User login
Quality Reporting Incentive Payments Surge
A Centers for Medicare & Medicaid Services (CMS) report that shows a nearly 300% increase in bonus payments under Medicare's Physician Quality Reporting Initiative (PQRI) is further evidence that hospitalists are embracing pay-for-reporting measures, according to the chair of SHM's Performance and Standards Committee.
Patrick Torcson, MD, MMM, FACP, director of hospital medicine at St. Tammany Parish Hospital in Covington, La., says increased usage of pay incentives to push quality reform is "past that tipping point, but what's really unknown right now is what's going to happen with the healthcare reform in front of us right now."
"It's an evolution for physicians to accept that pay for performance, starting with pay for reporting, is here to stay," Dr. Torcson says. "It's really a matter of the practice management that's necessary to include performance reporting as part of the workflow of how you take care of patients and report your billing claims."
In 2008, CMS paid $92 million in bonuses under the PQRI program, an increase from $36 million in 2007. However, the program was only active for the second half of 2007, so Dr. Torcson cautions against reading too much into the increase. Still, CMS reported that payments were distributed to more than 85,500 physicians with an average payment of $1,000. In Dr. Torcson's 10-hospitalist group, the average bonus was $1,400. He predicts an average 2009 payment of $2,400 for members of his group.
Dr. Torcson expects more hospitalists will use the incentive program once more HM-specific performance measures are put in place, including yardsticks focused on care transitions and inpatient management of heart failure.
"This truly is the platform for the future pay-for-performance model that's going to affect every hospitalist," he adds. "I can't see any reason to ignore it.”
For more information about reporting PQRI measures, visit the CMS Web site and check out the PQRI toolkit. Visit SHM's Web site for information about getting your hospitalist program started in Medicare's voluntary pay-for-reporting program.
A Centers for Medicare & Medicaid Services (CMS) report that shows a nearly 300% increase in bonus payments under Medicare's Physician Quality Reporting Initiative (PQRI) is further evidence that hospitalists are embracing pay-for-reporting measures, according to the chair of SHM's Performance and Standards Committee.
Patrick Torcson, MD, MMM, FACP, director of hospital medicine at St. Tammany Parish Hospital in Covington, La., says increased usage of pay incentives to push quality reform is "past that tipping point, but what's really unknown right now is what's going to happen with the healthcare reform in front of us right now."
"It's an evolution for physicians to accept that pay for performance, starting with pay for reporting, is here to stay," Dr. Torcson says. "It's really a matter of the practice management that's necessary to include performance reporting as part of the workflow of how you take care of patients and report your billing claims."
In 2008, CMS paid $92 million in bonuses under the PQRI program, an increase from $36 million in 2007. However, the program was only active for the second half of 2007, so Dr. Torcson cautions against reading too much into the increase. Still, CMS reported that payments were distributed to more than 85,500 physicians with an average payment of $1,000. In Dr. Torcson's 10-hospitalist group, the average bonus was $1,400. He predicts an average 2009 payment of $2,400 for members of his group.
Dr. Torcson expects more hospitalists will use the incentive program once more HM-specific performance measures are put in place, including yardsticks focused on care transitions and inpatient management of heart failure.
"This truly is the platform for the future pay-for-performance model that's going to affect every hospitalist," he adds. "I can't see any reason to ignore it.”
For more information about reporting PQRI measures, visit the CMS Web site and check out the PQRI toolkit. Visit SHM's Web site for information about getting your hospitalist program started in Medicare's voluntary pay-for-reporting program.
A Centers for Medicare & Medicaid Services (CMS) report that shows a nearly 300% increase in bonus payments under Medicare's Physician Quality Reporting Initiative (PQRI) is further evidence that hospitalists are embracing pay-for-reporting measures, according to the chair of SHM's Performance and Standards Committee.
Patrick Torcson, MD, MMM, FACP, director of hospital medicine at St. Tammany Parish Hospital in Covington, La., says increased usage of pay incentives to push quality reform is "past that tipping point, but what's really unknown right now is what's going to happen with the healthcare reform in front of us right now."
"It's an evolution for physicians to accept that pay for performance, starting with pay for reporting, is here to stay," Dr. Torcson says. "It's really a matter of the practice management that's necessary to include performance reporting as part of the workflow of how you take care of patients and report your billing claims."
In 2008, CMS paid $92 million in bonuses under the PQRI program, an increase from $36 million in 2007. However, the program was only active for the second half of 2007, so Dr. Torcson cautions against reading too much into the increase. Still, CMS reported that payments were distributed to more than 85,500 physicians with an average payment of $1,000. In Dr. Torcson's 10-hospitalist group, the average bonus was $1,400. He predicts an average 2009 payment of $2,400 for members of his group.
Dr. Torcson expects more hospitalists will use the incentive program once more HM-specific performance measures are put in place, including yardsticks focused on care transitions and inpatient management of heart failure.
"This truly is the platform for the future pay-for-performance model that's going to affect every hospitalist," he adds. "I can't see any reason to ignore it.”
For more information about reporting PQRI measures, visit the CMS Web site and check out the PQRI toolkit. Visit SHM's Web site for information about getting your hospitalist program started in Medicare's voluntary pay-for-reporting program.
In the Literature: The Latest Research You Need to Know
Clinical question: How adequately do hospital discharge summaries document laboratory tests with pending results?
Background: Discharge summaries commonly lack important clinical and administrative information. Poor communication among hospital providers about tests that are pending at hospital discharge represents a patient-safety concern.
Study design: Retrospective cohort.
Setting: Two academic medical centers.
Synopsis: Discharge summaries were reviewed for 668 patients who had laboratory test results pending at hospital discharge. A total of 2,927 results were pending at discharge, most often corresponding to microbiology (47.7%), hematology (17.1%), or chemistry (10.8%) studies. Among the pending tests, 296 (10%) were rated as “actionable,” meaning they required a change in therapy, a follow-up test, or an outpatient visit. Only 168 (25%) of the 668 discharge summaries mentioned any pending tests. Information about the outpatient provider or clinic to which test results could be sent did not appear in 33% of the discharge summaries.
The study did not determine whether the laboratory test results received appropriate follow up and did not assess clinical outcomes. Other types of tests (e.g., radiology studies) were not analyzed.
Bottom line: Hospital discharge summaries often omit information about pending laboratory test results or the outpatient provider to whom such tests results could be sent.
Citation: Were MC, Li X, Kesterson J, et al. Adequacy of hospital discharge summaries in documenting tests with pending results and outpatient follow-up providers. J Gen Intern Med. 2009;24(6):1002-1006.
Reviewed for TH eWire by Kelly Cunningham, MD, Elizabeth Rice, MD, Eduard Vasilevskis, MD, Joshua LaBrin, MD, Kelly Sopko, MD, Shelley Ellis, MD, MPH, Sunil Kripalani, MD, MSc; Section of Hospital Medicine, Vanderbilt University
For more reviews of HM-related literature, visit www.the-hospitalist.org.
Clinical question: How adequately do hospital discharge summaries document laboratory tests with pending results?
Background: Discharge summaries commonly lack important clinical and administrative information. Poor communication among hospital providers about tests that are pending at hospital discharge represents a patient-safety concern.
Study design: Retrospective cohort.
Setting: Two academic medical centers.
Synopsis: Discharge summaries were reviewed for 668 patients who had laboratory test results pending at hospital discharge. A total of 2,927 results were pending at discharge, most often corresponding to microbiology (47.7%), hematology (17.1%), or chemistry (10.8%) studies. Among the pending tests, 296 (10%) were rated as “actionable,” meaning they required a change in therapy, a follow-up test, or an outpatient visit. Only 168 (25%) of the 668 discharge summaries mentioned any pending tests. Information about the outpatient provider or clinic to which test results could be sent did not appear in 33% of the discharge summaries.
The study did not determine whether the laboratory test results received appropriate follow up and did not assess clinical outcomes. Other types of tests (e.g., radiology studies) were not analyzed.
Bottom line: Hospital discharge summaries often omit information about pending laboratory test results or the outpatient provider to whom such tests results could be sent.
Citation: Were MC, Li X, Kesterson J, et al. Adequacy of hospital discharge summaries in documenting tests with pending results and outpatient follow-up providers. J Gen Intern Med. 2009;24(6):1002-1006.
Reviewed for TH eWire by Kelly Cunningham, MD, Elizabeth Rice, MD, Eduard Vasilevskis, MD, Joshua LaBrin, MD, Kelly Sopko, MD, Shelley Ellis, MD, MPH, Sunil Kripalani, MD, MSc; Section of Hospital Medicine, Vanderbilt University
For more reviews of HM-related literature, visit www.the-hospitalist.org.
Clinical question: How adequately do hospital discharge summaries document laboratory tests with pending results?
Background: Discharge summaries commonly lack important clinical and administrative information. Poor communication among hospital providers about tests that are pending at hospital discharge represents a patient-safety concern.
Study design: Retrospective cohort.
Setting: Two academic medical centers.
Synopsis: Discharge summaries were reviewed for 668 patients who had laboratory test results pending at hospital discharge. A total of 2,927 results were pending at discharge, most often corresponding to microbiology (47.7%), hematology (17.1%), or chemistry (10.8%) studies. Among the pending tests, 296 (10%) were rated as “actionable,” meaning they required a change in therapy, a follow-up test, or an outpatient visit. Only 168 (25%) of the 668 discharge summaries mentioned any pending tests. Information about the outpatient provider or clinic to which test results could be sent did not appear in 33% of the discharge summaries.
The study did not determine whether the laboratory test results received appropriate follow up and did not assess clinical outcomes. Other types of tests (e.g., radiology studies) were not analyzed.
Bottom line: Hospital discharge summaries often omit information about pending laboratory test results or the outpatient provider to whom such tests results could be sent.
Citation: Were MC, Li X, Kesterson J, et al. Adequacy of hospital discharge summaries in documenting tests with pending results and outpatient follow-up providers. J Gen Intern Med. 2009;24(6):1002-1006.
Reviewed for TH eWire by Kelly Cunningham, MD, Elizabeth Rice, MD, Eduard Vasilevskis, MD, Joshua LaBrin, MD, Kelly Sopko, MD, Shelley Ellis, MD, MPH, Sunil Kripalani, MD, MSc; Section of Hospital Medicine, Vanderbilt University
For more reviews of HM-related literature, visit www.the-hospitalist.org.
Opacity Overlying Vertebral Column on CRX
In the evaluation of patients presenting with complaints referable to the chest, the chest radiograph (CXR) is an important and almost universal component of the initial assessment.
Chest radiography is normally performed with both posterior‐anterior (PA) and lateral projections.1 The lateral projection is generally accepted as an indispensable component because it allows better visualization of certain structures including the lower lobes, areas of which are partially obscured by the heart or hemidiaphragms on the PA projection. As such, some radiographic findings are only apparent on the lateral projection. As well, when an abnormality is discovered on the PA projection, the orthogonal orientation of the lateral projection often allows lesion localization.
Together with information gleaned from a thorough history and physical examination, the results of chest radiography often inform initial management when a diagnosis has been established, and the need for additional investigations when the diagnosis remains in question. In the hospital setting, the CXR is often reviewed first by physicians who are not radiologists (eg, internists, emergency physicians, and trainees at various stages of training) when evaluating a patient.
We undertook the current study to investigate the test characteristics (sensitivity, specificity, and likelihood ratio [LR]), and precision of 1 particular finding on lateral chest radiography as interpreted by nonradiologist physicians in the hospital setting. On a normal lateral CXR, one should observe progressive superior‐inferior vertebral radiolucency (Figure 1A). Observed opacity overlying the vertebral column obscuring this progression is usually abnormal and suggestive of pathology in the lower lobes of the lungs or associated structures (Figure 1B). A review of the literature yielded only 1 study of this finding,2 which used a case‐control design and lacked a true gold standard investigation necessary for calculation of meaningful test characteristics. In fact, few studies have compared findings on chest radiography with more definitive investigations,3, 4 and none have examined the predictive value of this finding by nonradiologist observers using a reference standard investigation such as computed tomography (CT) of the chest.
Methods
The radiology Picture Archiving and Communication System (PACS) used at our institution allows us to search for exams by date and study type. We retrospectively identified all patients seen at 1 of 3 university‐affiliated tertiary care adult teaching hospitals (Toronto General, Toronto Western, and Mount Sinai Hospitals) within an 8‐month period (January 1, 2006 to August 31, 2006) who underwent a 2‐view CXR (PA and lateral views). (Note that in this study, the terms radiograph, x‐ray, and plain film are used synonymously.) We then determined which of these patients had a subsequent CT within 24 hours of the x‐ray, resulting in a sample of 370 patients for this study. These patients primarily included patients presenting to the emergency department, and inpatients, with a very small number of outpatients. The majority of the index CXRs were performed for chief complaints of dyspnea, chest pain, cough, or for follow‐up of a previous CXR. However, many were simply performed routinely for admission. Patients with prosthetic devices or appliances obscuring the vertebral column were excluded.
After several training sessions by an experienced internist (A.S.D.), 2 authors (D.R.M., M.E.D.) independently reviewed each lateral CXR using standard 17‐inch displays and documented the presence or absence of abnormal radioopacity obscuring the superior to inferior progression of vertebral radiolucency. These 2 authors were fourth‐year medical students at the time the study began and first‐year trainees in internal medicine when it ended. The presence of abnormal opacity overlying the vertebral column was recorded as a positive test while the absence of this finding was recorded as a negative test.
Observed opacity overlying the vertebral column on lateral CXRs was considered abnormal when it did not represent manifestations of normal anatomical structures. However, the finding of opacity overlying the vertebral column of little diagnostic significance, such as prominent pulmonary vessels, degenerative bony changes, or the finding of a tortuous aorta, were considered normal in this study. Corresponding PA CXRs were also available for viewing. In most cases, the authors viewed both the lateral and PA CXRs, reflecting their use in clinical practice. However, in cases of obvious abnormality on the lateral CXR, only that projection was viewed. No clinical information was made available to the observers of the lateral CXR and they were blinded to the results of CT imaging of the chest. All 370 cases were reviewed by both observers (D.R.M. and M.E.D.). For the purpose of calculating test characteristics and LRs, cases of disagreement between the 3 lateral CXR observers were resolved by independent review by a third author (A.S.D.), a general internist with over 20 years of experience interpreting the lateral CXR.
A fourth author (M.O.B) reviewed the chest CT reports for each patient and recorded the mention of the presence or absence of various pathologies in the lower lobes of the lungs and associated structures in those reports. No clinical information was made available to this author and he was blinded to the results of lateral CXR. All CT investigations were originally interpreted by a university‐affiliated chest radiology faculty member at the time of the investigation. Table 1 lists all relevant chest CT findings in our sample that were recorded as disease‐positive for the purpose of dichotomizing the results of the reference standard, and enabling calculation of test characteristics (Table 2). Notable chest CT findings that were not recorded as disease‐positive for this purpose included mediastinal lymphadenopathy, subpleural density, lytic vertebral lesions, cystic or emphysematous changes, and pneumothorax. Dependent atelectasis was included within the disease‐positive category, though some cases may not have been pathological. It should be pointed out that there may be some variation in terminology used between staff radiologists (eg, reticulation by one radiologist may be called minor densities by another radiologist).
| Number of Cases | CXR (+) | CXR () | LR (+)* | LR ()* | |
|---|---|---|---|---|---|
| |||||
| Disease‐positive/abnormal findings | |||||
| Atelectasis or fibrosis including usual interstitial pneumonitis | 215 | 191 | 24 | 3.1 | 0.16 |
| Effusion, loculated effusion, empyema or fluid collections in fissures | 83 | 79 | 4 | 3.3 | 0.07 |
| Consolidation, airspace disease, mucous plugging or postradiation opacities | 57 | 54 | 3 | 3.3 | 0.07 |
| Ground glass opacity | 50 | 42 | 8 | 2.9 | 0.23 |
| Nodule or mass >5 mm | 48 | 44 | 4 | 3.1 | 0.12 |
| Pulmonary embolus | 22 | 18 | 4 | 2.8 | 0.26 |
| Bronchiectasis or bronchial dilation | 14 | 13 | 1 | 3.2 | 0.10 |
| Reticulation | 10 | 9 | 1 | 3.1 | 0.14 |
| Sclerotic bone lesion | 10 | 10 | 0 | 3.4 | 0 |
| Pulmonary edema or septal thickening | 8 | 8 | 0 | 3.4 | 0 |
| Interlobular septal thickening | 8 | 7 | 1 | 3.0 | 0.18 |
| Pleural plaque or calcification | 6 | 5 | 1 | 2.9 | 0.24 |
| Abnormal hemidiaphragm | 5 | 5 | 0 | 3.4 | 0 |
| Hydrothorax | 3 | 3 | 0 | 3.4 | 0 |
| Cavitary lesion | 2 | 2 | 0 | 3.4 | 0 |
| Pleural thickening | 1 | 1 | 0 | 3.4 | 0 |
| Vertebral compression fracture(s) | 1 | 1 | 0 | 3.4 | 0 |
| Bronchial obstruction | 1 | 1 | 0 | 3.4 | 0 |
| Bronchial wall thickening | 1 | 1 | 0 | 3.4 | 0 |
| Any abnormal CT finding | 289 | 251 | 38 | 2.9 | 0.19 |
| Disease‐negative/normal findings | |||||
| Normal | 81 | 24 | 57 | ||
| Overall LR | 2.9 (2.14.1) | 0.19 (0.130.26) | |||
| Abnormal Chest CT | Normal Chest CT | |
|---|---|---|
| ||
| Abnormal lateral CXR | 251 | 24 |
| Normal lateral CXR | 38 | 57 |
Using the chest CT report as the reference standard for abnormal opacity overlying the vertebral column on lateral chest radiography, we calculated the sensitivity, specificity, and positive and negative LRs (LR+ and LR, respectively) with 95% confidence intervals (CIs) for individual and summary CT‐documented pathologies.5 For this purpose, we constructed a 2 2 table (Table 2) for summary CT‐documented abnormal findings, in which patients with any abnormal CT finding were considered disease‐positive and compared with patients whose CTs were interpreted as normal, considered disease‐negative. We also constructed 2 2 tables for each of the individual CT‐documented pathologies using data from Table 1, in which only the patients with the abnormal CT finding of interest (eg, consolidation) were considered disease‐positive and compared with patients whose CTs were interpreted as normal, considered disease‐negative. In this case, patients with abnormal CT findings (eg, atelectasis, effusion) other than the finding of interest were excluded from the analysis. This secondary analysis is an attempt to estimate the variability of the accuracy of the finding in question across different diagnoses, and not to derive precise estimates of LRs given the small sample sizes for some individual findings.
Of the 370 original patients, we selected a sample of 100 patients by random number assignment whose lateral CXRs were reviewed a second time by the same observers to quantify intraobserver variability. Interobserver variability was quantified by comparing the data of the 2 independent lateral CXR observers on all 370 patients. In both cases, we calculated simple agreement and kappa statistics as measures of precision.6 Our chest CT observer also identified a sample of 10 CT investigations by random number assignment and reviewed the images in a blinded fashion to quantify interobserver variability in CT findings (ie, a comparison of the original CT report with our chest CT observer's interpretation).
We obtained approval from the relevant research ethics boards for the hospitals in which our study population was identified and have endeavored to comply with the Standards for Reporting of Diagnostic Accuracy (STARD) initiative.7 All statistical analyses were performed using R version 2.018 (Free Software Foundation, Boston, MA) and WinBUGS version 1.4. (MRC Biostatistics Unit, Cambridge, UK)9
Results
The identified study sample of 370 patients was 52% male and had an average age of 58 17 years (range, 18 to 96 years). Of the 370 patients, 81 (21.9%) were found to have a normal chest CT, 118 (31.9%) had a single CT finding in the lower lobes designated as disease‐positive, and 171 (46.2%) had 2 or more lower‐lobe CT findings. Overall, 78.1% had 1 or more CT findings considered disease‐positive.
Abnormal opacity overlying the vertebral column on lateral chest radiography had a sensitivity of 86.9% (95% CI, 82.5%‐90.3%) and specificity of 70.4% (95% CI, 59.7%‐79.2%) for CT‐documented lower‐lobe and associated structural pathology (Table 2). The summary LR+ for abnormal opacity overlying the vertebral column on lateral chest radiography was 2.9 (95% CI, 2.1‐4.1) and the summary LR for the absence of this finding was 0.19 (95% CI, 0.13‐0.26). LRs for individual CT‐documented pathologies were very similar to the summary LRs, with a range for LR+s between 2.8 and 3.4, and a range for LRs between 0 and 0.26 (Table 1).
Intraobserver simple agreement and kappa statistics for each of the lateral CXR observers were 79% ( = 0.56) and 81% ( = 0.58), respectively. Interobserver simple agreement between the lateral CXR observers, as well as the associated kappa statistic, were similar at 77% ( = 0.52). Compared with the original chest CT reports generated by university‐affiliated radiology faculty members, the blinded review of 10 randomly‐identified CT investigations by our chest CT observer (M.O.B.) yielded 100% agreement.
Discussion
This study fills a gap in the literature by providing evidence of the accuracy and precision of a particular finding on lateral chest radiography: namely, observed radioopacity obscuring the normal succession of superior‐inferior vertebral radiolucency.
Our investigation of this finding's test characteristics reveal that abnormal opacity overlying the vertebral column on lateral chest radiography is a more sensitive than specific finding, and thus in general more useful for ruling out the presence of disease than ruling it in. But it is our calculated LRs that allow application of this finding's predictive value to clinical scenarios in practice.
LRs are a powerful method of applying new information to the pretest probability of disease, to arrive at the posttest probability. If the summary point estimate LRs of our study are applied to a hypothetical pretest probability of 50% for any CT‐documented pathology, abnormal opacity overlying the vertebral column (LR+ 2.9) gives a posttest probability of 75%, and the absence of this finding (LR 0.19) gives a posttest probability of 16%. In some cases, these posttest probabilities may be high enough to stop investigating and start treating, or low enough to stop investigating.
We also calculated LRs for each subgroup of CT‐documented pathology by comparing only patients with the CT finding of interest and patients with CTs interpreted as normal. While the validity of these calculations is compromised by ignoring the patients in the other subgroups of diagnoses in the calculation, the stability of these LR estimates suggests that the finding and summary LRs can be used for a variety of diagnoses. The individual LRs, however, should not be used in arriving at posttest probabilities of individual pathologies.
Our calculated kappa statistics, a measure of chance‐corrected agreement, quantified the precision of abnormal opacity overlying the vertebral column noted by nonradiologist observers. The kappa statistics associated with intraobserver and interobserver variability for abnormal opacity overlying the vertebral column are indicative of moderate agreement, which is similar to the precision of many other investigational findings in common usage.
This study does have some limitations related to its design. First, CT was used as the gold standard in this study. Ideally, a combination of CT and more invasive measures such as lung biopsy would have been used; however, for ethical and logistical reasons this was obviously not possible. Second, when designing the study we had to decide whether or not to repeat the interpretation of CT images with observers we could ensure were blinded to the corresponding CXRs. We chose not to repeat the interpretation of CT images, and instead used the report of the staff chest radiologist who read the imaging study at the time it was performed. The person reviewing the report of the CT was blinded to the CXR. Our reasons for not rereading each of the CT images with a blinded study radiologist are as follows. First, the chest radiologists who reviewed the CT images at the time they were done were completely unaware of our hypothesis regarding the utility of the lateral CXR (our study took place after the CTs were interpreted). Second, the radiologists tell us that when they interpret CTs they rarely rely on findings in the CXR to help with those interpretations. For these 2 reasons, the original interpretation is very close to complete blinding. In addition, the individuals who interpret and write reports on chest CTs are all expert staff radiologists with considerable experience in this area. A study radiologist (likely a radiology resident) would not have been as proficient. Finally, in performing any study one must weigh the costs with the benefits of any methodological decision, reinterpretation of 370 chest CTs would have required an enormous amount of time. Finally, our small sample of 10 comparing official reports to the reinterpretation of the scans themselves supported the view that we did not need to review all 370 cases again.
Approximately three‐quarters of our study population was found to have CT‐documented disease. However, this is not surprising given our method of patient selection. Because the sample was collected from clinical practice, it is likely that only patients who exhibited a finding on the CXR that required delineation went on to have the reference standard investigation (CT). This study is therefore subject to workup bias. Workup bias in this scenario could work in 1 of 2 directions. In one situation, some patients would have a clear pathology or diagnosis based on the CXR, such that a CT was unnecessary and therefore not performed. In this case, our study would have underestimated the sensitivity of the sign being studied because a group of true positives would have been left out of the sample. In the second situation, patients with true pathology and a normal CXR (false negatives) fail to undergo CT. In this case, our study would have overestimated the sensitivity. We are not sure which effect of workup bias predominates in the study, but in either case an independent, prospective comparison of these imaging modalities in all patients who had CXRs was not feasible for ethical reasons. If we were to apply the reference standard investigation to all those patients, the potential for harm from excess radiation10 would be too great. As such, our cohort of patients is the best possible sample that can be studied.
Another feature of this study is that it intentionally used nonradiologist (budding internist) interpreters of the lateral CXRs, thus defining its generalizability. We did so for 2 reasons. First, the sign studied is likely too basic to be of relevance to radiologists. Second, it is intended to be used by internists, emergency physicians, and nonradiology trainees at all levels, who are required to make initial treatment decisions based on their preliminary interpretation of x‐rays, particularly in the hospital setting. Therefore, we decided our results would be more externally valid and applicable if the interpreters of the x‐rays and use of the x‐ray sign in this study was by trainees.
Abnormal opacity overlying the vertebral column on lateral chest radiography is a clinically useful finding that can help nonradiologist physicians determine initial management or the need for further investigation when diagnostic uncertainty remains. This study provides evidence that this finding is both reliable and useful for ruling the presence of lower‐lobe and associated structural pathology out, and somewhat useful for ruling the presence of such pathology in.
Acknowledgements
The authors thank Dr. Meyer Balter for his comments on an earlier version of this work.
- ,,,.Efficacy of routine screening and lateral chest radiographs in a hospital‐based population.N Engl J Med.1974;291:1001–1004.
- ,,, et al.Diagnosing left lower lobe pneumonia: usefulness of the ‘spine sign’ on lateral chest radiographs.J Fam Pract.1996;43:242–248.
- ,,, et al.Digital storage phosphor imaging versus conventional film radiography in CT‐documented chest disease.Radiology.1990;174:207–210.
- ,,,,.Chest imaging with a selenium detector versus conventional film radiography: a CT‐controlled study.Radiology.1996;200:687–690.
- .A primer on the precision and accuracy of the clinical examination.JAMA.1992;267:2638–2644.
- ,,, et al.Tips for learners of evidence‐based medicine: 3. Measures of observer variability (kappa statistic).CMAJ.2004;171:1369–1373.
- ,,, et al.Towards complete and accurate reporting of studies of diagnostic accuracy: the STARD initiative.Ann Intern Med.2003;138:40–44.
- R Development Core Team.R: A Language and Environment for Statistical Computing.Vienna, Austria:R Foundation for Statistical Computing;2004.
- ,,,.WinBUGS Version 1.4.1 User Manual.Cambridge, England:MRC Biostatistics Unit;2004.
- ,.Computed tomography—an increasing source of radiation exposure.N Engl J Med.2007;357(22):2277–2284.
In the evaluation of patients presenting with complaints referable to the chest, the chest radiograph (CXR) is an important and almost universal component of the initial assessment.
Chest radiography is normally performed with both posterior‐anterior (PA) and lateral projections.1 The lateral projection is generally accepted as an indispensable component because it allows better visualization of certain structures including the lower lobes, areas of which are partially obscured by the heart or hemidiaphragms on the PA projection. As such, some radiographic findings are only apparent on the lateral projection. As well, when an abnormality is discovered on the PA projection, the orthogonal orientation of the lateral projection often allows lesion localization.
Together with information gleaned from a thorough history and physical examination, the results of chest radiography often inform initial management when a diagnosis has been established, and the need for additional investigations when the diagnosis remains in question. In the hospital setting, the CXR is often reviewed first by physicians who are not radiologists (eg, internists, emergency physicians, and trainees at various stages of training) when evaluating a patient.
We undertook the current study to investigate the test characteristics (sensitivity, specificity, and likelihood ratio [LR]), and precision of 1 particular finding on lateral chest radiography as interpreted by nonradiologist physicians in the hospital setting. On a normal lateral CXR, one should observe progressive superior‐inferior vertebral radiolucency (Figure 1A). Observed opacity overlying the vertebral column obscuring this progression is usually abnormal and suggestive of pathology in the lower lobes of the lungs or associated structures (Figure 1B). A review of the literature yielded only 1 study of this finding,2 which used a case‐control design and lacked a true gold standard investigation necessary for calculation of meaningful test characteristics. In fact, few studies have compared findings on chest radiography with more definitive investigations,3, 4 and none have examined the predictive value of this finding by nonradiologist observers using a reference standard investigation such as computed tomography (CT) of the chest.
Methods
The radiology Picture Archiving and Communication System (PACS) used at our institution allows us to search for exams by date and study type. We retrospectively identified all patients seen at 1 of 3 university‐affiliated tertiary care adult teaching hospitals (Toronto General, Toronto Western, and Mount Sinai Hospitals) within an 8‐month period (January 1, 2006 to August 31, 2006) who underwent a 2‐view CXR (PA and lateral views). (Note that in this study, the terms radiograph, x‐ray, and plain film are used synonymously.) We then determined which of these patients had a subsequent CT within 24 hours of the x‐ray, resulting in a sample of 370 patients for this study. These patients primarily included patients presenting to the emergency department, and inpatients, with a very small number of outpatients. The majority of the index CXRs were performed for chief complaints of dyspnea, chest pain, cough, or for follow‐up of a previous CXR. However, many were simply performed routinely for admission. Patients with prosthetic devices or appliances obscuring the vertebral column were excluded.
After several training sessions by an experienced internist (A.S.D.), 2 authors (D.R.M., M.E.D.) independently reviewed each lateral CXR using standard 17‐inch displays and documented the presence or absence of abnormal radioopacity obscuring the superior to inferior progression of vertebral radiolucency. These 2 authors were fourth‐year medical students at the time the study began and first‐year trainees in internal medicine when it ended. The presence of abnormal opacity overlying the vertebral column was recorded as a positive test while the absence of this finding was recorded as a negative test.
Observed opacity overlying the vertebral column on lateral CXRs was considered abnormal when it did not represent manifestations of normal anatomical structures. However, the finding of opacity overlying the vertebral column of little diagnostic significance, such as prominent pulmonary vessels, degenerative bony changes, or the finding of a tortuous aorta, were considered normal in this study. Corresponding PA CXRs were also available for viewing. In most cases, the authors viewed both the lateral and PA CXRs, reflecting their use in clinical practice. However, in cases of obvious abnormality on the lateral CXR, only that projection was viewed. No clinical information was made available to the observers of the lateral CXR and they were blinded to the results of CT imaging of the chest. All 370 cases were reviewed by both observers (D.R.M. and M.E.D.). For the purpose of calculating test characteristics and LRs, cases of disagreement between the 3 lateral CXR observers were resolved by independent review by a third author (A.S.D.), a general internist with over 20 years of experience interpreting the lateral CXR.
A fourth author (M.O.B) reviewed the chest CT reports for each patient and recorded the mention of the presence or absence of various pathologies in the lower lobes of the lungs and associated structures in those reports. No clinical information was made available to this author and he was blinded to the results of lateral CXR. All CT investigations were originally interpreted by a university‐affiliated chest radiology faculty member at the time of the investigation. Table 1 lists all relevant chest CT findings in our sample that were recorded as disease‐positive for the purpose of dichotomizing the results of the reference standard, and enabling calculation of test characteristics (Table 2). Notable chest CT findings that were not recorded as disease‐positive for this purpose included mediastinal lymphadenopathy, subpleural density, lytic vertebral lesions, cystic or emphysematous changes, and pneumothorax. Dependent atelectasis was included within the disease‐positive category, though some cases may not have been pathological. It should be pointed out that there may be some variation in terminology used between staff radiologists (eg, reticulation by one radiologist may be called minor densities by another radiologist).
| Number of Cases | CXR (+) | CXR () | LR (+)* | LR ()* | |
|---|---|---|---|---|---|
| |||||
| Disease‐positive/abnormal findings | |||||
| Atelectasis or fibrosis including usual interstitial pneumonitis | 215 | 191 | 24 | 3.1 | 0.16 |
| Effusion, loculated effusion, empyema or fluid collections in fissures | 83 | 79 | 4 | 3.3 | 0.07 |
| Consolidation, airspace disease, mucous plugging or postradiation opacities | 57 | 54 | 3 | 3.3 | 0.07 |
| Ground glass opacity | 50 | 42 | 8 | 2.9 | 0.23 |
| Nodule or mass >5 mm | 48 | 44 | 4 | 3.1 | 0.12 |
| Pulmonary embolus | 22 | 18 | 4 | 2.8 | 0.26 |
| Bronchiectasis or bronchial dilation | 14 | 13 | 1 | 3.2 | 0.10 |
| Reticulation | 10 | 9 | 1 | 3.1 | 0.14 |
| Sclerotic bone lesion | 10 | 10 | 0 | 3.4 | 0 |
| Pulmonary edema or septal thickening | 8 | 8 | 0 | 3.4 | 0 |
| Interlobular septal thickening | 8 | 7 | 1 | 3.0 | 0.18 |
| Pleural plaque or calcification | 6 | 5 | 1 | 2.9 | 0.24 |
| Abnormal hemidiaphragm | 5 | 5 | 0 | 3.4 | 0 |
| Hydrothorax | 3 | 3 | 0 | 3.4 | 0 |
| Cavitary lesion | 2 | 2 | 0 | 3.4 | 0 |
| Pleural thickening | 1 | 1 | 0 | 3.4 | 0 |
| Vertebral compression fracture(s) | 1 | 1 | 0 | 3.4 | 0 |
| Bronchial obstruction | 1 | 1 | 0 | 3.4 | 0 |
| Bronchial wall thickening | 1 | 1 | 0 | 3.4 | 0 |
| Any abnormal CT finding | 289 | 251 | 38 | 2.9 | 0.19 |
| Disease‐negative/normal findings | |||||
| Normal | 81 | 24 | 57 | ||
| Overall LR | 2.9 (2.14.1) | 0.19 (0.130.26) | |||
| Abnormal Chest CT | Normal Chest CT | |
|---|---|---|
| ||
| Abnormal lateral CXR | 251 | 24 |
| Normal lateral CXR | 38 | 57 |
Using the chest CT report as the reference standard for abnormal opacity overlying the vertebral column on lateral chest radiography, we calculated the sensitivity, specificity, and positive and negative LRs (LR+ and LR, respectively) with 95% confidence intervals (CIs) for individual and summary CT‐documented pathologies.5 For this purpose, we constructed a 2 2 table (Table 2) for summary CT‐documented abnormal findings, in which patients with any abnormal CT finding were considered disease‐positive and compared with patients whose CTs were interpreted as normal, considered disease‐negative. We also constructed 2 2 tables for each of the individual CT‐documented pathologies using data from Table 1, in which only the patients with the abnormal CT finding of interest (eg, consolidation) were considered disease‐positive and compared with patients whose CTs were interpreted as normal, considered disease‐negative. In this case, patients with abnormal CT findings (eg, atelectasis, effusion) other than the finding of interest were excluded from the analysis. This secondary analysis is an attempt to estimate the variability of the accuracy of the finding in question across different diagnoses, and not to derive precise estimates of LRs given the small sample sizes for some individual findings.
Of the 370 original patients, we selected a sample of 100 patients by random number assignment whose lateral CXRs were reviewed a second time by the same observers to quantify intraobserver variability. Interobserver variability was quantified by comparing the data of the 2 independent lateral CXR observers on all 370 patients. In both cases, we calculated simple agreement and kappa statistics as measures of precision.6 Our chest CT observer also identified a sample of 10 CT investigations by random number assignment and reviewed the images in a blinded fashion to quantify interobserver variability in CT findings (ie, a comparison of the original CT report with our chest CT observer's interpretation).
We obtained approval from the relevant research ethics boards for the hospitals in which our study population was identified and have endeavored to comply with the Standards for Reporting of Diagnostic Accuracy (STARD) initiative.7 All statistical analyses were performed using R version 2.018 (Free Software Foundation, Boston, MA) and WinBUGS version 1.4. (MRC Biostatistics Unit, Cambridge, UK)9
Results
The identified study sample of 370 patients was 52% male and had an average age of 58 17 years (range, 18 to 96 years). Of the 370 patients, 81 (21.9%) were found to have a normal chest CT, 118 (31.9%) had a single CT finding in the lower lobes designated as disease‐positive, and 171 (46.2%) had 2 or more lower‐lobe CT findings. Overall, 78.1% had 1 or more CT findings considered disease‐positive.
Abnormal opacity overlying the vertebral column on lateral chest radiography had a sensitivity of 86.9% (95% CI, 82.5%‐90.3%) and specificity of 70.4% (95% CI, 59.7%‐79.2%) for CT‐documented lower‐lobe and associated structural pathology (Table 2). The summary LR+ for abnormal opacity overlying the vertebral column on lateral chest radiography was 2.9 (95% CI, 2.1‐4.1) and the summary LR for the absence of this finding was 0.19 (95% CI, 0.13‐0.26). LRs for individual CT‐documented pathologies were very similar to the summary LRs, with a range for LR+s between 2.8 and 3.4, and a range for LRs between 0 and 0.26 (Table 1).
Intraobserver simple agreement and kappa statistics for each of the lateral CXR observers were 79% ( = 0.56) and 81% ( = 0.58), respectively. Interobserver simple agreement between the lateral CXR observers, as well as the associated kappa statistic, were similar at 77% ( = 0.52). Compared with the original chest CT reports generated by university‐affiliated radiology faculty members, the blinded review of 10 randomly‐identified CT investigations by our chest CT observer (M.O.B.) yielded 100% agreement.
Discussion
This study fills a gap in the literature by providing evidence of the accuracy and precision of a particular finding on lateral chest radiography: namely, observed radioopacity obscuring the normal succession of superior‐inferior vertebral radiolucency.
Our investigation of this finding's test characteristics reveal that abnormal opacity overlying the vertebral column on lateral chest radiography is a more sensitive than specific finding, and thus in general more useful for ruling out the presence of disease than ruling it in. But it is our calculated LRs that allow application of this finding's predictive value to clinical scenarios in practice.
LRs are a powerful method of applying new information to the pretest probability of disease, to arrive at the posttest probability. If the summary point estimate LRs of our study are applied to a hypothetical pretest probability of 50% for any CT‐documented pathology, abnormal opacity overlying the vertebral column (LR+ 2.9) gives a posttest probability of 75%, and the absence of this finding (LR 0.19) gives a posttest probability of 16%. In some cases, these posttest probabilities may be high enough to stop investigating and start treating, or low enough to stop investigating.
We also calculated LRs for each subgroup of CT‐documented pathology by comparing only patients with the CT finding of interest and patients with CTs interpreted as normal. While the validity of these calculations is compromised by ignoring the patients in the other subgroups of diagnoses in the calculation, the stability of these LR estimates suggests that the finding and summary LRs can be used for a variety of diagnoses. The individual LRs, however, should not be used in arriving at posttest probabilities of individual pathologies.
Our calculated kappa statistics, a measure of chance‐corrected agreement, quantified the precision of abnormal opacity overlying the vertebral column noted by nonradiologist observers. The kappa statistics associated with intraobserver and interobserver variability for abnormal opacity overlying the vertebral column are indicative of moderate agreement, which is similar to the precision of many other investigational findings in common usage.
This study does have some limitations related to its design. First, CT was used as the gold standard in this study. Ideally, a combination of CT and more invasive measures such as lung biopsy would have been used; however, for ethical and logistical reasons this was obviously not possible. Second, when designing the study we had to decide whether or not to repeat the interpretation of CT images with observers we could ensure were blinded to the corresponding CXRs. We chose not to repeat the interpretation of CT images, and instead used the report of the staff chest radiologist who read the imaging study at the time it was performed. The person reviewing the report of the CT was blinded to the CXR. Our reasons for not rereading each of the CT images with a blinded study radiologist are as follows. First, the chest radiologists who reviewed the CT images at the time they were done were completely unaware of our hypothesis regarding the utility of the lateral CXR (our study took place after the CTs were interpreted). Second, the radiologists tell us that when they interpret CTs they rarely rely on findings in the CXR to help with those interpretations. For these 2 reasons, the original interpretation is very close to complete blinding. In addition, the individuals who interpret and write reports on chest CTs are all expert staff radiologists with considerable experience in this area. A study radiologist (likely a radiology resident) would not have been as proficient. Finally, in performing any study one must weigh the costs with the benefits of any methodological decision, reinterpretation of 370 chest CTs would have required an enormous amount of time. Finally, our small sample of 10 comparing official reports to the reinterpretation of the scans themselves supported the view that we did not need to review all 370 cases again.
Approximately three‐quarters of our study population was found to have CT‐documented disease. However, this is not surprising given our method of patient selection. Because the sample was collected from clinical practice, it is likely that only patients who exhibited a finding on the CXR that required delineation went on to have the reference standard investigation (CT). This study is therefore subject to workup bias. Workup bias in this scenario could work in 1 of 2 directions. In one situation, some patients would have a clear pathology or diagnosis based on the CXR, such that a CT was unnecessary and therefore not performed. In this case, our study would have underestimated the sensitivity of the sign being studied because a group of true positives would have been left out of the sample. In the second situation, patients with true pathology and a normal CXR (false negatives) fail to undergo CT. In this case, our study would have overestimated the sensitivity. We are not sure which effect of workup bias predominates in the study, but in either case an independent, prospective comparison of these imaging modalities in all patients who had CXRs was not feasible for ethical reasons. If we were to apply the reference standard investigation to all those patients, the potential for harm from excess radiation10 would be too great. As such, our cohort of patients is the best possible sample that can be studied.
Another feature of this study is that it intentionally used nonradiologist (budding internist) interpreters of the lateral CXRs, thus defining its generalizability. We did so for 2 reasons. First, the sign studied is likely too basic to be of relevance to radiologists. Second, it is intended to be used by internists, emergency physicians, and nonradiology trainees at all levels, who are required to make initial treatment decisions based on their preliminary interpretation of x‐rays, particularly in the hospital setting. Therefore, we decided our results would be more externally valid and applicable if the interpreters of the x‐rays and use of the x‐ray sign in this study was by trainees.
Abnormal opacity overlying the vertebral column on lateral chest radiography is a clinically useful finding that can help nonradiologist physicians determine initial management or the need for further investigation when diagnostic uncertainty remains. This study provides evidence that this finding is both reliable and useful for ruling the presence of lower‐lobe and associated structural pathology out, and somewhat useful for ruling the presence of such pathology in.
Acknowledgements
The authors thank Dr. Meyer Balter for his comments on an earlier version of this work.
In the evaluation of patients presenting with complaints referable to the chest, the chest radiograph (CXR) is an important and almost universal component of the initial assessment.
Chest radiography is normally performed with both posterior‐anterior (PA) and lateral projections.1 The lateral projection is generally accepted as an indispensable component because it allows better visualization of certain structures including the lower lobes, areas of which are partially obscured by the heart or hemidiaphragms on the PA projection. As such, some radiographic findings are only apparent on the lateral projection. As well, when an abnormality is discovered on the PA projection, the orthogonal orientation of the lateral projection often allows lesion localization.
Together with information gleaned from a thorough history and physical examination, the results of chest radiography often inform initial management when a diagnosis has been established, and the need for additional investigations when the diagnosis remains in question. In the hospital setting, the CXR is often reviewed first by physicians who are not radiologists (eg, internists, emergency physicians, and trainees at various stages of training) when evaluating a patient.
We undertook the current study to investigate the test characteristics (sensitivity, specificity, and likelihood ratio [LR]), and precision of 1 particular finding on lateral chest radiography as interpreted by nonradiologist physicians in the hospital setting. On a normal lateral CXR, one should observe progressive superior‐inferior vertebral radiolucency (Figure 1A). Observed opacity overlying the vertebral column obscuring this progression is usually abnormal and suggestive of pathology in the lower lobes of the lungs or associated structures (Figure 1B). A review of the literature yielded only 1 study of this finding,2 which used a case‐control design and lacked a true gold standard investigation necessary for calculation of meaningful test characteristics. In fact, few studies have compared findings on chest radiography with more definitive investigations,3, 4 and none have examined the predictive value of this finding by nonradiologist observers using a reference standard investigation such as computed tomography (CT) of the chest.
Methods
The radiology Picture Archiving and Communication System (PACS) used at our institution allows us to search for exams by date and study type. We retrospectively identified all patients seen at 1 of 3 university‐affiliated tertiary care adult teaching hospitals (Toronto General, Toronto Western, and Mount Sinai Hospitals) within an 8‐month period (January 1, 2006 to August 31, 2006) who underwent a 2‐view CXR (PA and lateral views). (Note that in this study, the terms radiograph, x‐ray, and plain film are used synonymously.) We then determined which of these patients had a subsequent CT within 24 hours of the x‐ray, resulting in a sample of 370 patients for this study. These patients primarily included patients presenting to the emergency department, and inpatients, with a very small number of outpatients. The majority of the index CXRs were performed for chief complaints of dyspnea, chest pain, cough, or for follow‐up of a previous CXR. However, many were simply performed routinely for admission. Patients with prosthetic devices or appliances obscuring the vertebral column were excluded.
After several training sessions by an experienced internist (A.S.D.), 2 authors (D.R.M., M.E.D.) independently reviewed each lateral CXR using standard 17‐inch displays and documented the presence or absence of abnormal radioopacity obscuring the superior to inferior progression of vertebral radiolucency. These 2 authors were fourth‐year medical students at the time the study began and first‐year trainees in internal medicine when it ended. The presence of abnormal opacity overlying the vertebral column was recorded as a positive test while the absence of this finding was recorded as a negative test.
Observed opacity overlying the vertebral column on lateral CXRs was considered abnormal when it did not represent manifestations of normal anatomical structures. However, the finding of opacity overlying the vertebral column of little diagnostic significance, such as prominent pulmonary vessels, degenerative bony changes, or the finding of a tortuous aorta, were considered normal in this study. Corresponding PA CXRs were also available for viewing. In most cases, the authors viewed both the lateral and PA CXRs, reflecting their use in clinical practice. However, in cases of obvious abnormality on the lateral CXR, only that projection was viewed. No clinical information was made available to the observers of the lateral CXR and they were blinded to the results of CT imaging of the chest. All 370 cases were reviewed by both observers (D.R.M. and M.E.D.). For the purpose of calculating test characteristics and LRs, cases of disagreement between the 3 lateral CXR observers were resolved by independent review by a third author (A.S.D.), a general internist with over 20 years of experience interpreting the lateral CXR.
A fourth author (M.O.B) reviewed the chest CT reports for each patient and recorded the mention of the presence or absence of various pathologies in the lower lobes of the lungs and associated structures in those reports. No clinical information was made available to this author and he was blinded to the results of lateral CXR. All CT investigations were originally interpreted by a university‐affiliated chest radiology faculty member at the time of the investigation. Table 1 lists all relevant chest CT findings in our sample that were recorded as disease‐positive for the purpose of dichotomizing the results of the reference standard, and enabling calculation of test characteristics (Table 2). Notable chest CT findings that were not recorded as disease‐positive for this purpose included mediastinal lymphadenopathy, subpleural density, lytic vertebral lesions, cystic or emphysematous changes, and pneumothorax. Dependent atelectasis was included within the disease‐positive category, though some cases may not have been pathological. It should be pointed out that there may be some variation in terminology used between staff radiologists (eg, reticulation by one radiologist may be called minor densities by another radiologist).
| Number of Cases | CXR (+) | CXR () | LR (+)* | LR ()* | |
|---|---|---|---|---|---|
| |||||
| Disease‐positive/abnormal findings | |||||
| Atelectasis or fibrosis including usual interstitial pneumonitis | 215 | 191 | 24 | 3.1 | 0.16 |
| Effusion, loculated effusion, empyema or fluid collections in fissures | 83 | 79 | 4 | 3.3 | 0.07 |
| Consolidation, airspace disease, mucous plugging or postradiation opacities | 57 | 54 | 3 | 3.3 | 0.07 |
| Ground glass opacity | 50 | 42 | 8 | 2.9 | 0.23 |
| Nodule or mass >5 mm | 48 | 44 | 4 | 3.1 | 0.12 |
| Pulmonary embolus | 22 | 18 | 4 | 2.8 | 0.26 |
| Bronchiectasis or bronchial dilation | 14 | 13 | 1 | 3.2 | 0.10 |
| Reticulation | 10 | 9 | 1 | 3.1 | 0.14 |
| Sclerotic bone lesion | 10 | 10 | 0 | 3.4 | 0 |
| Pulmonary edema or septal thickening | 8 | 8 | 0 | 3.4 | 0 |
| Interlobular septal thickening | 8 | 7 | 1 | 3.0 | 0.18 |
| Pleural plaque or calcification | 6 | 5 | 1 | 2.9 | 0.24 |
| Abnormal hemidiaphragm | 5 | 5 | 0 | 3.4 | 0 |
| Hydrothorax | 3 | 3 | 0 | 3.4 | 0 |
| Cavitary lesion | 2 | 2 | 0 | 3.4 | 0 |
| Pleural thickening | 1 | 1 | 0 | 3.4 | 0 |
| Vertebral compression fracture(s) | 1 | 1 | 0 | 3.4 | 0 |
| Bronchial obstruction | 1 | 1 | 0 | 3.4 | 0 |
| Bronchial wall thickening | 1 | 1 | 0 | 3.4 | 0 |
| Any abnormal CT finding | 289 | 251 | 38 | 2.9 | 0.19 |
| Disease‐negative/normal findings | |||||
| Normal | 81 | 24 | 57 | ||
| Overall LR | 2.9 (2.14.1) | 0.19 (0.130.26) | |||
| Abnormal Chest CT | Normal Chest CT | |
|---|---|---|
| ||
| Abnormal lateral CXR | 251 | 24 |
| Normal lateral CXR | 38 | 57 |
Using the chest CT report as the reference standard for abnormal opacity overlying the vertebral column on lateral chest radiography, we calculated the sensitivity, specificity, and positive and negative LRs (LR+ and LR, respectively) with 95% confidence intervals (CIs) for individual and summary CT‐documented pathologies.5 For this purpose, we constructed a 2 2 table (Table 2) for summary CT‐documented abnormal findings, in which patients with any abnormal CT finding were considered disease‐positive and compared with patients whose CTs were interpreted as normal, considered disease‐negative. We also constructed 2 2 tables for each of the individual CT‐documented pathologies using data from Table 1, in which only the patients with the abnormal CT finding of interest (eg, consolidation) were considered disease‐positive and compared with patients whose CTs were interpreted as normal, considered disease‐negative. In this case, patients with abnormal CT findings (eg, atelectasis, effusion) other than the finding of interest were excluded from the analysis. This secondary analysis is an attempt to estimate the variability of the accuracy of the finding in question across different diagnoses, and not to derive precise estimates of LRs given the small sample sizes for some individual findings.
Of the 370 original patients, we selected a sample of 100 patients by random number assignment whose lateral CXRs were reviewed a second time by the same observers to quantify intraobserver variability. Interobserver variability was quantified by comparing the data of the 2 independent lateral CXR observers on all 370 patients. In both cases, we calculated simple agreement and kappa statistics as measures of precision.6 Our chest CT observer also identified a sample of 10 CT investigations by random number assignment and reviewed the images in a blinded fashion to quantify interobserver variability in CT findings (ie, a comparison of the original CT report with our chest CT observer's interpretation).
We obtained approval from the relevant research ethics boards for the hospitals in which our study population was identified and have endeavored to comply with the Standards for Reporting of Diagnostic Accuracy (STARD) initiative.7 All statistical analyses were performed using R version 2.018 (Free Software Foundation, Boston, MA) and WinBUGS version 1.4. (MRC Biostatistics Unit, Cambridge, UK)9
Results
The identified study sample of 370 patients was 52% male and had an average age of 58 17 years (range, 18 to 96 years). Of the 370 patients, 81 (21.9%) were found to have a normal chest CT, 118 (31.9%) had a single CT finding in the lower lobes designated as disease‐positive, and 171 (46.2%) had 2 or more lower‐lobe CT findings. Overall, 78.1% had 1 or more CT findings considered disease‐positive.
Abnormal opacity overlying the vertebral column on lateral chest radiography had a sensitivity of 86.9% (95% CI, 82.5%‐90.3%) and specificity of 70.4% (95% CI, 59.7%‐79.2%) for CT‐documented lower‐lobe and associated structural pathology (Table 2). The summary LR+ for abnormal opacity overlying the vertebral column on lateral chest radiography was 2.9 (95% CI, 2.1‐4.1) and the summary LR for the absence of this finding was 0.19 (95% CI, 0.13‐0.26). LRs for individual CT‐documented pathologies were very similar to the summary LRs, with a range for LR+s between 2.8 and 3.4, and a range for LRs between 0 and 0.26 (Table 1).
Intraobserver simple agreement and kappa statistics for each of the lateral CXR observers were 79% ( = 0.56) and 81% ( = 0.58), respectively. Interobserver simple agreement between the lateral CXR observers, as well as the associated kappa statistic, were similar at 77% ( = 0.52). Compared with the original chest CT reports generated by university‐affiliated radiology faculty members, the blinded review of 10 randomly‐identified CT investigations by our chest CT observer (M.O.B.) yielded 100% agreement.
Discussion
This study fills a gap in the literature by providing evidence of the accuracy and precision of a particular finding on lateral chest radiography: namely, observed radioopacity obscuring the normal succession of superior‐inferior vertebral radiolucency.
Our investigation of this finding's test characteristics reveal that abnormal opacity overlying the vertebral column on lateral chest radiography is a more sensitive than specific finding, and thus in general more useful for ruling out the presence of disease than ruling it in. But it is our calculated LRs that allow application of this finding's predictive value to clinical scenarios in practice.
LRs are a powerful method of applying new information to the pretest probability of disease, to arrive at the posttest probability. If the summary point estimate LRs of our study are applied to a hypothetical pretest probability of 50% for any CT‐documented pathology, abnormal opacity overlying the vertebral column (LR+ 2.9) gives a posttest probability of 75%, and the absence of this finding (LR 0.19) gives a posttest probability of 16%. In some cases, these posttest probabilities may be high enough to stop investigating and start treating, or low enough to stop investigating.
We also calculated LRs for each subgroup of CT‐documented pathology by comparing only patients with the CT finding of interest and patients with CTs interpreted as normal. While the validity of these calculations is compromised by ignoring the patients in the other subgroups of diagnoses in the calculation, the stability of these LR estimates suggests that the finding and summary LRs can be used for a variety of diagnoses. The individual LRs, however, should not be used in arriving at posttest probabilities of individual pathologies.
Our calculated kappa statistics, a measure of chance‐corrected agreement, quantified the precision of abnormal opacity overlying the vertebral column noted by nonradiologist observers. The kappa statistics associated with intraobserver and interobserver variability for abnormal opacity overlying the vertebral column are indicative of moderate agreement, which is similar to the precision of many other investigational findings in common usage.
This study does have some limitations related to its design. First, CT was used as the gold standard in this study. Ideally, a combination of CT and more invasive measures such as lung biopsy would have been used; however, for ethical and logistical reasons this was obviously not possible. Second, when designing the study we had to decide whether or not to repeat the interpretation of CT images with observers we could ensure were blinded to the corresponding CXRs. We chose not to repeat the interpretation of CT images, and instead used the report of the staff chest radiologist who read the imaging study at the time it was performed. The person reviewing the report of the CT was blinded to the CXR. Our reasons for not rereading each of the CT images with a blinded study radiologist are as follows. First, the chest radiologists who reviewed the CT images at the time they were done were completely unaware of our hypothesis regarding the utility of the lateral CXR (our study took place after the CTs were interpreted). Second, the radiologists tell us that when they interpret CTs they rarely rely on findings in the CXR to help with those interpretations. For these 2 reasons, the original interpretation is very close to complete blinding. In addition, the individuals who interpret and write reports on chest CTs are all expert staff radiologists with considerable experience in this area. A study radiologist (likely a radiology resident) would not have been as proficient. Finally, in performing any study one must weigh the costs with the benefits of any methodological decision, reinterpretation of 370 chest CTs would have required an enormous amount of time. Finally, our small sample of 10 comparing official reports to the reinterpretation of the scans themselves supported the view that we did not need to review all 370 cases again.
Approximately three‐quarters of our study population was found to have CT‐documented disease. However, this is not surprising given our method of patient selection. Because the sample was collected from clinical practice, it is likely that only patients who exhibited a finding on the CXR that required delineation went on to have the reference standard investigation (CT). This study is therefore subject to workup bias. Workup bias in this scenario could work in 1 of 2 directions. In one situation, some patients would have a clear pathology or diagnosis based on the CXR, such that a CT was unnecessary and therefore not performed. In this case, our study would have underestimated the sensitivity of the sign being studied because a group of true positives would have been left out of the sample. In the second situation, patients with true pathology and a normal CXR (false negatives) fail to undergo CT. In this case, our study would have overestimated the sensitivity. We are not sure which effect of workup bias predominates in the study, but in either case an independent, prospective comparison of these imaging modalities in all patients who had CXRs was not feasible for ethical reasons. If we were to apply the reference standard investigation to all those patients, the potential for harm from excess radiation10 would be too great. As such, our cohort of patients is the best possible sample that can be studied.
Another feature of this study is that it intentionally used nonradiologist (budding internist) interpreters of the lateral CXRs, thus defining its generalizability. We did so for 2 reasons. First, the sign studied is likely too basic to be of relevance to radiologists. Second, it is intended to be used by internists, emergency physicians, and nonradiology trainees at all levels, who are required to make initial treatment decisions based on their preliminary interpretation of x‐rays, particularly in the hospital setting. Therefore, we decided our results would be more externally valid and applicable if the interpreters of the x‐rays and use of the x‐ray sign in this study was by trainees.
Abnormal opacity overlying the vertebral column on lateral chest radiography is a clinically useful finding that can help nonradiologist physicians determine initial management or the need for further investigation when diagnostic uncertainty remains. This study provides evidence that this finding is both reliable and useful for ruling the presence of lower‐lobe and associated structural pathology out, and somewhat useful for ruling the presence of such pathology in.
Acknowledgements
The authors thank Dr. Meyer Balter for his comments on an earlier version of this work.
- ,,,.Efficacy of routine screening and lateral chest radiographs in a hospital‐based population.N Engl J Med.1974;291:1001–1004.
- ,,, et al.Diagnosing left lower lobe pneumonia: usefulness of the ‘spine sign’ on lateral chest radiographs.J Fam Pract.1996;43:242–248.
- ,,, et al.Digital storage phosphor imaging versus conventional film radiography in CT‐documented chest disease.Radiology.1990;174:207–210.
- ,,,,.Chest imaging with a selenium detector versus conventional film radiography: a CT‐controlled study.Radiology.1996;200:687–690.
- .A primer on the precision and accuracy of the clinical examination.JAMA.1992;267:2638–2644.
- ,,, et al.Tips for learners of evidence‐based medicine: 3. Measures of observer variability (kappa statistic).CMAJ.2004;171:1369–1373.
- ,,, et al.Towards complete and accurate reporting of studies of diagnostic accuracy: the STARD initiative.Ann Intern Med.2003;138:40–44.
- R Development Core Team.R: A Language and Environment for Statistical Computing.Vienna, Austria:R Foundation for Statistical Computing;2004.
- ,,,.WinBUGS Version 1.4.1 User Manual.Cambridge, England:MRC Biostatistics Unit;2004.
- ,.Computed tomography—an increasing source of radiation exposure.N Engl J Med.2007;357(22):2277–2284.
- ,,,.Efficacy of routine screening and lateral chest radiographs in a hospital‐based population.N Engl J Med.1974;291:1001–1004.
- ,,, et al.Diagnosing left lower lobe pneumonia: usefulness of the ‘spine sign’ on lateral chest radiographs.J Fam Pract.1996;43:242–248.
- ,,, et al.Digital storage phosphor imaging versus conventional film radiography in CT‐documented chest disease.Radiology.1990;174:207–210.
- ,,,,.Chest imaging with a selenium detector versus conventional film radiography: a CT‐controlled study.Radiology.1996;200:687–690.
- .A primer on the precision and accuracy of the clinical examination.JAMA.1992;267:2638–2644.
- ,,, et al.Tips for learners of evidence‐based medicine: 3. Measures of observer variability (kappa statistic).CMAJ.2004;171:1369–1373.
- ,,, et al.Towards complete and accurate reporting of studies of diagnostic accuracy: the STARD initiative.Ann Intern Med.2003;138:40–44.
- R Development Core Team.R: A Language and Environment for Statistical Computing.Vienna, Austria:R Foundation for Statistical Computing;2004.
- ,,,.WinBUGS Version 1.4.1 User Manual.Cambridge, England:MRC Biostatistics Unit;2004.
- ,.Computed tomography—an increasing source of radiation exposure.N Engl J Med.2007;357(22):2277–2284.
Copyright © 2009 Society of Hospital Medicine
Inpatient Glucose Control
The past decade has seen an increase in the number of hospital discharges associated with a diabetes diagnosis.1, 2 Diabetes is the fourth leading comorbid condition associated with any hospital discharge in the United States.3 Nearly one‐third of diabetes patients require 2 or more hospitalizations in any given year,4 and inpatient stays account for the largest proportion of direct medical expenses incurred by persons with the disease.5
The hospital component of diabetes care has been receiving considerable attention. The advantage of effective inpatient diabetes managementwith particular attention to improving glycemic controlis evident for a number of clinical situations (eg, acute myocardial infarction, critically ill patients).68 National and regional organizations,912 and professional societies68, 12 have developed guidelines about management of inpatient hyperglycemia.
Despite increased awareness of the value of treating inpatient hyperglycemia, little is known about glucose control in U.S. hospitals. As hospitals begin to develop programs to improve inpatient glucose management, some method of standardized benchmarking should be put in place. Using information systems solutions to obtain point‐of‐care bedside glucose (POC‐BG) data, we previously reported on inpatient glucose control from a smaller number of U.S. hospitals.13, 14 We now provide data on a larger, more representative number of U.S. hospitals that gives a broader national view of the current status of inpatient glycemic control.
Patients and Methods
Data Collection
The hospitals in this study employed standard bedside glucose meters (ACCU‐CHEK Inform, Roche Diagnostics, Indianapolis, IN), downloaded to the Remote Automated Laboratory System‐Plus (RALS‐Plus; Medical Automation Systems, Charlottesville, VA), a well‐established POC test information management system.1315 Participating hospitals do not provide patient specific data (eg, age, sex, race, diagnosis codes), but individual patients can be selected based on a unique anonymous identifier. Data also includes date and time of the POC‐BG test, download location (nursing unit), and the test result. Patient‐level POC‐BG data was extracted by linking the POC‐BG data to the unique patient identifier. Adult inpatient data from January to December 2007 were collected. Out‐of‐range values of LO (<10 mg/dL) and HI (>600 mg/dL) were discarded. The number of HI/LO values totaled less than 0.4% of the measurements. Repeat measures, largely performed to verify hypoglycemia were found to be present for <3% of the measures and were retained in this analyses.
Hospital Selection
Participating hospitals were included through self‐selection based on interest and a willingness to complete a business agreement prior to a data collection deadline. All of the more than 1300 hospitals with RALS‐Plus capability were invited to participate in the RALS‐Annual Report,16 an ongoing benchmarking project of inpatient glucose control in U.S. hospitals; 126 hospitals agreed to participate. Hospitals provided written permission to remotely access their RALS‐Plus glucose data and combine it with other participating hospitals into an aggregate database. Confidentiality was guaranteed for the identity of participating hospitals and their data.
Characteristics of participating hospitals, including number of beds, type (academic, urban community, rural community), and region, were obtained via completion of a questionnaire. This information was verified by accessing the hospital website or consulting the 2008 Hospital Blue Book (Official National Edition; Billian Publishing, Inc., Atlanta, GA). For academic status, we used membership in the Association of American Medical Colleges' Council of Teaching Hospitals, which is limited to organizations having a documented affiliation agreement with a medical school. Our definition of hospital types for the 126 study hospitals was based on first selecting the academic hospitals as a separate subgroup. The remaining hospitals were then classified as urban community or rural community.
Statistical Analysis
Glucose data were normalized to patient‐day, and expressed according to the number of patient‐days during which measurements were obtained. Patient‐day analyses were conducted by first constructing a patient‐day POC‐BG mean. An average POC‐BG level was computed for each patient‐day by summing together the measurement occasions for a given patient‐day and dividing by the number of measurements that occurred on that day. These patient‐day averages were then aggregated to the hospital level, and averaged to compute the patient‐day‐weighted mean POC‐BG level for each hospital, using the patient‐day as the unit of analysis.
Because of variations in the definition of maximal recommended inpatient glucose levels,8, 9 we calculated proportion of patient‐days with a patient‐day‐weighted mean POC‐BG value above the cut points of >180, >200, >250, >300, >350, and >400 mg/dL.14, 17 Published studies on hypoglycemia also use various biochemical definitions of low glucose;1824 therefore, we determined percentages of patient days with at least 1 POC‐BG value below the different cut points (<70, <60, <50, and <40 mg/dL) as previously described.14, 17
Finally, we evaluated the relationship between hospital patient‐day‐weighted mean POC‐BG values (normalized to patient day as above) and specific hospital characteristics: number of hospital beds, hospital type (academic, urban community, rural community), and U.S. geographic region. Hospital groups were compared for continuous variables using Mann‐Whitney tests and categorical variables (hospital characteristics) by chi‐square tests. All analyses were done using SPSS 15.0 (SPSS, Chicago, IL). Statistics were calculated for intensive care unit (ICU) and non‐ICU locations separately.
Results
Characteristics of Participating Hospitals
Of the 126 participating hospitals (Table 1), 38.1% were <200 beds, 19.8% were 200 to 299 beds, 13.5% were 300 to 399 beds, and 28.6% were 400 beds; 54.8% were urban community hospitals, 36.5% were rural community, 8.7% were academic, 32.5% were located in the South, 29.4% in the Midwest, 22.2% in the West, and 15.9% in the Northeast. Using chi‐square comparison our study sample was found to be representative of the larger sample of hospitals that use RALS‐Plus with regards to bed number, hospital type, and region (P = not significant [NS]), but not representative of hospitals nationally in these categories (P < 0.05). The most notable difference was seen in hospital size, where the sample hospitals were disproportionately larger; a trait shared by RALS hospitals more generally.
| Study Hospitals | RALS‐Plus Hospitals | U.S. Hospitals | |
|---|---|---|---|
| |||
| Total | 126 | 1225 | 4936 |
| Number of beds, n (%) | |||
| <200 | 48 (38.1) | 510 (41.6) | 3532 (71.6) |
| 200‐299 | 25 (19.8) | 284 (23.2) | 619 (12.5) |
| 300‐399 | 17 (13.5) | 193 (15.8) | 368 (7.5) |
| 400 | 36 (28.6) | 238 (19.4) | 417 (8.4) |
| Hospital type, n (%) | |||
| Academic | 11 (8.7) | 74 (6.0) | 413 (8.4) |
| Urban | 69 (54.8) | 835 (68.2) | 2514 (50.9) |
| Rural | 46 (36.5) | 316 (25.8) | 2009 (40.7) |
| Region, n (%) | |||
| Northeast | 20 (15.9) | 206 (16.8) | 680 (13.8) |
| Midwest | 37 (29.4) | 520 (42.4) | 1422 (28.8) |
| South | 41 (32.5) | 259 (21.1) | 1919 (38.9) |
| West | 28 (22.2) | 239 (19.5) | 915 (18.5) |
Overall Glycemic Control
A total of 12,559,305 POC‐BG measurements (2,935,167 from the ICU and 9,624,138 from the non‐ICU) from 1,010,705 patients with 3,973,460 patient days were analyzed from 126 hospitals. The mean number of measurements was 20 per ICU patient and 9.5 for non‐ICU patients. The average number of measurements taken per patient‐day was 5 for the ICU patient and 3 for the non‐ICU patient.
Hospital hyperglycemia (>180 mg/dL) was 46.0% for ICU and 31.7% for non‐ICU. The patient‐day‐weighted mean POC‐BG for ICU measurements was 165 mg/dL (median = 164 mg/dL, SD 14.5) and 166 mg/dL (median = 167 mg/dL, SD 8) for non‐ICU. The distributions of patient‐day‐weighted mean POC‐BG values for ICU and non‐ICU settings are shown in Figure 1. The range of patient‐day‐weighted mean values was much wider for the ICU (126‐203 mg/dL) than in the non‐ICU (139‐186 mg/dL).
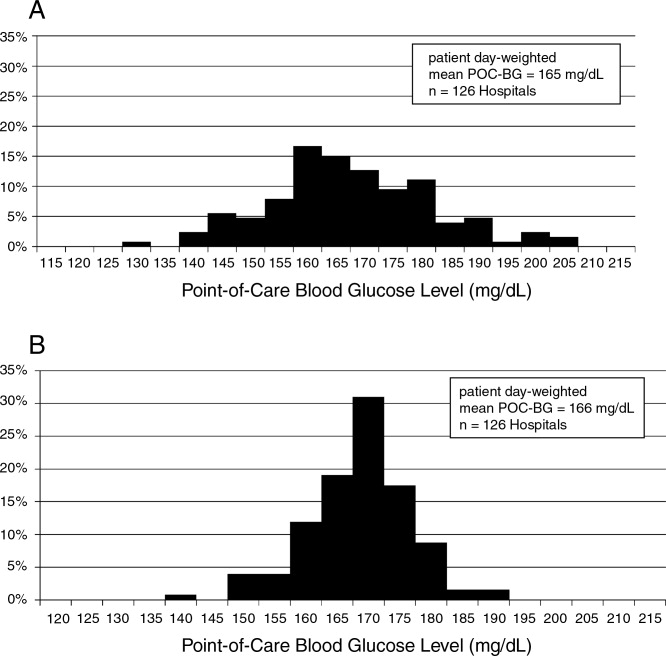
Hyperglycemia Prevalence
Of ICU patients, 60.6% had at least 1 POC‐BG value >180 mg/dL, as did 46.4% of non‐ICU patients. The proportion of patient‐days with a patient‐day‐weighted mean POC‐BG >180 mg/dL was 26.3% in the ICU setting (Figure 2A) and 31.3% in the non‐ICU (Figure 2B); the other cut points are also shown in Figure 2. The prevalence of patient‐days where hyperglycemia was more severe (>300 mg/dL) was low but nonetheless still detected in both the ICU and non‐ICU settings, although these differences appear to be less pronounced than in the ICU.
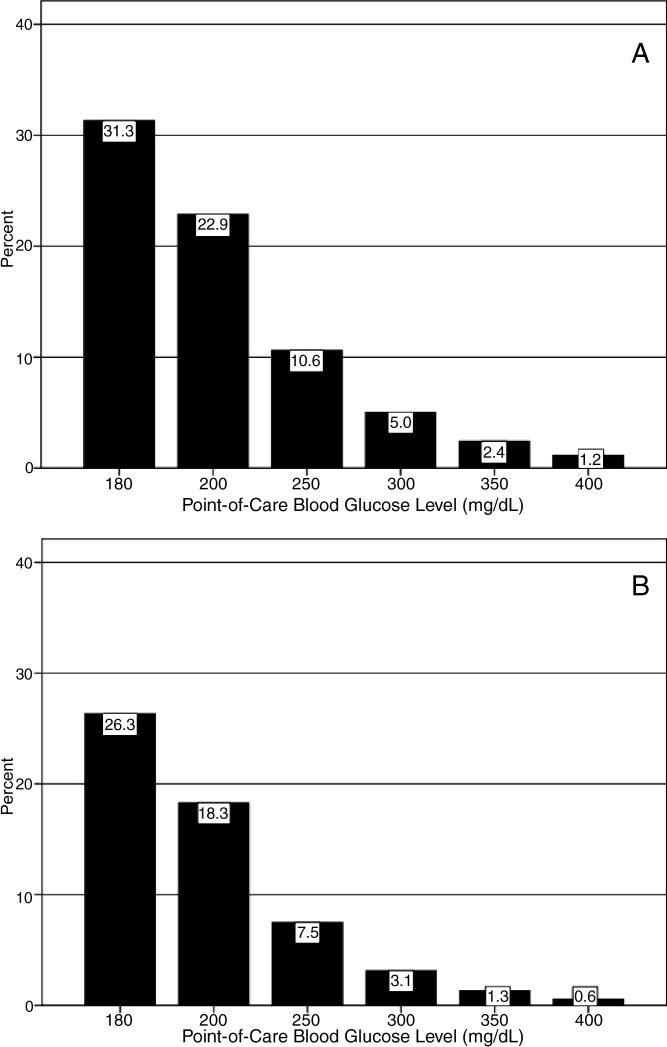
Hypoglycemia Rates
There were 21.3% of patients who had at least 1 POC‐BG value <70 mg/dL. Hospital hypoglycemia was low in both the ICU and non‐ICU measurement data, although the proportion of patient days with POC‐BG <70 mg/dL was higher in the ICU vs. the non‐ICU setting (Figure 3A,B). Hypoglycemia (<70 mg/dL) was detected in 10.1% of patient‐days (3.2% of all measures) in the ICU setting (Figure 3A) and 3.5% of patient‐days (4.2% of all measures) in the non‐ICU (Figure 3B). Moderate (<60 mg/dL) and more severe (<50 mg/dL and <40 mg/dL) hypoglycemia were very uncommon in both the ICU and non‐ICU.
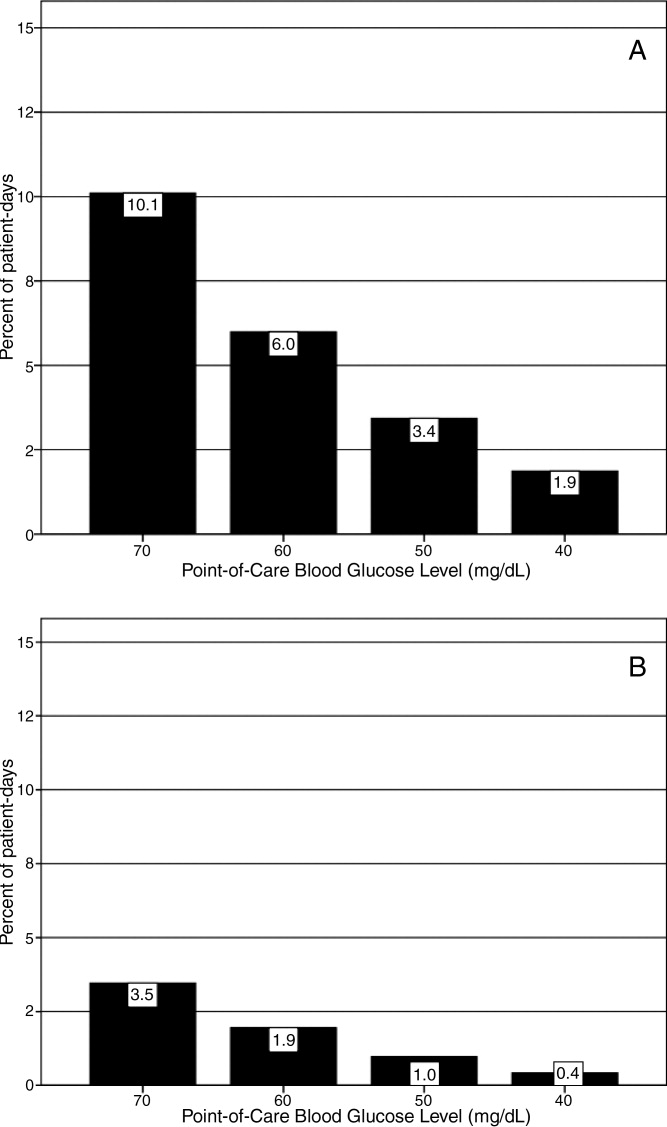
Relationship of Glucose Control with Hospital Characteristics
There was a significant relationship between the total number of hospital beds and patient‐day‐weighted mean POC‐BG values in the ICU (Figure 4A). In the ICU, hospitals with <200 beds had significantly higher patient‐day‐weighted mean POC‐BG levels than those with 200 to 299 beds (P < 0.05), 300 to 399 beds (P < 0.01), and 400 beds (P < 0.001). Rural hospitals (Figure 4B) also had higher patient‐day‐weighted mean POC‐BG values compared to urban community and academic hospitals (both P < 0.001). Finally, ICUs in hospitals in the West (Figure 4C, bottom panel) had significantly lower values than those in the Midwest and South (both P < 0.01).
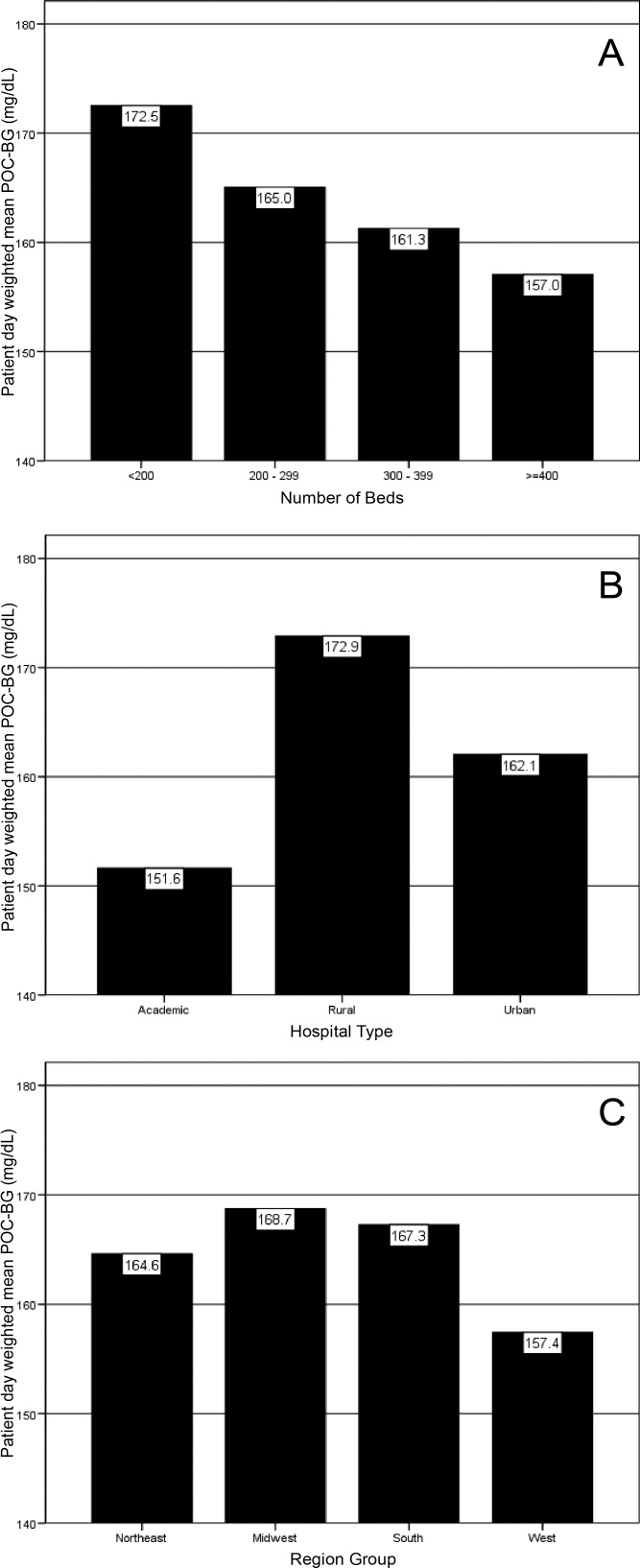
Differences in patient‐day‐weighted mean POC‐BG levels based on hospital characteristics were also observed for the non‐ICU (Figure 5), although these differences appear to be less pronounced than in the ICU. Hospitals with <200 beds (Figure 5A) had significantly higher patient‐day‐weighted mean POC‐BG values compared to hospitals with 300 to 399 beds (P < 0.05) and 400 beds (P < 0.001). Rural hospitals (Figure 5B) had significantly higher values than academic (P < 0.05) and urban community (P < 0.001) hospitals, and hospitals in the West (Figure 5C) had significantly lower values than those in the South and Northeast (both P < 0.05).
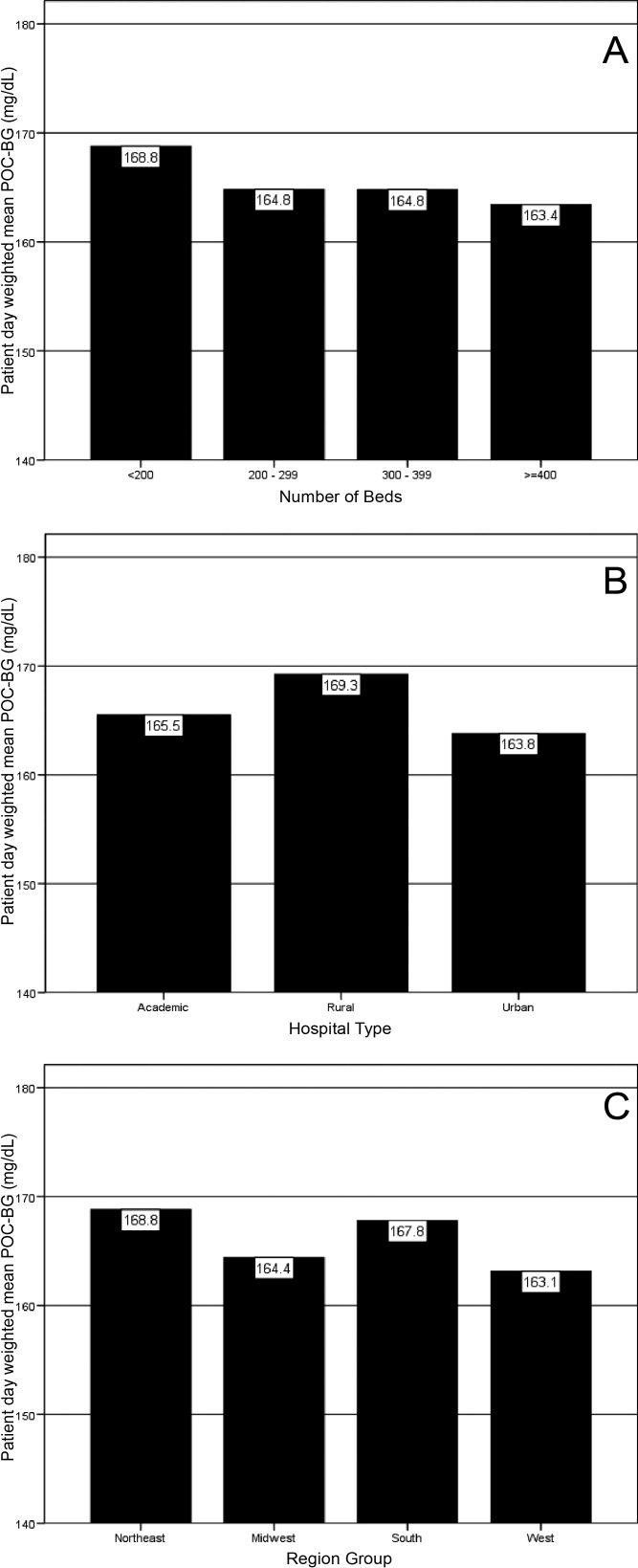
Discussion
Hospitalizations associated with diabetes pose a substantial burden on the U.S. health system.15 Recent consensus advocates good glucose control in the hospital to optimize outcomes for a number of clinical scenarios.68 Aside from a few institution‐specific studies,2527 the quality of diabetes treatment in U.S. hospitals is mostly unknown, but assessing the level of glycemic control will be a key metric that hospitals will need to track as they implement improvement programs targeting hospital hyperglycemia. Hospitals will need a way not just to track overall glucose levels, but also to monitor whether hypoglycemic events rise as they implement tight glycemic control initiatives. To our knowledge this is the first report on glycemic control from a large number of U.S. hospitals with diverse characteristics and from different geographic regions.
Debate continues as to what glucose targets for inpatients should be attained.28, 29 The overall patient‐day‐weighted mean POC‐BG was 170 mg/dL for the non‐ICU, and only a moderately lower 162 mg/dL in the ICU, despite much lower thresholds for ICU measurements in current suggested guidelines.8, 30 For the average hospital, over one‐third of non‐ICUs had patient‐day‐weighted mean POC‐BG levels that were >180 mg/dL and nearly one‐quarter had values >200 mg/dL. Similarly, nearly 40% of ICUs had patient‐day‐weighted mean POC‐BGs >180 mg/dL and over 30% were >200 mg/dL, indicating room for improvement in hospital ICU glucose control, at least in the hospitals sampled here. The range of patient‐day‐weighted mean POC‐BG levels for the ICU was broader than what was seen in the non‐ICU data, with the ICU data containing lower weighted mean POC‐BG values, and may indicate that hospitals are concentrating their efforts on adopting stricter glucose control measures in their ICUs.
Whether examining data from a single institution,17 from a larger group of hospitals,14 or now from 126 hospitals, one consistent finding has been the low prevalence of hypoglycemiaparticularly severe hypoglycemia (glucose <50 mg/dL or <40 mg/dL). Based on this larger sampling, however, hypoglycemia in the ICU, while still uncommon with respect to hyperglycemia, is more than double that of the non‐ICU. Fear of hypoglycemia is frequently mentioned as a barrier to attaining lower inpatient glucose levels.31 Although hypoglycemia frequency in the hospital is low, and even though recent data indicates that hypoglycemia is not perceived by practitioners as the number 1 barrier to successful inpatient diabetes management,3234 the possible association of severe low glucose levels to inpatient mortality18, 19, 21, 22, 24, 35 makes hypoglycemia a key counterbalance metric that hospitals will need to track as they implement glycemic control programs. In the ICU, higher glycemic targets may be needed to allay practitioner fears, and insulin administration protocols that have the best track record for minimizing hypoglycemia should be identified and promulgated.
Recent data showing increased risk of hospital hypoglycemia with attempts to better control hyperglycemia may unjustifiably deter practitioners and hospitals from implementing programs to better control inpatient glucose levels.24, 36 Unlike the outpatient setting, where patients can take measures to prevent hypoglycemia, hospitalized patients surrender control of their diabetes management to staff. Inpatient tight glycemic control initiatives cannot be instituted unless they are coupled with efforts to understand and correct system‐based problems that increase the risk of hypoglycemia. Recently published reports demonstrate that hypoglycemic events can be kept very low during treatment with an intensive insulin infusion protocol if expert rules are built into the algorithm that address hypoglycemia.37, 38 Thus, rather than abandon efforts at improving inpatient hyperglycemia over concerns about hypoglycemia, hospitals will need to develop methods to change their hypoglycemia policies from ones that typically just guide treatment to ones that incorporate preventive strategies.
Our data suggest a relationship between POC‐BG levels and hospital characteristics. Rural hospitals and hospitals with the least number of beds had higher POC‐BG levels compared to urban, academic, or larger hospitals, especially in the ICU setting. The reasons underlying these findings cannot be determined from this analysis, but it is possible that smaller hospitals and those located in rural areas do not have access to the diabetes experts (eg, endocrinologists or diabetes educators) to assist them in developing tight glycemic control programs. We also detected differences in patient‐day‐weighted mean POC‐BG data based on geographic region. Whether considering ICU or non‐ICU data, hospitals located in the West had lower glucose values compared to other regions. As with the other hospital characteristics, the explanation underlying these observations cannot be determined. It is possible that hospitals in the West are earlier‐adopters of tight glycemic control programs compared to other U.S. geographic regions. Further study is needed in a larger number of hospitals to confirm these findings.
These findings should be considered in light of the following limitations: unavailability to us of specific patient‐level information that would allow adjustment of data for such as variables as comorbidity; the fact that recommendations about glycemic targets in the hospital vary by organization,810, 30 which may result in hospitals aiming for different targets in different populations; and the controversy that continues on the benefits of glycemic control in the ICU, which may be dissuading facilities from implementing glucose control programs.39, 40 All that can be concluded from our analysis is that there is variation in the POC‐BG data based on hospital characteristics. We cannot state that one type of hospital is performing glycemic control better than another, particularly as some hospital types are underrepresented in our sample, and we cannot control for patient‐level data. Moreover, this statistical variation seen between different hospital types may not be of clinical importance in terms of being associated with different outcomes, or may simply be a result of different patterns of glucose monitoring in individual hospitals. However, the observed variation should prompt further investigation into the basis of differences (eg, some hospital types or regions may be further ahead in inpatient diabetes quality improvement initiatives than others).
There is no consensus about how best to summarize and report glycemic control in the hospital (so called glucometrics),41 and a variety of reporting measures have been suggested.20, 4245 We show data using one method: with the mean BG normalized to patient‐day as the unit of analysis; however, we found similar results when we used the patient or the glucose reading as the unit of analysis. As organizations move to develop standards for summarizing inpatient glucose data, consideration must be given to which measure is best correlated with hospital outcomes. In addition, when developing standards, it will be important to determine what type of data hospitals will find most clinically useful to track the impact of glucose control interventions. For instance, hospitals may wish to see data on the frequencies of glucose measurements that are above and below certain desired thresholds, which is one of the approaches that we have used in previous publications,14, 17, 26, 46 and which is currently provided as feedback to hospitals participating in RALS reporting.
The other issue to address in development of standards in inpatient glycemic control reporting is what method of glucose measurement should be used. Correlation between whole‐blood vs. POC‐BG values can be imprecise in the intensive care setting.41, 47 We have previously utilized bedside glucose measurements as our means of evaluating the status of inpatient glucose control,14, 17, 26 and bedside glucose measurements remain the mainstay of how practitioners judge the status of inpatient hyperglycemia and make therapeutic decisions about management. The hospitals participating in the process reviewed here all use the same system of bedside glucose monitoring and glucometer‐laboratory electronic interface. Until alternative clinical methods are developed to frequently sample glucose levels in a convenient and minimally invasive way at the bedside, current POC‐BG technology will continue to be the most utilized means of assessing hospital glucose management in the inpatient setting.
Electronic data warehouses such as RALS‐Plus are convenient sources of information in which to store data on the quality of inpatient diabetes care. Unlike chart abstraction which requires extensive man‐hours to extract data on a few patients, use of electronic data allows examination of large numbers of hospital cases. Queries of information systems could be automated, report cards potentially generated, and feedback given to providers and hospitals on the status of inpatient glycemic control.
Nonetheless, there are limitations to using electronic records as the sole method to assess inpatient diabetes care. Analysis of electronic records does not allow assessment of reasons underlying decision‐making behavior of clinicians (eg, why they did or did not change hyperglycemic therapy). Moreover, our electronic data does not permit an assessment of who had preexisting diabetes, who was admitted with new onset diabetes, or who developed hyperglycemia as a result of the hospital stay.
In addition to the above, while our sample was representative of other RALs participating hospitals, it was not entirely representative of all U.S. hospitals. Hospitals contributing data to this report were chosen by self‐selection rather than by random methods. Expanding hospital participation in this inpatient glucose assessment benchmarking process will be needed to determine if findings in this work can be generalized. Finally, our study was conducted using the hospital, rather than the patient, as the unit of analysis, as patient‐level characteristics (age, sex, race/ethnicity) were not provided by participating hospitals.
Despite these limitations and issues noted above, to our knowledge this report is the most extensive review of the state of blood glucose control in hospitals across the United States. While other commercial laboratory data management systems may exist in hospitals, their data has not been reported to date. Additionally, our analysis provides a first glimpse of inpatient glycemic control of a large number of U.S. hospitals of varying characteristics and different national regions. Increased hospital participation in data collection may allow the creation of a national benchmarking process for the development of best practices and improved inpatient hyperglycemia management.
- Centers for Disease Control and Prevention. Hospitalization for Diabetes as First‐Listed Diagnosis. Available at: http://www.cdc.gov/diabetes/statistics/dmfirst/index.htm. Accessed April2009.
- Centers for Disease Control and Prevention. Hospitalizations for Diabetes as Any‐Listed Diagnosis. Available at: http://www.cdc.gov/diabetes/statistics/dmany/index.htm. Accessed April2009.
- ,,,.Hospitalization in the United States, 1997.Rockville, MD:Agency for Healthcare Research and Quality;2000. HCUP Fact Book No. 1; AHRQ Publication No. 00‐0031.
- ,,,.Multiple hospitalizations for patients with diabetes.Diabetes Care.2003;26(5):1421–1426.
- American Diabetes Association.Economic costs of diabetes in the US in 2007.Diabetes Care.2008;31(3):596–615.
- ,,, et al.American Diabetes Association Diabetes in Hospitals Writing Committee: Management of diabetes and hyperglycemia in hospitals.Diabetes Care.2004;27:553–591.
- ACE Task Force on Inpatient Diabetes and Metabolic Control.American College of Endocrinology Position Statement on Inpatient Diabetes and Metabolic Control.Endocr Pract.2004;10:77–82.
- ACE/ADA Task Force on Inpatient Diabetes.American College of Endocrinology and American Diabetes Association consensus statement on inpatient diabetes and glycemic control.Endocr Pract.2006;12(4):459–468.
- Institute for Healthcare Improvement. Getting started kit: prevent surgical site infections. Available at: http://www.ihi.org/NR/rdonlyres/00EBAF1F‐A29F‐4822‐ABCE‐829573255AB8/0/SSIHowtoGuideFINAL.pdf. Accessed April2009.
- Institute for Healthcare Improvement. Implement Effective Glucose Control. Available at: http://www.ihi.org/IHI/Topics/CriticalCare/IntensiveCare/Changes/ImplementEffectiveGlucoseControl.htm. Accessed April2009.
- Joint Commission on Accreditation of Healthcare Organizations. Inpatient Diabetes Certification Addendum. Available at: http://www.jointcommission.org/CertificationPrograms/Inpatient+Diabetes. Accessed April2009.
- ,,, et al.Working to improve care of hospital hyperglycemia through statewide collaboration: the Georgia Hospital Association Diabetes Special Interest Group.Endocr Pract.2007;13:45–50.
- ,,,.Current state of inpatient diabetes burden and care, and goal of the conference.Endocr Pract.2006;12:S1–S10.
- ,,,,.Inpatient point‐of‐care bedside glucose testing: preliminary data on use of connectivity informatics to measure hospital glycemic control.Diabetes Technol Ther.2007;9:493–500.
- .Medical automation systems and a brief history of point‐of‐care informatics.Point Care.2007;6:154–159.
- Medical Automation Systems. RALS‐Report. Available at: http://www.rals.com/RALS‐Report.html. Accessed April2009.
- ,,, et al.Diabetes care in hospitalized non‐critically ill patients: more evidence for clinical inertia and negative therapeutic momentum.J Hosp Med.2007;2:203–211.
- ,,.Hypoglycemia in hospitalized patients. Causes and outcomes.N Engl J Med.1986;315(20):1245–1250.
- ,,,,,.Mortality in hospitalized patients with hypoglycemia and severe hyperglycemia.Mt Sinai J Med.1995;62(6):422–426.
- ,,.Glycemic control and sliding scale insulin use in medical inpatients with diabetes mellitus.Arch Intern Med.1997;157(5):545–552.
- ,,,,.Influence of individual characteristics on outcome of glycemic control in intensive care unit patients with or without diabetes mellitus.Mayo Clin Proc.2005;80(12):1558–1567.
- ,,, et al.Evaluation of short‐term consequences of hypoglycemia in an intensive care unit. [see Comment].Crit Care Med.2006;34(11):2714–2718.
- ,,, et al.Predisposing factors for hypoglycemia in the intensive care unit. [see Comment].Crit Care Med.2006;34(1):96–101.
- .Severe hypoglycemia in critically ill patients: risk factors and outcomes.Crit Care Med.2007;35(10):2262–2267.
- ,,,,.Unrecognized diabetes among hospitalized patients.Diabetes Care.1998;21(2):246–249.
- ,,, et al.Diabetes care in the non‐ICU setting: is there clinical inertia in the hospital?J Hosp Med.2006;1(3):151–160.
- ,,,,.Inpatient management of diabetes and hyperglycemia among general medicine patients at a large teaching hospital.J Hosp Med.2006;1(3):145–150.
- ,.Counterpoint: inpatient glucose management. A premature call to arms?Diabetes Care.2005;28:976–979.
- ,.Point: inpatient glucose management. The emperor finally has clothes.Diabetes Care.2005;28(4):973–975.
- ,,, et al.Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008.Crit Care Med.2008;36(1):296–327.
- ,,, et al.Hospital hypoglycemia: not only treatment but also prevention. American College of Endocrinology (ACE) Inpatient Diabetes and Metabolic Control Consensus Conference.Endocr Pract.2004;10(suppl 2):89–99.
- ,,, et al.Management of inpatient hyperglycemia: assessing perceptions and barriers to care among resident physicians.Endoc Pract.2007;13:117–125.
- ,,, et al.Beliefs about hospital diabetes and perceived barriers to glucose management among inpatient midlevel practitioners.Diabetes Educ.2008;34(1):75–83.
- ,,,.Perceptions of resident physicians about management of inpatient hyperglycemia in an urban hospital.J Hosp Med.2009;4(1):E1–E8.
- ,,.Hypoglycemia in hospitalized adult patients without diabetes.Endocr Pract.2005;11(2):91–96.
- ,,, et al.Intensive insulin therapy and pentastarch resuscitation in severe sepsis.N Engl J Med.2008;358(2):125–139.
- ,,, et al.Development and implementation of evidence‐based, IV insulin guidelines: a statewide collaborative approach.Insulin.2008;3:67–77.
- ,,, et al.Outcomes of a cardiothoracic intensive care web‐based online intravenous insulin infusion calculator study at a Medical University Hospital.Diabetes Technol Ther.2007;9(6):523–534.
- ,,.Benefits and risks of tight glucose control in critically ill adults. A meta‐analysis.JAMA.2008;300(8):933–944.
- ,.Tight glycemic control in critically ill adults.JAMA.2008;300(8):963–965.
- ,,, et al.“Glucometrics”—assessing the quality of inpatient glucose management.Diabetes Technol Ther.2006;8(5):560–569.
- ,,, et al.Glucometrics in patients hospitalized with acute myocardial infarction: defining the optimal outcomes‐based measure of risk. [see Comment].Circulation.2008;117(8):1018–1027.
- ,,.Hyperglycaemic index as a tool to assess glucose control: a retrospective study.Crit Care.2004;8(3):R122–R127.
- ,,,,.SHM glycemic control task force summary: practical recommendations for assessing the impact of glycemic control efforts.J Hosp Med.2008;3(S5):66–75.
- ,,, et al.Understanding and improving management of inpatient diabetes mellitus: The Mayo Clinic Arizona Experience.J Diabetes Sci Technol.2008;2:925–931.
- ,,, et al.Reliability of point‐of‐care testing for glucose measurement in critically ill adults.Crit Care Med.2005;33(12):2778–2785.
- ,,, et al.Accuracy of bedside glucometry in critically ill patients: influence of clinical characteristics and perfusion index.Mayo Clin Proc.2008;83:400–405.
The past decade has seen an increase in the number of hospital discharges associated with a diabetes diagnosis.1, 2 Diabetes is the fourth leading comorbid condition associated with any hospital discharge in the United States.3 Nearly one‐third of diabetes patients require 2 or more hospitalizations in any given year,4 and inpatient stays account for the largest proportion of direct medical expenses incurred by persons with the disease.5
The hospital component of diabetes care has been receiving considerable attention. The advantage of effective inpatient diabetes managementwith particular attention to improving glycemic controlis evident for a number of clinical situations (eg, acute myocardial infarction, critically ill patients).68 National and regional organizations,912 and professional societies68, 12 have developed guidelines about management of inpatient hyperglycemia.
Despite increased awareness of the value of treating inpatient hyperglycemia, little is known about glucose control in U.S. hospitals. As hospitals begin to develop programs to improve inpatient glucose management, some method of standardized benchmarking should be put in place. Using information systems solutions to obtain point‐of‐care bedside glucose (POC‐BG) data, we previously reported on inpatient glucose control from a smaller number of U.S. hospitals.13, 14 We now provide data on a larger, more representative number of U.S. hospitals that gives a broader national view of the current status of inpatient glycemic control.
Patients and Methods
Data Collection
The hospitals in this study employed standard bedside glucose meters (ACCU‐CHEK Inform, Roche Diagnostics, Indianapolis, IN), downloaded to the Remote Automated Laboratory System‐Plus (RALS‐Plus; Medical Automation Systems, Charlottesville, VA), a well‐established POC test information management system.1315 Participating hospitals do not provide patient specific data (eg, age, sex, race, diagnosis codes), but individual patients can be selected based on a unique anonymous identifier. Data also includes date and time of the POC‐BG test, download location (nursing unit), and the test result. Patient‐level POC‐BG data was extracted by linking the POC‐BG data to the unique patient identifier. Adult inpatient data from January to December 2007 were collected. Out‐of‐range values of LO (<10 mg/dL) and HI (>600 mg/dL) were discarded. The number of HI/LO values totaled less than 0.4% of the measurements. Repeat measures, largely performed to verify hypoglycemia were found to be present for <3% of the measures and were retained in this analyses.
Hospital Selection
Participating hospitals were included through self‐selection based on interest and a willingness to complete a business agreement prior to a data collection deadline. All of the more than 1300 hospitals with RALS‐Plus capability were invited to participate in the RALS‐Annual Report,16 an ongoing benchmarking project of inpatient glucose control in U.S. hospitals; 126 hospitals agreed to participate. Hospitals provided written permission to remotely access their RALS‐Plus glucose data and combine it with other participating hospitals into an aggregate database. Confidentiality was guaranteed for the identity of participating hospitals and their data.
Characteristics of participating hospitals, including number of beds, type (academic, urban community, rural community), and region, were obtained via completion of a questionnaire. This information was verified by accessing the hospital website or consulting the 2008 Hospital Blue Book (Official National Edition; Billian Publishing, Inc., Atlanta, GA). For academic status, we used membership in the Association of American Medical Colleges' Council of Teaching Hospitals, which is limited to organizations having a documented affiliation agreement with a medical school. Our definition of hospital types for the 126 study hospitals was based on first selecting the academic hospitals as a separate subgroup. The remaining hospitals were then classified as urban community or rural community.
Statistical Analysis
Glucose data were normalized to patient‐day, and expressed according to the number of patient‐days during which measurements were obtained. Patient‐day analyses were conducted by first constructing a patient‐day POC‐BG mean. An average POC‐BG level was computed for each patient‐day by summing together the measurement occasions for a given patient‐day and dividing by the number of measurements that occurred on that day. These patient‐day averages were then aggregated to the hospital level, and averaged to compute the patient‐day‐weighted mean POC‐BG level for each hospital, using the patient‐day as the unit of analysis.
Because of variations in the definition of maximal recommended inpatient glucose levels,8, 9 we calculated proportion of patient‐days with a patient‐day‐weighted mean POC‐BG value above the cut points of >180, >200, >250, >300, >350, and >400 mg/dL.14, 17 Published studies on hypoglycemia also use various biochemical definitions of low glucose;1824 therefore, we determined percentages of patient days with at least 1 POC‐BG value below the different cut points (<70, <60, <50, and <40 mg/dL) as previously described.14, 17
Finally, we evaluated the relationship between hospital patient‐day‐weighted mean POC‐BG values (normalized to patient day as above) and specific hospital characteristics: number of hospital beds, hospital type (academic, urban community, rural community), and U.S. geographic region. Hospital groups were compared for continuous variables using Mann‐Whitney tests and categorical variables (hospital characteristics) by chi‐square tests. All analyses were done using SPSS 15.0 (SPSS, Chicago, IL). Statistics were calculated for intensive care unit (ICU) and non‐ICU locations separately.
Results
Characteristics of Participating Hospitals
Of the 126 participating hospitals (Table 1), 38.1% were <200 beds, 19.8% were 200 to 299 beds, 13.5% were 300 to 399 beds, and 28.6% were 400 beds; 54.8% were urban community hospitals, 36.5% were rural community, 8.7% were academic, 32.5% were located in the South, 29.4% in the Midwest, 22.2% in the West, and 15.9% in the Northeast. Using chi‐square comparison our study sample was found to be representative of the larger sample of hospitals that use RALS‐Plus with regards to bed number, hospital type, and region (P = not significant [NS]), but not representative of hospitals nationally in these categories (P < 0.05). The most notable difference was seen in hospital size, where the sample hospitals were disproportionately larger; a trait shared by RALS hospitals more generally.
| Study Hospitals | RALS‐Plus Hospitals | U.S. Hospitals | |
|---|---|---|---|
| |||
| Total | 126 | 1225 | 4936 |
| Number of beds, n (%) | |||
| <200 | 48 (38.1) | 510 (41.6) | 3532 (71.6) |
| 200‐299 | 25 (19.8) | 284 (23.2) | 619 (12.5) |
| 300‐399 | 17 (13.5) | 193 (15.8) | 368 (7.5) |
| 400 | 36 (28.6) | 238 (19.4) | 417 (8.4) |
| Hospital type, n (%) | |||
| Academic | 11 (8.7) | 74 (6.0) | 413 (8.4) |
| Urban | 69 (54.8) | 835 (68.2) | 2514 (50.9) |
| Rural | 46 (36.5) | 316 (25.8) | 2009 (40.7) |
| Region, n (%) | |||
| Northeast | 20 (15.9) | 206 (16.8) | 680 (13.8) |
| Midwest | 37 (29.4) | 520 (42.4) | 1422 (28.8) |
| South | 41 (32.5) | 259 (21.1) | 1919 (38.9) |
| West | 28 (22.2) | 239 (19.5) | 915 (18.5) |
Overall Glycemic Control
A total of 12,559,305 POC‐BG measurements (2,935,167 from the ICU and 9,624,138 from the non‐ICU) from 1,010,705 patients with 3,973,460 patient days were analyzed from 126 hospitals. The mean number of measurements was 20 per ICU patient and 9.5 for non‐ICU patients. The average number of measurements taken per patient‐day was 5 for the ICU patient and 3 for the non‐ICU patient.
Hospital hyperglycemia (>180 mg/dL) was 46.0% for ICU and 31.7% for non‐ICU. The patient‐day‐weighted mean POC‐BG for ICU measurements was 165 mg/dL (median = 164 mg/dL, SD 14.5) and 166 mg/dL (median = 167 mg/dL, SD 8) for non‐ICU. The distributions of patient‐day‐weighted mean POC‐BG values for ICU and non‐ICU settings are shown in Figure 1. The range of patient‐day‐weighted mean values was much wider for the ICU (126‐203 mg/dL) than in the non‐ICU (139‐186 mg/dL).
Hyperglycemia Prevalence
Of ICU patients, 60.6% had at least 1 POC‐BG value >180 mg/dL, as did 46.4% of non‐ICU patients. The proportion of patient‐days with a patient‐day‐weighted mean POC‐BG >180 mg/dL was 26.3% in the ICU setting (Figure 2A) and 31.3% in the non‐ICU (Figure 2B); the other cut points are also shown in Figure 2. The prevalence of patient‐days where hyperglycemia was more severe (>300 mg/dL) was low but nonetheless still detected in both the ICU and non‐ICU settings, although these differences appear to be less pronounced than in the ICU.
Hypoglycemia Rates
There were 21.3% of patients who had at least 1 POC‐BG value <70 mg/dL. Hospital hypoglycemia was low in both the ICU and non‐ICU measurement data, although the proportion of patient days with POC‐BG <70 mg/dL was higher in the ICU vs. the non‐ICU setting (Figure 3A,B). Hypoglycemia (<70 mg/dL) was detected in 10.1% of patient‐days (3.2% of all measures) in the ICU setting (Figure 3A) and 3.5% of patient‐days (4.2% of all measures) in the non‐ICU (Figure 3B). Moderate (<60 mg/dL) and more severe (<50 mg/dL and <40 mg/dL) hypoglycemia were very uncommon in both the ICU and non‐ICU.
Relationship of Glucose Control with Hospital Characteristics
There was a significant relationship between the total number of hospital beds and patient‐day‐weighted mean POC‐BG values in the ICU (Figure 4A). In the ICU, hospitals with <200 beds had significantly higher patient‐day‐weighted mean POC‐BG levels than those with 200 to 299 beds (P < 0.05), 300 to 399 beds (P < 0.01), and 400 beds (P < 0.001). Rural hospitals (Figure 4B) also had higher patient‐day‐weighted mean POC‐BG values compared to urban community and academic hospitals (both P < 0.001). Finally, ICUs in hospitals in the West (Figure 4C, bottom panel) had significantly lower values than those in the Midwest and South (both P < 0.01).
Differences in patient‐day‐weighted mean POC‐BG levels based on hospital characteristics were also observed for the non‐ICU (Figure 5), although these differences appear to be less pronounced than in the ICU. Hospitals with <200 beds (Figure 5A) had significantly higher patient‐day‐weighted mean POC‐BG values compared to hospitals with 300 to 399 beds (P < 0.05) and 400 beds (P < 0.001). Rural hospitals (Figure 5B) had significantly higher values than academic (P < 0.05) and urban community (P < 0.001) hospitals, and hospitals in the West (Figure 5C) had significantly lower values than those in the South and Northeast (both P < 0.05).
Discussion
Hospitalizations associated with diabetes pose a substantial burden on the U.S. health system.15 Recent consensus advocates good glucose control in the hospital to optimize outcomes for a number of clinical scenarios.68 Aside from a few institution‐specific studies,2527 the quality of diabetes treatment in U.S. hospitals is mostly unknown, but assessing the level of glycemic control will be a key metric that hospitals will need to track as they implement improvement programs targeting hospital hyperglycemia. Hospitals will need a way not just to track overall glucose levels, but also to monitor whether hypoglycemic events rise as they implement tight glycemic control initiatives. To our knowledge this is the first report on glycemic control from a large number of U.S. hospitals with diverse characteristics and from different geographic regions.
Debate continues as to what glucose targets for inpatients should be attained.28, 29 The overall patient‐day‐weighted mean POC‐BG was 170 mg/dL for the non‐ICU, and only a moderately lower 162 mg/dL in the ICU, despite much lower thresholds for ICU measurements in current suggested guidelines.8, 30 For the average hospital, over one‐third of non‐ICUs had patient‐day‐weighted mean POC‐BG levels that were >180 mg/dL and nearly one‐quarter had values >200 mg/dL. Similarly, nearly 40% of ICUs had patient‐day‐weighted mean POC‐BGs >180 mg/dL and over 30% were >200 mg/dL, indicating room for improvement in hospital ICU glucose control, at least in the hospitals sampled here. The range of patient‐day‐weighted mean POC‐BG levels for the ICU was broader than what was seen in the non‐ICU data, with the ICU data containing lower weighted mean POC‐BG values, and may indicate that hospitals are concentrating their efforts on adopting stricter glucose control measures in their ICUs.
Whether examining data from a single institution,17 from a larger group of hospitals,14 or now from 126 hospitals, one consistent finding has been the low prevalence of hypoglycemiaparticularly severe hypoglycemia (glucose <50 mg/dL or <40 mg/dL). Based on this larger sampling, however, hypoglycemia in the ICU, while still uncommon with respect to hyperglycemia, is more than double that of the non‐ICU. Fear of hypoglycemia is frequently mentioned as a barrier to attaining lower inpatient glucose levels.31 Although hypoglycemia frequency in the hospital is low, and even though recent data indicates that hypoglycemia is not perceived by practitioners as the number 1 barrier to successful inpatient diabetes management,3234 the possible association of severe low glucose levels to inpatient mortality18, 19, 21, 22, 24, 35 makes hypoglycemia a key counterbalance metric that hospitals will need to track as they implement glycemic control programs. In the ICU, higher glycemic targets may be needed to allay practitioner fears, and insulin administration protocols that have the best track record for minimizing hypoglycemia should be identified and promulgated.
Recent data showing increased risk of hospital hypoglycemia with attempts to better control hyperglycemia may unjustifiably deter practitioners and hospitals from implementing programs to better control inpatient glucose levels.24, 36 Unlike the outpatient setting, where patients can take measures to prevent hypoglycemia, hospitalized patients surrender control of their diabetes management to staff. Inpatient tight glycemic control initiatives cannot be instituted unless they are coupled with efforts to understand and correct system‐based problems that increase the risk of hypoglycemia. Recently published reports demonstrate that hypoglycemic events can be kept very low during treatment with an intensive insulin infusion protocol if expert rules are built into the algorithm that address hypoglycemia.37, 38 Thus, rather than abandon efforts at improving inpatient hyperglycemia over concerns about hypoglycemia, hospitals will need to develop methods to change their hypoglycemia policies from ones that typically just guide treatment to ones that incorporate preventive strategies.
Our data suggest a relationship between POC‐BG levels and hospital characteristics. Rural hospitals and hospitals with the least number of beds had higher POC‐BG levels compared to urban, academic, or larger hospitals, especially in the ICU setting. The reasons underlying these findings cannot be determined from this analysis, but it is possible that smaller hospitals and those located in rural areas do not have access to the diabetes experts (eg, endocrinologists or diabetes educators) to assist them in developing tight glycemic control programs. We also detected differences in patient‐day‐weighted mean POC‐BG data based on geographic region. Whether considering ICU or non‐ICU data, hospitals located in the West had lower glucose values compared to other regions. As with the other hospital characteristics, the explanation underlying these observations cannot be determined. It is possible that hospitals in the West are earlier‐adopters of tight glycemic control programs compared to other U.S. geographic regions. Further study is needed in a larger number of hospitals to confirm these findings.
These findings should be considered in light of the following limitations: unavailability to us of specific patient‐level information that would allow adjustment of data for such as variables as comorbidity; the fact that recommendations about glycemic targets in the hospital vary by organization,810, 30 which may result in hospitals aiming for different targets in different populations; and the controversy that continues on the benefits of glycemic control in the ICU, which may be dissuading facilities from implementing glucose control programs.39, 40 All that can be concluded from our analysis is that there is variation in the POC‐BG data based on hospital characteristics. We cannot state that one type of hospital is performing glycemic control better than another, particularly as some hospital types are underrepresented in our sample, and we cannot control for patient‐level data. Moreover, this statistical variation seen between different hospital types may not be of clinical importance in terms of being associated with different outcomes, or may simply be a result of different patterns of glucose monitoring in individual hospitals. However, the observed variation should prompt further investigation into the basis of differences (eg, some hospital types or regions may be further ahead in inpatient diabetes quality improvement initiatives than others).
There is no consensus about how best to summarize and report glycemic control in the hospital (so called glucometrics),41 and a variety of reporting measures have been suggested.20, 4245 We show data using one method: with the mean BG normalized to patient‐day as the unit of analysis; however, we found similar results when we used the patient or the glucose reading as the unit of analysis. As organizations move to develop standards for summarizing inpatient glucose data, consideration must be given to which measure is best correlated with hospital outcomes. In addition, when developing standards, it will be important to determine what type of data hospitals will find most clinically useful to track the impact of glucose control interventions. For instance, hospitals may wish to see data on the frequencies of glucose measurements that are above and below certain desired thresholds, which is one of the approaches that we have used in previous publications,14, 17, 26, 46 and which is currently provided as feedback to hospitals participating in RALS reporting.
The other issue to address in development of standards in inpatient glycemic control reporting is what method of glucose measurement should be used. Correlation between whole‐blood vs. POC‐BG values can be imprecise in the intensive care setting.41, 47 We have previously utilized bedside glucose measurements as our means of evaluating the status of inpatient glucose control,14, 17, 26 and bedside glucose measurements remain the mainstay of how practitioners judge the status of inpatient hyperglycemia and make therapeutic decisions about management. The hospitals participating in the process reviewed here all use the same system of bedside glucose monitoring and glucometer‐laboratory electronic interface. Until alternative clinical methods are developed to frequently sample glucose levels in a convenient and minimally invasive way at the bedside, current POC‐BG technology will continue to be the most utilized means of assessing hospital glucose management in the inpatient setting.
Electronic data warehouses such as RALS‐Plus are convenient sources of information in which to store data on the quality of inpatient diabetes care. Unlike chart abstraction which requires extensive man‐hours to extract data on a few patients, use of electronic data allows examination of large numbers of hospital cases. Queries of information systems could be automated, report cards potentially generated, and feedback given to providers and hospitals on the status of inpatient glycemic control.
Nonetheless, there are limitations to using electronic records as the sole method to assess inpatient diabetes care. Analysis of electronic records does not allow assessment of reasons underlying decision‐making behavior of clinicians (eg, why they did or did not change hyperglycemic therapy). Moreover, our electronic data does not permit an assessment of who had preexisting diabetes, who was admitted with new onset diabetes, or who developed hyperglycemia as a result of the hospital stay.
In addition to the above, while our sample was representative of other RALs participating hospitals, it was not entirely representative of all U.S. hospitals. Hospitals contributing data to this report were chosen by self‐selection rather than by random methods. Expanding hospital participation in this inpatient glucose assessment benchmarking process will be needed to determine if findings in this work can be generalized. Finally, our study was conducted using the hospital, rather than the patient, as the unit of analysis, as patient‐level characteristics (age, sex, race/ethnicity) were not provided by participating hospitals.
Despite these limitations and issues noted above, to our knowledge this report is the most extensive review of the state of blood glucose control in hospitals across the United States. While other commercial laboratory data management systems may exist in hospitals, their data has not been reported to date. Additionally, our analysis provides a first glimpse of inpatient glycemic control of a large number of U.S. hospitals of varying characteristics and different national regions. Increased hospital participation in data collection may allow the creation of a national benchmarking process for the development of best practices and improved inpatient hyperglycemia management.
The past decade has seen an increase in the number of hospital discharges associated with a diabetes diagnosis.1, 2 Diabetes is the fourth leading comorbid condition associated with any hospital discharge in the United States.3 Nearly one‐third of diabetes patients require 2 or more hospitalizations in any given year,4 and inpatient stays account for the largest proportion of direct medical expenses incurred by persons with the disease.5
The hospital component of diabetes care has been receiving considerable attention. The advantage of effective inpatient diabetes managementwith particular attention to improving glycemic controlis evident for a number of clinical situations (eg, acute myocardial infarction, critically ill patients).68 National and regional organizations,912 and professional societies68, 12 have developed guidelines about management of inpatient hyperglycemia.
Despite increased awareness of the value of treating inpatient hyperglycemia, little is known about glucose control in U.S. hospitals. As hospitals begin to develop programs to improve inpatient glucose management, some method of standardized benchmarking should be put in place. Using information systems solutions to obtain point‐of‐care bedside glucose (POC‐BG) data, we previously reported on inpatient glucose control from a smaller number of U.S. hospitals.13, 14 We now provide data on a larger, more representative number of U.S. hospitals that gives a broader national view of the current status of inpatient glycemic control.
Patients and Methods
Data Collection
The hospitals in this study employed standard bedside glucose meters (ACCU‐CHEK Inform, Roche Diagnostics, Indianapolis, IN), downloaded to the Remote Automated Laboratory System‐Plus (RALS‐Plus; Medical Automation Systems, Charlottesville, VA), a well‐established POC test information management system.1315 Participating hospitals do not provide patient specific data (eg, age, sex, race, diagnosis codes), but individual patients can be selected based on a unique anonymous identifier. Data also includes date and time of the POC‐BG test, download location (nursing unit), and the test result. Patient‐level POC‐BG data was extracted by linking the POC‐BG data to the unique patient identifier. Adult inpatient data from January to December 2007 were collected. Out‐of‐range values of LO (<10 mg/dL) and HI (>600 mg/dL) were discarded. The number of HI/LO values totaled less than 0.4% of the measurements. Repeat measures, largely performed to verify hypoglycemia were found to be present for <3% of the measures and were retained in this analyses.
Hospital Selection
Participating hospitals were included through self‐selection based on interest and a willingness to complete a business agreement prior to a data collection deadline. All of the more than 1300 hospitals with RALS‐Plus capability were invited to participate in the RALS‐Annual Report,16 an ongoing benchmarking project of inpatient glucose control in U.S. hospitals; 126 hospitals agreed to participate. Hospitals provided written permission to remotely access their RALS‐Plus glucose data and combine it with other participating hospitals into an aggregate database. Confidentiality was guaranteed for the identity of participating hospitals and their data.
Characteristics of participating hospitals, including number of beds, type (academic, urban community, rural community), and region, were obtained via completion of a questionnaire. This information was verified by accessing the hospital website or consulting the 2008 Hospital Blue Book (Official National Edition; Billian Publishing, Inc., Atlanta, GA). For academic status, we used membership in the Association of American Medical Colleges' Council of Teaching Hospitals, which is limited to organizations having a documented affiliation agreement with a medical school. Our definition of hospital types for the 126 study hospitals was based on first selecting the academic hospitals as a separate subgroup. The remaining hospitals were then classified as urban community or rural community.
Statistical Analysis
Glucose data were normalized to patient‐day, and expressed according to the number of patient‐days during which measurements were obtained. Patient‐day analyses were conducted by first constructing a patient‐day POC‐BG mean. An average POC‐BG level was computed for each patient‐day by summing together the measurement occasions for a given patient‐day and dividing by the number of measurements that occurred on that day. These patient‐day averages were then aggregated to the hospital level, and averaged to compute the patient‐day‐weighted mean POC‐BG level for each hospital, using the patient‐day as the unit of analysis.
Because of variations in the definition of maximal recommended inpatient glucose levels,8, 9 we calculated proportion of patient‐days with a patient‐day‐weighted mean POC‐BG value above the cut points of >180, >200, >250, >300, >350, and >400 mg/dL.14, 17 Published studies on hypoglycemia also use various biochemical definitions of low glucose;1824 therefore, we determined percentages of patient days with at least 1 POC‐BG value below the different cut points (<70, <60, <50, and <40 mg/dL) as previously described.14, 17
Finally, we evaluated the relationship between hospital patient‐day‐weighted mean POC‐BG values (normalized to patient day as above) and specific hospital characteristics: number of hospital beds, hospital type (academic, urban community, rural community), and U.S. geographic region. Hospital groups were compared for continuous variables using Mann‐Whitney tests and categorical variables (hospital characteristics) by chi‐square tests. All analyses were done using SPSS 15.0 (SPSS, Chicago, IL). Statistics were calculated for intensive care unit (ICU) and non‐ICU locations separately.
Results
Characteristics of Participating Hospitals
Of the 126 participating hospitals (Table 1), 38.1% were <200 beds, 19.8% were 200 to 299 beds, 13.5% were 300 to 399 beds, and 28.6% were 400 beds; 54.8% were urban community hospitals, 36.5% were rural community, 8.7% were academic, 32.5% were located in the South, 29.4% in the Midwest, 22.2% in the West, and 15.9% in the Northeast. Using chi‐square comparison our study sample was found to be representative of the larger sample of hospitals that use RALS‐Plus with regards to bed number, hospital type, and region (P = not significant [NS]), but not representative of hospitals nationally in these categories (P < 0.05). The most notable difference was seen in hospital size, where the sample hospitals were disproportionately larger; a trait shared by RALS hospitals more generally.
| Study Hospitals | RALS‐Plus Hospitals | U.S. Hospitals | |
|---|---|---|---|
| |||
| Total | 126 | 1225 | 4936 |
| Number of beds, n (%) | |||
| <200 | 48 (38.1) | 510 (41.6) | 3532 (71.6) |
| 200‐299 | 25 (19.8) | 284 (23.2) | 619 (12.5) |
| 300‐399 | 17 (13.5) | 193 (15.8) | 368 (7.5) |
| 400 | 36 (28.6) | 238 (19.4) | 417 (8.4) |
| Hospital type, n (%) | |||
| Academic | 11 (8.7) | 74 (6.0) | 413 (8.4) |
| Urban | 69 (54.8) | 835 (68.2) | 2514 (50.9) |
| Rural | 46 (36.5) | 316 (25.8) | 2009 (40.7) |
| Region, n (%) | |||
| Northeast | 20 (15.9) | 206 (16.8) | 680 (13.8) |
| Midwest | 37 (29.4) | 520 (42.4) | 1422 (28.8) |
| South | 41 (32.5) | 259 (21.1) | 1919 (38.9) |
| West | 28 (22.2) | 239 (19.5) | 915 (18.5) |
Overall Glycemic Control
A total of 12,559,305 POC‐BG measurements (2,935,167 from the ICU and 9,624,138 from the non‐ICU) from 1,010,705 patients with 3,973,460 patient days were analyzed from 126 hospitals. The mean number of measurements was 20 per ICU patient and 9.5 for non‐ICU patients. The average number of measurements taken per patient‐day was 5 for the ICU patient and 3 for the non‐ICU patient.
Hospital hyperglycemia (>180 mg/dL) was 46.0% for ICU and 31.7% for non‐ICU. The patient‐day‐weighted mean POC‐BG for ICU measurements was 165 mg/dL (median = 164 mg/dL, SD 14.5) and 166 mg/dL (median = 167 mg/dL, SD 8) for non‐ICU. The distributions of patient‐day‐weighted mean POC‐BG values for ICU and non‐ICU settings are shown in Figure 1. The range of patient‐day‐weighted mean values was much wider for the ICU (126‐203 mg/dL) than in the non‐ICU (139‐186 mg/dL).
Hyperglycemia Prevalence
Of ICU patients, 60.6% had at least 1 POC‐BG value >180 mg/dL, as did 46.4% of non‐ICU patients. The proportion of patient‐days with a patient‐day‐weighted mean POC‐BG >180 mg/dL was 26.3% in the ICU setting (Figure 2A) and 31.3% in the non‐ICU (Figure 2B); the other cut points are also shown in Figure 2. The prevalence of patient‐days where hyperglycemia was more severe (>300 mg/dL) was low but nonetheless still detected in both the ICU and non‐ICU settings, although these differences appear to be less pronounced than in the ICU.
Hypoglycemia Rates
There were 21.3% of patients who had at least 1 POC‐BG value <70 mg/dL. Hospital hypoglycemia was low in both the ICU and non‐ICU measurement data, although the proportion of patient days with POC‐BG <70 mg/dL was higher in the ICU vs. the non‐ICU setting (Figure 3A,B). Hypoglycemia (<70 mg/dL) was detected in 10.1% of patient‐days (3.2% of all measures) in the ICU setting (Figure 3A) and 3.5% of patient‐days (4.2% of all measures) in the non‐ICU (Figure 3B). Moderate (<60 mg/dL) and more severe (<50 mg/dL and <40 mg/dL) hypoglycemia were very uncommon in both the ICU and non‐ICU.
Relationship of Glucose Control with Hospital Characteristics
There was a significant relationship between the total number of hospital beds and patient‐day‐weighted mean POC‐BG values in the ICU (Figure 4A). In the ICU, hospitals with <200 beds had significantly higher patient‐day‐weighted mean POC‐BG levels than those with 200 to 299 beds (P < 0.05), 300 to 399 beds (P < 0.01), and 400 beds (P < 0.001). Rural hospitals (Figure 4B) also had higher patient‐day‐weighted mean POC‐BG values compared to urban community and academic hospitals (both P < 0.001). Finally, ICUs in hospitals in the West (Figure 4C, bottom panel) had significantly lower values than those in the Midwest and South (both P < 0.01).
Differences in patient‐day‐weighted mean POC‐BG levels based on hospital characteristics were also observed for the non‐ICU (Figure 5), although these differences appear to be less pronounced than in the ICU. Hospitals with <200 beds (Figure 5A) had significantly higher patient‐day‐weighted mean POC‐BG values compared to hospitals with 300 to 399 beds (P < 0.05) and 400 beds (P < 0.001). Rural hospitals (Figure 5B) had significantly higher values than academic (P < 0.05) and urban community (P < 0.001) hospitals, and hospitals in the West (Figure 5C) had significantly lower values than those in the South and Northeast (both P < 0.05).
Discussion
Hospitalizations associated with diabetes pose a substantial burden on the U.S. health system.15 Recent consensus advocates good glucose control in the hospital to optimize outcomes for a number of clinical scenarios.68 Aside from a few institution‐specific studies,2527 the quality of diabetes treatment in U.S. hospitals is mostly unknown, but assessing the level of glycemic control will be a key metric that hospitals will need to track as they implement improvement programs targeting hospital hyperglycemia. Hospitals will need a way not just to track overall glucose levels, but also to monitor whether hypoglycemic events rise as they implement tight glycemic control initiatives. To our knowledge this is the first report on glycemic control from a large number of U.S. hospitals with diverse characteristics and from different geographic regions.
Debate continues as to what glucose targets for inpatients should be attained.28, 29 The overall patient‐day‐weighted mean POC‐BG was 170 mg/dL for the non‐ICU, and only a moderately lower 162 mg/dL in the ICU, despite much lower thresholds for ICU measurements in current suggested guidelines.8, 30 For the average hospital, over one‐third of non‐ICUs had patient‐day‐weighted mean POC‐BG levels that were >180 mg/dL and nearly one‐quarter had values >200 mg/dL. Similarly, nearly 40% of ICUs had patient‐day‐weighted mean POC‐BGs >180 mg/dL and over 30% were >200 mg/dL, indicating room for improvement in hospital ICU glucose control, at least in the hospitals sampled here. The range of patient‐day‐weighted mean POC‐BG levels for the ICU was broader than what was seen in the non‐ICU data, with the ICU data containing lower weighted mean POC‐BG values, and may indicate that hospitals are concentrating their efforts on adopting stricter glucose control measures in their ICUs.
Whether examining data from a single institution,17 from a larger group of hospitals,14 or now from 126 hospitals, one consistent finding has been the low prevalence of hypoglycemiaparticularly severe hypoglycemia (glucose <50 mg/dL or <40 mg/dL). Based on this larger sampling, however, hypoglycemia in the ICU, while still uncommon with respect to hyperglycemia, is more than double that of the non‐ICU. Fear of hypoglycemia is frequently mentioned as a barrier to attaining lower inpatient glucose levels.31 Although hypoglycemia frequency in the hospital is low, and even though recent data indicates that hypoglycemia is not perceived by practitioners as the number 1 barrier to successful inpatient diabetes management,3234 the possible association of severe low glucose levels to inpatient mortality18, 19, 21, 22, 24, 35 makes hypoglycemia a key counterbalance metric that hospitals will need to track as they implement glycemic control programs. In the ICU, higher glycemic targets may be needed to allay practitioner fears, and insulin administration protocols that have the best track record for minimizing hypoglycemia should be identified and promulgated.
Recent data showing increased risk of hospital hypoglycemia with attempts to better control hyperglycemia may unjustifiably deter practitioners and hospitals from implementing programs to better control inpatient glucose levels.24, 36 Unlike the outpatient setting, where patients can take measures to prevent hypoglycemia, hospitalized patients surrender control of their diabetes management to staff. Inpatient tight glycemic control initiatives cannot be instituted unless they are coupled with efforts to understand and correct system‐based problems that increase the risk of hypoglycemia. Recently published reports demonstrate that hypoglycemic events can be kept very low during treatment with an intensive insulin infusion protocol if expert rules are built into the algorithm that address hypoglycemia.37, 38 Thus, rather than abandon efforts at improving inpatient hyperglycemia over concerns about hypoglycemia, hospitals will need to develop methods to change their hypoglycemia policies from ones that typically just guide treatment to ones that incorporate preventive strategies.
Our data suggest a relationship between POC‐BG levels and hospital characteristics. Rural hospitals and hospitals with the least number of beds had higher POC‐BG levels compared to urban, academic, or larger hospitals, especially in the ICU setting. The reasons underlying these findings cannot be determined from this analysis, but it is possible that smaller hospitals and those located in rural areas do not have access to the diabetes experts (eg, endocrinologists or diabetes educators) to assist them in developing tight glycemic control programs. We also detected differences in patient‐day‐weighted mean POC‐BG data based on geographic region. Whether considering ICU or non‐ICU data, hospitals located in the West had lower glucose values compared to other regions. As with the other hospital characteristics, the explanation underlying these observations cannot be determined. It is possible that hospitals in the West are earlier‐adopters of tight glycemic control programs compared to other U.S. geographic regions. Further study is needed in a larger number of hospitals to confirm these findings.
These findings should be considered in light of the following limitations: unavailability to us of specific patient‐level information that would allow adjustment of data for such as variables as comorbidity; the fact that recommendations about glycemic targets in the hospital vary by organization,810, 30 which may result in hospitals aiming for different targets in different populations; and the controversy that continues on the benefits of glycemic control in the ICU, which may be dissuading facilities from implementing glucose control programs.39, 40 All that can be concluded from our analysis is that there is variation in the POC‐BG data based on hospital characteristics. We cannot state that one type of hospital is performing glycemic control better than another, particularly as some hospital types are underrepresented in our sample, and we cannot control for patient‐level data. Moreover, this statistical variation seen between different hospital types may not be of clinical importance in terms of being associated with different outcomes, or may simply be a result of different patterns of glucose monitoring in individual hospitals. However, the observed variation should prompt further investigation into the basis of differences (eg, some hospital types or regions may be further ahead in inpatient diabetes quality improvement initiatives than others).
There is no consensus about how best to summarize and report glycemic control in the hospital (so called glucometrics),41 and a variety of reporting measures have been suggested.20, 4245 We show data using one method: with the mean BG normalized to patient‐day as the unit of analysis; however, we found similar results when we used the patient or the glucose reading as the unit of analysis. As organizations move to develop standards for summarizing inpatient glucose data, consideration must be given to which measure is best correlated with hospital outcomes. In addition, when developing standards, it will be important to determine what type of data hospitals will find most clinically useful to track the impact of glucose control interventions. For instance, hospitals may wish to see data on the frequencies of glucose measurements that are above and below certain desired thresholds, which is one of the approaches that we have used in previous publications,14, 17, 26, 46 and which is currently provided as feedback to hospitals participating in RALS reporting.
The other issue to address in development of standards in inpatient glycemic control reporting is what method of glucose measurement should be used. Correlation between whole‐blood vs. POC‐BG values can be imprecise in the intensive care setting.41, 47 We have previously utilized bedside glucose measurements as our means of evaluating the status of inpatient glucose control,14, 17, 26 and bedside glucose measurements remain the mainstay of how practitioners judge the status of inpatient hyperglycemia and make therapeutic decisions about management. The hospitals participating in the process reviewed here all use the same system of bedside glucose monitoring and glucometer‐laboratory electronic interface. Until alternative clinical methods are developed to frequently sample glucose levels in a convenient and minimally invasive way at the bedside, current POC‐BG technology will continue to be the most utilized means of assessing hospital glucose management in the inpatient setting.
Electronic data warehouses such as RALS‐Plus are convenient sources of information in which to store data on the quality of inpatient diabetes care. Unlike chart abstraction which requires extensive man‐hours to extract data on a few patients, use of electronic data allows examination of large numbers of hospital cases. Queries of information systems could be automated, report cards potentially generated, and feedback given to providers and hospitals on the status of inpatient glycemic control.
Nonetheless, there are limitations to using electronic records as the sole method to assess inpatient diabetes care. Analysis of electronic records does not allow assessment of reasons underlying decision‐making behavior of clinicians (eg, why they did or did not change hyperglycemic therapy). Moreover, our electronic data does not permit an assessment of who had preexisting diabetes, who was admitted with new onset diabetes, or who developed hyperglycemia as a result of the hospital stay.
In addition to the above, while our sample was representative of other RALs participating hospitals, it was not entirely representative of all U.S. hospitals. Hospitals contributing data to this report were chosen by self‐selection rather than by random methods. Expanding hospital participation in this inpatient glucose assessment benchmarking process will be needed to determine if findings in this work can be generalized. Finally, our study was conducted using the hospital, rather than the patient, as the unit of analysis, as patient‐level characteristics (age, sex, race/ethnicity) were not provided by participating hospitals.
Despite these limitations and issues noted above, to our knowledge this report is the most extensive review of the state of blood glucose control in hospitals across the United States. While other commercial laboratory data management systems may exist in hospitals, their data has not been reported to date. Additionally, our analysis provides a first glimpse of inpatient glycemic control of a large number of U.S. hospitals of varying characteristics and different national regions. Increased hospital participation in data collection may allow the creation of a national benchmarking process for the development of best practices and improved inpatient hyperglycemia management.
- Centers for Disease Control and Prevention. Hospitalization for Diabetes as First‐Listed Diagnosis. Available at: http://www.cdc.gov/diabetes/statistics/dmfirst/index.htm. Accessed April2009.
- Centers for Disease Control and Prevention. Hospitalizations for Diabetes as Any‐Listed Diagnosis. Available at: http://www.cdc.gov/diabetes/statistics/dmany/index.htm. Accessed April2009.
- ,,,.Hospitalization in the United States, 1997.Rockville, MD:Agency for Healthcare Research and Quality;2000. HCUP Fact Book No. 1; AHRQ Publication No. 00‐0031.
- ,,,.Multiple hospitalizations for patients with diabetes.Diabetes Care.2003;26(5):1421–1426.
- American Diabetes Association.Economic costs of diabetes in the US in 2007.Diabetes Care.2008;31(3):596–615.
- ,,, et al.American Diabetes Association Diabetes in Hospitals Writing Committee: Management of diabetes and hyperglycemia in hospitals.Diabetes Care.2004;27:553–591.
- ACE Task Force on Inpatient Diabetes and Metabolic Control.American College of Endocrinology Position Statement on Inpatient Diabetes and Metabolic Control.Endocr Pract.2004;10:77–82.
- ACE/ADA Task Force on Inpatient Diabetes.American College of Endocrinology and American Diabetes Association consensus statement on inpatient diabetes and glycemic control.Endocr Pract.2006;12(4):459–468.
- Institute for Healthcare Improvement. Getting started kit: prevent surgical site infections. Available at: http://www.ihi.org/NR/rdonlyres/00EBAF1F‐A29F‐4822‐ABCE‐829573255AB8/0/SSIHowtoGuideFINAL.pdf. Accessed April2009.
- Institute for Healthcare Improvement. Implement Effective Glucose Control. Available at: http://www.ihi.org/IHI/Topics/CriticalCare/IntensiveCare/Changes/ImplementEffectiveGlucoseControl.htm. Accessed April2009.
- Joint Commission on Accreditation of Healthcare Organizations. Inpatient Diabetes Certification Addendum. Available at: http://www.jointcommission.org/CertificationPrograms/Inpatient+Diabetes. Accessed April2009.
- ,,, et al.Working to improve care of hospital hyperglycemia through statewide collaboration: the Georgia Hospital Association Diabetes Special Interest Group.Endocr Pract.2007;13:45–50.
- ,,,.Current state of inpatient diabetes burden and care, and goal of the conference.Endocr Pract.2006;12:S1–S10.
- ,,,,.Inpatient point‐of‐care bedside glucose testing: preliminary data on use of connectivity informatics to measure hospital glycemic control.Diabetes Technol Ther.2007;9:493–500.
- .Medical automation systems and a brief history of point‐of‐care informatics.Point Care.2007;6:154–159.
- Medical Automation Systems. RALS‐Report. Available at: http://www.rals.com/RALS‐Report.html. Accessed April2009.
- ,,, et al.Diabetes care in hospitalized non‐critically ill patients: more evidence for clinical inertia and negative therapeutic momentum.J Hosp Med.2007;2:203–211.
- ,,.Hypoglycemia in hospitalized patients. Causes and outcomes.N Engl J Med.1986;315(20):1245–1250.
- ,,,,,.Mortality in hospitalized patients with hypoglycemia and severe hyperglycemia.Mt Sinai J Med.1995;62(6):422–426.
- ,,.Glycemic control and sliding scale insulin use in medical inpatients with diabetes mellitus.Arch Intern Med.1997;157(5):545–552.
- ,,,,.Influence of individual characteristics on outcome of glycemic control in intensive care unit patients with or without diabetes mellitus.Mayo Clin Proc.2005;80(12):1558–1567.
- ,,, et al.Evaluation of short‐term consequences of hypoglycemia in an intensive care unit. [see Comment].Crit Care Med.2006;34(11):2714–2718.
- ,,, et al.Predisposing factors for hypoglycemia in the intensive care unit. [see Comment].Crit Care Med.2006;34(1):96–101.
- .Severe hypoglycemia in critically ill patients: risk factors and outcomes.Crit Care Med.2007;35(10):2262–2267.
- ,,,,.Unrecognized diabetes among hospitalized patients.Diabetes Care.1998;21(2):246–249.
- ,,, et al.Diabetes care in the non‐ICU setting: is there clinical inertia in the hospital?J Hosp Med.2006;1(3):151–160.
- ,,,,.Inpatient management of diabetes and hyperglycemia among general medicine patients at a large teaching hospital.J Hosp Med.2006;1(3):145–150.
- ,.Counterpoint: inpatient glucose management. A premature call to arms?Diabetes Care.2005;28:976–979.
- ,.Point: inpatient glucose management. The emperor finally has clothes.Diabetes Care.2005;28(4):973–975.
- ,,, et al.Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008.Crit Care Med.2008;36(1):296–327.
- ,,, et al.Hospital hypoglycemia: not only treatment but also prevention. American College of Endocrinology (ACE) Inpatient Diabetes and Metabolic Control Consensus Conference.Endocr Pract.2004;10(suppl 2):89–99.
- ,,, et al.Management of inpatient hyperglycemia: assessing perceptions and barriers to care among resident physicians.Endoc Pract.2007;13:117–125.
- ,,, et al.Beliefs about hospital diabetes and perceived barriers to glucose management among inpatient midlevel practitioners.Diabetes Educ.2008;34(1):75–83.
- ,,,.Perceptions of resident physicians about management of inpatient hyperglycemia in an urban hospital.J Hosp Med.2009;4(1):E1–E8.
- ,,.Hypoglycemia in hospitalized adult patients without diabetes.Endocr Pract.2005;11(2):91–96.
- ,,, et al.Intensive insulin therapy and pentastarch resuscitation in severe sepsis.N Engl J Med.2008;358(2):125–139.
- ,,, et al.Development and implementation of evidence‐based, IV insulin guidelines: a statewide collaborative approach.Insulin.2008;3:67–77.
- ,,, et al.Outcomes of a cardiothoracic intensive care web‐based online intravenous insulin infusion calculator study at a Medical University Hospital.Diabetes Technol Ther.2007;9(6):523–534.
- ,,.Benefits and risks of tight glucose control in critically ill adults. A meta‐analysis.JAMA.2008;300(8):933–944.
- ,.Tight glycemic control in critically ill adults.JAMA.2008;300(8):963–965.
- ,,, et al.“Glucometrics”—assessing the quality of inpatient glucose management.Diabetes Technol Ther.2006;8(5):560–569.
- ,,, et al.Glucometrics in patients hospitalized with acute myocardial infarction: defining the optimal outcomes‐based measure of risk. [see Comment].Circulation.2008;117(8):1018–1027.
- ,,.Hyperglycaemic index as a tool to assess glucose control: a retrospective study.Crit Care.2004;8(3):R122–R127.
- ,,,,.SHM glycemic control task force summary: practical recommendations for assessing the impact of glycemic control efforts.J Hosp Med.2008;3(S5):66–75.
- ,,, et al.Understanding and improving management of inpatient diabetes mellitus: The Mayo Clinic Arizona Experience.J Diabetes Sci Technol.2008;2:925–931.
- ,,, et al.Reliability of point‐of‐care testing for glucose measurement in critically ill adults.Crit Care Med.2005;33(12):2778–2785.
- ,,, et al.Accuracy of bedside glucometry in critically ill patients: influence of clinical characteristics and perfusion index.Mayo Clin Proc.2008;83:400–405.
- Centers for Disease Control and Prevention. Hospitalization for Diabetes as First‐Listed Diagnosis. Available at: http://www.cdc.gov/diabetes/statistics/dmfirst/index.htm. Accessed April2009.
- Centers for Disease Control and Prevention. Hospitalizations for Diabetes as Any‐Listed Diagnosis. Available at: http://www.cdc.gov/diabetes/statistics/dmany/index.htm. Accessed April2009.
- ,,,.Hospitalization in the United States, 1997.Rockville, MD:Agency for Healthcare Research and Quality;2000. HCUP Fact Book No. 1; AHRQ Publication No. 00‐0031.
- ,,,.Multiple hospitalizations for patients with diabetes.Diabetes Care.2003;26(5):1421–1426.
- American Diabetes Association.Economic costs of diabetes in the US in 2007.Diabetes Care.2008;31(3):596–615.
- ,,, et al.American Diabetes Association Diabetes in Hospitals Writing Committee: Management of diabetes and hyperglycemia in hospitals.Diabetes Care.2004;27:553–591.
- ACE Task Force on Inpatient Diabetes and Metabolic Control.American College of Endocrinology Position Statement on Inpatient Diabetes and Metabolic Control.Endocr Pract.2004;10:77–82.
- ACE/ADA Task Force on Inpatient Diabetes.American College of Endocrinology and American Diabetes Association consensus statement on inpatient diabetes and glycemic control.Endocr Pract.2006;12(4):459–468.
- Institute for Healthcare Improvement. Getting started kit: prevent surgical site infections. Available at: http://www.ihi.org/NR/rdonlyres/00EBAF1F‐A29F‐4822‐ABCE‐829573255AB8/0/SSIHowtoGuideFINAL.pdf. Accessed April2009.
- Institute for Healthcare Improvement. Implement Effective Glucose Control. Available at: http://www.ihi.org/IHI/Topics/CriticalCare/IntensiveCare/Changes/ImplementEffectiveGlucoseControl.htm. Accessed April2009.
- Joint Commission on Accreditation of Healthcare Organizations. Inpatient Diabetes Certification Addendum. Available at: http://www.jointcommission.org/CertificationPrograms/Inpatient+Diabetes. Accessed April2009.
- ,,, et al.Working to improve care of hospital hyperglycemia through statewide collaboration: the Georgia Hospital Association Diabetes Special Interest Group.Endocr Pract.2007;13:45–50.
- ,,,.Current state of inpatient diabetes burden and care, and goal of the conference.Endocr Pract.2006;12:S1–S10.
- ,,,,.Inpatient point‐of‐care bedside glucose testing: preliminary data on use of connectivity informatics to measure hospital glycemic control.Diabetes Technol Ther.2007;9:493–500.
- .Medical automation systems and a brief history of point‐of‐care informatics.Point Care.2007;6:154–159.
- Medical Automation Systems. RALS‐Report. Available at: http://www.rals.com/RALS‐Report.html. Accessed April2009.
- ,,, et al.Diabetes care in hospitalized non‐critically ill patients: more evidence for clinical inertia and negative therapeutic momentum.J Hosp Med.2007;2:203–211.
- ,,.Hypoglycemia in hospitalized patients. Causes and outcomes.N Engl J Med.1986;315(20):1245–1250.
- ,,,,,.Mortality in hospitalized patients with hypoglycemia and severe hyperglycemia.Mt Sinai J Med.1995;62(6):422–426.
- ,,.Glycemic control and sliding scale insulin use in medical inpatients with diabetes mellitus.Arch Intern Med.1997;157(5):545–552.
- ,,,,.Influence of individual characteristics on outcome of glycemic control in intensive care unit patients with or without diabetes mellitus.Mayo Clin Proc.2005;80(12):1558–1567.
- ,,, et al.Evaluation of short‐term consequences of hypoglycemia in an intensive care unit. [see Comment].Crit Care Med.2006;34(11):2714–2718.
- ,,, et al.Predisposing factors for hypoglycemia in the intensive care unit. [see Comment].Crit Care Med.2006;34(1):96–101.
- .Severe hypoglycemia in critically ill patients: risk factors and outcomes.Crit Care Med.2007;35(10):2262–2267.
- ,,,,.Unrecognized diabetes among hospitalized patients.Diabetes Care.1998;21(2):246–249.
- ,,, et al.Diabetes care in the non‐ICU setting: is there clinical inertia in the hospital?J Hosp Med.2006;1(3):151–160.
- ,,,,.Inpatient management of diabetes and hyperglycemia among general medicine patients at a large teaching hospital.J Hosp Med.2006;1(3):145–150.
- ,.Counterpoint: inpatient glucose management. A premature call to arms?Diabetes Care.2005;28:976–979.
- ,.Point: inpatient glucose management. The emperor finally has clothes.Diabetes Care.2005;28(4):973–975.
- ,,, et al.Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008.Crit Care Med.2008;36(1):296–327.
- ,,, et al.Hospital hypoglycemia: not only treatment but also prevention. American College of Endocrinology (ACE) Inpatient Diabetes and Metabolic Control Consensus Conference.Endocr Pract.2004;10(suppl 2):89–99.
- ,,, et al.Management of inpatient hyperglycemia: assessing perceptions and barriers to care among resident physicians.Endoc Pract.2007;13:117–125.
- ,,, et al.Beliefs about hospital diabetes and perceived barriers to glucose management among inpatient midlevel practitioners.Diabetes Educ.2008;34(1):75–83.
- ,,,.Perceptions of resident physicians about management of inpatient hyperglycemia in an urban hospital.J Hosp Med.2009;4(1):E1–E8.
- ,,.Hypoglycemia in hospitalized adult patients without diabetes.Endocr Pract.2005;11(2):91–96.
- ,,, et al.Intensive insulin therapy and pentastarch resuscitation in severe sepsis.N Engl J Med.2008;358(2):125–139.
- ,,, et al.Development and implementation of evidence‐based, IV insulin guidelines: a statewide collaborative approach.Insulin.2008;3:67–77.
- ,,, et al.Outcomes of a cardiothoracic intensive care web‐based online intravenous insulin infusion calculator study at a Medical University Hospital.Diabetes Technol Ther.2007;9(6):523–534.
- ,,.Benefits and risks of tight glucose control in critically ill adults. A meta‐analysis.JAMA.2008;300(8):933–944.
- ,.Tight glycemic control in critically ill adults.JAMA.2008;300(8):963–965.
- ,,, et al.“Glucometrics”—assessing the quality of inpatient glucose management.Diabetes Technol Ther.2006;8(5):560–569.
- ,,, et al.Glucometrics in patients hospitalized with acute myocardial infarction: defining the optimal outcomes‐based measure of risk. [see Comment].Circulation.2008;117(8):1018–1027.
- ,,.Hyperglycaemic index as a tool to assess glucose control: a retrospective study.Crit Care.2004;8(3):R122–R127.
- ,,,,.SHM glycemic control task force summary: practical recommendations for assessing the impact of glycemic control efforts.J Hosp Med.2008;3(S5):66–75.
- ,,, et al.Understanding and improving management of inpatient diabetes mellitus: The Mayo Clinic Arizona Experience.J Diabetes Sci Technol.2008;2:925–931.
- ,,, et al.Reliability of point‐of‐care testing for glucose measurement in critically ill adults.Crit Care Med.2005;33(12):2778–2785.
- ,,, et al.Accuracy of bedside glucometry in critically ill patients: influence of clinical characteristics and perfusion index.Mayo Clin Proc.2008;83:400–405.
Copyright © 2009 Society of Hospital Medicine
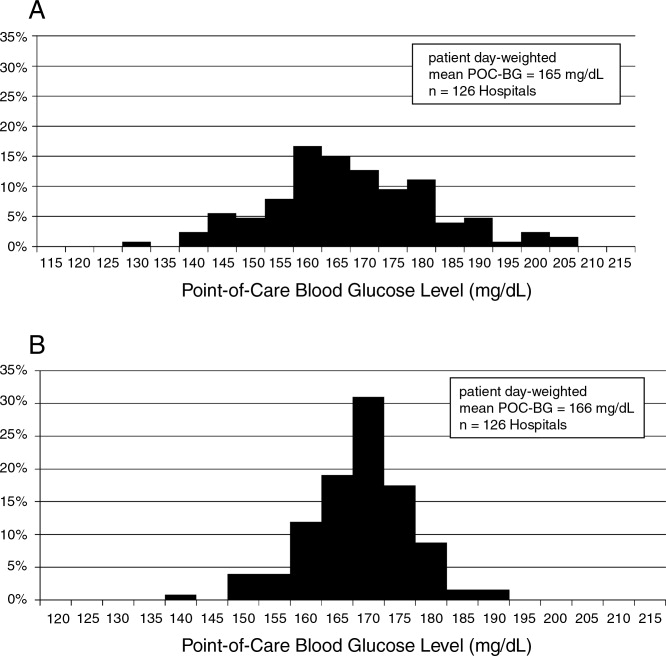
Flushing Out the Diagnosis
A 42‐year‐old woman with a history of mild asthma presented to the emergency department (ED) following 1 week of headache. She had been in her usual state of good health until 1 week prior to her presentation, when she noticed intermittent frontal headaches without neck stiffness or other neurologic symptoms. She then developed diffuse myalgias, fatigue, subjective fevers, and rigors for the 24 hours prior to presentation. On the morning of presentation, chest tightness, palpitations, and shortness of breath occurred. She used her albuterol metered‐dose inhaler without relief and went to the hospital.
Many of these features can be explained by a viral syndrome exacerbating underlying asthma or by a psychiatric condition such as anxiety or depression, but they may also be a harbinger of a systemic process, including infection, malignancy, or autoimmunity. Because the onset of headache is temporally distant from the other symptoms, I am more inclined to believe that it represents a primary intracranial process than I would if it were coincident with the onset of the other acute symptoms. If the fevers and rigors are verified, infection would be the initial concern. Failure to respond to her inhalers may either signify a severe asthma exacerbation or a nonbronchospastic cause of dyspnea.
She reported mild nausea, but denied photophobia, vomiting, abdominal pain, diarrhea, melena, or hematochezia. She did not have recent ill contacts, animal bites, or travel. Her medical history included asthma, diverticulitis, chronic right ankle pain, and obesity. She reported an allergic rash to amoxicillin. Her medications were sulindac and fluticasone/salmeterol, and albuterol metered‐dose inhalers. She worked as a preschool teacher and was married with 2 children. She denied any tobacco use and seldom drank alcoholic beverages. On exam, temperature was 36.7C, pulse was 107 beats per minute, blood pressure was 129/91 mm Hg, respiratory rate was 19 breaths per minute, and oxygen saturation was 98% while breathing ambient air. Her face and anterior neck were flushed and diaphoretic, and her sclerae were icteric. There was no nuchal rigidity. Her cardiac rhythm was regular without murmurs, lungs were clear to auscultation, and the abdomen was mildly tender to palpation in the epigastrium and right upper quadrant. The white blood cell (WBC) count was 9200/L, with 84% neutrophils, 3% lymphocytes, 6% monocytes, and 7% eosinophils. The hemoglobin was 14.8 g/dL and the platelet count was 166,000/L. Total serum bilirubin was 4.6 mg/dL, aspartate aminotransferase (AST) was 459 U/L (normal range, 8‐31), alanine aminotransferase (ALT) was 667 U/L (normal range, 7‐31), and alkaline phosphatase was 146 U/L (normal range, 39‐117). Serum electrolytes, creatinine, lactate, lipase, thyrotropin, coagulation studies, and cardiac enzymes were all normal. Urinalysis showed trace leukocyte esterase and bilirubin, as well as 3 WBCs and 2 red cells per high‐power field. Chest radiography and an electrocardiogram demonstrated no abnormalities.
The major findingwhich is critical to focusing problem‐solving in the face of a broad range of symptomsis her hepatitis. The common etiologies for hepatitis of this degree include viruses (hepatitis A and cytomegalovirus [CMV] should be considered given her work in preschool), toxins, autoimmunity, and vascular events. Liver disease in association with flushing raises the possibility of carcinoid syndrome with liver metastases. The lack of wheezing makes the bronchospasm of asthma or carcinoid less suitable explanations for her shortness of breath. Her eosinophilia is mild but probably is not accounted for alone by well‐controlled asthma in a person with no history of atopic disease. I would also ask her about any alternative and over‐the‐counter remedies. The paucity of lymphocytes raises the possibility of human immunodeficiency virus (HIV), Hodgkin's disease, or systemic lupus erythematosus. Although she does not have a documented fever or leukocytosis, she reported fevers and chills and is diaphoretic and tachycardic, so exclusion of biliary obstruction and cholangitis is the highest priority.
An abdominal ultrasound demonstrated hepatomegaly with moderate fatty infiltration and a normal gallbladder without pericholecystic fluid. The intrahepatic and extrahepatic biliary ducts were normal and the hepatic and portal veins were patent. Computed tomography of the abdomen showed slight thickening of the sigmoid colon wall. Ciprofloxacin and metronidazole were administered for possible diverticulitis. Over the first 48 hours of hospitalization her symptoms improved markedly. Her flushing resolved and she had no recorded fevers in the hospital. Serologies were negative for hepatitis A immunoglobulin M (IgM), hepatitis B surface antibody, hepatitis B surface antigen, and hepatitis C antibody. A monospot test was negative and the erythrocyte sedimentation rate was 11 mm/hour. Blood and urine cultures were negative. On the second hospital day the absolute eosinophil count rose to 855/L (15% of 5700 WBCs). On the fourth hospital day, the absolute eosinophil count was 1092/L, the total bilirubin was 1.9 mg/dL, and the AST and ALT were 174 U/L and 476 U/L, respectively. Antibiotics were stopped and she was discharged home.
Her prompt improvement suggests either a self‐limited condition or a response to the antibiotics. The rapid but incomplete resolution of her hepatitis is in keeping with a withdrawal of a toxin, relief of biliary obstruction, or a transient vascular event, and is less consistent with a viral hepatitis or an infiltrative process. With normal biliary system imaging, sterile blood cultures, and the absence of fever or leukocytosis, cholangitis is unlikely. Likewise, there is no suggestion of a vascular event, either obstructive or hemodynamic, that is impairing the liver.
A common cause of eosinophilia in hospitalized patients is medications, so it would be useful to monitor that count after the new antibiotics. At this point, I also wonder if the eosinophils are a feature of the underlying illness, as they were present to a modest degree on admission before any new medications were administered. The overlap of eosinophilia and hepatitis brings to mind a medication reaction (eg, to sulindac) or a hepatobiliary parasite, such as ascaris or clonorchis, for which she lacks a known exposure. Many patients experience flushing in the setting of fever or stress, but sustained flushing may suggest a systemic illness characterized by the release of vasoactive mediators such as carcinoid syndrome or mastocytosis. The latter might be considered more strongly if the eosinophilia is deemed to be primary (rather than reactive) after a thorough evaluation.
After 2 days at home, the patient had recurrence of subjective fevers, with chest, back, and abdominal pain, fatigue, loose stools, and rigors. She returned to the ED, where she was noted to have facial erythema and injected sclerae, but the remainder of her physical exam was normal. The total serum bilirubin was 1.1 mg/dL, AST was 156 U/L, ALT was 214 U/L, and alkaline phosphatase was 240 U/L. Serum lipase was normal. WBC count was 14,000/L, with 94% neutrophils, 3% lymphocytes, 2% monocytes, and 1% eosinophils. She was again treated empirically with ciprofloxacin and metronidazole. Endoscopic ultrasound was normal, with no evidence of gallbladder sludge or microlithiasis. Stool cultures, assay for Clostridium difficile, and examination for ova and parasites were negative. The 24‐hour urine demonstrated no elevation in 5‐hydroxyindoleacetic acid. An adrenocorticotropic hormone (ACTH) stimulation test was normal. HIV antibody was negative. Her symptoms improved within 2 days. The eosinophil count rose and peaked at 1541/L by the third hospital day, while the transaminase elevations resolved. Antibiotics were discontinued. A liver biopsy showed mixed macrovesicular and microvesicular fatty metamorphosis and steatohepatitis with eosinophils (Figures 1 and 2). She was discharged home on the sixth hospital day.

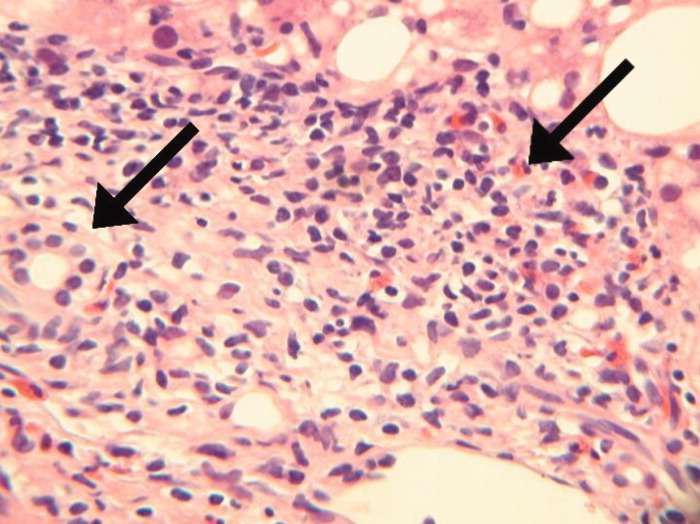
Her illness can now be characterized as relapsing inflammation, which given the frequency (over days) suggests either an indolent infectious focus that periodically causes systemic inflammation or reexposure to a toxic substance. The 2 most notable laboratory abnormalities, the hepatitis and the eosinophilia, persist but have differing trajectories. While the liver function tests have progressively normalized despite clinical relapses, the eosinophils have had a more fluctuating course characterized by increases during the hospitalization and higher levels during the second hospitalization. The absence of an infection, recurrent systemic inflammation, and eosinophilic hepatitis suggest a hypersensitivity reaction to a medication or other substance. She is most likely being reexposed at home, where her symptoms occur, and not in the hospital, where her symptoms resolve. Sulindac is a leading candidate, because nonsteroidal antiinflammatory drugs (NSAIDs) cause a number of hypersensitivity reactions and are frequently stopped when sick patients enter the hospital.
Seven days after discharge she developed acute onset of subjective fever, nausea, diffuse myalgias, and flushing, identical to the 2 prior episodes, and she again returned to the ED. Her temperature was 39.1C, heart rate was 120 beats per minute, blood pressure was 87/50 mm Hg, respiratory rate was 18 breaths per minute, and the oxygen saturation was 96% while breathing room air. She had diffuse flushing from her neck over her torso and was diaphoretic with injected sclera and conjunctiva. The WBC count was 11,400/L with 97% neutrophils and 3% lymphocytes. Total bilirubin was 0.8 mg/dL, AST was 134 U/L, ALT was 140 U/L, and alkaline phosphatase was 144 U/L. She was readmitted to the hospital. Following admission, she had no fevers, the flushing resolved, and AST and ALT levels decreased. The only treatment the patient received in the ED and during her hospital stay was acetaminophen as needed for pain or fever. The eosinophil count peaked at 1404/L by hospital day 4. Blood and urine cultures were negative. IgM antibodies to Epstein‐Barr virus were not detected, CMV DNA was not detected, and a rapid plasma reagin (RPR) test was nonreactive. Ferritin, ceruloplasmin, alpha‐1‐antitrypsin, and tryptase levels were normal. Antimitochondrial, antismooth muscle, antineutrophil cytoplasmic, and antinuclear antibodies were negative. There was no monoclonal band on serum protein electrophoresis. A blood smear for Borrelia detected no spirochetes.
A complete picture of the uncommon but classic flushing disorders, namely carcinoid, mastocytosis, and pheochromocytoma, has not emerged. The constellation of inflammation, mucosal and hepatic involvement, and eosinophilia are most consistent with a drug hypersensitivity reaction. Additionally, the recurrent inflammation is becoming more severe, as manifest by the fever and hemodynamic derangements, which suggests an increasing sensitization to the offending agent. I would review every drug she has received in the hospital, but given the recurrences after discharge her home medications are the most likely explanation. Of these, sulindac is the most likely culprit.
On further questioning, it was learned that the patient began taking sulindac 200 mg twice daily to treat her chronic ankle pain 6 weeks before the first admission. The medication had been stopped on each admission. She was instructed to discontinue sulindac. She has had no recurrences of symptoms and her hepatitis and eosinophilia have resolved.
DISCUSSION
This patient presented with recurrent skin findings, eosinophilia, hepatitis, and constitutional symptoms caused by hypersensitivity to sulindac. This drug‐induced hypersensitivity syndrome was originally described with anticonvulsant drugs (carbamazepine, phenytoin, and phenobarbitone) and named anticonvulsant hypersensitivity syndrome,1, 2 but has been observed with many other medications, including allopurinol, dapsone, minocycline, and nevirapine. The term drug rash with eosinophilia and systemic symptoms (DRESS) syndrome has been recently adopted to convey the cardinal features that characterize this disorder.3
DRESS syndrome is defined by rash, fever, and internal organ involvement.4 Also included in the diagnostic criteria are hematologic abnormalities (eosinophilia 1.5 109/mm3 or the presence of atypical lymphocytes) and lymphadenopathy.3 The multiorgan involvement distinguishes DRESS from other cutaneous drug eruptions. In a review of the French Pharmacovigilance Database for all cases of DRESS over a 15‐year period, 73% to 100% of patients were reported to have dermatologic abnormalities, most frequently a maculopapular rash or erythroderma. Less common skin findings include vesicles, bullae, pustules, erythroderma, and purpuric lesions. Liver abnormalities were observed in more than 60% of patients and were the most frequent systemic finding.5 Eosinophilia was the most common hematologic abnormality, present in more than 50% of cases. As this case underscores, DRESS syndrome typically begins 3 to 8 weeks after initiation of the drug because it is a delayed type IV hypersensitivity reaction.6 Fever can occur within hours on rechallenge because of the presence of memory T cells.
The main treatment for DRESS syndrome is withdrawal of the offending drug. Systemic corticosteroids have been recommended in cases with life‐threatening pulmonary or cardiac involvement, but have not been shown to be helpful in reversing renal or hepatic disease. Mortality, usually from end‐organ damage, occurs in about 10% of cases. The most common drugs are phenobarbital, carbamazepine, and phenytoin, with incidences of 1 in 5000 to 1 in 10,000. NSAIDs and antibiotics also have been implicated frequently. Human herpesvirus type 6 coinfection and genetically inherited slow acetylation have been associated with DRESS, although causal links have yet to be established.7, 8
The initial challenge in caring for a patient with multiple symptoms, exam findings, and test abnormalities is the coherent framing of the key clinical features that require explanation. This process, called problem representation, allows clinicians to search among a bounded list of possible diagnoses (or solutions) rather than invoking a differential diagnosis for every single abnormality. In searching for the proper diagnosis, this patient's clinical course required frequent reframing as more data became available.
Initially, the problem was framed as a 42‐year‐old woman with hepatitis. As the flushing and eosinophilia, which initially appeared to be transient and possibly nonspecific, became more prominent, the problem representation was revised to a 42‐year‐old woman with hepatitis, eosinophilia, and flushing. Since this triad did not immediately invoke a single diagnosis for the treating clinicians or the discussant, the differential diagnosis of hepatitis and eosinophilia and the differential diagnosis of flushing were considered in parallel.
Hepatitis and eosinophilia can occur coincidentally in the setting of parasitic infections, particularly helminths (ascaris, strongyloidiasis, and toxocaris) and liver flukes (opisthorchis and clonorchis), which invade the hepatobiliary system and induce a reactive eosinophilia. Some neoplasms, such as lymphomas and leukemias, and myeloproliferative disorders, including hypereosinophilic syndrome and mastocytosis, may have neoplastic cellular invasion of the liver and induce eosinophilia. Systemic drug hypersensitivity reactions are typically characterized by eosinophilia, transaminase elevations,9 and hepatitis on histology.10 As with this patient, liver biopsy in drug‐induced hepatitis shows a mixed microvesicular and macrovesicular steatosis, often with eosinophils.10
The flushing prompted a thorough but negative workup for the classic flushing disorders. The discussant's attempts to unify the flushing with the other clinical features illustrate how framing can affect our reasoning. Hepatitis, eosinophilia, and flushing defied an obvious single explanation and led the discussant down parallel diagnostic reasoning pathways. Although flushing is 1 of the well‐described dermatologic manifestations in drug‐hypersensitivity reactions, framing the central features as hepatitis, eosinophilia, and rash would have more readily suggested a drug reaction as a unifying diagnosis.11
The tempo and periodicity of this patient's illness provided the final formulation of a 42‐year‐old woman with hepatitis, eosinophilia, and flushing (or rash) that occurs every few days at home and resolves in the hospital. This formulation and the increasingly severe presentation, suggesting sensitization, were highly suggestive of an exogenous cause of her illness.
This case highlights how easily medication side effects can be overlooked during an extensive evaluation and how vigilant medication reconciliation coupled with an increased understanding of the spectrum of drug reactions can lead to early detection and prevention of potentially serious effects. In the case of DRESS, recognizing an association between a rash and organ involvement is central to making the diagnosis. Eosinophilia that accompanies a rash can further aid in narrowing the differential diagnosis.
The case also serves as a reminder of how framing with the slightest imprecision (eg, flushing instead of rash) can derail or delay the diagnostic process, yet is indispensable in tackling a complicated case. Finally, a time‐honored lesson in diagnosis is highlighted yet again: the diagnosis can usually be flushed out from the history.1214
Key Teaching Points
-
The constellation of skin findings, eosinophilia, organ involvement (particularly hepatitis), and constitutional symptoms should prompt consideration of DRESS syndrome and a hunt for a culprit drug.
-
Symptoms that resolve during hospitalization and repeatedly recur after discharge should prompt consideration of an exposure unique to the home, which may be environmental or pharmacologic.
-
Problem representation is critical in solving a complicated case, but adopting an inaccurate frame (representation) can derail or delay the diagnostic process.
The approach to clinical conundrums by an expert clinician is revealed through the presentation of an actual patient's case in an approach typical of a morning report. Similarly to patient care, sequential pieces of information are provided to the clinician, who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
- ,.Anticonvulsant hypersensitivity syndrome. In vitro assessment of risk.J Clin Invest.1988;82:1826–1832.
- ,,.Anticonvulsant hypersensitivity syndrome: incidence, prevention, and management.Drug Saf.1999;21:489–501.
- ,,,.Drug rash with eosinophilia and systemic symptoms vs toxic epidermal necrolysis: the dilemma of classification.Clin Dermatol.2005;23:311–314.
- ,.Management of drug rash with eosinophilia and systemic symptoms (DRESS syndrome): an update.Dermatology.2003;206:353–356.
- ,,,,,Blayac J‐P; Network of the French Pharmacovigilance Centers. Variability in the clinical pattern of cutaneous side‐effects of drugs with systemic symptoms: does a DRESS syndrome really exist?Br J Dermatol.2006;155:422–428.
- ,.The immunological and clinical spectrum of delayed drug‐induced exanthems.Curr Opin Allergy Clin Immunol.2004;4:411–419.
- ,,.Association between anticonvulsant hypersensitivity syndrome and human herpesvirus 6 reactivation and hypogammaglobulinemia.Arch Dermatol.2004;140:183–188.
- ,.Treatment of severe drug reactions: Stevens‐Johnson Syndrome, toxic epidermal necrolysis and hypersensitivity syndrome.Dermatol Online J.2002;8:5.
- ,.Drug reactions. In: Bolognia JL, Jorizzo JL, Rapini RP, eds.Dermatology.2nd ed.Spain:Mosby Elsevier;2008:310–311.
- Pathology Outlines. Liver and intrahepatic bile ducts—non tumor. Hepatitis (non‐infectious). Drug/toxin‐induced hepatitis. Available at: http://www.pathologyoutlines.com/liver.html#drugtoxin. Accessed August2009.
- ,,.The flushing patient: differential diagnosis, workup and treatment.J Am Acad Dermatol.2006;55(2):193–208.
- ,,,,.Relative contributions of history‐taking, physical examination, and laboratory investigation to diagnosis and management of medical outpatients.Br Med J.1975;2(5969):486–489.
- ,,,,.Contributions to the history, physical examination, and laboratory investigation in making medical diagnosis.West J Med.1992;156(2):163–165.
- ,.A study on relative contributions of the history, physical examination and investigations in making medical diagnosis.J Assoc Physicians India.2000;48(8):771–775.
A 42‐year‐old woman with a history of mild asthma presented to the emergency department (ED) following 1 week of headache. She had been in her usual state of good health until 1 week prior to her presentation, when she noticed intermittent frontal headaches without neck stiffness or other neurologic symptoms. She then developed diffuse myalgias, fatigue, subjective fevers, and rigors for the 24 hours prior to presentation. On the morning of presentation, chest tightness, palpitations, and shortness of breath occurred. She used her albuterol metered‐dose inhaler without relief and went to the hospital.
Many of these features can be explained by a viral syndrome exacerbating underlying asthma or by a psychiatric condition such as anxiety or depression, but they may also be a harbinger of a systemic process, including infection, malignancy, or autoimmunity. Because the onset of headache is temporally distant from the other symptoms, I am more inclined to believe that it represents a primary intracranial process than I would if it were coincident with the onset of the other acute symptoms. If the fevers and rigors are verified, infection would be the initial concern. Failure to respond to her inhalers may either signify a severe asthma exacerbation or a nonbronchospastic cause of dyspnea.
She reported mild nausea, but denied photophobia, vomiting, abdominal pain, diarrhea, melena, or hematochezia. She did not have recent ill contacts, animal bites, or travel. Her medical history included asthma, diverticulitis, chronic right ankle pain, and obesity. She reported an allergic rash to amoxicillin. Her medications were sulindac and fluticasone/salmeterol, and albuterol metered‐dose inhalers. She worked as a preschool teacher and was married with 2 children. She denied any tobacco use and seldom drank alcoholic beverages. On exam, temperature was 36.7C, pulse was 107 beats per minute, blood pressure was 129/91 mm Hg, respiratory rate was 19 breaths per minute, and oxygen saturation was 98% while breathing ambient air. Her face and anterior neck were flushed and diaphoretic, and her sclerae were icteric. There was no nuchal rigidity. Her cardiac rhythm was regular without murmurs, lungs were clear to auscultation, and the abdomen was mildly tender to palpation in the epigastrium and right upper quadrant. The white blood cell (WBC) count was 9200/L, with 84% neutrophils, 3% lymphocytes, 6% monocytes, and 7% eosinophils. The hemoglobin was 14.8 g/dL and the platelet count was 166,000/L. Total serum bilirubin was 4.6 mg/dL, aspartate aminotransferase (AST) was 459 U/L (normal range, 8‐31), alanine aminotransferase (ALT) was 667 U/L (normal range, 7‐31), and alkaline phosphatase was 146 U/L (normal range, 39‐117). Serum electrolytes, creatinine, lactate, lipase, thyrotropin, coagulation studies, and cardiac enzymes were all normal. Urinalysis showed trace leukocyte esterase and bilirubin, as well as 3 WBCs and 2 red cells per high‐power field. Chest radiography and an electrocardiogram demonstrated no abnormalities.
The major findingwhich is critical to focusing problem‐solving in the face of a broad range of symptomsis her hepatitis. The common etiologies for hepatitis of this degree include viruses (hepatitis A and cytomegalovirus [CMV] should be considered given her work in preschool), toxins, autoimmunity, and vascular events. Liver disease in association with flushing raises the possibility of carcinoid syndrome with liver metastases. The lack of wheezing makes the bronchospasm of asthma or carcinoid less suitable explanations for her shortness of breath. Her eosinophilia is mild but probably is not accounted for alone by well‐controlled asthma in a person with no history of atopic disease. I would also ask her about any alternative and over‐the‐counter remedies. The paucity of lymphocytes raises the possibility of human immunodeficiency virus (HIV), Hodgkin's disease, or systemic lupus erythematosus. Although she does not have a documented fever or leukocytosis, she reported fevers and chills and is diaphoretic and tachycardic, so exclusion of biliary obstruction and cholangitis is the highest priority.
An abdominal ultrasound demonstrated hepatomegaly with moderate fatty infiltration and a normal gallbladder without pericholecystic fluid. The intrahepatic and extrahepatic biliary ducts were normal and the hepatic and portal veins were patent. Computed tomography of the abdomen showed slight thickening of the sigmoid colon wall. Ciprofloxacin and metronidazole were administered for possible diverticulitis. Over the first 48 hours of hospitalization her symptoms improved markedly. Her flushing resolved and she had no recorded fevers in the hospital. Serologies were negative for hepatitis A immunoglobulin M (IgM), hepatitis B surface antibody, hepatitis B surface antigen, and hepatitis C antibody. A monospot test was negative and the erythrocyte sedimentation rate was 11 mm/hour. Blood and urine cultures were negative. On the second hospital day the absolute eosinophil count rose to 855/L (15% of 5700 WBCs). On the fourth hospital day, the absolute eosinophil count was 1092/L, the total bilirubin was 1.9 mg/dL, and the AST and ALT were 174 U/L and 476 U/L, respectively. Antibiotics were stopped and she was discharged home.
Her prompt improvement suggests either a self‐limited condition or a response to the antibiotics. The rapid but incomplete resolution of her hepatitis is in keeping with a withdrawal of a toxin, relief of biliary obstruction, or a transient vascular event, and is less consistent with a viral hepatitis or an infiltrative process. With normal biliary system imaging, sterile blood cultures, and the absence of fever or leukocytosis, cholangitis is unlikely. Likewise, there is no suggestion of a vascular event, either obstructive or hemodynamic, that is impairing the liver.
A common cause of eosinophilia in hospitalized patients is medications, so it would be useful to monitor that count after the new antibiotics. At this point, I also wonder if the eosinophils are a feature of the underlying illness, as they were present to a modest degree on admission before any new medications were administered. The overlap of eosinophilia and hepatitis brings to mind a medication reaction (eg, to sulindac) or a hepatobiliary parasite, such as ascaris or clonorchis, for which she lacks a known exposure. Many patients experience flushing in the setting of fever or stress, but sustained flushing may suggest a systemic illness characterized by the release of vasoactive mediators such as carcinoid syndrome or mastocytosis. The latter might be considered more strongly if the eosinophilia is deemed to be primary (rather than reactive) after a thorough evaluation.
After 2 days at home, the patient had recurrence of subjective fevers, with chest, back, and abdominal pain, fatigue, loose stools, and rigors. She returned to the ED, where she was noted to have facial erythema and injected sclerae, but the remainder of her physical exam was normal. The total serum bilirubin was 1.1 mg/dL, AST was 156 U/L, ALT was 214 U/L, and alkaline phosphatase was 240 U/L. Serum lipase was normal. WBC count was 14,000/L, with 94% neutrophils, 3% lymphocytes, 2% monocytes, and 1% eosinophils. She was again treated empirically with ciprofloxacin and metronidazole. Endoscopic ultrasound was normal, with no evidence of gallbladder sludge or microlithiasis. Stool cultures, assay for Clostridium difficile, and examination for ova and parasites were negative. The 24‐hour urine demonstrated no elevation in 5‐hydroxyindoleacetic acid. An adrenocorticotropic hormone (ACTH) stimulation test was normal. HIV antibody was negative. Her symptoms improved within 2 days. The eosinophil count rose and peaked at 1541/L by the third hospital day, while the transaminase elevations resolved. Antibiotics were discontinued. A liver biopsy showed mixed macrovesicular and microvesicular fatty metamorphosis and steatohepatitis with eosinophils (Figures 1 and 2). She was discharged home on the sixth hospital day.
Her illness can now be characterized as relapsing inflammation, which given the frequency (over days) suggests either an indolent infectious focus that periodically causes systemic inflammation or reexposure to a toxic substance. The 2 most notable laboratory abnormalities, the hepatitis and the eosinophilia, persist but have differing trajectories. While the liver function tests have progressively normalized despite clinical relapses, the eosinophils have had a more fluctuating course characterized by increases during the hospitalization and higher levels during the second hospitalization. The absence of an infection, recurrent systemic inflammation, and eosinophilic hepatitis suggest a hypersensitivity reaction to a medication or other substance. She is most likely being reexposed at home, where her symptoms occur, and not in the hospital, where her symptoms resolve. Sulindac is a leading candidate, because nonsteroidal antiinflammatory drugs (NSAIDs) cause a number of hypersensitivity reactions and are frequently stopped when sick patients enter the hospital.
Seven days after discharge she developed acute onset of subjective fever, nausea, diffuse myalgias, and flushing, identical to the 2 prior episodes, and she again returned to the ED. Her temperature was 39.1C, heart rate was 120 beats per minute, blood pressure was 87/50 mm Hg, respiratory rate was 18 breaths per minute, and the oxygen saturation was 96% while breathing room air. She had diffuse flushing from her neck over her torso and was diaphoretic with injected sclera and conjunctiva. The WBC count was 11,400/L with 97% neutrophils and 3% lymphocytes. Total bilirubin was 0.8 mg/dL, AST was 134 U/L, ALT was 140 U/L, and alkaline phosphatase was 144 U/L. She was readmitted to the hospital. Following admission, she had no fevers, the flushing resolved, and AST and ALT levels decreased. The only treatment the patient received in the ED and during her hospital stay was acetaminophen as needed for pain or fever. The eosinophil count peaked at 1404/L by hospital day 4. Blood and urine cultures were negative. IgM antibodies to Epstein‐Barr virus were not detected, CMV DNA was not detected, and a rapid plasma reagin (RPR) test was nonreactive. Ferritin, ceruloplasmin, alpha‐1‐antitrypsin, and tryptase levels were normal. Antimitochondrial, antismooth muscle, antineutrophil cytoplasmic, and antinuclear antibodies were negative. There was no monoclonal band on serum protein electrophoresis. A blood smear for Borrelia detected no spirochetes.
A complete picture of the uncommon but classic flushing disorders, namely carcinoid, mastocytosis, and pheochromocytoma, has not emerged. The constellation of inflammation, mucosal and hepatic involvement, and eosinophilia are most consistent with a drug hypersensitivity reaction. Additionally, the recurrent inflammation is becoming more severe, as manifest by the fever and hemodynamic derangements, which suggests an increasing sensitization to the offending agent. I would review every drug she has received in the hospital, but given the recurrences after discharge her home medications are the most likely explanation. Of these, sulindac is the most likely culprit.
On further questioning, it was learned that the patient began taking sulindac 200 mg twice daily to treat her chronic ankle pain 6 weeks before the first admission. The medication had been stopped on each admission. She was instructed to discontinue sulindac. She has had no recurrences of symptoms and her hepatitis and eosinophilia have resolved.
DISCUSSION
This patient presented with recurrent skin findings, eosinophilia, hepatitis, and constitutional symptoms caused by hypersensitivity to sulindac. This drug‐induced hypersensitivity syndrome was originally described with anticonvulsant drugs (carbamazepine, phenytoin, and phenobarbitone) and named anticonvulsant hypersensitivity syndrome,1, 2 but has been observed with many other medications, including allopurinol, dapsone, minocycline, and nevirapine. The term drug rash with eosinophilia and systemic symptoms (DRESS) syndrome has been recently adopted to convey the cardinal features that characterize this disorder.3
DRESS syndrome is defined by rash, fever, and internal organ involvement.4 Also included in the diagnostic criteria are hematologic abnormalities (eosinophilia 1.5 109/mm3 or the presence of atypical lymphocytes) and lymphadenopathy.3 The multiorgan involvement distinguishes DRESS from other cutaneous drug eruptions. In a review of the French Pharmacovigilance Database for all cases of DRESS over a 15‐year period, 73% to 100% of patients were reported to have dermatologic abnormalities, most frequently a maculopapular rash or erythroderma. Less common skin findings include vesicles, bullae, pustules, erythroderma, and purpuric lesions. Liver abnormalities were observed in more than 60% of patients and were the most frequent systemic finding.5 Eosinophilia was the most common hematologic abnormality, present in more than 50% of cases. As this case underscores, DRESS syndrome typically begins 3 to 8 weeks after initiation of the drug because it is a delayed type IV hypersensitivity reaction.6 Fever can occur within hours on rechallenge because of the presence of memory T cells.
The main treatment for DRESS syndrome is withdrawal of the offending drug. Systemic corticosteroids have been recommended in cases with life‐threatening pulmonary or cardiac involvement, but have not been shown to be helpful in reversing renal or hepatic disease. Mortality, usually from end‐organ damage, occurs in about 10% of cases. The most common drugs are phenobarbital, carbamazepine, and phenytoin, with incidences of 1 in 5000 to 1 in 10,000. NSAIDs and antibiotics also have been implicated frequently. Human herpesvirus type 6 coinfection and genetically inherited slow acetylation have been associated with DRESS, although causal links have yet to be established.7, 8
The initial challenge in caring for a patient with multiple symptoms, exam findings, and test abnormalities is the coherent framing of the key clinical features that require explanation. This process, called problem representation, allows clinicians to search among a bounded list of possible diagnoses (or solutions) rather than invoking a differential diagnosis for every single abnormality. In searching for the proper diagnosis, this patient's clinical course required frequent reframing as more data became available.
Initially, the problem was framed as a 42‐year‐old woman with hepatitis. As the flushing and eosinophilia, which initially appeared to be transient and possibly nonspecific, became more prominent, the problem representation was revised to a 42‐year‐old woman with hepatitis, eosinophilia, and flushing. Since this triad did not immediately invoke a single diagnosis for the treating clinicians or the discussant, the differential diagnosis of hepatitis and eosinophilia and the differential diagnosis of flushing were considered in parallel.
Hepatitis and eosinophilia can occur coincidentally in the setting of parasitic infections, particularly helminths (ascaris, strongyloidiasis, and toxocaris) and liver flukes (opisthorchis and clonorchis), which invade the hepatobiliary system and induce a reactive eosinophilia. Some neoplasms, such as lymphomas and leukemias, and myeloproliferative disorders, including hypereosinophilic syndrome and mastocytosis, may have neoplastic cellular invasion of the liver and induce eosinophilia. Systemic drug hypersensitivity reactions are typically characterized by eosinophilia, transaminase elevations,9 and hepatitis on histology.10 As with this patient, liver biopsy in drug‐induced hepatitis shows a mixed microvesicular and macrovesicular steatosis, often with eosinophils.10
The flushing prompted a thorough but negative workup for the classic flushing disorders. The discussant's attempts to unify the flushing with the other clinical features illustrate how framing can affect our reasoning. Hepatitis, eosinophilia, and flushing defied an obvious single explanation and led the discussant down parallel diagnostic reasoning pathways. Although flushing is 1 of the well‐described dermatologic manifestations in drug‐hypersensitivity reactions, framing the central features as hepatitis, eosinophilia, and rash would have more readily suggested a drug reaction as a unifying diagnosis.11
The tempo and periodicity of this patient's illness provided the final formulation of a 42‐year‐old woman with hepatitis, eosinophilia, and flushing (or rash) that occurs every few days at home and resolves in the hospital. This formulation and the increasingly severe presentation, suggesting sensitization, were highly suggestive of an exogenous cause of her illness.
This case highlights how easily medication side effects can be overlooked during an extensive evaluation and how vigilant medication reconciliation coupled with an increased understanding of the spectrum of drug reactions can lead to early detection and prevention of potentially serious effects. In the case of DRESS, recognizing an association between a rash and organ involvement is central to making the diagnosis. Eosinophilia that accompanies a rash can further aid in narrowing the differential diagnosis.
The case also serves as a reminder of how framing with the slightest imprecision (eg, flushing instead of rash) can derail or delay the diagnostic process, yet is indispensable in tackling a complicated case. Finally, a time‐honored lesson in diagnosis is highlighted yet again: the diagnosis can usually be flushed out from the history.1214
Key Teaching Points
-
The constellation of skin findings, eosinophilia, organ involvement (particularly hepatitis), and constitutional symptoms should prompt consideration of DRESS syndrome and a hunt for a culprit drug.
-
Symptoms that resolve during hospitalization and repeatedly recur after discharge should prompt consideration of an exposure unique to the home, which may be environmental or pharmacologic.
-
Problem representation is critical in solving a complicated case, but adopting an inaccurate frame (representation) can derail or delay the diagnostic process.
The approach to clinical conundrums by an expert clinician is revealed through the presentation of an actual patient's case in an approach typical of a morning report. Similarly to patient care, sequential pieces of information are provided to the clinician, who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
A 42‐year‐old woman with a history of mild asthma presented to the emergency department (ED) following 1 week of headache. She had been in her usual state of good health until 1 week prior to her presentation, when she noticed intermittent frontal headaches without neck stiffness or other neurologic symptoms. She then developed diffuse myalgias, fatigue, subjective fevers, and rigors for the 24 hours prior to presentation. On the morning of presentation, chest tightness, palpitations, and shortness of breath occurred. She used her albuterol metered‐dose inhaler without relief and went to the hospital.
Many of these features can be explained by a viral syndrome exacerbating underlying asthma or by a psychiatric condition such as anxiety or depression, but they may also be a harbinger of a systemic process, including infection, malignancy, or autoimmunity. Because the onset of headache is temporally distant from the other symptoms, I am more inclined to believe that it represents a primary intracranial process than I would if it were coincident with the onset of the other acute symptoms. If the fevers and rigors are verified, infection would be the initial concern. Failure to respond to her inhalers may either signify a severe asthma exacerbation or a nonbronchospastic cause of dyspnea.
She reported mild nausea, but denied photophobia, vomiting, abdominal pain, diarrhea, melena, or hematochezia. She did not have recent ill contacts, animal bites, or travel. Her medical history included asthma, diverticulitis, chronic right ankle pain, and obesity. She reported an allergic rash to amoxicillin. Her medications were sulindac and fluticasone/salmeterol, and albuterol metered‐dose inhalers. She worked as a preschool teacher and was married with 2 children. She denied any tobacco use and seldom drank alcoholic beverages. On exam, temperature was 36.7C, pulse was 107 beats per minute, blood pressure was 129/91 mm Hg, respiratory rate was 19 breaths per minute, and oxygen saturation was 98% while breathing ambient air. Her face and anterior neck were flushed and diaphoretic, and her sclerae were icteric. There was no nuchal rigidity. Her cardiac rhythm was regular without murmurs, lungs were clear to auscultation, and the abdomen was mildly tender to palpation in the epigastrium and right upper quadrant. The white blood cell (WBC) count was 9200/L, with 84% neutrophils, 3% lymphocytes, 6% monocytes, and 7% eosinophils. The hemoglobin was 14.8 g/dL and the platelet count was 166,000/L. Total serum bilirubin was 4.6 mg/dL, aspartate aminotransferase (AST) was 459 U/L (normal range, 8‐31), alanine aminotransferase (ALT) was 667 U/L (normal range, 7‐31), and alkaline phosphatase was 146 U/L (normal range, 39‐117). Serum electrolytes, creatinine, lactate, lipase, thyrotropin, coagulation studies, and cardiac enzymes were all normal. Urinalysis showed trace leukocyte esterase and bilirubin, as well as 3 WBCs and 2 red cells per high‐power field. Chest radiography and an electrocardiogram demonstrated no abnormalities.
The major findingwhich is critical to focusing problem‐solving in the face of a broad range of symptomsis her hepatitis. The common etiologies for hepatitis of this degree include viruses (hepatitis A and cytomegalovirus [CMV] should be considered given her work in preschool), toxins, autoimmunity, and vascular events. Liver disease in association with flushing raises the possibility of carcinoid syndrome with liver metastases. The lack of wheezing makes the bronchospasm of asthma or carcinoid less suitable explanations for her shortness of breath. Her eosinophilia is mild but probably is not accounted for alone by well‐controlled asthma in a person with no history of atopic disease. I would also ask her about any alternative and over‐the‐counter remedies. The paucity of lymphocytes raises the possibility of human immunodeficiency virus (HIV), Hodgkin's disease, or systemic lupus erythematosus. Although she does not have a documented fever or leukocytosis, she reported fevers and chills and is diaphoretic and tachycardic, so exclusion of biliary obstruction and cholangitis is the highest priority.
An abdominal ultrasound demonstrated hepatomegaly with moderate fatty infiltration and a normal gallbladder without pericholecystic fluid. The intrahepatic and extrahepatic biliary ducts were normal and the hepatic and portal veins were patent. Computed tomography of the abdomen showed slight thickening of the sigmoid colon wall. Ciprofloxacin and metronidazole were administered for possible diverticulitis. Over the first 48 hours of hospitalization her symptoms improved markedly. Her flushing resolved and she had no recorded fevers in the hospital. Serologies were negative for hepatitis A immunoglobulin M (IgM), hepatitis B surface antibody, hepatitis B surface antigen, and hepatitis C antibody. A monospot test was negative and the erythrocyte sedimentation rate was 11 mm/hour. Blood and urine cultures were negative. On the second hospital day the absolute eosinophil count rose to 855/L (15% of 5700 WBCs). On the fourth hospital day, the absolute eosinophil count was 1092/L, the total bilirubin was 1.9 mg/dL, and the AST and ALT were 174 U/L and 476 U/L, respectively. Antibiotics were stopped and she was discharged home.
Her prompt improvement suggests either a self‐limited condition or a response to the antibiotics. The rapid but incomplete resolution of her hepatitis is in keeping with a withdrawal of a toxin, relief of biliary obstruction, or a transient vascular event, and is less consistent with a viral hepatitis or an infiltrative process. With normal biliary system imaging, sterile blood cultures, and the absence of fever or leukocytosis, cholangitis is unlikely. Likewise, there is no suggestion of a vascular event, either obstructive or hemodynamic, that is impairing the liver.
A common cause of eosinophilia in hospitalized patients is medications, so it would be useful to monitor that count after the new antibiotics. At this point, I also wonder if the eosinophils are a feature of the underlying illness, as they were present to a modest degree on admission before any new medications were administered. The overlap of eosinophilia and hepatitis brings to mind a medication reaction (eg, to sulindac) or a hepatobiliary parasite, such as ascaris or clonorchis, for which she lacks a known exposure. Many patients experience flushing in the setting of fever or stress, but sustained flushing may suggest a systemic illness characterized by the release of vasoactive mediators such as carcinoid syndrome or mastocytosis. The latter might be considered more strongly if the eosinophilia is deemed to be primary (rather than reactive) after a thorough evaluation.
After 2 days at home, the patient had recurrence of subjective fevers, with chest, back, and abdominal pain, fatigue, loose stools, and rigors. She returned to the ED, where she was noted to have facial erythema and injected sclerae, but the remainder of her physical exam was normal. The total serum bilirubin was 1.1 mg/dL, AST was 156 U/L, ALT was 214 U/L, and alkaline phosphatase was 240 U/L. Serum lipase was normal. WBC count was 14,000/L, with 94% neutrophils, 3% lymphocytes, 2% monocytes, and 1% eosinophils. She was again treated empirically with ciprofloxacin and metronidazole. Endoscopic ultrasound was normal, with no evidence of gallbladder sludge or microlithiasis. Stool cultures, assay for Clostridium difficile, and examination for ova and parasites were negative. The 24‐hour urine demonstrated no elevation in 5‐hydroxyindoleacetic acid. An adrenocorticotropic hormone (ACTH) stimulation test was normal. HIV antibody was negative. Her symptoms improved within 2 days. The eosinophil count rose and peaked at 1541/L by the third hospital day, while the transaminase elevations resolved. Antibiotics were discontinued. A liver biopsy showed mixed macrovesicular and microvesicular fatty metamorphosis and steatohepatitis with eosinophils (Figures 1 and 2). She was discharged home on the sixth hospital day.
Her illness can now be characterized as relapsing inflammation, which given the frequency (over days) suggests either an indolent infectious focus that periodically causes systemic inflammation or reexposure to a toxic substance. The 2 most notable laboratory abnormalities, the hepatitis and the eosinophilia, persist but have differing trajectories. While the liver function tests have progressively normalized despite clinical relapses, the eosinophils have had a more fluctuating course characterized by increases during the hospitalization and higher levels during the second hospitalization. The absence of an infection, recurrent systemic inflammation, and eosinophilic hepatitis suggest a hypersensitivity reaction to a medication or other substance. She is most likely being reexposed at home, where her symptoms occur, and not in the hospital, where her symptoms resolve. Sulindac is a leading candidate, because nonsteroidal antiinflammatory drugs (NSAIDs) cause a number of hypersensitivity reactions and are frequently stopped when sick patients enter the hospital.
Seven days after discharge she developed acute onset of subjective fever, nausea, diffuse myalgias, and flushing, identical to the 2 prior episodes, and she again returned to the ED. Her temperature was 39.1C, heart rate was 120 beats per minute, blood pressure was 87/50 mm Hg, respiratory rate was 18 breaths per minute, and the oxygen saturation was 96% while breathing room air. She had diffuse flushing from her neck over her torso and was diaphoretic with injected sclera and conjunctiva. The WBC count was 11,400/L with 97% neutrophils and 3% lymphocytes. Total bilirubin was 0.8 mg/dL, AST was 134 U/L, ALT was 140 U/L, and alkaline phosphatase was 144 U/L. She was readmitted to the hospital. Following admission, she had no fevers, the flushing resolved, and AST and ALT levels decreased. The only treatment the patient received in the ED and during her hospital stay was acetaminophen as needed for pain or fever. The eosinophil count peaked at 1404/L by hospital day 4. Blood and urine cultures were negative. IgM antibodies to Epstein‐Barr virus were not detected, CMV DNA was not detected, and a rapid plasma reagin (RPR) test was nonreactive. Ferritin, ceruloplasmin, alpha‐1‐antitrypsin, and tryptase levels were normal. Antimitochondrial, antismooth muscle, antineutrophil cytoplasmic, and antinuclear antibodies were negative. There was no monoclonal band on serum protein electrophoresis. A blood smear for Borrelia detected no spirochetes.
A complete picture of the uncommon but classic flushing disorders, namely carcinoid, mastocytosis, and pheochromocytoma, has not emerged. The constellation of inflammation, mucosal and hepatic involvement, and eosinophilia are most consistent with a drug hypersensitivity reaction. Additionally, the recurrent inflammation is becoming more severe, as manifest by the fever and hemodynamic derangements, which suggests an increasing sensitization to the offending agent. I would review every drug she has received in the hospital, but given the recurrences after discharge her home medications are the most likely explanation. Of these, sulindac is the most likely culprit.
On further questioning, it was learned that the patient began taking sulindac 200 mg twice daily to treat her chronic ankle pain 6 weeks before the first admission. The medication had been stopped on each admission. She was instructed to discontinue sulindac. She has had no recurrences of symptoms and her hepatitis and eosinophilia have resolved.
DISCUSSION
This patient presented with recurrent skin findings, eosinophilia, hepatitis, and constitutional symptoms caused by hypersensitivity to sulindac. This drug‐induced hypersensitivity syndrome was originally described with anticonvulsant drugs (carbamazepine, phenytoin, and phenobarbitone) and named anticonvulsant hypersensitivity syndrome,1, 2 but has been observed with many other medications, including allopurinol, dapsone, minocycline, and nevirapine. The term drug rash with eosinophilia and systemic symptoms (DRESS) syndrome has been recently adopted to convey the cardinal features that characterize this disorder.3
DRESS syndrome is defined by rash, fever, and internal organ involvement.4 Also included in the diagnostic criteria are hematologic abnormalities (eosinophilia 1.5 109/mm3 or the presence of atypical lymphocytes) and lymphadenopathy.3 The multiorgan involvement distinguishes DRESS from other cutaneous drug eruptions. In a review of the French Pharmacovigilance Database for all cases of DRESS over a 15‐year period, 73% to 100% of patients were reported to have dermatologic abnormalities, most frequently a maculopapular rash or erythroderma. Less common skin findings include vesicles, bullae, pustules, erythroderma, and purpuric lesions. Liver abnormalities were observed in more than 60% of patients and were the most frequent systemic finding.5 Eosinophilia was the most common hematologic abnormality, present in more than 50% of cases. As this case underscores, DRESS syndrome typically begins 3 to 8 weeks after initiation of the drug because it is a delayed type IV hypersensitivity reaction.6 Fever can occur within hours on rechallenge because of the presence of memory T cells.
The main treatment for DRESS syndrome is withdrawal of the offending drug. Systemic corticosteroids have been recommended in cases with life‐threatening pulmonary or cardiac involvement, but have not been shown to be helpful in reversing renal or hepatic disease. Mortality, usually from end‐organ damage, occurs in about 10% of cases. The most common drugs are phenobarbital, carbamazepine, and phenytoin, with incidences of 1 in 5000 to 1 in 10,000. NSAIDs and antibiotics also have been implicated frequently. Human herpesvirus type 6 coinfection and genetically inherited slow acetylation have been associated with DRESS, although causal links have yet to be established.7, 8
The initial challenge in caring for a patient with multiple symptoms, exam findings, and test abnormalities is the coherent framing of the key clinical features that require explanation. This process, called problem representation, allows clinicians to search among a bounded list of possible diagnoses (or solutions) rather than invoking a differential diagnosis for every single abnormality. In searching for the proper diagnosis, this patient's clinical course required frequent reframing as more data became available.
Initially, the problem was framed as a 42‐year‐old woman with hepatitis. As the flushing and eosinophilia, which initially appeared to be transient and possibly nonspecific, became more prominent, the problem representation was revised to a 42‐year‐old woman with hepatitis, eosinophilia, and flushing. Since this triad did not immediately invoke a single diagnosis for the treating clinicians or the discussant, the differential diagnosis of hepatitis and eosinophilia and the differential diagnosis of flushing were considered in parallel.
Hepatitis and eosinophilia can occur coincidentally in the setting of parasitic infections, particularly helminths (ascaris, strongyloidiasis, and toxocaris) and liver flukes (opisthorchis and clonorchis), which invade the hepatobiliary system and induce a reactive eosinophilia. Some neoplasms, such as lymphomas and leukemias, and myeloproliferative disorders, including hypereosinophilic syndrome and mastocytosis, may have neoplastic cellular invasion of the liver and induce eosinophilia. Systemic drug hypersensitivity reactions are typically characterized by eosinophilia, transaminase elevations,9 and hepatitis on histology.10 As with this patient, liver biopsy in drug‐induced hepatitis shows a mixed microvesicular and macrovesicular steatosis, often with eosinophils.10
The flushing prompted a thorough but negative workup for the classic flushing disorders. The discussant's attempts to unify the flushing with the other clinical features illustrate how framing can affect our reasoning. Hepatitis, eosinophilia, and flushing defied an obvious single explanation and led the discussant down parallel diagnostic reasoning pathways. Although flushing is 1 of the well‐described dermatologic manifestations in drug‐hypersensitivity reactions, framing the central features as hepatitis, eosinophilia, and rash would have more readily suggested a drug reaction as a unifying diagnosis.11
The tempo and periodicity of this patient's illness provided the final formulation of a 42‐year‐old woman with hepatitis, eosinophilia, and flushing (or rash) that occurs every few days at home and resolves in the hospital. This formulation and the increasingly severe presentation, suggesting sensitization, were highly suggestive of an exogenous cause of her illness.
This case highlights how easily medication side effects can be overlooked during an extensive evaluation and how vigilant medication reconciliation coupled with an increased understanding of the spectrum of drug reactions can lead to early detection and prevention of potentially serious effects. In the case of DRESS, recognizing an association between a rash and organ involvement is central to making the diagnosis. Eosinophilia that accompanies a rash can further aid in narrowing the differential diagnosis.
The case also serves as a reminder of how framing with the slightest imprecision (eg, flushing instead of rash) can derail or delay the diagnostic process, yet is indispensable in tackling a complicated case. Finally, a time‐honored lesson in diagnosis is highlighted yet again: the diagnosis can usually be flushed out from the history.1214
Key Teaching Points
-
The constellation of skin findings, eosinophilia, organ involvement (particularly hepatitis), and constitutional symptoms should prompt consideration of DRESS syndrome and a hunt for a culprit drug.
-
Symptoms that resolve during hospitalization and repeatedly recur after discharge should prompt consideration of an exposure unique to the home, which may be environmental or pharmacologic.
-
Problem representation is critical in solving a complicated case, but adopting an inaccurate frame (representation) can derail or delay the diagnostic process.
The approach to clinical conundrums by an expert clinician is revealed through the presentation of an actual patient's case in an approach typical of a morning report. Similarly to patient care, sequential pieces of information are provided to the clinician, who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
- ,.Anticonvulsant hypersensitivity syndrome. In vitro assessment of risk.J Clin Invest.1988;82:1826–1832.
- ,,.Anticonvulsant hypersensitivity syndrome: incidence, prevention, and management.Drug Saf.1999;21:489–501.
- ,,,.Drug rash with eosinophilia and systemic symptoms vs toxic epidermal necrolysis: the dilemma of classification.Clin Dermatol.2005;23:311–314.
- ,.Management of drug rash with eosinophilia and systemic symptoms (DRESS syndrome): an update.Dermatology.2003;206:353–356.
- ,,,,,Blayac J‐P; Network of the French Pharmacovigilance Centers. Variability in the clinical pattern of cutaneous side‐effects of drugs with systemic symptoms: does a DRESS syndrome really exist?Br J Dermatol.2006;155:422–428.
- ,.The immunological and clinical spectrum of delayed drug‐induced exanthems.Curr Opin Allergy Clin Immunol.2004;4:411–419.
- ,,.Association between anticonvulsant hypersensitivity syndrome and human herpesvirus 6 reactivation and hypogammaglobulinemia.Arch Dermatol.2004;140:183–188.
- ,.Treatment of severe drug reactions: Stevens‐Johnson Syndrome, toxic epidermal necrolysis and hypersensitivity syndrome.Dermatol Online J.2002;8:5.
- ,.Drug reactions. In: Bolognia JL, Jorizzo JL, Rapini RP, eds.Dermatology.2nd ed.Spain:Mosby Elsevier;2008:310–311.
- Pathology Outlines. Liver and intrahepatic bile ducts—non tumor. Hepatitis (non‐infectious). Drug/toxin‐induced hepatitis. Available at: http://www.pathologyoutlines.com/liver.html#drugtoxin. Accessed August2009.
- ,,.The flushing patient: differential diagnosis, workup and treatment.J Am Acad Dermatol.2006;55(2):193–208.
- ,,,,.Relative contributions of history‐taking, physical examination, and laboratory investigation to diagnosis and management of medical outpatients.Br Med J.1975;2(5969):486–489.
- ,,,,.Contributions to the history, physical examination, and laboratory investigation in making medical diagnosis.West J Med.1992;156(2):163–165.
- ,.A study on relative contributions of the history, physical examination and investigations in making medical diagnosis.J Assoc Physicians India.2000;48(8):771–775.
- ,.Anticonvulsant hypersensitivity syndrome. In vitro assessment of risk.J Clin Invest.1988;82:1826–1832.
- ,,.Anticonvulsant hypersensitivity syndrome: incidence, prevention, and management.Drug Saf.1999;21:489–501.
- ,,,.Drug rash with eosinophilia and systemic symptoms vs toxic epidermal necrolysis: the dilemma of classification.Clin Dermatol.2005;23:311–314.
- ,.Management of drug rash with eosinophilia and systemic symptoms (DRESS syndrome): an update.Dermatology.2003;206:353–356.
- ,,,,,Blayac J‐P; Network of the French Pharmacovigilance Centers. Variability in the clinical pattern of cutaneous side‐effects of drugs with systemic symptoms: does a DRESS syndrome really exist?Br J Dermatol.2006;155:422–428.
- ,.The immunological and clinical spectrum of delayed drug‐induced exanthems.Curr Opin Allergy Clin Immunol.2004;4:411–419.
- ,,.Association between anticonvulsant hypersensitivity syndrome and human herpesvirus 6 reactivation and hypogammaglobulinemia.Arch Dermatol.2004;140:183–188.
- ,.Treatment of severe drug reactions: Stevens‐Johnson Syndrome, toxic epidermal necrolysis and hypersensitivity syndrome.Dermatol Online J.2002;8:5.
- ,.Drug reactions. In: Bolognia JL, Jorizzo JL, Rapini RP, eds.Dermatology.2nd ed.Spain:Mosby Elsevier;2008:310–311.
- Pathology Outlines. Liver and intrahepatic bile ducts—non tumor. Hepatitis (non‐infectious). Drug/toxin‐induced hepatitis. Available at: http://www.pathologyoutlines.com/liver.html#drugtoxin. Accessed August2009.
- ,,.The flushing patient: differential diagnosis, workup and treatment.J Am Acad Dermatol.2006;55(2):193–208.
- ,,,,.Relative contributions of history‐taking, physical examination, and laboratory investigation to diagnosis and management of medical outpatients.Br Med J.1975;2(5969):486–489.
- ,,,,.Contributions to the history, physical examination, and laboratory investigation in making medical diagnosis.West J Med.1992;156(2):163–165.
- ,.A study on relative contributions of the history, physical examination and investigations in making medical diagnosis.J Assoc Physicians India.2000;48(8):771–775.
Bilateral Adrenal Hemorrhage Complication
A 52‐year‐old man presented to the emergency department (ED) from a skilled nursing facility with a complaint of bilateral upper‐quadrant abdominal pain of 48 hours' duration. The pain was sharp, nonradiating, constant, and was associated with nausea, vomiting, and constipation. The patient denied any fever, back pain, dysuria, melena, or hematochezia. In the rehabilitation facility the patient had been initially evaluated for this pain. He was given laxatives and stool softeners for presumed constipation but these measures had not been effective. A computed tomography (CT) scan of the abdomen had only showed stool in the colon and he was sent to the ED for further evaluation.
Apart from severe degenerative joint disease in both his knees he was in good health. He was in the skilled nursing facility (SNF) for rehabilitation for bilateral knee replacement surgery done 9 days prior to this presentation. His postoperative course was unremarkable. He had been maintained on prophylaxis for venous thromboembolism with enoxaparin since postoperative day 1 at a daily dose of 40 mg subcutaneously, and was transferred to the SNF on postoperative day 6 on the same dose. His was receiving oxycodone and Tylenol for pain. He was on no other medications.
Vital signs on presentation revealed a temperature of 97.5F, a heart rate of 100 beats per minute, a respiratory rate of 16 breaths per minute, and a blood pressure of 136/69 mmHg. He was alert and oriented and in mild distress from the abdominal pain. Examination was normal except for tenderness in the upper quadrants of the abdomen though no rigidity or rebound tenderness were noted. Routine chemistries were normal except for sodium of 134 mg/dL. His white count, hemoglobin, hematocrit, and platelet levels were noted to be at 17.5K/L, 10 g/dL, 30%, and 345K/L, respectively, and were stable with regard to his discharge laboratory values. His serum eosinophil level was normal. A complete workup for hypercoagulable state and bleeding disorders including assays for antibodies associated with heparin‐induced thrombocytopenia were negative. He was admitted for further evaluation and treatment.
The patient had another CT scan of the abdomen (Figure 1), which when compared to the one done at the SNF 2 days prior showed markedly enlarged bilateral adrenal glands suggestive of bilateral acute adrenal hemorrhage. The enoxaparin was discontinued and empiric steroid replacement therapy was begun. A random cortisol level was normal but a cosyntropin stimulation test showed an absolute increase in cortisol level of only 0.8 g/dL at both 30 and 60 minutes after administration of 250 g of cosyntropin. An investigation was undertaken to determine if the patient had any prior risk factors for bleeding. There was no evidence of infection and a comprehensive evaluation for bleeding, and coagulation disorders was normal. The bilateral adrenal hemorrhage was attributed to the use of enoxaparin in the postoperative setting. Unfortunately, the patient subsequently developed a deep venous thrombosis in his lower extremity and an inferior vena cava (IVC) filter was placed before discharge. He was doing well 6 months later, and is still continued on glucocorticoid and mineralocorticoid replacement therapy and follows up with endocrinology as an outpatient.
Discussion
Bilateral adrenal hemorrhage is usually associated with massive sepsis from Gram‐negative organisms such as Neisseria meningitides, Pseudomonas aeroginosa, Escherichia coli, and Bacteroides fragilis. Rupert Waterhouse, in 1911, was the first person to describe a patient with severe meningococcal sepsis resulting in acute adrenal hemorrhage and collapse. This was also later described independently by Carl Friderichsen in 1918, and is now referred to as the Waterhouse‐Friderichsen syndrome. Other causes include antiphospholipid antibody syndrome, heparin‐associated thrombocytopenia (HIT), and severe physical stress. Bilateral adrenal hemorrhage can also spontaneously occur in the postoperative period, especially after cardiothoracic or orthopedic surgery. This phenomenon may be related to the frequent use of prophylactic anticoagulants after these types of procedures.
The first case report of bilateral adrenal hemorrhage secondary to use of anticoagulants was described in 1947, and the first case report of successful resuscitation after corticosteroid administration in a patient with bilateral adrenal hemorrhage secondary to anticoagulant use was described by Thorn in 1956.1 A review of the literature demonstrates multiple case reports of adrenal hemorrhage reported in the postoperative period, particularly after joint arthroplasty, and especially after knee replacement surgeries. Most of the recent cases have been associated with use of prophylactic low‐dose heparin or low‐molecular‐weight heparin at the time of adrenal hemorrhage. In a study of 157 case reports of individuals with bilateral hemorrhage (including 22 autopsies), 48 cases were associated with administration of anticoagulants, although the dose and effect were not specified.2 Amador et al.1 showed that out of 4325 autopsies performed from 1949 to 1962 in their institution, 30 cases were found of bilateral hemorrhage, of which 10 were receiving heparin at presumably prophylactic doses; 5 of these patients were also receiving dicumarol.
Mayo Clinic investigators performed a retrospective review of all cases of adrenal hemorrhage over a period of 25 years at their hospital, and found 141 cases of adrenal hemorrhage, of which 78 were bilateral and 63 were unilateral,3 and in 67 patients the condition was diagnosed at autopsy. In this study 14 patients had adrenal hemorrhage in the postoperative period in the absence of lupus anticoagulant or HIT; there was no specific mention in this study of the use of postoperative anticoagulants. Finally, a multicenter case control study was undertaken by Kovacs et al.4 to assess putative risk factors for development of bilateral massive adrenal hemorrhage. In the multivariate analysis, thrombocytopenia, exposure to heparin, and sepsis were found to be strongly associated with risk of hemorrhage. Of 23 patients with bilateral, massive adrenal hemorrhage, 16 had been exposed to heparin, and at least 6 were on exclusively subcutaneous heparin. The authors concluded that heparin exposure was a much bigger risk factor than other coagulopathies, and those exposed to heparin of any route or type for 4 to 6 days and those exposed for more than 6 days were about 17 and 34 times, respectively, more likely to develop bilateral hemorrhage than those who had less than 4 days or no exposure.
The clinical presentation of adrenal insufficiency due to bilateral adrenal hemorrhage is often nonspecific. Symptoms may include abdominal pain, back pain, fever, nausea, vomiting, weakness, obtundation, confusion, and hypotensionall of which are also common postoperative symptoms and can be missed or ignored.5 Rao et al.6 profiled the clinical presentation of 64 cases of bilateral hemorrhage and found the following: abdominal, flank, back, or chest pain (86%); anorexia, nausea, or vomiting (47%); psychiatric symptoms (42%); fever (66%); hypotension recognized before shock episode (19%); and abdominal rigidity or rebound (22%). Adrenal insufficiency becomes clinically evident once 90% of the gland is destroyed. About 50% of patients do not manifest typical laboratory abnormalities, so a high degree of suspicion is necessary to diagnose the condition.3 Also, the laboratory diagnosis of adrenal insufficiency using random cortisol levels is unreliable, as reference ranges in patients experiencing stress (as in the postoperative period) have not been well studied or established. In patients with bilateral hemorrhage postoperatively on prophylactic anticoagulants, the coagulation profile is usually within normal limits and there is typically no evidence of spontaneous bleeding elsewhere. In later stages, the typical laboratory findings of abnormal adrenal function such as hypokalemia, hyponatremia, declining cortisol levels, and an inappropriate response to adrenocorticotropic hormone stimulation test may be seen. A significant drop in hemoglobin secondary to hemorrhage may also be encountered in some patients secondary to the bleed.
CT is the most reliable and extensively used imaging modality for making the diagnosis, although magnetic resonance imaging (MRI) or ultrasound may also be utilized. Early in the course of adrenal hemorrhage, CT findings may be negative, and repeated imaging is appropriate when clinical suspicion is high. The presence of bilateral adrenal enlargement with increased signal attenuation suggests bilateral adrenal hemorrhage. MRI can both characterize adrenal hematomas, and estimate their age.7, 8
Postoperative adrenal hemorrhage and insufficiency is easily treatable and has excellent outcomes; survivors will need lifelong corticosteroid replacement (and usually mineralocorticoid replacement as well). In the Mayo Clinic study, survival was 100% with treatment vs. 17% without treatment. In comparison, sepsis‐induced or stress‐induced adrenal insufficiency has poor outcomes despite adequate treatment (9% survival with treatment vs. 6% survival without treatment).3 Death can occur within hours to days of symptoms if untreated. Treatment includes timely initiation of adrenal hormone replacement and reversal of coagulopathies.
Postoperative venous thromboembolism (VTE) prophylaxis with anticoagulants is the appropriate care in many cases, but, along with the postoperative state itself, also appears to be a risk factor for this unusual condition. Postoperative bilateral adrenal hemorrhage is rare and potentially fatal. Early identification and prompt initiation of steroid replacement therapy and reversal of coagulopathies can prove to be lifesaving. Making this diagnosis can be very challenging, as the clinical presentation and laboratory findings of adrenal hemorrhage are vague and nonspecific and mimic many nonlife threatening postoperative complications. Radiological diagnosis by CT may initially be normal and thus further confound the diagnosis. Hence, providers should remain vigilant for associated complications even with low‐dose prophylactic heparin or low‐molecular‐weight heparin in postoperative patients, and prompt, presumptive treatment with corticosteroids should be started while awaiting confirmation by imaging and laboratory testing.
- .Adrenal hemorrhage during anticoagulant therapy. A clinical and pathological study of ten cases.Ann Intern Med.1965;63(4):559–571.
- ,,,,,.Adrenal hemorrhage in the adult.Medicine.1978;57(3):211–221.
- ,,.Adrenal hemorrhage: a 25‐year experience at the Mayo Clinic.Mayo Clin Proc.2001;76(2):161–168.
- ,,.Bilateral massive adrenal hemorrhage. Assessment of putative risk factors by the case‐control method.Medicine.2001;80(1):45–53.
- .Bilateral massive adrenal hemorrhage.Med Clin North Am.1995;79(1):107–129.
- ,,.Bilateral massive adrenal hemorrhage: early recognition and treatment.Ann Intern Med.1989;110(3):227–235.
- ,,, et al.Imaging of nontraumatic hemorrhage of the adrenal gland.Radiographics.1999;19(4):949–963.
- ,,,,.Spontaneous unilateral adrenal hemorrhage: computerized tomography and magnetic resonance imaging findings in 8 cases.J Urol.1995;154(5):1647–1651.
A 52‐year‐old man presented to the emergency department (ED) from a skilled nursing facility with a complaint of bilateral upper‐quadrant abdominal pain of 48 hours' duration. The pain was sharp, nonradiating, constant, and was associated with nausea, vomiting, and constipation. The patient denied any fever, back pain, dysuria, melena, or hematochezia. In the rehabilitation facility the patient had been initially evaluated for this pain. He was given laxatives and stool softeners for presumed constipation but these measures had not been effective. A computed tomography (CT) scan of the abdomen had only showed stool in the colon and he was sent to the ED for further evaluation.
Apart from severe degenerative joint disease in both his knees he was in good health. He was in the skilled nursing facility (SNF) for rehabilitation for bilateral knee replacement surgery done 9 days prior to this presentation. His postoperative course was unremarkable. He had been maintained on prophylaxis for venous thromboembolism with enoxaparin since postoperative day 1 at a daily dose of 40 mg subcutaneously, and was transferred to the SNF on postoperative day 6 on the same dose. His was receiving oxycodone and Tylenol for pain. He was on no other medications.
Vital signs on presentation revealed a temperature of 97.5F, a heart rate of 100 beats per minute, a respiratory rate of 16 breaths per minute, and a blood pressure of 136/69 mmHg. He was alert and oriented and in mild distress from the abdominal pain. Examination was normal except for tenderness in the upper quadrants of the abdomen though no rigidity or rebound tenderness were noted. Routine chemistries were normal except for sodium of 134 mg/dL. His white count, hemoglobin, hematocrit, and platelet levels were noted to be at 17.5K/L, 10 g/dL, 30%, and 345K/L, respectively, and were stable with regard to his discharge laboratory values. His serum eosinophil level was normal. A complete workup for hypercoagulable state and bleeding disorders including assays for antibodies associated with heparin‐induced thrombocytopenia were negative. He was admitted for further evaluation and treatment.
The patient had another CT scan of the abdomen (Figure 1), which when compared to the one done at the SNF 2 days prior showed markedly enlarged bilateral adrenal glands suggestive of bilateral acute adrenal hemorrhage. The enoxaparin was discontinued and empiric steroid replacement therapy was begun. A random cortisol level was normal but a cosyntropin stimulation test showed an absolute increase in cortisol level of only 0.8 g/dL at both 30 and 60 minutes after administration of 250 g of cosyntropin. An investigation was undertaken to determine if the patient had any prior risk factors for bleeding. There was no evidence of infection and a comprehensive evaluation for bleeding, and coagulation disorders was normal. The bilateral adrenal hemorrhage was attributed to the use of enoxaparin in the postoperative setting. Unfortunately, the patient subsequently developed a deep venous thrombosis in his lower extremity and an inferior vena cava (IVC) filter was placed before discharge. He was doing well 6 months later, and is still continued on glucocorticoid and mineralocorticoid replacement therapy and follows up with endocrinology as an outpatient.
Discussion
Bilateral adrenal hemorrhage is usually associated with massive sepsis from Gram‐negative organisms such as Neisseria meningitides, Pseudomonas aeroginosa, Escherichia coli, and Bacteroides fragilis. Rupert Waterhouse, in 1911, was the first person to describe a patient with severe meningococcal sepsis resulting in acute adrenal hemorrhage and collapse. This was also later described independently by Carl Friderichsen in 1918, and is now referred to as the Waterhouse‐Friderichsen syndrome. Other causes include antiphospholipid antibody syndrome, heparin‐associated thrombocytopenia (HIT), and severe physical stress. Bilateral adrenal hemorrhage can also spontaneously occur in the postoperative period, especially after cardiothoracic or orthopedic surgery. This phenomenon may be related to the frequent use of prophylactic anticoagulants after these types of procedures.
The first case report of bilateral adrenal hemorrhage secondary to use of anticoagulants was described in 1947, and the first case report of successful resuscitation after corticosteroid administration in a patient with bilateral adrenal hemorrhage secondary to anticoagulant use was described by Thorn in 1956.1 A review of the literature demonstrates multiple case reports of adrenal hemorrhage reported in the postoperative period, particularly after joint arthroplasty, and especially after knee replacement surgeries. Most of the recent cases have been associated with use of prophylactic low‐dose heparin or low‐molecular‐weight heparin at the time of adrenal hemorrhage. In a study of 157 case reports of individuals with bilateral hemorrhage (including 22 autopsies), 48 cases were associated with administration of anticoagulants, although the dose and effect were not specified.2 Amador et al.1 showed that out of 4325 autopsies performed from 1949 to 1962 in their institution, 30 cases were found of bilateral hemorrhage, of which 10 were receiving heparin at presumably prophylactic doses; 5 of these patients were also receiving dicumarol.
Mayo Clinic investigators performed a retrospective review of all cases of adrenal hemorrhage over a period of 25 years at their hospital, and found 141 cases of adrenal hemorrhage, of which 78 were bilateral and 63 were unilateral,3 and in 67 patients the condition was diagnosed at autopsy. In this study 14 patients had adrenal hemorrhage in the postoperative period in the absence of lupus anticoagulant or HIT; there was no specific mention in this study of the use of postoperative anticoagulants. Finally, a multicenter case control study was undertaken by Kovacs et al.4 to assess putative risk factors for development of bilateral massive adrenal hemorrhage. In the multivariate analysis, thrombocytopenia, exposure to heparin, and sepsis were found to be strongly associated with risk of hemorrhage. Of 23 patients with bilateral, massive adrenal hemorrhage, 16 had been exposed to heparin, and at least 6 were on exclusively subcutaneous heparin. The authors concluded that heparin exposure was a much bigger risk factor than other coagulopathies, and those exposed to heparin of any route or type for 4 to 6 days and those exposed for more than 6 days were about 17 and 34 times, respectively, more likely to develop bilateral hemorrhage than those who had less than 4 days or no exposure.
The clinical presentation of adrenal insufficiency due to bilateral adrenal hemorrhage is often nonspecific. Symptoms may include abdominal pain, back pain, fever, nausea, vomiting, weakness, obtundation, confusion, and hypotensionall of which are also common postoperative symptoms and can be missed or ignored.5 Rao et al.6 profiled the clinical presentation of 64 cases of bilateral hemorrhage and found the following: abdominal, flank, back, or chest pain (86%); anorexia, nausea, or vomiting (47%); psychiatric symptoms (42%); fever (66%); hypotension recognized before shock episode (19%); and abdominal rigidity or rebound (22%). Adrenal insufficiency becomes clinically evident once 90% of the gland is destroyed. About 50% of patients do not manifest typical laboratory abnormalities, so a high degree of suspicion is necessary to diagnose the condition.3 Also, the laboratory diagnosis of adrenal insufficiency using random cortisol levels is unreliable, as reference ranges in patients experiencing stress (as in the postoperative period) have not been well studied or established. In patients with bilateral hemorrhage postoperatively on prophylactic anticoagulants, the coagulation profile is usually within normal limits and there is typically no evidence of spontaneous bleeding elsewhere. In later stages, the typical laboratory findings of abnormal adrenal function such as hypokalemia, hyponatremia, declining cortisol levels, and an inappropriate response to adrenocorticotropic hormone stimulation test may be seen. A significant drop in hemoglobin secondary to hemorrhage may also be encountered in some patients secondary to the bleed.
CT is the most reliable and extensively used imaging modality for making the diagnosis, although magnetic resonance imaging (MRI) or ultrasound may also be utilized. Early in the course of adrenal hemorrhage, CT findings may be negative, and repeated imaging is appropriate when clinical suspicion is high. The presence of bilateral adrenal enlargement with increased signal attenuation suggests bilateral adrenal hemorrhage. MRI can both characterize adrenal hematomas, and estimate their age.7, 8
Postoperative adrenal hemorrhage and insufficiency is easily treatable and has excellent outcomes; survivors will need lifelong corticosteroid replacement (and usually mineralocorticoid replacement as well). In the Mayo Clinic study, survival was 100% with treatment vs. 17% without treatment. In comparison, sepsis‐induced or stress‐induced adrenal insufficiency has poor outcomes despite adequate treatment (9% survival with treatment vs. 6% survival without treatment).3 Death can occur within hours to days of symptoms if untreated. Treatment includes timely initiation of adrenal hormone replacement and reversal of coagulopathies.
Postoperative venous thromboembolism (VTE) prophylaxis with anticoagulants is the appropriate care in many cases, but, along with the postoperative state itself, also appears to be a risk factor for this unusual condition. Postoperative bilateral adrenal hemorrhage is rare and potentially fatal. Early identification and prompt initiation of steroid replacement therapy and reversal of coagulopathies can prove to be lifesaving. Making this diagnosis can be very challenging, as the clinical presentation and laboratory findings of adrenal hemorrhage are vague and nonspecific and mimic many nonlife threatening postoperative complications. Radiological diagnosis by CT may initially be normal and thus further confound the diagnosis. Hence, providers should remain vigilant for associated complications even with low‐dose prophylactic heparin or low‐molecular‐weight heparin in postoperative patients, and prompt, presumptive treatment with corticosteroids should be started while awaiting confirmation by imaging and laboratory testing.
A 52‐year‐old man presented to the emergency department (ED) from a skilled nursing facility with a complaint of bilateral upper‐quadrant abdominal pain of 48 hours' duration. The pain was sharp, nonradiating, constant, and was associated with nausea, vomiting, and constipation. The patient denied any fever, back pain, dysuria, melena, or hematochezia. In the rehabilitation facility the patient had been initially evaluated for this pain. He was given laxatives and stool softeners for presumed constipation but these measures had not been effective. A computed tomography (CT) scan of the abdomen had only showed stool in the colon and he was sent to the ED for further evaluation.
Apart from severe degenerative joint disease in both his knees he was in good health. He was in the skilled nursing facility (SNF) for rehabilitation for bilateral knee replacement surgery done 9 days prior to this presentation. His postoperative course was unremarkable. He had been maintained on prophylaxis for venous thromboembolism with enoxaparin since postoperative day 1 at a daily dose of 40 mg subcutaneously, and was transferred to the SNF on postoperative day 6 on the same dose. His was receiving oxycodone and Tylenol for pain. He was on no other medications.
Vital signs on presentation revealed a temperature of 97.5F, a heart rate of 100 beats per minute, a respiratory rate of 16 breaths per minute, and a blood pressure of 136/69 mmHg. He was alert and oriented and in mild distress from the abdominal pain. Examination was normal except for tenderness in the upper quadrants of the abdomen though no rigidity or rebound tenderness were noted. Routine chemistries were normal except for sodium of 134 mg/dL. His white count, hemoglobin, hematocrit, and platelet levels were noted to be at 17.5K/L, 10 g/dL, 30%, and 345K/L, respectively, and were stable with regard to his discharge laboratory values. His serum eosinophil level was normal. A complete workup for hypercoagulable state and bleeding disorders including assays for antibodies associated with heparin‐induced thrombocytopenia were negative. He was admitted for further evaluation and treatment.
The patient had another CT scan of the abdomen (Figure 1), which when compared to the one done at the SNF 2 days prior showed markedly enlarged bilateral adrenal glands suggestive of bilateral acute adrenal hemorrhage. The enoxaparin was discontinued and empiric steroid replacement therapy was begun. A random cortisol level was normal but a cosyntropin stimulation test showed an absolute increase in cortisol level of only 0.8 g/dL at both 30 and 60 minutes after administration of 250 g of cosyntropin. An investigation was undertaken to determine if the patient had any prior risk factors for bleeding. There was no evidence of infection and a comprehensive evaluation for bleeding, and coagulation disorders was normal. The bilateral adrenal hemorrhage was attributed to the use of enoxaparin in the postoperative setting. Unfortunately, the patient subsequently developed a deep venous thrombosis in his lower extremity and an inferior vena cava (IVC) filter was placed before discharge. He was doing well 6 months later, and is still continued on glucocorticoid and mineralocorticoid replacement therapy and follows up with endocrinology as an outpatient.
Discussion
Bilateral adrenal hemorrhage is usually associated with massive sepsis from Gram‐negative organisms such as Neisseria meningitides, Pseudomonas aeroginosa, Escherichia coli, and Bacteroides fragilis. Rupert Waterhouse, in 1911, was the first person to describe a patient with severe meningococcal sepsis resulting in acute adrenal hemorrhage and collapse. This was also later described independently by Carl Friderichsen in 1918, and is now referred to as the Waterhouse‐Friderichsen syndrome. Other causes include antiphospholipid antibody syndrome, heparin‐associated thrombocytopenia (HIT), and severe physical stress. Bilateral adrenal hemorrhage can also spontaneously occur in the postoperative period, especially after cardiothoracic or orthopedic surgery. This phenomenon may be related to the frequent use of prophylactic anticoagulants after these types of procedures.
The first case report of bilateral adrenal hemorrhage secondary to use of anticoagulants was described in 1947, and the first case report of successful resuscitation after corticosteroid administration in a patient with bilateral adrenal hemorrhage secondary to anticoagulant use was described by Thorn in 1956.1 A review of the literature demonstrates multiple case reports of adrenal hemorrhage reported in the postoperative period, particularly after joint arthroplasty, and especially after knee replacement surgeries. Most of the recent cases have been associated with use of prophylactic low‐dose heparin or low‐molecular‐weight heparin at the time of adrenal hemorrhage. In a study of 157 case reports of individuals with bilateral hemorrhage (including 22 autopsies), 48 cases were associated with administration of anticoagulants, although the dose and effect were not specified.2 Amador et al.1 showed that out of 4325 autopsies performed from 1949 to 1962 in their institution, 30 cases were found of bilateral hemorrhage, of which 10 were receiving heparin at presumably prophylactic doses; 5 of these patients were also receiving dicumarol.
Mayo Clinic investigators performed a retrospective review of all cases of adrenal hemorrhage over a period of 25 years at their hospital, and found 141 cases of adrenal hemorrhage, of which 78 were bilateral and 63 were unilateral,3 and in 67 patients the condition was diagnosed at autopsy. In this study 14 patients had adrenal hemorrhage in the postoperative period in the absence of lupus anticoagulant or HIT; there was no specific mention in this study of the use of postoperative anticoagulants. Finally, a multicenter case control study was undertaken by Kovacs et al.4 to assess putative risk factors for development of bilateral massive adrenal hemorrhage. In the multivariate analysis, thrombocytopenia, exposure to heparin, and sepsis were found to be strongly associated with risk of hemorrhage. Of 23 patients with bilateral, massive adrenal hemorrhage, 16 had been exposed to heparin, and at least 6 were on exclusively subcutaneous heparin. The authors concluded that heparin exposure was a much bigger risk factor than other coagulopathies, and those exposed to heparin of any route or type for 4 to 6 days and those exposed for more than 6 days were about 17 and 34 times, respectively, more likely to develop bilateral hemorrhage than those who had less than 4 days or no exposure.
The clinical presentation of adrenal insufficiency due to bilateral adrenal hemorrhage is often nonspecific. Symptoms may include abdominal pain, back pain, fever, nausea, vomiting, weakness, obtundation, confusion, and hypotensionall of which are also common postoperative symptoms and can be missed or ignored.5 Rao et al.6 profiled the clinical presentation of 64 cases of bilateral hemorrhage and found the following: abdominal, flank, back, or chest pain (86%); anorexia, nausea, or vomiting (47%); psychiatric symptoms (42%); fever (66%); hypotension recognized before shock episode (19%); and abdominal rigidity or rebound (22%). Adrenal insufficiency becomes clinically evident once 90% of the gland is destroyed. About 50% of patients do not manifest typical laboratory abnormalities, so a high degree of suspicion is necessary to diagnose the condition.3 Also, the laboratory diagnosis of adrenal insufficiency using random cortisol levels is unreliable, as reference ranges in patients experiencing stress (as in the postoperative period) have not been well studied or established. In patients with bilateral hemorrhage postoperatively on prophylactic anticoagulants, the coagulation profile is usually within normal limits and there is typically no evidence of spontaneous bleeding elsewhere. In later stages, the typical laboratory findings of abnormal adrenal function such as hypokalemia, hyponatremia, declining cortisol levels, and an inappropriate response to adrenocorticotropic hormone stimulation test may be seen. A significant drop in hemoglobin secondary to hemorrhage may also be encountered in some patients secondary to the bleed.
CT is the most reliable and extensively used imaging modality for making the diagnosis, although magnetic resonance imaging (MRI) or ultrasound may also be utilized. Early in the course of adrenal hemorrhage, CT findings may be negative, and repeated imaging is appropriate when clinical suspicion is high. The presence of bilateral adrenal enlargement with increased signal attenuation suggests bilateral adrenal hemorrhage. MRI can both characterize adrenal hematomas, and estimate their age.7, 8
Postoperative adrenal hemorrhage and insufficiency is easily treatable and has excellent outcomes; survivors will need lifelong corticosteroid replacement (and usually mineralocorticoid replacement as well). In the Mayo Clinic study, survival was 100% with treatment vs. 17% without treatment. In comparison, sepsis‐induced or stress‐induced adrenal insufficiency has poor outcomes despite adequate treatment (9% survival with treatment vs. 6% survival without treatment).3 Death can occur within hours to days of symptoms if untreated. Treatment includes timely initiation of adrenal hormone replacement and reversal of coagulopathies.
Postoperative venous thromboembolism (VTE) prophylaxis with anticoagulants is the appropriate care in many cases, but, along with the postoperative state itself, also appears to be a risk factor for this unusual condition. Postoperative bilateral adrenal hemorrhage is rare and potentially fatal. Early identification and prompt initiation of steroid replacement therapy and reversal of coagulopathies can prove to be lifesaving. Making this diagnosis can be very challenging, as the clinical presentation and laboratory findings of adrenal hemorrhage are vague and nonspecific and mimic many nonlife threatening postoperative complications. Radiological diagnosis by CT may initially be normal and thus further confound the diagnosis. Hence, providers should remain vigilant for associated complications even with low‐dose prophylactic heparin or low‐molecular‐weight heparin in postoperative patients, and prompt, presumptive treatment with corticosteroids should be started while awaiting confirmation by imaging and laboratory testing.
- .Adrenal hemorrhage during anticoagulant therapy. A clinical and pathological study of ten cases.Ann Intern Med.1965;63(4):559–571.
- ,,,,,.Adrenal hemorrhage in the adult.Medicine.1978;57(3):211–221.
- ,,.Adrenal hemorrhage: a 25‐year experience at the Mayo Clinic.Mayo Clin Proc.2001;76(2):161–168.
- ,,.Bilateral massive adrenal hemorrhage. Assessment of putative risk factors by the case‐control method.Medicine.2001;80(1):45–53.
- .Bilateral massive adrenal hemorrhage.Med Clin North Am.1995;79(1):107–129.
- ,,.Bilateral massive adrenal hemorrhage: early recognition and treatment.Ann Intern Med.1989;110(3):227–235.
- ,,, et al.Imaging of nontraumatic hemorrhage of the adrenal gland.Radiographics.1999;19(4):949–963.
- ,,,,.Spontaneous unilateral adrenal hemorrhage: computerized tomography and magnetic resonance imaging findings in 8 cases.J Urol.1995;154(5):1647–1651.
- .Adrenal hemorrhage during anticoagulant therapy. A clinical and pathological study of ten cases.Ann Intern Med.1965;63(4):559–571.
- ,,,,,.Adrenal hemorrhage in the adult.Medicine.1978;57(3):211–221.
- ,,.Adrenal hemorrhage: a 25‐year experience at the Mayo Clinic.Mayo Clin Proc.2001;76(2):161–168.
- ,,.Bilateral massive adrenal hemorrhage. Assessment of putative risk factors by the case‐control method.Medicine.2001;80(1):45–53.
- .Bilateral massive adrenal hemorrhage.Med Clin North Am.1995;79(1):107–129.
- ,,.Bilateral massive adrenal hemorrhage: early recognition and treatment.Ann Intern Med.1989;110(3):227–235.
- ,,, et al.Imaging of nontraumatic hemorrhage of the adrenal gland.Radiographics.1999;19(4):949–963.
- ,,,,.Spontaneous unilateral adrenal hemorrhage: computerized tomography and magnetic resonance imaging findings in 8 cases.J Urol.1995;154(5):1647–1651.
Metastatic Lobular Breast Carcinoma
Gastric outlet obstruction (GOO) is frequently a diagnostic dilemma as malignancies have surpassed benign diseases as etiologies of GOO.1, 2 A case is presented of a previously healthy patient with persistent vomiting who was sequentially diagnosed with peptic ulcer disease (PUD), pancreatitis, and cholecystitis. Unfortunately, the diagnostic workup was less straightforward than initially suspected, as she was eventually diagnosed with a malignant GOO.
To the best of our knowledge, this is the second case in which GOO was the presenting manifestation of a previously undiagnosed metastatic lobular breast carcinoma.1 Although gastrointestinal involvement may be a late manifestation of metastatic breast carcinoma that almost always follows after spread to other sites, this case illustrates GOO as a presenting manifestation.3 Perhaps the most salient teaching point, consistent with recent literature, is that endoscopic biopsies in the workup of malignant GOO are often misleading and delay diagnosis.4
Case Report
A 44‐year‐old female with a history of fibrocystic breast disease presented with 1 month of right upper quadrant abdominal pain and nonbilious emesis of undigested food occurring several hours postprandially. Gallstones were demonstrated on an abdominal sonogram, and esophagogastroduodenoscopy revealed a normal proximal esophagus, distal esophagitis, and a Schatzki ring. An 8‐mm duodenal bulb ulcer was biopsied with benign results, but no duodenal obstruction or narrowing was visualized. Therapy for presumptive Helicobacter pylori infection and PUD was initiated, but she was hospitalized shortly later with persistent vomiting and acute renal failure. An abdominal computed tomography (CT) scan showed evidence of pancreatitis but a normal biliary system and normal small and large bowels. There was no clinical jaundice, and hepatic function tests were normal. After medical therapy, an open cholecystectomy was performed because of dense adhesions of the large and small bowels to the liver and gallbladder. No gross abnormalities of the common bile duct or intestines were described.
With the persistence of intractable vomiting, abdominal and pelvic CT scans were repeated and revealed duodenal thickening and luminal narrowing. Follow‐up abdominal magnetic resonance imaging (Figure 1) demonstrated an infiltrating duodenal mass with a resultant high‐grade GOO. Histological examination from repeat endoscopic biopsies of the duodenal mass revealed signet ring cells infiltrating the lamina propria with positive estrogen and progesterone receptors. Upon presentation to the surgical service, a physical examination revealed a right breast mass, and a subsequent breast biopsy diagnosed lobular breast carcinoma with 10% estrogen receptor and 5% progesterone receptor and histology identical to that of the duodenal mass. Immunohistochemical assays confirmed primary breast carcinoma with duodenal metastasis. A lumpectomy was performed, and docetaxel was initiated for stage IV invasive lobular breast carcinoma. A gastrostomy and duodenal stents were placed for the GOO with resolution of the vomiting, and she received hospice and palliative care.

Discussion
Prior to the advent of histamine blockers, PUD was the most common cause of GOO.1 Currently, malignancy accounts for 60% of cases of GOO.13 To the best of our knowledge, this patient's presentation represents the second case in which the initial manifestation of an undiagnosed metastatic breast disease was GOO.1 The diagnosis was both challenging and unusual because of the patient's other organic diseases (gallbladder disease, pancreatic disease, and PUD), which distracted from the underlying diagnosis of malignant GOO.
GOO is a clinical syndrome of diverse etiologies and pathogenesis that is characterized by mechanical impediment of gastric emptying. GOO is divided into 2 well‐defined groups: benign and malignant causes.14 Benign causes include: PUD, gastric polyps, pyloric stenosis, congenital duodenal webs, gallstone obstruction, pancreatic pseudocysts, and bezoars. Gastric cancer is the most common malignant cause and is followed by duodenal carcinoma, pancreatic carcinoma, cholangiocarcinoma, and metastatic disease of the gastric outlet.
Because of the stomach's significant capacity to distend, malignant GOO is often undetected clinically until a high‐grade obstruction develops.13 In patients with a previous diagnosis of carcinoma, nausea and vomiting can be mistakenly attributed to radiation or chemotherapy. Characteristic symptoms include nonbilious emesis of undigested food, early satiety, epigastric fullness, and abdominal pain.13
This case presentation is consistent with recent literature, which reports a surprising lack of reliability in diagnosing malignant GOO by endoscopy.4 In 1 study, endoscopic biopsy for detection of malignant GOO was associated with poor sensitivity (37%) in comparison with surgical biopsy.4 The authors recommended that patients who have a high clinical suspicion of malignant GOO (older patients and those without PUD) and who have initially benign biopsies be considered for surgical exploration prior to medical therapy or undergo repeat endoscopy with jumbo biopsies.4
Alternatively, endoscopic ultrasound has been advocated for detecting early mucosal gastric or duodenal cancer in patients without ulcerous changes on endoscopy. Radiographic features associated with submucosal tumor infiltration include irregular narrowing and budding signs.5 As conventional CT is considered suboptimal for the detection of gastric or intestinal carcinomas, multidetector‐row CT with multiplanar reconstruction has enhanced the overall ability to detect early gastric cancer and advanced gastric cancers with a sensitivity of 96.2%.6
Conclusion
The preceding case demonstrates valuable teaching points encountered in diagnosing malignant GOO. In patients with intractable vomiting severe enough to produce renal failure, other organic causes should be considered before one proceeds directly to cholecystectomy. This case further confirms that endoscopic biopsy is often alarmingly inadequate for diagnosing malignant GOO.46 Thus, if worrisome symptoms persist, the provider should not be comforted by normal endoscopy and should escalate investigations accordingly. More clinical trials should evaluate the roles of endoscopic ultrasound and multidetector‐row CT in the early detection of gastric and duodenal carcinoma in patients with normal endoscopic biopsies, which may have led to a more timely diagnosis in this patient.5, 6
- ,,, et al.Previously undiagnosed infiltrating lobular carcinoma of the breast presenting as a gastric outlet obstruction.Am J Gastroenterol.2001;12:3475–3477.
- ,,, et al.Breast cancer masquerading as primary gastric carcinoma.Aust N Z J Surg.1986;56:398–399.
- ,,, et al.The spectrum of gastrointestinal metastases of breast carcinoma: stomach.Gastrointest Endosc.1992;38:130–135.
- ,,.Gastric outlet obstruction with benign endoscopic biopsy should be further explored for malignancy.Gastrointest Endosc.1998;48:497–502.
- ,.The accuracy of endoscopic ultrasonography in differentiating mucosal from deeper gastric cancer.Am J Gastroenterol.2008;103:1801–1809.
- ,,, et al.Diagnosis of gastric cancer with MDCT using the water filling method and multiplanar reconstruction: CT histologic correlation.Am J Roentgenol.2005;185:1152–1158.
Gastric outlet obstruction (GOO) is frequently a diagnostic dilemma as malignancies have surpassed benign diseases as etiologies of GOO.1, 2 A case is presented of a previously healthy patient with persistent vomiting who was sequentially diagnosed with peptic ulcer disease (PUD), pancreatitis, and cholecystitis. Unfortunately, the diagnostic workup was less straightforward than initially suspected, as she was eventually diagnosed with a malignant GOO.
To the best of our knowledge, this is the second case in which GOO was the presenting manifestation of a previously undiagnosed metastatic lobular breast carcinoma.1 Although gastrointestinal involvement may be a late manifestation of metastatic breast carcinoma that almost always follows after spread to other sites, this case illustrates GOO as a presenting manifestation.3 Perhaps the most salient teaching point, consistent with recent literature, is that endoscopic biopsies in the workup of malignant GOO are often misleading and delay diagnosis.4
Case Report
A 44‐year‐old female with a history of fibrocystic breast disease presented with 1 month of right upper quadrant abdominal pain and nonbilious emesis of undigested food occurring several hours postprandially. Gallstones were demonstrated on an abdominal sonogram, and esophagogastroduodenoscopy revealed a normal proximal esophagus, distal esophagitis, and a Schatzki ring. An 8‐mm duodenal bulb ulcer was biopsied with benign results, but no duodenal obstruction or narrowing was visualized. Therapy for presumptive Helicobacter pylori infection and PUD was initiated, but she was hospitalized shortly later with persistent vomiting and acute renal failure. An abdominal computed tomography (CT) scan showed evidence of pancreatitis but a normal biliary system and normal small and large bowels. There was no clinical jaundice, and hepatic function tests were normal. After medical therapy, an open cholecystectomy was performed because of dense adhesions of the large and small bowels to the liver and gallbladder. No gross abnormalities of the common bile duct or intestines were described.
With the persistence of intractable vomiting, abdominal and pelvic CT scans were repeated and revealed duodenal thickening and luminal narrowing. Follow‐up abdominal magnetic resonance imaging (Figure 1) demonstrated an infiltrating duodenal mass with a resultant high‐grade GOO. Histological examination from repeat endoscopic biopsies of the duodenal mass revealed signet ring cells infiltrating the lamina propria with positive estrogen and progesterone receptors. Upon presentation to the surgical service, a physical examination revealed a right breast mass, and a subsequent breast biopsy diagnosed lobular breast carcinoma with 10% estrogen receptor and 5% progesterone receptor and histology identical to that of the duodenal mass. Immunohistochemical assays confirmed primary breast carcinoma with duodenal metastasis. A lumpectomy was performed, and docetaxel was initiated for stage IV invasive lobular breast carcinoma. A gastrostomy and duodenal stents were placed for the GOO with resolution of the vomiting, and she received hospice and palliative care.
Discussion
Prior to the advent of histamine blockers, PUD was the most common cause of GOO.1 Currently, malignancy accounts for 60% of cases of GOO.13 To the best of our knowledge, this patient's presentation represents the second case in which the initial manifestation of an undiagnosed metastatic breast disease was GOO.1 The diagnosis was both challenging and unusual because of the patient's other organic diseases (gallbladder disease, pancreatic disease, and PUD), which distracted from the underlying diagnosis of malignant GOO.
GOO is a clinical syndrome of diverse etiologies and pathogenesis that is characterized by mechanical impediment of gastric emptying. GOO is divided into 2 well‐defined groups: benign and malignant causes.14 Benign causes include: PUD, gastric polyps, pyloric stenosis, congenital duodenal webs, gallstone obstruction, pancreatic pseudocysts, and bezoars. Gastric cancer is the most common malignant cause and is followed by duodenal carcinoma, pancreatic carcinoma, cholangiocarcinoma, and metastatic disease of the gastric outlet.
Because of the stomach's significant capacity to distend, malignant GOO is often undetected clinically until a high‐grade obstruction develops.13 In patients with a previous diagnosis of carcinoma, nausea and vomiting can be mistakenly attributed to radiation or chemotherapy. Characteristic symptoms include nonbilious emesis of undigested food, early satiety, epigastric fullness, and abdominal pain.13
This case presentation is consistent with recent literature, which reports a surprising lack of reliability in diagnosing malignant GOO by endoscopy.4 In 1 study, endoscopic biopsy for detection of malignant GOO was associated with poor sensitivity (37%) in comparison with surgical biopsy.4 The authors recommended that patients who have a high clinical suspicion of malignant GOO (older patients and those without PUD) and who have initially benign biopsies be considered for surgical exploration prior to medical therapy or undergo repeat endoscopy with jumbo biopsies.4
Alternatively, endoscopic ultrasound has been advocated for detecting early mucosal gastric or duodenal cancer in patients without ulcerous changes on endoscopy. Radiographic features associated with submucosal tumor infiltration include irregular narrowing and budding signs.5 As conventional CT is considered suboptimal for the detection of gastric or intestinal carcinomas, multidetector‐row CT with multiplanar reconstruction has enhanced the overall ability to detect early gastric cancer and advanced gastric cancers with a sensitivity of 96.2%.6
Conclusion
The preceding case demonstrates valuable teaching points encountered in diagnosing malignant GOO. In patients with intractable vomiting severe enough to produce renal failure, other organic causes should be considered before one proceeds directly to cholecystectomy. This case further confirms that endoscopic biopsy is often alarmingly inadequate for diagnosing malignant GOO.46 Thus, if worrisome symptoms persist, the provider should not be comforted by normal endoscopy and should escalate investigations accordingly. More clinical trials should evaluate the roles of endoscopic ultrasound and multidetector‐row CT in the early detection of gastric and duodenal carcinoma in patients with normal endoscopic biopsies, which may have led to a more timely diagnosis in this patient.5, 6
Gastric outlet obstruction (GOO) is frequently a diagnostic dilemma as malignancies have surpassed benign diseases as etiologies of GOO.1, 2 A case is presented of a previously healthy patient with persistent vomiting who was sequentially diagnosed with peptic ulcer disease (PUD), pancreatitis, and cholecystitis. Unfortunately, the diagnostic workup was less straightforward than initially suspected, as she was eventually diagnosed with a malignant GOO.
To the best of our knowledge, this is the second case in which GOO was the presenting manifestation of a previously undiagnosed metastatic lobular breast carcinoma.1 Although gastrointestinal involvement may be a late manifestation of metastatic breast carcinoma that almost always follows after spread to other sites, this case illustrates GOO as a presenting manifestation.3 Perhaps the most salient teaching point, consistent with recent literature, is that endoscopic biopsies in the workup of malignant GOO are often misleading and delay diagnosis.4
Case Report
A 44‐year‐old female with a history of fibrocystic breast disease presented with 1 month of right upper quadrant abdominal pain and nonbilious emesis of undigested food occurring several hours postprandially. Gallstones were demonstrated on an abdominal sonogram, and esophagogastroduodenoscopy revealed a normal proximal esophagus, distal esophagitis, and a Schatzki ring. An 8‐mm duodenal bulb ulcer was biopsied with benign results, but no duodenal obstruction or narrowing was visualized. Therapy for presumptive Helicobacter pylori infection and PUD was initiated, but she was hospitalized shortly later with persistent vomiting and acute renal failure. An abdominal computed tomography (CT) scan showed evidence of pancreatitis but a normal biliary system and normal small and large bowels. There was no clinical jaundice, and hepatic function tests were normal. After medical therapy, an open cholecystectomy was performed because of dense adhesions of the large and small bowels to the liver and gallbladder. No gross abnormalities of the common bile duct or intestines were described.
With the persistence of intractable vomiting, abdominal and pelvic CT scans were repeated and revealed duodenal thickening and luminal narrowing. Follow‐up abdominal magnetic resonance imaging (Figure 1) demonstrated an infiltrating duodenal mass with a resultant high‐grade GOO. Histological examination from repeat endoscopic biopsies of the duodenal mass revealed signet ring cells infiltrating the lamina propria with positive estrogen and progesterone receptors. Upon presentation to the surgical service, a physical examination revealed a right breast mass, and a subsequent breast biopsy diagnosed lobular breast carcinoma with 10% estrogen receptor and 5% progesterone receptor and histology identical to that of the duodenal mass. Immunohistochemical assays confirmed primary breast carcinoma with duodenal metastasis. A lumpectomy was performed, and docetaxel was initiated for stage IV invasive lobular breast carcinoma. A gastrostomy and duodenal stents were placed for the GOO with resolution of the vomiting, and she received hospice and palliative care.
Discussion
Prior to the advent of histamine blockers, PUD was the most common cause of GOO.1 Currently, malignancy accounts for 60% of cases of GOO.13 To the best of our knowledge, this patient's presentation represents the second case in which the initial manifestation of an undiagnosed metastatic breast disease was GOO.1 The diagnosis was both challenging and unusual because of the patient's other organic diseases (gallbladder disease, pancreatic disease, and PUD), which distracted from the underlying diagnosis of malignant GOO.
GOO is a clinical syndrome of diverse etiologies and pathogenesis that is characterized by mechanical impediment of gastric emptying. GOO is divided into 2 well‐defined groups: benign and malignant causes.14 Benign causes include: PUD, gastric polyps, pyloric stenosis, congenital duodenal webs, gallstone obstruction, pancreatic pseudocysts, and bezoars. Gastric cancer is the most common malignant cause and is followed by duodenal carcinoma, pancreatic carcinoma, cholangiocarcinoma, and metastatic disease of the gastric outlet.
Because of the stomach's significant capacity to distend, malignant GOO is often undetected clinically until a high‐grade obstruction develops.13 In patients with a previous diagnosis of carcinoma, nausea and vomiting can be mistakenly attributed to radiation or chemotherapy. Characteristic symptoms include nonbilious emesis of undigested food, early satiety, epigastric fullness, and abdominal pain.13
This case presentation is consistent with recent literature, which reports a surprising lack of reliability in diagnosing malignant GOO by endoscopy.4 In 1 study, endoscopic biopsy for detection of malignant GOO was associated with poor sensitivity (37%) in comparison with surgical biopsy.4 The authors recommended that patients who have a high clinical suspicion of malignant GOO (older patients and those without PUD) and who have initially benign biopsies be considered for surgical exploration prior to medical therapy or undergo repeat endoscopy with jumbo biopsies.4
Alternatively, endoscopic ultrasound has been advocated for detecting early mucosal gastric or duodenal cancer in patients without ulcerous changes on endoscopy. Radiographic features associated with submucosal tumor infiltration include irregular narrowing and budding signs.5 As conventional CT is considered suboptimal for the detection of gastric or intestinal carcinomas, multidetector‐row CT with multiplanar reconstruction has enhanced the overall ability to detect early gastric cancer and advanced gastric cancers with a sensitivity of 96.2%.6
Conclusion
The preceding case demonstrates valuable teaching points encountered in diagnosing malignant GOO. In patients with intractable vomiting severe enough to produce renal failure, other organic causes should be considered before one proceeds directly to cholecystectomy. This case further confirms that endoscopic biopsy is often alarmingly inadequate for diagnosing malignant GOO.46 Thus, if worrisome symptoms persist, the provider should not be comforted by normal endoscopy and should escalate investigations accordingly. More clinical trials should evaluate the roles of endoscopic ultrasound and multidetector‐row CT in the early detection of gastric and duodenal carcinoma in patients with normal endoscopic biopsies, which may have led to a more timely diagnosis in this patient.5, 6
- ,,, et al.Previously undiagnosed infiltrating lobular carcinoma of the breast presenting as a gastric outlet obstruction.Am J Gastroenterol.2001;12:3475–3477.
- ,,, et al.Breast cancer masquerading as primary gastric carcinoma.Aust N Z J Surg.1986;56:398–399.
- ,,, et al.The spectrum of gastrointestinal metastases of breast carcinoma: stomach.Gastrointest Endosc.1992;38:130–135.
- ,,.Gastric outlet obstruction with benign endoscopic biopsy should be further explored for malignancy.Gastrointest Endosc.1998;48:497–502.
- ,.The accuracy of endoscopic ultrasonography in differentiating mucosal from deeper gastric cancer.Am J Gastroenterol.2008;103:1801–1809.
- ,,, et al.Diagnosis of gastric cancer with MDCT using the water filling method and multiplanar reconstruction: CT histologic correlation.Am J Roentgenol.2005;185:1152–1158.
- ,,, et al.Previously undiagnosed infiltrating lobular carcinoma of the breast presenting as a gastric outlet obstruction.Am J Gastroenterol.2001;12:3475–3477.
- ,,, et al.Breast cancer masquerading as primary gastric carcinoma.Aust N Z J Surg.1986;56:398–399.
- ,,, et al.The spectrum of gastrointestinal metastases of breast carcinoma: stomach.Gastrointest Endosc.1992;38:130–135.
- ,,.Gastric outlet obstruction with benign endoscopic biopsy should be further explored for malignancy.Gastrointest Endosc.1998;48:497–502.
- ,.The accuracy of endoscopic ultrasonography in differentiating mucosal from deeper gastric cancer.Am J Gastroenterol.2008;103:1801–1809.
- ,,, et al.Diagnosis of gastric cancer with MDCT using the water filling method and multiplanar reconstruction: CT histologic correlation.Am J Roentgenol.2005;185:1152–1158.

Patient Satisfaction—Hospitalists
Patient satisfaction is an important issue for hospitals, as it may affect the decision to seek care at one institution over another, but it may soon have direct implications for hospital reimbursement with the recent proposals for Value Based Purchasing (VBP) models by the Centers for Medicare and Medicaid Services (CMS). Up to 5% of inpatient Medicare reimbursement would be linked to performance measures, 40% of which could come from percentile outcomes on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) alone.1 HCAHPS scores are now available for individual hospitals at the Hospital Compare website maintained by CMS (
While the information garnered from the HCAHPS provides an external perception of hospital quality, the questions are broad and do not identify specific reasons for reduced satisfaction. Many have suggested that the incorporation of surveys already administered at hospitals may be required for successful HCAHPS administration in order to overcome the limitations inherent in its design.2
In order to identify explanatory factors for low HCAHPS scores, we decided to incorporate a technique known as a cognitive interview (CI). The CI is widely used as an evaluative tool for survey questions because of its ability to allow the interviewer to discern the processes that lead to responses.3 Up to this point, the focus of this CI method has been on the ability of the subject to comprehend and answer the questions.4 However, when a CI subject is answering a question, there is a large amount of information presented to the interviewer about the topic that is typically regarded as supplementary because of the focus on these specific issues.5 This study reports the supplemental information that may provide insight as to why patients answered as they did. Our goal was to gain further understanding of factors that may underlie HCAHPS responses.
Materials and Methods
Overview
The premise behind every step in the development and implementation of the interview process was to increase the comfort level of the patients with the process as well as take as much of the cognitive burden off of the patients as possible while maintaining the integrity of the questioning.
The study was developed and conducted in May and June 2008. The duration of the study and number of participants were based on time constraints on personnel and limited funding for the study.
Development of the Interview
We used the HCAHPS questions as a starting point to launch the development of our interview. Because the purpose of this study was to generate hypotheses regarding issues affecting patient satisfaction, we used a loose approach to questioning that gave the interview subject a greater degree of freedom with their answers than in a measurement study. This freedom of response eliminated the need to take minor comprehension issues into account, which would have been cause for concern using a standard survey.5
We focused on what the patients thought or felt in order to avoid making them feel overburdened for factual recall. There were some questions for which this was not possible (eg, the questions about medication). After the questions were reworded, their comprehension level was confirmed to be appropriate for the local community (grade 3‐6) using the Flesch Reading Ease and Flesch‐Kincaid grade level equations (data not shown).
The questions were then grouped from least cognitively intense to most cognitively intense surrounding any particular issue, which was generally least specific to most specific. This process of ordering questions has been shown to increase the accuracy of self reports,6 which is advantageous in our situation because it increases the amount of potentially useful information the patients include in their perception analysis. Every major section change started with at least 1 general question without specific aim in order to facilitate free response (full interview is included as Appendix 1).
For classic quantitative analysis, the 4 HCAHPS categories (always, usually, sometimes, never) were presented for most of the questions. They are reported in this work as Top Box, (ie, always), or Not Top Box (any other response). Top Box responses are the ratings most widely reported in HCAHPS surveys, and this dichotomy makes it easier to code and review answers. However, when we felt that quantitatively we wanted a more superficial inquiry, a 2‐category yes/no system was used. The interviews were also designed to be less than 1 hour in length, which has been shown to be appropriate in other kinds of cognitive studies in the medical field.7
The questions in the About You section of the HCAHPS were largely excluded with the exception of the education demographic question (for a full HCAHPS survey see Goldstein et al.).2 The community that we studied is quite homogeneously Caucasian and non‐Hispanic. Education level is the only remaining HCAHPS demographic variable, and our subjects had education levels comparable to those reported in HCAHPS for this hospital. Our data are primarily qualitative and were not weighted as the HCAHPS data were.8
Conducting the Interviews
The interviews were conducted by the principal researcher (A.B.) (the use of a single interviewer eliminates potential bias between interviewers on interview delivery) on medical and surgical inpatients in general inpatient and intensive care units who were at least 18 years old, not suffering significant discomfort, and able to comprehend questions and provide meaningful answers. The nurse managers on the inpatient units were asked to identify patients who fit these criteria. Of the 50 patients typically present on medical/surgical services, about 10 would be suitable for interview. The researcher would then select up to 5 patients each weekday from those actually present in their rooms, explain that he was doing research for the hospital, and ask if the patient would participate. The range of the number of selected patients depended upon the willingness of the available patients to participate and the amount of time it took to conduct the interviews. If the patient accepted, the researcher then emphasized that participation was completely optional and would have no effect on the medical care the patient would receive, that the identity of the patient would never be shared, and that the information provided would be used internally and possibly for anonymous external reporting. The researcher then asked if the patient would still like to continue. This protocol was approved by the hospital Institutional Review Board.
The patients were then instructed to think aloud as they answered questions and given Think Aloud Training using established methods.9 There were 4 instructions or questions in the training that were used sequentially, as follows: (1) Try to picture the place where you live, and think about how many windows there are in that place. As you count up the windows, tell me what you are seeing and thinking about;9 (2) I want you to think about the last school you personally went to and studied at. Think about yourself walking into the main building. Tell me what you are seeing and thinking about as you walk through the doors; (3) Now I want you to think about your favorite food. Can you tell me about it? and (4) I want you to think about a pot of flowers. Tell me about what you think and see as you walk up and smell the flowers. While the patients were thinking, the interviewer followed up with spontaneous general verbal probes (eg, Can you tell me what you are thinking?). After the patients were responding adequately to the training instructions, we proceeded to the interview.
The interviews were conducted by asking the patients the designed questions using a Think Aloud CI technique and spontaneous verbal probing in the instance of a seeming lack of information, inconsistency in information offered by the patient, indicative body language (eg, seeming uncomfortable), hesitation indicating the patient was not rendering all of the information that he or she was thinking, or if a common specific issue had been previously identified. Because we were looking for issues adversely affecting patient satisfaction, we decided to optimize our effort by focusing on questions to which patients responded negatively or hesitantly. However, as time permitted we also gave attention to questions patients answered immediately and positively.
Data Collection
Data were collected on interview sheets containing the questions asked to the patients with the Top Box/Not Top Box coding method described above, as well as a section for qualitative data gleaned from the cognitive elements of the interview. Recordings and full transcriptions were not performed to avoid raising patient concerns, which held the potential to negatively impact participation. All records of participant names were kept solely by the principal investigator to avoid duplicate interviews and were destroyed at the conclusion of the interview process.
Analysis
The data was collected from the interview sheets and then compiled into a spreadsheet. The classic quantitative data was compiled into raw totals and percentages. The qualitative data from the cognitive portion was then considered both separately, based on the question, and as a group. Both authors reviewed the data and identified significant items in both the qualitative and quantitative data, based on their ability to provide useful hypotheses regarding higher or lower levels of satisfaction. Also, because of the nature of the CI, useful information can come from as few as 1 respondent,9 so potentially useful individual comments were pulled out of the qualitative data as well.
It is important to note that this study is not a means of measuring patient satisfaction, but rather a means of determining elements and specific issues affecting patient satisfaction. Answers in this study cannot be considered equivalent to answers on the HCAHPS or any other patient satisfaction survey.
Results
Response Rate
There were 57 eligible patients who were asked to participate in this study. Availability of the patients identified as eligible limited the number of participants. Of the 57, 50 accepted. Of the 50 who accepted, 1 was rejected because the patient had only been at the hospital for a few hours and had not seen a physician yet, and 5 more opted to stop before the interview was completed. The 1 that was rejected was not included in the analysis, but the 5 that were left incomplete were included for the questions that had been answered.
Responsiveness to Questions
Patients were asked Did you get all of your questions answered? (Table 1). The responsiveness to questions by our staff was largely satisfactory, but the qualitative data yielded an interesting finding in that 3 of the 6 patients who rendered Not Top Box answers cited problems with question delivery. One patient said, The doctor was just in and out, and I didn't have time to ask questions. Another said, I think of questions 20 minutes after the doctor leaves. In other parts of the interview, 2 more patients mentioned not having questions ready when their attending physician was there, and then not being able to ask them, 1 of them saying, It was my own fault (when I did not get information I wanted) because I didn't ask all of the questions.
| Questions Asked of Patients | Responses | Number | Qualitative Subtheme |
|---|---|---|---|
| |||
| Did you get all of your questions answered? | Always | 41 | Difficulty with question delivery: (eg, I think of questions 20 minutes after the doctor leaves.) |
| Never, sometimes, usually | 6 | ||
| Total | 47 | ||
| Did anyone tell you what [the new medicine] was before they gave it to you? | Yes | 29 | |
| No | 2 | ||
| Total | 31 | ||
| Did anyone tell you about any side effects of the medicine? | Yes | 17 | Lack of communication regarding medicines with few major side effects: (eg, Tylenol or Advil) |
| No | 13 | ||
| Total | 31 | ||
| Do you feel the doctors spend enough time with you? | Yes | 37 | For example: (My doctor) didn't consult me and he didn't inform me. |
| No | 8 | ||
| Total | 45 | ||
| Do you feel the doctors know you as a person? | Yes | 29 | Physician behaviors may influence: (eg, He treats me as a person.) |
| No | 16 | ||
| Total | 45 | ||
| Do you feel the doctors treat you with respect? | Always | 40 | Physician behaviors may influence: (eg, I feel talked down too, like I can't handle the answers.) |
| Never, sometimes, usually | 6 | ||
| Total | 46 | ||
| Do you think the doctors listen carefully to you? | Always | 33 | For example: He had so much on his mind. |
| Never, sometimes, usually | 13 | ||
| Total | 46 | ||
Communication Regarding Medication
There are 2 important questions regarding this issue. Patients who reported taking new medication during their current hospital stay were asked, Did anyone tell you what [the new medication] was for before they gave it to you? and then, Did anyone tell you about any side effects of the medicine? (Table 1). From this we can see that, generally, patients are informed about new medications, but there seems to be a lack of informing the patients regarding side effects of new medications. Interestingly, 8 of the patients who reported that they were not told about side effects raised concerns about medications that have few major side effects. It is important to note that this issue was not initially known and the kind of medication the patients were given was seldom freely offered. We began specifically probing for it after a patient offered the information without prompting, so the actual number of these instances could be much higher.
Perception of Time Spent
We asked our subjects Do you feel the doctors spend enough time with you? (Table 1). The sensitivity of the quantitative data was decreased by using a 2‐category approach, but frequency estimation about an issue of time seemed an unnecessarily awkward approach considering that the more valuable information comes from the qualitative section of the interview.
The perception of enough time spent by physicians was not felt by all of the subjects. Three of the patients who answered No had mentioned a specific need that was not met, all 3 of which were issues with information and communication. The hospitalist changed all of my medicationshe didn't consult me, and he didn't inform me, said 1 patient. Another said, I don't really know who my doctor is, in reference to his attending hospitalist. There was another patient who answered No who felt that the physicians were just mechanically trying to treat his condition and discharge him as soon as possible. I think the hospital is getting the doctors to push people outthey need the beds. Also, 2 patients who answered Yes acknowledged that the doctors spent all the time they needed to for the patients' situations, and 1 patient who answered Yes mentioned a specific personal accommodation the physician made, specifically that the physician prays with the patient.
Personal Connections
This question was, Do you feel the doctors know you as a person? and was included to attempt to probe into the depth of the personal connections formed by our physicians. The standard quantitative data (Table 1) shows there were a significant number of patients who did not feel their physicians knew them as a person. Six of the patients who answered No said they felt the physicians were just doing their job. What else are you besides a body and a diagnosis? 1 patient asked. They are doing their job, said another. Six patients who answered Yes cited how their physicians acted toward them as the reason. One patient responded, One doctor carries on extra conversation with me. He knows me as a person. Another patient plainly said, He treats me as a person. Yet another said, They seem to respect my situation and my need for their services.
Nonclinical Competency
Two questions elicited significant information relevant to hospitalists on this issue, the first being Do you feel the doctors treat you with respect? and the second being Do you think the doctors listen carefully to you? (Table 1).
The standard quantitative data for the first question shows that, generally, our patients felt as though the doctors were treating them with respect. Interestingly, the qualitative portion of the study shows that all 6 patients who rendered Not Top Box answers mentioned either being talked down to or not being responded to by their physicians. The hospitalist treated me as I expected, as [a generic 50‐year‐old], remarked 1 patient about her hospitalist, by whom she felt ignored. I feel talked down too, like I can't handle the answers. I feel like I don't always get the full truth, said another patient regarding her physician telling her about her medical condition. It seems like the doctor put me off, said a third patient regarding his physician's willingness to treat him.
The quantitative data for the second question shows much weaker performance with regard to the perception of the doctors listening to the patients. The qualitative portion of the study shows that 3 patients mentioned how much their physicians had on their minds. One patient said, He was thinking so many things at the same time, and another plainly said, He had so much on his mind. Four patients mentioned not feeling responded to by their physicians. A patient commented, I would say something (to the doctor), and then my dad would [sic] re‐say it, and the doctor would respond when my dad said it, but not when I did. Another patient responded, I would ask (the doctors) to do something, and they wouldn't do it.
Discussion
Because of the limitations inherent in typical survey measures of investigation, we employed a CI technique. The objective was to generate hypotheses as to why patients may report reduced satisfaction with various aspects of hospitalization. The data set gleaned from this study was sizable, and held information pertinent to all parts of the hospital. The results reported in this article are focused on hospitalists.
The quantity of time hospitalists spend with patients may not be as important to the patients as the quality of interaction. Other studies have shown similar results, illustrating that the key factor in a patients' opinion of a visit with a physician was the perception of being taken seriously.10 The perception of being talked down to (as noted by Levy11) and the perception of not being responded to or focused on are the key negative factors for patients. By interacting with patients in a way that makes them feel valued, focused on, and responded to, physicians may improve patient satisfaction without requiring increased amounts of time spent with them.
Patient complaints that physicians do not respond to them may partially reflect inability to ask all of their questions. Hospitals may wish to consider methods to improve the ability of the patients to ask questions in the small amount of time available for physicians to talk with them (eg, placing notebooks by patients' bedsides and repeatedly encouraging them to write their questions down). This concept has also been endorsed as a means of improving the quality of care and reducing medical mistakes.12
Hospitalists and other physicians may positively impact the communication about medication issues by establishing a protocol for communicating major as well as minor side effects or even the lack of side effects of medication to patients. The challenge lies in determining the level of incidence that is significant enough (eg, 10%, 5%, or 1%) to warrant explaining minor side effects.
The findings of this study are limited by its small size, qualitative nature, nonrepresentative population, and loose approach to questioning. The patient responses were transcribed manually by the interviewer, leaving the possibility that some responses were not accurately recorded. Our survey instrument is not validated, and the results may not generalize to other settings. Instead of taking these findings as conclusive, we present them as suggestions for improvement that may be validated by further research.
Acknowledgements
The authors Tom Quinn and Toni Murdough for their contributions in developing the survey instrument.
Appendix
Appendix 1. Interview questions in the order they were presented to the patients
Background Questions
What is your name?
About how many hospital visits have you had in the last 6 months?
What is the highest grade or level of school that you have completed?
General Hospital Questions
What are the most important things you want in a hospital?
What do you think about the reputation of the hospital?
How has your stay here at the hospital been?
While you've been here, have you had any pain? Were you given any pain medicine? How well was your pain controlled? (The first two questions were for screening, the last question was for coding)
During this hospital stay, were you given any medicine that you had not taken before? Did anyone tell you what it was for before they gave it to you? Did anyone tell you about any side effects of the medicine? (First question for screening, last two for coding)
Do you think your room and bathroom are clean? Has it been that way the whole time you've been here?
Do you think this hospital has all the equipment needed for your treatment?
Do you feel you've been able to rest while you've been here?
Have you ever pressed the call button? How fast did the help come? Did it come as soon as you wanted it? (The first question was for screening, the second for insight, the third for coding)
While you were here at the hospital, did you ever need help getting to the bathroom or using a bedpan? How fast did you get help? Did help come as soon as you wanted it? (The first question was for screening, the second for insight, the third for coding)
Do you feel the staff paid attention to you?
Did you get all of your questions answered?
Have you had any problems here at the hospital? Did anybody help you with it? (The first question was for screening, the second for coding)
Nursing Staff Questions
What do you think about your nurses?
Do you feel the nurses treat you with respect?
Do you think the nurses listen carefully to you?
Did the nurses explain things in a way you could understand?
Did you get all the information you wanted from the nurses about your tests or treatments?
Do the nurses make you feel calm and safe while you are here at the hospital?
Do you feel the nurses know you as a person?
Do the nurses seem interested in doing things for you?
Do you feel the nurses spend enough time with you?
Have you ever had a change of nurses while you were here? Do you feel like the new nurse knew what the other nurse knew about you? Did the new nurse seem to know your situation? (The first question is for screening, the next two for coding)
What do you feel about the skill of your nurses here at the hospital?
Physician Staff Questions
What do you think about your doctors?
Do you feel the doctors treat you with respect?
Do you think the doctors listen carefully to you?
Did the doctors explain things in a way you could understand?
Did you get all the information you wanted from the doctors about your tests or treatments?
Do the doctors make you feel calm and safe while you are here at the hospital?
Do you feel the doctors know you as a person?
Did the doctors seem interested in doing things for you?
Do you feel the doctors spend enough time with you?
Have you ever been switched between doctors here at the hospital? Do you feel like the new doctor knew what the other doctor knew about you? Did the new doctor seem to know your situation? (The first question was for screening, the next two for coding)
Were you ever switched from your primary doctor to a doctor here at the hospital? Do you feel like the new doctor knew what your primary doctor knew about your medical situation? (The first question was for screening, the second question for coding)
What do you feel about the skill of your doctors here at the hospital?
Cumulative Hospital Questions
Did you see any hospital staff disagree with each other about your medical treatment?
On a scale of 1‐10, how would you rate the hospital?
Is there anything that we haven't talked about that would keep you from rating us a 10?
Would you recommend this hospital to your friends and family?
What can we do to make this the best hospital around?
Patient satisfaction is an important issue for hospitals, as it may affect the decision to seek care at one institution over another, but it may soon have direct implications for hospital reimbursement with the recent proposals for Value Based Purchasing (VBP) models by the Centers for Medicare and Medicaid Services (CMS). Up to 5% of inpatient Medicare reimbursement would be linked to performance measures, 40% of which could come from percentile outcomes on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) alone.1 HCAHPS scores are now available for individual hospitals at the Hospital Compare website maintained by CMS (
While the information garnered from the HCAHPS provides an external perception of hospital quality, the questions are broad and do not identify specific reasons for reduced satisfaction. Many have suggested that the incorporation of surveys already administered at hospitals may be required for successful HCAHPS administration in order to overcome the limitations inherent in its design.2
In order to identify explanatory factors for low HCAHPS scores, we decided to incorporate a technique known as a cognitive interview (CI). The CI is widely used as an evaluative tool for survey questions because of its ability to allow the interviewer to discern the processes that lead to responses.3 Up to this point, the focus of this CI method has been on the ability of the subject to comprehend and answer the questions.4 However, when a CI subject is answering a question, there is a large amount of information presented to the interviewer about the topic that is typically regarded as supplementary because of the focus on these specific issues.5 This study reports the supplemental information that may provide insight as to why patients answered as they did. Our goal was to gain further understanding of factors that may underlie HCAHPS responses.
Materials and Methods
Overview
The premise behind every step in the development and implementation of the interview process was to increase the comfort level of the patients with the process as well as take as much of the cognitive burden off of the patients as possible while maintaining the integrity of the questioning.
The study was developed and conducted in May and June 2008. The duration of the study and number of participants were based on time constraints on personnel and limited funding for the study.
Development of the Interview
We used the HCAHPS questions as a starting point to launch the development of our interview. Because the purpose of this study was to generate hypotheses regarding issues affecting patient satisfaction, we used a loose approach to questioning that gave the interview subject a greater degree of freedom with their answers than in a measurement study. This freedom of response eliminated the need to take minor comprehension issues into account, which would have been cause for concern using a standard survey.5
We focused on what the patients thought or felt in order to avoid making them feel overburdened for factual recall. There were some questions for which this was not possible (eg, the questions about medication). After the questions were reworded, their comprehension level was confirmed to be appropriate for the local community (grade 3‐6) using the Flesch Reading Ease and Flesch‐Kincaid grade level equations (data not shown).
The questions were then grouped from least cognitively intense to most cognitively intense surrounding any particular issue, which was generally least specific to most specific. This process of ordering questions has been shown to increase the accuracy of self reports,6 which is advantageous in our situation because it increases the amount of potentially useful information the patients include in their perception analysis. Every major section change started with at least 1 general question without specific aim in order to facilitate free response (full interview is included as Appendix 1).
For classic quantitative analysis, the 4 HCAHPS categories (always, usually, sometimes, never) were presented for most of the questions. They are reported in this work as Top Box, (ie, always), or Not Top Box (any other response). Top Box responses are the ratings most widely reported in HCAHPS surveys, and this dichotomy makes it easier to code and review answers. However, when we felt that quantitatively we wanted a more superficial inquiry, a 2‐category yes/no system was used. The interviews were also designed to be less than 1 hour in length, which has been shown to be appropriate in other kinds of cognitive studies in the medical field.7
The questions in the About You section of the HCAHPS were largely excluded with the exception of the education demographic question (for a full HCAHPS survey see Goldstein et al.).2 The community that we studied is quite homogeneously Caucasian and non‐Hispanic. Education level is the only remaining HCAHPS demographic variable, and our subjects had education levels comparable to those reported in HCAHPS for this hospital. Our data are primarily qualitative and were not weighted as the HCAHPS data were.8
Conducting the Interviews
The interviews were conducted by the principal researcher (A.B.) (the use of a single interviewer eliminates potential bias between interviewers on interview delivery) on medical and surgical inpatients in general inpatient and intensive care units who were at least 18 years old, not suffering significant discomfort, and able to comprehend questions and provide meaningful answers. The nurse managers on the inpatient units were asked to identify patients who fit these criteria. Of the 50 patients typically present on medical/surgical services, about 10 would be suitable for interview. The researcher would then select up to 5 patients each weekday from those actually present in their rooms, explain that he was doing research for the hospital, and ask if the patient would participate. The range of the number of selected patients depended upon the willingness of the available patients to participate and the amount of time it took to conduct the interviews. If the patient accepted, the researcher then emphasized that participation was completely optional and would have no effect on the medical care the patient would receive, that the identity of the patient would never be shared, and that the information provided would be used internally and possibly for anonymous external reporting. The researcher then asked if the patient would still like to continue. This protocol was approved by the hospital Institutional Review Board.
The patients were then instructed to think aloud as they answered questions and given Think Aloud Training using established methods.9 There were 4 instructions or questions in the training that were used sequentially, as follows: (1) Try to picture the place where you live, and think about how many windows there are in that place. As you count up the windows, tell me what you are seeing and thinking about;9 (2) I want you to think about the last school you personally went to and studied at. Think about yourself walking into the main building. Tell me what you are seeing and thinking about as you walk through the doors; (3) Now I want you to think about your favorite food. Can you tell me about it? and (4) I want you to think about a pot of flowers. Tell me about what you think and see as you walk up and smell the flowers. While the patients were thinking, the interviewer followed up with spontaneous general verbal probes (eg, Can you tell me what you are thinking?). After the patients were responding adequately to the training instructions, we proceeded to the interview.
The interviews were conducted by asking the patients the designed questions using a Think Aloud CI technique and spontaneous verbal probing in the instance of a seeming lack of information, inconsistency in information offered by the patient, indicative body language (eg, seeming uncomfortable), hesitation indicating the patient was not rendering all of the information that he or she was thinking, or if a common specific issue had been previously identified. Because we were looking for issues adversely affecting patient satisfaction, we decided to optimize our effort by focusing on questions to which patients responded negatively or hesitantly. However, as time permitted we also gave attention to questions patients answered immediately and positively.
Data Collection
Data were collected on interview sheets containing the questions asked to the patients with the Top Box/Not Top Box coding method described above, as well as a section for qualitative data gleaned from the cognitive elements of the interview. Recordings and full transcriptions were not performed to avoid raising patient concerns, which held the potential to negatively impact participation. All records of participant names were kept solely by the principal investigator to avoid duplicate interviews and were destroyed at the conclusion of the interview process.
Analysis
The data was collected from the interview sheets and then compiled into a spreadsheet. The classic quantitative data was compiled into raw totals and percentages. The qualitative data from the cognitive portion was then considered both separately, based on the question, and as a group. Both authors reviewed the data and identified significant items in both the qualitative and quantitative data, based on their ability to provide useful hypotheses regarding higher or lower levels of satisfaction. Also, because of the nature of the CI, useful information can come from as few as 1 respondent,9 so potentially useful individual comments were pulled out of the qualitative data as well.
It is important to note that this study is not a means of measuring patient satisfaction, but rather a means of determining elements and specific issues affecting patient satisfaction. Answers in this study cannot be considered equivalent to answers on the HCAHPS or any other patient satisfaction survey.
Results
Response Rate
There were 57 eligible patients who were asked to participate in this study. Availability of the patients identified as eligible limited the number of participants. Of the 57, 50 accepted. Of the 50 who accepted, 1 was rejected because the patient had only been at the hospital for a few hours and had not seen a physician yet, and 5 more opted to stop before the interview was completed. The 1 that was rejected was not included in the analysis, but the 5 that were left incomplete were included for the questions that had been answered.
Responsiveness to Questions
Patients were asked Did you get all of your questions answered? (Table 1). The responsiveness to questions by our staff was largely satisfactory, but the qualitative data yielded an interesting finding in that 3 of the 6 patients who rendered Not Top Box answers cited problems with question delivery. One patient said, The doctor was just in and out, and I didn't have time to ask questions. Another said, I think of questions 20 minutes after the doctor leaves. In other parts of the interview, 2 more patients mentioned not having questions ready when their attending physician was there, and then not being able to ask them, 1 of them saying, It was my own fault (when I did not get information I wanted) because I didn't ask all of the questions.
| Questions Asked of Patients | Responses | Number | Qualitative Subtheme |
|---|---|---|---|
| |||
| Did you get all of your questions answered? | Always | 41 | Difficulty with question delivery: (eg, I think of questions 20 minutes after the doctor leaves.) |
| Never, sometimes, usually | 6 | ||
| Total | 47 | ||
| Did anyone tell you what [the new medicine] was before they gave it to you? | Yes | 29 | |
| No | 2 | ||
| Total | 31 | ||
| Did anyone tell you about any side effects of the medicine? | Yes | 17 | Lack of communication regarding medicines with few major side effects: (eg, Tylenol or Advil) |
| No | 13 | ||
| Total | 31 | ||
| Do you feel the doctors spend enough time with you? | Yes | 37 | For example: (My doctor) didn't consult me and he didn't inform me. |
| No | 8 | ||
| Total | 45 | ||
| Do you feel the doctors know you as a person? | Yes | 29 | Physician behaviors may influence: (eg, He treats me as a person.) |
| No | 16 | ||
| Total | 45 | ||
| Do you feel the doctors treat you with respect? | Always | 40 | Physician behaviors may influence: (eg, I feel talked down too, like I can't handle the answers.) |
| Never, sometimes, usually | 6 | ||
| Total | 46 | ||
| Do you think the doctors listen carefully to you? | Always | 33 | For example: He had so much on his mind. |
| Never, sometimes, usually | 13 | ||
| Total | 46 | ||
Communication Regarding Medication
There are 2 important questions regarding this issue. Patients who reported taking new medication during their current hospital stay were asked, Did anyone tell you what [the new medication] was for before they gave it to you? and then, Did anyone tell you about any side effects of the medicine? (Table 1). From this we can see that, generally, patients are informed about new medications, but there seems to be a lack of informing the patients regarding side effects of new medications. Interestingly, 8 of the patients who reported that they were not told about side effects raised concerns about medications that have few major side effects. It is important to note that this issue was not initially known and the kind of medication the patients were given was seldom freely offered. We began specifically probing for it after a patient offered the information without prompting, so the actual number of these instances could be much higher.
Perception of Time Spent
We asked our subjects Do you feel the doctors spend enough time with you? (Table 1). The sensitivity of the quantitative data was decreased by using a 2‐category approach, but frequency estimation about an issue of time seemed an unnecessarily awkward approach considering that the more valuable information comes from the qualitative section of the interview.
The perception of enough time spent by physicians was not felt by all of the subjects. Three of the patients who answered No had mentioned a specific need that was not met, all 3 of which were issues with information and communication. The hospitalist changed all of my medicationshe didn't consult me, and he didn't inform me, said 1 patient. Another said, I don't really know who my doctor is, in reference to his attending hospitalist. There was another patient who answered No who felt that the physicians were just mechanically trying to treat his condition and discharge him as soon as possible. I think the hospital is getting the doctors to push people outthey need the beds. Also, 2 patients who answered Yes acknowledged that the doctors spent all the time they needed to for the patients' situations, and 1 patient who answered Yes mentioned a specific personal accommodation the physician made, specifically that the physician prays with the patient.
Personal Connections
This question was, Do you feel the doctors know you as a person? and was included to attempt to probe into the depth of the personal connections formed by our physicians. The standard quantitative data (Table 1) shows there were a significant number of patients who did not feel their physicians knew them as a person. Six of the patients who answered No said they felt the physicians were just doing their job. What else are you besides a body and a diagnosis? 1 patient asked. They are doing their job, said another. Six patients who answered Yes cited how their physicians acted toward them as the reason. One patient responded, One doctor carries on extra conversation with me. He knows me as a person. Another patient plainly said, He treats me as a person. Yet another said, They seem to respect my situation and my need for their services.
Nonclinical Competency
Two questions elicited significant information relevant to hospitalists on this issue, the first being Do you feel the doctors treat you with respect? and the second being Do you think the doctors listen carefully to you? (Table 1).
The standard quantitative data for the first question shows that, generally, our patients felt as though the doctors were treating them with respect. Interestingly, the qualitative portion of the study shows that all 6 patients who rendered Not Top Box answers mentioned either being talked down to or not being responded to by their physicians. The hospitalist treated me as I expected, as [a generic 50‐year‐old], remarked 1 patient about her hospitalist, by whom she felt ignored. I feel talked down too, like I can't handle the answers. I feel like I don't always get the full truth, said another patient regarding her physician telling her about her medical condition. It seems like the doctor put me off, said a third patient regarding his physician's willingness to treat him.
The quantitative data for the second question shows much weaker performance with regard to the perception of the doctors listening to the patients. The qualitative portion of the study shows that 3 patients mentioned how much their physicians had on their minds. One patient said, He was thinking so many things at the same time, and another plainly said, He had so much on his mind. Four patients mentioned not feeling responded to by their physicians. A patient commented, I would say something (to the doctor), and then my dad would [sic] re‐say it, and the doctor would respond when my dad said it, but not when I did. Another patient responded, I would ask (the doctors) to do something, and they wouldn't do it.
Discussion
Because of the limitations inherent in typical survey measures of investigation, we employed a CI technique. The objective was to generate hypotheses as to why patients may report reduced satisfaction with various aspects of hospitalization. The data set gleaned from this study was sizable, and held information pertinent to all parts of the hospital. The results reported in this article are focused on hospitalists.
The quantity of time hospitalists spend with patients may not be as important to the patients as the quality of interaction. Other studies have shown similar results, illustrating that the key factor in a patients' opinion of a visit with a physician was the perception of being taken seriously.10 The perception of being talked down to (as noted by Levy11) and the perception of not being responded to or focused on are the key negative factors for patients. By interacting with patients in a way that makes them feel valued, focused on, and responded to, physicians may improve patient satisfaction without requiring increased amounts of time spent with them.
Patient complaints that physicians do not respond to them may partially reflect inability to ask all of their questions. Hospitals may wish to consider methods to improve the ability of the patients to ask questions in the small amount of time available for physicians to talk with them (eg, placing notebooks by patients' bedsides and repeatedly encouraging them to write their questions down). This concept has also been endorsed as a means of improving the quality of care and reducing medical mistakes.12
Hospitalists and other physicians may positively impact the communication about medication issues by establishing a protocol for communicating major as well as minor side effects or even the lack of side effects of medication to patients. The challenge lies in determining the level of incidence that is significant enough (eg, 10%, 5%, or 1%) to warrant explaining minor side effects.
The findings of this study are limited by its small size, qualitative nature, nonrepresentative population, and loose approach to questioning. The patient responses were transcribed manually by the interviewer, leaving the possibility that some responses were not accurately recorded. Our survey instrument is not validated, and the results may not generalize to other settings. Instead of taking these findings as conclusive, we present them as suggestions for improvement that may be validated by further research.
Acknowledgements
The authors Tom Quinn and Toni Murdough for their contributions in developing the survey instrument.
Appendix
Appendix 1. Interview questions in the order they were presented to the patients
Background Questions
What is your name?
About how many hospital visits have you had in the last 6 months?
What is the highest grade or level of school that you have completed?
General Hospital Questions
What are the most important things you want in a hospital?
What do you think about the reputation of the hospital?
How has your stay here at the hospital been?
While you've been here, have you had any pain? Were you given any pain medicine? How well was your pain controlled? (The first two questions were for screening, the last question was for coding)
During this hospital stay, were you given any medicine that you had not taken before? Did anyone tell you what it was for before they gave it to you? Did anyone tell you about any side effects of the medicine? (First question for screening, last two for coding)
Do you think your room and bathroom are clean? Has it been that way the whole time you've been here?
Do you think this hospital has all the equipment needed for your treatment?
Do you feel you've been able to rest while you've been here?
Have you ever pressed the call button? How fast did the help come? Did it come as soon as you wanted it? (The first question was for screening, the second for insight, the third for coding)
While you were here at the hospital, did you ever need help getting to the bathroom or using a bedpan? How fast did you get help? Did help come as soon as you wanted it? (The first question was for screening, the second for insight, the third for coding)
Do you feel the staff paid attention to you?
Did you get all of your questions answered?
Have you had any problems here at the hospital? Did anybody help you with it? (The first question was for screening, the second for coding)
Nursing Staff Questions
What do you think about your nurses?
Do you feel the nurses treat you with respect?
Do you think the nurses listen carefully to you?
Did the nurses explain things in a way you could understand?
Did you get all the information you wanted from the nurses about your tests or treatments?
Do the nurses make you feel calm and safe while you are here at the hospital?
Do you feel the nurses know you as a person?
Do the nurses seem interested in doing things for you?
Do you feel the nurses spend enough time with you?
Have you ever had a change of nurses while you were here? Do you feel like the new nurse knew what the other nurse knew about you? Did the new nurse seem to know your situation? (The first question is for screening, the next two for coding)
What do you feel about the skill of your nurses here at the hospital?
Physician Staff Questions
What do you think about your doctors?
Do you feel the doctors treat you with respect?
Do you think the doctors listen carefully to you?
Did the doctors explain things in a way you could understand?
Did you get all the information you wanted from the doctors about your tests or treatments?
Do the doctors make you feel calm and safe while you are here at the hospital?
Do you feel the doctors know you as a person?
Did the doctors seem interested in doing things for you?
Do you feel the doctors spend enough time with you?
Have you ever been switched between doctors here at the hospital? Do you feel like the new doctor knew what the other doctor knew about you? Did the new doctor seem to know your situation? (The first question was for screening, the next two for coding)
Were you ever switched from your primary doctor to a doctor here at the hospital? Do you feel like the new doctor knew what your primary doctor knew about your medical situation? (The first question was for screening, the second question for coding)
What do you feel about the skill of your doctors here at the hospital?
Cumulative Hospital Questions
Did you see any hospital staff disagree with each other about your medical treatment?
On a scale of 1‐10, how would you rate the hospital?
Is there anything that we haven't talked about that would keep you from rating us a 10?
Would you recommend this hospital to your friends and family?
What can we do to make this the best hospital around?
Patient satisfaction is an important issue for hospitals, as it may affect the decision to seek care at one institution over another, but it may soon have direct implications for hospital reimbursement with the recent proposals for Value Based Purchasing (VBP) models by the Centers for Medicare and Medicaid Services (CMS). Up to 5% of inpatient Medicare reimbursement would be linked to performance measures, 40% of which could come from percentile outcomes on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) alone.1 HCAHPS scores are now available for individual hospitals at the Hospital Compare website maintained by CMS (
While the information garnered from the HCAHPS provides an external perception of hospital quality, the questions are broad and do not identify specific reasons for reduced satisfaction. Many have suggested that the incorporation of surveys already administered at hospitals may be required for successful HCAHPS administration in order to overcome the limitations inherent in its design.2
In order to identify explanatory factors for low HCAHPS scores, we decided to incorporate a technique known as a cognitive interview (CI). The CI is widely used as an evaluative tool for survey questions because of its ability to allow the interviewer to discern the processes that lead to responses.3 Up to this point, the focus of this CI method has been on the ability of the subject to comprehend and answer the questions.4 However, when a CI subject is answering a question, there is a large amount of information presented to the interviewer about the topic that is typically regarded as supplementary because of the focus on these specific issues.5 This study reports the supplemental information that may provide insight as to why patients answered as they did. Our goal was to gain further understanding of factors that may underlie HCAHPS responses.
Materials and Methods
Overview
The premise behind every step in the development and implementation of the interview process was to increase the comfort level of the patients with the process as well as take as much of the cognitive burden off of the patients as possible while maintaining the integrity of the questioning.
The study was developed and conducted in May and June 2008. The duration of the study and number of participants were based on time constraints on personnel and limited funding for the study.
Development of the Interview
We used the HCAHPS questions as a starting point to launch the development of our interview. Because the purpose of this study was to generate hypotheses regarding issues affecting patient satisfaction, we used a loose approach to questioning that gave the interview subject a greater degree of freedom with their answers than in a measurement study. This freedom of response eliminated the need to take minor comprehension issues into account, which would have been cause for concern using a standard survey.5
We focused on what the patients thought or felt in order to avoid making them feel overburdened for factual recall. There were some questions for which this was not possible (eg, the questions about medication). After the questions were reworded, their comprehension level was confirmed to be appropriate for the local community (grade 3‐6) using the Flesch Reading Ease and Flesch‐Kincaid grade level equations (data not shown).
The questions were then grouped from least cognitively intense to most cognitively intense surrounding any particular issue, which was generally least specific to most specific. This process of ordering questions has been shown to increase the accuracy of self reports,6 which is advantageous in our situation because it increases the amount of potentially useful information the patients include in their perception analysis. Every major section change started with at least 1 general question without specific aim in order to facilitate free response (full interview is included as Appendix 1).
For classic quantitative analysis, the 4 HCAHPS categories (always, usually, sometimes, never) were presented for most of the questions. They are reported in this work as Top Box, (ie, always), or Not Top Box (any other response). Top Box responses are the ratings most widely reported in HCAHPS surveys, and this dichotomy makes it easier to code and review answers. However, when we felt that quantitatively we wanted a more superficial inquiry, a 2‐category yes/no system was used. The interviews were also designed to be less than 1 hour in length, which has been shown to be appropriate in other kinds of cognitive studies in the medical field.7
The questions in the About You section of the HCAHPS were largely excluded with the exception of the education demographic question (for a full HCAHPS survey see Goldstein et al.).2 The community that we studied is quite homogeneously Caucasian and non‐Hispanic. Education level is the only remaining HCAHPS demographic variable, and our subjects had education levels comparable to those reported in HCAHPS for this hospital. Our data are primarily qualitative and were not weighted as the HCAHPS data were.8
Conducting the Interviews
The interviews were conducted by the principal researcher (A.B.) (the use of a single interviewer eliminates potential bias between interviewers on interview delivery) on medical and surgical inpatients in general inpatient and intensive care units who were at least 18 years old, not suffering significant discomfort, and able to comprehend questions and provide meaningful answers. The nurse managers on the inpatient units were asked to identify patients who fit these criteria. Of the 50 patients typically present on medical/surgical services, about 10 would be suitable for interview. The researcher would then select up to 5 patients each weekday from those actually present in their rooms, explain that he was doing research for the hospital, and ask if the patient would participate. The range of the number of selected patients depended upon the willingness of the available patients to participate and the amount of time it took to conduct the interviews. If the patient accepted, the researcher then emphasized that participation was completely optional and would have no effect on the medical care the patient would receive, that the identity of the patient would never be shared, and that the information provided would be used internally and possibly for anonymous external reporting. The researcher then asked if the patient would still like to continue. This protocol was approved by the hospital Institutional Review Board.
The patients were then instructed to think aloud as they answered questions and given Think Aloud Training using established methods.9 There were 4 instructions or questions in the training that were used sequentially, as follows: (1) Try to picture the place where you live, and think about how many windows there are in that place. As you count up the windows, tell me what you are seeing and thinking about;9 (2) I want you to think about the last school you personally went to and studied at. Think about yourself walking into the main building. Tell me what you are seeing and thinking about as you walk through the doors; (3) Now I want you to think about your favorite food. Can you tell me about it? and (4) I want you to think about a pot of flowers. Tell me about what you think and see as you walk up and smell the flowers. While the patients were thinking, the interviewer followed up with spontaneous general verbal probes (eg, Can you tell me what you are thinking?). After the patients were responding adequately to the training instructions, we proceeded to the interview.
The interviews were conducted by asking the patients the designed questions using a Think Aloud CI technique and spontaneous verbal probing in the instance of a seeming lack of information, inconsistency in information offered by the patient, indicative body language (eg, seeming uncomfortable), hesitation indicating the patient was not rendering all of the information that he or she was thinking, or if a common specific issue had been previously identified. Because we were looking for issues adversely affecting patient satisfaction, we decided to optimize our effort by focusing on questions to which patients responded negatively or hesitantly. However, as time permitted we also gave attention to questions patients answered immediately and positively.
Data Collection
Data were collected on interview sheets containing the questions asked to the patients with the Top Box/Not Top Box coding method described above, as well as a section for qualitative data gleaned from the cognitive elements of the interview. Recordings and full transcriptions were not performed to avoid raising patient concerns, which held the potential to negatively impact participation. All records of participant names were kept solely by the principal investigator to avoid duplicate interviews and were destroyed at the conclusion of the interview process.
Analysis
The data was collected from the interview sheets and then compiled into a spreadsheet. The classic quantitative data was compiled into raw totals and percentages. The qualitative data from the cognitive portion was then considered both separately, based on the question, and as a group. Both authors reviewed the data and identified significant items in both the qualitative and quantitative data, based on their ability to provide useful hypotheses regarding higher or lower levels of satisfaction. Also, because of the nature of the CI, useful information can come from as few as 1 respondent,9 so potentially useful individual comments were pulled out of the qualitative data as well.
It is important to note that this study is not a means of measuring patient satisfaction, but rather a means of determining elements and specific issues affecting patient satisfaction. Answers in this study cannot be considered equivalent to answers on the HCAHPS or any other patient satisfaction survey.
Results
Response Rate
There were 57 eligible patients who were asked to participate in this study. Availability of the patients identified as eligible limited the number of participants. Of the 57, 50 accepted. Of the 50 who accepted, 1 was rejected because the patient had only been at the hospital for a few hours and had not seen a physician yet, and 5 more opted to stop before the interview was completed. The 1 that was rejected was not included in the analysis, but the 5 that were left incomplete were included for the questions that had been answered.
Responsiveness to Questions
Patients were asked Did you get all of your questions answered? (Table 1). The responsiveness to questions by our staff was largely satisfactory, but the qualitative data yielded an interesting finding in that 3 of the 6 patients who rendered Not Top Box answers cited problems with question delivery. One patient said, The doctor was just in and out, and I didn't have time to ask questions. Another said, I think of questions 20 minutes after the doctor leaves. In other parts of the interview, 2 more patients mentioned not having questions ready when their attending physician was there, and then not being able to ask them, 1 of them saying, It was my own fault (when I did not get information I wanted) because I didn't ask all of the questions.
| Questions Asked of Patients | Responses | Number | Qualitative Subtheme |
|---|---|---|---|
| |||
| Did you get all of your questions answered? | Always | 41 | Difficulty with question delivery: (eg, I think of questions 20 minutes after the doctor leaves.) |
| Never, sometimes, usually | 6 | ||
| Total | 47 | ||
| Did anyone tell you what [the new medicine] was before they gave it to you? | Yes | 29 | |
| No | 2 | ||
| Total | 31 | ||
| Did anyone tell you about any side effects of the medicine? | Yes | 17 | Lack of communication regarding medicines with few major side effects: (eg, Tylenol or Advil) |
| No | 13 | ||
| Total | 31 | ||
| Do you feel the doctors spend enough time with you? | Yes | 37 | For example: (My doctor) didn't consult me and he didn't inform me. |
| No | 8 | ||
| Total | 45 | ||
| Do you feel the doctors know you as a person? | Yes | 29 | Physician behaviors may influence: (eg, He treats me as a person.) |
| No | 16 | ||
| Total | 45 | ||
| Do you feel the doctors treat you with respect? | Always | 40 | Physician behaviors may influence: (eg, I feel talked down too, like I can't handle the answers.) |
| Never, sometimes, usually | 6 | ||
| Total | 46 | ||
| Do you think the doctors listen carefully to you? | Always | 33 | For example: He had so much on his mind. |
| Never, sometimes, usually | 13 | ||
| Total | 46 | ||
Communication Regarding Medication
There are 2 important questions regarding this issue. Patients who reported taking new medication during their current hospital stay were asked, Did anyone tell you what [the new medication] was for before they gave it to you? and then, Did anyone tell you about any side effects of the medicine? (Table 1). From this we can see that, generally, patients are informed about new medications, but there seems to be a lack of informing the patients regarding side effects of new medications. Interestingly, 8 of the patients who reported that they were not told about side effects raised concerns about medications that have few major side effects. It is important to note that this issue was not initially known and the kind of medication the patients were given was seldom freely offered. We began specifically probing for it after a patient offered the information without prompting, so the actual number of these instances could be much higher.
Perception of Time Spent
We asked our subjects Do you feel the doctors spend enough time with you? (Table 1). The sensitivity of the quantitative data was decreased by using a 2‐category approach, but frequency estimation about an issue of time seemed an unnecessarily awkward approach considering that the more valuable information comes from the qualitative section of the interview.
The perception of enough time spent by physicians was not felt by all of the subjects. Three of the patients who answered No had mentioned a specific need that was not met, all 3 of which were issues with information and communication. The hospitalist changed all of my medicationshe didn't consult me, and he didn't inform me, said 1 patient. Another said, I don't really know who my doctor is, in reference to his attending hospitalist. There was another patient who answered No who felt that the physicians were just mechanically trying to treat his condition and discharge him as soon as possible. I think the hospital is getting the doctors to push people outthey need the beds. Also, 2 patients who answered Yes acknowledged that the doctors spent all the time they needed to for the patients' situations, and 1 patient who answered Yes mentioned a specific personal accommodation the physician made, specifically that the physician prays with the patient.
Personal Connections
This question was, Do you feel the doctors know you as a person? and was included to attempt to probe into the depth of the personal connections formed by our physicians. The standard quantitative data (Table 1) shows there were a significant number of patients who did not feel their physicians knew them as a person. Six of the patients who answered No said they felt the physicians were just doing their job. What else are you besides a body and a diagnosis? 1 patient asked. They are doing their job, said another. Six patients who answered Yes cited how their physicians acted toward them as the reason. One patient responded, One doctor carries on extra conversation with me. He knows me as a person. Another patient plainly said, He treats me as a person. Yet another said, They seem to respect my situation and my need for their services.
Nonclinical Competency
Two questions elicited significant information relevant to hospitalists on this issue, the first being Do you feel the doctors treat you with respect? and the second being Do you think the doctors listen carefully to you? (Table 1).
The standard quantitative data for the first question shows that, generally, our patients felt as though the doctors were treating them with respect. Interestingly, the qualitative portion of the study shows that all 6 patients who rendered Not Top Box answers mentioned either being talked down to or not being responded to by their physicians. The hospitalist treated me as I expected, as [a generic 50‐year‐old], remarked 1 patient about her hospitalist, by whom she felt ignored. I feel talked down too, like I can't handle the answers. I feel like I don't always get the full truth, said another patient regarding her physician telling her about her medical condition. It seems like the doctor put me off, said a third patient regarding his physician's willingness to treat him.
The quantitative data for the second question shows much weaker performance with regard to the perception of the doctors listening to the patients. The qualitative portion of the study shows that 3 patients mentioned how much their physicians had on their minds. One patient said, He was thinking so many things at the same time, and another plainly said, He had so much on his mind. Four patients mentioned not feeling responded to by their physicians. A patient commented, I would say something (to the doctor), and then my dad would [sic] re‐say it, and the doctor would respond when my dad said it, but not when I did. Another patient responded, I would ask (the doctors) to do something, and they wouldn't do it.
Discussion
Because of the limitations inherent in typical survey measures of investigation, we employed a CI technique. The objective was to generate hypotheses as to why patients may report reduced satisfaction with various aspects of hospitalization. The data set gleaned from this study was sizable, and held information pertinent to all parts of the hospital. The results reported in this article are focused on hospitalists.
The quantity of time hospitalists spend with patients may not be as important to the patients as the quality of interaction. Other studies have shown similar results, illustrating that the key factor in a patients' opinion of a visit with a physician was the perception of being taken seriously.10 The perception of being talked down to (as noted by Levy11) and the perception of not being responded to or focused on are the key negative factors for patients. By interacting with patients in a way that makes them feel valued, focused on, and responded to, physicians may improve patient satisfaction without requiring increased amounts of time spent with them.
Patient complaints that physicians do not respond to them may partially reflect inability to ask all of their questions. Hospitals may wish to consider methods to improve the ability of the patients to ask questions in the small amount of time available for physicians to talk with them (eg, placing notebooks by patients' bedsides and repeatedly encouraging them to write their questions down). This concept has also been endorsed as a means of improving the quality of care and reducing medical mistakes.12
Hospitalists and other physicians may positively impact the communication about medication issues by establishing a protocol for communicating major as well as minor side effects or even the lack of side effects of medication to patients. The challenge lies in determining the level of incidence that is significant enough (eg, 10%, 5%, or 1%) to warrant explaining minor side effects.
The findings of this study are limited by its small size, qualitative nature, nonrepresentative population, and loose approach to questioning. The patient responses were transcribed manually by the interviewer, leaving the possibility that some responses were not accurately recorded. Our survey instrument is not validated, and the results may not generalize to other settings. Instead of taking these findings as conclusive, we present them as suggestions for improvement that may be validated by further research.
Acknowledgements
The authors Tom Quinn and Toni Murdough for their contributions in developing the survey instrument.
Appendix
Appendix 1. Interview questions in the order they were presented to the patients
Background Questions
What is your name?
About how many hospital visits have you had in the last 6 months?
What is the highest grade or level of school that you have completed?
General Hospital Questions
What are the most important things you want in a hospital?
What do you think about the reputation of the hospital?
How has your stay here at the hospital been?
While you've been here, have you had any pain? Were you given any pain medicine? How well was your pain controlled? (The first two questions were for screening, the last question was for coding)
During this hospital stay, were you given any medicine that you had not taken before? Did anyone tell you what it was for before they gave it to you? Did anyone tell you about any side effects of the medicine? (First question for screening, last two for coding)
Do you think your room and bathroom are clean? Has it been that way the whole time you've been here?
Do you think this hospital has all the equipment needed for your treatment?
Do you feel you've been able to rest while you've been here?
Have you ever pressed the call button? How fast did the help come? Did it come as soon as you wanted it? (The first question was for screening, the second for insight, the third for coding)
While you were here at the hospital, did you ever need help getting to the bathroom or using a bedpan? How fast did you get help? Did help come as soon as you wanted it? (The first question was for screening, the second for insight, the third for coding)
Do you feel the staff paid attention to you?
Did you get all of your questions answered?
Have you had any problems here at the hospital? Did anybody help you with it? (The first question was for screening, the second for coding)
Nursing Staff Questions
What do you think about your nurses?
Do you feel the nurses treat you with respect?
Do you think the nurses listen carefully to you?
Did the nurses explain things in a way you could understand?
Did you get all the information you wanted from the nurses about your tests or treatments?
Do the nurses make you feel calm and safe while you are here at the hospital?
Do you feel the nurses know you as a person?
Do the nurses seem interested in doing things for you?
Do you feel the nurses spend enough time with you?
Have you ever had a change of nurses while you were here? Do you feel like the new nurse knew what the other nurse knew about you? Did the new nurse seem to know your situation? (The first question is for screening, the next two for coding)
What do you feel about the skill of your nurses here at the hospital?
Physician Staff Questions
What do you think about your doctors?
Do you feel the doctors treat you with respect?
Do you think the doctors listen carefully to you?
Did the doctors explain things in a way you could understand?
Did you get all the information you wanted from the doctors about your tests or treatments?
Do the doctors make you feel calm and safe while you are here at the hospital?
Do you feel the doctors know you as a person?
Did the doctors seem interested in doing things for you?
Do you feel the doctors spend enough time with you?
Have you ever been switched between doctors here at the hospital? Do you feel like the new doctor knew what the other doctor knew about you? Did the new doctor seem to know your situation? (The first question was for screening, the next two for coding)
Were you ever switched from your primary doctor to a doctor here at the hospital? Do you feel like the new doctor knew what your primary doctor knew about your medical situation? (The first question was for screening, the second question for coding)
What do you feel about the skill of your doctors here at the hospital?
Cumulative Hospital Questions
Did you see any hospital staff disagree with each other about your medical treatment?
On a scale of 1‐10, how would you rate the hospital?
Is there anything that we haven't talked about that would keep you from rating us a 10?
Would you recommend this hospital to your friends and family?
What can we do to make this the best hospital around?
Copyright © 2009 Society of Hospital Medicine
Continuing Medical Education Program in
If you wish to receive credit for this activity, which beginson the next page, please refer to the website:
Accreditation and Designation Statement
Blackwell Futura Media Services designates this educational activity for a 1 AMA PRA Category 1 Credit. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Educational Objectives
Continuous participation in the Journal of Hospital Medicine CME program will enable learners to be better able to:
-
Interpret clinical guidelines and their applications for higher quality and more efficient care for all hospitalized patients.
-
Describe the standard of care for common illnesses and conditions treated in the hospital; such as pneumonia, COPD exacerbation, acute coronary syndrome, HF exacerbation, glycemic control, venous thromboembolic disease, stroke, etc.
-
Discuss evidence‐based recommendations involving transitions of care, including the hospital discharge process.
-
Gain insights into the roles of hospitalists as medical educators, researchers, medical ethicists, palliative care providers, and hospital‐based geriatricians.
-
Incorporate best practices for hospitalist administration, including quality improvement, patient safety, practice management, leadership, and demonstrating hospitalist value.
-
Identify evidence‐based best practices and trends for both adult and pediatric hospital medicine.
Instructions on Receiving Credit
For information on applicability and acceptance of continuing medical education credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within the time designated on the title page; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity during the valid credit period that is noted on the title page.
Follow these steps to earn credit:
-
Log on to www.blackwellpublishing.com/cme.
-
Read the target audience, learning objectives, and author disclosures.
-
Read the article in print or online format.
-
Reflect on the article.
-
Access the CME Exam, and choose the best answer to each question.
-
Complete the required evaluation component of the activity.
If you wish to receive credit for this activity, which beginson the next page, please refer to the website:
Accreditation and Designation Statement
Blackwell Futura Media Services designates this educational activity for a 1 AMA PRA Category 1 Credit. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Educational Objectives
Continuous participation in the Journal of Hospital Medicine CME program will enable learners to be better able to:
-
Interpret clinical guidelines and their applications for higher quality and more efficient care for all hospitalized patients.
-
Describe the standard of care for common illnesses and conditions treated in the hospital; such as pneumonia, COPD exacerbation, acute coronary syndrome, HF exacerbation, glycemic control, venous thromboembolic disease, stroke, etc.
-
Discuss evidence‐based recommendations involving transitions of care, including the hospital discharge process.
-
Gain insights into the roles of hospitalists as medical educators, researchers, medical ethicists, palliative care providers, and hospital‐based geriatricians.
-
Incorporate best practices for hospitalist administration, including quality improvement, patient safety, practice management, leadership, and demonstrating hospitalist value.
-
Identify evidence‐based best practices and trends for both adult and pediatric hospital medicine.
Instructions on Receiving Credit
For information on applicability and acceptance of continuing medical education credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within the time designated on the title page; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity during the valid credit period that is noted on the title page.
Follow these steps to earn credit:
-
Log on to www.blackwellpublishing.com/cme.
-
Read the target audience, learning objectives, and author disclosures.
-
Read the article in print or online format.
-
Reflect on the article.
-
Access the CME Exam, and choose the best answer to each question.
-
Complete the required evaluation component of the activity.
If you wish to receive credit for this activity, which beginson the next page, please refer to the website:
Accreditation and Designation Statement
Blackwell Futura Media Services designates this educational activity for a 1 AMA PRA Category 1 Credit. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Educational Objectives
Continuous participation in the Journal of Hospital Medicine CME program will enable learners to be better able to:
-
Interpret clinical guidelines and their applications for higher quality and more efficient care for all hospitalized patients.
-
Describe the standard of care for common illnesses and conditions treated in the hospital; such as pneumonia, COPD exacerbation, acute coronary syndrome, HF exacerbation, glycemic control, venous thromboembolic disease, stroke, etc.
-
Discuss evidence‐based recommendations involving transitions of care, including the hospital discharge process.
-
Gain insights into the roles of hospitalists as medical educators, researchers, medical ethicists, palliative care providers, and hospital‐based geriatricians.
-
Incorporate best practices for hospitalist administration, including quality improvement, patient safety, practice management, leadership, and demonstrating hospitalist value.
-
Identify evidence‐based best practices and trends for both adult and pediatric hospital medicine.
Instructions on Receiving Credit
For information on applicability and acceptance of continuing medical education credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within the time designated on the title page; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity during the valid credit period that is noted on the title page.
Follow these steps to earn credit:
-
Log on to www.blackwellpublishing.com/cme.
-
Read the target audience, learning objectives, and author disclosures.
-
Read the article in print or online format.
-
Reflect on the article.
-
Access the CME Exam, and choose the best answer to each question.
-
Complete the required evaluation component of the activity.
Periprocedural Antithrombotic Management
The management of patients on long‐term antithrombotic therapy (vitamin K antagonists [VKA] or antiplatelet agents) who may require temporary disruption for an invasive procedure is challenging. Management is controversial due to methodologically limited prospective data and varied consensus opinions. Yet periprocedural anticoagulation management is a commonly encountered clinical problem. It is estimated that there are 2.5 million patients on long‐term VKA therapy in North America1 and 41% of the U.S. population over age 40 years is on antiplatelet therapy.2 Further, the need for temporary disruption of these therapies for an invasive procedure is frequent. As an example, in 1 European study, approximately 15% of patients on long‐term VKA required a major surgical procedure in 4 years of follow‐up.3 The role of the hospitalist physician in managing these patients is increasing as hospitalists care for an increasing number of surgical patients and provide periprocedural consultation both in and out of the hospital. Therefore, it is imperative for the hospitalist physician to be proficient in making thoughtful and individualized recommendations on the appropriate management of periprocedural anticoagulants, drawing from the available literature and evidence‐based practice guidelines. Importantly, the Society of Hospital Medicine has cited perioperative management as an important core competency.4
The hospitalist physician is likely to encounter numerous periprocedural scenarios, including the management of antiplatelet agents, identifying low bleeding risk procedures wherein interruption of anticoagulants is unnecessary, and recognizing patients with a low short‐term thromboembolic risk where anticoagulants can be disrupted without the need for heparin or low molecular weight heparin (LMWH) in the periprocedural period (defined as bridging therapy). Further, all other clinical scenarios require both a careful individualized assessment of the patient's risk of periprocedural bleeding and thromboembolism and a thoughtful discussion with all involved parties. This discussion may involve the person performing the procedure, the anesthesiologist, and the patient. The purpose of this work is to explore these relevant areas through a review of the literature with a particular focus on the recently published 2008 American College of Chest Physicians (ACCP) evidence‐based clinical practice guidelines.
We reviewed medical literature from 1990 through May 2008 with the following key words: bridging, anticoagulation, perioperative, antiplatelet, heparin, and low molecular weight heparin. Individual studies were then independently reviewed by the authors. Studies that were felt relevant to a hospitalist physician were retrieved and reviewed. If there was uncertainty regarding applicability to a hospitalist setting, a second author's opinion was rendered. Additionally, we reviewed 1 author's personal reference list of articles relating to periprocedural anticoagulation that has been compiled over the past 10 years. This list and the reference lists of retrieved articles were also reviewed. Data were summarized to answer 4 clinically relevant questions:
-
What is the optimal management of antiplatelet therapy in the periprocedural period?
-
Are there very low‐bleeding risk procedures that do not require interruption of oral anticoagulation?
-
Are there low thromboembolic risk populations who do not require periprocedural bridging?
-
How do you manage patients who must discontinue anticoagulants but are at an increased thrombotic risk?
Clinical Question #1: What Is the Optimal Management of Antiplatelet Therapy in the Periprocedural Period?
The optimal management of oral antiplatelet therapy in the periprocedural period is not well studied. Most reviews, expert recommendations, and consensus statements either do not comment on periprocedural antiplatelet management or recommend the routine discontinuation of therapy at least 7 days prior to surgery.3, 5, 6 However, as the 2008 ACCP guidelines highlight, the recommendation to routinely discontinue antiplatelet therapy 7 days prior to the procedure is an oversimplification.1 In the era of both bare metal cardiac stents and drug‐eluting stents, the optimal management of these patients requires that 2 primary questions be asked: (1) Is this a low‐bleeding risk procedure whereby antiplatelet therapy can be continued? (2) Does the patient have a coronary stent whereby the continuation of antiplatelet therapy or delay of the intervention is necessary?
In the context of ongoing aspirin therapy, certain procedures have a low risk of significant hemorrhagic complications. These low bleeding risk procedures include cataract surgery, cutaneous surgery, oral surgery, and endoscopic procedures, including those with mucosal biopsies.710 Patients undergoing these procedures may safely continue low dose aspirin therapy, especially if they have a high‐risk indication for their aspirin such as recent myocardial infarction, stroke, or the presence of a coronary stent.5, 710 Whether these procedures can be safely performed in the setting of a thienopyridine or combination antiplatelet therapy is uncertain.
In the past several decades, the management of obstructive coronary artery disease has undergone a major evolution. Placement of coronary stents has become commonplace, and there are now several million patients with drug‐eluting stents.11 The major complication of these devices is stent thrombosis, which results in death or myocardial infarction in up to 64% of patients.12 Fortunately, dual antiplatelet therapy (aspirin and a thienopyridine such as clopidogrel) markedly reduces this risk.13 Current guidelines recommend using combination antiplatelet therapy for at least 4 to 6 weeks and ideally up to 12 months after placement of a bare metal stent and at least 12 months after placement of either a sirolimus‐ or paclitaxel‐eluting stent.1, 14 During this period of dual antiplatelet therapy, the premature discontinuation of the thienopyridine may be catastrophic. To guide clinicians in managing these patients in the periprocedural period, recent consensus guidelines recommend the following:1, 12
-
In patients who are expected to need an invasive surgical procedure in the next 12 months, consideration should be given to avoiding drug‐eluting stents.
-
Elective procedures which have an increased risk of bleeding should be deferred for at least 6 weeks after bare metal stent implantation and 12 months after drug‐eluting stent implantation.
-
For patients undergoing a surgical procedure within 6 weeks of bare metal stent implantation and 12 months of drug‐eluting stent implantation, continuation of aspirin and clopidogrel is recommended. If bleeding risk prohibits this, then a cardiologist should be consulted.
-
In patients with a drug‐eluting stent who need to undergo a procedure whereby the thienopyridine needs to be discontinued, aspirin should be continued if at all possible, and the thienopyridine should be resumed as soon as possible after the procedure. It may be reasonable to consider a loading dose of clopidogrel, up to 600 mg, in this setting, although prospective supportive data is lacking.1
It is important to recognize that delayed stent thrombosis is now reported well beyond 1 year after drug‐eluting stent implantation, and that there may not be a diminution in risk after the initial 12 months.1517 Until additional data is available, it seems prudent, if possible, to at least continue aspirin in the periprocedural period in these patients. If bleeding concerns obviate this, then antiplatelet therapy should be discontinued and resumed as soon as possible.
For patients on chronic antiplatelet therapy who do not have a cardiac stent and who are not undergoing a low‐bleeding‐risk procedure, the risks and benefits of the continuation or discontinuation of antiplatelet therapy in the periprocedural period are uncertain as absolute risks in the periprocedural period have not been well studied. Relative risks/benefits, however, can be estimated from prior studies. Aspirin leads to an approximate 25% relative risk reduction in cardiac or thrombotic event rates compared to placebo.14, 18 Although important, the absolute benefit of 1 week of therapy (vs. no therapy during the periprocedural period) is estimated to be small. The small absolute benefit of continued aspirin therapy may be offset by an increase in significant bleeding events. Although, not well studied, continued aspirin increases significant bleeding by 50% with absolute event rates varying by type of procedure.8 In some procedures, such as intracranial surgery or transurethral prostatectomy, this bleeding risk is prohibitive. For others, the risk may be modest and the decision to continue vs. discontinue aspirin therapy may be at the discretion of the person performing the procedure. In general, for most patients who do not have a coronary stent and have not had a recent (past 3 months) myocardial infarction or stroke, discontinuation of antiplatelet therapy 7 to 10 days prior to the procedure seems prudent. The primary exceptions are patients who are undergoing percutaneous coronary intervention or coronary artery bypass grafting. For these procedures continuing aspirin is recommended.1 Figure 1 outlines a proposed management strategy based upon available evidence and guidelines.
Clinical Question #2: Are There Very‐Low‐Bleeding‐Risk Procedures That Do Not Require Interruption of Oral Anticoagulation?
Some procedures are associated with a low‐enough risk of bleeding that it is safe to proceed without interrupting VKA anticoagulation. This approach spares the risk and cost that occur with the holding of oral anticoagulants and institution of bridging therapy. When considering this strategy, it is important that the specialist performing the procedure is included in the discussion. Dental, dermatologic, and cataract procedures are common outpatient procedures that are associated with low bleeding risk. The relative safety of these procedures in patients who are anticoagulated is discussed thoroughly in the ACCP guidelines.1 Other low‐bleeding‐risk procedures for which a hospitalist may be consulted include certain endoscopic procedures, paracentesis, central venous catheter placement, and arthrocentesis.
The American Society for Gastrointestinal Endoscopy has published guidelines recommending that anticoagulation can be safely continued in patients undergoing the following endoscopic procedures with a low bleeding risk: esophagogastroduodenoscopy (EGD), flexible sigmoidoscopy, and colonoscopy, all with or without mucosal biopsy; enteroscopy, biliary/pancreatic stent placement, endoscopic ultrasound without biopsy, and endoscopic retrograde cholangiopancreatography (ERCP) without sphincterotomy.19 Conversely, high‐risk procedures for which interruption of anticoagulation is recommended include polypectomy, biliary sphincterotomy, variceal treatment, percutaneous endoscopic gastrostomy (PEG) placement, dilation of strictures, and endoscopic ultrasound‐guided fine‐needle aspiration.
Limited data suggest that paracentesis, central venous catheter placement, and arthrocentesis may be safe to perform in the setting of anticoagulation. For patients undergoing paracentesis there is little evidence in anticoagulated patients; however, it is probably safe to continue anticoagulation as studies have demonstrated the safety of this procedure in patients with significant thrombocytopenia and coagulopathy.20, 21 Limited data also supports that central venous catheter placement may be safely performed in the setting of abnormal coagulation tests, although some recommend avoiding the subclavian site due to the risk of hemothorax and the inability to apply adequate compression.2226 With regard to arthrocentesis, multiple authors have endorsed the idea that joint and soft‐tissue aspirations and injections present a low risk of serious bleeding even with anticoagulation.2729 This is supported by limited data.30, 31
Other procedures such as lumbar puncture, thoracentesis, and cardiac catheterization are somewhat more controversial in the anticoagulated patient. Anticoagulation should generally be interrupted for lumbar puncture,29, 32 as 1 study involving patients who were started on heparin immediately after the procedure had a 2% incidence of spinal hematoma and 6.7% major complication rate.33 With regard to thoracentesis, evidence is very limited, but experts generally accept that it may be safely performed in patients with mild coagulopathy.34, 35 One frequently‐cited study found no bleeding complications in 57 patients with mild elevation in prothrombin time, which correlated to an International Normalized Ratio of approximately 2.2 or less.36 A recent report also revealed no serious bleeding complications in 33 thoracenteses performed on patients receiving full anticoagulation with warfarin, heparin, and/or low molecular weight heparin.37
Therapeutic anticoagulation has traditionally been felt to be a relative contraindication to cardiac catheterization.38, 39 In spite of this, several observational studies have suggested it may be safely performed using a standard approach,40 using vascular closure devices,41 or using a radial artery approach instead of the more commonly used femoral site.4244 The small size of these observational reports, the diagnostic rather than therapeutic nature of most cases, the limited use of other antithrombotic and antiplatelet medications, and the experience required to use the transradial approach are all major limitations preventing widespread acceptance of cardiac catheterization in therapeutically anticoagulated patients.
In summary, there are numerous procedures that may be safely pursued in the setting of therapeutic anticoagulation. However, for most of these procedures the data is somewhat limited. As such, it is paramount for the hospitalist physician to recognize these clinical scenarios and to discuss management options with the patient and the person performing the procedure, if applicable.
Clinical Question #3: Are There LowThromboembolic‐Risk Populations Who Do Not Require Periprocedural Bridging?
Although it has previously been noted that there is a wide variation of opinion on when and how to perform periprocedural bridging, it is generally agreed that in the following conditions the risk of thrombosis is low enough that bridging with full dose heparin or LMWH is not necessary:1, 5, 4549
-
Atrial fibrillation without previous stroke or transient ischemic attack (TIA) and no more than 2 additional thrombotic risk factors on the CHADS2 scoring system (Table 1).
-
A single venous thromboembolic event that occurred greater than 12 months ago with no ongoing risk factors such as active malignancy, high risk thrombophilia, or the antiphospholipid antibody syndrome.
-
Bileaflet aortic valve without the presence of additional risk factors (ie, patients 75 years of age with the absence of atrial fibrillation, prior stroke or transient ischemic attack, hypertension, diabetes, or congestive heart failure).
| CHADS2 Score* | Annual Risk of Stroke (%) |
|---|---|
| |
| 0 | 1.9 |
| 1 | 2.8 |
| 2 | 4.0 |
| 3 | 5.9 |
| 4 | 8.5 |
| 5 | 12.5 |
| 6 | 18.2 |
Clinical Question #4: How Do You Manage Patients Who Must Discontinue Anticoagulants But Are at an Increased Thrombotic Risk?
When anticoagulation must be held and the patient does not have a very low thromboembolic risk, a decision of whether or not to use bridging anticoagulation must be made. The current ACCP guideline gives grade 1C and 2C recommendations (evidence from observational studies, case series, or controlled trials with serious flaws) regarding for whom and how to implement bridging.1 The grade C designation is due to a lack of high‐quality randomized clinical trials. As such, the clinician must carefully consider an individual patient's estimated thromboembolic risk, procedurally‐related bleeding risk, patient‐related bleeding risk factors, and the patient's values regarding concerns of thromboembolism or bleeding. In these situations it is also imperative that the person performing the procedure is involved in the risk‐to‐benefit discussion.
When evaluating an individual patient's risk of thromboembolism, clinicians sometimes estimate the perioperative risk by prorating the annual incidence of thromboembolic complications to the few days that anticoagulation is withheld.67 Making this extrapolation discounts the effect of a potential increase in thromboembolic risk induced by surgery. As an example, an average patient with atrial fibrillation who has a 5% predicted annual stroke rate would be estimated to have a stroke risk of 0.05% if they are not anticoagulated for 4 days. However, studies have shown that the actual rate of perioperative thromboembolism is approximately 1%.1 With these limitations and uncertainties in mind, and until there is better prospective outcomes data, we must consider relative risks in the context of absolute event rate estimates when deciding a perioperative anticoagulant management plan. The estimated annual incidence of thrombosis without anticoagulation for various indications and the current guideline recommendations are presented in Table 2.
| Practice Guideline Preferred Management Recommendations | ||||
|---|---|---|---|---|
| Indication for chronic anticoagulation | Estimated Annual Thrombotic Risk Without Anticoagulation | ACCP*1 | ACC/AHA45, 46 | British Haematologic Society70 |
| ||||
| Dual prosthetic or older‐generation valve | >10% | Bridge | Bridge | Bridge |
| VTE within 3 months or severe thrombophilias | Bridge | N/A | Bridge | |
| Pregnancy with prosthetic valve | Bridge | Bridge | N/A | |
| Bileaflet valve in the mitral position | Bridge | Bridge | Prophylaxis | |
| Valve with acute embolism 6 months | Bridge | N/A | Bridge | |
| A‐fib valvular or CHADS2 score 5‐6 | Bridge | Consider bridging | N/A | |
| Recurrent venous thromboembolism | 4‐10% | Bridge | N/A | N/A |
| VTE within 3‐12 months or active cancer | Bridge | N/A | Prophylaxis | |
| Bileaflet aortic valve with additional risk factors | Bridge | Bridge | Prophylaxis | |
| A‐fib CHADS2 score 3‐4 | Bridge | Consider bridging | N/A | |
| Bileaflet aortic valve without additional risk factors | 4% | Prophylaxis or no bridging | No bridging | Prophylaxis |
| VTE >12 months | Prophylaxis or no bridging | N/A | Prophylaxis | |
| A‐fib CHADS2 score 0‐2 and no previous CVA/TIA | Prophylaxis or no bridging | No bridging | N/A | |
In addition to thromboembolic risk, we must also consider the bleeding risk associated with the procedure/surgery. Importantly, therapeutic heparin started early in the postoperative period is associated with major bleeding event rates as high as 10% to 20%.1, 50 Once a major bleeding event occurs, this will often lead to an extended interruption of anticoagulant therapy, placing the patient at a more prolonged risk of an associated thromboembolic event. For this reason, the resumption of full‐dose anticoagulation with LMWH/heparin should be delayed for at least 48 hours in most patients undergoing a surgery or procedure associated with an increased risk of bleeding. Examples of these higher‐bleeding‐risk procedures include major thoracic surgery, intracranial or spinal surgery, major vascular surgery, major orthopedic surgery, urologic surgery involving the bladder or prostrate, major oncologic surgery, reconstructive plastic surgery, colonoscopy with associated polypectomy, renal or prostate biopsies, and placement of a cardiac pacemaker/defibrillator.1, 5157
Taken together, these uncertainties surrounding thromboembolic and bleeding risk estimates imply that there are multiple options for periprocedural management. Several studies, many of which included patients with mechanical heart valves, have shown similar safety and efficacy between LMWH and intravenous (IV) unfractionated heparin.5864 Table 3 summarizes these studies. The ACCP recommends bridging with LMWH over IV unfractionated heparin due to equal efficacy and cost savings with LMWH.1 When bridging is used, careful attention must be given to the timing and dose of anticoagulation in both the preoperative and postoperative periods. Table 4 lists dosing of commonly used LMWHs in North America. When using LMWHs in the preprocedural setting it is important to note that unacceptably high levels of anticoagulation remain present when a patient is given a full once‐daily LMWH dose the morning prior to the procedure or when a full‐dose, twice‐daily LMWH dose is given the evening prior to the procedure.65, 66 For this reason, the ACCP recommends administering the last preoperative dose 24 hours before surgery and if full‐dose once‐daily LMWH is used, the dose should be decreased by one‐half on the day before the surgery in order to ensure that no residual anticoagulant effect remains at the time of surgery.
| AuthorReference/Study Type | Number of Patients | Patient Population | Type of Procedure | Bridging Strategy | Major Bleeds | Minor Bleeds | TE Rate |
|---|---|---|---|---|---|---|---|
| |||||||
| Turpie and Douketis63/single arm cohort | 174 | 66% aortic valve; 34% mitral or dual prosthetic valve | Not specified | Enoxaparin 1 mg/kg twice daily | 2.3% | Not specified | None |
| Kovacs et al.61/single arm cohort | 224 | Prosthetic heart valves or a‐fib plus 1 major risk factor | 67 surgical; 157 nonsurgical | Preoperative bridging with dalteparin 200 IU/kg daily; dose reduced to 100 IU/kg on preoperative day 1; restarted at 100 IU/kg on POD 1; dose reduced to 5000 IU daily if high risk for bleeding | 6.7%; 8/15 occurred intraoperatively or 6 hours postoperatively; 2/15 occurred after 4 weeks | Not specified | 3.6%; 6/8 episodes occurred after warfarin held secondary to bleeding; 2/8 thrombotic episodes judged to be due to cardioembolism |
| Douketis et al.59/prospective registry | 650 | A‐fib 58%; mechanical heart valve 33% | 251 surgical; 399 nonsurgical | Dalteparin 100 IU/kg twice daily; held after high bleeding risk procedure and patients with poor hemostasis | 0.92% | 5.9% | 0.6% |
| Spyropolous et al.62/prospective registry; 14 centers in United States and Canada | 901 | UFH: 40% mechanical valves, 33% a‐fib; LMWH: 24% mechanical valve, 40% a‐fib | 394 surgical; 507 nonsurgical | LMWH mostly given twice daily 80%; UFH 20% | 5.5% UFH; 3.3% LMWH | 9.1% UFH; 12.0% LMWH | 2.4% UFH; 0.9% LMWH |
| Dunn et al.66/prospective cohort | 260 | A‐fib 68% or prior DVT 37% (excluding prosthetic heart valves) | 105 surgical; 145 nonsurgical | Enoxaparin 1.5 mg/kg daily | 3.5% overall; minor surgery/procedures 0.9%; major surgery 28% | 42% | 1.9%; 1/5 events occurred after bleeding led to withdrawal of AC |
| Omran et al.77/prospective registry | 779 | Various indications | Major and minor procedures | All patients bridged with enoxaparin; moderate TE risk 1 mg/kg daily; high TE risk 1 mg/kg twice daily | 0.5%; all in high‐risk group | 5.9% | 0 |
| Garcia et al.71/prospective, observational cohort of 101 sites in United States | 1024 patients with 1293 interruptions of AC | A‐fib 53%; VTE 14%; prosthetic valve 13% | Outpatient procedures only | At discretion of provider. Bridging performed in 8.3% of interruptions; 3% a‐fib, 10% VTE, and 29% mechanical valves | 0.6%; 4/6 patients with major bleed received bridging | 1.7%;10/17 patients with minor bleed received bridging | 0.7%; no events in patients who were bridged |
| Wysokinski et al.64/prospective cohort | 345 consecutive patients undergoing 386 procedures | 100% nonvalvular a‐fib | Major and minor surgeries/procedures | Individualized in AC clinic; 52% of patients bridged | 2.7%; no difference whether patient received bridging or not | 3.0%; 10/11 occurred in bridged patients | 1.1%; no difference in bridged vs. nonbridged patients |
| Low Molecular Weight Heparin | Subcutaneous Dose |
|---|---|
| |
| Dalteparin | |
| Low dose (prophylaxis dose) | 5,000 IU once daily |
| Full dose | 100 IU/kg twice daily or 200 IU/kg once daily |
| Enoxaparin | |
| Low dose (prophylaxis dose) | 30 mg twice daily or 40mg daily |
| Full dose | 1 mg/kg twice daily or 1.5 mg/kg once daily |
| Tinzaparin (full dose) | 175 IU/kg once daily |
In the postprocedural setting, timing and dose of anticoagulant is important, as major bleeding with the use of therapeutic anticoagulation can occur in up to 10% to 20% of cases. When restarting anticoagulation after the procedure, it is important to evaluate intraoperative hemostasis and to consider patient‐related factors that may further increase bleeding risk. These include advanced age, concomitant antiplatelet or nonsteroidal antiinflammatory medications, renal insufficiency, placement of spinal/epidural catheter, worsening liver disease, or the presence of other comorbid illnesses such as cancer.30, 67, 68 The ACCP recommends withholding full‐dose anticoagulation for at least 48 to 72 hours in patients who are felt to be at a high risk for postoperative bleeding.1 Figure 2 is a proposed management approach to the use of bridging anticoagulants that is consistent with the 2008 ACCP recommendations.
CONCLUSION
The evaluation and management of patients on long‐term antiplatelet or VKA therapy who require an invasive procedure or surgery is a common, complicated, and controversial area. Importantly, it is an area in which the hospitalist physician must be adept. Although there remain many unanswered clinical questions, an evolving literature base and recent practice guidelines can help guide management decisions.
- ,,, et al.The Perioperative Management of Antithrombotic Therapy: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th Edition).Chest.2008;133(6_suppl):299S–339S.
- ,,,,.Aspirin use among adults aged 40 and older in the United States: results of a national survey.Am J Prev Med.2007;32(5):403–407.
- ,.Oral anticoagulation in surgical procedures: risks and recommendations.Br J Haematol.2003;123(4):676–682.
- Perioperative medicine.J Hosp Med.2006;1(supp 1):30–31.
- .Perioperative anticoagulation management in patients who are receiving oral anticoagulant therapy: a practical guide for clinicians.Thromb Res.2002;108(1):3–13.
- ,,,.Periprocedural bridging therapy in patients receiving chronic oral anticoagulation therapy.Curr Med Res Opin.2006;22(6):1109–1122.
- ,,,,.Effect of aspirin intake on bleeding during cataract surgery.J Cataract Refract Surg.1998;24(9):1243–1246.
- ,,,.Low‐dose aspirin for secondary cardiovascular prevention–cardiovascular risks after its perioperative withdrawal versus bleeding risks with its continuation—review and meta‐analysis.J Intern Med.2005;257(5):399–414.
- ,,.Aspirin does not increase bleeding complications after transbronchial biopsy.Chest.2002;122(4):1461–1464.
- ,.The management of patients on anticoagulants prior to cutaneous surgery: case report of a thromboembolic complication, review of the literature, and evidence‐based recommendations.Plast Reconstr Surg.2006;118(5):110e–117e.
- .Unanswered questions—drug‐eluting stents and the risk of late thrombosis.N Engl J Med.2007;356(10):981–984.
- ,,, et al.Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians.Circulation.2007;115(6):813–818.
- ,,, et al.The Primary and Secondary Prevention of Coronary Artery Disease: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th Edition).Chest.2008;133(6_suppl):776S–814S.
- ,,, et al.2007 Focused Update of the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: 2007 Writing Group to Review New Evidence and Update the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention, Writing on Behalf of the 2005 Writing Committee.Circulation.2008;117(2):261–295.
- ,,,,,.Late thrombosis of drug‐eluting stents: a meta‐analysis of randomized clinical trials.Am J Med.2006;119(12):1056–1061.
- ,,, et al.Early and late coronary stent thrombosis of sirolimus‐eluting and paclitaxel‐eluting stents in routine clinical practice: data from a large two‐institutional cohort study.Lancet.2007;369(9562):667–678.
- ,,, et al.Clopidogrel use and long‐term clinical outcomes after drug‐eluting stent implantation.JAMA.2007;297(2):159–168.
- Collaborative overview of randomised trials of antiplatelet therapy—I: Prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in various categories of patients.Antiplatelet Trialists' Collaboration.Br Med J (Clin Res Ed).1994;308(6921):81–106.
- ,,, et al.Guideline on the management of anticoagulation and antiplatelet therapy for endoscopic procedures.Gastrointest Endosc.2002;55(7):775–779.
- ,.Severe haemorrhage following abdominal paracentesis for ascites in patients with liver disease.Aliment Pharmacol Ther.2005;21(5):525–529.
- ,,, et al.Performance standards for therapeutic abdominal paracentesis.Hepatology.2004;40(2):484–488.
- ,.Percutaneous cannulation of the internal jugular vein in patients with coagulopathies: an experience based on 1,000 attempts.Anesthesiology.1982;56(4):321–323.
- ,,,,,.Central venous catheterization in patients with coagulopathy.Arch Surg.1992;127(3):273–275.
- ,,.Central venous catheter placement in patients with disorders of hemostasis.Chest.1996;110(1):185–188.
- ,,.US‐guided placement of central vein catheters in patients with disorders of hemostasis.Eur J Radiol.2008;65(2):253–256.
- ,.Central venous cannulation in patients with liver disease and coagulopathy—a prospective audit.Intensive Care Med.1999;25(5):481–485.
- ,.Perioperative management of patients receiving oral anticoagulants: a systematic review.Arch Intern Med.2003;163(8):901–908.
- ,,, et al.Kelley's Textbook of Rheumatology.7th ed.Philadelphia, PA:Elsevier Saunders;2005.
- ,.Clinical Procedures in Emergency Medicine.4th ed.Philadelphia, PA:W.B. Saunders;2004.
- ,.A prospective study of the safety of joint and soft tissue aspirations and injections in patients taking warfarin sodium.Arthritis Rheum.1998;41(4):736–739.
- ,,, et al.[Frequency of the bleeding risk in patients receiving warfarin submitted to arthrocentesis of the knee].Reumatismo.2003;55(3):159–163.
- .Textbook of Critical Care.5th ed.Philadelphia, PA:Elsevier Saunders;2005.
- ,.Complications of lumbar puncture followed by anticoagulation.Stroke.1981;12(6):879–881.
- ,,,.Mason, Murray and Nadel's Textbook of Respiratory Medicine.4th ed.Philadelphia, PA:Elsevier Saunders;2005.
- ,,.Videos in clinical medicine. Thoracentesis.N Engl J Med.2006;355(15):e16.
- ,.Lack of increased bleeding after paracentesis and thoracentesis in patients with mild coagulation abnormalities.Transfusion.1991;31(2):164–171.
- .Risk of bleeding during thoracentesis in anticoagulated patients.Chest.2006;130(4):141S–d‐2.
- ,,, et al.Guidelines for prevention of thromboembolic events in valvular heart disease. Study Group of the Working Group on Valvular Heart Disease of the European Society of Cardiology.Eur Heart J.1995;16(10):1320–1330.
- ,.Coronary angiography and intravascular ultrasonography. In: Braunwald E, Zipes DP, Libby P, eds.Heart Disease: A Textbook of Cardiovascular Medicine.6th ed.Philadelphia, PA:WB Saunders;2001:387–421.
- ,,, et al.Effectiveness of manual pressure hemostasis following transfemoral coronary angiography in patients on therapeutic warfarin anticoagulation.Am J Cardiol.2006;97(4):485–488.
- ,,,,,.Elective coronary angiography and percutaneous coronary intervention during uninterrupted warfarin therapy.Catheter Cardiovasc Interv.2003;60(2):180–184.
- ,,,.Coronary angiography in the fully anticoagulated patient: the transradial route is successful and safe.Catheter Cardiovasc Interv.2003;58(1):8–10.
- ,,,,.Percutaneous left and right heart catheterization in fully anticoagulated patients utilizing the radial artery and forearm vein: a two‐center experience.J Interv Cardiol.2006;19(3):258–263.
- ,,, et al.[Safety of diagnostic transradial catheterization in patients undergoing long‐term anticoagulation with coumarin derivatives].Rev Esp Cardiol.2007;60(9):988–991. [Spanish]
- ,,,,,,,,,,,,,2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Valvular Heart Disease).J Am Coll Cardiol.2008;52:e1–142.
- ,,, et al.ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: executive summary. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation): developed in Collaboration With the North American Society of Pacing and Electrophysiology.J Am Coll Cardiol.2001;38(4):1231–1266.
- .Periprocedural thromboprophylaxis in patients receiving chronic anticoagulation therapy.Am Heart J.2004;147(1):3–15.
- ,.Management of anticoagulation before and after elective surgery.N Engl J Med.1997;336(21):1506–1511.
- ,,,,,.Modern management of prosthetic valve anticoagulation.Mayo Clin Proc.1998;73(7):665–680.
- ,.Anticoagulant‐related bleeding: clinical epidemiology, prediction, and prevention.Am J Med.1993;95(3):315–328.
- ,,,,,.Reconstruction of musculoskeletal defects following oncologic resection in 76 patients.Ann Plast Surg.2006;57(2):190–194.
- ,,,,.Biopsy of the prostate guided by transrectal ultrasound: relation between warfarin use and incidence of bleeding complications.Clin Radiol.2005;60(4):459–463; discussion 457‐458.
- ,.Anticoagulation in neurosurgical patients.Neurosurgery.1999;45(4):838–847; discussion 847‐848.
- ,,,,.Post‐operative blood loss after transurethral prostatectomy is dependent on in situ fibrinolysis.Br J Urol.1997;80(6):889–893.
- ,,.Complications of heparin therapy after total joint arthroplasty.J Bone Joint Surg.1989;71(8):1130–1134.
- ,,,,,.Postpolypectomy lower GI bleeding: descriptive analysis.Gastrointest Endosc.2000;51(6):690–696.
- ,,, et al.Pocket hematoma after pacemaker or implantable cardioverter defibrillator surgery: influence of patient morbidity, operation strategy, and perioperative antiplatelet/anticoagulation therapy.Chest.2004;126(4):1177–1186.
- ,,.[Perioperative bridging with enoxaparin. results of the prospective BRAVE registry with 779 patients].Med Klin (Munich).2007;102(10):809–815. [German]
- ,,.Low molecular weight heparin as bridging anticoagulation during interruption of warfarin: assessment of a standardized periprocedural anticoagulation regimen.Arch Intern Med.2004;164(12):1319–1326.
- ,,.Bridging therapy in patients on long‐term oral anticoagulants who require surgery: the Prospective Peri‐operative Enoxaparin Cohort Trial (PROSPECT).J Thromb Haemost.2007;5(11):2211–2218.
- ,,, et al.Single‐arm study of bridging therapy with low molecular weight heparin for patients at risk of arterial embolism who require temporary interruption of warfarin.Circulation.2004;110(12):1658–1663.
- ,,,.Costs and clinical outcomes associated with low molecular weight heparin vs unfractionated heparin for perioperative bridging in patients receiving long‐term oral anticoagulant therapy.Chest.2004;125(5):1642–1650.
- ,.Enoxaparin is effective and safe as bridging anticoagulation in patients with a mechanical prosthetic heart valve who require temporary interruption of warfarin because of surgery or an invasive procedure. [Abstract #703]. ASH Annual Meeting Abstracts.Blood.2004;104:202A.
- ,,, et al.Periprocedural anticoagulation management of patients with nonvalvular atrial fibrillation.Mayo Clin Proc.2008;83(6):639–645.
- ,,,.Bridging anticoagulation with low molecular weight heparin after interruption of warfarin therapy is associated with a residual anticoagulant effect prior to surgery.Thromb Haemost.2005;94(3):528–531.
- ,,, et al.Brief communication: preoperative anticoagulant activity after bridging low molecular weight heparin for temporary interruption of warfarin.Ann Intern Med.2007;146(3):184–187.
- National Institute for Clinical Excellence. Atrial fibrillation: national clinical guideline for management in primary and secondary care.2006. Available at: http://www.nice.org.uk/nicemedia/pdf/cg036fullguideline. pdf. Accessed May 2009.
- ,,, et al.Clinical outcomes with unfractionated heparin or low molecular weight heparin as bridging therapy in patients on long‐term oral anticoagulants: the REGIMEN registry.J Thromb Haemost.2006;4(6):1246–1252.
- ,,,,,.Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation.JAMA.2001;285(22):2864–2870.
- ,,.Guidelines on oral anticoagulation (warfarin). 3rd ed. 2005 update.Br J Haematol.2006;132(3):277–285.
- ,,, et al.Risk of thromboembolism with short‐term interruption of warfarin therapy.Arch Intern Med.2008;168(1):63–69.
The management of patients on long‐term antithrombotic therapy (vitamin K antagonists [VKA] or antiplatelet agents) who may require temporary disruption for an invasive procedure is challenging. Management is controversial due to methodologically limited prospective data and varied consensus opinions. Yet periprocedural anticoagulation management is a commonly encountered clinical problem. It is estimated that there are 2.5 million patients on long‐term VKA therapy in North America1 and 41% of the U.S. population over age 40 years is on antiplatelet therapy.2 Further, the need for temporary disruption of these therapies for an invasive procedure is frequent. As an example, in 1 European study, approximately 15% of patients on long‐term VKA required a major surgical procedure in 4 years of follow‐up.3 The role of the hospitalist physician in managing these patients is increasing as hospitalists care for an increasing number of surgical patients and provide periprocedural consultation both in and out of the hospital. Therefore, it is imperative for the hospitalist physician to be proficient in making thoughtful and individualized recommendations on the appropriate management of periprocedural anticoagulants, drawing from the available literature and evidence‐based practice guidelines. Importantly, the Society of Hospital Medicine has cited perioperative management as an important core competency.4
The hospitalist physician is likely to encounter numerous periprocedural scenarios, including the management of antiplatelet agents, identifying low bleeding risk procedures wherein interruption of anticoagulants is unnecessary, and recognizing patients with a low short‐term thromboembolic risk where anticoagulants can be disrupted without the need for heparin or low molecular weight heparin (LMWH) in the periprocedural period (defined as bridging therapy). Further, all other clinical scenarios require both a careful individualized assessment of the patient's risk of periprocedural bleeding and thromboembolism and a thoughtful discussion with all involved parties. This discussion may involve the person performing the procedure, the anesthesiologist, and the patient. The purpose of this work is to explore these relevant areas through a review of the literature with a particular focus on the recently published 2008 American College of Chest Physicians (ACCP) evidence‐based clinical practice guidelines.
We reviewed medical literature from 1990 through May 2008 with the following key words: bridging, anticoagulation, perioperative, antiplatelet, heparin, and low molecular weight heparin. Individual studies were then independently reviewed by the authors. Studies that were felt relevant to a hospitalist physician were retrieved and reviewed. If there was uncertainty regarding applicability to a hospitalist setting, a second author's opinion was rendered. Additionally, we reviewed 1 author's personal reference list of articles relating to periprocedural anticoagulation that has been compiled over the past 10 years. This list and the reference lists of retrieved articles were also reviewed. Data were summarized to answer 4 clinically relevant questions:
-
What is the optimal management of antiplatelet therapy in the periprocedural period?
-
Are there very low‐bleeding risk procedures that do not require interruption of oral anticoagulation?
-
Are there low thromboembolic risk populations who do not require periprocedural bridging?
-
How do you manage patients who must discontinue anticoagulants but are at an increased thrombotic risk?
Clinical Question #1: What Is the Optimal Management of Antiplatelet Therapy in the Periprocedural Period?
The optimal management of oral antiplatelet therapy in the periprocedural period is not well studied. Most reviews, expert recommendations, and consensus statements either do not comment on periprocedural antiplatelet management or recommend the routine discontinuation of therapy at least 7 days prior to surgery.3, 5, 6 However, as the 2008 ACCP guidelines highlight, the recommendation to routinely discontinue antiplatelet therapy 7 days prior to the procedure is an oversimplification.1 In the era of both bare metal cardiac stents and drug‐eluting stents, the optimal management of these patients requires that 2 primary questions be asked: (1) Is this a low‐bleeding risk procedure whereby antiplatelet therapy can be continued? (2) Does the patient have a coronary stent whereby the continuation of antiplatelet therapy or delay of the intervention is necessary?
In the context of ongoing aspirin therapy, certain procedures have a low risk of significant hemorrhagic complications. These low bleeding risk procedures include cataract surgery, cutaneous surgery, oral surgery, and endoscopic procedures, including those with mucosal biopsies.710 Patients undergoing these procedures may safely continue low dose aspirin therapy, especially if they have a high‐risk indication for their aspirin such as recent myocardial infarction, stroke, or the presence of a coronary stent.5, 710 Whether these procedures can be safely performed in the setting of a thienopyridine or combination antiplatelet therapy is uncertain.
In the past several decades, the management of obstructive coronary artery disease has undergone a major evolution. Placement of coronary stents has become commonplace, and there are now several million patients with drug‐eluting stents.11 The major complication of these devices is stent thrombosis, which results in death or myocardial infarction in up to 64% of patients.12 Fortunately, dual antiplatelet therapy (aspirin and a thienopyridine such as clopidogrel) markedly reduces this risk.13 Current guidelines recommend using combination antiplatelet therapy for at least 4 to 6 weeks and ideally up to 12 months after placement of a bare metal stent and at least 12 months after placement of either a sirolimus‐ or paclitaxel‐eluting stent.1, 14 During this period of dual antiplatelet therapy, the premature discontinuation of the thienopyridine may be catastrophic. To guide clinicians in managing these patients in the periprocedural period, recent consensus guidelines recommend the following:1, 12
-
In patients who are expected to need an invasive surgical procedure in the next 12 months, consideration should be given to avoiding drug‐eluting stents.
-
Elective procedures which have an increased risk of bleeding should be deferred for at least 6 weeks after bare metal stent implantation and 12 months after drug‐eluting stent implantation.
-
For patients undergoing a surgical procedure within 6 weeks of bare metal stent implantation and 12 months of drug‐eluting stent implantation, continuation of aspirin and clopidogrel is recommended. If bleeding risk prohibits this, then a cardiologist should be consulted.
-
In patients with a drug‐eluting stent who need to undergo a procedure whereby the thienopyridine needs to be discontinued, aspirin should be continued if at all possible, and the thienopyridine should be resumed as soon as possible after the procedure. It may be reasonable to consider a loading dose of clopidogrel, up to 600 mg, in this setting, although prospective supportive data is lacking.1
It is important to recognize that delayed stent thrombosis is now reported well beyond 1 year after drug‐eluting stent implantation, and that there may not be a diminution in risk after the initial 12 months.1517 Until additional data is available, it seems prudent, if possible, to at least continue aspirin in the periprocedural period in these patients. If bleeding concerns obviate this, then antiplatelet therapy should be discontinued and resumed as soon as possible.
For patients on chronic antiplatelet therapy who do not have a cardiac stent and who are not undergoing a low‐bleeding‐risk procedure, the risks and benefits of the continuation or discontinuation of antiplatelet therapy in the periprocedural period are uncertain as absolute risks in the periprocedural period have not been well studied. Relative risks/benefits, however, can be estimated from prior studies. Aspirin leads to an approximate 25% relative risk reduction in cardiac or thrombotic event rates compared to placebo.14, 18 Although important, the absolute benefit of 1 week of therapy (vs. no therapy during the periprocedural period) is estimated to be small. The small absolute benefit of continued aspirin therapy may be offset by an increase in significant bleeding events. Although, not well studied, continued aspirin increases significant bleeding by 50% with absolute event rates varying by type of procedure.8 In some procedures, such as intracranial surgery or transurethral prostatectomy, this bleeding risk is prohibitive. For others, the risk may be modest and the decision to continue vs. discontinue aspirin therapy may be at the discretion of the person performing the procedure. In general, for most patients who do not have a coronary stent and have not had a recent (past 3 months) myocardial infarction or stroke, discontinuation of antiplatelet therapy 7 to 10 days prior to the procedure seems prudent. The primary exceptions are patients who are undergoing percutaneous coronary intervention or coronary artery bypass grafting. For these procedures continuing aspirin is recommended.1 Figure 1 outlines a proposed management strategy based upon available evidence and guidelines.
Clinical Question #2: Are There Very‐Low‐Bleeding‐Risk Procedures That Do Not Require Interruption of Oral Anticoagulation?
Some procedures are associated with a low‐enough risk of bleeding that it is safe to proceed without interrupting VKA anticoagulation. This approach spares the risk and cost that occur with the holding of oral anticoagulants and institution of bridging therapy. When considering this strategy, it is important that the specialist performing the procedure is included in the discussion. Dental, dermatologic, and cataract procedures are common outpatient procedures that are associated with low bleeding risk. The relative safety of these procedures in patients who are anticoagulated is discussed thoroughly in the ACCP guidelines.1 Other low‐bleeding‐risk procedures for which a hospitalist may be consulted include certain endoscopic procedures, paracentesis, central venous catheter placement, and arthrocentesis.
The American Society for Gastrointestinal Endoscopy has published guidelines recommending that anticoagulation can be safely continued in patients undergoing the following endoscopic procedures with a low bleeding risk: esophagogastroduodenoscopy (EGD), flexible sigmoidoscopy, and colonoscopy, all with or without mucosal biopsy; enteroscopy, biliary/pancreatic stent placement, endoscopic ultrasound without biopsy, and endoscopic retrograde cholangiopancreatography (ERCP) without sphincterotomy.19 Conversely, high‐risk procedures for which interruption of anticoagulation is recommended include polypectomy, biliary sphincterotomy, variceal treatment, percutaneous endoscopic gastrostomy (PEG) placement, dilation of strictures, and endoscopic ultrasound‐guided fine‐needle aspiration.
Limited data suggest that paracentesis, central venous catheter placement, and arthrocentesis may be safe to perform in the setting of anticoagulation. For patients undergoing paracentesis there is little evidence in anticoagulated patients; however, it is probably safe to continue anticoagulation as studies have demonstrated the safety of this procedure in patients with significant thrombocytopenia and coagulopathy.20, 21 Limited data also supports that central venous catheter placement may be safely performed in the setting of abnormal coagulation tests, although some recommend avoiding the subclavian site due to the risk of hemothorax and the inability to apply adequate compression.2226 With regard to arthrocentesis, multiple authors have endorsed the idea that joint and soft‐tissue aspirations and injections present a low risk of serious bleeding even with anticoagulation.2729 This is supported by limited data.30, 31
Other procedures such as lumbar puncture, thoracentesis, and cardiac catheterization are somewhat more controversial in the anticoagulated patient. Anticoagulation should generally be interrupted for lumbar puncture,29, 32 as 1 study involving patients who were started on heparin immediately after the procedure had a 2% incidence of spinal hematoma and 6.7% major complication rate.33 With regard to thoracentesis, evidence is very limited, but experts generally accept that it may be safely performed in patients with mild coagulopathy.34, 35 One frequently‐cited study found no bleeding complications in 57 patients with mild elevation in prothrombin time, which correlated to an International Normalized Ratio of approximately 2.2 or less.36 A recent report also revealed no serious bleeding complications in 33 thoracenteses performed on patients receiving full anticoagulation with warfarin, heparin, and/or low molecular weight heparin.37
Therapeutic anticoagulation has traditionally been felt to be a relative contraindication to cardiac catheterization.38, 39 In spite of this, several observational studies have suggested it may be safely performed using a standard approach,40 using vascular closure devices,41 or using a radial artery approach instead of the more commonly used femoral site.4244 The small size of these observational reports, the diagnostic rather than therapeutic nature of most cases, the limited use of other antithrombotic and antiplatelet medications, and the experience required to use the transradial approach are all major limitations preventing widespread acceptance of cardiac catheterization in therapeutically anticoagulated patients.
In summary, there are numerous procedures that may be safely pursued in the setting of therapeutic anticoagulation. However, for most of these procedures the data is somewhat limited. As such, it is paramount for the hospitalist physician to recognize these clinical scenarios and to discuss management options with the patient and the person performing the procedure, if applicable.
Clinical Question #3: Are There LowThromboembolic‐Risk Populations Who Do Not Require Periprocedural Bridging?
Although it has previously been noted that there is a wide variation of opinion on when and how to perform periprocedural bridging, it is generally agreed that in the following conditions the risk of thrombosis is low enough that bridging with full dose heparin or LMWH is not necessary:1, 5, 4549
-
Atrial fibrillation without previous stroke or transient ischemic attack (TIA) and no more than 2 additional thrombotic risk factors on the CHADS2 scoring system (Table 1).
-
A single venous thromboembolic event that occurred greater than 12 months ago with no ongoing risk factors such as active malignancy, high risk thrombophilia, or the antiphospholipid antibody syndrome.
-
Bileaflet aortic valve without the presence of additional risk factors (ie, patients 75 years of age with the absence of atrial fibrillation, prior stroke or transient ischemic attack, hypertension, diabetes, or congestive heart failure).
| CHADS2 Score* | Annual Risk of Stroke (%) |
|---|---|
| |
| 0 | 1.9 |
| 1 | 2.8 |
| 2 | 4.0 |
| 3 | 5.9 |
| 4 | 8.5 |
| 5 | 12.5 |
| 6 | 18.2 |
Clinical Question #4: How Do You Manage Patients Who Must Discontinue Anticoagulants But Are at an Increased Thrombotic Risk?
When anticoagulation must be held and the patient does not have a very low thromboembolic risk, a decision of whether or not to use bridging anticoagulation must be made. The current ACCP guideline gives grade 1C and 2C recommendations (evidence from observational studies, case series, or controlled trials with serious flaws) regarding for whom and how to implement bridging.1 The grade C designation is due to a lack of high‐quality randomized clinical trials. As such, the clinician must carefully consider an individual patient's estimated thromboembolic risk, procedurally‐related bleeding risk, patient‐related bleeding risk factors, and the patient's values regarding concerns of thromboembolism or bleeding. In these situations it is also imperative that the person performing the procedure is involved in the risk‐to‐benefit discussion.
When evaluating an individual patient's risk of thromboembolism, clinicians sometimes estimate the perioperative risk by prorating the annual incidence of thromboembolic complications to the few days that anticoagulation is withheld.67 Making this extrapolation discounts the effect of a potential increase in thromboembolic risk induced by surgery. As an example, an average patient with atrial fibrillation who has a 5% predicted annual stroke rate would be estimated to have a stroke risk of 0.05% if they are not anticoagulated for 4 days. However, studies have shown that the actual rate of perioperative thromboembolism is approximately 1%.1 With these limitations and uncertainties in mind, and until there is better prospective outcomes data, we must consider relative risks in the context of absolute event rate estimates when deciding a perioperative anticoagulant management plan. The estimated annual incidence of thrombosis without anticoagulation for various indications and the current guideline recommendations are presented in Table 2.
| Practice Guideline Preferred Management Recommendations | ||||
|---|---|---|---|---|
| Indication for chronic anticoagulation | Estimated Annual Thrombotic Risk Without Anticoagulation | ACCP*1 | ACC/AHA45, 46 | British Haematologic Society70 |
| ||||
| Dual prosthetic or older‐generation valve | >10% | Bridge | Bridge | Bridge |
| VTE within 3 months or severe thrombophilias | Bridge | N/A | Bridge | |
| Pregnancy with prosthetic valve | Bridge | Bridge | N/A | |
| Bileaflet valve in the mitral position | Bridge | Bridge | Prophylaxis | |
| Valve with acute embolism 6 months | Bridge | N/A | Bridge | |
| A‐fib valvular or CHADS2 score 5‐6 | Bridge | Consider bridging | N/A | |
| Recurrent venous thromboembolism | 4‐10% | Bridge | N/A | N/A |
| VTE within 3‐12 months or active cancer | Bridge | N/A | Prophylaxis | |
| Bileaflet aortic valve with additional risk factors | Bridge | Bridge | Prophylaxis | |
| A‐fib CHADS2 score 3‐4 | Bridge | Consider bridging | N/A | |
| Bileaflet aortic valve without additional risk factors | 4% | Prophylaxis or no bridging | No bridging | Prophylaxis |
| VTE >12 months | Prophylaxis or no bridging | N/A | Prophylaxis | |
| A‐fib CHADS2 score 0‐2 and no previous CVA/TIA | Prophylaxis or no bridging | No bridging | N/A | |
In addition to thromboembolic risk, we must also consider the bleeding risk associated with the procedure/surgery. Importantly, therapeutic heparin started early in the postoperative period is associated with major bleeding event rates as high as 10% to 20%.1, 50 Once a major bleeding event occurs, this will often lead to an extended interruption of anticoagulant therapy, placing the patient at a more prolonged risk of an associated thromboembolic event. For this reason, the resumption of full‐dose anticoagulation with LMWH/heparin should be delayed for at least 48 hours in most patients undergoing a surgery or procedure associated with an increased risk of bleeding. Examples of these higher‐bleeding‐risk procedures include major thoracic surgery, intracranial or spinal surgery, major vascular surgery, major orthopedic surgery, urologic surgery involving the bladder or prostrate, major oncologic surgery, reconstructive plastic surgery, colonoscopy with associated polypectomy, renal or prostate biopsies, and placement of a cardiac pacemaker/defibrillator.1, 5157
Taken together, these uncertainties surrounding thromboembolic and bleeding risk estimates imply that there are multiple options for periprocedural management. Several studies, many of which included patients with mechanical heart valves, have shown similar safety and efficacy between LMWH and intravenous (IV) unfractionated heparin.5864 Table 3 summarizes these studies. The ACCP recommends bridging with LMWH over IV unfractionated heparin due to equal efficacy and cost savings with LMWH.1 When bridging is used, careful attention must be given to the timing and dose of anticoagulation in both the preoperative and postoperative periods. Table 4 lists dosing of commonly used LMWHs in North America. When using LMWHs in the preprocedural setting it is important to note that unacceptably high levels of anticoagulation remain present when a patient is given a full once‐daily LMWH dose the morning prior to the procedure or when a full‐dose, twice‐daily LMWH dose is given the evening prior to the procedure.65, 66 For this reason, the ACCP recommends administering the last preoperative dose 24 hours before surgery and if full‐dose once‐daily LMWH is used, the dose should be decreased by one‐half on the day before the surgery in order to ensure that no residual anticoagulant effect remains at the time of surgery.
| AuthorReference/Study Type | Number of Patients | Patient Population | Type of Procedure | Bridging Strategy | Major Bleeds | Minor Bleeds | TE Rate |
|---|---|---|---|---|---|---|---|
| |||||||
| Turpie and Douketis63/single arm cohort | 174 | 66% aortic valve; 34% mitral or dual prosthetic valve | Not specified | Enoxaparin 1 mg/kg twice daily | 2.3% | Not specified | None |
| Kovacs et al.61/single arm cohort | 224 | Prosthetic heart valves or a‐fib plus 1 major risk factor | 67 surgical; 157 nonsurgical | Preoperative bridging with dalteparin 200 IU/kg daily; dose reduced to 100 IU/kg on preoperative day 1; restarted at 100 IU/kg on POD 1; dose reduced to 5000 IU daily if high risk for bleeding | 6.7%; 8/15 occurred intraoperatively or 6 hours postoperatively; 2/15 occurred after 4 weeks | Not specified | 3.6%; 6/8 episodes occurred after warfarin held secondary to bleeding; 2/8 thrombotic episodes judged to be due to cardioembolism |
| Douketis et al.59/prospective registry | 650 | A‐fib 58%; mechanical heart valve 33% | 251 surgical; 399 nonsurgical | Dalteparin 100 IU/kg twice daily; held after high bleeding risk procedure and patients with poor hemostasis | 0.92% | 5.9% | 0.6% |
| Spyropolous et al.62/prospective registry; 14 centers in United States and Canada | 901 | UFH: 40% mechanical valves, 33% a‐fib; LMWH: 24% mechanical valve, 40% a‐fib | 394 surgical; 507 nonsurgical | LMWH mostly given twice daily 80%; UFH 20% | 5.5% UFH; 3.3% LMWH | 9.1% UFH; 12.0% LMWH | 2.4% UFH; 0.9% LMWH |
| Dunn et al.66/prospective cohort | 260 | A‐fib 68% or prior DVT 37% (excluding prosthetic heart valves) | 105 surgical; 145 nonsurgical | Enoxaparin 1.5 mg/kg daily | 3.5% overall; minor surgery/procedures 0.9%; major surgery 28% | 42% | 1.9%; 1/5 events occurred after bleeding led to withdrawal of AC |
| Omran et al.77/prospective registry | 779 | Various indications | Major and minor procedures | All patients bridged with enoxaparin; moderate TE risk 1 mg/kg daily; high TE risk 1 mg/kg twice daily | 0.5%; all in high‐risk group | 5.9% | 0 |
| Garcia et al.71/prospective, observational cohort of 101 sites in United States | 1024 patients with 1293 interruptions of AC | A‐fib 53%; VTE 14%; prosthetic valve 13% | Outpatient procedures only | At discretion of provider. Bridging performed in 8.3% of interruptions; 3% a‐fib, 10% VTE, and 29% mechanical valves | 0.6%; 4/6 patients with major bleed received bridging | 1.7%;10/17 patients with minor bleed received bridging | 0.7%; no events in patients who were bridged |
| Wysokinski et al.64/prospective cohort | 345 consecutive patients undergoing 386 procedures | 100% nonvalvular a‐fib | Major and minor surgeries/procedures | Individualized in AC clinic; 52% of patients bridged | 2.7%; no difference whether patient received bridging or not | 3.0%; 10/11 occurred in bridged patients | 1.1%; no difference in bridged vs. nonbridged patients |
| Low Molecular Weight Heparin | Subcutaneous Dose |
|---|---|
| |
| Dalteparin | |
| Low dose (prophylaxis dose) | 5,000 IU once daily |
| Full dose | 100 IU/kg twice daily or 200 IU/kg once daily |
| Enoxaparin | |
| Low dose (prophylaxis dose) | 30 mg twice daily or 40mg daily |
| Full dose | 1 mg/kg twice daily or 1.5 mg/kg once daily |
| Tinzaparin (full dose) | 175 IU/kg once daily |
In the postprocedural setting, timing and dose of anticoagulant is important, as major bleeding with the use of therapeutic anticoagulation can occur in up to 10% to 20% of cases. When restarting anticoagulation after the procedure, it is important to evaluate intraoperative hemostasis and to consider patient‐related factors that may further increase bleeding risk. These include advanced age, concomitant antiplatelet or nonsteroidal antiinflammatory medications, renal insufficiency, placement of spinal/epidural catheter, worsening liver disease, or the presence of other comorbid illnesses such as cancer.30, 67, 68 The ACCP recommends withholding full‐dose anticoagulation for at least 48 to 72 hours in patients who are felt to be at a high risk for postoperative bleeding.1 Figure 2 is a proposed management approach to the use of bridging anticoagulants that is consistent with the 2008 ACCP recommendations.
CONCLUSION
The evaluation and management of patients on long‐term antiplatelet or VKA therapy who require an invasive procedure or surgery is a common, complicated, and controversial area. Importantly, it is an area in which the hospitalist physician must be adept. Although there remain many unanswered clinical questions, an evolving literature base and recent practice guidelines can help guide management decisions.
The management of patients on long‐term antithrombotic therapy (vitamin K antagonists [VKA] or antiplatelet agents) who may require temporary disruption for an invasive procedure is challenging. Management is controversial due to methodologically limited prospective data and varied consensus opinions. Yet periprocedural anticoagulation management is a commonly encountered clinical problem. It is estimated that there are 2.5 million patients on long‐term VKA therapy in North America1 and 41% of the U.S. population over age 40 years is on antiplatelet therapy.2 Further, the need for temporary disruption of these therapies for an invasive procedure is frequent. As an example, in 1 European study, approximately 15% of patients on long‐term VKA required a major surgical procedure in 4 years of follow‐up.3 The role of the hospitalist physician in managing these patients is increasing as hospitalists care for an increasing number of surgical patients and provide periprocedural consultation both in and out of the hospital. Therefore, it is imperative for the hospitalist physician to be proficient in making thoughtful and individualized recommendations on the appropriate management of periprocedural anticoagulants, drawing from the available literature and evidence‐based practice guidelines. Importantly, the Society of Hospital Medicine has cited perioperative management as an important core competency.4
The hospitalist physician is likely to encounter numerous periprocedural scenarios, including the management of antiplatelet agents, identifying low bleeding risk procedures wherein interruption of anticoagulants is unnecessary, and recognizing patients with a low short‐term thromboembolic risk where anticoagulants can be disrupted without the need for heparin or low molecular weight heparin (LMWH) in the periprocedural period (defined as bridging therapy). Further, all other clinical scenarios require both a careful individualized assessment of the patient's risk of periprocedural bleeding and thromboembolism and a thoughtful discussion with all involved parties. This discussion may involve the person performing the procedure, the anesthesiologist, and the patient. The purpose of this work is to explore these relevant areas through a review of the literature with a particular focus on the recently published 2008 American College of Chest Physicians (ACCP) evidence‐based clinical practice guidelines.
We reviewed medical literature from 1990 through May 2008 with the following key words: bridging, anticoagulation, perioperative, antiplatelet, heparin, and low molecular weight heparin. Individual studies were then independently reviewed by the authors. Studies that were felt relevant to a hospitalist physician were retrieved and reviewed. If there was uncertainty regarding applicability to a hospitalist setting, a second author's opinion was rendered. Additionally, we reviewed 1 author's personal reference list of articles relating to periprocedural anticoagulation that has been compiled over the past 10 years. This list and the reference lists of retrieved articles were also reviewed. Data were summarized to answer 4 clinically relevant questions:
-
What is the optimal management of antiplatelet therapy in the periprocedural period?
-
Are there very low‐bleeding risk procedures that do not require interruption of oral anticoagulation?
-
Are there low thromboembolic risk populations who do not require periprocedural bridging?
-
How do you manage patients who must discontinue anticoagulants but are at an increased thrombotic risk?
Clinical Question #1: What Is the Optimal Management of Antiplatelet Therapy in the Periprocedural Period?
The optimal management of oral antiplatelet therapy in the periprocedural period is not well studied. Most reviews, expert recommendations, and consensus statements either do not comment on periprocedural antiplatelet management or recommend the routine discontinuation of therapy at least 7 days prior to surgery.3, 5, 6 However, as the 2008 ACCP guidelines highlight, the recommendation to routinely discontinue antiplatelet therapy 7 days prior to the procedure is an oversimplification.1 In the era of both bare metal cardiac stents and drug‐eluting stents, the optimal management of these patients requires that 2 primary questions be asked: (1) Is this a low‐bleeding risk procedure whereby antiplatelet therapy can be continued? (2) Does the patient have a coronary stent whereby the continuation of antiplatelet therapy or delay of the intervention is necessary?
In the context of ongoing aspirin therapy, certain procedures have a low risk of significant hemorrhagic complications. These low bleeding risk procedures include cataract surgery, cutaneous surgery, oral surgery, and endoscopic procedures, including those with mucosal biopsies.710 Patients undergoing these procedures may safely continue low dose aspirin therapy, especially if they have a high‐risk indication for their aspirin such as recent myocardial infarction, stroke, or the presence of a coronary stent.5, 710 Whether these procedures can be safely performed in the setting of a thienopyridine or combination antiplatelet therapy is uncertain.
In the past several decades, the management of obstructive coronary artery disease has undergone a major evolution. Placement of coronary stents has become commonplace, and there are now several million patients with drug‐eluting stents.11 The major complication of these devices is stent thrombosis, which results in death or myocardial infarction in up to 64% of patients.12 Fortunately, dual antiplatelet therapy (aspirin and a thienopyridine such as clopidogrel) markedly reduces this risk.13 Current guidelines recommend using combination antiplatelet therapy for at least 4 to 6 weeks and ideally up to 12 months after placement of a bare metal stent and at least 12 months after placement of either a sirolimus‐ or paclitaxel‐eluting stent.1, 14 During this period of dual antiplatelet therapy, the premature discontinuation of the thienopyridine may be catastrophic. To guide clinicians in managing these patients in the periprocedural period, recent consensus guidelines recommend the following:1, 12
-
In patients who are expected to need an invasive surgical procedure in the next 12 months, consideration should be given to avoiding drug‐eluting stents.
-
Elective procedures which have an increased risk of bleeding should be deferred for at least 6 weeks after bare metal stent implantation and 12 months after drug‐eluting stent implantation.
-
For patients undergoing a surgical procedure within 6 weeks of bare metal stent implantation and 12 months of drug‐eluting stent implantation, continuation of aspirin and clopidogrel is recommended. If bleeding risk prohibits this, then a cardiologist should be consulted.
-
In patients with a drug‐eluting stent who need to undergo a procedure whereby the thienopyridine needs to be discontinued, aspirin should be continued if at all possible, and the thienopyridine should be resumed as soon as possible after the procedure. It may be reasonable to consider a loading dose of clopidogrel, up to 600 mg, in this setting, although prospective supportive data is lacking.1
It is important to recognize that delayed stent thrombosis is now reported well beyond 1 year after drug‐eluting stent implantation, and that there may not be a diminution in risk after the initial 12 months.1517 Until additional data is available, it seems prudent, if possible, to at least continue aspirin in the periprocedural period in these patients. If bleeding concerns obviate this, then antiplatelet therapy should be discontinued and resumed as soon as possible.
For patients on chronic antiplatelet therapy who do not have a cardiac stent and who are not undergoing a low‐bleeding‐risk procedure, the risks and benefits of the continuation or discontinuation of antiplatelet therapy in the periprocedural period are uncertain as absolute risks in the periprocedural period have not been well studied. Relative risks/benefits, however, can be estimated from prior studies. Aspirin leads to an approximate 25% relative risk reduction in cardiac or thrombotic event rates compared to placebo.14, 18 Although important, the absolute benefit of 1 week of therapy (vs. no therapy during the periprocedural period) is estimated to be small. The small absolute benefit of continued aspirin therapy may be offset by an increase in significant bleeding events. Although, not well studied, continued aspirin increases significant bleeding by 50% with absolute event rates varying by type of procedure.8 In some procedures, such as intracranial surgery or transurethral prostatectomy, this bleeding risk is prohibitive. For others, the risk may be modest and the decision to continue vs. discontinue aspirin therapy may be at the discretion of the person performing the procedure. In general, for most patients who do not have a coronary stent and have not had a recent (past 3 months) myocardial infarction or stroke, discontinuation of antiplatelet therapy 7 to 10 days prior to the procedure seems prudent. The primary exceptions are patients who are undergoing percutaneous coronary intervention or coronary artery bypass grafting. For these procedures continuing aspirin is recommended.1 Figure 1 outlines a proposed management strategy based upon available evidence and guidelines.
Clinical Question #2: Are There Very‐Low‐Bleeding‐Risk Procedures That Do Not Require Interruption of Oral Anticoagulation?
Some procedures are associated with a low‐enough risk of bleeding that it is safe to proceed without interrupting VKA anticoagulation. This approach spares the risk and cost that occur with the holding of oral anticoagulants and institution of bridging therapy. When considering this strategy, it is important that the specialist performing the procedure is included in the discussion. Dental, dermatologic, and cataract procedures are common outpatient procedures that are associated with low bleeding risk. The relative safety of these procedures in patients who are anticoagulated is discussed thoroughly in the ACCP guidelines.1 Other low‐bleeding‐risk procedures for which a hospitalist may be consulted include certain endoscopic procedures, paracentesis, central venous catheter placement, and arthrocentesis.
The American Society for Gastrointestinal Endoscopy has published guidelines recommending that anticoagulation can be safely continued in patients undergoing the following endoscopic procedures with a low bleeding risk: esophagogastroduodenoscopy (EGD), flexible sigmoidoscopy, and colonoscopy, all with or without mucosal biopsy; enteroscopy, biliary/pancreatic stent placement, endoscopic ultrasound without biopsy, and endoscopic retrograde cholangiopancreatography (ERCP) without sphincterotomy.19 Conversely, high‐risk procedures for which interruption of anticoagulation is recommended include polypectomy, biliary sphincterotomy, variceal treatment, percutaneous endoscopic gastrostomy (PEG) placement, dilation of strictures, and endoscopic ultrasound‐guided fine‐needle aspiration.
Limited data suggest that paracentesis, central venous catheter placement, and arthrocentesis may be safe to perform in the setting of anticoagulation. For patients undergoing paracentesis there is little evidence in anticoagulated patients; however, it is probably safe to continue anticoagulation as studies have demonstrated the safety of this procedure in patients with significant thrombocytopenia and coagulopathy.20, 21 Limited data also supports that central venous catheter placement may be safely performed in the setting of abnormal coagulation tests, although some recommend avoiding the subclavian site due to the risk of hemothorax and the inability to apply adequate compression.2226 With regard to arthrocentesis, multiple authors have endorsed the idea that joint and soft‐tissue aspirations and injections present a low risk of serious bleeding even with anticoagulation.2729 This is supported by limited data.30, 31
Other procedures such as lumbar puncture, thoracentesis, and cardiac catheterization are somewhat more controversial in the anticoagulated patient. Anticoagulation should generally be interrupted for lumbar puncture,29, 32 as 1 study involving patients who were started on heparin immediately after the procedure had a 2% incidence of spinal hematoma and 6.7% major complication rate.33 With regard to thoracentesis, evidence is very limited, but experts generally accept that it may be safely performed in patients with mild coagulopathy.34, 35 One frequently‐cited study found no bleeding complications in 57 patients with mild elevation in prothrombin time, which correlated to an International Normalized Ratio of approximately 2.2 or less.36 A recent report also revealed no serious bleeding complications in 33 thoracenteses performed on patients receiving full anticoagulation with warfarin, heparin, and/or low molecular weight heparin.37
Therapeutic anticoagulation has traditionally been felt to be a relative contraindication to cardiac catheterization.38, 39 In spite of this, several observational studies have suggested it may be safely performed using a standard approach,40 using vascular closure devices,41 or using a radial artery approach instead of the more commonly used femoral site.4244 The small size of these observational reports, the diagnostic rather than therapeutic nature of most cases, the limited use of other antithrombotic and antiplatelet medications, and the experience required to use the transradial approach are all major limitations preventing widespread acceptance of cardiac catheterization in therapeutically anticoagulated patients.
In summary, there are numerous procedures that may be safely pursued in the setting of therapeutic anticoagulation. However, for most of these procedures the data is somewhat limited. As such, it is paramount for the hospitalist physician to recognize these clinical scenarios and to discuss management options with the patient and the person performing the procedure, if applicable.
Clinical Question #3: Are There LowThromboembolic‐Risk Populations Who Do Not Require Periprocedural Bridging?
Although it has previously been noted that there is a wide variation of opinion on when and how to perform periprocedural bridging, it is generally agreed that in the following conditions the risk of thrombosis is low enough that bridging with full dose heparin or LMWH is not necessary:1, 5, 4549
-
Atrial fibrillation without previous stroke or transient ischemic attack (TIA) and no more than 2 additional thrombotic risk factors on the CHADS2 scoring system (Table 1).
-
A single venous thromboembolic event that occurred greater than 12 months ago with no ongoing risk factors such as active malignancy, high risk thrombophilia, or the antiphospholipid antibody syndrome.
-
Bileaflet aortic valve without the presence of additional risk factors (ie, patients 75 years of age with the absence of atrial fibrillation, prior stroke or transient ischemic attack, hypertension, diabetes, or congestive heart failure).
| CHADS2 Score* | Annual Risk of Stroke (%) |
|---|---|
| |
| 0 | 1.9 |
| 1 | 2.8 |
| 2 | 4.0 |
| 3 | 5.9 |
| 4 | 8.5 |
| 5 | 12.5 |
| 6 | 18.2 |
Clinical Question #4: How Do You Manage Patients Who Must Discontinue Anticoagulants But Are at an Increased Thrombotic Risk?
When anticoagulation must be held and the patient does not have a very low thromboembolic risk, a decision of whether or not to use bridging anticoagulation must be made. The current ACCP guideline gives grade 1C and 2C recommendations (evidence from observational studies, case series, or controlled trials with serious flaws) regarding for whom and how to implement bridging.1 The grade C designation is due to a lack of high‐quality randomized clinical trials. As such, the clinician must carefully consider an individual patient's estimated thromboembolic risk, procedurally‐related bleeding risk, patient‐related bleeding risk factors, and the patient's values regarding concerns of thromboembolism or bleeding. In these situations it is also imperative that the person performing the procedure is involved in the risk‐to‐benefit discussion.
When evaluating an individual patient's risk of thromboembolism, clinicians sometimes estimate the perioperative risk by prorating the annual incidence of thromboembolic complications to the few days that anticoagulation is withheld.67 Making this extrapolation discounts the effect of a potential increase in thromboembolic risk induced by surgery. As an example, an average patient with atrial fibrillation who has a 5% predicted annual stroke rate would be estimated to have a stroke risk of 0.05% if they are not anticoagulated for 4 days. However, studies have shown that the actual rate of perioperative thromboembolism is approximately 1%.1 With these limitations and uncertainties in mind, and until there is better prospective outcomes data, we must consider relative risks in the context of absolute event rate estimates when deciding a perioperative anticoagulant management plan. The estimated annual incidence of thrombosis without anticoagulation for various indications and the current guideline recommendations are presented in Table 2.
| Practice Guideline Preferred Management Recommendations | ||||
|---|---|---|---|---|
| Indication for chronic anticoagulation | Estimated Annual Thrombotic Risk Without Anticoagulation | ACCP*1 | ACC/AHA45, 46 | British Haematologic Society70 |
| ||||
| Dual prosthetic or older‐generation valve | >10% | Bridge | Bridge | Bridge |
| VTE within 3 months or severe thrombophilias | Bridge | N/A | Bridge | |
| Pregnancy with prosthetic valve | Bridge | Bridge | N/A | |
| Bileaflet valve in the mitral position | Bridge | Bridge | Prophylaxis | |
| Valve with acute embolism 6 months | Bridge | N/A | Bridge | |
| A‐fib valvular or CHADS2 score 5‐6 | Bridge | Consider bridging | N/A | |
| Recurrent venous thromboembolism | 4‐10% | Bridge | N/A | N/A |
| VTE within 3‐12 months or active cancer | Bridge | N/A | Prophylaxis | |
| Bileaflet aortic valve with additional risk factors | Bridge | Bridge | Prophylaxis | |
| A‐fib CHADS2 score 3‐4 | Bridge | Consider bridging | N/A | |
| Bileaflet aortic valve without additional risk factors | 4% | Prophylaxis or no bridging | No bridging | Prophylaxis |
| VTE >12 months | Prophylaxis or no bridging | N/A | Prophylaxis | |
| A‐fib CHADS2 score 0‐2 and no previous CVA/TIA | Prophylaxis or no bridging | No bridging | N/A | |
In addition to thromboembolic risk, we must also consider the bleeding risk associated with the procedure/surgery. Importantly, therapeutic heparin started early in the postoperative period is associated with major bleeding event rates as high as 10% to 20%.1, 50 Once a major bleeding event occurs, this will often lead to an extended interruption of anticoagulant therapy, placing the patient at a more prolonged risk of an associated thromboembolic event. For this reason, the resumption of full‐dose anticoagulation with LMWH/heparin should be delayed for at least 48 hours in most patients undergoing a surgery or procedure associated with an increased risk of bleeding. Examples of these higher‐bleeding‐risk procedures include major thoracic surgery, intracranial or spinal surgery, major vascular surgery, major orthopedic surgery, urologic surgery involving the bladder or prostrate, major oncologic surgery, reconstructive plastic surgery, colonoscopy with associated polypectomy, renal or prostate biopsies, and placement of a cardiac pacemaker/defibrillator.1, 5157
Taken together, these uncertainties surrounding thromboembolic and bleeding risk estimates imply that there are multiple options for periprocedural management. Several studies, many of which included patients with mechanical heart valves, have shown similar safety and efficacy between LMWH and intravenous (IV) unfractionated heparin.5864 Table 3 summarizes these studies. The ACCP recommends bridging with LMWH over IV unfractionated heparin due to equal efficacy and cost savings with LMWH.1 When bridging is used, careful attention must be given to the timing and dose of anticoagulation in both the preoperative and postoperative periods. Table 4 lists dosing of commonly used LMWHs in North America. When using LMWHs in the preprocedural setting it is important to note that unacceptably high levels of anticoagulation remain present when a patient is given a full once‐daily LMWH dose the morning prior to the procedure or when a full‐dose, twice‐daily LMWH dose is given the evening prior to the procedure.65, 66 For this reason, the ACCP recommends administering the last preoperative dose 24 hours before surgery and if full‐dose once‐daily LMWH is used, the dose should be decreased by one‐half on the day before the surgery in order to ensure that no residual anticoagulant effect remains at the time of surgery.
| AuthorReference/Study Type | Number of Patients | Patient Population | Type of Procedure | Bridging Strategy | Major Bleeds | Minor Bleeds | TE Rate |
|---|---|---|---|---|---|---|---|
| |||||||
| Turpie and Douketis63/single arm cohort | 174 | 66% aortic valve; 34% mitral or dual prosthetic valve | Not specified | Enoxaparin 1 mg/kg twice daily | 2.3% | Not specified | None |
| Kovacs et al.61/single arm cohort | 224 | Prosthetic heart valves or a‐fib plus 1 major risk factor | 67 surgical; 157 nonsurgical | Preoperative bridging with dalteparin 200 IU/kg daily; dose reduced to 100 IU/kg on preoperative day 1; restarted at 100 IU/kg on POD 1; dose reduced to 5000 IU daily if high risk for bleeding | 6.7%; 8/15 occurred intraoperatively or 6 hours postoperatively; 2/15 occurred after 4 weeks | Not specified | 3.6%; 6/8 episodes occurred after warfarin held secondary to bleeding; 2/8 thrombotic episodes judged to be due to cardioembolism |
| Douketis et al.59/prospective registry | 650 | A‐fib 58%; mechanical heart valve 33% | 251 surgical; 399 nonsurgical | Dalteparin 100 IU/kg twice daily; held after high bleeding risk procedure and patients with poor hemostasis | 0.92% | 5.9% | 0.6% |
| Spyropolous et al.62/prospective registry; 14 centers in United States and Canada | 901 | UFH: 40% mechanical valves, 33% a‐fib; LMWH: 24% mechanical valve, 40% a‐fib | 394 surgical; 507 nonsurgical | LMWH mostly given twice daily 80%; UFH 20% | 5.5% UFH; 3.3% LMWH | 9.1% UFH; 12.0% LMWH | 2.4% UFH; 0.9% LMWH |
| Dunn et al.66/prospective cohort | 260 | A‐fib 68% or prior DVT 37% (excluding prosthetic heart valves) | 105 surgical; 145 nonsurgical | Enoxaparin 1.5 mg/kg daily | 3.5% overall; minor surgery/procedures 0.9%; major surgery 28% | 42% | 1.9%; 1/5 events occurred after bleeding led to withdrawal of AC |
| Omran et al.77/prospective registry | 779 | Various indications | Major and minor procedures | All patients bridged with enoxaparin; moderate TE risk 1 mg/kg daily; high TE risk 1 mg/kg twice daily | 0.5%; all in high‐risk group | 5.9% | 0 |
| Garcia et al.71/prospective, observational cohort of 101 sites in United States | 1024 patients with 1293 interruptions of AC | A‐fib 53%; VTE 14%; prosthetic valve 13% | Outpatient procedures only | At discretion of provider. Bridging performed in 8.3% of interruptions; 3% a‐fib, 10% VTE, and 29% mechanical valves | 0.6%; 4/6 patients with major bleed received bridging | 1.7%;10/17 patients with minor bleed received bridging | 0.7%; no events in patients who were bridged |
| Wysokinski et al.64/prospective cohort | 345 consecutive patients undergoing 386 procedures | 100% nonvalvular a‐fib | Major and minor surgeries/procedures | Individualized in AC clinic; 52% of patients bridged | 2.7%; no difference whether patient received bridging or not | 3.0%; 10/11 occurred in bridged patients | 1.1%; no difference in bridged vs. nonbridged patients |
| Low Molecular Weight Heparin | Subcutaneous Dose |
|---|---|
| |
| Dalteparin | |
| Low dose (prophylaxis dose) | 5,000 IU once daily |
| Full dose | 100 IU/kg twice daily or 200 IU/kg once daily |
| Enoxaparin | |
| Low dose (prophylaxis dose) | 30 mg twice daily or 40mg daily |
| Full dose | 1 mg/kg twice daily or 1.5 mg/kg once daily |
| Tinzaparin (full dose) | 175 IU/kg once daily |
In the postprocedural setting, timing and dose of anticoagulant is important, as major bleeding with the use of therapeutic anticoagulation can occur in up to 10% to 20% of cases. When restarting anticoagulation after the procedure, it is important to evaluate intraoperative hemostasis and to consider patient‐related factors that may further increase bleeding risk. These include advanced age, concomitant antiplatelet or nonsteroidal antiinflammatory medications, renal insufficiency, placement of spinal/epidural catheter, worsening liver disease, or the presence of other comorbid illnesses such as cancer.30, 67, 68 The ACCP recommends withholding full‐dose anticoagulation for at least 48 to 72 hours in patients who are felt to be at a high risk for postoperative bleeding.1 Figure 2 is a proposed management approach to the use of bridging anticoagulants that is consistent with the 2008 ACCP recommendations.
CONCLUSION
The evaluation and management of patients on long‐term antiplatelet or VKA therapy who require an invasive procedure or surgery is a common, complicated, and controversial area. Importantly, it is an area in which the hospitalist physician must be adept. Although there remain many unanswered clinical questions, an evolving literature base and recent practice guidelines can help guide management decisions.
- ,,, et al.The Perioperative Management of Antithrombotic Therapy: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th Edition).Chest.2008;133(6_suppl):299S–339S.
- ,,,,.Aspirin use among adults aged 40 and older in the United States: results of a national survey.Am J Prev Med.2007;32(5):403–407.
- ,.Oral anticoagulation in surgical procedures: risks and recommendations.Br J Haematol.2003;123(4):676–682.
- Perioperative medicine.J Hosp Med.2006;1(supp 1):30–31.
- .Perioperative anticoagulation management in patients who are receiving oral anticoagulant therapy: a practical guide for clinicians.Thromb Res.2002;108(1):3–13.
- ,,,.Periprocedural bridging therapy in patients receiving chronic oral anticoagulation therapy.Curr Med Res Opin.2006;22(6):1109–1122.
- ,,,,.Effect of aspirin intake on bleeding during cataract surgery.J Cataract Refract Surg.1998;24(9):1243–1246.
- ,,,.Low‐dose aspirin for secondary cardiovascular prevention–cardiovascular risks after its perioperative withdrawal versus bleeding risks with its continuation—review and meta‐analysis.J Intern Med.2005;257(5):399–414.
- ,,.Aspirin does not increase bleeding complications after transbronchial biopsy.Chest.2002;122(4):1461–1464.
- ,.The management of patients on anticoagulants prior to cutaneous surgery: case report of a thromboembolic complication, review of the literature, and evidence‐based recommendations.Plast Reconstr Surg.2006;118(5):110e–117e.
- .Unanswered questions—drug‐eluting stents and the risk of late thrombosis.N Engl J Med.2007;356(10):981–984.
- ,,, et al.Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians.Circulation.2007;115(6):813–818.
- ,,, et al.The Primary and Secondary Prevention of Coronary Artery Disease: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th Edition).Chest.2008;133(6_suppl):776S–814S.
- ,,, et al.2007 Focused Update of the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: 2007 Writing Group to Review New Evidence and Update the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention, Writing on Behalf of the 2005 Writing Committee.Circulation.2008;117(2):261–295.
- ,,,,,.Late thrombosis of drug‐eluting stents: a meta‐analysis of randomized clinical trials.Am J Med.2006;119(12):1056–1061.
- ,,, et al.Early and late coronary stent thrombosis of sirolimus‐eluting and paclitaxel‐eluting stents in routine clinical practice: data from a large two‐institutional cohort study.Lancet.2007;369(9562):667–678.
- ,,, et al.Clopidogrel use and long‐term clinical outcomes after drug‐eluting stent implantation.JAMA.2007;297(2):159–168.
- Collaborative overview of randomised trials of antiplatelet therapy—I: Prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in various categories of patients.Antiplatelet Trialists' Collaboration.Br Med J (Clin Res Ed).1994;308(6921):81–106.
- ,,, et al.Guideline on the management of anticoagulation and antiplatelet therapy for endoscopic procedures.Gastrointest Endosc.2002;55(7):775–779.
- ,.Severe haemorrhage following abdominal paracentesis for ascites in patients with liver disease.Aliment Pharmacol Ther.2005;21(5):525–529.
- ,,, et al.Performance standards for therapeutic abdominal paracentesis.Hepatology.2004;40(2):484–488.
- ,.Percutaneous cannulation of the internal jugular vein in patients with coagulopathies: an experience based on 1,000 attempts.Anesthesiology.1982;56(4):321–323.
- ,,,,,.Central venous catheterization in patients with coagulopathy.Arch Surg.1992;127(3):273–275.
- ,,.Central venous catheter placement in patients with disorders of hemostasis.Chest.1996;110(1):185–188.
- ,,.US‐guided placement of central vein catheters in patients with disorders of hemostasis.Eur J Radiol.2008;65(2):253–256.
- ,.Central venous cannulation in patients with liver disease and coagulopathy—a prospective audit.Intensive Care Med.1999;25(5):481–485.
- ,.Perioperative management of patients receiving oral anticoagulants: a systematic review.Arch Intern Med.2003;163(8):901–908.
- ,,, et al.Kelley's Textbook of Rheumatology.7th ed.Philadelphia, PA:Elsevier Saunders;2005.
- ,.Clinical Procedures in Emergency Medicine.4th ed.Philadelphia, PA:W.B. Saunders;2004.
- ,.A prospective study of the safety of joint and soft tissue aspirations and injections in patients taking warfarin sodium.Arthritis Rheum.1998;41(4):736–739.
- ,,, et al.[Frequency of the bleeding risk in patients receiving warfarin submitted to arthrocentesis of the knee].Reumatismo.2003;55(3):159–163.
- .Textbook of Critical Care.5th ed.Philadelphia, PA:Elsevier Saunders;2005.
- ,.Complications of lumbar puncture followed by anticoagulation.Stroke.1981;12(6):879–881.
- ,,,.Mason, Murray and Nadel's Textbook of Respiratory Medicine.4th ed.Philadelphia, PA:Elsevier Saunders;2005.
- ,,.Videos in clinical medicine. Thoracentesis.N Engl J Med.2006;355(15):e16.
- ,.Lack of increased bleeding after paracentesis and thoracentesis in patients with mild coagulation abnormalities.Transfusion.1991;31(2):164–171.
- .Risk of bleeding during thoracentesis in anticoagulated patients.Chest.2006;130(4):141S–d‐2.
- ,,, et al.Guidelines for prevention of thromboembolic events in valvular heart disease. Study Group of the Working Group on Valvular Heart Disease of the European Society of Cardiology.Eur Heart J.1995;16(10):1320–1330.
- ,.Coronary angiography and intravascular ultrasonography. In: Braunwald E, Zipes DP, Libby P, eds.Heart Disease: A Textbook of Cardiovascular Medicine.6th ed.Philadelphia, PA:WB Saunders;2001:387–421.
- ,,, et al.Effectiveness of manual pressure hemostasis following transfemoral coronary angiography in patients on therapeutic warfarin anticoagulation.Am J Cardiol.2006;97(4):485–488.
- ,,,,,.Elective coronary angiography and percutaneous coronary intervention during uninterrupted warfarin therapy.Catheter Cardiovasc Interv.2003;60(2):180–184.
- ,,,.Coronary angiography in the fully anticoagulated patient: the transradial route is successful and safe.Catheter Cardiovasc Interv.2003;58(1):8–10.
- ,,,,.Percutaneous left and right heart catheterization in fully anticoagulated patients utilizing the radial artery and forearm vein: a two‐center experience.J Interv Cardiol.2006;19(3):258–263.
- ,,, et al.[Safety of diagnostic transradial catheterization in patients undergoing long‐term anticoagulation with coumarin derivatives].Rev Esp Cardiol.2007;60(9):988–991. [Spanish]
- ,,,,,,,,,,,,,2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Valvular Heart Disease).J Am Coll Cardiol.2008;52:e1–142.
- ,,, et al.ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: executive summary. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation): developed in Collaboration With the North American Society of Pacing and Electrophysiology.J Am Coll Cardiol.2001;38(4):1231–1266.
- .Periprocedural thromboprophylaxis in patients receiving chronic anticoagulation therapy.Am Heart J.2004;147(1):3–15.
- ,.Management of anticoagulation before and after elective surgery.N Engl J Med.1997;336(21):1506–1511.
- ,,,,,.Modern management of prosthetic valve anticoagulation.Mayo Clin Proc.1998;73(7):665–680.
- ,.Anticoagulant‐related bleeding: clinical epidemiology, prediction, and prevention.Am J Med.1993;95(3):315–328.
- ,,,,,.Reconstruction of musculoskeletal defects following oncologic resection in 76 patients.Ann Plast Surg.2006;57(2):190–194.
- ,,,,.Biopsy of the prostate guided by transrectal ultrasound: relation between warfarin use and incidence of bleeding complications.Clin Radiol.2005;60(4):459–463; discussion 457‐458.
- ,.Anticoagulation in neurosurgical patients.Neurosurgery.1999;45(4):838–847; discussion 847‐848.
- ,,,,.Post‐operative blood loss after transurethral prostatectomy is dependent on in situ fibrinolysis.Br J Urol.1997;80(6):889–893.
- ,,.Complications of heparin therapy after total joint arthroplasty.J Bone Joint Surg.1989;71(8):1130–1134.
- ,,,,,.Postpolypectomy lower GI bleeding: descriptive analysis.Gastrointest Endosc.2000;51(6):690–696.
- ,,, et al.Pocket hematoma after pacemaker or implantable cardioverter defibrillator surgery: influence of patient morbidity, operation strategy, and perioperative antiplatelet/anticoagulation therapy.Chest.2004;126(4):1177–1186.
- ,,.[Perioperative bridging with enoxaparin. results of the prospective BRAVE registry with 779 patients].Med Klin (Munich).2007;102(10):809–815. [German]
- ,,.Low molecular weight heparin as bridging anticoagulation during interruption of warfarin: assessment of a standardized periprocedural anticoagulation regimen.Arch Intern Med.2004;164(12):1319–1326.
- ,,.Bridging therapy in patients on long‐term oral anticoagulants who require surgery: the Prospective Peri‐operative Enoxaparin Cohort Trial (PROSPECT).J Thromb Haemost.2007;5(11):2211–2218.
- ,,, et al.Single‐arm study of bridging therapy with low molecular weight heparin for patients at risk of arterial embolism who require temporary interruption of warfarin.Circulation.2004;110(12):1658–1663.
- ,,,.Costs and clinical outcomes associated with low molecular weight heparin vs unfractionated heparin for perioperative bridging in patients receiving long‐term oral anticoagulant therapy.Chest.2004;125(5):1642–1650.
- ,.Enoxaparin is effective and safe as bridging anticoagulation in patients with a mechanical prosthetic heart valve who require temporary interruption of warfarin because of surgery or an invasive procedure. [Abstract #703]. ASH Annual Meeting Abstracts.Blood.2004;104:202A.
- ,,, et al.Periprocedural anticoagulation management of patients with nonvalvular atrial fibrillation.Mayo Clin Proc.2008;83(6):639–645.
- ,,,.Bridging anticoagulation with low molecular weight heparin after interruption of warfarin therapy is associated with a residual anticoagulant effect prior to surgery.Thromb Haemost.2005;94(3):528–531.
- ,,, et al.Brief communication: preoperative anticoagulant activity after bridging low molecular weight heparin for temporary interruption of warfarin.Ann Intern Med.2007;146(3):184–187.
- National Institute for Clinical Excellence. Atrial fibrillation: national clinical guideline for management in primary and secondary care.2006. Available at: http://www.nice.org.uk/nicemedia/pdf/cg036fullguideline. pdf. Accessed May 2009.
- ,,, et al.Clinical outcomes with unfractionated heparin or low molecular weight heparin as bridging therapy in patients on long‐term oral anticoagulants: the REGIMEN registry.J Thromb Haemost.2006;4(6):1246–1252.
- ,,,,,.Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation.JAMA.2001;285(22):2864–2870.
- ,,.Guidelines on oral anticoagulation (warfarin). 3rd ed. 2005 update.Br J Haematol.2006;132(3):277–285.
- ,,, et al.Risk of thromboembolism with short‐term interruption of warfarin therapy.Arch Intern Med.2008;168(1):63–69.
- ,,, et al.The Perioperative Management of Antithrombotic Therapy: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th Edition).Chest.2008;133(6_suppl):299S–339S.
- ,,,,.Aspirin use among adults aged 40 and older in the United States: results of a national survey.Am J Prev Med.2007;32(5):403–407.
- ,.Oral anticoagulation in surgical procedures: risks and recommendations.Br J Haematol.2003;123(4):676–682.
- Perioperative medicine.J Hosp Med.2006;1(supp 1):30–31.
- .Perioperative anticoagulation management in patients who are receiving oral anticoagulant therapy: a practical guide for clinicians.Thromb Res.2002;108(1):3–13.
- ,,,.Periprocedural bridging therapy in patients receiving chronic oral anticoagulation therapy.Curr Med Res Opin.2006;22(6):1109–1122.
- ,,,,.Effect of aspirin intake on bleeding during cataract surgery.J Cataract Refract Surg.1998;24(9):1243–1246.
- ,,,.Low‐dose aspirin for secondary cardiovascular prevention–cardiovascular risks after its perioperative withdrawal versus bleeding risks with its continuation—review and meta‐analysis.J Intern Med.2005;257(5):399–414.
- ,,.Aspirin does not increase bleeding complications after transbronchial biopsy.Chest.2002;122(4):1461–1464.
- ,.The management of patients on anticoagulants prior to cutaneous surgery: case report of a thromboembolic complication, review of the literature, and evidence‐based recommendations.Plast Reconstr Surg.2006;118(5):110e–117e.
- .Unanswered questions—drug‐eluting stents and the risk of late thrombosis.N Engl J Med.2007;356(10):981–984.
- ,,, et al.Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians.Circulation.2007;115(6):813–818.
- ,,, et al.The Primary and Secondary Prevention of Coronary Artery Disease: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th Edition).Chest.2008;133(6_suppl):776S–814S.
- ,,, et al.2007 Focused Update of the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: 2007 Writing Group to Review New Evidence and Update the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention, Writing on Behalf of the 2005 Writing Committee.Circulation.2008;117(2):261–295.
- ,,,,,.Late thrombosis of drug‐eluting stents: a meta‐analysis of randomized clinical trials.Am J Med.2006;119(12):1056–1061.
- ,,, et al.Early and late coronary stent thrombosis of sirolimus‐eluting and paclitaxel‐eluting stents in routine clinical practice: data from a large two‐institutional cohort study.Lancet.2007;369(9562):667–678.
- ,,, et al.Clopidogrel use and long‐term clinical outcomes after drug‐eluting stent implantation.JAMA.2007;297(2):159–168.
- Collaborative overview of randomised trials of antiplatelet therapy—I: Prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in various categories of patients.Antiplatelet Trialists' Collaboration.Br Med J (Clin Res Ed).1994;308(6921):81–106.
- ,,, et al.Guideline on the management of anticoagulation and antiplatelet therapy for endoscopic procedures.Gastrointest Endosc.2002;55(7):775–779.
- ,.Severe haemorrhage following abdominal paracentesis for ascites in patients with liver disease.Aliment Pharmacol Ther.2005;21(5):525–529.
- ,,, et al.Performance standards for therapeutic abdominal paracentesis.Hepatology.2004;40(2):484–488.
- ,.Percutaneous cannulation of the internal jugular vein in patients with coagulopathies: an experience based on 1,000 attempts.Anesthesiology.1982;56(4):321–323.
- ,,,,,.Central venous catheterization in patients with coagulopathy.Arch Surg.1992;127(3):273–275.
- ,,.Central venous catheter placement in patients with disorders of hemostasis.Chest.1996;110(1):185–188.
- ,,.US‐guided placement of central vein catheters in patients with disorders of hemostasis.Eur J Radiol.2008;65(2):253–256.
- ,.Central venous cannulation in patients with liver disease and coagulopathy—a prospective audit.Intensive Care Med.1999;25(5):481–485.
- ,.Perioperative management of patients receiving oral anticoagulants: a systematic review.Arch Intern Med.2003;163(8):901–908.
- ,,, et al.Kelley's Textbook of Rheumatology.7th ed.Philadelphia, PA:Elsevier Saunders;2005.
- ,.Clinical Procedures in Emergency Medicine.4th ed.Philadelphia, PA:W.B. Saunders;2004.
- ,.A prospective study of the safety of joint and soft tissue aspirations and injections in patients taking warfarin sodium.Arthritis Rheum.1998;41(4):736–739.
- ,,, et al.[Frequency of the bleeding risk in patients receiving warfarin submitted to arthrocentesis of the knee].Reumatismo.2003;55(3):159–163.
- .Textbook of Critical Care.5th ed.Philadelphia, PA:Elsevier Saunders;2005.
- ,.Complications of lumbar puncture followed by anticoagulation.Stroke.1981;12(6):879–881.
- ,,,.Mason, Murray and Nadel's Textbook of Respiratory Medicine.4th ed.Philadelphia, PA:Elsevier Saunders;2005.
- ,,.Videos in clinical medicine. Thoracentesis.N Engl J Med.2006;355(15):e16.
- ,.Lack of increased bleeding after paracentesis and thoracentesis in patients with mild coagulation abnormalities.Transfusion.1991;31(2):164–171.
- .Risk of bleeding during thoracentesis in anticoagulated patients.Chest.2006;130(4):141S–d‐2.
- ,,, et al.Guidelines for prevention of thromboembolic events in valvular heart disease. Study Group of the Working Group on Valvular Heart Disease of the European Society of Cardiology.Eur Heart J.1995;16(10):1320–1330.
- ,.Coronary angiography and intravascular ultrasonography. In: Braunwald E, Zipes DP, Libby P, eds.Heart Disease: A Textbook of Cardiovascular Medicine.6th ed.Philadelphia, PA:WB Saunders;2001:387–421.
- ,,, et al.Effectiveness of manual pressure hemostasis following transfemoral coronary angiography in patients on therapeutic warfarin anticoagulation.Am J Cardiol.2006;97(4):485–488.
- ,,,,,.Elective coronary angiography and percutaneous coronary intervention during uninterrupted warfarin therapy.Catheter Cardiovasc Interv.2003;60(2):180–184.
- ,,,.Coronary angiography in the fully anticoagulated patient: the transradial route is successful and safe.Catheter Cardiovasc Interv.2003;58(1):8–10.
- ,,,,.Percutaneous left and right heart catheterization in fully anticoagulated patients utilizing the radial artery and forearm vein: a two‐center experience.J Interv Cardiol.2006;19(3):258–263.
- ,,, et al.[Safety of diagnostic transradial catheterization in patients undergoing long‐term anticoagulation with coumarin derivatives].Rev Esp Cardiol.2007;60(9):988–991. [Spanish]
- ,,,,,,,,,,,,,2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Valvular Heart Disease).J Am Coll Cardiol.2008;52:e1–142.
- ,,, et al.ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: executive summary. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation): developed in Collaboration With the North American Society of Pacing and Electrophysiology.J Am Coll Cardiol.2001;38(4):1231–1266.
- .Periprocedural thromboprophylaxis in patients receiving chronic anticoagulation therapy.Am Heart J.2004;147(1):3–15.
- ,.Management of anticoagulation before and after elective surgery.N Engl J Med.1997;336(21):1506–1511.
- ,,,,,.Modern management of prosthetic valve anticoagulation.Mayo Clin Proc.1998;73(7):665–680.
- ,.Anticoagulant‐related bleeding: clinical epidemiology, prediction, and prevention.Am J Med.1993;95(3):315–328.
- ,,,,,.Reconstruction of musculoskeletal defects following oncologic resection in 76 patients.Ann Plast Surg.2006;57(2):190–194.
- ,,,,.Biopsy of the prostate guided by transrectal ultrasound: relation between warfarin use and incidence of bleeding complications.Clin Radiol.2005;60(4):459–463; discussion 457‐458.
- ,.Anticoagulation in neurosurgical patients.Neurosurgery.1999;45(4):838–847; discussion 847‐848.
- ,,,,.Post‐operative blood loss after transurethral prostatectomy is dependent on in situ fibrinolysis.Br J Urol.1997;80(6):889–893.
- ,,.Complications of heparin therapy after total joint arthroplasty.J Bone Joint Surg.1989;71(8):1130–1134.
- ,,,,,.Postpolypectomy lower GI bleeding: descriptive analysis.Gastrointest Endosc.2000;51(6):690–696.
- ,,, et al.Pocket hematoma after pacemaker or implantable cardioverter defibrillator surgery: influence of patient morbidity, operation strategy, and perioperative antiplatelet/anticoagulation therapy.Chest.2004;126(4):1177–1186.
- ,,.[Perioperative bridging with enoxaparin. results of the prospective BRAVE registry with 779 patients].Med Klin (Munich).2007;102(10):809–815. [German]
- ,,.Low molecular weight heparin as bridging anticoagulation during interruption of warfarin: assessment of a standardized periprocedural anticoagulation regimen.Arch Intern Med.2004;164(12):1319–1326.
- ,,.Bridging therapy in patients on long‐term oral anticoagulants who require surgery: the Prospective Peri‐operative Enoxaparin Cohort Trial (PROSPECT).J Thromb Haemost.2007;5(11):2211–2218.
- ,,, et al.Single‐arm study of bridging therapy with low molecular weight heparin for patients at risk of arterial embolism who require temporary interruption of warfarin.Circulation.2004;110(12):1658–1663.
- ,,,.Costs and clinical outcomes associated with low molecular weight heparin vs unfractionated heparin for perioperative bridging in patients receiving long‐term oral anticoagulant therapy.Chest.2004;125(5):1642–1650.
- ,.Enoxaparin is effective and safe as bridging anticoagulation in patients with a mechanical prosthetic heart valve who require temporary interruption of warfarin because of surgery or an invasive procedure. [Abstract #703]. ASH Annual Meeting Abstracts.Blood.2004;104:202A.
- ,,, et al.Periprocedural anticoagulation management of patients with nonvalvular atrial fibrillation.Mayo Clin Proc.2008;83(6):639–645.
- ,,,.Bridging anticoagulation with low molecular weight heparin after interruption of warfarin therapy is associated with a residual anticoagulant effect prior to surgery.Thromb Haemost.2005;94(3):528–531.
- ,,, et al.Brief communication: preoperative anticoagulant activity after bridging low molecular weight heparin for temporary interruption of warfarin.Ann Intern Med.2007;146(3):184–187.
- National Institute for Clinical Excellence. Atrial fibrillation: national clinical guideline for management in primary and secondary care.2006. Available at: http://www.nice.org.uk/nicemedia/pdf/cg036fullguideline. pdf. Accessed May 2009.
- ,,, et al.Clinical outcomes with unfractionated heparin or low molecular weight heparin as bridging therapy in patients on long‐term oral anticoagulants: the REGIMEN registry.J Thromb Haemost.2006;4(6):1246–1252.
- ,,,,,.Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation.JAMA.2001;285(22):2864–2870.
- ,,.Guidelines on oral anticoagulation (warfarin). 3rd ed. 2005 update.Br J Haematol.2006;132(3):277–285.
- ,,, et al.Risk of thromboembolism with short‐term interruption of warfarin therapy.Arch Intern Med.2008;168(1):63–69.