User login
Predictors of Unplanned Postoperative Visits in a Veterans Affairs Hand Surgery Practice
Predictors of Unplanned Postoperative Visits in a Veterans Affairs Hand Surgery Practice
Patients make unplanned appointments after elective soft tissue hand surgery for real or perceived complications when they experience pain, anxiety, or fear. Unplanned appointments can create travel and financial burdens for patients and families. These appointments take time away from scheduled appointments and can contribute to late arrivals and delays in other clinics. Unscheduled appointments contribute to poor access when staff are diverted from scheduled appointments. If predictive factors can be identified, unplanned appointments may either be ameliorated or avoided with better perioperative risk management or education.
Methods
The US Department of Veterans Affairs (VA) North Florida/South Georgia Veterans Health System (NFSGVAHS) and University of Florida Institutional Review Board approved a retrospective chart review of all plastic surgery cases performed at the Malcom Randall VA Medical Center (MRVAMC) and Lake City VAMC operating rooms from July 1, 2018, through December 31, 2019, and January 1, 2021, through June 30, 2022 (nonurgent surgeries were discouraged during the COVID-19 pandemic). Elective soft tissue hand surgery cases were identified based on the operative description found in the Surgical Service Surgeon Staffing Report reviewed monthly by the Service Chief. Potential indicators of unplanned visits were recorded, including age; sex; diagnosis of diabetes, depression, anxiety, or posttraumatic stress disorder (PTSD); current smoking status; and residential zip code. We used the first 3 digits of the patients’ zip codes, which indicate region, as an estimate of proximity to the MRVAMC, which has a 50-county catchment area across North Florida and South Georgia. Diagnoses were found on the “problem list” from the electronic health record documented in the history and physical examinations before surgery. Clinic notes were examined for 3 months postsurgery to identify unplanned postoperative visits and the reason for the appointment. A χ2 analysis was conducted using Excel Version 2402. P < .05 was used to determine whether age (> 60 years), sex, proximity to MRVAMC, diabetes, smoking, depression, anxiety, or PTSD were statistically significant independent risk factors for these appointments.
Results
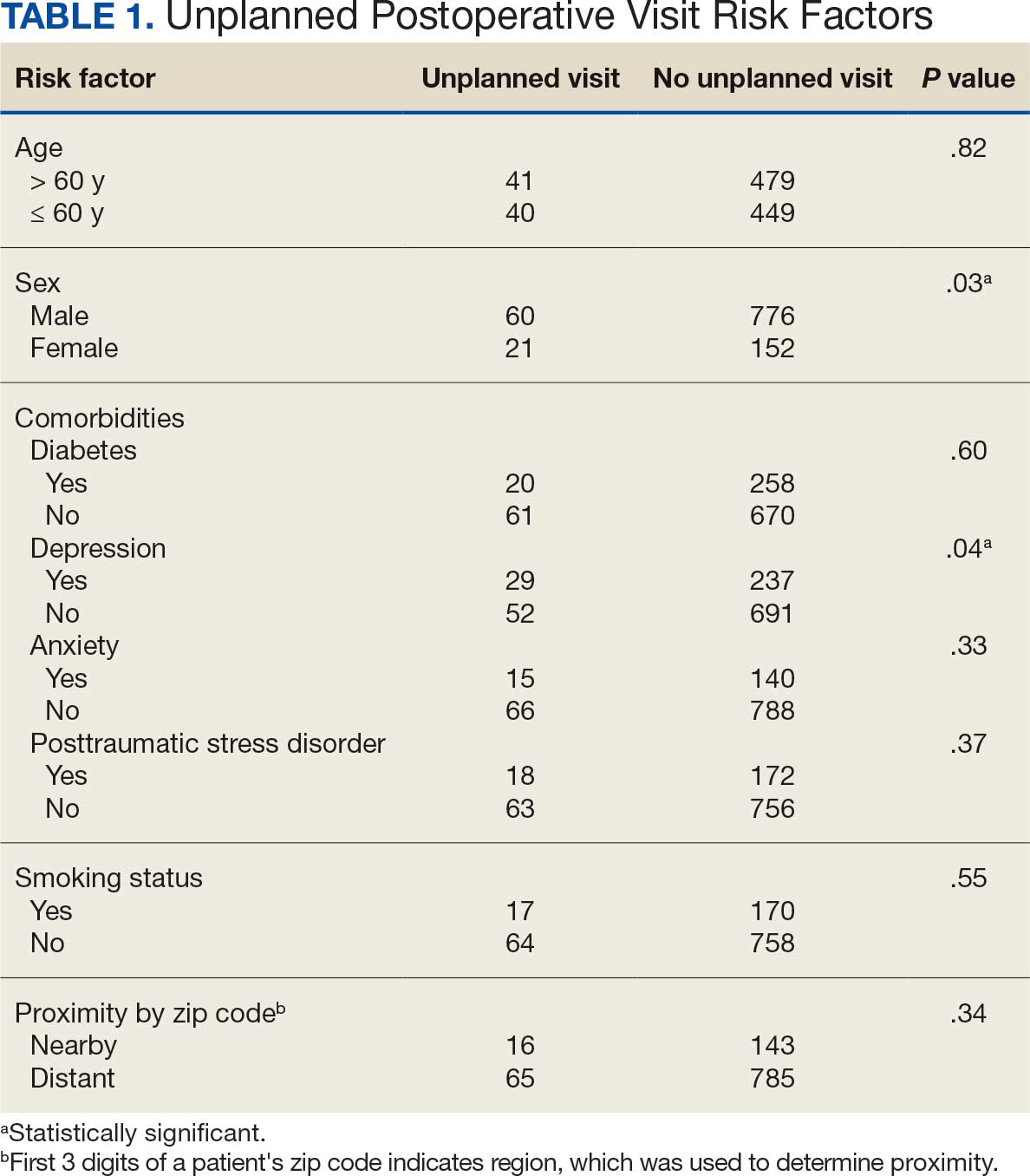
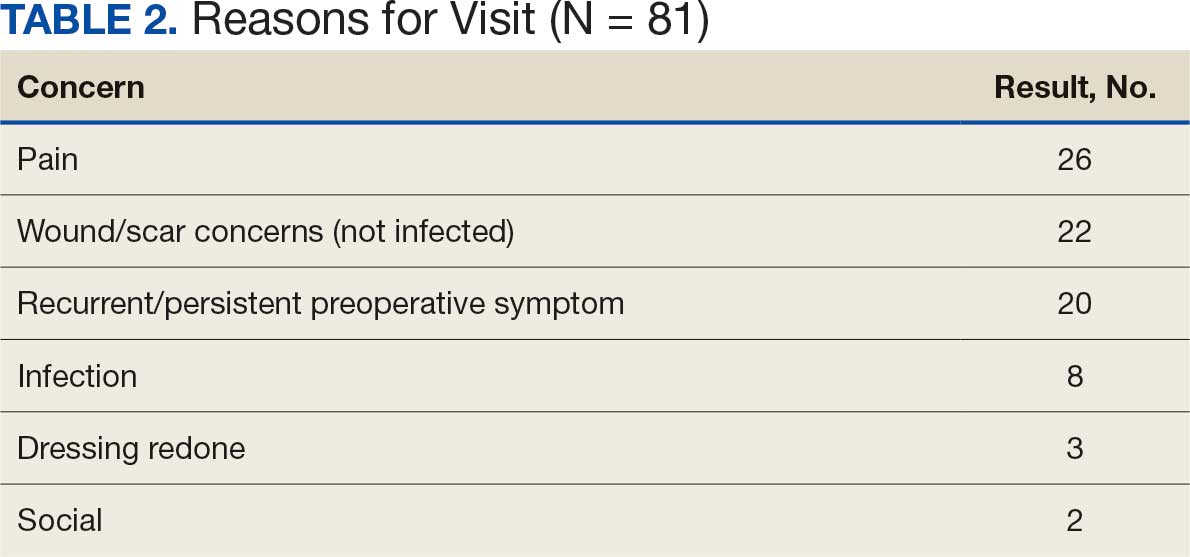
A total of 1009 elective soft tissue hand surgeries at MRVAMC were reviewed. The patients median age was 61 years. Patients included 173 women (17.1%) and 836 men (82.9%). Eighty-one patients (8.0%) returned for unplanned visits. Age (P = .82); proximity to MRVAMC (P = .34); and diabetes (P = .60), smoking (P = .55), anxiety (P = .33), or PTSD (P = .37) were not statistically significant predictors of unplanned appointments. Depression diagnosis (P = .04) and female sex (P = .03) were found to be independent risk factors for an unplanned appointment (Table 1). The most common indication for the requested appointment was pain-related, followed closely by noninfectious wound concerns and persistent symptoms (Table 2).
Discussion
Improved access, quality, and efficiency for patients are goals for the VA.1-3 The MRVAMC Plastic and Hand Surgery service provides care for the NFSGVAHS and receives an average of 15 to 20 consultation requests daily. The Veterans Health Administration is frequently challenged by staff shortages, and surgical services struggle to respond to consultation requests and treat patients within reasonable time frames.4,5
The objective of this study was to identify risk factors for unplanned postoperative appointments following elective hand surgery. Unplanned appointments prevent scheduled patients from being seen on time and contribute to backlogs and delays. When patients schedule multiple appointments on the same day, delays in the first clinic’s scheduled appointments create delays for the second and third clinics. Hand surgery clinics can provide a better experience for patients and staff by identifying and mitigating factors prompting unplanned visits.
We anticipated that wound complications would prompt unscheduled visits. Diabetes is a known risk factor for wound healing complications after plastic and hand surgery.6,7 A hemoglobin A1c (HbA1c) screening protocol used by the NFSGVAHS plastic surgery service since 2015 to identify poorly controlled patients with diabetes before surgery may partially explain this finding.8 We did not find a statistically significant difference between patients with diabetes and patients without diabetes for scheduling unplanned appointments. The plastic surgery service does not perform elective hand surgery unless the patient’s HbA1c level is < 9%, or violate the flexor sheath unless HbA1c level is < 8%. However, Zhuang et al found an increase in soft tissue infections after hand surgery with HbA1c levels ≥ 7%.9
Smoking is a potential factor in postoperative hand surgery complications.10,11 Lans et al found an increased incidence of 30-day emergency room visits in current and former smokers after outpatient upper extremity fracture surgery.12 The MRVAMC Plastic Surgery Service counsels patients about the risk of skin necrosis and delayed wound healing, but does not cancel cases or obtain laboratory values to verify abstinence in patients undergoing hand surgery. The VA has multiple resources available for patients interested in smoking cessation through mental health services.13
MRVAMC patients have been known to resist returning for scheduled appointments due to the costs or availability of transportation. We suspected that patients who lived further from MRVAMC would be less likely to return for unscheduled visits. We used the first 3 digits of the patients’ mailing zip code to estimate residential proximity to MRVAMC. An acknowledged limitation to this approach is that some veterans have primary addresses in other regions but still spend significant time in the MRVAMC catchment area and use the facility for their health care during the winter months. These “snowbirds” might reside near the facility despite having official addresses that are more distant. Additionally, there was no increased risk of unplanned visits after hand surgery in patients aged > 61 years (the median age of study participants) (P = .82). Dependence on a third party for transportation in older veterans could impact this finding.
Based on the observation that most patients needed reassurance rather than an intervention when they returned for unscheduled appointments, diagnoses of depression, anxiety, and PTSD were evaluated as separate predictive factors. In previous research, anxiety was found to be a risk factor for problematic recovery following carpal tunnel surgery.14 In the current study, depression was found to be a statistically significant predictor of unscheduled postoperative appointments (P = .04), while anxiety (P = .33) and PTSD (P = .37) were not statistically significant predictors. This is consistent with other studies that have found preexisting depression can predict complications after hand surgery.15,16 Vranceanu et al found that depression predicted pain intensity and disability after elective hand surgery.16 Similarly, Oflazoglu et al found a 12% incidence of depression based on the Patient Health Questionnaire-9 in new and returning hand patients who presented to an academic practice.17 They suggest patients should be assessed at all levels of care and that those with poor responses to surgical or nonsurgical management should be evaluated for depression. MRVAMC has a large mental health service consisting of psychiatrists, psychologists, addiction specialists, social workers, and homeless outreach, and patients tend to already have a diagnosis and mental health practitioner when they present to the clinic.
Recent studies found that wound problems, pain, and stiffness were the most common reasons for return visits.18,19 Shetty et al identified younger age, worse preoperative pain scores, and poor access to transportation as predictors of preventable emergency room visits, which generate higher health care expenditures than an office visit.19 Our study’s top reasons for appointments (pain, wound/scar concerns, persistent symptoms) can be addressed with additional presurgery patient and family education. Additionally, clinicians encourage nonnarcotic pain management strategies including anti-inflammatories, acetaminophen, elevation, splinting, and hand therapy, and the hospital employs experienced, fellowship-trained anesthesia block faculty who help limit perioperative narcotic use. Patients are advised that pain can be used to guide them through the postoperative recovery by preventing overuse and alerting them to a problem that would be masked with narcotics, and long-standing problems such as chronic nerve compressions may continue to cause pain after surgery.
Patients and families can be given consistent and repetitive verbal and written information, instructions, and expectations at the initial consultation, preoperative appointment, and on the day of surgery. Postoperatively, outside their scheduled appointments, patients are encouraged to use the My HealtheVet secure messaging system or call the clinic to access an experienced registered nurse before making a long drive. Access to virtual or phone visits can reduce emergent in-person visits in a VA population.20
Ozdag et al found that 42% of patients who had elective carpal tunnel surgery made unplanned electronic messages or phone contact within 2 weeks postsurgery. The authors point out the uncompensated administrative burden on the staff answering these messages and suggest pre-empting the contacts with more up-front education regarding postoperative pain expectations and management strategies.21
Fisher et al found that attending hand therapy reduced the number of emergency department visits in postoperative infection cases.22 At MRVAMC, a postoperative emergency department visit for a patient prompts an urgent unplanned appointment to the plastic surgery clinic, often on the same day. The MRVAMC occupational therapy clinic employed 3 on-site certified hand therapists during the study period. Because all hand surgery patients at the clinic receive hand therapy on the same day as their first postoperative appointment, attendance at hand therapy was not evaluated as a predictor of unplanned visits. Scheduled hand therapy is another point of contact where the clinic can provide reassurance and patient education.
While females made up 17.1% of the patients in this study, they constituted 12.5% of all veterans in Florida in fiscal year 2023.23 This study found that women were more likely to present for unplanned postoperative appointments (P = .03). This is consistent with existing literature which has found that women are higher users of health care and office-based appointments.24,25 This finding suggests the need for further study into whether our methods of communicating instructions to female patients undergoing plastic surgery may not be optimal.
Strengths and Limitations
As a retrospective review, the authors used information documented by multiple different health care practitioners, including trainees. The electronic medical record problem lists and templates provide consistency of information; however, less seasoned clinicians may interpret what they see and hear differently from more experienced clinicians in the postoperative setting. This study occurred in one part of the country with demographics that may not mirror other VA systems or the general population. The authors hope this study can be a starting point for other health care facilities to investigate ways to minimize the burden of unscheduled appointments. A strength of the study is that it was conducted within a closed system, as patients tend to stay within the VA system and documentation and communication among clinicians, even outside the immediate facility, are easily accessed through the electronic health record.
Conclusions
This study found that depression diagnosis and female sex are statistically significant predictors of unplanned postoperative visits after elective soft tissue hand surgery. More effective patient education during the preoperative period, particularly in patients with depression, may be warranted.
- Apaydin EA, Paige NM, Begashaw MM, et al. Veterans Health Administration (VA) vs. non-VA healthcare quality: a systematic review. J Gen Intern Med. 2023;38:2179-2188. doi:10.1007/s11606-023-08207-2
- Blegen M, Ko J, Salzman G, et al. Comparing quality of surgical care between the US Department of Veterans Affairs and non-Veterans Affairs settings: a systematic review. J Am Coll Surg. 2023;237:352-361. doi:10.1097/XCS.0000000000000720
- Valsangkar NP, Eppstein AC, Lawson RA, et al. Effect of lean processes on surgical wait times and efficiency in a tertiary care veterans affairs medical center. JAMA Surg. 2017;152:42-47. doi:10.1001/jamasurg.2016.2808
- National Association of Veterans Affairs Physicians and Dentists. Physicians remain at top of staffing shortage in VA. NAVAPD. December 20, 2023. Accessed March 16, 2026. https://www.navapd.org/news/physicians-remain-at-top-of-staffing-shortage-in-va
- OIG Determination of Veterans Health Administration’s severe occupational staffing shortages fiscal year 2024. Veterans Affairs Office of Inspector General. August 7, 2024. Accessed February 4, 2026. https://www.vaoig.gov/reports/national-healthcare-review/oig-determination-veterans-health-administrations-severe-0
- Goltsman D, Morrison KA, Ascherman JA. Defining the association between diabetes and plastic surgery outcomes: an analysis of nearly 40,000 patients. Plast Reconstr Surg Glob Open. 2017;5:e1461. doi:10.1097/GOX.0000000000001461 7.
- Cox CT, Sierra S, Egan A, et al. Elevated hemoglobin A1c and the risk of postoperative complications in elective hand and upper extremity surgery. Cureus. 2023;15:e48373. doi:10.7759/cureus.48373
- Coady-Fariborzian L, Anstead C. HbA1c and infection in diabetic elective hand surgery: a Veterans Affair Medical Center experience 2012-2018. Hand (NY). 2023;18:994-998. doi:10.1177/1558944720937363<
- Zhuang T, Shapiro LM, Fogel N, et al. Perioperative laboratory markers as risk factors for surgical site infection after elective hand surgery. J Hand Surg Am. 2021;46:675-684. doi:10.1016/j.jhsa.2021.04.001
- Cho BH, Aziz KT, Giladi AM. The impact of smoking on early postoperative complications in hand surgery. J Hand Surg Am. 2021;46:336.e1-336.e11. doi:10.1016/j.jhsa.2020.07.01411.
- Del Core MA, Ahn J, Golden AS, et al. Effect of smoking on short-term postoperative complications after elective upper extremity surgery. Hand (N Y). 2022;17:231-238. doi:10.1177/1558944720926638
- Lans J, Beagles CB, Watkins IT, et al. Unplanned postoperative emergency department visits after upper extremity fracture surgery. J Orthop Trauma. 2025;39:22-27. doi:10.1097/BOT.0000000000002925
- Tobacco and health - how to quit. US Dept of Veterans Affairs. Updated October 29, 2025. Accessed February 4, 2026. https://www.mentalhealth.va.gov/quit-tobacco/how-to-quit.asp
- Ryan C, Miner H, Ramachandran S, et al. General anxiety is associated with problematic initial recovery after carpal tunnel release. Clin Orthop Relat Res. 2022;480:1576-1581. doi:10.1097/CORR.0000000000002115
- Crijns TJ, Bernstein DN, Ring D, et al. Depression and pain interference correlate with physical function in patients recovering from hand surgery. Hand (N Y). 2019;14:830-835. doi:10.1177/1558944718777814
- Vranceanu AM, Jupiter JB, Mudgal CS, et al. Predictors of pain intensity and disability after minor hand surgery. J Hand Surg Am. 2010;35:956-960. doi:10.1016/j.jhsa.2010.02.00117.
- Oflazoglu K, Mellema JJ, Menendez ME, et al. Prevalence of and factors associated with major depression in patients with upper extremity conditions. J Hand Surg Am. 2016;41:263-269. doi:10.1016/j.jhsa.2015.11.019
- Townsend CB, Henry TW, Lutsky KF, et al. Unplanned office visits following outpatient hand surgery. Hand (N Y). 2022;17:1264-1268. doi:10.1177/15589447211028932
- Shetty PN, Guarino GM, Zhang G, et al. Risk factors for preventable emergency department use after outpatient hand surgery. J Hand Surg Am. 2022;47:855-864. doi:10.1016/j.jhsa.2022.05.012
- Sommers-Olson B, Christianson J, Neumann T, et al. Reducing nonemergent visits to the emergency department in a Veterans Affairs multistate system. J Emerg Nurs. 2023;49:539-545. doi:10.1016/j.jen.2023.02.010
- Ozdag Y, Manzar S, El Koussaify J, et al. Unplanned postoperative phone calls and electronic messages for patients with and without opioid prescriptions after carpal tunnel release. J Hand Surg Glob Online. 2024;6:363-368. doi:10.1016/j.jhsg.2024.02.006
- Fisher AH, Gandhi J, Nelson Z, et al. Immediate interventions after surgery to reduce readmission for upper extremity infections. Ann Plast Surg. 2022;88:S163-S169. doi:10.1097/SAP.0000000000003141
- Florida Department of Veterans Affairs Fast Facts. Florida Department of Veterans Affairs. Accessed February 4, 2026. https://floridavets.org/our-veterans/profilefast-facts/
- Bertakis KD, Azari R, Helms LJ, et al. Gender differences in the utilization of health care services. J Fam Pract. 2000;49:147-152.
- Ashman JJ, Santo L, Okeyode T. Characteristics of office-based physician visits, 2018. NCHS Data Brief. 2021;408:1-8.
Patients make unplanned appointments after elective soft tissue hand surgery for real or perceived complications when they experience pain, anxiety, or fear. Unplanned appointments can create travel and financial burdens for patients and families. These appointments take time away from scheduled appointments and can contribute to late arrivals and delays in other clinics. Unscheduled appointments contribute to poor access when staff are diverted from scheduled appointments. If predictive factors can be identified, unplanned appointments may either be ameliorated or avoided with better perioperative risk management or education.
Methods
The US Department of Veterans Affairs (VA) North Florida/South Georgia Veterans Health System (NFSGVAHS) and University of Florida Institutional Review Board approved a retrospective chart review of all plastic surgery cases performed at the Malcom Randall VA Medical Center (MRVAMC) and Lake City VAMC operating rooms from July 1, 2018, through December 31, 2019, and January 1, 2021, through June 30, 2022 (nonurgent surgeries were discouraged during the COVID-19 pandemic). Elective soft tissue hand surgery cases were identified based on the operative description found in the Surgical Service Surgeon Staffing Report reviewed monthly by the Service Chief. Potential indicators of unplanned visits were recorded, including age; sex; diagnosis of diabetes, depression, anxiety, or posttraumatic stress disorder (PTSD); current smoking status; and residential zip code. We used the first 3 digits of the patients’ zip codes, which indicate region, as an estimate of proximity to the MRVAMC, which has a 50-county catchment area across North Florida and South Georgia. Diagnoses were found on the “problem list” from the electronic health record documented in the history and physical examinations before surgery. Clinic notes were examined for 3 months postsurgery to identify unplanned postoperative visits and the reason for the appointment. A χ2 analysis was conducted using Excel Version 2402. P < .05 was used to determine whether age (> 60 years), sex, proximity to MRVAMC, diabetes, smoking, depression, anxiety, or PTSD were statistically significant independent risk factors for these appointments.
Results
A total of 1009 elective soft tissue hand surgeries at MRVAMC were reviewed. The patients median age was 61 years. Patients included 173 women (17.1%) and 836 men (82.9%). Eighty-one patients (8.0%) returned for unplanned visits. Age (P = .82); proximity to MRVAMC (P = .34); and diabetes (P = .60), smoking (P = .55), anxiety (P = .33), or PTSD (P = .37) were not statistically significant predictors of unplanned appointments. Depression diagnosis (P = .04) and female sex (P = .03) were found to be independent risk factors for an unplanned appointment (Table 1). The most common indication for the requested appointment was pain-related, followed closely by noninfectious wound concerns and persistent symptoms (Table 2).
Discussion
Improved access, quality, and efficiency for patients are goals for the VA.1-3 The MRVAMC Plastic and Hand Surgery service provides care for the NFSGVAHS and receives an average of 15 to 20 consultation requests daily. The Veterans Health Administration is frequently challenged by staff shortages, and surgical services struggle to respond to consultation requests and treat patients within reasonable time frames.4,5
The objective of this study was to identify risk factors for unplanned postoperative appointments following elective hand surgery. Unplanned appointments prevent scheduled patients from being seen on time and contribute to backlogs and delays. When patients schedule multiple appointments on the same day, delays in the first clinic’s scheduled appointments create delays for the second and third clinics. Hand surgery clinics can provide a better experience for patients and staff by identifying and mitigating factors prompting unplanned visits.
We anticipated that wound complications would prompt unscheduled visits. Diabetes is a known risk factor for wound healing complications after plastic and hand surgery.6,7 A hemoglobin A1c (HbA1c) screening protocol used by the NFSGVAHS plastic surgery service since 2015 to identify poorly controlled patients with diabetes before surgery may partially explain this finding.8 We did not find a statistically significant difference between patients with diabetes and patients without diabetes for scheduling unplanned appointments. The plastic surgery service does not perform elective hand surgery unless the patient’s HbA1c level is < 9%, or violate the flexor sheath unless HbA1c level is < 8%. However, Zhuang et al found an increase in soft tissue infections after hand surgery with HbA1c levels ≥ 7%.9
Smoking is a potential factor in postoperative hand surgery complications.10,11 Lans et al found an increased incidence of 30-day emergency room visits in current and former smokers after outpatient upper extremity fracture surgery.12 The MRVAMC Plastic Surgery Service counsels patients about the risk of skin necrosis and delayed wound healing, but does not cancel cases or obtain laboratory values to verify abstinence in patients undergoing hand surgery. The VA has multiple resources available for patients interested in smoking cessation through mental health services.13
MRVAMC patients have been known to resist returning for scheduled appointments due to the costs or availability of transportation. We suspected that patients who lived further from MRVAMC would be less likely to return for unscheduled visits. We used the first 3 digits of the patients’ mailing zip code to estimate residential proximity to MRVAMC. An acknowledged limitation to this approach is that some veterans have primary addresses in other regions but still spend significant time in the MRVAMC catchment area and use the facility for their health care during the winter months. These “snowbirds” might reside near the facility despite having official addresses that are more distant. Additionally, there was no increased risk of unplanned visits after hand surgery in patients aged > 61 years (the median age of study participants) (P = .82). Dependence on a third party for transportation in older veterans could impact this finding.
Based on the observation that most patients needed reassurance rather than an intervention when they returned for unscheduled appointments, diagnoses of depression, anxiety, and PTSD were evaluated as separate predictive factors. In previous research, anxiety was found to be a risk factor for problematic recovery following carpal tunnel surgery.14 In the current study, depression was found to be a statistically significant predictor of unscheduled postoperative appointments (P = .04), while anxiety (P = .33) and PTSD (P = .37) were not statistically significant predictors. This is consistent with other studies that have found preexisting depression can predict complications after hand surgery.15,16 Vranceanu et al found that depression predicted pain intensity and disability after elective hand surgery.16 Similarly, Oflazoglu et al found a 12% incidence of depression based on the Patient Health Questionnaire-9 in new and returning hand patients who presented to an academic practice.17 They suggest patients should be assessed at all levels of care and that those with poor responses to surgical or nonsurgical management should be evaluated for depression. MRVAMC has a large mental health service consisting of psychiatrists, psychologists, addiction specialists, social workers, and homeless outreach, and patients tend to already have a diagnosis and mental health practitioner when they present to the clinic.
Recent studies found that wound problems, pain, and stiffness were the most common reasons for return visits.18,19 Shetty et al identified younger age, worse preoperative pain scores, and poor access to transportation as predictors of preventable emergency room visits, which generate higher health care expenditures than an office visit.19 Our study’s top reasons for appointments (pain, wound/scar concerns, persistent symptoms) can be addressed with additional presurgery patient and family education. Additionally, clinicians encourage nonnarcotic pain management strategies including anti-inflammatories, acetaminophen, elevation, splinting, and hand therapy, and the hospital employs experienced, fellowship-trained anesthesia block faculty who help limit perioperative narcotic use. Patients are advised that pain can be used to guide them through the postoperative recovery by preventing overuse and alerting them to a problem that would be masked with narcotics, and long-standing problems such as chronic nerve compressions may continue to cause pain after surgery.
Patients and families can be given consistent and repetitive verbal and written information, instructions, and expectations at the initial consultation, preoperative appointment, and on the day of surgery. Postoperatively, outside their scheduled appointments, patients are encouraged to use the My HealtheVet secure messaging system or call the clinic to access an experienced registered nurse before making a long drive. Access to virtual or phone visits can reduce emergent in-person visits in a VA population.20
Ozdag et al found that 42% of patients who had elective carpal tunnel surgery made unplanned electronic messages or phone contact within 2 weeks postsurgery. The authors point out the uncompensated administrative burden on the staff answering these messages and suggest pre-empting the contacts with more up-front education regarding postoperative pain expectations and management strategies.21
Fisher et al found that attending hand therapy reduced the number of emergency department visits in postoperative infection cases.22 At MRVAMC, a postoperative emergency department visit for a patient prompts an urgent unplanned appointment to the plastic surgery clinic, often on the same day. The MRVAMC occupational therapy clinic employed 3 on-site certified hand therapists during the study period. Because all hand surgery patients at the clinic receive hand therapy on the same day as their first postoperative appointment, attendance at hand therapy was not evaluated as a predictor of unplanned visits. Scheduled hand therapy is another point of contact where the clinic can provide reassurance and patient education.
While females made up 17.1% of the patients in this study, they constituted 12.5% of all veterans in Florida in fiscal year 2023.23 This study found that women were more likely to present for unplanned postoperative appointments (P = .03). This is consistent with existing literature which has found that women are higher users of health care and office-based appointments.24,25 This finding suggests the need for further study into whether our methods of communicating instructions to female patients undergoing plastic surgery may not be optimal.
Strengths and Limitations
As a retrospective review, the authors used information documented by multiple different health care practitioners, including trainees. The electronic medical record problem lists and templates provide consistency of information; however, less seasoned clinicians may interpret what they see and hear differently from more experienced clinicians in the postoperative setting. This study occurred in one part of the country with demographics that may not mirror other VA systems or the general population. The authors hope this study can be a starting point for other health care facilities to investigate ways to minimize the burden of unscheduled appointments. A strength of the study is that it was conducted within a closed system, as patients tend to stay within the VA system and documentation and communication among clinicians, even outside the immediate facility, are easily accessed through the electronic health record.
Conclusions
This study found that depression diagnosis and female sex are statistically significant predictors of unplanned postoperative visits after elective soft tissue hand surgery. More effective patient education during the preoperative period, particularly in patients with depression, may be warranted.
Patients make unplanned appointments after elective soft tissue hand surgery for real or perceived complications when they experience pain, anxiety, or fear. Unplanned appointments can create travel and financial burdens for patients and families. These appointments take time away from scheduled appointments and can contribute to late arrivals and delays in other clinics. Unscheduled appointments contribute to poor access when staff are diverted from scheduled appointments. If predictive factors can be identified, unplanned appointments may either be ameliorated or avoided with better perioperative risk management or education.
Methods
The US Department of Veterans Affairs (VA) North Florida/South Georgia Veterans Health System (NFSGVAHS) and University of Florida Institutional Review Board approved a retrospective chart review of all plastic surgery cases performed at the Malcom Randall VA Medical Center (MRVAMC) and Lake City VAMC operating rooms from July 1, 2018, through December 31, 2019, and January 1, 2021, through June 30, 2022 (nonurgent surgeries were discouraged during the COVID-19 pandemic). Elective soft tissue hand surgery cases were identified based on the operative description found in the Surgical Service Surgeon Staffing Report reviewed monthly by the Service Chief. Potential indicators of unplanned visits were recorded, including age; sex; diagnosis of diabetes, depression, anxiety, or posttraumatic stress disorder (PTSD); current smoking status; and residential zip code. We used the first 3 digits of the patients’ zip codes, which indicate region, as an estimate of proximity to the MRVAMC, which has a 50-county catchment area across North Florida and South Georgia. Diagnoses were found on the “problem list” from the electronic health record documented in the history and physical examinations before surgery. Clinic notes were examined for 3 months postsurgery to identify unplanned postoperative visits and the reason for the appointment. A χ2 analysis was conducted using Excel Version 2402. P < .05 was used to determine whether age (> 60 years), sex, proximity to MRVAMC, diabetes, smoking, depression, anxiety, or PTSD were statistically significant independent risk factors for these appointments.
Results
A total of 1009 elective soft tissue hand surgeries at MRVAMC were reviewed. The patients median age was 61 years. Patients included 173 women (17.1%) and 836 men (82.9%). Eighty-one patients (8.0%) returned for unplanned visits. Age (P = .82); proximity to MRVAMC (P = .34); and diabetes (P = .60), smoking (P = .55), anxiety (P = .33), or PTSD (P = .37) were not statistically significant predictors of unplanned appointments. Depression diagnosis (P = .04) and female sex (P = .03) were found to be independent risk factors for an unplanned appointment (Table 1). The most common indication for the requested appointment was pain-related, followed closely by noninfectious wound concerns and persistent symptoms (Table 2).
Discussion
Improved access, quality, and efficiency for patients are goals for the VA.1-3 The MRVAMC Plastic and Hand Surgery service provides care for the NFSGVAHS and receives an average of 15 to 20 consultation requests daily. The Veterans Health Administration is frequently challenged by staff shortages, and surgical services struggle to respond to consultation requests and treat patients within reasonable time frames.4,5
The objective of this study was to identify risk factors for unplanned postoperative appointments following elective hand surgery. Unplanned appointments prevent scheduled patients from being seen on time and contribute to backlogs and delays. When patients schedule multiple appointments on the same day, delays in the first clinic’s scheduled appointments create delays for the second and third clinics. Hand surgery clinics can provide a better experience for patients and staff by identifying and mitigating factors prompting unplanned visits.
We anticipated that wound complications would prompt unscheduled visits. Diabetes is a known risk factor for wound healing complications after plastic and hand surgery.6,7 A hemoglobin A1c (HbA1c) screening protocol used by the NFSGVAHS plastic surgery service since 2015 to identify poorly controlled patients with diabetes before surgery may partially explain this finding.8 We did not find a statistically significant difference between patients with diabetes and patients without diabetes for scheduling unplanned appointments. The plastic surgery service does not perform elective hand surgery unless the patient’s HbA1c level is < 9%, or violate the flexor sheath unless HbA1c level is < 8%. However, Zhuang et al found an increase in soft tissue infections after hand surgery with HbA1c levels ≥ 7%.9
Smoking is a potential factor in postoperative hand surgery complications.10,11 Lans et al found an increased incidence of 30-day emergency room visits in current and former smokers after outpatient upper extremity fracture surgery.12 The MRVAMC Plastic Surgery Service counsels patients about the risk of skin necrosis and delayed wound healing, but does not cancel cases or obtain laboratory values to verify abstinence in patients undergoing hand surgery. The VA has multiple resources available for patients interested in smoking cessation through mental health services.13
MRVAMC patients have been known to resist returning for scheduled appointments due to the costs or availability of transportation. We suspected that patients who lived further from MRVAMC would be less likely to return for unscheduled visits. We used the first 3 digits of the patients’ mailing zip code to estimate residential proximity to MRVAMC. An acknowledged limitation to this approach is that some veterans have primary addresses in other regions but still spend significant time in the MRVAMC catchment area and use the facility for their health care during the winter months. These “snowbirds” might reside near the facility despite having official addresses that are more distant. Additionally, there was no increased risk of unplanned visits after hand surgery in patients aged > 61 years (the median age of study participants) (P = .82). Dependence on a third party for transportation in older veterans could impact this finding.
Based on the observation that most patients needed reassurance rather than an intervention when they returned for unscheduled appointments, diagnoses of depression, anxiety, and PTSD were evaluated as separate predictive factors. In previous research, anxiety was found to be a risk factor for problematic recovery following carpal tunnel surgery.14 In the current study, depression was found to be a statistically significant predictor of unscheduled postoperative appointments (P = .04), while anxiety (P = .33) and PTSD (P = .37) were not statistically significant predictors. This is consistent with other studies that have found preexisting depression can predict complications after hand surgery.15,16 Vranceanu et al found that depression predicted pain intensity and disability after elective hand surgery.16 Similarly, Oflazoglu et al found a 12% incidence of depression based on the Patient Health Questionnaire-9 in new and returning hand patients who presented to an academic practice.17 They suggest patients should be assessed at all levels of care and that those with poor responses to surgical or nonsurgical management should be evaluated for depression. MRVAMC has a large mental health service consisting of psychiatrists, psychologists, addiction specialists, social workers, and homeless outreach, and patients tend to already have a diagnosis and mental health practitioner when they present to the clinic.
Recent studies found that wound problems, pain, and stiffness were the most common reasons for return visits.18,19 Shetty et al identified younger age, worse preoperative pain scores, and poor access to transportation as predictors of preventable emergency room visits, which generate higher health care expenditures than an office visit.19 Our study’s top reasons for appointments (pain, wound/scar concerns, persistent symptoms) can be addressed with additional presurgery patient and family education. Additionally, clinicians encourage nonnarcotic pain management strategies including anti-inflammatories, acetaminophen, elevation, splinting, and hand therapy, and the hospital employs experienced, fellowship-trained anesthesia block faculty who help limit perioperative narcotic use. Patients are advised that pain can be used to guide them through the postoperative recovery by preventing overuse and alerting them to a problem that would be masked with narcotics, and long-standing problems such as chronic nerve compressions may continue to cause pain after surgery.
Patients and families can be given consistent and repetitive verbal and written information, instructions, and expectations at the initial consultation, preoperative appointment, and on the day of surgery. Postoperatively, outside their scheduled appointments, patients are encouraged to use the My HealtheVet secure messaging system or call the clinic to access an experienced registered nurse before making a long drive. Access to virtual or phone visits can reduce emergent in-person visits in a VA population.20
Ozdag et al found that 42% of patients who had elective carpal tunnel surgery made unplanned electronic messages or phone contact within 2 weeks postsurgery. The authors point out the uncompensated administrative burden on the staff answering these messages and suggest pre-empting the contacts with more up-front education regarding postoperative pain expectations and management strategies.21
Fisher et al found that attending hand therapy reduced the number of emergency department visits in postoperative infection cases.22 At MRVAMC, a postoperative emergency department visit for a patient prompts an urgent unplanned appointment to the plastic surgery clinic, often on the same day. The MRVAMC occupational therapy clinic employed 3 on-site certified hand therapists during the study period. Because all hand surgery patients at the clinic receive hand therapy on the same day as their first postoperative appointment, attendance at hand therapy was not evaluated as a predictor of unplanned visits. Scheduled hand therapy is another point of contact where the clinic can provide reassurance and patient education.
While females made up 17.1% of the patients in this study, they constituted 12.5% of all veterans in Florida in fiscal year 2023.23 This study found that women were more likely to present for unplanned postoperative appointments (P = .03). This is consistent with existing literature which has found that women are higher users of health care and office-based appointments.24,25 This finding suggests the need for further study into whether our methods of communicating instructions to female patients undergoing plastic surgery may not be optimal.
Strengths and Limitations
As a retrospective review, the authors used information documented by multiple different health care practitioners, including trainees. The electronic medical record problem lists and templates provide consistency of information; however, less seasoned clinicians may interpret what they see and hear differently from more experienced clinicians in the postoperative setting. This study occurred in one part of the country with demographics that may not mirror other VA systems or the general population. The authors hope this study can be a starting point for other health care facilities to investigate ways to minimize the burden of unscheduled appointments. A strength of the study is that it was conducted within a closed system, as patients tend to stay within the VA system and documentation and communication among clinicians, even outside the immediate facility, are easily accessed through the electronic health record.
Conclusions
This study found that depression diagnosis and female sex are statistically significant predictors of unplanned postoperative visits after elective soft tissue hand surgery. More effective patient education during the preoperative period, particularly in patients with depression, may be warranted.
- Apaydin EA, Paige NM, Begashaw MM, et al. Veterans Health Administration (VA) vs. non-VA healthcare quality: a systematic review. J Gen Intern Med. 2023;38:2179-2188. doi:10.1007/s11606-023-08207-2
- Blegen M, Ko J, Salzman G, et al. Comparing quality of surgical care between the US Department of Veterans Affairs and non-Veterans Affairs settings: a systematic review. J Am Coll Surg. 2023;237:352-361. doi:10.1097/XCS.0000000000000720
- Valsangkar NP, Eppstein AC, Lawson RA, et al. Effect of lean processes on surgical wait times and efficiency in a tertiary care veterans affairs medical center. JAMA Surg. 2017;152:42-47. doi:10.1001/jamasurg.2016.2808
- National Association of Veterans Affairs Physicians and Dentists. Physicians remain at top of staffing shortage in VA. NAVAPD. December 20, 2023. Accessed March 16, 2026. https://www.navapd.org/news/physicians-remain-at-top-of-staffing-shortage-in-va
- OIG Determination of Veterans Health Administration’s severe occupational staffing shortages fiscal year 2024. Veterans Affairs Office of Inspector General. August 7, 2024. Accessed February 4, 2026. https://www.vaoig.gov/reports/national-healthcare-review/oig-determination-veterans-health-administrations-severe-0
- Goltsman D, Morrison KA, Ascherman JA. Defining the association between diabetes and plastic surgery outcomes: an analysis of nearly 40,000 patients. Plast Reconstr Surg Glob Open. 2017;5:e1461. doi:10.1097/GOX.0000000000001461 7.
- Cox CT, Sierra S, Egan A, et al. Elevated hemoglobin A1c and the risk of postoperative complications in elective hand and upper extremity surgery. Cureus. 2023;15:e48373. doi:10.7759/cureus.48373
- Coady-Fariborzian L, Anstead C. HbA1c and infection in diabetic elective hand surgery: a Veterans Affair Medical Center experience 2012-2018. Hand (NY). 2023;18:994-998. doi:10.1177/1558944720937363<
- Zhuang T, Shapiro LM, Fogel N, et al. Perioperative laboratory markers as risk factors for surgical site infection after elective hand surgery. J Hand Surg Am. 2021;46:675-684. doi:10.1016/j.jhsa.2021.04.001
- Cho BH, Aziz KT, Giladi AM. The impact of smoking on early postoperative complications in hand surgery. J Hand Surg Am. 2021;46:336.e1-336.e11. doi:10.1016/j.jhsa.2020.07.01411.
- Del Core MA, Ahn J, Golden AS, et al. Effect of smoking on short-term postoperative complications after elective upper extremity surgery. Hand (N Y). 2022;17:231-238. doi:10.1177/1558944720926638
- Lans J, Beagles CB, Watkins IT, et al. Unplanned postoperative emergency department visits after upper extremity fracture surgery. J Orthop Trauma. 2025;39:22-27. doi:10.1097/BOT.0000000000002925
- Tobacco and health - how to quit. US Dept of Veterans Affairs. Updated October 29, 2025. Accessed February 4, 2026. https://www.mentalhealth.va.gov/quit-tobacco/how-to-quit.asp
- Ryan C, Miner H, Ramachandran S, et al. General anxiety is associated with problematic initial recovery after carpal tunnel release. Clin Orthop Relat Res. 2022;480:1576-1581. doi:10.1097/CORR.0000000000002115
- Crijns TJ, Bernstein DN, Ring D, et al. Depression and pain interference correlate with physical function in patients recovering from hand surgery. Hand (N Y). 2019;14:830-835. doi:10.1177/1558944718777814
- Vranceanu AM, Jupiter JB, Mudgal CS, et al. Predictors of pain intensity and disability after minor hand surgery. J Hand Surg Am. 2010;35:956-960. doi:10.1016/j.jhsa.2010.02.00117.
- Oflazoglu K, Mellema JJ, Menendez ME, et al. Prevalence of and factors associated with major depression in patients with upper extremity conditions. J Hand Surg Am. 2016;41:263-269. doi:10.1016/j.jhsa.2015.11.019
- Townsend CB, Henry TW, Lutsky KF, et al. Unplanned office visits following outpatient hand surgery. Hand (N Y). 2022;17:1264-1268. doi:10.1177/15589447211028932
- Shetty PN, Guarino GM, Zhang G, et al. Risk factors for preventable emergency department use after outpatient hand surgery. J Hand Surg Am. 2022;47:855-864. doi:10.1016/j.jhsa.2022.05.012
- Sommers-Olson B, Christianson J, Neumann T, et al. Reducing nonemergent visits to the emergency department in a Veterans Affairs multistate system. J Emerg Nurs. 2023;49:539-545. doi:10.1016/j.jen.2023.02.010
- Ozdag Y, Manzar S, El Koussaify J, et al. Unplanned postoperative phone calls and electronic messages for patients with and without opioid prescriptions after carpal tunnel release. J Hand Surg Glob Online. 2024;6:363-368. doi:10.1016/j.jhsg.2024.02.006
- Fisher AH, Gandhi J, Nelson Z, et al. Immediate interventions after surgery to reduce readmission for upper extremity infections. Ann Plast Surg. 2022;88:S163-S169. doi:10.1097/SAP.0000000000003141
- Florida Department of Veterans Affairs Fast Facts. Florida Department of Veterans Affairs. Accessed February 4, 2026. https://floridavets.org/our-veterans/profilefast-facts/
- Bertakis KD, Azari R, Helms LJ, et al. Gender differences in the utilization of health care services. J Fam Pract. 2000;49:147-152.
- Ashman JJ, Santo L, Okeyode T. Characteristics of office-based physician visits, 2018. NCHS Data Brief. 2021;408:1-8.
- Apaydin EA, Paige NM, Begashaw MM, et al. Veterans Health Administration (VA) vs. non-VA healthcare quality: a systematic review. J Gen Intern Med. 2023;38:2179-2188. doi:10.1007/s11606-023-08207-2
- Blegen M, Ko J, Salzman G, et al. Comparing quality of surgical care between the US Department of Veterans Affairs and non-Veterans Affairs settings: a systematic review. J Am Coll Surg. 2023;237:352-361. doi:10.1097/XCS.0000000000000720
- Valsangkar NP, Eppstein AC, Lawson RA, et al. Effect of lean processes on surgical wait times and efficiency in a tertiary care veterans affairs medical center. JAMA Surg. 2017;152:42-47. doi:10.1001/jamasurg.2016.2808
- National Association of Veterans Affairs Physicians and Dentists. Physicians remain at top of staffing shortage in VA. NAVAPD. December 20, 2023. Accessed March 16, 2026. https://www.navapd.org/news/physicians-remain-at-top-of-staffing-shortage-in-va
- OIG Determination of Veterans Health Administration’s severe occupational staffing shortages fiscal year 2024. Veterans Affairs Office of Inspector General. August 7, 2024. Accessed February 4, 2026. https://www.vaoig.gov/reports/national-healthcare-review/oig-determination-veterans-health-administrations-severe-0
- Goltsman D, Morrison KA, Ascherman JA. Defining the association between diabetes and plastic surgery outcomes: an analysis of nearly 40,000 patients. Plast Reconstr Surg Glob Open. 2017;5:e1461. doi:10.1097/GOX.0000000000001461 7.
- Cox CT, Sierra S, Egan A, et al. Elevated hemoglobin A1c and the risk of postoperative complications in elective hand and upper extremity surgery. Cureus. 2023;15:e48373. doi:10.7759/cureus.48373
- Coady-Fariborzian L, Anstead C. HbA1c and infection in diabetic elective hand surgery: a Veterans Affair Medical Center experience 2012-2018. Hand (NY). 2023;18:994-998. doi:10.1177/1558944720937363<
- Zhuang T, Shapiro LM, Fogel N, et al. Perioperative laboratory markers as risk factors for surgical site infection after elective hand surgery. J Hand Surg Am. 2021;46:675-684. doi:10.1016/j.jhsa.2021.04.001
- Cho BH, Aziz KT, Giladi AM. The impact of smoking on early postoperative complications in hand surgery. J Hand Surg Am. 2021;46:336.e1-336.e11. doi:10.1016/j.jhsa.2020.07.01411.
- Del Core MA, Ahn J, Golden AS, et al. Effect of smoking on short-term postoperative complications after elective upper extremity surgery. Hand (N Y). 2022;17:231-238. doi:10.1177/1558944720926638
- Lans J, Beagles CB, Watkins IT, et al. Unplanned postoperative emergency department visits after upper extremity fracture surgery. J Orthop Trauma. 2025;39:22-27. doi:10.1097/BOT.0000000000002925
- Tobacco and health - how to quit. US Dept of Veterans Affairs. Updated October 29, 2025. Accessed February 4, 2026. https://www.mentalhealth.va.gov/quit-tobacco/how-to-quit.asp
- Ryan C, Miner H, Ramachandran S, et al. General anxiety is associated with problematic initial recovery after carpal tunnel release. Clin Orthop Relat Res. 2022;480:1576-1581. doi:10.1097/CORR.0000000000002115
- Crijns TJ, Bernstein DN, Ring D, et al. Depression and pain interference correlate with physical function in patients recovering from hand surgery. Hand (N Y). 2019;14:830-835. doi:10.1177/1558944718777814
- Vranceanu AM, Jupiter JB, Mudgal CS, et al. Predictors of pain intensity and disability after minor hand surgery. J Hand Surg Am. 2010;35:956-960. doi:10.1016/j.jhsa.2010.02.00117.
- Oflazoglu K, Mellema JJ, Menendez ME, et al. Prevalence of and factors associated with major depression in patients with upper extremity conditions. J Hand Surg Am. 2016;41:263-269. doi:10.1016/j.jhsa.2015.11.019
- Townsend CB, Henry TW, Lutsky KF, et al. Unplanned office visits following outpatient hand surgery. Hand (N Y). 2022;17:1264-1268. doi:10.1177/15589447211028932
- Shetty PN, Guarino GM, Zhang G, et al. Risk factors for preventable emergency department use after outpatient hand surgery. J Hand Surg Am. 2022;47:855-864. doi:10.1016/j.jhsa.2022.05.012
- Sommers-Olson B, Christianson J, Neumann T, et al. Reducing nonemergent visits to the emergency department in a Veterans Affairs multistate system. J Emerg Nurs. 2023;49:539-545. doi:10.1016/j.jen.2023.02.010
- Ozdag Y, Manzar S, El Koussaify J, et al. Unplanned postoperative phone calls and electronic messages for patients with and without opioid prescriptions after carpal tunnel release. J Hand Surg Glob Online. 2024;6:363-368. doi:10.1016/j.jhsg.2024.02.006
- Fisher AH, Gandhi J, Nelson Z, et al. Immediate interventions after surgery to reduce readmission for upper extremity infections. Ann Plast Surg. 2022;88:S163-S169. doi:10.1097/SAP.0000000000003141
- Florida Department of Veterans Affairs Fast Facts. Florida Department of Veterans Affairs. Accessed February 4, 2026. https://floridavets.org/our-veterans/profilefast-facts/
- Bertakis KD, Azari R, Helms LJ, et al. Gender differences in the utilization of health care services. J Fam Pract. 2000;49:147-152.
- Ashman JJ, Santo L, Okeyode T. Characteristics of office-based physician visits, 2018. NCHS Data Brief. 2021;408:1-8.
Predictors of Unplanned Postoperative Visits in a Veterans Affairs Hand Surgery Practice
Predictors of Unplanned Postoperative Visits in a Veterans Affairs Hand Surgery Practice

To Hold or Not to Hold GLP-1s Before Surgery
This transcript has been edited for clarity.
Recently, there have been two somewhat conflicting recommendations about how to deal with our patients who are on incretin hormone therapy before undergoing elective surgical procedures.
First, the FDA [Food and Drug Administration] has updated the package inserts for all of these incretins, meaning the glucagon-like peptide-1 (GLP-1) receptor agonists and the dual glucose-dependent insulinotropic (GIP)/GLP-1 receptor agonist tirzepatide, with a warning about pulmonary aspiration during general anesthesia or deep sedation. They instruct patients to let healthcare providers know of any planned surgeries or procedures. This has come about because of postmarketing experience in which patients who are on GLP-1 receptor agonists have had residual gastric contents found despite reported adherence to preoperative fasting recommendations.
The problem with this is that the FDA says they don’t really actually know what to tell us to do or not to do because we don’t have knowledge as to how to truly mitigate the risk for pulmonary aspiration during general anesthesia or deep sedation. They don’t know if modifying preoperative fasting recommendations should be changed or if temporary discontinuation of the drugs could reduce this problem. They really don’t know what to tell us to do except to tell us that this is a problem we should discuss with our patients.
At about the same time, a society guideline— and this was from a number of different societies, including the American Society of Anesthesiologists — stated that most patients should continue taking their GLP-1 receptor agonist before elective surgery.
This struck me as somewhat discordant from what the FDA said, although the FDA also says they don’t know quite what to tell us to do. This clinical guideline goes into a bit more detail, and what they think might be a good idea is that patients who are at the highest risk for GI side effects should follow a liquid diet for 24 hours before the procedure.
They basically look at who is at highest risk, and they say the following: Patients in the escalation phase of their incretin therapy — that is, early in treatment when the dose is increasing — are most likely to have delays in gastric emptying because that effect is lessened over time. They say that the elective surgery should be deferred until the escalation phase has passed and the GI symptoms have dissipated.
They’re very clear that patients who have significant GI symptoms, including nausea, vomiting, abdominal pain, constipation, and shortness of breath, should wait until their symptoms have dissipated.
They think this is something that would be good no matter what dose of drug these patients are on. They do say that you tend to see more issues with gastric emptying in patients at the highest dose of a GLP-1 receptor agonist. They also mention other medical conditions that may slow gastric emptying, such as Parkinson’s disease, which may further modify the perioperative management plan.
Their proposed solutions that sort of correspond with my proposed solutions include assessing the patient. Obviously, if a patient is going up on the dose of these drugs or having many GI side effects, that’s someone who you probably don’t want to send for elective surgery if you don’t have to. However, if you need to — and possibly in everybody — you might want to withhold the drug for 10-14 days preoperatively to make sure they don’t have significant GI side effects as they’re preparing for their procedure.
One of the things the anesthesiology group was worried about was that glucose levels would go up and patients would have hyperglycemia going into surgery. I’m not so worried about holding a dose or two of one of these agents. I don’t see much hyperglycemia occurring. If it does, you can treat it in other ways.
If it’s somebody where you think they’re having symptoms but they want to have the procedure anyway, you can put them on a liquid diet for 24 hours or so, so that there’s less of a risk for retained gastric contents, at least solid gastric contents. Anesthesiologists can help with this as well because in many cases, they can do a point-of-care gastric ultrasound to check for retained food or fluid.
I know this is sort of vague because I don’t have clear recommendations, but I do think it’s important to talk with your patients to assess whether they’re having signs or symptoms of gastroparesis. I think it’s not unreasonable to hold the incretin hormone therapy for one or two doses before a procedure if you have that opportunity, and be sure that the anesthesiologist and surgery team are aware of the fact that the patient has been on one of these agents so that they’re a little more aware of the risk for aspiration.
Anne L. Peters, Professor, Department of Clinical Medicine, Keck School of Medicine; Director, University of Southern California Westside Center for Diabetes, University of Southern California, Los Angeles, California, has disclosed the following relevant financial relationships: Serve(d) on the advisory board for Abbott Diabetes Care; Becton Dickinson; Boehringer Ingelheim Pharmaceuticals, Inc.; Eli Lilly and Company; Lexicon Pharmaceuticals, Inc.; Livongo; Medscape; Merck & Co., Inc.; Novo Nordisk; Omada Health; OptumHealth; sanofi; Zafgen Received research support from: Dexcom; MannKind Corporation; Astra Zeneca. Serve(d) as a member of a speakers bureau for: Novo Nordisk.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Recently, there have been two somewhat conflicting recommendations about how to deal with our patients who are on incretin hormone therapy before undergoing elective surgical procedures.
First, the FDA [Food and Drug Administration] has updated the package inserts for all of these incretins, meaning the glucagon-like peptide-1 (GLP-1) receptor agonists and the dual glucose-dependent insulinotropic (GIP)/GLP-1 receptor agonist tirzepatide, with a warning about pulmonary aspiration during general anesthesia or deep sedation. They instruct patients to let healthcare providers know of any planned surgeries or procedures. This has come about because of postmarketing experience in which patients who are on GLP-1 receptor agonists have had residual gastric contents found despite reported adherence to preoperative fasting recommendations.
The problem with this is that the FDA says they don’t really actually know what to tell us to do or not to do because we don’t have knowledge as to how to truly mitigate the risk for pulmonary aspiration during general anesthesia or deep sedation. They don’t know if modifying preoperative fasting recommendations should be changed or if temporary discontinuation of the drugs could reduce this problem. They really don’t know what to tell us to do except to tell us that this is a problem we should discuss with our patients.
At about the same time, a society guideline— and this was from a number of different societies, including the American Society of Anesthesiologists — stated that most patients should continue taking their GLP-1 receptor agonist before elective surgery.
This struck me as somewhat discordant from what the FDA said, although the FDA also says they don’t know quite what to tell us to do. This clinical guideline goes into a bit more detail, and what they think might be a good idea is that patients who are at the highest risk for GI side effects should follow a liquid diet for 24 hours before the procedure.
They basically look at who is at highest risk, and they say the following: Patients in the escalation phase of their incretin therapy — that is, early in treatment when the dose is increasing — are most likely to have delays in gastric emptying because that effect is lessened over time. They say that the elective surgery should be deferred until the escalation phase has passed and the GI symptoms have dissipated.
They’re very clear that patients who have significant GI symptoms, including nausea, vomiting, abdominal pain, constipation, and shortness of breath, should wait until their symptoms have dissipated.
They think this is something that would be good no matter what dose of drug these patients are on. They do say that you tend to see more issues with gastric emptying in patients at the highest dose of a GLP-1 receptor agonist. They also mention other medical conditions that may slow gastric emptying, such as Parkinson’s disease, which may further modify the perioperative management plan.
Their proposed solutions that sort of correspond with my proposed solutions include assessing the patient. Obviously, if a patient is going up on the dose of these drugs or having many GI side effects, that’s someone who you probably don’t want to send for elective surgery if you don’t have to. However, if you need to — and possibly in everybody — you might want to withhold the drug for 10-14 days preoperatively to make sure they don’t have significant GI side effects as they’re preparing for their procedure.
One of the things the anesthesiology group was worried about was that glucose levels would go up and patients would have hyperglycemia going into surgery. I’m not so worried about holding a dose or two of one of these agents. I don’t see much hyperglycemia occurring. If it does, you can treat it in other ways.
If it’s somebody where you think they’re having symptoms but they want to have the procedure anyway, you can put them on a liquid diet for 24 hours or so, so that there’s less of a risk for retained gastric contents, at least solid gastric contents. Anesthesiologists can help with this as well because in many cases, they can do a point-of-care gastric ultrasound to check for retained food or fluid.
I know this is sort of vague because I don’t have clear recommendations, but I do think it’s important to talk with your patients to assess whether they’re having signs or symptoms of gastroparesis. I think it’s not unreasonable to hold the incretin hormone therapy for one or two doses before a procedure if you have that opportunity, and be sure that the anesthesiologist and surgery team are aware of the fact that the patient has been on one of these agents so that they’re a little more aware of the risk for aspiration.
Anne L. Peters, Professor, Department of Clinical Medicine, Keck School of Medicine; Director, University of Southern California Westside Center for Diabetes, University of Southern California, Los Angeles, California, has disclosed the following relevant financial relationships: Serve(d) on the advisory board for Abbott Diabetes Care; Becton Dickinson; Boehringer Ingelheim Pharmaceuticals, Inc.; Eli Lilly and Company; Lexicon Pharmaceuticals, Inc.; Livongo; Medscape; Merck & Co., Inc.; Novo Nordisk; Omada Health; OptumHealth; sanofi; Zafgen Received research support from: Dexcom; MannKind Corporation; Astra Zeneca. Serve(d) as a member of a speakers bureau for: Novo Nordisk.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Recently, there have been two somewhat conflicting recommendations about how to deal with our patients who are on incretin hormone therapy before undergoing elective surgical procedures.
First, the FDA [Food and Drug Administration] has updated the package inserts for all of these incretins, meaning the glucagon-like peptide-1 (GLP-1) receptor agonists and the dual glucose-dependent insulinotropic (GIP)/GLP-1 receptor agonist tirzepatide, with a warning about pulmonary aspiration during general anesthesia or deep sedation. They instruct patients to let healthcare providers know of any planned surgeries or procedures. This has come about because of postmarketing experience in which patients who are on GLP-1 receptor agonists have had residual gastric contents found despite reported adherence to preoperative fasting recommendations.
The problem with this is that the FDA says they don’t really actually know what to tell us to do or not to do because we don’t have knowledge as to how to truly mitigate the risk for pulmonary aspiration during general anesthesia or deep sedation. They don’t know if modifying preoperative fasting recommendations should be changed or if temporary discontinuation of the drugs could reduce this problem. They really don’t know what to tell us to do except to tell us that this is a problem we should discuss with our patients.
At about the same time, a society guideline— and this was from a number of different societies, including the American Society of Anesthesiologists — stated that most patients should continue taking their GLP-1 receptor agonist before elective surgery.
This struck me as somewhat discordant from what the FDA said, although the FDA also says they don’t know quite what to tell us to do. This clinical guideline goes into a bit more detail, and what they think might be a good idea is that patients who are at the highest risk for GI side effects should follow a liquid diet for 24 hours before the procedure.
They basically look at who is at highest risk, and they say the following: Patients in the escalation phase of their incretin therapy — that is, early in treatment when the dose is increasing — are most likely to have delays in gastric emptying because that effect is lessened over time. They say that the elective surgery should be deferred until the escalation phase has passed and the GI symptoms have dissipated.
They’re very clear that patients who have significant GI symptoms, including nausea, vomiting, abdominal pain, constipation, and shortness of breath, should wait until their symptoms have dissipated.
They think this is something that would be good no matter what dose of drug these patients are on. They do say that you tend to see more issues with gastric emptying in patients at the highest dose of a GLP-1 receptor agonist. They also mention other medical conditions that may slow gastric emptying, such as Parkinson’s disease, which may further modify the perioperative management plan.
Their proposed solutions that sort of correspond with my proposed solutions include assessing the patient. Obviously, if a patient is going up on the dose of these drugs or having many GI side effects, that’s someone who you probably don’t want to send for elective surgery if you don’t have to. However, if you need to — and possibly in everybody — you might want to withhold the drug for 10-14 days preoperatively to make sure they don’t have significant GI side effects as they’re preparing for their procedure.
One of the things the anesthesiology group was worried about was that glucose levels would go up and patients would have hyperglycemia going into surgery. I’m not so worried about holding a dose or two of one of these agents. I don’t see much hyperglycemia occurring. If it does, you can treat it in other ways.
If it’s somebody where you think they’re having symptoms but they want to have the procedure anyway, you can put them on a liquid diet for 24 hours or so, so that there’s less of a risk for retained gastric contents, at least solid gastric contents. Anesthesiologists can help with this as well because in many cases, they can do a point-of-care gastric ultrasound to check for retained food or fluid.
I know this is sort of vague because I don’t have clear recommendations, but I do think it’s important to talk with your patients to assess whether they’re having signs or symptoms of gastroparesis. I think it’s not unreasonable to hold the incretin hormone therapy for one or two doses before a procedure if you have that opportunity, and be sure that the anesthesiologist and surgery team are aware of the fact that the patient has been on one of these agents so that they’re a little more aware of the risk for aspiration.
Anne L. Peters, Professor, Department of Clinical Medicine, Keck School of Medicine; Director, University of Southern California Westside Center for Diabetes, University of Southern California, Los Angeles, California, has disclosed the following relevant financial relationships: Serve(d) on the advisory board for Abbott Diabetes Care; Becton Dickinson; Boehringer Ingelheim Pharmaceuticals, Inc.; Eli Lilly and Company; Lexicon Pharmaceuticals, Inc.; Livongo; Medscape; Merck & Co., Inc.; Novo Nordisk; Omada Health; OptumHealth; sanofi; Zafgen Received research support from: Dexcom; MannKind Corporation; Astra Zeneca. Serve(d) as a member of a speakers bureau for: Novo Nordisk.
A version of this article first appeared on Medscape.com.
Hemorrhoidal Disease Management: When and How to Intervene
according to Vincent de Parades, MD, PhD, of Hôpital Paris Saint-Joseph in France. In his presentation at France’s annual general medicine conference (JNMG 2024) on the management of hemorrhoidal disease, he noted, “this [NSAID and analgesic] treatment is highly effective, initially relieving pain and reducing edema, though the clot takes longer to resolve.” In cases where residual skin tags (marisques) remain after an episode, resection may be considered if they cause discomfort.
While patients often turn to over-the-counter topical treatments during flare-ups, de Parades noted that these have not been proven effective for hemorrhoidal disease. For hemorrhoidal thrombosis, however, a topical treatment with a corticosteroid and anesthetic may be prescribed.
No NSAIDs for Abscesses
In addition to NSAIDs, a local treatment may provide soothing benefits, especially when combined with topical application, as highlighted by Nadia Fathallah, MD, of Hôpital Paris Saint-Joseph, who joined de Parades in the presentation. “I recommend massaging the ointment to help dissolve the thrombus,” she added. However, “NSAIDs should not be prescribed in the case of an abscess,” cautioned de Parades, emphasizing that “any patient with a painful anal swelling needs an examination.” When in doubt, administer an analgesic and reexamine the patient 1-2 days later. If an abscess is present, it will not resolve on its own, and pain will persist.
The two proctologists reviewed various interventions for managing hemorrhoidal conditions, underscoring the benefits of minimally invasive surgery as an alternative to hemorrhoidectomy for treating grade 2 or 3 hemorrhoidal prolapse.
Hemorrhoidal disease involves abnormal dilation of the vascular system in the anus and rectum. External hemorrhoids affect the external vascular plexus, while internal hemorrhoids occur in the upper part of the anal canal at the internal plexus.
Hygiene and Dietary Guidelines
Common symptoms include light to heavy bleeding during bowel movements and the sensation of a lump inside the anus. In some cases, this is accompanied by throbbing pain, which suggests hemorrhoidal thrombosis, a condition often associated with a painful external swelling. Hemorrhoidal prolapse, meanwhile, is characterized by the protrusion of internal hemorrhoids and is classified into four grades:
- Grade 1: Hemorrhoids emerge during straining but do not protrude externally.
- Grade 2: Hemorrhoids protrude but spontaneously retract after straining.
- Grade 3: Hemorrhoids protrude with straining and require manual reinsertion.
- Grade 4: Prolapse is permanent.
In all cases, medical treatment is recommended as the initial approach. European guidelines recommend to first implement lifestyle and dietary measures, encouraging regular physical activity and adequate water and fiber intake to promote intestinal transit. Laxatives may also be recommended.
Elastic Band Ligation
For hemorrhoidal thrombosis, NSAIDs and nonopioid analgesics are recommended as first-line treatments. For patients with contraindications to NSAIDs, such as pregnant women, corticosteroid treatment may be administered, although it is less effective. Routine incision is no longer recommended, according to de Parades.
For prolapsed internal hemorrhoids, instrumental treatment is recommended as a second-line option if medical management fails for grades 1 and 2, or for isolated grade 3 hemorrhoids. With sclerotherapy injections largely phased out, two options remain: Infrared photocoagulation and elastic band ligation.
The objective of instrumental treatment is to create a scar at the top of the hemorrhoidal plexus to reduce vascularization and secure the hemorrhoid to the rectal wall. When correctly performed above the insensitive mucosal area in the anal canal, the procedure is painless.
Ligation involves placing an elastic band at the base of the hemorrhoid, with the intervention taking only a few minutes. “Within 4 weeks, the hemorrhoid disappears,” explained de Parades. Photocoagulation is a more superficial treatment requiring several spaced sessions, mainly to address bleeding.
Advances in Minimally Invasive Surgery
Surgery is recommended if instrumental treatment fails and as a first-line option for circular grade 3 hemorrhoids (multiple hemorrhoidal masses) and grade 4 cases.
Milligan-Morgan hemorrhoidectomy is considered the “gold standard” surgical technique and is used primarily for grades 2, 3, and 4 cases. This technique involves resecting the three main hemorrhoidal bundles while preserving surrounding tissue, providing a “radical and definitive” treatment.
While effective in the long term, hemorrhoid bundle resection requires a lengthy healing process and typically requires the patient to take 15-20 days off work. It is also not recommended for people who engage in anal intercourse, as “removing hemorrhoidal tissue can reduce flexibility and sensation in the anal canal,” Fathallah noted.
Another widely used technique in France is Doppler-guided hemorrhoidal artery ligation, which selectively reduces blood flow to the hemorrhoidal plexus. It is often combined with a mucopexy to secure the prolapse above the anal canal and restore normal anatomy.
Minimally invasive surgery is today increasingly considered an alternative to hemorrhoidectomy for treating grade 2 or 3 hemorrhoidal prolapse.
Laser and radiofrequency techniques induce submucosal coagulation, reducing arterial flow and creating fibrous tissue to retract the hemorrhoidal bundle. Because the procedure is applied above the anal canal, “it is associated with little or no pain.”
Hemorrhoidal Embolization
Recent studies have validated the benefits of minimally invasive surgery for this condition. In a French multicenter study, radiofrequency treatment significantly improved quality of life 3 months post operation, requiring only 4 days off work. The vast majority of patients said they were satisfied with the results.
The procedure is less uncomfortable than hemorrhoidectomy and allows for quicker recovery, but it carries a risk for recurrence. In the French study, nearly 8% of patients required reoperation within a year, mostly by hemorrhoidectomy. “The estimated recurrence rate is 20%-30% over 10 years,” said de Parades.
Overall, the specialist emphasized the value of surgery, including hemorrhoidectomy, in treating hemorrhoidal prolapse. With substantial benefits from minimally invasive options, “patients should be referred early” to prevent prolapse progression “that might leave no choice but hemorrhoidectomy.”
Finally, another technique is available for bleeding without prolapse: Hemorrhoidal embolization. Practiced for about a decade, the procedure involves blocking blood flow to the hemorrhoids by inserting tiny metal coils through a catheter, which is inserted via a transcutaneous route through an artery in the arm.
This story was translated from Medscape’s French edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version appeared on Medscape.com.
according to Vincent de Parades, MD, PhD, of Hôpital Paris Saint-Joseph in France. In his presentation at France’s annual general medicine conference (JNMG 2024) on the management of hemorrhoidal disease, he noted, “this [NSAID and analgesic] treatment is highly effective, initially relieving pain and reducing edema, though the clot takes longer to resolve.” In cases where residual skin tags (marisques) remain after an episode, resection may be considered if they cause discomfort.
While patients often turn to over-the-counter topical treatments during flare-ups, de Parades noted that these have not been proven effective for hemorrhoidal disease. For hemorrhoidal thrombosis, however, a topical treatment with a corticosteroid and anesthetic may be prescribed.
No NSAIDs for Abscesses
In addition to NSAIDs, a local treatment may provide soothing benefits, especially when combined with topical application, as highlighted by Nadia Fathallah, MD, of Hôpital Paris Saint-Joseph, who joined de Parades in the presentation. “I recommend massaging the ointment to help dissolve the thrombus,” she added. However, “NSAIDs should not be prescribed in the case of an abscess,” cautioned de Parades, emphasizing that “any patient with a painful anal swelling needs an examination.” When in doubt, administer an analgesic and reexamine the patient 1-2 days later. If an abscess is present, it will not resolve on its own, and pain will persist.
The two proctologists reviewed various interventions for managing hemorrhoidal conditions, underscoring the benefits of minimally invasive surgery as an alternative to hemorrhoidectomy for treating grade 2 or 3 hemorrhoidal prolapse.
Hemorrhoidal disease involves abnormal dilation of the vascular system in the anus and rectum. External hemorrhoids affect the external vascular plexus, while internal hemorrhoids occur in the upper part of the anal canal at the internal plexus.
Hygiene and Dietary Guidelines
Common symptoms include light to heavy bleeding during bowel movements and the sensation of a lump inside the anus. In some cases, this is accompanied by throbbing pain, which suggests hemorrhoidal thrombosis, a condition often associated with a painful external swelling. Hemorrhoidal prolapse, meanwhile, is characterized by the protrusion of internal hemorrhoids and is classified into four grades:
- Grade 1: Hemorrhoids emerge during straining but do not protrude externally.
- Grade 2: Hemorrhoids protrude but spontaneously retract after straining.
- Grade 3: Hemorrhoids protrude with straining and require manual reinsertion.
- Grade 4: Prolapse is permanent.
In all cases, medical treatment is recommended as the initial approach. European guidelines recommend to first implement lifestyle and dietary measures, encouraging regular physical activity and adequate water and fiber intake to promote intestinal transit. Laxatives may also be recommended.
Elastic Band Ligation
For hemorrhoidal thrombosis, NSAIDs and nonopioid analgesics are recommended as first-line treatments. For patients with contraindications to NSAIDs, such as pregnant women, corticosteroid treatment may be administered, although it is less effective. Routine incision is no longer recommended, according to de Parades.
For prolapsed internal hemorrhoids, instrumental treatment is recommended as a second-line option if medical management fails for grades 1 and 2, or for isolated grade 3 hemorrhoids. With sclerotherapy injections largely phased out, two options remain: Infrared photocoagulation and elastic band ligation.
The objective of instrumental treatment is to create a scar at the top of the hemorrhoidal plexus to reduce vascularization and secure the hemorrhoid to the rectal wall. When correctly performed above the insensitive mucosal area in the anal canal, the procedure is painless.
Ligation involves placing an elastic band at the base of the hemorrhoid, with the intervention taking only a few minutes. “Within 4 weeks, the hemorrhoid disappears,” explained de Parades. Photocoagulation is a more superficial treatment requiring several spaced sessions, mainly to address bleeding.
Advances in Minimally Invasive Surgery
Surgery is recommended if instrumental treatment fails and as a first-line option for circular grade 3 hemorrhoids (multiple hemorrhoidal masses) and grade 4 cases.
Milligan-Morgan hemorrhoidectomy is considered the “gold standard” surgical technique and is used primarily for grades 2, 3, and 4 cases. This technique involves resecting the three main hemorrhoidal bundles while preserving surrounding tissue, providing a “radical and definitive” treatment.
While effective in the long term, hemorrhoid bundle resection requires a lengthy healing process and typically requires the patient to take 15-20 days off work. It is also not recommended for people who engage in anal intercourse, as “removing hemorrhoidal tissue can reduce flexibility and sensation in the anal canal,” Fathallah noted.
Another widely used technique in France is Doppler-guided hemorrhoidal artery ligation, which selectively reduces blood flow to the hemorrhoidal plexus. It is often combined with a mucopexy to secure the prolapse above the anal canal and restore normal anatomy.
Minimally invasive surgery is today increasingly considered an alternative to hemorrhoidectomy for treating grade 2 or 3 hemorrhoidal prolapse.
Laser and radiofrequency techniques induce submucosal coagulation, reducing arterial flow and creating fibrous tissue to retract the hemorrhoidal bundle. Because the procedure is applied above the anal canal, “it is associated with little or no pain.”
Hemorrhoidal Embolization
Recent studies have validated the benefits of minimally invasive surgery for this condition. In a French multicenter study, radiofrequency treatment significantly improved quality of life 3 months post operation, requiring only 4 days off work. The vast majority of patients said they were satisfied with the results.
The procedure is less uncomfortable than hemorrhoidectomy and allows for quicker recovery, but it carries a risk for recurrence. In the French study, nearly 8% of patients required reoperation within a year, mostly by hemorrhoidectomy. “The estimated recurrence rate is 20%-30% over 10 years,” said de Parades.
Overall, the specialist emphasized the value of surgery, including hemorrhoidectomy, in treating hemorrhoidal prolapse. With substantial benefits from minimally invasive options, “patients should be referred early” to prevent prolapse progression “that might leave no choice but hemorrhoidectomy.”
Finally, another technique is available for bleeding without prolapse: Hemorrhoidal embolization. Practiced for about a decade, the procedure involves blocking blood flow to the hemorrhoids by inserting tiny metal coils through a catheter, which is inserted via a transcutaneous route through an artery in the arm.
This story was translated from Medscape’s French edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version appeared on Medscape.com.
according to Vincent de Parades, MD, PhD, of Hôpital Paris Saint-Joseph in France. In his presentation at France’s annual general medicine conference (JNMG 2024) on the management of hemorrhoidal disease, he noted, “this [NSAID and analgesic] treatment is highly effective, initially relieving pain and reducing edema, though the clot takes longer to resolve.” In cases where residual skin tags (marisques) remain after an episode, resection may be considered if they cause discomfort.
While patients often turn to over-the-counter topical treatments during flare-ups, de Parades noted that these have not been proven effective for hemorrhoidal disease. For hemorrhoidal thrombosis, however, a topical treatment with a corticosteroid and anesthetic may be prescribed.
No NSAIDs for Abscesses
In addition to NSAIDs, a local treatment may provide soothing benefits, especially when combined with topical application, as highlighted by Nadia Fathallah, MD, of Hôpital Paris Saint-Joseph, who joined de Parades in the presentation. “I recommend massaging the ointment to help dissolve the thrombus,” she added. However, “NSAIDs should not be prescribed in the case of an abscess,” cautioned de Parades, emphasizing that “any patient with a painful anal swelling needs an examination.” When in doubt, administer an analgesic and reexamine the patient 1-2 days later. If an abscess is present, it will not resolve on its own, and pain will persist.
The two proctologists reviewed various interventions for managing hemorrhoidal conditions, underscoring the benefits of minimally invasive surgery as an alternative to hemorrhoidectomy for treating grade 2 or 3 hemorrhoidal prolapse.
Hemorrhoidal disease involves abnormal dilation of the vascular system in the anus and rectum. External hemorrhoids affect the external vascular plexus, while internal hemorrhoids occur in the upper part of the anal canal at the internal plexus.
Hygiene and Dietary Guidelines
Common symptoms include light to heavy bleeding during bowel movements and the sensation of a lump inside the anus. In some cases, this is accompanied by throbbing pain, which suggests hemorrhoidal thrombosis, a condition often associated with a painful external swelling. Hemorrhoidal prolapse, meanwhile, is characterized by the protrusion of internal hemorrhoids and is classified into four grades:
- Grade 1: Hemorrhoids emerge during straining but do not protrude externally.
- Grade 2: Hemorrhoids protrude but spontaneously retract after straining.
- Grade 3: Hemorrhoids protrude with straining and require manual reinsertion.
- Grade 4: Prolapse is permanent.
In all cases, medical treatment is recommended as the initial approach. European guidelines recommend to first implement lifestyle and dietary measures, encouraging regular physical activity and adequate water and fiber intake to promote intestinal transit. Laxatives may also be recommended.
Elastic Band Ligation
For hemorrhoidal thrombosis, NSAIDs and nonopioid analgesics are recommended as first-line treatments. For patients with contraindications to NSAIDs, such as pregnant women, corticosteroid treatment may be administered, although it is less effective. Routine incision is no longer recommended, according to de Parades.
For prolapsed internal hemorrhoids, instrumental treatment is recommended as a second-line option if medical management fails for grades 1 and 2, or for isolated grade 3 hemorrhoids. With sclerotherapy injections largely phased out, two options remain: Infrared photocoagulation and elastic band ligation.
The objective of instrumental treatment is to create a scar at the top of the hemorrhoidal plexus to reduce vascularization and secure the hemorrhoid to the rectal wall. When correctly performed above the insensitive mucosal area in the anal canal, the procedure is painless.
Ligation involves placing an elastic band at the base of the hemorrhoid, with the intervention taking only a few minutes. “Within 4 weeks, the hemorrhoid disappears,” explained de Parades. Photocoagulation is a more superficial treatment requiring several spaced sessions, mainly to address bleeding.
Advances in Minimally Invasive Surgery
Surgery is recommended if instrumental treatment fails and as a first-line option for circular grade 3 hemorrhoids (multiple hemorrhoidal masses) and grade 4 cases.
Milligan-Morgan hemorrhoidectomy is considered the “gold standard” surgical technique and is used primarily for grades 2, 3, and 4 cases. This technique involves resecting the three main hemorrhoidal bundles while preserving surrounding tissue, providing a “radical and definitive” treatment.
While effective in the long term, hemorrhoid bundle resection requires a lengthy healing process and typically requires the patient to take 15-20 days off work. It is also not recommended for people who engage in anal intercourse, as “removing hemorrhoidal tissue can reduce flexibility and sensation in the anal canal,” Fathallah noted.
Another widely used technique in France is Doppler-guided hemorrhoidal artery ligation, which selectively reduces blood flow to the hemorrhoidal plexus. It is often combined with a mucopexy to secure the prolapse above the anal canal and restore normal anatomy.
Minimally invasive surgery is today increasingly considered an alternative to hemorrhoidectomy for treating grade 2 or 3 hemorrhoidal prolapse.
Laser and radiofrequency techniques induce submucosal coagulation, reducing arterial flow and creating fibrous tissue to retract the hemorrhoidal bundle. Because the procedure is applied above the anal canal, “it is associated with little or no pain.”
Hemorrhoidal Embolization
Recent studies have validated the benefits of minimally invasive surgery for this condition. In a French multicenter study, radiofrequency treatment significantly improved quality of life 3 months post operation, requiring only 4 days off work. The vast majority of patients said they were satisfied with the results.
The procedure is less uncomfortable than hemorrhoidectomy and allows for quicker recovery, but it carries a risk for recurrence. In the French study, nearly 8% of patients required reoperation within a year, mostly by hemorrhoidectomy. “The estimated recurrence rate is 20%-30% over 10 years,” said de Parades.
Overall, the specialist emphasized the value of surgery, including hemorrhoidectomy, in treating hemorrhoidal prolapse. With substantial benefits from minimally invasive options, “patients should be referred early” to prevent prolapse progression “that might leave no choice but hemorrhoidectomy.”
Finally, another technique is available for bleeding without prolapse: Hemorrhoidal embolization. Practiced for about a decade, the procedure involves blocking blood flow to the hemorrhoids by inserting tiny metal coils through a catheter, which is inserted via a transcutaneous route through an artery in the arm.
This story was translated from Medscape’s French edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version appeared on Medscape.com.
How to Manage Patients on GLP-1s Before Surgery
, as does the US Food and Drug Administration’s (FDA’s) labeling for the drugs. The changes can be challenging to keep up with, and endocrinologists seem to be making their own decisions based on clinical experience and their interpretations of the potential impact and value of the emerging information.
The latest FDA label change warns about the risk for pulmonary aspiration but notes “insufficient” data to inform recommendations to mitigate the risk in vulnerable patients. Yet, the latest multi-society guidance, led by the American Society of Anesthesiologists (ASA) and based on consensus, not evidence, has nuanced advice for managing patients at risk.
Does the FDA’s label change make a difference regarding the multi-society guidance, which was published earlier? “The answer is no,” Girish Joshi, MD, vice chair, ASA Committee on Practice Parameters, told this news organization. “The concern of increased pulmonary aspiration in patients who are on GLP-1 receptor agonists has been known, and that concern still exists. So, we started with not an assumption but the premise that patients on GLP-1 receptor agonists are at a higher risk of aspiration during sedation, analgesia, and/or general anesthesia. The FDA basically confirms what we say in the guidance.”
Joshi, professor in the Anesthesiology and Pain Management Department at UT Southwestern Medical Center, Dallas, aimed to make the guidance, which was published simultaneously in several society journals, more implementable with a letter to the editor of Anesthesiology. The key, he said, is to identify patients at higher risk for aspiration; all others would follow treatment as usual.
The letter highlights three overarching recommendations and then expands upon them: Standardized preoperative assessment for risk for delayed gastric emptying (yes/no); selective preoperative care plan based on delayed gastric emptying assessment and shared decision-making; and on the day of the procedure, reassess for delayed gastric emptying and mitigate risk if there is clinical concern.
But it seems as though, for now, endocrinologists are managing these patients as they see fit, within the parameters of any institutional guidance requirements. Here is what they said about their practice:
Amy E. Rothberg, MD, DABOM, director of the Weight Management Program & Rewind at the University of Michigan, Ann Arbor, Michigan, said, “I think it makes sense to inform our patients of the labeling and rare but potential adverse effects if they intend to undergo anesthesia for a scheduled procedure/surgery. There is never no risk of aspiration during anesthesia.”
“I find it a bit curious that ASA implies that those who experience GI side effects are more likely than those who do not to have this potential risk. I doubt there is evidence that those without GI side effects are necessarily ‘safer’ and a study to determine that is unlikely to take be conducted.”
“My institution does require a 1-week pause on GLP-1s for those undergoing anesthesia for surgery,” she added. “That’s not evidence-based either, but probably reduces the risk of aspiration during anesthesia — but I don’t know what the actual denominator is for aspiration in those who continued vs those who took a pause from GLP-1s. Pausing does certainly (anecdotally) increase the traffic of communications between physicians and their patients about what to do in the interval.”
Anne Peters, MD, a professor of clinical medicine and a clinical scholar at the Keck School of Medicine of the University of Southern California, Los Angeles, said, “The FDA label change is a warning that really doesn’t say exactly who on GLP-1 RAs is at highest risk or what to do, and if any intervention has been shown to help. The ASA recommendations seem much more nuanced and practical, including point-of-care gastric ultrasound to see if there is retained food/fluid prior to surgery.”
“In my practice, I individualize what I say, depending on the person and the circumstance,” she said. “Mostly, I have people hold one dose before planned surgery, so they have been 10 days at least without a dose. But if worried about gastrointestinal symptoms or gastroparesis, I have them do a clear liquid diet for 24 hours presurgery. Or at least avoid heavy fat meals the day before.”
“There is a risk of aspiration with anything that slows gastric emptying — maybe even in patients with gastroparesis at baseline due to physiologic, not pharmacological, reasons — and anesthesiologists should be aware of the need to assess patients individually.”
Michael A. Weintraub, MD, of NYU Langone Health Diabetes & Endocrine Associates in New York City, observed, “The risk of a pulmonary aspiration event with GLP-1 medication is quite rare, but not zero. On the other hand, stopping the GLP-1 can cause hyperglycemia or rebound weight gain. Furthermore, it can become complicated to restart GLP1 dosing, particularly given the existing medication shortages.”
“In most cases, stopping a weekly GLP-1 medication 1 week prior to the procedure minimizes the risks of pulmonary aspiration and prevents any worsening hyperglycemia or weight gain,” he said. However, taking the drug 7 days prior to the procedure is optimal. “That way, they would be due for the next dose on the day of the procedure, and taking it the day following procedure minimizes disruption in their once-weekly regimen.”
Malini Gupta, MD, director of G2Endo Endocrinology & Metabolism, Memphis, Tennessee, advised that physicians weigh the risk of stopping the medication (which can cause a glycemic spike) vs risk for aspiration.
“In my opinion, all patients should follow a strict liquid diet or NPO status prior to a surgery to further decrease the risk of aspiration,” she said. “I generally hold the GLP-1 RA for a week before a surgery. If additional glycemic control is necessary, I will add to or adjust one of the patient’s other diabetes medications.”
Jaime Almandoz, MD, associate professor of medicine and medical director of the Weight Wellness Program in Dallas, said, “As endocrinologists, we typically rely on our anesthesia colleagues for guidance on perioperative management. In light of emerging guidelines for holding GLP-1 medications, we also recommend patients adopt a liquid diet 24 hours prior to surgery, along with the fasting protocol.”
“For those managing diabetes with GLP-1 therapies, it is crucial to establish a blood sugar management plan while off these medications, especially during fasting or postoperative periods, which can be further influenced by many factors, including nausea, pain medications, and antibiotics after the procedure.”
Joshi added that at Parkland Hospital in Dallas, “we do a huge number of cases using the same information. We identify patients who are at risk, and then we tell our proceduralists and our surgeons if they’re in the escalating phase of the dosing or if they have GI symptoms; don’t even schedule them as an elective case; wait till the escalation phase is over and then schedule them.”
“That way,” he said, “it becomes logistically easy to manage because the recommendation from the group is that patients who are at higher risk should receive a 24-hour liquid diet — the same as colonoscopy. But sometimes it can be challenging to do so.”
Joshi has received honoraria for consultation from Merck Sharp & Dohme, Vertex Pharmaceuticals, and Haisco-USA Pharmaceuticals. Gupta is on the speakers bureau for Amgen (Tepezza) and IBSA (Tirosint) and is a creative consultant for AbbVie. Almandoz serves on advisory boards for Novo Nordisk, Eli Lilly, and Boehringer Ingelheim. The other experts declared no relevant relationships.
A version of this article first appeared on Medscape.com.
, as does the US Food and Drug Administration’s (FDA’s) labeling for the drugs. The changes can be challenging to keep up with, and endocrinologists seem to be making their own decisions based on clinical experience and their interpretations of the potential impact and value of the emerging information.
The latest FDA label change warns about the risk for pulmonary aspiration but notes “insufficient” data to inform recommendations to mitigate the risk in vulnerable patients. Yet, the latest multi-society guidance, led by the American Society of Anesthesiologists (ASA) and based on consensus, not evidence, has nuanced advice for managing patients at risk.
Does the FDA’s label change make a difference regarding the multi-society guidance, which was published earlier? “The answer is no,” Girish Joshi, MD, vice chair, ASA Committee on Practice Parameters, told this news organization. “The concern of increased pulmonary aspiration in patients who are on GLP-1 receptor agonists has been known, and that concern still exists. So, we started with not an assumption but the premise that patients on GLP-1 receptor agonists are at a higher risk of aspiration during sedation, analgesia, and/or general anesthesia. The FDA basically confirms what we say in the guidance.”
Joshi, professor in the Anesthesiology and Pain Management Department at UT Southwestern Medical Center, Dallas, aimed to make the guidance, which was published simultaneously in several society journals, more implementable with a letter to the editor of Anesthesiology. The key, he said, is to identify patients at higher risk for aspiration; all others would follow treatment as usual.
The letter highlights three overarching recommendations and then expands upon them: Standardized preoperative assessment for risk for delayed gastric emptying (yes/no); selective preoperative care plan based on delayed gastric emptying assessment and shared decision-making; and on the day of the procedure, reassess for delayed gastric emptying and mitigate risk if there is clinical concern.
But it seems as though, for now, endocrinologists are managing these patients as they see fit, within the parameters of any institutional guidance requirements. Here is what they said about their practice:
Amy E. Rothberg, MD, DABOM, director of the Weight Management Program & Rewind at the University of Michigan, Ann Arbor, Michigan, said, “I think it makes sense to inform our patients of the labeling and rare but potential adverse effects if they intend to undergo anesthesia for a scheduled procedure/surgery. There is never no risk of aspiration during anesthesia.”
“I find it a bit curious that ASA implies that those who experience GI side effects are more likely than those who do not to have this potential risk. I doubt there is evidence that those without GI side effects are necessarily ‘safer’ and a study to determine that is unlikely to take be conducted.”
“My institution does require a 1-week pause on GLP-1s for those undergoing anesthesia for surgery,” she added. “That’s not evidence-based either, but probably reduces the risk of aspiration during anesthesia — but I don’t know what the actual denominator is for aspiration in those who continued vs those who took a pause from GLP-1s. Pausing does certainly (anecdotally) increase the traffic of communications between physicians and their patients about what to do in the interval.”
Anne Peters, MD, a professor of clinical medicine and a clinical scholar at the Keck School of Medicine of the University of Southern California, Los Angeles, said, “The FDA label change is a warning that really doesn’t say exactly who on GLP-1 RAs is at highest risk or what to do, and if any intervention has been shown to help. The ASA recommendations seem much more nuanced and practical, including point-of-care gastric ultrasound to see if there is retained food/fluid prior to surgery.”
“In my practice, I individualize what I say, depending on the person and the circumstance,” she said. “Mostly, I have people hold one dose before planned surgery, so they have been 10 days at least without a dose. But if worried about gastrointestinal symptoms or gastroparesis, I have them do a clear liquid diet for 24 hours presurgery. Or at least avoid heavy fat meals the day before.”
“There is a risk of aspiration with anything that slows gastric emptying — maybe even in patients with gastroparesis at baseline due to physiologic, not pharmacological, reasons — and anesthesiologists should be aware of the need to assess patients individually.”
Michael A. Weintraub, MD, of NYU Langone Health Diabetes & Endocrine Associates in New York City, observed, “The risk of a pulmonary aspiration event with GLP-1 medication is quite rare, but not zero. On the other hand, stopping the GLP-1 can cause hyperglycemia or rebound weight gain. Furthermore, it can become complicated to restart GLP1 dosing, particularly given the existing medication shortages.”
“In most cases, stopping a weekly GLP-1 medication 1 week prior to the procedure minimizes the risks of pulmonary aspiration and prevents any worsening hyperglycemia or weight gain,” he said. However, taking the drug 7 days prior to the procedure is optimal. “That way, they would be due for the next dose on the day of the procedure, and taking it the day following procedure minimizes disruption in their once-weekly regimen.”
Malini Gupta, MD, director of G2Endo Endocrinology & Metabolism, Memphis, Tennessee, advised that physicians weigh the risk of stopping the medication (which can cause a glycemic spike) vs risk for aspiration.
“In my opinion, all patients should follow a strict liquid diet or NPO status prior to a surgery to further decrease the risk of aspiration,” she said. “I generally hold the GLP-1 RA for a week before a surgery. If additional glycemic control is necessary, I will add to or adjust one of the patient’s other diabetes medications.”
Jaime Almandoz, MD, associate professor of medicine and medical director of the Weight Wellness Program in Dallas, said, “As endocrinologists, we typically rely on our anesthesia colleagues for guidance on perioperative management. In light of emerging guidelines for holding GLP-1 medications, we also recommend patients adopt a liquid diet 24 hours prior to surgery, along with the fasting protocol.”
“For those managing diabetes with GLP-1 therapies, it is crucial to establish a blood sugar management plan while off these medications, especially during fasting or postoperative periods, which can be further influenced by many factors, including nausea, pain medications, and antibiotics after the procedure.”
Joshi added that at Parkland Hospital in Dallas, “we do a huge number of cases using the same information. We identify patients who are at risk, and then we tell our proceduralists and our surgeons if they’re in the escalating phase of the dosing or if they have GI symptoms; don’t even schedule them as an elective case; wait till the escalation phase is over and then schedule them.”
“That way,” he said, “it becomes logistically easy to manage because the recommendation from the group is that patients who are at higher risk should receive a 24-hour liquid diet — the same as colonoscopy. But sometimes it can be challenging to do so.”
Joshi has received honoraria for consultation from Merck Sharp & Dohme, Vertex Pharmaceuticals, and Haisco-USA Pharmaceuticals. Gupta is on the speakers bureau for Amgen (Tepezza) and IBSA (Tirosint) and is a creative consultant for AbbVie. Almandoz serves on advisory boards for Novo Nordisk, Eli Lilly, and Boehringer Ingelheim. The other experts declared no relevant relationships.
A version of this article first appeared on Medscape.com.
, as does the US Food and Drug Administration’s (FDA’s) labeling for the drugs. The changes can be challenging to keep up with, and endocrinologists seem to be making their own decisions based on clinical experience and their interpretations of the potential impact and value of the emerging information.
The latest FDA label change warns about the risk for pulmonary aspiration but notes “insufficient” data to inform recommendations to mitigate the risk in vulnerable patients. Yet, the latest multi-society guidance, led by the American Society of Anesthesiologists (ASA) and based on consensus, not evidence, has nuanced advice for managing patients at risk.
Does the FDA’s label change make a difference regarding the multi-society guidance, which was published earlier? “The answer is no,” Girish Joshi, MD, vice chair, ASA Committee on Practice Parameters, told this news organization. “The concern of increased pulmonary aspiration in patients who are on GLP-1 receptor agonists has been known, and that concern still exists. So, we started with not an assumption but the premise that patients on GLP-1 receptor agonists are at a higher risk of aspiration during sedation, analgesia, and/or general anesthesia. The FDA basically confirms what we say in the guidance.”
Joshi, professor in the Anesthesiology and Pain Management Department at UT Southwestern Medical Center, Dallas, aimed to make the guidance, which was published simultaneously in several society journals, more implementable with a letter to the editor of Anesthesiology. The key, he said, is to identify patients at higher risk for aspiration; all others would follow treatment as usual.
The letter highlights three overarching recommendations and then expands upon them: Standardized preoperative assessment for risk for delayed gastric emptying (yes/no); selective preoperative care plan based on delayed gastric emptying assessment and shared decision-making; and on the day of the procedure, reassess for delayed gastric emptying and mitigate risk if there is clinical concern.
But it seems as though, for now, endocrinologists are managing these patients as they see fit, within the parameters of any institutional guidance requirements. Here is what they said about their practice:
Amy E. Rothberg, MD, DABOM, director of the Weight Management Program & Rewind at the University of Michigan, Ann Arbor, Michigan, said, “I think it makes sense to inform our patients of the labeling and rare but potential adverse effects if they intend to undergo anesthesia for a scheduled procedure/surgery. There is never no risk of aspiration during anesthesia.”
“I find it a bit curious that ASA implies that those who experience GI side effects are more likely than those who do not to have this potential risk. I doubt there is evidence that those without GI side effects are necessarily ‘safer’ and a study to determine that is unlikely to take be conducted.”
“My institution does require a 1-week pause on GLP-1s for those undergoing anesthesia for surgery,” she added. “That’s not evidence-based either, but probably reduces the risk of aspiration during anesthesia — but I don’t know what the actual denominator is for aspiration in those who continued vs those who took a pause from GLP-1s. Pausing does certainly (anecdotally) increase the traffic of communications between physicians and their patients about what to do in the interval.”
Anne Peters, MD, a professor of clinical medicine and a clinical scholar at the Keck School of Medicine of the University of Southern California, Los Angeles, said, “The FDA label change is a warning that really doesn’t say exactly who on GLP-1 RAs is at highest risk or what to do, and if any intervention has been shown to help. The ASA recommendations seem much more nuanced and practical, including point-of-care gastric ultrasound to see if there is retained food/fluid prior to surgery.”
“In my practice, I individualize what I say, depending on the person and the circumstance,” she said. “Mostly, I have people hold one dose before planned surgery, so they have been 10 days at least without a dose. But if worried about gastrointestinal symptoms or gastroparesis, I have them do a clear liquid diet for 24 hours presurgery. Or at least avoid heavy fat meals the day before.”
“There is a risk of aspiration with anything that slows gastric emptying — maybe even in patients with gastroparesis at baseline due to physiologic, not pharmacological, reasons — and anesthesiologists should be aware of the need to assess patients individually.”
Michael A. Weintraub, MD, of NYU Langone Health Diabetes & Endocrine Associates in New York City, observed, “The risk of a pulmonary aspiration event with GLP-1 medication is quite rare, but not zero. On the other hand, stopping the GLP-1 can cause hyperglycemia or rebound weight gain. Furthermore, it can become complicated to restart GLP1 dosing, particularly given the existing medication shortages.”
“In most cases, stopping a weekly GLP-1 medication 1 week prior to the procedure minimizes the risks of pulmonary aspiration and prevents any worsening hyperglycemia or weight gain,” he said. However, taking the drug 7 days prior to the procedure is optimal. “That way, they would be due for the next dose on the day of the procedure, and taking it the day following procedure minimizes disruption in their once-weekly regimen.”
Malini Gupta, MD, director of G2Endo Endocrinology & Metabolism, Memphis, Tennessee, advised that physicians weigh the risk of stopping the medication (which can cause a glycemic spike) vs risk for aspiration.
“In my opinion, all patients should follow a strict liquid diet or NPO status prior to a surgery to further decrease the risk of aspiration,” she said. “I generally hold the GLP-1 RA for a week before a surgery. If additional glycemic control is necessary, I will add to or adjust one of the patient’s other diabetes medications.”
Jaime Almandoz, MD, associate professor of medicine and medical director of the Weight Wellness Program in Dallas, said, “As endocrinologists, we typically rely on our anesthesia colleagues for guidance on perioperative management. In light of emerging guidelines for holding GLP-1 medications, we also recommend patients adopt a liquid diet 24 hours prior to surgery, along with the fasting protocol.”
“For those managing diabetes with GLP-1 therapies, it is crucial to establish a blood sugar management plan while off these medications, especially during fasting or postoperative periods, which can be further influenced by many factors, including nausea, pain medications, and antibiotics after the procedure.”
Joshi added that at Parkland Hospital in Dallas, “we do a huge number of cases using the same information. We identify patients who are at risk, and then we tell our proceduralists and our surgeons if they’re in the escalating phase of the dosing or if they have GI symptoms; don’t even schedule them as an elective case; wait till the escalation phase is over and then schedule them.”
“That way,” he said, “it becomes logistically easy to manage because the recommendation from the group is that patients who are at higher risk should receive a 24-hour liquid diet — the same as colonoscopy. But sometimes it can be challenging to do so.”
Joshi has received honoraria for consultation from Merck Sharp & Dohme, Vertex Pharmaceuticals, and Haisco-USA Pharmaceuticals. Gupta is on the speakers bureau for Amgen (Tepezza) and IBSA (Tirosint) and is a creative consultant for AbbVie. Almandoz serves on advisory boards for Novo Nordisk, Eli Lilly, and Boehringer Ingelheim. The other experts declared no relevant relationships.
A version of this article first appeared on Medscape.com.
Does Radiation Timing Affect QOL After Prostate Surgery?
TOPLINE:
METHODOLOGY:
- Delaying radiotherapy after prostatectomy can help avoid overtreatment and mitigate genitourinary and erectile toxic effects. However, few studies have compared long-term patient-reported health-related quality-of-life outcomes on the basis of the timing of postprostatectomy radiotherapy.
- Researchers evaluated 1203 men (median age, 60.5 years; 92% were White and 6.8% were Black) with localized prostate cancer who underwent radical prostatectomy from the PROST-QA (2003-2006) and RP2 Consortium (2010-2013). Among these patients, 1082 underwent surgery only, 57 received early radiotherapy (within 12 months of surgery), and 64 underwent late radiotherapy (12 months or more after surgery).
- Patients who received early radiotherapy were more likely to receive androgen deprivation therapy than those who underwent late radiotherapy (40.4% vs 12.5%; P < .001).
- Primary outcome was health-related quality of life measured using the Expanded Prostate Cancer Index Composite at baseline, 2, 6, and 12 months, and annually after that. Health-related quality-of-life measures included sexual function, urinary incontinence, urinary irritation and/or obstruction, and bowel or rectal function.
- The median follow-up duration was 85.6 months.
TAKEAWAY:
- Postprostatectomy radiotherapy was associated with a significantly greater decline in health-related quality of life across all domains, including sexual function and urinary incontinence.
- Patients who received early radiation initially experienced worse urinary incontinence and sexual health, compared with patients in the late group, but the early group also had higher-risk disease and were more likely to receive concurrent androgen deprivation therapy.
- In the long term, the early radiotherapy group experienced more pronounced recovery of sexual function, urinary irritation, and urinary incontinence than the late radiotherapy group.
- Ultimately, patients in the early radiotherapy group had similar, potentially better, long-term health-related quality-of-life domain scores than those in the late group over the long term. For instance, the likelihood of being pad free increased for patients treated early with radiation, while it decreased for those treated late. In patients who received early radiation, the rate of freedom from pad use increased from 39% before radiation to 67% at the sixth follow-up visit after radiation, while it decreased from 73% to 48% in those who received late radiation.
IN PRACTICE:
“Long-term patient-reported sexual, incontinence, and urinary irritative outcomes did not significantly differ between early vs late postprostatectomy [radiotherapy],” the authors said. In fact, “men receiving early [radiation] experienced greater recovery of these toxicity domains and achieved similar, and possibly better, domain scores as those receiving late [radiation] at long-term follow-up.” Overall, “these results may help guide treatment counseling and support consideration of early [radiotherapy] after prostatectomy for men at particularly high risk of recurrence and metastasis.”
SOURCE:
The study, led by Sagar A. Patel, MD, MSc, Emory University in Atlanta, was published online in JAMA Network Open.
LIMITATIONS:
The early and late postprostatectomy radiotherapy groups were relatively small and underpowered to detect statistically significant differences between groups. The study has a nonrandomized design, which may introduce unaccounted for imbalances among the different groups. The study did not directly compare health-related quality of life between patients receiving adjuvant vs salvage radiotherapy.
DISCLOSURES:
This study received funding from National Institutes of Health grants and the Paul Calabresi Career Development Award for Clinical Oncology. Several authors reported receiving personal fees, grants, and having other ties with various sources. Additional disclosures are noted in the original article.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Delaying radiotherapy after prostatectomy can help avoid overtreatment and mitigate genitourinary and erectile toxic effects. However, few studies have compared long-term patient-reported health-related quality-of-life outcomes on the basis of the timing of postprostatectomy radiotherapy.
- Researchers evaluated 1203 men (median age, 60.5 years; 92% were White and 6.8% were Black) with localized prostate cancer who underwent radical prostatectomy from the PROST-QA (2003-2006) and RP2 Consortium (2010-2013). Among these patients, 1082 underwent surgery only, 57 received early radiotherapy (within 12 months of surgery), and 64 underwent late radiotherapy (12 months or more after surgery).
- Patients who received early radiotherapy were more likely to receive androgen deprivation therapy than those who underwent late radiotherapy (40.4% vs 12.5%; P < .001).
- Primary outcome was health-related quality of life measured using the Expanded Prostate Cancer Index Composite at baseline, 2, 6, and 12 months, and annually after that. Health-related quality-of-life measures included sexual function, urinary incontinence, urinary irritation and/or obstruction, and bowel or rectal function.
- The median follow-up duration was 85.6 months.
TAKEAWAY:
- Postprostatectomy radiotherapy was associated with a significantly greater decline in health-related quality of life across all domains, including sexual function and urinary incontinence.
- Patients who received early radiation initially experienced worse urinary incontinence and sexual health, compared with patients in the late group, but the early group also had higher-risk disease and were more likely to receive concurrent androgen deprivation therapy.
- In the long term, the early radiotherapy group experienced more pronounced recovery of sexual function, urinary irritation, and urinary incontinence than the late radiotherapy group.
- Ultimately, patients in the early radiotherapy group had similar, potentially better, long-term health-related quality-of-life domain scores than those in the late group over the long term. For instance, the likelihood of being pad free increased for patients treated early with radiation, while it decreased for those treated late. In patients who received early radiation, the rate of freedom from pad use increased from 39% before radiation to 67% at the sixth follow-up visit after radiation, while it decreased from 73% to 48% in those who received late radiation.
IN PRACTICE:
“Long-term patient-reported sexual, incontinence, and urinary irritative outcomes did not significantly differ between early vs late postprostatectomy [radiotherapy],” the authors said. In fact, “men receiving early [radiation] experienced greater recovery of these toxicity domains and achieved similar, and possibly better, domain scores as those receiving late [radiation] at long-term follow-up.” Overall, “these results may help guide treatment counseling and support consideration of early [radiotherapy] after prostatectomy for men at particularly high risk of recurrence and metastasis.”
SOURCE:
The study, led by Sagar A. Patel, MD, MSc, Emory University in Atlanta, was published online in JAMA Network Open.
LIMITATIONS:
The early and late postprostatectomy radiotherapy groups were relatively small and underpowered to detect statistically significant differences between groups. The study has a nonrandomized design, which may introduce unaccounted for imbalances among the different groups. The study did not directly compare health-related quality of life between patients receiving adjuvant vs salvage radiotherapy.
DISCLOSURES:
This study received funding from National Institutes of Health grants and the Paul Calabresi Career Development Award for Clinical Oncology. Several authors reported receiving personal fees, grants, and having other ties with various sources. Additional disclosures are noted in the original article.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Delaying radiotherapy after prostatectomy can help avoid overtreatment and mitigate genitourinary and erectile toxic effects. However, few studies have compared long-term patient-reported health-related quality-of-life outcomes on the basis of the timing of postprostatectomy radiotherapy.
- Researchers evaluated 1203 men (median age, 60.5 years; 92% were White and 6.8% were Black) with localized prostate cancer who underwent radical prostatectomy from the PROST-QA (2003-2006) and RP2 Consortium (2010-2013). Among these patients, 1082 underwent surgery only, 57 received early radiotherapy (within 12 months of surgery), and 64 underwent late radiotherapy (12 months or more after surgery).
- Patients who received early radiotherapy were more likely to receive androgen deprivation therapy than those who underwent late radiotherapy (40.4% vs 12.5%; P < .001).
- Primary outcome was health-related quality of life measured using the Expanded Prostate Cancer Index Composite at baseline, 2, 6, and 12 months, and annually after that. Health-related quality-of-life measures included sexual function, urinary incontinence, urinary irritation and/or obstruction, and bowel or rectal function.
- The median follow-up duration was 85.6 months.
TAKEAWAY:
- Postprostatectomy radiotherapy was associated with a significantly greater decline in health-related quality of life across all domains, including sexual function and urinary incontinence.
- Patients who received early radiation initially experienced worse urinary incontinence and sexual health, compared with patients in the late group, but the early group also had higher-risk disease and were more likely to receive concurrent androgen deprivation therapy.
- In the long term, the early radiotherapy group experienced more pronounced recovery of sexual function, urinary irritation, and urinary incontinence than the late radiotherapy group.
- Ultimately, patients in the early radiotherapy group had similar, potentially better, long-term health-related quality-of-life domain scores than those in the late group over the long term. For instance, the likelihood of being pad free increased for patients treated early with radiation, while it decreased for those treated late. In patients who received early radiation, the rate of freedom from pad use increased from 39% before radiation to 67% at the sixth follow-up visit after radiation, while it decreased from 73% to 48% in those who received late radiation.
IN PRACTICE:
“Long-term patient-reported sexual, incontinence, and urinary irritative outcomes did not significantly differ between early vs late postprostatectomy [radiotherapy],” the authors said. In fact, “men receiving early [radiation] experienced greater recovery of these toxicity domains and achieved similar, and possibly better, domain scores as those receiving late [radiation] at long-term follow-up.” Overall, “these results may help guide treatment counseling and support consideration of early [radiotherapy] after prostatectomy for men at particularly high risk of recurrence and metastasis.”
SOURCE:
The study, led by Sagar A. Patel, MD, MSc, Emory University in Atlanta, was published online in JAMA Network Open.
LIMITATIONS:
The early and late postprostatectomy radiotherapy groups were relatively small and underpowered to detect statistically significant differences between groups. The study has a nonrandomized design, which may introduce unaccounted for imbalances among the different groups. The study did not directly compare health-related quality of life between patients receiving adjuvant vs salvage radiotherapy.
DISCLOSURES:
This study received funding from National Institutes of Health grants and the Paul Calabresi Career Development Award for Clinical Oncology. Several authors reported receiving personal fees, grants, and having other ties with various sources. Additional disclosures are noted in the original article.
A version of this article appeared on Medscape.com.
GLP-1 RAs Safe in the Perioperative Period: New Guidance
The new guidance, contrasting with earlier recommendations, says these incrementally used agents can be taken up until the day of surgery, but patients are advised to follow a liquid diet for 24 hours before the procedure. The decision to proceed with endoscopy and other procedures should be based on shared decision-making with the patient and interdisciplinary care teams in conjunction with minimization of the aspiration risk from delayed gastric emptying, the guidance stresses.
The five endorsing organizations are the American Society for Metabolic and Bariatric Surgery, American Society of Anesthesiologists (ASA), American Gastroenterological Association, International Society of Perioperative Care of Patients with Obesity, and Society of American Gastrointestinal and Endoscopic Surgeons. The societies emphasize that the statement is intended as guidance only and is not an evidence-based formal guideline.
GLP-1 RAs are known to delay gastric emptying, raising concerns about regurgitation, aspiration, and airway compromise during anesthesia. Rare serious adverse events have also been observed, prompting the ASA in 2023 to recommend holding these agents for 1 week for the injectable form and 1 day for the oral form before all procedures requiring anesthesia.

That abundance of caution, however, had negative impacts of its own. “This guidance has led to cancellations and postponements of many endoscopic and surgical procedures or required patients to undergo general anesthesia who may otherwise have had their procedures performed under moderate sedation,” said guidance coauthor Allison R. Schulman, MD, MPH, an associate professor of medicine and surgery and chief of endoscopy at the University of Michigan in Ann Arbor. “Nearly all institutions have been forced to revise preprocedural protocols, despite a lack of high-level evidence to suggest that these adjustments are necessary.”
“Studies have yielded mixed results as to whether patients on GLP-1s are at increased risk of these events, and the limited data available are inconsistent,” Schulman said. “As a result, there are inconsistencies in the recommendations from various societies leading to growing uncertainty with proceduralists on how to provide safe, effective, and timely procedural care to patients taking GLP-1 RAs.”
The new joint-society guidance may alleviate some of the uncertainty. Among the recommendations:
- Continuing GLP-1 RAs in the perioperative period should be based on shared decision-making with the patient and all care teams balancing the metabolic need for the GLP-1 RA with individual patient risk.
- Certain variables may increase the risk for delayed gastric emptying and aspiration with the periprocedural use of GLP-1 RAs: escalation phase — This phase vs the maintenance phase is associated with a higher risk for delayed gastric emptying; higher dose — the higher the dose, the greater the risk for gastrointestinal (GI) side effects; weekly dosing — GI side effects are more common with weekly vs daily formulations; presence of GI symptoms — nausea, vomiting, abdominal pain, dyspepsia, and constipation may suggest delayed gastric emptying; and medical problems beyond GLP-1 RA indications with GI effects — assess for such conditions as bowel dysmotility, gastroparesis, and Parkinson’s disease.
- Risk factors should be assessed in advance to allow sufficient time to adjust preoperative care, including diet modification and medication bridging if GLP-1 RA cessation is deemed advisable.
- If retained gastric contents are a concern on the day of a procedure, point-of-care gastric ultrasound could be used to assess aspiration risk, resources permitting.
- The aspiration risk from delayed gastric emptying should be minimized by preoperative diet modification and/or altering the anesthesia plan to consider rapid sequence induction of general anesthesia for tracheal intubation. A 24-hour preoperative liquid diet, as before colonoscopy and bariatric surgery, can be utilized when delayed gastric emptying is a concern.
- When concern about retained gastric contents exists on procedure day, providers should engage patients in a shared decision-making model and consider the benefits and risks of rapid-sequence induction of general anesthesia for tracheal intubation to minimize aspiration risk vs procedure cancellation.
“Safe continuation of surgery and gastrointestinal endoscopy, and prevention of procedure cancellation, for patients on GLP-1 RAs can be prioritized following the recommendations above, as would occur for other patient populations with gastroparesis,” the guidance panel wrote.

Commenting on the statement but not involved in it, David B. Purow, MD, managing director of the Digestive Health Center at Northwell Health/Huntington Hospital in Huntington, New York, said the recommendations will encourage clinicians to be more discerning about actual risk in individual cases rather than follow the previous blanket recommendation to stop these agents before procedures requiring sedation.
While GLP-1 RAs were prescribed for the relatively small number of patients with diabetes, he said, the risk was not apparent but became clearer with the widespread use of these agents for weight loss — often unregulated and undisclosed to care providers.
“The pendulum shifted too far the other way, and now it’s shifted back,” he said in an interview. “The new guidance is great because now we can be more thoughtful about managing individual patients.” He cited, for instance, the recommendations on the greater risk in patients in the dose escalation phase or on higher doses, and the risk-reducing measure of a liquid diet for 24 hours before surgery.
His center is already using point-of-care ultrasound and recently had a case in which a patient who forgot and took his GLP-1 RA before a scheduled procedure was found on ultrasound to have a full stomach. “In some cases, these drugs can cause an almost gastroparesis level of delayed emptying,” Purow said.
Purow thinks this early guidance will probably progress to firm guidelines within a year. Schulman is more cautious. “Our understanding of this complex topic is increasing rapidly, and ongoing clinical research will ultimately lead to evidence-based guidelines in this changing landscape,” she said.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. Schulman is a consultant for Apollo Endosurgery, Boston Scientific, Olympus, Microtech, and Fractyl. Purow had no competing interests to declare.
A version of this article first appeared on Medscape.com.
The new guidance, contrasting with earlier recommendations, says these incrementally used agents can be taken up until the day of surgery, but patients are advised to follow a liquid diet for 24 hours before the procedure. The decision to proceed with endoscopy and other procedures should be based on shared decision-making with the patient and interdisciplinary care teams in conjunction with minimization of the aspiration risk from delayed gastric emptying, the guidance stresses.
The five endorsing organizations are the American Society for Metabolic and Bariatric Surgery, American Society of Anesthesiologists (ASA), American Gastroenterological Association, International Society of Perioperative Care of Patients with Obesity, and Society of American Gastrointestinal and Endoscopic Surgeons. The societies emphasize that the statement is intended as guidance only and is not an evidence-based formal guideline.
GLP-1 RAs are known to delay gastric emptying, raising concerns about regurgitation, aspiration, and airway compromise during anesthesia. Rare serious adverse events have also been observed, prompting the ASA in 2023 to recommend holding these agents for 1 week for the injectable form and 1 day for the oral form before all procedures requiring anesthesia.
That abundance of caution, however, had negative impacts of its own. “This guidance has led to cancellations and postponements of many endoscopic and surgical procedures or required patients to undergo general anesthesia who may otherwise have had their procedures performed under moderate sedation,” said guidance coauthor Allison R. Schulman, MD, MPH, an associate professor of medicine and surgery and chief of endoscopy at the University of Michigan in Ann Arbor. “Nearly all institutions have been forced to revise preprocedural protocols, despite a lack of high-level evidence to suggest that these adjustments are necessary.”
“Studies have yielded mixed results as to whether patients on GLP-1s are at increased risk of these events, and the limited data available are inconsistent,” Schulman said. “As a result, there are inconsistencies in the recommendations from various societies leading to growing uncertainty with proceduralists on how to provide safe, effective, and timely procedural care to patients taking GLP-1 RAs.”
The new joint-society guidance may alleviate some of the uncertainty. Among the recommendations:
- Continuing GLP-1 RAs in the perioperative period should be based on shared decision-making with the patient and all care teams balancing the metabolic need for the GLP-1 RA with individual patient risk.
- Certain variables may increase the risk for delayed gastric emptying and aspiration with the periprocedural use of GLP-1 RAs: escalation phase — This phase vs the maintenance phase is associated with a higher risk for delayed gastric emptying; higher dose — the higher the dose, the greater the risk for gastrointestinal (GI) side effects; weekly dosing — GI side effects are more common with weekly vs daily formulations; presence of GI symptoms — nausea, vomiting, abdominal pain, dyspepsia, and constipation may suggest delayed gastric emptying; and medical problems beyond GLP-1 RA indications with GI effects — assess for such conditions as bowel dysmotility, gastroparesis, and Parkinson’s disease.
- Risk factors should be assessed in advance to allow sufficient time to adjust preoperative care, including diet modification and medication bridging if GLP-1 RA cessation is deemed advisable.
- If retained gastric contents are a concern on the day of a procedure, point-of-care gastric ultrasound could be used to assess aspiration risk, resources permitting.
- The aspiration risk from delayed gastric emptying should be minimized by preoperative diet modification and/or altering the anesthesia plan to consider rapid sequence induction of general anesthesia for tracheal intubation. A 24-hour preoperative liquid diet, as before colonoscopy and bariatric surgery, can be utilized when delayed gastric emptying is a concern.
- When concern about retained gastric contents exists on procedure day, providers should engage patients in a shared decision-making model and consider the benefits and risks of rapid-sequence induction of general anesthesia for tracheal intubation to minimize aspiration risk vs procedure cancellation.
“Safe continuation of surgery and gastrointestinal endoscopy, and prevention of procedure cancellation, for patients on GLP-1 RAs can be prioritized following the recommendations above, as would occur for other patient populations with gastroparesis,” the guidance panel wrote.
Commenting on the statement but not involved in it, David B. Purow, MD, managing director of the Digestive Health Center at Northwell Health/Huntington Hospital in Huntington, New York, said the recommendations will encourage clinicians to be more discerning about actual risk in individual cases rather than follow the previous blanket recommendation to stop these agents before procedures requiring sedation.
While GLP-1 RAs were prescribed for the relatively small number of patients with diabetes, he said, the risk was not apparent but became clearer with the widespread use of these agents for weight loss — often unregulated and undisclosed to care providers.
“The pendulum shifted too far the other way, and now it’s shifted back,” he said in an interview. “The new guidance is great because now we can be more thoughtful about managing individual patients.” He cited, for instance, the recommendations on the greater risk in patients in the dose escalation phase or on higher doses, and the risk-reducing measure of a liquid diet for 24 hours before surgery.
His center is already using point-of-care ultrasound and recently had a case in which a patient who forgot and took his GLP-1 RA before a scheduled procedure was found on ultrasound to have a full stomach. “In some cases, these drugs can cause an almost gastroparesis level of delayed emptying,” Purow said.
Purow thinks this early guidance will probably progress to firm guidelines within a year. Schulman is more cautious. “Our understanding of this complex topic is increasing rapidly, and ongoing clinical research will ultimately lead to evidence-based guidelines in this changing landscape,” she said.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. Schulman is a consultant for Apollo Endosurgery, Boston Scientific, Olympus, Microtech, and Fractyl. Purow had no competing interests to declare.
A version of this article first appeared on Medscape.com.
The new guidance, contrasting with earlier recommendations, says these incrementally used agents can be taken up until the day of surgery, but patients are advised to follow a liquid diet for 24 hours before the procedure. The decision to proceed with endoscopy and other procedures should be based on shared decision-making with the patient and interdisciplinary care teams in conjunction with minimization of the aspiration risk from delayed gastric emptying, the guidance stresses.
The five endorsing organizations are the American Society for Metabolic and Bariatric Surgery, American Society of Anesthesiologists (ASA), American Gastroenterological Association, International Society of Perioperative Care of Patients with Obesity, and Society of American Gastrointestinal and Endoscopic Surgeons. The societies emphasize that the statement is intended as guidance only and is not an evidence-based formal guideline.
GLP-1 RAs are known to delay gastric emptying, raising concerns about regurgitation, aspiration, and airway compromise during anesthesia. Rare serious adverse events have also been observed, prompting the ASA in 2023 to recommend holding these agents for 1 week for the injectable form and 1 day for the oral form before all procedures requiring anesthesia.
That abundance of caution, however, had negative impacts of its own. “This guidance has led to cancellations and postponements of many endoscopic and surgical procedures or required patients to undergo general anesthesia who may otherwise have had their procedures performed under moderate sedation,” said guidance coauthor Allison R. Schulman, MD, MPH, an associate professor of medicine and surgery and chief of endoscopy at the University of Michigan in Ann Arbor. “Nearly all institutions have been forced to revise preprocedural protocols, despite a lack of high-level evidence to suggest that these adjustments are necessary.”
“Studies have yielded mixed results as to whether patients on GLP-1s are at increased risk of these events, and the limited data available are inconsistent,” Schulman said. “As a result, there are inconsistencies in the recommendations from various societies leading to growing uncertainty with proceduralists on how to provide safe, effective, and timely procedural care to patients taking GLP-1 RAs.”
The new joint-society guidance may alleviate some of the uncertainty. Among the recommendations:
- Continuing GLP-1 RAs in the perioperative period should be based on shared decision-making with the patient and all care teams balancing the metabolic need for the GLP-1 RA with individual patient risk.
- Certain variables may increase the risk for delayed gastric emptying and aspiration with the periprocedural use of GLP-1 RAs: escalation phase — This phase vs the maintenance phase is associated with a higher risk for delayed gastric emptying; higher dose — the higher the dose, the greater the risk for gastrointestinal (GI) side effects; weekly dosing — GI side effects are more common with weekly vs daily formulations; presence of GI symptoms — nausea, vomiting, abdominal pain, dyspepsia, and constipation may suggest delayed gastric emptying; and medical problems beyond GLP-1 RA indications with GI effects — assess for such conditions as bowel dysmotility, gastroparesis, and Parkinson’s disease.
- Risk factors should be assessed in advance to allow sufficient time to adjust preoperative care, including diet modification and medication bridging if GLP-1 RA cessation is deemed advisable.
- If retained gastric contents are a concern on the day of a procedure, point-of-care gastric ultrasound could be used to assess aspiration risk, resources permitting.
- The aspiration risk from delayed gastric emptying should be minimized by preoperative diet modification and/or altering the anesthesia plan to consider rapid sequence induction of general anesthesia for tracheal intubation. A 24-hour preoperative liquid diet, as before colonoscopy and bariatric surgery, can be utilized when delayed gastric emptying is a concern.
- When concern about retained gastric contents exists on procedure day, providers should engage patients in a shared decision-making model and consider the benefits and risks of rapid-sequence induction of general anesthesia for tracheal intubation to minimize aspiration risk vs procedure cancellation.
“Safe continuation of surgery and gastrointestinal endoscopy, and prevention of procedure cancellation, for patients on GLP-1 RAs can be prioritized following the recommendations above, as would occur for other patient populations with gastroparesis,” the guidance panel wrote.
Commenting on the statement but not involved in it, David B. Purow, MD, managing director of the Digestive Health Center at Northwell Health/Huntington Hospital in Huntington, New York, said the recommendations will encourage clinicians to be more discerning about actual risk in individual cases rather than follow the previous blanket recommendation to stop these agents before procedures requiring sedation.
While GLP-1 RAs were prescribed for the relatively small number of patients with diabetes, he said, the risk was not apparent but became clearer with the widespread use of these agents for weight loss — often unregulated and undisclosed to care providers.
“The pendulum shifted too far the other way, and now it’s shifted back,” he said in an interview. “The new guidance is great because now we can be more thoughtful about managing individual patients.” He cited, for instance, the recommendations on the greater risk in patients in the dose escalation phase or on higher doses, and the risk-reducing measure of a liquid diet for 24 hours before surgery.
His center is already using point-of-care ultrasound and recently had a case in which a patient who forgot and took his GLP-1 RA before a scheduled procedure was found on ultrasound to have a full stomach. “In some cases, these drugs can cause an almost gastroparesis level of delayed emptying,” Purow said.
Purow thinks this early guidance will probably progress to firm guidelines within a year. Schulman is more cautious. “Our understanding of this complex topic is increasing rapidly, and ongoing clinical research will ultimately lead to evidence-based guidelines in this changing landscape,” she said.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. Schulman is a consultant for Apollo Endosurgery, Boston Scientific, Olympus, Microtech, and Fractyl. Purow had no competing interests to declare.
A version of this article first appeared on Medscape.com.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Short-Course Vasoconstrictors After EVL: Time for a New Standard of Care?
PHILADELPHIA — without raising the risk for rebleeding, if the initial ligation successfully controls bleeding.
“This approach would allow earlier discharge from the hospital and reduce the risk of adverse events, all without sacrificing treatment efficacy or compromising patient safety,” Sushrut Ingawale, MD, MBBS, Quinnipiac University School of Medicine, North Haven, and St. Vincent’s Medical Center, Bridgeport, both in Connecticut, said in a presentation at the annual meeting of the American College of Gastroenterology (ACG).
Ingawale called for a “re-evaluation of existing protocols, emphasizing the potential to update current protocols to reflect shorter, more personalized” duration of vasoconstrictor therapy in these patients.

Commenting on this research, Nancy Reau, MD, AGAF, of Rush University in Chicago, Illinois, said: “We should always question the standard of care.”
“Vasoconstrictors for 5 days is the standard of care, but this could lead to prolonged hospitalization in patients who are otherwise doing well after endoscopic intervention. Recognizing that a shorter course of vasoconstrictor treatment may have equal outcome is very important though it may not be appropriate for all patients, especially those at high risk for rebleeding,” said Reau.
Outdated Guidelines?
In his presentation, Ingawale noted that current guidelines that recommend continuing vasoconstrictors, like octreotide or terlipressin, for at least 3-5 days after EVL for acute variceal bleeding are based primarily on old studies in which sclerotherapy was the primary hemostatic method.
The study team assessed comparative outcomes based on the duration of vasoconstrictors after EVL for acute variceal bleeding in a systematic review and network meta-analysis of 11 randomized controlled trials.
The studies had a total of 816 patients who were grouped based on the duration vasoconstrictor therapy: 24 hours or less (group 1), 24-72 hours (group 2), and 72-120 hours (group 3).
There was no significant difference in the risk for rebleeding in group 1 (risk ratio [RR], 1.36; 95% CI, 0.48-3.52) and group 2 (RR, 1.34; 95% CI, 0.42-4.54) vs group 3.
“This finding was even consistent when we compared individual durations” of 0, 12, 24, 48, and 72 hours vs 120 hours, Ingawale said.
There was also no statistically significant difference in the 5-day mortality risk between group 1 (RR, 0.66; 95% CI, 0.09-2.52) and group 2 (RR, 1.08; 95% CI, 0.15-6.43) or the 30-day mortality risk between group 1 (RR, 1.18; 95% CI, 0.51-2.51) and group 2 (RR, 0.98; 95% CI, 0.36-2.52) vs group 3.
Rapidly Evolving Area
“Our network meta-analysis did not show any benefit of continuing vasoconstrictors after EVL,” the researchers wrote in their conference abstract. Despite historical precedent, shorter durations may be adequate, “potentially enabling earlier hospital discharge without compromising patient outcomes.”
Ingawale suggested future research should look to identify the subset of patients at a risk for failure to control bleeding who might benefit from the continuation of vasoconstrictors.
“Management of complications of portal hypertension are rapidly evolving and this study will add to the data that drives our guidelines. Seeing this data in a peer reviewed publication will add the necessary validity to impact a change in the treatment paradigm,” Reau said.
The study had no specific funding. Ingawale had no relevant financial relationships. Reau disclosed various relationships with AbbVie, Gilead, Arbutus, Intercept, and Salix.
A version of this article first appeared on Medscape.com.
PHILADELPHIA — without raising the risk for rebleeding, if the initial ligation successfully controls bleeding.
“This approach would allow earlier discharge from the hospital and reduce the risk of adverse events, all without sacrificing treatment efficacy or compromising patient safety,” Sushrut Ingawale, MD, MBBS, Quinnipiac University School of Medicine, North Haven, and St. Vincent’s Medical Center, Bridgeport, both in Connecticut, said in a presentation at the annual meeting of the American College of Gastroenterology (ACG).
Ingawale called for a “re-evaluation of existing protocols, emphasizing the potential to update current protocols to reflect shorter, more personalized” duration of vasoconstrictor therapy in these patients.
Commenting on this research, Nancy Reau, MD, AGAF, of Rush University in Chicago, Illinois, said: “We should always question the standard of care.”
“Vasoconstrictors for 5 days is the standard of care, but this could lead to prolonged hospitalization in patients who are otherwise doing well after endoscopic intervention. Recognizing that a shorter course of vasoconstrictor treatment may have equal outcome is very important though it may not be appropriate for all patients, especially those at high risk for rebleeding,” said Reau.
Outdated Guidelines?
In his presentation, Ingawale noted that current guidelines that recommend continuing vasoconstrictors, like octreotide or terlipressin, for at least 3-5 days after EVL for acute variceal bleeding are based primarily on old studies in which sclerotherapy was the primary hemostatic method.
The study team assessed comparative outcomes based on the duration of vasoconstrictors after EVL for acute variceal bleeding in a systematic review and network meta-analysis of 11 randomized controlled trials.
The studies had a total of 816 patients who were grouped based on the duration vasoconstrictor therapy: 24 hours or less (group 1), 24-72 hours (group 2), and 72-120 hours (group 3).
There was no significant difference in the risk for rebleeding in group 1 (risk ratio [RR], 1.36; 95% CI, 0.48-3.52) and group 2 (RR, 1.34; 95% CI, 0.42-4.54) vs group 3.
“This finding was even consistent when we compared individual durations” of 0, 12, 24, 48, and 72 hours vs 120 hours, Ingawale said.
There was also no statistically significant difference in the 5-day mortality risk between group 1 (RR, 0.66; 95% CI, 0.09-2.52) and group 2 (RR, 1.08; 95% CI, 0.15-6.43) or the 30-day mortality risk between group 1 (RR, 1.18; 95% CI, 0.51-2.51) and group 2 (RR, 0.98; 95% CI, 0.36-2.52) vs group 3.
Rapidly Evolving Area
“Our network meta-analysis did not show any benefit of continuing vasoconstrictors after EVL,” the researchers wrote in their conference abstract. Despite historical precedent, shorter durations may be adequate, “potentially enabling earlier hospital discharge without compromising patient outcomes.”
Ingawale suggested future research should look to identify the subset of patients at a risk for failure to control bleeding who might benefit from the continuation of vasoconstrictors.
“Management of complications of portal hypertension are rapidly evolving and this study will add to the data that drives our guidelines. Seeing this data in a peer reviewed publication will add the necessary validity to impact a change in the treatment paradigm,” Reau said.
The study had no specific funding. Ingawale had no relevant financial relationships. Reau disclosed various relationships with AbbVie, Gilead, Arbutus, Intercept, and Salix.
A version of this article first appeared on Medscape.com.
PHILADELPHIA — without raising the risk for rebleeding, if the initial ligation successfully controls bleeding.
“This approach would allow earlier discharge from the hospital and reduce the risk of adverse events, all without sacrificing treatment efficacy or compromising patient safety,” Sushrut Ingawale, MD, MBBS, Quinnipiac University School of Medicine, North Haven, and St. Vincent’s Medical Center, Bridgeport, both in Connecticut, said in a presentation at the annual meeting of the American College of Gastroenterology (ACG).
Ingawale called for a “re-evaluation of existing protocols, emphasizing the potential to update current protocols to reflect shorter, more personalized” duration of vasoconstrictor therapy in these patients.
Commenting on this research, Nancy Reau, MD, AGAF, of Rush University in Chicago, Illinois, said: “We should always question the standard of care.”
“Vasoconstrictors for 5 days is the standard of care, but this could lead to prolonged hospitalization in patients who are otherwise doing well after endoscopic intervention. Recognizing that a shorter course of vasoconstrictor treatment may have equal outcome is very important though it may not be appropriate for all patients, especially those at high risk for rebleeding,” said Reau.
Outdated Guidelines?
In his presentation, Ingawale noted that current guidelines that recommend continuing vasoconstrictors, like octreotide or terlipressin, for at least 3-5 days after EVL for acute variceal bleeding are based primarily on old studies in which sclerotherapy was the primary hemostatic method.
The study team assessed comparative outcomes based on the duration of vasoconstrictors after EVL for acute variceal bleeding in a systematic review and network meta-analysis of 11 randomized controlled trials.
The studies had a total of 816 patients who were grouped based on the duration vasoconstrictor therapy: 24 hours or less (group 1), 24-72 hours (group 2), and 72-120 hours (group 3).
There was no significant difference in the risk for rebleeding in group 1 (risk ratio [RR], 1.36; 95% CI, 0.48-3.52) and group 2 (RR, 1.34; 95% CI, 0.42-4.54) vs group 3.
“This finding was even consistent when we compared individual durations” of 0, 12, 24, 48, and 72 hours vs 120 hours, Ingawale said.
There was also no statistically significant difference in the 5-day mortality risk between group 1 (RR, 0.66; 95% CI, 0.09-2.52) and group 2 (RR, 1.08; 95% CI, 0.15-6.43) or the 30-day mortality risk between group 1 (RR, 1.18; 95% CI, 0.51-2.51) and group 2 (RR, 0.98; 95% CI, 0.36-2.52) vs group 3.
Rapidly Evolving Area
“Our network meta-analysis did not show any benefit of continuing vasoconstrictors after EVL,” the researchers wrote in their conference abstract. Despite historical precedent, shorter durations may be adequate, “potentially enabling earlier hospital discharge without compromising patient outcomes.”
Ingawale suggested future research should look to identify the subset of patients at a risk for failure to control bleeding who might benefit from the continuation of vasoconstrictors.
“Management of complications of portal hypertension are rapidly evolving and this study will add to the data that drives our guidelines. Seeing this data in a peer reviewed publication will add the necessary validity to impact a change in the treatment paradigm,” Reau said.
The study had no specific funding. Ingawale had no relevant financial relationships. Reau disclosed various relationships with AbbVie, Gilead, Arbutus, Intercept, and Salix.
A version of this article first appeared on Medscape.com.
FROM ACG 2024
American Diabetes Association Advises on Hospital CGM Use
, based in part on data collected during the COVID-19 pandemic.
The statement, Consensus Considerations and Good Practice Points for Use of Continuous Glucose Monitoring Systems in Hospital Settings, was published on October 25, 2024, in Diabetes Care.
“This is something that requires close collaboration with many groups in the hospital ... There needs to be really good guidance within the hospital as to when it can be used, in which patients, and what checks and balances need to be in place,” statement lead author Julie L.V. Shaw, PhD, Laboratory Director at Renfrew Victoria Hospital and St. Francis Memorial Hospital, Ottawa, Ontario, Canada, told this news organization.
CGM use in the outpatient setting continues to grow, among people with type 2 as well as type 1 diabetes. The devices are worn on the body for up to 15 days via a subcutaneously-inserted sensor that detects glucose in interstitial fluid every 1-15 minutes. The readings generally track with blood glucose levels, although discrepancies can occur and may be even more relevant in hospital settings.
About 1 in 4 hospitalized patients have diabetes and/or hyperglycemia. During the COVID-19 pandemic, the US Food and Drug Administration (FDA) and Health Canada temporarily authorized the use of CGM systems in hospitals to supplement point-of-care glucose testing, as an emergency measure to reduce healthcare worker exposure and preserve personal protective equipment. That FDA authorization expired on November 7, 2023, and currently hospital CGM use in the United States is technically off-label, although it is often allowed for patients who already use CGM systems.
The new statement summarizes clinical study data and also addresses the potential benefits of CGM systems for inpatients, existing guidance, analytical and clinical evaluation of CGM performance, safety factors, staff training, clinical workflow, and hospital policies. Also covered are issues around quality assurance, integration of CGM data into electronic health records, cost considerations, and barriers to implementation.
The “good practice points for consideration” in the document are as follows:
- If healthcare professionals want to use CGM systems beyond their intended use, eg, to replace or reduce point-of-care glucose measurements, analytical and clinical performance should be assessed.
- The Clinical and Laboratory Standards Institute (CLSI) 2nd Edition of POCT05 — Performance Metrics for Continuous Interstitial Glucose Monitoring provides helpful guidance.
- Potential interferences that preclude patients from being eligible for CGM should be noted, and staff must be aware that CGM can’t be used for clinical decision-making in these patients.
- A CGM system and/or inpatient glycemia management committee should oversee the development and implementation of hospital-approved policies and procedures for CGM use in the hospital. This committee should have representatives from nursing leadership, physician leadership (e.g., endocrinologists, internal medicine specialists, hospitalists), laboratory, information services, hospital administration, pharmacy, and risk management/legal.
- Policies for patient-owned and hospital-owned CGM devices should be developed, and staff should be trained in their use.
“During the pandemic, there was a lot of research on CGM use in the hospital setting, so we could look at how it works and was it safe. I think we have some good data to show where it can be used,” said Shaw, who also heads the Division of Biochemistry at the Ottawa Hospital. She added, “There’s quite a bit we still don’t know, but I think with some guidance in place about when not to use it, there are certainly patient populations who could benefit from it in the hospital setting.”
Shaw had no disclosures. Another author is general manager and medical director of the Institute for Diabetes Technology (IfDT), which carries out clinical studies, eg, with medical devices for diabetes therapy, on its own initiative and on behalf of various companies. Another author is an IfDT employee. Other authors have received speakers’ honoraria or consulting fees in the last 3 years from Abbott, Berlin-Chemie, BOYDSense, Dexcom, Lilly Deutschland, Novo Nordisk, Perfood, PharmaSens, Roche, Sinocare, Terumo, and Ypsomed.
A version of this article appeared on Medscape.com.
, based in part on data collected during the COVID-19 pandemic.
The statement, Consensus Considerations and Good Practice Points for Use of Continuous Glucose Monitoring Systems in Hospital Settings, was published on October 25, 2024, in Diabetes Care.
“This is something that requires close collaboration with many groups in the hospital ... There needs to be really good guidance within the hospital as to when it can be used, in which patients, and what checks and balances need to be in place,” statement lead author Julie L.V. Shaw, PhD, Laboratory Director at Renfrew Victoria Hospital and St. Francis Memorial Hospital, Ottawa, Ontario, Canada, told this news organization.
CGM use in the outpatient setting continues to grow, among people with type 2 as well as type 1 diabetes. The devices are worn on the body for up to 15 days via a subcutaneously-inserted sensor that detects glucose in interstitial fluid every 1-15 minutes. The readings generally track with blood glucose levels, although discrepancies can occur and may be even more relevant in hospital settings.
About 1 in 4 hospitalized patients have diabetes and/or hyperglycemia. During the COVID-19 pandemic, the US Food and Drug Administration (FDA) and Health Canada temporarily authorized the use of CGM systems in hospitals to supplement point-of-care glucose testing, as an emergency measure to reduce healthcare worker exposure and preserve personal protective equipment. That FDA authorization expired on November 7, 2023, and currently hospital CGM use in the United States is technically off-label, although it is often allowed for patients who already use CGM systems.
The new statement summarizes clinical study data and also addresses the potential benefits of CGM systems for inpatients, existing guidance, analytical and clinical evaluation of CGM performance, safety factors, staff training, clinical workflow, and hospital policies. Also covered are issues around quality assurance, integration of CGM data into electronic health records, cost considerations, and barriers to implementation.
The “good practice points for consideration” in the document are as follows:
- If healthcare professionals want to use CGM systems beyond their intended use, eg, to replace or reduce point-of-care glucose measurements, analytical and clinical performance should be assessed.
- The Clinical and Laboratory Standards Institute (CLSI) 2nd Edition of POCT05 — Performance Metrics for Continuous Interstitial Glucose Monitoring provides helpful guidance.
- Potential interferences that preclude patients from being eligible for CGM should be noted, and staff must be aware that CGM can’t be used for clinical decision-making in these patients.
- A CGM system and/or inpatient glycemia management committee should oversee the development and implementation of hospital-approved policies and procedures for CGM use in the hospital. This committee should have representatives from nursing leadership, physician leadership (e.g., endocrinologists, internal medicine specialists, hospitalists), laboratory, information services, hospital administration, pharmacy, and risk management/legal.
- Policies for patient-owned and hospital-owned CGM devices should be developed, and staff should be trained in their use.
“During the pandemic, there was a lot of research on CGM use in the hospital setting, so we could look at how it works and was it safe. I think we have some good data to show where it can be used,” said Shaw, who also heads the Division of Biochemistry at the Ottawa Hospital. She added, “There’s quite a bit we still don’t know, but I think with some guidance in place about when not to use it, there are certainly patient populations who could benefit from it in the hospital setting.”
Shaw had no disclosures. Another author is general manager and medical director of the Institute for Diabetes Technology (IfDT), which carries out clinical studies, eg, with medical devices for diabetes therapy, on its own initiative and on behalf of various companies. Another author is an IfDT employee. Other authors have received speakers’ honoraria or consulting fees in the last 3 years from Abbott, Berlin-Chemie, BOYDSense, Dexcom, Lilly Deutschland, Novo Nordisk, Perfood, PharmaSens, Roche, Sinocare, Terumo, and Ypsomed.
A version of this article appeared on Medscape.com.
, based in part on data collected during the COVID-19 pandemic.
The statement, Consensus Considerations and Good Practice Points for Use of Continuous Glucose Monitoring Systems in Hospital Settings, was published on October 25, 2024, in Diabetes Care.
“This is something that requires close collaboration with many groups in the hospital ... There needs to be really good guidance within the hospital as to when it can be used, in which patients, and what checks and balances need to be in place,” statement lead author Julie L.V. Shaw, PhD, Laboratory Director at Renfrew Victoria Hospital and St. Francis Memorial Hospital, Ottawa, Ontario, Canada, told this news organization.
CGM use in the outpatient setting continues to grow, among people with type 2 as well as type 1 diabetes. The devices are worn on the body for up to 15 days via a subcutaneously-inserted sensor that detects glucose in interstitial fluid every 1-15 minutes. The readings generally track with blood glucose levels, although discrepancies can occur and may be even more relevant in hospital settings.
About 1 in 4 hospitalized patients have diabetes and/or hyperglycemia. During the COVID-19 pandemic, the US Food and Drug Administration (FDA) and Health Canada temporarily authorized the use of CGM systems in hospitals to supplement point-of-care glucose testing, as an emergency measure to reduce healthcare worker exposure and preserve personal protective equipment. That FDA authorization expired on November 7, 2023, and currently hospital CGM use in the United States is technically off-label, although it is often allowed for patients who already use CGM systems.
The new statement summarizes clinical study data and also addresses the potential benefits of CGM systems for inpatients, existing guidance, analytical and clinical evaluation of CGM performance, safety factors, staff training, clinical workflow, and hospital policies. Also covered are issues around quality assurance, integration of CGM data into electronic health records, cost considerations, and barriers to implementation.
The “good practice points for consideration” in the document are as follows:
- If healthcare professionals want to use CGM systems beyond their intended use, eg, to replace or reduce point-of-care glucose measurements, analytical and clinical performance should be assessed.
- The Clinical and Laboratory Standards Institute (CLSI) 2nd Edition of POCT05 — Performance Metrics for Continuous Interstitial Glucose Monitoring provides helpful guidance.
- Potential interferences that preclude patients from being eligible for CGM should be noted, and staff must be aware that CGM can’t be used for clinical decision-making in these patients.
- A CGM system and/or inpatient glycemia management committee should oversee the development and implementation of hospital-approved policies and procedures for CGM use in the hospital. This committee should have representatives from nursing leadership, physician leadership (e.g., endocrinologists, internal medicine specialists, hospitalists), laboratory, information services, hospital administration, pharmacy, and risk management/legal.
- Policies for patient-owned and hospital-owned CGM devices should be developed, and staff should be trained in their use.
“During the pandemic, there was a lot of research on CGM use in the hospital setting, so we could look at how it works and was it safe. I think we have some good data to show where it can be used,” said Shaw, who also heads the Division of Biochemistry at the Ottawa Hospital. She added, “There’s quite a bit we still don’t know, but I think with some guidance in place about when not to use it, there are certainly patient populations who could benefit from it in the hospital setting.”
Shaw had no disclosures. Another author is general manager and medical director of the Institute for Diabetes Technology (IfDT), which carries out clinical studies, eg, with medical devices for diabetes therapy, on its own initiative and on behalf of various companies. Another author is an IfDT employee. Other authors have received speakers’ honoraria or consulting fees in the last 3 years from Abbott, Berlin-Chemie, BOYDSense, Dexcom, Lilly Deutschland, Novo Nordisk, Perfood, PharmaSens, Roche, Sinocare, Terumo, and Ypsomed.
A version of this article appeared on Medscape.com.
NCCRT Confirmed as Best Approach in Locally Advanced, Resectable ESCC
confirmed the first randomized trial to directly compare the two approaches.
Yaoyao Zhu, MD, Department of Radiation Oncology, Shanghai Pulmonary Hospital, Shanghai, China, presented the new research at the annual World Conference on Lung Cancer on September 10.
Based on the findings, neoadjuvant concurrent chemoradiotherapy (NCCRT) followed by surgical resection “should be regarded as the standard of care for patients with locally advanced esophageal squamous cell carcinoma (ESCC) in the Chinese population,” Dr. Zhu said.
Different Approaches in ESCC
Dr. Zhu began her presentation by underscoring that in Western countries, NCCRT followed by surgery has been the standard treatment for locally advanced, resectable esophageal cancer since the publication of the CROSS trial in 2012, which compared neoadjuvant therapy plus surgery with surgery alone.
This demonstrated that preoperative chemoradiotherapy improved survival by 34% in patients with potentially curable esophageal or esophagogastric junction cancer, while adverse event rates were deemed “acceptable.”
In contrast, in most centers in China, clinicians opt for performing surgery followed by ASCRT.
Dr. Zhu pointed out that as previous randomized controlled trials have used surgery alone as the comparator arm, it has not been shown definitively that NCCRT plus surgery is superior to surgery followed by ASCRT.
The researchers, therefore, conducted the NEOTERIC trial, which enrolled patients with clinically resectable, locally advanced ESCC, defined as clinical stage T1-2N1M0 or T3-4N0-1M0.
They were randomized to one of two arms. The NCCRT arm involved 6 weeks of carboplatin plus paclitaxel chemotherapy alongside radiotherapy delivered as 50.4 Gy over 28 fractions. After an interval of 4-6 weeks, the patients underwent surgery, followed by an optional two cycles of carboplatin plus paclitaxel 4-6 weeks later.
In the ASCRT arm, patients underwent surgery straightaway, waited for 4-6 weeks, then had two cycles of carboplatin plus paclitaxel 3 weeks apart, followed by the same radiotherapy regimen as in the first arm. About 2-4 weeks later, patients could then undergo another two cycles of carboplatin plus paclitaxel.
More Than Doubling of Survival Outcomes
One hundred patients were assigned to NCCRT and 104 to ASCRT. There were no significant differences between the groups in terms of their baseline characteristics.
The vast majority of patients were men, just over two thirds were smokers, and the median age was around 60 years. The median tumor length was approximately 5 cm, and around half of tumors were located in the middle third of the esophagus.
Median disease-free survival was markedly longer with NCCRT, at 51.0 months vs 14.0 months in the ASCRT arm (P = .01). Similarly, median overall survival was far longer with neoadjuvant therapy, at 79.0 months, vs 38.0 months when waiting until after surgery to provide chemoradiotherapy (P = .025).
There were no significant differences in postsurgical complications between the two arms, and no significant differences in rates of grade 3-4 hematologic and nonhematologic toxicities. There were also no chemoradiotherapy-related deaths.
The most common toxicities across the two study arms were esophagitis, neutropenia, thrombocytopenia, and leukopenia.
Overall, the rates of recurrence were significantly lower with NCCRT than with ASCRT (58.0% vs 66.3%; P = .020). This included significant reductions in both locoregional (P = .012) and distant recurrence (P = .009).
Jaffer A. Ajani, MD, University of Texas MD Anderson Cancer Center, Houston, underlined that the experimental arm of the trial, with neoadjuvant chemoradiotherapy, “has been the standard of care in the United States for a long time, particularly for squamous carcinoma.”
However, he said in an interview that it is not a standard of care in China and clinicians continue with adjuvant therapy. This is despite a recent study conducted in Hong Kong that concluded that patients should not be given any treatment after surgery “because they do worse” than those given neoadjuvant therapy, he continued.
While Dr. Ajani noted that the current analysis is underpowered to provide a definitive conclusion, it remains “an important study for Chinese patients.
“Hopefully, it will be well advertised in China, and all the providers switch [to NCCRT]. This could push them to abandon what in the West was considered harmful.”
Dr. Ajani explained the reason neoadjuvant therapy performs better than adjuvant chemoradiotherapy is it “may be mopping up some of the micro metastatic disease, which is difficult to do after surgery,” especially as many patients cannot tolerate postoperative treatment.
“It may be that the majority of patients don’t even get [adjuvant therapy], and those who get it don’t seem to benefit.”
Vishwanath Sathyanarayanan, MD, PhD, Senior Consultant, Professor and Academic Advisor, Department of Medical Oncology, Apollo Cancer Centers, Bangalore, India, agreed that the study reinforces that “NCCRT continues to remain the standard of care in locally advanced resectable esophageal squamous cell carcinoma.”
Consequently, there are “no implications for clinical practice” for providers in the West from these study results, “particularly as NCCRT significantly improves outcomes vs ASCRT with a similar toxicity profile,” he said in an interview.
No funding was declared. Dr. Zhu declared no relevant financial relationships.
A version of this article appeared on Medscape.com.
confirmed the first randomized trial to directly compare the two approaches.
Yaoyao Zhu, MD, Department of Radiation Oncology, Shanghai Pulmonary Hospital, Shanghai, China, presented the new research at the annual World Conference on Lung Cancer on September 10.
Based on the findings, neoadjuvant concurrent chemoradiotherapy (NCCRT) followed by surgical resection “should be regarded as the standard of care for patients with locally advanced esophageal squamous cell carcinoma (ESCC) in the Chinese population,” Dr. Zhu said.
Different Approaches in ESCC
Dr. Zhu began her presentation by underscoring that in Western countries, NCCRT followed by surgery has been the standard treatment for locally advanced, resectable esophageal cancer since the publication of the CROSS trial in 2012, which compared neoadjuvant therapy plus surgery with surgery alone.
This demonstrated that preoperative chemoradiotherapy improved survival by 34% in patients with potentially curable esophageal or esophagogastric junction cancer, while adverse event rates were deemed “acceptable.”
In contrast, in most centers in China, clinicians opt for performing surgery followed by ASCRT.
Dr. Zhu pointed out that as previous randomized controlled trials have used surgery alone as the comparator arm, it has not been shown definitively that NCCRT plus surgery is superior to surgery followed by ASCRT.
The researchers, therefore, conducted the NEOTERIC trial, which enrolled patients with clinically resectable, locally advanced ESCC, defined as clinical stage T1-2N1M0 or T3-4N0-1M0.
They were randomized to one of two arms. The NCCRT arm involved 6 weeks of carboplatin plus paclitaxel chemotherapy alongside radiotherapy delivered as 50.4 Gy over 28 fractions. After an interval of 4-6 weeks, the patients underwent surgery, followed by an optional two cycles of carboplatin plus paclitaxel 4-6 weeks later.
In the ASCRT arm, patients underwent surgery straightaway, waited for 4-6 weeks, then had two cycles of carboplatin plus paclitaxel 3 weeks apart, followed by the same radiotherapy regimen as in the first arm. About 2-4 weeks later, patients could then undergo another two cycles of carboplatin plus paclitaxel.
More Than Doubling of Survival Outcomes
One hundred patients were assigned to NCCRT and 104 to ASCRT. There were no significant differences between the groups in terms of their baseline characteristics.
The vast majority of patients were men, just over two thirds were smokers, and the median age was around 60 years. The median tumor length was approximately 5 cm, and around half of tumors were located in the middle third of the esophagus.
Median disease-free survival was markedly longer with NCCRT, at 51.0 months vs 14.0 months in the ASCRT arm (P = .01). Similarly, median overall survival was far longer with neoadjuvant therapy, at 79.0 months, vs 38.0 months when waiting until after surgery to provide chemoradiotherapy (P = .025).
There were no significant differences in postsurgical complications between the two arms, and no significant differences in rates of grade 3-4 hematologic and nonhematologic toxicities. There were also no chemoradiotherapy-related deaths.
The most common toxicities across the two study arms were esophagitis, neutropenia, thrombocytopenia, and leukopenia.
Overall, the rates of recurrence were significantly lower with NCCRT than with ASCRT (58.0% vs 66.3%; P = .020). This included significant reductions in both locoregional (P = .012) and distant recurrence (P = .009).
Jaffer A. Ajani, MD, University of Texas MD Anderson Cancer Center, Houston, underlined that the experimental arm of the trial, with neoadjuvant chemoradiotherapy, “has been the standard of care in the United States for a long time, particularly for squamous carcinoma.”
However, he said in an interview that it is not a standard of care in China and clinicians continue with adjuvant therapy. This is despite a recent study conducted in Hong Kong that concluded that patients should not be given any treatment after surgery “because they do worse” than those given neoadjuvant therapy, he continued.
While Dr. Ajani noted that the current analysis is underpowered to provide a definitive conclusion, it remains “an important study for Chinese patients.
“Hopefully, it will be well advertised in China, and all the providers switch [to NCCRT]. This could push them to abandon what in the West was considered harmful.”
Dr. Ajani explained the reason neoadjuvant therapy performs better than adjuvant chemoradiotherapy is it “may be mopping up some of the micro metastatic disease, which is difficult to do after surgery,” especially as many patients cannot tolerate postoperative treatment.
“It may be that the majority of patients don’t even get [adjuvant therapy], and those who get it don’t seem to benefit.”
Vishwanath Sathyanarayanan, MD, PhD, Senior Consultant, Professor and Academic Advisor, Department of Medical Oncology, Apollo Cancer Centers, Bangalore, India, agreed that the study reinforces that “NCCRT continues to remain the standard of care in locally advanced resectable esophageal squamous cell carcinoma.”
Consequently, there are “no implications for clinical practice” for providers in the West from these study results, “particularly as NCCRT significantly improves outcomes vs ASCRT with a similar toxicity profile,” he said in an interview.
No funding was declared. Dr. Zhu declared no relevant financial relationships.
A version of this article appeared on Medscape.com.
confirmed the first randomized trial to directly compare the two approaches.
Yaoyao Zhu, MD, Department of Radiation Oncology, Shanghai Pulmonary Hospital, Shanghai, China, presented the new research at the annual World Conference on Lung Cancer on September 10.
Based on the findings, neoadjuvant concurrent chemoradiotherapy (NCCRT) followed by surgical resection “should be regarded as the standard of care for patients with locally advanced esophageal squamous cell carcinoma (ESCC) in the Chinese population,” Dr. Zhu said.
Different Approaches in ESCC
Dr. Zhu began her presentation by underscoring that in Western countries, NCCRT followed by surgery has been the standard treatment for locally advanced, resectable esophageal cancer since the publication of the CROSS trial in 2012, which compared neoadjuvant therapy plus surgery with surgery alone.
This demonstrated that preoperative chemoradiotherapy improved survival by 34% in patients with potentially curable esophageal or esophagogastric junction cancer, while adverse event rates were deemed “acceptable.”
In contrast, in most centers in China, clinicians opt for performing surgery followed by ASCRT.
Dr. Zhu pointed out that as previous randomized controlled trials have used surgery alone as the comparator arm, it has not been shown definitively that NCCRT plus surgery is superior to surgery followed by ASCRT.
The researchers, therefore, conducted the NEOTERIC trial, which enrolled patients with clinically resectable, locally advanced ESCC, defined as clinical stage T1-2N1M0 or T3-4N0-1M0.
They were randomized to one of two arms. The NCCRT arm involved 6 weeks of carboplatin plus paclitaxel chemotherapy alongside radiotherapy delivered as 50.4 Gy over 28 fractions. After an interval of 4-6 weeks, the patients underwent surgery, followed by an optional two cycles of carboplatin plus paclitaxel 4-6 weeks later.
In the ASCRT arm, patients underwent surgery straightaway, waited for 4-6 weeks, then had two cycles of carboplatin plus paclitaxel 3 weeks apart, followed by the same radiotherapy regimen as in the first arm. About 2-4 weeks later, patients could then undergo another two cycles of carboplatin plus paclitaxel.
More Than Doubling of Survival Outcomes
One hundred patients were assigned to NCCRT and 104 to ASCRT. There were no significant differences between the groups in terms of their baseline characteristics.
The vast majority of patients were men, just over two thirds were smokers, and the median age was around 60 years. The median tumor length was approximately 5 cm, and around half of tumors were located in the middle third of the esophagus.
Median disease-free survival was markedly longer with NCCRT, at 51.0 months vs 14.0 months in the ASCRT arm (P = .01). Similarly, median overall survival was far longer with neoadjuvant therapy, at 79.0 months, vs 38.0 months when waiting until after surgery to provide chemoradiotherapy (P = .025).
There were no significant differences in postsurgical complications between the two arms, and no significant differences in rates of grade 3-4 hematologic and nonhematologic toxicities. There were also no chemoradiotherapy-related deaths.
The most common toxicities across the two study arms were esophagitis, neutropenia, thrombocytopenia, and leukopenia.
Overall, the rates of recurrence were significantly lower with NCCRT than with ASCRT (58.0% vs 66.3%; P = .020). This included significant reductions in both locoregional (P = .012) and distant recurrence (P = .009).
Jaffer A. Ajani, MD, University of Texas MD Anderson Cancer Center, Houston, underlined that the experimental arm of the trial, with neoadjuvant chemoradiotherapy, “has been the standard of care in the United States for a long time, particularly for squamous carcinoma.”
However, he said in an interview that it is not a standard of care in China and clinicians continue with adjuvant therapy. This is despite a recent study conducted in Hong Kong that concluded that patients should not be given any treatment after surgery “because they do worse” than those given neoadjuvant therapy, he continued.
While Dr. Ajani noted that the current analysis is underpowered to provide a definitive conclusion, it remains “an important study for Chinese patients.
“Hopefully, it will be well advertised in China, and all the providers switch [to NCCRT]. This could push them to abandon what in the West was considered harmful.”
Dr. Ajani explained the reason neoadjuvant therapy performs better than adjuvant chemoradiotherapy is it “may be mopping up some of the micro metastatic disease, which is difficult to do after surgery,” especially as many patients cannot tolerate postoperative treatment.
“It may be that the majority of patients don’t even get [adjuvant therapy], and those who get it don’t seem to benefit.”
Vishwanath Sathyanarayanan, MD, PhD, Senior Consultant, Professor and Academic Advisor, Department of Medical Oncology, Apollo Cancer Centers, Bangalore, India, agreed that the study reinforces that “NCCRT continues to remain the standard of care in locally advanced resectable esophageal squamous cell carcinoma.”
Consequently, there are “no implications for clinical practice” for providers in the West from these study results, “particularly as NCCRT significantly improves outcomes vs ASCRT with a similar toxicity profile,” he said in an interview.
No funding was declared. Dr. Zhu declared no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM WCLC 2024
ACG/ASGE Task Force Identifies 19 Indicators for Achieving Quality GI Endoscopy
— most of which have a performance target > 98%, implying they should be achieved in nearly every case.
The task force’s work was published online in The American Journal of Gastroenterology.
“The purpose of this paper is to delineate all of the steps that the endoscopist should be thinking about before they perform any endoscopy,” task force member Nicholas Shaheen, MD, MPH, Division of Gastroenterology and Hepatology, the University of North Carolina at Chapel Hill, said in an interview.
“Some of these are straightforward — for instance, did we get informed consent? Others are more nuanced — did we appropriately plan for sedation for the procedure, or did we give the right antibiotics before the procedure to prevent an infectious complication after?
“While the vast majority of endoscopists do these measures with every procedure, especially in unusual circumstances or when the procedure is an emergency, they can be overlooked. Having these quality indicators listed in one place should minimize these omissions,” Dr. Shaheen said.
Four Priority Indicators
The update represents the third iteration of the ACG/ASGE quality indicators on GI endoscopic procedures, the most recent of which was published nearly a decade ago.
As in preceding versions, the task force “prioritized indicators that have wide-ranging clinical implications and have been validated in clinical studies.” There are 19 in total, divided into three time periods: Preprocedure (8), intraprocedure (4), and postprocedure (7).
While all 19 indicators are intended to serve as a framework for continual quality improvement efforts among endoscopists and units, the task force recognized a subset of 4 they identified as being a particular priority:
- Frequency with which endoscopy is performed for an indication that is included in a published standard list of appropriate indications and the indication is documented (performance target > 95%)
- Frequency with which prophylactic antibiotics are administered for appropriate indications (performance target > 98%)
- Frequency with which a plan for the management of antithrombotic therapy is formulated and documented before the procedure (performance target = 95%)
- Frequency with which adverse events are documented (performance target > 98%)
Room for Improvement
There remains a lack of compliance with some of these indicators, the task force said.
“Procedures are still performed for questionable indications, adverse events are not always captured and documented, and communication between the endoscopist and patient and/or involved clinicians is sometimes lacking.
“For these reasons, strict attention to the quality indicators in this document and an active plan for improvement in areas of measured deficiency should be a central pillar of the successful practice of endoscopy,” they wrote.
The task force advised that quality improvement efforts initially focus on the four priority indicators and then progress to include other indicators once it is determined that endoscopists are performing above recommended thresholds, either at baseline or after corrective interventions.
Reached for comment, Ashwin N. Ananthakrishnan, MD, MPH, AGAF, a gastroenterologist with Massachusetts General Hospital and Harvard Medical School, both in Boston, Massachusetts, said in an interview that these updated recommendations are “important and commonsense standard procedures that should be followed for all procedures.”
“We recognize endoscopic evaluation plays an important role in the assessment of GI illnesses, but there are also both risks and costs to this as a diagnostic and therapeutic intervention. Thus, it is important to make sure these standards are met, to optimize the outcomes of our patients,” said Dr. Ananthakrishnan, who was not involved in this work.
In a separate statement, the American Gastroenterological Association affirmed that is committed to supporting gastroenterologists in providing high-quality care via improved patients outcomes, increased efficiency and cost-effectiveness. AGA encouraged GIs to visit gastro.org/quality to learn more and find quality measures on topics including Barrett’s esophagus, inflammatory bowel disease, acute pancreatitis, and gastric intestinal metaplasia.
This work had no financial support. Dr. Shaheen and Dr. Ananthakrishnan disclosed having no relevant competing interests.
A version of this article first appeared on Medscape.com.
— most of which have a performance target > 98%, implying they should be achieved in nearly every case.
The task force’s work was published online in The American Journal of Gastroenterology.
“The purpose of this paper is to delineate all of the steps that the endoscopist should be thinking about before they perform any endoscopy,” task force member Nicholas Shaheen, MD, MPH, Division of Gastroenterology and Hepatology, the University of North Carolina at Chapel Hill, said in an interview.
“Some of these are straightforward — for instance, did we get informed consent? Others are more nuanced — did we appropriately plan for sedation for the procedure, or did we give the right antibiotics before the procedure to prevent an infectious complication after?
“While the vast majority of endoscopists do these measures with every procedure, especially in unusual circumstances or when the procedure is an emergency, they can be overlooked. Having these quality indicators listed in one place should minimize these omissions,” Dr. Shaheen said.
Four Priority Indicators
The update represents the third iteration of the ACG/ASGE quality indicators on GI endoscopic procedures, the most recent of which was published nearly a decade ago.
As in preceding versions, the task force “prioritized indicators that have wide-ranging clinical implications and have been validated in clinical studies.” There are 19 in total, divided into three time periods: Preprocedure (8), intraprocedure (4), and postprocedure (7).
While all 19 indicators are intended to serve as a framework for continual quality improvement efforts among endoscopists and units, the task force recognized a subset of 4 they identified as being a particular priority:
- Frequency with which endoscopy is performed for an indication that is included in a published standard list of appropriate indications and the indication is documented (performance target > 95%)
- Frequency with which prophylactic antibiotics are administered for appropriate indications (performance target > 98%)
- Frequency with which a plan for the management of antithrombotic therapy is formulated and documented before the procedure (performance target = 95%)
- Frequency with which adverse events are documented (performance target > 98%)
Room for Improvement
There remains a lack of compliance with some of these indicators, the task force said.
“Procedures are still performed for questionable indications, adverse events are not always captured and documented, and communication between the endoscopist and patient and/or involved clinicians is sometimes lacking.
“For these reasons, strict attention to the quality indicators in this document and an active plan for improvement in areas of measured deficiency should be a central pillar of the successful practice of endoscopy,” they wrote.
The task force advised that quality improvement efforts initially focus on the four priority indicators and then progress to include other indicators once it is determined that endoscopists are performing above recommended thresholds, either at baseline or after corrective interventions.
Reached for comment, Ashwin N. Ananthakrishnan, MD, MPH, AGAF, a gastroenterologist with Massachusetts General Hospital and Harvard Medical School, both in Boston, Massachusetts, said in an interview that these updated recommendations are “important and commonsense standard procedures that should be followed for all procedures.”
“We recognize endoscopic evaluation plays an important role in the assessment of GI illnesses, but there are also both risks and costs to this as a diagnostic and therapeutic intervention. Thus, it is important to make sure these standards are met, to optimize the outcomes of our patients,” said Dr. Ananthakrishnan, who was not involved in this work.
In a separate statement, the American Gastroenterological Association affirmed that is committed to supporting gastroenterologists in providing high-quality care via improved patients outcomes, increased efficiency and cost-effectiveness. AGA encouraged GIs to visit gastro.org/quality to learn more and find quality measures on topics including Barrett’s esophagus, inflammatory bowel disease, acute pancreatitis, and gastric intestinal metaplasia.
This work had no financial support. Dr. Shaheen and Dr. Ananthakrishnan disclosed having no relevant competing interests.
A version of this article first appeared on Medscape.com.
— most of which have a performance target > 98%, implying they should be achieved in nearly every case.
The task force’s work was published online in The American Journal of Gastroenterology.
“The purpose of this paper is to delineate all of the steps that the endoscopist should be thinking about before they perform any endoscopy,” task force member Nicholas Shaheen, MD, MPH, Division of Gastroenterology and Hepatology, the University of North Carolina at Chapel Hill, said in an interview.
“Some of these are straightforward — for instance, did we get informed consent? Others are more nuanced — did we appropriately plan for sedation for the procedure, or did we give the right antibiotics before the procedure to prevent an infectious complication after?
“While the vast majority of endoscopists do these measures with every procedure, especially in unusual circumstances or when the procedure is an emergency, they can be overlooked. Having these quality indicators listed in one place should minimize these omissions,” Dr. Shaheen said.
Four Priority Indicators
The update represents the third iteration of the ACG/ASGE quality indicators on GI endoscopic procedures, the most recent of which was published nearly a decade ago.
As in preceding versions, the task force “prioritized indicators that have wide-ranging clinical implications and have been validated in clinical studies.” There are 19 in total, divided into three time periods: Preprocedure (8), intraprocedure (4), and postprocedure (7).
While all 19 indicators are intended to serve as a framework for continual quality improvement efforts among endoscopists and units, the task force recognized a subset of 4 they identified as being a particular priority:
- Frequency with which endoscopy is performed for an indication that is included in a published standard list of appropriate indications and the indication is documented (performance target > 95%)
- Frequency with which prophylactic antibiotics are administered for appropriate indications (performance target > 98%)
- Frequency with which a plan for the management of antithrombotic therapy is formulated and documented before the procedure (performance target = 95%)
- Frequency with which adverse events are documented (performance target > 98%)
Room for Improvement
There remains a lack of compliance with some of these indicators, the task force said.
“Procedures are still performed for questionable indications, adverse events are not always captured and documented, and communication between the endoscopist and patient and/or involved clinicians is sometimes lacking.
“For these reasons, strict attention to the quality indicators in this document and an active plan for improvement in areas of measured deficiency should be a central pillar of the successful practice of endoscopy,” they wrote.
The task force advised that quality improvement efforts initially focus on the four priority indicators and then progress to include other indicators once it is determined that endoscopists are performing above recommended thresholds, either at baseline or after corrective interventions.
Reached for comment, Ashwin N. Ananthakrishnan, MD, MPH, AGAF, a gastroenterologist with Massachusetts General Hospital and Harvard Medical School, both in Boston, Massachusetts, said in an interview that these updated recommendations are “important and commonsense standard procedures that should be followed for all procedures.”
“We recognize endoscopic evaluation plays an important role in the assessment of GI illnesses, but there are also both risks and costs to this as a diagnostic and therapeutic intervention. Thus, it is important to make sure these standards are met, to optimize the outcomes of our patients,” said Dr. Ananthakrishnan, who was not involved in this work.
In a separate statement, the American Gastroenterological Association affirmed that is committed to supporting gastroenterologists in providing high-quality care via improved patients outcomes, increased efficiency and cost-effectiveness. AGA encouraged GIs to visit gastro.org/quality to learn more and find quality measures on topics including Barrett’s esophagus, inflammatory bowel disease, acute pancreatitis, and gastric intestinal metaplasia.
This work had no financial support. Dr. Shaheen and Dr. Ananthakrishnan disclosed having no relevant competing interests.
A version of this article first appeared on Medscape.com.
FROM THE AMERICAN JOURNAL OF GASTROENTEROLOGY