User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
MS CONFERENCE NEWS

- Common MS treatment wears off more quickly in Black patients
- A less expensive, more convenient treatment option for MS?
- Investigational drug reduces brain lesions in highly active MS
- Evobrutinib may lower nerve damage biomarker levels
- Disease progression and therapy response vary in MS by ethnicity
- Some MS treatments may heighten COVID risk
- Natalizumab postinfusion reactions
- Common MS treatment wears off more quickly in Black patients
- A less expensive, more convenient treatment option for MS?
- Investigational drug reduces brain lesions in highly active MS
- Evobrutinib may lower nerve damage biomarker levels
- Disease progression and therapy response vary in MS by ethnicity
- Some MS treatments may heighten COVID risk
- Natalizumab postinfusion reactions
- Common MS treatment wears off more quickly in Black patients
- A less expensive, more convenient treatment option for MS?
- Investigational drug reduces brain lesions in highly active MS
- Evobrutinib may lower nerve damage biomarker levels
- Disease progression and therapy response vary in MS by ethnicity
- Some MS treatments may heighten COVID risk
- Natalizumab postinfusion reactions
Physicians question the future of TNF inhibitors for psoriasis, PsA
Tumor necrosis factor inhibitors have long been the go-to treatment of choice for patients with psoriasis and psoriatic arthritis (PsA). They’ve served patients well since etanercept was first approved for PsA in 2002, but today, with the availability of more attractive interleukin-17 and IL-23 inhibitors, dermatologists and rheumatologists are asking whether it’s time to reconsider the use of TNF inhibitors as first-line therapy in psoriasis and PsA.

“TNF inhibitors have served psoriasis patients well for many years. The question is, ‘Is it time to move on from them as first-line agents for psoriasis?’ ” said April W. Armstrong, MD, MPH, a dermatologist and associate dean for clinical research at the University of Southern California, Los Angeles. Dr. Armstrong participated in a point/counterpoint debate about the merits of IL-17 and IL-23 inhibitors over TNF inhibitors at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis. “For the majority of our patients, IL-17 and IL-23 inhibitors are probably rationally better than TNF inhibitors as first-line agents for moderate to severe plaque psoriasis,” she said.
In this debate, dermatologists and rheumatologists cited studies showing the safety and efficacy of IL-17 and IL-23 inhibitors over TNF inhibitors. TNF inhibitors include etanercept (Enbrel and biosimilars), infliximab (Remicade and biosimilars), adalimumab (Humira and biosimilars), certolizumab pegol (Cimzia), and golimumab (Simponi). IL-12/23 inhibitors are limited to ustekinumab (Stelara). IL-17 inhibitors include secukinumab (Cosentyx), ixekizumab (Taltz), and brodalumab (Siliq). IL-23 inhibitors include guselkumab (Tremfya), tildrakizumab (Ilumya), and risankizumab (Skyrizi).
TNF inhibitors are recommended by the American College of Rheumatology as first-line therapy for treatment-naive patients with active PsA, and they, along with IL-12/23, IL-17, and IL-23 inhibitors are all recommended by the American Academy of Dermatology as monotherapy treatment options in adult patients with moderate to severe plaque psoriasis. However, some studies have shown that non–TNF-inhibitor biologics have a higher efficacy than TNF inhibitors in some cases for some patients, such as those with moderate to severe psoriasis alone or for musculoskeletal efficacy in patients with PsA who have peripheral arthritis, enthesitis, dactylitis, or axial manifestations.
Favorable characteristics of non–TNF-inhibitor biologics
Dr. Armstrong cited a number of head-to-head trials to support her view that IL-17 and IL-23 inhibitors are better than TNF inhibitors as first-line agents for patients with moderate to severe plaque psoriasis. In the first head-to-head study of its kind in patients with moderate to severe psoriasis, ustekinumab proved superior to etanercept. Guselkumab was shown to be superior to adalimumab for patients with moderate to severe psoriasis. Tildrakizumab also proved superior to etanercept for patients with psoriasis. Risankizumab bested adalimumab in patients with moderate to severe psoriasis. Ixekizumab proved superior to etanercept in two pivotal studies of patients with widespread moderate-to-severe psoriasis.
IL-23 and IL-17 inhibitors tend to have less frequent maintenance dosing, with IL-17 inhibitors being once every 2 or 4 weeks and IL-23 inhibitors once every 8 or 12 weeks, compared with frequencies ranging from every week to every 8 weeks with TNF inhibitors, Dr. Armstrong said.
IL-17 and IL-23 inhibitors also appear to have fewer safety concerns than TNF inhibitors, although there is less long-term data for them overall and there are some notable exceptions in certain patient populations. TNF inhibitors should be avoided in patients with a history of demyelinating disease or hepatitis B virus infection, and they are not preferred in patients who have a history of latent tuberculosis or advanced heart failure. IL-17 inhibitors should not be used in patients with a history of inflammatory bowel disease, and their use is associated with a higher rate of oral candidiasis. IL-23 inhibitors have a good safety profile overall, she said.
“The IL-17/23 axis is very important to psoriatic arthritis and should be the focus of our treatments” for PsA, said Deepak Jadon, MBBCh, MRCP, PhD, a rheumatologist and director of the rheumatology research unit at Addenbrooke’s Hospital, Cambridge (England) University Hospitals NHS Foundation Trust. In his presentation, he proposed that IL-17 inhibitors and IL-23 inhibitors be used as first-line therapies in PsA ahead of TNF inhibitors.
One reason to go with IL-17 and IL-23 inhibitors may be to ”get it right immunologically the first time,” Dr. Jadon said. He cited evidence showing substantially better response to guselkumab when given to biologic-naive patients with PsA versus those who had a inadequate response to TNF inhibitors, as well as data indicating better response with secukinumab regardless of previous TNF inhibitor use.
IL-17 inhibitors target more domains of psoriatic disease than do TNF inhibitors, he said, noting that “they have excellent musculoskeletal efficacy in patients with moderate skin psoriasis, not just those with severe psoriasis.” Ixekizumab proved superior to adalimumab in biologic-naive patients with PsA. The results of this study also indicated that IL-17 inhibitors should not be reserved only for patients with severe psoriasis since a higher percentage of patients with moderate psoriasis who were taking ixekizumab achieved very low PsA activity. Secukinumab also beat adalimumab in a head-to-head comparison and showed a greater impact on some measures of health-related quality of life.
IL-17 inhibitors also do not require concomitant methotrexate, he said, “which is a major bonus for our patients. All of my patients wish to stop methotrexate even if tolerated. Not having to cope with prescribed methotrexate improves risk of adverse events and frequency of blood test monitoring.”
IL-17 and IL-23 inhibitors appear to have good efficacy against axial disease in patients with PsA. Randomized trial results for secukinumab versus placebo show high percentages of patients improving either 20% or 40% in Assessment in Spondyloarthritis International Society response criteria and reduced inflammatory MRI lesions in the spine and sacroiliac joints. Analyses of trial results in guselkumab-treated patients with axial manifestations of PsA have shown the IL-23 inhibitor’s efficacy versus placebo across different measures of disease activity.
Dr. Jadon also cited real-world data showing that patients stay longer on IL-17 and IL-12/23 inhibitors versus TNF inhibitors. A 2016 study of patients with psoriasis in the PSOLAR registry showed that patients persisted on treatment longer with ustekinumab than with adalimumab, etanercept, or infliximab. Similarly, a 2020 study of patients with psoriasis from the British Association of Dermatologists Biologics and Immunomodulators Register found that both ustekinumab and secukinumab had better sustained drug survival than did adalimumab.
Accessibility weighs heavily in using TNF inhibitor first
Clinical trials data show that IL-17 inhibitors outperform TNF inhibitors for psoriasis, but in clinical practice, TNF inhibitors still perform very well in individual patients and are well tolerated, said Amit Garg, MD, founding chair of the department of dermatology at Hofstra University, Hempstead, N.Y.

He argued in favor of TNF inhibitors as first-line therapy over IL-17 inhibitors for psoriasis. In this case, treatment decisions often come down to accessibility, Dr. Garg said. Not all insurance companies cover the cost of the newer IL-23 inhibitors. Plus, access to TNF inhibitors is widespread and costs are generally lower.
“As a physician, I don’t have complete autonomy in prescribing what I want. The reality is whether it be because of cross indication or discount pricing, [TNF inhibitors] – in particular adalimumab – is widely available on all plans and is usually the preferred treatment plan, at least in our area,” he said. “I’m not a big fan of plans that allow drugs at low or no cost for a year or 2, and then abandon the patients at that point thereafter. I like to use something that insurance will cover sustainably, and, quite frankly, TNFs have served well in that regard.”
However, TNF inhibitors are associated with more safety signals, plus they carry a greater risk of infection, leading to tolerability and persistence issues with patients.
“Psoriasis is a lifelong disease. I wish I could tell you that every drug is going to work well forever for individual patients, but I don’t think we know that yet. From my perspective, for efficacy, general well tolerance, convenience, and access, TNFs are still an important part of our ability to treat psoriasis effectively. I have no problem starting there and transitioning as needed for individual patients.
“In my experience, I think patients on TNFs generally do well. We don’t always get the patients clear and certainly there’s drop off of efficacy over time, but I’m not sure that’s a rationale for [changing treatment],” Dr. Garg said.
Ying Ying (Katy) Leung, MD, a rheumatologist with Singapore General Hospital, and a member of the GRAPPA peripheral arthritis working group, argued against the use of IL-17 and IL-23 inhibitors as first-line treatment for PsA over TNF inhibitors. She reasoned that TNF blockers are more accessible, have more long-term safety data (including data indicating safety during pregnancy), and have better cardiovascular protection. She also noted that GRAPPA treatment recommendations strongly advise using TNF blockers (or IL-17 inhibitors) for treatment-naive patients with PsA.
“Accessibility is very important as I learned along the way of leading the peripheral arthritis [GRAPPA] working group. Accessibility [issues] can be coming from a lot of sources, but if you don’t take good care of accessibility, you might be developing a guideline that is way out of reality and nobody is going to use it,” she said.
In her native Singapore, Dr. Leung said that patients pay for biologics out of pocket, so cost is a key factor for her patients. She stated that adalimumab is available as a biosimilar at about $200 monthly for patients with PsA in Singapore, while the average monthly costs are $1,400 for originator infliximab and $1,500 for originator etanercept. By comparison, secukinumab sells for about $750 monthly, ixekizumab $540 monthly, and guselkumab $2,000 monthly.
Treatment choices should be aligned with the disease manifestations of PsA, Dr. Leung said, keeping in mind that accessibility and individual patient needs and preferences should be considered as well. She conducted an informal comparison that found TNF inhibitors are most effective for patients with uveitis or inflammatory bowel disease. Evidence from head-to-head studies indicates that TNF inhibitors and IL-17 inhibitors have similar efficacy for peripheral arthritis, enthesitis, and dactylitis. But caution is warranted, she suggested, for determining the best biologics for axial disease because no head-to-head comparison trials have been conducted for IL-17 or IL-23 inhibitors versus TNF inhibitors.
Dr. Armstrong has been a consultant to AbbVie, Bristol-Myers Squibb, Dermira, Genzyme, Incyte, Janssen, Leo Pharma, Eli Lilly, Novartis, Pfizer, and UCB. Dr. Jadon has been a consultant to, has been on speakers bureaus for, and has received grant/research support from AbbVie, Amgen, Celgene, Celltrion, Gilead, Janssen, Eli Lilly, MSD, Novartis, Pfizer, Roche, Sandoz, and UCB. Dr. Garg has consulted for AbbVie, Boehringer Ingelheim, Janssen, and UCB. Dr. Leung has been a consultant to AbbVie, Boehringer Ingelheim, Janssen, Eli Lilly, Novartis, and Pfizer. She has been on speakers bureaus for AbbVie, Janssen Eli Lilly, and Novartis. She has received grant/research support from Pfizer and conference support from AbbVie,
Tumor necrosis factor inhibitors have long been the go-to treatment of choice for patients with psoriasis and psoriatic arthritis (PsA). They’ve served patients well since etanercept was first approved for PsA in 2002, but today, with the availability of more attractive interleukin-17 and IL-23 inhibitors, dermatologists and rheumatologists are asking whether it’s time to reconsider the use of TNF inhibitors as first-line therapy in psoriasis and PsA.
“TNF inhibitors have served psoriasis patients well for many years. The question is, ‘Is it time to move on from them as first-line agents for psoriasis?’ ” said April W. Armstrong, MD, MPH, a dermatologist and associate dean for clinical research at the University of Southern California, Los Angeles. Dr. Armstrong participated in a point/counterpoint debate about the merits of IL-17 and IL-23 inhibitors over TNF inhibitors at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis. “For the majority of our patients, IL-17 and IL-23 inhibitors are probably rationally better than TNF inhibitors as first-line agents for moderate to severe plaque psoriasis,” she said.
In this debate, dermatologists and rheumatologists cited studies showing the safety and efficacy of IL-17 and IL-23 inhibitors over TNF inhibitors. TNF inhibitors include etanercept (Enbrel and biosimilars), infliximab (Remicade and biosimilars), adalimumab (Humira and biosimilars), certolizumab pegol (Cimzia), and golimumab (Simponi). IL-12/23 inhibitors are limited to ustekinumab (Stelara). IL-17 inhibitors include secukinumab (Cosentyx), ixekizumab (Taltz), and brodalumab (Siliq). IL-23 inhibitors include guselkumab (Tremfya), tildrakizumab (Ilumya), and risankizumab (Skyrizi).
TNF inhibitors are recommended by the American College of Rheumatology as first-line therapy for treatment-naive patients with active PsA, and they, along with IL-12/23, IL-17, and IL-23 inhibitors are all recommended by the American Academy of Dermatology as monotherapy treatment options in adult patients with moderate to severe plaque psoriasis. However, some studies have shown that non–TNF-inhibitor biologics have a higher efficacy than TNF inhibitors in some cases for some patients, such as those with moderate to severe psoriasis alone or for musculoskeletal efficacy in patients with PsA who have peripheral arthritis, enthesitis, dactylitis, or axial manifestations.
Favorable characteristics of non–TNF-inhibitor biologics
Dr. Armstrong cited a number of head-to-head trials to support her view that IL-17 and IL-23 inhibitors are better than TNF inhibitors as first-line agents for patients with moderate to severe plaque psoriasis. In the first head-to-head study of its kind in patients with moderate to severe psoriasis, ustekinumab proved superior to etanercept. Guselkumab was shown to be superior to adalimumab for patients with moderate to severe psoriasis. Tildrakizumab also proved superior to etanercept for patients with psoriasis. Risankizumab bested adalimumab in patients with moderate to severe psoriasis. Ixekizumab proved superior to etanercept in two pivotal studies of patients with widespread moderate-to-severe psoriasis.
IL-23 and IL-17 inhibitors tend to have less frequent maintenance dosing, with IL-17 inhibitors being once every 2 or 4 weeks and IL-23 inhibitors once every 8 or 12 weeks, compared with frequencies ranging from every week to every 8 weeks with TNF inhibitors, Dr. Armstrong said.
IL-17 and IL-23 inhibitors also appear to have fewer safety concerns than TNF inhibitors, although there is less long-term data for them overall and there are some notable exceptions in certain patient populations. TNF inhibitors should be avoided in patients with a history of demyelinating disease or hepatitis B virus infection, and they are not preferred in patients who have a history of latent tuberculosis or advanced heart failure. IL-17 inhibitors should not be used in patients with a history of inflammatory bowel disease, and their use is associated with a higher rate of oral candidiasis. IL-23 inhibitors have a good safety profile overall, she said.
“The IL-17/23 axis is very important to psoriatic arthritis and should be the focus of our treatments” for PsA, said Deepak Jadon, MBBCh, MRCP, PhD, a rheumatologist and director of the rheumatology research unit at Addenbrooke’s Hospital, Cambridge (England) University Hospitals NHS Foundation Trust. In his presentation, he proposed that IL-17 inhibitors and IL-23 inhibitors be used as first-line therapies in PsA ahead of TNF inhibitors.
One reason to go with IL-17 and IL-23 inhibitors may be to ”get it right immunologically the first time,” Dr. Jadon said. He cited evidence showing substantially better response to guselkumab when given to biologic-naive patients with PsA versus those who had a inadequate response to TNF inhibitors, as well as data indicating better response with secukinumab regardless of previous TNF inhibitor use.
IL-17 inhibitors target more domains of psoriatic disease than do TNF inhibitors, he said, noting that “they have excellent musculoskeletal efficacy in patients with moderate skin psoriasis, not just those with severe psoriasis.” Ixekizumab proved superior to adalimumab in biologic-naive patients with PsA. The results of this study also indicated that IL-17 inhibitors should not be reserved only for patients with severe psoriasis since a higher percentage of patients with moderate psoriasis who were taking ixekizumab achieved very low PsA activity. Secukinumab also beat adalimumab in a head-to-head comparison and showed a greater impact on some measures of health-related quality of life.
IL-17 inhibitors also do not require concomitant methotrexate, he said, “which is a major bonus for our patients. All of my patients wish to stop methotrexate even if tolerated. Not having to cope with prescribed methotrexate improves risk of adverse events and frequency of blood test monitoring.”
IL-17 and IL-23 inhibitors appear to have good efficacy against axial disease in patients with PsA. Randomized trial results for secukinumab versus placebo show high percentages of patients improving either 20% or 40% in Assessment in Spondyloarthritis International Society response criteria and reduced inflammatory MRI lesions in the spine and sacroiliac joints. Analyses of trial results in guselkumab-treated patients with axial manifestations of PsA have shown the IL-23 inhibitor’s efficacy versus placebo across different measures of disease activity.
Dr. Jadon also cited real-world data showing that patients stay longer on IL-17 and IL-12/23 inhibitors versus TNF inhibitors. A 2016 study of patients with psoriasis in the PSOLAR registry showed that patients persisted on treatment longer with ustekinumab than with adalimumab, etanercept, or infliximab. Similarly, a 2020 study of patients with psoriasis from the British Association of Dermatologists Biologics and Immunomodulators Register found that both ustekinumab and secukinumab had better sustained drug survival than did adalimumab.
Accessibility weighs heavily in using TNF inhibitor first
Clinical trials data show that IL-17 inhibitors outperform TNF inhibitors for psoriasis, but in clinical practice, TNF inhibitors still perform very well in individual patients and are well tolerated, said Amit Garg, MD, founding chair of the department of dermatology at Hofstra University, Hempstead, N.Y.
He argued in favor of TNF inhibitors as first-line therapy over IL-17 inhibitors for psoriasis. In this case, treatment decisions often come down to accessibility, Dr. Garg said. Not all insurance companies cover the cost of the newer IL-23 inhibitors. Plus, access to TNF inhibitors is widespread and costs are generally lower.
“As a physician, I don’t have complete autonomy in prescribing what I want. The reality is whether it be because of cross indication or discount pricing, [TNF inhibitors] – in particular adalimumab – is widely available on all plans and is usually the preferred treatment plan, at least in our area,” he said. “I’m not a big fan of plans that allow drugs at low or no cost for a year or 2, and then abandon the patients at that point thereafter. I like to use something that insurance will cover sustainably, and, quite frankly, TNFs have served well in that regard.”
However, TNF inhibitors are associated with more safety signals, plus they carry a greater risk of infection, leading to tolerability and persistence issues with patients.
“Psoriasis is a lifelong disease. I wish I could tell you that every drug is going to work well forever for individual patients, but I don’t think we know that yet. From my perspective, for efficacy, general well tolerance, convenience, and access, TNFs are still an important part of our ability to treat psoriasis effectively. I have no problem starting there and transitioning as needed for individual patients.
“In my experience, I think patients on TNFs generally do well. We don’t always get the patients clear and certainly there’s drop off of efficacy over time, but I’m not sure that’s a rationale for [changing treatment],” Dr. Garg said.
Ying Ying (Katy) Leung, MD, a rheumatologist with Singapore General Hospital, and a member of the GRAPPA peripheral arthritis working group, argued against the use of IL-17 and IL-23 inhibitors as first-line treatment for PsA over TNF inhibitors. She reasoned that TNF blockers are more accessible, have more long-term safety data (including data indicating safety during pregnancy), and have better cardiovascular protection. She also noted that GRAPPA treatment recommendations strongly advise using TNF blockers (or IL-17 inhibitors) for treatment-naive patients with PsA.
“Accessibility is very important as I learned along the way of leading the peripheral arthritis [GRAPPA] working group. Accessibility [issues] can be coming from a lot of sources, but if you don’t take good care of accessibility, you might be developing a guideline that is way out of reality and nobody is going to use it,” she said.
In her native Singapore, Dr. Leung said that patients pay for biologics out of pocket, so cost is a key factor for her patients. She stated that adalimumab is available as a biosimilar at about $200 monthly for patients with PsA in Singapore, while the average monthly costs are $1,400 for originator infliximab and $1,500 for originator etanercept. By comparison, secukinumab sells for about $750 monthly, ixekizumab $540 monthly, and guselkumab $2,000 monthly.
Treatment choices should be aligned with the disease manifestations of PsA, Dr. Leung said, keeping in mind that accessibility and individual patient needs and preferences should be considered as well. She conducted an informal comparison that found TNF inhibitors are most effective for patients with uveitis or inflammatory bowel disease. Evidence from head-to-head studies indicates that TNF inhibitors and IL-17 inhibitors have similar efficacy for peripheral arthritis, enthesitis, and dactylitis. But caution is warranted, she suggested, for determining the best biologics for axial disease because no head-to-head comparison trials have been conducted for IL-17 or IL-23 inhibitors versus TNF inhibitors.
Dr. Armstrong has been a consultant to AbbVie, Bristol-Myers Squibb, Dermira, Genzyme, Incyte, Janssen, Leo Pharma, Eli Lilly, Novartis, Pfizer, and UCB. Dr. Jadon has been a consultant to, has been on speakers bureaus for, and has received grant/research support from AbbVie, Amgen, Celgene, Celltrion, Gilead, Janssen, Eli Lilly, MSD, Novartis, Pfizer, Roche, Sandoz, and UCB. Dr. Garg has consulted for AbbVie, Boehringer Ingelheim, Janssen, and UCB. Dr. Leung has been a consultant to AbbVie, Boehringer Ingelheim, Janssen, Eli Lilly, Novartis, and Pfizer. She has been on speakers bureaus for AbbVie, Janssen Eli Lilly, and Novartis. She has received grant/research support from Pfizer and conference support from AbbVie,
Tumor necrosis factor inhibitors have long been the go-to treatment of choice for patients with psoriasis and psoriatic arthritis (PsA). They’ve served patients well since etanercept was first approved for PsA in 2002, but today, with the availability of more attractive interleukin-17 and IL-23 inhibitors, dermatologists and rheumatologists are asking whether it’s time to reconsider the use of TNF inhibitors as first-line therapy in psoriasis and PsA.
“TNF inhibitors have served psoriasis patients well for many years. The question is, ‘Is it time to move on from them as first-line agents for psoriasis?’ ” said April W. Armstrong, MD, MPH, a dermatologist and associate dean for clinical research at the University of Southern California, Los Angeles. Dr. Armstrong participated in a point/counterpoint debate about the merits of IL-17 and IL-23 inhibitors over TNF inhibitors at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis. “For the majority of our patients, IL-17 and IL-23 inhibitors are probably rationally better than TNF inhibitors as first-line agents for moderate to severe plaque psoriasis,” she said.
In this debate, dermatologists and rheumatologists cited studies showing the safety and efficacy of IL-17 and IL-23 inhibitors over TNF inhibitors. TNF inhibitors include etanercept (Enbrel and biosimilars), infliximab (Remicade and biosimilars), adalimumab (Humira and biosimilars), certolizumab pegol (Cimzia), and golimumab (Simponi). IL-12/23 inhibitors are limited to ustekinumab (Stelara). IL-17 inhibitors include secukinumab (Cosentyx), ixekizumab (Taltz), and brodalumab (Siliq). IL-23 inhibitors include guselkumab (Tremfya), tildrakizumab (Ilumya), and risankizumab (Skyrizi).
TNF inhibitors are recommended by the American College of Rheumatology as first-line therapy for treatment-naive patients with active PsA, and they, along with IL-12/23, IL-17, and IL-23 inhibitors are all recommended by the American Academy of Dermatology as monotherapy treatment options in adult patients with moderate to severe plaque psoriasis. However, some studies have shown that non–TNF-inhibitor biologics have a higher efficacy than TNF inhibitors in some cases for some patients, such as those with moderate to severe psoriasis alone or for musculoskeletal efficacy in patients with PsA who have peripheral arthritis, enthesitis, dactylitis, or axial manifestations.
Favorable characteristics of non–TNF-inhibitor biologics
Dr. Armstrong cited a number of head-to-head trials to support her view that IL-17 and IL-23 inhibitors are better than TNF inhibitors as first-line agents for patients with moderate to severe plaque psoriasis. In the first head-to-head study of its kind in patients with moderate to severe psoriasis, ustekinumab proved superior to etanercept. Guselkumab was shown to be superior to adalimumab for patients with moderate to severe psoriasis. Tildrakizumab also proved superior to etanercept for patients with psoriasis. Risankizumab bested adalimumab in patients with moderate to severe psoriasis. Ixekizumab proved superior to etanercept in two pivotal studies of patients with widespread moderate-to-severe psoriasis.
IL-23 and IL-17 inhibitors tend to have less frequent maintenance dosing, with IL-17 inhibitors being once every 2 or 4 weeks and IL-23 inhibitors once every 8 or 12 weeks, compared with frequencies ranging from every week to every 8 weeks with TNF inhibitors, Dr. Armstrong said.
IL-17 and IL-23 inhibitors also appear to have fewer safety concerns than TNF inhibitors, although there is less long-term data for them overall and there are some notable exceptions in certain patient populations. TNF inhibitors should be avoided in patients with a history of demyelinating disease or hepatitis B virus infection, and they are not preferred in patients who have a history of latent tuberculosis or advanced heart failure. IL-17 inhibitors should not be used in patients with a history of inflammatory bowel disease, and their use is associated with a higher rate of oral candidiasis. IL-23 inhibitors have a good safety profile overall, she said.
“The IL-17/23 axis is very important to psoriatic arthritis and should be the focus of our treatments” for PsA, said Deepak Jadon, MBBCh, MRCP, PhD, a rheumatologist and director of the rheumatology research unit at Addenbrooke’s Hospital, Cambridge (England) University Hospitals NHS Foundation Trust. In his presentation, he proposed that IL-17 inhibitors and IL-23 inhibitors be used as first-line therapies in PsA ahead of TNF inhibitors.
One reason to go with IL-17 and IL-23 inhibitors may be to ”get it right immunologically the first time,” Dr. Jadon said. He cited evidence showing substantially better response to guselkumab when given to biologic-naive patients with PsA versus those who had a inadequate response to TNF inhibitors, as well as data indicating better response with secukinumab regardless of previous TNF inhibitor use.
IL-17 inhibitors target more domains of psoriatic disease than do TNF inhibitors, he said, noting that “they have excellent musculoskeletal efficacy in patients with moderate skin psoriasis, not just those with severe psoriasis.” Ixekizumab proved superior to adalimumab in biologic-naive patients with PsA. The results of this study also indicated that IL-17 inhibitors should not be reserved only for patients with severe psoriasis since a higher percentage of patients with moderate psoriasis who were taking ixekizumab achieved very low PsA activity. Secukinumab also beat adalimumab in a head-to-head comparison and showed a greater impact on some measures of health-related quality of life.
IL-17 inhibitors also do not require concomitant methotrexate, he said, “which is a major bonus for our patients. All of my patients wish to stop methotrexate even if tolerated. Not having to cope with prescribed methotrexate improves risk of adverse events and frequency of blood test monitoring.”
IL-17 and IL-23 inhibitors appear to have good efficacy against axial disease in patients with PsA. Randomized trial results for secukinumab versus placebo show high percentages of patients improving either 20% or 40% in Assessment in Spondyloarthritis International Society response criteria and reduced inflammatory MRI lesions in the spine and sacroiliac joints. Analyses of trial results in guselkumab-treated patients with axial manifestations of PsA have shown the IL-23 inhibitor’s efficacy versus placebo across different measures of disease activity.
Dr. Jadon also cited real-world data showing that patients stay longer on IL-17 and IL-12/23 inhibitors versus TNF inhibitors. A 2016 study of patients with psoriasis in the PSOLAR registry showed that patients persisted on treatment longer with ustekinumab than with adalimumab, etanercept, or infliximab. Similarly, a 2020 study of patients with psoriasis from the British Association of Dermatologists Biologics and Immunomodulators Register found that both ustekinumab and secukinumab had better sustained drug survival than did adalimumab.
Accessibility weighs heavily in using TNF inhibitor first
Clinical trials data show that IL-17 inhibitors outperform TNF inhibitors for psoriasis, but in clinical practice, TNF inhibitors still perform very well in individual patients and are well tolerated, said Amit Garg, MD, founding chair of the department of dermatology at Hofstra University, Hempstead, N.Y.
He argued in favor of TNF inhibitors as first-line therapy over IL-17 inhibitors for psoriasis. In this case, treatment decisions often come down to accessibility, Dr. Garg said. Not all insurance companies cover the cost of the newer IL-23 inhibitors. Plus, access to TNF inhibitors is widespread and costs are generally lower.
“As a physician, I don’t have complete autonomy in prescribing what I want. The reality is whether it be because of cross indication or discount pricing, [TNF inhibitors] – in particular adalimumab – is widely available on all plans and is usually the preferred treatment plan, at least in our area,” he said. “I’m not a big fan of plans that allow drugs at low or no cost for a year or 2, and then abandon the patients at that point thereafter. I like to use something that insurance will cover sustainably, and, quite frankly, TNFs have served well in that regard.”
However, TNF inhibitors are associated with more safety signals, plus they carry a greater risk of infection, leading to tolerability and persistence issues with patients.
“Psoriasis is a lifelong disease. I wish I could tell you that every drug is going to work well forever for individual patients, but I don’t think we know that yet. From my perspective, for efficacy, general well tolerance, convenience, and access, TNFs are still an important part of our ability to treat psoriasis effectively. I have no problem starting there and transitioning as needed for individual patients.
“In my experience, I think patients on TNFs generally do well. We don’t always get the patients clear and certainly there’s drop off of efficacy over time, but I’m not sure that’s a rationale for [changing treatment],” Dr. Garg said.
Ying Ying (Katy) Leung, MD, a rheumatologist with Singapore General Hospital, and a member of the GRAPPA peripheral arthritis working group, argued against the use of IL-17 and IL-23 inhibitors as first-line treatment for PsA over TNF inhibitors. She reasoned that TNF blockers are more accessible, have more long-term safety data (including data indicating safety during pregnancy), and have better cardiovascular protection. She also noted that GRAPPA treatment recommendations strongly advise using TNF blockers (or IL-17 inhibitors) for treatment-naive patients with PsA.
“Accessibility is very important as I learned along the way of leading the peripheral arthritis [GRAPPA] working group. Accessibility [issues] can be coming from a lot of sources, but if you don’t take good care of accessibility, you might be developing a guideline that is way out of reality and nobody is going to use it,” she said.
In her native Singapore, Dr. Leung said that patients pay for biologics out of pocket, so cost is a key factor for her patients. She stated that adalimumab is available as a biosimilar at about $200 monthly for patients with PsA in Singapore, while the average monthly costs are $1,400 for originator infliximab and $1,500 for originator etanercept. By comparison, secukinumab sells for about $750 monthly, ixekizumab $540 monthly, and guselkumab $2,000 monthly.
Treatment choices should be aligned with the disease manifestations of PsA, Dr. Leung said, keeping in mind that accessibility and individual patient needs and preferences should be considered as well. She conducted an informal comparison that found TNF inhibitors are most effective for patients with uveitis or inflammatory bowel disease. Evidence from head-to-head studies indicates that TNF inhibitors and IL-17 inhibitors have similar efficacy for peripheral arthritis, enthesitis, and dactylitis. But caution is warranted, she suggested, for determining the best biologics for axial disease because no head-to-head comparison trials have been conducted for IL-17 or IL-23 inhibitors versus TNF inhibitors.
Dr. Armstrong has been a consultant to AbbVie, Bristol-Myers Squibb, Dermira, Genzyme, Incyte, Janssen, Leo Pharma, Eli Lilly, Novartis, Pfizer, and UCB. Dr. Jadon has been a consultant to, has been on speakers bureaus for, and has received grant/research support from AbbVie, Amgen, Celgene, Celltrion, Gilead, Janssen, Eli Lilly, MSD, Novartis, Pfizer, Roche, Sandoz, and UCB. Dr. Garg has consulted for AbbVie, Boehringer Ingelheim, Janssen, and UCB. Dr. Leung has been a consultant to AbbVie, Boehringer Ingelheim, Janssen, Eli Lilly, Novartis, and Pfizer. She has been on speakers bureaus for AbbVie, Janssen Eli Lilly, and Novartis. She has received grant/research support from Pfizer and conference support from AbbVie,
FROM THE GRAPPA 2021 ANNUAL MEETING
COVID-19 tied to acceleration of Alzheimer’s disease pathology
, a new study shows.
These results suggest that COVID-19 may accelerate Alzheimer’s disease symptoms and pathology, said study investigator Thomas Wisniewski, MD, professor of neurology, pathology, and psychiatry at New York University.
The findings were presented here at the Alzheimer’s Association International Conference (AAIC) 2021.
Strong correlation
There’s a clear association between SARS-CoV-2 infection and Alzheimer’s disease-related dementia. Patients with Alzheimer’s disease are at threefold higher risk for the infection and have a twofold higher risk for death, Dr. Wisniewski told meeting delegates.
He and his colleagues conducted a prospective study of patients who had tested positive for SARS-CoV-2 and who experienced neurologic sequelae and SARS-CoV-2 patients who were without neurologic sequelae. All patients were hospitalized from March 10 to May 20, 2020. This was during a period when New York City was overwhelmed by COVID: About 35% of hospitalized patients had COVID.
Of those who experienced neurologic events, the most common “by far and away” (51%) was toxic metabolic encephalopathy (TME), said Dr. Wisniewski. Other associations included seizures, hypoxic/anoxic injury, and ischemic stroke.
The most common TMEs were septic and hypoxic ischemia. In most patients (78%), TME had more than one cause.
Researchers followed 196 patients with COVID and neurologic complications (case patients) and 186 matched control patients who had no neurologic complications over a period of 6 months.
“Unfortunately, both groups had poor outcomes,” said Dr. Wisniewski. About 50% had impaired cognition, and 56% experienced limitations in activities of daily living.
However, those patients with COVID-19 who had neurologic sequelae “fared even worse,” said Dr. Wisniewski. Compared with control patients, they had twofold worse Modified Rankin Scale scores and worse scores on activity of daily living, and they were much less likely to return to work.
Mechanisms by which COVID-19 affects longer-term cognitive dysfunction are unclear, but inflammation likely plays a role.
The research team compared a number of Alzheimer’s disease plasma biomarkers in 158 patients with COVID-19 who had neurologic symptoms and 152 COVID patients with COVID but no neurologic symptoms. They found marked elevations of neurofilament light, a marker of neuronal injury, in those with symptoms (P = .0003) as well as increased glial fibrillary acid protein, a marker of neuroinflammation (P = .0098).
Ubiquitin carboxyl-terminal hydrolase L1, another marker of neuronal injury, was also elevated in those with neurologic symptoms. Regarding Alzheimer’s disease pathology, total tau (t-tau) and phosphorylated tau “also tracked with neurological sequelae,” said Dr. Wisniewski.
There was no difference in levels of amyloid beta 40 (A beta 40) between groups. However, A beta 42 plasma levels were significantly lower in those with neurologic effects, suggesting higher levels in the brain. In addition, the ratio of t-tau to A beta 42 “clearly differentiated the two groups,” he said.
“Serum biomarkers of neuroinflammation and neuronal injury and Alzheimer’s disease correlate strongly, perhaps suggesting that folks with COVID infection and neurological sequelae may have an acceleration of Alzheimer’s disease symptoms and pathology,” he said. “That’s something that needs longer follow-up.”
Important differentiation
Commenting on the research, Rebecca Edelmayer, PhD, senior director of scientific engagement, Alzheimer’s Association, said the study provides important information. The inclusion of plasma biomarkers in this research is “really critical to tease out what’s the impact of COVID itself on the brain,” said Dr. Edelmayer.
“We’re in an era of biomarkers when it comes to Alzheimer’s disease and other dementias, and being able to define those changes that are happening in the brain over time is going to be really critical and aid in early detection and accurate diagnoses,” she said.
What is still to be learned is what these biomarkers reveal long term, said Dr. Edelmayer. “Do those biological markers change? Do they go back to normal? A lot of that is still unknown,” she said.
She noted that many diseases that are linked to inflammation produce similar biomarkers in the brain – for example, neurofilament light.
With other viral infections, such as severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS), similar associations between the infection and cognition have been reported, said Dr. Edelmayer.
“But there are still a lot of questions around cause and effect. Is it really a direct effect of the virus on the brain itself? Is it an effect of having an enormous amount of inflammation going on in the body? A lot of that still needs to be teased out,” she commented.
The study was supported by the National Institutes of Health, the Alzheimer’s Association, and the State of New York. Dr. Wisniewski has consulted for Grifols, Amylon Pharmaceuticals, and Alzamed Neuro; 30 NYU patents are related to AD therapeutics.
A version of this article first appeared on Medscape.com.
, a new study shows.
These results suggest that COVID-19 may accelerate Alzheimer’s disease symptoms and pathology, said study investigator Thomas Wisniewski, MD, professor of neurology, pathology, and psychiatry at New York University.
The findings were presented here at the Alzheimer’s Association International Conference (AAIC) 2021.
Strong correlation
There’s a clear association between SARS-CoV-2 infection and Alzheimer’s disease-related dementia. Patients with Alzheimer’s disease are at threefold higher risk for the infection and have a twofold higher risk for death, Dr. Wisniewski told meeting delegates.
He and his colleagues conducted a prospective study of patients who had tested positive for SARS-CoV-2 and who experienced neurologic sequelae and SARS-CoV-2 patients who were without neurologic sequelae. All patients were hospitalized from March 10 to May 20, 2020. This was during a period when New York City was overwhelmed by COVID: About 35% of hospitalized patients had COVID.
Of those who experienced neurologic events, the most common “by far and away” (51%) was toxic metabolic encephalopathy (TME), said Dr. Wisniewski. Other associations included seizures, hypoxic/anoxic injury, and ischemic stroke.
The most common TMEs were septic and hypoxic ischemia. In most patients (78%), TME had more than one cause.
Researchers followed 196 patients with COVID and neurologic complications (case patients) and 186 matched control patients who had no neurologic complications over a period of 6 months.
“Unfortunately, both groups had poor outcomes,” said Dr. Wisniewski. About 50% had impaired cognition, and 56% experienced limitations in activities of daily living.
However, those patients with COVID-19 who had neurologic sequelae “fared even worse,” said Dr. Wisniewski. Compared with control patients, they had twofold worse Modified Rankin Scale scores and worse scores on activity of daily living, and they were much less likely to return to work.
Mechanisms by which COVID-19 affects longer-term cognitive dysfunction are unclear, but inflammation likely plays a role.
The research team compared a number of Alzheimer’s disease plasma biomarkers in 158 patients with COVID-19 who had neurologic symptoms and 152 COVID patients with COVID but no neurologic symptoms. They found marked elevations of neurofilament light, a marker of neuronal injury, in those with symptoms (P = .0003) as well as increased glial fibrillary acid protein, a marker of neuroinflammation (P = .0098).
Ubiquitin carboxyl-terminal hydrolase L1, another marker of neuronal injury, was also elevated in those with neurologic symptoms. Regarding Alzheimer’s disease pathology, total tau (t-tau) and phosphorylated tau “also tracked with neurological sequelae,” said Dr. Wisniewski.
There was no difference in levels of amyloid beta 40 (A beta 40) between groups. However, A beta 42 plasma levels were significantly lower in those with neurologic effects, suggesting higher levels in the brain. In addition, the ratio of t-tau to A beta 42 “clearly differentiated the two groups,” he said.
“Serum biomarkers of neuroinflammation and neuronal injury and Alzheimer’s disease correlate strongly, perhaps suggesting that folks with COVID infection and neurological sequelae may have an acceleration of Alzheimer’s disease symptoms and pathology,” he said. “That’s something that needs longer follow-up.”
Important differentiation
Commenting on the research, Rebecca Edelmayer, PhD, senior director of scientific engagement, Alzheimer’s Association, said the study provides important information. The inclusion of plasma biomarkers in this research is “really critical to tease out what’s the impact of COVID itself on the brain,” said Dr. Edelmayer.
“We’re in an era of biomarkers when it comes to Alzheimer’s disease and other dementias, and being able to define those changes that are happening in the brain over time is going to be really critical and aid in early detection and accurate diagnoses,” she said.
What is still to be learned is what these biomarkers reveal long term, said Dr. Edelmayer. “Do those biological markers change? Do they go back to normal? A lot of that is still unknown,” she said.
She noted that many diseases that are linked to inflammation produce similar biomarkers in the brain – for example, neurofilament light.
With other viral infections, such as severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS), similar associations between the infection and cognition have been reported, said Dr. Edelmayer.
“But there are still a lot of questions around cause and effect. Is it really a direct effect of the virus on the brain itself? Is it an effect of having an enormous amount of inflammation going on in the body? A lot of that still needs to be teased out,” she commented.
The study was supported by the National Institutes of Health, the Alzheimer’s Association, and the State of New York. Dr. Wisniewski has consulted for Grifols, Amylon Pharmaceuticals, and Alzamed Neuro; 30 NYU patents are related to AD therapeutics.
A version of this article first appeared on Medscape.com.
, a new study shows.
These results suggest that COVID-19 may accelerate Alzheimer’s disease symptoms and pathology, said study investigator Thomas Wisniewski, MD, professor of neurology, pathology, and psychiatry at New York University.
The findings were presented here at the Alzheimer’s Association International Conference (AAIC) 2021.
Strong correlation
There’s a clear association between SARS-CoV-2 infection and Alzheimer’s disease-related dementia. Patients with Alzheimer’s disease are at threefold higher risk for the infection and have a twofold higher risk for death, Dr. Wisniewski told meeting delegates.
He and his colleagues conducted a prospective study of patients who had tested positive for SARS-CoV-2 and who experienced neurologic sequelae and SARS-CoV-2 patients who were without neurologic sequelae. All patients were hospitalized from March 10 to May 20, 2020. This was during a period when New York City was overwhelmed by COVID: About 35% of hospitalized patients had COVID.
Of those who experienced neurologic events, the most common “by far and away” (51%) was toxic metabolic encephalopathy (TME), said Dr. Wisniewski. Other associations included seizures, hypoxic/anoxic injury, and ischemic stroke.
The most common TMEs were septic and hypoxic ischemia. In most patients (78%), TME had more than one cause.
Researchers followed 196 patients with COVID and neurologic complications (case patients) and 186 matched control patients who had no neurologic complications over a period of 6 months.
“Unfortunately, both groups had poor outcomes,” said Dr. Wisniewski. About 50% had impaired cognition, and 56% experienced limitations in activities of daily living.
However, those patients with COVID-19 who had neurologic sequelae “fared even worse,” said Dr. Wisniewski. Compared with control patients, they had twofold worse Modified Rankin Scale scores and worse scores on activity of daily living, and they were much less likely to return to work.
Mechanisms by which COVID-19 affects longer-term cognitive dysfunction are unclear, but inflammation likely plays a role.
The research team compared a number of Alzheimer’s disease plasma biomarkers in 158 patients with COVID-19 who had neurologic symptoms and 152 COVID patients with COVID but no neurologic symptoms. They found marked elevations of neurofilament light, a marker of neuronal injury, in those with symptoms (P = .0003) as well as increased glial fibrillary acid protein, a marker of neuroinflammation (P = .0098).
Ubiquitin carboxyl-terminal hydrolase L1, another marker of neuronal injury, was also elevated in those with neurologic symptoms. Regarding Alzheimer’s disease pathology, total tau (t-tau) and phosphorylated tau “also tracked with neurological sequelae,” said Dr. Wisniewski.
There was no difference in levels of amyloid beta 40 (A beta 40) between groups. However, A beta 42 plasma levels were significantly lower in those with neurologic effects, suggesting higher levels in the brain. In addition, the ratio of t-tau to A beta 42 “clearly differentiated the two groups,” he said.
“Serum biomarkers of neuroinflammation and neuronal injury and Alzheimer’s disease correlate strongly, perhaps suggesting that folks with COVID infection and neurological sequelae may have an acceleration of Alzheimer’s disease symptoms and pathology,” he said. “That’s something that needs longer follow-up.”
Important differentiation
Commenting on the research, Rebecca Edelmayer, PhD, senior director of scientific engagement, Alzheimer’s Association, said the study provides important information. The inclusion of plasma biomarkers in this research is “really critical to tease out what’s the impact of COVID itself on the brain,” said Dr. Edelmayer.
“We’re in an era of biomarkers when it comes to Alzheimer’s disease and other dementias, and being able to define those changes that are happening in the brain over time is going to be really critical and aid in early detection and accurate diagnoses,” she said.
What is still to be learned is what these biomarkers reveal long term, said Dr. Edelmayer. “Do those biological markers change? Do they go back to normal? A lot of that is still unknown,” she said.
She noted that many diseases that are linked to inflammation produce similar biomarkers in the brain – for example, neurofilament light.
With other viral infections, such as severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS), similar associations between the infection and cognition have been reported, said Dr. Edelmayer.
“But there are still a lot of questions around cause and effect. Is it really a direct effect of the virus on the brain itself? Is it an effect of having an enormous amount of inflammation going on in the body? A lot of that still needs to be teased out,” she commented.
The study was supported by the National Institutes of Health, the Alzheimer’s Association, and the State of New York. Dr. Wisniewski has consulted for Grifols, Amylon Pharmaceuticals, and Alzamed Neuro; 30 NYU patents are related to AD therapeutics.
A version of this article first appeared on Medscape.com.
From AAIC 2021
‘Alarming’ data on early cognitive decline in transgender adults
, new research shows.
Investigators found transgender adults – individuals who identify with a gender different than the one assigned to them at birth – were nearly twice as likely to report subjective cognitive decline and more than twice as likely to report SCD-related functional limitations – such as reduced ability to work, volunteer, or be social – than cisgender adults.

“Trans populations are disproportionately impacted by health disparities and also risk factors for dementia. Putting these pieces together, I wasn’t surprised by their greater risk of cognitive decline,” said study investigator Ethan Cicero, PhD, RN, an assistant professor at Emory University, Atlanta.
The findings were presented at the 2021 Alzheimer’s Association International Conference.
‘Alarming’ finding
SCD is a self-reported experience of worsening memory or thinking and is one of the first clinical manifestations of Alzheimer’s disease and related dementia (ADRD). Yet there is limited research into cognitive impairment among transgender adults.
The researchers examined SCD and associated functional limitations among transgender and cisgender adults older than age 45 years who provided health and health behavior data as part of the Behavioral Risk Factor Surveillance System (BRFSS) surveys (2015-2019).
The sample included 386,529 adults of whom 1,302 identified as transgender and 385,227 as cisgender.
Roughly 17% of transgender adults reported SCD, which is significantly higher than the 10.6% rate for cisgender adults (P < .001).
Compared with cisgender adults reporting SCD, transgender adults reporting SCD were younger (mean age 61.9 vs. 65.2 years, P = .0005), more likely to be in a racial/ethnic minority group (37.3% vs. 19.5%, P < .0001), have a high school degree or less (59.6% vs. 43.4%, P = .0003), be uninsured (17% vs. 5.5%, P = .0007) and have a depressive disorder (58.8% vs. 45.7%, P = .0028).
The fact that transgender people who reported SCD were about 3 years younger than cisgender people who reported SCD is “somewhat alarming and a red flag to ask middle-aged trans adults about their brain health and not just older or elderly trans adults,” said Dr. Cicero.
The study also showed that transgender adults reporting SCD were 2.3 times more likely to report related social and self-care limitations when compared with cisgender adults reporting SCD.
The findings align with a study reported at AAIC 2019, which showed that sexual or gender minorities (SGM) are almost 30% more likely to report subjective cognitive decline compared with the non-SGM population.
Cause unclear
“We are not certain what may be causing the elevated subjective cognitive decline rates among transgender adults. We postulate that it may be in part due to anti-transgender stigma and prejudice that expose transgender people to high rates of mistreatment and discrimination where they live, work, learn, seek health care, and age,” Dr. Cicero said.
“More research is needed to identify and target preventive intervention strategies, develop culturally relevant screenings, and shape policies to improve the health and well-being of the transgender population,” he added.
Weighing in on the study, Rebecca Edelmayer, PhD, senior director of scientific engagement at the Alzheimer’s Association, said “researchers have only just started to explore the experiences of dementia within the lesbian, gay, and bisexual community, but this is the first time we are seeing some specific research that’s looking at cognition in transgender individuals and gender nonbinary individuals.”
“We don’t know exactly why transgender and gender nonbinary individuals experience greater rates of subjective cognitive decline, but we do know that they have greater rates of health disparities that are considered risk factors for dementia, including higher rates of cardiovascular disease, depression, diabetes, tobacco and alcohol use, and obesity,” Dr. Edelmayer said.
“Alzheimer’s and dementia do not discriminate. Neither can we,” Maria C. Carrillo, PhD, chief science officer for the Alzheimer’s Association, said in a statement.
“The Alzheimer’s Association advocates for more research to better understand the cognitive and emotional needs of transgender and nonbinary individuals so that our nation’s health care providers can offer them culturally sensitive care,” said Dr. Carrillo.
The study had no specific funding. Dr. Cicero, Dr. Carrillo, and Dr. Edelmayer have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research shows.
Investigators found transgender adults – individuals who identify with a gender different than the one assigned to them at birth – were nearly twice as likely to report subjective cognitive decline and more than twice as likely to report SCD-related functional limitations – such as reduced ability to work, volunteer, or be social – than cisgender adults.
“Trans populations are disproportionately impacted by health disparities and also risk factors for dementia. Putting these pieces together, I wasn’t surprised by their greater risk of cognitive decline,” said study investigator Ethan Cicero, PhD, RN, an assistant professor at Emory University, Atlanta.
The findings were presented at the 2021 Alzheimer’s Association International Conference.
‘Alarming’ finding
SCD is a self-reported experience of worsening memory or thinking and is one of the first clinical manifestations of Alzheimer’s disease and related dementia (ADRD). Yet there is limited research into cognitive impairment among transgender adults.
The researchers examined SCD and associated functional limitations among transgender and cisgender adults older than age 45 years who provided health and health behavior data as part of the Behavioral Risk Factor Surveillance System (BRFSS) surveys (2015-2019).
The sample included 386,529 adults of whom 1,302 identified as transgender and 385,227 as cisgender.
Roughly 17% of transgender adults reported SCD, which is significantly higher than the 10.6% rate for cisgender adults (P < .001).
Compared with cisgender adults reporting SCD, transgender adults reporting SCD were younger (mean age 61.9 vs. 65.2 years, P = .0005), more likely to be in a racial/ethnic minority group (37.3% vs. 19.5%, P < .0001), have a high school degree or less (59.6% vs. 43.4%, P = .0003), be uninsured (17% vs. 5.5%, P = .0007) and have a depressive disorder (58.8% vs. 45.7%, P = .0028).
The fact that transgender people who reported SCD were about 3 years younger than cisgender people who reported SCD is “somewhat alarming and a red flag to ask middle-aged trans adults about their brain health and not just older or elderly trans adults,” said Dr. Cicero.
The study also showed that transgender adults reporting SCD were 2.3 times more likely to report related social and self-care limitations when compared with cisgender adults reporting SCD.
The findings align with a study reported at AAIC 2019, which showed that sexual or gender minorities (SGM) are almost 30% more likely to report subjective cognitive decline compared with the non-SGM population.
Cause unclear
“We are not certain what may be causing the elevated subjective cognitive decline rates among transgender adults. We postulate that it may be in part due to anti-transgender stigma and prejudice that expose transgender people to high rates of mistreatment and discrimination where they live, work, learn, seek health care, and age,” Dr. Cicero said.
“More research is needed to identify and target preventive intervention strategies, develop culturally relevant screenings, and shape policies to improve the health and well-being of the transgender population,” he added.
Weighing in on the study, Rebecca Edelmayer, PhD, senior director of scientific engagement at the Alzheimer’s Association, said “researchers have only just started to explore the experiences of dementia within the lesbian, gay, and bisexual community, but this is the first time we are seeing some specific research that’s looking at cognition in transgender individuals and gender nonbinary individuals.”
“We don’t know exactly why transgender and gender nonbinary individuals experience greater rates of subjective cognitive decline, but we do know that they have greater rates of health disparities that are considered risk factors for dementia, including higher rates of cardiovascular disease, depression, diabetes, tobacco and alcohol use, and obesity,” Dr. Edelmayer said.
“Alzheimer’s and dementia do not discriminate. Neither can we,” Maria C. Carrillo, PhD, chief science officer for the Alzheimer’s Association, said in a statement.
“The Alzheimer’s Association advocates for more research to better understand the cognitive and emotional needs of transgender and nonbinary individuals so that our nation’s health care providers can offer them culturally sensitive care,” said Dr. Carrillo.
The study had no specific funding. Dr. Cicero, Dr. Carrillo, and Dr. Edelmayer have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research shows.
Investigators found transgender adults – individuals who identify with a gender different than the one assigned to them at birth – were nearly twice as likely to report subjective cognitive decline and more than twice as likely to report SCD-related functional limitations – such as reduced ability to work, volunteer, or be social – than cisgender adults.
“Trans populations are disproportionately impacted by health disparities and also risk factors for dementia. Putting these pieces together, I wasn’t surprised by their greater risk of cognitive decline,” said study investigator Ethan Cicero, PhD, RN, an assistant professor at Emory University, Atlanta.
The findings were presented at the 2021 Alzheimer’s Association International Conference.
‘Alarming’ finding
SCD is a self-reported experience of worsening memory or thinking and is one of the first clinical manifestations of Alzheimer’s disease and related dementia (ADRD). Yet there is limited research into cognitive impairment among transgender adults.
The researchers examined SCD and associated functional limitations among transgender and cisgender adults older than age 45 years who provided health and health behavior data as part of the Behavioral Risk Factor Surveillance System (BRFSS) surveys (2015-2019).
The sample included 386,529 adults of whom 1,302 identified as transgender and 385,227 as cisgender.
Roughly 17% of transgender adults reported SCD, which is significantly higher than the 10.6% rate for cisgender adults (P < .001).
Compared with cisgender adults reporting SCD, transgender adults reporting SCD were younger (mean age 61.9 vs. 65.2 years, P = .0005), more likely to be in a racial/ethnic minority group (37.3% vs. 19.5%, P < .0001), have a high school degree or less (59.6% vs. 43.4%, P = .0003), be uninsured (17% vs. 5.5%, P = .0007) and have a depressive disorder (58.8% vs. 45.7%, P = .0028).
The fact that transgender people who reported SCD were about 3 years younger than cisgender people who reported SCD is “somewhat alarming and a red flag to ask middle-aged trans adults about their brain health and not just older or elderly trans adults,” said Dr. Cicero.
The study also showed that transgender adults reporting SCD were 2.3 times more likely to report related social and self-care limitations when compared with cisgender adults reporting SCD.
The findings align with a study reported at AAIC 2019, which showed that sexual or gender minorities (SGM) are almost 30% more likely to report subjective cognitive decline compared with the non-SGM population.
Cause unclear
“We are not certain what may be causing the elevated subjective cognitive decline rates among transgender adults. We postulate that it may be in part due to anti-transgender stigma and prejudice that expose transgender people to high rates of mistreatment and discrimination where they live, work, learn, seek health care, and age,” Dr. Cicero said.
“More research is needed to identify and target preventive intervention strategies, develop culturally relevant screenings, and shape policies to improve the health and well-being of the transgender population,” he added.
Weighing in on the study, Rebecca Edelmayer, PhD, senior director of scientific engagement at the Alzheimer’s Association, said “researchers have only just started to explore the experiences of dementia within the lesbian, gay, and bisexual community, but this is the first time we are seeing some specific research that’s looking at cognition in transgender individuals and gender nonbinary individuals.”
“We don’t know exactly why transgender and gender nonbinary individuals experience greater rates of subjective cognitive decline, but we do know that they have greater rates of health disparities that are considered risk factors for dementia, including higher rates of cardiovascular disease, depression, diabetes, tobacco and alcohol use, and obesity,” Dr. Edelmayer said.
“Alzheimer’s and dementia do not discriminate. Neither can we,” Maria C. Carrillo, PhD, chief science officer for the Alzheimer’s Association, said in a statement.
“The Alzheimer’s Association advocates for more research to better understand the cognitive and emotional needs of transgender and nonbinary individuals so that our nation’s health care providers can offer them culturally sensitive care,” said Dr. Carrillo.
The study had no specific funding. Dr. Cicero, Dr. Carrillo, and Dr. Edelmayer have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
From AAIC 2021
Low-dose aspirin linked to lower dementia risk in some
, according to a retrospective analysis of two large cohorts. The association with all-cause dementia was weak, but much more pronounced in subjects with coronary heart disease.
The results underscore that individuals with cardiovascular disease risk factors should be prescribed LDASA, and they should be encouraged to be compliant. The study differed from previous observational and randomized, controlled trials, which yielded mixed results. Many looked at individuals older than age 65. The pathological changes associated with dementia may occur up to 2 decades before symptom onset, and it appears that LDASA cannot counter cognitive decline after a diagnosis is made. “The use of LDASA at this age may be already too late,” said Thi Ngoc Mai Nguyen, a PhD student at Network Aging Research, Heidelberg University, Germany. She presented the results at the 2021 Alzheimer’s Association International Conference.
Previous studies also included individuals using LDASA to prevent cardiovascular disease, and they didn’t always adjust for these risk factors. The current work used two large databases, UK Biobank and ESTHER, with a follow-up time of over 10 years for both. “We were able to balance out the distribution of measured baseline covariates (to be) similar between LDASA users and nonusers, and thus, we were able to adjust for confounders more comprehensively,” said Ms. Nguyen.
Not yet a definitive answer
Although the findings are promising, Ms. Nguyen noted that the study is not the final word. “Residual confounding is possible, and causation cannot be tested. The only way to answer this is to have clinical trials with at least 10 years of follow-up,” said Ms. Nguyen. She plans to conduct similar studies in non-White populations, and also to examine whether LDASA can help preserve cognitive function in middle-age adults.
The study is interesting, said Claire Sexton, DPhil, who was asked to comment, but she suggested that it is not practice changing. “There is not evidence from the dementia science perspective that should go against whatever the recommendations are for cardiovascular risk,” said Dr. Sexton, director of scientific programs and outreach at the Alzheimer’s Association. “I don’t think this study alone can provide a definitive answer on low-dose aspirin and its association with dementia and Alzheimer’s disease, but it’s an important addition to the literature,” she added.
Meta-analysis data
The researchers examined two prospective cohort studies, and combined them into a meta-analysis. It included the ESTHER cohort from Saarland, Germany, with 5,258 individuals and 14.3 years of follow-up, and the UK Biobank cohort, with 305,394 individuals and 11.6 years of follow-up. Subjects selected for analysis were 55 years old or older.
The meta-analysis showed no significant association between LDASA use and reduced risk of Alzheimer’s disease, but there was an association between LDASA use and all-cause dementia (hazard ratio [HR], 0.96; 95% confidence interval [CI], 0.93-0.99).
There were no sex differences with respect to Alzheimer’s dementia, but in males, LDASA was associated with lower risk of vascular dementia (HR, 0.85; 95% CI, 0.79-0.93) and all-cause dementia (HR, 0.87; 95% CI, 0.83-0.92). However, in females, LDASA was tied to greater risk of both vascular dementia (HR, 1.13; 95% CI, 1.02-1.24) and all-cause dementia (HR, 1.07; 95% CI, 1.02-1.13).
The strongest association between LDASA and reduced dementia risk was found in subjects with coronary heart disease (HR, 0.69; 95% CI, 0.59-0.80).
The researchers also used UK Biobank primary care data to analyze associations between longer use of LDASA and reduced dementia risk. Those who used LDASA for 0-5 years were at a higher than average risk of all-cause dementia (HR, 2.80; 95% CI, 2.48-3.16), Alzheimer’s disease (HR, 2.26; 95% CI, 1.84-2.77), and vascular dementia (HR, 3.79; 95% CI, 3.17-4.53). Long-term LDASA users, defined as 10 years or longer, had a lower risk of all-cause dementia (HR, 0.51; 95% CI, 0.47-0.56), Alzheimer’s disease (HR, 0.58; 95% CI, 0.51-0.68), and vascular dementia (HR, 0.48; 95% CI, 0.42-0.56).
Dr. Nguyen and Dr. Sexton have no relevant financial disclosures.
, according to a retrospective analysis of two large cohorts. The association with all-cause dementia was weak, but much more pronounced in subjects with coronary heart disease.
The results underscore that individuals with cardiovascular disease risk factors should be prescribed LDASA, and they should be encouraged to be compliant. The study differed from previous observational and randomized, controlled trials, which yielded mixed results. Many looked at individuals older than age 65. The pathological changes associated with dementia may occur up to 2 decades before symptom onset, and it appears that LDASA cannot counter cognitive decline after a diagnosis is made. “The use of LDASA at this age may be already too late,” said Thi Ngoc Mai Nguyen, a PhD student at Network Aging Research, Heidelberg University, Germany. She presented the results at the 2021 Alzheimer’s Association International Conference.
Previous studies also included individuals using LDASA to prevent cardiovascular disease, and they didn’t always adjust for these risk factors. The current work used two large databases, UK Biobank and ESTHER, with a follow-up time of over 10 years for both. “We were able to balance out the distribution of measured baseline covariates (to be) similar between LDASA users and nonusers, and thus, we were able to adjust for confounders more comprehensively,” said Ms. Nguyen.
Not yet a definitive answer
Although the findings are promising, Ms. Nguyen noted that the study is not the final word. “Residual confounding is possible, and causation cannot be tested. The only way to answer this is to have clinical trials with at least 10 years of follow-up,” said Ms. Nguyen. She plans to conduct similar studies in non-White populations, and also to examine whether LDASA can help preserve cognitive function in middle-age adults.
The study is interesting, said Claire Sexton, DPhil, who was asked to comment, but she suggested that it is not practice changing. “There is not evidence from the dementia science perspective that should go against whatever the recommendations are for cardiovascular risk,” said Dr. Sexton, director of scientific programs and outreach at the Alzheimer’s Association. “I don’t think this study alone can provide a definitive answer on low-dose aspirin and its association with dementia and Alzheimer’s disease, but it’s an important addition to the literature,” she added.
Meta-analysis data
The researchers examined two prospective cohort studies, and combined them into a meta-analysis. It included the ESTHER cohort from Saarland, Germany, with 5,258 individuals and 14.3 years of follow-up, and the UK Biobank cohort, with 305,394 individuals and 11.6 years of follow-up. Subjects selected for analysis were 55 years old or older.
The meta-analysis showed no significant association between LDASA use and reduced risk of Alzheimer’s disease, but there was an association between LDASA use and all-cause dementia (hazard ratio [HR], 0.96; 95% confidence interval [CI], 0.93-0.99).
There were no sex differences with respect to Alzheimer’s dementia, but in males, LDASA was associated with lower risk of vascular dementia (HR, 0.85; 95% CI, 0.79-0.93) and all-cause dementia (HR, 0.87; 95% CI, 0.83-0.92). However, in females, LDASA was tied to greater risk of both vascular dementia (HR, 1.13; 95% CI, 1.02-1.24) and all-cause dementia (HR, 1.07; 95% CI, 1.02-1.13).
The strongest association between LDASA and reduced dementia risk was found in subjects with coronary heart disease (HR, 0.69; 95% CI, 0.59-0.80).
The researchers also used UK Biobank primary care data to analyze associations between longer use of LDASA and reduced dementia risk. Those who used LDASA for 0-5 years were at a higher than average risk of all-cause dementia (HR, 2.80; 95% CI, 2.48-3.16), Alzheimer’s disease (HR, 2.26; 95% CI, 1.84-2.77), and vascular dementia (HR, 3.79; 95% CI, 3.17-4.53). Long-term LDASA users, defined as 10 years or longer, had a lower risk of all-cause dementia (HR, 0.51; 95% CI, 0.47-0.56), Alzheimer’s disease (HR, 0.58; 95% CI, 0.51-0.68), and vascular dementia (HR, 0.48; 95% CI, 0.42-0.56).
Dr. Nguyen and Dr. Sexton have no relevant financial disclosures.
, according to a retrospective analysis of two large cohorts. The association with all-cause dementia was weak, but much more pronounced in subjects with coronary heart disease.
The results underscore that individuals with cardiovascular disease risk factors should be prescribed LDASA, and they should be encouraged to be compliant. The study differed from previous observational and randomized, controlled trials, which yielded mixed results. Many looked at individuals older than age 65. The pathological changes associated with dementia may occur up to 2 decades before symptom onset, and it appears that LDASA cannot counter cognitive decline after a diagnosis is made. “The use of LDASA at this age may be already too late,” said Thi Ngoc Mai Nguyen, a PhD student at Network Aging Research, Heidelberg University, Germany. She presented the results at the 2021 Alzheimer’s Association International Conference.
Previous studies also included individuals using LDASA to prevent cardiovascular disease, and they didn’t always adjust for these risk factors. The current work used two large databases, UK Biobank and ESTHER, with a follow-up time of over 10 years for both. “We were able to balance out the distribution of measured baseline covariates (to be) similar between LDASA users and nonusers, and thus, we were able to adjust for confounders more comprehensively,” said Ms. Nguyen.
Not yet a definitive answer
Although the findings are promising, Ms. Nguyen noted that the study is not the final word. “Residual confounding is possible, and causation cannot be tested. The only way to answer this is to have clinical trials with at least 10 years of follow-up,” said Ms. Nguyen. She plans to conduct similar studies in non-White populations, and also to examine whether LDASA can help preserve cognitive function in middle-age adults.
The study is interesting, said Claire Sexton, DPhil, who was asked to comment, but she suggested that it is not practice changing. “There is not evidence from the dementia science perspective that should go against whatever the recommendations are for cardiovascular risk,” said Dr. Sexton, director of scientific programs and outreach at the Alzheimer’s Association. “I don’t think this study alone can provide a definitive answer on low-dose aspirin and its association with dementia and Alzheimer’s disease, but it’s an important addition to the literature,” she added.
Meta-analysis data
The researchers examined two prospective cohort studies, and combined them into a meta-analysis. It included the ESTHER cohort from Saarland, Germany, with 5,258 individuals and 14.3 years of follow-up, and the UK Biobank cohort, with 305,394 individuals and 11.6 years of follow-up. Subjects selected for analysis were 55 years old or older.
The meta-analysis showed no significant association between LDASA use and reduced risk of Alzheimer’s disease, but there was an association between LDASA use and all-cause dementia (hazard ratio [HR], 0.96; 95% confidence interval [CI], 0.93-0.99).
There were no sex differences with respect to Alzheimer’s dementia, but in males, LDASA was associated with lower risk of vascular dementia (HR, 0.85; 95% CI, 0.79-0.93) and all-cause dementia (HR, 0.87; 95% CI, 0.83-0.92). However, in females, LDASA was tied to greater risk of both vascular dementia (HR, 1.13; 95% CI, 1.02-1.24) and all-cause dementia (HR, 1.07; 95% CI, 1.02-1.13).
The strongest association between LDASA and reduced dementia risk was found in subjects with coronary heart disease (HR, 0.69; 95% CI, 0.59-0.80).
The researchers also used UK Biobank primary care data to analyze associations between longer use of LDASA and reduced dementia risk. Those who used LDASA for 0-5 years were at a higher than average risk of all-cause dementia (HR, 2.80; 95% CI, 2.48-3.16), Alzheimer’s disease (HR, 2.26; 95% CI, 1.84-2.77), and vascular dementia (HR, 3.79; 95% CI, 3.17-4.53). Long-term LDASA users, defined as 10 years or longer, had a lower risk of all-cause dementia (HR, 0.51; 95% CI, 0.47-0.56), Alzheimer’s disease (HR, 0.58; 95% CI, 0.51-0.68), and vascular dementia (HR, 0.48; 95% CI, 0.42-0.56).
Dr. Nguyen and Dr. Sexton have no relevant financial disclosures.
FROM AAIC 2021
C. diff eradication not necessary for clinical cure of recurrent infections with fecal transplant
It’s not necessary to completely eradicate all Clostridioides difficile to successfully treat recurrent C. difficile infections with fecal microbiota transplant (FMT), according to a study presented online July 12 at the European Congress of Clinical Microbiology & Infectious Diseases.
C. difficile colonization persisted for 3 weeks after FMT in about one-quarter of patients, but it’s not clear whether this is a persistent infection, a newly acquired infection, or partial persistence of a mixed infection, said Elisabeth Terveer, MD, a medical microbiologist at Leiden (the Netherlands) University Medical Center. In addition, “82% of patients with detectable C. diff do not relapse, so it’s absolutely not necessary for a cure,” she said.
Several mechanisms explain why FMT is a highly effective therapy for recurrent C. difficile infections, including restoration of bacterial metabolism in the gut, immune modulation, and direct competition between bacteria, Dr. Terveer said, but it’s less clear whether eradication of C. difficile spores is among these mechanisms.
Between May 2016 and April 2020, the researchers analyzed fecal samples from 84 patients who took vancomycin for at least 4 days before undergoing FMT. The researchers took fecal samples from patients before FMT and 3 weeks after FMT to culture them and the donor samples for presence of C. difficile, and they assessed clinical outcomes at 3 weeks and 6 months after FMT.
After antibiotic treatment but prior to FMT, 19% of patients (n = 16) still had a toxigenic C. difficile culture while the other 81% had a negative culture. None of the donor samples had a positive C. difficile culture. After FMT treatment, five patients who had a positive pre-FMT culture remained positive, and the other 11 were negative. Among the 81% of patients (n = 68) who had a negative culture just before FMT, 22 had a positive culture and 46 had a negative culture after FMT. Overall, 26% of patients post FMT had a positive C. difficile culture, a finding that was 10-fold higher than another study that assessed C. difficile with PCR testing, Dr. Terveer said.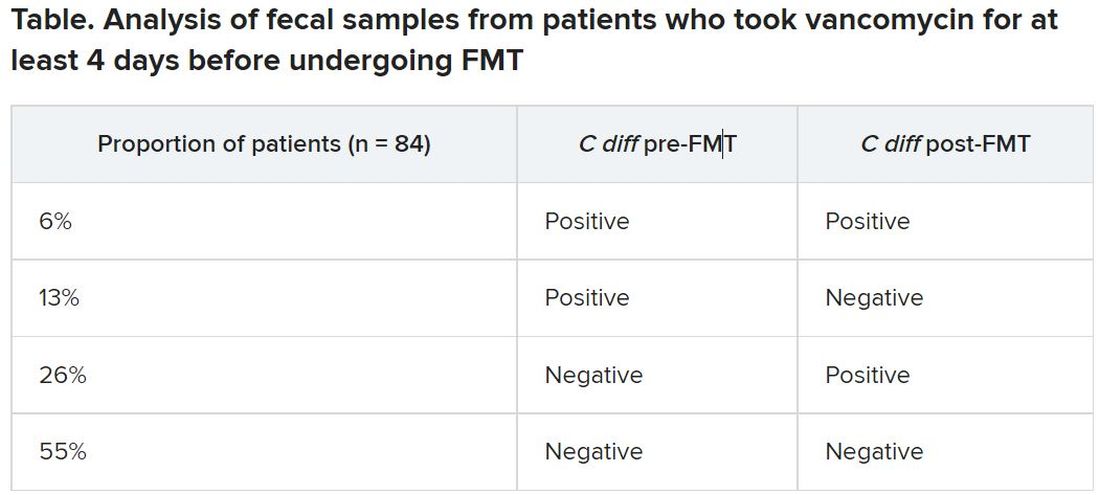
The clinical cure rate after FMT was 94%, and five patients had relapses within 2 months of their FMT. These relapses were more prevalent in patients with a positive C. difficile culture prior to FMT (odds ratio [OR], 7.6; P = .045) and a positive C. difficile culture after FMT (OR, 13.6; P = .016). Still, 82% of patients who had a positive C. difficile culture post FMT remained clinically cured 2 months later.
It’s unclear why 19% of patients had a positive culture after their antibiotic pretreatment prior to FMT, Dr. Terveer said, but it may be because the pretreatment was of such a short duration.
“I think the advice should be: Give a full anti–C. diff antibiotic course to treat the C. diff infection, and then give FMT afterward to restore the microbiota and prevent further relapses,” Dr. Terveer told attendees.
Dimitri Drekonja, MD, chief of the Minneapolis VA Infectious Disease Section, said the findings were not necessarily surprising, but it would have been interesting for the researchers to have conducted DNA sequencing of the patients’ fecal samples post FMT to see what the biological diversity looked like.
“One school of thought has been that you have to repopulate the normal diverse microbiota of the colon” with FMT, and the other “is that you need to get rid of the C. diff that›s there,” Dr. Drekonja, who was not involved in the study, said in an interview. “I think more people think it’s the diverse microbiota because if it’s just getting rid of C. diff, we can get do that with antibiotics – but that gets rid of the other organisms.”
As long as you have a diverse microbiota post FMT, Dr. Drekonja said, then “having a few residual organisms, even if they get magnified in the culture process, is probably not that big a deal.”
But there’s a third school of thought that Dr. Drekonja said he himself falls into: “I don’t really care how it works, just that in well-done trials, it does work.” As long as large, robust, well-blinded trials show that FMT works, “I’m open to all sorts of ideas of what the mechanism is,” he said. “The main thing is that it does or doesn’t work.”
These findings basically reinforce current guidance not to test patients’ stools if they are asymptomatic, Dr. Drekonja said. In the past, clinicians sometimes tested patients’ stool after therapy to ensure the C. difficile was eradicated, regardless of whether the patient had symptoms of infection, he said.
“We’ve since become much more attuned that there are lots of people who have detectable C. diff in their stool without any symptoms,” whether detectable by culture or PCR, Dr. Drekonja said. “Generally, if you’re doing well and you’re not having diarrhea, don’t test, and if someone does test and finds it, pretend you didn’t see the test,” he advised. “This is a big part of diagnostic stewardship, which is: You don’t go testing people who are doing well.”
The Netherlands Donor Feces Bank used in the research is funded by a grant from Vedanta Biosciences. Dr. Drekonja had no disclosures.
Help your patients understand their C. difficile diagnosis by sharing patient education from the AGA GI Patient Center: www.gastro.org/Cdiff.
A version of this article first appeared on Medscape.com.
It’s not necessary to completely eradicate all Clostridioides difficile to successfully treat recurrent C. difficile infections with fecal microbiota transplant (FMT), according to a study presented online July 12 at the European Congress of Clinical Microbiology & Infectious Diseases.
C. difficile colonization persisted for 3 weeks after FMT in about one-quarter of patients, but it’s not clear whether this is a persistent infection, a newly acquired infection, or partial persistence of a mixed infection, said Elisabeth Terveer, MD, a medical microbiologist at Leiden (the Netherlands) University Medical Center. In addition, “82% of patients with detectable C. diff do not relapse, so it’s absolutely not necessary for a cure,” she said.
Several mechanisms explain why FMT is a highly effective therapy for recurrent C. difficile infections, including restoration of bacterial metabolism in the gut, immune modulation, and direct competition between bacteria, Dr. Terveer said, but it’s less clear whether eradication of C. difficile spores is among these mechanisms.
Between May 2016 and April 2020, the researchers analyzed fecal samples from 84 patients who took vancomycin for at least 4 days before undergoing FMT. The researchers took fecal samples from patients before FMT and 3 weeks after FMT to culture them and the donor samples for presence of C. difficile, and they assessed clinical outcomes at 3 weeks and 6 months after FMT.
After antibiotic treatment but prior to FMT, 19% of patients (n = 16) still had a toxigenic C. difficile culture while the other 81% had a negative culture. None of the donor samples had a positive C. difficile culture. After FMT treatment, five patients who had a positive pre-FMT culture remained positive, and the other 11 were negative. Among the 81% of patients (n = 68) who had a negative culture just before FMT, 22 had a positive culture and 46 had a negative culture after FMT. Overall, 26% of patients post FMT had a positive C. difficile culture, a finding that was 10-fold higher than another study that assessed C. difficile with PCR testing, Dr. Terveer said.
The clinical cure rate after FMT was 94%, and five patients had relapses within 2 months of their FMT. These relapses were more prevalent in patients with a positive C. difficile culture prior to FMT (odds ratio [OR], 7.6; P = .045) and a positive C. difficile culture after FMT (OR, 13.6; P = .016). Still, 82% of patients who had a positive C. difficile culture post FMT remained clinically cured 2 months later.
It’s unclear why 19% of patients had a positive culture after their antibiotic pretreatment prior to FMT, Dr. Terveer said, but it may be because the pretreatment was of such a short duration.
“I think the advice should be: Give a full anti–C. diff antibiotic course to treat the C. diff infection, and then give FMT afterward to restore the microbiota and prevent further relapses,” Dr. Terveer told attendees.
Dimitri Drekonja, MD, chief of the Minneapolis VA Infectious Disease Section, said the findings were not necessarily surprising, but it would have been interesting for the researchers to have conducted DNA sequencing of the patients’ fecal samples post FMT to see what the biological diversity looked like.
“One school of thought has been that you have to repopulate the normal diverse microbiota of the colon” with FMT, and the other “is that you need to get rid of the C. diff that›s there,” Dr. Drekonja, who was not involved in the study, said in an interview. “I think more people think it’s the diverse microbiota because if it’s just getting rid of C. diff, we can get do that with antibiotics – but that gets rid of the other organisms.”
As long as you have a diverse microbiota post FMT, Dr. Drekonja said, then “having a few residual organisms, even if they get magnified in the culture process, is probably not that big a deal.”
But there’s a third school of thought that Dr. Drekonja said he himself falls into: “I don’t really care how it works, just that in well-done trials, it does work.” As long as large, robust, well-blinded trials show that FMT works, “I’m open to all sorts of ideas of what the mechanism is,” he said. “The main thing is that it does or doesn’t work.”
These findings basically reinforce current guidance not to test patients’ stools if they are asymptomatic, Dr. Drekonja said. In the past, clinicians sometimes tested patients’ stool after therapy to ensure the C. difficile was eradicated, regardless of whether the patient had symptoms of infection, he said.
“We’ve since become much more attuned that there are lots of people who have detectable C. diff in their stool without any symptoms,” whether detectable by culture or PCR, Dr. Drekonja said. “Generally, if you’re doing well and you’re not having diarrhea, don’t test, and if someone does test and finds it, pretend you didn’t see the test,” he advised. “This is a big part of diagnostic stewardship, which is: You don’t go testing people who are doing well.”
The Netherlands Donor Feces Bank used in the research is funded by a grant from Vedanta Biosciences. Dr. Drekonja had no disclosures.
Help your patients understand their C. difficile diagnosis by sharing patient education from the AGA GI Patient Center: www.gastro.org/Cdiff.
A version of this article first appeared on Medscape.com.
It’s not necessary to completely eradicate all Clostridioides difficile to successfully treat recurrent C. difficile infections with fecal microbiota transplant (FMT), according to a study presented online July 12 at the European Congress of Clinical Microbiology & Infectious Diseases.
C. difficile colonization persisted for 3 weeks after FMT in about one-quarter of patients, but it’s not clear whether this is a persistent infection, a newly acquired infection, or partial persistence of a mixed infection, said Elisabeth Terveer, MD, a medical microbiologist at Leiden (the Netherlands) University Medical Center. In addition, “82% of patients with detectable C. diff do not relapse, so it’s absolutely not necessary for a cure,” she said.
Several mechanisms explain why FMT is a highly effective therapy for recurrent C. difficile infections, including restoration of bacterial metabolism in the gut, immune modulation, and direct competition between bacteria, Dr. Terveer said, but it’s less clear whether eradication of C. difficile spores is among these mechanisms.
Between May 2016 and April 2020, the researchers analyzed fecal samples from 84 patients who took vancomycin for at least 4 days before undergoing FMT. The researchers took fecal samples from patients before FMT and 3 weeks after FMT to culture them and the donor samples for presence of C. difficile, and they assessed clinical outcomes at 3 weeks and 6 months after FMT.
After antibiotic treatment but prior to FMT, 19% of patients (n = 16) still had a toxigenic C. difficile culture while the other 81% had a negative culture. None of the donor samples had a positive C. difficile culture. After FMT treatment, five patients who had a positive pre-FMT culture remained positive, and the other 11 were negative. Among the 81% of patients (n = 68) who had a negative culture just before FMT, 22 had a positive culture and 46 had a negative culture after FMT. Overall, 26% of patients post FMT had a positive C. difficile culture, a finding that was 10-fold higher than another study that assessed C. difficile with PCR testing, Dr. Terveer said.
The clinical cure rate after FMT was 94%, and five patients had relapses within 2 months of their FMT. These relapses were more prevalent in patients with a positive C. difficile culture prior to FMT (odds ratio [OR], 7.6; P = .045) and a positive C. difficile culture after FMT (OR, 13.6; P = .016). Still, 82% of patients who had a positive C. difficile culture post FMT remained clinically cured 2 months later.
It’s unclear why 19% of patients had a positive culture after their antibiotic pretreatment prior to FMT, Dr. Terveer said, but it may be because the pretreatment was of such a short duration.
“I think the advice should be: Give a full anti–C. diff antibiotic course to treat the C. diff infection, and then give FMT afterward to restore the microbiota and prevent further relapses,” Dr. Terveer told attendees.
Dimitri Drekonja, MD, chief of the Minneapolis VA Infectious Disease Section, said the findings were not necessarily surprising, but it would have been interesting for the researchers to have conducted DNA sequencing of the patients’ fecal samples post FMT to see what the biological diversity looked like.
“One school of thought has been that you have to repopulate the normal diverse microbiota of the colon” with FMT, and the other “is that you need to get rid of the C. diff that›s there,” Dr. Drekonja, who was not involved in the study, said in an interview. “I think more people think it’s the diverse microbiota because if it’s just getting rid of C. diff, we can get do that with antibiotics – but that gets rid of the other organisms.”
As long as you have a diverse microbiota post FMT, Dr. Drekonja said, then “having a few residual organisms, even if they get magnified in the culture process, is probably not that big a deal.”
But there’s a third school of thought that Dr. Drekonja said he himself falls into: “I don’t really care how it works, just that in well-done trials, it does work.” As long as large, robust, well-blinded trials show that FMT works, “I’m open to all sorts of ideas of what the mechanism is,” he said. “The main thing is that it does or doesn’t work.”
These findings basically reinforce current guidance not to test patients’ stools if they are asymptomatic, Dr. Drekonja said. In the past, clinicians sometimes tested patients’ stool after therapy to ensure the C. difficile was eradicated, regardless of whether the patient had symptoms of infection, he said.
“We’ve since become much more attuned that there are lots of people who have detectable C. diff in their stool without any symptoms,” whether detectable by culture or PCR, Dr. Drekonja said. “Generally, if you’re doing well and you’re not having diarrhea, don’t test, and if someone does test and finds it, pretend you didn’t see the test,” he advised. “This is a big part of diagnostic stewardship, which is: You don’t go testing people who are doing well.”
The Netherlands Donor Feces Bank used in the research is funded by a grant from Vedanta Biosciences. Dr. Drekonja had no disclosures.
Help your patients understand their C. difficile diagnosis by sharing patient education from the AGA GI Patient Center: www.gastro.org/Cdiff.
A version of this article first appeared on Medscape.com.
Short sleep is linked to future dementia
, according to a new analysis of data from the Whitehall II cohort study.

Previous work had identified links between short sleep duration and dementia risk, but few studies examined sleep habits long before onset of dementia. Those that did produced inconsistent results, according to Séverine Sabia, PhD, who is a research associate at Inserm (France) and the University College London.
“One potential reason for these inconstancies is the large range of ages of the study populations, and the small number of participants within each sleep duration group. The novelty of our study is to examine this association among almost 8,000 participants with a follow-up of 30 years, using repeated measures of sleep duration starting in midlife to consider sleep duration at specific ages,” Dr. Sabia said in an interview. She presented the research at the 2021 Alzheimer’s Association International Conference.
Those previous studies found a U-shaped association between sleep duration and dementia risk, with lowest risk associated with 7-8 hours of sleep, but greater risk for shorter and longer durations. However, because the studies had follow-up periods shorter than 10 years, they are at greater risk of reverse causation bias. Longer follow-up studies tended to have small sample sizes or to focus on older adults.
The longer follow-up in the current study makes for a more compelling case, said Claire Sexton, DPhil, director of Scientific Programs & Outreach for the Alzheimer’s Association. Observations of short or long sleep closer to the onset of symptoms could just be a warning sign of dementia. “But looking at age 50, age 60 ... if you’re seeing those relationships, then it’s less likely that it is just purely prodromal,” said Dr. Sexton. But it still doesn’t necessarily confirm causation. “It could also be a risk factor,” Dr. Sexton added.
Multifactorial risk
Dr. Sabia also noted that the magnitude of risk was similar to that seen with smoking or obesity, and many factors play a role in dementia risk. “Even if the risk of dementia was 30% higher in those with persistent short sleep duration, in absolute terms, the percentage of those with persistent short duration who developed dementia was 8%, and 6% in those with persistent sleep duration of 7 hours. Dementia is a multifactorial disease, which means that several factors are likely to influence its onset. Sleep duration is one of them, but if a person has poor sleep and does not manage to increase it, there are other important prevention measures. It is important to keep a healthy lifestyle and cardiometabolic measures in the normal range. All together it is likely to be beneficial for brain health in later life,” she said.
Dr. Sexton agreed. “With sleep we’re still trying to tease apart what aspect of sleep is important. Is it the sleep duration? Is it the quality of sleep? Is it certain sleep stages?” she said.
Regardless of sleep’s potential influence on dementia risk, both Dr. Sexton and Dr. Sabia noted the importance of sleep for general health. “These types of problems are very prevalent, so it’s good for people to be aware of them. And then if they notice any problems with their sleep, or any changes, to go and see their health care provider, and to be discussing them, and then to be investigating the cause, and to see whether changes in sleep hygiene and treatments for insomnia could address these sleep problems,” said Dr. Sexton.
Decades of data
During the Whitehall II study, researchers assessed average sleep duration (“How many hours of sleep do you have on an average weeknight?”) six times over 30 years of follow-up. Dr. Sabia’s group extracted self-reported sleep duration data at ages 50, 60, and 70. Short sleep duration was defined as fewer than 5 hours, or 6 hours. Normal sleep duration was defined as 7 hours. Long duration was defined as 8 hours or more.
A questioner during the Q&A period noted that this grouping is a little unusual. Many studies define 7-8 hours as normal. Dr. Sabia answered that they were unable to examine periods of 9 hours or more due to the nature of the data, and the lowest associated risk was found at 7 hours.
The researchers analyzed data from 7,959 participants (33.0% women). At age 50, compared with 7 hours of sleep, 6 or few hours of sleep was associated with a higher risk of dementia over the ensuing 25 years of follow-up (hazard ratio [HR], 1.22; 95% confidence interval [CI], 1.01-1.48). The same was true at age 60 (15 years of follow-up HR, 1.37; 95% CI, 1.10-1.72). There was a trend at age 70 (8 years follow-up; HR, 1.24; 95% CI, 0.98-1.57). For 8 or more hours of sleep, there were trends toward increased risk at age 50 (HR, 1.25; 95% CI, 0.98-1.60). Long sleep at age 60 and 70 was associated with heightened risk, but the confidence intervals were well outside statistical significance.
Twenty percent of participants had persistent short sleep over the course of follow-up, 37% had persistent normal sleep, and 7% had persistent long sleep. Seven percent of participants experienced a change from normal sleep to short sleep, 16% had a change from short sleep to normal sleep, and 13% had a change from normal sleep to long sleep.
Persistent short sleep between age 50 and 70 was associated with a 30% increased risk of dementia (HR, 1.30; 95% CI, 1.00-1.69). There were no statistically significant associations between dementia risk and any of the changing sleep pattern groups.
Dr. Sabia and Dr. Sexton have no relevant financial disclosures.
, according to a new analysis of data from the Whitehall II cohort study.
Previous work had identified links between short sleep duration and dementia risk, but few studies examined sleep habits long before onset of dementia. Those that did produced inconsistent results, according to Séverine Sabia, PhD, who is a research associate at Inserm (France) and the University College London.
“One potential reason for these inconstancies is the large range of ages of the study populations, and the small number of participants within each sleep duration group. The novelty of our study is to examine this association among almost 8,000 participants with a follow-up of 30 years, using repeated measures of sleep duration starting in midlife to consider sleep duration at specific ages,” Dr. Sabia said in an interview. She presented the research at the 2021 Alzheimer’s Association International Conference.
Those previous studies found a U-shaped association between sleep duration and dementia risk, with lowest risk associated with 7-8 hours of sleep, but greater risk for shorter and longer durations. However, because the studies had follow-up periods shorter than 10 years, they are at greater risk of reverse causation bias. Longer follow-up studies tended to have small sample sizes or to focus on older adults.
The longer follow-up in the current study makes for a more compelling case, said Claire Sexton, DPhil, director of Scientific Programs & Outreach for the Alzheimer’s Association. Observations of short or long sleep closer to the onset of symptoms could just be a warning sign of dementia. “But looking at age 50, age 60 ... if you’re seeing those relationships, then it’s less likely that it is just purely prodromal,” said Dr. Sexton. But it still doesn’t necessarily confirm causation. “It could also be a risk factor,” Dr. Sexton added.
Multifactorial risk
Dr. Sabia also noted that the magnitude of risk was similar to that seen with smoking or obesity, and many factors play a role in dementia risk. “Even if the risk of dementia was 30% higher in those with persistent short sleep duration, in absolute terms, the percentage of those with persistent short duration who developed dementia was 8%, and 6% in those with persistent sleep duration of 7 hours. Dementia is a multifactorial disease, which means that several factors are likely to influence its onset. Sleep duration is one of them, but if a person has poor sleep and does not manage to increase it, there are other important prevention measures. It is important to keep a healthy lifestyle and cardiometabolic measures in the normal range. All together it is likely to be beneficial for brain health in later life,” she said.
Dr. Sexton agreed. “With sleep we’re still trying to tease apart what aspect of sleep is important. Is it the sleep duration? Is it the quality of sleep? Is it certain sleep stages?” she said.
Regardless of sleep’s potential influence on dementia risk, both Dr. Sexton and Dr. Sabia noted the importance of sleep for general health. “These types of problems are very prevalent, so it’s good for people to be aware of them. And then if they notice any problems with their sleep, or any changes, to go and see their health care provider, and to be discussing them, and then to be investigating the cause, and to see whether changes in sleep hygiene and treatments for insomnia could address these sleep problems,” said Dr. Sexton.
Decades of data
During the Whitehall II study, researchers assessed average sleep duration (“How many hours of sleep do you have on an average weeknight?”) six times over 30 years of follow-up. Dr. Sabia’s group extracted self-reported sleep duration data at ages 50, 60, and 70. Short sleep duration was defined as fewer than 5 hours, or 6 hours. Normal sleep duration was defined as 7 hours. Long duration was defined as 8 hours or more.
A questioner during the Q&A period noted that this grouping is a little unusual. Many studies define 7-8 hours as normal. Dr. Sabia answered that they were unable to examine periods of 9 hours or more due to the nature of the data, and the lowest associated risk was found at 7 hours.
The researchers analyzed data from 7,959 participants (33.0% women). At age 50, compared with 7 hours of sleep, 6 or few hours of sleep was associated with a higher risk of dementia over the ensuing 25 years of follow-up (hazard ratio [HR], 1.22; 95% confidence interval [CI], 1.01-1.48). The same was true at age 60 (15 years of follow-up HR, 1.37; 95% CI, 1.10-1.72). There was a trend at age 70 (8 years follow-up; HR, 1.24; 95% CI, 0.98-1.57). For 8 or more hours of sleep, there were trends toward increased risk at age 50 (HR, 1.25; 95% CI, 0.98-1.60). Long sleep at age 60 and 70 was associated with heightened risk, but the confidence intervals were well outside statistical significance.
Twenty percent of participants had persistent short sleep over the course of follow-up, 37% had persistent normal sleep, and 7% had persistent long sleep. Seven percent of participants experienced a change from normal sleep to short sleep, 16% had a change from short sleep to normal sleep, and 13% had a change from normal sleep to long sleep.
Persistent short sleep between age 50 and 70 was associated with a 30% increased risk of dementia (HR, 1.30; 95% CI, 1.00-1.69). There were no statistically significant associations between dementia risk and any of the changing sleep pattern groups.
Dr. Sabia and Dr. Sexton have no relevant financial disclosures.
, according to a new analysis of data from the Whitehall II cohort study.
Previous work had identified links between short sleep duration and dementia risk, but few studies examined sleep habits long before onset of dementia. Those that did produced inconsistent results, according to Séverine Sabia, PhD, who is a research associate at Inserm (France) and the University College London.
“One potential reason for these inconstancies is the large range of ages of the study populations, and the small number of participants within each sleep duration group. The novelty of our study is to examine this association among almost 8,000 participants with a follow-up of 30 years, using repeated measures of sleep duration starting in midlife to consider sleep duration at specific ages,” Dr. Sabia said in an interview. She presented the research at the 2021 Alzheimer’s Association International Conference.
Those previous studies found a U-shaped association between sleep duration and dementia risk, with lowest risk associated with 7-8 hours of sleep, but greater risk for shorter and longer durations. However, because the studies had follow-up periods shorter than 10 years, they are at greater risk of reverse causation bias. Longer follow-up studies tended to have small sample sizes or to focus on older adults.
The longer follow-up in the current study makes for a more compelling case, said Claire Sexton, DPhil, director of Scientific Programs & Outreach for the Alzheimer’s Association. Observations of short or long sleep closer to the onset of symptoms could just be a warning sign of dementia. “But looking at age 50, age 60 ... if you’re seeing those relationships, then it’s less likely that it is just purely prodromal,” said Dr. Sexton. But it still doesn’t necessarily confirm causation. “It could also be a risk factor,” Dr. Sexton added.
Multifactorial risk
Dr. Sabia also noted that the magnitude of risk was similar to that seen with smoking or obesity, and many factors play a role in dementia risk. “Even if the risk of dementia was 30% higher in those with persistent short sleep duration, in absolute terms, the percentage of those with persistent short duration who developed dementia was 8%, and 6% in those with persistent sleep duration of 7 hours. Dementia is a multifactorial disease, which means that several factors are likely to influence its onset. Sleep duration is one of them, but if a person has poor sleep and does not manage to increase it, there are other important prevention measures. It is important to keep a healthy lifestyle and cardiometabolic measures in the normal range. All together it is likely to be beneficial for brain health in later life,” she said.
Dr. Sexton agreed. “With sleep we’re still trying to tease apart what aspect of sleep is important. Is it the sleep duration? Is it the quality of sleep? Is it certain sleep stages?” she said.
Regardless of sleep’s potential influence on dementia risk, both Dr. Sexton and Dr. Sabia noted the importance of sleep for general health. “These types of problems are very prevalent, so it’s good for people to be aware of them. And then if they notice any problems with their sleep, or any changes, to go and see their health care provider, and to be discussing them, and then to be investigating the cause, and to see whether changes in sleep hygiene and treatments for insomnia could address these sleep problems,” said Dr. Sexton.
Decades of data
During the Whitehall II study, researchers assessed average sleep duration (“How many hours of sleep do you have on an average weeknight?”) six times over 30 years of follow-up. Dr. Sabia’s group extracted self-reported sleep duration data at ages 50, 60, and 70. Short sleep duration was defined as fewer than 5 hours, or 6 hours. Normal sleep duration was defined as 7 hours. Long duration was defined as 8 hours or more.
A questioner during the Q&A period noted that this grouping is a little unusual. Many studies define 7-8 hours as normal. Dr. Sabia answered that they were unable to examine periods of 9 hours or more due to the nature of the data, and the lowest associated risk was found at 7 hours.
The researchers analyzed data from 7,959 participants (33.0% women). At age 50, compared with 7 hours of sleep, 6 or few hours of sleep was associated with a higher risk of dementia over the ensuing 25 years of follow-up (hazard ratio [HR], 1.22; 95% confidence interval [CI], 1.01-1.48). The same was true at age 60 (15 years of follow-up HR, 1.37; 95% CI, 1.10-1.72). There was a trend at age 70 (8 years follow-up; HR, 1.24; 95% CI, 0.98-1.57). For 8 or more hours of sleep, there were trends toward increased risk at age 50 (HR, 1.25; 95% CI, 0.98-1.60). Long sleep at age 60 and 70 was associated with heightened risk, but the confidence intervals were well outside statistical significance.
Twenty percent of participants had persistent short sleep over the course of follow-up, 37% had persistent normal sleep, and 7% had persistent long sleep. Seven percent of participants experienced a change from normal sleep to short sleep, 16% had a change from short sleep to normal sleep, and 13% had a change from normal sleep to long sleep.
Persistent short sleep between age 50 and 70 was associated with a 30% increased risk of dementia (HR, 1.30; 95% CI, 1.00-1.69). There were no statistically significant associations between dementia risk and any of the changing sleep pattern groups.
Dr. Sabia and Dr. Sexton have no relevant financial disclosures.
FROM AAIC 2021
DOACs best aspirin after ventricular ablation: STROKE-VT
Catheter ablation has been around a lot longer for ventricular arrhythmia than for atrial fibrillation, but far less is settled about what antithrombotic therapy should follow ventricular ablations, as there have been no big, randomized trials for guidance.
But the evidence base grew stronger this week, and it favors postprocedure treatment with a direct oral anticoagulant (DOAC) over antiplatelet therapy with aspirin for patients undergoing radiofrequency (RF) ablation to treat left ventricular (LV) arrhythmias.
The 30-day risk for ischemic stroke or transient ischemia attack (TIA) was sharply higher for patients who took daily aspirin after RF ablation for ventricular tachycardia (VT) or premature ventricular contractions (PVC) in a multicenter randomized trial.
Those of its 246 patients who received aspirin were also far more likely to show asymptomatic lesions on cerebral MRI scans performed both 24 hours and 30 days after the procedure.
The findings show the importance of DOAC therapy after ventricular ablation procedures, a setting for which there are no evidence-based guidelines, “to mitigate the risk of systemic thromboembolic events,” said Dhanunjaya Lakkireddy, MD, Kansas City Heart Rhythm Institute, Overland Park. He spoke at a media presentation on the trial, called STROKE-VT, during the Heart Rhythm Society 2021 Scientific Sessions, held virtually and on-site in Boston.
The risk for stroke and TIA went up in association with several procedural issues, including some that operators might be able to change in order to reach for better outcomes, Dr. Lakkireddy observed.
“Prolonged radiofrequency ablation times, especially in those with low left ventricle ejection fractions, are definitely higher risk,” as are procedures that involved the retrograde transaortic approach for advancing the ablation catheter, rather than a trans-septal approach.
The retrograde transaortic approach should be avoided in such procedures, “whenever it can be avoided,” said Dr. Lakkireddy, who formally presented STROKE-VT at the HRS sessions and is lead author on its report published about the same time in JACC: Clinical Electrophysiology.
The trial has limitations, but “it’s a very important study, and I think that this could become our standard of care for managing anticoagulation after VT and PVC left-sided ablations,” Mina K. Chung, MD, Cleveland Clinic, said as an invited discussant after Dr. Lakkireddy’s presentation.
How patients are treated with antithrombotics after ventricular ablations can vary widely, sometimes based on the operator’s “subjective feeling of how extensive the ablation is,” Christine M. Albert, MD, MPH, Cedars-Sinai Medical Center, Los Angeles, not involved in the study, said during the STROKE-VT media briefing.
That’s consistent with the guidelines, which propose oral anticoagulation therapy after more extensive ventricular ablations and antiplatelets when the ablation is more limited – based more on consensus than firm evidence – as described by Jeffrey R. Winterfield, MD, Medical University of South Carolina, Charleston, and Usha Tedrow, MD, MSc, Brigham and Women’s Hospital, Boston, in an accompanying editorial.
“This is really the first randomized trial data, that I know of, that we have on this. So I do think it will be guideline-influencing,” Dr. Albert said.
“This should change practice,” agreed Jonathan P. Piccini, MD, MHS, Duke University, Durham, N.C., also not part of STROKE-VT. “A lot of evidence in the trial is consistent and provides a compelling story, not to mention that, in my opinion, the study probably underestimates the value of DOACs,” he told this news organization.
That’s because patients assigned to DOACs had far longer ablation times, “so their risk was even greater than in the aspirin arm,” Dr. Piccini said. Ablation times averaged 2,095 seconds in the DOAC group, compared with only 1,708 seconds in the aspirin group, probably because the preponderance of VT over PVC ablations for those getting a DOAC was even greater in the aspirin group.
Of the 246 patients assigned to either aspirin or a DOAC, usually a factor Xa inhibitor, 75% had undergone VT ablation and the remainder ablation for PVCs. Their mean age was 60 years and only 18% were women. None had experienced a cerebrovascular event in the previous 3 months.
The 30-day odds ratio for TIA or ischemic stroke in patients who received aspirin, compared with a DOAC, was 12.6 (95% confidence interval, 4.10-39.11; P < .001).
The corresponding OR for asymptomatic cerebral lesions by MRI at 24 hours was 2.15 (95% CI, 1.02-4.54; P = .04) and at 30 days was 3.48 (95% CI, 1.38-8.80; P = .008).
The rate of stroke or TIA was similar in patients who underwent ablation for VT and for PVCs (14% vs. 16%, respectively; P = .70). There were fewer asymptomatic cerebrovascular events by MRI at 24 hours for those undergoing VT ablations (14.7% and 25.8%, respectively; P = .046); but difference between rates attenuated by 30 days (11.4% and 14.5%, respectively; P = .52).
The OR for TIA or stroke associated with the retrograde transaortic approach, performed in about 40% of the patients, compared with the trans-septal approach in the remainder was 2.60 (95% CI, 1.06-6.37; P = .04).
“The study tells us it’s safe and indeed preferable to anticoagulate after an ablation procedure. But the more important finding, perhaps, wasn’t the one related to the core hypothesis. And that was the effect of retrograde access,” Paul A. Friedman, MD, Mayo Clinic, Rochester, Minn., said as an invited discussant after Dr. Lakkireddy’s formal presentation of the trial.
Whether a ventricular ablation is performed using the retrograde transaortic or trans-septal approach often depends on the location of the ablation targets in the left ventricle. But in some cases it’s a matter of operator preference, Dr. Piccini observed.
“There are some situations where, really, it is better to do retrograde aortic, and there are some cases that are better to do trans-septal. But now there’s going to be a higher burden of proof,” he said. Given the findings of STROKE-VT, operators may need to consider that a ventricular ablation procedure that can be done by the trans-septal route perhaps ought to be consistently done that way.
Dr. Lakkireddy discloses financial relationships with Boston Scientific, Biosense Webster, Janssen Pharmaceuticals, and more. Dr. Chung had “nothing relevant to disclose.” Dr. Piccini discloses receiving honoraria or speaking or consulting fees from Sanofi, Abbott, ARCA Biopharma, Medtronic, Philips, Biotronik, Allergan, LivaNova, and Myokardia; and research in conjunction with Bayer Healthcare, Abbott, Boston Scientific, and Philips. Dr. Friedman discloses conducting research in conjunction with Medtronic and Abbott; holding intellectual property rights with AliveCor, Inference, Medicool, Eko, and Anumana; and receiving honoraria or speaking or consulting fees from Boston Scientific. Dr. Winterfield and Dr. Tedrow had no disclosures.
A version of this article first appeared on Medscape.com.
Catheter ablation has been around a lot longer for ventricular arrhythmia than for atrial fibrillation, but far less is settled about what antithrombotic therapy should follow ventricular ablations, as there have been no big, randomized trials for guidance.
But the evidence base grew stronger this week, and it favors postprocedure treatment with a direct oral anticoagulant (DOAC) over antiplatelet therapy with aspirin for patients undergoing radiofrequency (RF) ablation to treat left ventricular (LV) arrhythmias.
The 30-day risk for ischemic stroke or transient ischemia attack (TIA) was sharply higher for patients who took daily aspirin after RF ablation for ventricular tachycardia (VT) or premature ventricular contractions (PVC) in a multicenter randomized trial.
Those of its 246 patients who received aspirin were also far more likely to show asymptomatic lesions on cerebral MRI scans performed both 24 hours and 30 days after the procedure.
The findings show the importance of DOAC therapy after ventricular ablation procedures, a setting for which there are no evidence-based guidelines, “to mitigate the risk of systemic thromboembolic events,” said Dhanunjaya Lakkireddy, MD, Kansas City Heart Rhythm Institute, Overland Park. He spoke at a media presentation on the trial, called STROKE-VT, during the Heart Rhythm Society 2021 Scientific Sessions, held virtually and on-site in Boston.
The risk for stroke and TIA went up in association with several procedural issues, including some that operators might be able to change in order to reach for better outcomes, Dr. Lakkireddy observed.
“Prolonged radiofrequency ablation times, especially in those with low left ventricle ejection fractions, are definitely higher risk,” as are procedures that involved the retrograde transaortic approach for advancing the ablation catheter, rather than a trans-septal approach.
The retrograde transaortic approach should be avoided in such procedures, “whenever it can be avoided,” said Dr. Lakkireddy, who formally presented STROKE-VT at the HRS sessions and is lead author on its report published about the same time in JACC: Clinical Electrophysiology.
The trial has limitations, but “it’s a very important study, and I think that this could become our standard of care for managing anticoagulation after VT and PVC left-sided ablations,” Mina K. Chung, MD, Cleveland Clinic, said as an invited discussant after Dr. Lakkireddy’s presentation.
How patients are treated with antithrombotics after ventricular ablations can vary widely, sometimes based on the operator’s “subjective feeling of how extensive the ablation is,” Christine M. Albert, MD, MPH, Cedars-Sinai Medical Center, Los Angeles, not involved in the study, said during the STROKE-VT media briefing.
That’s consistent with the guidelines, which propose oral anticoagulation therapy after more extensive ventricular ablations and antiplatelets when the ablation is more limited – based more on consensus than firm evidence – as described by Jeffrey R. Winterfield, MD, Medical University of South Carolina, Charleston, and Usha Tedrow, MD, MSc, Brigham and Women’s Hospital, Boston, in an accompanying editorial.
“This is really the first randomized trial data, that I know of, that we have on this. So I do think it will be guideline-influencing,” Dr. Albert said.
“This should change practice,” agreed Jonathan P. Piccini, MD, MHS, Duke University, Durham, N.C., also not part of STROKE-VT. “A lot of evidence in the trial is consistent and provides a compelling story, not to mention that, in my opinion, the study probably underestimates the value of DOACs,” he told this news organization.
That’s because patients assigned to DOACs had far longer ablation times, “so their risk was even greater than in the aspirin arm,” Dr. Piccini said. Ablation times averaged 2,095 seconds in the DOAC group, compared with only 1,708 seconds in the aspirin group, probably because the preponderance of VT over PVC ablations for those getting a DOAC was even greater in the aspirin group.
Of the 246 patients assigned to either aspirin or a DOAC, usually a factor Xa inhibitor, 75% had undergone VT ablation and the remainder ablation for PVCs. Their mean age was 60 years and only 18% were women. None had experienced a cerebrovascular event in the previous 3 months.
The 30-day odds ratio for TIA or ischemic stroke in patients who received aspirin, compared with a DOAC, was 12.6 (95% confidence interval, 4.10-39.11; P < .001).
The corresponding OR for asymptomatic cerebral lesions by MRI at 24 hours was 2.15 (95% CI, 1.02-4.54; P = .04) and at 30 days was 3.48 (95% CI, 1.38-8.80; P = .008).
The rate of stroke or TIA was similar in patients who underwent ablation for VT and for PVCs (14% vs. 16%, respectively; P = .70). There were fewer asymptomatic cerebrovascular events by MRI at 24 hours for those undergoing VT ablations (14.7% and 25.8%, respectively; P = .046); but difference between rates attenuated by 30 days (11.4% and 14.5%, respectively; P = .52).
The OR for TIA or stroke associated with the retrograde transaortic approach, performed in about 40% of the patients, compared with the trans-septal approach in the remainder was 2.60 (95% CI, 1.06-6.37; P = .04).
“The study tells us it’s safe and indeed preferable to anticoagulate after an ablation procedure. But the more important finding, perhaps, wasn’t the one related to the core hypothesis. And that was the effect of retrograde access,” Paul A. Friedman, MD, Mayo Clinic, Rochester, Minn., said as an invited discussant after Dr. Lakkireddy’s formal presentation of the trial.
Whether a ventricular ablation is performed using the retrograde transaortic or trans-septal approach often depends on the location of the ablation targets in the left ventricle. But in some cases it’s a matter of operator preference, Dr. Piccini observed.
“There are some situations where, really, it is better to do retrograde aortic, and there are some cases that are better to do trans-septal. But now there’s going to be a higher burden of proof,” he said. Given the findings of STROKE-VT, operators may need to consider that a ventricular ablation procedure that can be done by the trans-septal route perhaps ought to be consistently done that way.
Dr. Lakkireddy discloses financial relationships with Boston Scientific, Biosense Webster, Janssen Pharmaceuticals, and more. Dr. Chung had “nothing relevant to disclose.” Dr. Piccini discloses receiving honoraria or speaking or consulting fees from Sanofi, Abbott, ARCA Biopharma, Medtronic, Philips, Biotronik, Allergan, LivaNova, and Myokardia; and research in conjunction with Bayer Healthcare, Abbott, Boston Scientific, and Philips. Dr. Friedman discloses conducting research in conjunction with Medtronic and Abbott; holding intellectual property rights with AliveCor, Inference, Medicool, Eko, and Anumana; and receiving honoraria or speaking or consulting fees from Boston Scientific. Dr. Winterfield and Dr. Tedrow had no disclosures.
A version of this article first appeared on Medscape.com.
Catheter ablation has been around a lot longer for ventricular arrhythmia than for atrial fibrillation, but far less is settled about what antithrombotic therapy should follow ventricular ablations, as there have been no big, randomized trials for guidance.
But the evidence base grew stronger this week, and it favors postprocedure treatment with a direct oral anticoagulant (DOAC) over antiplatelet therapy with aspirin for patients undergoing radiofrequency (RF) ablation to treat left ventricular (LV) arrhythmias.
The 30-day risk for ischemic stroke or transient ischemia attack (TIA) was sharply higher for patients who took daily aspirin after RF ablation for ventricular tachycardia (VT) or premature ventricular contractions (PVC) in a multicenter randomized trial.
Those of its 246 patients who received aspirin were also far more likely to show asymptomatic lesions on cerebral MRI scans performed both 24 hours and 30 days after the procedure.
The findings show the importance of DOAC therapy after ventricular ablation procedures, a setting for which there are no evidence-based guidelines, “to mitigate the risk of systemic thromboembolic events,” said Dhanunjaya Lakkireddy, MD, Kansas City Heart Rhythm Institute, Overland Park. He spoke at a media presentation on the trial, called STROKE-VT, during the Heart Rhythm Society 2021 Scientific Sessions, held virtually and on-site in Boston.
The risk for stroke and TIA went up in association with several procedural issues, including some that operators might be able to change in order to reach for better outcomes, Dr. Lakkireddy observed.
“Prolonged radiofrequency ablation times, especially in those with low left ventricle ejection fractions, are definitely higher risk,” as are procedures that involved the retrograde transaortic approach for advancing the ablation catheter, rather than a trans-septal approach.
The retrograde transaortic approach should be avoided in such procedures, “whenever it can be avoided,” said Dr. Lakkireddy, who formally presented STROKE-VT at the HRS sessions and is lead author on its report published about the same time in JACC: Clinical Electrophysiology.
The trial has limitations, but “it’s a very important study, and I think that this could become our standard of care for managing anticoagulation after VT and PVC left-sided ablations,” Mina K. Chung, MD, Cleveland Clinic, said as an invited discussant after Dr. Lakkireddy’s presentation.
How patients are treated with antithrombotics after ventricular ablations can vary widely, sometimes based on the operator’s “subjective feeling of how extensive the ablation is,” Christine M. Albert, MD, MPH, Cedars-Sinai Medical Center, Los Angeles, not involved in the study, said during the STROKE-VT media briefing.
That’s consistent with the guidelines, which propose oral anticoagulation therapy after more extensive ventricular ablations and antiplatelets when the ablation is more limited – based more on consensus than firm evidence – as described by Jeffrey R. Winterfield, MD, Medical University of South Carolina, Charleston, and Usha Tedrow, MD, MSc, Brigham and Women’s Hospital, Boston, in an accompanying editorial.
“This is really the first randomized trial data, that I know of, that we have on this. So I do think it will be guideline-influencing,” Dr. Albert said.
“This should change practice,” agreed Jonathan P. Piccini, MD, MHS, Duke University, Durham, N.C., also not part of STROKE-VT. “A lot of evidence in the trial is consistent and provides a compelling story, not to mention that, in my opinion, the study probably underestimates the value of DOACs,” he told this news organization.
That’s because patients assigned to DOACs had far longer ablation times, “so their risk was even greater than in the aspirin arm,” Dr. Piccini said. Ablation times averaged 2,095 seconds in the DOAC group, compared with only 1,708 seconds in the aspirin group, probably because the preponderance of VT over PVC ablations for those getting a DOAC was even greater in the aspirin group.
Of the 246 patients assigned to either aspirin or a DOAC, usually a factor Xa inhibitor, 75% had undergone VT ablation and the remainder ablation for PVCs. Their mean age was 60 years and only 18% were women. None had experienced a cerebrovascular event in the previous 3 months.
The 30-day odds ratio for TIA or ischemic stroke in patients who received aspirin, compared with a DOAC, was 12.6 (95% confidence interval, 4.10-39.11; P < .001).
The corresponding OR for asymptomatic cerebral lesions by MRI at 24 hours was 2.15 (95% CI, 1.02-4.54; P = .04) and at 30 days was 3.48 (95% CI, 1.38-8.80; P = .008).
The rate of stroke or TIA was similar in patients who underwent ablation for VT and for PVCs (14% vs. 16%, respectively; P = .70). There were fewer asymptomatic cerebrovascular events by MRI at 24 hours for those undergoing VT ablations (14.7% and 25.8%, respectively; P = .046); but difference between rates attenuated by 30 days (11.4% and 14.5%, respectively; P = .52).
The OR for TIA or stroke associated with the retrograde transaortic approach, performed in about 40% of the patients, compared with the trans-septal approach in the remainder was 2.60 (95% CI, 1.06-6.37; P = .04).
“The study tells us it’s safe and indeed preferable to anticoagulate after an ablation procedure. But the more important finding, perhaps, wasn’t the one related to the core hypothesis. And that was the effect of retrograde access,” Paul A. Friedman, MD, Mayo Clinic, Rochester, Minn., said as an invited discussant after Dr. Lakkireddy’s formal presentation of the trial.
Whether a ventricular ablation is performed using the retrograde transaortic or trans-septal approach often depends on the location of the ablation targets in the left ventricle. But in some cases it’s a matter of operator preference, Dr. Piccini observed.
“There are some situations where, really, it is better to do retrograde aortic, and there are some cases that are better to do trans-septal. But now there’s going to be a higher burden of proof,” he said. Given the findings of STROKE-VT, operators may need to consider that a ventricular ablation procedure that can be done by the trans-septal route perhaps ought to be consistently done that way.
Dr. Lakkireddy discloses financial relationships with Boston Scientific, Biosense Webster, Janssen Pharmaceuticals, and more. Dr. Chung had “nothing relevant to disclose.” Dr. Piccini discloses receiving honoraria or speaking or consulting fees from Sanofi, Abbott, ARCA Biopharma, Medtronic, Philips, Biotronik, Allergan, LivaNova, and Myokardia; and research in conjunction with Bayer Healthcare, Abbott, Boston Scientific, and Philips. Dr. Friedman discloses conducting research in conjunction with Medtronic and Abbott; holding intellectual property rights with AliveCor, Inference, Medicool, Eko, and Anumana; and receiving honoraria or speaking or consulting fees from Boston Scientific. Dr. Winterfield and Dr. Tedrow had no disclosures.
A version of this article first appeared on Medscape.com.
Inflammatory diet is linked to dementia
according to a new analysis of longitudinal data from the Framingham Heart Study Offspring Cohort.

The lack of an association with Alzheimer’s disease was a surprise because amyloid-beta prompts microglia and astrocytes to release markers of systemic inflammation, according to Debora Melo van Lent, PhD, who is a postdoctoral fellow at the University of Texas Health San Antonio – Glenn Biggs Institute for Alzheimer’s and Neurodegenerative Diseases. “We expected to see a relationship between higher DII scores and an increased risk for incident Alzheimer’s disease,” said Dr. Melo van Lent, who presented the findings at the 2021 Alzheimer’s Association International Conference.
Dr. Melo van Lent added that the most likely explanation is that the study was underpowered to produce a positive association, and the team is conducting further study in a larger population.
A modifiable risk factor
The study is the first to look at all-cause dementia and Alzheimer’s disease dementia and their association with DII, Dr. Melo van Lent said.
“As diet is a modifiable risk factor, we can actually do something about it. If we take a closer look at five components of the DII which are most anti-inflammatory, these components are present in green leafy vegetables, vegetables, fruit, soy, whole grains, and green and black tea. Most of these components are included in the Mediterranean diet. When we look at the three most proinflammatory components, they are present in high caloric products; such as butter or margarine, pastries and sweets, fried snacks, and red or processed meat. These components are present in ‘Western diets,’ which are discouraged,” said Dr. Melo van Lent.
The researchers analyzed data from 1,486 participants who were free of dementia, stroke, or other neurologic diseases at baseline. They analyzed DII scores both in a continuous range and divided into quartiles, using the first quartile as a reference.
The mean age of participants was 69 years, and 53% were women. During follow-up, 11.3% developed AD dementia, and 14.8% developed non-AD dementia.
In the continuous model, DII was associated with increased risk of all-cause dementia after adjusting for age, sex, APOE E4 status, body mass index, smoking, physical activity index score, total energy intake, lipid-lowering medications, and total cholesterol to HDL cholesterol ratio (hazard ratio, 1.18; P =.001). In the quartile analysis, after adjustments, compared with quartile 1, there was an increased risk of all-cause dementia for those in quartile 3 (HR, 1.69; P =.020) and quartile 4 (HR, 1.84; P =.013).
In the continuous analysis, after adjustments, there was an association between DII score and Alzheimer’s dementia (HR, 1.15; P =.020). In the quartile analysis, no associations were significant, though there was a trend of quartile 4 versus quartile 1 (HR, 1.65; P =.077).
The researchers found no significant interactions between higher DII scores and sex, the APOE E4 allele, or physical activity with respect to all-cause dementia or Alzheimer’s dementia.
Intertwined variables
The results were interesting, but cause and effect relationships can be difficult to tease out from such a study, according to Claire Sexton, DPhil, director of scientific programs and outreach at the Alzheimer’s Association, who was asked to comment on the study. Dr. Sexton noted that individuals who eat well are more likely to have energy to exercise, which could in turn help them to sleep better, and all of those factors could be involved in reducing dementia risk. “They’re all kind of intertwined. So in this study, they were taking into account physical activity, but they can’t take into account every single variable. It’s important for them to be followed up by randomized control trials.”
Dr. Sexton also referenced the U.S. Pointer study being conducted by the Alzheimer’s Association, which is examining various interventions related to diet, physical activity, and cognitive stimulation. “Whether intervening and improving people’s health behaviors then goes on to reduce their risk for dementia is a key question. We still need more results from studies to be reporting out before we get definitive answers,” she said.
The study was funded by the ASPEN Rhoads Research Foundation. Dr. Melo van Lent and Dr. Sexton have no relevant financial disclosures.
according to a new analysis of longitudinal data from the Framingham Heart Study Offspring Cohort.
The lack of an association with Alzheimer’s disease was a surprise because amyloid-beta prompts microglia and astrocytes to release markers of systemic inflammation, according to Debora Melo van Lent, PhD, who is a postdoctoral fellow at the University of Texas Health San Antonio – Glenn Biggs Institute for Alzheimer’s and Neurodegenerative Diseases. “We expected to see a relationship between higher DII scores and an increased risk for incident Alzheimer’s disease,” said Dr. Melo van Lent, who presented the findings at the 2021 Alzheimer’s Association International Conference.
Dr. Melo van Lent added that the most likely explanation is that the study was underpowered to produce a positive association, and the team is conducting further study in a larger population.
A modifiable risk factor
The study is the first to look at all-cause dementia and Alzheimer’s disease dementia and their association with DII, Dr. Melo van Lent said.
“As diet is a modifiable risk factor, we can actually do something about it. If we take a closer look at five components of the DII which are most anti-inflammatory, these components are present in green leafy vegetables, vegetables, fruit, soy, whole grains, and green and black tea. Most of these components are included in the Mediterranean diet. When we look at the three most proinflammatory components, they are present in high caloric products; such as butter or margarine, pastries and sweets, fried snacks, and red or processed meat. These components are present in ‘Western diets,’ which are discouraged,” said Dr. Melo van Lent.
The researchers analyzed data from 1,486 participants who were free of dementia, stroke, or other neurologic diseases at baseline. They analyzed DII scores both in a continuous range and divided into quartiles, using the first quartile as a reference.
The mean age of participants was 69 years, and 53% were women. During follow-up, 11.3% developed AD dementia, and 14.8% developed non-AD dementia.
In the continuous model, DII was associated with increased risk of all-cause dementia after adjusting for age, sex, APOE E4 status, body mass index, smoking, physical activity index score, total energy intake, lipid-lowering medications, and total cholesterol to HDL cholesterol ratio (hazard ratio, 1.18; P =.001). In the quartile analysis, after adjustments, compared with quartile 1, there was an increased risk of all-cause dementia for those in quartile 3 (HR, 1.69; P =.020) and quartile 4 (HR, 1.84; P =.013).
In the continuous analysis, after adjustments, there was an association between DII score and Alzheimer’s dementia (HR, 1.15; P =.020). In the quartile analysis, no associations were significant, though there was a trend of quartile 4 versus quartile 1 (HR, 1.65; P =.077).
The researchers found no significant interactions between higher DII scores and sex, the APOE E4 allele, or physical activity with respect to all-cause dementia or Alzheimer’s dementia.
Intertwined variables
The results were interesting, but cause and effect relationships can be difficult to tease out from such a study, according to Claire Sexton, DPhil, director of scientific programs and outreach at the Alzheimer’s Association, who was asked to comment on the study. Dr. Sexton noted that individuals who eat well are more likely to have energy to exercise, which could in turn help them to sleep better, and all of those factors could be involved in reducing dementia risk. “They’re all kind of intertwined. So in this study, they were taking into account physical activity, but they can’t take into account every single variable. It’s important for them to be followed up by randomized control trials.”
Dr. Sexton also referenced the U.S. Pointer study being conducted by the Alzheimer’s Association, which is examining various interventions related to diet, physical activity, and cognitive stimulation. “Whether intervening and improving people’s health behaviors then goes on to reduce their risk for dementia is a key question. We still need more results from studies to be reporting out before we get definitive answers,” she said.
The study was funded by the ASPEN Rhoads Research Foundation. Dr. Melo van Lent and Dr. Sexton have no relevant financial disclosures.
according to a new analysis of longitudinal data from the Framingham Heart Study Offspring Cohort.
The lack of an association with Alzheimer’s disease was a surprise because amyloid-beta prompts microglia and astrocytes to release markers of systemic inflammation, according to Debora Melo van Lent, PhD, who is a postdoctoral fellow at the University of Texas Health San Antonio – Glenn Biggs Institute for Alzheimer’s and Neurodegenerative Diseases. “We expected to see a relationship between higher DII scores and an increased risk for incident Alzheimer’s disease,” said Dr. Melo van Lent, who presented the findings at the 2021 Alzheimer’s Association International Conference.
Dr. Melo van Lent added that the most likely explanation is that the study was underpowered to produce a positive association, and the team is conducting further study in a larger population.
A modifiable risk factor
The study is the first to look at all-cause dementia and Alzheimer’s disease dementia and their association with DII, Dr. Melo van Lent said.
“As diet is a modifiable risk factor, we can actually do something about it. If we take a closer look at five components of the DII which are most anti-inflammatory, these components are present in green leafy vegetables, vegetables, fruit, soy, whole grains, and green and black tea. Most of these components are included in the Mediterranean diet. When we look at the three most proinflammatory components, they are present in high caloric products; such as butter or margarine, pastries and sweets, fried snacks, and red or processed meat. These components are present in ‘Western diets,’ which are discouraged,” said Dr. Melo van Lent.
The researchers analyzed data from 1,486 participants who were free of dementia, stroke, or other neurologic diseases at baseline. They analyzed DII scores both in a continuous range and divided into quartiles, using the first quartile as a reference.
The mean age of participants was 69 years, and 53% were women. During follow-up, 11.3% developed AD dementia, and 14.8% developed non-AD dementia.
In the continuous model, DII was associated with increased risk of all-cause dementia after adjusting for age, sex, APOE E4 status, body mass index, smoking, physical activity index score, total energy intake, lipid-lowering medications, and total cholesterol to HDL cholesterol ratio (hazard ratio, 1.18; P =.001). In the quartile analysis, after adjustments, compared with quartile 1, there was an increased risk of all-cause dementia for those in quartile 3 (HR, 1.69; P =.020) and quartile 4 (HR, 1.84; P =.013).
In the continuous analysis, after adjustments, there was an association between DII score and Alzheimer’s dementia (HR, 1.15; P =.020). In the quartile analysis, no associations were significant, though there was a trend of quartile 4 versus quartile 1 (HR, 1.65; P =.077).
The researchers found no significant interactions between higher DII scores and sex, the APOE E4 allele, or physical activity with respect to all-cause dementia or Alzheimer’s dementia.
Intertwined variables
The results were interesting, but cause and effect relationships can be difficult to tease out from such a study, according to Claire Sexton, DPhil, director of scientific programs and outreach at the Alzheimer’s Association, who was asked to comment on the study. Dr. Sexton noted that individuals who eat well are more likely to have energy to exercise, which could in turn help them to sleep better, and all of those factors could be involved in reducing dementia risk. “They’re all kind of intertwined. So in this study, they were taking into account physical activity, but they can’t take into account every single variable. It’s important for them to be followed up by randomized control trials.”
Dr. Sexton also referenced the U.S. Pointer study being conducted by the Alzheimer’s Association, which is examining various interventions related to diet, physical activity, and cognitive stimulation. “Whether intervening and improving people’s health behaviors then goes on to reduce their risk for dementia is a key question. We still need more results from studies to be reporting out before we get definitive answers,” she said.
The study was funded by the ASPEN Rhoads Research Foundation. Dr. Melo van Lent and Dr. Sexton have no relevant financial disclosures.
FROM AAIC 2021
Alzheimer’s disease plasma biomarkers may be nuanced
Such tests are likely to be widely available in the near future.

But work remains to be done to translate findings from academic studies to the more general population. A key consideration is that plasma levels of these biomarkers could be affected by other conditions, which could in turn skew test results, according to Michelle Mielke, PhD, who spoke on the topic at the 2021 Alzheimer’s Association International Conference.
“The markers, which we’ve published on as well, look really promising. But they have primarily been looked at in more specialty clinics or memory clinics, and have not been examined in the general community. The goal of this presentation was really just to take a look at this in the community, in older individuals that have multiple comorbidities, and to understand what factors might affect the levels of these markers. Because as we do go forward and develop cut points, we are going to have to consider these aspects,” said Dr. Mielke in an interview. She is a professor of epidemiology and neurology at the Mayo Clinic in Rochester, Minn.
Case in point
To illustrate the point, Dr. Mielke presented data from her group, which analyzed P-tau 181 and P-tau 217 data from 1,329 Mayo clinic patients. Of that total, 1,161 were cognitively unimpaired (CU), 153 had mild cognitive impairment (MCI), and 15 had dementia. The median age was 67, 55% were male, and 26% had the APOE e4 allele.
After adjustment for age and sex, there were statistically significantly elevated levels of both biomarkers among patients who had tested positive for amyloid and patients who had had a stroke or myocardial infarction, and in the presence of chronic kidney disease (CKD). There also was a trend towards an increase of biomarker levels with increasing body mass index. The differences remained even after the analysis was restricted to individuals who were amyloid negative.
The researchers then looked more closely at the impact of CKD, stroke, and MI on P-tau cut points and the ability to predict abnormal amyloid positron emission tomography (PET) scans. They defined an abnormal range as 1.96 standard deviation units beyond the mean among amyloid-negative individuals who are cognitively impaired. They excluded subjects with those risk factors and then established new cut points in the absence of the factors. The approach led to a significant change for the cutoff of P-tau 181 values, from 1.57 pg/mL or greater for individuals without stroke, MI, or CKD, and 1.75 pg/mL or greater for individuals with one such factor. There was little difference in the cutoff value for P-tau 217, from 0.25 pg/mL to 0.26 pg/mL.
Among people without a history of stroke, MI, or CKD, a P-tau 181 cutoff of 1.57 pg/mL or greater had an area under the receiving operating characteristic (AUROC) value of 0.717 (95% confidence interval, 0.691-0.744), compared with an AUROC of 0.687 (95% CI, 0.662-0.712) at a cutoff of 1.75 pg/mL or greater among people with those conditions. For P-tau 217, the values were 0.737 pg/mL (95% CI, 0.712-0.762) and 0.724 pg/mL (95% CI, 0.699-0.748), respectively.
“The sensitivity was better when they excluded those individuals with these conditions. Specificity was slightly, but not significantly, lower,” said Dr. Mielke during her talk.
Other considerations
Dr. Mielke added that it will be important to account for these and other factors when applying biomarkers in community settings, but they should also be considered in the context of health care disparities. Stroke, MI, and CKD are more common in African Americans, for example, suggesting that there could be racial differences in biomarker levels, though she said the difference in biomarker levels would be more likely attributable to the underlying comorbidities than race per se. “As shown, these factors can affect the consideration of an accuracy of cut points for clinical use. So I think future discussions will be needed as to how best to determine the cut points, and how to base them off of (different) populations,” said Dr. Mielke.
These sorts of refinements are important, according to Christopher Weber, PhD, who was asked for comment. “We have learned the importance of an early and accurate diagnosis. The blood test is a biomarker that does detect the hallmarks of Alzheimer’s disease sometimes up to decades before symptoms even appear,” said Dr. Weber, who is director of Global Science Initiatives at the Alzheimer’s Association.
But “there’s a lot more that we need to learn regarding when exactly to use them, who they’re appropriate for. And I think validation is the key to these blood biomarkers,” Dr. Weber added.
Dr. Mielke has been a consultant with the Brain Protection Company and Biogen. Dr. Weber has no relevant financial disclosures.
Such tests are likely to be widely available in the near future.
But work remains to be done to translate findings from academic studies to the more general population. A key consideration is that plasma levels of these biomarkers could be affected by other conditions, which could in turn skew test results, according to Michelle Mielke, PhD, who spoke on the topic at the 2021 Alzheimer’s Association International Conference.
“The markers, which we’ve published on as well, look really promising. But they have primarily been looked at in more specialty clinics or memory clinics, and have not been examined in the general community. The goal of this presentation was really just to take a look at this in the community, in older individuals that have multiple comorbidities, and to understand what factors might affect the levels of these markers. Because as we do go forward and develop cut points, we are going to have to consider these aspects,” said Dr. Mielke in an interview. She is a professor of epidemiology and neurology at the Mayo Clinic in Rochester, Minn.
Case in point
To illustrate the point, Dr. Mielke presented data from her group, which analyzed P-tau 181 and P-tau 217 data from 1,329 Mayo clinic patients. Of that total, 1,161 were cognitively unimpaired (CU), 153 had mild cognitive impairment (MCI), and 15 had dementia. The median age was 67, 55% were male, and 26% had the APOE e4 allele.
After adjustment for age and sex, there were statistically significantly elevated levels of both biomarkers among patients who had tested positive for amyloid and patients who had had a stroke or myocardial infarction, and in the presence of chronic kidney disease (CKD). There also was a trend towards an increase of biomarker levels with increasing body mass index. The differences remained even after the analysis was restricted to individuals who were amyloid negative.
The researchers then looked more closely at the impact of CKD, stroke, and MI on P-tau cut points and the ability to predict abnormal amyloid positron emission tomography (PET) scans. They defined an abnormal range as 1.96 standard deviation units beyond the mean among amyloid-negative individuals who are cognitively impaired. They excluded subjects with those risk factors and then established new cut points in the absence of the factors. The approach led to a significant change for the cutoff of P-tau 181 values, from 1.57 pg/mL or greater for individuals without stroke, MI, or CKD, and 1.75 pg/mL or greater for individuals with one such factor. There was little difference in the cutoff value for P-tau 217, from 0.25 pg/mL to 0.26 pg/mL.
Among people without a history of stroke, MI, or CKD, a P-tau 181 cutoff of 1.57 pg/mL or greater had an area under the receiving operating characteristic (AUROC) value of 0.717 (95% confidence interval, 0.691-0.744), compared with an AUROC of 0.687 (95% CI, 0.662-0.712) at a cutoff of 1.75 pg/mL or greater among people with those conditions. For P-tau 217, the values were 0.737 pg/mL (95% CI, 0.712-0.762) and 0.724 pg/mL (95% CI, 0.699-0.748), respectively.
“The sensitivity was better when they excluded those individuals with these conditions. Specificity was slightly, but not significantly, lower,” said Dr. Mielke during her talk.
Other considerations
Dr. Mielke added that it will be important to account for these and other factors when applying biomarkers in community settings, but they should also be considered in the context of health care disparities. Stroke, MI, and CKD are more common in African Americans, for example, suggesting that there could be racial differences in biomarker levels, though she said the difference in biomarker levels would be more likely attributable to the underlying comorbidities than race per se. “As shown, these factors can affect the consideration of an accuracy of cut points for clinical use. So I think future discussions will be needed as to how best to determine the cut points, and how to base them off of (different) populations,” said Dr. Mielke.
These sorts of refinements are important, according to Christopher Weber, PhD, who was asked for comment. “We have learned the importance of an early and accurate diagnosis. The blood test is a biomarker that does detect the hallmarks of Alzheimer’s disease sometimes up to decades before symptoms even appear,” said Dr. Weber, who is director of Global Science Initiatives at the Alzheimer’s Association.
But “there’s a lot more that we need to learn regarding when exactly to use them, who they’re appropriate for. And I think validation is the key to these blood biomarkers,” Dr. Weber added.
Dr. Mielke has been a consultant with the Brain Protection Company and Biogen. Dr. Weber has no relevant financial disclosures.
Such tests are likely to be widely available in the near future.
But work remains to be done to translate findings from academic studies to the more general population. A key consideration is that plasma levels of these biomarkers could be affected by other conditions, which could in turn skew test results, according to Michelle Mielke, PhD, who spoke on the topic at the 2021 Alzheimer’s Association International Conference.
“The markers, which we’ve published on as well, look really promising. But they have primarily been looked at in more specialty clinics or memory clinics, and have not been examined in the general community. The goal of this presentation was really just to take a look at this in the community, in older individuals that have multiple comorbidities, and to understand what factors might affect the levels of these markers. Because as we do go forward and develop cut points, we are going to have to consider these aspects,” said Dr. Mielke in an interview. She is a professor of epidemiology and neurology at the Mayo Clinic in Rochester, Minn.
Case in point
To illustrate the point, Dr. Mielke presented data from her group, which analyzed P-tau 181 and P-tau 217 data from 1,329 Mayo clinic patients. Of that total, 1,161 were cognitively unimpaired (CU), 153 had mild cognitive impairment (MCI), and 15 had dementia. The median age was 67, 55% were male, and 26% had the APOE e4 allele.
After adjustment for age and sex, there were statistically significantly elevated levels of both biomarkers among patients who had tested positive for amyloid and patients who had had a stroke or myocardial infarction, and in the presence of chronic kidney disease (CKD). There also was a trend towards an increase of biomarker levels with increasing body mass index. The differences remained even after the analysis was restricted to individuals who were amyloid negative.
The researchers then looked more closely at the impact of CKD, stroke, and MI on P-tau cut points and the ability to predict abnormal amyloid positron emission tomography (PET) scans. They defined an abnormal range as 1.96 standard deviation units beyond the mean among amyloid-negative individuals who are cognitively impaired. They excluded subjects with those risk factors and then established new cut points in the absence of the factors. The approach led to a significant change for the cutoff of P-tau 181 values, from 1.57 pg/mL or greater for individuals without stroke, MI, or CKD, and 1.75 pg/mL or greater for individuals with one such factor. There was little difference in the cutoff value for P-tau 217, from 0.25 pg/mL to 0.26 pg/mL.
Among people without a history of stroke, MI, or CKD, a P-tau 181 cutoff of 1.57 pg/mL or greater had an area under the receiving operating characteristic (AUROC) value of 0.717 (95% confidence interval, 0.691-0.744), compared with an AUROC of 0.687 (95% CI, 0.662-0.712) at a cutoff of 1.75 pg/mL or greater among people with those conditions. For P-tau 217, the values were 0.737 pg/mL (95% CI, 0.712-0.762) and 0.724 pg/mL (95% CI, 0.699-0.748), respectively.
“The sensitivity was better when they excluded those individuals with these conditions. Specificity was slightly, but not significantly, lower,” said Dr. Mielke during her talk.
Other considerations
Dr. Mielke added that it will be important to account for these and other factors when applying biomarkers in community settings, but they should also be considered in the context of health care disparities. Stroke, MI, and CKD are more common in African Americans, for example, suggesting that there could be racial differences in biomarker levels, though she said the difference in biomarker levels would be more likely attributable to the underlying comorbidities than race per se. “As shown, these factors can affect the consideration of an accuracy of cut points for clinical use. So I think future discussions will be needed as to how best to determine the cut points, and how to base them off of (different) populations,” said Dr. Mielke.
These sorts of refinements are important, according to Christopher Weber, PhD, who was asked for comment. “We have learned the importance of an early and accurate diagnosis. The blood test is a biomarker that does detect the hallmarks of Alzheimer’s disease sometimes up to decades before symptoms even appear,” said Dr. Weber, who is director of Global Science Initiatives at the Alzheimer’s Association.
But “there’s a lot more that we need to learn regarding when exactly to use them, who they’re appropriate for. And I think validation is the key to these blood biomarkers,” Dr. Weber added.
Dr. Mielke has been a consultant with the Brain Protection Company and Biogen. Dr. Weber has no relevant financial disclosures.
FROM AAIC 2021