User login
Heart transplantation: Preop LVAD erases adverse impact of pulmonary hypertension
COLORADO SPRINGS – Reconsideration of the role of pulmonary hypertension in heart transplant outcomes is appropriate in the emerging era of the use of left ventricular assist devices (LVADs) as bridge to transplant, according to Ann C. Gaffey, MD, of the University of Pennsylvania, Philadelphia.
“Pulmonary hypertension secondary to congestive heart failure more than likely can be reversed to the values acceptable for heart transplant by the use of an LVAD. For bridge-to-transplant patients, pretransplant pulmonary hypertension does not affect recipient outcomes post transplantation,” she said at the annual meeting of the Western Thoracic Surgical Association.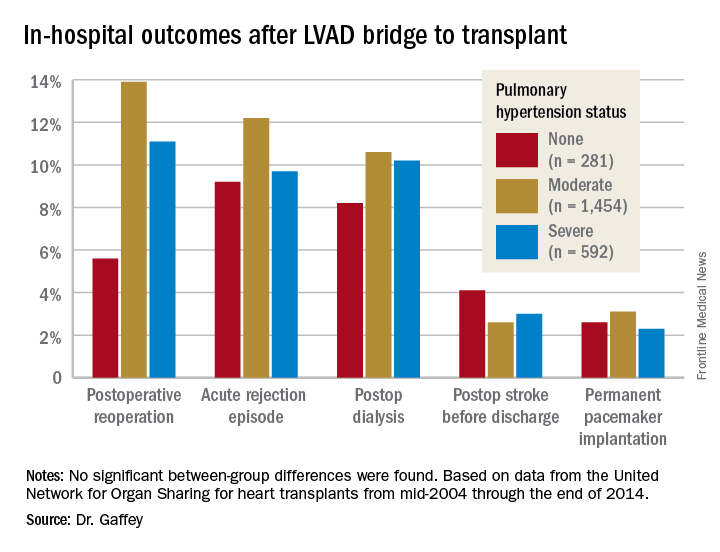
Vasodilators are prescribed in an effort to reduce PH; however, 40% of patients with PH are unresponsive to the medications and have therefore been excluded from consideration as potential candidates for a donor heart.
But the growing use of LVADs as a bridge to transplant has changed all that, Dr. Gaffey said. As supporting evidence, she presented a retrospective analysis of the United Network for Organ Sharing database on adult heart transplants from mid-2004 through the end of 2014.
The review turned up 3,951 heart transplant recipients who had been bridged to transplant with an LVAD. Dr. Gaffey and her coinvestigators divided them into three groups: 281 patients without pretransplant PH; 1,454 with moderate PH as defined by 1-3 Wood units; and 592 with severe PH and more than 3 Wood units.
The three groups didn’t differ in terms of age, sex, wait-list time, or the prevalence of diabetes or renal, liver, or cerebrovascular disease. Nor did their donors differ in age, sex, left ventricular function, or allograft ischemic time.
Key in-hospital outcomes were similar between the groups with no, mild, and severe PH.
Moreover, there was no between-group difference in the rate of rejection at 1 year. Five-year survival rates were closely similar in the three groups, in the mid-70s.
Audience member Nahush A. Mokadam, MD, rose to praise Dr. Gaffey’s report.
“This is a great and important study. I think as a group we have been too conservative with pulmonary hypertension, so thank you for shining a good light on it,” said Dr. Mokadam of the University of Washington, Seattle.
Dr. Gaffey reported having no financial conflicts regarding the study, which was conducted free of commercial support.
COLORADO SPRINGS – Reconsideration of the role of pulmonary hypertension in heart transplant outcomes is appropriate in the emerging era of the use of left ventricular assist devices (LVADs) as bridge to transplant, according to Ann C. Gaffey, MD, of the University of Pennsylvania, Philadelphia.
“Pulmonary hypertension secondary to congestive heart failure more than likely can be reversed to the values acceptable for heart transplant by the use of an LVAD. For bridge-to-transplant patients, pretransplant pulmonary hypertension does not affect recipient outcomes post transplantation,” she said at the annual meeting of the Western Thoracic Surgical Association.
Vasodilators are prescribed in an effort to reduce PH; however, 40% of patients with PH are unresponsive to the medications and have therefore been excluded from consideration as potential candidates for a donor heart.
But the growing use of LVADs as a bridge to transplant has changed all that, Dr. Gaffey said. As supporting evidence, she presented a retrospective analysis of the United Network for Organ Sharing database on adult heart transplants from mid-2004 through the end of 2014.
The review turned up 3,951 heart transplant recipients who had been bridged to transplant with an LVAD. Dr. Gaffey and her coinvestigators divided them into three groups: 281 patients without pretransplant PH; 1,454 with moderate PH as defined by 1-3 Wood units; and 592 with severe PH and more than 3 Wood units.
The three groups didn’t differ in terms of age, sex, wait-list time, or the prevalence of diabetes or renal, liver, or cerebrovascular disease. Nor did their donors differ in age, sex, left ventricular function, or allograft ischemic time.
Key in-hospital outcomes were similar between the groups with no, mild, and severe PH.
Moreover, there was no between-group difference in the rate of rejection at 1 year. Five-year survival rates were closely similar in the three groups, in the mid-70s.
Audience member Nahush A. Mokadam, MD, rose to praise Dr. Gaffey’s report.
“This is a great and important study. I think as a group we have been too conservative with pulmonary hypertension, so thank you for shining a good light on it,” said Dr. Mokadam of the University of Washington, Seattle.
Dr. Gaffey reported having no financial conflicts regarding the study, which was conducted free of commercial support.
COLORADO SPRINGS – Reconsideration of the role of pulmonary hypertension in heart transplant outcomes is appropriate in the emerging era of the use of left ventricular assist devices (LVADs) as bridge to transplant, according to Ann C. Gaffey, MD, of the University of Pennsylvania, Philadelphia.
“Pulmonary hypertension secondary to congestive heart failure more than likely can be reversed to the values acceptable for heart transplant by the use of an LVAD. For bridge-to-transplant patients, pretransplant pulmonary hypertension does not affect recipient outcomes post transplantation,” she said at the annual meeting of the Western Thoracic Surgical Association.
Vasodilators are prescribed in an effort to reduce PH; however, 40% of patients with PH are unresponsive to the medications and have therefore been excluded from consideration as potential candidates for a donor heart.
But the growing use of LVADs as a bridge to transplant has changed all that, Dr. Gaffey said. As supporting evidence, she presented a retrospective analysis of the United Network for Organ Sharing database on adult heart transplants from mid-2004 through the end of 2014.
The review turned up 3,951 heart transplant recipients who had been bridged to transplant with an LVAD. Dr. Gaffey and her coinvestigators divided them into three groups: 281 patients without pretransplant PH; 1,454 with moderate PH as defined by 1-3 Wood units; and 592 with severe PH and more than 3 Wood units.
The three groups didn’t differ in terms of age, sex, wait-list time, or the prevalence of diabetes or renal, liver, or cerebrovascular disease. Nor did their donors differ in age, sex, left ventricular function, or allograft ischemic time.
Key in-hospital outcomes were similar between the groups with no, mild, and severe PH.
Moreover, there was no between-group difference in the rate of rejection at 1 year. Five-year survival rates were closely similar in the three groups, in the mid-70s.
Audience member Nahush A. Mokadam, MD, rose to praise Dr. Gaffey’s report.
“This is a great and important study. I think as a group we have been too conservative with pulmonary hypertension, so thank you for shining a good light on it,” said Dr. Mokadam of the University of Washington, Seattle.
Dr. Gaffey reported having no financial conflicts regarding the study, which was conducted free of commercial support.
AT THE WTSA ANNUAL MEETING
Key clinical point:
Major finding: It’s time to reconsider the practice of excluding patients with pulmonary hypertension from consideration for a donor heart.
Data source: A retrospective analysis of the United Network for Organ Sharing database including outcomes out to 5 years on 3,951 heart transplant recipients who had been bridged to transplant with an LVAD, most of whom had moderate or severe pulmonary hypertension before transplant.
Disclosures: This study was conducted free of commercial support. The presenter reported having no relevant financial conflicts of interest.
VIDEO: U.S. hypertension guidelines reset threshold to 130/80 mm Hg
ANAHEIM, CALIF. – Thirty million Americans became hypertensive overnight on Nov. 13 with the introduction of new high blood pressure guidelines from the American College of Cardiology and American Heart Association.
That happened by resetting the definition of adult hypertension from the long-standing threshold of 140/90 mm Hg to a blood pressure at or above 130/80 mm Hg, a change that jumps the U.S. adult prevalence of hypertension from roughly 32% to 46%. Nearly half of all U.S. adults now have hypertension, bringing the total national hypertensive population to a staggering 103 million.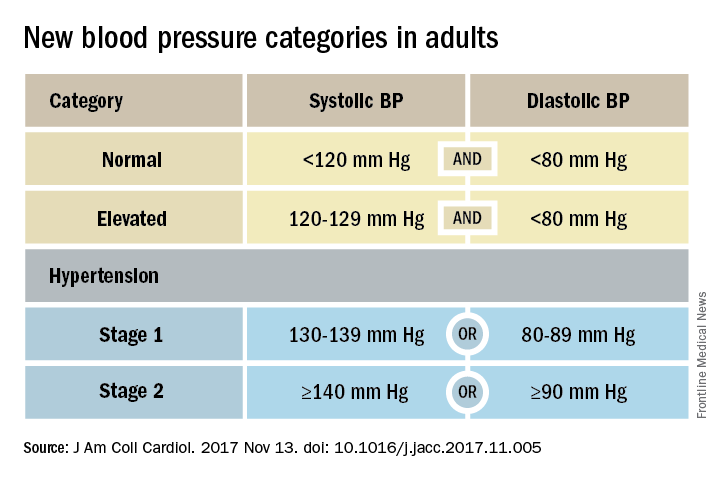
Goal is to transform care
But the new guidelines (J Am Coll Cardiol. 2017 Nov 13. doi: 10.1016/j.jacc.2017.11.005) for preventing, detecting, evaluating, and managing adult hypertension do lots more than just shake up the epidemiology of high blood pressure. With 106 total recommendations, the guidelines seek to transform every aspect of blood pressure in American medical practice, starting with how it’s measured and stretching to redefine applications of medical systems to try to ensure that every person with a blood pressure that truly falls outside the redefined limits gets a comprehensive package of interventions.
Many of these are “seismic changes,” said Lawrence J. Appel, MD. He particularly cited as seismic the new classification of stage 1 hypertension as a pressure at or above 130/80 mm Hg, the emphasis on using some form of out-of-office blood pressure measurement to confirm a diagnosis, the use of risk assessment when deciding whether to treat certain patients with drugs, and the same blood pressure goal of less than 130/80 mm Hg for all hypertensives, regardless of age, as long as they remain ambulatory and community dwelling.
One goal for all adults
“The systolic blood pressure goal for older people has gone from 140 mm Hg to 150 mm Hg and now to 130 mm Hg in the space of 2-3 years,” commented Dr. Appel, professor of epidemiology at Johns Hopkins University in Baltimore and not involved in the guideline-writing process.
In fact, the guidelines simplified the treatment goal all around, to less than 130/80 mm Hg for patients with diabetes, those with chronic kidney disease, and the elderly; that goal remains the same for all adults.
“It will be clearer and easier now that everyone should be less than 130/80 mm Hg. You won’t need to remember a second target,” said Sandra J. Taler, MD, a nephrologist and professor of medicine at the Mayo Clinic in Rochester, Minn., and a member of the guidelines task force.
“Some people may be upset that we changed the rules on them. They had normal blood pressure yesterday, and today it’s high. But it’s a good awakening, especially for using lifestyle interventions,” Dr. Taler said in an interview.
Preferred intervention: Lifestyle, not drugs
Lifestyle optimization is repeatedly cited as the cornerstone of intervention for everyone, including those with elevated blood pressure with a systolic pressure of 120-129 mm Hg, and as the only endorsed intervention for patients with hypertension of 130-139 mm Hg but below a 10% risk for a cardiovascular disease event during the next 10 years on the American College of Cardiology’s online risk calculator. The guidelines list six lifestyle goals: weight loss, following a DASH diet, reducing sodium, enhancing potassium, 90-150 min/wk of physical activity, and moderate alcohol intake.

Team-based care essential
The guidelines also put unprecedented emphasis on using a team-based management approach, which means having nurses, nurse practitioners, pharmacists, dietitians, and other clinicians, allowing for more frequent and focused care. Dr. Whelton and others cited in particular the VA Health System and Kaiser-Permanente as operating team-based and system-driven blood pressure management programs that have resulted in control rates for more than 90% of hypertensive patients. The team-based approach is also a key in the Target:BP program that the American Heart Association and American Medical Association founded. Target:BP will be instrumental in promoting implementation of the new guidelines, Dr. Carey said. Another systems recommendation is that every patient with hypertension should have a “clear, detailed, and current evidence-based plan of care.”
“Using nurse practitioners, physician assistants, and pharmacists has been shown to improve blood pressure levels,” and health systems that use this approach have had “great success,” commented Donald M. Lloyd-Jones, MD, professor and chairman of preventive medicine at Northwestern University in Chicago and not part of the guidelines task force. Some systems have used this approach to achieve high levels of blood pressure control. Now that financial penalties and incentives from payers also exist to push for higher levels of blood pressure control, the alignment of financial and health incentives should result in big changes, Dr. Lloyd-Jones predicted in a video interview.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
ANAHEIM, CALIF. – Thirty million Americans became hypertensive overnight on Nov. 13 with the introduction of new high blood pressure guidelines from the American College of Cardiology and American Heart Association.
That happened by resetting the definition of adult hypertension from the long-standing threshold of 140/90 mm Hg to a blood pressure at or above 130/80 mm Hg, a change that jumps the U.S. adult prevalence of hypertension from roughly 32% to 46%. Nearly half of all U.S. adults now have hypertension, bringing the total national hypertensive population to a staggering 103 million.
Goal is to transform care
But the new guidelines (J Am Coll Cardiol. 2017 Nov 13. doi: 10.1016/j.jacc.2017.11.005) for preventing, detecting, evaluating, and managing adult hypertension do lots more than just shake up the epidemiology of high blood pressure. With 106 total recommendations, the guidelines seek to transform every aspect of blood pressure in American medical practice, starting with how it’s measured and stretching to redefine applications of medical systems to try to ensure that every person with a blood pressure that truly falls outside the redefined limits gets a comprehensive package of interventions.
Many of these are “seismic changes,” said Lawrence J. Appel, MD. He particularly cited as seismic the new classification of stage 1 hypertension as a pressure at or above 130/80 mm Hg, the emphasis on using some form of out-of-office blood pressure measurement to confirm a diagnosis, the use of risk assessment when deciding whether to treat certain patients with drugs, and the same blood pressure goal of less than 130/80 mm Hg for all hypertensives, regardless of age, as long as they remain ambulatory and community dwelling.
One goal for all adults
“The systolic blood pressure goal for older people has gone from 140 mm Hg to 150 mm Hg and now to 130 mm Hg in the space of 2-3 years,” commented Dr. Appel, professor of epidemiology at Johns Hopkins University in Baltimore and not involved in the guideline-writing process.
In fact, the guidelines simplified the treatment goal all around, to less than 130/80 mm Hg for patients with diabetes, those with chronic kidney disease, and the elderly; that goal remains the same for all adults.
“It will be clearer and easier now that everyone should be less than 130/80 mm Hg. You won’t need to remember a second target,” said Sandra J. Taler, MD, a nephrologist and professor of medicine at the Mayo Clinic in Rochester, Minn., and a member of the guidelines task force.
“Some people may be upset that we changed the rules on them. They had normal blood pressure yesterday, and today it’s high. But it’s a good awakening, especially for using lifestyle interventions,” Dr. Taler said in an interview.
Preferred intervention: Lifestyle, not drugs
Lifestyle optimization is repeatedly cited as the cornerstone of intervention for everyone, including those with elevated blood pressure with a systolic pressure of 120-129 mm Hg, and as the only endorsed intervention for patients with hypertension of 130-139 mm Hg but below a 10% risk for a cardiovascular disease event during the next 10 years on the American College of Cardiology’s online risk calculator. The guidelines list six lifestyle goals: weight loss, following a DASH diet, reducing sodium, enhancing potassium, 90-150 min/wk of physical activity, and moderate alcohol intake.
Team-based care essential
The guidelines also put unprecedented emphasis on using a team-based management approach, which means having nurses, nurse practitioners, pharmacists, dietitians, and other clinicians, allowing for more frequent and focused care. Dr. Whelton and others cited in particular the VA Health System and Kaiser-Permanente as operating team-based and system-driven blood pressure management programs that have resulted in control rates for more than 90% of hypertensive patients. The team-based approach is also a key in the Target:BP program that the American Heart Association and American Medical Association founded. Target:BP will be instrumental in promoting implementation of the new guidelines, Dr. Carey said. Another systems recommendation is that every patient with hypertension should have a “clear, detailed, and current evidence-based plan of care.”
“Using nurse practitioners, physician assistants, and pharmacists has been shown to improve blood pressure levels,” and health systems that use this approach have had “great success,” commented Donald M. Lloyd-Jones, MD, professor and chairman of preventive medicine at Northwestern University in Chicago and not part of the guidelines task force. Some systems have used this approach to achieve high levels of blood pressure control. Now that financial penalties and incentives from payers also exist to push for higher levels of blood pressure control, the alignment of financial and health incentives should result in big changes, Dr. Lloyd-Jones predicted in a video interview.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
ANAHEIM, CALIF. – Thirty million Americans became hypertensive overnight on Nov. 13 with the introduction of new high blood pressure guidelines from the American College of Cardiology and American Heart Association.
That happened by resetting the definition of adult hypertension from the long-standing threshold of 140/90 mm Hg to a blood pressure at or above 130/80 mm Hg, a change that jumps the U.S. adult prevalence of hypertension from roughly 32% to 46%. Nearly half of all U.S. adults now have hypertension, bringing the total national hypertensive population to a staggering 103 million.
Goal is to transform care
But the new guidelines (J Am Coll Cardiol. 2017 Nov 13. doi: 10.1016/j.jacc.2017.11.005) for preventing, detecting, evaluating, and managing adult hypertension do lots more than just shake up the epidemiology of high blood pressure. With 106 total recommendations, the guidelines seek to transform every aspect of blood pressure in American medical practice, starting with how it’s measured and stretching to redefine applications of medical systems to try to ensure that every person with a blood pressure that truly falls outside the redefined limits gets a comprehensive package of interventions.
Many of these are “seismic changes,” said Lawrence J. Appel, MD. He particularly cited as seismic the new classification of stage 1 hypertension as a pressure at or above 130/80 mm Hg, the emphasis on using some form of out-of-office blood pressure measurement to confirm a diagnosis, the use of risk assessment when deciding whether to treat certain patients with drugs, and the same blood pressure goal of less than 130/80 mm Hg for all hypertensives, regardless of age, as long as they remain ambulatory and community dwelling.
One goal for all adults
“The systolic blood pressure goal for older people has gone from 140 mm Hg to 150 mm Hg and now to 130 mm Hg in the space of 2-3 years,” commented Dr. Appel, professor of epidemiology at Johns Hopkins University in Baltimore and not involved in the guideline-writing process.
In fact, the guidelines simplified the treatment goal all around, to less than 130/80 mm Hg for patients with diabetes, those with chronic kidney disease, and the elderly; that goal remains the same for all adults.
“It will be clearer and easier now that everyone should be less than 130/80 mm Hg. You won’t need to remember a second target,” said Sandra J. Taler, MD, a nephrologist and professor of medicine at the Mayo Clinic in Rochester, Minn., and a member of the guidelines task force.
“Some people may be upset that we changed the rules on them. They had normal blood pressure yesterday, and today it’s high. But it’s a good awakening, especially for using lifestyle interventions,” Dr. Taler said in an interview.
Preferred intervention: Lifestyle, not drugs
Lifestyle optimization is repeatedly cited as the cornerstone of intervention for everyone, including those with elevated blood pressure with a systolic pressure of 120-129 mm Hg, and as the only endorsed intervention for patients with hypertension of 130-139 mm Hg but below a 10% risk for a cardiovascular disease event during the next 10 years on the American College of Cardiology’s online risk calculator. The guidelines list six lifestyle goals: weight loss, following a DASH diet, reducing sodium, enhancing potassium, 90-150 min/wk of physical activity, and moderate alcohol intake.
Team-based care essential
The guidelines also put unprecedented emphasis on using a team-based management approach, which means having nurses, nurse practitioners, pharmacists, dietitians, and other clinicians, allowing for more frequent and focused care. Dr. Whelton and others cited in particular the VA Health System and Kaiser-Permanente as operating team-based and system-driven blood pressure management programs that have resulted in control rates for more than 90% of hypertensive patients. The team-based approach is also a key in the Target:BP program that the American Heart Association and American Medical Association founded. Target:BP will be instrumental in promoting implementation of the new guidelines, Dr. Carey said. Another systems recommendation is that every patient with hypertension should have a “clear, detailed, and current evidence-based plan of care.”
“Using nurse practitioners, physician assistants, and pharmacists has been shown to improve blood pressure levels,” and health systems that use this approach have had “great success,” commented Donald M. Lloyd-Jones, MD, professor and chairman of preventive medicine at Northwestern University in Chicago and not part of the guidelines task force. Some systems have used this approach to achieve high levels of blood pressure control. Now that financial penalties and incentives from payers also exist to push for higher levels of blood pressure control, the alignment of financial and health incentives should result in big changes, Dr. Lloyd-Jones predicted in a video interview.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE AHA SCIENTIFIC SESSIONS
VIDEO: Evidence mounts for pulmonary embolism benefit from catheter thrombolysis
TORONTO – Catheter-directed thrombolysis of pulmonary embolism using an ultrasound-assisted device led to significantly better outcomes in patients hospitalized for pulmonary embolism, compared with conventional systemic thrombolytic treatment, in a propensity score–adjusted analysis of nearly 3,400 patients.
Catheter-directed thrombolysis (CDT) “represents an opportunity to locally treat pulmonary embolism with significant thrombus burden with lower bleeding complications,” Abhishek Mishra, MD, said at the CHEST annual meeting. “I think we are underusing CDT,” said Dr. Mishra, a cardiovascular disease physician at Guthrie Robert Packer Hospital in Sayre, Pa.
Although one CDT device, the EKOS endovascular system that uses ultrasound to facilitate pulmonary embolism (PE) thrombolysis, received Food & Drug Administration approval for U.S. marketing in 2014, the trials that have compared it with systemic thrombolysis have been small, noted Dr. Mishra, and none have looked at whether CDT improves patient survival, compared with standard treatments. The largest report on CDT treatment of PE came from a single-arm, uncontrolled study with 150 patients who received ultrasound-facilitated CDT (JACC Cardiovasc Interv. 2015 Aug;8[10]:1382-92).
To better document the incremental benefit from CDT, Dr. Mishra and his associates used data collected by the Nationwide Readmissions Database during 2013 and 2014, both before and after a CDT device became available for U.S. use. From among 4,426 patients hospitalized with a primary diagnosis of PE and treated with thrombolytic therapy, they used propensity score matching to compare 2,256 patients treated with systemic thrombolysis with 1,128 matched patients treated with CDT using tissue plasminogen activator.
The analysis showed that in-hospital death was 15% in the systemic patients and 6% in the CDT group, a relative risk reduction of 63%, and 30-day readmissions occurred in 11% of the systemic patients and in 8% of those treated with CDT, a 30% relative risk reduction. Both were statistically significant differences for the study’s two primary endpoints, Dr. Mishra reported at the meeting. Rates of intracerebral hemorrhage and gastrointestinal bleeds were both numerically lower with CDT, and significantly lower for gastrointestinal bleeds.
The researchers also ran a multivariate analysis on their data that showed CDT was linked with significant relative reductions of about 60% for both in-hospital death and 30-day readmissions, compared with patients on systemic therapy. The results Dr. Mishra reported also appeared in a published report (Am J Cardiol. 2017 Nov 1;120[9]:1653-61).
These findings help buttress the case for using CDT for at least some PE patients. “The key is which patients need it. What is the best way to stratify patients?” commented Victor F. Tapson, MD, a pulmonologist at Cedars-Sinai Medical Center in Los Angeles.
“Patients with PE and a normal right ventricle generally don’t need anything more aggressive than anticoagulation, and really sick patients with massive PE need systemic thrombolytics. Intermediate-risk patients” are best suited to CDT, but “the problem is that intermediate-risk patients are heterogeneous,” Dr. Tapson said in a video interview. Future studies should establish a more specific subgroup of intermediate-risk patients who benefit from routinely employed CDT, he suggested.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
BY MITCHEL L. ZOLER
Frontline Medical News
BY MITCHEL L. ZOLER
Frontline Medical News
BY MITCHEL L. ZOLER
Frontline Medical News
TORONTO – Catheter-directed thrombolysis of pulmonary embolism using an ultrasound-assisted device led to significantly better outcomes in patients hospitalized for pulmonary embolism, compared with conventional systemic thrombolytic treatment, in a propensity score–adjusted analysis of nearly 3,400 patients.
Catheter-directed thrombolysis (CDT) “represents an opportunity to locally treat pulmonary embolism with significant thrombus burden with lower bleeding complications,” Abhishek Mishra, MD, said at the CHEST annual meeting. “I think we are underusing CDT,” said Dr. Mishra, a cardiovascular disease physician at Guthrie Robert Packer Hospital in Sayre, Pa.
Although one CDT device, the EKOS endovascular system that uses ultrasound to facilitate pulmonary embolism (PE) thrombolysis, received Food & Drug Administration approval for U.S. marketing in 2014, the trials that have compared it with systemic thrombolysis have been small, noted Dr. Mishra, and none have looked at whether CDT improves patient survival, compared with standard treatments. The largest report on CDT treatment of PE came from a single-arm, uncontrolled study with 150 patients who received ultrasound-facilitated CDT (JACC Cardiovasc Interv. 2015 Aug;8[10]:1382-92).
To better document the incremental benefit from CDT, Dr. Mishra and his associates used data collected by the Nationwide Readmissions Database during 2013 and 2014, both before and after a CDT device became available for U.S. use. From among 4,426 patients hospitalized with a primary diagnosis of PE and treated with thrombolytic therapy, they used propensity score matching to compare 2,256 patients treated with systemic thrombolysis with 1,128 matched patients treated with CDT using tissue plasminogen activator.
The analysis showed that in-hospital death was 15% in the systemic patients and 6% in the CDT group, a relative risk reduction of 63%, and 30-day readmissions occurred in 11% of the systemic patients and in 8% of those treated with CDT, a 30% relative risk reduction. Both were statistically significant differences for the study’s two primary endpoints, Dr. Mishra reported at the meeting. Rates of intracerebral hemorrhage and gastrointestinal bleeds were both numerically lower with CDT, and significantly lower for gastrointestinal bleeds.
The researchers also ran a multivariate analysis on their data that showed CDT was linked with significant relative reductions of about 60% for both in-hospital death and 30-day readmissions, compared with patients on systemic therapy. The results Dr. Mishra reported also appeared in a published report (Am J Cardiol. 2017 Nov 1;120[9]:1653-61).
These findings help buttress the case for using CDT for at least some PE patients. “The key is which patients need it. What is the best way to stratify patients?” commented Victor F. Tapson, MD, a pulmonologist at Cedars-Sinai Medical Center in Los Angeles.
“Patients with PE and a normal right ventricle generally don’t need anything more aggressive than anticoagulation, and really sick patients with massive PE need systemic thrombolytics. Intermediate-risk patients” are best suited to CDT, but “the problem is that intermediate-risk patients are heterogeneous,” Dr. Tapson said in a video interview. Future studies should establish a more specific subgroup of intermediate-risk patients who benefit from routinely employed CDT, he suggested.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
TORONTO – Catheter-directed thrombolysis of pulmonary embolism using an ultrasound-assisted device led to significantly better outcomes in patients hospitalized for pulmonary embolism, compared with conventional systemic thrombolytic treatment, in a propensity score–adjusted analysis of nearly 3,400 patients.
Catheter-directed thrombolysis (CDT) “represents an opportunity to locally treat pulmonary embolism with significant thrombus burden with lower bleeding complications,” Abhishek Mishra, MD, said at the CHEST annual meeting. “I think we are underusing CDT,” said Dr. Mishra, a cardiovascular disease physician at Guthrie Robert Packer Hospital in Sayre, Pa.
Although one CDT device, the EKOS endovascular system that uses ultrasound to facilitate pulmonary embolism (PE) thrombolysis, received Food & Drug Administration approval for U.S. marketing in 2014, the trials that have compared it with systemic thrombolysis have been small, noted Dr. Mishra, and none have looked at whether CDT improves patient survival, compared with standard treatments. The largest report on CDT treatment of PE came from a single-arm, uncontrolled study with 150 patients who received ultrasound-facilitated CDT (JACC Cardiovasc Interv. 2015 Aug;8[10]:1382-92).
To better document the incremental benefit from CDT, Dr. Mishra and his associates used data collected by the Nationwide Readmissions Database during 2013 and 2014, both before and after a CDT device became available for U.S. use. From among 4,426 patients hospitalized with a primary diagnosis of PE and treated with thrombolytic therapy, they used propensity score matching to compare 2,256 patients treated with systemic thrombolysis with 1,128 matched patients treated with CDT using tissue plasminogen activator.
The analysis showed that in-hospital death was 15% in the systemic patients and 6% in the CDT group, a relative risk reduction of 63%, and 30-day readmissions occurred in 11% of the systemic patients and in 8% of those treated with CDT, a 30% relative risk reduction. Both were statistically significant differences for the study’s two primary endpoints, Dr. Mishra reported at the meeting. Rates of intracerebral hemorrhage and gastrointestinal bleeds were both numerically lower with CDT, and significantly lower for gastrointestinal bleeds.
The researchers also ran a multivariate analysis on their data that showed CDT was linked with significant relative reductions of about 60% for both in-hospital death and 30-day readmissions, compared with patients on systemic therapy. The results Dr. Mishra reported also appeared in a published report (Am J Cardiol. 2017 Nov 1;120[9]:1653-61).
These findings help buttress the case for using CDT for at least some PE patients. “The key is which patients need it. What is the best way to stratify patients?” commented Victor F. Tapson, MD, a pulmonologist at Cedars-Sinai Medical Center in Los Angeles.
“Patients with PE and a normal right ventricle generally don’t need anything more aggressive than anticoagulation, and really sick patients with massive PE need systemic thrombolytics. Intermediate-risk patients” are best suited to CDT, but “the problem is that intermediate-risk patients are heterogeneous,” Dr. Tapson said in a video interview. Future studies should establish a more specific subgroup of intermediate-risk patients who benefit from routinely employed CDT, he suggested.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AT CHEST 2017
Key clinical point:
Major finding: Catheter-directed thrombolysis cut in-hospital mortality by 63%, compared with conventional systemic thrombolysis.
Data source: The National Readmission Database, which included 4,426 patients hospitalized during 2013 and 2014 with primary pulmonary embolism and treated with thrombolysis.
Disclosures: Dr. Mishra had no disclosures. Dr. Tapson has been a consultant to and had received research funding from Ekos/BTG, a company that markets a catheter-directed thrombolysis device. He has also ties to Daiichi Sankyo, Inari, Janssen, and Portola.

Late-Breaking Science preview: Wednesday, Nov. 15
The final Late-Breaking Science session delves into innovative therapies and novel applications, including two phase 1-2 stem cell trials, an early trial in toxin treatments to prevent atrial fibrillation, a phase 1 test of an interatrial shunt device for heart failure with preserved ejection fraction, and more:
- TNT-POAF: Nathan Waldron, MD, of Duke University, Durham, N.C., will present results of a trial aiming to prevent postoperative atrial fibrillation with the use of temporary toxin treatment.
- REDUCE LAP–HF 1: In what the investigators call the first randomized controlled trial of a device-based therapy to reduce left atrial pressure in HFpEF, an inter-atrial shunt device designed to provide continuous and dynamic decompression of the left atrium. Sanjiv J Shah, MD, of Northwestern University will present the study, which holds the hypothesis that the device may reduce symptoms and slow the progression of heart failure.
- PROPEL: This study tested the hypothesis that granulocyte-macrophage colony-stimulating factor (GM-CSF) combined with supervised treadmill exercise in patients with peripheral artery disease would significantly improve functional performance more than GM-CSF alone or supervised treadmill exercise alone. Mary McDermott, MD, of Northwestern University, Chicago, will present the primary endpoint of change in 6-minute walk performance at 12-weeks’ follow-up, as well as several secondary outcomes.
- ALLSTAR: Timothy Henry, MD, of the Cedars-Sinai Heart Institute, Los Angeles, will present the phase 1-2 ALLSTAR (Allogeneic Heart Stem Cells to Achieve Myocardial Regeneration) study, which compared allogeneic cardiosphere-derived cells (CAP-1002) to placebo in order to find whether it is safe and effective in decreasing infarct size in patients with an MI.
- HOPE-Duchenne: This phase 1-2 study randomized men with cardiomyopathy secondary to Duchenne muscular dystrophy to receive CAP-1002 cells or usual care; its primary outcome is safety. Ronald Victor, MD, will present the results.
chackett@frontlinemedcom.com
On Twitter @cardionews
The final Late-Breaking Science session delves into innovative therapies and novel applications, including two phase 1-2 stem cell trials, an early trial in toxin treatments to prevent atrial fibrillation, a phase 1 test of an interatrial shunt device for heart failure with preserved ejection fraction, and more:
- TNT-POAF: Nathan Waldron, MD, of Duke University, Durham, N.C., will present results of a trial aiming to prevent postoperative atrial fibrillation with the use of temporary toxin treatment.
- REDUCE LAP–HF 1: In what the investigators call the first randomized controlled trial of a device-based therapy to reduce left atrial pressure in HFpEF, an inter-atrial shunt device designed to provide continuous and dynamic decompression of the left atrium. Sanjiv J Shah, MD, of Northwestern University will present the study, which holds the hypothesis that the device may reduce symptoms and slow the progression of heart failure.
- PROPEL: This study tested the hypothesis that granulocyte-macrophage colony-stimulating factor (GM-CSF) combined with supervised treadmill exercise in patients with peripheral artery disease would significantly improve functional performance more than GM-CSF alone or supervised treadmill exercise alone. Mary McDermott, MD, of Northwestern University, Chicago, will present the primary endpoint of change in 6-minute walk performance at 12-weeks’ follow-up, as well as several secondary outcomes.
- ALLSTAR: Timothy Henry, MD, of the Cedars-Sinai Heart Institute, Los Angeles, will present the phase 1-2 ALLSTAR (Allogeneic Heart Stem Cells to Achieve Myocardial Regeneration) study, which compared allogeneic cardiosphere-derived cells (CAP-1002) to placebo in order to find whether it is safe and effective in decreasing infarct size in patients with an MI.
- HOPE-Duchenne: This phase 1-2 study randomized men with cardiomyopathy secondary to Duchenne muscular dystrophy to receive CAP-1002 cells or usual care; its primary outcome is safety. Ronald Victor, MD, will present the results.
chackett@frontlinemedcom.com
On Twitter @cardionews
The final Late-Breaking Science session delves into innovative therapies and novel applications, including two phase 1-2 stem cell trials, an early trial in toxin treatments to prevent atrial fibrillation, a phase 1 test of an interatrial shunt device for heart failure with preserved ejection fraction, and more:
- TNT-POAF: Nathan Waldron, MD, of Duke University, Durham, N.C., will present results of a trial aiming to prevent postoperative atrial fibrillation with the use of temporary toxin treatment.
- REDUCE LAP–HF 1: In what the investigators call the first randomized controlled trial of a device-based therapy to reduce left atrial pressure in HFpEF, an inter-atrial shunt device designed to provide continuous and dynamic decompression of the left atrium. Sanjiv J Shah, MD, of Northwestern University will present the study, which holds the hypothesis that the device may reduce symptoms and slow the progression of heart failure.
- PROPEL: This study tested the hypothesis that granulocyte-macrophage colony-stimulating factor (GM-CSF) combined with supervised treadmill exercise in patients with peripheral artery disease would significantly improve functional performance more than GM-CSF alone or supervised treadmill exercise alone. Mary McDermott, MD, of Northwestern University, Chicago, will present the primary endpoint of change in 6-minute walk performance at 12-weeks’ follow-up, as well as several secondary outcomes.
- ALLSTAR: Timothy Henry, MD, of the Cedars-Sinai Heart Institute, Los Angeles, will present the phase 1-2 ALLSTAR (Allogeneic Heart Stem Cells to Achieve Myocardial Regeneration) study, which compared allogeneic cardiosphere-derived cells (CAP-1002) to placebo in order to find whether it is safe and effective in decreasing infarct size in patients with an MI.
- HOPE-Duchenne: This phase 1-2 study randomized men with cardiomyopathy secondary to Duchenne muscular dystrophy to receive CAP-1002 cells or usual care; its primary outcome is safety. Ronald Victor, MD, will present the results.
chackett@frontlinemedcom.com
On Twitter @cardionews
CV outcomes better with SGLT2 inhibitor than DPP4 inhibitor in T2DM study
LISBON – The sodium-glucose co-transporter 2 (SGLT-2) inhibitor dapagliflozin (Farxiga) posed a lower risk of cardiovascular events and all-cause mortality in patients with type 2 diabetes mellitus (T2DM) compared with dipeptidyl peptidase-4 inhibitors in a large real-world, observational study.
In CVD-REAL NORDIC, treatment with the SGLT-2 inhibitor reduced the incidence of major cardiovascular adverse events by 21% as compared to DDP-4 inhibitors (hazard ratio, 0.79; 95% confidence interval, 0.67-0.94; P = .006).

Anna Norhammar, MD, PhD, of the Institute of Medicine, Cardiology Unit, at Karolinska Institutet in Stockholm, presented the findings at the annual meeting of the European Association for the Study of Diabetes.
She said: “These results are in line with previous clinical trials and meta-analyses, but extend the results to a broader CV risk population and with a commonly used comparator.”
Indeed, the findings build on those from the widely reported EMPA-REG Outcome (New Engl J Med. 2015;373;2117-8) and CANVAS (New Engl J Med. 2017;377:644-7) randomized controlled trials. These trials respectively showed empagliflozin and canagliflozin significantly reduced the risk for MACE and heart failure in patients with T2DM versus placebo. As the majority of patients in these trials had established CV disease, this suggested a class effect for SGLT2 inhibitors, Dr. Norhammar explained.
CVD-REAL NORDIC is part of a larger, multinational, observational, comparative effectiveness study looking at the real-world effect of SGLT2 inhibitors versus other glucose-lowering drugs on CV outcomes in patients with T2DM. Altogether around 90,000 patients have been recruited in Sweden, Norway, and Denmark.
Previously, Dr. Norhammar and co-investigators have reported that SGLT2 inhibitors lowered MACE (HR, 0.78; 95% CI 0.69–0.87, P less than .0001) and heart failure hospitalization (HR, 0.70; 95% CI 0.61–0.81, P less than .0001) relative to all glucose-lowering drugs (Lancet Diabetes Endocrinol. 2017;709–17).
“However, the comparator group used in that study, other [glucose-lowering drugs], consisted of almost 50% patients with T2DM treated with insulin or sul[f]onylureas,” they wrote in Diabetes, Obesity and Metabolism (8 Sep., doi: 10.1111/dom.13077). Insulin or sulfonylureas, they add, “have been shown to have increased associated CV risks” compared with DPP4 inhibitors and it is “not fully clear to what extent this could have influenced risk estimates.”
Furthermore, the CVD-NORDIC investigators note that the comparator group reflected real-world practice and it is important to look at treatment strategies more specifically, hence why they decided to do an analysis comparing SGLT2 and DPP4 inhibitors.
The study population for the current analysis consisted of 40,909 patients with T2DM who were newly initiated on either dapagliflozin (n=10,227) or a DPP4 inhibitor (n=30,682) between 2012 and 2015. The mean age was 61 years, and around 23% had prior CV disease and 5% had previous heart failure.
After a mean follow-up of 11.3 months, 177 MACE events had occurred among the 10,227 dapagliflozin-treated patients and 695 among the 30,681 DPP4 inhibitor-treated patients, giving respective event rates of 1.86 and 2.34 per 100 patient years. MACE was defined as a composite of nonfatal myocardial infarction, nonfatal stroke, and CV mortality.
“Dapagliflozin is the most commonly used SGLT2 inhibitor in the Nordic countries,” Dr. Norhammar said, explaining why this particular SGLT2 inhibitor was used in the analysis.
While there was a clear benefit of using dapagliflozin over DPP4 inhibitors in terms of MACE, heart failure hospitalization, and all-cause mortality, there was a “neutral” effect on atrial fibrillation and severe hypoglycaemia, with respective HRs of 0.92 (95% CI 0.76–1.12; P = .41) and 0.94 (95% CI 0.74–1.19; P = .62).
Dr. Norhammar said these “neutral results for atrial fibrillation and severe hypoglycaemia,” were “in line with expectations, and suggest a low likelihood of confounding.”
As this was an observational study, one of the limitations is that could be confounding factors that could not be adequately matched in the analysis. The events were not adjudicated and the study didn’t look at safety.
Dr. Norhammar noted that the results of the DECLARE-TIMI 58 trials were now needed to see if the potential CV benefits of using an SGLT2 inhibitor over other gluc0se-lowering medications might extend into patients at lower CV risk.
AstraZeneca supported the study.
Dr. Norhammar disclosed acting as a consultant to and receiving honoraria from AstraZeneca, Boehringer-Ingelheim, Eli Lilly, Novo Nordisk, and MSD Sweden.
LISBON – The sodium-glucose co-transporter 2 (SGLT-2) inhibitor dapagliflozin (Farxiga) posed a lower risk of cardiovascular events and all-cause mortality in patients with type 2 diabetes mellitus (T2DM) compared with dipeptidyl peptidase-4 inhibitors in a large real-world, observational study.
In CVD-REAL NORDIC, treatment with the SGLT-2 inhibitor reduced the incidence of major cardiovascular adverse events by 21% as compared to DDP-4 inhibitors (hazard ratio, 0.79; 95% confidence interval, 0.67-0.94; P = .006).
Anna Norhammar, MD, PhD, of the Institute of Medicine, Cardiology Unit, at Karolinska Institutet in Stockholm, presented the findings at the annual meeting of the European Association for the Study of Diabetes.
She said: “These results are in line with previous clinical trials and meta-analyses, but extend the results to a broader CV risk population and with a commonly used comparator.”
Indeed, the findings build on those from the widely reported EMPA-REG Outcome (New Engl J Med. 2015;373;2117-8) and CANVAS (New Engl J Med. 2017;377:644-7) randomized controlled trials. These trials respectively showed empagliflozin and canagliflozin significantly reduced the risk for MACE and heart failure in patients with T2DM versus placebo. As the majority of patients in these trials had established CV disease, this suggested a class effect for SGLT2 inhibitors, Dr. Norhammar explained.
CVD-REAL NORDIC is part of a larger, multinational, observational, comparative effectiveness study looking at the real-world effect of SGLT2 inhibitors versus other glucose-lowering drugs on CV outcomes in patients with T2DM. Altogether around 90,000 patients have been recruited in Sweden, Norway, and Denmark.
Previously, Dr. Norhammar and co-investigators have reported that SGLT2 inhibitors lowered MACE (HR, 0.78; 95% CI 0.69–0.87, P less than .0001) and heart failure hospitalization (HR, 0.70; 95% CI 0.61–0.81, P less than .0001) relative to all glucose-lowering drugs (Lancet Diabetes Endocrinol. 2017;709–17).
“However, the comparator group used in that study, other [glucose-lowering drugs], consisted of almost 50% patients with T2DM treated with insulin or sul[f]onylureas,” they wrote in Diabetes, Obesity and Metabolism (8 Sep., doi: 10.1111/dom.13077). Insulin or sulfonylureas, they add, “have been shown to have increased associated CV risks” compared with DPP4 inhibitors and it is “not fully clear to what extent this could have influenced risk estimates.”
Furthermore, the CVD-NORDIC investigators note that the comparator group reflected real-world practice and it is important to look at treatment strategies more specifically, hence why they decided to do an analysis comparing SGLT2 and DPP4 inhibitors.
The study population for the current analysis consisted of 40,909 patients with T2DM who were newly initiated on either dapagliflozin (n=10,227) or a DPP4 inhibitor (n=30,682) between 2012 and 2015. The mean age was 61 years, and around 23% had prior CV disease and 5% had previous heart failure.
After a mean follow-up of 11.3 months, 177 MACE events had occurred among the 10,227 dapagliflozin-treated patients and 695 among the 30,681 DPP4 inhibitor-treated patients, giving respective event rates of 1.86 and 2.34 per 100 patient years. MACE was defined as a composite of nonfatal myocardial infarction, nonfatal stroke, and CV mortality.
“Dapagliflozin is the most commonly used SGLT2 inhibitor in the Nordic countries,” Dr. Norhammar said, explaining why this particular SGLT2 inhibitor was used in the analysis.
While there was a clear benefit of using dapagliflozin over DPP4 inhibitors in terms of MACE, heart failure hospitalization, and all-cause mortality, there was a “neutral” effect on atrial fibrillation and severe hypoglycaemia, with respective HRs of 0.92 (95% CI 0.76–1.12; P = .41) and 0.94 (95% CI 0.74–1.19; P = .62).
Dr. Norhammar said these “neutral results for atrial fibrillation and severe hypoglycaemia,” were “in line with expectations, and suggest a low likelihood of confounding.”
As this was an observational study, one of the limitations is that could be confounding factors that could not be adequately matched in the analysis. The events were not adjudicated and the study didn’t look at safety.
Dr. Norhammar noted that the results of the DECLARE-TIMI 58 trials were now needed to see if the potential CV benefits of using an SGLT2 inhibitor over other gluc0se-lowering medications might extend into patients at lower CV risk.
AstraZeneca supported the study.
Dr. Norhammar disclosed acting as a consultant to and receiving honoraria from AstraZeneca, Boehringer-Ingelheim, Eli Lilly, Novo Nordisk, and MSD Sweden.
LISBON – The sodium-glucose co-transporter 2 (SGLT-2) inhibitor dapagliflozin (Farxiga) posed a lower risk of cardiovascular events and all-cause mortality in patients with type 2 diabetes mellitus (T2DM) compared with dipeptidyl peptidase-4 inhibitors in a large real-world, observational study.
In CVD-REAL NORDIC, treatment with the SGLT-2 inhibitor reduced the incidence of major cardiovascular adverse events by 21% as compared to DDP-4 inhibitors (hazard ratio, 0.79; 95% confidence interval, 0.67-0.94; P = .006).
Anna Norhammar, MD, PhD, of the Institute of Medicine, Cardiology Unit, at Karolinska Institutet in Stockholm, presented the findings at the annual meeting of the European Association for the Study of Diabetes.
She said: “These results are in line with previous clinical trials and meta-analyses, but extend the results to a broader CV risk population and with a commonly used comparator.”
Indeed, the findings build on those from the widely reported EMPA-REG Outcome (New Engl J Med. 2015;373;2117-8) and CANVAS (New Engl J Med. 2017;377:644-7) randomized controlled trials. These trials respectively showed empagliflozin and canagliflozin significantly reduced the risk for MACE and heart failure in patients with T2DM versus placebo. As the majority of patients in these trials had established CV disease, this suggested a class effect for SGLT2 inhibitors, Dr. Norhammar explained.
CVD-REAL NORDIC is part of a larger, multinational, observational, comparative effectiveness study looking at the real-world effect of SGLT2 inhibitors versus other glucose-lowering drugs on CV outcomes in patients with T2DM. Altogether around 90,000 patients have been recruited in Sweden, Norway, and Denmark.
Previously, Dr. Norhammar and co-investigators have reported that SGLT2 inhibitors lowered MACE (HR, 0.78; 95% CI 0.69–0.87, P less than .0001) and heart failure hospitalization (HR, 0.70; 95% CI 0.61–0.81, P less than .0001) relative to all glucose-lowering drugs (Lancet Diabetes Endocrinol. 2017;709–17).
“However, the comparator group used in that study, other [glucose-lowering drugs], consisted of almost 50% patients with T2DM treated with insulin or sul[f]onylureas,” they wrote in Diabetes, Obesity and Metabolism (8 Sep., doi: 10.1111/dom.13077). Insulin or sulfonylureas, they add, “have been shown to have increased associated CV risks” compared with DPP4 inhibitors and it is “not fully clear to what extent this could have influenced risk estimates.”
Furthermore, the CVD-NORDIC investigators note that the comparator group reflected real-world practice and it is important to look at treatment strategies more specifically, hence why they decided to do an analysis comparing SGLT2 and DPP4 inhibitors.
The study population for the current analysis consisted of 40,909 patients with T2DM who were newly initiated on either dapagliflozin (n=10,227) or a DPP4 inhibitor (n=30,682) between 2012 and 2015. The mean age was 61 years, and around 23% had prior CV disease and 5% had previous heart failure.
After a mean follow-up of 11.3 months, 177 MACE events had occurred among the 10,227 dapagliflozin-treated patients and 695 among the 30,681 DPP4 inhibitor-treated patients, giving respective event rates of 1.86 and 2.34 per 100 patient years. MACE was defined as a composite of nonfatal myocardial infarction, nonfatal stroke, and CV mortality.
“Dapagliflozin is the most commonly used SGLT2 inhibitor in the Nordic countries,” Dr. Norhammar said, explaining why this particular SGLT2 inhibitor was used in the analysis.
While there was a clear benefit of using dapagliflozin over DPP4 inhibitors in terms of MACE, heart failure hospitalization, and all-cause mortality, there was a “neutral” effect on atrial fibrillation and severe hypoglycaemia, with respective HRs of 0.92 (95% CI 0.76–1.12; P = .41) and 0.94 (95% CI 0.74–1.19; P = .62).
Dr. Norhammar said these “neutral results for atrial fibrillation and severe hypoglycaemia,” were “in line with expectations, and suggest a low likelihood of confounding.”
As this was an observational study, one of the limitations is that could be confounding factors that could not be adequately matched in the analysis. The events were not adjudicated and the study didn’t look at safety.
Dr. Norhammar noted that the results of the DECLARE-TIMI 58 trials were now needed to see if the potential CV benefits of using an SGLT2 inhibitor over other gluc0se-lowering medications might extend into patients at lower CV risk.
AstraZeneca supported the study.
Dr. Norhammar disclosed acting as a consultant to and receiving honoraria from AstraZeneca, Boehringer-Ingelheim, Eli Lilly, Novo Nordisk, and MSD Sweden.
AT EASD 2017
Key clinical point:
Major finding: Hazard ratios for MACE, heart failure hospitalization, and all-cause mortality were a respective 0.79, 0.62, and 0.59, comparing SGLT2 with DPP4 inhibitors.
Data source: CVD-NORDIC, part of a multinational, observational study comparing the real-world effect of SGLT2 inhibitors versus other glucose-lowering drugs on CV outcomes in patients with T2DM.
Disclosures: AstraZeneca supported the study. The presenting author disclosed acting as a consultant to and receiving honoraria from AstraZeneca, Boehringer-Ingelheim, Eli Lilly, Novo Nordisk, and MSD Sweden.
Why VADS is gaining ground in pediatrics
The miniaturization of continuous-flow ventricular assist devices has launched the era of continuous-flow VAD support in pediatric patients, and the trend may accelerate with the introduction of a continuous-flow device designed specifically for small children. In an expert opinion in the Journal of Thoracic and Cardiovascular Surgery, Iki Adachi, MD, of Baylor College of Medicine in Houston, said the emerging science of continuous-flow VADs in children promises to solve problems like device size mismatch, hospital-only VADs, and chronic therapy (J Thorac Cardiovasc Surg. 2017 Oct;154:1358-61). “With ongoing device miniaturization, enthusiasm has been growing among pediatric physicians for the use of continuous-flow VADs in children,” Dr. Adachi said. He noted the introduction of a continuous-flow device for small children, the Infant Jarvik 2015, “may further accelerate the trend.”
Dr. Adachi cited PediMACS reports that stated that more than half of the long-term devices now registered are continuous-flow devices, and that continuous-flow VADs comprised 62% of all durable VAD implants in the third quarter of 2016. “With the encouraging results recorded to date, the use of continuous-flow devices in the pediatric population is rapidly increasing,” he said.
Miniaturization has addressed the problem of size mismatch when using continuous-flow VAD devices in children, he said, noting that use of the Infant Jarvik device may be expanded even further to children as small at 8 kg or less. The PumpKIN trial(Pumps for Kids, Infants, and Neonates), which is evaluating the Infant Jarvik 2015 vs. the Berlin Heart EXCOR, could provide answers on the feasibility of continuous-flow VADs in small children.
“Based on experience with the chronic animal model, I believe that the Infant Jarvik device will properly fit the patients included in the trial,” he said.
Continuous-flow VAD in children also holds potential for managing these patients outside the hospital setting. “Outpatient management of children with continuous-flow VADs has been shown to be feasible,” he said, adding that the PediMACS registry has reported that only 45% of patients have been managed this way. “Nonetheless, with maturation of the pediatric field, outpatient management will become routine rather than the exception,” he said.
Greater use of continuous-flow VADs also may create opportunities to improve the status and suitability for transplantation of children with severe heart failure, he said. He gave as an example his group’s practice at Houston’s Texas Children’s Hospital, which is to deactivate patients on the transplant wait list for 3 months once they start continuous-flow VAD support. “A postoperative ‘grace period’ affords protected opportunities for both physical and psychological recovery,” he said. This timeout of sorts also affords the care team time to assess the myocardium for possible functional recovery.
In patients who are not good candidates for transplantation, durable continuous-flow VADs may provide chronic therapy, and in time, these patients may become suitable transplant candidates, said Dr. Adachi. “Bypassing such an unfavorable period for transplantation with prolonged VAD support may be a reasonable approach,” he said.
Patients with failing single-ventricle circulation also may benefit from VAD support, although the challenges facing this population are more profound than in other groups, Dr. Adachi said. VAD support for single-ventricle disease is sparse, but these patients require careful evaluation of the nature of their condition. “If systolic dysfunction is the predominant cause of circulatory failure, then VAD support for the failing systemic ventricle will likely improve hemodynamics,” said Dr. Adachi. VAD support also could help the patient move through the various stages of palliation.
“Again, the emphasis is not just on simply keeping the patient alive until a donor organ becomes available; rather, attention is refocused on overall health beyond survival, which may eventually affect transplantation candidacy and even post transplantation outcome,” Dr. Adachi concluded.
Dr. Adachi serves as a consultant and proctor for Berlin Heart and HeartWare, and as a consultant for the New England Research Institute related to the PumpKIN trial.
The miniaturization of continuous-flow ventricular assist devices has launched the era of continuous-flow VAD support in pediatric patients, and the trend may accelerate with the introduction of a continuous-flow device designed specifically for small children. In an expert opinion in the Journal of Thoracic and Cardiovascular Surgery, Iki Adachi, MD, of Baylor College of Medicine in Houston, said the emerging science of continuous-flow VADs in children promises to solve problems like device size mismatch, hospital-only VADs, and chronic therapy (J Thorac Cardiovasc Surg. 2017 Oct;154:1358-61). “With ongoing device miniaturization, enthusiasm has been growing among pediatric physicians for the use of continuous-flow VADs in children,” Dr. Adachi said. He noted the introduction of a continuous-flow device for small children, the Infant Jarvik 2015, “may further accelerate the trend.”
Dr. Adachi cited PediMACS reports that stated that more than half of the long-term devices now registered are continuous-flow devices, and that continuous-flow VADs comprised 62% of all durable VAD implants in the third quarter of 2016. “With the encouraging results recorded to date, the use of continuous-flow devices in the pediatric population is rapidly increasing,” he said.
Miniaturization has addressed the problem of size mismatch when using continuous-flow VAD devices in children, he said, noting that use of the Infant Jarvik device may be expanded even further to children as small at 8 kg or less. The PumpKIN trial(Pumps for Kids, Infants, and Neonates), which is evaluating the Infant Jarvik 2015 vs. the Berlin Heart EXCOR, could provide answers on the feasibility of continuous-flow VADs in small children.
“Based on experience with the chronic animal model, I believe that the Infant Jarvik device will properly fit the patients included in the trial,” he said.
Continuous-flow VAD in children also holds potential for managing these patients outside the hospital setting. “Outpatient management of children with continuous-flow VADs has been shown to be feasible,” he said, adding that the PediMACS registry has reported that only 45% of patients have been managed this way. “Nonetheless, with maturation of the pediatric field, outpatient management will become routine rather than the exception,” he said.
Greater use of continuous-flow VADs also may create opportunities to improve the status and suitability for transplantation of children with severe heart failure, he said. He gave as an example his group’s practice at Houston’s Texas Children’s Hospital, which is to deactivate patients on the transplant wait list for 3 months once they start continuous-flow VAD support. “A postoperative ‘grace period’ affords protected opportunities for both physical and psychological recovery,” he said. This timeout of sorts also affords the care team time to assess the myocardium for possible functional recovery.
In patients who are not good candidates for transplantation, durable continuous-flow VADs may provide chronic therapy, and in time, these patients may become suitable transplant candidates, said Dr. Adachi. “Bypassing such an unfavorable period for transplantation with prolonged VAD support may be a reasonable approach,” he said.
Patients with failing single-ventricle circulation also may benefit from VAD support, although the challenges facing this population are more profound than in other groups, Dr. Adachi said. VAD support for single-ventricle disease is sparse, but these patients require careful evaluation of the nature of their condition. “If systolic dysfunction is the predominant cause of circulatory failure, then VAD support for the failing systemic ventricle will likely improve hemodynamics,” said Dr. Adachi. VAD support also could help the patient move through the various stages of palliation.
“Again, the emphasis is not just on simply keeping the patient alive until a donor organ becomes available; rather, attention is refocused on overall health beyond survival, which may eventually affect transplantation candidacy and even post transplantation outcome,” Dr. Adachi concluded.
Dr. Adachi serves as a consultant and proctor for Berlin Heart and HeartWare, and as a consultant for the New England Research Institute related to the PumpKIN trial.
The miniaturization of continuous-flow ventricular assist devices has launched the era of continuous-flow VAD support in pediatric patients, and the trend may accelerate with the introduction of a continuous-flow device designed specifically for small children. In an expert opinion in the Journal of Thoracic and Cardiovascular Surgery, Iki Adachi, MD, of Baylor College of Medicine in Houston, said the emerging science of continuous-flow VADs in children promises to solve problems like device size mismatch, hospital-only VADs, and chronic therapy (J Thorac Cardiovasc Surg. 2017 Oct;154:1358-61). “With ongoing device miniaturization, enthusiasm has been growing among pediatric physicians for the use of continuous-flow VADs in children,” Dr. Adachi said. He noted the introduction of a continuous-flow device for small children, the Infant Jarvik 2015, “may further accelerate the trend.”
Dr. Adachi cited PediMACS reports that stated that more than half of the long-term devices now registered are continuous-flow devices, and that continuous-flow VADs comprised 62% of all durable VAD implants in the third quarter of 2016. “With the encouraging results recorded to date, the use of continuous-flow devices in the pediatric population is rapidly increasing,” he said.
Miniaturization has addressed the problem of size mismatch when using continuous-flow VAD devices in children, he said, noting that use of the Infant Jarvik device may be expanded even further to children as small at 8 kg or less. The PumpKIN trial(Pumps for Kids, Infants, and Neonates), which is evaluating the Infant Jarvik 2015 vs. the Berlin Heart EXCOR, could provide answers on the feasibility of continuous-flow VADs in small children.
“Based on experience with the chronic animal model, I believe that the Infant Jarvik device will properly fit the patients included in the trial,” he said.
Continuous-flow VAD in children also holds potential for managing these patients outside the hospital setting. “Outpatient management of children with continuous-flow VADs has been shown to be feasible,” he said, adding that the PediMACS registry has reported that only 45% of patients have been managed this way. “Nonetheless, with maturation of the pediatric field, outpatient management will become routine rather than the exception,” he said.
Greater use of continuous-flow VADs also may create opportunities to improve the status and suitability for transplantation of children with severe heart failure, he said. He gave as an example his group’s practice at Houston’s Texas Children’s Hospital, which is to deactivate patients on the transplant wait list for 3 months once they start continuous-flow VAD support. “A postoperative ‘grace period’ affords protected opportunities for both physical and psychological recovery,” he said. This timeout of sorts also affords the care team time to assess the myocardium for possible functional recovery.
In patients who are not good candidates for transplantation, durable continuous-flow VADs may provide chronic therapy, and in time, these patients may become suitable transplant candidates, said Dr. Adachi. “Bypassing such an unfavorable period for transplantation with prolonged VAD support may be a reasonable approach,” he said.
Patients with failing single-ventricle circulation also may benefit from VAD support, although the challenges facing this population are more profound than in other groups, Dr. Adachi said. VAD support for single-ventricle disease is sparse, but these patients require careful evaluation of the nature of their condition. “If systolic dysfunction is the predominant cause of circulatory failure, then VAD support for the failing systemic ventricle will likely improve hemodynamics,” said Dr. Adachi. VAD support also could help the patient move through the various stages of palliation.
“Again, the emphasis is not just on simply keeping the patient alive until a donor organ becomes available; rather, attention is refocused on overall health beyond survival, which may eventually affect transplantation candidacy and even post transplantation outcome,” Dr. Adachi concluded.
Dr. Adachi serves as a consultant and proctor for Berlin Heart and HeartWare, and as a consultant for the New England Research Institute related to the PumpKIN trial.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Advances in continuous-flow ventricular assist devices (VADs) promise a paradigm shift in pediatrics.
Major finding: Device miniaturization is solving problems such as size mismatch, inpatients on VADs, and chronic therapy.
Data source: Expert opinion drawing on PediMACS reports and published trials of continuous-flow VAD.
Disclosures: Dr. Adachi serves as a consultant and proctor for Berlin Heart and HeartWare and as a consultant for the New England Research Institute related to the PumpKIN trial.
Cardiogenic shock boosts PAH readmissions 10-fold
TORONTO – Cardiogenic shock, acute kidney injury, and chronic obstructive pulmonary disease were the top drivers of 30-day rehospitalizations in U.S. patients after an index hospitalization for pulmonary artery hypertension, based on an analysis of U.S. national data from 2013.
An episode of cardiogenic shock boosted 30-day rehospitalizations nearly 10-fold in recently discharged pulmonary artery hypertension (PAH) patients. A history of chronic obstructive pulmonary disease (COPD) linked with a threefold higher rehospitalization rate, and acute kidney injury linked with a doubled number of 30-day rehospitalizations, Kshitij Chatterjee, MD, said at the CHEST annual meeting.

The powerful impact of cardiogenic shock in particular suggests that interventions that improve patient compliance with stabilizing treatments following an index PAH hospitalization might be effective at preventing a patient’s quick return to the hospital. Contacting PAH patients a week after their index hospitalization discharge to make sure they are compliant with their diuretic regimen, for example, might help prevent a decompensation that then leads to cardiogenic shock and a return trip to the hospital, Dr. Chatterjee suggested.
Follow-up of PAH patients after an index hospitalization “is probably the single most important thing, because it can help with compliance,” he said in an interview.
The rehospitalizations he studied could be for any cause. His analysis showed that the most common cause of rehospitalization was heart failure, which caused 23% of the rehospitalizations, followed by pulmonary hypertension that caused 20%, and acute kidney injury, responsible for 11% of the 30-day rehospitalizations.
Dr. Chatterjee’s study used data collected during 2013 in the National Readmissions Database, run by the federal Agency for Healthcare Quality and Research. During that period, 776 patients entered a U.S. hospital with a primary diagnosis of PAH. During the 30 days following discharge, 114 (15%) returned to the hospital. During the second hospitalization 8% died, and the median length of stay for those who remained alive was 7 days.
Dr. Chatterjee highlighted that the modest number of index hospitalizations for PAH, as well as 30-day rehospitalizations he found in 2013, make it highly unlikely that PAH rehospitalizations will become a target for Medicare penalties as has been done for heart failure, pneumonia, COPD, and a few other disorders. But he stressed that patients with PAH who need rehospitalization generally have a highly compromised quality of life that potentially could be avoided by better management, which could prevent the need for rehospitalization.
Dr. Chatterjee had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
TORONTO – Cardiogenic shock, acute kidney injury, and chronic obstructive pulmonary disease were the top drivers of 30-day rehospitalizations in U.S. patients after an index hospitalization for pulmonary artery hypertension, based on an analysis of U.S. national data from 2013.
An episode of cardiogenic shock boosted 30-day rehospitalizations nearly 10-fold in recently discharged pulmonary artery hypertension (PAH) patients. A history of chronic obstructive pulmonary disease (COPD) linked with a threefold higher rehospitalization rate, and acute kidney injury linked with a doubled number of 30-day rehospitalizations, Kshitij Chatterjee, MD, said at the CHEST annual meeting.
The powerful impact of cardiogenic shock in particular suggests that interventions that improve patient compliance with stabilizing treatments following an index PAH hospitalization might be effective at preventing a patient’s quick return to the hospital. Contacting PAH patients a week after their index hospitalization discharge to make sure they are compliant with their diuretic regimen, for example, might help prevent a decompensation that then leads to cardiogenic shock and a return trip to the hospital, Dr. Chatterjee suggested.
Follow-up of PAH patients after an index hospitalization “is probably the single most important thing, because it can help with compliance,” he said in an interview.
The rehospitalizations he studied could be for any cause. His analysis showed that the most common cause of rehospitalization was heart failure, which caused 23% of the rehospitalizations, followed by pulmonary hypertension that caused 20%, and acute kidney injury, responsible for 11% of the 30-day rehospitalizations.
Dr. Chatterjee’s study used data collected during 2013 in the National Readmissions Database, run by the federal Agency for Healthcare Quality and Research. During that period, 776 patients entered a U.S. hospital with a primary diagnosis of PAH. During the 30 days following discharge, 114 (15%) returned to the hospital. During the second hospitalization 8% died, and the median length of stay for those who remained alive was 7 days.
Dr. Chatterjee highlighted that the modest number of index hospitalizations for PAH, as well as 30-day rehospitalizations he found in 2013, make it highly unlikely that PAH rehospitalizations will become a target for Medicare penalties as has been done for heart failure, pneumonia, COPD, and a few other disorders. But he stressed that patients with PAH who need rehospitalization generally have a highly compromised quality of life that potentially could be avoided by better management, which could prevent the need for rehospitalization.
Dr. Chatterjee had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
TORONTO – Cardiogenic shock, acute kidney injury, and chronic obstructive pulmonary disease were the top drivers of 30-day rehospitalizations in U.S. patients after an index hospitalization for pulmonary artery hypertension, based on an analysis of U.S. national data from 2013.
An episode of cardiogenic shock boosted 30-day rehospitalizations nearly 10-fold in recently discharged pulmonary artery hypertension (PAH) patients. A history of chronic obstructive pulmonary disease (COPD) linked with a threefold higher rehospitalization rate, and acute kidney injury linked with a doubled number of 30-day rehospitalizations, Kshitij Chatterjee, MD, said at the CHEST annual meeting.
The powerful impact of cardiogenic shock in particular suggests that interventions that improve patient compliance with stabilizing treatments following an index PAH hospitalization might be effective at preventing a patient’s quick return to the hospital. Contacting PAH patients a week after their index hospitalization discharge to make sure they are compliant with their diuretic regimen, for example, might help prevent a decompensation that then leads to cardiogenic shock and a return trip to the hospital, Dr. Chatterjee suggested.
Follow-up of PAH patients after an index hospitalization “is probably the single most important thing, because it can help with compliance,” he said in an interview.
The rehospitalizations he studied could be for any cause. His analysis showed that the most common cause of rehospitalization was heart failure, which caused 23% of the rehospitalizations, followed by pulmonary hypertension that caused 20%, and acute kidney injury, responsible for 11% of the 30-day rehospitalizations.
Dr. Chatterjee’s study used data collected during 2013 in the National Readmissions Database, run by the federal Agency for Healthcare Quality and Research. During that period, 776 patients entered a U.S. hospital with a primary diagnosis of PAH. During the 30 days following discharge, 114 (15%) returned to the hospital. During the second hospitalization 8% died, and the median length of stay for those who remained alive was 7 days.
Dr. Chatterjee highlighted that the modest number of index hospitalizations for PAH, as well as 30-day rehospitalizations he found in 2013, make it highly unlikely that PAH rehospitalizations will become a target for Medicare penalties as has been done for heart failure, pneumonia, COPD, and a few other disorders. But he stressed that patients with PAH who need rehospitalization generally have a highly compromised quality of life that potentially could be avoided by better management, which could prevent the need for rehospitalization.
Dr. Chatterjee had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AT CHEST 2017
Key clinical point:
Major finding: Patients with cardiogenic shock following PAH hospitalization had a 9.7-fold increased rate of 30-day rehospitalization, compared with patients without shock.
Data source: The National Readmissions Database, which included 776 index U.S. hospitalizations for pulmonary arterial hospitalization during 2013.
Disclosures: Dr. Chatterjee had no disclosures.

Generic, brand-name levothyroxine have similar cardiovascular outcomes
VICTORIA, B.C. – Hypothyroid patients have similar cardiovascular outcomes in the shorter term whether they take generic or brand-name levothyroxine, results of a retrospective propensity-matched cohort study reported at the annual meeting of the American Thyroid Association suggest.
Investigators led by Robert Smallridge, MD, an endocrinologist at the Mayo Clinic, in Jacksonville, Fla., used a large administrative database to study nearly 88,000 treatment-naive hypothyroid patients (most having benign thyroid disease) who started levothyroxine.

However, monthly total medication costs with the brand-name medication were more than twice those with the generic.
“I don’t think we are ready yet to say everybody ought to be on generic,” Dr. Smallridge said in an interview, citing the limited treatment duration captured in the study because patients switched medications or changed insurers. “But I think, at least in the short term, it’s giving us some data that we can build upon.”
He and his coinvestigators plan additional analyses looking at longer-term users, other types of thyroid hormone preparations, and the very small group of patients who had thyroid cancer.
“I primarily take care of cancer patients, and we purposely push these patients to slightly lower [thyroid-stimulating hormone levels] in general, which presumably is going to increase your risk of atrial fibrillation and could affect these events,” he said. “The numbers are somewhat smaller, clearly, but I’d like to see that explored also, to see if there is a difference between brand and generics in that subset who are probably getting a little bit more thyroid medication.”
Both hypothyroidism and its overtreatment with thyroid hormone therapy can increase cardiovascular risk, Dr. Smallridge noted.
For the study, the investigators analyzed data from a large administrative claims database (OptumLabs Data Warehouse) for the years 2006-2014. Patients having any prior use of any thyroid hormone preparation, amiodarone, or lithium were excluded. And patients were censored if they left the insurance plan, stopped treatment, or switched medication category.
The investigators identified 201,056 hypothyroid patients who started some type of thyroid hormone therapy. The majority (70.8%) started generic levothyroxine, and 22.1% started brand-name levothyroxine (Synthroid, Levoxyl, Tirosint, Unithroid). The small remaining group started another thyroid extract, triiodothyronine (T3), or a compounded preparation.
Primary care physicians were the main identifiable prescribers (60.3%), followed by endocrinologists (10.8%). “Endocrinologists tended to prescribe brand significantly more than the primary care physicians,” Dr. Smallridge said.
The investigators used propensity matching on a variety of factors (age, sex, race, census region, Charlson comorbidity index, year of index prescription, and a dozen baseline comorbidities) to compare patients starting brand-name versus generic levothyroxine. Outcomes were assessed during a median follow-up of 1 year (range, 0-9.3 years).
Event rates per 1,000 patient-years with branded versus generic levothyroxine were similar for atrial fibrillation (2.19 vs. 1.82; hazard ratio, 1.22, P = .19), myocardial infarction (1.83 vs. 2.12; HR, 0.86, P = .35), and congestive heart failure (2.00 vs. 2.27; HR, 0.88, P = .41). There was a borderline-significant difference on hospitalization for stroke, with marginally lower risk with brand-name levothyroxine (2.38 vs. 3.10; HR, 0.77; P = .05).
Findings were essentially the same in age-stratified analyses, splitting patients into subgroups younger and older than age 65.
When average 30-day costs were compared for users of branded versus generic levothyroxine, total cost for the branded drug was more than twice as high ($18.47 vs. $8.18).
“Thyroid preparations have been the most prescribed drug in the United States for several recent years. In the neighborhood of 25 million different patients a year take thyroid medications,” Dr. Smallridge said. “In terms of the dollars spent, it’s considerably less than some of the other drugs out there. But because of sheer numbers of patients, in terms of impact on health care dollars, it’s still a significant amount of money. And this is a lifelong treatment – once you go on thyroid hormones, you’re on them for life.”
The study had several strengths. “This is a very large, diverse, real-world population across the entire country with a wide range of ages,” Dr. Smallridge explained. “We got pharmacy claims documenting that they were continuing to get the refills, although we didn’t do pill counts, so we don’t know whether they were taking the medication. And a really important thing was the propensity score matching.”
At the same time, limitations included possible variations in coding and billing, and some residual confounding. “Key issues are that we need more data on longer-term follow-up, and we didn’t have lab values,” he added.
Dr. Smallridge reported that he had no relevant conflicts of interest.
VICTORIA, B.C. – Hypothyroid patients have similar cardiovascular outcomes in the shorter term whether they take generic or brand-name levothyroxine, results of a retrospective propensity-matched cohort study reported at the annual meeting of the American Thyroid Association suggest.
Investigators led by Robert Smallridge, MD, an endocrinologist at the Mayo Clinic, in Jacksonville, Fla., used a large administrative database to study nearly 88,000 treatment-naive hypothyroid patients (most having benign thyroid disease) who started levothyroxine.
However, monthly total medication costs with the brand-name medication were more than twice those with the generic.
“I don’t think we are ready yet to say everybody ought to be on generic,” Dr. Smallridge said in an interview, citing the limited treatment duration captured in the study because patients switched medications or changed insurers. “But I think, at least in the short term, it’s giving us some data that we can build upon.”
He and his coinvestigators plan additional analyses looking at longer-term users, other types of thyroid hormone preparations, and the very small group of patients who had thyroid cancer.
“I primarily take care of cancer patients, and we purposely push these patients to slightly lower [thyroid-stimulating hormone levels] in general, which presumably is going to increase your risk of atrial fibrillation and could affect these events,” he said. “The numbers are somewhat smaller, clearly, but I’d like to see that explored also, to see if there is a difference between brand and generics in that subset who are probably getting a little bit more thyroid medication.”
Both hypothyroidism and its overtreatment with thyroid hormone therapy can increase cardiovascular risk, Dr. Smallridge noted.
For the study, the investigators analyzed data from a large administrative claims database (OptumLabs Data Warehouse) for the years 2006-2014. Patients having any prior use of any thyroid hormone preparation, amiodarone, or lithium were excluded. And patients were censored if they left the insurance plan, stopped treatment, or switched medication category.
The investigators identified 201,056 hypothyroid patients who started some type of thyroid hormone therapy. The majority (70.8%) started generic levothyroxine, and 22.1% started brand-name levothyroxine (Synthroid, Levoxyl, Tirosint, Unithroid). The small remaining group started another thyroid extract, triiodothyronine (T3), or a compounded preparation.
Primary care physicians were the main identifiable prescribers (60.3%), followed by endocrinologists (10.8%). “Endocrinologists tended to prescribe brand significantly more than the primary care physicians,” Dr. Smallridge said.
The investigators used propensity matching on a variety of factors (age, sex, race, census region, Charlson comorbidity index, year of index prescription, and a dozen baseline comorbidities) to compare patients starting brand-name versus generic levothyroxine. Outcomes were assessed during a median follow-up of 1 year (range, 0-9.3 years).
Event rates per 1,000 patient-years with branded versus generic levothyroxine were similar for atrial fibrillation (2.19 vs. 1.82; hazard ratio, 1.22, P = .19), myocardial infarction (1.83 vs. 2.12; HR, 0.86, P = .35), and congestive heart failure (2.00 vs. 2.27; HR, 0.88, P = .41). There was a borderline-significant difference on hospitalization for stroke, with marginally lower risk with brand-name levothyroxine (2.38 vs. 3.10; HR, 0.77; P = .05).
Findings were essentially the same in age-stratified analyses, splitting patients into subgroups younger and older than age 65.
When average 30-day costs were compared for users of branded versus generic levothyroxine, total cost for the branded drug was more than twice as high ($18.47 vs. $8.18).
“Thyroid preparations have been the most prescribed drug in the United States for several recent years. In the neighborhood of 25 million different patients a year take thyroid medications,” Dr. Smallridge said. “In terms of the dollars spent, it’s considerably less than some of the other drugs out there. But because of sheer numbers of patients, in terms of impact on health care dollars, it’s still a significant amount of money. And this is a lifelong treatment – once you go on thyroid hormones, you’re on them for life.”
The study had several strengths. “This is a very large, diverse, real-world population across the entire country with a wide range of ages,” Dr. Smallridge explained. “We got pharmacy claims documenting that they were continuing to get the refills, although we didn’t do pill counts, so we don’t know whether they were taking the medication. And a really important thing was the propensity score matching.”
At the same time, limitations included possible variations in coding and billing, and some residual confounding. “Key issues are that we need more data on longer-term follow-up, and we didn’t have lab values,” he added.
Dr. Smallridge reported that he had no relevant conflicts of interest.
VICTORIA, B.C. – Hypothyroid patients have similar cardiovascular outcomes in the shorter term whether they take generic or brand-name levothyroxine, results of a retrospective propensity-matched cohort study reported at the annual meeting of the American Thyroid Association suggest.
Investigators led by Robert Smallridge, MD, an endocrinologist at the Mayo Clinic, in Jacksonville, Fla., used a large administrative database to study nearly 88,000 treatment-naive hypothyroid patients (most having benign thyroid disease) who started levothyroxine.
However, monthly total medication costs with the brand-name medication were more than twice those with the generic.
“I don’t think we are ready yet to say everybody ought to be on generic,” Dr. Smallridge said in an interview, citing the limited treatment duration captured in the study because patients switched medications or changed insurers. “But I think, at least in the short term, it’s giving us some data that we can build upon.”
He and his coinvestigators plan additional analyses looking at longer-term users, other types of thyroid hormone preparations, and the very small group of patients who had thyroid cancer.
“I primarily take care of cancer patients, and we purposely push these patients to slightly lower [thyroid-stimulating hormone levels] in general, which presumably is going to increase your risk of atrial fibrillation and could affect these events,” he said. “The numbers are somewhat smaller, clearly, but I’d like to see that explored also, to see if there is a difference between brand and generics in that subset who are probably getting a little bit more thyroid medication.”
Both hypothyroidism and its overtreatment with thyroid hormone therapy can increase cardiovascular risk, Dr. Smallridge noted.
For the study, the investigators analyzed data from a large administrative claims database (OptumLabs Data Warehouse) for the years 2006-2014. Patients having any prior use of any thyroid hormone preparation, amiodarone, or lithium were excluded. And patients were censored if they left the insurance plan, stopped treatment, or switched medication category.
The investigators identified 201,056 hypothyroid patients who started some type of thyroid hormone therapy. The majority (70.8%) started generic levothyroxine, and 22.1% started brand-name levothyroxine (Synthroid, Levoxyl, Tirosint, Unithroid). The small remaining group started another thyroid extract, triiodothyronine (T3), or a compounded preparation.
Primary care physicians were the main identifiable prescribers (60.3%), followed by endocrinologists (10.8%). “Endocrinologists tended to prescribe brand significantly more than the primary care physicians,” Dr. Smallridge said.
The investigators used propensity matching on a variety of factors (age, sex, race, census region, Charlson comorbidity index, year of index prescription, and a dozen baseline comorbidities) to compare patients starting brand-name versus generic levothyroxine. Outcomes were assessed during a median follow-up of 1 year (range, 0-9.3 years).
Event rates per 1,000 patient-years with branded versus generic levothyroxine were similar for atrial fibrillation (2.19 vs. 1.82; hazard ratio, 1.22, P = .19), myocardial infarction (1.83 vs. 2.12; HR, 0.86, P = .35), and congestive heart failure (2.00 vs. 2.27; HR, 0.88, P = .41). There was a borderline-significant difference on hospitalization for stroke, with marginally lower risk with brand-name levothyroxine (2.38 vs. 3.10; HR, 0.77; P = .05).
Findings were essentially the same in age-stratified analyses, splitting patients into subgroups younger and older than age 65.
When average 30-day costs were compared for users of branded versus generic levothyroxine, total cost for the branded drug was more than twice as high ($18.47 vs. $8.18).
“Thyroid preparations have been the most prescribed drug in the United States for several recent years. In the neighborhood of 25 million different patients a year take thyroid medications,” Dr. Smallridge said. “In terms of the dollars spent, it’s considerably less than some of the other drugs out there. But because of sheer numbers of patients, in terms of impact on health care dollars, it’s still a significant amount of money. And this is a lifelong treatment – once you go on thyroid hormones, you’re on them for life.”
The study had several strengths. “This is a very large, diverse, real-world population across the entire country with a wide range of ages,” Dr. Smallridge explained. “We got pharmacy claims documenting that they were continuing to get the refills, although we didn’t do pill counts, so we don’t know whether they were taking the medication. And a really important thing was the propensity score matching.”
At the same time, limitations included possible variations in coding and billing, and some residual confounding. “Key issues are that we need more data on longer-term follow-up, and we didn’t have lab values,” he added.
Dr. Smallridge reported that he had no relevant conflicts of interest.
AT ATA 2017
Key clinical point:
Major finding: Patients taking brand-name versus generic levothyroxine had similar risks of hospitalization for atrial fibrillation (HR, 1.22; P = .19), myocardial infarction (0.86; P = .35), congestive heart failure (0.88; P = .41), and stroke (0.77; P = .05).
Data source: A retrospective cohort study of 87,902 propensity-matched hypothyroid patients starting generic or brand-name levothyroxine.
Disclosures: Dr. Smallridge reported that he had no relevant conflicts of interest.
New appropriate use criteria reframe severe aortic stenosis
New appropriate use criteria (AUC) for severe aortic stenosis (AS) run the full gamut of clinical scenarios and treatment options.
“Cardiology is seeing a radical change in the management of aortic stenosis. This new document incorporates all therapies currently available in the world,” said Vinod H. Thourani, MD, who served on the AUC’s writing group on behalf of the American College of Cardiology. “The AUC highlights state-of-the-art therapy for aortic stenosis and, even more importantly, helps clarify the right indications for surgical and transcatheter valve replacement.”

Surgical risk is assessed based on the Society of Thoracic Surgeons Predicted Risk of Mortality score plus additional anatomic and functional considerations that should be assessed by a multidisciplinary heart team. The AUC repeatedly emphasizes this team’s importance. “Multiple comorbidities can change the pathway of treating AS, and this determination is best made by a heart team that at least includes a noninvasive cardiologist, an interventional cardiologist, and a cardiac surgeon,” Dr. Thourani said. “That’s how patients get the best care.”
Historically, aortic stenosis typically was managed medically or with balloon aortic valvuloplasty (BAV) or open aortic valve replacement, Dr. Thourani said. However, BAV is less common now, and indications for surgical or transcatheter aortic valve replacement (SAVR or TAVR) are expanding. Balloon aortic valvuloplasty sometimes does provide palliative treatment or serve as a bridge to a decision, the AUC states. For example, for a high-risk patient with severe aortic stenosis and severe secondary mitral regurgitation, BAV can help the heart team decide whether TAVR alone will improve mitral regurgitation or whether a double valve procedure is preferable.
Regardless of risk score, the AUC considers a wait-and-see approach as potentially appropriate for patients with asymptomatic high-grade AS whose left ventricular ejection fraction is at least 50%, peak aortic valve velocity is 4.0-4.9 m/sec, and exercise stress test is normal and with no predictors of symptom onset or rapid progression. Asymptomatic patients who are likely to become symptomatic but who have a low risk of sudden death are candidates for intervention (rated “appropriate”) or medical management (“may be appropriate”). In contrast, a positive stress test in an otherwise asymptomatic patient merits consideration of SAVR or TAVR regardless of surgical risk. The recommendations for asymptomatic patients reflect a lack of head-to-head trials in this population, Dr. Thourani said. “We don’t have good randomized data to show one therapy is better than another.”
Symptomatic, high-gradient, severe AS with associated coronary artery disease merits consideration of SAVR with coronary artery bypass graft or, in some cases, TAVR with percutaneous coronary intervention, according to the AUC. Less evidence supports SAVR with PCI. “Optimal management of coronary artery disease in patients with AS is a complex decision process requiring clinical, anatomical, and technical considerations that is best achieved with close collaboration between heart team members,” the authors stress.
The document covers other valvular and structural heart conditions that commonly accompany severe AS, such as symptomatic AS with bicuspid aortic valve and ascending aortic dilation. “Although there remains an increasing prevalence of transcatheter valve usage in bicuspid aortic valve, the standard of care remains surgical therapy, especially in patients who have a dilated aorta,” Dr. Thourani said.
For the first time, the AUC also addresses failing aortic valve prostheses, presenting six relevant clinical scenarios. The AUC consistently recommends SAVR, although the use of TAVR has “dramatically increased” in these patients, Dr. Thourani said. “Long-term data are still pending, but TAVR appears to be a less morbid procedure, when done appropriately.”
The societies involved in creating the AUC statement were the American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, European Association for Cardio-Thoracic Surgery, Heart Valve Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons.
Dr. Thourani disclosed ties to Edwards Lifesciences, St. Jude Medical, Abbott, Boston Scientific, and Medtronic.
New appropriate use criteria (AUC) for severe aortic stenosis (AS) run the full gamut of clinical scenarios and treatment options.
“Cardiology is seeing a radical change in the management of aortic stenosis. This new document incorporates all therapies currently available in the world,” said Vinod H. Thourani, MD, who served on the AUC’s writing group on behalf of the American College of Cardiology. “The AUC highlights state-of-the-art therapy for aortic stenosis and, even more importantly, helps clarify the right indications for surgical and transcatheter valve replacement.”
Surgical risk is assessed based on the Society of Thoracic Surgeons Predicted Risk of Mortality score plus additional anatomic and functional considerations that should be assessed by a multidisciplinary heart team. The AUC repeatedly emphasizes this team’s importance. “Multiple comorbidities can change the pathway of treating AS, and this determination is best made by a heart team that at least includes a noninvasive cardiologist, an interventional cardiologist, and a cardiac surgeon,” Dr. Thourani said. “That’s how patients get the best care.”
Historically, aortic stenosis typically was managed medically or with balloon aortic valvuloplasty (BAV) or open aortic valve replacement, Dr. Thourani said. However, BAV is less common now, and indications for surgical or transcatheter aortic valve replacement (SAVR or TAVR) are expanding. Balloon aortic valvuloplasty sometimes does provide palliative treatment or serve as a bridge to a decision, the AUC states. For example, for a high-risk patient with severe aortic stenosis and severe secondary mitral regurgitation, BAV can help the heart team decide whether TAVR alone will improve mitral regurgitation or whether a double valve procedure is preferable.
Regardless of risk score, the AUC considers a wait-and-see approach as potentially appropriate for patients with asymptomatic high-grade AS whose left ventricular ejection fraction is at least 50%, peak aortic valve velocity is 4.0-4.9 m/sec, and exercise stress test is normal and with no predictors of symptom onset or rapid progression. Asymptomatic patients who are likely to become symptomatic but who have a low risk of sudden death are candidates for intervention (rated “appropriate”) or medical management (“may be appropriate”). In contrast, a positive stress test in an otherwise asymptomatic patient merits consideration of SAVR or TAVR regardless of surgical risk. The recommendations for asymptomatic patients reflect a lack of head-to-head trials in this population, Dr. Thourani said. “We don’t have good randomized data to show one therapy is better than another.”
Symptomatic, high-gradient, severe AS with associated coronary artery disease merits consideration of SAVR with coronary artery bypass graft or, in some cases, TAVR with percutaneous coronary intervention, according to the AUC. Less evidence supports SAVR with PCI. “Optimal management of coronary artery disease in patients with AS is a complex decision process requiring clinical, anatomical, and technical considerations that is best achieved with close collaboration between heart team members,” the authors stress.
The document covers other valvular and structural heart conditions that commonly accompany severe AS, such as symptomatic AS with bicuspid aortic valve and ascending aortic dilation. “Although there remains an increasing prevalence of transcatheter valve usage in bicuspid aortic valve, the standard of care remains surgical therapy, especially in patients who have a dilated aorta,” Dr. Thourani said.
For the first time, the AUC also addresses failing aortic valve prostheses, presenting six relevant clinical scenarios. The AUC consistently recommends SAVR, although the use of TAVR has “dramatically increased” in these patients, Dr. Thourani said. “Long-term data are still pending, but TAVR appears to be a less morbid procedure, when done appropriately.”
The societies involved in creating the AUC statement were the American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, European Association for Cardio-Thoracic Surgery, Heart Valve Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons.
Dr. Thourani disclosed ties to Edwards Lifesciences, St. Jude Medical, Abbott, Boston Scientific, and Medtronic.
New appropriate use criteria (AUC) for severe aortic stenosis (AS) run the full gamut of clinical scenarios and treatment options.
“Cardiology is seeing a radical change in the management of aortic stenosis. This new document incorporates all therapies currently available in the world,” said Vinod H. Thourani, MD, who served on the AUC’s writing group on behalf of the American College of Cardiology. “The AUC highlights state-of-the-art therapy for aortic stenosis and, even more importantly, helps clarify the right indications for surgical and transcatheter valve replacement.”
Surgical risk is assessed based on the Society of Thoracic Surgeons Predicted Risk of Mortality score plus additional anatomic and functional considerations that should be assessed by a multidisciplinary heart team. The AUC repeatedly emphasizes this team’s importance. “Multiple comorbidities can change the pathway of treating AS, and this determination is best made by a heart team that at least includes a noninvasive cardiologist, an interventional cardiologist, and a cardiac surgeon,” Dr. Thourani said. “That’s how patients get the best care.”
Historically, aortic stenosis typically was managed medically or with balloon aortic valvuloplasty (BAV) or open aortic valve replacement, Dr. Thourani said. However, BAV is less common now, and indications for surgical or transcatheter aortic valve replacement (SAVR or TAVR) are expanding. Balloon aortic valvuloplasty sometimes does provide palliative treatment or serve as a bridge to a decision, the AUC states. For example, for a high-risk patient with severe aortic stenosis and severe secondary mitral regurgitation, BAV can help the heart team decide whether TAVR alone will improve mitral regurgitation or whether a double valve procedure is preferable.
Regardless of risk score, the AUC considers a wait-and-see approach as potentially appropriate for patients with asymptomatic high-grade AS whose left ventricular ejection fraction is at least 50%, peak aortic valve velocity is 4.0-4.9 m/sec, and exercise stress test is normal and with no predictors of symptom onset or rapid progression. Asymptomatic patients who are likely to become symptomatic but who have a low risk of sudden death are candidates for intervention (rated “appropriate”) or medical management (“may be appropriate”). In contrast, a positive stress test in an otherwise asymptomatic patient merits consideration of SAVR or TAVR regardless of surgical risk. The recommendations for asymptomatic patients reflect a lack of head-to-head trials in this population, Dr. Thourani said. “We don’t have good randomized data to show one therapy is better than another.”
Symptomatic, high-gradient, severe AS with associated coronary artery disease merits consideration of SAVR with coronary artery bypass graft or, in some cases, TAVR with percutaneous coronary intervention, according to the AUC. Less evidence supports SAVR with PCI. “Optimal management of coronary artery disease in patients with AS is a complex decision process requiring clinical, anatomical, and technical considerations that is best achieved with close collaboration between heart team members,” the authors stress.
The document covers other valvular and structural heart conditions that commonly accompany severe AS, such as symptomatic AS with bicuspid aortic valve and ascending aortic dilation. “Although there remains an increasing prevalence of transcatheter valve usage in bicuspid aortic valve, the standard of care remains surgical therapy, especially in patients who have a dilated aorta,” Dr. Thourani said.
For the first time, the AUC also addresses failing aortic valve prostheses, presenting six relevant clinical scenarios. The AUC consistently recommends SAVR, although the use of TAVR has “dramatically increased” in these patients, Dr. Thourani said. “Long-term data are still pending, but TAVR appears to be a less morbid procedure, when done appropriately.”
The societies involved in creating the AUC statement were the American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, European Association for Cardio-Thoracic Surgery, Heart Valve Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons.
Dr. Thourani disclosed ties to Edwards Lifesciences, St. Jude Medical, Abbott, Boston Scientific, and Medtronic.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY

Role grows for heart failure patient-reported outcomes
DALLAS – The Food and Drug Administration is keenly seeking patient-reported outcomes as endpoints in cardiovascular drug or device trials, particularly for heart failure patients, but the bar remains high for getting such an outcome into labeling, said agency officials who regulate cardiovascular disease therapies.
The FDA issued guidance nearly 8 years ago on how to integrate patient-reported outcome (PRO) measures into medical product development, but so far no heart failure drug nor device has met the agency’s standards for documented success in improving a PRO, despite the clear need for these patients to receive patient-centered care, clinicians said.

“We don’t yet have a patient-reported outcome in a label for heart failure,” Paul A. Heidenreich, MD, said during a session on PROs at the annual scientific meeting of the Heart Failure Society of America. He voiced hope that a PRO might end up on the label of a heart failure drug or device sometime in 2018. “Almost half of FDA submissions now include a PRO” as part of the data package, added Dr. Heidenreich, a cardiologist and professor of medicine at Stanford (Calif.) University.
For years, PROs for heart failure weren’t often used in trials, and they remain largely absent from routine practice – an absence Dr. Heidenreich lamented. “Just focusing on mortality in heart failure is really not patient centered,” he said.
Heart failure physicians “are very good at disease-centered care” that focuses on survival and reducing hospitalizations, but “survival is often not as important to patients,” noted Mary Norine Walsh, MD, medical director of the heart failure and cardiac transplantation program at St. Vincent Medical Group in Indianapolis. She suggested “tailoring treatment to improve patient symptoms, physical function, and quality of life” without necessarily reducing hospital readmissions or increasing survival rates. “Self-reported measures have more meaning for patients,” she said, and called for using PROs to better target interventions to the patients who can most benefit from them.
Two FDA representatives who spoke during the session agreed on the importance of PROs and attested to the agency’s interest in greater reliance on them.
“PROs are a critical complement to the other measures made in device trials,” said Bram Zuckerman, MD, director of the FDA’s division of cardiovascular devices. “We need PRO information because it reflects important aspects of patients’ health-related quality of life.”
The most commonly used PRO measures in device trials today are the Kansas City Cardiomyopathy Questionnaire (J Am Coll Cardiol. 2000 Apr;35[5]:1245-55) and the Minnesota Living With Heart Failure questionnaire, he noted.
“Neither is perfect, but there is a track record in heart failure device development that these two PROs can be helpful.” The FDA’s cardiovascular device division “wants to use PRO information,” Dr. Zuckerman said.
“All-cause mortality is the most unbiased endpoint, but there is interest in PROs,” agreed Ebony Dashiell-Aje, PhD, from the FDA’s office of new drugs in the Center for Drug Evaluation and Research. She highlighted the encouragement that the FDA gave to drug and device developers to include PROs in trials, both in its 2009 guidance document as well as in a “roadmap” from the agency on how to measure PROs in clinical trials. “Unfortunately, in heart failure we struggle to find tools that can adequately measure the patient’s perspective and be sensitive enough to detect a treatment benefit,” she said.

Norman Stockbridge, MD, director of the division of cardiovascular and renal products in the agency’s Office of Drug Evaluation, cited even bigger barriers to FDA approval of PROs as labeled effects from drugs or devices.
Getting a PRO endpoint supported by clinical-trial results that qualify it for an FDA label faces two big challenges. One challenge, he said, is “how much of an effect we need to see in a complex scoring algorithm to know that patients actually received some benefit in a disease that often varies from day to day and from week to week.” The second challenge is that, “in a disease with a high background rate of bad outcomes, you need some evidence that the benefit [from the treatment] is worth any risk,” which is something that can be hard to prove in heart failure when many patients don’t live more than 2 years with the disease, Dr. Stockbridge said in an interview.
“You need to be able to make the argument that the [PRO] benefit is likely perceptible to patients, but that is only half the problem. The other half is whether the developer can rule out that survival is not less than it would have been with no treatment. If patients take this, will they feel better but have a greater risk of being hurt?”

So far, no drug or device developer has succeeded in proving this to the FDA, despite the agency’s 2009 guidance on how it could be done.
That guidance “is one of the two worst and most destructive guidance documents we ever published,” Dr. Stockbridge declared.
Dr. Walsh, Dr. Heidenreich, Dr. Zuckerman, Dr. Dashiell-Aje, and Dr. Stockbridge had no relevant disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
DALLAS – The Food and Drug Administration is keenly seeking patient-reported outcomes as endpoints in cardiovascular drug or device trials, particularly for heart failure patients, but the bar remains high for getting such an outcome into labeling, said agency officials who regulate cardiovascular disease therapies.
The FDA issued guidance nearly 8 years ago on how to integrate patient-reported outcome (PRO) measures into medical product development, but so far no heart failure drug nor device has met the agency’s standards for documented success in improving a PRO, despite the clear need for these patients to receive patient-centered care, clinicians said.
“We don’t yet have a patient-reported outcome in a label for heart failure,” Paul A. Heidenreich, MD, said during a session on PROs at the annual scientific meeting of the Heart Failure Society of America. He voiced hope that a PRO might end up on the label of a heart failure drug or device sometime in 2018. “Almost half of FDA submissions now include a PRO” as part of the data package, added Dr. Heidenreich, a cardiologist and professor of medicine at Stanford (Calif.) University.
For years, PROs for heart failure weren’t often used in trials, and they remain largely absent from routine practice – an absence Dr. Heidenreich lamented. “Just focusing on mortality in heart failure is really not patient centered,” he said.
Heart failure physicians “are very good at disease-centered care” that focuses on survival and reducing hospitalizations, but “survival is often not as important to patients,” noted Mary Norine Walsh, MD, medical director of the heart failure and cardiac transplantation program at St. Vincent Medical Group in Indianapolis. She suggested “tailoring treatment to improve patient symptoms, physical function, and quality of life” without necessarily reducing hospital readmissions or increasing survival rates. “Self-reported measures have more meaning for patients,” she said, and called for using PROs to better target interventions to the patients who can most benefit from them.
Two FDA representatives who spoke during the session agreed on the importance of PROs and attested to the agency’s interest in greater reliance on them.
“PROs are a critical complement to the other measures made in device trials,” said Bram Zuckerman, MD, director of the FDA’s division of cardiovascular devices. “We need PRO information because it reflects important aspects of patients’ health-related quality of life.”
The most commonly used PRO measures in device trials today are the Kansas City Cardiomyopathy Questionnaire (J Am Coll Cardiol. 2000 Apr;35[5]:1245-55) and the Minnesota Living With Heart Failure questionnaire, he noted.
“Neither is perfect, but there is a track record in heart failure device development that these two PROs can be helpful.” The FDA’s cardiovascular device division “wants to use PRO information,” Dr. Zuckerman said.
“All-cause mortality is the most unbiased endpoint, but there is interest in PROs,” agreed Ebony Dashiell-Aje, PhD, from the FDA’s office of new drugs in the Center for Drug Evaluation and Research. She highlighted the encouragement that the FDA gave to drug and device developers to include PROs in trials, both in its 2009 guidance document as well as in a “roadmap” from the agency on how to measure PROs in clinical trials. “Unfortunately, in heart failure we struggle to find tools that can adequately measure the patient’s perspective and be sensitive enough to detect a treatment benefit,” she said.
Norman Stockbridge, MD, director of the division of cardiovascular and renal products in the agency’s Office of Drug Evaluation, cited even bigger barriers to FDA approval of PROs as labeled effects from drugs or devices.
Getting a PRO endpoint supported by clinical-trial results that qualify it for an FDA label faces two big challenges. One challenge, he said, is “how much of an effect we need to see in a complex scoring algorithm to know that patients actually received some benefit in a disease that often varies from day to day and from week to week.” The second challenge is that, “in a disease with a high background rate of bad outcomes, you need some evidence that the benefit [from the treatment] is worth any risk,” which is something that can be hard to prove in heart failure when many patients don’t live more than 2 years with the disease, Dr. Stockbridge said in an interview.
“You need to be able to make the argument that the [PRO] benefit is likely perceptible to patients, but that is only half the problem. The other half is whether the developer can rule out that survival is not less than it would have been with no treatment. If patients take this, will they feel better but have a greater risk of being hurt?”
So far, no drug or device developer has succeeded in proving this to the FDA, despite the agency’s 2009 guidance on how it could be done.
That guidance “is one of the two worst and most destructive guidance documents we ever published,” Dr. Stockbridge declared.
Dr. Walsh, Dr. Heidenreich, Dr. Zuckerman, Dr. Dashiell-Aje, and Dr. Stockbridge had no relevant disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
DALLAS – The Food and Drug Administration is keenly seeking patient-reported outcomes as endpoints in cardiovascular drug or device trials, particularly for heart failure patients, but the bar remains high for getting such an outcome into labeling, said agency officials who regulate cardiovascular disease therapies.
The FDA issued guidance nearly 8 years ago on how to integrate patient-reported outcome (PRO) measures into medical product development, but so far no heart failure drug nor device has met the agency’s standards for documented success in improving a PRO, despite the clear need for these patients to receive patient-centered care, clinicians said.
“We don’t yet have a patient-reported outcome in a label for heart failure,” Paul A. Heidenreich, MD, said during a session on PROs at the annual scientific meeting of the Heart Failure Society of America. He voiced hope that a PRO might end up on the label of a heart failure drug or device sometime in 2018. “Almost half of FDA submissions now include a PRO” as part of the data package, added Dr. Heidenreich, a cardiologist and professor of medicine at Stanford (Calif.) University.
For years, PROs for heart failure weren’t often used in trials, and they remain largely absent from routine practice – an absence Dr. Heidenreich lamented. “Just focusing on mortality in heart failure is really not patient centered,” he said.
Heart failure physicians “are very good at disease-centered care” that focuses on survival and reducing hospitalizations, but “survival is often not as important to patients,” noted Mary Norine Walsh, MD, medical director of the heart failure and cardiac transplantation program at St. Vincent Medical Group in Indianapolis. She suggested “tailoring treatment to improve patient symptoms, physical function, and quality of life” without necessarily reducing hospital readmissions or increasing survival rates. “Self-reported measures have more meaning for patients,” she said, and called for using PROs to better target interventions to the patients who can most benefit from them.
Two FDA representatives who spoke during the session agreed on the importance of PROs and attested to the agency’s interest in greater reliance on them.
“PROs are a critical complement to the other measures made in device trials,” said Bram Zuckerman, MD, director of the FDA’s division of cardiovascular devices. “We need PRO information because it reflects important aspects of patients’ health-related quality of life.”
The most commonly used PRO measures in device trials today are the Kansas City Cardiomyopathy Questionnaire (J Am Coll Cardiol. 2000 Apr;35[5]:1245-55) and the Minnesota Living With Heart Failure questionnaire, he noted.
“Neither is perfect, but there is a track record in heart failure device development that these two PROs can be helpful.” The FDA’s cardiovascular device division “wants to use PRO information,” Dr. Zuckerman said.
“All-cause mortality is the most unbiased endpoint, but there is interest in PROs,” agreed Ebony Dashiell-Aje, PhD, from the FDA’s office of new drugs in the Center for Drug Evaluation and Research. She highlighted the encouragement that the FDA gave to drug and device developers to include PROs in trials, both in its 2009 guidance document as well as in a “roadmap” from the agency on how to measure PROs in clinical trials. “Unfortunately, in heart failure we struggle to find tools that can adequately measure the patient’s perspective and be sensitive enough to detect a treatment benefit,” she said.
Norman Stockbridge, MD, director of the division of cardiovascular and renal products in the agency’s Office of Drug Evaluation, cited even bigger barriers to FDA approval of PROs as labeled effects from drugs or devices.
Getting a PRO endpoint supported by clinical-trial results that qualify it for an FDA label faces two big challenges. One challenge, he said, is “how much of an effect we need to see in a complex scoring algorithm to know that patients actually received some benefit in a disease that often varies from day to day and from week to week.” The second challenge is that, “in a disease with a high background rate of bad outcomes, you need some evidence that the benefit [from the treatment] is worth any risk,” which is something that can be hard to prove in heart failure when many patients don’t live more than 2 years with the disease, Dr. Stockbridge said in an interview.
“You need to be able to make the argument that the [PRO] benefit is likely perceptible to patients, but that is only half the problem. The other half is whether the developer can rule out that survival is not less than it would have been with no treatment. If patients take this, will they feel better but have a greater risk of being hurt?”
So far, no drug or device developer has succeeded in proving this to the FDA, despite the agency’s 2009 guidance on how it could be done.
That guidance “is one of the two worst and most destructive guidance documents we ever published,” Dr. Stockbridge declared.
Dr. Walsh, Dr. Heidenreich, Dr. Zuckerman, Dr. Dashiell-Aje, and Dr. Stockbridge had no relevant disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE HFSA ANNUAL SCIENTIFIC MEETING