User login
Everolimus fails to improve HCC survival
Everolimus failed to improve overall survival among patients with advanced hepatocellular carcinoma in a large international phase III clinical trial, according to a report published online July 1 in JAMA.
Everolimus – which targets the mTOR pathway that is a key regulator of cellular growth, proliferation, angiogenesis, and survival – had shown promise in numerous preclinical, phase I, and phase II studies. So the Everolimus for Liver Cancer Evaluation (EVOLVE-1) trial was designed to compare the drug’s efficacy and safety against that of a matching placebo in patients whose HCC was refractory to, or who were intolerant of, sorafenib, said Dr. Andrew X. Zhu of Massachusetts General Hospital Cancer Center and Harvard Medical School, Boston, and his associates.
Sorafenib is the only systemic therapy shown to improve survival in advanced HCC, but its benefits are "transient and modest," and it produces significant adverse events, according to the researchers. In this study, sorafenib was discontinued because of disease progression in 81% of patients and because of intolerance in 19%, they noted.
In EVOLVE-1, 546 patients were enrolled during a 2-year period at 111 medical centers in 17 countries, randomly assigned in a double-blind fashion to receive either 7.5 mg oral everolimus (362 subjects) or placebo (184 subjects) daily, and followed for a median of 2.5 years (range, 14.8-36.6 months). The trial was sponsored by Novartis, maker of everolimus.
HCC was associated with hepatitis B virus in 26.2% of the patients, hepatitis C virus in 25.1%, and alcohol abuse in 20.0%. There were 303 deaths (83.7%) in the active-treatment group and 151 (82.1%) in the placebo group.
At 5 months, the primary endpoint of estimated overall survival was not significantly different between patients taking everolimus (67.0%) and those taking placebo (65.6%); the rates also were not significantly different at 7 months (53.4% and 51.4%, respectively). Median overall survival time was 7.6 months for everolimus and 7.3 months with placebo, also a nonsignificant difference, Dr. Zhu and his associates said (JAMA 2014 July 1 [doi:10.1001/jama.2014.7189]).
These findings were consistent across all but one subgroup of patients. Secondary endpoints, including time to disease progression, rate of complete response (0% in both groups), and time to deterioration in quality of life, also were not significantly different between the two study groups.
Serious adverse events, including adverse events leading to treatment discontinuation, were more common with everolimus than with placebo. These included asthenia, anemia, decreased appetite, resurgence of HBV, ascites, and thrombocytopenia.
Thus, "despite the strong scientific rationale and preclinical data," everolimus failed to improve outcomes in advanced HCC, the investigators said.
However, "given the immunosuppressive and antitumor effects of mTOR inhibitors, the potential benefits of this class of agents in the adjuvant setting are being assessed in a phase-III trial of sirolimus for patients with HCC after liver transplantation," they added.
Everolimus failed to improve overall survival among patients with advanced hepatocellular carcinoma in a large international phase III clinical trial, according to a report published online July 1 in JAMA.
Everolimus – which targets the mTOR pathway that is a key regulator of cellular growth, proliferation, angiogenesis, and survival – had shown promise in numerous preclinical, phase I, and phase II studies. So the Everolimus for Liver Cancer Evaluation (EVOLVE-1) trial was designed to compare the drug’s efficacy and safety against that of a matching placebo in patients whose HCC was refractory to, or who were intolerant of, sorafenib, said Dr. Andrew X. Zhu of Massachusetts General Hospital Cancer Center and Harvard Medical School, Boston, and his associates.
Sorafenib is the only systemic therapy shown to improve survival in advanced HCC, but its benefits are "transient and modest," and it produces significant adverse events, according to the researchers. In this study, sorafenib was discontinued because of disease progression in 81% of patients and because of intolerance in 19%, they noted.
In EVOLVE-1, 546 patients were enrolled during a 2-year period at 111 medical centers in 17 countries, randomly assigned in a double-blind fashion to receive either 7.5 mg oral everolimus (362 subjects) or placebo (184 subjects) daily, and followed for a median of 2.5 years (range, 14.8-36.6 months). The trial was sponsored by Novartis, maker of everolimus.
HCC was associated with hepatitis B virus in 26.2% of the patients, hepatitis C virus in 25.1%, and alcohol abuse in 20.0%. There were 303 deaths (83.7%) in the active-treatment group and 151 (82.1%) in the placebo group.
At 5 months, the primary endpoint of estimated overall survival was not significantly different between patients taking everolimus (67.0%) and those taking placebo (65.6%); the rates also were not significantly different at 7 months (53.4% and 51.4%, respectively). Median overall survival time was 7.6 months for everolimus and 7.3 months with placebo, also a nonsignificant difference, Dr. Zhu and his associates said (JAMA 2014 July 1 [doi:10.1001/jama.2014.7189]).
These findings were consistent across all but one subgroup of patients. Secondary endpoints, including time to disease progression, rate of complete response (0% in both groups), and time to deterioration in quality of life, also were not significantly different between the two study groups.
Serious adverse events, including adverse events leading to treatment discontinuation, were more common with everolimus than with placebo. These included asthenia, anemia, decreased appetite, resurgence of HBV, ascites, and thrombocytopenia.
Thus, "despite the strong scientific rationale and preclinical data," everolimus failed to improve outcomes in advanced HCC, the investigators said.
However, "given the immunosuppressive and antitumor effects of mTOR inhibitors, the potential benefits of this class of agents in the adjuvant setting are being assessed in a phase-III trial of sirolimus for patients with HCC after liver transplantation," they added.
Everolimus failed to improve overall survival among patients with advanced hepatocellular carcinoma in a large international phase III clinical trial, according to a report published online July 1 in JAMA.
Everolimus – which targets the mTOR pathway that is a key regulator of cellular growth, proliferation, angiogenesis, and survival – had shown promise in numerous preclinical, phase I, and phase II studies. So the Everolimus for Liver Cancer Evaluation (EVOLVE-1) trial was designed to compare the drug’s efficacy and safety against that of a matching placebo in patients whose HCC was refractory to, or who were intolerant of, sorafenib, said Dr. Andrew X. Zhu of Massachusetts General Hospital Cancer Center and Harvard Medical School, Boston, and his associates.
Sorafenib is the only systemic therapy shown to improve survival in advanced HCC, but its benefits are "transient and modest," and it produces significant adverse events, according to the researchers. In this study, sorafenib was discontinued because of disease progression in 81% of patients and because of intolerance in 19%, they noted.
In EVOLVE-1, 546 patients were enrolled during a 2-year period at 111 medical centers in 17 countries, randomly assigned in a double-blind fashion to receive either 7.5 mg oral everolimus (362 subjects) or placebo (184 subjects) daily, and followed for a median of 2.5 years (range, 14.8-36.6 months). The trial was sponsored by Novartis, maker of everolimus.
HCC was associated with hepatitis B virus in 26.2% of the patients, hepatitis C virus in 25.1%, and alcohol abuse in 20.0%. There were 303 deaths (83.7%) in the active-treatment group and 151 (82.1%) in the placebo group.
At 5 months, the primary endpoint of estimated overall survival was not significantly different between patients taking everolimus (67.0%) and those taking placebo (65.6%); the rates also were not significantly different at 7 months (53.4% and 51.4%, respectively). Median overall survival time was 7.6 months for everolimus and 7.3 months with placebo, also a nonsignificant difference, Dr. Zhu and his associates said (JAMA 2014 July 1 [doi:10.1001/jama.2014.7189]).
These findings were consistent across all but one subgroup of patients. Secondary endpoints, including time to disease progression, rate of complete response (0% in both groups), and time to deterioration in quality of life, also were not significantly different between the two study groups.
Serious adverse events, including adverse events leading to treatment discontinuation, were more common with everolimus than with placebo. These included asthenia, anemia, decreased appetite, resurgence of HBV, ascites, and thrombocytopenia.
Thus, "despite the strong scientific rationale and preclinical data," everolimus failed to improve outcomes in advanced HCC, the investigators said.
However, "given the immunosuppressive and antitumor effects of mTOR inhibitors, the potential benefits of this class of agents in the adjuvant setting are being assessed in a phase-III trial of sirolimus for patients with HCC after liver transplantation," they added.
FROM JAMA
Key clinical point: Despite the "strong scientific rationale and preclinical data," everolimus failed to improve outcomes in advanced HCC.
Major finding: At 5 months, the primary endpoint of estimated overall survival was not significantly different between patients taking everolimus (67.0%) and those taking placebo (65.6%); the rates also were not significantly different at 7 months (53.4% and 51.4%, respectively).
Data source: An international prospective, double-blind placebo-controlled phase III clinical trial of 546 patients with advanced hepatocellular carcinoma who were followed for a median of 2.5 years.
Disclosures: EVOLVE-1 was sponsored by Novartis. Dr. Zhu reported serving as a consultant to Sanofi-Aventis, Exelixis, Eisai, and Daiichi Sankyo; his associates reported ties to numerous industry sources.
Nucleoside analogues’ benefits in HBV vary
Nucleoside analogues are effective at preventing hepatocellular carcinoma in hepatitis B, but all are not equal when it comes to overall mortality and liver transplant, according to two new studies in the July issue of Gastroenterology.
In the first study, Dr. Chun-Ying Wu of the National Yang-Ming University, in Taipei, Taiwan, and his colleagues examined the long-term protective effects of nucleoside analogue therapy among chronic hepatitis B patients (doi.org/10.1053/j.gastro.2014.03.048).
They conducted a retrospective nationwide cohort study using data from Taiwan’s National Health Insurance Research Database, collecting records from 1997 through 2010 on patients with chronic hepatitis B.
In total, Dr. Wu looked at 21,595 patients who had been treated for at least 90 days with nucleoside analogues and the same number of propensity-matched patients who had not; patients with hepatitis C, HIV, or cancer developed before the index date were excluded from the analysis.
Among the treated patients, 19,063 received only one nucleoside analogue, including lamivudine (n = 12,938), entecavir (5,748), and telbivudine (377). The remaining 2,532 patients received more than one.
Over a mean follow-up period of 3.46 years and 5.24 years for the treated and untreated cohorts, respectively, the authors found that patients treated with nucleoside analogues had a significantly lower incidence of hepatocellular carcinoma (HCC) (n = 992, or 4.6%), compared with their untreated counterparts (n = 4,454, or 20.6%).
Patients treated with nucleoside analogues also demonstrated a much-lower 7-year cumulative incidence of HCC, compared with untreated patients (7.32% vs. 22.70%; P less than .001).
That translated to an average annual incidence of HCC of 1.05% and 3.24% for treated and untreated patients, respectively.
Dr. Wu and his colleagues disclosed no personal conflicts of interest; they wrote that their work received support from Taiwan’s National Health Research Institutes, the Taipei Veterans General Hospital and Department of Health, and the National Yang-Ming University.
The second study, led by Dr. Young-Suk Lim of the Asan Medical Center, in Seoul, sought to determine which nucleoside analogue offered better protection against not only HCC, but also liver transplant and mortality: entecavir, or the "less potent" lamivudine.
In that report, the researchers conducted a retrospective analysis of 5,374 consecutive adult patients with chronic hepatitis B, treated with entecavir (n = 2,000) or lamivudine (n = 3,374) at a single center in Seoul between 1999 and 2011 (doi.org/10.1053/j.gastro.2014.02.033).
The researchers found that, when looking at propensity-matched pairs, after 3 years of follow-up the risk of death or transplantation diverged significantly: Compared with the lamivudine cohort, entecavir patients had a hazard ratio for these outcomes of 0.49 (95% confidence interval, 0.37-0.64; P less than .001).
On the other hand, looking at the risk for HCC development, there was no significant difference between groups (HR, 1.01; 95% CI, 0.80-1.27; P = .95).
When an adjusted analysis of matched pairs with cirrhosis at study baseline was undertaken, the results were similar: entecavir was associated with a significantly lower risk of death or transplantation, compared with lamivudine (HR, 0.42; 95% CI, 0.31-0.57; P less than .001), but not HCC (HR, 1.00; 95% CI, 0.78-1.28; P = .999).
An analysis of patients without baseline cirrhosis, however, showed no difference between any of the outcomes: transplant, death, or HCC.
"These results advocate current practice guidelines that recommend the use of two potent antiviral agents (that is, entecavir and tenofovir) as first-line drugs for the treatment of chronic hepatitis B," wrote the authors.
"Further longer-term studies on patients of other races or ethnicity, and studies using other potent antiviral agents such as tenofovir, are warranted."
Dr. Lim disclosed financial relationships with Bayer Healthcare, Bristol-Myers Squibb (maker of entecavir), Gilead Science and Novartis; the investigators stated that their study received funding from the Asan Medical Center and the Korean Association for the Study of Liver.
Current guidelines recommend the high-genetic barrier entecavir (nucleoside) or tenofovir (nucleotide) as first-line options for the treatment of chronic hepatitis B (CHB). However, data on their effect on major long-term outcomes and mostly on hepatocellular carcinoma (HCC) have been limited. Moreover, lamivudine, a nucleoside with a low-genetic barrier to resistance, may be still used as first-line therapy in some countries because of its lower direct cost. These two interesting studies using carefully matched large patient cohorts provide important information for these issues.
The first study from Taiwan showed that therapy with nucleoside analogues (lamivudine, entecavir, and telbivudine) decreases the HCC risk in CHB patients, compared with untreated controls (7-year cumulative HCC incidence: 7.3% vs. 22.7%). The second study from Korea showed that entecavir is superior to lamivudine in reducing mortality and liver transplant by approximately 50%, but offers no additional benefit for HCC prevention. The benefit from entecavir was obvious in patients with baseline cirrhosis and not in noncirrhotics who are at low short- or medium-term risk for major outcomes anyway. Since these and other similar studies in CHB come from Asian cohorts, additional long-term outcome data in white patients will be useful.
These results further support previous reports that antiviral therapy reduces but do not eliminate the HCC risk in CHB patients, in whom HCC surveillance should continue if they are at increased baseline HCC risk regardless of viral suppression under treatment. In addition, such findings reinforce the current recommendations for use of high-genetic barrier agents as first-line treatment in CHB.
Dr. George Papatheodoridis is associate professor in medicine and gastroenterology, Athens University, director of the academic department of gastroenterology, Laiko General Hospital of Athens. He is an adviser/lecturer for Bristol-Meyers Squibb, Gilead, Merck, Novartis, Roche; and he has received research grants from Bristol-Meyers Squibb, Gilead, and Roche.
Current guidelines recommend the high-genetic barrier entecavir (nucleoside) or tenofovir (nucleotide) as first-line options for the treatment of chronic hepatitis B (CHB). However, data on their effect on major long-term outcomes and mostly on hepatocellular carcinoma (HCC) have been limited. Moreover, lamivudine, a nucleoside with a low-genetic barrier to resistance, may be still used as first-line therapy in some countries because of its lower direct cost. These two interesting studies using carefully matched large patient cohorts provide important information for these issues.
The first study from Taiwan showed that therapy with nucleoside analogues (lamivudine, entecavir, and telbivudine) decreases the HCC risk in CHB patients, compared with untreated controls (7-year cumulative HCC incidence: 7.3% vs. 22.7%). The second study from Korea showed that entecavir is superior to lamivudine in reducing mortality and liver transplant by approximately 50%, but offers no additional benefit for HCC prevention. The benefit from entecavir was obvious in patients with baseline cirrhosis and not in noncirrhotics who are at low short- or medium-term risk for major outcomes anyway. Since these and other similar studies in CHB come from Asian cohorts, additional long-term outcome data in white patients will be useful.
These results further support previous reports that antiviral therapy reduces but do not eliminate the HCC risk in CHB patients, in whom HCC surveillance should continue if they are at increased baseline HCC risk regardless of viral suppression under treatment. In addition, such findings reinforce the current recommendations for use of high-genetic barrier agents as first-line treatment in CHB.
Dr. George Papatheodoridis is associate professor in medicine and gastroenterology, Athens University, director of the academic department of gastroenterology, Laiko General Hospital of Athens. He is an adviser/lecturer for Bristol-Meyers Squibb, Gilead, Merck, Novartis, Roche; and he has received research grants from Bristol-Meyers Squibb, Gilead, and Roche.
Current guidelines recommend the high-genetic barrier entecavir (nucleoside) or tenofovir (nucleotide) as first-line options for the treatment of chronic hepatitis B (CHB). However, data on their effect on major long-term outcomes and mostly on hepatocellular carcinoma (HCC) have been limited. Moreover, lamivudine, a nucleoside with a low-genetic barrier to resistance, may be still used as first-line therapy in some countries because of its lower direct cost. These two interesting studies using carefully matched large patient cohorts provide important information for these issues.
The first study from Taiwan showed that therapy with nucleoside analogues (lamivudine, entecavir, and telbivudine) decreases the HCC risk in CHB patients, compared with untreated controls (7-year cumulative HCC incidence: 7.3% vs. 22.7%). The second study from Korea showed that entecavir is superior to lamivudine in reducing mortality and liver transplant by approximately 50%, but offers no additional benefit for HCC prevention. The benefit from entecavir was obvious in patients with baseline cirrhosis and not in noncirrhotics who are at low short- or medium-term risk for major outcomes anyway. Since these and other similar studies in CHB come from Asian cohorts, additional long-term outcome data in white patients will be useful.
These results further support previous reports that antiviral therapy reduces but do not eliminate the HCC risk in CHB patients, in whom HCC surveillance should continue if they are at increased baseline HCC risk regardless of viral suppression under treatment. In addition, such findings reinforce the current recommendations for use of high-genetic barrier agents as first-line treatment in CHB.
Dr. George Papatheodoridis is associate professor in medicine and gastroenterology, Athens University, director of the academic department of gastroenterology, Laiko General Hospital of Athens. He is an adviser/lecturer for Bristol-Meyers Squibb, Gilead, Merck, Novartis, Roche; and he has received research grants from Bristol-Meyers Squibb, Gilead, and Roche.
Nucleoside analogues are effective at preventing hepatocellular carcinoma in hepatitis B, but all are not equal when it comes to overall mortality and liver transplant, according to two new studies in the July issue of Gastroenterology.
In the first study, Dr. Chun-Ying Wu of the National Yang-Ming University, in Taipei, Taiwan, and his colleagues examined the long-term protective effects of nucleoside analogue therapy among chronic hepatitis B patients (doi.org/10.1053/j.gastro.2014.03.048).
They conducted a retrospective nationwide cohort study using data from Taiwan’s National Health Insurance Research Database, collecting records from 1997 through 2010 on patients with chronic hepatitis B.
In total, Dr. Wu looked at 21,595 patients who had been treated for at least 90 days with nucleoside analogues and the same number of propensity-matched patients who had not; patients with hepatitis C, HIV, or cancer developed before the index date were excluded from the analysis.
Among the treated patients, 19,063 received only one nucleoside analogue, including lamivudine (n = 12,938), entecavir (5,748), and telbivudine (377). The remaining 2,532 patients received more than one.
Over a mean follow-up period of 3.46 years and 5.24 years for the treated and untreated cohorts, respectively, the authors found that patients treated with nucleoside analogues had a significantly lower incidence of hepatocellular carcinoma (HCC) (n = 992, or 4.6%), compared with their untreated counterparts (n = 4,454, or 20.6%).
Patients treated with nucleoside analogues also demonstrated a much-lower 7-year cumulative incidence of HCC, compared with untreated patients (7.32% vs. 22.70%; P less than .001).
That translated to an average annual incidence of HCC of 1.05% and 3.24% for treated and untreated patients, respectively.
Dr. Wu and his colleagues disclosed no personal conflicts of interest; they wrote that their work received support from Taiwan’s National Health Research Institutes, the Taipei Veterans General Hospital and Department of Health, and the National Yang-Ming University.
The second study, led by Dr. Young-Suk Lim of the Asan Medical Center, in Seoul, sought to determine which nucleoside analogue offered better protection against not only HCC, but also liver transplant and mortality: entecavir, or the "less potent" lamivudine.
In that report, the researchers conducted a retrospective analysis of 5,374 consecutive adult patients with chronic hepatitis B, treated with entecavir (n = 2,000) or lamivudine (n = 3,374) at a single center in Seoul between 1999 and 2011 (doi.org/10.1053/j.gastro.2014.02.033).
The researchers found that, when looking at propensity-matched pairs, after 3 years of follow-up the risk of death or transplantation diverged significantly: Compared with the lamivudine cohort, entecavir patients had a hazard ratio for these outcomes of 0.49 (95% confidence interval, 0.37-0.64; P less than .001).
On the other hand, looking at the risk for HCC development, there was no significant difference between groups (HR, 1.01; 95% CI, 0.80-1.27; P = .95).
When an adjusted analysis of matched pairs with cirrhosis at study baseline was undertaken, the results were similar: entecavir was associated with a significantly lower risk of death or transplantation, compared with lamivudine (HR, 0.42; 95% CI, 0.31-0.57; P less than .001), but not HCC (HR, 1.00; 95% CI, 0.78-1.28; P = .999).
An analysis of patients without baseline cirrhosis, however, showed no difference between any of the outcomes: transplant, death, or HCC.
"These results advocate current practice guidelines that recommend the use of two potent antiviral agents (that is, entecavir and tenofovir) as first-line drugs for the treatment of chronic hepatitis B," wrote the authors.
"Further longer-term studies on patients of other races or ethnicity, and studies using other potent antiviral agents such as tenofovir, are warranted."
Dr. Lim disclosed financial relationships with Bayer Healthcare, Bristol-Myers Squibb (maker of entecavir), Gilead Science and Novartis; the investigators stated that their study received funding from the Asan Medical Center and the Korean Association for the Study of Liver.
Nucleoside analogues are effective at preventing hepatocellular carcinoma in hepatitis B, but all are not equal when it comes to overall mortality and liver transplant, according to two new studies in the July issue of Gastroenterology.
In the first study, Dr. Chun-Ying Wu of the National Yang-Ming University, in Taipei, Taiwan, and his colleagues examined the long-term protective effects of nucleoside analogue therapy among chronic hepatitis B patients (doi.org/10.1053/j.gastro.2014.03.048).
They conducted a retrospective nationwide cohort study using data from Taiwan’s National Health Insurance Research Database, collecting records from 1997 through 2010 on patients with chronic hepatitis B.
In total, Dr. Wu looked at 21,595 patients who had been treated for at least 90 days with nucleoside analogues and the same number of propensity-matched patients who had not; patients with hepatitis C, HIV, or cancer developed before the index date were excluded from the analysis.
Among the treated patients, 19,063 received only one nucleoside analogue, including lamivudine (n = 12,938), entecavir (5,748), and telbivudine (377). The remaining 2,532 patients received more than one.
Over a mean follow-up period of 3.46 years and 5.24 years for the treated and untreated cohorts, respectively, the authors found that patients treated with nucleoside analogues had a significantly lower incidence of hepatocellular carcinoma (HCC) (n = 992, or 4.6%), compared with their untreated counterparts (n = 4,454, or 20.6%).
Patients treated with nucleoside analogues also demonstrated a much-lower 7-year cumulative incidence of HCC, compared with untreated patients (7.32% vs. 22.70%; P less than .001).
That translated to an average annual incidence of HCC of 1.05% and 3.24% for treated and untreated patients, respectively.
Dr. Wu and his colleagues disclosed no personal conflicts of interest; they wrote that their work received support from Taiwan’s National Health Research Institutes, the Taipei Veterans General Hospital and Department of Health, and the National Yang-Ming University.
The second study, led by Dr. Young-Suk Lim of the Asan Medical Center, in Seoul, sought to determine which nucleoside analogue offered better protection against not only HCC, but also liver transplant and mortality: entecavir, or the "less potent" lamivudine.
In that report, the researchers conducted a retrospective analysis of 5,374 consecutive adult patients with chronic hepatitis B, treated with entecavir (n = 2,000) or lamivudine (n = 3,374) at a single center in Seoul between 1999 and 2011 (doi.org/10.1053/j.gastro.2014.02.033).
The researchers found that, when looking at propensity-matched pairs, after 3 years of follow-up the risk of death or transplantation diverged significantly: Compared with the lamivudine cohort, entecavir patients had a hazard ratio for these outcomes of 0.49 (95% confidence interval, 0.37-0.64; P less than .001).
On the other hand, looking at the risk for HCC development, there was no significant difference between groups (HR, 1.01; 95% CI, 0.80-1.27; P = .95).
When an adjusted analysis of matched pairs with cirrhosis at study baseline was undertaken, the results were similar: entecavir was associated with a significantly lower risk of death or transplantation, compared with lamivudine (HR, 0.42; 95% CI, 0.31-0.57; P less than .001), but not HCC (HR, 1.00; 95% CI, 0.78-1.28; P = .999).
An analysis of patients without baseline cirrhosis, however, showed no difference between any of the outcomes: transplant, death, or HCC.
"These results advocate current practice guidelines that recommend the use of two potent antiviral agents (that is, entecavir and tenofovir) as first-line drugs for the treatment of chronic hepatitis B," wrote the authors.
"Further longer-term studies on patients of other races or ethnicity, and studies using other potent antiviral agents such as tenofovir, are warranted."
Dr. Lim disclosed financial relationships with Bayer Healthcare, Bristol-Myers Squibb (maker of entecavir), Gilead Science and Novartis; the investigators stated that their study received funding from the Asan Medical Center and the Korean Association for the Study of Liver.
FROM GASTROENTEROLOGY
Key clinical point: Entecavir treatment in HBV reduces the risk of transplant and death.
Major finding: HBV patients treated with nucleoside analogues had a significantly lower incidence of hepatocellular carcinoma (4.6%), compared with untreated counterparts (20.6%): Compared with lamivudine, patients given entecavir, specifically, had an HR of 0.49 for transplant and death.
Data sources: A retrospective nationwide cohort study of hepatitis B patients in Taiwan’s National Health Insurance Research Database, for one, and a retrospective analysis of 5,374 hepatitis B patients treated at a single center in Seoul.
Disclosures: Dr. Wu and his colleagues disclosed no personal conflicts of interest; they wrote that their work received support from Taiwan’s National Health Research Institutes, the Taipei Veterans General Hospital and Department of Health, and the National Yang-Ming University. Dr. Lim disclosed financial relationships with Bayer Healthcare, Bristol-Myers Squibb (maker of entecavir), Gilead Science, and Novartis. The investigators stated that their study received funding from the Asan Medical Center and the Korean Association for the Study of Liver.
Increased intestinal permeability is central to alcoholic hepatitis
CHICAGO – Why is it that only about 20% of individuals who consume 10 or more alcoholic drinks daily for years on end will develop alcoholic hepatitis?
New insight into the mechanism of this disease points to markedly increased intestinal permeability as playing a key role. Increased intestinal permeability is consistently present in patients with alcoholic hepatitis, but not in heavy drinkers without the disease or in normal healthy controls, Dr. George Holman reported at the annual Digestive Disease Week.

"Our study suggests that intestinal permeability is disrupted in alcoholic hepatitis. We speculate that increased intestinal permeability allows passage of lipopolysaccharides from gut bacteria into the serum. These endotoxins are carried to the liver and cause subsequent hepatic inflammation," according to Dr. Holman of the University of New Mexico, Albuquerque.
Alcoholic hepatitis is characterized by steatohepatitis and rapid clinical decompensation. It is typically seen only in patients who have consumed more than 100 g of alcohol – that’s roughly 10 drinks – daily for years.
Dr. Holman presented a prospective case-control study involving 22 patients hospitalized for severe alcoholic hepatitis and 33 healthy volunteers. The study hypothesis was that patients with alcoholic hepatitis have defective intestinal barrier function which allows gut-derived bacterial endotoxins, known as lipopolysaccharides, to enter the systemic circulation, leading to a resultant inflammatory response in the liver.
To test this hypothesis, the investigators utilized urinary excretion of lactulose and mannitol as intestinal permeability markers. They also measured serum lipopolysaccharide levels as well as circulating levels of the proinflammatory cytokines interleukin-6 and tumor necrosis factor–alpha.
The alcoholic hepatitis group showed on average an eightfold increase in intestinal permeability as measured by the lactulose/mannitol excretion ratio, compared with controls. Also, a near-perfect linear correlation was found between the degree of intestinal permeability and the magnitude of the elevation in serum lipopolysaccharide levels. Paralleling these increases in intestinal permeability and lipopolysaccharides, serum levels of interleukin-6 and tumor necrosis factor–alpha were also significantly higher in the alcoholic hepatitis patients than in controls. These data, taken as a whole, point to increased intestinal permeability as a pathogenic factor resulting in endotoxemia and immune activation, he said.
Also worthy of note, intestinal permeability tracked with MELD (model for end-stage liver disease) scores such that as intestinal permeability increased, MELD scores climbed nearly exponentially, Dr. Holman continued.
Audience members wondered whether treating alcoholic hepatitis patients, typically with prednisone or pentoxifylline, had a favorable impact upon their abnormal intestinal permeability. Dr. Holman replied that although he and his coinvestigators had planned to look at this issue, follow-up simply wasn’t possible. This was a very sick patient cohort – their mean alcohol consumption was 26 drinks daily for years – and despite treatment, nearly half of them were dead within several months. However, other investigators have previously shown that alcoholic hepatitis patients who respond favorably to treatment and are able to leave the hospital show a decrease in their previously high endotoxin levels, while more severely affected patients do not.
The cause of the defective intestinal barrier that figures prominently in alcoholic hepatitis remains a mystery. Other studies have shown that individuals who drink heavily without developing alcoholic liver injury don’t have increased intestinal permeability. Thus, increased intestinal permeability is not caused by heavy alcohol use. Some other as yet unidentified factor must be causing it, Dr. Holman concluded.
This study was supported by university research funds. Dr. Holman reported having no financial conflicts.
CHICAGO – Why is it that only about 20% of individuals who consume 10 or more alcoholic drinks daily for years on end will develop alcoholic hepatitis?
New insight into the mechanism of this disease points to markedly increased intestinal permeability as playing a key role. Increased intestinal permeability is consistently present in patients with alcoholic hepatitis, but not in heavy drinkers without the disease or in normal healthy controls, Dr. George Holman reported at the annual Digestive Disease Week.
"Our study suggests that intestinal permeability is disrupted in alcoholic hepatitis. We speculate that increased intestinal permeability allows passage of lipopolysaccharides from gut bacteria into the serum. These endotoxins are carried to the liver and cause subsequent hepatic inflammation," according to Dr. Holman of the University of New Mexico, Albuquerque.
Alcoholic hepatitis is characterized by steatohepatitis and rapid clinical decompensation. It is typically seen only in patients who have consumed more than 100 g of alcohol – that’s roughly 10 drinks – daily for years.
Dr. Holman presented a prospective case-control study involving 22 patients hospitalized for severe alcoholic hepatitis and 33 healthy volunteers. The study hypothesis was that patients with alcoholic hepatitis have defective intestinal barrier function which allows gut-derived bacterial endotoxins, known as lipopolysaccharides, to enter the systemic circulation, leading to a resultant inflammatory response in the liver.
To test this hypothesis, the investigators utilized urinary excretion of lactulose and mannitol as intestinal permeability markers. They also measured serum lipopolysaccharide levels as well as circulating levels of the proinflammatory cytokines interleukin-6 and tumor necrosis factor–alpha.
The alcoholic hepatitis group showed on average an eightfold increase in intestinal permeability as measured by the lactulose/mannitol excretion ratio, compared with controls. Also, a near-perfect linear correlation was found between the degree of intestinal permeability and the magnitude of the elevation in serum lipopolysaccharide levels. Paralleling these increases in intestinal permeability and lipopolysaccharides, serum levels of interleukin-6 and tumor necrosis factor–alpha were also significantly higher in the alcoholic hepatitis patients than in controls. These data, taken as a whole, point to increased intestinal permeability as a pathogenic factor resulting in endotoxemia and immune activation, he said.
Also worthy of note, intestinal permeability tracked with MELD (model for end-stage liver disease) scores such that as intestinal permeability increased, MELD scores climbed nearly exponentially, Dr. Holman continued.
Audience members wondered whether treating alcoholic hepatitis patients, typically with prednisone or pentoxifylline, had a favorable impact upon their abnormal intestinal permeability. Dr. Holman replied that although he and his coinvestigators had planned to look at this issue, follow-up simply wasn’t possible. This was a very sick patient cohort – their mean alcohol consumption was 26 drinks daily for years – and despite treatment, nearly half of them were dead within several months. However, other investigators have previously shown that alcoholic hepatitis patients who respond favorably to treatment and are able to leave the hospital show a decrease in their previously high endotoxin levels, while more severely affected patients do not.
The cause of the defective intestinal barrier that figures prominently in alcoholic hepatitis remains a mystery. Other studies have shown that individuals who drink heavily without developing alcoholic liver injury don’t have increased intestinal permeability. Thus, increased intestinal permeability is not caused by heavy alcohol use. Some other as yet unidentified factor must be causing it, Dr. Holman concluded.
This study was supported by university research funds. Dr. Holman reported having no financial conflicts.
CHICAGO – Why is it that only about 20% of individuals who consume 10 or more alcoholic drinks daily for years on end will develop alcoholic hepatitis?
New insight into the mechanism of this disease points to markedly increased intestinal permeability as playing a key role. Increased intestinal permeability is consistently present in patients with alcoholic hepatitis, but not in heavy drinkers without the disease or in normal healthy controls, Dr. George Holman reported at the annual Digestive Disease Week.
"Our study suggests that intestinal permeability is disrupted in alcoholic hepatitis. We speculate that increased intestinal permeability allows passage of lipopolysaccharides from gut bacteria into the serum. These endotoxins are carried to the liver and cause subsequent hepatic inflammation," according to Dr. Holman of the University of New Mexico, Albuquerque.
Alcoholic hepatitis is characterized by steatohepatitis and rapid clinical decompensation. It is typically seen only in patients who have consumed more than 100 g of alcohol – that’s roughly 10 drinks – daily for years.
Dr. Holman presented a prospective case-control study involving 22 patients hospitalized for severe alcoholic hepatitis and 33 healthy volunteers. The study hypothesis was that patients with alcoholic hepatitis have defective intestinal barrier function which allows gut-derived bacterial endotoxins, known as lipopolysaccharides, to enter the systemic circulation, leading to a resultant inflammatory response in the liver.
To test this hypothesis, the investigators utilized urinary excretion of lactulose and mannitol as intestinal permeability markers. They also measured serum lipopolysaccharide levels as well as circulating levels of the proinflammatory cytokines interleukin-6 and tumor necrosis factor–alpha.
The alcoholic hepatitis group showed on average an eightfold increase in intestinal permeability as measured by the lactulose/mannitol excretion ratio, compared with controls. Also, a near-perfect linear correlation was found between the degree of intestinal permeability and the magnitude of the elevation in serum lipopolysaccharide levels. Paralleling these increases in intestinal permeability and lipopolysaccharides, serum levels of interleukin-6 and tumor necrosis factor–alpha were also significantly higher in the alcoholic hepatitis patients than in controls. These data, taken as a whole, point to increased intestinal permeability as a pathogenic factor resulting in endotoxemia and immune activation, he said.
Also worthy of note, intestinal permeability tracked with MELD (model for end-stage liver disease) scores such that as intestinal permeability increased, MELD scores climbed nearly exponentially, Dr. Holman continued.
Audience members wondered whether treating alcoholic hepatitis patients, typically with prednisone or pentoxifylline, had a favorable impact upon their abnormal intestinal permeability. Dr. Holman replied that although he and his coinvestigators had planned to look at this issue, follow-up simply wasn’t possible. This was a very sick patient cohort – their mean alcohol consumption was 26 drinks daily for years – and despite treatment, nearly half of them were dead within several months. However, other investigators have previously shown that alcoholic hepatitis patients who respond favorably to treatment and are able to leave the hospital show a decrease in their previously high endotoxin levels, while more severely affected patients do not.
The cause of the defective intestinal barrier that figures prominently in alcoholic hepatitis remains a mystery. Other studies have shown that individuals who drink heavily without developing alcoholic liver injury don’t have increased intestinal permeability. Thus, increased intestinal permeability is not caused by heavy alcohol use. Some other as yet unidentified factor must be causing it, Dr. Holman concluded.
This study was supported by university research funds. Dr. Holman reported having no financial conflicts.
AT DDW 2014
Key clinical point: Endotoxins from gut bacteria may inflame the liver via increased intestinal permeability in alcoholic hepatitis.
Major finding: Alcoholic hepatitis is distinguished by a defective intestinal barrier as manifest in an eightfold increase in intestinal permeability in affected patients, compared with normal controls.
Data source: This was a prospective case-control study involving 22 patients hospitalized for alcoholic hepatitis and 33 healthy controls.
Disclosures: The study was supported by university research funds. The presenter reported having no financial conflicts of interest.

Medicare to cover hepatitis C screening
Medicare will cover screening for hepatitis C virus infection in high-risk beneficiaries, including a one-time screening for all beneficiaries born between 1946 and 1964, according to a national coverage decision announced June 2.
High risk is defined in the coverage memo as persons who have "a current or past history of illicit injection drug use; and persons who have a history of receiving a blood transfusion prior to 1992." To be covered, screening must be ordered by the beneficiary’s primary care physician or another practitioner within the primary care setting.

Annual rescreening is also covered for high-risk beneficiaries who continue to use illicit injection drugs, according to the decision memo.
The Centers for Medicare & Medicaid Services proposed the coverage, which follows U.S. Preventive Services Task Force recommendations for screening in March. That proposal followed an overwhelmingly positive response to the agency’s initial consideration of coverage for HCV screening in September 2013.
Treatment options for hepatitis C are expanding, with FDA approving three protease inhibitors in recent years – boceprevir (Victrelis), telaprevir (Incivek), and simeprevir (Olysio) – for treatment of patients with genotype 1 infection. Each of these treatments can be used in combination with pegylated interferon and ribavirin for the treatment of genotype 1 infection.
Last year, FDA approved sofosbuvir (Sovaldi), indicated for infections from genotypes 1, 2, 3, or 4, although access is hindered by its cost: $84,000 for a 12-week course of treatment ($1,000 a pill).
Medicare will cover screening for hepatitis C virus infection in high-risk beneficiaries, including a one-time screening for all beneficiaries born between 1946 and 1964, according to a national coverage decision announced June 2.
High risk is defined in the coverage memo as persons who have "a current or past history of illicit injection drug use; and persons who have a history of receiving a blood transfusion prior to 1992." To be covered, screening must be ordered by the beneficiary’s primary care physician or another practitioner within the primary care setting.
Annual rescreening is also covered for high-risk beneficiaries who continue to use illicit injection drugs, according to the decision memo.
The Centers for Medicare & Medicaid Services proposed the coverage, which follows U.S. Preventive Services Task Force recommendations for screening in March. That proposal followed an overwhelmingly positive response to the agency’s initial consideration of coverage for HCV screening in September 2013.
Treatment options for hepatitis C are expanding, with FDA approving three protease inhibitors in recent years – boceprevir (Victrelis), telaprevir (Incivek), and simeprevir (Olysio) – for treatment of patients with genotype 1 infection. Each of these treatments can be used in combination with pegylated interferon and ribavirin for the treatment of genotype 1 infection.
Last year, FDA approved sofosbuvir (Sovaldi), indicated for infections from genotypes 1, 2, 3, or 4, although access is hindered by its cost: $84,000 for a 12-week course of treatment ($1,000 a pill).
Medicare will cover screening for hepatitis C virus infection in high-risk beneficiaries, including a one-time screening for all beneficiaries born between 1946 and 1964, according to a national coverage decision announced June 2.
High risk is defined in the coverage memo as persons who have "a current or past history of illicit injection drug use; and persons who have a history of receiving a blood transfusion prior to 1992." To be covered, screening must be ordered by the beneficiary’s primary care physician or another practitioner within the primary care setting.
Annual rescreening is also covered for high-risk beneficiaries who continue to use illicit injection drugs, according to the decision memo.
The Centers for Medicare & Medicaid Services proposed the coverage, which follows U.S. Preventive Services Task Force recommendations for screening in March. That proposal followed an overwhelmingly positive response to the agency’s initial consideration of coverage for HCV screening in September 2013.
Treatment options for hepatitis C are expanding, with FDA approving three protease inhibitors in recent years – boceprevir (Victrelis), telaprevir (Incivek), and simeprevir (Olysio) – for treatment of patients with genotype 1 infection. Each of these treatments can be used in combination with pegylated interferon and ribavirin for the treatment of genotype 1 infection.
Last year, FDA approved sofosbuvir (Sovaldi), indicated for infections from genotypes 1, 2, 3, or 4, although access is hindered by its cost: $84,000 for a 12-week course of treatment ($1,000 a pill).

Stop beta-blockers in spontaneous bacterial peritonitis
Nonselective beta-blockers are contraindicated in cirrhosis with spontaneous bacterial peritonitis, wrote Dr. Mattias Mandorfer and his colleagues in the June issue of Gastroenterology (doi: 10.1053/j.gastro.2014.03.005).
Indeed, in a retrospective analysis, the drugs increased the length of hospitalization and the rate of hepatorenal syndrome, while decreasing overall transplant-free survival.
"These observations suggest that nonselective beta-blocker treatment should be discontinued at the first development of spontaneous bacterial peritonitis (SBP), raising the question of whether to permanently discontinue or to restart ... treatment after resolving the SBP episode," they added.
Dr. Mandorfer, of the Medical University of Vienna, and his colleagues followed 607 consecutive cirrhosis patients who underwent their first paracentesis at that institution between 2006 and 2011.
Overall, 245 patients were taking beta-blockers, including propranolol, with doses ranging from 20 to 120 mg, and carvedilol, with doses between 6.25 and 25 mg.
Spontaneous bacterial peritonitis was defined as an ascitic polymorphonuclear neutrophil count greater than 250 cells/mL with no evident source of infection.
A total of 182 cases of a first SBP infection were detected during the study period and included for analysis (86 in beta-blocker patients), with incidence rates comparable between beta-blocker and non–beta-blocker cohorts (0.107 vs, 0.117 per person-year, respectively).
The authors found that a higher proportion of beta-blocker patients were hemodynamically unstable, with 38% registering mean systolic arterial pressures less than 100 mm Hg at the time of first paracentesis during an SBP episode, compared with 18% of non–beta-blocker patients (P = .002).
And although variceal bleeding rates were similar between cohorts, beta-blocker patients tallied overall longer durations of hospitalization than did their untreated counterparts (33.4 vs. 28.8 days per person-year).
Looking at the development of hepatorenal syndrome, Dr. Mandorfer also noted that the incidence was significantly higher in patients taking beta-blockers (24%) than in patients who were not (11%; P = .027).
Perhaps most importantly, while beta-blocker treatment was associated with improved transplant-free survival generally, after SBP diagnosis, taking beta-blockers resulted in a lower transplant-free survival (hazard ratio, 1.58; 95% confidence interval, 1.098-2.274; P = .014) after adjustment for the presence of varices and the Child-Pugh score.
According to Dr. Mandorfer, the present study adds another voice to the "lively debate" that began after a 2010 study showed that beta-blockers had deleterious effects on survival (Hepatology 2010;52:1017-22).
And while these findings support the "window hypothesis," which posits that the optimal "window" for beta-blocker treatment opens at the diagnosis of cirrhosis but closes at the development of SBP, "whether the therapeutic window for [beta-blocker] treatment reopens after resolving the SBP episode remains unclear," they wrote.
Indeed, "The development of bacterial infections might define a distinct group of critically ill patients with cirrhosis with a highly restricted prognosis in which maintaining the circulatory reserve is crucial not only during the acute phase of infection but also later on," they added.
"Prospective studies are highly encouraged to investigate the appropriate, stage-dependent use of this cornerstone in the treatment of portal hypertension."
The authors stated that they had no conflicts of interest and disclosed no funding for this study.
The beta-blocker controversy continues in this issue of Gastroenterology, with an exciting study from Mandorfer and colleagues on the detrimental effect of beta-blocker treatment after the development of spontaneous bacterial peritonitis in patients with cirrhosis. In this retrospective cohort study, nonselective beta-blockers were shown to increase transplant-free survival in patients without SBP. However, following the first diagnosis of SBP, nonselective beta-blockers were associated with hemodynamic compromise and decreased blood pressures, reduced transplant-free survival, increased hospitalization rates, and increased incidence of hepatorenal syndrome and acute kidney injury. The authors conclude that patients with cirrhosis and SBP should not receive beta-blocker therapy.
The clinical implications of this study are far-reaching. Beta-blockers are well established in the primary and secondary prevention of variceal hemorrhage in patients with cirrhosis, and critics are likely to point out the retrospective nature of this study. However, several recent and similarly controversial studies have also suggested harm with beta-blocker therapy in patients with advanced cirrhosis. This has led to the proposal of a "window hypothesis," in which beta-blockers improve survival within a limited window in the natural history of cirrhosis.
The current study adds to the mounting body of evidence in support of the "window hypothesis," and suggests furthermore that the therapeutic window closes at the first onset of SBP. Whether or not the window reopens is up for debate; however, it is increasingly clear that beta-blocker therapy in patients with cirrhosis is only beneficial within a small window of opportunity, quite possibly smaller than previously thought.
Dr. Phillip S. Ge and Dr. Bruce A. Runyon are with the division of digestive diseases/hepatology, Santa Monica-UCLA [University of California, Los Angeles] Medical Center. The authors disclosed no potential conflicts of interest.
The beta-blocker controversy continues in this issue of Gastroenterology, with an exciting study from Mandorfer and colleagues on the detrimental effect of beta-blocker treatment after the development of spontaneous bacterial peritonitis in patients with cirrhosis. In this retrospective cohort study, nonselective beta-blockers were shown to increase transplant-free survival in patients without SBP. However, following the first diagnosis of SBP, nonselective beta-blockers were associated with hemodynamic compromise and decreased blood pressures, reduced transplant-free survival, increased hospitalization rates, and increased incidence of hepatorenal syndrome and acute kidney injury. The authors conclude that patients with cirrhosis and SBP should not receive beta-blocker therapy.
The clinical implications of this study are far-reaching. Beta-blockers are well established in the primary and secondary prevention of variceal hemorrhage in patients with cirrhosis, and critics are likely to point out the retrospective nature of this study. However, several recent and similarly controversial studies have also suggested harm with beta-blocker therapy in patients with advanced cirrhosis. This has led to the proposal of a "window hypothesis," in which beta-blockers improve survival within a limited window in the natural history of cirrhosis.
The current study adds to the mounting body of evidence in support of the "window hypothesis," and suggests furthermore that the therapeutic window closes at the first onset of SBP. Whether or not the window reopens is up for debate; however, it is increasingly clear that beta-blocker therapy in patients with cirrhosis is only beneficial within a small window of opportunity, quite possibly smaller than previously thought.
Dr. Phillip S. Ge and Dr. Bruce A. Runyon are with the division of digestive diseases/hepatology, Santa Monica-UCLA [University of California, Los Angeles] Medical Center. The authors disclosed no potential conflicts of interest.
The beta-blocker controversy continues in this issue of Gastroenterology, with an exciting study from Mandorfer and colleagues on the detrimental effect of beta-blocker treatment after the development of spontaneous bacterial peritonitis in patients with cirrhosis. In this retrospective cohort study, nonselective beta-blockers were shown to increase transplant-free survival in patients without SBP. However, following the first diagnosis of SBP, nonselective beta-blockers were associated with hemodynamic compromise and decreased blood pressures, reduced transplant-free survival, increased hospitalization rates, and increased incidence of hepatorenal syndrome and acute kidney injury. The authors conclude that patients with cirrhosis and SBP should not receive beta-blocker therapy.
The clinical implications of this study are far-reaching. Beta-blockers are well established in the primary and secondary prevention of variceal hemorrhage in patients with cirrhosis, and critics are likely to point out the retrospective nature of this study. However, several recent and similarly controversial studies have also suggested harm with beta-blocker therapy in patients with advanced cirrhosis. This has led to the proposal of a "window hypothesis," in which beta-blockers improve survival within a limited window in the natural history of cirrhosis.
The current study adds to the mounting body of evidence in support of the "window hypothesis," and suggests furthermore that the therapeutic window closes at the first onset of SBP. Whether or not the window reopens is up for debate; however, it is increasingly clear that beta-blocker therapy in patients with cirrhosis is only beneficial within a small window of opportunity, quite possibly smaller than previously thought.
Dr. Phillip S. Ge and Dr. Bruce A. Runyon are with the division of digestive diseases/hepatology, Santa Monica-UCLA [University of California, Los Angeles] Medical Center. The authors disclosed no potential conflicts of interest.
Nonselective beta-blockers are contraindicated in cirrhosis with spontaneous bacterial peritonitis, wrote Dr. Mattias Mandorfer and his colleagues in the June issue of Gastroenterology (doi: 10.1053/j.gastro.2014.03.005).
Indeed, in a retrospective analysis, the drugs increased the length of hospitalization and the rate of hepatorenal syndrome, while decreasing overall transplant-free survival.
"These observations suggest that nonselective beta-blocker treatment should be discontinued at the first development of spontaneous bacterial peritonitis (SBP), raising the question of whether to permanently discontinue or to restart ... treatment after resolving the SBP episode," they added.
Dr. Mandorfer, of the Medical University of Vienna, and his colleagues followed 607 consecutive cirrhosis patients who underwent their first paracentesis at that institution between 2006 and 2011.
Overall, 245 patients were taking beta-blockers, including propranolol, with doses ranging from 20 to 120 mg, and carvedilol, with doses between 6.25 and 25 mg.
Spontaneous bacterial peritonitis was defined as an ascitic polymorphonuclear neutrophil count greater than 250 cells/mL with no evident source of infection.
A total of 182 cases of a first SBP infection were detected during the study period and included for analysis (86 in beta-blocker patients), with incidence rates comparable between beta-blocker and non–beta-blocker cohorts (0.107 vs, 0.117 per person-year, respectively).
The authors found that a higher proportion of beta-blocker patients were hemodynamically unstable, with 38% registering mean systolic arterial pressures less than 100 mm Hg at the time of first paracentesis during an SBP episode, compared with 18% of non–beta-blocker patients (P = .002).
And although variceal bleeding rates were similar between cohorts, beta-blocker patients tallied overall longer durations of hospitalization than did their untreated counterparts (33.4 vs. 28.8 days per person-year).
Looking at the development of hepatorenal syndrome, Dr. Mandorfer also noted that the incidence was significantly higher in patients taking beta-blockers (24%) than in patients who were not (11%; P = .027).
Perhaps most importantly, while beta-blocker treatment was associated with improved transplant-free survival generally, after SBP diagnosis, taking beta-blockers resulted in a lower transplant-free survival (hazard ratio, 1.58; 95% confidence interval, 1.098-2.274; P = .014) after adjustment for the presence of varices and the Child-Pugh score.
According to Dr. Mandorfer, the present study adds another voice to the "lively debate" that began after a 2010 study showed that beta-blockers had deleterious effects on survival (Hepatology 2010;52:1017-22).
And while these findings support the "window hypothesis," which posits that the optimal "window" for beta-blocker treatment opens at the diagnosis of cirrhosis but closes at the development of SBP, "whether the therapeutic window for [beta-blocker] treatment reopens after resolving the SBP episode remains unclear," they wrote.
Indeed, "The development of bacterial infections might define a distinct group of critically ill patients with cirrhosis with a highly restricted prognosis in which maintaining the circulatory reserve is crucial not only during the acute phase of infection but also later on," they added.
"Prospective studies are highly encouraged to investigate the appropriate, stage-dependent use of this cornerstone in the treatment of portal hypertension."
The authors stated that they had no conflicts of interest and disclosed no funding for this study.
Nonselective beta-blockers are contraindicated in cirrhosis with spontaneous bacterial peritonitis, wrote Dr. Mattias Mandorfer and his colleagues in the June issue of Gastroenterology (doi: 10.1053/j.gastro.2014.03.005).
Indeed, in a retrospective analysis, the drugs increased the length of hospitalization and the rate of hepatorenal syndrome, while decreasing overall transplant-free survival.
"These observations suggest that nonselective beta-blocker treatment should be discontinued at the first development of spontaneous bacterial peritonitis (SBP), raising the question of whether to permanently discontinue or to restart ... treatment after resolving the SBP episode," they added.
Dr. Mandorfer, of the Medical University of Vienna, and his colleagues followed 607 consecutive cirrhosis patients who underwent their first paracentesis at that institution between 2006 and 2011.
Overall, 245 patients were taking beta-blockers, including propranolol, with doses ranging from 20 to 120 mg, and carvedilol, with doses between 6.25 and 25 mg.
Spontaneous bacterial peritonitis was defined as an ascitic polymorphonuclear neutrophil count greater than 250 cells/mL with no evident source of infection.
A total of 182 cases of a first SBP infection were detected during the study period and included for analysis (86 in beta-blocker patients), with incidence rates comparable between beta-blocker and non–beta-blocker cohorts (0.107 vs, 0.117 per person-year, respectively).
The authors found that a higher proportion of beta-blocker patients were hemodynamically unstable, with 38% registering mean systolic arterial pressures less than 100 mm Hg at the time of first paracentesis during an SBP episode, compared with 18% of non–beta-blocker patients (P = .002).
And although variceal bleeding rates were similar between cohorts, beta-blocker patients tallied overall longer durations of hospitalization than did their untreated counterparts (33.4 vs. 28.8 days per person-year).
Looking at the development of hepatorenal syndrome, Dr. Mandorfer also noted that the incidence was significantly higher in patients taking beta-blockers (24%) than in patients who were not (11%; P = .027).
Perhaps most importantly, while beta-blocker treatment was associated with improved transplant-free survival generally, after SBP diagnosis, taking beta-blockers resulted in a lower transplant-free survival (hazard ratio, 1.58; 95% confidence interval, 1.098-2.274; P = .014) after adjustment for the presence of varices and the Child-Pugh score.
According to Dr. Mandorfer, the present study adds another voice to the "lively debate" that began after a 2010 study showed that beta-blockers had deleterious effects on survival (Hepatology 2010;52:1017-22).
And while these findings support the "window hypothesis," which posits that the optimal "window" for beta-blocker treatment opens at the diagnosis of cirrhosis but closes at the development of SBP, "whether the therapeutic window for [beta-blocker] treatment reopens after resolving the SBP episode remains unclear," they wrote.
Indeed, "The development of bacterial infections might define a distinct group of critically ill patients with cirrhosis with a highly restricted prognosis in which maintaining the circulatory reserve is crucial not only during the acute phase of infection but also later on," they added.
"Prospective studies are highly encouraged to investigate the appropriate, stage-dependent use of this cornerstone in the treatment of portal hypertension."
The authors stated that they had no conflicts of interest and disclosed no funding for this study.
FROM GASTROENTEROLOGY
Major finding: Beta-blockers were linked to lower transplant-free survival among spontaneous bacterial peritonitis patients (hazard ratio, 1.58).
Data source: A retrospective analysis of more than 600 patients at a single center in Vienna.
Disclosures: The authors stated that they had no conflicts of interest and disclosed no funding for this study.
Less risk of esophageal bleed with rifaximin
CHICAGO – Patients with cirrhosis and medium to large esophageal varices were 81% less likely to develop a first esophageal variceal bleed within 5 years if they took rifaximin to manage hepatic encephalopathy, a retrospective study of 238 patients found.
Of the 97 patients who received rifaximin (a nonabsorbable antibiotic with broad-spectrum activity), 94% remained free of variceal hemorrhage at 3 years, 4 years, and 5 years after their sentinel endoscopy, the historic cohort study showed. Among the 141 patients who were not on rifaximin, 75% had not developed a variceal bleed within 3 years, and 58% had no variceal bleeds at years 4 and 5, Dr. Bradley Confer and his associates reported.

The cumulative incidence of esophageal variceal bleed was 11% in 5 years, or 4% for patients on rifaximin and 16% for those not on rifaximin, said Dr. Confer of the Cleveland Clinic.
Those statistically significant differences between groups suggest that rifaximin use decreases the risk of a first esophageal bleed and decreases the time to a first bleed in cirrhotic patients with medium to large varices, but a larger prospective randomized trial would be needed to confirm that, he said at the annual Digestive Disease Week.
All patients were treated with nonselective beta-blocker medications, esophageal band ligation, or a combination of both and were followed to the time of a first esophageal variceal bleed, liver transplant, last follow-up, or death. Beta-blockers were used by 63% of patients, and 87% underwent at least one banding procedure. Patients on rifaximin used the drug for a median of 9 months.
Although five factors were associated with the risk for a first variceal hemorrhage in a univariate analysis, only three remained significant after a multivariate analysis that adjusted for the use of beta-blockers and band ligation: rifaximin use (associated with an 81% decrease in risk), age (a 20% increase in risk with 5 additional years of age), and the patient’s International Normalized Ratio (which can be associated with more than a sixfold increase in bleed risk).
Previous data suggest that cirrhotic patients with medium to large esophageal varices still have a 10%-20% risk of developing a first esophageal variceal bleed even after treatment with either nonselective beta-blockers or band ligation. Many patients do not tolerate nonselective beta-blockers well, and the drugs may negatively affect a subgroup of patients with cirrhosis, he said. Repeating variceal ligation is a costly and invasive management strategy.
The investigators turned their attention to rifaximin after separate data showed that 4 weeks of use were associated with a significant decrease in hepatic venous pressure gradient in patients with alcoholic cirrhosis. They evaluated records on 1,121 patients with cirrhosis who underwent esophagogastroduodenoscopy in 2008-2011 and excluded any with no varices, small varices, a history of esophageal variceal bleeding, or noncirrhotic portal hypertension, or who received a transjugular intrahepatic portosystemic shunt.
The mean age at the time of esophagogastroduodenoscopy was 53 years, and 72% of patients were male. They had an average Model for End-Stage Liver Disease score of 14.3 and an average Child-Pugh score of 8.7. Compared with patients not on rifaximin, those who got the antibiotic were significantly less likely to use nonselective beta-blockers and were sicker, Dr. Confer said, with significantly higher serum creatinine levels, lower serum albumin, and a greater likelihood of hepatic encephalopathy at baseline.
Dr. Confer reported having no financial disclosures.
On Twitter @sherryboschert
This article was updated on June 26, 2014.
CHICAGO – Patients with cirrhosis and medium to large esophageal varices were 81% less likely to develop a first esophageal variceal bleed within 5 years if they took rifaximin to manage hepatic encephalopathy, a retrospective study of 238 patients found.
Of the 97 patients who received rifaximin (a nonabsorbable antibiotic with broad-spectrum activity), 94% remained free of variceal hemorrhage at 3 years, 4 years, and 5 years after their sentinel endoscopy, the historic cohort study showed. Among the 141 patients who were not on rifaximin, 75% had not developed a variceal bleed within 3 years, and 58% had no variceal bleeds at years 4 and 5, Dr. Bradley Confer and his associates reported.
The cumulative incidence of esophageal variceal bleed was 11% in 5 years, or 4% for patients on rifaximin and 16% for those not on rifaximin, said Dr. Confer of the Cleveland Clinic.
Those statistically significant differences between groups suggest that rifaximin use decreases the risk of a first esophageal bleed and decreases the time to a first bleed in cirrhotic patients with medium to large varices, but a larger prospective randomized trial would be needed to confirm that, he said at the annual Digestive Disease Week.
All patients were treated with nonselective beta-blocker medications, esophageal band ligation, or a combination of both and were followed to the time of a first esophageal variceal bleed, liver transplant, last follow-up, or death. Beta-blockers were used by 63% of patients, and 87% underwent at least one banding procedure. Patients on rifaximin used the drug for a median of 9 months.
Although five factors were associated with the risk for a first variceal hemorrhage in a univariate analysis, only three remained significant after a multivariate analysis that adjusted for the use of beta-blockers and band ligation: rifaximin use (associated with an 81% decrease in risk), age (a 20% increase in risk with 5 additional years of age), and the patient’s International Normalized Ratio (which can be associated with more than a sixfold increase in bleed risk).
Previous data suggest that cirrhotic patients with medium to large esophageal varices still have a 10%-20% risk of developing a first esophageal variceal bleed even after treatment with either nonselective beta-blockers or band ligation. Many patients do not tolerate nonselective beta-blockers well, and the drugs may negatively affect a subgroup of patients with cirrhosis, he said. Repeating variceal ligation is a costly and invasive management strategy.
The investigators turned their attention to rifaximin after separate data showed that 4 weeks of use were associated with a significant decrease in hepatic venous pressure gradient in patients with alcoholic cirrhosis. They evaluated records on 1,121 patients with cirrhosis who underwent esophagogastroduodenoscopy in 2008-2011 and excluded any with no varices, small varices, a history of esophageal variceal bleeding, or noncirrhotic portal hypertension, or who received a transjugular intrahepatic portosystemic shunt.
The mean age at the time of esophagogastroduodenoscopy was 53 years, and 72% of patients were male. They had an average Model for End-Stage Liver Disease score of 14.3 and an average Child-Pugh score of 8.7. Compared with patients not on rifaximin, those who got the antibiotic were significantly less likely to use nonselective beta-blockers and were sicker, Dr. Confer said, with significantly higher serum creatinine levels, lower serum albumin, and a greater likelihood of hepatic encephalopathy at baseline.
Dr. Confer reported having no financial disclosures.
On Twitter @sherryboschert
This article was updated on June 26, 2014.
CHICAGO – Patients with cirrhosis and medium to large esophageal varices were 81% less likely to develop a first esophageal variceal bleed within 5 years if they took rifaximin to manage hepatic encephalopathy, a retrospective study of 238 patients found.
Of the 97 patients who received rifaximin (a nonabsorbable antibiotic with broad-spectrum activity), 94% remained free of variceal hemorrhage at 3 years, 4 years, and 5 years after their sentinel endoscopy, the historic cohort study showed. Among the 141 patients who were not on rifaximin, 75% had not developed a variceal bleed within 3 years, and 58% had no variceal bleeds at years 4 and 5, Dr. Bradley Confer and his associates reported.
The cumulative incidence of esophageal variceal bleed was 11% in 5 years, or 4% for patients on rifaximin and 16% for those not on rifaximin, said Dr. Confer of the Cleveland Clinic.
Those statistically significant differences between groups suggest that rifaximin use decreases the risk of a first esophageal bleed and decreases the time to a first bleed in cirrhotic patients with medium to large varices, but a larger prospective randomized trial would be needed to confirm that, he said at the annual Digestive Disease Week.
All patients were treated with nonselective beta-blocker medications, esophageal band ligation, or a combination of both and were followed to the time of a first esophageal variceal bleed, liver transplant, last follow-up, or death. Beta-blockers were used by 63% of patients, and 87% underwent at least one banding procedure. Patients on rifaximin used the drug for a median of 9 months.
Although five factors were associated with the risk for a first variceal hemorrhage in a univariate analysis, only three remained significant after a multivariate analysis that adjusted for the use of beta-blockers and band ligation: rifaximin use (associated with an 81% decrease in risk), age (a 20% increase in risk with 5 additional years of age), and the patient’s International Normalized Ratio (which can be associated with more than a sixfold increase in bleed risk).
Previous data suggest that cirrhotic patients with medium to large esophageal varices still have a 10%-20% risk of developing a first esophageal variceal bleed even after treatment with either nonselective beta-blockers or band ligation. Many patients do not tolerate nonselective beta-blockers well, and the drugs may negatively affect a subgroup of patients with cirrhosis, he said. Repeating variceal ligation is a costly and invasive management strategy.
The investigators turned their attention to rifaximin after separate data showed that 4 weeks of use were associated with a significant decrease in hepatic venous pressure gradient in patients with alcoholic cirrhosis. They evaluated records on 1,121 patients with cirrhosis who underwent esophagogastroduodenoscopy in 2008-2011 and excluded any with no varices, small varices, a history of esophageal variceal bleeding, or noncirrhotic portal hypertension, or who received a transjugular intrahepatic portosystemic shunt.
The mean age at the time of esophagogastroduodenoscopy was 53 years, and 72% of patients were male. They had an average Model for End-Stage Liver Disease score of 14.3 and an average Child-Pugh score of 8.7. Compared with patients not on rifaximin, those who got the antibiotic were significantly less likely to use nonselective beta-blockers and were sicker, Dr. Confer said, with significantly higher serum creatinine levels, lower serum albumin, and a greater likelihood of hepatic encephalopathy at baseline.
Dr. Confer reported having no financial disclosures.
On Twitter @sherryboschert
This article was updated on June 26, 2014.
AT DDW 2014
Key clinical point: Rifaximin may decrease the risk for esophageal variceal bleed in cirrhotic patients with medium to large esophageal varices.
Major finding: The 5-year risk of a first esophageal variceal bleed was 81% lower in patients on rifaximin, compared with those not on rifaximin.
Data source: A retrospective cohort study of 238 patients with cirrhosis and medium to large esophageal varices treated with nonselective beta-blockers and/or esophageal band ligation, 41% of whom also took rifaximin to manage hepatic encephalopathy.
Disclosures: Dr. Confer reported having no financial disclosures.

Liver cancer without cirrhosis surprisingly common: Is NAFLD the cause?
CHICAGO – A full 13% of patients diagnosed with hepatocellular carcinoma did not have underlying cirrhosis in a national sample of 1,500 veterans.
Although hepatocellular carcinoma (HCC) in patients with cirrhosis typically arises against a background of alcohol abuse or hepatitis C virus infection, this entity was strongly associated with nonalcoholic fatty liver disease (NAFLD) and idiopathic HCC.
"While this represents a small proportion, this poses a logistical problem for HCC surveillance, given the large population with NAFLD and no real identifying features of who is going to develop HCC," Dr. Sahil Mittal said at the annual Digestive Disease Week.

Despite a threefold increase in HCC in the United States over the last 3 decades and emerging evidence for NAFLD presenting in the absence of cirrhosis, this is the first study to assess the prevalence and risk factors for HCC without cirrhosis in a national sample of HCC patients, he said.
The investigators, led by Dr. Hashem B. El-Serag, section chief, gastroenterology and hepatology, Baylor College of Medicine, Houston, performed a chart review of 1,500 veterans with a confirmed diagnosis of HCC randomly selected between 2005 and 2011. Of these, cirrhosis was absent in 43 (3%), highly improbable in 151 (10%), and definite in 1,201 (80%), with the diagnosis unclear because of insufficient data in 105 (7%).
As expected, HCC patients with cirrhosis were significantly more likely than those with no or probable no cirrhosis to abuse alcohol (84% vs. 67.4% vs. 63.6%; P less than .01) and to have hepatitis C infection (72.2% vs. 42% vs. 44.4%; P less than .01), said Dr. Mittal, also with Baylor’s College of Medicine.
Hepatitis B infection was similar in all three groups (5% vs. 4.7% vs. 2%).
In contrast, NAFLD was more common in patients with no or probably no cirrhosis than in those with cirrhosis (14% vs. 20.5% vs. 5.8%; P less than .01), as was idiopathic HCC (18.6% vs. 27.8% vs. 8.2%; P less than .01), he said.
"NAFLD is associated with a significantly increased risk of HCC in the absence of cirrhosis, compared with hepatitis C or alcohol," he said.
With regard to clinical factors, sex and race did not differ between groups. However, the no and probably no cirrhosis patients were significantly older than were those with HCC accompanied by cirrhosis (65.5 years, vs. 69.7 years vs. 62.6 years) and significantly more likely to have comorbidities associated with metabolic syndrome, such as hypertension (88.4% vs. 86.8% vs. 72.6%), myocardial infarction (11.6% vs. 18.5% vs. 7.5%), and peripheral vascular disease (11.6% vs. 20% vs. 9.5%), Dr. Mittal reported. The differences among groups were statistically significant with P values of less than .01.
The investigators then performed logistic regression analysis to examine predictors of HCC without cirrhosis. After adjustment for confounders, they found NAFLD was more than threefold likely (odds ratio, 3.1) and idiopathic HCC more than twofold likely (OR, 2.8) in patients with HCC without cirrhosis, compared with patients with hepatitis C–related HCC.
This entity of HCC in the absence of cirrhosis was also associated with the metabolic syndrome–related comorbidities of hypertension (OR, 1.8) and myocardial infarction (OR, 1.8).
The findings suggest that the risk of HCC in patients with NAFLD is increased not only because of progression to cirrhosis, but possibly through other alternative noncirrhosis pathways, Dr. Mittal said in an interview. This has important implications for understanding the pathogenesis of HCC, as well as for HCC screening in NAFLD patients.
"Due to the high prevalence of NAFLD in the general population, conventional screening by ultrasonography may not be a feasible strategy, especially if one cannot rely on cirrhosis as the main predisposing lesion to HCC," he said. "Studies are needed to identify risk factors and biomarkers that can identify NAFLD patients at higher risk of developing HCC. Future research is also needed to investigate the role of chemoprevention."
Dr. Mittal reported no conflicting interests. Lead author Dr. El-Serag reported consulting fees and grant/research support from Gilead Sciences.
CHICAGO – A full 13% of patients diagnosed with hepatocellular carcinoma did not have underlying cirrhosis in a national sample of 1,500 veterans.
Although hepatocellular carcinoma (HCC) in patients with cirrhosis typically arises against a background of alcohol abuse or hepatitis C virus infection, this entity was strongly associated with nonalcoholic fatty liver disease (NAFLD) and idiopathic HCC.
"While this represents a small proportion, this poses a logistical problem for HCC surveillance, given the large population with NAFLD and no real identifying features of who is going to develop HCC," Dr. Sahil Mittal said at the annual Digestive Disease Week.
Despite a threefold increase in HCC in the United States over the last 3 decades and emerging evidence for NAFLD presenting in the absence of cirrhosis, this is the first study to assess the prevalence and risk factors for HCC without cirrhosis in a national sample of HCC patients, he said.
The investigators, led by Dr. Hashem B. El-Serag, section chief, gastroenterology and hepatology, Baylor College of Medicine, Houston, performed a chart review of 1,500 veterans with a confirmed diagnosis of HCC randomly selected between 2005 and 2011. Of these, cirrhosis was absent in 43 (3%), highly improbable in 151 (10%), and definite in 1,201 (80%), with the diagnosis unclear because of insufficient data in 105 (7%).
As expected, HCC patients with cirrhosis were significantly more likely than those with no or probable no cirrhosis to abuse alcohol (84% vs. 67.4% vs. 63.6%; P less than .01) and to have hepatitis C infection (72.2% vs. 42% vs. 44.4%; P less than .01), said Dr. Mittal, also with Baylor’s College of Medicine.
Hepatitis B infection was similar in all three groups (5% vs. 4.7% vs. 2%).
In contrast, NAFLD was more common in patients with no or probably no cirrhosis than in those with cirrhosis (14% vs. 20.5% vs. 5.8%; P less than .01), as was idiopathic HCC (18.6% vs. 27.8% vs. 8.2%; P less than .01), he said.
"NAFLD is associated with a significantly increased risk of HCC in the absence of cirrhosis, compared with hepatitis C or alcohol," he said.
With regard to clinical factors, sex and race did not differ between groups. However, the no and probably no cirrhosis patients were significantly older than were those with HCC accompanied by cirrhosis (65.5 years, vs. 69.7 years vs. 62.6 years) and significantly more likely to have comorbidities associated with metabolic syndrome, such as hypertension (88.4% vs. 86.8% vs. 72.6%), myocardial infarction (11.6% vs. 18.5% vs. 7.5%), and peripheral vascular disease (11.6% vs. 20% vs. 9.5%), Dr. Mittal reported. The differences among groups were statistically significant with P values of less than .01.
The investigators then performed logistic regression analysis to examine predictors of HCC without cirrhosis. After adjustment for confounders, they found NAFLD was more than threefold likely (odds ratio, 3.1) and idiopathic HCC more than twofold likely (OR, 2.8) in patients with HCC without cirrhosis, compared with patients with hepatitis C–related HCC.
This entity of HCC in the absence of cirrhosis was also associated with the metabolic syndrome–related comorbidities of hypertension (OR, 1.8) and myocardial infarction (OR, 1.8).
The findings suggest that the risk of HCC in patients with NAFLD is increased not only because of progression to cirrhosis, but possibly through other alternative noncirrhosis pathways, Dr. Mittal said in an interview. This has important implications for understanding the pathogenesis of HCC, as well as for HCC screening in NAFLD patients.
"Due to the high prevalence of NAFLD in the general population, conventional screening by ultrasonography may not be a feasible strategy, especially if one cannot rely on cirrhosis as the main predisposing lesion to HCC," he said. "Studies are needed to identify risk factors and biomarkers that can identify NAFLD patients at higher risk of developing HCC. Future research is also needed to investigate the role of chemoprevention."
Dr. Mittal reported no conflicting interests. Lead author Dr. El-Serag reported consulting fees and grant/research support from Gilead Sciences.
CHICAGO – A full 13% of patients diagnosed with hepatocellular carcinoma did not have underlying cirrhosis in a national sample of 1,500 veterans.
Although hepatocellular carcinoma (HCC) in patients with cirrhosis typically arises against a background of alcohol abuse or hepatitis C virus infection, this entity was strongly associated with nonalcoholic fatty liver disease (NAFLD) and idiopathic HCC.
"While this represents a small proportion, this poses a logistical problem for HCC surveillance, given the large population with NAFLD and no real identifying features of who is going to develop HCC," Dr. Sahil Mittal said at the annual Digestive Disease Week.
Despite a threefold increase in HCC in the United States over the last 3 decades and emerging evidence for NAFLD presenting in the absence of cirrhosis, this is the first study to assess the prevalence and risk factors for HCC without cirrhosis in a national sample of HCC patients, he said.
The investigators, led by Dr. Hashem B. El-Serag, section chief, gastroenterology and hepatology, Baylor College of Medicine, Houston, performed a chart review of 1,500 veterans with a confirmed diagnosis of HCC randomly selected between 2005 and 2011. Of these, cirrhosis was absent in 43 (3%), highly improbable in 151 (10%), and definite in 1,201 (80%), with the diagnosis unclear because of insufficient data in 105 (7%).
As expected, HCC patients with cirrhosis were significantly more likely than those with no or probable no cirrhosis to abuse alcohol (84% vs. 67.4% vs. 63.6%; P less than .01) and to have hepatitis C infection (72.2% vs. 42% vs. 44.4%; P less than .01), said Dr. Mittal, also with Baylor’s College of Medicine.
Hepatitis B infection was similar in all three groups (5% vs. 4.7% vs. 2%).
In contrast, NAFLD was more common in patients with no or probably no cirrhosis than in those with cirrhosis (14% vs. 20.5% vs. 5.8%; P less than .01), as was idiopathic HCC (18.6% vs. 27.8% vs. 8.2%; P less than .01), he said.
"NAFLD is associated with a significantly increased risk of HCC in the absence of cirrhosis, compared with hepatitis C or alcohol," he said.
With regard to clinical factors, sex and race did not differ between groups. However, the no and probably no cirrhosis patients were significantly older than were those with HCC accompanied by cirrhosis (65.5 years, vs. 69.7 years vs. 62.6 years) and significantly more likely to have comorbidities associated with metabolic syndrome, such as hypertension (88.4% vs. 86.8% vs. 72.6%), myocardial infarction (11.6% vs. 18.5% vs. 7.5%), and peripheral vascular disease (11.6% vs. 20% vs. 9.5%), Dr. Mittal reported. The differences among groups were statistically significant with P values of less than .01.
The investigators then performed logistic regression analysis to examine predictors of HCC without cirrhosis. After adjustment for confounders, they found NAFLD was more than threefold likely (odds ratio, 3.1) and idiopathic HCC more than twofold likely (OR, 2.8) in patients with HCC without cirrhosis, compared with patients with hepatitis C–related HCC.
This entity of HCC in the absence of cirrhosis was also associated with the metabolic syndrome–related comorbidities of hypertension (OR, 1.8) and myocardial infarction (OR, 1.8).
The findings suggest that the risk of HCC in patients with NAFLD is increased not only because of progression to cirrhosis, but possibly through other alternative noncirrhosis pathways, Dr. Mittal said in an interview. This has important implications for understanding the pathogenesis of HCC, as well as for HCC screening in NAFLD patients.
"Due to the high prevalence of NAFLD in the general population, conventional screening by ultrasonography may not be a feasible strategy, especially if one cannot rely on cirrhosis as the main predisposing lesion to HCC," he said. "Studies are needed to identify risk factors and biomarkers that can identify NAFLD patients at higher risk of developing HCC. Future research is also needed to investigate the role of chemoprevention."
Dr. Mittal reported no conflicting interests. Lead author Dr. El-Serag reported consulting fees and grant/research support from Gilead Sciences.
AT DDW 2014
Key clinical point: A significant proportion of NAFLD-related HCC patients have no cirrhosis at presentation, so clinicians need to maintain a high index of suspicion.
Major finding: Up to 13% of patients with HCC in the United States may not have underlying cirrhosis.
Data source: A retrospective cohort study of 1,500 veterans with HCC.
Disclosures: Dr. Mittal reported no conflicting interests. Lead author Dr. El-Serag reported consulting fees and grant/research support from Gilead Sciences.

Hepatitis B screening recommended for high-risk patients
Physicians should screen all asymptomatic but high-risk adolescents and adults for hepatitis B virus infection, according to an updated recommendation by the U.S. Preventive Services Task Force that was published online May 27 in Annals of Internal Medicine.
Since the last USPSTF recommendation on HBV screening in 2004, which focused on the general population and didn’t advocate screening of this subset of patients, research has documented that antiviral treatment improves both intermediate outcomes such as virologic and histologic responses and long-term outcomes such as prevention of hepatocellular carcinoma, cirrhosis, and end-stage liver disease.

Given this effectiveness, along with the 98% sensitivity and specificity of HBV screening tests, the group has now issued a level B recommendation that high-risk patients be screened, said Dr. Michael L. LeFevre, chair of the USPSTF and professor of family and community medicine at the University of Missouri, Columbia, and his associates.
High-risk patients include the following:
• People born in regions where the prevalence of HBV infection is 2% or greater, such as sub-Saharan Africa, central and southeast Asia, China, the Pacific Islands, and parts of Latin America. People born in these areas account for 47%-95% of the chronic HBV infection in the United States.
• American-born children of parents from these regions, who may not have been vaccinated in infancy.
• HIV-positive persons.
• IV-drug users.
• Household contacts of people with HBV infection.
• Men who have sex with men.
The updated USPSTF recommendations are in line with those of the Centers for Disease Control and Prevention, the American Association for the Study of Liver Diseases, the Institute of Medicine, and the American Academy of Family Physicians. The CDC additionally recommends HBV screening for blood, organ, or tissue donors; people with occupational or other exposure to infectious blood or body fluids; and patients receiving hemodialysis, cytotoxic therapy, or immunosuppressive therapy.
The USPSTF still does not recommend HBV screening for the general population. The prevalence of the infection is low in the U.S. general population, and most members of the general population who are infected with HBV do not develop the chronic form of the infection and do not develop complications like hepatocellular carcinoma or cirrhosis. The potential harms of general screening, then, probably exceed the potential benefits, Dr. LeFevre and his associates noted (Ann Intern. Med. 2014 May 27 [doi:10.7326/M14-1018]).
The USPSTF has separate recommendations regarding hepatitis B in pregnant women. These, along with the updated recommendations for high-risk patients, are available at www.uspreventiveservicestaskforce.org.
The USPSTF is a voluntary group funded by the Agency for Healthcare Research and Quality but otherwise independent of the federal government. Dr. LeFevre and his associates reported no potential financial conflicts of interest.
These "long overdue" recommendations are "a dramatic and welcome upgrade from the 2004 USPSTF guidelines, which issued a grade D recommendation against screening asymptomatic persons for HBV infection," said Dr. Ruma Rajbhandari and Dr. Raymond T. Chung.
"Many would argue that the USPSTF should have endorsed screening for HBV infection in high-risk populations a decade ago," they wrote. The group lagged far behind the American Association for the Study of Liver Diseases’ recommendations in 2001 and the CDC’s recommendations in 2005. "We may have thus missed an opportunity to screen many high-risk persons in the United States," Dr. Rajbhandari and Dr. Chung said.
The USPSTF update "would be more useful if they provided a clearer definition of the high-risk patient. ... We worry that busy generalist clinicians do not have the time to estimate their patients’ risks for HBV infection." Physicians may find it more helpful to look up the CDC’s table listing all the factors that render a patient high risk, they added.
Dr. Rajbhandari and Dr. Chung are with the liver center and gastrointestinal division at Massachusetts General Hospital, Boston. They reported no relevant conflicts of interest. These remarks were taken from their editorial accompanying Dr. Lefevre’s report (Ann. Intern. Med. 2014 May 27 [doi:10.7326/M14-1153]).
These "long overdue" recommendations are "a dramatic and welcome upgrade from the 2004 USPSTF guidelines, which issued a grade D recommendation against screening asymptomatic persons for HBV infection," said Dr. Ruma Rajbhandari and Dr. Raymond T. Chung.
"Many would argue that the USPSTF should have endorsed screening for HBV infection in high-risk populations a decade ago," they wrote. The group lagged far behind the American Association for the Study of Liver Diseases’ recommendations in 2001 and the CDC’s recommendations in 2005. "We may have thus missed an opportunity to screen many high-risk persons in the United States," Dr. Rajbhandari and Dr. Chung said.
The USPSTF update "would be more useful if they provided a clearer definition of the high-risk patient. ... We worry that busy generalist clinicians do not have the time to estimate their patients’ risks for HBV infection." Physicians may find it more helpful to look up the CDC’s table listing all the factors that render a patient high risk, they added.
Dr. Rajbhandari and Dr. Chung are with the liver center and gastrointestinal division at Massachusetts General Hospital, Boston. They reported no relevant conflicts of interest. These remarks were taken from their editorial accompanying Dr. Lefevre’s report (Ann. Intern. Med. 2014 May 27 [doi:10.7326/M14-1153]).
These "long overdue" recommendations are "a dramatic and welcome upgrade from the 2004 USPSTF guidelines, which issued a grade D recommendation against screening asymptomatic persons for HBV infection," said Dr. Ruma Rajbhandari and Dr. Raymond T. Chung.
"Many would argue that the USPSTF should have endorsed screening for HBV infection in high-risk populations a decade ago," they wrote. The group lagged far behind the American Association for the Study of Liver Diseases’ recommendations in 2001 and the CDC’s recommendations in 2005. "We may have thus missed an opportunity to screen many high-risk persons in the United States," Dr. Rajbhandari and Dr. Chung said.
The USPSTF update "would be more useful if they provided a clearer definition of the high-risk patient. ... We worry that busy generalist clinicians do not have the time to estimate their patients’ risks for HBV infection." Physicians may find it more helpful to look up the CDC’s table listing all the factors that render a patient high risk, they added.
Dr. Rajbhandari and Dr. Chung are with the liver center and gastrointestinal division at Massachusetts General Hospital, Boston. They reported no relevant conflicts of interest. These remarks were taken from their editorial accompanying Dr. Lefevre’s report (Ann. Intern. Med. 2014 May 27 [doi:10.7326/M14-1153]).
Physicians should screen all asymptomatic but high-risk adolescents and adults for hepatitis B virus infection, according to an updated recommendation by the U.S. Preventive Services Task Force that was published online May 27 in Annals of Internal Medicine.
Since the last USPSTF recommendation on HBV screening in 2004, which focused on the general population and didn’t advocate screening of this subset of patients, research has documented that antiviral treatment improves both intermediate outcomes such as virologic and histologic responses and long-term outcomes such as prevention of hepatocellular carcinoma, cirrhosis, and end-stage liver disease.
Given this effectiveness, along with the 98% sensitivity and specificity of HBV screening tests, the group has now issued a level B recommendation that high-risk patients be screened, said Dr. Michael L. LeFevre, chair of the USPSTF and professor of family and community medicine at the University of Missouri, Columbia, and his associates.
High-risk patients include the following:
• People born in regions where the prevalence of HBV infection is 2% or greater, such as sub-Saharan Africa, central and southeast Asia, China, the Pacific Islands, and parts of Latin America. People born in these areas account for 47%-95% of the chronic HBV infection in the United States.
• American-born children of parents from these regions, who may not have been vaccinated in infancy.
• HIV-positive persons.
• IV-drug users.
• Household contacts of people with HBV infection.
• Men who have sex with men.
The updated USPSTF recommendations are in line with those of the Centers for Disease Control and Prevention, the American Association for the Study of Liver Diseases, the Institute of Medicine, and the American Academy of Family Physicians. The CDC additionally recommends HBV screening for blood, organ, or tissue donors; people with occupational or other exposure to infectious blood or body fluids; and patients receiving hemodialysis, cytotoxic therapy, or immunosuppressive therapy.
The USPSTF still does not recommend HBV screening for the general population. The prevalence of the infection is low in the U.S. general population, and most members of the general population who are infected with HBV do not develop the chronic form of the infection and do not develop complications like hepatocellular carcinoma or cirrhosis. The potential harms of general screening, then, probably exceed the potential benefits, Dr. LeFevre and his associates noted (Ann Intern. Med. 2014 May 27 [doi:10.7326/M14-1018]).
The USPSTF has separate recommendations regarding hepatitis B in pregnant women. These, along with the updated recommendations for high-risk patients, are available at www.uspreventiveservicestaskforce.org.
The USPSTF is a voluntary group funded by the Agency for Healthcare Research and Quality but otherwise independent of the federal government. Dr. LeFevre and his associates reported no potential financial conflicts of interest.
Physicians should screen all asymptomatic but high-risk adolescents and adults for hepatitis B virus infection, according to an updated recommendation by the U.S. Preventive Services Task Force that was published online May 27 in Annals of Internal Medicine.
Since the last USPSTF recommendation on HBV screening in 2004, which focused on the general population and didn’t advocate screening of this subset of patients, research has documented that antiviral treatment improves both intermediate outcomes such as virologic and histologic responses and long-term outcomes such as prevention of hepatocellular carcinoma, cirrhosis, and end-stage liver disease.
Given this effectiveness, along with the 98% sensitivity and specificity of HBV screening tests, the group has now issued a level B recommendation that high-risk patients be screened, said Dr. Michael L. LeFevre, chair of the USPSTF and professor of family and community medicine at the University of Missouri, Columbia, and his associates.
High-risk patients include the following:
• People born in regions where the prevalence of HBV infection is 2% or greater, such as sub-Saharan Africa, central and southeast Asia, China, the Pacific Islands, and parts of Latin America. People born in these areas account for 47%-95% of the chronic HBV infection in the United States.
• American-born children of parents from these regions, who may not have been vaccinated in infancy.
• HIV-positive persons.
• IV-drug users.
• Household contacts of people with HBV infection.
• Men who have sex with men.
The updated USPSTF recommendations are in line with those of the Centers for Disease Control and Prevention, the American Association for the Study of Liver Diseases, the Institute of Medicine, and the American Academy of Family Physicians. The CDC additionally recommends HBV screening for blood, organ, or tissue donors; people with occupational or other exposure to infectious blood or body fluids; and patients receiving hemodialysis, cytotoxic therapy, or immunosuppressive therapy.
The USPSTF still does not recommend HBV screening for the general population. The prevalence of the infection is low in the U.S. general population, and most members of the general population who are infected with HBV do not develop the chronic form of the infection and do not develop complications like hepatocellular carcinoma or cirrhosis. The potential harms of general screening, then, probably exceed the potential benefits, Dr. LeFevre and his associates noted (Ann Intern. Med. 2014 May 27 [doi:10.7326/M14-1018]).
The USPSTF has separate recommendations regarding hepatitis B in pregnant women. These, along with the updated recommendations for high-risk patients, are available at www.uspreventiveservicestaskforce.org.
The USPSTF is a voluntary group funded by the Agency for Healthcare Research and Quality but otherwise independent of the federal government. Dr. LeFevre and his associates reported no potential financial conflicts of interest.
FROM ANNALS OF INTERNAL MEDICINE
Key clinical point: HBV screening is appropriate in all at-risk populations.
Major finding: Physicians should screen all adolescents and adults at high risk for HBV infection, including those born in regions where the virus is endemic, American-born children of such parents, household contacts of people with HBV, people with HIV, IV-drug users, and men who have sex with men.
Data source: A comprehensive review of the literature since 2004 regarding the benefits and harms of screening high-risk patients for HBV infection, and a compilation of recommendations for screening high-risk patients.
Disclosures: The USPSTF is a voluntary group funded by the Agency for Healthcare Research and Quality but otherwise independent of the federal government. Dr. LeFevre and his associates reported no potential financial conflicts of interest.

PEARL-II: Oral ‘3D’ regimen effective in hepatitis C with prior treatment failure
CHICAGO – The investigational "3D" combination of oral antiviral drugs achieved a cure rate that was nothing short of sensational in the phase III PEARL-II trial involving noncirrhotic patients with hepatitis C genotype 1b who had previously failed pegylated interferon–based therapy.
Moreover, these results were achieved without the use of daily oral ribavirin, formerly a standard part of hepatitis C therapy, and one responsible for a substantial burden of side effects.

Genotype 1b is the most prevalent form of hepatitis C disease worldwide. While it is especially common in Europe and Japan, genotype 1b also accounts for about one-third of cases of HCV in the United States.
The so-called 3D regimen is an all-oral combination of three direct-acting antiviral agents: ombitasvir, dasabuvir, and ABT-450. Each of these agents inhibits the viral life cycle at a different point, Dr. Peter Ferenci explained in presenting the PEARL-II results at the annual Digestive Disease Week.
PEARL-II was an open-label, 12-week trial which asked the question, what added benefit does daily oral ribavirin provide in conjunction with 3D therapy in noncirrhotic HCV genotype 1b patients previously treated unsuccessfully with a pegylated interferon/ribavirin regimen? The answer, as it turns out, is none.
The 186 participants were randomized to the 3D regimen with or without oral ribavirin. The oral 3D regimen consists of ABT-450 (150 mg)/ritonavir (100 mg)/ombitasvir (25 mg), formulated as a single once-daily pill plus dasabuvir at 250 mg twice daily.
The primary endpoint – a sustained virologic response 12 weeks after completion of the 12-week course of treatment – was achieved in 96.6% of the ribavirin group and 100% who didn’t receive ribavirin. Both rates are superior to the historical sustained virologic response rate seen in studies of the former state-of-the-art regimen of telaprevir plus pegylated interferon and ribavirin, noted Dr. Ferenci of the Medical University of Vienna.
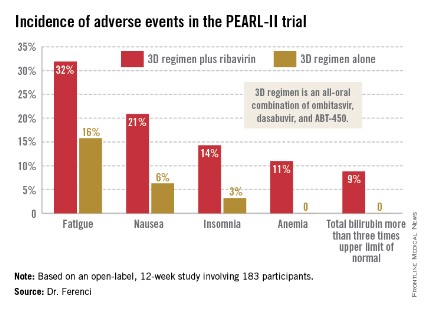
There were no virologic failures in PEARL-II. Two patients stopped the study drugs: one who developed pancreatitis deemed unrelated to treatment and another with anxiety, tachycardia, shortness of breath, and fever considered possibly treatment related.
Results of 3D therapy were equally good in men and women and in former relapsers, nonresponders, and partial responders to pegylated interferon-based regimens.
Treatment-related adverse events were more frequent in the ribavirin study arm (see graphic), but were generally mild and manageable.
Asked if in light of the impressive study results he thought physicians should hold off on treating PEARL-II–type patients until the 3D regimen receives marketing approval, Dr. Ferenci replied, "I think if you really need to treat a patient now, you have to use what exists. But I think in half a year your options will change."
PEARL-II was a companion trial to PEARL-III, conducted in previously untreated patients with HCV 1b infection (N. Engl. J. Med. 2014 [doi:10.1056/NEJMoa1402338]). Both studies were sponsored by AbbVie. Dr. Ferenci reported serving on advisory panels for roughly a dozen pharmaceutical companies.
daily oral ribavirin, formerly a standard part of hepatitis C therapy, Europe and Japan, HCV, ombitasvir, dasabuvir, ABT-450, Dr. Peter Ferenci, annual Digestive Disease Week,
CHICAGO – The investigational "3D" combination of oral antiviral drugs achieved a cure rate that was nothing short of sensational in the phase III PEARL-II trial involving noncirrhotic patients with hepatitis C genotype 1b who had previously failed pegylated interferon–based therapy.
Moreover, these results were achieved without the use of daily oral ribavirin, formerly a standard part of hepatitis C therapy, and one responsible for a substantial burden of side effects.
Genotype 1b is the most prevalent form of hepatitis C disease worldwide. While it is especially common in Europe and Japan, genotype 1b also accounts for about one-third of cases of HCV in the United States.
The so-called 3D regimen is an all-oral combination of three direct-acting antiviral agents: ombitasvir, dasabuvir, and ABT-450. Each of these agents inhibits the viral life cycle at a different point, Dr. Peter Ferenci explained in presenting the PEARL-II results at the annual Digestive Disease Week.
PEARL-II was an open-label, 12-week trial which asked the question, what added benefit does daily oral ribavirin provide in conjunction with 3D therapy in noncirrhotic HCV genotype 1b patients previously treated unsuccessfully with a pegylated interferon/ribavirin regimen? The answer, as it turns out, is none.
The 186 participants were randomized to the 3D regimen with or without oral ribavirin. The oral 3D regimen consists of ABT-450 (150 mg)/ritonavir (100 mg)/ombitasvir (25 mg), formulated as a single once-daily pill plus dasabuvir at 250 mg twice daily.
The primary endpoint – a sustained virologic response 12 weeks after completion of the 12-week course of treatment – was achieved in 96.6% of the ribavirin group and 100% who didn’t receive ribavirin. Both rates are superior to the historical sustained virologic response rate seen in studies of the former state-of-the-art regimen of telaprevir plus pegylated interferon and ribavirin, noted Dr. Ferenci of the Medical University of Vienna.
There were no virologic failures in PEARL-II. Two patients stopped the study drugs: one who developed pancreatitis deemed unrelated to treatment and another with anxiety, tachycardia, shortness of breath, and fever considered possibly treatment related.
Results of 3D therapy were equally good in men and women and in former relapsers, nonresponders, and partial responders to pegylated interferon-based regimens.
Treatment-related adverse events were more frequent in the ribavirin study arm (see graphic), but were generally mild and manageable.
Asked if in light of the impressive study results he thought physicians should hold off on treating PEARL-II–type patients until the 3D regimen receives marketing approval, Dr. Ferenci replied, "I think if you really need to treat a patient now, you have to use what exists. But I think in half a year your options will change."
PEARL-II was a companion trial to PEARL-III, conducted in previously untreated patients with HCV 1b infection (N. Engl. J. Med. 2014 [doi:10.1056/NEJMoa1402338]). Both studies were sponsored by AbbVie. Dr. Ferenci reported serving on advisory panels for roughly a dozen pharmaceutical companies.
CHICAGO – The investigational "3D" combination of oral antiviral drugs achieved a cure rate that was nothing short of sensational in the phase III PEARL-II trial involving noncirrhotic patients with hepatitis C genotype 1b who had previously failed pegylated interferon–based therapy.
Moreover, these results were achieved without the use of daily oral ribavirin, formerly a standard part of hepatitis C therapy, and one responsible for a substantial burden of side effects.
Genotype 1b is the most prevalent form of hepatitis C disease worldwide. While it is especially common in Europe and Japan, genotype 1b also accounts for about one-third of cases of HCV in the United States.
The so-called 3D regimen is an all-oral combination of three direct-acting antiviral agents: ombitasvir, dasabuvir, and ABT-450. Each of these agents inhibits the viral life cycle at a different point, Dr. Peter Ferenci explained in presenting the PEARL-II results at the annual Digestive Disease Week.
PEARL-II was an open-label, 12-week trial which asked the question, what added benefit does daily oral ribavirin provide in conjunction with 3D therapy in noncirrhotic HCV genotype 1b patients previously treated unsuccessfully with a pegylated interferon/ribavirin regimen? The answer, as it turns out, is none.
The 186 participants were randomized to the 3D regimen with or without oral ribavirin. The oral 3D regimen consists of ABT-450 (150 mg)/ritonavir (100 mg)/ombitasvir (25 mg), formulated as a single once-daily pill plus dasabuvir at 250 mg twice daily.
The primary endpoint – a sustained virologic response 12 weeks after completion of the 12-week course of treatment – was achieved in 96.6% of the ribavirin group and 100% who didn’t receive ribavirin. Both rates are superior to the historical sustained virologic response rate seen in studies of the former state-of-the-art regimen of telaprevir plus pegylated interferon and ribavirin, noted Dr. Ferenci of the Medical University of Vienna.
There were no virologic failures in PEARL-II. Two patients stopped the study drugs: one who developed pancreatitis deemed unrelated to treatment and another with anxiety, tachycardia, shortness of breath, and fever considered possibly treatment related.
Results of 3D therapy were equally good in men and women and in former relapsers, nonresponders, and partial responders to pegylated interferon-based regimens.
Treatment-related adverse events were more frequent in the ribavirin study arm (see graphic), but were generally mild and manageable.
Asked if in light of the impressive study results he thought physicians should hold off on treating PEARL-II–type patients until the 3D regimen receives marketing approval, Dr. Ferenci replied, "I think if you really need to treat a patient now, you have to use what exists. But I think in half a year your options will change."
PEARL-II was a companion trial to PEARL-III, conducted in previously untreated patients with HCV 1b infection (N. Engl. J. Med. 2014 [doi:10.1056/NEJMoa1402338]). Both studies were sponsored by AbbVie. Dr. Ferenci reported serving on advisory panels for roughly a dozen pharmaceutical companies.
daily oral ribavirin, formerly a standard part of hepatitis C therapy, Europe and Japan, HCV, ombitasvir, dasabuvir, ABT-450, Dr. Peter Ferenci, annual Digestive Disease Week,
daily oral ribavirin, formerly a standard part of hepatitis C therapy, Europe and Japan, HCV, ombitasvir, dasabuvir, ABT-450, Dr. Peter Ferenci, annual Digestive Disease Week,
AT DDW 2014
Major finding: Noncirrhotic patients with hepatitis C genotype 1b disease who had failed previous pegylated interferon–based therapy had a 100% sustained virologic response rate 12 weeks after the conclusion of a 12-week course of all-oral therapy with three direct-acting antiviral agents without daily ribavirin and a 96.6% rate if they did get ribavirin.
Data source: This was an open-label, 12-week, phase III trial including 186 patients.
Disclosures: The study was sponsored by AbbVie. The presenter reported serving on advisory panels for about a dozen pharmaceutical companies.
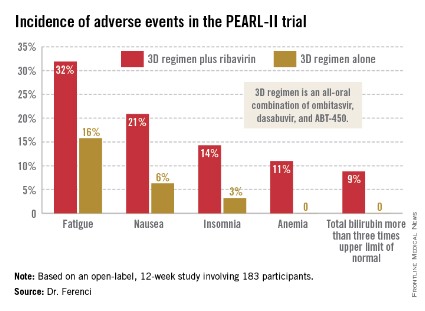
VIDEO: PCPs fuzzy on HCC surveillance in cirrhosis
CHICAGO – Several medical societies recommend that patients with cirrhosis undergo ultrasound surveillance for hepatocellular carcinoma every 6 months, but studies suggest less than 20% receive surveillance. The most common reason for failure to get the screening is lack of provider recommendation.
In a video interview with us at the annual Digestive Disease Week, Dr. Eimile Dalton-Fitzgerald of the University of Texas Southwestern Medical Center at Dallas delves into primary care provider (PCP) practice patterns, knowledge, and attitudes regarding hepatocellular carcinoma (HCC) surveillance gleaned from a survey of 77 PCPs in a large safety-net hospital in Dallas County, Texas.
Though most PCPs surveyed believe HCC surveillance is their responsibility (90%) and is effective for early tumor detection in cirrhosis (85%), many had misconceptions about the appropriate surveillance test choice.
PCPs also report several barriers to HCC surveillance, including not being up to date with surveillance guidelines (68%), difficulty with patient communication (56%), and having more important issues to manage in the clinic (52%).
A full 87% also said they’re influenced by a lack of recommendations from the U.S. Preventive Services Task Force, which has yet to weigh in on the issue.
Dr. Dalton-Fitzgerald reported no conflicting interests.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – Several medical societies recommend that patients with cirrhosis undergo ultrasound surveillance for hepatocellular carcinoma every 6 months, but studies suggest less than 20% receive surveillance. The most common reason for failure to get the screening is lack of provider recommendation.
In a video interview with us at the annual Digestive Disease Week, Dr. Eimile Dalton-Fitzgerald of the University of Texas Southwestern Medical Center at Dallas delves into primary care provider (PCP) practice patterns, knowledge, and attitudes regarding hepatocellular carcinoma (HCC) surveillance gleaned from a survey of 77 PCPs in a large safety-net hospital in Dallas County, Texas.
Though most PCPs surveyed believe HCC surveillance is their responsibility (90%) and is effective for early tumor detection in cirrhosis (85%), many had misconceptions about the appropriate surveillance test choice.
PCPs also report several barriers to HCC surveillance, including not being up to date with surveillance guidelines (68%), difficulty with patient communication (56%), and having more important issues to manage in the clinic (52%).
A full 87% also said they’re influenced by a lack of recommendations from the U.S. Preventive Services Task Force, which has yet to weigh in on the issue.
Dr. Dalton-Fitzgerald reported no conflicting interests.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – Several medical societies recommend that patients with cirrhosis undergo ultrasound surveillance for hepatocellular carcinoma every 6 months, but studies suggest less than 20% receive surveillance. The most common reason for failure to get the screening is lack of provider recommendation.
In a video interview with us at the annual Digestive Disease Week, Dr. Eimile Dalton-Fitzgerald of the University of Texas Southwestern Medical Center at Dallas delves into primary care provider (PCP) practice patterns, knowledge, and attitudes regarding hepatocellular carcinoma (HCC) surveillance gleaned from a survey of 77 PCPs in a large safety-net hospital in Dallas County, Texas.
Though most PCPs surveyed believe HCC surveillance is their responsibility (90%) and is effective for early tumor detection in cirrhosis (85%), many had misconceptions about the appropriate surveillance test choice.
PCPs also report several barriers to HCC surveillance, including not being up to date with surveillance guidelines (68%), difficulty with patient communication (56%), and having more important issues to manage in the clinic (52%).
A full 87% also said they’re influenced by a lack of recommendations from the U.S. Preventive Services Task Force, which has yet to weigh in on the issue.
Dr. Dalton-Fitzgerald reported no conflicting interests.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT DDW 2014
