User login
Transplantation palliative care: The time is ripe
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3

What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3
What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3
What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
SVS Now Accepting Abstracts for VAM 2017
Abstracts for the 2017 Vascular Annual Meeting are now being accepted. The submission site opened Monday, Nov. 14 for the meeting, to be held May 31 to June 3, 2017, in San Diego. Plenary sessions and exhibits will be June 1 to 3.
Participants may submit abstracts into any of 14 categories and a number of presentation types, including videos. In 2016, organizers selected approximately two-thirds of the submitted abstracts, and this year the VAM Program Committee is seeking additional venues for people to present their work in, including more sessions and other presentation formats.
Click here for abstract guidelines and more information. Abstracts themselves may be submitted here.
Abstracts for the 2017 Vascular Annual Meeting are now being accepted. The submission site opened Monday, Nov. 14 for the meeting, to be held May 31 to June 3, 2017, in San Diego. Plenary sessions and exhibits will be June 1 to 3.
Participants may submit abstracts into any of 14 categories and a number of presentation types, including videos. In 2016, organizers selected approximately two-thirds of the submitted abstracts, and this year the VAM Program Committee is seeking additional venues for people to present their work in, including more sessions and other presentation formats.
Click here for abstract guidelines and more information. Abstracts themselves may be submitted here.
Abstracts for the 2017 Vascular Annual Meeting are now being accepted. The submission site opened Monday, Nov. 14 for the meeting, to be held May 31 to June 3, 2017, in San Diego. Plenary sessions and exhibits will be June 1 to 3.
Participants may submit abstracts into any of 14 categories and a number of presentation types, including videos. In 2016, organizers selected approximately two-thirds of the submitted abstracts, and this year the VAM Program Committee is seeking additional venues for people to present their work in, including more sessions and other presentation formats.
Click here for abstract guidelines and more information. Abstracts themselves may be submitted here.
Best Practices: Protecting Dry Vulnerable Skin with CeraVe® Healing Ointment
A supplement to Dermatology News. This advertising supplement is sponsored by Valeant Pharmaceuticals.

- Reinforcing the Skin Barrier
- NEA Seal of Acceptance
- A Preventative Approach to Dry, Cracked Skin
- CeraVe Ointment in the Clinical Setting
Faculty/Faculty Disclosure
Sheila Fallon Friedlander, MD
Professor of Clinical Dermatology & Pediatrics
Director, Pediatric Dermatology Fellowship Training Program
University of California at San Diego School of Medicine
Rady Children’s Hospital,
San Diego, California
Dr. Friedlander was compensated for her participation in the development of this article.
CeraVe is a registered trademark of Valeant Pharmaceuticals International, Inc. or its affiliates.
A supplement to Dermatology News. This advertising supplement is sponsored by Valeant Pharmaceuticals.
- Reinforcing the Skin Barrier
- NEA Seal of Acceptance
- A Preventative Approach to Dry, Cracked Skin
- CeraVe Ointment in the Clinical Setting
Faculty/Faculty Disclosure
Sheila Fallon Friedlander, MD
Professor of Clinical Dermatology & Pediatrics
Director, Pediatric Dermatology Fellowship Training Program
University of California at San Diego School of Medicine
Rady Children’s Hospital,
San Diego, California
Dr. Friedlander was compensated for her participation in the development of this article.
CeraVe is a registered trademark of Valeant Pharmaceuticals International, Inc. or its affiliates.
A supplement to Dermatology News. This advertising supplement is sponsored by Valeant Pharmaceuticals.
- Reinforcing the Skin Barrier
- NEA Seal of Acceptance
- A Preventative Approach to Dry, Cracked Skin
- CeraVe Ointment in the Clinical Setting
Faculty/Faculty Disclosure
Sheila Fallon Friedlander, MD
Professor of Clinical Dermatology & Pediatrics
Director, Pediatric Dermatology Fellowship Training Program
University of California at San Diego School of Medicine
Rady Children’s Hospital,
San Diego, California
Dr. Friedlander was compensated for her participation in the development of this article.
CeraVe is a registered trademark of Valeant Pharmaceuticals International, Inc. or its affiliates.

Beyond Weight Loss: The Expanding Role of GLP-1s in Oncology
Beyond Weight Loss: The Expanding Role of GLP-1s in Oncology
This transcript has been edited for clarity.
Coral Olazagasti, MD: Hi, everyone. Good afternoon. My name is Dr Coral Olazagasti, and I’m a medical oncologist from the University of Miami. I’m excited to be here with my colleague and my friend, Carolina. Dr Bernabe, Can you please introduce yourself?
Carolina Bernabe, MD: I am Dr Carolina Bernabe. I’m one of the gastrointestinal (GI) oncologists at Montefiore Einstein Comprehensive Cancer Center. Thank you for having me today.
Olazagasti: We’re excited because we know that there has been excitement and interest in GLP-1s in cancer. You would think, like, “Hmm, let’s just combine a GI oncologist with a thoracic oncologist to talk about GLP-1s.”
I wanted to bring the conversation to the GLP-1s because we know that it’s been becoming a boom. You see it in your home because your husband is an endocrinologist, and many people are on these drugs. It’s been remarkable, the use and the benefits that we’ve seen so far. Then to know that they might have a benefit in cancer, I think it’s wonderful and very interesting.
What are your thoughts?
Bernabe: When looking at the data on how many patients are using this medication, you’re talking about 12% of the whole US population, which is, like, 44 million people. That’s crazy. Looking at the abstracts that were presented here at ASCO, they looked at these numbers and looked at these patients with cancer, which is around 1000 patients, and then they were evaluating what is the benefit of GLP-1s. You had a chance to look at the abstract, I think?
Olazagasti: Yeah. We have a retrospective study where the authors review a database. There were around 1000 patients, like you said, on GLP-1s with a history of cancer, and the benefit was profound. They found at 24 months there was an overall survival benefit, not only for breast but also prostate cancer, in patients on GLP-1s. Granted, I know that we’re looking into retrospective studies, but I think it makes you wonder if we’re seeing these trends in a retrospective fashion in breast and prostate, where else are we seeing it? I think it’s just a matter of looking at the data.
Bernabe: Even though it was a retrospective analysis, they also did this propensity score where it’s like matching, and that tries to create kind of a randomized clinical trial.
Olazagasti: After adjusting, it was for age and other factors.
Bernabe: Correct.
Olazagasti: The benefits were sustained, so I think it’s wonderful.
What about the other abstract? There was also another abstract. This one was in patients that had a history of cancer and were on GLP-1s, but they also were on immune checkpoint inhibitors. This database covered more patients. I think it was around 3800 patients that were in this particular retrospective study. That study found that not only were the patients having benefits of survival those patients on immune checkpoint inhibitors and GLP-1s, but also we’re seeing that the patients had lower rates of immune-related adverse events. It’s just mind-blowing to me.
Bernabe: Completely agree with you. We are seeing the benefit not only in the survival, who knows, maybe some decrease in the inflammatory component on cancer and tumor microenvironment, but also we’re seeing less events related to immunotherapy and less immune toxicity, right, that we’re always worried about and the patients need to start using a steroid. Maybe in the future, this can be used as a steroid-sparing agent. It’s wonderful news.
Olazagasti: Yeah, I know. We’ve been seeing data from rheumatologic disorders that GLP-1s help with that inflammation, so you’re right. Sometimes autoimmune diseases are our limiting factor to be able to offer these patients immunotherapy, and oftentimes our only choices are chemotherapy.
Bernabe: It opens a window.
Olazagasti: It may be allowing them a possibility of controlling their autoimmune disease while also being able to challenge them. I’m so excited. I think we’re going to start seeing these studies planned and designed in a prospective fashion, so I wonder how these data are going to look in the long term.
Bernabe: I think this is just the tip of an iceberg and will open up the opportunities to further prospective studies and trials.
Olazagasti: There’s a large amount of excitement also for patients, at least in the thoracic space, where with many of these drugs — especially TKIs, like lorlatinib for ALK-positive lung cancer — you have a large amount of edema. Even in patients with docetaxel, too, you have some swelling. With that agent that I mentioned, lorlatinib, patients also had high cholesterol levels, and that’s really a challenge.
I’m interested to see what the role will be of GLP-1s in these cohorts of patients. Is this going to be something where not only do they hopefully derive a survival benefit, but also in the side effect profile and in quality of life?
I’m excited to see. It’s crazy to be an oncologist in 2026, and so it’s honestly such a pleasure for me to see science advancing. At the end of the day, we want to make sure that the studies and the discoveries that we have are applicable to our patients and are something that we can incorporate outside of clinical trials and into the real world.
Bernabe: Especially this drug that is already popular, right? Now we’re seeing an extra benefit on top of all the weight loss and decrease in inflammation in general.
Olazagasti: Thank you for this wonderful discussion, and thank you for watching our video. Have a great day.
Bernabe: Thank you for having me.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Coral Olazagasti, MD: Hi, everyone. Good afternoon. My name is Dr Coral Olazagasti, and I’m a medical oncologist from the University of Miami. I’m excited to be here with my colleague and my friend, Carolina. Dr Bernabe, Can you please introduce yourself?
Carolina Bernabe, MD: I am Dr Carolina Bernabe. I’m one of the gastrointestinal (GI) oncologists at Montefiore Einstein Comprehensive Cancer Center. Thank you for having me today.
Olazagasti: We’re excited because we know that there has been excitement and interest in GLP-1s in cancer. You would think, like, “Hmm, let’s just combine a GI oncologist with a thoracic oncologist to talk about GLP-1s.”
I wanted to bring the conversation to the GLP-1s because we know that it’s been becoming a boom. You see it in your home because your husband is an endocrinologist, and many people are on these drugs. It’s been remarkable, the use and the benefits that we’ve seen so far. Then to know that they might have a benefit in cancer, I think it’s wonderful and very interesting.
What are your thoughts?
Bernabe: When looking at the data on how many patients are using this medication, you’re talking about 12% of the whole US population, which is, like, 44 million people. That’s crazy. Looking at the abstracts that were presented here at ASCO, they looked at these numbers and looked at these patients with cancer, which is around 1000 patients, and then they were evaluating what is the benefit of GLP-1s. You had a chance to look at the abstract, I think?
Olazagasti: Yeah. We have a retrospective study where the authors review a database. There were around 1000 patients, like you said, on GLP-1s with a history of cancer, and the benefit was profound. They found at 24 months there was an overall survival benefit, not only for breast but also prostate cancer, in patients on GLP-1s. Granted, I know that we’re looking into retrospective studies, but I think it makes you wonder if we’re seeing these trends in a retrospective fashion in breast and prostate, where else are we seeing it? I think it’s just a matter of looking at the data.
Bernabe: Even though it was a retrospective analysis, they also did this propensity score where it’s like matching, and that tries to create kind of a randomized clinical trial.
Olazagasti: After adjusting, it was for age and other factors.
Bernabe: Correct.
Olazagasti: The benefits were sustained, so I think it’s wonderful.
What about the other abstract? There was also another abstract. This one was in patients that had a history of cancer and were on GLP-1s, but they also were on immune checkpoint inhibitors. This database covered more patients. I think it was around 3800 patients that were in this particular retrospective study. That study found that not only were the patients having benefits of survival those patients on immune checkpoint inhibitors and GLP-1s, but also we’re seeing that the patients had lower rates of immune-related adverse events. It’s just mind-blowing to me.
Bernabe: Completely agree with you. We are seeing the benefit not only in the survival, who knows, maybe some decrease in the inflammatory component on cancer and tumor microenvironment, but also we’re seeing less events related to immunotherapy and less immune toxicity, right, that we’re always worried about and the patients need to start using a steroid. Maybe in the future, this can be used as a steroid-sparing agent. It’s wonderful news.
Olazagasti: Yeah, I know. We’ve been seeing data from rheumatologic disorders that GLP-1s help with that inflammation, so you’re right. Sometimes autoimmune diseases are our limiting factor to be able to offer these patients immunotherapy, and oftentimes our only choices are chemotherapy.
Bernabe: It opens a window.
Olazagasti: It may be allowing them a possibility of controlling their autoimmune disease while also being able to challenge them. I’m so excited. I think we’re going to start seeing these studies planned and designed in a prospective fashion, so I wonder how these data are going to look in the long term.
Bernabe: I think this is just the tip of an iceberg and will open up the opportunities to further prospective studies and trials.
Olazagasti: There’s a large amount of excitement also for patients, at least in the thoracic space, where with many of these drugs — especially TKIs, like lorlatinib for ALK-positive lung cancer — you have a large amount of edema. Even in patients with docetaxel, too, you have some swelling. With that agent that I mentioned, lorlatinib, patients also had high cholesterol levels, and that’s really a challenge.
I’m interested to see what the role will be of GLP-1s in these cohorts of patients. Is this going to be something where not only do they hopefully derive a survival benefit, but also in the side effect profile and in quality of life?
I’m excited to see. It’s crazy to be an oncologist in 2026, and so it’s honestly such a pleasure for me to see science advancing. At the end of the day, we want to make sure that the studies and the discoveries that we have are applicable to our patients and are something that we can incorporate outside of clinical trials and into the real world.
Bernabe: Especially this drug that is already popular, right? Now we’re seeing an extra benefit on top of all the weight loss and decrease in inflammation in general.
Olazagasti: Thank you for this wonderful discussion, and thank you for watching our video. Have a great day.
Bernabe: Thank you for having me.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Coral Olazagasti, MD: Hi, everyone. Good afternoon. My name is Dr Coral Olazagasti, and I’m a medical oncologist from the University of Miami. I’m excited to be here with my colleague and my friend, Carolina. Dr Bernabe, Can you please introduce yourself?
Carolina Bernabe, MD: I am Dr Carolina Bernabe. I’m one of the gastrointestinal (GI) oncologists at Montefiore Einstein Comprehensive Cancer Center. Thank you for having me today.
Olazagasti: We’re excited because we know that there has been excitement and interest in GLP-1s in cancer. You would think, like, “Hmm, let’s just combine a GI oncologist with a thoracic oncologist to talk about GLP-1s.”
I wanted to bring the conversation to the GLP-1s because we know that it’s been becoming a boom. You see it in your home because your husband is an endocrinologist, and many people are on these drugs. It’s been remarkable, the use and the benefits that we’ve seen so far. Then to know that they might have a benefit in cancer, I think it’s wonderful and very interesting.
What are your thoughts?
Bernabe: When looking at the data on how many patients are using this medication, you’re talking about 12% of the whole US population, which is, like, 44 million people. That’s crazy. Looking at the abstracts that were presented here at ASCO, they looked at these numbers and looked at these patients with cancer, which is around 1000 patients, and then they were evaluating what is the benefit of GLP-1s. You had a chance to look at the abstract, I think?
Olazagasti: Yeah. We have a retrospective study where the authors review a database. There were around 1000 patients, like you said, on GLP-1s with a history of cancer, and the benefit was profound. They found at 24 months there was an overall survival benefit, not only for breast but also prostate cancer, in patients on GLP-1s. Granted, I know that we’re looking into retrospective studies, but I think it makes you wonder if we’re seeing these trends in a retrospective fashion in breast and prostate, where else are we seeing it? I think it’s just a matter of looking at the data.
Bernabe: Even though it was a retrospective analysis, they also did this propensity score where it’s like matching, and that tries to create kind of a randomized clinical trial.
Olazagasti: After adjusting, it was for age and other factors.
Bernabe: Correct.
Olazagasti: The benefits were sustained, so I think it’s wonderful.
What about the other abstract? There was also another abstract. This one was in patients that had a history of cancer and were on GLP-1s, but they also were on immune checkpoint inhibitors. This database covered more patients. I think it was around 3800 patients that were in this particular retrospective study. That study found that not only were the patients having benefits of survival those patients on immune checkpoint inhibitors and GLP-1s, but also we’re seeing that the patients had lower rates of immune-related adverse events. It’s just mind-blowing to me.
Bernabe: Completely agree with you. We are seeing the benefit not only in the survival, who knows, maybe some decrease in the inflammatory component on cancer and tumor microenvironment, but also we’re seeing less events related to immunotherapy and less immune toxicity, right, that we’re always worried about and the patients need to start using a steroid. Maybe in the future, this can be used as a steroid-sparing agent. It’s wonderful news.
Olazagasti: Yeah, I know. We’ve been seeing data from rheumatologic disorders that GLP-1s help with that inflammation, so you’re right. Sometimes autoimmune diseases are our limiting factor to be able to offer these patients immunotherapy, and oftentimes our only choices are chemotherapy.
Bernabe: It opens a window.
Olazagasti: It may be allowing them a possibility of controlling their autoimmune disease while also being able to challenge them. I’m so excited. I think we’re going to start seeing these studies planned and designed in a prospective fashion, so I wonder how these data are going to look in the long term.
Bernabe: I think this is just the tip of an iceberg and will open up the opportunities to further prospective studies and trials.
Olazagasti: There’s a large amount of excitement also for patients, at least in the thoracic space, where with many of these drugs — especially TKIs, like lorlatinib for ALK-positive lung cancer — you have a large amount of edema. Even in patients with docetaxel, too, you have some swelling. With that agent that I mentioned, lorlatinib, patients also had high cholesterol levels, and that’s really a challenge.
I’m interested to see what the role will be of GLP-1s in these cohorts of patients. Is this going to be something where not only do they hopefully derive a survival benefit, but also in the side effect profile and in quality of life?
I’m excited to see. It’s crazy to be an oncologist in 2026, and so it’s honestly such a pleasure for me to see science advancing. At the end of the day, we want to make sure that the studies and the discoveries that we have are applicable to our patients and are something that we can incorporate outside of clinical trials and into the real world.
Bernabe: Especially this drug that is already popular, right? Now we’re seeing an extra benefit on top of all the weight loss and decrease in inflammation in general.
Olazagasti: Thank you for this wonderful discussion, and thank you for watching our video. Have a great day.
Bernabe: Thank you for having me.
A version of this article first appeared on Medscape.com.
Beyond Weight Loss: The Expanding Role of GLP-1s in Oncology
Beyond Weight Loss: The Expanding Role of GLP-1s in Oncology

Managing Requests for Medical Aid in Dying Within the Veterans Health Administration
Managing Requests for Medical Aid in Dying Within the Veterans Health Administration
Requests for medical aid in dying (MAID) within the Veterans Health Administration (VHA) present unique ethical, legal, and clinical challenges. MAID is a process in which a physician provides a terminally ill patient with the means to end their own life. It is expressly prohibited by federal law, including within the US Department of Veterans Affairs (VA), regardless of its legality at the state level.1 MAID is also prohibited within community care institutions funded by the VA. The American Medical Association, American Geriatrics Society, and American Academy of Hospice and Palliative Medicine have adopted neutral positions regarding MAID due to varying opinions among their respective members.2-4 VHA palliative care clinicians are trained to identify and honor preferences for care and alleviate physical and emotional distress, which may complicate the management of MAID requests. Veterans can request MAID due to their desire for autonomy and pain relief, but the VHA prohibits clinicians from honoring these specific preferences. The inability to help veterans achieve their care preferences conflicts with the core mission of palliative care to reduce suffering and respect end-of-life wishes.
This case report describes the management of a veteran who requested MAID while also exhibiting active suicidal ideation. The patient’s distress stemmed from fears of impending loss of autonomy and functional decline, factors frequently linked to requests for MAID in terminally ill patients.5,6 Addressing the veteran’s request for MAID required balancing respect for patient autonomy and concerns about future suffering with the VA mission to protect veterans from self-harm and provide mental health care for suicidal ideation. This case highlights the importance of nuanced clinical approaches, ethical reflection, and interdisciplinary collaboration in navigating such complex scenarios. Informed consent was obtained from the patient’s family and health care agent (HCA) to publish this report.
Case Presentation
A 73-year-old male veteran, with Parkinson disease (PD), diagnosed at age 52 years, was referred to palliative care following diagnosis of a glioblastoma multiforme (GBM). The patient also had a history of major depressive disorder (MDD), suicidal ideation (SI), benign prostatic hypertrophy, and migraines. He was divorced, had no children, and his only sibling (sister) was deceased. His brother-in-law served as his HCA.
The patient had many close friends in the community, was an architect by training, and was active in the removal of barriers and increasing access for people with disabilities. Since 2010, about 7 years before his PD diagnosis, the patient used psychiatry and psychology resources to treat MDD, functional decline, and SI. He was hospitalized in 2016 after self-administration of heroin. During the hospitalization the patient received a high risk for suicide label. He articulated a firm and long-standing belief in his right to die and shared plans to end his life when he experienced a significant decline in his independence and quality of life (QoL).
When diagnosed with PD, the patient shared that his QoL was of utmost importance. He was aware that he would have significant physical decline as PD progressed and felt like there would be a point when his QoL would not be acceptable. When that happened, he wanted to end his life by available means. He was followed closely by his VHA care team for physical and emotional distress.
When diagnosed with a GBM in 2023, the patient declined treatment and was referred to palliative care, which had sporadically treated him for PD-related distress prior to 2023. During his previous palliative care visits, the patient had discussed a desire to engage in MAID when his functional status declined. After the GBM diagnosis, he reported no acute intent to harm himself with heroin, but planned to travel to Vermont for MAID when he felt he no longer had an adequate QoL based on functional capability.
Pharmacologic and nonpharmacologic approaches were used to treat the patient’s pain. He reported significant benefit from biofeedback therapy provided by the VA Headache Center of Excellence. This work also reconnected him to meditation, which he used daily to relieve pain and distress. The patient managed head pain with nonpharmacologic and pharmacologic interventions for 6 months and reported satisfaction with his QoL.
After 6 months, imaging showed progression of the brain tumor, which was associated with more fatigue and memory decline. At that time, the patient was enrolled in home hospice and reported continued intent to pursue MAID in Vermont but had not taken steps toward carrying it out. The patient understood the VA could not assist him in pursuing MAID; however, his care team was able to assist him in sharing his preferences for care with his loved ones and health care power of attorney.
He experienced rapid functional and cognitive decline due to progression of the GBM and was admitted to the VA Connecticut Healthcare System (VACHS) acute care unit where he exhibited confusion and screened positive for delirium using the Confusion Assessment Method.7 His physical and cognitive deterioration was likely due to the progressive brain tumor, and the patient lacked the capacity to make complex medical decisions. Formal consent was obtained from his HCA to transfer him to inpatient hospice. Psychiatry followed the patient throughout.
After 4 weeks of hospice care, the patient had a witnessed suicide attempt while the nurse was assisting him in the bathroom. The patient attempted to use hospital pajamas to hang himself when he wrapped a hospital gown around his neck and stated he was trying to tie a knot. Due to his confusion and delirium, the patient was unable to express his reasoning for the suicide attempt. He was seen by the Psychiatry service, which determined that his suicide risk was low to intermediate. The Psychiatry service did not recommend a 1:1 safety sitter, but suggested medication changes. Levetiracetam was discontinued, and valproate 500 mg orally twice daily was initiated for seizure prevention.
The hospice team was informed of the suicide attempt and psychiatry recommendations. The suicide prevention team was also updated following this event and agreed with psychiatry recommendations. The patient continued to decline, was no longer able to get out of bed, and had minimal speech. The patient received comfort medications, including intravenous morphine 2 mg and lorazepam 0.5 mg as needed ≤ 4 times daily. He died 8 days later.
Discussion
Chronic medical illness has been associated with increased suicide risk.8-10 The increased risk of suicide in chronically ill patients has been described as having as a bidirectional relationship with MDD, with depression not only increasing the risk of chronic medical illness but new-onset chronic medical illness being associated with new onset depression.11,12 Chronic medical conditions are associated with numerous psychiatric disorders, and the presence of a comorbid psychiatric illness is associated with higher rates of hospitalization, emergency department visits, and increased health care costs.13 Research has found that the association between suicide risk and chronic medical illness remains even after accounting for comorbid mental health disorders.14 This has been postulated to be due to a multitude of interpersonal, behavioral, cognitive, and affective factors (eg, perceived burdensomeness, loneliness, stress, pain catastrophizing, self-criticism).15 Additionally, some researchers have questioned whether suicidality constitutes a distinct mental disorder.16
Patients with cancer are at increased risk for suicidal ideation (including passive death wishes) and suicide attempts.17,18 Recent data indicate that compared with the general population, there is an 85% increased risk of suicide mortality in patients with cancer.19 Studies show the incidence of suicide is greater for individuals with cancer compared with the general population, with standardized mortality ratios ranging from 1.4 to 5.7.20-22
Among patients with cancer, suicide risk is associated with several factors: worse prognosis, older age, male sex, living in a socioeconomically vulnerable environment, and increased communication about suicidal intent prior to death.23-25 Just as the prevalence of suicidal ideation in people with cancer varies widely, reported rates of suicidality in caregivers of patients with cancer range from 2.7% to 71%.17,26 A survey of health care workers indicated the following reasons patients with cancer may die by suicide or seek aid in assisted suicide: social isolation, pain, physical impairment, loss of autonomy and meaning, terminal illness, and psychic distress and desperation.27
As with cancer, patients with PD exhibit increased suicidal ideation compared with the general population.28,29 Two studies found the suicide rate in individuals with PD is about twice as high as it is in the general population.30,31 Among people with PD, male sex, younger age, initial onset of motor symptoms in the upper or both upper and lower extremities, history of depression or any psychiatric diagnosis, delusions, higher levodopa dosing, and urban residence have been clinically correlated with suicide. Jumping has been a frequent method of suicide.30,31
Some research has evaluated the perspectives of loved ones after a patient chooses MAID. A study in the Netherlands found that 92% of relatives surveyed believed that access to MAID improved QoL and reduced pain at the end of life.32 In another, family members of individuals who used MAID reported higher quality on items related to physical symptom control and preparedness for death, compared with individuals who did not pursue MAID or who requested but did not receive it. There were no differences on items assessing connectedness to their loved one, being unafraid of death, level of consciousness, or global quality of death items.33 Another study found no significant differences in depression rates, grief, or use of mental health services among Oregon families whose loved ones died using MAID compared with those who did not.34
The higher suicide rate among terminally ill patients highlights the complex issue of MAID and the right to die. It is important to differentiate between euthanasia and medically-assisted dying. Euthanasia is an act whereby a person other than the patient acts to cause death. In MAID, the patient is provided with a medication that they self-administer. Recent Gallup polls found that > 70% of Americans believe physicians should be “allowed by law to end the patient’s life by some painless means if the patient and his or her family request it.”35
It is important to acknowledge MAID in the context of chronic suicidality, like in the case described in this article. It is imperative not to dismiss reports of suicidality in this population. Ignoring reports of suicidal ideation may lead to decreased access to pharmacologic and nonpharmacologic interventions. It is also important to maintain a timeline of symptom occurrence and to differentiate between chronic suicidality and the desire to die associated with having a terminal illness. A thorough assessment is necessary to assess whether the patient’s decision stems from a calculated decision with preserved capacity or from underlying mental health conditions. Other factors that may lead the patient to a hastened death (ie, pain, poor psychosocial support, delirium, cognitive impairment, incomplete understanding of treatment/prognosis) need to be addressed prior to finalizing choices. In this case, an assessment was performed by psychiatry, psychology, social work, and chaplains to ensure comprehensive evaluation.
The VHA offers resources to assist individuals experiencing suicidal ideation, including suicide prevention coordinators who work directly with veterans and offer consultation to teams working with veterans at risk for suicide. Support for VHA clinicians who treat veterans considering MAID may help address any moral distress. In this case, the care team met early for overnight sign-out, had daily core hospice team meetings, as-needed safety huddles, and weekly care plan meetings to ensure maximal physical and emotional comfort for the patient. These meetings cultivate open, honest, and transparent discussions regarding any staff concerns or personal distress around the plan of care. The VACHS chief well-being officer was also available for all staff.
A systematic review of the impact of MAID on clinicians found that MAID legislation influenced emotional responses. For countries whose MAID legislation emphasized alleviation from pain in addition to terminal illness, clinicians reported more emotional reflection. Whereas, in countries where MAID legislation is stricter and can be applied solely for terminal illness, clinicians reported a stronger and more polarizing range of emotions.36 This highlights the potential influence of the context in which clinicians work on their emotional experience with MAID. Given that MAID is not permitted in the VA, staff members may experience heightened emotional responses. In a survey of US adults, there was an interest in using MAID but there were knowledge deficits regarding the process and legality.37
Legal aspects come into play as well with regards to MAID. Eligibility requires the patient be aged ≥ 18 years, be terminally ill with a prognosis of ≤ 6 months, have the capacity to make their own health care decision, and be able to self-administer the medication. States also may have residency restrictions. Special care and adequate education are needed, as having anyone but the patient administer the medication may be considered criminal. Furthermore, since MAID is not allowed federally, this creates further distress in VHA clinicians entrusted to minimizing pain for patients.
Strategies to support veterans given prohibition of MAID include: conversations about the patient’s values, clarifying reasons for request, assessing all domains of distress, affirming concerns with compassion and nonjudgment, addressing any pain using pharmacologic and nonpharmacologic interventions, providing education on other permissible options for end-of-life care, and consulting other specialties.38
End-of-life options permitted by the VA include withholding/ withdrawing life-sustaining treatments, palliative sedation, and voluntary stopping of eating and drinking.39 Given the complexities of MAID, the VHA should initiate discussions of MAID, educate clinicians on what they can and cannot do as federal employees, and establish committees to discuss approaches that could minimize pain for patients and clinician distress.
Conclusions
Caring for veterans who request MAID requires clinicians to navigate a complex intersection of ethical obligations, legal constraints, and patient preferences. Within the VHA, where MAID is prohibited, clinicians must balance respect for patient autonomy with adherence to VA regulations. Comprehensive assessment to identify sources of distress, interdisciplinary collaboration, and recognition of permissible alternatives that align with patients’ values are essential to provide effective end-of-life care at the VHA for individuals considering MAID. As requests for MAID continue to emerge in clinical practice, the VHA has an opportunity to strengthen clinician education, clarify institutional expectations, and promote supportive structures that reduce both patient suffering and clinician moral distress.
- Meisel A, Snyder L, Quill T; American College of Physicians-- American Society of Internal Medicine End-of-Life Care Consensus Panel. Seven legal barriers to end-of- life care: myths, realities, and grains of truth. JAMA. 2000;284:2495-2501. doi:10.1001/jama.284.19.2495
- Physician-Assisted Suicide. American Medical Association Code of Medical Ethics. 2025. Accessed May 6, 2026. https://code-medical-ethics.ama-assn.org/ethics-opinions /physician-assisted-suicide
- Youngner SJ, Thoman R. AGS survey actually supports engaged neutrality for physician-assisted death. J Am Geriatr Soc. 2020;68:2140-2141. doi:10.1111/jgs.16679
- Physician-Assisted Dying. American Academy of Hospice and Palliative Medicine. Updated 2007. Accessed May 6, 2026. https://aahpm.org/advocacy/where-we-stand/pad/
- Ganzini L, Goy ER, Dobscha SK. Why Oregon patients request assisted death: family members’ views. J Gen Intern Med. 2008;23:154-157. doi:10.1007/s11606-007-0476-x
- Pearlman RA, Hsu C, Starks H, et al. Motivations for physician-assisted suicide: patient and family voices. J Gen Intern Med. 2005;20:234-239. doi:10.1111/j.1525-1497.2005.40225.x
- Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the Confusion Assessment Method. A new method for detection of delirium. Ann Intern Med. 1990;113:941- 948. doi:10.7326/0003-4819-113-12-941
- Fässberg MM, Cheung G, Canetto SS, et al. A systematic review of physical illness, functional disability, and suicidal behaviour among older adults.
Aging Ment Health. 2016;20:166-194. doi:10.1080/13607863.2015.1083945 - Gürhan N, Bes¸er NG, Polat Ü, et al. Suicide risk and depression in individuals with chronic illness. Community Ment Health J. 2019;55:840-848. doi:10.1007/s10597-019-00388-7
- Kye SY, Park K. Suicidal ideation and suicidal attempts among adults with chronic diseases: a crosssectional study. Compr Psychiatry. 2017;73:160-167. doi:10.1016/j.comppsych.2016.12.001
- Patten SB. Long-term medical conditions and major depression in a Canadian population study at waves 1 and 2. J Affect Disord. 2001;63:35-41. doi:10.1016/s0165-0327(00)00186-5
- Van der Kooy K, van Hout H, Marwijk H, et al. Depression and the risk for cardiovascular diseases: systematic review and meta analysis. Int J Geriatr Psychiatry. 2007;22:613- 626. doi:10.1002/gps.1723
- Sporinova B, Manns B, Tonelli M, et al. Association of mental health disorders with health care utilization and costs among adults with chronic disease. JAMA Netw Open. 2019;2:e199910. doi:10.1001/jamanetworkopen.2019.9910
- Ahmedani BK, Peterson EL, Hu Y, et al. Major physical health conditions and risk of suicide. Am J Prev Med. 2017;53:308-315. doi:10.1016/j.amepre.2017.04.001
- Rogers ML, Joiner TE, Shahar G. Suicidality in chronic illness: an overview of cognitive-affective and interpersonal factors. J Clin Psychol Med Settings. 2021;28:137-148. doi:10.1007/s10880-020-09749-x
- Sisti D, Mann JJ, Oquendo MA. Toward a distinct mental disorder—suicidal behavior. JAMA Psychiatry. 2020;77:661-662. doi:10.1001/jamapsychiatry.2020.0111
- Kolva E, Hoffecker L, Cox-Martin E. Suicidal ideation in patients with cancer: a systematic review of prevalence, risk factors, intervention and assessment. Palliat Support Care. 2020;18:206-219. doi:10.1017/S1478951519000610
- Zaorsky NG, Zhang Y, Tuanquin L, et al. Suicide among cancer patients. Nat Commun. 2019;10:207. doi:10.1038/s41467-018-08170-1
- Heinrich M, Hofmann L, Baurecht H, et al. Suicide risk and mortality among patients with cancer. Nat Med. 2022;28:852-859. doi:10.1038/s41591-022-01745-y
- Yousaf U, Christensen ML, Engholm G, et al. Suicides among Danish cancer patients 1971-1999. Br J Cancer. 2005;92:995-1000. doi:10.1038/sj.bjc.6602424
- Misono S, Weiss NS, Fann JR, et al. Incidence of suicide in persons with cancer. J Clin Oncol. 2008;26:4731-4738. doi:10.1200/JCO.2007.13.8941
- Björkenstam C, Edberg A, Ayoubi S, et al. Are cancer patients at higher suicide risk than the general population?. Scand J Public Health. 2005;33:208-214. doi:10.1080/14034940410019226
- Kinslow CJ, Kumar P, Olfson M, et al. Prognosis and risk of suicide after cancer diagnosis. Cancer. 2024;130:588-596. doi:10.1002/cncr.35118
- Men VY, Emery CR, Yip PSF. Characteristics of cancer patients who died by suicide: a quantitative study of 15-year coronial records. Psychooncology. 2021;30:1051-1058. doi:10.1002/pon.5634
- Abdel-Rahman O. Socioeconomic predictors of suicide risk among cancer patients in the United States: a population- based study. Cancer Epidemiol. 2019;63:101601. doi:10.1016/j.canep.2019.101601
- O’Dwyer ST, Janssens A, Sansom A, et al. Suicidality in family caregivers of people with long-term illnesses and disabilities: a scoping review. Compr Psychiatry. 2021;110:152261. doi:10.1016/j.comppsych.2021.152261
- Senf B, Maiwurm P, Fettel J. Attitudes and opinions towards suicidality in professionals working with oncology patients: results from an online survey. Support Care Cancer. 2022;30:1775-1786. doi:10.1007/s00520-021-06590-2
- Berardelli I, Belvisi D, Nardella A, et al. Suicide in Parkinson’s disease: a systematic review. CNS Neurol Disord Drug Targets. 2019;18:466-477. doi:10.2174/1871527318666190703093345
- Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry. 1999;56:617-626. doi:10.1001/archpsyc.56.7.617
- Chen YY, Yu S, Hu YH, et al. Risk of suicide among patients with Parkinson disease. JAMA Psychiatry. 2021;78:293-301. doi:10.1001/jamapsychiatry.2020.4001
- Lee T, Lee HB, Ahn MH, et al. Increased suicide risk and clinical correlates of suicide among patients with Parkinson’s disease. Parkinsonism Relat Disord. 2016;32:102- 107. doi:10.1016/j.parkreldis.2016.09.006
- Georges JJ, Onwuteaka-Philipsen BD, Muller MT, et al. Relatives’ perspective on the terminally ill patients who died after euthanasia or physician-assisted suicide: a retrospective cross-sectional interview study in the Netherlands. Death Stud. 2007;31:1-15. doi:10.1080/07481180600985041
- Smith KA, Goy ER, Harvath TA, et al. Quality of death and dying in patients who request physician-assisted death. J Palliat Med. 2011;14:445-450. doi:10.1089/jpm.2010.0425
- Ganzini L, Goy ER, Dobscha SK, et al. Mental health outcomes of family members of Oregonians who request physician aid in dying. J Pain Symptom Manage. 2009;38:807-815. doi:10.1016/j.jpainsymman.2009.04.026
- Yi R. Most Americans favor legal euthanasia. Gallup. August 8, 2024. Accessed May 6, 2026. https://news.gallup .com/poll/648215/americans-favor-legal-euthanasia.aspx
- Dholakia SY, Bagheri A, Simpson A. Emotional impact on healthcare providers involved in medical assistance in dying (MAiD): a systematic review and qualitative meta-synthesis. BMJ Open. 2022;12:e058523. doi:10.1136/bmjopen-2021-058523
- Kozlov E, Luth EA, Nemeth S, et al. Knowl - edge of and preferences for medical aid in dying. JAMA Netw Open. 2025;8:e2461495. doi:10.1001/jamanetworkopen.2024.61495
- Geppert C; Veterans Administration National Center for Ethics in Health Care. Medical aid in dying in the VA. Presented at: VISN 1 Palliative Care Summit, September 2024.
- National Ethics Committee, Veterans Health Administration. The ethics of palliative sedation as a therapy of last resort. Am J Hosp Palliat Care. 2006;23:483-491. doi:10.1177/1049909106294883
Requests for medical aid in dying (MAID) within the Veterans Health Administration (VHA) present unique ethical, legal, and clinical challenges. MAID is a process in which a physician provides a terminally ill patient with the means to end their own life. It is expressly prohibited by federal law, including within the US Department of Veterans Affairs (VA), regardless of its legality at the state level.1 MAID is also prohibited within community care institutions funded by the VA. The American Medical Association, American Geriatrics Society, and American Academy of Hospice and Palliative Medicine have adopted neutral positions regarding MAID due to varying opinions among their respective members.2-4 VHA palliative care clinicians are trained to identify and honor preferences for care and alleviate physical and emotional distress, which may complicate the management of MAID requests. Veterans can request MAID due to their desire for autonomy and pain relief, but the VHA prohibits clinicians from honoring these specific preferences. The inability to help veterans achieve their care preferences conflicts with the core mission of palliative care to reduce suffering and respect end-of-life wishes.
This case report describes the management of a veteran who requested MAID while also exhibiting active suicidal ideation. The patient’s distress stemmed from fears of impending loss of autonomy and functional decline, factors frequently linked to requests for MAID in terminally ill patients.5,6 Addressing the veteran’s request for MAID required balancing respect for patient autonomy and concerns about future suffering with the VA mission to protect veterans from self-harm and provide mental health care for suicidal ideation. This case highlights the importance of nuanced clinical approaches, ethical reflection, and interdisciplinary collaboration in navigating such complex scenarios. Informed consent was obtained from the patient’s family and health care agent (HCA) to publish this report.
Case Presentation
A 73-year-old male veteran, with Parkinson disease (PD), diagnosed at age 52 years, was referred to palliative care following diagnosis of a glioblastoma multiforme (GBM). The patient also had a history of major depressive disorder (MDD), suicidal ideation (SI), benign prostatic hypertrophy, and migraines. He was divorced, had no children, and his only sibling (sister) was deceased. His brother-in-law served as his HCA.
The patient had many close friends in the community, was an architect by training, and was active in the removal of barriers and increasing access for people with disabilities. Since 2010, about 7 years before his PD diagnosis, the patient used psychiatry and psychology resources to treat MDD, functional decline, and SI. He was hospitalized in 2016 after self-administration of heroin. During the hospitalization the patient received a high risk for suicide label. He articulated a firm and long-standing belief in his right to die and shared plans to end his life when he experienced a significant decline in his independence and quality of life (QoL).
When diagnosed with PD, the patient shared that his QoL was of utmost importance. He was aware that he would have significant physical decline as PD progressed and felt like there would be a point when his QoL would not be acceptable. When that happened, he wanted to end his life by available means. He was followed closely by his VHA care team for physical and emotional distress.
When diagnosed with a GBM in 2023, the patient declined treatment and was referred to palliative care, which had sporadically treated him for PD-related distress prior to 2023. During his previous palliative care visits, the patient had discussed a desire to engage in MAID when his functional status declined. After the GBM diagnosis, he reported no acute intent to harm himself with heroin, but planned to travel to Vermont for MAID when he felt he no longer had an adequate QoL based on functional capability.
Pharmacologic and nonpharmacologic approaches were used to treat the patient’s pain. He reported significant benefit from biofeedback therapy provided by the VA Headache Center of Excellence. This work also reconnected him to meditation, which he used daily to relieve pain and distress. The patient managed head pain with nonpharmacologic and pharmacologic interventions for 6 months and reported satisfaction with his QoL.
After 6 months, imaging showed progression of the brain tumor, which was associated with more fatigue and memory decline. At that time, the patient was enrolled in home hospice and reported continued intent to pursue MAID in Vermont but had not taken steps toward carrying it out. The patient understood the VA could not assist him in pursuing MAID; however, his care team was able to assist him in sharing his preferences for care with his loved ones and health care power of attorney.
He experienced rapid functional and cognitive decline due to progression of the GBM and was admitted to the VA Connecticut Healthcare System (VACHS) acute care unit where he exhibited confusion and screened positive for delirium using the Confusion Assessment Method.7 His physical and cognitive deterioration was likely due to the progressive brain tumor, and the patient lacked the capacity to make complex medical decisions. Formal consent was obtained from his HCA to transfer him to inpatient hospice. Psychiatry followed the patient throughout.
After 4 weeks of hospice care, the patient had a witnessed suicide attempt while the nurse was assisting him in the bathroom. The patient attempted to use hospital pajamas to hang himself when he wrapped a hospital gown around his neck and stated he was trying to tie a knot. Due to his confusion and delirium, the patient was unable to express his reasoning for the suicide attempt. He was seen by the Psychiatry service, which determined that his suicide risk was low to intermediate. The Psychiatry service did not recommend a 1:1 safety sitter, but suggested medication changes. Levetiracetam was discontinued, and valproate 500 mg orally twice daily was initiated for seizure prevention.
The hospice team was informed of the suicide attempt and psychiatry recommendations. The suicide prevention team was also updated following this event and agreed with psychiatry recommendations. The patient continued to decline, was no longer able to get out of bed, and had minimal speech. The patient received comfort medications, including intravenous morphine 2 mg and lorazepam 0.5 mg as needed ≤ 4 times daily. He died 8 days later.
Discussion
Chronic medical illness has been associated with increased suicide risk.8-10 The increased risk of suicide in chronically ill patients has been described as having as a bidirectional relationship with MDD, with depression not only increasing the risk of chronic medical illness but new-onset chronic medical illness being associated with new onset depression.11,12 Chronic medical conditions are associated with numerous psychiatric disorders, and the presence of a comorbid psychiatric illness is associated with higher rates of hospitalization, emergency department visits, and increased health care costs.13 Research has found that the association between suicide risk and chronic medical illness remains even after accounting for comorbid mental health disorders.14 This has been postulated to be due to a multitude of interpersonal, behavioral, cognitive, and affective factors (eg, perceived burdensomeness, loneliness, stress, pain catastrophizing, self-criticism).15 Additionally, some researchers have questioned whether suicidality constitutes a distinct mental disorder.16
Patients with cancer are at increased risk for suicidal ideation (including passive death wishes) and suicide attempts.17,18 Recent data indicate that compared with the general population, there is an 85% increased risk of suicide mortality in patients with cancer.19 Studies show the incidence of suicide is greater for individuals with cancer compared with the general population, with standardized mortality ratios ranging from 1.4 to 5.7.20-22
Among patients with cancer, suicide risk is associated with several factors: worse prognosis, older age, male sex, living in a socioeconomically vulnerable environment, and increased communication about suicidal intent prior to death.23-25 Just as the prevalence of suicidal ideation in people with cancer varies widely, reported rates of suicidality in caregivers of patients with cancer range from 2.7% to 71%.17,26 A survey of health care workers indicated the following reasons patients with cancer may die by suicide or seek aid in assisted suicide: social isolation, pain, physical impairment, loss of autonomy and meaning, terminal illness, and psychic distress and desperation.27
As with cancer, patients with PD exhibit increased suicidal ideation compared with the general population.28,29 Two studies found the suicide rate in individuals with PD is about twice as high as it is in the general population.30,31 Among people with PD, male sex, younger age, initial onset of motor symptoms in the upper or both upper and lower extremities, history of depression or any psychiatric diagnosis, delusions, higher levodopa dosing, and urban residence have been clinically correlated with suicide. Jumping has been a frequent method of suicide.30,31
Some research has evaluated the perspectives of loved ones after a patient chooses MAID. A study in the Netherlands found that 92% of relatives surveyed believed that access to MAID improved QoL and reduced pain at the end of life.32 In another, family members of individuals who used MAID reported higher quality on items related to physical symptom control and preparedness for death, compared with individuals who did not pursue MAID or who requested but did not receive it. There were no differences on items assessing connectedness to their loved one, being unafraid of death, level of consciousness, or global quality of death items.33 Another study found no significant differences in depression rates, grief, or use of mental health services among Oregon families whose loved ones died using MAID compared with those who did not.34
The higher suicide rate among terminally ill patients highlights the complex issue of MAID and the right to die. It is important to differentiate between euthanasia and medically-assisted dying. Euthanasia is an act whereby a person other than the patient acts to cause death. In MAID, the patient is provided with a medication that they self-administer. Recent Gallup polls found that > 70% of Americans believe physicians should be “allowed by law to end the patient’s life by some painless means if the patient and his or her family request it.”35
It is important to acknowledge MAID in the context of chronic suicidality, like in the case described in this article. It is imperative not to dismiss reports of suicidality in this population. Ignoring reports of suicidal ideation may lead to decreased access to pharmacologic and nonpharmacologic interventions. It is also important to maintain a timeline of symptom occurrence and to differentiate between chronic suicidality and the desire to die associated with having a terminal illness. A thorough assessment is necessary to assess whether the patient’s decision stems from a calculated decision with preserved capacity or from underlying mental health conditions. Other factors that may lead the patient to a hastened death (ie, pain, poor psychosocial support, delirium, cognitive impairment, incomplete understanding of treatment/prognosis) need to be addressed prior to finalizing choices. In this case, an assessment was performed by psychiatry, psychology, social work, and chaplains to ensure comprehensive evaluation.
The VHA offers resources to assist individuals experiencing suicidal ideation, including suicide prevention coordinators who work directly with veterans and offer consultation to teams working with veterans at risk for suicide. Support for VHA clinicians who treat veterans considering MAID may help address any moral distress. In this case, the care team met early for overnight sign-out, had daily core hospice team meetings, as-needed safety huddles, and weekly care plan meetings to ensure maximal physical and emotional comfort for the patient. These meetings cultivate open, honest, and transparent discussions regarding any staff concerns or personal distress around the plan of care. The VACHS chief well-being officer was also available for all staff.
A systematic review of the impact of MAID on clinicians found that MAID legislation influenced emotional responses. For countries whose MAID legislation emphasized alleviation from pain in addition to terminal illness, clinicians reported more emotional reflection. Whereas, in countries where MAID legislation is stricter and can be applied solely for terminal illness, clinicians reported a stronger and more polarizing range of emotions.36 This highlights the potential influence of the context in which clinicians work on their emotional experience with MAID. Given that MAID is not permitted in the VA, staff members may experience heightened emotional responses. In a survey of US adults, there was an interest in using MAID but there were knowledge deficits regarding the process and legality.37
Legal aspects come into play as well with regards to MAID. Eligibility requires the patient be aged ≥ 18 years, be terminally ill with a prognosis of ≤ 6 months, have the capacity to make their own health care decision, and be able to self-administer the medication. States also may have residency restrictions. Special care and adequate education are needed, as having anyone but the patient administer the medication may be considered criminal. Furthermore, since MAID is not allowed federally, this creates further distress in VHA clinicians entrusted to minimizing pain for patients.
Strategies to support veterans given prohibition of MAID include: conversations about the patient’s values, clarifying reasons for request, assessing all domains of distress, affirming concerns with compassion and nonjudgment, addressing any pain using pharmacologic and nonpharmacologic interventions, providing education on other permissible options for end-of-life care, and consulting other specialties.38
End-of-life options permitted by the VA include withholding/ withdrawing life-sustaining treatments, palliative sedation, and voluntary stopping of eating and drinking.39 Given the complexities of MAID, the VHA should initiate discussions of MAID, educate clinicians on what they can and cannot do as federal employees, and establish committees to discuss approaches that could minimize pain for patients and clinician distress.
Conclusions
Caring for veterans who request MAID requires clinicians to navigate a complex intersection of ethical obligations, legal constraints, and patient preferences. Within the VHA, where MAID is prohibited, clinicians must balance respect for patient autonomy with adherence to VA regulations. Comprehensive assessment to identify sources of distress, interdisciplinary collaboration, and recognition of permissible alternatives that align with patients’ values are essential to provide effective end-of-life care at the VHA for individuals considering MAID. As requests for MAID continue to emerge in clinical practice, the VHA has an opportunity to strengthen clinician education, clarify institutional expectations, and promote supportive structures that reduce both patient suffering and clinician moral distress.
Requests for medical aid in dying (MAID) within the Veterans Health Administration (VHA) present unique ethical, legal, and clinical challenges. MAID is a process in which a physician provides a terminally ill patient with the means to end their own life. It is expressly prohibited by federal law, including within the US Department of Veterans Affairs (VA), regardless of its legality at the state level.1 MAID is also prohibited within community care institutions funded by the VA. The American Medical Association, American Geriatrics Society, and American Academy of Hospice and Palliative Medicine have adopted neutral positions regarding MAID due to varying opinions among their respective members.2-4 VHA palliative care clinicians are trained to identify and honor preferences for care and alleviate physical and emotional distress, which may complicate the management of MAID requests. Veterans can request MAID due to their desire for autonomy and pain relief, but the VHA prohibits clinicians from honoring these specific preferences. The inability to help veterans achieve their care preferences conflicts with the core mission of palliative care to reduce suffering and respect end-of-life wishes.
This case report describes the management of a veteran who requested MAID while also exhibiting active suicidal ideation. The patient’s distress stemmed from fears of impending loss of autonomy and functional decline, factors frequently linked to requests for MAID in terminally ill patients.5,6 Addressing the veteran’s request for MAID required balancing respect for patient autonomy and concerns about future suffering with the VA mission to protect veterans from self-harm and provide mental health care for suicidal ideation. This case highlights the importance of nuanced clinical approaches, ethical reflection, and interdisciplinary collaboration in navigating such complex scenarios. Informed consent was obtained from the patient’s family and health care agent (HCA) to publish this report.
Case Presentation
A 73-year-old male veteran, with Parkinson disease (PD), diagnosed at age 52 years, was referred to palliative care following diagnosis of a glioblastoma multiforme (GBM). The patient also had a history of major depressive disorder (MDD), suicidal ideation (SI), benign prostatic hypertrophy, and migraines. He was divorced, had no children, and his only sibling (sister) was deceased. His brother-in-law served as his HCA.
The patient had many close friends in the community, was an architect by training, and was active in the removal of barriers and increasing access for people with disabilities. Since 2010, about 7 years before his PD diagnosis, the patient used psychiatry and psychology resources to treat MDD, functional decline, and SI. He was hospitalized in 2016 after self-administration of heroin. During the hospitalization the patient received a high risk for suicide label. He articulated a firm and long-standing belief in his right to die and shared plans to end his life when he experienced a significant decline in his independence and quality of life (QoL).
When diagnosed with PD, the patient shared that his QoL was of utmost importance. He was aware that he would have significant physical decline as PD progressed and felt like there would be a point when his QoL would not be acceptable. When that happened, he wanted to end his life by available means. He was followed closely by his VHA care team for physical and emotional distress.
When diagnosed with a GBM in 2023, the patient declined treatment and was referred to palliative care, which had sporadically treated him for PD-related distress prior to 2023. During his previous palliative care visits, the patient had discussed a desire to engage in MAID when his functional status declined. After the GBM diagnosis, he reported no acute intent to harm himself with heroin, but planned to travel to Vermont for MAID when he felt he no longer had an adequate QoL based on functional capability.
Pharmacologic and nonpharmacologic approaches were used to treat the patient’s pain. He reported significant benefit from biofeedback therapy provided by the VA Headache Center of Excellence. This work also reconnected him to meditation, which he used daily to relieve pain and distress. The patient managed head pain with nonpharmacologic and pharmacologic interventions for 6 months and reported satisfaction with his QoL.
After 6 months, imaging showed progression of the brain tumor, which was associated with more fatigue and memory decline. At that time, the patient was enrolled in home hospice and reported continued intent to pursue MAID in Vermont but had not taken steps toward carrying it out. The patient understood the VA could not assist him in pursuing MAID; however, his care team was able to assist him in sharing his preferences for care with his loved ones and health care power of attorney.
He experienced rapid functional and cognitive decline due to progression of the GBM and was admitted to the VA Connecticut Healthcare System (VACHS) acute care unit where he exhibited confusion and screened positive for delirium using the Confusion Assessment Method.7 His physical and cognitive deterioration was likely due to the progressive brain tumor, and the patient lacked the capacity to make complex medical decisions. Formal consent was obtained from his HCA to transfer him to inpatient hospice. Psychiatry followed the patient throughout.
After 4 weeks of hospice care, the patient had a witnessed suicide attempt while the nurse was assisting him in the bathroom. The patient attempted to use hospital pajamas to hang himself when he wrapped a hospital gown around his neck and stated he was trying to tie a knot. Due to his confusion and delirium, the patient was unable to express his reasoning for the suicide attempt. He was seen by the Psychiatry service, which determined that his suicide risk was low to intermediate. The Psychiatry service did not recommend a 1:1 safety sitter, but suggested medication changes. Levetiracetam was discontinued, and valproate 500 mg orally twice daily was initiated for seizure prevention.
The hospice team was informed of the suicide attempt and psychiatry recommendations. The suicide prevention team was also updated following this event and agreed with psychiatry recommendations. The patient continued to decline, was no longer able to get out of bed, and had minimal speech. The patient received comfort medications, including intravenous morphine 2 mg and lorazepam 0.5 mg as needed ≤ 4 times daily. He died 8 days later.
Discussion
Chronic medical illness has been associated with increased suicide risk.8-10 The increased risk of suicide in chronically ill patients has been described as having as a bidirectional relationship with MDD, with depression not only increasing the risk of chronic medical illness but new-onset chronic medical illness being associated with new onset depression.11,12 Chronic medical conditions are associated with numerous psychiatric disorders, and the presence of a comorbid psychiatric illness is associated with higher rates of hospitalization, emergency department visits, and increased health care costs.13 Research has found that the association between suicide risk and chronic medical illness remains even after accounting for comorbid mental health disorders.14 This has been postulated to be due to a multitude of interpersonal, behavioral, cognitive, and affective factors (eg, perceived burdensomeness, loneliness, stress, pain catastrophizing, self-criticism).15 Additionally, some researchers have questioned whether suicidality constitutes a distinct mental disorder.16
Patients with cancer are at increased risk for suicidal ideation (including passive death wishes) and suicide attempts.17,18 Recent data indicate that compared with the general population, there is an 85% increased risk of suicide mortality in patients with cancer.19 Studies show the incidence of suicide is greater for individuals with cancer compared with the general population, with standardized mortality ratios ranging from 1.4 to 5.7.20-22
Among patients with cancer, suicide risk is associated with several factors: worse prognosis, older age, male sex, living in a socioeconomically vulnerable environment, and increased communication about suicidal intent prior to death.23-25 Just as the prevalence of suicidal ideation in people with cancer varies widely, reported rates of suicidality in caregivers of patients with cancer range from 2.7% to 71%.17,26 A survey of health care workers indicated the following reasons patients with cancer may die by suicide or seek aid in assisted suicide: social isolation, pain, physical impairment, loss of autonomy and meaning, terminal illness, and psychic distress and desperation.27
As with cancer, patients with PD exhibit increased suicidal ideation compared with the general population.28,29 Two studies found the suicide rate in individuals with PD is about twice as high as it is in the general population.30,31 Among people with PD, male sex, younger age, initial onset of motor symptoms in the upper or both upper and lower extremities, history of depression or any psychiatric diagnosis, delusions, higher levodopa dosing, and urban residence have been clinically correlated with suicide. Jumping has been a frequent method of suicide.30,31
Some research has evaluated the perspectives of loved ones after a patient chooses MAID. A study in the Netherlands found that 92% of relatives surveyed believed that access to MAID improved QoL and reduced pain at the end of life.32 In another, family members of individuals who used MAID reported higher quality on items related to physical symptom control and preparedness for death, compared with individuals who did not pursue MAID or who requested but did not receive it. There were no differences on items assessing connectedness to their loved one, being unafraid of death, level of consciousness, or global quality of death items.33 Another study found no significant differences in depression rates, grief, or use of mental health services among Oregon families whose loved ones died using MAID compared with those who did not.34
The higher suicide rate among terminally ill patients highlights the complex issue of MAID and the right to die. It is important to differentiate between euthanasia and medically-assisted dying. Euthanasia is an act whereby a person other than the patient acts to cause death. In MAID, the patient is provided with a medication that they self-administer. Recent Gallup polls found that > 70% of Americans believe physicians should be “allowed by law to end the patient’s life by some painless means if the patient and his or her family request it.”35
It is important to acknowledge MAID in the context of chronic suicidality, like in the case described in this article. It is imperative not to dismiss reports of suicidality in this population. Ignoring reports of suicidal ideation may lead to decreased access to pharmacologic and nonpharmacologic interventions. It is also important to maintain a timeline of symptom occurrence and to differentiate between chronic suicidality and the desire to die associated with having a terminal illness. A thorough assessment is necessary to assess whether the patient’s decision stems from a calculated decision with preserved capacity or from underlying mental health conditions. Other factors that may lead the patient to a hastened death (ie, pain, poor psychosocial support, delirium, cognitive impairment, incomplete understanding of treatment/prognosis) need to be addressed prior to finalizing choices. In this case, an assessment was performed by psychiatry, psychology, social work, and chaplains to ensure comprehensive evaluation.
The VHA offers resources to assist individuals experiencing suicidal ideation, including suicide prevention coordinators who work directly with veterans and offer consultation to teams working with veterans at risk for suicide. Support for VHA clinicians who treat veterans considering MAID may help address any moral distress. In this case, the care team met early for overnight sign-out, had daily core hospice team meetings, as-needed safety huddles, and weekly care plan meetings to ensure maximal physical and emotional comfort for the patient. These meetings cultivate open, honest, and transparent discussions regarding any staff concerns or personal distress around the plan of care. The VACHS chief well-being officer was also available for all staff.
A systematic review of the impact of MAID on clinicians found that MAID legislation influenced emotional responses. For countries whose MAID legislation emphasized alleviation from pain in addition to terminal illness, clinicians reported more emotional reflection. Whereas, in countries where MAID legislation is stricter and can be applied solely for terminal illness, clinicians reported a stronger and more polarizing range of emotions.36 This highlights the potential influence of the context in which clinicians work on their emotional experience with MAID. Given that MAID is not permitted in the VA, staff members may experience heightened emotional responses. In a survey of US adults, there was an interest in using MAID but there were knowledge deficits regarding the process and legality.37
Legal aspects come into play as well with regards to MAID. Eligibility requires the patient be aged ≥ 18 years, be terminally ill with a prognosis of ≤ 6 months, have the capacity to make their own health care decision, and be able to self-administer the medication. States also may have residency restrictions. Special care and adequate education are needed, as having anyone but the patient administer the medication may be considered criminal. Furthermore, since MAID is not allowed federally, this creates further distress in VHA clinicians entrusted to minimizing pain for patients.
Strategies to support veterans given prohibition of MAID include: conversations about the patient’s values, clarifying reasons for request, assessing all domains of distress, affirming concerns with compassion and nonjudgment, addressing any pain using pharmacologic and nonpharmacologic interventions, providing education on other permissible options for end-of-life care, and consulting other specialties.38
End-of-life options permitted by the VA include withholding/ withdrawing life-sustaining treatments, palliative sedation, and voluntary stopping of eating and drinking.39 Given the complexities of MAID, the VHA should initiate discussions of MAID, educate clinicians on what they can and cannot do as federal employees, and establish committees to discuss approaches that could minimize pain for patients and clinician distress.
Conclusions
Caring for veterans who request MAID requires clinicians to navigate a complex intersection of ethical obligations, legal constraints, and patient preferences. Within the VHA, where MAID is prohibited, clinicians must balance respect for patient autonomy with adherence to VA regulations. Comprehensive assessment to identify sources of distress, interdisciplinary collaboration, and recognition of permissible alternatives that align with patients’ values are essential to provide effective end-of-life care at the VHA for individuals considering MAID. As requests for MAID continue to emerge in clinical practice, the VHA has an opportunity to strengthen clinician education, clarify institutional expectations, and promote supportive structures that reduce both patient suffering and clinician moral distress.
- Meisel A, Snyder L, Quill T; American College of Physicians-- American Society of Internal Medicine End-of-Life Care Consensus Panel. Seven legal barriers to end-of- life care: myths, realities, and grains of truth. JAMA. 2000;284:2495-2501. doi:10.1001/jama.284.19.2495
- Physician-Assisted Suicide. American Medical Association Code of Medical Ethics. 2025. Accessed May 6, 2026. https://code-medical-ethics.ama-assn.org/ethics-opinions /physician-assisted-suicide
- Youngner SJ, Thoman R. AGS survey actually supports engaged neutrality for physician-assisted death. J Am Geriatr Soc. 2020;68:2140-2141. doi:10.1111/jgs.16679
- Physician-Assisted Dying. American Academy of Hospice and Palliative Medicine. Updated 2007. Accessed May 6, 2026. https://aahpm.org/advocacy/where-we-stand/pad/
- Ganzini L, Goy ER, Dobscha SK. Why Oregon patients request assisted death: family members’ views. J Gen Intern Med. 2008;23:154-157. doi:10.1007/s11606-007-0476-x
- Pearlman RA, Hsu C, Starks H, et al. Motivations for physician-assisted suicide: patient and family voices. J Gen Intern Med. 2005;20:234-239. doi:10.1111/j.1525-1497.2005.40225.x
- Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the Confusion Assessment Method. A new method for detection of delirium. Ann Intern Med. 1990;113:941- 948. doi:10.7326/0003-4819-113-12-941
- Fässberg MM, Cheung G, Canetto SS, et al. A systematic review of physical illness, functional disability, and suicidal behaviour among older adults.
Aging Ment Health. 2016;20:166-194. doi:10.1080/13607863.2015.1083945 - Gürhan N, Bes¸er NG, Polat Ü, et al. Suicide risk and depression in individuals with chronic illness. Community Ment Health J. 2019;55:840-848. doi:10.1007/s10597-019-00388-7
- Kye SY, Park K. Suicidal ideation and suicidal attempts among adults with chronic diseases: a crosssectional study. Compr Psychiatry. 2017;73:160-167. doi:10.1016/j.comppsych.2016.12.001
- Patten SB. Long-term medical conditions and major depression in a Canadian population study at waves 1 and 2. J Affect Disord. 2001;63:35-41. doi:10.1016/s0165-0327(00)00186-5
- Van der Kooy K, van Hout H, Marwijk H, et al. Depression and the risk for cardiovascular diseases: systematic review and meta analysis. Int J Geriatr Psychiatry. 2007;22:613- 626. doi:10.1002/gps.1723
- Sporinova B, Manns B, Tonelli M, et al. Association of mental health disorders with health care utilization and costs among adults with chronic disease. JAMA Netw Open. 2019;2:e199910. doi:10.1001/jamanetworkopen.2019.9910
- Ahmedani BK, Peterson EL, Hu Y, et al. Major physical health conditions and risk of suicide. Am J Prev Med. 2017;53:308-315. doi:10.1016/j.amepre.2017.04.001
- Rogers ML, Joiner TE, Shahar G. Suicidality in chronic illness: an overview of cognitive-affective and interpersonal factors. J Clin Psychol Med Settings. 2021;28:137-148. doi:10.1007/s10880-020-09749-x
- Sisti D, Mann JJ, Oquendo MA. Toward a distinct mental disorder—suicidal behavior. JAMA Psychiatry. 2020;77:661-662. doi:10.1001/jamapsychiatry.2020.0111
- Kolva E, Hoffecker L, Cox-Martin E. Suicidal ideation in patients with cancer: a systematic review of prevalence, risk factors, intervention and assessment. Palliat Support Care. 2020;18:206-219. doi:10.1017/S1478951519000610
- Zaorsky NG, Zhang Y, Tuanquin L, et al. Suicide among cancer patients. Nat Commun. 2019;10:207. doi:10.1038/s41467-018-08170-1
- Heinrich M, Hofmann L, Baurecht H, et al. Suicide risk and mortality among patients with cancer. Nat Med. 2022;28:852-859. doi:10.1038/s41591-022-01745-y
- Yousaf U, Christensen ML, Engholm G, et al. Suicides among Danish cancer patients 1971-1999. Br J Cancer. 2005;92:995-1000. doi:10.1038/sj.bjc.6602424
- Misono S, Weiss NS, Fann JR, et al. Incidence of suicide in persons with cancer. J Clin Oncol. 2008;26:4731-4738. doi:10.1200/JCO.2007.13.8941
- Björkenstam C, Edberg A, Ayoubi S, et al. Are cancer patients at higher suicide risk than the general population?. Scand J Public Health. 2005;33:208-214. doi:10.1080/14034940410019226
- Kinslow CJ, Kumar P, Olfson M, et al. Prognosis and risk of suicide after cancer diagnosis. Cancer. 2024;130:588-596. doi:10.1002/cncr.35118
- Men VY, Emery CR, Yip PSF. Characteristics of cancer patients who died by suicide: a quantitative study of 15-year coronial records. Psychooncology. 2021;30:1051-1058. doi:10.1002/pon.5634
- Abdel-Rahman O. Socioeconomic predictors of suicide risk among cancer patients in the United States: a population- based study. Cancer Epidemiol. 2019;63:101601. doi:10.1016/j.canep.2019.101601
- O’Dwyer ST, Janssens A, Sansom A, et al. Suicidality in family caregivers of people with long-term illnesses and disabilities: a scoping review. Compr Psychiatry. 2021;110:152261. doi:10.1016/j.comppsych.2021.152261
- Senf B, Maiwurm P, Fettel J. Attitudes and opinions towards suicidality in professionals working with oncology patients: results from an online survey. Support Care Cancer. 2022;30:1775-1786. doi:10.1007/s00520-021-06590-2
- Berardelli I, Belvisi D, Nardella A, et al. Suicide in Parkinson’s disease: a systematic review. CNS Neurol Disord Drug Targets. 2019;18:466-477. doi:10.2174/1871527318666190703093345
- Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry. 1999;56:617-626. doi:10.1001/archpsyc.56.7.617
- Chen YY, Yu S, Hu YH, et al. Risk of suicide among patients with Parkinson disease. JAMA Psychiatry. 2021;78:293-301. doi:10.1001/jamapsychiatry.2020.4001
- Lee T, Lee HB, Ahn MH, et al. Increased suicide risk and clinical correlates of suicide among patients with Parkinson’s disease. Parkinsonism Relat Disord. 2016;32:102- 107. doi:10.1016/j.parkreldis.2016.09.006
- Georges JJ, Onwuteaka-Philipsen BD, Muller MT, et al. Relatives’ perspective on the terminally ill patients who died after euthanasia or physician-assisted suicide: a retrospective cross-sectional interview study in the Netherlands. Death Stud. 2007;31:1-15. doi:10.1080/07481180600985041
- Smith KA, Goy ER, Harvath TA, et al. Quality of death and dying in patients who request physician-assisted death. J Palliat Med. 2011;14:445-450. doi:10.1089/jpm.2010.0425
- Ganzini L, Goy ER, Dobscha SK, et al. Mental health outcomes of family members of Oregonians who request physician aid in dying. J Pain Symptom Manage. 2009;38:807-815. doi:10.1016/j.jpainsymman.2009.04.026
- Yi R. Most Americans favor legal euthanasia. Gallup. August 8, 2024. Accessed May 6, 2026. https://news.gallup .com/poll/648215/americans-favor-legal-euthanasia.aspx
- Dholakia SY, Bagheri A, Simpson A. Emotional impact on healthcare providers involved in medical assistance in dying (MAiD): a systematic review and qualitative meta-synthesis. BMJ Open. 2022;12:e058523. doi:10.1136/bmjopen-2021-058523
- Kozlov E, Luth EA, Nemeth S, et al. Knowl - edge of and preferences for medical aid in dying. JAMA Netw Open. 2025;8:e2461495. doi:10.1001/jamanetworkopen.2024.61495
- Geppert C; Veterans Administration National Center for Ethics in Health Care. Medical aid in dying in the VA. Presented at: VISN 1 Palliative Care Summit, September 2024.
- National Ethics Committee, Veterans Health Administration. The ethics of palliative sedation as a therapy of last resort. Am J Hosp Palliat Care. 2006;23:483-491. doi:10.1177/1049909106294883
- Meisel A, Snyder L, Quill T; American College of Physicians-- American Society of Internal Medicine End-of-Life Care Consensus Panel. Seven legal barriers to end-of- life care: myths, realities, and grains of truth. JAMA. 2000;284:2495-2501. doi:10.1001/jama.284.19.2495
- Physician-Assisted Suicide. American Medical Association Code of Medical Ethics. 2025. Accessed May 6, 2026. https://code-medical-ethics.ama-assn.org/ethics-opinions /physician-assisted-suicide
- Youngner SJ, Thoman R. AGS survey actually supports engaged neutrality for physician-assisted death. J Am Geriatr Soc. 2020;68:2140-2141. doi:10.1111/jgs.16679
- Physician-Assisted Dying. American Academy of Hospice and Palliative Medicine. Updated 2007. Accessed May 6, 2026. https://aahpm.org/advocacy/where-we-stand/pad/
- Ganzini L, Goy ER, Dobscha SK. Why Oregon patients request assisted death: family members’ views. J Gen Intern Med. 2008;23:154-157. doi:10.1007/s11606-007-0476-x
- Pearlman RA, Hsu C, Starks H, et al. Motivations for physician-assisted suicide: patient and family voices. J Gen Intern Med. 2005;20:234-239. doi:10.1111/j.1525-1497.2005.40225.x
- Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the Confusion Assessment Method. A new method for detection of delirium. Ann Intern Med. 1990;113:941- 948. doi:10.7326/0003-4819-113-12-941
- Fässberg MM, Cheung G, Canetto SS, et al. A systematic review of physical illness, functional disability, and suicidal behaviour among older adults.
Aging Ment Health. 2016;20:166-194. doi:10.1080/13607863.2015.1083945 - Gürhan N, Bes¸er NG, Polat Ü, et al. Suicide risk and depression in individuals with chronic illness. Community Ment Health J. 2019;55:840-848. doi:10.1007/s10597-019-00388-7
- Kye SY, Park K. Suicidal ideation and suicidal attempts among adults with chronic diseases: a crosssectional study. Compr Psychiatry. 2017;73:160-167. doi:10.1016/j.comppsych.2016.12.001
- Patten SB. Long-term medical conditions and major depression in a Canadian population study at waves 1 and 2. J Affect Disord. 2001;63:35-41. doi:10.1016/s0165-0327(00)00186-5
- Van der Kooy K, van Hout H, Marwijk H, et al. Depression and the risk for cardiovascular diseases: systematic review and meta analysis. Int J Geriatr Psychiatry. 2007;22:613- 626. doi:10.1002/gps.1723
- Sporinova B, Manns B, Tonelli M, et al. Association of mental health disorders with health care utilization and costs among adults with chronic disease. JAMA Netw Open. 2019;2:e199910. doi:10.1001/jamanetworkopen.2019.9910
- Ahmedani BK, Peterson EL, Hu Y, et al. Major physical health conditions and risk of suicide. Am J Prev Med. 2017;53:308-315. doi:10.1016/j.amepre.2017.04.001
- Rogers ML, Joiner TE, Shahar G. Suicidality in chronic illness: an overview of cognitive-affective and interpersonal factors. J Clin Psychol Med Settings. 2021;28:137-148. doi:10.1007/s10880-020-09749-x
- Sisti D, Mann JJ, Oquendo MA. Toward a distinct mental disorder—suicidal behavior. JAMA Psychiatry. 2020;77:661-662. doi:10.1001/jamapsychiatry.2020.0111
- Kolva E, Hoffecker L, Cox-Martin E. Suicidal ideation in patients with cancer: a systematic review of prevalence, risk factors, intervention and assessment. Palliat Support Care. 2020;18:206-219. doi:10.1017/S1478951519000610
- Zaorsky NG, Zhang Y, Tuanquin L, et al. Suicide among cancer patients. Nat Commun. 2019;10:207. doi:10.1038/s41467-018-08170-1
- Heinrich M, Hofmann L, Baurecht H, et al. Suicide risk and mortality among patients with cancer. Nat Med. 2022;28:852-859. doi:10.1038/s41591-022-01745-y
- Yousaf U, Christensen ML, Engholm G, et al. Suicides among Danish cancer patients 1971-1999. Br J Cancer. 2005;92:995-1000. doi:10.1038/sj.bjc.6602424
- Misono S, Weiss NS, Fann JR, et al. Incidence of suicide in persons with cancer. J Clin Oncol. 2008;26:4731-4738. doi:10.1200/JCO.2007.13.8941
- Björkenstam C, Edberg A, Ayoubi S, et al. Are cancer patients at higher suicide risk than the general population?. Scand J Public Health. 2005;33:208-214. doi:10.1080/14034940410019226
- Kinslow CJ, Kumar P, Olfson M, et al. Prognosis and risk of suicide after cancer diagnosis. Cancer. 2024;130:588-596. doi:10.1002/cncr.35118
- Men VY, Emery CR, Yip PSF. Characteristics of cancer patients who died by suicide: a quantitative study of 15-year coronial records. Psychooncology. 2021;30:1051-1058. doi:10.1002/pon.5634
- Abdel-Rahman O. Socioeconomic predictors of suicide risk among cancer patients in the United States: a population- based study. Cancer Epidemiol. 2019;63:101601. doi:10.1016/j.canep.2019.101601
- O’Dwyer ST, Janssens A, Sansom A, et al. Suicidality in family caregivers of people with long-term illnesses and disabilities: a scoping review. Compr Psychiatry. 2021;110:152261. doi:10.1016/j.comppsych.2021.152261
- Senf B, Maiwurm P, Fettel J. Attitudes and opinions towards suicidality in professionals working with oncology patients: results from an online survey. Support Care Cancer. 2022;30:1775-1786. doi:10.1007/s00520-021-06590-2
- Berardelli I, Belvisi D, Nardella A, et al. Suicide in Parkinson’s disease: a systematic review. CNS Neurol Disord Drug Targets. 2019;18:466-477. doi:10.2174/1871527318666190703093345
- Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry. 1999;56:617-626. doi:10.1001/archpsyc.56.7.617
- Chen YY, Yu S, Hu YH, et al. Risk of suicide among patients with Parkinson disease. JAMA Psychiatry. 2021;78:293-301. doi:10.1001/jamapsychiatry.2020.4001
- Lee T, Lee HB, Ahn MH, et al. Increased suicide risk and clinical correlates of suicide among patients with Parkinson’s disease. Parkinsonism Relat Disord. 2016;32:102- 107. doi:10.1016/j.parkreldis.2016.09.006
- Georges JJ, Onwuteaka-Philipsen BD, Muller MT, et al. Relatives’ perspective on the terminally ill patients who died after euthanasia or physician-assisted suicide: a retrospective cross-sectional interview study in the Netherlands. Death Stud. 2007;31:1-15. doi:10.1080/07481180600985041
- Smith KA, Goy ER, Harvath TA, et al. Quality of death and dying in patients who request physician-assisted death. J Palliat Med. 2011;14:445-450. doi:10.1089/jpm.2010.0425
- Ganzini L, Goy ER, Dobscha SK, et al. Mental health outcomes of family members of Oregonians who request physician aid in dying. J Pain Symptom Manage. 2009;38:807-815. doi:10.1016/j.jpainsymman.2009.04.026
- Yi R. Most Americans favor legal euthanasia. Gallup. August 8, 2024. Accessed May 6, 2026. https://news.gallup .com/poll/648215/americans-favor-legal-euthanasia.aspx
- Dholakia SY, Bagheri A, Simpson A. Emotional impact on healthcare providers involved in medical assistance in dying (MAiD): a systematic review and qualitative meta-synthesis. BMJ Open. 2022;12:e058523. doi:10.1136/bmjopen-2021-058523
- Kozlov E, Luth EA, Nemeth S, et al. Knowl - edge of and preferences for medical aid in dying. JAMA Netw Open. 2025;8:e2461495. doi:10.1001/jamanetworkopen.2024.61495
- Geppert C; Veterans Administration National Center for Ethics in Health Care. Medical aid in dying in the VA. Presented at: VISN 1 Palliative Care Summit, September 2024.
- National Ethics Committee, Veterans Health Administration. The ethics of palliative sedation as a therapy of last resort. Am J Hosp Palliat Care. 2006;23:483-491. doi:10.1177/1049909106294883
Managing Requests for Medical Aid in Dying Within the Veterans Health Administration
Managing Requests for Medical Aid in Dying Within the Veterans Health Administration

Assessment of False-Positive Fentanyl Results on Urine Drug Screens in Veterans
Assessment of False-Positive Fentanyl Results on Urine Drug Screens in Veterans
A urine drug screen (UDS) is commonly performed to evaluate illicit and prescribed drug use in patients to guide treatment decisions and ensure patient safety. Common uses include evaluating medication adherence, identifying ingested substances in cases of intoxication or overdose, ruling out substance-induced disorders, and screening for illicit drug use. There is a potential for false-positive or false-negative results due to the qualitative and nonspecific nature of UDSs.1 These results can be verified with confirmatory testing using gas chromatography/mass spectrometry or liquid chromatography/ tandem mass spectrometry by identifying specific molecular structures and quantifying the amount of drug or substance present in the sample.1
An April 2023 memorandum instructed all US Department of Veterans Affairs (VA) medical centers and community-based outpatient clinics (CBOC) to have fentanyl urine testing readily available.2 Some facilities added fentanyl to a standard UDS, while others created a separate quick order. The memorandum led to increased fentanyl testing. As a result, unexpected positive fentanyl UDS results are more common. Some facilities have an automatic fentanyl confirmation test that is ordered after a positive fentanyl UDS. However, a positive result for fentanyl on a UDS does not automatically result in confirmation testing at all VA facilities. Without automatic confirmation testing, a clinician must decide to order a fentanyl confirmation test following the positive result. Therefore, the true rate of false-positive results for fentanyl is unknown because confirmation testing is not ordered for every positive UDS.
False-positive results can have unintended consequences, including discontinuation of prescribed medications, patient stigma, and inappropriate recommendations for substance use treatment. False-positive results may contribute to unnecessary health care costs and adversely affect patients’ lives. Previous research has reported false-positive fentanyl UDS results for patients taking risperidone, ziprasidone, and labetalol.3-5 Studies have found that loperamide and high-concentration methamphetamine samples could cause false-positive fentanyl UDS results.6,7 Wang et al evaluated the performance of the SEFRIA fentanyl immunoassay using the 1 ng/mL cutoff cleared by the US Food and Drug Administration (FDA). The study of 410 patients found a 38% false-positive rate; concomitant use of trazodone, labetalol, and haloperidol accounted for 230 (56%) of the false-positive results.8 Limited data evaluating false-positive results for the current SEFRIA fentanyl testing assay suggest the need for additional research. This study aims to add to data on false-positive results for fentanyl on UDS samples and potential causes.
Methods
A retrospective, multicenter observational cohort study was conducted that included patients at 3 VA MidSouth Healthcare Network VA medical centers located in Tennessee with their associated CBOCs from August 1, 2023, to August 1, 2024 who had positive fentanyl UDS results. The primary outcome was the rate of false-positive fentanyl UDS results when confirmation testing was performed. Secondary outcomes included the rate of confirmation testing, prescribed medications used by patients with false-positive UDS results, and the rate of follow-up in the electronic health record (EHR) on results of confirmation testing. Confirmations were primarily obtained for positive results and not all UDSs. Therefore, it was not possible in this retrospective study to obtain the true measure of false-negative or true-negative results.
A structured query language query was performed to identify patients with a UDS positive for fentanyl from August 1, 2023, to August 1, 2024. Patients were enrolled if they were aged ≥ 18 years with a UDS positive for fentanyl. Patients were excluded from the primary outcome analysis if results for the confirmatory testing were unquantifiable or could not be found.
Study Intervention
This was a descriptive study with no comparator group. The rate of confirmed false-positive results for fentanyl, rate of confirmation testing for patients with positive fentanyl UDS results, rate of follow-up on confirmation results, and prescribed medications in patients with false-positive fentanyl results were evaluated. For true-positive results, follow-up was defined as documentation in the EHR reporting fentanyl use or illicit substance use likely to be laced with fentanyl at the time of the UDS or documentation of the confirmation result. For false-positive results, follow-up was defined as documentation in the EHR of the confirmation result.
Statistical Analysis
Descriptive statistics including means and percentages were used to analyze demographic data. Continuous variables and parametric data are presented as mean (SD) and nominal data as percentages. All statistical analyses were completed using Excel. The SEFRIA fentanyl immunoassay was used at each study site. Facilities 1 and 2 were combined for the primary outcome analysis because they used the same fentanyl immunoassay cutoff level of 1 ng/mL. Facility 3 used a cutoff level of 2 ng/mL and was analyzed separately.
Results
A total of 1228 UDS tests were positive for fentanyl, including 618 at facility 1, 308 at facility 2, and 302 at facility 3 (Figure 1). Patients were predominantly male and White, with a mean age of 55 years, though age and race varied by location (Table 1). Patients may have had ≥ 1 UDS. Of 1228 UDSs recorded in the EHR, 578 were sent for confirmation testing and 546 had confirmation results available in the EHR (84 at facility 1, 271 at facility 2, and 191 at facility 3). Of 546 confirmation tests, 186 were negative for fentanyl, indicating a false-positive rate of 34.1%. Most confirmation tests (43%) were requested for patients seen in a mental health clinic.
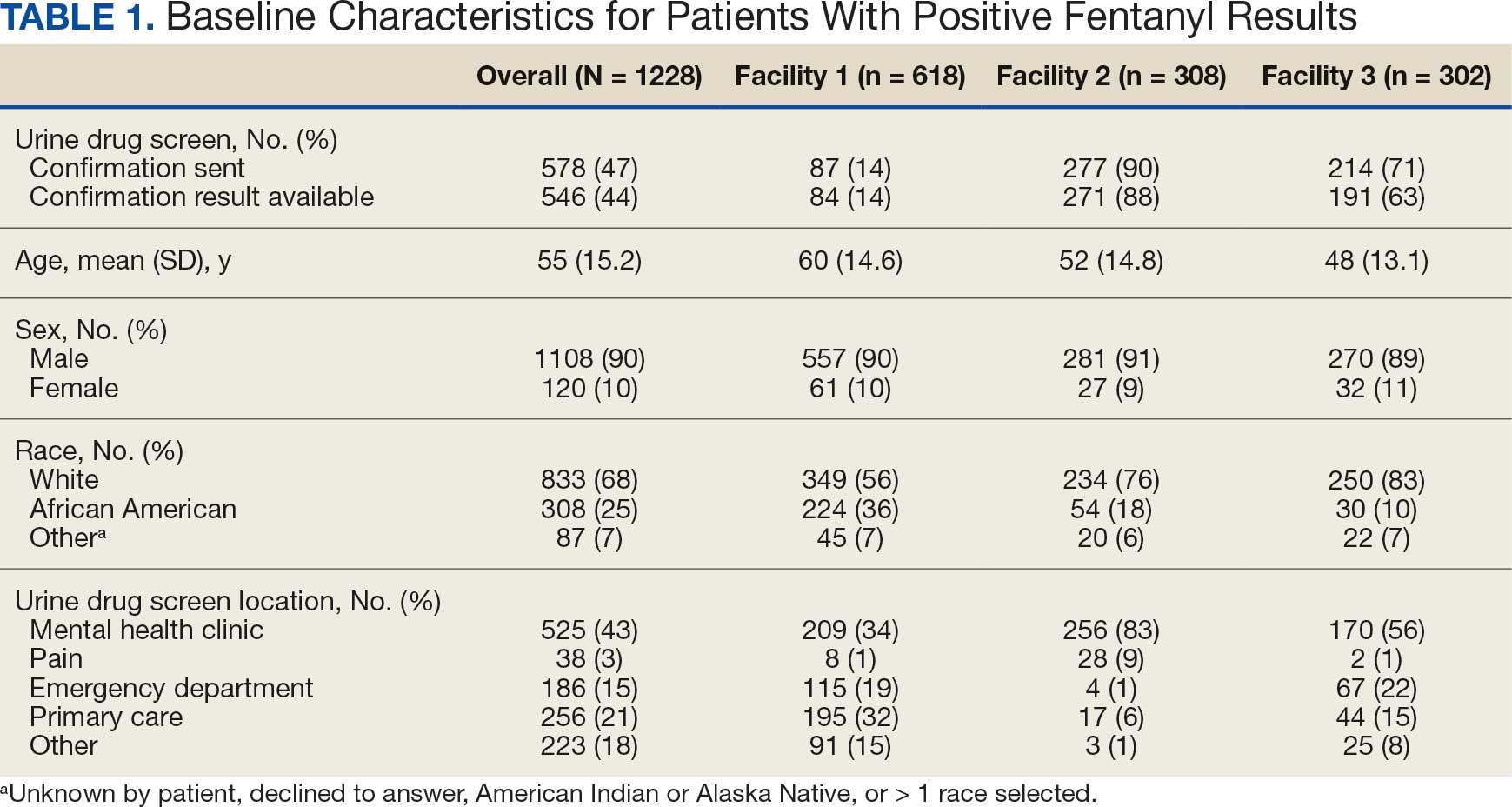
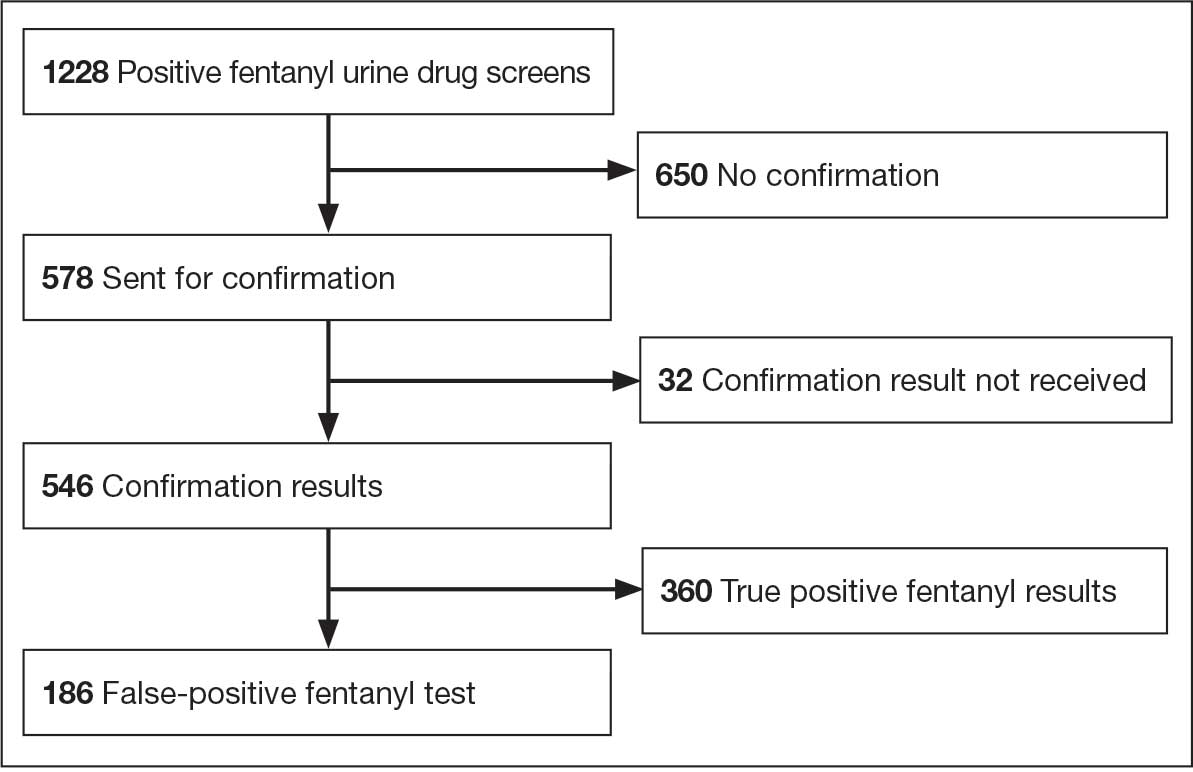
The combined false-positive rate was 49.9% for 355 UDS confirmation results at facilities 1 and 2 (70.2% and 43.5%, respectively) and 4.7% for 191 UDS confirmation results at facility 3, which used the higher 2 ng/mL cutoff level (Figure 2). Confirmation testing was ordered for 578 tests (47.1%). There were 87 confirmation tests (14.1%) at facility 1, 277 tests (89.9%) at facility 2, and 214 (70.9%) at facility 3 (Figure 3). Follow-up after confirmation tests was completed for 406 patients (74.4%): 56 follow-ups (66.7%) at facility 1, 190 follow-ups (70.1%) at facility 2, and 160 follow-ups (83.8%) at facility 3 (Figure 4). Trazodone was the most commonly prescribed medication for patients with false-positive fentanyl UDS results. Trazodone was prescribed to 153 patients (82,3%), followed by 116 patients (62.4%) prescribed naloxone, 86 patients (46.2%) prescribed or with reported use of acetaminophen, 72 patients (38.7%) prescribed nicotine replacement products, and 64 patients (34.4%) prescribed omeprazole (Table 2).
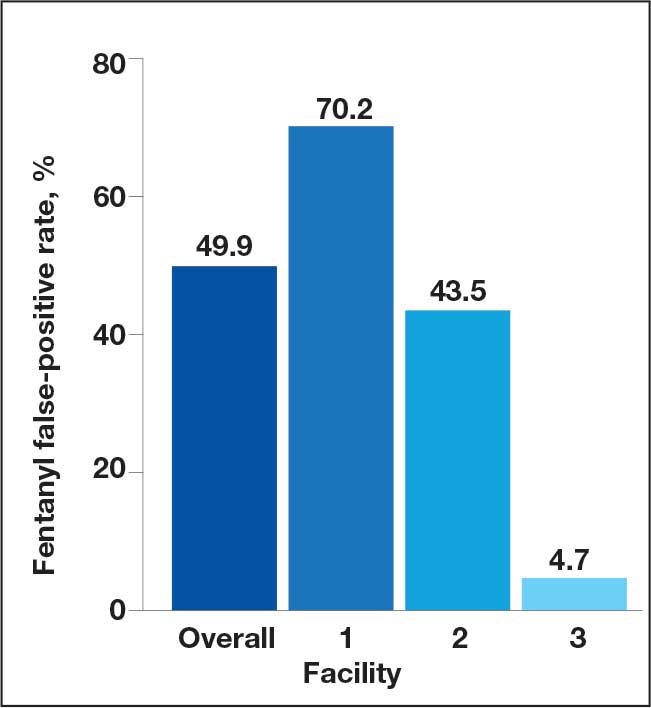
Confirmed Fentanyl False-Positive Rate
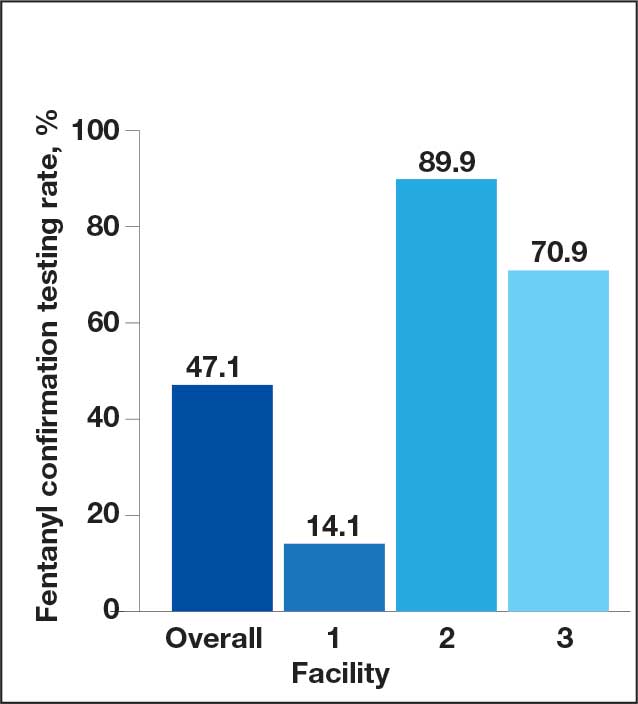
Confirmation Testing
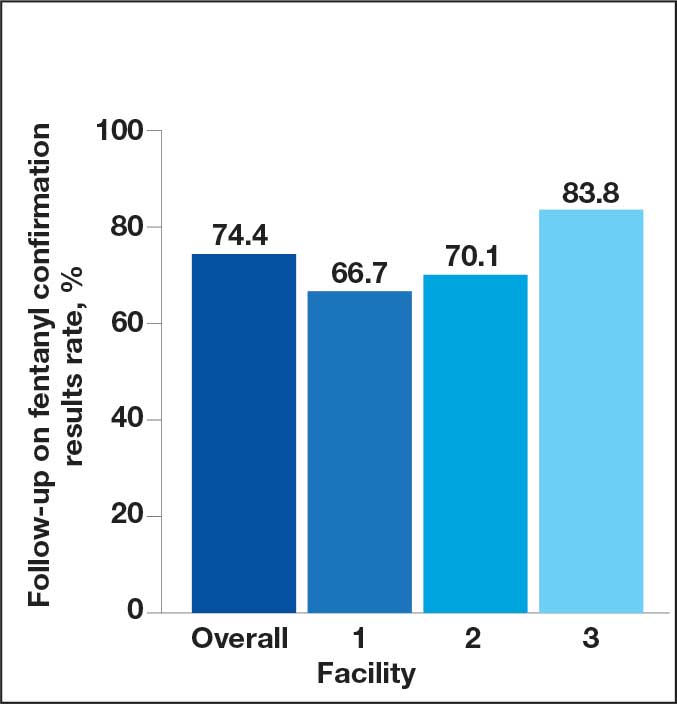
Fentanyl Confirmation Results
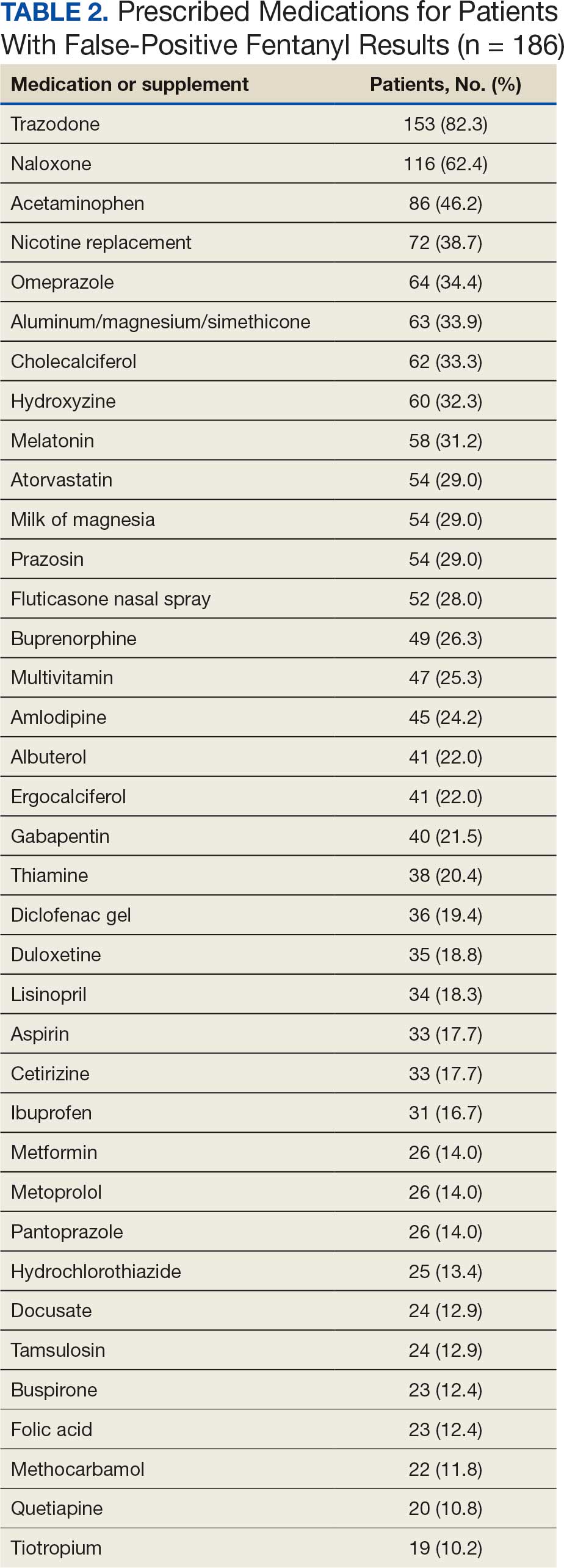
Discussion
There are several factors to note when interpreting the study results. First, facilities 1 and 2 used the FDA-cleared 1 ng/mL cutoff for positive results on the SEFRIA fentanyl immunoassay, whereas facility 3 used a cutoff level of 2 ng/mL. Second, during the study period, facilities 1 and 3 included fentanyl as part of their standard UDS; facility 2 required a separate fentanyl UDS order. Third, facility 2 had automatic confirmation testing for positive results on individually ordered fentanyl UDS tests. Finally, confirmation tests were primarily obtained for positive fentanyl results and not all UDSs, which limited the analyses that could be performed.
This study found a high rate of false-positive fentanyl UDS results at facilities 1 and 2 and a very low rate at facility 3, likely due to the higher cutoff level. Facility 3 used the higher cutoff level due to previously observed high rates of false-positive results. While a higher cutoff level can decrease the rate of false-positive results, it also may increase the rate of false-negative results.
Studies have found false-positive rates ranging from 3% to 45% with the SEFRIA immunoassay FDA-cleared 1 ng/mL cutoff. Increasing the cutoff to 1.3 ng/mL decreased the false-positive rate from 38% to 7.5% in a study by Wang et al.8-11 Manar et al evaluated fentanyl assays in 42 samples using a 2 ng/mL cutoff for the SEFRIA assay and reported a false-positive rate of 0 and a false-negative rate of 22.5%.12 Given the high rate of false-positive rates demonstrated in studies using the current FDA-recommended 1 ng/mL cutoff, additional studies evaluating different cutoff levels may be beneficial to determine the best cutoff level to reduce false-positive results without significantly increasing false-negative rates. While data on the impact of using a higher cutoff level are limited, the results of our study have led to discussions at VA MidSouth Healthcare Network facilities regarding use of different cutoff levels.
There was a low rate of confirmation testing at facility 1 compared with facilities 2 and 3. Only facility 2 had automatic confirmation testing during the study period. Pharmacists at facility 3 reviewed UDS results without needing a consultation and, during the study period, could order fentanyl UDS confirmations. Another factor that may have contributed to the disparity in confirmation testing between facilities is the location of the UDS order. Most UDS samples at facilities 2 and 3 were ordered for patients seen in mental health clinics, whereas many facility 1 orders were placed in primary care or the emergency department (ED).
Given these results, education may be indicated regarding the risk of false-positive results and the importance of confirmation testing in primary care and the ED. Facility 1 and 3 did not have automatic fentanyl confirmation testing during the study; however, facility 3 implemented automatic confirmation shortly after the study period and facility 1 implemented automatic confirmation testing for a positive fentanyl UDS result after evaluation of the study data.
Although follow-up on confirmation UDS results was fairly high, it was highest at facility 3, which does not require a consultation for pharmacist UDS result evaluations. Given the high rate of false-positive results for fentanyl, confirmation testing for a positive UDS and follow-up on confirmation results is an important step to consider. The higher rate of follow-up at the facility where pharmacists had more autonomous involvement shows the benefits of having pharmacists provide comprehensive patient care. Implementing similar protocols across all facilities may improve follow-up, which may improve patient care and safety given the implications of false-positive results.
Trazodone was prescribed in 82.3% of all patients with false-positive fentanyl tests. Even at facility 3, with the higher fentanyl immunoassay cutoff level, trazodone was prescribed in 77.8% of patients with false-positive results. While this retrospective study does not show causation, it does align with the findings reported by Wang et al, adding to the data implicating trazodone as a potential cause for false-positive fentanyl UDS results. The high incidence of trazodone prescriptions in patients with false-positive UDS results at facility 3 strengthens this association, indicating that even when using a higher cutoff level, trazodone may be implicated.
While there was a high rate of confirmed false-positive results in this study, there was also a potential for undetected true-positive results. The SEFRIA fentanyl immunoassay is sensitive to multiple fentanyl analogues. Williams et al showed that the SEFRIA immunoassay detected 57 of 58 fentanyl analogues tested; norsufentanil was the only analogue it did not detect.13 Most of the confirmatory tests reviewed during this study did not include all fentanyl analogues, only fentanyl and norfentanyl. Given the increased prevalence of synthetic fentanyl analogues, this is an important consideration because some identified false-positive results could potentially be undetected true-positive results for a fentanyl analogue. Switching to a more comprehensive confirmation test that includes more fentanyl analogues may reduce the risk of undetected positive results and, therefore, reduce the observed rate of false-positive UDS results.
Strengths and Limitations
Patient medications were only identified if they were documented in the EHR at the time of UDS results, which could have missed over-the-counter medications or medications prescribed outside the VA; this limits identification and implication of medications as possibly contributing to false-positive results. Only samples sent for confirmation were evaluated for true- or false-positive results; therefore, the true rate of false-positive results could not be determined. UDS confirmation tests only analyzed for fentanyl and norfentanyl, which left the potential for undetected true-positive results for other fentanyl analogues. Use of EHR data for the analysis leaves the potential for documentation errors and undetected bias.
This study adds to limited data on false-positive results for fentanyl on UDS samples. It included a large sample size of patients across multiple sites. Additionally, it included results using multiple cutoff levels on the SEFRIA fentanyl immunoassay, adding to limited data in this area.
Conclusions
This retrospective study found evidence that automatic confirmation testing should be considered for positive fentanyl UDS tests due to the high rate of false-positive results. Facility 1 began automatic confirmation testing due to the findings of this study. Facilities should consider switching to a more comprehensive confirmation test that includes more fentanyl analogues to reduce the risk of undetected true-positive results. This study also adds to the data implicating trazodone in fentanyl UDS false-positive results due to high incidence of trazodone prescriptions among patients in the study with false-positive UDS results. Future considerations include investigating different cutoff levels for the SEFRIA fentanyl immunoassay to reduce false-positive results as data are currently limited.
- Kale N. Urine drug tests: ordering and interpreting results. Am Fam Physician. 2019;99:33-39.
- Scavella E. US Department of Veterans Affairs, Assistant Under Secretary for Health for Clinical Services/Chief Medical Officer. Veterans Health Administration memorandum: urine toxicology screening (inpatient, residential, and outpatient substance use disorder [SUD] and mental health treatment programs) (VIEWS 9897520). April 18, 2023.
- Shroitman NK, Peles E, Even-Tov S, et al. Falsepositive fentanyl screening kit results duringWang D, Sun Q, Schneider R, et al. Understanding FDA-cleared fentanyl testing: a clinical evaluation of the SEFRIA fentanyl immunoassay. Drug Alcohol Depend. 2024;259:111287. doi:10.1016/j.drugalcdep.2024.111287 treatment with long-term injectable risperidone (Risperdal- Consta). Psychiatry Res. 2021;305:114246. doi:10.1016/j.psychres.2021.114246
- Waters K, Tewksbury A. A false-positive fentanyl result on urine drug screen in a patient treated with ziprasidone. J Am Pharm Assoc (2003). 2022;62:1707-1710. doi:10.1016/j.japh.2022.05.011
- Wanar A, Isley BC, Saia K, et al. False-positive fentanyl urine detection after initiation of labetalol treatment for hypertension in pregnancy: a case report. J Addict Med. 2022;16:e417-e419. doi:10.1097/ADM.0000000000001010
- Geno KA, Badea A, Lynch KL, et al. An opioid hiding in plain sight: loperamide-induced false-positive fentanyl and buprenorphine immunoassay results. J Appl Lab Med. 2022;7:1318-1328. doi:10.1093/jalm/jfac065
- Abbott DL, Limoges JF, Virkler KJ, et al. ELISA screens for fentanyl in urine are susceptible to false-positives in highconcentration methamphetamine samples. J Anal Toxicol. 2022;46:457-459. doi:10.1093/jat/bkab033
- Wang D, Sun Q, Schneider R, et al. Understanding FDA-cleared fentanyl testing: a clinical evaluation of the SEFRIA fentanyl immunoassay. Drug Alcohol Depend. 2024;259:111287. doi:10.1016/j.drugalcdep.2024.111287
- Mills CM, Dryja PC, Champion-Lyons E, et al. Performance of fentanyl immunoassays in an ED patient population. J Appl Lab Med. 2024;9:886-894. doi:10.1093/jalm/jfae022
- Feng S, Rutledge TJ, Manzoni M, et al. Performance of 2 fentanyl immunoassays against a liquid chromatography- tandem mass spectrometry method. J Anal Toxicol. 2021;45:117-123. doi:10.1093/jat/bkaa053
- Laryea ET, Nichols JH. Evaluation of a rapid drug test device for urine fentanyl compared with mass spectrometry and 2 urine fentanyl assays. J Appl Lab Med. 2024;9:1020-1024. doi:10.1093/jalm/jfae059
- Manar S, George B, Huang R. B-336 comparison of the LZI fentanyl enzyme immunoassay with ARKII and SEFRIA fentanyl assays on Beckman AU analyzer. Clin Chem. 2023;69:hvad097.655. doi:10.1093/clinchem/hvad097.655
- Williams GR, Akala M, Wolf CE. Detection of 58 fentanyl analogs using ARK fentanyl II and Immunalysis fentanyl immunoassays. Clin Biochem. 2023;113:45-51. doi:10.1016/j.clinbiochem.2023.01.001
A urine drug screen (UDS) is commonly performed to evaluate illicit and prescribed drug use in patients to guide treatment decisions and ensure patient safety. Common uses include evaluating medication adherence, identifying ingested substances in cases of intoxication or overdose, ruling out substance-induced disorders, and screening for illicit drug use. There is a potential for false-positive or false-negative results due to the qualitative and nonspecific nature of UDSs.1 These results can be verified with confirmatory testing using gas chromatography/mass spectrometry or liquid chromatography/ tandem mass spectrometry by identifying specific molecular structures and quantifying the amount of drug or substance present in the sample.1
An April 2023 memorandum instructed all US Department of Veterans Affairs (VA) medical centers and community-based outpatient clinics (CBOC) to have fentanyl urine testing readily available.2 Some facilities added fentanyl to a standard UDS, while others created a separate quick order. The memorandum led to increased fentanyl testing. As a result, unexpected positive fentanyl UDS results are more common. Some facilities have an automatic fentanyl confirmation test that is ordered after a positive fentanyl UDS. However, a positive result for fentanyl on a UDS does not automatically result in confirmation testing at all VA facilities. Without automatic confirmation testing, a clinician must decide to order a fentanyl confirmation test following the positive result. Therefore, the true rate of false-positive results for fentanyl is unknown because confirmation testing is not ordered for every positive UDS.
False-positive results can have unintended consequences, including discontinuation of prescribed medications, patient stigma, and inappropriate recommendations for substance use treatment. False-positive results may contribute to unnecessary health care costs and adversely affect patients’ lives. Previous research has reported false-positive fentanyl UDS results for patients taking risperidone, ziprasidone, and labetalol.3-5 Studies have found that loperamide and high-concentration methamphetamine samples could cause false-positive fentanyl UDS results.6,7 Wang et al evaluated the performance of the SEFRIA fentanyl immunoassay using the 1 ng/mL cutoff cleared by the US Food and Drug Administration (FDA). The study of 410 patients found a 38% false-positive rate; concomitant use of trazodone, labetalol, and haloperidol accounted for 230 (56%) of the false-positive results.8 Limited data evaluating false-positive results for the current SEFRIA fentanyl testing assay suggest the need for additional research. This study aims to add to data on false-positive results for fentanyl on UDS samples and potential causes.
Methods
A retrospective, multicenter observational cohort study was conducted that included patients at 3 VA MidSouth Healthcare Network VA medical centers located in Tennessee with their associated CBOCs from August 1, 2023, to August 1, 2024 who had positive fentanyl UDS results. The primary outcome was the rate of false-positive fentanyl UDS results when confirmation testing was performed. Secondary outcomes included the rate of confirmation testing, prescribed medications used by patients with false-positive UDS results, and the rate of follow-up in the electronic health record (EHR) on results of confirmation testing. Confirmations were primarily obtained for positive results and not all UDSs. Therefore, it was not possible in this retrospective study to obtain the true measure of false-negative or true-negative results.
A structured query language query was performed to identify patients with a UDS positive for fentanyl from August 1, 2023, to August 1, 2024. Patients were enrolled if they were aged ≥ 18 years with a UDS positive for fentanyl. Patients were excluded from the primary outcome analysis if results for the confirmatory testing were unquantifiable or could not be found.
Study Intervention
This was a descriptive study with no comparator group. The rate of confirmed false-positive results for fentanyl, rate of confirmation testing for patients with positive fentanyl UDS results, rate of follow-up on confirmation results, and prescribed medications in patients with false-positive fentanyl results were evaluated. For true-positive results, follow-up was defined as documentation in the EHR reporting fentanyl use or illicit substance use likely to be laced with fentanyl at the time of the UDS or documentation of the confirmation result. For false-positive results, follow-up was defined as documentation in the EHR of the confirmation result.
Statistical Analysis
Descriptive statistics including means and percentages were used to analyze demographic data. Continuous variables and parametric data are presented as mean (SD) and nominal data as percentages. All statistical analyses were completed using Excel. The SEFRIA fentanyl immunoassay was used at each study site. Facilities 1 and 2 were combined for the primary outcome analysis because they used the same fentanyl immunoassay cutoff level of 1 ng/mL. Facility 3 used a cutoff level of 2 ng/mL and was analyzed separately.
Results
A total of 1228 UDS tests were positive for fentanyl, including 618 at facility 1, 308 at facility 2, and 302 at facility 3 (Figure 1). Patients were predominantly male and White, with a mean age of 55 years, though age and race varied by location (Table 1). Patients may have had ≥ 1 UDS. Of 1228 UDSs recorded in the EHR, 578 were sent for confirmation testing and 546 had confirmation results available in the EHR (84 at facility 1, 271 at facility 2, and 191 at facility 3). Of 546 confirmation tests, 186 were negative for fentanyl, indicating a false-positive rate of 34.1%. Most confirmation tests (43%) were requested for patients seen in a mental health clinic.
The combined false-positive rate was 49.9% for 355 UDS confirmation results at facilities 1 and 2 (70.2% and 43.5%, respectively) and 4.7% for 191 UDS confirmation results at facility 3, which used the higher 2 ng/mL cutoff level (Figure 2). Confirmation testing was ordered for 578 tests (47.1%). There were 87 confirmation tests (14.1%) at facility 1, 277 tests (89.9%) at facility 2, and 214 (70.9%) at facility 3 (Figure 3). Follow-up after confirmation tests was completed for 406 patients (74.4%): 56 follow-ups (66.7%) at facility 1, 190 follow-ups (70.1%) at facility 2, and 160 follow-ups (83.8%) at facility 3 (Figure 4). Trazodone was the most commonly prescribed medication for patients with false-positive fentanyl UDS results. Trazodone was prescribed to 153 patients (82,3%), followed by 116 patients (62.4%) prescribed naloxone, 86 patients (46.2%) prescribed or with reported use of acetaminophen, 72 patients (38.7%) prescribed nicotine replacement products, and 64 patients (34.4%) prescribed omeprazole (Table 2).
Confirmed Fentanyl False-Positive Rate
Confirmation Testing
Fentanyl Confirmation Results
Discussion
There are several factors to note when interpreting the study results. First, facilities 1 and 2 used the FDA-cleared 1 ng/mL cutoff for positive results on the SEFRIA fentanyl immunoassay, whereas facility 3 used a cutoff level of 2 ng/mL. Second, during the study period, facilities 1 and 3 included fentanyl as part of their standard UDS; facility 2 required a separate fentanyl UDS order. Third, facility 2 had automatic confirmation testing for positive results on individually ordered fentanyl UDS tests. Finally, confirmation tests were primarily obtained for positive fentanyl results and not all UDSs, which limited the analyses that could be performed.
This study found a high rate of false-positive fentanyl UDS results at facilities 1 and 2 and a very low rate at facility 3, likely due to the higher cutoff level. Facility 3 used the higher cutoff level due to previously observed high rates of false-positive results. While a higher cutoff level can decrease the rate of false-positive results, it also may increase the rate of false-negative results.
Studies have found false-positive rates ranging from 3% to 45% with the SEFRIA immunoassay FDA-cleared 1 ng/mL cutoff. Increasing the cutoff to 1.3 ng/mL decreased the false-positive rate from 38% to 7.5% in a study by Wang et al.8-11 Manar et al evaluated fentanyl assays in 42 samples using a 2 ng/mL cutoff for the SEFRIA assay and reported a false-positive rate of 0 and a false-negative rate of 22.5%.12 Given the high rate of false-positive rates demonstrated in studies using the current FDA-recommended 1 ng/mL cutoff, additional studies evaluating different cutoff levels may be beneficial to determine the best cutoff level to reduce false-positive results without significantly increasing false-negative rates. While data on the impact of using a higher cutoff level are limited, the results of our study have led to discussions at VA MidSouth Healthcare Network facilities regarding use of different cutoff levels.
There was a low rate of confirmation testing at facility 1 compared with facilities 2 and 3. Only facility 2 had automatic confirmation testing during the study period. Pharmacists at facility 3 reviewed UDS results without needing a consultation and, during the study period, could order fentanyl UDS confirmations. Another factor that may have contributed to the disparity in confirmation testing between facilities is the location of the UDS order. Most UDS samples at facilities 2 and 3 were ordered for patients seen in mental health clinics, whereas many facility 1 orders were placed in primary care or the emergency department (ED).
Given these results, education may be indicated regarding the risk of false-positive results and the importance of confirmation testing in primary care and the ED. Facility 1 and 3 did not have automatic fentanyl confirmation testing during the study; however, facility 3 implemented automatic confirmation shortly after the study period and facility 1 implemented automatic confirmation testing for a positive fentanyl UDS result after evaluation of the study data.
Although follow-up on confirmation UDS results was fairly high, it was highest at facility 3, which does not require a consultation for pharmacist UDS result evaluations. Given the high rate of false-positive results for fentanyl, confirmation testing for a positive UDS and follow-up on confirmation results is an important step to consider. The higher rate of follow-up at the facility where pharmacists had more autonomous involvement shows the benefits of having pharmacists provide comprehensive patient care. Implementing similar protocols across all facilities may improve follow-up, which may improve patient care and safety given the implications of false-positive results.
Trazodone was prescribed in 82.3% of all patients with false-positive fentanyl tests. Even at facility 3, with the higher fentanyl immunoassay cutoff level, trazodone was prescribed in 77.8% of patients with false-positive results. While this retrospective study does not show causation, it does align with the findings reported by Wang et al, adding to the data implicating trazodone as a potential cause for false-positive fentanyl UDS results. The high incidence of trazodone prescriptions in patients with false-positive UDS results at facility 3 strengthens this association, indicating that even when using a higher cutoff level, trazodone may be implicated.
While there was a high rate of confirmed false-positive results in this study, there was also a potential for undetected true-positive results. The SEFRIA fentanyl immunoassay is sensitive to multiple fentanyl analogues. Williams et al showed that the SEFRIA immunoassay detected 57 of 58 fentanyl analogues tested; norsufentanil was the only analogue it did not detect.13 Most of the confirmatory tests reviewed during this study did not include all fentanyl analogues, only fentanyl and norfentanyl. Given the increased prevalence of synthetic fentanyl analogues, this is an important consideration because some identified false-positive results could potentially be undetected true-positive results for a fentanyl analogue. Switching to a more comprehensive confirmation test that includes more fentanyl analogues may reduce the risk of undetected positive results and, therefore, reduce the observed rate of false-positive UDS results.
Strengths and Limitations
Patient medications were only identified if they were documented in the EHR at the time of UDS results, which could have missed over-the-counter medications or medications prescribed outside the VA; this limits identification and implication of medications as possibly contributing to false-positive results. Only samples sent for confirmation were evaluated for true- or false-positive results; therefore, the true rate of false-positive results could not be determined. UDS confirmation tests only analyzed for fentanyl and norfentanyl, which left the potential for undetected true-positive results for other fentanyl analogues. Use of EHR data for the analysis leaves the potential for documentation errors and undetected bias.
This study adds to limited data on false-positive results for fentanyl on UDS samples. It included a large sample size of patients across multiple sites. Additionally, it included results using multiple cutoff levels on the SEFRIA fentanyl immunoassay, adding to limited data in this area.
Conclusions
This retrospective study found evidence that automatic confirmation testing should be considered for positive fentanyl UDS tests due to the high rate of false-positive results. Facility 1 began automatic confirmation testing due to the findings of this study. Facilities should consider switching to a more comprehensive confirmation test that includes more fentanyl analogues to reduce the risk of undetected true-positive results. This study also adds to the data implicating trazodone in fentanyl UDS false-positive results due to high incidence of trazodone prescriptions among patients in the study with false-positive UDS results. Future considerations include investigating different cutoff levels for the SEFRIA fentanyl immunoassay to reduce false-positive results as data are currently limited.
A urine drug screen (UDS) is commonly performed to evaluate illicit and prescribed drug use in patients to guide treatment decisions and ensure patient safety. Common uses include evaluating medication adherence, identifying ingested substances in cases of intoxication or overdose, ruling out substance-induced disorders, and screening for illicit drug use. There is a potential for false-positive or false-negative results due to the qualitative and nonspecific nature of UDSs.1 These results can be verified with confirmatory testing using gas chromatography/mass spectrometry or liquid chromatography/ tandem mass spectrometry by identifying specific molecular structures and quantifying the amount of drug or substance present in the sample.1
An April 2023 memorandum instructed all US Department of Veterans Affairs (VA) medical centers and community-based outpatient clinics (CBOC) to have fentanyl urine testing readily available.2 Some facilities added fentanyl to a standard UDS, while others created a separate quick order. The memorandum led to increased fentanyl testing. As a result, unexpected positive fentanyl UDS results are more common. Some facilities have an automatic fentanyl confirmation test that is ordered after a positive fentanyl UDS. However, a positive result for fentanyl on a UDS does not automatically result in confirmation testing at all VA facilities. Without automatic confirmation testing, a clinician must decide to order a fentanyl confirmation test following the positive result. Therefore, the true rate of false-positive results for fentanyl is unknown because confirmation testing is not ordered for every positive UDS.
False-positive results can have unintended consequences, including discontinuation of prescribed medications, patient stigma, and inappropriate recommendations for substance use treatment. False-positive results may contribute to unnecessary health care costs and adversely affect patients’ lives. Previous research has reported false-positive fentanyl UDS results for patients taking risperidone, ziprasidone, and labetalol.3-5 Studies have found that loperamide and high-concentration methamphetamine samples could cause false-positive fentanyl UDS results.6,7 Wang et al evaluated the performance of the SEFRIA fentanyl immunoassay using the 1 ng/mL cutoff cleared by the US Food and Drug Administration (FDA). The study of 410 patients found a 38% false-positive rate; concomitant use of trazodone, labetalol, and haloperidol accounted for 230 (56%) of the false-positive results.8 Limited data evaluating false-positive results for the current SEFRIA fentanyl testing assay suggest the need for additional research. This study aims to add to data on false-positive results for fentanyl on UDS samples and potential causes.
Methods
A retrospective, multicenter observational cohort study was conducted that included patients at 3 VA MidSouth Healthcare Network VA medical centers located in Tennessee with their associated CBOCs from August 1, 2023, to August 1, 2024 who had positive fentanyl UDS results. The primary outcome was the rate of false-positive fentanyl UDS results when confirmation testing was performed. Secondary outcomes included the rate of confirmation testing, prescribed medications used by patients with false-positive UDS results, and the rate of follow-up in the electronic health record (EHR) on results of confirmation testing. Confirmations were primarily obtained for positive results and not all UDSs. Therefore, it was not possible in this retrospective study to obtain the true measure of false-negative or true-negative results.
A structured query language query was performed to identify patients with a UDS positive for fentanyl from August 1, 2023, to August 1, 2024. Patients were enrolled if they were aged ≥ 18 years with a UDS positive for fentanyl. Patients were excluded from the primary outcome analysis if results for the confirmatory testing were unquantifiable or could not be found.
Study Intervention
This was a descriptive study with no comparator group. The rate of confirmed false-positive results for fentanyl, rate of confirmation testing for patients with positive fentanyl UDS results, rate of follow-up on confirmation results, and prescribed medications in patients with false-positive fentanyl results were evaluated. For true-positive results, follow-up was defined as documentation in the EHR reporting fentanyl use or illicit substance use likely to be laced with fentanyl at the time of the UDS or documentation of the confirmation result. For false-positive results, follow-up was defined as documentation in the EHR of the confirmation result.
Statistical Analysis
Descriptive statistics including means and percentages were used to analyze demographic data. Continuous variables and parametric data are presented as mean (SD) and nominal data as percentages. All statistical analyses were completed using Excel. The SEFRIA fentanyl immunoassay was used at each study site. Facilities 1 and 2 were combined for the primary outcome analysis because they used the same fentanyl immunoassay cutoff level of 1 ng/mL. Facility 3 used a cutoff level of 2 ng/mL and was analyzed separately.
Results
A total of 1228 UDS tests were positive for fentanyl, including 618 at facility 1, 308 at facility 2, and 302 at facility 3 (Figure 1). Patients were predominantly male and White, with a mean age of 55 years, though age and race varied by location (Table 1). Patients may have had ≥ 1 UDS. Of 1228 UDSs recorded in the EHR, 578 were sent for confirmation testing and 546 had confirmation results available in the EHR (84 at facility 1, 271 at facility 2, and 191 at facility 3). Of 546 confirmation tests, 186 were negative for fentanyl, indicating a false-positive rate of 34.1%. Most confirmation tests (43%) were requested for patients seen in a mental health clinic.
The combined false-positive rate was 49.9% for 355 UDS confirmation results at facilities 1 and 2 (70.2% and 43.5%, respectively) and 4.7% for 191 UDS confirmation results at facility 3, which used the higher 2 ng/mL cutoff level (Figure 2). Confirmation testing was ordered for 578 tests (47.1%). There were 87 confirmation tests (14.1%) at facility 1, 277 tests (89.9%) at facility 2, and 214 (70.9%) at facility 3 (Figure 3). Follow-up after confirmation tests was completed for 406 patients (74.4%): 56 follow-ups (66.7%) at facility 1, 190 follow-ups (70.1%) at facility 2, and 160 follow-ups (83.8%) at facility 3 (Figure 4). Trazodone was the most commonly prescribed medication for patients with false-positive fentanyl UDS results. Trazodone was prescribed to 153 patients (82,3%), followed by 116 patients (62.4%) prescribed naloxone, 86 patients (46.2%) prescribed or with reported use of acetaminophen, 72 patients (38.7%) prescribed nicotine replacement products, and 64 patients (34.4%) prescribed omeprazole (Table 2).
Confirmed Fentanyl False-Positive Rate
Confirmation Testing
Fentanyl Confirmation Results
Discussion
There are several factors to note when interpreting the study results. First, facilities 1 and 2 used the FDA-cleared 1 ng/mL cutoff for positive results on the SEFRIA fentanyl immunoassay, whereas facility 3 used a cutoff level of 2 ng/mL. Second, during the study period, facilities 1 and 3 included fentanyl as part of their standard UDS; facility 2 required a separate fentanyl UDS order. Third, facility 2 had automatic confirmation testing for positive results on individually ordered fentanyl UDS tests. Finally, confirmation tests were primarily obtained for positive fentanyl results and not all UDSs, which limited the analyses that could be performed.
This study found a high rate of false-positive fentanyl UDS results at facilities 1 and 2 and a very low rate at facility 3, likely due to the higher cutoff level. Facility 3 used the higher cutoff level due to previously observed high rates of false-positive results. While a higher cutoff level can decrease the rate of false-positive results, it also may increase the rate of false-negative results.
Studies have found false-positive rates ranging from 3% to 45% with the SEFRIA immunoassay FDA-cleared 1 ng/mL cutoff. Increasing the cutoff to 1.3 ng/mL decreased the false-positive rate from 38% to 7.5% in a study by Wang et al.8-11 Manar et al evaluated fentanyl assays in 42 samples using a 2 ng/mL cutoff for the SEFRIA assay and reported a false-positive rate of 0 and a false-negative rate of 22.5%.12 Given the high rate of false-positive rates demonstrated in studies using the current FDA-recommended 1 ng/mL cutoff, additional studies evaluating different cutoff levels may be beneficial to determine the best cutoff level to reduce false-positive results without significantly increasing false-negative rates. While data on the impact of using a higher cutoff level are limited, the results of our study have led to discussions at VA MidSouth Healthcare Network facilities regarding use of different cutoff levels.
There was a low rate of confirmation testing at facility 1 compared with facilities 2 and 3. Only facility 2 had automatic confirmation testing during the study period. Pharmacists at facility 3 reviewed UDS results without needing a consultation and, during the study period, could order fentanyl UDS confirmations. Another factor that may have contributed to the disparity in confirmation testing between facilities is the location of the UDS order. Most UDS samples at facilities 2 and 3 were ordered for patients seen in mental health clinics, whereas many facility 1 orders were placed in primary care or the emergency department (ED).
Given these results, education may be indicated regarding the risk of false-positive results and the importance of confirmation testing in primary care and the ED. Facility 1 and 3 did not have automatic fentanyl confirmation testing during the study; however, facility 3 implemented automatic confirmation shortly after the study period and facility 1 implemented automatic confirmation testing for a positive fentanyl UDS result after evaluation of the study data.
Although follow-up on confirmation UDS results was fairly high, it was highest at facility 3, which does not require a consultation for pharmacist UDS result evaluations. Given the high rate of false-positive results for fentanyl, confirmation testing for a positive UDS and follow-up on confirmation results is an important step to consider. The higher rate of follow-up at the facility where pharmacists had more autonomous involvement shows the benefits of having pharmacists provide comprehensive patient care. Implementing similar protocols across all facilities may improve follow-up, which may improve patient care and safety given the implications of false-positive results.
Trazodone was prescribed in 82.3% of all patients with false-positive fentanyl tests. Even at facility 3, with the higher fentanyl immunoassay cutoff level, trazodone was prescribed in 77.8% of patients with false-positive results. While this retrospective study does not show causation, it does align with the findings reported by Wang et al, adding to the data implicating trazodone as a potential cause for false-positive fentanyl UDS results. The high incidence of trazodone prescriptions in patients with false-positive UDS results at facility 3 strengthens this association, indicating that even when using a higher cutoff level, trazodone may be implicated.
While there was a high rate of confirmed false-positive results in this study, there was also a potential for undetected true-positive results. The SEFRIA fentanyl immunoassay is sensitive to multiple fentanyl analogues. Williams et al showed that the SEFRIA immunoassay detected 57 of 58 fentanyl analogues tested; norsufentanil was the only analogue it did not detect.13 Most of the confirmatory tests reviewed during this study did not include all fentanyl analogues, only fentanyl and norfentanyl. Given the increased prevalence of synthetic fentanyl analogues, this is an important consideration because some identified false-positive results could potentially be undetected true-positive results for a fentanyl analogue. Switching to a more comprehensive confirmation test that includes more fentanyl analogues may reduce the risk of undetected positive results and, therefore, reduce the observed rate of false-positive UDS results.
Strengths and Limitations
Patient medications were only identified if they were documented in the EHR at the time of UDS results, which could have missed over-the-counter medications or medications prescribed outside the VA; this limits identification and implication of medications as possibly contributing to false-positive results. Only samples sent for confirmation were evaluated for true- or false-positive results; therefore, the true rate of false-positive results could not be determined. UDS confirmation tests only analyzed for fentanyl and norfentanyl, which left the potential for undetected true-positive results for other fentanyl analogues. Use of EHR data for the analysis leaves the potential for documentation errors and undetected bias.
This study adds to limited data on false-positive results for fentanyl on UDS samples. It included a large sample size of patients across multiple sites. Additionally, it included results using multiple cutoff levels on the SEFRIA fentanyl immunoassay, adding to limited data in this area.
Conclusions
This retrospective study found evidence that automatic confirmation testing should be considered for positive fentanyl UDS tests due to the high rate of false-positive results. Facility 1 began automatic confirmation testing due to the findings of this study. Facilities should consider switching to a more comprehensive confirmation test that includes more fentanyl analogues to reduce the risk of undetected true-positive results. This study also adds to the data implicating trazodone in fentanyl UDS false-positive results due to high incidence of trazodone prescriptions among patients in the study with false-positive UDS results. Future considerations include investigating different cutoff levels for the SEFRIA fentanyl immunoassay to reduce false-positive results as data are currently limited.
- Kale N. Urine drug tests: ordering and interpreting results. Am Fam Physician. 2019;99:33-39.
- Scavella E. US Department of Veterans Affairs, Assistant Under Secretary for Health for Clinical Services/Chief Medical Officer. Veterans Health Administration memorandum: urine toxicology screening (inpatient, residential, and outpatient substance use disorder [SUD] and mental health treatment programs) (VIEWS 9897520). April 18, 2023.
- Shroitman NK, Peles E, Even-Tov S, et al. Falsepositive fentanyl screening kit results duringWang D, Sun Q, Schneider R, et al. Understanding FDA-cleared fentanyl testing: a clinical evaluation of the SEFRIA fentanyl immunoassay. Drug Alcohol Depend. 2024;259:111287. doi:10.1016/j.drugalcdep.2024.111287 treatment with long-term injectable risperidone (Risperdal- Consta). Psychiatry Res. 2021;305:114246. doi:10.1016/j.psychres.2021.114246
- Waters K, Tewksbury A. A false-positive fentanyl result on urine drug screen in a patient treated with ziprasidone. J Am Pharm Assoc (2003). 2022;62:1707-1710. doi:10.1016/j.japh.2022.05.011
- Wanar A, Isley BC, Saia K, et al. False-positive fentanyl urine detection after initiation of labetalol treatment for hypertension in pregnancy: a case report. J Addict Med. 2022;16:e417-e419. doi:10.1097/ADM.0000000000001010
- Geno KA, Badea A, Lynch KL, et al. An opioid hiding in plain sight: loperamide-induced false-positive fentanyl and buprenorphine immunoassay results. J Appl Lab Med. 2022;7:1318-1328. doi:10.1093/jalm/jfac065
- Abbott DL, Limoges JF, Virkler KJ, et al. ELISA screens for fentanyl in urine are susceptible to false-positives in highconcentration methamphetamine samples. J Anal Toxicol. 2022;46:457-459. doi:10.1093/jat/bkab033
- Wang D, Sun Q, Schneider R, et al. Understanding FDA-cleared fentanyl testing: a clinical evaluation of the SEFRIA fentanyl immunoassay. Drug Alcohol Depend. 2024;259:111287. doi:10.1016/j.drugalcdep.2024.111287
- Mills CM, Dryja PC, Champion-Lyons E, et al. Performance of fentanyl immunoassays in an ED patient population. J Appl Lab Med. 2024;9:886-894. doi:10.1093/jalm/jfae022
- Feng S, Rutledge TJ, Manzoni M, et al. Performance of 2 fentanyl immunoassays against a liquid chromatography- tandem mass spectrometry method. J Anal Toxicol. 2021;45:117-123. doi:10.1093/jat/bkaa053
- Laryea ET, Nichols JH. Evaluation of a rapid drug test device for urine fentanyl compared with mass spectrometry and 2 urine fentanyl assays. J Appl Lab Med. 2024;9:1020-1024. doi:10.1093/jalm/jfae059
- Manar S, George B, Huang R. B-336 comparison of the LZI fentanyl enzyme immunoassay with ARKII and SEFRIA fentanyl assays on Beckman AU analyzer. Clin Chem. 2023;69:hvad097.655. doi:10.1093/clinchem/hvad097.655
- Williams GR, Akala M, Wolf CE. Detection of 58 fentanyl analogs using ARK fentanyl II and Immunalysis fentanyl immunoassays. Clin Biochem. 2023;113:45-51. doi:10.1016/j.clinbiochem.2023.01.001
- Kale N. Urine drug tests: ordering and interpreting results. Am Fam Physician. 2019;99:33-39.
- Scavella E. US Department of Veterans Affairs, Assistant Under Secretary for Health for Clinical Services/Chief Medical Officer. Veterans Health Administration memorandum: urine toxicology screening (inpatient, residential, and outpatient substance use disorder [SUD] and mental health treatment programs) (VIEWS 9897520). April 18, 2023.
- Shroitman NK, Peles E, Even-Tov S, et al. Falsepositive fentanyl screening kit results duringWang D, Sun Q, Schneider R, et al. Understanding FDA-cleared fentanyl testing: a clinical evaluation of the SEFRIA fentanyl immunoassay. Drug Alcohol Depend. 2024;259:111287. doi:10.1016/j.drugalcdep.2024.111287 treatment with long-term injectable risperidone (Risperdal- Consta). Psychiatry Res. 2021;305:114246. doi:10.1016/j.psychres.2021.114246
- Waters K, Tewksbury A. A false-positive fentanyl result on urine drug screen in a patient treated with ziprasidone. J Am Pharm Assoc (2003). 2022;62:1707-1710. doi:10.1016/j.japh.2022.05.011
- Wanar A, Isley BC, Saia K, et al. False-positive fentanyl urine detection after initiation of labetalol treatment for hypertension in pregnancy: a case report. J Addict Med. 2022;16:e417-e419. doi:10.1097/ADM.0000000000001010
- Geno KA, Badea A, Lynch KL, et al. An opioid hiding in plain sight: loperamide-induced false-positive fentanyl and buprenorphine immunoassay results. J Appl Lab Med. 2022;7:1318-1328. doi:10.1093/jalm/jfac065
- Abbott DL, Limoges JF, Virkler KJ, et al. ELISA screens for fentanyl in urine are susceptible to false-positives in highconcentration methamphetamine samples. J Anal Toxicol. 2022;46:457-459. doi:10.1093/jat/bkab033
- Wang D, Sun Q, Schneider R, et al. Understanding FDA-cleared fentanyl testing: a clinical evaluation of the SEFRIA fentanyl immunoassay. Drug Alcohol Depend. 2024;259:111287. doi:10.1016/j.drugalcdep.2024.111287
- Mills CM, Dryja PC, Champion-Lyons E, et al. Performance of fentanyl immunoassays in an ED patient population. J Appl Lab Med. 2024;9:886-894. doi:10.1093/jalm/jfae022
- Feng S, Rutledge TJ, Manzoni M, et al. Performance of 2 fentanyl immunoassays against a liquid chromatography- tandem mass spectrometry method. J Anal Toxicol. 2021;45:117-123. doi:10.1093/jat/bkaa053
- Laryea ET, Nichols JH. Evaluation of a rapid drug test device for urine fentanyl compared with mass spectrometry and 2 urine fentanyl assays. J Appl Lab Med. 2024;9:1020-1024. doi:10.1093/jalm/jfae059
- Manar S, George B, Huang R. B-336 comparison of the LZI fentanyl enzyme immunoassay with ARKII and SEFRIA fentanyl assays on Beckman AU analyzer. Clin Chem. 2023;69:hvad097.655. doi:10.1093/clinchem/hvad097.655
- Williams GR, Akala M, Wolf CE. Detection of 58 fentanyl analogs using ARK fentanyl II and Immunalysis fentanyl immunoassays. Clin Biochem. 2023;113:45-51. doi:10.1016/j.clinbiochem.2023.01.001
Assessment of False-Positive Fentanyl Results on Urine Drug Screens in Veterans
Assessment of False-Positive Fentanyl Results on Urine Drug Screens in Veterans

VA Advanced Training for Clinician Researchers and Data Scientists in Mental Health
VA Advanced Training for Clinician Researchers and Data Scientists in Mental Health
The US Department of Veterans Affairs (VA) mission realizes President Abraham Lincoln’s promise to “to care for him who shall have borne the battle, and for his widow, and his orphan.”1 Evidence-based care fulfills this promise and is the backbone of Veterans Health Administration (VHA) mental health care.2,3 To ensure veterans receive state-of-the-art clinical care, a skilled workforce and investment in data-driven approaches are necessary to identify best treatments and strategies to implement them in practice.
Through scientific and clinical training tailored to VA, the 23 VA Advanced Fellowships have secured a steady flow of highly trained PhD professionals (ie, psychologists and other allied health professionals), and medical doctors (ie, psychiatrists and neurologists) into the VA workforce.4 The VA Advanced Fellows are funded by the Office of Academic Affiliations (OAA) and offer 2-year training opportunities for postresidency MDs and postdoctoral PhDs. This article describes a VA Advanced Fellowship in mental health as an example of how these programs can have a broad and positive impact on the VA health care system.
Advanced Fellows Program
The VA Advanced Fellowship in Mental Illness Research and Treatment (AF MIRT), formerly known as the VA Special Fellowship Program in Advanced Psychiatry and Psychology, educates and trains clinician and nonclinician researchers to meet VA priority mental health care needs.5 Clinical AF MIRT fellows dedicate 75% of their time to training and research activities and 25% to direct clinical services. Data science fellows complete projects that inform veteran clinical care through qualitative data collection, program evaluation, and analysis of large datasets. The full translational pathway to evidence-based clinical care is represented by fellow research spanning basic animal models, genetics, and neuroimaging to implementation science and applied clinical care for veterans.
In 2025, AF MIRT marked its 25th year of training postdoctoral-level mental health scientific practitioners and scholars. This investment in clinical research training has had profound benefits for innovation and retention of clinicians and scientists within the VA system. As of April 1, 2026, AF MIRT trained 700 fellows, including 152 MD or MD/PhD fellows, 544 PhD or PsyD fellows, 3 PharmDs fellows, and 1 doctor of nursing practice fellow.
Fellowship Structure
The AF MIRT coordinating center provides key administrative support to fellowship site directors and topical didactic training to Advanced Fellows, ensuring consistent standard of quality training across locations in 15 states and 4 times zones. The training provided by the AF MIRT coordinating center deepens the nationally-mandated focus of local translational clinical centers (eg, Mental Illness Research Education and Clinical Centers, Centers of Excellence) on posttraumatic stress disorder (PTSD), serious mental illness, dementia, and other areas.
The AF MIRT coordinating center also promotes VA workforce sustainability. Advanced Fellows in programs with a coordinating center are much more likely to be retained in VA for postfellowship employment compared with fellows in programs without such a coordinating center (60% vs 38%) according to unpublished Office of Academic Affiliations data (Joel Schmidt, oral communication, May 15, 2025). The AF MIRT coordinating center provides central standardization and uses evidence-based approaches to ensure fellows receive consistent support, resources, and training. More specifically, the coordinating center develops and delivers a standardized, core curriculum to the program’s 28 sites. The program pioneered video delivery of integrated didactics that enlist national experts, many of them VA researchers and clinicians themselves. Didactics include high priority veteran mental health topics, such as suicide prevention, new and emerging evidence-based treatments (eg, neurostimulation for treatment resistant PTSD, psychotherapeutic approaches for traumatic brain injury), and VA health system considerations for mental health treatment delivery.
This curated didactic series also covers professional and technical issues, such as statistical and methodological considerations for clinical trials, scientific writing, and grant-writing skill development. These offerings support the career pathways of advanced fellows to pursue careers as researchers, scientifically-informed clinicians, or data scientists at VA or academic medical centers. The coordinating center prepares fellows to apply for mentored career award funding or independent investigator awards through the VA, National Institutes of Health (NIH), US Department of Defense, and other organizations by offering an annual mock grant review session and monthly reviews and discussions of fellows’ grant applications.
AF MIRT continuously fine tunes the didactic series curriculum based on feedback from fellows on how the program meets their training needs. For example, learning about the strategies Advanced Fellows used to remain productive during COVID-19 pandemic lockdowns revealed a strong trend toward use of secondary data (eg, publicly available data or VA electronic health record data). This fueled curriculum adjustments to include more topics relevant to fellow interests and needs for accessing secondary data resources for high priority veteran mental health topics.6
VA Advanced Fellowships Successes
From July 2020 to June 2025, MIRT advanced fellows published 906 peer-reviewed articles in psychiatry, psychology, and other disciplines. Each year, about 20 to 25 articles are published in high-impact journals. In this 5-year period, fellows have received 153 grants (114 VA grants) as principal investigators– many examining new innovations to improve the quality of care of veterans. Of the 165 fellows who graduated since 2020, 63% continued working in veteran health care: 38% transitioned to full-time VA employment and 25% moved to VA employment with an academic-affiliated role. Nineteen percent transitioned to academic positions, 12% transitioned to the private sector, and 5% transitioned to other government, industry, or nonprofit employment where these professionals contribute to scientific and clinical innovation benefiting the US public; 1% did not provide postfellowship employment information. The Figure displays geographic locations of graduated fellows’ postfellowship employment from July 2020 to June 2025.
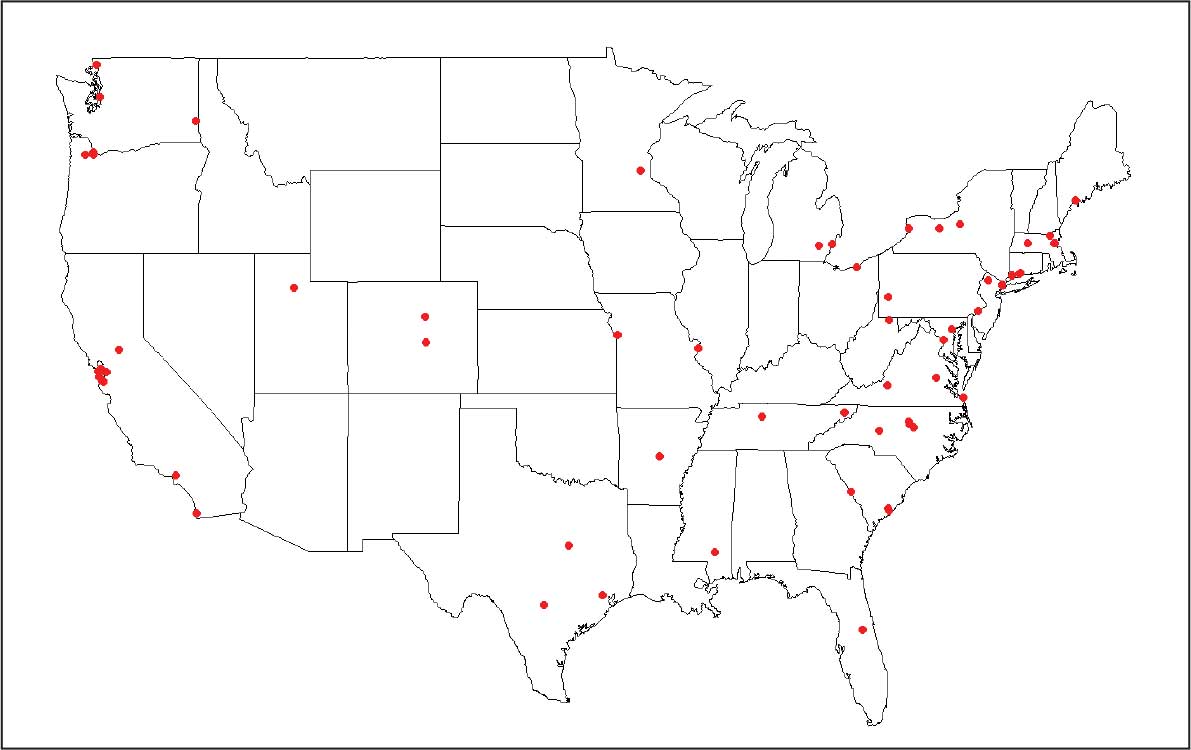
employment across all settings, July 2020 to June 2025.
The accomplishments of fellows are wide-ranging and aligned with VA’s mission. Each year, roughly 15 fellows receive new investigator awards, travel awards, and poster or presentation awards from prominent professional societies. Fellows have obtained VA Career Development Awards in diverse topics, including suicide prevention through clinician resources and training programs, firearm safety discussions, digital phenotyping and neuroimaging to enhance social integration in veterans with schizophrenia, rapid transcranial magnetic stimulation to treat nicotine use and PTSD, and evidence-based psychotherapy techniques for female veterans experiencing issues in menopause.
Several recent MIRT fellows have also received highly competitive NIH K Career Development Awards. One notable example is a fellow who studied pharmacologic approaches for treatment-resistant depression informed by novel brain circuit findings, first testing these approaches in community samples through a NIH K grant and translating findings to veterans. Fellows have gone on to become directors of important national research centers and studies, chairs of academic departments, and presidents of national medical organizations. Importantly, many MIRT fellows have become local directors and mentors to a new generation of VA fellows and researchers.
Conclusions
The AF MIRT coordinating center supports the VA’s mission of fulfilling President Lincoln’s promise to care for veterans. There are multiple benefits to evidence-based work that helps veterans and fosters a highly skilled VA workforce. Veterans are at the center of the MIRT data-driven approach, which is critical given their complex needs. Approaches to building the AF MIRT’s evidence base include randomized controlled trials open to veteran participants; program evaluation of current local, regional, or national VHA clinical services through measurement-based care and evaluation of national clinician training programs; and even smaller quality improvement projects in local VA clinics. These efforts support effective, efficient, and accessible provision of treatments that benefit veterans.
- US Department of Veterans Affairs. Our VA mission and core values. Updated April 17, 2025. Accessed March 2, 2026. https://department.va.gov/icare/
- Holliday R, Holder N. VA is a leader in mental health and social service research and operations. Fed Pract. 2025;42:S5. doi:10.12788/fp.0578
- Zeiss AM, Karlin BE. Integrating mental health and primary care services in the Department of Veterans Affairs health care system. J Clin Psychol Med Settings. 2008;15:73-78. doi:10.1007/s10880-008-9100-4
- O’Hara R, Cassidy-Eagle EL, Beaudreau SA, et al. Increasing the ranks of academic researchers in mental health: a multisite approach to postdoctoral fellowship training. Acad Med. 2010;85:41-47. doi:10.1097/ACM.0b013e3181c47c51
- US Department of Veterans Affairs. Office of Academic Affiliations. Updated March 13, 2025. Accessed March 2, 2026. https://www.va.gov/oaa/advancedfellowships /advanced-fellowships.asp
- Hantke NC, Samarina V, Hallmayer J, et al. Preparing the next generation of academic researchers during the pandemic: lessons from a national mental health research postdoctoral fellowship. Acad Psychiatry. 2022;46:466- 469. doi:10.1007/s40596-022-01613-4
The US Department of Veterans Affairs (VA) mission realizes President Abraham Lincoln’s promise to “to care for him who shall have borne the battle, and for his widow, and his orphan.”1 Evidence-based care fulfills this promise and is the backbone of Veterans Health Administration (VHA) mental health care.2,3 To ensure veterans receive state-of-the-art clinical care, a skilled workforce and investment in data-driven approaches are necessary to identify best treatments and strategies to implement them in practice.
Through scientific and clinical training tailored to VA, the 23 VA Advanced Fellowships have secured a steady flow of highly trained PhD professionals (ie, psychologists and other allied health professionals), and medical doctors (ie, psychiatrists and neurologists) into the VA workforce.4 The VA Advanced Fellows are funded by the Office of Academic Affiliations (OAA) and offer 2-year training opportunities for postresidency MDs and postdoctoral PhDs. This article describes a VA Advanced Fellowship in mental health as an example of how these programs can have a broad and positive impact on the VA health care system.
Advanced Fellows Program
The VA Advanced Fellowship in Mental Illness Research and Treatment (AF MIRT), formerly known as the VA Special Fellowship Program in Advanced Psychiatry and Psychology, educates and trains clinician and nonclinician researchers to meet VA priority mental health care needs.5 Clinical AF MIRT fellows dedicate 75% of their time to training and research activities and 25% to direct clinical services. Data science fellows complete projects that inform veteran clinical care through qualitative data collection, program evaluation, and analysis of large datasets. The full translational pathway to evidence-based clinical care is represented by fellow research spanning basic animal models, genetics, and neuroimaging to implementation science and applied clinical care for veterans.
In 2025, AF MIRT marked its 25th year of training postdoctoral-level mental health scientific practitioners and scholars. This investment in clinical research training has had profound benefits for innovation and retention of clinicians and scientists within the VA system. As of April 1, 2026, AF MIRT trained 700 fellows, including 152 MD or MD/PhD fellows, 544 PhD or PsyD fellows, 3 PharmDs fellows, and 1 doctor of nursing practice fellow.
Fellowship Structure
The AF MIRT coordinating center provides key administrative support to fellowship site directors and topical didactic training to Advanced Fellows, ensuring consistent standard of quality training across locations in 15 states and 4 times zones. The training provided by the AF MIRT coordinating center deepens the nationally-mandated focus of local translational clinical centers (eg, Mental Illness Research Education and Clinical Centers, Centers of Excellence) on posttraumatic stress disorder (PTSD), serious mental illness, dementia, and other areas.
The AF MIRT coordinating center also promotes VA workforce sustainability. Advanced Fellows in programs with a coordinating center are much more likely to be retained in VA for postfellowship employment compared with fellows in programs without such a coordinating center (60% vs 38%) according to unpublished Office of Academic Affiliations data (Joel Schmidt, oral communication, May 15, 2025). The AF MIRT coordinating center provides central standardization and uses evidence-based approaches to ensure fellows receive consistent support, resources, and training. More specifically, the coordinating center develops and delivers a standardized, core curriculum to the program’s 28 sites. The program pioneered video delivery of integrated didactics that enlist national experts, many of them VA researchers and clinicians themselves. Didactics include high priority veteran mental health topics, such as suicide prevention, new and emerging evidence-based treatments (eg, neurostimulation for treatment resistant PTSD, psychotherapeutic approaches for traumatic brain injury), and VA health system considerations for mental health treatment delivery.
This curated didactic series also covers professional and technical issues, such as statistical and methodological considerations for clinical trials, scientific writing, and grant-writing skill development. These offerings support the career pathways of advanced fellows to pursue careers as researchers, scientifically-informed clinicians, or data scientists at VA or academic medical centers. The coordinating center prepares fellows to apply for mentored career award funding or independent investigator awards through the VA, National Institutes of Health (NIH), US Department of Defense, and other organizations by offering an annual mock grant review session and monthly reviews and discussions of fellows’ grant applications.
AF MIRT continuously fine tunes the didactic series curriculum based on feedback from fellows on how the program meets their training needs. For example, learning about the strategies Advanced Fellows used to remain productive during COVID-19 pandemic lockdowns revealed a strong trend toward use of secondary data (eg, publicly available data or VA electronic health record data). This fueled curriculum adjustments to include more topics relevant to fellow interests and needs for accessing secondary data resources for high priority veteran mental health topics.6
VA Advanced Fellowships Successes
From July 2020 to June 2025, MIRT advanced fellows published 906 peer-reviewed articles in psychiatry, psychology, and other disciplines. Each year, about 20 to 25 articles are published in high-impact journals. In this 5-year period, fellows have received 153 grants (114 VA grants) as principal investigators– many examining new innovations to improve the quality of care of veterans. Of the 165 fellows who graduated since 2020, 63% continued working in veteran health care: 38% transitioned to full-time VA employment and 25% moved to VA employment with an academic-affiliated role. Nineteen percent transitioned to academic positions, 12% transitioned to the private sector, and 5% transitioned to other government, industry, or nonprofit employment where these professionals contribute to scientific and clinical innovation benefiting the US public; 1% did not provide postfellowship employment information. The Figure displays geographic locations of graduated fellows’ postfellowship employment from July 2020 to June 2025.
employment across all settings, July 2020 to June 2025.
The accomplishments of fellows are wide-ranging and aligned with VA’s mission. Each year, roughly 15 fellows receive new investigator awards, travel awards, and poster or presentation awards from prominent professional societies. Fellows have obtained VA Career Development Awards in diverse topics, including suicide prevention through clinician resources and training programs, firearm safety discussions, digital phenotyping and neuroimaging to enhance social integration in veterans with schizophrenia, rapid transcranial magnetic stimulation to treat nicotine use and PTSD, and evidence-based psychotherapy techniques for female veterans experiencing issues in menopause.
Several recent MIRT fellows have also received highly competitive NIH K Career Development Awards. One notable example is a fellow who studied pharmacologic approaches for treatment-resistant depression informed by novel brain circuit findings, first testing these approaches in community samples through a NIH K grant and translating findings to veterans. Fellows have gone on to become directors of important national research centers and studies, chairs of academic departments, and presidents of national medical organizations. Importantly, many MIRT fellows have become local directors and mentors to a new generation of VA fellows and researchers.
Conclusions
The AF MIRT coordinating center supports the VA’s mission of fulfilling President Lincoln’s promise to care for veterans. There are multiple benefits to evidence-based work that helps veterans and fosters a highly skilled VA workforce. Veterans are at the center of the MIRT data-driven approach, which is critical given their complex needs. Approaches to building the AF MIRT’s evidence base include randomized controlled trials open to veteran participants; program evaluation of current local, regional, or national VHA clinical services through measurement-based care and evaluation of national clinician training programs; and even smaller quality improvement projects in local VA clinics. These efforts support effective, efficient, and accessible provision of treatments that benefit veterans.
The US Department of Veterans Affairs (VA) mission realizes President Abraham Lincoln’s promise to “to care for him who shall have borne the battle, and for his widow, and his orphan.”1 Evidence-based care fulfills this promise and is the backbone of Veterans Health Administration (VHA) mental health care.2,3 To ensure veterans receive state-of-the-art clinical care, a skilled workforce and investment in data-driven approaches are necessary to identify best treatments and strategies to implement them in practice.
Through scientific and clinical training tailored to VA, the 23 VA Advanced Fellowships have secured a steady flow of highly trained PhD professionals (ie, psychologists and other allied health professionals), and medical doctors (ie, psychiatrists and neurologists) into the VA workforce.4 The VA Advanced Fellows are funded by the Office of Academic Affiliations (OAA) and offer 2-year training opportunities for postresidency MDs and postdoctoral PhDs. This article describes a VA Advanced Fellowship in mental health as an example of how these programs can have a broad and positive impact on the VA health care system.
Advanced Fellows Program
The VA Advanced Fellowship in Mental Illness Research and Treatment (AF MIRT), formerly known as the VA Special Fellowship Program in Advanced Psychiatry and Psychology, educates and trains clinician and nonclinician researchers to meet VA priority mental health care needs.5 Clinical AF MIRT fellows dedicate 75% of their time to training and research activities and 25% to direct clinical services. Data science fellows complete projects that inform veteran clinical care through qualitative data collection, program evaluation, and analysis of large datasets. The full translational pathway to evidence-based clinical care is represented by fellow research spanning basic animal models, genetics, and neuroimaging to implementation science and applied clinical care for veterans.
In 2025, AF MIRT marked its 25th year of training postdoctoral-level mental health scientific practitioners and scholars. This investment in clinical research training has had profound benefits for innovation and retention of clinicians and scientists within the VA system. As of April 1, 2026, AF MIRT trained 700 fellows, including 152 MD or MD/PhD fellows, 544 PhD or PsyD fellows, 3 PharmDs fellows, and 1 doctor of nursing practice fellow.
Fellowship Structure
The AF MIRT coordinating center provides key administrative support to fellowship site directors and topical didactic training to Advanced Fellows, ensuring consistent standard of quality training across locations in 15 states and 4 times zones. The training provided by the AF MIRT coordinating center deepens the nationally-mandated focus of local translational clinical centers (eg, Mental Illness Research Education and Clinical Centers, Centers of Excellence) on posttraumatic stress disorder (PTSD), serious mental illness, dementia, and other areas.
The AF MIRT coordinating center also promotes VA workforce sustainability. Advanced Fellows in programs with a coordinating center are much more likely to be retained in VA for postfellowship employment compared with fellows in programs without such a coordinating center (60% vs 38%) according to unpublished Office of Academic Affiliations data (Joel Schmidt, oral communication, May 15, 2025). The AF MIRT coordinating center provides central standardization and uses evidence-based approaches to ensure fellows receive consistent support, resources, and training. More specifically, the coordinating center develops and delivers a standardized, core curriculum to the program’s 28 sites. The program pioneered video delivery of integrated didactics that enlist national experts, many of them VA researchers and clinicians themselves. Didactics include high priority veteran mental health topics, such as suicide prevention, new and emerging evidence-based treatments (eg, neurostimulation for treatment resistant PTSD, psychotherapeutic approaches for traumatic brain injury), and VA health system considerations for mental health treatment delivery.
This curated didactic series also covers professional and technical issues, such as statistical and methodological considerations for clinical trials, scientific writing, and grant-writing skill development. These offerings support the career pathways of advanced fellows to pursue careers as researchers, scientifically-informed clinicians, or data scientists at VA or academic medical centers. The coordinating center prepares fellows to apply for mentored career award funding or independent investigator awards through the VA, National Institutes of Health (NIH), US Department of Defense, and other organizations by offering an annual mock grant review session and monthly reviews and discussions of fellows’ grant applications.
AF MIRT continuously fine tunes the didactic series curriculum based on feedback from fellows on how the program meets their training needs. For example, learning about the strategies Advanced Fellows used to remain productive during COVID-19 pandemic lockdowns revealed a strong trend toward use of secondary data (eg, publicly available data or VA electronic health record data). This fueled curriculum adjustments to include more topics relevant to fellow interests and needs for accessing secondary data resources for high priority veteran mental health topics.6
VA Advanced Fellowships Successes
From July 2020 to June 2025, MIRT advanced fellows published 906 peer-reviewed articles in psychiatry, psychology, and other disciplines. Each year, about 20 to 25 articles are published in high-impact journals. In this 5-year period, fellows have received 153 grants (114 VA grants) as principal investigators– many examining new innovations to improve the quality of care of veterans. Of the 165 fellows who graduated since 2020, 63% continued working in veteran health care: 38% transitioned to full-time VA employment and 25% moved to VA employment with an academic-affiliated role. Nineteen percent transitioned to academic positions, 12% transitioned to the private sector, and 5% transitioned to other government, industry, or nonprofit employment where these professionals contribute to scientific and clinical innovation benefiting the US public; 1% did not provide postfellowship employment information. The Figure displays geographic locations of graduated fellows’ postfellowship employment from July 2020 to June 2025.
employment across all settings, July 2020 to June 2025.
The accomplishments of fellows are wide-ranging and aligned with VA’s mission. Each year, roughly 15 fellows receive new investigator awards, travel awards, and poster or presentation awards from prominent professional societies. Fellows have obtained VA Career Development Awards in diverse topics, including suicide prevention through clinician resources and training programs, firearm safety discussions, digital phenotyping and neuroimaging to enhance social integration in veterans with schizophrenia, rapid transcranial magnetic stimulation to treat nicotine use and PTSD, and evidence-based psychotherapy techniques for female veterans experiencing issues in menopause.
Several recent MIRT fellows have also received highly competitive NIH K Career Development Awards. One notable example is a fellow who studied pharmacologic approaches for treatment-resistant depression informed by novel brain circuit findings, first testing these approaches in community samples through a NIH K grant and translating findings to veterans. Fellows have gone on to become directors of important national research centers and studies, chairs of academic departments, and presidents of national medical organizations. Importantly, many MIRT fellows have become local directors and mentors to a new generation of VA fellows and researchers.
Conclusions
The AF MIRT coordinating center supports the VA’s mission of fulfilling President Lincoln’s promise to care for veterans. There are multiple benefits to evidence-based work that helps veterans and fosters a highly skilled VA workforce. Veterans are at the center of the MIRT data-driven approach, which is critical given their complex needs. Approaches to building the AF MIRT’s evidence base include randomized controlled trials open to veteran participants; program evaluation of current local, regional, or national VHA clinical services through measurement-based care and evaluation of national clinician training programs; and even smaller quality improvement projects in local VA clinics. These efforts support effective, efficient, and accessible provision of treatments that benefit veterans.
- US Department of Veterans Affairs. Our VA mission and core values. Updated April 17, 2025. Accessed March 2, 2026. https://department.va.gov/icare/
- Holliday R, Holder N. VA is a leader in mental health and social service research and operations. Fed Pract. 2025;42:S5. doi:10.12788/fp.0578
- Zeiss AM, Karlin BE. Integrating mental health and primary care services in the Department of Veterans Affairs health care system. J Clin Psychol Med Settings. 2008;15:73-78. doi:10.1007/s10880-008-9100-4
- O’Hara R, Cassidy-Eagle EL, Beaudreau SA, et al. Increasing the ranks of academic researchers in mental health: a multisite approach to postdoctoral fellowship training. Acad Med. 2010;85:41-47. doi:10.1097/ACM.0b013e3181c47c51
- US Department of Veterans Affairs. Office of Academic Affiliations. Updated March 13, 2025. Accessed March 2, 2026. https://www.va.gov/oaa/advancedfellowships /advanced-fellowships.asp
- Hantke NC, Samarina V, Hallmayer J, et al. Preparing the next generation of academic researchers during the pandemic: lessons from a national mental health research postdoctoral fellowship. Acad Psychiatry. 2022;46:466- 469. doi:10.1007/s40596-022-01613-4
- US Department of Veterans Affairs. Our VA mission and core values. Updated April 17, 2025. Accessed March 2, 2026. https://department.va.gov/icare/
- Holliday R, Holder N. VA is a leader in mental health and social service research and operations. Fed Pract. 2025;42:S5. doi:10.12788/fp.0578
- Zeiss AM, Karlin BE. Integrating mental health and primary care services in the Department of Veterans Affairs health care system. J Clin Psychol Med Settings. 2008;15:73-78. doi:10.1007/s10880-008-9100-4
- O’Hara R, Cassidy-Eagle EL, Beaudreau SA, et al. Increasing the ranks of academic researchers in mental health: a multisite approach to postdoctoral fellowship training. Acad Med. 2010;85:41-47. doi:10.1097/ACM.0b013e3181c47c51
- US Department of Veterans Affairs. Office of Academic Affiliations. Updated March 13, 2025. Accessed March 2, 2026. https://www.va.gov/oaa/advancedfellowships /advanced-fellowships.asp
- Hantke NC, Samarina V, Hallmayer J, et al. Preparing the next generation of academic researchers during the pandemic: lessons from a national mental health research postdoctoral fellowship. Acad Psychiatry. 2022;46:466- 469. doi:10.1007/s40596-022-01613-4
VA Advanced Training for Clinician Researchers and Data Scientists in Mental Health
VA Advanced Training for Clinician Researchers and Data Scientists in Mental Health

The Home Improvements and Structural Alterations Program: Overview and Future Implications
The Home Improvements and Structural Alterations Program: Overview and Future Implications
The Veterans Health Administration (VHA) Home Improvements and Structural Alterations (HISA) program is a primary means through which veterans can obtain home modifications necessary to continue safe and independent living in their home, including fall risk reduction and accessibility to essential parts of the home. However, not all eligible veterans who may benefit from this program participate, for a variety of reasons.1-6 Historically, the HISA program has been administered in a decentralized and nonstandardized fashion dictated by the organizational structure of each US Department of Veterans Affairs (VA) medical center (VAMC) within a certain region or Veterans Integrated Service Network (VISN). Previous research found differential access to the HISA program by younger veterans, women, minorities, veterans with certain disability types, and veterans living in rural vs urban settings. These disparities in access and use of benefits conferred by the HISA program suggests an area of unmet need, which may improve veterans’ health care outcomes and reduce costs associated with their care.2-8
The purpose of this article is to provide information to improve equitable provision and effective eligible use of resources available through the HISA program in a more generalizable manner by providing insight to highlight common program process deficiencies and care provision gaps relevant to VAMCs nationwide. This information can be used to inform the VA Physical Medicine and Rehabilitation (PM&R) and Prosthetic and Sensory Aid Service (PSAS) national policy initiatives, as well as hiring practices, clinic organization, specific care provision, and administrative goals and metrics at each VISN and at the VA Healthcare System level.
Methods
Veterans who participated in the HISA program, VHA administrators, and VHA clinicians from select VAMCs were identified and interviewed to better understand what helps increase access to the program, barriers to access, and how existing program components and processes impact use of the service. These interviews were taken from a directed convenience sample of selected VAMCs. To obtain this directed convenience sample, 167 VAMCs that participated in the HISA program were categorized as facilities that provided either a high or low number of HISA program prescriptions based on data from 2010 to 2018. Ten facilities from the top quartiles and 10 from the bottom quartiles of prescribing locations were selected. This facility selection was driven by the proportion of rural veterans served by each facility, favoring those serving a greater proportion of rural veterans, as well geographic location, with the aim of avoiding overrepresentation of any specific region. The convenience sample included 45 individuals (20 VHA employees and 25 veterans) across 22 states from the Northeast, West, South, and Midwest US Census regions.
Interview Process
Interviews underwent a coding process. The development of topical themes followed a systematic, 2-phase approach. Initially, researchers analyzed responses to semistructured interview questions addressing specific aspects of the HISA program, such as program awareness and accessibility. These responses naturally clustered into preliminary categories based on the interview guide structure. For example, responses related to program discovery formed a marketing-related category, while recommendations about program implementation contributed to a training and development category.
Following this initial categorization, the research team conducted a more rigorous coding process. A team of 3 researchers systematically reviewed assigned interview transcripts to extract practical recommendations for the guide. The researchers first identified relevant responses individually and then convened during group meetings to discuss and finalize selections. This second phase refined the preliminary categorization while maintaining alignment with the original interview structure.
This approach allowed the team to preserve the practical utility of participant feedback while ensuring methodological rigor in the analysis process. Resulting themes reflect both the structured nature of the original inquiry and the practical recommendations identified for improving the HISA program. Information on the following areas were collected: education about the HISA program, the contracting process, use of telehealth, interaction between VHA clinical care and the PSAS, marketing of the program, program funding, and revising the application process.
Results
Interview respondents provided several recommendations for improving the HISA program (Table). Regarding training and education, respondents noted deficiencies in VHA employee communication about the HISA program to veterans. Some employees did not know details or were unaware the HISA program existed. Additionally, a lack of knowledge about HISA program alternatives, including other available programs for obtaining home modifications or other durable medical equipment alternatives (eg, provision of a portable ramp rather than construction of a permanent one), was apparent. It was strongly recommended to provide additional education to effectively disseminate knowledge about the HISA program. Specifically, VHA employees, especially those in Primary Care, Geriatrics, Home Based Primary Care, the Caregiver Support Program, and Blind Rehabilitation Services, require greater awareness of the program and its processes.
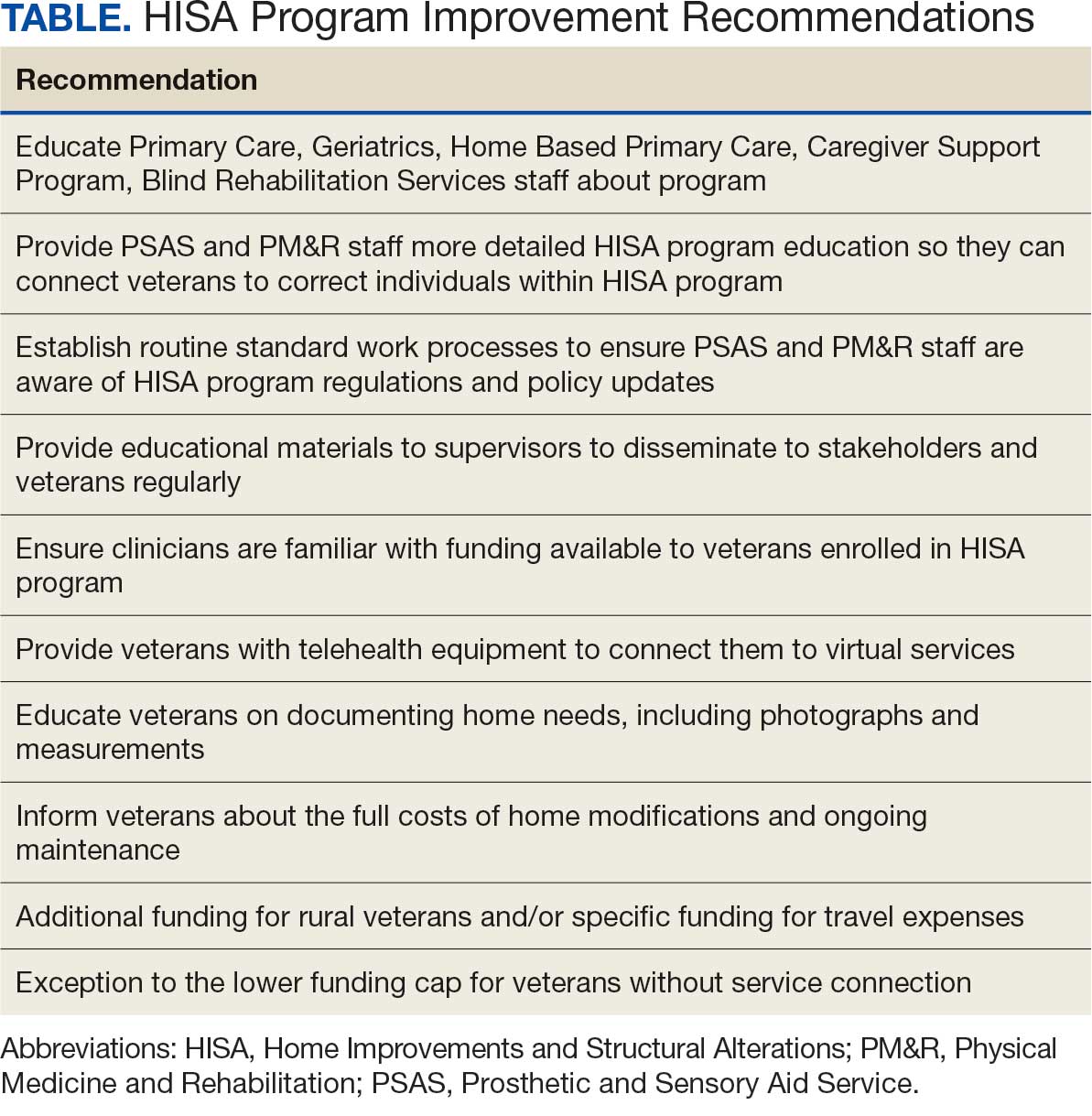
PSAS and PM&R professionals, including physicians, nurse practitioners, physician assistants, and physical and occupational therapists, would be expected to have some knowledge of the HISA program, and therefore be more likely to connect a veteran with it. However, they may lack specific details about the program such as correct contact persons in the other service (PSAS or PM&R, respectively), facility- specific processes, such as how to enter a HISA consultation within the veteran’s electronic health record, how the entered consultation would progress through the system and avoid cancellation, and what should routinely be done to avoid HISA consultation cancellation, such as referral to Occupational Therapy for a functional assessment so appropriate durable medical equipment can be trialed with the veteran prior to proceeding with more costly and time-consuming home modifications.
In addition, there is no routine standard work process to ensure that PM&R staff are aware of updates in HISA program regulations and policy. Further recommendations in this area include having supervisory employees in PSAS and PM&R work both individually and together to develop effective information dissemination methods for key stakeholders. These include targeted in-services (ie, educational trainings often scheduled and conducted during recurring meetings), whether faceto- face or virtually in real time, or recorded, that occur on an ongoing and regular basis with sister services such as Primary Care, Geriatrics, Home Based Primary Care, the Caregiver Support Program, and Blind Rehabilitation Services (eg, the facility Vision Impairment Services Team coordinator). Regularly updated educational materials should be provided to veterans and VHA adjacent stakeholders such as Veteran Service Organizations and Veteran County Service Officers, via a variety of platforms.
Successfully navigating the provision of home modifications via the HISA program involves identifying a contractor to perform the home modification and obtaining service and construction plan pricing. A key barrier in this area is that veterans and VHA clinicians perceive the funds available through HISA as insufficient, regardless of whether they have serviceconnected status or not. Service connection refers to designation of ≥ 1 medical conditions determined to be related to military service and thus eligible to receive VHA care.9 Service-connected veterans receive a lifetime maximum award of $6800 from HISA while veterans without service connection receive a lifetime maximum award of $2000.1,2
Rural veterans face a greater challenge than urban veterans, as there are fewer contractors located nearby. Thus, providing higher funding for rural veterans, or specific funding such as for travel expenses, would be especially helpful to find a willing contractor to perform home medications.1 The current requirement of working with a licensed contractor was also a barrier, especially for smaller jobs, and could result in VHA employees (including clinicians) feeling pressured to become overly involved to assist veterans to move through the process.
To that point, respondents requested resources such as a regularly updated list of licensed contractors in the area, especially those familiar with working with the HISA program, be provided to veterans and their assisting groups. In addition, respondents asked that VHA take on greater responsibility and liability with regard to contractors accessing HISA funding, such as not releasing final payment until VHA approved the completed home modification. On the other hand, respondents also expressed concerns about the length of time associated with HISA program payment and noted it should be sped up to allow contractors who participate to receive payment sooner, which many believed would increase the number of contractors willing to take on this work.
The role of telehealth was noted as a great facilitator of increased access to care, especially following the COVID-19 pandemic. Telehealth modalities adapted for the HISA program could help increase access to the program and improve processing speed. Barriers include lack of appropriate veteran telehealth equipment and poor understanding of information needed to move the process forward. Recommendations included providing veterans tablets to connect to virtual services, and developing information on home measurements needed, assistance in obtaining and sending photographs, and detailed information on successfully using telehealth for the HISA application process. Of note, some clinicians, representing home-based primary care, prosthetics services, geriatrics, rehabilitation therapy, mobile clinic, and the telehealth division, and including both clinical staff (eg, occupational therapists) and nonclinical staff (eg, prosthetics representatives and administrative personnel), have found patients expressed comparable satisfaction with the process whether faceto- face or via telehealth.
The essential relationship between PSAS and PM&R regarding the HISA program was a key finding. Both services are integral to helping veterans successfully obtain home modifications via the HISA program.1,2 Barriers include insufficient communication and a lack of clearly defined points of contact for each service, poorly defined roles, and inefficiencies because 2 services are involved in navigating the process. Recommendations therefore include addressing these issues, such as adopting a case management or liaison model between the services to better manage the process.
Respondents indicated that insufficient program funding was a concern. Veterans living in poorer quality housing, such as older homes, often require more expensive home modifications, necessitating greater out-of-pocket expenses. Veterans and VHA employees advocated for the creation of an exception to the lower funding cap for veterans without service connection in cases of financial hardship. Overall, the funding limits for both service-connected veterans and those without service connection were thought to be insufficient, especially as the COVID-19 pandemic increased the cost of construction materials.
Respondents also noted that veterans would benefit from clear messaging that receiving HISA funds does not impact eligibility for other VA benefits and services. Veterans must understand that home modifications work must be approved by VHA before being started and should be aware that if their disability rating increases so that they become eligible for the higher level service-connected benefits, they would then become eligible for the higher maximum benefit. Respondents recommended veterans should receive assistance in understanding the full costs of the home modification and ongoing maintenance, and the HISA research team recommended that the National Program develop a fact sheet that can be used to advise veterans.
Respondents consistently indicated that information about the HISA program was not disseminated effectively to key internal and external stakeholders, and opportunities to highlight the program on VHA websites, brochures throughout VHA facilities, and other outlets such as direct mailing should be used. Veterans who have used the program are overwhelmingly older (mean age 71 years), White, and male, suggesting missed opportunities and unmet need for underrepresented groups. Therefore, targeted marketing interventions would especially benefit these groups.
Respondents also noted inefficiencies throughout the HISA program application process and advocated for changes such as national standard operating procedures (SOPs) to guide navigation through the HISA process. The national SOPs could include home evaluation prior to HISA application submission, clearly identified points of contact for the HISA program in PSAS and PM&R, and standardized documentation.
Future Directions
Information from respondents provided several avenues for future studies. Recommendations were obtained from each of the 7 broad topical areas: training and educational needs, potential, contracting challenges and opportunities, telehealth as a conduit to facilitate the availability of the HISA program, PSAS, and clinical services collaboration, marketing, need for increased funding, and revision of the application process. Input from stakeholders can help direct efficient use of resources to guide future studies for the greatest impact and highlight current and future priorities. Easy areas of intervention indicated by respondents include creating a national standard work process regarding the HISA program with standardized educational materials for key stakeholders, revised at regular intervals, and readily available on national websites. A pre- and postimplementation survey could help provide quantifiable information about the benefits of such an intervention.
Conclusions
A qualitative analysis of interviews with veterans and VHA clinicians provides evidence of potential barriers for the HISA program. Addressing these barriers could allow HISA to better meet the VHA goal of providing home modifications that allow veterans to live safely and independently in their homes. There is a need for ongoing review and assessment of the program to ensure optimization and efficient use of resources across the spectrum of veteran needs.
- Semeah LM, Ahrentzen S, Jia H, et al. The Home Improvements and Structural Alterations Benefits Program: veterans with disabilities and home accessibility. J Disabil Policy Stud. 2017;28:43-51. doi:10.1177/1044207317696275
- Semeah LM, Wang X, Cowper Ripley DC, et al. Improving health through a home modification service for veterans. In: Fiedler BA, ed. Three Facets of Public Health and Paths to Improvements. 2020:381-416. doi:10.1016/B978-0-12-819008-1.00014-6
- Semeah LM, Ganesh SP, Wang X, et al. Home modification and health services utilization by rural and urban veterans with disabilities. Housing Policy Debate. 2021;31:862-874. doi:10.1080/10511482.2020.1858923
- Semeah LM, Orozco T, Wang X, et al. Home modifications for rural veterans with disabilities. Fed Pract. 2021;38:300- 310. doi:10.12788/fp.0153
- Semeah LM, Orozco T, Wang X, et al. Predictors of countylevel home modification use across the US. Fed Pract. 2022;39:274-280. doi:10.12788/fp.0279
- Semeah LM, Orozco T, Wang X, et al. Rural and urban home modification program users: a comparative study. HERD. 2023;16:223-235. doi:10.1177/19375867221142627
- US Department of of Veterans Affairs. Home Improvements and Structural Alterations (HISA) benefits program: final rule. Fed Regist. 2014;79:71658-71663
- US Department of Veterans Affairs. Home Improvement and Structural Alterations (HISA): increase in the limit for home improvement and structural alterations (HISA)-VA: final regulations. Fed Regist. 1993;58:25565.
- US Department of Veterans Affairs. Eligibility for VA disability benefits. Updated April 25, 2025. Accessed April 1, 2026. https://www.va.gov/disability/eligibility
The Veterans Health Administration (VHA) Home Improvements and Structural Alterations (HISA) program is a primary means through which veterans can obtain home modifications necessary to continue safe and independent living in their home, including fall risk reduction and accessibility to essential parts of the home. However, not all eligible veterans who may benefit from this program participate, for a variety of reasons.1-6 Historically, the HISA program has been administered in a decentralized and nonstandardized fashion dictated by the organizational structure of each US Department of Veterans Affairs (VA) medical center (VAMC) within a certain region or Veterans Integrated Service Network (VISN). Previous research found differential access to the HISA program by younger veterans, women, minorities, veterans with certain disability types, and veterans living in rural vs urban settings. These disparities in access and use of benefits conferred by the HISA program suggests an area of unmet need, which may improve veterans’ health care outcomes and reduce costs associated with their care.2-8
The purpose of this article is to provide information to improve equitable provision and effective eligible use of resources available through the HISA program in a more generalizable manner by providing insight to highlight common program process deficiencies and care provision gaps relevant to VAMCs nationwide. This information can be used to inform the VA Physical Medicine and Rehabilitation (PM&R) and Prosthetic and Sensory Aid Service (PSAS) national policy initiatives, as well as hiring practices, clinic organization, specific care provision, and administrative goals and metrics at each VISN and at the VA Healthcare System level.
Methods
Veterans who participated in the HISA program, VHA administrators, and VHA clinicians from select VAMCs were identified and interviewed to better understand what helps increase access to the program, barriers to access, and how existing program components and processes impact use of the service. These interviews were taken from a directed convenience sample of selected VAMCs. To obtain this directed convenience sample, 167 VAMCs that participated in the HISA program were categorized as facilities that provided either a high or low number of HISA program prescriptions based on data from 2010 to 2018. Ten facilities from the top quartiles and 10 from the bottom quartiles of prescribing locations were selected. This facility selection was driven by the proportion of rural veterans served by each facility, favoring those serving a greater proportion of rural veterans, as well geographic location, with the aim of avoiding overrepresentation of any specific region. The convenience sample included 45 individuals (20 VHA employees and 25 veterans) across 22 states from the Northeast, West, South, and Midwest US Census regions.
Interview Process
Interviews underwent a coding process. The development of topical themes followed a systematic, 2-phase approach. Initially, researchers analyzed responses to semistructured interview questions addressing specific aspects of the HISA program, such as program awareness and accessibility. These responses naturally clustered into preliminary categories based on the interview guide structure. For example, responses related to program discovery formed a marketing-related category, while recommendations about program implementation contributed to a training and development category.
Following this initial categorization, the research team conducted a more rigorous coding process. A team of 3 researchers systematically reviewed assigned interview transcripts to extract practical recommendations for the guide. The researchers first identified relevant responses individually and then convened during group meetings to discuss and finalize selections. This second phase refined the preliminary categorization while maintaining alignment with the original interview structure.
This approach allowed the team to preserve the practical utility of participant feedback while ensuring methodological rigor in the analysis process. Resulting themes reflect both the structured nature of the original inquiry and the practical recommendations identified for improving the HISA program. Information on the following areas were collected: education about the HISA program, the contracting process, use of telehealth, interaction between VHA clinical care and the PSAS, marketing of the program, program funding, and revising the application process.
Results
Interview respondents provided several recommendations for improving the HISA program (Table). Regarding training and education, respondents noted deficiencies in VHA employee communication about the HISA program to veterans. Some employees did not know details or were unaware the HISA program existed. Additionally, a lack of knowledge about HISA program alternatives, including other available programs for obtaining home modifications or other durable medical equipment alternatives (eg, provision of a portable ramp rather than construction of a permanent one), was apparent. It was strongly recommended to provide additional education to effectively disseminate knowledge about the HISA program. Specifically, VHA employees, especially those in Primary Care, Geriatrics, Home Based Primary Care, the Caregiver Support Program, and Blind Rehabilitation Services, require greater awareness of the program and its processes.
PSAS and PM&R professionals, including physicians, nurse practitioners, physician assistants, and physical and occupational therapists, would be expected to have some knowledge of the HISA program, and therefore be more likely to connect a veteran with it. However, they may lack specific details about the program such as correct contact persons in the other service (PSAS or PM&R, respectively), facility- specific processes, such as how to enter a HISA consultation within the veteran’s electronic health record, how the entered consultation would progress through the system and avoid cancellation, and what should routinely be done to avoid HISA consultation cancellation, such as referral to Occupational Therapy for a functional assessment so appropriate durable medical equipment can be trialed with the veteran prior to proceeding with more costly and time-consuming home modifications.
In addition, there is no routine standard work process to ensure that PM&R staff are aware of updates in HISA program regulations and policy. Further recommendations in this area include having supervisory employees in PSAS and PM&R work both individually and together to develop effective information dissemination methods for key stakeholders. These include targeted in-services (ie, educational trainings often scheduled and conducted during recurring meetings), whether faceto- face or virtually in real time, or recorded, that occur on an ongoing and regular basis with sister services such as Primary Care, Geriatrics, Home Based Primary Care, the Caregiver Support Program, and Blind Rehabilitation Services (eg, the facility Vision Impairment Services Team coordinator). Regularly updated educational materials should be provided to veterans and VHA adjacent stakeholders such as Veteran Service Organizations and Veteran County Service Officers, via a variety of platforms.
Successfully navigating the provision of home modifications via the HISA program involves identifying a contractor to perform the home modification and obtaining service and construction plan pricing. A key barrier in this area is that veterans and VHA clinicians perceive the funds available through HISA as insufficient, regardless of whether they have serviceconnected status or not. Service connection refers to designation of ≥ 1 medical conditions determined to be related to military service and thus eligible to receive VHA care.9 Service-connected veterans receive a lifetime maximum award of $6800 from HISA while veterans without service connection receive a lifetime maximum award of $2000.1,2
Rural veterans face a greater challenge than urban veterans, as there are fewer contractors located nearby. Thus, providing higher funding for rural veterans, or specific funding such as for travel expenses, would be especially helpful to find a willing contractor to perform home medications.1 The current requirement of working with a licensed contractor was also a barrier, especially for smaller jobs, and could result in VHA employees (including clinicians) feeling pressured to become overly involved to assist veterans to move through the process.
To that point, respondents requested resources such as a regularly updated list of licensed contractors in the area, especially those familiar with working with the HISA program, be provided to veterans and their assisting groups. In addition, respondents asked that VHA take on greater responsibility and liability with regard to contractors accessing HISA funding, such as not releasing final payment until VHA approved the completed home modification. On the other hand, respondents also expressed concerns about the length of time associated with HISA program payment and noted it should be sped up to allow contractors who participate to receive payment sooner, which many believed would increase the number of contractors willing to take on this work.
The role of telehealth was noted as a great facilitator of increased access to care, especially following the COVID-19 pandemic. Telehealth modalities adapted for the HISA program could help increase access to the program and improve processing speed. Barriers include lack of appropriate veteran telehealth equipment and poor understanding of information needed to move the process forward. Recommendations included providing veterans tablets to connect to virtual services, and developing information on home measurements needed, assistance in obtaining and sending photographs, and detailed information on successfully using telehealth for the HISA application process. Of note, some clinicians, representing home-based primary care, prosthetics services, geriatrics, rehabilitation therapy, mobile clinic, and the telehealth division, and including both clinical staff (eg, occupational therapists) and nonclinical staff (eg, prosthetics representatives and administrative personnel), have found patients expressed comparable satisfaction with the process whether faceto- face or via telehealth.
The essential relationship between PSAS and PM&R regarding the HISA program was a key finding. Both services are integral to helping veterans successfully obtain home modifications via the HISA program.1,2 Barriers include insufficient communication and a lack of clearly defined points of contact for each service, poorly defined roles, and inefficiencies because 2 services are involved in navigating the process. Recommendations therefore include addressing these issues, such as adopting a case management or liaison model between the services to better manage the process.
Respondents indicated that insufficient program funding was a concern. Veterans living in poorer quality housing, such as older homes, often require more expensive home modifications, necessitating greater out-of-pocket expenses. Veterans and VHA employees advocated for the creation of an exception to the lower funding cap for veterans without service connection in cases of financial hardship. Overall, the funding limits for both service-connected veterans and those without service connection were thought to be insufficient, especially as the COVID-19 pandemic increased the cost of construction materials.
Respondents also noted that veterans would benefit from clear messaging that receiving HISA funds does not impact eligibility for other VA benefits and services. Veterans must understand that home modifications work must be approved by VHA before being started and should be aware that if their disability rating increases so that they become eligible for the higher level service-connected benefits, they would then become eligible for the higher maximum benefit. Respondents recommended veterans should receive assistance in understanding the full costs of the home modification and ongoing maintenance, and the HISA research team recommended that the National Program develop a fact sheet that can be used to advise veterans.
Respondents consistently indicated that information about the HISA program was not disseminated effectively to key internal and external stakeholders, and opportunities to highlight the program on VHA websites, brochures throughout VHA facilities, and other outlets such as direct mailing should be used. Veterans who have used the program are overwhelmingly older (mean age 71 years), White, and male, suggesting missed opportunities and unmet need for underrepresented groups. Therefore, targeted marketing interventions would especially benefit these groups.
Respondents also noted inefficiencies throughout the HISA program application process and advocated for changes such as national standard operating procedures (SOPs) to guide navigation through the HISA process. The national SOPs could include home evaluation prior to HISA application submission, clearly identified points of contact for the HISA program in PSAS and PM&R, and standardized documentation.
Future Directions
Information from respondents provided several avenues for future studies. Recommendations were obtained from each of the 7 broad topical areas: training and educational needs, potential, contracting challenges and opportunities, telehealth as a conduit to facilitate the availability of the HISA program, PSAS, and clinical services collaboration, marketing, need for increased funding, and revision of the application process. Input from stakeholders can help direct efficient use of resources to guide future studies for the greatest impact and highlight current and future priorities. Easy areas of intervention indicated by respondents include creating a national standard work process regarding the HISA program with standardized educational materials for key stakeholders, revised at regular intervals, and readily available on national websites. A pre- and postimplementation survey could help provide quantifiable information about the benefits of such an intervention.
Conclusions
A qualitative analysis of interviews with veterans and VHA clinicians provides evidence of potential barriers for the HISA program. Addressing these barriers could allow HISA to better meet the VHA goal of providing home modifications that allow veterans to live safely and independently in their homes. There is a need for ongoing review and assessment of the program to ensure optimization and efficient use of resources across the spectrum of veteran needs.
The Veterans Health Administration (VHA) Home Improvements and Structural Alterations (HISA) program is a primary means through which veterans can obtain home modifications necessary to continue safe and independent living in their home, including fall risk reduction and accessibility to essential parts of the home. However, not all eligible veterans who may benefit from this program participate, for a variety of reasons.1-6 Historically, the HISA program has been administered in a decentralized and nonstandardized fashion dictated by the organizational structure of each US Department of Veterans Affairs (VA) medical center (VAMC) within a certain region or Veterans Integrated Service Network (VISN). Previous research found differential access to the HISA program by younger veterans, women, minorities, veterans with certain disability types, and veterans living in rural vs urban settings. These disparities in access and use of benefits conferred by the HISA program suggests an area of unmet need, which may improve veterans’ health care outcomes and reduce costs associated with their care.2-8
The purpose of this article is to provide information to improve equitable provision and effective eligible use of resources available through the HISA program in a more generalizable manner by providing insight to highlight common program process deficiencies and care provision gaps relevant to VAMCs nationwide. This information can be used to inform the VA Physical Medicine and Rehabilitation (PM&R) and Prosthetic and Sensory Aid Service (PSAS) national policy initiatives, as well as hiring practices, clinic organization, specific care provision, and administrative goals and metrics at each VISN and at the VA Healthcare System level.
Methods
Veterans who participated in the HISA program, VHA administrators, and VHA clinicians from select VAMCs were identified and interviewed to better understand what helps increase access to the program, barriers to access, and how existing program components and processes impact use of the service. These interviews were taken from a directed convenience sample of selected VAMCs. To obtain this directed convenience sample, 167 VAMCs that participated in the HISA program were categorized as facilities that provided either a high or low number of HISA program prescriptions based on data from 2010 to 2018. Ten facilities from the top quartiles and 10 from the bottom quartiles of prescribing locations were selected. This facility selection was driven by the proportion of rural veterans served by each facility, favoring those serving a greater proportion of rural veterans, as well geographic location, with the aim of avoiding overrepresentation of any specific region. The convenience sample included 45 individuals (20 VHA employees and 25 veterans) across 22 states from the Northeast, West, South, and Midwest US Census regions.
Interview Process
Interviews underwent a coding process. The development of topical themes followed a systematic, 2-phase approach. Initially, researchers analyzed responses to semistructured interview questions addressing specific aspects of the HISA program, such as program awareness and accessibility. These responses naturally clustered into preliminary categories based on the interview guide structure. For example, responses related to program discovery formed a marketing-related category, while recommendations about program implementation contributed to a training and development category.
Following this initial categorization, the research team conducted a more rigorous coding process. A team of 3 researchers systematically reviewed assigned interview transcripts to extract practical recommendations for the guide. The researchers first identified relevant responses individually and then convened during group meetings to discuss and finalize selections. This second phase refined the preliminary categorization while maintaining alignment with the original interview structure.
This approach allowed the team to preserve the practical utility of participant feedback while ensuring methodological rigor in the analysis process. Resulting themes reflect both the structured nature of the original inquiry and the practical recommendations identified for improving the HISA program. Information on the following areas were collected: education about the HISA program, the contracting process, use of telehealth, interaction between VHA clinical care and the PSAS, marketing of the program, program funding, and revising the application process.
Results
Interview respondents provided several recommendations for improving the HISA program (Table). Regarding training and education, respondents noted deficiencies in VHA employee communication about the HISA program to veterans. Some employees did not know details or were unaware the HISA program existed. Additionally, a lack of knowledge about HISA program alternatives, including other available programs for obtaining home modifications or other durable medical equipment alternatives (eg, provision of a portable ramp rather than construction of a permanent one), was apparent. It was strongly recommended to provide additional education to effectively disseminate knowledge about the HISA program. Specifically, VHA employees, especially those in Primary Care, Geriatrics, Home Based Primary Care, the Caregiver Support Program, and Blind Rehabilitation Services, require greater awareness of the program and its processes.
PSAS and PM&R professionals, including physicians, nurse practitioners, physician assistants, and physical and occupational therapists, would be expected to have some knowledge of the HISA program, and therefore be more likely to connect a veteran with it. However, they may lack specific details about the program such as correct contact persons in the other service (PSAS or PM&R, respectively), facility- specific processes, such as how to enter a HISA consultation within the veteran’s electronic health record, how the entered consultation would progress through the system and avoid cancellation, and what should routinely be done to avoid HISA consultation cancellation, such as referral to Occupational Therapy for a functional assessment so appropriate durable medical equipment can be trialed with the veteran prior to proceeding with more costly and time-consuming home modifications.
In addition, there is no routine standard work process to ensure that PM&R staff are aware of updates in HISA program regulations and policy. Further recommendations in this area include having supervisory employees in PSAS and PM&R work both individually and together to develop effective information dissemination methods for key stakeholders. These include targeted in-services (ie, educational trainings often scheduled and conducted during recurring meetings), whether faceto- face or virtually in real time, or recorded, that occur on an ongoing and regular basis with sister services such as Primary Care, Geriatrics, Home Based Primary Care, the Caregiver Support Program, and Blind Rehabilitation Services (eg, the facility Vision Impairment Services Team coordinator). Regularly updated educational materials should be provided to veterans and VHA adjacent stakeholders such as Veteran Service Organizations and Veteran County Service Officers, via a variety of platforms.
Successfully navigating the provision of home modifications via the HISA program involves identifying a contractor to perform the home modification and obtaining service and construction plan pricing. A key barrier in this area is that veterans and VHA clinicians perceive the funds available through HISA as insufficient, regardless of whether they have serviceconnected status or not. Service connection refers to designation of ≥ 1 medical conditions determined to be related to military service and thus eligible to receive VHA care.9 Service-connected veterans receive a lifetime maximum award of $6800 from HISA while veterans without service connection receive a lifetime maximum award of $2000.1,2
Rural veterans face a greater challenge than urban veterans, as there are fewer contractors located nearby. Thus, providing higher funding for rural veterans, or specific funding such as for travel expenses, would be especially helpful to find a willing contractor to perform home medications.1 The current requirement of working with a licensed contractor was also a barrier, especially for smaller jobs, and could result in VHA employees (including clinicians) feeling pressured to become overly involved to assist veterans to move through the process.
To that point, respondents requested resources such as a regularly updated list of licensed contractors in the area, especially those familiar with working with the HISA program, be provided to veterans and their assisting groups. In addition, respondents asked that VHA take on greater responsibility and liability with regard to contractors accessing HISA funding, such as not releasing final payment until VHA approved the completed home modification. On the other hand, respondents also expressed concerns about the length of time associated with HISA program payment and noted it should be sped up to allow contractors who participate to receive payment sooner, which many believed would increase the number of contractors willing to take on this work.
The role of telehealth was noted as a great facilitator of increased access to care, especially following the COVID-19 pandemic. Telehealth modalities adapted for the HISA program could help increase access to the program and improve processing speed. Barriers include lack of appropriate veteran telehealth equipment and poor understanding of information needed to move the process forward. Recommendations included providing veterans tablets to connect to virtual services, and developing information on home measurements needed, assistance in obtaining and sending photographs, and detailed information on successfully using telehealth for the HISA application process. Of note, some clinicians, representing home-based primary care, prosthetics services, geriatrics, rehabilitation therapy, mobile clinic, and the telehealth division, and including both clinical staff (eg, occupational therapists) and nonclinical staff (eg, prosthetics representatives and administrative personnel), have found patients expressed comparable satisfaction with the process whether faceto- face or via telehealth.
The essential relationship between PSAS and PM&R regarding the HISA program was a key finding. Both services are integral to helping veterans successfully obtain home modifications via the HISA program.1,2 Barriers include insufficient communication and a lack of clearly defined points of contact for each service, poorly defined roles, and inefficiencies because 2 services are involved in navigating the process. Recommendations therefore include addressing these issues, such as adopting a case management or liaison model between the services to better manage the process.
Respondents indicated that insufficient program funding was a concern. Veterans living in poorer quality housing, such as older homes, often require more expensive home modifications, necessitating greater out-of-pocket expenses. Veterans and VHA employees advocated for the creation of an exception to the lower funding cap for veterans without service connection in cases of financial hardship. Overall, the funding limits for both service-connected veterans and those without service connection were thought to be insufficient, especially as the COVID-19 pandemic increased the cost of construction materials.
Respondents also noted that veterans would benefit from clear messaging that receiving HISA funds does not impact eligibility for other VA benefits and services. Veterans must understand that home modifications work must be approved by VHA before being started and should be aware that if their disability rating increases so that they become eligible for the higher level service-connected benefits, they would then become eligible for the higher maximum benefit. Respondents recommended veterans should receive assistance in understanding the full costs of the home modification and ongoing maintenance, and the HISA research team recommended that the National Program develop a fact sheet that can be used to advise veterans.
Respondents consistently indicated that information about the HISA program was not disseminated effectively to key internal and external stakeholders, and opportunities to highlight the program on VHA websites, brochures throughout VHA facilities, and other outlets such as direct mailing should be used. Veterans who have used the program are overwhelmingly older (mean age 71 years), White, and male, suggesting missed opportunities and unmet need for underrepresented groups. Therefore, targeted marketing interventions would especially benefit these groups.
Respondents also noted inefficiencies throughout the HISA program application process and advocated for changes such as national standard operating procedures (SOPs) to guide navigation through the HISA process. The national SOPs could include home evaluation prior to HISA application submission, clearly identified points of contact for the HISA program in PSAS and PM&R, and standardized documentation.
Future Directions
Information from respondents provided several avenues for future studies. Recommendations were obtained from each of the 7 broad topical areas: training and educational needs, potential, contracting challenges and opportunities, telehealth as a conduit to facilitate the availability of the HISA program, PSAS, and clinical services collaboration, marketing, need for increased funding, and revision of the application process. Input from stakeholders can help direct efficient use of resources to guide future studies for the greatest impact and highlight current and future priorities. Easy areas of intervention indicated by respondents include creating a national standard work process regarding the HISA program with standardized educational materials for key stakeholders, revised at regular intervals, and readily available on national websites. A pre- and postimplementation survey could help provide quantifiable information about the benefits of such an intervention.
Conclusions
A qualitative analysis of interviews with veterans and VHA clinicians provides evidence of potential barriers for the HISA program. Addressing these barriers could allow HISA to better meet the VHA goal of providing home modifications that allow veterans to live safely and independently in their homes. There is a need for ongoing review and assessment of the program to ensure optimization and efficient use of resources across the spectrum of veteran needs.
- Semeah LM, Ahrentzen S, Jia H, et al. The Home Improvements and Structural Alterations Benefits Program: veterans with disabilities and home accessibility. J Disabil Policy Stud. 2017;28:43-51. doi:10.1177/1044207317696275
- Semeah LM, Wang X, Cowper Ripley DC, et al. Improving health through a home modification service for veterans. In: Fiedler BA, ed. Three Facets of Public Health and Paths to Improvements. 2020:381-416. doi:10.1016/B978-0-12-819008-1.00014-6
- Semeah LM, Ganesh SP, Wang X, et al. Home modification and health services utilization by rural and urban veterans with disabilities. Housing Policy Debate. 2021;31:862-874. doi:10.1080/10511482.2020.1858923
- Semeah LM, Orozco T, Wang X, et al. Home modifications for rural veterans with disabilities. Fed Pract. 2021;38:300- 310. doi:10.12788/fp.0153
- Semeah LM, Orozco T, Wang X, et al. Predictors of countylevel home modification use across the US. Fed Pract. 2022;39:274-280. doi:10.12788/fp.0279
- Semeah LM, Orozco T, Wang X, et al. Rural and urban home modification program users: a comparative study. HERD. 2023;16:223-235. doi:10.1177/19375867221142627
- US Department of of Veterans Affairs. Home Improvements and Structural Alterations (HISA) benefits program: final rule. Fed Regist. 2014;79:71658-71663
- US Department of Veterans Affairs. Home Improvement and Structural Alterations (HISA): increase in the limit for home improvement and structural alterations (HISA)-VA: final regulations. Fed Regist. 1993;58:25565.
- US Department of Veterans Affairs. Eligibility for VA disability benefits. Updated April 25, 2025. Accessed April 1, 2026. https://www.va.gov/disability/eligibility
- Semeah LM, Ahrentzen S, Jia H, et al. The Home Improvements and Structural Alterations Benefits Program: veterans with disabilities and home accessibility. J Disabil Policy Stud. 2017;28:43-51. doi:10.1177/1044207317696275
- Semeah LM, Wang X, Cowper Ripley DC, et al. Improving health through a home modification service for veterans. In: Fiedler BA, ed. Three Facets of Public Health and Paths to Improvements. 2020:381-416. doi:10.1016/B978-0-12-819008-1.00014-6
- Semeah LM, Ganesh SP, Wang X, et al. Home modification and health services utilization by rural and urban veterans with disabilities. Housing Policy Debate. 2021;31:862-874. doi:10.1080/10511482.2020.1858923
- Semeah LM, Orozco T, Wang X, et al. Home modifications for rural veterans with disabilities. Fed Pract. 2021;38:300- 310. doi:10.12788/fp.0153
- Semeah LM, Orozco T, Wang X, et al. Predictors of countylevel home modification use across the US. Fed Pract. 2022;39:274-280. doi:10.12788/fp.0279
- Semeah LM, Orozco T, Wang X, et al. Rural and urban home modification program users: a comparative study. HERD. 2023;16:223-235. doi:10.1177/19375867221142627
- US Department of of Veterans Affairs. Home Improvements and Structural Alterations (HISA) benefits program: final rule. Fed Regist. 2014;79:71658-71663
- US Department of Veterans Affairs. Home Improvement and Structural Alterations (HISA): increase in the limit for home improvement and structural alterations (HISA)-VA: final regulations. Fed Regist. 1993;58:25565.
- US Department of Veterans Affairs. Eligibility for VA disability benefits. Updated April 25, 2025. Accessed April 1, 2026. https://www.va.gov/disability/eligibility
The Home Improvements and Structural Alterations Program: Overview and Future Implications
The Home Improvements and Structural Alterations Program: Overview and Future Implications
