User login
Understanding Physicians’ Attitudes toward Safety Culture
Results from a survey to assess physicians’ and medical trainees’ perceptions and attitudes about the culture of patient safety at the University of California at San Francisco (UCSF) Medical Center were reported at HM11 in Dallas by Patrick Kneeland, MD, who has since moved to Providence Regional Medical Center’s Everett Clinic in Seattle, where he co-chairs the Medical Quality Review Committee.
“We were interested in perceptions about what most determines a safety culture within a hospital,” and about differences and similarities between faculty, fellows, and residents, Dr. Kneeland explains. A positive safety culture is essential to enhancing patient safety, and it requires support and commitment at multiple levels.
Dr. Kneeland and colleagues used an established, validated instrument, the federal Agency for Healthcare Research and Quality’s “Hospital Survey on Patient Safety Culture,” which is used by hospitals to assess their staffs’ attitudes toward safety. But the UCSF team
modified the instrument to include additional survey dimensions, such as trainee supervision, event disclosure to patients, and physician-to-physician handoffs.1 Of 290 physicians surveyed in UCSF’s Department of Medicine, 53% completed the survey.
“What was surprising from our survey was the overall high degree of agreement, but with some interesting differences,” Dr. Kneeland explains. In terms of the overall rating of safety culture, on a 1-to-5 scale with five being the highest, fellows rated the safety culture the highest, followed by faculty, and then residents. “Even though, across the board, 70 percent or more said adverse events should be disclosed to patients, only half of the trainees felt encouraged to do so, and half felt there is some danger in doing so,” he says.
Findings led to a major educational initiative around error disclosure, and to having the chief residents openly discuss overnight adverse patient events at morning rounds. The goal is to make event reporting part of customary practice. UCSF plans to repeat the survey in five years, using the initial results as a benchmark, Dr. Kneeland adds.
For more information or to request a copy of the modified survey, email Dr. Kneeland at Patrick.Kneeland@providence.org.
Larry Beresford is a freelance writer in Oakland, Calif.
Reference
Results from a survey to assess physicians’ and medical trainees’ perceptions and attitudes about the culture of patient safety at the University of California at San Francisco (UCSF) Medical Center were reported at HM11 in Dallas by Patrick Kneeland, MD, who has since moved to Providence Regional Medical Center’s Everett Clinic in Seattle, where he co-chairs the Medical Quality Review Committee.
“We were interested in perceptions about what most determines a safety culture within a hospital,” and about differences and similarities between faculty, fellows, and residents, Dr. Kneeland explains. A positive safety culture is essential to enhancing patient safety, and it requires support and commitment at multiple levels.
Dr. Kneeland and colleagues used an established, validated instrument, the federal Agency for Healthcare Research and Quality’s “Hospital Survey on Patient Safety Culture,” which is used by hospitals to assess their staffs’ attitudes toward safety. But the UCSF team
modified the instrument to include additional survey dimensions, such as trainee supervision, event disclosure to patients, and physician-to-physician handoffs.1 Of 290 physicians surveyed in UCSF’s Department of Medicine, 53% completed the survey.
“What was surprising from our survey was the overall high degree of agreement, but with some interesting differences,” Dr. Kneeland explains. In terms of the overall rating of safety culture, on a 1-to-5 scale with five being the highest, fellows rated the safety culture the highest, followed by faculty, and then residents. “Even though, across the board, 70 percent or more said adverse events should be disclosed to patients, only half of the trainees felt encouraged to do so, and half felt there is some danger in doing so,” he says.
Findings led to a major educational initiative around error disclosure, and to having the chief residents openly discuss overnight adverse patient events at morning rounds. The goal is to make event reporting part of customary practice. UCSF plans to repeat the survey in five years, using the initial results as a benchmark, Dr. Kneeland adds.
For more information or to request a copy of the modified survey, email Dr. Kneeland at Patrick.Kneeland@providence.org.
Larry Beresford is a freelance writer in Oakland, Calif.
Reference
Results from a survey to assess physicians’ and medical trainees’ perceptions and attitudes about the culture of patient safety at the University of California at San Francisco (UCSF) Medical Center were reported at HM11 in Dallas by Patrick Kneeland, MD, who has since moved to Providence Regional Medical Center’s Everett Clinic in Seattle, where he co-chairs the Medical Quality Review Committee.
“We were interested in perceptions about what most determines a safety culture within a hospital,” and about differences and similarities between faculty, fellows, and residents, Dr. Kneeland explains. A positive safety culture is essential to enhancing patient safety, and it requires support and commitment at multiple levels.
Dr. Kneeland and colleagues used an established, validated instrument, the federal Agency for Healthcare Research and Quality’s “Hospital Survey on Patient Safety Culture,” which is used by hospitals to assess their staffs’ attitudes toward safety. But the UCSF team
modified the instrument to include additional survey dimensions, such as trainee supervision, event disclosure to patients, and physician-to-physician handoffs.1 Of 290 physicians surveyed in UCSF’s Department of Medicine, 53% completed the survey.
“What was surprising from our survey was the overall high degree of agreement, but with some interesting differences,” Dr. Kneeland explains. In terms of the overall rating of safety culture, on a 1-to-5 scale with five being the highest, fellows rated the safety culture the highest, followed by faculty, and then residents. “Even though, across the board, 70 percent or more said adverse events should be disclosed to patients, only half of the trainees felt encouraged to do so, and half felt there is some danger in doing so,” he says.
Findings led to a major educational initiative around error disclosure, and to having the chief residents openly discuss overnight adverse patient events at morning rounds. The goal is to make event reporting part of customary practice. UCSF plans to repeat the survey in five years, using the initial results as a benchmark, Dr. Kneeland adds.
For more information or to request a copy of the modified survey, email Dr. Kneeland at Patrick.Kneeland@providence.org.
Larry Beresford is a freelance writer in Oakland, Calif.
Reference
By the Numbers: 8.3%
8.3%1 in 12 adults ages 21 and older Discharged from the hospital to the community were readmitted within 30 days, according to the National Institute for Health Care Reform. One in 3 (32.9%) were readmitted within one year, suggesting that a significant number of patients remain at risk for readmission far beyond the typically measured 30-day window.
8.3%1 in 12 adults ages 21 and older Discharged from the hospital to the community were readmitted within 30 days, according to the National Institute for Health Care Reform. One in 3 (32.9%) were readmitted within one year, suggesting that a significant number of patients remain at risk for readmission far beyond the typically measured 30-day window.
8.3%1 in 12 adults ages 21 and older Discharged from the hospital to the community were readmitted within 30 days, according to the National Institute for Health Care Reform. One in 3 (32.9%) were readmitted within one year, suggesting that a significant number of patients remain at risk for readmission far beyond the typically measured 30-day window.
WIN WHITCOMB: CMS Core Measures Program a Win-Win for Hospitalists

EDITOR’S NOTE: This month, we introduce a new column, “On the Horizon: Quality, Systems, Safety.” Herein, author Win Whitcomb, MD, MHM, one of SHM’s founders and medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., will deliver his views on all things quality and monitor the major issues affecting hospitalists today. As a companion to Dr. Whitcomb’s perspectives, you’ll find “The View from the Center.” “The View” will on occasion provide readers with news and details of how SHM’s Center for Hospital Innovation and Improvement (“the center”) is addressing implementation of healthcare reform, planning programs to improve quality and safety of care, and influencing decisions that will affect hospital medicine for years to come.
Burke Kealey, MD, SFHM, SHM board member and medical director with HealthPartners in Minneapolis, once remarked, “The core measures program is one of the greatest gifts hospital medicine has been given.” Scoring high on the Centers for Medicare & Medicaid Services (CMS) core measures has been a no-brainer for many hospitalist programs over the years; this success has allowed hospitalists to distinguish themselves from traditional PCPs in the hospital.
Looking back, many of us saw the huge opportunity created by the core measures a decade ago. What could be so hard about writing for a flu shot or ordering an echocardiogram? We joined teams, and put systems in place to ensure high performance and, ahem, figured out how to jump through documentation hoops. (Who disputes that quality improvement is two parts better care, one part managing the medical record?)
The result? A bonanza for hospitalists (as overachievers) in the process measures known as the CMS core measures. Admittedly, some of us have struggled more than others in achieving high performance on some of the measures. For example, we couldn’t for the life of us figure out how to excel in “discharge instructions” for heart failure patients at my hospital because we stunk at medication reconciliation. And, being the team sport that QI is, some of these struggles have been beyond hospitalists’ influence.
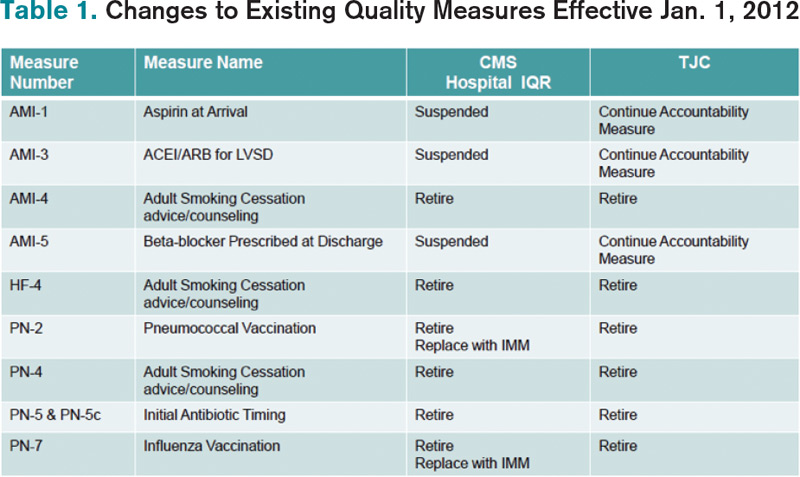
Well, times are changing, and a good number of core measures (the CMS Inpatient Quality Reporting, or IQR, Program) recently have been retired or suspended. Table 1 outlines the retired or suspended CMS measures; The Joint Commission is retiring many, but not all, of the same measures. To clarify, CMS uses Hospital IQR measures for reporting on the public website hospitalcompare.hhs.gov and, beginning in 2013, a subset will make up part of the value-based purchasing program (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1, or visit www.hospitalmedicine.org/vbp). For the commission, the measures are used as part of the survey process for hospital accreditation.
Timeline
The changes described in Table 1 denote measures that will be retired or suspended from the FY14 Hospital IQR measure set, and were reflected in hospital discharges effective Jan. 1, 2012. In other words, the changes are reflected in CMS’ collection of data from hospitals as of this year.
A few words of explanation of the table terms: “AMI,” of course, stands for acute myocardial infarction, “HF” is heart failure, and “PN” is pneumonia.
“Retire” means just that. Let’s hope so, and not what Michael Jordan meant when calling it quits the first time to try out baseball.
“Suspended” means CMS is retaining the measure in the IQR program but is not collecting data until such time that evidence shows hospital performance has unacceptably declined. Win’s word: Hard to know exactly what that means. It scares me enough that my hospital will continue data collection for internal purposes and not take our eye off the ball regarding performance.
“IMM” is short for global immunization and means that influenza and pneumococcal vaccine administration will be tracked on all hospital patients, not just those with pneumonia, who meet the age and high-risk criteria. Win’s word: You read that correctly. All inpatients require these vaccinations if they meet the criteria.
“Accountability measures” became part of The Joint Commission’s accreditation process Jan. 1. According to the commission’s website, they refer to a subset of core measures resulting in “the greatest positive impact on patient outcomes when hospitals demonstrate improvement on them.” Each accountability measure must meet these four criteria:
RESEARCH: There is strong evidence that compliance with this process of care improves outcomes.
PROXIMITY: The process being measured is “close” to the outcome (i.e. relatively few steps between the process and outcome).
ACCURACY: The measure accurately reflects that the process actually has been provided. Win’s word: In = “aspirin on arrival” and “ACE/ARB for LVSD.” Out = “smoking cessation counseling.” For smoking cessation, who knows if this was actually provided or the box was simply checked?
ADVERSE EFFECTS: The measure minimizes adverse effects. Win’s word: The “initial antibiotic timing” measure probably reduced diagnostic accuracy of pneumonia. See ya.
The other core measures will remain in their current form for now. Going forward, the IQR program provides hospitalists new opportunities to shine. These went into effect Jan. 1:
- Admit decision time to ED departure for admitted patients;
- Median time from ED arrival to ED departure for admitted patients; and
- Catheter-associated UTI rates.
As with all the measures, working in teams will be essential to success in these new measures. So go out there and hit a few more home runs (or at least a base hit or two). The season is well underway.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder of SHM and an expert in quality improvement and hospitalist practice management. Write to him at wfwhit@comcast.net.
EDITOR’S NOTE: This month, we introduce a new column, “On the Horizon: Quality, Systems, Safety.” Herein, author Win Whitcomb, MD, MHM, one of SHM’s founders and medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., will deliver his views on all things quality and monitor the major issues affecting hospitalists today. As a companion to Dr. Whitcomb’s perspectives, you’ll find “The View from the Center.” “The View” will on occasion provide readers with news and details of how SHM’s Center for Hospital Innovation and Improvement (“the center”) is addressing implementation of healthcare reform, planning programs to improve quality and safety of care, and influencing decisions that will affect hospital medicine for years to come.
Burke Kealey, MD, SFHM, SHM board member and medical director with HealthPartners in Minneapolis, once remarked, “The core measures program is one of the greatest gifts hospital medicine has been given.” Scoring high on the Centers for Medicare & Medicaid Services (CMS) core measures has been a no-brainer for many hospitalist programs over the years; this success has allowed hospitalists to distinguish themselves from traditional PCPs in the hospital.
Looking back, many of us saw the huge opportunity created by the core measures a decade ago. What could be so hard about writing for a flu shot or ordering an echocardiogram? We joined teams, and put systems in place to ensure high performance and, ahem, figured out how to jump through documentation hoops. (Who disputes that quality improvement is two parts better care, one part managing the medical record?)
The result? A bonanza for hospitalists (as overachievers) in the process measures known as the CMS core measures. Admittedly, some of us have struggled more than others in achieving high performance on some of the measures. For example, we couldn’t for the life of us figure out how to excel in “discharge instructions” for heart failure patients at my hospital because we stunk at medication reconciliation. And, being the team sport that QI is, some of these struggles have been beyond hospitalists’ influence.
Well, times are changing, and a good number of core measures (the CMS Inpatient Quality Reporting, or IQR, Program) recently have been retired or suspended. Table 1 outlines the retired or suspended CMS measures; The Joint Commission is retiring many, but not all, of the same measures. To clarify, CMS uses Hospital IQR measures for reporting on the public website hospitalcompare.hhs.gov and, beginning in 2013, a subset will make up part of the value-based purchasing program (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1, or visit www.hospitalmedicine.org/vbp). For the commission, the measures are used as part of the survey process for hospital accreditation.
Timeline
The changes described in Table 1 denote measures that will be retired or suspended from the FY14 Hospital IQR measure set, and were reflected in hospital discharges effective Jan. 1, 2012. In other words, the changes are reflected in CMS’ collection of data from hospitals as of this year.
A few words of explanation of the table terms: “AMI,” of course, stands for acute myocardial infarction, “HF” is heart failure, and “PN” is pneumonia.
“Retire” means just that. Let’s hope so, and not what Michael Jordan meant when calling it quits the first time to try out baseball.
“Suspended” means CMS is retaining the measure in the IQR program but is not collecting data until such time that evidence shows hospital performance has unacceptably declined. Win’s word: Hard to know exactly what that means. It scares me enough that my hospital will continue data collection for internal purposes and not take our eye off the ball regarding performance.
“IMM” is short for global immunization and means that influenza and pneumococcal vaccine administration will be tracked on all hospital patients, not just those with pneumonia, who meet the age and high-risk criteria. Win’s word: You read that correctly. All inpatients require these vaccinations if they meet the criteria.
“Accountability measures” became part of The Joint Commission’s accreditation process Jan. 1. According to the commission’s website, they refer to a subset of core measures resulting in “the greatest positive impact on patient outcomes when hospitals demonstrate improvement on them.” Each accountability measure must meet these four criteria:
RESEARCH: There is strong evidence that compliance with this process of care improves outcomes.
PROXIMITY: The process being measured is “close” to the outcome (i.e. relatively few steps between the process and outcome).
ACCURACY: The measure accurately reflects that the process actually has been provided. Win’s word: In = “aspirin on arrival” and “ACE/ARB for LVSD.” Out = “smoking cessation counseling.” For smoking cessation, who knows if this was actually provided or the box was simply checked?
ADVERSE EFFECTS: The measure minimizes adverse effects. Win’s word: The “initial antibiotic timing” measure probably reduced diagnostic accuracy of pneumonia. See ya.
The other core measures will remain in their current form for now. Going forward, the IQR program provides hospitalists new opportunities to shine. These went into effect Jan. 1:
- Admit decision time to ED departure for admitted patients;
- Median time from ED arrival to ED departure for admitted patients; and
- Catheter-associated UTI rates.
As with all the measures, working in teams will be essential to success in these new measures. So go out there and hit a few more home runs (or at least a base hit or two). The season is well underway.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder of SHM and an expert in quality improvement and hospitalist practice management. Write to him at wfwhit@comcast.net.
EDITOR’S NOTE: This month, we introduce a new column, “On the Horizon: Quality, Systems, Safety.” Herein, author Win Whitcomb, MD, MHM, one of SHM’s founders and medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., will deliver his views on all things quality and monitor the major issues affecting hospitalists today. As a companion to Dr. Whitcomb’s perspectives, you’ll find “The View from the Center.” “The View” will on occasion provide readers with news and details of how SHM’s Center for Hospital Innovation and Improvement (“the center”) is addressing implementation of healthcare reform, planning programs to improve quality and safety of care, and influencing decisions that will affect hospital medicine for years to come.
Burke Kealey, MD, SFHM, SHM board member and medical director with HealthPartners in Minneapolis, once remarked, “The core measures program is one of the greatest gifts hospital medicine has been given.” Scoring high on the Centers for Medicare & Medicaid Services (CMS) core measures has been a no-brainer for many hospitalist programs over the years; this success has allowed hospitalists to distinguish themselves from traditional PCPs in the hospital.
Looking back, many of us saw the huge opportunity created by the core measures a decade ago. What could be so hard about writing for a flu shot or ordering an echocardiogram? We joined teams, and put systems in place to ensure high performance and, ahem, figured out how to jump through documentation hoops. (Who disputes that quality improvement is two parts better care, one part managing the medical record?)
The result? A bonanza for hospitalists (as overachievers) in the process measures known as the CMS core measures. Admittedly, some of us have struggled more than others in achieving high performance on some of the measures. For example, we couldn’t for the life of us figure out how to excel in “discharge instructions” for heart failure patients at my hospital because we stunk at medication reconciliation. And, being the team sport that QI is, some of these struggles have been beyond hospitalists’ influence.
Well, times are changing, and a good number of core measures (the CMS Inpatient Quality Reporting, or IQR, Program) recently have been retired or suspended. Table 1 outlines the retired or suspended CMS measures; The Joint Commission is retiring many, but not all, of the same measures. To clarify, CMS uses Hospital IQR measures for reporting on the public website hospitalcompare.hhs.gov and, beginning in 2013, a subset will make up part of the value-based purchasing program (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1, or visit www.hospitalmedicine.org/vbp). For the commission, the measures are used as part of the survey process for hospital accreditation.
Timeline
The changes described in Table 1 denote measures that will be retired or suspended from the FY14 Hospital IQR measure set, and were reflected in hospital discharges effective Jan. 1, 2012. In other words, the changes are reflected in CMS’ collection of data from hospitals as of this year.
A few words of explanation of the table terms: “AMI,” of course, stands for acute myocardial infarction, “HF” is heart failure, and “PN” is pneumonia.
“Retire” means just that. Let’s hope so, and not what Michael Jordan meant when calling it quits the first time to try out baseball.
“Suspended” means CMS is retaining the measure in the IQR program but is not collecting data until such time that evidence shows hospital performance has unacceptably declined. Win’s word: Hard to know exactly what that means. It scares me enough that my hospital will continue data collection for internal purposes and not take our eye off the ball regarding performance.
“IMM” is short for global immunization and means that influenza and pneumococcal vaccine administration will be tracked on all hospital patients, not just those with pneumonia, who meet the age and high-risk criteria. Win’s word: You read that correctly. All inpatients require these vaccinations if they meet the criteria.
“Accountability measures” became part of The Joint Commission’s accreditation process Jan. 1. According to the commission’s website, they refer to a subset of core measures resulting in “the greatest positive impact on patient outcomes when hospitals demonstrate improvement on them.” Each accountability measure must meet these four criteria:
RESEARCH: There is strong evidence that compliance with this process of care improves outcomes.
PROXIMITY: The process being measured is “close” to the outcome (i.e. relatively few steps between the process and outcome).
ACCURACY: The measure accurately reflects that the process actually has been provided. Win’s word: In = “aspirin on arrival” and “ACE/ARB for LVSD.” Out = “smoking cessation counseling.” For smoking cessation, who knows if this was actually provided or the box was simply checked?
ADVERSE EFFECTS: The measure minimizes adverse effects. Win’s word: The “initial antibiotic timing” measure probably reduced diagnostic accuracy of pneumonia. See ya.
The other core measures will remain in their current form for now. Going forward, the IQR program provides hospitalists new opportunities to shine. These went into effect Jan. 1:
- Admit decision time to ED departure for admitted patients;
- Median time from ED arrival to ED departure for admitted patients; and
- Catheter-associated UTI rates.
As with all the measures, working in teams will be essential to success in these new measures. So go out there and hit a few more home runs (or at least a base hit or two). The season is well underway.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder of SHM and an expert in quality improvement and hospitalist practice management. Write to him at wfwhit@comcast.net.
The Society of Hospital Medicine's Physician Editors Contribute in Ways Large, Small, Significant

Mark and Jeff set the bar: What are we going to do for hospital medicine?
“Write an article, about a thousand words long. Just make sure you turn it in on time every month.” These were verbatim the instructions I received from the editorial staff about a year ago before I started writing this monthly column in The Hospitalist. Most hospitalists, even those in academia, don’t write an article every month. In fact, for most hospitalists, it’s probably been years, possibly decades, since they have penned a piece for publication. The last probably was turned in for a grade.
Well, the good news was that I was given carte blanche to write about topics of my choice. I thought that was a good idea until it came time to write my first column. Yikes! What do I write about? It certainly was easier in school when I was told I had to write about specific topics─say, why Napoleon scapegoated Snowball in Orwell’s “Animal Farm.” Now, not only did I have to write, but I also had to come up with the topic.
Partly because of my obligation to The Hospitalist, I have developed great admiration for interesting, prolific writers. What else did I learn from writing this column? I found out that it is hard to write in a vacuum. Although I knew the editorial staff would be proofreading my language and grammar, I didn’t expect them to give me feedback about content or style.
Soon after my first column, I started putting my email address at the end of the column. Some of the best feedback I received this year as SHM president came because I listed my email address with this column. Secretly, I am hoping that future SHM presidents will do the same and that SHM members will take advantage of the opportunity to communicate with their president.
There is a lesson to be learned here: In order to improve, all of us need consistent, timely, constructive feedback. I have enjoyed writing this monthly column and thank everyone at SHM and The Hospitalist for this opportunity. It was not always easy coming up with a topic or finding the time to string together coherent ideas on a keyboard.
As challenging as it has been at times for me, I think about what Jeff Glasheen has done for the past five years as physician editor of The Hospitalist. Not only did Jeff produce a monthly column five times longer than I did, he also worked tirelessly with the editorial staff to shape, expand, and improve the content of The Hospitalist. Under his leadership, we finally have a professional magazine with content that the advertisers can be proud of. He did this on top of his day job as chief of the hospitalist program at University of Colorado Denver. I won’t elaborate on his multiple other SHM commitments, which including roles as course director of the Academic Hospitalist Academy and chair of the Academic Hospitalist Committee. By the way, Jeff was HM12 course director, too. I’d like to take this opportunity to thank him for his service.
Jeff has been a tireless advocate not only for SHM, but for our profession. Enjoy Jeff’s column this month (see "The End," p. 52). I don’t know ahead of time what he will write about, but rest assured, it will be timely and interesting. This will be Jeff’s final column as physician editor of The Hospitalist. He recently made the decision to step down and hand over the reins to another incredibly talented hospitalist, Danielle Scheurer.
Luckily, Jeff is not one to rest on his laurels. He will be joining the editorial staff of the Journal of Hospital Medicine. Jeff has been the face of The Hospitalist for so long that it will be hard to think of The Hospitalist without him. Danielle, I’m sure, will do a great job. She also knows she has massive shoes to fill.
What I just said about Jeff can and should be said also for Mark Williams, who recently stepped down as JHM’s editor in chief. As the first editor of our field’s preeminent scientific journal, Mark set a high standard. His successor, Andy Auerbach, will be challenged to surpass this high standard. Like Jeff, Mark’s leadership of JHM was only the tip of the iceberg. Mark has done virtually everything there is do at SHM, including serving as an annual meeting course director, SHM board member, and SHM president. Mark is a recognized national leader in transitions of care and was instrumental in development of SHM’s Project BOOST. All of us owe Mark and Jeff a tremendous debt of gratitude. I am a big fan of both of them and feel fortunate to know both HM leaders.
My expectation is that Mark and Jeff, like others who have been so influential in our field—Jeff Wiese, Tina Budnitz, and Larry Wellikson among them—will one day join the Wachters, Nelsons, and Whitcombs as Masters in Hospital Medicine. The views and ideas in The Hospitalist and JHM formulated and shaped the ideas of this young profession. Over the past few years, nobody’s voice has been louder than those of our editors, Mark Williams and Jeff Glasheen.
The field of hospital medicine and our professional society, the Society of Hospital Medicine, has been blessed with visionary leaders, hard-working volunteers, and a talented staff in its first 15 years. They have laid a solid foundation for our field. HM and SHM will continue to grow only if we are able to produce high-value care for our patients. Our ability to increase healthcare value will be based on our ability to improve the quality of care for patients inside and outside the hospital. Individuals like Mark and Jeff have shown us the way. The challenge is for individuals like you and me to help them carry the torch over the next decade and beyond.
I welcome your feedback. Email me at josephli@hospitalmedicine.org; catch me on Twitter: @_JosephLi; or contact me via LinkedIn at Joseph Li.
Dr. Li is president of SHM.
Mark and Jeff set the bar: What are we going to do for hospital medicine?
“Write an article, about a thousand words long. Just make sure you turn it in on time every month.” These were verbatim the instructions I received from the editorial staff about a year ago before I started writing this monthly column in The Hospitalist. Most hospitalists, even those in academia, don’t write an article every month. In fact, for most hospitalists, it’s probably been years, possibly decades, since they have penned a piece for publication. The last probably was turned in for a grade.
Well, the good news was that I was given carte blanche to write about topics of my choice. I thought that was a good idea until it came time to write my first column. Yikes! What do I write about? It certainly was easier in school when I was told I had to write about specific topics─say, why Napoleon scapegoated Snowball in Orwell’s “Animal Farm.” Now, not only did I have to write, but I also had to come up with the topic.
Partly because of my obligation to The Hospitalist, I have developed great admiration for interesting, prolific writers. What else did I learn from writing this column? I found out that it is hard to write in a vacuum. Although I knew the editorial staff would be proofreading my language and grammar, I didn’t expect them to give me feedback about content or style.
Soon after my first column, I started putting my email address at the end of the column. Some of the best feedback I received this year as SHM president came because I listed my email address with this column. Secretly, I am hoping that future SHM presidents will do the same and that SHM members will take advantage of the opportunity to communicate with their president.
There is a lesson to be learned here: In order to improve, all of us need consistent, timely, constructive feedback. I have enjoyed writing this monthly column and thank everyone at SHM and The Hospitalist for this opportunity. It was not always easy coming up with a topic or finding the time to string together coherent ideas on a keyboard.
As challenging as it has been at times for me, I think about what Jeff Glasheen has done for the past five years as physician editor of The Hospitalist. Not only did Jeff produce a monthly column five times longer than I did, he also worked tirelessly with the editorial staff to shape, expand, and improve the content of The Hospitalist. Under his leadership, we finally have a professional magazine with content that the advertisers can be proud of. He did this on top of his day job as chief of the hospitalist program at University of Colorado Denver. I won’t elaborate on his multiple other SHM commitments, which including roles as course director of the Academic Hospitalist Academy and chair of the Academic Hospitalist Committee. By the way, Jeff was HM12 course director, too. I’d like to take this opportunity to thank him for his service.
Jeff has been a tireless advocate not only for SHM, but for our profession. Enjoy Jeff’s column this month (see "The End," p. 52). I don’t know ahead of time what he will write about, but rest assured, it will be timely and interesting. This will be Jeff’s final column as physician editor of The Hospitalist. He recently made the decision to step down and hand over the reins to another incredibly talented hospitalist, Danielle Scheurer.
Luckily, Jeff is not one to rest on his laurels. He will be joining the editorial staff of the Journal of Hospital Medicine. Jeff has been the face of The Hospitalist for so long that it will be hard to think of The Hospitalist without him. Danielle, I’m sure, will do a great job. She also knows she has massive shoes to fill.
What I just said about Jeff can and should be said also for Mark Williams, who recently stepped down as JHM’s editor in chief. As the first editor of our field’s preeminent scientific journal, Mark set a high standard. His successor, Andy Auerbach, will be challenged to surpass this high standard. Like Jeff, Mark’s leadership of JHM was only the tip of the iceberg. Mark has done virtually everything there is do at SHM, including serving as an annual meeting course director, SHM board member, and SHM president. Mark is a recognized national leader in transitions of care and was instrumental in development of SHM’s Project BOOST. All of us owe Mark and Jeff a tremendous debt of gratitude. I am a big fan of both of them and feel fortunate to know both HM leaders.
My expectation is that Mark and Jeff, like others who have been so influential in our field—Jeff Wiese, Tina Budnitz, and Larry Wellikson among them—will one day join the Wachters, Nelsons, and Whitcombs as Masters in Hospital Medicine. The views and ideas in The Hospitalist and JHM formulated and shaped the ideas of this young profession. Over the past few years, nobody’s voice has been louder than those of our editors, Mark Williams and Jeff Glasheen.
The field of hospital medicine and our professional society, the Society of Hospital Medicine, has been blessed with visionary leaders, hard-working volunteers, and a talented staff in its first 15 years. They have laid a solid foundation for our field. HM and SHM will continue to grow only if we are able to produce high-value care for our patients. Our ability to increase healthcare value will be based on our ability to improve the quality of care for patients inside and outside the hospital. Individuals like Mark and Jeff have shown us the way. The challenge is for individuals like you and me to help them carry the torch over the next decade and beyond.
I welcome your feedback. Email me at josephli@hospitalmedicine.org; catch me on Twitter: @_JosephLi; or contact me via LinkedIn at Joseph Li.
Dr. Li is president of SHM.
Mark and Jeff set the bar: What are we going to do for hospital medicine?
“Write an article, about a thousand words long. Just make sure you turn it in on time every month.” These were verbatim the instructions I received from the editorial staff about a year ago before I started writing this monthly column in The Hospitalist. Most hospitalists, even those in academia, don’t write an article every month. In fact, for most hospitalists, it’s probably been years, possibly decades, since they have penned a piece for publication. The last probably was turned in for a grade.
Well, the good news was that I was given carte blanche to write about topics of my choice. I thought that was a good idea until it came time to write my first column. Yikes! What do I write about? It certainly was easier in school when I was told I had to write about specific topics─say, why Napoleon scapegoated Snowball in Orwell’s “Animal Farm.” Now, not only did I have to write, but I also had to come up with the topic.
Partly because of my obligation to The Hospitalist, I have developed great admiration for interesting, prolific writers. What else did I learn from writing this column? I found out that it is hard to write in a vacuum. Although I knew the editorial staff would be proofreading my language and grammar, I didn’t expect them to give me feedback about content or style.
Soon after my first column, I started putting my email address at the end of the column. Some of the best feedback I received this year as SHM president came because I listed my email address with this column. Secretly, I am hoping that future SHM presidents will do the same and that SHM members will take advantage of the opportunity to communicate with their president.
There is a lesson to be learned here: In order to improve, all of us need consistent, timely, constructive feedback. I have enjoyed writing this monthly column and thank everyone at SHM and The Hospitalist for this opportunity. It was not always easy coming up with a topic or finding the time to string together coherent ideas on a keyboard.
As challenging as it has been at times for me, I think about what Jeff Glasheen has done for the past five years as physician editor of The Hospitalist. Not only did Jeff produce a monthly column five times longer than I did, he also worked tirelessly with the editorial staff to shape, expand, and improve the content of The Hospitalist. Under his leadership, we finally have a professional magazine with content that the advertisers can be proud of. He did this on top of his day job as chief of the hospitalist program at University of Colorado Denver. I won’t elaborate on his multiple other SHM commitments, which including roles as course director of the Academic Hospitalist Academy and chair of the Academic Hospitalist Committee. By the way, Jeff was HM12 course director, too. I’d like to take this opportunity to thank him for his service.
Jeff has been a tireless advocate not only for SHM, but for our profession. Enjoy Jeff’s column this month (see "The End," p. 52). I don’t know ahead of time what he will write about, but rest assured, it will be timely and interesting. This will be Jeff’s final column as physician editor of The Hospitalist. He recently made the decision to step down and hand over the reins to another incredibly talented hospitalist, Danielle Scheurer.
Luckily, Jeff is not one to rest on his laurels. He will be joining the editorial staff of the Journal of Hospital Medicine. Jeff has been the face of The Hospitalist for so long that it will be hard to think of The Hospitalist without him. Danielle, I’m sure, will do a great job. She also knows she has massive shoes to fill.
What I just said about Jeff can and should be said also for Mark Williams, who recently stepped down as JHM’s editor in chief. As the first editor of our field’s preeminent scientific journal, Mark set a high standard. His successor, Andy Auerbach, will be challenged to surpass this high standard. Like Jeff, Mark’s leadership of JHM was only the tip of the iceberg. Mark has done virtually everything there is do at SHM, including serving as an annual meeting course director, SHM board member, and SHM president. Mark is a recognized national leader in transitions of care and was instrumental in development of SHM’s Project BOOST. All of us owe Mark and Jeff a tremendous debt of gratitude. I am a big fan of both of them and feel fortunate to know both HM leaders.
My expectation is that Mark and Jeff, like others who have been so influential in our field—Jeff Wiese, Tina Budnitz, and Larry Wellikson among them—will one day join the Wachters, Nelsons, and Whitcombs as Masters in Hospital Medicine. The views and ideas in The Hospitalist and JHM formulated and shaped the ideas of this young profession. Over the past few years, nobody’s voice has been louder than those of our editors, Mark Williams and Jeff Glasheen.
The field of hospital medicine and our professional society, the Society of Hospital Medicine, has been blessed with visionary leaders, hard-working volunteers, and a talented staff in its first 15 years. They have laid a solid foundation for our field. HM and SHM will continue to grow only if we are able to produce high-value care for our patients. Our ability to increase healthcare value will be based on our ability to improve the quality of care for patients inside and outside the hospital. Individuals like Mark and Jeff have shown us the way. The challenge is for individuals like you and me to help them carry the torch over the next decade and beyond.
I welcome your feedback. Email me at josephli@hospitalmedicine.org; catch me on Twitter: @_JosephLi; or contact me via LinkedIn at Joseph Li.
Dr. Li is president of SHM.
JEFF GLASHEEN: What's Been, What's Next, and a Hogan Update

By now you are no doubt aware that the world will soon end. And by soon, I don’t mean Dec. 21, 2012, as predicted by the Mayans—rather, July 21, the date the Weekly World News recently reported that the Earth will hurdle into the planet Nibiru, no doubt inconveniencing my son’s tee-ball game and upending my father’s 72nd annual failed attempt at pulling off the white T, black socks, and sandals look at the beach.
The tabloid also reports that Elvis was spotted pilfering a Vegas buffet (photos of inexplicably barren shrimp cocktail containers support their case), a manigator is loose in Alabama (heads up if you’re reading this in Mobile!), and that duck hunters mistakenly shot an angel (bad move angering the angels right before Doomsday).
OK, maybe you don’t believe that the world will end in 2012. But one thing that will end is my tenure as physician editor of The Hospitalist. The date: March 31, 2012. Yes, after nearly five years, I’m passing the baton and moving on before my editing career takes on an overweight, beefy side-burned, flowing-jumpsuit-in-Vegas course of its own.
And after editing and writing columns for 55 issues of the definitive publication in hospital medicine, what question do I get the most?
How’s Hogan?
History Through Headlines
Looking back at my columns, I now see that some themes developed. I touched on disease states (Spanish Flu Redux?), obesity (Fight the Losing Battle), electronic health records (Only Fools Rush In), patient satisfaction (Doctor Remodel), physician burnout (Left Turns), and healthcare reform (Get Well Now). I wrote about the births of my children, Greyson (Lesson of the Titanic) and Kaiya (Undercover, MD), Grey’s trip to the ED (Mind Games & Silence), and the myriad ways my father can irritate from the backseat of a car (Minivan, Major Lesson).
But over the years, I also increasingly wrote about patient safety (Bueller … Bueller?; Handless Employees; Designed to Harm; A Run For Safety), quality improvement (Something Interesting Happened; Quality Defined) and the need for hospitalists to lead these imperatives (Exceed Acceptable; Promise or Insanity?; Subsidy or Payment?; Fiddling As HM Burns).
And along the way, my monologue turned into a dialogue. I remember the first email that proved someone other than my coerced wife read my column. Then again, I shouldn’t have been surprised that my dad emailed to tell me to stop writing about him.
But then it happened again. And again. And again.
I was surprised to hear from so many readers. People wrote that they, too, had embarrassingly misdiagnosed their child’s croup as a life-threatening disorder, were struggling with burnout and balance, didn’t like the new ABIM recognition of focused practice in hospital medicine (Urban Legends; Certified Special), and, in the case of my chair of medicine, that they could not achieve my challenge (Transitions Telethon) to call every PCP on discharge for one week.
Readers wrote that I made them laugh, that a story touched them, or that they were angry. One was upset that I called childbirth a “miracle,” another that I was too forgiving about the new duty hours (Rise of the Napturnist), and my father that I still hadn’t stopped writing about him.
But none of this generated the interest that Hogan did.
What Would Hogan Want?
In August 2009, I wrote The Anvil of Indecision column about my dog, Hogan, and our experience with his incidentally discovered 5-cm lung mass. It was my first personal foray into end-of-life decision-making, and it came in the form of a 10-year-old Weimaraner. Hogan was present for many of the most important strata of my life—his rings counting my single-guy resident days, early hospitalist career, marriage, a few relocations, and the births of my kids. And along the way, he was the one constant, the glue that kept my life together.
Best friends are like that.
As I noted in that column, my wife and I struggled with “how much physical distress, how much intervention we afford to an older, sleep-most-of-the-day arthritic dog.” Not knowing if the mass was benign or malignant, should we work it up or just let nature sort it out? If we treated, should we diagnose and stage the tumor, blindly surgically remove it, or just give palliative chemotherapy? What if it was isolated and surgery would be curative? What if it was metastatic and surgery just added morbidity? What if this was benign and Hogan died in the operating room? What would Hogan want? Hogan trusted me to make the right decision.
Best friends are like that.
This was the easiest column I’d ever typed but the hardest I’d ever written. I wrote it in about an hour and then cried about it for two days. I was distraught, miserable, and unmoored in the way that only pet-lovers who have faced the demise of a loved one can understand.
I was truly confounded, and the act of writing was cathartic. It was my first venture beyond standard professional content. I spent two weeks deciding if I could really publish it. It was difficult, I found, to expose myself—to be vulnerable in this manner.
No one can beat you up for saying we should care about patient safety and improve quality. Dedicating an entire column to a dog? What if my peers, the society, my bosses found it immature or self-pitying? What if they didn’t get it?
Within days of publishing the column about Hogan, I’d received hundreds of comments from readers, most relating their similar experiences, all expressing support—by far more interest than I got about anything else I’d written.
Turns out, you got it.
What’s Next?
I wonder what my next 55 columns would have looked like. I surely would continue to discuss HM’s struggles to operationalize the quality and safety promise we hold. This should continue to be our singular goal.
I’d likely write about bundled payments and ACOs. I believe these are potential game-changers in much the same way the prospective payment system was in the 1980s. The latter laid the groundwork for hospitalists. Will new payment models prove a boon or a death knell?
I’d spill ink, no doubt, about the financing of HM groups. As hospital reimbursement fades, can hospitalist salaries be far behind? Will this push us toward more encounters and more shifts, leaving less time for meaningful process improvement work, less time for personal and professional balance, less satisfaction in our careers?
I would wrestle with how we can attract the best and brightest to our field. Who will fill the next 20,000 hospitalist positions?
I would, no doubt, chronicle the tribulations of my kids (a record to be leveraged when I look to move in with them in 2040), send a few more barbs my father’s way (payback for the 1980s, Dad!), and deprecate a few of my future dimwitted moves.
And I might even devote a few more inches of column to Hogan.
Because, you see, Hogan is doing well. He’s cancer-free nearly three years after surgery and chemotherapy for metastatic pulmonary adenocarcinoma. I’ll skip the details and just say “thanks.”
Thanks for asking. Thanks for reading.
Dr. Glasheen is physician editor of The Hospitalist.
By now you are no doubt aware that the world will soon end. And by soon, I don’t mean Dec. 21, 2012, as predicted by the Mayans—rather, July 21, the date the Weekly World News recently reported that the Earth will hurdle into the planet Nibiru, no doubt inconveniencing my son’s tee-ball game and upending my father’s 72nd annual failed attempt at pulling off the white T, black socks, and sandals look at the beach.
The tabloid also reports that Elvis was spotted pilfering a Vegas buffet (photos of inexplicably barren shrimp cocktail containers support their case), a manigator is loose in Alabama (heads up if you’re reading this in Mobile!), and that duck hunters mistakenly shot an angel (bad move angering the angels right before Doomsday).
OK, maybe you don’t believe that the world will end in 2012. But one thing that will end is my tenure as physician editor of The Hospitalist. The date: March 31, 2012. Yes, after nearly five years, I’m passing the baton and moving on before my editing career takes on an overweight, beefy side-burned, flowing-jumpsuit-in-Vegas course of its own.
And after editing and writing columns for 55 issues of the definitive publication in hospital medicine, what question do I get the most?
How’s Hogan?
History Through Headlines
Looking back at my columns, I now see that some themes developed. I touched on disease states (Spanish Flu Redux?), obesity (Fight the Losing Battle), electronic health records (Only Fools Rush In), patient satisfaction (Doctor Remodel), physician burnout (Left Turns), and healthcare reform (Get Well Now). I wrote about the births of my children, Greyson (Lesson of the Titanic) and Kaiya (Undercover, MD), Grey’s trip to the ED (Mind Games & Silence), and the myriad ways my father can irritate from the backseat of a car (Minivan, Major Lesson).
But over the years, I also increasingly wrote about patient safety (Bueller … Bueller?; Handless Employees; Designed to Harm; A Run For Safety), quality improvement (Something Interesting Happened; Quality Defined) and the need for hospitalists to lead these imperatives (Exceed Acceptable; Promise or Insanity?; Subsidy or Payment?; Fiddling As HM Burns).
And along the way, my monologue turned into a dialogue. I remember the first email that proved someone other than my coerced wife read my column. Then again, I shouldn’t have been surprised that my dad emailed to tell me to stop writing about him.
But then it happened again. And again. And again.
I was surprised to hear from so many readers. People wrote that they, too, had embarrassingly misdiagnosed their child’s croup as a life-threatening disorder, were struggling with burnout and balance, didn’t like the new ABIM recognition of focused practice in hospital medicine (Urban Legends; Certified Special), and, in the case of my chair of medicine, that they could not achieve my challenge (Transitions Telethon) to call every PCP on discharge for one week.
Readers wrote that I made them laugh, that a story touched them, or that they were angry. One was upset that I called childbirth a “miracle,” another that I was too forgiving about the new duty hours (Rise of the Napturnist), and my father that I still hadn’t stopped writing about him.
But none of this generated the interest that Hogan did.
What Would Hogan Want?
In August 2009, I wrote The Anvil of Indecision column about my dog, Hogan, and our experience with his incidentally discovered 5-cm lung mass. It was my first personal foray into end-of-life decision-making, and it came in the form of a 10-year-old Weimaraner. Hogan was present for many of the most important strata of my life—his rings counting my single-guy resident days, early hospitalist career, marriage, a few relocations, and the births of my kids. And along the way, he was the one constant, the glue that kept my life together.
Best friends are like that.
As I noted in that column, my wife and I struggled with “how much physical distress, how much intervention we afford to an older, sleep-most-of-the-day arthritic dog.” Not knowing if the mass was benign or malignant, should we work it up or just let nature sort it out? If we treated, should we diagnose and stage the tumor, blindly surgically remove it, or just give palliative chemotherapy? What if it was isolated and surgery would be curative? What if it was metastatic and surgery just added morbidity? What if this was benign and Hogan died in the operating room? What would Hogan want? Hogan trusted me to make the right decision.
Best friends are like that.
This was the easiest column I’d ever typed but the hardest I’d ever written. I wrote it in about an hour and then cried about it for two days. I was distraught, miserable, and unmoored in the way that only pet-lovers who have faced the demise of a loved one can understand.
I was truly confounded, and the act of writing was cathartic. It was my first venture beyond standard professional content. I spent two weeks deciding if I could really publish it. It was difficult, I found, to expose myself—to be vulnerable in this manner.
No one can beat you up for saying we should care about patient safety and improve quality. Dedicating an entire column to a dog? What if my peers, the society, my bosses found it immature or self-pitying? What if they didn’t get it?
Within days of publishing the column about Hogan, I’d received hundreds of comments from readers, most relating their similar experiences, all expressing support—by far more interest than I got about anything else I’d written.
Turns out, you got it.
What’s Next?
I wonder what my next 55 columns would have looked like. I surely would continue to discuss HM’s struggles to operationalize the quality and safety promise we hold. This should continue to be our singular goal.
I’d likely write about bundled payments and ACOs. I believe these are potential game-changers in much the same way the prospective payment system was in the 1980s. The latter laid the groundwork for hospitalists. Will new payment models prove a boon or a death knell?
I’d spill ink, no doubt, about the financing of HM groups. As hospital reimbursement fades, can hospitalist salaries be far behind? Will this push us toward more encounters and more shifts, leaving less time for meaningful process improvement work, less time for personal and professional balance, less satisfaction in our careers?
I would wrestle with how we can attract the best and brightest to our field. Who will fill the next 20,000 hospitalist positions?
I would, no doubt, chronicle the tribulations of my kids (a record to be leveraged when I look to move in with them in 2040), send a few more barbs my father’s way (payback for the 1980s, Dad!), and deprecate a few of my future dimwitted moves.
And I might even devote a few more inches of column to Hogan.
Because, you see, Hogan is doing well. He’s cancer-free nearly three years after surgery and chemotherapy for metastatic pulmonary adenocarcinoma. I’ll skip the details and just say “thanks.”
Thanks for asking. Thanks for reading.
Dr. Glasheen is physician editor of The Hospitalist.
By now you are no doubt aware that the world will soon end. And by soon, I don’t mean Dec. 21, 2012, as predicted by the Mayans—rather, July 21, the date the Weekly World News recently reported that the Earth will hurdle into the planet Nibiru, no doubt inconveniencing my son’s tee-ball game and upending my father’s 72nd annual failed attempt at pulling off the white T, black socks, and sandals look at the beach.
The tabloid also reports that Elvis was spotted pilfering a Vegas buffet (photos of inexplicably barren shrimp cocktail containers support their case), a manigator is loose in Alabama (heads up if you’re reading this in Mobile!), and that duck hunters mistakenly shot an angel (bad move angering the angels right before Doomsday).
OK, maybe you don’t believe that the world will end in 2012. But one thing that will end is my tenure as physician editor of The Hospitalist. The date: March 31, 2012. Yes, after nearly five years, I’m passing the baton and moving on before my editing career takes on an overweight, beefy side-burned, flowing-jumpsuit-in-Vegas course of its own.
And after editing and writing columns for 55 issues of the definitive publication in hospital medicine, what question do I get the most?
How’s Hogan?
History Through Headlines
Looking back at my columns, I now see that some themes developed. I touched on disease states (Spanish Flu Redux?), obesity (Fight the Losing Battle), electronic health records (Only Fools Rush In), patient satisfaction (Doctor Remodel), physician burnout (Left Turns), and healthcare reform (Get Well Now). I wrote about the births of my children, Greyson (Lesson of the Titanic) and Kaiya (Undercover, MD), Grey’s trip to the ED (Mind Games & Silence), and the myriad ways my father can irritate from the backseat of a car (Minivan, Major Lesson).
But over the years, I also increasingly wrote about patient safety (Bueller … Bueller?; Handless Employees; Designed to Harm; A Run For Safety), quality improvement (Something Interesting Happened; Quality Defined) and the need for hospitalists to lead these imperatives (Exceed Acceptable; Promise or Insanity?; Subsidy or Payment?; Fiddling As HM Burns).
And along the way, my monologue turned into a dialogue. I remember the first email that proved someone other than my coerced wife read my column. Then again, I shouldn’t have been surprised that my dad emailed to tell me to stop writing about him.
But then it happened again. And again. And again.
I was surprised to hear from so many readers. People wrote that they, too, had embarrassingly misdiagnosed their child’s croup as a life-threatening disorder, were struggling with burnout and balance, didn’t like the new ABIM recognition of focused practice in hospital medicine (Urban Legends; Certified Special), and, in the case of my chair of medicine, that they could not achieve my challenge (Transitions Telethon) to call every PCP on discharge for one week.
Readers wrote that I made them laugh, that a story touched them, or that they were angry. One was upset that I called childbirth a “miracle,” another that I was too forgiving about the new duty hours (Rise of the Napturnist), and my father that I still hadn’t stopped writing about him.
But none of this generated the interest that Hogan did.
What Would Hogan Want?
In August 2009, I wrote The Anvil of Indecision column about my dog, Hogan, and our experience with his incidentally discovered 5-cm lung mass. It was my first personal foray into end-of-life decision-making, and it came in the form of a 10-year-old Weimaraner. Hogan was present for many of the most important strata of my life—his rings counting my single-guy resident days, early hospitalist career, marriage, a few relocations, and the births of my kids. And along the way, he was the one constant, the glue that kept my life together.
Best friends are like that.
As I noted in that column, my wife and I struggled with “how much physical distress, how much intervention we afford to an older, sleep-most-of-the-day arthritic dog.” Not knowing if the mass was benign or malignant, should we work it up or just let nature sort it out? If we treated, should we diagnose and stage the tumor, blindly surgically remove it, or just give palliative chemotherapy? What if it was isolated and surgery would be curative? What if it was metastatic and surgery just added morbidity? What if this was benign and Hogan died in the operating room? What would Hogan want? Hogan trusted me to make the right decision.
Best friends are like that.
This was the easiest column I’d ever typed but the hardest I’d ever written. I wrote it in about an hour and then cried about it for two days. I was distraught, miserable, and unmoored in the way that only pet-lovers who have faced the demise of a loved one can understand.
I was truly confounded, and the act of writing was cathartic. It was my first venture beyond standard professional content. I spent two weeks deciding if I could really publish it. It was difficult, I found, to expose myself—to be vulnerable in this manner.
No one can beat you up for saying we should care about patient safety and improve quality. Dedicating an entire column to a dog? What if my peers, the society, my bosses found it immature or self-pitying? What if they didn’t get it?
Within days of publishing the column about Hogan, I’d received hundreds of comments from readers, most relating their similar experiences, all expressing support—by far more interest than I got about anything else I’d written.
Turns out, you got it.
What’s Next?
I wonder what my next 55 columns would have looked like. I surely would continue to discuss HM’s struggles to operationalize the quality and safety promise we hold. This should continue to be our singular goal.
I’d likely write about bundled payments and ACOs. I believe these are potential game-changers in much the same way the prospective payment system was in the 1980s. The latter laid the groundwork for hospitalists. Will new payment models prove a boon or a death knell?
I’d spill ink, no doubt, about the financing of HM groups. As hospital reimbursement fades, can hospitalist salaries be far behind? Will this push us toward more encounters and more shifts, leaving less time for meaningful process improvement work, less time for personal and professional balance, less satisfaction in our careers?
I would wrestle with how we can attract the best and brightest to our field. Who will fill the next 20,000 hospitalist positions?
I would, no doubt, chronicle the tribulations of my kids (a record to be leveraged when I look to move in with them in 2040), send a few more barbs my father’s way (payback for the 1980s, Dad!), and deprecate a few of my future dimwitted moves.
And I might even devote a few more inches of column to Hogan.
Because, you see, Hogan is doing well. He’s cancer-free nearly three years after surgery and chemotherapy for metastatic pulmonary adenocarcinoma. I’ll skip the details and just say “thanks.”
Thanks for asking. Thanks for reading.
Dr. Glasheen is physician editor of The Hospitalist.
JOHN NELSON: Morning Discharges and Length of Stay

Last month, I discussed ED, or “front end,” throughput. This month I will focus on what can be thought of as the two components of “back end” throughput: effective management of length of stay (LOS) and patient discharge in the morning rather than late in the day.
How many times have you heard a well-intentioned administrator ask: “We can’t get patients from the ED to ward more quickly unless we can discharge patients earlier in the day to make beds available. So please round on your potential discharges and get the D/C order written early”?
Easier said than done. But not impossible, if you’re willing to make some adjustments in how you organize your work.
Strategies Re-examined
I provided a list of strategies in my April 2009 column (see “Early-Day Discharge Strategies,” p. 48), and in May 2010 I described in greater detail two ideas that can help with early-morning discharge. The easiest of these is to increase the portion of patients who discharge early in the day. To do this, hospitalists should write in the order section of the chart (not just the progress notes where it can be missed by nursing staff) an order like “possible disch tomorrow” or “Probably discharge Thurs or Fri.” That will help hospital staff anticipate and prepare for discharge, and there is little cost if the patient isn’t ready on the day forecast.
More difficult, but more effective, is fully preparing a patient’s discharge a day ahead of time. I do this on about half or more of my patients and, despite having no rigorous data to prove it, I’m convinced that it makes for better discharges and transitions, and it’s a real stress-reliever for me. My mornings are much less hectic, as I rarely have to devote 30-60 minutes to a discharge while other patients are waiting to be rounded on. And it helps me uncover loose ends like the need to get additional chest imaging to evaluate a possible lung lesion early enough that I can order the additional test without delaying discharge (it can be done the night before).
Note that when billing the discharge visit only, the time spent on the day of discharge counts as billable time. So preparing everything the day before will mean that nearly all discharges will be billed at the lower level: 99238 rather than 99239. You will have to decide for yourself whether losing the ability to bill some discharges at the higher level is worth it. Most hospitals probably will be willing to make up the lost professional fee revenue if it led to a meaningful improvement in the portion of patients with discharge orders early in the day.
One CMS administrator told my consulting partner, Leslie Flores, that discharge summaries can’t be dictated on a day prior to discharge because they have to include all information related to the hospital stay, including any relevant information from the night before discharge. The administrator said that CMS would view this as a surgeon dictating an operative report before performing the operation. (Are there surgeons who are actually doing that?) I think care is better when I do a discharge summary unhurried and with few interruptions in the evening before discharge rather than the busy morning of the discharge day. And I can always add an addendum (and often do) at the time of actual discharge. So you might want to ask your hospital compliance expert about dictating a D/C summary the day before discharge.
A Tricky Proposition
It is pretty easy for administrators to think that the time of day a discharge order is written is nearly always up to the doctor and how they organize their day. To them, it might seem reasonable to expect more than 50% of discharge orders to be written before 10 a.m. or earlier. But wait … it is more complicated than that.
The same administrators care a lot about LOS, which is most commonly reported in days but can also be measured in hours. So the time of day a discharge order is written, arguably the most important determinant of when a patient will vacate a room, is a determinant of LOS. If we’re really managing LOS optimally, we should discharge a patient at the first moment it is clinically appropriate, which means discharging at any hour of the day or night. (Of course, no one is proposing that we discharge and expect patients to vacate rooms in the middle of the night. Yet.)
But that would mean only a small portion of patients would end up with early-morning discharge orders. So excellent LOS management and a high portion of discharge orders written early in the day are incompatible. Setting the target percentage of early-a.m. discharge orders too high probably will increase LOS and defeat the original objective.
Benefits and Costs of Improved Throughput
Let’s say you’re sold on the value of improving throughput. It should lead to improved efficiency and financial performance for your hospital. I suspect it will improve quality and reduce iatrogenesis for some patients, but risk more readmissions and quality lapses or errors for others. And as every department tries to improve their own throughput, there will be a tendency to push problems off on others. For example, it is easy to improve ED throughput if the ED doctor just does a lot less evaluation and sends patients upstairs without much of a workup. Example: “The patient has fever and low sats, so I know he’s going to be admitted. Why should I keep him in the ED to do a workup?”
In fact, I think we should move away from using the ED as a triage unit and send some patients directly from ED triage to the inpatient unit. But we’ll need to put in place systems that make that safe and ensure good care. I don’t think any hospital has such systems in place now.
Let’s say that by 2013 most hospitals have dramatically improved their throughput, have short ED admit decision time to ED departure, and many patients are discharged and vacate their rooms early in the day. And let’s say we’ve been able to do that while maintaining or improving quality of care (we must!). We’ll then have happy patients and hospital administrators, and can bring up this improved performance when negotiating for hospital financial support for our practice. Everyone is happy, right?
Well, won’t this increase marginal or unnecessary admissions and readmissions, and lead to overall increased hospital utilization? After all, if it becomes really quick and easy to admit a patient to the hospital, won’t we do it more often? I think we will, but would never propose that we maintain poor throughput to keep a lid on costs and inappropriate utilization. But we’d better come up with other ways, or improved throughput will just be one more factor contributing to escalating healthcare costs.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm.
Last month, I discussed ED, or “front end,” throughput. This month I will focus on what can be thought of as the two components of “back end” throughput: effective management of length of stay (LOS) and patient discharge in the morning rather than late in the day.
How many times have you heard a well-intentioned administrator ask: “We can’t get patients from the ED to ward more quickly unless we can discharge patients earlier in the day to make beds available. So please round on your potential discharges and get the D/C order written early”?
Easier said than done. But not impossible, if you’re willing to make some adjustments in how you organize your work.
Strategies Re-examined
I provided a list of strategies in my April 2009 column (see “Early-Day Discharge Strategies,” p. 48), and in May 2010 I described in greater detail two ideas that can help with early-morning discharge. The easiest of these is to increase the portion of patients who discharge early in the day. To do this, hospitalists should write in the order section of the chart (not just the progress notes where it can be missed by nursing staff) an order like “possible disch tomorrow” or “Probably discharge Thurs or Fri.” That will help hospital staff anticipate and prepare for discharge, and there is little cost if the patient isn’t ready on the day forecast.
More difficult, but more effective, is fully preparing a patient’s discharge a day ahead of time. I do this on about half or more of my patients and, despite having no rigorous data to prove it, I’m convinced that it makes for better discharges and transitions, and it’s a real stress-reliever for me. My mornings are much less hectic, as I rarely have to devote 30-60 minutes to a discharge while other patients are waiting to be rounded on. And it helps me uncover loose ends like the need to get additional chest imaging to evaluate a possible lung lesion early enough that I can order the additional test without delaying discharge (it can be done the night before).
Note that when billing the discharge visit only, the time spent on the day of discharge counts as billable time. So preparing everything the day before will mean that nearly all discharges will be billed at the lower level: 99238 rather than 99239. You will have to decide for yourself whether losing the ability to bill some discharges at the higher level is worth it. Most hospitals probably will be willing to make up the lost professional fee revenue if it led to a meaningful improvement in the portion of patients with discharge orders early in the day.
One CMS administrator told my consulting partner, Leslie Flores, that discharge summaries can’t be dictated on a day prior to discharge because they have to include all information related to the hospital stay, including any relevant information from the night before discharge. The administrator said that CMS would view this as a surgeon dictating an operative report before performing the operation. (Are there surgeons who are actually doing that?) I think care is better when I do a discharge summary unhurried and with few interruptions in the evening before discharge rather than the busy morning of the discharge day. And I can always add an addendum (and often do) at the time of actual discharge. So you might want to ask your hospital compliance expert about dictating a D/C summary the day before discharge.
A Tricky Proposition
It is pretty easy for administrators to think that the time of day a discharge order is written is nearly always up to the doctor and how they organize their day. To them, it might seem reasonable to expect more than 50% of discharge orders to be written before 10 a.m. or earlier. But wait … it is more complicated than that.
The same administrators care a lot about LOS, which is most commonly reported in days but can also be measured in hours. So the time of day a discharge order is written, arguably the most important determinant of when a patient will vacate a room, is a determinant of LOS. If we’re really managing LOS optimally, we should discharge a patient at the first moment it is clinically appropriate, which means discharging at any hour of the day or night. (Of course, no one is proposing that we discharge and expect patients to vacate rooms in the middle of the night. Yet.)
But that would mean only a small portion of patients would end up with early-morning discharge orders. So excellent LOS management and a high portion of discharge orders written early in the day are incompatible. Setting the target percentage of early-a.m. discharge orders too high probably will increase LOS and defeat the original objective.
Benefits and Costs of Improved Throughput
Let’s say you’re sold on the value of improving throughput. It should lead to improved efficiency and financial performance for your hospital. I suspect it will improve quality and reduce iatrogenesis for some patients, but risk more readmissions and quality lapses or errors for others. And as every department tries to improve their own throughput, there will be a tendency to push problems off on others. For example, it is easy to improve ED throughput if the ED doctor just does a lot less evaluation and sends patients upstairs without much of a workup. Example: “The patient has fever and low sats, so I know he’s going to be admitted. Why should I keep him in the ED to do a workup?”
In fact, I think we should move away from using the ED as a triage unit and send some patients directly from ED triage to the inpatient unit. But we’ll need to put in place systems that make that safe and ensure good care. I don’t think any hospital has such systems in place now.
Let’s say that by 2013 most hospitals have dramatically improved their throughput, have short ED admit decision time to ED departure, and many patients are discharged and vacate their rooms early in the day. And let’s say we’ve been able to do that while maintaining or improving quality of care (we must!). We’ll then have happy patients and hospital administrators, and can bring up this improved performance when negotiating for hospital financial support for our practice. Everyone is happy, right?
Well, won’t this increase marginal or unnecessary admissions and readmissions, and lead to overall increased hospital utilization? After all, if it becomes really quick and easy to admit a patient to the hospital, won’t we do it more often? I think we will, but would never propose that we maintain poor throughput to keep a lid on costs and inappropriate utilization. But we’d better come up with other ways, or improved throughput will just be one more factor contributing to escalating healthcare costs.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm.
Last month, I discussed ED, or “front end,” throughput. This month I will focus on what can be thought of as the two components of “back end” throughput: effective management of length of stay (LOS) and patient discharge in the morning rather than late in the day.
How many times have you heard a well-intentioned administrator ask: “We can’t get patients from the ED to ward more quickly unless we can discharge patients earlier in the day to make beds available. So please round on your potential discharges and get the D/C order written early”?
Easier said than done. But not impossible, if you’re willing to make some adjustments in how you organize your work.
Strategies Re-examined
I provided a list of strategies in my April 2009 column (see “Early-Day Discharge Strategies,” p. 48), and in May 2010 I described in greater detail two ideas that can help with early-morning discharge. The easiest of these is to increase the portion of patients who discharge early in the day. To do this, hospitalists should write in the order section of the chart (not just the progress notes where it can be missed by nursing staff) an order like “possible disch tomorrow” or “Probably discharge Thurs or Fri.” That will help hospital staff anticipate and prepare for discharge, and there is little cost if the patient isn’t ready on the day forecast.
More difficult, but more effective, is fully preparing a patient’s discharge a day ahead of time. I do this on about half or more of my patients and, despite having no rigorous data to prove it, I’m convinced that it makes for better discharges and transitions, and it’s a real stress-reliever for me. My mornings are much less hectic, as I rarely have to devote 30-60 minutes to a discharge while other patients are waiting to be rounded on. And it helps me uncover loose ends like the need to get additional chest imaging to evaluate a possible lung lesion early enough that I can order the additional test without delaying discharge (it can be done the night before).
Note that when billing the discharge visit only, the time spent on the day of discharge counts as billable time. So preparing everything the day before will mean that nearly all discharges will be billed at the lower level: 99238 rather than 99239. You will have to decide for yourself whether losing the ability to bill some discharges at the higher level is worth it. Most hospitals probably will be willing to make up the lost professional fee revenue if it led to a meaningful improvement in the portion of patients with discharge orders early in the day.
One CMS administrator told my consulting partner, Leslie Flores, that discharge summaries can’t be dictated on a day prior to discharge because they have to include all information related to the hospital stay, including any relevant information from the night before discharge. The administrator said that CMS would view this as a surgeon dictating an operative report before performing the operation. (Are there surgeons who are actually doing that?) I think care is better when I do a discharge summary unhurried and with few interruptions in the evening before discharge rather than the busy morning of the discharge day. And I can always add an addendum (and often do) at the time of actual discharge. So you might want to ask your hospital compliance expert about dictating a D/C summary the day before discharge.
A Tricky Proposition
It is pretty easy for administrators to think that the time of day a discharge order is written is nearly always up to the doctor and how they organize their day. To them, it might seem reasonable to expect more than 50% of discharge orders to be written before 10 a.m. or earlier. But wait … it is more complicated than that.
The same administrators care a lot about LOS, which is most commonly reported in days but can also be measured in hours. So the time of day a discharge order is written, arguably the most important determinant of when a patient will vacate a room, is a determinant of LOS. If we’re really managing LOS optimally, we should discharge a patient at the first moment it is clinically appropriate, which means discharging at any hour of the day or night. (Of course, no one is proposing that we discharge and expect patients to vacate rooms in the middle of the night. Yet.)
But that would mean only a small portion of patients would end up with early-morning discharge orders. So excellent LOS management and a high portion of discharge orders written early in the day are incompatible. Setting the target percentage of early-a.m. discharge orders too high probably will increase LOS and defeat the original objective.
Benefits and Costs of Improved Throughput
Let’s say you’re sold on the value of improving throughput. It should lead to improved efficiency and financial performance for your hospital. I suspect it will improve quality and reduce iatrogenesis for some patients, but risk more readmissions and quality lapses or errors for others. And as every department tries to improve their own throughput, there will be a tendency to push problems off on others. For example, it is easy to improve ED throughput if the ED doctor just does a lot less evaluation and sends patients upstairs without much of a workup. Example: “The patient has fever and low sats, so I know he’s going to be admitted. Why should I keep him in the ED to do a workup?”
In fact, I think we should move away from using the ED as a triage unit and send some patients directly from ED triage to the inpatient unit. But we’ll need to put in place systems that make that safe and ensure good care. I don’t think any hospital has such systems in place now.
Let’s say that by 2013 most hospitals have dramatically improved their throughput, have short ED admit decision time to ED departure, and many patients are discharged and vacate their rooms early in the day. And let’s say we’ve been able to do that while maintaining or improving quality of care (we must!). We’ll then have happy patients and hospital administrators, and can bring up this improved performance when negotiating for hospital financial support for our practice. Everyone is happy, right?
Well, won’t this increase marginal or unnecessary admissions and readmissions, and lead to overall increased hospital utilization? After all, if it becomes really quick and easy to admit a patient to the hospital, won’t we do it more often? I think we will, but would never propose that we maintain poor throughput to keep a lid on costs and inappropriate utilization. But we’d better come up with other ways, or improved throughput will just be one more factor contributing to escalating healthcare costs.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm.
C-Suite Vocabulary for Hospitalists
The Nuance of C-Suite Vocabulary
I have just become the leader of our hospitalist group and had the most amazing meeting with the hospital administrators. They seem to be speaking English, but I didn’t understand a thing. Can you help?
—B.N.L., Bellingham, Wash.
Dr. Hospitalist responds:
Ah, congrats on your first exposure to corporate jargon—otherwise known as admino-babble. Having survived numerous boardroom encounters with members of the corporate tribe to which you refer, I am, sad to say, now fluent in this most obtuse way of communicating. Herewith, a glossary that is gloriously non-alphabetical. Please note, I have heard all of these terms in person; this is not just some list I parroted off the Web:
Circle back: We don’t have any answers, but this meeting has gone on too long, so let’s talk about it next time.
Close the loop: Finish what you were thinking.
Failure of messaging: Things did not get explained very well. Formerly known as: It’s not you, it’s me.
Low-hanging fruit: The easy victories. Otherwise known as the stuff you already did for the hospital but never thought to get contractually paid for.
Value-add: Something that adds value. Hmm.
Corner case: An argument for something that isn’t likely to happen anyway. Otherwise known as “a long run for a short slide.”
Ping me offline: Send me an email/text after the meeting. LOL.
Straw man: An example that is thrown together just for the sake of discussion, and is not expected to stand up to scrutiny. Cousin to “laying down a marker.”
Cascading failures: Major, major problems. Example: “Our census just increased 50%, which means we don’t have time to get the discharges done, which means the census will stay high, which means ... ”
Granularity: The details.
Drill down: No, thanks, I just got granularity on that.
Deep dive: How cool is this? We now have three ways of saying the same thing.
Brand refresh: Marketing-speak for “The CEO doesn’t like our logo.”
Bandwidth: The capacity to take on more work. Old saying: “Yeah, I can do that.”
Contextualize: To add meaning to a discussion. (Is this actually a word?)
Deliverable: Those things in the contract that you said you would do, only now in writing.
Open the kimono: Umm, I’m afraid to say anything here. Use the Internet at your peril.
Visibility: The ability to not only recognize a problem, but understand it as well. “We don’t have visibility on that process.”
SWOT analysis: Strengths, Weaknesses, Opportunities, Threats—a way to characterize the current state of your hospitalist group.
30,000-foot view: Opposite of granular. The view the upper management likes to have. Apparently it’s not enough, because there is now even a “50,000-foot view.”
Win-win: Where everybody is happy. Somehow used often in negotiations, when in actuality the hallmark of a good negotiation is that both sides think they could have gotten a little bit more.
Deck, or slide deck: One of those interminable PowerPoint presentations.
Elevator test: An idea or concept that can be explained to someone important during the course of a brief elevator ride.
Pushback: Disagreement. “We’re likely to get some pushback from the ED docs if you want them to write admission orders.”
Right-size the organization: Everybody is going to get fired. Update your resume.
Off-path: When things aren’t going your way.
Off-budget: For you, it means losing money; for them, it just means not making enough.
Opportunities and synergies: Things that might happen but rarely do.
Boil the ocean: Do the impossible. “Let’s not try to boil the ocean here, maybe just harvest the low-hanging fruit.”
Amazingly, there are many more terms available. Please do remember all this in your new role. And here’s one more definition for good measure:
The consultant: Someone who takes a subject you understand and makes it sound confusing, and for these efforts is paid fantastically well.
Best of luck out there!
The Nuance of C-Suite Vocabulary
I have just become the leader of our hospitalist group and had the most amazing meeting with the hospital administrators. They seem to be speaking English, but I didn’t understand a thing. Can you help?
—B.N.L., Bellingham, Wash.
Dr. Hospitalist responds:
Ah, congrats on your first exposure to corporate jargon—otherwise known as admino-babble. Having survived numerous boardroom encounters with members of the corporate tribe to which you refer, I am, sad to say, now fluent in this most obtuse way of communicating. Herewith, a glossary that is gloriously non-alphabetical. Please note, I have heard all of these terms in person; this is not just some list I parroted off the Web:
Circle back: We don’t have any answers, but this meeting has gone on too long, so let’s talk about it next time.
Close the loop: Finish what you were thinking.
Failure of messaging: Things did not get explained very well. Formerly known as: It’s not you, it’s me.
Low-hanging fruit: The easy victories. Otherwise known as the stuff you already did for the hospital but never thought to get contractually paid for.
Value-add: Something that adds value. Hmm.
Corner case: An argument for something that isn’t likely to happen anyway. Otherwise known as “a long run for a short slide.”
Ping me offline: Send me an email/text after the meeting. LOL.
Straw man: An example that is thrown together just for the sake of discussion, and is not expected to stand up to scrutiny. Cousin to “laying down a marker.”
Cascading failures: Major, major problems. Example: “Our census just increased 50%, which means we don’t have time to get the discharges done, which means the census will stay high, which means ... ”
Granularity: The details.
Drill down: No, thanks, I just got granularity on that.
Deep dive: How cool is this? We now have three ways of saying the same thing.
Brand refresh: Marketing-speak for “The CEO doesn’t like our logo.”
Bandwidth: The capacity to take on more work. Old saying: “Yeah, I can do that.”
Contextualize: To add meaning to a discussion. (Is this actually a word?)
Deliverable: Those things in the contract that you said you would do, only now in writing.
Open the kimono: Umm, I’m afraid to say anything here. Use the Internet at your peril.
Visibility: The ability to not only recognize a problem, but understand it as well. “We don’t have visibility on that process.”
SWOT analysis: Strengths, Weaknesses, Opportunities, Threats—a way to characterize the current state of your hospitalist group.
30,000-foot view: Opposite of granular. The view the upper management likes to have. Apparently it’s not enough, because there is now even a “50,000-foot view.”
Win-win: Where everybody is happy. Somehow used often in negotiations, when in actuality the hallmark of a good negotiation is that both sides think they could have gotten a little bit more.
Deck, or slide deck: One of those interminable PowerPoint presentations.
Elevator test: An idea or concept that can be explained to someone important during the course of a brief elevator ride.
Pushback: Disagreement. “We’re likely to get some pushback from the ED docs if you want them to write admission orders.”
Right-size the organization: Everybody is going to get fired. Update your resume.
Off-path: When things aren’t going your way.
Off-budget: For you, it means losing money; for them, it just means not making enough.
Opportunities and synergies: Things that might happen but rarely do.
Boil the ocean: Do the impossible. “Let’s not try to boil the ocean here, maybe just harvest the low-hanging fruit.”
Amazingly, there are many more terms available. Please do remember all this in your new role. And here’s one more definition for good measure:
The consultant: Someone who takes a subject you understand and makes it sound confusing, and for these efforts is paid fantastically well.
Best of luck out there!
The Nuance of C-Suite Vocabulary
I have just become the leader of our hospitalist group and had the most amazing meeting with the hospital administrators. They seem to be speaking English, but I didn’t understand a thing. Can you help?
—B.N.L., Bellingham, Wash.
Dr. Hospitalist responds:
Ah, congrats on your first exposure to corporate jargon—otherwise known as admino-babble. Having survived numerous boardroom encounters with members of the corporate tribe to which you refer, I am, sad to say, now fluent in this most obtuse way of communicating. Herewith, a glossary that is gloriously non-alphabetical. Please note, I have heard all of these terms in person; this is not just some list I parroted off the Web:
Circle back: We don’t have any answers, but this meeting has gone on too long, so let’s talk about it next time.
Close the loop: Finish what you were thinking.
Failure of messaging: Things did not get explained very well. Formerly known as: It’s not you, it’s me.
Low-hanging fruit: The easy victories. Otherwise known as the stuff you already did for the hospital but never thought to get contractually paid for.
Value-add: Something that adds value. Hmm.
Corner case: An argument for something that isn’t likely to happen anyway. Otherwise known as “a long run for a short slide.”
Ping me offline: Send me an email/text after the meeting. LOL.
Straw man: An example that is thrown together just for the sake of discussion, and is not expected to stand up to scrutiny. Cousin to “laying down a marker.”
Cascading failures: Major, major problems. Example: “Our census just increased 50%, which means we don’t have time to get the discharges done, which means the census will stay high, which means ... ”
Granularity: The details.
Drill down: No, thanks, I just got granularity on that.
Deep dive: How cool is this? We now have three ways of saying the same thing.
Brand refresh: Marketing-speak for “The CEO doesn’t like our logo.”
Bandwidth: The capacity to take on more work. Old saying: “Yeah, I can do that.”
Contextualize: To add meaning to a discussion. (Is this actually a word?)
Deliverable: Those things in the contract that you said you would do, only now in writing.
Open the kimono: Umm, I’m afraid to say anything here. Use the Internet at your peril.
Visibility: The ability to not only recognize a problem, but understand it as well. “We don’t have visibility on that process.”
SWOT analysis: Strengths, Weaknesses, Opportunities, Threats—a way to characterize the current state of your hospitalist group.
30,000-foot view: Opposite of granular. The view the upper management likes to have. Apparently it’s not enough, because there is now even a “50,000-foot view.”
Win-win: Where everybody is happy. Somehow used often in negotiations, when in actuality the hallmark of a good negotiation is that both sides think they could have gotten a little bit more.
Deck, or slide deck: One of those interminable PowerPoint presentations.
Elevator test: An idea or concept that can be explained to someone important during the course of a brief elevator ride.
Pushback: Disagreement. “We’re likely to get some pushback from the ED docs if you want them to write admission orders.”
Right-size the organization: Everybody is going to get fired. Update your resume.
Off-path: When things aren’t going your way.
Off-budget: For you, it means losing money; for them, it just means not making enough.
Opportunities and synergies: Things that might happen but rarely do.
Boil the ocean: Do the impossible. “Let’s not try to boil the ocean here, maybe just harvest the low-hanging fruit.”
Amazingly, there are many more terms available. Please do remember all this in your new role. And here’s one more definition for good measure:
The consultant: Someone who takes a subject you understand and makes it sound confusing, and for these efforts is paid fantastically well.
Best of luck out there!
How Prepared are Hospitalists to Handle Infectious Disease Cases?
Hospitalists routinely have to handle infection cases, but how well trained are they to do so, and how well prepared are the hospitals they work in to support them on difficult cases?
It depends on training and the institution, but both areas have room for improvement, says a physician who has had feet on both sides of the fence.
Leland Allen, MD, says there is no easy answer on whether hospitalists have enough baseline training.
“What I see locally in Birmingham is that there is a wide variation in the training,” he says. “The hospitalists that I see that are family-practice-trained, just as the nature of the family practice training [goes], have a whole lot of outpatient experience. And so these people don’t have nearly the inpatient experience in their training that people trained in internal medicine do.”

—Leland Allen, MD, infectious-disease physician, Shelby Baptist Medical Center, Birmingham, Ala.
Some hospitalists, Dr. Allen says, are as proficient in dealing with inpatient ID cases as he is. Others are clueless, he says. “It really just depends on the training. It would be nice if there was some standardization of training, rather than just kind of catch-as-catch-can.”
As for ID resources available at hospitals, Dr. Allen says, “there is potential in any hospital to have an excellent backbone program of infection control.” But that depends on the availability of ID experts and the willingness of hospital administration to invest in the program.
“A well-developed, well-maintained infection-control program, with a good infection-control nurse, can really help a hospitalist to understand the types of infections that they’re up against in that particular institution,” Dr. Allen explains. “It really pays off down the road for the hospital with reduced infection rates, and also physicians who are practicing in the hospital, in terms of making their life a little bit easier.”
And with changes in Medicare reimbursement for hospital-acquired infections, he says, “it really behooves a hospital to spend some money up front.”
Hospitalists routinely have to handle infection cases, but how well trained are they to do so, and how well prepared are the hospitals they work in to support them on difficult cases?
It depends on training and the institution, but both areas have room for improvement, says a physician who has had feet on both sides of the fence.
Leland Allen, MD, says there is no easy answer on whether hospitalists have enough baseline training.
“What I see locally in Birmingham is that there is a wide variation in the training,” he says. “The hospitalists that I see that are family-practice-trained, just as the nature of the family practice training [goes], have a whole lot of outpatient experience. And so these people don’t have nearly the inpatient experience in their training that people trained in internal medicine do.”
—Leland Allen, MD, infectious-disease physician, Shelby Baptist Medical Center, Birmingham, Ala.
Some hospitalists, Dr. Allen says, are as proficient in dealing with inpatient ID cases as he is. Others are clueless, he says. “It really just depends on the training. It would be nice if there was some standardization of training, rather than just kind of catch-as-catch-can.”
As for ID resources available at hospitals, Dr. Allen says, “there is potential in any hospital to have an excellent backbone program of infection control.” But that depends on the availability of ID experts and the willingness of hospital administration to invest in the program.
“A well-developed, well-maintained infection-control program, with a good infection-control nurse, can really help a hospitalist to understand the types of infections that they’re up against in that particular institution,” Dr. Allen explains. “It really pays off down the road for the hospital with reduced infection rates, and also physicians who are practicing in the hospital, in terms of making their life a little bit easier.”
And with changes in Medicare reimbursement for hospital-acquired infections, he says, “it really behooves a hospital to spend some money up front.”
Hospitalists routinely have to handle infection cases, but how well trained are they to do so, and how well prepared are the hospitals they work in to support them on difficult cases?
It depends on training and the institution, but both areas have room for improvement, says a physician who has had feet on both sides of the fence.
Leland Allen, MD, says there is no easy answer on whether hospitalists have enough baseline training.
“What I see locally in Birmingham is that there is a wide variation in the training,” he says. “The hospitalists that I see that are family-practice-trained, just as the nature of the family practice training [goes], have a whole lot of outpatient experience. And so these people don’t have nearly the inpatient experience in their training that people trained in internal medicine do.”
—Leland Allen, MD, infectious-disease physician, Shelby Baptist Medical Center, Birmingham, Ala.
Some hospitalists, Dr. Allen says, are as proficient in dealing with inpatient ID cases as he is. Others are clueless, he says. “It really just depends on the training. It would be nice if there was some standardization of training, rather than just kind of catch-as-catch-can.”
As for ID resources available at hospitals, Dr. Allen says, “there is potential in any hospital to have an excellent backbone program of infection control.” But that depends on the availability of ID experts and the willingness of hospital administration to invest in the program.
“A well-developed, well-maintained infection-control program, with a good infection-control nurse, can really help a hospitalist to understand the types of infections that they’re up against in that particular institution,” Dr. Allen explains. “It really pays off down the road for the hospital with reduced infection rates, and also physicians who are practicing in the hospital, in terms of making their life a little bit easier.”
And with changes in Medicare reimbursement for hospital-acquired infections, he says, “it really behooves a hospital to spend some money up front.”
Experts Urge Hospitalists To Be Good Antimicrobial Stewards
It might seem basic, but ID experts say it’s too important not to repeat it over and over again: Hospitalists have to take care to narrowly tailor patients’ antibiotic treatments.
Starting a patient on broad-spectrum therapies might be necessary, but once the culprit is identified, the therapy should be honed, they say.
“I think frequently people who get started on antibiotics empirically in the emergency room, they’ll come into the hospital and they’ll kind of stay on them because folks are sometimes afraid to stop them,” Dr. Chansolme says. “But don’t be afraid to do that, particularly in this era of multi-drug resistance.”
Dr. Allen says scaling down treatment might not be easy in the middle of a busy day, but that it must be done.
“The path of least resistance is always to do nothing,” he says. “Even sometimes when you’re 100% certain [about the precise bug requiring
treatment], there’s this little voice in the back of your head going, ‘Yeah, but what if?’ It really does take some thought, and [courage], to stop antibiotics when the patient’s getting better on the current therapy.”
Dr. Gupta of the CDC says HM programs are in prime position to influence a hospital’s practices. “It’s important to remember appropriate use of antimicrobials and treatment and prevention of hospital-acquired infections when they are practicing that they’re often influencing physicians and training,” he says.
The experts raise a few red flags and offer tips that, if followed, should help hospitalists improve their antimicrobial stewardship:
Dr. Chansolme cautions that “not all fluoroquinolones are created equal” and are not interchangeable. In particular, he notes, moxifloxacin is not good for pseudomonas and doesn’t cover UTIs.
- Dr. Allen says that metronidazole does not have to be given if you’re already giving Zosyn or a carbapenem—it doesn’t add anything to the treatment.
- Dr. Allen also says it’s important to remember that cellulitis is almost always just a gram-positive infection, and does not require a very broad-spectrum antibiotic, a mistake he often sees.
- Dr. Orenstein says hospitalists should be on the lookout for the procalcitonin test, a laboratory study based on a prohormone that tends to be elevated in the setting of bacterial infections. The test can be used to possibly shorten the length of time a patient is given an antibiotic in certain cases.
“If elevated and you followed it, you could use it as a marker for when you could stop your antibiotics,” Dr. Orenstein said.
He says the test generally has been shown to allow doctors to shorten the course of antibiotics by one or two days, which can save on cost and length of stay.
“People need to be aware of it,” he says, “as I think a lot of places will be using it. It’s not quite ready for prime time.”
It might seem basic, but ID experts say it’s too important not to repeat it over and over again: Hospitalists have to take care to narrowly tailor patients’ antibiotic treatments.
Starting a patient on broad-spectrum therapies might be necessary, but once the culprit is identified, the therapy should be honed, they say.
“I think frequently people who get started on antibiotics empirically in the emergency room, they’ll come into the hospital and they’ll kind of stay on them because folks are sometimes afraid to stop them,” Dr. Chansolme says. “But don’t be afraid to do that, particularly in this era of multi-drug resistance.”
Dr. Allen says scaling down treatment might not be easy in the middle of a busy day, but that it must be done.
“The path of least resistance is always to do nothing,” he says. “Even sometimes when you’re 100% certain [about the precise bug requiring
treatment], there’s this little voice in the back of your head going, ‘Yeah, but what if?’ It really does take some thought, and [courage], to stop antibiotics when the patient’s getting better on the current therapy.”
Dr. Gupta of the CDC says HM programs are in prime position to influence a hospital’s practices. “It’s important to remember appropriate use of antimicrobials and treatment and prevention of hospital-acquired infections when they are practicing that they’re often influencing physicians and training,” he says.
The experts raise a few red flags and offer tips that, if followed, should help hospitalists improve their antimicrobial stewardship:
Dr. Chansolme cautions that “not all fluoroquinolones are created equal” and are not interchangeable. In particular, he notes, moxifloxacin is not good for pseudomonas and doesn’t cover UTIs.
- Dr. Allen says that metronidazole does not have to be given if you’re already giving Zosyn or a carbapenem—it doesn’t add anything to the treatment.
- Dr. Allen also says it’s important to remember that cellulitis is almost always just a gram-positive infection, and does not require a very broad-spectrum antibiotic, a mistake he often sees.
- Dr. Orenstein says hospitalists should be on the lookout for the procalcitonin test, a laboratory study based on a prohormone that tends to be elevated in the setting of bacterial infections. The test can be used to possibly shorten the length of time a patient is given an antibiotic in certain cases.
“If elevated and you followed it, you could use it as a marker for when you could stop your antibiotics,” Dr. Orenstein said.
He says the test generally has been shown to allow doctors to shorten the course of antibiotics by one or two days, which can save on cost and length of stay.
“People need to be aware of it,” he says, “as I think a lot of places will be using it. It’s not quite ready for prime time.”
It might seem basic, but ID experts say it’s too important not to repeat it over and over again: Hospitalists have to take care to narrowly tailor patients’ antibiotic treatments.
Starting a patient on broad-spectrum therapies might be necessary, but once the culprit is identified, the therapy should be honed, they say.
“I think frequently people who get started on antibiotics empirically in the emergency room, they’ll come into the hospital and they’ll kind of stay on them because folks are sometimes afraid to stop them,” Dr. Chansolme says. “But don’t be afraid to do that, particularly in this era of multi-drug resistance.”
Dr. Allen says scaling down treatment might not be easy in the middle of a busy day, but that it must be done.
“The path of least resistance is always to do nothing,” he says. “Even sometimes when you’re 100% certain [about the precise bug requiring
treatment], there’s this little voice in the back of your head going, ‘Yeah, but what if?’ It really does take some thought, and [courage], to stop antibiotics when the patient’s getting better on the current therapy.”
Dr. Gupta of the CDC says HM programs are in prime position to influence a hospital’s practices. “It’s important to remember appropriate use of antimicrobials and treatment and prevention of hospital-acquired infections when they are practicing that they’re often influencing physicians and training,” he says.
The experts raise a few red flags and offer tips that, if followed, should help hospitalists improve their antimicrobial stewardship:
Dr. Chansolme cautions that “not all fluoroquinolones are created equal” and are not interchangeable. In particular, he notes, moxifloxacin is not good for pseudomonas and doesn’t cover UTIs.
- Dr. Allen says that metronidazole does not have to be given if you’re already giving Zosyn or a carbapenem—it doesn’t add anything to the treatment.
- Dr. Allen also says it’s important to remember that cellulitis is almost always just a gram-positive infection, and does not require a very broad-spectrum antibiotic, a mistake he often sees.
- Dr. Orenstein says hospitalists should be on the lookout for the procalcitonin test, a laboratory study based on a prohormone that tends to be elevated in the setting of bacterial infections. The test can be used to possibly shorten the length of time a patient is given an antibiotic in certain cases.
“If elevated and you followed it, you could use it as a marker for when you could stop your antibiotics,” Dr. Orenstein said.
He says the test generally has been shown to allow doctors to shorten the course of antibiotics by one or two days, which can save on cost and length of stay.
“People need to be aware of it,” he says, “as I think a lot of places will be using it. It’s not quite ready for prime time.”
Leadership Tools for Hospitalists
- Command of Clinical Care. “First and foremost, you have to be a good hospitalist,” Dr. George says. “You cannot lead a group of physicians unless they respect the quality of your medical care.”
- Transformational leadership. “This is inspiring members of an organization toward a common vision and getting workers to invest energies beyond their own self-interest,” Dr. Carnes says. “That includes things like mentoring your subordinates and taking a personal interest in trying to form a community.”
- Vision/strategic thinking. “You need to understand where your organization is today and envision what the threats to the organization could be or the opportunities for the organization,” Dr. Gorman says. “If a leader doesn’t have an idea of the direction they should go, then they can’t really lead anywhere.”
- Communication. “You have to be able to communicate with a large, diverse audience that includes your colleagues, the administration of the hospital, providers in the community, and your supervisor or direct report,” Dr. Bell says.
- Active listening. “This is really being able to listen to what an individual is saying and what they’re not saying, and to set aside your own preconceived notions, opinions, filters, and judgments, so that you’re truly hearing what the other person has to say,” Cannon says.
- Consensus-building. “A good leader has the ability to work with others, break down barriers, and get that buy-in,” Dr. Ammann says. “The more people you can bring into a project to work on it together, the better.”
- Determination. “If you have a goal, you have to really be steadfast in achieving it,” Dr. Satpathy says. “You’re going to have so many pitfalls along the way that you can’t ever just say, ‘This isn’t going to work.’”
- Open-mindedness. “You have to be able to be unbiased─i.e., try to evaluate whatever the circumstance is from more than one perspective,” Dr. Bell says. “When an issue or problem is brought to you, you really need to hear both sides of the story before you reach a conclusion.”
- Willingness to seek advice. “If you have a view of where you want to go and you’re not getting there, find the right people who can give you some thoughts on how you can approach the issue,” Dr. Gorman says.
- Managerial competence. “If the practice is not financially viable, then the practice will cease to exist,” Dr. Bell says. “So you have to understand the balance between the financial realities and clinical needs of the practice.”
- Command of Clinical Care. “First and foremost, you have to be a good hospitalist,” Dr. George says. “You cannot lead a group of physicians unless they respect the quality of your medical care.”
- Transformational leadership. “This is inspiring members of an organization toward a common vision and getting workers to invest energies beyond their own self-interest,” Dr. Carnes says. “That includes things like mentoring your subordinates and taking a personal interest in trying to form a community.”
- Vision/strategic thinking. “You need to understand where your organization is today and envision what the threats to the organization could be or the opportunities for the organization,” Dr. Gorman says. “If a leader doesn’t have an idea of the direction they should go, then they can’t really lead anywhere.”
- Communication. “You have to be able to communicate with a large, diverse audience that includes your colleagues, the administration of the hospital, providers in the community, and your supervisor or direct report,” Dr. Bell says.
- Active listening. “This is really being able to listen to what an individual is saying and what they’re not saying, and to set aside your own preconceived notions, opinions, filters, and judgments, so that you’re truly hearing what the other person has to say,” Cannon says.
- Consensus-building. “A good leader has the ability to work with others, break down barriers, and get that buy-in,” Dr. Ammann says. “The more people you can bring into a project to work on it together, the better.”
- Determination. “If you have a goal, you have to really be steadfast in achieving it,” Dr. Satpathy says. “You’re going to have so many pitfalls along the way that you can’t ever just say, ‘This isn’t going to work.’”
- Open-mindedness. “You have to be able to be unbiased─i.e., try to evaluate whatever the circumstance is from more than one perspective,” Dr. Bell says. “When an issue or problem is brought to you, you really need to hear both sides of the story before you reach a conclusion.”
- Willingness to seek advice. “If you have a view of where you want to go and you’re not getting there, find the right people who can give you some thoughts on how you can approach the issue,” Dr. Gorman says.
- Managerial competence. “If the practice is not financially viable, then the practice will cease to exist,” Dr. Bell says. “So you have to understand the balance between the financial realities and clinical needs of the practice.”
- Command of Clinical Care. “First and foremost, you have to be a good hospitalist,” Dr. George says. “You cannot lead a group of physicians unless they respect the quality of your medical care.”
- Transformational leadership. “This is inspiring members of an organization toward a common vision and getting workers to invest energies beyond their own self-interest,” Dr. Carnes says. “That includes things like mentoring your subordinates and taking a personal interest in trying to form a community.”
- Vision/strategic thinking. “You need to understand where your organization is today and envision what the threats to the organization could be or the opportunities for the organization,” Dr. Gorman says. “If a leader doesn’t have an idea of the direction they should go, then they can’t really lead anywhere.”
- Communication. “You have to be able to communicate with a large, diverse audience that includes your colleagues, the administration of the hospital, providers in the community, and your supervisor or direct report,” Dr. Bell says.
- Active listening. “This is really being able to listen to what an individual is saying and what they’re not saying, and to set aside your own preconceived notions, opinions, filters, and judgments, so that you’re truly hearing what the other person has to say,” Cannon says.
- Consensus-building. “A good leader has the ability to work with others, break down barriers, and get that buy-in,” Dr. Ammann says. “The more people you can bring into a project to work on it together, the better.”
- Determination. “If you have a goal, you have to really be steadfast in achieving it,” Dr. Satpathy says. “You’re going to have so many pitfalls along the way that you can’t ever just say, ‘This isn’t going to work.’”
- Open-mindedness. “You have to be able to be unbiased─i.e., try to evaluate whatever the circumstance is from more than one perspective,” Dr. Bell says. “When an issue or problem is brought to you, you really need to hear both sides of the story before you reach a conclusion.”
- Willingness to seek advice. “If you have a view of where you want to go and you’re not getting there, find the right people who can give you some thoughts on how you can approach the issue,” Dr. Gorman says.
- Managerial competence. “If the practice is not financially viable, then the practice will cease to exist,” Dr. Bell says. “So you have to understand the balance between the financial realities and clinical needs of the practice.”