blood levels. But it’s more complicated than that at the tissue level.
What we and other groups are working on right now is trying to understand if the manganese levels change in the gut and what happens in inflammation. The gut is a particularly interesting area for manganese, in that much of the manganese that we eat is excreted. We only absorb a small amount of it. And so, manganese levels within the gut lumen may actually be quite high – and may be even higher in inflammation. But there are things we don’t understand about that and how it relates to mucosal levels of manganese and Crohn’s disease. The ileum, the site of the Crohn’s disease that’s specifically associated with this mutation, might be particularly sensitive to changes in the manganese levels or the downstream processes that changing manganese availability affects.
One of those processes is glycosylation. Manganese is important to properly glycosylate your proteins. Many enzymes help cells put sugars on proteins, and many of those enzymes need manganese to do it. Glycosylation of proteins is important so cells know where those proteins should go, and the sugars help them stay where they need to be. When you change protein glycosylation, you can stress the cells. We know individuals who carry this mutation have changes in the glycosylation of their proteins. What we’re working on right now is understanding which key proteins might change when that happens, and why that’s a potential problem, especially in the ileum.
Q: How might your research inform clinical practice?
Dr. Melia: We’ve seen significant progress in new medications and new pathways that have emerged. We still have this fundamental problem that our immune-targeting medicines are only helping about 50% of the patients.
It’s critical that we begin to identify new pathways. And my hope is that in studying genes like the ZIP8 (SLC39A8), which is associated with the dysregulated processing of manganese, we can understand different pathways and mechanisms to target.
As an example, if we could help correct the glycosylation problem, that would help to boost the barrier function of the gut and perhaps decrease the activation of those immune cells, because you’re just reinforcing the barrier integrity of the gut.
We want to target that glycosylation problem as we would treat patients with congenital disorders of glycosylation by giving supplemental sugars. We think this problem of glycosylation extends beyond patients with the ZIP8 mutation, but it is also really important for patients with the mutation. So, the goal would be to use ZIP8 genetics to help prioritize patients for therapy targeting this problem.
Q: You’re involved in the American Gastroenterological Association Future Leaders Program. What is your role in this program? Why is it important?
Dr. Melia: I was very grateful for the opportunity to participate in the AGA’s Future Leaders Program. I think it was exceedingly valuable for two main reasons. One, it really offered an insight into the role of the AGA and the important role that the AGA plays in the careers of gastroenterologists. Two, it was such a unique opportunity to work with colleagues nationwide and to build a network of individuals who are all at a similar stage in their careers. It was a very inspiring group to meet and to have the opportunity to work with as part of that program, and I thank the AGA for supporting such an initiative.
Q: What teacher or mentor had the greatest impact on you?
Dr. Melia: I have been blessed by many clinical and research mentors through my career. I was inspired to do science at the lab of Ramnik Xavier, MD, at Massachusetts General Hospital. At Johns Hopkins, I credit Cindy Sears, MD, and Anne Marie O’Broin Lennon, MBBCh, PhD, as two physician scientists who have really shaped how I have tried to integrate my clinical and research career.
LIGHTNING ROUND
Do you prefer texting or talking?
Texting
If you weren’t a gastroenterologist, what would you be?
Teacher
What was the last movie you watched?
Great Bear Rainforest
What is your most favorite city in the U.S.?
Surry, Maine
What song do you absolutely have to sing along with when you hear it?
Any song by Whitney Houston.
Are you an introvert or extrovert?
Introvert
How many cups of coffee do you drink per day?
One
FDA approves mirikizumab for ulcerative colitis
Mirikizumab is a humanized monoclonal antibody that targets the p19 subunit of IL-23, a key player in UC-related inflammation. It’s the first IL-23 inhibitor to be approved in the United States for UC. The drug is administered intravenously.
The approval of mirikizumab represents a “novel scientific advancement, providing a treatment that may offer relief from three key symptoms – stool frequency, rectal bleeding, and bowel urgency – regardless of past biologic use,” Bruce Sands, MD, chief of the division of gastroenterology, Icahn School of Medicine at Mount Sinai, who worked on the pivotal trials, said in a news release.
Last April, the FDA withheld approval of the drug, citing issues related to the proposed manufacturing of the drug. The agency did not express concerns about safety or efficacy data, Eli Lilly confirmed.
The FDA approval was based on results from the phase 3 LUCENT-1 induction and LUCENT-2 maintenance trials, published in the New England Journal of Medicine.
All patients in the LUCENT program had moderately to severely active UC and had experienced treatment failure or could not tolerate past treatments, including biologic therapies.
The induction trial enrolled 1,281 patients; 544 patients who had a response to mirikizumab were enrolled in the maintenance phase.
The trials showed that mirikizumab achieved primary and secondary endpoints, including sustained clinical remission and significantly improved bowel urgency.
“Bowel urgency is one of the most disruptive symptoms for patients with ulcerative colitis,” Michael Osso, president and chief executive officer of the Crohn’s and Colitis Foundation, said in the news release.
Mirikizumab offers “new hope for those who have tried other therapies and still find themselves making accommodations for the uncertainty of bowel urgency–related accidents and other symptoms associated with ulcerative colitis,” Mr. Osso added.
The most common adverse reactions associated with mirikizumab were upper respiratory infections, injection site reactions, arthralgia, rash, headache, and herpes viral infection.
The drug label contains warnings and precautions related to hypersensitivity reactions, risk of infection, tuberculosis, hepatotoxicity, and immunizations.
A version of this article was originally published on Medscape.com .
Mirikizumab is a humanized monoclonal antibody that targets the p19 subunit of IL-23, a key player in UC-related inflammation. It’s the first IL-23 inhibitor to be approved in the United States for UC. The drug is administered intravenously.
The approval of mirikizumab represents a “novel scientific advancement, providing a treatment that may offer relief from three key symptoms – stool frequency, rectal bleeding, and bowel urgency – regardless of past biologic use,” Bruce Sands, MD, chief of the division of gastroenterology, Icahn School of Medicine at Mount Sinai, who worked on the pivotal trials, said in a news release.
Last April, the FDA withheld approval of the drug, citing issues related to the proposed manufacturing of the drug. The agency did not express concerns about safety or efficacy data, Eli Lilly confirmed.
The FDA approval was based on results from the phase 3 LUCENT-1 induction and LUCENT-2 maintenance trials, published in the New England Journal of Medicine.
All patients in the LUCENT program had moderately to severely active UC and had experienced treatment failure or could not tolerate past treatments, including biologic therapies.
The induction trial enrolled 1,281 patients; 544 patients who had a response to mirikizumab were enrolled in the maintenance phase.
The trials showed that mirikizumab achieved primary and secondary endpoints, including sustained clinical remission and significantly improved bowel urgency.
“Bowel urgency is one of the most disruptive symptoms for patients with ulcerative colitis,” Michael Osso, president and chief executive officer of the Crohn’s and Colitis Foundation, said in the news release.
Mirikizumab offers “new hope for those who have tried other therapies and still find themselves making accommodations for the uncertainty of bowel urgency–related accidents and other symptoms associated with ulcerative colitis,” Mr. Osso added.
The most common adverse reactions associated with mirikizumab were upper respiratory infections, injection site reactions, arthralgia, rash, headache, and herpes viral infection.
The drug label contains warnings and precautions related to hypersensitivity reactions, risk of infection, tuberculosis, hepatotoxicity, and immunizations.
A version of this article was originally published on Medscape.com .
Mirikizumab is a humanized monoclonal antibody that targets the p19 subunit of IL-23, a key player in UC-related inflammation. It’s the first IL-23 inhibitor to be approved in the United States for UC. The drug is administered intravenously.
The approval of mirikizumab represents a “novel scientific advancement, providing a treatment that may offer relief from three key symptoms – stool frequency, rectal bleeding, and bowel urgency – regardless of past biologic use,” Bruce Sands, MD, chief of the division of gastroenterology, Icahn School of Medicine at Mount Sinai, who worked on the pivotal trials, said in a news release.
Last April, the FDA withheld approval of the drug, citing issues related to the proposed manufacturing of the drug. The agency did not express concerns about safety or efficacy data, Eli Lilly confirmed.
The FDA approval was based on results from the phase 3 LUCENT-1 induction and LUCENT-2 maintenance trials, published in the New England Journal of Medicine.
All patients in the LUCENT program had moderately to severely active UC and had experienced treatment failure or could not tolerate past treatments, including biologic therapies.
The induction trial enrolled 1,281 patients; 544 patients who had a response to mirikizumab were enrolled in the maintenance phase.
The trials showed that mirikizumab achieved primary and secondary endpoints, including sustained clinical remission and significantly improved bowel urgency.
“Bowel urgency is one of the most disruptive symptoms for patients with ulcerative colitis,” Michael Osso, president and chief executive officer of the Crohn’s and Colitis Foundation, said in the news release.
Mirikizumab offers “new hope for those who have tried other therapies and still find themselves making accommodations for the uncertainty of bowel urgency–related accidents and other symptoms associated with ulcerative colitis,” Mr. Osso added.
The most common adverse reactions associated with mirikizumab were upper respiratory infections, injection site reactions, arthralgia, rash, headache, and herpes viral infection.
The drug label contains warnings and precautions related to hypersensitivity reactions, risk of infection, tuberculosis, hepatotoxicity, and immunizations.
A version of this article was originally published on Medscape.com .
RSV more common in IBD
A study presented this week in Vancouver at the ACG: American College of Gastroenterology annual meeting suggests that
RSV has historically been recognized in young and elderly populations and in patients who have received organ transplants. In fact, there is a body of literature that highlights the morbidity and mortality impact on immunocompromised organ transplant patients, but there is little research on the impact of RSV on patients with IBD.
For patients with inflammatory bowel disease (IBD), particularly those with comorbidities, an RSV infection can turn serious, said Ryan Smith, MD, a gastroenterology and hepatology fellow with the University of Wisconsin–Madison, who presented the study at the meeting.
“These patients are known to be at increased risk for infections, especially respiratory infections, with diseases such as influenza, pneumococcal pneumonia, and PJP (pneumocystis jirovecii pneumonia) being big risks,” he said during his presentation.
The Smith et al. study was a retrospective cohort study using data from the global TriNetX research network. It included an IBD cohort of 206,475 patients and a control cohort of 4.2 million patients without IBD.
Researchers found higher rates of RSV diagnoses in IBD cohorts across age groups (P <.0001 for all groups), but also when comorbidities were present. Patients with IBD who were being treated with immunomodulators or anti-TNF therapy were at increased risk for infection, but not just any infection – serious infections, Dr. Smith said.
“This risk [in general] seems to exist across all age groups from our youngest to our elderly populations And, this risk increases for our patients with underlying comorbidities in our inflammatory bowel disease group,” he said.
Among patients 18 and younger, 0.36% of the IBD cohort were at increased risk of RSV infection, compared with 0.16% of the control group. Among those 18-49 years old, the risk was 0.26% of the IBD cohort and 0.15% of the control group. Among patients older than 65 years, the risk was 0.55% for patients with IBD, compared with 0.24% of the control group.
In terms of hospitalizations, 47.3% of the patients 18 years old and younger were hospitalized, compared with 39.7% of the control group. For those 65 years and older, 56.4% of the IBD cohort were hospitalized, compared with 47.3% of the control group. The mortality rate in the IBD cohort was 4.7%.
New RSV vaccines approved this year
RSV is relatively common in the United States and accounts for approximately 1.4 million outpatient visits each year, but health care officials are concerned that number will rise this year as the 2023-2024 RSV season gets underway. In September, the Centers for Disease Control and Prevention issued a statement saying there has already been an increase in RSV activity in the southeastern part of the United States.
In May, the Food and Drug Administration approved Arexvy (GSK) for the prevention of RSV-related lower respiratory tract disease for use in adults ages 60 years and older. Also approved in May was Abrysvo (Pfizer) for pregnant women to prevent RSV-related lower respiratory tract disease (LRTD) and severe LRTD in infants from birth through 6 months of age.
The Centers for Disease Control and Prevention recommends that adults 60 years or older receive a single dose of RSV vaccine “using shared clinical decision-making and prioritizing those at highest risk for severe disease.” It also recommendeds a new immunization starting this fall to help protect all infants under 8 months and babies between 8 and 19 months who are at increased risk of severe RSV disease.
Patients who are eligible for the RSV vaccination should get it, said Freddy Caldera, DO, a physician-scientist in gastroenterology and hepatology at the University of Wisconsin–Madison and lead author of the IBD study presented at ACG. The study is intended to help clinicians who treat patients with IBD address questions from patients about the recently introduced RSV vaccines.
At this point, Dr. Caldera said, there is not enough evidence to say all adults with IBD should get RSV vaccinations. More work needs to be done to address this question, such as a replication of the findings of the work presented at ACG, he said. And in many cases too, insurers may not cover the RSV vaccine. In regards to other patients, the data presented at ACG can be part of a larger conversation between clinicians and patients.
Fielding questions from patients
In an interview, Jessica Philpott, MD, PhD, a gastroenterologist at Cleveland Clinic, described the study findings as an important attempt to understand the risk for RSV among patients with IBD.
Dr. Philpott said she is already getting questions from her patients about RSV vaccinations. Many patients with IBD are immunocompromised and thus have been interested in following up after learning about the new RSV vaccinations, especially after seeing news reports about rising cases, she said. “Certainly, every week I receive messages about the RSV vaccine” from patients, she said.
Dr. Philpott also said it’s too early to make blanket recommendations about RSV vaccinations for adults with IBS, as it is going to take some time to understand how these products work for these patients, she said.
But people with IBD know they already may be at high risk and will factor that in as they weigh whether to seek RSV vaccination, especially given its low risk for side effects, Dr. Philpott said. Patients with IBD who would not have insurance coverage for the vaccine may consider taking it anyway, she said.
“We would advocate to get this covered by their insurance because we have this data that shows they’re at greater risks than the average population,” she said.
This study received no outside funding. Dr. Smith indicated no relevant financial relationships. Dr. Caldera has served as a consultant for GlaxoSmithKline. Francis Farraye has served on a GSK advisory committee.
A study presented this week in Vancouver at the ACG: American College of Gastroenterology annual meeting suggests that
RSV has historically been recognized in young and elderly populations and in patients who have received organ transplants. In fact, there is a body of literature that highlights the morbidity and mortality impact on immunocompromised organ transplant patients, but there is little research on the impact of RSV on patients with IBD.
For patients with inflammatory bowel disease (IBD), particularly those with comorbidities, an RSV infection can turn serious, said Ryan Smith, MD, a gastroenterology and hepatology fellow with the University of Wisconsin–Madison, who presented the study at the meeting.
“These patients are known to be at increased risk for infections, especially respiratory infections, with diseases such as influenza, pneumococcal pneumonia, and PJP (pneumocystis jirovecii pneumonia) being big risks,” he said during his presentation.
The Smith et al. study was a retrospective cohort study using data from the global TriNetX research network. It included an IBD cohort of 206,475 patients and a control cohort of 4.2 million patients without IBD.
Researchers found higher rates of RSV diagnoses in IBD cohorts across age groups (P <.0001 for all groups), but also when comorbidities were present. Patients with IBD who were being treated with immunomodulators or anti-TNF therapy were at increased risk for infection, but not just any infection – serious infections, Dr. Smith said.
“This risk [in general] seems to exist across all age groups from our youngest to our elderly populations And, this risk increases for our patients with underlying comorbidities in our inflammatory bowel disease group,” he said.
Among patients 18 and younger, 0.36% of the IBD cohort were at increased risk of RSV infection, compared with 0.16% of the control group. Among those 18-49 years old, the risk was 0.26% of the IBD cohort and 0.15% of the control group. Among patients older than 65 years, the risk was 0.55% for patients with IBD, compared with 0.24% of the control group.
In terms of hospitalizations, 47.3% of the patients 18 years old and younger were hospitalized, compared with 39.7% of the control group. For those 65 years and older, 56.4% of the IBD cohort were hospitalized, compared with 47.3% of the control group. The mortality rate in the IBD cohort was 4.7%.
New RSV vaccines approved this year
RSV is relatively common in the United States and accounts for approximately 1.4 million outpatient visits each year, but health care officials are concerned that number will rise this year as the 2023-2024 RSV season gets underway. In September, the Centers for Disease Control and Prevention issued a statement saying there has already been an increase in RSV activity in the southeastern part of the United States.
In May, the Food and Drug Administration approved Arexvy (GSK) for the prevention of RSV-related lower respiratory tract disease for use in adults ages 60 years and older. Also approved in May was Abrysvo (Pfizer) for pregnant women to prevent RSV-related lower respiratory tract disease (LRTD) and severe LRTD in infants from birth through 6 months of age.
The Centers for Disease Control and Prevention recommends that adults 60 years or older receive a single dose of RSV vaccine “using shared clinical decision-making and prioritizing those at highest risk for severe disease.” It also recommendeds a new immunization starting this fall to help protect all infants under 8 months and babies between 8 and 19 months who are at increased risk of severe RSV disease.
Patients who are eligible for the RSV vaccination should get it, said Freddy Caldera, DO, a physician-scientist in gastroenterology and hepatology at the University of Wisconsin–Madison and lead author of the IBD study presented at ACG. The study is intended to help clinicians who treat patients with IBD address questions from patients about the recently introduced RSV vaccines.
At this point, Dr. Caldera said, there is not enough evidence to say all adults with IBD should get RSV vaccinations. More work needs to be done to address this question, such as a replication of the findings of the work presented at ACG, he said. And in many cases too, insurers may not cover the RSV vaccine. In regards to other patients, the data presented at ACG can be part of a larger conversation between clinicians and patients.
Fielding questions from patients
In an interview, Jessica Philpott, MD, PhD, a gastroenterologist at Cleveland Clinic, described the study findings as an important attempt to understand the risk for RSV among patients with IBD.
Dr. Philpott said she is already getting questions from her patients about RSV vaccinations. Many patients with IBD are immunocompromised and thus have been interested in following up after learning about the new RSV vaccinations, especially after seeing news reports about rising cases, she said. “Certainly, every week I receive messages about the RSV vaccine” from patients, she said.
Dr. Philpott also said it’s too early to make blanket recommendations about RSV vaccinations for adults with IBS, as it is going to take some time to understand how these products work for these patients, she said.
But people with IBD know they already may be at high risk and will factor that in as they weigh whether to seek RSV vaccination, especially given its low risk for side effects, Dr. Philpott said. Patients with IBD who would not have insurance coverage for the vaccine may consider taking it anyway, she said.
“We would advocate to get this covered by their insurance because we have this data that shows they’re at greater risks than the average population,” she said.
This study received no outside funding. Dr. Smith indicated no relevant financial relationships. Dr. Caldera has served as a consultant for GlaxoSmithKline. Francis Farraye has served on a GSK advisory committee.
A study presented this week in Vancouver at the ACG: American College of Gastroenterology annual meeting suggests that
RSV has historically been recognized in young and elderly populations and in patients who have received organ transplants. In fact, there is a body of literature that highlights the morbidity and mortality impact on immunocompromised organ transplant patients, but there is little research on the impact of RSV on patients with IBD.
For patients with inflammatory bowel disease (IBD), particularly those with comorbidities, an RSV infection can turn serious, said Ryan Smith, MD, a gastroenterology and hepatology fellow with the University of Wisconsin–Madison, who presented the study at the meeting.
“These patients are known to be at increased risk for infections, especially respiratory infections, with diseases such as influenza, pneumococcal pneumonia, and PJP (pneumocystis jirovecii pneumonia) being big risks,” he said during his presentation.
The Smith et al. study was a retrospective cohort study using data from the global TriNetX research network. It included an IBD cohort of 206,475 patients and a control cohort of 4.2 million patients without IBD.
Researchers found higher rates of RSV diagnoses in IBD cohorts across age groups (P <.0001 for all groups), but also when comorbidities were present. Patients with IBD who were being treated with immunomodulators or anti-TNF therapy were at increased risk for infection, but not just any infection – serious infections, Dr. Smith said.
“This risk [in general] seems to exist across all age groups from our youngest to our elderly populations And, this risk increases for our patients with underlying comorbidities in our inflammatory bowel disease group,” he said.
Among patients 18 and younger, 0.36% of the IBD cohort were at increased risk of RSV infection, compared with 0.16% of the control group. Among those 18-49 years old, the risk was 0.26% of the IBD cohort and 0.15% of the control group. Among patients older than 65 years, the risk was 0.55% for patients with IBD, compared with 0.24% of the control group.
In terms of hospitalizations, 47.3% of the patients 18 years old and younger were hospitalized, compared with 39.7% of the control group. For those 65 years and older, 56.4% of the IBD cohort were hospitalized, compared with 47.3% of the control group. The mortality rate in the IBD cohort was 4.7%.
New RSV vaccines approved this year
RSV is relatively common in the United States and accounts for approximately 1.4 million outpatient visits each year, but health care officials are concerned that number will rise this year as the 2023-2024 RSV season gets underway. In September, the Centers for Disease Control and Prevention issued a statement saying there has already been an increase in RSV activity in the southeastern part of the United States.
In May, the Food and Drug Administration approved Arexvy (GSK) for the prevention of RSV-related lower respiratory tract disease for use in adults ages 60 years and older. Also approved in May was Abrysvo (Pfizer) for pregnant women to prevent RSV-related lower respiratory tract disease (LRTD) and severe LRTD in infants from birth through 6 months of age.
The Centers for Disease Control and Prevention recommends that adults 60 years or older receive a single dose of RSV vaccine “using shared clinical decision-making and prioritizing those at highest risk for severe disease.” It also recommendeds a new immunization starting this fall to help protect all infants under 8 months and babies between 8 and 19 months who are at increased risk of severe RSV disease.
Patients who are eligible for the RSV vaccination should get it, said Freddy Caldera, DO, a physician-scientist in gastroenterology and hepatology at the University of Wisconsin–Madison and lead author of the IBD study presented at ACG. The study is intended to help clinicians who treat patients with IBD address questions from patients about the recently introduced RSV vaccines.
At this point, Dr. Caldera said, there is not enough evidence to say all adults with IBD should get RSV vaccinations. More work needs to be done to address this question, such as a replication of the findings of the work presented at ACG, he said. And in many cases too, insurers may not cover the RSV vaccine. In regards to other patients, the data presented at ACG can be part of a larger conversation between clinicians and patients.
Fielding questions from patients
In an interview, Jessica Philpott, MD, PhD, a gastroenterologist at Cleveland Clinic, described the study findings as an important attempt to understand the risk for RSV among patients with IBD.
Dr. Philpott said she is already getting questions from her patients about RSV vaccinations. Many patients with IBD are immunocompromised and thus have been interested in following up after learning about the new RSV vaccinations, especially after seeing news reports about rising cases, she said. “Certainly, every week I receive messages about the RSV vaccine” from patients, she said.
Dr. Philpott also said it’s too early to make blanket recommendations about RSV vaccinations for adults with IBS, as it is going to take some time to understand how these products work for these patients, she said.
But people with IBD know they already may be at high risk and will factor that in as they weigh whether to seek RSV vaccination, especially given its low risk for side effects, Dr. Philpott said. Patients with IBD who would not have insurance coverage for the vaccine may consider taking it anyway, she said.
“We would advocate to get this covered by their insurance because we have this data that shows they’re at greater risks than the average population,” she said.
This study received no outside funding. Dr. Smith indicated no relevant financial relationships. Dr. Caldera has served as a consultant for GlaxoSmithKline. Francis Farraye has served on a GSK advisory committee.
FROM ACG 2023
New study ties ultra-processed foods to IBD
, suggesting another field for inquiry about the potential role of industrial-produced edible food products in IBD.
The study, which was a meta-analysis of four studies, found a 47% greater risk of IBD in adults who consumed high levels of ultra-processed foods, compared with adults in reference groups.
“Our data are also consistent with other observational studies that found increased consumption of junk food, along with reduced intakes of fresh fruit and vegetables, are associated with the development of IBD. Because Americans consume over 60% of their calories in the form of ultra-processed foods, reductions in this level of consumption could meaningfully decrease the incidence of IBD,” wrote authors who were led by Eric Hecht, MD, PhD, MPH, president and executive director of the nonprofit Institute of Etiological Research, Boca Raton, Fla.
The potential effect of poor diet on the gut is a critical public health question, he said. Diet may be just one possible contributor to inflammatory bowel disease. Other contributors include genetics and having a compromised immune system.
Dr. Hecht and colleagues began this study with a search on the PubMed database of published research on IBD that included details of diet. Of 10 relevant studies, 4 studies met the inclusion criteria for the analysis.
The four studies included 652,880 adults, 2,240 cases of IBD with a follow-up period ranging from 2.3 to 22.3 years. Statistically significant elevated risks for both Crohn’s disease and ulcerative colitis were documented in the studies. There was a relative risk of 1.47 (95% confidence interval, 1.29-1.66) for IBD; 1.94 (95% CI, 1.45-2.58) for Crohn’s disease, and 1.26 (95% CI, 1.10-1.45) for ulcerative colitis.
Findings from the 4 studies
Chen et al. reported, in the Journal of Crohn’s and Colitis, the results of a cross-sectional and prospective cohort study of 187,854 adults who were followed for an average of 10 years. They found that a higher intake of ultra-processed foods was associated with a higher incidence of Crohn’s disease but not ulcerative colitis. It also found that people who were already diagnosed with an IBD consumed more ultra-processed foods than did those without a diagnosis. The authors called for further studies to address the impact of UPF intake.
Vasseur et al. documented, in Inflammatory Bowel Diseases, research drawn from the NutriNet-Santé Study, a large French web-based prospective study. It did not find that ultra-processed foods were significantly associated with the risk of incident IBD. But the authors noted that certain types of food items or dietary patterns could partly explain the increase in the incidence of IBD observed in several countries, saying that further large-scale studies would be needed to support pathophysiological assumptions made about the dietary risk factors and IBD.
In September 2020 in Gastroenterology, Lo et al. used data from the Nurses’ Health Study (1984-2014), Nurses’ Health Study II (1991-2015), and Health Professionals Follow-up Study (1986-2012). The authors reported finding dietary patterns associated with high inflammatory potential to be associated with increased risk of Crohn’s disease but not ulcerative colitis.
In October 2021 in Gastroenterology, Narula et al. reported finding no significant association between certain dietary patterns and risk of ulcerative colitis. There was some signal for Crohn’s disease, in keeping with findings from earlier research. Longer term follow-up is needed to clarify whether the observed excess risk for Crohn’s disease becomes more evident as more cases accumulate.
However, in an email interview with GI & Hepatology News, Neeraj Narula, MD, MPH, of McMaster University, Hamilton, Ont., cited two of his other published works that did make a connection between diet and IBD. In July 2021 in BMJ, he and colleagues reported findings of a prospective cohort study that found that higher intake of ultra-processed food was positively associated with risk of IBD. Further studies are needed to identify the contributory factors within ultra-processed foods, they wrote. He and colleagues published a meta-analysis of 5 cohort studies which concluded that higher ultra-processed food and lower unprocessed/minimally processed food intakes were associated with higher risk of Crohn’s disease but not ulcerative colitis.
Study limitations
Aviva Musicus, ScD, the science director for the nonprofit Center for Science in the Public Interest (CSPI), said the Dr. Hecht et al. meta-analysis suggests there could be a signal in the association between higher ultra-processed food consumption and IBD, but there’s also a lot of “noise” in this presentation.
It’s not clear from these analyses presented what might be driving the relationship between IBD and ultra-processed food, she said. “Is it the nutrient content of these foods, given that many are high in added sugar, sodium, and saturated fat and low in dietary fiber (potential risk factors for IBD)? Is it the emulsifiers used in some of these foods, or other chemicals added during processing? Or, is it something else?” Dr. Musicus said.
She said further studies are needed on the issue of ultra-processed food and IBD.
“I wasn’t convinced by the conclusion of this research abstract. It’s not clear to me that general reductions in UPF (ultra-processed foods) consumption could meaningfully decrease the incidence of IBD, given that it may be a subset of these (somewhat heterogeneous) foods driving the associations, and people may not reduce their consumption of that specific subset upon hearing this news,” Dr. Musicus said.
“However, we already know that consumers can reduce chronic disease risk by eating more vegetables, fruits, whole grains, and legumes (good sources of dietary fiber) and limiting consumption of added sugars, sodium, and saturated fat,” she added.
Miguel Regueiro, MD, chair of the Digestive Disease and Surgery Institute at Cleveland Clinic, agreed with the need for further study. There are limitations with the methodology used in the research from Dr. Hecht and colleagues, he said.
“Meta-analyses aren’t perfect and I think we all acknowledge that,” he said, adding that the Hecht poster provides “a larger perspective on the topic.”
There’s widespread agreement that ultraprocessed foods are not healthy, raising heart and cancer risks, he said. In counseling his patients, Dr. Regueiro said he acknowledges the challenges many people face in trying to pursue a healthier diet. Ultraprocessed foods tend to be cheap and readily available, and many people need help in spotting them, such as learning to look at labels for unfamiliar terms.
“What I tell my own patients in the clinic is to really try to clean up the diet as much as possible and in a realistic way,” he said.
The authors of the ACG poster did not report any financial conflicts. Dr. Hecht said he founded the Institute for Etiological Research to pursue questions about public health. Its funders include the Bertarelli Foundation.
, suggesting another field for inquiry about the potential role of industrial-produced edible food products in IBD.
The study, which was a meta-analysis of four studies, found a 47% greater risk of IBD in adults who consumed high levels of ultra-processed foods, compared with adults in reference groups.
“Our data are also consistent with other observational studies that found increased consumption of junk food, along with reduced intakes of fresh fruit and vegetables, are associated with the development of IBD. Because Americans consume over 60% of their calories in the form of ultra-processed foods, reductions in this level of consumption could meaningfully decrease the incidence of IBD,” wrote authors who were led by Eric Hecht, MD, PhD, MPH, president and executive director of the nonprofit Institute of Etiological Research, Boca Raton, Fla.
The potential effect of poor diet on the gut is a critical public health question, he said. Diet may be just one possible contributor to inflammatory bowel disease. Other contributors include genetics and having a compromised immune system.
Dr. Hecht and colleagues began this study with a search on the PubMed database of published research on IBD that included details of diet. Of 10 relevant studies, 4 studies met the inclusion criteria for the analysis.
The four studies included 652,880 adults, 2,240 cases of IBD with a follow-up period ranging from 2.3 to 22.3 years. Statistically significant elevated risks for both Crohn’s disease and ulcerative colitis were documented in the studies. There was a relative risk of 1.47 (95% confidence interval, 1.29-1.66) for IBD; 1.94 (95% CI, 1.45-2.58) for Crohn’s disease, and 1.26 (95% CI, 1.10-1.45) for ulcerative colitis.
Findings from the 4 studies
Chen et al. reported, in the Journal of Crohn’s and Colitis, the results of a cross-sectional and prospective cohort study of 187,854 adults who were followed for an average of 10 years. They found that a higher intake of ultra-processed foods was associated with a higher incidence of Crohn’s disease but not ulcerative colitis. It also found that people who were already diagnosed with an IBD consumed more ultra-processed foods than did those without a diagnosis. The authors called for further studies to address the impact of UPF intake.
Vasseur et al. documented, in Inflammatory Bowel Diseases, research drawn from the NutriNet-Santé Study, a large French web-based prospective study. It did not find that ultra-processed foods were significantly associated with the risk of incident IBD. But the authors noted that certain types of food items or dietary patterns could partly explain the increase in the incidence of IBD observed in several countries, saying that further large-scale studies would be needed to support pathophysiological assumptions made about the dietary risk factors and IBD.
In September 2020 in Gastroenterology, Lo et al. used data from the Nurses’ Health Study (1984-2014), Nurses’ Health Study II (1991-2015), and Health Professionals Follow-up Study (1986-2012). The authors reported finding dietary patterns associated with high inflammatory potential to be associated with increased risk of Crohn’s disease but not ulcerative colitis.
In October 2021 in Gastroenterology, Narula et al. reported finding no significant association between certain dietary patterns and risk of ulcerative colitis. There was some signal for Crohn’s disease, in keeping with findings from earlier research. Longer term follow-up is needed to clarify whether the observed excess risk for Crohn’s disease becomes more evident as more cases accumulate.
However, in an email interview with GI & Hepatology News, Neeraj Narula, MD, MPH, of McMaster University, Hamilton, Ont., cited two of his other published works that did make a connection between diet and IBD. In July 2021 in BMJ, he and colleagues reported findings of a prospective cohort study that found that higher intake of ultra-processed food was positively associated with risk of IBD. Further studies are needed to identify the contributory factors within ultra-processed foods, they wrote. He and colleagues published a meta-analysis of 5 cohort studies which concluded that higher ultra-processed food and lower unprocessed/minimally processed food intakes were associated with higher risk of Crohn’s disease but not ulcerative colitis.
Study limitations
Aviva Musicus, ScD, the science director for the nonprofit Center for Science in the Public Interest (CSPI), said the Dr. Hecht et al. meta-analysis suggests there could be a signal in the association between higher ultra-processed food consumption and IBD, but there’s also a lot of “noise” in this presentation.
It’s not clear from these analyses presented what might be driving the relationship between IBD and ultra-processed food, she said. “Is it the nutrient content of these foods, given that many are high in added sugar, sodium, and saturated fat and low in dietary fiber (potential risk factors for IBD)? Is it the emulsifiers used in some of these foods, or other chemicals added during processing? Or, is it something else?” Dr. Musicus said.
She said further studies are needed on the issue of ultra-processed food and IBD.
“I wasn’t convinced by the conclusion of this research abstract. It’s not clear to me that general reductions in UPF (ultra-processed foods) consumption could meaningfully decrease the incidence of IBD, given that it may be a subset of these (somewhat heterogeneous) foods driving the associations, and people may not reduce their consumption of that specific subset upon hearing this news,” Dr. Musicus said.
“However, we already know that consumers can reduce chronic disease risk by eating more vegetables, fruits, whole grains, and legumes (good sources of dietary fiber) and limiting consumption of added sugars, sodium, and saturated fat,” she added.
Miguel Regueiro, MD, chair of the Digestive Disease and Surgery Institute at Cleveland Clinic, agreed with the need for further study. There are limitations with the methodology used in the research from Dr. Hecht and colleagues, he said.
“Meta-analyses aren’t perfect and I think we all acknowledge that,” he said, adding that the Hecht poster provides “a larger perspective on the topic.”
There’s widespread agreement that ultraprocessed foods are not healthy, raising heart and cancer risks, he said. In counseling his patients, Dr. Regueiro said he acknowledges the challenges many people face in trying to pursue a healthier diet. Ultraprocessed foods tend to be cheap and readily available, and many people need help in spotting them, such as learning to look at labels for unfamiliar terms.
“What I tell my own patients in the clinic is to really try to clean up the diet as much as possible and in a realistic way,” he said.
The authors of the ACG poster did not report any financial conflicts. Dr. Hecht said he founded the Institute for Etiological Research to pursue questions about public health. Its funders include the Bertarelli Foundation.
, suggesting another field for inquiry about the potential role of industrial-produced edible food products in IBD.
The study, which was a meta-analysis of four studies, found a 47% greater risk of IBD in adults who consumed high levels of ultra-processed foods, compared with adults in reference groups.
“Our data are also consistent with other observational studies that found increased consumption of junk food, along with reduced intakes of fresh fruit and vegetables, are associated with the development of IBD. Because Americans consume over 60% of their calories in the form of ultra-processed foods, reductions in this level of consumption could meaningfully decrease the incidence of IBD,” wrote authors who were led by Eric Hecht, MD, PhD, MPH, president and executive director of the nonprofit Institute of Etiological Research, Boca Raton, Fla.
The potential effect of poor diet on the gut is a critical public health question, he said. Diet may be just one possible contributor to inflammatory bowel disease. Other contributors include genetics and having a compromised immune system.
Dr. Hecht and colleagues began this study with a search on the PubMed database of published research on IBD that included details of diet. Of 10 relevant studies, 4 studies met the inclusion criteria for the analysis.
The four studies included 652,880 adults, 2,240 cases of IBD with a follow-up period ranging from 2.3 to 22.3 years. Statistically significant elevated risks for both Crohn’s disease and ulcerative colitis were documented in the studies. There was a relative risk of 1.47 (95% confidence interval, 1.29-1.66) for IBD; 1.94 (95% CI, 1.45-2.58) for Crohn’s disease, and 1.26 (95% CI, 1.10-1.45) for ulcerative colitis.
Findings from the 4 studies
Chen et al. reported, in the Journal of Crohn’s and Colitis, the results of a cross-sectional and prospective cohort study of 187,854 adults who were followed for an average of 10 years. They found that a higher intake of ultra-processed foods was associated with a higher incidence of Crohn’s disease but not ulcerative colitis. It also found that people who were already diagnosed with an IBD consumed more ultra-processed foods than did those without a diagnosis. The authors called for further studies to address the impact of UPF intake.
Vasseur et al. documented, in Inflammatory Bowel Diseases, research drawn from the NutriNet-Santé Study, a large French web-based prospective study. It did not find that ultra-processed foods were significantly associated with the risk of incident IBD. But the authors noted that certain types of food items or dietary patterns could partly explain the increase in the incidence of IBD observed in several countries, saying that further large-scale studies would be needed to support pathophysiological assumptions made about the dietary risk factors and IBD.
In September 2020 in Gastroenterology, Lo et al. used data from the Nurses’ Health Study (1984-2014), Nurses’ Health Study II (1991-2015), and Health Professionals Follow-up Study (1986-2012). The authors reported finding dietary patterns associated with high inflammatory potential to be associated with increased risk of Crohn’s disease but not ulcerative colitis.
In October 2021 in Gastroenterology, Narula et al. reported finding no significant association between certain dietary patterns and risk of ulcerative colitis. There was some signal for Crohn’s disease, in keeping with findings from earlier research. Longer term follow-up is needed to clarify whether the observed excess risk for Crohn’s disease becomes more evident as more cases accumulate.
However, in an email interview with GI & Hepatology News, Neeraj Narula, MD, MPH, of McMaster University, Hamilton, Ont., cited two of his other published works that did make a connection between diet and IBD. In July 2021 in BMJ, he and colleagues reported findings of a prospective cohort study that found that higher intake of ultra-processed food was positively associated with risk of IBD. Further studies are needed to identify the contributory factors within ultra-processed foods, they wrote. He and colleagues published a meta-analysis of 5 cohort studies which concluded that higher ultra-processed food and lower unprocessed/minimally processed food intakes were associated with higher risk of Crohn’s disease but not ulcerative colitis.
Study limitations
Aviva Musicus, ScD, the science director for the nonprofit Center for Science in the Public Interest (CSPI), said the Dr. Hecht et al. meta-analysis suggests there could be a signal in the association between higher ultra-processed food consumption and IBD, but there’s also a lot of “noise” in this presentation.
It’s not clear from these analyses presented what might be driving the relationship between IBD and ultra-processed food, she said. “Is it the nutrient content of these foods, given that many are high in added sugar, sodium, and saturated fat and low in dietary fiber (potential risk factors for IBD)? Is it the emulsifiers used in some of these foods, or other chemicals added during processing? Or, is it something else?” Dr. Musicus said.
She said further studies are needed on the issue of ultra-processed food and IBD.
“I wasn’t convinced by the conclusion of this research abstract. It’s not clear to me that general reductions in UPF (ultra-processed foods) consumption could meaningfully decrease the incidence of IBD, given that it may be a subset of these (somewhat heterogeneous) foods driving the associations, and people may not reduce their consumption of that specific subset upon hearing this news,” Dr. Musicus said.
“However, we already know that consumers can reduce chronic disease risk by eating more vegetables, fruits, whole grains, and legumes (good sources of dietary fiber) and limiting consumption of added sugars, sodium, and saturated fat,” she added.
Miguel Regueiro, MD, chair of the Digestive Disease and Surgery Institute at Cleveland Clinic, agreed with the need for further study. There are limitations with the methodology used in the research from Dr. Hecht and colleagues, he said.
“Meta-analyses aren’t perfect and I think we all acknowledge that,” he said, adding that the Hecht poster provides “a larger perspective on the topic.”
There’s widespread agreement that ultraprocessed foods are not healthy, raising heart and cancer risks, he said. In counseling his patients, Dr. Regueiro said he acknowledges the challenges many people face in trying to pursue a healthier diet. Ultraprocessed foods tend to be cheap and readily available, and many people need help in spotting them, such as learning to look at labels for unfamiliar terms.
“What I tell my own patients in the clinic is to really try to clean up the diet as much as possible and in a realistic way,” he said.
The authors of the ACG poster did not report any financial conflicts. Dr. Hecht said he founded the Institute for Etiological Research to pursue questions about public health. Its funders include the Bertarelli Foundation.
FROM ACG 2023
FDA approves subcutaneous infliximab for IBD
Infliximab-dyyb is a subcutaneous formulation of Celltrion’s infliximab. The FDA approval provides an alternative administration option for delivering the drug, which blocks the action of tumor necrosis factor alpha.
The new formulation was approved based on phase 3 pivotal trials that evaluated the safety and efficacy of infliximab-dyyb as maintenance therapy in patients with moderately to severely active UC (LIBERTY-UC) and CD (LIBERTY-CD).
In both 54-week trials, infliximab-dyyb demonstrated superiority to placebo in the primary endpoints of clinical remission (UC and CD) and endoscopic response (CD) when given as maintenance therapy after induction therapy with IV infliximab.
The overall safety profile of infliximab-dyyb was similar to that of the placebo during the maintenance period in both studies, with no new safety signals seen.
In the randomized, placebo-controlled, double-blind LIBERTY-UC study, 438 patients with moderately to severely active UC after induction therapy with IV infliximab were randomly assigned at week 10. The rate of clinical remission at week 54 was significantly greater with infliximab-dyyb (43.2%), compared with placebo (20.8%).
The most common adverse events were COVID-19, anemia, arthralgia, injection site reaction, increased alanine aminotransferase, and abdominal pain.
In the similarly designed LIBERTY-CD study, 343 patients with moderately to severely active CD after induction therapy were randomly assigned at week 10. At week 54, the clinical remission rate was greater with infliximab-dyyb (62.3%) than with placebo (32.1%).
In parallel, the endoscopic response rate at week 54 was also greater in the infliximab-dyyb arm than in the placebo arm (51.1% vs. 17.9%, respectively).
The safety profile during the maintenance phase was generally comparable between the two trial arms. The most common adverse events were COVID-19, upper respiratory tract infection, headache, injection site reaction, diarrhea, increased alanine aminotransferase, increased blood creatine phosphokinase, neutropenia, hypertension, urinary tract infection, dizziness, and leukopenia.
Full prescribing information is available online.
“As someone dedicated to improving the lives of patients with IBD, I am excited to see data supporting the efficacy and safety of a new formulation offering convenience and improved access to a well-known and proven drug,” Andres Yarur, MD, of Cedars-Sinai Medical Center, Los Angeles, said in a news release.
The data “validate a convenient treatment option that could allow more patients in the United States to have greater control of their disease management,” added Jean-Frederic Colombel, MD, of Icahn School of Medicine at Mount Sinai, New York.
A version of this article first appeared on Medscape.com.
Infliximab-dyyb is a subcutaneous formulation of Celltrion’s infliximab. The FDA approval provides an alternative administration option for delivering the drug, which blocks the action of tumor necrosis factor alpha.
The new formulation was approved based on phase 3 pivotal trials that evaluated the safety and efficacy of infliximab-dyyb as maintenance therapy in patients with moderately to severely active UC (LIBERTY-UC) and CD (LIBERTY-CD).
In both 54-week trials, infliximab-dyyb demonstrated superiority to placebo in the primary endpoints of clinical remission (UC and CD) and endoscopic response (CD) when given as maintenance therapy after induction therapy with IV infliximab.
The overall safety profile of infliximab-dyyb was similar to that of the placebo during the maintenance period in both studies, with no new safety signals seen.
In the randomized, placebo-controlled, double-blind LIBERTY-UC study, 438 patients with moderately to severely active UC after induction therapy with IV infliximab were randomly assigned at week 10. The rate of clinical remission at week 54 was significantly greater with infliximab-dyyb (43.2%), compared with placebo (20.8%).
The most common adverse events were COVID-19, anemia, arthralgia, injection site reaction, increased alanine aminotransferase, and abdominal pain.
In the similarly designed LIBERTY-CD study, 343 patients with moderately to severely active CD after induction therapy were randomly assigned at week 10. At week 54, the clinical remission rate was greater with infliximab-dyyb (62.3%) than with placebo (32.1%).
In parallel, the endoscopic response rate at week 54 was also greater in the infliximab-dyyb arm than in the placebo arm (51.1% vs. 17.9%, respectively).
The safety profile during the maintenance phase was generally comparable between the two trial arms. The most common adverse events were COVID-19, upper respiratory tract infection, headache, injection site reaction, diarrhea, increased alanine aminotransferase, increased blood creatine phosphokinase, neutropenia, hypertension, urinary tract infection, dizziness, and leukopenia.
Full prescribing information is available online.
“As someone dedicated to improving the lives of patients with IBD, I am excited to see data supporting the efficacy and safety of a new formulation offering convenience and improved access to a well-known and proven drug,” Andres Yarur, MD, of Cedars-Sinai Medical Center, Los Angeles, said in a news release.
The data “validate a convenient treatment option that could allow more patients in the United States to have greater control of their disease management,” added Jean-Frederic Colombel, MD, of Icahn School of Medicine at Mount Sinai, New York.
A version of this article first appeared on Medscape.com.
Infliximab-dyyb is a subcutaneous formulation of Celltrion’s infliximab. The FDA approval provides an alternative administration option for delivering the drug, which blocks the action of tumor necrosis factor alpha.
The new formulation was approved based on phase 3 pivotal trials that evaluated the safety and efficacy of infliximab-dyyb as maintenance therapy in patients with moderately to severely active UC (LIBERTY-UC) and CD (LIBERTY-CD).
In both 54-week trials, infliximab-dyyb demonstrated superiority to placebo in the primary endpoints of clinical remission (UC and CD) and endoscopic response (CD) when given as maintenance therapy after induction therapy with IV infliximab.
The overall safety profile of infliximab-dyyb was similar to that of the placebo during the maintenance period in both studies, with no new safety signals seen.
In the randomized, placebo-controlled, double-blind LIBERTY-UC study, 438 patients with moderately to severely active UC after induction therapy with IV infliximab were randomly assigned at week 10. The rate of clinical remission at week 54 was significantly greater with infliximab-dyyb (43.2%), compared with placebo (20.8%).
The most common adverse events were COVID-19, anemia, arthralgia, injection site reaction, increased alanine aminotransferase, and abdominal pain.
In the similarly designed LIBERTY-CD study, 343 patients with moderately to severely active CD after induction therapy were randomly assigned at week 10. At week 54, the clinical remission rate was greater with infliximab-dyyb (62.3%) than with placebo (32.1%).
In parallel, the endoscopic response rate at week 54 was also greater in the infliximab-dyyb arm than in the placebo arm (51.1% vs. 17.9%, respectively).
The safety profile during the maintenance phase was generally comparable between the two trial arms. The most common adverse events were COVID-19, upper respiratory tract infection, headache, injection site reaction, diarrhea, increased alanine aminotransferase, increased blood creatine phosphokinase, neutropenia, hypertension, urinary tract infection, dizziness, and leukopenia.
Full prescribing information is available online.
“As someone dedicated to improving the lives of patients with IBD, I am excited to see data supporting the efficacy and safety of a new formulation offering convenience and improved access to a well-known and proven drug,” Andres Yarur, MD, of Cedars-Sinai Medical Center, Los Angeles, said in a news release.
The data “validate a convenient treatment option that could allow more patients in the United States to have greater control of their disease management,” added Jean-Frederic Colombel, MD, of Icahn School of Medicine at Mount Sinai, New York.
A version of this article first appeared on Medscape.com.
Two-thirds with microscopic colitis respond to bile acid sequestrants
, based on a recent retrospective study from the Mayo Clinic.
The findings support use of BAS in patients with microscopic colitis who fail first-line therapy, or have intolerance to those agents, wrote researchers who were led by Darrell S. Pardi, MD, AGAF, a gastroenterologist with Mayo Clinic, Rochester, Minn. To date, the American Gastroenterological Association (AGA) has refrained from issuing any recommendations for BAS monotherapy in microscopic colitis (MC), the study authors wrote, citing a lack of relevant data.
The AGA recommends budesonide as first-line therapy for patients with moderate to severe symptoms of microscopic colitis. However, the treatment is associated with a high rate of relapse (40%-81%) once the patient stops taking the drug. Its long-term use is associated with a risk of side effects.
“At present, there are no randomized controlled trials that have evaluated the efficacy of BAS monotherapy for MC,” the investigators wrote in Clinical Gastroenterology and Hepatology. “Studies investigating the role of BAM [bile acid malabsorption] in MC are comprised of small cohorts and have shown inconsistent results. Patients without BAM may also respond to BAS therapy. Therefore, the role of BAM and treatment with BAS in MC merits further investigation.”
The study analyzed data from 282 patients (88.3% women) with microscopic colitis treated between 2010 to 2020. Bile acid malabsorption was defined by elevated serum 7⍺-hydroxy-4-cholesten-3-one or by fecal testing. After a median follow-up of 4.5 years, cholestyramine was the most prescribed BAS (64.9%), followed by colesevelam (21.6%) and colestipol (13.5%). Approximately half of the patients achieved a complete response (49.3%), while 16.3% had a partial response. Nonresponders accounted for 24.8% of the population, and 9.6% of patients did not tolerate BAS therapy. These outcomes were not significantly impacted by BAS dose or combination with other agents. Additional logistic regression analysis revealed no predictors of response.
After discontinuing BAS, 41.6% of patients had recurrence in a median of 21 weeks, ranging from 1 to 172 weeks.
“Consistent with prior studies evaluating the clinical course of MC and similar to the high rate of recurrence after discontinuation of budesonide, relapse was common after cessation of BAS therapy,” the investigators noted.
Still, the findings suggest that BAS is a valid second-line option with a favorable risk-benefit profile, and an elevated dose appears unnecessary to achieve clinical response.
“These results suggest that BAS may be considered as a treatment option in those that do not respond to first-line options or have intolerance to these agents,” the researchers wrote.
They suggested that BAS may be particularly useful as long-term maintenance therapy for patients wishing to avoid prolonged corticosteroid exposure.
“However, BAS have the potential to interfere with the administration and absorption of other medications, particularly in older populations with polypharmacy,” the researchers wrote. “Patients should thus be closely monitored for drug interactions, especially those taking concurrent medications. BAS should be administered separately from other medications to avoid the potential for drug interactions.”
Ideally, prospective studies will be conducted to confirm these findings, and to identify the subset of patients who are most likely to respond to BAS, the investigators concluded.
Dr. Pardi has grant funding from Pfizer, Vedanta, Seres, Finch, Applied Molecular Transport, and Takeda; and has consulted for Vedanta, Seres, Phantom Pharmaceuticals, Abbvie, Immunic, and Otsuka.
Despite being increasingly recognized and diagnosed, there remains a scantiness of studies addressing therapeutic options in microscopic colitis (MC). Oral budesonide is recommended as first-line option; however, there is a high relapse rate after budesonide discontinuation, some patients are intolerant, and there is concern for steroid toxicity associated with long-term exposure.
While the cause of MC remains elusive, there is a rationale to suggest that bile acids may play a role in disease pathogenesis. Not only are BA important signaling molecules, acting in inflammation and metabolism, but also prior small studies reported on BA malabsorption co-existing in MC, with variable response rates to BA sequestrants.
This retrospective large study of 282 patients with MC showed that almost two-thirds of patients will present a complete or partial response to BA sequestrant therapy (cholestyramine, colesevelam, and colestipol). For those that relapsed following BA therapy discontinuation, re-treatment was successful in the majority of cases.
Therapy was well tolerated, however caution is needed, as it can interfere with absorption of other medications, and in the long-term also with fat-soluble vitamins. It remains to be determined which patients could benefit the most from BA therapy, since no predictors of response were identified, nor was response associated with BA malabsorption. Nonetheless, this study shows that BA therapy could be an attractive option for steroid-dependent, steroid refractory or intolerant MC patients potentially worth trying before embarking on immunosuppressive or biological therapy. It also highlights the need for carefully conducted clinical trials exploring other options beyond budesonide for this chronic and debilitating condition.
Joana Torres, MD, PhD, is a consultant gastroenterologist at Hospital Beatriz Angelo and Hospital da Luz in Portugal and assistant professor in Uniersidade de Lisboa, Portugal. She has no conflicts.
Despite being increasingly recognized and diagnosed, there remains a scantiness of studies addressing therapeutic options in microscopic colitis (MC). Oral budesonide is recommended as first-line option; however, there is a high relapse rate after budesonide discontinuation, some patients are intolerant, and there is concern for steroid toxicity associated with long-term exposure.
While the cause of MC remains elusive, there is a rationale to suggest that bile acids may play a role in disease pathogenesis. Not only are BA important signaling molecules, acting in inflammation and metabolism, but also prior small studies reported on BA malabsorption co-existing in MC, with variable response rates to BA sequestrants.
This retrospective large study of 282 patients with MC showed that almost two-thirds of patients will present a complete or partial response to BA sequestrant therapy (cholestyramine, colesevelam, and colestipol). For those that relapsed following BA therapy discontinuation, re-treatment was successful in the majority of cases.
Therapy was well tolerated, however caution is needed, as it can interfere with absorption of other medications, and in the long-term also with fat-soluble vitamins. It remains to be determined which patients could benefit the most from BA therapy, since no predictors of response were identified, nor was response associated with BA malabsorption. Nonetheless, this study shows that BA therapy could be an attractive option for steroid-dependent, steroid refractory or intolerant MC patients potentially worth trying before embarking on immunosuppressive or biological therapy. It also highlights the need for carefully conducted clinical trials exploring other options beyond budesonide for this chronic and debilitating condition.
Joana Torres, MD, PhD, is a consultant gastroenterologist at Hospital Beatriz Angelo and Hospital da Luz in Portugal and assistant professor in Uniersidade de Lisboa, Portugal. She has no conflicts.
Despite being increasingly recognized and diagnosed, there remains a scantiness of studies addressing therapeutic options in microscopic colitis (MC). Oral budesonide is recommended as first-line option; however, there is a high relapse rate after budesonide discontinuation, some patients are intolerant, and there is concern for steroid toxicity associated with long-term exposure.
While the cause of MC remains elusive, there is a rationale to suggest that bile acids may play a role in disease pathogenesis. Not only are BA important signaling molecules, acting in inflammation and metabolism, but also prior small studies reported on BA malabsorption co-existing in MC, with variable response rates to BA sequestrants.
This retrospective large study of 282 patients with MC showed that almost two-thirds of patients will present a complete or partial response to BA sequestrant therapy (cholestyramine, colesevelam, and colestipol). For those that relapsed following BA therapy discontinuation, re-treatment was successful in the majority of cases.
Therapy was well tolerated, however caution is needed, as it can interfere with absorption of other medications, and in the long-term also with fat-soluble vitamins. It remains to be determined which patients could benefit the most from BA therapy, since no predictors of response were identified, nor was response associated with BA malabsorption. Nonetheless, this study shows that BA therapy could be an attractive option for steroid-dependent, steroid refractory or intolerant MC patients potentially worth trying before embarking on immunosuppressive or biological therapy. It also highlights the need for carefully conducted clinical trials exploring other options beyond budesonide for this chronic and debilitating condition.
Joana Torres, MD, PhD, is a consultant gastroenterologist at Hospital Beatriz Angelo and Hospital da Luz in Portugal and assistant professor in Uniersidade de Lisboa, Portugal. She has no conflicts.
, based on a recent retrospective study from the Mayo Clinic.
The findings support use of BAS in patients with microscopic colitis who fail first-line therapy, or have intolerance to those agents, wrote researchers who were led by Darrell S. Pardi, MD, AGAF, a gastroenterologist with Mayo Clinic, Rochester, Minn. To date, the American Gastroenterological Association (AGA) has refrained from issuing any recommendations for BAS monotherapy in microscopic colitis (MC), the study authors wrote, citing a lack of relevant data.
The AGA recommends budesonide as first-line therapy for patients with moderate to severe symptoms of microscopic colitis. However, the treatment is associated with a high rate of relapse (40%-81%) once the patient stops taking the drug. Its long-term use is associated with a risk of side effects.
“At present, there are no randomized controlled trials that have evaluated the efficacy of BAS monotherapy for MC,” the investigators wrote in Clinical Gastroenterology and Hepatology. “Studies investigating the role of BAM [bile acid malabsorption] in MC are comprised of small cohorts and have shown inconsistent results. Patients without BAM may also respond to BAS therapy. Therefore, the role of BAM and treatment with BAS in MC merits further investigation.”
The study analyzed data from 282 patients (88.3% women) with microscopic colitis treated between 2010 to 2020. Bile acid malabsorption was defined by elevated serum 7⍺-hydroxy-4-cholesten-3-one or by fecal testing. After a median follow-up of 4.5 years, cholestyramine was the most prescribed BAS (64.9%), followed by colesevelam (21.6%) and colestipol (13.5%). Approximately half of the patients achieved a complete response (49.3%), while 16.3% had a partial response. Nonresponders accounted for 24.8% of the population, and 9.6% of patients did not tolerate BAS therapy. These outcomes were not significantly impacted by BAS dose or combination with other agents. Additional logistic regression analysis revealed no predictors of response.
After discontinuing BAS, 41.6% of patients had recurrence in a median of 21 weeks, ranging from 1 to 172 weeks.
“Consistent with prior studies evaluating the clinical course of MC and similar to the high rate of recurrence after discontinuation of budesonide, relapse was common after cessation of BAS therapy,” the investigators noted.
Still, the findings suggest that BAS is a valid second-line option with a favorable risk-benefit profile, and an elevated dose appears unnecessary to achieve clinical response.
“These results suggest that BAS may be considered as a treatment option in those that do not respond to first-line options or have intolerance to these agents,” the researchers wrote.
They suggested that BAS may be particularly useful as long-term maintenance therapy for patients wishing to avoid prolonged corticosteroid exposure.
“However, BAS have the potential to interfere with the administration and absorption of other medications, particularly in older populations with polypharmacy,” the researchers wrote. “Patients should thus be closely monitored for drug interactions, especially those taking concurrent medications. BAS should be administered separately from other medications to avoid the potential for drug interactions.”
Ideally, prospective studies will be conducted to confirm these findings, and to identify the subset of patients who are most likely to respond to BAS, the investigators concluded.
Dr. Pardi has grant funding from Pfizer, Vedanta, Seres, Finch, Applied Molecular Transport, and Takeda; and has consulted for Vedanta, Seres, Phantom Pharmaceuticals, Abbvie, Immunic, and Otsuka.
, based on a recent retrospective study from the Mayo Clinic.
The findings support use of BAS in patients with microscopic colitis who fail first-line therapy, or have intolerance to those agents, wrote researchers who were led by Darrell S. Pardi, MD, AGAF, a gastroenterologist with Mayo Clinic, Rochester, Minn. To date, the American Gastroenterological Association (AGA) has refrained from issuing any recommendations for BAS monotherapy in microscopic colitis (MC), the study authors wrote, citing a lack of relevant data.
The AGA recommends budesonide as first-line therapy for patients with moderate to severe symptoms of microscopic colitis. However, the treatment is associated with a high rate of relapse (40%-81%) once the patient stops taking the drug. Its long-term use is associated with a risk of side effects.
“At present, there are no randomized controlled trials that have evaluated the efficacy of BAS monotherapy for MC,” the investigators wrote in Clinical Gastroenterology and Hepatology. “Studies investigating the role of BAM [bile acid malabsorption] in MC are comprised of small cohorts and have shown inconsistent results. Patients without BAM may also respond to BAS therapy. Therefore, the role of BAM and treatment with BAS in MC merits further investigation.”
The study analyzed data from 282 patients (88.3% women) with microscopic colitis treated between 2010 to 2020. Bile acid malabsorption was defined by elevated serum 7⍺-hydroxy-4-cholesten-3-one or by fecal testing. After a median follow-up of 4.5 years, cholestyramine was the most prescribed BAS (64.9%), followed by colesevelam (21.6%) and colestipol (13.5%). Approximately half of the patients achieved a complete response (49.3%), while 16.3% had a partial response. Nonresponders accounted for 24.8% of the population, and 9.6% of patients did not tolerate BAS therapy. These outcomes were not significantly impacted by BAS dose or combination with other agents. Additional logistic regression analysis revealed no predictors of response.
After discontinuing BAS, 41.6% of patients had recurrence in a median of 21 weeks, ranging from 1 to 172 weeks.
“Consistent with prior studies evaluating the clinical course of MC and similar to the high rate of recurrence after discontinuation of budesonide, relapse was common after cessation of BAS therapy,” the investigators noted.
Still, the findings suggest that BAS is a valid second-line option with a favorable risk-benefit profile, and an elevated dose appears unnecessary to achieve clinical response.
“These results suggest that BAS may be considered as a treatment option in those that do not respond to first-line options or have intolerance to these agents,” the researchers wrote.
They suggested that BAS may be particularly useful as long-term maintenance therapy for patients wishing to avoid prolonged corticosteroid exposure.
“However, BAS have the potential to interfere with the administration and absorption of other medications, particularly in older populations with polypharmacy,” the researchers wrote. “Patients should thus be closely monitored for drug interactions, especially those taking concurrent medications. BAS should be administered separately from other medications to avoid the potential for drug interactions.”
Ideally, prospective studies will be conducted to confirm these findings, and to identify the subset of patients who are most likely to respond to BAS, the investigators concluded.
Dr. Pardi has grant funding from Pfizer, Vedanta, Seres, Finch, Applied Molecular Transport, and Takeda; and has consulted for Vedanta, Seres, Phantom Pharmaceuticals, Abbvie, Immunic, and Otsuka.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Low-certainty evidence supports probiotics for IBS
or very low certainty, with many studies suffering from bias, according to a recent review and meta-analysis.
These shortcomings in the probiotic research landscape should be kept in mind when making treatment recommendations, reported researchers who were led by Alexander C. Ford, MBChB, of the Leeds Gastroenterology Institute, University of Leeds (England). They suggested these issues need to be addressed in the methodology of future clinical trials.
“Although multiple probiotics have been tested in IBS in randomized clinical trials, understanding of which probiotics may be beneficial is limited,” the investigators wrote in Gastroenterology.
They noted that previous efforts – including their own – to meta-analyze these findings have been hindered by a scarcity of trial data coupled with heterogeneity across probiotic strains, combinations, and doses, resulting in clinical uncertainty.
“Making recommendations concerning which probiotics, or combinations of probiotics, are beneficial according to IBS subtype or individual symptom has been difficult to date,” they wrote.
To narrow this knowledge gap, the researchers conducted an updated systematic review and meta-analysis with newly identified trials.
“There is continued interest in the role of probiotics in the management of IBS, as evidenced by the publication of more than 20 new randomized clinical trials since the prior version of this meta-analysis in 2018,” they wrote.
The new dataset included 82 RCTs comprising 10,332 patients with IBS. Along with safety, three separate efficacy endpoints were evaluated: global symptoms, abdominal pain, and abdominal bloating or distension.
For global symptoms, moderate-certainty evidence supported the efficacy of Escherichia coli strains; low-certainty data supported Lactobacillus plantarum 299V and other Lactobacillus strains; and very-low-certainty evidence supported Bacillus, LacClean Gold S, and Duolac 7s strains, and combination probiotics.
For abdominal pain, low-certainty evidence supported Bifidobacterium strains and Saccharomyces cerevisiae I-3856. Very-low-certainty data supported Lactobacillus, Saccharomyces, and Bacillus strains, and combination probiotics.
Very-low-certainty evidence supported the benefits of Bacillus strains and combination probiotics for alleviating abdominal bloating or distension.
In a safety analysis of 55 trials involving more than 7,000 patients, risk of adverse events was no higher for probiotics than placebo.
“Our analyses provide some support for the use of certain probiotics in IBS, and also for particular strains for specific symptoms,” the investigators wrote. “However, there is a paucity of data for their use in patients with IBS-C [IBS with constipation], with only seven RCTs reporting efficacy in this subtype, and no evidence of efficacy in any of these analyses. Their use in patients with IBS-C is, therefore, not supported by current evidence.”
A broader discussion in the publication called out the general lack of high certainty evidence in this area of clinical research.
“Only 24 of 82 eligible RCTs were low risk of bias across all domains, and there was significant heterogeneity between trials in many of our analyses, as well as evidence of publication bias, or other small study effects, in some of our analyses,” the researchers wrote. “The fact that few of the included studies were low risk of bias across all domains should be borne in mind when making treatment recommendations.”
The investigators disclosed relationships with Salix, Biocodex, 4D Pharma, and others.
IBS patients frequently inquire about probiotics. As a clinician, this can be difficult to address. A search of the literature yields numerous small trials. Turning to the guidelines does not help, as the AGA Clinical Practice Guidelines on Probiotics offer no recommendations for IBS because of the low quality of evidence. Nevertheless, we have patients who want to try probiotics. Some of these patients have had inadequate responses to first-line therapies and/or prefer a nonpharmacologic approach.

For example, the strain with the most trials was Lactobacillus plantarum 299V. The dose used (10 billion CFU once daily) is commercially available (Jarrow Formulas Ideal Bowel Support® LP299V®). Bacillus strains were also promising for global symptoms, abdominal pain and bloating. Two trials used the same strain and dose, Bacillus coagulans MTCC 5856, 2 billion CFU once daily, also commercially available (LactoSpore). Both can be purchased via major online retailers for $10-$13 for a 30-day supply. I am glad to have something to recommend however conditionally.
Elizabeth (Beth) Videlock, MD, PhD is assistant professor of medicine in the Vatche and Tamar Manoukian Division of Digestive Diseases at the University of California, Los Angeles, and a staff physician in gastroenterology in the Greater Los Angeles Veterans Affairs Healthcare System. She is co-lead of the neurodevelopmental and neurodegenerative diseases research program of the Goodman-Luskin Microbiome Center at UCLA. She has no relevant disclosures.
IBS patients frequently inquire about probiotics. As a clinician, this can be difficult to address. A search of the literature yields numerous small trials. Turning to the guidelines does not help, as the AGA Clinical Practice Guidelines on Probiotics offer no recommendations for IBS because of the low quality of evidence. Nevertheless, we have patients who want to try probiotics. Some of these patients have had inadequate responses to first-line therapies and/or prefer a nonpharmacologic approach.
For example, the strain with the most trials was Lactobacillus plantarum 299V. The dose used (10 billion CFU once daily) is commercially available (Jarrow Formulas Ideal Bowel Support® LP299V®). Bacillus strains were also promising for global symptoms, abdominal pain and bloating. Two trials used the same strain and dose, Bacillus coagulans MTCC 5856, 2 billion CFU once daily, also commercially available (LactoSpore). Both can be purchased via major online retailers for $10-$13 for a 30-day supply. I am glad to have something to recommend however conditionally.
Elizabeth (Beth) Videlock, MD, PhD is assistant professor of medicine in the Vatche and Tamar Manoukian Division of Digestive Diseases at the University of California, Los Angeles, and a staff physician in gastroenterology in the Greater Los Angeles Veterans Affairs Healthcare System. She is co-lead of the neurodevelopmental and neurodegenerative diseases research program of the Goodman-Luskin Microbiome Center at UCLA. She has no relevant disclosures.
IBS patients frequently inquire about probiotics. As a clinician, this can be difficult to address. A search of the literature yields numerous small trials. Turning to the guidelines does not help, as the AGA Clinical Practice Guidelines on Probiotics offer no recommendations for IBS because of the low quality of evidence. Nevertheless, we have patients who want to try probiotics. Some of these patients have had inadequate responses to first-line therapies and/or prefer a nonpharmacologic approach.
For example, the strain with the most trials was Lactobacillus plantarum 299V. The dose used (10 billion CFU once daily) is commercially available (Jarrow Formulas Ideal Bowel Support® LP299V®). Bacillus strains were also promising for global symptoms, abdominal pain and bloating. Two trials used the same strain and dose, Bacillus coagulans MTCC 5856, 2 billion CFU once daily, also commercially available (LactoSpore). Both can be purchased via major online retailers for $10-$13 for a 30-day supply. I am glad to have something to recommend however conditionally.
Elizabeth (Beth) Videlock, MD, PhD is assistant professor of medicine in the Vatche and Tamar Manoukian Division of Digestive Diseases at the University of California, Los Angeles, and a staff physician in gastroenterology in the Greater Los Angeles Veterans Affairs Healthcare System. She is co-lead of the neurodevelopmental and neurodegenerative diseases research program of the Goodman-Luskin Microbiome Center at UCLA. She has no relevant disclosures.
or very low certainty, with many studies suffering from bias, according to a recent review and meta-analysis.
These shortcomings in the probiotic research landscape should be kept in mind when making treatment recommendations, reported researchers who were led by Alexander C. Ford, MBChB, of the Leeds Gastroenterology Institute, University of Leeds (England). They suggested these issues need to be addressed in the methodology of future clinical trials.
“Although multiple probiotics have been tested in IBS in randomized clinical trials, understanding of which probiotics may be beneficial is limited,” the investigators wrote in Gastroenterology.
They noted that previous efforts – including their own – to meta-analyze these findings have been hindered by a scarcity of trial data coupled with heterogeneity across probiotic strains, combinations, and doses, resulting in clinical uncertainty.
“Making recommendations concerning which probiotics, or combinations of probiotics, are beneficial according to IBS subtype or individual symptom has been difficult to date,” they wrote.
To narrow this knowledge gap, the researchers conducted an updated systematic review and meta-analysis with newly identified trials.
“There is continued interest in the role of probiotics in the management of IBS, as evidenced by the publication of more than 20 new randomized clinical trials since the prior version of this meta-analysis in 2018,” they wrote.
The new dataset included 82 RCTs comprising 10,332 patients with IBS. Along with safety, three separate efficacy endpoints were evaluated: global symptoms, abdominal pain, and abdominal bloating or distension.
For global symptoms, moderate-certainty evidence supported the efficacy of Escherichia coli strains; low-certainty data supported Lactobacillus plantarum 299V and other Lactobacillus strains; and very-low-certainty evidence supported Bacillus, LacClean Gold S, and Duolac 7s strains, and combination probiotics.
For abdominal pain, low-certainty evidence supported Bifidobacterium strains and Saccharomyces cerevisiae I-3856. Very-low-certainty data supported Lactobacillus, Saccharomyces, and Bacillus strains, and combination probiotics.
Very-low-certainty evidence supported the benefits of Bacillus strains and combination probiotics for alleviating abdominal bloating or distension.
In a safety analysis of 55 trials involving more than 7,000 patients, risk of adverse events was no higher for probiotics than placebo.
“Our analyses provide some support for the use of certain probiotics in IBS, and also for particular strains for specific symptoms,” the investigators wrote. “However, there is a paucity of data for their use in patients with IBS-C [IBS with constipation], with only seven RCTs reporting efficacy in this subtype, and no evidence of efficacy in any of these analyses. Their use in patients with IBS-C is, therefore, not supported by current evidence.”
A broader discussion in the publication called out the general lack of high certainty evidence in this area of clinical research.
“Only 24 of 82 eligible RCTs were low risk of bias across all domains, and there was significant heterogeneity between trials in many of our analyses, as well as evidence of publication bias, or other small study effects, in some of our analyses,” the researchers wrote. “The fact that few of the included studies were low risk of bias across all domains should be borne in mind when making treatment recommendations.”
The investigators disclosed relationships with Salix, Biocodex, 4D Pharma, and others.
or very low certainty, with many studies suffering from bias, according to a recent review and meta-analysis.
These shortcomings in the probiotic research landscape should be kept in mind when making treatment recommendations, reported researchers who were led by Alexander C. Ford, MBChB, of the Leeds Gastroenterology Institute, University of Leeds (England). They suggested these issues need to be addressed in the methodology of future clinical trials.
“Although multiple probiotics have been tested in IBS in randomized clinical trials, understanding of which probiotics may be beneficial is limited,” the investigators wrote in Gastroenterology.
They noted that previous efforts – including their own – to meta-analyze these findings have been hindered by a scarcity of trial data coupled with heterogeneity across probiotic strains, combinations, and doses, resulting in clinical uncertainty.
“Making recommendations concerning which probiotics, or combinations of probiotics, are beneficial according to IBS subtype or individual symptom has been difficult to date,” they wrote.
To narrow this knowledge gap, the researchers conducted an updated systematic review and meta-analysis with newly identified trials.
“There is continued interest in the role of probiotics in the management of IBS, as evidenced by the publication of more than 20 new randomized clinical trials since the prior version of this meta-analysis in 2018,” they wrote.
The new dataset included 82 RCTs comprising 10,332 patients with IBS. Along with safety, three separate efficacy endpoints were evaluated: global symptoms, abdominal pain, and abdominal bloating or distension.
For global symptoms, moderate-certainty evidence supported the efficacy of Escherichia coli strains; low-certainty data supported Lactobacillus plantarum 299V and other Lactobacillus strains; and very-low-certainty evidence supported Bacillus, LacClean Gold S, and Duolac 7s strains, and combination probiotics.
For abdominal pain, low-certainty evidence supported Bifidobacterium strains and Saccharomyces cerevisiae I-3856. Very-low-certainty data supported Lactobacillus, Saccharomyces, and Bacillus strains, and combination probiotics.
Very-low-certainty evidence supported the benefits of Bacillus strains and combination probiotics for alleviating abdominal bloating or distension.
In a safety analysis of 55 trials involving more than 7,000 patients, risk of adverse events was no higher for probiotics than placebo.
“Our analyses provide some support for the use of certain probiotics in IBS, and also for particular strains for specific symptoms,” the investigators wrote. “However, there is a paucity of data for their use in patients with IBS-C [IBS with constipation], with only seven RCTs reporting efficacy in this subtype, and no evidence of efficacy in any of these analyses. Their use in patients with IBS-C is, therefore, not supported by current evidence.”
A broader discussion in the publication called out the general lack of high certainty evidence in this area of clinical research.
“Only 24 of 82 eligible RCTs were low risk of bias across all domains, and there was significant heterogeneity between trials in many of our analyses, as well as evidence of publication bias, or other small study effects, in some of our analyses,” the researchers wrote. “The fact that few of the included studies were low risk of bias across all domains should be borne in mind when making treatment recommendations.”
The investigators disclosed relationships with Salix, Biocodex, 4D Pharma, and others.
FROM GASTROENTEROLOGY
FDA OKs subcutaneous vedolizumab for UC maintenance therapy
The Food and Drug Administration has approved the subcutaneous administration of vedolizumab (Entyvio SC, Takeda) for maintenance therapy in adults with moderately to severely active ulcerative colitis (UC) following induction therapy with intravenous administration of vedolizumab.
The FDA approved the intravenous formulation of the biologic in 2014 for patients with moderate to severe UC and Crohn’s disease who failed or cannot tolerate other therapies.
The approval of subcutaneous (SC) vedolizumab was based on results from the phase 3, randomized, double-blind, placebo-controlled VISIBLE 1 trial.
The trial assessed the safety and efficacy of maintenance therapy with SC vedolizumab in adult patients with moderately to severely active UC who achieved clinical response at week 6 following two doses of intravenous vedolizumab.
At week 6, 162 patients were randomly allocated (2:1) to vedolizumab or placebo by subcutaneous injection every 2 weeks. The primary endpoint was clinical remission at week 52, defined as a total Mayo score of 2 or less and no individual subscore greater than 1.
At week 52, nearly half (46%) of patients who received vedolizumab SC maintenance therapy achieved clinical remission, compared with 14% of those who received placebo SC (P < .001).
The safety profile of SC vedolizumab was “generally consistent” with that of intravenous vedolizumab, with the addition of injection-site reactions, the drugmaker, Takeda, said in a news release.
The most common adverse reactions with intravenous vedolizumab are nasopharyngitis, headache, arthralgia, nausea, pyrexia (fever), upper respiratory tract infection, fatigue, cough, bronchitis, influenza, back pain, rash, pruritus, sinusitis, oropharyngeal pain, and pain in the extremities.
SC vedolizumab “can provide physicians with an additional administration option for achieving remission in their moderate to severe ulcerative colitis patients,” according to Bruce E. Sands, MD, AGAF, chief of gastroenterology at the Icahn School of Medicine at Mount Sinai, New York. He provided a statement in the Takeda news release.
“I appreciate now having a subcutaneous administration option that provides a clinical profile consistent with Entyvio intravenous while also giving me and my appropriate UC patients a choice of how they receive their maintenance therapy,” Dr. Sands said.
The FDA is currently reviewing Takeda’s biologics license application for subcutaneous administration of vedolizumab in the treatment of adults with moderately to severely active Crohn’s disease.
Dr. Sands is a paid consultant of Takeda.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved the subcutaneous administration of vedolizumab (Entyvio SC, Takeda) for maintenance therapy in adults with moderately to severely active ulcerative colitis (UC) following induction therapy with intravenous administration of vedolizumab.
The FDA approved the intravenous formulation of the biologic in 2014 for patients with moderate to severe UC and Crohn’s disease who failed or cannot tolerate other therapies.
The approval of subcutaneous (SC) vedolizumab was based on results from the phase 3, randomized, double-blind, placebo-controlled VISIBLE 1 trial.
The trial assessed the safety and efficacy of maintenance therapy with SC vedolizumab in adult patients with moderately to severely active UC who achieved clinical response at week 6 following two doses of intravenous vedolizumab.
At week 6, 162 patients were randomly allocated (2:1) to vedolizumab or placebo by subcutaneous injection every 2 weeks. The primary endpoint was clinical remission at week 52, defined as a total Mayo score of 2 or less and no individual subscore greater than 1.
At week 52, nearly half (46%) of patients who received vedolizumab SC maintenance therapy achieved clinical remission, compared with 14% of those who received placebo SC (P < .001).
The safety profile of SC vedolizumab was “generally consistent” with that of intravenous vedolizumab, with the addition of injection-site reactions, the drugmaker, Takeda, said in a news release.
The most common adverse reactions with intravenous vedolizumab are nasopharyngitis, headache, arthralgia, nausea, pyrexia (fever), upper respiratory tract infection, fatigue, cough, bronchitis, influenza, back pain, rash, pruritus, sinusitis, oropharyngeal pain, and pain in the extremities.
SC vedolizumab “can provide physicians with an additional administration option for achieving remission in their moderate to severe ulcerative colitis patients,” according to Bruce E. Sands, MD, AGAF, chief of gastroenterology at the Icahn School of Medicine at Mount Sinai, New York. He provided a statement in the Takeda news release.
“I appreciate now having a subcutaneous administration option that provides a clinical profile consistent with Entyvio intravenous while also giving me and my appropriate UC patients a choice of how they receive their maintenance therapy,” Dr. Sands said.
The FDA is currently reviewing Takeda’s biologics license application for subcutaneous administration of vedolizumab in the treatment of adults with moderately to severely active Crohn’s disease.
Dr. Sands is a paid consultant of Takeda.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved the subcutaneous administration of vedolizumab (Entyvio SC, Takeda) for maintenance therapy in adults with moderately to severely active ulcerative colitis (UC) following induction therapy with intravenous administration of vedolizumab.
The FDA approved the intravenous formulation of the biologic in 2014 for patients with moderate to severe UC and Crohn’s disease who failed or cannot tolerate other therapies.
The approval of subcutaneous (SC) vedolizumab was based on results from the phase 3, randomized, double-blind, placebo-controlled VISIBLE 1 trial.
The trial assessed the safety and efficacy of maintenance therapy with SC vedolizumab in adult patients with moderately to severely active UC who achieved clinical response at week 6 following two doses of intravenous vedolizumab.
At week 6, 162 patients were randomly allocated (2:1) to vedolizumab or placebo by subcutaneous injection every 2 weeks. The primary endpoint was clinical remission at week 52, defined as a total Mayo score of 2 or less and no individual subscore greater than 1.
At week 52, nearly half (46%) of patients who received vedolizumab SC maintenance therapy achieved clinical remission, compared with 14% of those who received placebo SC (P < .001).
The safety profile of SC vedolizumab was “generally consistent” with that of intravenous vedolizumab, with the addition of injection-site reactions, the drugmaker, Takeda, said in a news release.
The most common adverse reactions with intravenous vedolizumab are nasopharyngitis, headache, arthralgia, nausea, pyrexia (fever), upper respiratory tract infection, fatigue, cough, bronchitis, influenza, back pain, rash, pruritus, sinusitis, oropharyngeal pain, and pain in the extremities.
SC vedolizumab “can provide physicians with an additional administration option for achieving remission in their moderate to severe ulcerative colitis patients,” according to Bruce E. Sands, MD, AGAF, chief of gastroenterology at the Icahn School of Medicine at Mount Sinai, New York. He provided a statement in the Takeda news release.
“I appreciate now having a subcutaneous administration option that provides a clinical profile consistent with Entyvio intravenous while also giving me and my appropriate UC patients a choice of how they receive their maintenance therapy,” Dr. Sands said.
The FDA is currently reviewing Takeda’s biologics license application for subcutaneous administration of vedolizumab in the treatment of adults with moderately to severely active Crohn’s disease.
Dr. Sands is a paid consultant of Takeda.
A version of this article first appeared on Medscape.com.
ChatGPT may aid decision-making in the ED for acute ulcerative colitis
(UC).
In a small study, ChatGPT version 4 (GPT-4) accurately gauged disease severity and made decisions about the need for hospitalization that were largely in line with expert gastroenterologists.
“Our findings suggest that GPT-4 has potential as a clinical decision-support tool in assessing UC severity and recommending suitable settings for further treatment,” say the authors, led by Asaf Levartovsky, MD, department of gastroenterology, Sheba Medical Center, Tel Aviv University.
The study was published online in the American Journal of Gastroenterology.
Assessing its potential
UC is a chronic inflammatory bowel disease known for episodes of flare-ups and remissions. Flare-ups often result in a trip to the ED, where staff must rapidly assess disease severity and need for hospital admission.
Dr. Levartovsky and colleagues explored how helpful GPT-4 could be in 20 distinct presentations of acute UC in the ED. They assessed the chatbot’s ability to determine the severity of disease and whether a specific presentation warranted hospital admission for further treatment.
They fed GPT-4 case summaries that included crucial data such as symptoms, vital signs, and laboratory results. For each case, they asked the chatbot to assess disease severity based on established criteria and recommend hospital admission or outpatient care.
The GPT-4 answers were compared with assessments made by gastroenterologists and the actual decision regarding hospitalization made by the physician in the ED.
Overall, ChatGPT categorized acute UC as severe in 12 patients, as moderate in 7, and as mild in 1. In each case, the chatbot provided a detailed answer depicting severity of every variable of the criteria and an overall severity classification.
ChatGPT’s assessments were consistent with gastroenterologists’ assessments 80% of the time, with a “high degree of reliability” between the two assessments, the study team reports.
The average correlation between ChatGPT and physician ratings was 0.839 (P < .001). Inconsistencies in four cases stemmed largely from inaccurate cut-off values for systemic variables (such as hemoglobin and tachycardia).
Following severity assessment, ChatGPT leaned toward hospital admission for 16 patients, whereas in actual clinical practice, only 12 patients were hospitalized. In one patient with moderate UC who was discharged, ChatGPT was in favor of hospitalization, based on the patient’s age and comorbid conditions. For two moderate UC cases, the chatbot recommended consultation with a health care professional for further evaluation and management, which the researchers deemed to be an indecisive response.
Based on their findings, the researchers say ChatGPT could serve as a real-time decision support tool – one that is not meant to replace physicians but rather enhance human decision-making.
They note that the small sample size is a limitation and that ChatGPT’s accuracy rate requires further validation across larger samples and diverse clinical scenarios.
The study had no specific funding. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
(UC).
In a small study, ChatGPT version 4 (GPT-4) accurately gauged disease severity and made decisions about the need for hospitalization that were largely in line with expert gastroenterologists.
“Our findings suggest that GPT-4 has potential as a clinical decision-support tool in assessing UC severity and recommending suitable settings for further treatment,” say the authors, led by Asaf Levartovsky, MD, department of gastroenterology, Sheba Medical Center, Tel Aviv University.
The study was published online in the American Journal of Gastroenterology.
Assessing its potential
UC is a chronic inflammatory bowel disease known for episodes of flare-ups and remissions. Flare-ups often result in a trip to the ED, where staff must rapidly assess disease severity and need for hospital admission.
Dr. Levartovsky and colleagues explored how helpful GPT-4 could be in 20 distinct presentations of acute UC in the ED. They assessed the chatbot’s ability to determine the severity of disease and whether a specific presentation warranted hospital admission for further treatment.
They fed GPT-4 case summaries that included crucial data such as symptoms, vital signs, and laboratory results. For each case, they asked the chatbot to assess disease severity based on established criteria and recommend hospital admission or outpatient care.
The GPT-4 answers were compared with assessments made by gastroenterologists and the actual decision regarding hospitalization made by the physician in the ED.
Overall, ChatGPT categorized acute UC as severe in 12 patients, as moderate in 7, and as mild in 1. In each case, the chatbot provided a detailed answer depicting severity of every variable of the criteria and an overall severity classification.
ChatGPT’s assessments were consistent with gastroenterologists’ assessments 80% of the time, with a “high degree of reliability” between the two assessments, the study team reports.
The average correlation between ChatGPT and physician ratings was 0.839 (P < .001). Inconsistencies in four cases stemmed largely from inaccurate cut-off values for systemic variables (such as hemoglobin and tachycardia).
Following severity assessment, ChatGPT leaned toward hospital admission for 16 patients, whereas in actual clinical practice, only 12 patients were hospitalized. In one patient with moderate UC who was discharged, ChatGPT was in favor of hospitalization, based on the patient’s age and comorbid conditions. For two moderate UC cases, the chatbot recommended consultation with a health care professional for further evaluation and management, which the researchers deemed to be an indecisive response.
Based on their findings, the researchers say ChatGPT could serve as a real-time decision support tool – one that is not meant to replace physicians but rather enhance human decision-making.
They note that the small sample size is a limitation and that ChatGPT’s accuracy rate requires further validation across larger samples and diverse clinical scenarios.
The study had no specific funding. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
(UC).
In a small study, ChatGPT version 4 (GPT-4) accurately gauged disease severity and made decisions about the need for hospitalization that were largely in line with expert gastroenterologists.
“Our findings suggest that GPT-4 has potential as a clinical decision-support tool in assessing UC severity and recommending suitable settings for further treatment,” say the authors, led by Asaf Levartovsky, MD, department of gastroenterology, Sheba Medical Center, Tel Aviv University.
The study was published online in the American Journal of Gastroenterology.
Assessing its potential
UC is a chronic inflammatory bowel disease known for episodes of flare-ups and remissions. Flare-ups often result in a trip to the ED, where staff must rapidly assess disease severity and need for hospital admission.
Dr. Levartovsky and colleagues explored how helpful GPT-4 could be in 20 distinct presentations of acute UC in the ED. They assessed the chatbot’s ability to determine the severity of disease and whether a specific presentation warranted hospital admission for further treatment.
They fed GPT-4 case summaries that included crucial data such as symptoms, vital signs, and laboratory results. For each case, they asked the chatbot to assess disease severity based on established criteria and recommend hospital admission or outpatient care.
The GPT-4 answers were compared with assessments made by gastroenterologists and the actual decision regarding hospitalization made by the physician in the ED.
Overall, ChatGPT categorized acute UC as severe in 12 patients, as moderate in 7, and as mild in 1. In each case, the chatbot provided a detailed answer depicting severity of every variable of the criteria and an overall severity classification.
ChatGPT’s assessments were consistent with gastroenterologists’ assessments 80% of the time, with a “high degree of reliability” between the two assessments, the study team reports.
The average correlation between ChatGPT and physician ratings was 0.839 (P < .001). Inconsistencies in four cases stemmed largely from inaccurate cut-off values for systemic variables (such as hemoglobin and tachycardia).
Following severity assessment, ChatGPT leaned toward hospital admission for 16 patients, whereas in actual clinical practice, only 12 patients were hospitalized. In one patient with moderate UC who was discharged, ChatGPT was in favor of hospitalization, based on the patient’s age and comorbid conditions. For two moderate UC cases, the chatbot recommended consultation with a health care professional for further evaluation and management, which the researchers deemed to be an indecisive response.
Based on their findings, the researchers say ChatGPT could serve as a real-time decision support tool – one that is not meant to replace physicians but rather enhance human decision-making.
They note that the small sample size is a limitation and that ChatGPT’s accuracy rate requires further validation across larger samples and diverse clinical scenarios.
The study had no specific funding. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE AMERICAN JOURNAL OF GASTROENTEROLOGY