User login
CHMP recommends extending brentuximab approval

Photo from Business Wire
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended extending the current conditional approval of brentuximab vedotin (Adcetris) to include the treatment of adults with CD30+ Hodgkin lymphoma (HL) at increased risk of relapse or progression following autologous stem cell transplant (ASCT).
The CHMP’s recommendation will now be reviewed by the European Commission (EC).
If the recommendation is formally adopted by the EC, brentuximab vedotin will be approved for the aforementioned indication in the 28 member states of the European Union as well as Norway, Liechtenstein, and Iceland.
Brentuximab vedotin already has conditional marketing authorization from the EC for 2 indications:
- To treat adults with relapsed or refractory CD30+ HL after ASCT or following at least 2 prior therapies when ASCT or multi-agent chemotherapy is not a treatment option
- To treat adults with relapsed or refractory systemic anaplastic large-cell lymphoma (sALCL).
In January 2016, the EC approved a Type II variation to include data on the retreatment of adult patients with HL or sALCL who previously responded to brentuximab vedotin and later relapsed.
Brentuximab vedotin is under joint development by Seattle Genetics and Takeda Pharmaceutical Company Limited.
AETHERA trial
The CHMP’s recommendation to extend the approval of brentuximab vedotin is based on results from the phase 3 AETHERA trial.
The trial was designed to compare brentuximab vedotin to placebo, both administered for up to 16 cycles (approximately 1 year) every 3 weeks following ASCT. Results from the trial were published in The Lancet in March 2015 and presented at the 2014 ASH Annual Meeting.
The study enrolled 329 HL patients at risk of relapse or progression, including 165 on the brentuximab vedotin arm and 164 on the placebo arm.
Patients were eligible for enrollment if they had a history of primary refractory HL, relapsed within a year of receiving frontline chemotherapy, and/or had disease outside of the lymph nodes at the time of pre-ASCT relapse.
Brentuximab vedotin conferred a significant increase in progression-free survival over placebo, with a hazard ratio of 0.57 (P=0.001). The median progression-free survival was 43 months for patients who received brentuximab vedotin and 24 months for those who received placebo.
The most common adverse events (≥20%), of any grade and regardless of causality, in the brentuximab vedotin arm were neutropenia (78%), peripheral sensory neuropathy (56%), thrombocytopenia (41%), anemia (27%), upper respiratory tract infection (26%), fatigue (24%), peripheral motor neuropathy (23%), nausea (22%), cough (21%), and diarrhea (20%).
The most common adverse events (≥20%), of any grade and regardless of causality, in the placebo arm were neutropenia (34%), upper respiratory tract infection (23%), and thrombocytopenia (20%).
In all, 67% of patients on the brentuximab vedotin arm experienced peripheral neuropathy. Of those patients, 85% had resolution (59%) or partial improvement (26%) in symptoms at the time of their last evaluation, with a median time to improvement of 23 weeks (range, 0.1-138). ![]()
Photo from Business Wire
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended extending the current conditional approval of brentuximab vedotin (Adcetris) to include the treatment of adults with CD30+ Hodgkin lymphoma (HL) at increased risk of relapse or progression following autologous stem cell transplant (ASCT).
The CHMP’s recommendation will now be reviewed by the European Commission (EC).
If the recommendation is formally adopted by the EC, brentuximab vedotin will be approved for the aforementioned indication in the 28 member states of the European Union as well as Norway, Liechtenstein, and Iceland.
Brentuximab vedotin already has conditional marketing authorization from the EC for 2 indications:
- To treat adults with relapsed or refractory CD30+ HL after ASCT or following at least 2 prior therapies when ASCT or multi-agent chemotherapy is not a treatment option
- To treat adults with relapsed or refractory systemic anaplastic large-cell lymphoma (sALCL).
In January 2016, the EC approved a Type II variation to include data on the retreatment of adult patients with HL or sALCL who previously responded to brentuximab vedotin and later relapsed.
Brentuximab vedotin is under joint development by Seattle Genetics and Takeda Pharmaceutical Company Limited.
AETHERA trial
The CHMP’s recommendation to extend the approval of brentuximab vedotin is based on results from the phase 3 AETHERA trial.
The trial was designed to compare brentuximab vedotin to placebo, both administered for up to 16 cycles (approximately 1 year) every 3 weeks following ASCT. Results from the trial were published in The Lancet in March 2015 and presented at the 2014 ASH Annual Meeting.
The study enrolled 329 HL patients at risk of relapse or progression, including 165 on the brentuximab vedotin arm and 164 on the placebo arm.
Patients were eligible for enrollment if they had a history of primary refractory HL, relapsed within a year of receiving frontline chemotherapy, and/or had disease outside of the lymph nodes at the time of pre-ASCT relapse.
Brentuximab vedotin conferred a significant increase in progression-free survival over placebo, with a hazard ratio of 0.57 (P=0.001). The median progression-free survival was 43 months for patients who received brentuximab vedotin and 24 months for those who received placebo.
The most common adverse events (≥20%), of any grade and regardless of causality, in the brentuximab vedotin arm were neutropenia (78%), peripheral sensory neuropathy (56%), thrombocytopenia (41%), anemia (27%), upper respiratory tract infection (26%), fatigue (24%), peripheral motor neuropathy (23%), nausea (22%), cough (21%), and diarrhea (20%).
The most common adverse events (≥20%), of any grade and regardless of causality, in the placebo arm were neutropenia (34%), upper respiratory tract infection (23%), and thrombocytopenia (20%).
In all, 67% of patients on the brentuximab vedotin arm experienced peripheral neuropathy. Of those patients, 85% had resolution (59%) or partial improvement (26%) in symptoms at the time of their last evaluation, with a median time to improvement of 23 weeks (range, 0.1-138). ![]()
Photo from Business Wire
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended extending the current conditional approval of brentuximab vedotin (Adcetris) to include the treatment of adults with CD30+ Hodgkin lymphoma (HL) at increased risk of relapse or progression following autologous stem cell transplant (ASCT).
The CHMP’s recommendation will now be reviewed by the European Commission (EC).
If the recommendation is formally adopted by the EC, brentuximab vedotin will be approved for the aforementioned indication in the 28 member states of the European Union as well as Norway, Liechtenstein, and Iceland.
Brentuximab vedotin already has conditional marketing authorization from the EC for 2 indications:
- To treat adults with relapsed or refractory CD30+ HL after ASCT or following at least 2 prior therapies when ASCT or multi-agent chemotherapy is not a treatment option
- To treat adults with relapsed or refractory systemic anaplastic large-cell lymphoma (sALCL).
In January 2016, the EC approved a Type II variation to include data on the retreatment of adult patients with HL or sALCL who previously responded to brentuximab vedotin and later relapsed.
Brentuximab vedotin is under joint development by Seattle Genetics and Takeda Pharmaceutical Company Limited.
AETHERA trial
The CHMP’s recommendation to extend the approval of brentuximab vedotin is based on results from the phase 3 AETHERA trial.
The trial was designed to compare brentuximab vedotin to placebo, both administered for up to 16 cycles (approximately 1 year) every 3 weeks following ASCT. Results from the trial were published in The Lancet in March 2015 and presented at the 2014 ASH Annual Meeting.
The study enrolled 329 HL patients at risk of relapse or progression, including 165 on the brentuximab vedotin arm and 164 on the placebo arm.
Patients were eligible for enrollment if they had a history of primary refractory HL, relapsed within a year of receiving frontline chemotherapy, and/or had disease outside of the lymph nodes at the time of pre-ASCT relapse.
Brentuximab vedotin conferred a significant increase in progression-free survival over placebo, with a hazard ratio of 0.57 (P=0.001). The median progression-free survival was 43 months for patients who received brentuximab vedotin and 24 months for those who received placebo.
The most common adverse events (≥20%), of any grade and regardless of causality, in the brentuximab vedotin arm were neutropenia (78%), peripheral sensory neuropathy (56%), thrombocytopenia (41%), anemia (27%), upper respiratory tract infection (26%), fatigue (24%), peripheral motor neuropathy (23%), nausea (22%), cough (21%), and diarrhea (20%).
The most common adverse events (≥20%), of any grade and regardless of causality, in the placebo arm were neutropenia (34%), upper respiratory tract infection (23%), and thrombocytopenia (20%).
In all, 67% of patients on the brentuximab vedotin arm experienced peripheral neuropathy. Of those patients, 85% had resolution (59%) or partial improvement (26%) in symptoms at the time of their last evaluation, with a median time to improvement of 23 weeks (range, 0.1-138). ![]()
Team describes mechanism of aggressive lymphomas

telomeres in green
Image by Claus Azzalin
Researchers say they have identified a mechanism by which defective telomere replication exacerbates tumor growth.
The team found that simultaneous inactivation of the telomere-binding factor POT1 and the tumor suppressor p53 accelerates the onset and increases the severity of T-cell lymphomas.
The research, published in Cell Reports, also suggests a possible way to fight these lymphomas—by targeting the ATR pathway.
The researchers knew that POT1 normally forms a protective cap around telomeres, stopping cell machinery from mistakenly damaging the DNA there and causing harmful mutations.
In fact, POT1 is so critical that cells without functional POT1 would rather die than pass on POT1 mutations. Stress in these cells leads to the activation of ATR, which triggers apoptosis.
However, recent research revealed recurrent mutations affecting POT1 in several cancers, including leukemia and melanoma.
“Somehow, those cells found a way to survive—and thrive,” said Eros Lazzerini Denchi, PhD, of The Scripps Research Institute in La Jolla, California.
“We thought that if we could understand how that happens, maybe we could find a way to kill those cells.”
Using a mouse model, the researchers found that mutations in POT1 lead to cancer when combined with a mutation in p53.
“The cells no longer have the mechanism for dying, and mice develop really aggressive thymic lymphomas,” Dr Lazzerini Denchi said.
When mutated, p53 overrides the protective cell death response initiated by ATR. Then, without POT1 creating a protective cap, the chromosomes are fused together and the DNA is rearranged, driving the accumulation of even more mutations. The mutant cells go on to proliferate and become aggressive tumors.
These findings led the researchers to consider a new strategy for killing these tumors.
They noted that all cells will die if they have no ATR. Since tumors with mutant POT1 already have low ATR levels, the researchers think a drug that knocks out the remaining ATR could kill tumors without affecting healthy cells.
The team plans to investigate this approach in future studies.
“This study shows that by looking at basic biological questions, we can potentially find new ways to treat cancer,” Dr Lazzerini Denchi concluded. ![]()
telomeres in green
Image by Claus Azzalin
Researchers say they have identified a mechanism by which defective telomere replication exacerbates tumor growth.
The team found that simultaneous inactivation of the telomere-binding factor POT1 and the tumor suppressor p53 accelerates the onset and increases the severity of T-cell lymphomas.
The research, published in Cell Reports, also suggests a possible way to fight these lymphomas—by targeting the ATR pathway.
The researchers knew that POT1 normally forms a protective cap around telomeres, stopping cell machinery from mistakenly damaging the DNA there and causing harmful mutations.
In fact, POT1 is so critical that cells without functional POT1 would rather die than pass on POT1 mutations. Stress in these cells leads to the activation of ATR, which triggers apoptosis.
However, recent research revealed recurrent mutations affecting POT1 in several cancers, including leukemia and melanoma.
“Somehow, those cells found a way to survive—and thrive,” said Eros Lazzerini Denchi, PhD, of The Scripps Research Institute in La Jolla, California.
“We thought that if we could understand how that happens, maybe we could find a way to kill those cells.”
Using a mouse model, the researchers found that mutations in POT1 lead to cancer when combined with a mutation in p53.
“The cells no longer have the mechanism for dying, and mice develop really aggressive thymic lymphomas,” Dr Lazzerini Denchi said.
When mutated, p53 overrides the protective cell death response initiated by ATR. Then, without POT1 creating a protective cap, the chromosomes are fused together and the DNA is rearranged, driving the accumulation of even more mutations. The mutant cells go on to proliferate and become aggressive tumors.
These findings led the researchers to consider a new strategy for killing these tumors.
They noted that all cells will die if they have no ATR. Since tumors with mutant POT1 already have low ATR levels, the researchers think a drug that knocks out the remaining ATR could kill tumors without affecting healthy cells.
The team plans to investigate this approach in future studies.
“This study shows that by looking at basic biological questions, we can potentially find new ways to treat cancer,” Dr Lazzerini Denchi concluded. ![]()
telomeres in green
Image by Claus Azzalin
Researchers say they have identified a mechanism by which defective telomere replication exacerbates tumor growth.
The team found that simultaneous inactivation of the telomere-binding factor POT1 and the tumor suppressor p53 accelerates the onset and increases the severity of T-cell lymphomas.
The research, published in Cell Reports, also suggests a possible way to fight these lymphomas—by targeting the ATR pathway.
The researchers knew that POT1 normally forms a protective cap around telomeres, stopping cell machinery from mistakenly damaging the DNA there and causing harmful mutations.
In fact, POT1 is so critical that cells without functional POT1 would rather die than pass on POT1 mutations. Stress in these cells leads to the activation of ATR, which triggers apoptosis.
However, recent research revealed recurrent mutations affecting POT1 in several cancers, including leukemia and melanoma.
“Somehow, those cells found a way to survive—and thrive,” said Eros Lazzerini Denchi, PhD, of The Scripps Research Institute in La Jolla, California.
“We thought that if we could understand how that happens, maybe we could find a way to kill those cells.”
Using a mouse model, the researchers found that mutations in POT1 lead to cancer when combined with a mutation in p53.
“The cells no longer have the mechanism for dying, and mice develop really aggressive thymic lymphomas,” Dr Lazzerini Denchi said.
When mutated, p53 overrides the protective cell death response initiated by ATR. Then, without POT1 creating a protective cap, the chromosomes are fused together and the DNA is rearranged, driving the accumulation of even more mutations. The mutant cells go on to proliferate and become aggressive tumors.
These findings led the researchers to consider a new strategy for killing these tumors.
They noted that all cells will die if they have no ATR. Since tumors with mutant POT1 already have low ATR levels, the researchers think a drug that knocks out the remaining ATR could kill tumors without affecting healthy cells.
The team plans to investigate this approach in future studies.
“This study shows that by looking at basic biological questions, we can potentially find new ways to treat cancer,” Dr Lazzerini Denchi concluded. ![]()
Why patients don’t report possible cancer symptoms

Photo courtesy of NIH
Worrying about wasting their doctor’s time is stopping people from reporting symptoms that might be related to cancer, according to a small study published in the British Journal of General Practice.
The goal of the study was to determine why some people are more likely than others to worry about wasting a general practitioner’s (GP’s) time and delay reporting possible cancer symptoms.
“People worrying about wasting their doctor’s time is one of the challenges we need to tackle when thinking about trying to diagnose cancer earlier,” said study author Katriina Whitaker, PhD, of the University of Surrey in the UK.
“We need to get to the root of the problem and find out why people are feeling worried. Not a lot of work has been done on this so far. Our study draws attention to some reasons patients put off going to their GP to check out possible cancer symptoms.”
For this study, Dr Whitaker and her colleagues conducted interviews with subjects in London, South East England, and North West England.
The subjects were recruited from a sample of 2042 adults, age 50 and older, who completed a survey that included a list of “cancer alarm symptoms.”
Ultimately, the researchers interviewed 62 subjects who had reported symptoms at baseline, were still present at the 3-month follow-up, and had agreed to be contacted.
The interviews revealed a few reasons why subjects were hesitant to report symptoms to their GP.
Some subjects felt that long waiting times for appointments indicated GPs were very busy, so they shouldn’t bother making an appointment unless symptoms seemed very serious.
Other subjects felt that seeking help when their symptoms did not seem serious—ie, persistent, worsening, or life-threatening—was a waste of a doctor’s time.
Still other subjects were hesitant to seek help because their doctors had been dismissive about symptoms in the past.
On the other hand, subjects who reported positive interactions with GPs or good relationships with them were less worried about time-wasting.
And other subjects weren’t worried about wasting their doctor’s time because they think of GPs as fulfilling a service financed by taxpayers.
“We’ve all had times where we’ve wondered if we should go to see a GP, but getting unusual or persistent changes checked out is really important,” said Julie Sharp, head of health and patient information at Cancer Research UK, which funded this study.
“Worrying about wasting a GP’s time should not put people off. Doctors are there to help spot cancer symptoms early when treatment is more likely to be successful, and delaying a visit could save up bigger problems for later. So if you’ve noticed anything that isn’t normal for you, make an appointment to see your doctor.” ![]()
Photo courtesy of NIH
Worrying about wasting their doctor’s time is stopping people from reporting symptoms that might be related to cancer, according to a small study published in the British Journal of General Practice.
The goal of the study was to determine why some people are more likely than others to worry about wasting a general practitioner’s (GP’s) time and delay reporting possible cancer symptoms.
“People worrying about wasting their doctor’s time is one of the challenges we need to tackle when thinking about trying to diagnose cancer earlier,” said study author Katriina Whitaker, PhD, of the University of Surrey in the UK.
“We need to get to the root of the problem and find out why people are feeling worried. Not a lot of work has been done on this so far. Our study draws attention to some reasons patients put off going to their GP to check out possible cancer symptoms.”
For this study, Dr Whitaker and her colleagues conducted interviews with subjects in London, South East England, and North West England.
The subjects were recruited from a sample of 2042 adults, age 50 and older, who completed a survey that included a list of “cancer alarm symptoms.”
Ultimately, the researchers interviewed 62 subjects who had reported symptoms at baseline, were still present at the 3-month follow-up, and had agreed to be contacted.
The interviews revealed a few reasons why subjects were hesitant to report symptoms to their GP.
Some subjects felt that long waiting times for appointments indicated GPs were very busy, so they shouldn’t bother making an appointment unless symptoms seemed very serious.
Other subjects felt that seeking help when their symptoms did not seem serious—ie, persistent, worsening, or life-threatening—was a waste of a doctor’s time.
Still other subjects were hesitant to seek help because their doctors had been dismissive about symptoms in the past.
On the other hand, subjects who reported positive interactions with GPs or good relationships with them were less worried about time-wasting.
And other subjects weren’t worried about wasting their doctor’s time because they think of GPs as fulfilling a service financed by taxpayers.
“We’ve all had times where we’ve wondered if we should go to see a GP, but getting unusual or persistent changes checked out is really important,” said Julie Sharp, head of health and patient information at Cancer Research UK, which funded this study.
“Worrying about wasting a GP’s time should not put people off. Doctors are there to help spot cancer symptoms early when treatment is more likely to be successful, and delaying a visit could save up bigger problems for later. So if you’ve noticed anything that isn’t normal for you, make an appointment to see your doctor.” ![]()
Photo courtesy of NIH
Worrying about wasting their doctor’s time is stopping people from reporting symptoms that might be related to cancer, according to a small study published in the British Journal of General Practice.
The goal of the study was to determine why some people are more likely than others to worry about wasting a general practitioner’s (GP’s) time and delay reporting possible cancer symptoms.
“People worrying about wasting their doctor’s time is one of the challenges we need to tackle when thinking about trying to diagnose cancer earlier,” said study author Katriina Whitaker, PhD, of the University of Surrey in the UK.
“We need to get to the root of the problem and find out why people are feeling worried. Not a lot of work has been done on this so far. Our study draws attention to some reasons patients put off going to their GP to check out possible cancer symptoms.”
For this study, Dr Whitaker and her colleagues conducted interviews with subjects in London, South East England, and North West England.
The subjects were recruited from a sample of 2042 adults, age 50 and older, who completed a survey that included a list of “cancer alarm symptoms.”
Ultimately, the researchers interviewed 62 subjects who had reported symptoms at baseline, were still present at the 3-month follow-up, and had agreed to be contacted.
The interviews revealed a few reasons why subjects were hesitant to report symptoms to their GP.
Some subjects felt that long waiting times for appointments indicated GPs were very busy, so they shouldn’t bother making an appointment unless symptoms seemed very serious.
Other subjects felt that seeking help when their symptoms did not seem serious—ie, persistent, worsening, or life-threatening—was a waste of a doctor’s time.
Still other subjects were hesitant to seek help because their doctors had been dismissive about symptoms in the past.
On the other hand, subjects who reported positive interactions with GPs or good relationships with them were less worried about time-wasting.
And other subjects weren’t worried about wasting their doctor’s time because they think of GPs as fulfilling a service financed by taxpayers.
“We’ve all had times where we’ve wondered if we should go to see a GP, but getting unusual or persistent changes checked out is really important,” said Julie Sharp, head of health and patient information at Cancer Research UK, which funded this study.
“Worrying about wasting a GP’s time should not put people off. Doctors are there to help spot cancer symptoms early when treatment is more likely to be successful, and delaying a visit could save up bigger problems for later. So if you’ve noticed anything that isn’t normal for you, make an appointment to see your doctor.” ![]()
ASCT still a player for multiple myeloma
Even in this era of novel therapies for multiple myeloma, for patients with newly diagnosed disease, autologous stem cell transplant (ASCT) after chemotherapy provides benefits in terms of disease progression and extent of response, compared with chemotherapy alone. The benefit of ASCT was especially pronounced among certain groups of high-risk patients.
Novel proteasome inhibitors and immunomodulators “have dramatically increased the complete response rate and significantly extended progression-free survival and overall survival in previously untreated multiple myeloma patients,” Dr. Michele Cavo, head of the Seragnoli Institute of Hematology at the University of Bologna School of Medicine in Italy, said at a presscast in advance of the annual meeting of the American Society of Clinical Oncology.
But questions remain about how these newer agents perform, compared with high-dose melphalan (HDM) followed by ASCT, traditionally seen as the standard of care for younger and fit patients with newly diagnosed disease.
EMN02/HO95 is a large, prospective, multicenter, intergroup, randomized phase III study that addresses this question, as well as single vs. double ASCT and the use of consolidation therapy or not. The study includes patients 65 years old or younger, and the trial protocol involves induction therapy with bortezomib (Velcade)–cyclophosphamide-dexamethasone (VCD) and subsequent collection of peripheral blood stem cells.
Patients were then randomly assigned to receive bortezomib-melphalan-prednisone (VMP) or HDM as intensification therapy in centers that had a single ASCT policy. For those centers doing double (tandem) ASCT procedures, the randomization was to VMP vs. HDM + single ASCT vs. HDM + double ASCT.
Patients in each treatment arm then underwent another randomization to consolidation therapy with bortezomib-lenalidomide (Revlimid)–dexamethasone or no consolidation. All patients received lenalidomide maintenance until disease progression or toxicity. At the time of a preliminary analysis of trial data in January 2016, results from the second randomization to consolidation or no consolidation therapy were not yet complete. This first prespecified interim analysis was performed after at least 33% of the required events had occurred.
Early results show ASCT benefit
Early results on 1,266 patients (VMP, n = 512; HDM, n = 754) show that a median progression-free survival (PFS) was not yet reached after a median follow-up of 23.9 months from the first randomization (to VMP vs. HDM+ASCT), the primary endpoint of the trial.
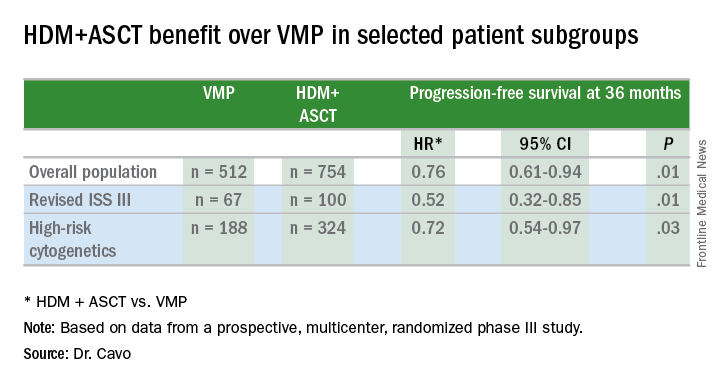
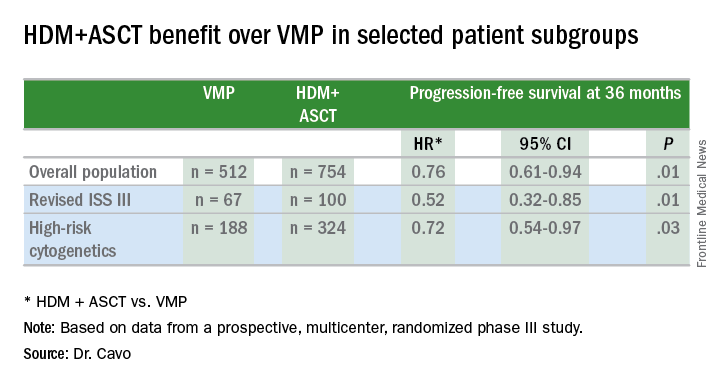
In the overall patient population, patients achieved a significant 24% benefit in PFS when given HDM+ASCT up front (hazard ratio, 0.76 vs. VMP), and this benefit extended to certain patient subgroups, as well.
“PFS benefit with bortezomib-based ASCT was of relevance for patients at high risk of early relapse, in particular for those with revised ISS [International Staging System] stage III and high-risk cytogenetic profiles, who had a relative reduction in the risk of progression or death of 48% and 28%, respectively,” Dr. Cavo said.
Other predictors of longer PFS were ISS stage I (HR, 0.44; 95% confidence interval, 0.28-067; P less than .0001), standard risk cytogenetics (HR, 0.57; 95% CI, 0.41-0.78; P less than .0001), randomization to the HDM+ASCT arm (HR, 0.61; 95% CI, 0.45-0.82; P = .001), and less than 60% bone marrow plasma cells (HR, 0.67; 95% CI, 0.48-0.99; P = .014).
More patients receiving ASCT up front had a significantly greater reduction in tumor volume of at least 90%, as indicated by the composite of very good partial remission, complete response, and stringent complete response, which was achieved in 74.0% in the VMP arm and in 84.4% of the HDM+ASCT arm (P less than .0001).
For patients at low risk of relapse, Dr. Cavo said longer follow up will be needed to compare the different arms of the study, and future analyses will delineate the effects of consolidation or no consolidation therapy and the use of the VMP regimen, compared with single or double ASCT.
ASCO president Dr. Julie Vose said that even with effective novel agents available, older, proven approaches still retain their value. “This study demonstrated that combining the best of both worlds – initial therapy with a novel agent followed by stem cell transplant – resulted in the best patient outcomes,” she said.
Even in this era of novel therapies for multiple myeloma, for patients with newly diagnosed disease, autologous stem cell transplant (ASCT) after chemotherapy provides benefits in terms of disease progression and extent of response, compared with chemotherapy alone. The benefit of ASCT was especially pronounced among certain groups of high-risk patients.
Novel proteasome inhibitors and immunomodulators “have dramatically increased the complete response rate and significantly extended progression-free survival and overall survival in previously untreated multiple myeloma patients,” Dr. Michele Cavo, head of the Seragnoli Institute of Hematology at the University of Bologna School of Medicine in Italy, said at a presscast in advance of the annual meeting of the American Society of Clinical Oncology.
But questions remain about how these newer agents perform, compared with high-dose melphalan (HDM) followed by ASCT, traditionally seen as the standard of care for younger and fit patients with newly diagnosed disease.
EMN02/HO95 is a large, prospective, multicenter, intergroup, randomized phase III study that addresses this question, as well as single vs. double ASCT and the use of consolidation therapy or not. The study includes patients 65 years old or younger, and the trial protocol involves induction therapy with bortezomib (Velcade)–cyclophosphamide-dexamethasone (VCD) and subsequent collection of peripheral blood stem cells.
Patients were then randomly assigned to receive bortezomib-melphalan-prednisone (VMP) or HDM as intensification therapy in centers that had a single ASCT policy. For those centers doing double (tandem) ASCT procedures, the randomization was to VMP vs. HDM + single ASCT vs. HDM + double ASCT.
Patients in each treatment arm then underwent another randomization to consolidation therapy with bortezomib-lenalidomide (Revlimid)–dexamethasone or no consolidation. All patients received lenalidomide maintenance until disease progression or toxicity. At the time of a preliminary analysis of trial data in January 2016, results from the second randomization to consolidation or no consolidation therapy were not yet complete. This first prespecified interim analysis was performed after at least 33% of the required events had occurred.
Early results show ASCT benefit
Early results on 1,266 patients (VMP, n = 512; HDM, n = 754) show that a median progression-free survival (PFS) was not yet reached after a median follow-up of 23.9 months from the first randomization (to VMP vs. HDM+ASCT), the primary endpoint of the trial.
In the overall patient population, patients achieved a significant 24% benefit in PFS when given HDM+ASCT up front (hazard ratio, 0.76 vs. VMP), and this benefit extended to certain patient subgroups, as well.
“PFS benefit with bortezomib-based ASCT was of relevance for patients at high risk of early relapse, in particular for those with revised ISS [International Staging System] stage III and high-risk cytogenetic profiles, who had a relative reduction in the risk of progression or death of 48% and 28%, respectively,” Dr. Cavo said.
Other predictors of longer PFS were ISS stage I (HR, 0.44; 95% confidence interval, 0.28-067; P less than .0001), standard risk cytogenetics (HR, 0.57; 95% CI, 0.41-0.78; P less than .0001), randomization to the HDM+ASCT arm (HR, 0.61; 95% CI, 0.45-0.82; P = .001), and less than 60% bone marrow plasma cells (HR, 0.67; 95% CI, 0.48-0.99; P = .014).
More patients receiving ASCT up front had a significantly greater reduction in tumor volume of at least 90%, as indicated by the composite of very good partial remission, complete response, and stringent complete response, which was achieved in 74.0% in the VMP arm and in 84.4% of the HDM+ASCT arm (P less than .0001).
For patients at low risk of relapse, Dr. Cavo said longer follow up will be needed to compare the different arms of the study, and future analyses will delineate the effects of consolidation or no consolidation therapy and the use of the VMP regimen, compared with single or double ASCT.
ASCO president Dr. Julie Vose said that even with effective novel agents available, older, proven approaches still retain their value. “This study demonstrated that combining the best of both worlds – initial therapy with a novel agent followed by stem cell transplant – resulted in the best patient outcomes,” she said.
Even in this era of novel therapies for multiple myeloma, for patients with newly diagnosed disease, autologous stem cell transplant (ASCT) after chemotherapy provides benefits in terms of disease progression and extent of response, compared with chemotherapy alone. The benefit of ASCT was especially pronounced among certain groups of high-risk patients.
Novel proteasome inhibitors and immunomodulators “have dramatically increased the complete response rate and significantly extended progression-free survival and overall survival in previously untreated multiple myeloma patients,” Dr. Michele Cavo, head of the Seragnoli Institute of Hematology at the University of Bologna School of Medicine in Italy, said at a presscast in advance of the annual meeting of the American Society of Clinical Oncology.
But questions remain about how these newer agents perform, compared with high-dose melphalan (HDM) followed by ASCT, traditionally seen as the standard of care for younger and fit patients with newly diagnosed disease.
EMN02/HO95 is a large, prospective, multicenter, intergroup, randomized phase III study that addresses this question, as well as single vs. double ASCT and the use of consolidation therapy or not. The study includes patients 65 years old or younger, and the trial protocol involves induction therapy with bortezomib (Velcade)–cyclophosphamide-dexamethasone (VCD) and subsequent collection of peripheral blood stem cells.
Patients were then randomly assigned to receive bortezomib-melphalan-prednisone (VMP) or HDM as intensification therapy in centers that had a single ASCT policy. For those centers doing double (tandem) ASCT procedures, the randomization was to VMP vs. HDM + single ASCT vs. HDM + double ASCT.
Patients in each treatment arm then underwent another randomization to consolidation therapy with bortezomib-lenalidomide (Revlimid)–dexamethasone or no consolidation. All patients received lenalidomide maintenance until disease progression or toxicity. At the time of a preliminary analysis of trial data in January 2016, results from the second randomization to consolidation or no consolidation therapy were not yet complete. This first prespecified interim analysis was performed after at least 33% of the required events had occurred.
Early results show ASCT benefit
Early results on 1,266 patients (VMP, n = 512; HDM, n = 754) show that a median progression-free survival (PFS) was not yet reached after a median follow-up of 23.9 months from the first randomization (to VMP vs. HDM+ASCT), the primary endpoint of the trial.
In the overall patient population, patients achieved a significant 24% benefit in PFS when given HDM+ASCT up front (hazard ratio, 0.76 vs. VMP), and this benefit extended to certain patient subgroups, as well.
“PFS benefit with bortezomib-based ASCT was of relevance for patients at high risk of early relapse, in particular for those with revised ISS [International Staging System] stage III and high-risk cytogenetic profiles, who had a relative reduction in the risk of progression or death of 48% and 28%, respectively,” Dr. Cavo said.
Other predictors of longer PFS were ISS stage I (HR, 0.44; 95% confidence interval, 0.28-067; P less than .0001), standard risk cytogenetics (HR, 0.57; 95% CI, 0.41-0.78; P less than .0001), randomization to the HDM+ASCT arm (HR, 0.61; 95% CI, 0.45-0.82; P = .001), and less than 60% bone marrow plasma cells (HR, 0.67; 95% CI, 0.48-0.99; P = .014).
More patients receiving ASCT up front had a significantly greater reduction in tumor volume of at least 90%, as indicated by the composite of very good partial remission, complete response, and stringent complete response, which was achieved in 74.0% in the VMP arm and in 84.4% of the HDM+ASCT arm (P less than .0001).
For patients at low risk of relapse, Dr. Cavo said longer follow up will be needed to compare the different arms of the study, and future analyses will delineate the effects of consolidation or no consolidation therapy and the use of the VMP regimen, compared with single or double ASCT.
ASCO president Dr. Julie Vose said that even with effective novel agents available, older, proven approaches still retain their value. “This study demonstrated that combining the best of both worlds – initial therapy with a novel agent followed by stem cell transplant – resulted in the best patient outcomes,” she said.
FROM THE 2016 ASCO ANNUAL MEETING
Key clinical point: ASCT bested bortezomib for newly diagnosed younger multiple myeloma patients.
Major finding: Multiple myeloma patients showed 24% PFS prolongation with up front HDM+ASCT.
Data source: EMN02/HO95, a prospective, multicenter, intergroup, randomized phase III study of 1,266 patients.
Disclosures: The study was funded by HOVON, the Hemato Oncology Foundation for Adults in the Netherlands. Dr. Cavo disclosed relationships with Janssen, Takeda, Amgen, Bristol-Myers Squibb, and Celgene. Dr. Vose disclosed relationships with Sanofi Aventis, Seattle Genetics, Acerta, Bristol-Myers Squibb, Celgene, Genentech, GlaxoSmithKline, Incyte, Janssen Biotech, Kite Pharma, Pharmacyclics, and Spectrum Pharmaceuticals.
Advances in the management of multiple myeloma
Multiple myeloma (MM) is a bone marrow- based malignancy of plasma cells that is diagnosed in over 30,000 patients annually in the United States. Despite the many recent advances in the treatment of MM, it remains an incurable disease. Thus, the need for the development of new effective therapies remains critical for these patients.
Smoldering MM
In general, it has not been shown that patients with smoldering MM (SMM) benefit from early treatment, but recent studies have identified a subset of patients who are at high-risk and may require therapy more quickly. Recent guidelines from the International Myeloma Working Group recommend immediate treatment of this subgroup of SMM.1 However, although findings in a Spanish study suggested that early treatment of high-risk SMM patients with the immunomodulatory agent (IMiD) lenalidomide and dexamethasone improves overall survival (OS),2 the design of that study limits its clinical applicability, and no other randomized trials have been completed to show the advantage of early therapy for these patients.
Specific drugs
The development of novel agents such as proteasome inhibitors (PIs), IMiDs, histone deacetylase inhibitors (HDACIs), and monoclonal antibodies (mAbs) in recent years has vastly changed the approach to the treatment of MM patients.
PIs that are cytotoxic to MM cells, such as bortezomib, have become a foundation for MM treatment over the past decade. However, patients develop drug resistance to bortezomib by acquiring gene mutations and through other mechanisms. In recent years, newer forms of PIs such as carfilzomib and the oral formulations ixazomib and oprozomib have been and are currently being developed.3 Preclinical studies have shown that resistance to one PI can be overcome with treatment with another PI.4
Click on the PDF icon at the top of this introduction to read the full article.
Multiple myeloma (MM) is a bone marrow- based malignancy of plasma cells that is diagnosed in over 30,000 patients annually in the United States. Despite the many recent advances in the treatment of MM, it remains an incurable disease. Thus, the need for the development of new effective therapies remains critical for these patients.
Smoldering MM
In general, it has not been shown that patients with smoldering MM (SMM) benefit from early treatment, but recent studies have identified a subset of patients who are at high-risk and may require therapy more quickly. Recent guidelines from the International Myeloma Working Group recommend immediate treatment of this subgroup of SMM.1 However, although findings in a Spanish study suggested that early treatment of high-risk SMM patients with the immunomodulatory agent (IMiD) lenalidomide and dexamethasone improves overall survival (OS),2 the design of that study limits its clinical applicability, and no other randomized trials have been completed to show the advantage of early therapy for these patients.
Specific drugs
The development of novel agents such as proteasome inhibitors (PIs), IMiDs, histone deacetylase inhibitors (HDACIs), and monoclonal antibodies (mAbs) in recent years has vastly changed the approach to the treatment of MM patients.
PIs that are cytotoxic to MM cells, such as bortezomib, have become a foundation for MM treatment over the past decade. However, patients develop drug resistance to bortezomib by acquiring gene mutations and through other mechanisms. In recent years, newer forms of PIs such as carfilzomib and the oral formulations ixazomib and oprozomib have been and are currently being developed.3 Preclinical studies have shown that resistance to one PI can be overcome with treatment with another PI.4
Click on the PDF icon at the top of this introduction to read the full article.
Multiple myeloma (MM) is a bone marrow- based malignancy of plasma cells that is diagnosed in over 30,000 patients annually in the United States. Despite the many recent advances in the treatment of MM, it remains an incurable disease. Thus, the need for the development of new effective therapies remains critical for these patients.
Smoldering MM
In general, it has not been shown that patients with smoldering MM (SMM) benefit from early treatment, but recent studies have identified a subset of patients who are at high-risk and may require therapy more quickly. Recent guidelines from the International Myeloma Working Group recommend immediate treatment of this subgroup of SMM.1 However, although findings in a Spanish study suggested that early treatment of high-risk SMM patients with the immunomodulatory agent (IMiD) lenalidomide and dexamethasone improves overall survival (OS),2 the design of that study limits its clinical applicability, and no other randomized trials have been completed to show the advantage of early therapy for these patients.
Specific drugs
The development of novel agents such as proteasome inhibitors (PIs), IMiDs, histone deacetylase inhibitors (HDACIs), and monoclonal antibodies (mAbs) in recent years has vastly changed the approach to the treatment of MM patients.
PIs that are cytotoxic to MM cells, such as bortezomib, have become a foundation for MM treatment over the past decade. However, patients develop drug resistance to bortezomib by acquiring gene mutations and through other mechanisms. In recent years, newer forms of PIs such as carfilzomib and the oral formulations ixazomib and oprozomib have been and are currently being developed.3 Preclinical studies have shown that resistance to one PI can be overcome with treatment with another PI.4
Click on the PDF icon at the top of this introduction to read the full article.
Enzastaurin flops as maintenance in treated DLBCL
Maintenance therapy with enzastaurin, an experimental agent directed against B-cell malignancies, did not improve disease-free survival among patients with high-risk diffuse large B-cell lymphomas following complete responses to chemotherapy with rituximab.
In a randomized, double-blind trial, after a median follow-up of 48 months, the hazard ratio for disease-free survival with enzastaurin vs. placebo, the primary endpoint, was 0.92 (P = .541), reported Dr. Michael Crump of Princess Margaret Cancer Centre in Toronto, and colleagues.
“The risk of treatment failure, however defined, is likely to be different in the subpopulation of patients who achieve remission after that treatment. Furthermore, identifying the value of specific biomarkers in predicting therapeutic response to novel targeted agents may be necessary in guiding future trials within defined subgroups of patients with DLBCL,” they wrote in the study, published online May 23 in Journal of Clinical Oncology.
Enzastaurin is a selective inhibitor of the protein kinase C-beta isoform (PKC-beta) expressed in both normal and malignant B cells. It has been shown to decrease tumor proliferation and induced apoptosis in cancer cells, and has been shown to have activity against relapsed or refractory DLBCL, mantle cell lymphoma, and follicular lymphoma, the authors explained.
Dr. Crump and colleagues conducted a phase III study to determine whether enzastaurin could be effective as maintenance therapy in patients with DLBCL at high risk for relapse after having had complete responses to first-line therapy with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP).
They enrolled 758 patients with stage II bulky DLBCL or stage III-IV disease who had three or more International Prognostic Index risk factors at diagnosis, and who had achieved either a confirmed or unconfirmed complete response after six to eight cycles of R-CHOP.
The patients were randomly assigned on a 2:1 basis to receive either oral enzastaurin 500 mg daily or placebo for 3 years, or until disease progression or unacceptable toxicity,
As noted, there was no significant difference in DFS with the active drug vs. placebo. In addition, in correlative analyses looking for biomarkers of response by cell of origin (i.e., germinal-center or non–germinal-center B cell) or by PKC-beta protein expression, the authors found no significant associations with either DFS or overall survival.
Enzastaurin was generally safe, with minor and manageable adverse events. More patients in the enzastaurin arm had episodes of QTc prolongation, but these did not require discontinuation of the drug.
Dr. Crump and coauthors disclosed consulting, advising, research funding and other relationships with various companies, including Eli Lilly. Five coauthors are Lilly employees.
Maintenance therapy with enzastaurin, an experimental agent directed against B-cell malignancies, did not improve disease-free survival among patients with high-risk diffuse large B-cell lymphomas following complete responses to chemotherapy with rituximab.
In a randomized, double-blind trial, after a median follow-up of 48 months, the hazard ratio for disease-free survival with enzastaurin vs. placebo, the primary endpoint, was 0.92 (P = .541), reported Dr. Michael Crump of Princess Margaret Cancer Centre in Toronto, and colleagues.
“The risk of treatment failure, however defined, is likely to be different in the subpopulation of patients who achieve remission after that treatment. Furthermore, identifying the value of specific biomarkers in predicting therapeutic response to novel targeted agents may be necessary in guiding future trials within defined subgroups of patients with DLBCL,” they wrote in the study, published online May 23 in Journal of Clinical Oncology.
Enzastaurin is a selective inhibitor of the protein kinase C-beta isoform (PKC-beta) expressed in both normal and malignant B cells. It has been shown to decrease tumor proliferation and induced apoptosis in cancer cells, and has been shown to have activity against relapsed or refractory DLBCL, mantle cell lymphoma, and follicular lymphoma, the authors explained.
Dr. Crump and colleagues conducted a phase III study to determine whether enzastaurin could be effective as maintenance therapy in patients with DLBCL at high risk for relapse after having had complete responses to first-line therapy with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP).
They enrolled 758 patients with stage II bulky DLBCL or stage III-IV disease who had three or more International Prognostic Index risk factors at diagnosis, and who had achieved either a confirmed or unconfirmed complete response after six to eight cycles of R-CHOP.
The patients were randomly assigned on a 2:1 basis to receive either oral enzastaurin 500 mg daily or placebo for 3 years, or until disease progression or unacceptable toxicity,
As noted, there was no significant difference in DFS with the active drug vs. placebo. In addition, in correlative analyses looking for biomarkers of response by cell of origin (i.e., germinal-center or non–germinal-center B cell) or by PKC-beta protein expression, the authors found no significant associations with either DFS or overall survival.
Enzastaurin was generally safe, with minor and manageable adverse events. More patients in the enzastaurin arm had episodes of QTc prolongation, but these did not require discontinuation of the drug.
Dr. Crump and coauthors disclosed consulting, advising, research funding and other relationships with various companies, including Eli Lilly. Five coauthors are Lilly employees.
Maintenance therapy with enzastaurin, an experimental agent directed against B-cell malignancies, did not improve disease-free survival among patients with high-risk diffuse large B-cell lymphomas following complete responses to chemotherapy with rituximab.
In a randomized, double-blind trial, after a median follow-up of 48 months, the hazard ratio for disease-free survival with enzastaurin vs. placebo, the primary endpoint, was 0.92 (P = .541), reported Dr. Michael Crump of Princess Margaret Cancer Centre in Toronto, and colleagues.
“The risk of treatment failure, however defined, is likely to be different in the subpopulation of patients who achieve remission after that treatment. Furthermore, identifying the value of specific biomarkers in predicting therapeutic response to novel targeted agents may be necessary in guiding future trials within defined subgroups of patients with DLBCL,” they wrote in the study, published online May 23 in Journal of Clinical Oncology.
Enzastaurin is a selective inhibitor of the protein kinase C-beta isoform (PKC-beta) expressed in both normal and malignant B cells. It has been shown to decrease tumor proliferation and induced apoptosis in cancer cells, and has been shown to have activity against relapsed or refractory DLBCL, mantle cell lymphoma, and follicular lymphoma, the authors explained.
Dr. Crump and colleagues conducted a phase III study to determine whether enzastaurin could be effective as maintenance therapy in patients with DLBCL at high risk for relapse after having had complete responses to first-line therapy with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP).
They enrolled 758 patients with stage II bulky DLBCL or stage III-IV disease who had three or more International Prognostic Index risk factors at diagnosis, and who had achieved either a confirmed or unconfirmed complete response after six to eight cycles of R-CHOP.
The patients were randomly assigned on a 2:1 basis to receive either oral enzastaurin 500 mg daily or placebo for 3 years, or until disease progression or unacceptable toxicity,
As noted, there was no significant difference in DFS with the active drug vs. placebo. In addition, in correlative analyses looking for biomarkers of response by cell of origin (i.e., germinal-center or non–germinal-center B cell) or by PKC-beta protein expression, the authors found no significant associations with either DFS or overall survival.
Enzastaurin was generally safe, with minor and manageable adverse events. More patients in the enzastaurin arm had episodes of QTc prolongation, but these did not require discontinuation of the drug.
Dr. Crump and coauthors disclosed consulting, advising, research funding and other relationships with various companies, including Eli Lilly. Five coauthors are Lilly employees.
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: The experimental agent enzastaurin was no better than placebo as maintenance therapy in patients who had achieved a complete response to R-CHOP.
Major finding: At 48 months median follow-up, the hazard ratio for enzastaurin was 0.92 (P = ns).
Data source: Randomized, double-blind, placebo controlled trial of 758 patients with diffuse large B-cell lymphoma in complete remission after first-line therapy with R-CHOP.
Disclosures: Dr. Crump and coauthors disclosed consulting, advising, research funding and other relationships with various companies, including Eli Lilly. Five coauthors are Lilly employees.
Study reveals how BET inhibitors kill cancer cells

Image courtesy of PNAS
Researchers say they have determined how BET inhibitors fight hematologic malignancies.
Previous studies showed that BET inhibitors are effective at halting tumor growth, but it wasn’t clear whether the drugs kill cancer cells outright or merely pause their growth.
The new study provides an answer and reveals potential ways in which cancer cells may develop resistance to BET inhibitors.
The findings have been published in Leukaemia.
Researchers tested the BET inhibitors JQ1 and IBET151 in a range of hematopoietic cancer cell lines (leukemias, lymphomas, and multiple myeloma) and in mice (with and without malignancy).
The team found that JQ1’s ability to kill cancer cells principally relies on the activation of BAX/BAK-dependent mitochondrial apoptosis. They said this is largely triggered by upregulation of the protein BIM when BET inhibitors suppress miR-17-92, a post-transcriptional repressor of BIM expression.
“We found that when apoptosis was impaired—for instance, by loss of BIM—the BET inhibitors were no longer effective,” said study author Zhen Xu, PhD, of Walter and Eliza Hall Institute of Medical Research in Melbourne, Victoria, Australia.
“This suggests that cancer cells that acquire mutations in genes that drive apoptosis will lose sensitivity to BET inhibitors and thus will be able to survive treatment, leading to disease relapse.”
The researchers also found that BET inhibitors could induce apoptosis in normal hematopoietic cells, particularly those of lymphoid origin. The team said this suggests the cells’ susceptibility to BET inhibitors did not arise from oncogenic transformation.
These findings could help researchers improve strategies for using BET inhibitors to treat cancers, according to study author Stefan Glaser, PhD, of the Walter and Eliza Hall Institute of Medical Research.
“Understanding how the drugs work gives us the opportunity to investigate new treatments—for example, by using combination therapies or altering the dosage and timing of treatment to prevent drug resistance from emerging,” Dr Glaser said. ![]()
Image courtesy of PNAS
Researchers say they have determined how BET inhibitors fight hematologic malignancies.
Previous studies showed that BET inhibitors are effective at halting tumor growth, but it wasn’t clear whether the drugs kill cancer cells outright or merely pause their growth.
The new study provides an answer and reveals potential ways in which cancer cells may develop resistance to BET inhibitors.
The findings have been published in Leukaemia.
Researchers tested the BET inhibitors JQ1 and IBET151 in a range of hematopoietic cancer cell lines (leukemias, lymphomas, and multiple myeloma) and in mice (with and without malignancy).
The team found that JQ1’s ability to kill cancer cells principally relies on the activation of BAX/BAK-dependent mitochondrial apoptosis. They said this is largely triggered by upregulation of the protein BIM when BET inhibitors suppress miR-17-92, a post-transcriptional repressor of BIM expression.
“We found that when apoptosis was impaired—for instance, by loss of BIM—the BET inhibitors were no longer effective,” said study author Zhen Xu, PhD, of Walter and Eliza Hall Institute of Medical Research in Melbourne, Victoria, Australia.
“This suggests that cancer cells that acquire mutations in genes that drive apoptosis will lose sensitivity to BET inhibitors and thus will be able to survive treatment, leading to disease relapse.”
The researchers also found that BET inhibitors could induce apoptosis in normal hematopoietic cells, particularly those of lymphoid origin. The team said this suggests the cells’ susceptibility to BET inhibitors did not arise from oncogenic transformation.
These findings could help researchers improve strategies for using BET inhibitors to treat cancers, according to study author Stefan Glaser, PhD, of the Walter and Eliza Hall Institute of Medical Research.
“Understanding how the drugs work gives us the opportunity to investigate new treatments—for example, by using combination therapies or altering the dosage and timing of treatment to prevent drug resistance from emerging,” Dr Glaser said. ![]()
Image courtesy of PNAS
Researchers say they have determined how BET inhibitors fight hematologic malignancies.
Previous studies showed that BET inhibitors are effective at halting tumor growth, but it wasn’t clear whether the drugs kill cancer cells outright or merely pause their growth.
The new study provides an answer and reveals potential ways in which cancer cells may develop resistance to BET inhibitors.
The findings have been published in Leukaemia.
Researchers tested the BET inhibitors JQ1 and IBET151 in a range of hematopoietic cancer cell lines (leukemias, lymphomas, and multiple myeloma) and in mice (with and without malignancy).
The team found that JQ1’s ability to kill cancer cells principally relies on the activation of BAX/BAK-dependent mitochondrial apoptosis. They said this is largely triggered by upregulation of the protein BIM when BET inhibitors suppress miR-17-92, a post-transcriptional repressor of BIM expression.
“We found that when apoptosis was impaired—for instance, by loss of BIM—the BET inhibitors were no longer effective,” said study author Zhen Xu, PhD, of Walter and Eliza Hall Institute of Medical Research in Melbourne, Victoria, Australia.
“This suggests that cancer cells that acquire mutations in genes that drive apoptosis will lose sensitivity to BET inhibitors and thus will be able to survive treatment, leading to disease relapse.”
The researchers also found that BET inhibitors could induce apoptosis in normal hematopoietic cells, particularly those of lymphoid origin. The team said this suggests the cells’ susceptibility to BET inhibitors did not arise from oncogenic transformation.
These findings could help researchers improve strategies for using BET inhibitors to treat cancers, according to study author Stefan Glaser, PhD, of the Walter and Eliza Hall Institute of Medical Research.
“Understanding how the drugs work gives us the opportunity to investigate new treatments—for example, by using combination therapies or altering the dosage and timing of treatment to prevent drug resistance from emerging,” Dr Glaser said. ![]()
Fertility concerns of female cancer survivors

Photo by Vera Kratochvil
A new study indicates that many young adult female cancer survivors do not receive adequate information about their fertility as part of their survivorship care, despite having concerns about their ability to bear children in the future.
The research, published in Cancer, suggests a need for better resources to support cancer survivors in making informed decisions about their reproductive options after they complete treatment.
To conduct this study, Catherine Benedict, PhD, of North Shore-Long Island Jewish Medical Center in Manhasset, New York, and her colleagues asked female cancer survivors to complete a web-based, anonymous survey.
There were 346 participants. They had an average age of 29.9 and had completed treatment an average of 4.9 years earlier.
The investigators focused on a subgroup of 179 women with uncertain fertility status who had not previously undergone or attempted fertility preservation, either before or after their cancer treatment, and who either wanted future children or were unsure.
Many of these women said they did not have enough information concerning their risk of infertility (58%), risk of early menopause (60%), options to assess their fertility (62%), options to preserve their fertility (51%), or options for alternative family building (43%).
The women’s greatest reproductive concerns were potential fertility problems and the health of a future child. Sixty-four percent of the women said they were concerned about not being able to have children (or more children), and 59% were worried about passing the risk of cancer on to their future children.
Only 13% of women said they were well informed about options for preserving fertility, and 74% were unclear about their personal values regarding fertility preservation.
Seventy percent of the women said they hadn’t received enough advice on fertility preservation, and 35% said they didn’t have enough support to make a decision about fertility preservation.
The investigators found a significant association between greater unmet information needs and higher levels of decisional conflict about fertility preservation (P<0.001).
On the other hand, having undergone a fertility evaluation after treatment was associated with lower decisional conflict (P=0.02).
The investigators said these findings establish the need for support services to help young female cancer survivors make decisions about fertility preservation and family-building as part of survivorship care.
The literature has largely focused on the clinical and support needs of women making fertility decisions before their treatment begins, but most patients do not preserve their fertility before treatment for a number of reasons, despite wanting children in the future.
“The potential loss of fertility has been described in the literature as being almost as painful, if not more so, than the cancer diagnosis itself,” Dr Benedict said.
“Failure to provide information and address concerns with respect to fertility-related decisions may have lasting consequences for young women who hope to move on from their cancer experience to achieve important life goals such as having children. For women at risk for early menopause, delaying fertility-related decisions may cause them to miss their narrowed window of opportunity to preserve their fertility, if desired.” ![]()
Photo by Vera Kratochvil
A new study indicates that many young adult female cancer survivors do not receive adequate information about their fertility as part of their survivorship care, despite having concerns about their ability to bear children in the future.
The research, published in Cancer, suggests a need for better resources to support cancer survivors in making informed decisions about their reproductive options after they complete treatment.
To conduct this study, Catherine Benedict, PhD, of North Shore-Long Island Jewish Medical Center in Manhasset, New York, and her colleagues asked female cancer survivors to complete a web-based, anonymous survey.
There were 346 participants. They had an average age of 29.9 and had completed treatment an average of 4.9 years earlier.
The investigators focused on a subgroup of 179 women with uncertain fertility status who had not previously undergone or attempted fertility preservation, either before or after their cancer treatment, and who either wanted future children or were unsure.
Many of these women said they did not have enough information concerning their risk of infertility (58%), risk of early menopause (60%), options to assess their fertility (62%), options to preserve their fertility (51%), or options for alternative family building (43%).
The women’s greatest reproductive concerns were potential fertility problems and the health of a future child. Sixty-four percent of the women said they were concerned about not being able to have children (or more children), and 59% were worried about passing the risk of cancer on to their future children.
Only 13% of women said they were well informed about options for preserving fertility, and 74% were unclear about their personal values regarding fertility preservation.
Seventy percent of the women said they hadn’t received enough advice on fertility preservation, and 35% said they didn’t have enough support to make a decision about fertility preservation.
The investigators found a significant association between greater unmet information needs and higher levels of decisional conflict about fertility preservation (P<0.001).
On the other hand, having undergone a fertility evaluation after treatment was associated with lower decisional conflict (P=0.02).
The investigators said these findings establish the need for support services to help young female cancer survivors make decisions about fertility preservation and family-building as part of survivorship care.
The literature has largely focused on the clinical and support needs of women making fertility decisions before their treatment begins, but most patients do not preserve their fertility before treatment for a number of reasons, despite wanting children in the future.
“The potential loss of fertility has been described in the literature as being almost as painful, if not more so, than the cancer diagnosis itself,” Dr Benedict said.
“Failure to provide information and address concerns with respect to fertility-related decisions may have lasting consequences for young women who hope to move on from their cancer experience to achieve important life goals such as having children. For women at risk for early menopause, delaying fertility-related decisions may cause them to miss their narrowed window of opportunity to preserve their fertility, if desired.” ![]()
Photo by Vera Kratochvil
A new study indicates that many young adult female cancer survivors do not receive adequate information about their fertility as part of their survivorship care, despite having concerns about their ability to bear children in the future.
The research, published in Cancer, suggests a need for better resources to support cancer survivors in making informed decisions about their reproductive options after they complete treatment.
To conduct this study, Catherine Benedict, PhD, of North Shore-Long Island Jewish Medical Center in Manhasset, New York, and her colleagues asked female cancer survivors to complete a web-based, anonymous survey.
There were 346 participants. They had an average age of 29.9 and had completed treatment an average of 4.9 years earlier.
The investigators focused on a subgroup of 179 women with uncertain fertility status who had not previously undergone or attempted fertility preservation, either before or after their cancer treatment, and who either wanted future children or were unsure.
Many of these women said they did not have enough information concerning their risk of infertility (58%), risk of early menopause (60%), options to assess their fertility (62%), options to preserve their fertility (51%), or options for alternative family building (43%).
The women’s greatest reproductive concerns were potential fertility problems and the health of a future child. Sixty-four percent of the women said they were concerned about not being able to have children (or more children), and 59% were worried about passing the risk of cancer on to their future children.
Only 13% of women said they were well informed about options for preserving fertility, and 74% were unclear about their personal values regarding fertility preservation.
Seventy percent of the women said they hadn’t received enough advice on fertility preservation, and 35% said they didn’t have enough support to make a decision about fertility preservation.
The investigators found a significant association between greater unmet information needs and higher levels of decisional conflict about fertility preservation (P<0.001).
On the other hand, having undergone a fertility evaluation after treatment was associated with lower decisional conflict (P=0.02).
The investigators said these findings establish the need for support services to help young female cancer survivors make decisions about fertility preservation and family-building as part of survivorship care.
The literature has largely focused on the clinical and support needs of women making fertility decisions before their treatment begins, but most patients do not preserve their fertility before treatment for a number of reasons, despite wanting children in the future.
“The potential loss of fertility has been described in the literature as being almost as painful, if not more so, than the cancer diagnosis itself,” Dr Benedict said.
“Failure to provide information and address concerns with respect to fertility-related decisions may have lasting consequences for young women who hope to move on from their cancer experience to achieve important life goals such as having children. For women at risk for early menopause, delaying fertility-related decisions may cause them to miss their narrowed window of opportunity to preserve their fertility, if desired.” ![]()
Method may produce better CAR-NKTs

Photo by Aaron Logan
Researchers say they have discovered a method for expanding natural killer T cells (NKTs) that ensures their persistence, thereby making NKTs more attractive as chimeric antigen receptor (CAR) carriers for cancer immunotherapy.
When transduced with a CD19-specific CAR, the researchers’ persistent NKTs produced sustained tumor regression in a mouse model of B-cell lymphoma.
The team described this work in the Journal of Clinical Investigation.
“NKT technology is quite powerful and offers a significant potential for treatment of cancer,” said study author Leonid Metelitsa, MD, PhD, of Baylor College of Medicine in Houston, Texas.
“But for it to be most effective, we have to find the best way to expand the cells ex vivo while preserving their ability to persist once delivered back to patients. If they can persist in the body for a long time, they have much longer therapeutic activity, and this is essential for fighting cancer.”
Molecule affects persistence
The researchers noted that central memory T cells are known for their ability to proliferate and persist, and these cells are characterized by expression of the surface molecule CD62L.
In this study, the team found that NKT cells freshly derived from blood did not express CD62L, or it was expressed at a very low level. However, after the researchers expanded NKT cells, they found that CD62L was expressed at higher levels.
“We consistently identified a subset of cells present at very high numbers after the first 12 days of expansion, and critical to this subset of cells was the presence of CD62L,” Dr Metelitsa said. “In fact, they became the majority of the new cells.”
In addition, Dr Metelitsa said that CD62L-positive NKT cells were responsible for further propagation of NKTs in culture, which is important for achieving large numbers of cells. However, extensive culture led to the eventual decline of CD62L expression in NKTs.
To test the role of CD62L in NKT-cell persistence, the researchers delivered CD62L-positive and CD62L-negative NKTs to immune-deficient NSG mice. They found that CD62L-positive NKTs persisted 5 times longer than CD62L-negative NKTs.
CAR-NKTs fight lymphoma
Next, the researchers transduced CD62L-positive and CD62L-negative NKTs with a CD19-specific CAR and delivered these cells to mice with B-cell lymphoma.
The team found that both CD62L-positve and CD62L-negative CAR-NKTs prolonged the survival of mice, when compared to controls (P<0.001).
However, only the CD62L-positive CAR-NKTs induced sustained tumor regression. Seven of 9 mice that received CD62L-positive CAR-NKTs lived, and 5 were tumor-free for at least 3 months. But all 10 mice that received CD62L-negative CAR-NKTs ultimately succumbed to tumor progression (P<0.001).
Costimulation improves NKTs/CAR-NKTs
The researchers then turned their focus to costimulation of NKTs in order to maintain the subset with a high percentage of CD62L-positive cells in prolonged culture. Costimulation involves the interaction of receptors on NKTs with activating molecules on an antigen-presenting cell to increase the NKTs’ immune functions.
“We have known that costimulation is an important part of immune response and immunotherapy, but, in this case, we did not know which costimulatory molecules would be important for the expansion and persistence of CD62L-positive NKT cells,” said Gengwen Tian, MD, of the Baylor College of Medicine.
After testing more than 100 combinations, the researchers discovered that combining an antigen-presenting molecule—CD1d—with 3 costimulatory molecules—CD86, 4-1BBL, and OX40L—induced prolonged persistence and better therapeutic activity of NKTs and CAR-NKTs in mouse models.
“When we developed an antigen-presenting cell clone that expressed CD1d with all of these costimulatory molecules at certain levels, NKT cells maintained a high percentage of CD62L even in a prolonged culture,” Dr Metelitsa said.
The researchers conducted in vivo testing of CAR-NKT cells that were expanded with the original method or with the costimulation method. And they found that costimulated cells had significantly higher therapeutic activity in mouse models of neuroblastoma and lymphoma.
“Our goal now is to optimize our NKT cell expansion protocol so that we can obtain FDA approval to initiate clinical trials,” Dr Metelitsa said. ![]()
Photo by Aaron Logan
Researchers say they have discovered a method for expanding natural killer T cells (NKTs) that ensures their persistence, thereby making NKTs more attractive as chimeric antigen receptor (CAR) carriers for cancer immunotherapy.
When transduced with a CD19-specific CAR, the researchers’ persistent NKTs produced sustained tumor regression in a mouse model of B-cell lymphoma.
The team described this work in the Journal of Clinical Investigation.
“NKT technology is quite powerful and offers a significant potential for treatment of cancer,” said study author Leonid Metelitsa, MD, PhD, of Baylor College of Medicine in Houston, Texas.
“But for it to be most effective, we have to find the best way to expand the cells ex vivo while preserving their ability to persist once delivered back to patients. If they can persist in the body for a long time, they have much longer therapeutic activity, and this is essential for fighting cancer.”
Molecule affects persistence
The researchers noted that central memory T cells are known for their ability to proliferate and persist, and these cells are characterized by expression of the surface molecule CD62L.
In this study, the team found that NKT cells freshly derived from blood did not express CD62L, or it was expressed at a very low level. However, after the researchers expanded NKT cells, they found that CD62L was expressed at higher levels.
“We consistently identified a subset of cells present at very high numbers after the first 12 days of expansion, and critical to this subset of cells was the presence of CD62L,” Dr Metelitsa said. “In fact, they became the majority of the new cells.”
In addition, Dr Metelitsa said that CD62L-positive NKT cells were responsible for further propagation of NKTs in culture, which is important for achieving large numbers of cells. However, extensive culture led to the eventual decline of CD62L expression in NKTs.
To test the role of CD62L in NKT-cell persistence, the researchers delivered CD62L-positive and CD62L-negative NKTs to immune-deficient NSG mice. They found that CD62L-positive NKTs persisted 5 times longer than CD62L-negative NKTs.
CAR-NKTs fight lymphoma
Next, the researchers transduced CD62L-positive and CD62L-negative NKTs with a CD19-specific CAR and delivered these cells to mice with B-cell lymphoma.
The team found that both CD62L-positve and CD62L-negative CAR-NKTs prolonged the survival of mice, when compared to controls (P<0.001).
However, only the CD62L-positive CAR-NKTs induced sustained tumor regression. Seven of 9 mice that received CD62L-positive CAR-NKTs lived, and 5 were tumor-free for at least 3 months. But all 10 mice that received CD62L-negative CAR-NKTs ultimately succumbed to tumor progression (P<0.001).
Costimulation improves NKTs/CAR-NKTs
The researchers then turned their focus to costimulation of NKTs in order to maintain the subset with a high percentage of CD62L-positive cells in prolonged culture. Costimulation involves the interaction of receptors on NKTs with activating molecules on an antigen-presenting cell to increase the NKTs’ immune functions.
“We have known that costimulation is an important part of immune response and immunotherapy, but, in this case, we did not know which costimulatory molecules would be important for the expansion and persistence of CD62L-positive NKT cells,” said Gengwen Tian, MD, of the Baylor College of Medicine.
After testing more than 100 combinations, the researchers discovered that combining an antigen-presenting molecule—CD1d—with 3 costimulatory molecules—CD86, 4-1BBL, and OX40L—induced prolonged persistence and better therapeutic activity of NKTs and CAR-NKTs in mouse models.
“When we developed an antigen-presenting cell clone that expressed CD1d with all of these costimulatory molecules at certain levels, NKT cells maintained a high percentage of CD62L even in a prolonged culture,” Dr Metelitsa said.
The researchers conducted in vivo testing of CAR-NKT cells that were expanded with the original method or with the costimulation method. And they found that costimulated cells had significantly higher therapeutic activity in mouse models of neuroblastoma and lymphoma.
“Our goal now is to optimize our NKT cell expansion protocol so that we can obtain FDA approval to initiate clinical trials,” Dr Metelitsa said. ![]()
Photo by Aaron Logan
Researchers say they have discovered a method for expanding natural killer T cells (NKTs) that ensures their persistence, thereby making NKTs more attractive as chimeric antigen receptor (CAR) carriers for cancer immunotherapy.
When transduced with a CD19-specific CAR, the researchers’ persistent NKTs produced sustained tumor regression in a mouse model of B-cell lymphoma.
The team described this work in the Journal of Clinical Investigation.
“NKT technology is quite powerful and offers a significant potential for treatment of cancer,” said study author Leonid Metelitsa, MD, PhD, of Baylor College of Medicine in Houston, Texas.
“But for it to be most effective, we have to find the best way to expand the cells ex vivo while preserving their ability to persist once delivered back to patients. If they can persist in the body for a long time, they have much longer therapeutic activity, and this is essential for fighting cancer.”
Molecule affects persistence
The researchers noted that central memory T cells are known for their ability to proliferate and persist, and these cells are characterized by expression of the surface molecule CD62L.
In this study, the team found that NKT cells freshly derived from blood did not express CD62L, or it was expressed at a very low level. However, after the researchers expanded NKT cells, they found that CD62L was expressed at higher levels.
“We consistently identified a subset of cells present at very high numbers after the first 12 days of expansion, and critical to this subset of cells was the presence of CD62L,” Dr Metelitsa said. “In fact, they became the majority of the new cells.”
In addition, Dr Metelitsa said that CD62L-positive NKT cells were responsible for further propagation of NKTs in culture, which is important for achieving large numbers of cells. However, extensive culture led to the eventual decline of CD62L expression in NKTs.
To test the role of CD62L in NKT-cell persistence, the researchers delivered CD62L-positive and CD62L-negative NKTs to immune-deficient NSG mice. They found that CD62L-positive NKTs persisted 5 times longer than CD62L-negative NKTs.
CAR-NKTs fight lymphoma
Next, the researchers transduced CD62L-positive and CD62L-negative NKTs with a CD19-specific CAR and delivered these cells to mice with B-cell lymphoma.
The team found that both CD62L-positve and CD62L-negative CAR-NKTs prolonged the survival of mice, when compared to controls (P<0.001).
However, only the CD62L-positive CAR-NKTs induced sustained tumor regression. Seven of 9 mice that received CD62L-positive CAR-NKTs lived, and 5 were tumor-free for at least 3 months. But all 10 mice that received CD62L-negative CAR-NKTs ultimately succumbed to tumor progression (P<0.001).
Costimulation improves NKTs/CAR-NKTs
The researchers then turned their focus to costimulation of NKTs in order to maintain the subset with a high percentage of CD62L-positive cells in prolonged culture. Costimulation involves the interaction of receptors on NKTs with activating molecules on an antigen-presenting cell to increase the NKTs’ immune functions.
“We have known that costimulation is an important part of immune response and immunotherapy, but, in this case, we did not know which costimulatory molecules would be important for the expansion and persistence of CD62L-positive NKT cells,” said Gengwen Tian, MD, of the Baylor College of Medicine.
After testing more than 100 combinations, the researchers discovered that combining an antigen-presenting molecule—CD1d—with 3 costimulatory molecules—CD86, 4-1BBL, and OX40L—induced prolonged persistence and better therapeutic activity of NKTs and CAR-NKTs in mouse models.
“When we developed an antigen-presenting cell clone that expressed CD1d with all of these costimulatory molecules at certain levels, NKT cells maintained a high percentage of CD62L even in a prolonged culture,” Dr Metelitsa said.
The researchers conducted in vivo testing of CAR-NKT cells that were expanded with the original method or with the costimulation method. And they found that costimulated cells had significantly higher therapeutic activity in mouse models of neuroblastoma and lymphoma.
“Our goal now is to optimize our NKT cell expansion protocol so that we can obtain FDA approval to initiate clinical trials,” Dr Metelitsa said. ![]()
HIV patients undertreated for lymphoma, other cancers
cultured lymphocyte
Image courtesy of the CDC
A new study suggests that cancer patients with HIV are less likely to receive cancer treatment, regardless of insurance status and comorbidities.
Patients with HIV were less likely than their HIV-free peers to receive treatment for Hodgkin lymphoma, diffuse large B-cell lymphoma, and 7 solid tumor malignancies.
Gita Suneja, MD, of the University of Utah in Salt Lake City, and her colleagues reported these findings in Cancer.
The team used the National Cancer Data Base to study non-elderly US adults diagnosed with 10 common cancers from 2003 to 2011. There were a total of 10,265 HIV-infected patients and 2,219,232 HIV-free patients.
The researchers examined associations between HIV status and lack of cancer treatment, taking into account insurance status and comorbidities.
The results showed a lack of treatment among HIV patients for all of the cancers studied except anal cancer (relative risk [RR]=1.20, P=0.333).
So HIV-infected patients were more likely to lack cancer treatment for:
- Hodgkin lymphoma (RR=1.92, P<0.001)
- Diffuse large B-cell lymphoma (RR=1.82, P<0.001)
- Head and neck cancer (RR=1.48, P=0.013)
- Upper gastrointestinal tract cancer (RR=2.62, P<0.001)
- Colorectal cancer (RR=1.70, P=0.006)
- Lung cancer (RR=2.46, P<0.001)
- Breast cancer (RR=2.14, P=0.015)
- Cervical cancer (RR=2.81, P<0.001)
- Prostate cancer (RR=2.16, P<0.001).
The researchers said factors that predicted a lack of cancer treatment among HIV-infected individuals varied between those with solid tumors and those with lymphomas.
Advanced stage at the time of cancer diagnosis (stage IV vs stage I) meant HIV patients with solid tumors were less likely to receive cancer treatment, but lymphoma patients were more likely to receive cancer treatment.
Having a higher modified Charlson-Deyo comorbidity score (1 or 2+ vs 0) predicted a lack of cancer treatment for HIV-infected patients with lymphoma but not those with solid tumors.
And older age (45-64 vs 18-44) was associated with a lack of treatment for HIV-infected patients regardless of cancer type, but this was only significant for lymphoma patients.
For the entire cohort, black race (vs white) and a lack of private insurance (Medicaid, Medicare, uninsured, or unknown insurance status) were significant predictors for a lack of cancer treatment among HIV patients.
Still, the researchers noted that, even among privately insured patients, HIV-infected individuals were less likely to receive cancer treatment.
Dr Suneja and her colleagues said several factors may contribute to these findings. For one, HIV-infected patients have historically been excluded from cancer clinical trials, thereby limiting the applicability of trial results for this population.
In addition, cancer treatment guidelines specific to HIV-infected patients are not available for most cancer types. And clinicians may lack experience treating HIV-infected patients with cancer.
Furthermore, the psychosocial and economic challenges associated with the dual management of cancer and HIV treatment may make adherence to treatment a challenge. ![]()
cultured lymphocyte
Image courtesy of the CDC
A new study suggests that cancer patients with HIV are less likely to receive cancer treatment, regardless of insurance status and comorbidities.
Patients with HIV were less likely than their HIV-free peers to receive treatment for Hodgkin lymphoma, diffuse large B-cell lymphoma, and 7 solid tumor malignancies.
Gita Suneja, MD, of the University of Utah in Salt Lake City, and her colleagues reported these findings in Cancer.
The team used the National Cancer Data Base to study non-elderly US adults diagnosed with 10 common cancers from 2003 to 2011. There were a total of 10,265 HIV-infected patients and 2,219,232 HIV-free patients.
The researchers examined associations between HIV status and lack of cancer treatment, taking into account insurance status and comorbidities.
The results showed a lack of treatment among HIV patients for all of the cancers studied except anal cancer (relative risk [RR]=1.20, P=0.333).
So HIV-infected patients were more likely to lack cancer treatment for:
- Hodgkin lymphoma (RR=1.92, P<0.001)
- Diffuse large B-cell lymphoma (RR=1.82, P<0.001)
- Head and neck cancer (RR=1.48, P=0.013)
- Upper gastrointestinal tract cancer (RR=2.62, P<0.001)
- Colorectal cancer (RR=1.70, P=0.006)
- Lung cancer (RR=2.46, P<0.001)
- Breast cancer (RR=2.14, P=0.015)
- Cervical cancer (RR=2.81, P<0.001)
- Prostate cancer (RR=2.16, P<0.001).
The researchers said factors that predicted a lack of cancer treatment among HIV-infected individuals varied between those with solid tumors and those with lymphomas.
Advanced stage at the time of cancer diagnosis (stage IV vs stage I) meant HIV patients with solid tumors were less likely to receive cancer treatment, but lymphoma patients were more likely to receive cancer treatment.
Having a higher modified Charlson-Deyo comorbidity score (1 or 2+ vs 0) predicted a lack of cancer treatment for HIV-infected patients with lymphoma but not those with solid tumors.
And older age (45-64 vs 18-44) was associated with a lack of treatment for HIV-infected patients regardless of cancer type, but this was only significant for lymphoma patients.
For the entire cohort, black race (vs white) and a lack of private insurance (Medicaid, Medicare, uninsured, or unknown insurance status) were significant predictors for a lack of cancer treatment among HIV patients.
Still, the researchers noted that, even among privately insured patients, HIV-infected individuals were less likely to receive cancer treatment.
Dr Suneja and her colleagues said several factors may contribute to these findings. For one, HIV-infected patients have historically been excluded from cancer clinical trials, thereby limiting the applicability of trial results for this population.
In addition, cancer treatment guidelines specific to HIV-infected patients are not available for most cancer types. And clinicians may lack experience treating HIV-infected patients with cancer.
Furthermore, the psychosocial and economic challenges associated with the dual management of cancer and HIV treatment may make adherence to treatment a challenge. ![]()
cultured lymphocyte
Image courtesy of the CDC
A new study suggests that cancer patients with HIV are less likely to receive cancer treatment, regardless of insurance status and comorbidities.
Patients with HIV were less likely than their HIV-free peers to receive treatment for Hodgkin lymphoma, diffuse large B-cell lymphoma, and 7 solid tumor malignancies.
Gita Suneja, MD, of the University of Utah in Salt Lake City, and her colleagues reported these findings in Cancer.
The team used the National Cancer Data Base to study non-elderly US adults diagnosed with 10 common cancers from 2003 to 2011. There were a total of 10,265 HIV-infected patients and 2,219,232 HIV-free patients.
The researchers examined associations between HIV status and lack of cancer treatment, taking into account insurance status and comorbidities.
The results showed a lack of treatment among HIV patients for all of the cancers studied except anal cancer (relative risk [RR]=1.20, P=0.333).
So HIV-infected patients were more likely to lack cancer treatment for:
- Hodgkin lymphoma (RR=1.92, P<0.001)
- Diffuse large B-cell lymphoma (RR=1.82, P<0.001)
- Head and neck cancer (RR=1.48, P=0.013)
- Upper gastrointestinal tract cancer (RR=2.62, P<0.001)
- Colorectal cancer (RR=1.70, P=0.006)
- Lung cancer (RR=2.46, P<0.001)
- Breast cancer (RR=2.14, P=0.015)
- Cervical cancer (RR=2.81, P<0.001)
- Prostate cancer (RR=2.16, P<0.001).
The researchers said factors that predicted a lack of cancer treatment among HIV-infected individuals varied between those with solid tumors and those with lymphomas.
Advanced stage at the time of cancer diagnosis (stage IV vs stage I) meant HIV patients with solid tumors were less likely to receive cancer treatment, but lymphoma patients were more likely to receive cancer treatment.
Having a higher modified Charlson-Deyo comorbidity score (1 or 2+ vs 0) predicted a lack of cancer treatment for HIV-infected patients with lymphoma but not those with solid tumors.
And older age (45-64 vs 18-44) was associated with a lack of treatment for HIV-infected patients regardless of cancer type, but this was only significant for lymphoma patients.
For the entire cohort, black race (vs white) and a lack of private insurance (Medicaid, Medicare, uninsured, or unknown insurance status) were significant predictors for a lack of cancer treatment among HIV patients.
Still, the researchers noted that, even among privately insured patients, HIV-infected individuals were less likely to receive cancer treatment.
Dr Suneja and her colleagues said several factors may contribute to these findings. For one, HIV-infected patients have historically been excluded from cancer clinical trials, thereby limiting the applicability of trial results for this population.
In addition, cancer treatment guidelines specific to HIV-infected patients are not available for most cancer types. And clinicians may lack experience treating HIV-infected patients with cancer.
Furthermore, the psychosocial and economic challenges associated with the dual management of cancer and HIV treatment may make adherence to treatment a challenge.