User login
OsteoArthritis Research Society International (OARSI): World Congress on Osteoarthritis
Harnessing the placebo effect in management of osteoarthritis
SEATTLE – When it comes to managing osteoarthritis, clinicians can use their interactions with patients to tap into a powerful placebo effect, according to Dr. Paul Dieppe, a professor of health and well-being at the University of Exeter, England.
“I am particularly excited to have the opportunity to talk to you about a phenomenology that I think is amongst the most important within medicine and an area that those of us interested in osteoarthritis could really exploit,” he said at the World Congress on Osteoarthritis. “We don’t have a treatment that’s better than placebo, so let’s use placebo.”
In the clinical trial context, the placebo effect – the response seen from giving a sham or dummy treatment, or in essence, doing nothing – has an effect size of about 0.5 for alleviating pain and stiffness from osteoarthritis (Ann. Rheum. Dis. 2008;67:1716-23). “That’s an effect size which is quite a lot bigger than the effect size of most of the standard interventions that we use, be they drug therapy, physical therapy, whatever. It’s not as big as joint replacement, although there we don’t have the appropriate data. But it is bigger than pretty much everything else. So ‘nothing’ is efficacious,” Dr. Dieppe commented.
On the other hand, effectiveness in the real-world setting is unknown and would require large pragmatic trials or Big Data analyses using registries. “But I think the effectiveness of ‘nothing’ is much, much greater than its efficacy in the very artificial circumstance of a clinical trial,” he said, a viewpoint based on his experience both as a clinician and as a patient with knee osteoarthritis.
“I prefer to call [the placebo effect] a healing response, and I’m not trying to be provocative using that term because I think we do have innate healing abilities in our bodies. I think that’s an evolutionary demand, and good interactions can activate that,” Dr. Dieppe maintained.
Compelling evidence suggests that healing does indeed work (Explore [NY] 2015;11:11-23). “We think that it’s mediated by focused attention with good intention of sensitive people,” he said. “Maybe that’s what a lot of you as therapists are actually doing. Maybe that is the basis of much of what we call the placebo effect.”
Clinicians should also be aware of the nocebo effect, what Dr. Dieppe referred to as the placebo effect’s evil twin, as it can negatively influence outcomes and is stronger (Am. J. Med. 2015;128:126-9). “The fact is that doing nothing ... can and often does make our patients much worse. This is most likely to occur when one or both people in a consultation are feeling unsafe or anxious. ... A lot of what we do in modern health care seems designed to make people anxious and to make them worse,” he elaborated at the meeting, which was sponsored by the Osteoarthritis Research Society International.
Many of the leading theories about the placebo and nocebo effects postulate that they relate to factors such as expectations or the release or blockage of natural endorphins. “These theories are basically saying that this is all about what’s going on in the brain of the patient,” Dr. Dieppe commented. “I think that’s wrong. ... It’s missing the point, completely, because the point is that this is about the quality of interactions between individuals. We are social beings, we are evolved as social beings, and our social interactions control a lot of what happens to us, not only psychologically but physiologically.”
He pointed to theories that instead focus on interactions, such as one pertaining to the concept of validation and invalidation (J. Clin. Psychol. 2006;62:459-80). “This theory goes beyond empathy and compassion, which are the usual sort of things evoked in this context, because you can be empathic and compassionate as much as you like, but if the patient in front of you doesn’t know you are being empathic or compassionate, then it’s no use at all. So validation, invalidation is more about have you successfully communicated that empathy and compassion to the other person or not. If you have, the person feels validated, they feel you genuinely do understand them, and you do genuinely care about them. If they are invalidated, they feel you haven’t understood them, and you don’t really care.” He added, “It depends very much on your behavior, as much as on what you say. Communication specialists tell us that 80% of communication to people is nonverbal.”
Another relevant theory here is the polyvagal theory of social interaction, which proposes that in addition to being hardwired for a fight or flight response, the autonomic nervous system is hardwired for a nurturing response (Cleve. Clin. J. Med. 2009;76 Suppl 2:S86-S90). Activation of this response has a calming physiologic effect and influences how messages are heard. “This nurturing response … is linked to communication strategies, so that you have to feel safe to be able to communicate well with another person,” Dr. Dieppe noted.
Taken together, these theories on interactions help explain “how we can make people better, how we can make people worse with ‘nothing,’ ” he maintained. “Of course, it’s not nothing – it’s the totality of our behavior with another person, and it’s crucial. And it can, in extreme cases, positively activate the innate healing response, or it can, as we often do sadly in clinical practice, activate an invalidation, fight-or-flight response, and make everything a lot worse.”
“There are colossal implications about how we behave when we are with patients,” Dr. Dieppe concluded. “I think basically, it’s just about our ability to be present for another human being in a nonjudgmental way. And that’s difficult, but that’s what we need to be able to do.”
SEATTLE – When it comes to managing osteoarthritis, clinicians can use their interactions with patients to tap into a powerful placebo effect, according to Dr. Paul Dieppe, a professor of health and well-being at the University of Exeter, England.
“I am particularly excited to have the opportunity to talk to you about a phenomenology that I think is amongst the most important within medicine and an area that those of us interested in osteoarthritis could really exploit,” he said at the World Congress on Osteoarthritis. “We don’t have a treatment that’s better than placebo, so let’s use placebo.”
In the clinical trial context, the placebo effect – the response seen from giving a sham or dummy treatment, or in essence, doing nothing – has an effect size of about 0.5 for alleviating pain and stiffness from osteoarthritis (Ann. Rheum. Dis. 2008;67:1716-23). “That’s an effect size which is quite a lot bigger than the effect size of most of the standard interventions that we use, be they drug therapy, physical therapy, whatever. It’s not as big as joint replacement, although there we don’t have the appropriate data. But it is bigger than pretty much everything else. So ‘nothing’ is efficacious,” Dr. Dieppe commented.
On the other hand, effectiveness in the real-world setting is unknown and would require large pragmatic trials or Big Data analyses using registries. “But I think the effectiveness of ‘nothing’ is much, much greater than its efficacy in the very artificial circumstance of a clinical trial,” he said, a viewpoint based on his experience both as a clinician and as a patient with knee osteoarthritis.
“I prefer to call [the placebo effect] a healing response, and I’m not trying to be provocative using that term because I think we do have innate healing abilities in our bodies. I think that’s an evolutionary demand, and good interactions can activate that,” Dr. Dieppe maintained.
Compelling evidence suggests that healing does indeed work (Explore [NY] 2015;11:11-23). “We think that it’s mediated by focused attention with good intention of sensitive people,” he said. “Maybe that’s what a lot of you as therapists are actually doing. Maybe that is the basis of much of what we call the placebo effect.”
Clinicians should also be aware of the nocebo effect, what Dr. Dieppe referred to as the placebo effect’s evil twin, as it can negatively influence outcomes and is stronger (Am. J. Med. 2015;128:126-9). “The fact is that doing nothing ... can and often does make our patients much worse. This is most likely to occur when one or both people in a consultation are feeling unsafe or anxious. ... A lot of what we do in modern health care seems designed to make people anxious and to make them worse,” he elaborated at the meeting, which was sponsored by the Osteoarthritis Research Society International.
Many of the leading theories about the placebo and nocebo effects postulate that they relate to factors such as expectations or the release or blockage of natural endorphins. “These theories are basically saying that this is all about what’s going on in the brain of the patient,” Dr. Dieppe commented. “I think that’s wrong. ... It’s missing the point, completely, because the point is that this is about the quality of interactions between individuals. We are social beings, we are evolved as social beings, and our social interactions control a lot of what happens to us, not only psychologically but physiologically.”
He pointed to theories that instead focus on interactions, such as one pertaining to the concept of validation and invalidation (J. Clin. Psychol. 2006;62:459-80). “This theory goes beyond empathy and compassion, which are the usual sort of things evoked in this context, because you can be empathic and compassionate as much as you like, but if the patient in front of you doesn’t know you are being empathic or compassionate, then it’s no use at all. So validation, invalidation is more about have you successfully communicated that empathy and compassion to the other person or not. If you have, the person feels validated, they feel you genuinely do understand them, and you do genuinely care about them. If they are invalidated, they feel you haven’t understood them, and you don’t really care.” He added, “It depends very much on your behavior, as much as on what you say. Communication specialists tell us that 80% of communication to people is nonverbal.”
Another relevant theory here is the polyvagal theory of social interaction, which proposes that in addition to being hardwired for a fight or flight response, the autonomic nervous system is hardwired for a nurturing response (Cleve. Clin. J. Med. 2009;76 Suppl 2:S86-S90). Activation of this response has a calming physiologic effect and influences how messages are heard. “This nurturing response … is linked to communication strategies, so that you have to feel safe to be able to communicate well with another person,” Dr. Dieppe noted.
Taken together, these theories on interactions help explain “how we can make people better, how we can make people worse with ‘nothing,’ ” he maintained. “Of course, it’s not nothing – it’s the totality of our behavior with another person, and it’s crucial. And it can, in extreme cases, positively activate the innate healing response, or it can, as we often do sadly in clinical practice, activate an invalidation, fight-or-flight response, and make everything a lot worse.”
“There are colossal implications about how we behave when we are with patients,” Dr. Dieppe concluded. “I think basically, it’s just about our ability to be present for another human being in a nonjudgmental way. And that’s difficult, but that’s what we need to be able to do.”
SEATTLE – When it comes to managing osteoarthritis, clinicians can use their interactions with patients to tap into a powerful placebo effect, according to Dr. Paul Dieppe, a professor of health and well-being at the University of Exeter, England.
“I am particularly excited to have the opportunity to talk to you about a phenomenology that I think is amongst the most important within medicine and an area that those of us interested in osteoarthritis could really exploit,” he said at the World Congress on Osteoarthritis. “We don’t have a treatment that’s better than placebo, so let’s use placebo.”
In the clinical trial context, the placebo effect – the response seen from giving a sham or dummy treatment, or in essence, doing nothing – has an effect size of about 0.5 for alleviating pain and stiffness from osteoarthritis (Ann. Rheum. Dis. 2008;67:1716-23). “That’s an effect size which is quite a lot bigger than the effect size of most of the standard interventions that we use, be they drug therapy, physical therapy, whatever. It’s not as big as joint replacement, although there we don’t have the appropriate data. But it is bigger than pretty much everything else. So ‘nothing’ is efficacious,” Dr. Dieppe commented.
On the other hand, effectiveness in the real-world setting is unknown and would require large pragmatic trials or Big Data analyses using registries. “But I think the effectiveness of ‘nothing’ is much, much greater than its efficacy in the very artificial circumstance of a clinical trial,” he said, a viewpoint based on his experience both as a clinician and as a patient with knee osteoarthritis.
“I prefer to call [the placebo effect] a healing response, and I’m not trying to be provocative using that term because I think we do have innate healing abilities in our bodies. I think that’s an evolutionary demand, and good interactions can activate that,” Dr. Dieppe maintained.
Compelling evidence suggests that healing does indeed work (Explore [NY] 2015;11:11-23). “We think that it’s mediated by focused attention with good intention of sensitive people,” he said. “Maybe that’s what a lot of you as therapists are actually doing. Maybe that is the basis of much of what we call the placebo effect.”
Clinicians should also be aware of the nocebo effect, what Dr. Dieppe referred to as the placebo effect’s evil twin, as it can negatively influence outcomes and is stronger (Am. J. Med. 2015;128:126-9). “The fact is that doing nothing ... can and often does make our patients much worse. This is most likely to occur when one or both people in a consultation are feeling unsafe or anxious. ... A lot of what we do in modern health care seems designed to make people anxious and to make them worse,” he elaborated at the meeting, which was sponsored by the Osteoarthritis Research Society International.
Many of the leading theories about the placebo and nocebo effects postulate that they relate to factors such as expectations or the release or blockage of natural endorphins. “These theories are basically saying that this is all about what’s going on in the brain of the patient,” Dr. Dieppe commented. “I think that’s wrong. ... It’s missing the point, completely, because the point is that this is about the quality of interactions between individuals. We are social beings, we are evolved as social beings, and our social interactions control a lot of what happens to us, not only psychologically but physiologically.”
He pointed to theories that instead focus on interactions, such as one pertaining to the concept of validation and invalidation (J. Clin. Psychol. 2006;62:459-80). “This theory goes beyond empathy and compassion, which are the usual sort of things evoked in this context, because you can be empathic and compassionate as much as you like, but if the patient in front of you doesn’t know you are being empathic or compassionate, then it’s no use at all. So validation, invalidation is more about have you successfully communicated that empathy and compassion to the other person or not. If you have, the person feels validated, they feel you genuinely do understand them, and you do genuinely care about them. If they are invalidated, they feel you haven’t understood them, and you don’t really care.” He added, “It depends very much on your behavior, as much as on what you say. Communication specialists tell us that 80% of communication to people is nonverbal.”
Another relevant theory here is the polyvagal theory of social interaction, which proposes that in addition to being hardwired for a fight or flight response, the autonomic nervous system is hardwired for a nurturing response (Cleve. Clin. J. Med. 2009;76 Suppl 2:S86-S90). Activation of this response has a calming physiologic effect and influences how messages are heard. “This nurturing response … is linked to communication strategies, so that you have to feel safe to be able to communicate well with another person,” Dr. Dieppe noted.
Taken together, these theories on interactions help explain “how we can make people better, how we can make people worse with ‘nothing,’ ” he maintained. “Of course, it’s not nothing – it’s the totality of our behavior with another person, and it’s crucial. And it can, in extreme cases, positively activate the innate healing response, or it can, as we often do sadly in clinical practice, activate an invalidation, fight-or-flight response, and make everything a lot worse.”
“There are colossal implications about how we behave when we are with patients,” Dr. Dieppe concluded. “I think basically, it’s just about our ability to be present for another human being in a nonjudgmental way. And that’s difficult, but that’s what we need to be able to do.”
AT OARSI 2015
OARSI: Set concrete walking goals in knee OA
SEATTLE – The pain of knee osteoarthritis is not exacerbated by regular exercise such as walking and may actually be relieved by it, according to several findings presented at the World Congress on Osteoarthritis.
“Physical activity is important for the reduction of knee pain and the prevention of functional limitation in knee osteoarthritis,” Daniel White, Sc.D., said.
“We should be recommending walking to people with painful knee osteoarthritis. Just as a preliminary goal, we can start with 3,000 steps per day and ultimately progress people to at least 6,000 steps per day,” he added.
National guidelines issued in 2008 for the general population call for at least 150 minutes per week of moderate to vigorous–intensity physical activity, according to Dr. White of the department of physical therapy at the University of Delaware in Newark. When that recommendation is applied to walking, which is the most common physical activity among older adults (Arthritis Care Res. 2014;66:139-46), it translates to a brisk pace that permits conversation but is exertional enough to cause sweating. Meeting the goal would mean approximately 100 steps per minute (Am. J. Prev. Med. 2009;36:410-5).
“The clinical hypothesis is that osteoarthritis pain is limiting your physical activity, but whether that has been empirically [established] has yet to be seen,” Dr. White said. For example, investigators for an Osteoarthritis Initiative study found that only 13% of men and 8% of women with knee osteoarthritis met the criteria for the national guideline (Arthritis Rheum. 2011;63:3372-82), but also noted that these values differed little from those of the general population. Data from the Multicenter Osteoarthritis Study found similarly low proportions, regardless of the presence of radiographic disease and the severity of knee pain (Arthritis Rheum. 2013;65:139-47). In a cohort that underwent total knee replacement, patients had more than 180% improvements in subjective pain and function at 6 months, yet their objectively measured time spent walking increased by only 5% (Clin. Orthop. Relat. Res. 2008;466:2201-8).
These findings suggest that osteoarthritis and pain may have a limited role in explaining physical inactivity, according to Dr. White. “An implication of this is that improvements in disease and pain may not lead to more physical activity; in other words, the pills you give to people to make them feel better or the exercises that they may do to improve their knee pain may not necessarily increase the amount of unstructured physical activity that people do on a day-to-day basis. Also, physical activity specifically may need to be targeted; you need to increase physical activity in a specific way rather than just expecting it to happen once the barriers of pain and disease are removed.”
Recommendations for physical activity must consider both potential risks and benefits, he noted. Data regarding its impact on structural changes in the knee are mixed. Conversely, there is substantial evidence that physical activity moderately reduces knee pain (Cochrane Database Syst Rev. 2015;1:CD004376) and lowers the likelihood of developing functional limitations in a dose-response manner (Arthritis Care Res. 2014;66:1328-36). And there are a variety of other health benefits, some of which may affect osteoarthritis, such as weight maintenance.
“In my mind, the benefits outweigh the risks for promoting physical activity in this patient population. And specifically, given that walking is the most common physical activity, from a clinical perspective, there is very strong evidence to recommend walking to this patient population,” Dr. White said at the meeting sponsored by the Osteoarthritis Research Society International.
He further endorsed use of a pedometer as a practical, objective way to measure this activity. “Regardless of what instrument or device you use, they all measure steps, and that is sort of the common denominator which is a very understandable outcome that patients can relate to, that clinicians understand,” he elaborated. Moreover, a meta-analysis has shown that interventions using pedometers achieve greater increases in walking (JAMA 2007;298:2296-304).
The above analysis of impact on functional limitations in people with knee osteoarthritis also helps to define target walking goals, according to Dr. White, who disclosed that he had no relevant conflicts of interest. The study showed that 95% of people who did not develop functional limitations walked at least 3,000 steps per day, and that 6,000 steps per day best discriminated between those who did and did not develop functional limitations.
Assuming that a moderate intensity of walking is 100 steps per minute, this step range translates to 30-60 minutes of walking per day, he said. As half of 60-year-olds in the general population already walk approximately 40-50 minutes daily as part of their usual activities (J. Gerontol. A Biol. Sci. Med. Sci. 2013;68:1426-32), they may need to add only 10 more minutes. And a recent report suggests that even people with severe knee osteoarthritis find this amount to be safe and feasible (Osteoarthritis Cartilage 2015 April 14 [doi:10.1016/j.joca.2015.04.001]).
SEATTLE – The pain of knee osteoarthritis is not exacerbated by regular exercise such as walking and may actually be relieved by it, according to several findings presented at the World Congress on Osteoarthritis.
“Physical activity is important for the reduction of knee pain and the prevention of functional limitation in knee osteoarthritis,” Daniel White, Sc.D., said.
“We should be recommending walking to people with painful knee osteoarthritis. Just as a preliminary goal, we can start with 3,000 steps per day and ultimately progress people to at least 6,000 steps per day,” he added.
National guidelines issued in 2008 for the general population call for at least 150 minutes per week of moderate to vigorous–intensity physical activity, according to Dr. White of the department of physical therapy at the University of Delaware in Newark. When that recommendation is applied to walking, which is the most common physical activity among older adults (Arthritis Care Res. 2014;66:139-46), it translates to a brisk pace that permits conversation but is exertional enough to cause sweating. Meeting the goal would mean approximately 100 steps per minute (Am. J. Prev. Med. 2009;36:410-5).
“The clinical hypothesis is that osteoarthritis pain is limiting your physical activity, but whether that has been empirically [established] has yet to be seen,” Dr. White said. For example, investigators for an Osteoarthritis Initiative study found that only 13% of men and 8% of women with knee osteoarthritis met the criteria for the national guideline (Arthritis Rheum. 2011;63:3372-82), but also noted that these values differed little from those of the general population. Data from the Multicenter Osteoarthritis Study found similarly low proportions, regardless of the presence of radiographic disease and the severity of knee pain (Arthritis Rheum. 2013;65:139-47). In a cohort that underwent total knee replacement, patients had more than 180% improvements in subjective pain and function at 6 months, yet their objectively measured time spent walking increased by only 5% (Clin. Orthop. Relat. Res. 2008;466:2201-8).
These findings suggest that osteoarthritis and pain may have a limited role in explaining physical inactivity, according to Dr. White. “An implication of this is that improvements in disease and pain may not lead to more physical activity; in other words, the pills you give to people to make them feel better or the exercises that they may do to improve their knee pain may not necessarily increase the amount of unstructured physical activity that people do on a day-to-day basis. Also, physical activity specifically may need to be targeted; you need to increase physical activity in a specific way rather than just expecting it to happen once the barriers of pain and disease are removed.”
Recommendations for physical activity must consider both potential risks and benefits, he noted. Data regarding its impact on structural changes in the knee are mixed. Conversely, there is substantial evidence that physical activity moderately reduces knee pain (Cochrane Database Syst Rev. 2015;1:CD004376) and lowers the likelihood of developing functional limitations in a dose-response manner (Arthritis Care Res. 2014;66:1328-36). And there are a variety of other health benefits, some of which may affect osteoarthritis, such as weight maintenance.
“In my mind, the benefits outweigh the risks for promoting physical activity in this patient population. And specifically, given that walking is the most common physical activity, from a clinical perspective, there is very strong evidence to recommend walking to this patient population,” Dr. White said at the meeting sponsored by the Osteoarthritis Research Society International.
He further endorsed use of a pedometer as a practical, objective way to measure this activity. “Regardless of what instrument or device you use, they all measure steps, and that is sort of the common denominator which is a very understandable outcome that patients can relate to, that clinicians understand,” he elaborated. Moreover, a meta-analysis has shown that interventions using pedometers achieve greater increases in walking (JAMA 2007;298:2296-304).
The above analysis of impact on functional limitations in people with knee osteoarthritis also helps to define target walking goals, according to Dr. White, who disclosed that he had no relevant conflicts of interest. The study showed that 95% of people who did not develop functional limitations walked at least 3,000 steps per day, and that 6,000 steps per day best discriminated between those who did and did not develop functional limitations.
Assuming that a moderate intensity of walking is 100 steps per minute, this step range translates to 30-60 minutes of walking per day, he said. As half of 60-year-olds in the general population already walk approximately 40-50 minutes daily as part of their usual activities (J. Gerontol. A Biol. Sci. Med. Sci. 2013;68:1426-32), they may need to add only 10 more minutes. And a recent report suggests that even people with severe knee osteoarthritis find this amount to be safe and feasible (Osteoarthritis Cartilage 2015 April 14 [doi:10.1016/j.joca.2015.04.001]).
SEATTLE – The pain of knee osteoarthritis is not exacerbated by regular exercise such as walking and may actually be relieved by it, according to several findings presented at the World Congress on Osteoarthritis.
“Physical activity is important for the reduction of knee pain and the prevention of functional limitation in knee osteoarthritis,” Daniel White, Sc.D., said.
“We should be recommending walking to people with painful knee osteoarthritis. Just as a preliminary goal, we can start with 3,000 steps per day and ultimately progress people to at least 6,000 steps per day,” he added.
National guidelines issued in 2008 for the general population call for at least 150 minutes per week of moderate to vigorous–intensity physical activity, according to Dr. White of the department of physical therapy at the University of Delaware in Newark. When that recommendation is applied to walking, which is the most common physical activity among older adults (Arthritis Care Res. 2014;66:139-46), it translates to a brisk pace that permits conversation but is exertional enough to cause sweating. Meeting the goal would mean approximately 100 steps per minute (Am. J. Prev. Med. 2009;36:410-5).
“The clinical hypothesis is that osteoarthritis pain is limiting your physical activity, but whether that has been empirically [established] has yet to be seen,” Dr. White said. For example, investigators for an Osteoarthritis Initiative study found that only 13% of men and 8% of women with knee osteoarthritis met the criteria for the national guideline (Arthritis Rheum. 2011;63:3372-82), but also noted that these values differed little from those of the general population. Data from the Multicenter Osteoarthritis Study found similarly low proportions, regardless of the presence of radiographic disease and the severity of knee pain (Arthritis Rheum. 2013;65:139-47). In a cohort that underwent total knee replacement, patients had more than 180% improvements in subjective pain and function at 6 months, yet their objectively measured time spent walking increased by only 5% (Clin. Orthop. Relat. Res. 2008;466:2201-8).
These findings suggest that osteoarthritis and pain may have a limited role in explaining physical inactivity, according to Dr. White. “An implication of this is that improvements in disease and pain may not lead to more physical activity; in other words, the pills you give to people to make them feel better or the exercises that they may do to improve their knee pain may not necessarily increase the amount of unstructured physical activity that people do on a day-to-day basis. Also, physical activity specifically may need to be targeted; you need to increase physical activity in a specific way rather than just expecting it to happen once the barriers of pain and disease are removed.”
Recommendations for physical activity must consider both potential risks and benefits, he noted. Data regarding its impact on structural changes in the knee are mixed. Conversely, there is substantial evidence that physical activity moderately reduces knee pain (Cochrane Database Syst Rev. 2015;1:CD004376) and lowers the likelihood of developing functional limitations in a dose-response manner (Arthritis Care Res. 2014;66:1328-36). And there are a variety of other health benefits, some of which may affect osteoarthritis, such as weight maintenance.
“In my mind, the benefits outweigh the risks for promoting physical activity in this patient population. And specifically, given that walking is the most common physical activity, from a clinical perspective, there is very strong evidence to recommend walking to this patient population,” Dr. White said at the meeting sponsored by the Osteoarthritis Research Society International.
He further endorsed use of a pedometer as a practical, objective way to measure this activity. “Regardless of what instrument or device you use, they all measure steps, and that is sort of the common denominator which is a very understandable outcome that patients can relate to, that clinicians understand,” he elaborated. Moreover, a meta-analysis has shown that interventions using pedometers achieve greater increases in walking (JAMA 2007;298:2296-304).
The above analysis of impact on functional limitations in people with knee osteoarthritis also helps to define target walking goals, according to Dr. White, who disclosed that he had no relevant conflicts of interest. The study showed that 95% of people who did not develop functional limitations walked at least 3,000 steps per day, and that 6,000 steps per day best discriminated between those who did and did not develop functional limitations.
Assuming that a moderate intensity of walking is 100 steps per minute, this step range translates to 30-60 minutes of walking per day, he said. As half of 60-year-olds in the general population already walk approximately 40-50 minutes daily as part of their usual activities (J. Gerontol. A Biol. Sci. Med. Sci. 2013;68:1426-32), they may need to add only 10 more minutes. And a recent report suggests that even people with severe knee osteoarthritis find this amount to be safe and feasible (Osteoarthritis Cartilage 2015 April 14 [doi:10.1016/j.joca.2015.04.001]).
EXPERT ANALYSIS FROM OARSI 2015

OARSI: CRP is prognostic marker in knee osteoarthritis
SEATTLE – C-reactive protein is associated with the presence and progression of bone marrow lesions in patients with osteoarthritis of the knee, according to data from a cohort study of 192 patients that were reported at the World Congress on Osteoarthritis.
“Osteoarthritis has predominantly been viewed as a degenerative joint disease driven by continued and irreversible deterioration of joints,” said lead investigator Zhaohua (Alex) Zhu, a PhD candidate at the Menzies Institute for Medical Research, University of Tasmania, Hobart, Australia. “However, current studies suggest a different way of understanding this disease, showing that the development of osteoarthritis may be in great part driven by a low-grade inflammatory process.”

He and his colleagues analyzed data from the randomized phase III VIDEO trial (Vitamin D Effect on Osteoarthritis), which enrolled patients aged 50-79 years who had symptomatic knee osteoarthritis and vitamin D deficiency. Analyses were based on 192 patients who had measurement of high-sensitivity C-reactive protein (CRP) and resistin (a proinflammatory cytokine secreted by adipose tissue) at baseline and again 2 years later.
Bone marrow lesions also were assessed at both time points with a modified version of the whole-organ magnetic resonance imaging score (WORMS). “Bone marrow lesions may represent areas of edema, inflammation, and remodeling,” Mr. Zhu explained. “Plenty of studies have shown that bone marrow lesions are linked to knee pain, cartilage volumes, and cartilage defect changes, so it’s a very important subchondral feature in knee osteoarthritis. But so far, the cause of bone marrow lesions remains unclear.”
Multivariate analyses showed that, as patients’ baseline CRP quartile increased, so did their odds of having total knee bone marrow lesions at that time (odds ratio, 1.45) and worsening of these lesions during follow-up (odds ratio, 1.56), according to data reported at the meeting, which was sponsored by the Osteoarthritis Research Society International. Additionally, the absolute change in CRP level during follow-up was positively associated with a worsening of lesions.
Associations for resistin were generally weaker or absent, with the only significant one seen between baseline quartile of that marker and bone marrow lesions at that time, reported Dr. Zhu.
In an interview, Dr. Timothy McAlindon, one of the session’s comoderators and professor of medicine at Tufts University in Boston, said that the study helps elucidate a possible role for adipose tissue, overweight, and adipocytokines in one subphenotype of osteoarthritis. “They found some associations, and I think those associations are probably the basis for further study and hopefully more understanding of what they mean,” he commented.
Dr. Rik Lories, the other session comoderator and professor at the University of Leuven (Belgium), noted that research on this topic is complicated. “You can ask questions about the chicken and the egg in this case because, if you are obese, you have a higher fat mass, so you are more likely to produce proinflammatory mediators, which can then induce your CRP. The fact that you have more inflammatory mediators could also contribute to the fact that you get these bone marrow lesions,” he elaborated. “But on the other hand, if you put more weight on your knees, the impact may also play a role. So it remains a very, very difficult thing to study and to come up with clear answers.”
Dr. Zhu disclosed no relevant conflicts of interest.
SEATTLE – C-reactive protein is associated with the presence and progression of bone marrow lesions in patients with osteoarthritis of the knee, according to data from a cohort study of 192 patients that were reported at the World Congress on Osteoarthritis.
“Osteoarthritis has predominantly been viewed as a degenerative joint disease driven by continued and irreversible deterioration of joints,” said lead investigator Zhaohua (Alex) Zhu, a PhD candidate at the Menzies Institute for Medical Research, University of Tasmania, Hobart, Australia. “However, current studies suggest a different way of understanding this disease, showing that the development of osteoarthritis may be in great part driven by a low-grade inflammatory process.”
He and his colleagues analyzed data from the randomized phase III VIDEO trial (Vitamin D Effect on Osteoarthritis), which enrolled patients aged 50-79 years who had symptomatic knee osteoarthritis and vitamin D deficiency. Analyses were based on 192 patients who had measurement of high-sensitivity C-reactive protein (CRP) and resistin (a proinflammatory cytokine secreted by adipose tissue) at baseline and again 2 years later.
Bone marrow lesions also were assessed at both time points with a modified version of the whole-organ magnetic resonance imaging score (WORMS). “Bone marrow lesions may represent areas of edema, inflammation, and remodeling,” Mr. Zhu explained. “Plenty of studies have shown that bone marrow lesions are linked to knee pain, cartilage volumes, and cartilage defect changes, so it’s a very important subchondral feature in knee osteoarthritis. But so far, the cause of bone marrow lesions remains unclear.”
Multivariate analyses showed that, as patients’ baseline CRP quartile increased, so did their odds of having total knee bone marrow lesions at that time (odds ratio, 1.45) and worsening of these lesions during follow-up (odds ratio, 1.56), according to data reported at the meeting, which was sponsored by the Osteoarthritis Research Society International. Additionally, the absolute change in CRP level during follow-up was positively associated with a worsening of lesions.
Associations for resistin were generally weaker or absent, with the only significant one seen between baseline quartile of that marker and bone marrow lesions at that time, reported Dr. Zhu.
In an interview, Dr. Timothy McAlindon, one of the session’s comoderators and professor of medicine at Tufts University in Boston, said that the study helps elucidate a possible role for adipose tissue, overweight, and adipocytokines in one subphenotype of osteoarthritis. “They found some associations, and I think those associations are probably the basis for further study and hopefully more understanding of what they mean,” he commented.
Dr. Rik Lories, the other session comoderator and professor at the University of Leuven (Belgium), noted that research on this topic is complicated. “You can ask questions about the chicken and the egg in this case because, if you are obese, you have a higher fat mass, so you are more likely to produce proinflammatory mediators, which can then induce your CRP. The fact that you have more inflammatory mediators could also contribute to the fact that you get these bone marrow lesions,” he elaborated. “But on the other hand, if you put more weight on your knees, the impact may also play a role. So it remains a very, very difficult thing to study and to come up with clear answers.”
Dr. Zhu disclosed no relevant conflicts of interest.
SEATTLE – C-reactive protein is associated with the presence and progression of bone marrow lesions in patients with osteoarthritis of the knee, according to data from a cohort study of 192 patients that were reported at the World Congress on Osteoarthritis.
“Osteoarthritis has predominantly been viewed as a degenerative joint disease driven by continued and irreversible deterioration of joints,” said lead investigator Zhaohua (Alex) Zhu, a PhD candidate at the Menzies Institute for Medical Research, University of Tasmania, Hobart, Australia. “However, current studies suggest a different way of understanding this disease, showing that the development of osteoarthritis may be in great part driven by a low-grade inflammatory process.”
He and his colleagues analyzed data from the randomized phase III VIDEO trial (Vitamin D Effect on Osteoarthritis), which enrolled patients aged 50-79 years who had symptomatic knee osteoarthritis and vitamin D deficiency. Analyses were based on 192 patients who had measurement of high-sensitivity C-reactive protein (CRP) and resistin (a proinflammatory cytokine secreted by adipose tissue) at baseline and again 2 years later.
Bone marrow lesions also were assessed at both time points with a modified version of the whole-organ magnetic resonance imaging score (WORMS). “Bone marrow lesions may represent areas of edema, inflammation, and remodeling,” Mr. Zhu explained. “Plenty of studies have shown that bone marrow lesions are linked to knee pain, cartilage volumes, and cartilage defect changes, so it’s a very important subchondral feature in knee osteoarthritis. But so far, the cause of bone marrow lesions remains unclear.”
Multivariate analyses showed that, as patients’ baseline CRP quartile increased, so did their odds of having total knee bone marrow lesions at that time (odds ratio, 1.45) and worsening of these lesions during follow-up (odds ratio, 1.56), according to data reported at the meeting, which was sponsored by the Osteoarthritis Research Society International. Additionally, the absolute change in CRP level during follow-up was positively associated with a worsening of lesions.
Associations for resistin were generally weaker or absent, with the only significant one seen between baseline quartile of that marker and bone marrow lesions at that time, reported Dr. Zhu.
In an interview, Dr. Timothy McAlindon, one of the session’s comoderators and professor of medicine at Tufts University in Boston, said that the study helps elucidate a possible role for adipose tissue, overweight, and adipocytokines in one subphenotype of osteoarthritis. “They found some associations, and I think those associations are probably the basis for further study and hopefully more understanding of what they mean,” he commented.
Dr. Rik Lories, the other session comoderator and professor at the University of Leuven (Belgium), noted that research on this topic is complicated. “You can ask questions about the chicken and the egg in this case because, if you are obese, you have a higher fat mass, so you are more likely to produce proinflammatory mediators, which can then induce your CRP. The fact that you have more inflammatory mediators could also contribute to the fact that you get these bone marrow lesions,” he elaborated. “But on the other hand, if you put more weight on your knees, the impact may also play a role. So it remains a very, very difficult thing to study and to come up with clear answers.”
Dr. Zhu disclosed no relevant conflicts of interest.
AT OARSI 2015
Key clinical point: CRP levels can help to identify patients at increased risk for progression of bone marrow lesions.
Major finding: As patients’ baseline CRP quartile increased, so did their odds of having bone marrow lesions (odds ratio, 1.45) and worsening of those lesions during follow-up (odds ratio, 1.56).
Data source: A cohort study from a randomized trial of 192 patients with knee osteoarthritis and vitamin D deficiency.
Disclosures: Dr. Zhu reported having no financial conflicts.

OARSI: Flex educational, motivational muscle when prescribing exercise for OA
SEATTLE – A new study using an analytic framework grounded in behavior change theory shows several modifiable ways to help patients with knee and/or hip osteoarthritis to exercise, the most influential being beliefs about exercise, medical advice, gym referral, supervision, and encouragement, according to a report at the World Congress on Osteoarthritis.
“Our study provides a comprehensive synthesis of the many barriers and facilitators faced by those with osteoarthritis regarding intentional exercise,” commented lead investigator Philippa Nicolson, a research scientist at the Centre for Health, Exercise & Sports Medicine, University of Melbourne.

“Importantly, exercise adherence is not a problem that patients can solve on their own. Clinicians must take an active and leading role in identifying and considering barriers and facilitators to exercise, and engage with patients to create a patient-centered exercise plan that suits each individual’s needs and circumstances,” she recommended. “Clinicians must also help patients to gain the knowledge and skills that they need in order to adhere to exercise in the long term.”
In an interview, Stephen P. Messier, Ph.D., session comoderator and professor and director of both the J.B. Snow Biomechanics Laboratory and the Wake Forest University Runners’ Clinic in Winston-Salem, N. C., said, “A lot of this is not new information, I would say, but it really is important that [clinicians] understand that people who have been sedentary all their lives need help. They can’t do it on their own.”
Critical issues are how to stay in contact with patients and give them ongoing support in the long term, he noted, adding that, with social media and other methods, physicians can give patients personal help in the beginning and then wean them off of that help but still stay in contact in some way so patients feel like they have someone to talk to and someone that cares.
The physician plays a key role in the process, all the way from prescribing exercise to identifying suitable facilities to monitoring progress. “When your doctor cares about it, then older folks are going to do it because they really pay attention to what the physician says,” Dr. Messier said.

Introducing the study, Ms. Nicolson commented, “Exercise is a core component of osteoarthritis management and is now recommended in all clinical guidelines. High-quality evidence for the benefits of exercise in improving pain and function for those with lower-limb osteoarthritis are well established. However, exercise is globally underutilized, and among those for whom exercise is prescribed, adherence is found to be poor, particularly in the long term.”
“Understanding the barriers and facilitators to exercise will allow clinicians to change their practice to better facilitate adherence and allow researchers to develop and evaluate behavioral interventions targeting improved adherence,” she explained. “Given that initiating and adhering to exercise often requires significant behavior change, the use of behavior change theory is essential. In order to facilitate people with osteoarthritis to exercise, we need to analyze the behaviors influencing exercise participation. Interventions based on behavior change theory have been found to be significantly more successful than those that are not.”
The investigators conducted a scoping review to identify exercise barriers and facilitators in this population. They identified 23 relevant articles on intentional exercise (supervised or not and prescribed or self-initiated) among a total of 4,633 patients aged 45 years or older with hip and/or knee osteoarthritis.
Most of the more than 200 barriers and facilitators extracted from the articles were modifiable, according to data reported at the meeting, which was sponsored by the Osteoarthritis Research Society International.
The investigators mapped these modifiable factors onto domains of the Theoretical Domains Framework, which integrates multiple behavior change theories into a single framework and is aimed at helping researchers identify processes that do and do not work (Implement. Sci. 2012;7:37). They found that the barriers and facilitators mapped onto all 14 domains.
Among highlights, the many barriers mapping onto the framework’s Environmental Context and Resources domain included having to descend hills or stairs during a walking program, inability to find a suitable exercise, and rigidity of the program. Facilitators mapping onto this domain included use of a pedometer, physical therapist guidance, and receipt of a gym referral from the doctor.
Barriers mapping onto the Beliefs About Consequences domain included a belief that exercise has limited benefit, fear about damaging the joint further, and concern about precipitating pain.
Facilitators mapping onto the Reinforcement domain included medical advice to exercise, telephone reinforcement, and getting physician encouragement.
“Our findings have a number of clinical implications,” commented Ms. Nicolson.
“Given the many barriers that we identified linking to a person’s environment and resources, this highlights the need for individualized exercise tailored to each person’s situation,” she said. “Many barriers also relate to a person’s beliefs about their ability and consequences of exercise … This highlights the need for thorough and accurate education to each and every patient about their capabilities and the likely benefits of exercise.”
“Reinforcement, both internal and external, was frequently identified as a facilitator to exercise. The use of such things as logbooks, diaries, ongoing encouragement, and clinician advice to exercise can utilize these facilitators,” she concluded.
Ms. Nicolson disclosed no relevant conflicts of interest.
SEATTLE – A new study using an analytic framework grounded in behavior change theory shows several modifiable ways to help patients with knee and/or hip osteoarthritis to exercise, the most influential being beliefs about exercise, medical advice, gym referral, supervision, and encouragement, according to a report at the World Congress on Osteoarthritis.
“Our study provides a comprehensive synthesis of the many barriers and facilitators faced by those with osteoarthritis regarding intentional exercise,” commented lead investigator Philippa Nicolson, a research scientist at the Centre for Health, Exercise & Sports Medicine, University of Melbourne.
“Importantly, exercise adherence is not a problem that patients can solve on their own. Clinicians must take an active and leading role in identifying and considering barriers and facilitators to exercise, and engage with patients to create a patient-centered exercise plan that suits each individual’s needs and circumstances,” she recommended. “Clinicians must also help patients to gain the knowledge and skills that they need in order to adhere to exercise in the long term.”
In an interview, Stephen P. Messier, Ph.D., session comoderator and professor and director of both the J.B. Snow Biomechanics Laboratory and the Wake Forest University Runners’ Clinic in Winston-Salem, N. C., said, “A lot of this is not new information, I would say, but it really is important that [clinicians] understand that people who have been sedentary all their lives need help. They can’t do it on their own.”
Critical issues are how to stay in contact with patients and give them ongoing support in the long term, he noted, adding that, with social media and other methods, physicians can give patients personal help in the beginning and then wean them off of that help but still stay in contact in some way so patients feel like they have someone to talk to and someone that cares.
The physician plays a key role in the process, all the way from prescribing exercise to identifying suitable facilities to monitoring progress. “When your doctor cares about it, then older folks are going to do it because they really pay attention to what the physician says,” Dr. Messier said.
Introducing the study, Ms. Nicolson commented, “Exercise is a core component of osteoarthritis management and is now recommended in all clinical guidelines. High-quality evidence for the benefits of exercise in improving pain and function for those with lower-limb osteoarthritis are well established. However, exercise is globally underutilized, and among those for whom exercise is prescribed, adherence is found to be poor, particularly in the long term.”
“Understanding the barriers and facilitators to exercise will allow clinicians to change their practice to better facilitate adherence and allow researchers to develop and evaluate behavioral interventions targeting improved adherence,” she explained. “Given that initiating and adhering to exercise often requires significant behavior change, the use of behavior change theory is essential. In order to facilitate people with osteoarthritis to exercise, we need to analyze the behaviors influencing exercise participation. Interventions based on behavior change theory have been found to be significantly more successful than those that are not.”
The investigators conducted a scoping review to identify exercise barriers and facilitators in this population. They identified 23 relevant articles on intentional exercise (supervised or not and prescribed or self-initiated) among a total of 4,633 patients aged 45 years or older with hip and/or knee osteoarthritis.
Most of the more than 200 barriers and facilitators extracted from the articles were modifiable, according to data reported at the meeting, which was sponsored by the Osteoarthritis Research Society International.
The investigators mapped these modifiable factors onto domains of the Theoretical Domains Framework, which integrates multiple behavior change theories into a single framework and is aimed at helping researchers identify processes that do and do not work (Implement. Sci. 2012;7:37). They found that the barriers and facilitators mapped onto all 14 domains.
Among highlights, the many barriers mapping onto the framework’s Environmental Context and Resources domain included having to descend hills or stairs during a walking program, inability to find a suitable exercise, and rigidity of the program. Facilitators mapping onto this domain included use of a pedometer, physical therapist guidance, and receipt of a gym referral from the doctor.
Barriers mapping onto the Beliefs About Consequences domain included a belief that exercise has limited benefit, fear about damaging the joint further, and concern about precipitating pain.
Facilitators mapping onto the Reinforcement domain included medical advice to exercise, telephone reinforcement, and getting physician encouragement.
“Our findings have a number of clinical implications,” commented Ms. Nicolson.
“Given the many barriers that we identified linking to a person’s environment and resources, this highlights the need for individualized exercise tailored to each person’s situation,” she said. “Many barriers also relate to a person’s beliefs about their ability and consequences of exercise … This highlights the need for thorough and accurate education to each and every patient about their capabilities and the likely benefits of exercise.”
“Reinforcement, both internal and external, was frequently identified as a facilitator to exercise. The use of such things as logbooks, diaries, ongoing encouragement, and clinician advice to exercise can utilize these facilitators,” she concluded.
Ms. Nicolson disclosed no relevant conflicts of interest.
SEATTLE – A new study using an analytic framework grounded in behavior change theory shows several modifiable ways to help patients with knee and/or hip osteoarthritis to exercise, the most influential being beliefs about exercise, medical advice, gym referral, supervision, and encouragement, according to a report at the World Congress on Osteoarthritis.
“Our study provides a comprehensive synthesis of the many barriers and facilitators faced by those with osteoarthritis regarding intentional exercise,” commented lead investigator Philippa Nicolson, a research scientist at the Centre for Health, Exercise & Sports Medicine, University of Melbourne.
“Importantly, exercise adherence is not a problem that patients can solve on their own. Clinicians must take an active and leading role in identifying and considering barriers and facilitators to exercise, and engage with patients to create a patient-centered exercise plan that suits each individual’s needs and circumstances,” she recommended. “Clinicians must also help patients to gain the knowledge and skills that they need in order to adhere to exercise in the long term.”
In an interview, Stephen P. Messier, Ph.D., session comoderator and professor and director of both the J.B. Snow Biomechanics Laboratory and the Wake Forest University Runners’ Clinic in Winston-Salem, N. C., said, “A lot of this is not new information, I would say, but it really is important that [clinicians] understand that people who have been sedentary all their lives need help. They can’t do it on their own.”
Critical issues are how to stay in contact with patients and give them ongoing support in the long term, he noted, adding that, with social media and other methods, physicians can give patients personal help in the beginning and then wean them off of that help but still stay in contact in some way so patients feel like they have someone to talk to and someone that cares.
The physician plays a key role in the process, all the way from prescribing exercise to identifying suitable facilities to monitoring progress. “When your doctor cares about it, then older folks are going to do it because they really pay attention to what the physician says,” Dr. Messier said.
Introducing the study, Ms. Nicolson commented, “Exercise is a core component of osteoarthritis management and is now recommended in all clinical guidelines. High-quality evidence for the benefits of exercise in improving pain and function for those with lower-limb osteoarthritis are well established. However, exercise is globally underutilized, and among those for whom exercise is prescribed, adherence is found to be poor, particularly in the long term.”
“Understanding the barriers and facilitators to exercise will allow clinicians to change their practice to better facilitate adherence and allow researchers to develop and evaluate behavioral interventions targeting improved adherence,” she explained. “Given that initiating and adhering to exercise often requires significant behavior change, the use of behavior change theory is essential. In order to facilitate people with osteoarthritis to exercise, we need to analyze the behaviors influencing exercise participation. Interventions based on behavior change theory have been found to be significantly more successful than those that are not.”
The investigators conducted a scoping review to identify exercise barriers and facilitators in this population. They identified 23 relevant articles on intentional exercise (supervised or not and prescribed or self-initiated) among a total of 4,633 patients aged 45 years or older with hip and/or knee osteoarthritis.
Most of the more than 200 barriers and facilitators extracted from the articles were modifiable, according to data reported at the meeting, which was sponsored by the Osteoarthritis Research Society International.
The investigators mapped these modifiable factors onto domains of the Theoretical Domains Framework, which integrates multiple behavior change theories into a single framework and is aimed at helping researchers identify processes that do and do not work (Implement. Sci. 2012;7:37). They found that the barriers and facilitators mapped onto all 14 domains.
Among highlights, the many barriers mapping onto the framework’s Environmental Context and Resources domain included having to descend hills or stairs during a walking program, inability to find a suitable exercise, and rigidity of the program. Facilitators mapping onto this domain included use of a pedometer, physical therapist guidance, and receipt of a gym referral from the doctor.
Barriers mapping onto the Beliefs About Consequences domain included a belief that exercise has limited benefit, fear about damaging the joint further, and concern about precipitating pain.
Facilitators mapping onto the Reinforcement domain included medical advice to exercise, telephone reinforcement, and getting physician encouragement.
“Our findings have a number of clinical implications,” commented Ms. Nicolson.
“Given the many barriers that we identified linking to a person’s environment and resources, this highlights the need for individualized exercise tailored to each person’s situation,” she said. “Many barriers also relate to a person’s beliefs about their ability and consequences of exercise … This highlights the need for thorough and accurate education to each and every patient about their capabilities and the likely benefits of exercise.”
“Reinforcement, both internal and external, was frequently identified as a facilitator to exercise. The use of such things as logbooks, diaries, ongoing encouragement, and clinician advice to exercise can utilize these facilitators,” she concluded.
Ms. Nicolson disclosed no relevant conflicts of interest.
AT OARSI 2015
Key clinical point: Patients with osteoarthritis need assistance and support to start and adhere to an exercise plan.
Major finding: Most of the more than 200 identified exercise barriers and facilitators were modifiable.
Data source: A scoping review of 23 studies on exercise involving a total of 4,633 patients with hip and/or knee osteoarthritis.
Disclosures: Ms. Nicolson reported having no financial conflicts.

OARSI: Chronic conditions complicate osteoarthritis treatment, compliance
SEATTLE – Patients with osteoarthritis often have other common chronic conditions, a scenario that has implications for both clinical care and research, according to Dr. Gillian Hawker.
“This is a critically important topic in our field,” she told attendees of the World Congress on Osteoarthritis. “We know from myriad studies that there are major challenges to the diagnosis and management of osteoarthritis ... But probably now what’s becoming a major issue is the high occurrence of coexisting medical problems, which have been shown to present competing demands to patients and physicians who are trying to balance a number of conditions in a single patient and contraindications to osteoarthritis therapies.”

Today, 90% of individuals aged 65 years and older with osteoarthritis have at least one other chronic condition, according to Dr. Hawker, the Sir John and Lady Eaton Professor and chair of medicine at the University of Toronto. Most commonly, those conditions are cardiovascular disease, diabetes, and hypertension, but about one-third of patients have depressed mood, which may affect adherence to and effectiveness of therapies.
Two main hypotheses have been proposed for the association of osteoarthritis and other common chronic conditions, according to Dr. Hawker. According to the first hypothesis, the shared risk factors of aging and obesity independently lead to both osteoarthritis, with resultant physical inactivity, and a cluster of metabolic perturbations including hypertension, hyperglycemia, and dyslipidemia. Collectively, these conditions increase risk for cardiovascular disease and diabetes.
In support of this hypothesis, “we have lots of data from qualitative research showing that people manage their osteoarthritis symptoms by giving up activities that exacerbate them, partly because they are afraid of taking painkillers and partly because nobody offers them anything that’s more effective,” Dr. Hawker noted. In addition, when patients juggle multiple health conditions, exercise is the most frequently dropped activity.
“Many have hypothesized that inability to walk, climb stairs, and be mobile would potentially impact the ability to self-manage physical activity, impacting numerous chronic conditions,” she said. Compelling evidence comes from research such as a cohort study of patients with symptomatic hip or knee osteoarthritis that found walking disability predicted a 30% increase in the risk of all-cause death and a 17% increase in the risk of cardiovascular events; among the subset with comorbid diabetes, walking disability and grip strength predicted the risk of hospitalization for diabetic complications (PLoS One 2014;9:e91286).
“These are large, well-controlled observational studies that do show consistent independent relationships between walking disability and cardiovascular events, diabetes complications, and all-cause death,” Dr. Hawker said, while acknowledging that the research is still hypothesis generating.
Of note, recent attention has focused on systemic inflammation and a metabolic osteoarthritis phenotype. When it comes to the pathogenesis of osteoarthritis, “we now are very comfortable understanding the local biomechanical effects separately from the systemic effects on our joints,” she said. Obesity is among the systemic factors implicated, with some data suggesting that adipokines affect joint tissues in a manner similar to mechanical stress.
According to the second main hypothesis proposed to explain the association between osteoarthritis and common chronic conditions, aging and obesity give rise to a cluster of metabolic factors (hypertension, hyperglycemia, and dyslipidemia) that independently increase the risk of symptomatic osteoarthritis. Again, the arthritis may result in the loss of physical activity and disability, which exacerbates the metabolic situation.
Evidence in support of this hypothesis comes from a variety of studies. For example, one has shown that the number of components of the metabolic syndrome is related to the adjusted risk of development and progression of knee osteoarthritis (Osteoarthritis Cartilage 2012;20:1217-26).
Overall, Dr. Hawker said, “we have some independent associations between metabolic syndrome and its components, and osteoarthritis – more so in the knee and hand, more so in women than in men, and more so in younger than in older individuals. And we have some data that suggest that symptomatic and disabling osteoarthritis has an association with increased risk of cardiovascular events and diabetes complications.” Here again, the studies have limitations, so the relative contributions of disability and systemic inflammation remain unknown, she cautioned.
Hypotheses aside, the association of osteoarthritis with common chronic conditions has implications for clinical care, Dr. Hawker said at the meeting, which was sponsored by the Osteoarthritis Research Society International. “Clearly, all of these data, irrespective of the relationships, point to a pivotal role for physical activity, a combination of physical activities,” she said, noting that benefits include reductions in both metabolic alterations and physical impairment, and possibly alleviation of depressed mood and improved sleep.
Osteoarthritis may be an independent risk factor for cardiovascular disease. “Many are suggesting that, in fact, if it is the fifth component of metabolic syndrome, this should really influence how we think about cardiovascular disease prevention, that osteoarthritis patients should be screened and we should be thinking more seriously about how we use various therapies,” such as nonsteroidal anti-inflammatory drugs, she said.
Dr. Hawker endorsed future research on these topics. “In the 2014 OARSI guidelines, we showed collectively as a community that we don’t have enough trials in this population, which is the majority of our patients with osteoarthritis. So yes, conservative therapy is good, but I’d say that we need way more evidence for effective interventions in the population with osteoarthritis who are living with other chronic conditions.”
Specifically needed are large prospective studies of the temporal relationships that look at mechanisms beyond age and body mass index, she explained. These studies should assess incidence and progression separately, structure and symptoms separately, and both weight-bearing and non–weight-bearing joints.
“To date, I haven’t seen any evidence to show that treatment of metabolic syndrome or its components influences the incidence or progression of osteoarthritis. And I think we should be thinking about asking those questions as they may in fact be modifiable risk factors for osteoarthritis,” she said.
Also needed are trials assessing the impact of aggressive treatment of osteoarthritis disability, according to Dr. Hawker, who disclosed that she had no relevant conflicts of interest. “If we reduce osteoarthritis disability, particularly walking disability, can we actually impact the outcomes of cardiovascular disease and diabetes? I think that’s an important question,” she concluded.
SEATTLE – Patients with osteoarthritis often have other common chronic conditions, a scenario that has implications for both clinical care and research, according to Dr. Gillian Hawker.
“This is a critically important topic in our field,” she told attendees of the World Congress on Osteoarthritis. “We know from myriad studies that there are major challenges to the diagnosis and management of osteoarthritis ... But probably now what’s becoming a major issue is the high occurrence of coexisting medical problems, which have been shown to present competing demands to patients and physicians who are trying to balance a number of conditions in a single patient and contraindications to osteoarthritis therapies.”
Today, 90% of individuals aged 65 years and older with osteoarthritis have at least one other chronic condition, according to Dr. Hawker, the Sir John and Lady Eaton Professor and chair of medicine at the University of Toronto. Most commonly, those conditions are cardiovascular disease, diabetes, and hypertension, but about one-third of patients have depressed mood, which may affect adherence to and effectiveness of therapies.
Two main hypotheses have been proposed for the association of osteoarthritis and other common chronic conditions, according to Dr. Hawker. According to the first hypothesis, the shared risk factors of aging and obesity independently lead to both osteoarthritis, with resultant physical inactivity, and a cluster of metabolic perturbations including hypertension, hyperglycemia, and dyslipidemia. Collectively, these conditions increase risk for cardiovascular disease and diabetes.
In support of this hypothesis, “we have lots of data from qualitative research showing that people manage their osteoarthritis symptoms by giving up activities that exacerbate them, partly because they are afraid of taking painkillers and partly because nobody offers them anything that’s more effective,” Dr. Hawker noted. In addition, when patients juggle multiple health conditions, exercise is the most frequently dropped activity.
“Many have hypothesized that inability to walk, climb stairs, and be mobile would potentially impact the ability to self-manage physical activity, impacting numerous chronic conditions,” she said. Compelling evidence comes from research such as a cohort study of patients with symptomatic hip or knee osteoarthritis that found walking disability predicted a 30% increase in the risk of all-cause death and a 17% increase in the risk of cardiovascular events; among the subset with comorbid diabetes, walking disability and grip strength predicted the risk of hospitalization for diabetic complications (PLoS One 2014;9:e91286).
“These are large, well-controlled observational studies that do show consistent independent relationships between walking disability and cardiovascular events, diabetes complications, and all-cause death,” Dr. Hawker said, while acknowledging that the research is still hypothesis generating.
Of note, recent attention has focused on systemic inflammation and a metabolic osteoarthritis phenotype. When it comes to the pathogenesis of osteoarthritis, “we now are very comfortable understanding the local biomechanical effects separately from the systemic effects on our joints,” she said. Obesity is among the systemic factors implicated, with some data suggesting that adipokines affect joint tissues in a manner similar to mechanical stress.
According to the second main hypothesis proposed to explain the association between osteoarthritis and common chronic conditions, aging and obesity give rise to a cluster of metabolic factors (hypertension, hyperglycemia, and dyslipidemia) that independently increase the risk of symptomatic osteoarthritis. Again, the arthritis may result in the loss of physical activity and disability, which exacerbates the metabolic situation.
Evidence in support of this hypothesis comes from a variety of studies. For example, one has shown that the number of components of the metabolic syndrome is related to the adjusted risk of development and progression of knee osteoarthritis (Osteoarthritis Cartilage 2012;20:1217-26).
Overall, Dr. Hawker said, “we have some independent associations between metabolic syndrome and its components, and osteoarthritis – more so in the knee and hand, more so in women than in men, and more so in younger than in older individuals. And we have some data that suggest that symptomatic and disabling osteoarthritis has an association with increased risk of cardiovascular events and diabetes complications.” Here again, the studies have limitations, so the relative contributions of disability and systemic inflammation remain unknown, she cautioned.
Hypotheses aside, the association of osteoarthritis with common chronic conditions has implications for clinical care, Dr. Hawker said at the meeting, which was sponsored by the Osteoarthritis Research Society International. “Clearly, all of these data, irrespective of the relationships, point to a pivotal role for physical activity, a combination of physical activities,” she said, noting that benefits include reductions in both metabolic alterations and physical impairment, and possibly alleviation of depressed mood and improved sleep.
Osteoarthritis may be an independent risk factor for cardiovascular disease. “Many are suggesting that, in fact, if it is the fifth component of metabolic syndrome, this should really influence how we think about cardiovascular disease prevention, that osteoarthritis patients should be screened and we should be thinking more seriously about how we use various therapies,” such as nonsteroidal anti-inflammatory drugs, she said.
Dr. Hawker endorsed future research on these topics. “In the 2014 OARSI guidelines, we showed collectively as a community that we don’t have enough trials in this population, which is the majority of our patients with osteoarthritis. So yes, conservative therapy is good, but I’d say that we need way more evidence for effective interventions in the population with osteoarthritis who are living with other chronic conditions.”
Specifically needed are large prospective studies of the temporal relationships that look at mechanisms beyond age and body mass index, she explained. These studies should assess incidence and progression separately, structure and symptoms separately, and both weight-bearing and non–weight-bearing joints.
“To date, I haven’t seen any evidence to show that treatment of metabolic syndrome or its components influences the incidence or progression of osteoarthritis. And I think we should be thinking about asking those questions as they may in fact be modifiable risk factors for osteoarthritis,” she said.
Also needed are trials assessing the impact of aggressive treatment of osteoarthritis disability, according to Dr. Hawker, who disclosed that she had no relevant conflicts of interest. “If we reduce osteoarthritis disability, particularly walking disability, can we actually impact the outcomes of cardiovascular disease and diabetes? I think that’s an important question,” she concluded.
SEATTLE – Patients with osteoarthritis often have other common chronic conditions, a scenario that has implications for both clinical care and research, according to Dr. Gillian Hawker.
“This is a critically important topic in our field,” she told attendees of the World Congress on Osteoarthritis. “We know from myriad studies that there are major challenges to the diagnosis and management of osteoarthritis ... But probably now what’s becoming a major issue is the high occurrence of coexisting medical problems, which have been shown to present competing demands to patients and physicians who are trying to balance a number of conditions in a single patient and contraindications to osteoarthritis therapies.”
Today, 90% of individuals aged 65 years and older with osteoarthritis have at least one other chronic condition, according to Dr. Hawker, the Sir John and Lady Eaton Professor and chair of medicine at the University of Toronto. Most commonly, those conditions are cardiovascular disease, diabetes, and hypertension, but about one-third of patients have depressed mood, which may affect adherence to and effectiveness of therapies.
Two main hypotheses have been proposed for the association of osteoarthritis and other common chronic conditions, according to Dr. Hawker. According to the first hypothesis, the shared risk factors of aging and obesity independently lead to both osteoarthritis, with resultant physical inactivity, and a cluster of metabolic perturbations including hypertension, hyperglycemia, and dyslipidemia. Collectively, these conditions increase risk for cardiovascular disease and diabetes.
In support of this hypothesis, “we have lots of data from qualitative research showing that people manage their osteoarthritis symptoms by giving up activities that exacerbate them, partly because they are afraid of taking painkillers and partly because nobody offers them anything that’s more effective,” Dr. Hawker noted. In addition, when patients juggle multiple health conditions, exercise is the most frequently dropped activity.
“Many have hypothesized that inability to walk, climb stairs, and be mobile would potentially impact the ability to self-manage physical activity, impacting numerous chronic conditions,” she said. Compelling evidence comes from research such as a cohort study of patients with symptomatic hip or knee osteoarthritis that found walking disability predicted a 30% increase in the risk of all-cause death and a 17% increase in the risk of cardiovascular events; among the subset with comorbid diabetes, walking disability and grip strength predicted the risk of hospitalization for diabetic complications (PLoS One 2014;9:e91286).
“These are large, well-controlled observational studies that do show consistent independent relationships between walking disability and cardiovascular events, diabetes complications, and all-cause death,” Dr. Hawker said, while acknowledging that the research is still hypothesis generating.
Of note, recent attention has focused on systemic inflammation and a metabolic osteoarthritis phenotype. When it comes to the pathogenesis of osteoarthritis, “we now are very comfortable understanding the local biomechanical effects separately from the systemic effects on our joints,” she said. Obesity is among the systemic factors implicated, with some data suggesting that adipokines affect joint tissues in a manner similar to mechanical stress.
According to the second main hypothesis proposed to explain the association between osteoarthritis and common chronic conditions, aging and obesity give rise to a cluster of metabolic factors (hypertension, hyperglycemia, and dyslipidemia) that independently increase the risk of symptomatic osteoarthritis. Again, the arthritis may result in the loss of physical activity and disability, which exacerbates the metabolic situation.
Evidence in support of this hypothesis comes from a variety of studies. For example, one has shown that the number of components of the metabolic syndrome is related to the adjusted risk of development and progression of knee osteoarthritis (Osteoarthritis Cartilage 2012;20:1217-26).
Overall, Dr. Hawker said, “we have some independent associations between metabolic syndrome and its components, and osteoarthritis – more so in the knee and hand, more so in women than in men, and more so in younger than in older individuals. And we have some data that suggest that symptomatic and disabling osteoarthritis has an association with increased risk of cardiovascular events and diabetes complications.” Here again, the studies have limitations, so the relative contributions of disability and systemic inflammation remain unknown, she cautioned.
Hypotheses aside, the association of osteoarthritis with common chronic conditions has implications for clinical care, Dr. Hawker said at the meeting, which was sponsored by the Osteoarthritis Research Society International. “Clearly, all of these data, irrespective of the relationships, point to a pivotal role for physical activity, a combination of physical activities,” she said, noting that benefits include reductions in both metabolic alterations and physical impairment, and possibly alleviation of depressed mood and improved sleep.
Osteoarthritis may be an independent risk factor for cardiovascular disease. “Many are suggesting that, in fact, if it is the fifth component of metabolic syndrome, this should really influence how we think about cardiovascular disease prevention, that osteoarthritis patients should be screened and we should be thinking more seriously about how we use various therapies,” such as nonsteroidal anti-inflammatory drugs, she said.
Dr. Hawker endorsed future research on these topics. “In the 2014 OARSI guidelines, we showed collectively as a community that we don’t have enough trials in this population, which is the majority of our patients with osteoarthritis. So yes, conservative therapy is good, but I’d say that we need way more evidence for effective interventions in the population with osteoarthritis who are living with other chronic conditions.”
Specifically needed are large prospective studies of the temporal relationships that look at mechanisms beyond age and body mass index, she explained. These studies should assess incidence and progression separately, structure and symptoms separately, and both weight-bearing and non–weight-bearing joints.
“To date, I haven’t seen any evidence to show that treatment of metabolic syndrome or its components influences the incidence or progression of osteoarthritis. And I think we should be thinking about asking those questions as they may in fact be modifiable risk factors for osteoarthritis,” she said.
Also needed are trials assessing the impact of aggressive treatment of osteoarthritis disability, according to Dr. Hawker, who disclosed that she had no relevant conflicts of interest. “If we reduce osteoarthritis disability, particularly walking disability, can we actually impact the outcomes of cardiovascular disease and diabetes? I think that’s an important question,” she concluded.
EXPERT ANALYSIS FROM OARSI 2015

BSR: Multiple benefits seen with intensive psoriatic arthritis therapy
MANCHESTER, U.K. – Multiple joint and skin benefits can be achieved by intensively treating patients with psoriatic arthritis until they achieve a set of minimal disease activity criteria, an expert said at the British Society for Rheumatology annual conference.
While data are mounting on the value of treating to target (otherwise known as tight control) in psoriatic arthritis (PsA), these data lag significantly behind that for inducing and maintaining remission in rheumatoid arthritis (RA), noted Dr. Philip Helliwell of the University of Leeds (England).
“There is half as much evidence in PsA as there is in rheumatoid arthritis,” he observed. “But we’ve also got a heterogeneous disease and what we are going to have to do moving forward is to find out how to treat different phenotypic expressions of psoriatic disease, and we’re beginning to work towards that now,” he said during a Special Interest Group on Spondyloarthropathies.
Dr. Helliwell is the principal investigator of the Tight Control of Psoriatic Arthritis (TICOPA) study, which he highlighted as an example of how targeting treatment to achieve minimal disease activity (MDA) criteria (Ann. Rheum. Dis. 2010;69:48-53) could be beneficial versus standard care.
A total of 206 patients with newly-diagnosed PsA were enrolled into the study and were randomized to receive either ‘tight control’ – meaning an intensive management strategy – or to standard care for 48 weeks.
Intensive treatment involved starting with methotrexate at a dose of 15 mg/kg per week and rapidly escalating to 25 mg/kg per week at 6 weeks if needed. If patients did not achieve five out of a set of seven MDA criteria for PsA, then methotrexate was continued and sulfasalazine was added and dose escalated after 4-8 weeks.
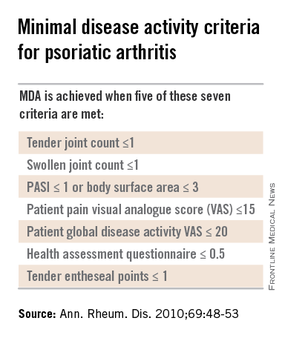
If MDA was still not achieved and criteria for biologics were not met according to NICE guidance, then alternatives were swapping out sulfasalazine for cyclosporine or leflunomide, again increasing the doses. Patients who did get put onto a biologic could switch to another anti-TNF if they did not respond after 12 weeks.
The primary endpoint data from the trial have been reported previously and showed that a higher proportion of patients in the intensive management group achieved ACR20 at 48 weeks, compared with those in the standard care group (62% vs. 45%, respectively; P = .02). A higher percentage of intensively managed patients also achieved ACR50 (51% vs. 25%; P = .0004) and ACR70 (38% vs. 17%, P = .002).
Skin symptoms, measured via the Psoriasis Area and Severity Index (PASI) showed significant improvement favoring intensive therapy over standard care. PASI20 was achieved by 72% of intensively managed patients versus 52% of those who received standard care. PASI75 was achieved by 59% versus 33%, respectively, and PASI90 by 40% versus 20%, respectively.
The full results of the study will be published soon in The Lancet and will include details of a variety of secondary outcomes and the cost-effectiveness of the intensive management strategy versus the standard care approach.
One of the key secondary outcomes of the trial was to look at the effects of the two treatment strategies on other PsA symptoms, such as enthesitis, dactylitis, and nail symptoms. No differences between the groups were observed, however, with similar decreases seen in the tight control and standard care groups.
There were no statistically significant differences in radiologic outcomes, which included baseline and end-of-treatment changes in the total modified Sharp van der Heijde (SVdH) score, the erosion score, and joint-space narrowing (JSN) score.
While this might seem somewhat disappointing, “there wasn’t a lot of radiologic progression going on anyway,” Dr. Helliwell pointed out. Overall, there was a difference of about 5% in the percentage of patients with at least one joint erosion at baseline and after 48 weeks of treatment.
The majority of radiographic change that did occur was JSN of the hands, Dr. Helliwell said, adding that patients with JSN tended to be slightly older than those without, although this observation did not reach statistical significance.
“We’ve since looked for associations with ACPA [anticitrullinated protein antibodies] – about 7% of our patients were ACPA positive – but there is no relationship,” he added. There was also no significant association between levels of C-reactive protein levels and erosive disease.
There was a trend suggesting that patients with erosions may be more likely to have polyarticular disease than oligoarticular disease, so a next step would be to look at radiologic progression in these two groups of patients in more detail.
More adverse events were seen in the tight control arm, compared with the standard care arm, including more serious adverse events, but not all of these were related to study treatment and many adverse events were those to be expected with methotrexate treatment, Dr. Helliwell observed.
But is the intensive approach cost-effective when compared to standard care? Data suggest that it is. Although the incremental cost-effectiveness ratio (ICER) initially exceeded the £20,000–£30,000 (about $31,000-$47,000) threshold used by the U.K. National Institute for Health and Care Excellence to judge if a new treatment is cost effective, allowing for certain factors enabled the ICER to be brought down to about £28,000 ($44,000), making it a cost-effective strategy.
PsA consists of five classical subtypes. The most common of these subtypes is polyarthritis (60% of patients), followed by oligoarthritis (30%). The remaining 10% of patients comprise those with arthritis mutilans, distal interphalangeal predominant disease, or spinal predominant disease. The clinical features of dactylitis and enthesitis are prevalent in about 40% and 50% of patients, respectively, and can occur in any subgroup.
Considering such heterogeneity in its presentation, the challenge now will be to determine if all clinical subgroups of PsA could benefit from treating to an MDA target with intensive management, or if one or other subgroups benefit more than another.
The TICOPA study was funded by Arthritis Research UK with support from Pfizer. Dr. Helliwell has received consulting fees from Pfizer.
Results of this study were published in the Lancet Sept. 30, 2015.
This article was updated October 6, 2015.
MANCHESTER, U.K. – Multiple joint and skin benefits can be achieved by intensively treating patients with psoriatic arthritis until they achieve a set of minimal disease activity criteria, an expert said at the British Society for Rheumatology annual conference.
While data are mounting on the value of treating to target (otherwise known as tight control) in psoriatic arthritis (PsA), these data lag significantly behind that for inducing and maintaining remission in rheumatoid arthritis (RA), noted Dr. Philip Helliwell of the University of Leeds (England).
“There is half as much evidence in PsA as there is in rheumatoid arthritis,” he observed. “But we’ve also got a heterogeneous disease and what we are going to have to do moving forward is to find out how to treat different phenotypic expressions of psoriatic disease, and we’re beginning to work towards that now,” he said during a Special Interest Group on Spondyloarthropathies.
Dr. Helliwell is the principal investigator of the Tight Control of Psoriatic Arthritis (TICOPA) study, which he highlighted as an example of how targeting treatment to achieve minimal disease activity (MDA) criteria (Ann. Rheum. Dis. 2010;69:48-53) could be beneficial versus standard care.
A total of 206 patients with newly-diagnosed PsA were enrolled into the study and were randomized to receive either ‘tight control’ – meaning an intensive management strategy – or to standard care for 48 weeks.
Intensive treatment involved starting with methotrexate at a dose of 15 mg/kg per week and rapidly escalating to 25 mg/kg per week at 6 weeks if needed. If patients did not achieve five out of a set of seven MDA criteria for PsA, then methotrexate was continued and sulfasalazine was added and dose escalated after 4-8 weeks.
If MDA was still not achieved and criteria for biologics were not met according to NICE guidance, then alternatives were swapping out sulfasalazine for cyclosporine or leflunomide, again increasing the doses. Patients who did get put onto a biologic could switch to another anti-TNF if they did not respond after 12 weeks.
The primary endpoint data from the trial have been reported previously and showed that a higher proportion of patients in the intensive management group achieved ACR20 at 48 weeks, compared with those in the standard care group (62% vs. 45%, respectively; P = .02). A higher percentage of intensively managed patients also achieved ACR50 (51% vs. 25%; P = .0004) and ACR70 (38% vs. 17%, P = .002).
Skin symptoms, measured via the Psoriasis Area and Severity Index (PASI) showed significant improvement favoring intensive therapy over standard care. PASI20 was achieved by 72% of intensively managed patients versus 52% of those who received standard care. PASI75 was achieved by 59% versus 33%, respectively, and PASI90 by 40% versus 20%, respectively.
The full results of the study will be published soon in The Lancet and will include details of a variety of secondary outcomes and the cost-effectiveness of the intensive management strategy versus the standard care approach.
One of the key secondary outcomes of the trial was to look at the effects of the two treatment strategies on other PsA symptoms, such as enthesitis, dactylitis, and nail symptoms. No differences between the groups were observed, however, with similar decreases seen in the tight control and standard care groups.
There were no statistically significant differences in radiologic outcomes, which included baseline and end-of-treatment changes in the total modified Sharp van der Heijde (SVdH) score, the erosion score, and joint-space narrowing (JSN) score.
While this might seem somewhat disappointing, “there wasn’t a lot of radiologic progression going on anyway,” Dr. Helliwell pointed out. Overall, there was a difference of about 5% in the percentage of patients with at least one joint erosion at baseline and after 48 weeks of treatment.
The majority of radiographic change that did occur was JSN of the hands, Dr. Helliwell said, adding that patients with JSN tended to be slightly older than those without, although this observation did not reach statistical significance.
“We’ve since looked for associations with ACPA [anticitrullinated protein antibodies] – about 7% of our patients were ACPA positive – but there is no relationship,” he added. There was also no significant association between levels of C-reactive protein levels and erosive disease.
There was a trend suggesting that patients with erosions may be more likely to have polyarticular disease than oligoarticular disease, so a next step would be to look at radiologic progression in these two groups of patients in more detail.
More adverse events were seen in the tight control arm, compared with the standard care arm, including more serious adverse events, but not all of these were related to study treatment and many adverse events were those to be expected with methotrexate treatment, Dr. Helliwell observed.
But is the intensive approach cost-effective when compared to standard care? Data suggest that it is. Although the incremental cost-effectiveness ratio (ICER) initially exceeded the £20,000–£30,000 (about $31,000-$47,000) threshold used by the U.K. National Institute for Health and Care Excellence to judge if a new treatment is cost effective, allowing for certain factors enabled the ICER to be brought down to about £28,000 ($44,000), making it a cost-effective strategy.
PsA consists of five classical subtypes. The most common of these subtypes is polyarthritis (60% of patients), followed by oligoarthritis (30%). The remaining 10% of patients comprise those with arthritis mutilans, distal interphalangeal predominant disease, or spinal predominant disease. The clinical features of dactylitis and enthesitis are prevalent in about 40% and 50% of patients, respectively, and can occur in any subgroup.
Considering such heterogeneity in its presentation, the challenge now will be to determine if all clinical subgroups of PsA could benefit from treating to an MDA target with intensive management, or if one or other subgroups benefit more than another.
The TICOPA study was funded by Arthritis Research UK with support from Pfizer. Dr. Helliwell has received consulting fees from Pfizer.
Results of this study were published in the Lancet Sept. 30, 2015.
This article was updated October 6, 2015.
MANCHESTER, U.K. – Multiple joint and skin benefits can be achieved by intensively treating patients with psoriatic arthritis until they achieve a set of minimal disease activity criteria, an expert said at the British Society for Rheumatology annual conference.
While data are mounting on the value of treating to target (otherwise known as tight control) in psoriatic arthritis (PsA), these data lag significantly behind that for inducing and maintaining remission in rheumatoid arthritis (RA), noted Dr. Philip Helliwell of the University of Leeds (England).
“There is half as much evidence in PsA as there is in rheumatoid arthritis,” he observed. “But we’ve also got a heterogeneous disease and what we are going to have to do moving forward is to find out how to treat different phenotypic expressions of psoriatic disease, and we’re beginning to work towards that now,” he said during a Special Interest Group on Spondyloarthropathies.
Dr. Helliwell is the principal investigator of the Tight Control of Psoriatic Arthritis (TICOPA) study, which he highlighted as an example of how targeting treatment to achieve minimal disease activity (MDA) criteria (Ann. Rheum. Dis. 2010;69:48-53) could be beneficial versus standard care.
A total of 206 patients with newly-diagnosed PsA were enrolled into the study and were randomized to receive either ‘tight control’ – meaning an intensive management strategy – or to standard care for 48 weeks.
Intensive treatment involved starting with methotrexate at a dose of 15 mg/kg per week and rapidly escalating to 25 mg/kg per week at 6 weeks if needed. If patients did not achieve five out of a set of seven MDA criteria for PsA, then methotrexate was continued and sulfasalazine was added and dose escalated after 4-8 weeks.
If MDA was still not achieved and criteria for biologics were not met according to NICE guidance, then alternatives were swapping out sulfasalazine for cyclosporine or leflunomide, again increasing the doses. Patients who did get put onto a biologic could switch to another anti-TNF if they did not respond after 12 weeks.
The primary endpoint data from the trial have been reported previously and showed that a higher proportion of patients in the intensive management group achieved ACR20 at 48 weeks, compared with those in the standard care group (62% vs. 45%, respectively; P = .02). A higher percentage of intensively managed patients also achieved ACR50 (51% vs. 25%; P = .0004) and ACR70 (38% vs. 17%, P = .002).
Skin symptoms, measured via the Psoriasis Area and Severity Index (PASI) showed significant improvement favoring intensive therapy over standard care. PASI20 was achieved by 72% of intensively managed patients versus 52% of those who received standard care. PASI75 was achieved by 59% versus 33%, respectively, and PASI90 by 40% versus 20%, respectively.
The full results of the study will be published soon in The Lancet and will include details of a variety of secondary outcomes and the cost-effectiveness of the intensive management strategy versus the standard care approach.
One of the key secondary outcomes of the trial was to look at the effects of the two treatment strategies on other PsA symptoms, such as enthesitis, dactylitis, and nail symptoms. No differences between the groups were observed, however, with similar decreases seen in the tight control and standard care groups.
There were no statistically significant differences in radiologic outcomes, which included baseline and end-of-treatment changes in the total modified Sharp van der Heijde (SVdH) score, the erosion score, and joint-space narrowing (JSN) score.
While this might seem somewhat disappointing, “there wasn’t a lot of radiologic progression going on anyway,” Dr. Helliwell pointed out. Overall, there was a difference of about 5% in the percentage of patients with at least one joint erosion at baseline and after 48 weeks of treatment.
The majority of radiographic change that did occur was JSN of the hands, Dr. Helliwell said, adding that patients with JSN tended to be slightly older than those without, although this observation did not reach statistical significance.
“We’ve since looked for associations with ACPA [anticitrullinated protein antibodies] – about 7% of our patients were ACPA positive – but there is no relationship,” he added. There was also no significant association between levels of C-reactive protein levels and erosive disease.
There was a trend suggesting that patients with erosions may be more likely to have polyarticular disease than oligoarticular disease, so a next step would be to look at radiologic progression in these two groups of patients in more detail.
More adverse events were seen in the tight control arm, compared with the standard care arm, including more serious adverse events, but not all of these were related to study treatment and many adverse events were those to be expected with methotrexate treatment, Dr. Helliwell observed.
But is the intensive approach cost-effective when compared to standard care? Data suggest that it is. Although the incremental cost-effectiveness ratio (ICER) initially exceeded the £20,000–£30,000 (about $31,000-$47,000) threshold used by the U.K. National Institute for Health and Care Excellence to judge if a new treatment is cost effective, allowing for certain factors enabled the ICER to be brought down to about £28,000 ($44,000), making it a cost-effective strategy.
PsA consists of five classical subtypes. The most common of these subtypes is polyarthritis (60% of patients), followed by oligoarthritis (30%). The remaining 10% of patients comprise those with arthritis mutilans, distal interphalangeal predominant disease, or spinal predominant disease. The clinical features of dactylitis and enthesitis are prevalent in about 40% and 50% of patients, respectively, and can occur in any subgroup.
Considering such heterogeneity in its presentation, the challenge now will be to determine if all clinical subgroups of PsA could benefit from treating to an MDA target with intensive management, or if one or other subgroups benefit more than another.
The TICOPA study was funded by Arthritis Research UK with support from Pfizer. Dr. Helliwell has received consulting fees from Pfizer.
Results of this study were published in the Lancet Sept. 30, 2015.
This article was updated October 6, 2015.
EXPERT ANALYSIS AT RHEUMATOLOGY 2015
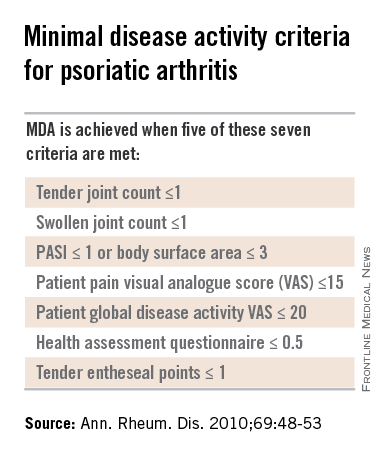
OARSI: Data further link hand osteoarthritis, cardiometabolic disease
SEATTLE – New data presented at the World Congress on Osteoarthritis further suggest that hand osteoarthritis and cardiometabolic disease may have a shared etiology or pathophysiology.
In a study of 869 patients with hand osteoarthritis, those with ischemic cardiac disease were more than three times as likely to have joint symptoms and had greater clinical progression. In addition, obese patients had more extensive radiographic disease in their hands.

The results add to previous data showing higher rates of ischemic cardiac events in patients with symptomatic hand osteoarthritis (Ann. Rheum. Dis. 2013;74:74-81), according to Dr. Alice Courties, a rheumatologist at Saint-Antoine Hospital, Université Paris 6, Assistance Publique–Hôpitaux de Paris.
“One hypothesis is that symptomatic hand osteoarthritis and cardiometabolic disease share a common background based on chronic low-grade inflammation,” she proposed.
In an interview, Dr. Lisa Mandl, a rheumatologist at the Hospital for Special Surgery, New York, and one of the session’s comoderators, said, “I think this study is confirmatory that inflammation may play a role in non–weight-bearing joints.” She noted that analyses stratified by anatomic subtype of hand osteoarthritis would have been additionally informative.

Dr. Nigel Arden, the other session comoderator and director of both Musculoskeletal Epidemiology and the Oxford Musculoskeletal BioBank at the University of Oxford (England) said, “I think the whole association of cardiovascular risk, metabolic syndrome, and osteoarthritis is very important, and very important in treating patients or intervention. And this [study] is an integral part of that work.”
Giving some background to the research, Dr. Courties noted that risk factors for the development of hand osteoarthritis have been identified, but factors associated with clinical and radiographic severity of disease and with progression remain poorly defined.
The investigators performed an ancillary study of patients enrolled in the phase III, randomized Strontium Ranelate in Knee Osteoarthritis (SEKOIA) trial, in which assessments included hand x-rays and hand symptoms. The trial was conducted by Servier, but the ancillary analysis was fully independent.

Cross-sectional analyses were based on 869 patients with hand osteoarthritis, defined as presence of at least two joints with a Kellgren-Lawrence score of 2 or higher. In terms of clinical severity, 26% of patients had symptomatic hand joints, defined as a Functional Index for Hand Osteoarthritis (FIHOA) score of 5 or greater; in terms of radiographic severity, the average summary Kellgren-Lawrence hand score was 21 out of 128 points.
Results of multivariate analyses showed that patients with ischemic heart disease were more likely to have symptomatic hand joints (odds ratio, 3.59), according to data reported at the meeting, which was sponsored by the Osteoarthritis Research Society International. Odds were also higher for postmenopausal women, and for patients who had depression, a higher Kellgren-Lawrence hand score, or more joints showing erosion.
Patients who were obese (a body-mass index of 30 kg/m2 or greater) had more severe radiographic disease assessed with the hand score (beta, 2.88 points). Severity was also greater for those who had symptomatic hand joints or a higher Kellgren-Lawrence knee score.
Longitudinal analyses were based on the 307 patients who were in the trial’s placebo group and had a mean follow-up of 2.6 years. Overall, 23% experienced clinical progression of their hand osteoarthritis, defined as a worsening of their FIHOA, and 72% experienced radiographic progression, defined as a worsening of their Kellgren-Lawrence hand score, reported Dr. Courties, who disclosed that she has received congress invitations from Pfizer, Biogaran, and Expanscience. Multivariate analysis here showed that patients with ischemic cardiac disease had greater clinical progression (beta, 2.31 points), while those with a higher hand score at baseline had greater radiographic progression.
SEATTLE – New data presented at the World Congress on Osteoarthritis further suggest that hand osteoarthritis and cardiometabolic disease may have a shared etiology or pathophysiology.
In a study of 869 patients with hand osteoarthritis, those with ischemic cardiac disease were more than three times as likely to have joint symptoms and had greater clinical progression. In addition, obese patients had more extensive radiographic disease in their hands.
The results add to previous data showing higher rates of ischemic cardiac events in patients with symptomatic hand osteoarthritis (Ann. Rheum. Dis. 2013;74:74-81), according to Dr. Alice Courties, a rheumatologist at Saint-Antoine Hospital, Université Paris 6, Assistance Publique–Hôpitaux de Paris.
“One hypothesis is that symptomatic hand osteoarthritis and cardiometabolic disease share a common background based on chronic low-grade inflammation,” she proposed.
In an interview, Dr. Lisa Mandl, a rheumatologist at the Hospital for Special Surgery, New York, and one of the session’s comoderators, said, “I think this study is confirmatory that inflammation may play a role in non–weight-bearing joints.” She noted that analyses stratified by anatomic subtype of hand osteoarthritis would have been additionally informative.
Dr. Nigel Arden, the other session comoderator and director of both Musculoskeletal Epidemiology and the Oxford Musculoskeletal BioBank at the University of Oxford (England) said, “I think the whole association of cardiovascular risk, metabolic syndrome, and osteoarthritis is very important, and very important in treating patients or intervention. And this [study] is an integral part of that work.”
Giving some background to the research, Dr. Courties noted that risk factors for the development of hand osteoarthritis have been identified, but factors associated with clinical and radiographic severity of disease and with progression remain poorly defined.
The investigators performed an ancillary study of patients enrolled in the phase III, randomized Strontium Ranelate in Knee Osteoarthritis (SEKOIA) trial, in which assessments included hand x-rays and hand symptoms. The trial was conducted by Servier, but the ancillary analysis was fully independent.
Cross-sectional analyses were based on 869 patients with hand osteoarthritis, defined as presence of at least two joints with a Kellgren-Lawrence score of 2 or higher. In terms of clinical severity, 26% of patients had symptomatic hand joints, defined as a Functional Index for Hand Osteoarthritis (FIHOA) score of 5 or greater; in terms of radiographic severity, the average summary Kellgren-Lawrence hand score was 21 out of 128 points.
Results of multivariate analyses showed that patients with ischemic heart disease were more likely to have symptomatic hand joints (odds ratio, 3.59), according to data reported at the meeting, which was sponsored by the Osteoarthritis Research Society International. Odds were also higher for postmenopausal women, and for patients who had depression, a higher Kellgren-Lawrence hand score, or more joints showing erosion.
Patients who were obese (a body-mass index of 30 kg/m2 or greater) had more severe radiographic disease assessed with the hand score (beta, 2.88 points). Severity was also greater for those who had symptomatic hand joints or a higher Kellgren-Lawrence knee score.
Longitudinal analyses were based on the 307 patients who were in the trial’s placebo group and had a mean follow-up of 2.6 years. Overall, 23% experienced clinical progression of their hand osteoarthritis, defined as a worsening of their FIHOA, and 72% experienced radiographic progression, defined as a worsening of their Kellgren-Lawrence hand score, reported Dr. Courties, who disclosed that she has received congress invitations from Pfizer, Biogaran, and Expanscience. Multivariate analysis here showed that patients with ischemic cardiac disease had greater clinical progression (beta, 2.31 points), while those with a higher hand score at baseline had greater radiographic progression.
SEATTLE – New data presented at the World Congress on Osteoarthritis further suggest that hand osteoarthritis and cardiometabolic disease may have a shared etiology or pathophysiology.
In a study of 869 patients with hand osteoarthritis, those with ischemic cardiac disease were more than three times as likely to have joint symptoms and had greater clinical progression. In addition, obese patients had more extensive radiographic disease in their hands.
The results add to previous data showing higher rates of ischemic cardiac events in patients with symptomatic hand osteoarthritis (Ann. Rheum. Dis. 2013;74:74-81), according to Dr. Alice Courties, a rheumatologist at Saint-Antoine Hospital, Université Paris 6, Assistance Publique–Hôpitaux de Paris.
“One hypothesis is that symptomatic hand osteoarthritis and cardiometabolic disease share a common background based on chronic low-grade inflammation,” she proposed.
In an interview, Dr. Lisa Mandl, a rheumatologist at the Hospital for Special Surgery, New York, and one of the session’s comoderators, said, “I think this study is confirmatory that inflammation may play a role in non–weight-bearing joints.” She noted that analyses stratified by anatomic subtype of hand osteoarthritis would have been additionally informative.
Dr. Nigel Arden, the other session comoderator and director of both Musculoskeletal Epidemiology and the Oxford Musculoskeletal BioBank at the University of Oxford (England) said, “I think the whole association of cardiovascular risk, metabolic syndrome, and osteoarthritis is very important, and very important in treating patients or intervention. And this [study] is an integral part of that work.”
Giving some background to the research, Dr. Courties noted that risk factors for the development of hand osteoarthritis have been identified, but factors associated with clinical and radiographic severity of disease and with progression remain poorly defined.
The investigators performed an ancillary study of patients enrolled in the phase III, randomized Strontium Ranelate in Knee Osteoarthritis (SEKOIA) trial, in which assessments included hand x-rays and hand symptoms. The trial was conducted by Servier, but the ancillary analysis was fully independent.
Cross-sectional analyses were based on 869 patients with hand osteoarthritis, defined as presence of at least two joints with a Kellgren-Lawrence score of 2 or higher. In terms of clinical severity, 26% of patients had symptomatic hand joints, defined as a Functional Index for Hand Osteoarthritis (FIHOA) score of 5 or greater; in terms of radiographic severity, the average summary Kellgren-Lawrence hand score was 21 out of 128 points.
Results of multivariate analyses showed that patients with ischemic heart disease were more likely to have symptomatic hand joints (odds ratio, 3.59), according to data reported at the meeting, which was sponsored by the Osteoarthritis Research Society International. Odds were also higher for postmenopausal women, and for patients who had depression, a higher Kellgren-Lawrence hand score, or more joints showing erosion.
Patients who were obese (a body-mass index of 30 kg/m2 or greater) had more severe radiographic disease assessed with the hand score (beta, 2.88 points). Severity was also greater for those who had symptomatic hand joints or a higher Kellgren-Lawrence knee score.
Longitudinal analyses were based on the 307 patients who were in the trial’s placebo group and had a mean follow-up of 2.6 years. Overall, 23% experienced clinical progression of their hand osteoarthritis, defined as a worsening of their FIHOA, and 72% experienced radiographic progression, defined as a worsening of their Kellgren-Lawrence hand score, reported Dr. Courties, who disclosed that she has received congress invitations from Pfizer, Biogaran, and Expanscience. Multivariate analysis here showed that patients with ischemic cardiac disease had greater clinical progression (beta, 2.31 points), while those with a higher hand score at baseline had greater radiographic progression.
AT OARSI 2015
Key clinical point: Chronic low-grade inflammation may play a role in both hand osteoarthritis and cardiometabolic disease.
Major finding: Ischemic cardiac disease was associated with clinical severity (odds ratio, 3.59) and clinical progression (beta, 2.31 points), while obesity was associated with radiographic severity (beta, 2.88 points).
Data source: A cohort study of 869 patients with radiographic hand osteoarthritis as well as knee osteoarthritis.
Disclosures: Dr. Courties disclosed that she has received congress invitations from Pfizer, Biogaran, and Expanscience. The SEKOIA trial was conducted by Servier, but this ancillary analysis was fully independent.

Obesity implicated in spinal degeneration
SEATTLE – Heavier individuals are more likely to have degenerative changes of the lumbar spine seen on MRI, according to findings from an analysis of 1,684 patients in the European Genodisc Study.
“BMI [body mass index] is associated with disc herniation and spinal stenosis. It is also associated with disc degeneration, but the coefficient is so small it’s unlikely to be clinically relevant,” lead investigator Dr. Anand Segar reported at the World Congress on Osteoarthritis.
“Age appears to be the most import factor in determining spinal degeneration,” he added. “Interestingly, smoking and work intensity were not associated with any outcomes.”

Although degenerative changes were worse and more prevalent at the lower lumbar levels, the associations of BMI with these changes were actually stronger at the upper three levels, according to Dr. Segar, who is a resident in the Nuffield Department of Orthopaedics, Rheumatology, and Musculoskeletal Sciences at the University of Oxford (England). Thus, “we further add to the thought of an upper spine phenotype, which has been described by other authors, and this needs further investigation,” he maintained.
Session comoderator Dr. Jeffrey N. Katz, professor of orthopedic surgery at Harvard Medical School and codirector of the Brigham Spine Center at Brigham and Women’s Hospital, Boston, asked, “Looking at the upper spine, were you able to exclude the possibility of scoliosis as a reason for transferring load to the upper rather than the lower spine? And in evaluating spinal stenosis and thinking about BMI as your primary predictor, did you make any accommodation for how you dealt with epidural fat in relation to spinal stenosis?”
The investigators did not specifically look at scoliosis, but it was uncommon in the study sample and therefore unlikely to have affected the findings, Dr. Segar replied. Similarly, they did not specifically evaluate epidural fat, “but my understanding from the literature is that epidural fat is not really associated with obesity, ... so I don’t think again it would have changed our results.”
The patients in Genodisc were recruited from tertiary spinal clinics in the United Kingdom, Hungary, Italy, and Slovenia.

They underwent MRI of the lumbar spine, and the scans were evaluated by a musculoskeletal radiologist. Disc degeneration was assessed with the 5-point Pfirrmann grading system, while disc herniation and spinal stenosis were simply scored as present or absent.
On average, the patients studied were 51 years old and had a BMI of 27.2 kg/m2, according to data reported at the meeting, which was sponsored by the Osteoarthritis Research Society International.
Results of multivariate analysis showed that each 5-kg/m2 increase in BMI was associated with a 0.04-unit increase in disc degeneration score, a 19% increase in the odds of disc herniation, and a 24% increase in the odds of spinal stenosis.
For comparison, each 10-year increment in age was associated with a 0.31-unit increase in disc degeneration score, a 30% decrease in the odds of disc herniation, and a more than a doubling of the odds of spinal stenosis.
The impact of BMI on the lumbar spine was greater at the upper three levels, reported Dr. Segar, who disclosed no relevant conflicts of interest. In analyses restricted to those levels, each 5-kg/m2 increase in BMI was associated with a 39% increase in the odds of disc herniation and a 65% increase in the odds of spinal stenosis.
SEATTLE – Heavier individuals are more likely to have degenerative changes of the lumbar spine seen on MRI, according to findings from an analysis of 1,684 patients in the European Genodisc Study.
“BMI [body mass index] is associated with disc herniation and spinal stenosis. It is also associated with disc degeneration, but the coefficient is so small it’s unlikely to be clinically relevant,” lead investigator Dr. Anand Segar reported at the World Congress on Osteoarthritis.
“Age appears to be the most import factor in determining spinal degeneration,” he added. “Interestingly, smoking and work intensity were not associated with any outcomes.”
Although degenerative changes were worse and more prevalent at the lower lumbar levels, the associations of BMI with these changes were actually stronger at the upper three levels, according to Dr. Segar, who is a resident in the Nuffield Department of Orthopaedics, Rheumatology, and Musculoskeletal Sciences at the University of Oxford (England). Thus, “we further add to the thought of an upper spine phenotype, which has been described by other authors, and this needs further investigation,” he maintained.
Session comoderator Dr. Jeffrey N. Katz, professor of orthopedic surgery at Harvard Medical School and codirector of the Brigham Spine Center at Brigham and Women’s Hospital, Boston, asked, “Looking at the upper spine, were you able to exclude the possibility of scoliosis as a reason for transferring load to the upper rather than the lower spine? And in evaluating spinal stenosis and thinking about BMI as your primary predictor, did you make any accommodation for how you dealt with epidural fat in relation to spinal stenosis?”
The investigators did not specifically look at scoliosis, but it was uncommon in the study sample and therefore unlikely to have affected the findings, Dr. Segar replied. Similarly, they did not specifically evaluate epidural fat, “but my understanding from the literature is that epidural fat is not really associated with obesity, ... so I don’t think again it would have changed our results.”
The patients in Genodisc were recruited from tertiary spinal clinics in the United Kingdom, Hungary, Italy, and Slovenia.
They underwent MRI of the lumbar spine, and the scans were evaluated by a musculoskeletal radiologist. Disc degeneration was assessed with the 5-point Pfirrmann grading system, while disc herniation and spinal stenosis were simply scored as present or absent.
On average, the patients studied were 51 years old and had a BMI of 27.2 kg/m2, according to data reported at the meeting, which was sponsored by the Osteoarthritis Research Society International.
Results of multivariate analysis showed that each 5-kg/m2 increase in BMI was associated with a 0.04-unit increase in disc degeneration score, a 19% increase in the odds of disc herniation, and a 24% increase in the odds of spinal stenosis.
For comparison, each 10-year increment in age was associated with a 0.31-unit increase in disc degeneration score, a 30% decrease in the odds of disc herniation, and a more than a doubling of the odds of spinal stenosis.
The impact of BMI on the lumbar spine was greater at the upper three levels, reported Dr. Segar, who disclosed no relevant conflicts of interest. In analyses restricted to those levels, each 5-kg/m2 increase in BMI was associated with a 39% increase in the odds of disc herniation and a 65% increase in the odds of spinal stenosis.
SEATTLE – Heavier individuals are more likely to have degenerative changes of the lumbar spine seen on MRI, according to findings from an analysis of 1,684 patients in the European Genodisc Study.
“BMI [body mass index] is associated with disc herniation and spinal stenosis. It is also associated with disc degeneration, but the coefficient is so small it’s unlikely to be clinically relevant,” lead investigator Dr. Anand Segar reported at the World Congress on Osteoarthritis.
“Age appears to be the most import factor in determining spinal degeneration,” he added. “Interestingly, smoking and work intensity were not associated with any outcomes.”
Although degenerative changes were worse and more prevalent at the lower lumbar levels, the associations of BMI with these changes were actually stronger at the upper three levels, according to Dr. Segar, who is a resident in the Nuffield Department of Orthopaedics, Rheumatology, and Musculoskeletal Sciences at the University of Oxford (England). Thus, “we further add to the thought of an upper spine phenotype, which has been described by other authors, and this needs further investigation,” he maintained.
Session comoderator Dr. Jeffrey N. Katz, professor of orthopedic surgery at Harvard Medical School and codirector of the Brigham Spine Center at Brigham and Women’s Hospital, Boston, asked, “Looking at the upper spine, were you able to exclude the possibility of scoliosis as a reason for transferring load to the upper rather than the lower spine? And in evaluating spinal stenosis and thinking about BMI as your primary predictor, did you make any accommodation for how you dealt with epidural fat in relation to spinal stenosis?”
The investigators did not specifically look at scoliosis, but it was uncommon in the study sample and therefore unlikely to have affected the findings, Dr. Segar replied. Similarly, they did not specifically evaluate epidural fat, “but my understanding from the literature is that epidural fat is not really associated with obesity, ... so I don’t think again it would have changed our results.”
The patients in Genodisc were recruited from tertiary spinal clinics in the United Kingdom, Hungary, Italy, and Slovenia.
They underwent MRI of the lumbar spine, and the scans were evaluated by a musculoskeletal radiologist. Disc degeneration was assessed with the 5-point Pfirrmann grading system, while disc herniation and spinal stenosis were simply scored as present or absent.
On average, the patients studied were 51 years old and had a BMI of 27.2 kg/m2, according to data reported at the meeting, which was sponsored by the Osteoarthritis Research Society International.
Results of multivariate analysis showed that each 5-kg/m2 increase in BMI was associated with a 0.04-unit increase in disc degeneration score, a 19% increase in the odds of disc herniation, and a 24% increase in the odds of spinal stenosis.
For comparison, each 10-year increment in age was associated with a 0.31-unit increase in disc degeneration score, a 30% decrease in the odds of disc herniation, and a more than a doubling of the odds of spinal stenosis.
The impact of BMI on the lumbar spine was greater at the upper three levels, reported Dr. Segar, who disclosed no relevant conflicts of interest. In analyses restricted to those levels, each 5-kg/m2 increase in BMI was associated with a 39% increase in the odds of disc herniation and a 65% increase in the odds of spinal stenosis.
AT OARSI 2015
Key clinical point: Heavier individuals are at increased risk for degenerative changes in the lumbar spine.
Major finding: Each 5-kg/m2 increase in BMI was associated with a 0.04-unit increase in disc degeneration score and with 19% and 24% increases in the odds of disc herniation and spinal stenosis, respectively.
Data source: A cohort study of 1,684 patients recruited from European spine clinics.
Disclosures: Dr. Segar disclosed having no relevant conflicts of interest.

OARSI: Hydroxychloroquine disappoints in hand osteoarthritis
SEATTLE – Hydroxychloroquine is not efficacious for treating primary hand osteoarthritis, according to results from the first randomized trial to test the disease-modifying antirheumatic drug in this patient population.
Findings reported at the World Congress on Osteoarthritis showed that after 24 weeks of treatment, scores for pain and hand function budged little from baseline whether patients took hydroxychloroquine (Plaquenil) or a placebo. And although the drug was generally well tolerated, patients in that group more commonly had allergic reactions and developed rashes.

“The results of our study do not support the prescription of hydroxychloroquine in patients with hand osteoarthritis,” concluded lead investigator WeiChing Lee, Pharm.D., hospital pharmacist at the Maasstad Hospital Rotterdam in the Netherlands.
During a question and answer period, however, session attendees pointed out some study limitations that may still leave the door open for hydroxychloroquine in this setting.
“Thank you for doing this trial. I’ve always wanted to see a randomized, controlled trial looking at this. I’m a little depressed that it’s negative,” commented session attendee Dr. Grace Lo of the Baylor College of Medicine in Houston. An older case series did suggest a benefit of hydroxychloroquine in patients with more severe disease, “so I was wondering why you specifically excluded those people from this study.”
“We believed that patients with very severe disease are not likely to benefit from hydroxychloroquine because it is in the end stage,” Dr. Lee replied.
Dr. Lo further wondered if outcomes had been assessed separately among patients with different anatomic types of hand osteoarthritis, such as carpometacarpal osteoarthritis versus osteoarthritis of the proximal and distal interphalangeal joints. The investigators have not performed those analyses, according to Dr. Lee. “You just need to see if there is a difference,” Dr. Lo recommended.
Another attendee noted that pain scores at baseline suggested some patients had little to no pain. “Did you do a subgroup analysis looking at higher pain scores at baseline versus lower pain scores?” he asked.
“Yes, we did a subanalysis of patients with a pain score of 60 mm or more versus less [on a 100-mm scale], and we saw it improved with more severe pain symptoms; there was a decrease of 15 mm in the pain scores in both the placebo and hydroxychloroquine groups,” Dr. Lee replied, and still no difference between groups.
“Were you surprised there was no placebo response?” that attendee further asked.
“Yes, we were. That was the reason why we did the subanalysis,” Dr. Lee said; results showed a placebo effect in the group with more severe pain but not in the group with less severe pain.
A third attendee asked, “Do you have any data on how much inflammation these patients actually had at baseline? Could the lack of effect be due to low inflammation at baseline?”
The investigators have not looked at inflammatory markers, Dr. Lee replied.

In an interview, Dr. Xavier Chevalier, session comoderator and head of the department of rheumatology at the Henri Mondor Hospital, University Paris XII, in Créteil, France, agreed with the attendees’ points. “Unfortunately, this is a negative trial, but I’m afraid that the level of pain was not really well defined at the beginning of the study,” he said. “And it’s a little bit of a shame that they didn’t include patients with a very high level of pain.”
Introducing the study, Dr. Lee noted, “The cause and pathophysiology of hand osteoarthritis have not been clarified yet, but it is clear that inflammation plays an important tole. So it is believed that anti-inflammatory drugs might be effective in treating hand osteoarthritis.”
“Hydroxychloroquine is an anti-inflammatory drug that has been used successfully in other rheumatic diseases. It is prescribed commonly in hand osteoarthritis, but this indication is off label and not well investigated,” she said.
The investigators recruited to the trial 202 patients who met American College of Rheumatology criteria for primary hand osteoarthritis from outpatient rheumatology clinics in the Netherlands.
The patients had had pain from their arthritis for at least 1 year and had nodules or Kellgren-Lawrence grade 1, 2, or 3 changes in at least two symptomatic joints; those with grade 4 changes were excluded. They were randomized evenly to treatment with hydroxychloroquine (400 mg daily) or placebo.
Pain at baseline averaged about 44 mm on the 100-mm Visual Analog Scale (VAS) pain scale in each group, according to data reported at the meeting sponsored by the Osteoarthritis Research Society International.
Intention-to-treat analyses showed that at 24 weeks, the VAS score had increased by 0.10 mm in the placebo group and decreased by 1.3 mm in the hydroxychloroquine group, but the difference was not significant, reported Dr. Lee, who disclosed that she had no relevant conflicts of interest.
The groups were likewise statistically indistinguishable with respect to the change from baseline in the Australian/Canadian Osteoarthritis Hand Index (AUSCAN) scores and in total scores on the short form of the Arthritis Impact Measurement Scales 2 (AIMS2-SF).
About a fifth of patients in each group experienced adverse events. The hydroxychloroquine group had more allergic reactions (three vs. none) and cases of rash/pruritus (eight vs. three).
Dr. Lee disclosed that she had no relevant conflicts of interest.
SEATTLE – Hydroxychloroquine is not efficacious for treating primary hand osteoarthritis, according to results from the first randomized trial to test the disease-modifying antirheumatic drug in this patient population.
Findings reported at the World Congress on Osteoarthritis showed that after 24 weeks of treatment, scores for pain and hand function budged little from baseline whether patients took hydroxychloroquine (Plaquenil) or a placebo. And although the drug was generally well tolerated, patients in that group more commonly had allergic reactions and developed rashes.
“The results of our study do not support the prescription of hydroxychloroquine in patients with hand osteoarthritis,” concluded lead investigator WeiChing Lee, Pharm.D., hospital pharmacist at the Maasstad Hospital Rotterdam in the Netherlands.
During a question and answer period, however, session attendees pointed out some study limitations that may still leave the door open for hydroxychloroquine in this setting.
“Thank you for doing this trial. I’ve always wanted to see a randomized, controlled trial looking at this. I’m a little depressed that it’s negative,” commented session attendee Dr. Grace Lo of the Baylor College of Medicine in Houston. An older case series did suggest a benefit of hydroxychloroquine in patients with more severe disease, “so I was wondering why you specifically excluded those people from this study.”
“We believed that patients with very severe disease are not likely to benefit from hydroxychloroquine because it is in the end stage,” Dr. Lee replied.
Dr. Lo further wondered if outcomes had been assessed separately among patients with different anatomic types of hand osteoarthritis, such as carpometacarpal osteoarthritis versus osteoarthritis of the proximal and distal interphalangeal joints. The investigators have not performed those analyses, according to Dr. Lee. “You just need to see if there is a difference,” Dr. Lo recommended.
Another attendee noted that pain scores at baseline suggested some patients had little to no pain. “Did you do a subgroup analysis looking at higher pain scores at baseline versus lower pain scores?” he asked.
“Yes, we did a subanalysis of patients with a pain score of 60 mm or more versus less [on a 100-mm scale], and we saw it improved with more severe pain symptoms; there was a decrease of 15 mm in the pain scores in both the placebo and hydroxychloroquine groups,” Dr. Lee replied, and still no difference between groups.
“Were you surprised there was no placebo response?” that attendee further asked.
“Yes, we were. That was the reason why we did the subanalysis,” Dr. Lee said; results showed a placebo effect in the group with more severe pain but not in the group with less severe pain.
A third attendee asked, “Do you have any data on how much inflammation these patients actually had at baseline? Could the lack of effect be due to low inflammation at baseline?”
The investigators have not looked at inflammatory markers, Dr. Lee replied.
In an interview, Dr. Xavier Chevalier, session comoderator and head of the department of rheumatology at the Henri Mondor Hospital, University Paris XII, in Créteil, France, agreed with the attendees’ points. “Unfortunately, this is a negative trial, but I’m afraid that the level of pain was not really well defined at the beginning of the study,” he said. “And it’s a little bit of a shame that they didn’t include patients with a very high level of pain.”
Introducing the study, Dr. Lee noted, “The cause and pathophysiology of hand osteoarthritis have not been clarified yet, but it is clear that inflammation plays an important tole. So it is believed that anti-inflammatory drugs might be effective in treating hand osteoarthritis.”
“Hydroxychloroquine is an anti-inflammatory drug that has been used successfully in other rheumatic diseases. It is prescribed commonly in hand osteoarthritis, but this indication is off label and not well investigated,” she said.
The investigators recruited to the trial 202 patients who met American College of Rheumatology criteria for primary hand osteoarthritis from outpatient rheumatology clinics in the Netherlands.
The patients had had pain from their arthritis for at least 1 year and had nodules or Kellgren-Lawrence grade 1, 2, or 3 changes in at least two symptomatic joints; those with grade 4 changes were excluded. They were randomized evenly to treatment with hydroxychloroquine (400 mg daily) or placebo.
Pain at baseline averaged about 44 mm on the 100-mm Visual Analog Scale (VAS) pain scale in each group, according to data reported at the meeting sponsored by the Osteoarthritis Research Society International.
Intention-to-treat analyses showed that at 24 weeks, the VAS score had increased by 0.10 mm in the placebo group and decreased by 1.3 mm in the hydroxychloroquine group, but the difference was not significant, reported Dr. Lee, who disclosed that she had no relevant conflicts of interest.
The groups were likewise statistically indistinguishable with respect to the change from baseline in the Australian/Canadian Osteoarthritis Hand Index (AUSCAN) scores and in total scores on the short form of the Arthritis Impact Measurement Scales 2 (AIMS2-SF).
About a fifth of patients in each group experienced adverse events. The hydroxychloroquine group had more allergic reactions (three vs. none) and cases of rash/pruritus (eight vs. three).
Dr. Lee disclosed that she had no relevant conflicts of interest.
SEATTLE – Hydroxychloroquine is not efficacious for treating primary hand osteoarthritis, according to results from the first randomized trial to test the disease-modifying antirheumatic drug in this patient population.
Findings reported at the World Congress on Osteoarthritis showed that after 24 weeks of treatment, scores for pain and hand function budged little from baseline whether patients took hydroxychloroquine (Plaquenil) or a placebo. And although the drug was generally well tolerated, patients in that group more commonly had allergic reactions and developed rashes.
“The results of our study do not support the prescription of hydroxychloroquine in patients with hand osteoarthritis,” concluded lead investigator WeiChing Lee, Pharm.D., hospital pharmacist at the Maasstad Hospital Rotterdam in the Netherlands.
During a question and answer period, however, session attendees pointed out some study limitations that may still leave the door open for hydroxychloroquine in this setting.
“Thank you for doing this trial. I’ve always wanted to see a randomized, controlled trial looking at this. I’m a little depressed that it’s negative,” commented session attendee Dr. Grace Lo of the Baylor College of Medicine in Houston. An older case series did suggest a benefit of hydroxychloroquine in patients with more severe disease, “so I was wondering why you specifically excluded those people from this study.”
“We believed that patients with very severe disease are not likely to benefit from hydroxychloroquine because it is in the end stage,” Dr. Lee replied.
Dr. Lo further wondered if outcomes had been assessed separately among patients with different anatomic types of hand osteoarthritis, such as carpometacarpal osteoarthritis versus osteoarthritis of the proximal and distal interphalangeal joints. The investigators have not performed those analyses, according to Dr. Lee. “You just need to see if there is a difference,” Dr. Lo recommended.
Another attendee noted that pain scores at baseline suggested some patients had little to no pain. “Did you do a subgroup analysis looking at higher pain scores at baseline versus lower pain scores?” he asked.
“Yes, we did a subanalysis of patients with a pain score of 60 mm or more versus less [on a 100-mm scale], and we saw it improved with more severe pain symptoms; there was a decrease of 15 mm in the pain scores in both the placebo and hydroxychloroquine groups,” Dr. Lee replied, and still no difference between groups.
“Were you surprised there was no placebo response?” that attendee further asked.
“Yes, we were. That was the reason why we did the subanalysis,” Dr. Lee said; results showed a placebo effect in the group with more severe pain but not in the group with less severe pain.
A third attendee asked, “Do you have any data on how much inflammation these patients actually had at baseline? Could the lack of effect be due to low inflammation at baseline?”
The investigators have not looked at inflammatory markers, Dr. Lee replied.
In an interview, Dr. Xavier Chevalier, session comoderator and head of the department of rheumatology at the Henri Mondor Hospital, University Paris XII, in Créteil, France, agreed with the attendees’ points. “Unfortunately, this is a negative trial, but I’m afraid that the level of pain was not really well defined at the beginning of the study,” he said. “And it’s a little bit of a shame that they didn’t include patients with a very high level of pain.”
Introducing the study, Dr. Lee noted, “The cause and pathophysiology of hand osteoarthritis have not been clarified yet, but it is clear that inflammation plays an important tole. So it is believed that anti-inflammatory drugs might be effective in treating hand osteoarthritis.”
“Hydroxychloroquine is an anti-inflammatory drug that has been used successfully in other rheumatic diseases. It is prescribed commonly in hand osteoarthritis, but this indication is off label and not well investigated,” she said.
The investigators recruited to the trial 202 patients who met American College of Rheumatology criteria for primary hand osteoarthritis from outpatient rheumatology clinics in the Netherlands.
The patients had had pain from their arthritis for at least 1 year and had nodules or Kellgren-Lawrence grade 1, 2, or 3 changes in at least two symptomatic joints; those with grade 4 changes were excluded. They were randomized evenly to treatment with hydroxychloroquine (400 mg daily) or placebo.
Pain at baseline averaged about 44 mm on the 100-mm Visual Analog Scale (VAS) pain scale in each group, according to data reported at the meeting sponsored by the Osteoarthritis Research Society International.
Intention-to-treat analyses showed that at 24 weeks, the VAS score had increased by 0.10 mm in the placebo group and decreased by 1.3 mm in the hydroxychloroquine group, but the difference was not significant, reported Dr. Lee, who disclosed that she had no relevant conflicts of interest.
The groups were likewise statistically indistinguishable with respect to the change from baseline in the Australian/Canadian Osteoarthritis Hand Index (AUSCAN) scores and in total scores on the short form of the Arthritis Impact Measurement Scales 2 (AIMS2-SF).
About a fifth of patients in each group experienced adverse events. The hydroxychloroquine group had more allergic reactions (three vs. none) and cases of rash/pruritus (eight vs. three).
Dr. Lee disclosed that she had no relevant conflicts of interest.
AT OARSI 2015
Key clinical point: Hydroxychloroquine was not efficacious for treating hand osteoarthritis.
Major finding: The change in VAS pain score did not differ significantly between the hydroxychloroquine and placebo groups.
Data source: A randomized phase III trial among 202 patients with mild to moderate hand osteoarthritis.
Disclosures: Dr. Lee disclosed that she had no relevant conflicts of interest.

OARSI: Pain of knee osteoarthritis is worse for smokers
SEATTLE – Smoking is related to prevalent and incident joint pain in patients who have knee osteoarthritis or are at high risk for it, but the mechanism of this association is unclear, in a study of 3,026 patients.
“Previous studies have shown that compared to nonsmokers, smokers have more musculoskeletal pain and report more severe pain,” Jingbo Niu, D.Sc. of the Clinical Epidemiology Research & Training Unit at Boston University reported at the World Congress on Osteoarthritis.

Possible mechanisms include down-regulation of the hypothalamic-pituitary-adrenal axis or triggering of nicotine-sensitive acetylcholine receptors in the dorsal root ganglion. “These factors may translate to a change in pain perception among smokers,” she said.
Dr. Niu and her colleagues analyzed data from the Multicenter Osteoarthritis Study (MOST), a prospective cohort study of risk factors for the development and progression of knee osteoarthritis and knee pain in patients initially aged 50-79 years. They performed cross-sectional analyses at baseline and at the 7-year follow-up visit, and longitudinal analyses for the interim period.
At baseline, 56% of the cohort were never-smokers, 38% were former smokers, and 6% were current smokers, reported Dr. Niu, who disclosed that she had no relevant conflicts of interest. Smoking intensity averaged 22 pack-years.
Study results showed that at baseline, current smokers had significantly more severe knee pain than did never-smokers, with an adjusted difference of 0.83 points on the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) knee pain scale.
Also at baseline, former smokers were more likely than were never-smokers to have widespread joint pain, defined as pain in all five regions of a joint pain homunculus (adjusted odds ratio, 1.3). And there was a dose-response relationship, whereby the greater the number of pack-years at baseline, the higher the risk of developing widespread joint pain during follow-up (P = .02).
However, neither smoking status nor smoking intensity was significantly associated with pain sensitization, assessed from the pressure pain threshold at the right wrist, according to the data reported at the meeting, which was sponsored by the Osteoarthritis Research Society International.
“We found smoking was related to knee pain severity and widespread pain, but not with pain sensitization,” Dr. Niu concluded.
“The number of current smokers in our analysis was limited,” she said. In addition, “subjects with knee pain were more likely to be recruited into the MOST study because they have a high risk of developing knee osteoarthritis. This inclusion criterion may lead to selection bias when we study knee pain and other pain-related outcomes.”
One session attendee noted that the confounders in the analyses did not include socioeconomic factors and recommended they be added. “Of course, smoking status could be confounded by socioeconomic factors, and couldn’t it just be that smoking is a surrogate measure?” he asked.
“It’s a good suggestion,” Dr. Niu agreed, noting that the data set has some socioeconomic measures, such as education, that could be incorporated into analyses.
In an interview, Dr. Timothy McAlindon, one of the session’s comoderators and a professor of medicine at Tufts University, Boston, said, “I think this is a very nicely done study looking at the association of smoking with pain in osteoarthritis.
“What they found is there is clearly a significant association of smoking with pain and incident widespread pain. What was less clear was the mechanistic relationship. Maybe they didn’t test the right mechanistic measures,” he proposed.
“If there is a causal relationship, it could perhaps suggest intervention. But I think that is very conjectural based on what they have done so far,” Dr. McAlindon concluded.
SEATTLE – Smoking is related to prevalent and incident joint pain in patients who have knee osteoarthritis or are at high risk for it, but the mechanism of this association is unclear, in a study of 3,026 patients.
“Previous studies have shown that compared to nonsmokers, smokers have more musculoskeletal pain and report more severe pain,” Jingbo Niu, D.Sc. of the Clinical Epidemiology Research & Training Unit at Boston University reported at the World Congress on Osteoarthritis.
Possible mechanisms include down-regulation of the hypothalamic-pituitary-adrenal axis or triggering of nicotine-sensitive acetylcholine receptors in the dorsal root ganglion. “These factors may translate to a change in pain perception among smokers,” she said.
Dr. Niu and her colleagues analyzed data from the Multicenter Osteoarthritis Study (MOST), a prospective cohort study of risk factors for the development and progression of knee osteoarthritis and knee pain in patients initially aged 50-79 years. They performed cross-sectional analyses at baseline and at the 7-year follow-up visit, and longitudinal analyses for the interim period.
At baseline, 56% of the cohort were never-smokers, 38% were former smokers, and 6% were current smokers, reported Dr. Niu, who disclosed that she had no relevant conflicts of interest. Smoking intensity averaged 22 pack-years.
Study results showed that at baseline, current smokers had significantly more severe knee pain than did never-smokers, with an adjusted difference of 0.83 points on the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) knee pain scale.
Also at baseline, former smokers were more likely than were never-smokers to have widespread joint pain, defined as pain in all five regions of a joint pain homunculus (adjusted odds ratio, 1.3). And there was a dose-response relationship, whereby the greater the number of pack-years at baseline, the higher the risk of developing widespread joint pain during follow-up (P = .02).
However, neither smoking status nor smoking intensity was significantly associated with pain sensitization, assessed from the pressure pain threshold at the right wrist, according to the data reported at the meeting, which was sponsored by the Osteoarthritis Research Society International.
“We found smoking was related to knee pain severity and widespread pain, but not with pain sensitization,” Dr. Niu concluded.
“The number of current smokers in our analysis was limited,” she said. In addition, “subjects with knee pain were more likely to be recruited into the MOST study because they have a high risk of developing knee osteoarthritis. This inclusion criterion may lead to selection bias when we study knee pain and other pain-related outcomes.”
One session attendee noted that the confounders in the analyses did not include socioeconomic factors and recommended they be added. “Of course, smoking status could be confounded by socioeconomic factors, and couldn’t it just be that smoking is a surrogate measure?” he asked.
“It’s a good suggestion,” Dr. Niu agreed, noting that the data set has some socioeconomic measures, such as education, that could be incorporated into analyses.
In an interview, Dr. Timothy McAlindon, one of the session’s comoderators and a professor of medicine at Tufts University, Boston, said, “I think this is a very nicely done study looking at the association of smoking with pain in osteoarthritis.
“What they found is there is clearly a significant association of smoking with pain and incident widespread pain. What was less clear was the mechanistic relationship. Maybe they didn’t test the right mechanistic measures,” he proposed.
“If there is a causal relationship, it could perhaps suggest intervention. But I think that is very conjectural based on what they have done so far,” Dr. McAlindon concluded.
SEATTLE – Smoking is related to prevalent and incident joint pain in patients who have knee osteoarthritis or are at high risk for it, but the mechanism of this association is unclear, in a study of 3,026 patients.
“Previous studies have shown that compared to nonsmokers, smokers have more musculoskeletal pain and report more severe pain,” Jingbo Niu, D.Sc. of the Clinical Epidemiology Research & Training Unit at Boston University reported at the World Congress on Osteoarthritis.
Possible mechanisms include down-regulation of the hypothalamic-pituitary-adrenal axis or triggering of nicotine-sensitive acetylcholine receptors in the dorsal root ganglion. “These factors may translate to a change in pain perception among smokers,” she said.
Dr. Niu and her colleagues analyzed data from the Multicenter Osteoarthritis Study (MOST), a prospective cohort study of risk factors for the development and progression of knee osteoarthritis and knee pain in patients initially aged 50-79 years. They performed cross-sectional analyses at baseline and at the 7-year follow-up visit, and longitudinal analyses for the interim period.
At baseline, 56% of the cohort were never-smokers, 38% were former smokers, and 6% were current smokers, reported Dr. Niu, who disclosed that she had no relevant conflicts of interest. Smoking intensity averaged 22 pack-years.
Study results showed that at baseline, current smokers had significantly more severe knee pain than did never-smokers, with an adjusted difference of 0.83 points on the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) knee pain scale.
Also at baseline, former smokers were more likely than were never-smokers to have widespread joint pain, defined as pain in all five regions of a joint pain homunculus (adjusted odds ratio, 1.3). And there was a dose-response relationship, whereby the greater the number of pack-years at baseline, the higher the risk of developing widespread joint pain during follow-up (P = .02).
However, neither smoking status nor smoking intensity was significantly associated with pain sensitization, assessed from the pressure pain threshold at the right wrist, according to the data reported at the meeting, which was sponsored by the Osteoarthritis Research Society International.
“We found smoking was related to knee pain severity and widespread pain, but not with pain sensitization,” Dr. Niu concluded.
“The number of current smokers in our analysis was limited,” she said. In addition, “subjects with knee pain were more likely to be recruited into the MOST study because they have a high risk of developing knee osteoarthritis. This inclusion criterion may lead to selection bias when we study knee pain and other pain-related outcomes.”
One session attendee noted that the confounders in the analyses did not include socioeconomic factors and recommended they be added. “Of course, smoking status could be confounded by socioeconomic factors, and couldn’t it just be that smoking is a surrogate measure?” he asked.
“It’s a good suggestion,” Dr. Niu agreed, noting that the data set has some socioeconomic measures, such as education, that could be incorporated into analyses.
In an interview, Dr. Timothy McAlindon, one of the session’s comoderators and a professor of medicine at Tufts University, Boston, said, “I think this is a very nicely done study looking at the association of smoking with pain in osteoarthritis.
“What they found is there is clearly a significant association of smoking with pain and incident widespread pain. What was less clear was the mechanistic relationship. Maybe they didn’t test the right mechanistic measures,” he proposed.
“If there is a causal relationship, it could perhaps suggest intervention. But I think that is very conjectural based on what they have done so far,” Dr. McAlindon concluded.
AT OARSI 2015
Key clinical point: Smoking is associated with prevalent and incident joint pain among older adults with knee osteoarthritis.
Major finding: Scores on the WOMAC knee pain scale were 0.83 points higher for current smokers than for never-smokers.
Data source: Cross-sectional and longitudinal analyses of a cohort of 3,026 patients with or at high risk for knee osteoarthritis.
Disclosures: Dr. Niu disclosed that she had no relevant conflicts of interest.
