User login
Impact of Lithium on Suicidality in the Veteran Population
Suicide is the tenth leading cause of death in the United States claiming nearly 48,000 individuals in 2019 and is the second leading cause of death among individuals aged 10 to 34 years.1 From 1999 to 2019, the suicide rate increased by 33%.1 In a retrospective study evaluating suicide risk in > 29,000 men, veterans had a greater risk for suicide in all age groups except for the oldest when compared with nonveterans.2 Another study of > 800,000 veterans found that younger veterans were most at risk for suicide.3 Veterans with completed suicides have a high incidence of affective disorders comorbid with substance use disorders, and therefore it is imperative to optimally treat these conditions to address suicidality.4 Additionally, a retrospective case-control study of veterans who died by suicide matched to controls identified that the cases had significantly higher rates of mental health conditions and suicidal ideation. Given that the veteran population is at higher risk of suicide, research of treatments to address suicidal ideation in veterans is needed.5
Lithium and Antisuicidal Properties
Lithium is the oldest treatment for bipolar disorder and is a long-standing first-line option due to its well-established efficacy as a mood stabilizer.6 Lithium’s antisuicidal properties separate it from the other pharmacologic options for bipolar disorder. A possible explanation for lithium’s unique antisuicidal properties is that these effects are mediated by its impact on aggression and impulsivity, which are both linked to an increased suicide risk.7,8 A meta-analysis by Baldessarini and colleagues demonstrated that patients with mood disorders who were prescribed lithium had a 5 times lower risk of suicide and attempts than did those not treated with lithium.9 Lithium’s current place in therapy is in the treatment of bipolar disorder and major depressive disorder augmentation.10-12Smith and colleagues found that in a cohort study of 21,194 veterans diagnosed with mental health conditions and initiated on lithium or valproate, there were no significant differences in associations with suicide observed between these agents over 365 days; however, there was a significant increased risk of suicide among patients discontinuing or modifying lithium within the first 180 days of treatment.13
Currently, lithium is thought to be underutilized at the US Department of Veterans Affairs (VA) Michael E. DeBakey VA Medical Center (MEDVAMC) in Houston, Texas, based on the number of prescriptions of lithium in the large population of veterans seen by mental health clinicians. MEDVAMC is a 538-bed academic teaching hospital serving approximately 130,000 veterans in southeast Texas. The Mental Health Care Line has 73 inpatient beds and an outpatient clinic serving > 12,000 patients annually. By retrospectively evaluating changes in suicidality in a sample of veterans prescribed lithium, we may be able to better understand the role that lithium plays in a population that has a higher suicide rate than does the general population. The primary objective of this study was to evaluate the change in number of suicide attempts from 3 months prior to lithium initiation to 3 months following a 6-month duration of lithium use. The secondary objective was to determine the change in suicidal ideation from the period prior to lithium use to the period following 6 months of lithium use.
Methods
This was a single-site, retrospective chart review conducted between October 2017 and April 2018. Prior to data collection, the MEDVAMC Research and Development committee approved the study as quality assurance research. Patients with an active lithium prescription were identified using the VA Lithium Lab Monitoring Dashboard, which includes all patients on lithium, their lithium level, and other data such as upcoming appointments.
Inclusion criteria consisted of adults who were aged ≥ 18 years, had an active lithium prescription on the date of data extraction, and had an active lithium prescription for at least 6 months. Patients were excluded if they had < 3 months of data before and/or after lithium was used for 6 months, and if they were initiated on lithium outside MEDVAMC. Cumulatively, patients had to have at least 12 months of data: 3 months prior to lithium use, at least 6 months of lithium use, and 9 months after lithium initiation.
Suicide Attempt and Suicidal Ideation Identification
When determining the number of suicide attempts, we recorded 4 data points: Veterans Crisis Line notes documenting suicide attempts, hospital admissions for suicide attempts, suicide behavior reports within the indicated time frame, and mental health progress notes documenting suicide attempts. Suicidal ideation was measured in 4 ways. First, we looked at the percentage of outpatient mental health progress notes documenting suicidal ideation. Second, using the Patient Health Questionnaire-9 (PHQ-9) depression assessments, we looked at the percentage of patients that indicated several days, more than half the days, or nearly every day to the question, “Thoughts that you would be better off dead or of hurting yourself in some way.”14 Third, we recorded the percentage of suicide risk assessments that patients responded yes to both questions on current preoccupation with suicidal thoughts and serious intent and plan to commit suicide with access to guns, stashed pills, or other means. Finally, we noted the percentage of suicide risk assessments where the assessment of risk was moderate or high.
A retrospective electronic health record (EHR) review was performed and the following information was obtained: patient demographics, lithium refill history, concomitant psychotropic medications and psychotherapy, lithium levels, comorbidities at lithium initiation, presence of a high-risk suicide flag in the EHR, suicide risk assessments, suicide behavior reports, Veteran Crisis Line notes, PHQ-9 assessments, and hospital admission and mental health outpatient notes. The lithium therapeutic range of 0.6-1.2 mmol/L is indicated for bipolar disorder and not other indications where the dose is typically titrated to effect rather than level. Medication possession ratio (MPR) was also calculated for lithium (sum of days’ supply for all fills in period ÷ number of days in period). A high-risk suicide flag alerts clinicians and staff that a mental health professional considers the veteran at risk for suicide.15 Statistical analysis was performed using the paired t test for means to assess proportional differences between variables for the primary and secondary outcomes. Descriptive statistics were used to describe the baseline characteristics.
Results
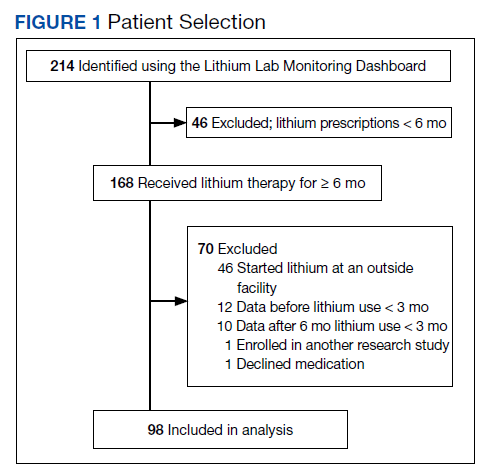
A total of 214 patients with an active prescription for lithium were identified on the Lithium Lab Monitoring Dashboard on October 31, 2017. After exclusion criteria were applied, 98 patients were included in the study (Figure 1). The 2 most common reasons for exclusion were due to patients not being on lithium for at least 6 months and being initiated on lithium at an outside facility. One patient was enrolled in a lithium research study (the medication ordered was lithium/placebo) and another patient refused all psychotropic medications according to the progress notes.
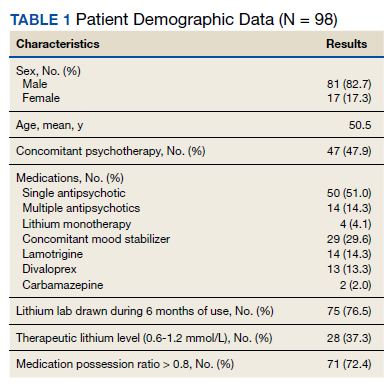
Most of the 98 patients (82.7%) were male with average age 50.5 years (Table 1). Almost half the patients (n = 47) were concomitantly participating in psychotherapy, and 50 (51.0%) patients received at least 1 antipsychotic medication. Twenty-nine patients had an active prescription for an additional mood stabilizer, and only 4 (4.1%) patients received lithium as monotherapy. Only 75 (76.5%) patients had a lithium level drawn during the 6 months of therapy, with 28 (37.3%) patients having a therapeutic lithium level (0.6 - 1.2 mmol/L). Seventy-one patients (72.4% ) were adherent to lithium therapy with a MPR > 0.8.16 Participants had 13 different psychiatric diagnoses at the time of lithium initiation; the most common were bipolar spectrum disorder (n = 38; 38.8%), depressive disorder (n = 27; 27.6%), and posttraumatic stress disorder (PTSD) (n = 26; 26.5%). Of note, 5 patients had a diagnosis of only PTSD without a concomitant mood disorder.
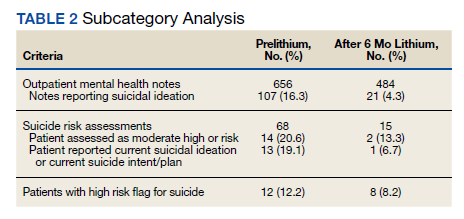
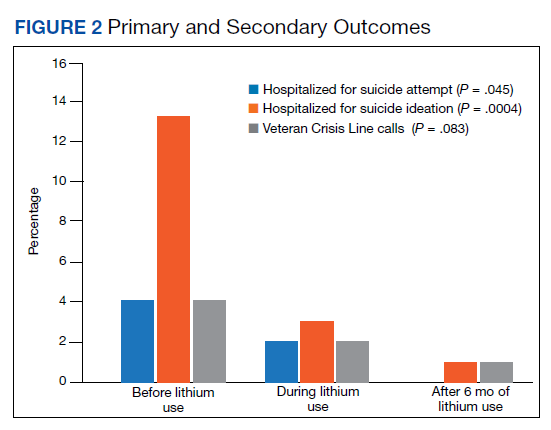
For the primary outcome, hospitalization for a suspected suicide attempt decreased from 4 (4.1%) before lithium use with a mean (SD) 0.04 (0.20) attempts per person to none within 3 months after lithium use for 6 months (t(97) = 2.03, P = .045) (Figure 2). The secondary outcome of hospitalization for suicidal ideations also decreased from 13 (13.3%) before lithium use with a mean (SD) 0.1 (0.3) ideations per person to 1 (1.0%) within 3 months after lithium use for 6 months with a mean (SD) 0.01 (0.1) ideations per person (t(97) = 3.68, P = .0004). Veteran Crisis Line calls also decreased from 4 (4.1%) with a mean (SD) 0.04 (0.2) calls per person to 1 (1.0%) within 3 months after 6 months of lithium with a mean (SD) 0.01 (0.1) calls per person (t(97) = 1.75, P = .08). The comparison of metrics from 3 months before lithium initiation and within 3 months after use saw decreases in all categories (Table 2). Outpatient notes documenting suicidal ideation decreased, as did the number of patients with a high-risk suicide flag.
Discussion
The results of this study suggest lithium may have a role in reducing suicidality in a veteran population. There was a statistically significant reduction in hospitalizations for suicide attempt and suicidal ideation after at least 6 months of lithium use. These results are comparable with a previously published study that observed significant decreases in suicidal behavior and/or hospitalization risks among veterans taking lithium compared with those not taking lithium.17 Our study was similar in respect to the reduced hospitalizations among a veteran population; however, the previous study did not report a difference in suicide attempts and lithium use. This could be related to the longer follow-up time in the previous study (3 years) vs our study (9 months).
Our study identified a significant reduction in Veteran Crisis Line calls after at least 6 months of lithium use. While a reduction in suicidal ideations could be implicated in the decrease in crisis line calls, there may be a confounding variable. It is possible that after lithium initiation, veterans had more frequent contact with health care practitioners due to laboratory test monitoring and follow-up visits and thus had concerns/crises addressed during these interactions ultimately leading to a decreased utilization of the crisis line. Interestingly, there was a reduction in mental health outpatient notes from the prelithium period to the 3-month period that followed 6 months of lithium therapy. However, our study did not report on the number of mental health outpatient notes or visits during the 6-month lithium duration. Additionally, time of year/season could have an impact on suicidality, but this relationship was not evaluated in this study.
The presence of high-risk suicide flags also decreased from the prelithium period to the period 3 months following 6 months of lithium use. High-risk flags are reviewed by the suicide prevention coordinators and mental health professionals every 90 days; therefore, the patients with flags had multiple opportunities for review and thus renewal or discontinuation during the study period. A similar rationale can be applied to the high-risk flag as with the Veteran Crisis Line reduction, although this change could also be representative of a decrease in suicidality. Our study is different from other lithium studies because it included patients with a multitude of psychiatric diagnoses rather than just mood disorders. Five of the patients had a diagnosis of only PTSD and no documented mood disorder at the time of lithium initiation. Additional research is needed on the impact of lithium on suicidality in veterans with PTSD and psychiatric conditions other than mood disorders.
Underutilization of Lithium
Despite widespread knowledge of lithium’s antisuicidal effects, it is underutilized as a mood stabilizer in the US.18 There are various modifiable barriers that impact the prescribing as well as use of lithium. Clinicians may not be fully aware of lithium’s antisuicidal properties and may also have a low level of confidence in patients’ likelihood of adherence to laboratory monitoring.18,19 Due to the narrow therapeutic index of lithium, the consequences of nonadherence to monitoring can be dangerous, which may deter mental health professionals from prescribing this antisuicidal agent. At MEDVAMC, only 72.4% of patients with a lithium prescription had a lithium level drawn within a 6-month period. This could be attributed to patient nonadherence (eg, the test was ordered but the patient did not go) or clinician nonadherence (eg, test was not ordered).
With increased clinician education as well as clinics dedicated to lithium management that allow for closer follow-up, facilities may see an increased level of comfort with lithium use. Lithium management clinics that provide close follow-up may also help address patient-related concerns about adverse effects and allow for close monitoring. To facilitate lithium monitoring at MEDVAMC, mental health practitioners and pharmacists developed a lithium test monitoring menu that serves as a “one-stop shop” for lithium baseline and ongoing test results.
In the future, we may study the impact of this test monitoring menu on lithium prescribing. One may also consider whether lithium levels need to be monitored at different frequencies (eg, less frequently for depression than bipolar disorder) depending on the diagnoses. A better understanding of the necessity for therapeutic monitoring may potentially reduce barriers to prescribing for patients who do not have indications that have a recommended therapeutic range (eg, bipolar disorder).
Lithium Adherence
A primary patient-related concern for low lithium utilization is poor adherence. In this sample, 71 patients (72.4%) were considered fully adherent. This was higher than the rate of 54.1% reported by Sajatovic and colleagues in a study evaluating adherence to lithium and other anticonvulsants in veterans with bipolar disorder.20 Patients’ beliefs about medications and overall health as well as knowledge of the illness and treatment may impact adherence.21 The literature indicates that strategies such as cognitive behavioral therapy (CBT) and didactic lectures positively impact patients’ attitudes about lithium, which ultimately influences adherence.21-23 Involving a family member or significant other in psychotherapy may also improve lithium adherence.21 Specifically in the VA, to address knowledge deficits and improve overall adherence, the Lithium Lab Monitoring Dashboard could be used to identify and invite new lithium starts to educational groups about lithium. These groups could also serve as lithium management clinics.
Limitations
There were several limitations to this study. This was a single-site, retrospective chart review with a small sample size. We studied a cross-section of veterans with only active prescriptions, which limited the sample size. The results should be interpreted cautiously because < 40% of patients who had a level drawn were in the therapeutic range. Patients whose lithium levels were outside of the therapeutic range may have not been fully adherent to the medication. Further analysis based on reason for lithium prescription (eg, bipolar disorder vs depression vs aggression/impulsivity in PTSD) may be helpful in better understanding the results.
Additionally, while we collected data on concomitant mood stabilizers and antipsychotics, we did not collect data on concurrent antidepressant therapy and only 4% of patients were on lithium monotherapy. Data regarding veterans undergoing concurrent CBT during their lithium trial were not assessed in this study and could be considered a confounding factor for future studies. We included any Veteran Crisis Line call in our results regardless of the reason for the call, which could have led to overreporting of this suicidality marker.
Given its small sample size, this study should be considered as hypothesis-generating. Further studies are needed to address lithium’s antisuicidal effects in specific diagnoses (eg, PTSD, anxiety, schizoaffective disorder) to better understand its place in therapy. Studies evaluating the relationship between dosing and suicidality may help provide insight into whether the antisuicidal effect of lithium is dose-dependent and whether a specific dose range rather than a therapeutic level should be targeted for antisuicidal purposes.
Conclusions
People treated for an affective disorder have a 30-times greater risk of suicide than do those in the general population; however, as lithium can reduce the risk of suicide and self-harm, it should continue to have an important role in clinical practice.24 At MEDVAMC, we observed a statistically significant reduction in hospitalization for suicide attempts and suicidal ideation in veterans prescribed lithium following nonfatal suicide behavior and suicidal ideation. Prospective randomized placebo-controlled studies are needed to better understand lithium’s antisuicidal effects.
1. Centers for Disease Control and Prevention. Preventing Suicide Fact Sheet. Updated April 2021. Accessed February 16, 2022. https://www.cdc.gov/suicide/pdf/preventing-suicide-factsheet-2021-508.pdf
2. Kaplan MS, McFarland BH, Huguet N, Valenstein M. Suicide risk and precipitating circumstances among young, middle-aged, and older male veterans. Am J Public Health. 2012;102 Suppl 1(Suppl 1):S131-S137. doi:10.2105/AJPH.2011.300445
3. Zivin K, Kim HM, McCarthy JF, et al. Suicide mortality among individuals receiving treatment for depression in the Veterans Affairs health system: associations with patient and treatment setting characteristics. Am J Public Health. 2007;97(12):2193-2198. doi:10.2105/AJPH.2007.115477
4. Lehmann L, McCormick RA, McCracken L. Suicidal behavior among patients in the VA health care system. Psychiatr Serv. 1995;46(10):1069-1071. doi:10.1176/ps.46.10.1069
5. Dobscha SK, Denneson LM, Kovas AE, et al. Correlates of suicide among veterans treated in primary care: case-control study of a nationally representative sample. J Gen Intern Med. 2014;29(suppl 4):853-860. doi:10.1007/s11606-014-3028-1
6. Malhi GS, Tanious M, Das P, Coulston CM, Berk M. Potential mechanisms of action of lithium in bipolar disorder. Current understanding. CNS Drugs. 2013;27(2):135-153. doi:10.1007/s40263-013-0039-0
7. Kovacsics CE, Gottesman II, Gould TD. Lithium’s antisuicidal efficacy: elucidation of neurobiological targets using endophenotype strategies. Annu Rev Pharmacol Toxicol. 2009;49:175-198. doi:10.1146/annurev.pharmtox.011008.145557
8. Mann JJ, Waternaux C, Haas GL, Malone KM. Toward a clinical model of suicidal behavior in psychiatric patients. Am J Psychiatry. 1999;156(2):181-189. doi:10.1176/ajp.156.2.181
9. Baldessarini RJ, Tondo L, Davis P, Pompili M, Goodwin FK, Hennen J. Decreased risk of suicides and attempts during long-term lithium treatment: a meta-analytic review [published correction appears in Bipolar Disord. 2007 May;9(3):314]. Bipolar Disord. 2006;8(5 Pt 2):625-639. doi:10.1111/j.1399-5618.2006.00344.x
10. Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018;20(2):97-170. doi:10.1111/bdi.12609
11. Stein G, Bernadt M. Lithium augmentation therapy in tricyclic-resistant depression. A controlled trial using lithium in low and normal doses. Br J Psychiatry. 1993;162:634-640. doi:10.1192/bjp.162.5.634
12. Bauer M, Bschor T, Kunz D, Berghöfer A, Ströhle A, Müller-Oerlinghausen B. Double-blind, placebo-controlled trial of the use of lithium to augment antidepressant medication in continuation treatment of unipolar major depression. Am J Psychiatry. 2000;157(9):1429-1435. doi:10.1176/appi.ajp.157.9.1429
13. Smith EG, Austin KL, Kim HM, et al. Suicide risk in Veterans Health Administration patients with mental health diagnoses initiating lithium or valproate: a historical prospective cohort study. BMC Psychiatry. 2014;14:357. Published 2014 Dec 17. doi:10.1186/s12888-014-0357-x
14. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606-613. doi:10.1046/j.1525-1497.2001.016009606.x
15. US Department of Veterans Affairs, Veterans Health Administration. Use of patient record flags to identify patients at high risk for suicide. VHA Directive 2008-036. Published July 18, 2008. Accessed February 7, 2022. www.va.gov/vhapublications/ViewPublication.asp?pub_ID=1719
16. Sylvia LG, Reilly-Harrington NA, Leon AC, et al. Medication adherence in a comparative effectiveness trial for bipolar disorder. Acta Psychiatr Scand. 2014;129(5):359-365. doi:10.1111/acps.12202
17. Yerevanian BI, Koek RJ, Mintz J. Bipolar pharmacotherapy and suicidal behavior. Part I: Lithium, divalproex and carbamazepine. J Affect Disord. 2007;103(1-3):5-11. doi:10.1016/j.jad.2007.05.019
18. Post RM. The New News about Lithium: An Underutilized Treatment in the United States. Neuropsychopharmacology. 2018;43(5):1174-1179. doi:10.1038/npp.2017.238
19. Öhlund L, Ott M, Oja S, et al. Reasons for lithium discontinuation in men and women with bipolar disorder: a retrospective cohort study [published correction appears in BMC Psychiatry. 2018 Oct 3;18(1):322]. BMC Psychiatry. 2018;18(1):37. Published 2018 Feb 7. doi:10.1186/s12888-018-1622-1
20. Sajatovic M, Valenstein M, Blow F, Ganoczy D, Ignacio R. Treatment adherence with lithium and anticonvulsant medications among patients with bipolar disorder. Psychiatr Serv. 2007;58(6):855-863. doi:10.1176/ps.2007.58.6.855
21. Chakrabarti S. Treatment-adherence in bipolar disorder: A patient-centred approach. World J Psychiatry. 2016;6(4):399-409. Published 2016 Dec 22. doi:10.5498/wjp.v6.i4.399
22. Gaudiano BA, Weinstock LM, Miller IW. Improving treatment adherence in bipolar disorder: a review of current psychosocial treatment efficacy and recommendations for future treatment development. Behav Modif. 2008;32(3):267-301. doi:10.1177/0145445507309023
23. Peet M, Harvey NS. Lithium maintenance: 1. A standard education programme for patients. Br J Psychiatry. 1991;158:197-200. doi:10.1192/bjp.158.2.197
24. Cipriani A, Hawton K, Stockton S, Geddes JR. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis. BMJ. 2013;346:f3646. doi:10.1136/bmj.f3646
Suicide is the tenth leading cause of death in the United States claiming nearly 48,000 individuals in 2019 and is the second leading cause of death among individuals aged 10 to 34 years.1 From 1999 to 2019, the suicide rate increased by 33%.1 In a retrospective study evaluating suicide risk in > 29,000 men, veterans had a greater risk for suicide in all age groups except for the oldest when compared with nonveterans.2 Another study of > 800,000 veterans found that younger veterans were most at risk for suicide.3 Veterans with completed suicides have a high incidence of affective disorders comorbid with substance use disorders, and therefore it is imperative to optimally treat these conditions to address suicidality.4 Additionally, a retrospective case-control study of veterans who died by suicide matched to controls identified that the cases had significantly higher rates of mental health conditions and suicidal ideation. Given that the veteran population is at higher risk of suicide, research of treatments to address suicidal ideation in veterans is needed.5
Lithium and Antisuicidal Properties
Lithium is the oldest treatment for bipolar disorder and is a long-standing first-line option due to its well-established efficacy as a mood stabilizer.6 Lithium’s antisuicidal properties separate it from the other pharmacologic options for bipolar disorder. A possible explanation for lithium’s unique antisuicidal properties is that these effects are mediated by its impact on aggression and impulsivity, which are both linked to an increased suicide risk.7,8 A meta-analysis by Baldessarini and colleagues demonstrated that patients with mood disorders who were prescribed lithium had a 5 times lower risk of suicide and attempts than did those not treated with lithium.9 Lithium’s current place in therapy is in the treatment of bipolar disorder and major depressive disorder augmentation.10-12Smith and colleagues found that in a cohort study of 21,194 veterans diagnosed with mental health conditions and initiated on lithium or valproate, there were no significant differences in associations with suicide observed between these agents over 365 days; however, there was a significant increased risk of suicide among patients discontinuing or modifying lithium within the first 180 days of treatment.13
Currently, lithium is thought to be underutilized at the US Department of Veterans Affairs (VA) Michael E. DeBakey VA Medical Center (MEDVAMC) in Houston, Texas, based on the number of prescriptions of lithium in the large population of veterans seen by mental health clinicians. MEDVAMC is a 538-bed academic teaching hospital serving approximately 130,000 veterans in southeast Texas. The Mental Health Care Line has 73 inpatient beds and an outpatient clinic serving > 12,000 patients annually. By retrospectively evaluating changes in suicidality in a sample of veterans prescribed lithium, we may be able to better understand the role that lithium plays in a population that has a higher suicide rate than does the general population. The primary objective of this study was to evaluate the change in number of suicide attempts from 3 months prior to lithium initiation to 3 months following a 6-month duration of lithium use. The secondary objective was to determine the change in suicidal ideation from the period prior to lithium use to the period following 6 months of lithium use.
Methods
This was a single-site, retrospective chart review conducted between October 2017 and April 2018. Prior to data collection, the MEDVAMC Research and Development committee approved the study as quality assurance research. Patients with an active lithium prescription were identified using the VA Lithium Lab Monitoring Dashboard, which includes all patients on lithium, their lithium level, and other data such as upcoming appointments.
Inclusion criteria consisted of adults who were aged ≥ 18 years, had an active lithium prescription on the date of data extraction, and had an active lithium prescription for at least 6 months. Patients were excluded if they had < 3 months of data before and/or after lithium was used for 6 months, and if they were initiated on lithium outside MEDVAMC. Cumulatively, patients had to have at least 12 months of data: 3 months prior to lithium use, at least 6 months of lithium use, and 9 months after lithium initiation.
Suicide Attempt and Suicidal Ideation Identification
When determining the number of suicide attempts, we recorded 4 data points: Veterans Crisis Line notes documenting suicide attempts, hospital admissions for suicide attempts, suicide behavior reports within the indicated time frame, and mental health progress notes documenting suicide attempts. Suicidal ideation was measured in 4 ways. First, we looked at the percentage of outpatient mental health progress notes documenting suicidal ideation. Second, using the Patient Health Questionnaire-9 (PHQ-9) depression assessments, we looked at the percentage of patients that indicated several days, more than half the days, or nearly every day to the question, “Thoughts that you would be better off dead or of hurting yourself in some way.”14 Third, we recorded the percentage of suicide risk assessments that patients responded yes to both questions on current preoccupation with suicidal thoughts and serious intent and plan to commit suicide with access to guns, stashed pills, or other means. Finally, we noted the percentage of suicide risk assessments where the assessment of risk was moderate or high.
A retrospective electronic health record (EHR) review was performed and the following information was obtained: patient demographics, lithium refill history, concomitant psychotropic medications and psychotherapy, lithium levels, comorbidities at lithium initiation, presence of a high-risk suicide flag in the EHR, suicide risk assessments, suicide behavior reports, Veteran Crisis Line notes, PHQ-9 assessments, and hospital admission and mental health outpatient notes. The lithium therapeutic range of 0.6-1.2 mmol/L is indicated for bipolar disorder and not other indications where the dose is typically titrated to effect rather than level. Medication possession ratio (MPR) was also calculated for lithium (sum of days’ supply for all fills in period ÷ number of days in period). A high-risk suicide flag alerts clinicians and staff that a mental health professional considers the veteran at risk for suicide.15 Statistical analysis was performed using the paired t test for means to assess proportional differences between variables for the primary and secondary outcomes. Descriptive statistics were used to describe the baseline characteristics.
Results
A total of 214 patients with an active prescription for lithium were identified on the Lithium Lab Monitoring Dashboard on October 31, 2017. After exclusion criteria were applied, 98 patients were included in the study (Figure 1). The 2 most common reasons for exclusion were due to patients not being on lithium for at least 6 months and being initiated on lithium at an outside facility. One patient was enrolled in a lithium research study (the medication ordered was lithium/placebo) and another patient refused all psychotropic medications according to the progress notes.
Most of the 98 patients (82.7%) were male with average age 50.5 years (Table 1). Almost half the patients (n = 47) were concomitantly participating in psychotherapy, and 50 (51.0%) patients received at least 1 antipsychotic medication. Twenty-nine patients had an active prescription for an additional mood stabilizer, and only 4 (4.1%) patients received lithium as monotherapy. Only 75 (76.5%) patients had a lithium level drawn during the 6 months of therapy, with 28 (37.3%) patients having a therapeutic lithium level (0.6 - 1.2 mmol/L). Seventy-one patients (72.4% ) were adherent to lithium therapy with a MPR > 0.8.16 Participants had 13 different psychiatric diagnoses at the time of lithium initiation; the most common were bipolar spectrum disorder (n = 38; 38.8%), depressive disorder (n = 27; 27.6%), and posttraumatic stress disorder (PTSD) (n = 26; 26.5%). Of note, 5 patients had a diagnosis of only PTSD without a concomitant mood disorder.
For the primary outcome, hospitalization for a suspected suicide attempt decreased from 4 (4.1%) before lithium use with a mean (SD) 0.04 (0.20) attempts per person to none within 3 months after lithium use for 6 months (t(97) = 2.03, P = .045) (Figure 2). The secondary outcome of hospitalization for suicidal ideations also decreased from 13 (13.3%) before lithium use with a mean (SD) 0.1 (0.3) ideations per person to 1 (1.0%) within 3 months after lithium use for 6 months with a mean (SD) 0.01 (0.1) ideations per person (t(97) = 3.68, P = .0004). Veteran Crisis Line calls also decreased from 4 (4.1%) with a mean (SD) 0.04 (0.2) calls per person to 1 (1.0%) within 3 months after 6 months of lithium with a mean (SD) 0.01 (0.1) calls per person (t(97) = 1.75, P = .08). The comparison of metrics from 3 months before lithium initiation and within 3 months after use saw decreases in all categories (Table 2). Outpatient notes documenting suicidal ideation decreased, as did the number of patients with a high-risk suicide flag.
Discussion
The results of this study suggest lithium may have a role in reducing suicidality in a veteran population. There was a statistically significant reduction in hospitalizations for suicide attempt and suicidal ideation after at least 6 months of lithium use. These results are comparable with a previously published study that observed significant decreases in suicidal behavior and/or hospitalization risks among veterans taking lithium compared with those not taking lithium.17 Our study was similar in respect to the reduced hospitalizations among a veteran population; however, the previous study did not report a difference in suicide attempts and lithium use. This could be related to the longer follow-up time in the previous study (3 years) vs our study (9 months).
Our study identified a significant reduction in Veteran Crisis Line calls after at least 6 months of lithium use. While a reduction in suicidal ideations could be implicated in the decrease in crisis line calls, there may be a confounding variable. It is possible that after lithium initiation, veterans had more frequent contact with health care practitioners due to laboratory test monitoring and follow-up visits and thus had concerns/crises addressed during these interactions ultimately leading to a decreased utilization of the crisis line. Interestingly, there was a reduction in mental health outpatient notes from the prelithium period to the 3-month period that followed 6 months of lithium therapy. However, our study did not report on the number of mental health outpatient notes or visits during the 6-month lithium duration. Additionally, time of year/season could have an impact on suicidality, but this relationship was not evaluated in this study.
The presence of high-risk suicide flags also decreased from the prelithium period to the period 3 months following 6 months of lithium use. High-risk flags are reviewed by the suicide prevention coordinators and mental health professionals every 90 days; therefore, the patients with flags had multiple opportunities for review and thus renewal or discontinuation during the study period. A similar rationale can be applied to the high-risk flag as with the Veteran Crisis Line reduction, although this change could also be representative of a decrease in suicidality. Our study is different from other lithium studies because it included patients with a multitude of psychiatric diagnoses rather than just mood disorders. Five of the patients had a diagnosis of only PTSD and no documented mood disorder at the time of lithium initiation. Additional research is needed on the impact of lithium on suicidality in veterans with PTSD and psychiatric conditions other than mood disorders.
Underutilization of Lithium
Despite widespread knowledge of lithium’s antisuicidal effects, it is underutilized as a mood stabilizer in the US.18 There are various modifiable barriers that impact the prescribing as well as use of lithium. Clinicians may not be fully aware of lithium’s antisuicidal properties and may also have a low level of confidence in patients’ likelihood of adherence to laboratory monitoring.18,19 Due to the narrow therapeutic index of lithium, the consequences of nonadherence to monitoring can be dangerous, which may deter mental health professionals from prescribing this antisuicidal agent. At MEDVAMC, only 72.4% of patients with a lithium prescription had a lithium level drawn within a 6-month period. This could be attributed to patient nonadherence (eg, the test was ordered but the patient did not go) or clinician nonadherence (eg, test was not ordered).
With increased clinician education as well as clinics dedicated to lithium management that allow for closer follow-up, facilities may see an increased level of comfort with lithium use. Lithium management clinics that provide close follow-up may also help address patient-related concerns about adverse effects and allow for close monitoring. To facilitate lithium monitoring at MEDVAMC, mental health practitioners and pharmacists developed a lithium test monitoring menu that serves as a “one-stop shop” for lithium baseline and ongoing test results.
In the future, we may study the impact of this test monitoring menu on lithium prescribing. One may also consider whether lithium levels need to be monitored at different frequencies (eg, less frequently for depression than bipolar disorder) depending on the diagnoses. A better understanding of the necessity for therapeutic monitoring may potentially reduce barriers to prescribing for patients who do not have indications that have a recommended therapeutic range (eg, bipolar disorder).
Lithium Adherence
A primary patient-related concern for low lithium utilization is poor adherence. In this sample, 71 patients (72.4%) were considered fully adherent. This was higher than the rate of 54.1% reported by Sajatovic and colleagues in a study evaluating adherence to lithium and other anticonvulsants in veterans with bipolar disorder.20 Patients’ beliefs about medications and overall health as well as knowledge of the illness and treatment may impact adherence.21 The literature indicates that strategies such as cognitive behavioral therapy (CBT) and didactic lectures positively impact patients’ attitudes about lithium, which ultimately influences adherence.21-23 Involving a family member or significant other in psychotherapy may also improve lithium adherence.21 Specifically in the VA, to address knowledge deficits and improve overall adherence, the Lithium Lab Monitoring Dashboard could be used to identify and invite new lithium starts to educational groups about lithium. These groups could also serve as lithium management clinics.
Limitations
There were several limitations to this study. This was a single-site, retrospective chart review with a small sample size. We studied a cross-section of veterans with only active prescriptions, which limited the sample size. The results should be interpreted cautiously because < 40% of patients who had a level drawn were in the therapeutic range. Patients whose lithium levels were outside of the therapeutic range may have not been fully adherent to the medication. Further analysis based on reason for lithium prescription (eg, bipolar disorder vs depression vs aggression/impulsivity in PTSD) may be helpful in better understanding the results.
Additionally, while we collected data on concomitant mood stabilizers and antipsychotics, we did not collect data on concurrent antidepressant therapy and only 4% of patients were on lithium monotherapy. Data regarding veterans undergoing concurrent CBT during their lithium trial were not assessed in this study and could be considered a confounding factor for future studies. We included any Veteran Crisis Line call in our results regardless of the reason for the call, which could have led to overreporting of this suicidality marker.
Given its small sample size, this study should be considered as hypothesis-generating. Further studies are needed to address lithium’s antisuicidal effects in specific diagnoses (eg, PTSD, anxiety, schizoaffective disorder) to better understand its place in therapy. Studies evaluating the relationship between dosing and suicidality may help provide insight into whether the antisuicidal effect of lithium is dose-dependent and whether a specific dose range rather than a therapeutic level should be targeted for antisuicidal purposes.
Conclusions
People treated for an affective disorder have a 30-times greater risk of suicide than do those in the general population; however, as lithium can reduce the risk of suicide and self-harm, it should continue to have an important role in clinical practice.24 At MEDVAMC, we observed a statistically significant reduction in hospitalization for suicide attempts and suicidal ideation in veterans prescribed lithium following nonfatal suicide behavior and suicidal ideation. Prospective randomized placebo-controlled studies are needed to better understand lithium’s antisuicidal effects.
Suicide is the tenth leading cause of death in the United States claiming nearly 48,000 individuals in 2019 and is the second leading cause of death among individuals aged 10 to 34 years.1 From 1999 to 2019, the suicide rate increased by 33%.1 In a retrospective study evaluating suicide risk in > 29,000 men, veterans had a greater risk for suicide in all age groups except for the oldest when compared with nonveterans.2 Another study of > 800,000 veterans found that younger veterans were most at risk for suicide.3 Veterans with completed suicides have a high incidence of affective disorders comorbid with substance use disorders, and therefore it is imperative to optimally treat these conditions to address suicidality.4 Additionally, a retrospective case-control study of veterans who died by suicide matched to controls identified that the cases had significantly higher rates of mental health conditions and suicidal ideation. Given that the veteran population is at higher risk of suicide, research of treatments to address suicidal ideation in veterans is needed.5
Lithium and Antisuicidal Properties
Lithium is the oldest treatment for bipolar disorder and is a long-standing first-line option due to its well-established efficacy as a mood stabilizer.6 Lithium’s antisuicidal properties separate it from the other pharmacologic options for bipolar disorder. A possible explanation for lithium’s unique antisuicidal properties is that these effects are mediated by its impact on aggression and impulsivity, which are both linked to an increased suicide risk.7,8 A meta-analysis by Baldessarini and colleagues demonstrated that patients with mood disorders who were prescribed lithium had a 5 times lower risk of suicide and attempts than did those not treated with lithium.9 Lithium’s current place in therapy is in the treatment of bipolar disorder and major depressive disorder augmentation.10-12Smith and colleagues found that in a cohort study of 21,194 veterans diagnosed with mental health conditions and initiated on lithium or valproate, there were no significant differences in associations with suicide observed between these agents over 365 days; however, there was a significant increased risk of suicide among patients discontinuing or modifying lithium within the first 180 days of treatment.13
Currently, lithium is thought to be underutilized at the US Department of Veterans Affairs (VA) Michael E. DeBakey VA Medical Center (MEDVAMC) in Houston, Texas, based on the number of prescriptions of lithium in the large population of veterans seen by mental health clinicians. MEDVAMC is a 538-bed academic teaching hospital serving approximately 130,000 veterans in southeast Texas. The Mental Health Care Line has 73 inpatient beds and an outpatient clinic serving > 12,000 patients annually. By retrospectively evaluating changes in suicidality in a sample of veterans prescribed lithium, we may be able to better understand the role that lithium plays in a population that has a higher suicide rate than does the general population. The primary objective of this study was to evaluate the change in number of suicide attempts from 3 months prior to lithium initiation to 3 months following a 6-month duration of lithium use. The secondary objective was to determine the change in suicidal ideation from the period prior to lithium use to the period following 6 months of lithium use.
Methods
This was a single-site, retrospective chart review conducted between October 2017 and April 2018. Prior to data collection, the MEDVAMC Research and Development committee approved the study as quality assurance research. Patients with an active lithium prescription were identified using the VA Lithium Lab Monitoring Dashboard, which includes all patients on lithium, their lithium level, and other data such as upcoming appointments.
Inclusion criteria consisted of adults who were aged ≥ 18 years, had an active lithium prescription on the date of data extraction, and had an active lithium prescription for at least 6 months. Patients were excluded if they had < 3 months of data before and/or after lithium was used for 6 months, and if they were initiated on lithium outside MEDVAMC. Cumulatively, patients had to have at least 12 months of data: 3 months prior to lithium use, at least 6 months of lithium use, and 9 months after lithium initiation.
Suicide Attempt and Suicidal Ideation Identification
When determining the number of suicide attempts, we recorded 4 data points: Veterans Crisis Line notes documenting suicide attempts, hospital admissions for suicide attempts, suicide behavior reports within the indicated time frame, and mental health progress notes documenting suicide attempts. Suicidal ideation was measured in 4 ways. First, we looked at the percentage of outpatient mental health progress notes documenting suicidal ideation. Second, using the Patient Health Questionnaire-9 (PHQ-9) depression assessments, we looked at the percentage of patients that indicated several days, more than half the days, or nearly every day to the question, “Thoughts that you would be better off dead or of hurting yourself in some way.”14 Third, we recorded the percentage of suicide risk assessments that patients responded yes to both questions on current preoccupation with suicidal thoughts and serious intent and plan to commit suicide with access to guns, stashed pills, or other means. Finally, we noted the percentage of suicide risk assessments where the assessment of risk was moderate or high.
A retrospective electronic health record (EHR) review was performed and the following information was obtained: patient demographics, lithium refill history, concomitant psychotropic medications and psychotherapy, lithium levels, comorbidities at lithium initiation, presence of a high-risk suicide flag in the EHR, suicide risk assessments, suicide behavior reports, Veteran Crisis Line notes, PHQ-9 assessments, and hospital admission and mental health outpatient notes. The lithium therapeutic range of 0.6-1.2 mmol/L is indicated for bipolar disorder and not other indications where the dose is typically titrated to effect rather than level. Medication possession ratio (MPR) was also calculated for lithium (sum of days’ supply for all fills in period ÷ number of days in period). A high-risk suicide flag alerts clinicians and staff that a mental health professional considers the veteran at risk for suicide.15 Statistical analysis was performed using the paired t test for means to assess proportional differences between variables for the primary and secondary outcomes. Descriptive statistics were used to describe the baseline characteristics.
Results
A total of 214 patients with an active prescription for lithium were identified on the Lithium Lab Monitoring Dashboard on October 31, 2017. After exclusion criteria were applied, 98 patients were included in the study (Figure 1). The 2 most common reasons for exclusion were due to patients not being on lithium for at least 6 months and being initiated on lithium at an outside facility. One patient was enrolled in a lithium research study (the medication ordered was lithium/placebo) and another patient refused all psychotropic medications according to the progress notes.
Most of the 98 patients (82.7%) were male with average age 50.5 years (Table 1). Almost half the patients (n = 47) were concomitantly participating in psychotherapy, and 50 (51.0%) patients received at least 1 antipsychotic medication. Twenty-nine patients had an active prescription for an additional mood stabilizer, and only 4 (4.1%) patients received lithium as monotherapy. Only 75 (76.5%) patients had a lithium level drawn during the 6 months of therapy, with 28 (37.3%) patients having a therapeutic lithium level (0.6 - 1.2 mmol/L). Seventy-one patients (72.4% ) were adherent to lithium therapy with a MPR > 0.8.16 Participants had 13 different psychiatric diagnoses at the time of lithium initiation; the most common were bipolar spectrum disorder (n = 38; 38.8%), depressive disorder (n = 27; 27.6%), and posttraumatic stress disorder (PTSD) (n = 26; 26.5%). Of note, 5 patients had a diagnosis of only PTSD without a concomitant mood disorder.
For the primary outcome, hospitalization for a suspected suicide attempt decreased from 4 (4.1%) before lithium use with a mean (SD) 0.04 (0.20) attempts per person to none within 3 months after lithium use for 6 months (t(97) = 2.03, P = .045) (Figure 2). The secondary outcome of hospitalization for suicidal ideations also decreased from 13 (13.3%) before lithium use with a mean (SD) 0.1 (0.3) ideations per person to 1 (1.0%) within 3 months after lithium use for 6 months with a mean (SD) 0.01 (0.1) ideations per person (t(97) = 3.68, P = .0004). Veteran Crisis Line calls also decreased from 4 (4.1%) with a mean (SD) 0.04 (0.2) calls per person to 1 (1.0%) within 3 months after 6 months of lithium with a mean (SD) 0.01 (0.1) calls per person (t(97) = 1.75, P = .08). The comparison of metrics from 3 months before lithium initiation and within 3 months after use saw decreases in all categories (Table 2). Outpatient notes documenting suicidal ideation decreased, as did the number of patients with a high-risk suicide flag.
Discussion
The results of this study suggest lithium may have a role in reducing suicidality in a veteran population. There was a statistically significant reduction in hospitalizations for suicide attempt and suicidal ideation after at least 6 months of lithium use. These results are comparable with a previously published study that observed significant decreases in suicidal behavior and/or hospitalization risks among veterans taking lithium compared with those not taking lithium.17 Our study was similar in respect to the reduced hospitalizations among a veteran population; however, the previous study did not report a difference in suicide attempts and lithium use. This could be related to the longer follow-up time in the previous study (3 years) vs our study (9 months).
Our study identified a significant reduction in Veteran Crisis Line calls after at least 6 months of lithium use. While a reduction in suicidal ideations could be implicated in the decrease in crisis line calls, there may be a confounding variable. It is possible that after lithium initiation, veterans had more frequent contact with health care practitioners due to laboratory test monitoring and follow-up visits and thus had concerns/crises addressed during these interactions ultimately leading to a decreased utilization of the crisis line. Interestingly, there was a reduction in mental health outpatient notes from the prelithium period to the 3-month period that followed 6 months of lithium therapy. However, our study did not report on the number of mental health outpatient notes or visits during the 6-month lithium duration. Additionally, time of year/season could have an impact on suicidality, but this relationship was not evaluated in this study.
The presence of high-risk suicide flags also decreased from the prelithium period to the period 3 months following 6 months of lithium use. High-risk flags are reviewed by the suicide prevention coordinators and mental health professionals every 90 days; therefore, the patients with flags had multiple opportunities for review and thus renewal or discontinuation during the study period. A similar rationale can be applied to the high-risk flag as with the Veteran Crisis Line reduction, although this change could also be representative of a decrease in suicidality. Our study is different from other lithium studies because it included patients with a multitude of psychiatric diagnoses rather than just mood disorders. Five of the patients had a diagnosis of only PTSD and no documented mood disorder at the time of lithium initiation. Additional research is needed on the impact of lithium on suicidality in veterans with PTSD and psychiatric conditions other than mood disorders.
Underutilization of Lithium
Despite widespread knowledge of lithium’s antisuicidal effects, it is underutilized as a mood stabilizer in the US.18 There are various modifiable barriers that impact the prescribing as well as use of lithium. Clinicians may not be fully aware of lithium’s antisuicidal properties and may also have a low level of confidence in patients’ likelihood of adherence to laboratory monitoring.18,19 Due to the narrow therapeutic index of lithium, the consequences of nonadherence to monitoring can be dangerous, which may deter mental health professionals from prescribing this antisuicidal agent. At MEDVAMC, only 72.4% of patients with a lithium prescription had a lithium level drawn within a 6-month period. This could be attributed to patient nonadherence (eg, the test was ordered but the patient did not go) or clinician nonadherence (eg, test was not ordered).
With increased clinician education as well as clinics dedicated to lithium management that allow for closer follow-up, facilities may see an increased level of comfort with lithium use. Lithium management clinics that provide close follow-up may also help address patient-related concerns about adverse effects and allow for close monitoring. To facilitate lithium monitoring at MEDVAMC, mental health practitioners and pharmacists developed a lithium test monitoring menu that serves as a “one-stop shop” for lithium baseline and ongoing test results.
In the future, we may study the impact of this test monitoring menu on lithium prescribing. One may also consider whether lithium levels need to be monitored at different frequencies (eg, less frequently for depression than bipolar disorder) depending on the diagnoses. A better understanding of the necessity for therapeutic monitoring may potentially reduce barriers to prescribing for patients who do not have indications that have a recommended therapeutic range (eg, bipolar disorder).
Lithium Adherence
A primary patient-related concern for low lithium utilization is poor adherence. In this sample, 71 patients (72.4%) were considered fully adherent. This was higher than the rate of 54.1% reported by Sajatovic and colleagues in a study evaluating adherence to lithium and other anticonvulsants in veterans with bipolar disorder.20 Patients’ beliefs about medications and overall health as well as knowledge of the illness and treatment may impact adherence.21 The literature indicates that strategies such as cognitive behavioral therapy (CBT) and didactic lectures positively impact patients’ attitudes about lithium, which ultimately influences adherence.21-23 Involving a family member or significant other in psychotherapy may also improve lithium adherence.21 Specifically in the VA, to address knowledge deficits and improve overall adherence, the Lithium Lab Monitoring Dashboard could be used to identify and invite new lithium starts to educational groups about lithium. These groups could also serve as lithium management clinics.
Limitations
There were several limitations to this study. This was a single-site, retrospective chart review with a small sample size. We studied a cross-section of veterans with only active prescriptions, which limited the sample size. The results should be interpreted cautiously because < 40% of patients who had a level drawn were in the therapeutic range. Patients whose lithium levels were outside of the therapeutic range may have not been fully adherent to the medication. Further analysis based on reason for lithium prescription (eg, bipolar disorder vs depression vs aggression/impulsivity in PTSD) may be helpful in better understanding the results.
Additionally, while we collected data on concomitant mood stabilizers and antipsychotics, we did not collect data on concurrent antidepressant therapy and only 4% of patients were on lithium monotherapy. Data regarding veterans undergoing concurrent CBT during their lithium trial were not assessed in this study and could be considered a confounding factor for future studies. We included any Veteran Crisis Line call in our results regardless of the reason for the call, which could have led to overreporting of this suicidality marker.
Given its small sample size, this study should be considered as hypothesis-generating. Further studies are needed to address lithium’s antisuicidal effects in specific diagnoses (eg, PTSD, anxiety, schizoaffective disorder) to better understand its place in therapy. Studies evaluating the relationship between dosing and suicidality may help provide insight into whether the antisuicidal effect of lithium is dose-dependent and whether a specific dose range rather than a therapeutic level should be targeted for antisuicidal purposes.
Conclusions
People treated for an affective disorder have a 30-times greater risk of suicide than do those in the general population; however, as lithium can reduce the risk of suicide and self-harm, it should continue to have an important role in clinical practice.24 At MEDVAMC, we observed a statistically significant reduction in hospitalization for suicide attempts and suicidal ideation in veterans prescribed lithium following nonfatal suicide behavior and suicidal ideation. Prospective randomized placebo-controlled studies are needed to better understand lithium’s antisuicidal effects.
1. Centers for Disease Control and Prevention. Preventing Suicide Fact Sheet. Updated April 2021. Accessed February 16, 2022. https://www.cdc.gov/suicide/pdf/preventing-suicide-factsheet-2021-508.pdf
2. Kaplan MS, McFarland BH, Huguet N, Valenstein M. Suicide risk and precipitating circumstances among young, middle-aged, and older male veterans. Am J Public Health. 2012;102 Suppl 1(Suppl 1):S131-S137. doi:10.2105/AJPH.2011.300445
3. Zivin K, Kim HM, McCarthy JF, et al. Suicide mortality among individuals receiving treatment for depression in the Veterans Affairs health system: associations with patient and treatment setting characteristics. Am J Public Health. 2007;97(12):2193-2198. doi:10.2105/AJPH.2007.115477
4. Lehmann L, McCormick RA, McCracken L. Suicidal behavior among patients in the VA health care system. Psychiatr Serv. 1995;46(10):1069-1071. doi:10.1176/ps.46.10.1069
5. Dobscha SK, Denneson LM, Kovas AE, et al. Correlates of suicide among veterans treated in primary care: case-control study of a nationally representative sample. J Gen Intern Med. 2014;29(suppl 4):853-860. doi:10.1007/s11606-014-3028-1
6. Malhi GS, Tanious M, Das P, Coulston CM, Berk M. Potential mechanisms of action of lithium in bipolar disorder. Current understanding. CNS Drugs. 2013;27(2):135-153. doi:10.1007/s40263-013-0039-0
7. Kovacsics CE, Gottesman II, Gould TD. Lithium’s antisuicidal efficacy: elucidation of neurobiological targets using endophenotype strategies. Annu Rev Pharmacol Toxicol. 2009;49:175-198. doi:10.1146/annurev.pharmtox.011008.145557
8. Mann JJ, Waternaux C, Haas GL, Malone KM. Toward a clinical model of suicidal behavior in psychiatric patients. Am J Psychiatry. 1999;156(2):181-189. doi:10.1176/ajp.156.2.181
9. Baldessarini RJ, Tondo L, Davis P, Pompili M, Goodwin FK, Hennen J. Decreased risk of suicides and attempts during long-term lithium treatment: a meta-analytic review [published correction appears in Bipolar Disord. 2007 May;9(3):314]. Bipolar Disord. 2006;8(5 Pt 2):625-639. doi:10.1111/j.1399-5618.2006.00344.x
10. Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018;20(2):97-170. doi:10.1111/bdi.12609
11. Stein G, Bernadt M. Lithium augmentation therapy in tricyclic-resistant depression. A controlled trial using lithium in low and normal doses. Br J Psychiatry. 1993;162:634-640. doi:10.1192/bjp.162.5.634
12. Bauer M, Bschor T, Kunz D, Berghöfer A, Ströhle A, Müller-Oerlinghausen B. Double-blind, placebo-controlled trial of the use of lithium to augment antidepressant medication in continuation treatment of unipolar major depression. Am J Psychiatry. 2000;157(9):1429-1435. doi:10.1176/appi.ajp.157.9.1429
13. Smith EG, Austin KL, Kim HM, et al. Suicide risk in Veterans Health Administration patients with mental health diagnoses initiating lithium or valproate: a historical prospective cohort study. BMC Psychiatry. 2014;14:357. Published 2014 Dec 17. doi:10.1186/s12888-014-0357-x
14. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606-613. doi:10.1046/j.1525-1497.2001.016009606.x
15. US Department of Veterans Affairs, Veterans Health Administration. Use of patient record flags to identify patients at high risk for suicide. VHA Directive 2008-036. Published July 18, 2008. Accessed February 7, 2022. www.va.gov/vhapublications/ViewPublication.asp?pub_ID=1719
16. Sylvia LG, Reilly-Harrington NA, Leon AC, et al. Medication adherence in a comparative effectiveness trial for bipolar disorder. Acta Psychiatr Scand. 2014;129(5):359-365. doi:10.1111/acps.12202
17. Yerevanian BI, Koek RJ, Mintz J. Bipolar pharmacotherapy and suicidal behavior. Part I: Lithium, divalproex and carbamazepine. J Affect Disord. 2007;103(1-3):5-11. doi:10.1016/j.jad.2007.05.019
18. Post RM. The New News about Lithium: An Underutilized Treatment in the United States. Neuropsychopharmacology. 2018;43(5):1174-1179. doi:10.1038/npp.2017.238
19. Öhlund L, Ott M, Oja S, et al. Reasons for lithium discontinuation in men and women with bipolar disorder: a retrospective cohort study [published correction appears in BMC Psychiatry. 2018 Oct 3;18(1):322]. BMC Psychiatry. 2018;18(1):37. Published 2018 Feb 7. doi:10.1186/s12888-018-1622-1
20. Sajatovic M, Valenstein M, Blow F, Ganoczy D, Ignacio R. Treatment adherence with lithium and anticonvulsant medications among patients with bipolar disorder. Psychiatr Serv. 2007;58(6):855-863. doi:10.1176/ps.2007.58.6.855
21. Chakrabarti S. Treatment-adherence in bipolar disorder: A patient-centred approach. World J Psychiatry. 2016;6(4):399-409. Published 2016 Dec 22. doi:10.5498/wjp.v6.i4.399
22. Gaudiano BA, Weinstock LM, Miller IW. Improving treatment adherence in bipolar disorder: a review of current psychosocial treatment efficacy and recommendations for future treatment development. Behav Modif. 2008;32(3):267-301. doi:10.1177/0145445507309023
23. Peet M, Harvey NS. Lithium maintenance: 1. A standard education programme for patients. Br J Psychiatry. 1991;158:197-200. doi:10.1192/bjp.158.2.197
24. Cipriani A, Hawton K, Stockton S, Geddes JR. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis. BMJ. 2013;346:f3646. doi:10.1136/bmj.f3646
1. Centers for Disease Control and Prevention. Preventing Suicide Fact Sheet. Updated April 2021. Accessed February 16, 2022. https://www.cdc.gov/suicide/pdf/preventing-suicide-factsheet-2021-508.pdf
2. Kaplan MS, McFarland BH, Huguet N, Valenstein M. Suicide risk and precipitating circumstances among young, middle-aged, and older male veterans. Am J Public Health. 2012;102 Suppl 1(Suppl 1):S131-S137. doi:10.2105/AJPH.2011.300445
3. Zivin K, Kim HM, McCarthy JF, et al. Suicide mortality among individuals receiving treatment for depression in the Veterans Affairs health system: associations with patient and treatment setting characteristics. Am J Public Health. 2007;97(12):2193-2198. doi:10.2105/AJPH.2007.115477
4. Lehmann L, McCormick RA, McCracken L. Suicidal behavior among patients in the VA health care system. Psychiatr Serv. 1995;46(10):1069-1071. doi:10.1176/ps.46.10.1069
5. Dobscha SK, Denneson LM, Kovas AE, et al. Correlates of suicide among veterans treated in primary care: case-control study of a nationally representative sample. J Gen Intern Med. 2014;29(suppl 4):853-860. doi:10.1007/s11606-014-3028-1
6. Malhi GS, Tanious M, Das P, Coulston CM, Berk M. Potential mechanisms of action of lithium in bipolar disorder. Current understanding. CNS Drugs. 2013;27(2):135-153. doi:10.1007/s40263-013-0039-0
7. Kovacsics CE, Gottesman II, Gould TD. Lithium’s antisuicidal efficacy: elucidation of neurobiological targets using endophenotype strategies. Annu Rev Pharmacol Toxicol. 2009;49:175-198. doi:10.1146/annurev.pharmtox.011008.145557
8. Mann JJ, Waternaux C, Haas GL, Malone KM. Toward a clinical model of suicidal behavior in psychiatric patients. Am J Psychiatry. 1999;156(2):181-189. doi:10.1176/ajp.156.2.181
9. Baldessarini RJ, Tondo L, Davis P, Pompili M, Goodwin FK, Hennen J. Decreased risk of suicides and attempts during long-term lithium treatment: a meta-analytic review [published correction appears in Bipolar Disord. 2007 May;9(3):314]. Bipolar Disord. 2006;8(5 Pt 2):625-639. doi:10.1111/j.1399-5618.2006.00344.x
10. Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018;20(2):97-170. doi:10.1111/bdi.12609
11. Stein G, Bernadt M. Lithium augmentation therapy in tricyclic-resistant depression. A controlled trial using lithium in low and normal doses. Br J Psychiatry. 1993;162:634-640. doi:10.1192/bjp.162.5.634
12. Bauer M, Bschor T, Kunz D, Berghöfer A, Ströhle A, Müller-Oerlinghausen B. Double-blind, placebo-controlled trial of the use of lithium to augment antidepressant medication in continuation treatment of unipolar major depression. Am J Psychiatry. 2000;157(9):1429-1435. doi:10.1176/appi.ajp.157.9.1429
13. Smith EG, Austin KL, Kim HM, et al. Suicide risk in Veterans Health Administration patients with mental health diagnoses initiating lithium or valproate: a historical prospective cohort study. BMC Psychiatry. 2014;14:357. Published 2014 Dec 17. doi:10.1186/s12888-014-0357-x
14. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606-613. doi:10.1046/j.1525-1497.2001.016009606.x
15. US Department of Veterans Affairs, Veterans Health Administration. Use of patient record flags to identify patients at high risk for suicide. VHA Directive 2008-036. Published July 18, 2008. Accessed February 7, 2022. www.va.gov/vhapublications/ViewPublication.asp?pub_ID=1719
16. Sylvia LG, Reilly-Harrington NA, Leon AC, et al. Medication adherence in a comparative effectiveness trial for bipolar disorder. Acta Psychiatr Scand. 2014;129(5):359-365. doi:10.1111/acps.12202
17. Yerevanian BI, Koek RJ, Mintz J. Bipolar pharmacotherapy and suicidal behavior. Part I: Lithium, divalproex and carbamazepine. J Affect Disord. 2007;103(1-3):5-11. doi:10.1016/j.jad.2007.05.019
18. Post RM. The New News about Lithium: An Underutilized Treatment in the United States. Neuropsychopharmacology. 2018;43(5):1174-1179. doi:10.1038/npp.2017.238
19. Öhlund L, Ott M, Oja S, et al. Reasons for lithium discontinuation in men and women with bipolar disorder: a retrospective cohort study [published correction appears in BMC Psychiatry. 2018 Oct 3;18(1):322]. BMC Psychiatry. 2018;18(1):37. Published 2018 Feb 7. doi:10.1186/s12888-018-1622-1
20. Sajatovic M, Valenstein M, Blow F, Ganoczy D, Ignacio R. Treatment adherence with lithium and anticonvulsant medications among patients with bipolar disorder. Psychiatr Serv. 2007;58(6):855-863. doi:10.1176/ps.2007.58.6.855
21. Chakrabarti S. Treatment-adherence in bipolar disorder: A patient-centred approach. World J Psychiatry. 2016;6(4):399-409. Published 2016 Dec 22. doi:10.5498/wjp.v6.i4.399
22. Gaudiano BA, Weinstock LM, Miller IW. Improving treatment adherence in bipolar disorder: a review of current psychosocial treatment efficacy and recommendations for future treatment development. Behav Modif. 2008;32(3):267-301. doi:10.1177/0145445507309023
23. Peet M, Harvey NS. Lithium maintenance: 1. A standard education programme for patients. Br J Psychiatry. 1991;158:197-200. doi:10.1192/bjp.158.2.197
24. Cipriani A, Hawton K, Stockton S, Geddes JR. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis. BMJ. 2013;346:f3646. doi:10.1136/bmj.f3646
Mindfulness intervention curbs opioid misuse, chronic pain
In a randomized clinical trial, 250 adults with both opioid misuse and chronic pain received either the intervention, called mindfulness-oriented recovery enhancement (MORE), or supportive psychotherapy.
Results showed the first group was twice as likely to reduce opioid misuse after 9 months than the latter group.

The intervention was developed by Eric Garland, PhD, director of the Center on Mindfulness and Integrative Health Intervention Development (C-MIIND), University of Utah, Salt Lake City. “As the largest and longest-term clinical trial of MORE ever conducted, this study definitively establishes the efficacy of MORE as a treatment for chronic pain and opioid misuse,” he told this news organization.
The findings were published online Feb. 28 in JAMA Internal Medicine.
Self-regulation
Study participants included 250 adults (64% women; mean age, 51.8 years) with co-occurring opioid misuse and chronic pain who were randomly allocated to receive MORE or supportive psychotherapy, which served as a control group.
Both interventions were delivered by trained clinical social workers in six primary care clinics in Utah to groups of 6-12 participants across 8 weekly 2-hour sessions.
The MORE intervention, detailed on Dr. Garland’s website, provides sequenced training in mindfulness, reappraisal, and savoring skills.
Mindfulness consisted of meditation on breathing and body sensations to strengthen self-regulation of compulsive opioid use and to mitigate pain and opioid craving by reinterpreting these experiences as innocuous sensory information.
Reappraisal consisted of reframing maladaptive thoughts to decrease negative emotions and engender meaning in life.
Savoring consisted of training in focusing awareness on pleasurable events and sensations to amplify positive emotions and reward.
Fewer depressive symptoms
Through 9 months of follow-up, the MORE group had about a twofold greater likelihood than the supportive psychotherapy group for reduction in opioid misuse (odds ratio [OR], 2.06; 95% confidence interval, 1.17-3.61; P = .01)
“MORE reduced opioid misuse by 45% 9 months after the end of treatment, more than doubling the effect of standard supportive psychotherapy and exceeding the effect size of other therapies for opioid misuse among people with chronic pain,” Dr. Garland said.
Members of the MORE group experienced greater reduction in pain severity and pain-related functional interference compared with members of the control group.
“MORE’s effect size on chronic pain symptoms was greater than that observed for CBT, the current gold standard psychological treatment for chronic pain,” Dr. Garland noted.
Compared with supportive psychotherapy, MORE decreased emotional distress, depressive symptoms, and real-time reports of opioid craving in daily life.
“Although nearly 70% of participants met criteria for depression at the beginning of the trial, on average, patients in MORE no longer exhibited symptoms consistent with major depressive disorder by the end of the study,” Dr. Garland said.
The current study builds on prior studies of MORE showing similar results, as reported previously by this news organization.
MORE can be successfully delivered in routine primary care, Dr. Garland noted. “In this trial, we delivered MORE in conference rooms, break rooms, and lunch rooms at community primary care clinics,” he added.
‘Powerful program’
To date, Dr. Garland has trained more than 450 physicians, nurses, social workers, and psychologists in health care systems across the country to implement MORE as an insurance-reimbursable group visit for patients in need.
One of them is Nancy Sudak, MD, chief well-being officer and director of integrative health, Essentia Health, Duluth, Minn.

“MORE is a very powerful program that teaches patients how to turn down the volume of their pain. I’ve been quite impressed by the power of MORE,” Dr. Sudak told this news organization
She noted that “buy-in” from patients is key – and the more a clinician knows a patient, the easier the buy-in.
“I recruited most of the patients in my groups from my own practice, so I already knew the patients quite well and there wasn’t really a need to sell it,” Dr. Sudak said.
“We have tried to operationalize it through our system and find that, as long as our recruitment techniques are robust enough, it’s not that hard to find patients to fill the groups, especially because chronic pain is just so common,” she added.
Dr. Sudak has found that patients who participate in MORE “bond and learn with each other and support each other. Patients love it, providers love it, and it’s a way to address isolation and loneliness” that can come with certain conditions.
“There are really only upsides to the group visit model and I think we’ll be seeing quite a bit more of it in the future,” she added.
Evidence-based data
Anna Parisi, PhD, is also delivering MORE to patients. She told this news organization, she was “really drawn” to the MORE program because oftentimes patients who require the most sophisticated therapies receive the ones with the least evidence.
This is often “what folks in the community are getting when they’re struggling with substance use,” added Dr. Parisi, a postdoctoral research associate working with Dr. Garland at the University of Utah. Dr. Parisi was not a coauthor on the current study.
“With MORE, all of the strategies and techniques are tied to mechanistic studies of their efficacy, so you know that what you’re delivering has a rationale behind it,” she said.
Like Dr. Sudak, Dr. Parisi said her patients, for the most part, have been receptive to the program. Although at first some were skeptical about mindfulness – with one patient using the term “tree-hugging” – they found immediate benefit even after the first session.
“That really helps them stay motivated to finish the program,” Dr. Parisi said.
This work was supported by a grant from the National Institute on Drug Abuse. Dr. Garland serves as director of the Center on Mindfulness and Integrative Health Intervention Development, which provides MORE, mindfulness-based therapy, and CBT in the context of research trials for no cost to research participants. He receives honoraria and payment for delivering seminars, lectures, and teaching engagements related to training clinicians in MORE and mindfulness and receives royalties from BehaVR and from the sales of books related to MORE outside the submitted work. Dr. Sudak and Dr. Parisi have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a randomized clinical trial, 250 adults with both opioid misuse and chronic pain received either the intervention, called mindfulness-oriented recovery enhancement (MORE), or supportive psychotherapy.
Results showed the first group was twice as likely to reduce opioid misuse after 9 months than the latter group.
The intervention was developed by Eric Garland, PhD, director of the Center on Mindfulness and Integrative Health Intervention Development (C-MIIND), University of Utah, Salt Lake City. “As the largest and longest-term clinical trial of MORE ever conducted, this study definitively establishes the efficacy of MORE as a treatment for chronic pain and opioid misuse,” he told this news organization.
The findings were published online Feb. 28 in JAMA Internal Medicine.
Self-regulation
Study participants included 250 adults (64% women; mean age, 51.8 years) with co-occurring opioid misuse and chronic pain who were randomly allocated to receive MORE or supportive psychotherapy, which served as a control group.
Both interventions were delivered by trained clinical social workers in six primary care clinics in Utah to groups of 6-12 participants across 8 weekly 2-hour sessions.
The MORE intervention, detailed on Dr. Garland’s website, provides sequenced training in mindfulness, reappraisal, and savoring skills.
Mindfulness consisted of meditation on breathing and body sensations to strengthen self-regulation of compulsive opioid use and to mitigate pain and opioid craving by reinterpreting these experiences as innocuous sensory information.
Reappraisal consisted of reframing maladaptive thoughts to decrease negative emotions and engender meaning in life.
Savoring consisted of training in focusing awareness on pleasurable events and sensations to amplify positive emotions and reward.
Fewer depressive symptoms
Through 9 months of follow-up, the MORE group had about a twofold greater likelihood than the supportive psychotherapy group for reduction in opioid misuse (odds ratio [OR], 2.06; 95% confidence interval, 1.17-3.61; P = .01)
“MORE reduced opioid misuse by 45% 9 months after the end of treatment, more than doubling the effect of standard supportive psychotherapy and exceeding the effect size of other therapies for opioid misuse among people with chronic pain,” Dr. Garland said.
Members of the MORE group experienced greater reduction in pain severity and pain-related functional interference compared with members of the control group.
“MORE’s effect size on chronic pain symptoms was greater than that observed for CBT, the current gold standard psychological treatment for chronic pain,” Dr. Garland noted.
Compared with supportive psychotherapy, MORE decreased emotional distress, depressive symptoms, and real-time reports of opioid craving in daily life.
“Although nearly 70% of participants met criteria for depression at the beginning of the trial, on average, patients in MORE no longer exhibited symptoms consistent with major depressive disorder by the end of the study,” Dr. Garland said.
The current study builds on prior studies of MORE showing similar results, as reported previously by this news organization.
MORE can be successfully delivered in routine primary care, Dr. Garland noted. “In this trial, we delivered MORE in conference rooms, break rooms, and lunch rooms at community primary care clinics,” he added.
‘Powerful program’
To date, Dr. Garland has trained more than 450 physicians, nurses, social workers, and psychologists in health care systems across the country to implement MORE as an insurance-reimbursable group visit for patients in need.
One of them is Nancy Sudak, MD, chief well-being officer and director of integrative health, Essentia Health, Duluth, Minn.
“MORE is a very powerful program that teaches patients how to turn down the volume of their pain. I’ve been quite impressed by the power of MORE,” Dr. Sudak told this news organization
She noted that “buy-in” from patients is key – and the more a clinician knows a patient, the easier the buy-in.
“I recruited most of the patients in my groups from my own practice, so I already knew the patients quite well and there wasn’t really a need to sell it,” Dr. Sudak said.
“We have tried to operationalize it through our system and find that, as long as our recruitment techniques are robust enough, it’s not that hard to find patients to fill the groups, especially because chronic pain is just so common,” she added.
Dr. Sudak has found that patients who participate in MORE “bond and learn with each other and support each other. Patients love it, providers love it, and it’s a way to address isolation and loneliness” that can come with certain conditions.
“There are really only upsides to the group visit model and I think we’ll be seeing quite a bit more of it in the future,” she added.
Evidence-based data
Anna Parisi, PhD, is also delivering MORE to patients. She told this news organization, she was “really drawn” to the MORE program because oftentimes patients who require the most sophisticated therapies receive the ones with the least evidence.
This is often “what folks in the community are getting when they’re struggling with substance use,” added Dr. Parisi, a postdoctoral research associate working with Dr. Garland at the University of Utah. Dr. Parisi was not a coauthor on the current study.
“With MORE, all of the strategies and techniques are tied to mechanistic studies of their efficacy, so you know that what you’re delivering has a rationale behind it,” she said.
Like Dr. Sudak, Dr. Parisi said her patients, for the most part, have been receptive to the program. Although at first some were skeptical about mindfulness – with one patient using the term “tree-hugging” – they found immediate benefit even after the first session.
“That really helps them stay motivated to finish the program,” Dr. Parisi said.
This work was supported by a grant from the National Institute on Drug Abuse. Dr. Garland serves as director of the Center on Mindfulness and Integrative Health Intervention Development, which provides MORE, mindfulness-based therapy, and CBT in the context of research trials for no cost to research participants. He receives honoraria and payment for delivering seminars, lectures, and teaching engagements related to training clinicians in MORE and mindfulness and receives royalties from BehaVR and from the sales of books related to MORE outside the submitted work. Dr. Sudak and Dr. Parisi have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a randomized clinical trial, 250 adults with both opioid misuse and chronic pain received either the intervention, called mindfulness-oriented recovery enhancement (MORE), or supportive psychotherapy.
Results showed the first group was twice as likely to reduce opioid misuse after 9 months than the latter group.
The intervention was developed by Eric Garland, PhD, director of the Center on Mindfulness and Integrative Health Intervention Development (C-MIIND), University of Utah, Salt Lake City. “As the largest and longest-term clinical trial of MORE ever conducted, this study definitively establishes the efficacy of MORE as a treatment for chronic pain and opioid misuse,” he told this news organization.
The findings were published online Feb. 28 in JAMA Internal Medicine.
Self-regulation
Study participants included 250 adults (64% women; mean age, 51.8 years) with co-occurring opioid misuse and chronic pain who were randomly allocated to receive MORE or supportive psychotherapy, which served as a control group.
Both interventions were delivered by trained clinical social workers in six primary care clinics in Utah to groups of 6-12 participants across 8 weekly 2-hour sessions.
The MORE intervention, detailed on Dr. Garland’s website, provides sequenced training in mindfulness, reappraisal, and savoring skills.
Mindfulness consisted of meditation on breathing and body sensations to strengthen self-regulation of compulsive opioid use and to mitigate pain and opioid craving by reinterpreting these experiences as innocuous sensory information.
Reappraisal consisted of reframing maladaptive thoughts to decrease negative emotions and engender meaning in life.
Savoring consisted of training in focusing awareness on pleasurable events and sensations to amplify positive emotions and reward.
Fewer depressive symptoms
Through 9 months of follow-up, the MORE group had about a twofold greater likelihood than the supportive psychotherapy group for reduction in opioid misuse (odds ratio [OR], 2.06; 95% confidence interval, 1.17-3.61; P = .01)
“MORE reduced opioid misuse by 45% 9 months after the end of treatment, more than doubling the effect of standard supportive psychotherapy and exceeding the effect size of other therapies for opioid misuse among people with chronic pain,” Dr. Garland said.
Members of the MORE group experienced greater reduction in pain severity and pain-related functional interference compared with members of the control group.
“MORE’s effect size on chronic pain symptoms was greater than that observed for CBT, the current gold standard psychological treatment for chronic pain,” Dr. Garland noted.
Compared with supportive psychotherapy, MORE decreased emotional distress, depressive symptoms, and real-time reports of opioid craving in daily life.
“Although nearly 70% of participants met criteria for depression at the beginning of the trial, on average, patients in MORE no longer exhibited symptoms consistent with major depressive disorder by the end of the study,” Dr. Garland said.
The current study builds on prior studies of MORE showing similar results, as reported previously by this news organization.
MORE can be successfully delivered in routine primary care, Dr. Garland noted. “In this trial, we delivered MORE in conference rooms, break rooms, and lunch rooms at community primary care clinics,” he added.
‘Powerful program’
To date, Dr. Garland has trained more than 450 physicians, nurses, social workers, and psychologists in health care systems across the country to implement MORE as an insurance-reimbursable group visit for patients in need.
One of them is Nancy Sudak, MD, chief well-being officer and director of integrative health, Essentia Health, Duluth, Minn.
“MORE is a very powerful program that teaches patients how to turn down the volume of their pain. I’ve been quite impressed by the power of MORE,” Dr. Sudak told this news organization
She noted that “buy-in” from patients is key – and the more a clinician knows a patient, the easier the buy-in.
“I recruited most of the patients in my groups from my own practice, so I already knew the patients quite well and there wasn’t really a need to sell it,” Dr. Sudak said.
“We have tried to operationalize it through our system and find that, as long as our recruitment techniques are robust enough, it’s not that hard to find patients to fill the groups, especially because chronic pain is just so common,” she added.
Dr. Sudak has found that patients who participate in MORE “bond and learn with each other and support each other. Patients love it, providers love it, and it’s a way to address isolation and loneliness” that can come with certain conditions.
“There are really only upsides to the group visit model and I think we’ll be seeing quite a bit more of it in the future,” she added.
Evidence-based data
Anna Parisi, PhD, is also delivering MORE to patients. She told this news organization, she was “really drawn” to the MORE program because oftentimes patients who require the most sophisticated therapies receive the ones with the least evidence.
This is often “what folks in the community are getting when they’re struggling with substance use,” added Dr. Parisi, a postdoctoral research associate working with Dr. Garland at the University of Utah. Dr. Parisi was not a coauthor on the current study.
“With MORE, all of the strategies and techniques are tied to mechanistic studies of their efficacy, so you know that what you’re delivering has a rationale behind it,” she said.
Like Dr. Sudak, Dr. Parisi said her patients, for the most part, have been receptive to the program. Although at first some were skeptical about mindfulness – with one patient using the term “tree-hugging” – they found immediate benefit even after the first session.
“That really helps them stay motivated to finish the program,” Dr. Parisi said.
This work was supported by a grant from the National Institute on Drug Abuse. Dr. Garland serves as director of the Center on Mindfulness and Integrative Health Intervention Development, which provides MORE, mindfulness-based therapy, and CBT in the context of research trials for no cost to research participants. He receives honoraria and payment for delivering seminars, lectures, and teaching engagements related to training clinicians in MORE and mindfulness and receives royalties from BehaVR and from the sales of books related to MORE outside the submitted work. Dr. Sudak and Dr. Parisi have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
‘Robust’ increase in tics during the pandemic explained?
The findings should help answer questions surrounding a recent increase in tic disorders, lead author Jessica Frey, MD, a movement disorders fellow at the University of Florida, Gainesville, told this news organization.

“We’re trying to learn why there are new-onset explosive tic disorders [or] functional tic disorders, and to find ways to educate patients, parents, and the general public about what Tourette syndrome looks like – and how we can help patients have a better quality of life,” Dr. Frey said.
The findings will be presented at the American Academy of Neurology 2022 annual meeting in April.
‘Robust’ increase
A neurologic disorder that causes sudden repetitive involuntary muscle movements and sounds, Tourette syndrome typically develops in childhood, worsens in adolescence, and improves or completely disappears in adulthood, Dr. Frey noted.
The condition is often negatively portrayed in films, showing people using obscene gestures or vulgar language, she said. Although social media can be an “empowering tool” for tic sufferers, it is unregulated and can be a vehicle for “false information,” she added.
Dr. Frey noted that during the pandemic there has been a “robust” increase in use by teens of social media, particularly TikTok. At the same time, there have been reports of teen girls experiencing “explosive tic onset” that mimics videos from TikTok influencers.
The new analysis included 20 teens with a tic disorder, ranging in age from 11 to 21 years (average age, 16 years). About 45% of participants identified as male, 45% as female, and 10% as nonbinary.
The nature of the tic disorder varied widely among participants. Some had experienced tics for many years, while others only developed tics during the pandemic.
Participants completed a detailed survey, part of which inquired about where they received information about tics, such as from a doctor, media, parents, or teachers.
They were also asked to rank various social media platforms, including Tik Tok, Facebook, and YouTube on a five-point Likert scale as an information source about tics.
In addition, the survey inquired about tic severity and frequency, quality of life, and whether the pandemic or social media affected respondents’ tics.
Worsens quality of life
Results showed 65% of respondents used social media at least four to five times per day for an average of 5.6 hours per day. Approximately 90% reported increased use of social media during COVID.
Only 5% of participants reported using social media to provide information about tics.
About half of respondents indicated social media adversely affected their tics, and 85% said their tic frequency worsened during COVID.
Dr. Frey noted that because teens had to attend school virtually, that may have led to increased hours spent online.
There was no significant correlation between social media use and self-reported frequency of tics since the onset of COVID (Pearson correlation coefficient [R], –0.0055, P = .982).
However, there was a statistically significant correlation between social media use and tic severity (R, –0.496, P = .026) and quality of life (R, –0.447, P = .048).
These results suggest teenagers did not develop more tics, but rather the tics they already had worsened and affected their quality of life, Dr. Frey noted. She added that teens sometimes injure themselves while experiencing tics.
The full study has now enrolled 50 participants, and investigators anticipate that number to go up to 80. “We’re hoping to see more patterns emerge when we have a larger cohort of data available,” said Dr. Frey.
Asking parents to weigh in on the impact of social media on their child’s tic condition would be “a great idea for a follow-up study,” she added.
Symptoms exacerbated
Commenting on the findings, Tamara Pringsheim, MD, professor in the department of clinical neurosciences, psychiatry, pediatrics, and community health sciences at the University of Calgary (Alta.), said she also has noticed the impact of increased social media use on young patients with tics during the pandemic.

“Many young people report that seeing other people with tics, or ticlike behaviors, can exacerbate their own symptoms,” said Dr. Pringsheim, who is the university’s program lead on Tourette and pediatric movement disorders.
She noted a principle of the Comprehensive Behavioral Intervention for Tics, which is a nonpharmacologic technique demonstrated to reduce tic severity, is to identify antecedents or triggers for tics, and to learn to manage them. It might be a good idea to remind young patients of this principle, said Dr. Pringsheim, who was not associated with the current research.
“I suggest to young people who report specific social media content as a trigger for symptoms to recognize the effect of the exposure on their symptoms and make an informed choice about what they view and how much time they spend on social media,” she added.
The study did not receive any outside funding support. Dr. Frey has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The findings should help answer questions surrounding a recent increase in tic disorders, lead author Jessica Frey, MD, a movement disorders fellow at the University of Florida, Gainesville, told this news organization.
“We’re trying to learn why there are new-onset explosive tic disorders [or] functional tic disorders, and to find ways to educate patients, parents, and the general public about what Tourette syndrome looks like – and how we can help patients have a better quality of life,” Dr. Frey said.
The findings will be presented at the American Academy of Neurology 2022 annual meeting in April.
‘Robust’ increase
A neurologic disorder that causes sudden repetitive involuntary muscle movements and sounds, Tourette syndrome typically develops in childhood, worsens in adolescence, and improves or completely disappears in adulthood, Dr. Frey noted.
The condition is often negatively portrayed in films, showing people using obscene gestures or vulgar language, she said. Although social media can be an “empowering tool” for tic sufferers, it is unregulated and can be a vehicle for “false information,” she added.
Dr. Frey noted that during the pandemic there has been a “robust” increase in use by teens of social media, particularly TikTok. At the same time, there have been reports of teen girls experiencing “explosive tic onset” that mimics videos from TikTok influencers.
The new analysis included 20 teens with a tic disorder, ranging in age from 11 to 21 years (average age, 16 years). About 45% of participants identified as male, 45% as female, and 10% as nonbinary.
The nature of the tic disorder varied widely among participants. Some had experienced tics for many years, while others only developed tics during the pandemic.
Participants completed a detailed survey, part of which inquired about where they received information about tics, such as from a doctor, media, parents, or teachers.
They were also asked to rank various social media platforms, including Tik Tok, Facebook, and YouTube on a five-point Likert scale as an information source about tics.
In addition, the survey inquired about tic severity and frequency, quality of life, and whether the pandemic or social media affected respondents’ tics.
Worsens quality of life
Results showed 65% of respondents used social media at least four to five times per day for an average of 5.6 hours per day. Approximately 90% reported increased use of social media during COVID.
Only 5% of participants reported using social media to provide information about tics.
About half of respondents indicated social media adversely affected their tics, and 85% said their tic frequency worsened during COVID.
Dr. Frey noted that because teens had to attend school virtually, that may have led to increased hours spent online.
There was no significant correlation between social media use and self-reported frequency of tics since the onset of COVID (Pearson correlation coefficient [R], –0.0055, P = .982).
However, there was a statistically significant correlation between social media use and tic severity (R, –0.496, P = .026) and quality of life (R, –0.447, P = .048).
These results suggest teenagers did not develop more tics, but rather the tics they already had worsened and affected their quality of life, Dr. Frey noted. She added that teens sometimes injure themselves while experiencing tics.
The full study has now enrolled 50 participants, and investigators anticipate that number to go up to 80. “We’re hoping to see more patterns emerge when we have a larger cohort of data available,” said Dr. Frey.
Asking parents to weigh in on the impact of social media on their child’s tic condition would be “a great idea for a follow-up study,” she added.
Symptoms exacerbated
Commenting on the findings, Tamara Pringsheim, MD, professor in the department of clinical neurosciences, psychiatry, pediatrics, and community health sciences at the University of Calgary (Alta.), said she also has noticed the impact of increased social media use on young patients with tics during the pandemic.
“Many young people report that seeing other people with tics, or ticlike behaviors, can exacerbate their own symptoms,” said Dr. Pringsheim, who is the university’s program lead on Tourette and pediatric movement disorders.
She noted a principle of the Comprehensive Behavioral Intervention for Tics, which is a nonpharmacologic technique demonstrated to reduce tic severity, is to identify antecedents or triggers for tics, and to learn to manage them. It might be a good idea to remind young patients of this principle, said Dr. Pringsheim, who was not associated with the current research.
“I suggest to young people who report specific social media content as a trigger for symptoms to recognize the effect of the exposure on their symptoms and make an informed choice about what they view and how much time they spend on social media,” she added.
The study did not receive any outside funding support. Dr. Frey has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The findings should help answer questions surrounding a recent increase in tic disorders, lead author Jessica Frey, MD, a movement disorders fellow at the University of Florida, Gainesville, told this news organization.
“We’re trying to learn why there are new-onset explosive tic disorders [or] functional tic disorders, and to find ways to educate patients, parents, and the general public about what Tourette syndrome looks like – and how we can help patients have a better quality of life,” Dr. Frey said.
The findings will be presented at the American Academy of Neurology 2022 annual meeting in April.
‘Robust’ increase
A neurologic disorder that causes sudden repetitive involuntary muscle movements and sounds, Tourette syndrome typically develops in childhood, worsens in adolescence, and improves or completely disappears in adulthood, Dr. Frey noted.
The condition is often negatively portrayed in films, showing people using obscene gestures or vulgar language, she said. Although social media can be an “empowering tool” for tic sufferers, it is unregulated and can be a vehicle for “false information,” she added.
Dr. Frey noted that during the pandemic there has been a “robust” increase in use by teens of social media, particularly TikTok. At the same time, there have been reports of teen girls experiencing “explosive tic onset” that mimics videos from TikTok influencers.
The new analysis included 20 teens with a tic disorder, ranging in age from 11 to 21 years (average age, 16 years). About 45% of participants identified as male, 45% as female, and 10% as nonbinary.
The nature of the tic disorder varied widely among participants. Some had experienced tics for many years, while others only developed tics during the pandemic.
Participants completed a detailed survey, part of which inquired about where they received information about tics, such as from a doctor, media, parents, or teachers.
They were also asked to rank various social media platforms, including Tik Tok, Facebook, and YouTube on a five-point Likert scale as an information source about tics.
In addition, the survey inquired about tic severity and frequency, quality of life, and whether the pandemic or social media affected respondents’ tics.
Worsens quality of life
Results showed 65% of respondents used social media at least four to five times per day for an average of 5.6 hours per day. Approximately 90% reported increased use of social media during COVID.
Only 5% of participants reported using social media to provide information about tics.
About half of respondents indicated social media adversely affected their tics, and 85% said their tic frequency worsened during COVID.
Dr. Frey noted that because teens had to attend school virtually, that may have led to increased hours spent online.
There was no significant correlation between social media use and self-reported frequency of tics since the onset of COVID (Pearson correlation coefficient [R], –0.0055, P = .982).
However, there was a statistically significant correlation between social media use and tic severity (R, –0.496, P = .026) and quality of life (R, –0.447, P = .048).
These results suggest teenagers did not develop more tics, but rather the tics they already had worsened and affected their quality of life, Dr. Frey noted. She added that teens sometimes injure themselves while experiencing tics.
The full study has now enrolled 50 participants, and investigators anticipate that number to go up to 80. “We’re hoping to see more patterns emerge when we have a larger cohort of data available,” said Dr. Frey.
Asking parents to weigh in on the impact of social media on their child’s tic condition would be “a great idea for a follow-up study,” she added.
Symptoms exacerbated
Commenting on the findings, Tamara Pringsheim, MD, professor in the department of clinical neurosciences, psychiatry, pediatrics, and community health sciences at the University of Calgary (Alta.), said she also has noticed the impact of increased social media use on young patients with tics during the pandemic.
“Many young people report that seeing other people with tics, or ticlike behaviors, can exacerbate their own symptoms,” said Dr. Pringsheim, who is the university’s program lead on Tourette and pediatric movement disorders.
She noted a principle of the Comprehensive Behavioral Intervention for Tics, which is a nonpharmacologic technique demonstrated to reduce tic severity, is to identify antecedents or triggers for tics, and to learn to manage them. It might be a good idea to remind young patients of this principle, said Dr. Pringsheim, who was not associated with the current research.
“I suggest to young people who report specific social media content as a trigger for symptoms to recognize the effect of the exposure on their symptoms and make an informed choice about what they view and how much time they spend on social media,” she added.
The study did not receive any outside funding support. Dr. Frey has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Self-care tips for clinicians as COVID-19 lingers
LAS VEGAS – according to Jon A. Levenson, MD.
“There are those who will need mental health treatment, so creating an easy way to reach out for help and facilitate linkage with care is critically important,” Dr. Levenson, associate professor of psychiatry at Columbia University Irving Medical Center, New York, said during an annual psychopharmacology update held by the Nevada Psychiatric Association. “The vast majority of our workforce will thrive with proper support. But what can each of us do to take care of ourselves?”

Step one is to recognize common stress reactions as well as signs of distress. He offered the oxygen mask metaphor, the idea that before we can take care of and support anyone else, we must first take care of ourselves. “When people are stressed, they don’t always think about the oxygen mask metaphor,” Dr. Levenson said. Step two is to practice and model self-care by adopting principles often discussed in acceptance and commitment therapy: to focus on what you can control, not on what you can’t control.
“We can’t control the amount of toilet paper at the grocery store, how long the pandemic will last, or how others have reacted,” Dr. Levenson said. “We also can’t control other people’s motives, predict what will happen, or the actions of others, including whether they will follow social distancing guidelines or not.”
How about what we can control? One is a positive attitude, “which can sustain people during times of intense stress,” he said. “Other things that we can do include turn off the news and find fun and enriching activities to do at home, whether it be playing a game with family or reaching out to friends through an iPad or a smartphone. You can also follow [Centers for Disease Control and Prevention] recommendations, control your own social distancing, and limit social media activity, which can be stressful. We can also control our kindness and grace.” He added that resilience does not mean “snapping back” to how you were before the pandemic, but rather “learning to integrate the adverse experiences into who you are and growing with them, which is sometimes known as posttraumatic growth.”
Dr. Levenson encouraged health care workers to use their coping resources, connect to others, and cultivate their values and purpose in life as they navigate these challenging times. “You also want to promote realistic optimism; find a way to stay positive,” he said. “We emphasize to our staff that while you won’t forget this time, focus on what you can control – your positive relationships – and remind yourself of your values and sources of gratitude. Figure out, and reflect on, what you care about, and then care about it. Remind yourself in a deliberate, purposeful way what anchors you to your job, which in the health care setting tends to be a desire to care for others, to assist those in need, and to work in teams. We also encourage staff to refrain from judgment. Guilt is a normal and near-universal response to this stressor, but there are many ways to contribute without a judgmental or guilty tone.”
Other tips for self-support are to remind yourself that it is not selfish to take breaks. “The needs of your patients are not more important than your own needs,” Dr. Levenson said. “Working nonstop can put you at higher risk for stress, exhaustion, and illness. You may need to give yourself more time to step back and recover from workplace challenges or extended coverage for peers; this is important. We remind our staff that your work may feel more emotionally draining than usual because everything is more intense overall during the COVID-19 pandemic. This reminder helps staff normalize what they already may be experiencing, and in turn, to further support each other.”
Soothing activities to relieve stress include meditation, prayer, deep and slow breathing, relaxation exercises, yoga, mindfulness, stretching, staying hydrated, eating healthfully, exercise, and getting sufficient sleep. Other stress management tips include avoiding excessive alcohol intake, reaching out to others, asking for assistance, and delegating when possible. “We want to promote psychological flexibility: the ability to stay in contact with the present moment,” he said. “We encourage our peers to be aware of unpleasant thoughts and feelings, and to try to redirect negative thought patterns to a proactive problem-solving approach; this includes choosing one’s behaviors based on the situation and personal values.”
Dr. Levenson reported having no disclosures related to his presentation.
LAS VEGAS – according to Jon A. Levenson, MD.
“There are those who will need mental health treatment, so creating an easy way to reach out for help and facilitate linkage with care is critically important,” Dr. Levenson, associate professor of psychiatry at Columbia University Irving Medical Center, New York, said during an annual psychopharmacology update held by the Nevada Psychiatric Association. “The vast majority of our workforce will thrive with proper support. But what can each of us do to take care of ourselves?”
Step one is to recognize common stress reactions as well as signs of distress. He offered the oxygen mask metaphor, the idea that before we can take care of and support anyone else, we must first take care of ourselves. “When people are stressed, they don’t always think about the oxygen mask metaphor,” Dr. Levenson said. Step two is to practice and model self-care by adopting principles often discussed in acceptance and commitment therapy: to focus on what you can control, not on what you can’t control.
“We can’t control the amount of toilet paper at the grocery store, how long the pandemic will last, or how others have reacted,” Dr. Levenson said. “We also can’t control other people’s motives, predict what will happen, or the actions of others, including whether they will follow social distancing guidelines or not.”
How about what we can control? One is a positive attitude, “which can sustain people during times of intense stress,” he said. “Other things that we can do include turn off the news and find fun and enriching activities to do at home, whether it be playing a game with family or reaching out to friends through an iPad or a smartphone. You can also follow [Centers for Disease Control and Prevention] recommendations, control your own social distancing, and limit social media activity, which can be stressful. We can also control our kindness and grace.” He added that resilience does not mean “snapping back” to how you were before the pandemic, but rather “learning to integrate the adverse experiences into who you are and growing with them, which is sometimes known as posttraumatic growth.”
Dr. Levenson encouraged health care workers to use their coping resources, connect to others, and cultivate their values and purpose in life as they navigate these challenging times. “You also want to promote realistic optimism; find a way to stay positive,” he said. “We emphasize to our staff that while you won’t forget this time, focus on what you can control – your positive relationships – and remind yourself of your values and sources of gratitude. Figure out, and reflect on, what you care about, and then care about it. Remind yourself in a deliberate, purposeful way what anchors you to your job, which in the health care setting tends to be a desire to care for others, to assist those in need, and to work in teams. We also encourage staff to refrain from judgment. Guilt is a normal and near-universal response to this stressor, but there are many ways to contribute without a judgmental or guilty tone.”
Other tips for self-support are to remind yourself that it is not selfish to take breaks. “The needs of your patients are not more important than your own needs,” Dr. Levenson said. “Working nonstop can put you at higher risk for stress, exhaustion, and illness. You may need to give yourself more time to step back and recover from workplace challenges or extended coverage for peers; this is important. We remind our staff that your work may feel more emotionally draining than usual because everything is more intense overall during the COVID-19 pandemic. This reminder helps staff normalize what they already may be experiencing, and in turn, to further support each other.”
Soothing activities to relieve stress include meditation, prayer, deep and slow breathing, relaxation exercises, yoga, mindfulness, stretching, staying hydrated, eating healthfully, exercise, and getting sufficient sleep. Other stress management tips include avoiding excessive alcohol intake, reaching out to others, asking for assistance, and delegating when possible. “We want to promote psychological flexibility: the ability to stay in contact with the present moment,” he said. “We encourage our peers to be aware of unpleasant thoughts and feelings, and to try to redirect negative thought patterns to a proactive problem-solving approach; this includes choosing one’s behaviors based on the situation and personal values.”
Dr. Levenson reported having no disclosures related to his presentation.
LAS VEGAS – according to Jon A. Levenson, MD.
“There are those who will need mental health treatment, so creating an easy way to reach out for help and facilitate linkage with care is critically important,” Dr. Levenson, associate professor of psychiatry at Columbia University Irving Medical Center, New York, said during an annual psychopharmacology update held by the Nevada Psychiatric Association. “The vast majority of our workforce will thrive with proper support. But what can each of us do to take care of ourselves?”
Step one is to recognize common stress reactions as well as signs of distress. He offered the oxygen mask metaphor, the idea that before we can take care of and support anyone else, we must first take care of ourselves. “When people are stressed, they don’t always think about the oxygen mask metaphor,” Dr. Levenson said. Step two is to practice and model self-care by adopting principles often discussed in acceptance and commitment therapy: to focus on what you can control, not on what you can’t control.
“We can’t control the amount of toilet paper at the grocery store, how long the pandemic will last, or how others have reacted,” Dr. Levenson said. “We also can’t control other people’s motives, predict what will happen, or the actions of others, including whether they will follow social distancing guidelines or not.”
How about what we can control? One is a positive attitude, “which can sustain people during times of intense stress,” he said. “Other things that we can do include turn off the news and find fun and enriching activities to do at home, whether it be playing a game with family or reaching out to friends through an iPad or a smartphone. You can also follow [Centers for Disease Control and Prevention] recommendations, control your own social distancing, and limit social media activity, which can be stressful. We can also control our kindness and grace.” He added that resilience does not mean “snapping back” to how you were before the pandemic, but rather “learning to integrate the adverse experiences into who you are and growing with them, which is sometimes known as posttraumatic growth.”
Dr. Levenson encouraged health care workers to use their coping resources, connect to others, and cultivate their values and purpose in life as they navigate these challenging times. “You also want to promote realistic optimism; find a way to stay positive,” he said. “We emphasize to our staff that while you won’t forget this time, focus on what you can control – your positive relationships – and remind yourself of your values and sources of gratitude. Figure out, and reflect on, what you care about, and then care about it. Remind yourself in a deliberate, purposeful way what anchors you to your job, which in the health care setting tends to be a desire to care for others, to assist those in need, and to work in teams. We also encourage staff to refrain from judgment. Guilt is a normal and near-universal response to this stressor, but there are many ways to contribute without a judgmental or guilty tone.”
Other tips for self-support are to remind yourself that it is not selfish to take breaks. “The needs of your patients are not more important than your own needs,” Dr. Levenson said. “Working nonstop can put you at higher risk for stress, exhaustion, and illness. You may need to give yourself more time to step back and recover from workplace challenges or extended coverage for peers; this is important. We remind our staff that your work may feel more emotionally draining than usual because everything is more intense overall during the COVID-19 pandemic. This reminder helps staff normalize what they already may be experiencing, and in turn, to further support each other.”
Soothing activities to relieve stress include meditation, prayer, deep and slow breathing, relaxation exercises, yoga, mindfulness, stretching, staying hydrated, eating healthfully, exercise, and getting sufficient sleep. Other stress management tips include avoiding excessive alcohol intake, reaching out to others, asking for assistance, and delegating when possible. “We want to promote psychological flexibility: the ability to stay in contact with the present moment,” he said. “We encourage our peers to be aware of unpleasant thoughts and feelings, and to try to redirect negative thought patterns to a proactive problem-solving approach; this includes choosing one’s behaviors based on the situation and personal values.”
Dr. Levenson reported having no disclosures related to his presentation.
AT NPA 2022
Mental illness tied to increased dementia risk
Results of a large, longitudinal, population-based study show that individuals hospitalized for a mental health disorder had a fourfold increased relative risk (RR) for developing dementia, compared with those who were not hospitalized with a mental illness.
In addition, those with dementia plus a mental disorder developed dementia almost 6 years earlier than those without a mental illness.
The findings were consistent among men and women, in patients with early- and late-onset dementia, in those with Alzheimer’s and non-Alzheimer’s dementia, and across all mental health disorders – and remained so after accounting for pre-existing physical illness and socioeconomic factors.
“Dementia is not typically treated until later in life, but our study suggests that we need to be thinking about dementia prevention much earlier in the life course,” study investigator Leah Richmond-Rakerd, PhD, assistant professor, department of psychology, University of Michigan, said in an interview.
“Supporting young people’s mental health could be a window of opportunity to help reduce the burden of dementia in older adults,” she said.
The findings were published online Feb. 16.
Underappreciated risk factor
“Recognition of the outsized influence of dementia on later-life functioning has fueled research into modifiable risk factors and prevention targets,” the investigators write.
Previous research suggests mental disorders may “comprise an underappreciated category of modifiable risk factors.” However, those studies focused primarily on midlife and older individuals, not on capturing mental disorders during young adulthood, which is the time of “peak prevalence,” they add. In addition, most studies have not explored the full range of mental disorders.
Dr. Richmond-Rakerd noted that it is well known that mental health disorders peak in adolescence and young adulthood – and are treatable.
“If the same people who have mental disorders when they are young tend to develop dementia when they are older, that would mean that preventing mental health problems in younger people might reduce or delay the burden of dementia in older people,” she said.
The investigators assessed records from the New Zealand Integrated Data Infrastructure, which is a de-identified register that includes the entire New Zealand population. They also examined information about hospitalizations and diagnoses from records kept by the New Zealand Ministry of Health.
The researchers followed 1,711,386 individuals born between 1928 and 1967 (50.6% men, aged 21 to 60 years at baseline) for 30 years. The population was subdivided into age groups based on birth years: 1928-1937 (14.8%), 1938-1947 (20.85%), 1948-1957 (29.35%), and 1958-1967 (35.1%).
Earlier onset
During the study period, 3.8% of individuals were identified as having a mental disorder, and 2% were identified as having dementia. Similar percentages of men and women had a mental disorder, and similar percentages had dementia.
Dementia was “over-represented” among participants with versus without a mental disorder (6.1% vs. 1.8%). This finding held across all age groups.
Those diagnosed with a mental disorder were also more likely to develop dementia, compared with their peers without a mental disorder (RR, 3.51; 95% confidence interval, 3.39-3.64), which is a larger association than that between physical diseases and dementia (RR, 1.19; 95% CI, 1.16-1.21).
These associations were present in both sexes and in all age groups, although the associations were stronger in more recently born cohorts.
A sixfold higher risk for dementia remained even after adjusting for pre-existing physical illnesses (HR, 6.49; 95% CI, 6.25-6.73); and the elevated risk was evident across different lengths of follow-up from the index mental disorder.
When the researchers focused specifically on individuals diagnosed with dementia, they found that those diagnosed with a mental disorder developed dementia a mean of 5.60 years earlier than those without a mental disorder diagnosis – an association observed across both sexes and all age groups.
“Individuals diagnosed with psychotic, substance use, mood, neurotic, and all other mental disorders and who engaged in self-harm were all more likely than those without a mental disorder to be diagnosed with subsequent dementia, even after accounting for their physical disease histories,” the investigators write.
Although there was a link between mental disorders in both Alzheimer’s and non-Alzheimer’s dementias, the association was larger in non-Alzheimer’s.
The researchers note that the study has several limitations, including the fact that it was conducted in New Zealand and therefore the results may not be generalizable to other regions. In addition, inpatient hospital records do not capture less severe mental disorder cases treated in the outpatient setting.
Dr. Richmond-Rakerd suggested several potential mechanisms that could account for the link between mental illness and dementia, including poor lifestyle choices and metabolic side effects associated with some psychiatric medications.
“There could also be shared risk factors for both mental disorders and dementia, such as shared genetics, or individuals may experience a lifelong brain vulnerability that shows up as mental health problems earlier in life and shows up as dementia later in life,” she said.
An important risk factor
Commenting for this article, Ken Duckworth, MD, chief medical officer of the National Alliance on Mental Illness, said a major strength of the study was its longitudinal scope and large population size.
He described the study as allowing clinicians to “watch the movie,” as opposed to looking at a “snapshot” of data.
“Although you can learn things from snapshots, a large, comprehensive public health system looking at 30 years of claims – something not possible in the U.S. because of our more fragmented health care system – offers more insight,” said Dr. Duckworth, who was not involved with the research.
The investigators are “painting a picture of a correlation of risk, and to me, that’s the beginning of further inquiry,” he added. “Would preventive efforts targeting dementia, such as exercise and socialization, be helpful? It’s a great study that raises these interesting questions.”
Also commenting in an interview, Claire Sexton, DPhil, director of scientific programs and outreach at the Alzheimer’s Association, said the study “adds a wealth of data to our understanding” of mental disorders as a dementia risk factor.
However, the study was observational, so “the findings cannot imply causation, [and just] because someone has depression, that does not mean they will go on to develop Alzheimer’s,” said Dr. Sexton, who also was not involved with the research.
Still, “these data support the idea that taking care of one’s mental health is incredibly important for overall wellbeing. For providers, it’s important to have mental health evaluation be a part of your patient’s regular checkups,” she added.
Dr. Richmond-Rakerd noted that even if mental health conditions are not a causal risk factor for dementia, “the presence of a mental health problem is still an important indicator of risk. Mental health providers may wish to target other risk factors for dementia that are more common in individuals with mental health conditions, such as social disconnection.”
The study was funded by grants from the National Institute on Aging, the U.K. Medical Research Council, the National Institute of Child Health and Development through the Duke Population Research Center, and the National Institute on Aging through the Center for Advancing Sociodemographic and Economic Study of Alzheimer’s Disease and Related Dementias. Dr. Richmond-Rakerd reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Sexton and Dr. Duckworth report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Results of a large, longitudinal, population-based study show that individuals hospitalized for a mental health disorder had a fourfold increased relative risk (RR) for developing dementia, compared with those who were not hospitalized with a mental illness.
In addition, those with dementia plus a mental disorder developed dementia almost 6 years earlier than those without a mental illness.
The findings were consistent among men and women, in patients with early- and late-onset dementia, in those with Alzheimer’s and non-Alzheimer’s dementia, and across all mental health disorders – and remained so after accounting for pre-existing physical illness and socioeconomic factors.
“Dementia is not typically treated until later in life, but our study suggests that we need to be thinking about dementia prevention much earlier in the life course,” study investigator Leah Richmond-Rakerd, PhD, assistant professor, department of psychology, University of Michigan, said in an interview.
“Supporting young people’s mental health could be a window of opportunity to help reduce the burden of dementia in older adults,” she said.
The findings were published online Feb. 16.
Underappreciated risk factor
“Recognition of the outsized influence of dementia on later-life functioning has fueled research into modifiable risk factors and prevention targets,” the investigators write.
Previous research suggests mental disorders may “comprise an underappreciated category of modifiable risk factors.” However, those studies focused primarily on midlife and older individuals, not on capturing mental disorders during young adulthood, which is the time of “peak prevalence,” they add. In addition, most studies have not explored the full range of mental disorders.
Dr. Richmond-Rakerd noted that it is well known that mental health disorders peak in adolescence and young adulthood – and are treatable.
“If the same people who have mental disorders when they are young tend to develop dementia when they are older, that would mean that preventing mental health problems in younger people might reduce or delay the burden of dementia in older people,” she said.
The investigators assessed records from the New Zealand Integrated Data Infrastructure, which is a de-identified register that includes the entire New Zealand population. They also examined information about hospitalizations and diagnoses from records kept by the New Zealand Ministry of Health.
The researchers followed 1,711,386 individuals born between 1928 and 1967 (50.6% men, aged 21 to 60 years at baseline) for 30 years. The population was subdivided into age groups based on birth years: 1928-1937 (14.8%), 1938-1947 (20.85%), 1948-1957 (29.35%), and 1958-1967 (35.1%).
Earlier onset
During the study period, 3.8% of individuals were identified as having a mental disorder, and 2% were identified as having dementia. Similar percentages of men and women had a mental disorder, and similar percentages had dementia.
Dementia was “over-represented” among participants with versus without a mental disorder (6.1% vs. 1.8%). This finding held across all age groups.
Those diagnosed with a mental disorder were also more likely to develop dementia, compared with their peers without a mental disorder (RR, 3.51; 95% confidence interval, 3.39-3.64), which is a larger association than that between physical diseases and dementia (RR, 1.19; 95% CI, 1.16-1.21).
These associations were present in both sexes and in all age groups, although the associations were stronger in more recently born cohorts.
A sixfold higher risk for dementia remained even after adjusting for pre-existing physical illnesses (HR, 6.49; 95% CI, 6.25-6.73); and the elevated risk was evident across different lengths of follow-up from the index mental disorder.
When the researchers focused specifically on individuals diagnosed with dementia, they found that those diagnosed with a mental disorder developed dementia a mean of 5.60 years earlier than those without a mental disorder diagnosis – an association observed across both sexes and all age groups.
“Individuals diagnosed with psychotic, substance use, mood, neurotic, and all other mental disorders and who engaged in self-harm were all more likely than those without a mental disorder to be diagnosed with subsequent dementia, even after accounting for their physical disease histories,” the investigators write.
Although there was a link between mental disorders in both Alzheimer’s and non-Alzheimer’s dementias, the association was larger in non-Alzheimer’s.
The researchers note that the study has several limitations, including the fact that it was conducted in New Zealand and therefore the results may not be generalizable to other regions. In addition, inpatient hospital records do not capture less severe mental disorder cases treated in the outpatient setting.
Dr. Richmond-Rakerd suggested several potential mechanisms that could account for the link between mental illness and dementia, including poor lifestyle choices and metabolic side effects associated with some psychiatric medications.
“There could also be shared risk factors for both mental disorders and dementia, such as shared genetics, or individuals may experience a lifelong brain vulnerability that shows up as mental health problems earlier in life and shows up as dementia later in life,” she said.
An important risk factor
Commenting for this article, Ken Duckworth, MD, chief medical officer of the National Alliance on Mental Illness, said a major strength of the study was its longitudinal scope and large population size.
He described the study as allowing clinicians to “watch the movie,” as opposed to looking at a “snapshot” of data.
“Although you can learn things from snapshots, a large, comprehensive public health system looking at 30 years of claims – something not possible in the U.S. because of our more fragmented health care system – offers more insight,” said Dr. Duckworth, who was not involved with the research.
The investigators are “painting a picture of a correlation of risk, and to me, that’s the beginning of further inquiry,” he added. “Would preventive efforts targeting dementia, such as exercise and socialization, be helpful? It’s a great study that raises these interesting questions.”
Also commenting in an interview, Claire Sexton, DPhil, director of scientific programs and outreach at the Alzheimer’s Association, said the study “adds a wealth of data to our understanding” of mental disorders as a dementia risk factor.
However, the study was observational, so “the findings cannot imply causation, [and just] because someone has depression, that does not mean they will go on to develop Alzheimer’s,” said Dr. Sexton, who also was not involved with the research.
Still, “these data support the idea that taking care of one’s mental health is incredibly important for overall wellbeing. For providers, it’s important to have mental health evaluation be a part of your patient’s regular checkups,” she added.
Dr. Richmond-Rakerd noted that even if mental health conditions are not a causal risk factor for dementia, “the presence of a mental health problem is still an important indicator of risk. Mental health providers may wish to target other risk factors for dementia that are more common in individuals with mental health conditions, such as social disconnection.”
The study was funded by grants from the National Institute on Aging, the U.K. Medical Research Council, the National Institute of Child Health and Development through the Duke Population Research Center, and the National Institute on Aging through the Center for Advancing Sociodemographic and Economic Study of Alzheimer’s Disease and Related Dementias. Dr. Richmond-Rakerd reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Sexton and Dr. Duckworth report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Results of a large, longitudinal, population-based study show that individuals hospitalized for a mental health disorder had a fourfold increased relative risk (RR) for developing dementia, compared with those who were not hospitalized with a mental illness.
In addition, those with dementia plus a mental disorder developed dementia almost 6 years earlier than those without a mental illness.
The findings were consistent among men and women, in patients with early- and late-onset dementia, in those with Alzheimer’s and non-Alzheimer’s dementia, and across all mental health disorders – and remained so after accounting for pre-existing physical illness and socioeconomic factors.
“Dementia is not typically treated until later in life, but our study suggests that we need to be thinking about dementia prevention much earlier in the life course,” study investigator Leah Richmond-Rakerd, PhD, assistant professor, department of psychology, University of Michigan, said in an interview.
“Supporting young people’s mental health could be a window of opportunity to help reduce the burden of dementia in older adults,” she said.
The findings were published online Feb. 16.
Underappreciated risk factor
“Recognition of the outsized influence of dementia on later-life functioning has fueled research into modifiable risk factors and prevention targets,” the investigators write.
Previous research suggests mental disorders may “comprise an underappreciated category of modifiable risk factors.” However, those studies focused primarily on midlife and older individuals, not on capturing mental disorders during young adulthood, which is the time of “peak prevalence,” they add. In addition, most studies have not explored the full range of mental disorders.
Dr. Richmond-Rakerd noted that it is well known that mental health disorders peak in adolescence and young adulthood – and are treatable.
“If the same people who have mental disorders when they are young tend to develop dementia when they are older, that would mean that preventing mental health problems in younger people might reduce or delay the burden of dementia in older people,” she said.
The investigators assessed records from the New Zealand Integrated Data Infrastructure, which is a de-identified register that includes the entire New Zealand population. They also examined information about hospitalizations and diagnoses from records kept by the New Zealand Ministry of Health.
The researchers followed 1,711,386 individuals born between 1928 and 1967 (50.6% men, aged 21 to 60 years at baseline) for 30 years. The population was subdivided into age groups based on birth years: 1928-1937 (14.8%), 1938-1947 (20.85%), 1948-1957 (29.35%), and 1958-1967 (35.1%).
Earlier onset
During the study period, 3.8% of individuals were identified as having a mental disorder, and 2% were identified as having dementia. Similar percentages of men and women had a mental disorder, and similar percentages had dementia.
Dementia was “over-represented” among participants with versus without a mental disorder (6.1% vs. 1.8%). This finding held across all age groups.
Those diagnosed with a mental disorder were also more likely to develop dementia, compared with their peers without a mental disorder (RR, 3.51; 95% confidence interval, 3.39-3.64), which is a larger association than that between physical diseases and dementia (RR, 1.19; 95% CI, 1.16-1.21).
These associations were present in both sexes and in all age groups, although the associations were stronger in more recently born cohorts.
A sixfold higher risk for dementia remained even after adjusting for pre-existing physical illnesses (HR, 6.49; 95% CI, 6.25-6.73); and the elevated risk was evident across different lengths of follow-up from the index mental disorder.
When the researchers focused specifically on individuals diagnosed with dementia, they found that those diagnosed with a mental disorder developed dementia a mean of 5.60 years earlier than those without a mental disorder diagnosis – an association observed across both sexes and all age groups.
“Individuals diagnosed with psychotic, substance use, mood, neurotic, and all other mental disorders and who engaged in self-harm were all more likely than those without a mental disorder to be diagnosed with subsequent dementia, even after accounting for their physical disease histories,” the investigators write.
Although there was a link between mental disorders in both Alzheimer’s and non-Alzheimer’s dementias, the association was larger in non-Alzheimer’s.
The researchers note that the study has several limitations, including the fact that it was conducted in New Zealand and therefore the results may not be generalizable to other regions. In addition, inpatient hospital records do not capture less severe mental disorder cases treated in the outpatient setting.
Dr. Richmond-Rakerd suggested several potential mechanisms that could account for the link between mental illness and dementia, including poor lifestyle choices and metabolic side effects associated with some psychiatric medications.
“There could also be shared risk factors for both mental disorders and dementia, such as shared genetics, or individuals may experience a lifelong brain vulnerability that shows up as mental health problems earlier in life and shows up as dementia later in life,” she said.
An important risk factor
Commenting for this article, Ken Duckworth, MD, chief medical officer of the National Alliance on Mental Illness, said a major strength of the study was its longitudinal scope and large population size.
He described the study as allowing clinicians to “watch the movie,” as opposed to looking at a “snapshot” of data.
“Although you can learn things from snapshots, a large, comprehensive public health system looking at 30 years of claims – something not possible in the U.S. because of our more fragmented health care system – offers more insight,” said Dr. Duckworth, who was not involved with the research.
The investigators are “painting a picture of a correlation of risk, and to me, that’s the beginning of further inquiry,” he added. “Would preventive efforts targeting dementia, such as exercise and socialization, be helpful? It’s a great study that raises these interesting questions.”
Also commenting in an interview, Claire Sexton, DPhil, director of scientific programs and outreach at the Alzheimer’s Association, said the study “adds a wealth of data to our understanding” of mental disorders as a dementia risk factor.
However, the study was observational, so “the findings cannot imply causation, [and just] because someone has depression, that does not mean they will go on to develop Alzheimer’s,” said Dr. Sexton, who also was not involved with the research.
Still, “these data support the idea that taking care of one’s mental health is incredibly important for overall wellbeing. For providers, it’s important to have mental health evaluation be a part of your patient’s regular checkups,” she added.
Dr. Richmond-Rakerd noted that even if mental health conditions are not a causal risk factor for dementia, “the presence of a mental health problem is still an important indicator of risk. Mental health providers may wish to target other risk factors for dementia that are more common in individuals with mental health conditions, such as social disconnection.”
The study was funded by grants from the National Institute on Aging, the U.K. Medical Research Council, the National Institute of Child Health and Development through the Duke Population Research Center, and the National Institute on Aging through the Center for Advancing Sociodemographic and Economic Study of Alzheimer’s Disease and Related Dementias. Dr. Richmond-Rakerd reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Sexton and Dr. Duckworth report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA PSYCHIATRY
Columbia names interim chair of psychiatry after Twitter controversy
Helen Blair Simpson, MD, PhD, will take over for Jeffrey Lieberman, MD, who was suspended over a tweet he sent that was widely condemned as both racist and sexist.

She will also serve as interim director of the New York State Psychiatric Institute and interim psychiatrist-in-chief at New York–Presbyterian/Columbia University Irving Medical Center, the email stated.
All appointments were effective on Feb. 28.
Latest response
Dr. Simpson, who joined the faculty at Columbia in 1999, previously served as a professor and vice chair of research for the psychiatry department, director of Columbia’s Center for Obsessive-Compulsive and Related Disorders, and director of psychiatry research at the New York State Psychiatric Institute. Dr. Simpson is associate editor of JAMA Psychiatry and is president-elect of the Anxiety and Depression Association of America.
Her research has been continuously funded by the National Institute of Mental Health since 1999, and she has advised both the World Health Organization and the American Psychiatric Association on the diagnosis and treatment of OCD.
Dr. Simpson has a bachelor’s degree in biology from Yale University and completed an MD-PhD program at The Rockefeller University and Weill Cornell Medicine, New York. She did her residency in psychiatry at New York–Presbyterian.
The announcement is Columbia’s latest response to the furor that erupted on social media following Dr. Lieberman’s tweet about Sudanese model Nyakim Gatwech, in which he wrote, “Whether a work of art or a freak of nature she’s a beautiful sight to behold.”
Twitter reacted immediately and negatively to the tweet, which even Dr. Lieberman later acknowledged was “racist and sexist” in an email apology he sent Feb. 22 to faculty and staff in the department of psychiatry.
As reported by this news organization, Columbia suspended Dr. Lieberman from his chair position on Feb. 23 and permanently removed him from the post of psychiatrist-in-chief at New York–Presbyterian Hospital/Columbia University Irving Medical Center. Lieberman also resigned as executive director of the New York State Psychiatric Institute.
The email announcing Simpson’s appointment was signed by Katrina Armstrong, MD, incoming CEO, Columbia University Irving Medical Center and dean of the Faculties of Health Sciences and the Vagelos College of Physicians and Surgeons; Anil K. Rustgi, MD, interim executive vice president and dean of the Faculties of Health Sciences and Medicine; Steven J. Corwin, MD; president and CEO, New York–Presbyterian; and Ann Marie Sullivan, MD, commissioner of the New York State Office of Mental Health.
This is a developing story.
A version of this article first appeared on Medscape.com.
Helen Blair Simpson, MD, PhD, will take over for Jeffrey Lieberman, MD, who was suspended over a tweet he sent that was widely condemned as both racist and sexist.
She will also serve as interim director of the New York State Psychiatric Institute and interim psychiatrist-in-chief at New York–Presbyterian/Columbia University Irving Medical Center, the email stated.
All appointments were effective on Feb. 28.
Latest response
Dr. Simpson, who joined the faculty at Columbia in 1999, previously served as a professor and vice chair of research for the psychiatry department, director of Columbia’s Center for Obsessive-Compulsive and Related Disorders, and director of psychiatry research at the New York State Psychiatric Institute. Dr. Simpson is associate editor of JAMA Psychiatry and is president-elect of the Anxiety and Depression Association of America.
Her research has been continuously funded by the National Institute of Mental Health since 1999, and she has advised both the World Health Organization and the American Psychiatric Association on the diagnosis and treatment of OCD.
Dr. Simpson has a bachelor’s degree in biology from Yale University and completed an MD-PhD program at The Rockefeller University and Weill Cornell Medicine, New York. She did her residency in psychiatry at New York–Presbyterian.
The announcement is Columbia’s latest response to the furor that erupted on social media following Dr. Lieberman’s tweet about Sudanese model Nyakim Gatwech, in which he wrote, “Whether a work of art or a freak of nature she’s a beautiful sight to behold.”
Twitter reacted immediately and negatively to the tweet, which even Dr. Lieberman later acknowledged was “racist and sexist” in an email apology he sent Feb. 22 to faculty and staff in the department of psychiatry.
As reported by this news organization, Columbia suspended Dr. Lieberman from his chair position on Feb. 23 and permanently removed him from the post of psychiatrist-in-chief at New York–Presbyterian Hospital/Columbia University Irving Medical Center. Lieberman also resigned as executive director of the New York State Psychiatric Institute.
The email announcing Simpson’s appointment was signed by Katrina Armstrong, MD, incoming CEO, Columbia University Irving Medical Center and dean of the Faculties of Health Sciences and the Vagelos College of Physicians and Surgeons; Anil K. Rustgi, MD, interim executive vice president and dean of the Faculties of Health Sciences and Medicine; Steven J. Corwin, MD; president and CEO, New York–Presbyterian; and Ann Marie Sullivan, MD, commissioner of the New York State Office of Mental Health.
This is a developing story.
A version of this article first appeared on Medscape.com.
Helen Blair Simpson, MD, PhD, will take over for Jeffrey Lieberman, MD, who was suspended over a tweet he sent that was widely condemned as both racist and sexist.
She will also serve as interim director of the New York State Psychiatric Institute and interim psychiatrist-in-chief at New York–Presbyterian/Columbia University Irving Medical Center, the email stated.
All appointments were effective on Feb. 28.
Latest response
Dr. Simpson, who joined the faculty at Columbia in 1999, previously served as a professor and vice chair of research for the psychiatry department, director of Columbia’s Center for Obsessive-Compulsive and Related Disorders, and director of psychiatry research at the New York State Psychiatric Institute. Dr. Simpson is associate editor of JAMA Psychiatry and is president-elect of the Anxiety and Depression Association of America.
Her research has been continuously funded by the National Institute of Mental Health since 1999, and she has advised both the World Health Organization and the American Psychiatric Association on the diagnosis and treatment of OCD.
Dr. Simpson has a bachelor’s degree in biology from Yale University and completed an MD-PhD program at The Rockefeller University and Weill Cornell Medicine, New York. She did her residency in psychiatry at New York–Presbyterian.
The announcement is Columbia’s latest response to the furor that erupted on social media following Dr. Lieberman’s tweet about Sudanese model Nyakim Gatwech, in which he wrote, “Whether a work of art or a freak of nature she’s a beautiful sight to behold.”
Twitter reacted immediately and negatively to the tweet, which even Dr. Lieberman later acknowledged was “racist and sexist” in an email apology he sent Feb. 22 to faculty and staff in the department of psychiatry.
As reported by this news organization, Columbia suspended Dr. Lieberman from his chair position on Feb. 23 and permanently removed him from the post of psychiatrist-in-chief at New York–Presbyterian Hospital/Columbia University Irving Medical Center. Lieberman also resigned as executive director of the New York State Psychiatric Institute.
The email announcing Simpson’s appointment was signed by Katrina Armstrong, MD, incoming CEO, Columbia University Irving Medical Center and dean of the Faculties of Health Sciences and the Vagelos College of Physicians and Surgeons; Anil K. Rustgi, MD, interim executive vice president and dean of the Faculties of Health Sciences and Medicine; Steven J. Corwin, MD; president and CEO, New York–Presbyterian; and Ann Marie Sullivan, MD, commissioner of the New York State Office of Mental Health.
This is a developing story.
A version of this article first appeared on Medscape.com.
The importance of a post-COVID wellness program for medical staff
LAS VEGAS – , according to Jon A. Levenson, MD.
“We can learn from previous pandemics and epidemics, which will be important for us going forward from COVID-19,” Dr. Levenson, associate professor of psychiatry at Columbia University Irving Medical Center, New York, said during an annual psychopharmacology update held by the Nevada Psychiatric Association.
During the severe acute respiratory syndrome (SARS) epidemic in 2005, 68% of health care workers reported significant job-related stress, including increased workload, changing work duties, redeployment, shortage of medical supplies, concerns about insufficient personal protective equipment (PPE), lack of safety at work, absence of effective treatment protocols, inconsistent organizational support and information and misinformation from hospital management, and witnessing intense pain, isolation, and loss on a daily basis with few opportunities to take breaks (Psychiatr Serv. 2020 Oct 6. doi: 10.1176/appi.ps.202000274).
Personal concerns associated with psychopathological symptoms included spreading infection to family members; feeling responsibility for family members’ social isolation; self-isolating to avoid infecting family, which can lead to increased loneliness and sadness. “For those who were working remotely, this level of work is hard and challenging,” Dr. Levenson said. “For those who are parents, the 24-hour childcare responsibilities exist on top of work. They often found they can’t unwind with friends.”
Across SARS, MERS, Ebola, and swine flu, a wide range of prevalence in symptoms of distress, stress, anxiety, depressive symptoms, and substance use emerged, he continued. During COVID-19, at least three studies reported significant percentages of distress, depression, anxiety, insomnia, and PTSD among health care workers (JAMA Netw Open. 2020;3[3]:e203976, Front Psychol. 2020 Dec 8;11:608986., and Gen Hosp Psychiatry. Sep-Oct 2020;66:1-8).
“Who is at most-increased risk?” Dr. Levenson asked. “Women; those who are younger and have fewer years of work experience; those working on the front lines such as nurses and advanced practice professionals; and people with preexisting vulnerabilities to psychiatric disorders including anxiety, depression, obsessional symptoms, substance use, suicidal behavior, and impulse control disorders are likely to be especially vulnerable to stress-related symptoms.”
At CUIMC, there were certain “tipping points,” to the vulnerability of health care worker well-being in the early stage of the COVID-19 pandemic, he said, including the loss of an emergency medicine physician colleague from death by suicide. “On the national level there were so many other issues going on such as health care disparities of the COVID-19 infection itself, the murder of George Floyd in Minneapolis, other issues of racial injustice, a tense political climate with an upcoming election at the time, and other factors related to the natural climate concerns,” he said. This prompted several faculty members in the CUIMC department of psychiatry including Claude Ann Mellins, PhD, Laurel S. Mayer, MD, and Lourival Baptista-Neto, MD, to partner with ColumbiaDoctors and New York-Presbyterian Hospital and develop a model of care for health care workers known as CopeColumbia, a virtual program intended to address staff burnout and fatigue, with an emphasis on prevention and promotion of resilience.* It launched in March of 2020 and consists of 1:1 peer support, a peer support group program, town halls/webinars, and an active web site.
The 1:1 peer support sessions typically last 20-30 minutes and provide easy access for all distressed hospital and medical center staff. “We have a phone line staffed by Columbia psychiatrists and psychologists so that a distressed staff member can reach support directly,” he said. The format of these sessions includes a brief discussion of challenges and brainstorming around potential coping strategies. “This is not a psychotherapy session,” Dr. Levenson said. “Each session can be individualized to further assess the type of distress or to implement rating scales such as the Generalized Anxiety Disorder-7 scale to assess for signs and symptoms consistent with GAD. There are options to schedule a second or third peer support session, or a prompt referral within Columbia psychiatry when indicated.”
A typical peer support group meeting lasts about 30 minutes and comprises individual divisions or departments. Some goals of the peer groups are to discuss unique challenges of the work environment and to encourage the members of the group to come up with solutions; to promote team support and coping; to teach resilience-enhancing strategies from empirically based treatments such as CBT, “and to end each meeting with expressions of gratitude and of thanks within the group,” he said.
According to Dr. Levenson, sample questions CopeColumbia faculty use to facilitate coping, include “which coping skills are working for you?”; “Are you able to be present?”; “Have you honored loss with any specific ways or traditions?”; “Do you have any work buddies who support you and vice versa?”; “Can your work community build off each other’s individual strengths to help both the individual and the work group cope optimally?”; and “How can your work team help facilitate each other to best support each other?”
Other aspects of the CopeColumbia program include town halls/grand rounds that range from 30 to 60 minutes in length. “It may be a virtual presentation from a mental health professional on specific aspects of coping such as relaxation techniques,” he said. “The focus is how to manage stress, anxiety, trauma, loss, and grief. It also includes an active Q&A to engage staff participants. The advantage of this format is that you can reach many staff in an entire department.” The program also has an active web site for staff with both internal and external support links including mindfulness, meditation, exercise, parenting suggestions/caregiving, and other resources to promote well-being and resilience for staff and family.
To date, certain themes emerged from the 1:1 and peer support group sessions, including expressions of difficulty adapting to “such a new reality,” compared with the pre-COVID era. “Staff would often express anticipatory anxiety and uncertainty, such as is there going to be another surge of COVID-19 cases, and will there be a change in policies?” Dr. Levenson said. “There was a lot of expression of stress and frustration related to politicizing the virus and public containment strategies, both on a local and national level.”
Staff also mentioned the loss of usual coping strategies because of prolonged social isolation, especially for those doing remote work, and the loss of usual support resources that have helped them in the past. “They also reported delayed trauma and grief reactions, including symptoms of depression, anxiety, and posttraumatic stress,” he said. “Health care workers with children mentioned high levels of stress related to childcare, increased workload, and what seems like an impossible work-life balance.” Many reported exhaustion and irritability, “which could affect and cause tension within the work group and challenges to effective team cohesion,” he said. “There were also stressors related to the impact of racial injustices and the [presidential] election that could exacerbate the impact of COVID-19.”
Dr. Levenson hopes that CopeColumbia serves as a model for other health care systems looking for ways to support the mental well-being of their employees. “We want to promote the message that emotional health should have the same priority level as physical health,” he said. “The term that I like to use is total health. Addressing the well-being of health care workers is critical for a healthy workforce and for delivering high-quality patient care.”
He reported having no relevant financial disclosures related to his presentation.
Correction, 2/28/22: An earlier version of this article misstated Dr. Lourival Baptista-Neto's name.
LAS VEGAS – , according to Jon A. Levenson, MD.
“We can learn from previous pandemics and epidemics, which will be important for us going forward from COVID-19,” Dr. Levenson, associate professor of psychiatry at Columbia University Irving Medical Center, New York, said during an annual psychopharmacology update held by the Nevada Psychiatric Association.
During the severe acute respiratory syndrome (SARS) epidemic in 2005, 68% of health care workers reported significant job-related stress, including increased workload, changing work duties, redeployment, shortage of medical supplies, concerns about insufficient personal protective equipment (PPE), lack of safety at work, absence of effective treatment protocols, inconsistent organizational support and information and misinformation from hospital management, and witnessing intense pain, isolation, and loss on a daily basis with few opportunities to take breaks (Psychiatr Serv. 2020 Oct 6. doi: 10.1176/appi.ps.202000274).
Personal concerns associated with psychopathological symptoms included spreading infection to family members; feeling responsibility for family members’ social isolation; self-isolating to avoid infecting family, which can lead to increased loneliness and sadness. “For those who were working remotely, this level of work is hard and challenging,” Dr. Levenson said. “For those who are parents, the 24-hour childcare responsibilities exist on top of work. They often found they can’t unwind with friends.”
Across SARS, MERS, Ebola, and swine flu, a wide range of prevalence in symptoms of distress, stress, anxiety, depressive symptoms, and substance use emerged, he continued. During COVID-19, at least three studies reported significant percentages of distress, depression, anxiety, insomnia, and PTSD among health care workers (JAMA Netw Open. 2020;3[3]:e203976, Front Psychol. 2020 Dec 8;11:608986., and Gen Hosp Psychiatry. Sep-Oct 2020;66:1-8).
“Who is at most-increased risk?” Dr. Levenson asked. “Women; those who are younger and have fewer years of work experience; those working on the front lines such as nurses and advanced practice professionals; and people with preexisting vulnerabilities to psychiatric disorders including anxiety, depression, obsessional symptoms, substance use, suicidal behavior, and impulse control disorders are likely to be especially vulnerable to stress-related symptoms.”
At CUIMC, there were certain “tipping points,” to the vulnerability of health care worker well-being in the early stage of the COVID-19 pandemic, he said, including the loss of an emergency medicine physician colleague from death by suicide. “On the national level there were so many other issues going on such as health care disparities of the COVID-19 infection itself, the murder of George Floyd in Minneapolis, other issues of racial injustice, a tense political climate with an upcoming election at the time, and other factors related to the natural climate concerns,” he said. This prompted several faculty members in the CUIMC department of psychiatry including Claude Ann Mellins, PhD, Laurel S. Mayer, MD, and Lourival Baptista-Neto, MD, to partner with ColumbiaDoctors and New York-Presbyterian Hospital and develop a model of care for health care workers known as CopeColumbia, a virtual program intended to address staff burnout and fatigue, with an emphasis on prevention and promotion of resilience.* It launched in March of 2020 and consists of 1:1 peer support, a peer support group program, town halls/webinars, and an active web site.
The 1:1 peer support sessions typically last 20-30 minutes and provide easy access for all distressed hospital and medical center staff. “We have a phone line staffed by Columbia psychiatrists and psychologists so that a distressed staff member can reach support directly,” he said. The format of these sessions includes a brief discussion of challenges and brainstorming around potential coping strategies. “This is not a psychotherapy session,” Dr. Levenson said. “Each session can be individualized to further assess the type of distress or to implement rating scales such as the Generalized Anxiety Disorder-7 scale to assess for signs and symptoms consistent with GAD. There are options to schedule a second or third peer support session, or a prompt referral within Columbia psychiatry when indicated.”
A typical peer support group meeting lasts about 30 minutes and comprises individual divisions or departments. Some goals of the peer groups are to discuss unique challenges of the work environment and to encourage the members of the group to come up with solutions; to promote team support and coping; to teach resilience-enhancing strategies from empirically based treatments such as CBT, “and to end each meeting with expressions of gratitude and of thanks within the group,” he said.
According to Dr. Levenson, sample questions CopeColumbia faculty use to facilitate coping, include “which coping skills are working for you?”; “Are you able to be present?”; “Have you honored loss with any specific ways or traditions?”; “Do you have any work buddies who support you and vice versa?”; “Can your work community build off each other’s individual strengths to help both the individual and the work group cope optimally?”; and “How can your work team help facilitate each other to best support each other?”
Other aspects of the CopeColumbia program include town halls/grand rounds that range from 30 to 60 minutes in length. “It may be a virtual presentation from a mental health professional on specific aspects of coping such as relaxation techniques,” he said. “The focus is how to manage stress, anxiety, trauma, loss, and grief. It also includes an active Q&A to engage staff participants. The advantage of this format is that you can reach many staff in an entire department.” The program also has an active web site for staff with both internal and external support links including mindfulness, meditation, exercise, parenting suggestions/caregiving, and other resources to promote well-being and resilience for staff and family.
To date, certain themes emerged from the 1:1 and peer support group sessions, including expressions of difficulty adapting to “such a new reality,” compared with the pre-COVID era. “Staff would often express anticipatory anxiety and uncertainty, such as is there going to be another surge of COVID-19 cases, and will there be a change in policies?” Dr. Levenson said. “There was a lot of expression of stress and frustration related to politicizing the virus and public containment strategies, both on a local and national level.”
Staff also mentioned the loss of usual coping strategies because of prolonged social isolation, especially for those doing remote work, and the loss of usual support resources that have helped them in the past. “They also reported delayed trauma and grief reactions, including symptoms of depression, anxiety, and posttraumatic stress,” he said. “Health care workers with children mentioned high levels of stress related to childcare, increased workload, and what seems like an impossible work-life balance.” Many reported exhaustion and irritability, “which could affect and cause tension within the work group and challenges to effective team cohesion,” he said. “There were also stressors related to the impact of racial injustices and the [presidential] election that could exacerbate the impact of COVID-19.”
Dr. Levenson hopes that CopeColumbia serves as a model for other health care systems looking for ways to support the mental well-being of their employees. “We want to promote the message that emotional health should have the same priority level as physical health,” he said. “The term that I like to use is total health. Addressing the well-being of health care workers is critical for a healthy workforce and for delivering high-quality patient care.”
He reported having no relevant financial disclosures related to his presentation.
Correction, 2/28/22: An earlier version of this article misstated Dr. Lourival Baptista-Neto's name.
LAS VEGAS – , according to Jon A. Levenson, MD.
“We can learn from previous pandemics and epidemics, which will be important for us going forward from COVID-19,” Dr. Levenson, associate professor of psychiatry at Columbia University Irving Medical Center, New York, said during an annual psychopharmacology update held by the Nevada Psychiatric Association.
During the severe acute respiratory syndrome (SARS) epidemic in 2005, 68% of health care workers reported significant job-related stress, including increased workload, changing work duties, redeployment, shortage of medical supplies, concerns about insufficient personal protective equipment (PPE), lack of safety at work, absence of effective treatment protocols, inconsistent organizational support and information and misinformation from hospital management, and witnessing intense pain, isolation, and loss on a daily basis with few opportunities to take breaks (Psychiatr Serv. 2020 Oct 6. doi: 10.1176/appi.ps.202000274).
Personal concerns associated with psychopathological symptoms included spreading infection to family members; feeling responsibility for family members’ social isolation; self-isolating to avoid infecting family, which can lead to increased loneliness and sadness. “For those who were working remotely, this level of work is hard and challenging,” Dr. Levenson said. “For those who are parents, the 24-hour childcare responsibilities exist on top of work. They often found they can’t unwind with friends.”
Across SARS, MERS, Ebola, and swine flu, a wide range of prevalence in symptoms of distress, stress, anxiety, depressive symptoms, and substance use emerged, he continued. During COVID-19, at least three studies reported significant percentages of distress, depression, anxiety, insomnia, and PTSD among health care workers (JAMA Netw Open. 2020;3[3]:e203976, Front Psychol. 2020 Dec 8;11:608986., and Gen Hosp Psychiatry. Sep-Oct 2020;66:1-8).
“Who is at most-increased risk?” Dr. Levenson asked. “Women; those who are younger and have fewer years of work experience; those working on the front lines such as nurses and advanced practice professionals; and people with preexisting vulnerabilities to psychiatric disorders including anxiety, depression, obsessional symptoms, substance use, suicidal behavior, and impulse control disorders are likely to be especially vulnerable to stress-related symptoms.”
At CUIMC, there were certain “tipping points,” to the vulnerability of health care worker well-being in the early stage of the COVID-19 pandemic, he said, including the loss of an emergency medicine physician colleague from death by suicide. “On the national level there were so many other issues going on such as health care disparities of the COVID-19 infection itself, the murder of George Floyd in Minneapolis, other issues of racial injustice, a tense political climate with an upcoming election at the time, and other factors related to the natural climate concerns,” he said. This prompted several faculty members in the CUIMC department of psychiatry including Claude Ann Mellins, PhD, Laurel S. Mayer, MD, and Lourival Baptista-Neto, MD, to partner with ColumbiaDoctors and New York-Presbyterian Hospital and develop a model of care for health care workers known as CopeColumbia, a virtual program intended to address staff burnout and fatigue, with an emphasis on prevention and promotion of resilience.* It launched in March of 2020 and consists of 1:1 peer support, a peer support group program, town halls/webinars, and an active web site.
The 1:1 peer support sessions typically last 20-30 minutes and provide easy access for all distressed hospital and medical center staff. “We have a phone line staffed by Columbia psychiatrists and psychologists so that a distressed staff member can reach support directly,” he said. The format of these sessions includes a brief discussion of challenges and brainstorming around potential coping strategies. “This is not a psychotherapy session,” Dr. Levenson said. “Each session can be individualized to further assess the type of distress or to implement rating scales such as the Generalized Anxiety Disorder-7 scale to assess for signs and symptoms consistent with GAD. There are options to schedule a second or third peer support session, or a prompt referral within Columbia psychiatry when indicated.”
A typical peer support group meeting lasts about 30 minutes and comprises individual divisions or departments. Some goals of the peer groups are to discuss unique challenges of the work environment and to encourage the members of the group to come up with solutions; to promote team support and coping; to teach resilience-enhancing strategies from empirically based treatments such as CBT, “and to end each meeting with expressions of gratitude and of thanks within the group,” he said.
According to Dr. Levenson, sample questions CopeColumbia faculty use to facilitate coping, include “which coping skills are working for you?”; “Are you able to be present?”; “Have you honored loss with any specific ways or traditions?”; “Do you have any work buddies who support you and vice versa?”; “Can your work community build off each other’s individual strengths to help both the individual and the work group cope optimally?”; and “How can your work team help facilitate each other to best support each other?”
Other aspects of the CopeColumbia program include town halls/grand rounds that range from 30 to 60 minutes in length. “It may be a virtual presentation from a mental health professional on specific aspects of coping such as relaxation techniques,” he said. “The focus is how to manage stress, anxiety, trauma, loss, and grief. It also includes an active Q&A to engage staff participants. The advantage of this format is that you can reach many staff in an entire department.” The program also has an active web site for staff with both internal and external support links including mindfulness, meditation, exercise, parenting suggestions/caregiving, and other resources to promote well-being and resilience for staff and family.
To date, certain themes emerged from the 1:1 and peer support group sessions, including expressions of difficulty adapting to “such a new reality,” compared with the pre-COVID era. “Staff would often express anticipatory anxiety and uncertainty, such as is there going to be another surge of COVID-19 cases, and will there be a change in policies?” Dr. Levenson said. “There was a lot of expression of stress and frustration related to politicizing the virus and public containment strategies, both on a local and national level.”
Staff also mentioned the loss of usual coping strategies because of prolonged social isolation, especially for those doing remote work, and the loss of usual support resources that have helped them in the past. “They also reported delayed trauma and grief reactions, including symptoms of depression, anxiety, and posttraumatic stress,” he said. “Health care workers with children mentioned high levels of stress related to childcare, increased workload, and what seems like an impossible work-life balance.” Many reported exhaustion and irritability, “which could affect and cause tension within the work group and challenges to effective team cohesion,” he said. “There were also stressors related to the impact of racial injustices and the [presidential] election that could exacerbate the impact of COVID-19.”
Dr. Levenson hopes that CopeColumbia serves as a model for other health care systems looking for ways to support the mental well-being of their employees. “We want to promote the message that emotional health should have the same priority level as physical health,” he said. “The term that I like to use is total health. Addressing the well-being of health care workers is critical for a healthy workforce and for delivering high-quality patient care.”
He reported having no relevant financial disclosures related to his presentation.
Correction, 2/28/22: An earlier version of this article misstated Dr. Lourival Baptista-Neto's name.
FROM NPA 2022
Triaging neurocognitive screening after SARS-CoV-2 infection
The study covered in this summary was published in Research Square as a preprint and has not yet been peer reviewed.
Key takeaways
- Focal cognitive deficits are more prevalent in hospitalized patients than ambulatory patients.
- Objective neurocognitive measures can supply crucial information to guide clinical decisions regarding the need for further imaging or neurologic workup and should be included as endpoints in clinical trials.
Why this matters
- Cognitive complaints commonly occur in patients convalescing from COVID-19, although their cause is frequently unclear.
- The researchers evaluated factors that play a role in cognitive impairment in ambulatory versus hospitalized patients during the subacute stage of recovery.
- These results underscore the significance of assessing both subjective and objective complaints in ascertaining the prevalence of cognitive impairment in recovering patients and research participants.
- The drivers of cognitive complaints are likely different in hospitalized COVID-19 patients in comparison with ambulatory COVID-19 patients, so it’s important to understand these factors in making treatment decisions.
- Biopsychosocial factors appear to be a powerful driver of cognitive complaints in recovering ambulatory patients. They can be treated with interventions targeting anxiety, depression, sleep disturbances, and pain, which may prove to be the most efficient and cost-effective approach to prevent disability in individuals with mild manifestations of COVID-19.
- Objective neurocognitive deficits were more prevalent in hospitalized patients – a marker of greater disease severity – with mainly deficits in memory and psychomotor speed. Factors that contribute to focal cognitive deficits in these individuals are emerging and represent a noteworthy realm for future investigation.
Study design
- The trial prospectively recruited patients from a hospital-wide registry at the Mayo Clinic in Jacksonville, Fla.
- All patients tested positive for SARS-CoV-2 infection on a real-time reverse transcriptase polymerase chain-reaction assay between June 2020 and March 2021.
- Patients were 18 years of age or older.
- The researchers excluded those with a pre-existing major neurocognitive disorder.
- To participate, patients needed access to a desktop or laptop computer to complete a test and survey.
- They responded to a comprehensive neuropsychological questionnaire and a computerized cognitive screen using a remote telemedicine platform.
- The researchers compared rates of subjective and objective neuropsychological impairment between the ambulatory and hospitalized groups. Factors linked to impairment were analyzed separately within each group.
Key results
- After laboratory confirmation of SARS-CoV-2 infection, a total of 102 patients (76 ambulatory, 26 hospitalized) completed the symptom inventory and neurocognitive tests in 24 ± 22 days.
- Hospitalized and ambulatory patients self-reported high rates of cognitive impairment (27%-40%). There were no variations between the groups.
- However, hospitalized patients had more significant rates of objective impairment in visual memory (30% vs. 4%; P = .001) and psychomotor speed (41% vs. 15%; P = .008).
- Objective cognitive test performance was linked to anxiety, depression, fatigue, and pain in the ambulatory but not the hospitalized group.
Limitations
- The sample size of hospitalized patients was small.
- A larger fraction of hospitalized patients in the sample completed outcome assessments, compared with ambulatory patients, indicating that remote computerized testing did not present a disproportionate access barrier for patients with more severe illness.
- Owing to limited instances of delirium, seizures, and stroke, it was not possible to directly consider the contributions of these events to post–COVID-19 subjective complaints and objective impairment.
- The researchers depended on a 45-minute computerized test battery, which eliminates exposure risk and is available to patients in remote locations, but it necessitates computer literacy and access to a home desktop computer. While this requirement may have skewed the sample toward a more socioeconomically advantaged and younger population, there were no differences in age, race, or ethnicity between those who completed the computerized outcome assessments and those who did not. For patients who are able to give consent electronically, computerized testing does not pose an additional barrier.
- As a result of this study’s cross-sectional nature, the researchers could not comment on the natural history and long-term risk of COVID-19 cognitive impairment. It will be crucial to monitor cognitive progression at future time points to assess the rate and predictors of cognitive normalization versus decline.
Study disclosures
- Gregory S. Day, a coauthor, owns stock (greater than $10,000) in ANI Pharmaceuticals, a generic pharmaceutical company. He serves as a topic editor for DynaMed (EBSCO), overseeing development of evidence-based educational content, a consultant for Parabon Nanolabs (advice relevant to National Institutes of Health small business grant submission), and as the clinical director of the Anti-NMDA Receptor Encephalitis Foundation, Canada (uncompensated). The other authors have disclosed no relevant financial relationships.
This is a summary of a preprint research study, “Neurocognitive Screening in Patients Following SARS-CoV-2 Infection: Tools for Triage,” written by Karen Blackmon from Mayo Clinic in Florida, on medRxiv. This study has not yet been peer reviewed. The full text of the study can be found on medRxiv.org. A version of this article first appeared on Medscape.com.
The study covered in this summary was published in Research Square as a preprint and has not yet been peer reviewed.
Key takeaways
- Focal cognitive deficits are more prevalent in hospitalized patients than ambulatory patients.
- Objective neurocognitive measures can supply crucial information to guide clinical decisions regarding the need for further imaging or neurologic workup and should be included as endpoints in clinical trials.
Why this matters
- Cognitive complaints commonly occur in patients convalescing from COVID-19, although their cause is frequently unclear.
- The researchers evaluated factors that play a role in cognitive impairment in ambulatory versus hospitalized patients during the subacute stage of recovery.
- These results underscore the significance of assessing both subjective and objective complaints in ascertaining the prevalence of cognitive impairment in recovering patients and research participants.
- The drivers of cognitive complaints are likely different in hospitalized COVID-19 patients in comparison with ambulatory COVID-19 patients, so it’s important to understand these factors in making treatment decisions.
- Biopsychosocial factors appear to be a powerful driver of cognitive complaints in recovering ambulatory patients. They can be treated with interventions targeting anxiety, depression, sleep disturbances, and pain, which may prove to be the most efficient and cost-effective approach to prevent disability in individuals with mild manifestations of COVID-19.
- Objective neurocognitive deficits were more prevalent in hospitalized patients – a marker of greater disease severity – with mainly deficits in memory and psychomotor speed. Factors that contribute to focal cognitive deficits in these individuals are emerging and represent a noteworthy realm for future investigation.
Study design
- The trial prospectively recruited patients from a hospital-wide registry at the Mayo Clinic in Jacksonville, Fla.
- All patients tested positive for SARS-CoV-2 infection on a real-time reverse transcriptase polymerase chain-reaction assay between June 2020 and March 2021.
- Patients were 18 years of age or older.
- The researchers excluded those with a pre-existing major neurocognitive disorder.
- To participate, patients needed access to a desktop or laptop computer to complete a test and survey.
- They responded to a comprehensive neuropsychological questionnaire and a computerized cognitive screen using a remote telemedicine platform.
- The researchers compared rates of subjective and objective neuropsychological impairment between the ambulatory and hospitalized groups. Factors linked to impairment were analyzed separately within each group.
Key results
- After laboratory confirmation of SARS-CoV-2 infection, a total of 102 patients (76 ambulatory, 26 hospitalized) completed the symptom inventory and neurocognitive tests in 24 ± 22 days.
- Hospitalized and ambulatory patients self-reported high rates of cognitive impairment (27%-40%). There were no variations between the groups.
- However, hospitalized patients had more significant rates of objective impairment in visual memory (30% vs. 4%; P = .001) and psychomotor speed (41% vs. 15%; P = .008).
- Objective cognitive test performance was linked to anxiety, depression, fatigue, and pain in the ambulatory but not the hospitalized group.
Limitations
- The sample size of hospitalized patients was small.
- A larger fraction of hospitalized patients in the sample completed outcome assessments, compared with ambulatory patients, indicating that remote computerized testing did not present a disproportionate access barrier for patients with more severe illness.
- Owing to limited instances of delirium, seizures, and stroke, it was not possible to directly consider the contributions of these events to post–COVID-19 subjective complaints and objective impairment.
- The researchers depended on a 45-minute computerized test battery, which eliminates exposure risk and is available to patients in remote locations, but it necessitates computer literacy and access to a home desktop computer. While this requirement may have skewed the sample toward a more socioeconomically advantaged and younger population, there were no differences in age, race, or ethnicity between those who completed the computerized outcome assessments and those who did not. For patients who are able to give consent electronically, computerized testing does not pose an additional barrier.
- As a result of this study’s cross-sectional nature, the researchers could not comment on the natural history and long-term risk of COVID-19 cognitive impairment. It will be crucial to monitor cognitive progression at future time points to assess the rate and predictors of cognitive normalization versus decline.
Study disclosures
- Gregory S. Day, a coauthor, owns stock (greater than $10,000) in ANI Pharmaceuticals, a generic pharmaceutical company. He serves as a topic editor for DynaMed (EBSCO), overseeing development of evidence-based educational content, a consultant for Parabon Nanolabs (advice relevant to National Institutes of Health small business grant submission), and as the clinical director of the Anti-NMDA Receptor Encephalitis Foundation, Canada (uncompensated). The other authors have disclosed no relevant financial relationships.
This is a summary of a preprint research study, “Neurocognitive Screening in Patients Following SARS-CoV-2 Infection: Tools for Triage,” written by Karen Blackmon from Mayo Clinic in Florida, on medRxiv. This study has not yet been peer reviewed. The full text of the study can be found on medRxiv.org. A version of this article first appeared on Medscape.com.
The study covered in this summary was published in Research Square as a preprint and has not yet been peer reviewed.
Key takeaways
- Focal cognitive deficits are more prevalent in hospitalized patients than ambulatory patients.
- Objective neurocognitive measures can supply crucial information to guide clinical decisions regarding the need for further imaging or neurologic workup and should be included as endpoints in clinical trials.
Why this matters
- Cognitive complaints commonly occur in patients convalescing from COVID-19, although their cause is frequently unclear.
- The researchers evaluated factors that play a role in cognitive impairment in ambulatory versus hospitalized patients during the subacute stage of recovery.
- These results underscore the significance of assessing both subjective and objective complaints in ascertaining the prevalence of cognitive impairment in recovering patients and research participants.
- The drivers of cognitive complaints are likely different in hospitalized COVID-19 patients in comparison with ambulatory COVID-19 patients, so it’s important to understand these factors in making treatment decisions.
- Biopsychosocial factors appear to be a powerful driver of cognitive complaints in recovering ambulatory patients. They can be treated with interventions targeting anxiety, depression, sleep disturbances, and pain, which may prove to be the most efficient and cost-effective approach to prevent disability in individuals with mild manifestations of COVID-19.
- Objective neurocognitive deficits were more prevalent in hospitalized patients – a marker of greater disease severity – with mainly deficits in memory and psychomotor speed. Factors that contribute to focal cognitive deficits in these individuals are emerging and represent a noteworthy realm for future investigation.
Study design
- The trial prospectively recruited patients from a hospital-wide registry at the Mayo Clinic in Jacksonville, Fla.
- All patients tested positive for SARS-CoV-2 infection on a real-time reverse transcriptase polymerase chain-reaction assay between June 2020 and March 2021.
- Patients were 18 years of age or older.
- The researchers excluded those with a pre-existing major neurocognitive disorder.
- To participate, patients needed access to a desktop or laptop computer to complete a test and survey.
- They responded to a comprehensive neuropsychological questionnaire and a computerized cognitive screen using a remote telemedicine platform.
- The researchers compared rates of subjective and objective neuropsychological impairment between the ambulatory and hospitalized groups. Factors linked to impairment were analyzed separately within each group.
Key results
- After laboratory confirmation of SARS-CoV-2 infection, a total of 102 patients (76 ambulatory, 26 hospitalized) completed the symptom inventory and neurocognitive tests in 24 ± 22 days.
- Hospitalized and ambulatory patients self-reported high rates of cognitive impairment (27%-40%). There were no variations between the groups.
- However, hospitalized patients had more significant rates of objective impairment in visual memory (30% vs. 4%; P = .001) and psychomotor speed (41% vs. 15%; P = .008).
- Objective cognitive test performance was linked to anxiety, depression, fatigue, and pain in the ambulatory but not the hospitalized group.
Limitations
- The sample size of hospitalized patients was small.
- A larger fraction of hospitalized patients in the sample completed outcome assessments, compared with ambulatory patients, indicating that remote computerized testing did not present a disproportionate access barrier for patients with more severe illness.
- Owing to limited instances of delirium, seizures, and stroke, it was not possible to directly consider the contributions of these events to post–COVID-19 subjective complaints and objective impairment.
- The researchers depended on a 45-minute computerized test battery, which eliminates exposure risk and is available to patients in remote locations, but it necessitates computer literacy and access to a home desktop computer. While this requirement may have skewed the sample toward a more socioeconomically advantaged and younger population, there were no differences in age, race, or ethnicity between those who completed the computerized outcome assessments and those who did not. For patients who are able to give consent electronically, computerized testing does not pose an additional barrier.
- As a result of this study’s cross-sectional nature, the researchers could not comment on the natural history and long-term risk of COVID-19 cognitive impairment. It will be crucial to monitor cognitive progression at future time points to assess the rate and predictors of cognitive normalization versus decline.
Study disclosures
- Gregory S. Day, a coauthor, owns stock (greater than $10,000) in ANI Pharmaceuticals, a generic pharmaceutical company. He serves as a topic editor for DynaMed (EBSCO), overseeing development of evidence-based educational content, a consultant for Parabon Nanolabs (advice relevant to National Institutes of Health small business grant submission), and as the clinical director of the Anti-NMDA Receptor Encephalitis Foundation, Canada (uncompensated). The other authors have disclosed no relevant financial relationships.
This is a summary of a preprint research study, “Neurocognitive Screening in Patients Following SARS-CoV-2 Infection: Tools for Triage,” written by Karen Blackmon from Mayo Clinic in Florida, on medRxiv. This study has not yet been peer reviewed. The full text of the study can be found on medRxiv.org. A version of this article first appeared on Medscape.com.
Five million children have lost a caregiver to COVID-19
As the COVID-19 pandemic enters its third year, the death toll continues to rise and with it, the number of children who may be left without anyone to care for them.
By Oct. 31, 2021, more than 5 million people worldwide had died from COVID-19, and about 5.2 million children had lost a parent or caregiver, according to new research published in the Lancet Child and Adolescent Health.
Of particular note, wrote the authors, was how the number of affected children surged during the latter part of their study period. During the first 14 months of the pandemic (March 1, 2020, to April 30, 2021), 2,737,300 children were affected by COVID-19-related caregiver death. But that number jumped by 90% during the next 6 months, from April 30 to Oct. 31, 2021, to 5,209,000. Essentially, the number of children who were affected nearly doubled, compared with those observed during that first year.
To put these numbers into perspective, study author Charles Nelson, PhD, professor of pediatrics and neuroscience and professor of psychology in the department of psychiatry at Harvard Medical School, Boston, compared it to the HIV/AIDS pandemic. “The current worldwide estimate is now approaching 6 million,” he said. “For HIV, it took 10 years before the number of orphans hit 5 million but for COVID it took 2 years. This should provide some perspective.”
Dr. Nelson pointed out that there are many other differences between the two pandemics. “There was no vaccine for HIV/AIDS, in contrast to the last year or so for COVID, when illness and death could largely be prevented,” he explained. “The politics surrounding HIV-related deaths seemed ‘relatively’ apolitical compared to COVID.”
Another major difference is that children whose parents had HIV were allowed to visit their parents, but for COVID-19, isolation was in place so many children could not see their parents before they died.
There is also more misinformation versus lack of information about COVID-19, compared to HIV/AIDS. “As an example, one young girl who lost her father to COVID was told by her classmates that her father hadn’t really died, he just abandoned the family,” Dr. Nelson said.
Minority communities face heaviest loss
A “companion study” was conducted by the Centers for Disease Control and Prevention, which looked at parental/caregiver death just within the United States. During the period between April 1, 2020, through June 30, 2021, the researchers found that more than 140,000 children under the age of 18 years had lost a parent, custodial grandparent, or grandparent caregiver because of COVID-19. In addition, there were significant racial, ethnic, and geographic disparities in COVID-19–associated death of caregivers, and the highest burden of death was observed in the Southern states along the U.S.-Mexican border for Hispanic children, Southeastern states for Black children, and in states with tribal areas for American Indian/Alaska Native populations. Overall, almost two-thirds (65%) of the children who lost a primary caregiver belonged to a racial or ethnic minority.
But as with the international data, the number of affected children has continued to rise since the end of the original study period. “Seth Flaxman, at Imperial College London, has updated the figures as of end of December for the U.S.,” said Dr. Nelson. The 140,000 has increased to 222,718 who lost a primary or secondary caregiver.
In addition, 192,449 lost a primary caregiver, 175,151 lost a parent, and 30,269 lost a secondary caregiver.
The rate, unfortunately, remains disproportionate to minorities. These data do reflect the inequities that have been observed since the beginning of the pandemic, as COVID-19 unequally affected many racial and ethnic minority groups and put them at a higher risk of severe illness and death. “Native Americans are four times more likely than Whites to be orphaned, and Black and Hispanic children 2.5 times more likely,” said Dr. Nelson.
The COVID Collaborative, a diverse group of leading experts from a wide range of disciplines including health, education, and economics, is working to develop consensus recommendations on pandemic-related issues such as vaccination of children who have lost caregivers. In December 2021, they released Hidden Pain: Children Who Lost a Parent or Caretaker to COVID-19 and What the Nation Can Do to Help Them, a report providing estimates of the number of children who lost a caregiver and concrete recommendations to support them.
“The death of an adult caregiver is life-altering for any child regardless of the circumstances or cause,” said Dan Treglia, PhD, associate professor of practice at the University of Pennsylvania, Philadelphia, and a contributor to Hidden Pain. “Traumatic grief is more common in sudden deaths like accidents where support systems are unable to mobilize in anticipation of the death and COVID-19 patients who die are typically in the hospital for barely a week before they pass.”
This suggests that responses to COVID-19 deaths may be more typical of sudden deaths than those of chronic illness such as cancer, he noted, adding that the pandemic has hindered the systems that children and their caregivers would normally rely on for support.
“Social distancing, for example, has limited informal community relationships critical for emotional health and in the current National Emergency in Children’s Mental Health, as noted by the American Academy of Pediatrics, among others, formal community-based and clinical services are overwhelmed,” said Dr. Treglia.
The authors of Hidden Pain note that the children most likely to lose a parent or other caregiver are generally the most likely to have faced “significant previous adversities that hinder their ability to successfully adapt to new experiences of adversity or trauma.” Studies have now revealed the magnitude of COVID-19–associated parent and caregiver death, and Dr. Treglia pointed out that action is needed from federal, state, and local policymakers to help children who have lost a caregiver to COVID-19.
Solutions needed now
“Their whole world has collapsed around them, as they have lost a provider of love, affection, developmental support, and in many cases a provider of critical financial support,” he said. “The federal government has an unparalleled ability to direct resources and attention and shape policy at lower levels of government, and its leadership is critical if we want to ensure care for COVID-bereaved children in all corners of the country.”
At least one state thus far is moving toward legislation to help this population. In California, a state with a high number of children who have lost a caregiver, the Hope, Opportunity, Perseverance, and Empowerment (HOPE) for Children Act has been introduced into the state legislature. If passed into law, children who lost a parent or caregiver to COVID-19 and are in the state’s foster care system or a low-income household would be eligible for a state-funded trust fund.
But while this is a start, the consequences of caregiver loss go far beyond the economics, and can include depression, PTSD, substance use disorder, lower levels of educational attainment, and subsequent lower levels of employment. However, most children (90%-95%) will experience a normative course of grief, according to the COVID Collaboration, which can be managed through family and social support systems. Community-based interventions, such as grief camps, peer support groups, or a mentoring program can also be very helpful.
Camp Erin, for example, is a bereavement camp for children aged 6-17 years. It is run by Eluna, a national nonprofit that supports children and families impacted by grief or addiction. “Camp Erin is the largest national bereavement program for children who are grieving the loss of a family member or caregiver, or other significant person in their lives,” said Mary FitzGerald, CEO of Eluna. “Many families needed help with these new dynamics of loss due to COVID.”
Led by bereavement professionals and volunteers, Camp Erin is a weekend experience that combines grief education and emotional support with traditional and fun activities. “It’s a safe environment for children to explore grief, and be with other children who are also grieving,” said Ms. FitzGerald. “There are 33 locations and it’s free of charge.”
Dr. Treglia emphasized the necessity of providing immediate financial assistance through well-established funding streams. “For example, Temporary Assistance to Needy Families, Supplemental Nutritional Assistance Program, and Social Security Survivor’s Benefits are a good start to reinforce their economic stability and keep financial disaster from piling onto their personal tragedy,” he said. “We also need to buttress community-based organizations and schools to ensure they have the resources and grief competence to identify bereaved children and can either provide services directly or refer them to organizations that can.”
He added that the infrastructure and knowledge already exist and “it’s a matter of making strategic investments at the necessary scale.”
As the COVID-19 pandemic enters its third year, the death toll continues to rise and with it, the number of children who may be left without anyone to care for them.
By Oct. 31, 2021, more than 5 million people worldwide had died from COVID-19, and about 5.2 million children had lost a parent or caregiver, according to new research published in the Lancet Child and Adolescent Health.
Of particular note, wrote the authors, was how the number of affected children surged during the latter part of their study period. During the first 14 months of the pandemic (March 1, 2020, to April 30, 2021), 2,737,300 children were affected by COVID-19-related caregiver death. But that number jumped by 90% during the next 6 months, from April 30 to Oct. 31, 2021, to 5,209,000. Essentially, the number of children who were affected nearly doubled, compared with those observed during that first year.
To put these numbers into perspective, study author Charles Nelson, PhD, professor of pediatrics and neuroscience and professor of psychology in the department of psychiatry at Harvard Medical School, Boston, compared it to the HIV/AIDS pandemic. “The current worldwide estimate is now approaching 6 million,” he said. “For HIV, it took 10 years before the number of orphans hit 5 million but for COVID it took 2 years. This should provide some perspective.”
Dr. Nelson pointed out that there are many other differences between the two pandemics. “There was no vaccine for HIV/AIDS, in contrast to the last year or so for COVID, when illness and death could largely be prevented,” he explained. “The politics surrounding HIV-related deaths seemed ‘relatively’ apolitical compared to COVID.”
Another major difference is that children whose parents had HIV were allowed to visit their parents, but for COVID-19, isolation was in place so many children could not see their parents before they died.
There is also more misinformation versus lack of information about COVID-19, compared to HIV/AIDS. “As an example, one young girl who lost her father to COVID was told by her classmates that her father hadn’t really died, he just abandoned the family,” Dr. Nelson said.
Minority communities face heaviest loss
A “companion study” was conducted by the Centers for Disease Control and Prevention, which looked at parental/caregiver death just within the United States. During the period between April 1, 2020, through June 30, 2021, the researchers found that more than 140,000 children under the age of 18 years had lost a parent, custodial grandparent, or grandparent caregiver because of COVID-19. In addition, there were significant racial, ethnic, and geographic disparities in COVID-19–associated death of caregivers, and the highest burden of death was observed in the Southern states along the U.S.-Mexican border for Hispanic children, Southeastern states for Black children, and in states with tribal areas for American Indian/Alaska Native populations. Overall, almost two-thirds (65%) of the children who lost a primary caregiver belonged to a racial or ethnic minority.
But as with the international data, the number of affected children has continued to rise since the end of the original study period. “Seth Flaxman, at Imperial College London, has updated the figures as of end of December for the U.S.,” said Dr. Nelson. The 140,000 has increased to 222,718 who lost a primary or secondary caregiver.
In addition, 192,449 lost a primary caregiver, 175,151 lost a parent, and 30,269 lost a secondary caregiver.
The rate, unfortunately, remains disproportionate to minorities. These data do reflect the inequities that have been observed since the beginning of the pandemic, as COVID-19 unequally affected many racial and ethnic minority groups and put them at a higher risk of severe illness and death. “Native Americans are four times more likely than Whites to be orphaned, and Black and Hispanic children 2.5 times more likely,” said Dr. Nelson.
The COVID Collaborative, a diverse group of leading experts from a wide range of disciplines including health, education, and economics, is working to develop consensus recommendations on pandemic-related issues such as vaccination of children who have lost caregivers. In December 2021, they released Hidden Pain: Children Who Lost a Parent or Caretaker to COVID-19 and What the Nation Can Do to Help Them, a report providing estimates of the number of children who lost a caregiver and concrete recommendations to support them.
“The death of an adult caregiver is life-altering for any child regardless of the circumstances or cause,” said Dan Treglia, PhD, associate professor of practice at the University of Pennsylvania, Philadelphia, and a contributor to Hidden Pain. “Traumatic grief is more common in sudden deaths like accidents where support systems are unable to mobilize in anticipation of the death and COVID-19 patients who die are typically in the hospital for barely a week before they pass.”
This suggests that responses to COVID-19 deaths may be more typical of sudden deaths than those of chronic illness such as cancer, he noted, adding that the pandemic has hindered the systems that children and their caregivers would normally rely on for support.
“Social distancing, for example, has limited informal community relationships critical for emotional health and in the current National Emergency in Children’s Mental Health, as noted by the American Academy of Pediatrics, among others, formal community-based and clinical services are overwhelmed,” said Dr. Treglia.
The authors of Hidden Pain note that the children most likely to lose a parent or other caregiver are generally the most likely to have faced “significant previous adversities that hinder their ability to successfully adapt to new experiences of adversity or trauma.” Studies have now revealed the magnitude of COVID-19–associated parent and caregiver death, and Dr. Treglia pointed out that action is needed from federal, state, and local policymakers to help children who have lost a caregiver to COVID-19.
Solutions needed now
“Their whole world has collapsed around them, as they have lost a provider of love, affection, developmental support, and in many cases a provider of critical financial support,” he said. “The federal government has an unparalleled ability to direct resources and attention and shape policy at lower levels of government, and its leadership is critical if we want to ensure care for COVID-bereaved children in all corners of the country.”
At least one state thus far is moving toward legislation to help this population. In California, a state with a high number of children who have lost a caregiver, the Hope, Opportunity, Perseverance, and Empowerment (HOPE) for Children Act has been introduced into the state legislature. If passed into law, children who lost a parent or caregiver to COVID-19 and are in the state’s foster care system or a low-income household would be eligible for a state-funded trust fund.
But while this is a start, the consequences of caregiver loss go far beyond the economics, and can include depression, PTSD, substance use disorder, lower levels of educational attainment, and subsequent lower levels of employment. However, most children (90%-95%) will experience a normative course of grief, according to the COVID Collaboration, which can be managed through family and social support systems. Community-based interventions, such as grief camps, peer support groups, or a mentoring program can also be very helpful.
Camp Erin, for example, is a bereavement camp for children aged 6-17 years. It is run by Eluna, a national nonprofit that supports children and families impacted by grief or addiction. “Camp Erin is the largest national bereavement program for children who are grieving the loss of a family member or caregiver, or other significant person in their lives,” said Mary FitzGerald, CEO of Eluna. “Many families needed help with these new dynamics of loss due to COVID.”
Led by bereavement professionals and volunteers, Camp Erin is a weekend experience that combines grief education and emotional support with traditional and fun activities. “It’s a safe environment for children to explore grief, and be with other children who are also grieving,” said Ms. FitzGerald. “There are 33 locations and it’s free of charge.”
Dr. Treglia emphasized the necessity of providing immediate financial assistance through well-established funding streams. “For example, Temporary Assistance to Needy Families, Supplemental Nutritional Assistance Program, and Social Security Survivor’s Benefits are a good start to reinforce their economic stability and keep financial disaster from piling onto their personal tragedy,” he said. “We also need to buttress community-based organizations and schools to ensure they have the resources and grief competence to identify bereaved children and can either provide services directly or refer them to organizations that can.”
He added that the infrastructure and knowledge already exist and “it’s a matter of making strategic investments at the necessary scale.”
As the COVID-19 pandemic enters its third year, the death toll continues to rise and with it, the number of children who may be left without anyone to care for them.
By Oct. 31, 2021, more than 5 million people worldwide had died from COVID-19, and about 5.2 million children had lost a parent or caregiver, according to new research published in the Lancet Child and Adolescent Health.
Of particular note, wrote the authors, was how the number of affected children surged during the latter part of their study period. During the first 14 months of the pandemic (March 1, 2020, to April 30, 2021), 2,737,300 children were affected by COVID-19-related caregiver death. But that number jumped by 90% during the next 6 months, from April 30 to Oct. 31, 2021, to 5,209,000. Essentially, the number of children who were affected nearly doubled, compared with those observed during that first year.
To put these numbers into perspective, study author Charles Nelson, PhD, professor of pediatrics and neuroscience and professor of psychology in the department of psychiatry at Harvard Medical School, Boston, compared it to the HIV/AIDS pandemic. “The current worldwide estimate is now approaching 6 million,” he said. “For HIV, it took 10 years before the number of orphans hit 5 million but for COVID it took 2 years. This should provide some perspective.”
Dr. Nelson pointed out that there are many other differences between the two pandemics. “There was no vaccine for HIV/AIDS, in contrast to the last year or so for COVID, when illness and death could largely be prevented,” he explained. “The politics surrounding HIV-related deaths seemed ‘relatively’ apolitical compared to COVID.”
Another major difference is that children whose parents had HIV were allowed to visit their parents, but for COVID-19, isolation was in place so many children could not see their parents before they died.
There is also more misinformation versus lack of information about COVID-19, compared to HIV/AIDS. “As an example, one young girl who lost her father to COVID was told by her classmates that her father hadn’t really died, he just abandoned the family,” Dr. Nelson said.
Minority communities face heaviest loss
A “companion study” was conducted by the Centers for Disease Control and Prevention, which looked at parental/caregiver death just within the United States. During the period between April 1, 2020, through June 30, 2021, the researchers found that more than 140,000 children under the age of 18 years had lost a parent, custodial grandparent, or grandparent caregiver because of COVID-19. In addition, there were significant racial, ethnic, and geographic disparities in COVID-19–associated death of caregivers, and the highest burden of death was observed in the Southern states along the U.S.-Mexican border for Hispanic children, Southeastern states for Black children, and in states with tribal areas for American Indian/Alaska Native populations. Overall, almost two-thirds (65%) of the children who lost a primary caregiver belonged to a racial or ethnic minority.
But as with the international data, the number of affected children has continued to rise since the end of the original study period. “Seth Flaxman, at Imperial College London, has updated the figures as of end of December for the U.S.,” said Dr. Nelson. The 140,000 has increased to 222,718 who lost a primary or secondary caregiver.
In addition, 192,449 lost a primary caregiver, 175,151 lost a parent, and 30,269 lost a secondary caregiver.
The rate, unfortunately, remains disproportionate to minorities. These data do reflect the inequities that have been observed since the beginning of the pandemic, as COVID-19 unequally affected many racial and ethnic minority groups and put them at a higher risk of severe illness and death. “Native Americans are four times more likely than Whites to be orphaned, and Black and Hispanic children 2.5 times more likely,” said Dr. Nelson.
The COVID Collaborative, a diverse group of leading experts from a wide range of disciplines including health, education, and economics, is working to develop consensus recommendations on pandemic-related issues such as vaccination of children who have lost caregivers. In December 2021, they released Hidden Pain: Children Who Lost a Parent or Caretaker to COVID-19 and What the Nation Can Do to Help Them, a report providing estimates of the number of children who lost a caregiver and concrete recommendations to support them.
“The death of an adult caregiver is life-altering for any child regardless of the circumstances or cause,” said Dan Treglia, PhD, associate professor of practice at the University of Pennsylvania, Philadelphia, and a contributor to Hidden Pain. “Traumatic grief is more common in sudden deaths like accidents where support systems are unable to mobilize in anticipation of the death and COVID-19 patients who die are typically in the hospital for barely a week before they pass.”
This suggests that responses to COVID-19 deaths may be more typical of sudden deaths than those of chronic illness such as cancer, he noted, adding that the pandemic has hindered the systems that children and their caregivers would normally rely on for support.
“Social distancing, for example, has limited informal community relationships critical for emotional health and in the current National Emergency in Children’s Mental Health, as noted by the American Academy of Pediatrics, among others, formal community-based and clinical services are overwhelmed,” said Dr. Treglia.
The authors of Hidden Pain note that the children most likely to lose a parent or other caregiver are generally the most likely to have faced “significant previous adversities that hinder their ability to successfully adapt to new experiences of adversity or trauma.” Studies have now revealed the magnitude of COVID-19–associated parent and caregiver death, and Dr. Treglia pointed out that action is needed from federal, state, and local policymakers to help children who have lost a caregiver to COVID-19.
Solutions needed now
“Their whole world has collapsed around them, as they have lost a provider of love, affection, developmental support, and in many cases a provider of critical financial support,” he said. “The federal government has an unparalleled ability to direct resources and attention and shape policy at lower levels of government, and its leadership is critical if we want to ensure care for COVID-bereaved children in all corners of the country.”
At least one state thus far is moving toward legislation to help this population. In California, a state with a high number of children who have lost a caregiver, the Hope, Opportunity, Perseverance, and Empowerment (HOPE) for Children Act has been introduced into the state legislature. If passed into law, children who lost a parent or caregiver to COVID-19 and are in the state’s foster care system or a low-income household would be eligible for a state-funded trust fund.
But while this is a start, the consequences of caregiver loss go far beyond the economics, and can include depression, PTSD, substance use disorder, lower levels of educational attainment, and subsequent lower levels of employment. However, most children (90%-95%) will experience a normative course of grief, according to the COVID Collaboration, which can be managed through family and social support systems. Community-based interventions, such as grief camps, peer support groups, or a mentoring program can also be very helpful.
Camp Erin, for example, is a bereavement camp for children aged 6-17 years. It is run by Eluna, a national nonprofit that supports children and families impacted by grief or addiction. “Camp Erin is the largest national bereavement program for children who are grieving the loss of a family member or caregiver, or other significant person in their lives,” said Mary FitzGerald, CEO of Eluna. “Many families needed help with these new dynamics of loss due to COVID.”
Led by bereavement professionals and volunteers, Camp Erin is a weekend experience that combines grief education and emotional support with traditional and fun activities. “It’s a safe environment for children to explore grief, and be with other children who are also grieving,” said Ms. FitzGerald. “There are 33 locations and it’s free of charge.”
Dr. Treglia emphasized the necessity of providing immediate financial assistance through well-established funding streams. “For example, Temporary Assistance to Needy Families, Supplemental Nutritional Assistance Program, and Social Security Survivor’s Benefits are a good start to reinforce their economic stability and keep financial disaster from piling onto their personal tragedy,” he said. “We also need to buttress community-based organizations and schools to ensure they have the resources and grief competence to identify bereaved children and can either provide services directly or refer them to organizations that can.”
He added that the infrastructure and knowledge already exist and “it’s a matter of making strategic investments at the necessary scale.”
FROM THE LANCET CHILD AND ADOLESCENT HEALTH
PTSD symptoms common in families of COVID-19 patients
The pandemic has significantly affected the mental health of family members of patients with COVID-19, including high rates of posttraumatic stress disorder (PTSD), anxiety, and depression, new research suggests.
They also had a higher prevalence of depression and anxiety symptoms.
The results illustrate how the mental health of families has been adversely affected by strict isolation measures instituted at the height of the COVID pandemic, lead author Elie Azoulay, MD, PhD, professor of medicine at Diderot University and director of the Medical Intensive Care Unit, Saint Louis Hospital, Paris, told this news organization.
Such restrictions were unnecessary, Dr. Azoulay noted, adding that everyone, including health care professionals, benefits when families are allowed to interact with their loved ones in the ICU.
He added the study findings also emphasize the importance of social supports.
“We need to develop and really increase what we can do for family members” of patients staying in the ICU, said Dr. Azoulay.
The findings were published online Feb. 18 in JAMA.
Twenty-three ICUs in France
The study included adult family members of patients admitted with ARDS to 23 ICUs in France from January to October 2020.
Patients had a partial pressure of arterial oxygen to fraction of inspired oxygen ratio (PaO2/FiO2) of less than 300, and bilateral opacities on chest radiography not fully explained by cardiac failure or fluid overload.
Two trained clinical psychologists interviewed family members and patients by telephone a median of 112 days after ICU discharge. During this interview, participants completed the Impact of Event Scale Revised (IES-R) and the Hospital Anxiety and Depression Scale (HADS).
The IES-R score ranges from 0 (best) to 88 (worst) with a score of more than 22 indicating presence of PTSD-related symptoms of clinical concern. The HADS has separate subscales for anxiety and depression, with a score of 7 or greater on a 21-point scale indicating symptoms of anxiety or depression.
Family members also rated social supports on a scale from 0 (extremely limited) to 10 (extremely effective). Dr. Azoulay noted that social support is the subjective perception of the extent to which friends, mental health specialists, and others are available and helpful.
Investigators divided patients into two groups depending on whether or not the cause of ARDS was COVID-19. Causes other than COVID-19 mainly included community-acquired pneumonia and influenza.
The primary outcome was the prevalence of PTSD-related symptoms among family members. Secondary outcomes were the prevalence of anxiety and depression in family members.
The analysis included 303 family members of patients with COVID-19 ARDS and 214 family members of patients with non–COVID-19 ARDS. Almost half of the family members were spouses.
Those with family members with COVID-19 were younger than the non-COVID group (median age, 50 vs. 55 years). They were less frequently allowed to visit the ICU (35% vs. 88%) and more commonly received patient information by phone (84% vs. 20%).
Better strategies needed
Results showed PTSD symptoms were significantly more common in family members of patients with than without COVID-10 (35% vs. 19%; difference of 16%; 95% confidence interval, 8%-24%; P < .001).
Anxiety symptoms were significantly more common in the COVID-19 group (41% vs. 34%; difference of 8%; 95% CI, 0%-16%; P = .05), as were depression symptoms (31% vs. 18%; difference of 13%; 95% CI, 6%-21%; P < .001).
About 26% of the hospitalized relatives died. PTSD symptoms were more common among bereaved family members of patients who died from COVID-19 than of patients without COVID-19 (63% vs. 39%; difference of 24%; 95% CI, 7%-40%; P = .008).
In the COVID-19 group, significantly fewer family members reported having attended the funeral (77% vs. 91%, P = .04). This could be because of concerns over transmitting the virus, the investigators noted.
After adjustment for age, sex, and level of social support in a multivariable analysis, COVID-19 ARDS was significantly associated with increased risk for PTSD-related symptoms in family members (odds ratio, 2.05; 95% CI, 1.30-3.23; P =.002).
Other factors independently associated with PTSD symptoms were age, level of social support, and being male.
Factors associated with anxiety included having COVID-19 ARDS, age, being male, and level of social support. COVID-19 ARDS and level of social support were independently associated with depression.
Although isolation measures were implemented to prevent viral transmission during the pandemic, severely restricting family members from interacting with their sick loved ones in the ICU is “very destructive [and] deeply distressing,” said Dr. Azoulay. “It’s almost cruel.”
Fear may be at the heart of the “psycho-trauma” experienced by family members, he said.
“I would say one of the main sources is fear of getting infected, fear of abandoning family members, fear of leaving the kids alone without any support, and fear of infecting others,” he added.
Health care providers should develop strategies to better communicate with family members, who also feel a lot of guilt when they’re unable to be with their sick loved ones, said Dr. Azoulay.
‘Element of fear’
Commenting on the findings for this news organization, O. Joseph Bienvenu, MD, PhD, professor of psychiatry and behavioral sciences at Johns Hopkins Medicine, Baltimore, called the study “solid” and noted the lead author is “a well-recognized clinical researcher.”
It was “remarkable” that investigators were able to include a control group of family members of patients with ARDS not due to COVID-19, added Dr. Bienvenu, who was not involved with the research.
“It sounds like the bottom line is COVID adds an additional element of fear in loved ones,” he said.
Dr. Bienvenu added this fits with his own clinical experience – and noted that some COVID-19 follow-up clinics now include family members in their assessments and care.
“I think this study nicely illustrates the utility of this,” he concluded.
The study received funding from the French Ministry of Health. Dr. Azoulay reported receipt of personal fees from lectures from Pfizer, Gilead, Baxter, and Alexion, and institutional research grants from Merck Sharp and Dohme, Pfizer, Baxter, and Alexion. Dr. Bienvenu has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The pandemic has significantly affected the mental health of family members of patients with COVID-19, including high rates of posttraumatic stress disorder (PTSD), anxiety, and depression, new research suggests.
They also had a higher prevalence of depression and anxiety symptoms.
The results illustrate how the mental health of families has been adversely affected by strict isolation measures instituted at the height of the COVID pandemic, lead author Elie Azoulay, MD, PhD, professor of medicine at Diderot University and director of the Medical Intensive Care Unit, Saint Louis Hospital, Paris, told this news organization.
Such restrictions were unnecessary, Dr. Azoulay noted, adding that everyone, including health care professionals, benefits when families are allowed to interact with their loved ones in the ICU.
He added the study findings also emphasize the importance of social supports.
“We need to develop and really increase what we can do for family members” of patients staying in the ICU, said Dr. Azoulay.
The findings were published online Feb. 18 in JAMA.
Twenty-three ICUs in France
The study included adult family members of patients admitted with ARDS to 23 ICUs in France from January to October 2020.
Patients had a partial pressure of arterial oxygen to fraction of inspired oxygen ratio (PaO2/FiO2) of less than 300, and bilateral opacities on chest radiography not fully explained by cardiac failure or fluid overload.
Two trained clinical psychologists interviewed family members and patients by telephone a median of 112 days after ICU discharge. During this interview, participants completed the Impact of Event Scale Revised (IES-R) and the Hospital Anxiety and Depression Scale (HADS).
The IES-R score ranges from 0 (best) to 88 (worst) with a score of more than 22 indicating presence of PTSD-related symptoms of clinical concern. The HADS has separate subscales for anxiety and depression, with a score of 7 or greater on a 21-point scale indicating symptoms of anxiety or depression.
Family members also rated social supports on a scale from 0 (extremely limited) to 10 (extremely effective). Dr. Azoulay noted that social support is the subjective perception of the extent to which friends, mental health specialists, and others are available and helpful.
Investigators divided patients into two groups depending on whether or not the cause of ARDS was COVID-19. Causes other than COVID-19 mainly included community-acquired pneumonia and influenza.
The primary outcome was the prevalence of PTSD-related symptoms among family members. Secondary outcomes were the prevalence of anxiety and depression in family members.
The analysis included 303 family members of patients with COVID-19 ARDS and 214 family members of patients with non–COVID-19 ARDS. Almost half of the family members were spouses.
Those with family members with COVID-19 were younger than the non-COVID group (median age, 50 vs. 55 years). They were less frequently allowed to visit the ICU (35% vs. 88%) and more commonly received patient information by phone (84% vs. 20%).
Better strategies needed
Results showed PTSD symptoms were significantly more common in family members of patients with than without COVID-10 (35% vs. 19%; difference of 16%; 95% confidence interval, 8%-24%; P < .001).
Anxiety symptoms were significantly more common in the COVID-19 group (41% vs. 34%; difference of 8%; 95% CI, 0%-16%; P = .05), as were depression symptoms (31% vs. 18%; difference of 13%; 95% CI, 6%-21%; P < .001).
About 26% of the hospitalized relatives died. PTSD symptoms were more common among bereaved family members of patients who died from COVID-19 than of patients without COVID-19 (63% vs. 39%; difference of 24%; 95% CI, 7%-40%; P = .008).
In the COVID-19 group, significantly fewer family members reported having attended the funeral (77% vs. 91%, P = .04). This could be because of concerns over transmitting the virus, the investigators noted.
After adjustment for age, sex, and level of social support in a multivariable analysis, COVID-19 ARDS was significantly associated with increased risk for PTSD-related symptoms in family members (odds ratio, 2.05; 95% CI, 1.30-3.23; P =.002).
Other factors independently associated with PTSD symptoms were age, level of social support, and being male.
Factors associated with anxiety included having COVID-19 ARDS, age, being male, and level of social support. COVID-19 ARDS and level of social support were independently associated with depression.
Although isolation measures were implemented to prevent viral transmission during the pandemic, severely restricting family members from interacting with their sick loved ones in the ICU is “very destructive [and] deeply distressing,” said Dr. Azoulay. “It’s almost cruel.”
Fear may be at the heart of the “psycho-trauma” experienced by family members, he said.
“I would say one of the main sources is fear of getting infected, fear of abandoning family members, fear of leaving the kids alone without any support, and fear of infecting others,” he added.
Health care providers should develop strategies to better communicate with family members, who also feel a lot of guilt when they’re unable to be with their sick loved ones, said Dr. Azoulay.
‘Element of fear’
Commenting on the findings for this news organization, O. Joseph Bienvenu, MD, PhD, professor of psychiatry and behavioral sciences at Johns Hopkins Medicine, Baltimore, called the study “solid” and noted the lead author is “a well-recognized clinical researcher.”
It was “remarkable” that investigators were able to include a control group of family members of patients with ARDS not due to COVID-19, added Dr. Bienvenu, who was not involved with the research.
“It sounds like the bottom line is COVID adds an additional element of fear in loved ones,” he said.
Dr. Bienvenu added this fits with his own clinical experience – and noted that some COVID-19 follow-up clinics now include family members in their assessments and care.
“I think this study nicely illustrates the utility of this,” he concluded.
The study received funding from the French Ministry of Health. Dr. Azoulay reported receipt of personal fees from lectures from Pfizer, Gilead, Baxter, and Alexion, and institutional research grants from Merck Sharp and Dohme, Pfizer, Baxter, and Alexion. Dr. Bienvenu has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The pandemic has significantly affected the mental health of family members of patients with COVID-19, including high rates of posttraumatic stress disorder (PTSD), anxiety, and depression, new research suggests.
They also had a higher prevalence of depression and anxiety symptoms.
The results illustrate how the mental health of families has been adversely affected by strict isolation measures instituted at the height of the COVID pandemic, lead author Elie Azoulay, MD, PhD, professor of medicine at Diderot University and director of the Medical Intensive Care Unit, Saint Louis Hospital, Paris, told this news organization.
Such restrictions were unnecessary, Dr. Azoulay noted, adding that everyone, including health care professionals, benefits when families are allowed to interact with their loved ones in the ICU.
He added the study findings also emphasize the importance of social supports.
“We need to develop and really increase what we can do for family members” of patients staying in the ICU, said Dr. Azoulay.
The findings were published online Feb. 18 in JAMA.
Twenty-three ICUs in France
The study included adult family members of patients admitted with ARDS to 23 ICUs in France from January to October 2020.
Patients had a partial pressure of arterial oxygen to fraction of inspired oxygen ratio (PaO2/FiO2) of less than 300, and bilateral opacities on chest radiography not fully explained by cardiac failure or fluid overload.
Two trained clinical psychologists interviewed family members and patients by telephone a median of 112 days after ICU discharge. During this interview, participants completed the Impact of Event Scale Revised (IES-R) and the Hospital Anxiety and Depression Scale (HADS).
The IES-R score ranges from 0 (best) to 88 (worst) with a score of more than 22 indicating presence of PTSD-related symptoms of clinical concern. The HADS has separate subscales for anxiety and depression, with a score of 7 or greater on a 21-point scale indicating symptoms of anxiety or depression.
Family members also rated social supports on a scale from 0 (extremely limited) to 10 (extremely effective). Dr. Azoulay noted that social support is the subjective perception of the extent to which friends, mental health specialists, and others are available and helpful.
Investigators divided patients into two groups depending on whether or not the cause of ARDS was COVID-19. Causes other than COVID-19 mainly included community-acquired pneumonia and influenza.
The primary outcome was the prevalence of PTSD-related symptoms among family members. Secondary outcomes were the prevalence of anxiety and depression in family members.
The analysis included 303 family members of patients with COVID-19 ARDS and 214 family members of patients with non–COVID-19 ARDS. Almost half of the family members were spouses.
Those with family members with COVID-19 were younger than the non-COVID group (median age, 50 vs. 55 years). They were less frequently allowed to visit the ICU (35% vs. 88%) and more commonly received patient information by phone (84% vs. 20%).
Better strategies needed
Results showed PTSD symptoms were significantly more common in family members of patients with than without COVID-10 (35% vs. 19%; difference of 16%; 95% confidence interval, 8%-24%; P < .001).
Anxiety symptoms were significantly more common in the COVID-19 group (41% vs. 34%; difference of 8%; 95% CI, 0%-16%; P = .05), as were depression symptoms (31% vs. 18%; difference of 13%; 95% CI, 6%-21%; P < .001).
About 26% of the hospitalized relatives died. PTSD symptoms were more common among bereaved family members of patients who died from COVID-19 than of patients without COVID-19 (63% vs. 39%; difference of 24%; 95% CI, 7%-40%; P = .008).
In the COVID-19 group, significantly fewer family members reported having attended the funeral (77% vs. 91%, P = .04). This could be because of concerns over transmitting the virus, the investigators noted.
After adjustment for age, sex, and level of social support in a multivariable analysis, COVID-19 ARDS was significantly associated with increased risk for PTSD-related symptoms in family members (odds ratio, 2.05; 95% CI, 1.30-3.23; P =.002).
Other factors independently associated with PTSD symptoms were age, level of social support, and being male.
Factors associated with anxiety included having COVID-19 ARDS, age, being male, and level of social support. COVID-19 ARDS and level of social support were independently associated with depression.
Although isolation measures were implemented to prevent viral transmission during the pandemic, severely restricting family members from interacting with their sick loved ones in the ICU is “very destructive [and] deeply distressing,” said Dr. Azoulay. “It’s almost cruel.”
Fear may be at the heart of the “psycho-trauma” experienced by family members, he said.
“I would say one of the main sources is fear of getting infected, fear of abandoning family members, fear of leaving the kids alone without any support, and fear of infecting others,” he added.
Health care providers should develop strategies to better communicate with family members, who also feel a lot of guilt when they’re unable to be with their sick loved ones, said Dr. Azoulay.
‘Element of fear’
Commenting on the findings for this news organization, O. Joseph Bienvenu, MD, PhD, professor of psychiatry and behavioral sciences at Johns Hopkins Medicine, Baltimore, called the study “solid” and noted the lead author is “a well-recognized clinical researcher.”
It was “remarkable” that investigators were able to include a control group of family members of patients with ARDS not due to COVID-19, added Dr. Bienvenu, who was not involved with the research.
“It sounds like the bottom line is COVID adds an additional element of fear in loved ones,” he said.
Dr. Bienvenu added this fits with his own clinical experience – and noted that some COVID-19 follow-up clinics now include family members in their assessments and care.
“I think this study nicely illustrates the utility of this,” he concluded.
The study received funding from the French Ministry of Health. Dr. Azoulay reported receipt of personal fees from lectures from Pfizer, Gilead, Baxter, and Alexion, and institutional research grants from Merck Sharp and Dohme, Pfizer, Baxter, and Alexion. Dr. Bienvenu has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA