User login
American Association of Diabetes Educators (AADE): Annual Meeting
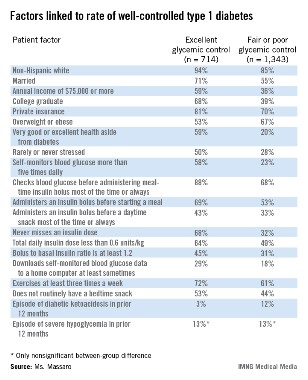
Correlates of excellent type 1 diabetes control found
PHILADELPHIA – U.S. patients with type 1 diabetes who maintain excellent glycemic control have the best diabetes-control practices, use a pump, and have higher incomes and educational attainment, compared with patients who maintain fair or poor glycemic control, based on data collected from more than 2,000 registry patients.
Patients with excellent control had, by definition, the lowest levels of hemoglobin A1c, and also had a quarter of the episodes of diabetic ketoacidosis as did the patients who maintained fair or poor glycemic control, Elaine Massaro, R.N., said at the annual meeting of the American Association of Diabetes Educators.

But better glycemic control did not result in an increased incidence of severe hypoglycemic episodes; the rate of severe hypoglycemia was 13% during the preceding 12 months among patients with excellent glycemic control and those with fair or poor control, said Ms. Massaro, an advanced practice nurse at Northwestern University in Chicago.
Between September 2010 and May 2013, more than 26,000 U.S. adult and pediatric patients with type 1 diabetes treated at any of 70 participating centers enrolled in the T1D Exchange Clinic Registry. From the total group of enrollees, Ms. Massaro and her associates identified 714 patients (3%) who, at their entry examination, were at least 26 years old, had been diagnosed with type 1 diabetes for at least 2 years, were not using a real-time continuous glucose monitor, and had excellent glycemic control, with a HbA1c of less than 6.5%. The researchers also identified a second subgroup of 1,343 (5%) from the registered patients who matched the first group by age, duration of diagnosis, and lack of continuous monitoring, but differed by having fair or poor glycemic control, with a HbA1c of 8.5% or higher.

Comparison of these two subgroups identified several factors that significantly correlated with excellent glycemic control. For example, 68% of patients with excellent control never missed an insulin dose, compared with 32% of those with fair or poor control. The prevalence of patients who said they self-monitored their blood glucose more than five times a day was 58% among those with excellent control and 23% among those with fair or poor control.
Four times as many patients with fair or poor control reported having an episode of diabetic ketoacidosis during the prior 12 months, compared with patients who maintained excellent glycemic control (12% vs. 3%).
The analysis failed to find any correlation between the level of glycemic control and the type of insulin that patients used, or whether they administered a long-acting insulin formulation once or twice a day. The results also showed that insulin pump use was significantly more prevalent among patients with excellent glycemic control than among those with fair or poor control, but Ms. Massaro did not report specific rates of pump use in the two subgroups.
Ms. Massaro had no disclosures.
On Twitter @mitchelzoler
PHILADELPHIA – U.S. patients with type 1 diabetes who maintain excellent glycemic control have the best diabetes-control practices, use a pump, and have higher incomes and educational attainment, compared with patients who maintain fair or poor glycemic control, based on data collected from more than 2,000 registry patients.
Patients with excellent control had, by definition, the lowest levels of hemoglobin A1c, and also had a quarter of the episodes of diabetic ketoacidosis as did the patients who maintained fair or poor glycemic control, Elaine Massaro, R.N., said at the annual meeting of the American Association of Diabetes Educators.
But better glycemic control did not result in an increased incidence of severe hypoglycemic episodes; the rate of severe hypoglycemia was 13% during the preceding 12 months among patients with excellent glycemic control and those with fair or poor control, said Ms. Massaro, an advanced practice nurse at Northwestern University in Chicago.
Between September 2010 and May 2013, more than 26,000 U.S. adult and pediatric patients with type 1 diabetes treated at any of 70 participating centers enrolled in the T1D Exchange Clinic Registry. From the total group of enrollees, Ms. Massaro and her associates identified 714 patients (3%) who, at their entry examination, were at least 26 years old, had been diagnosed with type 1 diabetes for at least 2 years, were not using a real-time continuous glucose monitor, and had excellent glycemic control, with a HbA1c of less than 6.5%. The researchers also identified a second subgroup of 1,343 (5%) from the registered patients who matched the first group by age, duration of diagnosis, and lack of continuous monitoring, but differed by having fair or poor glycemic control, with a HbA1c of 8.5% or higher.
Comparison of these two subgroups identified several factors that significantly correlated with excellent glycemic control. For example, 68% of patients with excellent control never missed an insulin dose, compared with 32% of those with fair or poor control. The prevalence of patients who said they self-monitored their blood glucose more than five times a day was 58% among those with excellent control and 23% among those with fair or poor control.
Four times as many patients with fair or poor control reported having an episode of diabetic ketoacidosis during the prior 12 months, compared with patients who maintained excellent glycemic control (12% vs. 3%).
The analysis failed to find any correlation between the level of glycemic control and the type of insulin that patients used, or whether they administered a long-acting insulin formulation once or twice a day. The results also showed that insulin pump use was significantly more prevalent among patients with excellent glycemic control than among those with fair or poor control, but Ms. Massaro did not report specific rates of pump use in the two subgroups.
Ms. Massaro had no disclosures.
On Twitter @mitchelzoler
PHILADELPHIA – U.S. patients with type 1 diabetes who maintain excellent glycemic control have the best diabetes-control practices, use a pump, and have higher incomes and educational attainment, compared with patients who maintain fair or poor glycemic control, based on data collected from more than 2,000 registry patients.
Patients with excellent control had, by definition, the lowest levels of hemoglobin A1c, and also had a quarter of the episodes of diabetic ketoacidosis as did the patients who maintained fair or poor glycemic control, Elaine Massaro, R.N., said at the annual meeting of the American Association of Diabetes Educators.
But better glycemic control did not result in an increased incidence of severe hypoglycemic episodes; the rate of severe hypoglycemia was 13% during the preceding 12 months among patients with excellent glycemic control and those with fair or poor control, said Ms. Massaro, an advanced practice nurse at Northwestern University in Chicago.
Between September 2010 and May 2013, more than 26,000 U.S. adult and pediatric patients with type 1 diabetes treated at any of 70 participating centers enrolled in the T1D Exchange Clinic Registry. From the total group of enrollees, Ms. Massaro and her associates identified 714 patients (3%) who, at their entry examination, were at least 26 years old, had been diagnosed with type 1 diabetes for at least 2 years, were not using a real-time continuous glucose monitor, and had excellent glycemic control, with a HbA1c of less than 6.5%. The researchers also identified a second subgroup of 1,343 (5%) from the registered patients who matched the first group by age, duration of diagnosis, and lack of continuous monitoring, but differed by having fair or poor glycemic control, with a HbA1c of 8.5% or higher.
Comparison of these two subgroups identified several factors that significantly correlated with excellent glycemic control. For example, 68% of patients with excellent control never missed an insulin dose, compared with 32% of those with fair or poor control. The prevalence of patients who said they self-monitored their blood glucose more than five times a day was 58% among those with excellent control and 23% among those with fair or poor control.
Four times as many patients with fair or poor control reported having an episode of diabetic ketoacidosis during the prior 12 months, compared with patients who maintained excellent glycemic control (12% vs. 3%).
The analysis failed to find any correlation between the level of glycemic control and the type of insulin that patients used, or whether they administered a long-acting insulin formulation once or twice a day. The results also showed that insulin pump use was significantly more prevalent among patients with excellent glycemic control than among those with fair or poor control, but Ms. Massaro did not report specific rates of pump use in the two subgroups.
Ms. Massaro had no disclosures.
On Twitter @mitchelzoler
AT AADE 13
Major finding: Of patients with excellent type 1 diabetes control, 68% never miss an insulin dose, compared with 32% of patients with fair or poor control.
Data source: Data came from 2,057 U.S. patients with type 1 diabetes and excellent or fair-to-poor glycemic control enrolled in a nationwide patient registry.
Disclosures: Ms. Massaro had no disclosures.
Multidisciplinary approach maintains weight loss in diabetes patients
PHILADELPHIA – A multidisciplinary approach to weight loss and maintenance in obese patients with diabetes produced sustained weight loss and biomarker improvements that lasted for 4 years in 57 of 119 patients (48%) followed that long.
The 57 patients who maintained their weight loss had an average reduction of 24 pounds, 10% of their baseline weight, 4 years after they entered the single-center program and began the 12-week weight-loss phase, Gillian Arathuzik, R.N., said at the annual meeting of the American Association of Diabetes Educators.
The 62 patients (52%) who were unable to maintain their initial weight loss had an average 8-pound loss after 4 years, about 3% of their baseline weight.
All these patients participated in the Weight Achievement and Intensive Treatment (Why WAIT) program, run since 2005 at the Joslin Diabetes Center in Boston, said Ms. Arathuzik, a nutrition diabetes educator at Joslin.
Why WAIT includes intensive diabetes treatment, a structured diet intervention, an individualized exercise plan, cognitive behavioral support, and group education. "The big challenge is maintaining initial weight loss," she said.
The starting diet involves daily restriction of about 1,000 calories, with a weight-loss goal of 7%-10%. The composition is 40% carbohydrate, 30% protein, and 30% fat. "Reducing carbohydrates and increasing protein and fat make patients feel satisfied. The program wouldn’t be successful if patients felt hungry all the time," said Amanda Kirpitch, R.D., a nutrition and diabetes counselor who also works at Joslin. The diet is high in fiber and in mono- and polyunsaturated fatty acids, and low in saturated fatty acids and sodium. The initial diet uses one or two meal-replacement drinks per day, which "establish structure and are satisfying," said Ms. Kirpitch.
"We discuss with patients what [aspect of their diet] is a struggle and what works for them and can be maintained. We try to think about what they can manage 10 years out. And we try to limit their diet monotony. We encourage patients to tell us what drives them off track," she said.
The exercise program starts slowly, aimed at a goal of 60-90 minutes six or seven times a week for weight loss, and 30 minutes five times a week for fitness and weight maintenance. These target amounts can be achieved in several exercise periods that last 10 minutes, and are regarded as a goal that may not be realistic for all participants. "Our target is 60 minutes six times a week," said Ms. Kirpitch. Each patient receives an individualized exercise plan that can include aerobic classes, resistance and strength training, and flexibility exercises. Resistance training is important because it decreases loss of lean body mass and increases muscle mass, fat oxidation, and energy expenditure. The ideal long-term goal for patients is to perform 10-12 resistance training exercises three or four times a week. "We use exercise as medicine," she said.
Cognitive behavioral support occurs during 30- to 60-minute sessions facilitated by a psychologist. The focus is on realistic and attainable goals with long-term sustainability. Sessions deal with relapse prevention, mastering unique challenges, planning ahead, and managing automatic, negative thoughts.
Medical management of patients is assessed by a consulting physician who tries to "make the regimen more weight-loss friendly," said Ms. Arathuzik. The weight-neutral drug metformin is usually the first-line oral agent, followed by a glucagonlike peptide–1 agonist such as exenatide (Byetta) or liraglutide (Victoza) as the preferred second agent because of their weight-loss effect. The dipeptidyl peptidase–4 inhibitors, such as sitagliptin (Januvia) and linagliptin (Tradjenta), are good tertiary oral drugs, as they are also weight neutral. Drugs that cause modest or significant weight gain, such as sulfonylureas or thiazolidinediones, are stopped or reduced. Patients on insulin may be able to have their dosage lowered, and the insulin type changed to detemir (Levemir), which causes more modest weight gain than other insulin types.
By the end of the initial, 12-week intervention "most patients are on fewer medications, and some are totally off medications," said Ms. Arathuzik.
The 119 obese patients with either type 1 or type 2 diabetes enrolled in Why WAIT averaged about 54 years old, had a mean weight of about 245 pounds, and had diabetes for an average of about 8 years. Most patients had a sharp drop in weight during their 12 weeks in the active phase, with an average loss of about 25 pounds among all 119 patients.
Weight loss was greatest in the 48% of patients who went on to maintain their loss through 4 years. The average weight loss in this subgroup reached a maximum of about 32 pounds at 6 months after the start of intervention. This subgroup then began to gradually gain weight, gaining an average of about 6 pounds over the next 18 months, so after 2 years their average loss from baseline was about 24 pounds. These patients then maintained this amount of loss through the next 2 years of follow-up.
In contrast, the 52% of patients who did not maintain their initial loss had a lower initial loss that averaged 20 pounds after 12 weeks and then quickly rebounded to an average net loss of about 6 pounds by 1 year after the intervention began. The patients in this group then stayed at an average loss of about 3-8 pounds through the remaining 3 years of follow-up.
The entire group of program participants averaged a sharp, roughly 1-percentage-point drop in their hemoglobin A1c level, from a starting level of about 7.4% to about 6.4% by the end of the initial 12-week intervention. The levels then rebounded just as sharply in both subgroups. However, by the end of 4 years, patients in the subgroup that maintained weight loss had an average HbA1c of 6.9%, significantly below the average 8.0% level in patients who regained much of their weight.
Ms. Arathuzik speculated that many patients had a sharp drop and then a rebound in their HbA1c levels because of the "huge" reduction in drug treatment many patients had when their weight initially dropped. The reduced need for medications initially cut annual costs by an average of more than $500 per patient. But their need for treatment increased once their weight rose again.
The patients who successfully maintained their weight loss also showed an average decline in their blood pressure of about 4/2 mm Hg at 4 years compared with baseline. Patients in both groups had an average drop in their low density lipoprotein (LDL) cholesterol of 6-9 mg/dL after 4 years, and an average increase in their high density lipoprotein (HDL) cholesterol of about 7 mg/dL, compared with baseline after 4 years.
Future research will examine ways to maintain patients in diabetes remission through weight loss, she said. Another area for further research is to find factors that identify patients who will maintain their weight loss. "We have been bad at predicting who will maintain their loss and who will regain weight," Ms. Arathuzik said in an interview.
Ms. Arathuzik and Ms. Kirpitch said that they had no disclosures.
On Twitter @mitchelzoler
PHILADELPHIA – A multidisciplinary approach to weight loss and maintenance in obese patients with diabetes produced sustained weight loss and biomarker improvements that lasted for 4 years in 57 of 119 patients (48%) followed that long.
The 57 patients who maintained their weight loss had an average reduction of 24 pounds, 10% of their baseline weight, 4 years after they entered the single-center program and began the 12-week weight-loss phase, Gillian Arathuzik, R.N., said at the annual meeting of the American Association of Diabetes Educators.
The 62 patients (52%) who were unable to maintain their initial weight loss had an average 8-pound loss after 4 years, about 3% of their baseline weight.
All these patients participated in the Weight Achievement and Intensive Treatment (Why WAIT) program, run since 2005 at the Joslin Diabetes Center in Boston, said Ms. Arathuzik, a nutrition diabetes educator at Joslin.
Why WAIT includes intensive diabetes treatment, a structured diet intervention, an individualized exercise plan, cognitive behavioral support, and group education. "The big challenge is maintaining initial weight loss," she said.
The starting diet involves daily restriction of about 1,000 calories, with a weight-loss goal of 7%-10%. The composition is 40% carbohydrate, 30% protein, and 30% fat. "Reducing carbohydrates and increasing protein and fat make patients feel satisfied. The program wouldn’t be successful if patients felt hungry all the time," said Amanda Kirpitch, R.D., a nutrition and diabetes counselor who also works at Joslin. The diet is high in fiber and in mono- and polyunsaturated fatty acids, and low in saturated fatty acids and sodium. The initial diet uses one or two meal-replacement drinks per day, which "establish structure and are satisfying," said Ms. Kirpitch.
"We discuss with patients what [aspect of their diet] is a struggle and what works for them and can be maintained. We try to think about what they can manage 10 years out. And we try to limit their diet monotony. We encourage patients to tell us what drives them off track," she said.
The exercise program starts slowly, aimed at a goal of 60-90 minutes six or seven times a week for weight loss, and 30 minutes five times a week for fitness and weight maintenance. These target amounts can be achieved in several exercise periods that last 10 minutes, and are regarded as a goal that may not be realistic for all participants. "Our target is 60 minutes six times a week," said Ms. Kirpitch. Each patient receives an individualized exercise plan that can include aerobic classes, resistance and strength training, and flexibility exercises. Resistance training is important because it decreases loss of lean body mass and increases muscle mass, fat oxidation, and energy expenditure. The ideal long-term goal for patients is to perform 10-12 resistance training exercises three or four times a week. "We use exercise as medicine," she said.
Cognitive behavioral support occurs during 30- to 60-minute sessions facilitated by a psychologist. The focus is on realistic and attainable goals with long-term sustainability. Sessions deal with relapse prevention, mastering unique challenges, planning ahead, and managing automatic, negative thoughts.
Medical management of patients is assessed by a consulting physician who tries to "make the regimen more weight-loss friendly," said Ms. Arathuzik. The weight-neutral drug metformin is usually the first-line oral agent, followed by a glucagonlike peptide–1 agonist such as exenatide (Byetta) or liraglutide (Victoza) as the preferred second agent because of their weight-loss effect. The dipeptidyl peptidase–4 inhibitors, such as sitagliptin (Januvia) and linagliptin (Tradjenta), are good tertiary oral drugs, as they are also weight neutral. Drugs that cause modest or significant weight gain, such as sulfonylureas or thiazolidinediones, are stopped or reduced. Patients on insulin may be able to have their dosage lowered, and the insulin type changed to detemir (Levemir), which causes more modest weight gain than other insulin types.
By the end of the initial, 12-week intervention "most patients are on fewer medications, and some are totally off medications," said Ms. Arathuzik.
The 119 obese patients with either type 1 or type 2 diabetes enrolled in Why WAIT averaged about 54 years old, had a mean weight of about 245 pounds, and had diabetes for an average of about 8 years. Most patients had a sharp drop in weight during their 12 weeks in the active phase, with an average loss of about 25 pounds among all 119 patients.
Weight loss was greatest in the 48% of patients who went on to maintain their loss through 4 years. The average weight loss in this subgroup reached a maximum of about 32 pounds at 6 months after the start of intervention. This subgroup then began to gradually gain weight, gaining an average of about 6 pounds over the next 18 months, so after 2 years their average loss from baseline was about 24 pounds. These patients then maintained this amount of loss through the next 2 years of follow-up.
In contrast, the 52% of patients who did not maintain their initial loss had a lower initial loss that averaged 20 pounds after 12 weeks and then quickly rebounded to an average net loss of about 6 pounds by 1 year after the intervention began. The patients in this group then stayed at an average loss of about 3-8 pounds through the remaining 3 years of follow-up.
The entire group of program participants averaged a sharp, roughly 1-percentage-point drop in their hemoglobin A1c level, from a starting level of about 7.4% to about 6.4% by the end of the initial 12-week intervention. The levels then rebounded just as sharply in both subgroups. However, by the end of 4 years, patients in the subgroup that maintained weight loss had an average HbA1c of 6.9%, significantly below the average 8.0% level in patients who regained much of their weight.
Ms. Arathuzik speculated that many patients had a sharp drop and then a rebound in their HbA1c levels because of the "huge" reduction in drug treatment many patients had when their weight initially dropped. The reduced need for medications initially cut annual costs by an average of more than $500 per patient. But their need for treatment increased once their weight rose again.
The patients who successfully maintained their weight loss also showed an average decline in their blood pressure of about 4/2 mm Hg at 4 years compared with baseline. Patients in both groups had an average drop in their low density lipoprotein (LDL) cholesterol of 6-9 mg/dL after 4 years, and an average increase in their high density lipoprotein (HDL) cholesterol of about 7 mg/dL, compared with baseline after 4 years.
Future research will examine ways to maintain patients in diabetes remission through weight loss, she said. Another area for further research is to find factors that identify patients who will maintain their weight loss. "We have been bad at predicting who will maintain their loss and who will regain weight," Ms. Arathuzik said in an interview.
Ms. Arathuzik and Ms. Kirpitch said that they had no disclosures.
On Twitter @mitchelzoler
PHILADELPHIA – A multidisciplinary approach to weight loss and maintenance in obese patients with diabetes produced sustained weight loss and biomarker improvements that lasted for 4 years in 57 of 119 patients (48%) followed that long.
The 57 patients who maintained their weight loss had an average reduction of 24 pounds, 10% of their baseline weight, 4 years after they entered the single-center program and began the 12-week weight-loss phase, Gillian Arathuzik, R.N., said at the annual meeting of the American Association of Diabetes Educators.
The 62 patients (52%) who were unable to maintain their initial weight loss had an average 8-pound loss after 4 years, about 3% of their baseline weight.
All these patients participated in the Weight Achievement and Intensive Treatment (Why WAIT) program, run since 2005 at the Joslin Diabetes Center in Boston, said Ms. Arathuzik, a nutrition diabetes educator at Joslin.
Why WAIT includes intensive diabetes treatment, a structured diet intervention, an individualized exercise plan, cognitive behavioral support, and group education. "The big challenge is maintaining initial weight loss," she said.
The starting diet involves daily restriction of about 1,000 calories, with a weight-loss goal of 7%-10%. The composition is 40% carbohydrate, 30% protein, and 30% fat. "Reducing carbohydrates and increasing protein and fat make patients feel satisfied. The program wouldn’t be successful if patients felt hungry all the time," said Amanda Kirpitch, R.D., a nutrition and diabetes counselor who also works at Joslin. The diet is high in fiber and in mono- and polyunsaturated fatty acids, and low in saturated fatty acids and sodium. The initial diet uses one or two meal-replacement drinks per day, which "establish structure and are satisfying," said Ms. Kirpitch.
"We discuss with patients what [aspect of their diet] is a struggle and what works for them and can be maintained. We try to think about what they can manage 10 years out. And we try to limit their diet monotony. We encourage patients to tell us what drives them off track," she said.
The exercise program starts slowly, aimed at a goal of 60-90 minutes six or seven times a week for weight loss, and 30 minutes five times a week for fitness and weight maintenance. These target amounts can be achieved in several exercise periods that last 10 minutes, and are regarded as a goal that may not be realistic for all participants. "Our target is 60 minutes six times a week," said Ms. Kirpitch. Each patient receives an individualized exercise plan that can include aerobic classes, resistance and strength training, and flexibility exercises. Resistance training is important because it decreases loss of lean body mass and increases muscle mass, fat oxidation, and energy expenditure. The ideal long-term goal for patients is to perform 10-12 resistance training exercises three or four times a week. "We use exercise as medicine," she said.
Cognitive behavioral support occurs during 30- to 60-minute sessions facilitated by a psychologist. The focus is on realistic and attainable goals with long-term sustainability. Sessions deal with relapse prevention, mastering unique challenges, planning ahead, and managing automatic, negative thoughts.
Medical management of patients is assessed by a consulting physician who tries to "make the regimen more weight-loss friendly," said Ms. Arathuzik. The weight-neutral drug metformin is usually the first-line oral agent, followed by a glucagonlike peptide–1 agonist such as exenatide (Byetta) or liraglutide (Victoza) as the preferred second agent because of their weight-loss effect. The dipeptidyl peptidase–4 inhibitors, such as sitagliptin (Januvia) and linagliptin (Tradjenta), are good tertiary oral drugs, as they are also weight neutral. Drugs that cause modest or significant weight gain, such as sulfonylureas or thiazolidinediones, are stopped or reduced. Patients on insulin may be able to have their dosage lowered, and the insulin type changed to detemir (Levemir), which causes more modest weight gain than other insulin types.
By the end of the initial, 12-week intervention "most patients are on fewer medications, and some are totally off medications," said Ms. Arathuzik.
The 119 obese patients with either type 1 or type 2 diabetes enrolled in Why WAIT averaged about 54 years old, had a mean weight of about 245 pounds, and had diabetes for an average of about 8 years. Most patients had a sharp drop in weight during their 12 weeks in the active phase, with an average loss of about 25 pounds among all 119 patients.
Weight loss was greatest in the 48% of patients who went on to maintain their loss through 4 years. The average weight loss in this subgroup reached a maximum of about 32 pounds at 6 months after the start of intervention. This subgroup then began to gradually gain weight, gaining an average of about 6 pounds over the next 18 months, so after 2 years their average loss from baseline was about 24 pounds. These patients then maintained this amount of loss through the next 2 years of follow-up.
In contrast, the 52% of patients who did not maintain their initial loss had a lower initial loss that averaged 20 pounds after 12 weeks and then quickly rebounded to an average net loss of about 6 pounds by 1 year after the intervention began. The patients in this group then stayed at an average loss of about 3-8 pounds through the remaining 3 years of follow-up.
The entire group of program participants averaged a sharp, roughly 1-percentage-point drop in their hemoglobin A1c level, from a starting level of about 7.4% to about 6.4% by the end of the initial 12-week intervention. The levels then rebounded just as sharply in both subgroups. However, by the end of 4 years, patients in the subgroup that maintained weight loss had an average HbA1c of 6.9%, significantly below the average 8.0% level in patients who regained much of their weight.
Ms. Arathuzik speculated that many patients had a sharp drop and then a rebound in their HbA1c levels because of the "huge" reduction in drug treatment many patients had when their weight initially dropped. The reduced need for medications initially cut annual costs by an average of more than $500 per patient. But their need for treatment increased once their weight rose again.
The patients who successfully maintained their weight loss also showed an average decline in their blood pressure of about 4/2 mm Hg at 4 years compared with baseline. Patients in both groups had an average drop in their low density lipoprotein (LDL) cholesterol of 6-9 mg/dL after 4 years, and an average increase in their high density lipoprotein (HDL) cholesterol of about 7 mg/dL, compared with baseline after 4 years.
Future research will examine ways to maintain patients in diabetes remission through weight loss, she said. Another area for further research is to find factors that identify patients who will maintain their weight loss. "We have been bad at predicting who will maintain their loss and who will regain weight," Ms. Arathuzik said in an interview.
Ms. Arathuzik and Ms. Kirpitch said that they had no disclosures.
On Twitter @mitchelzoler
AT AADE 13
Major finding: Four years after intervention, 48% of patients maintained an average 10% weight loss, compared with their baseline weight.
Data source: Data came from 4-year follow-up of 119 obese patients with diabetes treated at one U.S. center since 2005.
Disclosures: Ms. Arathuzik and Ms. Kirpitch said that they had no disclosures.
Pilot study: Mindfulness stress reduction benefits diabetes patients
PHILADELPHIA – Eight weeks of training classes in mindfulness-based stress reduction plus at-home meditation sessions led to medium to large improvements in mindfulness, stress, and diabetes problems in a pilot study that enrolled six women with type 2 diabetes who were on oral medications.
The mindfulness stress-reduction program also was linked with an average 0.7% cut in hemoglobin A1c (HbA1c) levels in the six women who participated in the intervention, Monica DiNardo said at the annual meeting of the American Association of Diabetes Educators.
Based on these "encouraging" results in the pilot study, Ms. DiNardo, a nurse practitioner at the Veterans Affairs Medical Center in Pittsburgh, and her associates began a similar mindfulness intervention in 28 patients with diabetes treated there in a study that also included 7 control patients who did not undergo the intervention. Follow-up data from many of these patients will soon be analyzed, she said.

Results available so far also show that in the pilot study, as well as the study with 35 veterans, the mindfulness stress-reduction training and home-based sessions were feasible and well received by patients. In the pilot study, all six participants completed the mindfulness intervention and said that they would recommend it to others and that they intended to continue mindfulness on their own. Five of the six patients remained in the study through full follow-up. Among the veterans, 17 of the 35 participants have completed the study with full 3-month follow-up, with several of the others positioned for full follow-up.
Ms. DiNardo and her associates designed these studies to examine whether stress reduction with a mindfulness-based intervention was feasible and acceptable in patients with diabetes. Other research groups in Germany (Diabetes Care 2012;35:945-7) and the Netherlands (Diabetes Care 2013;36:823-30) recently reported improved outcomes in patients with diabetes who underwent mindfulness-based interventions.
The Pittsburgh researchers used mindfulness-based stress reduction training modeled on the work of Jon Kabat-Zinn, Ph.D., who first introduced this approach in the 1970s (JAMA 2008;300:1350-2). Ms. DiNardo described mindfulness as "self-regulated attention to the present moment experience with nonjudgmental acceptance of one’s thoughts, feelings, and physical sensations; attainment of a mental calmness that counteracts the stress response and develops into a permanent set of traits."
The six women with diabetes in the pilot study received weekly training modeled on the work of Dr. Kabat-Zinn during 90 minutes for 8 weeks. The classes were facilitated by a psychologist who had more than 15 years of experience with meditation. The participants were also asked to perform meditation at home during 40-minute sessions guided by a CD five to six times per week, and to maintain a diary of their home sessions.
The women had a median age of 56 years, their median HbA1c was 6.9%, their median body mass index was 38 kg/m2, and they had been diagnosed with type 2 diabetes for a median of about 5 years. All six women were college graduates, and all had annual incomes of more than $40,000.
The researchers measured outcomes using with five different indices along with HbA1c. The measured mindfulness with the Mindfulness Attention Awareness Scale and with the Five Facet Mindfulness Questionnaire, they measured stress with the Perceived Stress Scale and with the Pittsburgh Quality Sleep Index, and they measured diabetes-related distress with the Problem Areas in Diabetes Scale. In addition to seeing an average 0.7% reduction in HbA1c, the researchers also found medium to large improvements from baseline to follow-up in the Mindfulness Attention Awareness Scale, the Perceived Stress Scale, and the Problem Areas in Diabetes Scale.
Ms. DiNardo said that she had no disclosures.
On Twitter @mitchelzoler
PHILADELPHIA – Eight weeks of training classes in mindfulness-based stress reduction plus at-home meditation sessions led to medium to large improvements in mindfulness, stress, and diabetes problems in a pilot study that enrolled six women with type 2 diabetes who were on oral medications.
The mindfulness stress-reduction program also was linked with an average 0.7% cut in hemoglobin A1c (HbA1c) levels in the six women who participated in the intervention, Monica DiNardo said at the annual meeting of the American Association of Diabetes Educators.
Based on these "encouraging" results in the pilot study, Ms. DiNardo, a nurse practitioner at the Veterans Affairs Medical Center in Pittsburgh, and her associates began a similar mindfulness intervention in 28 patients with diabetes treated there in a study that also included 7 control patients who did not undergo the intervention. Follow-up data from many of these patients will soon be analyzed, she said.
Results available so far also show that in the pilot study, as well as the study with 35 veterans, the mindfulness stress-reduction training and home-based sessions were feasible and well received by patients. In the pilot study, all six participants completed the mindfulness intervention and said that they would recommend it to others and that they intended to continue mindfulness on their own. Five of the six patients remained in the study through full follow-up. Among the veterans, 17 of the 35 participants have completed the study with full 3-month follow-up, with several of the others positioned for full follow-up.
Ms. DiNardo and her associates designed these studies to examine whether stress reduction with a mindfulness-based intervention was feasible and acceptable in patients with diabetes. Other research groups in Germany (Diabetes Care 2012;35:945-7) and the Netherlands (Diabetes Care 2013;36:823-30) recently reported improved outcomes in patients with diabetes who underwent mindfulness-based interventions.
The Pittsburgh researchers used mindfulness-based stress reduction training modeled on the work of Jon Kabat-Zinn, Ph.D., who first introduced this approach in the 1970s (JAMA 2008;300:1350-2). Ms. DiNardo described mindfulness as "self-regulated attention to the present moment experience with nonjudgmental acceptance of one’s thoughts, feelings, and physical sensations; attainment of a mental calmness that counteracts the stress response and develops into a permanent set of traits."
The six women with diabetes in the pilot study received weekly training modeled on the work of Dr. Kabat-Zinn during 90 minutes for 8 weeks. The classes were facilitated by a psychologist who had more than 15 years of experience with meditation. The participants were also asked to perform meditation at home during 40-minute sessions guided by a CD five to six times per week, and to maintain a diary of their home sessions.
The women had a median age of 56 years, their median HbA1c was 6.9%, their median body mass index was 38 kg/m2, and they had been diagnosed with type 2 diabetes for a median of about 5 years. All six women were college graduates, and all had annual incomes of more than $40,000.
The researchers measured outcomes using with five different indices along with HbA1c. The measured mindfulness with the Mindfulness Attention Awareness Scale and with the Five Facet Mindfulness Questionnaire, they measured stress with the Perceived Stress Scale and with the Pittsburgh Quality Sleep Index, and they measured diabetes-related distress with the Problem Areas in Diabetes Scale. In addition to seeing an average 0.7% reduction in HbA1c, the researchers also found medium to large improvements from baseline to follow-up in the Mindfulness Attention Awareness Scale, the Perceived Stress Scale, and the Problem Areas in Diabetes Scale.
Ms. DiNardo said that she had no disclosures.
On Twitter @mitchelzoler
PHILADELPHIA – Eight weeks of training classes in mindfulness-based stress reduction plus at-home meditation sessions led to medium to large improvements in mindfulness, stress, and diabetes problems in a pilot study that enrolled six women with type 2 diabetes who were on oral medications.
The mindfulness stress-reduction program also was linked with an average 0.7% cut in hemoglobin A1c (HbA1c) levels in the six women who participated in the intervention, Monica DiNardo said at the annual meeting of the American Association of Diabetes Educators.
Based on these "encouraging" results in the pilot study, Ms. DiNardo, a nurse practitioner at the Veterans Affairs Medical Center in Pittsburgh, and her associates began a similar mindfulness intervention in 28 patients with diabetes treated there in a study that also included 7 control patients who did not undergo the intervention. Follow-up data from many of these patients will soon be analyzed, she said.
Results available so far also show that in the pilot study, as well as the study with 35 veterans, the mindfulness stress-reduction training and home-based sessions were feasible and well received by patients. In the pilot study, all six participants completed the mindfulness intervention and said that they would recommend it to others and that they intended to continue mindfulness on their own. Five of the six patients remained in the study through full follow-up. Among the veterans, 17 of the 35 participants have completed the study with full 3-month follow-up, with several of the others positioned for full follow-up.
Ms. DiNardo and her associates designed these studies to examine whether stress reduction with a mindfulness-based intervention was feasible and acceptable in patients with diabetes. Other research groups in Germany (Diabetes Care 2012;35:945-7) and the Netherlands (Diabetes Care 2013;36:823-30) recently reported improved outcomes in patients with diabetes who underwent mindfulness-based interventions.
The Pittsburgh researchers used mindfulness-based stress reduction training modeled on the work of Jon Kabat-Zinn, Ph.D., who first introduced this approach in the 1970s (JAMA 2008;300:1350-2). Ms. DiNardo described mindfulness as "self-regulated attention to the present moment experience with nonjudgmental acceptance of one’s thoughts, feelings, and physical sensations; attainment of a mental calmness that counteracts the stress response and develops into a permanent set of traits."
The six women with diabetes in the pilot study received weekly training modeled on the work of Dr. Kabat-Zinn during 90 minutes for 8 weeks. The classes were facilitated by a psychologist who had more than 15 years of experience with meditation. The participants were also asked to perform meditation at home during 40-minute sessions guided by a CD five to six times per week, and to maintain a diary of their home sessions.
The women had a median age of 56 years, their median HbA1c was 6.9%, their median body mass index was 38 kg/m2, and they had been diagnosed with type 2 diabetes for a median of about 5 years. All six women were college graduates, and all had annual incomes of more than $40,000.
The researchers measured outcomes using with five different indices along with HbA1c. The measured mindfulness with the Mindfulness Attention Awareness Scale and with the Five Facet Mindfulness Questionnaire, they measured stress with the Perceived Stress Scale and with the Pittsburgh Quality Sleep Index, and they measured diabetes-related distress with the Problem Areas in Diabetes Scale. In addition to seeing an average 0.7% reduction in HbA1c, the researchers also found medium to large improvements from baseline to follow-up in the Mindfulness Attention Awareness Scale, the Perceived Stress Scale, and the Problem Areas in Diabetes Scale.
Ms. DiNardo said that she had no disclosures.
On Twitter @mitchelzoler
AT AADE 2013
Major finding: Women with type-2 diabetes who received mindfulness-based stress-reduction training had an average 0.7% decrease in hemoglobin A1c.
Data source: Data came from six women with type 2 diabetes who received mindfulness-based stress-reduction training for 8 weeks at one U.S. center.
Disclosures: Ms. DiNardo said that she had no disclosures.

Nutrition society drafts diabetes-prevention recommendations
PHILADELPHIA – Weight loss is the cornerstone of lifestyle measures to prevent people with prediabetes from progressing to type 2 diabetes, but other dietary steps also help, according to draft recommendations from a working group of the Academy of Nutrition and Dietetics.
In addition to weight loss, the new recommendations call for a registered dietician nutritionist to provide medical nutrition therapy to people with prediabetes and to produce individualized plans for macronutrient distribution, Patricia Davidson, DCN, said at the annual meeting of the American Association of Diabetes Educators.

"A registered dietician nutritionist and certified diabetes educator who provides medical nutrition therapy as part of a diabetes management team plays an important role in preventing onset of type 2 diabetes," said Dr. Davidson, who practices in Westfield, N.J., and chaired the panel that drafted the recommendations.
The finalized, published version is planned for later this year, she said.
The draft recommendations also call for an attempt at reducing a person’s glycemic index and glycemic load. "Reducing glycemic load may or may not help, but it can’t hurt, so we try it," said Shelley Mesznik, a member of the recommendation panel and a registered dietician and certified diabetes educator in Mount Kisco, N.Y.
In addition, the recommendations call for consumption of vegetable protein rather than animal protein for prevention of diabetes, but say there is no evidence that the amount of particular fat types in the diet affects progression to diabetes. The recommendations say that while evidence supports physical activity as a means to prevent progression to metabolic syndrome (when done for 135-180 min/week), there is no documented effect of activity on development of diabetes.
Despite endorsing medical nutrition therapy, both speakers highlighted the primacy of weight loss, achieved by lifestyle modification or bariatric surgery.
"We definitely found that weight loss is the key," said Dr. Davidson.
"If a patient asks for a number, we say aim to lose 10%-15%, but we’re looking for trends in the right direction; loss is more important than the size of the loss," Ms. Mesznik said.
The recommendations specify that several of the more marginal interventions, such as reduced glycemic load and index, use of vegetable protein, and increased physical activity, have evidence for efficacy only in the context of concurrent weight loss.
The panel performed a literature review to determine whether diet can reduce the risk for development of type 2 diabetes. The evidence summaries drawn from this literature that form the bases for the recommendations are available only to members of the Academy of Nutrition and Dietetics, Dr. Davidson said.
The work group also addressed the definition of people at high risk for diabetes, and discussed the differences between patients at risk because of prediabetes – based on fasting or challenged glucose levels or blood level of hemoglobin A1c, and those at risk with metabolic syndrome. Most interventions discussed appear equally effective in both populations, except for exercise, which is more effective for metabolic syndrome.
The panel also commented on the growing prevalence of prediabetes. In 2010, the Centers for Disease Control and Prevention estimated that 79 million Americans aged 20 or older had prediabetes, which included about half of those aged 65 or older, said Ms. Mesznik. In 2009, the CDC estimated that about a third of Americans aged 20 years or older had metabolic syndrome.
Dr. Davidson and Ms. Mesznik had no disclosures.
On Twitter @mitchelzoler
PHILADELPHIA – Weight loss is the cornerstone of lifestyle measures to prevent people with prediabetes from progressing to type 2 diabetes, but other dietary steps also help, according to draft recommendations from a working group of the Academy of Nutrition and Dietetics.
In addition to weight loss, the new recommendations call for a registered dietician nutritionist to provide medical nutrition therapy to people with prediabetes and to produce individualized plans for macronutrient distribution, Patricia Davidson, DCN, said at the annual meeting of the American Association of Diabetes Educators.
"A registered dietician nutritionist and certified diabetes educator who provides medical nutrition therapy as part of a diabetes management team plays an important role in preventing onset of type 2 diabetes," said Dr. Davidson, who practices in Westfield, N.J., and chaired the panel that drafted the recommendations.
The finalized, published version is planned for later this year, she said.
The draft recommendations also call for an attempt at reducing a person’s glycemic index and glycemic load. "Reducing glycemic load may or may not help, but it can’t hurt, so we try it," said Shelley Mesznik, a member of the recommendation panel and a registered dietician and certified diabetes educator in Mount Kisco, N.Y.
In addition, the recommendations call for consumption of vegetable protein rather than animal protein for prevention of diabetes, but say there is no evidence that the amount of particular fat types in the diet affects progression to diabetes. The recommendations say that while evidence supports physical activity as a means to prevent progression to metabolic syndrome (when done for 135-180 min/week), there is no documented effect of activity on development of diabetes.
Despite endorsing medical nutrition therapy, both speakers highlighted the primacy of weight loss, achieved by lifestyle modification or bariatric surgery.
"We definitely found that weight loss is the key," said Dr. Davidson.
"If a patient asks for a number, we say aim to lose 10%-15%, but we’re looking for trends in the right direction; loss is more important than the size of the loss," Ms. Mesznik said.
The recommendations specify that several of the more marginal interventions, such as reduced glycemic load and index, use of vegetable protein, and increased physical activity, have evidence for efficacy only in the context of concurrent weight loss.
The panel performed a literature review to determine whether diet can reduce the risk for development of type 2 diabetes. The evidence summaries drawn from this literature that form the bases for the recommendations are available only to members of the Academy of Nutrition and Dietetics, Dr. Davidson said.
The work group also addressed the definition of people at high risk for diabetes, and discussed the differences between patients at risk because of prediabetes – based on fasting or challenged glucose levels or blood level of hemoglobin A1c, and those at risk with metabolic syndrome. Most interventions discussed appear equally effective in both populations, except for exercise, which is more effective for metabolic syndrome.
The panel also commented on the growing prevalence of prediabetes. In 2010, the Centers for Disease Control and Prevention estimated that 79 million Americans aged 20 or older had prediabetes, which included about half of those aged 65 or older, said Ms. Mesznik. In 2009, the CDC estimated that about a third of Americans aged 20 years or older had metabolic syndrome.
Dr. Davidson and Ms. Mesznik had no disclosures.
On Twitter @mitchelzoler
PHILADELPHIA – Weight loss is the cornerstone of lifestyle measures to prevent people with prediabetes from progressing to type 2 diabetes, but other dietary steps also help, according to draft recommendations from a working group of the Academy of Nutrition and Dietetics.
In addition to weight loss, the new recommendations call for a registered dietician nutritionist to provide medical nutrition therapy to people with prediabetes and to produce individualized plans for macronutrient distribution, Patricia Davidson, DCN, said at the annual meeting of the American Association of Diabetes Educators.
"A registered dietician nutritionist and certified diabetes educator who provides medical nutrition therapy as part of a diabetes management team plays an important role in preventing onset of type 2 diabetes," said Dr. Davidson, who practices in Westfield, N.J., and chaired the panel that drafted the recommendations.
The finalized, published version is planned for later this year, she said.
The draft recommendations also call for an attempt at reducing a person’s glycemic index and glycemic load. "Reducing glycemic load may or may not help, but it can’t hurt, so we try it," said Shelley Mesznik, a member of the recommendation panel and a registered dietician and certified diabetes educator in Mount Kisco, N.Y.
In addition, the recommendations call for consumption of vegetable protein rather than animal protein for prevention of diabetes, but say there is no evidence that the amount of particular fat types in the diet affects progression to diabetes. The recommendations say that while evidence supports physical activity as a means to prevent progression to metabolic syndrome (when done for 135-180 min/week), there is no documented effect of activity on development of diabetes.
Despite endorsing medical nutrition therapy, both speakers highlighted the primacy of weight loss, achieved by lifestyle modification or bariatric surgery.
"We definitely found that weight loss is the key," said Dr. Davidson.
"If a patient asks for a number, we say aim to lose 10%-15%, but we’re looking for trends in the right direction; loss is more important than the size of the loss," Ms. Mesznik said.
The recommendations specify that several of the more marginal interventions, such as reduced glycemic load and index, use of vegetable protein, and increased physical activity, have evidence for efficacy only in the context of concurrent weight loss.
The panel performed a literature review to determine whether diet can reduce the risk for development of type 2 diabetes. The evidence summaries drawn from this literature that form the bases for the recommendations are available only to members of the Academy of Nutrition and Dietetics, Dr. Davidson said.
The work group also addressed the definition of people at high risk for diabetes, and discussed the differences between patients at risk because of prediabetes – based on fasting or challenged glucose levels or blood level of hemoglobin A1c, and those at risk with metabolic syndrome. Most interventions discussed appear equally effective in both populations, except for exercise, which is more effective for metabolic syndrome.
The panel also commented on the growing prevalence of prediabetes. In 2010, the Centers for Disease Control and Prevention estimated that 79 million Americans aged 20 or older had prediabetes, which included about half of those aged 65 or older, said Ms. Mesznik. In 2009, the CDC estimated that about a third of Americans aged 20 years or older had metabolic syndrome.
Dr. Davidson and Ms. Mesznik had no disclosures.
On Twitter @mitchelzoler
EXPERT OPINION FROM AADE 2013
