User login
Many surgical residents consider quitting during training
A majority of general surgery residents seriously consider dropping out of their training, with female residents more likely to consider quitting, a new study in JAMA Surgery reveals.
According to a survey, 58.0% of the 288 respondents "seriously considered leaving training." The most frequent reasons cited for wanting to quit training were sleep deprivation on a specific rotation (50%), an undesirable future lifestyle (47%), and excessive work hours on a specific rotation (41.4%). Survey results were published online July 30 in JAMA Surgery (2014 [doi:10.1001/jamasurg.2014.935]).

Factors cited that ultimately keep general surgery residents from ending training are support from family or significant other (65%), support from other residents (63.5%), and perception of being better rested (58.9%).
"We believe that our survey findings highlight the fact that a desire to leave training may not be affected by job rigor alone but rather [by] program-specific or rotation-specific factors or dissatisfaction with a future career in general surgery," the report states. Dr. Edward Gifford of the department of surgery, University of California, Los Angeles, Medical Center, is the report’s lead author.
In addressing the factors that led to consideration for leaving training, the authors noted that "a potential remedy may be to identify those high work-hour rotations and modify them accordingly," though lifestyle concerns may be harder to address as practicing surgeons "continue to experience high levels of work-home conflicts and burnout."
For women specifically, another issue is "the paucity of female mentors in academic surgery," the report states. "Striving to increase the number of female faculty members within training programs and refining the mentor-mentee relationship with incoming residents may improve the outlook and productivity of future female surgeons."
Overall, while men’s thoughts of quitting decreased as their residency progressed, women’s considerations remained persistent. The report cites previous studies that reported that men and women view general surgery careers differently, including that it was not a welcoming career because of lifestyle challenges, particularly if the woman had children, limited flexible training, and lack of role models.
"These findings may explain why women in our survey continued to consider leaving residency throughout the duration of training and underscores the importance of supporting female residents through the difficult balance between motherhood and professional life," the report states.
The study was approved by the human subjects committee of the Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, Los Angeles. The authors reported no conflicts of interest.
Program directors at residency programs "must take a purposeful, proactive approach from the beginning of surgery residency that shows residents how they can achieve a healthy balance of work and life, create practices over which they have control, and live happy, productive lives," Dr. Karen Deveney writes in a commentary published online July 30 in JAMA Surgery 2014 [doi:10.1001/jamasurg.2014964]).
Dr. Deveney also cautioned about current surgeons being openly critical of their chosen profession. "We have failed our younger generation if we whine and complain about our wretched lives rather than taking steps that are available to use to be proactive, take control of our own fates, and realize what a privileged position we are in as surgeons. Women residents are particularly vulnerable to worries that they may not be able to juggle competing demands of their families and their careers and need to be matched with female surgeons in practice who have managed successfully to find that balance."
Dr. Deveney works in the department of surgery at the Oregon Health and Science University in Portland.
Program directors at residency programs "must take a purposeful, proactive approach from the beginning of surgery residency that shows residents how they can achieve a healthy balance of work and life, create practices over which they have control, and live happy, productive lives," Dr. Karen Deveney writes in a commentary published online July 30 in JAMA Surgery 2014 [doi:10.1001/jamasurg.2014964]).
Dr. Deveney also cautioned about current surgeons being openly critical of their chosen profession. "We have failed our younger generation if we whine and complain about our wretched lives rather than taking steps that are available to use to be proactive, take control of our own fates, and realize what a privileged position we are in as surgeons. Women residents are particularly vulnerable to worries that they may not be able to juggle competing demands of their families and their careers and need to be matched with female surgeons in practice who have managed successfully to find that balance."
Dr. Deveney works in the department of surgery at the Oregon Health and Science University in Portland.
Program directors at residency programs "must take a purposeful, proactive approach from the beginning of surgery residency that shows residents how they can achieve a healthy balance of work and life, create practices over which they have control, and live happy, productive lives," Dr. Karen Deveney writes in a commentary published online July 30 in JAMA Surgery 2014 [doi:10.1001/jamasurg.2014964]).
Dr. Deveney also cautioned about current surgeons being openly critical of their chosen profession. "We have failed our younger generation if we whine and complain about our wretched lives rather than taking steps that are available to use to be proactive, take control of our own fates, and realize what a privileged position we are in as surgeons. Women residents are particularly vulnerable to worries that they may not be able to juggle competing demands of their families and their careers and need to be matched with female surgeons in practice who have managed successfully to find that balance."
Dr. Deveney works in the department of surgery at the Oregon Health and Science University in Portland.
A majority of general surgery residents seriously consider dropping out of their training, with female residents more likely to consider quitting, a new study in JAMA Surgery reveals.
According to a survey, 58.0% of the 288 respondents "seriously considered leaving training." The most frequent reasons cited for wanting to quit training were sleep deprivation on a specific rotation (50%), an undesirable future lifestyle (47%), and excessive work hours on a specific rotation (41.4%). Survey results were published online July 30 in JAMA Surgery (2014 [doi:10.1001/jamasurg.2014.935]).
Factors cited that ultimately keep general surgery residents from ending training are support from family or significant other (65%), support from other residents (63.5%), and perception of being better rested (58.9%).
"We believe that our survey findings highlight the fact that a desire to leave training may not be affected by job rigor alone but rather [by] program-specific or rotation-specific factors or dissatisfaction with a future career in general surgery," the report states. Dr. Edward Gifford of the department of surgery, University of California, Los Angeles, Medical Center, is the report’s lead author.
In addressing the factors that led to consideration for leaving training, the authors noted that "a potential remedy may be to identify those high work-hour rotations and modify them accordingly," though lifestyle concerns may be harder to address as practicing surgeons "continue to experience high levels of work-home conflicts and burnout."
For women specifically, another issue is "the paucity of female mentors in academic surgery," the report states. "Striving to increase the number of female faculty members within training programs and refining the mentor-mentee relationship with incoming residents may improve the outlook and productivity of future female surgeons."
Overall, while men’s thoughts of quitting decreased as their residency progressed, women’s considerations remained persistent. The report cites previous studies that reported that men and women view general surgery careers differently, including that it was not a welcoming career because of lifestyle challenges, particularly if the woman had children, limited flexible training, and lack of role models.
"These findings may explain why women in our survey continued to consider leaving residency throughout the duration of training and underscores the importance of supporting female residents through the difficult balance between motherhood and professional life," the report states.
The study was approved by the human subjects committee of the Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, Los Angeles. The authors reported no conflicts of interest.
A majority of general surgery residents seriously consider dropping out of their training, with female residents more likely to consider quitting, a new study in JAMA Surgery reveals.
According to a survey, 58.0% of the 288 respondents "seriously considered leaving training." The most frequent reasons cited for wanting to quit training were sleep deprivation on a specific rotation (50%), an undesirable future lifestyle (47%), and excessive work hours on a specific rotation (41.4%). Survey results were published online July 30 in JAMA Surgery (2014 [doi:10.1001/jamasurg.2014.935]).
Factors cited that ultimately keep general surgery residents from ending training are support from family or significant other (65%), support from other residents (63.5%), and perception of being better rested (58.9%).
"We believe that our survey findings highlight the fact that a desire to leave training may not be affected by job rigor alone but rather [by] program-specific or rotation-specific factors or dissatisfaction with a future career in general surgery," the report states. Dr. Edward Gifford of the department of surgery, University of California, Los Angeles, Medical Center, is the report’s lead author.
In addressing the factors that led to consideration for leaving training, the authors noted that "a potential remedy may be to identify those high work-hour rotations and modify them accordingly," though lifestyle concerns may be harder to address as practicing surgeons "continue to experience high levels of work-home conflicts and burnout."
For women specifically, another issue is "the paucity of female mentors in academic surgery," the report states. "Striving to increase the number of female faculty members within training programs and refining the mentor-mentee relationship with incoming residents may improve the outlook and productivity of future female surgeons."
Overall, while men’s thoughts of quitting decreased as their residency progressed, women’s considerations remained persistent. The report cites previous studies that reported that men and women view general surgery careers differently, including that it was not a welcoming career because of lifestyle challenges, particularly if the woman had children, limited flexible training, and lack of role models.
"These findings may explain why women in our survey continued to consider leaving residency throughout the duration of training and underscores the importance of supporting female residents through the difficult balance between motherhood and professional life," the report states.
The study was approved by the human subjects committee of the Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, Los Angeles. The authors reported no conflicts of interest.
FROM JAMA Surgery
Major finding: More than half of survey respondents (58%) considered quitting their general surgery residency, an issue more persistent with female respondents.
Data source: Analysis of 288 responses to a survey of general surgery residents in 13 residency programs across different regions (West, Southwest, Midwest, and Northeast) and training centers (university programs, independent programs, or hybrid university-affiliated programs without an onsite university or medical school).
Disclosures: The study was approved by the human subjects committee of the Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, Los Angeles. The authors reported no conflicts of interest.

Weathering the ‘Perfect Storm?’
The era of the Affordable Care Act is upon us, and short of an unlikely repeal following midterm elections, this will remain the law of the land. As surgical residents, most of us have neither the time nor mental stamina to become significantly entrenched in politics. As a result, many of us know less about the impact that the Affordable Care Act will have on our future livelihood than many of the Senators did when they passed the bill on December 24, 2009. While most of the public focus has been on the individual mandate, pre-existing conditions, and insurance exchanges, further hidden from the public eye are the methods by which our fundamental model for health care reimbursement will change.
Much of the mystery was dispelled for me this May, when I heard a lecture entitled "The Perfect Storm: The Affordable Care Act and the Repeal of the SGR" by Dr. Jeffrey Rich. Dr. Rich’s presentation was the 2014 Norman E. Shumway, MD, Visiting Professorship Lecture at Stanford (Calif.) University, a webcast of which is available at http://ctsurgery.stanford.edu/media/.

Dr. Rich has a unique perspective on the issue of health care reimbursement, as he has served both as president of STS from 2012-2013 and director of the Center for Medicare Management, part of the Centers for Medicare & Medicaid Services, in 2008, in the political tumult leading up to the passage of the Affordable Care Act. On top of this, he has remained a practicing cardiothoracic surgeon in the Sentara Health System and sits as director-at-large for the Virginia Cardiac Surgery Quality Initiative. It is impossible to overstate the impact that he and his staff have had on the future of health care reimbursement. His recent lecture highlighted the ideological change in payment models that the Affordable Care Act embodies, along with the carrots and the sticks that the government will be wielding over the next 5 years to change physician and hospital behavior. This, along with the untenable continuation of the Sustainable Growth Rate (SGR) with all of its problems, portends huge swings both positive and negative for the reimbursement of all doctors, and cardiothoracic surgeons in particular. Early adopters may find themselves with a much-needed windfall, while those who do not anticipate the changes may find themselves in dire financial straits.
First, let us examine where we stand. The United States spends 17.6% of its gross domestic product (GDP) on health care. The nearest rival sits at 12%. State and federal government together spent $1.5 trillion on health care in 2013. Add private insurance into the mix and the figure is $2.8 trillion. Our life expectancy has not followed the money, and the rate of increase in health care spending is far outstripping inflation and the growth in our GDP. Our spending has increased exponentially since the passage of the Social Security Amendments of 1965 and shows no sign of slowing down. These statistics are well publicized, and should no longer be a surprise to anyone.
Keeping in mind that hindsight is 20/20, it seems obvious how we got here. The private health insurance industry took off during WWII, when competitive wage controls were put in place to keep skilled laborers in jobs supporting the war effort. To compete for laborers, private sector employers began offering health insurance policies. Shortly thereafter, public pressure to provide a health care safety net culminated in the creation of Medicare and Medicaid in 1965, and our complex public/private health insurance environment was born. For the first decade or so, physician reimbursement was based on "reasonable charge," meaning that doctors sent a bill to Medicare and, if it was considered reasonable, the doctor was paid. This fee-for-service model can be seen as a blank check of sorts, in that it contained few stipulations to withhold repayment for redundant or unnecessary tests and procedures. Expenses associated with complications also were reimbursable. The incentive to "do more" was set. It is worth noting that the Social Security Amendments of 1965 are federal law, and the law stipulates that reimbursement is tied to the amount of work that a physician performs, which also forbids associating reimbursement with the quality of work that the physician produces. It takes an act of Congress to change such law.
The Affordable Care Act is that act. Dr. Rich’s work at CMS paved the way for the inclusion of "Title III: Improving the quality and efficiency of health care," which allows Medicare and Medicaid reimbursements to be altered based on efficiency and outcomes, moving away (although not disintegrating) the fee-for-service model. It incentivizes the development of Accountable Care Organizations and Clinically Integrated Networks to encourage cross-specialty collaboration within the fee-for-service model and lays the groundwork for physician and hospital reimbursement to be based on high-quality, efficient, and appropriate care.
This is the most comprehensive change to the status quo, but it is by no means the first. By 1975, the federal government could see that open fee-for-service was leading to skyrocketing health care costs. It began experimenting with ways to curb physician charges. It pegged reimbursements to the Medicare Economic Index (still used to update hospital reimbursements by 3.2%-3.6% per year) and then tried basing reimbursement on relative value units. Costs continued to rise. Thirty years after the 1965 law, as health care spending continued to spiral out of control, the Sustainable Growth Rate was applied to physician repayment as an attempt to reel it in. The basic premise was that increased costs from increased patient and procedure volume would be curbed by decreasing the reimbursement per procedure.
The sustainable growth model essentially placed a spending target that would grow in step with GDP using the total expenditures beginning in 1996 as a benchmark. If, during a given year, spending outstripped the target, the following year a compensatory decrease in physician reimbursement would be enacted. If spending were less than the target, then physician payments would increase. Expenditures have exceeded the target every year since 2002, and each year our spending gets further and further from the benchmark, compounding the penalty. If the SGR penalties were allowed, it is estimated that physician repayment would drop by 25%-35% in the next few years. Each time the penalty is about to be applied, a fix is passed by Congress, saving our livelihoods at the last minute. Although we should be thankful not to take a 35% pay cut, the SGR and its fixes increased physician repayment by a mere 5.1% between 1992 and 2012. For comparison, Social Security benefits, adjusted annually to compensate increasing cost of living, have risen 52.9% in the same period. Meanwhile, as I mentioned earlier, hospital reimbursement continues to be tied to the Medicare Economic Index, which yields a fairly predictable payment increase of 3.2%-3.6% each year. The Affordable Care Act operates as a law separate from the SGR law, though the two are closely intertwined.
Title III of the Affordable Care Act provides a number of new incentives and penalties that will help make efficiency and quality goals that affect profit at least as much as procedural volume. It will impact hospitals and physicians in a number of new and potentially positive ways. Most immediately concerning to hospitals and medical groups are the incentives for quality. With value-based purchasing, Medicare will withhold 2% of diagnosis-related group (DRG) reimbursements to hospitals at the beginning of a year, giving them the chance to earn it back at the end of the year if they meet quality and efficiency performance goals. The top performers will receive a bonus from the funds collected from those who do not meet goals, making this a budget-neutral operation. Cardiothoracic surgeons will feel this scrutiny early, as the first five DRGs subject to the law are acute myocardial infarction, heart failure, pneumonia, surgeries, and health care–associated infections. As time passes, more diagnoses will be added.
Payments will be based on bundled care, meaning that a hospital will be paid one sum to cover the peri-admission period, starting from 3 days prior to 30 days after admission. Complications, readmissions, and repeat tests will not generate additional funds for the hospital. You can expect that daily chest x-rays and multiple echocardiograms will generate a lot of e-mails to attending physicians. Other preventable hospital-acquired conditions, such as catheter-associated urinary tract infections and pressure ulcers, if present in rates beyond the norm for the country, could cut reimbursements an additional 1%. Patient satisfaction scores will influence hospital reimbursement. Readmission rates beyond the specified cutoff for each admission will result in a 3% hospital pay cut, again, starting with the same set of diagnoses. When meaningful use of electronic health records incentives are factored in, hospitals are looking at a 7% swing on reimbursements for the DRGs listed above by 2017. Hospitals typically operate on a profit margin around 3.5%.
On the individual physician level, there are a number of changes. Already in place was a bonus for participating in physician quality reporting systems (PQRS), such as the STS database. By 2016 the bonus for participating will become a 2% pay cut for not participating. Thankfully, our specialty has been forward thinking in this regard, and the majority of cardiothoracic practices already participate in the STS database. Similar to value-based purchasing, the physician value modifier will apply a 2% bonus or penalty to reimbursements, based on a broad spectrum of quality measures, including patient safety, population and community health, total cost per patient by condition, and patient experience. Again, this will be budget neutral. When all of the items are tallied, the lowest-performing providers could see a 6% decrease in their personal reimbursement.
The SGR has not been fixed with the Affordable Care Act. Dr. Rich, in his role as STS president, provided testimony to Congress leading up to the most recent attempt to reform the law. Part of the main thrust of his testimony was that each specialty needs to set its own outcomes standards through database-driven research. Incentives for improved outcomes need to be in place for all members of the heart team, not just the physicians. All three of the proposed bills that followed his testimony included such incentives, but they also included even more dismal updates to physician payments than we have seen in the past 20 years. For better or for worse, none of the bills passed, and we can look forward to more anxiety as we await the next SGR patch. Whatever durable solution passes will likely focus on these new models of payment but without a significant boost in hospital income.
Currently, the alternative payment model (APM) pilot programs are still being developed. CMS has a $10 billion budget to fund the pilot programs, and consulting groups that advised the agency chose cardiothoracic surgery as a top priority for APM development. Current discussions indicate that participants in APMs could get a 5% bonus and would not be subject to the physician value modifier.
So how does this apply to us residents? Despite our ground-level perspective, we must recognize that we are straddling two drastically different eras in the practice of medicine. It will be the duty of all of us, not just our attendings, to reduce our costs and provide better patient care. This may mean using our stethoscope more effectively or making those extra phone calls to avoid unnecessary or repeated tests. We need to rebel against the ideology of physician shift work by owning our patients, but still work effectively in that system. When it comes time to seek our first jobs, we should focus not just on the department that we will work on, but its context within the local hospital system. The most vibrant department within an unresponsive hospital system will drown in the future penalties, and likewise for an unenthusiastic department within a forward-thinking system. In short, we need to start training ourselves to be keener, sharper, and more agile physicians, and to position ourselves within like-minded environments. Perhaps more important than any of these, we need to reclaim the right to shape our own profession. In recent history there has not been a better opportunity for cardiothoracic surgeons as a group to assert themselves as adept physicians and leaders. Whether we become head of CMS, participate in STS fly-ins to Capitol Hill, write our congressman about the issues we face, or engage our hospitals to anticipate the coming changes, it is up to us to ensure that we have a future.
Dr. Zeigler is one of the outgoing resident medical editors for Thoracic Surgery News.
The era of the Affordable Care Act is upon us, and short of an unlikely repeal following midterm elections, this will remain the law of the land. As surgical residents, most of us have neither the time nor mental stamina to become significantly entrenched in politics. As a result, many of us know less about the impact that the Affordable Care Act will have on our future livelihood than many of the Senators did when they passed the bill on December 24, 2009. While most of the public focus has been on the individual mandate, pre-existing conditions, and insurance exchanges, further hidden from the public eye are the methods by which our fundamental model for health care reimbursement will change.
Much of the mystery was dispelled for me this May, when I heard a lecture entitled "The Perfect Storm: The Affordable Care Act and the Repeal of the SGR" by Dr. Jeffrey Rich. Dr. Rich’s presentation was the 2014 Norman E. Shumway, MD, Visiting Professorship Lecture at Stanford (Calif.) University, a webcast of which is available at http://ctsurgery.stanford.edu/media/.
Dr. Rich has a unique perspective on the issue of health care reimbursement, as he has served both as president of STS from 2012-2013 and director of the Center for Medicare Management, part of the Centers for Medicare & Medicaid Services, in 2008, in the political tumult leading up to the passage of the Affordable Care Act. On top of this, he has remained a practicing cardiothoracic surgeon in the Sentara Health System and sits as director-at-large for the Virginia Cardiac Surgery Quality Initiative. It is impossible to overstate the impact that he and his staff have had on the future of health care reimbursement. His recent lecture highlighted the ideological change in payment models that the Affordable Care Act embodies, along with the carrots and the sticks that the government will be wielding over the next 5 years to change physician and hospital behavior. This, along with the untenable continuation of the Sustainable Growth Rate (SGR) with all of its problems, portends huge swings both positive and negative for the reimbursement of all doctors, and cardiothoracic surgeons in particular. Early adopters may find themselves with a much-needed windfall, while those who do not anticipate the changes may find themselves in dire financial straits.
First, let us examine where we stand. The United States spends 17.6% of its gross domestic product (GDP) on health care. The nearest rival sits at 12%. State and federal government together spent $1.5 trillion on health care in 2013. Add private insurance into the mix and the figure is $2.8 trillion. Our life expectancy has not followed the money, and the rate of increase in health care spending is far outstripping inflation and the growth in our GDP. Our spending has increased exponentially since the passage of the Social Security Amendments of 1965 and shows no sign of slowing down. These statistics are well publicized, and should no longer be a surprise to anyone.
Keeping in mind that hindsight is 20/20, it seems obvious how we got here. The private health insurance industry took off during WWII, when competitive wage controls were put in place to keep skilled laborers in jobs supporting the war effort. To compete for laborers, private sector employers began offering health insurance policies. Shortly thereafter, public pressure to provide a health care safety net culminated in the creation of Medicare and Medicaid in 1965, and our complex public/private health insurance environment was born. For the first decade or so, physician reimbursement was based on "reasonable charge," meaning that doctors sent a bill to Medicare and, if it was considered reasonable, the doctor was paid. This fee-for-service model can be seen as a blank check of sorts, in that it contained few stipulations to withhold repayment for redundant or unnecessary tests and procedures. Expenses associated with complications also were reimbursable. The incentive to "do more" was set. It is worth noting that the Social Security Amendments of 1965 are federal law, and the law stipulates that reimbursement is tied to the amount of work that a physician performs, which also forbids associating reimbursement with the quality of work that the physician produces. It takes an act of Congress to change such law.
The Affordable Care Act is that act. Dr. Rich’s work at CMS paved the way for the inclusion of "Title III: Improving the quality and efficiency of health care," which allows Medicare and Medicaid reimbursements to be altered based on efficiency and outcomes, moving away (although not disintegrating) the fee-for-service model. It incentivizes the development of Accountable Care Organizations and Clinically Integrated Networks to encourage cross-specialty collaboration within the fee-for-service model and lays the groundwork for physician and hospital reimbursement to be based on high-quality, efficient, and appropriate care.
This is the most comprehensive change to the status quo, but it is by no means the first. By 1975, the federal government could see that open fee-for-service was leading to skyrocketing health care costs. It began experimenting with ways to curb physician charges. It pegged reimbursements to the Medicare Economic Index (still used to update hospital reimbursements by 3.2%-3.6% per year) and then tried basing reimbursement on relative value units. Costs continued to rise. Thirty years after the 1965 law, as health care spending continued to spiral out of control, the Sustainable Growth Rate was applied to physician repayment as an attempt to reel it in. The basic premise was that increased costs from increased patient and procedure volume would be curbed by decreasing the reimbursement per procedure.
The sustainable growth model essentially placed a spending target that would grow in step with GDP using the total expenditures beginning in 1996 as a benchmark. If, during a given year, spending outstripped the target, the following year a compensatory decrease in physician reimbursement would be enacted. If spending were less than the target, then physician payments would increase. Expenditures have exceeded the target every year since 2002, and each year our spending gets further and further from the benchmark, compounding the penalty. If the SGR penalties were allowed, it is estimated that physician repayment would drop by 25%-35% in the next few years. Each time the penalty is about to be applied, a fix is passed by Congress, saving our livelihoods at the last minute. Although we should be thankful not to take a 35% pay cut, the SGR and its fixes increased physician repayment by a mere 5.1% between 1992 and 2012. For comparison, Social Security benefits, adjusted annually to compensate increasing cost of living, have risen 52.9% in the same period. Meanwhile, as I mentioned earlier, hospital reimbursement continues to be tied to the Medicare Economic Index, which yields a fairly predictable payment increase of 3.2%-3.6% each year. The Affordable Care Act operates as a law separate from the SGR law, though the two are closely intertwined.
Title III of the Affordable Care Act provides a number of new incentives and penalties that will help make efficiency and quality goals that affect profit at least as much as procedural volume. It will impact hospitals and physicians in a number of new and potentially positive ways. Most immediately concerning to hospitals and medical groups are the incentives for quality. With value-based purchasing, Medicare will withhold 2% of diagnosis-related group (DRG) reimbursements to hospitals at the beginning of a year, giving them the chance to earn it back at the end of the year if they meet quality and efficiency performance goals. The top performers will receive a bonus from the funds collected from those who do not meet goals, making this a budget-neutral operation. Cardiothoracic surgeons will feel this scrutiny early, as the first five DRGs subject to the law are acute myocardial infarction, heart failure, pneumonia, surgeries, and health care–associated infections. As time passes, more diagnoses will be added.
Payments will be based on bundled care, meaning that a hospital will be paid one sum to cover the peri-admission period, starting from 3 days prior to 30 days after admission. Complications, readmissions, and repeat tests will not generate additional funds for the hospital. You can expect that daily chest x-rays and multiple echocardiograms will generate a lot of e-mails to attending physicians. Other preventable hospital-acquired conditions, such as catheter-associated urinary tract infections and pressure ulcers, if present in rates beyond the norm for the country, could cut reimbursements an additional 1%. Patient satisfaction scores will influence hospital reimbursement. Readmission rates beyond the specified cutoff for each admission will result in a 3% hospital pay cut, again, starting with the same set of diagnoses. When meaningful use of electronic health records incentives are factored in, hospitals are looking at a 7% swing on reimbursements for the DRGs listed above by 2017. Hospitals typically operate on a profit margin around 3.5%.
On the individual physician level, there are a number of changes. Already in place was a bonus for participating in physician quality reporting systems (PQRS), such as the STS database. By 2016 the bonus for participating will become a 2% pay cut for not participating. Thankfully, our specialty has been forward thinking in this regard, and the majority of cardiothoracic practices already participate in the STS database. Similar to value-based purchasing, the physician value modifier will apply a 2% bonus or penalty to reimbursements, based on a broad spectrum of quality measures, including patient safety, population and community health, total cost per patient by condition, and patient experience. Again, this will be budget neutral. When all of the items are tallied, the lowest-performing providers could see a 6% decrease in their personal reimbursement.
The SGR has not been fixed with the Affordable Care Act. Dr. Rich, in his role as STS president, provided testimony to Congress leading up to the most recent attempt to reform the law. Part of the main thrust of his testimony was that each specialty needs to set its own outcomes standards through database-driven research. Incentives for improved outcomes need to be in place for all members of the heart team, not just the physicians. All three of the proposed bills that followed his testimony included such incentives, but they also included even more dismal updates to physician payments than we have seen in the past 20 years. For better or for worse, none of the bills passed, and we can look forward to more anxiety as we await the next SGR patch. Whatever durable solution passes will likely focus on these new models of payment but without a significant boost in hospital income.
Currently, the alternative payment model (APM) pilot programs are still being developed. CMS has a $10 billion budget to fund the pilot programs, and consulting groups that advised the agency chose cardiothoracic surgery as a top priority for APM development. Current discussions indicate that participants in APMs could get a 5% bonus and would not be subject to the physician value modifier.
So how does this apply to us residents? Despite our ground-level perspective, we must recognize that we are straddling two drastically different eras in the practice of medicine. It will be the duty of all of us, not just our attendings, to reduce our costs and provide better patient care. This may mean using our stethoscope more effectively or making those extra phone calls to avoid unnecessary or repeated tests. We need to rebel against the ideology of physician shift work by owning our patients, but still work effectively in that system. When it comes time to seek our first jobs, we should focus not just on the department that we will work on, but its context within the local hospital system. The most vibrant department within an unresponsive hospital system will drown in the future penalties, and likewise for an unenthusiastic department within a forward-thinking system. In short, we need to start training ourselves to be keener, sharper, and more agile physicians, and to position ourselves within like-minded environments. Perhaps more important than any of these, we need to reclaim the right to shape our own profession. In recent history there has not been a better opportunity for cardiothoracic surgeons as a group to assert themselves as adept physicians and leaders. Whether we become head of CMS, participate in STS fly-ins to Capitol Hill, write our congressman about the issues we face, or engage our hospitals to anticipate the coming changes, it is up to us to ensure that we have a future.
Dr. Zeigler is one of the outgoing resident medical editors for Thoracic Surgery News.
The era of the Affordable Care Act is upon us, and short of an unlikely repeal following midterm elections, this will remain the law of the land. As surgical residents, most of us have neither the time nor mental stamina to become significantly entrenched in politics. As a result, many of us know less about the impact that the Affordable Care Act will have on our future livelihood than many of the Senators did when they passed the bill on December 24, 2009. While most of the public focus has been on the individual mandate, pre-existing conditions, and insurance exchanges, further hidden from the public eye are the methods by which our fundamental model for health care reimbursement will change.
Much of the mystery was dispelled for me this May, when I heard a lecture entitled "The Perfect Storm: The Affordable Care Act and the Repeal of the SGR" by Dr. Jeffrey Rich. Dr. Rich’s presentation was the 2014 Norman E. Shumway, MD, Visiting Professorship Lecture at Stanford (Calif.) University, a webcast of which is available at http://ctsurgery.stanford.edu/media/.
Dr. Rich has a unique perspective on the issue of health care reimbursement, as he has served both as president of STS from 2012-2013 and director of the Center for Medicare Management, part of the Centers for Medicare & Medicaid Services, in 2008, in the political tumult leading up to the passage of the Affordable Care Act. On top of this, he has remained a practicing cardiothoracic surgeon in the Sentara Health System and sits as director-at-large for the Virginia Cardiac Surgery Quality Initiative. It is impossible to overstate the impact that he and his staff have had on the future of health care reimbursement. His recent lecture highlighted the ideological change in payment models that the Affordable Care Act embodies, along with the carrots and the sticks that the government will be wielding over the next 5 years to change physician and hospital behavior. This, along with the untenable continuation of the Sustainable Growth Rate (SGR) with all of its problems, portends huge swings both positive and negative for the reimbursement of all doctors, and cardiothoracic surgeons in particular. Early adopters may find themselves with a much-needed windfall, while those who do not anticipate the changes may find themselves in dire financial straits.
First, let us examine where we stand. The United States spends 17.6% of its gross domestic product (GDP) on health care. The nearest rival sits at 12%. State and federal government together spent $1.5 trillion on health care in 2013. Add private insurance into the mix and the figure is $2.8 trillion. Our life expectancy has not followed the money, and the rate of increase in health care spending is far outstripping inflation and the growth in our GDP. Our spending has increased exponentially since the passage of the Social Security Amendments of 1965 and shows no sign of slowing down. These statistics are well publicized, and should no longer be a surprise to anyone.
Keeping in mind that hindsight is 20/20, it seems obvious how we got here. The private health insurance industry took off during WWII, when competitive wage controls were put in place to keep skilled laborers in jobs supporting the war effort. To compete for laborers, private sector employers began offering health insurance policies. Shortly thereafter, public pressure to provide a health care safety net culminated in the creation of Medicare and Medicaid in 1965, and our complex public/private health insurance environment was born. For the first decade or so, physician reimbursement was based on "reasonable charge," meaning that doctors sent a bill to Medicare and, if it was considered reasonable, the doctor was paid. This fee-for-service model can be seen as a blank check of sorts, in that it contained few stipulations to withhold repayment for redundant or unnecessary tests and procedures. Expenses associated with complications also were reimbursable. The incentive to "do more" was set. It is worth noting that the Social Security Amendments of 1965 are federal law, and the law stipulates that reimbursement is tied to the amount of work that a physician performs, which also forbids associating reimbursement with the quality of work that the physician produces. It takes an act of Congress to change such law.
The Affordable Care Act is that act. Dr. Rich’s work at CMS paved the way for the inclusion of "Title III: Improving the quality and efficiency of health care," which allows Medicare and Medicaid reimbursements to be altered based on efficiency and outcomes, moving away (although not disintegrating) the fee-for-service model. It incentivizes the development of Accountable Care Organizations and Clinically Integrated Networks to encourage cross-specialty collaboration within the fee-for-service model and lays the groundwork for physician and hospital reimbursement to be based on high-quality, efficient, and appropriate care.
This is the most comprehensive change to the status quo, but it is by no means the first. By 1975, the federal government could see that open fee-for-service was leading to skyrocketing health care costs. It began experimenting with ways to curb physician charges. It pegged reimbursements to the Medicare Economic Index (still used to update hospital reimbursements by 3.2%-3.6% per year) and then tried basing reimbursement on relative value units. Costs continued to rise. Thirty years after the 1965 law, as health care spending continued to spiral out of control, the Sustainable Growth Rate was applied to physician repayment as an attempt to reel it in. The basic premise was that increased costs from increased patient and procedure volume would be curbed by decreasing the reimbursement per procedure.
The sustainable growth model essentially placed a spending target that would grow in step with GDP using the total expenditures beginning in 1996 as a benchmark. If, during a given year, spending outstripped the target, the following year a compensatory decrease in physician reimbursement would be enacted. If spending were less than the target, then physician payments would increase. Expenditures have exceeded the target every year since 2002, and each year our spending gets further and further from the benchmark, compounding the penalty. If the SGR penalties were allowed, it is estimated that physician repayment would drop by 25%-35% in the next few years. Each time the penalty is about to be applied, a fix is passed by Congress, saving our livelihoods at the last minute. Although we should be thankful not to take a 35% pay cut, the SGR and its fixes increased physician repayment by a mere 5.1% between 1992 and 2012. For comparison, Social Security benefits, adjusted annually to compensate increasing cost of living, have risen 52.9% in the same period. Meanwhile, as I mentioned earlier, hospital reimbursement continues to be tied to the Medicare Economic Index, which yields a fairly predictable payment increase of 3.2%-3.6% each year. The Affordable Care Act operates as a law separate from the SGR law, though the two are closely intertwined.
Title III of the Affordable Care Act provides a number of new incentives and penalties that will help make efficiency and quality goals that affect profit at least as much as procedural volume. It will impact hospitals and physicians in a number of new and potentially positive ways. Most immediately concerning to hospitals and medical groups are the incentives for quality. With value-based purchasing, Medicare will withhold 2% of diagnosis-related group (DRG) reimbursements to hospitals at the beginning of a year, giving them the chance to earn it back at the end of the year if they meet quality and efficiency performance goals. The top performers will receive a bonus from the funds collected from those who do not meet goals, making this a budget-neutral operation. Cardiothoracic surgeons will feel this scrutiny early, as the first five DRGs subject to the law are acute myocardial infarction, heart failure, pneumonia, surgeries, and health care–associated infections. As time passes, more diagnoses will be added.
Payments will be based on bundled care, meaning that a hospital will be paid one sum to cover the peri-admission period, starting from 3 days prior to 30 days after admission. Complications, readmissions, and repeat tests will not generate additional funds for the hospital. You can expect that daily chest x-rays and multiple echocardiograms will generate a lot of e-mails to attending physicians. Other preventable hospital-acquired conditions, such as catheter-associated urinary tract infections and pressure ulcers, if present in rates beyond the norm for the country, could cut reimbursements an additional 1%. Patient satisfaction scores will influence hospital reimbursement. Readmission rates beyond the specified cutoff for each admission will result in a 3% hospital pay cut, again, starting with the same set of diagnoses. When meaningful use of electronic health records incentives are factored in, hospitals are looking at a 7% swing on reimbursements for the DRGs listed above by 2017. Hospitals typically operate on a profit margin around 3.5%.
On the individual physician level, there are a number of changes. Already in place was a bonus for participating in physician quality reporting systems (PQRS), such as the STS database. By 2016 the bonus for participating will become a 2% pay cut for not participating. Thankfully, our specialty has been forward thinking in this regard, and the majority of cardiothoracic practices already participate in the STS database. Similar to value-based purchasing, the physician value modifier will apply a 2% bonus or penalty to reimbursements, based on a broad spectrum of quality measures, including patient safety, population and community health, total cost per patient by condition, and patient experience. Again, this will be budget neutral. When all of the items are tallied, the lowest-performing providers could see a 6% decrease in their personal reimbursement.
The SGR has not been fixed with the Affordable Care Act. Dr. Rich, in his role as STS president, provided testimony to Congress leading up to the most recent attempt to reform the law. Part of the main thrust of his testimony was that each specialty needs to set its own outcomes standards through database-driven research. Incentives for improved outcomes need to be in place for all members of the heart team, not just the physicians. All three of the proposed bills that followed his testimony included such incentives, but they also included even more dismal updates to physician payments than we have seen in the past 20 years. For better or for worse, none of the bills passed, and we can look forward to more anxiety as we await the next SGR patch. Whatever durable solution passes will likely focus on these new models of payment but without a significant boost in hospital income.
Currently, the alternative payment model (APM) pilot programs are still being developed. CMS has a $10 billion budget to fund the pilot programs, and consulting groups that advised the agency chose cardiothoracic surgery as a top priority for APM development. Current discussions indicate that participants in APMs could get a 5% bonus and would not be subject to the physician value modifier.
So how does this apply to us residents? Despite our ground-level perspective, we must recognize that we are straddling two drastically different eras in the practice of medicine. It will be the duty of all of us, not just our attendings, to reduce our costs and provide better patient care. This may mean using our stethoscope more effectively or making those extra phone calls to avoid unnecessary or repeated tests. We need to rebel against the ideology of physician shift work by owning our patients, but still work effectively in that system. When it comes time to seek our first jobs, we should focus not just on the department that we will work on, but its context within the local hospital system. The most vibrant department within an unresponsive hospital system will drown in the future penalties, and likewise for an unenthusiastic department within a forward-thinking system. In short, we need to start training ourselves to be keener, sharper, and more agile physicians, and to position ourselves within like-minded environments. Perhaps more important than any of these, we need to reclaim the right to shape our own profession. In recent history there has not been a better opportunity for cardiothoracic surgeons as a group to assert themselves as adept physicians and leaders. Whether we become head of CMS, participate in STS fly-ins to Capitol Hill, write our congressman about the issues we face, or engage our hospitals to anticipate the coming changes, it is up to us to ensure that we have a future.
Dr. Zeigler is one of the outgoing resident medical editors for Thoracic Surgery News.

Residents, postop complications linked
BOSTON – Resident participation in emergency general surgery cases was independently associated with a host of complications – pulmonary embolism, surgical site infections, and unplanned reoperation in a secondary analysis of the American College of Surgeons prospective National Surgical Quality Improvement database.
Adequate exposure of residents to emergency general surgery is crucial for surgical training, but academic operating teams should be mindful of this association, Dr. George Kasotakis said at the annual meeting of the American Surgical Association.

Three papers have shown resident participation modestly increases complications in elective surgery, but their impact is not well understood for emergency general surgery, where patient physiology is typically deranged and timely surgery is imperative.
Dr. Kasotakis and his colleagues at Boston University identified 141,010 patients who underwent emergency general surgery procedures in the 2005-2010 American College of Surgeons prospective National Surgical Quality Improvement database. Because of the nonrandom assignment of more complex cases to resident participation, patients were matched 1:1 based on age; gender; use of alcohol, tobacco, and steroids; inpatient status; obesity; diabetes; renal failure; cardiopulmonary disease; and expected probability for morbidity and mortality. Regression models were fitted for each outcome and adjusted for the same risk factors and operative time.
The most common procedures were appendectomy (40%), exploratory laparotomy (8.75%), bowel resection (9.2%), cholecystectomy (6%), and lysis of adhesions (6%).
Thirty-day mortality was similar with and without residents (3.25% vs. 2.96%; P = .082), but hospital length of stay was longer by about a half a day with residents (4.97 days vs. 4.59 days; P = .019), said Dr. Kasotakis, an acute care surgeon and intensivist.
Resident participation added about 20 minutes to operative (75 minutes vs. 59 minutes; P less than .001) and anesthesia (122 minutes vs. 100 minutes; P less than .001) times.
Intraoperative transfusions were more common with residents (3.43% vs. 2.55%; P less than .001), perhaps because of longer operating room times, and, as a result, fewer postoperative transfusions were needed (1.12% vs. 1.28% P = .031), he said. Unplanned reoperations, however, were more common with residents, as well (4.22% vs. 3.80%; P = .002).
Postsurgical superficial wound infections (3.5% vs. 2.78%; P less than .001) and organ space surgical site infections (2.27% vs. 1.77%; P less than .001) were more common in the resident group, while wound dehiscence was not (0.63% vs. 0.69%; P = .266), Dr. Kasotakis noted.
Pulmonary complications were significantly more common in the resident group including postoperative pneumonia (1.85% vs. 1.67%; P = .04), reintubation (1.64% vs. 1.15%; P less than .001), and mechanical ventilation for more than 48 hours (2.87% vs. 2.06%; P less than .001).
The same was true for deep vein thrombosis (DVT) (0.80% vs. 0.62%; P = .002) and pulmonary embolism (PE) (0.43% vs. 0.28%; P less than .001).
Urinary tract infections (UTI) were higher with resident participation (1.45% vs. 1.14%; P less than .001), as was sepsis (2.42% vs. 2.13%; P = .005), likely because of the increase in surgical infections, Dr. Kasotakis said.
Thankfully, significant cardiac complications and septic shock were not more common with residents, he said.
Adjusted analyses
After adjustment for operative duration, case complexity and pre-existing comorbidities, residents did not increase length of stay (odds ratio, 0.07; P = .242) or septic events (OR, 1.07; P = .155), but their participation was still independently associated with about 20% more superficial surgical site infections (odds ratio, 1.23; P less than .001), organ space infections (OR, 1.21; P less than .001), UTIs (OR, 1.23; P = .001), and intraoperative transfusions (OR, 1.20; P = .001), he said.
Also, about 8% more patients required a return trip to the operating room when residents participated (OR, 1.08; P = .041).
"These outcomes can perhaps be attributed to their underdeveloped surgical skills," Dr. Kasotakis said.
The incidence of DVT and PE were also higher by about 25% (OR, 1.25; P = .011) and 40% (OR, 1.42; P = .005), respectively, perhaps because of delayed DVT prophylaxis initiation because of concerns of hemostasis or missed doses due to additional return trips to the emergency department, he suggested.
Interestingly, reintubation and prolonged mechanical ventilation rates were increased by about 40% (OR, 1.38; OR, 1.43; both P less than .001), perhaps because of prolonged operative times or greater resuscitation requirements, he added.
Dr. Kasotakis was quick to point out that this was a secondary analysis of a data set not originally intended to assess the effect of trainee participation, that no information was available on the degree of resident involvement during surgery or in perioperative care, and that participating institutions were skewed toward tertiary centers, which typically receive more complex cases.
"Staff surgeons should supervise as needed and minimize unnecessary [emergency department] time. And residents, for their part, should be well prepared for emergency procedures through simulation training and aim to maximize their operating room efficiency," he suggested.
The results sparked a flurry of rebuttals led off by discussant Dr. Julie Ann Sosa, Duke University, Durham, N.C.,who said they conflict with other analyses showing little to no impact from residents in elective cases.
"If not interpreted with care, policy makers, payers, and the public could construe that surgical care at academic health centers is compromised by trainees, which could have unfortunate ramifications for everyone in the room as well as the trainees and the patients," she said.
Dr. Sosa expressed concern about drawing causal inferences from an observational study in the setting of possible selection bias and said attempts to match for case complexity using CPT codes do not necessarily account for say, "the difference between a routine appendectomy that takes 15-30 minutes and a complex one that takes 3 hours for a perforation."
Some attendees questioned why the authors didn’t match the institutions in the analysis and chose to ascribe all of the outcomes to residents, with a round of applause following the suggestion that the paper should be titled "Academic centers increase emergency surgery complications." Other attendees questioned whether the poor outcomes reflect resident training and supervision.
Dr. George Velmahos, Massachusetts General Hospital, Boston, questioned whether hospitals have a medical/legal responsibility to inform patients that a resident is in the operating room and may impact outcomes.
Dr. Kasotakis said that institutions may want to add a clause to consent paperwork stating that residents and trainees will be participating.
The complete manuscript of this study and its presentation at the American Surgical Association’s 134th Annual Meeting is anticipated to be published in the Annals of Surgery, pending editorial review.
Dr. Kasotakis reported no conflicts.

|
| Dr. Sapan S. Desai |
While it is tempting to value the very high sample sizes reported in studies that utilize administrative database sources such as NSQIP, it is with great caution that we should interpret the results of these studies. Databases are a valuable source of determining incidence, costs, and even some correlations among various factors. Correlations, however, do not imply causation. For instance, one could say that there is a high correlation between the number of taxis on the street after 3 a.m. and the number of crimes, but that does not mean that taxi drivers transform into criminals during the hour of the wolf.
Databases are a blunt tool for identifying trends in data over large samples and over many years. However, as noted in the study presented by Dr. Kasotakis, the NSQIP does not track the extent of resident participation in operative cases. In fact, the exact variable that is tracked is entitled "ATTEND" in position 16 of the NSQIP and is as follows: 1) Attending & Resident in OR, 2) Attending Alone, and 3) Attending Not Present, but Available. It does not characterize the amount of the case completed by the resident, nor does it state the level of training of the resident. It does not mention whether medical students, visitors, nurse trainees, PAs, new scrub techs, or other personnel are present. In fact, there is no way to know who did what during the case, which is a requirement in order to be able to reliably and accurately determine that the resident is the culprit for longer case times and more intraoperative transfusions. This specific variable has insufficient granularity: the conclusion that "[adding] a clause to consent paperwork stating that residents and trainees will be participating in the case" due to the "underdeveloped surgical skills" of trainees, among other factors, is invalid.
As Dr. Sosa indicated, it is dangerous to imply that these correlations somehow imply causation, as this may lead to adverse impacts on training and negatively impact patient care far more than a possible 20 minute increase in the duration of an operation. The sole utility of this paper is that it is hypothesis generating; only a properly designed prospective study can truly study the positive and negative impacts on patient care due to resident education in the operating room. The question is, do we really want to know the answer to this question and will it truly affect what we do now?
Sapan S. Desai, M.D., is the resident medical editor for Vascular Specialist.
|
|
| Dr. Sapan S. Desai |
While it is tempting to value the very high sample sizes reported in studies that utilize administrative database sources such as NSQIP, it is with great caution that we should interpret the results of these studies. Databases are a valuable source of determining incidence, costs, and even some correlations among various factors. Correlations, however, do not imply causation. For instance, one could say that there is a high correlation between the number of taxis on the street after 3 a.m. and the number of crimes, but that does not mean that taxi drivers transform into criminals during the hour of the wolf.
Databases are a blunt tool for identifying trends in data over large samples and over many years. However, as noted in the study presented by Dr. Kasotakis, the NSQIP does not track the extent of resident participation in operative cases. In fact, the exact variable that is tracked is entitled "ATTEND" in position 16 of the NSQIP and is as follows: 1) Attending & Resident in OR, 2) Attending Alone, and 3) Attending Not Present, but Available. It does not characterize the amount of the case completed by the resident, nor does it state the level of training of the resident. It does not mention whether medical students, visitors, nurse trainees, PAs, new scrub techs, or other personnel are present. In fact, there is no way to know who did what during the case, which is a requirement in order to be able to reliably and accurately determine that the resident is the culprit for longer case times and more intraoperative transfusions. This specific variable has insufficient granularity: the conclusion that "[adding] a clause to consent paperwork stating that residents and trainees will be participating in the case" due to the "underdeveloped surgical skills" of trainees, among other factors, is invalid.
As Dr. Sosa indicated, it is dangerous to imply that these correlations somehow imply causation, as this may lead to adverse impacts on training and negatively impact patient care far more than a possible 20 minute increase in the duration of an operation. The sole utility of this paper is that it is hypothesis generating; only a properly designed prospective study can truly study the positive and negative impacts on patient care due to resident education in the operating room. The question is, do we really want to know the answer to this question and will it truly affect what we do now?
Sapan S. Desai, M.D., is the resident medical editor for Vascular Specialist.
|
|
| Dr. Sapan S. Desai |
While it is tempting to value the very high sample sizes reported in studies that utilize administrative database sources such as NSQIP, it is with great caution that we should interpret the results of these studies. Databases are a valuable source of determining incidence, costs, and even some correlations among various factors. Correlations, however, do not imply causation. For instance, one could say that there is a high correlation between the number of taxis on the street after 3 a.m. and the number of crimes, but that does not mean that taxi drivers transform into criminals during the hour of the wolf.
Databases are a blunt tool for identifying trends in data over large samples and over many years. However, as noted in the study presented by Dr. Kasotakis, the NSQIP does not track the extent of resident participation in operative cases. In fact, the exact variable that is tracked is entitled "ATTEND" in position 16 of the NSQIP and is as follows: 1) Attending & Resident in OR, 2) Attending Alone, and 3) Attending Not Present, but Available. It does not characterize the amount of the case completed by the resident, nor does it state the level of training of the resident. It does not mention whether medical students, visitors, nurse trainees, PAs, new scrub techs, or other personnel are present. In fact, there is no way to know who did what during the case, which is a requirement in order to be able to reliably and accurately determine that the resident is the culprit for longer case times and more intraoperative transfusions. This specific variable has insufficient granularity: the conclusion that "[adding] a clause to consent paperwork stating that residents and trainees will be participating in the case" due to the "underdeveloped surgical skills" of trainees, among other factors, is invalid.
As Dr. Sosa indicated, it is dangerous to imply that these correlations somehow imply causation, as this may lead to adverse impacts on training and negatively impact patient care far more than a possible 20 minute increase in the duration of an operation. The sole utility of this paper is that it is hypothesis generating; only a properly designed prospective study can truly study the positive and negative impacts on patient care due to resident education in the operating room. The question is, do we really want to know the answer to this question and will it truly affect what we do now?
Sapan S. Desai, M.D., is the resident medical editor for Vascular Specialist.
BOSTON – Resident participation in emergency general surgery cases was independently associated with a host of complications – pulmonary embolism, surgical site infections, and unplanned reoperation in a secondary analysis of the American College of Surgeons prospective National Surgical Quality Improvement database.
Adequate exposure of residents to emergency general surgery is crucial for surgical training, but academic operating teams should be mindful of this association, Dr. George Kasotakis said at the annual meeting of the American Surgical Association.
Three papers have shown resident participation modestly increases complications in elective surgery, but their impact is not well understood for emergency general surgery, where patient physiology is typically deranged and timely surgery is imperative.
Dr. Kasotakis and his colleagues at Boston University identified 141,010 patients who underwent emergency general surgery procedures in the 2005-2010 American College of Surgeons prospective National Surgical Quality Improvement database. Because of the nonrandom assignment of more complex cases to resident participation, patients were matched 1:1 based on age; gender; use of alcohol, tobacco, and steroids; inpatient status; obesity; diabetes; renal failure; cardiopulmonary disease; and expected probability for morbidity and mortality. Regression models were fitted for each outcome and adjusted for the same risk factors and operative time.
The most common procedures were appendectomy (40%), exploratory laparotomy (8.75%), bowel resection (9.2%), cholecystectomy (6%), and lysis of adhesions (6%).
Thirty-day mortality was similar with and without residents (3.25% vs. 2.96%; P = .082), but hospital length of stay was longer by about a half a day with residents (4.97 days vs. 4.59 days; P = .019), said Dr. Kasotakis, an acute care surgeon and intensivist.
Resident participation added about 20 minutes to operative (75 minutes vs. 59 minutes; P less than .001) and anesthesia (122 minutes vs. 100 minutes; P less than .001) times.
Intraoperative transfusions were more common with residents (3.43% vs. 2.55%; P less than .001), perhaps because of longer operating room times, and, as a result, fewer postoperative transfusions were needed (1.12% vs. 1.28% P = .031), he said. Unplanned reoperations, however, were more common with residents, as well (4.22% vs. 3.80%; P = .002).
Postsurgical superficial wound infections (3.5% vs. 2.78%; P less than .001) and organ space surgical site infections (2.27% vs. 1.77%; P less than .001) were more common in the resident group, while wound dehiscence was not (0.63% vs. 0.69%; P = .266), Dr. Kasotakis noted.
Pulmonary complications were significantly more common in the resident group including postoperative pneumonia (1.85% vs. 1.67%; P = .04), reintubation (1.64% vs. 1.15%; P less than .001), and mechanical ventilation for more than 48 hours (2.87% vs. 2.06%; P less than .001).
The same was true for deep vein thrombosis (DVT) (0.80% vs. 0.62%; P = .002) and pulmonary embolism (PE) (0.43% vs. 0.28%; P less than .001).
Urinary tract infections (UTI) were higher with resident participation (1.45% vs. 1.14%; P less than .001), as was sepsis (2.42% vs. 2.13%; P = .005), likely because of the increase in surgical infections, Dr. Kasotakis said.
Thankfully, significant cardiac complications and septic shock were not more common with residents, he said.
Adjusted analyses
After adjustment for operative duration, case complexity and pre-existing comorbidities, residents did not increase length of stay (odds ratio, 0.07; P = .242) or septic events (OR, 1.07; P = .155), but their participation was still independently associated with about 20% more superficial surgical site infections (odds ratio, 1.23; P less than .001), organ space infections (OR, 1.21; P less than .001), UTIs (OR, 1.23; P = .001), and intraoperative transfusions (OR, 1.20; P = .001), he said.
Also, about 8% more patients required a return trip to the operating room when residents participated (OR, 1.08; P = .041).
"These outcomes can perhaps be attributed to their underdeveloped surgical skills," Dr. Kasotakis said.
The incidence of DVT and PE were also higher by about 25% (OR, 1.25; P = .011) and 40% (OR, 1.42; P = .005), respectively, perhaps because of delayed DVT prophylaxis initiation because of concerns of hemostasis or missed doses due to additional return trips to the emergency department, he suggested.
Interestingly, reintubation and prolonged mechanical ventilation rates were increased by about 40% (OR, 1.38; OR, 1.43; both P less than .001), perhaps because of prolonged operative times or greater resuscitation requirements, he added.
Dr. Kasotakis was quick to point out that this was a secondary analysis of a data set not originally intended to assess the effect of trainee participation, that no information was available on the degree of resident involvement during surgery or in perioperative care, and that participating institutions were skewed toward tertiary centers, which typically receive more complex cases.
"Staff surgeons should supervise as needed and minimize unnecessary [emergency department] time. And residents, for their part, should be well prepared for emergency procedures through simulation training and aim to maximize their operating room efficiency," he suggested.
The results sparked a flurry of rebuttals led off by discussant Dr. Julie Ann Sosa, Duke University, Durham, N.C.,who said they conflict with other analyses showing little to no impact from residents in elective cases.
"If not interpreted with care, policy makers, payers, and the public could construe that surgical care at academic health centers is compromised by trainees, which could have unfortunate ramifications for everyone in the room as well as the trainees and the patients," she said.
Dr. Sosa expressed concern about drawing causal inferences from an observational study in the setting of possible selection bias and said attempts to match for case complexity using CPT codes do not necessarily account for say, "the difference between a routine appendectomy that takes 15-30 minutes and a complex one that takes 3 hours for a perforation."
Some attendees questioned why the authors didn’t match the institutions in the analysis and chose to ascribe all of the outcomes to residents, with a round of applause following the suggestion that the paper should be titled "Academic centers increase emergency surgery complications." Other attendees questioned whether the poor outcomes reflect resident training and supervision.
Dr. George Velmahos, Massachusetts General Hospital, Boston, questioned whether hospitals have a medical/legal responsibility to inform patients that a resident is in the operating room and may impact outcomes.
Dr. Kasotakis said that institutions may want to add a clause to consent paperwork stating that residents and trainees will be participating.
The complete manuscript of this study and its presentation at the American Surgical Association’s 134th Annual Meeting is anticipated to be published in the Annals of Surgery, pending editorial review.
Dr. Kasotakis reported no conflicts.
BOSTON – Resident participation in emergency general surgery cases was independently associated with a host of complications – pulmonary embolism, surgical site infections, and unplanned reoperation in a secondary analysis of the American College of Surgeons prospective National Surgical Quality Improvement database.
Adequate exposure of residents to emergency general surgery is crucial for surgical training, but academic operating teams should be mindful of this association, Dr. George Kasotakis said at the annual meeting of the American Surgical Association.
Three papers have shown resident participation modestly increases complications in elective surgery, but their impact is not well understood for emergency general surgery, where patient physiology is typically deranged and timely surgery is imperative.
Dr. Kasotakis and his colleagues at Boston University identified 141,010 patients who underwent emergency general surgery procedures in the 2005-2010 American College of Surgeons prospective National Surgical Quality Improvement database. Because of the nonrandom assignment of more complex cases to resident participation, patients were matched 1:1 based on age; gender; use of alcohol, tobacco, and steroids; inpatient status; obesity; diabetes; renal failure; cardiopulmonary disease; and expected probability for morbidity and mortality. Regression models were fitted for each outcome and adjusted for the same risk factors and operative time.
The most common procedures were appendectomy (40%), exploratory laparotomy (8.75%), bowel resection (9.2%), cholecystectomy (6%), and lysis of adhesions (6%).
Thirty-day mortality was similar with and without residents (3.25% vs. 2.96%; P = .082), but hospital length of stay was longer by about a half a day with residents (4.97 days vs. 4.59 days; P = .019), said Dr. Kasotakis, an acute care surgeon and intensivist.
Resident participation added about 20 minutes to operative (75 minutes vs. 59 minutes; P less than .001) and anesthesia (122 minutes vs. 100 minutes; P less than .001) times.
Intraoperative transfusions were more common with residents (3.43% vs. 2.55%; P less than .001), perhaps because of longer operating room times, and, as a result, fewer postoperative transfusions were needed (1.12% vs. 1.28% P = .031), he said. Unplanned reoperations, however, were more common with residents, as well (4.22% vs. 3.80%; P = .002).
Postsurgical superficial wound infections (3.5% vs. 2.78%; P less than .001) and organ space surgical site infections (2.27% vs. 1.77%; P less than .001) were more common in the resident group, while wound dehiscence was not (0.63% vs. 0.69%; P = .266), Dr. Kasotakis noted.
Pulmonary complications were significantly more common in the resident group including postoperative pneumonia (1.85% vs. 1.67%; P = .04), reintubation (1.64% vs. 1.15%; P less than .001), and mechanical ventilation for more than 48 hours (2.87% vs. 2.06%; P less than .001).
The same was true for deep vein thrombosis (DVT) (0.80% vs. 0.62%; P = .002) and pulmonary embolism (PE) (0.43% vs. 0.28%; P less than .001).
Urinary tract infections (UTI) were higher with resident participation (1.45% vs. 1.14%; P less than .001), as was sepsis (2.42% vs. 2.13%; P = .005), likely because of the increase in surgical infections, Dr. Kasotakis said.
Thankfully, significant cardiac complications and septic shock were not more common with residents, he said.
Adjusted analyses
After adjustment for operative duration, case complexity and pre-existing comorbidities, residents did not increase length of stay (odds ratio, 0.07; P = .242) or septic events (OR, 1.07; P = .155), but their participation was still independently associated with about 20% more superficial surgical site infections (odds ratio, 1.23; P less than .001), organ space infections (OR, 1.21; P less than .001), UTIs (OR, 1.23; P = .001), and intraoperative transfusions (OR, 1.20; P = .001), he said.
Also, about 8% more patients required a return trip to the operating room when residents participated (OR, 1.08; P = .041).
"These outcomes can perhaps be attributed to their underdeveloped surgical skills," Dr. Kasotakis said.
The incidence of DVT and PE were also higher by about 25% (OR, 1.25; P = .011) and 40% (OR, 1.42; P = .005), respectively, perhaps because of delayed DVT prophylaxis initiation because of concerns of hemostasis or missed doses due to additional return trips to the emergency department, he suggested.
Interestingly, reintubation and prolonged mechanical ventilation rates were increased by about 40% (OR, 1.38; OR, 1.43; both P less than .001), perhaps because of prolonged operative times or greater resuscitation requirements, he added.
Dr. Kasotakis was quick to point out that this was a secondary analysis of a data set not originally intended to assess the effect of trainee participation, that no information was available on the degree of resident involvement during surgery or in perioperative care, and that participating institutions were skewed toward tertiary centers, which typically receive more complex cases.
"Staff surgeons should supervise as needed and minimize unnecessary [emergency department] time. And residents, for their part, should be well prepared for emergency procedures through simulation training and aim to maximize their operating room efficiency," he suggested.
The results sparked a flurry of rebuttals led off by discussant Dr. Julie Ann Sosa, Duke University, Durham, N.C.,who said they conflict with other analyses showing little to no impact from residents in elective cases.
"If not interpreted with care, policy makers, payers, and the public could construe that surgical care at academic health centers is compromised by trainees, which could have unfortunate ramifications for everyone in the room as well as the trainees and the patients," she said.
Dr. Sosa expressed concern about drawing causal inferences from an observational study in the setting of possible selection bias and said attempts to match for case complexity using CPT codes do not necessarily account for say, "the difference between a routine appendectomy that takes 15-30 minutes and a complex one that takes 3 hours for a perforation."
Some attendees questioned why the authors didn’t match the institutions in the analysis and chose to ascribe all of the outcomes to residents, with a round of applause following the suggestion that the paper should be titled "Academic centers increase emergency surgery complications." Other attendees questioned whether the poor outcomes reflect resident training and supervision.
Dr. George Velmahos, Massachusetts General Hospital, Boston, questioned whether hospitals have a medical/legal responsibility to inform patients that a resident is in the operating room and may impact outcomes.
Dr. Kasotakis said that institutions may want to add a clause to consent paperwork stating that residents and trainees will be participating.
The complete manuscript of this study and its presentation at the American Surgical Association’s 134th Annual Meeting is anticipated to be published in the Annals of Surgery, pending editorial review.
Dr. Kasotakis reported no conflicts.
Major finding: Rates were significantly higher with resident participation than without for DVT (0.80% vs. 0.62%; P = .002) and PE (0.43% vs. 0.28%; P less than .001).
Data source: A secondary analysis of 141,010 emergency general surgery cases in the prospective ACS NSQIP database.
Disclosures: Dr. Kasotakis and his coauthors reported no conflicting interests.

Mentorship: An essential key to growth and success
In 2011, an article titled "Building a Successful Career: Advice From Leaders in Thoracic Surgery" was published in Thoracic Surgical Clinics of North America.1 In developing this paper, Dr. Sean Grondin states, "I have been fortunate to have had mentors who have guided me through my surgical training and early years of practice," and he continues, "I realize how much I have learned from and been influenced by the experience and guidance of other surgeons."
Based on his experiences, Dr. Grondin selected a group of 20 outstanding leaders in thoracic surgery, and asked them to each write a short summary of what they deemed to be key elements for developing a successful thoracic surgical career. The inspiration for the paper was an appreciation for mentorship and a desire to further disseminate the influences of the greats in our field; it is both revealing and remarkably appropriate that, in their responses, the majority of the recognized leaders discussed the importance of cultivating strong mentorship relationships, with the word "mentor" mentioned 34 times in the article. The importance of having strong mentors to guide oneself in career development is highlighted over and over again.

In his comments, Dr. Douglas Mathisen states, "Residency training usually introduces you to the most important mentors in your life. They will be the ones who nurture you, educate you, and point you in the right direction. They are likely to bring out the desire in you to become an academic surgeon and educator."
Advice for success from Dr. Valerie Rusch included eight key points, one of which focused on mentorship: "Peer review and senior advice are frequently helpful, and most senior academic physicians are delighted to provide this. Mentors may be surgeons but are also often found in other specialties or even nonclinical settings." And, from the mentors’ perspective, Dr. F.G. Pearson remarks, "In a residency training program, the opportunity to act as a meaningful mentor is a gift and a rewarding opportunity."
For a cardiothoracic surgeon’s individual success, it is clear that having (and utilizing) the right mentors can make a significant impact. Further, when one considers the success of a group of individuals, it is equally important that mentorship relationships are present and strong. In the summer of 2011, the Senior Tour (a group of retired cardiothoracic surgeons committed to education and service for their profession) was asked by the Joint Council on Thoracic Surgery Education to visit 10 thoracic surgical training programs that were considered above average according to a poll taken of thoracic surgical residents in the fall of 2010 by the Thoracic Surgery Residents Association.2
As they summarized their findings, they noted that the top programs possessed many common features leading to superior training in cardiac and general thoracic surgery. The authors specifically noted seven key factors, and, among them, was "a significant emphasis on mentorship, with the program director playing the primary roles and with voluntary relationships between residents and other faculty and with mentorship also including involvement in job finding."
If mentorship is so important to success in this career path, exactly what opportunities exist for trainees seeking mentorship? A Google search for ["mentor" AND "thoracic surgery"] yields a number of results, with ultimate direction leading to essentially two organizations: the AATS and Women in Thoracic Surgery (WTS).
From the AATS website, there is a list of names and contact information for mentors who have been selected or self-nominated for prospective candidates for thoracic surgery residency. These mentors are available to offer guidance, recommendations, and research opportunities, as well as clinical rotations in cardiothoracic surgery (http://aats.org/TSR/contactsMentors.cgi).
A number of opportunities for mentorship are also available through WTS. There is a formal mentoring program, aiming to pair women interested in cardiothoracic surgical careers with established WTS members. Dr. Shanda Blackmon, the Mentoring Chair for the WTS, reflects on the program, stating, "Many surgeons think that mentorship has to be a formal relationship at the same institution. What we have learned at WTS is that mentorship relationships can be equally effective even when they are not formal and the mentor is not from the same institution." She continues, reporting that, "in the survey we conducted through WTS, we discovered that mentorship was one of the most important factors to young surgeons aspiring to start a career in thoracic surgery." It is for this reason that WTS places such emphasis on helping trainees find and sustain mentorship opportunities.
WTS specifically offers scholarships to the Society of Thoracic Surgeons meeting, the Scanlan/WTS Traveling Mentorship, the Carolyn Reed Award, a list of mentors online, and resident mentors. (Further details of all of these programs can be found at www.wtsnet.org.) WTS provides a number of opportunities for female trainees to connect with female mentors. But is it absolutely necessary to find mentors who are "like you"?
Dr. Jennifer Lawton, president of WTS, acknowledges that everyone needs mentoring, but urges that "mentoring of women and minorities is particularly important in order to take advantage of the vast array of benefits to be gained by ethnic, racial, and gender diversity in the workplace."
She continues: "If we don’t see others successful in a chosen field, we do not perceive the goal attainable for ourselves. I have seen this many times in cardiothoracic surgery and women. Women who are not exposed to female mentors have expressed concern that practice in the field is not possible for women (especially those who aspire to have a family)." And, further, she explains that "we are typically more comfortable in mentoring situations with others like ourselves (similar challenges, needs, concerns). Surveys demonstrate that medical students often choose fields of interest because of mentors. For these reasons, it is important for individuals to find mentors who are similar to themselves."
Additional formal mentoring programs exist, and include the Brooks Scholarship through the Southern Thoracic Surgical Association (STSA), the Society of Thoracic Surgeons Looking to the Future scholarship program, the AATS Member for a Day program, and more.
Exactly what should one hope to get out of a mentorship relationship? The truth is, it really depends on the stage of career and the specific needs of the mentee. Mentorship needs change over time, and even well-established mentoring relationships will evolve and adjust along with participants in the interaction.
Sarah Schubert is a fourth-year medical student at Penn State, who has matched into the I-6 program at the University of Virginia and is the current recipient of the Scanlan/WTS scholarship. This award provides trainees with an opportunity to gain exposure to women cardiothoracic surgeon mentors by visiting a WTS member for an elective period. Ms. Schubert reports that she applied for the scholarship because she "wanted to work with and learn from a highly successful female cardiac surgeon in hopes of initiating and developing a professional relationship with a woman in the field."
As a medical student, she has fairly basic mentorship needs. She tells us that "right now, I need mentors who can serve as good role models – in the OR, with patients, with colleagues and trainees, and in their personal lives outside the hospital. As I prepare to enter residency, I anticipate that I will need to further develop my patient care skills and operative techniques, as well as skills to manage time and obligations. Knowing and working with people who have already figured out how to juggle those different obligations will be immensely helpful." Other medical students may be looking for advice on interviewing and ranking residency programs, and, like Ms. Schubert, may be interested in tips on how to get a great start in internship.
For individuals deep in the throes of cardiothoracic training, the needs are clearly different. Dr. Ryan Shelstad, a first-year fellow at the University of Colorado, states: "In my mind, the primary objective of clinical fellowship is acquisition of technical skills and clinical decision making in CT surgery. Thus, mentorship at this stage follows this objective." He continues, "CT fellowship is a relatively short time to achieve this goal as well as position oneself to successfully transition to a faculty position or private practice, which is the second objective—and area for mentoring."
Dr. Shelstad acknowledges and explains the transition in his mentorship needs, "I think earlier in training, mentorship focused on career choice, research, and transition to a fellowship. Much was focused on getting to the next step. While that is still important, now is the time to focus on the clinical aspects of CT surgery that I will use the rest of my career." And, certainly, the specific mentoring needs will continue to change with time.
Dr. Lawton, who holds the rank of professor at Washington University, St. Louis, states that, "after reaching full professor, surgeons need mentoring and sponsoring to reach goals such as dean positions, leadership positions, national organization officer positions, etc. We also all continually need mosaic mentoring that evolves over time (someone to mentor for research career aspects, managing work-life balance issues, family issues, teaching issues, financial issues, etc.). As we progress in our careers, we have the opportunity to also be mentored in other areas by younger generations."
Wait, did she just say that progressing surgeons can be mentored by younger generations? Yes, she did. And not only can seasoned surgeons be mentored by younger surgeons, they also stand to gain considerably from their own mentees. Dr. Lawton further states, "There is always reciprocal gain in a mentoring relationship for the mentor. There is no better joy than to see a mentee succeed and be fulfilled and happy in her chosen field. For some, this provides a rich legacy of trainees and mentees to provide continued enrichment, excitement, and a source of tremendous pride in later years." In the previously mentioned article by Grondin, Dr. Gail Darling states, "Academic careers are usually measured in papers published, grants awarded, invited lectures, and academic standing. Equally important are the students we teach and motivate toward careers in surgery, residents and fellows we have taught and mentored who will provide care to patients and who will go out and teach new generations of surgeons who will in turn provide care."
Once mentorship bonds have been established, it is critical to cultivate these relationships and to gain the most possible from these interactions. When asked how he has achieved these ends, Dr. Shelstad replies, "You and your mentors have the same goal: mutual success. Work hard for your mentors, and they will work hard for you. I would encourage explicit discussion of goals and expectations to ensure you and a potential mentor are on the same page. Mentorship is essential to success in cardiothoracic surgery."
Without a doubt, participation in mentorship relationships is a key element of success at every stage of the career and development of a cardiothoracic surgeon. Outstanding programs already exist to support modern trainees, and further efforts will certainly be met with great enthusiasm. Also apparent is the need for ongoing, career-long mentorship – and the paucity of formal programs to support it. This need may be a great opportunity for the establishment of future programming.
On a personal note, when reflecting on mentorship, I think of a statement made by Benjamin Franklin: "Tell me and I forget, teach me and I may remember, involve me and I learn." To those incredible individuals who have taken the time, effort, and interest to truly involve me, I have immense gratitude. I will aim for the rest of my career to make it worth your while, with hopes to bring you pride and inspire others as you have inspired me. To all who have taken time to truly involve any student, resident, or junior colleague – you have motivated us and given strength to the ongoing legacy of our amazing field.
Citations
1. Grondin SC. Building a Successful Career: Advice From Leaders in Thoracic Surgery. Thorac. Surg. Clin. 2011;21(3):395-415.
2. J. Thorac. Cardiovasc. Surg. 2014;147(1):15-17.
In 2011, an article titled "Building a Successful Career: Advice From Leaders in Thoracic Surgery" was published in Thoracic Surgical Clinics of North America.1 In developing this paper, Dr. Sean Grondin states, "I have been fortunate to have had mentors who have guided me through my surgical training and early years of practice," and he continues, "I realize how much I have learned from and been influenced by the experience and guidance of other surgeons."
Based on his experiences, Dr. Grondin selected a group of 20 outstanding leaders in thoracic surgery, and asked them to each write a short summary of what they deemed to be key elements for developing a successful thoracic surgical career. The inspiration for the paper was an appreciation for mentorship and a desire to further disseminate the influences of the greats in our field; it is both revealing and remarkably appropriate that, in their responses, the majority of the recognized leaders discussed the importance of cultivating strong mentorship relationships, with the word "mentor" mentioned 34 times in the article. The importance of having strong mentors to guide oneself in career development is highlighted over and over again.
In his comments, Dr. Douglas Mathisen states, "Residency training usually introduces you to the most important mentors in your life. They will be the ones who nurture you, educate you, and point you in the right direction. They are likely to bring out the desire in you to become an academic surgeon and educator."
Advice for success from Dr. Valerie Rusch included eight key points, one of which focused on mentorship: "Peer review and senior advice are frequently helpful, and most senior academic physicians are delighted to provide this. Mentors may be surgeons but are also often found in other specialties or even nonclinical settings." And, from the mentors’ perspective, Dr. F.G. Pearson remarks, "In a residency training program, the opportunity to act as a meaningful mentor is a gift and a rewarding opportunity."
For a cardiothoracic surgeon’s individual success, it is clear that having (and utilizing) the right mentors can make a significant impact. Further, when one considers the success of a group of individuals, it is equally important that mentorship relationships are present and strong. In the summer of 2011, the Senior Tour (a group of retired cardiothoracic surgeons committed to education and service for their profession) was asked by the Joint Council on Thoracic Surgery Education to visit 10 thoracic surgical training programs that were considered above average according to a poll taken of thoracic surgical residents in the fall of 2010 by the Thoracic Surgery Residents Association.2
As they summarized their findings, they noted that the top programs possessed many common features leading to superior training in cardiac and general thoracic surgery. The authors specifically noted seven key factors, and, among them, was "a significant emphasis on mentorship, with the program director playing the primary roles and with voluntary relationships between residents and other faculty and with mentorship also including involvement in job finding."
If mentorship is so important to success in this career path, exactly what opportunities exist for trainees seeking mentorship? A Google search for ["mentor" AND "thoracic surgery"] yields a number of results, with ultimate direction leading to essentially two organizations: the AATS and Women in Thoracic Surgery (WTS).
From the AATS website, there is a list of names and contact information for mentors who have been selected or self-nominated for prospective candidates for thoracic surgery residency. These mentors are available to offer guidance, recommendations, and research opportunities, as well as clinical rotations in cardiothoracic surgery (http://aats.org/TSR/contactsMentors.cgi).
A number of opportunities for mentorship are also available through WTS. There is a formal mentoring program, aiming to pair women interested in cardiothoracic surgical careers with established WTS members. Dr. Shanda Blackmon, the Mentoring Chair for the WTS, reflects on the program, stating, "Many surgeons think that mentorship has to be a formal relationship at the same institution. What we have learned at WTS is that mentorship relationships can be equally effective even when they are not formal and the mentor is not from the same institution." She continues, reporting that, "in the survey we conducted through WTS, we discovered that mentorship was one of the most important factors to young surgeons aspiring to start a career in thoracic surgery." It is for this reason that WTS places such emphasis on helping trainees find and sustain mentorship opportunities.
WTS specifically offers scholarships to the Society of Thoracic Surgeons meeting, the Scanlan/WTS Traveling Mentorship, the Carolyn Reed Award, a list of mentors online, and resident mentors. (Further details of all of these programs can be found at www.wtsnet.org.) WTS provides a number of opportunities for female trainees to connect with female mentors. But is it absolutely necessary to find mentors who are "like you"?
Dr. Jennifer Lawton, president of WTS, acknowledges that everyone needs mentoring, but urges that "mentoring of women and minorities is particularly important in order to take advantage of the vast array of benefits to be gained by ethnic, racial, and gender diversity in the workplace."
She continues: "If we don’t see others successful in a chosen field, we do not perceive the goal attainable for ourselves. I have seen this many times in cardiothoracic surgery and women. Women who are not exposed to female mentors have expressed concern that practice in the field is not possible for women (especially those who aspire to have a family)." And, further, she explains that "we are typically more comfortable in mentoring situations with others like ourselves (similar challenges, needs, concerns). Surveys demonstrate that medical students often choose fields of interest because of mentors. For these reasons, it is important for individuals to find mentors who are similar to themselves."
Additional formal mentoring programs exist, and include the Brooks Scholarship through the Southern Thoracic Surgical Association (STSA), the Society of Thoracic Surgeons Looking to the Future scholarship program, the AATS Member for a Day program, and more.
Exactly what should one hope to get out of a mentorship relationship? The truth is, it really depends on the stage of career and the specific needs of the mentee. Mentorship needs change over time, and even well-established mentoring relationships will evolve and adjust along with participants in the interaction.
Sarah Schubert is a fourth-year medical student at Penn State, who has matched into the I-6 program at the University of Virginia and is the current recipient of the Scanlan/WTS scholarship. This award provides trainees with an opportunity to gain exposure to women cardiothoracic surgeon mentors by visiting a WTS member for an elective period. Ms. Schubert reports that she applied for the scholarship because she "wanted to work with and learn from a highly successful female cardiac surgeon in hopes of initiating and developing a professional relationship with a woman in the field."
As a medical student, she has fairly basic mentorship needs. She tells us that "right now, I need mentors who can serve as good role models – in the OR, with patients, with colleagues and trainees, and in their personal lives outside the hospital. As I prepare to enter residency, I anticipate that I will need to further develop my patient care skills and operative techniques, as well as skills to manage time and obligations. Knowing and working with people who have already figured out how to juggle those different obligations will be immensely helpful." Other medical students may be looking for advice on interviewing and ranking residency programs, and, like Ms. Schubert, may be interested in tips on how to get a great start in internship.
For individuals deep in the throes of cardiothoracic training, the needs are clearly different. Dr. Ryan Shelstad, a first-year fellow at the University of Colorado, states: "In my mind, the primary objective of clinical fellowship is acquisition of technical skills and clinical decision making in CT surgery. Thus, mentorship at this stage follows this objective." He continues, "CT fellowship is a relatively short time to achieve this goal as well as position oneself to successfully transition to a faculty position or private practice, which is the second objective—and area for mentoring."
Dr. Shelstad acknowledges and explains the transition in his mentorship needs, "I think earlier in training, mentorship focused on career choice, research, and transition to a fellowship. Much was focused on getting to the next step. While that is still important, now is the time to focus on the clinical aspects of CT surgery that I will use the rest of my career." And, certainly, the specific mentoring needs will continue to change with time.
Dr. Lawton, who holds the rank of professor at Washington University, St. Louis, states that, "after reaching full professor, surgeons need mentoring and sponsoring to reach goals such as dean positions, leadership positions, national organization officer positions, etc. We also all continually need mosaic mentoring that evolves over time (someone to mentor for research career aspects, managing work-life balance issues, family issues, teaching issues, financial issues, etc.). As we progress in our careers, we have the opportunity to also be mentored in other areas by younger generations."
Wait, did she just say that progressing surgeons can be mentored by younger generations? Yes, she did. And not only can seasoned surgeons be mentored by younger surgeons, they also stand to gain considerably from their own mentees. Dr. Lawton further states, "There is always reciprocal gain in a mentoring relationship for the mentor. There is no better joy than to see a mentee succeed and be fulfilled and happy in her chosen field. For some, this provides a rich legacy of trainees and mentees to provide continued enrichment, excitement, and a source of tremendous pride in later years." In the previously mentioned article by Grondin, Dr. Gail Darling states, "Academic careers are usually measured in papers published, grants awarded, invited lectures, and academic standing. Equally important are the students we teach and motivate toward careers in surgery, residents and fellows we have taught and mentored who will provide care to patients and who will go out and teach new generations of surgeons who will in turn provide care."
Once mentorship bonds have been established, it is critical to cultivate these relationships and to gain the most possible from these interactions. When asked how he has achieved these ends, Dr. Shelstad replies, "You and your mentors have the same goal: mutual success. Work hard for your mentors, and they will work hard for you. I would encourage explicit discussion of goals and expectations to ensure you and a potential mentor are on the same page. Mentorship is essential to success in cardiothoracic surgery."
Without a doubt, participation in mentorship relationships is a key element of success at every stage of the career and development of a cardiothoracic surgeon. Outstanding programs already exist to support modern trainees, and further efforts will certainly be met with great enthusiasm. Also apparent is the need for ongoing, career-long mentorship – and the paucity of formal programs to support it. This need may be a great opportunity for the establishment of future programming.
On a personal note, when reflecting on mentorship, I think of a statement made by Benjamin Franklin: "Tell me and I forget, teach me and I may remember, involve me and I learn." To those incredible individuals who have taken the time, effort, and interest to truly involve me, I have immense gratitude. I will aim for the rest of my career to make it worth your while, with hopes to bring you pride and inspire others as you have inspired me. To all who have taken time to truly involve any student, resident, or junior colleague – you have motivated us and given strength to the ongoing legacy of our amazing field.
Citations
1. Grondin SC. Building a Successful Career: Advice From Leaders in Thoracic Surgery. Thorac. Surg. Clin. 2011;21(3):395-415.
2. J. Thorac. Cardiovasc. Surg. 2014;147(1):15-17.
In 2011, an article titled "Building a Successful Career: Advice From Leaders in Thoracic Surgery" was published in Thoracic Surgical Clinics of North America.1 In developing this paper, Dr. Sean Grondin states, "I have been fortunate to have had mentors who have guided me through my surgical training and early years of practice," and he continues, "I realize how much I have learned from and been influenced by the experience and guidance of other surgeons."
Based on his experiences, Dr. Grondin selected a group of 20 outstanding leaders in thoracic surgery, and asked them to each write a short summary of what they deemed to be key elements for developing a successful thoracic surgical career. The inspiration for the paper was an appreciation for mentorship and a desire to further disseminate the influences of the greats in our field; it is both revealing and remarkably appropriate that, in their responses, the majority of the recognized leaders discussed the importance of cultivating strong mentorship relationships, with the word "mentor" mentioned 34 times in the article. The importance of having strong mentors to guide oneself in career development is highlighted over and over again.
In his comments, Dr. Douglas Mathisen states, "Residency training usually introduces you to the most important mentors in your life. They will be the ones who nurture you, educate you, and point you in the right direction. They are likely to bring out the desire in you to become an academic surgeon and educator."
Advice for success from Dr. Valerie Rusch included eight key points, one of which focused on mentorship: "Peer review and senior advice are frequently helpful, and most senior academic physicians are delighted to provide this. Mentors may be surgeons but are also often found in other specialties or even nonclinical settings." And, from the mentors’ perspective, Dr. F.G. Pearson remarks, "In a residency training program, the opportunity to act as a meaningful mentor is a gift and a rewarding opportunity."
For a cardiothoracic surgeon’s individual success, it is clear that having (and utilizing) the right mentors can make a significant impact. Further, when one considers the success of a group of individuals, it is equally important that mentorship relationships are present and strong. In the summer of 2011, the Senior Tour (a group of retired cardiothoracic surgeons committed to education and service for their profession) was asked by the Joint Council on Thoracic Surgery Education to visit 10 thoracic surgical training programs that were considered above average according to a poll taken of thoracic surgical residents in the fall of 2010 by the Thoracic Surgery Residents Association.2
As they summarized their findings, they noted that the top programs possessed many common features leading to superior training in cardiac and general thoracic surgery. The authors specifically noted seven key factors, and, among them, was "a significant emphasis on mentorship, with the program director playing the primary roles and with voluntary relationships between residents and other faculty and with mentorship also including involvement in job finding."
If mentorship is so important to success in this career path, exactly what opportunities exist for trainees seeking mentorship? A Google search for ["mentor" AND "thoracic surgery"] yields a number of results, with ultimate direction leading to essentially two organizations: the AATS and Women in Thoracic Surgery (WTS).
From the AATS website, there is a list of names and contact information for mentors who have been selected or self-nominated for prospective candidates for thoracic surgery residency. These mentors are available to offer guidance, recommendations, and research opportunities, as well as clinical rotations in cardiothoracic surgery (http://aats.org/TSR/contactsMentors.cgi).
A number of opportunities for mentorship are also available through WTS. There is a formal mentoring program, aiming to pair women interested in cardiothoracic surgical careers with established WTS members. Dr. Shanda Blackmon, the Mentoring Chair for the WTS, reflects on the program, stating, "Many surgeons think that mentorship has to be a formal relationship at the same institution. What we have learned at WTS is that mentorship relationships can be equally effective even when they are not formal and the mentor is not from the same institution." She continues, reporting that, "in the survey we conducted through WTS, we discovered that mentorship was one of the most important factors to young surgeons aspiring to start a career in thoracic surgery." It is for this reason that WTS places such emphasis on helping trainees find and sustain mentorship opportunities.
WTS specifically offers scholarships to the Society of Thoracic Surgeons meeting, the Scanlan/WTS Traveling Mentorship, the Carolyn Reed Award, a list of mentors online, and resident mentors. (Further details of all of these programs can be found at www.wtsnet.org.) WTS provides a number of opportunities for female trainees to connect with female mentors. But is it absolutely necessary to find mentors who are "like you"?
Dr. Jennifer Lawton, president of WTS, acknowledges that everyone needs mentoring, but urges that "mentoring of women and minorities is particularly important in order to take advantage of the vast array of benefits to be gained by ethnic, racial, and gender diversity in the workplace."
She continues: "If we don’t see others successful in a chosen field, we do not perceive the goal attainable for ourselves. I have seen this many times in cardiothoracic surgery and women. Women who are not exposed to female mentors have expressed concern that practice in the field is not possible for women (especially those who aspire to have a family)." And, further, she explains that "we are typically more comfortable in mentoring situations with others like ourselves (similar challenges, needs, concerns). Surveys demonstrate that medical students often choose fields of interest because of mentors. For these reasons, it is important for individuals to find mentors who are similar to themselves."
Additional formal mentoring programs exist, and include the Brooks Scholarship through the Southern Thoracic Surgical Association (STSA), the Society of Thoracic Surgeons Looking to the Future scholarship program, the AATS Member for a Day program, and more.
Exactly what should one hope to get out of a mentorship relationship? The truth is, it really depends on the stage of career and the specific needs of the mentee. Mentorship needs change over time, and even well-established mentoring relationships will evolve and adjust along with participants in the interaction.
Sarah Schubert is a fourth-year medical student at Penn State, who has matched into the I-6 program at the University of Virginia and is the current recipient of the Scanlan/WTS scholarship. This award provides trainees with an opportunity to gain exposure to women cardiothoracic surgeon mentors by visiting a WTS member for an elective period. Ms. Schubert reports that she applied for the scholarship because she "wanted to work with and learn from a highly successful female cardiac surgeon in hopes of initiating and developing a professional relationship with a woman in the field."
As a medical student, she has fairly basic mentorship needs. She tells us that "right now, I need mentors who can serve as good role models – in the OR, with patients, with colleagues and trainees, and in their personal lives outside the hospital. As I prepare to enter residency, I anticipate that I will need to further develop my patient care skills and operative techniques, as well as skills to manage time and obligations. Knowing and working with people who have already figured out how to juggle those different obligations will be immensely helpful." Other medical students may be looking for advice on interviewing and ranking residency programs, and, like Ms. Schubert, may be interested in tips on how to get a great start in internship.
For individuals deep in the throes of cardiothoracic training, the needs are clearly different. Dr. Ryan Shelstad, a first-year fellow at the University of Colorado, states: "In my mind, the primary objective of clinical fellowship is acquisition of technical skills and clinical decision making in CT surgery. Thus, mentorship at this stage follows this objective." He continues, "CT fellowship is a relatively short time to achieve this goal as well as position oneself to successfully transition to a faculty position or private practice, which is the second objective—and area for mentoring."
Dr. Shelstad acknowledges and explains the transition in his mentorship needs, "I think earlier in training, mentorship focused on career choice, research, and transition to a fellowship. Much was focused on getting to the next step. While that is still important, now is the time to focus on the clinical aspects of CT surgery that I will use the rest of my career." And, certainly, the specific mentoring needs will continue to change with time.
Dr. Lawton, who holds the rank of professor at Washington University, St. Louis, states that, "after reaching full professor, surgeons need mentoring and sponsoring to reach goals such as dean positions, leadership positions, national organization officer positions, etc. We also all continually need mosaic mentoring that evolves over time (someone to mentor for research career aspects, managing work-life balance issues, family issues, teaching issues, financial issues, etc.). As we progress in our careers, we have the opportunity to also be mentored in other areas by younger generations."
Wait, did she just say that progressing surgeons can be mentored by younger generations? Yes, she did. And not only can seasoned surgeons be mentored by younger surgeons, they also stand to gain considerably from their own mentees. Dr. Lawton further states, "There is always reciprocal gain in a mentoring relationship for the mentor. There is no better joy than to see a mentee succeed and be fulfilled and happy in her chosen field. For some, this provides a rich legacy of trainees and mentees to provide continued enrichment, excitement, and a source of tremendous pride in later years." In the previously mentioned article by Grondin, Dr. Gail Darling states, "Academic careers are usually measured in papers published, grants awarded, invited lectures, and academic standing. Equally important are the students we teach and motivate toward careers in surgery, residents and fellows we have taught and mentored who will provide care to patients and who will go out and teach new generations of surgeons who will in turn provide care."
Once mentorship bonds have been established, it is critical to cultivate these relationships and to gain the most possible from these interactions. When asked how he has achieved these ends, Dr. Shelstad replies, "You and your mentors have the same goal: mutual success. Work hard for your mentors, and they will work hard for you. I would encourage explicit discussion of goals and expectations to ensure you and a potential mentor are on the same page. Mentorship is essential to success in cardiothoracic surgery."
Without a doubt, participation in mentorship relationships is a key element of success at every stage of the career and development of a cardiothoracic surgeon. Outstanding programs already exist to support modern trainees, and further efforts will certainly be met with great enthusiasm. Also apparent is the need for ongoing, career-long mentorship – and the paucity of formal programs to support it. This need may be a great opportunity for the establishment of future programming.
On a personal note, when reflecting on mentorship, I think of a statement made by Benjamin Franklin: "Tell me and I forget, teach me and I may remember, involve me and I learn." To those incredible individuals who have taken the time, effort, and interest to truly involve me, I have immense gratitude. I will aim for the rest of my career to make it worth your while, with hopes to bring you pride and inspire others as you have inspired me. To all who have taken time to truly involve any student, resident, or junior colleague – you have motivated us and given strength to the ongoing legacy of our amazing field.
Citations
1. Grondin SC. Building a Successful Career: Advice From Leaders in Thoracic Surgery. Thorac. Surg. Clin. 2011;21(3):395-415.
2. J. Thorac. Cardiovasc. Surg. 2014;147(1):15-17.

Attendings in 'simultaneous' ORs
TORONTO – In academic medical centers, attending cardiothoracic surgeons often perform simultaneous procedures in different operating rooms as a means of increasing training opportunities for surgical fellows and to decrease hospital costs. However, the practice of running simultaneous operating rooms did not appear to affect perioperative timing or negatively affect patient outcomes, according to the results of a single institution review by Dr. Kenan W. Yount.
He and his colleagues at the University of Virginia, Charlottesville, wanted to examine their own data in guiding hospital policy as several major centers have recently proposed implementing a 1:1 ratio of attending surgeon-to-operating room.

In his presentation, Dr. Yount discussed the results of their review study, which categorized 1,377 cardiac and 1,682 general thoracic operations performed from July 2011 to July 2013 by attending, case type, and whether the attending was simultaneously supervising two surgeries. "Our institution adheres to a strict policy of attending surgeon oversight of and involvement in the critical and key portions of all operations," said Dr. Yount.
They compared operative duration, starting and closing times, postoperative complications, and 30-day mortality in each category. They also compared rates postoperative complications, hospital length of stay, and operative mortality in each category.
Interestingly, timing effects varied between the two overall types of surgery. Running two rooms had no effect on room start times, but thoracic rooms finished 16 minutes later than scheduled. Across six surgeons and 15 operation types, however, there were no differences in operative times.
"Furthermore, running two rooms was not associated with any differences in operative duration, morbidity, or mortality in our multivariate regression analyses, and there were no statistically significant differences in observed outcomes in any category," Dr. Yount said.
"In academic cardiothoracic surgical centers that rely on surgical support from fellowship training, the practice of running simultaneous operating rooms can be efficient and does not appear to negatively impact patient outcomes," said Dr. Yount. "In addition, the practice did not significantly increase operative duration or dramatically [affect] operating room starting or closing times," he concluded.
In discussing the implications of these results, he said, "Obviously, there are caveats: Attendings must be intimately involved in operations and scrubbed for every key and critical portion of the operation; also operations being scheduled in separate rooms must be done so with reasonable foresight."
As long as institutions are following these practices, he concluded, "It would appear that lens of current policy efforts is too narrow by focusing on perception. The debate should be refocused by challenging training programs to strengthen attending involvement and ensure the requisite competence of their trainees."
Dr. Yount reported no relevant disclosures.
TORONTO – In academic medical centers, attending cardiothoracic surgeons often perform simultaneous procedures in different operating rooms as a means of increasing training opportunities for surgical fellows and to decrease hospital costs. However, the practice of running simultaneous operating rooms did not appear to affect perioperative timing or negatively affect patient outcomes, according to the results of a single institution review by Dr. Kenan W. Yount.
He and his colleagues at the University of Virginia, Charlottesville, wanted to examine their own data in guiding hospital policy as several major centers have recently proposed implementing a 1:1 ratio of attending surgeon-to-operating room.
In his presentation, Dr. Yount discussed the results of their review study, which categorized 1,377 cardiac and 1,682 general thoracic operations performed from July 2011 to July 2013 by attending, case type, and whether the attending was simultaneously supervising two surgeries. "Our institution adheres to a strict policy of attending surgeon oversight of and involvement in the critical and key portions of all operations," said Dr. Yount.
They compared operative duration, starting and closing times, postoperative complications, and 30-day mortality in each category. They also compared rates postoperative complications, hospital length of stay, and operative mortality in each category.
Interestingly, timing effects varied between the two overall types of surgery. Running two rooms had no effect on room start times, but thoracic rooms finished 16 minutes later than scheduled. Across six surgeons and 15 operation types, however, there were no differences in operative times.
"Furthermore, running two rooms was not associated with any differences in operative duration, morbidity, or mortality in our multivariate regression analyses, and there were no statistically significant differences in observed outcomes in any category," Dr. Yount said.
"In academic cardiothoracic surgical centers that rely on surgical support from fellowship training, the practice of running simultaneous operating rooms can be efficient and does not appear to negatively impact patient outcomes," said Dr. Yount. "In addition, the practice did not significantly increase operative duration or dramatically [affect] operating room starting or closing times," he concluded.
In discussing the implications of these results, he said, "Obviously, there are caveats: Attendings must be intimately involved in operations and scrubbed for every key and critical portion of the operation; also operations being scheduled in separate rooms must be done so with reasonable foresight."
As long as institutions are following these practices, he concluded, "It would appear that lens of current policy efforts is too narrow by focusing on perception. The debate should be refocused by challenging training programs to strengthen attending involvement and ensure the requisite competence of their trainees."
Dr. Yount reported no relevant disclosures.
TORONTO – In academic medical centers, attending cardiothoracic surgeons often perform simultaneous procedures in different operating rooms as a means of increasing training opportunities for surgical fellows and to decrease hospital costs. However, the practice of running simultaneous operating rooms did not appear to affect perioperative timing or negatively affect patient outcomes, according to the results of a single institution review by Dr. Kenan W. Yount.
He and his colleagues at the University of Virginia, Charlottesville, wanted to examine their own data in guiding hospital policy as several major centers have recently proposed implementing a 1:1 ratio of attending surgeon-to-operating room.
In his presentation, Dr. Yount discussed the results of their review study, which categorized 1,377 cardiac and 1,682 general thoracic operations performed from July 2011 to July 2013 by attending, case type, and whether the attending was simultaneously supervising two surgeries. "Our institution adheres to a strict policy of attending surgeon oversight of and involvement in the critical and key portions of all operations," said Dr. Yount.
They compared operative duration, starting and closing times, postoperative complications, and 30-day mortality in each category. They also compared rates postoperative complications, hospital length of stay, and operative mortality in each category.
Interestingly, timing effects varied between the two overall types of surgery. Running two rooms had no effect on room start times, but thoracic rooms finished 16 minutes later than scheduled. Across six surgeons and 15 operation types, however, there were no differences in operative times.
"Furthermore, running two rooms was not associated with any differences in operative duration, morbidity, or mortality in our multivariate regression analyses, and there were no statistically significant differences in observed outcomes in any category," Dr. Yount said.
"In academic cardiothoracic surgical centers that rely on surgical support from fellowship training, the practice of running simultaneous operating rooms can be efficient and does not appear to negatively impact patient outcomes," said Dr. Yount. "In addition, the practice did not significantly increase operative duration or dramatically [affect] operating room starting or closing times," he concluded.
In discussing the implications of these results, he said, "Obviously, there are caveats: Attendings must be intimately involved in operations and scrubbed for every key and critical portion of the operation; also operations being scheduled in separate rooms must be done so with reasonable foresight."
As long as institutions are following these practices, he concluded, "It would appear that lens of current policy efforts is too narrow by focusing on perception. The debate should be refocused by challenging training programs to strengthen attending involvement and ensure the requisite competence of their trainees."
Dr. Yount reported no relevant disclosures.
Major finding: Running two rooms was not associated with any differences in operative duration, morbidity, or mortality in multivariate regression analyses, and there were no statistically significant differences in observed outcomes in any category.
Data source: The study reviewed 1,377 cardiac and 1682 general thoracic operations performed from July 2011 to July 2013 by attending, case type, and whether the attending was simultaneously supervising two surgeries.
Disclosures: Dr. Yount had no disclosures.

Training for minimally invasive cardiac surgery
Minimally invasive cardiac surgery has experienced a meteoric rise since its development in the 1990s. The first thoracic aortic stent graft was placed in July 1992, at Stanford (Calif.) University. Five years later, the Stanford group published their approach to mitral valve surgery through a right anterior thoracotomy. Just a year later, Dr. Alain Carpentier performed the first robotic-assisted mitral valve operation.1 There has been an explosion of new techniques, broadening the cardiac surgeon’s armamentarium far beyond the typical median sternotomy and occasional left thoracotomy.

While many of these techniques will undoubtedly become historical footnotes, it is clear that minimally invasive cardiac surgery is here to stay, as 20% of mitral repairs are performed with some element of minimally invasive technique. Similarly, thoracic endovascular aortic repair has become a well-established treatment for aneurysmal disease and dissection of the thoracic aorta, and is rapidly catching up with open repair as the treatment of choice.2
Training has also changed. The last decade brought a surge of applications to traditional fellowship programs, and the integrated thoracic surgery programs graduated their first trainees last year. With the variety of new operations and techniques, novel training formats, and professional goals for cardiothoracic surgery trainees, how can we be sure that young cardiac surgeons are learning the skills they need to succeed in the coming decades?
To ask how new surgeons should learn, you must start by asking what needs to be learned. After I asked a number of different surgeons in a variety of practice set-ups, the answer became obvious, and it is deceptively basic. The purpose of training is simply to ensure that each trainee can do all of the commonly performed operations of their specialty. This includes open valve and coronary surgery on the cardiac side, while for thoracic surgery, this includes all of the traditional lung and esophageal resections, chest wall and pleural operations, and importantly, the widely practiced VATS lobectomy. When I asked about more advanced VATS skills and minimally invasive cardiac skills, I was always told that those would be icing on the cake, as it were, to make a graduate more valuable to a potential employer. The first step in learning a minimally invasive operation is to understand the traditional, open approach, and VATS lung surgery is no different.
The VATS lobectomy has been a recent but well-received addition to the expected repertoire of graduates, and Dr. Chadrick Denlinger, associate professor of surgery at the Medical University of South Carolina, Charleston, allows his chief residents to take other trainees through the case, and expects that all new graduates can do one. Across the coast, Dr. Joseph Woo, newly appointed chair of cardiovascular surgery at Stanford, agrees. This expectation alone informs us that our specialty is dynamic and that the definition of an essential skill is in constant flux. On the other hand, cardiac surgery has no touchstone or standard minimally invasive procedure. However, Dr. Woo explains, the ABTS has set its recommendations in anticipation of the continued success of minimally invasive approaches to cardiovascular problems. The board doesn’t require mastery of any specific minimally invasive cardiac operation by the end of a training program, but it does require that we are exposed to a number of different endovascular and nontraditional approaches to coronary, valve, and aortic surgery. Coupled with our presumed mastery of the standard, open operations, we should then have the basic skills necessary to learn whatever minimally invasive operations we like, depending on our interests and our post-training mentorship.
Of course, the safety and efficacy of thoracic aortic stent grafting and minimally invasive mitral surgery have already been proven to some degree, and the operations aren’t going away anytime soon.3,4 So what is stopping us from learning this stuff during our training? The answer is complicated. Dr. Woo cites the lack of visualization for two surgeons, the difficulty in preventing and controlling technical complications in a limited field, and the very nature the operations themselves.
Take, for example, the minimally invasive mitral valve repair. Its open counterpart requires a skill set that few trainees, if any, can claim mastery of until the very end of their training. The skill required, patient selection, and pathology treated make the operation sort of a "boutique" treatment. The patients that are offered right thoracotomy approach tend to be younger, less symptomatic, and with less complex disease. They have higher expectations. As Dr. Woo put it, "if you perform an absolutely perfect repair, then you’ve only done your job. But there is no way to do any better." With that sort of standard, many attending surgeons are hesitant to hand over the instruments to a trainee. Furthermore, not every resident’s technical ability lines up with what is required of that interest, and more importantly, not every resident is interested. Because of the highly specialized nature of the operation, the relatively smaller patient base, and the technical difficulty involved, it is often up to the highly motivated fellow or resident to gravitate to these repairs and seek out the training on their own.
Dr. James Fann, cofounder of the annual TSDA boot camp and a national surgical education leader, has some perspective on the matter. If residents are interested in gaining added endovascular or minimally invasive skills, he suggests, they first have to prove themselves in the operating room. When they’ve mastered the skills for an open technique and have proven they can get out of trouble, then an attending might feel comfortable letting them take on these more complex cases. It takes a combination of skill and interest – and as only a minority of trainees will have both, most training programs do not require that every TEVAR or mini-mitral be staffed with a resident.
It seems that simulation does not provide an easy shortcut beyond this approach, though it does have a role. To be honest, I expected Dr. Fann to preach the simulation gospel, and tell me about some incredible TEVAR or TAVR simulator he was getting ready to unveil, but his response was far more measured. "The role of simulation," he said, "is not to teach a resident how to operate. It is an adjunct – a tool that can be used to identify and address specific technical issues outside of the operating room." He reinforced the importance of mastering traditional surgical techniques before embarking on miniaturization. Simulation can help trainees operate more efficiently and effectively, but it cannot and should not replace mentored operative experience.
MICS simulation does exist, as anyone who has worked with Dr. L. Wiley Nifong and Dr. Randolph Chitwood’s high-fidelity tissue simulators for minimally invasive mitral valve repair knows. Simbionix USA (Cleveland) has just obtained FDA clearance for its TEVAR simulator that can be tailored to rehearse an upcoming case using a patient’s CT scan. On the lower end of the cost spectrum, a Dutch group and a separate Hannover group have developed low-cost, reproducible models of mini-mitral surgery that can be built from materials from a hardware store.5 Again, all of these tools are designed to be adjuncts to experiential training and mentorship, not mentors in and of themselves.
Residents can and should be exposed to TEVAR, TAVR, mini-mitral repair, and other less invasive approaches that are offered at their institution if they are interested. These, along with any other skills beyond traditional open techniques, make the surgeon better. More importantly, they help the trainee gain the basic wire and small incision skills they will need to learn quickly any newly developed operations that the changing specialty requires. They may not master the skills as a resident, but they are that much more prepared to hone those skills with their mentors when that time comes. In fact, the faculty I spoke with placed far more emphasis on mentorship after residency than aggressive residency training, simulation, and superfellowship as the key to gaining these advanced skills. Trainees should be soaking up all of the skills that they possibly can while they can, and if one is smart, ambitious, and skilled enough to become technically proficient at a more technically advanced skill, it certainly makes them a more desirable surgeon. For most of us, however, it is more important to realize that the training never truly ends, to take advantage of the opportunities afforded by residency, and to continue getting those reps in the OR.
References
1. Cardiac Surgery in the Adult, 4e. New York, N.Y.: McGraw-Hill; 2012.
2. J. Thorac. Cardiovasc. Surg. 2012; 144:612-16.
3. Circulation 2013;6:407-16.
4. Ann. Cardiothorac. Surg. 2013;2:744-50.
5. Interact. Cardiovasc. Thorac. Surg. 2013;16:97-101.
Minimally invasive cardiac surgery has experienced a meteoric rise since its development in the 1990s. The first thoracic aortic stent graft was placed in July 1992, at Stanford (Calif.) University. Five years later, the Stanford group published their approach to mitral valve surgery through a right anterior thoracotomy. Just a year later, Dr. Alain Carpentier performed the first robotic-assisted mitral valve operation.1 There has been an explosion of new techniques, broadening the cardiac surgeon’s armamentarium far beyond the typical median sternotomy and occasional left thoracotomy.
While many of these techniques will undoubtedly become historical footnotes, it is clear that minimally invasive cardiac surgery is here to stay, as 20% of mitral repairs are performed with some element of minimally invasive technique. Similarly, thoracic endovascular aortic repair has become a well-established treatment for aneurysmal disease and dissection of the thoracic aorta, and is rapidly catching up with open repair as the treatment of choice.2
Training has also changed. The last decade brought a surge of applications to traditional fellowship programs, and the integrated thoracic surgery programs graduated their first trainees last year. With the variety of new operations and techniques, novel training formats, and professional goals for cardiothoracic surgery trainees, how can we be sure that young cardiac surgeons are learning the skills they need to succeed in the coming decades?
To ask how new surgeons should learn, you must start by asking what needs to be learned. After I asked a number of different surgeons in a variety of practice set-ups, the answer became obvious, and it is deceptively basic. The purpose of training is simply to ensure that each trainee can do all of the commonly performed operations of their specialty. This includes open valve and coronary surgery on the cardiac side, while for thoracic surgery, this includes all of the traditional lung and esophageal resections, chest wall and pleural operations, and importantly, the widely practiced VATS lobectomy. When I asked about more advanced VATS skills and minimally invasive cardiac skills, I was always told that those would be icing on the cake, as it were, to make a graduate more valuable to a potential employer. The first step in learning a minimally invasive operation is to understand the traditional, open approach, and VATS lung surgery is no different.
The VATS lobectomy has been a recent but well-received addition to the expected repertoire of graduates, and Dr. Chadrick Denlinger, associate professor of surgery at the Medical University of South Carolina, Charleston, allows his chief residents to take other trainees through the case, and expects that all new graduates can do one. Across the coast, Dr. Joseph Woo, newly appointed chair of cardiovascular surgery at Stanford, agrees. This expectation alone informs us that our specialty is dynamic and that the definition of an essential skill is in constant flux. On the other hand, cardiac surgery has no touchstone or standard minimally invasive procedure. However, Dr. Woo explains, the ABTS has set its recommendations in anticipation of the continued success of minimally invasive approaches to cardiovascular problems. The board doesn’t require mastery of any specific minimally invasive cardiac operation by the end of a training program, but it does require that we are exposed to a number of different endovascular and nontraditional approaches to coronary, valve, and aortic surgery. Coupled with our presumed mastery of the standard, open operations, we should then have the basic skills necessary to learn whatever minimally invasive operations we like, depending on our interests and our post-training mentorship.
Of course, the safety and efficacy of thoracic aortic stent grafting and minimally invasive mitral surgery have already been proven to some degree, and the operations aren’t going away anytime soon.3,4 So what is stopping us from learning this stuff during our training? The answer is complicated. Dr. Woo cites the lack of visualization for two surgeons, the difficulty in preventing and controlling technical complications in a limited field, and the very nature the operations themselves.
Take, for example, the minimally invasive mitral valve repair. Its open counterpart requires a skill set that few trainees, if any, can claim mastery of until the very end of their training. The skill required, patient selection, and pathology treated make the operation sort of a "boutique" treatment. The patients that are offered right thoracotomy approach tend to be younger, less symptomatic, and with less complex disease. They have higher expectations. As Dr. Woo put it, "if you perform an absolutely perfect repair, then you’ve only done your job. But there is no way to do any better." With that sort of standard, many attending surgeons are hesitant to hand over the instruments to a trainee. Furthermore, not every resident’s technical ability lines up with what is required of that interest, and more importantly, not every resident is interested. Because of the highly specialized nature of the operation, the relatively smaller patient base, and the technical difficulty involved, it is often up to the highly motivated fellow or resident to gravitate to these repairs and seek out the training on their own.
Dr. James Fann, cofounder of the annual TSDA boot camp and a national surgical education leader, has some perspective on the matter. If residents are interested in gaining added endovascular or minimally invasive skills, he suggests, they first have to prove themselves in the operating room. When they’ve mastered the skills for an open technique and have proven they can get out of trouble, then an attending might feel comfortable letting them take on these more complex cases. It takes a combination of skill and interest – and as only a minority of trainees will have both, most training programs do not require that every TEVAR or mini-mitral be staffed with a resident.
It seems that simulation does not provide an easy shortcut beyond this approach, though it does have a role. To be honest, I expected Dr. Fann to preach the simulation gospel, and tell me about some incredible TEVAR or TAVR simulator he was getting ready to unveil, but his response was far more measured. "The role of simulation," he said, "is not to teach a resident how to operate. It is an adjunct – a tool that can be used to identify and address specific technical issues outside of the operating room." He reinforced the importance of mastering traditional surgical techniques before embarking on miniaturization. Simulation can help trainees operate more efficiently and effectively, but it cannot and should not replace mentored operative experience.
MICS simulation does exist, as anyone who has worked with Dr. L. Wiley Nifong and Dr. Randolph Chitwood’s high-fidelity tissue simulators for minimally invasive mitral valve repair knows. Simbionix USA (Cleveland) has just obtained FDA clearance for its TEVAR simulator that can be tailored to rehearse an upcoming case using a patient’s CT scan. On the lower end of the cost spectrum, a Dutch group and a separate Hannover group have developed low-cost, reproducible models of mini-mitral surgery that can be built from materials from a hardware store.5 Again, all of these tools are designed to be adjuncts to experiential training and mentorship, not mentors in and of themselves.
Residents can and should be exposed to TEVAR, TAVR, mini-mitral repair, and other less invasive approaches that are offered at their institution if they are interested. These, along with any other skills beyond traditional open techniques, make the surgeon better. More importantly, they help the trainee gain the basic wire and small incision skills they will need to learn quickly any newly developed operations that the changing specialty requires. They may not master the skills as a resident, but they are that much more prepared to hone those skills with their mentors when that time comes. In fact, the faculty I spoke with placed far more emphasis on mentorship after residency than aggressive residency training, simulation, and superfellowship as the key to gaining these advanced skills. Trainees should be soaking up all of the skills that they possibly can while they can, and if one is smart, ambitious, and skilled enough to become technically proficient at a more technically advanced skill, it certainly makes them a more desirable surgeon. For most of us, however, it is more important to realize that the training never truly ends, to take advantage of the opportunities afforded by residency, and to continue getting those reps in the OR.
References
1. Cardiac Surgery in the Adult, 4e. New York, N.Y.: McGraw-Hill; 2012.
2. J. Thorac. Cardiovasc. Surg. 2012; 144:612-16.
3. Circulation 2013;6:407-16.
4. Ann. Cardiothorac. Surg. 2013;2:744-50.
5. Interact. Cardiovasc. Thorac. Surg. 2013;16:97-101.
Minimally invasive cardiac surgery has experienced a meteoric rise since its development in the 1990s. The first thoracic aortic stent graft was placed in July 1992, at Stanford (Calif.) University. Five years later, the Stanford group published their approach to mitral valve surgery through a right anterior thoracotomy. Just a year later, Dr. Alain Carpentier performed the first robotic-assisted mitral valve operation.1 There has been an explosion of new techniques, broadening the cardiac surgeon’s armamentarium far beyond the typical median sternotomy and occasional left thoracotomy.
While many of these techniques will undoubtedly become historical footnotes, it is clear that minimally invasive cardiac surgery is here to stay, as 20% of mitral repairs are performed with some element of minimally invasive technique. Similarly, thoracic endovascular aortic repair has become a well-established treatment for aneurysmal disease and dissection of the thoracic aorta, and is rapidly catching up with open repair as the treatment of choice.2
Training has also changed. The last decade brought a surge of applications to traditional fellowship programs, and the integrated thoracic surgery programs graduated their first trainees last year. With the variety of new operations and techniques, novel training formats, and professional goals for cardiothoracic surgery trainees, how can we be sure that young cardiac surgeons are learning the skills they need to succeed in the coming decades?
To ask how new surgeons should learn, you must start by asking what needs to be learned. After I asked a number of different surgeons in a variety of practice set-ups, the answer became obvious, and it is deceptively basic. The purpose of training is simply to ensure that each trainee can do all of the commonly performed operations of their specialty. This includes open valve and coronary surgery on the cardiac side, while for thoracic surgery, this includes all of the traditional lung and esophageal resections, chest wall and pleural operations, and importantly, the widely practiced VATS lobectomy. When I asked about more advanced VATS skills and minimally invasive cardiac skills, I was always told that those would be icing on the cake, as it were, to make a graduate more valuable to a potential employer. The first step in learning a minimally invasive operation is to understand the traditional, open approach, and VATS lung surgery is no different.
The VATS lobectomy has been a recent but well-received addition to the expected repertoire of graduates, and Dr. Chadrick Denlinger, associate professor of surgery at the Medical University of South Carolina, Charleston, allows his chief residents to take other trainees through the case, and expects that all new graduates can do one. Across the coast, Dr. Joseph Woo, newly appointed chair of cardiovascular surgery at Stanford, agrees. This expectation alone informs us that our specialty is dynamic and that the definition of an essential skill is in constant flux. On the other hand, cardiac surgery has no touchstone or standard minimally invasive procedure. However, Dr. Woo explains, the ABTS has set its recommendations in anticipation of the continued success of minimally invasive approaches to cardiovascular problems. The board doesn’t require mastery of any specific minimally invasive cardiac operation by the end of a training program, but it does require that we are exposed to a number of different endovascular and nontraditional approaches to coronary, valve, and aortic surgery. Coupled with our presumed mastery of the standard, open operations, we should then have the basic skills necessary to learn whatever minimally invasive operations we like, depending on our interests and our post-training mentorship.
Of course, the safety and efficacy of thoracic aortic stent grafting and minimally invasive mitral surgery have already been proven to some degree, and the operations aren’t going away anytime soon.3,4 So what is stopping us from learning this stuff during our training? The answer is complicated. Dr. Woo cites the lack of visualization for two surgeons, the difficulty in preventing and controlling technical complications in a limited field, and the very nature the operations themselves.
Take, for example, the minimally invasive mitral valve repair. Its open counterpart requires a skill set that few trainees, if any, can claim mastery of until the very end of their training. The skill required, patient selection, and pathology treated make the operation sort of a "boutique" treatment. The patients that are offered right thoracotomy approach tend to be younger, less symptomatic, and with less complex disease. They have higher expectations. As Dr. Woo put it, "if you perform an absolutely perfect repair, then you’ve only done your job. But there is no way to do any better." With that sort of standard, many attending surgeons are hesitant to hand over the instruments to a trainee. Furthermore, not every resident’s technical ability lines up with what is required of that interest, and more importantly, not every resident is interested. Because of the highly specialized nature of the operation, the relatively smaller patient base, and the technical difficulty involved, it is often up to the highly motivated fellow or resident to gravitate to these repairs and seek out the training on their own.
Dr. James Fann, cofounder of the annual TSDA boot camp and a national surgical education leader, has some perspective on the matter. If residents are interested in gaining added endovascular or minimally invasive skills, he suggests, they first have to prove themselves in the operating room. When they’ve mastered the skills for an open technique and have proven they can get out of trouble, then an attending might feel comfortable letting them take on these more complex cases. It takes a combination of skill and interest – and as only a minority of trainees will have both, most training programs do not require that every TEVAR or mini-mitral be staffed with a resident.
It seems that simulation does not provide an easy shortcut beyond this approach, though it does have a role. To be honest, I expected Dr. Fann to preach the simulation gospel, and tell me about some incredible TEVAR or TAVR simulator he was getting ready to unveil, but his response was far more measured. "The role of simulation," he said, "is not to teach a resident how to operate. It is an adjunct – a tool that can be used to identify and address specific technical issues outside of the operating room." He reinforced the importance of mastering traditional surgical techniques before embarking on miniaturization. Simulation can help trainees operate more efficiently and effectively, but it cannot and should not replace mentored operative experience.
MICS simulation does exist, as anyone who has worked with Dr. L. Wiley Nifong and Dr. Randolph Chitwood’s high-fidelity tissue simulators for minimally invasive mitral valve repair knows. Simbionix USA (Cleveland) has just obtained FDA clearance for its TEVAR simulator that can be tailored to rehearse an upcoming case using a patient’s CT scan. On the lower end of the cost spectrum, a Dutch group and a separate Hannover group have developed low-cost, reproducible models of mini-mitral surgery that can be built from materials from a hardware store.5 Again, all of these tools are designed to be adjuncts to experiential training and mentorship, not mentors in and of themselves.
Residents can and should be exposed to TEVAR, TAVR, mini-mitral repair, and other less invasive approaches that are offered at their institution if they are interested. These, along with any other skills beyond traditional open techniques, make the surgeon better. More importantly, they help the trainee gain the basic wire and small incision skills they will need to learn quickly any newly developed operations that the changing specialty requires. They may not master the skills as a resident, but they are that much more prepared to hone those skills with their mentors when that time comes. In fact, the faculty I spoke with placed far more emphasis on mentorship after residency than aggressive residency training, simulation, and superfellowship as the key to gaining these advanced skills. Trainees should be soaking up all of the skills that they possibly can while they can, and if one is smart, ambitious, and skilled enough to become technically proficient at a more technically advanced skill, it certainly makes them a more desirable surgeon. For most of us, however, it is more important to realize that the training never truly ends, to take advantage of the opportunities afforded by residency, and to continue getting those reps in the OR.
References
1. Cardiac Surgery in the Adult, 4e. New York, N.Y.: McGraw-Hill; 2012.
2. J. Thorac. Cardiovasc. Surg. 2012; 144:612-16.
3. Circulation 2013;6:407-16.
4. Ann. Cardiothorac. Surg. 2013;2:744-50.
5. Interact. Cardiovasc. Thorac. Surg. 2013;16:97-101.

TSRA - Advocates for the CT Surgical Trainee
The Thoracic Surgery Residents Association currently serves as the largest, official representative organization for cardiothoracic surgery trainees in the United States. The mission of the TSRA is to represent the interest of all cardiothoracic surgery residents through the improvement of thoracic surgery education and partnership with the Thoracic Surgery Directors Association (TSDA). Resident membership in the TSRA commences upon enrollment in an Accreditation Council of Graduate Medical Education (ACGME) accredited thoracic surgery residency program and remains until completion of thoracic residency or subsequent advanced fellowship training. The TSRA also provides resident representation directly to several important national organizations, including the American Association for Thoracic Surgery (AATS), Society of Thoracic Surgeons (STS), Joint Council for Thoracic Surgical Education, American Association of Medical Colleges, ACGME, Thoracic Surgery Residency Review Committee, and CTSNet.
The TSRA organizes two exciting resident forums held during the annual AATS and STS meetings. These forums provide direct interaction between residents, invited speakers, and representatives of the AATS, STS, and TSDA. All residents attending the conferences are invited and encouraged to attend and participate.
The TSRA values professional mentorship. Thus, each year, the TSRA formally recognizes surgeons who have made outstanding contributions to cardiothoracic surgery education. The Socrates Award is presented to a surgical educator who has demonstrated a significant commitment to excellence in resident education. The Dr. Dwight C. McGoon Award is presented to an individual who has significantly contributed to the clinical and educational development of thoracic surgery residents through inspiring academic and political contributions to the specialty.
The TSRA has taken leadership in the development of several new and exciting projects designed to facilitate and compliment resident education. Through the contribution of hundreds of different thoracic surgical trainees across the United States, the TSRA has produced a series of resources to assist residents in their training and board preparation. Our flagship project culminated in the publishing of the TSRA Review of Cardiothoracic Surgery, which has now been in circulation for over three years. Available in both print and electronic media, this review source has been utilized by CT residents not only in the United States, but also in several other countries as well. Last spring, the TSRA continued these efforts with the publishing of the 2nd and 3rd installments of our cardiothoracic surgical review series, TSRA Primer of Cardiothoracic Surgery and TSRA Clinical Scenarios in Cardiothoracic Surgery. TSRA Primer is an exciting, multimedia-based resource designed for Junior level CT residents and beginning fellows focused upon enhancing an underlying foundation of basic cardiothoracic surgical knowledge. TSRA Clinical Scenarios provides the first available, comprehensive review designed to assist residents to work through common clinical scenarios encountered in CT training, clinical practice, and on the oral boards.
This spring, the TSRA will launch the new TSRA Operative Dictations in Cardiothoracic Surgery, a review of key operative indications and steps for a variety of adult cardiac, general thoracic, and congenital operations as well example templates to assist in operative dictations, and the TSRA Journal Club, an online resource that offers residents an easily accessible library of seminal and current journal articles in the areas of cardiac, thoracic, and congenital heart surgery.
The TSRA is an entirely resident run organization that strongly encourages the active participation of all CT surgical trainees. To learn more about our organization, visit our webpage (www.tsranet.org) and/or on visit us on Facebook (www.facebook.com/thoracicsurgeryresidentsassociation).
The Thoracic Surgery Residents Association currently serves as the largest, official representative organization for cardiothoracic surgery trainees in the United States. The mission of the TSRA is to represent the interest of all cardiothoracic surgery residents through the improvement of thoracic surgery education and partnership with the Thoracic Surgery Directors Association (TSDA). Resident membership in the TSRA commences upon enrollment in an Accreditation Council of Graduate Medical Education (ACGME) accredited thoracic surgery residency program and remains until completion of thoracic residency or subsequent advanced fellowship training. The TSRA also provides resident representation directly to several important national organizations, including the American Association for Thoracic Surgery (AATS), Society of Thoracic Surgeons (STS), Joint Council for Thoracic Surgical Education, American Association of Medical Colleges, ACGME, Thoracic Surgery Residency Review Committee, and CTSNet.
The TSRA organizes two exciting resident forums held during the annual AATS and STS meetings. These forums provide direct interaction between residents, invited speakers, and representatives of the AATS, STS, and TSDA. All residents attending the conferences are invited and encouraged to attend and participate.
The TSRA values professional mentorship. Thus, each year, the TSRA formally recognizes surgeons who have made outstanding contributions to cardiothoracic surgery education. The Socrates Award is presented to a surgical educator who has demonstrated a significant commitment to excellence in resident education. The Dr. Dwight C. McGoon Award is presented to an individual who has significantly contributed to the clinical and educational development of thoracic surgery residents through inspiring academic and political contributions to the specialty.
The TSRA has taken leadership in the development of several new and exciting projects designed to facilitate and compliment resident education. Through the contribution of hundreds of different thoracic surgical trainees across the United States, the TSRA has produced a series of resources to assist residents in their training and board preparation. Our flagship project culminated in the publishing of the TSRA Review of Cardiothoracic Surgery, which has now been in circulation for over three years. Available in both print and electronic media, this review source has been utilized by CT residents not only in the United States, but also in several other countries as well. Last spring, the TSRA continued these efforts with the publishing of the 2nd and 3rd installments of our cardiothoracic surgical review series, TSRA Primer of Cardiothoracic Surgery and TSRA Clinical Scenarios in Cardiothoracic Surgery. TSRA Primer is an exciting, multimedia-based resource designed for Junior level CT residents and beginning fellows focused upon enhancing an underlying foundation of basic cardiothoracic surgical knowledge. TSRA Clinical Scenarios provides the first available, comprehensive review designed to assist residents to work through common clinical scenarios encountered in CT training, clinical practice, and on the oral boards.
This spring, the TSRA will launch the new TSRA Operative Dictations in Cardiothoracic Surgery, a review of key operative indications and steps for a variety of adult cardiac, general thoracic, and congenital operations as well example templates to assist in operative dictations, and the TSRA Journal Club, an online resource that offers residents an easily accessible library of seminal and current journal articles in the areas of cardiac, thoracic, and congenital heart surgery.
The TSRA is an entirely resident run organization that strongly encourages the active participation of all CT surgical trainees. To learn more about our organization, visit our webpage (www.tsranet.org) and/or on visit us on Facebook (www.facebook.com/thoracicsurgeryresidentsassociation).
The Thoracic Surgery Residents Association currently serves as the largest, official representative organization for cardiothoracic surgery trainees in the United States. The mission of the TSRA is to represent the interest of all cardiothoracic surgery residents through the improvement of thoracic surgery education and partnership with the Thoracic Surgery Directors Association (TSDA). Resident membership in the TSRA commences upon enrollment in an Accreditation Council of Graduate Medical Education (ACGME) accredited thoracic surgery residency program and remains until completion of thoracic residency or subsequent advanced fellowship training. The TSRA also provides resident representation directly to several important national organizations, including the American Association for Thoracic Surgery (AATS), Society of Thoracic Surgeons (STS), Joint Council for Thoracic Surgical Education, American Association of Medical Colleges, ACGME, Thoracic Surgery Residency Review Committee, and CTSNet.
The TSRA organizes two exciting resident forums held during the annual AATS and STS meetings. These forums provide direct interaction between residents, invited speakers, and representatives of the AATS, STS, and TSDA. All residents attending the conferences are invited and encouraged to attend and participate.
The TSRA values professional mentorship. Thus, each year, the TSRA formally recognizes surgeons who have made outstanding contributions to cardiothoracic surgery education. The Socrates Award is presented to a surgical educator who has demonstrated a significant commitment to excellence in resident education. The Dr. Dwight C. McGoon Award is presented to an individual who has significantly contributed to the clinical and educational development of thoracic surgery residents through inspiring academic and political contributions to the specialty.
The TSRA has taken leadership in the development of several new and exciting projects designed to facilitate and compliment resident education. Through the contribution of hundreds of different thoracic surgical trainees across the United States, the TSRA has produced a series of resources to assist residents in their training and board preparation. Our flagship project culminated in the publishing of the TSRA Review of Cardiothoracic Surgery, which has now been in circulation for over three years. Available in both print and electronic media, this review source has been utilized by CT residents not only in the United States, but also in several other countries as well. Last spring, the TSRA continued these efforts with the publishing of the 2nd and 3rd installments of our cardiothoracic surgical review series, TSRA Primer of Cardiothoracic Surgery and TSRA Clinical Scenarios in Cardiothoracic Surgery. TSRA Primer is an exciting, multimedia-based resource designed for Junior level CT residents and beginning fellows focused upon enhancing an underlying foundation of basic cardiothoracic surgical knowledge. TSRA Clinical Scenarios provides the first available, comprehensive review designed to assist residents to work through common clinical scenarios encountered in CT training, clinical practice, and on the oral boards.
This spring, the TSRA will launch the new TSRA Operative Dictations in Cardiothoracic Surgery, a review of key operative indications and steps for a variety of adult cardiac, general thoracic, and congenital operations as well example templates to assist in operative dictations, and the TSRA Journal Club, an online resource that offers residents an easily accessible library of seminal and current journal articles in the areas of cardiac, thoracic, and congenital heart surgery.
The TSRA is an entirely resident run organization that strongly encourages the active participation of all CT surgical trainees. To learn more about our organization, visit our webpage (www.tsranet.org) and/or on visit us on Facebook (www.facebook.com/thoracicsurgeryresidentsassociation).
Commentary: Performing clinical research as a CT trainee
"Why do I need to do research if I’m going into private practice anyway?"
I have heard this question multiple times throughout my career as a resident, fellow, and attending thoracic surgeon. The truth is, there are multiple reasons, any of which is sufficient to justify your participation in clinical research during training. First, and perhaps most importantly, it teaches you to critically appraise the literature. This is a skill that will serve you well throughout your career, guiding your clinical decision-making, regardless if you choose private practice or academic surgery. Another reason is that performing clinical research allows you to become a content expert on a specific topic early in your career. This knowledge base is something that will serve as a foundation for ongoing learning and may help in designing future studies. Once your project is complete, it will be your ticket to attend and present at regional, national, or international meetings. There is no better forum to gain public recognition for your investigative efforts and network with potential future partners than societal meetings. Formal and informal interviews routinely occur at these gatherings and you do not want to be left out because you chose not to participate in research as a trainee. Finally, it is your responsibility to the patients that you have sworn to treat. There are many ways to care for patients, and pushing back the frontiers of medical knowledge is as important as the day-to-day tasks that you perform on the ward or in the operating room.

So, now that you have decided that you want to participate in a research project as a trainee, how do you make it happen? Before you begin a project, you will have to choose a mentor, a topic, a clear, novel question, and the appropriate study design. Chances are that at some point, a mentor helped guide you toward a career in cardiothoracic surgery. A research mentor is just as important as a clinical mentor for a young surgeon.
The most important trait that you should seek out in a research mentor is the ability to delineate important questions. All too often, residents and fellows are approached by attending surgeons with good intentions, but bad research ideas. Trainees then feel obligated to take them up on the project (in order to not appear like a slacker) and for various reasons, it does not result in an abstract, presentation, or publication. In fact, all it results in is frustration, a distaste for investigation, and wasted time. The bottom line is that only you can protect your time, and as a surgical trainee, you must guard it ferociously. Look for a mentor who is an expert in your field of interest and who has a track record of publications.
He or she must be a logical thinker who can help you delineate a clear, novel question, choose the appropriate study design, guide your writing of the manuscript, and direct your submission to the appropriate meetings and journals. Finally, your mentor must be dedicated to your success. We are all busy, but if your mentor cannot find the time to routinely meet with you at every step of your project, you need to find a new mentor.
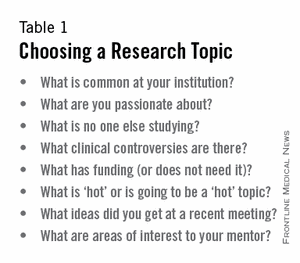
Choosing a clear, novel clinical question starts with choosing an appropriate topic (Table 1). With the right topic and question, the hypothesis is obvious, it is easy to define your endpoints, and your study design will fall into place. But with the wrong question, your study will lack focus, it will be difficult to explain the relevance of your study, and you will not want to present your data on the podium. An example of a good question is "Do patients with a given disease treated with operation X live longer than those treated with operation Y?" Stay away from the lure of "Let’s review our experience of operation X..." or "Why don’t I see how many of operation Y we’ve done over the past 10 years..." These topics are vague and do not ask a specific question. There must be a clear hypothesis for any study that is expected to produce meaningful results.
Once you have chosen an appropriate question, you must decide on a study design. Although case reports are marginally publishable, they will not answer your clinical questions. For many reasons, randomized, controlled trials, the gold standard of research, are difficult to design, carry out, and complete in your short time as a trainee. The good news is that well-designed and sufficiently powered observational studies often give similar results as randomized, controlled studies. Examples of common observational study designs include cohort studies, case control studies, and cross-sectional studies (Table 2). Each study design is different and your mentor should be able to help you decide which is the best to answer the question you want to ask.
When designing a study, one of the most important principles is defining a priori endpoints. Every study will have one primary endpoint that reflects the hypothesis. Secondary endpoints are interesting and potentially helpful, but are not the main message. It will be important to meet with a statistician before you start data collection. Understanding the statistics to be used will allow you to collect your data in the correct way (categorical vs. continuous, etc.). Reviewing charts is very time consuming and you have to do everything in your power to ensure you only do it once.
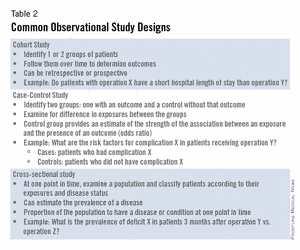
The next step is to create a research proposal. To do this, you will need to go to the literature, and see what published data relate to your study. Perhaps there are previous studies examining your question with conflicting results. Or if your question has not been previously investigated, what supporting literature suggests that yours is the next logical study? Your proposal should include a background section (1-2 paragraphs), hypothesis (1 sentence), the specific aims of the study (1-3 sentences), methods (2-4 paragraphs), anticipated results (1 paragraph), proposed timeline, and anticipated meeting to which it will be submitted. Your mentor will revise and critique the proposal and eventually give you a signature of approval.
This proposal serves many purposes. It will allow you to fully understand the study before you begin, some form of it is usually required for the Institutional Review Board (IRB) application, it will serve as the outline for your eventual manuscript, and it sets a timeline for completion of the project. Without an agreed upon deadline, too many good studies are left in various states of completion when the trainee moves on, and are never finished. The deadline should be based on the meeting that you and your mentor agree is appropriate for reporting your results.
Most would agree that data collection is the most painful part of doing clinical research. However, there are a few tricks to ease your pain. First, there are many databases available that you may be able to harvest data from to minimize your chart work (Table 3). Before you hit the charts, it is essential to think through every step of the project.
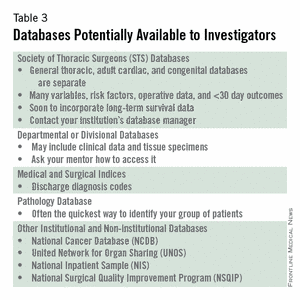
Anticipate problems (where in the chart will you locate each data point), do not collect unnecessary data points (postoperative data #3 serum [Na+] when looking at survival of thoracoscopic vs. open lobectomy), meet with your statistician beforehand to collect data for the correct analysis, collect the raw data (creatinine and weight, not presence of renal failure and obesity). Finally, be sure that your data are backed up in multiple places. Some prefer to collect data on paper then enter it later into a spreadsheet. This ensures a hard copy of the data regardless of whether the electronic version is lost.
After the data are collected and the statistics are done, you will be faced with interpreting your results and composing an abstract and manuscript. If your study is focused and hypothesis driven, this step should be fairly straightforward.
Schedule time with your mentor and discuss the results to ensure your interpretation of the data is correct. Next, using your proposal as an outline, put together a rough draft of a manuscript.
Remember that manuscripts are the currency of academia. If you do not present and publish your work, you have not fully capitalized on the hard work you have put in to your study. Your mentor will need to revise your manuscript repeatedly; use it as a learning experience for critiquing the literature and writing future manuscripts. He or she likely knows what editors and readers will be looking for in your finished product.
Remember, you will need multiple revisions of the abstract and manuscript, so plan adequate time prior to your deadline for writing. Most institutions have medical illustrators available for hire; consider including a drawing or photograph if it legitimately adds content to your manuscript.
The final step in the process is presenting your work in front of experts who likely know more about cardiothoracic surgery than you. Just remember, no one knows more about your data than you. Prepare relentlessly for your talk, take a deep breath before you walk on stage, speak with confidence, and if you don’t know the answer to a given question from the audience, admit it. Soon enough you will be the expert in the audience asking the tough questions.
Then spend as much time as possible after the session speaking with audience members about you and your study. You will meet lifelong colleagues, and maybe even your future partner. For many, research is a rewarding lifelong endeavor. For others, it is a means of learning to critically appraise the literature and landing a job. Either way, you cannot afford not to do research as a trainee.
Acknowledgement: I would like to thank my friend and colleague, Dr. Stephen H. McKellar (University of Utah), for his advice on performing research as a cardiothoracic trainee.
Dr. Seder is in the department of cardiovascular and thoracic surgery at Rush University Medical Center.
"Why do I need to do research if I’m going into private practice anyway?"
I have heard this question multiple times throughout my career as a resident, fellow, and attending thoracic surgeon. The truth is, there are multiple reasons, any of which is sufficient to justify your participation in clinical research during training. First, and perhaps most importantly, it teaches you to critically appraise the literature. This is a skill that will serve you well throughout your career, guiding your clinical decision-making, regardless if you choose private practice or academic surgery. Another reason is that performing clinical research allows you to become a content expert on a specific topic early in your career. This knowledge base is something that will serve as a foundation for ongoing learning and may help in designing future studies. Once your project is complete, it will be your ticket to attend and present at regional, national, or international meetings. There is no better forum to gain public recognition for your investigative efforts and network with potential future partners than societal meetings. Formal and informal interviews routinely occur at these gatherings and you do not want to be left out because you chose not to participate in research as a trainee. Finally, it is your responsibility to the patients that you have sworn to treat. There are many ways to care for patients, and pushing back the frontiers of medical knowledge is as important as the day-to-day tasks that you perform on the ward or in the operating room.
So, now that you have decided that you want to participate in a research project as a trainee, how do you make it happen? Before you begin a project, you will have to choose a mentor, a topic, a clear, novel question, and the appropriate study design. Chances are that at some point, a mentor helped guide you toward a career in cardiothoracic surgery. A research mentor is just as important as a clinical mentor for a young surgeon.
The most important trait that you should seek out in a research mentor is the ability to delineate important questions. All too often, residents and fellows are approached by attending surgeons with good intentions, but bad research ideas. Trainees then feel obligated to take them up on the project (in order to not appear like a slacker) and for various reasons, it does not result in an abstract, presentation, or publication. In fact, all it results in is frustration, a distaste for investigation, and wasted time. The bottom line is that only you can protect your time, and as a surgical trainee, you must guard it ferociously. Look for a mentor who is an expert in your field of interest and who has a track record of publications.
He or she must be a logical thinker who can help you delineate a clear, novel question, choose the appropriate study design, guide your writing of the manuscript, and direct your submission to the appropriate meetings and journals. Finally, your mentor must be dedicated to your success. We are all busy, but if your mentor cannot find the time to routinely meet with you at every step of your project, you need to find a new mentor.
Choosing a clear, novel clinical question starts with choosing an appropriate topic (Table 1). With the right topic and question, the hypothesis is obvious, it is easy to define your endpoints, and your study design will fall into place. But with the wrong question, your study will lack focus, it will be difficult to explain the relevance of your study, and you will not want to present your data on the podium. An example of a good question is "Do patients with a given disease treated with operation X live longer than those treated with operation Y?" Stay away from the lure of "Let’s review our experience of operation X..." or "Why don’t I see how many of operation Y we’ve done over the past 10 years..." These topics are vague and do not ask a specific question. There must be a clear hypothesis for any study that is expected to produce meaningful results.
Once you have chosen an appropriate question, you must decide on a study design. Although case reports are marginally publishable, they will not answer your clinical questions. For many reasons, randomized, controlled trials, the gold standard of research, are difficult to design, carry out, and complete in your short time as a trainee. The good news is that well-designed and sufficiently powered observational studies often give similar results as randomized, controlled studies. Examples of common observational study designs include cohort studies, case control studies, and cross-sectional studies (Table 2). Each study design is different and your mentor should be able to help you decide which is the best to answer the question you want to ask.
When designing a study, one of the most important principles is defining a priori endpoints. Every study will have one primary endpoint that reflects the hypothesis. Secondary endpoints are interesting and potentially helpful, but are not the main message. It will be important to meet with a statistician before you start data collection. Understanding the statistics to be used will allow you to collect your data in the correct way (categorical vs. continuous, etc.). Reviewing charts is very time consuming and you have to do everything in your power to ensure you only do it once.
The next step is to create a research proposal. To do this, you will need to go to the literature, and see what published data relate to your study. Perhaps there are previous studies examining your question with conflicting results. Or if your question has not been previously investigated, what supporting literature suggests that yours is the next logical study? Your proposal should include a background section (1-2 paragraphs), hypothesis (1 sentence), the specific aims of the study (1-3 sentences), methods (2-4 paragraphs), anticipated results (1 paragraph), proposed timeline, and anticipated meeting to which it will be submitted. Your mentor will revise and critique the proposal and eventually give you a signature of approval.
This proposal serves many purposes. It will allow you to fully understand the study before you begin, some form of it is usually required for the Institutional Review Board (IRB) application, it will serve as the outline for your eventual manuscript, and it sets a timeline for completion of the project. Without an agreed upon deadline, too many good studies are left in various states of completion when the trainee moves on, and are never finished. The deadline should be based on the meeting that you and your mentor agree is appropriate for reporting your results.
Most would agree that data collection is the most painful part of doing clinical research. However, there are a few tricks to ease your pain. First, there are many databases available that you may be able to harvest data from to minimize your chart work (Table 3). Before you hit the charts, it is essential to think through every step of the project.
Anticipate problems (where in the chart will you locate each data point), do not collect unnecessary data points (postoperative data #3 serum [Na+] when looking at survival of thoracoscopic vs. open lobectomy), meet with your statistician beforehand to collect data for the correct analysis, collect the raw data (creatinine and weight, not presence of renal failure and obesity). Finally, be sure that your data are backed up in multiple places. Some prefer to collect data on paper then enter it later into a spreadsheet. This ensures a hard copy of the data regardless of whether the electronic version is lost.
After the data are collected and the statistics are done, you will be faced with interpreting your results and composing an abstract and manuscript. If your study is focused and hypothesis driven, this step should be fairly straightforward.
Schedule time with your mentor and discuss the results to ensure your interpretation of the data is correct. Next, using your proposal as an outline, put together a rough draft of a manuscript.
Remember that manuscripts are the currency of academia. If you do not present and publish your work, you have not fully capitalized on the hard work you have put in to your study. Your mentor will need to revise your manuscript repeatedly; use it as a learning experience for critiquing the literature and writing future manuscripts. He or she likely knows what editors and readers will be looking for in your finished product.
Remember, you will need multiple revisions of the abstract and manuscript, so plan adequate time prior to your deadline for writing. Most institutions have medical illustrators available for hire; consider including a drawing or photograph if it legitimately adds content to your manuscript.
The final step in the process is presenting your work in front of experts who likely know more about cardiothoracic surgery than you. Just remember, no one knows more about your data than you. Prepare relentlessly for your talk, take a deep breath before you walk on stage, speak with confidence, and if you don’t know the answer to a given question from the audience, admit it. Soon enough you will be the expert in the audience asking the tough questions.
Then spend as much time as possible after the session speaking with audience members about you and your study. You will meet lifelong colleagues, and maybe even your future partner. For many, research is a rewarding lifelong endeavor. For others, it is a means of learning to critically appraise the literature and landing a job. Either way, you cannot afford not to do research as a trainee.
Acknowledgement: I would like to thank my friend and colleague, Dr. Stephen H. McKellar (University of Utah), for his advice on performing research as a cardiothoracic trainee.
Dr. Seder is in the department of cardiovascular and thoracic surgery at Rush University Medical Center.
"Why do I need to do research if I’m going into private practice anyway?"
I have heard this question multiple times throughout my career as a resident, fellow, and attending thoracic surgeon. The truth is, there are multiple reasons, any of which is sufficient to justify your participation in clinical research during training. First, and perhaps most importantly, it teaches you to critically appraise the literature. This is a skill that will serve you well throughout your career, guiding your clinical decision-making, regardless if you choose private practice or academic surgery. Another reason is that performing clinical research allows you to become a content expert on a specific topic early in your career. This knowledge base is something that will serve as a foundation for ongoing learning and may help in designing future studies. Once your project is complete, it will be your ticket to attend and present at regional, national, or international meetings. There is no better forum to gain public recognition for your investigative efforts and network with potential future partners than societal meetings. Formal and informal interviews routinely occur at these gatherings and you do not want to be left out because you chose not to participate in research as a trainee. Finally, it is your responsibility to the patients that you have sworn to treat. There are many ways to care for patients, and pushing back the frontiers of medical knowledge is as important as the day-to-day tasks that you perform on the ward or in the operating room.
So, now that you have decided that you want to participate in a research project as a trainee, how do you make it happen? Before you begin a project, you will have to choose a mentor, a topic, a clear, novel question, and the appropriate study design. Chances are that at some point, a mentor helped guide you toward a career in cardiothoracic surgery. A research mentor is just as important as a clinical mentor for a young surgeon.
The most important trait that you should seek out in a research mentor is the ability to delineate important questions. All too often, residents and fellows are approached by attending surgeons with good intentions, but bad research ideas. Trainees then feel obligated to take them up on the project (in order to not appear like a slacker) and for various reasons, it does not result in an abstract, presentation, or publication. In fact, all it results in is frustration, a distaste for investigation, and wasted time. The bottom line is that only you can protect your time, and as a surgical trainee, you must guard it ferociously. Look for a mentor who is an expert in your field of interest and who has a track record of publications.
He or she must be a logical thinker who can help you delineate a clear, novel question, choose the appropriate study design, guide your writing of the manuscript, and direct your submission to the appropriate meetings and journals. Finally, your mentor must be dedicated to your success. We are all busy, but if your mentor cannot find the time to routinely meet with you at every step of your project, you need to find a new mentor.
Choosing a clear, novel clinical question starts with choosing an appropriate topic (Table 1). With the right topic and question, the hypothesis is obvious, it is easy to define your endpoints, and your study design will fall into place. But with the wrong question, your study will lack focus, it will be difficult to explain the relevance of your study, and you will not want to present your data on the podium. An example of a good question is "Do patients with a given disease treated with operation X live longer than those treated with operation Y?" Stay away from the lure of "Let’s review our experience of operation X..." or "Why don’t I see how many of operation Y we’ve done over the past 10 years..." These topics are vague and do not ask a specific question. There must be a clear hypothesis for any study that is expected to produce meaningful results.
Once you have chosen an appropriate question, you must decide on a study design. Although case reports are marginally publishable, they will not answer your clinical questions. For many reasons, randomized, controlled trials, the gold standard of research, are difficult to design, carry out, and complete in your short time as a trainee. The good news is that well-designed and sufficiently powered observational studies often give similar results as randomized, controlled studies. Examples of common observational study designs include cohort studies, case control studies, and cross-sectional studies (Table 2). Each study design is different and your mentor should be able to help you decide which is the best to answer the question you want to ask.
When designing a study, one of the most important principles is defining a priori endpoints. Every study will have one primary endpoint that reflects the hypothesis. Secondary endpoints are interesting and potentially helpful, but are not the main message. It will be important to meet with a statistician before you start data collection. Understanding the statistics to be used will allow you to collect your data in the correct way (categorical vs. continuous, etc.). Reviewing charts is very time consuming and you have to do everything in your power to ensure you only do it once.
The next step is to create a research proposal. To do this, you will need to go to the literature, and see what published data relate to your study. Perhaps there are previous studies examining your question with conflicting results. Or if your question has not been previously investigated, what supporting literature suggests that yours is the next logical study? Your proposal should include a background section (1-2 paragraphs), hypothesis (1 sentence), the specific aims of the study (1-3 sentences), methods (2-4 paragraphs), anticipated results (1 paragraph), proposed timeline, and anticipated meeting to which it will be submitted. Your mentor will revise and critique the proposal and eventually give you a signature of approval.
This proposal serves many purposes. It will allow you to fully understand the study before you begin, some form of it is usually required for the Institutional Review Board (IRB) application, it will serve as the outline for your eventual manuscript, and it sets a timeline for completion of the project. Without an agreed upon deadline, too many good studies are left in various states of completion when the trainee moves on, and are never finished. The deadline should be based on the meeting that you and your mentor agree is appropriate for reporting your results.
Most would agree that data collection is the most painful part of doing clinical research. However, there are a few tricks to ease your pain. First, there are many databases available that you may be able to harvest data from to minimize your chart work (Table 3). Before you hit the charts, it is essential to think through every step of the project.
Anticipate problems (where in the chart will you locate each data point), do not collect unnecessary data points (postoperative data #3 serum [Na+] when looking at survival of thoracoscopic vs. open lobectomy), meet with your statistician beforehand to collect data for the correct analysis, collect the raw data (creatinine and weight, not presence of renal failure and obesity). Finally, be sure that your data are backed up in multiple places. Some prefer to collect data on paper then enter it later into a spreadsheet. This ensures a hard copy of the data regardless of whether the electronic version is lost.
After the data are collected and the statistics are done, you will be faced with interpreting your results and composing an abstract and manuscript. If your study is focused and hypothesis driven, this step should be fairly straightforward.
Schedule time with your mentor and discuss the results to ensure your interpretation of the data is correct. Next, using your proposal as an outline, put together a rough draft of a manuscript.
Remember that manuscripts are the currency of academia. If you do not present and publish your work, you have not fully capitalized on the hard work you have put in to your study. Your mentor will need to revise your manuscript repeatedly; use it as a learning experience for critiquing the literature and writing future manuscripts. He or she likely knows what editors and readers will be looking for in your finished product.
Remember, you will need multiple revisions of the abstract and manuscript, so plan adequate time prior to your deadline for writing. Most institutions have medical illustrators available for hire; consider including a drawing or photograph if it legitimately adds content to your manuscript.
The final step in the process is presenting your work in front of experts who likely know more about cardiothoracic surgery than you. Just remember, no one knows more about your data than you. Prepare relentlessly for your talk, take a deep breath before you walk on stage, speak with confidence, and if you don’t know the answer to a given question from the audience, admit it. Soon enough you will be the expert in the audience asking the tough questions.
Then spend as much time as possible after the session speaking with audience members about you and your study. You will meet lifelong colleagues, and maybe even your future partner. For many, research is a rewarding lifelong endeavor. For others, it is a means of learning to critically appraise the literature and landing a job. Either way, you cannot afford not to do research as a trainee.
Acknowledgement: I would like to thank my friend and colleague, Dr. Stephen H. McKellar (University of Utah), for his advice on performing research as a cardiothoracic trainee.
Dr. Seder is in the department of cardiovascular and thoracic surgery at Rush University Medical Center.
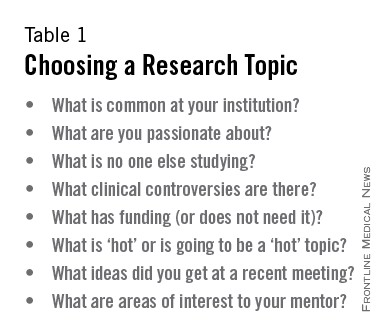
STS Resident Symposium 2014
The 2014 Residents’ Symposium at the STS 50th Annual Meeting in Orlando was heavily attended and greatly appreciated by current thoracic surgical trainees.
This outstanding forum boasted several experienced and informative speakers, with the overall goals of helping residents to find the right job and transition to practice.
Moderated by Dr. Sidhu Gangadharan, Dr. Sandra Starnes, and Dr. Ara A. Vaporciyan, this session addressed several key foci, specifically aiming to help residents plan a successful job search, negotiate important elements of a contract, plan for ways to bring new technologies into a practice, recognize the legal issues of billing and coding, and identify the important aspects of early career development. This phenomenal collection of talks featured a number of key speakers, who provided tips and recommendations received with great interest by the resident participants.

The symposium was kicked off by Dr. Danny Chu of the University of Pittsburgh Medical Center, who spoke on how to find a job position. He shared his personal experiences and gave attendees an overview of the actual job-search process. He provided several tips for finding the best job. He stated that since, "good positions are almost never advertised until they are filled, it helps to have a big network." He explained that, "in such a small community, there are literally 3 degrees of separation, and everyone knows everyone. In addition to being a good surgeon, being a nice and affable person will get you a good position." His top tips for finding a job are to "Work hard, be nice, and be social." Dr. Chu concluded his presentation by explaining that there’s no magic formula for finding a job, but that it’s very much like dating. He warns that money is not everything, details are all negotiable, and one should be cautious in trusting others. In the end, he believes that "nice guys will win," and tells the group despite much anxiety, it will work out in the end.
This was followed by a talk from Dr. Christine Lau of the University of Virginia, Charlottesville, on interviewing and self-marketing. Dr. Lau provided her insights on how to best represent yourself in the interview process, with a number of great points about putting your best foot forward. She emphasized the importance of being prepared, and she strongly advised that, prior to going on an interview, you do your homework. "Know what the position entails," explained Dr. Lau, "and have a well-thought-out plan regarding what you uniquely bring to it."
She advised speaking to a number of people in advance in order to elucidate the specific needs of the group. And, while Dr. Lau encourages you to have a clear explanation as to how you might meet the expectations of the job, she offered a reminder of the importance of being honest. "Yes, you want to explain how you fit into the spot; however, if it’s not a good fit, don’t try to be something that you’re not. You won’t be happy in the long run, and neither will they." Dr. Lau also offered some advice regarding the concept of specialization.
"Everybody wants to have a niche. But you don’t need to force yourself to differentiate early on." She continued, "If your interests and skills are broad at this point, that’s not a bad thing. You can always morph later."
Dr. Faiz Bhora of Columbia University, N.Y., wrapped up the first session with a discussion of contract negotiations – helping attendees prioritize what’s worth fighting for, how to fight for it, and how to avoid going so far as to negotiate oneself out of a job.
After the opportunity to partake in both small and large group sessions and a short break, the symposium resumed, with the second half focusing on the transition from trainee to attending surgeon.
Dr. Edward Chen of Emory University in Atlanta provided suggestions for adding new technologies to one’s practice and the effective team interactions required to do so. He listed several key strategies that he feels are critical to a successful transition. Communication, communication, and communication were at the top of his list. He advised that it’s a two-way street and that ample meetings may be necessary regarding one’s needs and expectations. He warned not to make any assumptions and to be flexible about adapting to the system that is in place. He also stressed the importance of a willingness to educate the staff about specific technology – in the ICU, in the OR, and on the ward. Dr. Chen also spoke about professional behavior and team building once one is out in the real world.
His advice to trainees entering practice entails the following three recommendations: "1) Make patient care your absolute top priority. 2) Treat everyone around you with utmost respect and dignity. Care about and find value in all team members, even those who are not the strongest members. Always have your team member’s back and never openly criticize anyone. And 3) embrace your new institution and new team members." These suggestions are useful for trainees entering their first job; however, they are also incredibly practical advice for anybody working on a medical team, regardless of the environment or their role on the team.
Dr. Francis C. Nichols, from the Mayo Clinic, in Rochester, Minn., gave a great update on the new ICD-10, explaining key differences between previous coding systems and the new one.
He provided attendees with a helpful understanding of the importance of appropriate coding and billing strategies, and offered tips for accurately optimizing one’s ability to bill for provided services.
Finally, this wonderful series of brief lectures was finished off with a top-notch presentation from Dr. Elizabeth A. David of the University of California, Davis, who spoke about the various means of developing your career in the early years. She provided insight and details about developing reasonable, achievable 5- and 10-year plans; finding mentors (both within and outside of one’s institution); and how not to fail as a junior attending. The most important thing that you should do as a junior attending, according to Dr. David, is to make sure that your patients do well. She recommends, "Check everything, be vigilant, make sure your outcomes are yours, and be available to your patients and your referring physicians."
When asked what she wishes she’d known before venturing into practice, Dr. David states, "I wish I had known how hard I was going to work as a junior faculty member. People had told me that the first year would be a hard year, but it never really sunk in until I was experiencing it." She continues, "my first year was definitely a challenging year, but like all things you work hard for – it was very rewarding!"
Likewise, the symposium was incredibly rewarding. States Dr. Michelle Ellis, a finishing fellow at the University of Michigan, Ann Arbor, "I enjoyed the symposium very much. It was timely and relevant. I would definitely recommend it to other residents and fellows. I especially liked the break-out sessions which allowed for detailed discussion."
Dr. Antonoff is a second-year, thoracic-track trainee at Washington University in St Louis.
The 2014 Residents’ Symposium at the STS 50th Annual Meeting in Orlando was heavily attended and greatly appreciated by current thoracic surgical trainees.
This outstanding forum boasted several experienced and informative speakers, with the overall goals of helping residents to find the right job and transition to practice.
Moderated by Dr. Sidhu Gangadharan, Dr. Sandra Starnes, and Dr. Ara A. Vaporciyan, this session addressed several key foci, specifically aiming to help residents plan a successful job search, negotiate important elements of a contract, plan for ways to bring new technologies into a practice, recognize the legal issues of billing and coding, and identify the important aspects of early career development. This phenomenal collection of talks featured a number of key speakers, who provided tips and recommendations received with great interest by the resident participants.
The symposium was kicked off by Dr. Danny Chu of the University of Pittsburgh Medical Center, who spoke on how to find a job position. He shared his personal experiences and gave attendees an overview of the actual job-search process. He provided several tips for finding the best job. He stated that since, "good positions are almost never advertised until they are filled, it helps to have a big network." He explained that, "in such a small community, there are literally 3 degrees of separation, and everyone knows everyone. In addition to being a good surgeon, being a nice and affable person will get you a good position." His top tips for finding a job are to "Work hard, be nice, and be social." Dr. Chu concluded his presentation by explaining that there’s no magic formula for finding a job, but that it’s very much like dating. He warns that money is not everything, details are all negotiable, and one should be cautious in trusting others. In the end, he believes that "nice guys will win," and tells the group despite much anxiety, it will work out in the end.
This was followed by a talk from Dr. Christine Lau of the University of Virginia, Charlottesville, on interviewing and self-marketing. Dr. Lau provided her insights on how to best represent yourself in the interview process, with a number of great points about putting your best foot forward. She emphasized the importance of being prepared, and she strongly advised that, prior to going on an interview, you do your homework. "Know what the position entails," explained Dr. Lau, "and have a well-thought-out plan regarding what you uniquely bring to it."
She advised speaking to a number of people in advance in order to elucidate the specific needs of the group. And, while Dr. Lau encourages you to have a clear explanation as to how you might meet the expectations of the job, she offered a reminder of the importance of being honest. "Yes, you want to explain how you fit into the spot; however, if it’s not a good fit, don’t try to be something that you’re not. You won’t be happy in the long run, and neither will they." Dr. Lau also offered some advice regarding the concept of specialization.
"Everybody wants to have a niche. But you don’t need to force yourself to differentiate early on." She continued, "If your interests and skills are broad at this point, that’s not a bad thing. You can always morph later."
Dr. Faiz Bhora of Columbia University, N.Y., wrapped up the first session with a discussion of contract negotiations – helping attendees prioritize what’s worth fighting for, how to fight for it, and how to avoid going so far as to negotiate oneself out of a job.
After the opportunity to partake in both small and large group sessions and a short break, the symposium resumed, with the second half focusing on the transition from trainee to attending surgeon.
Dr. Edward Chen of Emory University in Atlanta provided suggestions for adding new technologies to one’s practice and the effective team interactions required to do so. He listed several key strategies that he feels are critical to a successful transition. Communication, communication, and communication were at the top of his list. He advised that it’s a two-way street and that ample meetings may be necessary regarding one’s needs and expectations. He warned not to make any assumptions and to be flexible about adapting to the system that is in place. He also stressed the importance of a willingness to educate the staff about specific technology – in the ICU, in the OR, and on the ward. Dr. Chen also spoke about professional behavior and team building once one is out in the real world.
His advice to trainees entering practice entails the following three recommendations: "1) Make patient care your absolute top priority. 2) Treat everyone around you with utmost respect and dignity. Care about and find value in all team members, even those who are not the strongest members. Always have your team member’s back and never openly criticize anyone. And 3) embrace your new institution and new team members." These suggestions are useful for trainees entering their first job; however, they are also incredibly practical advice for anybody working on a medical team, regardless of the environment or their role on the team.
Dr. Francis C. Nichols, from the Mayo Clinic, in Rochester, Minn., gave a great update on the new ICD-10, explaining key differences between previous coding systems and the new one.
He provided attendees with a helpful understanding of the importance of appropriate coding and billing strategies, and offered tips for accurately optimizing one’s ability to bill for provided services.
Finally, this wonderful series of brief lectures was finished off with a top-notch presentation from Dr. Elizabeth A. David of the University of California, Davis, who spoke about the various means of developing your career in the early years. She provided insight and details about developing reasonable, achievable 5- and 10-year plans; finding mentors (both within and outside of one’s institution); and how not to fail as a junior attending. The most important thing that you should do as a junior attending, according to Dr. David, is to make sure that your patients do well. She recommends, "Check everything, be vigilant, make sure your outcomes are yours, and be available to your patients and your referring physicians."
When asked what she wishes she’d known before venturing into practice, Dr. David states, "I wish I had known how hard I was going to work as a junior faculty member. People had told me that the first year would be a hard year, but it never really sunk in until I was experiencing it." She continues, "my first year was definitely a challenging year, but like all things you work hard for – it was very rewarding!"
Likewise, the symposium was incredibly rewarding. States Dr. Michelle Ellis, a finishing fellow at the University of Michigan, Ann Arbor, "I enjoyed the symposium very much. It was timely and relevant. I would definitely recommend it to other residents and fellows. I especially liked the break-out sessions which allowed for detailed discussion."
Dr. Antonoff is a second-year, thoracic-track trainee at Washington University in St Louis.
The 2014 Residents’ Symposium at the STS 50th Annual Meeting in Orlando was heavily attended and greatly appreciated by current thoracic surgical trainees.
This outstanding forum boasted several experienced and informative speakers, with the overall goals of helping residents to find the right job and transition to practice.
Moderated by Dr. Sidhu Gangadharan, Dr. Sandra Starnes, and Dr. Ara A. Vaporciyan, this session addressed several key foci, specifically aiming to help residents plan a successful job search, negotiate important elements of a contract, plan for ways to bring new technologies into a practice, recognize the legal issues of billing and coding, and identify the important aspects of early career development. This phenomenal collection of talks featured a number of key speakers, who provided tips and recommendations received with great interest by the resident participants.
The symposium was kicked off by Dr. Danny Chu of the University of Pittsburgh Medical Center, who spoke on how to find a job position. He shared his personal experiences and gave attendees an overview of the actual job-search process. He provided several tips for finding the best job. He stated that since, "good positions are almost never advertised until they are filled, it helps to have a big network." He explained that, "in such a small community, there are literally 3 degrees of separation, and everyone knows everyone. In addition to being a good surgeon, being a nice and affable person will get you a good position." His top tips for finding a job are to "Work hard, be nice, and be social." Dr. Chu concluded his presentation by explaining that there’s no magic formula for finding a job, but that it’s very much like dating. He warns that money is not everything, details are all negotiable, and one should be cautious in trusting others. In the end, he believes that "nice guys will win," and tells the group despite much anxiety, it will work out in the end.
This was followed by a talk from Dr. Christine Lau of the University of Virginia, Charlottesville, on interviewing and self-marketing. Dr. Lau provided her insights on how to best represent yourself in the interview process, with a number of great points about putting your best foot forward. She emphasized the importance of being prepared, and she strongly advised that, prior to going on an interview, you do your homework. "Know what the position entails," explained Dr. Lau, "and have a well-thought-out plan regarding what you uniquely bring to it."
She advised speaking to a number of people in advance in order to elucidate the specific needs of the group. And, while Dr. Lau encourages you to have a clear explanation as to how you might meet the expectations of the job, she offered a reminder of the importance of being honest. "Yes, you want to explain how you fit into the spot; however, if it’s not a good fit, don’t try to be something that you’re not. You won’t be happy in the long run, and neither will they." Dr. Lau also offered some advice regarding the concept of specialization.
"Everybody wants to have a niche. But you don’t need to force yourself to differentiate early on." She continued, "If your interests and skills are broad at this point, that’s not a bad thing. You can always morph later."
Dr. Faiz Bhora of Columbia University, N.Y., wrapped up the first session with a discussion of contract negotiations – helping attendees prioritize what’s worth fighting for, how to fight for it, and how to avoid going so far as to negotiate oneself out of a job.
After the opportunity to partake in both small and large group sessions and a short break, the symposium resumed, with the second half focusing on the transition from trainee to attending surgeon.
Dr. Edward Chen of Emory University in Atlanta provided suggestions for adding new technologies to one’s practice and the effective team interactions required to do so. He listed several key strategies that he feels are critical to a successful transition. Communication, communication, and communication were at the top of his list. He advised that it’s a two-way street and that ample meetings may be necessary regarding one’s needs and expectations. He warned not to make any assumptions and to be flexible about adapting to the system that is in place. He also stressed the importance of a willingness to educate the staff about specific technology – in the ICU, in the OR, and on the ward. Dr. Chen also spoke about professional behavior and team building once one is out in the real world.
His advice to trainees entering practice entails the following three recommendations: "1) Make patient care your absolute top priority. 2) Treat everyone around you with utmost respect and dignity. Care about and find value in all team members, even those who are not the strongest members. Always have your team member’s back and never openly criticize anyone. And 3) embrace your new institution and new team members." These suggestions are useful for trainees entering their first job; however, they are also incredibly practical advice for anybody working on a medical team, regardless of the environment or their role on the team.
Dr. Francis C. Nichols, from the Mayo Clinic, in Rochester, Minn., gave a great update on the new ICD-10, explaining key differences between previous coding systems and the new one.
He provided attendees with a helpful understanding of the importance of appropriate coding and billing strategies, and offered tips for accurately optimizing one’s ability to bill for provided services.
Finally, this wonderful series of brief lectures was finished off with a top-notch presentation from Dr. Elizabeth A. David of the University of California, Davis, who spoke about the various means of developing your career in the early years. She provided insight and details about developing reasonable, achievable 5- and 10-year plans; finding mentors (both within and outside of one’s institution); and how not to fail as a junior attending. The most important thing that you should do as a junior attending, according to Dr. David, is to make sure that your patients do well. She recommends, "Check everything, be vigilant, make sure your outcomes are yours, and be available to your patients and your referring physicians."
When asked what she wishes she’d known before venturing into practice, Dr. David states, "I wish I had known how hard I was going to work as a junior faculty member. People had told me that the first year would be a hard year, but it never really sunk in until I was experiencing it." She continues, "my first year was definitely a challenging year, but like all things you work hard for – it was very rewarding!"
Likewise, the symposium was incredibly rewarding. States Dr. Michelle Ellis, a finishing fellow at the University of Michigan, Ann Arbor, "I enjoyed the symposium very much. It was timely and relevant. I would definitely recommend it to other residents and fellows. I especially liked the break-out sessions which allowed for detailed discussion."
Dr. Antonoff is a second-year, thoracic-track trainee at Washington University in St Louis.

On the Go Education: Mobile software in cardiothoracic training
In nearly every facet of our lives, our mobile devices have taken over. Managing our calendars, organizing our contacts, and planning our driving directions -- our devices have become invaluable and ubiquitously present. While the ease of use of smartphones and tablets puts the power of portable computing in the hands of everyone, mobile software seems to be particularly appreciated by young professionals, who seek the convenience of on-the-go functionality and feel comfortable with computing in the palms of their hands. Throughout the world of education and a breadth of academic fields, advanced software programs have gained momentum, recognized for their ability to provide up-to-date, on-the-ground information.
In recent years, there has been an explosion of new software programs applicable to the field of cardiothoracic surgery, and these applications have been well received by modern trainees.
"Mobile apps are incredibly convenient because they provide a means of accessing information while on the go," states Jonathan Spicer, a thoracic trainee at M.D. Anderson Cancer Center in Houston.
He continues, "Having the capacity to look up helpful information from my phone while in the operating room, on the ward, or in transit is particularly helpful."
In this article, we aim to highlight some of the more exciting and innovative mobile software programs available today for those interested in expanding their knowledge in cardiothoracic surgery or looking for an easy-to-access resource.
iBronch (Edward Bender), $0.99: iBronch is one of the many outstanding thoracic surgical apps developed by Ed Bender. This program aims to guide learners through the basic anatomy of the trachea and bronchial tree, with correlation of simultaneous images from a fiberoptic bronchoscope and along an anatomic airway diagram. Branches of the pulmonary tree are labeled on the schematic and the bronchoscopy images. This app is particularly useful for those trainees gaining comfort with bronchoscopic procedures; however, its utility may be less significant for more advanced learners. Regardless, this is a great program, quite helpful for the intended audience.
Thoracic Lymph Node Map (RADIOLOGiQ, LLC), Free: This app provides a color-coded lymph node map, associated with computed tomography images and adapted from the International Association for the Study of Lung Cancer (IASLC) lung cancer project. This program provides excellent illustrations of the anatomic definitions for each of the intrathoracic lymph node stations. This is helpful both in examining imaging studies of actual patients and in the operating room.
CT Journals (Edward Bender), Free: This software program serves as a scholarly journal aggregator for the field of cardiothoracic surgery. The app displays feeds for journals of interest, with inclusion of those relevant periodicals with the most readership and highest impact factors. Not only can one access the articles while online, abstracts can be saved for future use offline. This is a great resource, but users should be aware that access to the full articles is available only for those who have active accounts providing them access to the specific journals.
CTSNetWiki (Edward Bender), Free: Cardiothoracic Surgery Notes is an online review developed and maintained by residents in thoracic surgical training. This resource is a tremendous repository of information, compiling graphics, text, and other multimedia content on a breadth of topics. This app allows general review of a wide variety of cardiothoracic surgical problems and is appropriate for both the novice learner and as a review for those who are further along in their training.
SESATS IX (Edward Bender), Free: Perhaps the most valuable mobile software application out there, the Self Education Self Assessment in Thoracic Surgery (SESATS) IX application contains actual questions from previous versions of the SESATS. The mobile app even includes the associated images, videos, and CT scans that correspond with the questions. Although the program does not contain the latest version of SESATS, the utility of this app cannot be overestimated. This program is enormously helpful for self-testing, on-the-go topic-specific learning, and exam preparation. This is a real gem of a find, and it comes with a strong recommendation to all trainees for its download and use.
TSRA Primer of Cardiothoracic Surgery (Thoracic Surgery Residents' Association), $4.99: Produced by CT residents for CT residents, this is probably the most useful resource for the intern, junior resident, or new fellow who needs to brush up on the basics before rounds, in between consults, and before assisting in the OR. It's not comprehensive, but it is full of clinical pearls covering all the major divisions of cardiothoracic surgery. Many cardiac residents, especially younger integrated residents, have been waiting for a straightforward, practical tutorial like this for years. Beautiful and often interactive illustrations and videos really make this iBook memorable.
NCCN Guidelines (TIP Medical Communications), Free: Available for Android and iOS, this compendium of NCCN guidelines for 56 cancers and cancer-related topics is indispensible for trainees. The utility of having up-to-date, in-depth guidelines for diagnosis and staging of all commonly encountered malignancies cannot be overstated. Additional topics ranging from management of cancer-related emesis to lung cancer screening guidelines polish it off. A must have for anyone who treats cancer, not just thoracic surgeons.
CathSource (ECGSource, LLC), $3.99: Available for Android and iOS, CathSource is a mobile app that aims to teach cardiovascular medicine fellows about coronary anatomy, angiogram projections, and catheter-based hemodynamic measurements. Luckily, CT trainees stand to benefit from the app as well. It seems to be most helpful for learning coronary anatomy on the different projections, but it also has exhaustive hemodynamic formulae and tracings for more detailed review. The app has over 30 videos of normal and abnormal findings.
EchoSource (ECGSource, LLC), $4.99:It's the same idea as above, but -- you guessed it -- for echocardiography. Both are good tools, especially for residents who teach. Both apps take simple, conceptual drawings to start and expand them with real imaging. Residents who have spent a good deal of time in learning cath and echo may find these apps less useful.
Pocket Heart (PocketAnatomy), $9.99: This is an interactive, 3D heart model with a fairly detailed presentation of cardiac anatomy and added features such as pinning quizzes and case studies. While cardiothoracic residents ought to have the anatomy down, the app can be used to teach patients and families about various anatomical aspects of cardiac disease. The graphics leave a little to be desired, but anyone who teaches medical students or patients frequently will enjoy having this easy-to-understand tool handy.

This list of cardiothoracic-specific mobile applications is by no means exhaustive. Each physician's needs will be different, and the options are countless. Countless risk calculators, mnemonic databases, formula compendiums, and pharmacologic formularies clutter the app store. Note-taking suites such as OneNote and Evernote (personal favorite of both of the authors) can help turn the most hare-brained resident into a paragon of organizational excellence. Journal citation managers such as EndNote, Dropbox, Mendeley, and Yep can help organize and manage that virtual pile of unread but probably important journal articles that keeps building up in your inbox. Even the humble iBooks app can be used to read and mark up pdf files on the fly, all while syncing with your library on your home computer. Many hospital EMRs have mobile platforms with various levels of functionality for tablets and smartphones.
What is obvious is that mobile computing technology is rapidly changing medicine and surgery in many ways. Although each one of us strives to be a complete physician, utterly self-reliant and assured of one's clinical knowledge, we all must learn the basics first. Whether at the bus stop, in a resident lounge, or in the operating room, these mobile technologies help us to learn more efficiently while on the go.
If there are any gems we have forgotten to highlight, please send an e-mail to Thoracic Surgery News and we will try to present them in the future. We hope that the residents reading this column can find a new app they didn't know they needed, one that will energize them and push their learning to a new height. Just don't forget to look up once in a while.
Dr. Antonoff is a 2nd-year, Thoracic-track trainee at Washington University in St Louis. Dr. Zeigler is a 3rd-year, integrated Cardiothoracic Surgery trainee at Stanford (Calif.) University. They reported no relevant financial conflicts.
In nearly every facet of our lives, our mobile devices have taken over. Managing our calendars, organizing our contacts, and planning our driving directions -- our devices have become invaluable and ubiquitously present. While the ease of use of smartphones and tablets puts the power of portable computing in the hands of everyone, mobile software seems to be particularly appreciated by young professionals, who seek the convenience of on-the-go functionality and feel comfortable with computing in the palms of their hands. Throughout the world of education and a breadth of academic fields, advanced software programs have gained momentum, recognized for their ability to provide up-to-date, on-the-ground information.
In recent years, there has been an explosion of new software programs applicable to the field of cardiothoracic surgery, and these applications have been well received by modern trainees.
"Mobile apps are incredibly convenient because they provide a means of accessing information while on the go," states Jonathan Spicer, a thoracic trainee at M.D. Anderson Cancer Center in Houston.
He continues, "Having the capacity to look up helpful information from my phone while in the operating room, on the ward, or in transit is particularly helpful."
In this article, we aim to highlight some of the more exciting and innovative mobile software programs available today for those interested in expanding their knowledge in cardiothoracic surgery or looking for an easy-to-access resource.
iBronch (Edward Bender), $0.99: iBronch is one of the many outstanding thoracic surgical apps developed by Ed Bender. This program aims to guide learners through the basic anatomy of the trachea and bronchial tree, with correlation of simultaneous images from a fiberoptic bronchoscope and along an anatomic airway diagram. Branches of the pulmonary tree are labeled on the schematic and the bronchoscopy images. This app is particularly useful for those trainees gaining comfort with bronchoscopic procedures; however, its utility may be less significant for more advanced learners. Regardless, this is a great program, quite helpful for the intended audience.
Thoracic Lymph Node Map (RADIOLOGiQ, LLC), Free: This app provides a color-coded lymph node map, associated with computed tomography images and adapted from the International Association for the Study of Lung Cancer (IASLC) lung cancer project. This program provides excellent illustrations of the anatomic definitions for each of the intrathoracic lymph node stations. This is helpful both in examining imaging studies of actual patients and in the operating room.
CT Journals (Edward Bender), Free: This software program serves as a scholarly journal aggregator for the field of cardiothoracic surgery. The app displays feeds for journals of interest, with inclusion of those relevant periodicals with the most readership and highest impact factors. Not only can one access the articles while online, abstracts can be saved for future use offline. This is a great resource, but users should be aware that access to the full articles is available only for those who have active accounts providing them access to the specific journals.
CTSNetWiki (Edward Bender), Free: Cardiothoracic Surgery Notes is an online review developed and maintained by residents in thoracic surgical training. This resource is a tremendous repository of information, compiling graphics, text, and other multimedia content on a breadth of topics. This app allows general review of a wide variety of cardiothoracic surgical problems and is appropriate for both the novice learner and as a review for those who are further along in their training.
SESATS IX (Edward Bender), Free: Perhaps the most valuable mobile software application out there, the Self Education Self Assessment in Thoracic Surgery (SESATS) IX application contains actual questions from previous versions of the SESATS. The mobile app even includes the associated images, videos, and CT scans that correspond with the questions. Although the program does not contain the latest version of SESATS, the utility of this app cannot be overestimated. This program is enormously helpful for self-testing, on-the-go topic-specific learning, and exam preparation. This is a real gem of a find, and it comes with a strong recommendation to all trainees for its download and use.
TSRA Primer of Cardiothoracic Surgery (Thoracic Surgery Residents' Association), $4.99: Produced by CT residents for CT residents, this is probably the most useful resource for the intern, junior resident, or new fellow who needs to brush up on the basics before rounds, in between consults, and before assisting in the OR. It's not comprehensive, but it is full of clinical pearls covering all the major divisions of cardiothoracic surgery. Many cardiac residents, especially younger integrated residents, have been waiting for a straightforward, practical tutorial like this for years. Beautiful and often interactive illustrations and videos really make this iBook memorable.
NCCN Guidelines (TIP Medical Communications), Free: Available for Android and iOS, this compendium of NCCN guidelines for 56 cancers and cancer-related topics is indispensible for trainees. The utility of having up-to-date, in-depth guidelines for diagnosis and staging of all commonly encountered malignancies cannot be overstated. Additional topics ranging from management of cancer-related emesis to lung cancer screening guidelines polish it off. A must have for anyone who treats cancer, not just thoracic surgeons.
CathSource (ECGSource, LLC), $3.99: Available for Android and iOS, CathSource is a mobile app that aims to teach cardiovascular medicine fellows about coronary anatomy, angiogram projections, and catheter-based hemodynamic measurements. Luckily, CT trainees stand to benefit from the app as well. It seems to be most helpful for learning coronary anatomy on the different projections, but it also has exhaustive hemodynamic formulae and tracings for more detailed review. The app has over 30 videos of normal and abnormal findings.
EchoSource (ECGSource, LLC), $4.99:It's the same idea as above, but -- you guessed it -- for echocardiography. Both are good tools, especially for residents who teach. Both apps take simple, conceptual drawings to start and expand them with real imaging. Residents who have spent a good deal of time in learning cath and echo may find these apps less useful.
Pocket Heart (PocketAnatomy), $9.99: This is an interactive, 3D heart model with a fairly detailed presentation of cardiac anatomy and added features such as pinning quizzes and case studies. While cardiothoracic residents ought to have the anatomy down, the app can be used to teach patients and families about various anatomical aspects of cardiac disease. The graphics leave a little to be desired, but anyone who teaches medical students or patients frequently will enjoy having this easy-to-understand tool handy.
This list of cardiothoracic-specific mobile applications is by no means exhaustive. Each physician's needs will be different, and the options are countless. Countless risk calculators, mnemonic databases, formula compendiums, and pharmacologic formularies clutter the app store. Note-taking suites such as OneNote and Evernote (personal favorite of both of the authors) can help turn the most hare-brained resident into a paragon of organizational excellence. Journal citation managers such as EndNote, Dropbox, Mendeley, and Yep can help organize and manage that virtual pile of unread but probably important journal articles that keeps building up in your inbox. Even the humble iBooks app can be used to read and mark up pdf files on the fly, all while syncing with your library on your home computer. Many hospital EMRs have mobile platforms with various levels of functionality for tablets and smartphones.
What is obvious is that mobile computing technology is rapidly changing medicine and surgery in many ways. Although each one of us strives to be a complete physician, utterly self-reliant and assured of one's clinical knowledge, we all must learn the basics first. Whether at the bus stop, in a resident lounge, or in the operating room, these mobile technologies help us to learn more efficiently while on the go.
If there are any gems we have forgotten to highlight, please send an e-mail to Thoracic Surgery News and we will try to present them in the future. We hope that the residents reading this column can find a new app they didn't know they needed, one that will energize them and push their learning to a new height. Just don't forget to look up once in a while.
Dr. Antonoff is a 2nd-year, Thoracic-track trainee at Washington University in St Louis. Dr. Zeigler is a 3rd-year, integrated Cardiothoracic Surgery trainee at Stanford (Calif.) University. They reported no relevant financial conflicts.
In nearly every facet of our lives, our mobile devices have taken over. Managing our calendars, organizing our contacts, and planning our driving directions -- our devices have become invaluable and ubiquitously present. While the ease of use of smartphones and tablets puts the power of portable computing in the hands of everyone, mobile software seems to be particularly appreciated by young professionals, who seek the convenience of on-the-go functionality and feel comfortable with computing in the palms of their hands. Throughout the world of education and a breadth of academic fields, advanced software programs have gained momentum, recognized for their ability to provide up-to-date, on-the-ground information.
In recent years, there has been an explosion of new software programs applicable to the field of cardiothoracic surgery, and these applications have been well received by modern trainees.
"Mobile apps are incredibly convenient because they provide a means of accessing information while on the go," states Jonathan Spicer, a thoracic trainee at M.D. Anderson Cancer Center in Houston.
He continues, "Having the capacity to look up helpful information from my phone while in the operating room, on the ward, or in transit is particularly helpful."
In this article, we aim to highlight some of the more exciting and innovative mobile software programs available today for those interested in expanding their knowledge in cardiothoracic surgery or looking for an easy-to-access resource.
iBronch (Edward Bender), $0.99: iBronch is one of the many outstanding thoracic surgical apps developed by Ed Bender. This program aims to guide learners through the basic anatomy of the trachea and bronchial tree, with correlation of simultaneous images from a fiberoptic bronchoscope and along an anatomic airway diagram. Branches of the pulmonary tree are labeled on the schematic and the bronchoscopy images. This app is particularly useful for those trainees gaining comfort with bronchoscopic procedures; however, its utility may be less significant for more advanced learners. Regardless, this is a great program, quite helpful for the intended audience.
Thoracic Lymph Node Map (RADIOLOGiQ, LLC), Free: This app provides a color-coded lymph node map, associated with computed tomography images and adapted from the International Association for the Study of Lung Cancer (IASLC) lung cancer project. This program provides excellent illustrations of the anatomic definitions for each of the intrathoracic lymph node stations. This is helpful both in examining imaging studies of actual patients and in the operating room.
CT Journals (Edward Bender), Free: This software program serves as a scholarly journal aggregator for the field of cardiothoracic surgery. The app displays feeds for journals of interest, with inclusion of those relevant periodicals with the most readership and highest impact factors. Not only can one access the articles while online, abstracts can be saved for future use offline. This is a great resource, but users should be aware that access to the full articles is available only for those who have active accounts providing them access to the specific journals.
CTSNetWiki (Edward Bender), Free: Cardiothoracic Surgery Notes is an online review developed and maintained by residents in thoracic surgical training. This resource is a tremendous repository of information, compiling graphics, text, and other multimedia content on a breadth of topics. This app allows general review of a wide variety of cardiothoracic surgical problems and is appropriate for both the novice learner and as a review for those who are further along in their training.
SESATS IX (Edward Bender), Free: Perhaps the most valuable mobile software application out there, the Self Education Self Assessment in Thoracic Surgery (SESATS) IX application contains actual questions from previous versions of the SESATS. The mobile app even includes the associated images, videos, and CT scans that correspond with the questions. Although the program does not contain the latest version of SESATS, the utility of this app cannot be overestimated. This program is enormously helpful for self-testing, on-the-go topic-specific learning, and exam preparation. This is a real gem of a find, and it comes with a strong recommendation to all trainees for its download and use.
TSRA Primer of Cardiothoracic Surgery (Thoracic Surgery Residents' Association), $4.99: Produced by CT residents for CT residents, this is probably the most useful resource for the intern, junior resident, or new fellow who needs to brush up on the basics before rounds, in between consults, and before assisting in the OR. It's not comprehensive, but it is full of clinical pearls covering all the major divisions of cardiothoracic surgery. Many cardiac residents, especially younger integrated residents, have been waiting for a straightforward, practical tutorial like this for years. Beautiful and often interactive illustrations and videos really make this iBook memorable.
NCCN Guidelines (TIP Medical Communications), Free: Available for Android and iOS, this compendium of NCCN guidelines for 56 cancers and cancer-related topics is indispensible for trainees. The utility of having up-to-date, in-depth guidelines for diagnosis and staging of all commonly encountered malignancies cannot be overstated. Additional topics ranging from management of cancer-related emesis to lung cancer screening guidelines polish it off. A must have for anyone who treats cancer, not just thoracic surgeons.
CathSource (ECGSource, LLC), $3.99: Available for Android and iOS, CathSource is a mobile app that aims to teach cardiovascular medicine fellows about coronary anatomy, angiogram projections, and catheter-based hemodynamic measurements. Luckily, CT trainees stand to benefit from the app as well. It seems to be most helpful for learning coronary anatomy on the different projections, but it also has exhaustive hemodynamic formulae and tracings for more detailed review. The app has over 30 videos of normal and abnormal findings.
EchoSource (ECGSource, LLC), $4.99:It's the same idea as above, but -- you guessed it -- for echocardiography. Both are good tools, especially for residents who teach. Both apps take simple, conceptual drawings to start and expand them with real imaging. Residents who have spent a good deal of time in learning cath and echo may find these apps less useful.
Pocket Heart (PocketAnatomy), $9.99: This is an interactive, 3D heart model with a fairly detailed presentation of cardiac anatomy and added features such as pinning quizzes and case studies. While cardiothoracic residents ought to have the anatomy down, the app can be used to teach patients and families about various anatomical aspects of cardiac disease. The graphics leave a little to be desired, but anyone who teaches medical students or patients frequently will enjoy having this easy-to-understand tool handy.
This list of cardiothoracic-specific mobile applications is by no means exhaustive. Each physician's needs will be different, and the options are countless. Countless risk calculators, mnemonic databases, formula compendiums, and pharmacologic formularies clutter the app store. Note-taking suites such as OneNote and Evernote (personal favorite of both of the authors) can help turn the most hare-brained resident into a paragon of organizational excellence. Journal citation managers such as EndNote, Dropbox, Mendeley, and Yep can help organize and manage that virtual pile of unread but probably important journal articles that keeps building up in your inbox. Even the humble iBooks app can be used to read and mark up pdf files on the fly, all while syncing with your library on your home computer. Many hospital EMRs have mobile platforms with various levels of functionality for tablets and smartphones.
What is obvious is that mobile computing technology is rapidly changing medicine and surgery in many ways. Although each one of us strives to be a complete physician, utterly self-reliant and assured of one's clinical knowledge, we all must learn the basics first. Whether at the bus stop, in a resident lounge, or in the operating room, these mobile technologies help us to learn more efficiently while on the go.
If there are any gems we have forgotten to highlight, please send an e-mail to Thoracic Surgery News and we will try to present them in the future. We hope that the residents reading this column can find a new app they didn't know they needed, one that will energize them and push their learning to a new height. Just don't forget to look up once in a while.
Dr. Antonoff is a 2nd-year, Thoracic-track trainee at Washington University in St Louis. Dr. Zeigler is a 3rd-year, integrated Cardiothoracic Surgery trainee at Stanford (Calif.) University. They reported no relevant financial conflicts.
