User login
FDA panel backs T-VEC for advanced melanoma, with precautions
SILVER SPRING, MD. – A Food and Drug Administration advisory panel supports approval of talimogene laherparepvec (T-VEC), an oncolytic immunotherapy, voting 22-1 that the overall risk-benefit profile is favorable for treatment of patients with injectable regionally or distantly metastatic melanoma.
At a joint meeting of the FDA’s Oncologic Drugs Advisory Committee and the Cellular, Tissue and Gene Therapies Advisory Committee on April 29, panelists agreed that it was clear that at least some subpopulations of patients can benefit from this treatment, but cautioned that while nonvisceral metastases may respond to treatment, it was not clear whether visceral metastases responded, and that it should not be used to treat visceral disease. They also recommended that labeling should discourage clinicians from using this treatment in patients with substantial metastatic disease.
T-VEC is a first-in-class oncolytic immunotherapy derived from herpes simplex virus type 1 (HSV-1) the virus that causes most cold sores. It has been genetically modified to attenuate its virulence and engineered to express granulocyte-macrophage colony-stimulating factor (GM-CSF), while remaining susceptible to antiviral treatments such as acyclovir. T-VEC is injected directly into cutaneous, subcutaneous, or nodal lesions, “resulting in selective lysis of the injected tumor cells (and not normal tissue),” which “results in the release and presentation of tumor-derived antigens and local expression of GM-CSF to initiate a systemic anti-tumor immune response that also induces regression of non-injected and distant lesions,” according to the Amgen briefing documents. If approved, this would be the first virus-based cancer treatment, the company noted.
The FDA panel looked at a phase III, open-label, multicenter randomized study that compared treatment with T-VEC to GM-CSF (administered subcutaneously) in 436 people with melanoma (stage IIIB/C or stage IV with limited visceral disease burden that was considered unresectable); the trial began before several targeted and biologic treatments that are now available for advanced melanoma were approved. About half the patients had been treated previously for melanoma and more than 20% were older than 75 years; 292 patients were treated with T-VEC (up to 4 mL injected into one or more subcutaneous or nodal melanoma lesions every 1 or 2 weeks until clinically relevant disease progression occurred or there was no more residual tumor to inject) and 141 received GM-CSF daily in the control arm (for 14 days and off for 14 days).
The primary efficacy endpoint was the durable response rate (DRR), defined as the proportion of patients with responses (complete or partial) “maintained continuously for 6 or more months and beginning at any point within 12 months of initiating therapy,” as assessed by a blinded independent committee. That endpoint was met by 16.3% of those treated with T-VEC vs. 2.1% of those on GM-CSF, a significant difference (P < .0001).
Other results included the overall response rate – complete or partial – which was 26.4% in the T-VEC group vs. 5.7% in the control group; Complete response was 10.8% among those on T-VEC, vs. 0.7% among those on GM-CSF.
Among the approximately 400 patients treated with T-VEC in this and five other studies, the most common adverse events were expected, namely, cellulitis and flu-like symptoms, and most adverse events were mild or moderate.
Disease progression and cellulitis were the most common serious adverse events and occurred more often among those on T-VEC (3.1% vs. 1.6%, and 2.4% vs. 0.8%, respectively). Fatal adverse events were higher among those on T-VEC (3.4% vs. 1.6%); disease progression was the most commonly reported.
Almost 6% of those on T-VEC reported herpetic events, mostly oral herpes, but there were no serious herpes complications or cases of secondary transmission. Amgen has proposed a risk management plan to address the risks of the treatment, including herpetic lesions, accidental exposures to health care professionals, and secondary transmission, and postmarketing studies.
Several panelists pointed out that the company‘s claims that T-VEC has a systemic effect was not necessarily substantiated by the data, and that the unresectable disease qualifier should be added to the indication. Other points made by panel members were that the dosing instructions were not sufficient, and that while the safety profile was acceptable, the risks of cellulitis and of shedding on family members, pregnant women, children, health care professionals, and other cancer patients were concerns. Panelists also noted that it is unclear how T-VEC compares to the other treatments that have been approved for advanced melanoma over the past several years.
“What’s very, very clear is there is a response of the injected lesions.” and local control of lesions is important to patients, said panelist Dr. Patrick Hwu, professor in the department of melanoma medical oncology, University of Texas M.D. Anderson Cancer Center, Houston. Based on the data, “this clearly ... will be among the least toxic agents for cancer given in the [melanoma] clinic,” compared to other treatments, he added.
The FDA usually follows advisory panels’ recommendations. An FDA decision on approval is expected by Oct. 27, 2015, according to Amgen. Panelists had no potential conflicts of interest related to this meeting.
SILVER SPRING, MD. – A Food and Drug Administration advisory panel supports approval of talimogene laherparepvec (T-VEC), an oncolytic immunotherapy, voting 22-1 that the overall risk-benefit profile is favorable for treatment of patients with injectable regionally or distantly metastatic melanoma.
At a joint meeting of the FDA’s Oncologic Drugs Advisory Committee and the Cellular, Tissue and Gene Therapies Advisory Committee on April 29, panelists agreed that it was clear that at least some subpopulations of patients can benefit from this treatment, but cautioned that while nonvisceral metastases may respond to treatment, it was not clear whether visceral metastases responded, and that it should not be used to treat visceral disease. They also recommended that labeling should discourage clinicians from using this treatment in patients with substantial metastatic disease.
T-VEC is a first-in-class oncolytic immunotherapy derived from herpes simplex virus type 1 (HSV-1) the virus that causes most cold sores. It has been genetically modified to attenuate its virulence and engineered to express granulocyte-macrophage colony-stimulating factor (GM-CSF), while remaining susceptible to antiviral treatments such as acyclovir. T-VEC is injected directly into cutaneous, subcutaneous, or nodal lesions, “resulting in selective lysis of the injected tumor cells (and not normal tissue),” which “results in the release and presentation of tumor-derived antigens and local expression of GM-CSF to initiate a systemic anti-tumor immune response that also induces regression of non-injected and distant lesions,” according to the Amgen briefing documents. If approved, this would be the first virus-based cancer treatment, the company noted.
The FDA panel looked at a phase III, open-label, multicenter randomized study that compared treatment with T-VEC to GM-CSF (administered subcutaneously) in 436 people with melanoma (stage IIIB/C or stage IV with limited visceral disease burden that was considered unresectable); the trial began before several targeted and biologic treatments that are now available for advanced melanoma were approved. About half the patients had been treated previously for melanoma and more than 20% were older than 75 years; 292 patients were treated with T-VEC (up to 4 mL injected into one or more subcutaneous or nodal melanoma lesions every 1 or 2 weeks until clinically relevant disease progression occurred or there was no more residual tumor to inject) and 141 received GM-CSF daily in the control arm (for 14 days and off for 14 days).
The primary efficacy endpoint was the durable response rate (DRR), defined as the proportion of patients with responses (complete or partial) “maintained continuously for 6 or more months and beginning at any point within 12 months of initiating therapy,” as assessed by a blinded independent committee. That endpoint was met by 16.3% of those treated with T-VEC vs. 2.1% of those on GM-CSF, a significant difference (P < .0001).
Other results included the overall response rate – complete or partial – which was 26.4% in the T-VEC group vs. 5.7% in the control group; Complete response was 10.8% among those on T-VEC, vs. 0.7% among those on GM-CSF.
Among the approximately 400 patients treated with T-VEC in this and five other studies, the most common adverse events were expected, namely, cellulitis and flu-like symptoms, and most adverse events were mild or moderate.
Disease progression and cellulitis were the most common serious adverse events and occurred more often among those on T-VEC (3.1% vs. 1.6%, and 2.4% vs. 0.8%, respectively). Fatal adverse events were higher among those on T-VEC (3.4% vs. 1.6%); disease progression was the most commonly reported.
Almost 6% of those on T-VEC reported herpetic events, mostly oral herpes, but there were no serious herpes complications or cases of secondary transmission. Amgen has proposed a risk management plan to address the risks of the treatment, including herpetic lesions, accidental exposures to health care professionals, and secondary transmission, and postmarketing studies.
Several panelists pointed out that the company‘s claims that T-VEC has a systemic effect was not necessarily substantiated by the data, and that the unresectable disease qualifier should be added to the indication. Other points made by panel members were that the dosing instructions were not sufficient, and that while the safety profile was acceptable, the risks of cellulitis and of shedding on family members, pregnant women, children, health care professionals, and other cancer patients were concerns. Panelists also noted that it is unclear how T-VEC compares to the other treatments that have been approved for advanced melanoma over the past several years.
“What’s very, very clear is there is a response of the injected lesions.” and local control of lesions is important to patients, said panelist Dr. Patrick Hwu, professor in the department of melanoma medical oncology, University of Texas M.D. Anderson Cancer Center, Houston. Based on the data, “this clearly ... will be among the least toxic agents for cancer given in the [melanoma] clinic,” compared to other treatments, he added.
The FDA usually follows advisory panels’ recommendations. An FDA decision on approval is expected by Oct. 27, 2015, according to Amgen. Panelists had no potential conflicts of interest related to this meeting.
SILVER SPRING, MD. – A Food and Drug Administration advisory panel supports approval of talimogene laherparepvec (T-VEC), an oncolytic immunotherapy, voting 22-1 that the overall risk-benefit profile is favorable for treatment of patients with injectable regionally or distantly metastatic melanoma.
At a joint meeting of the FDA’s Oncologic Drugs Advisory Committee and the Cellular, Tissue and Gene Therapies Advisory Committee on April 29, panelists agreed that it was clear that at least some subpopulations of patients can benefit from this treatment, but cautioned that while nonvisceral metastases may respond to treatment, it was not clear whether visceral metastases responded, and that it should not be used to treat visceral disease. They also recommended that labeling should discourage clinicians from using this treatment in patients with substantial metastatic disease.
T-VEC is a first-in-class oncolytic immunotherapy derived from herpes simplex virus type 1 (HSV-1) the virus that causes most cold sores. It has been genetically modified to attenuate its virulence and engineered to express granulocyte-macrophage colony-stimulating factor (GM-CSF), while remaining susceptible to antiviral treatments such as acyclovir. T-VEC is injected directly into cutaneous, subcutaneous, or nodal lesions, “resulting in selective lysis of the injected tumor cells (and not normal tissue),” which “results in the release and presentation of tumor-derived antigens and local expression of GM-CSF to initiate a systemic anti-tumor immune response that also induces regression of non-injected and distant lesions,” according to the Amgen briefing documents. If approved, this would be the first virus-based cancer treatment, the company noted.
The FDA panel looked at a phase III, open-label, multicenter randomized study that compared treatment with T-VEC to GM-CSF (administered subcutaneously) in 436 people with melanoma (stage IIIB/C or stage IV with limited visceral disease burden that was considered unresectable); the trial began before several targeted and biologic treatments that are now available for advanced melanoma were approved. About half the patients had been treated previously for melanoma and more than 20% were older than 75 years; 292 patients were treated with T-VEC (up to 4 mL injected into one or more subcutaneous or nodal melanoma lesions every 1 or 2 weeks until clinically relevant disease progression occurred or there was no more residual tumor to inject) and 141 received GM-CSF daily in the control arm (for 14 days and off for 14 days).
The primary efficacy endpoint was the durable response rate (DRR), defined as the proportion of patients with responses (complete or partial) “maintained continuously for 6 or more months and beginning at any point within 12 months of initiating therapy,” as assessed by a blinded independent committee. That endpoint was met by 16.3% of those treated with T-VEC vs. 2.1% of those on GM-CSF, a significant difference (P < .0001).
Other results included the overall response rate – complete or partial – which was 26.4% in the T-VEC group vs. 5.7% in the control group; Complete response was 10.8% among those on T-VEC, vs. 0.7% among those on GM-CSF.
Among the approximately 400 patients treated with T-VEC in this and five other studies, the most common adverse events were expected, namely, cellulitis and flu-like symptoms, and most adverse events were mild or moderate.
Disease progression and cellulitis were the most common serious adverse events and occurred more often among those on T-VEC (3.1% vs. 1.6%, and 2.4% vs. 0.8%, respectively). Fatal adverse events were higher among those on T-VEC (3.4% vs. 1.6%); disease progression was the most commonly reported.
Almost 6% of those on T-VEC reported herpetic events, mostly oral herpes, but there were no serious herpes complications or cases of secondary transmission. Amgen has proposed a risk management plan to address the risks of the treatment, including herpetic lesions, accidental exposures to health care professionals, and secondary transmission, and postmarketing studies.
Several panelists pointed out that the company‘s claims that T-VEC has a systemic effect was not necessarily substantiated by the data, and that the unresectable disease qualifier should be added to the indication. Other points made by panel members were that the dosing instructions were not sufficient, and that while the safety profile was acceptable, the risks of cellulitis and of shedding on family members, pregnant women, children, health care professionals, and other cancer patients were concerns. Panelists also noted that it is unclear how T-VEC compares to the other treatments that have been approved for advanced melanoma over the past several years.
“What’s very, very clear is there is a response of the injected lesions.” and local control of lesions is important to patients, said panelist Dr. Patrick Hwu, professor in the department of melanoma medical oncology, University of Texas M.D. Anderson Cancer Center, Houston. Based on the data, “this clearly ... will be among the least toxic agents for cancer given in the [melanoma] clinic,” compared to other treatments, he added.
The FDA usually follows advisory panels’ recommendations. An FDA decision on approval is expected by Oct. 27, 2015, according to Amgen. Panelists had no potential conflicts of interest related to this meeting.
AT AN FDA ADVISORY COMMITTEE MEETING
Imaging guides BCC laser ablation
KISSIMMEE, FLA. – Reflective confocal microscopic imaging successfully guided carbon dioxide laser ablation of basal cell carcinomas, and imaging results fully matched those from Mohs histology, a small study found.
“Our results suggest that reflective confocal microscopy can accurately guide carbon dioxide laser ablation of superficial and early nodular basal cell carcinomas,” said Dr. Brian Hibler of Memorial Sloan Kettering Cancer Center in New York. The technique provides a real-time, noninvasive way to delineate the tumor area before ablation and to check for residual tumor between passes with the laser, he said at the annual meeting of the American Society for Laser Medicine and surgery.
While conventional and Mohs microscopic surgeries remain the gold standard for removing basal carcinomas (BCC), surgery is not an option for some patients because of tumor location, comorbidities, or personal preferences, Dr. Hibler noted. Past studies have reported good clinical and cosmetic outcomes with laser ablation of BCCs, but use of the modality has been limited because there was no way to assess response without excision or biopsies. Reflective confocal microscopy (RCM) uses a low-powered laser system that provides cellular-level imaging and can distinguish BCCs, he said.
Dr. Hibler and his colleagues performed baseline RCM of eight BCCs (three on the trunk, three on the extremities, and two on the head and neck) from seven patients aged 29-83 years. Two patients were men and five were women. The patients then underwent carbon dioxide laser ablation with a wavelength of 10,600 nm, pulse duration of 750 microseconds, and fluence of 7.5 J/cm2, using a square pattern and density of 30%. If RCM revealed residual BCC, the researchers repeated the process up to two more times, for a maximum of three passes. They then removed the entire lesion using Mohs micrographic surgery, performing vertical histologic sectioning of the tissue.
Reflective confocal microscopy generated reliable cellular-level images in real time on the tumor surface and up to 150 mcm deep, Dr. Hibler reported. Tissue from BCCs appears as dense nodular areas with adjacent spaces and red blood cell trafficking, he noted. Microscopy results were consistent with Mohs histology findings in all eight cases, including six in which the tumor was completely removed and two with residual tumor. One of these two cases was the only infiltrative BCC in the series, while the other might have been tissue artifact, Dr. Hibler said.
Patients experienced no adverse effects from the interventions, Dr. Hibler reported. “Future studies are planned are planned without Mohs, so we can use reflective confocal microscopy to longitudinally monitor for recurrence,” he added.
The study won an award at the meeting.
Dr. Hibler reported no funding sources and made no disclosures.
KISSIMMEE, FLA. – Reflective confocal microscopic imaging successfully guided carbon dioxide laser ablation of basal cell carcinomas, and imaging results fully matched those from Mohs histology, a small study found.
“Our results suggest that reflective confocal microscopy can accurately guide carbon dioxide laser ablation of superficial and early nodular basal cell carcinomas,” said Dr. Brian Hibler of Memorial Sloan Kettering Cancer Center in New York. The technique provides a real-time, noninvasive way to delineate the tumor area before ablation and to check for residual tumor between passes with the laser, he said at the annual meeting of the American Society for Laser Medicine and surgery.
While conventional and Mohs microscopic surgeries remain the gold standard for removing basal carcinomas (BCC), surgery is not an option for some patients because of tumor location, comorbidities, or personal preferences, Dr. Hibler noted. Past studies have reported good clinical and cosmetic outcomes with laser ablation of BCCs, but use of the modality has been limited because there was no way to assess response without excision or biopsies. Reflective confocal microscopy (RCM) uses a low-powered laser system that provides cellular-level imaging and can distinguish BCCs, he said.
Dr. Hibler and his colleagues performed baseline RCM of eight BCCs (three on the trunk, three on the extremities, and two on the head and neck) from seven patients aged 29-83 years. Two patients were men and five were women. The patients then underwent carbon dioxide laser ablation with a wavelength of 10,600 nm, pulse duration of 750 microseconds, and fluence of 7.5 J/cm2, using a square pattern and density of 30%. If RCM revealed residual BCC, the researchers repeated the process up to two more times, for a maximum of three passes. They then removed the entire lesion using Mohs micrographic surgery, performing vertical histologic sectioning of the tissue.
Reflective confocal microscopy generated reliable cellular-level images in real time on the tumor surface and up to 150 mcm deep, Dr. Hibler reported. Tissue from BCCs appears as dense nodular areas with adjacent spaces and red blood cell trafficking, he noted. Microscopy results were consistent with Mohs histology findings in all eight cases, including six in which the tumor was completely removed and two with residual tumor. One of these two cases was the only infiltrative BCC in the series, while the other might have been tissue artifact, Dr. Hibler said.
Patients experienced no adverse effects from the interventions, Dr. Hibler reported. “Future studies are planned are planned without Mohs, so we can use reflective confocal microscopy to longitudinally monitor for recurrence,” he added.
The study won an award at the meeting.
Dr. Hibler reported no funding sources and made no disclosures.
KISSIMMEE, FLA. – Reflective confocal microscopic imaging successfully guided carbon dioxide laser ablation of basal cell carcinomas, and imaging results fully matched those from Mohs histology, a small study found.
“Our results suggest that reflective confocal microscopy can accurately guide carbon dioxide laser ablation of superficial and early nodular basal cell carcinomas,” said Dr. Brian Hibler of Memorial Sloan Kettering Cancer Center in New York. The technique provides a real-time, noninvasive way to delineate the tumor area before ablation and to check for residual tumor between passes with the laser, he said at the annual meeting of the American Society for Laser Medicine and surgery.
While conventional and Mohs microscopic surgeries remain the gold standard for removing basal carcinomas (BCC), surgery is not an option for some patients because of tumor location, comorbidities, or personal preferences, Dr. Hibler noted. Past studies have reported good clinical and cosmetic outcomes with laser ablation of BCCs, but use of the modality has been limited because there was no way to assess response without excision or biopsies. Reflective confocal microscopy (RCM) uses a low-powered laser system that provides cellular-level imaging and can distinguish BCCs, he said.
Dr. Hibler and his colleagues performed baseline RCM of eight BCCs (three on the trunk, three on the extremities, and two on the head and neck) from seven patients aged 29-83 years. Two patients were men and five were women. The patients then underwent carbon dioxide laser ablation with a wavelength of 10,600 nm, pulse duration of 750 microseconds, and fluence of 7.5 J/cm2, using a square pattern and density of 30%. If RCM revealed residual BCC, the researchers repeated the process up to two more times, for a maximum of three passes. They then removed the entire lesion using Mohs micrographic surgery, performing vertical histologic sectioning of the tissue.
Reflective confocal microscopy generated reliable cellular-level images in real time on the tumor surface and up to 150 mcm deep, Dr. Hibler reported. Tissue from BCCs appears as dense nodular areas with adjacent spaces and red blood cell trafficking, he noted. Microscopy results were consistent with Mohs histology findings in all eight cases, including six in which the tumor was completely removed and two with residual tumor. One of these two cases was the only infiltrative BCC in the series, while the other might have been tissue artifact, Dr. Hibler said.
Patients experienced no adverse effects from the interventions, Dr. Hibler reported. “Future studies are planned are planned without Mohs, so we can use reflective confocal microscopy to longitudinally monitor for recurrence,” he added.
The study won an award at the meeting.
Dr. Hibler reported no funding sources and made no disclosures.
Key clinical point: Reflective confocal microscopy offers noninvasive, real-time imaging to guide laser ablation of basal cell carcinomas.
Major finding: Results from RCM matched those from Mohs histology in all patients.
Data source: Prospective study of eight BCCs in seven patients.
Disclosures: Dr. Hibler reported no funding sources and made no disclosures.
Momentous Melanoma Marker Modality?
Clarke et al published a study online on March 2 in the Journal of Cutaneous Pathology regarding a novel diagnostic test for melanoma. Using quantitative reverse transcriptase–polymerase chain reaction targeting 23 preselected genes, biopsy samples from a variety of melanocytic skin lesions—464 lesions in a training set and 437 lesions in a separate validation set—were analyzed. The test assigned a single numeric score favoring either benign or malignant with sensitivity and specificity of 89% and 93%, respectively (training set), and 90% and 91%, respectively (validation set), when compared to expert consensus dermatopathology review.
What’s the issue?
Any clinician who biopsies multiple melanocytic lesions per day daydreams about a modality that will consistently and accurately distinguish the neoplasms that haunt us the most: the ones with no clear diagnosis and the lesions where intra- and interdepartmental histopathology results vary across the board. In fact, a patient recently told me that I “missed” her “dangerous” melanoma when our dermatopathology and outside consultant opinions stated that the lesion was a dysplastic nevus. The patient personally took the slides to another institution where they were deemed an “evolving” melanoma in situ. Are they all correct? How do we know that something is evolving? Which tumors will eventually be the sinister ones? If we don’t know, then how can a patient understand his/her predicament? What’s a clinician to do?
Reassuringly, in perusing the exhibit hall at the 73rd Annual Meeting of the American Academy of Dermatology, the climate has shifted somewhat. A new zone of molecular and genetic technology has emerged between the rows of pharmaceutical innovation and office supply hardware. The reverse transcriptase–polymerase chain reaction melanoma diagnostic test distinguishes itself with its large study set and measurement parameters, as it quantifies gene expression. Other adjunctive diagnostic modalities have been proven useful in atypical melanocytic proliferations, such as fluorescence in situ hybridization, comparative genomic hybridization, and DNA microarray technology, with focus on physical chromosomal copy alterations; however, it seems as though this new test provides a functional measure and straightforward plus/minus result that may be more universally and objectively relevant and interpretable from a simple skin biopsy. Perhaps the diagnostic technology has now outpaced our limited and confusing vocabulary for melanocytic lesions. Nonetheless, further clinical follow-up, prospective prognostic data, and cost analysis will define its evolving role. How do you think this gene signature test will ultimately influence our interpretation of melanocytic biopsy results?
Clarke et al published a study online on March 2 in the Journal of Cutaneous Pathology regarding a novel diagnostic test for melanoma. Using quantitative reverse transcriptase–polymerase chain reaction targeting 23 preselected genes, biopsy samples from a variety of melanocytic skin lesions—464 lesions in a training set and 437 lesions in a separate validation set—were analyzed. The test assigned a single numeric score favoring either benign or malignant with sensitivity and specificity of 89% and 93%, respectively (training set), and 90% and 91%, respectively (validation set), when compared to expert consensus dermatopathology review.
What’s the issue?
Any clinician who biopsies multiple melanocytic lesions per day daydreams about a modality that will consistently and accurately distinguish the neoplasms that haunt us the most: the ones with no clear diagnosis and the lesions where intra- and interdepartmental histopathology results vary across the board. In fact, a patient recently told me that I “missed” her “dangerous” melanoma when our dermatopathology and outside consultant opinions stated that the lesion was a dysplastic nevus. The patient personally took the slides to another institution where they were deemed an “evolving” melanoma in situ. Are they all correct? How do we know that something is evolving? Which tumors will eventually be the sinister ones? If we don’t know, then how can a patient understand his/her predicament? What’s a clinician to do?
Reassuringly, in perusing the exhibit hall at the 73rd Annual Meeting of the American Academy of Dermatology, the climate has shifted somewhat. A new zone of molecular and genetic technology has emerged between the rows of pharmaceutical innovation and office supply hardware. The reverse transcriptase–polymerase chain reaction melanoma diagnostic test distinguishes itself with its large study set and measurement parameters, as it quantifies gene expression. Other adjunctive diagnostic modalities have been proven useful in atypical melanocytic proliferations, such as fluorescence in situ hybridization, comparative genomic hybridization, and DNA microarray technology, with focus on physical chromosomal copy alterations; however, it seems as though this new test provides a functional measure and straightforward plus/minus result that may be more universally and objectively relevant and interpretable from a simple skin biopsy. Perhaps the diagnostic technology has now outpaced our limited and confusing vocabulary for melanocytic lesions. Nonetheless, further clinical follow-up, prospective prognostic data, and cost analysis will define its evolving role. How do you think this gene signature test will ultimately influence our interpretation of melanocytic biopsy results?
Clarke et al published a study online on March 2 in the Journal of Cutaneous Pathology regarding a novel diagnostic test for melanoma. Using quantitative reverse transcriptase–polymerase chain reaction targeting 23 preselected genes, biopsy samples from a variety of melanocytic skin lesions—464 lesions in a training set and 437 lesions in a separate validation set—were analyzed. The test assigned a single numeric score favoring either benign or malignant with sensitivity and specificity of 89% and 93%, respectively (training set), and 90% and 91%, respectively (validation set), when compared to expert consensus dermatopathology review.
What’s the issue?
Any clinician who biopsies multiple melanocytic lesions per day daydreams about a modality that will consistently and accurately distinguish the neoplasms that haunt us the most: the ones with no clear diagnosis and the lesions where intra- and interdepartmental histopathology results vary across the board. In fact, a patient recently told me that I “missed” her “dangerous” melanoma when our dermatopathology and outside consultant opinions stated that the lesion was a dysplastic nevus. The patient personally took the slides to another institution where they were deemed an “evolving” melanoma in situ. Are they all correct? How do we know that something is evolving? Which tumors will eventually be the sinister ones? If we don’t know, then how can a patient understand his/her predicament? What’s a clinician to do?
Reassuringly, in perusing the exhibit hall at the 73rd Annual Meeting of the American Academy of Dermatology, the climate has shifted somewhat. A new zone of molecular and genetic technology has emerged between the rows of pharmaceutical innovation and office supply hardware. The reverse transcriptase–polymerase chain reaction melanoma diagnostic test distinguishes itself with its large study set and measurement parameters, as it quantifies gene expression. Other adjunctive diagnostic modalities have been proven useful in atypical melanocytic proliferations, such as fluorescence in situ hybridization, comparative genomic hybridization, and DNA microarray technology, with focus on physical chromosomal copy alterations; however, it seems as though this new test provides a functional measure and straightforward plus/minus result that may be more universally and objectively relevant and interpretable from a simple skin biopsy. Perhaps the diagnostic technology has now outpaced our limited and confusing vocabulary for melanocytic lesions. Nonetheless, further clinical follow-up, prospective prognostic data, and cost analysis will define its evolving role. How do you think this gene signature test will ultimately influence our interpretation of melanocytic biopsy results?

Intradermal ALA-PDT linked to long-term remission in BCC
KISSIMMEE, FLA. – Using a needle-free device to inject nodular basal cell carcinomas with intralesional 5-aminolevulinic acid before photodynamic therapy led to complete, years-long remissions and few side effects in a small case series.
“This approach represents an interesting alternative to Mohs, for sure,” Dr. Daniel Barolet said at the annual meeting of the American Society for Laser Medicine and Surgery. “The secret is in the injector nozzle, which lets you inject with multiple openings to get the best uniformity around the tumor.”
Mohs micrographic surgery remains the standard for basal cell carcinoma (BCC) in high-risk sites, and the number of Mohs surgeries has approximately doubled since 2001, said Dr. Barolet, adjunct professor of dermatology at McGill University in Montreal.
Mohs, however, can cause scarring, and BCCs recur in about 4% of patients. In contrast, photodynamic therapy (PDT) is associated with less scarring and pain, fewer complications, shorter recovery times, and lower costs, although the recurrence rate is about 14%, he noted.
Since PDT alone does not efficiently penetrate thick tumor volumes, it works best with pretreatment using agents such as aminolevulinic acid (ALA).
Using needles to inject the tumor, however, can cause pain, vascular damage, vasoconstriction, deep purpura, necrosis, and infection. “Because of this, no-needle injection is an interesting avenue for PDT,” he noted. Needle-free devices currently are used to inject insulin and to administer some vaccines. They are “virtually painless,” noninvasive, and tissue sparing, he said.
To explore the potential role for needle-free injection in ALA-PDT, Dr. Barolot used a prototype high-speed jet to deliver intralesional 5-ALA in the nodular facial BCCs of four patients. He then performed photoactivation with a red light–emitting diode, with continuous wave at 630 nm, irradiance at 50 mW/cm2, and total fluence 50-100 J/cm2.
Patients had no evidence of clinical or histopathologic recurrence for up to 7 years after treatment, Dr. Barolet reported. They experienced mild crusting at treated sites for up to a week after treatment, but no other adverse effects. Two patients needed a second treatment 2 months after the initial treatment to achieve complete remission. “Excellent cosmesis was obtained,” he added, pointing to before and after photos that showed no evidence of lesions several months after treatment.
Multicenter clinical trials are needed to further evaluate the modality, but the preliminary data suggest that intralesional PDT is a reasonable alternative to Mohs for BCCs in high-risk body sites, as long as lesions are few in number and do not affect large areas of the body, Dr. Barolet said.
The modality is especially well suited to “tricky” areas of the body that are difficult to treat with Mohs, he said.
“Developing a user-friendly, disposable no-needle injector will make it much easier for users,” he added. For low-risk BCCs in low-risk sites, conventional treatments such as surgical excision remain the best option, he said.
Dr. Barolet reported no funding sources for the study and said he had no relevant financial disclosures.
KISSIMMEE, FLA. – Using a needle-free device to inject nodular basal cell carcinomas with intralesional 5-aminolevulinic acid before photodynamic therapy led to complete, years-long remissions and few side effects in a small case series.
“This approach represents an interesting alternative to Mohs, for sure,” Dr. Daniel Barolet said at the annual meeting of the American Society for Laser Medicine and Surgery. “The secret is in the injector nozzle, which lets you inject with multiple openings to get the best uniformity around the tumor.”
Mohs micrographic surgery remains the standard for basal cell carcinoma (BCC) in high-risk sites, and the number of Mohs surgeries has approximately doubled since 2001, said Dr. Barolet, adjunct professor of dermatology at McGill University in Montreal.
Mohs, however, can cause scarring, and BCCs recur in about 4% of patients. In contrast, photodynamic therapy (PDT) is associated with less scarring and pain, fewer complications, shorter recovery times, and lower costs, although the recurrence rate is about 14%, he noted.
Since PDT alone does not efficiently penetrate thick tumor volumes, it works best with pretreatment using agents such as aminolevulinic acid (ALA).
Using needles to inject the tumor, however, can cause pain, vascular damage, vasoconstriction, deep purpura, necrosis, and infection. “Because of this, no-needle injection is an interesting avenue for PDT,” he noted. Needle-free devices currently are used to inject insulin and to administer some vaccines. They are “virtually painless,” noninvasive, and tissue sparing, he said.
To explore the potential role for needle-free injection in ALA-PDT, Dr. Barolot used a prototype high-speed jet to deliver intralesional 5-ALA in the nodular facial BCCs of four patients. He then performed photoactivation with a red light–emitting diode, with continuous wave at 630 nm, irradiance at 50 mW/cm2, and total fluence 50-100 J/cm2.
Patients had no evidence of clinical or histopathologic recurrence for up to 7 years after treatment, Dr. Barolet reported. They experienced mild crusting at treated sites for up to a week after treatment, but no other adverse effects. Two patients needed a second treatment 2 months after the initial treatment to achieve complete remission. “Excellent cosmesis was obtained,” he added, pointing to before and after photos that showed no evidence of lesions several months after treatment.
Multicenter clinical trials are needed to further evaluate the modality, but the preliminary data suggest that intralesional PDT is a reasonable alternative to Mohs for BCCs in high-risk body sites, as long as lesions are few in number and do not affect large areas of the body, Dr. Barolet said.
The modality is especially well suited to “tricky” areas of the body that are difficult to treat with Mohs, he said.
“Developing a user-friendly, disposable no-needle injector will make it much easier for users,” he added. For low-risk BCCs in low-risk sites, conventional treatments such as surgical excision remain the best option, he said.
Dr. Barolet reported no funding sources for the study and said he had no relevant financial disclosures.
KISSIMMEE, FLA. – Using a needle-free device to inject nodular basal cell carcinomas with intralesional 5-aminolevulinic acid before photodynamic therapy led to complete, years-long remissions and few side effects in a small case series.
“This approach represents an interesting alternative to Mohs, for sure,” Dr. Daniel Barolet said at the annual meeting of the American Society for Laser Medicine and Surgery. “The secret is in the injector nozzle, which lets you inject with multiple openings to get the best uniformity around the tumor.”
Mohs micrographic surgery remains the standard for basal cell carcinoma (BCC) in high-risk sites, and the number of Mohs surgeries has approximately doubled since 2001, said Dr. Barolet, adjunct professor of dermatology at McGill University in Montreal.
Mohs, however, can cause scarring, and BCCs recur in about 4% of patients. In contrast, photodynamic therapy (PDT) is associated with less scarring and pain, fewer complications, shorter recovery times, and lower costs, although the recurrence rate is about 14%, he noted.
Since PDT alone does not efficiently penetrate thick tumor volumes, it works best with pretreatment using agents such as aminolevulinic acid (ALA).
Using needles to inject the tumor, however, can cause pain, vascular damage, vasoconstriction, deep purpura, necrosis, and infection. “Because of this, no-needle injection is an interesting avenue for PDT,” he noted. Needle-free devices currently are used to inject insulin and to administer some vaccines. They are “virtually painless,” noninvasive, and tissue sparing, he said.
To explore the potential role for needle-free injection in ALA-PDT, Dr. Barolot used a prototype high-speed jet to deliver intralesional 5-ALA in the nodular facial BCCs of four patients. He then performed photoactivation with a red light–emitting diode, with continuous wave at 630 nm, irradiance at 50 mW/cm2, and total fluence 50-100 J/cm2.
Patients had no evidence of clinical or histopathologic recurrence for up to 7 years after treatment, Dr. Barolet reported. They experienced mild crusting at treated sites for up to a week after treatment, but no other adverse effects. Two patients needed a second treatment 2 months after the initial treatment to achieve complete remission. “Excellent cosmesis was obtained,” he added, pointing to before and after photos that showed no evidence of lesions several months after treatment.
Multicenter clinical trials are needed to further evaluate the modality, but the preliminary data suggest that intralesional PDT is a reasonable alternative to Mohs for BCCs in high-risk body sites, as long as lesions are few in number and do not affect large areas of the body, Dr. Barolet said.
The modality is especially well suited to “tricky” areas of the body that are difficult to treat with Mohs, he said.
“Developing a user-friendly, disposable no-needle injector will make it much easier for users,” he added. For low-risk BCCs in low-risk sites, conventional treatments such as surgical excision remain the best option, he said.
Dr. Barolet reported no funding sources for the study and said he had no relevant financial disclosures.
AT LASER 2015
Key clinical point: Intralesional 5-ALA-PDT is a potential alternative to Mohs micrographic surgery for treating basal cell carcinomas in high-risk sites.
Major finding: Four treated patients experienced resolution of recurrent basal cell carcinomas for up to 7 years.
Data source: Series of four cases of recurrent nodular facial basal cell carcinomas.
Disclosures: Dr. Barolet reported no funding sources and declared no relevant financial disclosures.
Effectiveness and safety of ipilimumab therapy in advanced melanoma: evidence from clinical practice sites in the US
Class of 2015: New drugs projected to earn billions and billions
Of all drugs to be released in 2015, the melanoma drug Opdivo (nivolumab) is expected to have the brightest future, according to a report from Thomson Reuters.
With sales forecast to reach nearly $5.7 billion by 2019, Opdivo is at the head of a large 2015 “blockbuster” drug class. Opdivo is followed by a pair of drugs for the cardiovascular system: Praluent (alirocumab) for hypercholesterolemia with projected sales of $4.4 billion and LCZ-696 (sacubitril and valsartan) for chronic heart failure with projected 2019 sales of $3.7 billion, Thomson Reuters said.
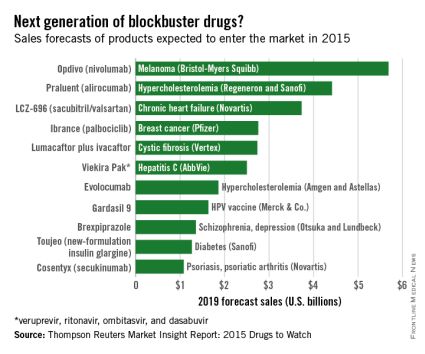
With estimated sales of $2.8 billion, the breast cancer drug Ibrance (palbociclib) is the second oncologic drug making the blockbuster list, with the first noncancer or non-CV drug – lumacaftor plus ivacaftor for cystic fibrosis – rounding out the Top 5 with projected sales of $2.7 billion by 2019.
Next comes Viekira Pak (ombitasvir, paritaprevir, and ritonavir tablets, copackaged with dasabuvir tablets), a hepatitis C virus drug with estimated 2019 sales of $2.5 billion, followed by the hypercholesterolemia/hyperlipidemia drug evolocumab, with projected sales of $1.9 billion. This $2.5 billion disparity between evolocumab and Praluent may be explained by Praluent’s arrival on the market a month sooner, and also because Praluent had a reduced rate of cardiac death, heart attack, and stroke in a phase III trial, a point likely to be relevant to most patients, according to the report.
Overall, 11 drugs are expected to reach $1 billion in sales by 2019, many more than the three blockbusters predicted from the 2014 stock of drugs. However, the two highest-selling new drugs from 2014, Sovaldi (sofosbuvir) and Harvoni (sofosbuvir plus ledipasvir) – both HCV drugs – are each predicted to reach sales of more than $10 billion by 2017, far exceeding anything from 2015, the report said.
The Thomson Reuters Market Insight Report used data collected from 2013 through early February 2015.
Of all drugs to be released in 2015, the melanoma drug Opdivo (nivolumab) is expected to have the brightest future, according to a report from Thomson Reuters.
With sales forecast to reach nearly $5.7 billion by 2019, Opdivo is at the head of a large 2015 “blockbuster” drug class. Opdivo is followed by a pair of drugs for the cardiovascular system: Praluent (alirocumab) for hypercholesterolemia with projected sales of $4.4 billion and LCZ-696 (sacubitril and valsartan) for chronic heart failure with projected 2019 sales of $3.7 billion, Thomson Reuters said.
With estimated sales of $2.8 billion, the breast cancer drug Ibrance (palbociclib) is the second oncologic drug making the blockbuster list, with the first noncancer or non-CV drug – lumacaftor plus ivacaftor for cystic fibrosis – rounding out the Top 5 with projected sales of $2.7 billion by 2019.
Next comes Viekira Pak (ombitasvir, paritaprevir, and ritonavir tablets, copackaged with dasabuvir tablets), a hepatitis C virus drug with estimated 2019 sales of $2.5 billion, followed by the hypercholesterolemia/hyperlipidemia drug evolocumab, with projected sales of $1.9 billion. This $2.5 billion disparity between evolocumab and Praluent may be explained by Praluent’s arrival on the market a month sooner, and also because Praluent had a reduced rate of cardiac death, heart attack, and stroke in a phase III trial, a point likely to be relevant to most patients, according to the report.
Overall, 11 drugs are expected to reach $1 billion in sales by 2019, many more than the three blockbusters predicted from the 2014 stock of drugs. However, the two highest-selling new drugs from 2014, Sovaldi (sofosbuvir) and Harvoni (sofosbuvir plus ledipasvir) – both HCV drugs – are each predicted to reach sales of more than $10 billion by 2017, far exceeding anything from 2015, the report said.
The Thomson Reuters Market Insight Report used data collected from 2013 through early February 2015.
Of all drugs to be released in 2015, the melanoma drug Opdivo (nivolumab) is expected to have the brightest future, according to a report from Thomson Reuters.
With sales forecast to reach nearly $5.7 billion by 2019, Opdivo is at the head of a large 2015 “blockbuster” drug class. Opdivo is followed by a pair of drugs for the cardiovascular system: Praluent (alirocumab) for hypercholesterolemia with projected sales of $4.4 billion and LCZ-696 (sacubitril and valsartan) for chronic heart failure with projected 2019 sales of $3.7 billion, Thomson Reuters said.
With estimated sales of $2.8 billion, the breast cancer drug Ibrance (palbociclib) is the second oncologic drug making the blockbuster list, with the first noncancer or non-CV drug – lumacaftor plus ivacaftor for cystic fibrosis – rounding out the Top 5 with projected sales of $2.7 billion by 2019.
Next comes Viekira Pak (ombitasvir, paritaprevir, and ritonavir tablets, copackaged with dasabuvir tablets), a hepatitis C virus drug with estimated 2019 sales of $2.5 billion, followed by the hypercholesterolemia/hyperlipidemia drug evolocumab, with projected sales of $1.9 billion. This $2.5 billion disparity between evolocumab and Praluent may be explained by Praluent’s arrival on the market a month sooner, and also because Praluent had a reduced rate of cardiac death, heart attack, and stroke in a phase III trial, a point likely to be relevant to most patients, according to the report.
Overall, 11 drugs are expected to reach $1 billion in sales by 2019, many more than the three blockbusters predicted from the 2014 stock of drugs. However, the two highest-selling new drugs from 2014, Sovaldi (sofosbuvir) and Harvoni (sofosbuvir plus ledipasvir) – both HCV drugs – are each predicted to reach sales of more than $10 billion by 2017, far exceeding anything from 2015, the report said.
The Thomson Reuters Market Insight Report used data collected from 2013 through early February 2015.
Pembrolizumab bests ipilimumab in advanced melanoma
Pembrolizumab was superior to ipilimumab, the standard of care, as first-line therapy for advanced melanoma in the phase III KEYNOTE-006 trial.
Pembrolizumab (Keytruda) hit all of its primary survival end points and nearly tripled response rates from 12% with ipilimumab (Yervoy) to 33% in the first frontline head-to-head comparison of the two immune checkpoint inhibitors.
Pembrolizumab reduced the risk of progression by 42% and the risk of death by 31% to 37%, compared with ipilimumab, study author Dr. Antoni Ribas reported at the annual meeting of the American Association for Cancer Research.

“We think that this data should change the paradigm of treatment for these patients, and the standard of care should quickly shift to giving PD-1 antibodies,” he said at a press briefing.
Pembrolizumab, a monoclonal antibody that inhibits programmed death receptor-1 (PD-1), is approved as second-line therapy for unresectable or metastatic melanoma after failing iplimumab or a BRAF inhibitor, if a BRAF V600 mutation is present.
Ipilimumab has been the gold standard against which everything else was measured, but “this is now expected to change the treatment landscape for melanoma. This is a very high impact trial,” Dr. Suzanne Topalian, director of the melanoma program at Johns Hopkins Sidney Kimmel Comprehensive Cancer Center in Baltimore, said during the briefing.
The 2011 approval of ipilimumab, a cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) inhibitor, as first-line therapy for advanced melanoma was a landmark moment, she said, not only for melanoma because it was the first drug ever to show a survival advantage in a randomized trial, but also for immunotherapy because it was the first checkpoint blocker to show such a benefit.
Results of the KEYSTONE-006 trial, simultaneously published on line (N. Engl. J. Med. 2015. DOI: 10.1056/NEJMoa1503093), prompted the safety monitoring committee to recommend stopping the trial early and allowing ipilimumab patients to receive pembrolizumab.

Lead investigator Dr. Caroline Robert, head of dermatology at Institut Gustave-Roussy in Paris, said in a statement that she hoped the results would accelerate regulatory approval of pembrolizumab in Europe, where the drug is still not on the market.
KEYNOTE-006 included 834 patients with unresectable, ipilimumab-naive, stage III or IV melanoma treated with no more than one previous systemic therapy who were randomly assigned to 10 mg/kg pembrolizumab either every 2 weeks or every 3 weeks or four cycles of 3 mg/kg ipilimumab every 3 weeks, until disease progression or unacceptable toxicity. Treatment response was assessed 12 weeks after randomization and every 6 weeks thereafter per RECIST guideline v1.1 by central review and per immune-related response criteria by investigator review.
Two-thirds of patients were treatment naive, 79% had PD-ligand 1(PD-L1)-positive tumors, and 36% had BRAF V600-mutant tumors.
At the first interim analysis after a median follow-up of 8 months, 6-month progression-free survival rates were 47.3% for pembrolizumab every 2 weeks, 46.4% for pembrolizumab every 3 weeks, and 26.5% for ipilimumab (Hazard ratio, 0.58; P < .001), Dr. Antoni Ribas of the University of California Los Angeles Jonsson Comprehensive Cancer Center, reported.
The benefit was seen across all prespecified subgroups, including PD-L1-positive and PD-L1-negative tumors.
At the time of the analysis, responses by RECIST were ongoing in 89.4% of patients treated with pembrolizumab every 2 weeks, 96.7% on pembrolizumab every 3 weeks, and 88% given ipilumumab.
The median duration of response was 251 days in the pembrolizumab every 2 weeks-arm, but had not been reached in the other two arms.
There has been no evidence of resistance, and only a small minority, perhaps 5-10% of patients, have escape lesions or progress after response, he said.
At the second interim analysis after a median follow-up of 13.8 months, 1-year overall survival rates were 74% for pembrolizumab every 2 weeks (HR, 0.63; P = .0005), 68.4% for pembrolizumab every 3 weeks (HR, 0.69; P = .0036), and 58.2% for ipilimumab. The survival benefit extended to all subgroups, except the 18% of patients with PD-L1-negative tumors, although sample sizes were small and confidence intervals wide.
Efficacy and tolerability was similar for both pembrolizumab dosing schedules, Dr. Ribas said. Treatment-related grade 3-4 adverse events were lower in the pembrolizumab every 2 and 3 weeks arms than with ipilimumab (13.3% vs. 10.1% vs. 20%), despite exposure to pembrolizumab being nearly 3 times as long (164 days vs. 151.5 days vs. 50 days).
When asked how the findings would change his practice tomorrow, Dr. Ribas said pembrolizumab should be used first line but that he will continue to use ipilimumab, either alone or in combination with a PD-1 inhibitor, because it can give durable responses. The critical unanswered question of what the most effective sequence or combination of checkpoint inhibitors is will take years to answer.
“This is just the start,” he said. “This is amazing that single-agent checkpoint blockade gives these responses in melanoma and as you will see in lung cancer, but the reality is that there’s two-thirds of patients who do not respond and we have to do something about that.”
The study was funded by Merck Sharp & Dohme. Dr. Ribas is a consultant to Merck, with the honoraria paid to his institution. Dr. Robert is a consultant with honoraria for MSD, Bristol Myers Squibb, Roche, Novartis, GlaxoSmithKline, and Amgen.
Pembrolizumab was superior to ipilimumab, the standard of care, as first-line therapy for advanced melanoma in the phase III KEYNOTE-006 trial.
Pembrolizumab (Keytruda) hit all of its primary survival end points and nearly tripled response rates from 12% with ipilimumab (Yervoy) to 33% in the first frontline head-to-head comparison of the two immune checkpoint inhibitors.
Pembrolizumab reduced the risk of progression by 42% and the risk of death by 31% to 37%, compared with ipilimumab, study author Dr. Antoni Ribas reported at the annual meeting of the American Association for Cancer Research.
“We think that this data should change the paradigm of treatment for these patients, and the standard of care should quickly shift to giving PD-1 antibodies,” he said at a press briefing.
Pembrolizumab, a monoclonal antibody that inhibits programmed death receptor-1 (PD-1), is approved as second-line therapy for unresectable or metastatic melanoma after failing iplimumab or a BRAF inhibitor, if a BRAF V600 mutation is present.
Ipilimumab has been the gold standard against which everything else was measured, but “this is now expected to change the treatment landscape for melanoma. This is a very high impact trial,” Dr. Suzanne Topalian, director of the melanoma program at Johns Hopkins Sidney Kimmel Comprehensive Cancer Center in Baltimore, said during the briefing.
The 2011 approval of ipilimumab, a cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) inhibitor, as first-line therapy for advanced melanoma was a landmark moment, she said, not only for melanoma because it was the first drug ever to show a survival advantage in a randomized trial, but also for immunotherapy because it was the first checkpoint blocker to show such a benefit.
Results of the KEYSTONE-006 trial, simultaneously published on line (N. Engl. J. Med. 2015. DOI: 10.1056/NEJMoa1503093), prompted the safety monitoring committee to recommend stopping the trial early and allowing ipilimumab patients to receive pembrolizumab.
Lead investigator Dr. Caroline Robert, head of dermatology at Institut Gustave-Roussy in Paris, said in a statement that she hoped the results would accelerate regulatory approval of pembrolizumab in Europe, where the drug is still not on the market.
KEYNOTE-006 included 834 patients with unresectable, ipilimumab-naive, stage III or IV melanoma treated with no more than one previous systemic therapy who were randomly assigned to 10 mg/kg pembrolizumab either every 2 weeks or every 3 weeks or four cycles of 3 mg/kg ipilimumab every 3 weeks, until disease progression or unacceptable toxicity. Treatment response was assessed 12 weeks after randomization and every 6 weeks thereafter per RECIST guideline v1.1 by central review and per immune-related response criteria by investigator review.
Two-thirds of patients were treatment naive, 79% had PD-ligand 1(PD-L1)-positive tumors, and 36% had BRAF V600-mutant tumors.
At the first interim analysis after a median follow-up of 8 months, 6-month progression-free survival rates were 47.3% for pembrolizumab every 2 weeks, 46.4% for pembrolizumab every 3 weeks, and 26.5% for ipilimumab (Hazard ratio, 0.58; P < .001), Dr. Antoni Ribas of the University of California Los Angeles Jonsson Comprehensive Cancer Center, reported.
The benefit was seen across all prespecified subgroups, including PD-L1-positive and PD-L1-negative tumors.
At the time of the analysis, responses by RECIST were ongoing in 89.4% of patients treated with pembrolizumab every 2 weeks, 96.7% on pembrolizumab every 3 weeks, and 88% given ipilumumab.
The median duration of response was 251 days in the pembrolizumab every 2 weeks-arm, but had not been reached in the other two arms.
There has been no evidence of resistance, and only a small minority, perhaps 5-10% of patients, have escape lesions or progress after response, he said.
At the second interim analysis after a median follow-up of 13.8 months, 1-year overall survival rates were 74% for pembrolizumab every 2 weeks (HR, 0.63; P = .0005), 68.4% for pembrolizumab every 3 weeks (HR, 0.69; P = .0036), and 58.2% for ipilimumab. The survival benefit extended to all subgroups, except the 18% of patients with PD-L1-negative tumors, although sample sizes were small and confidence intervals wide.
Efficacy and tolerability was similar for both pembrolizumab dosing schedules, Dr. Ribas said. Treatment-related grade 3-4 adverse events were lower in the pembrolizumab every 2 and 3 weeks arms than with ipilimumab (13.3% vs. 10.1% vs. 20%), despite exposure to pembrolizumab being nearly 3 times as long (164 days vs. 151.5 days vs. 50 days).
When asked how the findings would change his practice tomorrow, Dr. Ribas said pembrolizumab should be used first line but that he will continue to use ipilimumab, either alone or in combination with a PD-1 inhibitor, because it can give durable responses. The critical unanswered question of what the most effective sequence or combination of checkpoint inhibitors is will take years to answer.
“This is just the start,” he said. “This is amazing that single-agent checkpoint blockade gives these responses in melanoma and as you will see in lung cancer, but the reality is that there’s two-thirds of patients who do not respond and we have to do something about that.”
The study was funded by Merck Sharp & Dohme. Dr. Ribas is a consultant to Merck, with the honoraria paid to his institution. Dr. Robert is a consultant with honoraria for MSD, Bristol Myers Squibb, Roche, Novartis, GlaxoSmithKline, and Amgen.
Pembrolizumab was superior to ipilimumab, the standard of care, as first-line therapy for advanced melanoma in the phase III KEYNOTE-006 trial.
Pembrolizumab (Keytruda) hit all of its primary survival end points and nearly tripled response rates from 12% with ipilimumab (Yervoy) to 33% in the first frontline head-to-head comparison of the two immune checkpoint inhibitors.
Pembrolizumab reduced the risk of progression by 42% and the risk of death by 31% to 37%, compared with ipilimumab, study author Dr. Antoni Ribas reported at the annual meeting of the American Association for Cancer Research.
“We think that this data should change the paradigm of treatment for these patients, and the standard of care should quickly shift to giving PD-1 antibodies,” he said at a press briefing.
Pembrolizumab, a monoclonal antibody that inhibits programmed death receptor-1 (PD-1), is approved as second-line therapy for unresectable or metastatic melanoma after failing iplimumab or a BRAF inhibitor, if a BRAF V600 mutation is present.
Ipilimumab has been the gold standard against which everything else was measured, but “this is now expected to change the treatment landscape for melanoma. This is a very high impact trial,” Dr. Suzanne Topalian, director of the melanoma program at Johns Hopkins Sidney Kimmel Comprehensive Cancer Center in Baltimore, said during the briefing.
The 2011 approval of ipilimumab, a cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) inhibitor, as first-line therapy for advanced melanoma was a landmark moment, she said, not only for melanoma because it was the first drug ever to show a survival advantage in a randomized trial, but also for immunotherapy because it was the first checkpoint blocker to show such a benefit.
Results of the KEYSTONE-006 trial, simultaneously published on line (N. Engl. J. Med. 2015. DOI: 10.1056/NEJMoa1503093), prompted the safety monitoring committee to recommend stopping the trial early and allowing ipilimumab patients to receive pembrolizumab.
Lead investigator Dr. Caroline Robert, head of dermatology at Institut Gustave-Roussy in Paris, said in a statement that she hoped the results would accelerate regulatory approval of pembrolizumab in Europe, where the drug is still not on the market.
KEYNOTE-006 included 834 patients with unresectable, ipilimumab-naive, stage III or IV melanoma treated with no more than one previous systemic therapy who were randomly assigned to 10 mg/kg pembrolizumab either every 2 weeks or every 3 weeks or four cycles of 3 mg/kg ipilimumab every 3 weeks, until disease progression or unacceptable toxicity. Treatment response was assessed 12 weeks after randomization and every 6 weeks thereafter per RECIST guideline v1.1 by central review and per immune-related response criteria by investigator review.
Two-thirds of patients were treatment naive, 79% had PD-ligand 1(PD-L1)-positive tumors, and 36% had BRAF V600-mutant tumors.
At the first interim analysis after a median follow-up of 8 months, 6-month progression-free survival rates were 47.3% for pembrolizumab every 2 weeks, 46.4% for pembrolizumab every 3 weeks, and 26.5% for ipilimumab (Hazard ratio, 0.58; P < .001), Dr. Antoni Ribas of the University of California Los Angeles Jonsson Comprehensive Cancer Center, reported.
The benefit was seen across all prespecified subgroups, including PD-L1-positive and PD-L1-negative tumors.
At the time of the analysis, responses by RECIST were ongoing in 89.4% of patients treated with pembrolizumab every 2 weeks, 96.7% on pembrolizumab every 3 weeks, and 88% given ipilumumab.
The median duration of response was 251 days in the pembrolizumab every 2 weeks-arm, but had not been reached in the other two arms.
There has been no evidence of resistance, and only a small minority, perhaps 5-10% of patients, have escape lesions or progress after response, he said.
At the second interim analysis after a median follow-up of 13.8 months, 1-year overall survival rates were 74% for pembrolizumab every 2 weeks (HR, 0.63; P = .0005), 68.4% for pembrolizumab every 3 weeks (HR, 0.69; P = .0036), and 58.2% for ipilimumab. The survival benefit extended to all subgroups, except the 18% of patients with PD-L1-negative tumors, although sample sizes were small and confidence intervals wide.
Efficacy and tolerability was similar for both pembrolizumab dosing schedules, Dr. Ribas said. Treatment-related grade 3-4 adverse events were lower in the pembrolizumab every 2 and 3 weeks arms than with ipilimumab (13.3% vs. 10.1% vs. 20%), despite exposure to pembrolizumab being nearly 3 times as long (164 days vs. 151.5 days vs. 50 days).
When asked how the findings would change his practice tomorrow, Dr. Ribas said pembrolizumab should be used first line but that he will continue to use ipilimumab, either alone or in combination with a PD-1 inhibitor, because it can give durable responses. The critical unanswered question of what the most effective sequence or combination of checkpoint inhibitors is will take years to answer.
“This is just the start,” he said. “This is amazing that single-agent checkpoint blockade gives these responses in melanoma and as you will see in lung cancer, but the reality is that there’s two-thirds of patients who do not respond and we have to do something about that.”
The study was funded by Merck Sharp & Dohme. Dr. Ribas is a consultant to Merck, with the honoraria paid to his institution. Dr. Robert is a consultant with honoraria for MSD, Bristol Myers Squibb, Roche, Novartis, GlaxoSmithKline, and Amgen.
FROM THE AACR ANNUAL MEETING
Key clinical point: Pembrolizumab was superior to ipilimumab, the standard of care, for first-line treatment of advanced melanoma.
Major finding: Pembrolizumab reduced the risk of progression by 42% and the risk of death by 31% to 37% compared with ipilimumab.
Data source: Phase III, randomized, open-label trial in 834 patients with advanced melanoma with no more than one prior systemic therapy.
Disclosures: The study was funded by Merck Sharp & Dohme. Dr. Ribas is a consultant to Merck, with the honoraria paid to his institution. Dr. Robert is a consultant with honoraria for MSD, Bristol-Myers Squibb, Roche, Novartis, GlaxoSmithKline, and Amgen.

Sleep disorders in patients with cancer
Sleep disturbances are common among patients with cancer for many reasons. Sleep problems can be present at any stage during treatment for cancer and in some patients, sleep disturbance may be the presenting symptoms that lead to the diagnosis of some types of cancer. Poor sleep impairs quality of life In people with cancer, but most do not specifically complain of sleep problems unless they are explicitly asked. Insomnia and fatigue are most common sleep disorders in this cohort, although primary sleep disorders, including obstructive sleep apnea and restless legs syndrome, which are common in the general population, have not been carefully studied in the oncology setting despite significant their impairment of quality of life.
Click on the PDF icon at the top of this introduction to read the full article.
disorder
Sleep disturbances are common among patients with cancer for many reasons. Sleep problems can be present at any stage during treatment for cancer and in some patients, sleep disturbance may be the presenting symptoms that lead to the diagnosis of some types of cancer. Poor sleep impairs quality of life In people with cancer, but most do not specifically complain of sleep problems unless they are explicitly asked. Insomnia and fatigue are most common sleep disorders in this cohort, although primary sleep disorders, including obstructive sleep apnea and restless legs syndrome, which are common in the general population, have not been carefully studied in the oncology setting despite significant their impairment of quality of life.
Click on the PDF icon at the top of this introduction to read the full article.
Sleep disturbances are common among patients with cancer for many reasons. Sleep problems can be present at any stage during treatment for cancer and in some patients, sleep disturbance may be the presenting symptoms that lead to the diagnosis of some types of cancer. Poor sleep impairs quality of life In people with cancer, but most do not specifically complain of sleep problems unless they are explicitly asked. Insomnia and fatigue are most common sleep disorders in this cohort, although primary sleep disorders, including obstructive sleep apnea and restless legs syndrome, which are common in the general population, have not been carefully studied in the oncology setting despite significant their impairment of quality of life.
Click on the PDF icon at the top of this introduction to read the full article.
disorder
disorder
Update on Melanoma Guidelines: Report From the AAD Meeting
Melanoma was an important topic at multiple sessions of the 73rd Annual Meeting of the American Academy of Dermatology (AAD) in San Francisco, California. Dr. Susan M. Swetter reviews the AAD and National Comprehensive Cancer Network recommendations for biopsy of pigmented suspicious lesions. She also discusses when sentinel lymph node biopsies are recommended and factors that would indicate a patient needs a sentinel lymph node biopsy. Dr. Swetter also outlines surgical margins for melanoma and emphasizes that these are clinical margins taken at the time of surgery, not histologic margins. She concludes with a review of the melanoma subtype lentigo maligna.
Melanoma was an important topic at multiple sessions of the 73rd Annual Meeting of the American Academy of Dermatology (AAD) in San Francisco, California. Dr. Susan M. Swetter reviews the AAD and National Comprehensive Cancer Network recommendations for biopsy of pigmented suspicious lesions. She also discusses when sentinel lymph node biopsies are recommended and factors that would indicate a patient needs a sentinel lymph node biopsy. Dr. Swetter also outlines surgical margins for melanoma and emphasizes that these are clinical margins taken at the time of surgery, not histologic margins. She concludes with a review of the melanoma subtype lentigo maligna.
Melanoma was an important topic at multiple sessions of the 73rd Annual Meeting of the American Academy of Dermatology (AAD) in San Francisco, California. Dr. Susan M. Swetter reviews the AAD and National Comprehensive Cancer Network recommendations for biopsy of pigmented suspicious lesions. She also discusses when sentinel lymph node biopsies are recommended and factors that would indicate a patient needs a sentinel lymph node biopsy. Dr. Swetter also outlines surgical margins for melanoma and emphasizes that these are clinical margins taken at the time of surgery, not histologic margins. She concludes with a review of the melanoma subtype lentigo maligna.

New melanoma therapies may break the bank
HOUSTON – Newer systemic therapies for metastatic malignant melanoma have resulted in significant gains in survival, but at a cost that may be unsustainable in the near future, according to Dr. Jeffrey E. Gershenwald.
Up to one-half of all expenses related to the treatment of malignant melanoma are accounted for by the care of patients with advanced disease, yet patients with distant metastases (stage IV disease) account for only about 2% of all patients, said Dr. Gershenwald, professor of surgical oncology at the University of Texas M.D. Anderson Cancer Center, Houston.

“How best can we achieve the right therapy for the right patient at the right time, and as we learn more and more about some of the therapies, particularly in melanoma, for the right length of time? We can’t really afford to give treatments in perpetuity, so we need to know how long they actually need to be delivered in order to have optimal value for the patient,” he said at the annual Society of Surgical Oncology Cancer Symposium.
Over the last 3 decades, and particularly over the last 5 years, there have been tremendous forward strides in therapy. In 1975, when dacarbazine became the standard of care for metastatic melanoma, it was associated with response rates of only about 6%-15%, durable responses in only 5%-15% of patients, and a median overall survival of about 6-9 months, Dr. Gershenwald reported.
Treatment toxicities, but not response rates, increased with the introduction of interleukin-2 in 1998, which for want of a better drug became the new preferred treatment.
But with the introduction of new systemic therapies, such as immune checkpoint inhibitors (ipilimumab [Yervoy], nivolumab [Opdivo], and pembrolizumab [Keytruda]) and targeted agents (vemurafenib [Zelboraf], dabrafenib [Tafinlar], and trametinib [Mekinist]), response rates have soared, resulting in an improvement in 1-year survival rates from about 30% to 35% in 1970 to as high as 80% in clinical trials in 2014.
Increased survival, higher costs
Dr. Gershenwald pointed to a recently published cost-effectiveness analysis of treatment strategies for BRAF-mutated metastatic melanoma. In it, the authors noted that vemurafenib costs $13,000 per month, translating into $207,000 for a patient with median survival. Patients for whom vemurafenib fails are often put on ipilimumab, at $150,000 per course.
The authors calculated that the incremental cost-effectiveness ratio (ICER) for vemurafenib compared with dacarbazine was nearly $354,993 per quality-adjusted life-year (QALY) gained, a figure that is more than threefold higher than widely accepted thresholds for cost-effective treatment ($50,000-$100,000 per QALY gained).
The ICER for firstline vemurafenib followed by ipilimumab was $158,139, still well above the accepted limits.
The authors of the cost analysis noted that the treatments could become cost effective if drug prices were to drop significantly, or if clinical trials could establish whether it was possible to achieve a durable response without continued therapy.
Going forward, clinicians will need to consider disease burden, including both the extent and growth rate of the disease, as well as the risk of recurrence, in deciding whether to use adjuvant therapies, Dr. Gershenwald said.
In addition, clinical choices will be based on disease biology, predictors of response (although few such predictors currently exist), the likelihood of resistance, and drug toxicities, quality of life, and ease of administration, he said.
Dr. Gershenwald disclosed serving on a Merck advisory board.
HOUSTON – Newer systemic therapies for metastatic malignant melanoma have resulted in significant gains in survival, but at a cost that may be unsustainable in the near future, according to Dr. Jeffrey E. Gershenwald.
Up to one-half of all expenses related to the treatment of malignant melanoma are accounted for by the care of patients with advanced disease, yet patients with distant metastases (stage IV disease) account for only about 2% of all patients, said Dr. Gershenwald, professor of surgical oncology at the University of Texas M.D. Anderson Cancer Center, Houston.
“How best can we achieve the right therapy for the right patient at the right time, and as we learn more and more about some of the therapies, particularly in melanoma, for the right length of time? We can’t really afford to give treatments in perpetuity, so we need to know how long they actually need to be delivered in order to have optimal value for the patient,” he said at the annual Society of Surgical Oncology Cancer Symposium.
Over the last 3 decades, and particularly over the last 5 years, there have been tremendous forward strides in therapy. In 1975, when dacarbazine became the standard of care for metastatic melanoma, it was associated with response rates of only about 6%-15%, durable responses in only 5%-15% of patients, and a median overall survival of about 6-9 months, Dr. Gershenwald reported.
Treatment toxicities, but not response rates, increased with the introduction of interleukin-2 in 1998, which for want of a better drug became the new preferred treatment.
But with the introduction of new systemic therapies, such as immune checkpoint inhibitors (ipilimumab [Yervoy], nivolumab [Opdivo], and pembrolizumab [Keytruda]) and targeted agents (vemurafenib [Zelboraf], dabrafenib [Tafinlar], and trametinib [Mekinist]), response rates have soared, resulting in an improvement in 1-year survival rates from about 30% to 35% in 1970 to as high as 80% in clinical trials in 2014.
Increased survival, higher costs
Dr. Gershenwald pointed to a recently published cost-effectiveness analysis of treatment strategies for BRAF-mutated metastatic melanoma. In it, the authors noted that vemurafenib costs $13,000 per month, translating into $207,000 for a patient with median survival. Patients for whom vemurafenib fails are often put on ipilimumab, at $150,000 per course.
The authors calculated that the incremental cost-effectiveness ratio (ICER) for vemurafenib compared with dacarbazine was nearly $354,993 per quality-adjusted life-year (QALY) gained, a figure that is more than threefold higher than widely accepted thresholds for cost-effective treatment ($50,000-$100,000 per QALY gained).
The ICER for firstline vemurafenib followed by ipilimumab was $158,139, still well above the accepted limits.
The authors of the cost analysis noted that the treatments could become cost effective if drug prices were to drop significantly, or if clinical trials could establish whether it was possible to achieve a durable response without continued therapy.
Going forward, clinicians will need to consider disease burden, including both the extent and growth rate of the disease, as well as the risk of recurrence, in deciding whether to use adjuvant therapies, Dr. Gershenwald said.
In addition, clinical choices will be based on disease biology, predictors of response (although few such predictors currently exist), the likelihood of resistance, and drug toxicities, quality of life, and ease of administration, he said.
Dr. Gershenwald disclosed serving on a Merck advisory board.
HOUSTON – Newer systemic therapies for metastatic malignant melanoma have resulted in significant gains in survival, but at a cost that may be unsustainable in the near future, according to Dr. Jeffrey E. Gershenwald.
Up to one-half of all expenses related to the treatment of malignant melanoma are accounted for by the care of patients with advanced disease, yet patients with distant metastases (stage IV disease) account for only about 2% of all patients, said Dr. Gershenwald, professor of surgical oncology at the University of Texas M.D. Anderson Cancer Center, Houston.
“How best can we achieve the right therapy for the right patient at the right time, and as we learn more and more about some of the therapies, particularly in melanoma, for the right length of time? We can’t really afford to give treatments in perpetuity, so we need to know how long they actually need to be delivered in order to have optimal value for the patient,” he said at the annual Society of Surgical Oncology Cancer Symposium.
Over the last 3 decades, and particularly over the last 5 years, there have been tremendous forward strides in therapy. In 1975, when dacarbazine became the standard of care for metastatic melanoma, it was associated with response rates of only about 6%-15%, durable responses in only 5%-15% of patients, and a median overall survival of about 6-9 months, Dr. Gershenwald reported.
Treatment toxicities, but not response rates, increased with the introduction of interleukin-2 in 1998, which for want of a better drug became the new preferred treatment.
But with the introduction of new systemic therapies, such as immune checkpoint inhibitors (ipilimumab [Yervoy], nivolumab [Opdivo], and pembrolizumab [Keytruda]) and targeted agents (vemurafenib [Zelboraf], dabrafenib [Tafinlar], and trametinib [Mekinist]), response rates have soared, resulting in an improvement in 1-year survival rates from about 30% to 35% in 1970 to as high as 80% in clinical trials in 2014.
Increased survival, higher costs
Dr. Gershenwald pointed to a recently published cost-effectiveness analysis of treatment strategies for BRAF-mutated metastatic melanoma. In it, the authors noted that vemurafenib costs $13,000 per month, translating into $207,000 for a patient with median survival. Patients for whom vemurafenib fails are often put on ipilimumab, at $150,000 per course.
The authors calculated that the incremental cost-effectiveness ratio (ICER) for vemurafenib compared with dacarbazine was nearly $354,993 per quality-adjusted life-year (QALY) gained, a figure that is more than threefold higher than widely accepted thresholds for cost-effective treatment ($50,000-$100,000 per QALY gained).
The ICER for firstline vemurafenib followed by ipilimumab was $158,139, still well above the accepted limits.
The authors of the cost analysis noted that the treatments could become cost effective if drug prices were to drop significantly, or if clinical trials could establish whether it was possible to achieve a durable response without continued therapy.
Going forward, clinicians will need to consider disease burden, including both the extent and growth rate of the disease, as well as the risk of recurrence, in deciding whether to use adjuvant therapies, Dr. Gershenwald said.
In addition, clinical choices will be based on disease biology, predictors of response (although few such predictors currently exist), the likelihood of resistance, and drug toxicities, quality of life, and ease of administration, he said.
Dr. Gershenwald disclosed serving on a Merck advisory board.
AT SSO 2015
Key clinical point: Immunotherapies and targeted agents for metastatic melanoma are effective but very costly.
Major finding: The incremental cost-effectiveness ratio for vemurafenib, compared with dacarbazine, was nearly $354,993 per quality-adjusted life-year gained.
Data source: A review of data on the efficacy and costs of therapy for metastatic malignant melanoma.
Disclosures: Dr. Gershenwald disclosed serving on a Merck advisory board.
