User login
For MD-IQ use only
Two treatments show early promise for hypothalamic obesity
Two different agents showed potential for safely treating patients with hypothalamic obesity in two pilot studies with small numbers of patients.
One study prospectively randomized 21 adults with acquired hypothalamic obesity to treatment with placebo or Tesomet, a compound that combines the novel monoamine reuptake inhibitor tesofensine with metoprolol, a beta-blocker added to protect against adverse effects from tesofensine on heart rate and cardiac contractility. After 24 weeks of treatment, people on tesofensine/metoprolol had significant weight loss, compared with controls, while showing good tolerance with no significant effects on heart rate, blood pressure, or heart rhythm, Ulla Feldt-Rasmussen, MD, DMSc, reported at the annual meeting of the Endocrine Society.
The second report reviewed 18 children and adolescents with either acquired or genetic hypothalamic obesity who received open-label treatment with dextroamphetamine for an average of 20 months, and overall patients safely lost an average of 0.43 in their body mass index (BMI) standard deviation score, reported Jiska van Schaik, MD, in a separate talk at the meeting.
‘A supplement for lost satiety’
Patients with hypothalamic obesity face a dual problem from hypothalamic dysfunction that’s addressed by tesofensine, the weight-loss agent in Tesomet that increases hypothalamic levels of dopamine, serotonin, and noradrenaline by blocking reuptake, and thereby dulls appetite and food craving while also increasing fat metabolism, explained Dr. Feldt-Rasmussen, a professor of medical endocrinology at the University of Denmark and Rigshospitalet in Copenhagen. No treatment currently has regulatory approval for treating any form of hypothalamic obesity.
Tesofensine works as “a supplement for lost satiety, and satiety is what is lost” in patients with hypothalamic obesity as well in patients as Prader-Willi syndrome, the two disorders for which tesofensine/metoprolol is currently undergoing testing. “That’s the rationale, and it seems to work,” she declared during her talk. The formulation contains 0.5 mg tesofensine and 50 mg metoprolol administered orally once daily.
The study, run at Rigshospitalet, randomized 21 patients aged 18-75 years and with a BMI of at least 27 kg/m2who all had acquired hypothalamic obesity secondary to hypothalamic damage following cancer treatment. Patients averaged about 45 years of age, three-quarters were women, and their average BMI was about 37, with 90% having a BMI of at least 30.
The study’s design calls for 48-week follow-up; Dr. Feldt-Rasmussen presented the interim results after 24 weeks, with 18 of the 21 enrolled patients remaining in the study through 24 weeks. Three patients dropped out because of adverse events: one in the placebo arm, and two who received tesofensine/metoprolol.
Weight dropped by an average of 6.6 kg from baseline among the 11 patients who completed 24 weeks on tesofensine/metoprolol treatment, compared with no average change from baseline among the seven patients who completed the study on placebo, a significant difference. The researchers measured a validated, composite satiety score every 4 weeks, and found significantly more improvement among patients on tesofensine/metoprolol than in those on placebo during the study’s first half, but subsequently average scores among the actively treated patients fell to the same level of modest improvement as in the placebo patients.
Despite this, average weight loss in the patients on tesofensine/metoprolol steadily increased throughout the full 24 weeks.
Safety measures of diastolic blood pressure, heart rate, and corrected QT interval showed no significant between-group difference. Systolic pressure showed a transient average rise of 4 mm Hg above baseline in the tesofensine/metoprolol group, compared with a small dip in the control patients, but by 24 weeks average systolic blood pressure had reverted closer to baseline levels in both subgroups and showed no significant between-group difference. Two patients on tesofensine/metoprolol developed serious adverse events. In one patient these were not treatment related. The other patient developed anxiety after 8 weeks that was possibly treatment related but remained on treatment. Other adverse effects on tesofensine/metoprolol included dizziness, sleep disorder, and dry mouth, but all of these were mild and patients were willing to tolerate them to achieve their weight loss, Dr. Feldt-Rasmussen said.
Repurposing an ADHD treatment
Dextroamphetamine increases satiety and boosts resting energy expenditure, and is a common treatment for attention deficit hyperactivity disorder. Dr. van Schaik and coauthors reviewed 13 children and adolescents with acquired hypothalamic obesity and 5 with genetic hypothalamic obesity who received the treatment at either of two Dutch hospitals during 2014-2020. All 18 patients went on dextroamphetamine after other interventions had failed to produce improvement, said Dr. van Schaik, a researcher at University Medical Center and Wilhelmina Children’s Hospital in Utrecht, the Netherlands. The patients averaged about 13 years of age.
In addition to an overall effect on weight across all 18 subjects, the researchers found they could subdivide the full cohort into 10 responders (56%), 4 (22%) with weight stabilization on treatment, and 4 nonresponders (22%) who continued to gain weight despite treatment. The 10 responding patients had an average drop in their BMI standard deviation score of 0.91. All 10 responders had acquired hypothalamic obesity, and they averaged a 12.5 percentage point rise in their resting energy expenditure level, compared with baseline, while on treatment. The four whose weight stabilized on treatment included three patients with genetic hypothalamic obesity. The four nonresponders split into two with acquired hypothalamic obesity and two with the genetic form.
Thirteen patients (72%) had improvements in hyperphagia, energy, and behavior, and no patient had a serious adverse effect. One patient stopped treatment after 1 month because of elevated blood pressure.
“Dextroamphetamine may be promising, especially for acquired hypothalamic obesity,” Dr. van Schaik concluded, adding that prospective, controlled assessments are needed, and that a healthy lifestyle is the foundation of hypothalamic obesity treatment.
The Tesomet study was sponsored by Saniona, the company developing Tesomet. Dr Feldt-Rasmussen is an advisor to Saniona, and some of the coauthors on the study are Saniona employees. Dr. van Schaik had no disclosures.
Two different agents showed potential for safely treating patients with hypothalamic obesity in two pilot studies with small numbers of patients.
One study prospectively randomized 21 adults with acquired hypothalamic obesity to treatment with placebo or Tesomet, a compound that combines the novel monoamine reuptake inhibitor tesofensine with metoprolol, a beta-blocker added to protect against adverse effects from tesofensine on heart rate and cardiac contractility. After 24 weeks of treatment, people on tesofensine/metoprolol had significant weight loss, compared with controls, while showing good tolerance with no significant effects on heart rate, blood pressure, or heart rhythm, Ulla Feldt-Rasmussen, MD, DMSc, reported at the annual meeting of the Endocrine Society.
The second report reviewed 18 children and adolescents with either acquired or genetic hypothalamic obesity who received open-label treatment with dextroamphetamine for an average of 20 months, and overall patients safely lost an average of 0.43 in their body mass index (BMI) standard deviation score, reported Jiska van Schaik, MD, in a separate talk at the meeting.
‘A supplement for lost satiety’
Patients with hypothalamic obesity face a dual problem from hypothalamic dysfunction that’s addressed by tesofensine, the weight-loss agent in Tesomet that increases hypothalamic levels of dopamine, serotonin, and noradrenaline by blocking reuptake, and thereby dulls appetite and food craving while also increasing fat metabolism, explained Dr. Feldt-Rasmussen, a professor of medical endocrinology at the University of Denmark and Rigshospitalet in Copenhagen. No treatment currently has regulatory approval for treating any form of hypothalamic obesity.
Tesofensine works as “a supplement for lost satiety, and satiety is what is lost” in patients with hypothalamic obesity as well in patients as Prader-Willi syndrome, the two disorders for which tesofensine/metoprolol is currently undergoing testing. “That’s the rationale, and it seems to work,” she declared during her talk. The formulation contains 0.5 mg tesofensine and 50 mg metoprolol administered orally once daily.
The study, run at Rigshospitalet, randomized 21 patients aged 18-75 years and with a BMI of at least 27 kg/m2who all had acquired hypothalamic obesity secondary to hypothalamic damage following cancer treatment. Patients averaged about 45 years of age, three-quarters were women, and their average BMI was about 37, with 90% having a BMI of at least 30.
The study’s design calls for 48-week follow-up; Dr. Feldt-Rasmussen presented the interim results after 24 weeks, with 18 of the 21 enrolled patients remaining in the study through 24 weeks. Three patients dropped out because of adverse events: one in the placebo arm, and two who received tesofensine/metoprolol.
Weight dropped by an average of 6.6 kg from baseline among the 11 patients who completed 24 weeks on tesofensine/metoprolol treatment, compared with no average change from baseline among the seven patients who completed the study on placebo, a significant difference. The researchers measured a validated, composite satiety score every 4 weeks, and found significantly more improvement among patients on tesofensine/metoprolol than in those on placebo during the study’s first half, but subsequently average scores among the actively treated patients fell to the same level of modest improvement as in the placebo patients.
Despite this, average weight loss in the patients on tesofensine/metoprolol steadily increased throughout the full 24 weeks.
Safety measures of diastolic blood pressure, heart rate, and corrected QT interval showed no significant between-group difference. Systolic pressure showed a transient average rise of 4 mm Hg above baseline in the tesofensine/metoprolol group, compared with a small dip in the control patients, but by 24 weeks average systolic blood pressure had reverted closer to baseline levels in both subgroups and showed no significant between-group difference. Two patients on tesofensine/metoprolol developed serious adverse events. In one patient these were not treatment related. The other patient developed anxiety after 8 weeks that was possibly treatment related but remained on treatment. Other adverse effects on tesofensine/metoprolol included dizziness, sleep disorder, and dry mouth, but all of these were mild and patients were willing to tolerate them to achieve their weight loss, Dr. Feldt-Rasmussen said.
Repurposing an ADHD treatment
Dextroamphetamine increases satiety and boosts resting energy expenditure, and is a common treatment for attention deficit hyperactivity disorder. Dr. van Schaik and coauthors reviewed 13 children and adolescents with acquired hypothalamic obesity and 5 with genetic hypothalamic obesity who received the treatment at either of two Dutch hospitals during 2014-2020. All 18 patients went on dextroamphetamine after other interventions had failed to produce improvement, said Dr. van Schaik, a researcher at University Medical Center and Wilhelmina Children’s Hospital in Utrecht, the Netherlands. The patients averaged about 13 years of age.
In addition to an overall effect on weight across all 18 subjects, the researchers found they could subdivide the full cohort into 10 responders (56%), 4 (22%) with weight stabilization on treatment, and 4 nonresponders (22%) who continued to gain weight despite treatment. The 10 responding patients had an average drop in their BMI standard deviation score of 0.91. All 10 responders had acquired hypothalamic obesity, and they averaged a 12.5 percentage point rise in their resting energy expenditure level, compared with baseline, while on treatment. The four whose weight stabilized on treatment included three patients with genetic hypothalamic obesity. The four nonresponders split into two with acquired hypothalamic obesity and two with the genetic form.
Thirteen patients (72%) had improvements in hyperphagia, energy, and behavior, and no patient had a serious adverse effect. One patient stopped treatment after 1 month because of elevated blood pressure.
“Dextroamphetamine may be promising, especially for acquired hypothalamic obesity,” Dr. van Schaik concluded, adding that prospective, controlled assessments are needed, and that a healthy lifestyle is the foundation of hypothalamic obesity treatment.
The Tesomet study was sponsored by Saniona, the company developing Tesomet. Dr Feldt-Rasmussen is an advisor to Saniona, and some of the coauthors on the study are Saniona employees. Dr. van Schaik had no disclosures.
Two different agents showed potential for safely treating patients with hypothalamic obesity in two pilot studies with small numbers of patients.
One study prospectively randomized 21 adults with acquired hypothalamic obesity to treatment with placebo or Tesomet, a compound that combines the novel monoamine reuptake inhibitor tesofensine with metoprolol, a beta-blocker added to protect against adverse effects from tesofensine on heart rate and cardiac contractility. After 24 weeks of treatment, people on tesofensine/metoprolol had significant weight loss, compared with controls, while showing good tolerance with no significant effects on heart rate, blood pressure, or heart rhythm, Ulla Feldt-Rasmussen, MD, DMSc, reported at the annual meeting of the Endocrine Society.
The second report reviewed 18 children and adolescents with either acquired or genetic hypothalamic obesity who received open-label treatment with dextroamphetamine for an average of 20 months, and overall patients safely lost an average of 0.43 in their body mass index (BMI) standard deviation score, reported Jiska van Schaik, MD, in a separate talk at the meeting.
‘A supplement for lost satiety’
Patients with hypothalamic obesity face a dual problem from hypothalamic dysfunction that’s addressed by tesofensine, the weight-loss agent in Tesomet that increases hypothalamic levels of dopamine, serotonin, and noradrenaline by blocking reuptake, and thereby dulls appetite and food craving while also increasing fat metabolism, explained Dr. Feldt-Rasmussen, a professor of medical endocrinology at the University of Denmark and Rigshospitalet in Copenhagen. No treatment currently has regulatory approval for treating any form of hypothalamic obesity.
Tesofensine works as “a supplement for lost satiety, and satiety is what is lost” in patients with hypothalamic obesity as well in patients as Prader-Willi syndrome, the two disorders for which tesofensine/metoprolol is currently undergoing testing. “That’s the rationale, and it seems to work,” she declared during her talk. The formulation contains 0.5 mg tesofensine and 50 mg metoprolol administered orally once daily.
The study, run at Rigshospitalet, randomized 21 patients aged 18-75 years and with a BMI of at least 27 kg/m2who all had acquired hypothalamic obesity secondary to hypothalamic damage following cancer treatment. Patients averaged about 45 years of age, three-quarters were women, and their average BMI was about 37, with 90% having a BMI of at least 30.
The study’s design calls for 48-week follow-up; Dr. Feldt-Rasmussen presented the interim results after 24 weeks, with 18 of the 21 enrolled patients remaining in the study through 24 weeks. Three patients dropped out because of adverse events: one in the placebo arm, and two who received tesofensine/metoprolol.
Weight dropped by an average of 6.6 kg from baseline among the 11 patients who completed 24 weeks on tesofensine/metoprolol treatment, compared with no average change from baseline among the seven patients who completed the study on placebo, a significant difference. The researchers measured a validated, composite satiety score every 4 weeks, and found significantly more improvement among patients on tesofensine/metoprolol than in those on placebo during the study’s first half, but subsequently average scores among the actively treated patients fell to the same level of modest improvement as in the placebo patients.
Despite this, average weight loss in the patients on tesofensine/metoprolol steadily increased throughout the full 24 weeks.
Safety measures of diastolic blood pressure, heart rate, and corrected QT interval showed no significant between-group difference. Systolic pressure showed a transient average rise of 4 mm Hg above baseline in the tesofensine/metoprolol group, compared with a small dip in the control patients, but by 24 weeks average systolic blood pressure had reverted closer to baseline levels in both subgroups and showed no significant between-group difference. Two patients on tesofensine/metoprolol developed serious adverse events. In one patient these were not treatment related. The other patient developed anxiety after 8 weeks that was possibly treatment related but remained on treatment. Other adverse effects on tesofensine/metoprolol included dizziness, sleep disorder, and dry mouth, but all of these were mild and patients were willing to tolerate them to achieve their weight loss, Dr. Feldt-Rasmussen said.
Repurposing an ADHD treatment
Dextroamphetamine increases satiety and boosts resting energy expenditure, and is a common treatment for attention deficit hyperactivity disorder. Dr. van Schaik and coauthors reviewed 13 children and adolescents with acquired hypothalamic obesity and 5 with genetic hypothalamic obesity who received the treatment at either of two Dutch hospitals during 2014-2020. All 18 patients went on dextroamphetamine after other interventions had failed to produce improvement, said Dr. van Schaik, a researcher at University Medical Center and Wilhelmina Children’s Hospital in Utrecht, the Netherlands. The patients averaged about 13 years of age.
In addition to an overall effect on weight across all 18 subjects, the researchers found they could subdivide the full cohort into 10 responders (56%), 4 (22%) with weight stabilization on treatment, and 4 nonresponders (22%) who continued to gain weight despite treatment. The 10 responding patients had an average drop in their BMI standard deviation score of 0.91. All 10 responders had acquired hypothalamic obesity, and they averaged a 12.5 percentage point rise in their resting energy expenditure level, compared with baseline, while on treatment. The four whose weight stabilized on treatment included three patients with genetic hypothalamic obesity. The four nonresponders split into two with acquired hypothalamic obesity and two with the genetic form.
Thirteen patients (72%) had improvements in hyperphagia, energy, and behavior, and no patient had a serious adverse effect. One patient stopped treatment after 1 month because of elevated blood pressure.
“Dextroamphetamine may be promising, especially for acquired hypothalamic obesity,” Dr. van Schaik concluded, adding that prospective, controlled assessments are needed, and that a healthy lifestyle is the foundation of hypothalamic obesity treatment.
The Tesomet study was sponsored by Saniona, the company developing Tesomet. Dr Feldt-Rasmussen is an advisor to Saniona, and some of the coauthors on the study are Saniona employees. Dr. van Schaik had no disclosures.
FROM ENDO 2021
Possible obesity effect detected in cancer death rates
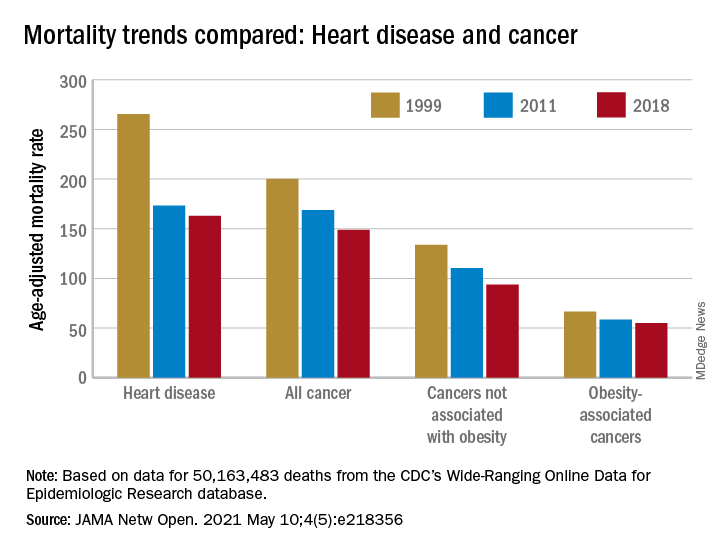
“By integrating 20 years of cancer mortality data, we demonstrated that trends in obesity-associated cancer mortality showed signs of recent deceleration, consistent with recent findings for heart disease mortality,” Christy L. Avery, PhD, and associates wrote in JAMA Network Open.
Improvements in mortality related to heart disease slowed after 2011, a phenomenon that has been associated with rising obesity rates. The age-adjusted mortality rate (AAMR) declined at an average of 3.8 deaths per 100,000 persons from 1999 to 2011 but only 0.7 deaths per 100,000 from 2011 to 2018, based on data from the Centers for Disease Control and Prevention’s Wide-Ranging Online Data for Epidemiologic Research (WONDER).
To understand trends in cancer mortality and their possible connection with obesity, data for 1999-2018 from the WONDER database were divided into obesity-associated and non–obesity-associated categories and compared with heart disease mortality, they explained. The database included more than 50 million deaths that matched inclusion criteria.
The analysis showed there was difference between obesity-associated and non–obesity-associated cancers that was obscured when all cancer deaths were considered together. The average annual change in AAMR for obesity-associated cancers slowed from –1.19 deaths per 100,000 in 1999-2011 to –0.83 in 2011-2018, Dr. Avery and associates reported.
For non–obesity-associated cancers, the annual change in AAMR increased from –1.62 per 100,000 for 1999-2011 to –2.29 for 2011-2018, following the trend for all cancers: –1.48 per 100,000 during 1999-2011 and –1.77 in 2011-2018, they said.
“The largest mortality decreases were observed for melanoma of the skin and lung cancer, two cancers not associated with obesity. For obesity-associated cancers, stable or increasing mortality rates have been observed for liver and pancreatic cancer among both men and women as well as for uterine cancer among women,” the investigators wrote.
Demographically, however, the slowing improvement in mortality for obesity-associated cancers did not follow the trend for heart disease. The deceleration for cancer was more pronounced for women and for non-Hispanic Whites and not seen at all in non-Hispanic Asian/Pacific Islander individuals. “For heart disease, evidence of a deceleration was consistent across sex, race, and ethnicity,” they said.
There are “longstanding disparities in obesity” among various populations in the United States, and the recent trend of obesity occurring earlier in life may be having an effect. “Whether the findings of decelerating mortality rates potentially signal a changing profile of cancer and heart disease mortality as the consequences of the obesity epidemic are realized remains to be seen,” they concluded.
The investigators reported receiving grants from the National Institutes of Health during the conduct of the study, but no other disclosures were reported.
“By integrating 20 years of cancer mortality data, we demonstrated that trends in obesity-associated cancer mortality showed signs of recent deceleration, consistent with recent findings for heart disease mortality,” Christy L. Avery, PhD, and associates wrote in JAMA Network Open.
Improvements in mortality related to heart disease slowed after 2011, a phenomenon that has been associated with rising obesity rates. The age-adjusted mortality rate (AAMR) declined at an average of 3.8 deaths per 100,000 persons from 1999 to 2011 but only 0.7 deaths per 100,000 from 2011 to 2018, based on data from the Centers for Disease Control and Prevention’s Wide-Ranging Online Data for Epidemiologic Research (WONDER).
To understand trends in cancer mortality and their possible connection with obesity, data for 1999-2018 from the WONDER database were divided into obesity-associated and non–obesity-associated categories and compared with heart disease mortality, they explained. The database included more than 50 million deaths that matched inclusion criteria.
The analysis showed there was difference between obesity-associated and non–obesity-associated cancers that was obscured when all cancer deaths were considered together. The average annual change in AAMR for obesity-associated cancers slowed from –1.19 deaths per 100,000 in 1999-2011 to –0.83 in 2011-2018, Dr. Avery and associates reported.
For non–obesity-associated cancers, the annual change in AAMR increased from –1.62 per 100,000 for 1999-2011 to –2.29 for 2011-2018, following the trend for all cancers: –1.48 per 100,000 during 1999-2011 and –1.77 in 2011-2018, they said.
“The largest mortality decreases were observed for melanoma of the skin and lung cancer, two cancers not associated with obesity. For obesity-associated cancers, stable or increasing mortality rates have been observed for liver and pancreatic cancer among both men and women as well as for uterine cancer among women,” the investigators wrote.
Demographically, however, the slowing improvement in mortality for obesity-associated cancers did not follow the trend for heart disease. The deceleration for cancer was more pronounced for women and for non-Hispanic Whites and not seen at all in non-Hispanic Asian/Pacific Islander individuals. “For heart disease, evidence of a deceleration was consistent across sex, race, and ethnicity,” they said.
There are “longstanding disparities in obesity” among various populations in the United States, and the recent trend of obesity occurring earlier in life may be having an effect. “Whether the findings of decelerating mortality rates potentially signal a changing profile of cancer and heart disease mortality as the consequences of the obesity epidemic are realized remains to be seen,” they concluded.
The investigators reported receiving grants from the National Institutes of Health during the conduct of the study, but no other disclosures were reported.
“By integrating 20 years of cancer mortality data, we demonstrated that trends in obesity-associated cancer mortality showed signs of recent deceleration, consistent with recent findings for heart disease mortality,” Christy L. Avery, PhD, and associates wrote in JAMA Network Open.
Improvements in mortality related to heart disease slowed after 2011, a phenomenon that has been associated with rising obesity rates. The age-adjusted mortality rate (AAMR) declined at an average of 3.8 deaths per 100,000 persons from 1999 to 2011 but only 0.7 deaths per 100,000 from 2011 to 2018, based on data from the Centers for Disease Control and Prevention’s Wide-Ranging Online Data for Epidemiologic Research (WONDER).
To understand trends in cancer mortality and their possible connection with obesity, data for 1999-2018 from the WONDER database were divided into obesity-associated and non–obesity-associated categories and compared with heart disease mortality, they explained. The database included more than 50 million deaths that matched inclusion criteria.
The analysis showed there was difference between obesity-associated and non–obesity-associated cancers that was obscured when all cancer deaths were considered together. The average annual change in AAMR for obesity-associated cancers slowed from –1.19 deaths per 100,000 in 1999-2011 to –0.83 in 2011-2018, Dr. Avery and associates reported.
For non–obesity-associated cancers, the annual change in AAMR increased from –1.62 per 100,000 for 1999-2011 to –2.29 for 2011-2018, following the trend for all cancers: –1.48 per 100,000 during 1999-2011 and –1.77 in 2011-2018, they said.
“The largest mortality decreases were observed for melanoma of the skin and lung cancer, two cancers not associated with obesity. For obesity-associated cancers, stable or increasing mortality rates have been observed for liver and pancreatic cancer among both men and women as well as for uterine cancer among women,” the investigators wrote.
Demographically, however, the slowing improvement in mortality for obesity-associated cancers did not follow the trend for heart disease. The deceleration for cancer was more pronounced for women and for non-Hispanic Whites and not seen at all in non-Hispanic Asian/Pacific Islander individuals. “For heart disease, evidence of a deceleration was consistent across sex, race, and ethnicity,” they said.
There are “longstanding disparities in obesity” among various populations in the United States, and the recent trend of obesity occurring earlier in life may be having an effect. “Whether the findings of decelerating mortality rates potentially signal a changing profile of cancer and heart disease mortality as the consequences of the obesity epidemic are realized remains to be seen,” they concluded.
The investigators reported receiving grants from the National Institutes of Health during the conduct of the study, but no other disclosures were reported.
FROM JAMA NETWORK OPEN
Novel hedgehog inhibitor strategies improve BCC outcomes
MD, a Mohs surgeon and chair of the department of dermatology at the Cleveland Clinic.

She and her colleagues have noticed an accelerated and durable response to hedgehog inhibitors after debulking and are studying cell signaling before and after debulking to better understand the issue.
Dr. Vidimos shared a remarkable case to illustrate the point during a clinical pearls talk at the annual meeting of the American College of Mohs Surgery.
An 82-year-old woman presented with a crusted, hemorrhagic, nodular basal cell carcinoma (BCC) that had overgrown over nearly her entire nose and left lower eyelid. A recurrence of a previous BCC, the tumor had been growing for a decade and had invaded her nasal bones but not the periorbital tissue.
An outside surgeon suggested a full rhinectomy and removal of the lower eyelid, but the woman refused.
Dr. Vidimos decided to treat her with vismodegib, but prior to doing so, she debulked the tumor to help with the pain and bleeding. She did not curette the portion of tumor extending through the ala into the nasal vestibule. “I let the vismodegib take care of that,” she said.
After 9 months, the tumor was virtually gone, with no recurrence after 3 years. Surgical debulking prior to hedgehog inhibition “reduces the tumor burden and may increase the efficacy and shorten the course of therapy,” Dr. Vidimos said.
The hedgehog inhibitors vismodegib (Erivedge) and sonidegib Odomzo are both approved for treating locally advanced BCC, with a complete response of 31% of locally advanced disease with vismodegib, according to one report.
But monotherapy is limited by intolerable side effects, most commonly muscle spasms, alopecia, and dysgeusia. To minimize the impact, Dr. Vidimos generally puts patients on treatment with Monday through Friday dosing and gives them the weekends off, a schedule she and her colleagues have reported works as well as daily dosing.
Still, many patients discontinue the drugs because of the side effects. Hedgehog inhibitors are also expensive and responses aren’t always durable. To increase efficacy and shorten the course of therapy, “we need alternative treatment strategies,” Dr. Vidimos said.
Up-front tumor debulking is one such strategy. Altered cell signaling pathways associated with tissue remodeling might improve response, and debulking may reduce the genetic heterogeneity of tumor cells, rendering remaining cells less resistant to hedgehog inhibition, she explained.
“It is exciting to see how tumor debulking may reduce tumor burden and heterogeneity, and thus lead to a durable response in extensive tumors,” said Vishal Patel, MD, assistant professor of dermatology and director of the cutaneous oncology program at George Washington University, Washington, who heard the presentation. “More investigation is needed to reproduce these results, but this approach may lead to improved outcomes with targeted therapies,” he said in an interview.
Combination therapy with other agents is another option, and there also seems to be a synergistic effect with radiation, with hedgehog inhibitors increasing cellular response to radiation therapy, Dr. Vidimos said.
Hedgehog inhibitors can also be used to shrink tumors before surgery. One small series found a 27% decrease in the area of the tumor after 3 to 6 months of preoperative vismodegib.
Dr. Vidimos shared another case to illustrate the point.
A 64-year-old woman fainted and presented to the ED with a hemoglobin of 3.2 mg/dL because of chronic blood loss from an ulcerated BCC on her upper back. The lesion measured 25 cm by 9 cm, and was 3.5 cm deep with no bone involvement. The woman was addicted to opioids by the time she presented.
She was started on vismodegib; the ulcer shrunk considerably after 6 months, and the woman underwent a resection. Only one small focus of BCC was found across 78 specimens submitted to Dr. Vidimos for Mohs reading.
Resection was followed by a muscle flap repair and radiation. At 5 and a half years, there is no evidence of disease; the only sign that the lesion had been there was a scar running along the woman’s upper spine.
The approach “was very successful for a very aggressive and worrisome tumor,” Dr. Vidimos said.
Dr. Vidimos did not have any relevant disclosures. Dr. Patel had no relevant disclosures.
MD, a Mohs surgeon and chair of the department of dermatology at the Cleveland Clinic.
She and her colleagues have noticed an accelerated and durable response to hedgehog inhibitors after debulking and are studying cell signaling before and after debulking to better understand the issue.
Dr. Vidimos shared a remarkable case to illustrate the point during a clinical pearls talk at the annual meeting of the American College of Mohs Surgery.
An 82-year-old woman presented with a crusted, hemorrhagic, nodular basal cell carcinoma (BCC) that had overgrown over nearly her entire nose and left lower eyelid. A recurrence of a previous BCC, the tumor had been growing for a decade and had invaded her nasal bones but not the periorbital tissue.
An outside surgeon suggested a full rhinectomy and removal of the lower eyelid, but the woman refused.
Dr. Vidimos decided to treat her with vismodegib, but prior to doing so, she debulked the tumor to help with the pain and bleeding. She did not curette the portion of tumor extending through the ala into the nasal vestibule. “I let the vismodegib take care of that,” she said.
After 9 months, the tumor was virtually gone, with no recurrence after 3 years. Surgical debulking prior to hedgehog inhibition “reduces the tumor burden and may increase the efficacy and shorten the course of therapy,” Dr. Vidimos said.
The hedgehog inhibitors vismodegib (Erivedge) and sonidegib Odomzo are both approved for treating locally advanced BCC, with a complete response of 31% of locally advanced disease with vismodegib, according to one report.
But monotherapy is limited by intolerable side effects, most commonly muscle spasms, alopecia, and dysgeusia. To minimize the impact, Dr. Vidimos generally puts patients on treatment with Monday through Friday dosing and gives them the weekends off, a schedule she and her colleagues have reported works as well as daily dosing.
Still, many patients discontinue the drugs because of the side effects. Hedgehog inhibitors are also expensive and responses aren’t always durable. To increase efficacy and shorten the course of therapy, “we need alternative treatment strategies,” Dr. Vidimos said.
Up-front tumor debulking is one such strategy. Altered cell signaling pathways associated with tissue remodeling might improve response, and debulking may reduce the genetic heterogeneity of tumor cells, rendering remaining cells less resistant to hedgehog inhibition, she explained.
“It is exciting to see how tumor debulking may reduce tumor burden and heterogeneity, and thus lead to a durable response in extensive tumors,” said Vishal Patel, MD, assistant professor of dermatology and director of the cutaneous oncology program at George Washington University, Washington, who heard the presentation. “More investigation is needed to reproduce these results, but this approach may lead to improved outcomes with targeted therapies,” he said in an interview.
Combination therapy with other agents is another option, and there also seems to be a synergistic effect with radiation, with hedgehog inhibitors increasing cellular response to radiation therapy, Dr. Vidimos said.
Hedgehog inhibitors can also be used to shrink tumors before surgery. One small series found a 27% decrease in the area of the tumor after 3 to 6 months of preoperative vismodegib.
Dr. Vidimos shared another case to illustrate the point.
A 64-year-old woman fainted and presented to the ED with a hemoglobin of 3.2 mg/dL because of chronic blood loss from an ulcerated BCC on her upper back. The lesion measured 25 cm by 9 cm, and was 3.5 cm deep with no bone involvement. The woman was addicted to opioids by the time she presented.
She was started on vismodegib; the ulcer shrunk considerably after 6 months, and the woman underwent a resection. Only one small focus of BCC was found across 78 specimens submitted to Dr. Vidimos for Mohs reading.
Resection was followed by a muscle flap repair and radiation. At 5 and a half years, there is no evidence of disease; the only sign that the lesion had been there was a scar running along the woman’s upper spine.
The approach “was very successful for a very aggressive and worrisome tumor,” Dr. Vidimos said.
Dr. Vidimos did not have any relevant disclosures. Dr. Patel had no relevant disclosures.
MD, a Mohs surgeon and chair of the department of dermatology at the Cleveland Clinic.
She and her colleagues have noticed an accelerated and durable response to hedgehog inhibitors after debulking and are studying cell signaling before and after debulking to better understand the issue.
Dr. Vidimos shared a remarkable case to illustrate the point during a clinical pearls talk at the annual meeting of the American College of Mohs Surgery.
An 82-year-old woman presented with a crusted, hemorrhagic, nodular basal cell carcinoma (BCC) that had overgrown over nearly her entire nose and left lower eyelid. A recurrence of a previous BCC, the tumor had been growing for a decade and had invaded her nasal bones but not the periorbital tissue.
An outside surgeon suggested a full rhinectomy and removal of the lower eyelid, but the woman refused.
Dr. Vidimos decided to treat her with vismodegib, but prior to doing so, she debulked the tumor to help with the pain and bleeding. She did not curette the portion of tumor extending through the ala into the nasal vestibule. “I let the vismodegib take care of that,” she said.
After 9 months, the tumor was virtually gone, with no recurrence after 3 years. Surgical debulking prior to hedgehog inhibition “reduces the tumor burden and may increase the efficacy and shorten the course of therapy,” Dr. Vidimos said.
The hedgehog inhibitors vismodegib (Erivedge) and sonidegib Odomzo are both approved for treating locally advanced BCC, with a complete response of 31% of locally advanced disease with vismodegib, according to one report.
But monotherapy is limited by intolerable side effects, most commonly muscle spasms, alopecia, and dysgeusia. To minimize the impact, Dr. Vidimos generally puts patients on treatment with Monday through Friday dosing and gives them the weekends off, a schedule she and her colleagues have reported works as well as daily dosing.
Still, many patients discontinue the drugs because of the side effects. Hedgehog inhibitors are also expensive and responses aren’t always durable. To increase efficacy and shorten the course of therapy, “we need alternative treatment strategies,” Dr. Vidimos said.
Up-front tumor debulking is one such strategy. Altered cell signaling pathways associated with tissue remodeling might improve response, and debulking may reduce the genetic heterogeneity of tumor cells, rendering remaining cells less resistant to hedgehog inhibition, she explained.
“It is exciting to see how tumor debulking may reduce tumor burden and heterogeneity, and thus lead to a durable response in extensive tumors,” said Vishal Patel, MD, assistant professor of dermatology and director of the cutaneous oncology program at George Washington University, Washington, who heard the presentation. “More investigation is needed to reproduce these results, but this approach may lead to improved outcomes with targeted therapies,” he said in an interview.
Combination therapy with other agents is another option, and there also seems to be a synergistic effect with radiation, with hedgehog inhibitors increasing cellular response to radiation therapy, Dr. Vidimos said.
Hedgehog inhibitors can also be used to shrink tumors before surgery. One small series found a 27% decrease in the area of the tumor after 3 to 6 months of preoperative vismodegib.
Dr. Vidimos shared another case to illustrate the point.
A 64-year-old woman fainted and presented to the ED with a hemoglobin of 3.2 mg/dL because of chronic blood loss from an ulcerated BCC on her upper back. The lesion measured 25 cm by 9 cm, and was 3.5 cm deep with no bone involvement. The woman was addicted to opioids by the time she presented.
She was started on vismodegib; the ulcer shrunk considerably after 6 months, and the woman underwent a resection. Only one small focus of BCC was found across 78 specimens submitted to Dr. Vidimos for Mohs reading.
Resection was followed by a muscle flap repair and radiation. At 5 and a half years, there is no evidence of disease; the only sign that the lesion had been there was a scar running along the woman’s upper spine.
The approach “was very successful for a very aggressive and worrisome tumor,” Dr. Vidimos said.
Dr. Vidimos did not have any relevant disclosures. Dr. Patel had no relevant disclosures.
FROM THE ACMS ANNUAL MEETING
Clinician well-being a top priority, Surgeon General says
Clinicians’ well-being is a “crisis” of grave import to the public health and a top issue that he hopes to get more squarely on the public radar screen, Surgeon General Vivek Murthy, MD, MBA, said May 6 in a “fireside chat” with SHM president Danielle Scheurer, MD, MSRC, SFHM, at SHM Converge, the annual conference of the Society of Hospital Medicine.

“This is a crisis that I don’t know that the country recognizes is fully important,” Dr. Murthy said. “I don’t think that most people in the public recognize just how extraordinarily difficult it is, for many clinicians, to come to practice. And if the clinicians continue to burn out at the rate that they are – in addition to the humanitarian crisis of people who are struggling that we should all feel concern about – it will impact care in a profound way.” He said part of his plan is a “national agenda” for clinician well-being, with a clear pathway for creating an environment more conducive to providing quality patient care.
Dr. Scheurer said that this was “welcome news and wonderful to hear.”
“Fortunately or unfortunately, now I do think it’s more in the front seat,” she said, adding that “this notion of ‘heal thyself,’ we know doesn’t work and these are really systemic ailments that we all have to tackle together.”
Dr. Murthy, a hospitalist by training, recently began his second term as Surgeon General, having served under President Obama and appointed to the post again by President Biden. This second appointment is different in the knowledge he has about the job from the start, in the enormity of the public health challenges posed by the COVID-19 pandemic, and in the political tenor of the country.
He said one of his main priorities is to “recenter our public health response” with scientists and public health leaders regaining their proper role.
“Have them be the voices that are actually speaking directly to the public, not in a way that’s biased by the politics or by politicians, but it’s really guided again by the science and substance of what we know needs to happen,” he said.
The response to COVID goes beyond continuing an aggressive vaccination and testing campaign, he said. The pandemic has given rise to worse mental health issues such as depression and anxiety, substance use disorders, and delays in care for other medical conditions for fear of infection – and these are all priorities, Dr. Murthy said.
One “silver lining” of the pandemic is the expansion of telehealth, but this needs refining and persistence to make it work optimally for all patients, he said.
“We have to ensure that that expansion continues and that it’s even – meaning that there are so many parts of the country where broadband access is a challenge for patients, so they don’t have the benefits of telemedicine,” he said. “We also need to ensure that these systems are integrated across our current systems, across hospitals so that we’re not creating more work for clinicians when it comes to utilizing this technology to reach their patients.”
Clinicians – typically viewed as coming to Capitol Hill only to push for higher payment or changes to medical liability laws – need to use their trusted voices to raise the profile of preventive care and identifying and fixing social barriers related to health, such as transportation issues and unsafe neighborhoods, Dr. Murthy said.
“No one really celebrates the heart attack that was prevented or the asthma that was prevented – we celebrate the illness that took place and was cured,” he said. “We know as clinicians that if you really want to reduce human suffering that you have to focus on the prevention side of the house, and I think that unless our colleagues in medicine and in public health come together and advocate for greater investments in prevention, or a national agenda around prevention, my worry is that it won’t naturally develop.”
On vaccine hesitancy, Dr. Murthy said that the United States needs to work more in increasing confidence that the vaccines will work, and in access to vaccines, but, mostly, in motivation.
“What we’ve learned is that ultimately trusted voices are what make all the difference when it comes to vaccination,” he said. “It’s one of these large, people-powered movements that we have to build in our community.”

Dr. Scheurer noted that, with hospitalists in 90% of U.S. hospitals, they can play a big role. “If we can all do our part then we’ll at least take the ball further down the field.”
Dr. Murthy added that, since residency, when he cared for young cancer patients near his own age, he has focused on “finding meaning now” in his work and life. The pandemic has reinforced this, and he doesn’t necessarily want life to go back to exactly how it was before the pandemic.
“Many of us are thinking – ‘Is there actually a better way for us to live our lives and design our workdays and our choices other than what we were doing prepandemic? Can we center our lives more around the people we love and care about, can we design our work to accommodate our family as opposed to the other way around, to always make our families accommodate our work?’ – These are the kinds of choices that we have to make as a society.”
Clinicians’ well-being is a “crisis” of grave import to the public health and a top issue that he hopes to get more squarely on the public radar screen, Surgeon General Vivek Murthy, MD, MBA, said May 6 in a “fireside chat” with SHM president Danielle Scheurer, MD, MSRC, SFHM, at SHM Converge, the annual conference of the Society of Hospital Medicine.
“This is a crisis that I don’t know that the country recognizes is fully important,” Dr. Murthy said. “I don’t think that most people in the public recognize just how extraordinarily difficult it is, for many clinicians, to come to practice. And if the clinicians continue to burn out at the rate that they are – in addition to the humanitarian crisis of people who are struggling that we should all feel concern about – it will impact care in a profound way.” He said part of his plan is a “national agenda” for clinician well-being, with a clear pathway for creating an environment more conducive to providing quality patient care.
Dr. Scheurer said that this was “welcome news and wonderful to hear.”
“Fortunately or unfortunately, now I do think it’s more in the front seat,” she said, adding that “this notion of ‘heal thyself,’ we know doesn’t work and these are really systemic ailments that we all have to tackle together.”
Dr. Murthy, a hospitalist by training, recently began his second term as Surgeon General, having served under President Obama and appointed to the post again by President Biden. This second appointment is different in the knowledge he has about the job from the start, in the enormity of the public health challenges posed by the COVID-19 pandemic, and in the political tenor of the country.
He said one of his main priorities is to “recenter our public health response” with scientists and public health leaders regaining their proper role.
“Have them be the voices that are actually speaking directly to the public, not in a way that’s biased by the politics or by politicians, but it’s really guided again by the science and substance of what we know needs to happen,” he said.
The response to COVID goes beyond continuing an aggressive vaccination and testing campaign, he said. The pandemic has given rise to worse mental health issues such as depression and anxiety, substance use disorders, and delays in care for other medical conditions for fear of infection – and these are all priorities, Dr. Murthy said.
One “silver lining” of the pandemic is the expansion of telehealth, but this needs refining and persistence to make it work optimally for all patients, he said.
“We have to ensure that that expansion continues and that it’s even – meaning that there are so many parts of the country where broadband access is a challenge for patients, so they don’t have the benefits of telemedicine,” he said. “We also need to ensure that these systems are integrated across our current systems, across hospitals so that we’re not creating more work for clinicians when it comes to utilizing this technology to reach their patients.”
Clinicians – typically viewed as coming to Capitol Hill only to push for higher payment or changes to medical liability laws – need to use their trusted voices to raise the profile of preventive care and identifying and fixing social barriers related to health, such as transportation issues and unsafe neighborhoods, Dr. Murthy said.
“No one really celebrates the heart attack that was prevented or the asthma that was prevented – we celebrate the illness that took place and was cured,” he said. “We know as clinicians that if you really want to reduce human suffering that you have to focus on the prevention side of the house, and I think that unless our colleagues in medicine and in public health come together and advocate for greater investments in prevention, or a national agenda around prevention, my worry is that it won’t naturally develop.”
On vaccine hesitancy, Dr. Murthy said that the United States needs to work more in increasing confidence that the vaccines will work, and in access to vaccines, but, mostly, in motivation.
“What we’ve learned is that ultimately trusted voices are what make all the difference when it comes to vaccination,” he said. “It’s one of these large, people-powered movements that we have to build in our community.”
Dr. Scheurer noted that, with hospitalists in 90% of U.S. hospitals, they can play a big role. “If we can all do our part then we’ll at least take the ball further down the field.”
Dr. Murthy added that, since residency, when he cared for young cancer patients near his own age, he has focused on “finding meaning now” in his work and life. The pandemic has reinforced this, and he doesn’t necessarily want life to go back to exactly how it was before the pandemic.
“Many of us are thinking – ‘Is there actually a better way for us to live our lives and design our workdays and our choices other than what we were doing prepandemic? Can we center our lives more around the people we love and care about, can we design our work to accommodate our family as opposed to the other way around, to always make our families accommodate our work?’ – These are the kinds of choices that we have to make as a society.”
Clinicians’ well-being is a “crisis” of grave import to the public health and a top issue that he hopes to get more squarely on the public radar screen, Surgeon General Vivek Murthy, MD, MBA, said May 6 in a “fireside chat” with SHM president Danielle Scheurer, MD, MSRC, SFHM, at SHM Converge, the annual conference of the Society of Hospital Medicine.
“This is a crisis that I don’t know that the country recognizes is fully important,” Dr. Murthy said. “I don’t think that most people in the public recognize just how extraordinarily difficult it is, for many clinicians, to come to practice. And if the clinicians continue to burn out at the rate that they are – in addition to the humanitarian crisis of people who are struggling that we should all feel concern about – it will impact care in a profound way.” He said part of his plan is a “national agenda” for clinician well-being, with a clear pathway for creating an environment more conducive to providing quality patient care.
Dr. Scheurer said that this was “welcome news and wonderful to hear.”
“Fortunately or unfortunately, now I do think it’s more in the front seat,” she said, adding that “this notion of ‘heal thyself,’ we know doesn’t work and these are really systemic ailments that we all have to tackle together.”
Dr. Murthy, a hospitalist by training, recently began his second term as Surgeon General, having served under President Obama and appointed to the post again by President Biden. This second appointment is different in the knowledge he has about the job from the start, in the enormity of the public health challenges posed by the COVID-19 pandemic, and in the political tenor of the country.
He said one of his main priorities is to “recenter our public health response” with scientists and public health leaders regaining their proper role.
“Have them be the voices that are actually speaking directly to the public, not in a way that’s biased by the politics or by politicians, but it’s really guided again by the science and substance of what we know needs to happen,” he said.
The response to COVID goes beyond continuing an aggressive vaccination and testing campaign, he said. The pandemic has given rise to worse mental health issues such as depression and anxiety, substance use disorders, and delays in care for other medical conditions for fear of infection – and these are all priorities, Dr. Murthy said.
One “silver lining” of the pandemic is the expansion of telehealth, but this needs refining and persistence to make it work optimally for all patients, he said.
“We have to ensure that that expansion continues and that it’s even – meaning that there are so many parts of the country where broadband access is a challenge for patients, so they don’t have the benefits of telemedicine,” he said. “We also need to ensure that these systems are integrated across our current systems, across hospitals so that we’re not creating more work for clinicians when it comes to utilizing this technology to reach their patients.”
Clinicians – typically viewed as coming to Capitol Hill only to push for higher payment or changes to medical liability laws – need to use their trusted voices to raise the profile of preventive care and identifying and fixing social barriers related to health, such as transportation issues and unsafe neighborhoods, Dr. Murthy said.
“No one really celebrates the heart attack that was prevented or the asthma that was prevented – we celebrate the illness that took place and was cured,” he said. “We know as clinicians that if you really want to reduce human suffering that you have to focus on the prevention side of the house, and I think that unless our colleagues in medicine and in public health come together and advocate for greater investments in prevention, or a national agenda around prevention, my worry is that it won’t naturally develop.”
On vaccine hesitancy, Dr. Murthy said that the United States needs to work more in increasing confidence that the vaccines will work, and in access to vaccines, but, mostly, in motivation.
“What we’ve learned is that ultimately trusted voices are what make all the difference when it comes to vaccination,” he said. “It’s one of these large, people-powered movements that we have to build in our community.”
Dr. Scheurer noted that, with hospitalists in 90% of U.S. hospitals, they can play a big role. “If we can all do our part then we’ll at least take the ball further down the field.”
Dr. Murthy added that, since residency, when he cared for young cancer patients near his own age, he has focused on “finding meaning now” in his work and life. The pandemic has reinforced this, and he doesn’t necessarily want life to go back to exactly how it was before the pandemic.
“Many of us are thinking – ‘Is there actually a better way for us to live our lives and design our workdays and our choices other than what we were doing prepandemic? Can we center our lives more around the people we love and care about, can we design our work to accommodate our family as opposed to the other way around, to always make our families accommodate our work?’ – These are the kinds of choices that we have to make as a society.”
FROM SHM CONVERGE 2021
Genital skin exams in girls: Conduct with care, look for signs of abuse
at the American Academy of Dermatology Virtual Meeting Experience.

“One in four adult women report being childhood victims of sexual abuse, which is just a staggering number. This is an opportunity for us to identify these patients early and give them the terminology to be able to report what is happening to them,” said pediatric dermatologist Kalyani Marathe, MD, MPH, director of the division of dermatology at Cincinnati Children’s Hospital. “We also have the chance to give them a sense of agency over their bodies.”
Dr. Marathe offered the following recommendations when performing a genital skin exam:
- Make sure a “chaperone” is present. “Chaperones are a must when you’re examining children and teens,” she said. “Ask whom they prefer. For prepubertal children, you’re going to usually use the parent who’s there with them. If the parent is their father, they might ask him to step behind the curtain, in which case you can bring over your nurse or medical assistant.” Teens may ask either parent to step out of the room, she said. In that case, a nurse, medical assistant, resident, or trainee can fill in. “If you have male residents or trainees with you and the patient really does not want to be examined by a male, honor their request. Do not force them.”
- Explain why the exam is being performed. Make sure the patient understands why she is being seen, Dr. Marathe advised. For example, say something like “your pediatrician told us that you have an itchy area” or “your mom told us that there’s some loss of color in that area, that you’re having a problem there.” She added that it’s helpful to explain the type of doctor you are, with a comment such as the following: “We’re examining you because we’re doctors who specialize in skin. ... We want to help you feel better and make sure that your skin heals and is healthy.”
- Ask both the child and the parent for permission to perform the exam. While this may seem trivial, “it’s very, very important in setting the right tone for the encounter,” she said. “If the child says yes, we turn to the mom and say: ‘Mom, is it okay for us to do this exam today?’ You can see visible relief on the part of the parent, and as the parent relaxes, the child relaxes. Just saying those few things really makes the encounter so much smoother.” However, “if they say no, you have to honor the response. ... You say: ‘Okay, we’re not going to do the exam today,” and see the patient in a few weeks. If it’s urgent, an exam under anesthesia may be an option, she added.
- Talk to the child about the terms they use for private parts. It can be helpful to ask: “Do you have any terms for your private area?” According to Dr. Marathe, “this is a good chance to educate them on the terms vulva and vagina since they may be using other terminology. Making sure that they have the correct terms will actually help patients identify and report abuse earlier.” Dr. Marathe recalled that a colleague had a patient who’d been calling her private area “pound cake” and had been “reporting to her teacher that someone had been touching her ‘pound cake.’ Her teacher did not know what she meant by that, and this led to a great delay in her childhood abuse being reported.”
- Talk about what will happen during the exam. “I like to show them any instruments that we’re going to be using,” Dr. Marathe said. “If we’re using a flashlight, for example, I like to show them a picture [of a flashlight] or show them that flashlight. If we’re using a camera to do digital photography, show them that. If we’re going to be using a Q-tip or a swab to demonstrate anything or to take a culture, I like to show them that beforehand to make sure that they know what we’re doing.” In regard to photography, “make sure the parent and child know where the photos are going to go, who’s going to see them, what are they going to be used for. If they’re going to be used for educational purposes, make sure they have given explicit permission for that and they know they’ll be deidentified.”
- Make it clear that the exam won’t be painful. It’s important to put both the patient and the parent at ease on this front, Dr. Marathe said. “A lot of parents are concerned that we’re going to do a speculum exam in their prepubertal child. So make sure that it’s clarified ahead of time that we’re not going to be doing a speculum exam.”
Commenting on this topic, Tor Shwayder, MD, a pediatric dermatologist at Henry Ford Health System, Detroit, urged colleagues to take action if they feel suspicious about a possible sign of child abuse, even if they’re far from certain that anything is wrong. “Don’t ignore those feelings in the back of the brain,” he said in an interview.
Most states have child-abuse hotlines for medical professionals, and major hospitals will have child-abuse teams, Dr. Shwayder said. He urged dermatologists to take advantage of these resources when appropriate. “The professionals on the other side of the 800 number or at the hospital will help you. You don’t have to decide immediately whether this is child abuse. You just need to have a suspicion.”
Dr. Marathe and Dr. Shwayder report no disclosures.
at the American Academy of Dermatology Virtual Meeting Experience.
“One in four adult women report being childhood victims of sexual abuse, which is just a staggering number. This is an opportunity for us to identify these patients early and give them the terminology to be able to report what is happening to them,” said pediatric dermatologist Kalyani Marathe, MD, MPH, director of the division of dermatology at Cincinnati Children’s Hospital. “We also have the chance to give them a sense of agency over their bodies.”
Dr. Marathe offered the following recommendations when performing a genital skin exam:
- Make sure a “chaperone” is present. “Chaperones are a must when you’re examining children and teens,” she said. “Ask whom they prefer. For prepubertal children, you’re going to usually use the parent who’s there with them. If the parent is their father, they might ask him to step behind the curtain, in which case you can bring over your nurse or medical assistant.” Teens may ask either parent to step out of the room, she said. In that case, a nurse, medical assistant, resident, or trainee can fill in. “If you have male residents or trainees with you and the patient really does not want to be examined by a male, honor their request. Do not force them.”
- Explain why the exam is being performed. Make sure the patient understands why she is being seen, Dr. Marathe advised. For example, say something like “your pediatrician told us that you have an itchy area” or “your mom told us that there’s some loss of color in that area, that you’re having a problem there.” She added that it’s helpful to explain the type of doctor you are, with a comment such as the following: “We’re examining you because we’re doctors who specialize in skin. ... We want to help you feel better and make sure that your skin heals and is healthy.”
- Ask both the child and the parent for permission to perform the exam. While this may seem trivial, “it’s very, very important in setting the right tone for the encounter,” she said. “If the child says yes, we turn to the mom and say: ‘Mom, is it okay for us to do this exam today?’ You can see visible relief on the part of the parent, and as the parent relaxes, the child relaxes. Just saying those few things really makes the encounter so much smoother.” However, “if they say no, you have to honor the response. ... You say: ‘Okay, we’re not going to do the exam today,” and see the patient in a few weeks. If it’s urgent, an exam under anesthesia may be an option, she added.
- Talk to the child about the terms they use for private parts. It can be helpful to ask: “Do you have any terms for your private area?” According to Dr. Marathe, “this is a good chance to educate them on the terms vulva and vagina since they may be using other terminology. Making sure that they have the correct terms will actually help patients identify and report abuse earlier.” Dr. Marathe recalled that a colleague had a patient who’d been calling her private area “pound cake” and had been “reporting to her teacher that someone had been touching her ‘pound cake.’ Her teacher did not know what she meant by that, and this led to a great delay in her childhood abuse being reported.”
- Talk about what will happen during the exam. “I like to show them any instruments that we’re going to be using,” Dr. Marathe said. “If we’re using a flashlight, for example, I like to show them a picture [of a flashlight] or show them that flashlight. If we’re using a camera to do digital photography, show them that. If we’re going to be using a Q-tip or a swab to demonstrate anything or to take a culture, I like to show them that beforehand to make sure that they know what we’re doing.” In regard to photography, “make sure the parent and child know where the photos are going to go, who’s going to see them, what are they going to be used for. If they’re going to be used for educational purposes, make sure they have given explicit permission for that and they know they’ll be deidentified.”
- Make it clear that the exam won’t be painful. It’s important to put both the patient and the parent at ease on this front, Dr. Marathe said. “A lot of parents are concerned that we’re going to do a speculum exam in their prepubertal child. So make sure that it’s clarified ahead of time that we’re not going to be doing a speculum exam.”
Commenting on this topic, Tor Shwayder, MD, a pediatric dermatologist at Henry Ford Health System, Detroit, urged colleagues to take action if they feel suspicious about a possible sign of child abuse, even if they’re far from certain that anything is wrong. “Don’t ignore those feelings in the back of the brain,” he said in an interview.
Most states have child-abuse hotlines for medical professionals, and major hospitals will have child-abuse teams, Dr. Shwayder said. He urged dermatologists to take advantage of these resources when appropriate. “The professionals on the other side of the 800 number or at the hospital will help you. You don’t have to decide immediately whether this is child abuse. You just need to have a suspicion.”
Dr. Marathe and Dr. Shwayder report no disclosures.
at the American Academy of Dermatology Virtual Meeting Experience.
“One in four adult women report being childhood victims of sexual abuse, which is just a staggering number. This is an opportunity for us to identify these patients early and give them the terminology to be able to report what is happening to them,” said pediatric dermatologist Kalyani Marathe, MD, MPH, director of the division of dermatology at Cincinnati Children’s Hospital. “We also have the chance to give them a sense of agency over their bodies.”
Dr. Marathe offered the following recommendations when performing a genital skin exam:
- Make sure a “chaperone” is present. “Chaperones are a must when you’re examining children and teens,” she said. “Ask whom they prefer. For prepubertal children, you’re going to usually use the parent who’s there with them. If the parent is their father, they might ask him to step behind the curtain, in which case you can bring over your nurse or medical assistant.” Teens may ask either parent to step out of the room, she said. In that case, a nurse, medical assistant, resident, or trainee can fill in. “If you have male residents or trainees with you and the patient really does not want to be examined by a male, honor their request. Do not force them.”
- Explain why the exam is being performed. Make sure the patient understands why she is being seen, Dr. Marathe advised. For example, say something like “your pediatrician told us that you have an itchy area” or “your mom told us that there’s some loss of color in that area, that you’re having a problem there.” She added that it’s helpful to explain the type of doctor you are, with a comment such as the following: “We’re examining you because we’re doctors who specialize in skin. ... We want to help you feel better and make sure that your skin heals and is healthy.”
- Ask both the child and the parent for permission to perform the exam. While this may seem trivial, “it’s very, very important in setting the right tone for the encounter,” she said. “If the child says yes, we turn to the mom and say: ‘Mom, is it okay for us to do this exam today?’ You can see visible relief on the part of the parent, and as the parent relaxes, the child relaxes. Just saying those few things really makes the encounter so much smoother.” However, “if they say no, you have to honor the response. ... You say: ‘Okay, we’re not going to do the exam today,” and see the patient in a few weeks. If it’s urgent, an exam under anesthesia may be an option, she added.
- Talk to the child about the terms they use for private parts. It can be helpful to ask: “Do you have any terms for your private area?” According to Dr. Marathe, “this is a good chance to educate them on the terms vulva and vagina since they may be using other terminology. Making sure that they have the correct terms will actually help patients identify and report abuse earlier.” Dr. Marathe recalled that a colleague had a patient who’d been calling her private area “pound cake” and had been “reporting to her teacher that someone had been touching her ‘pound cake.’ Her teacher did not know what she meant by that, and this led to a great delay in her childhood abuse being reported.”
- Talk about what will happen during the exam. “I like to show them any instruments that we’re going to be using,” Dr. Marathe said. “If we’re using a flashlight, for example, I like to show them a picture [of a flashlight] or show them that flashlight. If we’re using a camera to do digital photography, show them that. If we’re going to be using a Q-tip or a swab to demonstrate anything or to take a culture, I like to show them that beforehand to make sure that they know what we’re doing.” In regard to photography, “make sure the parent and child know where the photos are going to go, who’s going to see them, what are they going to be used for. If they’re going to be used for educational purposes, make sure they have given explicit permission for that and they know they’ll be deidentified.”
- Make it clear that the exam won’t be painful. It’s important to put both the patient and the parent at ease on this front, Dr. Marathe said. “A lot of parents are concerned that we’re going to do a speculum exam in their prepubertal child. So make sure that it’s clarified ahead of time that we’re not going to be doing a speculum exam.”
Commenting on this topic, Tor Shwayder, MD, a pediatric dermatologist at Henry Ford Health System, Detroit, urged colleagues to take action if they feel suspicious about a possible sign of child abuse, even if they’re far from certain that anything is wrong. “Don’t ignore those feelings in the back of the brain,” he said in an interview.
Most states have child-abuse hotlines for medical professionals, and major hospitals will have child-abuse teams, Dr. Shwayder said. He urged dermatologists to take advantage of these resources when appropriate. “The professionals on the other side of the 800 number or at the hospital will help you. You don’t have to decide immediately whether this is child abuse. You just need to have a suspicion.”
Dr. Marathe and Dr. Shwayder report no disclosures.
FROM AAD VMX 2021
AAD unveils new guidelines for actinic keratosis management
. They also conditionally recommend the use of photodynamic therapy (PDT) and diclofenac for the treatment of AK, both individually and as part of combination therapy regimens.
Those are two of 18 recommendations made by 14 members of the multidisciplinary work group that convened to assemble the AAD’s first-ever guidelines on the management of AKs, which were published online April 2 in the Journal of the American Academy of Dermatology. The group, cochaired by Daniel B. Eisen, MD, professor of clinical dermatology at the University of California, Davis, and Todd E. Schlesinger, MD, medical director of the Dermatology and Laser Center of Charleston, S.C., conducted a systematic review to address five clinical questions on the management of AKs in adults. The questions were: What are the efficacy, effectiveness, and adverse effects of surgical and chemical peel treatments for AK; of topically applied agents for AK; of energy devices and other miscellaneous treatments for AK; and of combination therapy for the treatment of AK? And what are the special considerations to be taken into account when treating AK in immunocompromised individuals?
Next, the work group applied the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach for assessing the certainty of the evidence and formulating and grading clinical recommendations based on relevant randomized trials in the medical literature.
“As a participant in the work group, I was impressed by the level of care and detail and the involvement of relevant stakeholders, including a patient advocate, as well as having the draft guidelines go out to the AAD membership at large, and evaluating every comment that came in,” Maryam Asgari, MD, MPH, professor of dermatology at Harvard University, Boston, said in an interview. “The academy sought stakeholder and leadership input in revising and revamping the guidelines. The AAD also made sure the work group had minimal conflicts of interest by requiring that the majority of experts convened did not have relevant financial conflicts of interest. That might not be the case in a publication such as a systematic review, where no threshold for financial conflict of interest for coauthorship is set.”
Of the 18 recommendations the work group made for patients with AKs, only four were ranked as “strong” based on the evidence reviewed, while the rest were ranked as “conditional.”
The strong recommendations include the use of UV protection, field treatment with 5-FU, field treatment with imiquimod, and the use of cryosurgery.
The first four conditional recommendations for patients with AKs include the use of diclofenac, treatment with cryosurgery over CO2 laser ablation, aminolevulinic acid (ALA)–red-light PDT, and 1- to 4-hour 5-ALA incubation time to enhance complete clearance with red-light PDT. The work group also conditionally recommends ALA-daylight PDT as less painful than but equally effective as ALA–red-light PDT.
In the clinical experience of Catherine M. DiGiorgio, MD, who was not involved in the guidelines, daylight PDT with ALA is a viable, cost-effective option. “Patients can come into the office, apply the ALA and then they go outside for 2 hours – not in direct sunlight but in a shady area,” Dr. DiGiorgio, a dermatologist who practices at the Boston Center for Facial Rejuvenation, said in an interview. “That’s a cost-effective treatment for patients who perhaps can’t afford some of the chemotherapy creams. I don’t think we’ve adopted ALA-daylight PDT here in the U.S. very much.”
The work group noted that topical 1% tirbanibulin ointment, a novel microtubule inhibitor, was approved for treatment of AKs on the face and scalp by the Food and Drug Administration after the guidelines had been put together.
Several trials of combination therapy were included in the review of evidence, prompting several recommendations. For example, the work group conditionally recommends combined 5-FU cream and cryosurgery over cryosurgery alone, based on moderate-quality evidence and conditionally recommends combined imiquimod and cryosurgery over cryosurgery alone based on low-quality evidence. In addition, the work group conditionally recommends against the use of 3% diclofenac in addition to cryosurgery, favoring cryosurgery alone based on low-quality evidence, and conditionally recommends against the use of imiquimod typically after ALA–blue-light PDT, based on moderate-quality data.
“The additional treatment with imiquimod was thought to add both expense and burden to the patient, which negates much of the perceived convenience of using PDT as a stand-alone treatment modality and which is not mitigated by the modest increase in lesion reduction,” the authors wrote.
The guidelines emphasize the importance of shared decision-making between patients and clinicians on the choice of therapy, a point that resonates with Dr. DiGiorgio. Success of a treatment can depend on whether a patient is willing to go through with it, she said. “Some patients don’t want to do a therapeutic topical like 5-FU. They prefer to come in and have cryotherapy done. Others prefer to not come in and have the cream at home and treat themselves.”
Assembling the guidelines exposed certain gaps in research, according to the work group. Of the 18 recommendations, seven were based on low-quality evidence, and there were not enough data to make guidelines for the treatment of AKs in immunocompromised individuals.
“I can’t tell you the number of times we in the committee sat back and said, ‘we need to have a randomized trial that looks at this, or compares this to that head on,’” Dr. Asgari said. Such limitations “give researchers direction for where the areas of study need to go to help us answer some of these management conundrums.”
She added that the new guidelines “give clinicians a leg to stand on” when an insurer pushes back on a recommended treatment for AK. “It gives you a way to have dialogue with insurers if you’re prescribing some of these treatments.”
The guidelines authors write that there is “strong theoretic rationale for the treatment of AK to prevent skin cancers” but acknowledge that only a few studies in the review “report the incidence of skin cancer as an outcome measure or have sufficient follow-up to viably measure carcinoma development.” In addition, “more long-term research is needed to validate our current understanding of skin cancer progression from AKs to keratinocyte carcinoma.”
Dr. DiGiorgio thinks about this differently. “I think treatment of AKs does prevent skin cancers,” she said. “We call them precancers as we’re treating our patients because we know a certain percentage of them can develop into skin cancers over time.”
The study was funded by internal funds from the AAD. Dr. Asgari disclosed that she serves as an investigator for Pfizer. Several of the other authors reported having financial disclosures.
Dr. DiGiorgio reported having no financial disclosures.
. They also conditionally recommend the use of photodynamic therapy (PDT) and diclofenac for the treatment of AK, both individually and as part of combination therapy regimens.
Those are two of 18 recommendations made by 14 members of the multidisciplinary work group that convened to assemble the AAD’s first-ever guidelines on the management of AKs, which were published online April 2 in the Journal of the American Academy of Dermatology. The group, cochaired by Daniel B. Eisen, MD, professor of clinical dermatology at the University of California, Davis, and Todd E. Schlesinger, MD, medical director of the Dermatology and Laser Center of Charleston, S.C., conducted a systematic review to address five clinical questions on the management of AKs in adults. The questions were: What are the efficacy, effectiveness, and adverse effects of surgical and chemical peel treatments for AK; of topically applied agents for AK; of energy devices and other miscellaneous treatments for AK; and of combination therapy for the treatment of AK? And what are the special considerations to be taken into account when treating AK in immunocompromised individuals?
Next, the work group applied the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach for assessing the certainty of the evidence and formulating and grading clinical recommendations based on relevant randomized trials in the medical literature.
“As a participant in the work group, I was impressed by the level of care and detail and the involvement of relevant stakeholders, including a patient advocate, as well as having the draft guidelines go out to the AAD membership at large, and evaluating every comment that came in,” Maryam Asgari, MD, MPH, professor of dermatology at Harvard University, Boston, said in an interview. “The academy sought stakeholder and leadership input in revising and revamping the guidelines. The AAD also made sure the work group had minimal conflicts of interest by requiring that the majority of experts convened did not have relevant financial conflicts of interest. That might not be the case in a publication such as a systematic review, where no threshold for financial conflict of interest for coauthorship is set.”
Of the 18 recommendations the work group made for patients with AKs, only four were ranked as “strong” based on the evidence reviewed, while the rest were ranked as “conditional.”
The strong recommendations include the use of UV protection, field treatment with 5-FU, field treatment with imiquimod, and the use of cryosurgery.
The first four conditional recommendations for patients with AKs include the use of diclofenac, treatment with cryosurgery over CO2 laser ablation, aminolevulinic acid (ALA)–red-light PDT, and 1- to 4-hour 5-ALA incubation time to enhance complete clearance with red-light PDT. The work group also conditionally recommends ALA-daylight PDT as less painful than but equally effective as ALA–red-light PDT.
In the clinical experience of Catherine M. DiGiorgio, MD, who was not involved in the guidelines, daylight PDT with ALA is a viable, cost-effective option. “Patients can come into the office, apply the ALA and then they go outside for 2 hours – not in direct sunlight but in a shady area,” Dr. DiGiorgio, a dermatologist who practices at the Boston Center for Facial Rejuvenation, said in an interview. “That’s a cost-effective treatment for patients who perhaps can’t afford some of the chemotherapy creams. I don’t think we’ve adopted ALA-daylight PDT here in the U.S. very much.”
The work group noted that topical 1% tirbanibulin ointment, a novel microtubule inhibitor, was approved for treatment of AKs on the face and scalp by the Food and Drug Administration after the guidelines had been put together.
Several trials of combination therapy were included in the review of evidence, prompting several recommendations. For example, the work group conditionally recommends combined 5-FU cream and cryosurgery over cryosurgery alone, based on moderate-quality evidence and conditionally recommends combined imiquimod and cryosurgery over cryosurgery alone based on low-quality evidence. In addition, the work group conditionally recommends against the use of 3% diclofenac in addition to cryosurgery, favoring cryosurgery alone based on low-quality evidence, and conditionally recommends against the use of imiquimod typically after ALA–blue-light PDT, based on moderate-quality data.
“The additional treatment with imiquimod was thought to add both expense and burden to the patient, which negates much of the perceived convenience of using PDT as a stand-alone treatment modality and which is not mitigated by the modest increase in lesion reduction,” the authors wrote.
The guidelines emphasize the importance of shared decision-making between patients and clinicians on the choice of therapy, a point that resonates with Dr. DiGiorgio. Success of a treatment can depend on whether a patient is willing to go through with it, she said. “Some patients don’t want to do a therapeutic topical like 5-FU. They prefer to come in and have cryotherapy done. Others prefer to not come in and have the cream at home and treat themselves.”
Assembling the guidelines exposed certain gaps in research, according to the work group. Of the 18 recommendations, seven were based on low-quality evidence, and there were not enough data to make guidelines for the treatment of AKs in immunocompromised individuals.
“I can’t tell you the number of times we in the committee sat back and said, ‘we need to have a randomized trial that looks at this, or compares this to that head on,’” Dr. Asgari said. Such limitations “give researchers direction for where the areas of study need to go to help us answer some of these management conundrums.”
She added that the new guidelines “give clinicians a leg to stand on” when an insurer pushes back on a recommended treatment for AK. “It gives you a way to have dialogue with insurers if you’re prescribing some of these treatments.”
The guidelines authors write that there is “strong theoretic rationale for the treatment of AK to prevent skin cancers” but acknowledge that only a few studies in the review “report the incidence of skin cancer as an outcome measure or have sufficient follow-up to viably measure carcinoma development.” In addition, “more long-term research is needed to validate our current understanding of skin cancer progression from AKs to keratinocyte carcinoma.”
Dr. DiGiorgio thinks about this differently. “I think treatment of AKs does prevent skin cancers,” she said. “We call them precancers as we’re treating our patients because we know a certain percentage of them can develop into skin cancers over time.”
The study was funded by internal funds from the AAD. Dr. Asgari disclosed that she serves as an investigator for Pfizer. Several of the other authors reported having financial disclosures.
Dr. DiGiorgio reported having no financial disclosures.
. They also conditionally recommend the use of photodynamic therapy (PDT) and diclofenac for the treatment of AK, both individually and as part of combination therapy regimens.
Those are two of 18 recommendations made by 14 members of the multidisciplinary work group that convened to assemble the AAD’s first-ever guidelines on the management of AKs, which were published online April 2 in the Journal of the American Academy of Dermatology. The group, cochaired by Daniel B. Eisen, MD, professor of clinical dermatology at the University of California, Davis, and Todd E. Schlesinger, MD, medical director of the Dermatology and Laser Center of Charleston, S.C., conducted a systematic review to address five clinical questions on the management of AKs in adults. The questions were: What are the efficacy, effectiveness, and adverse effects of surgical and chemical peel treatments for AK; of topically applied agents for AK; of energy devices and other miscellaneous treatments for AK; and of combination therapy for the treatment of AK? And what are the special considerations to be taken into account when treating AK in immunocompromised individuals?
Next, the work group applied the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach for assessing the certainty of the evidence and formulating and grading clinical recommendations based on relevant randomized trials in the medical literature.
“As a participant in the work group, I was impressed by the level of care and detail and the involvement of relevant stakeholders, including a patient advocate, as well as having the draft guidelines go out to the AAD membership at large, and evaluating every comment that came in,” Maryam Asgari, MD, MPH, professor of dermatology at Harvard University, Boston, said in an interview. “The academy sought stakeholder and leadership input in revising and revamping the guidelines. The AAD also made sure the work group had minimal conflicts of interest by requiring that the majority of experts convened did not have relevant financial conflicts of interest. That might not be the case in a publication such as a systematic review, where no threshold for financial conflict of interest for coauthorship is set.”
Of the 18 recommendations the work group made for patients with AKs, only four were ranked as “strong” based on the evidence reviewed, while the rest were ranked as “conditional.”
The strong recommendations include the use of UV protection, field treatment with 5-FU, field treatment with imiquimod, and the use of cryosurgery.
The first four conditional recommendations for patients with AKs include the use of diclofenac, treatment with cryosurgery over CO2 laser ablation, aminolevulinic acid (ALA)–red-light PDT, and 1- to 4-hour 5-ALA incubation time to enhance complete clearance with red-light PDT. The work group also conditionally recommends ALA-daylight PDT as less painful than but equally effective as ALA–red-light PDT.
In the clinical experience of Catherine M. DiGiorgio, MD, who was not involved in the guidelines, daylight PDT with ALA is a viable, cost-effective option. “Patients can come into the office, apply the ALA and then they go outside for 2 hours – not in direct sunlight but in a shady area,” Dr. DiGiorgio, a dermatologist who practices at the Boston Center for Facial Rejuvenation, said in an interview. “That’s a cost-effective treatment for patients who perhaps can’t afford some of the chemotherapy creams. I don’t think we’ve adopted ALA-daylight PDT here in the U.S. very much.”
The work group noted that topical 1% tirbanibulin ointment, a novel microtubule inhibitor, was approved for treatment of AKs on the face and scalp by the Food and Drug Administration after the guidelines had been put together.
Several trials of combination therapy were included in the review of evidence, prompting several recommendations. For example, the work group conditionally recommends combined 5-FU cream and cryosurgery over cryosurgery alone, based on moderate-quality evidence and conditionally recommends combined imiquimod and cryosurgery over cryosurgery alone based on low-quality evidence. In addition, the work group conditionally recommends against the use of 3% diclofenac in addition to cryosurgery, favoring cryosurgery alone based on low-quality evidence, and conditionally recommends against the use of imiquimod typically after ALA–blue-light PDT, based on moderate-quality data.
“The additional treatment with imiquimod was thought to add both expense and burden to the patient, which negates much of the perceived convenience of using PDT as a stand-alone treatment modality and which is not mitigated by the modest increase in lesion reduction,” the authors wrote.
The guidelines emphasize the importance of shared decision-making between patients and clinicians on the choice of therapy, a point that resonates with Dr. DiGiorgio. Success of a treatment can depend on whether a patient is willing to go through with it, she said. “Some patients don’t want to do a therapeutic topical like 5-FU. They prefer to come in and have cryotherapy done. Others prefer to not come in and have the cream at home and treat themselves.”
Assembling the guidelines exposed certain gaps in research, according to the work group. Of the 18 recommendations, seven were based on low-quality evidence, and there were not enough data to make guidelines for the treatment of AKs in immunocompromised individuals.
“I can’t tell you the number of times we in the committee sat back and said, ‘we need to have a randomized trial that looks at this, or compares this to that head on,’” Dr. Asgari said. Such limitations “give researchers direction for where the areas of study need to go to help us answer some of these management conundrums.”
She added that the new guidelines “give clinicians a leg to stand on” when an insurer pushes back on a recommended treatment for AK. “It gives you a way to have dialogue with insurers if you’re prescribing some of these treatments.”
The guidelines authors write that there is “strong theoretic rationale for the treatment of AK to prevent skin cancers” but acknowledge that only a few studies in the review “report the incidence of skin cancer as an outcome measure or have sufficient follow-up to viably measure carcinoma development.” In addition, “more long-term research is needed to validate our current understanding of skin cancer progression from AKs to keratinocyte carcinoma.”
Dr. DiGiorgio thinks about this differently. “I think treatment of AKs does prevent skin cancers,” she said. “We call them precancers as we’re treating our patients because we know a certain percentage of them can develop into skin cancers over time.”
The study was funded by internal funds from the AAD. Dr. Asgari disclosed that she serves as an investigator for Pfizer. Several of the other authors reported having financial disclosures.
Dr. DiGiorgio reported having no financial disclosures.
FROM JAAD
SHM Converge Daily News -- Day 3
Click here for the Friday issue of the SHM Converge Daily News newsletter.
Click here for the Friday issue of the SHM Converge Daily News newsletter.
Click here for the Friday issue of the SHM Converge Daily News newsletter.
COVID experience underscores ‘vital’ role of hospital medicine
While the COVID-19 pandemic has generated anxiety and confusion in medicine, one thing should bring a sense of clarity to hospitalists: They’re needed now more than ever.

Larry Wellikson, MD, MHM, the former, longtime CEO of the Society of Hospital Medicine, in a May 6 keynote speech at SHM Converge, the annual conference of the Society of Hospital Medicine, said the COVID-19 era has underscored the singular importance of the specialty.
“I think one thing that this recent pandemic has emphasized is just how important and vital hospitalists are to the United States’ health care system,” Dr. Wellikson said. “The response to the acute care needs in this pandemic would have been impossible in the health care system that existed before hospitalists. And so this is something that we should understand and appreciate.”
The “upheaval” experienced in hospital medicine continues a trend of change that will go on, both in the corporate health care landscape and in the role that hospitalists play in providing care, he said. Insurers have been merging and looking to consolidate. Hospital medicine companies have been merging, and “newfangled bedfellows” have been a trend, such as CVS stepping beyond its pharmacy role into an expanded health care role, Cigna buying Express Scripts, and an Amazon-Berkshire Hathaway-J.P. Morgan health care partnership that ultimately did not pan out, although that hasn’t ended Amazon’s presence in health care.
“You may not realize it, but Amazon is currently one of the largest hospital supply-chain companies,” Dr. Wellikson said. “They’re attempting to become a major pharmacy benefits manager and will only further enter into health care and into our personal and professional lives.”
New models of care point to the way of the future, he said. Mount Sinai’s continuing success with its Hospital at Home program – which involves an acute care nurse and team assigned to a patient in the home – introduces a concept that will be adopted more broadly, because of its cost savings and good outcomes, he said. Mergers of hospital systems, leading to excess hospital capacity, has given rise to what he calls “ED-plus,” or using formerly full-service hospitals as more focused centers – providing emergency, obstetrician, cardiology, x-ray, or orthopedics care, or whatever is needed in a given community.
An increasing focus on population health rather than procedures plays into the strengths of hospitalists, Dr. Wellikson said, and the need for their skills will continue to deepen.
When changes in reimbursement began about 4 years ago, specialties such as cardiology entered into new contracts with hospitals, but the facilities began to notice that many of the services – such as initial heart failure and chest pain management – can be provided by hospitalists.
“They’re signing fewer cardiologists and needing therefore to hire more hospitalists,” he said.
To keep readmissions low and subsequent costs down, hospitalists will continue to handle the first few postdischarge visits with patients, he said. This is crucial in bundled payment systems.
“Most of the savings in those systems comes from being very efficient in the initial postdischarge portion of people’s care,” Dr. Wellikson said.
At the same time, hospitalists are not in “unlimited supply.”
“I think every hospital medicine group should be assessing and working on improving their clinicians’ well-being,” he said. “We need to ration somewhat, so we’re deploying hospitalists for the things that only we can do.” He predicted that hospitalists will be required to work in the electronic medical record less frequently, with this task handled by others.
Dr. Wellikson also called on the specialty to continue to expand its racial and ethnic diversity so that it reflects the patient population it serves.
“We’re looking to create pathways to leadership for everyone and not just a tokenism moving forward,” he said.
The basic strengths of hospital medicine – its flexibility, professional culture, and youth – leave it well prepared for all of these changes, he said.
“There is a bright future and hospitalists are right in the middle of this – we’re not going to be marginalized or on the periphery,” Dr. Wellikson said. “If I had one message for all of you, I would say be relevant and add value and you will not only survive, but thrive.”
RIV winners announced
The winners of the 2021 RIV competition were also announced at the May 6 general session of Converge. There were two winners in each of the three categories, as follows:
RESEARCH
Overall: “Suboptimal Communication During Inter-Hospital Transfer,” Stephanie Mueller, MD, MPH, SFHM
Trainee: “Mentorship in Pediatric Hospital Medicine: A Survey of Division Directors,” Brandon Palmer, MD
INNOVATIONS
Overall: “Leveraging Artificial Intelligence for a Team-Based Approach to Advance Care Planning,” Ron Li, MD
Trainee: “A Trainee-Designed Initiative Reshapes Communication for Hospital Medicine Patients During COVID-19,” Smitha Ganeshan, MD, MBA
CLINICAL VIGNETTES
Adults: “Holy Spontaneous Heparin-Induced Thrombocytopenia,” Min Hwang
Pediatrics: “The Great Pretender: A Tale of Two Systems,” Shivani Desai, MD
While the COVID-19 pandemic has generated anxiety and confusion in medicine, one thing should bring a sense of clarity to hospitalists: They’re needed now more than ever.
Larry Wellikson, MD, MHM, the former, longtime CEO of the Society of Hospital Medicine, in a May 6 keynote speech at SHM Converge, the annual conference of the Society of Hospital Medicine, said the COVID-19 era has underscored the singular importance of the specialty.
“I think one thing that this recent pandemic has emphasized is just how important and vital hospitalists are to the United States’ health care system,” Dr. Wellikson said. “The response to the acute care needs in this pandemic would have been impossible in the health care system that existed before hospitalists. And so this is something that we should understand and appreciate.”
The “upheaval” experienced in hospital medicine continues a trend of change that will go on, both in the corporate health care landscape and in the role that hospitalists play in providing care, he said. Insurers have been merging and looking to consolidate. Hospital medicine companies have been merging, and “newfangled bedfellows” have been a trend, such as CVS stepping beyond its pharmacy role into an expanded health care role, Cigna buying Express Scripts, and an Amazon-Berkshire Hathaway-J.P. Morgan health care partnership that ultimately did not pan out, although that hasn’t ended Amazon’s presence in health care.
“You may not realize it, but Amazon is currently one of the largest hospital supply-chain companies,” Dr. Wellikson said. “They’re attempting to become a major pharmacy benefits manager and will only further enter into health care and into our personal and professional lives.”
New models of care point to the way of the future, he said. Mount Sinai’s continuing success with its Hospital at Home program – which involves an acute care nurse and team assigned to a patient in the home – introduces a concept that will be adopted more broadly, because of its cost savings and good outcomes, he said. Mergers of hospital systems, leading to excess hospital capacity, has given rise to what he calls “ED-plus,” or using formerly full-service hospitals as more focused centers – providing emergency, obstetrician, cardiology, x-ray, or orthopedics care, or whatever is needed in a given community.
An increasing focus on population health rather than procedures plays into the strengths of hospitalists, Dr. Wellikson said, and the need for their skills will continue to deepen.
When changes in reimbursement began about 4 years ago, specialties such as cardiology entered into new contracts with hospitals, but the facilities began to notice that many of the services – such as initial heart failure and chest pain management – can be provided by hospitalists.
“They’re signing fewer cardiologists and needing therefore to hire more hospitalists,” he said.
To keep readmissions low and subsequent costs down, hospitalists will continue to handle the first few postdischarge visits with patients, he said. This is crucial in bundled payment systems.
“Most of the savings in those systems comes from being very efficient in the initial postdischarge portion of people’s care,” Dr. Wellikson said.
At the same time, hospitalists are not in “unlimited supply.”
“I think every hospital medicine group should be assessing and working on improving their clinicians’ well-being,” he said. “We need to ration somewhat, so we’re deploying hospitalists for the things that only we can do.” He predicted that hospitalists will be required to work in the electronic medical record less frequently, with this task handled by others.
Dr. Wellikson also called on the specialty to continue to expand its racial and ethnic diversity so that it reflects the patient population it serves.
“We’re looking to create pathways to leadership for everyone and not just a tokenism moving forward,” he said.
The basic strengths of hospital medicine – its flexibility, professional culture, and youth – leave it well prepared for all of these changes, he said.
“There is a bright future and hospitalists are right in the middle of this – we’re not going to be marginalized or on the periphery,” Dr. Wellikson said. “If I had one message for all of you, I would say be relevant and add value and you will not only survive, but thrive.”
RIV winners announced
The winners of the 2021 RIV competition were also announced at the May 6 general session of Converge. There were two winners in each of the three categories, as follows:
RESEARCH
Overall: “Suboptimal Communication During Inter-Hospital Transfer,” Stephanie Mueller, MD, MPH, SFHM
Trainee: “Mentorship in Pediatric Hospital Medicine: A Survey of Division Directors,” Brandon Palmer, MD
INNOVATIONS
Overall: “Leveraging Artificial Intelligence for a Team-Based Approach to Advance Care Planning,” Ron Li, MD
Trainee: “A Trainee-Designed Initiative Reshapes Communication for Hospital Medicine Patients During COVID-19,” Smitha Ganeshan, MD, MBA
CLINICAL VIGNETTES
Adults: “Holy Spontaneous Heparin-Induced Thrombocytopenia,” Min Hwang
Pediatrics: “The Great Pretender: A Tale of Two Systems,” Shivani Desai, MD
While the COVID-19 pandemic has generated anxiety and confusion in medicine, one thing should bring a sense of clarity to hospitalists: They’re needed now more than ever.
Larry Wellikson, MD, MHM, the former, longtime CEO of the Society of Hospital Medicine, in a May 6 keynote speech at SHM Converge, the annual conference of the Society of Hospital Medicine, said the COVID-19 era has underscored the singular importance of the specialty.
“I think one thing that this recent pandemic has emphasized is just how important and vital hospitalists are to the United States’ health care system,” Dr. Wellikson said. “The response to the acute care needs in this pandemic would have been impossible in the health care system that existed before hospitalists. And so this is something that we should understand and appreciate.”
The “upheaval” experienced in hospital medicine continues a trend of change that will go on, both in the corporate health care landscape and in the role that hospitalists play in providing care, he said. Insurers have been merging and looking to consolidate. Hospital medicine companies have been merging, and “newfangled bedfellows” have been a trend, such as CVS stepping beyond its pharmacy role into an expanded health care role, Cigna buying Express Scripts, and an Amazon-Berkshire Hathaway-J.P. Morgan health care partnership that ultimately did not pan out, although that hasn’t ended Amazon’s presence in health care.
“You may not realize it, but Amazon is currently one of the largest hospital supply-chain companies,” Dr. Wellikson said. “They’re attempting to become a major pharmacy benefits manager and will only further enter into health care and into our personal and professional lives.”
New models of care point to the way of the future, he said. Mount Sinai’s continuing success with its Hospital at Home program – which involves an acute care nurse and team assigned to a patient in the home – introduces a concept that will be adopted more broadly, because of its cost savings and good outcomes, he said. Mergers of hospital systems, leading to excess hospital capacity, has given rise to what he calls “ED-plus,” or using formerly full-service hospitals as more focused centers – providing emergency, obstetrician, cardiology, x-ray, or orthopedics care, or whatever is needed in a given community.
An increasing focus on population health rather than procedures plays into the strengths of hospitalists, Dr. Wellikson said, and the need for their skills will continue to deepen.
When changes in reimbursement began about 4 years ago, specialties such as cardiology entered into new contracts with hospitals, but the facilities began to notice that many of the services – such as initial heart failure and chest pain management – can be provided by hospitalists.
“They’re signing fewer cardiologists and needing therefore to hire more hospitalists,” he said.
To keep readmissions low and subsequent costs down, hospitalists will continue to handle the first few postdischarge visits with patients, he said. This is crucial in bundled payment systems.
“Most of the savings in those systems comes from being very efficient in the initial postdischarge portion of people’s care,” Dr. Wellikson said.
At the same time, hospitalists are not in “unlimited supply.”
“I think every hospital medicine group should be assessing and working on improving their clinicians’ well-being,” he said. “We need to ration somewhat, so we’re deploying hospitalists for the things that only we can do.” He predicted that hospitalists will be required to work in the electronic medical record less frequently, with this task handled by others.
Dr. Wellikson also called on the specialty to continue to expand its racial and ethnic diversity so that it reflects the patient population it serves.
“We’re looking to create pathways to leadership for everyone and not just a tokenism moving forward,” he said.
The basic strengths of hospital medicine – its flexibility, professional culture, and youth – leave it well prepared for all of these changes, he said.
“There is a bright future and hospitalists are right in the middle of this – we’re not going to be marginalized or on the periphery,” Dr. Wellikson said. “If I had one message for all of you, I would say be relevant and add value and you will not only survive, but thrive.”
RIV winners announced
The winners of the 2021 RIV competition were also announced at the May 6 general session of Converge. There were two winners in each of the three categories, as follows:
RESEARCH
Overall: “Suboptimal Communication During Inter-Hospital Transfer,” Stephanie Mueller, MD, MPH, SFHM
Trainee: “Mentorship in Pediatric Hospital Medicine: A Survey of Division Directors,” Brandon Palmer, MD
INNOVATIONS
Overall: “Leveraging Artificial Intelligence for a Team-Based Approach to Advance Care Planning,” Ron Li, MD
Trainee: “A Trainee-Designed Initiative Reshapes Communication for Hospital Medicine Patients During COVID-19,” Smitha Ganeshan, MD, MBA
CLINICAL VIGNETTES
Adults: “Holy Spontaneous Heparin-Induced Thrombocytopenia,” Min Hwang
Pediatrics: “The Great Pretender: A Tale of Two Systems,” Shivani Desai, MD
FROM SHM CONVERGE 2021

Telehealth takeaways for hospitalists outlined
Although the COVID-19 pandemic put telehealth on fast forward, more than one third of patients in the United States engaged with telehealth services before February 2020, according to Ameet Doshi, MD, and Chrisanne Timpe, MD, of HealthPartners in Bloomington, Minn.
Broadly speaking, telehealth is “using virtual tools to evaluate, manage, and care for our patients, regardless of where they are located,” Dr. Doshi said during a May 6 session at SHM Converge, the annual conference of the Society of Hospital Medicine.
The entirety of telehealth includes remote ways to meet almost any patient demand, he said. Some common health terms are used interchangeably, but some use telehealth as a broad term for electronic health care services, while telemedicine may refer specifically to remote patient care, he said.
Telemedicine allows flexibility of delivering patient care in inpatient, outpatient, or at-home settings, said Dr. Doshi. To illustrate the current application of telemedicine, he used an example of a 25-bed critical access hospital serving a growing regional population in which outpatient volume is expanding and ambulatory care services are being added. In this example, inpatient volume is growing, but not enough to support an inpatient consult service, but telehealth access to specialists such as cardiology would be useful in this case, he said.
Hospitalist telehealth means “being able to provide services to changing patient populations regardless of location; we can bring services to where patients are,” said Dr. Doshi.
Benefits of telehealth to patients include less travel and easier access to care, benefits to clinicians include expanding services at lower financial costs, he said.
COVID-19 challenges and opportunities
The COVID-19 pandemic presented both challenges and opportunities for telehealth, Dr. Doshi said. One opportunity was the sudden broad acceptance of virtual care out of necessity and concern for patient and staff safety, and to preserve the use of personal protective equipment, he said. In addition, a loosening of regulatory and financial pressures allowed more institutions to expand and initiate telehealth services.
Challenges included technological limitations and, in some cases, the need to develop a telehealth infrastructure from scratch, Dr. Doshi explained. Concerns also remain regarding how telehealth will evolve in the post-pandemic future, he said.
In the meantime, Medicare data show the impact of the pandemic on telehealth services, said Dr. Doshi. A telehealth waiver issued in March 2020 led to an increase in virtual encounters, and Medicare data show approximately 25 million virtual Medicare encounters between March 2020 and October 2020, representing a 3,000% increase from the same period in 2019, he said.
“Telehealth is here to stay, so the questions are how to craft a hospitalist telehealth program and provide essential patient care,” he said.
Dr. Timpe shared some examples of the evolution of telehealth care during the pandemic, including a case of an asymptomatic but frail patient with diabetes, dementia, and coronary artery disease undergoing outpatient care for a foot infection. The patient presented to an emergency department but refused to be hospitalized because of family concerns about patient isolation (no visitors were allowed at the time) and the concerns about COVID-19 infection.
The need to help treat acutely ill patients such as this patient while avoiding hospital admission during and after the pandemic continues to lead to the development of telehealth programs, Dr. Timpe said. She shared details of the Hospital@Home program developed by her organization, Health Partners. The program is designed to treat acutely ill people in the home, if possible, and avoid the need for hospital admission. Patients receive daily medical management from a hospitalist and care from staff, including registered nurses and community paramedics. Services include provision of IV medications and fluids, but the staff also conduct labs and imaging services, Dr. Timpe said.
Conditions that the program has managed at patients’ homes include pneumonia, COPD, asthma, bronchitis, flu, COVID-19, congestive heart failure, cellulitis, and urinary tract infections, said Dr. Timpe.
“We do not accept people into the program who have treatment needs that can only be met in a hospital,” such as the need for blood products, vasopressor support, telemetry, or positive pressure support, she noted.
Between November 2019 and February 15, 2021, the Hospital@Home program has provided services to 132 patients for a total of 287 visits. The program has averted 50 emergency department visits and 40 hospitalizations, and shorted hospital stays in 57 cases, she noted.
Hospitalists are suited for telehealth for several reasons, including the ability to triage acutely ill patients, familiarity with resource utilization, and expertise in management of complex medical care, said Dr. Timpe.
Looking ahead
Dr. Doshi emphasized several ongoing issues regarding the future of telemedicine, primarily the need for standardized regulation and reimbursement; reduction of health equity disparity and attention to technological barriers (including access and technology literacy); and identification of the next frontiers in telehealth.
Research on the impact and effectiveness of telehealth is limited, but growing, and next frontiers might include making patients more active participants in telehealth via patient-operated kits, or the option of an open telemedicine marketplace, in which patients can select providers from across the country, he said. No matter where telehealth leads in the future, “we need to make sure we have a positive patient outcome,” he concluded.
Dr. Doshi and Dr. Timpe had no financial conflicts to disclose.
Although the COVID-19 pandemic put telehealth on fast forward, more than one third of patients in the United States engaged with telehealth services before February 2020, according to Ameet Doshi, MD, and Chrisanne Timpe, MD, of HealthPartners in Bloomington, Minn.
Broadly speaking, telehealth is “using virtual tools to evaluate, manage, and care for our patients, regardless of where they are located,” Dr. Doshi said during a May 6 session at SHM Converge, the annual conference of the Society of Hospital Medicine.
The entirety of telehealth includes remote ways to meet almost any patient demand, he said. Some common health terms are used interchangeably, but some use telehealth as a broad term for electronic health care services, while telemedicine may refer specifically to remote patient care, he said.
Telemedicine allows flexibility of delivering patient care in inpatient, outpatient, or at-home settings, said Dr. Doshi. To illustrate the current application of telemedicine, he used an example of a 25-bed critical access hospital serving a growing regional population in which outpatient volume is expanding and ambulatory care services are being added. In this example, inpatient volume is growing, but not enough to support an inpatient consult service, but telehealth access to specialists such as cardiology would be useful in this case, he said.
Hospitalist telehealth means “being able to provide services to changing patient populations regardless of location; we can bring services to where patients are,” said Dr. Doshi.
Benefits of telehealth to patients include less travel and easier access to care, benefits to clinicians include expanding services at lower financial costs, he said.
COVID-19 challenges and opportunities
The COVID-19 pandemic presented both challenges and opportunities for telehealth, Dr. Doshi said. One opportunity was the sudden broad acceptance of virtual care out of necessity and concern for patient and staff safety, and to preserve the use of personal protective equipment, he said. In addition, a loosening of regulatory and financial pressures allowed more institutions to expand and initiate telehealth services.
Challenges included technological limitations and, in some cases, the need to develop a telehealth infrastructure from scratch, Dr. Doshi explained. Concerns also remain regarding how telehealth will evolve in the post-pandemic future, he said.
In the meantime, Medicare data show the impact of the pandemic on telehealth services, said Dr. Doshi. A telehealth waiver issued in March 2020 led to an increase in virtual encounters, and Medicare data show approximately 25 million virtual Medicare encounters between March 2020 and October 2020, representing a 3,000% increase from the same period in 2019, he said.
“Telehealth is here to stay, so the questions are how to craft a hospitalist telehealth program and provide essential patient care,” he said.
Dr. Timpe shared some examples of the evolution of telehealth care during the pandemic, including a case of an asymptomatic but frail patient with diabetes, dementia, and coronary artery disease undergoing outpatient care for a foot infection. The patient presented to an emergency department but refused to be hospitalized because of family concerns about patient isolation (no visitors were allowed at the time) and the concerns about COVID-19 infection.
The need to help treat acutely ill patients such as this patient while avoiding hospital admission during and after the pandemic continues to lead to the development of telehealth programs, Dr. Timpe said. She shared details of the Hospital@Home program developed by her organization, Health Partners. The program is designed to treat acutely ill people in the home, if possible, and avoid the need for hospital admission. Patients receive daily medical management from a hospitalist and care from staff, including registered nurses and community paramedics. Services include provision of IV medications and fluids, but the staff also conduct labs and imaging services, Dr. Timpe said.
Conditions that the program has managed at patients’ homes include pneumonia, COPD, asthma, bronchitis, flu, COVID-19, congestive heart failure, cellulitis, and urinary tract infections, said Dr. Timpe.
“We do not accept people into the program who have treatment needs that can only be met in a hospital,” such as the need for blood products, vasopressor support, telemetry, or positive pressure support, she noted.
Between November 2019 and February 15, 2021, the Hospital@Home program has provided services to 132 patients for a total of 287 visits. The program has averted 50 emergency department visits and 40 hospitalizations, and shorted hospital stays in 57 cases, she noted.
Hospitalists are suited for telehealth for several reasons, including the ability to triage acutely ill patients, familiarity with resource utilization, and expertise in management of complex medical care, said Dr. Timpe.
Looking ahead
Dr. Doshi emphasized several ongoing issues regarding the future of telemedicine, primarily the need for standardized regulation and reimbursement; reduction of health equity disparity and attention to technological barriers (including access and technology literacy); and identification of the next frontiers in telehealth.
Research on the impact and effectiveness of telehealth is limited, but growing, and next frontiers might include making patients more active participants in telehealth via patient-operated kits, or the option of an open telemedicine marketplace, in which patients can select providers from across the country, he said. No matter where telehealth leads in the future, “we need to make sure we have a positive patient outcome,” he concluded.
Dr. Doshi and Dr. Timpe had no financial conflicts to disclose.
Although the COVID-19 pandemic put telehealth on fast forward, more than one third of patients in the United States engaged with telehealth services before February 2020, according to Ameet Doshi, MD, and Chrisanne Timpe, MD, of HealthPartners in Bloomington, Minn.
Broadly speaking, telehealth is “using virtual tools to evaluate, manage, and care for our patients, regardless of where they are located,” Dr. Doshi said during a May 6 session at SHM Converge, the annual conference of the Society of Hospital Medicine.
The entirety of telehealth includes remote ways to meet almost any patient demand, he said. Some common health terms are used interchangeably, but some use telehealth as a broad term for electronic health care services, while telemedicine may refer specifically to remote patient care, he said.
Telemedicine allows flexibility of delivering patient care in inpatient, outpatient, or at-home settings, said Dr. Doshi. To illustrate the current application of telemedicine, he used an example of a 25-bed critical access hospital serving a growing regional population in which outpatient volume is expanding and ambulatory care services are being added. In this example, inpatient volume is growing, but not enough to support an inpatient consult service, but telehealth access to specialists such as cardiology would be useful in this case, he said.
Hospitalist telehealth means “being able to provide services to changing patient populations regardless of location; we can bring services to where patients are,” said Dr. Doshi.
Benefits of telehealth to patients include less travel and easier access to care, benefits to clinicians include expanding services at lower financial costs, he said.
COVID-19 challenges and opportunities
The COVID-19 pandemic presented both challenges and opportunities for telehealth, Dr. Doshi said. One opportunity was the sudden broad acceptance of virtual care out of necessity and concern for patient and staff safety, and to preserve the use of personal protective equipment, he said. In addition, a loosening of regulatory and financial pressures allowed more institutions to expand and initiate telehealth services.
Challenges included technological limitations and, in some cases, the need to develop a telehealth infrastructure from scratch, Dr. Doshi explained. Concerns also remain regarding how telehealth will evolve in the post-pandemic future, he said.
In the meantime, Medicare data show the impact of the pandemic on telehealth services, said Dr. Doshi. A telehealth waiver issued in March 2020 led to an increase in virtual encounters, and Medicare data show approximately 25 million virtual Medicare encounters between March 2020 and October 2020, representing a 3,000% increase from the same period in 2019, he said.
“Telehealth is here to stay, so the questions are how to craft a hospitalist telehealth program and provide essential patient care,” he said.
Dr. Timpe shared some examples of the evolution of telehealth care during the pandemic, including a case of an asymptomatic but frail patient with diabetes, dementia, and coronary artery disease undergoing outpatient care for a foot infection. The patient presented to an emergency department but refused to be hospitalized because of family concerns about patient isolation (no visitors were allowed at the time) and the concerns about COVID-19 infection.
The need to help treat acutely ill patients such as this patient while avoiding hospital admission during and after the pandemic continues to lead to the development of telehealth programs, Dr. Timpe said. She shared details of the Hospital@Home program developed by her organization, Health Partners. The program is designed to treat acutely ill people in the home, if possible, and avoid the need for hospital admission. Patients receive daily medical management from a hospitalist and care from staff, including registered nurses and community paramedics. Services include provision of IV medications and fluids, but the staff also conduct labs and imaging services, Dr. Timpe said.
Conditions that the program has managed at patients’ homes include pneumonia, COPD, asthma, bronchitis, flu, COVID-19, congestive heart failure, cellulitis, and urinary tract infections, said Dr. Timpe.
“We do not accept people into the program who have treatment needs that can only be met in a hospital,” such as the need for blood products, vasopressor support, telemetry, or positive pressure support, she noted.
Between November 2019 and February 15, 2021, the Hospital@Home program has provided services to 132 patients for a total of 287 visits. The program has averted 50 emergency department visits and 40 hospitalizations, and shorted hospital stays in 57 cases, she noted.
Hospitalists are suited for telehealth for several reasons, including the ability to triage acutely ill patients, familiarity with resource utilization, and expertise in management of complex medical care, said Dr. Timpe.
Looking ahead
Dr. Doshi emphasized several ongoing issues regarding the future of telemedicine, primarily the need for standardized regulation and reimbursement; reduction of health equity disparity and attention to technological barriers (including access and technology literacy); and identification of the next frontiers in telehealth.
Research on the impact and effectiveness of telehealth is limited, but growing, and next frontiers might include making patients more active participants in telehealth via patient-operated kits, or the option of an open telemedicine marketplace, in which patients can select providers from across the country, he said. No matter where telehealth leads in the future, “we need to make sure we have a positive patient outcome,” he concluded.
Dr. Doshi and Dr. Timpe had no financial conflicts to disclose.
FROM SHM CONVERGE 2021
Prioritize goals of older patients with multimorbidities, gerontologist says
said Mary Tinetti, MD, Gladys Phillips Crofoot Professor of Medicine and Public Health and chief of geriatrics at Yale University, New Haven, Conn.

During a virtual presentation at the American College of Physicians annual Internal Medicine meeting, the gerontologist noted that primary care providers face a number of challenges when managing elderly patients with multimorbidity. These challenges include a lack of representative data in clinical trials, conflicting guideline recommendations, patient nonadherence, and decreased benefit from therapies due to competing conditions, she said.
“Trying to follow multiple guidelines can result in unintentional harms to these people with multiple conditions,” Dr. Tinetti said. She gave examples of the wide-ranging goals patients can have.
“Some [patients] will maximize the focus on function, regardless of how long they are likely to live,” Dr. Tinetti said. “Others will say symptom burden management is most important to them. And others will say they want to live as long as possible, and survival is most important, even if that means a reduction in their function. These individuals also vary in the care they are willing and able to receive to achieve the outcomes that matter most to them.”
For these reasons, Dr. Tinetti recommended patient priorities care, which she and her colleagues have been developing and implementing over the past 5-6 years.
“If the benefits and harms of addressing each condition in isolation is of uncertain benefit and potentially burdensome to both clinician and patient, and we know that patients vary in their health priorities ... then what else would you want to focus on in your 20-minute visit ... except each patient’s priorities?” Dr. Tinetti asked. “This is one solution to the challenge.”
What is patient priorities care?
Patient priorities care is a multidisciplinary, cyclical approach to clinical decision-making composed of three steps, Dr. Tinetti explained. First, a clinician identifies the patient’s health priorities. Second, this information is transmitted to comanaging providers, who decide which of their respective treatments are consistent with the patient’s priorities. And third, those decisions are disseminated to everyone involved in the patient’s care, both within and outside of the health care system, allowing all care providers to align with the patient’s priorities, she noted.
“Each person does that from their own expertise,” Dr. Tinetti said. “The social worker will do something different than the cardiologist, the physical therapist, the endocrinologist – but everybody is aiming at the same outcome – the patient’s priorities.”
In 2019, Dr. Tinetti led a nonrandomized clinical trial to test the feasibility of patient priorities care. The study involved 366 older adults with multimorbidity, among whom 203 received usual care, while 163 received this type of care. Patients in the latter group were twice as likely to have medications stopped, and significantly less likely to have self-management tasks added and diagnostic tests ordered.
How electronic health records can help
In an interview, Dr. Tinetti suggested that comanaging physicians communicate through electronic health records (EHRs), first to ensure that all care providers understand a patient’s goals, then to determine if recommended therapies align with those goals.
“It would be a little bit of a culture change to do that,” Dr. Tinetti said, “but the technology is there and it isn’t too terribly time consuming.”
She went on to suggest that primary care providers are typically best suited to coordinate this process; however, if a patient receives the majority of their care from a particular specialist, then that clinician may be the most suitable coordinator.
Systemic obstacles and solutions
According to Cynthia Boyd, MD, interim director of the division of geriatric medicine and gerontology, Johns Hopkins University, Baltimore, clinicians may encounter obstacles when implementing patient priorities care.
“Our health care system doesn’t always make it easy to do this,” Dr. Boyd said. “It’s important to acknowledge this because it can be hard to do. There’s no question,” Dr. Boyd said in an interview.
Among the headwinds that clinicians may face are clinical practice guidelines, the structure of electronic health records, and quality metrics focused on specific conditions, she explained.
“There’s a lot of things that push us – in primary care and other parts of medicine – away from the approach that’s best for people with multiple chronic conditions,” Dr. Boyd said.
Dr. Tinetti said a challenge to providing this care that she expects is for clinicians, regardless of specialty, “to feel uneasy” about transitioning away from a conventional approach.
Among Dr. Tinetti’s arguments in favor of providing patient priorities care is that “it’s going to bring more joy in practice because you’re really addressing what matters to that individual while also providing good care.”
To get the most out of patient priorities care, Dr. Boyd recommended that clinicians focus on ‘the 4 M’s’: what matters most, mentation, mobility, and medications.
In an effort to address the last of these on a broad scale, Dr. Boyd is co-leading the US Deprescribing Research Network(USDeN), which aims to “improve medication use among older adults and the outcomes that are important to them,” according to the USDeN website.
To encourage deprescribing on a day-to-day level, Dr. Boyd called for strong communication between co–managing providers.
In an ideal world, there would be a better way to communicate than largely via electronic health records, she said.
“We need more than the EHR to connect us. That’s why it’s really important for primary care providers and specialists to be able to have time to actually talk to each other. This gets into how we reimburse and organize the communication and cognitive aspects of care,” Dr. Boyd noted.
Dr. Tinetti disclosed support from the John A. Hartford Foundation, the Donaghue Foundation, the National Institute on Aging, and the Institute for Healthcare Improvement. Dr. Boyd disclosed a relationship with UpToDate, for which she coauthored a chapter on multimorbidity.
said Mary Tinetti, MD, Gladys Phillips Crofoot Professor of Medicine and Public Health and chief of geriatrics at Yale University, New Haven, Conn.
During a virtual presentation at the American College of Physicians annual Internal Medicine meeting, the gerontologist noted that primary care providers face a number of challenges when managing elderly patients with multimorbidity. These challenges include a lack of representative data in clinical trials, conflicting guideline recommendations, patient nonadherence, and decreased benefit from therapies due to competing conditions, she said.
“Trying to follow multiple guidelines can result in unintentional harms to these people with multiple conditions,” Dr. Tinetti said. She gave examples of the wide-ranging goals patients can have.
“Some [patients] will maximize the focus on function, regardless of how long they are likely to live,” Dr. Tinetti said. “Others will say symptom burden management is most important to them. And others will say they want to live as long as possible, and survival is most important, even if that means a reduction in their function. These individuals also vary in the care they are willing and able to receive to achieve the outcomes that matter most to them.”
For these reasons, Dr. Tinetti recommended patient priorities care, which she and her colleagues have been developing and implementing over the past 5-6 years.
“If the benefits and harms of addressing each condition in isolation is of uncertain benefit and potentially burdensome to both clinician and patient, and we know that patients vary in their health priorities ... then what else would you want to focus on in your 20-minute visit ... except each patient’s priorities?” Dr. Tinetti asked. “This is one solution to the challenge.”
What is patient priorities care?
Patient priorities care is a multidisciplinary, cyclical approach to clinical decision-making composed of three steps, Dr. Tinetti explained. First, a clinician identifies the patient’s health priorities. Second, this information is transmitted to comanaging providers, who decide which of their respective treatments are consistent with the patient’s priorities. And third, those decisions are disseminated to everyone involved in the patient’s care, both within and outside of the health care system, allowing all care providers to align with the patient’s priorities, she noted.
“Each person does that from their own expertise,” Dr. Tinetti said. “The social worker will do something different than the cardiologist, the physical therapist, the endocrinologist – but everybody is aiming at the same outcome – the patient’s priorities.”
In 2019, Dr. Tinetti led a nonrandomized clinical trial to test the feasibility of patient priorities care. The study involved 366 older adults with multimorbidity, among whom 203 received usual care, while 163 received this type of care. Patients in the latter group were twice as likely to have medications stopped, and significantly less likely to have self-management tasks added and diagnostic tests ordered.
How electronic health records can help
In an interview, Dr. Tinetti suggested that comanaging physicians communicate through electronic health records (EHRs), first to ensure that all care providers understand a patient’s goals, then to determine if recommended therapies align with those goals.
“It would be a little bit of a culture change to do that,” Dr. Tinetti said, “but the technology is there and it isn’t too terribly time consuming.”
She went on to suggest that primary care providers are typically best suited to coordinate this process; however, if a patient receives the majority of their care from a particular specialist, then that clinician may be the most suitable coordinator.
Systemic obstacles and solutions
According to Cynthia Boyd, MD, interim director of the division of geriatric medicine and gerontology, Johns Hopkins University, Baltimore, clinicians may encounter obstacles when implementing patient priorities care.
“Our health care system doesn’t always make it easy to do this,” Dr. Boyd said. “It’s important to acknowledge this because it can be hard to do. There’s no question,” Dr. Boyd said in an interview.
Among the headwinds that clinicians may face are clinical practice guidelines, the structure of electronic health records, and quality metrics focused on specific conditions, she explained.
“There’s a lot of things that push us – in primary care and other parts of medicine – away from the approach that’s best for people with multiple chronic conditions,” Dr. Boyd said.
Dr. Tinetti said a challenge to providing this care that she expects is for clinicians, regardless of specialty, “to feel uneasy” about transitioning away from a conventional approach.
Among Dr. Tinetti’s arguments in favor of providing patient priorities care is that “it’s going to bring more joy in practice because you’re really addressing what matters to that individual while also providing good care.”
To get the most out of patient priorities care, Dr. Boyd recommended that clinicians focus on ‘the 4 M’s’: what matters most, mentation, mobility, and medications.
In an effort to address the last of these on a broad scale, Dr. Boyd is co-leading the US Deprescribing Research Network(USDeN), which aims to “improve medication use among older adults and the outcomes that are important to them,” according to the USDeN website.
To encourage deprescribing on a day-to-day level, Dr. Boyd called for strong communication between co–managing providers.
In an ideal world, there would be a better way to communicate than largely via electronic health records, she said.
“We need more than the EHR to connect us. That’s why it’s really important for primary care providers and specialists to be able to have time to actually talk to each other. This gets into how we reimburse and organize the communication and cognitive aspects of care,” Dr. Boyd noted.
Dr. Tinetti disclosed support from the John A. Hartford Foundation, the Donaghue Foundation, the National Institute on Aging, and the Institute for Healthcare Improvement. Dr. Boyd disclosed a relationship with UpToDate, for which she coauthored a chapter on multimorbidity.
said Mary Tinetti, MD, Gladys Phillips Crofoot Professor of Medicine and Public Health and chief of geriatrics at Yale University, New Haven, Conn.
During a virtual presentation at the American College of Physicians annual Internal Medicine meeting, the gerontologist noted that primary care providers face a number of challenges when managing elderly patients with multimorbidity. These challenges include a lack of representative data in clinical trials, conflicting guideline recommendations, patient nonadherence, and decreased benefit from therapies due to competing conditions, she said.
“Trying to follow multiple guidelines can result in unintentional harms to these people with multiple conditions,” Dr. Tinetti said. She gave examples of the wide-ranging goals patients can have.
“Some [patients] will maximize the focus on function, regardless of how long they are likely to live,” Dr. Tinetti said. “Others will say symptom burden management is most important to them. And others will say they want to live as long as possible, and survival is most important, even if that means a reduction in their function. These individuals also vary in the care they are willing and able to receive to achieve the outcomes that matter most to them.”
For these reasons, Dr. Tinetti recommended patient priorities care, which she and her colleagues have been developing and implementing over the past 5-6 years.
“If the benefits and harms of addressing each condition in isolation is of uncertain benefit and potentially burdensome to both clinician and patient, and we know that patients vary in their health priorities ... then what else would you want to focus on in your 20-minute visit ... except each patient’s priorities?” Dr. Tinetti asked. “This is one solution to the challenge.”
What is patient priorities care?
Patient priorities care is a multidisciplinary, cyclical approach to clinical decision-making composed of three steps, Dr. Tinetti explained. First, a clinician identifies the patient’s health priorities. Second, this information is transmitted to comanaging providers, who decide which of their respective treatments are consistent with the patient’s priorities. And third, those decisions are disseminated to everyone involved in the patient’s care, both within and outside of the health care system, allowing all care providers to align with the patient’s priorities, she noted.
“Each person does that from their own expertise,” Dr. Tinetti said. “The social worker will do something different than the cardiologist, the physical therapist, the endocrinologist – but everybody is aiming at the same outcome – the patient’s priorities.”
In 2019, Dr. Tinetti led a nonrandomized clinical trial to test the feasibility of patient priorities care. The study involved 366 older adults with multimorbidity, among whom 203 received usual care, while 163 received this type of care. Patients in the latter group were twice as likely to have medications stopped, and significantly less likely to have self-management tasks added and diagnostic tests ordered.
How electronic health records can help
In an interview, Dr. Tinetti suggested that comanaging physicians communicate through electronic health records (EHRs), first to ensure that all care providers understand a patient’s goals, then to determine if recommended therapies align with those goals.
“It would be a little bit of a culture change to do that,” Dr. Tinetti said, “but the technology is there and it isn’t too terribly time consuming.”
She went on to suggest that primary care providers are typically best suited to coordinate this process; however, if a patient receives the majority of their care from a particular specialist, then that clinician may be the most suitable coordinator.
Systemic obstacles and solutions
According to Cynthia Boyd, MD, interim director of the division of geriatric medicine and gerontology, Johns Hopkins University, Baltimore, clinicians may encounter obstacles when implementing patient priorities care.
“Our health care system doesn’t always make it easy to do this,” Dr. Boyd said. “It’s important to acknowledge this because it can be hard to do. There’s no question,” Dr. Boyd said in an interview.
Among the headwinds that clinicians may face are clinical practice guidelines, the structure of electronic health records, and quality metrics focused on specific conditions, she explained.
“There’s a lot of things that push us – in primary care and other parts of medicine – away from the approach that’s best for people with multiple chronic conditions,” Dr. Boyd said.
Dr. Tinetti said a challenge to providing this care that she expects is for clinicians, regardless of specialty, “to feel uneasy” about transitioning away from a conventional approach.
Among Dr. Tinetti’s arguments in favor of providing patient priorities care is that “it’s going to bring more joy in practice because you’re really addressing what matters to that individual while also providing good care.”
To get the most out of patient priorities care, Dr. Boyd recommended that clinicians focus on ‘the 4 M’s’: what matters most, mentation, mobility, and medications.
In an effort to address the last of these on a broad scale, Dr. Boyd is co-leading the US Deprescribing Research Network(USDeN), which aims to “improve medication use among older adults and the outcomes that are important to them,” according to the USDeN website.
To encourage deprescribing on a day-to-day level, Dr. Boyd called for strong communication between co–managing providers.
In an ideal world, there would be a better way to communicate than largely via electronic health records, she said.
“We need more than the EHR to connect us. That’s why it’s really important for primary care providers and specialists to be able to have time to actually talk to each other. This gets into how we reimburse and organize the communication and cognitive aspects of care,” Dr. Boyd noted.
Dr. Tinetti disclosed support from the John A. Hartford Foundation, the Donaghue Foundation, the National Institute on Aging, and the Institute for Healthcare Improvement. Dr. Boyd disclosed a relationship with UpToDate, for which she coauthored a chapter on multimorbidity.
FROM INTERNAL MEDICINE 2021