User login
11 Things Neurologists Think Hospitalists Need To Know

11 Things: At a Glance
- You might be overdiagnosing transient ischemic attacks (TIA).
- Early mobilization after a stroke might be better for some patients.
- MRI is the best tool to evaluate TIA patients.
- Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
- Tracking the time a hospitalized patient was last seen to be normal is crucial.
- Consider neuromuscular disorders when a patient presents with weakness.
- Urinary tract infections (UTIs) are not the only cause of altered mental status.
- Take care in distinguishing aphasia from general confusion.
- A simple checklist might eliminate the need to consult the neurologist.
- Calling a neurologist earlier is way better than calling later.
- Hire a neurohospitalist if your institution doesn’t have one already.
When a patient is admitted to the hospital with neurological symptoms, such as altered mental status, he or she might not be the only one who is confused. Hospitalists might be a little confused, too.
Of all the subspecialties to which hospitalists are exposed, none might make them more uncomfortable than neurology. Because of what often is a dearth of training in this area, and because of the vexing and sometimes fleeting nature of symptoms, hospitalists might be inclined to lean on neurologists more than other specialists.
The Hospitalist spoke with a half-dozen experts, gathering their words of guidance and clinical tips. Here’s hoping they give you a little extra confidence the next time you see a patient with altered mental status.
You might be overdiagnosing transient ischemic attacks (TIA).
Ira Chang, MD, a neurohospitalist with Blue Sky Neurology in Englewood, Colo., and assistant clinical professor at the University of Colorado Health Sciences Center in Denver, says TIA is all too commonly a go-to diagnosis, frequently when there’s another cause.
“I think that hospitalists, and maybe medical internists in general, are very quick to diagnose anything that has a neurologic symptom that comes and goes as a TIA,” she says. “Patients have to have specific neurologic symptoms that we think are due to arterial blood flow or ischemia problems.”
Near-fainting spells and dizzy spells involving confusion commonly are diagnosed as TIA when these symptoms could be due to “a number of other causes,” Dr. Chang adds.

Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says the suspicion of a TIA should be greater if the patient is older or has traditional cardiovascular risk factors, such as hyptertension, diabetes, hyperlipidemia, or tobacco use.
A TIA typically causes symptoms referable to common arterial distributions. Carotid-distribution TIA often causes ipsilateral loss of vision and contralateral weakness or numbness. Posterior-circulation TIAs bring on symptoms such as ataxia, unilateral or bilateral limb weakness, diplopia, and slurred or slow speech.
TIA diagnoses can be tricky even for those trained in neurology, Dr. Barrett says.
“Even among fellowship-trained vascular neurologists, TIA can be a challenging diagnosis, often with poor inter-observer agreement,” he notes.
Early mobilization after a stroke might be better for some patients.
After receiving tissue plasminogen activator (tPA) therapy for stroke, patients historically were kept on bed rest for 24 hours to reduce the risk of hemorrhage. Evidence now is coming to light that some patients might benefit from getting out of bed sooner, Dr. Barrett says.1
“We’re learning that in selected patients, they can actually be mobilized at 12 hours,” he says. “In some cases, that would not only reduce the risk of complications related to immobilization like DVT but shorten length of stay. These are all important metrics for anybody who practices primarily within an inpatient setting.”
Early mobilization generally is more suitable for patients with less severe deficits and who are hemodynamically stable.
MRI is the best tool to evaluate TIA patients.
TIA patients who have transient symptoms and normal diffusion-weighted imaging (DWI) abnormalities on an MRI are at a very low risk. “Less than 1% of those patients have a stroke within the subsequent seven days,” Dr. Barrett says.2 “But those patients who do have a DWI abnormality, they’re at very high risk: 7.1% at seven days.
“The utility of MRI following TIA is becoming very much apparent. It is something that hospitalists should be aware of.”
Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
Patients experiencing confusion or speech disturbance or altered mentation—particularly if they’re elderly or have dementia—could be having a partial seizure, Dr. Chang says. Dementia patients have a 10% to 15% incidence of complex partial seizures, she says.
“I see that underdiagnosed a lot,” she says. “They keep coming back, and everybody diagnoses them with TIAs. So they keep getting put on aspirin, and they get switched to Aggrenox [to prevent clotting]. They keep coming back with the same symptoms.”
Tracking the time a hospitalized patient was last seen to be normal is crucial.
About 10% to 15% of strokes occur in patients who are in the hospital.
“While a lot of those strokes are perioperative, there also are patients who are going to be on hospitalist services,” says Eric Adelman, MD, assistant professor of neurology at the University of Michigan in Ann Arbor.

Hospitalists should note that patients suffering strokes are found not just in the ED but also on the floor, where all the tools for treatment might not be as readily available. That makes those cases a challenge and makes forethought that much more important, Dr. Adelman says.
“It’s a matter of trying to track down last normal times,” he says. “If they’re eligible for tPA and they’re within the therapeutic window, we should be able to do that within a hospital.”
Establishing a neurological baseline is particularly important for patients who are at higher stroke risk, like those with atrial fibrillation and other cardiovascular risk factors.
“In case something does happen,” Dr. Adelman says, “at least you have a baseline so you can [know that] at time X, we knew they had full strength in their right arm, and now they don’t.”
Consider neuromuscular disorders when a patient presents with weakness.
It’s safe to say some hospitalists might miss a neuromuscular disorder, Dr. Chang says.
“A lot of disorders that are harder for hospitalists to diagnose and that tend to take longer to call a neurologist [on] are things that are due to myasthenia gravis [a breakdown between nerves and muscles leading to muscle fatigue], myopathy, or ALS,” she says. “Many patients present with weakness. I think a lot of times there will be a lot of tests on and a lot of treatment for general medical conditions that can cause weakness.”
And that might be a case of misdirected attention. Patients with weakness accompanied by persistent swallowing problems, slurred speech with no other obvious cause, or the inability to lift their head off the bed without an obvious cause may end up with a neuromuscular diagnosis, she says.
It would be helpful to have a neurologist’s input in these cases, she says, where “nothing’s getting better, and three, four, five days later, the patient’s still weak.
“I think a neurologist would be more in tune with something like that,” she adds.
Urinary tract infections (UTIs) are not the only cause of altered mental status.
That might seem obvious, but too often, a UTI can be pegged as the source of altered mental status when it should not be, Dr. Chang says.
“We get a lot of people who come in with confusion and they have a slightly abnormal urinalysis and they diagnose them with UTI,” Dr. Chang says. “And it turns out that they actually had a stroke or they had a seizure.”
Significantly altered mentation should show a significantly abnormal urine with a positive culture, she says. “They ought to have significant laboratory support for a urinary tract infection.”
Dr. Barrett says a neurologic review of systems, or at least a neurologic exam, should be the physician’s guide.
“Those are key parts of a hospitalist’s practice,” he says, “because that’s what’s truly going to guide them to consider primary neurological causes of altered mental status.”
Take care in distinguishing aphasia from general confusion.
If a patient is still talking and is fairly fluent, that doesn’t mean they aren’t suffering from certain types of aphasia, a disorder caused by damage to parts of the brain that control language, Dr. Adelman says.
“Oftentimes, when you’re dealing with a patient with confusion, you want to make sure that it’s confusion, or encephalopathy, rather than a focal neurologic problem like aphasia,” he says. “Frequently patients with aphasia will have other symptoms such as a facial drop or weakness in the arm, but stroke can present as isolated aphasia.”
A good habit to get into is to determine whether the patient can repeat a phrase, follow a command, or name objects, he says. If they can, they probably do not have aphasia.
“The thing that you worry about with aphasia, particularly acute onset aphasia, is an ischemic stroke,” Dr. Adelman says.
A simple checklist might eliminate the need to consult the neurologist.
When Edgar Kenton, MD, now director of the stroke program at Geisinger Health System in Danville, Pa., was at Emory University Hospital in Atlanta, he found he was getting snowed under with consults from hospitalists. There were about 15 hospitalists for just one or two neurologists.
“There was no way I was able to see these patients, particularly in follow-up, because you might get five consults every day,” he says. “By the middle of the week, that’s 15 consults. You don’t get a chance to go back and see the patients because you’re just going from one consult to the other.”
The situation improved with a checklist of things to consider when a patient presents with altered mental status. Before seeking a consult, neurologists suggested the hospitalists check the electrolytes, blood pressure, and urine, and use CT scans as a screening test. That might uncover the root of the patient’s problems. If those are clear, by all means get the neurologist involved, he says.
“We were able to educate the hospitalists so they knew when to call; they knew when it was beyond their expertise to take care of the patient, so we weren’t getting called for every patient with altered mental status when all they needed to do was to check the electrolytes,” Dr. Kenton says.
Calling a neurologist earlier is way better than calling later.
Once the decision is made to consult with a neurologist, the consult should be done right away, Dr. Kenton says, not after a few days when symptoms don’t appear to be improving.
“We’ll get the call on a Friday afternoon because they thought, finally, ‘Well, you know, we need to get neurology involved because we a) haven’t solved the problem and b) there may be some other tests we should be getting,’” he says of common situations. “That has been a problem. If you don’t have a neurohospitalist involved day by day, working with the patient and the general hospitalist, neurology becomes an afterthought.”
He says accurate and early diagnosis is paramount to the patient.
“If the diagnosis is delayed, obviously there’s more insult to the patients, more persistent insult,” he says, noting the timing is particularly important in neurological conditions “because things can get bad in a hurry.”
He strongly urges hospitalists to consult with a neurologist before ordering an entire battery of tests.
At Geisinger, neurologists are encouraging hospitalists to chat informally with neurosurgeons about cases for guidance at the outset rather than after several days.
Hire a neurohospitalist if your institution doesn’t have one already.
At the top of the list of Dr. Kenton’s suggestions on caring for hospitalized neurology patients is this declaration: “Get a neurohospitalist.”
“It’s important to have the neurologist involved from the time the patient’s admitted,” he says. “That’s the value of connecting the general hospitalist with neurologists.”
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says his colleagues are team players and improve patient care.
“Neurology consultations can be called very quickly, and a nice partnership can develop between internal medicine hospitalists and neurohospitalists to care for those patients who have those medical and neurologic problems,” he says.
He also says having a neurohospitalist on board can ease some of the tension.
“No longer if there’s a neurologic condition does a hospitalist have to think about, ‘Well, does this rise to the level of something that I need to get the neurologist to drive across the city to come see?’” he explains. “‘Or is this something we should try to manage ourselves?’”
Tom Collins is a freelance writer in South Florida.
“Neurophobia” a Challenge for Hospitalists, Other Physicians

The unease that many hospitalists, internal-medicine doctors, and other providers feel about treating neurologic conditions is so readily recognized that a term has been coined to describe it: “neurophobia.”
The term has been used in published literature for at least two decades. A 2010 survey found that medical students and residents felt that neurology was the specialty they had the least knowledge about and was the one that was the most difficult.3 And trainees had the least confidence in treating patients with neurological complaints.
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says internal-medicine hospitalists are “increasingly feeling uncomfortable with requests that they have to care for patients with a wide range of primary neurologic conditions in some instances.”
That has helped lead to the emergence of neurohospitalists, he says.
John Vazquez, MD, medical director of the division hospital medicine of Emory University Hospital in Atlanta, says neurophobia is real.
“Every hospitalist has different subspecialty areas that they’re less comfortable with, and I think neurology specifically is one that does scare a lot of hospitalists,” he says. “I think on one side there are hospitalists that might ignore a neurologic problem because they don’t really know what they don’t know. On the other side are the hospitalists who I think are just concerned that they don’t know the field very well and may not feel comfortable.”
Dr. Vazquez did rotations in nephrology, pulmonology, cardiology, and rheumatology but, like many hospitalists, not neurology.
“Neurology is not one that you have to go through,” he says.
He made these suggestions:
- Know what you don’t know and get guidance when necessary.
- Do your own neurologic assessment. Even if a neurologist decides confusion is due to a patient being elderly and having a urinary tract infection, that doesn’t mean that they didn’t actually have a stroke. So if something seems not quite right, be willing to challenge the neurologist.
- Use the resources available to widen your knowledge base.
“You can utilize the consultants for your own education if you have neurologists in your hospital, and many at least have some that rotate in,” Dr. Vazquez says. “You can pick their brain on what they would do with different strokes and what’s the newest thing and ongoing treatment and whatever it is you’re concerned about.”
—Thomas R. Collins
John Vazquez, MD, of Emory University Hospital talks about neurophobia and provides tips for adjusting to the discomfort of working with neurology patients.
References
- Bernhardt J, Dewey H, Thrift A, Collier J, Donnan G. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke. 2008;39;390-396.
- Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs. time-defined TIA: a multicenter study. Neurology. 2011;77(13):1222-1228.
- Zinchuk AV, Flanagan EP, Tubridy NJ, Miller WA, McCullough LD. Attitudes of US medical trainees towards neurology education: “Neurophobia”—a global issue. BMC Med Educ. 2010;10:49.
11 Things: At a Glance
- You might be overdiagnosing transient ischemic attacks (TIA).
- Early mobilization after a stroke might be better for some patients.
- MRI is the best tool to evaluate TIA patients.
- Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
- Tracking the time a hospitalized patient was last seen to be normal is crucial.
- Consider neuromuscular disorders when a patient presents with weakness.
- Urinary tract infections (UTIs) are not the only cause of altered mental status.
- Take care in distinguishing aphasia from general confusion.
- A simple checklist might eliminate the need to consult the neurologist.
- Calling a neurologist earlier is way better than calling later.
- Hire a neurohospitalist if your institution doesn’t have one already.
When a patient is admitted to the hospital with neurological symptoms, such as altered mental status, he or she might not be the only one who is confused. Hospitalists might be a little confused, too.
Of all the subspecialties to which hospitalists are exposed, none might make them more uncomfortable than neurology. Because of what often is a dearth of training in this area, and because of the vexing and sometimes fleeting nature of symptoms, hospitalists might be inclined to lean on neurologists more than other specialists.
The Hospitalist spoke with a half-dozen experts, gathering their words of guidance and clinical tips. Here’s hoping they give you a little extra confidence the next time you see a patient with altered mental status.
You might be overdiagnosing transient ischemic attacks (TIA).
Ira Chang, MD, a neurohospitalist with Blue Sky Neurology in Englewood, Colo., and assistant clinical professor at the University of Colorado Health Sciences Center in Denver, says TIA is all too commonly a go-to diagnosis, frequently when there’s another cause.
“I think that hospitalists, and maybe medical internists in general, are very quick to diagnose anything that has a neurologic symptom that comes and goes as a TIA,” she says. “Patients have to have specific neurologic symptoms that we think are due to arterial blood flow or ischemia problems.”
Near-fainting spells and dizzy spells involving confusion commonly are diagnosed as TIA when these symptoms could be due to “a number of other causes,” Dr. Chang adds.
Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says the suspicion of a TIA should be greater if the patient is older or has traditional cardiovascular risk factors, such as hyptertension, diabetes, hyperlipidemia, or tobacco use.
A TIA typically causes symptoms referable to common arterial distributions. Carotid-distribution TIA often causes ipsilateral loss of vision and contralateral weakness or numbness. Posterior-circulation TIAs bring on symptoms such as ataxia, unilateral or bilateral limb weakness, diplopia, and slurred or slow speech.
TIA diagnoses can be tricky even for those trained in neurology, Dr. Barrett says.
“Even among fellowship-trained vascular neurologists, TIA can be a challenging diagnosis, often with poor inter-observer agreement,” he notes.
Early mobilization after a stroke might be better for some patients.
After receiving tissue plasminogen activator (tPA) therapy for stroke, patients historically were kept on bed rest for 24 hours to reduce the risk of hemorrhage. Evidence now is coming to light that some patients might benefit from getting out of bed sooner, Dr. Barrett says.1
“We’re learning that in selected patients, they can actually be mobilized at 12 hours,” he says. “In some cases, that would not only reduce the risk of complications related to immobilization like DVT but shorten length of stay. These are all important metrics for anybody who practices primarily within an inpatient setting.”
Early mobilization generally is more suitable for patients with less severe deficits and who are hemodynamically stable.
MRI is the best tool to evaluate TIA patients.
TIA patients who have transient symptoms and normal diffusion-weighted imaging (DWI) abnormalities on an MRI are at a very low risk. “Less than 1% of those patients have a stroke within the subsequent seven days,” Dr. Barrett says.2 “But those patients who do have a DWI abnormality, they’re at very high risk: 7.1% at seven days.
“The utility of MRI following TIA is becoming very much apparent. It is something that hospitalists should be aware of.”
Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
Patients experiencing confusion or speech disturbance or altered mentation—particularly if they’re elderly or have dementia—could be having a partial seizure, Dr. Chang says. Dementia patients have a 10% to 15% incidence of complex partial seizures, she says.
“I see that underdiagnosed a lot,” she says. “They keep coming back, and everybody diagnoses them with TIAs. So they keep getting put on aspirin, and they get switched to Aggrenox [to prevent clotting]. They keep coming back with the same symptoms.”
Tracking the time a hospitalized patient was last seen to be normal is crucial.
About 10% to 15% of strokes occur in patients who are in the hospital.
“While a lot of those strokes are perioperative, there also are patients who are going to be on hospitalist services,” says Eric Adelman, MD, assistant professor of neurology at the University of Michigan in Ann Arbor.
Hospitalists should note that patients suffering strokes are found not just in the ED but also on the floor, where all the tools for treatment might not be as readily available. That makes those cases a challenge and makes forethought that much more important, Dr. Adelman says.
“It’s a matter of trying to track down last normal times,” he says. “If they’re eligible for tPA and they’re within the therapeutic window, we should be able to do that within a hospital.”
Establishing a neurological baseline is particularly important for patients who are at higher stroke risk, like those with atrial fibrillation and other cardiovascular risk factors.
“In case something does happen,” Dr. Adelman says, “at least you have a baseline so you can [know that] at time X, we knew they had full strength in their right arm, and now they don’t.”
Consider neuromuscular disorders when a patient presents with weakness.
It’s safe to say some hospitalists might miss a neuromuscular disorder, Dr. Chang says.
“A lot of disorders that are harder for hospitalists to diagnose and that tend to take longer to call a neurologist [on] are things that are due to myasthenia gravis [a breakdown between nerves and muscles leading to muscle fatigue], myopathy, or ALS,” she says. “Many patients present with weakness. I think a lot of times there will be a lot of tests on and a lot of treatment for general medical conditions that can cause weakness.”
And that might be a case of misdirected attention. Patients with weakness accompanied by persistent swallowing problems, slurred speech with no other obvious cause, or the inability to lift their head off the bed without an obvious cause may end up with a neuromuscular diagnosis, she says.
It would be helpful to have a neurologist’s input in these cases, she says, where “nothing’s getting better, and three, four, five days later, the patient’s still weak.
“I think a neurologist would be more in tune with something like that,” she adds.
Urinary tract infections (UTIs) are not the only cause of altered mental status.
That might seem obvious, but too often, a UTI can be pegged as the source of altered mental status when it should not be, Dr. Chang says.
“We get a lot of people who come in with confusion and they have a slightly abnormal urinalysis and they diagnose them with UTI,” Dr. Chang says. “And it turns out that they actually had a stroke or they had a seizure.”
Significantly altered mentation should show a significantly abnormal urine with a positive culture, she says. “They ought to have significant laboratory support for a urinary tract infection.”
Dr. Barrett says a neurologic review of systems, or at least a neurologic exam, should be the physician’s guide.
“Those are key parts of a hospitalist’s practice,” he says, “because that’s what’s truly going to guide them to consider primary neurological causes of altered mental status.”
Take care in distinguishing aphasia from general confusion.
If a patient is still talking and is fairly fluent, that doesn’t mean they aren’t suffering from certain types of aphasia, a disorder caused by damage to parts of the brain that control language, Dr. Adelman says.
“Oftentimes, when you’re dealing with a patient with confusion, you want to make sure that it’s confusion, or encephalopathy, rather than a focal neurologic problem like aphasia,” he says. “Frequently patients with aphasia will have other symptoms such as a facial drop or weakness in the arm, but stroke can present as isolated aphasia.”
A good habit to get into is to determine whether the patient can repeat a phrase, follow a command, or name objects, he says. If they can, they probably do not have aphasia.
“The thing that you worry about with aphasia, particularly acute onset aphasia, is an ischemic stroke,” Dr. Adelman says.
A simple checklist might eliminate the need to consult the neurologist.
When Edgar Kenton, MD, now director of the stroke program at Geisinger Health System in Danville, Pa., was at Emory University Hospital in Atlanta, he found he was getting snowed under with consults from hospitalists. There were about 15 hospitalists for just one or two neurologists.
“There was no way I was able to see these patients, particularly in follow-up, because you might get five consults every day,” he says. “By the middle of the week, that’s 15 consults. You don’t get a chance to go back and see the patients because you’re just going from one consult to the other.”
The situation improved with a checklist of things to consider when a patient presents with altered mental status. Before seeking a consult, neurologists suggested the hospitalists check the electrolytes, blood pressure, and urine, and use CT scans as a screening test. That might uncover the root of the patient’s problems. If those are clear, by all means get the neurologist involved, he says.
“We were able to educate the hospitalists so they knew when to call; they knew when it was beyond their expertise to take care of the patient, so we weren’t getting called for every patient with altered mental status when all they needed to do was to check the electrolytes,” Dr. Kenton says.
Calling a neurologist earlier is way better than calling later.
Once the decision is made to consult with a neurologist, the consult should be done right away, Dr. Kenton says, not after a few days when symptoms don’t appear to be improving.
“We’ll get the call on a Friday afternoon because they thought, finally, ‘Well, you know, we need to get neurology involved because we a) haven’t solved the problem and b) there may be some other tests we should be getting,’” he says of common situations. “That has been a problem. If you don’t have a neurohospitalist involved day by day, working with the patient and the general hospitalist, neurology becomes an afterthought.”
He says accurate and early diagnosis is paramount to the patient.
“If the diagnosis is delayed, obviously there’s more insult to the patients, more persistent insult,” he says, noting the timing is particularly important in neurological conditions “because things can get bad in a hurry.”
He strongly urges hospitalists to consult with a neurologist before ordering an entire battery of tests.
At Geisinger, neurologists are encouraging hospitalists to chat informally with neurosurgeons about cases for guidance at the outset rather than after several days.
Hire a neurohospitalist if your institution doesn’t have one already.
At the top of the list of Dr. Kenton’s suggestions on caring for hospitalized neurology patients is this declaration: “Get a neurohospitalist.”
“It’s important to have the neurologist involved from the time the patient’s admitted,” he says. “That’s the value of connecting the general hospitalist with neurologists.”
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says his colleagues are team players and improve patient care.
“Neurology consultations can be called very quickly, and a nice partnership can develop between internal medicine hospitalists and neurohospitalists to care for those patients who have those medical and neurologic problems,” he says.
He also says having a neurohospitalist on board can ease some of the tension.
“No longer if there’s a neurologic condition does a hospitalist have to think about, ‘Well, does this rise to the level of something that I need to get the neurologist to drive across the city to come see?’” he explains. “‘Or is this something we should try to manage ourselves?’”
Tom Collins is a freelance writer in South Florida.
“Neurophobia” a Challenge for Hospitalists, Other Physicians
The unease that many hospitalists, internal-medicine doctors, and other providers feel about treating neurologic conditions is so readily recognized that a term has been coined to describe it: “neurophobia.”
The term has been used in published literature for at least two decades. A 2010 survey found that medical students and residents felt that neurology was the specialty they had the least knowledge about and was the one that was the most difficult.3 And trainees had the least confidence in treating patients with neurological complaints.
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says internal-medicine hospitalists are “increasingly feeling uncomfortable with requests that they have to care for patients with a wide range of primary neurologic conditions in some instances.”
That has helped lead to the emergence of neurohospitalists, he says.
John Vazquez, MD, medical director of the division hospital medicine of Emory University Hospital in Atlanta, says neurophobia is real.
“Every hospitalist has different subspecialty areas that they’re less comfortable with, and I think neurology specifically is one that does scare a lot of hospitalists,” he says. “I think on one side there are hospitalists that might ignore a neurologic problem because they don’t really know what they don’t know. On the other side are the hospitalists who I think are just concerned that they don’t know the field very well and may not feel comfortable.”
Dr. Vazquez did rotations in nephrology, pulmonology, cardiology, and rheumatology but, like many hospitalists, not neurology.
“Neurology is not one that you have to go through,” he says.
He made these suggestions:
- Know what you don’t know and get guidance when necessary.
- Do your own neurologic assessment. Even if a neurologist decides confusion is due to a patient being elderly and having a urinary tract infection, that doesn’t mean that they didn’t actually have a stroke. So if something seems not quite right, be willing to challenge the neurologist.
- Use the resources available to widen your knowledge base.
“You can utilize the consultants for your own education if you have neurologists in your hospital, and many at least have some that rotate in,” Dr. Vazquez says. “You can pick their brain on what they would do with different strokes and what’s the newest thing and ongoing treatment and whatever it is you’re concerned about.”
—Thomas R. Collins
John Vazquez, MD, of Emory University Hospital talks about neurophobia and provides tips for adjusting to the discomfort of working with neurology patients.
References
- Bernhardt J, Dewey H, Thrift A, Collier J, Donnan G. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke. 2008;39;390-396.
- Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs. time-defined TIA: a multicenter study. Neurology. 2011;77(13):1222-1228.
- Zinchuk AV, Flanagan EP, Tubridy NJ, Miller WA, McCullough LD. Attitudes of US medical trainees towards neurology education: “Neurophobia”—a global issue. BMC Med Educ. 2010;10:49.
11 Things: At a Glance
- You might be overdiagnosing transient ischemic attacks (TIA).
- Early mobilization after a stroke might be better for some patients.
- MRI is the best tool to evaluate TIA patients.
- Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
- Tracking the time a hospitalized patient was last seen to be normal is crucial.
- Consider neuromuscular disorders when a patient presents with weakness.
- Urinary tract infections (UTIs) are not the only cause of altered mental status.
- Take care in distinguishing aphasia from general confusion.
- A simple checklist might eliminate the need to consult the neurologist.
- Calling a neurologist earlier is way better than calling later.
- Hire a neurohospitalist if your institution doesn’t have one already.
When a patient is admitted to the hospital with neurological symptoms, such as altered mental status, he or she might not be the only one who is confused. Hospitalists might be a little confused, too.
Of all the subspecialties to which hospitalists are exposed, none might make them more uncomfortable than neurology. Because of what often is a dearth of training in this area, and because of the vexing and sometimes fleeting nature of symptoms, hospitalists might be inclined to lean on neurologists more than other specialists.
The Hospitalist spoke with a half-dozen experts, gathering their words of guidance and clinical tips. Here’s hoping they give you a little extra confidence the next time you see a patient with altered mental status.
You might be overdiagnosing transient ischemic attacks (TIA).
Ira Chang, MD, a neurohospitalist with Blue Sky Neurology in Englewood, Colo., and assistant clinical professor at the University of Colorado Health Sciences Center in Denver, says TIA is all too commonly a go-to diagnosis, frequently when there’s another cause.
“I think that hospitalists, and maybe medical internists in general, are very quick to diagnose anything that has a neurologic symptom that comes and goes as a TIA,” she says. “Patients have to have specific neurologic symptoms that we think are due to arterial blood flow or ischemia problems.”
Near-fainting spells and dizzy spells involving confusion commonly are diagnosed as TIA when these symptoms could be due to “a number of other causes,” Dr. Chang adds.
Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says the suspicion of a TIA should be greater if the patient is older or has traditional cardiovascular risk factors, such as hyptertension, diabetes, hyperlipidemia, or tobacco use.
A TIA typically causes symptoms referable to common arterial distributions. Carotid-distribution TIA often causes ipsilateral loss of vision and contralateral weakness or numbness. Posterior-circulation TIAs bring on symptoms such as ataxia, unilateral or bilateral limb weakness, diplopia, and slurred or slow speech.
TIA diagnoses can be tricky even for those trained in neurology, Dr. Barrett says.
“Even among fellowship-trained vascular neurologists, TIA can be a challenging diagnosis, often with poor inter-observer agreement,” he notes.
Early mobilization after a stroke might be better for some patients.
After receiving tissue plasminogen activator (tPA) therapy for stroke, patients historically were kept on bed rest for 24 hours to reduce the risk of hemorrhage. Evidence now is coming to light that some patients might benefit from getting out of bed sooner, Dr. Barrett says.1
“We’re learning that in selected patients, they can actually be mobilized at 12 hours,” he says. “In some cases, that would not only reduce the risk of complications related to immobilization like DVT but shorten length of stay. These are all important metrics for anybody who practices primarily within an inpatient setting.”
Early mobilization generally is more suitable for patients with less severe deficits and who are hemodynamically stable.
MRI is the best tool to evaluate TIA patients.
TIA patients who have transient symptoms and normal diffusion-weighted imaging (DWI) abnormalities on an MRI are at a very low risk. “Less than 1% of those patients have a stroke within the subsequent seven days,” Dr. Barrett says.2 “But those patients who do have a DWI abnormality, they’re at very high risk: 7.1% at seven days.
“The utility of MRI following TIA is becoming very much apparent. It is something that hospitalists should be aware of.”
Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
Patients experiencing confusion or speech disturbance or altered mentation—particularly if they’re elderly or have dementia—could be having a partial seizure, Dr. Chang says. Dementia patients have a 10% to 15% incidence of complex partial seizures, she says.
“I see that underdiagnosed a lot,” she says. “They keep coming back, and everybody diagnoses them with TIAs. So they keep getting put on aspirin, and they get switched to Aggrenox [to prevent clotting]. They keep coming back with the same symptoms.”
Tracking the time a hospitalized patient was last seen to be normal is crucial.
About 10% to 15% of strokes occur in patients who are in the hospital.
“While a lot of those strokes are perioperative, there also are patients who are going to be on hospitalist services,” says Eric Adelman, MD, assistant professor of neurology at the University of Michigan in Ann Arbor.
Hospitalists should note that patients suffering strokes are found not just in the ED but also on the floor, where all the tools for treatment might not be as readily available. That makes those cases a challenge and makes forethought that much more important, Dr. Adelman says.
“It’s a matter of trying to track down last normal times,” he says. “If they’re eligible for tPA and they’re within the therapeutic window, we should be able to do that within a hospital.”
Establishing a neurological baseline is particularly important for patients who are at higher stroke risk, like those with atrial fibrillation and other cardiovascular risk factors.
“In case something does happen,” Dr. Adelman says, “at least you have a baseline so you can [know that] at time X, we knew they had full strength in their right arm, and now they don’t.”
Consider neuromuscular disorders when a patient presents with weakness.
It’s safe to say some hospitalists might miss a neuromuscular disorder, Dr. Chang says.
“A lot of disorders that are harder for hospitalists to diagnose and that tend to take longer to call a neurologist [on] are things that are due to myasthenia gravis [a breakdown between nerves and muscles leading to muscle fatigue], myopathy, or ALS,” she says. “Many patients present with weakness. I think a lot of times there will be a lot of tests on and a lot of treatment for general medical conditions that can cause weakness.”
And that might be a case of misdirected attention. Patients with weakness accompanied by persistent swallowing problems, slurred speech with no other obvious cause, or the inability to lift their head off the bed without an obvious cause may end up with a neuromuscular diagnosis, she says.
It would be helpful to have a neurologist’s input in these cases, she says, where “nothing’s getting better, and three, four, five days later, the patient’s still weak.
“I think a neurologist would be more in tune with something like that,” she adds.
Urinary tract infections (UTIs) are not the only cause of altered mental status.
That might seem obvious, but too often, a UTI can be pegged as the source of altered mental status when it should not be, Dr. Chang says.
“We get a lot of people who come in with confusion and they have a slightly abnormal urinalysis and they diagnose them with UTI,” Dr. Chang says. “And it turns out that they actually had a stroke or they had a seizure.”
Significantly altered mentation should show a significantly abnormal urine with a positive culture, she says. “They ought to have significant laboratory support for a urinary tract infection.”
Dr. Barrett says a neurologic review of systems, or at least a neurologic exam, should be the physician’s guide.
“Those are key parts of a hospitalist’s practice,” he says, “because that’s what’s truly going to guide them to consider primary neurological causes of altered mental status.”
Take care in distinguishing aphasia from general confusion.
If a patient is still talking and is fairly fluent, that doesn’t mean they aren’t suffering from certain types of aphasia, a disorder caused by damage to parts of the brain that control language, Dr. Adelman says.
“Oftentimes, when you’re dealing with a patient with confusion, you want to make sure that it’s confusion, or encephalopathy, rather than a focal neurologic problem like aphasia,” he says. “Frequently patients with aphasia will have other symptoms such as a facial drop or weakness in the arm, but stroke can present as isolated aphasia.”
A good habit to get into is to determine whether the patient can repeat a phrase, follow a command, or name objects, he says. If they can, they probably do not have aphasia.
“The thing that you worry about with aphasia, particularly acute onset aphasia, is an ischemic stroke,” Dr. Adelman says.
A simple checklist might eliminate the need to consult the neurologist.
When Edgar Kenton, MD, now director of the stroke program at Geisinger Health System in Danville, Pa., was at Emory University Hospital in Atlanta, he found he was getting snowed under with consults from hospitalists. There were about 15 hospitalists for just one or two neurologists.
“There was no way I was able to see these patients, particularly in follow-up, because you might get five consults every day,” he says. “By the middle of the week, that’s 15 consults. You don’t get a chance to go back and see the patients because you’re just going from one consult to the other.”
The situation improved with a checklist of things to consider when a patient presents with altered mental status. Before seeking a consult, neurologists suggested the hospitalists check the electrolytes, blood pressure, and urine, and use CT scans as a screening test. That might uncover the root of the patient’s problems. If those are clear, by all means get the neurologist involved, he says.
“We were able to educate the hospitalists so they knew when to call; they knew when it was beyond their expertise to take care of the patient, so we weren’t getting called for every patient with altered mental status when all they needed to do was to check the electrolytes,” Dr. Kenton says.
Calling a neurologist earlier is way better than calling later.
Once the decision is made to consult with a neurologist, the consult should be done right away, Dr. Kenton says, not after a few days when symptoms don’t appear to be improving.
“We’ll get the call on a Friday afternoon because they thought, finally, ‘Well, you know, we need to get neurology involved because we a) haven’t solved the problem and b) there may be some other tests we should be getting,’” he says of common situations. “That has been a problem. If you don’t have a neurohospitalist involved day by day, working with the patient and the general hospitalist, neurology becomes an afterthought.”
He says accurate and early diagnosis is paramount to the patient.
“If the diagnosis is delayed, obviously there’s more insult to the patients, more persistent insult,” he says, noting the timing is particularly important in neurological conditions “because things can get bad in a hurry.”
He strongly urges hospitalists to consult with a neurologist before ordering an entire battery of tests.
At Geisinger, neurologists are encouraging hospitalists to chat informally with neurosurgeons about cases for guidance at the outset rather than after several days.
Hire a neurohospitalist if your institution doesn’t have one already.
At the top of the list of Dr. Kenton’s suggestions on caring for hospitalized neurology patients is this declaration: “Get a neurohospitalist.”
“It’s important to have the neurologist involved from the time the patient’s admitted,” he says. “That’s the value of connecting the general hospitalist with neurologists.”
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says his colleagues are team players and improve patient care.
“Neurology consultations can be called very quickly, and a nice partnership can develop between internal medicine hospitalists and neurohospitalists to care for those patients who have those medical and neurologic problems,” he says.
He also says having a neurohospitalist on board can ease some of the tension.
“No longer if there’s a neurologic condition does a hospitalist have to think about, ‘Well, does this rise to the level of something that I need to get the neurologist to drive across the city to come see?’” he explains. “‘Or is this something we should try to manage ourselves?’”
Tom Collins is a freelance writer in South Florida.
“Neurophobia” a Challenge for Hospitalists, Other Physicians
The unease that many hospitalists, internal-medicine doctors, and other providers feel about treating neurologic conditions is so readily recognized that a term has been coined to describe it: “neurophobia.”
The term has been used in published literature for at least two decades. A 2010 survey found that medical students and residents felt that neurology was the specialty they had the least knowledge about and was the one that was the most difficult.3 And trainees had the least confidence in treating patients with neurological complaints.
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says internal-medicine hospitalists are “increasingly feeling uncomfortable with requests that they have to care for patients with a wide range of primary neurologic conditions in some instances.”
That has helped lead to the emergence of neurohospitalists, he says.
John Vazquez, MD, medical director of the division hospital medicine of Emory University Hospital in Atlanta, says neurophobia is real.
“Every hospitalist has different subspecialty areas that they’re less comfortable with, and I think neurology specifically is one that does scare a lot of hospitalists,” he says. “I think on one side there are hospitalists that might ignore a neurologic problem because they don’t really know what they don’t know. On the other side are the hospitalists who I think are just concerned that they don’t know the field very well and may not feel comfortable.”
Dr. Vazquez did rotations in nephrology, pulmonology, cardiology, and rheumatology but, like many hospitalists, not neurology.
“Neurology is not one that you have to go through,” he says.
He made these suggestions:
- Know what you don’t know and get guidance when necessary.
- Do your own neurologic assessment. Even if a neurologist decides confusion is due to a patient being elderly and having a urinary tract infection, that doesn’t mean that they didn’t actually have a stroke. So if something seems not quite right, be willing to challenge the neurologist.
- Use the resources available to widen your knowledge base.
“You can utilize the consultants for your own education if you have neurologists in your hospital, and many at least have some that rotate in,” Dr. Vazquez says. “You can pick their brain on what they would do with different strokes and what’s the newest thing and ongoing treatment and whatever it is you’re concerned about.”
—Thomas R. Collins
John Vazquez, MD, of Emory University Hospital talks about neurophobia and provides tips for adjusting to the discomfort of working with neurology patients.
References
- Bernhardt J, Dewey H, Thrift A, Collier J, Donnan G. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke. 2008;39;390-396.
- Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs. time-defined TIA: a multicenter study. Neurology. 2011;77(13):1222-1228.
- Zinchuk AV, Flanagan EP, Tubridy NJ, Miller WA, McCullough LD. Attitudes of US medical trainees towards neurology education: “Neurophobia”—a global issue. BMC Med Educ. 2010;10:49.
Obituary: Laura Mirkinson, MD, MSc, FAAP
Laura Mirkinson, MD, MSc, FAAP, pediatric hospitalist and a founder of the American Academy of Pediatrics’ (AAP) Section on Hospital Medicine Executive Committee, died April 29 of ovarian cancer. She was 60.
Dr. Mirkinson received her medical degree from Uniformed Services University of the Health Sciences (USUHS) in Bethesda, Md., before serving her pediatrics residency at Bethesda Naval Hospital and Walter Reed Army Medical Center. She served as an active-duty medical officer in the U.S. Naval Medical Corps Reserves before retiring as a captain in 2000. She then worked at Children’s Hospital of Washington and the pediatric hospitalist group at Holy Cross Hospital in Silver Spring, Md.
Dr. Mirkinson played a role in the development of pediatric hospital medicine during and after her military service. In 2007, she was elected chief of pediatrics at Blythedale Children’s Hospital in Valhalla, N.Y. She also served as director of education for the AAP’s Section on Hospital Medicine and was its second chairperson, following the section’s co-founder Jack Percelay, MD, FAAP. Through this work, she helped promote the AAP Section on Hospital Medicine newsletter, as well as the Hospital Pediatrics journal.
Dr. Mirkinson’s colleagues and students remember her as a caring, insightful teacher and mentor who offered wise advice on all matters professional and personal. Her devotion to patient care was evident throughout her career. Even in her administrative roles, she would often practice clinical medicine to help fill scheduling gaps or cover other physicians’ vacations.
Laura Mirkinson, MD, MSc, FAAP, pediatric hospitalist and a founder of the American Academy of Pediatrics’ (AAP) Section on Hospital Medicine Executive Committee, died April 29 of ovarian cancer. She was 60.
Dr. Mirkinson received her medical degree from Uniformed Services University of the Health Sciences (USUHS) in Bethesda, Md., before serving her pediatrics residency at Bethesda Naval Hospital and Walter Reed Army Medical Center. She served as an active-duty medical officer in the U.S. Naval Medical Corps Reserves before retiring as a captain in 2000. She then worked at Children’s Hospital of Washington and the pediatric hospitalist group at Holy Cross Hospital in Silver Spring, Md.
Dr. Mirkinson played a role in the development of pediatric hospital medicine during and after her military service. In 2007, she was elected chief of pediatrics at Blythedale Children’s Hospital in Valhalla, N.Y. She also served as director of education for the AAP’s Section on Hospital Medicine and was its second chairperson, following the section’s co-founder Jack Percelay, MD, FAAP. Through this work, she helped promote the AAP Section on Hospital Medicine newsletter, as well as the Hospital Pediatrics journal.
Dr. Mirkinson’s colleagues and students remember her as a caring, insightful teacher and mentor who offered wise advice on all matters professional and personal. Her devotion to patient care was evident throughout her career. Even in her administrative roles, she would often practice clinical medicine to help fill scheduling gaps or cover other physicians’ vacations.
Laura Mirkinson, MD, MSc, FAAP, pediatric hospitalist and a founder of the American Academy of Pediatrics’ (AAP) Section on Hospital Medicine Executive Committee, died April 29 of ovarian cancer. She was 60.
Dr. Mirkinson received her medical degree from Uniformed Services University of the Health Sciences (USUHS) in Bethesda, Md., before serving her pediatrics residency at Bethesda Naval Hospital and Walter Reed Army Medical Center. She served as an active-duty medical officer in the U.S. Naval Medical Corps Reserves before retiring as a captain in 2000. She then worked at Children’s Hospital of Washington and the pediatric hospitalist group at Holy Cross Hospital in Silver Spring, Md.
Dr. Mirkinson played a role in the development of pediatric hospital medicine during and after her military service. In 2007, she was elected chief of pediatrics at Blythedale Children’s Hospital in Valhalla, N.Y. She also served as director of education for the AAP’s Section on Hospital Medicine and was its second chairperson, following the section’s co-founder Jack Percelay, MD, FAAP. Through this work, she helped promote the AAP Section on Hospital Medicine newsletter, as well as the Hospital Pediatrics journal.
Dr. Mirkinson’s colleagues and students remember her as a caring, insightful teacher and mentor who offered wise advice on all matters professional and personal. Her devotion to patient care was evident throughout her career. Even in her administrative roles, she would often practice clinical medicine to help fill scheduling gaps or cover other physicians’ vacations.
Reviews of Research on Steroids and VTE Risk, Epidural Catheterization, and Beta-Blockers During Noncardiac Surgery
In This Edition
Literature At A Glance
A guide to this month’s studies
- Steroids may increase VTE risk
- Mortality rates rise at critical-care hospitals
- Physicians don’t discuss advance-care planning with elderly, families
- Ultrasound imaging for lumbar puncture, epidural catheterization
- Financial impact of surgical complications on hospitals
- Lab test fees and frequency of test ordering
- Inpatient elderly multidisciplinary teams reduce readmissions
- Use of beta-blockers in high-risk patients during noncardiac surgery
- Patient-centered decision-making and health-care outcomes
- Adverse surgical outcomes in patients with schizophrenia
Steroids May Increase VTE Risk
Clinical question: Is exogenous glucocorticoid administration associated with an increased risk of VTE?
Background: Endogenous hypercortisolism is linked to increased VTE rates, and pathophysiologic data exist to suggest glucocorticoids increase clotting, but few studies have measured the clinical link between glucocorticoid administration and VTE events.
Study design: Case-control study.
Setting: Denmark.
Synopsis: The authors analyzed Danish national registries, which include information on diagnoses and prescriptions. The study selection period was Jan. 1, 2005, to Dec. 31, 2011. During this period, 38,675 cases of VTE (both DVT and pulmonary embolism) were identified in the population of Denmark. These cases were matched with 387,650 controls. Three routes of glucocorticoid use were studied: systemic (oral and intravenous), inhaled, and intestinal-acting. Cases were classified as present (within 90 days of VTE event), recent (91 to 365 days), or former (over 365 days) users of glucocorticoids. Categories were also created for new versus continuous users.
Glucocorticoid use was associated with a significant increase in VTE occurrence. The strongest link was in new and recent users, and the effect diminished over time. Key limitations of the study included its reliance on registry data, as well as the fact that cases had more comorbid conditions than controls (e.g. recent infection, chronic illnesses).
Bottom line: Recipients of glucocorticoids had an increased risk of VTE; the effect was strongest in new and recent users.
Citation: Johannesdottir SA, Horvath-Puho E, Dekkers OM, et al. Use of glucocorticoids and risk of venous thromboembolism. JAMA Intern Med. 2013;173(9):743-752.
Mortality Rates Rise at Critical-Access Hospitals
Clinical question: How have trends in mortality changed in the past decade at critical-access hospitals when compared to other hospitals?
Background: Hospitals are designated as critical-access hospitals (CAH) by meeting certain requirements—namely, rural setting, small number of beds, and minimum distance from the nearest hospital. Because of the intrinsic challenges they face, CAHs are exempt from certain quality measures. Little data exist on patient outcomes at CAHs.
Study design: Retrospective observational study.
Setting: All nonfederal hospitals in the U.S. that provide acute care to Medicare beneficiaries.
Synopsis: Using Medicare data, risk-adjusted 30-day mortality rates were calculated at critical-access hospitals and non-critical-access hospitals from 2002 to 2010 for three conditions: acute myocardial infarction, congestive heart failure, and pneumonia. Mortality trends across these conditions were compared at baseline and over time. In 2002, CAHs had mortality rates comparable with non-CAHs. From 2002 to 2010, mortality rates increased by 0.1% per year at CAHs and decreased by 0.2% per year at non-CAHs, resulting in a mortality difference between these two hospital groups at the end of the study period. The authors postulate that differences in policy initiatives, enforcement of quality measures, and access to technology may play a role.
This study is limited in its ability to explain the findings. Notably, within the CAHs, the authors found that 48% did improve from 2002 to 2010; there were no significant differences in hospital characteristics between the CAHs that did and did not improve. The reasons for the overall widening gap between CAHs and non-CAHs, therefore, merit further investigation.
Bottom line: From 2002 to 2010, mortality rates at U.S. critical-access hospitals rose while rates fell at non-critical access hospitals.
Citation: Joynt KE, Orav EJ, Jha AK. Mortality rates for Medicare beneficiaries admitted to critical access and non-critical access hospitals, 2002-2010. JAMA. 2013;309(13):1379-1387.
Physicians Fail to Discuss Advance-Care Planning with Hospitalized Elderly, Relatives
Clinical question: Do elderly patients who are at high risk for death have documented advance-care plans, and do their physicians discuss goals of care with them?
Background: While studies indicate that most sick, elderly patients prefer a better quality of life to life-sustaining treatment, many patients still die in the hospital, often in the ICU. It is unclear whether this is due to the absence of advance-care planning or the lack of communicating goals of care.
Study design: Multicenter prospective cohort study.
Setting: Canada.
Synopsis: A validated questionnaire was used to evaluate advance-care planning both before hospitalization and on admission. Patients and their families were enrolled if they were considered at high risk for dying, including patients with advanced disease, or aged >80 years. Of the 278 patients enrolled, 76.3% had thought about advance-care planning. Approximately 47.9% of patients had written an advance-care plan, and 73.3% had formally documented a surrogate health-care decision-maker. Only a quarter of patients reported that they had been asked about advance-care planning on admission to the hospital. Patients’ stated preferences for end-of-life care were notably incongruent with goals-of-care orders documented in the hospital records. While 28% of patients preferred comfort-only care, this was documented in the hospital records for only 4.5% of patients.
In this study of mostly white, English-speaking hospitalized patients, many had considered and made advance-care plans but few had discussed this with their health-care providers. Not surprisingly, the goals-of-care orders that were documented did not match patients’ previously stated end-of-life preferences.
Bottom line: Physicians routinely fail to discuss patients’ advance-care planning, which may have profound effects on their inpatient care.
Citation: Heyland DK, Barwich D, Pichora D, et al. Failure to engage hospitalized elderly patients and their families in advance care planning. JAMA Intern Med. 2013;173(9):778-787.
Ultrasound Use Reduces Lumbar Puncture and Epidural Catheterization Failure
Clinical question: Does ultrasound imaging for lumbar puncture and epidural catheterization reduce risk of procedure failures?
Background: Numerous studies have compared ultrasound-guided lumbar puncture and epidural catheterization with standard techniques, but they have been underpowered to evaluate whether ultrasound use reduces lumbar puncture and epidural catheterization failure.
Study design: Systematic review and meta-analysis of randomized controlled trials.
Setting: Hospitals in North America, Europe, and Asia.
Synopsis: Among 14 trials, a total of 1,334 patients (including one pediatric study group) were randomly assigned either to receive ultrasound imaging or to a control group (using manual palpation or loss of resistance). Ultrasound imaging comprised a preprocedure marking approach, real-time visual guidance, or both. In the 12 trials in which the primary outcome was available, ultrasound imaging significantly reduced the risk of failed procedures with a risk ratio of 0.21 (95% confidence interval 0.10 to 0.43). A total of 16 ultrasound-guided procedures were needed to avoid one procedure failure. Ultrasound guidance also reduced the number of traumatic procedures, needle reinsertions, and needle redirections. These results were consistent across multiple subgroup analyses.
Only one of the studies included in the meta-analysis was double-blind, and in all of the studies, ultrasound imaging was performed by a clinician with high-level ultrasound experience. While this study suggests that ultrasound does reduce the frequency of procedure failure, the investigators did not include cost-effectiveness analyses.
Bottom line: Ultrasound imaging likely reduces the failure of lumbar puncture and epidural catheterization, but future research will be necessary to evaluate the cost-effectiveness of ultrasound use for these procedures.
Citation: Shaikh F, Brzezinski J, Alexander S, et al. Ultrasound imaging for lumbar punctures and epidural catheterisations: systematic review and meta-analysis. BMJ. 2013;346:f1720.
Surgical Complications might Be Financially Advantageous for Hospitals
Clinical question: What is the impact of surgical complications on hospital finances?
Background: Surgical complications are common and lead to longer lengths of stay and higher costs. Strategies are available to reduce postsurgical complications but have not been universally adopted.
Study design: Observational study.
Setting: Twelve hospitals in one nonprofit Southern hospital system, which includes academic, nonacademic, and rural settings.
Synopsis: Researchers identified 34,526 patients who underwent surgery in 2010, excluding patients undergoing Caesarean section. Of those, 1,820 procedures (5.3%) were associated with at least one complication. The most frequent complications were surgical-site infection, other infections, pneumonia, and thromboembolic disease. The mortality rate for patients with complications was 12.3% compared with 0.6% for those without. Length of stay was four times longer for patients with complications.
Complications were associated with a higher total cost of hospitalization, with a differential of $37,917. This translated into a higher contribution to the margin. The cost differential varied by insurance type, with higher contributions under Medicare and private insurance but not with Medicaid.
The study had the benefit of using a large administrative database; however, this may have underestimated the actual rate of postoperative complications. The study supports the paradox in which quality-improvement (QI) programs that reduce surgical complications and improve postoperative mortality may negatively affect a hospital’s financial performance.
Bottom line: Surgical complications lead to higher mortality for patients but a financial benefit for hospitals.
Citation: Eappen S, Lane BH, Rosenberg B, et al. Relationship between occurrence of surgical complications and hospital finances. JAMA. 2013;309(5):1509-1606.
Showing Lab Test Fees May Decrease Frequency Of Test Ordering
Clinical question: Does information on the cost of a lab test lead to lowered ordering frequency among internal-medicine residents?
Background: Lab test overuse is common; some studies estimate that 70% of lab tests do not affect care. Strategies to reduce frequency of unnecessary lab tests are needed.
Study design: Randomized controlled trial.
Setting: Johns Hopkins Hospital, a 1,051-bed academic medical center in Baltimore.
Synopsis: Researchers used an administrative database to identify the 35 most frequently ordered and the 35 most expensive tests (each ordered at least 50 times). They randomized tests to an active arm, which displayed the Medicare allowable fee at the time of order entry within the computerized physician order entry, and a control arm. A total of 1,166,753 tests were ordered during the baseline and intervention period. Many more tests were ordered in the active group relative to the control group, a consequence of the randomization process. Relative to a six-month baseline period, tests in the active group were ordered 9.1% less frequently; control-group tests were ordered 5.1% more frequently. Charges decreased by $3.79 per patient-day in the active group and increased by $0.52 per patient-day in the control group.
This study reflects a low-cost strategy to reduce lab testing and associated costs. It is unknown whether only unnecessary tests were averted, or if there was any effect on the quality of care. The durability of the intervention and its applicability to other settings and with other types of providers is unclear.
Bottom line: Showing the fee associated with lab tests may decrease the frequency of ordering these tests and the resultant costs.
Citation: Feldman LS, Shihab HM, Thiemann D, et al. Impact of providing fee data on laboratory test ordering: a controlled clinical trial. JAMA Intern Med. 2013;173(10):903-908.
Inpatient Elderly Multidisciplinary-Team-Based Unit Reduces Readmissions
Clinical question: Can an inpatient unit that uses interdisciplinary rounds and a team approach reduce 30-day readmissions and lower cost compared with usual care?
Background: Elderly patients are at risk for adverse outcomes including delirium, deconditioning, and undernutrition. The Acute Care for Elders (ACE) model is designed as a team-based approach to improve communication between clinicians and to begin discharge planning soon after admission. ACE units have been shown to improve specific outcomes in older adults, but the impact on cost is less clear.
Study design: Retrospective cohort study.
Setting: University of Alabama at Birmingham Acute Care for Elders unit.
Synopsis: The analysis of cost data extrapolated from administrative sources indicated an average of $371 in variable cost savings per patient, and therefore an expected $148,400 savings for 400 patients admitted to this unit. The rate of 30-day readmissions was significantly lower in the ACE model: 7.9% versus 12.8% in patients receiving usual care.
Limitations of this study relate both to its design and single-center location. It is unclear which aspect of this ACE unit was helpful in the studied outcomes, and how this specific program would be reproduced at another institution. There were also some costs associated with the ACE-unit staffing, which may have resulted in an overestimation of the cost savings.
Bottom line: ACE units appear to improve outcomes and may lower cost, but further investigation is needed.
Citation: Flood KL, MacLennan PA, McGrew D, Green D, Dodd C, Brown CJ. Effects of an acute care for elders unit on costs and 30-day readmissions. JAMA. 2013 April 22 [Epub ahead of print].
Continue Beta-Blockers in High-Risk Patients During Noncardiac Surgery
Clinical question: Does exposure to a beta-blocker at the time of noncardiac surgery have an association with mortality, cardiac arrest, or Q-wave myocardial infarction (MI)?
Background: Exposure to beta-blockers perioperatively is controversial. The authors suggest that a randomized trial would be difficult, as one might need to withhold beta-blockers from stable patients. The American Heart Association and American College of Cardiology currently recommend continuation of pre-existing beta-blockades perioperatively.
Study design: Retrospective, propensity-matched cohort analysis.
Setting: One hundred four Veterans Affairs (VA) medical centers from January 2005 to August 2010.
Synopsis: Exposure for any reason to beta-blockers around nonvascular surgery appears to lower the risk of mortality and cardiac arrest, particularly in patients with higher revised cardiac risk index factors. Stopping beta-blockers in this same period was associated with increased mortality. The reasons for beta-blocker use in the exposed cohort were not well-established or -stratified.
Limitations include that the exposed cohort had a higher rate of cardiovascular disease and comorbidities and were generally older. Duration of exposure to beta-blockers was mixed, although more than 75% had a prescription for more than three months, with less than 2% for several days. Some of the matched cohort appears to have had beta-blocker exposure, thus diminishing the potential impact.
Bottom line: In this retrospective analysis, there is an association between beta-blocker use during noncardiac, nonvascular surgery and lower mortality, as well as lower rates of cardiac arrest and Q-wave MI, particularly among higher-risk patients.
Citation: London MJ, Hur K, Schwartz G, Henderson WG. Association of perioperative beta-blockade with mortality and cardiovascular morbidity following major noncardiac surgery. JAMA. 2013;309(16):1704-1713.
Patient-Centered Decision-Making and Health-Care Outcomes
Clinical question: Does recognition of contextual domains in the care plan lead to resolution of patients’ presenting problems?
Background: Patient-centered decision-making, or contextualization of care, adapts best evidence to the care of the individual patient. Examples of contextual domains include access to care, social support, and financial situation. Contextual errors (e.g. unrecognized domains) are, on average, more costly than errors in evidenced-based medicine.
Study design: Observational study.
Setting: VA ambulatory-care centers.
Synopsis: A total of 548 patient-derived audio recordings of physician encounters that included contextual red flags (e.g. missed appointments, HbA1c >8%) were reviewed at two VA hospital ambulatory-care centers using the content coding for contextualization of care (4C) method. Prospectively determined good and poor outcomes were derived from specific red flags (e.g. keeping next appointment, decrease in HbA1c). Of the 548 red flags, 208 were associated with contextual domains using the 4C method. Some 59% of physicians recognized contextual domains in care-plan development, leading to good outcomes in 71% of red flags. As many as 41% of physicians did not recognize contextual domains, leading to poor outcomes in 54% of red-flag instances.
Hospitalists should be aware of contextual domains and red flags (e.g. readmissions), and this study provides a method of evaluating patient-centered decision-making in the hospital setting. However, the inherently subjective 4C method may underestimate the number of contextual domains.
Bottom line: Recognition and incorporation of contextual domains in care-plan development in the ambulatory setting are associated with improved contextual red flag outcomes.
Citation: Weiner SJ, Schwartz A, Sharma G, et al. Patient-centered decision making and health care outcomes: an observational study. Ann Intern Med. 2013;158:573-579.
Adverse Surgical Outcomes in Schizophrenia Patients
Clinical question: What is the full spectrum of postoperative complications and mortality in schizophrenic patients receiving in-hospital major surgery?
Background: Schizophrenia affects an estimated 4 to 7 per 1,000 persons worldwide, and patients with schizophrenia are at increased risk of diabetes, cardiovascular disease, and stroke with subsequent increased mortality risk. The correlation between severity of mental illness and postoperative in-hospital mortality has not been validated in previous studies.
Study design: Population-based, cross-sectional study.
Setting: Taiwan hospitals.
Synopsis: Using the Taiwan National Health Insurance Research Database, researchers examined claims from 2004 to 2007 and retrospectively identified 8,967 schizophrenic patients who underwent major inpatient surgery and were hospitalized for more than one day. Primary outcomes included acute myocardial infarction, acute renal failure, stroke, and in-hospital mortality within 30 days. Postoperative complications and mortality rates were compared between schizophrenic patients and patients without mental illness.
Schizophrenic patients had higher rates of many primary outcomes, including 30-day postoperative mortality, compared with patients without mental illness, after adjusting for sex, age, surgery type, and hospital setting. The risk for 30-day mortality rose with the number of preoperative schizophrenia-related services provided. Limitations include the nature of retrospective analysis and generalizability.
Bottom line: Compared to patients without mental illness, schizophrenic patients have an increased risk of acute renal failure, pneumonia, septicemia, and 30-day mortality in the postoperative setting, with higher mortality rates in schizophrenic patients with more severe disease.
Citation: Liao CC, Shen WW, Chang CC, Chang H, Chen T. Surgical adverse outcomes in patients with schizophrenia. Ann Surg. 2013;257:433-438.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Steroids may increase VTE risk
- Mortality rates rise at critical-care hospitals
- Physicians don’t discuss advance-care planning with elderly, families
- Ultrasound imaging for lumbar puncture, epidural catheterization
- Financial impact of surgical complications on hospitals
- Lab test fees and frequency of test ordering
- Inpatient elderly multidisciplinary teams reduce readmissions
- Use of beta-blockers in high-risk patients during noncardiac surgery
- Patient-centered decision-making and health-care outcomes
- Adverse surgical outcomes in patients with schizophrenia
Steroids May Increase VTE Risk
Clinical question: Is exogenous glucocorticoid administration associated with an increased risk of VTE?
Background: Endogenous hypercortisolism is linked to increased VTE rates, and pathophysiologic data exist to suggest glucocorticoids increase clotting, but few studies have measured the clinical link between glucocorticoid administration and VTE events.
Study design: Case-control study.
Setting: Denmark.
Synopsis: The authors analyzed Danish national registries, which include information on diagnoses and prescriptions. The study selection period was Jan. 1, 2005, to Dec. 31, 2011. During this period, 38,675 cases of VTE (both DVT and pulmonary embolism) were identified in the population of Denmark. These cases were matched with 387,650 controls. Three routes of glucocorticoid use were studied: systemic (oral and intravenous), inhaled, and intestinal-acting. Cases were classified as present (within 90 days of VTE event), recent (91 to 365 days), or former (over 365 days) users of glucocorticoids. Categories were also created for new versus continuous users.
Glucocorticoid use was associated with a significant increase in VTE occurrence. The strongest link was in new and recent users, and the effect diminished over time. Key limitations of the study included its reliance on registry data, as well as the fact that cases had more comorbid conditions than controls (e.g. recent infection, chronic illnesses).
Bottom line: Recipients of glucocorticoids had an increased risk of VTE; the effect was strongest in new and recent users.
Citation: Johannesdottir SA, Horvath-Puho E, Dekkers OM, et al. Use of glucocorticoids and risk of venous thromboembolism. JAMA Intern Med. 2013;173(9):743-752.
Mortality Rates Rise at Critical-Access Hospitals
Clinical question: How have trends in mortality changed in the past decade at critical-access hospitals when compared to other hospitals?
Background: Hospitals are designated as critical-access hospitals (CAH) by meeting certain requirements—namely, rural setting, small number of beds, and minimum distance from the nearest hospital. Because of the intrinsic challenges they face, CAHs are exempt from certain quality measures. Little data exist on patient outcomes at CAHs.
Study design: Retrospective observational study.
Setting: All nonfederal hospitals in the U.S. that provide acute care to Medicare beneficiaries.
Synopsis: Using Medicare data, risk-adjusted 30-day mortality rates were calculated at critical-access hospitals and non-critical-access hospitals from 2002 to 2010 for three conditions: acute myocardial infarction, congestive heart failure, and pneumonia. Mortality trends across these conditions were compared at baseline and over time. In 2002, CAHs had mortality rates comparable with non-CAHs. From 2002 to 2010, mortality rates increased by 0.1% per year at CAHs and decreased by 0.2% per year at non-CAHs, resulting in a mortality difference between these two hospital groups at the end of the study period. The authors postulate that differences in policy initiatives, enforcement of quality measures, and access to technology may play a role.
This study is limited in its ability to explain the findings. Notably, within the CAHs, the authors found that 48% did improve from 2002 to 2010; there were no significant differences in hospital characteristics between the CAHs that did and did not improve. The reasons for the overall widening gap between CAHs and non-CAHs, therefore, merit further investigation.
Bottom line: From 2002 to 2010, mortality rates at U.S. critical-access hospitals rose while rates fell at non-critical access hospitals.
Citation: Joynt KE, Orav EJ, Jha AK. Mortality rates for Medicare beneficiaries admitted to critical access and non-critical access hospitals, 2002-2010. JAMA. 2013;309(13):1379-1387.
Physicians Fail to Discuss Advance-Care Planning with Hospitalized Elderly, Relatives
Clinical question: Do elderly patients who are at high risk for death have documented advance-care plans, and do their physicians discuss goals of care with them?
Background: While studies indicate that most sick, elderly patients prefer a better quality of life to life-sustaining treatment, many patients still die in the hospital, often in the ICU. It is unclear whether this is due to the absence of advance-care planning or the lack of communicating goals of care.
Study design: Multicenter prospective cohort study.
Setting: Canada.
Synopsis: A validated questionnaire was used to evaluate advance-care planning both before hospitalization and on admission. Patients and their families were enrolled if they were considered at high risk for dying, including patients with advanced disease, or aged >80 years. Of the 278 patients enrolled, 76.3% had thought about advance-care planning. Approximately 47.9% of patients had written an advance-care plan, and 73.3% had formally documented a surrogate health-care decision-maker. Only a quarter of patients reported that they had been asked about advance-care planning on admission to the hospital. Patients’ stated preferences for end-of-life care were notably incongruent with goals-of-care orders documented in the hospital records. While 28% of patients preferred comfort-only care, this was documented in the hospital records for only 4.5% of patients.
In this study of mostly white, English-speaking hospitalized patients, many had considered and made advance-care plans but few had discussed this with their health-care providers. Not surprisingly, the goals-of-care orders that were documented did not match patients’ previously stated end-of-life preferences.
Bottom line: Physicians routinely fail to discuss patients’ advance-care planning, which may have profound effects on their inpatient care.
Citation: Heyland DK, Barwich D, Pichora D, et al. Failure to engage hospitalized elderly patients and their families in advance care planning. JAMA Intern Med. 2013;173(9):778-787.
Ultrasound Use Reduces Lumbar Puncture and Epidural Catheterization Failure
Clinical question: Does ultrasound imaging for lumbar puncture and epidural catheterization reduce risk of procedure failures?
Background: Numerous studies have compared ultrasound-guided lumbar puncture and epidural catheterization with standard techniques, but they have been underpowered to evaluate whether ultrasound use reduces lumbar puncture and epidural catheterization failure.
Study design: Systematic review and meta-analysis of randomized controlled trials.
Setting: Hospitals in North America, Europe, and Asia.
Synopsis: Among 14 trials, a total of 1,334 patients (including one pediatric study group) were randomly assigned either to receive ultrasound imaging or to a control group (using manual palpation or loss of resistance). Ultrasound imaging comprised a preprocedure marking approach, real-time visual guidance, or both. In the 12 trials in which the primary outcome was available, ultrasound imaging significantly reduced the risk of failed procedures with a risk ratio of 0.21 (95% confidence interval 0.10 to 0.43). A total of 16 ultrasound-guided procedures were needed to avoid one procedure failure. Ultrasound guidance also reduced the number of traumatic procedures, needle reinsertions, and needle redirections. These results were consistent across multiple subgroup analyses.
Only one of the studies included in the meta-analysis was double-blind, and in all of the studies, ultrasound imaging was performed by a clinician with high-level ultrasound experience. While this study suggests that ultrasound does reduce the frequency of procedure failure, the investigators did not include cost-effectiveness analyses.
Bottom line: Ultrasound imaging likely reduces the failure of lumbar puncture and epidural catheterization, but future research will be necessary to evaluate the cost-effectiveness of ultrasound use for these procedures.
Citation: Shaikh F, Brzezinski J, Alexander S, et al. Ultrasound imaging for lumbar punctures and epidural catheterisations: systematic review and meta-analysis. BMJ. 2013;346:f1720.
Surgical Complications might Be Financially Advantageous for Hospitals
Clinical question: What is the impact of surgical complications on hospital finances?
Background: Surgical complications are common and lead to longer lengths of stay and higher costs. Strategies are available to reduce postsurgical complications but have not been universally adopted.
Study design: Observational study.
Setting: Twelve hospitals in one nonprofit Southern hospital system, which includes academic, nonacademic, and rural settings.
Synopsis: Researchers identified 34,526 patients who underwent surgery in 2010, excluding patients undergoing Caesarean section. Of those, 1,820 procedures (5.3%) were associated with at least one complication. The most frequent complications were surgical-site infection, other infections, pneumonia, and thromboembolic disease. The mortality rate for patients with complications was 12.3% compared with 0.6% for those without. Length of stay was four times longer for patients with complications.
Complications were associated with a higher total cost of hospitalization, with a differential of $37,917. This translated into a higher contribution to the margin. The cost differential varied by insurance type, with higher contributions under Medicare and private insurance but not with Medicaid.
The study had the benefit of using a large administrative database; however, this may have underestimated the actual rate of postoperative complications. The study supports the paradox in which quality-improvement (QI) programs that reduce surgical complications and improve postoperative mortality may negatively affect a hospital’s financial performance.
Bottom line: Surgical complications lead to higher mortality for patients but a financial benefit for hospitals.
Citation: Eappen S, Lane BH, Rosenberg B, et al. Relationship between occurrence of surgical complications and hospital finances. JAMA. 2013;309(5):1509-1606.
Showing Lab Test Fees May Decrease Frequency Of Test Ordering
Clinical question: Does information on the cost of a lab test lead to lowered ordering frequency among internal-medicine residents?
Background: Lab test overuse is common; some studies estimate that 70% of lab tests do not affect care. Strategies to reduce frequency of unnecessary lab tests are needed.
Study design: Randomized controlled trial.
Setting: Johns Hopkins Hospital, a 1,051-bed academic medical center in Baltimore.
Synopsis: Researchers used an administrative database to identify the 35 most frequently ordered and the 35 most expensive tests (each ordered at least 50 times). They randomized tests to an active arm, which displayed the Medicare allowable fee at the time of order entry within the computerized physician order entry, and a control arm. A total of 1,166,753 tests were ordered during the baseline and intervention period. Many more tests were ordered in the active group relative to the control group, a consequence of the randomization process. Relative to a six-month baseline period, tests in the active group were ordered 9.1% less frequently; control-group tests were ordered 5.1% more frequently. Charges decreased by $3.79 per patient-day in the active group and increased by $0.52 per patient-day in the control group.
This study reflects a low-cost strategy to reduce lab testing and associated costs. It is unknown whether only unnecessary tests were averted, or if there was any effect on the quality of care. The durability of the intervention and its applicability to other settings and with other types of providers is unclear.
Bottom line: Showing the fee associated with lab tests may decrease the frequency of ordering these tests and the resultant costs.
Citation: Feldman LS, Shihab HM, Thiemann D, et al. Impact of providing fee data on laboratory test ordering: a controlled clinical trial. JAMA Intern Med. 2013;173(10):903-908.
Inpatient Elderly Multidisciplinary-Team-Based Unit Reduces Readmissions
Clinical question: Can an inpatient unit that uses interdisciplinary rounds and a team approach reduce 30-day readmissions and lower cost compared with usual care?
Background: Elderly patients are at risk for adverse outcomes including delirium, deconditioning, and undernutrition. The Acute Care for Elders (ACE) model is designed as a team-based approach to improve communication between clinicians and to begin discharge planning soon after admission. ACE units have been shown to improve specific outcomes in older adults, but the impact on cost is less clear.
Study design: Retrospective cohort study.
Setting: University of Alabama at Birmingham Acute Care for Elders unit.
Synopsis: The analysis of cost data extrapolated from administrative sources indicated an average of $371 in variable cost savings per patient, and therefore an expected $148,400 savings for 400 patients admitted to this unit. The rate of 30-day readmissions was significantly lower in the ACE model: 7.9% versus 12.8% in patients receiving usual care.
Limitations of this study relate both to its design and single-center location. It is unclear which aspect of this ACE unit was helpful in the studied outcomes, and how this specific program would be reproduced at another institution. There were also some costs associated with the ACE-unit staffing, which may have resulted in an overestimation of the cost savings.
Bottom line: ACE units appear to improve outcomes and may lower cost, but further investigation is needed.
Citation: Flood KL, MacLennan PA, McGrew D, Green D, Dodd C, Brown CJ. Effects of an acute care for elders unit on costs and 30-day readmissions. JAMA. 2013 April 22 [Epub ahead of print].
Continue Beta-Blockers in High-Risk Patients During Noncardiac Surgery
Clinical question: Does exposure to a beta-blocker at the time of noncardiac surgery have an association with mortality, cardiac arrest, or Q-wave myocardial infarction (MI)?
Background: Exposure to beta-blockers perioperatively is controversial. The authors suggest that a randomized trial would be difficult, as one might need to withhold beta-blockers from stable patients. The American Heart Association and American College of Cardiology currently recommend continuation of pre-existing beta-blockades perioperatively.
Study design: Retrospective, propensity-matched cohort analysis.
Setting: One hundred four Veterans Affairs (VA) medical centers from January 2005 to August 2010.
Synopsis: Exposure for any reason to beta-blockers around nonvascular surgery appears to lower the risk of mortality and cardiac arrest, particularly in patients with higher revised cardiac risk index factors. Stopping beta-blockers in this same period was associated with increased mortality. The reasons for beta-blocker use in the exposed cohort were not well-established or -stratified.
Limitations include that the exposed cohort had a higher rate of cardiovascular disease and comorbidities and were generally older. Duration of exposure to beta-blockers was mixed, although more than 75% had a prescription for more than three months, with less than 2% for several days. Some of the matched cohort appears to have had beta-blocker exposure, thus diminishing the potential impact.
Bottom line: In this retrospective analysis, there is an association between beta-blocker use during noncardiac, nonvascular surgery and lower mortality, as well as lower rates of cardiac arrest and Q-wave MI, particularly among higher-risk patients.
Citation: London MJ, Hur K, Schwartz G, Henderson WG. Association of perioperative beta-blockade with mortality and cardiovascular morbidity following major noncardiac surgery. JAMA. 2013;309(16):1704-1713.
Patient-Centered Decision-Making and Health-Care Outcomes
Clinical question: Does recognition of contextual domains in the care plan lead to resolution of patients’ presenting problems?
Background: Patient-centered decision-making, or contextualization of care, adapts best evidence to the care of the individual patient. Examples of contextual domains include access to care, social support, and financial situation. Contextual errors (e.g. unrecognized domains) are, on average, more costly than errors in evidenced-based medicine.
Study design: Observational study.
Setting: VA ambulatory-care centers.
Synopsis: A total of 548 patient-derived audio recordings of physician encounters that included contextual red flags (e.g. missed appointments, HbA1c >8%) were reviewed at two VA hospital ambulatory-care centers using the content coding for contextualization of care (4C) method. Prospectively determined good and poor outcomes were derived from specific red flags (e.g. keeping next appointment, decrease in HbA1c). Of the 548 red flags, 208 were associated with contextual domains using the 4C method. Some 59% of physicians recognized contextual domains in care-plan development, leading to good outcomes in 71% of red flags. As many as 41% of physicians did not recognize contextual domains, leading to poor outcomes in 54% of red-flag instances.
Hospitalists should be aware of contextual domains and red flags (e.g. readmissions), and this study provides a method of evaluating patient-centered decision-making in the hospital setting. However, the inherently subjective 4C method may underestimate the number of contextual domains.
Bottom line: Recognition and incorporation of contextual domains in care-plan development in the ambulatory setting are associated with improved contextual red flag outcomes.
Citation: Weiner SJ, Schwartz A, Sharma G, et al. Patient-centered decision making and health care outcomes: an observational study. Ann Intern Med. 2013;158:573-579.
Adverse Surgical Outcomes in Schizophrenia Patients
Clinical question: What is the full spectrum of postoperative complications and mortality in schizophrenic patients receiving in-hospital major surgery?
Background: Schizophrenia affects an estimated 4 to 7 per 1,000 persons worldwide, and patients with schizophrenia are at increased risk of diabetes, cardiovascular disease, and stroke with subsequent increased mortality risk. The correlation between severity of mental illness and postoperative in-hospital mortality has not been validated in previous studies.
Study design: Population-based, cross-sectional study.
Setting: Taiwan hospitals.
Synopsis: Using the Taiwan National Health Insurance Research Database, researchers examined claims from 2004 to 2007 and retrospectively identified 8,967 schizophrenic patients who underwent major inpatient surgery and were hospitalized for more than one day. Primary outcomes included acute myocardial infarction, acute renal failure, stroke, and in-hospital mortality within 30 days. Postoperative complications and mortality rates were compared between schizophrenic patients and patients without mental illness.
Schizophrenic patients had higher rates of many primary outcomes, including 30-day postoperative mortality, compared with patients without mental illness, after adjusting for sex, age, surgery type, and hospital setting. The risk for 30-day mortality rose with the number of preoperative schizophrenia-related services provided. Limitations include the nature of retrospective analysis and generalizability.
Bottom line: Compared to patients without mental illness, schizophrenic patients have an increased risk of acute renal failure, pneumonia, septicemia, and 30-day mortality in the postoperative setting, with higher mortality rates in schizophrenic patients with more severe disease.
Citation: Liao CC, Shen WW, Chang CC, Chang H, Chen T. Surgical adverse outcomes in patients with schizophrenia. Ann Surg. 2013;257:433-438.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Steroids may increase VTE risk
- Mortality rates rise at critical-care hospitals
- Physicians don’t discuss advance-care planning with elderly, families
- Ultrasound imaging for lumbar puncture, epidural catheterization
- Financial impact of surgical complications on hospitals
- Lab test fees and frequency of test ordering
- Inpatient elderly multidisciplinary teams reduce readmissions
- Use of beta-blockers in high-risk patients during noncardiac surgery
- Patient-centered decision-making and health-care outcomes
- Adverse surgical outcomes in patients with schizophrenia
Steroids May Increase VTE Risk
Clinical question: Is exogenous glucocorticoid administration associated with an increased risk of VTE?
Background: Endogenous hypercortisolism is linked to increased VTE rates, and pathophysiologic data exist to suggest glucocorticoids increase clotting, but few studies have measured the clinical link between glucocorticoid administration and VTE events.
Study design: Case-control study.
Setting: Denmark.
Synopsis: The authors analyzed Danish national registries, which include information on diagnoses and prescriptions. The study selection period was Jan. 1, 2005, to Dec. 31, 2011. During this period, 38,675 cases of VTE (both DVT and pulmonary embolism) were identified in the population of Denmark. These cases were matched with 387,650 controls. Three routes of glucocorticoid use were studied: systemic (oral and intravenous), inhaled, and intestinal-acting. Cases were classified as present (within 90 days of VTE event), recent (91 to 365 days), or former (over 365 days) users of glucocorticoids. Categories were also created for new versus continuous users.
Glucocorticoid use was associated with a significant increase in VTE occurrence. The strongest link was in new and recent users, and the effect diminished over time. Key limitations of the study included its reliance on registry data, as well as the fact that cases had more comorbid conditions than controls (e.g. recent infection, chronic illnesses).
Bottom line: Recipients of glucocorticoids had an increased risk of VTE; the effect was strongest in new and recent users.
Citation: Johannesdottir SA, Horvath-Puho E, Dekkers OM, et al. Use of glucocorticoids and risk of venous thromboembolism. JAMA Intern Med. 2013;173(9):743-752.
Mortality Rates Rise at Critical-Access Hospitals
Clinical question: How have trends in mortality changed in the past decade at critical-access hospitals when compared to other hospitals?
Background: Hospitals are designated as critical-access hospitals (CAH) by meeting certain requirements—namely, rural setting, small number of beds, and minimum distance from the nearest hospital. Because of the intrinsic challenges they face, CAHs are exempt from certain quality measures. Little data exist on patient outcomes at CAHs.
Study design: Retrospective observational study.
Setting: All nonfederal hospitals in the U.S. that provide acute care to Medicare beneficiaries.
Synopsis: Using Medicare data, risk-adjusted 30-day mortality rates were calculated at critical-access hospitals and non-critical-access hospitals from 2002 to 2010 for three conditions: acute myocardial infarction, congestive heart failure, and pneumonia. Mortality trends across these conditions were compared at baseline and over time. In 2002, CAHs had mortality rates comparable with non-CAHs. From 2002 to 2010, mortality rates increased by 0.1% per year at CAHs and decreased by 0.2% per year at non-CAHs, resulting in a mortality difference between these two hospital groups at the end of the study period. The authors postulate that differences in policy initiatives, enforcement of quality measures, and access to technology may play a role.
This study is limited in its ability to explain the findings. Notably, within the CAHs, the authors found that 48% did improve from 2002 to 2010; there were no significant differences in hospital characteristics between the CAHs that did and did not improve. The reasons for the overall widening gap between CAHs and non-CAHs, therefore, merit further investigation.
Bottom line: From 2002 to 2010, mortality rates at U.S. critical-access hospitals rose while rates fell at non-critical access hospitals.
Citation: Joynt KE, Orav EJ, Jha AK. Mortality rates for Medicare beneficiaries admitted to critical access and non-critical access hospitals, 2002-2010. JAMA. 2013;309(13):1379-1387.
Physicians Fail to Discuss Advance-Care Planning with Hospitalized Elderly, Relatives
Clinical question: Do elderly patients who are at high risk for death have documented advance-care plans, and do their physicians discuss goals of care with them?
Background: While studies indicate that most sick, elderly patients prefer a better quality of life to life-sustaining treatment, many patients still die in the hospital, often in the ICU. It is unclear whether this is due to the absence of advance-care planning or the lack of communicating goals of care.
Study design: Multicenter prospective cohort study.
Setting: Canada.
Synopsis: A validated questionnaire was used to evaluate advance-care planning both before hospitalization and on admission. Patients and their families were enrolled if they were considered at high risk for dying, including patients with advanced disease, or aged >80 years. Of the 278 patients enrolled, 76.3% had thought about advance-care planning. Approximately 47.9% of patients had written an advance-care plan, and 73.3% had formally documented a surrogate health-care decision-maker. Only a quarter of patients reported that they had been asked about advance-care planning on admission to the hospital. Patients’ stated preferences for end-of-life care were notably incongruent with goals-of-care orders documented in the hospital records. While 28% of patients preferred comfort-only care, this was documented in the hospital records for only 4.5% of patients.
In this study of mostly white, English-speaking hospitalized patients, many had considered and made advance-care plans but few had discussed this with their health-care providers. Not surprisingly, the goals-of-care orders that were documented did not match patients’ previously stated end-of-life preferences.
Bottom line: Physicians routinely fail to discuss patients’ advance-care planning, which may have profound effects on their inpatient care.
Citation: Heyland DK, Barwich D, Pichora D, et al. Failure to engage hospitalized elderly patients and their families in advance care planning. JAMA Intern Med. 2013;173(9):778-787.
Ultrasound Use Reduces Lumbar Puncture and Epidural Catheterization Failure
Clinical question: Does ultrasound imaging for lumbar puncture and epidural catheterization reduce risk of procedure failures?
Background: Numerous studies have compared ultrasound-guided lumbar puncture and epidural catheterization with standard techniques, but they have been underpowered to evaluate whether ultrasound use reduces lumbar puncture and epidural catheterization failure.
Study design: Systematic review and meta-analysis of randomized controlled trials.
Setting: Hospitals in North America, Europe, and Asia.
Synopsis: Among 14 trials, a total of 1,334 patients (including one pediatric study group) were randomly assigned either to receive ultrasound imaging or to a control group (using manual palpation or loss of resistance). Ultrasound imaging comprised a preprocedure marking approach, real-time visual guidance, or both. In the 12 trials in which the primary outcome was available, ultrasound imaging significantly reduced the risk of failed procedures with a risk ratio of 0.21 (95% confidence interval 0.10 to 0.43). A total of 16 ultrasound-guided procedures were needed to avoid one procedure failure. Ultrasound guidance also reduced the number of traumatic procedures, needle reinsertions, and needle redirections. These results were consistent across multiple subgroup analyses.
Only one of the studies included in the meta-analysis was double-blind, and in all of the studies, ultrasound imaging was performed by a clinician with high-level ultrasound experience. While this study suggests that ultrasound does reduce the frequency of procedure failure, the investigators did not include cost-effectiveness analyses.
Bottom line: Ultrasound imaging likely reduces the failure of lumbar puncture and epidural catheterization, but future research will be necessary to evaluate the cost-effectiveness of ultrasound use for these procedures.
Citation: Shaikh F, Brzezinski J, Alexander S, et al. Ultrasound imaging for lumbar punctures and epidural catheterisations: systematic review and meta-analysis. BMJ. 2013;346:f1720.
Surgical Complications might Be Financially Advantageous for Hospitals
Clinical question: What is the impact of surgical complications on hospital finances?
Background: Surgical complications are common and lead to longer lengths of stay and higher costs. Strategies are available to reduce postsurgical complications but have not been universally adopted.
Study design: Observational study.
Setting: Twelve hospitals in one nonprofit Southern hospital system, which includes academic, nonacademic, and rural settings.
Synopsis: Researchers identified 34,526 patients who underwent surgery in 2010, excluding patients undergoing Caesarean section. Of those, 1,820 procedures (5.3%) were associated with at least one complication. The most frequent complications were surgical-site infection, other infections, pneumonia, and thromboembolic disease. The mortality rate for patients with complications was 12.3% compared with 0.6% for those without. Length of stay was four times longer for patients with complications.
Complications were associated with a higher total cost of hospitalization, with a differential of $37,917. This translated into a higher contribution to the margin. The cost differential varied by insurance type, with higher contributions under Medicare and private insurance but not with Medicaid.
The study had the benefit of using a large administrative database; however, this may have underestimated the actual rate of postoperative complications. The study supports the paradox in which quality-improvement (QI) programs that reduce surgical complications and improve postoperative mortality may negatively affect a hospital’s financial performance.
Bottom line: Surgical complications lead to higher mortality for patients but a financial benefit for hospitals.
Citation: Eappen S, Lane BH, Rosenberg B, et al. Relationship between occurrence of surgical complications and hospital finances. JAMA. 2013;309(5):1509-1606.
Showing Lab Test Fees May Decrease Frequency Of Test Ordering
Clinical question: Does information on the cost of a lab test lead to lowered ordering frequency among internal-medicine residents?
Background: Lab test overuse is common; some studies estimate that 70% of lab tests do not affect care. Strategies to reduce frequency of unnecessary lab tests are needed.
Study design: Randomized controlled trial.
Setting: Johns Hopkins Hospital, a 1,051-bed academic medical center in Baltimore.
Synopsis: Researchers used an administrative database to identify the 35 most frequently ordered and the 35 most expensive tests (each ordered at least 50 times). They randomized tests to an active arm, which displayed the Medicare allowable fee at the time of order entry within the computerized physician order entry, and a control arm. A total of 1,166,753 tests were ordered during the baseline and intervention period. Many more tests were ordered in the active group relative to the control group, a consequence of the randomization process. Relative to a six-month baseline period, tests in the active group were ordered 9.1% less frequently; control-group tests were ordered 5.1% more frequently. Charges decreased by $3.79 per patient-day in the active group and increased by $0.52 per patient-day in the control group.
This study reflects a low-cost strategy to reduce lab testing and associated costs. It is unknown whether only unnecessary tests were averted, or if there was any effect on the quality of care. The durability of the intervention and its applicability to other settings and with other types of providers is unclear.
Bottom line: Showing the fee associated with lab tests may decrease the frequency of ordering these tests and the resultant costs.
Citation: Feldman LS, Shihab HM, Thiemann D, et al. Impact of providing fee data on laboratory test ordering: a controlled clinical trial. JAMA Intern Med. 2013;173(10):903-908.
Inpatient Elderly Multidisciplinary-Team-Based Unit Reduces Readmissions
Clinical question: Can an inpatient unit that uses interdisciplinary rounds and a team approach reduce 30-day readmissions and lower cost compared with usual care?
Background: Elderly patients are at risk for adverse outcomes including delirium, deconditioning, and undernutrition. The Acute Care for Elders (ACE) model is designed as a team-based approach to improve communication between clinicians and to begin discharge planning soon after admission. ACE units have been shown to improve specific outcomes in older adults, but the impact on cost is less clear.
Study design: Retrospective cohort study.
Setting: University of Alabama at Birmingham Acute Care for Elders unit.
Synopsis: The analysis of cost data extrapolated from administrative sources indicated an average of $371 in variable cost savings per patient, and therefore an expected $148,400 savings for 400 patients admitted to this unit. The rate of 30-day readmissions was significantly lower in the ACE model: 7.9% versus 12.8% in patients receiving usual care.
Limitations of this study relate both to its design and single-center location. It is unclear which aspect of this ACE unit was helpful in the studied outcomes, and how this specific program would be reproduced at another institution. There were also some costs associated with the ACE-unit staffing, which may have resulted in an overestimation of the cost savings.
Bottom line: ACE units appear to improve outcomes and may lower cost, but further investigation is needed.
Citation: Flood KL, MacLennan PA, McGrew D, Green D, Dodd C, Brown CJ. Effects of an acute care for elders unit on costs and 30-day readmissions. JAMA. 2013 April 22 [Epub ahead of print].
Continue Beta-Blockers in High-Risk Patients During Noncardiac Surgery
Clinical question: Does exposure to a beta-blocker at the time of noncardiac surgery have an association with mortality, cardiac arrest, or Q-wave myocardial infarction (MI)?
Background: Exposure to beta-blockers perioperatively is controversial. The authors suggest that a randomized trial would be difficult, as one might need to withhold beta-blockers from stable patients. The American Heart Association and American College of Cardiology currently recommend continuation of pre-existing beta-blockades perioperatively.
Study design: Retrospective, propensity-matched cohort analysis.
Setting: One hundred four Veterans Affairs (VA) medical centers from January 2005 to August 2010.
Synopsis: Exposure for any reason to beta-blockers around nonvascular surgery appears to lower the risk of mortality and cardiac arrest, particularly in patients with higher revised cardiac risk index factors. Stopping beta-blockers in this same period was associated with increased mortality. The reasons for beta-blocker use in the exposed cohort were not well-established or -stratified.
Limitations include that the exposed cohort had a higher rate of cardiovascular disease and comorbidities and were generally older. Duration of exposure to beta-blockers was mixed, although more than 75% had a prescription for more than three months, with less than 2% for several days. Some of the matched cohort appears to have had beta-blocker exposure, thus diminishing the potential impact.
Bottom line: In this retrospective analysis, there is an association between beta-blocker use during noncardiac, nonvascular surgery and lower mortality, as well as lower rates of cardiac arrest and Q-wave MI, particularly among higher-risk patients.
Citation: London MJ, Hur K, Schwartz G, Henderson WG. Association of perioperative beta-blockade with mortality and cardiovascular morbidity following major noncardiac surgery. JAMA. 2013;309(16):1704-1713.
Patient-Centered Decision-Making and Health-Care Outcomes
Clinical question: Does recognition of contextual domains in the care plan lead to resolution of patients’ presenting problems?
Background: Patient-centered decision-making, or contextualization of care, adapts best evidence to the care of the individual patient. Examples of contextual domains include access to care, social support, and financial situation. Contextual errors (e.g. unrecognized domains) are, on average, more costly than errors in evidenced-based medicine.
Study design: Observational study.
Setting: VA ambulatory-care centers.
Synopsis: A total of 548 patient-derived audio recordings of physician encounters that included contextual red flags (e.g. missed appointments, HbA1c >8%) were reviewed at two VA hospital ambulatory-care centers using the content coding for contextualization of care (4C) method. Prospectively determined good and poor outcomes were derived from specific red flags (e.g. keeping next appointment, decrease in HbA1c). Of the 548 red flags, 208 were associated with contextual domains using the 4C method. Some 59% of physicians recognized contextual domains in care-plan development, leading to good outcomes in 71% of red flags. As many as 41% of physicians did not recognize contextual domains, leading to poor outcomes in 54% of red-flag instances.
Hospitalists should be aware of contextual domains and red flags (e.g. readmissions), and this study provides a method of evaluating patient-centered decision-making in the hospital setting. However, the inherently subjective 4C method may underestimate the number of contextual domains.
Bottom line: Recognition and incorporation of contextual domains in care-plan development in the ambulatory setting are associated with improved contextual red flag outcomes.
Citation: Weiner SJ, Schwartz A, Sharma G, et al. Patient-centered decision making and health care outcomes: an observational study. Ann Intern Med. 2013;158:573-579.
Adverse Surgical Outcomes in Schizophrenia Patients
Clinical question: What is the full spectrum of postoperative complications and mortality in schizophrenic patients receiving in-hospital major surgery?
Background: Schizophrenia affects an estimated 4 to 7 per 1,000 persons worldwide, and patients with schizophrenia are at increased risk of diabetes, cardiovascular disease, and stroke with subsequent increased mortality risk. The correlation between severity of mental illness and postoperative in-hospital mortality has not been validated in previous studies.
Study design: Population-based, cross-sectional study.
Setting: Taiwan hospitals.
Synopsis: Using the Taiwan National Health Insurance Research Database, researchers examined claims from 2004 to 2007 and retrospectively identified 8,967 schizophrenic patients who underwent major inpatient surgery and were hospitalized for more than one day. Primary outcomes included acute myocardial infarction, acute renal failure, stroke, and in-hospital mortality within 30 days. Postoperative complications and mortality rates were compared between schizophrenic patients and patients without mental illness.
Schizophrenic patients had higher rates of many primary outcomes, including 30-day postoperative mortality, compared with patients without mental illness, after adjusting for sex, age, surgery type, and hospital setting. The risk for 30-day mortality rose with the number of preoperative schizophrenia-related services provided. Limitations include the nature of retrospective analysis and generalizability.
Bottom line: Compared to patients without mental illness, schizophrenic patients have an increased risk of acute renal failure, pneumonia, septicemia, and 30-day mortality in the postoperative setting, with higher mortality rates in schizophrenic patients with more severe disease.
Citation: Liao CC, Shen WW, Chang CC, Chang H, Chen T. Surgical adverse outcomes in patients with schizophrenia. Ann Surg. 2013;257:433-438.
Observation Status Designation in Pediatric Hospitals Is Costly

Clinical question: What are the costs associated with observation-status hospital stays compared to inpatient-status stays in pediatric hospitals?
Background: Observation status is a designation for hospitalizations that are typically shorter than 48 hours and do not meet criteria for inpatient status. It is considered to be outpatient for evaluation and management (E/M) coding. A designation of observation status for a hospital stay can have significant effects on out-of-pocket costs for patients and reimbursements to physicians and hospitals. It also can affect readmission and length-of-stay data, as observation-status hospital stays are often excluded from a hospital’s inpatient data.
Study design: Multicenter retrospective cohort study.
Setting: Thirty-three freestanding children’s hospitals.
Synopsis: Researchers reviewed data obtained from the Pediatric Health Information System (PHIS), which contains demographic and resource utilization date from 43 freestanding children’s hospitals in the U.S. Resource utilization data were reviewed from 33 of 43 hospitals in PHIS that reported data regarding observation- versus inpatient-status stays. Data were then limited to observation-status stays £2 days, which made up 97.8% of all observation-status stays. These were then compared to a corresponding cohort of inpatient-status stays of £2 days (47.5% of inpatient-status stays), excluding any patient who had spent time in an ICU.
Hospitalization costs were analyzed and separated into room and nonroom costs, as well as in aggregate. These were further subdivided into costs for four common diagnoses (asthma, gastroenteritis, bronchiolitis, and seizure) and were risk-adjusted.
Observation status was used variably between hospitals (2% to 45%) and within hospitals. There was significant overlap in costs of observation-status and inpatient-status stays, which persisted when accounting for nonroom costs and within the diagnosis subgroups. Although average severity-adjusted costs for observation-status stays were consistently less than those for inpatient-status stays, the dollar amounts were small.
Bottom line: Observation-status designation is used inconsistently in pediatric hospitals, and their costs overlap substantially with inpatient-status stays.
Citation: Fieldston ES, Shah SS, Hall M. Resource utilization for observation-status stays at children’s hospitals. Pediatrics. 2013;131;1050-1058.
Reviewed by Pediatric Editor Weijen Chang, MD, SFHM, FACP, associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital.
Clinical question: What are the costs associated with observation-status hospital stays compared to inpatient-status stays in pediatric hospitals?
Background: Observation status is a designation for hospitalizations that are typically shorter than 48 hours and do not meet criteria for inpatient status. It is considered to be outpatient for evaluation and management (E/M) coding. A designation of observation status for a hospital stay can have significant effects on out-of-pocket costs for patients and reimbursements to physicians and hospitals. It also can affect readmission and length-of-stay data, as observation-status hospital stays are often excluded from a hospital’s inpatient data.
Study design: Multicenter retrospective cohort study.
Setting: Thirty-three freestanding children’s hospitals.
Synopsis: Researchers reviewed data obtained from the Pediatric Health Information System (PHIS), which contains demographic and resource utilization date from 43 freestanding children’s hospitals in the U.S. Resource utilization data were reviewed from 33 of 43 hospitals in PHIS that reported data regarding observation- versus inpatient-status stays. Data were then limited to observation-status stays £2 days, which made up 97.8% of all observation-status stays. These were then compared to a corresponding cohort of inpatient-status stays of £2 days (47.5% of inpatient-status stays), excluding any patient who had spent time in an ICU.
Hospitalization costs were analyzed and separated into room and nonroom costs, as well as in aggregate. These were further subdivided into costs for four common diagnoses (asthma, gastroenteritis, bronchiolitis, and seizure) and were risk-adjusted.
Observation status was used variably between hospitals (2% to 45%) and within hospitals. There was significant overlap in costs of observation-status and inpatient-status stays, which persisted when accounting for nonroom costs and within the diagnosis subgroups. Although average severity-adjusted costs for observation-status stays were consistently less than those for inpatient-status stays, the dollar amounts were small.
Bottom line: Observation-status designation is used inconsistently in pediatric hospitals, and their costs overlap substantially with inpatient-status stays.
Citation: Fieldston ES, Shah SS, Hall M. Resource utilization for observation-status stays at children’s hospitals. Pediatrics. 2013;131;1050-1058.
Reviewed by Pediatric Editor Weijen Chang, MD, SFHM, FACP, associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital.
Clinical question: What are the costs associated with observation-status hospital stays compared to inpatient-status stays in pediatric hospitals?
Background: Observation status is a designation for hospitalizations that are typically shorter than 48 hours and do not meet criteria for inpatient status. It is considered to be outpatient for evaluation and management (E/M) coding. A designation of observation status for a hospital stay can have significant effects on out-of-pocket costs for patients and reimbursements to physicians and hospitals. It also can affect readmission and length-of-stay data, as observation-status hospital stays are often excluded from a hospital’s inpatient data.
Study design: Multicenter retrospective cohort study.
Setting: Thirty-three freestanding children’s hospitals.
Synopsis: Researchers reviewed data obtained from the Pediatric Health Information System (PHIS), which contains demographic and resource utilization date from 43 freestanding children’s hospitals in the U.S. Resource utilization data were reviewed from 33 of 43 hospitals in PHIS that reported data regarding observation- versus inpatient-status stays. Data were then limited to observation-status stays £2 days, which made up 97.8% of all observation-status stays. These were then compared to a corresponding cohort of inpatient-status stays of £2 days (47.5% of inpatient-status stays), excluding any patient who had spent time in an ICU.
Hospitalization costs were analyzed and separated into room and nonroom costs, as well as in aggregate. These were further subdivided into costs for four common diagnoses (asthma, gastroenteritis, bronchiolitis, and seizure) and were risk-adjusted.
Observation status was used variably between hospitals (2% to 45%) and within hospitals. There was significant overlap in costs of observation-status and inpatient-status stays, which persisted when accounting for nonroom costs and within the diagnosis subgroups. Although average severity-adjusted costs for observation-status stays were consistently less than those for inpatient-status stays, the dollar amounts were small.
Bottom line: Observation-status designation is used inconsistently in pediatric hospitals, and their costs overlap substantially with inpatient-status stays.
Citation: Fieldston ES, Shah SS, Hall M. Resource utilization for observation-status stays at children’s hospitals. Pediatrics. 2013;131;1050-1058.
Reviewed by Pediatric Editor Weijen Chang, MD, SFHM, FACP, associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital.
How to Manage Pain in Patients with Renal Insufficiency or End-Stage Renal Disease on Dialysis?

Case
A 70-year-old male with ESRD on hemodialysis presents with methicillin-resistant Staphylococcus aureus (MRSA) bacteremia and ankle pain after a fall. An MRI of his ankle is negative, and he is started on acetaminophen and lidocaine patches, which result in adequate pain relief of the ankle. He later develops significant neuropathic pain in both arms, and a CT scan of the cervical spine reveals a cervical abscess and osteomyelitis. The patient desires pain relief but adamantly refuses narcotics, stating: “I don’t want to get addicted.” How can his pain be managed?
Overview
Pain is a common problem in patients with renal insufficiency and end-stage renal disease (ESRD) and can have a significant effect on the patient’s quality of life.1 When assessing a patient’s pain, assess both the severity of the pain (such as on an analogue scale, 0-10) and the characteristics of the pain. Pain is most commonly characterized as nociceptive, neuropathic, or both. Nociceptive pain can be further classified as arising from either somatic or visceral sources, and is often described as dull, throbbing, cramping, and/or pressurelike.1 Neuropathic pain is often described as tingling, numbing, burning, and/or stabbing.
It is a challenge to manage pain in patients with renal insufficiency and dialysis. Renal insufficiency affects the pharmacokinetic properties of most pain medications, including their distribution, clearance, and excretion. The magnitude of the effect of renal insufficiency on drug metabolism varies depending on the agent itself, its metabolite, and the extent of renal failure.3 Multiple factors should be considered when prescribing pain medications for patients on dialysis, including the properties of the parent drug and its metabolites; the physical properties of the dialysis equipment, such as the filter pore size, the flow rate, and the efficiency of the technique used; and the dialysis method (intermittent versus continuous).3 Table 1 provides the recommended dosing of the most commonly prescribed agents, based on the degree of renal impairment. A modified World Health Organization (WHO) ladder has been suggested to treat pain in patients with ESRD, which can lead to effective pain relief in as many as 96% of patients (see Figure 1).2

*Beginning dose: If switching from IR to ER, calculate 24-hour total dose.
**For patients with creatinine clearances (CrCl) of 15 mL/min or less, the daily dosage should be adjusted proportionally (e.g. patients with a CrCl of 7.5 mL/min should receive one-half the dose of a patient with a CrCl of 15 mL/min).
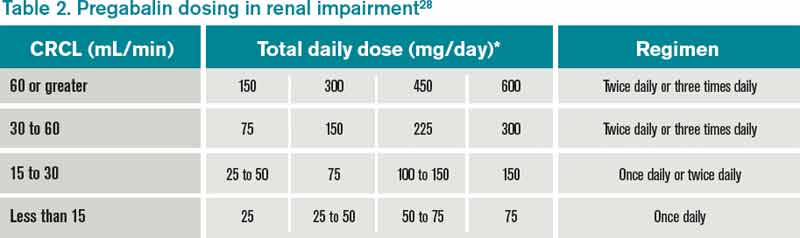
Review of Data
Nonopioid options. Nonopioids, such as acetaminophen and NSAIDs, have no associated tolerance but have a ceiling effect for analgesia, and NSAIDs are associated with dose-dependent acute renal failure, gastrointestinal ulceration and bleeding, and cardiac events. The nonopioids that are considered safe options in patients with renal insufficiency include acetaminophen, ibuprofen, and fenoprofen (Nalfon). However, in the elderly, American Geriatric Society (AGS) guidelines currently recommend avoiding all NSAIDs due to their safety profile in the geriatric population.4 Although all NSAIDs can potentially be used for pain, selected NSAIDs with an FDA indication for acute or chronic pain were included for this review.
Acetaminophen (APAP) is a dialyzable compound that is metabolized in the liver to five inactive metabolites. The terminal elimination half-life of its sulfate and glucuronide metabolites are prolonged in patients with renal failure; therefore, the dosing interval of APAP should be increased to six to eight hours in renally impaired patients.5,6,7 Overall, acetaminophen is considered one of the safest agents to use for the treatment of pain, in renal patients and otherwise, as long as dosing is below the minimal daily dose (see Table 1).
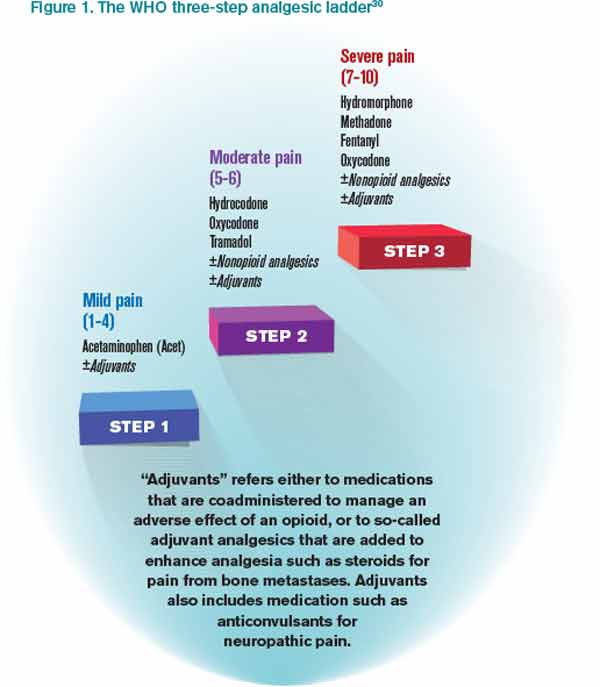
Ibuprofen is metabolized in the liver to inactive compounds. It does not accumulate in renal insufficiency, and two of the inactive compounds are dialyzable.8 It is considered a safe option for the treatment of pain in patients with renal insufficiency or dialysis.9
Fenoprofen is metabolized in the liver to inactive compounds. Renal impairment is likely to cause the accumulation of the inactive metabolites but not the parent compound, so dose reduction is not necessary with the use of this agent in renal insufficiency or dialysis.6
Mefenamic acid (Ponstel) is metabolized in the liver. Mefenamic acid can further deteriorate renal function in patients with underlying renal disease.12 However, the nephrotoxic potential of this agent is of little consideration in ESRD patients on dialysis, and therefore no dosage adjustments are necessary in these patients.6
Ketoprofen is metabolized in the liver, where approximately 80% of the dose is excreted in the urine as a glucuronide metabolite. Dose reduction is recommended in renal insufficiency and dialysis, as it not dialyzable.8
Ketorolac accumulates in renal insufficiency; therefore, it is contraindicated in these patients and in patients at risk for renal failure, including those with volume depletion.10 Ketorolac is unlikely to be removed by dialysis and so should be avoided.10,11
Naproxen is metabolized in the liver to inactive compounds. Use of naproxen is not recommended in patients with moderate to severe renal impairment. If therapy must be initiated, close monitoring of the patient’s renal function is recommended.13
Celecoxib is the only cyclooxygenase-2 (COX-2) inhibitor available in the U.S. It is metabolized extensively by the liver and is unlikely to be removed by dialysis. Therefore, use of COX-2 inhibitors should be avoided in severe renal impairment and in those on dialysis.14,15
Opioid options. The use of opioids in the renally impaired population is challenging, as one must balance opioid-related adverse events with adequate pain control. As such, it is recommended to start with lower-than-recommended doses and slowly titrate up the dose while extending the dosing interval. This will help limit adverse effects, such as respiratory depression and hypotension.3
Hydrocodone is metabolized to hydromorphone (Dilaudid), which is then metabolized to its major metabolite hydromorphine-3-glucuronide (H3G) and minor metabolite hydromorphine-6-hydroxy, all of which are excreted renally along with the parent compound. H3G has no analgesic properties, but it can potentially cause neuroexcitation, agitation, confusion, and hallucination. Hydromorphone has been used safely in patients with renal insufficiency and dialysis, as it is expected to be dialyzable. 16,17
Tramadol is metabolized in the liver, producing one active compound. Approximately 30% of the tramadol dose is excreted unchanged in the urine, whereas 60% of the dose is excreted as metabolites. It is recommended to reduce the dose and increase the dosing interval in patients with renal insufficiency, but tramadol is generally well-tolerated in patients with renal insufficiency and dialysis. It is significantly removed by hemodialysis; therefore, redosing after a session may be necessary.18,19
Oxycodone can be used in patients with mild to moderate renal insufficiency but should be used at reduced dosing; it has been associated with significant sedation with usual doses in renal failure patients.16 Its use is generally not recommended in dialysis patients due to lack of data.3
Methadone and its metabolites are excreted in the urine and feces. Methadone has been used safely in patients with renal insufficiency, but it is poorly removed by dialysis and no specific recommendations are available regarding its dosing in dialysis.3,16
Fentanyl is primarily metabolized in the liver to inactive metabolites. Fentanyl clearance is reduced in patients with moderate to severe uremia (BUN >60 mg/dL). It is not expected that fentanyl be dialyzable because of its pharmacokinetic properties (high protein-binding, low water solubility, high molecular weight, and high volume of distribution). Data suggests that fentanyl can be used at usual doses in mild to moderate renal insufficiency and in dialysis patients, although reduced doses may be prudent. Such patients should be monitored for signs of gradual accumulation of the parent drug.3,16
Morphine is metabolized in the liver to morphine-6-glucuronide (M6G) and morphine-3-glucuronide (M3G), all of which are excreted renally, along with the parent compound. Only M6G has analgesic properties, and when it accumulates, it can lead to CNS depression. M3G is associated with behavioral excitation, a side effect that is further magnified in patients with renal insufficiency. Although morphine is dialyzable, it should generally be avoided in patients with any level of renal insufficiency.16,17,20,21
Codeine is metabolized to several active metabolites, all of which are renally excreted. Lower-than-usual doses are recommended in patients with renal insufficiency, and it should be avoided altogether in dialysis patients.3,16
Meperidine is metabolized in the liver to various metabolites, primarily normeperidine, which is toxic and has a long half-life, five to 10 times longer then meperidine. Meperidine should not be used in patients with renal insufficiency or dialysis.3
Adjunctive therapeutic options. Lidocaine patches currently are only FDA-indicated for postherpetic neuralgia but are used for a wide variety of local pain syndromes. Absorption of lidocaine is determined by the duration of application and the surface area over which it is applied. There is no appreciable accumulation of lidocaine or its metabolites in renal insufficiency; therefore, dose adjustments are not required.22,23
Gabapentin is FDA-indicated for partial seizures and postherpetic neuralgia but is also used for a wide variety of neuropathic pain syndromes, including postoperative pain.24 Gabapentin is not metabolized and is excreted in the urine unchanged. Renal clearance of gabapentin is reduced by 40% and the elimination half-life is increased up to 52 hours in renal insufficiency, but it is dialyzable. Therefore, dose adjustments are required with gabapentin in patients with moderate to severe renal insufficiency, and supplemental doses should be administered in patients after receiving dialysis.25-27
Pregabalin is structurally related to gabapentin and is indicated for a variety of neuropathic pain conditions. Pregabalin is 90% excreted unchanged in the urine, and approximately 50% of drug is removed after four hours of hemodialysis. Dose adjustments are required in patients with moderate to severe renal insufficiency, and supplemental doses should be administered in patients after receiving dialysis.28
Antidepressant options. Amitriptyline, nortryptiline, and desipramine are the tricyclic antidepressants (TCAs) commonly used for neuropathic pain. TCAs are metabolized in the liver to inactive metabolites, with the exception of amitriptyline, which is metabolized to nortryptiline. Common side effects reported with TCAs include postural hypotension and anticholinergic side effects, such as constipation, urinary retention, blurred vision, dry mouth, delirium, and sedation. It is unlikely that the TCAs can be removed by dialysis. It is suggested that the dosage be reduced in renal insufficiency and that anticholinergic side effects be monitored.29
Back to the Case
The patient’s ankle pain was controlled with acetaminophen and lidocaine patches. For the neuropathic pain in his upper extremities, tramadol was started at 25 mg oral every 12 hours and increased to 50 mg oral every eight hours (below the maximum of 200 mg a day). The tramadol did not result in adequate pain relief, so gabapentin 100 mg at bedtime was initiated, then increased to twice daily over three days with some relief.
A geriatric consult was obtained to help educate him regarding addiction to opioids, as well as to explore goals of care, but he continued to insist on the use of a non-narcotic regimen for his pain.
Bottom Line
Pain management in patients with renal insufficiency and dialysis can be challenging, but there are a number of safe non-narcotic and narcotic pain regimens that can be safely used in this patient population.
Dr. Harisingani is a board-certified hospitalist at Long Island Jewish Medical Center in New Hyde Park, N.Y., and Drs. Saad and Cassagnol are assistant clinical professors at St. Johns University College of Pharmacy and Health Sciences in Jamaica, N.Y., and clinical pharmacy coordinators at Long Island Jewish Medical Center.
References
- Mid-Atlantic Renal Coalition and the Kidney End-of-Life Coalition. Clinical algorithm & preferred medications to treat pain in dialysis patients. Coalition for Supportive Care of Kidney Patients website. Available at: http://www.kidneysupportivecare.org/Physicians-Clinicians/Pain—Symptom-Management.aspx. Accessed Nov. 18, 2012.
- Barakzoy AS, Moss AH. Efficacy of the World Health Organization analgesic ladder to treat pain in end-stage renal disease. J Am Soc Nephrol. 2006;17(11):3198-3203.
- Johnson SJ. Opioid safety in patients with renal or hepatic dysfunction. Pain Treatment Topics website. Available at: http://pain-topics.org/pdf/Opioids-Renal-Hepatic-Dysfunction.pdf. Accessed Nov. 28, 2012.
- Ferrell B, Argoff CE, Epplin J, et al. American Geriatrics Society Panel on Pharmacological Management of Persistent Pain in Older Persons. Pharmacological management of persistent pain in older persons. J Am Geriatr Soc. 2009;57(8):1331-1346.
- Prescott LF, Speirs GC, Critchley JA, Temple RM, Winney RJ. Paracetamol disposition and metabolite kinetics in patients with chronic renal failure. Eur J Clin Pharmacol. 1989;36(3):291-297.
- Launay-Vacher V, Karie S, Fau JB, Izzedine H, Deray G. Treatment of pain in patients with renal insufficiency: the World Health Organization three-step ladder adapted. J Pain. 2006;6(3):137-148.
- Berg KJ, Djøseland O, Gjellan A, et al. Acute effects of paracetamol on prostaglandin synthesis and renal function in normal man and in patients with renal failure. Clin Nephrol. 1990;34:255-262.
- Delbarre F, Roucayrol JC, Amor B, et al. Pharmacokinetic study of ketoprofen (19.583 R.P.) in man using the tritiated compound. Scand J Rheumatol Suppl. 1976;1976(0):45-52.
- Shen CH, Hung CJ, Wu CC, Huang HW, Ho WM. Rhabdomyolysis-induced acute renal failure after morphine overdose—a case report. Acta Anaesthesiol Sin. 1999;37(3):159-162.
- Ketorolac tromethamine oral tablets [package insert]. St. Louis: Ethex Corp.: 2008.
- Brocks DR, Jamali F. Clinical pharmacokinetics of ketorolac tromethamine. Clin Pharmacokinet. 1992;23:415-427. Erratum in: Clin Pharmacokinet. 1999;24(3):270.
- Ponstel [package insert]. Alpharetta, GA: First Horizon Pharmaceutical Corp.; 2006.
- Naprosyn [package insert]. Nutley, NJ: Roche Laboratories Inc.; 2008.
- Celebrex [package insert]. New York: G.D. Searle LLC; 2011.
- Catella-Lawson F, McAdam B, Morrison BW, et al. Effects of specific inhibition of cyclooygenase-2 on sodium balance, hemodynamics, and vasoactive eicosanoids. J Pharmacol Exp Ther. 1999;289:735-741.
- Dean M. Opioids in renal failure and dialysis patients. J Pain Symptom Manage. 2004;28(5):497-504.
- Lee MA, Leng ME, Tiernan EJ. Retrospective study of the use of hydromorphone in palliative care patients with normal and abnormal urea and creatinine. Palliat Med. 2001;15(1):26-34.
- Gibson TP. Pharmacokinetics, efficacy, and safety of analgesia with a focus on tramadol HCI. Am J. Med. 1996;101(1A):47S-53S.
- Izzedine H, Launay-Vacher V, Abbara C, Aymard G, Bassilios N, Deray G. Pharmacokinetics of tramadol in a hemodialysis patient. Nephron. 2002;92(3):755-756.
- Hasselström J, Säwe J. Morphine pharmacokinetics and metabolism in humans. Enterohepatic cycling and relative contribution of metabolites to active opioid concentrations. Clin Pharmacokinet. 1993;24(4):344-354.
- Andersen G, Christrup L, Sjøgren P. Relationships among morphine metabolism, pain and side effects during long-term treatment: an update. J Pain Symptom Manage. 2003;25(1):74-91.
- Lidoderm [package insert]. Chadds Ford, PA: Endo Pharmaceuticals Inc.; 2010.
- Carter GT, Galer BS. Advances in the management of neuropathic pain. Phys Med Rehabil Clin N Am. 2001;12(2):447-459.
- Ho KY, Gan TJ, Habib AS. Gabapentin and postoperative pain—a systematic review of randomized controlled trials. Pain. 2006;15:126(1-3):91-101.
- Neurontin [package insert]. New York: Parke-Davis; 2010.
- Pandey CK, Priye S, Singh S, et al. Preemptive use of gabapentin significantly decreases postoperative pain and rescue analgesic requirements in laparoscopic cholecystectomy. Can J Anaesth. 2004;51(4):358-363.
- Srivastava U, Kumar A, Saxena S, et al: Effect of preoperative gabapentin on postoperative pain and tramadol consumption after minilap open cholecystectomy: a randomized double-blind, placebo-controlled trial. Eur J Anaesthesiol. 2010;27(N4):331-335.
- Lyrica [package insert]. New York: Pfizer Inc.; 2012.
- Broadbent A, Khor K, Heaney A. Palliation and chronic renal failure: opioid and other palliative medications—dosage guidelines. Progress in Palliative Care. 2003;11(4):183-190(8).
- Nayak-Rao S. Achieving effective pain relief in patients with chronic kidney disease: a review of analgesics in renal failure. J Nephrol. 2011;24(1):35-40.
- Wolters Kluwer Health. Facts & comparisons. Wolters Kluwer Health website. Available at: http://www.factsandcomparisons.com. Accessed Jan. 14, 2013.
- Lexicomp. Lexicomp Online. Lexicomp website. Available at: http://www.lexi.com/institutions/products/online/.
Case
A 70-year-old male with ESRD on hemodialysis presents with methicillin-resistant Staphylococcus aureus (MRSA) bacteremia and ankle pain after a fall. An MRI of his ankle is negative, and he is started on acetaminophen and lidocaine patches, which result in adequate pain relief of the ankle. He later develops significant neuropathic pain in both arms, and a CT scan of the cervical spine reveals a cervical abscess and osteomyelitis. The patient desires pain relief but adamantly refuses narcotics, stating: “I don’t want to get addicted.” How can his pain be managed?
Overview
Pain is a common problem in patients with renal insufficiency and end-stage renal disease (ESRD) and can have a significant effect on the patient’s quality of life.1 When assessing a patient’s pain, assess both the severity of the pain (such as on an analogue scale, 0-10) and the characteristics of the pain. Pain is most commonly characterized as nociceptive, neuropathic, or both. Nociceptive pain can be further classified as arising from either somatic or visceral sources, and is often described as dull, throbbing, cramping, and/or pressurelike.1 Neuropathic pain is often described as tingling, numbing, burning, and/or stabbing.
It is a challenge to manage pain in patients with renal insufficiency and dialysis. Renal insufficiency affects the pharmacokinetic properties of most pain medications, including their distribution, clearance, and excretion. The magnitude of the effect of renal insufficiency on drug metabolism varies depending on the agent itself, its metabolite, and the extent of renal failure.3 Multiple factors should be considered when prescribing pain medications for patients on dialysis, including the properties of the parent drug and its metabolites; the physical properties of the dialysis equipment, such as the filter pore size, the flow rate, and the efficiency of the technique used; and the dialysis method (intermittent versus continuous).3 Table 1 provides the recommended dosing of the most commonly prescribed agents, based on the degree of renal impairment. A modified World Health Organization (WHO) ladder has been suggested to treat pain in patients with ESRD, which can lead to effective pain relief in as many as 96% of patients (see Figure 1).2
*Beginning dose: If switching from IR to ER, calculate 24-hour total dose.
**For patients with creatinine clearances (CrCl) of 15 mL/min or less, the daily dosage should be adjusted proportionally (e.g. patients with a CrCl of 7.5 mL/min should receive one-half the dose of a patient with a CrCl of 15 mL/min).
Review of Data
Nonopioid options. Nonopioids, such as acetaminophen and NSAIDs, have no associated tolerance but have a ceiling effect for analgesia, and NSAIDs are associated with dose-dependent acute renal failure, gastrointestinal ulceration and bleeding, and cardiac events. The nonopioids that are considered safe options in patients with renal insufficiency include acetaminophen, ibuprofen, and fenoprofen (Nalfon). However, in the elderly, American Geriatric Society (AGS) guidelines currently recommend avoiding all NSAIDs due to their safety profile in the geriatric population.4 Although all NSAIDs can potentially be used for pain, selected NSAIDs with an FDA indication for acute or chronic pain were included for this review.
Acetaminophen (APAP) is a dialyzable compound that is metabolized in the liver to five inactive metabolites. The terminal elimination half-life of its sulfate and glucuronide metabolites are prolonged in patients with renal failure; therefore, the dosing interval of APAP should be increased to six to eight hours in renally impaired patients.5,6,7 Overall, acetaminophen is considered one of the safest agents to use for the treatment of pain, in renal patients and otherwise, as long as dosing is below the minimal daily dose (see Table 1).
Ibuprofen is metabolized in the liver to inactive compounds. It does not accumulate in renal insufficiency, and two of the inactive compounds are dialyzable.8 It is considered a safe option for the treatment of pain in patients with renal insufficiency or dialysis.9
Fenoprofen is metabolized in the liver to inactive compounds. Renal impairment is likely to cause the accumulation of the inactive metabolites but not the parent compound, so dose reduction is not necessary with the use of this agent in renal insufficiency or dialysis.6
Mefenamic acid (Ponstel) is metabolized in the liver. Mefenamic acid can further deteriorate renal function in patients with underlying renal disease.12 However, the nephrotoxic potential of this agent is of little consideration in ESRD patients on dialysis, and therefore no dosage adjustments are necessary in these patients.6
Ketoprofen is metabolized in the liver, where approximately 80% of the dose is excreted in the urine as a glucuronide metabolite. Dose reduction is recommended in renal insufficiency and dialysis, as it not dialyzable.8
Ketorolac accumulates in renal insufficiency; therefore, it is contraindicated in these patients and in patients at risk for renal failure, including those with volume depletion.10 Ketorolac is unlikely to be removed by dialysis and so should be avoided.10,11
Naproxen is metabolized in the liver to inactive compounds. Use of naproxen is not recommended in patients with moderate to severe renal impairment. If therapy must be initiated, close monitoring of the patient’s renal function is recommended.13
Celecoxib is the only cyclooxygenase-2 (COX-2) inhibitor available in the U.S. It is metabolized extensively by the liver and is unlikely to be removed by dialysis. Therefore, use of COX-2 inhibitors should be avoided in severe renal impairment and in those on dialysis.14,15
Opioid options. The use of opioids in the renally impaired population is challenging, as one must balance opioid-related adverse events with adequate pain control. As such, it is recommended to start with lower-than-recommended doses and slowly titrate up the dose while extending the dosing interval. This will help limit adverse effects, such as respiratory depression and hypotension.3
Hydrocodone is metabolized to hydromorphone (Dilaudid), which is then metabolized to its major metabolite hydromorphine-3-glucuronide (H3G) and minor metabolite hydromorphine-6-hydroxy, all of which are excreted renally along with the parent compound. H3G has no analgesic properties, but it can potentially cause neuroexcitation, agitation, confusion, and hallucination. Hydromorphone has been used safely in patients with renal insufficiency and dialysis, as it is expected to be dialyzable. 16,17
Tramadol is metabolized in the liver, producing one active compound. Approximately 30% of the tramadol dose is excreted unchanged in the urine, whereas 60% of the dose is excreted as metabolites. It is recommended to reduce the dose and increase the dosing interval in patients with renal insufficiency, but tramadol is generally well-tolerated in patients with renal insufficiency and dialysis. It is significantly removed by hemodialysis; therefore, redosing after a session may be necessary.18,19
Oxycodone can be used in patients with mild to moderate renal insufficiency but should be used at reduced dosing; it has been associated with significant sedation with usual doses in renal failure patients.16 Its use is generally not recommended in dialysis patients due to lack of data.3
Methadone and its metabolites are excreted in the urine and feces. Methadone has been used safely in patients with renal insufficiency, but it is poorly removed by dialysis and no specific recommendations are available regarding its dosing in dialysis.3,16
Fentanyl is primarily metabolized in the liver to inactive metabolites. Fentanyl clearance is reduced in patients with moderate to severe uremia (BUN >60 mg/dL). It is not expected that fentanyl be dialyzable because of its pharmacokinetic properties (high protein-binding, low water solubility, high molecular weight, and high volume of distribution). Data suggests that fentanyl can be used at usual doses in mild to moderate renal insufficiency and in dialysis patients, although reduced doses may be prudent. Such patients should be monitored for signs of gradual accumulation of the parent drug.3,16
Morphine is metabolized in the liver to morphine-6-glucuronide (M6G) and morphine-3-glucuronide (M3G), all of which are excreted renally, along with the parent compound. Only M6G has analgesic properties, and when it accumulates, it can lead to CNS depression. M3G is associated with behavioral excitation, a side effect that is further magnified in patients with renal insufficiency. Although morphine is dialyzable, it should generally be avoided in patients with any level of renal insufficiency.16,17,20,21
Codeine is metabolized to several active metabolites, all of which are renally excreted. Lower-than-usual doses are recommended in patients with renal insufficiency, and it should be avoided altogether in dialysis patients.3,16
Meperidine is metabolized in the liver to various metabolites, primarily normeperidine, which is toxic and has a long half-life, five to 10 times longer then meperidine. Meperidine should not be used in patients with renal insufficiency or dialysis.3
Adjunctive therapeutic options. Lidocaine patches currently are only FDA-indicated for postherpetic neuralgia but are used for a wide variety of local pain syndromes. Absorption of lidocaine is determined by the duration of application and the surface area over which it is applied. There is no appreciable accumulation of lidocaine or its metabolites in renal insufficiency; therefore, dose adjustments are not required.22,23
Gabapentin is FDA-indicated for partial seizures and postherpetic neuralgia but is also used for a wide variety of neuropathic pain syndromes, including postoperative pain.24 Gabapentin is not metabolized and is excreted in the urine unchanged. Renal clearance of gabapentin is reduced by 40% and the elimination half-life is increased up to 52 hours in renal insufficiency, but it is dialyzable. Therefore, dose adjustments are required with gabapentin in patients with moderate to severe renal insufficiency, and supplemental doses should be administered in patients after receiving dialysis.25-27
Pregabalin is structurally related to gabapentin and is indicated for a variety of neuropathic pain conditions. Pregabalin is 90% excreted unchanged in the urine, and approximately 50% of drug is removed after four hours of hemodialysis. Dose adjustments are required in patients with moderate to severe renal insufficiency, and supplemental doses should be administered in patients after receiving dialysis.28
Antidepressant options. Amitriptyline, nortryptiline, and desipramine are the tricyclic antidepressants (TCAs) commonly used for neuropathic pain. TCAs are metabolized in the liver to inactive metabolites, with the exception of amitriptyline, which is metabolized to nortryptiline. Common side effects reported with TCAs include postural hypotension and anticholinergic side effects, such as constipation, urinary retention, blurred vision, dry mouth, delirium, and sedation. It is unlikely that the TCAs can be removed by dialysis. It is suggested that the dosage be reduced in renal insufficiency and that anticholinergic side effects be monitored.29
Back to the Case
The patient’s ankle pain was controlled with acetaminophen and lidocaine patches. For the neuropathic pain in his upper extremities, tramadol was started at 25 mg oral every 12 hours and increased to 50 mg oral every eight hours (below the maximum of 200 mg a day). The tramadol did not result in adequate pain relief, so gabapentin 100 mg at bedtime was initiated, then increased to twice daily over three days with some relief.
A geriatric consult was obtained to help educate him regarding addiction to opioids, as well as to explore goals of care, but he continued to insist on the use of a non-narcotic regimen for his pain.
Bottom Line
Pain management in patients with renal insufficiency and dialysis can be challenging, but there are a number of safe non-narcotic and narcotic pain regimens that can be safely used in this patient population.
Dr. Harisingani is a board-certified hospitalist at Long Island Jewish Medical Center in New Hyde Park, N.Y., and Drs. Saad and Cassagnol are assistant clinical professors at St. Johns University College of Pharmacy and Health Sciences in Jamaica, N.Y., and clinical pharmacy coordinators at Long Island Jewish Medical Center.
References
- Mid-Atlantic Renal Coalition and the Kidney End-of-Life Coalition. Clinical algorithm & preferred medications to treat pain in dialysis patients. Coalition for Supportive Care of Kidney Patients website. Available at: http://www.kidneysupportivecare.org/Physicians-Clinicians/Pain—Symptom-Management.aspx. Accessed Nov. 18, 2012.
- Barakzoy AS, Moss AH. Efficacy of the World Health Organization analgesic ladder to treat pain in end-stage renal disease. J Am Soc Nephrol. 2006;17(11):3198-3203.
- Johnson SJ. Opioid safety in patients with renal or hepatic dysfunction. Pain Treatment Topics website. Available at: http://pain-topics.org/pdf/Opioids-Renal-Hepatic-Dysfunction.pdf. Accessed Nov. 28, 2012.
- Ferrell B, Argoff CE, Epplin J, et al. American Geriatrics Society Panel on Pharmacological Management of Persistent Pain in Older Persons. Pharmacological management of persistent pain in older persons. J Am Geriatr Soc. 2009;57(8):1331-1346.
- Prescott LF, Speirs GC, Critchley JA, Temple RM, Winney RJ. Paracetamol disposition and metabolite kinetics in patients with chronic renal failure. Eur J Clin Pharmacol. 1989;36(3):291-297.
- Launay-Vacher V, Karie S, Fau JB, Izzedine H, Deray G. Treatment of pain in patients with renal insufficiency: the World Health Organization three-step ladder adapted. J Pain. 2006;6(3):137-148.
- Berg KJ, Djøseland O, Gjellan A, et al. Acute effects of paracetamol on prostaglandin synthesis and renal function in normal man and in patients with renal failure. Clin Nephrol. 1990;34:255-262.
- Delbarre F, Roucayrol JC, Amor B, et al. Pharmacokinetic study of ketoprofen (19.583 R.P.) in man using the tritiated compound. Scand J Rheumatol Suppl. 1976;1976(0):45-52.
- Shen CH, Hung CJ, Wu CC, Huang HW, Ho WM. Rhabdomyolysis-induced acute renal failure after morphine overdose—a case report. Acta Anaesthesiol Sin. 1999;37(3):159-162.
- Ketorolac tromethamine oral tablets [package insert]. St. Louis: Ethex Corp.: 2008.
- Brocks DR, Jamali F. Clinical pharmacokinetics of ketorolac tromethamine. Clin Pharmacokinet. 1992;23:415-427. Erratum in: Clin Pharmacokinet. 1999;24(3):270.
- Ponstel [package insert]. Alpharetta, GA: First Horizon Pharmaceutical Corp.; 2006.
- Naprosyn [package insert]. Nutley, NJ: Roche Laboratories Inc.; 2008.
- Celebrex [package insert]. New York: G.D. Searle LLC; 2011.
- Catella-Lawson F, McAdam B, Morrison BW, et al. Effects of specific inhibition of cyclooygenase-2 on sodium balance, hemodynamics, and vasoactive eicosanoids. J Pharmacol Exp Ther. 1999;289:735-741.
- Dean M. Opioids in renal failure and dialysis patients. J Pain Symptom Manage. 2004;28(5):497-504.
- Lee MA, Leng ME, Tiernan EJ. Retrospective study of the use of hydromorphone in palliative care patients with normal and abnormal urea and creatinine. Palliat Med. 2001;15(1):26-34.
- Gibson TP. Pharmacokinetics, efficacy, and safety of analgesia with a focus on tramadol HCI. Am J. Med. 1996;101(1A):47S-53S.
- Izzedine H, Launay-Vacher V, Abbara C, Aymard G, Bassilios N, Deray G. Pharmacokinetics of tramadol in a hemodialysis patient. Nephron. 2002;92(3):755-756.
- Hasselström J, Säwe J. Morphine pharmacokinetics and metabolism in humans. Enterohepatic cycling and relative contribution of metabolites to active opioid concentrations. Clin Pharmacokinet. 1993;24(4):344-354.
- Andersen G, Christrup L, Sjøgren P. Relationships among morphine metabolism, pain and side effects during long-term treatment: an update. J Pain Symptom Manage. 2003;25(1):74-91.
- Lidoderm [package insert]. Chadds Ford, PA: Endo Pharmaceuticals Inc.; 2010.
- Carter GT, Galer BS. Advances in the management of neuropathic pain. Phys Med Rehabil Clin N Am. 2001;12(2):447-459.
- Ho KY, Gan TJ, Habib AS. Gabapentin and postoperative pain—a systematic review of randomized controlled trials. Pain. 2006;15:126(1-3):91-101.
- Neurontin [package insert]. New York: Parke-Davis; 2010.
- Pandey CK, Priye S, Singh S, et al. Preemptive use of gabapentin significantly decreases postoperative pain and rescue analgesic requirements in laparoscopic cholecystectomy. Can J Anaesth. 2004;51(4):358-363.
- Srivastava U, Kumar A, Saxena S, et al: Effect of preoperative gabapentin on postoperative pain and tramadol consumption after minilap open cholecystectomy: a randomized double-blind, placebo-controlled trial. Eur J Anaesthesiol. 2010;27(N4):331-335.
- Lyrica [package insert]. New York: Pfizer Inc.; 2012.
- Broadbent A, Khor K, Heaney A. Palliation and chronic renal failure: opioid and other palliative medications—dosage guidelines. Progress in Palliative Care. 2003;11(4):183-190(8).
- Nayak-Rao S. Achieving effective pain relief in patients with chronic kidney disease: a review of analgesics in renal failure. J Nephrol. 2011;24(1):35-40.
- Wolters Kluwer Health. Facts & comparisons. Wolters Kluwer Health website. Available at: http://www.factsandcomparisons.com. Accessed Jan. 14, 2013.
- Lexicomp. Lexicomp Online. Lexicomp website. Available at: http://www.lexi.com/institutions/products/online/.
Case
A 70-year-old male with ESRD on hemodialysis presents with methicillin-resistant Staphylococcus aureus (MRSA) bacteremia and ankle pain after a fall. An MRI of his ankle is negative, and he is started on acetaminophen and lidocaine patches, which result in adequate pain relief of the ankle. He later develops significant neuropathic pain in both arms, and a CT scan of the cervical spine reveals a cervical abscess and osteomyelitis. The patient desires pain relief but adamantly refuses narcotics, stating: “I don’t want to get addicted.” How can his pain be managed?
Overview
Pain is a common problem in patients with renal insufficiency and end-stage renal disease (ESRD) and can have a significant effect on the patient’s quality of life.1 When assessing a patient’s pain, assess both the severity of the pain (such as on an analogue scale, 0-10) and the characteristics of the pain. Pain is most commonly characterized as nociceptive, neuropathic, or both. Nociceptive pain can be further classified as arising from either somatic or visceral sources, and is often described as dull, throbbing, cramping, and/or pressurelike.1 Neuropathic pain is often described as tingling, numbing, burning, and/or stabbing.
It is a challenge to manage pain in patients with renal insufficiency and dialysis. Renal insufficiency affects the pharmacokinetic properties of most pain medications, including their distribution, clearance, and excretion. The magnitude of the effect of renal insufficiency on drug metabolism varies depending on the agent itself, its metabolite, and the extent of renal failure.3 Multiple factors should be considered when prescribing pain medications for patients on dialysis, including the properties of the parent drug and its metabolites; the physical properties of the dialysis equipment, such as the filter pore size, the flow rate, and the efficiency of the technique used; and the dialysis method (intermittent versus continuous).3 Table 1 provides the recommended dosing of the most commonly prescribed agents, based on the degree of renal impairment. A modified World Health Organization (WHO) ladder has been suggested to treat pain in patients with ESRD, which can lead to effective pain relief in as many as 96% of patients (see Figure 1).2
*Beginning dose: If switching from IR to ER, calculate 24-hour total dose.
**For patients with creatinine clearances (CrCl) of 15 mL/min or less, the daily dosage should be adjusted proportionally (e.g. patients with a CrCl of 7.5 mL/min should receive one-half the dose of a patient with a CrCl of 15 mL/min).
Review of Data
Nonopioid options. Nonopioids, such as acetaminophen and NSAIDs, have no associated tolerance but have a ceiling effect for analgesia, and NSAIDs are associated with dose-dependent acute renal failure, gastrointestinal ulceration and bleeding, and cardiac events. The nonopioids that are considered safe options in patients with renal insufficiency include acetaminophen, ibuprofen, and fenoprofen (Nalfon). However, in the elderly, American Geriatric Society (AGS) guidelines currently recommend avoiding all NSAIDs due to their safety profile in the geriatric population.4 Although all NSAIDs can potentially be used for pain, selected NSAIDs with an FDA indication for acute or chronic pain were included for this review.
Acetaminophen (APAP) is a dialyzable compound that is metabolized in the liver to five inactive metabolites. The terminal elimination half-life of its sulfate and glucuronide metabolites are prolonged in patients with renal failure; therefore, the dosing interval of APAP should be increased to six to eight hours in renally impaired patients.5,6,7 Overall, acetaminophen is considered one of the safest agents to use for the treatment of pain, in renal patients and otherwise, as long as dosing is below the minimal daily dose (see Table 1).
Ibuprofen is metabolized in the liver to inactive compounds. It does not accumulate in renal insufficiency, and two of the inactive compounds are dialyzable.8 It is considered a safe option for the treatment of pain in patients with renal insufficiency or dialysis.9
Fenoprofen is metabolized in the liver to inactive compounds. Renal impairment is likely to cause the accumulation of the inactive metabolites but not the parent compound, so dose reduction is not necessary with the use of this agent in renal insufficiency or dialysis.6
Mefenamic acid (Ponstel) is metabolized in the liver. Mefenamic acid can further deteriorate renal function in patients with underlying renal disease.12 However, the nephrotoxic potential of this agent is of little consideration in ESRD patients on dialysis, and therefore no dosage adjustments are necessary in these patients.6
Ketoprofen is metabolized in the liver, where approximately 80% of the dose is excreted in the urine as a glucuronide metabolite. Dose reduction is recommended in renal insufficiency and dialysis, as it not dialyzable.8
Ketorolac accumulates in renal insufficiency; therefore, it is contraindicated in these patients and in patients at risk for renal failure, including those with volume depletion.10 Ketorolac is unlikely to be removed by dialysis and so should be avoided.10,11
Naproxen is metabolized in the liver to inactive compounds. Use of naproxen is not recommended in patients with moderate to severe renal impairment. If therapy must be initiated, close monitoring of the patient’s renal function is recommended.13
Celecoxib is the only cyclooxygenase-2 (COX-2) inhibitor available in the U.S. It is metabolized extensively by the liver and is unlikely to be removed by dialysis. Therefore, use of COX-2 inhibitors should be avoided in severe renal impairment and in those on dialysis.14,15
Opioid options. The use of opioids in the renally impaired population is challenging, as one must balance opioid-related adverse events with adequate pain control. As such, it is recommended to start with lower-than-recommended doses and slowly titrate up the dose while extending the dosing interval. This will help limit adverse effects, such as respiratory depression and hypotension.3
Hydrocodone is metabolized to hydromorphone (Dilaudid), which is then metabolized to its major metabolite hydromorphine-3-glucuronide (H3G) and minor metabolite hydromorphine-6-hydroxy, all of which are excreted renally along with the parent compound. H3G has no analgesic properties, but it can potentially cause neuroexcitation, agitation, confusion, and hallucination. Hydromorphone has been used safely in patients with renal insufficiency and dialysis, as it is expected to be dialyzable. 16,17
Tramadol is metabolized in the liver, producing one active compound. Approximately 30% of the tramadol dose is excreted unchanged in the urine, whereas 60% of the dose is excreted as metabolites. It is recommended to reduce the dose and increase the dosing interval in patients with renal insufficiency, but tramadol is generally well-tolerated in patients with renal insufficiency and dialysis. It is significantly removed by hemodialysis; therefore, redosing after a session may be necessary.18,19
Oxycodone can be used in patients with mild to moderate renal insufficiency but should be used at reduced dosing; it has been associated with significant sedation with usual doses in renal failure patients.16 Its use is generally not recommended in dialysis patients due to lack of data.3
Methadone and its metabolites are excreted in the urine and feces. Methadone has been used safely in patients with renal insufficiency, but it is poorly removed by dialysis and no specific recommendations are available regarding its dosing in dialysis.3,16
Fentanyl is primarily metabolized in the liver to inactive metabolites. Fentanyl clearance is reduced in patients with moderate to severe uremia (BUN >60 mg/dL). It is not expected that fentanyl be dialyzable because of its pharmacokinetic properties (high protein-binding, low water solubility, high molecular weight, and high volume of distribution). Data suggests that fentanyl can be used at usual doses in mild to moderate renal insufficiency and in dialysis patients, although reduced doses may be prudent. Such patients should be monitored for signs of gradual accumulation of the parent drug.3,16
Morphine is metabolized in the liver to morphine-6-glucuronide (M6G) and morphine-3-glucuronide (M3G), all of which are excreted renally, along with the parent compound. Only M6G has analgesic properties, and when it accumulates, it can lead to CNS depression. M3G is associated with behavioral excitation, a side effect that is further magnified in patients with renal insufficiency. Although morphine is dialyzable, it should generally be avoided in patients with any level of renal insufficiency.16,17,20,21
Codeine is metabolized to several active metabolites, all of which are renally excreted. Lower-than-usual doses are recommended in patients with renal insufficiency, and it should be avoided altogether in dialysis patients.3,16
Meperidine is metabolized in the liver to various metabolites, primarily normeperidine, which is toxic and has a long half-life, five to 10 times longer then meperidine. Meperidine should not be used in patients with renal insufficiency or dialysis.3
Adjunctive therapeutic options. Lidocaine patches currently are only FDA-indicated for postherpetic neuralgia but are used for a wide variety of local pain syndromes. Absorption of lidocaine is determined by the duration of application and the surface area over which it is applied. There is no appreciable accumulation of lidocaine or its metabolites in renal insufficiency; therefore, dose adjustments are not required.22,23
Gabapentin is FDA-indicated for partial seizures and postherpetic neuralgia but is also used for a wide variety of neuropathic pain syndromes, including postoperative pain.24 Gabapentin is not metabolized and is excreted in the urine unchanged. Renal clearance of gabapentin is reduced by 40% and the elimination half-life is increased up to 52 hours in renal insufficiency, but it is dialyzable. Therefore, dose adjustments are required with gabapentin in patients with moderate to severe renal insufficiency, and supplemental doses should be administered in patients after receiving dialysis.25-27
Pregabalin is structurally related to gabapentin and is indicated for a variety of neuropathic pain conditions. Pregabalin is 90% excreted unchanged in the urine, and approximately 50% of drug is removed after four hours of hemodialysis. Dose adjustments are required in patients with moderate to severe renal insufficiency, and supplemental doses should be administered in patients after receiving dialysis.28
Antidepressant options. Amitriptyline, nortryptiline, and desipramine are the tricyclic antidepressants (TCAs) commonly used for neuropathic pain. TCAs are metabolized in the liver to inactive metabolites, with the exception of amitriptyline, which is metabolized to nortryptiline. Common side effects reported with TCAs include postural hypotension and anticholinergic side effects, such as constipation, urinary retention, blurred vision, dry mouth, delirium, and sedation. It is unlikely that the TCAs can be removed by dialysis. It is suggested that the dosage be reduced in renal insufficiency and that anticholinergic side effects be monitored.29
Back to the Case
The patient’s ankle pain was controlled with acetaminophen and lidocaine patches. For the neuropathic pain in his upper extremities, tramadol was started at 25 mg oral every 12 hours and increased to 50 mg oral every eight hours (below the maximum of 200 mg a day). The tramadol did not result in adequate pain relief, so gabapentin 100 mg at bedtime was initiated, then increased to twice daily over three days with some relief.
A geriatric consult was obtained to help educate him regarding addiction to opioids, as well as to explore goals of care, but he continued to insist on the use of a non-narcotic regimen for his pain.
Bottom Line
Pain management in patients with renal insufficiency and dialysis can be challenging, but there are a number of safe non-narcotic and narcotic pain regimens that can be safely used in this patient population.
Dr. Harisingani is a board-certified hospitalist at Long Island Jewish Medical Center in New Hyde Park, N.Y., and Drs. Saad and Cassagnol are assistant clinical professors at St. Johns University College of Pharmacy and Health Sciences in Jamaica, N.Y., and clinical pharmacy coordinators at Long Island Jewish Medical Center.
References
- Mid-Atlantic Renal Coalition and the Kidney End-of-Life Coalition. Clinical algorithm & preferred medications to treat pain in dialysis patients. Coalition for Supportive Care of Kidney Patients website. Available at: http://www.kidneysupportivecare.org/Physicians-Clinicians/Pain—Symptom-Management.aspx. Accessed Nov. 18, 2012.
- Barakzoy AS, Moss AH. Efficacy of the World Health Organization analgesic ladder to treat pain in end-stage renal disease. J Am Soc Nephrol. 2006;17(11):3198-3203.
- Johnson SJ. Opioid safety in patients with renal or hepatic dysfunction. Pain Treatment Topics website. Available at: http://pain-topics.org/pdf/Opioids-Renal-Hepatic-Dysfunction.pdf. Accessed Nov. 28, 2012.
- Ferrell B, Argoff CE, Epplin J, et al. American Geriatrics Society Panel on Pharmacological Management of Persistent Pain in Older Persons. Pharmacological management of persistent pain in older persons. J Am Geriatr Soc. 2009;57(8):1331-1346.
- Prescott LF, Speirs GC, Critchley JA, Temple RM, Winney RJ. Paracetamol disposition and metabolite kinetics in patients with chronic renal failure. Eur J Clin Pharmacol. 1989;36(3):291-297.
- Launay-Vacher V, Karie S, Fau JB, Izzedine H, Deray G. Treatment of pain in patients with renal insufficiency: the World Health Organization three-step ladder adapted. J Pain. 2006;6(3):137-148.
- Berg KJ, Djøseland O, Gjellan A, et al. Acute effects of paracetamol on prostaglandin synthesis and renal function in normal man and in patients with renal failure. Clin Nephrol. 1990;34:255-262.
- Delbarre F, Roucayrol JC, Amor B, et al. Pharmacokinetic study of ketoprofen (19.583 R.P.) in man using the tritiated compound. Scand J Rheumatol Suppl. 1976;1976(0):45-52.
- Shen CH, Hung CJ, Wu CC, Huang HW, Ho WM. Rhabdomyolysis-induced acute renal failure after morphine overdose—a case report. Acta Anaesthesiol Sin. 1999;37(3):159-162.
- Ketorolac tromethamine oral tablets [package insert]. St. Louis: Ethex Corp.: 2008.
- Brocks DR, Jamali F. Clinical pharmacokinetics of ketorolac tromethamine. Clin Pharmacokinet. 1992;23:415-427. Erratum in: Clin Pharmacokinet. 1999;24(3):270.
- Ponstel [package insert]. Alpharetta, GA: First Horizon Pharmaceutical Corp.; 2006.
- Naprosyn [package insert]. Nutley, NJ: Roche Laboratories Inc.; 2008.
- Celebrex [package insert]. New York: G.D. Searle LLC; 2011.
- Catella-Lawson F, McAdam B, Morrison BW, et al. Effects of specific inhibition of cyclooygenase-2 on sodium balance, hemodynamics, and vasoactive eicosanoids. J Pharmacol Exp Ther. 1999;289:735-741.
- Dean M. Opioids in renal failure and dialysis patients. J Pain Symptom Manage. 2004;28(5):497-504.
- Lee MA, Leng ME, Tiernan EJ. Retrospective study of the use of hydromorphone in palliative care patients with normal and abnormal urea and creatinine. Palliat Med. 2001;15(1):26-34.
- Gibson TP. Pharmacokinetics, efficacy, and safety of analgesia with a focus on tramadol HCI. Am J. Med. 1996;101(1A):47S-53S.
- Izzedine H, Launay-Vacher V, Abbara C, Aymard G, Bassilios N, Deray G. Pharmacokinetics of tramadol in a hemodialysis patient. Nephron. 2002;92(3):755-756.
- Hasselström J, Säwe J. Morphine pharmacokinetics and metabolism in humans. Enterohepatic cycling and relative contribution of metabolites to active opioid concentrations. Clin Pharmacokinet. 1993;24(4):344-354.
- Andersen G, Christrup L, Sjøgren P. Relationships among morphine metabolism, pain and side effects during long-term treatment: an update. J Pain Symptom Manage. 2003;25(1):74-91.
- Lidoderm [package insert]. Chadds Ford, PA: Endo Pharmaceuticals Inc.; 2010.
- Carter GT, Galer BS. Advances in the management of neuropathic pain. Phys Med Rehabil Clin N Am. 2001;12(2):447-459.
- Ho KY, Gan TJ, Habib AS. Gabapentin and postoperative pain—a systematic review of randomized controlled trials. Pain. 2006;15:126(1-3):91-101.
- Neurontin [package insert]. New York: Parke-Davis; 2010.
- Pandey CK, Priye S, Singh S, et al. Preemptive use of gabapentin significantly decreases postoperative pain and rescue analgesic requirements in laparoscopic cholecystectomy. Can J Anaesth. 2004;51(4):358-363.
- Srivastava U, Kumar A, Saxena S, et al: Effect of preoperative gabapentin on postoperative pain and tramadol consumption after minilap open cholecystectomy: a randomized double-blind, placebo-controlled trial. Eur J Anaesthesiol. 2010;27(N4):331-335.
- Lyrica [package insert]. New York: Pfizer Inc.; 2012.
- Broadbent A, Khor K, Heaney A. Palliation and chronic renal failure: opioid and other palliative medications—dosage guidelines. Progress in Palliative Care. 2003;11(4):183-190(8).
- Nayak-Rao S. Achieving effective pain relief in patients with chronic kidney disease: a review of analgesics in renal failure. J Nephrol. 2011;24(1):35-40.
- Wolters Kluwer Health. Facts & comparisons. Wolters Kluwer Health website. Available at: http://www.factsandcomparisons.com. Accessed Jan. 14, 2013.
- Lexicomp. Lexicomp Online. Lexicomp website. Available at: http://www.lexi.com/institutions/products/online/.
American College of Gastroenterology Releases C. Diff Recommendations
Clostridium difficile infection (CDI) is a common and costly bacterial illness in hospitalized patients, involving 1% of U.S. hospital stays with an aggregate cost of $8.2 billion annually.1 The spore-forming, gram-positive bacillus is spread by the fecal-oral route; in health-care settings, it is often transmitted by hand carriage and contamination of environmental surfaces. C. diff produces toxins that can cause a spectrum of diseases, including asymptomatic carriage, mild to severe diarrhea, colitis, and pseudomembranous colitis, which in severe cases can lead to sepsis, colectomy, or death.
CDI is defined as the acute onset of diarrhea in a patient with documented toxigenic C. diff or C. diff toxin, without any other clear cause of diarrhea.2 In the past decade, CDI has increased in frequency and severity, with most experts thinking it is related to a particularly virulent strain known as BI/NAP1/027.3 Antibiotic exposure is the most significant and modifiable risk factor for CDI, with increasing age, gastric acid suppression, and immunocompromised states also placing patients at increased risk for developing infection.
Guideline Analysis
In February, the American College of Gastroenterology (ACG) released guidelines for diagnostic testing and pharmacologic therapy for CDI, management of complicated and recurrent disease, and infection control and prevention.2 Previous recommendations for the prevention, diagnosis, and treatment of CDI have been provided by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and a collaboration of the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA).4,5 Recommendations addressing CDI in infants and children are also available.6 The 2013 ACG guidelines are the first from this group to address CDI and are intended to supplement previously published guidelines.
Diagnostic testing. The ACG guidelines emphasize that only stools from patients with diarrhea be tested for C. diff and/or its toxin. Colonization with C. diff is common, and performing tests in asymptomatic patients may complicate clinical care. Rarely, patients with CDI will develop ileus, and in those cases, rectal swab may be performed, but in nearly all circumstances, only diarrheal stools warrant testing. The authors also strongly discourage repeat testing after a negative test and testing for cure following treatment and resolution of symptoms. All of these recommendations are consistent with the SHEA-IDSA guidelines and reflect moderate- to high-quality evidence.
Recognizing that diagnostic testing for C. diff continues to evolve, the ACG makes specific recommendations regarding the use of newer tests, such as nucleic acid amplification and glutamate dehydrogenase detection. These are favored over toxin A and B enzyme immunoassay testing due to higher sensitivity.
Management of mild, moderate, and severe CDI. As with prior guidelines, the 2013 ACG guidelines stratify treatment recommendations by disease severity. Mild to moderate disease, which includes diarrhea only (mild) or diarrhea with signs and symptoms not meeting criteria for severe or complicated CDI (moderate), should be treated with metronidazole 500 mg orally three times daily for 10 days. Oral vancomycin should only be used in patients with mild to moderate disease who fail to respond after five to seven days of metronidazole or in those who are intolerant to metronidazole, or pregnant or breastfeeding. Although fidaxomicin is FDA-approved to treat mild to moderate CDI, the ACG does not make a formal recommendation on its use, given its high cost and limited data to support its effectiveness.
The ACG defines severe disease as CDI in patients with albumin <3 g/dL, and either WBC ≥15,000 cells/mm3 or abdominal tenderness. Though this definition of severe disease differs from the ESCMID and SHEA-IDSA definitions, which include elevated creatinine (>50% greater than premorbid level) instead of low albumin, the treatment recommendation is the same: vancomycin 125 mg orally four times daily for 10 days. While vancomycin and metronidazole are equally effective in mild to moderate CDI, there is some evidence to suggest that vancomycin is more effective in severe disease.7
Regardless of disease severity, one of the strongest recommendations is to discontinue any inciting antibiotics. This point, along with the recommendation to avoid anti-peristaltic agents, has also been emphasized in prior guidelines. Additionally, the authors note that although providers commonly prescribe treatment for 14 days, there is no evidence to suggest that a 14-day treatment course is more efficacious than a 10-day course for either metronidazole or vancomycin.
Management of severe and complicated CDI. Severe and complicated disease refers to CDI in patients meeting at least one of the following criteria: admission to the ICU, hypotension, fever ≥38.5°C, ileus or significant abdominal distention, mental status changes, WBC ≥35,000 or <2,000 cells/mm3, serum lactate >2.2 mmol/L, or end-stage organ failure. This definition is more specific than the SHEA-IDSA guidelines, which categorize severe and complicated disease as situations where shock, ileus, or megacolon are present. The recommended treatment is combined therapy with oral vancomycin 125 mg four times daily, plus intravenous metronidazole 500 mg three times daily. Surgical consultation should be obtained in all patients with complicated CDI. Colectomy should be considered in patients with evidence of severe sepsis, leukocytosis of ≥50,000, lactate ≥5 mmol/L, and failure to improve with medical therapy.
Patients with ileus or history of bowel surgery in whom oral antibiotics may not reach the colon should have vancomycin per rectum (enema of 500 mg in 100 mL to 500 mL of normal saline every six hours) added to the above treatments, regardless of disease severity.
Management of recurrent CDI. Consistent with previously published guidelines, the ACG recommends that the first recurrence of CDI be treated with the same regimen that was used for the initial episode. Second recurrences should be treated with a pulsed oral vancomycin regimen. Data are lacking regarding specific taper regimens, but the ACG suggests vancomycin 125 mg four times daily for 10 days, followed by a 125 mg dose every three days for 10 doses. For additional recurrences, fecal microbiota transplant may be considered. Reports suggest that this practice is safe and effective, but data from randomized controlled trials are lacking.
There is limited evidence to support the use of other antibiotics (e.g. rifampin, rifamixin), probiotics, or immunotherapy in the prevention of recurrent CDI.
Management of CDI in patients with comorbid conditions. A unique feature of the 2013 ACG guidelines is the incorporation of recommendations for patient groups who are at elevated risk for developing CDI or associated complications. Patients with inflammatory bowel disease (IBD) are one such group, as they often have underlying colonic inflammation and ongoing immunosuppression. The authors recommend that patients presenting with IBD flares be tested for C. diff. Other immunocompromised populations, including patients with malignancy, exposure to chemotherapy or corticosteroids, organ transplantation, and cirrhosis, should also be tested for CDI when presenting with diarrheal illness. Similarly, pregnant and peripartum women are considered high-risk and should undergo early testing and prompt initiation of treatment for CDI in the setting of diarrhea.
Infection control and prevention. Like SHEA-IDSA, the ACG recommends a hospital-based infection control program, antibiotic stewardship, and strict use of contact precautions for patients with known or suspected CDI. Contact precautions should be continued at minimum for the duration of diarrhea. Patients should be placed in private rooms and disposable equipment should be used, when possible. Disinfection of environmental surfaces is critical, as the environment is a common source of nosocomial infection. Disinfectants should have an Environmental Protection Agency-registered C. diff sporicidal label claim or contain a minimum concentration of chlorine solution. Important: Hand-washing with soap and water is required, as alcohol-based antiseptics are not active against C. diff spores.
HM Takeaways
The 2013 ACG guidelines for the diagnosis, treatment, and prevention of CDI are generally consistent with previously published guidelines from ESCMID and SHEA-IDSA. Ongoing points of emphasis are the following:
- Only test patients with diarrhea;
- Do not repeat testing after a negative test or after completion of treatment;
- Promptly discontinue any inciting antibiotics;
- Avoid use of anti-peristaltic agents; and
- Treat based on disease severity.
Hospitalists should be aware of criteria that place patients into the severe and complicated category, and understand that initial treatment should be provided for a 10-day course. These guidelines also highlight the need for a high index of suspicion and low threshold for empiric treatment in immunocompromised patients.
Finally, hospitalists should be attentive to antibiotic stewardship and strictly adhere to contact precautions and hand hygiene with soap and water, as these behaviors have been shown to prevent and control CDI.
Dr. Cunningham Sponsler is a hospitalist in the section of hospital medicine at Vanderbilt University in Nashville, Tenn.
References 1. Lucado J, Gould C, Elixhauser A. Clostridium difficile infections (CDI) in hospital stays, 2009. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb124.pdf. Accessed June 17, 2013.
2. Surawicz CM, Brandt LJ, Binion DJ, et al. Guidelines for diagnosis, treatment and prevention of Clostridium difficile infections. Am J Gastroenterol. 2013;108:478-498.
3. Freeman J, Bauer MP, Baines SD, et al. The changing epidemiology of Clostridium difficile infections. Clin Microbiol Rev. 2010;23:529-549.
4. Bauer MP, Kuijper EJ, van Dissel JT. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): treatment guidance for Clostridium difficile infection (CDI). Clin Microbiol Infect. 2009;15:1067-1079.
5. Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control and Hosp Epidemiol. 2010;31:431-455.
6. Committee on Infectious Diseases. Clostridium difficile infection in infants and children. Pediatrics. 2013;131:196-200.
7. Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45:302-307.
Clostridium difficile infection (CDI) is a common and costly bacterial illness in hospitalized patients, involving 1% of U.S. hospital stays with an aggregate cost of $8.2 billion annually.1 The spore-forming, gram-positive bacillus is spread by the fecal-oral route; in health-care settings, it is often transmitted by hand carriage and contamination of environmental surfaces. C. diff produces toxins that can cause a spectrum of diseases, including asymptomatic carriage, mild to severe diarrhea, colitis, and pseudomembranous colitis, which in severe cases can lead to sepsis, colectomy, or death.
CDI is defined as the acute onset of diarrhea in a patient with documented toxigenic C. diff or C. diff toxin, without any other clear cause of diarrhea.2 In the past decade, CDI has increased in frequency and severity, with most experts thinking it is related to a particularly virulent strain known as BI/NAP1/027.3 Antibiotic exposure is the most significant and modifiable risk factor for CDI, with increasing age, gastric acid suppression, and immunocompromised states also placing patients at increased risk for developing infection.
Guideline Analysis
In February, the American College of Gastroenterology (ACG) released guidelines for diagnostic testing and pharmacologic therapy for CDI, management of complicated and recurrent disease, and infection control and prevention.2 Previous recommendations for the prevention, diagnosis, and treatment of CDI have been provided by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and a collaboration of the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA).4,5 Recommendations addressing CDI in infants and children are also available.6 The 2013 ACG guidelines are the first from this group to address CDI and are intended to supplement previously published guidelines.
Diagnostic testing. The ACG guidelines emphasize that only stools from patients with diarrhea be tested for C. diff and/or its toxin. Colonization with C. diff is common, and performing tests in asymptomatic patients may complicate clinical care. Rarely, patients with CDI will develop ileus, and in those cases, rectal swab may be performed, but in nearly all circumstances, only diarrheal stools warrant testing. The authors also strongly discourage repeat testing after a negative test and testing for cure following treatment and resolution of symptoms. All of these recommendations are consistent with the SHEA-IDSA guidelines and reflect moderate- to high-quality evidence.
Recognizing that diagnostic testing for C. diff continues to evolve, the ACG makes specific recommendations regarding the use of newer tests, such as nucleic acid amplification and glutamate dehydrogenase detection. These are favored over toxin A and B enzyme immunoassay testing due to higher sensitivity.
Management of mild, moderate, and severe CDI. As with prior guidelines, the 2013 ACG guidelines stratify treatment recommendations by disease severity. Mild to moderate disease, which includes diarrhea only (mild) or diarrhea with signs and symptoms not meeting criteria for severe or complicated CDI (moderate), should be treated with metronidazole 500 mg orally three times daily for 10 days. Oral vancomycin should only be used in patients with mild to moderate disease who fail to respond after five to seven days of metronidazole or in those who are intolerant to metronidazole, or pregnant or breastfeeding. Although fidaxomicin is FDA-approved to treat mild to moderate CDI, the ACG does not make a formal recommendation on its use, given its high cost and limited data to support its effectiveness.
The ACG defines severe disease as CDI in patients with albumin <3 g/dL, and either WBC ≥15,000 cells/mm3 or abdominal tenderness. Though this definition of severe disease differs from the ESCMID and SHEA-IDSA definitions, which include elevated creatinine (>50% greater than premorbid level) instead of low albumin, the treatment recommendation is the same: vancomycin 125 mg orally four times daily for 10 days. While vancomycin and metronidazole are equally effective in mild to moderate CDI, there is some evidence to suggest that vancomycin is more effective in severe disease.7
Regardless of disease severity, one of the strongest recommendations is to discontinue any inciting antibiotics. This point, along with the recommendation to avoid anti-peristaltic agents, has also been emphasized in prior guidelines. Additionally, the authors note that although providers commonly prescribe treatment for 14 days, there is no evidence to suggest that a 14-day treatment course is more efficacious than a 10-day course for either metronidazole or vancomycin.
Management of severe and complicated CDI. Severe and complicated disease refers to CDI in patients meeting at least one of the following criteria: admission to the ICU, hypotension, fever ≥38.5°C, ileus or significant abdominal distention, mental status changes, WBC ≥35,000 or <2,000 cells/mm3, serum lactate >2.2 mmol/L, or end-stage organ failure. This definition is more specific than the SHEA-IDSA guidelines, which categorize severe and complicated disease as situations where shock, ileus, or megacolon are present. The recommended treatment is combined therapy with oral vancomycin 125 mg four times daily, plus intravenous metronidazole 500 mg three times daily. Surgical consultation should be obtained in all patients with complicated CDI. Colectomy should be considered in patients with evidence of severe sepsis, leukocytosis of ≥50,000, lactate ≥5 mmol/L, and failure to improve with medical therapy.
Patients with ileus or history of bowel surgery in whom oral antibiotics may not reach the colon should have vancomycin per rectum (enema of 500 mg in 100 mL to 500 mL of normal saline every six hours) added to the above treatments, regardless of disease severity.
Management of recurrent CDI. Consistent with previously published guidelines, the ACG recommends that the first recurrence of CDI be treated with the same regimen that was used for the initial episode. Second recurrences should be treated with a pulsed oral vancomycin regimen. Data are lacking regarding specific taper regimens, but the ACG suggests vancomycin 125 mg four times daily for 10 days, followed by a 125 mg dose every three days for 10 doses. For additional recurrences, fecal microbiota transplant may be considered. Reports suggest that this practice is safe and effective, but data from randomized controlled trials are lacking.
There is limited evidence to support the use of other antibiotics (e.g. rifampin, rifamixin), probiotics, or immunotherapy in the prevention of recurrent CDI.
Management of CDI in patients with comorbid conditions. A unique feature of the 2013 ACG guidelines is the incorporation of recommendations for patient groups who are at elevated risk for developing CDI or associated complications. Patients with inflammatory bowel disease (IBD) are one such group, as they often have underlying colonic inflammation and ongoing immunosuppression. The authors recommend that patients presenting with IBD flares be tested for C. diff. Other immunocompromised populations, including patients with malignancy, exposure to chemotherapy or corticosteroids, organ transplantation, and cirrhosis, should also be tested for CDI when presenting with diarrheal illness. Similarly, pregnant and peripartum women are considered high-risk and should undergo early testing and prompt initiation of treatment for CDI in the setting of diarrhea.
Infection control and prevention. Like SHEA-IDSA, the ACG recommends a hospital-based infection control program, antibiotic stewardship, and strict use of contact precautions for patients with known or suspected CDI. Contact precautions should be continued at minimum for the duration of diarrhea. Patients should be placed in private rooms and disposable equipment should be used, when possible. Disinfection of environmental surfaces is critical, as the environment is a common source of nosocomial infection. Disinfectants should have an Environmental Protection Agency-registered C. diff sporicidal label claim or contain a minimum concentration of chlorine solution. Important: Hand-washing with soap and water is required, as alcohol-based antiseptics are not active against C. diff spores.
HM Takeaways
The 2013 ACG guidelines for the diagnosis, treatment, and prevention of CDI are generally consistent with previously published guidelines from ESCMID and SHEA-IDSA. Ongoing points of emphasis are the following:
- Only test patients with diarrhea;
- Do not repeat testing after a negative test or after completion of treatment;
- Promptly discontinue any inciting antibiotics;
- Avoid use of anti-peristaltic agents; and
- Treat based on disease severity.
Hospitalists should be aware of criteria that place patients into the severe and complicated category, and understand that initial treatment should be provided for a 10-day course. These guidelines also highlight the need for a high index of suspicion and low threshold for empiric treatment in immunocompromised patients.
Finally, hospitalists should be attentive to antibiotic stewardship and strictly adhere to contact precautions and hand hygiene with soap and water, as these behaviors have been shown to prevent and control CDI.
Dr. Cunningham Sponsler is a hospitalist in the section of hospital medicine at Vanderbilt University in Nashville, Tenn.
References 1. Lucado J, Gould C, Elixhauser A. Clostridium difficile infections (CDI) in hospital stays, 2009. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb124.pdf. Accessed June 17, 2013.
2. Surawicz CM, Brandt LJ, Binion DJ, et al. Guidelines for diagnosis, treatment and prevention of Clostridium difficile infections. Am J Gastroenterol. 2013;108:478-498.
3. Freeman J, Bauer MP, Baines SD, et al. The changing epidemiology of Clostridium difficile infections. Clin Microbiol Rev. 2010;23:529-549.
4. Bauer MP, Kuijper EJ, van Dissel JT. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): treatment guidance for Clostridium difficile infection (CDI). Clin Microbiol Infect. 2009;15:1067-1079.
5. Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control and Hosp Epidemiol. 2010;31:431-455.
6. Committee on Infectious Diseases. Clostridium difficile infection in infants and children. Pediatrics. 2013;131:196-200.
7. Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45:302-307.
Clostridium difficile infection (CDI) is a common and costly bacterial illness in hospitalized patients, involving 1% of U.S. hospital stays with an aggregate cost of $8.2 billion annually.1 The spore-forming, gram-positive bacillus is spread by the fecal-oral route; in health-care settings, it is often transmitted by hand carriage and contamination of environmental surfaces. C. diff produces toxins that can cause a spectrum of diseases, including asymptomatic carriage, mild to severe diarrhea, colitis, and pseudomembranous colitis, which in severe cases can lead to sepsis, colectomy, or death.
CDI is defined as the acute onset of diarrhea in a patient with documented toxigenic C. diff or C. diff toxin, without any other clear cause of diarrhea.2 In the past decade, CDI has increased in frequency and severity, with most experts thinking it is related to a particularly virulent strain known as BI/NAP1/027.3 Antibiotic exposure is the most significant and modifiable risk factor for CDI, with increasing age, gastric acid suppression, and immunocompromised states also placing patients at increased risk for developing infection.
Guideline Analysis
In February, the American College of Gastroenterology (ACG) released guidelines for diagnostic testing and pharmacologic therapy for CDI, management of complicated and recurrent disease, and infection control and prevention.2 Previous recommendations for the prevention, diagnosis, and treatment of CDI have been provided by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and a collaboration of the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA).4,5 Recommendations addressing CDI in infants and children are also available.6 The 2013 ACG guidelines are the first from this group to address CDI and are intended to supplement previously published guidelines.
Diagnostic testing. The ACG guidelines emphasize that only stools from patients with diarrhea be tested for C. diff and/or its toxin. Colonization with C. diff is common, and performing tests in asymptomatic patients may complicate clinical care. Rarely, patients with CDI will develop ileus, and in those cases, rectal swab may be performed, but in nearly all circumstances, only diarrheal stools warrant testing. The authors also strongly discourage repeat testing after a negative test and testing for cure following treatment and resolution of symptoms. All of these recommendations are consistent with the SHEA-IDSA guidelines and reflect moderate- to high-quality evidence.
Recognizing that diagnostic testing for C. diff continues to evolve, the ACG makes specific recommendations regarding the use of newer tests, such as nucleic acid amplification and glutamate dehydrogenase detection. These are favored over toxin A and B enzyme immunoassay testing due to higher sensitivity.
Management of mild, moderate, and severe CDI. As with prior guidelines, the 2013 ACG guidelines stratify treatment recommendations by disease severity. Mild to moderate disease, which includes diarrhea only (mild) or diarrhea with signs and symptoms not meeting criteria for severe or complicated CDI (moderate), should be treated with metronidazole 500 mg orally three times daily for 10 days. Oral vancomycin should only be used in patients with mild to moderate disease who fail to respond after five to seven days of metronidazole or in those who are intolerant to metronidazole, or pregnant or breastfeeding. Although fidaxomicin is FDA-approved to treat mild to moderate CDI, the ACG does not make a formal recommendation on its use, given its high cost and limited data to support its effectiveness.
The ACG defines severe disease as CDI in patients with albumin <3 g/dL, and either WBC ≥15,000 cells/mm3 or abdominal tenderness. Though this definition of severe disease differs from the ESCMID and SHEA-IDSA definitions, which include elevated creatinine (>50% greater than premorbid level) instead of low albumin, the treatment recommendation is the same: vancomycin 125 mg orally four times daily for 10 days. While vancomycin and metronidazole are equally effective in mild to moderate CDI, there is some evidence to suggest that vancomycin is more effective in severe disease.7
Regardless of disease severity, one of the strongest recommendations is to discontinue any inciting antibiotics. This point, along with the recommendation to avoid anti-peristaltic agents, has also been emphasized in prior guidelines. Additionally, the authors note that although providers commonly prescribe treatment for 14 days, there is no evidence to suggest that a 14-day treatment course is more efficacious than a 10-day course for either metronidazole or vancomycin.
Management of severe and complicated CDI. Severe and complicated disease refers to CDI in patients meeting at least one of the following criteria: admission to the ICU, hypotension, fever ≥38.5°C, ileus or significant abdominal distention, mental status changes, WBC ≥35,000 or <2,000 cells/mm3, serum lactate >2.2 mmol/L, or end-stage organ failure. This definition is more specific than the SHEA-IDSA guidelines, which categorize severe and complicated disease as situations where shock, ileus, or megacolon are present. The recommended treatment is combined therapy with oral vancomycin 125 mg four times daily, plus intravenous metronidazole 500 mg three times daily. Surgical consultation should be obtained in all patients with complicated CDI. Colectomy should be considered in patients with evidence of severe sepsis, leukocytosis of ≥50,000, lactate ≥5 mmol/L, and failure to improve with medical therapy.
Patients with ileus or history of bowel surgery in whom oral antibiotics may not reach the colon should have vancomycin per rectum (enema of 500 mg in 100 mL to 500 mL of normal saline every six hours) added to the above treatments, regardless of disease severity.
Management of recurrent CDI. Consistent with previously published guidelines, the ACG recommends that the first recurrence of CDI be treated with the same regimen that was used for the initial episode. Second recurrences should be treated with a pulsed oral vancomycin regimen. Data are lacking regarding specific taper regimens, but the ACG suggests vancomycin 125 mg four times daily for 10 days, followed by a 125 mg dose every three days for 10 doses. For additional recurrences, fecal microbiota transplant may be considered. Reports suggest that this practice is safe and effective, but data from randomized controlled trials are lacking.
There is limited evidence to support the use of other antibiotics (e.g. rifampin, rifamixin), probiotics, or immunotherapy in the prevention of recurrent CDI.
Management of CDI in patients with comorbid conditions. A unique feature of the 2013 ACG guidelines is the incorporation of recommendations for patient groups who are at elevated risk for developing CDI or associated complications. Patients with inflammatory bowel disease (IBD) are one such group, as they often have underlying colonic inflammation and ongoing immunosuppression. The authors recommend that patients presenting with IBD flares be tested for C. diff. Other immunocompromised populations, including patients with malignancy, exposure to chemotherapy or corticosteroids, organ transplantation, and cirrhosis, should also be tested for CDI when presenting with diarrheal illness. Similarly, pregnant and peripartum women are considered high-risk and should undergo early testing and prompt initiation of treatment for CDI in the setting of diarrhea.
Infection control and prevention. Like SHEA-IDSA, the ACG recommends a hospital-based infection control program, antibiotic stewardship, and strict use of contact precautions for patients with known or suspected CDI. Contact precautions should be continued at minimum for the duration of diarrhea. Patients should be placed in private rooms and disposable equipment should be used, when possible. Disinfection of environmental surfaces is critical, as the environment is a common source of nosocomial infection. Disinfectants should have an Environmental Protection Agency-registered C. diff sporicidal label claim or contain a minimum concentration of chlorine solution. Important: Hand-washing with soap and water is required, as alcohol-based antiseptics are not active against C. diff spores.
HM Takeaways
The 2013 ACG guidelines for the diagnosis, treatment, and prevention of CDI are generally consistent with previously published guidelines from ESCMID and SHEA-IDSA. Ongoing points of emphasis are the following:
- Only test patients with diarrhea;
- Do not repeat testing after a negative test or after completion of treatment;
- Promptly discontinue any inciting antibiotics;
- Avoid use of anti-peristaltic agents; and
- Treat based on disease severity.
Hospitalists should be aware of criteria that place patients into the severe and complicated category, and understand that initial treatment should be provided for a 10-day course. These guidelines also highlight the need for a high index of suspicion and low threshold for empiric treatment in immunocompromised patients.
Finally, hospitalists should be attentive to antibiotic stewardship and strictly adhere to contact precautions and hand hygiene with soap and water, as these behaviors have been shown to prevent and control CDI.
Dr. Cunningham Sponsler is a hospitalist in the section of hospital medicine at Vanderbilt University in Nashville, Tenn.
References 1. Lucado J, Gould C, Elixhauser A. Clostridium difficile infections (CDI) in hospital stays, 2009. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb124.pdf. Accessed June 17, 2013.
2. Surawicz CM, Brandt LJ, Binion DJ, et al. Guidelines for diagnosis, treatment and prevention of Clostridium difficile infections. Am J Gastroenterol. 2013;108:478-498.
3. Freeman J, Bauer MP, Baines SD, et al. The changing epidemiology of Clostridium difficile infections. Clin Microbiol Rev. 2010;23:529-549.
4. Bauer MP, Kuijper EJ, van Dissel JT. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): treatment guidance for Clostridium difficile infection (CDI). Clin Microbiol Infect. 2009;15:1067-1079.
5. Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control and Hosp Epidemiol. 2010;31:431-455.
6. Committee on Infectious Diseases. Clostridium difficile infection in infants and children. Pediatrics. 2013;131:196-200.
7. Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45:302-307.
Pediatric Hospital Medicine Aims to Define Itself

Legend has it that Alexander the Great once was confronted with an intricate knot tying up a sacred ox cart in the palace of the Phrygians, whom he was trying to conquer. When his attempts to untie the knot proved unsuccessful, he drew his sword and sliced it in half, thus providing a rapid if inelegant solution.
Pediatric hospital medicine (PHM) now finds itself facing a similar dilemma in its attempts to define its “kingdom.” The question: Who will become citizens of this kingdom—and who will be left outside the gates? And will this intricate knot be unraveled or simply cut?
In some ways, the mere posing of this question signifies the success PHM has forged for itself over the past decade. At its core, the question of how to define the identity, and thus the training, of a pediatric hospitalist is rooted in noble ideals: excellence in the management of hospitalized children, robust training in quality improvement, patient safety, and cost-effective care.1 Yet this question also stirs up more base feelings frequently articulated in many a physician lounge: territoriality, inadequacy, feeling excluded.
Nevertheless, the question must be answered.
In many ways, the situation in which PHM finds itself mirrors the dilemma facing pediatrics itself in its infancy. As Borden Veeder, the first president of the American Board of Pediatrics (ABP), wrote in the 1930s, “There were no legal or medical requirements relating to the training and education of specialists—all a man licensed to practice medicine had to do was to announce himself as a surgeon, internist, pediatrician, etc., as he preferred.”2 In 1933, the ABP was incorporated, with representatives from the American Academy of Pediatrics (AAP), the American Medical Association (AMA) section on pediatrics, and the American Pediatric Society.
Facing a similar state of confusion, hospitalist leaders of the PHM community in 2010 formed the Strategic Planning Committee (STP) to evaluate training and certification options for PHM as a distinct discipline.3 Co-chairs of the STP Committee were chosen by consensus from a group composed of one representative each from the AAP Section on Hospital Medicine (AAP SOHM), the Academic Pediatric Association (APA), and SHM. The STP identified various training and/or certification options that could define PHM as a subspecialty. A survey with these options was distributed to the PHM community via the listservs of the APA, the AAP SOHM, and the AAP. The results:3
- 33% of respondents preferred Recognition of Focused Practice through the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC);
- 30% preferred a two-year fellowship; and
- 17% suggested an HM track within pediatric residency.
Yet at the PHM Leaders Conference in Chapel Hill, N.C., in April, “there was overwhelming consensus that an MOC program could not provide the rigor to insure [sic] that all pediatric hospitalists would meet a standard.”4 Further, “there was overwhelming consensus that a standardized training program resulting in certification was the best option to assure adequate training in the PHM Core Competencies and provide the public with a meaningful definition of a pediatric hospitalist” and “that the duration of such training should be two years.” Why, one might ask, would those present feel so strongly that the MOC model would be inadequate?
Many concerns regarding MOC were voiced, including whether MOC addresses a knowledge gap after residency (which it does to some extent through ongoing recertification requirements), whether it ensures public trust (but it had “positive potential”), and whether it addressed core competencies (to which the leadership present answered “yes, if rigorous”).4
The perception that the Focused Practice in Hospital Medicine (FPHM) MOC was “not a successful model so far in adult hospital medicine” seemed to weigh heavily on the minds of those in attendance. This perception may have arisen from data showing a somewhat low number of adult hospitalists (363 completed, 527 in process) having successfully completed the FPHM MOC to date. Of note, the possibility of a FPHM MOC for PHM was considered a “non-starter” by the ABP representatives, who in turn attributed this determination to the American Board of Medical Specialties (ABMS).5
There are, of course, many reasons for the low turnout for adult FPHM MOC. Candidates must have been previously certified in internal medicine of family medicine, and thus entry into the FPHM MOC would only arise at recertification or if one decided to seek FPHM certification “early”—that is, prior to the need for recertification. Being not only a Procrastination Club president but also a client, I was not among the 67 virtuous hospitalists who were among the first class of FPHM diplomates in 2011.6 The FPHM MOC also initially was more rigorous than the traditional IM recertification, in that it required completion of a practice-improvement module (PIM) every three years versus every 10 years (in 2014, both the traditional IM and FPHM MOC programs will require PIM completion every 5 years). Without a clearly mandated requirement from most HM groups, at the inception of the FPHM MOC one would be entering a more rigorous recertification process without a clear benefit.
This lack of a requirement from adult HM groups for completion or entry into the FPHM MOC, in turn, arises from a straightforward issue: workforce. Requiring all hospitalists in your HM group to have completed or entered FPHM MOC is a bar most directors and chiefs are not prepared to raise given its potential to shrink their applicant pool. With only 32 to 35 graduates of pediatric HM fellowship programs yearly, workforce issues should clearly be of concern to the PHM community given the current estimates that pediatric hospitalists number anywhere from 1,500 to 3,000.6,7
Is the adult FPHM MOC process perfect? Nothing created by so many committees and professional societies could ever be, but as a first iteration, it certainly created a relatively sturdy straw man. Could the PHM community create a FPHM MOC upon this model that was refined and tailored to their needs? Creating and requiring completion of a robust PHM-specific curriculum via required self-evaluation modules, requiring not only patient encounter thresholds but also evidence of quality care, and developing PIMs specific to PHM would all go a long way to making a FPHM MOC an acceptable alternative for pediatric hospitalist “designation.”
In any case, the gauntlet seems to have been thrown down already in Chapel Hill in favor of a two-year fellowship leading to certification. I admire those present for advocating a training and certification that provides the least compromise in defining the path of future pediatric hospitalists. But I suspect that the answer to the problem of PHM’s future may not be so simple as a single sharp-edged solution and might lie in a more complex array of options for future pediatric hospitalists.
Dr. Chang is pediatric editor of The Hospitalist. He is associate clinical professor of medicine and pediatrics at the University of California at San Diego (UCSD) School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital. Send comments and questions to wwch@ucsd.edu.
References
- Maniscalco J, Fisher ES. Pediatric hospital medicine and education: why we can’t stand still. JAMA Pediatr. 2013;167:412-413.
- Brownlee RC. The American Board of Pediatrics: its origin and early history. Pediatrics. 1994;94:732-735.
- Maloney CG, Mendez SS, Quinonez RA, et al. The Strategic Planning Committee report: the first step in a journey to recognize pediatric hospital medicine as a distinct discipline. Hospital Pediatrics. 2012;2:187-190.
- Strategic Planning Committee. Strategic planning for the future of pediatric hospital medicine. Strategic Planning Committee website. Available at: http://stpcommittee.blogspot.com/2013/04/phm-leadership-conference-april-4-5.htmlfiles/97/phm-leadership-conference-april-4-5.html. Accessed July 4, 2013.
- Fisher ES. (2013) Email sent to Chang WW. 25 June.
- Carris J. Defining moment: focused practice in HM. The Hospitalist website. Available at: http://www.the-hospitalist.org/details/article/1018793/Defining_Moment_Focused_Practice_in_HM.html. Accessed June 15, 2013.
- American Academy of Pediatrics. PHM fellowship info. American Academy of Pediatrics website. Available at: http://www.aap.org/en-us/about-the-aap/Committees-Councils-Sections/Section-on-Hospital-Medicine.html. Accessed June 15, 2013.
- Rauch DA, Lye PS, Carlson D, et al. Pediatric hospital medicine: a strategic planning roundtable to chart the future. J Hosp Med. 2012;7:329-334.
Legend has it that Alexander the Great once was confronted with an intricate knot tying up a sacred ox cart in the palace of the Phrygians, whom he was trying to conquer. When his attempts to untie the knot proved unsuccessful, he drew his sword and sliced it in half, thus providing a rapid if inelegant solution.
Pediatric hospital medicine (PHM) now finds itself facing a similar dilemma in its attempts to define its “kingdom.” The question: Who will become citizens of this kingdom—and who will be left outside the gates? And will this intricate knot be unraveled or simply cut?
In some ways, the mere posing of this question signifies the success PHM has forged for itself over the past decade. At its core, the question of how to define the identity, and thus the training, of a pediatric hospitalist is rooted in noble ideals: excellence in the management of hospitalized children, robust training in quality improvement, patient safety, and cost-effective care.1 Yet this question also stirs up more base feelings frequently articulated in many a physician lounge: territoriality, inadequacy, feeling excluded.
Nevertheless, the question must be answered.
In many ways, the situation in which PHM finds itself mirrors the dilemma facing pediatrics itself in its infancy. As Borden Veeder, the first president of the American Board of Pediatrics (ABP), wrote in the 1930s, “There were no legal or medical requirements relating to the training and education of specialists—all a man licensed to practice medicine had to do was to announce himself as a surgeon, internist, pediatrician, etc., as he preferred.”2 In 1933, the ABP was incorporated, with representatives from the American Academy of Pediatrics (AAP), the American Medical Association (AMA) section on pediatrics, and the American Pediatric Society.
Facing a similar state of confusion, hospitalist leaders of the PHM community in 2010 formed the Strategic Planning Committee (STP) to evaluate training and certification options for PHM as a distinct discipline.3 Co-chairs of the STP Committee were chosen by consensus from a group composed of one representative each from the AAP Section on Hospital Medicine (AAP SOHM), the Academic Pediatric Association (APA), and SHM. The STP identified various training and/or certification options that could define PHM as a subspecialty. A survey with these options was distributed to the PHM community via the listservs of the APA, the AAP SOHM, and the AAP. The results:3
- 33% of respondents preferred Recognition of Focused Practice through the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC);
- 30% preferred a two-year fellowship; and
- 17% suggested an HM track within pediatric residency.
Yet at the PHM Leaders Conference in Chapel Hill, N.C., in April, “there was overwhelming consensus that an MOC program could not provide the rigor to insure [sic] that all pediatric hospitalists would meet a standard.”4 Further, “there was overwhelming consensus that a standardized training program resulting in certification was the best option to assure adequate training in the PHM Core Competencies and provide the public with a meaningful definition of a pediatric hospitalist” and “that the duration of such training should be two years.” Why, one might ask, would those present feel so strongly that the MOC model would be inadequate?
Many concerns regarding MOC were voiced, including whether MOC addresses a knowledge gap after residency (which it does to some extent through ongoing recertification requirements), whether it ensures public trust (but it had “positive potential”), and whether it addressed core competencies (to which the leadership present answered “yes, if rigorous”).4
The perception that the Focused Practice in Hospital Medicine (FPHM) MOC was “not a successful model so far in adult hospital medicine” seemed to weigh heavily on the minds of those in attendance. This perception may have arisen from data showing a somewhat low number of adult hospitalists (363 completed, 527 in process) having successfully completed the FPHM MOC to date. Of note, the possibility of a FPHM MOC for PHM was considered a “non-starter” by the ABP representatives, who in turn attributed this determination to the American Board of Medical Specialties (ABMS).5
There are, of course, many reasons for the low turnout for adult FPHM MOC. Candidates must have been previously certified in internal medicine of family medicine, and thus entry into the FPHM MOC would only arise at recertification or if one decided to seek FPHM certification “early”—that is, prior to the need for recertification. Being not only a Procrastination Club president but also a client, I was not among the 67 virtuous hospitalists who were among the first class of FPHM diplomates in 2011.6 The FPHM MOC also initially was more rigorous than the traditional IM recertification, in that it required completion of a practice-improvement module (PIM) every three years versus every 10 years (in 2014, both the traditional IM and FPHM MOC programs will require PIM completion every 5 years). Without a clearly mandated requirement from most HM groups, at the inception of the FPHM MOC one would be entering a more rigorous recertification process without a clear benefit.
This lack of a requirement from adult HM groups for completion or entry into the FPHM MOC, in turn, arises from a straightforward issue: workforce. Requiring all hospitalists in your HM group to have completed or entered FPHM MOC is a bar most directors and chiefs are not prepared to raise given its potential to shrink their applicant pool. With only 32 to 35 graduates of pediatric HM fellowship programs yearly, workforce issues should clearly be of concern to the PHM community given the current estimates that pediatric hospitalists number anywhere from 1,500 to 3,000.6,7
Is the adult FPHM MOC process perfect? Nothing created by so many committees and professional societies could ever be, but as a first iteration, it certainly created a relatively sturdy straw man. Could the PHM community create a FPHM MOC upon this model that was refined and tailored to their needs? Creating and requiring completion of a robust PHM-specific curriculum via required self-evaluation modules, requiring not only patient encounter thresholds but also evidence of quality care, and developing PIMs specific to PHM would all go a long way to making a FPHM MOC an acceptable alternative for pediatric hospitalist “designation.”
In any case, the gauntlet seems to have been thrown down already in Chapel Hill in favor of a two-year fellowship leading to certification. I admire those present for advocating a training and certification that provides the least compromise in defining the path of future pediatric hospitalists. But I suspect that the answer to the problem of PHM’s future may not be so simple as a single sharp-edged solution and might lie in a more complex array of options for future pediatric hospitalists.
Dr. Chang is pediatric editor of The Hospitalist. He is associate clinical professor of medicine and pediatrics at the University of California at San Diego (UCSD) School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital. Send comments and questions to wwch@ucsd.edu.
References
- Maniscalco J, Fisher ES. Pediatric hospital medicine and education: why we can’t stand still. JAMA Pediatr. 2013;167:412-413.
- Brownlee RC. The American Board of Pediatrics: its origin and early history. Pediatrics. 1994;94:732-735.
- Maloney CG, Mendez SS, Quinonez RA, et al. The Strategic Planning Committee report: the first step in a journey to recognize pediatric hospital medicine as a distinct discipline. Hospital Pediatrics. 2012;2:187-190.
- Strategic Planning Committee. Strategic planning for the future of pediatric hospital medicine. Strategic Planning Committee website. Available at: http://stpcommittee.blogspot.com/2013/04/phm-leadership-conference-april-4-5.htmlfiles/97/phm-leadership-conference-april-4-5.html. Accessed July 4, 2013.
- Fisher ES. (2013) Email sent to Chang WW. 25 June.
- Carris J. Defining moment: focused practice in HM. The Hospitalist website. Available at: http://www.the-hospitalist.org/details/article/1018793/Defining_Moment_Focused_Practice_in_HM.html. Accessed June 15, 2013.
- American Academy of Pediatrics. PHM fellowship info. American Academy of Pediatrics website. Available at: http://www.aap.org/en-us/about-the-aap/Committees-Councils-Sections/Section-on-Hospital-Medicine.html. Accessed June 15, 2013.
- Rauch DA, Lye PS, Carlson D, et al. Pediatric hospital medicine: a strategic planning roundtable to chart the future. J Hosp Med. 2012;7:329-334.
Legend has it that Alexander the Great once was confronted with an intricate knot tying up a sacred ox cart in the palace of the Phrygians, whom he was trying to conquer. When his attempts to untie the knot proved unsuccessful, he drew his sword and sliced it in half, thus providing a rapid if inelegant solution.
Pediatric hospital medicine (PHM) now finds itself facing a similar dilemma in its attempts to define its “kingdom.” The question: Who will become citizens of this kingdom—and who will be left outside the gates? And will this intricate knot be unraveled or simply cut?
In some ways, the mere posing of this question signifies the success PHM has forged for itself over the past decade. At its core, the question of how to define the identity, and thus the training, of a pediatric hospitalist is rooted in noble ideals: excellence in the management of hospitalized children, robust training in quality improvement, patient safety, and cost-effective care.1 Yet this question also stirs up more base feelings frequently articulated in many a physician lounge: territoriality, inadequacy, feeling excluded.
Nevertheless, the question must be answered.
In many ways, the situation in which PHM finds itself mirrors the dilemma facing pediatrics itself in its infancy. As Borden Veeder, the first president of the American Board of Pediatrics (ABP), wrote in the 1930s, “There were no legal or medical requirements relating to the training and education of specialists—all a man licensed to practice medicine had to do was to announce himself as a surgeon, internist, pediatrician, etc., as he preferred.”2 In 1933, the ABP was incorporated, with representatives from the American Academy of Pediatrics (AAP), the American Medical Association (AMA) section on pediatrics, and the American Pediatric Society.
Facing a similar state of confusion, hospitalist leaders of the PHM community in 2010 formed the Strategic Planning Committee (STP) to evaluate training and certification options for PHM as a distinct discipline.3 Co-chairs of the STP Committee were chosen by consensus from a group composed of one representative each from the AAP Section on Hospital Medicine (AAP SOHM), the Academic Pediatric Association (APA), and SHM. The STP identified various training and/or certification options that could define PHM as a subspecialty. A survey with these options was distributed to the PHM community via the listservs of the APA, the AAP SOHM, and the AAP. The results:3
- 33% of respondents preferred Recognition of Focused Practice through the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC);
- 30% preferred a two-year fellowship; and
- 17% suggested an HM track within pediatric residency.
Yet at the PHM Leaders Conference in Chapel Hill, N.C., in April, “there was overwhelming consensus that an MOC program could not provide the rigor to insure [sic] that all pediatric hospitalists would meet a standard.”4 Further, “there was overwhelming consensus that a standardized training program resulting in certification was the best option to assure adequate training in the PHM Core Competencies and provide the public with a meaningful definition of a pediatric hospitalist” and “that the duration of such training should be two years.” Why, one might ask, would those present feel so strongly that the MOC model would be inadequate?
Many concerns regarding MOC were voiced, including whether MOC addresses a knowledge gap after residency (which it does to some extent through ongoing recertification requirements), whether it ensures public trust (but it had “positive potential”), and whether it addressed core competencies (to which the leadership present answered “yes, if rigorous”).4
The perception that the Focused Practice in Hospital Medicine (FPHM) MOC was “not a successful model so far in adult hospital medicine” seemed to weigh heavily on the minds of those in attendance. This perception may have arisen from data showing a somewhat low number of adult hospitalists (363 completed, 527 in process) having successfully completed the FPHM MOC to date. Of note, the possibility of a FPHM MOC for PHM was considered a “non-starter” by the ABP representatives, who in turn attributed this determination to the American Board of Medical Specialties (ABMS).5
There are, of course, many reasons for the low turnout for adult FPHM MOC. Candidates must have been previously certified in internal medicine of family medicine, and thus entry into the FPHM MOC would only arise at recertification or if one decided to seek FPHM certification “early”—that is, prior to the need for recertification. Being not only a Procrastination Club president but also a client, I was not among the 67 virtuous hospitalists who were among the first class of FPHM diplomates in 2011.6 The FPHM MOC also initially was more rigorous than the traditional IM recertification, in that it required completion of a practice-improvement module (PIM) every three years versus every 10 years (in 2014, both the traditional IM and FPHM MOC programs will require PIM completion every 5 years). Without a clearly mandated requirement from most HM groups, at the inception of the FPHM MOC one would be entering a more rigorous recertification process without a clear benefit.
This lack of a requirement from adult HM groups for completion or entry into the FPHM MOC, in turn, arises from a straightforward issue: workforce. Requiring all hospitalists in your HM group to have completed or entered FPHM MOC is a bar most directors and chiefs are not prepared to raise given its potential to shrink their applicant pool. With only 32 to 35 graduates of pediatric HM fellowship programs yearly, workforce issues should clearly be of concern to the PHM community given the current estimates that pediatric hospitalists number anywhere from 1,500 to 3,000.6,7
Is the adult FPHM MOC process perfect? Nothing created by so many committees and professional societies could ever be, but as a first iteration, it certainly created a relatively sturdy straw man. Could the PHM community create a FPHM MOC upon this model that was refined and tailored to their needs? Creating and requiring completion of a robust PHM-specific curriculum via required self-evaluation modules, requiring not only patient encounter thresholds but also evidence of quality care, and developing PIMs specific to PHM would all go a long way to making a FPHM MOC an acceptable alternative for pediatric hospitalist “designation.”
In any case, the gauntlet seems to have been thrown down already in Chapel Hill in favor of a two-year fellowship leading to certification. I admire those present for advocating a training and certification that provides the least compromise in defining the path of future pediatric hospitalists. But I suspect that the answer to the problem of PHM’s future may not be so simple as a single sharp-edged solution and might lie in a more complex array of options for future pediatric hospitalists.
Dr. Chang is pediatric editor of The Hospitalist. He is associate clinical professor of medicine and pediatrics at the University of California at San Diego (UCSD) School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital. Send comments and questions to wwch@ucsd.edu.
References
- Maniscalco J, Fisher ES. Pediatric hospital medicine and education: why we can’t stand still. JAMA Pediatr. 2013;167:412-413.
- Brownlee RC. The American Board of Pediatrics: its origin and early history. Pediatrics. 1994;94:732-735.
- Maloney CG, Mendez SS, Quinonez RA, et al. The Strategic Planning Committee report: the first step in a journey to recognize pediatric hospital medicine as a distinct discipline. Hospital Pediatrics. 2012;2:187-190.
- Strategic Planning Committee. Strategic planning for the future of pediatric hospital medicine. Strategic Planning Committee website. Available at: http://stpcommittee.blogspot.com/2013/04/phm-leadership-conference-april-4-5.htmlfiles/97/phm-leadership-conference-april-4-5.html. Accessed July 4, 2013.
- Fisher ES. (2013) Email sent to Chang WW. 25 June.
- Carris J. Defining moment: focused practice in HM. The Hospitalist website. Available at: http://www.the-hospitalist.org/details/article/1018793/Defining_Moment_Focused_Practice_in_HM.html. Accessed June 15, 2013.
- American Academy of Pediatrics. PHM fellowship info. American Academy of Pediatrics website. Available at: http://www.aap.org/en-us/about-the-aap/Committees-Councils-Sections/Section-on-Hospital-Medicine.html. Accessed June 15, 2013.
- Rauch DA, Lye PS, Carlson D, et al. Pediatric hospital medicine: a strategic planning roundtable to chart the future. J Hosp Med. 2012;7:329-334.
Proton-Pump Inhibitors Associated with Increased Mortality Risk
Clinical question: Is the use of proton-pump inhibitors (PPIs) associated with risk of mortality or combined risk of death or rehospitalization in older patients discharged from acute-care hospitals?
Background: Previous studies have shown that the use of PPIs could be associated with increased mortality in institutionalized older people and in patients discharged from acute-care hospitals. Older patients could be more vulnerable to adverse effects of PPIs, such as drug-drug interactions and absorption of nutrients, because of the higher incidence of polypharmacy and malnutrition in the elderly.
Study design: Prospective cohort.
Setting: Eleven acute-care medical wards participating in the Italian study Pharmacosurveillance in the Elderly Care.
Synopsis: All patients aged 65 years or older consecutively admitted to participating wards from April to June 2007 underwent screening. Excluding patients who refused, died during hospitalization, or were admitted to long-term care or rehabilitation units, a total of 491 patients were analyzed. The study team administered questionnaires during admission and conducted follow-up visits every three months for one year after discharge. Outcomes included one-year survival of patients discharged from acute-care medical wards and the combined endpoint of death or rehospitalization.
Overall, 174 patients (35.4%) had PPI exposure. After adjusting for age, cognitive impairment, disability, comorbidities, nutritional status, and number of drugs prescribed, patients exposed to PPIs had a significantly increased risk of death (adjusted HR 1.51, 95% CI 1.03-2.77). This association was strongest among patients receiving high-dose PPIs. No such association was found when considering the combined endpoint (HR 1.49, 95% CI 0.98-2.17). Limitations of the study include observational design, small size, potential for confounding by indication for PPI, and indeterminate PPI use prior to index hospitalization. Finally, the finding of an association between PPIs and increased mortality does not equate to a causative relationship between the two variables.
Bottom line: Proton-pump inhibitor use in older patients discharged from acute-care hospitals is associated with increased all-cause mortality at one year.
Citation: Maggio M, Corsonello A, Ceda GP, et al. Proton-pump inhibitors and risk of 1-year mortality and rehospitalization in older patients discharged from acute care hospitals. JAMA Intern Med. 2013;173(7):518-523.
Clinical question: Is the use of proton-pump inhibitors (PPIs) associated with risk of mortality or combined risk of death or rehospitalization in older patients discharged from acute-care hospitals?
Background: Previous studies have shown that the use of PPIs could be associated with increased mortality in institutionalized older people and in patients discharged from acute-care hospitals. Older patients could be more vulnerable to adverse effects of PPIs, such as drug-drug interactions and absorption of nutrients, because of the higher incidence of polypharmacy and malnutrition in the elderly.
Study design: Prospective cohort.
Setting: Eleven acute-care medical wards participating in the Italian study Pharmacosurveillance in the Elderly Care.
Synopsis: All patients aged 65 years or older consecutively admitted to participating wards from April to June 2007 underwent screening. Excluding patients who refused, died during hospitalization, or were admitted to long-term care or rehabilitation units, a total of 491 patients were analyzed. The study team administered questionnaires during admission and conducted follow-up visits every three months for one year after discharge. Outcomes included one-year survival of patients discharged from acute-care medical wards and the combined endpoint of death or rehospitalization.
Overall, 174 patients (35.4%) had PPI exposure. After adjusting for age, cognitive impairment, disability, comorbidities, nutritional status, and number of drugs prescribed, patients exposed to PPIs had a significantly increased risk of death (adjusted HR 1.51, 95% CI 1.03-2.77). This association was strongest among patients receiving high-dose PPIs. No such association was found when considering the combined endpoint (HR 1.49, 95% CI 0.98-2.17). Limitations of the study include observational design, small size, potential for confounding by indication for PPI, and indeterminate PPI use prior to index hospitalization. Finally, the finding of an association between PPIs and increased mortality does not equate to a causative relationship between the two variables.
Bottom line: Proton-pump inhibitor use in older patients discharged from acute-care hospitals is associated with increased all-cause mortality at one year.
Citation: Maggio M, Corsonello A, Ceda GP, et al. Proton-pump inhibitors and risk of 1-year mortality and rehospitalization in older patients discharged from acute care hospitals. JAMA Intern Med. 2013;173(7):518-523.
Clinical question: Is the use of proton-pump inhibitors (PPIs) associated with risk of mortality or combined risk of death or rehospitalization in older patients discharged from acute-care hospitals?
Background: Previous studies have shown that the use of PPIs could be associated with increased mortality in institutionalized older people and in patients discharged from acute-care hospitals. Older patients could be more vulnerable to adverse effects of PPIs, such as drug-drug interactions and absorption of nutrients, because of the higher incidence of polypharmacy and malnutrition in the elderly.
Study design: Prospective cohort.
Setting: Eleven acute-care medical wards participating in the Italian study Pharmacosurveillance in the Elderly Care.
Synopsis: All patients aged 65 years or older consecutively admitted to participating wards from April to June 2007 underwent screening. Excluding patients who refused, died during hospitalization, or were admitted to long-term care or rehabilitation units, a total of 491 patients were analyzed. The study team administered questionnaires during admission and conducted follow-up visits every three months for one year after discharge. Outcomes included one-year survival of patients discharged from acute-care medical wards and the combined endpoint of death or rehospitalization.
Overall, 174 patients (35.4%) had PPI exposure. After adjusting for age, cognitive impairment, disability, comorbidities, nutritional status, and number of drugs prescribed, patients exposed to PPIs had a significantly increased risk of death (adjusted HR 1.51, 95% CI 1.03-2.77). This association was strongest among patients receiving high-dose PPIs. No such association was found when considering the combined endpoint (HR 1.49, 95% CI 0.98-2.17). Limitations of the study include observational design, small size, potential for confounding by indication for PPI, and indeterminate PPI use prior to index hospitalization. Finally, the finding of an association between PPIs and increased mortality does not equate to a causative relationship between the two variables.
Bottom line: Proton-pump inhibitor use in older patients discharged from acute-care hospitals is associated with increased all-cause mortality at one year.
Citation: Maggio M, Corsonello A, Ceda GP, et al. Proton-pump inhibitors and risk of 1-year mortality and rehospitalization in older patients discharged from acute care hospitals. JAMA Intern Med. 2013;173(7):518-523.
Diabetes Mellitus Does Not Increase Risk of Surgical Complications after Elective Total Knee Replacement Surgery
Clinical question: Does uncontrolled diabetes mellitus increase risk for post-operative complications after elective joint replacement surgery?
Background: Several previous studies suggested that patients with uncontrolled diabetes could be at higher risk of postoperative complications and have worse functional outcomes after joint replacement surgery than patients without diabetes. Preoperative glycemic control is a potentially modifiable risk factor in patients undergoing elective joint replacement surgery. Demand for elective joint replacement is expected to increase over time, and reducing the risk of postoperative complications is essential in order to optimize functional outcomes and reduce healthcare costs.
Study design: Retrospective cohort.
Setting: Five regions of the Kaiser Permanente healthcare system.
Synopsis: The study included 40,491 patients aged 18 years and older who underwent primary knee replacement between January 2001 and December 2009 in five regions of the Kaiser Permanente system. Patients were identified using the Kaiser Permanente Total Joint Replacement Registry. Clinical information on each patient was collected from two years before the procedure to one year after the procedure using Kaiser Permanente electronic health records. Subjects were classified as nondiabetic (81.3%), diabetic with good glycemic control (12.5%), or diabetic with poor glycemic control (6.2%). Glycemic control status was assessed using the latest hemoglobin A1c (HbA1c) value measured prior to the date of the index surgery, with HbA1c <7.0% defined as good glycemic control. Outcomes included revision arthroplasty, deep infection, DVT or PE, incident myocardial infarction, and rehospitalization.
There was no significant association identified between uncontrolled diabetes and any of the five outcomes.
Limitations of the study include retrospective design, rarity of all outcomes except all-cause rehospitalization, and the small number of patients with uncontrolled diabetes in the cohort. In addition, functional outcomes were not assessed in this study.
Bottom line: The effect of uncontrolled diabetes on the risk of adverse surgical outcomes following elective joint replacement remains unclear based on currently published data; more studies are needed.
Citation: Adams AL, Paxton EW, Wang JQ, et al. Surgical outcomes of total knee replacement according to diabetes status and glycemic control, 2001-2009. J Bone Joint Surg Am. 2013;95:481-487.
Clinical question: Does uncontrolled diabetes mellitus increase risk for post-operative complications after elective joint replacement surgery?
Background: Several previous studies suggested that patients with uncontrolled diabetes could be at higher risk of postoperative complications and have worse functional outcomes after joint replacement surgery than patients without diabetes. Preoperative glycemic control is a potentially modifiable risk factor in patients undergoing elective joint replacement surgery. Demand for elective joint replacement is expected to increase over time, and reducing the risk of postoperative complications is essential in order to optimize functional outcomes and reduce healthcare costs.
Study design: Retrospective cohort.
Setting: Five regions of the Kaiser Permanente healthcare system.
Synopsis: The study included 40,491 patients aged 18 years and older who underwent primary knee replacement between January 2001 and December 2009 in five regions of the Kaiser Permanente system. Patients were identified using the Kaiser Permanente Total Joint Replacement Registry. Clinical information on each patient was collected from two years before the procedure to one year after the procedure using Kaiser Permanente electronic health records. Subjects were classified as nondiabetic (81.3%), diabetic with good glycemic control (12.5%), or diabetic with poor glycemic control (6.2%). Glycemic control status was assessed using the latest hemoglobin A1c (HbA1c) value measured prior to the date of the index surgery, with HbA1c <7.0% defined as good glycemic control. Outcomes included revision arthroplasty, deep infection, DVT or PE, incident myocardial infarction, and rehospitalization.
There was no significant association identified between uncontrolled diabetes and any of the five outcomes.
Limitations of the study include retrospective design, rarity of all outcomes except all-cause rehospitalization, and the small number of patients with uncontrolled diabetes in the cohort. In addition, functional outcomes were not assessed in this study.
Bottom line: The effect of uncontrolled diabetes on the risk of adverse surgical outcomes following elective joint replacement remains unclear based on currently published data; more studies are needed.
Citation: Adams AL, Paxton EW, Wang JQ, et al. Surgical outcomes of total knee replacement according to diabetes status and glycemic control, 2001-2009. J Bone Joint Surg Am. 2013;95:481-487.
Clinical question: Does uncontrolled diabetes mellitus increase risk for post-operative complications after elective joint replacement surgery?
Background: Several previous studies suggested that patients with uncontrolled diabetes could be at higher risk of postoperative complications and have worse functional outcomes after joint replacement surgery than patients without diabetes. Preoperative glycemic control is a potentially modifiable risk factor in patients undergoing elective joint replacement surgery. Demand for elective joint replacement is expected to increase over time, and reducing the risk of postoperative complications is essential in order to optimize functional outcomes and reduce healthcare costs.
Study design: Retrospective cohort.
Setting: Five regions of the Kaiser Permanente healthcare system.
Synopsis: The study included 40,491 patients aged 18 years and older who underwent primary knee replacement between January 2001 and December 2009 in five regions of the Kaiser Permanente system. Patients were identified using the Kaiser Permanente Total Joint Replacement Registry. Clinical information on each patient was collected from two years before the procedure to one year after the procedure using Kaiser Permanente electronic health records. Subjects were classified as nondiabetic (81.3%), diabetic with good glycemic control (12.5%), or diabetic with poor glycemic control (6.2%). Glycemic control status was assessed using the latest hemoglobin A1c (HbA1c) value measured prior to the date of the index surgery, with HbA1c <7.0% defined as good glycemic control. Outcomes included revision arthroplasty, deep infection, DVT or PE, incident myocardial infarction, and rehospitalization.
There was no significant association identified between uncontrolled diabetes and any of the five outcomes.
Limitations of the study include retrospective design, rarity of all outcomes except all-cause rehospitalization, and the small number of patients with uncontrolled diabetes in the cohort. In addition, functional outcomes were not assessed in this study.
Bottom line: The effect of uncontrolled diabetes on the risk of adverse surgical outcomes following elective joint replacement remains unclear based on currently published data; more studies are needed.
Citation: Adams AL, Paxton EW, Wang JQ, et al. Surgical outcomes of total knee replacement according to diabetes status and glycemic control, 2001-2009. J Bone Joint Surg Am. 2013;95:481-487.
Elevated Lactate Levels Correlate with Adverse Outcomes in Acute PE
Clinical question: Are high plasma lactate levels associated with mortality and clinical deterioration among patients with acute pulmonary embolism (PE)?
Background: Prognostic clinical markers are limited in patients presenting with acute PE, especially among normotensive individuals. Plasma lactate concentration is a marker of tissue hypoperfusion that has been used to risk-stratify patients with sepsis and trauma. It is unknown whether elevated lactate levels predict poor outcomes in acute PE.
Study design: Prospective cohort.
Setting: ED in a large teaching hospital in Italy.
Synopsis: Consecutive adult patients with acute PE diagnosed by spiral computed tomography or lung scan were included. Plasma lactate levels were tested in all patients at presentation, and levels of ≥2 mmol/L were considered abnormal. The primary endpoint was all-cause death within 30 days, and the secondary endpoint was the composite of all-cause death and PE-related clinical deterioration and death.
Of the 270 patients, 81 (30%) had abnormal lactate levels, though only 12 (4.4%) had shock or hypotension. Patients with elevated lactate had higher mortality compared with patients with lower levels (17.3% vs. 1.6%, OR 12.95, 95% CI 3.43-58.73). Plasma lactate ≥2 mmol/L was associated with higher all-cause mortality (HR 11.67, 95% CI 3.32-41.03) and the composite endpoint (HR 8.14, 95% CI 3.83-17.34). This association was independent of the presence of hypotension, right ventricular dysfunction, or elevated troponin.
Limitations include the single study site (which limits generalizability of the findings) and that lactate levels were only checked once (which might not have fully reflected each patient’s clinical picture). The authors suggest that plasma lactate levels might have utility in determining which patients should be treated more aggressively for PE.
Bottom line: In patients presenting with acute PE, elevated plasma lactate levels are associated with increased risk of short-term mortality and morbidity, independent of the presence of hypotension or markers of right ventricular injury.
Citation: Vanni S, Viviani G, Baioni M, et al. Prognostic value of plasma lactate levels among patients with acute pulmonary embolism: the thrombo-embolism lactate outcome study. Ann Emerg Med. 2013;61:330-338.
Clinical question: Are high plasma lactate levels associated with mortality and clinical deterioration among patients with acute pulmonary embolism (PE)?
Background: Prognostic clinical markers are limited in patients presenting with acute PE, especially among normotensive individuals. Plasma lactate concentration is a marker of tissue hypoperfusion that has been used to risk-stratify patients with sepsis and trauma. It is unknown whether elevated lactate levels predict poor outcomes in acute PE.
Study design: Prospective cohort.
Setting: ED in a large teaching hospital in Italy.
Synopsis: Consecutive adult patients with acute PE diagnosed by spiral computed tomography or lung scan were included. Plasma lactate levels were tested in all patients at presentation, and levels of ≥2 mmol/L were considered abnormal. The primary endpoint was all-cause death within 30 days, and the secondary endpoint was the composite of all-cause death and PE-related clinical deterioration and death.
Of the 270 patients, 81 (30%) had abnormal lactate levels, though only 12 (4.4%) had shock or hypotension. Patients with elevated lactate had higher mortality compared with patients with lower levels (17.3% vs. 1.6%, OR 12.95, 95% CI 3.43-58.73). Plasma lactate ≥2 mmol/L was associated with higher all-cause mortality (HR 11.67, 95% CI 3.32-41.03) and the composite endpoint (HR 8.14, 95% CI 3.83-17.34). This association was independent of the presence of hypotension, right ventricular dysfunction, or elevated troponin.
Limitations include the single study site (which limits generalizability of the findings) and that lactate levels were only checked once (which might not have fully reflected each patient’s clinical picture). The authors suggest that plasma lactate levels might have utility in determining which patients should be treated more aggressively for PE.
Bottom line: In patients presenting with acute PE, elevated plasma lactate levels are associated with increased risk of short-term mortality and morbidity, independent of the presence of hypotension or markers of right ventricular injury.
Citation: Vanni S, Viviani G, Baioni M, et al. Prognostic value of plasma lactate levels among patients with acute pulmonary embolism: the thrombo-embolism lactate outcome study. Ann Emerg Med. 2013;61:330-338.
Clinical question: Are high plasma lactate levels associated with mortality and clinical deterioration among patients with acute pulmonary embolism (PE)?
Background: Prognostic clinical markers are limited in patients presenting with acute PE, especially among normotensive individuals. Plasma lactate concentration is a marker of tissue hypoperfusion that has been used to risk-stratify patients with sepsis and trauma. It is unknown whether elevated lactate levels predict poor outcomes in acute PE.
Study design: Prospective cohort.
Setting: ED in a large teaching hospital in Italy.
Synopsis: Consecutive adult patients with acute PE diagnosed by spiral computed tomography or lung scan were included. Plasma lactate levels were tested in all patients at presentation, and levels of ≥2 mmol/L were considered abnormal. The primary endpoint was all-cause death within 30 days, and the secondary endpoint was the composite of all-cause death and PE-related clinical deterioration and death.
Of the 270 patients, 81 (30%) had abnormal lactate levels, though only 12 (4.4%) had shock or hypotension. Patients with elevated lactate had higher mortality compared with patients with lower levels (17.3% vs. 1.6%, OR 12.95, 95% CI 3.43-58.73). Plasma lactate ≥2 mmol/L was associated with higher all-cause mortality (HR 11.67, 95% CI 3.32-41.03) and the composite endpoint (HR 8.14, 95% CI 3.83-17.34). This association was independent of the presence of hypotension, right ventricular dysfunction, or elevated troponin.
Limitations include the single study site (which limits generalizability of the findings) and that lactate levels were only checked once (which might not have fully reflected each patient’s clinical picture). The authors suggest that plasma lactate levels might have utility in determining which patients should be treated more aggressively for PE.
Bottom line: In patients presenting with acute PE, elevated plasma lactate levels are associated with increased risk of short-term mortality and morbidity, independent of the presence of hypotension or markers of right ventricular injury.
Citation: Vanni S, Viviani G, Baioni M, et al. Prognostic value of plasma lactate levels among patients with acute pulmonary embolism: the thrombo-embolism lactate outcome study. Ann Emerg Med. 2013;61:330-338.