User login
Morphology of Mycosis Fungoides and Sézary Syndrome in Skin of Color
Mycosis fungoides (MF) and Sézary syndrome (SS) are non-Hodgkin T-cell lymphomas that make up the majority of cutaneous T-cell lymphomas. These conditions commonly affect Black patients, with an incidence rate of 12.6 cases of cutaneous T-cell lymphomas per million individuals vs 9.8 per million individuals in non–skin of color (SoC) patients.1 However, educational resources tend to focus on the clinical manifestations of MF/SS in lighter skin types, describing MF as erythematous patches, plaques, or tumors presenting in non–sun-exposed areas of the skin and SS as generalized erythroderma.2 Skin of color, comprised of Fitzpatrick skin types (FSTs) IV to VI,3 is poorly represented across dermatology textbooks,4,5 medical student resources,6 and peer-reviewed publications,7 raising awareness for the need to address this disparity.
Skin of color patients with MF/SS display variable morphologies, including features such as hyperpigmentation and hypopigmentation,8 the latter being exceedingly rare in non-SoC patients.9 Familiarity with these differences among providers is essential to allow for equitable diagnosis and treatment across all skin types, especially in light of data predicting that by 2044 more than 50% of the US population will be people of color.10 Patients with SoC are of many ethnic and racial backgrounds, including Black, Hispanic, American Indian, Pacific Islander, and Asian.11
Along with morphologic differences, there also are several racial disparities in the prognosis and survival of patients with MF/SS. Black patients diagnosed with MF present with greater body surface area affected, and Black women with MF have reduced survival rates compared to their White counterparts.12 Given these racial disparities in survival and representation in educational resources, we aimed to quantify the frequency of various morphologic characteristics of MF/SS in patients with SoC vs non-SoC patients to facilitate better recognition of early MF/SS in SoC patients by medical providers.
Methods
We performed a retrospective chart review following approval from the institutional review board at Northwestern University (Chicago, Illinois). We identified all patients with FSTs IV to VI and biopsy-proven MF/SS who had been clinically photographed in our clinic from January 1998 to December 2019. Only photographs that were high quality enough to review morphologic features were included in our review. Fitzpatrick skin type was determined based on electronic medical record documentation. If photographs were available from multiple visits for the same patient, only those showing posttreatment nonactive lesions were included. Additionally, 36 patients with FSTs I to III (non-SoC) and biopsy-proven MF/SS were included in our review as a comparison with the SoC cohort. The primary outcomes for this study included the presence of scale, erythema, hyperpigmentation, hypopigmentation, violaceous color, lichenification, silver hue, dyschromia, alopecia, poikiloderma, atrophy, and ulceration in active lesions. Dyschromia was defined by the presence of both hypopigmentation and hyperpigmentation. Poikiloderma was defined by hypopigmentation and hyperpigmentation, telangiectasia, and atrophy. Secondary outcomes included evaluation of those same characteristics in posttreatment nonactive lesions. All photographs were independently assessed by 3 authors (M.L.E., C.J.W., J.M.M.), and discrepancies were resolved by further review of the photograph in question and discussion.
Statistical Analysis—Summary statistics were applied to describe demographic and clinical characteristics. The χ2 test was used for categorical variables. Results achieving P<.05 were considered statistically significant.

Results
We reviewed photographs of 111 patients across all skin types (8, FST I; 12, FST II; 16, FST III; 17, FST IV; 44, FST V; 14, FST VI). The cohort was 47% female, and the mean age was 49.7 years (range, 15–86 years). The majority of the cohort had early-stage MF (stage IA or IB). There were more cases of SS in the SoC cohort than the non-SoC cohort (Table). Only 5 photographs had discrepancies and required discussion among the reviewers to achieve consensus.
![Frequency of morphologic features found in skin of color (SoC [Fitzpatrick skin types IV–VI]) vs non-SoC (Fitzpatrick skin types I–III) patients with mycosis fungoides/Sézary syndrome](https://cdn.mdedge.com/files/s3fs-public/Espinosa_1.JPG "Frequency of morphologic features found in skin of color (SoC [Fitzpatrick skin types IV–VI]) vs non-SoC (Fitzpatrick skin types I–III) patients with mycosis fungoides/Sézary syndrome")
Regarding morphologic characteristics in active lesions (Figure 1), scale was present in almost all patients (99% in SoC, 94% in non-SoC). Erythema was present in nearly all non-SoC patients (94%) but only in 69% of SoC patients (P=.003). Poikiloderma also was found to be present at higher frequencies in non-SoC patients compared with SoC patients (19% and 4%, respectively [P=.008]). However, hyperpigmentation (80% vs 39%), lichenification (43% vs 17%), and silver hue (25% vs 3%) were more common in SoC patients than non-SoC patients (P<.05). There were no significant differences in the remaining features, including hypopigmentation (39% vs 25%), dyschromia (24% vs 19%), violaceous color (44% vs 25%), atrophy (11% vs 22%), alopecia (23% vs 31%), and ulceration (16% vs 8%) between SoC and non-SoC patients (P>.05). Photographs of MF in patients with SoC can be seen in Figure 2.
![Representative photographs of mycosis fungoides (MF) in skin of color (Fitzpatrick skin types [FSTs] IV–VI)](https://cdn.mdedge.com/files/s3fs-public/CT109003003_e_Fig2_ABCDE.JPG "Representative photographs of mycosis fungoides (MF) in skin of color (Fitzpatrick skin types [FSTs] IV–VI)")
Posttreatment (nonactive) photographs were available for 26 patients (6 non-SoC, 20 SoC). We found that across all FST groups, hyperpigmentation was more common than hypopigmentation in areas of previously active disease. Statistical analysis was not completed given that few non-SoC photographs were available for comparison.
Comment
This qualitative review demonstrates the heterogeneity of MF/SS in SoC patients and that these conditions do not present in this population with the classic erythematous patches and plaques found in non-SoC patients. We found that hyperpigmentation, lichenification, and silver hue were present at higher rates in patients with FSTs IV to VI compared to those with FSTs I to III, which had higher rates of erythema and poikiloderma. Familiarity with these morphologic features along with increased exposure to clinical photographs of MF/SS in SoC patients will aid in the visual recognition required for this diagnosis, since erythema is harder to identify in darker skin types. Recognizing the unique findings of MF in patients with SoC as well as in patients with lighter skin types will enable earlier diagnosis and treatment of MF/SS across all skin types. If MF is diagnosed and treated early, life expectancy is similar to that of patients without MF.13 However, the 5-year survival rate for advanced-stage MF/SS is 52% across all skin types, and studies have found that Black patients with advanced-stage disease have worse outcomes despite accounting for demographic factors and tumor stage.14,15 Given the worse outcomes in SoC patients with advanced-stage MF/SS, earlier diagnosis could help address this disparity.8,13,14 Similar morphologic features could be used in diagnosing other inflammatory conditions; studies have shown that the lack of recognition of erythema in Black children has led to delayed diagnosis of atopic dermatitis and subsequent inadequate treatment.16,17
The morphologic presentation of MF/SS in SoC patients also can influence an optimal treatment plan for this population. Hypopigmented MF responds better to phototherapy than hyperpigmented MF, as phototherapy has been shown to have decreased efficacy with increasing FST.18 Therefore, for patients with FSTs IV to VI, topical agents such as nitrogen mustard or bexarotene may be more suitable treatment options, as the efficacy of these treatments is independent of skin color.8 However, nitrogen mustard commonly leads to postinflammatory hyperpigmentation, and topical bexarotene may lead to erythema or irritation; therefore, providers must counsel patients on these possible side effects. For refractory disease, adjunct systemic treatments such as oral bexarotene, subcutaneous interferon, methotrexate, or radiation therapy may be considered.8
In addition to aiding in the prompt diagnosis and treatment of MF/SS in SoC patients, our findings may be used to better assess the extent of disease and distinguish between active MF/SS lesions vs xerosis cutis or residual dyschromia from previously treated lesions. It is important to note that these morphologic features must be taken into account with a complete history and work-up. The differential diagnosis of MF/SS includes conditions such as atopic dermatitis, psoriasis, tinea corporis, and drug reactions, which may have similar morphology in SoC.19
Limitations of our study include the single-center design and the use of photographs instead of in-person examination; however, our cutaneous lymphoma clinic serves a diverse patient population, and our 3 reviewers rated the photographs independently. Discussion amongst the reviewers to address discrepancies was only required for 5 photographs, indicating the high inter-reviewer reliability. Additionally, the original purpose of FST was to assess for the propensity of the skin to burn when undergoing phototherapy, not to serve as a marker for skin color. We recommend trainees and clinicians be mindful about the purpose of FST and to use inclusive language (eg, using the terms skin irritation, skin tenderness, or skin becoming darker from the sun instead of tanning) when determining FST in darker-skinned individuals.20 Future directions include examining if certain treatments are associated with prolonged dyschromia.
Conclusion
In our single-institution retrospective study, we found differences in the morphologic presentation of MF/SS in SoC patients vs non-SoC patients. While erythema is a common feature in non-SoC patients, clinical features of hyperpigmentation, lichenification, and silver hue should be carefully evaluated in the diagnosis of MF/SS in SoC patients. Knowledge of the heterogenous presentation of MF/SS in patients with SoC allows for expedited diagnosis and treatment, leading to better clinical outcomes. Valuable resources, including Taylor and Kelly’s Dermatology for Skin of Color, the Skin of Color Society, and VisualDx educate providers on how dermatologic conditions present in darker skin types. However, there is still work to be done to enhance diversity in educational resources in order to provide equitable care to patients of all skin types.
- Korgavkar K, Xiong M, Weinstock M. Changing incidence trends of cutaneous T-cell lymphoma. JAMA Dermatol. 2013;149:1295-1299. doi:10.1001/jamadermatol.2013.5526
- Jawed SI, Myskowski PL, Horwitz S, et al. Primary cutaneous T-cell lymphoma (mycosis fungoides and Sézary syndrome): part I. diagnosis: clinical and histopathologic features and new molecular and biologic markers. J Am Acad Dermatol. 2014;70:205.E1-E16; quiz 221-222. doi:10.1016/j.jaad.2013.07.049
- Tull RZ, Kerby E, Subash JJ, et al. Ethnic skin centers in the United States: where are we in 2020?. J Am Acad Dermatol. 2020;83:1757-1759. doi:10.1016/j.jaad.2020.03.054
- Adelekun A, Onyekaba G, Lipoff JB. Skin color in dermatology textbooks: an updated evaluation and analysis. J Am Acad Dermatol. 2021;84:194-196. doi:10.1016/j.jaad.2020.04.084
- Ebede T, Papier A. Disparities in dermatology educational resources. J Am Acad Dermatol. 2006;55:687-690. doi:10.1016/j.jaad.2005.10.068
- Jones VA, Clark KA, Shobajo MT, et al. Skin of color representation in medical education: an analysis of popular preparatory materials used for United States medical licensing examinations. J Am Acad Dermatol. 2021;85:773-775. doi:10.1016/j.jaad.2020.07.112
- Montgomery SN, Elbuluk N. A quantitative analysis of research publications focused on the top chief complaints in skin of color patients. J Am Acad Dermatol. 2021;85:241-242. doi:10.1016/j.jaad.2020.08.031
- Hinds GA, Heald P. Cutaneous T-cell lymphoma in skin of color. J Am Acad Dermatol. 2009;60:359-375; quiz 376-378. doi:10.1016/j.jaad.2008.10.031
- Ardigó M, Borroni G, Muscardin L, et al. Hypopigmented mycosis fungoides in Caucasian patients: a clinicopathologic study of 7 cases. J Am Acad Dermatol. 2003;49:264-270. doi:10.1067/s0190-9622(03)00907-1
- Colby SL, Ortman JM. Projections of the size and composition of the U.S. population: 2014 to 2060. United States Census Bureau website. Updated October 8, 2021. Accessed February 28, 2022. https://www.census.gov/library/publications/2015/demo/p25-1143.html
- Taylor SC, Kyei A. Defining skin of color. In: Kelly AP, Taylor SC, Lim HW, et al, eds. Taylor and Kelly’s Dermatology for Skin of Color. 2nd ed. McGraw-Hill Education; 2016.
- Huang AH, Kwatra SG, Khanna R, et al. Racial disparities in the clinical presentation and prognosis of patients with mycosis fungoides. J Natl Med Assoc. 2019;111:633-639. doi:10.1016/j.jnma.2019.08.006
- Kim YH, Jensen RA, Watanabe GL, et al. Clinical stage IA (limited patch and plaque) mycosis fungoides. a long-term outcome analysis. Arch Dermatol. 1996;132:1309-1313.
- Scarisbrick JJ, Prince HM, Vermeer MH, et al. Cutaneous lymphoma international consortium study of outcome in advanced stages of mycosis fungoides and Sézary syndrome: effect of specific prognostic markers on survival and development of a prognostic model. J Clin Oncol. 2015;33:3766-3773. doi:10.1200/JCO.2015.61.7142
- Nath SK, Yu JB, Wilson LD. Poorer prognosis of African-American patients with mycosis fungoides: an analysis of the SEER dataset, 1988 to 2008. Clin Lymphoma Myeloma Leuk. 2014;14:419-423. doi:10.1016/j.clml.2013.12.018
- Ben-Gashir MA, Hay RJ. Reliance on erythema scores may mask severe atopic dermatitis in black children compared with their white counterparts. Br J Dermatol. 2002;147:920-925. doi:10.1046/j.1365-2133.2002.04965.x
- Poladian K, De Souza B, McMichael AJ. Atopic dermatitis in adolescents with skin of color. Cutis. 2019;104:164-168.
- Yones SS, Palmer RA, Garibaldinos TT, et al. Randomized double-blind trial of the treatment of chronic plaque psoriasis: efficacy of psoralen-UV-A therapy vs narrowband UV-B therapy. Arch Dermatol. 2006;142:836-842. doi:10.1001/archderm.142.7.836
- Currimbhoy S, Pandya AG. Cutaneous T-cell lymphoma. In: Kelly AP, Taylor SC, Lim HW, et al, eds. Taylor and Kelly’s Dermatology for Skin of Color. 2nd ed. McGraw-Hill Education; 2016.
- Ware OR, Dawson JE, Shinohara MM, et al. Racial limitations of Fitzpatrick skin type. Cutis. 2020;105:77-80.
Mycosis fungoides (MF) and Sézary syndrome (SS) are non-Hodgkin T-cell lymphomas that make up the majority of cutaneous T-cell lymphomas. These conditions commonly affect Black patients, with an incidence rate of 12.6 cases of cutaneous T-cell lymphomas per million individuals vs 9.8 per million individuals in non–skin of color (SoC) patients.1 However, educational resources tend to focus on the clinical manifestations of MF/SS in lighter skin types, describing MF as erythematous patches, plaques, or tumors presenting in non–sun-exposed areas of the skin and SS as generalized erythroderma.2 Skin of color, comprised of Fitzpatrick skin types (FSTs) IV to VI,3 is poorly represented across dermatology textbooks,4,5 medical student resources,6 and peer-reviewed publications,7 raising awareness for the need to address this disparity.
Skin of color patients with MF/SS display variable morphologies, including features such as hyperpigmentation and hypopigmentation,8 the latter being exceedingly rare in non-SoC patients.9 Familiarity with these differences among providers is essential to allow for equitable diagnosis and treatment across all skin types, especially in light of data predicting that by 2044 more than 50% of the US population will be people of color.10 Patients with SoC are of many ethnic and racial backgrounds, including Black, Hispanic, American Indian, Pacific Islander, and Asian.11
Along with morphologic differences, there also are several racial disparities in the prognosis and survival of patients with MF/SS. Black patients diagnosed with MF present with greater body surface area affected, and Black women with MF have reduced survival rates compared to their White counterparts.12 Given these racial disparities in survival and representation in educational resources, we aimed to quantify the frequency of various morphologic characteristics of MF/SS in patients with SoC vs non-SoC patients to facilitate better recognition of early MF/SS in SoC patients by medical providers.
Methods
We performed a retrospective chart review following approval from the institutional review board at Northwestern University (Chicago, Illinois). We identified all patients with FSTs IV to VI and biopsy-proven MF/SS who had been clinically photographed in our clinic from January 1998 to December 2019. Only photographs that were high quality enough to review morphologic features were included in our review. Fitzpatrick skin type was determined based on electronic medical record documentation. If photographs were available from multiple visits for the same patient, only those showing posttreatment nonactive lesions were included. Additionally, 36 patients with FSTs I to III (non-SoC) and biopsy-proven MF/SS were included in our review as a comparison with the SoC cohort. The primary outcomes for this study included the presence of scale, erythema, hyperpigmentation, hypopigmentation, violaceous color, lichenification, silver hue, dyschromia, alopecia, poikiloderma, atrophy, and ulceration in active lesions. Dyschromia was defined by the presence of both hypopigmentation and hyperpigmentation. Poikiloderma was defined by hypopigmentation and hyperpigmentation, telangiectasia, and atrophy. Secondary outcomes included evaluation of those same characteristics in posttreatment nonactive lesions. All photographs were independently assessed by 3 authors (M.L.E., C.J.W., J.M.M.), and discrepancies were resolved by further review of the photograph in question and discussion.
Statistical Analysis—Summary statistics were applied to describe demographic and clinical characteristics. The χ2 test was used for categorical variables. Results achieving P<.05 were considered statistically significant.
Results
We reviewed photographs of 111 patients across all skin types (8, FST I; 12, FST II; 16, FST III; 17, FST IV; 44, FST V; 14, FST VI). The cohort was 47% female, and the mean age was 49.7 years (range, 15–86 years). The majority of the cohort had early-stage MF (stage IA or IB). There were more cases of SS in the SoC cohort than the non-SoC cohort (Table). Only 5 photographs had discrepancies and required discussion among the reviewers to achieve consensus.
Regarding morphologic characteristics in active lesions (Figure 1), scale was present in almost all patients (99% in SoC, 94% in non-SoC). Erythema was present in nearly all non-SoC patients (94%) but only in 69% of SoC patients (P=.003). Poikiloderma also was found to be present at higher frequencies in non-SoC patients compared with SoC patients (19% and 4%, respectively [P=.008]). However, hyperpigmentation (80% vs 39%), lichenification (43% vs 17%), and silver hue (25% vs 3%) were more common in SoC patients than non-SoC patients (P<.05). There were no significant differences in the remaining features, including hypopigmentation (39% vs 25%), dyschromia (24% vs 19%), violaceous color (44% vs 25%), atrophy (11% vs 22%), alopecia (23% vs 31%), and ulceration (16% vs 8%) between SoC and non-SoC patients (P>.05). Photographs of MF in patients with SoC can be seen in Figure 2.
Posttreatment (nonactive) photographs were available for 26 patients (6 non-SoC, 20 SoC). We found that across all FST groups, hyperpigmentation was more common than hypopigmentation in areas of previously active disease. Statistical analysis was not completed given that few non-SoC photographs were available for comparison.
Comment
This qualitative review demonstrates the heterogeneity of MF/SS in SoC patients and that these conditions do not present in this population with the classic erythematous patches and plaques found in non-SoC patients. We found that hyperpigmentation, lichenification, and silver hue were present at higher rates in patients with FSTs IV to VI compared to those with FSTs I to III, which had higher rates of erythema and poikiloderma. Familiarity with these morphologic features along with increased exposure to clinical photographs of MF/SS in SoC patients will aid in the visual recognition required for this diagnosis, since erythema is harder to identify in darker skin types. Recognizing the unique findings of MF in patients with SoC as well as in patients with lighter skin types will enable earlier diagnosis and treatment of MF/SS across all skin types. If MF is diagnosed and treated early, life expectancy is similar to that of patients without MF.13 However, the 5-year survival rate for advanced-stage MF/SS is 52% across all skin types, and studies have found that Black patients with advanced-stage disease have worse outcomes despite accounting for demographic factors and tumor stage.14,15 Given the worse outcomes in SoC patients with advanced-stage MF/SS, earlier diagnosis could help address this disparity.8,13,14 Similar morphologic features could be used in diagnosing other inflammatory conditions; studies have shown that the lack of recognition of erythema in Black children has led to delayed diagnosis of atopic dermatitis and subsequent inadequate treatment.16,17
The morphologic presentation of MF/SS in SoC patients also can influence an optimal treatment plan for this population. Hypopigmented MF responds better to phototherapy than hyperpigmented MF, as phototherapy has been shown to have decreased efficacy with increasing FST.18 Therefore, for patients with FSTs IV to VI, topical agents such as nitrogen mustard or bexarotene may be more suitable treatment options, as the efficacy of these treatments is independent of skin color.8 However, nitrogen mustard commonly leads to postinflammatory hyperpigmentation, and topical bexarotene may lead to erythema or irritation; therefore, providers must counsel patients on these possible side effects. For refractory disease, adjunct systemic treatments such as oral bexarotene, subcutaneous interferon, methotrexate, or radiation therapy may be considered.8
In addition to aiding in the prompt diagnosis and treatment of MF/SS in SoC patients, our findings may be used to better assess the extent of disease and distinguish between active MF/SS lesions vs xerosis cutis or residual dyschromia from previously treated lesions. It is important to note that these morphologic features must be taken into account with a complete history and work-up. The differential diagnosis of MF/SS includes conditions such as atopic dermatitis, psoriasis, tinea corporis, and drug reactions, which may have similar morphology in SoC.19
Limitations of our study include the single-center design and the use of photographs instead of in-person examination; however, our cutaneous lymphoma clinic serves a diverse patient population, and our 3 reviewers rated the photographs independently. Discussion amongst the reviewers to address discrepancies was only required for 5 photographs, indicating the high inter-reviewer reliability. Additionally, the original purpose of FST was to assess for the propensity of the skin to burn when undergoing phototherapy, not to serve as a marker for skin color. We recommend trainees and clinicians be mindful about the purpose of FST and to use inclusive language (eg, using the terms skin irritation, skin tenderness, or skin becoming darker from the sun instead of tanning) when determining FST in darker-skinned individuals.20 Future directions include examining if certain treatments are associated with prolonged dyschromia.
Conclusion
In our single-institution retrospective study, we found differences in the morphologic presentation of MF/SS in SoC patients vs non-SoC patients. While erythema is a common feature in non-SoC patients, clinical features of hyperpigmentation, lichenification, and silver hue should be carefully evaluated in the diagnosis of MF/SS in SoC patients. Knowledge of the heterogenous presentation of MF/SS in patients with SoC allows for expedited diagnosis and treatment, leading to better clinical outcomes. Valuable resources, including Taylor and Kelly’s Dermatology for Skin of Color, the Skin of Color Society, and VisualDx educate providers on how dermatologic conditions present in darker skin types. However, there is still work to be done to enhance diversity in educational resources in order to provide equitable care to patients of all skin types.
Mycosis fungoides (MF) and Sézary syndrome (SS) are non-Hodgkin T-cell lymphomas that make up the majority of cutaneous T-cell lymphomas. These conditions commonly affect Black patients, with an incidence rate of 12.6 cases of cutaneous T-cell lymphomas per million individuals vs 9.8 per million individuals in non–skin of color (SoC) patients.1 However, educational resources tend to focus on the clinical manifestations of MF/SS in lighter skin types, describing MF as erythematous patches, plaques, or tumors presenting in non–sun-exposed areas of the skin and SS as generalized erythroderma.2 Skin of color, comprised of Fitzpatrick skin types (FSTs) IV to VI,3 is poorly represented across dermatology textbooks,4,5 medical student resources,6 and peer-reviewed publications,7 raising awareness for the need to address this disparity.
Skin of color patients with MF/SS display variable morphologies, including features such as hyperpigmentation and hypopigmentation,8 the latter being exceedingly rare in non-SoC patients.9 Familiarity with these differences among providers is essential to allow for equitable diagnosis and treatment across all skin types, especially in light of data predicting that by 2044 more than 50% of the US population will be people of color.10 Patients with SoC are of many ethnic and racial backgrounds, including Black, Hispanic, American Indian, Pacific Islander, and Asian.11
Along with morphologic differences, there also are several racial disparities in the prognosis and survival of patients with MF/SS. Black patients diagnosed with MF present with greater body surface area affected, and Black women with MF have reduced survival rates compared to their White counterparts.12 Given these racial disparities in survival and representation in educational resources, we aimed to quantify the frequency of various morphologic characteristics of MF/SS in patients with SoC vs non-SoC patients to facilitate better recognition of early MF/SS in SoC patients by medical providers.
Methods
We performed a retrospective chart review following approval from the institutional review board at Northwestern University (Chicago, Illinois). We identified all patients with FSTs IV to VI and biopsy-proven MF/SS who had been clinically photographed in our clinic from January 1998 to December 2019. Only photographs that were high quality enough to review morphologic features were included in our review. Fitzpatrick skin type was determined based on electronic medical record documentation. If photographs were available from multiple visits for the same patient, only those showing posttreatment nonactive lesions were included. Additionally, 36 patients with FSTs I to III (non-SoC) and biopsy-proven MF/SS were included in our review as a comparison with the SoC cohort. The primary outcomes for this study included the presence of scale, erythema, hyperpigmentation, hypopigmentation, violaceous color, lichenification, silver hue, dyschromia, alopecia, poikiloderma, atrophy, and ulceration in active lesions. Dyschromia was defined by the presence of both hypopigmentation and hyperpigmentation. Poikiloderma was defined by hypopigmentation and hyperpigmentation, telangiectasia, and atrophy. Secondary outcomes included evaluation of those same characteristics in posttreatment nonactive lesions. All photographs were independently assessed by 3 authors (M.L.E., C.J.W., J.M.M.), and discrepancies were resolved by further review of the photograph in question and discussion.
Statistical Analysis—Summary statistics were applied to describe demographic and clinical characteristics. The χ2 test was used for categorical variables. Results achieving P<.05 were considered statistically significant.
Results
We reviewed photographs of 111 patients across all skin types (8, FST I; 12, FST II; 16, FST III; 17, FST IV; 44, FST V; 14, FST VI). The cohort was 47% female, and the mean age was 49.7 years (range, 15–86 years). The majority of the cohort had early-stage MF (stage IA or IB). There were more cases of SS in the SoC cohort than the non-SoC cohort (Table). Only 5 photographs had discrepancies and required discussion among the reviewers to achieve consensus.
Regarding morphologic characteristics in active lesions (Figure 1), scale was present in almost all patients (99% in SoC, 94% in non-SoC). Erythema was present in nearly all non-SoC patients (94%) but only in 69% of SoC patients (P=.003). Poikiloderma also was found to be present at higher frequencies in non-SoC patients compared with SoC patients (19% and 4%, respectively [P=.008]). However, hyperpigmentation (80% vs 39%), lichenification (43% vs 17%), and silver hue (25% vs 3%) were more common in SoC patients than non-SoC patients (P<.05). There were no significant differences in the remaining features, including hypopigmentation (39% vs 25%), dyschromia (24% vs 19%), violaceous color (44% vs 25%), atrophy (11% vs 22%), alopecia (23% vs 31%), and ulceration (16% vs 8%) between SoC and non-SoC patients (P>.05). Photographs of MF in patients with SoC can be seen in Figure 2.
Posttreatment (nonactive) photographs were available for 26 patients (6 non-SoC, 20 SoC). We found that across all FST groups, hyperpigmentation was more common than hypopigmentation in areas of previously active disease. Statistical analysis was not completed given that few non-SoC photographs were available for comparison.
Comment
This qualitative review demonstrates the heterogeneity of MF/SS in SoC patients and that these conditions do not present in this population with the classic erythematous patches and plaques found in non-SoC patients. We found that hyperpigmentation, lichenification, and silver hue were present at higher rates in patients with FSTs IV to VI compared to those with FSTs I to III, which had higher rates of erythema and poikiloderma. Familiarity with these morphologic features along with increased exposure to clinical photographs of MF/SS in SoC patients will aid in the visual recognition required for this diagnosis, since erythema is harder to identify in darker skin types. Recognizing the unique findings of MF in patients with SoC as well as in patients with lighter skin types will enable earlier diagnosis and treatment of MF/SS across all skin types. If MF is diagnosed and treated early, life expectancy is similar to that of patients without MF.13 However, the 5-year survival rate for advanced-stage MF/SS is 52% across all skin types, and studies have found that Black patients with advanced-stage disease have worse outcomes despite accounting for demographic factors and tumor stage.14,15 Given the worse outcomes in SoC patients with advanced-stage MF/SS, earlier diagnosis could help address this disparity.8,13,14 Similar morphologic features could be used in diagnosing other inflammatory conditions; studies have shown that the lack of recognition of erythema in Black children has led to delayed diagnosis of atopic dermatitis and subsequent inadequate treatment.16,17
The morphologic presentation of MF/SS in SoC patients also can influence an optimal treatment plan for this population. Hypopigmented MF responds better to phototherapy than hyperpigmented MF, as phototherapy has been shown to have decreased efficacy with increasing FST.18 Therefore, for patients with FSTs IV to VI, topical agents such as nitrogen mustard or bexarotene may be more suitable treatment options, as the efficacy of these treatments is independent of skin color.8 However, nitrogen mustard commonly leads to postinflammatory hyperpigmentation, and topical bexarotene may lead to erythema or irritation; therefore, providers must counsel patients on these possible side effects. For refractory disease, adjunct systemic treatments such as oral bexarotene, subcutaneous interferon, methotrexate, or radiation therapy may be considered.8
In addition to aiding in the prompt diagnosis and treatment of MF/SS in SoC patients, our findings may be used to better assess the extent of disease and distinguish between active MF/SS lesions vs xerosis cutis or residual dyschromia from previously treated lesions. It is important to note that these morphologic features must be taken into account with a complete history and work-up. The differential diagnosis of MF/SS includes conditions such as atopic dermatitis, psoriasis, tinea corporis, and drug reactions, which may have similar morphology in SoC.19
Limitations of our study include the single-center design and the use of photographs instead of in-person examination; however, our cutaneous lymphoma clinic serves a diverse patient population, and our 3 reviewers rated the photographs independently. Discussion amongst the reviewers to address discrepancies was only required for 5 photographs, indicating the high inter-reviewer reliability. Additionally, the original purpose of FST was to assess for the propensity of the skin to burn when undergoing phototherapy, not to serve as a marker for skin color. We recommend trainees and clinicians be mindful about the purpose of FST and to use inclusive language (eg, using the terms skin irritation, skin tenderness, or skin becoming darker from the sun instead of tanning) when determining FST in darker-skinned individuals.20 Future directions include examining if certain treatments are associated with prolonged dyschromia.
Conclusion
In our single-institution retrospective study, we found differences in the morphologic presentation of MF/SS in SoC patients vs non-SoC patients. While erythema is a common feature in non-SoC patients, clinical features of hyperpigmentation, lichenification, and silver hue should be carefully evaluated in the diagnosis of MF/SS in SoC patients. Knowledge of the heterogenous presentation of MF/SS in patients with SoC allows for expedited diagnosis and treatment, leading to better clinical outcomes. Valuable resources, including Taylor and Kelly’s Dermatology for Skin of Color, the Skin of Color Society, and VisualDx educate providers on how dermatologic conditions present in darker skin types. However, there is still work to be done to enhance diversity in educational resources in order to provide equitable care to patients of all skin types.
- Korgavkar K, Xiong M, Weinstock M. Changing incidence trends of cutaneous T-cell lymphoma. JAMA Dermatol. 2013;149:1295-1299. doi:10.1001/jamadermatol.2013.5526
- Jawed SI, Myskowski PL, Horwitz S, et al. Primary cutaneous T-cell lymphoma (mycosis fungoides and Sézary syndrome): part I. diagnosis: clinical and histopathologic features and new molecular and biologic markers. J Am Acad Dermatol. 2014;70:205.E1-E16; quiz 221-222. doi:10.1016/j.jaad.2013.07.049
- Tull RZ, Kerby E, Subash JJ, et al. Ethnic skin centers in the United States: where are we in 2020?. J Am Acad Dermatol. 2020;83:1757-1759. doi:10.1016/j.jaad.2020.03.054
- Adelekun A, Onyekaba G, Lipoff JB. Skin color in dermatology textbooks: an updated evaluation and analysis. J Am Acad Dermatol. 2021;84:194-196. doi:10.1016/j.jaad.2020.04.084
- Ebede T, Papier A. Disparities in dermatology educational resources. J Am Acad Dermatol. 2006;55:687-690. doi:10.1016/j.jaad.2005.10.068
- Jones VA, Clark KA, Shobajo MT, et al. Skin of color representation in medical education: an analysis of popular preparatory materials used for United States medical licensing examinations. J Am Acad Dermatol. 2021;85:773-775. doi:10.1016/j.jaad.2020.07.112
- Montgomery SN, Elbuluk N. A quantitative analysis of research publications focused on the top chief complaints in skin of color patients. J Am Acad Dermatol. 2021;85:241-242. doi:10.1016/j.jaad.2020.08.031
- Hinds GA, Heald P. Cutaneous T-cell lymphoma in skin of color. J Am Acad Dermatol. 2009;60:359-375; quiz 376-378. doi:10.1016/j.jaad.2008.10.031
- Ardigó M, Borroni G, Muscardin L, et al. Hypopigmented mycosis fungoides in Caucasian patients: a clinicopathologic study of 7 cases. J Am Acad Dermatol. 2003;49:264-270. doi:10.1067/s0190-9622(03)00907-1
- Colby SL, Ortman JM. Projections of the size and composition of the U.S. population: 2014 to 2060. United States Census Bureau website. Updated October 8, 2021. Accessed February 28, 2022. https://www.census.gov/library/publications/2015/demo/p25-1143.html
- Taylor SC, Kyei A. Defining skin of color. In: Kelly AP, Taylor SC, Lim HW, et al, eds. Taylor and Kelly’s Dermatology for Skin of Color. 2nd ed. McGraw-Hill Education; 2016.
- Huang AH, Kwatra SG, Khanna R, et al. Racial disparities in the clinical presentation and prognosis of patients with mycosis fungoides. J Natl Med Assoc. 2019;111:633-639. doi:10.1016/j.jnma.2019.08.006
- Kim YH, Jensen RA, Watanabe GL, et al. Clinical stage IA (limited patch and plaque) mycosis fungoides. a long-term outcome analysis. Arch Dermatol. 1996;132:1309-1313.
- Scarisbrick JJ, Prince HM, Vermeer MH, et al. Cutaneous lymphoma international consortium study of outcome in advanced stages of mycosis fungoides and Sézary syndrome: effect of specific prognostic markers on survival and development of a prognostic model. J Clin Oncol. 2015;33:3766-3773. doi:10.1200/JCO.2015.61.7142
- Nath SK, Yu JB, Wilson LD. Poorer prognosis of African-American patients with mycosis fungoides: an analysis of the SEER dataset, 1988 to 2008. Clin Lymphoma Myeloma Leuk. 2014;14:419-423. doi:10.1016/j.clml.2013.12.018
- Ben-Gashir MA, Hay RJ. Reliance on erythema scores may mask severe atopic dermatitis in black children compared with their white counterparts. Br J Dermatol. 2002;147:920-925. doi:10.1046/j.1365-2133.2002.04965.x
- Poladian K, De Souza B, McMichael AJ. Atopic dermatitis in adolescents with skin of color. Cutis. 2019;104:164-168.
- Yones SS, Palmer RA, Garibaldinos TT, et al. Randomized double-blind trial of the treatment of chronic plaque psoriasis: efficacy of psoralen-UV-A therapy vs narrowband UV-B therapy. Arch Dermatol. 2006;142:836-842. doi:10.1001/archderm.142.7.836
- Currimbhoy S, Pandya AG. Cutaneous T-cell lymphoma. In: Kelly AP, Taylor SC, Lim HW, et al, eds. Taylor and Kelly’s Dermatology for Skin of Color. 2nd ed. McGraw-Hill Education; 2016.
- Ware OR, Dawson JE, Shinohara MM, et al. Racial limitations of Fitzpatrick skin type. Cutis. 2020;105:77-80.
- Korgavkar K, Xiong M, Weinstock M. Changing incidence trends of cutaneous T-cell lymphoma. JAMA Dermatol. 2013;149:1295-1299. doi:10.1001/jamadermatol.2013.5526
- Jawed SI, Myskowski PL, Horwitz S, et al. Primary cutaneous T-cell lymphoma (mycosis fungoides and Sézary syndrome): part I. diagnosis: clinical and histopathologic features and new molecular and biologic markers. J Am Acad Dermatol. 2014;70:205.E1-E16; quiz 221-222. doi:10.1016/j.jaad.2013.07.049
- Tull RZ, Kerby E, Subash JJ, et al. Ethnic skin centers in the United States: where are we in 2020?. J Am Acad Dermatol. 2020;83:1757-1759. doi:10.1016/j.jaad.2020.03.054
- Adelekun A, Onyekaba G, Lipoff JB. Skin color in dermatology textbooks: an updated evaluation and analysis. J Am Acad Dermatol. 2021;84:194-196. doi:10.1016/j.jaad.2020.04.084
- Ebede T, Papier A. Disparities in dermatology educational resources. J Am Acad Dermatol. 2006;55:687-690. doi:10.1016/j.jaad.2005.10.068
- Jones VA, Clark KA, Shobajo MT, et al. Skin of color representation in medical education: an analysis of popular preparatory materials used for United States medical licensing examinations. J Am Acad Dermatol. 2021;85:773-775. doi:10.1016/j.jaad.2020.07.112
- Montgomery SN, Elbuluk N. A quantitative analysis of research publications focused on the top chief complaints in skin of color patients. J Am Acad Dermatol. 2021;85:241-242. doi:10.1016/j.jaad.2020.08.031
- Hinds GA, Heald P. Cutaneous T-cell lymphoma in skin of color. J Am Acad Dermatol. 2009;60:359-375; quiz 376-378. doi:10.1016/j.jaad.2008.10.031
- Ardigó M, Borroni G, Muscardin L, et al. Hypopigmented mycosis fungoides in Caucasian patients: a clinicopathologic study of 7 cases. J Am Acad Dermatol. 2003;49:264-270. doi:10.1067/s0190-9622(03)00907-1
- Colby SL, Ortman JM. Projections of the size and composition of the U.S. population: 2014 to 2060. United States Census Bureau website. Updated October 8, 2021. Accessed February 28, 2022. https://www.census.gov/library/publications/2015/demo/p25-1143.html
- Taylor SC, Kyei A. Defining skin of color. In: Kelly AP, Taylor SC, Lim HW, et al, eds. Taylor and Kelly’s Dermatology for Skin of Color. 2nd ed. McGraw-Hill Education; 2016.
- Huang AH, Kwatra SG, Khanna R, et al. Racial disparities in the clinical presentation and prognosis of patients with mycosis fungoides. J Natl Med Assoc. 2019;111:633-639. doi:10.1016/j.jnma.2019.08.006
- Kim YH, Jensen RA, Watanabe GL, et al. Clinical stage IA (limited patch and plaque) mycosis fungoides. a long-term outcome analysis. Arch Dermatol. 1996;132:1309-1313.
- Scarisbrick JJ, Prince HM, Vermeer MH, et al. Cutaneous lymphoma international consortium study of outcome in advanced stages of mycosis fungoides and Sézary syndrome: effect of specific prognostic markers on survival and development of a prognostic model. J Clin Oncol. 2015;33:3766-3773. doi:10.1200/JCO.2015.61.7142
- Nath SK, Yu JB, Wilson LD. Poorer prognosis of African-American patients with mycosis fungoides: an analysis of the SEER dataset, 1988 to 2008. Clin Lymphoma Myeloma Leuk. 2014;14:419-423. doi:10.1016/j.clml.2013.12.018
- Ben-Gashir MA, Hay RJ. Reliance on erythema scores may mask severe atopic dermatitis in black children compared with their white counterparts. Br J Dermatol. 2002;147:920-925. doi:10.1046/j.1365-2133.2002.04965.x
- Poladian K, De Souza B, McMichael AJ. Atopic dermatitis in adolescents with skin of color. Cutis. 2019;104:164-168.
- Yones SS, Palmer RA, Garibaldinos TT, et al. Randomized double-blind trial of the treatment of chronic plaque psoriasis: efficacy of psoralen-UV-A therapy vs narrowband UV-B therapy. Arch Dermatol. 2006;142:836-842. doi:10.1001/archderm.142.7.836
- Currimbhoy S, Pandya AG. Cutaneous T-cell lymphoma. In: Kelly AP, Taylor SC, Lim HW, et al, eds. Taylor and Kelly’s Dermatology for Skin of Color. 2nd ed. McGraw-Hill Education; 2016.
- Ware OR, Dawson JE, Shinohara MM, et al. Racial limitations of Fitzpatrick skin type. Cutis. 2020;105:77-80.
Practice Points
- Dermatologists should be familiar with the variable morphology of mycosis fungoides (MF)/Sézary syndrome (SS) exhibited by patients of all skin types to ensure prompt diagnosis and treatment.
- Patients with skin of color (SoC)(Fitzpatrick skin types IV–VI) with MF/SS are more likely than non-SoC patients (Fitzpatrick skin types I–III) to present with hyperpigmentation, a silver hue, and lichenification, whereas non-SoC patients commonly present with erythema and poikiloderma.
 who presented with hypopigmented scaly patches on the abdomen")
Women still missing from CV clinical trial leadership
Although women were well represented on panels, and chaired or cochaired sessions, thanks to the ACC’s ongoing efforts to promote gender diversity and inclusion, they rarely got to give the big talks.
“Unfortunately, women continue to be underrepresented among CV clinical trial leadership, leading to a lack of subject diversity,” Mary Norine Walsh, MD, medical director of heart failure and cardiac transplantation at Ascension St. Vincent Heart Center, Indianapolis, Ind., wrote in a review published online Feb. 28 in the Journal of the American College of Cardiology.
An analysis of cardiovascular trials published during the past 4 years showed that women comprised only 10.1% of clinical trial leadership committees, and more than half of the trials had no women at all as part of the trial leadership team. About 10% of the trials had a woman as first or senior author.
In an interview, Dr. Walsh said she was prompted to write her review because she found the absence of women presenters at ACC 21 so striking.
“ACC 21 was held virtually because of COVID. This gave me the opportunity to easily view all of the research sessions. I attended all of the late-breaking clinical trials and featured clinical research sessions live while they were being presented, and it slowly dawned on me as I was watching that the vast majority of the presenters were men,” she said.
“The ACC does what it can to ensure a good gender mix of panelists and session chairs, but what it cannot control is who presents the data. The fact that 93% of these talks were given by men was astonishing to me,” Dr. Walsh said.
Of the three trials presented by women, one was on sex-specific outcomes in high-risk patients receiving ticagrelor with or without aspirin after percutaneous coronary intervention (a subanalysis of the TWILIGHT study); one was on the impact of COVID-19 on the global cardiovascular workforce (the ACC 2020 Well Being Study); and one was on the prevention of cardiac dysfunction during adjuvanttherapy with candesartan and metoprolol (the PRADA study).
Most of the presenters were regulars at the ACC podium. As Dr. Walsh observed: “This was assuredly not the inaugural turn at the international podium for these male trial presenters.”
So why are women so noticeably absent among the leaders of cardiovascular clinical trials research?
The root cause for this underrepresentation begins with the low number of women who lead clinical trials in cardiovascular medicine and surgery, and the fact that there are fewer female cardiologists than male cardiologists to begin with.
Then there is the lack of mentorship, which, Dr. Walsh said, “really does occur along gendered lines, with men mentoring men.”
In addition, industry-funded trials tend to feed a nondiverse investigator pipeline and other research collaborations often encompass established networks, Dr. Walsh noted.
“When industry is embarking on a new trial of a drug or device, it tends to lean back on who they have had led before. It really gets down to who you know, so getting new people in is fairly difficult,” she said.
Several initiatives to increase diversity in CV clinical trial leadership are ongoing by the ACC and other organizations.
For example, Women as One gives “escalator awards” to boost or escalate the training of highly qualified female cardiologists through targeted funding, mentorship, and networking.
The ACC’s “Clinical Trial Research: Upping Your Game” program aims to develop and train the next generation of a diverse and inclusive clinical trials workforce, focusing not only on women but on other traditionally underrepresented groups.
“We’re now in our third cohort of investigators who are early in their careers. We’re arming them with the skills to become successful in becoming investigators and then going up the chain to trial leadership. We are focusing our efforts on those who are underrepresented in cardiology – women, native Americans, Latinx, and Black investigators. We are hoping to increase diversity through that way, but more still needs to be done,” she said.
Trial sponsors, whether federally funded or industry sponsored, need to insist on diversity of the trial steering committee, and principal investigators need to consider diversity.
“A rethinking of who is eligible to present important trial results is needed,” Dr. Walsh said.
“The informal, or formal, pecking order of CV trial leadership needs to be reworked. All members of the steering committee should be possible presenters, and women should not be asked to report late-breaking results of trials that are reporting sex-specific results or data that are pertinent only to a female population.”
A version of this article first appeared on Medscape.com.
Although women were well represented on panels, and chaired or cochaired sessions, thanks to the ACC’s ongoing efforts to promote gender diversity and inclusion, they rarely got to give the big talks.
“Unfortunately, women continue to be underrepresented among CV clinical trial leadership, leading to a lack of subject diversity,” Mary Norine Walsh, MD, medical director of heart failure and cardiac transplantation at Ascension St. Vincent Heart Center, Indianapolis, Ind., wrote in a review published online Feb. 28 in the Journal of the American College of Cardiology.
An analysis of cardiovascular trials published during the past 4 years showed that women comprised only 10.1% of clinical trial leadership committees, and more than half of the trials had no women at all as part of the trial leadership team. About 10% of the trials had a woman as first or senior author.
In an interview, Dr. Walsh said she was prompted to write her review because she found the absence of women presenters at ACC 21 so striking.
“ACC 21 was held virtually because of COVID. This gave me the opportunity to easily view all of the research sessions. I attended all of the late-breaking clinical trials and featured clinical research sessions live while they were being presented, and it slowly dawned on me as I was watching that the vast majority of the presenters were men,” she said.
“The ACC does what it can to ensure a good gender mix of panelists and session chairs, but what it cannot control is who presents the data. The fact that 93% of these talks were given by men was astonishing to me,” Dr. Walsh said.
Of the three trials presented by women, one was on sex-specific outcomes in high-risk patients receiving ticagrelor with or without aspirin after percutaneous coronary intervention (a subanalysis of the TWILIGHT study); one was on the impact of COVID-19 on the global cardiovascular workforce (the ACC 2020 Well Being Study); and one was on the prevention of cardiac dysfunction during adjuvanttherapy with candesartan and metoprolol (the PRADA study).
Most of the presenters were regulars at the ACC podium. As Dr. Walsh observed: “This was assuredly not the inaugural turn at the international podium for these male trial presenters.”
So why are women so noticeably absent among the leaders of cardiovascular clinical trials research?
The root cause for this underrepresentation begins with the low number of women who lead clinical trials in cardiovascular medicine and surgery, and the fact that there are fewer female cardiologists than male cardiologists to begin with.
Then there is the lack of mentorship, which, Dr. Walsh said, “really does occur along gendered lines, with men mentoring men.”
In addition, industry-funded trials tend to feed a nondiverse investigator pipeline and other research collaborations often encompass established networks, Dr. Walsh noted.
“When industry is embarking on a new trial of a drug or device, it tends to lean back on who they have had led before. It really gets down to who you know, so getting new people in is fairly difficult,” she said.
Several initiatives to increase diversity in CV clinical trial leadership are ongoing by the ACC and other organizations.
For example, Women as One gives “escalator awards” to boost or escalate the training of highly qualified female cardiologists through targeted funding, mentorship, and networking.
The ACC’s “Clinical Trial Research: Upping Your Game” program aims to develop and train the next generation of a diverse and inclusive clinical trials workforce, focusing not only on women but on other traditionally underrepresented groups.
“We’re now in our third cohort of investigators who are early in their careers. We’re arming them with the skills to become successful in becoming investigators and then going up the chain to trial leadership. We are focusing our efforts on those who are underrepresented in cardiology – women, native Americans, Latinx, and Black investigators. We are hoping to increase diversity through that way, but more still needs to be done,” she said.
Trial sponsors, whether federally funded or industry sponsored, need to insist on diversity of the trial steering committee, and principal investigators need to consider diversity.
“A rethinking of who is eligible to present important trial results is needed,” Dr. Walsh said.
“The informal, or formal, pecking order of CV trial leadership needs to be reworked. All members of the steering committee should be possible presenters, and women should not be asked to report late-breaking results of trials that are reporting sex-specific results or data that are pertinent only to a female population.”
A version of this article first appeared on Medscape.com.
Although women were well represented on panels, and chaired or cochaired sessions, thanks to the ACC’s ongoing efforts to promote gender diversity and inclusion, they rarely got to give the big talks.
“Unfortunately, women continue to be underrepresented among CV clinical trial leadership, leading to a lack of subject diversity,” Mary Norine Walsh, MD, medical director of heart failure and cardiac transplantation at Ascension St. Vincent Heart Center, Indianapolis, Ind., wrote in a review published online Feb. 28 in the Journal of the American College of Cardiology.
An analysis of cardiovascular trials published during the past 4 years showed that women comprised only 10.1% of clinical trial leadership committees, and more than half of the trials had no women at all as part of the trial leadership team. About 10% of the trials had a woman as first or senior author.
In an interview, Dr. Walsh said she was prompted to write her review because she found the absence of women presenters at ACC 21 so striking.
“ACC 21 was held virtually because of COVID. This gave me the opportunity to easily view all of the research sessions. I attended all of the late-breaking clinical trials and featured clinical research sessions live while they were being presented, and it slowly dawned on me as I was watching that the vast majority of the presenters were men,” she said.
“The ACC does what it can to ensure a good gender mix of panelists and session chairs, but what it cannot control is who presents the data. The fact that 93% of these talks were given by men was astonishing to me,” Dr. Walsh said.
Of the three trials presented by women, one was on sex-specific outcomes in high-risk patients receiving ticagrelor with or without aspirin after percutaneous coronary intervention (a subanalysis of the TWILIGHT study); one was on the impact of COVID-19 on the global cardiovascular workforce (the ACC 2020 Well Being Study); and one was on the prevention of cardiac dysfunction during adjuvanttherapy with candesartan and metoprolol (the PRADA study).
Most of the presenters were regulars at the ACC podium. As Dr. Walsh observed: “This was assuredly not the inaugural turn at the international podium for these male trial presenters.”
So why are women so noticeably absent among the leaders of cardiovascular clinical trials research?
The root cause for this underrepresentation begins with the low number of women who lead clinical trials in cardiovascular medicine and surgery, and the fact that there are fewer female cardiologists than male cardiologists to begin with.
Then there is the lack of mentorship, which, Dr. Walsh said, “really does occur along gendered lines, with men mentoring men.”
In addition, industry-funded trials tend to feed a nondiverse investigator pipeline and other research collaborations often encompass established networks, Dr. Walsh noted.
“When industry is embarking on a new trial of a drug or device, it tends to lean back on who they have had led before. It really gets down to who you know, so getting new people in is fairly difficult,” she said.
Several initiatives to increase diversity in CV clinical trial leadership are ongoing by the ACC and other organizations.
For example, Women as One gives “escalator awards” to boost or escalate the training of highly qualified female cardiologists through targeted funding, mentorship, and networking.
The ACC’s “Clinical Trial Research: Upping Your Game” program aims to develop and train the next generation of a diverse and inclusive clinical trials workforce, focusing not only on women but on other traditionally underrepresented groups.
“We’re now in our third cohort of investigators who are early in their careers. We’re arming them with the skills to become successful in becoming investigators and then going up the chain to trial leadership. We are focusing our efforts on those who are underrepresented in cardiology – women, native Americans, Latinx, and Black investigators. We are hoping to increase diversity through that way, but more still needs to be done,” she said.
Trial sponsors, whether federally funded or industry sponsored, need to insist on diversity of the trial steering committee, and principal investigators need to consider diversity.
“A rethinking of who is eligible to present important trial results is needed,” Dr. Walsh said.
“The informal, or formal, pecking order of CV trial leadership needs to be reworked. All members of the steering committee should be possible presenters, and women should not be asked to report late-breaking results of trials that are reporting sex-specific results or data that are pertinent only to a female population.”
A version of this article first appeared on Medscape.com.
Discoid lupus
THE COMPARISON
A Multicolored (pink, brown, and white) indurated plaques in a butterfly distribution on the face of a 30-year-old woman with a darker skin tone.
B Pink, elevated, indurated plaques with hypopigmentation in a butterfly distribution on the face of a 19-year-old woman with a lighter skin tone.
Cutaneous lupus erythematosus may occur with or without systemic lupus erythematosus. Discoid lupus erythematosus (DLE), a form of chronic cutaneous lupus, is most commonly found on the scalp, face, and ears.1

Epidemiology
DLE is most common in adult women (age range, 20–40 years).2 It occurs more frequently in women of African descent.3,4
Key clinical features in people with darker skin tones
Clinical features of DLE lesions include erythema, induration, follicular plugging, dyspigmentation, and scarring alopecia.1 In patients of African descent, lesions may be annular and hypopigmented to depigmented centrally with a border of hyperpigmentation. Active lesions may be painful and/or pruritic.2
DLE lesions occur in photodistributed areas, although not exclusively. Photoprotective clothing and sunscreen are an important part of the treatment plan.1 Although sunscreen is recommended for patients with DLE, those with darker skin tones may find some sunscreens cosmetically unappealing due to a mismatch with their normal skin color.5 Tinted sunscreens may be beneficial additions.
Worth noting
Approximately 5% to 25% of patients with cutaneous lupus go on to develop systemic lupus erythematosus.6
Health disparity highlight
Discoid lesions may cause cutaneous scars that are quite disfiguring and may negatively impact quality of life. Some patients may have a few scattered lesions, whereas others have extensive disease covering most of the scalp. DLE lesions of the scalp have classic clinical features including hair loss, erythema, hypopigmentation, and hyperpigmentation. The clinician’s comfort with performing a scalp examination with cultural humility is an important acquired skill and is especially important when the examination is performed on patients with more tightly coiled hair.7 For example, physicians may adopt the “compliment, discuss, and suggest” method when counseling patients.8
1. Bolognia JL, Jorizzo JJ, Schaffer JV, et al. Dermatology. 3rd ed. Elsevier; 2012.
2. Otberg N, Wu W-Y, McElwee KJ, et al. Diagnosis and management of primary cicatricial alopecia: part I. Skinmed. 2008;7:19-26. doi:10.1111/j.1540-9740.2007.07163.x
3. Callen JP. Chronic cutaneous lupus erythematosus. clinical, laboratory, therapeutic, and prognostic examination of 62 patients. Arch Dermatol. 1982;118:412-416. doi:10.1001/archderm.118.6.412
4. McCarty DJ, Manzi S, Medsger TA Jr, et al. Incidence of systemic lupus erythematosus. race and gender differences. Arthritis Rheum. 1995;38:1260-1270. doi:10.1002/art.1780380914
5. Morquette AJ, Waples ER, Heath CR. The importance of cosmetically elegant sunscreen in skin of color populations. J Cosmet Dermatol. In press.
6. Zhou W, Wu H, Zhao M, et al. New insights into the progression from cutaneous lupus to systemic lupus erythematosus. Expert Rev Clin Immunol. 2020;16:829-837. doi:10.1080/17446 66X.2020.1805316
7. Grayson C, Heath C. An approach to examining tightly coiled hair among patients with hair loss in race-discordant patient-physician interactions. JAMA Dermatol. 2021;157:505-506. doi:10.1001/jamadermatol.2021.0338
8. Grayson C, Heath CR. Counseling about traction alopecia: a “compliment, discuss, and suggest” method. Cutis. 2021;108:20-22.
THE COMPARISON
A Multicolored (pink, brown, and white) indurated plaques in a butterfly distribution on the face of a 30-year-old woman with a darker skin tone.
B Pink, elevated, indurated plaques with hypopigmentation in a butterfly distribution on the face of a 19-year-old woman with a lighter skin tone.
Cutaneous lupus erythematosus may occur with or without systemic lupus erythematosus. Discoid lupus erythematosus (DLE), a form of chronic cutaneous lupus, is most commonly found on the scalp, face, and ears.1
Epidemiology
DLE is most common in adult women (age range, 20–40 years).2 It occurs more frequently in women of African descent.3,4
Key clinical features in people with darker skin tones
Clinical features of DLE lesions include erythema, induration, follicular plugging, dyspigmentation, and scarring alopecia.1 In patients of African descent, lesions may be annular and hypopigmented to depigmented centrally with a border of hyperpigmentation. Active lesions may be painful and/or pruritic.2
DLE lesions occur in photodistributed areas, although not exclusively. Photoprotective clothing and sunscreen are an important part of the treatment plan.1 Although sunscreen is recommended for patients with DLE, those with darker skin tones may find some sunscreens cosmetically unappealing due to a mismatch with their normal skin color.5 Tinted sunscreens may be beneficial additions.
Worth noting
Approximately 5% to 25% of patients with cutaneous lupus go on to develop systemic lupus erythematosus.6
Health disparity highlight
Discoid lesions may cause cutaneous scars that are quite disfiguring and may negatively impact quality of life. Some patients may have a few scattered lesions, whereas others have extensive disease covering most of the scalp. DLE lesions of the scalp have classic clinical features including hair loss, erythema, hypopigmentation, and hyperpigmentation. The clinician’s comfort with performing a scalp examination with cultural humility is an important acquired skill and is especially important when the examination is performed on patients with more tightly coiled hair.7 For example, physicians may adopt the “compliment, discuss, and suggest” method when counseling patients.8
THE COMPARISON
A Multicolored (pink, brown, and white) indurated plaques in a butterfly distribution on the face of a 30-year-old woman with a darker skin tone.
B Pink, elevated, indurated plaques with hypopigmentation in a butterfly distribution on the face of a 19-year-old woman with a lighter skin tone.
Cutaneous lupus erythematosus may occur with or without systemic lupus erythematosus. Discoid lupus erythematosus (DLE), a form of chronic cutaneous lupus, is most commonly found on the scalp, face, and ears.1
Epidemiology
DLE is most common in adult women (age range, 20–40 years).2 It occurs more frequently in women of African descent.3,4
Key clinical features in people with darker skin tones
Clinical features of DLE lesions include erythema, induration, follicular plugging, dyspigmentation, and scarring alopecia.1 In patients of African descent, lesions may be annular and hypopigmented to depigmented centrally with a border of hyperpigmentation. Active lesions may be painful and/or pruritic.2
DLE lesions occur in photodistributed areas, although not exclusively. Photoprotective clothing and sunscreen are an important part of the treatment plan.1 Although sunscreen is recommended for patients with DLE, those with darker skin tones may find some sunscreens cosmetically unappealing due to a mismatch with their normal skin color.5 Tinted sunscreens may be beneficial additions.
Worth noting
Approximately 5% to 25% of patients with cutaneous lupus go on to develop systemic lupus erythematosus.6
Health disparity highlight
Discoid lesions may cause cutaneous scars that are quite disfiguring and may negatively impact quality of life. Some patients may have a few scattered lesions, whereas others have extensive disease covering most of the scalp. DLE lesions of the scalp have classic clinical features including hair loss, erythema, hypopigmentation, and hyperpigmentation. The clinician’s comfort with performing a scalp examination with cultural humility is an important acquired skill and is especially important when the examination is performed on patients with more tightly coiled hair.7 For example, physicians may adopt the “compliment, discuss, and suggest” method when counseling patients.8
1. Bolognia JL, Jorizzo JJ, Schaffer JV, et al. Dermatology. 3rd ed. Elsevier; 2012.
2. Otberg N, Wu W-Y, McElwee KJ, et al. Diagnosis and management of primary cicatricial alopecia: part I. Skinmed. 2008;7:19-26. doi:10.1111/j.1540-9740.2007.07163.x
3. Callen JP. Chronic cutaneous lupus erythematosus. clinical, laboratory, therapeutic, and prognostic examination of 62 patients. Arch Dermatol. 1982;118:412-416. doi:10.1001/archderm.118.6.412
4. McCarty DJ, Manzi S, Medsger TA Jr, et al. Incidence of systemic lupus erythematosus. race and gender differences. Arthritis Rheum. 1995;38:1260-1270. doi:10.1002/art.1780380914
5. Morquette AJ, Waples ER, Heath CR. The importance of cosmetically elegant sunscreen in skin of color populations. J Cosmet Dermatol. In press.
6. Zhou W, Wu H, Zhao M, et al. New insights into the progression from cutaneous lupus to systemic lupus erythematosus. Expert Rev Clin Immunol. 2020;16:829-837. doi:10.1080/17446 66X.2020.1805316
7. Grayson C, Heath C. An approach to examining tightly coiled hair among patients with hair loss in race-discordant patient-physician interactions. JAMA Dermatol. 2021;157:505-506. doi:10.1001/jamadermatol.2021.0338
8. Grayson C, Heath CR. Counseling about traction alopecia: a “compliment, discuss, and suggest” method. Cutis. 2021;108:20-22.
1. Bolognia JL, Jorizzo JJ, Schaffer JV, et al. Dermatology. 3rd ed. Elsevier; 2012.
2. Otberg N, Wu W-Y, McElwee KJ, et al. Diagnosis and management of primary cicatricial alopecia: part I. Skinmed. 2008;7:19-26. doi:10.1111/j.1540-9740.2007.07163.x
3. Callen JP. Chronic cutaneous lupus erythematosus. clinical, laboratory, therapeutic, and prognostic examination of 62 patients. Arch Dermatol. 1982;118:412-416. doi:10.1001/archderm.118.6.412
4. McCarty DJ, Manzi S, Medsger TA Jr, et al. Incidence of systemic lupus erythematosus. race and gender differences. Arthritis Rheum. 1995;38:1260-1270. doi:10.1002/art.1780380914
5. Morquette AJ, Waples ER, Heath CR. The importance of cosmetically elegant sunscreen in skin of color populations. J Cosmet Dermatol. In press.
6. Zhou W, Wu H, Zhao M, et al. New insights into the progression from cutaneous lupus to systemic lupus erythematosus. Expert Rev Clin Immunol. 2020;16:829-837. doi:10.1080/17446 66X.2020.1805316
7. Grayson C, Heath C. An approach to examining tightly coiled hair among patients with hair loss in race-discordant patient-physician interactions. JAMA Dermatol. 2021;157:505-506. doi:10.1001/jamadermatol.2021.0338
8. Grayson C, Heath CR. Counseling about traction alopecia: a “compliment, discuss, and suggest” method. Cutis. 2021;108:20-22.
 indurated plaques in a butterfly distribution on the face of a 30-year-old woman with a darker skin tone")
All in the family
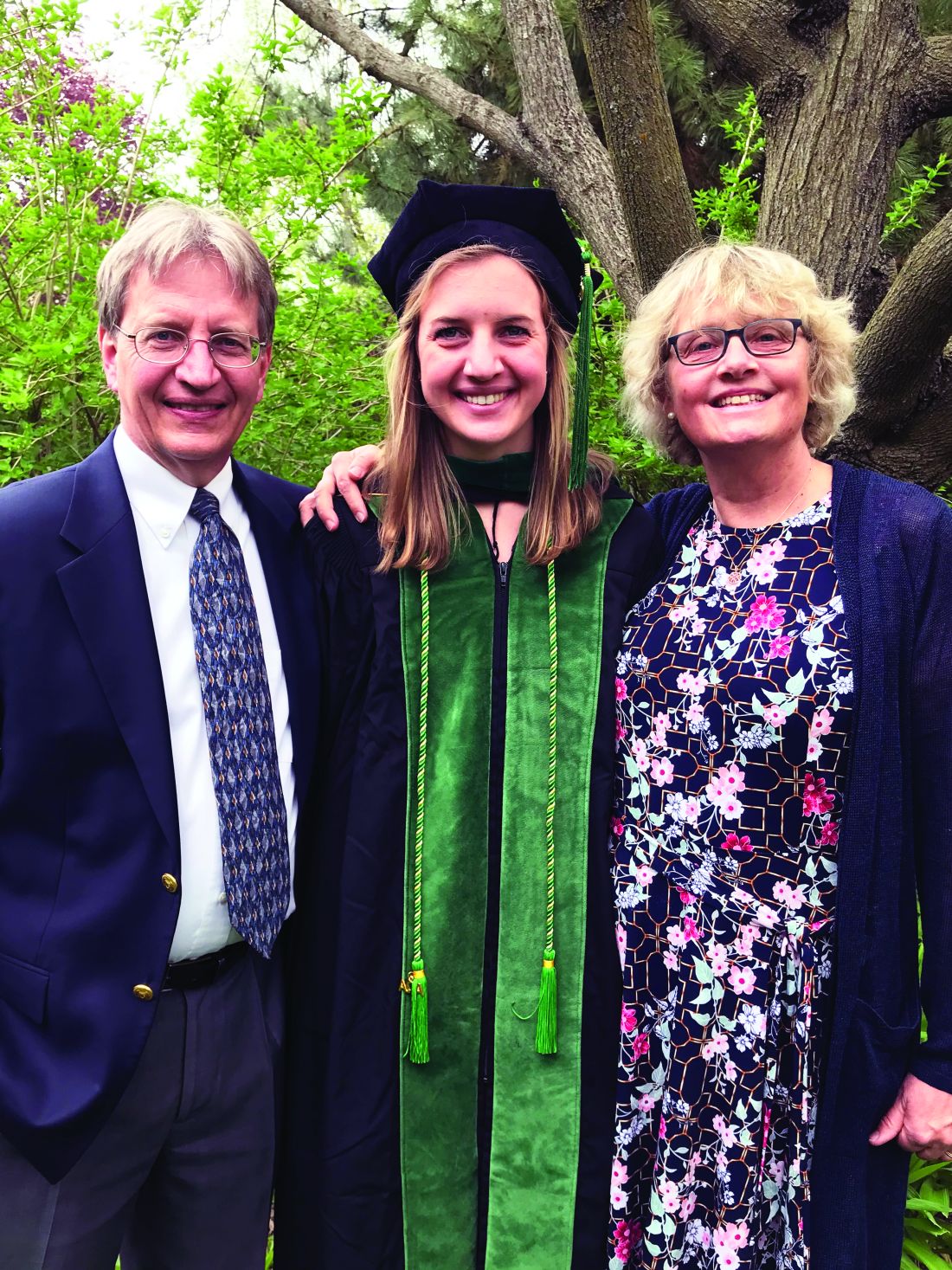
Six female doctors from two families share their journeys through medicine.
When Annie Uhing, MD, is stressed about work, she can call her mom. She and her mom are close, yes, but her mom is also a physician and understands the ups and downs of medical education and the unique challenges of being a woman in medicine.
“My mom and I were talking about this the other day – I don’t think we know any other mother-daughter pairs of doctors,” said Dr. Uhing.
In the United States, the number of female physicians has risen steadily since the mid- and late-20th century. As of 2019, women made up more than half of medical school classes across the country and 36.3% of the physician workforce.
Still, most female physicians are concentrated in a handful of specialties (such as pediatrics and obstetrics and gynecology) while the percentages of women in other areas remains extremely low (urology and orthopedic surgery). Many female physicians share anecdotal stories about not being taken seriously, like when a patient mistook them for a nurse, or preferred the advice of a male colleague to their own.
To celebrate International Women’s Day, this news organization talked to two families of female doctors about their experiences in medicine and how they inspire and support one another inside and outside the hospital.
Deborah, Charlene, and Annie
When Deborah Gaebler-Spira, MD, started medical school at the University of Illinois in 1975, women made up just 15% of her class. “For me, the idea that as a woman you could have a vocation that could be quite meaningful and self-directed – that was very important,” said Dr. Gaebler-Spira, now a pediatric rehabilitation physician at the Shirley Ryan Ability Lab and professor at Northwestern University in Chicago.
She blocked out a lot of discouragement along the way. In undergrad, the dean of the college warned Dr. Gaebler-Spira she’d never make it as a doctor. In medical school interviews, administrators could be hostile. “There was this feeling that you were taking a place of someone who really deserved it,” she said. When selecting a residency, Dr. Gaebler-Spira decided against a career in obstetrics because of the overt misogyny in the field at the time.
Instead, she went into pediatrics and physical medicine and rehabilitation, eventually working to become an expert in cerebral palsy. Along the way, Dr. Gaebler-Spira made lifelong friends with other female physicians and found strong female mentors, including Billie Adams, MD, and Helen Emery, MD.
When her sister, Charlene Gaebler-Uhing, MD, also decided to go into medicine, Dr. Gaebler-Spira said she “thought it was a sign of sanity as she was always much more competitive than I was! And if I could do it, no question she was able!”
Dr. Gaebler-Uhing, now an adolescent medicine specialist at Children’s Wisconsin in Milwaukee, followed her older sister’s footsteps to medical school in 1983, after first considering a career in social work.
While there were now more women going into medicine – her medical school class was about 25% women – problems persisted. During clinical rotations in residency, Dr. Gaebler-Uhing was often the only woman on a team and made the conscious decision to go professionally by her nickname, Charlie. “If a woman’s name was on the consult, her opinion and insights did not get the same value or respect as a male physician’s,” she said. “The only way they knew I was a woman was if they really knew me.”
The Gaebler sisters leaned on each other professionally and personally throughout their careers. When both sisters practiced in Chicago, they referred patients to one another. And Dr. Gaebler-Uhing said her older sister was a great role model for how to balance the dual roles of physician and parent, as few of the older female doctors who trained her were married or had a child.
Now Dr. Gaebler-Uhing’s daughter, Annie Uhing, MD, is entering medicine herself. She is currently pediatric resident at the University of Wisconsin American Family Hospital. She plans to do a chief year and then a pediatric endocrinology fellowship.
Growing up, Dr. Uhing wasn’t always sure she wanted to work as much as her parents, who are both doctors. But her mom provided a great example few of her friends had at home: “If you want to work, you should work and do what you want to do and it’s not wrong to want to have a really high-powered job as a woman,” said Dr. Uhing.
Kathryn, Susan, and Rita
The three sisters Kathryn Hudson, MD, Susan Schmidt, MD, and Rita Butler, MD, were inspired to go into medicine by their mother, Rita Watson, MD, who was one of the first female interventional cardiologists in the United States.
“I think we had a front row seat to what being a doctor was like,” said Dr. Hudson, a hematologist and oncologist and director of survivorship at Texas Oncology in Austin. Both parents were MDs – their dad was a pharmaceutical researcher at Merck – and they would excitedly discuss patient cases and drug development at the dinner table, said Dr. Butler, an interventional cardiology fellow at the Lankenau Heart Institute in Wynnewood, Pa.
All three sisters have vivid memories of ‘Take Your Daughter to Work Day’ at their mom’s hospital. “I remember going to Take Your Daughter to Work Day with her and watching her in action and thinking, oh my gosh, my mom is so cool and I want to be like her,” said Dr. Schmidt, a pediatric critical care specialist at St. Christopher’s Hospital for Children in Philadelphia. “I’ve always felt special that my mom was doing something really cool and really saving lives,” said Dr. Schmidt.
Their fourth sibling, John, isn’t a physician and “I honestly wonder if it’s because he never went to Take Your Daughter to Work Day!” said Dr. Butler.
Having a mother who had both a high-powered medical career and a family helped the three women know they could do the same. “It is a difficult journey, don’t get me wrong, but I never questioned that I could do it because my mom did it first,” said Dr. Hudson.
As adults, the sisters confide in one another as they navigate modern motherhood and careers, switching between discussing medical cases and parenting advice.
As hard as their mom worked while they were growing up, she didn’t have the pressure of living up to the “super mom” ideal we have now, said Dr. Butler. “Everyone wants women to work like they don’t have kids and everyone wants women to parent like they don’t have a job,” she said. Having two sisters who can provide reassurance and advice in that area goes a long way, she said.
“I think sharing that experience of navigating motherhood, a medical career, and marriage, and adult life with sisters who are going through all the same things is really special and I feel really fortunate for that,” said Dr. Schmidt.
*This story was updated on 3/8/2022.
Six female doctors from two families share their journeys through medicine.
Six female doctors from two families share their journeys through medicine.
When Annie Uhing, MD, is stressed about work, she can call her mom. She and her mom are close, yes, but her mom is also a physician and understands the ups and downs of medical education and the unique challenges of being a woman in medicine.
“My mom and I were talking about this the other day – I don’t think we know any other mother-daughter pairs of doctors,” said Dr. Uhing.
In the United States, the number of female physicians has risen steadily since the mid- and late-20th century. As of 2019, women made up more than half of medical school classes across the country and 36.3% of the physician workforce.
Still, most female physicians are concentrated in a handful of specialties (such as pediatrics and obstetrics and gynecology) while the percentages of women in other areas remains extremely low (urology and orthopedic surgery). Many female physicians share anecdotal stories about not being taken seriously, like when a patient mistook them for a nurse, or preferred the advice of a male colleague to their own.
To celebrate International Women’s Day, this news organization talked to two families of female doctors about their experiences in medicine and how they inspire and support one another inside and outside the hospital.
Deborah, Charlene, and Annie
When Deborah Gaebler-Spira, MD, started medical school at the University of Illinois in 1975, women made up just 15% of her class. “For me, the idea that as a woman you could have a vocation that could be quite meaningful and self-directed – that was very important,” said Dr. Gaebler-Spira, now a pediatric rehabilitation physician at the Shirley Ryan Ability Lab and professor at Northwestern University in Chicago.
She blocked out a lot of discouragement along the way. In undergrad, the dean of the college warned Dr. Gaebler-Spira she’d never make it as a doctor. In medical school interviews, administrators could be hostile. “There was this feeling that you were taking a place of someone who really deserved it,” she said. When selecting a residency, Dr. Gaebler-Spira decided against a career in obstetrics because of the overt misogyny in the field at the time.
Instead, she went into pediatrics and physical medicine and rehabilitation, eventually working to become an expert in cerebral palsy. Along the way, Dr. Gaebler-Spira made lifelong friends with other female physicians and found strong female mentors, including Billie Adams, MD, and Helen Emery, MD.
When her sister, Charlene Gaebler-Uhing, MD, also decided to go into medicine, Dr. Gaebler-Spira said she “thought it was a sign of sanity as she was always much more competitive than I was! And if I could do it, no question she was able!”
Dr. Gaebler-Uhing, now an adolescent medicine specialist at Children’s Wisconsin in Milwaukee, followed her older sister’s footsteps to medical school in 1983, after first considering a career in social work.
While there were now more women going into medicine – her medical school class was about 25% women – problems persisted. During clinical rotations in residency, Dr. Gaebler-Uhing was often the only woman on a team and made the conscious decision to go professionally by her nickname, Charlie. “If a woman’s name was on the consult, her opinion and insights did not get the same value or respect as a male physician’s,” she said. “The only way they knew I was a woman was if they really knew me.”
The Gaebler sisters leaned on each other professionally and personally throughout their careers. When both sisters practiced in Chicago, they referred patients to one another. And Dr. Gaebler-Uhing said her older sister was a great role model for how to balance the dual roles of physician and parent, as few of the older female doctors who trained her were married or had a child.
Now Dr. Gaebler-Uhing’s daughter, Annie Uhing, MD, is entering medicine herself. She is currently pediatric resident at the University of Wisconsin American Family Hospital. She plans to do a chief year and then a pediatric endocrinology fellowship.
Growing up, Dr. Uhing wasn’t always sure she wanted to work as much as her parents, who are both doctors. But her mom provided a great example few of her friends had at home: “If you want to work, you should work and do what you want to do and it’s not wrong to want to have a really high-powered job as a woman,” said Dr. Uhing.
Kathryn, Susan, and Rita
The three sisters Kathryn Hudson, MD, Susan Schmidt, MD, and Rita Butler, MD, were inspired to go into medicine by their mother, Rita Watson, MD, who was one of the first female interventional cardiologists in the United States.
“I think we had a front row seat to what being a doctor was like,” said Dr. Hudson, a hematologist and oncologist and director of survivorship at Texas Oncology in Austin. Both parents were MDs – their dad was a pharmaceutical researcher at Merck – and they would excitedly discuss patient cases and drug development at the dinner table, said Dr. Butler, an interventional cardiology fellow at the Lankenau Heart Institute in Wynnewood, Pa.
All three sisters have vivid memories of ‘Take Your Daughter to Work Day’ at their mom’s hospital. “I remember going to Take Your Daughter to Work Day with her and watching her in action and thinking, oh my gosh, my mom is so cool and I want to be like her,” said Dr. Schmidt, a pediatric critical care specialist at St. Christopher’s Hospital for Children in Philadelphia. “I’ve always felt special that my mom was doing something really cool and really saving lives,” said Dr. Schmidt.
Their fourth sibling, John, isn’t a physician and “I honestly wonder if it’s because he never went to Take Your Daughter to Work Day!” said Dr. Butler.
Having a mother who had both a high-powered medical career and a family helped the three women know they could do the same. “It is a difficult journey, don’t get me wrong, but I never questioned that I could do it because my mom did it first,” said Dr. Hudson.
As adults, the sisters confide in one another as they navigate modern motherhood and careers, switching between discussing medical cases and parenting advice.
As hard as their mom worked while they were growing up, she didn’t have the pressure of living up to the “super mom” ideal we have now, said Dr. Butler. “Everyone wants women to work like they don’t have kids and everyone wants women to parent like they don’t have a job,” she said. Having two sisters who can provide reassurance and advice in that area goes a long way, she said.
“I think sharing that experience of navigating motherhood, a medical career, and marriage, and adult life with sisters who are going through all the same things is really special and I feel really fortunate for that,” said Dr. Schmidt.
*This story was updated on 3/8/2022.
When Annie Uhing, MD, is stressed about work, she can call her mom. She and her mom are close, yes, but her mom is also a physician and understands the ups and downs of medical education and the unique challenges of being a woman in medicine.
“My mom and I were talking about this the other day – I don’t think we know any other mother-daughter pairs of doctors,” said Dr. Uhing.
In the United States, the number of female physicians has risen steadily since the mid- and late-20th century. As of 2019, women made up more than half of medical school classes across the country and 36.3% of the physician workforce.
Still, most female physicians are concentrated in a handful of specialties (such as pediatrics and obstetrics and gynecology) while the percentages of women in other areas remains extremely low (urology and orthopedic surgery). Many female physicians share anecdotal stories about not being taken seriously, like when a patient mistook them for a nurse, or preferred the advice of a male colleague to their own.
To celebrate International Women’s Day, this news organization talked to two families of female doctors about their experiences in medicine and how they inspire and support one another inside and outside the hospital.
Deborah, Charlene, and Annie
When Deborah Gaebler-Spira, MD, started medical school at the University of Illinois in 1975, women made up just 15% of her class. “For me, the idea that as a woman you could have a vocation that could be quite meaningful and self-directed – that was very important,” said Dr. Gaebler-Spira, now a pediatric rehabilitation physician at the Shirley Ryan Ability Lab and professor at Northwestern University in Chicago.
She blocked out a lot of discouragement along the way. In undergrad, the dean of the college warned Dr. Gaebler-Spira she’d never make it as a doctor. In medical school interviews, administrators could be hostile. “There was this feeling that you were taking a place of someone who really deserved it,” she said. When selecting a residency, Dr. Gaebler-Spira decided against a career in obstetrics because of the overt misogyny in the field at the time.
Instead, she went into pediatrics and physical medicine and rehabilitation, eventually working to become an expert in cerebral palsy. Along the way, Dr. Gaebler-Spira made lifelong friends with other female physicians and found strong female mentors, including Billie Adams, MD, and Helen Emery, MD.
When her sister, Charlene Gaebler-Uhing, MD, also decided to go into medicine, Dr. Gaebler-Spira said she “thought it was a sign of sanity as she was always much more competitive than I was! And if I could do it, no question she was able!”
Dr. Gaebler-Uhing, now an adolescent medicine specialist at Children’s Wisconsin in Milwaukee, followed her older sister’s footsteps to medical school in 1983, after first considering a career in social work.
While there were now more women going into medicine – her medical school class was about 25% women – problems persisted. During clinical rotations in residency, Dr. Gaebler-Uhing was often the only woman on a team and made the conscious decision to go professionally by her nickname, Charlie. “If a woman’s name was on the consult, her opinion and insights did not get the same value or respect as a male physician’s,” she said. “The only way they knew I was a woman was if they really knew me.”
The Gaebler sisters leaned on each other professionally and personally throughout their careers. When both sisters practiced in Chicago, they referred patients to one another. And Dr. Gaebler-Uhing said her older sister was a great role model for how to balance the dual roles of physician and parent, as few of the older female doctors who trained her were married or had a child.
Now Dr. Gaebler-Uhing’s daughter, Annie Uhing, MD, is entering medicine herself. She is currently pediatric resident at the University of Wisconsin American Family Hospital. She plans to do a chief year and then a pediatric endocrinology fellowship.
Growing up, Dr. Uhing wasn’t always sure she wanted to work as much as her parents, who are both doctors. But her mom provided a great example few of her friends had at home: “If you want to work, you should work and do what you want to do and it’s not wrong to want to have a really high-powered job as a woman,” said Dr. Uhing.
Kathryn, Susan, and Rita
The three sisters Kathryn Hudson, MD, Susan Schmidt, MD, and Rita Butler, MD, were inspired to go into medicine by their mother, Rita Watson, MD, who was one of the first female interventional cardiologists in the United States.
“I think we had a front row seat to what being a doctor was like,” said Dr. Hudson, a hematologist and oncologist and director of survivorship at Texas Oncology in Austin. Both parents were MDs – their dad was a pharmaceutical researcher at Merck – and they would excitedly discuss patient cases and drug development at the dinner table, said Dr. Butler, an interventional cardiology fellow at the Lankenau Heart Institute in Wynnewood, Pa.
All three sisters have vivid memories of ‘Take Your Daughter to Work Day’ at their mom’s hospital. “I remember going to Take Your Daughter to Work Day with her and watching her in action and thinking, oh my gosh, my mom is so cool and I want to be like her,” said Dr. Schmidt, a pediatric critical care specialist at St. Christopher’s Hospital for Children in Philadelphia. “I’ve always felt special that my mom was doing something really cool and really saving lives,” said Dr. Schmidt.
Their fourth sibling, John, isn’t a physician and “I honestly wonder if it’s because he never went to Take Your Daughter to Work Day!” said Dr. Butler.
Having a mother who had both a high-powered medical career and a family helped the three women know they could do the same. “It is a difficult journey, don’t get me wrong, but I never questioned that I could do it because my mom did it first,” said Dr. Hudson.
As adults, the sisters confide in one another as they navigate modern motherhood and careers, switching between discussing medical cases and parenting advice.
As hard as their mom worked while they were growing up, she didn’t have the pressure of living up to the “super mom” ideal we have now, said Dr. Butler. “Everyone wants women to work like they don’t have kids and everyone wants women to parent like they don’t have a job,” she said. Having two sisters who can provide reassurance and advice in that area goes a long way, she said.
“I think sharing that experience of navigating motherhood, a medical career, and marriage, and adult life with sisters who are going through all the same things is really special and I feel really fortunate for that,” said Dr. Schmidt.
*This story was updated on 3/8/2022.
Discoid Lupus

THE COMPARISON
A Multicolored (pink, brown, and white) indurated plaques in a butterfly distribution on the face of a 30-year-old woman with a darker skin tone.
B Pink, elevated, indurated plaques with hypopigmentation in a butterfly distribution on the face of a 19-year-old woman with a lighter skin tone.
Cutaneous lupus erythematosus may occur with or without systemic lupus erythematosus. Discoid lupus erythematosus (DLE), a form of chronic cutaneous lupus, is most commonly found on the scalp, face, and ears.1
Epidemiology
Discoid lupus erythematosus is most common in adult women (age range, 20–40 years).2 It occurs more frequently in women of African descent.3,4
Key clinical features in people with darker skin tones:
Clinical features of DLE lesions include erythema, induration, follicular plugging, dyspigmentation, and scarring alopecia.1 In patients of African descent, lesions may be annular and hypopigmented to depigmented centrally with a border of hyperpigmentation. Active lesions may be painful and/or pruritic.2
Discoid lupus erythematosus lesions occur in photodistributed areas, although not exclusively. Photoprotective clothing and sunscreen are an important part of the treatment plan.1 Although sunscreen is recommended for patients with DLE, those with darker skin tones may find some sunscreens cosmetically unappealing due to a mismatch with their normal skin color.5 Tinted sunscreens may be beneficial additions.
Worth noting
Approximately 5% to 25% of patients with cutaneous lupus go on to develop systemic lupus erythematosus.6
Health disparity highlight
Discoid lesions may cause cutaneous scars that are quite disfiguring and may negatively impact quality of life. Some patients may have a few scattered lesions, whereas others have extensive disease covering most of the scalp. Discoid lupus erythematosus lesions of the scalp have classic clinical features including hair loss, erythema, hypopigmentation, and hyperpigmentation. The clinician’s comfort with performing a scalp examination with cultural humility is an important acquired skill and is especially important when the examination is performed on patients with more tightly coiled hair.7 For example, physicians may adopt the “compliment, discuss, and suggest” method when counseling patients.8
- Bolognia JL, Jorizzo JJ, Schaffer JV, et al. Dermatology. 3rd ed. Elsevier; 2012.
- Otberg N, Wu W-Y, McElwee KJ, et al. Diagnosis and management of primary cicatricial alopecia: part I. Skinmed. 2008;7:19-26. doi:10.1111/j.1540-9740.2007.07163.x
- Callen JP. Chronic cutaneous lupus erythematosus. clinical, laboratory, therapeutic, and prognostic examination of 62 patients. Arch Dermatol. 1982;118:412-416. doi:10.1001/archderm.118.6.412
- McCarty DJ, Manzi S, Medsger TA Jr, et al. Incidence of systemic lupus erythematosus. race and gender differences. Arthritis Rheum. 1995;38:1260-1270. doi:10.1002/art.1780380914
- Morquette AJ, Waples ER, Heath CR. The importance of cosmetically elegant sunscreen in skin of color populations. J Cosmet Dermatol. In press.
- Zhou W, Wu H, Zhao M, et al. New insights into the progression from cutaneous lupus to systemic lupus erythematosus. Expert Rev Clin Immunol. 2020;16:829-837. doi:10.1080/17446 66X.2020.1805316
- Grayson C, Heath C. An approach to examining tightly coiled hair among patients with hair loss in race-discordant patientphysician interactions. JAMA Dermatol. 2021;157:505-506. doi:10.1001/jamadermatol.2021.0338
- Grayson C, Heath CR. Counseling about traction alopecia: a “compliment, discuss, and suggest” method. Cutis. 2021;108:20-22.
THE COMPARISON
A Multicolored (pink, brown, and white) indurated plaques in a butterfly distribution on the face of a 30-year-old woman with a darker skin tone.
B Pink, elevated, indurated plaques with hypopigmentation in a butterfly distribution on the face of a 19-year-old woman with a lighter skin tone.
Cutaneous lupus erythematosus may occur with or without systemic lupus erythematosus. Discoid lupus erythematosus (DLE), a form of chronic cutaneous lupus, is most commonly found on the scalp, face, and ears.1
Epidemiology
Discoid lupus erythematosus is most common in adult women (age range, 20–40 years).2 It occurs more frequently in women of African descent.3,4
Key clinical features in people with darker skin tones:
Clinical features of DLE lesions include erythema, induration, follicular plugging, dyspigmentation, and scarring alopecia.1 In patients of African descent, lesions may be annular and hypopigmented to depigmented centrally with a border of hyperpigmentation. Active lesions may be painful and/or pruritic.2
Discoid lupus erythematosus lesions occur in photodistributed areas, although not exclusively. Photoprotective clothing and sunscreen are an important part of the treatment plan.1 Although sunscreen is recommended for patients with DLE, those with darker skin tones may find some sunscreens cosmetically unappealing due to a mismatch with their normal skin color.5 Tinted sunscreens may be beneficial additions.
Worth noting
Approximately 5% to 25% of patients with cutaneous lupus go on to develop systemic lupus erythematosus.6
Health disparity highlight
Discoid lesions may cause cutaneous scars that are quite disfiguring and may negatively impact quality of life. Some patients may have a few scattered lesions, whereas others have extensive disease covering most of the scalp. Discoid lupus erythematosus lesions of the scalp have classic clinical features including hair loss, erythema, hypopigmentation, and hyperpigmentation. The clinician’s comfort with performing a scalp examination with cultural humility is an important acquired skill and is especially important when the examination is performed on patients with more tightly coiled hair.7 For example, physicians may adopt the “compliment, discuss, and suggest” method when counseling patients.8
THE COMPARISON
A Multicolored (pink, brown, and white) indurated plaques in a butterfly distribution on the face of a 30-year-old woman with a darker skin tone.
B Pink, elevated, indurated plaques with hypopigmentation in a butterfly distribution on the face of a 19-year-old woman with a lighter skin tone.
Cutaneous lupus erythematosus may occur with or without systemic lupus erythematosus. Discoid lupus erythematosus (DLE), a form of chronic cutaneous lupus, is most commonly found on the scalp, face, and ears.1
Epidemiology
Discoid lupus erythematosus is most common in adult women (age range, 20–40 years).2 It occurs more frequently in women of African descent.3,4
Key clinical features in people with darker skin tones:
Clinical features of DLE lesions include erythema, induration, follicular plugging, dyspigmentation, and scarring alopecia.1 In patients of African descent, lesions may be annular and hypopigmented to depigmented centrally with a border of hyperpigmentation. Active lesions may be painful and/or pruritic.2
Discoid lupus erythematosus lesions occur in photodistributed areas, although not exclusively. Photoprotective clothing and sunscreen are an important part of the treatment plan.1 Although sunscreen is recommended for patients with DLE, those with darker skin tones may find some sunscreens cosmetically unappealing due to a mismatch with their normal skin color.5 Tinted sunscreens may be beneficial additions.
Worth noting
Approximately 5% to 25% of patients with cutaneous lupus go on to develop systemic lupus erythematosus.6
Health disparity highlight
Discoid lesions may cause cutaneous scars that are quite disfiguring and may negatively impact quality of life. Some patients may have a few scattered lesions, whereas others have extensive disease covering most of the scalp. Discoid lupus erythematosus lesions of the scalp have classic clinical features including hair loss, erythema, hypopigmentation, and hyperpigmentation. The clinician’s comfort with performing a scalp examination with cultural humility is an important acquired skill and is especially important when the examination is performed on patients with more tightly coiled hair.7 For example, physicians may adopt the “compliment, discuss, and suggest” method when counseling patients.8
- Bolognia JL, Jorizzo JJ, Schaffer JV, et al. Dermatology. 3rd ed. Elsevier; 2012.
- Otberg N, Wu W-Y, McElwee KJ, et al. Diagnosis and management of primary cicatricial alopecia: part I. Skinmed. 2008;7:19-26. doi:10.1111/j.1540-9740.2007.07163.x
- Callen JP. Chronic cutaneous lupus erythematosus. clinical, laboratory, therapeutic, and prognostic examination of 62 patients. Arch Dermatol. 1982;118:412-416. doi:10.1001/archderm.118.6.412
- McCarty DJ, Manzi S, Medsger TA Jr, et al. Incidence of systemic lupus erythematosus. race and gender differences. Arthritis Rheum. 1995;38:1260-1270. doi:10.1002/art.1780380914
- Morquette AJ, Waples ER, Heath CR. The importance of cosmetically elegant sunscreen in skin of color populations. J Cosmet Dermatol. In press.
- Zhou W, Wu H, Zhao M, et al. New insights into the progression from cutaneous lupus to systemic lupus erythematosus. Expert Rev Clin Immunol. 2020;16:829-837. doi:10.1080/17446 66X.2020.1805316
- Grayson C, Heath C. An approach to examining tightly coiled hair among patients with hair loss in race-discordant patientphysician interactions. JAMA Dermatol. 2021;157:505-506. doi:10.1001/jamadermatol.2021.0338
- Grayson C, Heath CR. Counseling about traction alopecia: a “compliment, discuss, and suggest” method. Cutis. 2021;108:20-22.
- Bolognia JL, Jorizzo JJ, Schaffer JV, et al. Dermatology. 3rd ed. Elsevier; 2012.
- Otberg N, Wu W-Y, McElwee KJ, et al. Diagnosis and management of primary cicatricial alopecia: part I. Skinmed. 2008;7:19-26. doi:10.1111/j.1540-9740.2007.07163.x
- Callen JP. Chronic cutaneous lupus erythematosus. clinical, laboratory, therapeutic, and prognostic examination of 62 patients. Arch Dermatol. 1982;118:412-416. doi:10.1001/archderm.118.6.412
- McCarty DJ, Manzi S, Medsger TA Jr, et al. Incidence of systemic lupus erythematosus. race and gender differences. Arthritis Rheum. 1995;38:1260-1270. doi:10.1002/art.1780380914
- Morquette AJ, Waples ER, Heath CR. The importance of cosmetically elegant sunscreen in skin of color populations. J Cosmet Dermatol. In press.
- Zhou W, Wu H, Zhao M, et al. New insights into the progression from cutaneous lupus to systemic lupus erythematosus. Expert Rev Clin Immunol. 2020;16:829-837. doi:10.1080/17446 66X.2020.1805316
- Grayson C, Heath C. An approach to examining tightly coiled hair among patients with hair loss in race-discordant patientphysician interactions. JAMA Dermatol. 2021;157:505-506. doi:10.1001/jamadermatol.2021.0338
- Grayson C, Heath CR. Counseling about traction alopecia: a “compliment, discuss, and suggest” method. Cutis. 2021;108:20-22.
 indurated plaques in a butterfly distribution on the face of a 30-year-old woman with a darker skin tone")
Columbia names interim chair of psychiatry after Twitter controversy
Helen Blair Simpson, MD, PhD, will take over for Jeffrey Lieberman, MD, who was suspended over a tweet he sent that was widely condemned as both racist and sexist.

She will also serve as interim director of the New York State Psychiatric Institute and interim psychiatrist-in-chief at New York–Presbyterian/Columbia University Irving Medical Center, the email stated.
All appointments were effective on Feb. 28.
Latest response
Dr. Simpson, who joined the faculty at Columbia in 1999, previously served as a professor and vice chair of research for the psychiatry department, director of Columbia’s Center for Obsessive-Compulsive and Related Disorders, and director of psychiatry research at the New York State Psychiatric Institute. Dr. Simpson is associate editor of JAMA Psychiatry and is president-elect of the Anxiety and Depression Association of America.
Her research has been continuously funded by the National Institute of Mental Health since 1999, and she has advised both the World Health Organization and the American Psychiatric Association on the diagnosis and treatment of OCD.
Dr. Simpson has a bachelor’s degree in biology from Yale University and completed an MD-PhD program at The Rockefeller University and Weill Cornell Medicine, New York. She did her residency in psychiatry at New York–Presbyterian.
The announcement is Columbia’s latest response to the furor that erupted on social media following Dr. Lieberman’s tweet about Sudanese model Nyakim Gatwech, in which he wrote, “Whether a work of art or a freak of nature she’s a beautiful sight to behold.”
Twitter reacted immediately and negatively to the tweet, which even Dr. Lieberman later acknowledged was “racist and sexist” in an email apology he sent Feb. 22 to faculty and staff in the department of psychiatry.
As reported by this news organization, Columbia suspended Dr. Lieberman from his chair position on Feb. 23 and permanently removed him from the post of psychiatrist-in-chief at New York–Presbyterian Hospital/Columbia University Irving Medical Center. Lieberman also resigned as executive director of the New York State Psychiatric Institute.
The email announcing Simpson’s appointment was signed by Katrina Armstrong, MD, incoming CEO, Columbia University Irving Medical Center and dean of the Faculties of Health Sciences and the Vagelos College of Physicians and Surgeons; Anil K. Rustgi, MD, interim executive vice president and dean of the Faculties of Health Sciences and Medicine; Steven J. Corwin, MD; president and CEO, New York–Presbyterian; and Ann Marie Sullivan, MD, commissioner of the New York State Office of Mental Health.
This is a developing story.
A version of this article first appeared on Medscape.com.
Helen Blair Simpson, MD, PhD, will take over for Jeffrey Lieberman, MD, who was suspended over a tweet he sent that was widely condemned as both racist and sexist.
She will also serve as interim director of the New York State Psychiatric Institute and interim psychiatrist-in-chief at New York–Presbyterian/Columbia University Irving Medical Center, the email stated.
All appointments were effective on Feb. 28.
Latest response
Dr. Simpson, who joined the faculty at Columbia in 1999, previously served as a professor and vice chair of research for the psychiatry department, director of Columbia’s Center for Obsessive-Compulsive and Related Disorders, and director of psychiatry research at the New York State Psychiatric Institute. Dr. Simpson is associate editor of JAMA Psychiatry and is president-elect of the Anxiety and Depression Association of America.
Her research has been continuously funded by the National Institute of Mental Health since 1999, and she has advised both the World Health Organization and the American Psychiatric Association on the diagnosis and treatment of OCD.
Dr. Simpson has a bachelor’s degree in biology from Yale University and completed an MD-PhD program at The Rockefeller University and Weill Cornell Medicine, New York. She did her residency in psychiatry at New York–Presbyterian.
The announcement is Columbia’s latest response to the furor that erupted on social media following Dr. Lieberman’s tweet about Sudanese model Nyakim Gatwech, in which he wrote, “Whether a work of art or a freak of nature she’s a beautiful sight to behold.”
Twitter reacted immediately and negatively to the tweet, which even Dr. Lieberman later acknowledged was “racist and sexist” in an email apology he sent Feb. 22 to faculty and staff in the department of psychiatry.
As reported by this news organization, Columbia suspended Dr. Lieberman from his chair position on Feb. 23 and permanently removed him from the post of psychiatrist-in-chief at New York–Presbyterian Hospital/Columbia University Irving Medical Center. Lieberman also resigned as executive director of the New York State Psychiatric Institute.
The email announcing Simpson’s appointment was signed by Katrina Armstrong, MD, incoming CEO, Columbia University Irving Medical Center and dean of the Faculties of Health Sciences and the Vagelos College of Physicians and Surgeons; Anil K. Rustgi, MD, interim executive vice president and dean of the Faculties of Health Sciences and Medicine; Steven J. Corwin, MD; president and CEO, New York–Presbyterian; and Ann Marie Sullivan, MD, commissioner of the New York State Office of Mental Health.
This is a developing story.
A version of this article first appeared on Medscape.com.
Helen Blair Simpson, MD, PhD, will take over for Jeffrey Lieberman, MD, who was suspended over a tweet he sent that was widely condemned as both racist and sexist.
She will also serve as interim director of the New York State Psychiatric Institute and interim psychiatrist-in-chief at New York–Presbyterian/Columbia University Irving Medical Center, the email stated.
All appointments were effective on Feb. 28.
Latest response
Dr. Simpson, who joined the faculty at Columbia in 1999, previously served as a professor and vice chair of research for the psychiatry department, director of Columbia’s Center for Obsessive-Compulsive and Related Disorders, and director of psychiatry research at the New York State Psychiatric Institute. Dr. Simpson is associate editor of JAMA Psychiatry and is president-elect of the Anxiety and Depression Association of America.
Her research has been continuously funded by the National Institute of Mental Health since 1999, and she has advised both the World Health Organization and the American Psychiatric Association on the diagnosis and treatment of OCD.
Dr. Simpson has a bachelor’s degree in biology from Yale University and completed an MD-PhD program at The Rockefeller University and Weill Cornell Medicine, New York. She did her residency in psychiatry at New York–Presbyterian.
The announcement is Columbia’s latest response to the furor that erupted on social media following Dr. Lieberman’s tweet about Sudanese model Nyakim Gatwech, in which he wrote, “Whether a work of art or a freak of nature she’s a beautiful sight to behold.”
Twitter reacted immediately and negatively to the tweet, which even Dr. Lieberman later acknowledged was “racist and sexist” in an email apology he sent Feb. 22 to faculty and staff in the department of psychiatry.
As reported by this news organization, Columbia suspended Dr. Lieberman from his chair position on Feb. 23 and permanently removed him from the post of psychiatrist-in-chief at New York–Presbyterian Hospital/Columbia University Irving Medical Center. Lieberman also resigned as executive director of the New York State Psychiatric Institute.
The email announcing Simpson’s appointment was signed by Katrina Armstrong, MD, incoming CEO, Columbia University Irving Medical Center and dean of the Faculties of Health Sciences and the Vagelos College of Physicians and Surgeons; Anil K. Rustgi, MD, interim executive vice president and dean of the Faculties of Health Sciences and Medicine; Steven J. Corwin, MD; president and CEO, New York–Presbyterian; and Ann Marie Sullivan, MD, commissioner of the New York State Office of Mental Health.
This is a developing story.
A version of this article first appeared on Medscape.com.
Health disparities exist all over rheumatology: What can be done?
Disparities in health care exist in every specialty. In rheumatology, health disparities look like lack of access to care and lack of education on the part of rheumatologists and their patients, according to a speaker at the 2022 Rheumatology Winter Clinical Symposium.
Health disparities can affect people based on their racial or ethnic group, gender, sexual orientation, a mental or physical disability, socioeconomic status, or religion, Alvin Wells, MD, PhD, director of the department of rheumatology at Advocate Aurora Health in Franklin, Wisc., said in his presentation. But a person’s environment also plays a role – “where you live, work, play, and worship.”
Social determinants of health can affect short-term and long-term health outcomes, functioning, and quality of life, he noted. “It’s economic stability, it’s access not only to health care, but also to education. And indeed, in my lifetime, as you know, some individuals weren’t allowed to read and write. They weren’t allowed to go to schools. You didn’t get the same type of education, and so that made a dramatic impact in moving forward with future, subsequent generations.”
In a survey of executives, clinical leaders, and clinicians in NEJM Catalyst Innovations in Care Delivery, 48% said widespread disparities in care delivery were present in their organizations. According to the social psychologist James S. House, PhD, some of these disparities like race/ethnicity, socioeconomic status, genetics, and geography are fixed, while others like psychosocial, medical care/insurance, and environmental hazards are modifiable. While factors like education, work, and location might be modifiable for some patients, others don’t have the ability to make these changes, Dr. Wells explained. “It’s not that easy when you think about it.”
Within rheumatology, racial and ethnic disparities exist in rheumatoid arthritis when it comes to disease activity and use of disease-modifying antirheumatic drugs. Disparities in outcomes based on race and geographic location have also been identified for patients with systemic lupus erythematosus, lupus nephritis, and based on race in osteoarthritis and psoriatic arthritis. “Where people live, where they reside, where their zip code is,” makes a difference for patients with rheumatic diseases, Dr. Wells said.
“We’ve heard at this meeting [about] some amazing drugs in treating our patients, both [for] skin and joint disease, but not everybody has the same kind of access,” he said.
What actions can medical stakeholders take?
Health equity should be a “desirable goal” for patients who experience health disparities, but it needs to be a “continuous effort,” Dr. Wells said. Focusing on the “how” of eliminating disparities should be a focus rather than checking a box.
Pharmacoequity is also a component of health equity, according to Dr. Wells. Where a person lives can affect their health based on their neighborhood’s level of air pollution, access to green space, and food deserts, but where a person lives also affects what parts of the health system they have access to, according to an editorial published in Circulation: Cardiovascular Quality and Outcomes. When patients aren’t taking their medication, it might be because that person doesn’t have easy access to a pharmacy, noted Dr. Wells. “It really kind of blows you away when you look at the data.”
Different stakeholders in medicine can tackle various aspects of this problem. For example, health care organizations and medical schools can make long-term commitments to prioritizing health equality, Dr. Wells said. “You want to make this a part of your practice, your group, or your university. And then once you get a process in place, don’t just check that box and move on. You want to see it. If you haven’t reached your goal, you need to revamp. If you met your goal, how do [you] improve upon that?”
Medical schools can also do better at improving misconceptions about patients of different races and ethnicities. Dr. Wells cited a striking paper published in Proceedings of the National Academy of Sciences of the U.S.A. that compared false beliefs in biological differences between Black and White people held by White laypeople and medical students. The study found that 58% of laypeople and 40% of first-year medical students believed that Black people have thicker skin than White people. “It’s absolutely amazing when you think about what medical schools can do,” he said.
Increased access to care is another area for improvement, Dr. Wells noted. “If you take people who are uninsured and you look at their health once they get Medicare, the gaps begin to close between the different races.”
In terms of individual actions, Dr. Wells noted that researchers and clinicians can help to make clinical trials better represent the overall population. At your practice, “treat all your patients like a VIP.” Instead of being concerned about the cost of a treatment, ask “is your patient worth it?”
“I have one of my patients on Medicaid. She’s on a biologic drug. And one of the VPs of my hospital is on the same drug. We don’t treat them any differently.”
The private sector is also acting, Dr. Wells said. He cited Novartis’ pledge to partner with 26 historically Black colleges to improve disparities in health and education. “We need to see more of that done from corporate America.”
Are there any short-term solutions?
Eric Ruderman, MD, professor of rheumatology at Northwestern University, Chicago, commented that institutions have been forming committees and focus groups, but “not a lot of action.”
“They’re checking boxes,” he said, “which is very frustrating.” What can rheumatologists do in the short term, he asked?
Dr. Wells noted that there has been some success in using a “carrot” model of using payment models to reduce racial disparities. For example, a recent study analyzing the effects of the Comprehensive Care for Joint Replacement model highlighted the need for payment reform that incentivizes clinicians to spend wisely on patient treatment. Under a payment model that rewards clinicians for treating patients cost effectively, “if I do a great job cost effectively, I could just have more of that money back to my group,” he said.
George Martin, MD, a clinical dermatologist practicing in Maui, recalled the disparity in health care he observed as a child growing up in Philadelphia. “There’s really, within the city, there’s two different levels of health care,” he said. “There’s a tremendous disparity in the quality of the physician in hospital, and way out in the community. Because that’s the point of contact. That’s when either you’re going to prescribe a biologic, or [you’re] going to give them some aspirin and tell them go home. That’s where it starts, point of contact.”
Dr. Wells agreed that it is a big challenge, noting that cities also contribute to pollution, crowding, and other factors that adversely impact health care.
“It’s a shared responsibility. How do we solve that?” Dr. Martin asked. “And if you tell me, I’m going to give you a Nobel Prize.”
Dr. Wells reported he is a reviewer for the Journal of Racial and Ethnic Disparities.
Disparities in health care exist in every specialty. In rheumatology, health disparities look like lack of access to care and lack of education on the part of rheumatologists and their patients, according to a speaker at the 2022 Rheumatology Winter Clinical Symposium.
Health disparities can affect people based on their racial or ethnic group, gender, sexual orientation, a mental or physical disability, socioeconomic status, or religion, Alvin Wells, MD, PhD, director of the department of rheumatology at Advocate Aurora Health in Franklin, Wisc., said in his presentation. But a person’s environment also plays a role – “where you live, work, play, and worship.”
Social determinants of health can affect short-term and long-term health outcomes, functioning, and quality of life, he noted. “It’s economic stability, it’s access not only to health care, but also to education. And indeed, in my lifetime, as you know, some individuals weren’t allowed to read and write. They weren’t allowed to go to schools. You didn’t get the same type of education, and so that made a dramatic impact in moving forward with future, subsequent generations.”
In a survey of executives, clinical leaders, and clinicians in NEJM Catalyst Innovations in Care Delivery, 48% said widespread disparities in care delivery were present in their organizations. According to the social psychologist James S. House, PhD, some of these disparities like race/ethnicity, socioeconomic status, genetics, and geography are fixed, while others like psychosocial, medical care/insurance, and environmental hazards are modifiable. While factors like education, work, and location might be modifiable for some patients, others don’t have the ability to make these changes, Dr. Wells explained. “It’s not that easy when you think about it.”
Within rheumatology, racial and ethnic disparities exist in rheumatoid arthritis when it comes to disease activity and use of disease-modifying antirheumatic drugs. Disparities in outcomes based on race and geographic location have also been identified for patients with systemic lupus erythematosus, lupus nephritis, and based on race in osteoarthritis and psoriatic arthritis. “Where people live, where they reside, where their zip code is,” makes a difference for patients with rheumatic diseases, Dr. Wells said.
“We’ve heard at this meeting [about] some amazing drugs in treating our patients, both [for] skin and joint disease, but not everybody has the same kind of access,” he said.
What actions can medical stakeholders take?
Health equity should be a “desirable goal” for patients who experience health disparities, but it needs to be a “continuous effort,” Dr. Wells said. Focusing on the “how” of eliminating disparities should be a focus rather than checking a box.
Pharmacoequity is also a component of health equity, according to Dr. Wells. Where a person lives can affect their health based on their neighborhood’s level of air pollution, access to green space, and food deserts, but where a person lives also affects what parts of the health system they have access to, according to an editorial published in Circulation: Cardiovascular Quality and Outcomes. When patients aren’t taking their medication, it might be because that person doesn’t have easy access to a pharmacy, noted Dr. Wells. “It really kind of blows you away when you look at the data.”
Different stakeholders in medicine can tackle various aspects of this problem. For example, health care organizations and medical schools can make long-term commitments to prioritizing health equality, Dr. Wells said. “You want to make this a part of your practice, your group, or your university. And then once you get a process in place, don’t just check that box and move on. You want to see it. If you haven’t reached your goal, you need to revamp. If you met your goal, how do [you] improve upon that?”
Medical schools can also do better at improving misconceptions about patients of different races and ethnicities. Dr. Wells cited a striking paper published in Proceedings of the National Academy of Sciences of the U.S.A. that compared false beliefs in biological differences between Black and White people held by White laypeople and medical students. The study found that 58% of laypeople and 40% of first-year medical students believed that Black people have thicker skin than White people. “It’s absolutely amazing when you think about what medical schools can do,” he said.
Increased access to care is another area for improvement, Dr. Wells noted. “If you take people who are uninsured and you look at their health once they get Medicare, the gaps begin to close between the different races.”
In terms of individual actions, Dr. Wells noted that researchers and clinicians can help to make clinical trials better represent the overall population. At your practice, “treat all your patients like a VIP.” Instead of being concerned about the cost of a treatment, ask “is your patient worth it?”
“I have one of my patients on Medicaid. She’s on a biologic drug. And one of the VPs of my hospital is on the same drug. We don’t treat them any differently.”
The private sector is also acting, Dr. Wells said. He cited Novartis’ pledge to partner with 26 historically Black colleges to improve disparities in health and education. “We need to see more of that done from corporate America.”
Are there any short-term solutions?
Eric Ruderman, MD, professor of rheumatology at Northwestern University, Chicago, commented that institutions have been forming committees and focus groups, but “not a lot of action.”
“They’re checking boxes,” he said, “which is very frustrating.” What can rheumatologists do in the short term, he asked?
Dr. Wells noted that there has been some success in using a “carrot” model of using payment models to reduce racial disparities. For example, a recent study analyzing the effects of the Comprehensive Care for Joint Replacement model highlighted the need for payment reform that incentivizes clinicians to spend wisely on patient treatment. Under a payment model that rewards clinicians for treating patients cost effectively, “if I do a great job cost effectively, I could just have more of that money back to my group,” he said.
George Martin, MD, a clinical dermatologist practicing in Maui, recalled the disparity in health care he observed as a child growing up in Philadelphia. “There’s really, within the city, there’s two different levels of health care,” he said. “There’s a tremendous disparity in the quality of the physician in hospital, and way out in the community. Because that’s the point of contact. That’s when either you’re going to prescribe a biologic, or [you’re] going to give them some aspirin and tell them go home. That’s where it starts, point of contact.”
Dr. Wells agreed that it is a big challenge, noting that cities also contribute to pollution, crowding, and other factors that adversely impact health care.
“It’s a shared responsibility. How do we solve that?” Dr. Martin asked. “And if you tell me, I’m going to give you a Nobel Prize.”
Dr. Wells reported he is a reviewer for the Journal of Racial and Ethnic Disparities.
Disparities in health care exist in every specialty. In rheumatology, health disparities look like lack of access to care and lack of education on the part of rheumatologists and their patients, according to a speaker at the 2022 Rheumatology Winter Clinical Symposium.
Health disparities can affect people based on their racial or ethnic group, gender, sexual orientation, a mental or physical disability, socioeconomic status, or religion, Alvin Wells, MD, PhD, director of the department of rheumatology at Advocate Aurora Health in Franklin, Wisc., said in his presentation. But a person’s environment also plays a role – “where you live, work, play, and worship.”
Social determinants of health can affect short-term and long-term health outcomes, functioning, and quality of life, he noted. “It’s economic stability, it’s access not only to health care, but also to education. And indeed, in my lifetime, as you know, some individuals weren’t allowed to read and write. They weren’t allowed to go to schools. You didn’t get the same type of education, and so that made a dramatic impact in moving forward with future, subsequent generations.”
In a survey of executives, clinical leaders, and clinicians in NEJM Catalyst Innovations in Care Delivery, 48% said widespread disparities in care delivery were present in their organizations. According to the social psychologist James S. House, PhD, some of these disparities like race/ethnicity, socioeconomic status, genetics, and geography are fixed, while others like psychosocial, medical care/insurance, and environmental hazards are modifiable. While factors like education, work, and location might be modifiable for some patients, others don’t have the ability to make these changes, Dr. Wells explained. “It’s not that easy when you think about it.”
Within rheumatology, racial and ethnic disparities exist in rheumatoid arthritis when it comes to disease activity and use of disease-modifying antirheumatic drugs. Disparities in outcomes based on race and geographic location have also been identified for patients with systemic lupus erythematosus, lupus nephritis, and based on race in osteoarthritis and psoriatic arthritis. “Where people live, where they reside, where their zip code is,” makes a difference for patients with rheumatic diseases, Dr. Wells said.
“We’ve heard at this meeting [about] some amazing drugs in treating our patients, both [for] skin and joint disease, but not everybody has the same kind of access,” he said.
What actions can medical stakeholders take?
Health equity should be a “desirable goal” for patients who experience health disparities, but it needs to be a “continuous effort,” Dr. Wells said. Focusing on the “how” of eliminating disparities should be a focus rather than checking a box.
Pharmacoequity is also a component of health equity, according to Dr. Wells. Where a person lives can affect their health based on their neighborhood’s level of air pollution, access to green space, and food deserts, but where a person lives also affects what parts of the health system they have access to, according to an editorial published in Circulation: Cardiovascular Quality and Outcomes. When patients aren’t taking their medication, it might be because that person doesn’t have easy access to a pharmacy, noted Dr. Wells. “It really kind of blows you away when you look at the data.”
Different stakeholders in medicine can tackle various aspects of this problem. For example, health care organizations and medical schools can make long-term commitments to prioritizing health equality, Dr. Wells said. “You want to make this a part of your practice, your group, or your university. And then once you get a process in place, don’t just check that box and move on. You want to see it. If you haven’t reached your goal, you need to revamp. If you met your goal, how do [you] improve upon that?”
Medical schools can also do better at improving misconceptions about patients of different races and ethnicities. Dr. Wells cited a striking paper published in Proceedings of the National Academy of Sciences of the U.S.A. that compared false beliefs in biological differences between Black and White people held by White laypeople and medical students. The study found that 58% of laypeople and 40% of first-year medical students believed that Black people have thicker skin than White people. “It’s absolutely amazing when you think about what medical schools can do,” he said.
Increased access to care is another area for improvement, Dr. Wells noted. “If you take people who are uninsured and you look at their health once they get Medicare, the gaps begin to close between the different races.”
In terms of individual actions, Dr. Wells noted that researchers and clinicians can help to make clinical trials better represent the overall population. At your practice, “treat all your patients like a VIP.” Instead of being concerned about the cost of a treatment, ask “is your patient worth it?”
“I have one of my patients on Medicaid. She’s on a biologic drug. And one of the VPs of my hospital is on the same drug. We don’t treat them any differently.”
The private sector is also acting, Dr. Wells said. He cited Novartis’ pledge to partner with 26 historically Black colleges to improve disparities in health and education. “We need to see more of that done from corporate America.”
Are there any short-term solutions?
Eric Ruderman, MD, professor of rheumatology at Northwestern University, Chicago, commented that institutions have been forming committees and focus groups, but “not a lot of action.”
“They’re checking boxes,” he said, “which is very frustrating.” What can rheumatologists do in the short term, he asked?
Dr. Wells noted that there has been some success in using a “carrot” model of using payment models to reduce racial disparities. For example, a recent study analyzing the effects of the Comprehensive Care for Joint Replacement model highlighted the need for payment reform that incentivizes clinicians to spend wisely on patient treatment. Under a payment model that rewards clinicians for treating patients cost effectively, “if I do a great job cost effectively, I could just have more of that money back to my group,” he said.
George Martin, MD, a clinical dermatologist practicing in Maui, recalled the disparity in health care he observed as a child growing up in Philadelphia. “There’s really, within the city, there’s two different levels of health care,” he said. “There’s a tremendous disparity in the quality of the physician in hospital, and way out in the community. Because that’s the point of contact. That’s when either you’re going to prescribe a biologic, or [you’re] going to give them some aspirin and tell them go home. That’s where it starts, point of contact.”
Dr. Wells agreed that it is a big challenge, noting that cities also contribute to pollution, crowding, and other factors that adversely impact health care.
“It’s a shared responsibility. How do we solve that?” Dr. Martin asked. “And if you tell me, I’m going to give you a Nobel Prize.”
Dr. Wells reported he is a reviewer for the Journal of Racial and Ethnic Disparities.
FROM RWCS 2022
Epidural may lower odds of severe maternal birth complications
Use of neuraxial analgesia for vaginal delivery is associated with a 14% decreased risk for severe maternal morbidity, in part from a reduction in postpartum hemorrhage, new research shows.
The findings indicate that increasing the use of epidural or combined spinal-epidural analgesia may improve maternal health outcomes, especially for Hispanic, Black, and uninsured women who are less likely than White women to receive these interventions, according to the researchers, who published their findings online in JAMA Network Open.
About 80% of non-Hispanic White women receive neuraxial analgesia during labor in the United States, compared with 70% of non-Hispanic Black women and 65% of Hispanic women, according to birth certificate data. Among women without health insurance, half receive epidurals.
Programs that inform pregnant women about epidural use, expand Medicaid, and provide in-house obstetric anesthesia teams “may improve patient participation in clinical decision making and access to care,” study author Guohua Li, MD, DrPH, of Columbia University, New York, said in a statement about the research.
Earlier data from France showed that neuraxial analgesia is associated with reduced risk for severe postpartum hemorrhage. To examine the association between labor neuraxial analgesia and severe maternal morbidity in the United States, Dr. Li and colleagues analyzed more than 575,000 vaginal deliveries in New York hospitals between 2010 and 2017; about half (47.4%) of the women received epidurals during labor.
The researchers focused on severe maternal morbidity, including 16 complications, such as heart failure and sepsis, and five procedures, including hysterectomy and ventilation.
They also considered patient characteristics and comorbidities and hospital-related factors to identify patients who were at higher risk for injury or death.
Severe maternal morbidity occurred in 1.3% of the women. Of the 7,712 women with severe morbidity, more than one in three (35.6%) experienced postpartum hemorrhage.
The overall incidence of severe maternal morbidity was 1.3% among women who received an epidural injection and 1.4% among those who did not. In a weighted analysis, the adjusted odds ratio of severe maternal morbidity associated with epidurals was 0.86 (95% confidence interval, 0.82-0.90).
The study is limited by its observational design and does not prove causation, the authors acknowledged.
“Labor neuraxial analgesia may facilitate early evaluation and management of the third stage of labor to avoid escalation of postpartum hemorrhaging into grave complications and death,” study author Jean Guglielminotti, MD, PhD, an anesthesiologist at Columbia University, said in a statement.
Concerning trends
The Department of Health & Human Services has labeled severe maternal morbidity a public health priority. Recent data from the Centers for Disease Control and Prevention show an increase in maternal mortality rates and worsening disparities by race and ethnicity.
According to the CDC, 861 women died of maternal causes in 2020, up from 754 in 2019. The rate of maternal mortality increased from 20.1 to 23.8 deaths per 100,000 live births.
For Black women, however, the maternal mortality rate was far higher: 55.3 deaths per 100,000 live births – nearly triple the figure of 19.1 per 100,000 for White women. Between 2019 and 2020, the mortality rate increased significantly for Black and Hispanic women, but not White mothers.
Researchers affiliated with University of Toronto and the Hospital for Sick Children agreed in an accompanying editorial that more access to neuraxial labor analgesia for vaginal delivery might improve maternal health outcomes and “may be a strategy well worth pursuing in public health policy.”
The intervention is relatively safe and can “alleviate discomfort and distress,” they wrote.
Neuraxial anesthesia in surgical procedures has been shown to decrease the risk for complications like deep vein thrombosis, pulmonary embolus, transfusion requirements, and kidney failure, said editorialists Evelina Pankiv, MD; Alan Yang, MSc; and Kazuyoshi Aoyama, MD, PhD.
Benefits potentially could stem from improving blood flow, mitigating hypercoagulation, or reducing surgical stress response. But there are rare risks to consider as well, including hemorrhage, infection, and neurologic injury, they added.
Guglielminotti disclosed grants from the National Institute on Minority Health and Health Disparities. Dr. Aoyama reported receiving grants from the Perioperative Services Facilitator Grant Program and Hospital for Sick Children. The other authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Use of neuraxial analgesia for vaginal delivery is associated with a 14% decreased risk for severe maternal morbidity, in part from a reduction in postpartum hemorrhage, new research shows.
The findings indicate that increasing the use of epidural or combined spinal-epidural analgesia may improve maternal health outcomes, especially for Hispanic, Black, and uninsured women who are less likely than White women to receive these interventions, according to the researchers, who published their findings online in JAMA Network Open.
About 80% of non-Hispanic White women receive neuraxial analgesia during labor in the United States, compared with 70% of non-Hispanic Black women and 65% of Hispanic women, according to birth certificate data. Among women without health insurance, half receive epidurals.
Programs that inform pregnant women about epidural use, expand Medicaid, and provide in-house obstetric anesthesia teams “may improve patient participation in clinical decision making and access to care,” study author Guohua Li, MD, DrPH, of Columbia University, New York, said in a statement about the research.
Earlier data from France showed that neuraxial analgesia is associated with reduced risk for severe postpartum hemorrhage. To examine the association between labor neuraxial analgesia and severe maternal morbidity in the United States, Dr. Li and colleagues analyzed more than 575,000 vaginal deliveries in New York hospitals between 2010 and 2017; about half (47.4%) of the women received epidurals during labor.
The researchers focused on severe maternal morbidity, including 16 complications, such as heart failure and sepsis, and five procedures, including hysterectomy and ventilation.
They also considered patient characteristics and comorbidities and hospital-related factors to identify patients who were at higher risk for injury or death.
Severe maternal morbidity occurred in 1.3% of the women. Of the 7,712 women with severe morbidity, more than one in three (35.6%) experienced postpartum hemorrhage.
The overall incidence of severe maternal morbidity was 1.3% among women who received an epidural injection and 1.4% among those who did not. In a weighted analysis, the adjusted odds ratio of severe maternal morbidity associated with epidurals was 0.86 (95% confidence interval, 0.82-0.90).
The study is limited by its observational design and does not prove causation, the authors acknowledged.
“Labor neuraxial analgesia may facilitate early evaluation and management of the third stage of labor to avoid escalation of postpartum hemorrhaging into grave complications and death,” study author Jean Guglielminotti, MD, PhD, an anesthesiologist at Columbia University, said in a statement.
Concerning trends
The Department of Health & Human Services has labeled severe maternal morbidity a public health priority. Recent data from the Centers for Disease Control and Prevention show an increase in maternal mortality rates and worsening disparities by race and ethnicity.
According to the CDC, 861 women died of maternal causes in 2020, up from 754 in 2019. The rate of maternal mortality increased from 20.1 to 23.8 deaths per 100,000 live births.
For Black women, however, the maternal mortality rate was far higher: 55.3 deaths per 100,000 live births – nearly triple the figure of 19.1 per 100,000 for White women. Between 2019 and 2020, the mortality rate increased significantly for Black and Hispanic women, but not White mothers.
Researchers affiliated with University of Toronto and the Hospital for Sick Children agreed in an accompanying editorial that more access to neuraxial labor analgesia for vaginal delivery might improve maternal health outcomes and “may be a strategy well worth pursuing in public health policy.”
The intervention is relatively safe and can “alleviate discomfort and distress,” they wrote.
Neuraxial anesthesia in surgical procedures has been shown to decrease the risk for complications like deep vein thrombosis, pulmonary embolus, transfusion requirements, and kidney failure, said editorialists Evelina Pankiv, MD; Alan Yang, MSc; and Kazuyoshi Aoyama, MD, PhD.
Benefits potentially could stem from improving blood flow, mitigating hypercoagulation, or reducing surgical stress response. But there are rare risks to consider as well, including hemorrhage, infection, and neurologic injury, they added.
Guglielminotti disclosed grants from the National Institute on Minority Health and Health Disparities. Dr. Aoyama reported receiving grants from the Perioperative Services Facilitator Grant Program and Hospital for Sick Children. The other authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Use of neuraxial analgesia for vaginal delivery is associated with a 14% decreased risk for severe maternal morbidity, in part from a reduction in postpartum hemorrhage, new research shows.
The findings indicate that increasing the use of epidural or combined spinal-epidural analgesia may improve maternal health outcomes, especially for Hispanic, Black, and uninsured women who are less likely than White women to receive these interventions, according to the researchers, who published their findings online in JAMA Network Open.
About 80% of non-Hispanic White women receive neuraxial analgesia during labor in the United States, compared with 70% of non-Hispanic Black women and 65% of Hispanic women, according to birth certificate data. Among women without health insurance, half receive epidurals.
Programs that inform pregnant women about epidural use, expand Medicaid, and provide in-house obstetric anesthesia teams “may improve patient participation in clinical decision making and access to care,” study author Guohua Li, MD, DrPH, of Columbia University, New York, said in a statement about the research.
Earlier data from France showed that neuraxial analgesia is associated with reduced risk for severe postpartum hemorrhage. To examine the association between labor neuraxial analgesia and severe maternal morbidity in the United States, Dr. Li and colleagues analyzed more than 575,000 vaginal deliveries in New York hospitals between 2010 and 2017; about half (47.4%) of the women received epidurals during labor.
The researchers focused on severe maternal morbidity, including 16 complications, such as heart failure and sepsis, and five procedures, including hysterectomy and ventilation.
They also considered patient characteristics and comorbidities and hospital-related factors to identify patients who were at higher risk for injury or death.
Severe maternal morbidity occurred in 1.3% of the women. Of the 7,712 women with severe morbidity, more than one in three (35.6%) experienced postpartum hemorrhage.
The overall incidence of severe maternal morbidity was 1.3% among women who received an epidural injection and 1.4% among those who did not. In a weighted analysis, the adjusted odds ratio of severe maternal morbidity associated with epidurals was 0.86 (95% confidence interval, 0.82-0.90).
The study is limited by its observational design and does not prove causation, the authors acknowledged.
“Labor neuraxial analgesia may facilitate early evaluation and management of the third stage of labor to avoid escalation of postpartum hemorrhaging into grave complications and death,” study author Jean Guglielminotti, MD, PhD, an anesthesiologist at Columbia University, said in a statement.
Concerning trends
The Department of Health & Human Services has labeled severe maternal morbidity a public health priority. Recent data from the Centers for Disease Control and Prevention show an increase in maternal mortality rates and worsening disparities by race and ethnicity.
According to the CDC, 861 women died of maternal causes in 2020, up from 754 in 2019. The rate of maternal mortality increased from 20.1 to 23.8 deaths per 100,000 live births.
For Black women, however, the maternal mortality rate was far higher: 55.3 deaths per 100,000 live births – nearly triple the figure of 19.1 per 100,000 for White women. Between 2019 and 2020, the mortality rate increased significantly for Black and Hispanic women, but not White mothers.
Researchers affiliated with University of Toronto and the Hospital for Sick Children agreed in an accompanying editorial that more access to neuraxial labor analgesia for vaginal delivery might improve maternal health outcomes and “may be a strategy well worth pursuing in public health policy.”
The intervention is relatively safe and can “alleviate discomfort and distress,” they wrote.
Neuraxial anesthesia in surgical procedures has been shown to decrease the risk for complications like deep vein thrombosis, pulmonary embolus, transfusion requirements, and kidney failure, said editorialists Evelina Pankiv, MD; Alan Yang, MSc; and Kazuyoshi Aoyama, MD, PhD.
Benefits potentially could stem from improving blood flow, mitigating hypercoagulation, or reducing surgical stress response. But there are rare risks to consider as well, including hemorrhage, infection, and neurologic injury, they added.
Guglielminotti disclosed grants from the National Institute on Minority Health and Health Disparities. Dr. Aoyama reported receiving grants from the Perioperative Services Facilitator Grant Program and Hospital for Sick Children. The other authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Former APA president suspended by Columbia for ‘racist’ tweet
The university had not confirmed the suspension to this news organization by press time, but a letter from the school’s leadership notifying staff of the suspension was posted on Twitter the morning of Feb. 23 by addiction psychiatrist Jeremy Kidd, MD, who is a colleague of Dr. Lieberman’s at Columbia.
The suspension comes in the wake of Dr. Lieberman’s Feb. 21 tweet that drew immediate backlash by Twitter users who characterized it as racist and misogynist.
Dr. Lieberman, a former president of the American Psychiatric Association, reportedly deleted the tweet and his entire Twitter account soon after, according to NewsOne.
However, the tweet was captured by others, including Jack Turban, MD, a child psychiatry fellow at Stanford University. In Turban’s retweet, Dr. Lieberman commented on a tweet about a black model, noting, “whether a work of art or a freak of nature she’s a beautiful sight to behold.”
The response on Twitter was swift. “My ancestors would roll over in their graves if I refrained from commentary on how anti-Blackness shows up in ‘compliments,’” tweeted Jessica Isom, MD, MPH, a psychiatrist at Yale University.
Dr. Turban speculated that there will be no consequences for Dr. Lieberman, adding in his tweet, “He will continue to make the hiring decisions (including for faculty candidates who are women of color).”
Apology letter?
David Pagliaccio, a research scientist at the New York State Psychiatric Institute, posted what appeared to be an apology letter from Dr. Lieberman, although it could not be verified by this news organization.
In it, Dr. Lieberman was quoted as saying, “Yesterday, I tweeted from my personal account a message that was racist and sexist,” adding that prejudices he didn’t know he had held had been exposed, “and I’m deeply ashamed and very sorry.”
“I’ve hurt many, and I am beginning to understand the work ahead to make needed personal changes and over time to regain your trust,” Dr. Lieberman added.
Dr. Kidd called the suspension “absolutely the right move.” He added in his tweet that it “is only the beginning of what Columbia must do to heal & earn the trust our patients & trainees place in us every day.”
This news organization’s queries to Columbia University and to Dr. Lieberman were not returned by press time.
Dr. Lieberman is also director of the New York State Psychiatric Institute, was an advisory board member for Medscape Psychiatry and a frequent columnist for Medscape Medical News (sister organizations of MDedge.com), and was a consultant for Clinical Psychiatry.
A version of this article first appeared on Medscape.com.
The university had not confirmed the suspension to this news organization by press time, but a letter from the school’s leadership notifying staff of the suspension was posted on Twitter the morning of Feb. 23 by addiction psychiatrist Jeremy Kidd, MD, who is a colleague of Dr. Lieberman’s at Columbia.
The suspension comes in the wake of Dr. Lieberman’s Feb. 21 tweet that drew immediate backlash by Twitter users who characterized it as racist and misogynist.
Dr. Lieberman, a former president of the American Psychiatric Association, reportedly deleted the tweet and his entire Twitter account soon after, according to NewsOne.
However, the tweet was captured by others, including Jack Turban, MD, a child psychiatry fellow at Stanford University. In Turban’s retweet, Dr. Lieberman commented on a tweet about a black model, noting, “whether a work of art or a freak of nature she’s a beautiful sight to behold.”
The response on Twitter was swift. “My ancestors would roll over in their graves if I refrained from commentary on how anti-Blackness shows up in ‘compliments,’” tweeted Jessica Isom, MD, MPH, a psychiatrist at Yale University.
Dr. Turban speculated that there will be no consequences for Dr. Lieberman, adding in his tweet, “He will continue to make the hiring decisions (including for faculty candidates who are women of color).”
Apology letter?
David Pagliaccio, a research scientist at the New York State Psychiatric Institute, posted what appeared to be an apology letter from Dr. Lieberman, although it could not be verified by this news organization.
In it, Dr. Lieberman was quoted as saying, “Yesterday, I tweeted from my personal account a message that was racist and sexist,” adding that prejudices he didn’t know he had held had been exposed, “and I’m deeply ashamed and very sorry.”
“I’ve hurt many, and I am beginning to understand the work ahead to make needed personal changes and over time to regain your trust,” Dr. Lieberman added.
Dr. Kidd called the suspension “absolutely the right move.” He added in his tweet that it “is only the beginning of what Columbia must do to heal & earn the trust our patients & trainees place in us every day.”
This news organization’s queries to Columbia University and to Dr. Lieberman were not returned by press time.
Dr. Lieberman is also director of the New York State Psychiatric Institute, was an advisory board member for Medscape Psychiatry and a frequent columnist for Medscape Medical News (sister organizations of MDedge.com), and was a consultant for Clinical Psychiatry.
A version of this article first appeared on Medscape.com.
The university had not confirmed the suspension to this news organization by press time, but a letter from the school’s leadership notifying staff of the suspension was posted on Twitter the morning of Feb. 23 by addiction psychiatrist Jeremy Kidd, MD, who is a colleague of Dr. Lieberman’s at Columbia.
The suspension comes in the wake of Dr. Lieberman’s Feb. 21 tweet that drew immediate backlash by Twitter users who characterized it as racist and misogynist.
Dr. Lieberman, a former president of the American Psychiatric Association, reportedly deleted the tweet and his entire Twitter account soon after, according to NewsOne.
However, the tweet was captured by others, including Jack Turban, MD, a child psychiatry fellow at Stanford University. In Turban’s retweet, Dr. Lieberman commented on a tweet about a black model, noting, “whether a work of art or a freak of nature she’s a beautiful sight to behold.”
The response on Twitter was swift. “My ancestors would roll over in their graves if I refrained from commentary on how anti-Blackness shows up in ‘compliments,’” tweeted Jessica Isom, MD, MPH, a psychiatrist at Yale University.
Dr. Turban speculated that there will be no consequences for Dr. Lieberman, adding in his tweet, “He will continue to make the hiring decisions (including for faculty candidates who are women of color).”
Apology letter?
David Pagliaccio, a research scientist at the New York State Psychiatric Institute, posted what appeared to be an apology letter from Dr. Lieberman, although it could not be verified by this news organization.
In it, Dr. Lieberman was quoted as saying, “Yesterday, I tweeted from my personal account a message that was racist and sexist,” adding that prejudices he didn’t know he had held had been exposed, “and I’m deeply ashamed and very sorry.”
“I’ve hurt many, and I am beginning to understand the work ahead to make needed personal changes and over time to regain your trust,” Dr. Lieberman added.
Dr. Kidd called the suspension “absolutely the right move.” He added in his tweet that it “is only the beginning of what Columbia must do to heal & earn the trust our patients & trainees place in us every day.”
This news organization’s queries to Columbia University and to Dr. Lieberman were not returned by press time.
Dr. Lieberman is also director of the New York State Psychiatric Institute, was an advisory board member for Medscape Psychiatry and a frequent columnist for Medscape Medical News (sister organizations of MDedge.com), and was a consultant for Clinical Psychiatry.
A version of this article first appeared on Medscape.com.
Poor trial representation tied to worse breast cancer survival
Women with early-stage breast cancer who are poorly represented in clinical trials have worse survival than their well-represented peers, according to a real-world analysis.
The study shows that more than half of women with early breast cancer are not well represented in clinical trials because of age, comorbidities, or race, yet they receive therapies based on the results of these trials.
“The most interesting finding is that patients with comorbidities resulting in lab abnormalities that would typically exclude them from receiving medication on a trial are still frequently receiving these medications and have an almost threefold higher mortality,” Gabrielle Rocque, MD, with the division of hematology and oncology, University of Alabama at Birmingham, told this news organization.
“We need to do a deeper dive to better understand what is driving this mortality difference and test specific medications in patients with these conditions to understand the optimal treatment for this population,” Dr. Rocque added.
The study was published Feb. 1 in JCO Oncology Practice.
Many patient groups are not well represented in clinical trials, including patients of color, older patients, and those with comorbidities, and it remains unclear how treatment outcomes may differ among these patients, compared with those who are well represented in trials.
To investigate, Dr. Rocque and colleagues looked at 11,770 women diagnosed with stage I-III breast cancer between 2005 and 2015 in the American Society of Clinical Oncology CancerLinQ database.
White women between 45 and 69 years of age with no comorbid conditions were considered well represented and made up 48% of the cohort.
Non-White women and/or those younger than 45 years or older than 70 were considered under represented and made up 45% of the cohort. The unrepresented group (7%) included women with comorbidities – such as liver disease, renal insufficiency, thrombocytopenia, anemia, or uncontrolled diabetes – or concurrent cancer.
The majority of the women received a high-intensity chemotherapy regimen, including 58% of unrepresented, 66% of underrepresented, and 63% of well-represented patients.
Compared with well-represented women, unrepresented women had a higher risk of death at 5 years (adjusted hazard ratio, 2.71; 95% confidence interval, 2.08-3.52).
Overall, the team found no significant increase in the risk of death at 5 years in underrepresented vs. well-represented women (aHR, 1.19; 95% CI, 0.98-1.45). However, that risk varied with age. Among underrepresented women, those aged 70 and older had more than a twofold higher risk of 5-year mortality (aHR, 2.21), while those younger than 45 had a lower risk of 5-year mortality (aHR, 0.63), compared with those aged 45-69 years.
For three cancer subtypes, unrepresented patients had a greater than twofold higher risk of 5-year mortality, compared with well-represented patients (aHR, 2.50 for HER2-positive disease; aHR, 2.54 for HR-positive/HER2-negative disease; and aHR, 2.75 for triple-negative disease).
Underrepresented patients with HR-positive/HER2-negative disease had a 38% increased risk of 5-year mortality, compared with their well-represented peers (aHR, 1.38). However, there were no significant differences in 5-year mortality for underrepresented vs. well-represented patients with HER2-positive or triple-negative subtypes.
Risky business?
This analysis shows that unrepresented populations receive common treatment regimens at a similar rate as well-represented patients, the researchers note.
“By excluding patients with differing clinical conditions from trials but including them in the population to which drugs can be disseminated, one runs the risk of inadvertently causing injury,” the authors caution.
“To inform the practice of evidence-based medicine in an equitable manner, our findings support a need to both expand clinical trial inclusion criteria and report on clinical trial outcomes by clinical and demographic characteristics,” Dr. Rocque and colleagues conclude.
Charles Shapiro, MD, professor of medicine, hematology, and medical oncology, Icahn School of Medicine at Mount Sinai, New York, is not surprised by the findings of this study.
“We know that clinical trials are too restrictive and include only a selected population largely without comorbidities, but in the real world, people have comorbidities,” Dr. Shapiro, who was not involved in the research, told this news organization.
The study “starkly illustrates” the poorer survival of populations not represented in clinical trials.
“It could be that we need to change clinical trials, maybe ask fewer questions or maybe ask more important questions and loosen the eligibility up, because in the real world, there are people with comorbidities and people who are over 70,” Dr. Shapiro stated.
Are strides being made to change that? “Not really,” Dr. Shapiro said in an interview.
The study was supported by grants from the Robert Wood Johnson Foundation and the American Cancer Society. Dr. Rocque has served as a consultant or advisor for Pfizer; has received research funding from Carevive Systems, Genentech, and Pfizer; and has received travel, accommodations, and expenses from Carevive. Dr. Shapiro has financial relationships with UptoDate, 2nd MD, and Anthenum.
A version of this article first appeared on Medscape.com.
Women with early-stage breast cancer who are poorly represented in clinical trials have worse survival than their well-represented peers, according to a real-world analysis.
The study shows that more than half of women with early breast cancer are not well represented in clinical trials because of age, comorbidities, or race, yet they receive therapies based on the results of these trials.
“The most interesting finding is that patients with comorbidities resulting in lab abnormalities that would typically exclude them from receiving medication on a trial are still frequently receiving these medications and have an almost threefold higher mortality,” Gabrielle Rocque, MD, with the division of hematology and oncology, University of Alabama at Birmingham, told this news organization.
“We need to do a deeper dive to better understand what is driving this mortality difference and test specific medications in patients with these conditions to understand the optimal treatment for this population,” Dr. Rocque added.
The study was published Feb. 1 in JCO Oncology Practice.
Many patient groups are not well represented in clinical trials, including patients of color, older patients, and those with comorbidities, and it remains unclear how treatment outcomes may differ among these patients, compared with those who are well represented in trials.
To investigate, Dr. Rocque and colleagues looked at 11,770 women diagnosed with stage I-III breast cancer between 2005 and 2015 in the American Society of Clinical Oncology CancerLinQ database.
White women between 45 and 69 years of age with no comorbid conditions were considered well represented and made up 48% of the cohort.
Non-White women and/or those younger than 45 years or older than 70 were considered under represented and made up 45% of the cohort. The unrepresented group (7%) included women with comorbidities – such as liver disease, renal insufficiency, thrombocytopenia, anemia, or uncontrolled diabetes – or concurrent cancer.
The majority of the women received a high-intensity chemotherapy regimen, including 58% of unrepresented, 66% of underrepresented, and 63% of well-represented patients.
Compared with well-represented women, unrepresented women had a higher risk of death at 5 years (adjusted hazard ratio, 2.71; 95% confidence interval, 2.08-3.52).
Overall, the team found no significant increase in the risk of death at 5 years in underrepresented vs. well-represented women (aHR, 1.19; 95% CI, 0.98-1.45). However, that risk varied with age. Among underrepresented women, those aged 70 and older had more than a twofold higher risk of 5-year mortality (aHR, 2.21), while those younger than 45 had a lower risk of 5-year mortality (aHR, 0.63), compared with those aged 45-69 years.
For three cancer subtypes, unrepresented patients had a greater than twofold higher risk of 5-year mortality, compared with well-represented patients (aHR, 2.50 for HER2-positive disease; aHR, 2.54 for HR-positive/HER2-negative disease; and aHR, 2.75 for triple-negative disease).
Underrepresented patients with HR-positive/HER2-negative disease had a 38% increased risk of 5-year mortality, compared with their well-represented peers (aHR, 1.38). However, there were no significant differences in 5-year mortality for underrepresented vs. well-represented patients with HER2-positive or triple-negative subtypes.
Risky business?
This analysis shows that unrepresented populations receive common treatment regimens at a similar rate as well-represented patients, the researchers note.
“By excluding patients with differing clinical conditions from trials but including them in the population to which drugs can be disseminated, one runs the risk of inadvertently causing injury,” the authors caution.
“To inform the practice of evidence-based medicine in an equitable manner, our findings support a need to both expand clinical trial inclusion criteria and report on clinical trial outcomes by clinical and demographic characteristics,” Dr. Rocque and colleagues conclude.
Charles Shapiro, MD, professor of medicine, hematology, and medical oncology, Icahn School of Medicine at Mount Sinai, New York, is not surprised by the findings of this study.
“We know that clinical trials are too restrictive and include only a selected population largely without comorbidities, but in the real world, people have comorbidities,” Dr. Shapiro, who was not involved in the research, told this news organization.
The study “starkly illustrates” the poorer survival of populations not represented in clinical trials.
“It could be that we need to change clinical trials, maybe ask fewer questions or maybe ask more important questions and loosen the eligibility up, because in the real world, there are people with comorbidities and people who are over 70,” Dr. Shapiro stated.
Are strides being made to change that? “Not really,” Dr. Shapiro said in an interview.
The study was supported by grants from the Robert Wood Johnson Foundation and the American Cancer Society. Dr. Rocque has served as a consultant or advisor for Pfizer; has received research funding from Carevive Systems, Genentech, and Pfizer; and has received travel, accommodations, and expenses from Carevive. Dr. Shapiro has financial relationships with UptoDate, 2nd MD, and Anthenum.
A version of this article first appeared on Medscape.com.
Women with early-stage breast cancer who are poorly represented in clinical trials have worse survival than their well-represented peers, according to a real-world analysis.
The study shows that more than half of women with early breast cancer are not well represented in clinical trials because of age, comorbidities, or race, yet they receive therapies based on the results of these trials.
“The most interesting finding is that patients with comorbidities resulting in lab abnormalities that would typically exclude them from receiving medication on a trial are still frequently receiving these medications and have an almost threefold higher mortality,” Gabrielle Rocque, MD, with the division of hematology and oncology, University of Alabama at Birmingham, told this news organization.
“We need to do a deeper dive to better understand what is driving this mortality difference and test specific medications in patients with these conditions to understand the optimal treatment for this population,” Dr. Rocque added.
The study was published Feb. 1 in JCO Oncology Practice.
Many patient groups are not well represented in clinical trials, including patients of color, older patients, and those with comorbidities, and it remains unclear how treatment outcomes may differ among these patients, compared with those who are well represented in trials.
To investigate, Dr. Rocque and colleagues looked at 11,770 women diagnosed with stage I-III breast cancer between 2005 and 2015 in the American Society of Clinical Oncology CancerLinQ database.
White women between 45 and 69 years of age with no comorbid conditions were considered well represented and made up 48% of the cohort.
Non-White women and/or those younger than 45 years or older than 70 were considered under represented and made up 45% of the cohort. The unrepresented group (7%) included women with comorbidities – such as liver disease, renal insufficiency, thrombocytopenia, anemia, or uncontrolled diabetes – or concurrent cancer.
The majority of the women received a high-intensity chemotherapy regimen, including 58% of unrepresented, 66% of underrepresented, and 63% of well-represented patients.
Compared with well-represented women, unrepresented women had a higher risk of death at 5 years (adjusted hazard ratio, 2.71; 95% confidence interval, 2.08-3.52).
Overall, the team found no significant increase in the risk of death at 5 years in underrepresented vs. well-represented women (aHR, 1.19; 95% CI, 0.98-1.45). However, that risk varied with age. Among underrepresented women, those aged 70 and older had more than a twofold higher risk of 5-year mortality (aHR, 2.21), while those younger than 45 had a lower risk of 5-year mortality (aHR, 0.63), compared with those aged 45-69 years.
For three cancer subtypes, unrepresented patients had a greater than twofold higher risk of 5-year mortality, compared with well-represented patients (aHR, 2.50 for HER2-positive disease; aHR, 2.54 for HR-positive/HER2-negative disease; and aHR, 2.75 for triple-negative disease).
Underrepresented patients with HR-positive/HER2-negative disease had a 38% increased risk of 5-year mortality, compared with their well-represented peers (aHR, 1.38). However, there were no significant differences in 5-year mortality for underrepresented vs. well-represented patients with HER2-positive or triple-negative subtypes.
Risky business?
This analysis shows that unrepresented populations receive common treatment regimens at a similar rate as well-represented patients, the researchers note.
“By excluding patients with differing clinical conditions from trials but including them in the population to which drugs can be disseminated, one runs the risk of inadvertently causing injury,” the authors caution.
“To inform the practice of evidence-based medicine in an equitable manner, our findings support a need to both expand clinical trial inclusion criteria and report on clinical trial outcomes by clinical and demographic characteristics,” Dr. Rocque and colleagues conclude.
Charles Shapiro, MD, professor of medicine, hematology, and medical oncology, Icahn School of Medicine at Mount Sinai, New York, is not surprised by the findings of this study.
“We know that clinical trials are too restrictive and include only a selected population largely without comorbidities, but in the real world, people have comorbidities,” Dr. Shapiro, who was not involved in the research, told this news organization.
The study “starkly illustrates” the poorer survival of populations not represented in clinical trials.
“It could be that we need to change clinical trials, maybe ask fewer questions or maybe ask more important questions and loosen the eligibility up, because in the real world, there are people with comorbidities and people who are over 70,” Dr. Shapiro stated.
Are strides being made to change that? “Not really,” Dr. Shapiro said in an interview.
The study was supported by grants from the Robert Wood Johnson Foundation and the American Cancer Society. Dr. Rocque has served as a consultant or advisor for Pfizer; has received research funding from Carevive Systems, Genentech, and Pfizer; and has received travel, accommodations, and expenses from Carevive. Dr. Shapiro has financial relationships with UptoDate, 2nd MD, and Anthenum.
A version of this article first appeared on Medscape.com.
FROM JCO ONCOLOGY PRACTICE