User login
Which code for Gartner’s duct cyst procedure?
But if it was a marsupialization procedure in which the cyst was drained first and then the walls of the cyst were sewn in place to form a pouch, then the procedure should be coded using the unlisted code, 58999 (unlisted procedure, female genital system [nonobstetrical]).
The Gartner’s duct is usually located in the lateral wall of the vagina, so the code to report marsupialization of a Bartholin gland cyst, 56440, would not apply.
Be sure to let the payer know that the procedure is very similar to the 2 codes 56440 (Bartholin’s) and 57135 (excision). Code 56440 has 4.89 RVUs, while 57135 has 5.25 RVUs.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
But if it was a marsupialization procedure in which the cyst was drained first and then the walls of the cyst were sewn in place to form a pouch, then the procedure should be coded using the unlisted code, 58999 (unlisted procedure, female genital system [nonobstetrical]).
The Gartner’s duct is usually located in the lateral wall of the vagina, so the code to report marsupialization of a Bartholin gland cyst, 56440, would not apply.
Be sure to let the payer know that the procedure is very similar to the 2 codes 56440 (Bartholin’s) and 57135 (excision). Code 56440 has 4.89 RVUs, while 57135 has 5.25 RVUs.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
But if it was a marsupialization procedure in which the cyst was drained first and then the walls of the cyst were sewn in place to form a pouch, then the procedure should be coded using the unlisted code, 58999 (unlisted procedure, female genital system [nonobstetrical]).
The Gartner’s duct is usually located in the lateral wall of the vagina, so the code to report marsupialization of a Bartholin gland cyst, 56440, would not apply.
Be sure to let the payer know that the procedure is very similar to the 2 codes 56440 (Bartholin’s) and 57135 (excision). Code 56440 has 4.89 RVUs, while 57135 has 5.25 RVUs.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
Correct coding when the patient goes to ER
Timing is everything. Although the codes for observation care do not stipulate a time period, the record must clearly show that she was observed before a determination could be made to send her home or admit her to the hospital. This would include being seen first by you and then having nursing staff observe for problems prior to your deciding to send her home.
The observation codes require, at a minimum, documentation of a detailed history and exam (with any level of medical decision making). If your patient was admitted and discharged on the same service date, the codes you would select from are 99234-99236 (observation or inpatient hospital care, for the evaluation and management of a patient including admission and discharge on the same date).
If, on the other hand, you saw the patient, treated her, and then immediately released her to go home or you left orders to send her home after a test had been performed such as a nonstress test, you should consider this to be an outpatient service and you would report one of the established patient problem codes (99212-99215).
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
Timing is everything. Although the codes for observation care do not stipulate a time period, the record must clearly show that she was observed before a determination could be made to send her home or admit her to the hospital. This would include being seen first by you and then having nursing staff observe for problems prior to your deciding to send her home.
The observation codes require, at a minimum, documentation of a detailed history and exam (with any level of medical decision making). If your patient was admitted and discharged on the same service date, the codes you would select from are 99234-99236 (observation or inpatient hospital care, for the evaluation and management of a patient including admission and discharge on the same date).
If, on the other hand, you saw the patient, treated her, and then immediately released her to go home or you left orders to send her home after a test had been performed such as a nonstress test, you should consider this to be an outpatient service and you would report one of the established patient problem codes (99212-99215).
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
Timing is everything. Although the codes for observation care do not stipulate a time period, the record must clearly show that she was observed before a determination could be made to send her home or admit her to the hospital. This would include being seen first by you and then having nursing staff observe for problems prior to your deciding to send her home.
The observation codes require, at a minimum, documentation of a detailed history and exam (with any level of medical decision making). If your patient was admitted and discharged on the same service date, the codes you would select from are 99234-99236 (observation or inpatient hospital care, for the evaluation and management of a patient including admission and discharge on the same date).
If, on the other hand, you saw the patient, treated her, and then immediately released her to go home or you left orders to send her home after a test had been performed such as a nonstress test, you should consider this to be an outpatient service and you would report one of the established patient problem codes (99212-99215).
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
ICD code depends on why labor was induced
In either case, report the ICD-9-CM code that supports the type of preeclampsia (eg, 642.51, severe preeclampsia; delivered with or without mention of antepartum condition). But if labor was induced, add code 644.21 (early onset of delivery; delivered with or without mention of antepartum condition). This code represents premature labor with delivery before 37 completed weeks of gestation.
If the delivery was accomplished by performing a cesarean, in addition to an outcome code such as V27.0 (single liveborn), you might add a code if the patient had a previous cesarean delivery (654.21).
If this was her first cesarean delivery, only the preeclampsia and outcome diagnosis codes would be assigned.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
In either case, report the ICD-9-CM code that supports the type of preeclampsia (eg, 642.51, severe preeclampsia; delivered with or without mention of antepartum condition). But if labor was induced, add code 644.21 (early onset of delivery; delivered with or without mention of antepartum condition). This code represents premature labor with delivery before 37 completed weeks of gestation.
If the delivery was accomplished by performing a cesarean, in addition to an outcome code such as V27.0 (single liveborn), you might add a code if the patient had a previous cesarean delivery (654.21).
If this was her first cesarean delivery, only the preeclampsia and outcome diagnosis codes would be assigned.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
In either case, report the ICD-9-CM code that supports the type of preeclampsia (eg, 642.51, severe preeclampsia; delivered with or without mention of antepartum condition). But if labor was induced, add code 644.21 (early onset of delivery; delivered with or without mention of antepartum condition). This code represents premature labor with delivery before 37 completed weeks of gestation.
If the delivery was accomplished by performing a cesarean, in addition to an outcome code such as V27.0 (single liveborn), you might add a code if the patient had a previous cesarean delivery (654.21).
If this was her first cesarean delivery, only the preeclampsia and outcome diagnosis codes would be assigned.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
Use OB or GYN code if fetal pole is absent?
If the purpose of the ultrasound is only to check for fetal heart tones, then the correct code is 76815 (ultrasound, pregnant uterus, real time with image documentation limited [eg, fetal heart beat, placental location, fetal position and/or qualitative amniotic fluid volume], one or more fetuses).
While this scan could be performed transvaginally, the amount of work in checking only for fetal heart tones is significantly less than that involved in the OB transvaginal procedure.
Therefore, I recommend that you use the limited ultrasound code even if a vaginal probe was used.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
If the purpose of the ultrasound is only to check for fetal heart tones, then the correct code is 76815 (ultrasound, pregnant uterus, real time with image documentation limited [eg, fetal heart beat, placental location, fetal position and/or qualitative amniotic fluid volume], one or more fetuses).
While this scan could be performed transvaginally, the amount of work in checking only for fetal heart tones is significantly less than that involved in the OB transvaginal procedure.
Therefore, I recommend that you use the limited ultrasound code even if a vaginal probe was used.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
If the purpose of the ultrasound is only to check for fetal heart tones, then the correct code is 76815 (ultrasound, pregnant uterus, real time with image documentation limited [eg, fetal heart beat, placental location, fetal position and/or qualitative amniotic fluid volume], one or more fetuses).
While this scan could be performed transvaginally, the amount of work in checking only for fetal heart tones is significantly less than that involved in the OB transvaginal procedure.
Therefore, I recommend that you use the limited ultrasound code even if a vaginal probe was used.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
How do we code for new HPV vaccine?
- 90649 is the vaccine product code (human papilloma virus [HPV] vaccine, types 6, 11, 16, 18 [quadrivalent], 3-dose schedule, for intramuscular use). A 3-dose schedule means you will be billing for the procedure 3 times during a 6-month period.
- 90471 can also be reported for the administration of the vaccine. (Immunization administration [includes percutaneous, intradermal, subcutaneous, or intramuscular injections]; one vaccine [single or combination vaccine/toxoid])
Adding modifiers. CPT guidelines state that a modifier -51 (multiple procedure) would not be added to either of these codes, and of course if you provide a significant and separate evaluation and management (E/M) service at the time the vaccine is given, you may also bill an E/M code with a modifier -25 added to let the payer know that the E/M service was separate.
Note that almost no payers will pay separately for the E/M code 99211 plus an injection procedure because it represents a minimal, not a significant E/M service.
Insurance coverage unlikely, for now
Until such time as the CDC comes out with a recommendation for the vaccine, coverage is going to be a problem. Insurance plans can be expected to cover the cost of the vaccine only if the CDC Advisory Committee on Immunization Practices recommends HPV vaccination as standard.
Tell patients! Until then, you may want to advise your patients who are candidates for the vaccine that this vaccine may be an out-of-pocket expense for them. Merck, the company that produces the quadrivalent vaccine, has stated that the price will be $120 per injection. The company has indicated that they have created a new program to provide free vaccines including HPV vaccine, for uninsured adults unable to pay.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
- 90649 is the vaccine product code (human papilloma virus [HPV] vaccine, types 6, 11, 16, 18 [quadrivalent], 3-dose schedule, for intramuscular use). A 3-dose schedule means you will be billing for the procedure 3 times during a 6-month period.
- 90471 can also be reported for the administration of the vaccine. (Immunization administration [includes percutaneous, intradermal, subcutaneous, or intramuscular injections]; one vaccine [single or combination vaccine/toxoid])
Adding modifiers. CPT guidelines state that a modifier -51 (multiple procedure) would not be added to either of these codes, and of course if you provide a significant and separate evaluation and management (E/M) service at the time the vaccine is given, you may also bill an E/M code with a modifier -25 added to let the payer know that the E/M service was separate.
Note that almost no payers will pay separately for the E/M code 99211 plus an injection procedure because it represents a minimal, not a significant E/M service.
Insurance coverage unlikely, for now
Until such time as the CDC comes out with a recommendation for the vaccine, coverage is going to be a problem. Insurance plans can be expected to cover the cost of the vaccine only if the CDC Advisory Committee on Immunization Practices recommends HPV vaccination as standard.
Tell patients! Until then, you may want to advise your patients who are candidates for the vaccine that this vaccine may be an out-of-pocket expense for them. Merck, the company that produces the quadrivalent vaccine, has stated that the price will be $120 per injection. The company has indicated that they have created a new program to provide free vaccines including HPV vaccine, for uninsured adults unable to pay.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
- 90649 is the vaccine product code (human papilloma virus [HPV] vaccine, types 6, 11, 16, 18 [quadrivalent], 3-dose schedule, for intramuscular use). A 3-dose schedule means you will be billing for the procedure 3 times during a 6-month period.
- 90471 can also be reported for the administration of the vaccine. (Immunization administration [includes percutaneous, intradermal, subcutaneous, or intramuscular injections]; one vaccine [single or combination vaccine/toxoid])
Adding modifiers. CPT guidelines state that a modifier -51 (multiple procedure) would not be added to either of these codes, and of course if you provide a significant and separate evaluation and management (E/M) service at the time the vaccine is given, you may also bill an E/M code with a modifier -25 added to let the payer know that the E/M service was separate.
Note that almost no payers will pay separately for the E/M code 99211 plus an injection procedure because it represents a minimal, not a significant E/M service.
Insurance coverage unlikely, for now
Until such time as the CDC comes out with a recommendation for the vaccine, coverage is going to be a problem. Insurance plans can be expected to cover the cost of the vaccine only if the CDC Advisory Committee on Immunization Practices recommends HPV vaccination as standard.
Tell patients! Until then, you may want to advise your patients who are candidates for the vaccine that this vaccine may be an out-of-pocket expense for them. Merck, the company that produces the quadrivalent vaccine, has stated that the price will be $120 per injection. The company has indicated that they have created a new program to provide free vaccines including HPV vaccine, for uninsured adults unable to pay.
Ms. Witt, former program manager in the Department of Coding and Nomenclature at the American College of Obstetricians and Gynecologists, is an independent coding and documentation consultant. Reimbursement Adviser reflects the most commonly accepted interpretations of CPT-4 and ICD-9-CM coding. When in doubt on a coding or billing matter, check with your individual payer.
What best prevents exercise-induced bronchoconstriction for a child with asthma?
Inhaled short-acting beta-agonists (SABAs) are most effective in preventing exercise-induced bronchoconstriction, followed by inhaled mast cell stabilizers and anticholinergic agents (strength of recommendation [SOR]: A, multiple randomized control trials [RCTs]). Less evidence supports the use of leukotriene antagonists and inhaled corticosteroids, either individually or in combination (SOR: B). Underlying asthma, which commonly contributes to exercise-induced bronchoconstriction, should be diagnosed and controlled first (SOR: C).
Control the asthma and the need for pre-treatment often becomes unnecessary
Because truly isolated exercise-induced bronchoconstriction is uncommon in a nonasthmatic child, and because bronchospasm in a child during exercise more commonly indicates undiagnosed asthma, search for treatable asthma when a child wheezes with exercise. These children have sputum eosinophilia reflecting inflammation, and they are best served by addressing the underlying asthma with inhaled corticosteroids. Once the asthma is under control, their need for “the best pre-treatment” (a SABA) often becomes irrelevant. Ask the child whether he or she is having more shortness of breath and difficulty breathing after exercise than during exercise; this reveals those most likely to benefit from treatment.
Evidence summary
It is difficult to interpret studies on exercise-induced bronchoconstriction (the rather uncommon presence of exercise-induced bronchospasm in a nonasthmatic) and exercise-induced asthma (the more common situation of asthma worsened by exercise). Many studies include both types of patients.
A systematic review of 24 RCTs (of which 13 evaluated children) showed that SABAs, mast cell stabilizers, and anticholinergics provide a significant protective effect against exercise-induced bronchoconstriction with few adverse effects (the child subgroup analyses did not differ significantly from pooled results). Mast cell stabilizers were found less effective at attenuating bronchoconstriction than SABAs, with an average maximum decrease in the forced expiratory volume in 1 second (FEV1) of 11.9% compared with 4.6% for beta-agonists (child subgroup: weighted mean difference=7.3%; 95% confidence interval [CI], 3.9–10.7). Complete protection (defined in this study as maximum % decrease in FEV1 <15% post-exercise) and clinical protection (50% improvement over placebo) measures were included. Fewer children had complete protection (pooled: 66% vs 85%, odds ratio [OR]=0.3; 95% CI, 0.2–0.5) or clinical protection (pooled: 55% vs 77%, OR=0.4; 95% CI, 0.2–0.8).
Mast cell stabilizers were more effective than anticholinergic agents, with average maximum FEV1 decrease of 9.4% compared with 16.0% on anticholinergics (child subgroup: weighted mean difference=6.6%; 95% CI, 1.0–12.2). They also provided more individuals with complete protection (pooled: 73% vs 56%, OR=2.2; 95% CI, 1.3–3.7) and clinical protection (pooled: 73% vs 52%, OR=2.7; 95% CI, 1.1–6.4). Combining mast cell stabilizers with SABAs did not produce significant advantages in pulmonary function over SABAs alone. No significant subgroup differences were seen based on age, severity, or study quality.1
Another systematic review of 20 RCTs (15 studying children and 5 studying adults) with patients aged >6 years showed that 4 mg of nedocromil (Tilade) inhaled 15 to 60 minutes before exercise significantly reduced the severity and duration of exercise-induced bronchoconstriction compared with placebo. It had a greater effect on patients with severe exercise-induced bronchoconstriction (defined as an exercise-induced fall in lung function >30% from baseline).2
Eight RCTs (5 studying children) were included in a systematic review of patients aged >6 years that found no significant difference between nedocromil and cromoglycate with regards to decrease in FEV1, complete protection, clinical protection, or side effects.3
Leukotriene antagonists have been recommended on a trial basis with follow-up to evaluate the treatment response.4 Although there are several long-term studies of leukotriene antagonists for adults, few have studied children. A recent study assessed the effects of montelukast (Singulair) on 64 children with exercise-induced bronchoconstriction. After 8 weeks of treatment, the montelukast group showed significant improvements (compared with placebo) in asthma symptom scores (24.3±8.2 before vs 17.8±6.8 after 8 weeks of montelukast treatment, P<.05; vs 17.7±6.7 8 weeks after stopping treatment, P<.05), maximum percent fall in FEV1 after exercise (36.5±10.2% before vs 27.6±14.4% after 8 wks of treatment, P<.01; vs 26.7±19.4% 8 weeks after stopping treatment, P<.01), and time to recovery (41.8±8.1 min before vs 25.3±23.3 min after 8 weeks of treatment, P<.01; vs 27.7±26.5 min 8 weeks after stopping, P<.05).5
Therapies awaiting further study include a combination of budesonide (Pulmicort) and formoterol (Foradil), which is similar to the currently available preparation of fluticasone and salmeterol (Advair Diskus) but contains a long-acting beta-agonist with quicker onset. The phosphodiesterase-4 inhibitors roflumilast (Daxas) and cilomilast (Ariflo)—neither of which have been FDA-approved—and inhaled low-molecular-weight heparin have potential efficacy.6 Other options suggested for this problem—including inhaled furosemide, vitamin C, antihistamines, calcium channel blockers, and reduced dietary salt intake—need further study.7
Recommendations from others
Review articles on this topic suggest the following to prevent exercise-induced bronchoconstriction: controlling baseline asthma, avoiding known allergens, choosing appropriate sports with short bursts of activity, and selecting warm, humid environments for the activities.6-8 Some authorities recommend warm-up before athletic events to take advantage of a 30- to 90-minute refractory period. This can help prevent exercise-induced bronchoconstriction; however, effects vary considerably from person to person.7,8
The National Asthma Education and Prevention Program recommends prevention of exercise-induced bronchoconstriction by optimally controlling underlying asthma. If a patient remains symptomatic during exercise, you should review medication usage, understanding of dosage instructions, and administration technique before any changes in the treatment regimen.9
1. Spooner CH, Spooner GR, Rowe BH. Mast-cell stabilising agents to prevent exercise-induced bronchoconstriction. Cochrane Database Syst Rev 2003;(4):CD002307.
2. Spooner CH, Saunders LD, Rowe BH. Nedocromil sodium for preventing exercise-induced bronchoconstriction. Cochrane Database Syst Rev 2002;(1):CD001183.
3. Kelly K, Spooner CH, Rowe BH. Nedocromil sodium versus sodium cromoglycate for preventing exercise-induced bronchoconstriction in asthmatics. Cochrane Database Syst Rev 2000;(4):CD002731.
4. Moraes TJ, Selvadurai H. Management of exercise-induced bronchospasm in children: the role of leukotriene antagonists. Treat Respir Med 2004;3:9-15.
5. Kim JH, Lee SY, Kim HB, et al. Prolonged effect of montelukast in asthmatic children with exercise-induced bronchoconstriction. Pediatr Pulmonol 2005;39(2):162-166.
6. Storms WW. Asthma associated with exercise. Immunol Allergy Clin North Am 2005;25:31-43.
7. Sinha T, David AK. Recognition and management of exercise-induced bronchospasm. Am Fam Physician 2003;67(4):769-774, 675.
8. DYNAMED [database online]. Columbia, Mo: Dynamic Medical Information Systems, LLC;1995, continuous daily updating. Updated December 2, 2004.
9. Williams SG, Schmidt DK, Redd SC, Storms W. Key clinical activities for quality asthma care: recommendations of the National Asthma Education and Prevention Program. MMWR Recomm Rep 2003;52(RR-6):1-8.
Inhaled short-acting beta-agonists (SABAs) are most effective in preventing exercise-induced bronchoconstriction, followed by inhaled mast cell stabilizers and anticholinergic agents (strength of recommendation [SOR]: A, multiple randomized control trials [RCTs]). Less evidence supports the use of leukotriene antagonists and inhaled corticosteroids, either individually or in combination (SOR: B). Underlying asthma, which commonly contributes to exercise-induced bronchoconstriction, should be diagnosed and controlled first (SOR: C).
Control the asthma and the need for pre-treatment often becomes unnecessary
Because truly isolated exercise-induced bronchoconstriction is uncommon in a nonasthmatic child, and because bronchospasm in a child during exercise more commonly indicates undiagnosed asthma, search for treatable asthma when a child wheezes with exercise. These children have sputum eosinophilia reflecting inflammation, and they are best served by addressing the underlying asthma with inhaled corticosteroids. Once the asthma is under control, their need for “the best pre-treatment” (a SABA) often becomes irrelevant. Ask the child whether he or she is having more shortness of breath and difficulty breathing after exercise than during exercise; this reveals those most likely to benefit from treatment.
Evidence summary
It is difficult to interpret studies on exercise-induced bronchoconstriction (the rather uncommon presence of exercise-induced bronchospasm in a nonasthmatic) and exercise-induced asthma (the more common situation of asthma worsened by exercise). Many studies include both types of patients.
A systematic review of 24 RCTs (of which 13 evaluated children) showed that SABAs, mast cell stabilizers, and anticholinergics provide a significant protective effect against exercise-induced bronchoconstriction with few adverse effects (the child subgroup analyses did not differ significantly from pooled results). Mast cell stabilizers were found less effective at attenuating bronchoconstriction than SABAs, with an average maximum decrease in the forced expiratory volume in 1 second (FEV1) of 11.9% compared with 4.6% for beta-agonists (child subgroup: weighted mean difference=7.3%; 95% confidence interval [CI], 3.9–10.7). Complete protection (defined in this study as maximum % decrease in FEV1 <15% post-exercise) and clinical protection (50% improvement over placebo) measures were included. Fewer children had complete protection (pooled: 66% vs 85%, odds ratio [OR]=0.3; 95% CI, 0.2–0.5) or clinical protection (pooled: 55% vs 77%, OR=0.4; 95% CI, 0.2–0.8).
Mast cell stabilizers were more effective than anticholinergic agents, with average maximum FEV1 decrease of 9.4% compared with 16.0% on anticholinergics (child subgroup: weighted mean difference=6.6%; 95% CI, 1.0–12.2). They also provided more individuals with complete protection (pooled: 73% vs 56%, OR=2.2; 95% CI, 1.3–3.7) and clinical protection (pooled: 73% vs 52%, OR=2.7; 95% CI, 1.1–6.4). Combining mast cell stabilizers with SABAs did not produce significant advantages in pulmonary function over SABAs alone. No significant subgroup differences were seen based on age, severity, or study quality.1
Another systematic review of 20 RCTs (15 studying children and 5 studying adults) with patients aged >6 years showed that 4 mg of nedocromil (Tilade) inhaled 15 to 60 minutes before exercise significantly reduced the severity and duration of exercise-induced bronchoconstriction compared with placebo. It had a greater effect on patients with severe exercise-induced bronchoconstriction (defined as an exercise-induced fall in lung function >30% from baseline).2
Eight RCTs (5 studying children) were included in a systematic review of patients aged >6 years that found no significant difference between nedocromil and cromoglycate with regards to decrease in FEV1, complete protection, clinical protection, or side effects.3
Leukotriene antagonists have been recommended on a trial basis with follow-up to evaluate the treatment response.4 Although there are several long-term studies of leukotriene antagonists for adults, few have studied children. A recent study assessed the effects of montelukast (Singulair) on 64 children with exercise-induced bronchoconstriction. After 8 weeks of treatment, the montelukast group showed significant improvements (compared with placebo) in asthma symptom scores (24.3±8.2 before vs 17.8±6.8 after 8 weeks of montelukast treatment, P<.05; vs 17.7±6.7 8 weeks after stopping treatment, P<.05), maximum percent fall in FEV1 after exercise (36.5±10.2% before vs 27.6±14.4% after 8 wks of treatment, P<.01; vs 26.7±19.4% 8 weeks after stopping treatment, P<.01), and time to recovery (41.8±8.1 min before vs 25.3±23.3 min after 8 weeks of treatment, P<.01; vs 27.7±26.5 min 8 weeks after stopping, P<.05).5
Therapies awaiting further study include a combination of budesonide (Pulmicort) and formoterol (Foradil), which is similar to the currently available preparation of fluticasone and salmeterol (Advair Diskus) but contains a long-acting beta-agonist with quicker onset. The phosphodiesterase-4 inhibitors roflumilast (Daxas) and cilomilast (Ariflo)—neither of which have been FDA-approved—and inhaled low-molecular-weight heparin have potential efficacy.6 Other options suggested for this problem—including inhaled furosemide, vitamin C, antihistamines, calcium channel blockers, and reduced dietary salt intake—need further study.7
Recommendations from others
Review articles on this topic suggest the following to prevent exercise-induced bronchoconstriction: controlling baseline asthma, avoiding known allergens, choosing appropriate sports with short bursts of activity, and selecting warm, humid environments for the activities.6-8 Some authorities recommend warm-up before athletic events to take advantage of a 30- to 90-minute refractory period. This can help prevent exercise-induced bronchoconstriction; however, effects vary considerably from person to person.7,8
The National Asthma Education and Prevention Program recommends prevention of exercise-induced bronchoconstriction by optimally controlling underlying asthma. If a patient remains symptomatic during exercise, you should review medication usage, understanding of dosage instructions, and administration technique before any changes in the treatment regimen.9
Inhaled short-acting beta-agonists (SABAs) are most effective in preventing exercise-induced bronchoconstriction, followed by inhaled mast cell stabilizers and anticholinergic agents (strength of recommendation [SOR]: A, multiple randomized control trials [RCTs]). Less evidence supports the use of leukotriene antagonists and inhaled corticosteroids, either individually or in combination (SOR: B). Underlying asthma, which commonly contributes to exercise-induced bronchoconstriction, should be diagnosed and controlled first (SOR: C).
Control the asthma and the need for pre-treatment often becomes unnecessary
Because truly isolated exercise-induced bronchoconstriction is uncommon in a nonasthmatic child, and because bronchospasm in a child during exercise more commonly indicates undiagnosed asthma, search for treatable asthma when a child wheezes with exercise. These children have sputum eosinophilia reflecting inflammation, and they are best served by addressing the underlying asthma with inhaled corticosteroids. Once the asthma is under control, their need for “the best pre-treatment” (a SABA) often becomes irrelevant. Ask the child whether he or she is having more shortness of breath and difficulty breathing after exercise than during exercise; this reveals those most likely to benefit from treatment.
Evidence summary
It is difficult to interpret studies on exercise-induced bronchoconstriction (the rather uncommon presence of exercise-induced bronchospasm in a nonasthmatic) and exercise-induced asthma (the more common situation of asthma worsened by exercise). Many studies include both types of patients.
A systematic review of 24 RCTs (of which 13 evaluated children) showed that SABAs, mast cell stabilizers, and anticholinergics provide a significant protective effect against exercise-induced bronchoconstriction with few adverse effects (the child subgroup analyses did not differ significantly from pooled results). Mast cell stabilizers were found less effective at attenuating bronchoconstriction than SABAs, with an average maximum decrease in the forced expiratory volume in 1 second (FEV1) of 11.9% compared with 4.6% for beta-agonists (child subgroup: weighted mean difference=7.3%; 95% confidence interval [CI], 3.9–10.7). Complete protection (defined in this study as maximum % decrease in FEV1 <15% post-exercise) and clinical protection (50% improvement over placebo) measures were included. Fewer children had complete protection (pooled: 66% vs 85%, odds ratio [OR]=0.3; 95% CI, 0.2–0.5) or clinical protection (pooled: 55% vs 77%, OR=0.4; 95% CI, 0.2–0.8).
Mast cell stabilizers were more effective than anticholinergic agents, with average maximum FEV1 decrease of 9.4% compared with 16.0% on anticholinergics (child subgroup: weighted mean difference=6.6%; 95% CI, 1.0–12.2). They also provided more individuals with complete protection (pooled: 73% vs 56%, OR=2.2; 95% CI, 1.3–3.7) and clinical protection (pooled: 73% vs 52%, OR=2.7; 95% CI, 1.1–6.4). Combining mast cell stabilizers with SABAs did not produce significant advantages in pulmonary function over SABAs alone. No significant subgroup differences were seen based on age, severity, or study quality.1
Another systematic review of 20 RCTs (15 studying children and 5 studying adults) with patients aged >6 years showed that 4 mg of nedocromil (Tilade) inhaled 15 to 60 minutes before exercise significantly reduced the severity and duration of exercise-induced bronchoconstriction compared with placebo. It had a greater effect on patients with severe exercise-induced bronchoconstriction (defined as an exercise-induced fall in lung function >30% from baseline).2
Eight RCTs (5 studying children) were included in a systematic review of patients aged >6 years that found no significant difference between nedocromil and cromoglycate with regards to decrease in FEV1, complete protection, clinical protection, or side effects.3
Leukotriene antagonists have been recommended on a trial basis with follow-up to evaluate the treatment response.4 Although there are several long-term studies of leukotriene antagonists for adults, few have studied children. A recent study assessed the effects of montelukast (Singulair) on 64 children with exercise-induced bronchoconstriction. After 8 weeks of treatment, the montelukast group showed significant improvements (compared with placebo) in asthma symptom scores (24.3±8.2 before vs 17.8±6.8 after 8 weeks of montelukast treatment, P<.05; vs 17.7±6.7 8 weeks after stopping treatment, P<.05), maximum percent fall in FEV1 after exercise (36.5±10.2% before vs 27.6±14.4% after 8 wks of treatment, P<.01; vs 26.7±19.4% 8 weeks after stopping treatment, P<.01), and time to recovery (41.8±8.1 min before vs 25.3±23.3 min after 8 weeks of treatment, P<.01; vs 27.7±26.5 min 8 weeks after stopping, P<.05).5
Therapies awaiting further study include a combination of budesonide (Pulmicort) and formoterol (Foradil), which is similar to the currently available preparation of fluticasone and salmeterol (Advair Diskus) but contains a long-acting beta-agonist with quicker onset. The phosphodiesterase-4 inhibitors roflumilast (Daxas) and cilomilast (Ariflo)—neither of which have been FDA-approved—and inhaled low-molecular-weight heparin have potential efficacy.6 Other options suggested for this problem—including inhaled furosemide, vitamin C, antihistamines, calcium channel blockers, and reduced dietary salt intake—need further study.7
Recommendations from others
Review articles on this topic suggest the following to prevent exercise-induced bronchoconstriction: controlling baseline asthma, avoiding known allergens, choosing appropriate sports with short bursts of activity, and selecting warm, humid environments for the activities.6-8 Some authorities recommend warm-up before athletic events to take advantage of a 30- to 90-minute refractory period. This can help prevent exercise-induced bronchoconstriction; however, effects vary considerably from person to person.7,8
The National Asthma Education and Prevention Program recommends prevention of exercise-induced bronchoconstriction by optimally controlling underlying asthma. If a patient remains symptomatic during exercise, you should review medication usage, understanding of dosage instructions, and administration technique before any changes in the treatment regimen.9
1. Spooner CH, Spooner GR, Rowe BH. Mast-cell stabilising agents to prevent exercise-induced bronchoconstriction. Cochrane Database Syst Rev 2003;(4):CD002307.
2. Spooner CH, Saunders LD, Rowe BH. Nedocromil sodium for preventing exercise-induced bronchoconstriction. Cochrane Database Syst Rev 2002;(1):CD001183.
3. Kelly K, Spooner CH, Rowe BH. Nedocromil sodium versus sodium cromoglycate for preventing exercise-induced bronchoconstriction in asthmatics. Cochrane Database Syst Rev 2000;(4):CD002731.
4. Moraes TJ, Selvadurai H. Management of exercise-induced bronchospasm in children: the role of leukotriene antagonists. Treat Respir Med 2004;3:9-15.
5. Kim JH, Lee SY, Kim HB, et al. Prolonged effect of montelukast in asthmatic children with exercise-induced bronchoconstriction. Pediatr Pulmonol 2005;39(2):162-166.
6. Storms WW. Asthma associated with exercise. Immunol Allergy Clin North Am 2005;25:31-43.
7. Sinha T, David AK. Recognition and management of exercise-induced bronchospasm. Am Fam Physician 2003;67(4):769-774, 675.
8. DYNAMED [database online]. Columbia, Mo: Dynamic Medical Information Systems, LLC;1995, continuous daily updating. Updated December 2, 2004.
9. Williams SG, Schmidt DK, Redd SC, Storms W. Key clinical activities for quality asthma care: recommendations of the National Asthma Education and Prevention Program. MMWR Recomm Rep 2003;52(RR-6):1-8.
1. Spooner CH, Spooner GR, Rowe BH. Mast-cell stabilising agents to prevent exercise-induced bronchoconstriction. Cochrane Database Syst Rev 2003;(4):CD002307.
2. Spooner CH, Saunders LD, Rowe BH. Nedocromil sodium for preventing exercise-induced bronchoconstriction. Cochrane Database Syst Rev 2002;(1):CD001183.
3. Kelly K, Spooner CH, Rowe BH. Nedocromil sodium versus sodium cromoglycate for preventing exercise-induced bronchoconstriction in asthmatics. Cochrane Database Syst Rev 2000;(4):CD002731.
4. Moraes TJ, Selvadurai H. Management of exercise-induced bronchospasm in children: the role of leukotriene antagonists. Treat Respir Med 2004;3:9-15.
5. Kim JH, Lee SY, Kim HB, et al. Prolonged effect of montelukast in asthmatic children with exercise-induced bronchoconstriction. Pediatr Pulmonol 2005;39(2):162-166.
6. Storms WW. Asthma associated with exercise. Immunol Allergy Clin North Am 2005;25:31-43.
7. Sinha T, David AK. Recognition and management of exercise-induced bronchospasm. Am Fam Physician 2003;67(4):769-774, 675.
8. DYNAMED [database online]. Columbia, Mo: Dynamic Medical Information Systems, LLC;1995, continuous daily updating. Updated December 2, 2004.
9. Williams SG, Schmidt DK, Redd SC, Storms W. Key clinical activities for quality asthma care: recommendations of the National Asthma Education and Prevention Program. MMWR Recomm Rep 2003;52(RR-6):1-8.
Evidence-based answers from the Family Physicians Inquiries Network
Of time and wounds
Our last date
It was dusk, and I stared glumly at cold rain falling onto steaming rooftop vents outside the clouded window of my husband's hospital room. I was feeling more than a little sorry for myself. Out there, it was a Friday night full of the promise of weekend diversions. In here, it was much like the night before, and the night before thata waiting game.
Waiting to see if Doug would live or die. Waiting to see if he could overcome the terrible malaise that gripped his body and come home. Waiting to see if he would ever be able to move his arms and legs again.
Turning from the window, I found Doug awake. He had only been off the ventilator for a short time and wasn't able to talk. I had just come from work, having been away from him since late morning. It seemed as though there should be plenty of things to tell him, but patter about the office and traffic did not belong in this room, and he'd already heard endlessly that his family and friends were pulling hard for him.
So I held his hand and leaned on the side rail of his bed, getting my face as close to his as I could. We locked eyes and smiled, and words flowed silently between us, just as they had so many times over our 25 years of marriage. God, how I'd missed that!
The nurses had dimmed the lights in the ICU for the night, and though it was far from dark, the room had a nicer ambience than usual. Straightening up, I searched the channels on Doug's TV for something more suitable than CNN. Suddenly, there were Jake and Elwood sauntering into Aretha Franklin's eatery on their mission from God. Hey, Doug. I said, It's The Blues Brothers. Moments later, Aretha was belting out R‐E‐S‐P‐E‐C‐T, and I was gyrating. Doug was doing the only thing he could, swinging his head from side to side in time to the music.
It was just a tiny moment, a vignette unnoticed by anyone but us two in the life of that ICU. But it is the sweetest memory I have of that time. Just days before his death at age 55, the spark that was us had flamed briefly to life.
It was dusk, and I stared glumly at cold rain falling onto steaming rooftop vents outside the clouded window of my husband's hospital room. I was feeling more than a little sorry for myself. Out there, it was a Friday night full of the promise of weekend diversions. In here, it was much like the night before, and the night before thata waiting game.
Waiting to see if Doug would live or die. Waiting to see if he could overcome the terrible malaise that gripped his body and come home. Waiting to see if he would ever be able to move his arms and legs again.
Turning from the window, I found Doug awake. He had only been off the ventilator for a short time and wasn't able to talk. I had just come from work, having been away from him since late morning. It seemed as though there should be plenty of things to tell him, but patter about the office and traffic did not belong in this room, and he'd already heard endlessly that his family and friends were pulling hard for him.
So I held his hand and leaned on the side rail of his bed, getting my face as close to his as I could. We locked eyes and smiled, and words flowed silently between us, just as they had so many times over our 25 years of marriage. God, how I'd missed that!
The nurses had dimmed the lights in the ICU for the night, and though it was far from dark, the room had a nicer ambience than usual. Straightening up, I searched the channels on Doug's TV for something more suitable than CNN. Suddenly, there were Jake and Elwood sauntering into Aretha Franklin's eatery on their mission from God. Hey, Doug. I said, It's The Blues Brothers. Moments later, Aretha was belting out R‐E‐S‐P‐E‐C‐T, and I was gyrating. Doug was doing the only thing he could, swinging his head from side to side in time to the music.
It was just a tiny moment, a vignette unnoticed by anyone but us two in the life of that ICU. But it is the sweetest memory I have of that time. Just days before his death at age 55, the spark that was us had flamed briefly to life.
It was dusk, and I stared glumly at cold rain falling onto steaming rooftop vents outside the clouded window of my husband's hospital room. I was feeling more than a little sorry for myself. Out there, it was a Friday night full of the promise of weekend diversions. In here, it was much like the night before, and the night before thata waiting game.
Waiting to see if Doug would live or die. Waiting to see if he could overcome the terrible malaise that gripped his body and come home. Waiting to see if he would ever be able to move his arms and legs again.
Turning from the window, I found Doug awake. He had only been off the ventilator for a short time and wasn't able to talk. I had just come from work, having been away from him since late morning. It seemed as though there should be plenty of things to tell him, but patter about the office and traffic did not belong in this room, and he'd already heard endlessly that his family and friends were pulling hard for him.
So I held his hand and leaned on the side rail of his bed, getting my face as close to his as I could. We locked eyes and smiled, and words flowed silently between us, just as they had so many times over our 25 years of marriage. God, how I'd missed that!
The nurses had dimmed the lights in the ICU for the night, and though it was far from dark, the room had a nicer ambience than usual. Straightening up, I searched the channels on Doug's TV for something more suitable than CNN. Suddenly, there were Jake and Elwood sauntering into Aretha Franklin's eatery on their mission from God. Hey, Doug. I said, It's The Blues Brothers. Moments later, Aretha was belting out R‐E‐S‐P‐E‐C‐T, and I was gyrating. Doug was doing the only thing he could, swinging his head from side to side in time to the music.
It was just a tiny moment, a vignette unnoticed by anyone but us two in the life of that ICU. But it is the sweetest memory I have of that time. Just days before his death at age 55, the spark that was us had flamed briefly to life.
Handoffs
My dad was a hero. I suppose it's natural that I feel that way, growing up as I did in a small rural town where my father was the only doctor. Once, he was called to attend to a farmer who had climbed down from his combine, stating flatly that he was going to die. After this pronouncement, the farmer sat on the ground, where over the next hour he proceeded to do just that.
With the benefit of my own 30‐year career in medicine, it's easy to opine that this farmer probably had a pulmonary embolism from a lower extremity deep vein thrombosis (hours spent on the seat of a tractor are the rural equivalent of a long plane ride). I'm sure he was experiencing the feeling of impending doom that can signal such an event. What's harder to conjecture is how my father was able to quickly assess the situation, know his limitations, and still have the guts to carry on. There was no dialing 911, no starting of IVs, and no CPR once the chain of events started. Even if the doomed patient had been taken to the hospital, he would likely have died en route. If not, the personnel, equipment, and therapeutics there would not have been much more than those available in the wheat field. My father had all the tools he needed right there at the scene to bring comfort to that poor individual in the final moments of his life. He also had the courage to use them. What a hero!
Other events and memories of my father flash through my mind as I remember those times. Dozens of antibiotics rendered for cold virusesbut what a placebo effect from that big shot in the butt! Tonsillectomies performed right in the office, with a nurse‐anesthetist coming in once a week to render sedation. (That is until one of a set of twins transiently quit breathing, after which all surgeries were moved to the hospital!) A shot of adrenaline, given unsuccessfully, via the intracardiac route to a high school football player who suddenly collapsed on the 30‐yard line while the usually boisterous Friday‐night crowd watched in stunned horror. Countless hours waiting in the car for my dad to make house calls or finish rounds at the local hospital.
There, in that place and at that time, my dad was it. He embodied medical science, such as it was, in our little community. His black bag and bow tie helped complete the image. He did what he could, limited as it may have been, and he loved every minute of it. Sure, he sometimes complained. It was tough when a patient showed up at the back door and interrupted dinner. He didn't much like it when then‐president LBJ tried to socialize medicine with the Medicare Act. Most of all, he hated it when my mother insisted he take a job with regular hours at a VA hospital after he had two heart attacks and a bout with colon cancer. Mostly though, I remember a happy, self‐actualized guy, especially when he was at work.
My dad died when I was a freshman in medical school, so exactly what he thought about those times I really don't know. I do know, however, how much I loved him and how much I wanted to be just like him.
In medical school and later during my residency, I had other heroes. Appropriately, for someone who ended up an internist and hospitalist, most were master diagnosticians. There was J. Willis Hurst, the renowned cardiologist, who I once saw diagnose cardiac sarcoid solely on the basis of a 12‐lead electrocardiogram. And there was Jay Sanford, author of that little book on antibiotics known as the bugs and drugs book, tucked to this day into my lab coat pocket, who I once heard tell of going to war‐torn Vietnam to collect water samples in order to make the diagnosis of babesiosis. Finally, there was Walter McDonald, then chief of medicine at the Portland VA hospital, later executive vice‐president of the American College of Physicians, who, to a third‐year medical student like I was then, seemed omniscient about each case relayed to him at morning report. They all seemed so confident and clever; so dedicated, diligent, and proud. I wanted to be just like them.
Now, as a vice‐president for medical affairs, given the task of improving quality at a large teaching hospital, I herd cats. I recite from memory the embarrassing statistics on medical errors revealed by the Institute of Medicine in 1999. I plead for standardization and strive to eliminate variability in hospital practice. From the evidence, I extract guidelines and implement them via standard order sets. But frequently I look back and wonder.
Would the practice of medicine, where the goal is standardization and lack of variability, appeal to my older heroes? How would the practices of exceeding benchmarks, following pathways, and complying with indicators play to the icons of my past? Would they be satisfied to practice in today's health care environment? Or would they perish the thought if asked to standardize their orders and comply with best‐practice norms? After all, there was nothing normal about these guys! Sure they knew the literature and would be the first to insist that practice be evidenced based, but for them, that was never enough. What made them so attractive was their ability to go beyond what any of us able to read the journals could achieve. These men (and, sadly, most, but not all, were men) treasured autonomy, yearned for diagnostic brilliance, and doggedly pursued therapeutic breakthroughs. They set the standards that mere mortals like me aspired to achieve. They were heroes.
So we must be careful not to stifle genius while promoting compliance. We must not push the standardization of health care to a point where an individual's ability to rise above the pack is limited. We should remember that with decreased variability comes the risk of denying innovation. For keep in mind that improved methods like those of hospital medicine exist because those before us sought a better way. They were able to try, and sometimes fail, to use their intuition and individual street smarts and to take risks for the greater good. To use a tired phrase, they were able to think outside the box. In the name of quality, we must not further limit the confines of that box. We must assure that however much we strive to elevate the norm, we do not restrict those few who set the curve. We must allow for heroes.
I believe our profession can produce those who will carry the banner forward. I already have some new heroesDon Berwick, Peter Pronovost, and Bob Wachter. These individuals have demonstrated the ability to combine the patient‐centered care practiced by my father with the evidenced‐based knowledge and intuitive genius of my academic mentors. They are then able to apply this admixture of competencies to the problems facing health care today such as the deficiencies in patient safety and the inefficiencies of delivery.
New heroes will attract another generation of the best and the brightest, and the cycle will repeat. With careful foresight we can assure that this will happen. To do otherwise is unthinkable. We must have heroes.
My dad was a hero. I suppose it's natural that I feel that way, growing up as I did in a small rural town where my father was the only doctor. Once, he was called to attend to a farmer who had climbed down from his combine, stating flatly that he was going to die. After this pronouncement, the farmer sat on the ground, where over the next hour he proceeded to do just that.
With the benefit of my own 30‐year career in medicine, it's easy to opine that this farmer probably had a pulmonary embolism from a lower extremity deep vein thrombosis (hours spent on the seat of a tractor are the rural equivalent of a long plane ride). I'm sure he was experiencing the feeling of impending doom that can signal such an event. What's harder to conjecture is how my father was able to quickly assess the situation, know his limitations, and still have the guts to carry on. There was no dialing 911, no starting of IVs, and no CPR once the chain of events started. Even if the doomed patient had been taken to the hospital, he would likely have died en route. If not, the personnel, equipment, and therapeutics there would not have been much more than those available in the wheat field. My father had all the tools he needed right there at the scene to bring comfort to that poor individual in the final moments of his life. He also had the courage to use them. What a hero!
Other events and memories of my father flash through my mind as I remember those times. Dozens of antibiotics rendered for cold virusesbut what a placebo effect from that big shot in the butt! Tonsillectomies performed right in the office, with a nurse‐anesthetist coming in once a week to render sedation. (That is until one of a set of twins transiently quit breathing, after which all surgeries were moved to the hospital!) A shot of adrenaline, given unsuccessfully, via the intracardiac route to a high school football player who suddenly collapsed on the 30‐yard line while the usually boisterous Friday‐night crowd watched in stunned horror. Countless hours waiting in the car for my dad to make house calls or finish rounds at the local hospital.
There, in that place and at that time, my dad was it. He embodied medical science, such as it was, in our little community. His black bag and bow tie helped complete the image. He did what he could, limited as it may have been, and he loved every minute of it. Sure, he sometimes complained. It was tough when a patient showed up at the back door and interrupted dinner. He didn't much like it when then‐president LBJ tried to socialize medicine with the Medicare Act. Most of all, he hated it when my mother insisted he take a job with regular hours at a VA hospital after he had two heart attacks and a bout with colon cancer. Mostly though, I remember a happy, self‐actualized guy, especially when he was at work.
My dad died when I was a freshman in medical school, so exactly what he thought about those times I really don't know. I do know, however, how much I loved him and how much I wanted to be just like him.
In medical school and later during my residency, I had other heroes. Appropriately, for someone who ended up an internist and hospitalist, most were master diagnosticians. There was J. Willis Hurst, the renowned cardiologist, who I once saw diagnose cardiac sarcoid solely on the basis of a 12‐lead electrocardiogram. And there was Jay Sanford, author of that little book on antibiotics known as the bugs and drugs book, tucked to this day into my lab coat pocket, who I once heard tell of going to war‐torn Vietnam to collect water samples in order to make the diagnosis of babesiosis. Finally, there was Walter McDonald, then chief of medicine at the Portland VA hospital, later executive vice‐president of the American College of Physicians, who, to a third‐year medical student like I was then, seemed omniscient about each case relayed to him at morning report. They all seemed so confident and clever; so dedicated, diligent, and proud. I wanted to be just like them.
Now, as a vice‐president for medical affairs, given the task of improving quality at a large teaching hospital, I herd cats. I recite from memory the embarrassing statistics on medical errors revealed by the Institute of Medicine in 1999. I plead for standardization and strive to eliminate variability in hospital practice. From the evidence, I extract guidelines and implement them via standard order sets. But frequently I look back and wonder.
Would the practice of medicine, where the goal is standardization and lack of variability, appeal to my older heroes? How would the practices of exceeding benchmarks, following pathways, and complying with indicators play to the icons of my past? Would they be satisfied to practice in today's health care environment? Or would they perish the thought if asked to standardize their orders and comply with best‐practice norms? After all, there was nothing normal about these guys! Sure they knew the literature and would be the first to insist that practice be evidenced based, but for them, that was never enough. What made them so attractive was their ability to go beyond what any of us able to read the journals could achieve. These men (and, sadly, most, but not all, were men) treasured autonomy, yearned for diagnostic brilliance, and doggedly pursued therapeutic breakthroughs. They set the standards that mere mortals like me aspired to achieve. They were heroes.
So we must be careful not to stifle genius while promoting compliance. We must not push the standardization of health care to a point where an individual's ability to rise above the pack is limited. We should remember that with decreased variability comes the risk of denying innovation. For keep in mind that improved methods like those of hospital medicine exist because those before us sought a better way. They were able to try, and sometimes fail, to use their intuition and individual street smarts and to take risks for the greater good. To use a tired phrase, they were able to think outside the box. In the name of quality, we must not further limit the confines of that box. We must assure that however much we strive to elevate the norm, we do not restrict those few who set the curve. We must allow for heroes.
I believe our profession can produce those who will carry the banner forward. I already have some new heroesDon Berwick, Peter Pronovost, and Bob Wachter. These individuals have demonstrated the ability to combine the patient‐centered care practiced by my father with the evidenced‐based knowledge and intuitive genius of my academic mentors. They are then able to apply this admixture of competencies to the problems facing health care today such as the deficiencies in patient safety and the inefficiencies of delivery.
New heroes will attract another generation of the best and the brightest, and the cycle will repeat. With careful foresight we can assure that this will happen. To do otherwise is unthinkable. We must have heroes.
My dad was a hero. I suppose it's natural that I feel that way, growing up as I did in a small rural town where my father was the only doctor. Once, he was called to attend to a farmer who had climbed down from his combine, stating flatly that he was going to die. After this pronouncement, the farmer sat on the ground, where over the next hour he proceeded to do just that.
With the benefit of my own 30‐year career in medicine, it's easy to opine that this farmer probably had a pulmonary embolism from a lower extremity deep vein thrombosis (hours spent on the seat of a tractor are the rural equivalent of a long plane ride). I'm sure he was experiencing the feeling of impending doom that can signal such an event. What's harder to conjecture is how my father was able to quickly assess the situation, know his limitations, and still have the guts to carry on. There was no dialing 911, no starting of IVs, and no CPR once the chain of events started. Even if the doomed patient had been taken to the hospital, he would likely have died en route. If not, the personnel, equipment, and therapeutics there would not have been much more than those available in the wheat field. My father had all the tools he needed right there at the scene to bring comfort to that poor individual in the final moments of his life. He also had the courage to use them. What a hero!
Other events and memories of my father flash through my mind as I remember those times. Dozens of antibiotics rendered for cold virusesbut what a placebo effect from that big shot in the butt! Tonsillectomies performed right in the office, with a nurse‐anesthetist coming in once a week to render sedation. (That is until one of a set of twins transiently quit breathing, after which all surgeries were moved to the hospital!) A shot of adrenaline, given unsuccessfully, via the intracardiac route to a high school football player who suddenly collapsed on the 30‐yard line while the usually boisterous Friday‐night crowd watched in stunned horror. Countless hours waiting in the car for my dad to make house calls or finish rounds at the local hospital.
There, in that place and at that time, my dad was it. He embodied medical science, such as it was, in our little community. His black bag and bow tie helped complete the image. He did what he could, limited as it may have been, and he loved every minute of it. Sure, he sometimes complained. It was tough when a patient showed up at the back door and interrupted dinner. He didn't much like it when then‐president LBJ tried to socialize medicine with the Medicare Act. Most of all, he hated it when my mother insisted he take a job with regular hours at a VA hospital after he had two heart attacks and a bout with colon cancer. Mostly though, I remember a happy, self‐actualized guy, especially when he was at work.
My dad died when I was a freshman in medical school, so exactly what he thought about those times I really don't know. I do know, however, how much I loved him and how much I wanted to be just like him.
In medical school and later during my residency, I had other heroes. Appropriately, for someone who ended up an internist and hospitalist, most were master diagnosticians. There was J. Willis Hurst, the renowned cardiologist, who I once saw diagnose cardiac sarcoid solely on the basis of a 12‐lead electrocardiogram. And there was Jay Sanford, author of that little book on antibiotics known as the bugs and drugs book, tucked to this day into my lab coat pocket, who I once heard tell of going to war‐torn Vietnam to collect water samples in order to make the diagnosis of babesiosis. Finally, there was Walter McDonald, then chief of medicine at the Portland VA hospital, later executive vice‐president of the American College of Physicians, who, to a third‐year medical student like I was then, seemed omniscient about each case relayed to him at morning report. They all seemed so confident and clever; so dedicated, diligent, and proud. I wanted to be just like them.
Now, as a vice‐president for medical affairs, given the task of improving quality at a large teaching hospital, I herd cats. I recite from memory the embarrassing statistics on medical errors revealed by the Institute of Medicine in 1999. I plead for standardization and strive to eliminate variability in hospital practice. From the evidence, I extract guidelines and implement them via standard order sets. But frequently I look back and wonder.
Would the practice of medicine, where the goal is standardization and lack of variability, appeal to my older heroes? How would the practices of exceeding benchmarks, following pathways, and complying with indicators play to the icons of my past? Would they be satisfied to practice in today's health care environment? Or would they perish the thought if asked to standardize their orders and comply with best‐practice norms? After all, there was nothing normal about these guys! Sure they knew the literature and would be the first to insist that practice be evidenced based, but for them, that was never enough. What made them so attractive was their ability to go beyond what any of us able to read the journals could achieve. These men (and, sadly, most, but not all, were men) treasured autonomy, yearned for diagnostic brilliance, and doggedly pursued therapeutic breakthroughs. They set the standards that mere mortals like me aspired to achieve. They were heroes.
So we must be careful not to stifle genius while promoting compliance. We must not push the standardization of health care to a point where an individual's ability to rise above the pack is limited. We should remember that with decreased variability comes the risk of denying innovation. For keep in mind that improved methods like those of hospital medicine exist because those before us sought a better way. They were able to try, and sometimes fail, to use their intuition and individual street smarts and to take risks for the greater good. To use a tired phrase, they were able to think outside the box. In the name of quality, we must not further limit the confines of that box. We must assure that however much we strive to elevate the norm, we do not restrict those few who set the curve. We must allow for heroes.
I believe our profession can produce those who will carry the banner forward. I already have some new heroesDon Berwick, Peter Pronovost, and Bob Wachter. These individuals have demonstrated the ability to combine the patient‐centered care practiced by my father with the evidenced‐based knowledge and intuitive genius of my academic mentors. They are then able to apply this admixture of competencies to the problems facing health care today such as the deficiencies in patient safety and the inefficiencies of delivery.
New heroes will attract another generation of the best and the brightest, and the cycle will repeat. With careful foresight we can assure that this will happen. To do otherwise is unthinkable. We must have heroes.
Clinical Conundrum
A 47‐year‐old woman was brought to the emergency department by her family because of 1 week of abdominal pain. The pain had begun in the epigastrium but had spread across the abdomen. She described it as constant and 10 of 10 in intensity but could not identify aggravating or alleviating factors. She also complained of nausea and vomiting, beginning 4 days prior to presentation, occurring 25 times per day. She noted poor oral intake and mild diarrhea. She denied melena or hematochezia. She reported no recent fever, dysuria, chills, or night sweats; however, she reported upper respiratory symptoms 2 weeks prior to presentation. On the day of presentation, her family felt she was becoming increasingly lethargic.
Epigastric pain in a middle‐aged woman suggests several possible diagnoses. Conditions such as acute cholecystitis begin abruptly, whereas small bowel obstruction, appendicitis, and diverticulitis start gradually. Nausea and vomiting are common concomitants of abdominal pain and are nonspecific. The absence of fever and chills is reassuring. Of greatest concern is the mental status. Initially, I think of enterohemorrhagic E. coli syndromes with associated glomerulonephritis. With a more systemic metabolic abnormality such as this, the rapid development of the disease tends to exaggerate symptoms.
The patient had a history of nephrolithiasis and underwent total abdominal hysterectomy and bilateral salpingo‐oopherectomy secondary to uterine fibroids in the past. She took occasional acetaminophen, smoked two cigarettes per day, and rarely consumed alcohol. Temperature was 38.5C, heart rate was 160 beats/minute, respiratory rate was 28/minute, and blood pressure was 92/52 mm Hg; oxygen saturation was 100% breathing 2 L of oxygen by nasal cannula. She was a moderately obese African American woman in moderate distress, lying in bed moaning. Mucous membranes were dry. There was no lymphadenopathy or thyromegaly. Heart rate was regular without appreciable murmur, rub, or gallop. Lungs were clear. Abdomen was soft and nondistended, with diffuse tenderness to palpation; bowel sounds were present; there was no rebound or guarding. She had normal rectal tone with brown, guaiac‐negative stool. There was no costovertebral angle tenderness. She was oriented to person, place, and time but lethargic; deep tendon reflexes were 3+ bilaterally, and no focal signs were elicited.
Renal stones certainly produce abdominal pain, and the rare patient undergoes laparotomy for this reason. The hysterectomy tells us that small bowel obstruction could be a reason for her symptoms, although abnormal mental status would not be expected without additional problems such as infection. The tachycardia seems out of proportion to her temperature. Hyperpnea and absent respiratory symptoms, along with hypotension and tachycardia, suggest a sepsis syndrome. Her physical exam confirms dehydration. Examination of the abdomen makes me speculate about whether she has a nonsurgical cause of acute abdomen. The lethargy remains unexplained. Sepsis syndrome, possibly from a perinephric abscess, is my leading diagnosis.
White blood cell count was 15.9/mm3 with 78% neutrophils, a hemoglobin of 14.3 g/dL with a MCV of 76 and a platelet count of 320/mm3. Sodium was 159 mmol/L, chloride 128 mmol/L, bicarbonate 19 mmol/L, blood urea nitrogen 120 mmol/L, creatinine 3.1 mg/dL, calcium 11.7 mg/dL, albumin 3.3 g/dL, serum aspartate aminotransferase 65 U/L, serum alanine aminotransferase 72 U/L, total bilirubin 0.7 mg/dL, amylase 137 U/L (normal 30100), and lipase 92 IU/dL (normal 424). Urine obtained from a Foley catheter revealed negative nitrite and leukocyte esterase, 5075 red blood cells, and 1025 white blood cells per high‐powered field.
The elevated serum sodium is likely contributing to her abnormal mental status. It is unusual for a previously healthy and conscious woman to become this hypernatremic because persons with a normal mental status will defend their sodium balance strenuously, assuming regulatory mechanisms are intact. Generally, this level of hypernatremia indicates 2 things. One, a patient was not allowed, or did not seek access to, free water. The other is the presence of diabetes insipidus. It is unlikely she became this dehydrated from the initial gastrointestinal episode as described. The low MCV suggests she may be a thalassemia carrier, as microcytosis with iron deficiency typically does not occur until the patient is anemic, although she may be when rehydrated. Serum calcium, while elevated, also will likely return to the normal range with hydration. The metabolic abnormalities strongly suggest a problem in the central nervous system. The hematuria in the urinalysis continues to raise the possibility of nephrolithiasis as a cause of abdominal pain, though it does not fit well with the rest of the patient's clinical picture. The hematuria and pyuria both could still indicate a urinary tract infection such as pyelonephritis or perinephric abscess causing a sepsis syndrome.
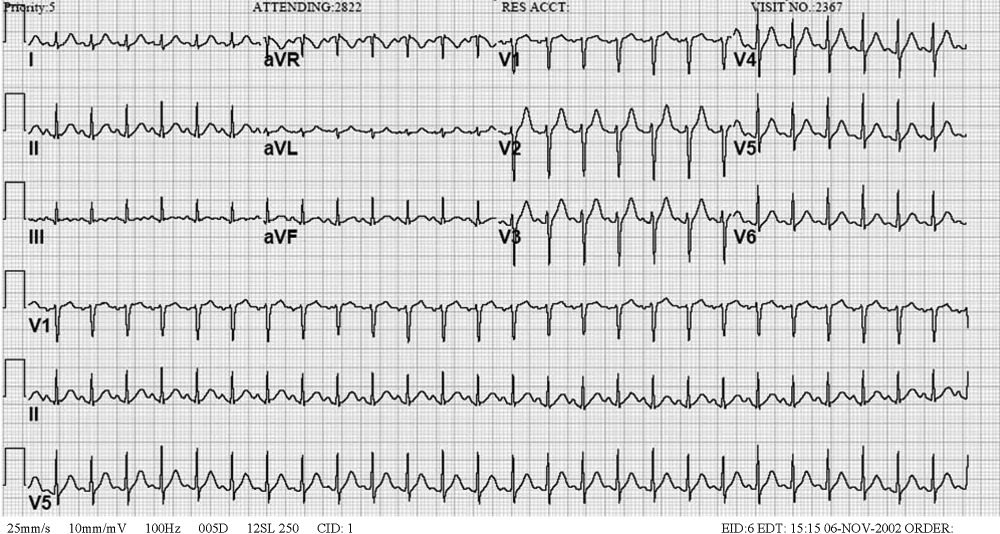
An acute abdominal series and chest radiograph revealed a paucity of gas in the abdomen but no free air under the diaphragm or active cardiopulmonary disease. Abdominal ultrasound showed cholelithiasis without biliary dilation. There was no evidence of hydronephrosis, hydroureter, or perinephric abscess. A noncontrast abdominal‐pelvic computed tomography (CT) scan demonstrated no peripancreatic stranding or fluid collection and no nephrolithiasis or fluid collection suggestive of abscess. The admission electrocardiogram, read as sinus tachycardia with a rate of 160, is displayed in Figure 1.
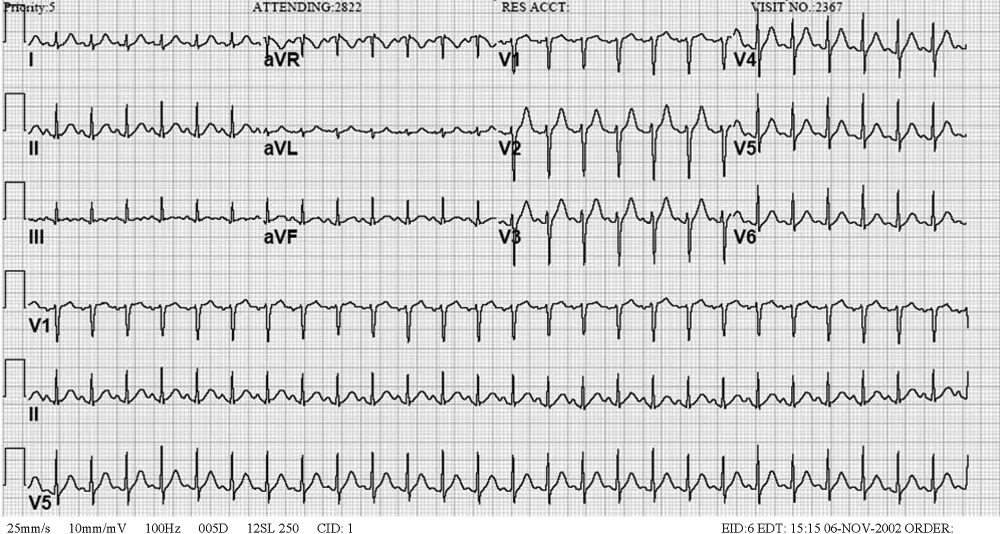
I have long believed that unexplained sinus tachycardia is one of the most ominous rhythms in clinical medicine; it is expected after vigorous exercise, among other situations, but not in the condition in which this woman finds herself. The nature of the tracing does not indicate the likelihood of a supraventricular arrhythmia, particularly atrial flutter, which should be considered given the rate. The absence of free air under the diaphragm on chest radiography is reassuring. Though the pancreatic enzymes are mildly elevated, they are usually far more striking in gallstone pancreatitis. Hypercalcemia may result in abdominal pain by several mechanisms. I remain concerned about her central nervous system.
The patient was admitted to the intensive care unit (ICU), where she received intravenous antibiotics and aggressive rehydration. The following morning, she continued to complain of abdominal pain. Her systolic blood pressure was 115 mmHg, and her heart rate ranged between 140 and 150 beats/minute. The remainder of her physical exam was unchanged. Repeat laboratory tests revealed a white blood cell count of 14.7/mm3, a blood urea nitrogen of 66 mg/dL, a creatinine of 1.3 mg.dL, amylase of 67 IU/L, and lipase of 70 IU/dL. A contrast‐enhanced abdominal‐pelvic CT scan did not reveal intra‐abdominal pathology. Blood and urine cultures obtained at admission were negative for any growth.
The patient was appropriately admitted to the ICU. When caring for a critically ill patient, establishing a diagnosis is less important initially than addressing treatable conditions with dispatch. The negative CT scans rule out previously entertained diagnoses like nephrolithiasis and perinephric abscess. It is possible that the initially positive urinalysis was a result of urinary catheter placement trauma. Given the course to date, I believe this patient likely has a nonsurgical cause of abdominal pain. I am considering entities such as lead intoxication, hypercalcemia, a tear of the rectus abdominus caused by vomiting, systemic vasculitis, or a hypercoagulable state leading to intra‐abdominal venous thrombosis.
By hospital day 3 her sodium decreased to 149 mmol/L and her creatinine was 1.0 mg/dL. Abdominal pain persisted, unchanged from admission. Her systolic blood pressure had stabilized at 120 mmHg, but the heart rate remained near 150 beats/minute. Her abdomen remained soft and nondistended on exam but diffusely tender to palpation. Her amylase and lipase continued to decrease, and her repeat electrocardiogram demonstrated tachycardia with a rate of 144.
We are gratified to see that her serum sodium has waned but not with the persistence of the tachycardia. It must be assumed that this patient has an infectious disease that we are not clever enough to diagnose at this time. I am also considering an autoimmune process, such as systemic lupus erythematosus. It is difficult to envision a neoplastic disorder causing these problems. The differential remains broad, however, because we have not ruled out metabolic or endocrine causes. It is difficult to imagine she could have Addison's diseasea common cause of severe abdominal pain, tachycardia, and hypotensiongiven her serum sodium level. Hyperthyroidism has been known to produce mild hypercalcemia and abdominal complaints and is an intriguing possibility. The striking elevation of her serum sodium makes me consider the possibility of a problem in the posterior pituitary gland such as sarcoidosis. I cannot explain how sarcoidosis would cause her abdominal pain, unless the hypercalcemia were related. The tachycardia remains of concern, especially if she is otherwise improving. Thus, I would likely administer a small dose of adenosine to ascertain that this is not a different supraventricular tachycardia. In sinus tachycardia, the rate is usually attendant to the clinical picture and thus begs explanation given her clinical improvement.
After receiving 6 mg of intravenous adenosine, the patient's heart rate declined; atrial flutter waves were observed.
This case nicely demonstrates a key teaching point: a fast regular heart rate of about 150, irrespective of the electrocardiogram, suggests atrial flutter. Who gets atrial flutter? Patients with chronic lung disease, myocardial ischemia (albeit rarely), alcohol‐induced cardiomyopathy, and infiltrative cardiac disorders do. Additionally, we also have to consider thyroid dysfunction.
If forced to come up with a single unifying diagnosis at this point, I would have to say this patient most likely has sarcoidosis because this entity would account for modest hypercalcemia, the myocardial conduction disturbance, and hypernatremia because of diabetes insipidus; furthermore, it would fit the patient's demographic profile. However, I am also concerned about hyperthyroidism and would not proceed until thyroid function studies were obtained.
Thyroid studies revealed thyroid stimulating hormone of less than 0.01 mU/L (normal range, 0.305.50), free thyroxine (T4) of 5.81 ng.dL (normal range, 0.731.79), free triiodothyronine (T3) of 15.7 pg/mL (normal range, 2.85.3), and total triiodothyronine (T3) of 218 ng/dL (normal range, 95170). The patient was diagnosed with thyroid crisis and was started on propranolol, propylthiouracil, hydrocortisone, and a saturated solution of potassium iodine. Thyroid stimulating immunoglobulins were obtained and found to be markedly elevated (3.4 TSI index; normal 1.3), suggestive of Grave's disease. Over the next several days, the patient's abdominal pain and tachycardia resolved. Her mental status returned to normal. A workup for her microcytic anemia revealed beta thalassemia trait. The patient was discharged home on hospital day 9 and has done well as an outpatient.
COMMENTARY
As Sir Zachary Cope stated in his classic text Cope's Early Diagnosis of the Acute Abdomen, [I]t is only by thorough history taking and physical examination that one can propound a diagnosis.1 When first presented with a patient whose chief complaint is abdominal pain, physicians tend to focus on the disorders of both the hollow and solid organs of the abdomen as potential sources of the pain. The differential diagnosis traditionally includes disorders such as cholecystitis, peptic ulcer disease, pancreatitis, small bowel obstruction, bowel ischemia or perforation, splenic abscess and infarct, nephrolithiasis, diverticulitis, and appendicitis, all of which were initially considered by the clinicians involved in this case. But as our discussant pointed out, in this case the differential needed to be broadened to include less common disorders, particularly given the patient's altered mental status, numerous electrolyte abnormalities, and lethargy and the lack of explanation provided by the physical examination and sophisticated imaging studies.
Specifically, a myriad of systemic diseases and metabolic derangements can cause abdominal complaints and mimic surgical abdominal disease, including hypercalcemia, acute intermittent porphyria, diabetic ketoacidosis, lead intoxication, familial Mediterranean fever, vasculopathies, adrenal insufficiency, and hyperthyroidism. Unfortunately, the frequency with which abdominal pain occurs in many of these less common disease processes and the pathophysiology that underlies its occurrence are not well defined. For example, abdominal pain is well described as a typical manifestation of both diabetic ketoacidosis and lead poisoning, but the pathophysiology behind its occurrence is poorly understood in both. Further, as a manifestation of thyrotoxicosis and as one of the diagnostic criteria for thyroid storm, the reported prevalence of abdominal pain in this condition is variable, ranging from rare to 20%47%.24 Also, although other gastrointestinal manifestations of hyperthyroidism (such as nausea, vomiting, and hyperdefecation) are thought to be the result of the effect of excess thyroid hormone on gastrointestinal motility, it is unclear whether this similar mechanism is responsible for the perception of abdominal pain.4
An important clue to the underlying diagnosis in this case was the patient's marked tachycardia. Classically, a persistent heart rate of 150 should raise suspicion of atrial flutter with a 2:1 conduction block, as was eventually discovered in this case. Adenosine, in addition to other vagal maneuvers such as carotid massage or Valsalva that also block atrioventricular (AV) node conduction, has been recognized as a safe and effective means of establishing a diagnosis in tachyarrhythmias.5 In AV nodal‐dependent tachycardias, such as AV node reentrant tachycardia or AV reentrant tachycardia, adenosine will often terminate the tachyarrhythmia by blocking the anterograde limb of the reentrant circuit. In AV nodeindependent tachyarrhythmias, such as atrial flutter or atrial fibrillation, adenosine will not terminate the rhythm. However, in the case of flutter, blocking the AV node will usually transiently unmask the underlying P waves, thereby facilitating the diagnosis.5, 6
In this patient, the discovery of atrial flutter was the main clue that thyrotoxicosis may provide the unifying diagnosis. Thyroid hormone has a direct positive cardiac chronotropic effect, resulting in the increased resting heart characteristic of thyrotoxicosis. Specifically, this hormone increases sinoatrial‐node firing, shortens the refractory period of conduction tissue within the heart, and decreases the electrical threshold for atrial excitation. In addition to predisposing to sinus tachycardia (the most common rhythm associated with this disorder), thyrotoxicosis is also associated with atrial tachycardias such as atrial flutter and, more classically, atrial fibrillation.7, 8 Though no studies have specifically evaluated the incidence of atrial flutter in thyrotoxicosis, atrial fibrillation has been found in 9%22% of these patients.7
Finally, several of the patient's electrolyte derangements could explain some of her clinical findings and are clues to the underlying diagnosis. She initially presented with a mild hypercalcemia that persisted even after hydration. Potential explanations include her severe dehydration or her underlying thyrotoxicosis because hypercalcemia is present in up to 20% of patients with hyperthyroidism.9, 10 However, the presence of significant hypercalcemia in the setting of thyrotoxicosis may actually make the diagnosis of thyrotoxicosis more difficult, masking the hypermetabolic signs and symptoms of the hyperthyroid state.11 Interestingly, coexistent primary hyperparathyroidism does occur in a few of these patients, but it likely was not an underlying cause in our patient given that her calcium normalized after receipt of propylthiouracil therapy.12
The patient's marked hypernatremia is more difficult to explain. She may have developed nephrogenic diabetes insipidus secondary to hypercalcemia, explained by a renal concentrating defect that can become evident once the calcium is persistently above 11 mg/dL.13 Combined with her altered mental status, which likely limited her ability to access free water, this may be enough to explain her marked hypernatremia. Her rapid improvement with rehydration is also consistent with this explanation, mediated through the improvement of her serum free calcium.
This case highlights the importance of using all the clinical clues provided by the history, physical exam, and laboratory and imaging studies when generating an initial differential diagnosis, as well as the importance of being willing to appropriately broaden and narrow the list of possibilities as a case evolves. When this patient was initially evaluated by physicians in the emergency department, they believed her symptoms were most consistent with generalized peritonitis that was likely secondary to an infectious or inflammatory intra‐abdominal process such as pancreatitis (especially in light of her mildly elevated lipase and amylase), appendicitis, or diverticulitis. When the medical team in the intensive care unit assumed care of this patient, members of the team failed to recognize several of the early clues, including the patient's markedly abnormal mental status, electrolyte derangements, and persistent tachycardia despite aggressive rehydration, which suggested the possibility of alternative, and less common, etiologies of her abdominal pain. Instead, they continued to aggressively pursue the possibility of the initial differential diagnosis, even repeating some of the previously negative studies from the emergency department. This case illustrates the importance of constantly reevaluating the available information from physical examination and laboratory and imaging studies and not falling victim to intellectual blind spots created by suggested diagnoses by other care providers. Fortunately for this patient, her thyroid crisis was diagnosed, albeit with some delay, before any long‐term complications occurred.
- Silen W, ed.Cope's Early Diagnosis of the Acute Abdomen.19th ed.New York:Oxford University Press;1995:4.
- ,.An unusual cause of abdominal pain in young woman.Ann Emerg Med.1991;20:574–582.
- .Vomiting, nausea and abdominal pain: unrecognized symptoms of thyrotoxicosis.J Fam Prac.1989;24:382–386.
- Powell DW,Alpers DH,Yamada,Owyang C,Laine L, eds.Textbook of Gastroenterology.3rd ed.Philadelphia, Pa:Lippincott Williams 783,2516.
- ,,.Usefulness of adenosine in diagnosis of tachyarrhythmias.Am J Cardiol.1995;75:952–955.
- ,,,,.Supraventricular tachycardia.Med Clin North Am.2001;85:193–223.
- .Thyrotoxicosis and the heart.N Engl J Med.1992;327:94–8.
- ,.Thyrotoxicosis and the heart.Endocrinol Metab Clin North Am.1998;27:51–62.
- ,,,.Treatment of thyrotoxic hypercalcemia with propranolol.N Engl J Med.1976;294:431.
- ,,,.Ionized and total plasma calcium and parathyroid hormone in hyperthyroidism.Ann Intern Med.1976;84:668.
- ,.Hypercalcemic crisis.Med Clin North Am.1995;79:79–92.
- ,,.Thyrotoxicosis, hypercalcemia, and secondary hyperparathyroidism.Arch Intern Med.1979;139:661–663.
- ,.Clinical Physiology of Acid‐Base and Electrolyte Disorders.5th ed.New York:McGraw‐Hill;2001:754–758.
A 47‐year‐old woman was brought to the emergency department by her family because of 1 week of abdominal pain. The pain had begun in the epigastrium but had spread across the abdomen. She described it as constant and 10 of 10 in intensity but could not identify aggravating or alleviating factors. She also complained of nausea and vomiting, beginning 4 days prior to presentation, occurring 25 times per day. She noted poor oral intake and mild diarrhea. She denied melena or hematochezia. She reported no recent fever, dysuria, chills, or night sweats; however, she reported upper respiratory symptoms 2 weeks prior to presentation. On the day of presentation, her family felt she was becoming increasingly lethargic.
Epigastric pain in a middle‐aged woman suggests several possible diagnoses. Conditions such as acute cholecystitis begin abruptly, whereas small bowel obstruction, appendicitis, and diverticulitis start gradually. Nausea and vomiting are common concomitants of abdominal pain and are nonspecific. The absence of fever and chills is reassuring. Of greatest concern is the mental status. Initially, I think of enterohemorrhagic E. coli syndromes with associated glomerulonephritis. With a more systemic metabolic abnormality such as this, the rapid development of the disease tends to exaggerate symptoms.
The patient had a history of nephrolithiasis and underwent total abdominal hysterectomy and bilateral salpingo‐oopherectomy secondary to uterine fibroids in the past. She took occasional acetaminophen, smoked two cigarettes per day, and rarely consumed alcohol. Temperature was 38.5C, heart rate was 160 beats/minute, respiratory rate was 28/minute, and blood pressure was 92/52 mm Hg; oxygen saturation was 100% breathing 2 L of oxygen by nasal cannula. She was a moderately obese African American woman in moderate distress, lying in bed moaning. Mucous membranes were dry. There was no lymphadenopathy or thyromegaly. Heart rate was regular without appreciable murmur, rub, or gallop. Lungs were clear. Abdomen was soft and nondistended, with diffuse tenderness to palpation; bowel sounds were present; there was no rebound or guarding. She had normal rectal tone with brown, guaiac‐negative stool. There was no costovertebral angle tenderness. She was oriented to person, place, and time but lethargic; deep tendon reflexes were 3+ bilaterally, and no focal signs were elicited.
Renal stones certainly produce abdominal pain, and the rare patient undergoes laparotomy for this reason. The hysterectomy tells us that small bowel obstruction could be a reason for her symptoms, although abnormal mental status would not be expected without additional problems such as infection. The tachycardia seems out of proportion to her temperature. Hyperpnea and absent respiratory symptoms, along with hypotension and tachycardia, suggest a sepsis syndrome. Her physical exam confirms dehydration. Examination of the abdomen makes me speculate about whether she has a nonsurgical cause of acute abdomen. The lethargy remains unexplained. Sepsis syndrome, possibly from a perinephric abscess, is my leading diagnosis.
White blood cell count was 15.9/mm3 with 78% neutrophils, a hemoglobin of 14.3 g/dL with a MCV of 76 and a platelet count of 320/mm3. Sodium was 159 mmol/L, chloride 128 mmol/L, bicarbonate 19 mmol/L, blood urea nitrogen 120 mmol/L, creatinine 3.1 mg/dL, calcium 11.7 mg/dL, albumin 3.3 g/dL, serum aspartate aminotransferase 65 U/L, serum alanine aminotransferase 72 U/L, total bilirubin 0.7 mg/dL, amylase 137 U/L (normal 30100), and lipase 92 IU/dL (normal 424). Urine obtained from a Foley catheter revealed negative nitrite and leukocyte esterase, 5075 red blood cells, and 1025 white blood cells per high‐powered field.
The elevated serum sodium is likely contributing to her abnormal mental status. It is unusual for a previously healthy and conscious woman to become this hypernatremic because persons with a normal mental status will defend their sodium balance strenuously, assuming regulatory mechanisms are intact. Generally, this level of hypernatremia indicates 2 things. One, a patient was not allowed, or did not seek access to, free water. The other is the presence of diabetes insipidus. It is unlikely she became this dehydrated from the initial gastrointestinal episode as described. The low MCV suggests she may be a thalassemia carrier, as microcytosis with iron deficiency typically does not occur until the patient is anemic, although she may be when rehydrated. Serum calcium, while elevated, also will likely return to the normal range with hydration. The metabolic abnormalities strongly suggest a problem in the central nervous system. The hematuria in the urinalysis continues to raise the possibility of nephrolithiasis as a cause of abdominal pain, though it does not fit well with the rest of the patient's clinical picture. The hematuria and pyuria both could still indicate a urinary tract infection such as pyelonephritis or perinephric abscess causing a sepsis syndrome.
An acute abdominal series and chest radiograph revealed a paucity of gas in the abdomen but no free air under the diaphragm or active cardiopulmonary disease. Abdominal ultrasound showed cholelithiasis without biliary dilation. There was no evidence of hydronephrosis, hydroureter, or perinephric abscess. A noncontrast abdominal‐pelvic computed tomography (CT) scan demonstrated no peripancreatic stranding or fluid collection and no nephrolithiasis or fluid collection suggestive of abscess. The admission electrocardiogram, read as sinus tachycardia with a rate of 160, is displayed in Figure 1.
I have long believed that unexplained sinus tachycardia is one of the most ominous rhythms in clinical medicine; it is expected after vigorous exercise, among other situations, but not in the condition in which this woman finds herself. The nature of the tracing does not indicate the likelihood of a supraventricular arrhythmia, particularly atrial flutter, which should be considered given the rate. The absence of free air under the diaphragm on chest radiography is reassuring. Though the pancreatic enzymes are mildly elevated, they are usually far more striking in gallstone pancreatitis. Hypercalcemia may result in abdominal pain by several mechanisms. I remain concerned about her central nervous system.
The patient was admitted to the intensive care unit (ICU), where she received intravenous antibiotics and aggressive rehydration. The following morning, she continued to complain of abdominal pain. Her systolic blood pressure was 115 mmHg, and her heart rate ranged between 140 and 150 beats/minute. The remainder of her physical exam was unchanged. Repeat laboratory tests revealed a white blood cell count of 14.7/mm3, a blood urea nitrogen of 66 mg/dL, a creatinine of 1.3 mg.dL, amylase of 67 IU/L, and lipase of 70 IU/dL. A contrast‐enhanced abdominal‐pelvic CT scan did not reveal intra‐abdominal pathology. Blood and urine cultures obtained at admission were negative for any growth.
The patient was appropriately admitted to the ICU. When caring for a critically ill patient, establishing a diagnosis is less important initially than addressing treatable conditions with dispatch. The negative CT scans rule out previously entertained diagnoses like nephrolithiasis and perinephric abscess. It is possible that the initially positive urinalysis was a result of urinary catheter placement trauma. Given the course to date, I believe this patient likely has a nonsurgical cause of abdominal pain. I am considering entities such as lead intoxication, hypercalcemia, a tear of the rectus abdominus caused by vomiting, systemic vasculitis, or a hypercoagulable state leading to intra‐abdominal venous thrombosis.
By hospital day 3 her sodium decreased to 149 mmol/L and her creatinine was 1.0 mg/dL. Abdominal pain persisted, unchanged from admission. Her systolic blood pressure had stabilized at 120 mmHg, but the heart rate remained near 150 beats/minute. Her abdomen remained soft and nondistended on exam but diffusely tender to palpation. Her amylase and lipase continued to decrease, and her repeat electrocardiogram demonstrated tachycardia with a rate of 144.
We are gratified to see that her serum sodium has waned but not with the persistence of the tachycardia. It must be assumed that this patient has an infectious disease that we are not clever enough to diagnose at this time. I am also considering an autoimmune process, such as systemic lupus erythematosus. It is difficult to envision a neoplastic disorder causing these problems. The differential remains broad, however, because we have not ruled out metabolic or endocrine causes. It is difficult to imagine she could have Addison's diseasea common cause of severe abdominal pain, tachycardia, and hypotensiongiven her serum sodium level. Hyperthyroidism has been known to produce mild hypercalcemia and abdominal complaints and is an intriguing possibility. The striking elevation of her serum sodium makes me consider the possibility of a problem in the posterior pituitary gland such as sarcoidosis. I cannot explain how sarcoidosis would cause her abdominal pain, unless the hypercalcemia were related. The tachycardia remains of concern, especially if she is otherwise improving. Thus, I would likely administer a small dose of adenosine to ascertain that this is not a different supraventricular tachycardia. In sinus tachycardia, the rate is usually attendant to the clinical picture and thus begs explanation given her clinical improvement.
After receiving 6 mg of intravenous adenosine, the patient's heart rate declined; atrial flutter waves were observed.
This case nicely demonstrates a key teaching point: a fast regular heart rate of about 150, irrespective of the electrocardiogram, suggests atrial flutter. Who gets atrial flutter? Patients with chronic lung disease, myocardial ischemia (albeit rarely), alcohol‐induced cardiomyopathy, and infiltrative cardiac disorders do. Additionally, we also have to consider thyroid dysfunction.
If forced to come up with a single unifying diagnosis at this point, I would have to say this patient most likely has sarcoidosis because this entity would account for modest hypercalcemia, the myocardial conduction disturbance, and hypernatremia because of diabetes insipidus; furthermore, it would fit the patient's demographic profile. However, I am also concerned about hyperthyroidism and would not proceed until thyroid function studies were obtained.
Thyroid studies revealed thyroid stimulating hormone of less than 0.01 mU/L (normal range, 0.305.50), free thyroxine (T4) of 5.81 ng.dL (normal range, 0.731.79), free triiodothyronine (T3) of 15.7 pg/mL (normal range, 2.85.3), and total triiodothyronine (T3) of 218 ng/dL (normal range, 95170). The patient was diagnosed with thyroid crisis and was started on propranolol, propylthiouracil, hydrocortisone, and a saturated solution of potassium iodine. Thyroid stimulating immunoglobulins were obtained and found to be markedly elevated (3.4 TSI index; normal 1.3), suggestive of Grave's disease. Over the next several days, the patient's abdominal pain and tachycardia resolved. Her mental status returned to normal. A workup for her microcytic anemia revealed beta thalassemia trait. The patient was discharged home on hospital day 9 and has done well as an outpatient.
COMMENTARY
As Sir Zachary Cope stated in his classic text Cope's Early Diagnosis of the Acute Abdomen, [I]t is only by thorough history taking and physical examination that one can propound a diagnosis.1 When first presented with a patient whose chief complaint is abdominal pain, physicians tend to focus on the disorders of both the hollow and solid organs of the abdomen as potential sources of the pain. The differential diagnosis traditionally includes disorders such as cholecystitis, peptic ulcer disease, pancreatitis, small bowel obstruction, bowel ischemia or perforation, splenic abscess and infarct, nephrolithiasis, diverticulitis, and appendicitis, all of which were initially considered by the clinicians involved in this case. But as our discussant pointed out, in this case the differential needed to be broadened to include less common disorders, particularly given the patient's altered mental status, numerous electrolyte abnormalities, and lethargy and the lack of explanation provided by the physical examination and sophisticated imaging studies.
Specifically, a myriad of systemic diseases and metabolic derangements can cause abdominal complaints and mimic surgical abdominal disease, including hypercalcemia, acute intermittent porphyria, diabetic ketoacidosis, lead intoxication, familial Mediterranean fever, vasculopathies, adrenal insufficiency, and hyperthyroidism. Unfortunately, the frequency with which abdominal pain occurs in many of these less common disease processes and the pathophysiology that underlies its occurrence are not well defined. For example, abdominal pain is well described as a typical manifestation of both diabetic ketoacidosis and lead poisoning, but the pathophysiology behind its occurrence is poorly understood in both. Further, as a manifestation of thyrotoxicosis and as one of the diagnostic criteria for thyroid storm, the reported prevalence of abdominal pain in this condition is variable, ranging from rare to 20%47%.24 Also, although other gastrointestinal manifestations of hyperthyroidism (such as nausea, vomiting, and hyperdefecation) are thought to be the result of the effect of excess thyroid hormone on gastrointestinal motility, it is unclear whether this similar mechanism is responsible for the perception of abdominal pain.4
An important clue to the underlying diagnosis in this case was the patient's marked tachycardia. Classically, a persistent heart rate of 150 should raise suspicion of atrial flutter with a 2:1 conduction block, as was eventually discovered in this case. Adenosine, in addition to other vagal maneuvers such as carotid massage or Valsalva that also block atrioventricular (AV) node conduction, has been recognized as a safe and effective means of establishing a diagnosis in tachyarrhythmias.5 In AV nodal‐dependent tachycardias, such as AV node reentrant tachycardia or AV reentrant tachycardia, adenosine will often terminate the tachyarrhythmia by blocking the anterograde limb of the reentrant circuit. In AV nodeindependent tachyarrhythmias, such as atrial flutter or atrial fibrillation, adenosine will not terminate the rhythm. However, in the case of flutter, blocking the AV node will usually transiently unmask the underlying P waves, thereby facilitating the diagnosis.5, 6
In this patient, the discovery of atrial flutter was the main clue that thyrotoxicosis may provide the unifying diagnosis. Thyroid hormone has a direct positive cardiac chronotropic effect, resulting in the increased resting heart characteristic of thyrotoxicosis. Specifically, this hormone increases sinoatrial‐node firing, shortens the refractory period of conduction tissue within the heart, and decreases the electrical threshold for atrial excitation. In addition to predisposing to sinus tachycardia (the most common rhythm associated with this disorder), thyrotoxicosis is also associated with atrial tachycardias such as atrial flutter and, more classically, atrial fibrillation.7, 8 Though no studies have specifically evaluated the incidence of atrial flutter in thyrotoxicosis, atrial fibrillation has been found in 9%22% of these patients.7
Finally, several of the patient's electrolyte derangements could explain some of her clinical findings and are clues to the underlying diagnosis. She initially presented with a mild hypercalcemia that persisted even after hydration. Potential explanations include her severe dehydration or her underlying thyrotoxicosis because hypercalcemia is present in up to 20% of patients with hyperthyroidism.9, 10 However, the presence of significant hypercalcemia in the setting of thyrotoxicosis may actually make the diagnosis of thyrotoxicosis more difficult, masking the hypermetabolic signs and symptoms of the hyperthyroid state.11 Interestingly, coexistent primary hyperparathyroidism does occur in a few of these patients, but it likely was not an underlying cause in our patient given that her calcium normalized after receipt of propylthiouracil therapy.12
The patient's marked hypernatremia is more difficult to explain. She may have developed nephrogenic diabetes insipidus secondary to hypercalcemia, explained by a renal concentrating defect that can become evident once the calcium is persistently above 11 mg/dL.13 Combined with her altered mental status, which likely limited her ability to access free water, this may be enough to explain her marked hypernatremia. Her rapid improvement with rehydration is also consistent with this explanation, mediated through the improvement of her serum free calcium.
This case highlights the importance of using all the clinical clues provided by the history, physical exam, and laboratory and imaging studies when generating an initial differential diagnosis, as well as the importance of being willing to appropriately broaden and narrow the list of possibilities as a case evolves. When this patient was initially evaluated by physicians in the emergency department, they believed her symptoms were most consistent with generalized peritonitis that was likely secondary to an infectious or inflammatory intra‐abdominal process such as pancreatitis (especially in light of her mildly elevated lipase and amylase), appendicitis, or diverticulitis. When the medical team in the intensive care unit assumed care of this patient, members of the team failed to recognize several of the early clues, including the patient's markedly abnormal mental status, electrolyte derangements, and persistent tachycardia despite aggressive rehydration, which suggested the possibility of alternative, and less common, etiologies of her abdominal pain. Instead, they continued to aggressively pursue the possibility of the initial differential diagnosis, even repeating some of the previously negative studies from the emergency department. This case illustrates the importance of constantly reevaluating the available information from physical examination and laboratory and imaging studies and not falling victim to intellectual blind spots created by suggested diagnoses by other care providers. Fortunately for this patient, her thyroid crisis was diagnosed, albeit with some delay, before any long‐term complications occurred.
A 47‐year‐old woman was brought to the emergency department by her family because of 1 week of abdominal pain. The pain had begun in the epigastrium but had spread across the abdomen. She described it as constant and 10 of 10 in intensity but could not identify aggravating or alleviating factors. She also complained of nausea and vomiting, beginning 4 days prior to presentation, occurring 25 times per day. She noted poor oral intake and mild diarrhea. She denied melena or hematochezia. She reported no recent fever, dysuria, chills, or night sweats; however, she reported upper respiratory symptoms 2 weeks prior to presentation. On the day of presentation, her family felt she was becoming increasingly lethargic.
Epigastric pain in a middle‐aged woman suggests several possible diagnoses. Conditions such as acute cholecystitis begin abruptly, whereas small bowel obstruction, appendicitis, and diverticulitis start gradually. Nausea and vomiting are common concomitants of abdominal pain and are nonspecific. The absence of fever and chills is reassuring. Of greatest concern is the mental status. Initially, I think of enterohemorrhagic E. coli syndromes with associated glomerulonephritis. With a more systemic metabolic abnormality such as this, the rapid development of the disease tends to exaggerate symptoms.
The patient had a history of nephrolithiasis and underwent total abdominal hysterectomy and bilateral salpingo‐oopherectomy secondary to uterine fibroids in the past. She took occasional acetaminophen, smoked two cigarettes per day, and rarely consumed alcohol. Temperature was 38.5C, heart rate was 160 beats/minute, respiratory rate was 28/minute, and blood pressure was 92/52 mm Hg; oxygen saturation was 100% breathing 2 L of oxygen by nasal cannula. She was a moderately obese African American woman in moderate distress, lying in bed moaning. Mucous membranes were dry. There was no lymphadenopathy or thyromegaly. Heart rate was regular without appreciable murmur, rub, or gallop. Lungs were clear. Abdomen was soft and nondistended, with diffuse tenderness to palpation; bowel sounds were present; there was no rebound or guarding. She had normal rectal tone with brown, guaiac‐negative stool. There was no costovertebral angle tenderness. She was oriented to person, place, and time but lethargic; deep tendon reflexes were 3+ bilaterally, and no focal signs were elicited.
Renal stones certainly produce abdominal pain, and the rare patient undergoes laparotomy for this reason. The hysterectomy tells us that small bowel obstruction could be a reason for her symptoms, although abnormal mental status would not be expected without additional problems such as infection. The tachycardia seems out of proportion to her temperature. Hyperpnea and absent respiratory symptoms, along with hypotension and tachycardia, suggest a sepsis syndrome. Her physical exam confirms dehydration. Examination of the abdomen makes me speculate about whether she has a nonsurgical cause of acute abdomen. The lethargy remains unexplained. Sepsis syndrome, possibly from a perinephric abscess, is my leading diagnosis.
White blood cell count was 15.9/mm3 with 78% neutrophils, a hemoglobin of 14.3 g/dL with a MCV of 76 and a platelet count of 320/mm3. Sodium was 159 mmol/L, chloride 128 mmol/L, bicarbonate 19 mmol/L, blood urea nitrogen 120 mmol/L, creatinine 3.1 mg/dL, calcium 11.7 mg/dL, albumin 3.3 g/dL, serum aspartate aminotransferase 65 U/L, serum alanine aminotransferase 72 U/L, total bilirubin 0.7 mg/dL, amylase 137 U/L (normal 30100), and lipase 92 IU/dL (normal 424). Urine obtained from a Foley catheter revealed negative nitrite and leukocyte esterase, 5075 red blood cells, and 1025 white blood cells per high‐powered field.
The elevated serum sodium is likely contributing to her abnormal mental status. It is unusual for a previously healthy and conscious woman to become this hypernatremic because persons with a normal mental status will defend their sodium balance strenuously, assuming regulatory mechanisms are intact. Generally, this level of hypernatremia indicates 2 things. One, a patient was not allowed, or did not seek access to, free water. The other is the presence of diabetes insipidus. It is unlikely she became this dehydrated from the initial gastrointestinal episode as described. The low MCV suggests she may be a thalassemia carrier, as microcytosis with iron deficiency typically does not occur until the patient is anemic, although she may be when rehydrated. Serum calcium, while elevated, also will likely return to the normal range with hydration. The metabolic abnormalities strongly suggest a problem in the central nervous system. The hematuria in the urinalysis continues to raise the possibility of nephrolithiasis as a cause of abdominal pain, though it does not fit well with the rest of the patient's clinical picture. The hematuria and pyuria both could still indicate a urinary tract infection such as pyelonephritis or perinephric abscess causing a sepsis syndrome.
An acute abdominal series and chest radiograph revealed a paucity of gas in the abdomen but no free air under the diaphragm or active cardiopulmonary disease. Abdominal ultrasound showed cholelithiasis without biliary dilation. There was no evidence of hydronephrosis, hydroureter, or perinephric abscess. A noncontrast abdominal‐pelvic computed tomography (CT) scan demonstrated no peripancreatic stranding or fluid collection and no nephrolithiasis or fluid collection suggestive of abscess. The admission electrocardiogram, read as sinus tachycardia with a rate of 160, is displayed in Figure 1.
I have long believed that unexplained sinus tachycardia is one of the most ominous rhythms in clinical medicine; it is expected after vigorous exercise, among other situations, but not in the condition in which this woman finds herself. The nature of the tracing does not indicate the likelihood of a supraventricular arrhythmia, particularly atrial flutter, which should be considered given the rate. The absence of free air under the diaphragm on chest radiography is reassuring. Though the pancreatic enzymes are mildly elevated, they are usually far more striking in gallstone pancreatitis. Hypercalcemia may result in abdominal pain by several mechanisms. I remain concerned about her central nervous system.
The patient was admitted to the intensive care unit (ICU), where she received intravenous antibiotics and aggressive rehydration. The following morning, she continued to complain of abdominal pain. Her systolic blood pressure was 115 mmHg, and her heart rate ranged between 140 and 150 beats/minute. The remainder of her physical exam was unchanged. Repeat laboratory tests revealed a white blood cell count of 14.7/mm3, a blood urea nitrogen of 66 mg/dL, a creatinine of 1.3 mg.dL, amylase of 67 IU/L, and lipase of 70 IU/dL. A contrast‐enhanced abdominal‐pelvic CT scan did not reveal intra‐abdominal pathology. Blood and urine cultures obtained at admission were negative for any growth.
The patient was appropriately admitted to the ICU. When caring for a critically ill patient, establishing a diagnosis is less important initially than addressing treatable conditions with dispatch. The negative CT scans rule out previously entertained diagnoses like nephrolithiasis and perinephric abscess. It is possible that the initially positive urinalysis was a result of urinary catheter placement trauma. Given the course to date, I believe this patient likely has a nonsurgical cause of abdominal pain. I am considering entities such as lead intoxication, hypercalcemia, a tear of the rectus abdominus caused by vomiting, systemic vasculitis, or a hypercoagulable state leading to intra‐abdominal venous thrombosis.
By hospital day 3 her sodium decreased to 149 mmol/L and her creatinine was 1.0 mg/dL. Abdominal pain persisted, unchanged from admission. Her systolic blood pressure had stabilized at 120 mmHg, but the heart rate remained near 150 beats/minute. Her abdomen remained soft and nondistended on exam but diffusely tender to palpation. Her amylase and lipase continued to decrease, and her repeat electrocardiogram demonstrated tachycardia with a rate of 144.
We are gratified to see that her serum sodium has waned but not with the persistence of the tachycardia. It must be assumed that this patient has an infectious disease that we are not clever enough to diagnose at this time. I am also considering an autoimmune process, such as systemic lupus erythematosus. It is difficult to envision a neoplastic disorder causing these problems. The differential remains broad, however, because we have not ruled out metabolic or endocrine causes. It is difficult to imagine she could have Addison's diseasea common cause of severe abdominal pain, tachycardia, and hypotensiongiven her serum sodium level. Hyperthyroidism has been known to produce mild hypercalcemia and abdominal complaints and is an intriguing possibility. The striking elevation of her serum sodium makes me consider the possibility of a problem in the posterior pituitary gland such as sarcoidosis. I cannot explain how sarcoidosis would cause her abdominal pain, unless the hypercalcemia were related. The tachycardia remains of concern, especially if she is otherwise improving. Thus, I would likely administer a small dose of adenosine to ascertain that this is not a different supraventricular tachycardia. In sinus tachycardia, the rate is usually attendant to the clinical picture and thus begs explanation given her clinical improvement.
After receiving 6 mg of intravenous adenosine, the patient's heart rate declined; atrial flutter waves were observed.
This case nicely demonstrates a key teaching point: a fast regular heart rate of about 150, irrespective of the electrocardiogram, suggests atrial flutter. Who gets atrial flutter? Patients with chronic lung disease, myocardial ischemia (albeit rarely), alcohol‐induced cardiomyopathy, and infiltrative cardiac disorders do. Additionally, we also have to consider thyroid dysfunction.
If forced to come up with a single unifying diagnosis at this point, I would have to say this patient most likely has sarcoidosis because this entity would account for modest hypercalcemia, the myocardial conduction disturbance, and hypernatremia because of diabetes insipidus; furthermore, it would fit the patient's demographic profile. However, I am also concerned about hyperthyroidism and would not proceed until thyroid function studies were obtained.
Thyroid studies revealed thyroid stimulating hormone of less than 0.01 mU/L (normal range, 0.305.50), free thyroxine (T4) of 5.81 ng.dL (normal range, 0.731.79), free triiodothyronine (T3) of 15.7 pg/mL (normal range, 2.85.3), and total triiodothyronine (T3) of 218 ng/dL (normal range, 95170). The patient was diagnosed with thyroid crisis and was started on propranolol, propylthiouracil, hydrocortisone, and a saturated solution of potassium iodine. Thyroid stimulating immunoglobulins were obtained and found to be markedly elevated (3.4 TSI index; normal 1.3), suggestive of Grave's disease. Over the next several days, the patient's abdominal pain and tachycardia resolved. Her mental status returned to normal. A workup for her microcytic anemia revealed beta thalassemia trait. The patient was discharged home on hospital day 9 and has done well as an outpatient.
COMMENTARY
As Sir Zachary Cope stated in his classic text Cope's Early Diagnosis of the Acute Abdomen, [I]t is only by thorough history taking and physical examination that one can propound a diagnosis.1 When first presented with a patient whose chief complaint is abdominal pain, physicians tend to focus on the disorders of both the hollow and solid organs of the abdomen as potential sources of the pain. The differential diagnosis traditionally includes disorders such as cholecystitis, peptic ulcer disease, pancreatitis, small bowel obstruction, bowel ischemia or perforation, splenic abscess and infarct, nephrolithiasis, diverticulitis, and appendicitis, all of which were initially considered by the clinicians involved in this case. But as our discussant pointed out, in this case the differential needed to be broadened to include less common disorders, particularly given the patient's altered mental status, numerous electrolyte abnormalities, and lethargy and the lack of explanation provided by the physical examination and sophisticated imaging studies.
Specifically, a myriad of systemic diseases and metabolic derangements can cause abdominal complaints and mimic surgical abdominal disease, including hypercalcemia, acute intermittent porphyria, diabetic ketoacidosis, lead intoxication, familial Mediterranean fever, vasculopathies, adrenal insufficiency, and hyperthyroidism. Unfortunately, the frequency with which abdominal pain occurs in many of these less common disease processes and the pathophysiology that underlies its occurrence are not well defined. For example, abdominal pain is well described as a typical manifestation of both diabetic ketoacidosis and lead poisoning, but the pathophysiology behind its occurrence is poorly understood in both. Further, as a manifestation of thyrotoxicosis and as one of the diagnostic criteria for thyroid storm, the reported prevalence of abdominal pain in this condition is variable, ranging from rare to 20%47%.24 Also, although other gastrointestinal manifestations of hyperthyroidism (such as nausea, vomiting, and hyperdefecation) are thought to be the result of the effect of excess thyroid hormone on gastrointestinal motility, it is unclear whether this similar mechanism is responsible for the perception of abdominal pain.4
An important clue to the underlying diagnosis in this case was the patient's marked tachycardia. Classically, a persistent heart rate of 150 should raise suspicion of atrial flutter with a 2:1 conduction block, as was eventually discovered in this case. Adenosine, in addition to other vagal maneuvers such as carotid massage or Valsalva that also block atrioventricular (AV) node conduction, has been recognized as a safe and effective means of establishing a diagnosis in tachyarrhythmias.5 In AV nodal‐dependent tachycardias, such as AV node reentrant tachycardia or AV reentrant tachycardia, adenosine will often terminate the tachyarrhythmia by blocking the anterograde limb of the reentrant circuit. In AV nodeindependent tachyarrhythmias, such as atrial flutter or atrial fibrillation, adenosine will not terminate the rhythm. However, in the case of flutter, blocking the AV node will usually transiently unmask the underlying P waves, thereby facilitating the diagnosis.5, 6
In this patient, the discovery of atrial flutter was the main clue that thyrotoxicosis may provide the unifying diagnosis. Thyroid hormone has a direct positive cardiac chronotropic effect, resulting in the increased resting heart characteristic of thyrotoxicosis. Specifically, this hormone increases sinoatrial‐node firing, shortens the refractory period of conduction tissue within the heart, and decreases the electrical threshold for atrial excitation. In addition to predisposing to sinus tachycardia (the most common rhythm associated with this disorder), thyrotoxicosis is also associated with atrial tachycardias such as atrial flutter and, more classically, atrial fibrillation.7, 8 Though no studies have specifically evaluated the incidence of atrial flutter in thyrotoxicosis, atrial fibrillation has been found in 9%22% of these patients.7
Finally, several of the patient's electrolyte derangements could explain some of her clinical findings and are clues to the underlying diagnosis. She initially presented with a mild hypercalcemia that persisted even after hydration. Potential explanations include her severe dehydration or her underlying thyrotoxicosis because hypercalcemia is present in up to 20% of patients with hyperthyroidism.9, 10 However, the presence of significant hypercalcemia in the setting of thyrotoxicosis may actually make the diagnosis of thyrotoxicosis more difficult, masking the hypermetabolic signs and symptoms of the hyperthyroid state.11 Interestingly, coexistent primary hyperparathyroidism does occur in a few of these patients, but it likely was not an underlying cause in our patient given that her calcium normalized after receipt of propylthiouracil therapy.12
The patient's marked hypernatremia is more difficult to explain. She may have developed nephrogenic diabetes insipidus secondary to hypercalcemia, explained by a renal concentrating defect that can become evident once the calcium is persistently above 11 mg/dL.13 Combined with her altered mental status, which likely limited her ability to access free water, this may be enough to explain her marked hypernatremia. Her rapid improvement with rehydration is also consistent with this explanation, mediated through the improvement of her serum free calcium.
This case highlights the importance of using all the clinical clues provided by the history, physical exam, and laboratory and imaging studies when generating an initial differential diagnosis, as well as the importance of being willing to appropriately broaden and narrow the list of possibilities as a case evolves. When this patient was initially evaluated by physicians in the emergency department, they believed her symptoms were most consistent with generalized peritonitis that was likely secondary to an infectious or inflammatory intra‐abdominal process such as pancreatitis (especially in light of her mildly elevated lipase and amylase), appendicitis, or diverticulitis. When the medical team in the intensive care unit assumed care of this patient, members of the team failed to recognize several of the early clues, including the patient's markedly abnormal mental status, electrolyte derangements, and persistent tachycardia despite aggressive rehydration, which suggested the possibility of alternative, and less common, etiologies of her abdominal pain. Instead, they continued to aggressively pursue the possibility of the initial differential diagnosis, even repeating some of the previously negative studies from the emergency department. This case illustrates the importance of constantly reevaluating the available information from physical examination and laboratory and imaging studies and not falling victim to intellectual blind spots created by suggested diagnoses by other care providers. Fortunately for this patient, her thyroid crisis was diagnosed, albeit with some delay, before any long‐term complications occurred.
- Silen W, ed.Cope's Early Diagnosis of the Acute Abdomen.19th ed.New York:Oxford University Press;1995:4.
- ,.An unusual cause of abdominal pain in young woman.Ann Emerg Med.1991;20:574–582.
- .Vomiting, nausea and abdominal pain: unrecognized symptoms of thyrotoxicosis.J Fam Prac.1989;24:382–386.
- Powell DW,Alpers DH,Yamada,Owyang C,Laine L, eds.Textbook of Gastroenterology.3rd ed.Philadelphia, Pa:Lippincott Williams 783,2516.
- ,,.Usefulness of adenosine in diagnosis of tachyarrhythmias.Am J Cardiol.1995;75:952–955.
- ,,,,.Supraventricular tachycardia.Med Clin North Am.2001;85:193–223.
- .Thyrotoxicosis and the heart.N Engl J Med.1992;327:94–8.
- ,.Thyrotoxicosis and the heart.Endocrinol Metab Clin North Am.1998;27:51–62.
- ,,,.Treatment of thyrotoxic hypercalcemia with propranolol.N Engl J Med.1976;294:431.
- ,,,.Ionized and total plasma calcium and parathyroid hormone in hyperthyroidism.Ann Intern Med.1976;84:668.
- ,.Hypercalcemic crisis.Med Clin North Am.1995;79:79–92.
- ,,.Thyrotoxicosis, hypercalcemia, and secondary hyperparathyroidism.Arch Intern Med.1979;139:661–663.
- ,.Clinical Physiology of Acid‐Base and Electrolyte Disorders.5th ed.New York:McGraw‐Hill;2001:754–758.
- Silen W, ed.Cope's Early Diagnosis of the Acute Abdomen.19th ed.New York:Oxford University Press;1995:4.
- ,.An unusual cause of abdominal pain in young woman.Ann Emerg Med.1991;20:574–582.
- .Vomiting, nausea and abdominal pain: unrecognized symptoms of thyrotoxicosis.J Fam Prac.1989;24:382–386.
- Powell DW,Alpers DH,Yamada,Owyang C,Laine L, eds.Textbook of Gastroenterology.3rd ed.Philadelphia, Pa:Lippincott Williams 783,2516.
- ,,.Usefulness of adenosine in diagnosis of tachyarrhythmias.Am J Cardiol.1995;75:952–955.
- ,,,,.Supraventricular tachycardia.Med Clin North Am.2001;85:193–223.
- .Thyrotoxicosis and the heart.N Engl J Med.1992;327:94–8.
- ,.Thyrotoxicosis and the heart.Endocrinol Metab Clin North Am.1998;27:51–62.
- ,,,.Treatment of thyrotoxic hypercalcemia with propranolol.N Engl J Med.1976;294:431.
- ,,,.Ionized and total plasma calcium and parathyroid hormone in hyperthyroidism.Ann Intern Med.1976;84:668.
- ,.Hypercalcemic crisis.Med Clin North Am.1995;79:79–92.
- ,,.Thyrotoxicosis, hypercalcemia, and secondary hyperparathyroidism.Arch Intern Med.1979;139:661–663.
- ,.Clinical Physiology of Acid‐Base and Electrolyte Disorders.5th ed.New York:McGraw‐Hill;2001:754–758.