User login
For MD-IQ use only
SCD, beta-thalassemia: CRISPR-based gene therapy `transformative’
Results from the prespecified interim analyses of the phase 3 CLIMB THAL-111 and CLIMB SCD-121 studies, presented at the European Hematology Association annual congress, show that patients with beta-thalassemia who received exa-cel were able to remain transfusion-free for up to 40.7 consecutive months, while in patients with sickle cell disease, the treatment likewise provided up to 36.5 months of freedom from vaso-occlusive crises.
The findings underscore that “exa-cel can provide a one-time, functional cure to patients with beta-thalassemia and sickle cell disease,” said coauthor Franco Locatelli, MD, of Catholic University of the Sacred Heart, Bambino Gesù Children’s Hospital, Rome.
In a comment, senior investigator Haydar Frangoul, MD, noted that, “with almost 4 years of follow-up on patients with beta-thalassemia and sickle cell disease, it appears that the benefit is holding.”
“The engraftment of our edited cells appears very stable over time. There is no reason to believe it will change,” said Dr. Frangoul, who is medical director of pediatric hematology/oncology, Sarah Cannon Center for Blood Cancer at The Children’s Hospital at TriStar Centennial, Nashville, Tenn.
Burden is high; current curative options have caveats
Patients with transfusion-dependent beta-thalassemia may require blood transfusions as often as every 2-5 weeks because of genetic mutations causing the absence of functional hemoglobin and subsequent depletions in red blood cells. And with hemoglobin being an iron-rich protein, patients are also at risk of an iron accumulation in the body, adding the possible need for uncomfortable iron chelation therapy to prevent organ damage.
The measures are burdensome, but the need is dire. Life expectancy in beta-thalassemia without them is only about 5 years.
With SCD, patients can face severe pain from vaso-occlusive crises as sickled red blood cells block blood flow, potentially causing hospitalization and complications including kidney failure or stroke.
A cure does already exist for both genetic disorders in the form of allogeneic stem cell transplantation. However, that option requires a matched related stem cell donor, and fewer than 20% of patients have accessibility to such donors.
Gene therapy
Gene therapy offers a potentially ideal alternative, providing a possible “functional cure” without the need for a donor, by instead harvesting patients’ cells, fixing the mutation and transferring them back to the patient.
The Food and Drug Administration already approved a first gene therapy, betibeglogene autotemcel (beti-cel), for children and adults with transfusion dependent beta-thalassemia, in August 2022.
While beti-cel utilizes a viral vector to insert functional copies of a modified gene into patients’ extracted hematopoietic stem cells before transfusing them back, exa-cel instead uses CRISPR-CAS9 technology to edit the gene, allowing the body to produce fetal hemoglobin, in an approach believed to be more precise and efficient.
“As we explain to patients, it’s a difference between gene addition, which is what beti-cel is, or gene editing, which is what exa-cel is,” Dr. Frangoul explained.
Phase 3 trial interim results
In investigating exa-cel for beta-thalassemia, the ongoing CLIMB THAL-111 has enrolled 48 patients with a mean baseline age of 20, with 16 between the ages of 12 and 18. Of the patients, 28 (58.3%) had severe genotypes of disease.
Among 27 patients who were evaluable for the study endpoints of the current interim analysis, 24 (88.9%), achieved the primary endpoint of maintaining a weighted average hemoglobin of at least 9 g/dL without the need for a transfusion for at least 12 months (P < .0001).
Patients who achieved the transfusion independence for at least 12 months remained transfusion-free for a mean duration of 20.5 months, with a range of 12.1-40.7 months.
Of 3 patients who did not achieve the 12-month transfusion-free endpoint, substantial reductions in transfusion volume were nevertheless achieved, of 70.3%, 79.6%, and 95.5%, among the 3.
And for the CLIMB SCD-121 trial of SCD, 35 participants have been dosed with exa-cel; in the primary efficacy set of 17 patients, 16 of the 17 (94.1%) achieved the primary endpoint of having no severe vaso-occlusive crises for at least 12 months (P < .0001).
All patients, however, achieved the secondary endpoint of being free from in-patient hospitalizations for severe vaso-occlusive crises for at least 12 months (P < .0001).
Patients who achieved freedom from vaso-occlusive crises for at least 12 months remained free of the events for a mean of 18.7 months, ranging from 13.1 months to 36.5 months.
Durability, patient-reported outcomes favorable
Importantly, in both studies, hemoglobin levels, as well as levels of the edited BCL11A alleles in bone marrow CD34+ and peripheral blood nucleated cells, showed sustained stability over time, indicating durable editing of the cells, Dr. Locatelli said.
In terms of patient-reported quality-of-life, measures significantly improved during both trials at 24 months of follow-up, with significant improvements on the EuroQol visual analog scale, Functional Assessment of Cancer Therapy–General, and the Bone Marrow Transplantation Subscale.
Safety results were consistent with those observed with myeloablative busulfan-based conditioning regimen and autologous transplantation procedures, with adverse events that were manageable.
In the beta-thalassemia study, two patients experienced serious adverse events that were determined to be related to exa-cel, including one patient having symptoms in the context of hemophagocytic lymphohistiocytosis.
For the other patient, the serious adverse events consisted of delayed engraftment and thrombocytopenia, each also considered related to busulfan. None of the patients with SCD had serious adverse events related to exa-cel.
All serious adverse events were resolved, with no reports of deaths, study discontinuations, or malignancies.
Potentially first ever CRISPR-based FDA approval
While CRISPR-CAS9 gene editing is being investigated in multiple other trials in humans for various disorders, to date none have received FDA approval, which would make an approval for exa-cel a landmark development.
The therapy is currently under review, and Dr. Frangoul said the FDA has stated that a decision on the indication for SCD is expected by Dec. 8, 2023, and for beta-thalassemia, by March 2024.
Commenting on the research, Raffaella Colombatti, MD, a pediatric hematologist-oncologist and assistant professor of pediatrics at the University of Padova (Italy), underscored the need for a better curative alternative.
“Unfortunately, the other curative option, bone marrow transplant, is not available for all candidates due to the lack of suitable donors,” Dr. Colombatti said in an interview.
“And, although there are promising results from alternative donors and new conditioning regimens, a further option for selected patients with sickle cell disease and thalassemia utilizing gene therapy and gene editing is needed.”
Caveats regarding gene therapy for the two diseases that still need consideration include: “long-term safety results are still not available and eligibility criteria still needs to be explored outside clinical trials,” she said.
Furthermore, “costs and sustainability are also an issue,” Dr. Colombatti added.
The price of gene therapy is not cheap. With beti-cel priced at more than $2 million for the treatment, its manufacturer, Bluebird Bio, has reportedly already indicated that it will not pursue marketing in Europe because of unfavorable reimbursement policies, and a similar high price is anticipated for exa-cel.
Overall, however, the findings bode well for groundbreaking improvements in treatment of the two red blood cell disorders, Michael J. Eckrich, MD, MPH, medical director of pediatric stem cell transplant & cellular therapy at Atrium Health Levine Children’s Hospital Cancer and Blood Disorders in Charlotte, N.C., said in an interview.
“I do think that this is transformative therapy and will change our approach for patients with severe sickle cell disease in need of transplant,” said Dr. Eckrich, who has also been an investigator on the research of exa-cel for sickle cell disease.
“It might not be hard to imagine, that with the progress in gene therapies and gene editing, that allogeneic transplant will soon become obsolete for patients with sickle cell disease and beta-thalassemia.”
Dr. Locatelli is on the advisory board for Vertex Pharma and the speaker’s bureau for BluebirdBio. Dr. Frangoul and Dr. Colombatti are or have been consultants for Vertex Pharma.
Results from the prespecified interim analyses of the phase 3 CLIMB THAL-111 and CLIMB SCD-121 studies, presented at the European Hematology Association annual congress, show that patients with beta-thalassemia who received exa-cel were able to remain transfusion-free for up to 40.7 consecutive months, while in patients with sickle cell disease, the treatment likewise provided up to 36.5 months of freedom from vaso-occlusive crises.
The findings underscore that “exa-cel can provide a one-time, functional cure to patients with beta-thalassemia and sickle cell disease,” said coauthor Franco Locatelli, MD, of Catholic University of the Sacred Heart, Bambino Gesù Children’s Hospital, Rome.
In a comment, senior investigator Haydar Frangoul, MD, noted that, “with almost 4 years of follow-up on patients with beta-thalassemia and sickle cell disease, it appears that the benefit is holding.”
“The engraftment of our edited cells appears very stable over time. There is no reason to believe it will change,” said Dr. Frangoul, who is medical director of pediatric hematology/oncology, Sarah Cannon Center for Blood Cancer at The Children’s Hospital at TriStar Centennial, Nashville, Tenn.
Burden is high; current curative options have caveats
Patients with transfusion-dependent beta-thalassemia may require blood transfusions as often as every 2-5 weeks because of genetic mutations causing the absence of functional hemoglobin and subsequent depletions in red blood cells. And with hemoglobin being an iron-rich protein, patients are also at risk of an iron accumulation in the body, adding the possible need for uncomfortable iron chelation therapy to prevent organ damage.
The measures are burdensome, but the need is dire. Life expectancy in beta-thalassemia without them is only about 5 years.
With SCD, patients can face severe pain from vaso-occlusive crises as sickled red blood cells block blood flow, potentially causing hospitalization and complications including kidney failure or stroke.
A cure does already exist for both genetic disorders in the form of allogeneic stem cell transplantation. However, that option requires a matched related stem cell donor, and fewer than 20% of patients have accessibility to such donors.
Gene therapy
Gene therapy offers a potentially ideal alternative, providing a possible “functional cure” without the need for a donor, by instead harvesting patients’ cells, fixing the mutation and transferring them back to the patient.
The Food and Drug Administration already approved a first gene therapy, betibeglogene autotemcel (beti-cel), for children and adults with transfusion dependent beta-thalassemia, in August 2022.
While beti-cel utilizes a viral vector to insert functional copies of a modified gene into patients’ extracted hematopoietic stem cells before transfusing them back, exa-cel instead uses CRISPR-CAS9 technology to edit the gene, allowing the body to produce fetal hemoglobin, in an approach believed to be more precise and efficient.
“As we explain to patients, it’s a difference between gene addition, which is what beti-cel is, or gene editing, which is what exa-cel is,” Dr. Frangoul explained.
Phase 3 trial interim results
In investigating exa-cel for beta-thalassemia, the ongoing CLIMB THAL-111 has enrolled 48 patients with a mean baseline age of 20, with 16 between the ages of 12 and 18. Of the patients, 28 (58.3%) had severe genotypes of disease.
Among 27 patients who were evaluable for the study endpoints of the current interim analysis, 24 (88.9%), achieved the primary endpoint of maintaining a weighted average hemoglobin of at least 9 g/dL without the need for a transfusion for at least 12 months (P < .0001).
Patients who achieved the transfusion independence for at least 12 months remained transfusion-free for a mean duration of 20.5 months, with a range of 12.1-40.7 months.
Of 3 patients who did not achieve the 12-month transfusion-free endpoint, substantial reductions in transfusion volume were nevertheless achieved, of 70.3%, 79.6%, and 95.5%, among the 3.
And for the CLIMB SCD-121 trial of SCD, 35 participants have been dosed with exa-cel; in the primary efficacy set of 17 patients, 16 of the 17 (94.1%) achieved the primary endpoint of having no severe vaso-occlusive crises for at least 12 months (P < .0001).
All patients, however, achieved the secondary endpoint of being free from in-patient hospitalizations for severe vaso-occlusive crises for at least 12 months (P < .0001).
Patients who achieved freedom from vaso-occlusive crises for at least 12 months remained free of the events for a mean of 18.7 months, ranging from 13.1 months to 36.5 months.
Durability, patient-reported outcomes favorable
Importantly, in both studies, hemoglobin levels, as well as levels of the edited BCL11A alleles in bone marrow CD34+ and peripheral blood nucleated cells, showed sustained stability over time, indicating durable editing of the cells, Dr. Locatelli said.
In terms of patient-reported quality-of-life, measures significantly improved during both trials at 24 months of follow-up, with significant improvements on the EuroQol visual analog scale, Functional Assessment of Cancer Therapy–General, and the Bone Marrow Transplantation Subscale.
Safety results were consistent with those observed with myeloablative busulfan-based conditioning regimen and autologous transplantation procedures, with adverse events that were manageable.
In the beta-thalassemia study, two patients experienced serious adverse events that were determined to be related to exa-cel, including one patient having symptoms in the context of hemophagocytic lymphohistiocytosis.
For the other patient, the serious adverse events consisted of delayed engraftment and thrombocytopenia, each also considered related to busulfan. None of the patients with SCD had serious adverse events related to exa-cel.
All serious adverse events were resolved, with no reports of deaths, study discontinuations, or malignancies.
Potentially first ever CRISPR-based FDA approval
While CRISPR-CAS9 gene editing is being investigated in multiple other trials in humans for various disorders, to date none have received FDA approval, which would make an approval for exa-cel a landmark development.
The therapy is currently under review, and Dr. Frangoul said the FDA has stated that a decision on the indication for SCD is expected by Dec. 8, 2023, and for beta-thalassemia, by March 2024.
Commenting on the research, Raffaella Colombatti, MD, a pediatric hematologist-oncologist and assistant professor of pediatrics at the University of Padova (Italy), underscored the need for a better curative alternative.
“Unfortunately, the other curative option, bone marrow transplant, is not available for all candidates due to the lack of suitable donors,” Dr. Colombatti said in an interview.
“And, although there are promising results from alternative donors and new conditioning regimens, a further option for selected patients with sickle cell disease and thalassemia utilizing gene therapy and gene editing is needed.”
Caveats regarding gene therapy for the two diseases that still need consideration include: “long-term safety results are still not available and eligibility criteria still needs to be explored outside clinical trials,” she said.
Furthermore, “costs and sustainability are also an issue,” Dr. Colombatti added.
The price of gene therapy is not cheap. With beti-cel priced at more than $2 million for the treatment, its manufacturer, Bluebird Bio, has reportedly already indicated that it will not pursue marketing in Europe because of unfavorable reimbursement policies, and a similar high price is anticipated for exa-cel.
Overall, however, the findings bode well for groundbreaking improvements in treatment of the two red blood cell disorders, Michael J. Eckrich, MD, MPH, medical director of pediatric stem cell transplant & cellular therapy at Atrium Health Levine Children’s Hospital Cancer and Blood Disorders in Charlotte, N.C., said in an interview.
“I do think that this is transformative therapy and will change our approach for patients with severe sickle cell disease in need of transplant,” said Dr. Eckrich, who has also been an investigator on the research of exa-cel for sickle cell disease.
“It might not be hard to imagine, that with the progress in gene therapies and gene editing, that allogeneic transplant will soon become obsolete for patients with sickle cell disease and beta-thalassemia.”
Dr. Locatelli is on the advisory board for Vertex Pharma and the speaker’s bureau for BluebirdBio. Dr. Frangoul and Dr. Colombatti are or have been consultants for Vertex Pharma.
Results from the prespecified interim analyses of the phase 3 CLIMB THAL-111 and CLIMB SCD-121 studies, presented at the European Hematology Association annual congress, show that patients with beta-thalassemia who received exa-cel were able to remain transfusion-free for up to 40.7 consecutive months, while in patients with sickle cell disease, the treatment likewise provided up to 36.5 months of freedom from vaso-occlusive crises.
The findings underscore that “exa-cel can provide a one-time, functional cure to patients with beta-thalassemia and sickle cell disease,” said coauthor Franco Locatelli, MD, of Catholic University of the Sacred Heart, Bambino Gesù Children’s Hospital, Rome.
In a comment, senior investigator Haydar Frangoul, MD, noted that, “with almost 4 years of follow-up on patients with beta-thalassemia and sickle cell disease, it appears that the benefit is holding.”
“The engraftment of our edited cells appears very stable over time. There is no reason to believe it will change,” said Dr. Frangoul, who is medical director of pediatric hematology/oncology, Sarah Cannon Center for Blood Cancer at The Children’s Hospital at TriStar Centennial, Nashville, Tenn.
Burden is high; current curative options have caveats
Patients with transfusion-dependent beta-thalassemia may require blood transfusions as often as every 2-5 weeks because of genetic mutations causing the absence of functional hemoglobin and subsequent depletions in red blood cells. And with hemoglobin being an iron-rich protein, patients are also at risk of an iron accumulation in the body, adding the possible need for uncomfortable iron chelation therapy to prevent organ damage.
The measures are burdensome, but the need is dire. Life expectancy in beta-thalassemia without them is only about 5 years.
With SCD, patients can face severe pain from vaso-occlusive crises as sickled red blood cells block blood flow, potentially causing hospitalization and complications including kidney failure or stroke.
A cure does already exist for both genetic disorders in the form of allogeneic stem cell transplantation. However, that option requires a matched related stem cell donor, and fewer than 20% of patients have accessibility to such donors.
Gene therapy
Gene therapy offers a potentially ideal alternative, providing a possible “functional cure” without the need for a donor, by instead harvesting patients’ cells, fixing the mutation and transferring them back to the patient.
The Food and Drug Administration already approved a first gene therapy, betibeglogene autotemcel (beti-cel), for children and adults with transfusion dependent beta-thalassemia, in August 2022.
While beti-cel utilizes a viral vector to insert functional copies of a modified gene into patients’ extracted hematopoietic stem cells before transfusing them back, exa-cel instead uses CRISPR-CAS9 technology to edit the gene, allowing the body to produce fetal hemoglobin, in an approach believed to be more precise and efficient.
“As we explain to patients, it’s a difference between gene addition, which is what beti-cel is, or gene editing, which is what exa-cel is,” Dr. Frangoul explained.
Phase 3 trial interim results
In investigating exa-cel for beta-thalassemia, the ongoing CLIMB THAL-111 has enrolled 48 patients with a mean baseline age of 20, with 16 between the ages of 12 and 18. Of the patients, 28 (58.3%) had severe genotypes of disease.
Among 27 patients who were evaluable for the study endpoints of the current interim analysis, 24 (88.9%), achieved the primary endpoint of maintaining a weighted average hemoglobin of at least 9 g/dL without the need for a transfusion for at least 12 months (P < .0001).
Patients who achieved the transfusion independence for at least 12 months remained transfusion-free for a mean duration of 20.5 months, with a range of 12.1-40.7 months.
Of 3 patients who did not achieve the 12-month transfusion-free endpoint, substantial reductions in transfusion volume were nevertheless achieved, of 70.3%, 79.6%, and 95.5%, among the 3.
And for the CLIMB SCD-121 trial of SCD, 35 participants have been dosed with exa-cel; in the primary efficacy set of 17 patients, 16 of the 17 (94.1%) achieved the primary endpoint of having no severe vaso-occlusive crises for at least 12 months (P < .0001).
All patients, however, achieved the secondary endpoint of being free from in-patient hospitalizations for severe vaso-occlusive crises for at least 12 months (P < .0001).
Patients who achieved freedom from vaso-occlusive crises for at least 12 months remained free of the events for a mean of 18.7 months, ranging from 13.1 months to 36.5 months.
Durability, patient-reported outcomes favorable
Importantly, in both studies, hemoglobin levels, as well as levels of the edited BCL11A alleles in bone marrow CD34+ and peripheral blood nucleated cells, showed sustained stability over time, indicating durable editing of the cells, Dr. Locatelli said.
In terms of patient-reported quality-of-life, measures significantly improved during both trials at 24 months of follow-up, with significant improvements on the EuroQol visual analog scale, Functional Assessment of Cancer Therapy–General, and the Bone Marrow Transplantation Subscale.
Safety results were consistent with those observed with myeloablative busulfan-based conditioning regimen and autologous transplantation procedures, with adverse events that were manageable.
In the beta-thalassemia study, two patients experienced serious adverse events that were determined to be related to exa-cel, including one patient having symptoms in the context of hemophagocytic lymphohistiocytosis.
For the other patient, the serious adverse events consisted of delayed engraftment and thrombocytopenia, each also considered related to busulfan. None of the patients with SCD had serious adverse events related to exa-cel.
All serious adverse events were resolved, with no reports of deaths, study discontinuations, or malignancies.
Potentially first ever CRISPR-based FDA approval
While CRISPR-CAS9 gene editing is being investigated in multiple other trials in humans for various disorders, to date none have received FDA approval, which would make an approval for exa-cel a landmark development.
The therapy is currently under review, and Dr. Frangoul said the FDA has stated that a decision on the indication for SCD is expected by Dec. 8, 2023, and for beta-thalassemia, by March 2024.
Commenting on the research, Raffaella Colombatti, MD, a pediatric hematologist-oncologist and assistant professor of pediatrics at the University of Padova (Italy), underscored the need for a better curative alternative.
“Unfortunately, the other curative option, bone marrow transplant, is not available for all candidates due to the lack of suitable donors,” Dr. Colombatti said in an interview.
“And, although there are promising results from alternative donors and new conditioning regimens, a further option for selected patients with sickle cell disease and thalassemia utilizing gene therapy and gene editing is needed.”
Caveats regarding gene therapy for the two diseases that still need consideration include: “long-term safety results are still not available and eligibility criteria still needs to be explored outside clinical trials,” she said.
Furthermore, “costs and sustainability are also an issue,” Dr. Colombatti added.
The price of gene therapy is not cheap. With beti-cel priced at more than $2 million for the treatment, its manufacturer, Bluebird Bio, has reportedly already indicated that it will not pursue marketing in Europe because of unfavorable reimbursement policies, and a similar high price is anticipated for exa-cel.
Overall, however, the findings bode well for groundbreaking improvements in treatment of the two red blood cell disorders, Michael J. Eckrich, MD, MPH, medical director of pediatric stem cell transplant & cellular therapy at Atrium Health Levine Children’s Hospital Cancer and Blood Disorders in Charlotte, N.C., said in an interview.
“I do think that this is transformative therapy and will change our approach for patients with severe sickle cell disease in need of transplant,” said Dr. Eckrich, who has also been an investigator on the research of exa-cel for sickle cell disease.
“It might not be hard to imagine, that with the progress in gene therapies and gene editing, that allogeneic transplant will soon become obsolete for patients with sickle cell disease and beta-thalassemia.”
Dr. Locatelli is on the advisory board for Vertex Pharma and the speaker’s bureau for BluebirdBio. Dr. Frangoul and Dr. Colombatti are or have been consultants for Vertex Pharma.
FROM EHA 2023
Death anxiety in psychiatry and society: Facing our fears and embracing life
Our fear of death is exposed often in medicine. It is not uncommon to hear the last moments of a patient’s life described as a series of futile, sterile medical interventions that attempt to prolong that life in quasi-sadistic fashion. So much effort is placed in making sure that “everything necessary” is tried that less emphasis is made on providing a comfortable death.
It seems obvious that a profession dedicated to prolonging health would have difficulty confronting death. But it should also be natural for psychiatry to be the specialty able to integrate this discomfort within the medical psyche.

Yet, in training, we have noted much more time spent on the assessment of capacity in patients in order to refuse medical intervention than on time spent educating about the importance to die at the right time, as suggested by Friedrich Nietzsche.1 A psychiatry resident may graduate knowing dozens of questions to assess the ability of a family member to consider the risk, benefits, and alternatives of continued intubation in a comatose patient, but may feel very ill-equipped in discussing the meaning of a rightful life and a rightful death.
Death anxiety can also come outside the context of not having endured enough traumas or successes in one’s life, or not having lived life right. As poignantly described by Dostoevsky in his 1864 novella, “Notes from the Underground,” death anxiety can manifest as a result of the deterministic nature of life.2 Doing everything which is expected of us can feel like a betrayal of our one chance to have lived life authentically. This concept is also particularly familiar to physicians, who may have – in part – chosen their career path in response to a recommendation from their parents, rather than a more authentic feeling. Dostoevsky goads us to transgress, to act in a rebellious way, to truly feel alive. This can serve as a solution for death anxiety – if you are scared to die then live, live your fullest. Even if that means doing the unexpected or changing your path.
The fear of being forgotten after death can also drive many to pursue a legacy. Even a parent choosing to have children and teaching them values and belief systems is a way of leaving behind a mark on the world. For some, finding ways for being remembered after death – whether through fame, fortune, or having children, is a way of dealing with death anxiety.
The Mexican holiday “Dia de los Muertos,” or Day of the Dead, and the Japanese holiday “Obon” are examples from cultures where deceased ancestors are celebrated through rituals and offerings. Such cultures may relieve the anxiety of death by suggesting that one’s descendants will still care for the departed, and their legacy may remain.
Coping with death anxiety
For others, the road to recovery from death anxiety may take a completely different approach. Some may find comfort in the position that, to extinguish death anxiety, one should not live to the fullest but accept the tragic and mostly inconsequential aspects of life. The philosophical movement of “absurdism” addresses this perspective.

In our modern world, where we are so deeply attached to finding the cause and reason for things, absurdism reminds us that most of our lives and world do not have to make sense. While Albert Camus, arguably the most famous of the absurdist philosophers, encourages us to create meaning and transcend the tragedy and randomness of life,3 some patients can also find comfort in the idea that life is absurd, and thus one should not judge one’s own life and not fear own’s inevitable death.
Death anxiety can also be therapeutic. Especially in the existential tradition, one can enlist the fear of death for motivation. Many patients come to see us with a lack of motivation or drive. They feel paralyzed by their predicament and mental illness. As in the experiments of Martin Seligman, PhD, who shocked animals at random, a human exposed to repeated failure and abuse can get a sense of learned helplessness.4 Such patients can be very hard to reach, yet ultimately their despondence is no match for the reality that life will end. Reminding a patient that any day spent not feeling alive might as well be a metaphor for death is a challenging interpretation, but one that can lead to significant growth.
When considering the fear of death, psychiatry has generally taken the position that it is pathological, a form of anxiety. Psychiatry argues that one should strive to find fulfillment and joy in life. It thus may be a surprise to find that this is not a universally shared perspective.
In his 2010 book, author Thomas Ligotti argues on behalf of pessimistic and antinatalist views.5 Throughout the book he emphasizes the suffering that life can offer and argues against the endless pursuit of more life. To some psychiatrists, such arguments will be understood as insulting to our profession. Some may even interpret his texts as an argument in favor of ending one’s life.
However, psychiatrists must ask themselves “what are my answers to those arguments?” Mr. Ligotti’s book is a series of arguments against the idea that life will be pleasurable. Understanding those arguments and formulating a rebuttal would be an important process for any mental health provider. It is foolish to think that our patients do not have a rich and complicated relationship to death, and that none of our patients find death attractive in some ways. After all, accepting our fears as an important part of our body is a natural coping skill, which can also be taught.6
Part of the difficulty in discussing death and the fear of death may come from society’s resistance at having complicated conversations. It is not uncommon, currently, to include trigger warnings at the mention of discussions about death, even abstract ones. While we appreciate and encourage the articulation of feelings that a discussion about death may raise, we worry that such trigger warnings may be a form of censure that only makes society more resistant to talk about those important topics.
For another example of the avoidance of discussions about death, recall the “death panel” debates of 2009.7 When the U.S. government considered encouraging physicians to have discussions with their patients about end-of-life care, politicians and pundits decried that such discussions were “death panels,” and claimed they were an encouragement to patients to “cut [their] life short.” Such public projection of one’s anxiety about death has made it particularly difficult for psychiatry to make meaningful progress.
Acknowledging and addressing the fear
Death anxiety is such a common aspect of human life that most religions make some effort to address this fear. Many do so by offering a form of afterlife, often one described in idyllic fashion without anxiety.
Heaven, if one believes in it, is appealing for the person dreading death anxiety. Heaven is often described as being offered to those who have lived a rightful life, thus relieving the anxiety regarding the decisions one has made. Reincarnation can also be interpreted as another way of calming death anxiety, by promising a continual repetition of chances at getting life right. However, for many patients, religion doesn’t have the appeal that it once had.
Ultimately, the fear of death is a complex and multifaceted issue that can manifest in various ways. The medical profession, especially psychiatry, has a responsibility to address this fear in patients, but it also struggles with its own discomfort with the topic. The importance of providing a comfortable death is often overshadowed by the emphasis on prolonging life, which may manifest as a series of futile medical interventions.
The fear of death can be therapeutic and motivating, but it can also be pathological and lead to a lack of motivation or drive. The philosophical movements of absurdism and antinatalism offer alternative perspectives on death and life, and it is important for mental health providers to understand and engage with these views.
Yet acknowledging and addressing the fear of death is an important aspect of mental health care and a crucial part of the human experience.
Dr. Akkoor is a psychiatry resident at the University of California, San Diego. She is interested in immigrant mental health, ethics, consultation-liaison psychiatry, and medical education. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. Dr. Badre and Dr. Akkoor have no conflicts of interest.
References
1. Nietzsche F. Thus Spoke Zarathustra. 1883-1892.
2. Dostoevsky F. Notes from the Underground. 1864.
3. Camus A. The Plague. 1947.
4. Seligman M. Helplessness: On depression, development, and death. 1975.
5. Ligotti T. The Conspiracy Against the Human Race. 2010.
6. Hayes SC. Behav Ther. 2016 Nov;47(6):869-85. doi: 10.1016/j.beth.2016.11.006.
7. Nyhan B. The Forum. 2010 April 27;8(1). doi: 10.2202/1540-8884.1354.
Our fear of death is exposed often in medicine. It is not uncommon to hear the last moments of a patient’s life described as a series of futile, sterile medical interventions that attempt to prolong that life in quasi-sadistic fashion. So much effort is placed in making sure that “everything necessary” is tried that less emphasis is made on providing a comfortable death.
It seems obvious that a profession dedicated to prolonging health would have difficulty confronting death. But it should also be natural for psychiatry to be the specialty able to integrate this discomfort within the medical psyche.
Yet, in training, we have noted much more time spent on the assessment of capacity in patients in order to refuse medical intervention than on time spent educating about the importance to die at the right time, as suggested by Friedrich Nietzsche.1 A psychiatry resident may graduate knowing dozens of questions to assess the ability of a family member to consider the risk, benefits, and alternatives of continued intubation in a comatose patient, but may feel very ill-equipped in discussing the meaning of a rightful life and a rightful death.
Death anxiety can also come outside the context of not having endured enough traumas or successes in one’s life, or not having lived life right. As poignantly described by Dostoevsky in his 1864 novella, “Notes from the Underground,” death anxiety can manifest as a result of the deterministic nature of life.2 Doing everything which is expected of us can feel like a betrayal of our one chance to have lived life authentically. This concept is also particularly familiar to physicians, who may have – in part – chosen their career path in response to a recommendation from their parents, rather than a more authentic feeling. Dostoevsky goads us to transgress, to act in a rebellious way, to truly feel alive. This can serve as a solution for death anxiety – if you are scared to die then live, live your fullest. Even if that means doing the unexpected or changing your path.
The fear of being forgotten after death can also drive many to pursue a legacy. Even a parent choosing to have children and teaching them values and belief systems is a way of leaving behind a mark on the world. For some, finding ways for being remembered after death – whether through fame, fortune, or having children, is a way of dealing with death anxiety.
The Mexican holiday “Dia de los Muertos,” or Day of the Dead, and the Japanese holiday “Obon” are examples from cultures where deceased ancestors are celebrated through rituals and offerings. Such cultures may relieve the anxiety of death by suggesting that one’s descendants will still care for the departed, and their legacy may remain.
Coping with death anxiety
For others, the road to recovery from death anxiety may take a completely different approach. Some may find comfort in the position that, to extinguish death anxiety, one should not live to the fullest but accept the tragic and mostly inconsequential aspects of life. The philosophical movement of “absurdism” addresses this perspective.
In our modern world, where we are so deeply attached to finding the cause and reason for things, absurdism reminds us that most of our lives and world do not have to make sense. While Albert Camus, arguably the most famous of the absurdist philosophers, encourages us to create meaning and transcend the tragedy and randomness of life,3 some patients can also find comfort in the idea that life is absurd, and thus one should not judge one’s own life and not fear own’s inevitable death.
Death anxiety can also be therapeutic. Especially in the existential tradition, one can enlist the fear of death for motivation. Many patients come to see us with a lack of motivation or drive. They feel paralyzed by their predicament and mental illness. As in the experiments of Martin Seligman, PhD, who shocked animals at random, a human exposed to repeated failure and abuse can get a sense of learned helplessness.4 Such patients can be very hard to reach, yet ultimately their despondence is no match for the reality that life will end. Reminding a patient that any day spent not feeling alive might as well be a metaphor for death is a challenging interpretation, but one that can lead to significant growth.
When considering the fear of death, psychiatry has generally taken the position that it is pathological, a form of anxiety. Psychiatry argues that one should strive to find fulfillment and joy in life. It thus may be a surprise to find that this is not a universally shared perspective.
In his 2010 book, author Thomas Ligotti argues on behalf of pessimistic and antinatalist views.5 Throughout the book he emphasizes the suffering that life can offer and argues against the endless pursuit of more life. To some psychiatrists, such arguments will be understood as insulting to our profession. Some may even interpret his texts as an argument in favor of ending one’s life.
However, psychiatrists must ask themselves “what are my answers to those arguments?” Mr. Ligotti’s book is a series of arguments against the idea that life will be pleasurable. Understanding those arguments and formulating a rebuttal would be an important process for any mental health provider. It is foolish to think that our patients do not have a rich and complicated relationship to death, and that none of our patients find death attractive in some ways. After all, accepting our fears as an important part of our body is a natural coping skill, which can also be taught.6
Part of the difficulty in discussing death and the fear of death may come from society’s resistance at having complicated conversations. It is not uncommon, currently, to include trigger warnings at the mention of discussions about death, even abstract ones. While we appreciate and encourage the articulation of feelings that a discussion about death may raise, we worry that such trigger warnings may be a form of censure that only makes society more resistant to talk about those important topics.
For another example of the avoidance of discussions about death, recall the “death panel” debates of 2009.7 When the U.S. government considered encouraging physicians to have discussions with their patients about end-of-life care, politicians and pundits decried that such discussions were “death panels,” and claimed they were an encouragement to patients to “cut [their] life short.” Such public projection of one’s anxiety about death has made it particularly difficult for psychiatry to make meaningful progress.
Acknowledging and addressing the fear
Death anxiety is such a common aspect of human life that most religions make some effort to address this fear. Many do so by offering a form of afterlife, often one described in idyllic fashion without anxiety.
Heaven, if one believes in it, is appealing for the person dreading death anxiety. Heaven is often described as being offered to those who have lived a rightful life, thus relieving the anxiety regarding the decisions one has made. Reincarnation can also be interpreted as another way of calming death anxiety, by promising a continual repetition of chances at getting life right. However, for many patients, religion doesn’t have the appeal that it once had.
Ultimately, the fear of death is a complex and multifaceted issue that can manifest in various ways. The medical profession, especially psychiatry, has a responsibility to address this fear in patients, but it also struggles with its own discomfort with the topic. The importance of providing a comfortable death is often overshadowed by the emphasis on prolonging life, which may manifest as a series of futile medical interventions.
The fear of death can be therapeutic and motivating, but it can also be pathological and lead to a lack of motivation or drive. The philosophical movements of absurdism and antinatalism offer alternative perspectives on death and life, and it is important for mental health providers to understand and engage with these views.
Yet acknowledging and addressing the fear of death is an important aspect of mental health care and a crucial part of the human experience.
Dr. Akkoor is a psychiatry resident at the University of California, San Diego. She is interested in immigrant mental health, ethics, consultation-liaison psychiatry, and medical education. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. Dr. Badre and Dr. Akkoor have no conflicts of interest.
References
1. Nietzsche F. Thus Spoke Zarathustra. 1883-1892.
2. Dostoevsky F. Notes from the Underground. 1864.
3. Camus A. The Plague. 1947.
4. Seligman M. Helplessness: On depression, development, and death. 1975.
5. Ligotti T. The Conspiracy Against the Human Race. 2010.
6. Hayes SC. Behav Ther. 2016 Nov;47(6):869-85. doi: 10.1016/j.beth.2016.11.006.
7. Nyhan B. The Forum. 2010 April 27;8(1). doi: 10.2202/1540-8884.1354.
Our fear of death is exposed often in medicine. It is not uncommon to hear the last moments of a patient’s life described as a series of futile, sterile medical interventions that attempt to prolong that life in quasi-sadistic fashion. So much effort is placed in making sure that “everything necessary” is tried that less emphasis is made on providing a comfortable death.
It seems obvious that a profession dedicated to prolonging health would have difficulty confronting death. But it should also be natural for psychiatry to be the specialty able to integrate this discomfort within the medical psyche.
Yet, in training, we have noted much more time spent on the assessment of capacity in patients in order to refuse medical intervention than on time spent educating about the importance to die at the right time, as suggested by Friedrich Nietzsche.1 A psychiatry resident may graduate knowing dozens of questions to assess the ability of a family member to consider the risk, benefits, and alternatives of continued intubation in a comatose patient, but may feel very ill-equipped in discussing the meaning of a rightful life and a rightful death.
Death anxiety can also come outside the context of not having endured enough traumas or successes in one’s life, or not having lived life right. As poignantly described by Dostoevsky in his 1864 novella, “Notes from the Underground,” death anxiety can manifest as a result of the deterministic nature of life.2 Doing everything which is expected of us can feel like a betrayal of our one chance to have lived life authentically. This concept is also particularly familiar to physicians, who may have – in part – chosen their career path in response to a recommendation from their parents, rather than a more authentic feeling. Dostoevsky goads us to transgress, to act in a rebellious way, to truly feel alive. This can serve as a solution for death anxiety – if you are scared to die then live, live your fullest. Even if that means doing the unexpected or changing your path.
The fear of being forgotten after death can also drive many to pursue a legacy. Even a parent choosing to have children and teaching them values and belief systems is a way of leaving behind a mark on the world. For some, finding ways for being remembered after death – whether through fame, fortune, or having children, is a way of dealing with death anxiety.
The Mexican holiday “Dia de los Muertos,” or Day of the Dead, and the Japanese holiday “Obon” are examples from cultures where deceased ancestors are celebrated through rituals and offerings. Such cultures may relieve the anxiety of death by suggesting that one’s descendants will still care for the departed, and their legacy may remain.
Coping with death anxiety
For others, the road to recovery from death anxiety may take a completely different approach. Some may find comfort in the position that, to extinguish death anxiety, one should not live to the fullest but accept the tragic and mostly inconsequential aspects of life. The philosophical movement of “absurdism” addresses this perspective.
In our modern world, where we are so deeply attached to finding the cause and reason for things, absurdism reminds us that most of our lives and world do not have to make sense. While Albert Camus, arguably the most famous of the absurdist philosophers, encourages us to create meaning and transcend the tragedy and randomness of life,3 some patients can also find comfort in the idea that life is absurd, and thus one should not judge one’s own life and not fear own’s inevitable death.
Death anxiety can also be therapeutic. Especially in the existential tradition, one can enlist the fear of death for motivation. Many patients come to see us with a lack of motivation or drive. They feel paralyzed by their predicament and mental illness. As in the experiments of Martin Seligman, PhD, who shocked animals at random, a human exposed to repeated failure and abuse can get a sense of learned helplessness.4 Such patients can be very hard to reach, yet ultimately their despondence is no match for the reality that life will end. Reminding a patient that any day spent not feeling alive might as well be a metaphor for death is a challenging interpretation, but one that can lead to significant growth.
When considering the fear of death, psychiatry has generally taken the position that it is pathological, a form of anxiety. Psychiatry argues that one should strive to find fulfillment and joy in life. It thus may be a surprise to find that this is not a universally shared perspective.
In his 2010 book, author Thomas Ligotti argues on behalf of pessimistic and antinatalist views.5 Throughout the book he emphasizes the suffering that life can offer and argues against the endless pursuit of more life. To some psychiatrists, such arguments will be understood as insulting to our profession. Some may even interpret his texts as an argument in favor of ending one’s life.
However, psychiatrists must ask themselves “what are my answers to those arguments?” Mr. Ligotti’s book is a series of arguments against the idea that life will be pleasurable. Understanding those arguments and formulating a rebuttal would be an important process for any mental health provider. It is foolish to think that our patients do not have a rich and complicated relationship to death, and that none of our patients find death attractive in some ways. After all, accepting our fears as an important part of our body is a natural coping skill, which can also be taught.6
Part of the difficulty in discussing death and the fear of death may come from society’s resistance at having complicated conversations. It is not uncommon, currently, to include trigger warnings at the mention of discussions about death, even abstract ones. While we appreciate and encourage the articulation of feelings that a discussion about death may raise, we worry that such trigger warnings may be a form of censure that only makes society more resistant to talk about those important topics.
For another example of the avoidance of discussions about death, recall the “death panel” debates of 2009.7 When the U.S. government considered encouraging physicians to have discussions with their patients about end-of-life care, politicians and pundits decried that such discussions were “death panels,” and claimed they were an encouragement to patients to “cut [their] life short.” Such public projection of one’s anxiety about death has made it particularly difficult for psychiatry to make meaningful progress.
Acknowledging and addressing the fear
Death anxiety is such a common aspect of human life that most religions make some effort to address this fear. Many do so by offering a form of afterlife, often one described in idyllic fashion without anxiety.
Heaven, if one believes in it, is appealing for the person dreading death anxiety. Heaven is often described as being offered to those who have lived a rightful life, thus relieving the anxiety regarding the decisions one has made. Reincarnation can also be interpreted as another way of calming death anxiety, by promising a continual repetition of chances at getting life right. However, for many patients, religion doesn’t have the appeal that it once had.
Ultimately, the fear of death is a complex and multifaceted issue that can manifest in various ways. The medical profession, especially psychiatry, has a responsibility to address this fear in patients, but it also struggles with its own discomfort with the topic. The importance of providing a comfortable death is often overshadowed by the emphasis on prolonging life, which may manifest as a series of futile medical interventions.
The fear of death can be therapeutic and motivating, but it can also be pathological and lead to a lack of motivation or drive. The philosophical movements of absurdism and antinatalism offer alternative perspectives on death and life, and it is important for mental health providers to understand and engage with these views.
Yet acknowledging and addressing the fear of death is an important aspect of mental health care and a crucial part of the human experience.
Dr. Akkoor is a psychiatry resident at the University of California, San Diego. She is interested in immigrant mental health, ethics, consultation-liaison psychiatry, and medical education. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. Dr. Badre and Dr. Akkoor have no conflicts of interest.
References
1. Nietzsche F. Thus Spoke Zarathustra. 1883-1892.
2. Dostoevsky F. Notes from the Underground. 1864.
3. Camus A. The Plague. 1947.
4. Seligman M. Helplessness: On depression, development, and death. 1975.
5. Ligotti T. The Conspiracy Against the Human Race. 2010.
6. Hayes SC. Behav Ther. 2016 Nov;47(6):869-85. doi: 10.1016/j.beth.2016.11.006.
7. Nyhan B. The Forum. 2010 April 27;8(1). doi: 10.2202/1540-8884.1354.
30 days in, UHC offers little guidance on advance notification
It’s been just over 1 month since UnitedHealthcare (UHC) launched its advance notification program requiring providers to record nonscreening colonoscopy and other gastroenterology procedures to be eligible for its 2024 Gold Card program.
The program, which will begin next year, may eliminate prior authorization requirements for providers who successfully complete the advance notification program this year. However, there is no guarantee that providers who complete the advance notification program will be enrolled in the Gold Card program, which means they would have to seek prior authorization for nonscreening procedures, according to the American Gastroenterological Association.
While UHC has provided some information about how advance notification works, there are many unanswered questions, said Barbara H. Jung, MD,AGAF, AGA president.

“UnitedHealthcare’s haphazard approach to rolling out a policy that will ultimately control patient access to critical, often lifesaving medical procedures are the opposite of what should be our common goal of expeditious access to essential care,” she said in a written statement.
The advance notification program was announced on June 1 when UHC said it was dropping its controversial prior authorization program, which was due to go into effect that day.
AGA is concerned that UHC’s advance notification program is merely a delay tactic because prior authorization may be required next year for providers who are not accepted into the Gold Card program. Providers who are not accepted into the program may face delays in administering procedures due to the need for prior authorizations. Thousands of endoscopies and colonoscopies could potentially be disrupted in the first month alone due to canceled procedures because of new prior authorization requirements, they said.
UHC has been trying to rein in health care costs by first considering prior authorizations for most gastrointestinal (GI) endoscopic procedures, except for screening colonoscopy, but ultimately adopting advance notification. Providers, UHC has said, don’t always follow evidence-based medicine treatment recommendations or they overutilize procedures. Their goal, according to a summary document it issued outlining changes to advance notification and prior authorization requirements, is “better care, improved health outcomes, and lower costs.”
“Clinical studies demonstrate overutilization of these procedures and lack of adherence to specialty society–endorsed guidelines and recommendations. Up to one-third of upper GI procedures and almost half of nonscreening colonoscopies performed for common clinical conditions are not consistent with clinical guidelines,” UHC stated in an FAQ. “A UHC review of upper endoscopy and lower endoscopy procedures performed in 2022 revealed two- to fivefold practice-level variation in the use of both procedure types, even after adjusting for member characteristics including age and comorbidities.”
However, according to a statement from the AGA, it has not seen utilization data specific to UHC: “It is clear that UHC does not currently have any data indicating significant overutilization of critical colonoscopy and endoscopy procedures and therefore no justification to impose burdensome barriers like prior authorization.” AGA also pointed to research showing there is an unmet need for colonoscopies in the United States, which suggests there is an underutilization of this crucial procedure.
“AGA has expressed its willingness to work collaboratively with UnitedHealthcare to address any concerns and educate physicians, but communication and transparency with the insurer are nearly nonexistent. Instead, the GI community is confronted with a nebulous concept called advance notification, which is not conducive to seamless patient care. Ultimately, it appears advance notification will form the basis of prior authorization, which we know can delay, disrupt, and deny timely care,” Dr. Jung said.
How advance notification works
Beginning June 1, providers have been asked to provide advance notification for nonscreening GI endoscopy procedures that include: esophagogastroduodenoscopy, capsule endoscopy, diagnostic colonoscopy and surveillance colonoscopy. The notification can be made by phone (866-889-8054) or through a UHC online portal at UHCprovider.com.
The AGA has said that some GI practices have found the portal to be confusing and it lacks a standard software application raising concerns for high error rates.
Advance notification applies to patients who have UHC commercial plans, including UnitedHealthcare, UnitedHealthcare Plan of the River Valley, Neighborhood Health Partnership, UnitedHealthcare Level Funded, and UnitedHealthcare Oxford Health Plans in all states, except Rhode Island, Kentucky, and New Mexico.
Providers who opt out of participating in advance notification will not be eligible to participate in the Gold Card program in 2024. The program will essentially allow providers to order most GI endoscopy procedures, except for screening colonoscopy, without prior authorization. However, UHC has not released any information about how it will implement its planned Gold Card prior authorization program or how many providers will be accepted into the program.
UHC has assured providers it will not issue medical necessity denials through this process, but it may ask providers to participate in a “comprehensive peer-to-peer discussion with a board-certified gastroenterologist around clinical guidelines.”
The fear for practices is that advance notification will be an onerous process adding burdensome paperwork that practices are not equipped to manage. UHC is the largest health insurer in the country representing 46% of the total market.
Lawrence Kim, MD, AGAF, vice president of AGA and a gastroenterologist practicing in Denver said that each physician in his practice does over 1,000 procedures annually and 25% of their patients carry UHC.
“We are currently completing 30-40 notifications a day, requiring two staff members to comply with this program. UHC is not asking for any clinical information, just procedure and diagnosis codes, and in some cases site of service. Therefore, the advance notification program as it stands will not provide UHC with any additional information beyond what they already have through claims data. This highlights the strain these requirements are putting on providers and practices for repetitive data,” he said.
For more details about UHC’s advance notification program, UHC has prepared this FAQ. To learn more about AGA’s advocacy, visit www.gastro.org/UHC.
It’s been just over 1 month since UnitedHealthcare (UHC) launched its advance notification program requiring providers to record nonscreening colonoscopy and other gastroenterology procedures to be eligible for its 2024 Gold Card program.
The program, which will begin next year, may eliminate prior authorization requirements for providers who successfully complete the advance notification program this year. However, there is no guarantee that providers who complete the advance notification program will be enrolled in the Gold Card program, which means they would have to seek prior authorization for nonscreening procedures, according to the American Gastroenterological Association.
While UHC has provided some information about how advance notification works, there are many unanswered questions, said Barbara H. Jung, MD,AGAF, AGA president.
“UnitedHealthcare’s haphazard approach to rolling out a policy that will ultimately control patient access to critical, often lifesaving medical procedures are the opposite of what should be our common goal of expeditious access to essential care,” she said in a written statement.
The advance notification program was announced on June 1 when UHC said it was dropping its controversial prior authorization program, which was due to go into effect that day.
AGA is concerned that UHC’s advance notification program is merely a delay tactic because prior authorization may be required next year for providers who are not accepted into the Gold Card program. Providers who are not accepted into the program may face delays in administering procedures due to the need for prior authorizations. Thousands of endoscopies and colonoscopies could potentially be disrupted in the first month alone due to canceled procedures because of new prior authorization requirements, they said.
UHC has been trying to rein in health care costs by first considering prior authorizations for most gastrointestinal (GI) endoscopic procedures, except for screening colonoscopy, but ultimately adopting advance notification. Providers, UHC has said, don’t always follow evidence-based medicine treatment recommendations or they overutilize procedures. Their goal, according to a summary document it issued outlining changes to advance notification and prior authorization requirements, is “better care, improved health outcomes, and lower costs.”
“Clinical studies demonstrate overutilization of these procedures and lack of adherence to specialty society–endorsed guidelines and recommendations. Up to one-third of upper GI procedures and almost half of nonscreening colonoscopies performed for common clinical conditions are not consistent with clinical guidelines,” UHC stated in an FAQ. “A UHC review of upper endoscopy and lower endoscopy procedures performed in 2022 revealed two- to fivefold practice-level variation in the use of both procedure types, even after adjusting for member characteristics including age and comorbidities.”
However, according to a statement from the AGA, it has not seen utilization data specific to UHC: “It is clear that UHC does not currently have any data indicating significant overutilization of critical colonoscopy and endoscopy procedures and therefore no justification to impose burdensome barriers like prior authorization.” AGA also pointed to research showing there is an unmet need for colonoscopies in the United States, which suggests there is an underutilization of this crucial procedure.
“AGA has expressed its willingness to work collaboratively with UnitedHealthcare to address any concerns and educate physicians, but communication and transparency with the insurer are nearly nonexistent. Instead, the GI community is confronted with a nebulous concept called advance notification, which is not conducive to seamless patient care. Ultimately, it appears advance notification will form the basis of prior authorization, which we know can delay, disrupt, and deny timely care,” Dr. Jung said.
How advance notification works
Beginning June 1, providers have been asked to provide advance notification for nonscreening GI endoscopy procedures that include: esophagogastroduodenoscopy, capsule endoscopy, diagnostic colonoscopy and surveillance colonoscopy. The notification can be made by phone (866-889-8054) or through a UHC online portal at UHCprovider.com.
The AGA has said that some GI practices have found the portal to be confusing and it lacks a standard software application raising concerns for high error rates.
Advance notification applies to patients who have UHC commercial plans, including UnitedHealthcare, UnitedHealthcare Plan of the River Valley, Neighborhood Health Partnership, UnitedHealthcare Level Funded, and UnitedHealthcare Oxford Health Plans in all states, except Rhode Island, Kentucky, and New Mexico.
Providers who opt out of participating in advance notification will not be eligible to participate in the Gold Card program in 2024. The program will essentially allow providers to order most GI endoscopy procedures, except for screening colonoscopy, without prior authorization. However, UHC has not released any information about how it will implement its planned Gold Card prior authorization program or how many providers will be accepted into the program.
UHC has assured providers it will not issue medical necessity denials through this process, but it may ask providers to participate in a “comprehensive peer-to-peer discussion with a board-certified gastroenterologist around clinical guidelines.”
The fear for practices is that advance notification will be an onerous process adding burdensome paperwork that practices are not equipped to manage. UHC is the largest health insurer in the country representing 46% of the total market.
Lawrence Kim, MD, AGAF, vice president of AGA and a gastroenterologist practicing in Denver said that each physician in his practice does over 1,000 procedures annually and 25% of their patients carry UHC.
“We are currently completing 30-40 notifications a day, requiring two staff members to comply with this program. UHC is not asking for any clinical information, just procedure and diagnosis codes, and in some cases site of service. Therefore, the advance notification program as it stands will not provide UHC with any additional information beyond what they already have through claims data. This highlights the strain these requirements are putting on providers and practices for repetitive data,” he said.
For more details about UHC’s advance notification program, UHC has prepared this FAQ. To learn more about AGA’s advocacy, visit www.gastro.org/UHC.
It’s been just over 1 month since UnitedHealthcare (UHC) launched its advance notification program requiring providers to record nonscreening colonoscopy and other gastroenterology procedures to be eligible for its 2024 Gold Card program.
The program, which will begin next year, may eliminate prior authorization requirements for providers who successfully complete the advance notification program this year. However, there is no guarantee that providers who complete the advance notification program will be enrolled in the Gold Card program, which means they would have to seek prior authorization for nonscreening procedures, according to the American Gastroenterological Association.
While UHC has provided some information about how advance notification works, there are many unanswered questions, said Barbara H. Jung, MD,AGAF, AGA president.
“UnitedHealthcare’s haphazard approach to rolling out a policy that will ultimately control patient access to critical, often lifesaving medical procedures are the opposite of what should be our common goal of expeditious access to essential care,” she said in a written statement.
The advance notification program was announced on June 1 when UHC said it was dropping its controversial prior authorization program, which was due to go into effect that day.
AGA is concerned that UHC’s advance notification program is merely a delay tactic because prior authorization may be required next year for providers who are not accepted into the Gold Card program. Providers who are not accepted into the program may face delays in administering procedures due to the need for prior authorizations. Thousands of endoscopies and colonoscopies could potentially be disrupted in the first month alone due to canceled procedures because of new prior authorization requirements, they said.
UHC has been trying to rein in health care costs by first considering prior authorizations for most gastrointestinal (GI) endoscopic procedures, except for screening colonoscopy, but ultimately adopting advance notification. Providers, UHC has said, don’t always follow evidence-based medicine treatment recommendations or they overutilize procedures. Their goal, according to a summary document it issued outlining changes to advance notification and prior authorization requirements, is “better care, improved health outcomes, and lower costs.”
“Clinical studies demonstrate overutilization of these procedures and lack of adherence to specialty society–endorsed guidelines and recommendations. Up to one-third of upper GI procedures and almost half of nonscreening colonoscopies performed for common clinical conditions are not consistent with clinical guidelines,” UHC stated in an FAQ. “A UHC review of upper endoscopy and lower endoscopy procedures performed in 2022 revealed two- to fivefold practice-level variation in the use of both procedure types, even after adjusting for member characteristics including age and comorbidities.”
However, according to a statement from the AGA, it has not seen utilization data specific to UHC: “It is clear that UHC does not currently have any data indicating significant overutilization of critical colonoscopy and endoscopy procedures and therefore no justification to impose burdensome barriers like prior authorization.” AGA also pointed to research showing there is an unmet need for colonoscopies in the United States, which suggests there is an underutilization of this crucial procedure.
“AGA has expressed its willingness to work collaboratively with UnitedHealthcare to address any concerns and educate physicians, but communication and transparency with the insurer are nearly nonexistent. Instead, the GI community is confronted with a nebulous concept called advance notification, which is not conducive to seamless patient care. Ultimately, it appears advance notification will form the basis of prior authorization, which we know can delay, disrupt, and deny timely care,” Dr. Jung said.
How advance notification works
Beginning June 1, providers have been asked to provide advance notification for nonscreening GI endoscopy procedures that include: esophagogastroduodenoscopy, capsule endoscopy, diagnostic colonoscopy and surveillance colonoscopy. The notification can be made by phone (866-889-8054) or through a UHC online portal at UHCprovider.com.
The AGA has said that some GI practices have found the portal to be confusing and it lacks a standard software application raising concerns for high error rates.
Advance notification applies to patients who have UHC commercial plans, including UnitedHealthcare, UnitedHealthcare Plan of the River Valley, Neighborhood Health Partnership, UnitedHealthcare Level Funded, and UnitedHealthcare Oxford Health Plans in all states, except Rhode Island, Kentucky, and New Mexico.
Providers who opt out of participating in advance notification will not be eligible to participate in the Gold Card program in 2024. The program will essentially allow providers to order most GI endoscopy procedures, except for screening colonoscopy, without prior authorization. However, UHC has not released any information about how it will implement its planned Gold Card prior authorization program or how many providers will be accepted into the program.
UHC has assured providers it will not issue medical necessity denials through this process, but it may ask providers to participate in a “comprehensive peer-to-peer discussion with a board-certified gastroenterologist around clinical guidelines.”
The fear for practices is that advance notification will be an onerous process adding burdensome paperwork that practices are not equipped to manage. UHC is the largest health insurer in the country representing 46% of the total market.
Lawrence Kim, MD, AGAF, vice president of AGA and a gastroenterologist practicing in Denver said that each physician in his practice does over 1,000 procedures annually and 25% of their patients carry UHC.
“We are currently completing 30-40 notifications a day, requiring two staff members to comply with this program. UHC is not asking for any clinical information, just procedure and diagnosis codes, and in some cases site of service. Therefore, the advance notification program as it stands will not provide UHC with any additional information beyond what they already have through claims data. This highlights the strain these requirements are putting on providers and practices for repetitive data,” he said.
For more details about UHC’s advance notification program, UHC has prepared this FAQ. To learn more about AGA’s advocacy, visit www.gastro.org/UHC.
Coffee’s brain-boosting effect goes beyond caffeine
“There is a widespread anticipation that coffee boosts alertness and psychomotor performance. By gaining a deeper understanding of the mechanisms underlying this biological phenomenon, we pave the way for investigating the factors that can influence it and even exploring the potential advantages of those mechanisms,” study investigator Nuno Sousa, MD, PhD, with the University of Minho, Braga, Portugal, said in a statement.
The study was published online in Frontiers in Behavioral Neuroscience.
Caffeine can’t take all the credit
Certain compounds in coffee, including caffeine and chlorogenic acids, have well-documented psychoactive effects, but the psychological impact of coffee/caffeine consumption as a whole remains a matter of debate.
The researchers investigated the neurobiological impact of coffee drinking on brain connectivity using resting-state functional MRI (fMRI).
They recruited 47 generally healthy adults (mean age, 30 years; 31 women) who regularly drank a minimum of one cup of coffee per day. Participants refrained from eating or drinking caffeinated beverages for at least 3 hours prior to undergoing fMRI.
To tease out the specific impact of caffeinated coffee intake, 30 habitual coffee drinkers (mean age, 32 years; 27 women) were given hot water containing the same amount of caffeine, but they were not given coffee.
The investigators conducted two fMRI scans – one before, and one 30 minutes after drinking coffee or caffeine-infused water.
Both drinking coffee and drinking plain caffeine in water led to a decrease in functional connectivity of the brain’s default mode network, which is typically active during self-reflection in resting states.
This finding suggests that consuming either coffee or caffeine heightened individuals’ readiness to transition from a state of rest to engaging in task-related activities, the researchers noted.
However, drinking a cup of coffee also boosted connectivity in the higher visual network and the right executive control network, which are linked to working memory, cognitive control, and goal-directed behavior – something that did not occur from drinking caffeinated water.
“Put simply, individuals exhibited a heightened state of preparedness, being more responsive and attentive to external stimuli after drinking coffee,” said first author Maria Picó-Pérez, PhD, with the University of Minho.
Given that some of the effects of coffee also occurred with caffeine alone, it’s “plausible to assume that other caffeinated beverages may share similar effects,” she added.
Still, certain effects were specific to coffee drinking, “likely influenced by factors such as the distinct aroma and taste of coffee or the psychological expectations associated with consuming this particular beverage,” the researcher wrote.
The investigators report that the observations could provide a scientific foundation for the common belief that coffee increases alertness and cognitive functioning. Further research is needed to differentiate the effects of caffeine from the overall experience of drinking coffee.
A limitation of the study is the absence of a nondrinker control sample (to rule out the withdrawal effect) or an alternative group that consumed decaffeinated coffee (to rule out the placebo effect of coffee intake) – something that should be considered in future studies, the researchers noted.
The study was funded by the Institute for the Scientific Information on Coffee. The authors declared no relevant conflicts of interest.
A version of this article originally appeared on Medscape.com.
“There is a widespread anticipation that coffee boosts alertness and psychomotor performance. By gaining a deeper understanding of the mechanisms underlying this biological phenomenon, we pave the way for investigating the factors that can influence it and even exploring the potential advantages of those mechanisms,” study investigator Nuno Sousa, MD, PhD, with the University of Minho, Braga, Portugal, said in a statement.
The study was published online in Frontiers in Behavioral Neuroscience.
Caffeine can’t take all the credit
Certain compounds in coffee, including caffeine and chlorogenic acids, have well-documented psychoactive effects, but the psychological impact of coffee/caffeine consumption as a whole remains a matter of debate.
The researchers investigated the neurobiological impact of coffee drinking on brain connectivity using resting-state functional MRI (fMRI).
They recruited 47 generally healthy adults (mean age, 30 years; 31 women) who regularly drank a minimum of one cup of coffee per day. Participants refrained from eating or drinking caffeinated beverages for at least 3 hours prior to undergoing fMRI.
To tease out the specific impact of caffeinated coffee intake, 30 habitual coffee drinkers (mean age, 32 years; 27 women) were given hot water containing the same amount of caffeine, but they were not given coffee.
The investigators conducted two fMRI scans – one before, and one 30 minutes after drinking coffee or caffeine-infused water.
Both drinking coffee and drinking plain caffeine in water led to a decrease in functional connectivity of the brain’s default mode network, which is typically active during self-reflection in resting states.
This finding suggests that consuming either coffee or caffeine heightened individuals’ readiness to transition from a state of rest to engaging in task-related activities, the researchers noted.
However, drinking a cup of coffee also boosted connectivity in the higher visual network and the right executive control network, which are linked to working memory, cognitive control, and goal-directed behavior – something that did not occur from drinking caffeinated water.
“Put simply, individuals exhibited a heightened state of preparedness, being more responsive and attentive to external stimuli after drinking coffee,” said first author Maria Picó-Pérez, PhD, with the University of Minho.
Given that some of the effects of coffee also occurred with caffeine alone, it’s “plausible to assume that other caffeinated beverages may share similar effects,” she added.
Still, certain effects were specific to coffee drinking, “likely influenced by factors such as the distinct aroma and taste of coffee or the psychological expectations associated with consuming this particular beverage,” the researcher wrote.
The investigators report that the observations could provide a scientific foundation for the common belief that coffee increases alertness and cognitive functioning. Further research is needed to differentiate the effects of caffeine from the overall experience of drinking coffee.
A limitation of the study is the absence of a nondrinker control sample (to rule out the withdrawal effect) or an alternative group that consumed decaffeinated coffee (to rule out the placebo effect of coffee intake) – something that should be considered in future studies, the researchers noted.
The study was funded by the Institute for the Scientific Information on Coffee. The authors declared no relevant conflicts of interest.
A version of this article originally appeared on Medscape.com.
“There is a widespread anticipation that coffee boosts alertness and psychomotor performance. By gaining a deeper understanding of the mechanisms underlying this biological phenomenon, we pave the way for investigating the factors that can influence it and even exploring the potential advantages of those mechanisms,” study investigator Nuno Sousa, MD, PhD, with the University of Minho, Braga, Portugal, said in a statement.
The study was published online in Frontiers in Behavioral Neuroscience.
Caffeine can’t take all the credit
Certain compounds in coffee, including caffeine and chlorogenic acids, have well-documented psychoactive effects, but the psychological impact of coffee/caffeine consumption as a whole remains a matter of debate.
The researchers investigated the neurobiological impact of coffee drinking on brain connectivity using resting-state functional MRI (fMRI).
They recruited 47 generally healthy adults (mean age, 30 years; 31 women) who regularly drank a minimum of one cup of coffee per day. Participants refrained from eating or drinking caffeinated beverages for at least 3 hours prior to undergoing fMRI.
To tease out the specific impact of caffeinated coffee intake, 30 habitual coffee drinkers (mean age, 32 years; 27 women) were given hot water containing the same amount of caffeine, but they were not given coffee.
The investigators conducted two fMRI scans – one before, and one 30 minutes after drinking coffee or caffeine-infused water.
Both drinking coffee and drinking plain caffeine in water led to a decrease in functional connectivity of the brain’s default mode network, which is typically active during self-reflection in resting states.
This finding suggests that consuming either coffee or caffeine heightened individuals’ readiness to transition from a state of rest to engaging in task-related activities, the researchers noted.
However, drinking a cup of coffee also boosted connectivity in the higher visual network and the right executive control network, which are linked to working memory, cognitive control, and goal-directed behavior – something that did not occur from drinking caffeinated water.
“Put simply, individuals exhibited a heightened state of preparedness, being more responsive and attentive to external stimuli after drinking coffee,” said first author Maria Picó-Pérez, PhD, with the University of Minho.
Given that some of the effects of coffee also occurred with caffeine alone, it’s “plausible to assume that other caffeinated beverages may share similar effects,” she added.
Still, certain effects were specific to coffee drinking, “likely influenced by factors such as the distinct aroma and taste of coffee or the psychological expectations associated with consuming this particular beverage,” the researcher wrote.
The investigators report that the observations could provide a scientific foundation for the common belief that coffee increases alertness and cognitive functioning. Further research is needed to differentiate the effects of caffeine from the overall experience of drinking coffee.
A limitation of the study is the absence of a nondrinker control sample (to rule out the withdrawal effect) or an alternative group that consumed decaffeinated coffee (to rule out the placebo effect of coffee intake) – something that should be considered in future studies, the researchers noted.
The study was funded by the Institute for the Scientific Information on Coffee. The authors declared no relevant conflicts of interest.
A version of this article originally appeared on Medscape.com.
FROM FRONTIERS IN BEHAVIORAL NEUROSCIENCE
Cardiorespiratory fitness linked to cancer risk, mortality?
TOPLINE:
a large Swedish cohort study suggests.
METHODOLOGY:
- A prospective cohort study included 177,709 Swedish men (mean age, 42; mean body mass index, 26 kg/m2) who completed an occupational health profile assessment and were followed for a mean of 9.6 years.
- CRF was assessed by determining maximal oxygen consumption during an aerobic fitness test, known as a submaximal Åstrand cycle ergometer test.
- Participants reported physical activity habits, lifestyle, and perceived health.
- Data on prostate, colon, and lung cancer incidence and mortality were derived from national registers.
- Outcomes from three higher CRF groups (low, > 25-35; moderate, > 35-45; high, > 45 mL/min per kg) were compared with those from the very low CRF group (25 mL/min per kg or less). Models were adjusted for various factors, including age, BMI, education, dietary habits, comorbidity, and smoking.
TAKEAWAY:
- During follow-up, investigators identified 1,918 prostate, 499 colon, and 283 lung cancer cases as well as 141 prostate, 207 lung, and 152 colon cancer deaths.
- In the fully adjusted model, higher CRF levels were associated with a significantly lower risk for colon cancer (hazard ratio, 0.72 for moderate; HR, 0.63 for high).
- In this model, higher CRF was also associated with a lower risk of death from prostate cancer (HR, 0.67 for low; HR, 0.57 for moderate; HR, 0.29 for high).
- For lung cancer mortality, only high CRF was associated with a significantly lower risk of death (HR, 0.41).
- An association between CRF and lung cancer incidence (HR, 0.99) and death (HR, 0.99) was only evident among adults aged 60 and older.
IN PRACTICE:
“The clinical implications of these findings further emphasize the importance of CRF for possibly reducing cancer incidence and mortality,” the authors concluded. “It is important for the general public to understand that higher-intensity [physical activity] has greater effects on CRF and is likely to be more protective against the risk of developing and dying from certain cancers.”
SOURCE:
The study was led by Elin Ekblom-Bak, PhD, from the Swedish School of Sport and Health Sciences, Stockholm. It was published online in JAMA Network Open.
LIMITATIONS:
The study was limited by voluntary participation, inclusion of only employed individuals, and estimations of CRF via submaximal tests. Data on smoking status were not optimal and there was a small number of cancer cases and deaths.
DISCLOSURES:
Funding was provided by the Swedish Cancer Society. The authors have reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
a large Swedish cohort study suggests.
METHODOLOGY:
- A prospective cohort study included 177,709 Swedish men (mean age, 42; mean body mass index, 26 kg/m2) who completed an occupational health profile assessment and were followed for a mean of 9.6 years.
- CRF was assessed by determining maximal oxygen consumption during an aerobic fitness test, known as a submaximal Åstrand cycle ergometer test.
- Participants reported physical activity habits, lifestyle, and perceived health.
- Data on prostate, colon, and lung cancer incidence and mortality were derived from national registers.
- Outcomes from three higher CRF groups (low, > 25-35; moderate, > 35-45; high, > 45 mL/min per kg) were compared with those from the very low CRF group (25 mL/min per kg or less). Models were adjusted for various factors, including age, BMI, education, dietary habits, comorbidity, and smoking.
TAKEAWAY:
- During follow-up, investigators identified 1,918 prostate, 499 colon, and 283 lung cancer cases as well as 141 prostate, 207 lung, and 152 colon cancer deaths.
- In the fully adjusted model, higher CRF levels were associated with a significantly lower risk for colon cancer (hazard ratio, 0.72 for moderate; HR, 0.63 for high).
- In this model, higher CRF was also associated with a lower risk of death from prostate cancer (HR, 0.67 for low; HR, 0.57 for moderate; HR, 0.29 for high).
- For lung cancer mortality, only high CRF was associated with a significantly lower risk of death (HR, 0.41).
- An association between CRF and lung cancer incidence (HR, 0.99) and death (HR, 0.99) was only evident among adults aged 60 and older.
IN PRACTICE:
“The clinical implications of these findings further emphasize the importance of CRF for possibly reducing cancer incidence and mortality,” the authors concluded. “It is important for the general public to understand that higher-intensity [physical activity] has greater effects on CRF and is likely to be more protective against the risk of developing and dying from certain cancers.”
SOURCE:
The study was led by Elin Ekblom-Bak, PhD, from the Swedish School of Sport and Health Sciences, Stockholm. It was published online in JAMA Network Open.
LIMITATIONS:
The study was limited by voluntary participation, inclusion of only employed individuals, and estimations of CRF via submaximal tests. Data on smoking status were not optimal and there was a small number of cancer cases and deaths.
DISCLOSURES:
Funding was provided by the Swedish Cancer Society. The authors have reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
a large Swedish cohort study suggests.
METHODOLOGY:
- A prospective cohort study included 177,709 Swedish men (mean age, 42; mean body mass index, 26 kg/m2) who completed an occupational health profile assessment and were followed for a mean of 9.6 years.
- CRF was assessed by determining maximal oxygen consumption during an aerobic fitness test, known as a submaximal Åstrand cycle ergometer test.
- Participants reported physical activity habits, lifestyle, and perceived health.
- Data on prostate, colon, and lung cancer incidence and mortality were derived from national registers.
- Outcomes from three higher CRF groups (low, > 25-35; moderate, > 35-45; high, > 45 mL/min per kg) were compared with those from the very low CRF group (25 mL/min per kg or less). Models were adjusted for various factors, including age, BMI, education, dietary habits, comorbidity, and smoking.
TAKEAWAY:
- During follow-up, investigators identified 1,918 prostate, 499 colon, and 283 lung cancer cases as well as 141 prostate, 207 lung, and 152 colon cancer deaths.
- In the fully adjusted model, higher CRF levels were associated with a significantly lower risk for colon cancer (hazard ratio, 0.72 for moderate; HR, 0.63 for high).
- In this model, higher CRF was also associated with a lower risk of death from prostate cancer (HR, 0.67 for low; HR, 0.57 for moderate; HR, 0.29 for high).
- For lung cancer mortality, only high CRF was associated with a significantly lower risk of death (HR, 0.41).
- An association between CRF and lung cancer incidence (HR, 0.99) and death (HR, 0.99) was only evident among adults aged 60 and older.
IN PRACTICE:
“The clinical implications of these findings further emphasize the importance of CRF for possibly reducing cancer incidence and mortality,” the authors concluded. “It is important for the general public to understand that higher-intensity [physical activity] has greater effects on CRF and is likely to be more protective against the risk of developing and dying from certain cancers.”
SOURCE:
The study was led by Elin Ekblom-Bak, PhD, from the Swedish School of Sport and Health Sciences, Stockholm. It was published online in JAMA Network Open.
LIMITATIONS:
The study was limited by voluntary participation, inclusion of only employed individuals, and estimations of CRF via submaximal tests. Data on smoking status were not optimal and there was a small number of cancer cases and deaths.
DISCLOSURES:
Funding was provided by the Swedish Cancer Society. The authors have reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
New and transitioning gastroenterologists face burnout too
The field of gastroenterology can be challenging, both professionally and personally, leading to burnout, especially for new and transitioning gastroenterologists. Burnout is a state of emotional, physical, and mental exhaustion caused by prolonged or excessive stress.1 It is characterized by emotional fatigue, depersonalization, and a reduced sense of personal accomplishment.2,3 This condition can have severe consequences for physicians and their patients.
More than 50% of physicians report meeting the criteria for burnout, which is pervasive in all medical professions.3 Survey results of 7,288 U.S. physicians showed that burnout and dissatisfaction with work-life balance are significantly higher than among other working U.S. adults.3

The long and often irregular work hours expected of gastroenterologists significantly contribute to burnout within our field. The physically, intellectually, and technically demanding reality of managing complex patients and making high stakes decisions at all hours has far-reaching consequences.3 Most gastroenterologists work between 55 and 60 hours per week.4 This sharply contrasts the average 43-hour work week for full-time employees in the United States.5 Gastroenterologists may experience inaccurate perceptions of their commitment to patients, education, and their families based solely on time observed on each activity.4 Higher education and professional degrees usually protect against burnout.3 However, a degree in medicine (MD or DO) increases the burnout risk.3
New gastroenterologists are learning a wide range of intricate procedures and becoming proficient in diagnosing and managing gastrointestinal disorders. Extensive career demands often coincide with intense family-forming years, creating tension for a physician’s finite time and energy. The culture of medicine demanding “patients come first” while attempting to be fully human can sometimes feel irreconcilable, leading to feelings of inadequacy and anxiety.3 Gastroenterology training takes 3 years because of the complexity, danger, and need for thousands of procedures to gain proficiency and competence to recognize when complications occur. Oversight is ubiquitous during training, making this the ideal time to learn from mistakes and formulate lifelong habits of constant improvement. However, perfectionist tendencies and the Hippocratic Oath can create unrealistic self expectations.6 The risk of potential litigation, simply missing a diagnosis, or causing actual patient harm is never far from a proceduralist’s mind.

The diversity of gastroenterology requires high clinical knowledge, expertise, and emotional intelligence. Leading potentially intense end-of-life, cancer, fertility, and risk-factor discussions can be all-consuming. Keeping up with the latest research, treatments, and techniques in the field can be daunting. Furthermore, gastroenterologists spend many hours each day on electronic medical records. Constant re-documentation of interactions, seemingly endless prior authorizations, disability forms, referrals, and simply re-addressing patient and family concerns can feel low value. This uncompensated work also creates moral injury as it takes away from direct patient care.
Striking a work-life balance
New gastroenterologists are advised to find work-life balance. However, they are also plagued by the massive professional demands being constantly placed on them. The desire to find the mythical “balance” may create a mindset of significant sacrifices in their private lives as the only way to achieve professional successes.7 When gastroenterologists do not prioritize time for personal activities, including exercise, health checks, hobbies, rest, relaxation, family, and friends, they can get caught in a vicious cycle of continuing to feel poorly, resulting in overcompensating by working more in order to feel “accomplished.” The perfectionist pressure to maintain high productivity and patient satisfaction can also further contribute to burnout.

Gastroenterology burnout can severely affect physicians’ health status, job performance, and patient satisfaction.9 It may erode professionalism, negatively influence the quality of care, increase the risk of medical errors, and promote early retirement.3 Burnout may also correlate with adverse personal consequences for physicians, such as broken relationships, problematic alcohol use, and suicidal ideation.3 Physician burnout and professional satisfaction have strategic importance to health care organizations.10 Less burned-out physicians have patient panels with higher adherence and satisfaction with medical care.10 With more physicians becoming employees, there are opportunities for accountability of organizational leadership.10 Interestingly, healthy well-being or burnout is contagious from leaders to their teams.10 A 2015 study by Shanafelt et al. found that at the work unit level, 11% and 47% of the variation in burnout and satisfaction, correlated with the leader’s relative scores.10
So, what can be done to prevent and treat burnout in new and transitioning gastroenterologists? The gastroenterologist may implement several strategies. It is essential for individuals to take responsibility for their well-being and to prioritize self-care by setting boundaries, practicing stress management techniques, and seeking support from colleagues and mental health professionals when needed. 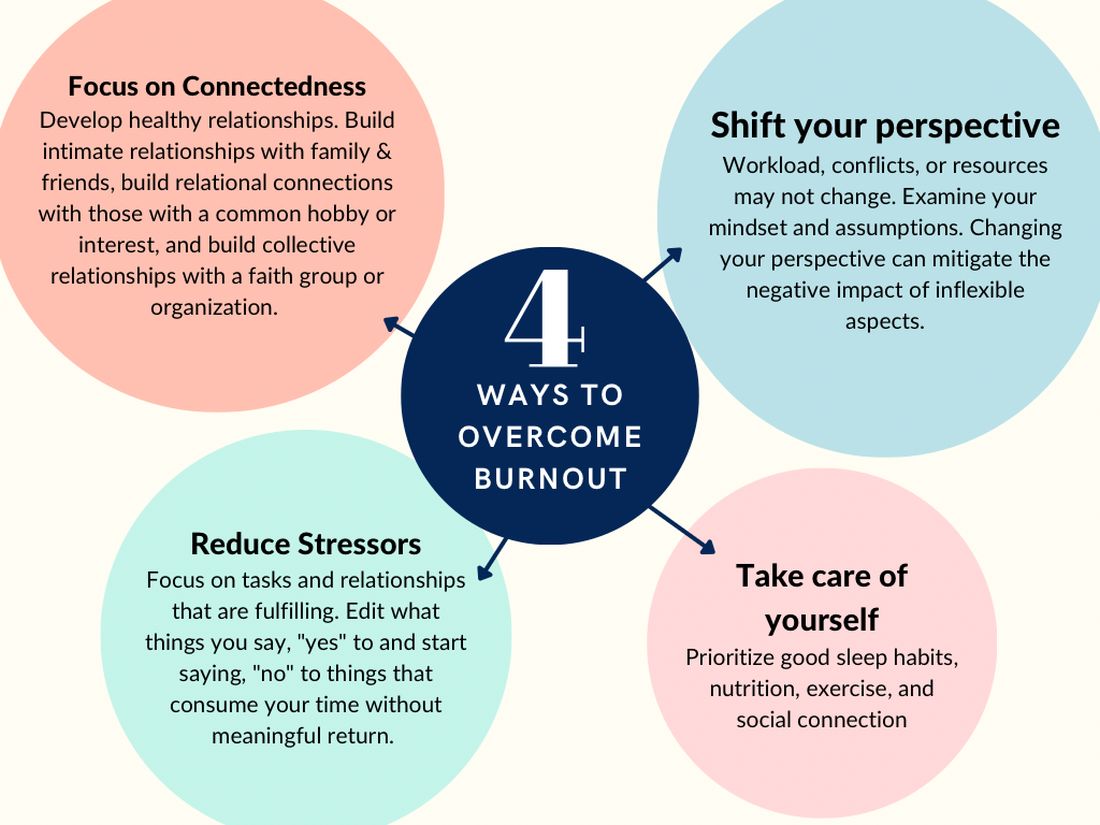
According to Dave et al. (2020), engagement in self-care practices such as mindfulness may offer advantages to gastroenterologists’ well-being and improved patient care.11
Burnout is not due to an individuals’ need for more resiliency. Instead, it developed from a systemic overwhelming of a health system near its breaking point. Recognizing that by 2033, there is a projected shortage of nearly 140,000 physicians in the United States, the U.S. Surgeon General, Dr. Vivek H. Murthy, issued a crisis advisory.12 This advisory highlights the urgent need to address the health worker burnout crisis nationwide that outlined “whole of society” efforts.12 Key components of the advisory on building a thriving health workforce included empowering health care workers, changing policies, reducing administrative burdens, prioritizing connections, and investing in our workforce.12
Provide access to mental health services
Institutions and practices would greatly benefit from providing access to mental health services, counseling, educational opportunities, potential mental health days, and mentorship programs. While the literature indicates that both individual-focused and structural or organizational strategies can result in clinically meaningful reductions in burnout among physicians, a meta-analysis revealed that corporate-led initiatives resulted in larger successes.12,13 Physicians who received support and resources from their institutions report lower levels of burnout and higher job satisfaction.2,3
New strategies to select and develop physician leaders who motivate, inspire, and effectively manage physicians may result in positive job satisfaction while decreasing employee burnout. Therefore, increased awareness of the importance of frontline leadership well-being and professional fulfillment of physicians working for a large health care organization is necessary.13 Robust and continual leadership training can ensure the entire team’s well-being, longevity, and success.13
Addressing the root causes of systemic burnout is imperative. Leadership could streamline administrative processes, optimize electronic medical records, delegate prior authorizations, and ensure staffing levels are appropriate to meet patient care demands. In a survey by Rao et al. (2017), the authors found that physicians who reported high levels of administrative burden and work overload were more likely to experience burnout.14
Institutions and practices should promote a culture of work-life balance by implementing flexible scheduling, promoting time off and vacation time, and encouraging regular exercise and healthy habits. The current compensation structure disincentivizes physicians from taking time away from patient care – this can be re-designed. Community and support mitigate burnout. Therefore, institutions and practices will benefit by intentionally providing opportunities for social connection and team building.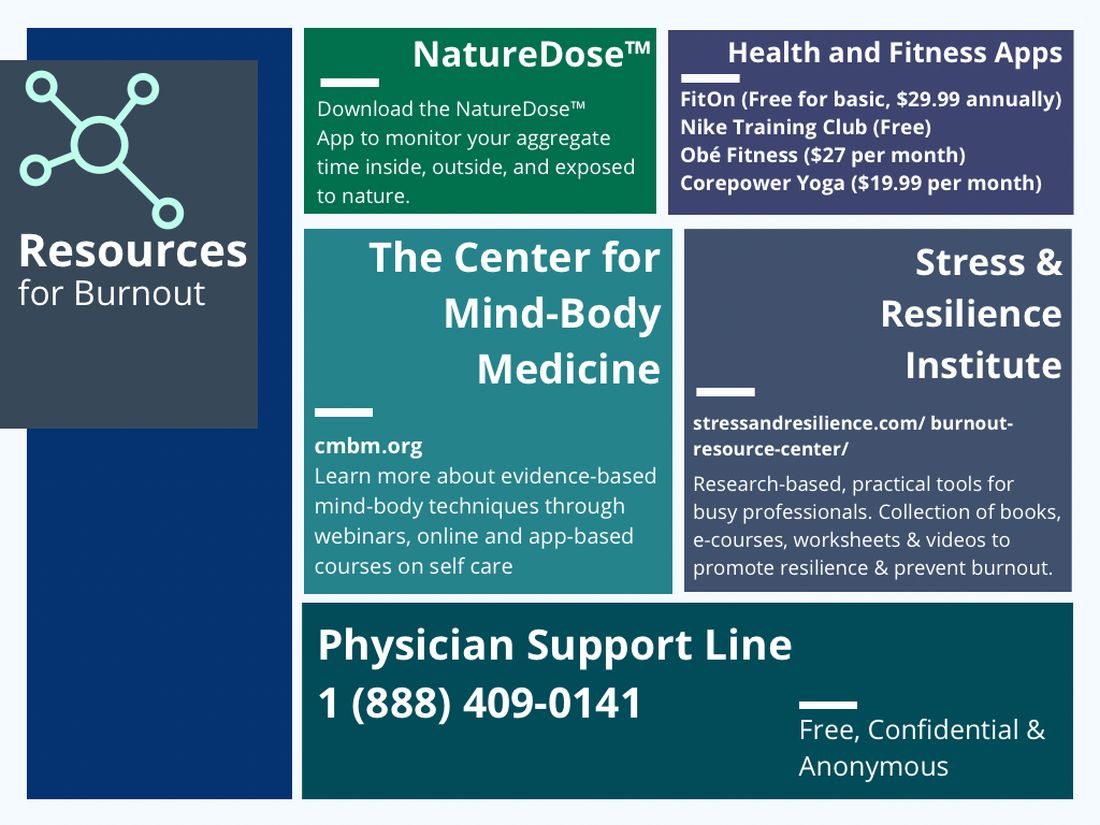
In reflection of the U.S. Surgeon General’s call for all of society to be part of the solution, we are pleased to see the Accreditation Council for Graduate Medical Education (ACGME) create mandatory 6 weeks of parental or caregiver leave for trainees.15 Continued positive pressure on overseeing agencies to minimize paperwork, preauthorizations, and non–value-added tasks to allow physicians to continue to provide medical services instead of documentation and auditing services would greatly positively impact all of health care. Therefore, communicating with legislators, policy makers, system leadership, and all health care societies to continue these improvements would be a wise use of time of resources.
In conclusion, burnout among new and transitioning gastroenterologists is a prevalent and concerning issue that can have severe consequences for both the individual and the health care system. Similar to the ergonomic considerations of being an endoscopist, A multifaceted approach to the well-being of all medical staff can help ensure the delivery of the highest quality patient care. By taking a proactive approach to preventing burnout, we can have a strong future for ourselves, our patients, and our profession.
Dr. Eboh is a gastroenterologist with Atrium Health, Charlotte, N.C.; Dr. Jaeger is with Baylor Scott & White Medical Center in Dallas. She is a gastroenterology fellow with Temple University Hospital, Philadelphia. Dr. Sears is clinical professor at Texas A&M University School of Medicine, and chief of gastroenterology at VA Central Texas Healthcare System. Dr. Sears owns GutGirlMD Consulting LLC, where she offers institutional and leadership coaching for physicians. Dr. Eboh on Instagram @Polyp.picker_EbohMD and on Twitter @PolypPicker_MD. Dr. Jaeger on Instagram @Doc.Tori.Fit and Twitter @DrToriJaeger. Dr. Sears is on Twitter @GutGirlMD.
References
1. Maslach C and Jackson S E. Maslach burnout inventory manual. Palo Alto, Calif: Consulting Psychologists Press, 1986.
2. Shanafelt TD et al. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014. Mayo Clin Proc. 2015 Dec 12;90:1600-13.
3. Shanafelt TD et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012 Oct 8;172(18):1377-85.
4. Elta G. The challenges of being a female gastroenterologist. Gastroenterol Clin North Am. 2011 Jun;40(2):441-7.
5. Gallup. Work and Workplace. 2023.
6. Gawande A. When doctors make mistakes. The New Yorker. 1999 Feb 1.
7. Buscarini E et al. Burnout among gastroenterologists: How to manage and prevent it. United European Gastroenterol J. 2020 Aug;8(7):832-4.
8. West CP et al. Interventions to prevent and reduce physician burnout: A systematic review and meta-analysis. Lancet. 2016 Nov 5;388(10057):2272-81.
9. Adarkwah CC et al. Burnout and work satisfaction are differentially associated in gastroenterologists in Germany. F1000Res. 2022 Mar 30;11:368. doi: 10.12688/f1000research.110296.3. eCollection 2022.
10. Shanafelt TD et al. Impact of organizational leadership on physician burnout and satisfaction. Mayo Clin Proc. 2015 Apr;90(4):432-40.
11. Umakant D et al. Mindfulness in gastroenterology training and practice: A personal perspective. Clin Exp Gastroenterol. 2020 Nov 4;13:497-502.
12. Murthy VH. Addressing Health Worker Burnout: The U.S. Surgeon General’s Advisory on Building a Thriving Health Workforce. The U.S. Department of Health and Human Services: Office of the U.S. Surgeon General, 2022.
13. Panagioti M et al. Controlled interventions to reduce burnout in physicians: A systematic review and meta-analysis. JAMA Intern Med. 2017 Feb 1;177(2):195-205.
14. Rao SK et al. The impact of administrative burden on academic physicians: Results of a hospital-wide physician survey. Acad Med. 2017 Feb;92(2):237-43.
15. ACGME. ACME Institutional Requirements 2021.
The field of gastroenterology can be challenging, both professionally and personally, leading to burnout, especially for new and transitioning gastroenterologists. Burnout is a state of emotional, physical, and mental exhaustion caused by prolonged or excessive stress.1 It is characterized by emotional fatigue, depersonalization, and a reduced sense of personal accomplishment.2,3 This condition can have severe consequences for physicians and their patients.
More than 50% of physicians report meeting the criteria for burnout, which is pervasive in all medical professions.3 Survey results of 7,288 U.S. physicians showed that burnout and dissatisfaction with work-life balance are significantly higher than among other working U.S. adults.3
The long and often irregular work hours expected of gastroenterologists significantly contribute to burnout within our field. The physically, intellectually, and technically demanding reality of managing complex patients and making high stakes decisions at all hours has far-reaching consequences.3 Most gastroenterologists work between 55 and 60 hours per week.4 This sharply contrasts the average 43-hour work week for full-time employees in the United States.5 Gastroenterologists may experience inaccurate perceptions of their commitment to patients, education, and their families based solely on time observed on each activity.4 Higher education and professional degrees usually protect against burnout.3 However, a degree in medicine (MD or DO) increases the burnout risk.3
New gastroenterologists are learning a wide range of intricate procedures and becoming proficient in diagnosing and managing gastrointestinal disorders. Extensive career demands often coincide with intense family-forming years, creating tension for a physician’s finite time and energy. The culture of medicine demanding “patients come first” while attempting to be fully human can sometimes feel irreconcilable, leading to feelings of inadequacy and anxiety.3 Gastroenterology training takes 3 years because of the complexity, danger, and need for thousands of procedures to gain proficiency and competence to recognize when complications occur. Oversight is ubiquitous during training, making this the ideal time to learn from mistakes and formulate lifelong habits of constant improvement. However, perfectionist tendencies and the Hippocratic Oath can create unrealistic self expectations.6 The risk of potential litigation, simply missing a diagnosis, or causing actual patient harm is never far from a proceduralist’s mind.
The diversity of gastroenterology requires high clinical knowledge, expertise, and emotional intelligence. Leading potentially intense end-of-life, cancer, fertility, and risk-factor discussions can be all-consuming. Keeping up with the latest research, treatments, and techniques in the field can be daunting. Furthermore, gastroenterologists spend many hours each day on electronic medical records. Constant re-documentation of interactions, seemingly endless prior authorizations, disability forms, referrals, and simply re-addressing patient and family concerns can feel low value. This uncompensated work also creates moral injury as it takes away from direct patient care.
Striking a work-life balance
New gastroenterologists are advised to find work-life balance. However, they are also plagued by the massive professional demands being constantly placed on them. The desire to find the mythical “balance” may create a mindset of significant sacrifices in their private lives as the only way to achieve professional successes.7 When gastroenterologists do not prioritize time for personal activities, including exercise, health checks, hobbies, rest, relaxation, family, and friends, they can get caught in a vicious cycle of continuing to feel poorly, resulting in overcompensating by working more in order to feel “accomplished.” The perfectionist pressure to maintain high productivity and patient satisfaction can also further contribute to burnout.
Gastroenterology burnout can severely affect physicians’ health status, job performance, and patient satisfaction.9 It may erode professionalism, negatively influence the quality of care, increase the risk of medical errors, and promote early retirement.3 Burnout may also correlate with adverse personal consequences for physicians, such as broken relationships, problematic alcohol use, and suicidal ideation.3 Physician burnout and professional satisfaction have strategic importance to health care organizations.10 Less burned-out physicians have patient panels with higher adherence and satisfaction with medical care.10 With more physicians becoming employees, there are opportunities for accountability of organizational leadership.10 Interestingly, healthy well-being or burnout is contagious from leaders to their teams.10 A 2015 study by Shanafelt et al. found that at the work unit level, 11% and 47% of the variation in burnout and satisfaction, correlated with the leader’s relative scores.10
So, what can be done to prevent and treat burnout in new and transitioning gastroenterologists? The gastroenterologist may implement several strategies. It is essential for individuals to take responsibility for their well-being and to prioritize self-care by setting boundaries, practicing stress management techniques, and seeking support from colleagues and mental health professionals when needed.
According to Dave et al. (2020), engagement in self-care practices such as mindfulness may offer advantages to gastroenterologists’ well-being and improved patient care.11
Burnout is not due to an individuals’ need for more resiliency. Instead, it developed from a systemic overwhelming of a health system near its breaking point. Recognizing that by 2033, there is a projected shortage of nearly 140,000 physicians in the United States, the U.S. Surgeon General, Dr. Vivek H. Murthy, issued a crisis advisory.12 This advisory highlights the urgent need to address the health worker burnout crisis nationwide that outlined “whole of society” efforts.12 Key components of the advisory on building a thriving health workforce included empowering health care workers, changing policies, reducing administrative burdens, prioritizing connections, and investing in our workforce.12
Provide access to mental health services
Institutions and practices would greatly benefit from providing access to mental health services, counseling, educational opportunities, potential mental health days, and mentorship programs. While the literature indicates that both individual-focused and structural or organizational strategies can result in clinically meaningful reductions in burnout among physicians, a meta-analysis revealed that corporate-led initiatives resulted in larger successes.12,13 Physicians who received support and resources from their institutions report lower levels of burnout and higher job satisfaction.2,3
New strategies to select and develop physician leaders who motivate, inspire, and effectively manage physicians may result in positive job satisfaction while decreasing employee burnout. Therefore, increased awareness of the importance of frontline leadership well-being and professional fulfillment of physicians working for a large health care organization is necessary.13 Robust and continual leadership training can ensure the entire team’s well-being, longevity, and success.13
Addressing the root causes of systemic burnout is imperative. Leadership could streamline administrative processes, optimize electronic medical records, delegate prior authorizations, and ensure staffing levels are appropriate to meet patient care demands. In a survey by Rao et al. (2017), the authors found that physicians who reported high levels of administrative burden and work overload were more likely to experience burnout.14
Institutions and practices should promote a culture of work-life balance by implementing flexible scheduling, promoting time off and vacation time, and encouraging regular exercise and healthy habits. The current compensation structure disincentivizes physicians from taking time away from patient care – this can be re-designed. Community and support mitigate burnout. Therefore, institutions and practices will benefit by intentionally providing opportunities for social connection and team building.
In reflection of the U.S. Surgeon General’s call for all of society to be part of the solution, we are pleased to see the Accreditation Council for Graduate Medical Education (ACGME) create mandatory 6 weeks of parental or caregiver leave for trainees.15 Continued positive pressure on overseeing agencies to minimize paperwork, preauthorizations, and non–value-added tasks to allow physicians to continue to provide medical services instead of documentation and auditing services would greatly positively impact all of health care. Therefore, communicating with legislators, policy makers, system leadership, and all health care societies to continue these improvements would be a wise use of time of resources.
In conclusion, burnout among new and transitioning gastroenterologists is a prevalent and concerning issue that can have severe consequences for both the individual and the health care system. Similar to the ergonomic considerations of being an endoscopist, A multifaceted approach to the well-being of all medical staff can help ensure the delivery of the highest quality patient care. By taking a proactive approach to preventing burnout, we can have a strong future for ourselves, our patients, and our profession.
Dr. Eboh is a gastroenterologist with Atrium Health, Charlotte, N.C.; Dr. Jaeger is with Baylor Scott & White Medical Center in Dallas. She is a gastroenterology fellow with Temple University Hospital, Philadelphia. Dr. Sears is clinical professor at Texas A&M University School of Medicine, and chief of gastroenterology at VA Central Texas Healthcare System. Dr. Sears owns GutGirlMD Consulting LLC, where she offers institutional and leadership coaching for physicians. Dr. Eboh on Instagram @Polyp.picker_EbohMD and on Twitter @PolypPicker_MD. Dr. Jaeger on Instagram @Doc.Tori.Fit and Twitter @DrToriJaeger. Dr. Sears is on Twitter @GutGirlMD.
References
1. Maslach C and Jackson S E. Maslach burnout inventory manual. Palo Alto, Calif: Consulting Psychologists Press, 1986.
2. Shanafelt TD et al. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014. Mayo Clin Proc. 2015 Dec 12;90:1600-13.
3. Shanafelt TD et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012 Oct 8;172(18):1377-85.
4. Elta G. The challenges of being a female gastroenterologist. Gastroenterol Clin North Am. 2011 Jun;40(2):441-7.
5. Gallup. Work and Workplace. 2023.
6. Gawande A. When doctors make mistakes. The New Yorker. 1999 Feb 1.
7. Buscarini E et al. Burnout among gastroenterologists: How to manage and prevent it. United European Gastroenterol J. 2020 Aug;8(7):832-4.
8. West CP et al. Interventions to prevent and reduce physician burnout: A systematic review and meta-analysis. Lancet. 2016 Nov 5;388(10057):2272-81.
9. Adarkwah CC et al. Burnout and work satisfaction are differentially associated in gastroenterologists in Germany. F1000Res. 2022 Mar 30;11:368. doi: 10.12688/f1000research.110296.3. eCollection 2022.
10. Shanafelt TD et al. Impact of organizational leadership on physician burnout and satisfaction. Mayo Clin Proc. 2015 Apr;90(4):432-40.
11. Umakant D et al. Mindfulness in gastroenterology training and practice: A personal perspective. Clin Exp Gastroenterol. 2020 Nov 4;13:497-502.
12. Murthy VH. Addressing Health Worker Burnout: The U.S. Surgeon General’s Advisory on Building a Thriving Health Workforce. The U.S. Department of Health and Human Services: Office of the U.S. Surgeon General, 2022.
13. Panagioti M et al. Controlled interventions to reduce burnout in physicians: A systematic review and meta-analysis. JAMA Intern Med. 2017 Feb 1;177(2):195-205.
14. Rao SK et al. The impact of administrative burden on academic physicians: Results of a hospital-wide physician survey. Acad Med. 2017 Feb;92(2):237-43.
15. ACGME. ACME Institutional Requirements 2021.
The field of gastroenterology can be challenging, both professionally and personally, leading to burnout, especially for new and transitioning gastroenterologists. Burnout is a state of emotional, physical, and mental exhaustion caused by prolonged or excessive stress.1 It is characterized by emotional fatigue, depersonalization, and a reduced sense of personal accomplishment.2,3 This condition can have severe consequences for physicians and their patients.
More than 50% of physicians report meeting the criteria for burnout, which is pervasive in all medical professions.3 Survey results of 7,288 U.S. physicians showed that burnout and dissatisfaction with work-life balance are significantly higher than among other working U.S. adults.3
The long and often irregular work hours expected of gastroenterologists significantly contribute to burnout within our field. The physically, intellectually, and technically demanding reality of managing complex patients and making high stakes decisions at all hours has far-reaching consequences.3 Most gastroenterologists work between 55 and 60 hours per week.4 This sharply contrasts the average 43-hour work week for full-time employees in the United States.5 Gastroenterologists may experience inaccurate perceptions of their commitment to patients, education, and their families based solely on time observed on each activity.4 Higher education and professional degrees usually protect against burnout.3 However, a degree in medicine (MD or DO) increases the burnout risk.3
New gastroenterologists are learning a wide range of intricate procedures and becoming proficient in diagnosing and managing gastrointestinal disorders. Extensive career demands often coincide with intense family-forming years, creating tension for a physician’s finite time and energy. The culture of medicine demanding “patients come first” while attempting to be fully human can sometimes feel irreconcilable, leading to feelings of inadequacy and anxiety.3 Gastroenterology training takes 3 years because of the complexity, danger, and need for thousands of procedures to gain proficiency and competence to recognize when complications occur. Oversight is ubiquitous during training, making this the ideal time to learn from mistakes and formulate lifelong habits of constant improvement. However, perfectionist tendencies and the Hippocratic Oath can create unrealistic self expectations.6 The risk of potential litigation, simply missing a diagnosis, or causing actual patient harm is never far from a proceduralist’s mind.
The diversity of gastroenterology requires high clinical knowledge, expertise, and emotional intelligence. Leading potentially intense end-of-life, cancer, fertility, and risk-factor discussions can be all-consuming. Keeping up with the latest research, treatments, and techniques in the field can be daunting. Furthermore, gastroenterologists spend many hours each day on electronic medical records. Constant re-documentation of interactions, seemingly endless prior authorizations, disability forms, referrals, and simply re-addressing patient and family concerns can feel low value. This uncompensated work also creates moral injury as it takes away from direct patient care.
Striking a work-life balance
New gastroenterologists are advised to find work-life balance. However, they are also plagued by the massive professional demands being constantly placed on them. The desire to find the mythical “balance” may create a mindset of significant sacrifices in their private lives as the only way to achieve professional successes.7 When gastroenterologists do not prioritize time for personal activities, including exercise, health checks, hobbies, rest, relaxation, family, and friends, they can get caught in a vicious cycle of continuing to feel poorly, resulting in overcompensating by working more in order to feel “accomplished.” The perfectionist pressure to maintain high productivity and patient satisfaction can also further contribute to burnout.
Gastroenterology burnout can severely affect physicians’ health status, job performance, and patient satisfaction.9 It may erode professionalism, negatively influence the quality of care, increase the risk of medical errors, and promote early retirement.3 Burnout may also correlate with adverse personal consequences for physicians, such as broken relationships, problematic alcohol use, and suicidal ideation.3 Physician burnout and professional satisfaction have strategic importance to health care organizations.10 Less burned-out physicians have patient panels with higher adherence and satisfaction with medical care.10 With more physicians becoming employees, there are opportunities for accountability of organizational leadership.10 Interestingly, healthy well-being or burnout is contagious from leaders to their teams.10 A 2015 study by Shanafelt et al. found that at the work unit level, 11% and 47% of the variation in burnout and satisfaction, correlated with the leader’s relative scores.10
So, what can be done to prevent and treat burnout in new and transitioning gastroenterologists? The gastroenterologist may implement several strategies. It is essential for individuals to take responsibility for their well-being and to prioritize self-care by setting boundaries, practicing stress management techniques, and seeking support from colleagues and mental health professionals when needed.
According to Dave et al. (2020), engagement in self-care practices such as mindfulness may offer advantages to gastroenterologists’ well-being and improved patient care.11
Burnout is not due to an individuals’ need for more resiliency. Instead, it developed from a systemic overwhelming of a health system near its breaking point. Recognizing that by 2033, there is a projected shortage of nearly 140,000 physicians in the United States, the U.S. Surgeon General, Dr. Vivek H. Murthy, issued a crisis advisory.12 This advisory highlights the urgent need to address the health worker burnout crisis nationwide that outlined “whole of society” efforts.12 Key components of the advisory on building a thriving health workforce included empowering health care workers, changing policies, reducing administrative burdens, prioritizing connections, and investing in our workforce.12
Provide access to mental health services
Institutions and practices would greatly benefit from providing access to mental health services, counseling, educational opportunities, potential mental health days, and mentorship programs. While the literature indicates that both individual-focused and structural or organizational strategies can result in clinically meaningful reductions in burnout among physicians, a meta-analysis revealed that corporate-led initiatives resulted in larger successes.12,13 Physicians who received support and resources from their institutions report lower levels of burnout and higher job satisfaction.2,3
New strategies to select and develop physician leaders who motivate, inspire, and effectively manage physicians may result in positive job satisfaction while decreasing employee burnout. Therefore, increased awareness of the importance of frontline leadership well-being and professional fulfillment of physicians working for a large health care organization is necessary.13 Robust and continual leadership training can ensure the entire team’s well-being, longevity, and success.13
Addressing the root causes of systemic burnout is imperative. Leadership could streamline administrative processes, optimize electronic medical records, delegate prior authorizations, and ensure staffing levels are appropriate to meet patient care demands. In a survey by Rao et al. (2017), the authors found that physicians who reported high levels of administrative burden and work overload were more likely to experience burnout.14
Institutions and practices should promote a culture of work-life balance by implementing flexible scheduling, promoting time off and vacation time, and encouraging regular exercise and healthy habits. The current compensation structure disincentivizes physicians from taking time away from patient care – this can be re-designed. Community and support mitigate burnout. Therefore, institutions and practices will benefit by intentionally providing opportunities for social connection and team building.
In reflection of the U.S. Surgeon General’s call for all of society to be part of the solution, we are pleased to see the Accreditation Council for Graduate Medical Education (ACGME) create mandatory 6 weeks of parental or caregiver leave for trainees.15 Continued positive pressure on overseeing agencies to minimize paperwork, preauthorizations, and non–value-added tasks to allow physicians to continue to provide medical services instead of documentation and auditing services would greatly positively impact all of health care. Therefore, communicating with legislators, policy makers, system leadership, and all health care societies to continue these improvements would be a wise use of time of resources.
In conclusion, burnout among new and transitioning gastroenterologists is a prevalent and concerning issue that can have severe consequences for both the individual and the health care system. Similar to the ergonomic considerations of being an endoscopist, A multifaceted approach to the well-being of all medical staff can help ensure the delivery of the highest quality patient care. By taking a proactive approach to preventing burnout, we can have a strong future for ourselves, our patients, and our profession.
Dr. Eboh is a gastroenterologist with Atrium Health, Charlotte, N.C.; Dr. Jaeger is with Baylor Scott & White Medical Center in Dallas. She is a gastroenterology fellow with Temple University Hospital, Philadelphia. Dr. Sears is clinical professor at Texas A&M University School of Medicine, and chief of gastroenterology at VA Central Texas Healthcare System. Dr. Sears owns GutGirlMD Consulting LLC, where she offers institutional and leadership coaching for physicians. Dr. Eboh on Instagram @Polyp.picker_EbohMD and on Twitter @PolypPicker_MD. Dr. Jaeger on Instagram @Doc.Tori.Fit and Twitter @DrToriJaeger. Dr. Sears is on Twitter @GutGirlMD.
References
1. Maslach C and Jackson S E. Maslach burnout inventory manual. Palo Alto, Calif: Consulting Psychologists Press, 1986.
2. Shanafelt TD et al. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014. Mayo Clin Proc. 2015 Dec 12;90:1600-13.
3. Shanafelt TD et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012 Oct 8;172(18):1377-85.
4. Elta G. The challenges of being a female gastroenterologist. Gastroenterol Clin North Am. 2011 Jun;40(2):441-7.
5. Gallup. Work and Workplace. 2023.
6. Gawande A. When doctors make mistakes. The New Yorker. 1999 Feb 1.
7. Buscarini E et al. Burnout among gastroenterologists: How to manage and prevent it. United European Gastroenterol J. 2020 Aug;8(7):832-4.
8. West CP et al. Interventions to prevent and reduce physician burnout: A systematic review and meta-analysis. Lancet. 2016 Nov 5;388(10057):2272-81.
9. Adarkwah CC et al. Burnout and work satisfaction are differentially associated in gastroenterologists in Germany. F1000Res. 2022 Mar 30;11:368. doi: 10.12688/f1000research.110296.3. eCollection 2022.
10. Shanafelt TD et al. Impact of organizational leadership on physician burnout and satisfaction. Mayo Clin Proc. 2015 Apr;90(4):432-40.
11. Umakant D et al. Mindfulness in gastroenterology training and practice: A personal perspective. Clin Exp Gastroenterol. 2020 Nov 4;13:497-502.
12. Murthy VH. Addressing Health Worker Burnout: The U.S. Surgeon General’s Advisory on Building a Thriving Health Workforce. The U.S. Department of Health and Human Services: Office of the U.S. Surgeon General, 2022.
13. Panagioti M et al. Controlled interventions to reduce burnout in physicians: A systematic review and meta-analysis. JAMA Intern Med. 2017 Feb 1;177(2):195-205.
14. Rao SK et al. The impact of administrative burden on academic physicians: Results of a hospital-wide physician survey. Acad Med. 2017 Feb;92(2):237-43.
15. ACGME. ACME Institutional Requirements 2021.
Developing training pathways in advanced endoscopic resection and third-space endoscopy in the U.S.
As a gastroenterology and hepatology fellow, choosing a career path was a daunting prospect. Despite the additional specialization, there seemed to be endless career options to consider. Did I want to join an academic, private, or hybrid practice? Should I subspecialize within the field? Was it important to incorporate research or teaching into my practice? What about opportunities to take on administrative or leadership roles?
Fellowship training at a large academic research institution provided me the opportunity to work with expert faculty in inflammatory bowel disease, esophageal disease, motility and functional gastrointestinal disease, pancreaticobiliary disease, and hepatology. I enjoyed seeing patients in each of these subspecialty clinics. But, by the end of my second year of GI fellowship, I still wasn’t sure what I wanted to do professionally.

A career in academic general gastroenterology seemed to be a good fit for my personality and goals. Rather than focusing on research, I chose to position myself as a clinician educator. I knew that having a subspecialty area of expertise would help improve my clinical practice and make me a more attractive candidate to academic centers. To help narrow my choice, I looked at the clinical enterprise at our institution and assessed where the unmet clinical needs were most acute. Simultaneously, I identified potential mentors to support and guide me through the transition from fellow to independent practitioner. I decided to focus on acquiring the skills to care for patients with anorectal diseases and lower-GI motility disorders, as this area met both of my criteria – excellent mentorship and an unmet clinical need. Under the guidance of Dr. Yolanda Scarlett, I spent my 3rd year in clinic learning to interpret anorectal manometry tests, defecograms, and sitz marker studies and treating patients with refractory constipation, fecal incontinence, and anal fissures.
With a plan to develop an expertise in anorectal diseases and low-GI motility disorders, I also wanted to focus on improving my endoscopic skills to graduate as well rounded a clinician as possible. To achieve this goal, I sought out a separate endoscopy mentor, Dr. Ian Grimm, the director of endoscopy at the University of North Carolina at Chapel Hill. Dr. Grimm, a classically trained advanced endoscopist performing endoscopic ultrasound (EUS) and endoscopic retrograde cholangiopancreatography (ERCP), had a burgeoning interest in endoscopic mucosal resection (EMR) and had just returned from a few months in Japan learning to perform endoscopic submucosal dissection (ESD) and peroral endoscopic myotomy (POEM).
When I began working with Dr. Grimm, I had not even heard the term third-space endoscopy and knew nothing about ESD or POEM. I spent as much time as possible watching and assisting Dr. Grimm with complex endoscopic mucosal resection (EMR) during the first few months of my 3rd year. Soon after my exposure to advanced endoscopic resection, it was clear that I wanted to learn and incorporate this into my clinical practice. I watched Dr. Grimm perform the first POEM at UNC in the fall of 2016 and by that time I was hooked on learning third-space endoscopy. I observed and assisted with as many EMR, ESD, and POEM cases as I could that year. In addition to the hands-on and cognitive training with Dr. Grimm, I attended national meetings and workshops focused on learning third-space endoscopy. In the spring of my 3rd year I was honored to be the first fellow to complete the Olympus master class in ESD – a 2-day hands-on training course sponsored by Olympus. By the end of that year, I was performing complex EMR with minimal assistance and had completed multiple ESDs and POEMs with cognitive supervision only.
After fellowship, I joined the UNC faculty as a general gastroenterologist with expertise in anorectal disease and lower-GI motility disorders. While I was comfortable performing complex EMR, I still needed additional training and supervision before I felt ready to independently perform ESD or POEM. With the gracious support and encouragement of our division chief, I continued third-space endoscopy training with Dr. Grimm during dedicated protected time 2 days each month. Over the ensuing 4 years, I transitioned to fully independent practice performing all types of advanced EMR and third-space endoscopy including complex EMR, ESD, endoscopic full-thickness resection (EFTR), submucosal tunnel endoscopic resection (STER), esophageal POEM, gastric POEM, and Zenker’s POEM.
As one of the first gastroenterologists in the United States to perform third-space endoscopy without any formal training in advanced pancreaticobiliary endoscopy, I believe learning advanced endoscopic resection and third-space endoscopy is best achieved through a training pathway separate from the conventional advanced endoscopy fellowship focused on teaching EUS and ERCP. Although there are transferable skills learned from EUS and ERCP to the techniques used in third-space endoscopy, there is nothing inherent to performing EUS or ERCP that enables one to learn how to perform an ESD or a POEM.
There is a robust training pathway to teach advanced pancreaticobiliary endoscopy, but no formal training pathway exists to teach third-space endoscopy in the United States. Historically, a small number of interested and motivated advanced pancreaticobiliary endoscopists sought out opportunities to learn third-space endoscopy after completion of their advanced endoscopy fellowship, in some cases many years after graduation. For these early adopters in the United States, the only training opportunities required travel to Japan or another Eastern country with arrangements made to observe and participate in third-space endoscopy cases with experts there. With increased recognition of the benefits of ESD and POEM over the past 5-10 years in the United States, there has been greater adoption of third-space endoscopy and with it, more training opportunities. Still, there are very few institutions with formalized training programs in advanced endoscopic resection and third-space endoscopy in the United States to date.
Proof that this model works
In Eastern countries such as Japan, training endoscopists to perform ESD and POEM has been successfully achieved through an apprenticeship model whereby an expert in third-space endoscopy closely supervises a trainee who gains greater autonomy with increasing experience and skill over time. My personal experience is proof that this model works. But, adopting such a model more widely in the United States may prove difficult. We lack a sufficient number of experienced third-space endoscopy operators and, given the challenges to appropriate reimbursement for third-space endoscopy in the United States, there is understandable resistance to accepting the prolonged training period necessary for technical mastery of this skill.
In part, a long training period is needed because of a relative paucity of appropriate target lesions for ESD and the rarity of achalasia in the United States. While there is consensus among experts regarding the benefits of ESD for resection of early gastric cancer (EGC), relatively few EGCs are found in the United States and indications for ESD outside resection of EGC are less well defined with less clear benefits over more widely performed piecemeal EMR. Despite these challenges, it is critical that we continue to develop dedicated training pathways to teach advanced endoscopic resection and third-space endoscopy in the United States. My practice has evolved considerably since completion of fellowship nearly 6 years ago, and I now focus almost exclusively on advanced endoscopic resection and third-space endoscopy. Recently, Dr. Grimm and I began an advanced endoscopic resection elective for the general GI fellows at UNC and we are excited to welcome our first advanced endoscopic resection and third-space endoscopy fellow to UNC this July.
While there are many possible avenues to expertise in advanced endoscopic resection, few will likely follow the same path that I have taken. Trainees who are interested in pursuing this subspecialty should seek out supportive mentors in a setting where there is already a robust case volume of esophageal motility disorders and endoscopic resections. Success requires the persistent motivation to seek out diverse opportunities for self-study, exposure to experts, data on developments in the field, and hands-on exposure to as many ex-vivo and in-vivo cases as possible.
Dr. Kroch is assistant professor of medicine in the division of gastroenterology and hepatology at the University of North Carolina at Chapel Hill. He disclosed having no conflicts of interest.
As a gastroenterology and hepatology fellow, choosing a career path was a daunting prospect. Despite the additional specialization, there seemed to be endless career options to consider. Did I want to join an academic, private, or hybrid practice? Should I subspecialize within the field? Was it important to incorporate research or teaching into my practice? What about opportunities to take on administrative or leadership roles?
Fellowship training at a large academic research institution provided me the opportunity to work with expert faculty in inflammatory bowel disease, esophageal disease, motility and functional gastrointestinal disease, pancreaticobiliary disease, and hepatology. I enjoyed seeing patients in each of these subspecialty clinics. But, by the end of my second year of GI fellowship, I still wasn’t sure what I wanted to do professionally.
A career in academic general gastroenterology seemed to be a good fit for my personality and goals. Rather than focusing on research, I chose to position myself as a clinician educator. I knew that having a subspecialty area of expertise would help improve my clinical practice and make me a more attractive candidate to academic centers. To help narrow my choice, I looked at the clinical enterprise at our institution and assessed where the unmet clinical needs were most acute. Simultaneously, I identified potential mentors to support and guide me through the transition from fellow to independent practitioner. I decided to focus on acquiring the skills to care for patients with anorectal diseases and lower-GI motility disorders, as this area met both of my criteria – excellent mentorship and an unmet clinical need. Under the guidance of Dr. Yolanda Scarlett, I spent my 3rd year in clinic learning to interpret anorectal manometry tests, defecograms, and sitz marker studies and treating patients with refractory constipation, fecal incontinence, and anal fissures.
With a plan to develop an expertise in anorectal diseases and low-GI motility disorders, I also wanted to focus on improving my endoscopic skills to graduate as well rounded a clinician as possible. To achieve this goal, I sought out a separate endoscopy mentor, Dr. Ian Grimm, the director of endoscopy at the University of North Carolina at Chapel Hill. Dr. Grimm, a classically trained advanced endoscopist performing endoscopic ultrasound (EUS) and endoscopic retrograde cholangiopancreatography (ERCP), had a burgeoning interest in endoscopic mucosal resection (EMR) and had just returned from a few months in Japan learning to perform endoscopic submucosal dissection (ESD) and peroral endoscopic myotomy (POEM).
When I began working with Dr. Grimm, I had not even heard the term third-space endoscopy and knew nothing about ESD or POEM. I spent as much time as possible watching and assisting Dr. Grimm with complex endoscopic mucosal resection (EMR) during the first few months of my 3rd year. Soon after my exposure to advanced endoscopic resection, it was clear that I wanted to learn and incorporate this into my clinical practice. I watched Dr. Grimm perform the first POEM at UNC in the fall of 2016 and by that time I was hooked on learning third-space endoscopy. I observed and assisted with as many EMR, ESD, and POEM cases as I could that year. In addition to the hands-on and cognitive training with Dr. Grimm, I attended national meetings and workshops focused on learning third-space endoscopy. In the spring of my 3rd year I was honored to be the first fellow to complete the Olympus master class in ESD – a 2-day hands-on training course sponsored by Olympus. By the end of that year, I was performing complex EMR with minimal assistance and had completed multiple ESDs and POEMs with cognitive supervision only.
After fellowship, I joined the UNC faculty as a general gastroenterologist with expertise in anorectal disease and lower-GI motility disorders. While I was comfortable performing complex EMR, I still needed additional training and supervision before I felt ready to independently perform ESD or POEM. With the gracious support and encouragement of our division chief, I continued third-space endoscopy training with Dr. Grimm during dedicated protected time 2 days each month. Over the ensuing 4 years, I transitioned to fully independent practice performing all types of advanced EMR and third-space endoscopy including complex EMR, ESD, endoscopic full-thickness resection (EFTR), submucosal tunnel endoscopic resection (STER), esophageal POEM, gastric POEM, and Zenker’s POEM.
As one of the first gastroenterologists in the United States to perform third-space endoscopy without any formal training in advanced pancreaticobiliary endoscopy, I believe learning advanced endoscopic resection and third-space endoscopy is best achieved through a training pathway separate from the conventional advanced endoscopy fellowship focused on teaching EUS and ERCP. Although there are transferable skills learned from EUS and ERCP to the techniques used in third-space endoscopy, there is nothing inherent to performing EUS or ERCP that enables one to learn how to perform an ESD or a POEM.
There is a robust training pathway to teach advanced pancreaticobiliary endoscopy, but no formal training pathway exists to teach third-space endoscopy in the United States. Historically, a small number of interested and motivated advanced pancreaticobiliary endoscopists sought out opportunities to learn third-space endoscopy after completion of their advanced endoscopy fellowship, in some cases many years after graduation. For these early adopters in the United States, the only training opportunities required travel to Japan or another Eastern country with arrangements made to observe and participate in third-space endoscopy cases with experts there. With increased recognition of the benefits of ESD and POEM over the past 5-10 years in the United States, there has been greater adoption of third-space endoscopy and with it, more training opportunities. Still, there are very few institutions with formalized training programs in advanced endoscopic resection and third-space endoscopy in the United States to date.
Proof that this model works
In Eastern countries such as Japan, training endoscopists to perform ESD and POEM has been successfully achieved through an apprenticeship model whereby an expert in third-space endoscopy closely supervises a trainee who gains greater autonomy with increasing experience and skill over time. My personal experience is proof that this model works. But, adopting such a model more widely in the United States may prove difficult. We lack a sufficient number of experienced third-space endoscopy operators and, given the challenges to appropriate reimbursement for third-space endoscopy in the United States, there is understandable resistance to accepting the prolonged training period necessary for technical mastery of this skill.
In part, a long training period is needed because of a relative paucity of appropriate target lesions for ESD and the rarity of achalasia in the United States. While there is consensus among experts regarding the benefits of ESD for resection of early gastric cancer (EGC), relatively few EGCs are found in the United States and indications for ESD outside resection of EGC are less well defined with less clear benefits over more widely performed piecemeal EMR. Despite these challenges, it is critical that we continue to develop dedicated training pathways to teach advanced endoscopic resection and third-space endoscopy in the United States. My practice has evolved considerably since completion of fellowship nearly 6 years ago, and I now focus almost exclusively on advanced endoscopic resection and third-space endoscopy. Recently, Dr. Grimm and I began an advanced endoscopic resection elective for the general GI fellows at UNC and we are excited to welcome our first advanced endoscopic resection and third-space endoscopy fellow to UNC this July.
While there are many possible avenues to expertise in advanced endoscopic resection, few will likely follow the same path that I have taken. Trainees who are interested in pursuing this subspecialty should seek out supportive mentors in a setting where there is already a robust case volume of esophageal motility disorders and endoscopic resections. Success requires the persistent motivation to seek out diverse opportunities for self-study, exposure to experts, data on developments in the field, and hands-on exposure to as many ex-vivo and in-vivo cases as possible.
Dr. Kroch is assistant professor of medicine in the division of gastroenterology and hepatology at the University of North Carolina at Chapel Hill. He disclosed having no conflicts of interest.
As a gastroenterology and hepatology fellow, choosing a career path was a daunting prospect. Despite the additional specialization, there seemed to be endless career options to consider. Did I want to join an academic, private, or hybrid practice? Should I subspecialize within the field? Was it important to incorporate research or teaching into my practice? What about opportunities to take on administrative or leadership roles?
Fellowship training at a large academic research institution provided me the opportunity to work with expert faculty in inflammatory bowel disease, esophageal disease, motility and functional gastrointestinal disease, pancreaticobiliary disease, and hepatology. I enjoyed seeing patients in each of these subspecialty clinics. But, by the end of my second year of GI fellowship, I still wasn’t sure what I wanted to do professionally.
A career in academic general gastroenterology seemed to be a good fit for my personality and goals. Rather than focusing on research, I chose to position myself as a clinician educator. I knew that having a subspecialty area of expertise would help improve my clinical practice and make me a more attractive candidate to academic centers. To help narrow my choice, I looked at the clinical enterprise at our institution and assessed where the unmet clinical needs were most acute. Simultaneously, I identified potential mentors to support and guide me through the transition from fellow to independent practitioner. I decided to focus on acquiring the skills to care for patients with anorectal diseases and lower-GI motility disorders, as this area met both of my criteria – excellent mentorship and an unmet clinical need. Under the guidance of Dr. Yolanda Scarlett, I spent my 3rd year in clinic learning to interpret anorectal manometry tests, defecograms, and sitz marker studies and treating patients with refractory constipation, fecal incontinence, and anal fissures.
With a plan to develop an expertise in anorectal diseases and low-GI motility disorders, I also wanted to focus on improving my endoscopic skills to graduate as well rounded a clinician as possible. To achieve this goal, I sought out a separate endoscopy mentor, Dr. Ian Grimm, the director of endoscopy at the University of North Carolina at Chapel Hill. Dr. Grimm, a classically trained advanced endoscopist performing endoscopic ultrasound (EUS) and endoscopic retrograde cholangiopancreatography (ERCP), had a burgeoning interest in endoscopic mucosal resection (EMR) and had just returned from a few months in Japan learning to perform endoscopic submucosal dissection (ESD) and peroral endoscopic myotomy (POEM).
When I began working with Dr. Grimm, I had not even heard the term third-space endoscopy and knew nothing about ESD or POEM. I spent as much time as possible watching and assisting Dr. Grimm with complex endoscopic mucosal resection (EMR) during the first few months of my 3rd year. Soon after my exposure to advanced endoscopic resection, it was clear that I wanted to learn and incorporate this into my clinical practice. I watched Dr. Grimm perform the first POEM at UNC in the fall of 2016 and by that time I was hooked on learning third-space endoscopy. I observed and assisted with as many EMR, ESD, and POEM cases as I could that year. In addition to the hands-on and cognitive training with Dr. Grimm, I attended national meetings and workshops focused on learning third-space endoscopy. In the spring of my 3rd year I was honored to be the first fellow to complete the Olympus master class in ESD – a 2-day hands-on training course sponsored by Olympus. By the end of that year, I was performing complex EMR with minimal assistance and had completed multiple ESDs and POEMs with cognitive supervision only.
After fellowship, I joined the UNC faculty as a general gastroenterologist with expertise in anorectal disease and lower-GI motility disorders. While I was comfortable performing complex EMR, I still needed additional training and supervision before I felt ready to independently perform ESD or POEM. With the gracious support and encouragement of our division chief, I continued third-space endoscopy training with Dr. Grimm during dedicated protected time 2 days each month. Over the ensuing 4 years, I transitioned to fully independent practice performing all types of advanced EMR and third-space endoscopy including complex EMR, ESD, endoscopic full-thickness resection (EFTR), submucosal tunnel endoscopic resection (STER), esophageal POEM, gastric POEM, and Zenker’s POEM.
As one of the first gastroenterologists in the United States to perform third-space endoscopy without any formal training in advanced pancreaticobiliary endoscopy, I believe learning advanced endoscopic resection and third-space endoscopy is best achieved through a training pathway separate from the conventional advanced endoscopy fellowship focused on teaching EUS and ERCP. Although there are transferable skills learned from EUS and ERCP to the techniques used in third-space endoscopy, there is nothing inherent to performing EUS or ERCP that enables one to learn how to perform an ESD or a POEM.
There is a robust training pathway to teach advanced pancreaticobiliary endoscopy, but no formal training pathway exists to teach third-space endoscopy in the United States. Historically, a small number of interested and motivated advanced pancreaticobiliary endoscopists sought out opportunities to learn third-space endoscopy after completion of their advanced endoscopy fellowship, in some cases many years after graduation. For these early adopters in the United States, the only training opportunities required travel to Japan or another Eastern country with arrangements made to observe and participate in third-space endoscopy cases with experts there. With increased recognition of the benefits of ESD and POEM over the past 5-10 years in the United States, there has been greater adoption of third-space endoscopy and with it, more training opportunities. Still, there are very few institutions with formalized training programs in advanced endoscopic resection and third-space endoscopy in the United States to date.
Proof that this model works
In Eastern countries such as Japan, training endoscopists to perform ESD and POEM has been successfully achieved through an apprenticeship model whereby an expert in third-space endoscopy closely supervises a trainee who gains greater autonomy with increasing experience and skill over time. My personal experience is proof that this model works. But, adopting such a model more widely in the United States may prove difficult. We lack a sufficient number of experienced third-space endoscopy operators and, given the challenges to appropriate reimbursement for third-space endoscopy in the United States, there is understandable resistance to accepting the prolonged training period necessary for technical mastery of this skill.
In part, a long training period is needed because of a relative paucity of appropriate target lesions for ESD and the rarity of achalasia in the United States. While there is consensus among experts regarding the benefits of ESD for resection of early gastric cancer (EGC), relatively few EGCs are found in the United States and indications for ESD outside resection of EGC are less well defined with less clear benefits over more widely performed piecemeal EMR. Despite these challenges, it is critical that we continue to develop dedicated training pathways to teach advanced endoscopic resection and third-space endoscopy in the United States. My practice has evolved considerably since completion of fellowship nearly 6 years ago, and I now focus almost exclusively on advanced endoscopic resection and third-space endoscopy. Recently, Dr. Grimm and I began an advanced endoscopic resection elective for the general GI fellows at UNC and we are excited to welcome our first advanced endoscopic resection and third-space endoscopy fellow to UNC this July.
While there are many possible avenues to expertise in advanced endoscopic resection, few will likely follow the same path that I have taken. Trainees who are interested in pursuing this subspecialty should seek out supportive mentors in a setting where there is already a robust case volume of esophageal motility disorders and endoscopic resections. Success requires the persistent motivation to seek out diverse opportunities for self-study, exposure to experts, data on developments in the field, and hands-on exposure to as many ex-vivo and in-vivo cases as possible.
Dr. Kroch is assistant professor of medicine in the division of gastroenterology and hepatology at the University of North Carolina at Chapel Hill. He disclosed having no conflicts of interest.
Finding the optimal fluid strategies for sepsis
The document offers guidance on the four forms of fluid use; assessing whether intravenous fluid administration is indicated; and fluid therapy goals, timing, type, and other clinical parameters. The recommendations are based on a literature search that included 28 randomized clinical trials, 7 secondary analyses of RCTs, 20 observational studies, 5 systematic reviews or meta-analyses, 1 scoping review, 1 practice guideline, and 14 references from a reference review.
“Our review highlights that crystalloids should remain the standard of care for most critically ill patients, especially during early resuscitation,” Fernando G. Zampieri, MD, PhD, assistant adjunct professor of critical care medicine at the University of Alberta and Alberta Health Services, both in Edmonton, said in an interview. “In particular, starches should not be used in critically ill patients. Balanced solutions might be better for most patients, except for patients with traumatic brain injury, where 0.9% saline is recommended.”
The review was published online in JAMA.
Four therapeutic phases
Approximately 20%-30% of patients admitted to an intensive care unit have sepsis, and fluid therapy is a key component of their treatment. Although intravenous fluid can increase cardiac output and blood pressure, maintain or increase intravascular fluid volume, and deliver medications, too much fluid or the wrong type of fluid may cause harm.
“Deciding which type of fluid is the best for a patient [with sepsis] can be challenging,” said Dr. Zampieri.
Fluid therapy can be conceptualized as encompassing four overlapping phases from early illness through resolution of sepsis, according to the review. These phases include resuscitation (rapidly administering fluid to restore perfusion), optimization (assessing risks and benefits of additional fluids to treat shock and ensure organ perfusion), stabilization (using fluid therapy only when there is a signal of fluid responsiveness), and evacuation (eliminating excess fluid accumulated during treatment).
The review described the studies that underpin its key recommendations for management in these phases. Three RCTs included 3,723 patients with sepsis who received 1-2 L of fluid. They found that goal-directed therapy with administration of fluid boluses to attain a central venous pressure of 8-12 mm Hg, vasopressors to attain a mean arterial blood pressure of 65-90 mm Hg, and red blood cell transfusions or inotropes to attain a central venous oxygen saturation of at least 70% did not decrease mortality, compared with unstructured clinical care (24.9% vs. 25.4%, P = .68).
One RCT with 1,563 patients with sepsis and hypotension who received 1 L of fluid found that favoring vasopressor treatment did not improve mortality, compared with further fluid administration (14.0% vs. 14.9%, P = .61).
In another RCT, among 1,554 patients with septic shock who were treated in the ICU with at least 1 L of fluid, restricting fluid administration in the absence of severe hypoperfusion did not reduce mortality, compared with more liberal fluid administration (42.3% vs. 42.1%, P = .96).
An RCT of 1,000 patients with acute respiratory distress during the evacuation phase found that limiting fluid administration and giving diuretics improved the number of days alive without mechanical ventilation, compared with fluid treatment to attain higher intracardiac pressure (14.6 vs. 12.1 days, P < .001).
This study also found that hydroxyethyl starch significantly increased the incidence of kidney replacement therapy, compared with saline (7.0% vs. 5.8%, P = .04), Ringer lactate, or Ringer acetate.
Ultrasonography lacks validation
The authors summarized the key concerns about fluid therapy. Fluid therapy should be initiated for patients with evidence of sepsis-induced hypoperfusion who are likely to have increased cardiac output with fluid administration. Fluid administration should be discontinued when evidence of hypoperfusion resolves, the patient no longer responds to fluid, or the patient shows evidence of fluid overload.
Balanced solutions should be selected over 0.9% saline for fluid therapy, according to the review. Hydroxyethyl starches should not be used.
Fluid removal should be considered after the resuscitation and optimization phases and when a patient has stabilized, the authors wrote. Diuretics are first-line therapy to facilitate fluid elimination.
Kidney replacement therapy may be considered for patients with severe acute kidney injury who have complications from fluid overload and are unresponsive to diuretic therapy.
“The use of ultrasonography as a bedside tool to guide fluid resuscitation is promising but lacks validation in robust randomized controlled trials,” said Dr. Zampieri. “Point-of-care ultrasound may be useful to assess causes of shock and [helping to exclude] a life-threatening diagnosis at presentation, such as cardiac tamponade.”
Pending the emergence of further evidence, the authors suggest that clinicians prescribe fluids judiciously, preferably at aliquots followed by frequent reassessment. “Defining a resuscitation target (such as capillary refill time or lactate, among others) and performing fluid challenges to correct them while no overt signs of fluid overload (such as pulmonary edema) occur is a common practice that is also sustained by clinical research,” said Dr. Zampieri.
He added that the review’s recommendations are based on research conducted mainly in high-income settings, and that generalizability will depend on factors such as local standards of care and resource availability.
“Our review provides an overall guidance, but caution is warranted before extrapolating the suggestion to every possible clinical scenario,” he concluded.
Fluids as drugs
Commenting on the review, Hernando Gomez, MD, MPH, an associate professor of critical care medicine at the University of Pittsburgh, said: “I agree with the conclusions and commend the authors for this very practical revision of the literature.” Dr. Gomez was not involved in the review.
“I would like to stress the point, however, that although fluids can be harmful, particularly when not indicated and when used in excess, fluid resuscitation in patients with sepsis who have evidence of hypoperfusion is paramount,” he said.
“The association between fluid accumulation and poor outcomes is truly a Goldilocks problem, often described in the literature as a ‘U’ shape, where too little fluid (i.e., a very restrictive strategy) or too much fluid (i.e., use in excess and in discordance with the patient’s needs) can be harmful,” said Dr. Gomez.
Furthermore, every strategy to assess fluid responsiveness has limitations. “It is key that clinicians resist the temptation to dismiss these limitations, because decisions made on flawed data are as dangerous as not assessing fluid responsiveness in the first place,” he said.
Based on the evidence, clinicians should “think of fluids as a drug and carefully assess risks and benefits before deciding to administer fluids to their patients,” Dr. Gomez added. It is also important to separate the question “Does my patient need fluids?” from the question “Is my patient fluid responsive?”
“These are two different questions that often get conflated,” Dr. Gomez said. “If a bolus of fluid given to a patient who needs fluids and is fluid-responsive does not improve tissue perfusion, then fluids should not be given.”
No funding was reported for the review. Dr. Zampieri reported receiving fluids and logistics from Baxter Hospitalar during the conduct of the BaSICS trial, personal fees from Bactiguard for statistical consulting and from Baxter for participating in an advisory board, grants from Ionis Pharmaceuticals outside the submitted work, and serving as lead investigator of the BaSICS trial. Dr. Gomez reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The document offers guidance on the four forms of fluid use; assessing whether intravenous fluid administration is indicated; and fluid therapy goals, timing, type, and other clinical parameters. The recommendations are based on a literature search that included 28 randomized clinical trials, 7 secondary analyses of RCTs, 20 observational studies, 5 systematic reviews or meta-analyses, 1 scoping review, 1 practice guideline, and 14 references from a reference review.
“Our review highlights that crystalloids should remain the standard of care for most critically ill patients, especially during early resuscitation,” Fernando G. Zampieri, MD, PhD, assistant adjunct professor of critical care medicine at the University of Alberta and Alberta Health Services, both in Edmonton, said in an interview. “In particular, starches should not be used in critically ill patients. Balanced solutions might be better for most patients, except for patients with traumatic brain injury, where 0.9% saline is recommended.”
The review was published online in JAMA.
Four therapeutic phases
Approximately 20%-30% of patients admitted to an intensive care unit have sepsis, and fluid therapy is a key component of their treatment. Although intravenous fluid can increase cardiac output and blood pressure, maintain or increase intravascular fluid volume, and deliver medications, too much fluid or the wrong type of fluid may cause harm.
“Deciding which type of fluid is the best for a patient [with sepsis] can be challenging,” said Dr. Zampieri.
Fluid therapy can be conceptualized as encompassing four overlapping phases from early illness through resolution of sepsis, according to the review. These phases include resuscitation (rapidly administering fluid to restore perfusion), optimization (assessing risks and benefits of additional fluids to treat shock and ensure organ perfusion), stabilization (using fluid therapy only when there is a signal of fluid responsiveness), and evacuation (eliminating excess fluid accumulated during treatment).
The review described the studies that underpin its key recommendations for management in these phases. Three RCTs included 3,723 patients with sepsis who received 1-2 L of fluid. They found that goal-directed therapy with administration of fluid boluses to attain a central venous pressure of 8-12 mm Hg, vasopressors to attain a mean arterial blood pressure of 65-90 mm Hg, and red blood cell transfusions or inotropes to attain a central venous oxygen saturation of at least 70% did not decrease mortality, compared with unstructured clinical care (24.9% vs. 25.4%, P = .68).
One RCT with 1,563 patients with sepsis and hypotension who received 1 L of fluid found that favoring vasopressor treatment did not improve mortality, compared with further fluid administration (14.0% vs. 14.9%, P = .61).
In another RCT, among 1,554 patients with septic shock who were treated in the ICU with at least 1 L of fluid, restricting fluid administration in the absence of severe hypoperfusion did not reduce mortality, compared with more liberal fluid administration (42.3% vs. 42.1%, P = .96).
An RCT of 1,000 patients with acute respiratory distress during the evacuation phase found that limiting fluid administration and giving diuretics improved the number of days alive without mechanical ventilation, compared with fluid treatment to attain higher intracardiac pressure (14.6 vs. 12.1 days, P < .001).
This study also found that hydroxyethyl starch significantly increased the incidence of kidney replacement therapy, compared with saline (7.0% vs. 5.8%, P = .04), Ringer lactate, or Ringer acetate.
Ultrasonography lacks validation
The authors summarized the key concerns about fluid therapy. Fluid therapy should be initiated for patients with evidence of sepsis-induced hypoperfusion who are likely to have increased cardiac output with fluid administration. Fluid administration should be discontinued when evidence of hypoperfusion resolves, the patient no longer responds to fluid, or the patient shows evidence of fluid overload.
Balanced solutions should be selected over 0.9% saline for fluid therapy, according to the review. Hydroxyethyl starches should not be used.
Fluid removal should be considered after the resuscitation and optimization phases and when a patient has stabilized, the authors wrote. Diuretics are first-line therapy to facilitate fluid elimination.
Kidney replacement therapy may be considered for patients with severe acute kidney injury who have complications from fluid overload and are unresponsive to diuretic therapy.
“The use of ultrasonography as a bedside tool to guide fluid resuscitation is promising but lacks validation in robust randomized controlled trials,” said Dr. Zampieri. “Point-of-care ultrasound may be useful to assess causes of shock and [helping to exclude] a life-threatening diagnosis at presentation, such as cardiac tamponade.”
Pending the emergence of further evidence, the authors suggest that clinicians prescribe fluids judiciously, preferably at aliquots followed by frequent reassessment. “Defining a resuscitation target (such as capillary refill time or lactate, among others) and performing fluid challenges to correct them while no overt signs of fluid overload (such as pulmonary edema) occur is a common practice that is also sustained by clinical research,” said Dr. Zampieri.
He added that the review’s recommendations are based on research conducted mainly in high-income settings, and that generalizability will depend on factors such as local standards of care and resource availability.
“Our review provides an overall guidance, but caution is warranted before extrapolating the suggestion to every possible clinical scenario,” he concluded.
Fluids as drugs
Commenting on the review, Hernando Gomez, MD, MPH, an associate professor of critical care medicine at the University of Pittsburgh, said: “I agree with the conclusions and commend the authors for this very practical revision of the literature.” Dr. Gomez was not involved in the review.
“I would like to stress the point, however, that although fluids can be harmful, particularly when not indicated and when used in excess, fluid resuscitation in patients with sepsis who have evidence of hypoperfusion is paramount,” he said.
“The association between fluid accumulation and poor outcomes is truly a Goldilocks problem, often described in the literature as a ‘U’ shape, where too little fluid (i.e., a very restrictive strategy) or too much fluid (i.e., use in excess and in discordance with the patient’s needs) can be harmful,” said Dr. Gomez.
Furthermore, every strategy to assess fluid responsiveness has limitations. “It is key that clinicians resist the temptation to dismiss these limitations, because decisions made on flawed data are as dangerous as not assessing fluid responsiveness in the first place,” he said.
Based on the evidence, clinicians should “think of fluids as a drug and carefully assess risks and benefits before deciding to administer fluids to their patients,” Dr. Gomez added. It is also important to separate the question “Does my patient need fluids?” from the question “Is my patient fluid responsive?”
“These are two different questions that often get conflated,” Dr. Gomez said. “If a bolus of fluid given to a patient who needs fluids and is fluid-responsive does not improve tissue perfusion, then fluids should not be given.”
No funding was reported for the review. Dr. Zampieri reported receiving fluids and logistics from Baxter Hospitalar during the conduct of the BaSICS trial, personal fees from Bactiguard for statistical consulting and from Baxter for participating in an advisory board, grants from Ionis Pharmaceuticals outside the submitted work, and serving as lead investigator of the BaSICS trial. Dr. Gomez reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The document offers guidance on the four forms of fluid use; assessing whether intravenous fluid administration is indicated; and fluid therapy goals, timing, type, and other clinical parameters. The recommendations are based on a literature search that included 28 randomized clinical trials, 7 secondary analyses of RCTs, 20 observational studies, 5 systematic reviews or meta-analyses, 1 scoping review, 1 practice guideline, and 14 references from a reference review.
“Our review highlights that crystalloids should remain the standard of care for most critically ill patients, especially during early resuscitation,” Fernando G. Zampieri, MD, PhD, assistant adjunct professor of critical care medicine at the University of Alberta and Alberta Health Services, both in Edmonton, said in an interview. “In particular, starches should not be used in critically ill patients. Balanced solutions might be better for most patients, except for patients with traumatic brain injury, where 0.9% saline is recommended.”
The review was published online in JAMA.
Four therapeutic phases
Approximately 20%-30% of patients admitted to an intensive care unit have sepsis, and fluid therapy is a key component of their treatment. Although intravenous fluid can increase cardiac output and blood pressure, maintain or increase intravascular fluid volume, and deliver medications, too much fluid or the wrong type of fluid may cause harm.
“Deciding which type of fluid is the best for a patient [with sepsis] can be challenging,” said Dr. Zampieri.
Fluid therapy can be conceptualized as encompassing four overlapping phases from early illness through resolution of sepsis, according to the review. These phases include resuscitation (rapidly administering fluid to restore perfusion), optimization (assessing risks and benefits of additional fluids to treat shock and ensure organ perfusion), stabilization (using fluid therapy only when there is a signal of fluid responsiveness), and evacuation (eliminating excess fluid accumulated during treatment).
The review described the studies that underpin its key recommendations for management in these phases. Three RCTs included 3,723 patients with sepsis who received 1-2 L of fluid. They found that goal-directed therapy with administration of fluid boluses to attain a central venous pressure of 8-12 mm Hg, vasopressors to attain a mean arterial blood pressure of 65-90 mm Hg, and red blood cell transfusions or inotropes to attain a central venous oxygen saturation of at least 70% did not decrease mortality, compared with unstructured clinical care (24.9% vs. 25.4%, P = .68).
One RCT with 1,563 patients with sepsis and hypotension who received 1 L of fluid found that favoring vasopressor treatment did not improve mortality, compared with further fluid administration (14.0% vs. 14.9%, P = .61).
In another RCT, among 1,554 patients with septic shock who were treated in the ICU with at least 1 L of fluid, restricting fluid administration in the absence of severe hypoperfusion did not reduce mortality, compared with more liberal fluid administration (42.3% vs. 42.1%, P = .96).
An RCT of 1,000 patients with acute respiratory distress during the evacuation phase found that limiting fluid administration and giving diuretics improved the number of days alive without mechanical ventilation, compared with fluid treatment to attain higher intracardiac pressure (14.6 vs. 12.1 days, P < .001).
This study also found that hydroxyethyl starch significantly increased the incidence of kidney replacement therapy, compared with saline (7.0% vs. 5.8%, P = .04), Ringer lactate, or Ringer acetate.
Ultrasonography lacks validation
The authors summarized the key concerns about fluid therapy. Fluid therapy should be initiated for patients with evidence of sepsis-induced hypoperfusion who are likely to have increased cardiac output with fluid administration. Fluid administration should be discontinued when evidence of hypoperfusion resolves, the patient no longer responds to fluid, or the patient shows evidence of fluid overload.
Balanced solutions should be selected over 0.9% saline for fluid therapy, according to the review. Hydroxyethyl starches should not be used.
Fluid removal should be considered after the resuscitation and optimization phases and when a patient has stabilized, the authors wrote. Diuretics are first-line therapy to facilitate fluid elimination.
Kidney replacement therapy may be considered for patients with severe acute kidney injury who have complications from fluid overload and are unresponsive to diuretic therapy.
“The use of ultrasonography as a bedside tool to guide fluid resuscitation is promising but lacks validation in robust randomized controlled trials,” said Dr. Zampieri. “Point-of-care ultrasound may be useful to assess causes of shock and [helping to exclude] a life-threatening diagnosis at presentation, such as cardiac tamponade.”
Pending the emergence of further evidence, the authors suggest that clinicians prescribe fluids judiciously, preferably at aliquots followed by frequent reassessment. “Defining a resuscitation target (such as capillary refill time or lactate, among others) and performing fluid challenges to correct them while no overt signs of fluid overload (such as pulmonary edema) occur is a common practice that is also sustained by clinical research,” said Dr. Zampieri.
He added that the review’s recommendations are based on research conducted mainly in high-income settings, and that generalizability will depend on factors such as local standards of care and resource availability.
“Our review provides an overall guidance, but caution is warranted before extrapolating the suggestion to every possible clinical scenario,” he concluded.
Fluids as drugs
Commenting on the review, Hernando Gomez, MD, MPH, an associate professor of critical care medicine at the University of Pittsburgh, said: “I agree with the conclusions and commend the authors for this very practical revision of the literature.” Dr. Gomez was not involved in the review.
“I would like to stress the point, however, that although fluids can be harmful, particularly when not indicated and when used in excess, fluid resuscitation in patients with sepsis who have evidence of hypoperfusion is paramount,” he said.
“The association between fluid accumulation and poor outcomes is truly a Goldilocks problem, often described in the literature as a ‘U’ shape, where too little fluid (i.e., a very restrictive strategy) or too much fluid (i.e., use in excess and in discordance with the patient’s needs) can be harmful,” said Dr. Gomez.
Furthermore, every strategy to assess fluid responsiveness has limitations. “It is key that clinicians resist the temptation to dismiss these limitations, because decisions made on flawed data are as dangerous as not assessing fluid responsiveness in the first place,” he said.
Based on the evidence, clinicians should “think of fluids as a drug and carefully assess risks and benefits before deciding to administer fluids to their patients,” Dr. Gomez added. It is also important to separate the question “Does my patient need fluids?” from the question “Is my patient fluid responsive?”
“These are two different questions that often get conflated,” Dr. Gomez said. “If a bolus of fluid given to a patient who needs fluids and is fluid-responsive does not improve tissue perfusion, then fluids should not be given.”
No funding was reported for the review. Dr. Zampieri reported receiving fluids and logistics from Baxter Hospitalar during the conduct of the BaSICS trial, personal fees from Bactiguard for statistical consulting and from Baxter for participating in an advisory board, grants from Ionis Pharmaceuticals outside the submitted work, and serving as lead investigator of the BaSICS trial. Dr. Gomez reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA
Peripartum cardiomyopathy raises risks at future pregnancy despite LV recovery
, a new study suggests.
Researchers looked at the long-term outcomes in a cohort of women who had developed PPCM and became pregnant again several years later, comparing those with LV function that had “normalized” in the interim against those with persisting LV dysfunction.
In their analysis, adverse maternal outcomes 5 years after an index pregnancy were significantly worse among those in whom LV dysfunction had persisted, compared with those with recovered LV function. The risk of relapsed PPCM persisted out to 8 years. Mortality remained high in both groups through the follow-up.
The study suggests that “women with PPCM need long-term follow-up by cardiology, as mortality does not abate over time,” Kalgi Modi, MD, Louisiana State University, Shreveport, said in an interview.
Women with a history of PPCM, she said, need “multidisciplinary and shared decision-making for family planning, because normalization of left ventricular function after index pregnancy does not guarantee a favorable outcome in the subsequent pregnancies.”
Dr. Modi is senior author on the study published online in the Journal of the American College of Cardiology.
The current findings are important to women with a history of PPCM who are “contemplating future pregnancy,” Afshan Hameed, MD, a maternal-fetal medicine specialist and cardiologist at the University of California, Irvine, said in an interview. The investigators suggest that “complete recovery of cardiac function after PPCM does not guarantee a favorable outcome in future pregnancy,” agreed Dr. Hameed, who was not involved in the current study. Future pregnancies must therefore “be highly discouraged or considered with caution even in patients who have recovered their cardiac function.”
To investigate the impact of PPCM on risk at subsequent pregnancies, the researchers studied 45 patients with PPCM who had gone on to have at least one more pregnancy, the first a median of 28 months later. Their mean age was 27 and 80% were Black; they were followed a median of 8 years.
Peripartum cardiomyopathy, defined as idiopathic heart failure with LV ejection fraction (LVEF) 45% or less in the last month of pregnancy through the following 5 months, was diagnosed post partum in 93.3% and antepartum in the remaining 6.7% (mean time of diagnosis, 6 weeks post partum).
The mean LVEF fell from 45.1% at the index pregnancy to 41.2% (P = .009) at subsequent pregnancies. The “recovery group” included the 30 women with LVEF recovery to 50% or higher after the index pregnancy, and the remaining 15 with persisting LV dysfunction – defined as LVEF < 50% – made up the “nonrecovery group.”
Recovery of LVEF was associated with a reduced risk of persisting LV dysfunction, the report states, at a hazard ratio of 0.08 (95% CI, 0.01-0.64; P = .02) after adjustment for hypertension, diabetes, and history of preeclampsia. But that risk went up sharply in association with illicit drug use, similarly adjusted, with an HR of 9.08 (95% CI, 1.38-59.8; P = .02).
The nonrecovery group, compared with the recovery group, experienced significantly higher rates of adverse maternal outcomes (53.3% vs. 20.0%; P = .04) – a composite endpoint that included relapse PPCM (33.3% vs. 3.3%; P = .01), HF (53.3% vs. 20.0%; P = .03), cardiogenic shock, thromboembolic events, and death – at 5 years. However, all-cause mortality was nonsignificantly different between the two groups (13.3% vs. 3.3%; P = .25)
All-cause mortality was nonsignificantly different between the two groups at a median of 8 years (20.0% vs. 20.0%; P = 1.00), and the difference in overall adverse maternal outcomes had gone from significant to nonsignificant (53.3% vs. 33.3%; P = .20). The difference in relapse PPCM between groups remained significant after 8 years (53.3% vs. 23.3%; P = .04)
The study is limited by its retrospective nature, a relatively small population, and lack of racial diversity, the report notes.
Indeed, most of the study’s subjects were Black, and previous studies have demonstrated a “different phenotypic presentation and outcome in African American women with PPCM, compared with non–African American women,” an accompanying editorial states.
Therefore, applicability of its findings to other populations “needs to be examined by urgently needed national prospective registries with long-term follow-up,” writes Uri Elkayam, MD, University of Southern California, Los Angeles.
Moreover, the study questions “whether the reverse remodeling and improvement of [LVEF] in women with PPCM represent a true recovery.” Prior studies “have shown an impaired contractile reserve as well as abnormal myocardial strain and reduced exercise capacity and even mortality in women with PPCM after RLV,” Dr. Elkayam notes.
It’s therefore possible – as with other forms of dilated cardiomyopathy – that LVEF normalization “does not represent a true recovery but a new steady state with subclinical myocardial dysfunction that is prone to development of recurrent [LV dysfunction] and clinical deterioration in response to various triggers such as long-standing hypertension, obesity, diabetes, illicit drug use,” and, “more importantly,” subsequent pregnancies.
The study points to “the need for a close long-term follow-up of women with PPCM” and provides “a rationale for early initiation of guideline-directed medical therapy after the diagnosis of PPCM and possible continuation even after improvement of LVEF.”
No funding source was reported. Dr. Modi and coauthors, Dr. Elkayam, and Dr. Hameed declare no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new study suggests.
Researchers looked at the long-term outcomes in a cohort of women who had developed PPCM and became pregnant again several years later, comparing those with LV function that had “normalized” in the interim against those with persisting LV dysfunction.
In their analysis, adverse maternal outcomes 5 years after an index pregnancy were significantly worse among those in whom LV dysfunction had persisted, compared with those with recovered LV function. The risk of relapsed PPCM persisted out to 8 years. Mortality remained high in both groups through the follow-up.
The study suggests that “women with PPCM need long-term follow-up by cardiology, as mortality does not abate over time,” Kalgi Modi, MD, Louisiana State University, Shreveport, said in an interview.
Women with a history of PPCM, she said, need “multidisciplinary and shared decision-making for family planning, because normalization of left ventricular function after index pregnancy does not guarantee a favorable outcome in the subsequent pregnancies.”
Dr. Modi is senior author on the study published online in the Journal of the American College of Cardiology.
The current findings are important to women with a history of PPCM who are “contemplating future pregnancy,” Afshan Hameed, MD, a maternal-fetal medicine specialist and cardiologist at the University of California, Irvine, said in an interview. The investigators suggest that “complete recovery of cardiac function after PPCM does not guarantee a favorable outcome in future pregnancy,” agreed Dr. Hameed, who was not involved in the current study. Future pregnancies must therefore “be highly discouraged or considered with caution even in patients who have recovered their cardiac function.”
To investigate the impact of PPCM on risk at subsequent pregnancies, the researchers studied 45 patients with PPCM who had gone on to have at least one more pregnancy, the first a median of 28 months later. Their mean age was 27 and 80% were Black; they were followed a median of 8 years.
Peripartum cardiomyopathy, defined as idiopathic heart failure with LV ejection fraction (LVEF) 45% or less in the last month of pregnancy through the following 5 months, was diagnosed post partum in 93.3% and antepartum in the remaining 6.7% (mean time of diagnosis, 6 weeks post partum).
The mean LVEF fell from 45.1% at the index pregnancy to 41.2% (P = .009) at subsequent pregnancies. The “recovery group” included the 30 women with LVEF recovery to 50% or higher after the index pregnancy, and the remaining 15 with persisting LV dysfunction – defined as LVEF < 50% – made up the “nonrecovery group.”
Recovery of LVEF was associated with a reduced risk of persisting LV dysfunction, the report states, at a hazard ratio of 0.08 (95% CI, 0.01-0.64; P = .02) after adjustment for hypertension, diabetes, and history of preeclampsia. But that risk went up sharply in association with illicit drug use, similarly adjusted, with an HR of 9.08 (95% CI, 1.38-59.8; P = .02).
The nonrecovery group, compared with the recovery group, experienced significantly higher rates of adverse maternal outcomes (53.3% vs. 20.0%; P = .04) – a composite endpoint that included relapse PPCM (33.3% vs. 3.3%; P = .01), HF (53.3% vs. 20.0%; P = .03), cardiogenic shock, thromboembolic events, and death – at 5 years. However, all-cause mortality was nonsignificantly different between the two groups (13.3% vs. 3.3%; P = .25)
All-cause mortality was nonsignificantly different between the two groups at a median of 8 years (20.0% vs. 20.0%; P = 1.00), and the difference in overall adverse maternal outcomes had gone from significant to nonsignificant (53.3% vs. 33.3%; P = .20). The difference in relapse PPCM between groups remained significant after 8 years (53.3% vs. 23.3%; P = .04)
The study is limited by its retrospective nature, a relatively small population, and lack of racial diversity, the report notes.
Indeed, most of the study’s subjects were Black, and previous studies have demonstrated a “different phenotypic presentation and outcome in African American women with PPCM, compared with non–African American women,” an accompanying editorial states.
Therefore, applicability of its findings to other populations “needs to be examined by urgently needed national prospective registries with long-term follow-up,” writes Uri Elkayam, MD, University of Southern California, Los Angeles.
Moreover, the study questions “whether the reverse remodeling and improvement of [LVEF] in women with PPCM represent a true recovery.” Prior studies “have shown an impaired contractile reserve as well as abnormal myocardial strain and reduced exercise capacity and even mortality in women with PPCM after RLV,” Dr. Elkayam notes.
It’s therefore possible – as with other forms of dilated cardiomyopathy – that LVEF normalization “does not represent a true recovery but a new steady state with subclinical myocardial dysfunction that is prone to development of recurrent [LV dysfunction] and clinical deterioration in response to various triggers such as long-standing hypertension, obesity, diabetes, illicit drug use,” and, “more importantly,” subsequent pregnancies.
The study points to “the need for a close long-term follow-up of women with PPCM” and provides “a rationale for early initiation of guideline-directed medical therapy after the diagnosis of PPCM and possible continuation even after improvement of LVEF.”
No funding source was reported. Dr. Modi and coauthors, Dr. Elkayam, and Dr. Hameed declare no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new study suggests.
Researchers looked at the long-term outcomes in a cohort of women who had developed PPCM and became pregnant again several years later, comparing those with LV function that had “normalized” in the interim against those with persisting LV dysfunction.
In their analysis, adverse maternal outcomes 5 years after an index pregnancy were significantly worse among those in whom LV dysfunction had persisted, compared with those with recovered LV function. The risk of relapsed PPCM persisted out to 8 years. Mortality remained high in both groups through the follow-up.
The study suggests that “women with PPCM need long-term follow-up by cardiology, as mortality does not abate over time,” Kalgi Modi, MD, Louisiana State University, Shreveport, said in an interview.
Women with a history of PPCM, she said, need “multidisciplinary and shared decision-making for family planning, because normalization of left ventricular function after index pregnancy does not guarantee a favorable outcome in the subsequent pregnancies.”
Dr. Modi is senior author on the study published online in the Journal of the American College of Cardiology.
The current findings are important to women with a history of PPCM who are “contemplating future pregnancy,” Afshan Hameed, MD, a maternal-fetal medicine specialist and cardiologist at the University of California, Irvine, said in an interview. The investigators suggest that “complete recovery of cardiac function after PPCM does not guarantee a favorable outcome in future pregnancy,” agreed Dr. Hameed, who was not involved in the current study. Future pregnancies must therefore “be highly discouraged or considered with caution even in patients who have recovered their cardiac function.”
To investigate the impact of PPCM on risk at subsequent pregnancies, the researchers studied 45 patients with PPCM who had gone on to have at least one more pregnancy, the first a median of 28 months later. Their mean age was 27 and 80% were Black; they were followed a median of 8 years.
Peripartum cardiomyopathy, defined as idiopathic heart failure with LV ejection fraction (LVEF) 45% or less in the last month of pregnancy through the following 5 months, was diagnosed post partum in 93.3% and antepartum in the remaining 6.7% (mean time of diagnosis, 6 weeks post partum).
The mean LVEF fell from 45.1% at the index pregnancy to 41.2% (P = .009) at subsequent pregnancies. The “recovery group” included the 30 women with LVEF recovery to 50% or higher after the index pregnancy, and the remaining 15 with persisting LV dysfunction – defined as LVEF < 50% – made up the “nonrecovery group.”
Recovery of LVEF was associated with a reduced risk of persisting LV dysfunction, the report states, at a hazard ratio of 0.08 (95% CI, 0.01-0.64; P = .02) after adjustment for hypertension, diabetes, and history of preeclampsia. But that risk went up sharply in association with illicit drug use, similarly adjusted, with an HR of 9.08 (95% CI, 1.38-59.8; P = .02).
The nonrecovery group, compared with the recovery group, experienced significantly higher rates of adverse maternal outcomes (53.3% vs. 20.0%; P = .04) – a composite endpoint that included relapse PPCM (33.3% vs. 3.3%; P = .01), HF (53.3% vs. 20.0%; P = .03), cardiogenic shock, thromboembolic events, and death – at 5 years. However, all-cause mortality was nonsignificantly different between the two groups (13.3% vs. 3.3%; P = .25)
All-cause mortality was nonsignificantly different between the two groups at a median of 8 years (20.0% vs. 20.0%; P = 1.00), and the difference in overall adverse maternal outcomes had gone from significant to nonsignificant (53.3% vs. 33.3%; P = .20). The difference in relapse PPCM between groups remained significant after 8 years (53.3% vs. 23.3%; P = .04)
The study is limited by its retrospective nature, a relatively small population, and lack of racial diversity, the report notes.
Indeed, most of the study’s subjects were Black, and previous studies have demonstrated a “different phenotypic presentation and outcome in African American women with PPCM, compared with non–African American women,” an accompanying editorial states.
Therefore, applicability of its findings to other populations “needs to be examined by urgently needed national prospective registries with long-term follow-up,” writes Uri Elkayam, MD, University of Southern California, Los Angeles.
Moreover, the study questions “whether the reverse remodeling and improvement of [LVEF] in women with PPCM represent a true recovery.” Prior studies “have shown an impaired contractile reserve as well as abnormal myocardial strain and reduced exercise capacity and even mortality in women with PPCM after RLV,” Dr. Elkayam notes.
It’s therefore possible – as with other forms of dilated cardiomyopathy – that LVEF normalization “does not represent a true recovery but a new steady state with subclinical myocardial dysfunction that is prone to development of recurrent [LV dysfunction] and clinical deterioration in response to various triggers such as long-standing hypertension, obesity, diabetes, illicit drug use,” and, “more importantly,” subsequent pregnancies.
The study points to “the need for a close long-term follow-up of women with PPCM” and provides “a rationale for early initiation of guideline-directed medical therapy after the diagnosis of PPCM and possible continuation even after improvement of LVEF.”
No funding source was reported. Dr. Modi and coauthors, Dr. Elkayam, and Dr. Hameed declare no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Family doctors provide most care for several chronic diseases
A population-based retrospective cohort study examined data from nearly 1 million patients with common chronic conditions in Alberta, Canada. Family doctors were the sole providers of care for 85.7% of patients with hypertension and 70.9% of those with diabetes.
The study is part of efforts to encourage more research “by primary care, for primary care,” study author Jessica Kirkwood, MD, family physician and assistant professor of family medicine at the University of Alberta, Edmonton, said in an interview. The prevalence of primary care involvement demonstrates the importance of involving family physicians in creating guidelines for management and developing clinical trials, Dr. Kirkwood said.
The study was published in Canadian Family Physician.
Who provides care?
The study focused on care provided from 2013 to 2017 for seven chronic conditions. The information collected consisted of data from administrative health databases, which track medical services provided by Alberta’s government-funded universal health care system.
Most patients’ care was managed by family physicians alone in four of the conditions studied: hypertension (85.7%), diabetes (70.9%), chronic obstructive pulmonary disease (59.8%), and asthma (65.5%).
Specialists were more involved in the remaining three diseases. They provided the sole management in 49.1% of patients with ischemic heart disease, 42.2% of those with chronic kidney disease, and 35.6% of those with heart failure. For these conditions, family physicians remained involved in the care for a large proportion of patients. Specialist involvement may be more common with these diseases because they sometimes involve interventions that only specialists offer, like angiography and dialysis, said Dr. Kirkwood.
The study also found that nurse practitioners were involved in care for very few patients (less than 1%), in accordance with the small number of nurse practitioners working in primary care settings.
Dr. Kirkwood acknowledged that the data come with certain limitations because they were not intended for research purposes. One limitation is that some conditions may not have been recorded because of “shadow billing.” Salaried physicians and practitioners do not have an incentive to include all diagnostic codes in their records. By comparison, clinicians operating under a fee-for-service model would be likely to indicate all diagnoses.
Developing guidelines
Despite the widespread management of chronic conditions by family physicians, these doctors represented about 17% of the experts who contribute to guidelines and recommendations, according to a 2015 study that the investigators cited.
“Frankly, that’s concerning,” said Dr. Kirkwood, regarding the disconnect between the people creating the recommendations and the people using them. The guidelines should include the perspective of clinicians who regularly work with patients, she said. Providing that perspective would also make the design of clinical trials on interventions more informative, the researchers concluded.
“I know as a family doctor myself that some recommendations are completely overwhelming,” especially given the range of issues that primary care clinicians see, said Dr. Kirkwood. Including primary care representatives who are familiar with the demands of the position “hopefully will make the recommendations much more applicable to the people that they will affect,” she said.
Dr. Kirkwood also noted the need for sufficient support for family doctors to contribute to guideline creation and research, especially for doctors in rural communities who are not already affiliated with a university.
The involvement of primary care providers in research settings is a primary goal of Patients, Experience, Evidence and Research (PEER), a primary care-led group that collaborates with the College of Family Physicians of Canada. The current investigators are members of PEER.
Additional conditions
Commenting on the study, Martin Fortin, MD, clinical teaching professor at the University of Sherbrooke, Quebec, said, “This is a good opportunity to advocate for more studies to be done in the primary care context, where the majority of chronic disease management is done.”
However, Dr. Fortin wishes that more diagnoses had been included in the study, such as mental health and musculoskeletal conditions like back pain and osteoarthritis. These conditions are also commonly seen by primary care clinicians, according to Dr. Fortin.
Because the number of conditions studied is limited, the data may not reflect the true prevalence of multimorbidity, Dr. Fortin added.
Primary care doctors provide a broad perspective on the overall health of patients, compared with specialists who focus on particular conditions. Similarly, during drug trials, pharmaceutical companies aim to reduce complicating factors, even though the medications are prescribed for conditions where multimorbidity is common. “Medication should be tested in the real environment,” said Dr. Fortin.
Ultimately, he added, the study cannot address the complexity of the patients, but it nevertheless sheds light on who is providing care and where the research on these conditions should be done.
The study was conducted without outside funding. Dr. Kirkwood and Dr. Fortin reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A population-based retrospective cohort study examined data from nearly 1 million patients with common chronic conditions in Alberta, Canada. Family doctors were the sole providers of care for 85.7% of patients with hypertension and 70.9% of those with diabetes.
The study is part of efforts to encourage more research “by primary care, for primary care,” study author Jessica Kirkwood, MD, family physician and assistant professor of family medicine at the University of Alberta, Edmonton, said in an interview. The prevalence of primary care involvement demonstrates the importance of involving family physicians in creating guidelines for management and developing clinical trials, Dr. Kirkwood said.
The study was published in Canadian Family Physician.
Who provides care?
The study focused on care provided from 2013 to 2017 for seven chronic conditions. The information collected consisted of data from administrative health databases, which track medical services provided by Alberta’s government-funded universal health care system.
Most patients’ care was managed by family physicians alone in four of the conditions studied: hypertension (85.7%), diabetes (70.9%), chronic obstructive pulmonary disease (59.8%), and asthma (65.5%).
Specialists were more involved in the remaining three diseases. They provided the sole management in 49.1% of patients with ischemic heart disease, 42.2% of those with chronic kidney disease, and 35.6% of those with heart failure. For these conditions, family physicians remained involved in the care for a large proportion of patients. Specialist involvement may be more common with these diseases because they sometimes involve interventions that only specialists offer, like angiography and dialysis, said Dr. Kirkwood.
The study also found that nurse practitioners were involved in care for very few patients (less than 1%), in accordance with the small number of nurse practitioners working in primary care settings.
Dr. Kirkwood acknowledged that the data come with certain limitations because they were not intended for research purposes. One limitation is that some conditions may not have been recorded because of “shadow billing.” Salaried physicians and practitioners do not have an incentive to include all diagnostic codes in their records. By comparison, clinicians operating under a fee-for-service model would be likely to indicate all diagnoses.
Developing guidelines
Despite the widespread management of chronic conditions by family physicians, these doctors represented about 17% of the experts who contribute to guidelines and recommendations, according to a 2015 study that the investigators cited.
“Frankly, that’s concerning,” said Dr. Kirkwood, regarding the disconnect between the people creating the recommendations and the people using them. The guidelines should include the perspective of clinicians who regularly work with patients, she said. Providing that perspective would also make the design of clinical trials on interventions more informative, the researchers concluded.
“I know as a family doctor myself that some recommendations are completely overwhelming,” especially given the range of issues that primary care clinicians see, said Dr. Kirkwood. Including primary care representatives who are familiar with the demands of the position “hopefully will make the recommendations much more applicable to the people that they will affect,” she said.
Dr. Kirkwood also noted the need for sufficient support for family doctors to contribute to guideline creation and research, especially for doctors in rural communities who are not already affiliated with a university.
The involvement of primary care providers in research settings is a primary goal of Patients, Experience, Evidence and Research (PEER), a primary care-led group that collaborates with the College of Family Physicians of Canada. The current investigators are members of PEER.
Additional conditions
Commenting on the study, Martin Fortin, MD, clinical teaching professor at the University of Sherbrooke, Quebec, said, “This is a good opportunity to advocate for more studies to be done in the primary care context, where the majority of chronic disease management is done.”
However, Dr. Fortin wishes that more diagnoses had been included in the study, such as mental health and musculoskeletal conditions like back pain and osteoarthritis. These conditions are also commonly seen by primary care clinicians, according to Dr. Fortin.
Because the number of conditions studied is limited, the data may not reflect the true prevalence of multimorbidity, Dr. Fortin added.
Primary care doctors provide a broad perspective on the overall health of patients, compared with specialists who focus on particular conditions. Similarly, during drug trials, pharmaceutical companies aim to reduce complicating factors, even though the medications are prescribed for conditions where multimorbidity is common. “Medication should be tested in the real environment,” said Dr. Fortin.
Ultimately, he added, the study cannot address the complexity of the patients, but it nevertheless sheds light on who is providing care and where the research on these conditions should be done.
The study was conducted without outside funding. Dr. Kirkwood and Dr. Fortin reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A population-based retrospective cohort study examined data from nearly 1 million patients with common chronic conditions in Alberta, Canada. Family doctors were the sole providers of care for 85.7% of patients with hypertension and 70.9% of those with diabetes.
The study is part of efforts to encourage more research “by primary care, for primary care,” study author Jessica Kirkwood, MD, family physician and assistant professor of family medicine at the University of Alberta, Edmonton, said in an interview. The prevalence of primary care involvement demonstrates the importance of involving family physicians in creating guidelines for management and developing clinical trials, Dr. Kirkwood said.
The study was published in Canadian Family Physician.
Who provides care?
The study focused on care provided from 2013 to 2017 for seven chronic conditions. The information collected consisted of data from administrative health databases, which track medical services provided by Alberta’s government-funded universal health care system.
Most patients’ care was managed by family physicians alone in four of the conditions studied: hypertension (85.7%), diabetes (70.9%), chronic obstructive pulmonary disease (59.8%), and asthma (65.5%).
Specialists were more involved in the remaining three diseases. They provided the sole management in 49.1% of patients with ischemic heart disease, 42.2% of those with chronic kidney disease, and 35.6% of those with heart failure. For these conditions, family physicians remained involved in the care for a large proportion of patients. Specialist involvement may be more common with these diseases because they sometimes involve interventions that only specialists offer, like angiography and dialysis, said Dr. Kirkwood.
The study also found that nurse practitioners were involved in care for very few patients (less than 1%), in accordance with the small number of nurse practitioners working in primary care settings.
Dr. Kirkwood acknowledged that the data come with certain limitations because they were not intended for research purposes. One limitation is that some conditions may not have been recorded because of “shadow billing.” Salaried physicians and practitioners do not have an incentive to include all diagnostic codes in their records. By comparison, clinicians operating under a fee-for-service model would be likely to indicate all diagnoses.
Developing guidelines
Despite the widespread management of chronic conditions by family physicians, these doctors represented about 17% of the experts who contribute to guidelines and recommendations, according to a 2015 study that the investigators cited.
“Frankly, that’s concerning,” said Dr. Kirkwood, regarding the disconnect between the people creating the recommendations and the people using them. The guidelines should include the perspective of clinicians who regularly work with patients, she said. Providing that perspective would also make the design of clinical trials on interventions more informative, the researchers concluded.
“I know as a family doctor myself that some recommendations are completely overwhelming,” especially given the range of issues that primary care clinicians see, said Dr. Kirkwood. Including primary care representatives who are familiar with the demands of the position “hopefully will make the recommendations much more applicable to the people that they will affect,” she said.
Dr. Kirkwood also noted the need for sufficient support for family doctors to contribute to guideline creation and research, especially for doctors in rural communities who are not already affiliated with a university.
The involvement of primary care providers in research settings is a primary goal of Patients, Experience, Evidence and Research (PEER), a primary care-led group that collaborates with the College of Family Physicians of Canada. The current investigators are members of PEER.
Additional conditions
Commenting on the study, Martin Fortin, MD, clinical teaching professor at the University of Sherbrooke, Quebec, said, “This is a good opportunity to advocate for more studies to be done in the primary care context, where the majority of chronic disease management is done.”
However, Dr. Fortin wishes that more diagnoses had been included in the study, such as mental health and musculoskeletal conditions like back pain and osteoarthritis. These conditions are also commonly seen by primary care clinicians, according to Dr. Fortin.
Because the number of conditions studied is limited, the data may not reflect the true prevalence of multimorbidity, Dr. Fortin added.
Primary care doctors provide a broad perspective on the overall health of patients, compared with specialists who focus on particular conditions. Similarly, during drug trials, pharmaceutical companies aim to reduce complicating factors, even though the medications are prescribed for conditions where multimorbidity is common. “Medication should be tested in the real environment,” said Dr. Fortin.
Ultimately, he added, the study cannot address the complexity of the patients, but it nevertheless sheds light on who is providing care and where the research on these conditions should be done.
The study was conducted without outside funding. Dr. Kirkwood and Dr. Fortin reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CANADIAN FAMILY PHYSICIAN