User login
The Official Newspaper of the American Association for Thoracic Surgery
Hospitals Teaching CT Surgery Excel At Lung Resection
SAN FRANCISCO - Pulmonary resection outcomes vary with respect to the kind of hospital in which the procedure is performed, particularly whether it is a teaching hospital, according to Dr. Castigliano M. Bhamidipati, of the University of Virginia Medical School, Charlottesville.
"In comparison to other hospitals, including general surgery teaching hospitals, cardiothoracic surgery teaching hospitals have lower morbidity and mortality," Dr. Bhamidipati said at the AATS annual meeting.
He and his colleagues examined the results of pulmonary resections performed at cardiothoracic (CT) teaching, general surgery (GS) teaching, nonsurgical (NS) teaching, and nonteaching (NT) hospitals.
The researchers evaluated the discharge records of nearly 500,000 adults who underwent either pneumonectomy, segmentectomy, lobar resections, or nonanatomic resections in an all-payer inpatient database for the time period between 2003 and 2009, according to Dr. Bhamidipati.
The hospital's teaching status as used in the study was determined by a linkage to the Association of American Medical Colleges’ Graduate Medical Education Tracking System.
The researchers examined patient demographics, risk factors, and hospital characteristics, and used multiple logistic regression models to examine in-hospital mortality, occurrence of any complications, and failure to rescue (death following a complication).
The mean annual percent of pulmonary resection volume among hospitals was CT (16%), GS (17%), NS (28%), and NT (39%).
The average age of pulmonary resection recipients among hospitals was similar, as were their mean number of comorbidities. The CT hospitals treated the smallest number of Medicare patients and the highest number of patients with Medicaid, a significant difference, said Dr. Bhamidipati.
He reported that the unadjusted mortality for all procedures was significantly lowest at the CT hospitals (CT: 2.6%; GS: 2.8%; NS: 3.4%; NT 3.6%).
Similarly, any complication was also least likely to occur at a CT hospital (CT: 20.5%, GS: 23.5%, NS: 24.6%, NT: 24.9%), he added.
Unadjusted procedural complications were found to be similar across hospitals, although pulmonary complications were significantly less likely to occur at CT hospitals compared with the others, according to Dr. Bhamidipati.
Following case-mix adjustment, the risk of having any complication after segmentectomy or nonanatomic resection was found to be significantly lower at CT hospitals than at the GS hospitals, he said.
In addition, among the pneumonectomy recipients, CT teaching status independently and significantly reduced the adjusted odds ratio (AOR) of failure to rescue by more than 25% compared with NS (AOR 0.34 vs. AOR 0.62).
Similarly, for the pneumonectomy patients, performance of the surgery at CT centers significantly lowered the AOR of death by more than 30% compared with GS hospitals (AOR 0.33 vs. AOR 0.69).
"These results support using CT hospital teaching status as an independent prognosticator of outcomes in pulmonary resections," concluded Dr. Bhamidipati.
Dr. Bhamidipati reported that he and his colleagues had no relevant disclosures.
SAN FRANCISCO - Pulmonary resection outcomes vary with respect to the kind of hospital in which the procedure is performed, particularly whether it is a teaching hospital, according to Dr. Castigliano M. Bhamidipati, of the University of Virginia Medical School, Charlottesville.
"In comparison to other hospitals, including general surgery teaching hospitals, cardiothoracic surgery teaching hospitals have lower morbidity and mortality," Dr. Bhamidipati said at the AATS annual meeting.
He and his colleagues examined the results of pulmonary resections performed at cardiothoracic (CT) teaching, general surgery (GS) teaching, nonsurgical (NS) teaching, and nonteaching (NT) hospitals.
The researchers evaluated the discharge records of nearly 500,000 adults who underwent either pneumonectomy, segmentectomy, lobar resections, or nonanatomic resections in an all-payer inpatient database for the time period between 2003 and 2009, according to Dr. Bhamidipati.
The hospital's teaching status as used in the study was determined by a linkage to the Association of American Medical Colleges’ Graduate Medical Education Tracking System.
The researchers examined patient demographics, risk factors, and hospital characteristics, and used multiple logistic regression models to examine in-hospital mortality, occurrence of any complications, and failure to rescue (death following a complication).
The mean annual percent of pulmonary resection volume among hospitals was CT (16%), GS (17%), NS (28%), and NT (39%).
The average age of pulmonary resection recipients among hospitals was similar, as were their mean number of comorbidities. The CT hospitals treated the smallest number of Medicare patients and the highest number of patients with Medicaid, a significant difference, said Dr. Bhamidipati.
He reported that the unadjusted mortality for all procedures was significantly lowest at the CT hospitals (CT: 2.6%; GS: 2.8%; NS: 3.4%; NT 3.6%).
Similarly, any complication was also least likely to occur at a CT hospital (CT: 20.5%, GS: 23.5%, NS: 24.6%, NT: 24.9%), he added.
Unadjusted procedural complications were found to be similar across hospitals, although pulmonary complications were significantly less likely to occur at CT hospitals compared with the others, according to Dr. Bhamidipati.
Following case-mix adjustment, the risk of having any complication after segmentectomy or nonanatomic resection was found to be significantly lower at CT hospitals than at the GS hospitals, he said.
In addition, among the pneumonectomy recipients, CT teaching status independently and significantly reduced the adjusted odds ratio (AOR) of failure to rescue by more than 25% compared with NS (AOR 0.34 vs. AOR 0.62).
Similarly, for the pneumonectomy patients, performance of the surgery at CT centers significantly lowered the AOR of death by more than 30% compared with GS hospitals (AOR 0.33 vs. AOR 0.69).
"These results support using CT hospital teaching status as an independent prognosticator of outcomes in pulmonary resections," concluded Dr. Bhamidipati.
Dr. Bhamidipati reported that he and his colleagues had no relevant disclosures.
SAN FRANCISCO - Pulmonary resection outcomes vary with respect to the kind of hospital in which the procedure is performed, particularly whether it is a teaching hospital, according to Dr. Castigliano M. Bhamidipati, of the University of Virginia Medical School, Charlottesville.
"In comparison to other hospitals, including general surgery teaching hospitals, cardiothoracic surgery teaching hospitals have lower morbidity and mortality," Dr. Bhamidipati said at the AATS annual meeting.
He and his colleagues examined the results of pulmonary resections performed at cardiothoracic (CT) teaching, general surgery (GS) teaching, nonsurgical (NS) teaching, and nonteaching (NT) hospitals.
The researchers evaluated the discharge records of nearly 500,000 adults who underwent either pneumonectomy, segmentectomy, lobar resections, or nonanatomic resections in an all-payer inpatient database for the time period between 2003 and 2009, according to Dr. Bhamidipati.
The hospital's teaching status as used in the study was determined by a linkage to the Association of American Medical Colleges’ Graduate Medical Education Tracking System.
The researchers examined patient demographics, risk factors, and hospital characteristics, and used multiple logistic regression models to examine in-hospital mortality, occurrence of any complications, and failure to rescue (death following a complication).
The mean annual percent of pulmonary resection volume among hospitals was CT (16%), GS (17%), NS (28%), and NT (39%).
The average age of pulmonary resection recipients among hospitals was similar, as were their mean number of comorbidities. The CT hospitals treated the smallest number of Medicare patients and the highest number of patients with Medicaid, a significant difference, said Dr. Bhamidipati.
He reported that the unadjusted mortality for all procedures was significantly lowest at the CT hospitals (CT: 2.6%; GS: 2.8%; NS: 3.4%; NT 3.6%).
Similarly, any complication was also least likely to occur at a CT hospital (CT: 20.5%, GS: 23.5%, NS: 24.6%, NT: 24.9%), he added.
Unadjusted procedural complications were found to be similar across hospitals, although pulmonary complications were significantly less likely to occur at CT hospitals compared with the others, according to Dr. Bhamidipati.
Following case-mix adjustment, the risk of having any complication after segmentectomy or nonanatomic resection was found to be significantly lower at CT hospitals than at the GS hospitals, he said.
In addition, among the pneumonectomy recipients, CT teaching status independently and significantly reduced the adjusted odds ratio (AOR) of failure to rescue by more than 25% compared with NS (AOR 0.34 vs. AOR 0.62).
Similarly, for the pneumonectomy patients, performance of the surgery at CT centers significantly lowered the AOR of death by more than 30% compared with GS hospitals (AOR 0.33 vs. AOR 0.69).
"These results support using CT hospital teaching status as an independent prognosticator of outcomes in pulmonary resections," concluded Dr. Bhamidipati.
Dr. Bhamidipati reported that he and his colleagues had no relevant disclosures.
Race, Sex Affect Congenital Heart Surgery Outcomes
FT. LAUDERDALE, FLA. – Sex and race appear to play a role in outcomes following congenital heart surgery in children and adolescents, according to a new analysis of data from almost 21,000 patients.
Black patients had significantly greater rates of mortality and complications and a significantly longer length of postoperative stay than other races, while female patients had a significantly shorter length of stay than males, Dr. Daniel J. DiBardino reported at the annual meeting of the Society of Thoracic Surgeons.
"The analysis of demographic and clinical data from nearly 21,000 patients in the congenital heart surgery database revealed important associations between gender, race, and outcome," said Dr. DiBardino, who is a cardiac surgeon at the Blair E. Batson Children’s Hospital in Jackson, Miss.
Dr. DiBardino’s study was chosen as a 2011 Richard E. Clark Paper by the Society of Thoracic Surgeons.
The researchers used data from the Society of Thoracic Surgeons Congenital Heart Surgery Database (STS-CHSD). Patients were included in the analysis if they were less than 18 years of age and had undergone cardiac surgery between 2007 and 2009.
Exclusion criteria included centers with more than 15% of data missing for key variables and centers with very small samples (less than five cases).
Data collection included demographics (age, sex, weight, and race) and preoperative data (noncardiac/genetic abnormalities and STS-defined risk factors). Race was classified as white, black, Hispanic, and other.
Operations were classified by STAT Mortality category, which is "a complexity stratification tool based on empiric data from 80,000 cases in STS and EACTS (European Association for Cardio-Thoracic Surgery) databases," said Dr. DiBardino.
The researchers looked at hospital mortality, postoperative length of stay, and complications. Multivariable analyses included dichotomous variables (mortality, complications) and a continuous variable (postoperative length of stay). Models were adjusted for age, weight, noncardiac/genetic abnormalities, any other STS preoperative risk factor, and STAT Mortality category.
In all, 20,399 patients were included from 49 centers. Of these, 54% were male. In terms of race, 55% were white, 17% were black, 16% were Hispanic, and 12% were other.
Based on unadjusted outcomes, there were no differences between the sexes for in-hospital mortality or complications. However, females had significantly shorter postoperative stays. In terms of race, white patients had significantly lower mortality, shorter length of stay, and fewer complications than any of the other racial groups.
In the adjusted multivariate analysis, there was no difference for mortality between the sexes. However, black patients had a significantly greater mortality risk with an odds ratio of 1.67.
Females did have a significantly shorter mean length of stay – 0.8 fewer days. In terms of race, black patients had a significantly longer mean length of stay by 2.4 hospital days, compared with white patients. Hispanic patients also had a significantly longer mean length of stay by almost 1 hospital day.
There was no difference between the sexes in terms of the occurrence of complications. In terms of race, "black patients experienced significantly more complications than other races with an odds ratio of 1.15," according to Dr. DiBardino.
The study is unique with the respect to the use of multivariable models. The researchers measured the association of sex and race with outcomes within each center and then combined the results, in order to mitigate the potential center effects.
"Our results cannot be explained by the possibility that patients of certain races might be disproportionately treated at centers with poorer outcomes in general."
The evaluation of complex relationships between clinical variables and socioeconomic and other factors affecting health care remains a significant challenge.
Since some pertinent socioeconomic data are not collected in the STS-CHSD, an analysis of a linked data set, which capitalizes on the strengths of both the CHSD and those of an administrative claims data set may be the next logical step, said Dr. DiBardino.
Dr. DiBardino and his coinvestigators reported that they have no relevant disclosures.
FT. LAUDERDALE, FLA. – Sex and race appear to play a role in outcomes following congenital heart surgery in children and adolescents, according to a new analysis of data from almost 21,000 patients.
Black patients had significantly greater rates of mortality and complications and a significantly longer length of postoperative stay than other races, while female patients had a significantly shorter length of stay than males, Dr. Daniel J. DiBardino reported at the annual meeting of the Society of Thoracic Surgeons.
"The analysis of demographic and clinical data from nearly 21,000 patients in the congenital heart surgery database revealed important associations between gender, race, and outcome," said Dr. DiBardino, who is a cardiac surgeon at the Blair E. Batson Children’s Hospital in Jackson, Miss.
Dr. DiBardino’s study was chosen as a 2011 Richard E. Clark Paper by the Society of Thoracic Surgeons.
The researchers used data from the Society of Thoracic Surgeons Congenital Heart Surgery Database (STS-CHSD). Patients were included in the analysis if they were less than 18 years of age and had undergone cardiac surgery between 2007 and 2009.
Exclusion criteria included centers with more than 15% of data missing for key variables and centers with very small samples (less than five cases).
Data collection included demographics (age, sex, weight, and race) and preoperative data (noncardiac/genetic abnormalities and STS-defined risk factors). Race was classified as white, black, Hispanic, and other.
Operations were classified by STAT Mortality category, which is "a complexity stratification tool based on empiric data from 80,000 cases in STS and EACTS (European Association for Cardio-Thoracic Surgery) databases," said Dr. DiBardino.
The researchers looked at hospital mortality, postoperative length of stay, and complications. Multivariable analyses included dichotomous variables (mortality, complications) and a continuous variable (postoperative length of stay). Models were adjusted for age, weight, noncardiac/genetic abnormalities, any other STS preoperative risk factor, and STAT Mortality category.
In all, 20,399 patients were included from 49 centers. Of these, 54% were male. In terms of race, 55% were white, 17% were black, 16% were Hispanic, and 12% were other.
Based on unadjusted outcomes, there were no differences between the sexes for in-hospital mortality or complications. However, females had significantly shorter postoperative stays. In terms of race, white patients had significantly lower mortality, shorter length of stay, and fewer complications than any of the other racial groups.
In the adjusted multivariate analysis, there was no difference for mortality between the sexes. However, black patients had a significantly greater mortality risk with an odds ratio of 1.67.
Females did have a significantly shorter mean length of stay – 0.8 fewer days. In terms of race, black patients had a significantly longer mean length of stay by 2.4 hospital days, compared with white patients. Hispanic patients also had a significantly longer mean length of stay by almost 1 hospital day.
There was no difference between the sexes in terms of the occurrence of complications. In terms of race, "black patients experienced significantly more complications than other races with an odds ratio of 1.15," according to Dr. DiBardino.
The study is unique with the respect to the use of multivariable models. The researchers measured the association of sex and race with outcomes within each center and then combined the results, in order to mitigate the potential center effects.
"Our results cannot be explained by the possibility that patients of certain races might be disproportionately treated at centers with poorer outcomes in general."
The evaluation of complex relationships between clinical variables and socioeconomic and other factors affecting health care remains a significant challenge.
Since some pertinent socioeconomic data are not collected in the STS-CHSD, an analysis of a linked data set, which capitalizes on the strengths of both the CHSD and those of an administrative claims data set may be the next logical step, said Dr. DiBardino.
Dr. DiBardino and his coinvestigators reported that they have no relevant disclosures.
FT. LAUDERDALE, FLA. – Sex and race appear to play a role in outcomes following congenital heart surgery in children and adolescents, according to a new analysis of data from almost 21,000 patients.
Black patients had significantly greater rates of mortality and complications and a significantly longer length of postoperative stay than other races, while female patients had a significantly shorter length of stay than males, Dr. Daniel J. DiBardino reported at the annual meeting of the Society of Thoracic Surgeons.
"The analysis of demographic and clinical data from nearly 21,000 patients in the congenital heart surgery database revealed important associations between gender, race, and outcome," said Dr. DiBardino, who is a cardiac surgeon at the Blair E. Batson Children’s Hospital in Jackson, Miss.
Dr. DiBardino’s study was chosen as a 2011 Richard E. Clark Paper by the Society of Thoracic Surgeons.
The researchers used data from the Society of Thoracic Surgeons Congenital Heart Surgery Database (STS-CHSD). Patients were included in the analysis if they were less than 18 years of age and had undergone cardiac surgery between 2007 and 2009.
Exclusion criteria included centers with more than 15% of data missing for key variables and centers with very small samples (less than five cases).
Data collection included demographics (age, sex, weight, and race) and preoperative data (noncardiac/genetic abnormalities and STS-defined risk factors). Race was classified as white, black, Hispanic, and other.
Operations were classified by STAT Mortality category, which is "a complexity stratification tool based on empiric data from 80,000 cases in STS and EACTS (European Association for Cardio-Thoracic Surgery) databases," said Dr. DiBardino.
The researchers looked at hospital mortality, postoperative length of stay, and complications. Multivariable analyses included dichotomous variables (mortality, complications) and a continuous variable (postoperative length of stay). Models were adjusted for age, weight, noncardiac/genetic abnormalities, any other STS preoperative risk factor, and STAT Mortality category.
In all, 20,399 patients were included from 49 centers. Of these, 54% were male. In terms of race, 55% were white, 17% were black, 16% were Hispanic, and 12% were other.
Based on unadjusted outcomes, there were no differences between the sexes for in-hospital mortality or complications. However, females had significantly shorter postoperative stays. In terms of race, white patients had significantly lower mortality, shorter length of stay, and fewer complications than any of the other racial groups.
In the adjusted multivariate analysis, there was no difference for mortality between the sexes. However, black patients had a significantly greater mortality risk with an odds ratio of 1.67.
Females did have a significantly shorter mean length of stay – 0.8 fewer days. In terms of race, black patients had a significantly longer mean length of stay by 2.4 hospital days, compared with white patients. Hispanic patients also had a significantly longer mean length of stay by almost 1 hospital day.
There was no difference between the sexes in terms of the occurrence of complications. In terms of race, "black patients experienced significantly more complications than other races with an odds ratio of 1.15," according to Dr. DiBardino.
The study is unique with the respect to the use of multivariable models. The researchers measured the association of sex and race with outcomes within each center and then combined the results, in order to mitigate the potential center effects.
"Our results cannot be explained by the possibility that patients of certain races might be disproportionately treated at centers with poorer outcomes in general."
The evaluation of complex relationships between clinical variables and socioeconomic and other factors affecting health care remains a significant challenge.
Since some pertinent socioeconomic data are not collected in the STS-CHSD, an analysis of a linked data set, which capitalizes on the strengths of both the CHSD and those of an administrative claims data set may be the next logical step, said Dr. DiBardino.
Dr. DiBardino and his coinvestigators reported that they have no relevant disclosures.
Major Finding: In adjusted multivariate analyses, black patients had a significantly greater mortality risk (67%), a significantly longer mean length of stay by 2.4 hospital days, and a significantly greater risk of complications (15%). Female patients had a significantly shorter mean length of stay – 0.8 fewer days.
Data Source: The retrospective review included 20,399 patients younger than 18 years from 49 centers, collected in the Society of Thoracic Surgeons Congenital Heart Surgery Database.
Disclosures: Dr. DiBardino and his coinvestigators reported that they have no relevant disclosures.
CMS Releases TAVR Coverage Decision
Medicare will cover transcatheter aortic valve replacement, or TAVR, under certain conditions, including the presence of a heart team during the procedure and evaluation of the patient by two cardiac surgeons, according to an official document released on May 1.
The Centers for Medicare and Medicaid Services’ (CMS) final national coverage decision for TAVR arrives as planned, nearly 3 months after the agency released its coverage proposal.
"This decision is particularly important as it highlights cooperative efforts among CMS, the Food and Drug Administration (FDA), the Agency for Healthcare Research and Quality, medical societies, and the medical device industry," said CMS Acting Administrator Marilyn Tavenner in a statement.
Because TAVR is relatively new, the final decision uses "coverage with evidence development," meaning certain criteria must be met as a condition of coverage, according to the statement.
The criteria outlined by CMS include:
• Two cardiac surgeons independently examine the patient face-to-face and evaluate the patient’s suitability for open valve replacement surgery.
• Before and after the surgery, the patient is under the care of a heart team, which is "a cohesive, multidisciplinary, team of medical professionals. The heart team concept embodies collaboration and dedication across medical specialties to offer optimal patient-centered care," according to the decision document. The document breaks down these criteria by centers with or without previous TAVR clinical trial experience.
• The heart team’s interventional cardiologist(s) and cardiac surgeon(s) must work together on the intraoperative technical aspects of TAVR.
• The heart team and hospital are also participating in a prospective, national, audited registry.
The agency will cover the procedure in clinical trials that follow criteria listed in the decision memo.
Meanwhile, Medicare patients whose comorbidities would prevent them from benefiting from the procedure will not be covered.
CMS also responded to comments, making some changes.
For instance, 23 commenters had disagreed with the requirement that unlabeled uses of TAVR be covered in clinical studies that have superiority designs. Eight had requested that CMS remove the requirement, according to CMS’s final decision memo.
Among those commenters was Edwards Lifesciences, the maker of the Sapien valve.
"CMS’s proposed requirement limiting coverage for unlabeled uses to ‘superiority trials’ undermines the agency’s efforts to promote continued U.S.-based clinical investigations in Medicare beneficiaries aimed at better understanding key determinants of health and quality of life outcomes," according to Edwards’ comments.
"Noninferiority and other clinical trial designs play an important role in the advancement of medical technology," the company added, saying that if the proposed conditions aren’t revised, important, yet relatively small, patient populations may not be able to receive treatment.
Removing the requirement, CMS explained in its final decision memo that "while we believe superiority trial designs provide important advantages that are not completely addressed by non-inferiority design, we recognize that non-inferiority trials have a place in the conduct of medical device regulatory trials.
"Therefore, we believe a broad non-coverage of non-inferiority trials may have unintended consequences for certain important studies."
CMS opened the national coverage determination analysis in September 2011, before the Edwards Lifesciences Sapien valve was approved, in response to a request from the Society of Thoracic Surgeons and the American College of Cardiology to establish the criteria for national Medicare coverage of the minimally invasive valve procedure.
In the United States, the first valve to be used for TAVR (the Edwards Lifesciences Sapien valve) was approved in November 2011 for use in inoperable patients with severe aortic stenosis.
The FDA’s Circulatory System Devices Panel will be meeting in order to evaluate the Sapien valve’s performance in severe aortic stenosis patients who are at high surgical risk for use in this application on June 13. Medtronic’s CoreValve is also in being studied in large U.S. trials.
Medicare will cover transcatheter aortic valve replacement, or TAVR, under certain conditions, including the presence of a heart team during the procedure and evaluation of the patient by two cardiac surgeons, according to an official document released on May 1.
The Centers for Medicare and Medicaid Services’ (CMS) final national coverage decision for TAVR arrives as planned, nearly 3 months after the agency released its coverage proposal.
"This decision is particularly important as it highlights cooperative efforts among CMS, the Food and Drug Administration (FDA), the Agency for Healthcare Research and Quality, medical societies, and the medical device industry," said CMS Acting Administrator Marilyn Tavenner in a statement.
Because TAVR is relatively new, the final decision uses "coverage with evidence development," meaning certain criteria must be met as a condition of coverage, according to the statement.
The criteria outlined by CMS include:
• Two cardiac surgeons independently examine the patient face-to-face and evaluate the patient’s suitability for open valve replacement surgery.
• Before and after the surgery, the patient is under the care of a heart team, which is "a cohesive, multidisciplinary, team of medical professionals. The heart team concept embodies collaboration and dedication across medical specialties to offer optimal patient-centered care," according to the decision document. The document breaks down these criteria by centers with or without previous TAVR clinical trial experience.
• The heart team’s interventional cardiologist(s) and cardiac surgeon(s) must work together on the intraoperative technical aspects of TAVR.
• The heart team and hospital are also participating in a prospective, national, audited registry.
The agency will cover the procedure in clinical trials that follow criteria listed in the decision memo.
Meanwhile, Medicare patients whose comorbidities would prevent them from benefiting from the procedure will not be covered.
CMS also responded to comments, making some changes.
For instance, 23 commenters had disagreed with the requirement that unlabeled uses of TAVR be covered in clinical studies that have superiority designs. Eight had requested that CMS remove the requirement, according to CMS’s final decision memo.
Among those commenters was Edwards Lifesciences, the maker of the Sapien valve.
"CMS’s proposed requirement limiting coverage for unlabeled uses to ‘superiority trials’ undermines the agency’s efforts to promote continued U.S.-based clinical investigations in Medicare beneficiaries aimed at better understanding key determinants of health and quality of life outcomes," according to Edwards’ comments.
"Noninferiority and other clinical trial designs play an important role in the advancement of medical technology," the company added, saying that if the proposed conditions aren’t revised, important, yet relatively small, patient populations may not be able to receive treatment.
Removing the requirement, CMS explained in its final decision memo that "while we believe superiority trial designs provide important advantages that are not completely addressed by non-inferiority design, we recognize that non-inferiority trials have a place in the conduct of medical device regulatory trials.
"Therefore, we believe a broad non-coverage of non-inferiority trials may have unintended consequences for certain important studies."
CMS opened the national coverage determination analysis in September 2011, before the Edwards Lifesciences Sapien valve was approved, in response to a request from the Society of Thoracic Surgeons and the American College of Cardiology to establish the criteria for national Medicare coverage of the minimally invasive valve procedure.
In the United States, the first valve to be used for TAVR (the Edwards Lifesciences Sapien valve) was approved in November 2011 for use in inoperable patients with severe aortic stenosis.
The FDA’s Circulatory System Devices Panel will be meeting in order to evaluate the Sapien valve’s performance in severe aortic stenosis patients who are at high surgical risk for use in this application on June 13. Medtronic’s CoreValve is also in being studied in large U.S. trials.
Medicare will cover transcatheter aortic valve replacement, or TAVR, under certain conditions, including the presence of a heart team during the procedure and evaluation of the patient by two cardiac surgeons, according to an official document released on May 1.
The Centers for Medicare and Medicaid Services’ (CMS) final national coverage decision for TAVR arrives as planned, nearly 3 months after the agency released its coverage proposal.
"This decision is particularly important as it highlights cooperative efforts among CMS, the Food and Drug Administration (FDA), the Agency for Healthcare Research and Quality, medical societies, and the medical device industry," said CMS Acting Administrator Marilyn Tavenner in a statement.
Because TAVR is relatively new, the final decision uses "coverage with evidence development," meaning certain criteria must be met as a condition of coverage, according to the statement.
The criteria outlined by CMS include:
• Two cardiac surgeons independently examine the patient face-to-face and evaluate the patient’s suitability for open valve replacement surgery.
• Before and after the surgery, the patient is under the care of a heart team, which is "a cohesive, multidisciplinary, team of medical professionals. The heart team concept embodies collaboration and dedication across medical specialties to offer optimal patient-centered care," according to the decision document. The document breaks down these criteria by centers with or without previous TAVR clinical trial experience.
• The heart team’s interventional cardiologist(s) and cardiac surgeon(s) must work together on the intraoperative technical aspects of TAVR.
• The heart team and hospital are also participating in a prospective, national, audited registry.
The agency will cover the procedure in clinical trials that follow criteria listed in the decision memo.
Meanwhile, Medicare patients whose comorbidities would prevent them from benefiting from the procedure will not be covered.
CMS also responded to comments, making some changes.
For instance, 23 commenters had disagreed with the requirement that unlabeled uses of TAVR be covered in clinical studies that have superiority designs. Eight had requested that CMS remove the requirement, according to CMS’s final decision memo.
Among those commenters was Edwards Lifesciences, the maker of the Sapien valve.
"CMS’s proposed requirement limiting coverage for unlabeled uses to ‘superiority trials’ undermines the agency’s efforts to promote continued U.S.-based clinical investigations in Medicare beneficiaries aimed at better understanding key determinants of health and quality of life outcomes," according to Edwards’ comments.
"Noninferiority and other clinical trial designs play an important role in the advancement of medical technology," the company added, saying that if the proposed conditions aren’t revised, important, yet relatively small, patient populations may not be able to receive treatment.
Removing the requirement, CMS explained in its final decision memo that "while we believe superiority trial designs provide important advantages that are not completely addressed by non-inferiority design, we recognize that non-inferiority trials have a place in the conduct of medical device regulatory trials.
"Therefore, we believe a broad non-coverage of non-inferiority trials may have unintended consequences for certain important studies."
CMS opened the national coverage determination analysis in September 2011, before the Edwards Lifesciences Sapien valve was approved, in response to a request from the Society of Thoracic Surgeons and the American College of Cardiology to establish the criteria for national Medicare coverage of the minimally invasive valve procedure.
In the United States, the first valve to be used for TAVR (the Edwards Lifesciences Sapien valve) was approved in November 2011 for use in inoperable patients with severe aortic stenosis.
The FDA’s Circulatory System Devices Panel will be meeting in order to evaluate the Sapien valve’s performance in severe aortic stenosis patients who are at high surgical risk for use in this application on June 13. Medtronic’s CoreValve is also in being studied in large U.S. trials.
Hospitals Teaching CT Surgery Excel At Lung Resection
SAN FRANCISCO - Pulmonary resection outcomes vary with respect to the kind of hospital in which the procedure is performed, particularly whether it is a teaching hospital, according to Dr. Castigliano M. Bhamidipati, of the University of Virginia Medical School, Charlottesville.
"In comparison to other hospitals, including general surgery teaching hospitals, cardiothoracic surgery teaching hospitals have lower morbidity and mortality," Dr. Bhamidipati said at the AATS annual meeting.
He and his colleagues examined the results of pulmonary resections performed at cardiothoracic (CT) teaching, general surgery (GS) teaching, nonsurgical (NS) teaching, and nonteaching (NT) hospitals.
The researchers evaluated the discharge records of nearly 500,000 adults who underwent either pneumonectomy, segmentectomy, lobar resections, or nonanatomic resections in an all-payer inpatient database for the time period between 2003 and 2009, according to Dr. Bhamidipati.
The hospital's teaching status as used in the study was determined by a linkage to the Association of American Medical Colleges’ Graduate Medical Education Tracking System.
The researchers examined patient demographics, risk factors, and hospital characteristics, and used multiple logistic regression models to examine in-hospital mortality, occurrence of any complications, and failure to rescue (death following a complication).
The mean annual percent of pulmonary resection volume among hospitals was CT (16%), GS (17%), NS (28%), and NT (39%).
The average age of pulmonary resection recipients among hospitals was similar, as were their mean number of comorbidities. The CT hospitals treated the smallest number of Medicare patients and the highest number of patients with Medicaid, a significant difference, said Dr. Bhamidipati.
He reported that the unadjusted mortality for all procedures was significantly lowest at the CT hospitals (CT: 2.6%; GS: 2.8%; NS: 3.4%; NT 3.6%).
Similarly, any complication was also least likely to occur at a CT hospital (CT: 20.5%, GS: 23.5%, NS: 24.6%, NT: 24.9%), he added.
Unadjusted procedural complications were found to be similar across hospitals, although pulmonary complications were significantly less likely to occur at CT hospitals compared with the others, according to Dr. Bhamidipati.
Following case-mix adjustment, the risk of having any complication after segmentectomy or nonanatomic resection was found to be significantly lower at CT hospitals than at the GS hospitals, he said.
In addition, among the pneumonectomy recipients, CT teaching status independently and significantly reduced the adjusted odds ratio (AOR) of failure to rescue by more than 25% compared with NS (AOR 0.34 vs. AOR 0.62).
Similarly, for the pneumonectomy patients, performance of the surgery at CT centers significantly lowered the AOR of death by more than 30% compared with GS hospitals (AOR 0.33 vs. AOR 0.69).
"These results support using CT hospital teaching status as an independent prognosticator of outcomes in pulmonary resections," concluded Dr. Bhamidipati.
Dr. Bhamidipati reported that he and his colleagues had no relevant disclosures.
SAN FRANCISCO - Pulmonary resection outcomes vary with respect to the kind of hospital in which the procedure is performed, particularly whether it is a teaching hospital, according to Dr. Castigliano M. Bhamidipati, of the University of Virginia Medical School, Charlottesville.
"In comparison to other hospitals, including general surgery teaching hospitals, cardiothoracic surgery teaching hospitals have lower morbidity and mortality," Dr. Bhamidipati said at the AATS annual meeting.
He and his colleagues examined the results of pulmonary resections performed at cardiothoracic (CT) teaching, general surgery (GS) teaching, nonsurgical (NS) teaching, and nonteaching (NT) hospitals.
The researchers evaluated the discharge records of nearly 500,000 adults who underwent either pneumonectomy, segmentectomy, lobar resections, or nonanatomic resections in an all-payer inpatient database for the time period between 2003 and 2009, according to Dr. Bhamidipati.
The hospital's teaching status as used in the study was determined by a linkage to the Association of American Medical Colleges’ Graduate Medical Education Tracking System.
The researchers examined patient demographics, risk factors, and hospital characteristics, and used multiple logistic regression models to examine in-hospital mortality, occurrence of any complications, and failure to rescue (death following a complication).
The mean annual percent of pulmonary resection volume among hospitals was CT (16%), GS (17%), NS (28%), and NT (39%).
The average age of pulmonary resection recipients among hospitals was similar, as were their mean number of comorbidities. The CT hospitals treated the smallest number of Medicare patients and the highest number of patients with Medicaid, a significant difference, said Dr. Bhamidipati.
He reported that the unadjusted mortality for all procedures was significantly lowest at the CT hospitals (CT: 2.6%; GS: 2.8%; NS: 3.4%; NT 3.6%).
Similarly, any complication was also least likely to occur at a CT hospital (CT: 20.5%, GS: 23.5%, NS: 24.6%, NT: 24.9%), he added.
Unadjusted procedural complications were found to be similar across hospitals, although pulmonary complications were significantly less likely to occur at CT hospitals compared with the others, according to Dr. Bhamidipati.
Following case-mix adjustment, the risk of having any complication after segmentectomy or nonanatomic resection was found to be significantly lower at CT hospitals than at the GS hospitals, he said.
In addition, among the pneumonectomy recipients, CT teaching status independently and significantly reduced the adjusted odds ratio (AOR) of failure to rescue by more than 25% compared with NS (AOR 0.34 vs. AOR 0.62).
Similarly, for the pneumonectomy patients, performance of the surgery at CT centers significantly lowered the AOR of death by more than 30% compared with GS hospitals (AOR 0.33 vs. AOR 0.69).
"These results support using CT hospital teaching status as an independent prognosticator of outcomes in pulmonary resections," concluded Dr. Bhamidipati.
Dr. Bhamidipati reported that he and his colleagues had no relevant disclosures.
SAN FRANCISCO - Pulmonary resection outcomes vary with respect to the kind of hospital in which the procedure is performed, particularly whether it is a teaching hospital, according to Dr. Castigliano M. Bhamidipati, of the University of Virginia Medical School, Charlottesville.
"In comparison to other hospitals, including general surgery teaching hospitals, cardiothoracic surgery teaching hospitals have lower morbidity and mortality," Dr. Bhamidipati said at the AATS annual meeting.
He and his colleagues examined the results of pulmonary resections performed at cardiothoracic (CT) teaching, general surgery (GS) teaching, nonsurgical (NS) teaching, and nonteaching (NT) hospitals.
The researchers evaluated the discharge records of nearly 500,000 adults who underwent either pneumonectomy, segmentectomy, lobar resections, or nonanatomic resections in an all-payer inpatient database for the time period between 2003 and 2009, according to Dr. Bhamidipati.
The hospital's teaching status as used in the study was determined by a linkage to the Association of American Medical Colleges’ Graduate Medical Education Tracking System.
The researchers examined patient demographics, risk factors, and hospital characteristics, and used multiple logistic regression models to examine in-hospital mortality, occurrence of any complications, and failure to rescue (death following a complication).
The mean annual percent of pulmonary resection volume among hospitals was CT (16%), GS (17%), NS (28%), and NT (39%).
The average age of pulmonary resection recipients among hospitals was similar, as were their mean number of comorbidities. The CT hospitals treated the smallest number of Medicare patients and the highest number of patients with Medicaid, a significant difference, said Dr. Bhamidipati.
He reported that the unadjusted mortality for all procedures was significantly lowest at the CT hospitals (CT: 2.6%; GS: 2.8%; NS: 3.4%; NT 3.6%).
Similarly, any complication was also least likely to occur at a CT hospital (CT: 20.5%, GS: 23.5%, NS: 24.6%, NT: 24.9%), he added.
Unadjusted procedural complications were found to be similar across hospitals, although pulmonary complications were significantly less likely to occur at CT hospitals compared with the others, according to Dr. Bhamidipati.
Following case-mix adjustment, the risk of having any complication after segmentectomy or nonanatomic resection was found to be significantly lower at CT hospitals than at the GS hospitals, he said.
In addition, among the pneumonectomy recipients, CT teaching status independently and significantly reduced the adjusted odds ratio (AOR) of failure to rescue by more than 25% compared with NS (AOR 0.34 vs. AOR 0.62).
Similarly, for the pneumonectomy patients, performance of the surgery at CT centers significantly lowered the AOR of death by more than 30% compared with GS hospitals (AOR 0.33 vs. AOR 0.69).
"These results support using CT hospital teaching status as an independent prognosticator of outcomes in pulmonary resections," concluded Dr. Bhamidipati.
Dr. Bhamidipati reported that he and his colleagues had no relevant disclosures.
Race, Sex Affect Congenital Heart Surgery Outcomes
FT. LAUDERDALE, FLA. – Sex and race appear to play a role in outcomes following congenital heart surgery in children and adolescents, according to a new analysis of data from almost 21,000 patients.
Black patients had significantly greater rates of mortality and complications and a significantly longer length of postoperative stay than other races, while female patients had a significantly shorter length of stay than males, Dr. Daniel J. DiBardino reported at the annual meeting of the Society of Thoracic Surgeons.
"The analysis of demographic and clinical data from nearly 21,000 patients in the congenital heart surgery database revealed important associations between gender, race, and outcome," said Dr. DiBardino, who is a cardiac surgeon at the Blair E. Batson Children’s Hospital in Jackson, Miss.
Dr. DiBardino’s study was chosen as a 2011 Richard E. Clark Paper by the Society of Thoracic Surgeons.
The researchers used data from the Society of Thoracic Surgeons Congenital Heart Surgery Database (STS-CHSD). Patients were included in the analysis if they were less than 18 years of age and had undergone cardiac surgery between 2007 and 2009.
Exclusion criteria included centers with more than 15% of data missing for key variables and centers with very small samples (less than five cases).
Data collection included demographics (age, sex, weight, and race) and preoperative data (noncardiac/genetic abnormalities and STS-defined risk factors). Race was classified as white, black, Hispanic, and other.
Operations were classified by STAT Mortality category, which is "a complexity stratification tool based on empiric data from 80,000 cases in STS and EACTS (European Association for Cardio-Thoracic Surgery) databases," said Dr. DiBardino.
The researchers looked at hospital mortality, postoperative length of stay, and complications. Multivariable analyses included dichotomous variables (mortality, complications) and a continuous variable (postoperative length of stay). Models were adjusted for age, weight, noncardiac/genetic abnormalities, any other STS preoperative risk factor, and STAT Mortality category.
In all, 20,399 patients were included from 49 centers. Of these, 54% were male. In terms of race, 55% were white, 17% were black, 16% were Hispanic, and 12% were other.
Based on unadjusted outcomes, there were no differences between the sexes for in-hospital mortality or complications. However, females had significantly shorter postoperative stays. In terms of race, white patients had significantly lower mortality, shorter length of stay, and fewer complications than any of the other racial groups.
In the adjusted multivariate analysis, there was no difference for mortality between the sexes. However, black patients had a significantly greater mortality risk with an odds ratio of 1.67.
Females did have a significantly shorter mean length of stay – 0.8 fewer days. In terms of race, black patients had a significantly longer mean length of stay by 2.4 hospital days, compared with white patients. Hispanic patients also had a significantly longer mean length of stay by almost 1 hospital day.
There was no difference between the sexes in terms of the occurrence of complications. In terms of race, "black patients experienced significantly more complications than other races with an odds ratio of 1.15," according to Dr. DiBardino.
The study is unique with the respect to the use of multivariable models. The researchers measured the association of sex and race with outcomes within each center and then combined the results, in order to mitigate the potential center effects.
"Our results cannot be explained by the possibility that patients of certain races might be disproportionately treated at centers with poorer outcomes in general."
The evaluation of complex relationships between clinical variables and socioeconomic and other factors affecting health care remains a significant challenge.
Since some pertinent socioeconomic data are not collected in the STS-CHSD, an analysis of a linked data set, which capitalizes on the strengths of both the CHSD and those of an administrative claims data set may be the next logical step, said Dr. DiBardino.
Dr. DiBardino and his coinvestigators reported that they have no relevant disclosures.
FT. LAUDERDALE, FLA. – Sex and race appear to play a role in outcomes following congenital heart surgery in children and adolescents, according to a new analysis of data from almost 21,000 patients.
Black patients had significantly greater rates of mortality and complications and a significantly longer length of postoperative stay than other races, while female patients had a significantly shorter length of stay than males, Dr. Daniel J. DiBardino reported at the annual meeting of the Society of Thoracic Surgeons.
"The analysis of demographic and clinical data from nearly 21,000 patients in the congenital heart surgery database revealed important associations between gender, race, and outcome," said Dr. DiBardino, who is a cardiac surgeon at the Blair E. Batson Children’s Hospital in Jackson, Miss.
Dr. DiBardino’s study was chosen as a 2011 Richard E. Clark Paper by the Society of Thoracic Surgeons.
The researchers used data from the Society of Thoracic Surgeons Congenital Heart Surgery Database (STS-CHSD). Patients were included in the analysis if they were less than 18 years of age and had undergone cardiac surgery between 2007 and 2009.
Exclusion criteria included centers with more than 15% of data missing for key variables and centers with very small samples (less than five cases).
Data collection included demographics (age, sex, weight, and race) and preoperative data (noncardiac/genetic abnormalities and STS-defined risk factors). Race was classified as white, black, Hispanic, and other.
Operations were classified by STAT Mortality category, which is "a complexity stratification tool based on empiric data from 80,000 cases in STS and EACTS (European Association for Cardio-Thoracic Surgery) databases," said Dr. DiBardino.
The researchers looked at hospital mortality, postoperative length of stay, and complications. Multivariable analyses included dichotomous variables (mortality, complications) and a continuous variable (postoperative length of stay). Models were adjusted for age, weight, noncardiac/genetic abnormalities, any other STS preoperative risk factor, and STAT Mortality category.
In all, 20,399 patients were included from 49 centers. Of these, 54% were male. In terms of race, 55% were white, 17% were black, 16% were Hispanic, and 12% were other.
Based on unadjusted outcomes, there were no differences between the sexes for in-hospital mortality or complications. However, females had significantly shorter postoperative stays. In terms of race, white patients had significantly lower mortality, shorter length of stay, and fewer complications than any of the other racial groups.
In the adjusted multivariate analysis, there was no difference for mortality between the sexes. However, black patients had a significantly greater mortality risk with an odds ratio of 1.67.
Females did have a significantly shorter mean length of stay – 0.8 fewer days. In terms of race, black patients had a significantly longer mean length of stay by 2.4 hospital days, compared with white patients. Hispanic patients also had a significantly longer mean length of stay by almost 1 hospital day.
There was no difference between the sexes in terms of the occurrence of complications. In terms of race, "black patients experienced significantly more complications than other races with an odds ratio of 1.15," according to Dr. DiBardino.
The study is unique with the respect to the use of multivariable models. The researchers measured the association of sex and race with outcomes within each center and then combined the results, in order to mitigate the potential center effects.
"Our results cannot be explained by the possibility that patients of certain races might be disproportionately treated at centers with poorer outcomes in general."
The evaluation of complex relationships between clinical variables and socioeconomic and other factors affecting health care remains a significant challenge.
Since some pertinent socioeconomic data are not collected in the STS-CHSD, an analysis of a linked data set, which capitalizes on the strengths of both the CHSD and those of an administrative claims data set may be the next logical step, said Dr. DiBardino.
Dr. DiBardino and his coinvestigators reported that they have no relevant disclosures.
FT. LAUDERDALE, FLA. – Sex and race appear to play a role in outcomes following congenital heart surgery in children and adolescents, according to a new analysis of data from almost 21,000 patients.
Black patients had significantly greater rates of mortality and complications and a significantly longer length of postoperative stay than other races, while female patients had a significantly shorter length of stay than males, Dr. Daniel J. DiBardino reported at the annual meeting of the Society of Thoracic Surgeons.
"The analysis of demographic and clinical data from nearly 21,000 patients in the congenital heart surgery database revealed important associations between gender, race, and outcome," said Dr. DiBardino, who is a cardiac surgeon at the Blair E. Batson Children’s Hospital in Jackson, Miss.
Dr. DiBardino’s study was chosen as a 2011 Richard E. Clark Paper by the Society of Thoracic Surgeons.
The researchers used data from the Society of Thoracic Surgeons Congenital Heart Surgery Database (STS-CHSD). Patients were included in the analysis if they were less than 18 years of age and had undergone cardiac surgery between 2007 and 2009.
Exclusion criteria included centers with more than 15% of data missing for key variables and centers with very small samples (less than five cases).
Data collection included demographics (age, sex, weight, and race) and preoperative data (noncardiac/genetic abnormalities and STS-defined risk factors). Race was classified as white, black, Hispanic, and other.
Operations were classified by STAT Mortality category, which is "a complexity stratification tool based on empiric data from 80,000 cases in STS and EACTS (European Association for Cardio-Thoracic Surgery) databases," said Dr. DiBardino.
The researchers looked at hospital mortality, postoperative length of stay, and complications. Multivariable analyses included dichotomous variables (mortality, complications) and a continuous variable (postoperative length of stay). Models were adjusted for age, weight, noncardiac/genetic abnormalities, any other STS preoperative risk factor, and STAT Mortality category.
In all, 20,399 patients were included from 49 centers. Of these, 54% were male. In terms of race, 55% were white, 17% were black, 16% were Hispanic, and 12% were other.
Based on unadjusted outcomes, there were no differences between the sexes for in-hospital mortality or complications. However, females had significantly shorter postoperative stays. In terms of race, white patients had significantly lower mortality, shorter length of stay, and fewer complications than any of the other racial groups.
In the adjusted multivariate analysis, there was no difference for mortality between the sexes. However, black patients had a significantly greater mortality risk with an odds ratio of 1.67.
Females did have a significantly shorter mean length of stay – 0.8 fewer days. In terms of race, black patients had a significantly longer mean length of stay by 2.4 hospital days, compared with white patients. Hispanic patients also had a significantly longer mean length of stay by almost 1 hospital day.
There was no difference between the sexes in terms of the occurrence of complications. In terms of race, "black patients experienced significantly more complications than other races with an odds ratio of 1.15," according to Dr. DiBardino.
The study is unique with the respect to the use of multivariable models. The researchers measured the association of sex and race with outcomes within each center and then combined the results, in order to mitigate the potential center effects.
"Our results cannot be explained by the possibility that patients of certain races might be disproportionately treated at centers with poorer outcomes in general."
The evaluation of complex relationships between clinical variables and socioeconomic and other factors affecting health care remains a significant challenge.
Since some pertinent socioeconomic data are not collected in the STS-CHSD, an analysis of a linked data set, which capitalizes on the strengths of both the CHSD and those of an administrative claims data set may be the next logical step, said Dr. DiBardino.
Dr. DiBardino and his coinvestigators reported that they have no relevant disclosures.
Major Finding: In adjusted multivariate analyses, black patients had a significantly greater mortality risk (67%), a significantly longer mean length of stay by 2.4 hospital days, and a significantly greater risk of complications (15%). Female patients had a significantly shorter mean length of stay – 0.8 fewer days.
Data Source: The retrospective review included 20,399 patients younger than 18 years from 49 centers, collected in the Society of Thoracic Surgeons Congenital Heart Surgery Database.
Disclosures: Dr. DiBardino and his coinvestigators reported that they have no relevant disclosures.
States Adopt Health Reform
Two years into the Affordable Care Act, almost every state in the union has implemented at least one item from the law’s early market reforms, the Patient’s Bill of Rights, an analysis from the Commonwealth Fund has found. Of the 49 states that have taken some action, 23 (and the District of Columbia) passed legislation or enacted regulations addressing at least one of the reforms. Twelve states addressed all reforms. An additional 15 issued guidance for insurers, and 11 states took no action but reported that regulators were reviewing insurers’ policy forms for compliance with reforms. Only Arizona has done nothing to enact ACA reforms
"The vast majority of states have been very busy on health reform, at least on these early market reforms,"said Katie Keith, lead author of the analysis in an interview.
As the law currently stands, if states don’t implement the Patient’s Bill of Rights by Jan. 1, 2014, the federal government will do it for them. States that have not acted on these ACA reforms already may have stronger patient protections or their laws already may allow ACA enforcement.
–Frances Correa
Two years into the Affordable Care Act, almost every state in the union has implemented at least one item from the law’s early market reforms, the Patient’s Bill of Rights, an analysis from the Commonwealth Fund has found. Of the 49 states that have taken some action, 23 (and the District of Columbia) passed legislation or enacted regulations addressing at least one of the reforms. Twelve states addressed all reforms. An additional 15 issued guidance for insurers, and 11 states took no action but reported that regulators were reviewing insurers’ policy forms for compliance with reforms. Only Arizona has done nothing to enact ACA reforms
"The vast majority of states have been very busy on health reform, at least on these early market reforms,"said Katie Keith, lead author of the analysis in an interview.
As the law currently stands, if states don’t implement the Patient’s Bill of Rights by Jan. 1, 2014, the federal government will do it for them. States that have not acted on these ACA reforms already may have stronger patient protections or their laws already may allow ACA enforcement.
–Frances Correa
Two years into the Affordable Care Act, almost every state in the union has implemented at least one item from the law’s early market reforms, the Patient’s Bill of Rights, an analysis from the Commonwealth Fund has found. Of the 49 states that have taken some action, 23 (and the District of Columbia) passed legislation or enacted regulations addressing at least one of the reforms. Twelve states addressed all reforms. An additional 15 issued guidance for insurers, and 11 states took no action but reported that regulators were reviewing insurers’ policy forms for compliance with reforms. Only Arizona has done nothing to enact ACA reforms
"The vast majority of states have been very busy on health reform, at least on these early market reforms,"said Katie Keith, lead author of the analysis in an interview.
As the law currently stands, if states don’t implement the Patient’s Bill of Rights by Jan. 1, 2014, the federal government will do it for them. States that have not acted on these ACA reforms already may have stronger patient protections or their laws already may allow ACA enforcement.
–Frances Correa
Surgical Coaching: A Timely Idea?
The role of a coach is to provide objective and constructive feedback on what he or she observes, helping the practitioner to recognize what is successful and what can be improved. Coaches do not judge or instruct; instead, they guide and facilitate. They act as collaborators and partners to assist in developing a better understanding of their own performance, and they help them to use their experience, knowledge, and abilities to provide the best care possible (Nursing Standard 2009;23:48-55). The focus should always be on the surgeon and not what the coach would do in a similar situation.
Coaching can be valuable for surgeons at all stages of their career (J. Am. Coll. Surg. 2012;214:115-24). It is easy to imagine the role of a coach in smoothing the increasingly jarring transition from training to independent practice. But experience in other areas suggests that established practitioners can also benefit.
As one develops expertise, actions become more automated and more experienced practitioners spend less time examining their approaches and actions (Fitts, P.M.; Posner, M.I.; Human Performance. Brooks/Cole Publishing Co.: Belmont, Calif., 1967; Work 2006;26:93-6). A coach can serve as a catalyst to jump-start introspection and further practice improvement.
The Importance of Adult Learning Theory
Until recently, medical education has not encompassed the proven principles by which adults learn. In 2007, Boonyasai and colleagues developed a list of adult learning principles based on major educational theories that could be applied in medicine (JAMA 2007;298:1023-37):
- Enabling adult learners to be active participants.
- Providing content relating to the learner’s current experiences.
- Assessing learners’ needs and tailoring teaching to their past experience.
- Allowing learners to identify and pursue their own learning goals.
- Allowing learners to practice their learning.
- Supporting learners during self-directed learning.
- Providing feedback to learners.
- Facilitating learner self-reflection.
- Role-modeling behaviors.
A coaching program would almost by definition include at least the first eight principles, so this list is likely to be an effective approach for improving performance.
What Makes a Good Coach?
The best athletic coaches were not always the standout athletes. They did, however, almost always participate in the sport they coach at a very high level. This is because the characteristics of a good athletic coach to do not necessarily parallel the characteristics of a good athlete, but an intimate knowledge of the skill set is critical.
Similarly, the most experienced and skilled surgeons will not necessarily make the best coaches, but a surgical coach by definition must be a surgeon. A surgical coach must develop an easy rapport and a trusting relationship with each surgeon. The coach must be empathetic and tactful, but also flexible – able to ask probing questions and make constructive comments (Consult. Psychol. J. Pract. Res.;2001;53:240-50). The best surgical coaches are likely to be experienced, thoughtful, inquisitive, nonjudgmental, and well respected by their colleagues.
The coach described by Atul Gawande in "Personal Best," his article on surgical coaching, embodied all of those qualities and excelled as a surgical coach (Gawande A. Personal Best. Top Athletes and Singers Have Coaches. Should You? New Yorker Oct. 3, 2011). When we questioned him about his deftness in this new role, he credited the light hand (socially) that he developed from years of intraoperative consults.
Coaches need time and flexibility in their schedule. For this reason, surgeons who are nearing retirement or who are newly retired may be good candidates to serve as coaches. Many of these surgeons are likely to have the experience and respect required for surgical coaching. The key is to ensure that they also have the flexibility, openness, and lack of judgment.
Another potential pool of coaches may be surgeons interested in a more flexible lifestyle for personal reasons, such as childrearing or caregiving for an ill or elderly family member. Surgical coaching can provide a way to remain engaged in surgery and continue to contribute to the field without the same demands as a busy surgical practice.
Some Basic Principles
Jim Knight has developed a paradigm that he terms "partnership learning" to coach teachers (Knight, J. Instructional Coaching: A Partnership Approach to Improving Instruction. Corwin Press: Thousand Oaks, Calif., 2007). He contrasts this with the "dominator approach" upon which most traditional professional development is based – for example, the situation in which a person gives a PowerPoint presentation to convey an "expert opinion" to a roomful of people. Sound familiar?
Instead, Mr. Knight advocates the use of core principles that will foster a partnership, the cornerstone of coaching (Knight, J. Partnership Learning. University of Kansas Center for Research on Learning: Lawrence, Kan., 2002). Here are some ways they could apply to surgical coaching:
- Equality – The opinions and approaches of the surgeon and the surgical coach are equally valuable.
- Choice – At a minimum, the surgeon should be allowed to choose the specific case and setting for each coaching session.
- Voice and dialogue – The surgeon should feel free to speak openly. Coaches should listen more than they talk. The coach should not control or dominate the interaction, but rather engage in a dialogue.
- Reflection – "Reflection on action" after an operation is likely to be more effective than "reflection in action" in the operating room so that the surgeon can concentrate fully on dissecting his or her own performance. In addition, coaching sessions can take place in a private, confidential setting away from patients and other providers. The use of video as a "thinking device" to prompt open dialogue holds significant promise.
- Praxis – Surgeons should be encouraged to explicitly think about how they will apply insights from the coaching session to their clinical practice.
Three other points deserve mention. Confidentiality and trust are critical, especially as surgeons acclimate to the idea of working with a coach. Additionally, the coaching style should be individualized and adapted to each surgeon throughout a coaching session. Such adaptability is an important characteristic of a successful coach. Finally, coaches should not have administrative oversight for the surgeon they are coaching. This is to ensure that the content of coaching sessions remain focused on performance improvement and not on performance evaluations or career development.
Will It Work?
There are very little empirical data on coaching in any discipline. What does exist tends to be exploratory and qualitative. However, Cornett and Knight describe several randomized trials, and a review in the field of education suggests that coaching will be successful (Cornett, J.; Knight, J. Research on Coaching:Approaches and Perspectives, 2009;192-216).
Researchers found that only 10% of teachers used a new skill in the classroom when they were provided with a verbal description. After modeling, practice, and feedback were added, the rate of adoption increased to 19%. It was only with the addition of peer coaching that an astounding 95% of teachers utilized the new skill. (Bush, R. N. Effective Staff Development in Making Our Schools More Effective: Proceedings of Three State Conferences. Far West Laboratories: San Francisco, 1984).
Other studies demonstrated that coaching increased skill transfer from 15% to 75%, compared with traditional approaches to professional development. Even more striking was the fact that these skills were still being used 6 months later. If we are even half as successful with coaching in surgery, results will be orders of magnitude better than any previous attempts at intraoperative performance improvement.
How Do We Move Forward?
The American College of Surgeons Division of Education – with its dedication to improving quality, safety, and education – is in a particularly strong position to develop surgical coaching and is exploring potential programs with us in Wisconsin and with others. Other surgical societies, including local and regional organizations, offer another opportunity to develop coaching programs. The state chapters of the American Academy of Pediatrics instituted a quality improvement initiative that included team coaching, and found several advantages to this approach over a national one (J. Contin. Educ. Health Profess. 2008;28:131-9).
Trust in, familiarity with, and participation in local/regional societies or state chapters is likely to increase acceptance and participation by practicing surgeons. The infrastructure of a regional society allows for participation across all practice settings – not just in large hospitals where a coach may be locally available – yet it is small enough to afford some level of familiarity, trust, and respect for the coach.
This type of cross-institutional collaboration may seem counterintuitive in light of the traditional competitive relationships of neighboring institutions; however, the success of programs such as the Surgical Care and Outcomes Assessment Program (SCOAP) in Washington State and the Michigan Surgical Collaboratives (MSQC and MSBC) suggests that as a discipline we are ready to work together to improve the quality and safety of surgical care.
Given the current paucity of data, we must continue to study any new programs or interventions, but surgical coaching seems like an idea whose time has come.
Acknowledgments
I would like to thank Atul Gawande, Yue-Yung Hu, Robert Osteen, and Michael Zinner for conversations and research that helped me formulate these ideas.☐
Dr. Greenberg is an associate professor of surgery, and director of the Wisconsin Surgical Outcomes Research Program at the University of Wisconsin, Madison.
The role of a coach is to provide objective and constructive feedback on what he or she observes, helping the practitioner to recognize what is successful and what can be improved. Coaches do not judge or instruct; instead, they guide and facilitate. They act as collaborators and partners to assist in developing a better understanding of their own performance, and they help them to use their experience, knowledge, and abilities to provide the best care possible (Nursing Standard 2009;23:48-55). The focus should always be on the surgeon and not what the coach would do in a similar situation.
Coaching can be valuable for surgeons at all stages of their career (J. Am. Coll. Surg. 2012;214:115-24). It is easy to imagine the role of a coach in smoothing the increasingly jarring transition from training to independent practice. But experience in other areas suggests that established practitioners can also benefit.
As one develops expertise, actions become more automated and more experienced practitioners spend less time examining their approaches and actions (Fitts, P.M.; Posner, M.I.; Human Performance. Brooks/Cole Publishing Co.: Belmont, Calif., 1967; Work 2006;26:93-6). A coach can serve as a catalyst to jump-start introspection and further practice improvement.
The Importance of Adult Learning Theory
Until recently, medical education has not encompassed the proven principles by which adults learn. In 2007, Boonyasai and colleagues developed a list of adult learning principles based on major educational theories that could be applied in medicine (JAMA 2007;298:1023-37):
- Enabling adult learners to be active participants.
- Providing content relating to the learner’s current experiences.
- Assessing learners’ needs and tailoring teaching to their past experience.
- Allowing learners to identify and pursue their own learning goals.
- Allowing learners to practice their learning.
- Supporting learners during self-directed learning.
- Providing feedback to learners.
- Facilitating learner self-reflection.
- Role-modeling behaviors.
A coaching program would almost by definition include at least the first eight principles, so this list is likely to be an effective approach for improving performance.
What Makes a Good Coach?
The best athletic coaches were not always the standout athletes. They did, however, almost always participate in the sport they coach at a very high level. This is because the characteristics of a good athletic coach to do not necessarily parallel the characteristics of a good athlete, but an intimate knowledge of the skill set is critical.
Similarly, the most experienced and skilled surgeons will not necessarily make the best coaches, but a surgical coach by definition must be a surgeon. A surgical coach must develop an easy rapport and a trusting relationship with each surgeon. The coach must be empathetic and tactful, but also flexible – able to ask probing questions and make constructive comments (Consult. Psychol. J. Pract. Res.;2001;53:240-50). The best surgical coaches are likely to be experienced, thoughtful, inquisitive, nonjudgmental, and well respected by their colleagues.
The coach described by Atul Gawande in "Personal Best," his article on surgical coaching, embodied all of those qualities and excelled as a surgical coach (Gawande A. Personal Best. Top Athletes and Singers Have Coaches. Should You? New Yorker Oct. 3, 2011). When we questioned him about his deftness in this new role, he credited the light hand (socially) that he developed from years of intraoperative consults.
Coaches need time and flexibility in their schedule. For this reason, surgeons who are nearing retirement or who are newly retired may be good candidates to serve as coaches. Many of these surgeons are likely to have the experience and respect required for surgical coaching. The key is to ensure that they also have the flexibility, openness, and lack of judgment.
Another potential pool of coaches may be surgeons interested in a more flexible lifestyle for personal reasons, such as childrearing or caregiving for an ill or elderly family member. Surgical coaching can provide a way to remain engaged in surgery and continue to contribute to the field without the same demands as a busy surgical practice.
Some Basic Principles
Jim Knight has developed a paradigm that he terms "partnership learning" to coach teachers (Knight, J. Instructional Coaching: A Partnership Approach to Improving Instruction. Corwin Press: Thousand Oaks, Calif., 2007). He contrasts this with the "dominator approach" upon which most traditional professional development is based – for example, the situation in which a person gives a PowerPoint presentation to convey an "expert opinion" to a roomful of people. Sound familiar?
Instead, Mr. Knight advocates the use of core principles that will foster a partnership, the cornerstone of coaching (Knight, J. Partnership Learning. University of Kansas Center for Research on Learning: Lawrence, Kan., 2002). Here are some ways they could apply to surgical coaching:
- Equality – The opinions and approaches of the surgeon and the surgical coach are equally valuable.
- Choice – At a minimum, the surgeon should be allowed to choose the specific case and setting for each coaching session.
- Voice and dialogue – The surgeon should feel free to speak openly. Coaches should listen more than they talk. The coach should not control or dominate the interaction, but rather engage in a dialogue.
- Reflection – "Reflection on action" after an operation is likely to be more effective than "reflection in action" in the operating room so that the surgeon can concentrate fully on dissecting his or her own performance. In addition, coaching sessions can take place in a private, confidential setting away from patients and other providers. The use of video as a "thinking device" to prompt open dialogue holds significant promise.
- Praxis – Surgeons should be encouraged to explicitly think about how they will apply insights from the coaching session to their clinical practice.
Three other points deserve mention. Confidentiality and trust are critical, especially as surgeons acclimate to the idea of working with a coach. Additionally, the coaching style should be individualized and adapted to each surgeon throughout a coaching session. Such adaptability is an important characteristic of a successful coach. Finally, coaches should not have administrative oversight for the surgeon they are coaching. This is to ensure that the content of coaching sessions remain focused on performance improvement and not on performance evaluations or career development.
Will It Work?
There are very little empirical data on coaching in any discipline. What does exist tends to be exploratory and qualitative. However, Cornett and Knight describe several randomized trials, and a review in the field of education suggests that coaching will be successful (Cornett, J.; Knight, J. Research on Coaching:Approaches and Perspectives, 2009;192-216).
Researchers found that only 10% of teachers used a new skill in the classroom when they were provided with a verbal description. After modeling, practice, and feedback were added, the rate of adoption increased to 19%. It was only with the addition of peer coaching that an astounding 95% of teachers utilized the new skill. (Bush, R. N. Effective Staff Development in Making Our Schools More Effective: Proceedings of Three State Conferences. Far West Laboratories: San Francisco, 1984).
Other studies demonstrated that coaching increased skill transfer from 15% to 75%, compared with traditional approaches to professional development. Even more striking was the fact that these skills were still being used 6 months later. If we are even half as successful with coaching in surgery, results will be orders of magnitude better than any previous attempts at intraoperative performance improvement.
How Do We Move Forward?
The American College of Surgeons Division of Education – with its dedication to improving quality, safety, and education – is in a particularly strong position to develop surgical coaching and is exploring potential programs with us in Wisconsin and with others. Other surgical societies, including local and regional organizations, offer another opportunity to develop coaching programs. The state chapters of the American Academy of Pediatrics instituted a quality improvement initiative that included team coaching, and found several advantages to this approach over a national one (J. Contin. Educ. Health Profess. 2008;28:131-9).
Trust in, familiarity with, and participation in local/regional societies or state chapters is likely to increase acceptance and participation by practicing surgeons. The infrastructure of a regional society allows for participation across all practice settings – not just in large hospitals where a coach may be locally available – yet it is small enough to afford some level of familiarity, trust, and respect for the coach.
This type of cross-institutional collaboration may seem counterintuitive in light of the traditional competitive relationships of neighboring institutions; however, the success of programs such as the Surgical Care and Outcomes Assessment Program (SCOAP) in Washington State and the Michigan Surgical Collaboratives (MSQC and MSBC) suggests that as a discipline we are ready to work together to improve the quality and safety of surgical care.
Given the current paucity of data, we must continue to study any new programs or interventions, but surgical coaching seems like an idea whose time has come.
Acknowledgments
I would like to thank Atul Gawande, Yue-Yung Hu, Robert Osteen, and Michael Zinner for conversations and research that helped me formulate these ideas.☐
Dr. Greenberg is an associate professor of surgery, and director of the Wisconsin Surgical Outcomes Research Program at the University of Wisconsin, Madison.
The role of a coach is to provide objective and constructive feedback on what he or she observes, helping the practitioner to recognize what is successful and what can be improved. Coaches do not judge or instruct; instead, they guide and facilitate. They act as collaborators and partners to assist in developing a better understanding of their own performance, and they help them to use their experience, knowledge, and abilities to provide the best care possible (Nursing Standard 2009;23:48-55). The focus should always be on the surgeon and not what the coach would do in a similar situation.
Coaching can be valuable for surgeons at all stages of their career (J. Am. Coll. Surg. 2012;214:115-24). It is easy to imagine the role of a coach in smoothing the increasingly jarring transition from training to independent practice. But experience in other areas suggests that established practitioners can also benefit.
As one develops expertise, actions become more automated and more experienced practitioners spend less time examining their approaches and actions (Fitts, P.M.; Posner, M.I.; Human Performance. Brooks/Cole Publishing Co.: Belmont, Calif., 1967; Work 2006;26:93-6). A coach can serve as a catalyst to jump-start introspection and further practice improvement.
The Importance of Adult Learning Theory
Until recently, medical education has not encompassed the proven principles by which adults learn. In 2007, Boonyasai and colleagues developed a list of adult learning principles based on major educational theories that could be applied in medicine (JAMA 2007;298:1023-37):
- Enabling adult learners to be active participants.
- Providing content relating to the learner’s current experiences.
- Assessing learners’ needs and tailoring teaching to their past experience.
- Allowing learners to identify and pursue their own learning goals.
- Allowing learners to practice their learning.
- Supporting learners during self-directed learning.
- Providing feedback to learners.
- Facilitating learner self-reflection.
- Role-modeling behaviors.
A coaching program would almost by definition include at least the first eight principles, so this list is likely to be an effective approach for improving performance.
What Makes a Good Coach?
The best athletic coaches were not always the standout athletes. They did, however, almost always participate in the sport they coach at a very high level. This is because the characteristics of a good athletic coach to do not necessarily parallel the characteristics of a good athlete, but an intimate knowledge of the skill set is critical.
Similarly, the most experienced and skilled surgeons will not necessarily make the best coaches, but a surgical coach by definition must be a surgeon. A surgical coach must develop an easy rapport and a trusting relationship with each surgeon. The coach must be empathetic and tactful, but also flexible – able to ask probing questions and make constructive comments (Consult. Psychol. J. Pract. Res.;2001;53:240-50). The best surgical coaches are likely to be experienced, thoughtful, inquisitive, nonjudgmental, and well respected by their colleagues.
The coach described by Atul Gawande in "Personal Best," his article on surgical coaching, embodied all of those qualities and excelled as a surgical coach (Gawande A. Personal Best. Top Athletes and Singers Have Coaches. Should You? New Yorker Oct. 3, 2011). When we questioned him about his deftness in this new role, he credited the light hand (socially) that he developed from years of intraoperative consults.
Coaches need time and flexibility in their schedule. For this reason, surgeons who are nearing retirement or who are newly retired may be good candidates to serve as coaches. Many of these surgeons are likely to have the experience and respect required for surgical coaching. The key is to ensure that they also have the flexibility, openness, and lack of judgment.
Another potential pool of coaches may be surgeons interested in a more flexible lifestyle for personal reasons, such as childrearing or caregiving for an ill or elderly family member. Surgical coaching can provide a way to remain engaged in surgery and continue to contribute to the field without the same demands as a busy surgical practice.
Some Basic Principles
Jim Knight has developed a paradigm that he terms "partnership learning" to coach teachers (Knight, J. Instructional Coaching: A Partnership Approach to Improving Instruction. Corwin Press: Thousand Oaks, Calif., 2007). He contrasts this with the "dominator approach" upon which most traditional professional development is based – for example, the situation in which a person gives a PowerPoint presentation to convey an "expert opinion" to a roomful of people. Sound familiar?
Instead, Mr. Knight advocates the use of core principles that will foster a partnership, the cornerstone of coaching (Knight, J. Partnership Learning. University of Kansas Center for Research on Learning: Lawrence, Kan., 2002). Here are some ways they could apply to surgical coaching:
- Equality – The opinions and approaches of the surgeon and the surgical coach are equally valuable.
- Choice – At a minimum, the surgeon should be allowed to choose the specific case and setting for each coaching session.
- Voice and dialogue – The surgeon should feel free to speak openly. Coaches should listen more than they talk. The coach should not control or dominate the interaction, but rather engage in a dialogue.
- Reflection – "Reflection on action" after an operation is likely to be more effective than "reflection in action" in the operating room so that the surgeon can concentrate fully on dissecting his or her own performance. In addition, coaching sessions can take place in a private, confidential setting away from patients and other providers. The use of video as a "thinking device" to prompt open dialogue holds significant promise.
- Praxis – Surgeons should be encouraged to explicitly think about how they will apply insights from the coaching session to their clinical practice.
Three other points deserve mention. Confidentiality and trust are critical, especially as surgeons acclimate to the idea of working with a coach. Additionally, the coaching style should be individualized and adapted to each surgeon throughout a coaching session. Such adaptability is an important characteristic of a successful coach. Finally, coaches should not have administrative oversight for the surgeon they are coaching. This is to ensure that the content of coaching sessions remain focused on performance improvement and not on performance evaluations or career development.
Will It Work?
There are very little empirical data on coaching in any discipline. What does exist tends to be exploratory and qualitative. However, Cornett and Knight describe several randomized trials, and a review in the field of education suggests that coaching will be successful (Cornett, J.; Knight, J. Research on Coaching:Approaches and Perspectives, 2009;192-216).
Researchers found that only 10% of teachers used a new skill in the classroom when they were provided with a verbal description. After modeling, practice, and feedback were added, the rate of adoption increased to 19%. It was only with the addition of peer coaching that an astounding 95% of teachers utilized the new skill. (Bush, R. N. Effective Staff Development in Making Our Schools More Effective: Proceedings of Three State Conferences. Far West Laboratories: San Francisco, 1984).
Other studies demonstrated that coaching increased skill transfer from 15% to 75%, compared with traditional approaches to professional development. Even more striking was the fact that these skills were still being used 6 months later. If we are even half as successful with coaching in surgery, results will be orders of magnitude better than any previous attempts at intraoperative performance improvement.
How Do We Move Forward?
The American College of Surgeons Division of Education – with its dedication to improving quality, safety, and education – is in a particularly strong position to develop surgical coaching and is exploring potential programs with us in Wisconsin and with others. Other surgical societies, including local and regional organizations, offer another opportunity to develop coaching programs. The state chapters of the American Academy of Pediatrics instituted a quality improvement initiative that included team coaching, and found several advantages to this approach over a national one (J. Contin. Educ. Health Profess. 2008;28:131-9).
Trust in, familiarity with, and participation in local/regional societies or state chapters is likely to increase acceptance and participation by practicing surgeons. The infrastructure of a regional society allows for participation across all practice settings – not just in large hospitals where a coach may be locally available – yet it is small enough to afford some level of familiarity, trust, and respect for the coach.
This type of cross-institutional collaboration may seem counterintuitive in light of the traditional competitive relationships of neighboring institutions; however, the success of programs such as the Surgical Care and Outcomes Assessment Program (SCOAP) in Washington State and the Michigan Surgical Collaboratives (MSQC and MSBC) suggests that as a discipline we are ready to work together to improve the quality and safety of surgical care.
Given the current paucity of data, we must continue to study any new programs or interventions, but surgical coaching seems like an idea whose time has come.
Acknowledgments
I would like to thank Atul Gawande, Yue-Yung Hu, Robert Osteen, and Michael Zinner for conversations and research that helped me formulate these ideas.☐
Dr. Greenberg is an associate professor of surgery, and director of the Wisconsin Surgical Outcomes Research Program at the University of Wisconsin, Madison.
Some Online Resources
AATS Resident Resources: www.aats.org/TSR/index.html
CTSNET Residents Section: www.ctsnet.org/sections/residents
Thoracic Surgery Directors Association: www.tsda.org
Thoracic Surgery News: www.thoracicsurgerynews.com
Thoracic Surgery Residents Association: www.tsranet.org
Thoracic Surgery Foundation for Research and Education: www.tsfre.org
AATS Resident Resources: www.aats.org/TSR/index.html
CTSNET Residents Section: www.ctsnet.org/sections/residents
Thoracic Surgery Directors Association: www.tsda.org
Thoracic Surgery News: www.thoracicsurgerynews.com
Thoracic Surgery Residents Association: www.tsranet.org
Thoracic Surgery Foundation for Research and Education: www.tsfre.org
AATS Resident Resources: www.aats.org/TSR/index.html
CTSNET Residents Section: www.ctsnet.org/sections/residents
Thoracic Surgery Directors Association: www.tsda.org
Thoracic Surgery News: www.thoracicsurgerynews.com
Thoracic Surgery Residents Association: www.tsranet.org
Thoracic Surgery Foundation for Research and Education: www.tsfre.org
NCCN Affirms CT Scans For Heavy Smokers
The benefits of routine lung cancer screening in high-risk individuals outweigh the potential risks, according to members of a National Comprehensive Cancer Network guidelines panel that recommended low-dose helical CT screening of two high-risk groups.
Mary E. Reid, Ph.D., of the Roswell Park Cancer Institute in Buffalo, N.Y., acknowledged the burdens – in particular, the cost and requisite resource utilization – associated with following all high-risk patients who screen positive. But, she said, "the evidence [in favor of] the recommendations is really strong and supports their implementation."
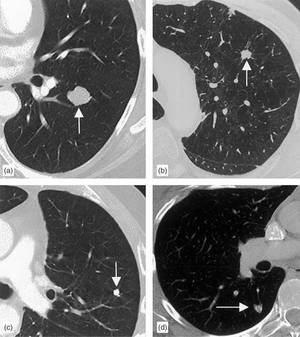
Lung cancer, she noted, is the only one of the top four deadliest cancers (lung, prostate, breast, and colorectal) that is not currently subject to routine screening.
Dr. Reid and colleagues on the National Comprehensive Cancer Network (NCCN) Guidelines Panel for Lung Cancer Screening presented the update at the NCCN annual conference March 14-18 in Hollywood, Fla. It had been issued in October 2011 and followed a New England Journal of Medicine report that low-dose CT screening of heavy smokers reduced lung cancer mortality by 20%, compared with annual chest x-rays, in the National Lung Screening Trial (NLST).
The revised guidelines recommend annual low-dose helical CT screening for the following two groups of high-risk individuals:
• Those aged 55-74 years with a minimum smoking history of 30 pack-years who either are current smokers or quit within the past 15 years.
• Those aged 50 years or older with a minimum smoking history of 20 pack-years plus one additional lung cancer risk factor, excluding secondhand exposure.
Evidence from the randomized, controlled NLST suggests that early detection via screening reduced lung-cancer specific mortality in the former risk group, which characterizes the NLST patient population. Specifically, 1 in 100 high-risk individuals who were enrolled in the study screened positive on their first low-dose CT exam, and one life was saved for every 320 high-risk individuals screened over 2 years (three screens) (N. Engl. J. Med. 2011;365:395-409). The NCCN recommendation for this group is category 1, the highest level.
The recommendation for annual screening in the second high-risk group is based on less-robust evidence and a nonuniform consensus of the NCCN panel members, Dr. Reid said. As such, it is a less-emphatic category 2B recommendation.
The NCCN screening recommendations have been deemed by some experts to be premature in the absence of cost-efficacy analysis, particularly because of the high false-positive rates observed in both the CT group (96.4%) and the radiography group (94.5%), as well as the potentially harmful effects of radiation exposure associated with low-dose CT screening.
Despite the favorable outcome of their study, the NLST authors stressed the need for rigorous cost-effectiveness analyses before the crafting of public policy recommendations. "The reductions in lung-cancer mortality must be weighed against the harms from positive screening results and overdiagnosis, as well as the costs," they wrote. "The cost component of low-dose CT screening includes not only the screening examination itself but also the diagnostic follow-up and treatment."
In addition to recommending appropriate candidates for routine screening and the proposed frequency of the scans, the new NCCN guidelines outline lung cancer risk factors, address the risks and benefits of screening as well as screening accuracy, and offer an algorithm for the evaluation and follow-up of positive screens. Specifically, the guidelines recommend the following:
• Basing the frequency of low-dose CT in high-risk patients on the size and status (solid, nonsolid, part-solid, ground-glass, ground-glass opacity) of the nodule on baseline CT.
• Excising all nodules that increase in size or become solid or part-solid during follow-up.
• Considering PET with CT for nodules 8 mm or larger at baseline.
• Performing biopsy or excision of nodules that are suspicious for lung cancer, based on PET with CT findings.
• Reexamining within 1 month solid endobronchial nodules with low-dose CT immediately after vigorous coughing.
• Counseling smokers to quit.
The NCCN is the first professional organization to recommend routine low-dose CT screening for individuals who are considered to be at high-risk for lung cancer, according to Dr. Reid. Last summer, the International Association for the Study of Lung Cancer issued a call for physicians to discuss lung cancer screening with patients who match the high-risk smoking history of those enrolled in the NSLT.
Dr. Reid reported having no financial conflicts of interest.
The benefits of routine lung cancer screening in high-risk individuals outweigh the potential risks, according to members of a National Comprehensive Cancer Network guidelines panel that recommended low-dose helical CT screening of two high-risk groups.
Mary E. Reid, Ph.D., of the Roswell Park Cancer Institute in Buffalo, N.Y., acknowledged the burdens – in particular, the cost and requisite resource utilization – associated with following all high-risk patients who screen positive. But, she said, "the evidence [in favor of] the recommendations is really strong and supports their implementation."
Lung cancer, she noted, is the only one of the top four deadliest cancers (lung, prostate, breast, and colorectal) that is not currently subject to routine screening.
Dr. Reid and colleagues on the National Comprehensive Cancer Network (NCCN) Guidelines Panel for Lung Cancer Screening presented the update at the NCCN annual conference March 14-18 in Hollywood, Fla. It had been issued in October 2011 and followed a New England Journal of Medicine report that low-dose CT screening of heavy smokers reduced lung cancer mortality by 20%, compared with annual chest x-rays, in the National Lung Screening Trial (NLST).
The revised guidelines recommend annual low-dose helical CT screening for the following two groups of high-risk individuals:
• Those aged 55-74 years with a minimum smoking history of 30 pack-years who either are current smokers or quit within the past 15 years.
• Those aged 50 years or older with a minimum smoking history of 20 pack-years plus one additional lung cancer risk factor, excluding secondhand exposure.
Evidence from the randomized, controlled NLST suggests that early detection via screening reduced lung-cancer specific mortality in the former risk group, which characterizes the NLST patient population. Specifically, 1 in 100 high-risk individuals who were enrolled in the study screened positive on their first low-dose CT exam, and one life was saved for every 320 high-risk individuals screened over 2 years (three screens) (N. Engl. J. Med. 2011;365:395-409). The NCCN recommendation for this group is category 1, the highest level.
The recommendation for annual screening in the second high-risk group is based on less-robust evidence and a nonuniform consensus of the NCCN panel members, Dr. Reid said. As such, it is a less-emphatic category 2B recommendation.
The NCCN screening recommendations have been deemed by some experts to be premature in the absence of cost-efficacy analysis, particularly because of the high false-positive rates observed in both the CT group (96.4%) and the radiography group (94.5%), as well as the potentially harmful effects of radiation exposure associated with low-dose CT screening.
Despite the favorable outcome of their study, the NLST authors stressed the need for rigorous cost-effectiveness analyses before the crafting of public policy recommendations. "The reductions in lung-cancer mortality must be weighed against the harms from positive screening results and overdiagnosis, as well as the costs," they wrote. "The cost component of low-dose CT screening includes not only the screening examination itself but also the diagnostic follow-up and treatment."
In addition to recommending appropriate candidates for routine screening and the proposed frequency of the scans, the new NCCN guidelines outline lung cancer risk factors, address the risks and benefits of screening as well as screening accuracy, and offer an algorithm for the evaluation and follow-up of positive screens. Specifically, the guidelines recommend the following:
• Basing the frequency of low-dose CT in high-risk patients on the size and status (solid, nonsolid, part-solid, ground-glass, ground-glass opacity) of the nodule on baseline CT.
• Excising all nodules that increase in size or become solid or part-solid during follow-up.
• Considering PET with CT for nodules 8 mm or larger at baseline.
• Performing biopsy or excision of nodules that are suspicious for lung cancer, based on PET with CT findings.
• Reexamining within 1 month solid endobronchial nodules with low-dose CT immediately after vigorous coughing.
• Counseling smokers to quit.
The NCCN is the first professional organization to recommend routine low-dose CT screening for individuals who are considered to be at high-risk for lung cancer, according to Dr. Reid. Last summer, the International Association for the Study of Lung Cancer issued a call for physicians to discuss lung cancer screening with patients who match the high-risk smoking history of those enrolled in the NSLT.
Dr. Reid reported having no financial conflicts of interest.
The benefits of routine lung cancer screening in high-risk individuals outweigh the potential risks, according to members of a National Comprehensive Cancer Network guidelines panel that recommended low-dose helical CT screening of two high-risk groups.
Mary E. Reid, Ph.D., of the Roswell Park Cancer Institute in Buffalo, N.Y., acknowledged the burdens – in particular, the cost and requisite resource utilization – associated with following all high-risk patients who screen positive. But, she said, "the evidence [in favor of] the recommendations is really strong and supports their implementation."
Lung cancer, she noted, is the only one of the top four deadliest cancers (lung, prostate, breast, and colorectal) that is not currently subject to routine screening.
Dr. Reid and colleagues on the National Comprehensive Cancer Network (NCCN) Guidelines Panel for Lung Cancer Screening presented the update at the NCCN annual conference March 14-18 in Hollywood, Fla. It had been issued in October 2011 and followed a New England Journal of Medicine report that low-dose CT screening of heavy smokers reduced lung cancer mortality by 20%, compared with annual chest x-rays, in the National Lung Screening Trial (NLST).
The revised guidelines recommend annual low-dose helical CT screening for the following two groups of high-risk individuals:
• Those aged 55-74 years with a minimum smoking history of 30 pack-years who either are current smokers or quit within the past 15 years.
• Those aged 50 years or older with a minimum smoking history of 20 pack-years plus one additional lung cancer risk factor, excluding secondhand exposure.
Evidence from the randomized, controlled NLST suggests that early detection via screening reduced lung-cancer specific mortality in the former risk group, which characterizes the NLST patient population. Specifically, 1 in 100 high-risk individuals who were enrolled in the study screened positive on their first low-dose CT exam, and one life was saved for every 320 high-risk individuals screened over 2 years (three screens) (N. Engl. J. Med. 2011;365:395-409). The NCCN recommendation for this group is category 1, the highest level.
The recommendation for annual screening in the second high-risk group is based on less-robust evidence and a nonuniform consensus of the NCCN panel members, Dr. Reid said. As such, it is a less-emphatic category 2B recommendation.
The NCCN screening recommendations have been deemed by some experts to be premature in the absence of cost-efficacy analysis, particularly because of the high false-positive rates observed in both the CT group (96.4%) and the radiography group (94.5%), as well as the potentially harmful effects of radiation exposure associated with low-dose CT screening.
Despite the favorable outcome of their study, the NLST authors stressed the need for rigorous cost-effectiveness analyses before the crafting of public policy recommendations. "The reductions in lung-cancer mortality must be weighed against the harms from positive screening results and overdiagnosis, as well as the costs," they wrote. "The cost component of low-dose CT screening includes not only the screening examination itself but also the diagnostic follow-up and treatment."
In addition to recommending appropriate candidates for routine screening and the proposed frequency of the scans, the new NCCN guidelines outline lung cancer risk factors, address the risks and benefits of screening as well as screening accuracy, and offer an algorithm for the evaluation and follow-up of positive screens. Specifically, the guidelines recommend the following:
• Basing the frequency of low-dose CT in high-risk patients on the size and status (solid, nonsolid, part-solid, ground-glass, ground-glass opacity) of the nodule on baseline CT.
• Excising all nodules that increase in size or become solid or part-solid during follow-up.
• Considering PET with CT for nodules 8 mm or larger at baseline.
• Performing biopsy or excision of nodules that are suspicious for lung cancer, based on PET with CT findings.
• Reexamining within 1 month solid endobronchial nodules with low-dose CT immediately after vigorous coughing.
• Counseling smokers to quit.
The NCCN is the first professional organization to recommend routine low-dose CT screening for individuals who are considered to be at high-risk for lung cancer, according to Dr. Reid. Last summer, the International Association for the Study of Lung Cancer issued a call for physicians to discuss lung cancer screening with patients who match the high-risk smoking history of those enrolled in the NSLT.
Dr. Reid reported having no financial conflicts of interest.
NCCN Affirms CT Scans For Heavy Smokers
The benefits of routine lung cancer screening in high-risk individuals outweigh the potential risks, according to members of a National Comprehensive Cancer Network guidelines panel that recommended low-dose helical CT screening of two high-risk groups.
Mary E. Reid, Ph.D., of the Roswell Park Cancer Institute in Buffalo, N.Y., acknowledged the burdens – in particular, the cost and requisite resource utilization – associated with following all high-risk patients who screen positive. But, she said, "the evidence [in favor of] the recommendations is really strong and supports their implementation."
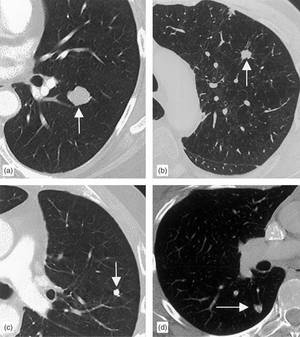
Lung cancer, she noted, is the only one of the top four deadliest cancers (lung, prostate, breast, and colorectal) that is not currently subject to routine screening.
Dr. Reid and colleagues on the National Comprehensive Cancer Network (NCCN) Guidelines Panel for Lung Cancer Screening presented the update at the NCCN annual conference March 14-18 in Hollywood, Fla. It had been issued in October 2011 and followed a New England Journal of Medicine report that low-dose CT screening of heavy smokers reduced lung cancer mortality by 20%, compared with annual chest x-rays, in the National Lung Screening Trial (NLST).
The revised guidelines recommend annual low-dose helical CT screening for the following two groups of high-risk individuals:
• Those aged 55-74 years with a minimum smoking history of 30 pack-years who either are current smokers or quit within the past 15 years.
• Those aged 50 years or older with a minimum smoking history of 20 pack-years plus one additional lung cancer risk factor, excluding secondhand exposure.
Evidence from the randomized, controlled NLST suggests that early detection via screening reduced lung-cancer specific mortality in the former risk group, which characterizes the NLST patient population. Specifically, 1 in 100 high-risk individuals who were enrolled in the study screened positive on their first low-dose CT exam, and one life was saved for every 320 high-risk individuals screened over 2 years (three screens) (N. Engl. J. Med. 2011;365:395-409). The NCCN recommendation for this group is category 1, the highest level.
The recommendation for annual screening in the second high-risk group is based on less-robust evidence and a nonuniform consensus of the NCCN panel members, Dr. Reid said. As such, it is a less-emphatic category 2B recommendation.
The NCCN screening recommendations have been deemed by some experts to be premature in the absence of cost-efficacy analysis, particularly because of the high false-positive rates observed in both the CT group (96.4%) and the radiography group (94.5%), as well as the potentially harmful effects of radiation exposure associated with low-dose CT screening.
Despite the favorable outcome of their study, the NLST authors stressed the need for rigorous cost-effectiveness analyses before the crafting of public policy recommendations. "The reductions in lung-cancer mortality must be weighed against the harms from positive screening results and overdiagnosis, as well as the costs," they wrote. "The cost component of low-dose CT screening includes not only the screening examination itself but also the diagnostic follow-up and treatment."
In addition to recommending appropriate candidates for routine screening and the proposed frequency of the scans, the new NCCN guidelines outline lung cancer risk factors, address the risks and benefits of screening as well as screening accuracy, and offer an algorithm for the evaluation and follow-up of positive screens. Specifically, the guidelines recommend the following:
• Basing the frequency of low-dose CT in high-risk patients on the size and status (solid, nonsolid, part-solid, ground-glass, ground-glass opacity) of the nodule on baseline CT.
• Excising all nodules that increase in size or become solid or part-solid during follow-up.
• Considering PET with CT for nodules 8 mm or larger at baseline.
• Performing biopsy or excision of nodules that are suspicious for lung cancer, based on PET with CT findings.
• Reexamining within 1 month solid endobronchial nodules with low-dose CT immediately after vigorous coughing.
• Counseling smokers to quit.
The NCCN is the first professional organization to recommend routine low-dose CT screening for individuals who are considered to be at high-risk for lung cancer, according to Dr. Reid. Last summer, the International Association for the Study of Lung Cancer issued a call for physicians to discuss lung cancer screening with patients who match the high-risk smoking history of those enrolled in the NSLT.
Dr. Reid reported having no financial conflicts of interest.
The benefits of routine lung cancer screening in high-risk individuals outweigh the potential risks, according to members of a National Comprehensive Cancer Network guidelines panel that recommended low-dose helical CT screening of two high-risk groups.
Mary E. Reid, Ph.D., of the Roswell Park Cancer Institute in Buffalo, N.Y., acknowledged the burdens – in particular, the cost and requisite resource utilization – associated with following all high-risk patients who screen positive. But, she said, "the evidence [in favor of] the recommendations is really strong and supports their implementation."
Lung cancer, she noted, is the only one of the top four deadliest cancers (lung, prostate, breast, and colorectal) that is not currently subject to routine screening.
Dr. Reid and colleagues on the National Comprehensive Cancer Network (NCCN) Guidelines Panel for Lung Cancer Screening presented the update at the NCCN annual conference March 14-18 in Hollywood, Fla. It had been issued in October 2011 and followed a New England Journal of Medicine report that low-dose CT screening of heavy smokers reduced lung cancer mortality by 20%, compared with annual chest x-rays, in the National Lung Screening Trial (NLST).
The revised guidelines recommend annual low-dose helical CT screening for the following two groups of high-risk individuals:
• Those aged 55-74 years with a minimum smoking history of 30 pack-years who either are current smokers or quit within the past 15 years.
• Those aged 50 years or older with a minimum smoking history of 20 pack-years plus one additional lung cancer risk factor, excluding secondhand exposure.
Evidence from the randomized, controlled NLST suggests that early detection via screening reduced lung-cancer specific mortality in the former risk group, which characterizes the NLST patient population. Specifically, 1 in 100 high-risk individuals who were enrolled in the study screened positive on their first low-dose CT exam, and one life was saved for every 320 high-risk individuals screened over 2 years (three screens) (N. Engl. J. Med. 2011;365:395-409). The NCCN recommendation for this group is category 1, the highest level.
The recommendation for annual screening in the second high-risk group is based on less-robust evidence and a nonuniform consensus of the NCCN panel members, Dr. Reid said. As such, it is a less-emphatic category 2B recommendation.
The NCCN screening recommendations have been deemed by some experts to be premature in the absence of cost-efficacy analysis, particularly because of the high false-positive rates observed in both the CT group (96.4%) and the radiography group (94.5%), as well as the potentially harmful effects of radiation exposure associated with low-dose CT screening.
Despite the favorable outcome of their study, the NLST authors stressed the need for rigorous cost-effectiveness analyses before the crafting of public policy recommendations. "The reductions in lung-cancer mortality must be weighed against the harms from positive screening results and overdiagnosis, as well as the costs," they wrote. "The cost component of low-dose CT screening includes not only the screening examination itself but also the diagnostic follow-up and treatment."
In addition to recommending appropriate candidates for routine screening and the proposed frequency of the scans, the new NCCN guidelines outline lung cancer risk factors, address the risks and benefits of screening as well as screening accuracy, and offer an algorithm for the evaluation and follow-up of positive screens. Specifically, the guidelines recommend the following:
• Basing the frequency of low-dose CT in high-risk patients on the size and status (solid, nonsolid, part-solid, ground-glass, ground-glass opacity) of the nodule on baseline CT.
• Excising all nodules that increase in size or become solid or part-solid during follow-up.
• Considering PET with CT for nodules 8 mm or larger at baseline.
• Performing biopsy or excision of nodules that are suspicious for lung cancer, based on PET with CT findings.
• Reexamining within 1 month solid endobronchial nodules with low-dose CT immediately after vigorous coughing.
• Counseling smokers to quit.
The NCCN is the first professional organization to recommend routine low-dose CT screening for individuals who are considered to be at high-risk for lung cancer, according to Dr. Reid. Last summer, the International Association for the Study of Lung Cancer issued a call for physicians to discuss lung cancer screening with patients who match the high-risk smoking history of those enrolled in the NSLT.
Dr. Reid reported having no financial conflicts of interest.
The benefits of routine lung cancer screening in high-risk individuals outweigh the potential risks, according to members of a National Comprehensive Cancer Network guidelines panel that recommended low-dose helical CT screening of two high-risk groups.
Mary E. Reid, Ph.D., of the Roswell Park Cancer Institute in Buffalo, N.Y., acknowledged the burdens – in particular, the cost and requisite resource utilization – associated with following all high-risk patients who screen positive. But, she said, "the evidence [in favor of] the recommendations is really strong and supports their implementation."
Lung cancer, she noted, is the only one of the top four deadliest cancers (lung, prostate, breast, and colorectal) that is not currently subject to routine screening.
Dr. Reid and colleagues on the National Comprehensive Cancer Network (NCCN) Guidelines Panel for Lung Cancer Screening presented the update at the NCCN annual conference March 14-18 in Hollywood, Fla. It had been issued in October 2011 and followed a New England Journal of Medicine report that low-dose CT screening of heavy smokers reduced lung cancer mortality by 20%, compared with annual chest x-rays, in the National Lung Screening Trial (NLST).
The revised guidelines recommend annual low-dose helical CT screening for the following two groups of high-risk individuals:
• Those aged 55-74 years with a minimum smoking history of 30 pack-years who either are current smokers or quit within the past 15 years.
• Those aged 50 years or older with a minimum smoking history of 20 pack-years plus one additional lung cancer risk factor, excluding secondhand exposure.
Evidence from the randomized, controlled NLST suggests that early detection via screening reduced lung-cancer specific mortality in the former risk group, which characterizes the NLST patient population. Specifically, 1 in 100 high-risk individuals who were enrolled in the study screened positive on their first low-dose CT exam, and one life was saved for every 320 high-risk individuals screened over 2 years (three screens) (N. Engl. J. Med. 2011;365:395-409). The NCCN recommendation for this group is category 1, the highest level.
The recommendation for annual screening in the second high-risk group is based on less-robust evidence and a nonuniform consensus of the NCCN panel members, Dr. Reid said. As such, it is a less-emphatic category 2B recommendation.
The NCCN screening recommendations have been deemed by some experts to be premature in the absence of cost-efficacy analysis, particularly because of the high false-positive rates observed in both the CT group (96.4%) and the radiography group (94.5%), as well as the potentially harmful effects of radiation exposure associated with low-dose CT screening.
Despite the favorable outcome of their study, the NLST authors stressed the need for rigorous cost-effectiveness analyses before the crafting of public policy recommendations. "The reductions in lung-cancer mortality must be weighed against the harms from positive screening results and overdiagnosis, as well as the costs," they wrote. "The cost component of low-dose CT screening includes not only the screening examination itself but also the diagnostic follow-up and treatment."
In addition to recommending appropriate candidates for routine screening and the proposed frequency of the scans, the new NCCN guidelines outline lung cancer risk factors, address the risks and benefits of screening as well as screening accuracy, and offer an algorithm for the evaluation and follow-up of positive screens. Specifically, the guidelines recommend the following:
• Basing the frequency of low-dose CT in high-risk patients on the size and status (solid, nonsolid, part-solid, ground-glass, ground-glass opacity) of the nodule on baseline CT.
• Excising all nodules that increase in size or become solid or part-solid during follow-up.
• Considering PET with CT for nodules 8 mm or larger at baseline.
• Performing biopsy or excision of nodules that are suspicious for lung cancer, based on PET with CT findings.
• Reexamining within 1 month solid endobronchial nodules with low-dose CT immediately after vigorous coughing.
• Counseling smokers to quit.
The NCCN is the first professional organization to recommend routine low-dose CT screening for individuals who are considered to be at high-risk for lung cancer, according to Dr. Reid. Last summer, the International Association for the Study of Lung Cancer issued a call for physicians to discuss lung cancer screening with patients who match the high-risk smoking history of those enrolled in the NSLT.
Dr. Reid reported having no financial conflicts of interest.