User login
Promising New Approach for Treating Cystic Fibrosis
In cystic fibrosis (CF), a defective gene makes a defective protein that causes acidic and sticky mucus that clogs the lungs and puts patients at risk for bacterial infections. Because different people have different protein mutations, and 10% of patients with CF make no protein at all, treatments are limited. But amphotericin apparently has the potential to work regardless of the mutation and even when the protein is missing. The researchers liken it to a “molecular prosthetic,” because it restores function much as a prosthetic device replaces a limb.
In the study, supported in part by the National Heart, Lung, and Blood Institute, researchers used lung tissue from patients with CF as well as animal models. Instead of trying to correct the protein or do gene therapy, which the researchers say is not yet effective in the lung, they used a small molecule protein that can perform the channel function of the missing or defective protein.
They found that amphotericin restored pH levels, improved viscosity, and increased antibacterial activity.
Amphotericin also can be delivered directly to the lungs to avoid common adverse effects, the researchers say. Although more studies are needed, according to the National Institute of Health, “experts are hopeful.”
In cystic fibrosis (CF), a defective gene makes a defective protein that causes acidic and sticky mucus that clogs the lungs and puts patients at risk for bacterial infections. Because different people have different protein mutations, and 10% of patients with CF make no protein at all, treatments are limited. But amphotericin apparently has the potential to work regardless of the mutation and even when the protein is missing. The researchers liken it to a “molecular prosthetic,” because it restores function much as a prosthetic device replaces a limb.
In the study, supported in part by the National Heart, Lung, and Blood Institute, researchers used lung tissue from patients with CF as well as animal models. Instead of trying to correct the protein or do gene therapy, which the researchers say is not yet effective in the lung, they used a small molecule protein that can perform the channel function of the missing or defective protein.
They found that amphotericin restored pH levels, improved viscosity, and increased antibacterial activity.
Amphotericin also can be delivered directly to the lungs to avoid common adverse effects, the researchers say. Although more studies are needed, according to the National Institute of Health, “experts are hopeful.”
In cystic fibrosis (CF), a defective gene makes a defective protein that causes acidic and sticky mucus that clogs the lungs and puts patients at risk for bacterial infections. Because different people have different protein mutations, and 10% of patients with CF make no protein at all, treatments are limited. But amphotericin apparently has the potential to work regardless of the mutation and even when the protein is missing. The researchers liken it to a “molecular prosthetic,” because it restores function much as a prosthetic device replaces a limb.
In the study, supported in part by the National Heart, Lung, and Blood Institute, researchers used lung tissue from patients with CF as well as animal models. Instead of trying to correct the protein or do gene therapy, which the researchers say is not yet effective in the lung, they used a small molecule protein that can perform the channel function of the missing or defective protein.
They found that amphotericin restored pH levels, improved viscosity, and increased antibacterial activity.
Amphotericin also can be delivered directly to the lungs to avoid common adverse effects, the researchers say. Although more studies are needed, according to the National Institute of Health, “experts are hopeful.”
Home oxygen therapy for children: New guidelines combine limited evidence, expert experience
Based on the very limited evidence available, an expert panel convened by the .
The guideline authors not only addressed specific indications for chronic lung and pulmonary vascular diseases, but also defined hypoxemia in children – noting that Medicare and Medicaid coverage determinations for home oxygen therapy in children are based on decades-old studies that lacked pediatric patients – and offer expert advice on how to wean and discontinue oxygen, when warranted.
The disease-specific recommendations on whether or not to prescribe home oxygen therapy are characterized either as strong, meaning that it’s the right course of action for at least 95% of patients; or conditional, meaning it might not be right for a “sizable minority” of patients, authors explained in the guideline.
Home oxygen therapy gets a strong recommendation, for example, in patients with cystic fibrosis complicated by severe chronic hypoxemia, but gets a conditional recommendation for sickle cell disease with severe chronic hypoxemia, according to the guideline, published in the American Journal of Respiratory and Critical Care Medicine.
Regardless of strong or conditional, the recommendations were largely based on “very low-quality evidence,” according to ad hoc subcommittee of the ATS Assembly on Pediatrics, cochaired by Don Hayes Jr., MD, of Nationwide Children’s Hospital, Columbus, Ohio, and Robin R. Deterding, MD, of Children’s Hospital Colorado, Denver.
“Despite widespread use of home oxygen therapy for various lung and pulmonary vascular diseases, there is a striking paucity of data regarding its implementation, efficacy, monitoring, and discontinuation,” Dr. Hayes, Dr. Deterding, and 20 additional committee members wrote in their report.
Accordingly, the panel sought to add expert opinion and experience to the limited evidence, in the hope that it would aid clinicians in the management of complex pediatric patients, they said.
One new tool they provide, toward that end, is a definition of hypoxemia in children based on oxygen saturation as quantified by pulse oximetry (SpO2).
Based on a review of 31 selected studies measuring oxygenation in healthy children, the expert panel defined hypoxemia (at or near sea level) as SpO2 of 90% or lower for 5% of the recording time in children under 1 year old, and an SpO2 of 93% or lower in older children; or alternately, as three independent measurements of SpO2 less than or equal to 90% in the younger children and 93% in the older children.
By contrast, an SpO2 of less than 88% is one of the indications for funding home oxygen therapy as determined by the Centers for Medicare & Medicaid Services for both pediatric and adult patients, according to the committee.
The CMS indications derived from “seminal studies” showing that continuous oxygen therapy reduced mortality in adults with chronic obstructive pulmonary disease, they said in the guideline document.
“Despite the lack of pediatric patients in these historic studies performed over 35 years ago, the CMS coverage determination for [home oxygen therapy] is the same for pediatric patients of all ages compared with adult patients,” they wrote in the report.
The committee unanimously agreed that 2 weeks of low SpO2 was “sufficient evidence” to indicate chronic hypoxemia, their report says.
Dr. Hayes reported no relationships with relevant commercial interests, while Dr. Deterding provided disclosures related to Boehringer Ingelheim, Novartis, and Elsevier Publishing, among others. Fellow committee members provided disclosures related to Shire Pharmaceuticals, United Therapeutics, and others as listed in the clinical practice guideline document.
SOURCE: Hayes D Jr. et al. J Respir Crit Care Med. 2019 Feb 1;199(3):e5-e23. doi: 10.1164/rccm.201812-2276ST.
It is unfortunate that over the course of a decade, the evidence base supporting home oxygen therapy in children has not substantially changed, according to Ian Balfour-Lynn, MD, a member of the American Thoracic Society (ATS) committee that developed the clinical practice guideline.
The ATS clinical practice guideline on home oxygen therapy for children echoes conclusions reached in a 2009 guideline published by the British Thoracic Society (BTS), he wrote in The Lancet Respiratory Medicine.
Dr. Balfour-Lynn, who chaired the BTS guideline committee, said new research is sorely needed, particularly in the prevention of preterm births, which he said constitute the commonest cause of home oxygen need among children, according to the Lancet report.
In addition, a large prospective trial is needed to evaluate strategies for weaning or discontinuing oxygen, he said, noting that the ATS recommendations on weaning were almost entirely based on the expert panel’s combined clinical experience.
Dr. Balfour-Lynn is a consultant in pediatric respiratory medicine at Royal Brompton Hospital, London. This summary of his opinions is based on his comments in a report that appeared March 8 in The Lancet Respiratory Medicine . He reported no relationships with commercial interests relevant to his work on the ATS clinical practice guideline.
It is unfortunate that over the course of a decade, the evidence base supporting home oxygen therapy in children has not substantially changed, according to Ian Balfour-Lynn, MD, a member of the American Thoracic Society (ATS) committee that developed the clinical practice guideline.
The ATS clinical practice guideline on home oxygen therapy for children echoes conclusions reached in a 2009 guideline published by the British Thoracic Society (BTS), he wrote in The Lancet Respiratory Medicine.
Dr. Balfour-Lynn, who chaired the BTS guideline committee, said new research is sorely needed, particularly in the prevention of preterm births, which he said constitute the commonest cause of home oxygen need among children, according to the Lancet report.
In addition, a large prospective trial is needed to evaluate strategies for weaning or discontinuing oxygen, he said, noting that the ATS recommendations on weaning were almost entirely based on the expert panel’s combined clinical experience.
Dr. Balfour-Lynn is a consultant in pediatric respiratory medicine at Royal Brompton Hospital, London. This summary of his opinions is based on his comments in a report that appeared March 8 in The Lancet Respiratory Medicine . He reported no relationships with commercial interests relevant to his work on the ATS clinical practice guideline.
It is unfortunate that over the course of a decade, the evidence base supporting home oxygen therapy in children has not substantially changed, according to Ian Balfour-Lynn, MD, a member of the American Thoracic Society (ATS) committee that developed the clinical practice guideline.
The ATS clinical practice guideline on home oxygen therapy for children echoes conclusions reached in a 2009 guideline published by the British Thoracic Society (BTS), he wrote in The Lancet Respiratory Medicine.
Dr. Balfour-Lynn, who chaired the BTS guideline committee, said new research is sorely needed, particularly in the prevention of preterm births, which he said constitute the commonest cause of home oxygen need among children, according to the Lancet report.
In addition, a large prospective trial is needed to evaluate strategies for weaning or discontinuing oxygen, he said, noting that the ATS recommendations on weaning were almost entirely based on the expert panel’s combined clinical experience.
Dr. Balfour-Lynn is a consultant in pediatric respiratory medicine at Royal Brompton Hospital, London. This summary of his opinions is based on his comments in a report that appeared March 8 in The Lancet Respiratory Medicine . He reported no relationships with commercial interests relevant to his work on the ATS clinical practice guideline.
Based on the very limited evidence available, an expert panel convened by the .
The guideline authors not only addressed specific indications for chronic lung and pulmonary vascular diseases, but also defined hypoxemia in children – noting that Medicare and Medicaid coverage determinations for home oxygen therapy in children are based on decades-old studies that lacked pediatric patients – and offer expert advice on how to wean and discontinue oxygen, when warranted.
The disease-specific recommendations on whether or not to prescribe home oxygen therapy are characterized either as strong, meaning that it’s the right course of action for at least 95% of patients; or conditional, meaning it might not be right for a “sizable minority” of patients, authors explained in the guideline.
Home oxygen therapy gets a strong recommendation, for example, in patients with cystic fibrosis complicated by severe chronic hypoxemia, but gets a conditional recommendation for sickle cell disease with severe chronic hypoxemia, according to the guideline, published in the American Journal of Respiratory and Critical Care Medicine.
Regardless of strong or conditional, the recommendations were largely based on “very low-quality evidence,” according to ad hoc subcommittee of the ATS Assembly on Pediatrics, cochaired by Don Hayes Jr., MD, of Nationwide Children’s Hospital, Columbus, Ohio, and Robin R. Deterding, MD, of Children’s Hospital Colorado, Denver.
“Despite widespread use of home oxygen therapy for various lung and pulmonary vascular diseases, there is a striking paucity of data regarding its implementation, efficacy, monitoring, and discontinuation,” Dr. Hayes, Dr. Deterding, and 20 additional committee members wrote in their report.
Accordingly, the panel sought to add expert opinion and experience to the limited evidence, in the hope that it would aid clinicians in the management of complex pediatric patients, they said.
One new tool they provide, toward that end, is a definition of hypoxemia in children based on oxygen saturation as quantified by pulse oximetry (SpO2).
Based on a review of 31 selected studies measuring oxygenation in healthy children, the expert panel defined hypoxemia (at or near sea level) as SpO2 of 90% or lower for 5% of the recording time in children under 1 year old, and an SpO2 of 93% or lower in older children; or alternately, as three independent measurements of SpO2 less than or equal to 90% in the younger children and 93% in the older children.
By contrast, an SpO2 of less than 88% is one of the indications for funding home oxygen therapy as determined by the Centers for Medicare & Medicaid Services for both pediatric and adult patients, according to the committee.
The CMS indications derived from “seminal studies” showing that continuous oxygen therapy reduced mortality in adults with chronic obstructive pulmonary disease, they said in the guideline document.
“Despite the lack of pediatric patients in these historic studies performed over 35 years ago, the CMS coverage determination for [home oxygen therapy] is the same for pediatric patients of all ages compared with adult patients,” they wrote in the report.
The committee unanimously agreed that 2 weeks of low SpO2 was “sufficient evidence” to indicate chronic hypoxemia, their report says.
Dr. Hayes reported no relationships with relevant commercial interests, while Dr. Deterding provided disclosures related to Boehringer Ingelheim, Novartis, and Elsevier Publishing, among others. Fellow committee members provided disclosures related to Shire Pharmaceuticals, United Therapeutics, and others as listed in the clinical practice guideline document.
SOURCE: Hayes D Jr. et al. J Respir Crit Care Med. 2019 Feb 1;199(3):e5-e23. doi: 10.1164/rccm.201812-2276ST.
Based on the very limited evidence available, an expert panel convened by the .
The guideline authors not only addressed specific indications for chronic lung and pulmonary vascular diseases, but also defined hypoxemia in children – noting that Medicare and Medicaid coverage determinations for home oxygen therapy in children are based on decades-old studies that lacked pediatric patients – and offer expert advice on how to wean and discontinue oxygen, when warranted.
The disease-specific recommendations on whether or not to prescribe home oxygen therapy are characterized either as strong, meaning that it’s the right course of action for at least 95% of patients; or conditional, meaning it might not be right for a “sizable minority” of patients, authors explained in the guideline.
Home oxygen therapy gets a strong recommendation, for example, in patients with cystic fibrosis complicated by severe chronic hypoxemia, but gets a conditional recommendation for sickle cell disease with severe chronic hypoxemia, according to the guideline, published in the American Journal of Respiratory and Critical Care Medicine.
Regardless of strong or conditional, the recommendations were largely based on “very low-quality evidence,” according to ad hoc subcommittee of the ATS Assembly on Pediatrics, cochaired by Don Hayes Jr., MD, of Nationwide Children’s Hospital, Columbus, Ohio, and Robin R. Deterding, MD, of Children’s Hospital Colorado, Denver.
“Despite widespread use of home oxygen therapy for various lung and pulmonary vascular diseases, there is a striking paucity of data regarding its implementation, efficacy, monitoring, and discontinuation,” Dr. Hayes, Dr. Deterding, and 20 additional committee members wrote in their report.
Accordingly, the panel sought to add expert opinion and experience to the limited evidence, in the hope that it would aid clinicians in the management of complex pediatric patients, they said.
One new tool they provide, toward that end, is a definition of hypoxemia in children based on oxygen saturation as quantified by pulse oximetry (SpO2).
Based on a review of 31 selected studies measuring oxygenation in healthy children, the expert panel defined hypoxemia (at or near sea level) as SpO2 of 90% or lower for 5% of the recording time in children under 1 year old, and an SpO2 of 93% or lower in older children; or alternately, as three independent measurements of SpO2 less than or equal to 90% in the younger children and 93% in the older children.
By contrast, an SpO2 of less than 88% is one of the indications for funding home oxygen therapy as determined by the Centers for Medicare & Medicaid Services for both pediatric and adult patients, according to the committee.
The CMS indications derived from “seminal studies” showing that continuous oxygen therapy reduced mortality in adults with chronic obstructive pulmonary disease, they said in the guideline document.
“Despite the lack of pediatric patients in these historic studies performed over 35 years ago, the CMS coverage determination for [home oxygen therapy] is the same for pediatric patients of all ages compared with adult patients,” they wrote in the report.
The committee unanimously agreed that 2 weeks of low SpO2 was “sufficient evidence” to indicate chronic hypoxemia, their report says.
Dr. Hayes reported no relationships with relevant commercial interests, while Dr. Deterding provided disclosures related to Boehringer Ingelheim, Novartis, and Elsevier Publishing, among others. Fellow committee members provided disclosures related to Shire Pharmaceuticals, United Therapeutics, and others as listed in the clinical practice guideline document.
SOURCE: Hayes D Jr. et al. J Respir Crit Care Med. 2019 Feb 1;199(3):e5-e23. doi: 10.1164/rccm.201812-2276ST.
FROM THE AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Survey: Americans support regulation of vaping products
Almost 70% of adults believe that the Food and Drug Administration should raise the legal age to purchase e-cigarettes and tobacco, according to a new survey by NORC at the University of Chicago, a nonpartisan research institution.
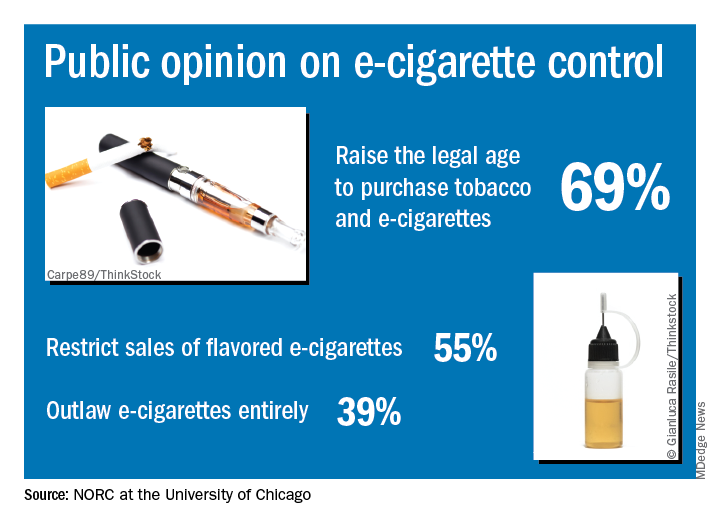
“Americans are particularly concerned about teens becoming newly addicted to e-cigarettes, and they support a range of actions the federal government could take to make vaping products less available, less addictive, and less appealing,” Caroline Pearson, senior vice president at NORC, said in a written statement.
The AmeriSpeak Spotlight on Health Poll, conducted Feb. 14-18, 2019 (margin of error, plus or minus 4.12%), showed that 69% of adults strongly or somewhat support raising the age limit to purchase e-cigarettes and tobacco and 55% support restricting sales of flavored e-cigarettes, NORC reported. Almost 40% of the 1,004 respondents expressed support for a complete ban on e-cigarettes.
Despite FDA efforts under Commissioner Scott Gottlieb, MD, to raise awareness of teen vaping, only 21% of those surveyed correctly responded that e-cigarettes generally contain more nicotine that regular cigarettes. Dr. Gottlieb announced his resignation recently, “but he indicated that the Trump Administration will continue efforts to increase regulation of e-cigarettes,” NORC said.
Almost 70% of adults believe that the Food and Drug Administration should raise the legal age to purchase e-cigarettes and tobacco, according to a new survey by NORC at the University of Chicago, a nonpartisan research institution.
“Americans are particularly concerned about teens becoming newly addicted to e-cigarettes, and they support a range of actions the federal government could take to make vaping products less available, less addictive, and less appealing,” Caroline Pearson, senior vice president at NORC, said in a written statement.
The AmeriSpeak Spotlight on Health Poll, conducted Feb. 14-18, 2019 (margin of error, plus or minus 4.12%), showed that 69% of adults strongly or somewhat support raising the age limit to purchase e-cigarettes and tobacco and 55% support restricting sales of flavored e-cigarettes, NORC reported. Almost 40% of the 1,004 respondents expressed support for a complete ban on e-cigarettes.
Despite FDA efforts under Commissioner Scott Gottlieb, MD, to raise awareness of teen vaping, only 21% of those surveyed correctly responded that e-cigarettes generally contain more nicotine that regular cigarettes. Dr. Gottlieb announced his resignation recently, “but he indicated that the Trump Administration will continue efforts to increase regulation of e-cigarettes,” NORC said.
Almost 70% of adults believe that the Food and Drug Administration should raise the legal age to purchase e-cigarettes and tobacco, according to a new survey by NORC at the University of Chicago, a nonpartisan research institution.
“Americans are particularly concerned about teens becoming newly addicted to e-cigarettes, and they support a range of actions the federal government could take to make vaping products less available, less addictive, and less appealing,” Caroline Pearson, senior vice president at NORC, said in a written statement.
The AmeriSpeak Spotlight on Health Poll, conducted Feb. 14-18, 2019 (margin of error, plus or minus 4.12%), showed that 69% of adults strongly or somewhat support raising the age limit to purchase e-cigarettes and tobacco and 55% support restricting sales of flavored e-cigarettes, NORC reported. Almost 40% of the 1,004 respondents expressed support for a complete ban on e-cigarettes.
Despite FDA efforts under Commissioner Scott Gottlieb, MD, to raise awareness of teen vaping, only 21% of those surveyed correctly responded that e-cigarettes generally contain more nicotine that regular cigarettes. Dr. Gottlieb announced his resignation recently, “but he indicated that the Trump Administration will continue efforts to increase regulation of e-cigarettes,” NORC said.
Flu activity levels down, but outpatient visits highest since 1998-99
Influenza activity measures declined for a third consecutive week, but levels are higher than usual at this point in the flu season, according to the Centers for Disease Control and Prevention.
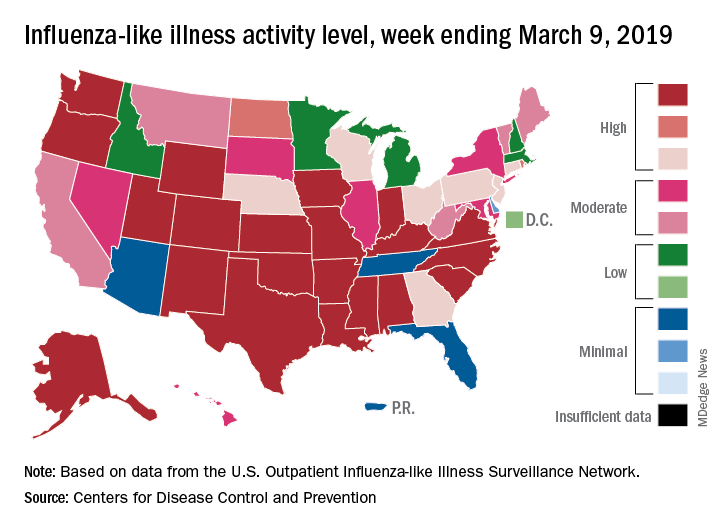
For the week ending March 9, an estimated 4.5% of outpatient visits were for influenza-like illness (ILI), which was down from 4.6% the previous week, the CDC’s influenza division reported March 15, but that is higher than the comparable week for any year since 1998-1999. During last year’s very severe flu season, the outpatient visit rate was just under 3.2% for the week ending March 10.
Although the number of states at level 10 on the CDC’s 1-10 scale remained at 21, the activity map actually looks more red than last week since Rhode Island and West Virgina were replaced by the much larger states of Iowa and Washington. The number of states in the high range (8-10), did go down from 32 to 30, data from the CDC’s Outpatient ILI Surveillance Network show.
Of those four deaths, only one occurred during the most recent reporting week, the CDC said.
Influenza activity measures declined for a third consecutive week, but levels are higher than usual at this point in the flu season, according to the Centers for Disease Control and Prevention.
For the week ending March 9, an estimated 4.5% of outpatient visits were for influenza-like illness (ILI), which was down from 4.6% the previous week, the CDC’s influenza division reported March 15, but that is higher than the comparable week for any year since 1998-1999. During last year’s very severe flu season, the outpatient visit rate was just under 3.2% for the week ending March 10.
Although the number of states at level 10 on the CDC’s 1-10 scale remained at 21, the activity map actually looks more red than last week since Rhode Island and West Virgina were replaced by the much larger states of Iowa and Washington. The number of states in the high range (8-10), did go down from 32 to 30, data from the CDC’s Outpatient ILI Surveillance Network show.
Of those four deaths, only one occurred during the most recent reporting week, the CDC said.
Influenza activity measures declined for a third consecutive week, but levels are higher than usual at this point in the flu season, according to the Centers for Disease Control and Prevention.
For the week ending March 9, an estimated 4.5% of outpatient visits were for influenza-like illness (ILI), which was down from 4.6% the previous week, the CDC’s influenza division reported March 15, but that is higher than the comparable week for any year since 1998-1999. During last year’s very severe flu season, the outpatient visit rate was just under 3.2% for the week ending March 10.
Although the number of states at level 10 on the CDC’s 1-10 scale remained at 21, the activity map actually looks more red than last week since Rhode Island and West Virgina were replaced by the much larger states of Iowa and Washington. The number of states in the high range (8-10), did go down from 32 to 30, data from the CDC’s Outpatient ILI Surveillance Network show.
Of those four deaths, only one occurred during the most recent reporting week, the CDC said.
Eisenmenger syndrome is a minefield for unwary physicians
SNOWMASS, COLO. – Interventions that are simple and straightforward for other patients – such as therapeutic phlebotomy, bronchoscopy, anticoagulation, administration of IV antibiotics – can quickly have catastrophic results in patients with Eisenmenger syndrome, Carole A. Warnes, MD, cautioned at the Annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.

This is why the 2018 ACC/American Heart Association guidelines on the management of patients with adult congenital heart disease recommend as a Class I indication that most patients with ACHD, including all those with Eisenmenger syndrome, be managed in collaboration with a cardiologist at a specialized ACHD center (Circulation. 2018 Aug 16. doi: 10.1161/CIR.0000000000000603), noted Dr. Warnes, professor of medicine at the Mayo Clinic in Rochester, Minn., and director of the Snowmass conference.
“There are lots of mistakes in diagnosis and management because so many physicians are unfamiliar with the kinds of problems these patients face,” the cardiologist said.
She cited as a real-world example a patient with Eisenmenger syndrome admitted for pneumonia. Twenty minutes after being placed on intravenous antibiotics she had a stroke. Why?
“She didn’t have an air filter on her IV line. Any air going into a cyanotic’s blood stream will go to the head and give them a stroke. Something that is simple – routine for other patients – may kill a patient with cyanotic heart disease,” Dr. Warnes said.
Another illustrative case: a patient with Eisenmenger syndrome presents with hemoptysis, an infiltrate in her right lung, a hemoglobin of 19.8 g/dL, and anemia. Should she undergo therapeutic phlebotomy? How about urgent bronchoscopy?
No and no, Dr. Warnes emphasized.
“You do not phlebotomize cyanotic patients unless they have symptoms of hyperviscosity, meaning terrible headache or poor concentration, along with a hemoglobin greater than 20 g/dL. They need that high hemoglobin. They may be blue, and you need those red cells to carry the oxygen around. Otherwise you may make them worse. And if you give them iron for their anemia, you will increase their risk of stroke,” she explained.
Hemoptysis in patients with Eisenmenger syndrome is a life-threatening warning sign. By the time Eisenmenger syndrome patients reach age 40 years, nearly all of them have experienced episodes of hemoptysis. And more and more patients with the syndrome are moving well beyond that milestone and surviving into their 60s and beyond.
“Many Eisenmenger syndrome patients are not dying when they’re 20 or 30. We can get them to a good old age,” according to Dr. Warnes, who founded the ACHD center at the Mayo Clinic.
Most of the time the cause of hemoptysis in patients with Eisenmenger syndrome is an intrapulmonary hemorrhage. Anticoagulation can turn that hemorrhage catastrophic. So can bronchoscopy. Indeed, the cause of death in roughly 30% of patients with this form of congenital heart disease is catastrophic hemoptysis.
“You bar the door from your friendly pulmonologist who wants to bronchoscope these patients. Bronchoscopy never does any good unless the patient is so hypoxic that you need to suck the blood out of their lungs,” Dr. Warnes emphasized.
Anticoagulation is ordinarily to be avoided in patients with Eisenmenger syndrome because of their bleeding risk, even when pulmonary thrombosis is suspected, she added.
So, to summarize: These patients basically need stabilizing, with no anticoagulation, no bronchoscopy, and no phlebotomy, she said.
Another danger zone for patients with Eisenmenger syndrome is pregnancy. The condition is associated with a 30% maternal mortality rate.
Dr. Warnes noted that, even at the Mayo Clinic, which has had a pioneering ACHD center for decades, awareness of key elements of management of affected patients is low among nonspecialists.
“As I’ve done my hospital services in the last couple of months, I sort of felt I was on patrol, snatching these patients from problems,” she recalled.
Dr. Warnes reported having no financial conflicts regarding her presentation.
SNOWMASS, COLO. – Interventions that are simple and straightforward for other patients – such as therapeutic phlebotomy, bronchoscopy, anticoagulation, administration of IV antibiotics – can quickly have catastrophic results in patients with Eisenmenger syndrome, Carole A. Warnes, MD, cautioned at the Annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.
This is why the 2018 ACC/American Heart Association guidelines on the management of patients with adult congenital heart disease recommend as a Class I indication that most patients with ACHD, including all those with Eisenmenger syndrome, be managed in collaboration with a cardiologist at a specialized ACHD center (Circulation. 2018 Aug 16. doi: 10.1161/CIR.0000000000000603), noted Dr. Warnes, professor of medicine at the Mayo Clinic in Rochester, Minn., and director of the Snowmass conference.
“There are lots of mistakes in diagnosis and management because so many physicians are unfamiliar with the kinds of problems these patients face,” the cardiologist said.
She cited as a real-world example a patient with Eisenmenger syndrome admitted for pneumonia. Twenty minutes after being placed on intravenous antibiotics she had a stroke. Why?
“She didn’t have an air filter on her IV line. Any air going into a cyanotic’s blood stream will go to the head and give them a stroke. Something that is simple – routine for other patients – may kill a patient with cyanotic heart disease,” Dr. Warnes said.
Another illustrative case: a patient with Eisenmenger syndrome presents with hemoptysis, an infiltrate in her right lung, a hemoglobin of 19.8 g/dL, and anemia. Should she undergo therapeutic phlebotomy? How about urgent bronchoscopy?
No and no, Dr. Warnes emphasized.
“You do not phlebotomize cyanotic patients unless they have symptoms of hyperviscosity, meaning terrible headache or poor concentration, along with a hemoglobin greater than 20 g/dL. They need that high hemoglobin. They may be blue, and you need those red cells to carry the oxygen around. Otherwise you may make them worse. And if you give them iron for their anemia, you will increase their risk of stroke,” she explained.
Hemoptysis in patients with Eisenmenger syndrome is a life-threatening warning sign. By the time Eisenmenger syndrome patients reach age 40 years, nearly all of them have experienced episodes of hemoptysis. And more and more patients with the syndrome are moving well beyond that milestone and surviving into their 60s and beyond.
“Many Eisenmenger syndrome patients are not dying when they’re 20 or 30. We can get them to a good old age,” according to Dr. Warnes, who founded the ACHD center at the Mayo Clinic.
Most of the time the cause of hemoptysis in patients with Eisenmenger syndrome is an intrapulmonary hemorrhage. Anticoagulation can turn that hemorrhage catastrophic. So can bronchoscopy. Indeed, the cause of death in roughly 30% of patients with this form of congenital heart disease is catastrophic hemoptysis.
“You bar the door from your friendly pulmonologist who wants to bronchoscope these patients. Bronchoscopy never does any good unless the patient is so hypoxic that you need to suck the blood out of their lungs,” Dr. Warnes emphasized.
Anticoagulation is ordinarily to be avoided in patients with Eisenmenger syndrome because of their bleeding risk, even when pulmonary thrombosis is suspected, she added.
So, to summarize: These patients basically need stabilizing, with no anticoagulation, no bronchoscopy, and no phlebotomy, she said.
Another danger zone for patients with Eisenmenger syndrome is pregnancy. The condition is associated with a 30% maternal mortality rate.
Dr. Warnes noted that, even at the Mayo Clinic, which has had a pioneering ACHD center for decades, awareness of key elements of management of affected patients is low among nonspecialists.
“As I’ve done my hospital services in the last couple of months, I sort of felt I was on patrol, snatching these patients from problems,” she recalled.
Dr. Warnes reported having no financial conflicts regarding her presentation.
SNOWMASS, COLO. – Interventions that are simple and straightforward for other patients – such as therapeutic phlebotomy, bronchoscopy, anticoagulation, administration of IV antibiotics – can quickly have catastrophic results in patients with Eisenmenger syndrome, Carole A. Warnes, MD, cautioned at the Annual Cardiovascular Conference at Snowmass sponsored by the American College of Cardiology.
This is why the 2018 ACC/American Heart Association guidelines on the management of patients with adult congenital heart disease recommend as a Class I indication that most patients with ACHD, including all those with Eisenmenger syndrome, be managed in collaboration with a cardiologist at a specialized ACHD center (Circulation. 2018 Aug 16. doi: 10.1161/CIR.0000000000000603), noted Dr. Warnes, professor of medicine at the Mayo Clinic in Rochester, Minn., and director of the Snowmass conference.
“There are lots of mistakes in diagnosis and management because so many physicians are unfamiliar with the kinds of problems these patients face,” the cardiologist said.
She cited as a real-world example a patient with Eisenmenger syndrome admitted for pneumonia. Twenty minutes after being placed on intravenous antibiotics she had a stroke. Why?
“She didn’t have an air filter on her IV line. Any air going into a cyanotic’s blood stream will go to the head and give them a stroke. Something that is simple – routine for other patients – may kill a patient with cyanotic heart disease,” Dr. Warnes said.
Another illustrative case: a patient with Eisenmenger syndrome presents with hemoptysis, an infiltrate in her right lung, a hemoglobin of 19.8 g/dL, and anemia. Should she undergo therapeutic phlebotomy? How about urgent bronchoscopy?
No and no, Dr. Warnes emphasized.
“You do not phlebotomize cyanotic patients unless they have symptoms of hyperviscosity, meaning terrible headache or poor concentration, along with a hemoglobin greater than 20 g/dL. They need that high hemoglobin. They may be blue, and you need those red cells to carry the oxygen around. Otherwise you may make them worse. And if you give them iron for their anemia, you will increase their risk of stroke,” she explained.
Hemoptysis in patients with Eisenmenger syndrome is a life-threatening warning sign. By the time Eisenmenger syndrome patients reach age 40 years, nearly all of them have experienced episodes of hemoptysis. And more and more patients with the syndrome are moving well beyond that milestone and surviving into their 60s and beyond.
“Many Eisenmenger syndrome patients are not dying when they’re 20 or 30. We can get them to a good old age,” according to Dr. Warnes, who founded the ACHD center at the Mayo Clinic.
Most of the time the cause of hemoptysis in patients with Eisenmenger syndrome is an intrapulmonary hemorrhage. Anticoagulation can turn that hemorrhage catastrophic. So can bronchoscopy. Indeed, the cause of death in roughly 30% of patients with this form of congenital heart disease is catastrophic hemoptysis.
“You bar the door from your friendly pulmonologist who wants to bronchoscope these patients. Bronchoscopy never does any good unless the patient is so hypoxic that you need to suck the blood out of their lungs,” Dr. Warnes emphasized.
Anticoagulation is ordinarily to be avoided in patients with Eisenmenger syndrome because of their bleeding risk, even when pulmonary thrombosis is suspected, she added.
So, to summarize: These patients basically need stabilizing, with no anticoagulation, no bronchoscopy, and no phlebotomy, she said.
Another danger zone for patients with Eisenmenger syndrome is pregnancy. The condition is associated with a 30% maternal mortality rate.
Dr. Warnes noted that, even at the Mayo Clinic, which has had a pioneering ACHD center for decades, awareness of key elements of management of affected patients is low among nonspecialists.
“As I’ve done my hospital services in the last couple of months, I sort of felt I was on patrol, snatching these patients from problems,” she recalled.
Dr. Warnes reported having no financial conflicts regarding her presentation.
REPORTING FROM ACC SNOWMASS 2019
Daily aspirin associated with lower risk of COPD flareup
Daily aspirin use could reduce the risk of acute exacerbations of chronic obstructive pulmonary disease, new data suggest.

Researchers reported the outcomes of an observational cohort study of 1,698 individuals with COPD, 45% of whom said they were taking daily aspirin at baseline. Their findings were published in Chest.
After a median follow up of 2.7 years, aspirin users had an overall 22% lower incidence of acute COPD exacerbations compared with nonusers. This was largely accounted for by a 25% reduction in moderate exacerbations, but there was no significant difference between aspirin users and nonusers in severe exacerbations.
A similar pattern was seen after just 1 year of follow-up, with an overall 30% reduction in the incidence of exacerbations, a 37% reduction in moderate exacerbations, but no significant reduction in severe exacerbations.
“Though aspirin use has previously been linked with reduced mortality risk in patients with COPD, to our knowledge, this is the first study to investigate the association of daily aspirin use with respiratory morbidity in COPD,” wrote Ashraf Fawzy, MD, of the division of pulmonary and critical care medicine at Johns Hopkins University, Baltimore, and his coauthors.
The association between aspirin use and reduced incidence of exacerbations was stronger among individuals with chronic bronchitis, which prompted the authors to suggest that future studies of aspirin in COPD should focus on participants with chronic bronchitis.
However, the association was not affected by COPD severity, emphysema presence or severity, or cardiometabolic phenotype.
Aspirin users reported better respiratory-specific quality of life than that of nonusers, including 34% lower odds of reporting moderate to severe dyspnea, and better baseline COPD health status.
“Findings of this study add to the existing literature by highlighting that aspirin use is also associated with reduced respiratory morbidity across several domains – including exacerbation risk, quality of life, and dyspnea – factors related to patient well-being and healthcare utilization,” the authors wrote.
Aspirin users were more likely to be white, male, and obese, and less likely to be smokers. They had better lung function but more cardiovascular comorbidities at baseline, although the aspirin users and nonusers were matched on baseline characteristics.
Speculating on the mechanisms by which aspirin might impact COPD exacerbations, the authors noted that the drug has both systemic and local pulmonary mechanisms of action.
For example, a pathway that results in elevated levels of a urinary metabolite in patients with COPD is irreversibly blocked by aspirin. Aspirin also attenuates the elevation of inflammatory markers interleukin-6 and C-reactive protein, which are part of the inflammatory phenotype of COPD. Aspirin has been shown to reduce proinflammatory cytokines in the lung.
The authors did note that aspirin use was self-reported, so they did not have data on dosage or duration of use.
The National Institutes of Health funded the study. Six authors declared advisory board positions, research support, and other funding from the pharmaceutical sector. One author was also a founder of a company commercializing lung image analysis software. No other conflicts of interest were declared.
SOURCE: Fawzy A et al. Chest. 2019 Mar;155(3): 519-27. doi: 10.1016/j.chest.2018.11.028.
Daily aspirin use could reduce the risk of acute exacerbations of chronic obstructive pulmonary disease, new data suggest.
Researchers reported the outcomes of an observational cohort study of 1,698 individuals with COPD, 45% of whom said they were taking daily aspirin at baseline. Their findings were published in Chest.
After a median follow up of 2.7 years, aspirin users had an overall 22% lower incidence of acute COPD exacerbations compared with nonusers. This was largely accounted for by a 25% reduction in moderate exacerbations, but there was no significant difference between aspirin users and nonusers in severe exacerbations.
A similar pattern was seen after just 1 year of follow-up, with an overall 30% reduction in the incidence of exacerbations, a 37% reduction in moderate exacerbations, but no significant reduction in severe exacerbations.
“Though aspirin use has previously been linked with reduced mortality risk in patients with COPD, to our knowledge, this is the first study to investigate the association of daily aspirin use with respiratory morbidity in COPD,” wrote Ashraf Fawzy, MD, of the division of pulmonary and critical care medicine at Johns Hopkins University, Baltimore, and his coauthors.
The association between aspirin use and reduced incidence of exacerbations was stronger among individuals with chronic bronchitis, which prompted the authors to suggest that future studies of aspirin in COPD should focus on participants with chronic bronchitis.
However, the association was not affected by COPD severity, emphysema presence or severity, or cardiometabolic phenotype.
Aspirin users reported better respiratory-specific quality of life than that of nonusers, including 34% lower odds of reporting moderate to severe dyspnea, and better baseline COPD health status.
“Findings of this study add to the existing literature by highlighting that aspirin use is also associated with reduced respiratory morbidity across several domains – including exacerbation risk, quality of life, and dyspnea – factors related to patient well-being and healthcare utilization,” the authors wrote.
Aspirin users were more likely to be white, male, and obese, and less likely to be smokers. They had better lung function but more cardiovascular comorbidities at baseline, although the aspirin users and nonusers were matched on baseline characteristics.
Speculating on the mechanisms by which aspirin might impact COPD exacerbations, the authors noted that the drug has both systemic and local pulmonary mechanisms of action.
For example, a pathway that results in elevated levels of a urinary metabolite in patients with COPD is irreversibly blocked by aspirin. Aspirin also attenuates the elevation of inflammatory markers interleukin-6 and C-reactive protein, which are part of the inflammatory phenotype of COPD. Aspirin has been shown to reduce proinflammatory cytokines in the lung.
The authors did note that aspirin use was self-reported, so they did not have data on dosage or duration of use.
The National Institutes of Health funded the study. Six authors declared advisory board positions, research support, and other funding from the pharmaceutical sector. One author was also a founder of a company commercializing lung image analysis software. No other conflicts of interest were declared.
SOURCE: Fawzy A et al. Chest. 2019 Mar;155(3): 519-27. doi: 10.1016/j.chest.2018.11.028.
Daily aspirin use could reduce the risk of acute exacerbations of chronic obstructive pulmonary disease, new data suggest.
Researchers reported the outcomes of an observational cohort study of 1,698 individuals with COPD, 45% of whom said they were taking daily aspirin at baseline. Their findings were published in Chest.
After a median follow up of 2.7 years, aspirin users had an overall 22% lower incidence of acute COPD exacerbations compared with nonusers. This was largely accounted for by a 25% reduction in moderate exacerbations, but there was no significant difference between aspirin users and nonusers in severe exacerbations.
A similar pattern was seen after just 1 year of follow-up, with an overall 30% reduction in the incidence of exacerbations, a 37% reduction in moderate exacerbations, but no significant reduction in severe exacerbations.
“Though aspirin use has previously been linked with reduced mortality risk in patients with COPD, to our knowledge, this is the first study to investigate the association of daily aspirin use with respiratory morbidity in COPD,” wrote Ashraf Fawzy, MD, of the division of pulmonary and critical care medicine at Johns Hopkins University, Baltimore, and his coauthors.
The association between aspirin use and reduced incidence of exacerbations was stronger among individuals with chronic bronchitis, which prompted the authors to suggest that future studies of aspirin in COPD should focus on participants with chronic bronchitis.
However, the association was not affected by COPD severity, emphysema presence or severity, or cardiometabolic phenotype.
Aspirin users reported better respiratory-specific quality of life than that of nonusers, including 34% lower odds of reporting moderate to severe dyspnea, and better baseline COPD health status.
“Findings of this study add to the existing literature by highlighting that aspirin use is also associated with reduced respiratory morbidity across several domains – including exacerbation risk, quality of life, and dyspnea – factors related to patient well-being and healthcare utilization,” the authors wrote.
Aspirin users were more likely to be white, male, and obese, and less likely to be smokers. They had better lung function but more cardiovascular comorbidities at baseline, although the aspirin users and nonusers were matched on baseline characteristics.
Speculating on the mechanisms by which aspirin might impact COPD exacerbations, the authors noted that the drug has both systemic and local pulmonary mechanisms of action.
For example, a pathway that results in elevated levels of a urinary metabolite in patients with COPD is irreversibly blocked by aspirin. Aspirin also attenuates the elevation of inflammatory markers interleukin-6 and C-reactive protein, which are part of the inflammatory phenotype of COPD. Aspirin has been shown to reduce proinflammatory cytokines in the lung.
The authors did note that aspirin use was self-reported, so they did not have data on dosage or duration of use.
The National Institutes of Health funded the study. Six authors declared advisory board positions, research support, and other funding from the pharmaceutical sector. One author was also a founder of a company commercializing lung image analysis software. No other conflicts of interest were declared.
SOURCE: Fawzy A et al. Chest. 2019 Mar;155(3): 519-27. doi: 10.1016/j.chest.2018.11.028.
FROM CHEST
Dupilumab to undergo FDA Priority Review for CRSwNP treatment
The Food and Drug Administration will conduct a Priority Review on the supplemental Biologics License Application (sBLA) for dupilumab (Dupixent) as an add-on treatment for adults with inadequately controlled severe chronic rhinosinusitis with nasal polyps (CRSwNP).

CRSwNP is a chronic disease of the upper airway in which patients can experience severe nasal obstruction with breathing difficulties, nasal discharge, reduction or loss of sense of smell and taste, and facial pain or pressure. There are currently no FDA-approved treatments for the disease, Regeneron said in the press release.
The sBLA is based on results from a pair of phase 3 trials in which patients with CRSwNP received either dupilumab plus a standard-of-care corticosteroid nasal spray or the standard-of-care spray alone. In results presented at the 2019 annual meeting of the American Academy of Allergy, Asthma, and Immunology, dupilumab plus the spray improved nasal polyp size, nasal congestion severity, chronic sinus disease, sense of smell, and comorbid asthma outcomes while reducing the need for corticosteroid use and nasal/sinus surgery.
Dupilumab is currently approved in the United States to treat moderate to severe atopic dermatitis in adults whose disease is poorly controlled with topical agents and as a maintenance treatment in combination with other asthma medications in patients aged 12 years and older whose disease is not controlled with their current prescription. The most common adverse events include injection-site reactions, oropharyngeal pain, and cold sores.
The target action date for the FDA decision is June 26, 2019, Regeneron said.
Find the full press release on the Regeneron website.
The Food and Drug Administration will conduct a Priority Review on the supplemental Biologics License Application (sBLA) for dupilumab (Dupixent) as an add-on treatment for adults with inadequately controlled severe chronic rhinosinusitis with nasal polyps (CRSwNP).
CRSwNP is a chronic disease of the upper airway in which patients can experience severe nasal obstruction with breathing difficulties, nasal discharge, reduction or loss of sense of smell and taste, and facial pain or pressure. There are currently no FDA-approved treatments for the disease, Regeneron said in the press release.
The sBLA is based on results from a pair of phase 3 trials in which patients with CRSwNP received either dupilumab plus a standard-of-care corticosteroid nasal spray or the standard-of-care spray alone. In results presented at the 2019 annual meeting of the American Academy of Allergy, Asthma, and Immunology, dupilumab plus the spray improved nasal polyp size, nasal congestion severity, chronic sinus disease, sense of smell, and comorbid asthma outcomes while reducing the need for corticosteroid use and nasal/sinus surgery.
Dupilumab is currently approved in the United States to treat moderate to severe atopic dermatitis in adults whose disease is poorly controlled with topical agents and as a maintenance treatment in combination with other asthma medications in patients aged 12 years and older whose disease is not controlled with their current prescription. The most common adverse events include injection-site reactions, oropharyngeal pain, and cold sores.
The target action date for the FDA decision is June 26, 2019, Regeneron said.
Find the full press release on the Regeneron website.
The Food and Drug Administration will conduct a Priority Review on the supplemental Biologics License Application (sBLA) for dupilumab (Dupixent) as an add-on treatment for adults with inadequately controlled severe chronic rhinosinusitis with nasal polyps (CRSwNP).
CRSwNP is a chronic disease of the upper airway in which patients can experience severe nasal obstruction with breathing difficulties, nasal discharge, reduction or loss of sense of smell and taste, and facial pain or pressure. There are currently no FDA-approved treatments for the disease, Regeneron said in the press release.
The sBLA is based on results from a pair of phase 3 trials in which patients with CRSwNP received either dupilumab plus a standard-of-care corticosteroid nasal spray or the standard-of-care spray alone. In results presented at the 2019 annual meeting of the American Academy of Allergy, Asthma, and Immunology, dupilumab plus the spray improved nasal polyp size, nasal congestion severity, chronic sinus disease, sense of smell, and comorbid asthma outcomes while reducing the need for corticosteroid use and nasal/sinus surgery.
Dupilumab is currently approved in the United States to treat moderate to severe atopic dermatitis in adults whose disease is poorly controlled with topical agents and as a maintenance treatment in combination with other asthma medications in patients aged 12 years and older whose disease is not controlled with their current prescription. The most common adverse events include injection-site reactions, oropharyngeal pain, and cold sores.
The target action date for the FDA decision is June 26, 2019, Regeneron said.
Find the full press release on the Regeneron website.
Flu activity down for a second straight week
A second straight week of reduced influenza activity suggests that the 2018-2019 flu season is on the decline, according to the most recent data from the Centers for Disease Control and Prevention.
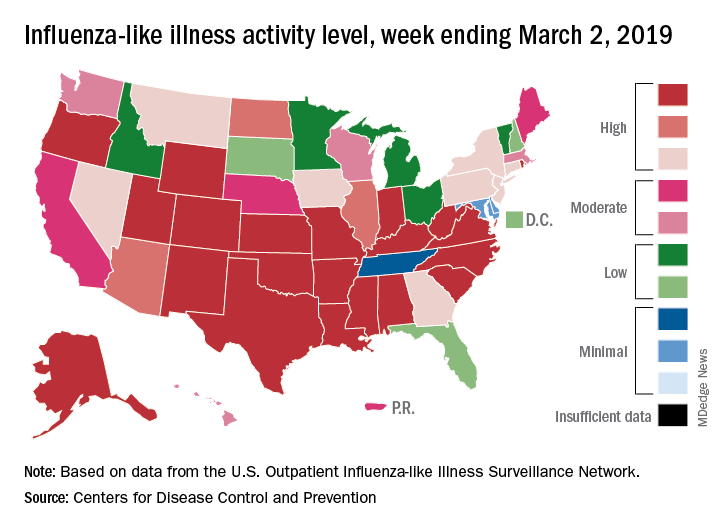
The proportion of outpatient visits for influenza-like illness (ILI) was 4.7% during the week ending March 2, which means that, thanks to a revision of the number for the previous week (Feb. 23) from 5.0% down to 4.9%, there have been two straight weeks of declines since outpatient visits reached a season-high 5.0% for the week ending Feb. 16, the CDC’s influenza division said March 8. The national baseline level is 2.2%.
This marks the second 2-week drop in ILI visits for the 2018-2019 season, as there was similar dip in the beginning of January before activity started rising again.
This compares with 24 the week before; 32 states were in the high range of 8-10, compared with the 33 reported last week, based on data from the Outpatient ILI Surveillance Network.
There were nine flu-related pediatric deaths reported during the week, with three occurring in the week ending March 2. To underscore the preliminary nature of these data, one of the deaths reported this week occurred in 2016. A total of 64 deaths in children have been associated with influenza so far for the 2018-2019 season, and the total for the 2015-2016 season is now 95, the CDC said.
A second straight week of reduced influenza activity suggests that the 2018-2019 flu season is on the decline, according to the most recent data from the Centers for Disease Control and Prevention.
The proportion of outpatient visits for influenza-like illness (ILI) was 4.7% during the week ending March 2, which means that, thanks to a revision of the number for the previous week (Feb. 23) from 5.0% down to 4.9%, there have been two straight weeks of declines since outpatient visits reached a season-high 5.0% for the week ending Feb. 16, the CDC’s influenza division said March 8. The national baseline level is 2.2%.
This marks the second 2-week drop in ILI visits for the 2018-2019 season, as there was similar dip in the beginning of January before activity started rising again.
This compares with 24 the week before; 32 states were in the high range of 8-10, compared with the 33 reported last week, based on data from the Outpatient ILI Surveillance Network.
There were nine flu-related pediatric deaths reported during the week, with three occurring in the week ending March 2. To underscore the preliminary nature of these data, one of the deaths reported this week occurred in 2016. A total of 64 deaths in children have been associated with influenza so far for the 2018-2019 season, and the total for the 2015-2016 season is now 95, the CDC said.
A second straight week of reduced influenza activity suggests that the 2018-2019 flu season is on the decline, according to the most recent data from the Centers for Disease Control and Prevention.
The proportion of outpatient visits for influenza-like illness (ILI) was 4.7% during the week ending March 2, which means that, thanks to a revision of the number for the previous week (Feb. 23) from 5.0% down to 4.9%, there have been two straight weeks of declines since outpatient visits reached a season-high 5.0% for the week ending Feb. 16, the CDC’s influenza division said March 8. The national baseline level is 2.2%.
This marks the second 2-week drop in ILI visits for the 2018-2019 season, as there was similar dip in the beginning of January before activity started rising again.
This compares with 24 the week before; 32 states were in the high range of 8-10, compared with the 33 reported last week, based on data from the Outpatient ILI Surveillance Network.
There were nine flu-related pediatric deaths reported during the week, with three occurring in the week ending March 2. To underscore the preliminary nature of these data, one of the deaths reported this week occurred in 2016. A total of 64 deaths in children have been associated with influenza so far for the 2018-2019 season, and the total for the 2015-2016 season is now 95, the CDC said.
Rounding team boosts ICU liberation efforts
SAN DIEGO – A rounding team formed to oversee implementation of a bundle of ICU interventions reduced the incidence of ventilator-associated pneumonia (VAP) and the number of ventilation days, as well as the ICU and hospital length of stay, according to a new study conducted at a level 1 trauma center in California. The rounding team worked toward optimal implementation of the Society of Critical Care Medicine’s ABCDEF bundle, part of the society’s ICU liberation initiative.
ABCDEF stands for: Assessment, prevention, and management of pain; Both spontaneous awakening and breathing trials; Choice of analgesia and sedation; Delirium assessment, prevention, and management; Early mobility and exercise; and Family engagement and empowerment.
The Community Regional Medical Center in Fresno, Calif., where the study was conducted, was chosen in 2015 to participate in the ICU liberation initiative. The facility serves a population of 3.2 million and sees just under 4,000 trauma patients per year.
After a 6-month retrospective analysis, the team members at the medical center realized they needed to improve ABCDEF implementation with respect to evaluating sedation practices and improving delirium assessment.
Before the start of the 17-month collaborative period, they formed an ICU liberation team called SMART, short for Sedation, Mobilization, Assessment Rounding Team, which included representatives from ICU nursing, pharmacy, respiratory therapy, physical therapy, physicians, and administration. They developed a daily rounding tool to help the team implement procedures, with the goal of reducing the continuous infusion of benzodiazepines and increasing intermittent dosing, the use of short-acting medications, and conducting spontaneous awakening and breathing trials. The SMART team made daily rounds to ensure that the ABCDEF bundle was being implemented.
The researchers then continued the analysis for another 12 months after the end of the initiative. During this last phase, the benefits of the SMART team became evident.
“Stick with it. Don’t let up. Don’t quit,” Wade Veneman, a respiratory therapist at the medical center, said in an interview. He presented the study at the Critical Care Congress sponsored by the Society of Critical Care Medicine. “It can be particularly difficult in the face of critical care providers who may be skeptical of new initiatives. They think it’s something new, and they hope that it goes away. But this is something we feel we’re going to keep for a long time,” he added.

Mr. Veneman hopes to implement the SMART program in the neurological critical care ICU. The medical director of that unit did not participate in the initial collaborative, but Mr. Veneman hopes to change that. “The data is going to show that his VAP and ventilator days are going up, and everywhere else they’re going down,” he said.
The researchers analyzed data on 1,127 mechanically ventilated patients in the ICU. At total of 197 patients were treated 6 months before the implementation of the collaborative, 519 during 17 months of collaborative implementation, and 411 in the 12 months after implementation. There were some differences between the populations: The before group was slightly younger than the after-implementation group (mean 41 vs. 44, P = .04), and the mean Injury Severity Score score was 24 in the before group, 22 during, and 20 after (P = .002). The researchers noted that the differences were clinically significant.
Benzodiazepine use declined, but the effect was statistically significant only in the after population. Continuous use declined from 87% before implementation to 83% during (P = .21) and 53% after (P less than .001). Intermittent use was 57% before implementation, increased to 61% during (P = .44), and fell to 44% after (P less than .001). Delirium assessment performance improved throughout, from 9% before implementation to 42% during (P less than .001) to 73% after implementation (P less than .001).
The VAP rate increased from 3.4% before the SMART program to 4.5% during implementation (P = .53), and then dropped to 0.9% afterward (P = .001). Ventilation days started at a mean of 10.5, then dropped to 9.5 during implementation (P = .30), and 8.2 after implementation (P = .027).
ICU length of stay improved from 10.7 before implementation to 9.3 afterward (P = .021), and overall hospital length of stay went from 17.3 days to 16.3 (P = .005).
The study was not funded. Mr. Veneman has no relevant financial disclosures.
SOURCE: Veneman W et al. CCC48, Abstract 63.
SAN DIEGO – A rounding team formed to oversee implementation of a bundle of ICU interventions reduced the incidence of ventilator-associated pneumonia (VAP) and the number of ventilation days, as well as the ICU and hospital length of stay, according to a new study conducted at a level 1 trauma center in California. The rounding team worked toward optimal implementation of the Society of Critical Care Medicine’s ABCDEF bundle, part of the society’s ICU liberation initiative.
ABCDEF stands for: Assessment, prevention, and management of pain; Both spontaneous awakening and breathing trials; Choice of analgesia and sedation; Delirium assessment, prevention, and management; Early mobility and exercise; and Family engagement and empowerment.
The Community Regional Medical Center in Fresno, Calif., where the study was conducted, was chosen in 2015 to participate in the ICU liberation initiative. The facility serves a population of 3.2 million and sees just under 4,000 trauma patients per year.
After a 6-month retrospective analysis, the team members at the medical center realized they needed to improve ABCDEF implementation with respect to evaluating sedation practices and improving delirium assessment.
Before the start of the 17-month collaborative period, they formed an ICU liberation team called SMART, short for Sedation, Mobilization, Assessment Rounding Team, which included representatives from ICU nursing, pharmacy, respiratory therapy, physical therapy, physicians, and administration. They developed a daily rounding tool to help the team implement procedures, with the goal of reducing the continuous infusion of benzodiazepines and increasing intermittent dosing, the use of short-acting medications, and conducting spontaneous awakening and breathing trials. The SMART team made daily rounds to ensure that the ABCDEF bundle was being implemented.
The researchers then continued the analysis for another 12 months after the end of the initiative. During this last phase, the benefits of the SMART team became evident.
“Stick with it. Don’t let up. Don’t quit,” Wade Veneman, a respiratory therapist at the medical center, said in an interview. He presented the study at the Critical Care Congress sponsored by the Society of Critical Care Medicine. “It can be particularly difficult in the face of critical care providers who may be skeptical of new initiatives. They think it’s something new, and they hope that it goes away. But this is something we feel we’re going to keep for a long time,” he added.
Mr. Veneman hopes to implement the SMART program in the neurological critical care ICU. The medical director of that unit did not participate in the initial collaborative, but Mr. Veneman hopes to change that. “The data is going to show that his VAP and ventilator days are going up, and everywhere else they’re going down,” he said.
The researchers analyzed data on 1,127 mechanically ventilated patients in the ICU. At total of 197 patients were treated 6 months before the implementation of the collaborative, 519 during 17 months of collaborative implementation, and 411 in the 12 months after implementation. There were some differences between the populations: The before group was slightly younger than the after-implementation group (mean 41 vs. 44, P = .04), and the mean Injury Severity Score score was 24 in the before group, 22 during, and 20 after (P = .002). The researchers noted that the differences were clinically significant.
Benzodiazepine use declined, but the effect was statistically significant only in the after population. Continuous use declined from 87% before implementation to 83% during (P = .21) and 53% after (P less than .001). Intermittent use was 57% before implementation, increased to 61% during (P = .44), and fell to 44% after (P less than .001). Delirium assessment performance improved throughout, from 9% before implementation to 42% during (P less than .001) to 73% after implementation (P less than .001).
The VAP rate increased from 3.4% before the SMART program to 4.5% during implementation (P = .53), and then dropped to 0.9% afterward (P = .001). Ventilation days started at a mean of 10.5, then dropped to 9.5 during implementation (P = .30), and 8.2 after implementation (P = .027).
ICU length of stay improved from 10.7 before implementation to 9.3 afterward (P = .021), and overall hospital length of stay went from 17.3 days to 16.3 (P = .005).
The study was not funded. Mr. Veneman has no relevant financial disclosures.
SOURCE: Veneman W et al. CCC48, Abstract 63.
SAN DIEGO – A rounding team formed to oversee implementation of a bundle of ICU interventions reduced the incidence of ventilator-associated pneumonia (VAP) and the number of ventilation days, as well as the ICU and hospital length of stay, according to a new study conducted at a level 1 trauma center in California. The rounding team worked toward optimal implementation of the Society of Critical Care Medicine’s ABCDEF bundle, part of the society’s ICU liberation initiative.
ABCDEF stands for: Assessment, prevention, and management of pain; Both spontaneous awakening and breathing trials; Choice of analgesia and sedation; Delirium assessment, prevention, and management; Early mobility and exercise; and Family engagement and empowerment.
The Community Regional Medical Center in Fresno, Calif., where the study was conducted, was chosen in 2015 to participate in the ICU liberation initiative. The facility serves a population of 3.2 million and sees just under 4,000 trauma patients per year.
After a 6-month retrospective analysis, the team members at the medical center realized they needed to improve ABCDEF implementation with respect to evaluating sedation practices and improving delirium assessment.
Before the start of the 17-month collaborative period, they formed an ICU liberation team called SMART, short for Sedation, Mobilization, Assessment Rounding Team, which included representatives from ICU nursing, pharmacy, respiratory therapy, physical therapy, physicians, and administration. They developed a daily rounding tool to help the team implement procedures, with the goal of reducing the continuous infusion of benzodiazepines and increasing intermittent dosing, the use of short-acting medications, and conducting spontaneous awakening and breathing trials. The SMART team made daily rounds to ensure that the ABCDEF bundle was being implemented.
The researchers then continued the analysis for another 12 months after the end of the initiative. During this last phase, the benefits of the SMART team became evident.
“Stick with it. Don’t let up. Don’t quit,” Wade Veneman, a respiratory therapist at the medical center, said in an interview. He presented the study at the Critical Care Congress sponsored by the Society of Critical Care Medicine. “It can be particularly difficult in the face of critical care providers who may be skeptical of new initiatives. They think it’s something new, and they hope that it goes away. But this is something we feel we’re going to keep for a long time,” he added.
Mr. Veneman hopes to implement the SMART program in the neurological critical care ICU. The medical director of that unit did not participate in the initial collaborative, but Mr. Veneman hopes to change that. “The data is going to show that his VAP and ventilator days are going up, and everywhere else they’re going down,” he said.
The researchers analyzed data on 1,127 mechanically ventilated patients in the ICU. At total of 197 patients were treated 6 months before the implementation of the collaborative, 519 during 17 months of collaborative implementation, and 411 in the 12 months after implementation. There were some differences between the populations: The before group was slightly younger than the after-implementation group (mean 41 vs. 44, P = .04), and the mean Injury Severity Score score was 24 in the before group, 22 during, and 20 after (P = .002). The researchers noted that the differences were clinically significant.
Benzodiazepine use declined, but the effect was statistically significant only in the after population. Continuous use declined from 87% before implementation to 83% during (P = .21) and 53% after (P less than .001). Intermittent use was 57% before implementation, increased to 61% during (P = .44), and fell to 44% after (P less than .001). Delirium assessment performance improved throughout, from 9% before implementation to 42% during (P less than .001) to 73% after implementation (P less than .001).
The VAP rate increased from 3.4% before the SMART program to 4.5% during implementation (P = .53), and then dropped to 0.9% afterward (P = .001). Ventilation days started at a mean of 10.5, then dropped to 9.5 during implementation (P = .30), and 8.2 after implementation (P = .027).
ICU length of stay improved from 10.7 before implementation to 9.3 afterward (P = .021), and overall hospital length of stay went from 17.3 days to 16.3 (P = .005).
The study was not funded. Mr. Veneman has no relevant financial disclosures.
SOURCE: Veneman W et al. CCC48, Abstract 63.
REPORTING FROM CCC48
Heart-harming toxins may hurt hookah smokers
Smoking a water pipe, or hookah, can result in significant inhalation of toxins and an increased risk for short- and long-term cardiovascular health problems, according to a scientific statement issued by the American Heart Association on March 8.

In the statement, published in the journal Circulation, Aruni Bhatnagar, PhD, of the University of Louisville (Ky.) and his colleagues reviewed the potential dangers of water pipe use and offered strategies for prevention.
Data from the 2016 National Youth Tobacco Survey showed that current use (defined as use within the past 30 days) of water pipes by high school students increased in a nonlinear trend from 4.1% in 2011 to 4.8% in 2016, with a peak of 9.4% in 2014. Water pipe tobacco is sold in flavors such as cherry, chocolate, and coffee that appeal to younger consumers, and epidemiology data suggest that youth view water pipes as safer than conventional cigarettes because the water “filters out toxins” according to the statement.
Findings from the National Adult Tobacco Survey showed an increase as well, from 1.5% during 2009-2010 to 3.2% during 2013-2014. Adults cite cultural and social influences, as well as psychological benefits of reduced stress and anger and improved concentration, which may be attributable to nicotine, the researchers noted.
Water pipe smoking involves placing charcoal briquettes on top of a tobacco-filled bowl with a stem immersed in water such that the smoke is pulled through and bubbles up through the water into a mouthpiece. and include tar, phenanthrene, carbon monoxide, heavy metals, and arsenic, as well as nicotine.
The patterns of exposure to toxins during water pipe smoking are unclear, the authors noted.
However, the risks for both short-term and long-term health effects are similar to those associated with cigarettes. “Overall, the short-term cardiovascular effects are consistent with the sympathomimetic effects of nicotine,” according to the statement.
Data on the long-term effects of water pipe smoking on cardiovascular health are limited, but “lifetime exposures exceeding 40 water pipe–years (2 water pipes per day for a total of 20 years or 1 water pipe for 40 years) are associated with a threefold increase in the odds of angiographically diagnosed coronary artery stenosis,” according to the statement. Additional research on long-term health effects may help guide regulation of water pipe products, the authors suggested.
The AHA statement encourages health care providers to take a proactive approach in addressing hookah use by asking patients about it, by advising those who use water pipes to quit, by assisting those who want to quit by providing counseling and social support, and by referring water pipe smokers to legitimate resources for information on the potential for addiction and health risks.
Dr. Bhatnagar received funding from the National Institutes of Health, but he had no other financial conflicts to disclose.
SOURCE: Bhatnagar A et al. Circulation. 2019 Mar 8. doi: 10.1161/CIR.0000000000000671.
Smoking a water pipe, or hookah, can result in significant inhalation of toxins and an increased risk for short- and long-term cardiovascular health problems, according to a scientific statement issued by the American Heart Association on March 8.
In the statement, published in the journal Circulation, Aruni Bhatnagar, PhD, of the University of Louisville (Ky.) and his colleagues reviewed the potential dangers of water pipe use and offered strategies for prevention.
Data from the 2016 National Youth Tobacco Survey showed that current use (defined as use within the past 30 days) of water pipes by high school students increased in a nonlinear trend from 4.1% in 2011 to 4.8% in 2016, with a peak of 9.4% in 2014. Water pipe tobacco is sold in flavors such as cherry, chocolate, and coffee that appeal to younger consumers, and epidemiology data suggest that youth view water pipes as safer than conventional cigarettes because the water “filters out toxins” according to the statement.
Findings from the National Adult Tobacco Survey showed an increase as well, from 1.5% during 2009-2010 to 3.2% during 2013-2014. Adults cite cultural and social influences, as well as psychological benefits of reduced stress and anger and improved concentration, which may be attributable to nicotine, the researchers noted.
Water pipe smoking involves placing charcoal briquettes on top of a tobacco-filled bowl with a stem immersed in water such that the smoke is pulled through and bubbles up through the water into a mouthpiece. and include tar, phenanthrene, carbon monoxide, heavy metals, and arsenic, as well as nicotine.
The patterns of exposure to toxins during water pipe smoking are unclear, the authors noted.
However, the risks for both short-term and long-term health effects are similar to those associated with cigarettes. “Overall, the short-term cardiovascular effects are consistent with the sympathomimetic effects of nicotine,” according to the statement.
Data on the long-term effects of water pipe smoking on cardiovascular health are limited, but “lifetime exposures exceeding 40 water pipe–years (2 water pipes per day for a total of 20 years or 1 water pipe for 40 years) are associated with a threefold increase in the odds of angiographically diagnosed coronary artery stenosis,” according to the statement. Additional research on long-term health effects may help guide regulation of water pipe products, the authors suggested.
The AHA statement encourages health care providers to take a proactive approach in addressing hookah use by asking patients about it, by advising those who use water pipes to quit, by assisting those who want to quit by providing counseling and social support, and by referring water pipe smokers to legitimate resources for information on the potential for addiction and health risks.
Dr. Bhatnagar received funding from the National Institutes of Health, but he had no other financial conflicts to disclose.
SOURCE: Bhatnagar A et al. Circulation. 2019 Mar 8. doi: 10.1161/CIR.0000000000000671.
Smoking a water pipe, or hookah, can result in significant inhalation of toxins and an increased risk for short- and long-term cardiovascular health problems, according to a scientific statement issued by the American Heart Association on March 8.
In the statement, published in the journal Circulation, Aruni Bhatnagar, PhD, of the University of Louisville (Ky.) and his colleagues reviewed the potential dangers of water pipe use and offered strategies for prevention.
Data from the 2016 National Youth Tobacco Survey showed that current use (defined as use within the past 30 days) of water pipes by high school students increased in a nonlinear trend from 4.1% in 2011 to 4.8% in 2016, with a peak of 9.4% in 2014. Water pipe tobacco is sold in flavors such as cherry, chocolate, and coffee that appeal to younger consumers, and epidemiology data suggest that youth view water pipes as safer than conventional cigarettes because the water “filters out toxins” according to the statement.
Findings from the National Adult Tobacco Survey showed an increase as well, from 1.5% during 2009-2010 to 3.2% during 2013-2014. Adults cite cultural and social influences, as well as psychological benefits of reduced stress and anger and improved concentration, which may be attributable to nicotine, the researchers noted.
Water pipe smoking involves placing charcoal briquettes on top of a tobacco-filled bowl with a stem immersed in water such that the smoke is pulled through and bubbles up through the water into a mouthpiece. and include tar, phenanthrene, carbon monoxide, heavy metals, and arsenic, as well as nicotine.
The patterns of exposure to toxins during water pipe smoking are unclear, the authors noted.
However, the risks for both short-term and long-term health effects are similar to those associated with cigarettes. “Overall, the short-term cardiovascular effects are consistent with the sympathomimetic effects of nicotine,” according to the statement.
Data on the long-term effects of water pipe smoking on cardiovascular health are limited, but “lifetime exposures exceeding 40 water pipe–years (2 water pipes per day for a total of 20 years or 1 water pipe for 40 years) are associated with a threefold increase in the odds of angiographically diagnosed coronary artery stenosis,” according to the statement. Additional research on long-term health effects may help guide regulation of water pipe products, the authors suggested.
The AHA statement encourages health care providers to take a proactive approach in addressing hookah use by asking patients about it, by advising those who use water pipes to quit, by assisting those who want to quit by providing counseling and social support, and by referring water pipe smokers to legitimate resources for information on the potential for addiction and health risks.
Dr. Bhatnagar received funding from the National Institutes of Health, but he had no other financial conflicts to disclose.
SOURCE: Bhatnagar A et al. Circulation. 2019 Mar 8. doi: 10.1161/CIR.0000000000000671.
FROM CIRCULATION