User login
Common parasite now tied to impaired cognitive function
Investigators reviewed and conducted a meta-analysis of 13 studies that encompassed more than 13,000 healthy adults and found a modest but significant association between T. gondii seropositivity and impaired performance on cognitive tests of processing speed, working memory, short-term verbal memory, and executive function. The average age of the persons in the studies was close to 50 years.
“Our findings show that T. gondii could have a negative but small effect on cognition,” study investigator Arjen Sutterland, MD, of the Amsterdam Neuroscience Research Institute and the Amsterdam Institute for Infection and Immunity, University of Amsterdam, said in an interview.
The study was published online July 14, 2021, in JAMA Psychiatry.
Mental illness link
T. gondii is “an intracellular parasite that produces quiescent infection in approximately 30% of humans worldwide,” the authors wrote. The parasite that causes the infection not only settles in muscle and liver tissue but also can cross the blood-brain barrier and settle quiescently in brain tissue. It can be spread through contact with cat feces or by consuming contaminated meat.
Previous research has shown that neurocognitive changes associated with toxoplasmosis can occur in humans, and meta-analyses suggest an association with neuropsychiatric disorders. Some research has also tied T. gondii infection to increased motor vehicle crashes and suicide attempts.
Dr. Sutterland said he had been inspired by the work of E. Fuller Torrey and Bob Yolken, who proposed the connection between T. gondii and schizophrenia.
Some years ago, Dr. Sutterland and his group analyzed the mental health consequences of T. gondii infection and found “several interesting associations,” but they were unable to “rule out reverse causation – i.e., people with mental health disorders more often get these infections – as well as determine the impact on the population of this common infection.”
For the current study, the investigators analyzed studies that examined specifically cognitive functioning in otherwise healthy individuals in relation to T. gondii infection, “because reverse causation would be less likely in this population and a grasp of global impact would become more clear.”
The researchers conducted a literature search of studies conducted through June 7, 2019, that analyzed cognitive function among healthy participants for whom data on T. gondii seropositivity were available.
A total of 13 studies (n = 13,289 participants; mean age, 46.7 years; 49.6% male) were used in the review and meta-analysis. Some of the studies enrolled a healthy population sample; other studies compared participants with and those without psychiatric disorders. From these, the researchers extracted only the data concerning healthy participants.
The studies analyzed four cognitive domains: processing speed, working memory, short-term verbal memory, and executive functioning.
All cognitive domains affected
Of all the participants, 22.6% had antibodies against T. gondii.
Participants who were seropositive for T. gondii had less favorable functioning in all cognitive domains, with “small but significant” differences. 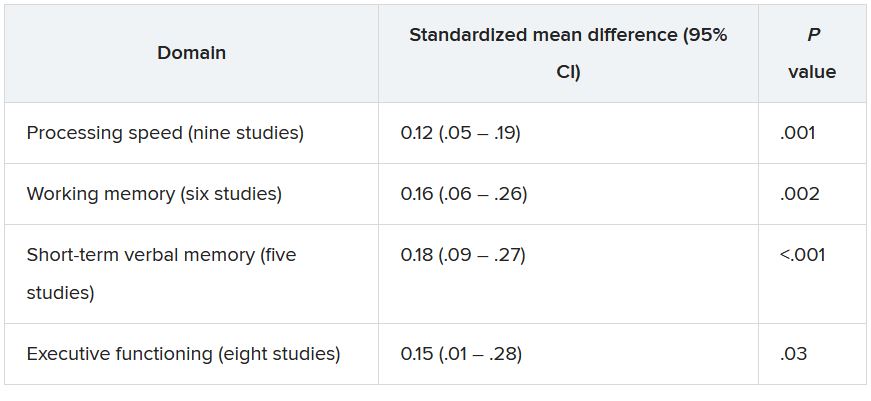
The researchers conducted a meta-regression analysis of mean age in the analysis of executive functioning and found greater effect sizes as age increased (Q = 6.17; R2 = 81%; P = .01).
The studies were of “high quality,” and there was “little suggestion of publication bias was detected,” the authors noted.
“Although the extent of the associations was modest, the ubiquitous prevalence of the quiescent infection worldwide ... suggests that the consequences for cognitive function of the population as a whole may be substantial, although it is difficult to quantify the global impact,” they wrote.
They note that because the studies were cross-sectional in nature, causality cannot be established.
Nevertheless, Dr. Sutterland suggested several possible mechanisms through which T. gondii might affect neurocognition.
“We know the parasite forms cysts in the brain and can influence dopaminergic neurotransmission, which, in turn, affects neurocognition. Alternatively, it is also possible that the immune response to the infection in the brain causes cognitive impairment. This remains an important question to explore further,” he said.
He noted that clinicians can reassure patients who test positive for T. gondii that although the infection can have a negative impact on cognition, the effect is “small.”
Prevention programs warranted
Commenting on the study in an interview, Shawn D. Gale, PhD, associate professor, department of psychology and neuroscience center, Brigham Young University, Provo, Utah, called it a “great meta-analysis.” He noted that his group is researching the subject and has obtained similar findings. A big plus is that the researchers assessed several cognitive domains, not just one.
Although the data showed “mild effects,” the findings could be important on a population level. Because 30% of the world’s population are seropositive for T. gondii, a potentially large number of people are at risk for cognitive impairment, noted Dr. Gale, who was not involved with the study.
“If you look at the United States, perhaps 10%-15% of people might test positive [for T. gondii], but in Germany and France, the number comes closer to 50%, and in other places in the world – especially countries that have a harder time economically – the rates are even higher. So if it can affect cognition, even a small effect is a big deal,” Dr. Gale said.
“I think prevention will be the most important thing, and perhaps down the road, I hope that a vaccine will be considered,” Dr. Gale added.
“These findings indicate that primary prevention of the infection could have substantial global impact on mental health” and that public health programs to prevent T. gondii “are warranted.”
These programs might consist of hygienic measures, especially after human contact with contaminated sources, as well as research into vaccine development.
No source of funding for the study was listed. The authors and Dr. Gale reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators reviewed and conducted a meta-analysis of 13 studies that encompassed more than 13,000 healthy adults and found a modest but significant association between T. gondii seropositivity and impaired performance on cognitive tests of processing speed, working memory, short-term verbal memory, and executive function. The average age of the persons in the studies was close to 50 years.
“Our findings show that T. gondii could have a negative but small effect on cognition,” study investigator Arjen Sutterland, MD, of the Amsterdam Neuroscience Research Institute and the Amsterdam Institute for Infection and Immunity, University of Amsterdam, said in an interview.
The study was published online July 14, 2021, in JAMA Psychiatry.
Mental illness link
T. gondii is “an intracellular parasite that produces quiescent infection in approximately 30% of humans worldwide,” the authors wrote. The parasite that causes the infection not only settles in muscle and liver tissue but also can cross the blood-brain barrier and settle quiescently in brain tissue. It can be spread through contact with cat feces or by consuming contaminated meat.
Previous research has shown that neurocognitive changes associated with toxoplasmosis can occur in humans, and meta-analyses suggest an association with neuropsychiatric disorders. Some research has also tied T. gondii infection to increased motor vehicle crashes and suicide attempts.
Dr. Sutterland said he had been inspired by the work of E. Fuller Torrey and Bob Yolken, who proposed the connection between T. gondii and schizophrenia.
Some years ago, Dr. Sutterland and his group analyzed the mental health consequences of T. gondii infection and found “several interesting associations,” but they were unable to “rule out reverse causation – i.e., people with mental health disorders more often get these infections – as well as determine the impact on the population of this common infection.”
For the current study, the investigators analyzed studies that examined specifically cognitive functioning in otherwise healthy individuals in relation to T. gondii infection, “because reverse causation would be less likely in this population and a grasp of global impact would become more clear.”
The researchers conducted a literature search of studies conducted through June 7, 2019, that analyzed cognitive function among healthy participants for whom data on T. gondii seropositivity were available.
A total of 13 studies (n = 13,289 participants; mean age, 46.7 years; 49.6% male) were used in the review and meta-analysis. Some of the studies enrolled a healthy population sample; other studies compared participants with and those without psychiatric disorders. From these, the researchers extracted only the data concerning healthy participants.
The studies analyzed four cognitive domains: processing speed, working memory, short-term verbal memory, and executive functioning.
All cognitive domains affected
Of all the participants, 22.6% had antibodies against T. gondii.
Participants who were seropositive for T. gondii had less favorable functioning in all cognitive domains, with “small but significant” differences.
The researchers conducted a meta-regression analysis of mean age in the analysis of executive functioning and found greater effect sizes as age increased (Q = 6.17; R2 = 81%; P = .01).
The studies were of “high quality,” and there was “little suggestion of publication bias was detected,” the authors noted.
“Although the extent of the associations was modest, the ubiquitous prevalence of the quiescent infection worldwide ... suggests that the consequences for cognitive function of the population as a whole may be substantial, although it is difficult to quantify the global impact,” they wrote.
They note that because the studies were cross-sectional in nature, causality cannot be established.
Nevertheless, Dr. Sutterland suggested several possible mechanisms through which T. gondii might affect neurocognition.
“We know the parasite forms cysts in the brain and can influence dopaminergic neurotransmission, which, in turn, affects neurocognition. Alternatively, it is also possible that the immune response to the infection in the brain causes cognitive impairment. This remains an important question to explore further,” he said.
He noted that clinicians can reassure patients who test positive for T. gondii that although the infection can have a negative impact on cognition, the effect is “small.”
Prevention programs warranted
Commenting on the study in an interview, Shawn D. Gale, PhD, associate professor, department of psychology and neuroscience center, Brigham Young University, Provo, Utah, called it a “great meta-analysis.” He noted that his group is researching the subject and has obtained similar findings. A big plus is that the researchers assessed several cognitive domains, not just one.
Although the data showed “mild effects,” the findings could be important on a population level. Because 30% of the world’s population are seropositive for T. gondii, a potentially large number of people are at risk for cognitive impairment, noted Dr. Gale, who was not involved with the study.
“If you look at the United States, perhaps 10%-15% of people might test positive [for T. gondii], but in Germany and France, the number comes closer to 50%, and in other places in the world – especially countries that have a harder time economically – the rates are even higher. So if it can affect cognition, even a small effect is a big deal,” Dr. Gale said.
“I think prevention will be the most important thing, and perhaps down the road, I hope that a vaccine will be considered,” Dr. Gale added.
“These findings indicate that primary prevention of the infection could have substantial global impact on mental health” and that public health programs to prevent T. gondii “are warranted.”
These programs might consist of hygienic measures, especially after human contact with contaminated sources, as well as research into vaccine development.
No source of funding for the study was listed. The authors and Dr. Gale reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators reviewed and conducted a meta-analysis of 13 studies that encompassed more than 13,000 healthy adults and found a modest but significant association between T. gondii seropositivity and impaired performance on cognitive tests of processing speed, working memory, short-term verbal memory, and executive function. The average age of the persons in the studies was close to 50 years.
“Our findings show that T. gondii could have a negative but small effect on cognition,” study investigator Arjen Sutterland, MD, of the Amsterdam Neuroscience Research Institute and the Amsterdam Institute for Infection and Immunity, University of Amsterdam, said in an interview.
The study was published online July 14, 2021, in JAMA Psychiatry.
Mental illness link
T. gondii is “an intracellular parasite that produces quiescent infection in approximately 30% of humans worldwide,” the authors wrote. The parasite that causes the infection not only settles in muscle and liver tissue but also can cross the blood-brain barrier and settle quiescently in brain tissue. It can be spread through contact with cat feces or by consuming contaminated meat.
Previous research has shown that neurocognitive changes associated with toxoplasmosis can occur in humans, and meta-analyses suggest an association with neuropsychiatric disorders. Some research has also tied T. gondii infection to increased motor vehicle crashes and suicide attempts.
Dr. Sutterland said he had been inspired by the work of E. Fuller Torrey and Bob Yolken, who proposed the connection between T. gondii and schizophrenia.
Some years ago, Dr. Sutterland and his group analyzed the mental health consequences of T. gondii infection and found “several interesting associations,” but they were unable to “rule out reverse causation – i.e., people with mental health disorders more often get these infections – as well as determine the impact on the population of this common infection.”
For the current study, the investigators analyzed studies that examined specifically cognitive functioning in otherwise healthy individuals in relation to T. gondii infection, “because reverse causation would be less likely in this population and a grasp of global impact would become more clear.”
The researchers conducted a literature search of studies conducted through June 7, 2019, that analyzed cognitive function among healthy participants for whom data on T. gondii seropositivity were available.
A total of 13 studies (n = 13,289 participants; mean age, 46.7 years; 49.6% male) were used in the review and meta-analysis. Some of the studies enrolled a healthy population sample; other studies compared participants with and those without psychiatric disorders. From these, the researchers extracted only the data concerning healthy participants.
The studies analyzed four cognitive domains: processing speed, working memory, short-term verbal memory, and executive functioning.
All cognitive domains affected
Of all the participants, 22.6% had antibodies against T. gondii.
Participants who were seropositive for T. gondii had less favorable functioning in all cognitive domains, with “small but significant” differences.
The researchers conducted a meta-regression analysis of mean age in the analysis of executive functioning and found greater effect sizes as age increased (Q = 6.17; R2 = 81%; P = .01).
The studies were of “high quality,” and there was “little suggestion of publication bias was detected,” the authors noted.
“Although the extent of the associations was modest, the ubiquitous prevalence of the quiescent infection worldwide ... suggests that the consequences for cognitive function of the population as a whole may be substantial, although it is difficult to quantify the global impact,” they wrote.
They note that because the studies were cross-sectional in nature, causality cannot be established.
Nevertheless, Dr. Sutterland suggested several possible mechanisms through which T. gondii might affect neurocognition.
“We know the parasite forms cysts in the brain and can influence dopaminergic neurotransmission, which, in turn, affects neurocognition. Alternatively, it is also possible that the immune response to the infection in the brain causes cognitive impairment. This remains an important question to explore further,” he said.
He noted that clinicians can reassure patients who test positive for T. gondii that although the infection can have a negative impact on cognition, the effect is “small.”
Prevention programs warranted
Commenting on the study in an interview, Shawn D. Gale, PhD, associate professor, department of psychology and neuroscience center, Brigham Young University, Provo, Utah, called it a “great meta-analysis.” He noted that his group is researching the subject and has obtained similar findings. A big plus is that the researchers assessed several cognitive domains, not just one.
Although the data showed “mild effects,” the findings could be important on a population level. Because 30% of the world’s population are seropositive for T. gondii, a potentially large number of people are at risk for cognitive impairment, noted Dr. Gale, who was not involved with the study.
“If you look at the United States, perhaps 10%-15% of people might test positive [for T. gondii], but in Germany and France, the number comes closer to 50%, and in other places in the world – especially countries that have a harder time economically – the rates are even higher. So if it can affect cognition, even a small effect is a big deal,” Dr. Gale said.
“I think prevention will be the most important thing, and perhaps down the road, I hope that a vaccine will be considered,” Dr. Gale added.
“These findings indicate that primary prevention of the infection could have substantial global impact on mental health” and that public health programs to prevent T. gondii “are warranted.”
These programs might consist of hygienic measures, especially after human contact with contaminated sources, as well as research into vaccine development.
No source of funding for the study was listed. The authors and Dr. Gale reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Twofold increased risk for death from COVID-19 in psych patients
compared with those without a psychiatric diagnosis, according to the results of the largest study of its kind to date.
These findings, the investigators noted, highlight the need to prioritize vaccination in patients with preexisting mental health disorders.
“We have proven beyond a shadow of a doubt that there are increased risks” among psychiatric patients who get COVID-19, study investigator Livia De Picker, MD, PhD, psychiatrist and postdoctoral researcher, University Psychiatric Hospital Campus Duffel and University of Antwerp (Belgium), told this news organization.
“Doctors need to look at these patients the same way they would other high-risk people, for example those with diabetes or chronic obstructive pulmonary disease,” all of whom should be protected against COVID-19, Dr. De Picker added.
The study was published online July 15, 2021, in Lancet Psychiatry.
Risk by mental illness type
The systematic review included 33 studies from 22 countries that reported risk estimates for mortality, hospitalization, and ICU admission in patients with confirmed SARS-CoV-2 infection. The meta-analysis included 23 of these studies with a total of 1.47 million participants. Of these, 43,938 had a psychiatric disorder.
The primary outcome was mortality after COVID-19. Secondary outcomes included hospitalization and ICU admission after COVID-19. Researchers adjusted for age, sex, and other covariates.
Results showed the presence of any comorbid mental illness was associated with an increased risk for death after SARS-CoV-2 infection (odds ratio, 2.00; 95% confidence interval, 1.58-2.54; P < .0001).
When researchers stratified mortality risk by psychiatric disorder type, the most robust associations were for psychotic and mood disorders. Substance use disorders, intellectual disabilities, and developmental disorders were associated with higher mortality only in crude estimates. There was no increased death risk associated with anxiety disorders.
“That there are differences between the various types of disorders was an interesting finding,” said Dr. De Picker, adding that previous research “just lumped together all diagnostic categories.”
Potential mechanisms
The study did not explore why psychiatric illness raise the risk for death in the setting of COVID-19, so potential mechanisms are purely speculative. However, the investigators believe it may reflect biological processes such as immune-inflammatory alterations.
Psychotic disorders and mood disorders in particular, are associated with immune changes, including immunogenetic abnormalities, raised cytokine concentrations, autoantibodies, acute-phase proteins, and aberrant counts of leukocyte cell types, said Dr. De Picker.
She likened this to elderly people being at increased risk following COVID-19 because their immune system is compromised and less able to fight infection.
There are likely other factors at play, said Dr. De Picker. These could include social isolation and lifestyle factors like poor diet, physical inactivity, high alcohol and tobacco use, and sleep disturbances.
In addition, psychiatric patients have a higher prevalence of comorbidities including diabetes, cardiovascular disease, and respiratory disease, which could also play a role.
The increased mortality might also reflect reduced access to care. “Some of these patients may be living in difficult socioeconomic conditions,” said Dr. De Picker.
She noted that, while the in-hospital mortality was not increased, the risk was significantly increased in samples that were outside of the hospital. This reinforces the need for providing close monitoring and early referral to hospital for psychiatric patients with COVID-19.
Mortality varied significantly among countries, with the lowest risk in Europe and the United States. This difference might be attributable to differences in health care systems and access to care, said Dr. De Picker.
Overall, the risk for hospitalization was about double for COVID patients with a mental illness, but when stratified by disorder, there was only a significantly increased risk for substance use and mood disorders. “But mood disorders were not even significant any more after adjusting for age, sex, and comorbid conditions, and we don’t see an increased risk for psychotic disorders whereas they had the highest mortality risks,” said Dr. De Picker.
Psych meds a risk factor?
The studies were primarily based on electronic medical records, so investigators were unable to carry out “a fine grain analysis” into clinical factors affecting outcomes, she noted.
Antipsychotics were consistently associated with an increased risk for mortality (adjusted OR, 2.43; 95% CI, 1.81-3.25), as were anxiolytics (aOR, 1.47; 95% CI, 1.15-1.88).
“There are some theoretical reasons why we believe there could be a risk associated with these drugs,” said Dr. De Picker. For example, antipsychotics can increase the risk for cardiac arrhythmias and thromboembolic events, and cause interactions with drugs used to treat COVID-19.
As for anxiolytics, especially benzodiazepines, these drugs are associated with respiratory risk and with all-cause mortality. “So you could imagine that someone who is infected with a respiratory virus and [is] then using these drugs on top of that would have a worse outcome,” said Dr. De Picker.
In contrast to antipsychotics and anxiolytics, antidepressants did not increase mortality risk.
Dr. De Picker noted a new study by French researchers showing a protective effect of certain serotonergic antidepressants on COVID outcomes, including mortality.
There was no robust evidence of an increased risk for ICU admission for patients with mental disorders. However, the authors noted some studies included small samples of patients with psychiatric disorders, “contributing to a low certainty of evidence for ICU admission.”
Dr. De Picker criticized COVID vaccine policies that don’t prioritize patients with psychiatric disorders. In many countries, groups that were initially green-lighted for the vaccine included health care workers, the elderly, and those with underlying conditions such as diabetes, obesity and even mild hypertension – but not mental illness, which is also an underlying risk.
‘Outstanding’ research
Commenting on the study for this news organization, Jonathan E. Alpert, MD, PhD, department of psychiatry and behavioral sciences, Montefiore Medical Center, New York, and chair of the American Psychiatric Association Council on Research, called it “outstanding” and the largest of its kind.
“There have been a number of studies that have come to similar conclusions, that people with psychiatric illness are at greater risk for poorer outcomes, but because any given study had a relatively limited sample, perhaps from one health system or one country, there were some inconsistencies,” said Dr. Alpert.
“This is the strongest report so far that has made the point that people with psychiatric illness are a vulnerable population for a negative outcome from COVID, including the most worrisome – mortality.”
The study helps drive home a “very important public health lesson” that applies to COVID-19 but goes “beyond,” said Dr. Alpert.
“As a society, we need to keep in mind that people with serious mental disorders are a vulnerable population for poorer outcomes in most general medical conditions,” he stressed, “whether it’s cancer or heart disease or diabetes, and special efforts need to be made to reach out to those populations.”
Dr. Alpert agreed that, at the start of the pandemic, psychiatric patients in the United States were not prioritized for vaccination, and although psychiatric patients may initially have found it difficult to navigate the health care system to learn where and how to get a COVID shot, today that barrier has mostly been removed.
“Our patients are at least as willing as any other subgroup to get the vaccine, and that includes people with psychotic disorders,” he said.
The study was supported by the European College of Neuropsychopharmacology Immuno-NeuroPsychiatry network and Fondazione Centro San Raffaele (Milan). Dr. De Picker reported receiving grants from Boehringer Ingelheim and Janssen outside the submitted work. She is a member of the European College of Neuropsychopharmacology Immuno-NeuroPsychiatry Thematic Working Group.
A version of this article first appeared on Medscape.com.
compared with those without a psychiatric diagnosis, according to the results of the largest study of its kind to date.
These findings, the investigators noted, highlight the need to prioritize vaccination in patients with preexisting mental health disorders.
“We have proven beyond a shadow of a doubt that there are increased risks” among psychiatric patients who get COVID-19, study investigator Livia De Picker, MD, PhD, psychiatrist and postdoctoral researcher, University Psychiatric Hospital Campus Duffel and University of Antwerp (Belgium), told this news organization.
“Doctors need to look at these patients the same way they would other high-risk people, for example those with diabetes or chronic obstructive pulmonary disease,” all of whom should be protected against COVID-19, Dr. De Picker added.
The study was published online July 15, 2021, in Lancet Psychiatry.
Risk by mental illness type
The systematic review included 33 studies from 22 countries that reported risk estimates for mortality, hospitalization, and ICU admission in patients with confirmed SARS-CoV-2 infection. The meta-analysis included 23 of these studies with a total of 1.47 million participants. Of these, 43,938 had a psychiatric disorder.
The primary outcome was mortality after COVID-19. Secondary outcomes included hospitalization and ICU admission after COVID-19. Researchers adjusted for age, sex, and other covariates.
Results showed the presence of any comorbid mental illness was associated with an increased risk for death after SARS-CoV-2 infection (odds ratio, 2.00; 95% confidence interval, 1.58-2.54; P < .0001).
When researchers stratified mortality risk by psychiatric disorder type, the most robust associations were for psychotic and mood disorders. Substance use disorders, intellectual disabilities, and developmental disorders were associated with higher mortality only in crude estimates. There was no increased death risk associated with anxiety disorders.
“That there are differences between the various types of disorders was an interesting finding,” said Dr. De Picker, adding that previous research “just lumped together all diagnostic categories.”
Potential mechanisms
The study did not explore why psychiatric illness raise the risk for death in the setting of COVID-19, so potential mechanisms are purely speculative. However, the investigators believe it may reflect biological processes such as immune-inflammatory alterations.
Psychotic disorders and mood disorders in particular, are associated with immune changes, including immunogenetic abnormalities, raised cytokine concentrations, autoantibodies, acute-phase proteins, and aberrant counts of leukocyte cell types, said Dr. De Picker.
She likened this to elderly people being at increased risk following COVID-19 because their immune system is compromised and less able to fight infection.
There are likely other factors at play, said Dr. De Picker. These could include social isolation and lifestyle factors like poor diet, physical inactivity, high alcohol and tobacco use, and sleep disturbances.
In addition, psychiatric patients have a higher prevalence of comorbidities including diabetes, cardiovascular disease, and respiratory disease, which could also play a role.
The increased mortality might also reflect reduced access to care. “Some of these patients may be living in difficult socioeconomic conditions,” said Dr. De Picker.
She noted that, while the in-hospital mortality was not increased, the risk was significantly increased in samples that were outside of the hospital. This reinforces the need for providing close monitoring and early referral to hospital for psychiatric patients with COVID-19.
Mortality varied significantly among countries, with the lowest risk in Europe and the United States. This difference might be attributable to differences in health care systems and access to care, said Dr. De Picker.
Overall, the risk for hospitalization was about double for COVID patients with a mental illness, but when stratified by disorder, there was only a significantly increased risk for substance use and mood disorders. “But mood disorders were not even significant any more after adjusting for age, sex, and comorbid conditions, and we don’t see an increased risk for psychotic disorders whereas they had the highest mortality risks,” said Dr. De Picker.
Psych meds a risk factor?
The studies were primarily based on electronic medical records, so investigators were unable to carry out “a fine grain analysis” into clinical factors affecting outcomes, she noted.
Antipsychotics were consistently associated with an increased risk for mortality (adjusted OR, 2.43; 95% CI, 1.81-3.25), as were anxiolytics (aOR, 1.47; 95% CI, 1.15-1.88).
“There are some theoretical reasons why we believe there could be a risk associated with these drugs,” said Dr. De Picker. For example, antipsychotics can increase the risk for cardiac arrhythmias and thromboembolic events, and cause interactions with drugs used to treat COVID-19.
As for anxiolytics, especially benzodiazepines, these drugs are associated with respiratory risk and with all-cause mortality. “So you could imagine that someone who is infected with a respiratory virus and [is] then using these drugs on top of that would have a worse outcome,” said Dr. De Picker.
In contrast to antipsychotics and anxiolytics, antidepressants did not increase mortality risk.
Dr. De Picker noted a new study by French researchers showing a protective effect of certain serotonergic antidepressants on COVID outcomes, including mortality.
There was no robust evidence of an increased risk for ICU admission for patients with mental disorders. However, the authors noted some studies included small samples of patients with psychiatric disorders, “contributing to a low certainty of evidence for ICU admission.”
Dr. De Picker criticized COVID vaccine policies that don’t prioritize patients with psychiatric disorders. In many countries, groups that were initially green-lighted for the vaccine included health care workers, the elderly, and those with underlying conditions such as diabetes, obesity and even mild hypertension – but not mental illness, which is also an underlying risk.
‘Outstanding’ research
Commenting on the study for this news organization, Jonathan E. Alpert, MD, PhD, department of psychiatry and behavioral sciences, Montefiore Medical Center, New York, and chair of the American Psychiatric Association Council on Research, called it “outstanding” and the largest of its kind.
“There have been a number of studies that have come to similar conclusions, that people with psychiatric illness are at greater risk for poorer outcomes, but because any given study had a relatively limited sample, perhaps from one health system or one country, there were some inconsistencies,” said Dr. Alpert.
“This is the strongest report so far that has made the point that people with psychiatric illness are a vulnerable population for a negative outcome from COVID, including the most worrisome – mortality.”
The study helps drive home a “very important public health lesson” that applies to COVID-19 but goes “beyond,” said Dr. Alpert.
“As a society, we need to keep in mind that people with serious mental disorders are a vulnerable population for poorer outcomes in most general medical conditions,” he stressed, “whether it’s cancer or heart disease or diabetes, and special efforts need to be made to reach out to those populations.”
Dr. Alpert agreed that, at the start of the pandemic, psychiatric patients in the United States were not prioritized for vaccination, and although psychiatric patients may initially have found it difficult to navigate the health care system to learn where and how to get a COVID shot, today that barrier has mostly been removed.
“Our patients are at least as willing as any other subgroup to get the vaccine, and that includes people with psychotic disorders,” he said.
The study was supported by the European College of Neuropsychopharmacology Immuno-NeuroPsychiatry network and Fondazione Centro San Raffaele (Milan). Dr. De Picker reported receiving grants from Boehringer Ingelheim and Janssen outside the submitted work. She is a member of the European College of Neuropsychopharmacology Immuno-NeuroPsychiatry Thematic Working Group.
A version of this article first appeared on Medscape.com.
compared with those without a psychiatric diagnosis, according to the results of the largest study of its kind to date.
These findings, the investigators noted, highlight the need to prioritize vaccination in patients with preexisting mental health disorders.
“We have proven beyond a shadow of a doubt that there are increased risks” among psychiatric patients who get COVID-19, study investigator Livia De Picker, MD, PhD, psychiatrist and postdoctoral researcher, University Psychiatric Hospital Campus Duffel and University of Antwerp (Belgium), told this news organization.
“Doctors need to look at these patients the same way they would other high-risk people, for example those with diabetes or chronic obstructive pulmonary disease,” all of whom should be protected against COVID-19, Dr. De Picker added.
The study was published online July 15, 2021, in Lancet Psychiatry.
Risk by mental illness type
The systematic review included 33 studies from 22 countries that reported risk estimates for mortality, hospitalization, and ICU admission in patients with confirmed SARS-CoV-2 infection. The meta-analysis included 23 of these studies with a total of 1.47 million participants. Of these, 43,938 had a psychiatric disorder.
The primary outcome was mortality after COVID-19. Secondary outcomes included hospitalization and ICU admission after COVID-19. Researchers adjusted for age, sex, and other covariates.
Results showed the presence of any comorbid mental illness was associated with an increased risk for death after SARS-CoV-2 infection (odds ratio, 2.00; 95% confidence interval, 1.58-2.54; P < .0001).
When researchers stratified mortality risk by psychiatric disorder type, the most robust associations were for psychotic and mood disorders. Substance use disorders, intellectual disabilities, and developmental disorders were associated with higher mortality only in crude estimates. There was no increased death risk associated with anxiety disorders.
“That there are differences between the various types of disorders was an interesting finding,” said Dr. De Picker, adding that previous research “just lumped together all diagnostic categories.”
Potential mechanisms
The study did not explore why psychiatric illness raise the risk for death in the setting of COVID-19, so potential mechanisms are purely speculative. However, the investigators believe it may reflect biological processes such as immune-inflammatory alterations.
Psychotic disorders and mood disorders in particular, are associated with immune changes, including immunogenetic abnormalities, raised cytokine concentrations, autoantibodies, acute-phase proteins, and aberrant counts of leukocyte cell types, said Dr. De Picker.
She likened this to elderly people being at increased risk following COVID-19 because their immune system is compromised and less able to fight infection.
There are likely other factors at play, said Dr. De Picker. These could include social isolation and lifestyle factors like poor diet, physical inactivity, high alcohol and tobacco use, and sleep disturbances.
In addition, psychiatric patients have a higher prevalence of comorbidities including diabetes, cardiovascular disease, and respiratory disease, which could also play a role.
The increased mortality might also reflect reduced access to care. “Some of these patients may be living in difficult socioeconomic conditions,” said Dr. De Picker.
She noted that, while the in-hospital mortality was not increased, the risk was significantly increased in samples that were outside of the hospital. This reinforces the need for providing close monitoring and early referral to hospital for psychiatric patients with COVID-19.
Mortality varied significantly among countries, with the lowest risk in Europe and the United States. This difference might be attributable to differences in health care systems and access to care, said Dr. De Picker.
Overall, the risk for hospitalization was about double for COVID patients with a mental illness, but when stratified by disorder, there was only a significantly increased risk for substance use and mood disorders. “But mood disorders were not even significant any more after adjusting for age, sex, and comorbid conditions, and we don’t see an increased risk for psychotic disorders whereas they had the highest mortality risks,” said Dr. De Picker.
Psych meds a risk factor?
The studies were primarily based on electronic medical records, so investigators were unable to carry out “a fine grain analysis” into clinical factors affecting outcomes, she noted.
Antipsychotics were consistently associated with an increased risk for mortality (adjusted OR, 2.43; 95% CI, 1.81-3.25), as were anxiolytics (aOR, 1.47; 95% CI, 1.15-1.88).
“There are some theoretical reasons why we believe there could be a risk associated with these drugs,” said Dr. De Picker. For example, antipsychotics can increase the risk for cardiac arrhythmias and thromboembolic events, and cause interactions with drugs used to treat COVID-19.
As for anxiolytics, especially benzodiazepines, these drugs are associated with respiratory risk and with all-cause mortality. “So you could imagine that someone who is infected with a respiratory virus and [is] then using these drugs on top of that would have a worse outcome,” said Dr. De Picker.
In contrast to antipsychotics and anxiolytics, antidepressants did not increase mortality risk.
Dr. De Picker noted a new study by French researchers showing a protective effect of certain serotonergic antidepressants on COVID outcomes, including mortality.
There was no robust evidence of an increased risk for ICU admission for patients with mental disorders. However, the authors noted some studies included small samples of patients with psychiatric disorders, “contributing to a low certainty of evidence for ICU admission.”
Dr. De Picker criticized COVID vaccine policies that don’t prioritize patients with psychiatric disorders. In many countries, groups that were initially green-lighted for the vaccine included health care workers, the elderly, and those with underlying conditions such as diabetes, obesity and even mild hypertension – but not mental illness, which is also an underlying risk.
‘Outstanding’ research
Commenting on the study for this news organization, Jonathan E. Alpert, MD, PhD, department of psychiatry and behavioral sciences, Montefiore Medical Center, New York, and chair of the American Psychiatric Association Council on Research, called it “outstanding” and the largest of its kind.
“There have been a number of studies that have come to similar conclusions, that people with psychiatric illness are at greater risk for poorer outcomes, but because any given study had a relatively limited sample, perhaps from one health system or one country, there were some inconsistencies,” said Dr. Alpert.
“This is the strongest report so far that has made the point that people with psychiatric illness are a vulnerable population for a negative outcome from COVID, including the most worrisome – mortality.”
The study helps drive home a “very important public health lesson” that applies to COVID-19 but goes “beyond,” said Dr. Alpert.
“As a society, we need to keep in mind that people with serious mental disorders are a vulnerable population for poorer outcomes in most general medical conditions,” he stressed, “whether it’s cancer or heart disease or diabetes, and special efforts need to be made to reach out to those populations.”
Dr. Alpert agreed that, at the start of the pandemic, psychiatric patients in the United States were not prioritized for vaccination, and although psychiatric patients may initially have found it difficult to navigate the health care system to learn where and how to get a COVID shot, today that barrier has mostly been removed.
“Our patients are at least as willing as any other subgroup to get the vaccine, and that includes people with psychotic disorders,” he said.
The study was supported by the European College of Neuropsychopharmacology Immuno-NeuroPsychiatry network and Fondazione Centro San Raffaele (Milan). Dr. De Picker reported receiving grants from Boehringer Ingelheim and Janssen outside the submitted work. She is a member of the European College of Neuropsychopharmacology Immuno-NeuroPsychiatry Thematic Working Group.
A version of this article first appeared on Medscape.com.
Grandmothers, the Friendship Bench, and wisdom
Is this model a blueprint for delivering mental health care?
The 4-year-old boy and his grandmother are out for stroll around the neighborhood, walking hand in hand.
“Let’s sit on the bench and talk,” the boy says.
“Okay,” says the grandmother and they climb up onto the high bench and look out across the quiet road to a small garden beyond.
“What would you like to talk about?” his grandmother asks.
“You first,” he says.
“Okay, let’s see ... the grandmother and the grandson are out for a walk and they see a bench to sit on. They climb up and look around. They see the daffodils and the white clouds in the blue sky. The breeze is blowing gently. It is a happy day. Your turn; what would you like to talk about?”
“Nanna and Papa.”
“Do you miss Papa?”
“Yes.”
“It has been a whole year since he died.”
“A long, long time.”
“He loved you very much.”
“Yes,” the boy replies.
“Nanna must miss him very much. She must be lonely without him.”
The boy nods.
They sit on for a while, watching the occasional car and the occasional bird pass by. The boy and the grandmother are quiet and contemplative.
“Okay, let’s go,” he says and jumps down, ready to continue their walk.
The Friendship Bench
It must have been such an experience that gave Dixon Chibanda, MD, MPH, PhD, a psychiatrist from Zimbabwe, his brilliant idea. He trained grandmothers in evidence-based talk therapy and sat them on a bench in the park with his patients.1,2 He founded the Friendship Bench in 2006 in the Harare township of Mbare with 14 grandmothers. There are more than 300 grandmothers sitting on benches, listening, and providing cognitive-behavioral therapy–informed interventions because he could find no therapists in the community and he found that, with a little training, these grandmothers could provide effective culturally sensitive interventions.
Originally, the sessions were conducted in Shona, the predominant native language in Zimbabwe, but since 2017, the sessions are also in English. By 2017, the Friendship Bench had helped more than 30,000 people. The method has been empirically vetted and expanded to countries beyond, including the United States. Dr. Chibanda’s Friendship Bench serves as a blueprint for any community interested in bringing affordable, accessible, and highly effective mental health services to its residents. Dr. Chibanda said: “Imagine if we could create a global network of grandmothers in every major city in the world.”3 Participants in this study reported that the Friendship Bench had a critical role in helping them accept their HIV status, citing the grandmothers’ empathic attitude, their normalization of the reality of living with HIV, and their encouragement of young people to socialize with peers and be free of guilt. Many recipients also described enhanced health and well-being.
Why grandmothers?
Have you heard of the evolutionary importance of grandmothers? The grandmother hypothesis is an adaptationist explanation for the fact that the human female lifespan extends beyond the period of fertility. A third of the average human female life span is post menopause. Does such a long female postreproductive life span have a reason, inquired Mwenza Blell, PhD.5
Peter B. Medawar, PhD,6 and Kristen Hawkes, PhD,7 suggested that grandparents influence their own fitness by their actions toward their grandchildren. International fieldwork has revealed that the situation is less clear than their hypothesis. In industrialized countries, grandmaternal support is often financial or emotional. Two meta-analyses of largely the same group of studies investigating grandmother effects have come up with differing conclusions. Rebecca Sear, PhD, and Ruth Mace, PhD, conclude that grandmothers are “almost universally” beneficial, while acknowledging some variation in the effects of paternal grandmothers.8 Maternal grandparents appear to invest more in their grandchildren than paternal grandparents. Beverly I. Strassmann, PhD, and Wendy M. Garrard, PhD, concluded that, in patrilineal societies, survival of maternal grandparents is associated with survival of grandchildren and suggest this may represent covert matriliny.9
Examining specific time periods, maternal grandmothers may have greatest effect on survival of grandchildren at the time of weaning, a time when increased pathogenic exposure is a threat to survival. Paternal grandmothers may influence the survival of grandchildren during the early period of life (1-12 months) and to influence the condition of their daughters-in-law during pregnancy. The fact that grandmothers share one X chromosome with their sons’ daughters, none with their sons’ sons, and have a 50% chance of sharing an X chromosome with their daughters’ children is suggested to explain the patterns of survival observed in these studies than a simple maternal/paternal division.

In low- and middle-income countries, grandmothers and older women are seen as owners of traditional knowledge, and influence many decisions about childcare, help with domestic work, and emotional support and advice.10 Studies find a significant positive impact on breastfeeding when grandmothers of the infants had their own breastfeeding experience or were positively inclined toward breastfeeding, although one Chinese study found that highly educated grandmothers were associated with decreased exclusive breastfeeding.11 Despite this, most health programs target individual new mothers, without an understanding of the family and who else influences decisions.
Grandchildren and grandparents benefit from intergenerational activities with improved health and well-being of both generations. When older adults are involved in raising children, there is a significant reduction in the incidence of behavioral problems in childhood and adolescence. Grandparents improve grandchild outcomes, when measured by coresidence, caregiving, financial, and other support. The grandchild outcomes include physical health, socioemotional well-being, and cognitive development.12
Are there ‘grandparent genes?’
Flavio Schwarz, PhD, and colleagues think that variants of APOE and CD33 protect against heart disease and Alzheimer’s disease, allowing older people to live longer with better functioning hearts and brains – thus enabling transfer of wisdom from older to younger generations.13 While this logic may be a bit of a stretch, it does lead to a more interesting question: What has wisdom got to do with it?
When I ask psychiatrists what they think about wisdom, they give a variety of answers. Dilip Jeste, MD, a geriatric psychiatrist who studies successful aging, helped develop a measurable vision of wisdom.14 Wisdom is defined as a “multidimensional human trait that includes good social decision-making and pragmatic knowledge of life, prosocial attitudes and behaviors such as empathy and compassion, emotional homeostasis with a tendency to favor positive emotions, reflection and self-understanding, acknowledgment of and coping effectively with uncertainty, and decisiveness.”15 Others suggest that they include spirituality, openness to new experience, and a sense of humor.16 A scale called the San Diego Wisdom scale (SD-WISE) was created, using 524 community-dwelling adults aged 25-104 years. These subjects comprised a high proportion of White adults and individuals with a higher education, thus lacking diversity. Lack of diversity perpetuates generalizations, and like all sociocultural constructs, truth is specific to the population studied. High scores on the SD-WISE are positively correlated with good mental health, self-ratings of successful aging, mastery, resilience, happiness, and satisfaction with life.
Which brings us back to the grandmothers on the bench: Can someone please give them the SD-WISE scale and confirm several hypotheses? I would like to know whether a pragmatic knowledge of life is a recognized grandmotherly quality, suitable for the bench.
Dr. Heru is professor of psychiatry at the University of Colorado at Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest.
References
1. Chibanda D. Bull World Health Organ. 2018 Jun 196(6):376-7.
2. Cavanaugh R. Lancet Psychiatry. 2017 Nov. doi: 10.1016/S2215-0366(17)30420-0.
3. Nuwer R. “How a bench and a team of grandmothers can tackle depression.” BBC. 2020 May 27.
4. Ouansafi I et al. PLoS One. 2021 Apr 22;16(4):e0250074.
5. Blell M. “Grandmother hypothesis, grandmother effect, and residence patterns.” Int Encyclopedia Anthropol. John Wiley & Sons, 2018.
6. Medawar PB. An Unsolved Problem of Biology. Routledge, 1957.
7. Hawkes K et al. Proc Nat Acad Sci. 1998 Feb 395(3):1336-9.
8. Sear R and Mace R. Evol Hum Behav. 2008;29(1):1-18.
9. Strassmann B and Garrard WM. Hum Nat. 2011 Jul;22(1-2):201-22.
10. Aubel J. BMJ Glob Health. 2021;6(2). doi 10.1136/bmjgh-2020-003808.
11. Negin J et al. BMJ Pregnancy Childbirth. 2016 Apr 7. doi: 10.1186/s12884-016-0880-5.
12. Sadruddin AFA. Soc Sci Med. 2019 Aug;239(4):112476.
13. Schwarz F et al. Proc Nat Acad Sci. 2016 Jan 5;113(1):74-9.
14. Jeste DV et al. Psychol Inquiry. 2020 Jun 22;31(2):134-43.
15. Meeks TW and Jeste DV. Arch Gen Psychiatry. 2009 Apr;66(4):355-65.
16. Bangen KJ et al. Am J Geriatr Psychiatry. 2013 Dec;21(12):1254-66.
Is this model a blueprint for delivering mental health care?
Is this model a blueprint for delivering mental health care?
The 4-year-old boy and his grandmother are out for stroll around the neighborhood, walking hand in hand.
“Let’s sit on the bench and talk,” the boy says.
“Okay,” says the grandmother and they climb up onto the high bench and look out across the quiet road to a small garden beyond.
“What would you like to talk about?” his grandmother asks.
“You first,” he says.
“Okay, let’s see ... the grandmother and the grandson are out for a walk and they see a bench to sit on. They climb up and look around. They see the daffodils and the white clouds in the blue sky. The breeze is blowing gently. It is a happy day. Your turn; what would you like to talk about?”
“Nanna and Papa.”
“Do you miss Papa?”
“Yes.”
“It has been a whole year since he died.”
“A long, long time.”
“He loved you very much.”
“Yes,” the boy replies.
“Nanna must miss him very much. She must be lonely without him.”
The boy nods.
They sit on for a while, watching the occasional car and the occasional bird pass by. The boy and the grandmother are quiet and contemplative.
“Okay, let’s go,” he says and jumps down, ready to continue their walk.
The Friendship Bench
It must have been such an experience that gave Dixon Chibanda, MD, MPH, PhD, a psychiatrist from Zimbabwe, his brilliant idea. He trained grandmothers in evidence-based talk therapy and sat them on a bench in the park with his patients.1,2 He founded the Friendship Bench in 2006 in the Harare township of Mbare with 14 grandmothers. There are more than 300 grandmothers sitting on benches, listening, and providing cognitive-behavioral therapy–informed interventions because he could find no therapists in the community and he found that, with a little training, these grandmothers could provide effective culturally sensitive interventions.
Originally, the sessions were conducted in Shona, the predominant native language in Zimbabwe, but since 2017, the sessions are also in English. By 2017, the Friendship Bench had helped more than 30,000 people. The method has been empirically vetted and expanded to countries beyond, including the United States. Dr. Chibanda’s Friendship Bench serves as a blueprint for any community interested in bringing affordable, accessible, and highly effective mental health services to its residents. Dr. Chibanda said: “Imagine if we could create a global network of grandmothers in every major city in the world.”3 Participants in this study reported that the Friendship Bench had a critical role in helping them accept their HIV status, citing the grandmothers’ empathic attitude, their normalization of the reality of living with HIV, and their encouragement of young people to socialize with peers and be free of guilt. Many recipients also described enhanced health and well-being.
Why grandmothers?
Have you heard of the evolutionary importance of grandmothers? The grandmother hypothesis is an adaptationist explanation for the fact that the human female lifespan extends beyond the period of fertility. A third of the average human female life span is post menopause. Does such a long female postreproductive life span have a reason, inquired Mwenza Blell, PhD.5
Peter B. Medawar, PhD,6 and Kristen Hawkes, PhD,7 suggested that grandparents influence their own fitness by their actions toward their grandchildren. International fieldwork has revealed that the situation is less clear than their hypothesis. In industrialized countries, grandmaternal support is often financial or emotional. Two meta-analyses of largely the same group of studies investigating grandmother effects have come up with differing conclusions. Rebecca Sear, PhD, and Ruth Mace, PhD, conclude that grandmothers are “almost universally” beneficial, while acknowledging some variation in the effects of paternal grandmothers.8 Maternal grandparents appear to invest more in their grandchildren than paternal grandparents. Beverly I. Strassmann, PhD, and Wendy M. Garrard, PhD, concluded that, in patrilineal societies, survival of maternal grandparents is associated with survival of grandchildren and suggest this may represent covert matriliny.9
Examining specific time periods, maternal grandmothers may have greatest effect on survival of grandchildren at the time of weaning, a time when increased pathogenic exposure is a threat to survival. Paternal grandmothers may influence the survival of grandchildren during the early period of life (1-12 months) and to influence the condition of their daughters-in-law during pregnancy. The fact that grandmothers share one X chromosome with their sons’ daughters, none with their sons’ sons, and have a 50% chance of sharing an X chromosome with their daughters’ children is suggested to explain the patterns of survival observed in these studies than a simple maternal/paternal division.
In low- and middle-income countries, grandmothers and older women are seen as owners of traditional knowledge, and influence many decisions about childcare, help with domestic work, and emotional support and advice.10 Studies find a significant positive impact on breastfeeding when grandmothers of the infants had their own breastfeeding experience or were positively inclined toward breastfeeding, although one Chinese study found that highly educated grandmothers were associated with decreased exclusive breastfeeding.11 Despite this, most health programs target individual new mothers, without an understanding of the family and who else influences decisions.
Grandchildren and grandparents benefit from intergenerational activities with improved health and well-being of both generations. When older adults are involved in raising children, there is a significant reduction in the incidence of behavioral problems in childhood and adolescence. Grandparents improve grandchild outcomes, when measured by coresidence, caregiving, financial, and other support. The grandchild outcomes include physical health, socioemotional well-being, and cognitive development.12
Are there ‘grandparent genes?’
Flavio Schwarz, PhD, and colleagues think that variants of APOE and CD33 protect against heart disease and Alzheimer’s disease, allowing older people to live longer with better functioning hearts and brains – thus enabling transfer of wisdom from older to younger generations.13 While this logic may be a bit of a stretch, it does lead to a more interesting question: What has wisdom got to do with it?
When I ask psychiatrists what they think about wisdom, they give a variety of answers. Dilip Jeste, MD, a geriatric psychiatrist who studies successful aging, helped develop a measurable vision of wisdom.14 Wisdom is defined as a “multidimensional human trait that includes good social decision-making and pragmatic knowledge of life, prosocial attitudes and behaviors such as empathy and compassion, emotional homeostasis with a tendency to favor positive emotions, reflection and self-understanding, acknowledgment of and coping effectively with uncertainty, and decisiveness.”15 Others suggest that they include spirituality, openness to new experience, and a sense of humor.16 A scale called the San Diego Wisdom scale (SD-WISE) was created, using 524 community-dwelling adults aged 25-104 years. These subjects comprised a high proportion of White adults and individuals with a higher education, thus lacking diversity. Lack of diversity perpetuates generalizations, and like all sociocultural constructs, truth is specific to the population studied. High scores on the SD-WISE are positively correlated with good mental health, self-ratings of successful aging, mastery, resilience, happiness, and satisfaction with life.
Which brings us back to the grandmothers on the bench: Can someone please give them the SD-WISE scale and confirm several hypotheses? I would like to know whether a pragmatic knowledge of life is a recognized grandmotherly quality, suitable for the bench.
Dr. Heru is professor of psychiatry at the University of Colorado at Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest.
References
1. Chibanda D. Bull World Health Organ. 2018 Jun 196(6):376-7.
2. Cavanaugh R. Lancet Psychiatry. 2017 Nov. doi: 10.1016/S2215-0366(17)30420-0.
3. Nuwer R. “How a bench and a team of grandmothers can tackle depression.” BBC. 2020 May 27.
4. Ouansafi I et al. PLoS One. 2021 Apr 22;16(4):e0250074.
5. Blell M. “Grandmother hypothesis, grandmother effect, and residence patterns.” Int Encyclopedia Anthropol. John Wiley & Sons, 2018.
6. Medawar PB. An Unsolved Problem of Biology. Routledge, 1957.
7. Hawkes K et al. Proc Nat Acad Sci. 1998 Feb 395(3):1336-9.
8. Sear R and Mace R. Evol Hum Behav. 2008;29(1):1-18.
9. Strassmann B and Garrard WM. Hum Nat. 2011 Jul;22(1-2):201-22.
10. Aubel J. BMJ Glob Health. 2021;6(2). doi 10.1136/bmjgh-2020-003808.
11. Negin J et al. BMJ Pregnancy Childbirth. 2016 Apr 7. doi: 10.1186/s12884-016-0880-5.
12. Sadruddin AFA. Soc Sci Med. 2019 Aug;239(4):112476.
13. Schwarz F et al. Proc Nat Acad Sci. 2016 Jan 5;113(1):74-9.
14. Jeste DV et al. Psychol Inquiry. 2020 Jun 22;31(2):134-43.
15. Meeks TW and Jeste DV. Arch Gen Psychiatry. 2009 Apr;66(4):355-65.
16. Bangen KJ et al. Am J Geriatr Psychiatry. 2013 Dec;21(12):1254-66.
The 4-year-old boy and his grandmother are out for stroll around the neighborhood, walking hand in hand.
“Let’s sit on the bench and talk,” the boy says.
“Okay,” says the grandmother and they climb up onto the high bench and look out across the quiet road to a small garden beyond.
“What would you like to talk about?” his grandmother asks.
“You first,” he says.
“Okay, let’s see ... the grandmother and the grandson are out for a walk and they see a bench to sit on. They climb up and look around. They see the daffodils and the white clouds in the blue sky. The breeze is blowing gently. It is a happy day. Your turn; what would you like to talk about?”
“Nanna and Papa.”
“Do you miss Papa?”
“Yes.”
“It has been a whole year since he died.”
“A long, long time.”
“He loved you very much.”
“Yes,” the boy replies.
“Nanna must miss him very much. She must be lonely without him.”
The boy nods.
They sit on for a while, watching the occasional car and the occasional bird pass by. The boy and the grandmother are quiet and contemplative.
“Okay, let’s go,” he says and jumps down, ready to continue their walk.
The Friendship Bench
It must have been such an experience that gave Dixon Chibanda, MD, MPH, PhD, a psychiatrist from Zimbabwe, his brilliant idea. He trained grandmothers in evidence-based talk therapy and sat them on a bench in the park with his patients.1,2 He founded the Friendship Bench in 2006 in the Harare township of Mbare with 14 grandmothers. There are more than 300 grandmothers sitting on benches, listening, and providing cognitive-behavioral therapy–informed interventions because he could find no therapists in the community and he found that, with a little training, these grandmothers could provide effective culturally sensitive interventions.
Originally, the sessions were conducted in Shona, the predominant native language in Zimbabwe, but since 2017, the sessions are also in English. By 2017, the Friendship Bench had helped more than 30,000 people. The method has been empirically vetted and expanded to countries beyond, including the United States. Dr. Chibanda’s Friendship Bench serves as a blueprint for any community interested in bringing affordable, accessible, and highly effective mental health services to its residents. Dr. Chibanda said: “Imagine if we could create a global network of grandmothers in every major city in the world.”3 Participants in this study reported that the Friendship Bench had a critical role in helping them accept their HIV status, citing the grandmothers’ empathic attitude, their normalization of the reality of living with HIV, and their encouragement of young people to socialize with peers and be free of guilt. Many recipients also described enhanced health and well-being.
Why grandmothers?
Have you heard of the evolutionary importance of grandmothers? The grandmother hypothesis is an adaptationist explanation for the fact that the human female lifespan extends beyond the period of fertility. A third of the average human female life span is post menopause. Does such a long female postreproductive life span have a reason, inquired Mwenza Blell, PhD.5
Peter B. Medawar, PhD,6 and Kristen Hawkes, PhD,7 suggested that grandparents influence their own fitness by their actions toward their grandchildren. International fieldwork has revealed that the situation is less clear than their hypothesis. In industrialized countries, grandmaternal support is often financial or emotional. Two meta-analyses of largely the same group of studies investigating grandmother effects have come up with differing conclusions. Rebecca Sear, PhD, and Ruth Mace, PhD, conclude that grandmothers are “almost universally” beneficial, while acknowledging some variation in the effects of paternal grandmothers.8 Maternal grandparents appear to invest more in their grandchildren than paternal grandparents. Beverly I. Strassmann, PhD, and Wendy M. Garrard, PhD, concluded that, in patrilineal societies, survival of maternal grandparents is associated with survival of grandchildren and suggest this may represent covert matriliny.9
Examining specific time periods, maternal grandmothers may have greatest effect on survival of grandchildren at the time of weaning, a time when increased pathogenic exposure is a threat to survival. Paternal grandmothers may influence the survival of grandchildren during the early period of life (1-12 months) and to influence the condition of their daughters-in-law during pregnancy. The fact that grandmothers share one X chromosome with their sons’ daughters, none with their sons’ sons, and have a 50% chance of sharing an X chromosome with their daughters’ children is suggested to explain the patterns of survival observed in these studies than a simple maternal/paternal division.
In low- and middle-income countries, grandmothers and older women are seen as owners of traditional knowledge, and influence many decisions about childcare, help with domestic work, and emotional support and advice.10 Studies find a significant positive impact on breastfeeding when grandmothers of the infants had their own breastfeeding experience or were positively inclined toward breastfeeding, although one Chinese study found that highly educated grandmothers were associated with decreased exclusive breastfeeding.11 Despite this, most health programs target individual new mothers, without an understanding of the family and who else influences decisions.
Grandchildren and grandparents benefit from intergenerational activities with improved health and well-being of both generations. When older adults are involved in raising children, there is a significant reduction in the incidence of behavioral problems in childhood and adolescence. Grandparents improve grandchild outcomes, when measured by coresidence, caregiving, financial, and other support. The grandchild outcomes include physical health, socioemotional well-being, and cognitive development.12
Are there ‘grandparent genes?’
Flavio Schwarz, PhD, and colleagues think that variants of APOE and CD33 protect against heart disease and Alzheimer’s disease, allowing older people to live longer with better functioning hearts and brains – thus enabling transfer of wisdom from older to younger generations.13 While this logic may be a bit of a stretch, it does lead to a more interesting question: What has wisdom got to do with it?
When I ask psychiatrists what they think about wisdom, they give a variety of answers. Dilip Jeste, MD, a geriatric psychiatrist who studies successful aging, helped develop a measurable vision of wisdom.14 Wisdom is defined as a “multidimensional human trait that includes good social decision-making and pragmatic knowledge of life, prosocial attitudes and behaviors such as empathy and compassion, emotional homeostasis with a tendency to favor positive emotions, reflection and self-understanding, acknowledgment of and coping effectively with uncertainty, and decisiveness.”15 Others suggest that they include spirituality, openness to new experience, and a sense of humor.16 A scale called the San Diego Wisdom scale (SD-WISE) was created, using 524 community-dwelling adults aged 25-104 years. These subjects comprised a high proportion of White adults and individuals with a higher education, thus lacking diversity. Lack of diversity perpetuates generalizations, and like all sociocultural constructs, truth is specific to the population studied. High scores on the SD-WISE are positively correlated with good mental health, self-ratings of successful aging, mastery, resilience, happiness, and satisfaction with life.
Which brings us back to the grandmothers on the bench: Can someone please give them the SD-WISE scale and confirm several hypotheses? I would like to know whether a pragmatic knowledge of life is a recognized grandmotherly quality, suitable for the bench.
Dr. Heru is professor of psychiatry at the University of Colorado at Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest.
References
1. Chibanda D. Bull World Health Organ. 2018 Jun 196(6):376-7.
2. Cavanaugh R. Lancet Psychiatry. 2017 Nov. doi: 10.1016/S2215-0366(17)30420-0.
3. Nuwer R. “How a bench and a team of grandmothers can tackle depression.” BBC. 2020 May 27.
4. Ouansafi I et al. PLoS One. 2021 Apr 22;16(4):e0250074.
5. Blell M. “Grandmother hypothesis, grandmother effect, and residence patterns.” Int Encyclopedia Anthropol. John Wiley & Sons, 2018.
6. Medawar PB. An Unsolved Problem of Biology. Routledge, 1957.
7. Hawkes K et al. Proc Nat Acad Sci. 1998 Feb 395(3):1336-9.
8. Sear R and Mace R. Evol Hum Behav. 2008;29(1):1-18.
9. Strassmann B and Garrard WM. Hum Nat. 2011 Jul;22(1-2):201-22.
10. Aubel J. BMJ Glob Health. 2021;6(2). doi 10.1136/bmjgh-2020-003808.
11. Negin J et al. BMJ Pregnancy Childbirth. 2016 Apr 7. doi: 10.1186/s12884-016-0880-5.
12. Sadruddin AFA. Soc Sci Med. 2019 Aug;239(4):112476.
13. Schwarz F et al. Proc Nat Acad Sci. 2016 Jan 5;113(1):74-9.
14. Jeste DV et al. Psychol Inquiry. 2020 Jun 22;31(2):134-43.
15. Meeks TW and Jeste DV. Arch Gen Psychiatry. 2009 Apr;66(4):355-65.
16. Bangen KJ et al. Am J Geriatr Psychiatry. 2013 Dec;21(12):1254-66.
Animal-assisted therapy could boost patients’ mental health
For me, vacation planning brings with it a bit of anxiety and stress – particularly as we navigate the many uncertainties around COVID-19.

Not only must my husband and I think about our own safety, we also have to make sure that our beloved dog, Samson, gets the proper care while we are away.
My husband adopted Samson, an 11-year-old mixed-breed rescue, when he was just a year old. He’s an important part of our family.
So, when booking our hotel room and flights, we also had to find someone we trust to care for Samson in our absence. Family members are not always an option, so we often rely on pet-sitting apps. We looked through profile after profile, contacted sitters, and interrogated them as if we were looking for care for a tiny human.
Eventually, we found a service that allows owners to use a mobile app that provides updates about how their pets are faring. While we were away, the sitter sent daily photos and videos of Samson that put our minds at ease.
As a registered nurse who works in an ICU, my own anxiety about leaving Samson reminded me about my patients’ reservations about leaving their pets during hospitalizations. Many of them share the same kinds of anxieties when they are separated from their beloved pets. Hospital visits are rarely planned. I have cared for patients who expressed concerns about their pets being home alone and needing to coordinate pet care. In some cases – to alleviate those patients’ anxieties – I have helped them contact friends and family members to assist with care.
Pets’ popularity grows in U.S.
According to the 2019-2020 National Pet Owners Survey, about 67% of U.S. households own a pet – which translates to about 84.9 million homes. During the height of COVID, Americans also acquired a greater number of smaller pets.1 In addition, when social restrictions increased, the demand for dog adoptions and the desire to serve as foster owners rose significantly.2 Last Chance Animal Rescue of Waldorf, Md., reportedly saw the adoption of dogs rise from 30%-40% in 2020. Another animal rescue operation, Lucky Dog, of Arlington, Va., in 2020 helped about 3,385 pets find adoption, up from about 1,800 in 2019.3 About two-thirds of all American households and roughly half of elderly individuals own pets.4

I am not surprised by those numbers. In my nursing practice, I face many stress-related factors, such as alternating day and night shifts, 12-hour shifts, strenuous physical work, and the psychological strain of attending to ill and dying patients. Interacting with Samson helps relieve that stress. The motion of petting Samson helps calm my heart rate and decreases my anxiety. In addition, Samson makes me smile – and excites almost all the people I interact with while he’s around. Of course, I’m not objective, but I view Samson’s impact on people as a symbol of the power of animal-assisted therapy (AAT).
AAT, defined as “the positive interaction between an animal and a patient within a therapeutic framework,”has proven to be an effective intervention for adults with intellectual disabilities who experience anxiety in an observational study.5 The intervention also has helped reduce cortisol levels in a study of nurses in physical medicine, internal medicine, and long-term care.6 Since most patient hospital stays are unplanned, there is a need to introduce AAT into hospital care. This would lessen anxiety in patients concerning their pets’ welfare.
We know that long-term hospital stays often cause adverse psychosocial effects on patients. Such stays can result in “hospitalization syndrome,” which is characterized by a gradual loss of cognition and orientation, an unwillingness to maintain contact with others or to engage in group therapy, and a loss of interest in their surroundings.7 The common causes for this syndrome are infection, medication, isolation, response to surgery, and dehydration. A consequence can be a permanent change in cognitive function or psychological impairment. However, my experience of practicing nursing for years has led me to discover that pets as an external stimulus can prevent the syndrome’s onset. This is because a large percentage of hospitalized patients have pets, and contact with a pet reminds them of home and the memories they share at home.
Introducing animal therapy into health care facilities could boost patients’ mental health – and ease their anxiety – by acting as a bridge between their present circumstances and the lives they have outside the establishment.
References
1. American Pet Owners Association. Will the COVID Pet Spike Last? State of the industry presentation. 2021 Mar 24.
2. Morgan L et al. Humanit Soc Sci Comm. 2020 Nov 24;7(144). doi: 10.1057/S41599-020-00649-x.
3. Hedgpeth D. So many pets have been adopted during the pandemic that shelters are running out. Washington Post. 2021 Jan 6.
4. Cherniack EP and Cherniack AR. Curr Gerontol Geriatr Res. 2014. doi: 10.1155/2014/623203.
5. Giuliani F and Jacquemettaz M. Eur J Integ Med. 2017 Sep;14;13-9.
6. Machová K et al. Int J Environ Res and Public Health. 2019 Oct;16(19):3670.
7. Machová K et al. Int J Environ Res Public Health. 2012 Apr;16(8):1362.
Ms. Scott is a registered nurse specializing in critical care and also has experience in nursing leadership. She has 8 years of experience in cardiothoracic ICUs. Ms. Scott received a bachelor of science in nursing degree from Queens University of Charlotte (N.C.), and a master of business administration in health care administration from the University of North Alabama, Florence. She has no conflicts of interest.
For me, vacation planning brings with it a bit of anxiety and stress – particularly as we navigate the many uncertainties around COVID-19.
Not only must my husband and I think about our own safety, we also have to make sure that our beloved dog, Samson, gets the proper care while we are away.
My husband adopted Samson, an 11-year-old mixed-breed rescue, when he was just a year old. He’s an important part of our family.
So, when booking our hotel room and flights, we also had to find someone we trust to care for Samson in our absence. Family members are not always an option, so we often rely on pet-sitting apps. We looked through profile after profile, contacted sitters, and interrogated them as if we were looking for care for a tiny human.
Eventually, we found a service that allows owners to use a mobile app that provides updates about how their pets are faring. While we were away, the sitter sent daily photos and videos of Samson that put our minds at ease.
As a registered nurse who works in an ICU, my own anxiety about leaving Samson reminded me about my patients’ reservations about leaving their pets during hospitalizations. Many of them share the same kinds of anxieties when they are separated from their beloved pets. Hospital visits are rarely planned. I have cared for patients who expressed concerns about their pets being home alone and needing to coordinate pet care. In some cases – to alleviate those patients’ anxieties – I have helped them contact friends and family members to assist with care.
Pets’ popularity grows in U.S.
According to the 2019-2020 National Pet Owners Survey, about 67% of U.S. households own a pet – which translates to about 84.9 million homes. During the height of COVID, Americans also acquired a greater number of smaller pets.1 In addition, when social restrictions increased, the demand for dog adoptions and the desire to serve as foster owners rose significantly.2 Last Chance Animal Rescue of Waldorf, Md., reportedly saw the adoption of dogs rise from 30%-40% in 2020. Another animal rescue operation, Lucky Dog, of Arlington, Va., in 2020 helped about 3,385 pets find adoption, up from about 1,800 in 2019.3 About two-thirds of all American households and roughly half of elderly individuals own pets.4
I am not surprised by those numbers. In my nursing practice, I face many stress-related factors, such as alternating day and night shifts, 12-hour shifts, strenuous physical work, and the psychological strain of attending to ill and dying patients. Interacting with Samson helps relieve that stress. The motion of petting Samson helps calm my heart rate and decreases my anxiety. In addition, Samson makes me smile – and excites almost all the people I interact with while he’s around. Of course, I’m not objective, but I view Samson’s impact on people as a symbol of the power of animal-assisted therapy (AAT).
AAT, defined as “the positive interaction between an animal and a patient within a therapeutic framework,”has proven to be an effective intervention for adults with intellectual disabilities who experience anxiety in an observational study.5 The intervention also has helped reduce cortisol levels in a study of nurses in physical medicine, internal medicine, and long-term care.6 Since most patient hospital stays are unplanned, there is a need to introduce AAT into hospital care. This would lessen anxiety in patients concerning their pets’ welfare.
We know that long-term hospital stays often cause adverse psychosocial effects on patients. Such stays can result in “hospitalization syndrome,” which is characterized by a gradual loss of cognition and orientation, an unwillingness to maintain contact with others or to engage in group therapy, and a loss of interest in their surroundings.7 The common causes for this syndrome are infection, medication, isolation, response to surgery, and dehydration. A consequence can be a permanent change in cognitive function or psychological impairment. However, my experience of practicing nursing for years has led me to discover that pets as an external stimulus can prevent the syndrome’s onset. This is because a large percentage of hospitalized patients have pets, and contact with a pet reminds them of home and the memories they share at home.
Introducing animal therapy into health care facilities could boost patients’ mental health – and ease their anxiety – by acting as a bridge between their present circumstances and the lives they have outside the establishment.
References
1. American Pet Owners Association. Will the COVID Pet Spike Last? State of the industry presentation. 2021 Mar 24.
2. Morgan L et al. Humanit Soc Sci Comm. 2020 Nov 24;7(144). doi: 10.1057/S41599-020-00649-x.
3. Hedgpeth D. So many pets have been adopted during the pandemic that shelters are running out. Washington Post. 2021 Jan 6.
4. Cherniack EP and Cherniack AR. Curr Gerontol Geriatr Res. 2014. doi: 10.1155/2014/623203.
5. Giuliani F and Jacquemettaz M. Eur J Integ Med. 2017 Sep;14;13-9.
6. Machová K et al. Int J Environ Res and Public Health. 2019 Oct;16(19):3670.
7. Machová K et al. Int J Environ Res Public Health. 2012 Apr;16(8):1362.
Ms. Scott is a registered nurse specializing in critical care and also has experience in nursing leadership. She has 8 years of experience in cardiothoracic ICUs. Ms. Scott received a bachelor of science in nursing degree from Queens University of Charlotte (N.C.), and a master of business administration in health care administration from the University of North Alabama, Florence. She has no conflicts of interest.
For me, vacation planning brings with it a bit of anxiety and stress – particularly as we navigate the many uncertainties around COVID-19.
Not only must my husband and I think about our own safety, we also have to make sure that our beloved dog, Samson, gets the proper care while we are away.
My husband adopted Samson, an 11-year-old mixed-breed rescue, when he was just a year old. He’s an important part of our family.
So, when booking our hotel room and flights, we also had to find someone we trust to care for Samson in our absence. Family members are not always an option, so we often rely on pet-sitting apps. We looked through profile after profile, contacted sitters, and interrogated them as if we were looking for care for a tiny human.
Eventually, we found a service that allows owners to use a mobile app that provides updates about how their pets are faring. While we were away, the sitter sent daily photos and videos of Samson that put our minds at ease.
As a registered nurse who works in an ICU, my own anxiety about leaving Samson reminded me about my patients’ reservations about leaving their pets during hospitalizations. Many of them share the same kinds of anxieties when they are separated from their beloved pets. Hospital visits are rarely planned. I have cared for patients who expressed concerns about their pets being home alone and needing to coordinate pet care. In some cases – to alleviate those patients’ anxieties – I have helped them contact friends and family members to assist with care.
Pets’ popularity grows in U.S.
According to the 2019-2020 National Pet Owners Survey, about 67% of U.S. households own a pet – which translates to about 84.9 million homes. During the height of COVID, Americans also acquired a greater number of smaller pets.1 In addition, when social restrictions increased, the demand for dog adoptions and the desire to serve as foster owners rose significantly.2 Last Chance Animal Rescue of Waldorf, Md., reportedly saw the adoption of dogs rise from 30%-40% in 2020. Another animal rescue operation, Lucky Dog, of Arlington, Va., in 2020 helped about 3,385 pets find adoption, up from about 1,800 in 2019.3 About two-thirds of all American households and roughly half of elderly individuals own pets.4
I am not surprised by those numbers. In my nursing practice, I face many stress-related factors, such as alternating day and night shifts, 12-hour shifts, strenuous physical work, and the psychological strain of attending to ill and dying patients. Interacting with Samson helps relieve that stress. The motion of petting Samson helps calm my heart rate and decreases my anxiety. In addition, Samson makes me smile – and excites almost all the people I interact with while he’s around. Of course, I’m not objective, but I view Samson’s impact on people as a symbol of the power of animal-assisted therapy (AAT).
AAT, defined as “the positive interaction between an animal and a patient within a therapeutic framework,”has proven to be an effective intervention for adults with intellectual disabilities who experience anxiety in an observational study.5 The intervention also has helped reduce cortisol levels in a study of nurses in physical medicine, internal medicine, and long-term care.6 Since most patient hospital stays are unplanned, there is a need to introduce AAT into hospital care. This would lessen anxiety in patients concerning their pets’ welfare.
We know that long-term hospital stays often cause adverse psychosocial effects on patients. Such stays can result in “hospitalization syndrome,” which is characterized by a gradual loss of cognition and orientation, an unwillingness to maintain contact with others or to engage in group therapy, and a loss of interest in their surroundings.7 The common causes for this syndrome are infection, medication, isolation, response to surgery, and dehydration. A consequence can be a permanent change in cognitive function or psychological impairment. However, my experience of practicing nursing for years has led me to discover that pets as an external stimulus can prevent the syndrome’s onset. This is because a large percentage of hospitalized patients have pets, and contact with a pet reminds them of home and the memories they share at home.
Introducing animal therapy into health care facilities could boost patients’ mental health – and ease their anxiety – by acting as a bridge between their present circumstances and the lives they have outside the establishment.
References
1. American Pet Owners Association. Will the COVID Pet Spike Last? State of the industry presentation. 2021 Mar 24.
2. Morgan L et al. Humanit Soc Sci Comm. 2020 Nov 24;7(144). doi: 10.1057/S41599-020-00649-x.
3. Hedgpeth D. So many pets have been adopted during the pandemic that shelters are running out. Washington Post. 2021 Jan 6.
4. Cherniack EP and Cherniack AR. Curr Gerontol Geriatr Res. 2014. doi: 10.1155/2014/623203.
5. Giuliani F and Jacquemettaz M. Eur J Integ Med. 2017 Sep;14;13-9.
6. Machová K et al. Int J Environ Res and Public Health. 2019 Oct;16(19):3670.
7. Machová K et al. Int J Environ Res Public Health. 2012 Apr;16(8):1362.
Ms. Scott is a registered nurse specializing in critical care and also has experience in nursing leadership. She has 8 years of experience in cardiothoracic ICUs. Ms. Scott received a bachelor of science in nursing degree from Queens University of Charlotte (N.C.), and a master of business administration in health care administration from the University of North Alabama, Florence. She has no conflicts of interest.
Legalization of cannabis tied to drop in opioid-related ED visits
State laws permitting recreational marijuana use have not led to an increase in opioid-related emergency department visits, as many had feared.
On the contrary, states that legalize recreational marijuana may see a short-term decrease in opioid-related ED visits in the first 6 months, after which rates may return to prelegalization levels, new research suggests.
Previous research suggests that individuals may reduce the use of opioids when they have an alternative and that cannabis can provide pain relief.
“At the same time, we often hear claims from politicians that we should not legalize cannabis because it may act as a ‘gateway drug’ that leads to use of other drugs,” lead researcher Coleman Drake, PhD, Department of Health Policy and Management, University of Pittsburgh Graduate School of Public Health, told this news organization.
“Our findings indicate that cannabis legalization does not effect any increase in opioid-related ED visits, contradicting the gateway drug explanation,” Dr. Drake said.
The study was published online July 12 in Health Economics.
Significant reduction
So far, 19 states have legalized recreational cannabis, meaning that nearly half of the U.S. population lives in a state that allows recreational cannabis use.
The investigators analyzed data on opioid-related ED visits from 29 states between 2011 and 2017. Four states – California, Maine, Massachusetts, and Nevada – legalized recreational marijuana during the study period; the remaining 25 states did not.
The four states with recreational cannabis laws experienced a 7.6% reduction in opioid-related ED visits for 6 months after the law went into effect in comparison with the states that did not legalize recreational marijuana.
“This isn’t trivial – a decline in opioid-related emergency department visits, even if only for 6 months, is a welcome public health development,” Dr. Drake said in a statement.
Not surprisingly, these effects are driven by men and adults aged 25 to 44 years. “These are populations that are more likely to use cannabis, and the reduction in opioid-related ED visits that we find is concentrated among them,” Dr. Drake told this news organization.
However, the downturn in opioid-related ED visits after making marijuana legal was only temporary.
“
Encouragingly, he said, the data show that opioid-related ED visits don’t increase above baseline after recreational marijuana laws are adopted.
“We conclude that cannabis legalization likely is not a panacea for the opioid epidemic, but there are some helpful effects,” Dr. Drake said in an interview.
The study was supported by the National Institute on Drug Abuse. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
State laws permitting recreational marijuana use have not led to an increase in opioid-related emergency department visits, as many had feared.
On the contrary, states that legalize recreational marijuana may see a short-term decrease in opioid-related ED visits in the first 6 months, after which rates may return to prelegalization levels, new research suggests.
Previous research suggests that individuals may reduce the use of opioids when they have an alternative and that cannabis can provide pain relief.
“At the same time, we often hear claims from politicians that we should not legalize cannabis because it may act as a ‘gateway drug’ that leads to use of other drugs,” lead researcher Coleman Drake, PhD, Department of Health Policy and Management, University of Pittsburgh Graduate School of Public Health, told this news organization.
“Our findings indicate that cannabis legalization does not effect any increase in opioid-related ED visits, contradicting the gateway drug explanation,” Dr. Drake said.
The study was published online July 12 in Health Economics.
Significant reduction
So far, 19 states have legalized recreational cannabis, meaning that nearly half of the U.S. population lives in a state that allows recreational cannabis use.
The investigators analyzed data on opioid-related ED visits from 29 states between 2011 and 2017. Four states – California, Maine, Massachusetts, and Nevada – legalized recreational marijuana during the study period; the remaining 25 states did not.
The four states with recreational cannabis laws experienced a 7.6% reduction in opioid-related ED visits for 6 months after the law went into effect in comparison with the states that did not legalize recreational marijuana.
“This isn’t trivial – a decline in opioid-related emergency department visits, even if only for 6 months, is a welcome public health development,” Dr. Drake said in a statement.
Not surprisingly, these effects are driven by men and adults aged 25 to 44 years. “These are populations that are more likely to use cannabis, and the reduction in opioid-related ED visits that we find is concentrated among them,” Dr. Drake told this news organization.
However, the downturn in opioid-related ED visits after making marijuana legal was only temporary.
“
Encouragingly, he said, the data show that opioid-related ED visits don’t increase above baseline after recreational marijuana laws are adopted.
“We conclude that cannabis legalization likely is not a panacea for the opioid epidemic, but there are some helpful effects,” Dr. Drake said in an interview.
The study was supported by the National Institute on Drug Abuse. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
State laws permitting recreational marijuana use have not led to an increase in opioid-related emergency department visits, as many had feared.
On the contrary, states that legalize recreational marijuana may see a short-term decrease in opioid-related ED visits in the first 6 months, after which rates may return to prelegalization levels, new research suggests.
Previous research suggests that individuals may reduce the use of opioids when they have an alternative and that cannabis can provide pain relief.
“At the same time, we often hear claims from politicians that we should not legalize cannabis because it may act as a ‘gateway drug’ that leads to use of other drugs,” lead researcher Coleman Drake, PhD, Department of Health Policy and Management, University of Pittsburgh Graduate School of Public Health, told this news organization.
“Our findings indicate that cannabis legalization does not effect any increase in opioid-related ED visits, contradicting the gateway drug explanation,” Dr. Drake said.
The study was published online July 12 in Health Economics.
Significant reduction
So far, 19 states have legalized recreational cannabis, meaning that nearly half of the U.S. population lives in a state that allows recreational cannabis use.
The investigators analyzed data on opioid-related ED visits from 29 states between 2011 and 2017. Four states – California, Maine, Massachusetts, and Nevada – legalized recreational marijuana during the study period; the remaining 25 states did not.
The four states with recreational cannabis laws experienced a 7.6% reduction in opioid-related ED visits for 6 months after the law went into effect in comparison with the states that did not legalize recreational marijuana.
“This isn’t trivial – a decline in opioid-related emergency department visits, even if only for 6 months, is a welcome public health development,” Dr. Drake said in a statement.
Not surprisingly, these effects are driven by men and adults aged 25 to 44 years. “These are populations that are more likely to use cannabis, and the reduction in opioid-related ED visits that we find is concentrated among them,” Dr. Drake told this news organization.
However, the downturn in opioid-related ED visits after making marijuana legal was only temporary.
“
Encouragingly, he said, the data show that opioid-related ED visits don’t increase above baseline after recreational marijuana laws are adopted.
“We conclude that cannabis legalization likely is not a panacea for the opioid epidemic, but there are some helpful effects,” Dr. Drake said in an interview.
The study was supported by the National Institute on Drug Abuse. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Mindfulness benefits kids with ADHD, and their families
Meditation, yoga, breathing exercises, and other mindfulness activities can help children with attention-deficit/hyperactivity disorder, but it’s not just the kids who benefit.
When families of children with ADHD complete a mindfulness program together, a new study suggests, children and parents can profit, with potential boosts to self-control, self-compassion, and psychological symptoms.
The findings do not suggest children should ditch medication in favor of focusing on the present moment. Instead, the study adds to growing evidence that mindfulness can be a helpful tool along with other strategies for children and adults with ADHD, said John Mitchell, PhD, a psychologist at Duke University, Durham, N.C., who was not involved with the new study. Mindfulness might help families ease stress and improve quality of life.
“We talk about ADHD because one person has that diagnosis, but we don’t live in bubbles,” he said. “We’re all interconnected and impact one another. And having treatments that acknowledge that and measuring that in the scientific literature is pretty important.”
Mindfulness training, which has its roots in Eastern traditions, generally aims to teach people how to be present in the moment and let go of judgment. Over the last couple of decades, researchers working on depression and other conditions have gathered evidence that practicing mindfulness can help in a variety of ways, including with the self-regulation of attention and emotions. It didn’t take long for those findings to draw interest from researchers who study ADHD, Dr. Mitchell said.
Research on mindfulness for ADHD started with adults, and results have been encouraging, Dr. Mitchell said. People who complete a mindfulness program tend to show some improvement in focus, impulsivity, and hyperactivity, studies show. In one small pilot study, Dr. Mitchell and colleagues reported improvements in symptoms and executive function in adults with ADHD.
Studies with children have lagged behind, but recent work has been promising. When looking at data from a number of studies, researchers have found small reductions in inattentiveness, hyperactivity, and impulsivity in young people with ADHD. Several randomized, controlled trials have also shown a reduction in symptoms as rated by parents and teachers.
Greater understanding, acceptance
In related research, there was a noticed reduction in stress among parents who get mindfulness training that teaches them to listen with their full attention, accept and develop compassion for themselves and their children, and regulate themselves within the relationship with their kids.
Still, first-line treatment for children with ADHD usually includes a combination of medication, cognitive behavioral therapy, and education, even though those strategies don’t always work well for everyone, says Corina Greven, PhD, a psychologist at Radboud (the Netherlands) University Medical Centre and Karakter Child and Adolescent Psychiatry.
Despite suggestive results, the data on mindfulness remains murky, in part because early studies that looked at mindfulness training for children with ADHD have been small. Few trials of mindfulness treatment for ADHD, Dr. Greven said, have included parents.
To fill in some of the gaps, Dr. Greven and colleagues conducted a trial with 103 families who had a child with ADHD between ages 8 and 16. Half of the families were randomly assigned simply to continue care as usual, which included medication for most.
The other half continued their usual care and also took part in a program called MYMind, which used mindfulness-based cognitive therapy for children and mindful parenting training for parents.
Families attended 90-minute group sessions once a week for 8 weeks, with an extra session 2 months later. The mindfulness group also completed homework every day that took about 30-45 minutes for parents and 15 minutes for children. Homework included workbooks and guided meditations.
In the short term, the team reported, children who received the mindfulness intervention showed small improvements in ADHD symptoms, anxiety, autistic symptoms, and problems falling asleep. One-third children who received mindfulness training improved on measures of self-control, Dr. Greven added, compared with just 1 in 10 who got only their usual care.
Benefits were larger and longer-lasting for parents. Compared with parents who didn’t get mindfulness training, those assigned to the mindfulness group improved in self-control, self-compassion, depression, anxiety, stress, well-being, and their own ADHD symptoms. Given a large genetic component to the disorder, it is common for parents of children with ADHD to have a diagnosis or ADHD symptoms as well. In addition, Dr. Greven said, families who completed the mindfulness-based intervention reported improvements in their relationships as well as acceptance of ADHD.
A new therapy?
The findings suggest new potential treatment options for children with ADHD, and for their parents, Dr. Greven said, as well as a need to study the condition more broadly. “Although parents of children with ADHD often have elevated parenting stress, anxiety, or their own ADHD symptoms, usual interventions for children with ADHD do not typically target parental mental health,” she said. “As researchers, we need to go broader than just looking at whether an intervention reduces symptoms and include additional outcomes that families find important.”
It will take more research to find out who is most likely to benefit from mindfulness training and how long those benefits last, but the new study is a useful starting point, experts say.
“Mindfulness training had potentially short-term and long-term beneficial effects to children with ADHD and their parents,” says Samuel Wong, MD, director of the JC School of Public Health and Primary Care at the Chinese University of Hong Kong. He says mindfulness is more likely to become an add-on than a replacement for other kinds of therapies.
“Clinicians may consider combining or adding family-based mindfulness training with current practice for children with ADHD who have residual symptoms with their current treatment,” he said.
Mindfulness training may help with issues beyond the classic symptoms that come with ADHD, Dr. Mitchell said, helping make family life better overall, even when some features of the disorder don’t budge much.
“With this study in particular, we see that we have some pretty promising effects that there may be something that will be beneficial above and beyond the core 18 DSM symptoms,” he said. “This is an important study, because it’s going to be a basis for the continuing evolution of the scientific research on this topic. It’s something to feel excited about.”
A version of this article first appeared on WebMD.com.
Meditation, yoga, breathing exercises, and other mindfulness activities can help children with attention-deficit/hyperactivity disorder, but it’s not just the kids who benefit.
When families of children with ADHD complete a mindfulness program together, a new study suggests, children and parents can profit, with potential boosts to self-control, self-compassion, and psychological symptoms.
The findings do not suggest children should ditch medication in favor of focusing on the present moment. Instead, the study adds to growing evidence that mindfulness can be a helpful tool along with other strategies for children and adults with ADHD, said John Mitchell, PhD, a psychologist at Duke University, Durham, N.C., who was not involved with the new study. Mindfulness might help families ease stress and improve quality of life.
“We talk about ADHD because one person has that diagnosis, but we don’t live in bubbles,” he said. “We’re all interconnected and impact one another. And having treatments that acknowledge that and measuring that in the scientific literature is pretty important.”
Mindfulness training, which has its roots in Eastern traditions, generally aims to teach people how to be present in the moment and let go of judgment. Over the last couple of decades, researchers working on depression and other conditions have gathered evidence that practicing mindfulness can help in a variety of ways, including with the self-regulation of attention and emotions. It didn’t take long for those findings to draw interest from researchers who study ADHD, Dr. Mitchell said.
Research on mindfulness for ADHD started with adults, and results have been encouraging, Dr. Mitchell said. People who complete a mindfulness program tend to show some improvement in focus, impulsivity, and hyperactivity, studies show. In one small pilot study, Dr. Mitchell and colleagues reported improvements in symptoms and executive function in adults with ADHD.
Studies with children have lagged behind, but recent work has been promising. When looking at data from a number of studies, researchers have found small reductions in inattentiveness, hyperactivity, and impulsivity in young people with ADHD. Several randomized, controlled trials have also shown a reduction in symptoms as rated by parents and teachers.
Greater understanding, acceptance
In related research, there was a noticed reduction in stress among parents who get mindfulness training that teaches them to listen with their full attention, accept and develop compassion for themselves and their children, and regulate themselves within the relationship with their kids.
Still, first-line treatment for children with ADHD usually includes a combination of medication, cognitive behavioral therapy, and education, even though those strategies don’t always work well for everyone, says Corina Greven, PhD, a psychologist at Radboud (the Netherlands) University Medical Centre and Karakter Child and Adolescent Psychiatry.
Despite suggestive results, the data on mindfulness remains murky, in part because early studies that looked at mindfulness training for children with ADHD have been small. Few trials of mindfulness treatment for ADHD, Dr. Greven said, have included parents.
To fill in some of the gaps, Dr. Greven and colleagues conducted a trial with 103 families who had a child with ADHD between ages 8 and 16. Half of the families were randomly assigned simply to continue care as usual, which included medication for most.
The other half continued their usual care and also took part in a program called MYMind, which used mindfulness-based cognitive therapy for children and mindful parenting training for parents.
Families attended 90-minute group sessions once a week for 8 weeks, with an extra session 2 months later. The mindfulness group also completed homework every day that took about 30-45 minutes for parents and 15 minutes for children. Homework included workbooks and guided meditations.
In the short term, the team reported, children who received the mindfulness intervention showed small improvements in ADHD symptoms, anxiety, autistic symptoms, and problems falling asleep. One-third children who received mindfulness training improved on measures of self-control, Dr. Greven added, compared with just 1 in 10 who got only their usual care.
Benefits were larger and longer-lasting for parents. Compared with parents who didn’t get mindfulness training, those assigned to the mindfulness group improved in self-control, self-compassion, depression, anxiety, stress, well-being, and their own ADHD symptoms. Given a large genetic component to the disorder, it is common for parents of children with ADHD to have a diagnosis or ADHD symptoms as well. In addition, Dr. Greven said, families who completed the mindfulness-based intervention reported improvements in their relationships as well as acceptance of ADHD.
A new therapy?
The findings suggest new potential treatment options for children with ADHD, and for their parents, Dr. Greven said, as well as a need to study the condition more broadly. “Although parents of children with ADHD often have elevated parenting stress, anxiety, or their own ADHD symptoms, usual interventions for children with ADHD do not typically target parental mental health,” she said. “As researchers, we need to go broader than just looking at whether an intervention reduces symptoms and include additional outcomes that families find important.”
It will take more research to find out who is most likely to benefit from mindfulness training and how long those benefits last, but the new study is a useful starting point, experts say.
“Mindfulness training had potentially short-term and long-term beneficial effects to children with ADHD and their parents,” says Samuel Wong, MD, director of the JC School of Public Health and Primary Care at the Chinese University of Hong Kong. He says mindfulness is more likely to become an add-on than a replacement for other kinds of therapies.
“Clinicians may consider combining or adding family-based mindfulness training with current practice for children with ADHD who have residual symptoms with their current treatment,” he said.
Mindfulness training may help with issues beyond the classic symptoms that come with ADHD, Dr. Mitchell said, helping make family life better overall, even when some features of the disorder don’t budge much.
“With this study in particular, we see that we have some pretty promising effects that there may be something that will be beneficial above and beyond the core 18 DSM symptoms,” he said. “This is an important study, because it’s going to be a basis for the continuing evolution of the scientific research on this topic. It’s something to feel excited about.”
A version of this article first appeared on WebMD.com.
Meditation, yoga, breathing exercises, and other mindfulness activities can help children with attention-deficit/hyperactivity disorder, but it’s not just the kids who benefit.
When families of children with ADHD complete a mindfulness program together, a new study suggests, children and parents can profit, with potential boosts to self-control, self-compassion, and psychological symptoms.
The findings do not suggest children should ditch medication in favor of focusing on the present moment. Instead, the study adds to growing evidence that mindfulness can be a helpful tool along with other strategies for children and adults with ADHD, said John Mitchell, PhD, a psychologist at Duke University, Durham, N.C., who was not involved with the new study. Mindfulness might help families ease stress and improve quality of life.
“We talk about ADHD because one person has that diagnosis, but we don’t live in bubbles,” he said. “We’re all interconnected and impact one another. And having treatments that acknowledge that and measuring that in the scientific literature is pretty important.”
Mindfulness training, which has its roots in Eastern traditions, generally aims to teach people how to be present in the moment and let go of judgment. Over the last couple of decades, researchers working on depression and other conditions have gathered evidence that practicing mindfulness can help in a variety of ways, including with the self-regulation of attention and emotions. It didn’t take long for those findings to draw interest from researchers who study ADHD, Dr. Mitchell said.
Research on mindfulness for ADHD started with adults, and results have been encouraging, Dr. Mitchell said. People who complete a mindfulness program tend to show some improvement in focus, impulsivity, and hyperactivity, studies show. In one small pilot study, Dr. Mitchell and colleagues reported improvements in symptoms and executive function in adults with ADHD.
Studies with children have lagged behind, but recent work has been promising. When looking at data from a number of studies, researchers have found small reductions in inattentiveness, hyperactivity, and impulsivity in young people with ADHD. Several randomized, controlled trials have also shown a reduction in symptoms as rated by parents and teachers.
Greater understanding, acceptance
In related research, there was a noticed reduction in stress among parents who get mindfulness training that teaches them to listen with their full attention, accept and develop compassion for themselves and their children, and regulate themselves within the relationship with their kids.
Still, first-line treatment for children with ADHD usually includes a combination of medication, cognitive behavioral therapy, and education, even though those strategies don’t always work well for everyone, says Corina Greven, PhD, a psychologist at Radboud (the Netherlands) University Medical Centre and Karakter Child and Adolescent Psychiatry.
Despite suggestive results, the data on mindfulness remains murky, in part because early studies that looked at mindfulness training for children with ADHD have been small. Few trials of mindfulness treatment for ADHD, Dr. Greven said, have included parents.
To fill in some of the gaps, Dr. Greven and colleagues conducted a trial with 103 families who had a child with ADHD between ages 8 and 16. Half of the families were randomly assigned simply to continue care as usual, which included medication for most.
The other half continued their usual care and also took part in a program called MYMind, which used mindfulness-based cognitive therapy for children and mindful parenting training for parents.
Families attended 90-minute group sessions once a week for 8 weeks, with an extra session 2 months later. The mindfulness group also completed homework every day that took about 30-45 minutes for parents and 15 minutes for children. Homework included workbooks and guided meditations.
In the short term, the team reported, children who received the mindfulness intervention showed small improvements in ADHD symptoms, anxiety, autistic symptoms, and problems falling asleep. One-third children who received mindfulness training improved on measures of self-control, Dr. Greven added, compared with just 1 in 10 who got only their usual care.
Benefits were larger and longer-lasting for parents. Compared with parents who didn’t get mindfulness training, those assigned to the mindfulness group improved in self-control, self-compassion, depression, anxiety, stress, well-being, and their own ADHD symptoms. Given a large genetic component to the disorder, it is common for parents of children with ADHD to have a diagnosis or ADHD symptoms as well. In addition, Dr. Greven said, families who completed the mindfulness-based intervention reported improvements in their relationships as well as acceptance of ADHD.
A new therapy?
The findings suggest new potential treatment options for children with ADHD, and for their parents, Dr. Greven said, as well as a need to study the condition more broadly. “Although parents of children with ADHD often have elevated parenting stress, anxiety, or their own ADHD symptoms, usual interventions for children with ADHD do not typically target parental mental health,” she said. “As researchers, we need to go broader than just looking at whether an intervention reduces symptoms and include additional outcomes that families find important.”
It will take more research to find out who is most likely to benefit from mindfulness training and how long those benefits last, but the new study is a useful starting point, experts say.
“Mindfulness training had potentially short-term and long-term beneficial effects to children with ADHD and their parents,” says Samuel Wong, MD, director of the JC School of Public Health and Primary Care at the Chinese University of Hong Kong. He says mindfulness is more likely to become an add-on than a replacement for other kinds of therapies.
“Clinicians may consider combining or adding family-based mindfulness training with current practice for children with ADHD who have residual symptoms with their current treatment,” he said.
Mindfulness training may help with issues beyond the classic symptoms that come with ADHD, Dr. Mitchell said, helping make family life better overall, even when some features of the disorder don’t budge much.
“With this study in particular, we see that we have some pretty promising effects that there may be something that will be beneficial above and beyond the core 18 DSM symptoms,” he said. “This is an important study, because it’s going to be a basis for the continuing evolution of the scientific research on this topic. It’s something to feel excited about.”
A version of this article first appeared on WebMD.com.
Health anxiety common as COVID restrictions loosen
As restrictions lift and mask mandates become scarce, Americans are filling their social calendars and booking vacations. While some are rejoicing, health care professionals say others are emerging from the pandemic with more health-related fears.
COVID-19 has caused more anxiety and depression for many over the course of the pandemic. A survey from the CDC and the Census Bureau found the percentage of adults with symptoms of an anxiety or depressive disorder increased from 36.4% to 41.5% from August 2020 to February 2021.
But this phenomenon will not just disappear as COVID-19 cases decrease, said Reese Druckenmiller, a clinical social worker for the Mayo Clinic Health System.
“There are still people out there not wanting to leave home,” she said. “Some folks inherently struggle with anxiety more than others, and we know anxiety can come from different experiences and traumas.
Though there is little research on the psychological effects of pandemic outbreaks, scientists are beginning to explore this. A recent review published in the International Journal of Cognitive Therapy concluded that, based on available research and the effects of previous pandemics, COVID-19 will likely have a significant effect on people’s mental health, particularly those who already have obsessive-compulsive disorder and health anxiety, along with people on the front line of health care.
According to the authors, since the virus doesn’t have symptoms among certain populations, there’s more anxiety about becoming infected and unknowingly spreading it to vulnerable people.
Not to mention the influx of anxiety-provoking news over the past year, Ms. Druckenmiller noted.
“One thing I noticed during the pandemic: The news changed. There were still regular news stories, but at the forefront of every single newscast was the numbers, how many people have died, how many people are hospitalized,” she said.
Some of Ms. Druckenmiller’s own patients who are more health-focused saw this as an added burden – another source of anxiety.
For those still uncomfortable with an abrupt reentry into public spaces, Ms. Druckenmiller recommended taking small steps. Start leaving the house every day, she suggested, even if it’s just for a walk. It is also important to be honest with loved ones about your own comfort level.
“Our brain is very flexible and fluid, but it also doesn’t just switch on a dime,” she said. “If I’ve been told over the past year this is a horrible thing that could kill me, my brain can’t adjust that fast. We need evidence through experience.”
A version of this article first appeared on WebMD.com.
As restrictions lift and mask mandates become scarce, Americans are filling their social calendars and booking vacations. While some are rejoicing, health care professionals say others are emerging from the pandemic with more health-related fears.
COVID-19 has caused more anxiety and depression for many over the course of the pandemic. A survey from the CDC and the Census Bureau found the percentage of adults with symptoms of an anxiety or depressive disorder increased from 36.4% to 41.5% from August 2020 to February 2021.
But this phenomenon will not just disappear as COVID-19 cases decrease, said Reese Druckenmiller, a clinical social worker for the Mayo Clinic Health System.
“There are still people out there not wanting to leave home,” she said. “Some folks inherently struggle with anxiety more than others, and we know anxiety can come from different experiences and traumas.
Though there is little research on the psychological effects of pandemic outbreaks, scientists are beginning to explore this. A recent review published in the International Journal of Cognitive Therapy concluded that, based on available research and the effects of previous pandemics, COVID-19 will likely have a significant effect on people’s mental health, particularly those who already have obsessive-compulsive disorder and health anxiety, along with people on the front line of health care.
According to the authors, since the virus doesn’t have symptoms among certain populations, there’s more anxiety about becoming infected and unknowingly spreading it to vulnerable people.
Not to mention the influx of anxiety-provoking news over the past year, Ms. Druckenmiller noted.
“One thing I noticed during the pandemic: The news changed. There were still regular news stories, but at the forefront of every single newscast was the numbers, how many people have died, how many people are hospitalized,” she said.
Some of Ms. Druckenmiller’s own patients who are more health-focused saw this as an added burden – another source of anxiety.
For those still uncomfortable with an abrupt reentry into public spaces, Ms. Druckenmiller recommended taking small steps. Start leaving the house every day, she suggested, even if it’s just for a walk. It is also important to be honest with loved ones about your own comfort level.
“Our brain is very flexible and fluid, but it also doesn’t just switch on a dime,” she said. “If I’ve been told over the past year this is a horrible thing that could kill me, my brain can’t adjust that fast. We need evidence through experience.”
A version of this article first appeared on WebMD.com.
As restrictions lift and mask mandates become scarce, Americans are filling their social calendars and booking vacations. While some are rejoicing, health care professionals say others are emerging from the pandemic with more health-related fears.
COVID-19 has caused more anxiety and depression for many over the course of the pandemic. A survey from the CDC and the Census Bureau found the percentage of adults with symptoms of an anxiety or depressive disorder increased from 36.4% to 41.5% from August 2020 to February 2021.
But this phenomenon will not just disappear as COVID-19 cases decrease, said Reese Druckenmiller, a clinical social worker for the Mayo Clinic Health System.
“There are still people out there not wanting to leave home,” she said. “Some folks inherently struggle with anxiety more than others, and we know anxiety can come from different experiences and traumas.
Though there is little research on the psychological effects of pandemic outbreaks, scientists are beginning to explore this. A recent review published in the International Journal of Cognitive Therapy concluded that, based on available research and the effects of previous pandemics, COVID-19 will likely have a significant effect on people’s mental health, particularly those who already have obsessive-compulsive disorder and health anxiety, along with people on the front line of health care.
According to the authors, since the virus doesn’t have symptoms among certain populations, there’s more anxiety about becoming infected and unknowingly spreading it to vulnerable people.
Not to mention the influx of anxiety-provoking news over the past year, Ms. Druckenmiller noted.
“One thing I noticed during the pandemic: The news changed. There were still regular news stories, but at the forefront of every single newscast was the numbers, how many people have died, how many people are hospitalized,” she said.
Some of Ms. Druckenmiller’s own patients who are more health-focused saw this as an added burden – another source of anxiety.
For those still uncomfortable with an abrupt reentry into public spaces, Ms. Druckenmiller recommended taking small steps. Start leaving the house every day, she suggested, even if it’s just for a walk. It is also important to be honest with loved ones about your own comfort level.
“Our brain is very flexible and fluid, but it also doesn’t just switch on a dime,” she said. “If I’ve been told over the past year this is a horrible thing that could kill me, my brain can’t adjust that fast. We need evidence through experience.”
A version of this article first appeared on WebMD.com.
Admissions for eating disorders double in pandemic
Medical admissions for adolescents with restrictive eating disorders more than doubled at one hospital during the first 12 months of the COVID-19 pandemic, relative to the average number of admissions in prior years, a new study shows.
Doctors are seeing similar increases across the United States and in other countries.
Providers and health care systems “may need to rapidly adapt in response to increasing demands for care during the COVID-19 pandemic,” the researchers said in their study, which was published online in Pediatrics.
To assess whether admission patterns among adolescents with restrictive eating disorders changed during the pandemic, Alana K. Otto, MD, MPH, with the division of adolescent medicine at the University of Michigan, Ann Arbor, and colleagues reviewed the charts of patients admitted to C.S. Mott Children’s Hospital, also in Ann Arbor.
Their analysis included 297 admissions among 248 patients aged 10-23 years between March 1, 2017, and March 31, 2021. Patients had an average age of about 15 years. Approximately 90% were female, and most had a diagnosis of anorexia nervosa or atypical anorexia nervosa.
Indications for medical admission included physiological instability (for example, heart rate less than 50 beats per minute while awake or blood pressure less than 90/40 mm Hg), electrolyte derangements, and acute medical complications of malnutrition such as syncope. Other possible indications included uncontrolled purging, body mass index less than 75% of the median for age and sex, acute food refusal, and failure of outpatient treatment.
Eating disorder–related admissions per month were stable prior to the pandemic. Admissions then decreased in April 2020, but subsequently increased significantly throughout the study period. In all, there were 125 admissions between April 1, 2020, and March 31, 2021. During the previous 3 years, the average number of admissions per year was 56.
Patients’ insurance status was one factor that differed before and during the pandemic. Prepandemic, about 20% of admissions were for adolescents with public insurance. During the pandemic, however, the proportion with public insurance was approximately 9%, the researchers noted. Other characteristics were generally similar.
The study was retrospective and relatively small and only looked at patients with restrictive eating disorders who were severely ill and admitted for medical stabilization. It does not reflect adolescents with eating disorders in different settings, the authors noted.
Primary care pediatricians should be familiar with indications for medical admission, such as severe bradycardia, as outlined by the Society for Adolescent Health and Medicine, they said.
Consistent trends
Unfortunately, the trend seems consistent across the nation, said Michaela M. Voss, MD, director of the the Eating Disorders Center at Children’s Mercy in Kansas City, Mo. “Our outpatient setting went from availability to get in immediately to a 6-month wait list.”
As in Michigan, Dr. Voss noted a drop in admissions as lockdowns started, followed by a spike in treatment demand that has not let up.
Dr. Voss described two of the more common presentations. In one, parents might note that their child had been getting into healthy eating and exercise before the pandemic and seemed fine. “But then COVID came, the lockdown happened, and they became overly obsessed with those things,” Dr. Voss said.
In the other presentation, kids with anxiety, depression, or OCD who lost access to their usual coping strategies and outlets developed eating disorders during the pandemic. “They focused on one of the few things they could during the lockdown, which was their own body, and then their anxiety, depression, [obsessive-compulsive disorder], and other mental health comorbidities presented as an eating disorder,” Dr. Voss said.
The increasing need for treatment over the course of the pandemic may reflect the time that it has taken for the disorders to develop, as well as the time that it takes parents to recognize the problem.
Not only are doctors seeing more cases, but patients are arriving sicker than usual, Dr. Voss said.
Major medical concerns for patients in starvation mode center on the heart, brain, and bones. In addition, refeeding syndrome poses an extreme risk, Dr. Voss noted.
The Academy for Eating Disorders has created a guide to help doctors recognize and manage risks for patients with eating disorders, which may be useful for primary care providers while they are trying to get a patient into more intensive treatment, Dr. Voss suggested. The American Academy of Pediatrics recently published a clinical report on the identification and management of eating disorders in children and adolescents.

At Johns Hopkins Hospital Children’s Center in Baltimore, “we have seen a pretty remarkable increase in the number of eating disorders in the child and adolescent space since COVID,” said Jennifer Leah Goetz, MD, a psychiatrist and medical director of the child and adolescent inpatient unit. “We have seen increasing numbers of kids presenting for acute medical stabilization and refeeding and for specific treatment for the eating disorder.”
It could be that, for people with a genetic predisposition to eating disorders, a confluence of factors related to the pandemic unmasked it. For example, children may have spent more time looking at themselves on virtual meeting platforms, which could stir lingering body image and appearance-related concerns in those who are vulnerable. And some teens who were not able to participate in athletics as usual started to watch what they eat more closely, Dr. Goetz said.
A treatment bottleneck
Patients with eating disorders “can be quite ill from a psychiatric and general medical perspective,” Dr. Goetz said. “Most psychiatrists are not particularly comfortable with the medical complications, and most internists or pediatricians are not particularly comfortable with the psychiatric complications. You end up with a patient population that can only see a really highly specialized group of individuals for care. And it is a problem. It was a problem before the pandemic, and it has been really exacerbated by what we have been going through with COVID.”

Natalie Muth, MD, MPH, RDN, a pediatrician at Children’s Primary Care Medical Group La Costa in Carlsbad, Calif., has also noticed the increase in eating disorders since COVID.
In-patient colleagues “have longer wait lists and more severe cases than they have ever seen previously,” said Dr. Muth, who chairs the American Academy of Pediatrics Section on Obesity and is an adjunct assistant professor at the University of California, Los Angeles. “In primary care, we are all having to better educate and prepare ourselves for identifying and managing patients with eating disorders.”
That could mean connecting with mental health professionals, registered dietitians, and higher levels of care. But that may be a challenge. “Accessing these resources has been more difficult due to the increasing incidence of eating disorders recently,” Dr. Muth said.
Dr. Voss acknowledged that childhood obesity is another concern for pediatricians. “However, there are appropriate and healthy and safe ways to address that,” she said. A patient with overweight or obesity who loses weight may not be doing so in a healthy way.
Clinicians should wonder if a patient’s weight is decreasing too fast. And they should ask patients questions that could help identify a problem, such as: What are they doing to cause the weight loss? Why do they want to lose the weight?
Dr. Voss added that eating disorders “do not discriminate.” While there may be a perception that all patients with eating disorders are White, upper middle–class females who are thin, “that is not the case,” Dr. Voss said. They “come in all genders, all races, all weight classes, and all ages,” she said, “and we see that variety.”
In general, there may be a need to shift how weight is discussed in clinics and society more broadly, Dr. Goetz said. Weight is an incredibly personal thing, and everyone’s genetics, metabolism, and life circumstances vary. At the same time, body mass index is not necessarily the best measure of a person’s health.
Asking a child, teen, or even an adult to go on a diet is not a benign intervention, Dr. Goetz noted. In addition, dieting is unlikely to help in the long term.
Emerging from lockdown, pressure to lose “COVID pounds” is a dangerous message for people with eating disorders, Dr. Goetz said. It also could be a dangerous message for people without eating disorders. “There are so many more interesting things about each one of us than our weight,” she added.
The study authors, Dr. Voss, Dr. Goetz, and Dr. Muth had no relevant disclosures.
Medical admissions for adolescents with restrictive eating disorders more than doubled at one hospital during the first 12 months of the COVID-19 pandemic, relative to the average number of admissions in prior years, a new study shows.
Doctors are seeing similar increases across the United States and in other countries.
Providers and health care systems “may need to rapidly adapt in response to increasing demands for care during the COVID-19 pandemic,” the researchers said in their study, which was published online in Pediatrics.
To assess whether admission patterns among adolescents with restrictive eating disorders changed during the pandemic, Alana K. Otto, MD, MPH, with the division of adolescent medicine at the University of Michigan, Ann Arbor, and colleagues reviewed the charts of patients admitted to C.S. Mott Children’s Hospital, also in Ann Arbor.
Their analysis included 297 admissions among 248 patients aged 10-23 years between March 1, 2017, and March 31, 2021. Patients had an average age of about 15 years. Approximately 90% were female, and most had a diagnosis of anorexia nervosa or atypical anorexia nervosa.
Indications for medical admission included physiological instability (for example, heart rate less than 50 beats per minute while awake or blood pressure less than 90/40 mm Hg), electrolyte derangements, and acute medical complications of malnutrition such as syncope. Other possible indications included uncontrolled purging, body mass index less than 75% of the median for age and sex, acute food refusal, and failure of outpatient treatment.
Eating disorder–related admissions per month were stable prior to the pandemic. Admissions then decreased in April 2020, but subsequently increased significantly throughout the study period. In all, there were 125 admissions between April 1, 2020, and March 31, 2021. During the previous 3 years, the average number of admissions per year was 56.
Patients’ insurance status was one factor that differed before and during the pandemic. Prepandemic, about 20% of admissions were for adolescents with public insurance. During the pandemic, however, the proportion with public insurance was approximately 9%, the researchers noted. Other characteristics were generally similar.
The study was retrospective and relatively small and only looked at patients with restrictive eating disorders who were severely ill and admitted for medical stabilization. It does not reflect adolescents with eating disorders in different settings, the authors noted.
Primary care pediatricians should be familiar with indications for medical admission, such as severe bradycardia, as outlined by the Society for Adolescent Health and Medicine, they said.
Consistent trends
Unfortunately, the trend seems consistent across the nation, said Michaela M. Voss, MD, director of the the Eating Disorders Center at Children’s Mercy in Kansas City, Mo. “Our outpatient setting went from availability to get in immediately to a 6-month wait list.”
As in Michigan, Dr. Voss noted a drop in admissions as lockdowns started, followed by a spike in treatment demand that has not let up.
Dr. Voss described two of the more common presentations. In one, parents might note that their child had been getting into healthy eating and exercise before the pandemic and seemed fine. “But then COVID came, the lockdown happened, and they became overly obsessed with those things,” Dr. Voss said.
In the other presentation, kids with anxiety, depression, or OCD who lost access to their usual coping strategies and outlets developed eating disorders during the pandemic. “They focused on one of the few things they could during the lockdown, which was their own body, and then their anxiety, depression, [obsessive-compulsive disorder], and other mental health comorbidities presented as an eating disorder,” Dr. Voss said.
The increasing need for treatment over the course of the pandemic may reflect the time that it has taken for the disorders to develop, as well as the time that it takes parents to recognize the problem.
Not only are doctors seeing more cases, but patients are arriving sicker than usual, Dr. Voss said.
Major medical concerns for patients in starvation mode center on the heart, brain, and bones. In addition, refeeding syndrome poses an extreme risk, Dr. Voss noted.
The Academy for Eating Disorders has created a guide to help doctors recognize and manage risks for patients with eating disorders, which may be useful for primary care providers while they are trying to get a patient into more intensive treatment, Dr. Voss suggested. The American Academy of Pediatrics recently published a clinical report on the identification and management of eating disorders in children and adolescents.
At Johns Hopkins Hospital Children’s Center in Baltimore, “we have seen a pretty remarkable increase in the number of eating disorders in the child and adolescent space since COVID,” said Jennifer Leah Goetz, MD, a psychiatrist and medical director of the child and adolescent inpatient unit. “We have seen increasing numbers of kids presenting for acute medical stabilization and refeeding and for specific treatment for the eating disorder.”
It could be that, for people with a genetic predisposition to eating disorders, a confluence of factors related to the pandemic unmasked it. For example, children may have spent more time looking at themselves on virtual meeting platforms, which could stir lingering body image and appearance-related concerns in those who are vulnerable. And some teens who were not able to participate in athletics as usual started to watch what they eat more closely, Dr. Goetz said.
A treatment bottleneck
Patients with eating disorders “can be quite ill from a psychiatric and general medical perspective,” Dr. Goetz said. “Most psychiatrists are not particularly comfortable with the medical complications, and most internists or pediatricians are not particularly comfortable with the psychiatric complications. You end up with a patient population that can only see a really highly specialized group of individuals for care. And it is a problem. It was a problem before the pandemic, and it has been really exacerbated by what we have been going through with COVID.”
Natalie Muth, MD, MPH, RDN, a pediatrician at Children’s Primary Care Medical Group La Costa in Carlsbad, Calif., has also noticed the increase in eating disorders since COVID.
In-patient colleagues “have longer wait lists and more severe cases than they have ever seen previously,” said Dr. Muth, who chairs the American Academy of Pediatrics Section on Obesity and is an adjunct assistant professor at the University of California, Los Angeles. “In primary care, we are all having to better educate and prepare ourselves for identifying and managing patients with eating disorders.”
That could mean connecting with mental health professionals, registered dietitians, and higher levels of care. But that may be a challenge. “Accessing these resources has been more difficult due to the increasing incidence of eating disorders recently,” Dr. Muth said.
Dr. Voss acknowledged that childhood obesity is another concern for pediatricians. “However, there are appropriate and healthy and safe ways to address that,” she said. A patient with overweight or obesity who loses weight may not be doing so in a healthy way.
Clinicians should wonder if a patient’s weight is decreasing too fast. And they should ask patients questions that could help identify a problem, such as: What are they doing to cause the weight loss? Why do they want to lose the weight?
Dr. Voss added that eating disorders “do not discriminate.” While there may be a perception that all patients with eating disorders are White, upper middle–class females who are thin, “that is not the case,” Dr. Voss said. They “come in all genders, all races, all weight classes, and all ages,” she said, “and we see that variety.”
In general, there may be a need to shift how weight is discussed in clinics and society more broadly, Dr. Goetz said. Weight is an incredibly personal thing, and everyone’s genetics, metabolism, and life circumstances vary. At the same time, body mass index is not necessarily the best measure of a person’s health.
Asking a child, teen, or even an adult to go on a diet is not a benign intervention, Dr. Goetz noted. In addition, dieting is unlikely to help in the long term.
Emerging from lockdown, pressure to lose “COVID pounds” is a dangerous message for people with eating disorders, Dr. Goetz said. It also could be a dangerous message for people without eating disorders. “There are so many more interesting things about each one of us than our weight,” she added.
The study authors, Dr. Voss, Dr. Goetz, and Dr. Muth had no relevant disclosures.
Medical admissions for adolescents with restrictive eating disorders more than doubled at one hospital during the first 12 months of the COVID-19 pandemic, relative to the average number of admissions in prior years, a new study shows.
Doctors are seeing similar increases across the United States and in other countries.
Providers and health care systems “may need to rapidly adapt in response to increasing demands for care during the COVID-19 pandemic,” the researchers said in their study, which was published online in Pediatrics.
To assess whether admission patterns among adolescents with restrictive eating disorders changed during the pandemic, Alana K. Otto, MD, MPH, with the division of adolescent medicine at the University of Michigan, Ann Arbor, and colleagues reviewed the charts of patients admitted to C.S. Mott Children’s Hospital, also in Ann Arbor.
Their analysis included 297 admissions among 248 patients aged 10-23 years between March 1, 2017, and March 31, 2021. Patients had an average age of about 15 years. Approximately 90% were female, and most had a diagnosis of anorexia nervosa or atypical anorexia nervosa.
Indications for medical admission included physiological instability (for example, heart rate less than 50 beats per minute while awake or blood pressure less than 90/40 mm Hg), electrolyte derangements, and acute medical complications of malnutrition such as syncope. Other possible indications included uncontrolled purging, body mass index less than 75% of the median for age and sex, acute food refusal, and failure of outpatient treatment.
Eating disorder–related admissions per month were stable prior to the pandemic. Admissions then decreased in April 2020, but subsequently increased significantly throughout the study period. In all, there were 125 admissions between April 1, 2020, and March 31, 2021. During the previous 3 years, the average number of admissions per year was 56.
Patients’ insurance status was one factor that differed before and during the pandemic. Prepandemic, about 20% of admissions were for adolescents with public insurance. During the pandemic, however, the proportion with public insurance was approximately 9%, the researchers noted. Other characteristics were generally similar.
The study was retrospective and relatively small and only looked at patients with restrictive eating disorders who were severely ill and admitted for medical stabilization. It does not reflect adolescents with eating disorders in different settings, the authors noted.
Primary care pediatricians should be familiar with indications for medical admission, such as severe bradycardia, as outlined by the Society for Adolescent Health and Medicine, they said.
Consistent trends
Unfortunately, the trend seems consistent across the nation, said Michaela M. Voss, MD, director of the the Eating Disorders Center at Children’s Mercy in Kansas City, Mo. “Our outpatient setting went from availability to get in immediately to a 6-month wait list.”
As in Michigan, Dr. Voss noted a drop in admissions as lockdowns started, followed by a spike in treatment demand that has not let up.
Dr. Voss described two of the more common presentations. In one, parents might note that their child had been getting into healthy eating and exercise before the pandemic and seemed fine. “But then COVID came, the lockdown happened, and they became overly obsessed with those things,” Dr. Voss said.
In the other presentation, kids with anxiety, depression, or OCD who lost access to their usual coping strategies and outlets developed eating disorders during the pandemic. “They focused on one of the few things they could during the lockdown, which was their own body, and then their anxiety, depression, [obsessive-compulsive disorder], and other mental health comorbidities presented as an eating disorder,” Dr. Voss said.
The increasing need for treatment over the course of the pandemic may reflect the time that it has taken for the disorders to develop, as well as the time that it takes parents to recognize the problem.
Not only are doctors seeing more cases, but patients are arriving sicker than usual, Dr. Voss said.
Major medical concerns for patients in starvation mode center on the heart, brain, and bones. In addition, refeeding syndrome poses an extreme risk, Dr. Voss noted.
The Academy for Eating Disorders has created a guide to help doctors recognize and manage risks for patients with eating disorders, which may be useful for primary care providers while they are trying to get a patient into more intensive treatment, Dr. Voss suggested. The American Academy of Pediatrics recently published a clinical report on the identification and management of eating disorders in children and adolescents.
At Johns Hopkins Hospital Children’s Center in Baltimore, “we have seen a pretty remarkable increase in the number of eating disorders in the child and adolescent space since COVID,” said Jennifer Leah Goetz, MD, a psychiatrist and medical director of the child and adolescent inpatient unit. “We have seen increasing numbers of kids presenting for acute medical stabilization and refeeding and for specific treatment for the eating disorder.”
It could be that, for people with a genetic predisposition to eating disorders, a confluence of factors related to the pandemic unmasked it. For example, children may have spent more time looking at themselves on virtual meeting platforms, which could stir lingering body image and appearance-related concerns in those who are vulnerable. And some teens who were not able to participate in athletics as usual started to watch what they eat more closely, Dr. Goetz said.
A treatment bottleneck
Patients with eating disorders “can be quite ill from a psychiatric and general medical perspective,” Dr. Goetz said. “Most psychiatrists are not particularly comfortable with the medical complications, and most internists or pediatricians are not particularly comfortable with the psychiatric complications. You end up with a patient population that can only see a really highly specialized group of individuals for care. And it is a problem. It was a problem before the pandemic, and it has been really exacerbated by what we have been going through with COVID.”
Natalie Muth, MD, MPH, RDN, a pediatrician at Children’s Primary Care Medical Group La Costa in Carlsbad, Calif., has also noticed the increase in eating disorders since COVID.
In-patient colleagues “have longer wait lists and more severe cases than they have ever seen previously,” said Dr. Muth, who chairs the American Academy of Pediatrics Section on Obesity and is an adjunct assistant professor at the University of California, Los Angeles. “In primary care, we are all having to better educate and prepare ourselves for identifying and managing patients with eating disorders.”
That could mean connecting with mental health professionals, registered dietitians, and higher levels of care. But that may be a challenge. “Accessing these resources has been more difficult due to the increasing incidence of eating disorders recently,” Dr. Muth said.
Dr. Voss acknowledged that childhood obesity is another concern for pediatricians. “However, there are appropriate and healthy and safe ways to address that,” she said. A patient with overweight or obesity who loses weight may not be doing so in a healthy way.
Clinicians should wonder if a patient’s weight is decreasing too fast. And they should ask patients questions that could help identify a problem, such as: What are they doing to cause the weight loss? Why do they want to lose the weight?
Dr. Voss added that eating disorders “do not discriminate.” While there may be a perception that all patients with eating disorders are White, upper middle–class females who are thin, “that is not the case,” Dr. Voss said. They “come in all genders, all races, all weight classes, and all ages,” she said, “and we see that variety.”
In general, there may be a need to shift how weight is discussed in clinics and society more broadly, Dr. Goetz said. Weight is an incredibly personal thing, and everyone’s genetics, metabolism, and life circumstances vary. At the same time, body mass index is not necessarily the best measure of a person’s health.
Asking a child, teen, or even an adult to go on a diet is not a benign intervention, Dr. Goetz noted. In addition, dieting is unlikely to help in the long term.
Emerging from lockdown, pressure to lose “COVID pounds” is a dangerous message for people with eating disorders, Dr. Goetz said. It also could be a dangerous message for people without eating disorders. “There are so many more interesting things about each one of us than our weight,” she added.
The study authors, Dr. Voss, Dr. Goetz, and Dr. Muth had no relevant disclosures.
FROM PEDIATRICS
Bullying in academic medicine rife, underreported
Bullying in academic medicine, especially among women, is rife, underreported, and remains largely unaddressed, new research suggests.
Investigators reviewed close to 70 studies, encompassing over 82,000 medical consultants or trainees in academic medical settings, and found that men were identified as the most common perpetrators – close to 70% of respondents – whereas women were the most common victims (56%).
Collectively, respondents in all of the studies identified the most common bullies to be consultants (54%), followed by residents (22%), and nurses (15%).
Disturbingly, less than one-third of victims overall reported that they were bullied, and close to 60% who formally reported the abuse said they did not have a positive outcome.
“We found that bullies are commonly men and senior consultants, while more than half of their victims are women,” senior author Harriette G.C. Van Spall, MD, MPH, associate professor of medicine and director of e-health and virtual care, Division of Cardiology, McMaster University, Hamilton, Ont., said in an interview.
“The greatest barriers to addressing academic bullying are the fear of reprisal, lack of impact of reporting, and non-enforcement of anti-bullying policies,” she added.
The study was published online July 12 in BMJ Open.
Personal experience
“Some behaviors were excruciating to deal with, protesting against them would bring more on, and every day was filled with dread. It took sheer will to show up at work to care for patients, to complete research I was leading, and to have hope, and my academic output, income, and personal well-being dropped during those years,” she added.
Dr. Van Spall thought the subject “merited research because our performance as clinicians, researchers, and educators relies on our work environment.”
To investigate, the researchers reviewed 68 studies (n = 82,349 respondents) conducted between 1999 and 2021 in academic medical settings, in which victims were either consultants or trainees. Many of the studies (31) were conducted in the U.S.
Other countries included the United Kingdom, Canada, Australia, Pakistan, Egypt, Iran, Turkey, New Zealand, Lithuania, Greece, India, Germany, Nigeria, Oman, and Finland.
Studies were required to describe the method and impact of bullying; characteristics of the perpetrators and victims; or interventions that were used to address the bullying.
“Bullying” was defined as “the abuse of authority by a perpetrator who targets the victim in an academic setting through punishing behaviors that include overwork, destabilization, and isolation in order to impede the education or career of the target.”
Systemic sexism
Bullying behaviors, reported in 28 studies (n = 35,779 respondents), were grouped into destabilization, threats to professional status, overwork, and isolation, with overwork found to be the most common form of bullying.
The most common impact of being bullied was psychological distress, reported by 39.1% of respondents in 14 studies, followed by considerations of quitting (35.9%; 7 studies), and worsening of clinical performance (34.6%, 8 studies).
“Among demographic groups, men were identified as the most common perpetrators (67.2% of 4,722 respondents in 5 studies) and women the most common victims (56.2% of 15,246 respondents in 27 studies),” the authors report.
“Academic medicine in many institutions is encumbered by systemic sexism that is evident in processes around remuneration, recognition, opportunities for advancement, and leadership positions,” said Dr. Van Spall.
“There are fewer women at decision-making tables in academic medicine, the climb is uphill at the best of times, and women are likely easier targets for bullies, as their voices are easier to drown out,” she added.
She noted that many men do “exhibit wonderful attributes of professionalism and decency,” but “some in positions of power are given impunity by virtue of other accomplishments.”
Multiple deterrents
Thirty-one studies (n = 15,868) described characteristics of the bullies and showed the most common to be consultants (53.6% [30 studies]), residents (22% [22 studies]), and nurses (14.9% [21 studies]).
Only a minority of victims (28.9% of 9,410 victims [10 studies]) formally reported the bullying. The researchers identified multiple deterrents to reporting.
When a formal complaint was submitted (n = 1,139 respondents), it most frequently had no perceived effect (35.6%); more than one-fifth (21.9%) experienced worsening of the bullying, and only 13.7% reported improvement.
The common institutional facilitators of bullying, described in 25 studies, included lack of enforcement of anti-bullying policies (13 studies), the hierarchical structure of medicine (7 studies), and normalization of bullying (10 studies).
Forty-nine studies looked at strategies to address academic bullying, including anti-bullying policies, mandatory workshops on mistreatment, establishing an anti-bullying oversight committee, and institutional support for victims. However, the studies testing the effectiveness of these interventions “had a high risk of bias.”
Support available
Commenting on the research for this news organization, Roberta Gebhard, DO, past president of the American Medical Women’s Association (AMWA) and a member of the advisory board for Physician Just Equity, called it a “good study, large, international, and well-written.”
Dr. Gebhard, a member of the Governing Council for the American Medical Association Women Physician Section, was not associated with this study but said she is currently researching women who left medical school and residency.
“A common reason for leaving is being bullied. Bullying is often not reported and if reported, often not addressed. Or, if addressed, the person who reports it is often retaliated against, which is a common experience, especially in women.”
She advised female physicians who are bullied to get support from other female physicians – for example, by joining the AMWA, which has an online women’s leadership group.
“Having other women physicians throughout the country you can call for advice and support can be helpful,” said Dr. Gebhard, a family practice physician based in Grand Island, New York.
Dr. Van Spall receives support from the Canadian Institutes of Health Research, the Heart and Stroke Foundation, the Women As One Escalator Award, and McMaster Department of Medicine. The study authors and Dr. Gebhard have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Bullying in academic medicine, especially among women, is rife, underreported, and remains largely unaddressed, new research suggests.
Investigators reviewed close to 70 studies, encompassing over 82,000 medical consultants or trainees in academic medical settings, and found that men were identified as the most common perpetrators – close to 70% of respondents – whereas women were the most common victims (56%).
Collectively, respondents in all of the studies identified the most common bullies to be consultants (54%), followed by residents (22%), and nurses (15%).
Disturbingly, less than one-third of victims overall reported that they were bullied, and close to 60% who formally reported the abuse said they did not have a positive outcome.
“We found that bullies are commonly men and senior consultants, while more than half of their victims are women,” senior author Harriette G.C. Van Spall, MD, MPH, associate professor of medicine and director of e-health and virtual care, Division of Cardiology, McMaster University, Hamilton, Ont., said in an interview.
“The greatest barriers to addressing academic bullying are the fear of reprisal, lack of impact of reporting, and non-enforcement of anti-bullying policies,” she added.
The study was published online July 12 in BMJ Open.
Personal experience
“Some behaviors were excruciating to deal with, protesting against them would bring more on, and every day was filled with dread. It took sheer will to show up at work to care for patients, to complete research I was leading, and to have hope, and my academic output, income, and personal well-being dropped during those years,” she added.
Dr. Van Spall thought the subject “merited research because our performance as clinicians, researchers, and educators relies on our work environment.”
To investigate, the researchers reviewed 68 studies (n = 82,349 respondents) conducted between 1999 and 2021 in academic medical settings, in which victims were either consultants or trainees. Many of the studies (31) were conducted in the U.S.
Other countries included the United Kingdom, Canada, Australia, Pakistan, Egypt, Iran, Turkey, New Zealand, Lithuania, Greece, India, Germany, Nigeria, Oman, and Finland.
Studies were required to describe the method and impact of bullying; characteristics of the perpetrators and victims; or interventions that were used to address the bullying.
“Bullying” was defined as “the abuse of authority by a perpetrator who targets the victim in an academic setting through punishing behaviors that include overwork, destabilization, and isolation in order to impede the education or career of the target.”
Systemic sexism
Bullying behaviors, reported in 28 studies (n = 35,779 respondents), were grouped into destabilization, threats to professional status, overwork, and isolation, with overwork found to be the most common form of bullying.
The most common impact of being bullied was psychological distress, reported by 39.1% of respondents in 14 studies, followed by considerations of quitting (35.9%; 7 studies), and worsening of clinical performance (34.6%, 8 studies).
“Among demographic groups, men were identified as the most common perpetrators (67.2% of 4,722 respondents in 5 studies) and women the most common victims (56.2% of 15,246 respondents in 27 studies),” the authors report.
“Academic medicine in many institutions is encumbered by systemic sexism that is evident in processes around remuneration, recognition, opportunities for advancement, and leadership positions,” said Dr. Van Spall.
“There are fewer women at decision-making tables in academic medicine, the climb is uphill at the best of times, and women are likely easier targets for bullies, as their voices are easier to drown out,” she added.
She noted that many men do “exhibit wonderful attributes of professionalism and decency,” but “some in positions of power are given impunity by virtue of other accomplishments.”
Multiple deterrents
Thirty-one studies (n = 15,868) described characteristics of the bullies and showed the most common to be consultants (53.6% [30 studies]), residents (22% [22 studies]), and nurses (14.9% [21 studies]).
Only a minority of victims (28.9% of 9,410 victims [10 studies]) formally reported the bullying. The researchers identified multiple deterrents to reporting.
When a formal complaint was submitted (n = 1,139 respondents), it most frequently had no perceived effect (35.6%); more than one-fifth (21.9%) experienced worsening of the bullying, and only 13.7% reported improvement.
The common institutional facilitators of bullying, described in 25 studies, included lack of enforcement of anti-bullying policies (13 studies), the hierarchical structure of medicine (7 studies), and normalization of bullying (10 studies).
Forty-nine studies looked at strategies to address academic bullying, including anti-bullying policies, mandatory workshops on mistreatment, establishing an anti-bullying oversight committee, and institutional support for victims. However, the studies testing the effectiveness of these interventions “had a high risk of bias.”
Support available
Commenting on the research for this news organization, Roberta Gebhard, DO, past president of the American Medical Women’s Association (AMWA) and a member of the advisory board for Physician Just Equity, called it a “good study, large, international, and well-written.”
Dr. Gebhard, a member of the Governing Council for the American Medical Association Women Physician Section, was not associated with this study but said she is currently researching women who left medical school and residency.
“A common reason for leaving is being bullied. Bullying is often not reported and if reported, often not addressed. Or, if addressed, the person who reports it is often retaliated against, which is a common experience, especially in women.”
She advised female physicians who are bullied to get support from other female physicians – for example, by joining the AMWA, which has an online women’s leadership group.
“Having other women physicians throughout the country you can call for advice and support can be helpful,” said Dr. Gebhard, a family practice physician based in Grand Island, New York.
Dr. Van Spall receives support from the Canadian Institutes of Health Research, the Heart and Stroke Foundation, the Women As One Escalator Award, and McMaster Department of Medicine. The study authors and Dr. Gebhard have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Bullying in academic medicine, especially among women, is rife, underreported, and remains largely unaddressed, new research suggests.
Investigators reviewed close to 70 studies, encompassing over 82,000 medical consultants or trainees in academic medical settings, and found that men were identified as the most common perpetrators – close to 70% of respondents – whereas women were the most common victims (56%).
Collectively, respondents in all of the studies identified the most common bullies to be consultants (54%), followed by residents (22%), and nurses (15%).
Disturbingly, less than one-third of victims overall reported that they were bullied, and close to 60% who formally reported the abuse said they did not have a positive outcome.
“We found that bullies are commonly men and senior consultants, while more than half of their victims are women,” senior author Harriette G.C. Van Spall, MD, MPH, associate professor of medicine and director of e-health and virtual care, Division of Cardiology, McMaster University, Hamilton, Ont., said in an interview.
“The greatest barriers to addressing academic bullying are the fear of reprisal, lack of impact of reporting, and non-enforcement of anti-bullying policies,” she added.
The study was published online July 12 in BMJ Open.
Personal experience
“Some behaviors were excruciating to deal with, protesting against them would bring more on, and every day was filled with dread. It took sheer will to show up at work to care for patients, to complete research I was leading, and to have hope, and my academic output, income, and personal well-being dropped during those years,” she added.
Dr. Van Spall thought the subject “merited research because our performance as clinicians, researchers, and educators relies on our work environment.”
To investigate, the researchers reviewed 68 studies (n = 82,349 respondents) conducted between 1999 and 2021 in academic medical settings, in which victims were either consultants or trainees. Many of the studies (31) were conducted in the U.S.
Other countries included the United Kingdom, Canada, Australia, Pakistan, Egypt, Iran, Turkey, New Zealand, Lithuania, Greece, India, Germany, Nigeria, Oman, and Finland.
Studies were required to describe the method and impact of bullying; characteristics of the perpetrators and victims; or interventions that were used to address the bullying.
“Bullying” was defined as “the abuse of authority by a perpetrator who targets the victim in an academic setting through punishing behaviors that include overwork, destabilization, and isolation in order to impede the education or career of the target.”
Systemic sexism
Bullying behaviors, reported in 28 studies (n = 35,779 respondents), were grouped into destabilization, threats to professional status, overwork, and isolation, with overwork found to be the most common form of bullying.
The most common impact of being bullied was psychological distress, reported by 39.1% of respondents in 14 studies, followed by considerations of quitting (35.9%; 7 studies), and worsening of clinical performance (34.6%, 8 studies).
“Among demographic groups, men were identified as the most common perpetrators (67.2% of 4,722 respondents in 5 studies) and women the most common victims (56.2% of 15,246 respondents in 27 studies),” the authors report.
“Academic medicine in many institutions is encumbered by systemic sexism that is evident in processes around remuneration, recognition, opportunities for advancement, and leadership positions,” said Dr. Van Spall.
“There are fewer women at decision-making tables in academic medicine, the climb is uphill at the best of times, and women are likely easier targets for bullies, as their voices are easier to drown out,” she added.
She noted that many men do “exhibit wonderful attributes of professionalism and decency,” but “some in positions of power are given impunity by virtue of other accomplishments.”
Multiple deterrents
Thirty-one studies (n = 15,868) described characteristics of the bullies and showed the most common to be consultants (53.6% [30 studies]), residents (22% [22 studies]), and nurses (14.9% [21 studies]).
Only a minority of victims (28.9% of 9,410 victims [10 studies]) formally reported the bullying. The researchers identified multiple deterrents to reporting.
When a formal complaint was submitted (n = 1,139 respondents), it most frequently had no perceived effect (35.6%); more than one-fifth (21.9%) experienced worsening of the bullying, and only 13.7% reported improvement.
The common institutional facilitators of bullying, described in 25 studies, included lack of enforcement of anti-bullying policies (13 studies), the hierarchical structure of medicine (7 studies), and normalization of bullying (10 studies).
Forty-nine studies looked at strategies to address academic bullying, including anti-bullying policies, mandatory workshops on mistreatment, establishing an anti-bullying oversight committee, and institutional support for victims. However, the studies testing the effectiveness of these interventions “had a high risk of bias.”
Support available
Commenting on the research for this news organization, Roberta Gebhard, DO, past president of the American Medical Women’s Association (AMWA) and a member of the advisory board for Physician Just Equity, called it a “good study, large, international, and well-written.”
Dr. Gebhard, a member of the Governing Council for the American Medical Association Women Physician Section, was not associated with this study but said she is currently researching women who left medical school and residency.
“A common reason for leaving is being bullied. Bullying is often not reported and if reported, often not addressed. Or, if addressed, the person who reports it is often retaliated against, which is a common experience, especially in women.”
She advised female physicians who are bullied to get support from other female physicians – for example, by joining the AMWA, which has an online women’s leadership group.
“Having other women physicians throughout the country you can call for advice and support can be helpful,” said Dr. Gebhard, a family practice physician based in Grand Island, New York.
Dr. Van Spall receives support from the Canadian Institutes of Health Research, the Heart and Stroke Foundation, the Women As One Escalator Award, and McMaster Department of Medicine. The study authors and Dr. Gebhard have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Talking about guns: Website helps physicians follow through on pledge
The group has developed a national resource for clinicians who wish to address the problem of gun violence deaths in the United States, which continue to mount by the day.
Signatures came quickly in 2018 after the Annals of Internal Medicine asked physicians to sign a formal pledge in which they commit to talking with their patients about firearms. To date, the list has grown to more than 3,600, and it remains open for additional signatories.
The effort built on data showing that before people commit violence with firearms, they often have notable risk factors that prompt them to see a physician.
At the time the pledge campaign was launched, frustration and despair had hit new highs after the school shooting of Feb. 14, 2018, in Parkland, Florida, in which 17 people were killed. That occurred just 4 months after the mass shooting in Las Vegas, Nevada, on Oct. 1, 2017, in which 58 people were gunned down.
An editorial by Garen J. Wintemute, MD, MPH, helped kick off the drive.
More deaths than WWII combat fatalities
Dr. Wintemute cited some grim statistics, writing that “nationwide in 2016, there was an average of 97 deaths from firearm violence per day: 35,476 altogether. In the 10 years ending with 2016, deaths of U.S. civilians from firearm violence exceeded American combat fatalities in World War II.”
Amy Barnhorst, MD, vice chair of psychiatry at UC Davis, who was one of the early signers of the pledge, told this news organization that data analyst Rocco Pallin, MPH, with the UC Davis Violence Prevention Research Program (VPRP), quickly started managing commitments to the pledge and developed a “What You Can Do” intervention for physicians looking for help on how to prevent firearm injury and death.
Those efforts snowballed, and a need arose for a centralized public resource. In 2019, the state of California gave $3.8 million to the VPRP, which helped launch the BulletPoints Project, which Dr. Barnhorst now directs.
The website provides clinicians with evidence-based direction on how to have the conversations with patients. It walks them through various scenarios and details what can be done if what they learn during a patient interview requires action.
Dr. Barnhorst said the team is working on formalized online educational courses for mental health professionals and medical clinicians that will be hosted through various national organizations.
Christine Laine, MD, editor-in-chief of the Annals of Internal Medicine, said in an interview that although almost 4,000 persons have made the pledge, that number should be higher. She notes that the American College of Physicians has about 165,000 members, and even that is only a fraction of all physicians and clinicians.
“Signing the pledge helps raise awareness that this is a public health issue and, within the realm of health care providers, that they should be counseling patients about reducing risk, the same way we counsel people to wear bike helmets and use seat belts,” she said.
Dr. Barnhorst says those who don’t want to sign the pledge usually cite time considerations and that they already talk with patients about a list of public health issues. They also say they don’t know how to have the conversations or what they should do if what they hear in the interviews requires action.
“We can’t do anything about the time, but we can do something about the resources,” Dr. Barnhorst said.
Some clinicians, she said, worry that patients will get angry if physicians ask about guns, or they believe it’s illegal to ask.
“But there’s no law preventing physicians from asking these questions,” she said.
Dr. Wintemute told this news organization that he is not discouraged that only about 4,000 have signed the pledge. Rather, he was encouraged that the signatures came so quickly. He also notes that the number of persons who are interested far exceeds the number who have made the pledge.
Boosting the pledge numbers will likely take a new push in the form of published articles, he added, and those are in the works.
Among the next steps is conducting pre- and post-tests to see whether BulletPoints is effectively conveying the information for users, he said.
Another is pushing for advances in petitioning for “extreme risk protection orders,” which would require a gun owner to temporarily relinquish any firearms and ammunition and not purchase additional firearms.
Dr. Wintemute said that currently, Maryland is the only state in which health care professionals can petition for extreme risk protection orders. In any state that has the law, a health care professional can contact law enforcement about “a person who is at very high risk for violence in the very near future” but who has not committed a crime and is not mentally ill and so cannot be legally detained.
For physicians to include gun counseling as a routine part of patient care will likely require hearing from peers who are finding the time to do this effectively and hearing that it matters, he said.
“It’s going to take that on-the-ground diffusion of information, just as it has with vaccine hesitancy,” he said.
He notes that data on how to stop firearm violence are sparse and approaches so far have extrapolated from information on how to stop other health threats, such as smoking and drinking.
But that is changing rapidly, he said: “There’s funding from the CDC for research into the kind of work we’re doing.”
Measuring the success of those efforts is difficult.
One sign of change in the past 3 years, Dr. Wintemute says, is that there’s recognition among health care professionals and the public that this fits into clinicians’ “lane.”
Mass shootings not the largest source of gun violence
Mass shootings continue to dominate news about fatal shootings, but Dr. Barnhorst notes that such shootings represent a very small part – reportedly 1% to 2% – of the firearm deaths in the United States. Almost two-thirds of the deaths are suicides. Domestic violence deaths make up another large sector.
But it’s the mass shootings that stick in the collective U.S. consciousness, and the rising and unrelenting numbers can lead to a sense of futility.
Dr. Barnhorst, Dr. Laine, and Dr. Wintemute acknowledge they don’t know to what degree physicians’ talking to patients about firearms can help. But they do not doubt it’s worthy of the effort.
Dr. Laine said that during the past year, COVID-19 overshadowed the focus on the pledge, but he notes the signup for the pledge remains open. Information on firearm injury is collected on the Annals website.
Dr. Barnhorst says there is no good answer to the question of how many lives need to be saved before talking with patients about firearms becomes worth the effort. “For me,” she said, “that number is very, very low.”
Dr. Laine puts the number at one.
“If a physician talking to their patients about firearms prevents one suicide, then the intervention is a success,” she said.
Dr. Laine, Dr. Barnhorst, and Dr. Wintemute report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The group has developed a national resource for clinicians who wish to address the problem of gun violence deaths in the United States, which continue to mount by the day.
Signatures came quickly in 2018 after the Annals of Internal Medicine asked physicians to sign a formal pledge in which they commit to talking with their patients about firearms. To date, the list has grown to more than 3,600, and it remains open for additional signatories.
The effort built on data showing that before people commit violence with firearms, they often have notable risk factors that prompt them to see a physician.
At the time the pledge campaign was launched, frustration and despair had hit new highs after the school shooting of Feb. 14, 2018, in Parkland, Florida, in which 17 people were killed. That occurred just 4 months after the mass shooting in Las Vegas, Nevada, on Oct. 1, 2017, in which 58 people were gunned down.
An editorial by Garen J. Wintemute, MD, MPH, helped kick off the drive.
More deaths than WWII combat fatalities
Dr. Wintemute cited some grim statistics, writing that “nationwide in 2016, there was an average of 97 deaths from firearm violence per day: 35,476 altogether. In the 10 years ending with 2016, deaths of U.S. civilians from firearm violence exceeded American combat fatalities in World War II.”
Amy Barnhorst, MD, vice chair of psychiatry at UC Davis, who was one of the early signers of the pledge, told this news organization that data analyst Rocco Pallin, MPH, with the UC Davis Violence Prevention Research Program (VPRP), quickly started managing commitments to the pledge and developed a “What You Can Do” intervention for physicians looking for help on how to prevent firearm injury and death.
Those efforts snowballed, and a need arose for a centralized public resource. In 2019, the state of California gave $3.8 million to the VPRP, which helped launch the BulletPoints Project, which Dr. Barnhorst now directs.
The website provides clinicians with evidence-based direction on how to have the conversations with patients. It walks them through various scenarios and details what can be done if what they learn during a patient interview requires action.
Dr. Barnhorst said the team is working on formalized online educational courses for mental health professionals and medical clinicians that will be hosted through various national organizations.
Christine Laine, MD, editor-in-chief of the Annals of Internal Medicine, said in an interview that although almost 4,000 persons have made the pledge, that number should be higher. She notes that the American College of Physicians has about 165,000 members, and even that is only a fraction of all physicians and clinicians.
“Signing the pledge helps raise awareness that this is a public health issue and, within the realm of health care providers, that they should be counseling patients about reducing risk, the same way we counsel people to wear bike helmets and use seat belts,” she said.
Dr. Barnhorst says those who don’t want to sign the pledge usually cite time considerations and that they already talk with patients about a list of public health issues. They also say they don’t know how to have the conversations or what they should do if what they hear in the interviews requires action.
“We can’t do anything about the time, but we can do something about the resources,” Dr. Barnhorst said.
Some clinicians, she said, worry that patients will get angry if physicians ask about guns, or they believe it’s illegal to ask.
“But there’s no law preventing physicians from asking these questions,” she said.
Dr. Wintemute told this news organization that he is not discouraged that only about 4,000 have signed the pledge. Rather, he was encouraged that the signatures came so quickly. He also notes that the number of persons who are interested far exceeds the number who have made the pledge.
Boosting the pledge numbers will likely take a new push in the form of published articles, he added, and those are in the works.
Among the next steps is conducting pre- and post-tests to see whether BulletPoints is effectively conveying the information for users, he said.
Another is pushing for advances in petitioning for “extreme risk protection orders,” which would require a gun owner to temporarily relinquish any firearms and ammunition and not purchase additional firearms.
Dr. Wintemute said that currently, Maryland is the only state in which health care professionals can petition for extreme risk protection orders. In any state that has the law, a health care professional can contact law enforcement about “a person who is at very high risk for violence in the very near future” but who has not committed a crime and is not mentally ill and so cannot be legally detained.
For physicians to include gun counseling as a routine part of patient care will likely require hearing from peers who are finding the time to do this effectively and hearing that it matters, he said.
“It’s going to take that on-the-ground diffusion of information, just as it has with vaccine hesitancy,” he said.
He notes that data on how to stop firearm violence are sparse and approaches so far have extrapolated from information on how to stop other health threats, such as smoking and drinking.
But that is changing rapidly, he said: “There’s funding from the CDC for research into the kind of work we’re doing.”
Measuring the success of those efforts is difficult.
One sign of change in the past 3 years, Dr. Wintemute says, is that there’s recognition among health care professionals and the public that this fits into clinicians’ “lane.”
Mass shootings not the largest source of gun violence
Mass shootings continue to dominate news about fatal shootings, but Dr. Barnhorst notes that such shootings represent a very small part – reportedly 1% to 2% – of the firearm deaths in the United States. Almost two-thirds of the deaths are suicides. Domestic violence deaths make up another large sector.
But it’s the mass shootings that stick in the collective U.S. consciousness, and the rising and unrelenting numbers can lead to a sense of futility.
Dr. Barnhorst, Dr. Laine, and Dr. Wintemute acknowledge they don’t know to what degree physicians’ talking to patients about firearms can help. But they do not doubt it’s worthy of the effort.
Dr. Laine said that during the past year, COVID-19 overshadowed the focus on the pledge, but he notes the signup for the pledge remains open. Information on firearm injury is collected on the Annals website.
Dr. Barnhorst says there is no good answer to the question of how many lives need to be saved before talking with patients about firearms becomes worth the effort. “For me,” she said, “that number is very, very low.”
Dr. Laine puts the number at one.
“If a physician talking to their patients about firearms prevents one suicide, then the intervention is a success,” she said.
Dr. Laine, Dr. Barnhorst, and Dr. Wintemute report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The group has developed a national resource for clinicians who wish to address the problem of gun violence deaths in the United States, which continue to mount by the day.
Signatures came quickly in 2018 after the Annals of Internal Medicine asked physicians to sign a formal pledge in which they commit to talking with their patients about firearms. To date, the list has grown to more than 3,600, and it remains open for additional signatories.
The effort built on data showing that before people commit violence with firearms, they often have notable risk factors that prompt them to see a physician.
At the time the pledge campaign was launched, frustration and despair had hit new highs after the school shooting of Feb. 14, 2018, in Parkland, Florida, in which 17 people were killed. That occurred just 4 months after the mass shooting in Las Vegas, Nevada, on Oct. 1, 2017, in which 58 people were gunned down.
An editorial by Garen J. Wintemute, MD, MPH, helped kick off the drive.
More deaths than WWII combat fatalities
Dr. Wintemute cited some grim statistics, writing that “nationwide in 2016, there was an average of 97 deaths from firearm violence per day: 35,476 altogether. In the 10 years ending with 2016, deaths of U.S. civilians from firearm violence exceeded American combat fatalities in World War II.”
Amy Barnhorst, MD, vice chair of psychiatry at UC Davis, who was one of the early signers of the pledge, told this news organization that data analyst Rocco Pallin, MPH, with the UC Davis Violence Prevention Research Program (VPRP), quickly started managing commitments to the pledge and developed a “What You Can Do” intervention for physicians looking for help on how to prevent firearm injury and death.
Those efforts snowballed, and a need arose for a centralized public resource. In 2019, the state of California gave $3.8 million to the VPRP, which helped launch the BulletPoints Project, which Dr. Barnhorst now directs.
The website provides clinicians with evidence-based direction on how to have the conversations with patients. It walks them through various scenarios and details what can be done if what they learn during a patient interview requires action.
Dr. Barnhorst said the team is working on formalized online educational courses for mental health professionals and medical clinicians that will be hosted through various national organizations.
Christine Laine, MD, editor-in-chief of the Annals of Internal Medicine, said in an interview that although almost 4,000 persons have made the pledge, that number should be higher. She notes that the American College of Physicians has about 165,000 members, and even that is only a fraction of all physicians and clinicians.
“Signing the pledge helps raise awareness that this is a public health issue and, within the realm of health care providers, that they should be counseling patients about reducing risk, the same way we counsel people to wear bike helmets and use seat belts,” she said.
Dr. Barnhorst says those who don’t want to sign the pledge usually cite time considerations and that they already talk with patients about a list of public health issues. They also say they don’t know how to have the conversations or what they should do if what they hear in the interviews requires action.
“We can’t do anything about the time, but we can do something about the resources,” Dr. Barnhorst said.
Some clinicians, she said, worry that patients will get angry if physicians ask about guns, or they believe it’s illegal to ask.
“But there’s no law preventing physicians from asking these questions,” she said.
Dr. Wintemute told this news organization that he is not discouraged that only about 4,000 have signed the pledge. Rather, he was encouraged that the signatures came so quickly. He also notes that the number of persons who are interested far exceeds the number who have made the pledge.
Boosting the pledge numbers will likely take a new push in the form of published articles, he added, and those are in the works.
Among the next steps is conducting pre- and post-tests to see whether BulletPoints is effectively conveying the information for users, he said.
Another is pushing for advances in petitioning for “extreme risk protection orders,” which would require a gun owner to temporarily relinquish any firearms and ammunition and not purchase additional firearms.
Dr. Wintemute said that currently, Maryland is the only state in which health care professionals can petition for extreme risk protection orders. In any state that has the law, a health care professional can contact law enforcement about “a person who is at very high risk for violence in the very near future” but who has not committed a crime and is not mentally ill and so cannot be legally detained.
For physicians to include gun counseling as a routine part of patient care will likely require hearing from peers who are finding the time to do this effectively and hearing that it matters, he said.
“It’s going to take that on-the-ground diffusion of information, just as it has with vaccine hesitancy,” he said.
He notes that data on how to stop firearm violence are sparse and approaches so far have extrapolated from information on how to stop other health threats, such as smoking and drinking.
But that is changing rapidly, he said: “There’s funding from the CDC for research into the kind of work we’re doing.”
Measuring the success of those efforts is difficult.
One sign of change in the past 3 years, Dr. Wintemute says, is that there’s recognition among health care professionals and the public that this fits into clinicians’ “lane.”
Mass shootings not the largest source of gun violence
Mass shootings continue to dominate news about fatal shootings, but Dr. Barnhorst notes that such shootings represent a very small part – reportedly 1% to 2% – of the firearm deaths in the United States. Almost two-thirds of the deaths are suicides. Domestic violence deaths make up another large sector.
But it’s the mass shootings that stick in the collective U.S. consciousness, and the rising and unrelenting numbers can lead to a sense of futility.
Dr. Barnhorst, Dr. Laine, and Dr. Wintemute acknowledge they don’t know to what degree physicians’ talking to patients about firearms can help. But they do not doubt it’s worthy of the effort.
Dr. Laine said that during the past year, COVID-19 overshadowed the focus on the pledge, but he notes the signup for the pledge remains open. Information on firearm injury is collected on the Annals website.
Dr. Barnhorst says there is no good answer to the question of how many lives need to be saved before talking with patients about firearms becomes worth the effort. “For me,” she said, “that number is very, very low.”
Dr. Laine puts the number at one.
“If a physician talking to their patients about firearms prevents one suicide, then the intervention is a success,” she said.
Dr. Laine, Dr. Barnhorst, and Dr. Wintemute report no relevant financial relationships.
A version of this article first appeared on Medscape.com.