User login
Nationwide study questions routine long-term beta-blocker post MI
Current American and European guidelines recommending long-term beta-blocker therapy following an acute MI appear to be obsolete in the modern reperfusion era, suggests an analysis of Danish registry data.
Those guidelines are based on old randomized trials of beta-blocker therapy conducted prior to introduction of routine percutaneous coronary intervention and modern multidrug optimal medical therapy for acute MI. There have been no prospective controlled studies in the reperfusion era. And a new Danish national observational study strongly suggests it’s time to reexamine the beta-blocker recommendation, Anders Holt, MD, said at the virtual annual congress of the European Society of Cardiology.
“Stable, optimally treated MI patients do not seem to benefit from beta-blocker treatment exceeding 3 months post hospitalization – bearing in mind this doesn’t apply to patients with other indications for beta-blockers, like heart failure or atrial fibrillation,” said Dr. Holt of Copenhagen University Hospital.
His analysis of Danish national registry data on more than 30,000 patients hospitalized for acute MI during 2003-2018 earned him the annual ESC Young Investigator Award in Population Science.
“This was a crisp and clear presentation of a very creative use of observational epidemiology to try to understand the length of therapy that may or may not be appropriate,” commented award session cochair Paul M. Ridker, MD, director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital and professor of medicine at Harvard Medical School, both in Boston.
Dr. Holt reported on 30,177 patients optimally treated for a first MI in Danish hospitals during 2003-2018, none of whom had a prior indication or contraindication for beta-blocker therapy. “Optimally treated” meant they underwent percutaneous coronary revascularization and were discharged on a statin and aspirin. As a study requirement, all had to be stable 90 days post hospitalization, at which point 24,770 of the patients were on long-term beta-blocker therapy, and 5,407 (18%) were not. The two groups were comparable in terms of age, sex, comorbidities, and baseline medications. All patients were followed through the registries for a maximum of 3 years, the duration of beta-blocker therapy post MI recommended in American Heart Association/American College of Cardiology guidelines. (The Danish Society of Cardiology recommends 2 years.)
At 3 years post MI, there was no between-group difference in a composite outcome comprising cardiovascular death, recurrent MI, heart failure, stroke, angina, or a cardiac procedure, with a rate of 22.9% in the beta-blocker group and 21.6% in patients not on long-term beta-blocker therapy. The rate of recurrent MI was identical at 6.7% in both groups. Cardiovascular death occurred during 3 years of follow-up in 1.4% of patients on beta-blocker therapy and 1.7% who weren’t, a nonsignificant difference.
“We saw no evidence of any cardioprotective effect, but no increased risk of adverse events resulting in hospitalization, either,” Dr. Holt observed. “I would like to acknowledge that no evidence of effect does not necessarily equal evidence of no effect, but even if there was an effect we can with fair certainty say that it’s probably quite minimal.”
He noted that the Danish registry data indicates that each year since 2012 has shown a growing trend for Danish patients to dispense with long-term beta-blocker therapy after an acute MI.
“This might indicate we are nudging toward a change in practice, where more physicians are thinking that long-term beta-blocker therapy might not be indicated for all MI patients in the reperfusion era,” according to Dr. Holt.
Asked by the four-judge award panel about the possibility of unmeasured confounding in this observational study, Dr Holt responded: “I would be very cautious about asking patients to stop beta-blocker therapy after 3 months just based on this observational data. We can’t speak to causality in an observational study.” But he added that “well-designed observational studies provide valuable data regarding this topic and should not be ignored. They should possibly influence the guidelines and the designs for upcoming randomized trials.”
He conducted several supplementary analyses designed to address the possibility of unevenly distributed unmeasured confounding in the registry study. These analyses proved reassuring. A positive exposure control analysis compared 3-year outcomes in patients who remained on long-term statin therapy and those who didn’t. As expected, outcomes were significantly better in those who did: a 3-year composite outcome rate of 22.1%, compared with 32.1% in patients not on a statin; a cardiovascular death rate of 1.3% with and 2.1% without statin therapy; a recurrent MI rate of 6.6%, compared with 10.1% without a statin; and a 2.8% all-cause mortality with and 5.4% without statin therapy.
In contrast, all-cause mortality was unaffected by whether or not patients were on long-term beta-blocker therapy. And in a negative exposure outcome analysis, no association was found between beta-blocker therapy and the risk of hospitalization for pneumonia, as to be expected if the beta-blocker and no-beta-blocker groups were comparable in key respects.
Dr. Holt reported having no financial conflicts regarding his study.
Current American and European guidelines recommending long-term beta-blocker therapy following an acute MI appear to be obsolete in the modern reperfusion era, suggests an analysis of Danish registry data.
Those guidelines are based on old randomized trials of beta-blocker therapy conducted prior to introduction of routine percutaneous coronary intervention and modern multidrug optimal medical therapy for acute MI. There have been no prospective controlled studies in the reperfusion era. And a new Danish national observational study strongly suggests it’s time to reexamine the beta-blocker recommendation, Anders Holt, MD, said at the virtual annual congress of the European Society of Cardiology.
“Stable, optimally treated MI patients do not seem to benefit from beta-blocker treatment exceeding 3 months post hospitalization – bearing in mind this doesn’t apply to patients with other indications for beta-blockers, like heart failure or atrial fibrillation,” said Dr. Holt of Copenhagen University Hospital.
His analysis of Danish national registry data on more than 30,000 patients hospitalized for acute MI during 2003-2018 earned him the annual ESC Young Investigator Award in Population Science.
“This was a crisp and clear presentation of a very creative use of observational epidemiology to try to understand the length of therapy that may or may not be appropriate,” commented award session cochair Paul M. Ridker, MD, director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital and professor of medicine at Harvard Medical School, both in Boston.
Dr. Holt reported on 30,177 patients optimally treated for a first MI in Danish hospitals during 2003-2018, none of whom had a prior indication or contraindication for beta-blocker therapy. “Optimally treated” meant they underwent percutaneous coronary revascularization and were discharged on a statin and aspirin. As a study requirement, all had to be stable 90 days post hospitalization, at which point 24,770 of the patients were on long-term beta-blocker therapy, and 5,407 (18%) were not. The two groups were comparable in terms of age, sex, comorbidities, and baseline medications. All patients were followed through the registries for a maximum of 3 years, the duration of beta-blocker therapy post MI recommended in American Heart Association/American College of Cardiology guidelines. (The Danish Society of Cardiology recommends 2 years.)
At 3 years post MI, there was no between-group difference in a composite outcome comprising cardiovascular death, recurrent MI, heart failure, stroke, angina, or a cardiac procedure, with a rate of 22.9% in the beta-blocker group and 21.6% in patients not on long-term beta-blocker therapy. The rate of recurrent MI was identical at 6.7% in both groups. Cardiovascular death occurred during 3 years of follow-up in 1.4% of patients on beta-blocker therapy and 1.7% who weren’t, a nonsignificant difference.
“We saw no evidence of any cardioprotective effect, but no increased risk of adverse events resulting in hospitalization, either,” Dr. Holt observed. “I would like to acknowledge that no evidence of effect does not necessarily equal evidence of no effect, but even if there was an effect we can with fair certainty say that it’s probably quite minimal.”
He noted that the Danish registry data indicates that each year since 2012 has shown a growing trend for Danish patients to dispense with long-term beta-blocker therapy after an acute MI.
“This might indicate we are nudging toward a change in practice, where more physicians are thinking that long-term beta-blocker therapy might not be indicated for all MI patients in the reperfusion era,” according to Dr. Holt.
Asked by the four-judge award panel about the possibility of unmeasured confounding in this observational study, Dr Holt responded: “I would be very cautious about asking patients to stop beta-blocker therapy after 3 months just based on this observational data. We can’t speak to causality in an observational study.” But he added that “well-designed observational studies provide valuable data regarding this topic and should not be ignored. They should possibly influence the guidelines and the designs for upcoming randomized trials.”
He conducted several supplementary analyses designed to address the possibility of unevenly distributed unmeasured confounding in the registry study. These analyses proved reassuring. A positive exposure control analysis compared 3-year outcomes in patients who remained on long-term statin therapy and those who didn’t. As expected, outcomes were significantly better in those who did: a 3-year composite outcome rate of 22.1%, compared with 32.1% in patients not on a statin; a cardiovascular death rate of 1.3% with and 2.1% without statin therapy; a recurrent MI rate of 6.6%, compared with 10.1% without a statin; and a 2.8% all-cause mortality with and 5.4% without statin therapy.
In contrast, all-cause mortality was unaffected by whether or not patients were on long-term beta-blocker therapy. And in a negative exposure outcome analysis, no association was found between beta-blocker therapy and the risk of hospitalization for pneumonia, as to be expected if the beta-blocker and no-beta-blocker groups were comparable in key respects.
Dr. Holt reported having no financial conflicts regarding his study.
Current American and European guidelines recommending long-term beta-blocker therapy following an acute MI appear to be obsolete in the modern reperfusion era, suggests an analysis of Danish registry data.
Those guidelines are based on old randomized trials of beta-blocker therapy conducted prior to introduction of routine percutaneous coronary intervention and modern multidrug optimal medical therapy for acute MI. There have been no prospective controlled studies in the reperfusion era. And a new Danish national observational study strongly suggests it’s time to reexamine the beta-blocker recommendation, Anders Holt, MD, said at the virtual annual congress of the European Society of Cardiology.
“Stable, optimally treated MI patients do not seem to benefit from beta-blocker treatment exceeding 3 months post hospitalization – bearing in mind this doesn’t apply to patients with other indications for beta-blockers, like heart failure or atrial fibrillation,” said Dr. Holt of Copenhagen University Hospital.
His analysis of Danish national registry data on more than 30,000 patients hospitalized for acute MI during 2003-2018 earned him the annual ESC Young Investigator Award in Population Science.
“This was a crisp and clear presentation of a very creative use of observational epidemiology to try to understand the length of therapy that may or may not be appropriate,” commented award session cochair Paul M. Ridker, MD, director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital and professor of medicine at Harvard Medical School, both in Boston.
Dr. Holt reported on 30,177 patients optimally treated for a first MI in Danish hospitals during 2003-2018, none of whom had a prior indication or contraindication for beta-blocker therapy. “Optimally treated” meant they underwent percutaneous coronary revascularization and were discharged on a statin and aspirin. As a study requirement, all had to be stable 90 days post hospitalization, at which point 24,770 of the patients were on long-term beta-blocker therapy, and 5,407 (18%) were not. The two groups were comparable in terms of age, sex, comorbidities, and baseline medications. All patients were followed through the registries for a maximum of 3 years, the duration of beta-blocker therapy post MI recommended in American Heart Association/American College of Cardiology guidelines. (The Danish Society of Cardiology recommends 2 years.)
At 3 years post MI, there was no between-group difference in a composite outcome comprising cardiovascular death, recurrent MI, heart failure, stroke, angina, or a cardiac procedure, with a rate of 22.9% in the beta-blocker group and 21.6% in patients not on long-term beta-blocker therapy. The rate of recurrent MI was identical at 6.7% in both groups. Cardiovascular death occurred during 3 years of follow-up in 1.4% of patients on beta-blocker therapy and 1.7% who weren’t, a nonsignificant difference.
“We saw no evidence of any cardioprotective effect, but no increased risk of adverse events resulting in hospitalization, either,” Dr. Holt observed. “I would like to acknowledge that no evidence of effect does not necessarily equal evidence of no effect, but even if there was an effect we can with fair certainty say that it’s probably quite minimal.”
He noted that the Danish registry data indicates that each year since 2012 has shown a growing trend for Danish patients to dispense with long-term beta-blocker therapy after an acute MI.
“This might indicate we are nudging toward a change in practice, where more physicians are thinking that long-term beta-blocker therapy might not be indicated for all MI patients in the reperfusion era,” according to Dr. Holt.
Asked by the four-judge award panel about the possibility of unmeasured confounding in this observational study, Dr Holt responded: “I would be very cautious about asking patients to stop beta-blocker therapy after 3 months just based on this observational data. We can’t speak to causality in an observational study.” But he added that “well-designed observational studies provide valuable data regarding this topic and should not be ignored. They should possibly influence the guidelines and the designs for upcoming randomized trials.”
He conducted several supplementary analyses designed to address the possibility of unevenly distributed unmeasured confounding in the registry study. These analyses proved reassuring. A positive exposure control analysis compared 3-year outcomes in patients who remained on long-term statin therapy and those who didn’t. As expected, outcomes were significantly better in those who did: a 3-year composite outcome rate of 22.1%, compared with 32.1% in patients not on a statin; a cardiovascular death rate of 1.3% with and 2.1% without statin therapy; a recurrent MI rate of 6.6%, compared with 10.1% without a statin; and a 2.8% all-cause mortality with and 5.4% without statin therapy.
In contrast, all-cause mortality was unaffected by whether or not patients were on long-term beta-blocker therapy. And in a negative exposure outcome analysis, no association was found between beta-blocker therapy and the risk of hospitalization for pneumonia, as to be expected if the beta-blocker and no-beta-blocker groups were comparable in key respects.
Dr. Holt reported having no financial conflicts regarding his study.
FROM ESC CONGRESS 2020
Pesco-Mediterranean diet, fasting ‘ideal’ to reduce CVD risk
A Pesco-Mediterranean diet consisting of plants, legumes, nuts, whole grains, extra-virgin olive oil (EVOO), moderate amounts of dairy products, and fish and/or seafood, together with intermittent fasting (also called time-restricted eating), can reduce risk for cardiovascular disease (CVD), according to a new review.
The authors presented the research and conceptual underpinnings of this approach, which “proposes that following a Pesco-Mediterranean diet with time-restricted eating is evidence-based and ideal for reducing cardiovascular risk,” study coauthor Sarah Smith, PhD, RN, of Saint Luke’s Mid America Heart Institute, Kansas City, Mo., said in an interview.
The review was published online September 14 in the Journal of the American College of Cardiology.
‘Omnivore’s dilemma’
A host of epidemiologic studies and randomized clinical trials support an association between the traditional Mediterranean diet and lower risk for all-cause and CVD mortality, coronary heart disease, metabolic syndrome, neurodegenerative diseases, and other adverse outcome. The diet has been subsequently endorsed by several sets of guidelines, including those from the Department of Health & Human Services and the Department of Agriculture, and the 2019 American Heart Association/American College of Cardiology primary prevention guidelines.
“Although humans are omnivores and can subsist on a myriad of foods, the ideal diet for health remains a dilemma for many people,” lead author James H. O’Keefe, MD, director of preventive cardiology at Saint Luke’s, said in a news release.
“Plant-rich diets reduce CVD risk; however, veganism is difficult to follow and can result in important nutrient deficiencies,” he stated.
On the other hand, “the standard American diet is high in red meat, especially processed meat from animals raised in inhumane conditions, fed unnatural foods, and often treated with hormones and antibiotics,” the authors pointed out.
Together with overconsumption of red meat, sugar and processed food contribute to poor health outcomes, Dr. Smith noted.
The review was designed to present the Pesco-Mediterranean diet as “a solution to the ‘omnivore’s dilemma’ about what to eat,” said Dr. O’Keefe.
Study coauthor Ibrahim M. Saeed, MD, a cardiologist at Saint Luke’s, added that the research “attempts to emphasize the results of landmark prospective trials that highlight good, healthy eating options rather than just [foods that people would] want to avoid.”
Key components
The traditional Mediterranean diet includes “unrestricted use of EVOO,” but the quality of the olive oil is “crucial” and it must be unrefined and cold pressed, the authors emphasized.
The “highly bioactive” polyphenols likely “underlie EVOO’s numerous cardiometabolic benefits,” the researchers wrote, noting that the 2014 PREDIMED trial provided “first-level scientific evidence of [EVOO’s] cardioprotective effects [if used] within the context of the Mediterranean diet.”
The authors recommend “generous use” of EVOO in salad dressings and vegetable dishes, pasta, rice, fish, sauces, or legumes.
They also review the role of tree nuts, noting that they are “nutrient-dense foods rich in unsaturated fats, fiber, protein, polyphenols, phytosterols, tocopherols, and nonsodium minerals” and have been shown beneficial in CVD prevention.
Legumes play a “central role” in the Mediterranean diet and are an “excellent source” of vegetable protein, folate, magnesium, and fiber. Legume consumption is associated with lowered risk for CVD, as well as improved blood glucose, cholesterol, blood pressure, and body weight, the authors stated.
Whole grains like barley, whole oats, brown rice, and quinoa are likewise central components of the traditional Mediterranean diet. The authors warned that refined grain products and commercial precooked pasta or pizza should be “consumed only in small amounts.”
Window of time
In time-restricted eating (which is one type of intermittent fasting), the daily intake of food is limited to a window of time, usually 6-12 hours each day, the authors explained.
When done regularly, this type of eating has been shown to both decrease intra-abdominal adipose tissue and reduce free-radical production. Additionally, it “elicits powerful cellular responses” that may reduce risks for systemic inflammation, diabetes, CVD, cancer, and neurodegenerative diseases.
However, the authors warned, the evidence supporting time-restricted eating is still preliminary.
‘Let food be thy medicine’
Andrew Freeman, MD, cochair of the ACC’s nutrition & lifestyle work group, cautioned that many American plant-based Mediterranean diets often include large amount of feta cheese and lamb and foods are often “heavily doused” in olive oil, while the traditional Mediterranean diet consists primarily of greens and lentils and is plant based.
“The goal would be to have a whole grain and leafy vegetables as the center of the meal, and – if an animal product such as fish is included – it should be limited to as little as possible and used as the garnish rather than the main dish,” he stated.
Moreover, fish are often exposed to large amount of toxins, heavy metals, and microplastics, so “don’t overdo eating fish,” he advised.
Dr. Freeman said that intermittent fasting “has a lot of promise and no harm” and concentrating food consumption during a shorter period in the day instead of “grazing throughout the day” will reduce constant snacking. “But don’t gorge yourself during those hours,” he warned.
Dr. Freeman concluded by citing the guidance of Hippocrates: “Let food be thy medicine.
“There’s some real truth to that,” he added.
No source of funding was listed. Dr. Smith and Dr. Freeman disclosed no relevant financial relationships. Dr. O’Keefe has a major ownership interest in CardioTabs, a supplement company that sells some products containing omega-3 fatty acids.
A version of this article originally appeared on Medscape.com.
A Pesco-Mediterranean diet consisting of plants, legumes, nuts, whole grains, extra-virgin olive oil (EVOO), moderate amounts of dairy products, and fish and/or seafood, together with intermittent fasting (also called time-restricted eating), can reduce risk for cardiovascular disease (CVD), according to a new review.
The authors presented the research and conceptual underpinnings of this approach, which “proposes that following a Pesco-Mediterranean diet with time-restricted eating is evidence-based and ideal for reducing cardiovascular risk,” study coauthor Sarah Smith, PhD, RN, of Saint Luke’s Mid America Heart Institute, Kansas City, Mo., said in an interview.
The review was published online September 14 in the Journal of the American College of Cardiology.
‘Omnivore’s dilemma’
A host of epidemiologic studies and randomized clinical trials support an association between the traditional Mediterranean diet and lower risk for all-cause and CVD mortality, coronary heart disease, metabolic syndrome, neurodegenerative diseases, and other adverse outcome. The diet has been subsequently endorsed by several sets of guidelines, including those from the Department of Health & Human Services and the Department of Agriculture, and the 2019 American Heart Association/American College of Cardiology primary prevention guidelines.
“Although humans are omnivores and can subsist on a myriad of foods, the ideal diet for health remains a dilemma for many people,” lead author James H. O’Keefe, MD, director of preventive cardiology at Saint Luke’s, said in a news release.
“Plant-rich diets reduce CVD risk; however, veganism is difficult to follow and can result in important nutrient deficiencies,” he stated.
On the other hand, “the standard American diet is high in red meat, especially processed meat from animals raised in inhumane conditions, fed unnatural foods, and often treated with hormones and antibiotics,” the authors pointed out.
Together with overconsumption of red meat, sugar and processed food contribute to poor health outcomes, Dr. Smith noted.
The review was designed to present the Pesco-Mediterranean diet as “a solution to the ‘omnivore’s dilemma’ about what to eat,” said Dr. O’Keefe.
Study coauthor Ibrahim M. Saeed, MD, a cardiologist at Saint Luke’s, added that the research “attempts to emphasize the results of landmark prospective trials that highlight good, healthy eating options rather than just [foods that people would] want to avoid.”
Key components
The traditional Mediterranean diet includes “unrestricted use of EVOO,” but the quality of the olive oil is “crucial” and it must be unrefined and cold pressed, the authors emphasized.
The “highly bioactive” polyphenols likely “underlie EVOO’s numerous cardiometabolic benefits,” the researchers wrote, noting that the 2014 PREDIMED trial provided “first-level scientific evidence of [EVOO’s] cardioprotective effects [if used] within the context of the Mediterranean diet.”
The authors recommend “generous use” of EVOO in salad dressings and vegetable dishes, pasta, rice, fish, sauces, or legumes.
They also review the role of tree nuts, noting that they are “nutrient-dense foods rich in unsaturated fats, fiber, protein, polyphenols, phytosterols, tocopherols, and nonsodium minerals” and have been shown beneficial in CVD prevention.
Legumes play a “central role” in the Mediterranean diet and are an “excellent source” of vegetable protein, folate, magnesium, and fiber. Legume consumption is associated with lowered risk for CVD, as well as improved blood glucose, cholesterol, blood pressure, and body weight, the authors stated.
Whole grains like barley, whole oats, brown rice, and quinoa are likewise central components of the traditional Mediterranean diet. The authors warned that refined grain products and commercial precooked pasta or pizza should be “consumed only in small amounts.”
Window of time
In time-restricted eating (which is one type of intermittent fasting), the daily intake of food is limited to a window of time, usually 6-12 hours each day, the authors explained.
When done regularly, this type of eating has been shown to both decrease intra-abdominal adipose tissue and reduce free-radical production. Additionally, it “elicits powerful cellular responses” that may reduce risks for systemic inflammation, diabetes, CVD, cancer, and neurodegenerative diseases.
However, the authors warned, the evidence supporting time-restricted eating is still preliminary.
‘Let food be thy medicine’
Andrew Freeman, MD, cochair of the ACC’s nutrition & lifestyle work group, cautioned that many American plant-based Mediterranean diets often include large amount of feta cheese and lamb and foods are often “heavily doused” in olive oil, while the traditional Mediterranean diet consists primarily of greens and lentils and is plant based.
“The goal would be to have a whole grain and leafy vegetables as the center of the meal, and – if an animal product such as fish is included – it should be limited to as little as possible and used as the garnish rather than the main dish,” he stated.
Moreover, fish are often exposed to large amount of toxins, heavy metals, and microplastics, so “don’t overdo eating fish,” he advised.
Dr. Freeman said that intermittent fasting “has a lot of promise and no harm” and concentrating food consumption during a shorter period in the day instead of “grazing throughout the day” will reduce constant snacking. “But don’t gorge yourself during those hours,” he warned.
Dr. Freeman concluded by citing the guidance of Hippocrates: “Let food be thy medicine.
“There’s some real truth to that,” he added.
No source of funding was listed. Dr. Smith and Dr. Freeman disclosed no relevant financial relationships. Dr. O’Keefe has a major ownership interest in CardioTabs, a supplement company that sells some products containing omega-3 fatty acids.
A version of this article originally appeared on Medscape.com.
A Pesco-Mediterranean diet consisting of plants, legumes, nuts, whole grains, extra-virgin olive oil (EVOO), moderate amounts of dairy products, and fish and/or seafood, together with intermittent fasting (also called time-restricted eating), can reduce risk for cardiovascular disease (CVD), according to a new review.
The authors presented the research and conceptual underpinnings of this approach, which “proposes that following a Pesco-Mediterranean diet with time-restricted eating is evidence-based and ideal for reducing cardiovascular risk,” study coauthor Sarah Smith, PhD, RN, of Saint Luke’s Mid America Heart Institute, Kansas City, Mo., said in an interview.
The review was published online September 14 in the Journal of the American College of Cardiology.
‘Omnivore’s dilemma’
A host of epidemiologic studies and randomized clinical trials support an association between the traditional Mediterranean diet and lower risk for all-cause and CVD mortality, coronary heart disease, metabolic syndrome, neurodegenerative diseases, and other adverse outcome. The diet has been subsequently endorsed by several sets of guidelines, including those from the Department of Health & Human Services and the Department of Agriculture, and the 2019 American Heart Association/American College of Cardiology primary prevention guidelines.
“Although humans are omnivores and can subsist on a myriad of foods, the ideal diet for health remains a dilemma for many people,” lead author James H. O’Keefe, MD, director of preventive cardiology at Saint Luke’s, said in a news release.
“Plant-rich diets reduce CVD risk; however, veganism is difficult to follow and can result in important nutrient deficiencies,” he stated.
On the other hand, “the standard American diet is high in red meat, especially processed meat from animals raised in inhumane conditions, fed unnatural foods, and often treated with hormones and antibiotics,” the authors pointed out.
Together with overconsumption of red meat, sugar and processed food contribute to poor health outcomes, Dr. Smith noted.
The review was designed to present the Pesco-Mediterranean diet as “a solution to the ‘omnivore’s dilemma’ about what to eat,” said Dr. O’Keefe.
Study coauthor Ibrahim M. Saeed, MD, a cardiologist at Saint Luke’s, added that the research “attempts to emphasize the results of landmark prospective trials that highlight good, healthy eating options rather than just [foods that people would] want to avoid.”
Key components
The traditional Mediterranean diet includes “unrestricted use of EVOO,” but the quality of the olive oil is “crucial” and it must be unrefined and cold pressed, the authors emphasized.
The “highly bioactive” polyphenols likely “underlie EVOO’s numerous cardiometabolic benefits,” the researchers wrote, noting that the 2014 PREDIMED trial provided “first-level scientific evidence of [EVOO’s] cardioprotective effects [if used] within the context of the Mediterranean diet.”
The authors recommend “generous use” of EVOO in salad dressings and vegetable dishes, pasta, rice, fish, sauces, or legumes.
They also review the role of tree nuts, noting that they are “nutrient-dense foods rich in unsaturated fats, fiber, protein, polyphenols, phytosterols, tocopherols, and nonsodium minerals” and have been shown beneficial in CVD prevention.
Legumes play a “central role” in the Mediterranean diet and are an “excellent source” of vegetable protein, folate, magnesium, and fiber. Legume consumption is associated with lowered risk for CVD, as well as improved blood glucose, cholesterol, blood pressure, and body weight, the authors stated.
Whole grains like barley, whole oats, brown rice, and quinoa are likewise central components of the traditional Mediterranean diet. The authors warned that refined grain products and commercial precooked pasta or pizza should be “consumed only in small amounts.”
Window of time
In time-restricted eating (which is one type of intermittent fasting), the daily intake of food is limited to a window of time, usually 6-12 hours each day, the authors explained.
When done regularly, this type of eating has been shown to both decrease intra-abdominal adipose tissue and reduce free-radical production. Additionally, it “elicits powerful cellular responses” that may reduce risks for systemic inflammation, diabetes, CVD, cancer, and neurodegenerative diseases.
However, the authors warned, the evidence supporting time-restricted eating is still preliminary.
‘Let food be thy medicine’
Andrew Freeman, MD, cochair of the ACC’s nutrition & lifestyle work group, cautioned that many American plant-based Mediterranean diets often include large amount of feta cheese and lamb and foods are often “heavily doused” in olive oil, while the traditional Mediterranean diet consists primarily of greens and lentils and is plant based.
“The goal would be to have a whole grain and leafy vegetables as the center of the meal, and – if an animal product such as fish is included – it should be limited to as little as possible and used as the garnish rather than the main dish,” he stated.
Moreover, fish are often exposed to large amount of toxins, heavy metals, and microplastics, so “don’t overdo eating fish,” he advised.
Dr. Freeman said that intermittent fasting “has a lot of promise and no harm” and concentrating food consumption during a shorter period in the day instead of “grazing throughout the day” will reduce constant snacking. “But don’t gorge yourself during those hours,” he warned.
Dr. Freeman concluded by citing the guidance of Hippocrates: “Let food be thy medicine.
“There’s some real truth to that,” he added.
No source of funding was listed. Dr. Smith and Dr. Freeman disclosed no relevant financial relationships. Dr. O’Keefe has a major ownership interest in CardioTabs, a supplement company that sells some products containing omega-3 fatty acids.
A version of this article originally appeared on Medscape.com.
Liberalized European sports cardiology guidelines break new ground
New guidelines on sports cardiology from the European Society of Cardiology break fresh ground by green-lighting participation in vigorous competitive sports by selected patients with stable coronary artery disease, heart failure, or mild arrhythmias.

These liberalized guidelines, released at the virtual annual congress of the European Society of Cardiology, thus move well beyond the standard exercise advice to engage in about 150 minutes per week of moderate physical activity, typically defined as brisk walking or its equivalent.
The guidelines reflect a conviction that exercise is powerful medicine for patients with cardiovascular disease and also affords a means to help curb the epidemics of diabetes and obesity that drive cardiovascular risk, according to Antonio Pelliccia, MD, who cochaired the 24-member task force of European and American experts that developed the guidelines.
In a session highlighting the new sports cardiology guidelines, Mats Borjesson, MD, head of the Center for Health and Performance at Gothenburg (Sweden) University, summarized the section devoted to patients with stable coronary artery disease: “If you have established CAD and a low risk of adverse events during exercise, you are eligible for high-intensity exercise and competitive sports. But if you have persistent ischemia despite medical treatment, or symptoms, then you’re only eligible for leisure-time subthreshold activity.”
Dr. Pelliccia put this new recommendation into context.
“We are not talking anymore in this particular disease just about cardiac rehabilitation or leisure-time activity, but we are also opening the border and talking about competitive sports activity in selected patients where you have the evidence for low risk of exercise-induced adverse events. This is a major achievement now for what is the major disease in our adult population,” said Dr. Pelliccia, chief of cardiology at the Institute of Sports Medicine and Science at the Italian National Olympic Committee and professor of sports cardiology at La Sapienza University of Rome.
The recommendation for individualized consideration of all types of exercise, even including vigorous competitive sports, in low-risk patients with CAD gets a class IIa, level of evidence (LOE) C recommendation in the new guidelines. That’s a big step down from a ringing class Ia endorsement, but since sports cardiology is a relatively young field with little evidence that’s based on randomized trials, the guidelines are rife with many other class IIa, LOE C recommendations as well.
“The level of evidence is rather low, so these guidelines are very much the personal perspective of the expert panel,” explained Martin Halle, MD, professor and head of the department of prevention, rehabilitation, and sports cardiology at Technical University of Munich.
The high-risk features for exercise-induced cardiac adverse events in patients with longstanding stable CAD, as cited in the guidelines, include a critical coronary stenosis, defined as a more than 70% lesion in a major coronary artery or a greater than 50% stenosis in the left main, and/or a fractional flow reserve score of less than 0.8; a left ventricular ejection fraction of 50% or less with wall-motion abnormalities; inducible myocardial ischemia on maximal exercise testing; nonsustained ventricular tachycardia; polymorphic or very frequent ventricular premature beats at rest and during maximum stress; and a recent acute coronary syndrome (ACS). These features call for an exercise prescription tailored to remain below the patient’s angina and ischemia thresholds.
“It’s important for cardiologists out there to understand that we definitely need a maximal exercise test. In somebody who is running and has an ACS and then wants to start running again, 200 watts on an ergometer is too low. We have to push them up to the end, and then if everything is okay – left ventricular function is okay, no ischemia, no arrhythmias under exercise testing – then it’s fine,” Dr. Halle said.
Dr. Pelliccia added that close follow-up is needed, because this is an evolving disease.”
Exercise and heart failure
Massimo F. Piepoli, MD, PhD, noted that the guidelines give a class IIb, LOE C recommendation for consideration of high-intensity recreational endurance and power sports in patients with heart failure with either midrange or preserved ejection fraction, provided they are stable, asymptomatic, on optimal guideline-directed medical therapy, and without abnormalities on a maximal exercise stress test.

However, such intense physical activity is not recommended in patients with heart failure with reduced ejection fraction, regardless of their symptom status, added Dr. Piepoli of Guglielmo da Saliceto Hospital in Placenza, Italy.
“We’re talking here, I think for the first time, about possible competitive sports participation in individuals with heart failure, depending on their clinical condition. We are really opening the barriers to sports participation, even in these patients in whom we never thought of it before,” Dr. Pelliccia observed.
Valvular heart disease and exercise
Guidelines panelist Sabiha Gati, MRCP, PhD, said asymptomatic individuals with mild valvular abnormalities can participate in all recreational and competitive sports; that’s a class I, LOE C recommendation.

“Moderate regurgitant lesions are better tolerated than stenotic lesions, and those with preserved systolic function, good functional capacity, without any exercise-induced arrhythmias or ischemia or abnormal hemodynamic response are considered to be low risk and can participate in all sports,” added Dr. Gati, a cardiologist at Royal Brompton Hospital, London.
The two most common valvular abnormalities encountered in clinical practice are bicuspid aortic valve and mitral valve prolapse. Dr. Gati noted that, while mitral valve prolapse has a benign prognosis in the great majority of affected individuals, the presence of specific features indicative of increased risk for sudden cardiac death precludes participation in strenuous exercise. These include T-wave inversion in the inferior leads on a 12-lead ECG, long QT, bileaflet mitral valve prolapse, basal inferolateral wall fibrosis, severe mitral regurgitation, or a family history of sudden cardiac death.
Bicuspid aortic valve has a prevalence of 1%-2% in the general population. It can be associated with aortic stenosis, aortic regurgitation, and increased risk of ascending aortic aneurysm and dissection. Since it remains unclear whether intensive exercise accelerates aortic dilatation, a cautious approach to sports participation is recommended in patients with an ascending aorta above the normal limit of 40 mm, she said.
The 80-page ESC sports cardiology guidelines, published online simultaneously with their presentation, cover a broad range of additional topics, including exercise recommendations for the general public, for the elderly, as well as for patients with cardiomyopathies, adult congenital heart disease, arrhythmias, and channelopathies. Gaps in evidence are also highlighted.
SOURCE: Pelliccia A. ESC 2020 and Eur Heart J. 2020 Aug 29. doi: 10.1093/eurheartj/ehaa605.
New guidelines on sports cardiology from the European Society of Cardiology break fresh ground by green-lighting participation in vigorous competitive sports by selected patients with stable coronary artery disease, heart failure, or mild arrhythmias.
These liberalized guidelines, released at the virtual annual congress of the European Society of Cardiology, thus move well beyond the standard exercise advice to engage in about 150 minutes per week of moderate physical activity, typically defined as brisk walking or its equivalent.
The guidelines reflect a conviction that exercise is powerful medicine for patients with cardiovascular disease and also affords a means to help curb the epidemics of diabetes and obesity that drive cardiovascular risk, according to Antonio Pelliccia, MD, who cochaired the 24-member task force of European and American experts that developed the guidelines.
In a session highlighting the new sports cardiology guidelines, Mats Borjesson, MD, head of the Center for Health and Performance at Gothenburg (Sweden) University, summarized the section devoted to patients with stable coronary artery disease: “If you have established CAD and a low risk of adverse events during exercise, you are eligible for high-intensity exercise and competitive sports. But if you have persistent ischemia despite medical treatment, or symptoms, then you’re only eligible for leisure-time subthreshold activity.”
Dr. Pelliccia put this new recommendation into context.
“We are not talking anymore in this particular disease just about cardiac rehabilitation or leisure-time activity, but we are also opening the border and talking about competitive sports activity in selected patients where you have the evidence for low risk of exercise-induced adverse events. This is a major achievement now for what is the major disease in our adult population,” said Dr. Pelliccia, chief of cardiology at the Institute of Sports Medicine and Science at the Italian National Olympic Committee and professor of sports cardiology at La Sapienza University of Rome.
The recommendation for individualized consideration of all types of exercise, even including vigorous competitive sports, in low-risk patients with CAD gets a class IIa, level of evidence (LOE) C recommendation in the new guidelines. That’s a big step down from a ringing class Ia endorsement, but since sports cardiology is a relatively young field with little evidence that’s based on randomized trials, the guidelines are rife with many other class IIa, LOE C recommendations as well.
“The level of evidence is rather low, so these guidelines are very much the personal perspective of the expert panel,” explained Martin Halle, MD, professor and head of the department of prevention, rehabilitation, and sports cardiology at Technical University of Munich.
The high-risk features for exercise-induced cardiac adverse events in patients with longstanding stable CAD, as cited in the guidelines, include a critical coronary stenosis, defined as a more than 70% lesion in a major coronary artery or a greater than 50% stenosis in the left main, and/or a fractional flow reserve score of less than 0.8; a left ventricular ejection fraction of 50% or less with wall-motion abnormalities; inducible myocardial ischemia on maximal exercise testing; nonsustained ventricular tachycardia; polymorphic or very frequent ventricular premature beats at rest and during maximum stress; and a recent acute coronary syndrome (ACS). These features call for an exercise prescription tailored to remain below the patient’s angina and ischemia thresholds.
“It’s important for cardiologists out there to understand that we definitely need a maximal exercise test. In somebody who is running and has an ACS and then wants to start running again, 200 watts on an ergometer is too low. We have to push them up to the end, and then if everything is okay – left ventricular function is okay, no ischemia, no arrhythmias under exercise testing – then it’s fine,” Dr. Halle said.
Dr. Pelliccia added that close follow-up is needed, because this is an evolving disease.”
Exercise and heart failure
Massimo F. Piepoli, MD, PhD, noted that the guidelines give a class IIb, LOE C recommendation for consideration of high-intensity recreational endurance and power sports in patients with heart failure with either midrange or preserved ejection fraction, provided they are stable, asymptomatic, on optimal guideline-directed medical therapy, and without abnormalities on a maximal exercise stress test.
However, such intense physical activity is not recommended in patients with heart failure with reduced ejection fraction, regardless of their symptom status, added Dr. Piepoli of Guglielmo da Saliceto Hospital in Placenza, Italy.
“We’re talking here, I think for the first time, about possible competitive sports participation in individuals with heart failure, depending on their clinical condition. We are really opening the barriers to sports participation, even in these patients in whom we never thought of it before,” Dr. Pelliccia observed.
Valvular heart disease and exercise
Guidelines panelist Sabiha Gati, MRCP, PhD, said asymptomatic individuals with mild valvular abnormalities can participate in all recreational and competitive sports; that’s a class I, LOE C recommendation.
“Moderate regurgitant lesions are better tolerated than stenotic lesions, and those with preserved systolic function, good functional capacity, without any exercise-induced arrhythmias or ischemia or abnormal hemodynamic response are considered to be low risk and can participate in all sports,” added Dr. Gati, a cardiologist at Royal Brompton Hospital, London.
The two most common valvular abnormalities encountered in clinical practice are bicuspid aortic valve and mitral valve prolapse. Dr. Gati noted that, while mitral valve prolapse has a benign prognosis in the great majority of affected individuals, the presence of specific features indicative of increased risk for sudden cardiac death precludes participation in strenuous exercise. These include T-wave inversion in the inferior leads on a 12-lead ECG, long QT, bileaflet mitral valve prolapse, basal inferolateral wall fibrosis, severe mitral regurgitation, or a family history of sudden cardiac death.
Bicuspid aortic valve has a prevalence of 1%-2% in the general population. It can be associated with aortic stenosis, aortic regurgitation, and increased risk of ascending aortic aneurysm and dissection. Since it remains unclear whether intensive exercise accelerates aortic dilatation, a cautious approach to sports participation is recommended in patients with an ascending aorta above the normal limit of 40 mm, she said.
The 80-page ESC sports cardiology guidelines, published online simultaneously with their presentation, cover a broad range of additional topics, including exercise recommendations for the general public, for the elderly, as well as for patients with cardiomyopathies, adult congenital heart disease, arrhythmias, and channelopathies. Gaps in evidence are also highlighted.
SOURCE: Pelliccia A. ESC 2020 and Eur Heart J. 2020 Aug 29. doi: 10.1093/eurheartj/ehaa605.
New guidelines on sports cardiology from the European Society of Cardiology break fresh ground by green-lighting participation in vigorous competitive sports by selected patients with stable coronary artery disease, heart failure, or mild arrhythmias.
These liberalized guidelines, released at the virtual annual congress of the European Society of Cardiology, thus move well beyond the standard exercise advice to engage in about 150 minutes per week of moderate physical activity, typically defined as brisk walking or its equivalent.
The guidelines reflect a conviction that exercise is powerful medicine for patients with cardiovascular disease and also affords a means to help curb the epidemics of diabetes and obesity that drive cardiovascular risk, according to Antonio Pelliccia, MD, who cochaired the 24-member task force of European and American experts that developed the guidelines.
In a session highlighting the new sports cardiology guidelines, Mats Borjesson, MD, head of the Center for Health and Performance at Gothenburg (Sweden) University, summarized the section devoted to patients with stable coronary artery disease: “If you have established CAD and a low risk of adverse events during exercise, you are eligible for high-intensity exercise and competitive sports. But if you have persistent ischemia despite medical treatment, or symptoms, then you’re only eligible for leisure-time subthreshold activity.”
Dr. Pelliccia put this new recommendation into context.
“We are not talking anymore in this particular disease just about cardiac rehabilitation or leisure-time activity, but we are also opening the border and talking about competitive sports activity in selected patients where you have the evidence for low risk of exercise-induced adverse events. This is a major achievement now for what is the major disease in our adult population,” said Dr. Pelliccia, chief of cardiology at the Institute of Sports Medicine and Science at the Italian National Olympic Committee and professor of sports cardiology at La Sapienza University of Rome.
The recommendation for individualized consideration of all types of exercise, even including vigorous competitive sports, in low-risk patients with CAD gets a class IIa, level of evidence (LOE) C recommendation in the new guidelines. That’s a big step down from a ringing class Ia endorsement, but since sports cardiology is a relatively young field with little evidence that’s based on randomized trials, the guidelines are rife with many other class IIa, LOE C recommendations as well.
“The level of evidence is rather low, so these guidelines are very much the personal perspective of the expert panel,” explained Martin Halle, MD, professor and head of the department of prevention, rehabilitation, and sports cardiology at Technical University of Munich.
The high-risk features for exercise-induced cardiac adverse events in patients with longstanding stable CAD, as cited in the guidelines, include a critical coronary stenosis, defined as a more than 70% lesion in a major coronary artery or a greater than 50% stenosis in the left main, and/or a fractional flow reserve score of less than 0.8; a left ventricular ejection fraction of 50% or less with wall-motion abnormalities; inducible myocardial ischemia on maximal exercise testing; nonsustained ventricular tachycardia; polymorphic or very frequent ventricular premature beats at rest and during maximum stress; and a recent acute coronary syndrome (ACS). These features call for an exercise prescription tailored to remain below the patient’s angina and ischemia thresholds.
“It’s important for cardiologists out there to understand that we definitely need a maximal exercise test. In somebody who is running and has an ACS and then wants to start running again, 200 watts on an ergometer is too low. We have to push them up to the end, and then if everything is okay – left ventricular function is okay, no ischemia, no arrhythmias under exercise testing – then it’s fine,” Dr. Halle said.
Dr. Pelliccia added that close follow-up is needed, because this is an evolving disease.”
Exercise and heart failure
Massimo F. Piepoli, MD, PhD, noted that the guidelines give a class IIb, LOE C recommendation for consideration of high-intensity recreational endurance and power sports in patients with heart failure with either midrange or preserved ejection fraction, provided they are stable, asymptomatic, on optimal guideline-directed medical therapy, and without abnormalities on a maximal exercise stress test.
However, such intense physical activity is not recommended in patients with heart failure with reduced ejection fraction, regardless of their symptom status, added Dr. Piepoli of Guglielmo da Saliceto Hospital in Placenza, Italy.
“We’re talking here, I think for the first time, about possible competitive sports participation in individuals with heart failure, depending on their clinical condition. We are really opening the barriers to sports participation, even in these patients in whom we never thought of it before,” Dr. Pelliccia observed.
Valvular heart disease and exercise
Guidelines panelist Sabiha Gati, MRCP, PhD, said asymptomatic individuals with mild valvular abnormalities can participate in all recreational and competitive sports; that’s a class I, LOE C recommendation.
“Moderate regurgitant lesions are better tolerated than stenotic lesions, and those with preserved systolic function, good functional capacity, without any exercise-induced arrhythmias or ischemia or abnormal hemodynamic response are considered to be low risk and can participate in all sports,” added Dr. Gati, a cardiologist at Royal Brompton Hospital, London.
The two most common valvular abnormalities encountered in clinical practice are bicuspid aortic valve and mitral valve prolapse. Dr. Gati noted that, while mitral valve prolapse has a benign prognosis in the great majority of affected individuals, the presence of specific features indicative of increased risk for sudden cardiac death precludes participation in strenuous exercise. These include T-wave inversion in the inferior leads on a 12-lead ECG, long QT, bileaflet mitral valve prolapse, basal inferolateral wall fibrosis, severe mitral regurgitation, or a family history of sudden cardiac death.
Bicuspid aortic valve has a prevalence of 1%-2% in the general population. It can be associated with aortic stenosis, aortic regurgitation, and increased risk of ascending aortic aneurysm and dissection. Since it remains unclear whether intensive exercise accelerates aortic dilatation, a cautious approach to sports participation is recommended in patients with an ascending aorta above the normal limit of 40 mm, she said.
The 80-page ESC sports cardiology guidelines, published online simultaneously with their presentation, cover a broad range of additional topics, including exercise recommendations for the general public, for the elderly, as well as for patients with cardiomyopathies, adult congenital heart disease, arrhythmias, and channelopathies. Gaps in evidence are also highlighted.
SOURCE: Pelliccia A. ESC 2020 and Eur Heart J. 2020 Aug 29. doi: 10.1093/eurheartj/ehaa605.
FROM ESC CONGRESS 2020
Biologics for psoriasis may also reduce coronary plaque
Biologics used as treatment for psoriasis may also help reduce lipid-rich necrotic core (LRNC), a high-risk plaque associated with cardiovascular events, recent research from a prospective, observational study suggests.
Cardiac CT scans performed on patients with psoriasis 1 year after starting biologic therapy revealed a reduction in LRNC, compared with patients who were not receiving biologics, according to Harry Choi, MD, of the National Heart, Lung, and Blood Institute at the National Institutes of Health and colleagues. The association with reduction in LRNC and biologic therapy remained significant when adjusted for type of biologic. “These findings demonstrate that LRNC may be modulated by the control of systemic inflammation,” the researchers wrote in their study, published Sept. 15 in Circulation: Cardiovascular Imaging.
Dr. Choi and colleagues evaluated 289 patients with psoriasis within the Psoriasis Atherosclerosis and Cardiometabolic Disease Initiative cohort. The patients had a mean age of 50 years and a mean body mass index of 29.4 kg/m2, as well as a mean Psoriasis Area and Severity Index (PASI) score of 6.0. At baseline, 29% of patients had hypertension, 41% had hyperlipidemia, their mean Framingham risk score was 1.9, and a three-quarters (212 of 289) had mild to moderate psoriasis.
Changes in LRNC were observed at 1 year, compared with baseline prior to and after receiving biologic therapy (124 patients) in comparison with patients who did not undergo biologic therapy (85 patients). Biologic therapies were grouped by type, which included anti–tumor necrosis factor (anti-TNF), anti–interleukin (IL)–12/23, and anti–IL-17 biologics.
There were a significant associations between LRNC and Framingham risk score (standardized beta coefficient, 0.12; 95% confidence interval, 0.00-0.15; P = .045) and severity of psoriasis (beta, 0.13; 95% CI, 0.01-0.26; P = .029) at baseline.
Key findings
The researchers found a significant reduction in LRNC 1 year after patients began biologic therapy (median, 2.97 mm2; interquartile range, 1.99-4.66), compared with baseline (median, 3.12 mm2; IQR, 1.84-4.35) (P = .028), while patients who did not receive biologic therapy had nonsignificantly higher LRNC after 1 year (median, 3.12 mm2; IQR, 1.82-4.60), compared with baseline measurements (median, 3.34 mm2; IQR, 2.04–4.74) (P = .06).
The results remained significant after the researchers adjusted for psoriasis severity, Framingham risk score, BMI, use of statins (beta, −0.09; 95% CI, −0.01 to −0.18; P = .033). Significant reductions in LRNC also remained when analyzing patients receiving anti-TNF, anti–IL-12/23, and anti–IL-17 biologics independently, and there were no significant between-group differences in reduction of LRNC.
The potential of biologics for improving vascular health
Discussing the study results in a press release from the American Heart Association, senior author Nehal N. Mehta, MD, MSCE, FAHA, chief of the Lab of Inflammation and Cardiometabolic Diseases at the NHLBI at NIH, compared the effect biologic therapy had on coronary plaque reduction with that of statins.
“There is approximately 6%-8% reduction in coronary plaque following therapy with statins. Similarly, our treatment with biologic therapy reduced coronary plaque by the same amount after one year. These findings suggest that biologic therapy to treat psoriasis may be just as beneficial as statin therapy on heart arteries,” Dr. Mehta said in the release.
In an interview, Nieca Goldberg, MD, medical director of NYU Women’s Heart Program at NYU Langone Health, echoed Dr. Mehta’s commments and said psoriasis carries the “potential to treat two conditions with the same drug.”
“We know conditions such as psoriatic arthritis and rheumatoid arthritis cause chronic inflammation. Chronic inflammation causes injury to blood vessels and high-risk coronary plaque. Individuals with these inflammatory conditions are at high risk for heart attack,” she said. “This study shows that biologic treatment for psoriatic arthritis can reduce the presence of high-risk plaque. It shows the potential to treat chronic inflammation and high-risk coronary plaque.”
While the results show an association between use of biologics and LRNC reduction, the study design was observational and patients had a short follow-up period. Dr. Goldberg noted more studies are needed to evaluate the effect of biologics on reducing cardiovascular events such as a myocardial infarction.
“We have never before been able to show healing of an inflamed plaque like this in humans. Biologic therapy reduces systemic inflammation and immune activation, and it has a favorable impact on improving overall vascular health,” Dr. Mehta said in the press release. “Imagine if we can treat both psoriasis and coronary heart disease with one therapy – that is the question to be asked in future studies.”
This study was funded with support from the NHLBI Intramural Research Program and the NIH Medical Research Scholars Program at the National Institutes of Health. One investigator reports financial relationships with numerous pharmaceutical companies. The other authors report no relevant conflicts of interest. Dr. Mehta also reports numerous such relationships. Dr. Goldberg reports no relevant conflicts of interest.
SOURCE: Choi H et al. Circ Cardiovasc Imaging. 2020 Sep;13(9):e011199.
Biologics used as treatment for psoriasis may also help reduce lipid-rich necrotic core (LRNC), a high-risk plaque associated with cardiovascular events, recent research from a prospective, observational study suggests.
Cardiac CT scans performed on patients with psoriasis 1 year after starting biologic therapy revealed a reduction in LRNC, compared with patients who were not receiving biologics, according to Harry Choi, MD, of the National Heart, Lung, and Blood Institute at the National Institutes of Health and colleagues. The association with reduction in LRNC and biologic therapy remained significant when adjusted for type of biologic. “These findings demonstrate that LRNC may be modulated by the control of systemic inflammation,” the researchers wrote in their study, published Sept. 15 in Circulation: Cardiovascular Imaging.
Dr. Choi and colleagues evaluated 289 patients with psoriasis within the Psoriasis Atherosclerosis and Cardiometabolic Disease Initiative cohort. The patients had a mean age of 50 years and a mean body mass index of 29.4 kg/m2, as well as a mean Psoriasis Area and Severity Index (PASI) score of 6.0. At baseline, 29% of patients had hypertension, 41% had hyperlipidemia, their mean Framingham risk score was 1.9, and a three-quarters (212 of 289) had mild to moderate psoriasis.
Changes in LRNC were observed at 1 year, compared with baseline prior to and after receiving biologic therapy (124 patients) in comparison with patients who did not undergo biologic therapy (85 patients). Biologic therapies were grouped by type, which included anti–tumor necrosis factor (anti-TNF), anti–interleukin (IL)–12/23, and anti–IL-17 biologics.
There were a significant associations between LRNC and Framingham risk score (standardized beta coefficient, 0.12; 95% confidence interval, 0.00-0.15; P = .045) and severity of psoriasis (beta, 0.13; 95% CI, 0.01-0.26; P = .029) at baseline.
Key findings
The researchers found a significant reduction in LRNC 1 year after patients began biologic therapy (median, 2.97 mm2; interquartile range, 1.99-4.66), compared with baseline (median, 3.12 mm2; IQR, 1.84-4.35) (P = .028), while patients who did not receive biologic therapy had nonsignificantly higher LRNC after 1 year (median, 3.12 mm2; IQR, 1.82-4.60), compared with baseline measurements (median, 3.34 mm2; IQR, 2.04–4.74) (P = .06).
The results remained significant after the researchers adjusted for psoriasis severity, Framingham risk score, BMI, use of statins (beta, −0.09; 95% CI, −0.01 to −0.18; P = .033). Significant reductions in LRNC also remained when analyzing patients receiving anti-TNF, anti–IL-12/23, and anti–IL-17 biologics independently, and there were no significant between-group differences in reduction of LRNC.
The potential of biologics for improving vascular health
Discussing the study results in a press release from the American Heart Association, senior author Nehal N. Mehta, MD, MSCE, FAHA, chief of the Lab of Inflammation and Cardiometabolic Diseases at the NHLBI at NIH, compared the effect biologic therapy had on coronary plaque reduction with that of statins.
“There is approximately 6%-8% reduction in coronary plaque following therapy with statins. Similarly, our treatment with biologic therapy reduced coronary plaque by the same amount after one year. These findings suggest that biologic therapy to treat psoriasis may be just as beneficial as statin therapy on heart arteries,” Dr. Mehta said in the release.
In an interview, Nieca Goldberg, MD, medical director of NYU Women’s Heart Program at NYU Langone Health, echoed Dr. Mehta’s commments and said psoriasis carries the “potential to treat two conditions with the same drug.”
“We know conditions such as psoriatic arthritis and rheumatoid arthritis cause chronic inflammation. Chronic inflammation causes injury to blood vessels and high-risk coronary plaque. Individuals with these inflammatory conditions are at high risk for heart attack,” she said. “This study shows that biologic treatment for psoriatic arthritis can reduce the presence of high-risk plaque. It shows the potential to treat chronic inflammation and high-risk coronary plaque.”
While the results show an association between use of biologics and LRNC reduction, the study design was observational and patients had a short follow-up period. Dr. Goldberg noted more studies are needed to evaluate the effect of biologics on reducing cardiovascular events such as a myocardial infarction.
“We have never before been able to show healing of an inflamed plaque like this in humans. Biologic therapy reduces systemic inflammation and immune activation, and it has a favorable impact on improving overall vascular health,” Dr. Mehta said in the press release. “Imagine if we can treat both psoriasis and coronary heart disease with one therapy – that is the question to be asked in future studies.”
This study was funded with support from the NHLBI Intramural Research Program and the NIH Medical Research Scholars Program at the National Institutes of Health. One investigator reports financial relationships with numerous pharmaceutical companies. The other authors report no relevant conflicts of interest. Dr. Mehta also reports numerous such relationships. Dr. Goldberg reports no relevant conflicts of interest.
SOURCE: Choi H et al. Circ Cardiovasc Imaging. 2020 Sep;13(9):e011199.
Biologics used as treatment for psoriasis may also help reduce lipid-rich necrotic core (LRNC), a high-risk plaque associated with cardiovascular events, recent research from a prospective, observational study suggests.
Cardiac CT scans performed on patients with psoriasis 1 year after starting biologic therapy revealed a reduction in LRNC, compared with patients who were not receiving biologics, according to Harry Choi, MD, of the National Heart, Lung, and Blood Institute at the National Institutes of Health and colleagues. The association with reduction in LRNC and biologic therapy remained significant when adjusted for type of biologic. “These findings demonstrate that LRNC may be modulated by the control of systemic inflammation,” the researchers wrote in their study, published Sept. 15 in Circulation: Cardiovascular Imaging.
Dr. Choi and colleagues evaluated 289 patients with psoriasis within the Psoriasis Atherosclerosis and Cardiometabolic Disease Initiative cohort. The patients had a mean age of 50 years and a mean body mass index of 29.4 kg/m2, as well as a mean Psoriasis Area and Severity Index (PASI) score of 6.0. At baseline, 29% of patients had hypertension, 41% had hyperlipidemia, their mean Framingham risk score was 1.9, and a three-quarters (212 of 289) had mild to moderate psoriasis.
Changes in LRNC were observed at 1 year, compared with baseline prior to and after receiving biologic therapy (124 patients) in comparison with patients who did not undergo biologic therapy (85 patients). Biologic therapies were grouped by type, which included anti–tumor necrosis factor (anti-TNF), anti–interleukin (IL)–12/23, and anti–IL-17 biologics.
There were a significant associations between LRNC and Framingham risk score (standardized beta coefficient, 0.12; 95% confidence interval, 0.00-0.15; P = .045) and severity of psoriasis (beta, 0.13; 95% CI, 0.01-0.26; P = .029) at baseline.
Key findings
The researchers found a significant reduction in LRNC 1 year after patients began biologic therapy (median, 2.97 mm2; interquartile range, 1.99-4.66), compared with baseline (median, 3.12 mm2; IQR, 1.84-4.35) (P = .028), while patients who did not receive biologic therapy had nonsignificantly higher LRNC after 1 year (median, 3.12 mm2; IQR, 1.82-4.60), compared with baseline measurements (median, 3.34 mm2; IQR, 2.04–4.74) (P = .06).
The results remained significant after the researchers adjusted for psoriasis severity, Framingham risk score, BMI, use of statins (beta, −0.09; 95% CI, −0.01 to −0.18; P = .033). Significant reductions in LRNC also remained when analyzing patients receiving anti-TNF, anti–IL-12/23, and anti–IL-17 biologics independently, and there were no significant between-group differences in reduction of LRNC.
The potential of biologics for improving vascular health
Discussing the study results in a press release from the American Heart Association, senior author Nehal N. Mehta, MD, MSCE, FAHA, chief of the Lab of Inflammation and Cardiometabolic Diseases at the NHLBI at NIH, compared the effect biologic therapy had on coronary plaque reduction with that of statins.
“There is approximately 6%-8% reduction in coronary plaque following therapy with statins. Similarly, our treatment with biologic therapy reduced coronary plaque by the same amount after one year. These findings suggest that biologic therapy to treat psoriasis may be just as beneficial as statin therapy on heart arteries,” Dr. Mehta said in the release.
In an interview, Nieca Goldberg, MD, medical director of NYU Women’s Heart Program at NYU Langone Health, echoed Dr. Mehta’s commments and said psoriasis carries the “potential to treat two conditions with the same drug.”
“We know conditions such as psoriatic arthritis and rheumatoid arthritis cause chronic inflammation. Chronic inflammation causes injury to blood vessels and high-risk coronary plaque. Individuals with these inflammatory conditions are at high risk for heart attack,” she said. “This study shows that biologic treatment for psoriatic arthritis can reduce the presence of high-risk plaque. It shows the potential to treat chronic inflammation and high-risk coronary plaque.”
While the results show an association between use of biologics and LRNC reduction, the study design was observational and patients had a short follow-up period. Dr. Goldberg noted more studies are needed to evaluate the effect of biologics on reducing cardiovascular events such as a myocardial infarction.
“We have never before been able to show healing of an inflamed plaque like this in humans. Biologic therapy reduces systemic inflammation and immune activation, and it has a favorable impact on improving overall vascular health,” Dr. Mehta said in the press release. “Imagine if we can treat both psoriasis and coronary heart disease with one therapy – that is the question to be asked in future studies.”
This study was funded with support from the NHLBI Intramural Research Program and the NIH Medical Research Scholars Program at the National Institutes of Health. One investigator reports financial relationships with numerous pharmaceutical companies. The other authors report no relevant conflicts of interest. Dr. Mehta also reports numerous such relationships. Dr. Goldberg reports no relevant conflicts of interest.
SOURCE: Choi H et al. Circ Cardiovasc Imaging. 2020 Sep;13(9):e011199.
FROM CIRCULATION: CARDIOVASCULAR IMAGING
Diffuse idiopathic skeletal hyperostosis heart risk higher than expected
More people with diffuse idiopathic skeletal hyperostosis (DISH) develop cardiovascular disease (CVD) than is predicted by the Framingham Risk Score, results of an observational study have shown.
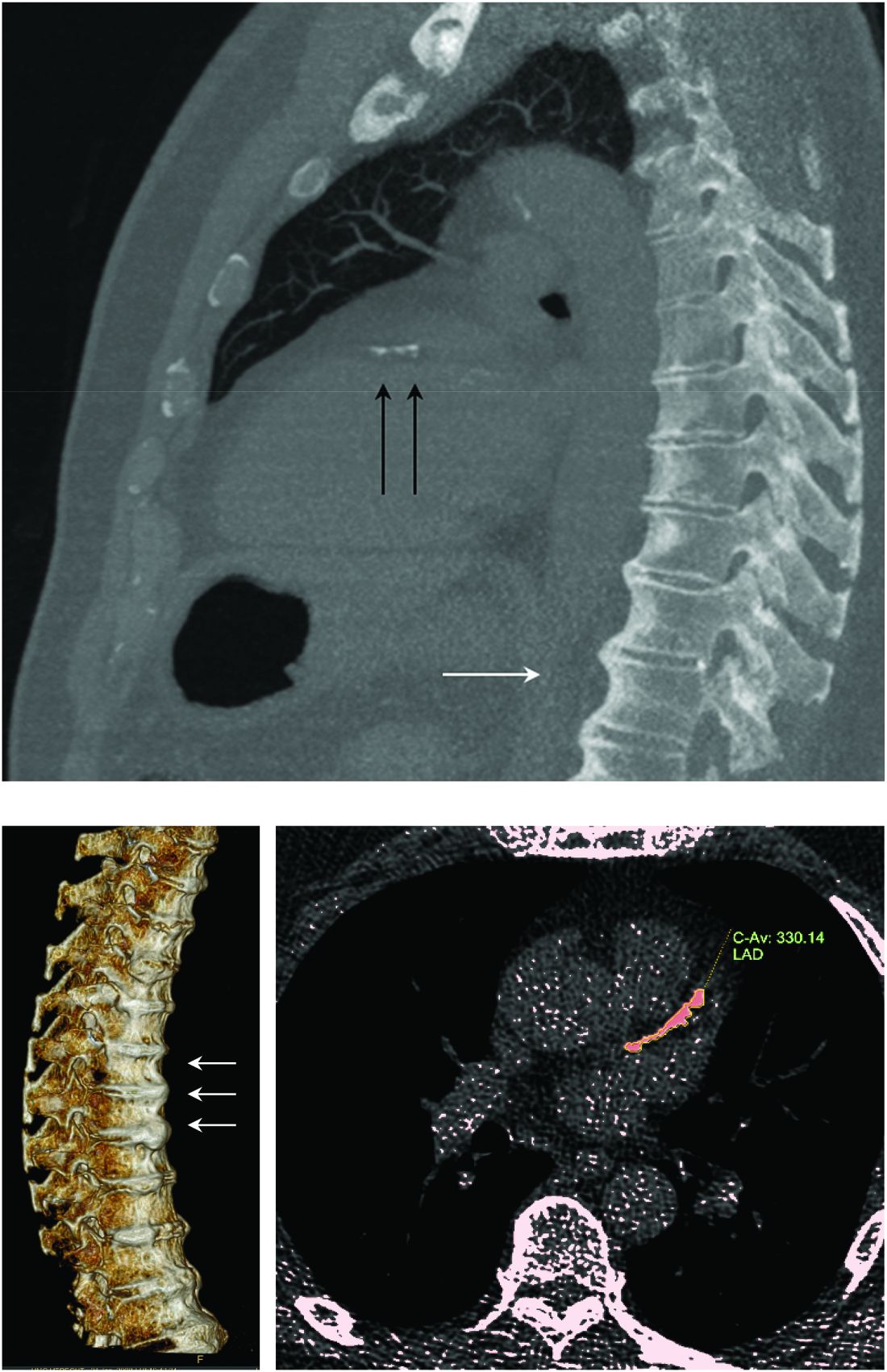
Notably, a higher rate of myocardial infarction (MI) was seen in those with DISH than in those without DISH over the 10-year follow-up period (24.4% vs. 4.3%; P = .0055).
“We propose more scrutiny is warranted in evaluating CV risk in these patients, more demanding treatment target goals should be established, and as a result, earlier and more aggressive preventive medical interventions instituted,” corresponding author Reuven Mader, MD, and associates wrote in Arthritis Research & Therapy.
“What Mader’s study is pointing out is that it’s worth the radiologist reporting [DISH],” Elizabeth A. Regan, MD, PhD, from the National Jewish Health Center in Denver, said in an interview.
DISH on a chest x-ray or CT scan should be another “red flag to be even more attentive to cardiovascular risk,” she added, particularly because studies have shown that people with DISH tend to be obese, have metabolic syndrome, or diabetes – all of which independently increase their risk for cardiovascular disease.
An old condition often found by accident
Physicians have known about DISH for many years, Dr. Mader of Ha’Emek Medical Center in Afula, Israel, observed in an interview. Historical evidence suggests it was present more than a thousand years ago, but it wasn’t until the 1950s that it gained scientific interest. Originally coined Forestier’s disease, it was renamed DISH in the late 1960s following the realization that it was not limited to the spine.
“It is a condition which is characterized by new bone formation,” Dr. Mader explained. This new bone formation has some predilection for the entheses – the tendons, ligaments, or joint capsules, that attach to the bone.
“Diagnosis of the disease is based mainly on radiographs, especially of the thoracic spine, and it requires the formation of bridges that connect at least four contiguous vertebra,” he continued.
“The bridges are usually right-sided and usually the intervertebral spaces are spared. Classically there is no involvement of the sacroiliac joints, although there are some changes that might involve the sacroiliac joints but in a different manner than in inflammatory sacroiliitis.”
DISH was originally thought to be a pain syndrome, which has “not played out,” Dr. Regan noted in her interview. While there may be people who experience pain as a result of DISH, most cases are asymptomatic and usually picked up incidentally on a chest x-ray or CT scan.
“It’s something that’s not obvious,” she said. One of the main problems it can cause is stiffness and lack of mobility in the spine and this can lead to quite severe fractures in some cases, such as during a car accident. Hence spinal surgeons and other orthopedic specialists, such as Dr. Regan, have also taken an interest in the condition.
“Apart from the thoracic spine, DISH may also involve the cervical spine; there have been many reports about difficulty in swallowing, breathing, and in the lumbar spine, spinal stenosis and so forth,” Dr. Mader said. The differential diagnosis includes ankylosing spondylitis, although there is some evidence that the two can coexist.
“The diagnosis depends on the alertness of the examining physician,” he added, noting that rheumatologists and other specialists would be “very aware of this condition” and “sensitive to changes that we see when we examine these patients.”
DISH and heightened cardiovascular risk
Previous work by Dr. Mader and associates has shown that people with DISH are more often affected by the metabolic syndrome than are those without DISH. The cross-sectional study had excluded those with preexisting CVD and found that people with DISH had a significantly higher Framingham Risk Score, compared with a control group of people with osteoarthritis and no DISH (P = .004), which in turn meant they had a significantly (P = .007) higher 10-year risk for developing CVD.
The aim of their most recent study was to compare the actual rate of CV events in 2016 versus those predicted by the Framingham Risk Score in 2006. To do this, they compared the available electronic medical records of 45 individuals with DISH and 47 without it.
The results showed that almost 39% of people with DISH had developed CVD, whereas the Framingham Risk Score had estimated that just under 27% would develop CVD.
For every 1% increase in the CVD risk calculated by the Framingham Risk Score, the odds of CVD increased by 4% in the DISH group versus the control group (P = .02).
While there was a significant (P < .003) difference in the Framingham Risk Score between the DISH and control groups in 2006 (28.6% vs. 17.8%), there was no overall statistical difference (P = .2) in the composite CVD outcome (38.8% vs. 25.5%) 10 years later, as calculated by the revised Framingham Risk Score, which included MI, cerebrovascular accident, transient ischemic attack, peripheral artery disease, and heart failure with preserved ejection fraction.
“We are dealing with patients who are in their 70s. So, it is expected that this group of patients will be more often affected by cardiovascular disease” than younger individuals, Dr. Mader observed. That said, the study’s findings “confirm the theory that patients with DISH have a high likelihood of developing cardiovascular disease,” he added, acknowledging that it was only the risk for MI that was statistically significantly higher in people with DISH than in the controls.
DISH and coronary artery calcification
“It might be even more interesting to have a different control population that had no osteoarthritis,” Dr. Regan observed.
As the associate director of the COPDGene study, Dr. Regan has access to data collected from a large cohort of people with chronic obstructive pulmonary disease (COPD; n = 2,728), around 13% of whom were identified as having DISH in one recent study.
In that study, the presence of DISH versus no DISH was associated with a 37% higher risk for having coronary artery calcification (CAC) – a marker for atherosclerosis and cardiovascular disease. Two-thirds of people with DISH had CAC, compared with 46.9% of those without DISH (P < .001). The prevalence of DISH was 8.8% in those without CAC, 12.8% in those with a CAC score of 1-100, 20% in those with a CAC score of 100-400, and 24.7% in those with a CAC score of more than 400, which is associated with a very high risk for coronary artery disease.
Dr. Regan observed that information on heart attacks and strokes were collected within the COPDGene study, so it would be possible to look at cardiovascular risk in their patients with DISH and confirm the findings of Mader and colleagues.
“I think the most important thing is recognizing that there are things going on in the spine that are important to people’s general health,” Dr. Regan said.
Dr. Mader noted: “It makes sense that patients with DISH should be more meticulously followed for at least the traditional risk factors and better treated because they are at a higher risk for these events.”
The study received no financial support. Neither Dr. Mader nor Dr. Regan had any conflicts of interest to disclose.
SOURCE: Glick K et al. Arthritis Res Ther. 2020. doi: 10.1186/s13075-020-02278-w.
More people with diffuse idiopathic skeletal hyperostosis (DISH) develop cardiovascular disease (CVD) than is predicted by the Framingham Risk Score, results of an observational study have shown.
Notably, a higher rate of myocardial infarction (MI) was seen in those with DISH than in those without DISH over the 10-year follow-up period (24.4% vs. 4.3%; P = .0055).
“We propose more scrutiny is warranted in evaluating CV risk in these patients, more demanding treatment target goals should be established, and as a result, earlier and more aggressive preventive medical interventions instituted,” corresponding author Reuven Mader, MD, and associates wrote in Arthritis Research & Therapy.
“What Mader’s study is pointing out is that it’s worth the radiologist reporting [DISH],” Elizabeth A. Regan, MD, PhD, from the National Jewish Health Center in Denver, said in an interview.
DISH on a chest x-ray or CT scan should be another “red flag to be even more attentive to cardiovascular risk,” she added, particularly because studies have shown that people with DISH tend to be obese, have metabolic syndrome, or diabetes – all of which independently increase their risk for cardiovascular disease.
An old condition often found by accident
Physicians have known about DISH for many years, Dr. Mader of Ha’Emek Medical Center in Afula, Israel, observed in an interview. Historical evidence suggests it was present more than a thousand years ago, but it wasn’t until the 1950s that it gained scientific interest. Originally coined Forestier’s disease, it was renamed DISH in the late 1960s following the realization that it was not limited to the spine.
“It is a condition which is characterized by new bone formation,” Dr. Mader explained. This new bone formation has some predilection for the entheses – the tendons, ligaments, or joint capsules, that attach to the bone.
“Diagnosis of the disease is based mainly on radiographs, especially of the thoracic spine, and it requires the formation of bridges that connect at least four contiguous vertebra,” he continued.
“The bridges are usually right-sided and usually the intervertebral spaces are spared. Classically there is no involvement of the sacroiliac joints, although there are some changes that might involve the sacroiliac joints but in a different manner than in inflammatory sacroiliitis.”
DISH was originally thought to be a pain syndrome, which has “not played out,” Dr. Regan noted in her interview. While there may be people who experience pain as a result of DISH, most cases are asymptomatic and usually picked up incidentally on a chest x-ray or CT scan.
“It’s something that’s not obvious,” she said. One of the main problems it can cause is stiffness and lack of mobility in the spine and this can lead to quite severe fractures in some cases, such as during a car accident. Hence spinal surgeons and other orthopedic specialists, such as Dr. Regan, have also taken an interest in the condition.
“Apart from the thoracic spine, DISH may also involve the cervical spine; there have been many reports about difficulty in swallowing, breathing, and in the lumbar spine, spinal stenosis and so forth,” Dr. Mader said. The differential diagnosis includes ankylosing spondylitis, although there is some evidence that the two can coexist.
“The diagnosis depends on the alertness of the examining physician,” he added, noting that rheumatologists and other specialists would be “very aware of this condition” and “sensitive to changes that we see when we examine these patients.”
DISH and heightened cardiovascular risk
Previous work by Dr. Mader and associates has shown that people with DISH are more often affected by the metabolic syndrome than are those without DISH. The cross-sectional study had excluded those with preexisting CVD and found that people with DISH had a significantly higher Framingham Risk Score, compared with a control group of people with osteoarthritis and no DISH (P = .004), which in turn meant they had a significantly (P = .007) higher 10-year risk for developing CVD.
The aim of their most recent study was to compare the actual rate of CV events in 2016 versus those predicted by the Framingham Risk Score in 2006. To do this, they compared the available electronic medical records of 45 individuals with DISH and 47 without it.
The results showed that almost 39% of people with DISH had developed CVD, whereas the Framingham Risk Score had estimated that just under 27% would develop CVD.
For every 1% increase in the CVD risk calculated by the Framingham Risk Score, the odds of CVD increased by 4% in the DISH group versus the control group (P = .02).
While there was a significant (P < .003) difference in the Framingham Risk Score between the DISH and control groups in 2006 (28.6% vs. 17.8%), there was no overall statistical difference (P = .2) in the composite CVD outcome (38.8% vs. 25.5%) 10 years later, as calculated by the revised Framingham Risk Score, which included MI, cerebrovascular accident, transient ischemic attack, peripheral artery disease, and heart failure with preserved ejection fraction.
“We are dealing with patients who are in their 70s. So, it is expected that this group of patients will be more often affected by cardiovascular disease” than younger individuals, Dr. Mader observed. That said, the study’s findings “confirm the theory that patients with DISH have a high likelihood of developing cardiovascular disease,” he added, acknowledging that it was only the risk for MI that was statistically significantly higher in people with DISH than in the controls.
DISH and coronary artery calcification
“It might be even more interesting to have a different control population that had no osteoarthritis,” Dr. Regan observed.
As the associate director of the COPDGene study, Dr. Regan has access to data collected from a large cohort of people with chronic obstructive pulmonary disease (COPD; n = 2,728), around 13% of whom were identified as having DISH in one recent study.
In that study, the presence of DISH versus no DISH was associated with a 37% higher risk for having coronary artery calcification (CAC) – a marker for atherosclerosis and cardiovascular disease. Two-thirds of people with DISH had CAC, compared with 46.9% of those without DISH (P < .001). The prevalence of DISH was 8.8% in those without CAC, 12.8% in those with a CAC score of 1-100, 20% in those with a CAC score of 100-400, and 24.7% in those with a CAC score of more than 400, which is associated with a very high risk for coronary artery disease.
Dr. Regan observed that information on heart attacks and strokes were collected within the COPDGene study, so it would be possible to look at cardiovascular risk in their patients with DISH and confirm the findings of Mader and colleagues.
“I think the most important thing is recognizing that there are things going on in the spine that are important to people’s general health,” Dr. Regan said.
Dr. Mader noted: “It makes sense that patients with DISH should be more meticulously followed for at least the traditional risk factors and better treated because they are at a higher risk for these events.”
The study received no financial support. Neither Dr. Mader nor Dr. Regan had any conflicts of interest to disclose.
SOURCE: Glick K et al. Arthritis Res Ther. 2020. doi: 10.1186/s13075-020-02278-w.
More people with diffuse idiopathic skeletal hyperostosis (DISH) develop cardiovascular disease (CVD) than is predicted by the Framingham Risk Score, results of an observational study have shown.
Notably, a higher rate of myocardial infarction (MI) was seen in those with DISH than in those without DISH over the 10-year follow-up period (24.4% vs. 4.3%; P = .0055).
“We propose more scrutiny is warranted in evaluating CV risk in these patients, more demanding treatment target goals should be established, and as a result, earlier and more aggressive preventive medical interventions instituted,” corresponding author Reuven Mader, MD, and associates wrote in Arthritis Research & Therapy.
“What Mader’s study is pointing out is that it’s worth the radiologist reporting [DISH],” Elizabeth A. Regan, MD, PhD, from the National Jewish Health Center in Denver, said in an interview.
DISH on a chest x-ray or CT scan should be another “red flag to be even more attentive to cardiovascular risk,” she added, particularly because studies have shown that people with DISH tend to be obese, have metabolic syndrome, or diabetes – all of which independently increase their risk for cardiovascular disease.
An old condition often found by accident
Physicians have known about DISH for many years, Dr. Mader of Ha’Emek Medical Center in Afula, Israel, observed in an interview. Historical evidence suggests it was present more than a thousand years ago, but it wasn’t until the 1950s that it gained scientific interest. Originally coined Forestier’s disease, it was renamed DISH in the late 1960s following the realization that it was not limited to the spine.
“It is a condition which is characterized by new bone formation,” Dr. Mader explained. This new bone formation has some predilection for the entheses – the tendons, ligaments, or joint capsules, that attach to the bone.
“Diagnosis of the disease is based mainly on radiographs, especially of the thoracic spine, and it requires the formation of bridges that connect at least four contiguous vertebra,” he continued.
“The bridges are usually right-sided and usually the intervertebral spaces are spared. Classically there is no involvement of the sacroiliac joints, although there are some changes that might involve the sacroiliac joints but in a different manner than in inflammatory sacroiliitis.”
DISH was originally thought to be a pain syndrome, which has “not played out,” Dr. Regan noted in her interview. While there may be people who experience pain as a result of DISH, most cases are asymptomatic and usually picked up incidentally on a chest x-ray or CT scan.
“It’s something that’s not obvious,” she said. One of the main problems it can cause is stiffness and lack of mobility in the spine and this can lead to quite severe fractures in some cases, such as during a car accident. Hence spinal surgeons and other orthopedic specialists, such as Dr. Regan, have also taken an interest in the condition.
“Apart from the thoracic spine, DISH may also involve the cervical spine; there have been many reports about difficulty in swallowing, breathing, and in the lumbar spine, spinal stenosis and so forth,” Dr. Mader said. The differential diagnosis includes ankylosing spondylitis, although there is some evidence that the two can coexist.
“The diagnosis depends on the alertness of the examining physician,” he added, noting that rheumatologists and other specialists would be “very aware of this condition” and “sensitive to changes that we see when we examine these patients.”
DISH and heightened cardiovascular risk
Previous work by Dr. Mader and associates has shown that people with DISH are more often affected by the metabolic syndrome than are those without DISH. The cross-sectional study had excluded those with preexisting CVD and found that people with DISH had a significantly higher Framingham Risk Score, compared with a control group of people with osteoarthritis and no DISH (P = .004), which in turn meant they had a significantly (P = .007) higher 10-year risk for developing CVD.
The aim of their most recent study was to compare the actual rate of CV events in 2016 versus those predicted by the Framingham Risk Score in 2006. To do this, they compared the available electronic medical records of 45 individuals with DISH and 47 without it.
The results showed that almost 39% of people with DISH had developed CVD, whereas the Framingham Risk Score had estimated that just under 27% would develop CVD.
For every 1% increase in the CVD risk calculated by the Framingham Risk Score, the odds of CVD increased by 4% in the DISH group versus the control group (P = .02).
While there was a significant (P < .003) difference in the Framingham Risk Score between the DISH and control groups in 2006 (28.6% vs. 17.8%), there was no overall statistical difference (P = .2) in the composite CVD outcome (38.8% vs. 25.5%) 10 years later, as calculated by the revised Framingham Risk Score, which included MI, cerebrovascular accident, transient ischemic attack, peripheral artery disease, and heart failure with preserved ejection fraction.
“We are dealing with patients who are in their 70s. So, it is expected that this group of patients will be more often affected by cardiovascular disease” than younger individuals, Dr. Mader observed. That said, the study’s findings “confirm the theory that patients with DISH have a high likelihood of developing cardiovascular disease,” he added, acknowledging that it was only the risk for MI that was statistically significantly higher in people with DISH than in the controls.
DISH and coronary artery calcification
“It might be even more interesting to have a different control population that had no osteoarthritis,” Dr. Regan observed.
As the associate director of the COPDGene study, Dr. Regan has access to data collected from a large cohort of people with chronic obstructive pulmonary disease (COPD; n = 2,728), around 13% of whom were identified as having DISH in one recent study.
In that study, the presence of DISH versus no DISH was associated with a 37% higher risk for having coronary artery calcification (CAC) – a marker for atherosclerosis and cardiovascular disease. Two-thirds of people with DISH had CAC, compared with 46.9% of those without DISH (P < .001). The prevalence of DISH was 8.8% in those without CAC, 12.8% in those with a CAC score of 1-100, 20% in those with a CAC score of 100-400, and 24.7% in those with a CAC score of more than 400, which is associated with a very high risk for coronary artery disease.
Dr. Regan observed that information on heart attacks and strokes were collected within the COPDGene study, so it would be possible to look at cardiovascular risk in their patients with DISH and confirm the findings of Mader and colleagues.
“I think the most important thing is recognizing that there are things going on in the spine that are important to people’s general health,” Dr. Regan said.
Dr. Mader noted: “It makes sense that patients with DISH should be more meticulously followed for at least the traditional risk factors and better treated because they are at a higher risk for these events.”
The study received no financial support. Neither Dr. Mader nor Dr. Regan had any conflicts of interest to disclose.
SOURCE: Glick K et al. Arthritis Res Ther. 2020. doi: 10.1186/s13075-020-02278-w.
FROM ARTHRITIS RESEARCH & THERAPY
Novel calculator predicts cancer risk in patients with CVD
Individualized 10-year and lifetime risks of cancer can now for the first time be estimated in patients with established cardiovascular disease, Cilie C. van ’t Klooster, MD, reported at the virtual annual congress of the European Society of Cardiology.

She and her coinvestigators have developed an easy-to-use predictive model that generates individualized risk estimates for total cancer, lung cancer, and colorectal cancer. The tool relies on nine readily available clinical variables: age, sex, smoking, weight, height, alcohol use, diabetes, antiplatelet drug use, and C-reactive protein level. The cancer risk calculator factors in an individual’s competing risk of death because of cardiovascular disease (CVD).
The risk calculator was developed using data on 7,280 patients with established CVD enrolled in the ongoing long-term Dutch UCC-SMART (Utrecht Cardiovascular Cohort – Second Manifestations of Arterial Disease) study, then independently validated in 9,322 patients in the double-blind CANTOS (Canakinumab Anti-Inflammatory Thrombosis Outcomes) trial, explained Dr. van ’t Klooster of Utrecht (the Netherlands) University.
Several other prediction models estimate the risk of a specific type of cancer, most commonly breast cancer or lung cancer. But the new Utrecht prediction tool is the first one to estimate total cancer risk. It’s also the first to apply specifically to patients with known CVD, thus filling an unmet need, because patients with established CVD are known to be on average at 19% increased risk of total cancer and 56% greater risk for lung cancer, compared with the general population. This is thought to be caused mainly by shared risk factors, including smoking, obesity, and low-grade systemic inflammation.
As the Utrecht/CANTOS analysis shows, however, that 19% increased relative risk for cancer in patients with CVD doesn’t tell the whole story. While the median lifetime and 10-year risks of total cancer in CANTOS were 26% and 10%, respectively, the individual patient risks for total cancer estimated using the Dutch prediction model ranged from 1% to 52% for lifetime and from 1% to 31% for 10-year risk. The same was true for lung cancer risk: median 5% lifetime and 2% 10-year risks, with individual patient risks ranging from 0% to 37% and from 0% to 24%. Likewise for colorectal cancer: a median 4% lifetime risk, ranging from 0% to 6%, and a median 2% risk over the next 10 years, with personalized risks ranging as high as 13% for lifetime risk and 6% for 10-year colorectal cancer risk.
The risk calculator performed “reasonably well,” according to Dr. van ’t Klooster. She pointed to a C-statistic of 0.74 for lung cancer, 0.63 for total cancer, and 0.64 for colorectal cancer. It’s possible the risk predictor’s performance could be further enhanced by incorporation of several potentially important factors that weren’t available in the UCC-SMART derivation cohort, including race, education level, and socioeconomic status, she added.
Potential applications for the risk calculator in clinical practice require further study, but include using the lifetime risk prediction for cancer as a motivational aid in conversations with patients about the importance of behavioral change in support of a healthier lifestyle. Also, a high predicted 10-year lung cancer risk could potentially be used to lower the threshold for a screening chest CT, resulting in earlier detection and treatment of lung cancer, Dr. van ’t Klooster noted.
In an interview, Bonnie Ky, MD, MSCE, praised the risk prediction study as rigorously executed, topical, and clinically significant.
“This paper signifies the overlap between our two disciplines of cancer and cardiovascular disease in terms of the risks that we face together when we care for this patient population,” said Dr. Ky, a cardiologist at the University of Pennsylvania, Philadelphia.
“Many of us in medicine believe in the importance of risk prediction: identifying who’s at high risk and doing everything we can to mitigate that risk. This paper speaks to that and moves us one step closer to accomplishing that aim,” added Dr. Ky, who is editor in chief of JACC: CardioOncology, which published the study simultaneously with Dr. van ’t Klooster’s presentation at ESC 2020. The paper provides direct access to the risk calculator.
Dr. van ’t Klooster reported having no financial conflicts regarding her study. UCC-SMART is funded by a Utrecht University grant, and CANTOS was funded by Novartis.
SOURCE: van ’t Klooster CC. ESC 2020 and JACC CardioOncol. 2020 Aug. doi: 10.1016/j.jaccao.2020.07.001.
Individualized 10-year and lifetime risks of cancer can now for the first time be estimated in patients with established cardiovascular disease, Cilie C. van ’t Klooster, MD, reported at the virtual annual congress of the European Society of Cardiology.
She and her coinvestigators have developed an easy-to-use predictive model that generates individualized risk estimates for total cancer, lung cancer, and colorectal cancer. The tool relies on nine readily available clinical variables: age, sex, smoking, weight, height, alcohol use, diabetes, antiplatelet drug use, and C-reactive protein level. The cancer risk calculator factors in an individual’s competing risk of death because of cardiovascular disease (CVD).
The risk calculator was developed using data on 7,280 patients with established CVD enrolled in the ongoing long-term Dutch UCC-SMART (Utrecht Cardiovascular Cohort – Second Manifestations of Arterial Disease) study, then independently validated in 9,322 patients in the double-blind CANTOS (Canakinumab Anti-Inflammatory Thrombosis Outcomes) trial, explained Dr. van ’t Klooster of Utrecht (the Netherlands) University.
Several other prediction models estimate the risk of a specific type of cancer, most commonly breast cancer or lung cancer. But the new Utrecht prediction tool is the first one to estimate total cancer risk. It’s also the first to apply specifically to patients with known CVD, thus filling an unmet need, because patients with established CVD are known to be on average at 19% increased risk of total cancer and 56% greater risk for lung cancer, compared with the general population. This is thought to be caused mainly by shared risk factors, including smoking, obesity, and low-grade systemic inflammation.
As the Utrecht/CANTOS analysis shows, however, that 19% increased relative risk for cancer in patients with CVD doesn’t tell the whole story. While the median lifetime and 10-year risks of total cancer in CANTOS were 26% and 10%, respectively, the individual patient risks for total cancer estimated using the Dutch prediction model ranged from 1% to 52% for lifetime and from 1% to 31% for 10-year risk. The same was true for lung cancer risk: median 5% lifetime and 2% 10-year risks, with individual patient risks ranging from 0% to 37% and from 0% to 24%. Likewise for colorectal cancer: a median 4% lifetime risk, ranging from 0% to 6%, and a median 2% risk over the next 10 years, with personalized risks ranging as high as 13% for lifetime risk and 6% for 10-year colorectal cancer risk.
The risk calculator performed “reasonably well,” according to Dr. van ’t Klooster. She pointed to a C-statistic of 0.74 for lung cancer, 0.63 for total cancer, and 0.64 for colorectal cancer. It’s possible the risk predictor’s performance could be further enhanced by incorporation of several potentially important factors that weren’t available in the UCC-SMART derivation cohort, including race, education level, and socioeconomic status, she added.
Potential applications for the risk calculator in clinical practice require further study, but include using the lifetime risk prediction for cancer as a motivational aid in conversations with patients about the importance of behavioral change in support of a healthier lifestyle. Also, a high predicted 10-year lung cancer risk could potentially be used to lower the threshold for a screening chest CT, resulting in earlier detection and treatment of lung cancer, Dr. van ’t Klooster noted.
In an interview, Bonnie Ky, MD, MSCE, praised the risk prediction study as rigorously executed, topical, and clinically significant.
“This paper signifies the overlap between our two disciplines of cancer and cardiovascular disease in terms of the risks that we face together when we care for this patient population,” said Dr. Ky, a cardiologist at the University of Pennsylvania, Philadelphia.
“Many of us in medicine believe in the importance of risk prediction: identifying who’s at high risk and doing everything we can to mitigate that risk. This paper speaks to that and moves us one step closer to accomplishing that aim,” added Dr. Ky, who is editor in chief of JACC: CardioOncology, which published the study simultaneously with Dr. van ’t Klooster’s presentation at ESC 2020. The paper provides direct access to the risk calculator.
Dr. van ’t Klooster reported having no financial conflicts regarding her study. UCC-SMART is funded by a Utrecht University grant, and CANTOS was funded by Novartis.
SOURCE: van ’t Klooster CC. ESC 2020 and JACC CardioOncol. 2020 Aug. doi: 10.1016/j.jaccao.2020.07.001.
Individualized 10-year and lifetime risks of cancer can now for the first time be estimated in patients with established cardiovascular disease, Cilie C. van ’t Klooster, MD, reported at the virtual annual congress of the European Society of Cardiology.
She and her coinvestigators have developed an easy-to-use predictive model that generates individualized risk estimates for total cancer, lung cancer, and colorectal cancer. The tool relies on nine readily available clinical variables: age, sex, smoking, weight, height, alcohol use, diabetes, antiplatelet drug use, and C-reactive protein level. The cancer risk calculator factors in an individual’s competing risk of death because of cardiovascular disease (CVD).
The risk calculator was developed using data on 7,280 patients with established CVD enrolled in the ongoing long-term Dutch UCC-SMART (Utrecht Cardiovascular Cohort – Second Manifestations of Arterial Disease) study, then independently validated in 9,322 patients in the double-blind CANTOS (Canakinumab Anti-Inflammatory Thrombosis Outcomes) trial, explained Dr. van ’t Klooster of Utrecht (the Netherlands) University.
Several other prediction models estimate the risk of a specific type of cancer, most commonly breast cancer or lung cancer. But the new Utrecht prediction tool is the first one to estimate total cancer risk. It’s also the first to apply specifically to patients with known CVD, thus filling an unmet need, because patients with established CVD are known to be on average at 19% increased risk of total cancer and 56% greater risk for lung cancer, compared with the general population. This is thought to be caused mainly by shared risk factors, including smoking, obesity, and low-grade systemic inflammation.
As the Utrecht/CANTOS analysis shows, however, that 19% increased relative risk for cancer in patients with CVD doesn’t tell the whole story. While the median lifetime and 10-year risks of total cancer in CANTOS were 26% and 10%, respectively, the individual patient risks for total cancer estimated using the Dutch prediction model ranged from 1% to 52% for lifetime and from 1% to 31% for 10-year risk. The same was true for lung cancer risk: median 5% lifetime and 2% 10-year risks, with individual patient risks ranging from 0% to 37% and from 0% to 24%. Likewise for colorectal cancer: a median 4% lifetime risk, ranging from 0% to 6%, and a median 2% risk over the next 10 years, with personalized risks ranging as high as 13% for lifetime risk and 6% for 10-year colorectal cancer risk.
The risk calculator performed “reasonably well,” according to Dr. van ’t Klooster. She pointed to a C-statistic of 0.74 for lung cancer, 0.63 for total cancer, and 0.64 for colorectal cancer. It’s possible the risk predictor’s performance could be further enhanced by incorporation of several potentially important factors that weren’t available in the UCC-SMART derivation cohort, including race, education level, and socioeconomic status, she added.
Potential applications for the risk calculator in clinical practice require further study, but include using the lifetime risk prediction for cancer as a motivational aid in conversations with patients about the importance of behavioral change in support of a healthier lifestyle. Also, a high predicted 10-year lung cancer risk could potentially be used to lower the threshold for a screening chest CT, resulting in earlier detection and treatment of lung cancer, Dr. van ’t Klooster noted.
In an interview, Bonnie Ky, MD, MSCE, praised the risk prediction study as rigorously executed, topical, and clinically significant.
“This paper signifies the overlap between our two disciplines of cancer and cardiovascular disease in terms of the risks that we face together when we care for this patient population,” said Dr. Ky, a cardiologist at the University of Pennsylvania, Philadelphia.
“Many of us in medicine believe in the importance of risk prediction: identifying who’s at high risk and doing everything we can to mitigate that risk. This paper speaks to that and moves us one step closer to accomplishing that aim,” added Dr. Ky, who is editor in chief of JACC: CardioOncology, which published the study simultaneously with Dr. van ’t Klooster’s presentation at ESC 2020. The paper provides direct access to the risk calculator.
Dr. van ’t Klooster reported having no financial conflicts regarding her study. UCC-SMART is funded by a Utrecht University grant, and CANTOS was funded by Novartis.
SOURCE: van ’t Klooster CC. ESC 2020 and JACC CardioOncol. 2020 Aug. doi: 10.1016/j.jaccao.2020.07.001.
FROM ESC CONGRESS 2020
Vascepa maker loses patent appeal, plans ‘vigorous’ fight
Amarin’s hopes of fending off generic competition for its blockbuster high-strength eicosapentaenoic acid product, icosapent ethyl (Vascepa), have dimmed following a decision by the U.S. Court of Appeals for the Federal Circuit in the company’s ongoing patent litigation.
The court upheld the March ruling by the District Court for the District of Nevada in favor of two generic companies in connection with their abbreviated new drug applications (ANDAs) for the product.
Amarin said it is currently reviewing its legal options and within 30 days expects to file a petition for an en banc review of the current decision by the full panel of 12 active judges at the Court of Appeals for the Federal Circuit.
“We are extremely disappointed with [the] ruling and plan to vigorously pursue available remedies,” John Thero, Amarin president and chief executive officer, said in a statement.
In 2012, Vascepa became the first and only prescription treatment approved by the Food and Drug Administration made up solely of the active ingredient icosapent ethyl, a unique form of eicosapentaenoic acid. It was initially approved for the reduction of very high triglyceride levels (≥500 mg/dL).
In late 2019, the FDA extended the indication to reduce the risk for cardiovascular events in people with elevated triglyceride levels and either established CV disease or diabetes with other CV risk factors.
The extended indication was based on results of the landmark REDUCE-IT trial, which showed a 25% relative risk reduction in major adverse CV events with icosapent ethyl, compared with placebo, in patients with triglyceride levels above 135 mg/dL and who had CV disease (70% of the study population), or who were high-risk primary-prevention patients with diabetes and one additional risk factor (30% of the study population).
According to Amarin, since its launch, Vascepa has been prescribed more than 8 million times.
The company said demand for the product in the United States remains “strong” and indicated that, despite the legal setback, it would continue promotional efforts. The company is also seeking additional regulatory approvals in China, Europe, and additional countries in the Middle East.
“We are particularly excited about the anticipated commercialization opportunities for Vascepa in Europe as we prepare for expected approval and launch in early 2021,” Mr. Thero said.
The company anticipates 10 years of market protection because of regulatory exclusivity in the European Union once approved, and said patent protection could extend into 2039.
Only Vascepa sold in the United States is subject to this litigation and judgment. No generic litigation is pending outside the United States, Amarin said.
A version of this article originally appeared on Medscape.com.
Amarin’s hopes of fending off generic competition for its blockbuster high-strength eicosapentaenoic acid product, icosapent ethyl (Vascepa), have dimmed following a decision by the U.S. Court of Appeals for the Federal Circuit in the company’s ongoing patent litigation.
The court upheld the March ruling by the District Court for the District of Nevada in favor of two generic companies in connection with their abbreviated new drug applications (ANDAs) for the product.
Amarin said it is currently reviewing its legal options and within 30 days expects to file a petition for an en banc review of the current decision by the full panel of 12 active judges at the Court of Appeals for the Federal Circuit.
“We are extremely disappointed with [the] ruling and plan to vigorously pursue available remedies,” John Thero, Amarin president and chief executive officer, said in a statement.
In 2012, Vascepa became the first and only prescription treatment approved by the Food and Drug Administration made up solely of the active ingredient icosapent ethyl, a unique form of eicosapentaenoic acid. It was initially approved for the reduction of very high triglyceride levels (≥500 mg/dL).
In late 2019, the FDA extended the indication to reduce the risk for cardiovascular events in people with elevated triglyceride levels and either established CV disease or diabetes with other CV risk factors.
The extended indication was based on results of the landmark REDUCE-IT trial, which showed a 25% relative risk reduction in major adverse CV events with icosapent ethyl, compared with placebo, in patients with triglyceride levels above 135 mg/dL and who had CV disease (70% of the study population), or who were high-risk primary-prevention patients with diabetes and one additional risk factor (30% of the study population).
According to Amarin, since its launch, Vascepa has been prescribed more than 8 million times.
The company said demand for the product in the United States remains “strong” and indicated that, despite the legal setback, it would continue promotional efforts. The company is also seeking additional regulatory approvals in China, Europe, and additional countries in the Middle East.
“We are particularly excited about the anticipated commercialization opportunities for Vascepa in Europe as we prepare for expected approval and launch in early 2021,” Mr. Thero said.
The company anticipates 10 years of market protection because of regulatory exclusivity in the European Union once approved, and said patent protection could extend into 2039.
Only Vascepa sold in the United States is subject to this litigation and judgment. No generic litigation is pending outside the United States, Amarin said.
A version of this article originally appeared on Medscape.com.
Amarin’s hopes of fending off generic competition for its blockbuster high-strength eicosapentaenoic acid product, icosapent ethyl (Vascepa), have dimmed following a decision by the U.S. Court of Appeals for the Federal Circuit in the company’s ongoing patent litigation.
The court upheld the March ruling by the District Court for the District of Nevada in favor of two generic companies in connection with their abbreviated new drug applications (ANDAs) for the product.
Amarin said it is currently reviewing its legal options and within 30 days expects to file a petition for an en banc review of the current decision by the full panel of 12 active judges at the Court of Appeals for the Federal Circuit.
“We are extremely disappointed with [the] ruling and plan to vigorously pursue available remedies,” John Thero, Amarin president and chief executive officer, said in a statement.
In 2012, Vascepa became the first and only prescription treatment approved by the Food and Drug Administration made up solely of the active ingredient icosapent ethyl, a unique form of eicosapentaenoic acid. It was initially approved for the reduction of very high triglyceride levels (≥500 mg/dL).
In late 2019, the FDA extended the indication to reduce the risk for cardiovascular events in people with elevated triglyceride levels and either established CV disease or diabetes with other CV risk factors.
The extended indication was based on results of the landmark REDUCE-IT trial, which showed a 25% relative risk reduction in major adverse CV events with icosapent ethyl, compared with placebo, in patients with triglyceride levels above 135 mg/dL and who had CV disease (70% of the study population), or who were high-risk primary-prevention patients with diabetes and one additional risk factor (30% of the study population).
According to Amarin, since its launch, Vascepa has been prescribed more than 8 million times.
The company said demand for the product in the United States remains “strong” and indicated that, despite the legal setback, it would continue promotional efforts. The company is also seeking additional regulatory approvals in China, Europe, and additional countries in the Middle East.
“We are particularly excited about the anticipated commercialization opportunities for Vascepa in Europe as we prepare for expected approval and launch in early 2021,” Mr. Thero said.
The company anticipates 10 years of market protection because of regulatory exclusivity in the European Union once approved, and said patent protection could extend into 2039.
Only Vascepa sold in the United States is subject to this litigation and judgment. No generic litigation is pending outside the United States, Amarin said.
A version of this article originally appeared on Medscape.com.
Final EVAPORATE results for Vascepa raise eyebrows
Final 18-month results of the EVAPORATE trial suggest icosapent ethyl (Vascepa) provides even greater slowing of coronary plaque progression when added to statins for patients with high triglyceride levels, but not all cardiologists are convinced.
The study was designed to explore a potential mechanism behind the cardiovascular event reduction in REDUCE-IT. Previously reported interim results showed that, after 9 months, the pharmaceutical-grade omega-3 fatty acid formation significantly slowed the progression of several plaque types but not the primary endpoint of change in low-attenuation plaque volume on multidetector CT.
From baseline to 18-month follow-up, however, the primary endpoint was significantly reduced by 17% in the icosapent ethyl group, whereas low-attenuation plaque volumes increased by 109% in the placebo group (P = .0061).
Significant declines were also seen with icosapent ethyl 4 g/day versus the mineral oil placebo for all other plaque types except dense calcium after adjustment for age, sex, diabetes, hypertension, and triglyceride levels at baseline:
- Dense calcium: –1% versus 15% (P = .0531).
- Fibro-fatty: –34% versus 32% (P = .0002).
- Fibrous: –20% versus 1% (P = .0028).
- Noncalcified: –19% versus 9% (P = .0005).
- Total plaque: –9% versus 11% (P = .0019).
The results parallel nicely with recent clinical data from REDUCE-IT REVASC, in which icosapent ethyl 4 g/day provided a very early benefit on first revascularization events that reached statistical significance after only 11 months (hazard ratio, 0.66), principal investigator Matthew Budoff, MD, director of cardiac CT at Harbor–University of California, Los Angeles, Medical Center in Torrance, Calif., said during the virtual European Society of Cardiology Congress 2020.
The findings were also published simultaneously in the European Heart Journal and quickly prompted a flurry of comments on social media.
Some were supportive. Christopher Cannon, MD, of Harvard Medical School, Boston; Dan Soffer, MD, a lipidologist at the University of Pennsylvania, Philadelphia; and Viet Le, MPAS, PA, a researcher at the Intermountain Heart Institute, Murray, Utah, took to Twitter to praise Dr. Budoff and the final results of the mechanistic study. Dr. Soffer called the study “elegant,” while Dr. Cannon said the results provide “important mechanistic data on plaque character.”
Others were highly critical, including a poll questioning whether the article should be retracted or revised.
Ibrahim H. Tanboga, MD, PhD, a cardiology professor and biostatistician at Hisar Intercontinental Hospital in Istanbul, questioned how the longitudinal change in low-attenuation plaque was possible clinically; his plot of the data showed these lesions getting worse in both arms before getting better in both arms.
A more volatile exchange concerned whether there were differences in the baseline characteristics between the two groups and whether the data might have been unblinded.
“I am sympathetic to the boss of a big laboratory [who] might not know how every step of the process was done and therefore might not be aware of opportunities for accidental bias. This can easily happen in a large and active department,” Darrel Francis, MD, professor of cardiology at the National Heart and Lung Institute, Imperial College, London, said in an interview.
An alternative explanation proffered on Twitter was that the interim analysis found no significant differences in baseline measures because it used nonparametric tests, whereas log transformation was applied to the final data. In any event, the tweets prompted a sharp rebuke from Dr. Budoff.
Dr. Francis raised another point of contention on Twitter regarding the degree of plaque progression in the placebo group.
In an interview, Dr. Francis pointed out that the final data represent the percentage change in the logarithm, not the actual percentage change in atheroma. So the increase in total atheroma volume in the placebo arm is not 11% but rather a scaling-up by 100.4 or 2.51, in other words, 151%.
He also offered a “less subtle feature of possible erroneous data,” in that the abstract reported low-attenuation plaque “more than doubles” in 18 months, which he described as a “ghastly supercharged version of Moore’s law for atheroma, instead of microchips.”
So “either it’s a mistake in the measurement or the placebo is harmful, because I can’t see how this is sustainable,” he said. “Why isn’t everyone dead from coronary disease?”
Concerns were raised previously over the possibility that the mineral oil placebo used in both EVAPORATE and REDUCE-IT could be having ill effects, notably, by increasing LDL cholesterol and C-reactive protein levels.
In an interview, Steven Nissen, MD, who is chair of cardiovascular medicine at the Cleveland Clinic and has been among the critics of the mineral oil placebo, also questioned the plaque progression over the 18 months.
“I’ve published more than dozen regression/progression trials, and we have never seen anything like this in a placebo group, ever,” he said. “If this was a clean placebo, why would this happen in a short amount of time?
“I’m concerned this is all about an increase, in the case of REDUCE-IT, in morbidity and mortality in the placebo group, and in the EVAPORATE trial, an increase in plaque in the placebo group,” Dr. Nissen said. “So this raises serious doubts about whether there is any benefit to icosapent ethyl.”
Asked about the 109% increase, Dr. Budoff said in an interview that low-attenuation plaque represents a much smaller quantity of overall plaque volume. “So the percentages might be exaggerated if you look at just percentage change because they;re small volumes.”
He also noted that previous trials that evaluated atherosclerosis progression used intravascular ultrasound (IVUS), whereas EVAPORATE is the first to make the transition to CT angiography-based analysis of plaque progression.
“I would point out that Dr. Nissen has only worked on intravascular ultrasound, which, while it’s parallel in its ability to measure plaque, measures different volumes and measures it in a totally different way,” said Dr. Budoff. “So I don’t think we can directly compare the results of CT angiography to Dr. Nissen’s examples of IVUS.”
During his presentation, Dr. Budoff highlighted their recent data showing a similar rate of plaque progression between the mineral oil placebo in EVAPORATE and a cellulose-based placebo in the Garlic5 study. “So we have high confidence that the benefits seen in this trial with icosapent ethyl represent icosapent ethyl’s beneficial effects on atherosclerosis and not harm of mineral oil,” he said.
Exactly how icosapent ethyl is slowing atherosclerosis, however, is not fully known, Dr. Budoff said in an interview. “It might be inflammation and oxidation; those have both been shown to be better with icosapent ethyl, but I don’t think we fully understand the implications of these results.”
Dr. Budoff dismissed tweets that suggest the data might have been unblinded as unprofessional and said they are requesting that Imperial College have Francis cease and desist.
“He doesn’t have the actual data, so there is no way to do statistics without the dataset. The whole thing is inappropriate,” Dr. Budoff said.
Amarin Pharma provided funding and drug for the trial. Dr. Budoff has received research funding from and has served as a speaker for Amarin Pharma, Amgen, AstraZeneca, Boehringer Ingelheim, Novo Nordisk, and Pfizer and has served as a speaker for Bristol-Myers Squibb. Dr. Francis has disclosed no relevant financial relationships..
A version of this article originally appeared on Medscape.com.
Final 18-month results of the EVAPORATE trial suggest icosapent ethyl (Vascepa) provides even greater slowing of coronary plaque progression when added to statins for patients with high triglyceride levels, but not all cardiologists are convinced.
The study was designed to explore a potential mechanism behind the cardiovascular event reduction in REDUCE-IT. Previously reported interim results showed that, after 9 months, the pharmaceutical-grade omega-3 fatty acid formation significantly slowed the progression of several plaque types but not the primary endpoint of change in low-attenuation plaque volume on multidetector CT.
From baseline to 18-month follow-up, however, the primary endpoint was significantly reduced by 17% in the icosapent ethyl group, whereas low-attenuation plaque volumes increased by 109% in the placebo group (P = .0061).
Significant declines were also seen with icosapent ethyl 4 g/day versus the mineral oil placebo for all other plaque types except dense calcium after adjustment for age, sex, diabetes, hypertension, and triglyceride levels at baseline:
- Dense calcium: –1% versus 15% (P = .0531).
- Fibro-fatty: –34% versus 32% (P = .0002).
- Fibrous: –20% versus 1% (P = .0028).
- Noncalcified: –19% versus 9% (P = .0005).
- Total plaque: –9% versus 11% (P = .0019).
The results parallel nicely with recent clinical data from REDUCE-IT REVASC, in which icosapent ethyl 4 g/day provided a very early benefit on first revascularization events that reached statistical significance after only 11 months (hazard ratio, 0.66), principal investigator Matthew Budoff, MD, director of cardiac CT at Harbor–University of California, Los Angeles, Medical Center in Torrance, Calif., said during the virtual European Society of Cardiology Congress 2020.
The findings were also published simultaneously in the European Heart Journal and quickly prompted a flurry of comments on social media.
Some were supportive. Christopher Cannon, MD, of Harvard Medical School, Boston; Dan Soffer, MD, a lipidologist at the University of Pennsylvania, Philadelphia; and Viet Le, MPAS, PA, a researcher at the Intermountain Heart Institute, Murray, Utah, took to Twitter to praise Dr. Budoff and the final results of the mechanistic study. Dr. Soffer called the study “elegant,” while Dr. Cannon said the results provide “important mechanistic data on plaque character.”
Others were highly critical, including a poll questioning whether the article should be retracted or revised.
Ibrahim H. Tanboga, MD, PhD, a cardiology professor and biostatistician at Hisar Intercontinental Hospital in Istanbul, questioned how the longitudinal change in low-attenuation plaque was possible clinically; his plot of the data showed these lesions getting worse in both arms before getting better in both arms.
A more volatile exchange concerned whether there were differences in the baseline characteristics between the two groups and whether the data might have been unblinded.
“I am sympathetic to the boss of a big laboratory [who] might not know how every step of the process was done and therefore might not be aware of opportunities for accidental bias. This can easily happen in a large and active department,” Darrel Francis, MD, professor of cardiology at the National Heart and Lung Institute, Imperial College, London, said in an interview.
An alternative explanation proffered on Twitter was that the interim analysis found no significant differences in baseline measures because it used nonparametric tests, whereas log transformation was applied to the final data. In any event, the tweets prompted a sharp rebuke from Dr. Budoff.
Dr. Francis raised another point of contention on Twitter regarding the degree of plaque progression in the placebo group.
In an interview, Dr. Francis pointed out that the final data represent the percentage change in the logarithm, not the actual percentage change in atheroma. So the increase in total atheroma volume in the placebo arm is not 11% but rather a scaling-up by 100.4 or 2.51, in other words, 151%.
He also offered a “less subtle feature of possible erroneous data,” in that the abstract reported low-attenuation plaque “more than doubles” in 18 months, which he described as a “ghastly supercharged version of Moore’s law for atheroma, instead of microchips.”
So “either it’s a mistake in the measurement or the placebo is harmful, because I can’t see how this is sustainable,” he said. “Why isn’t everyone dead from coronary disease?”
Concerns were raised previously over the possibility that the mineral oil placebo used in both EVAPORATE and REDUCE-IT could be having ill effects, notably, by increasing LDL cholesterol and C-reactive protein levels.
In an interview, Steven Nissen, MD, who is chair of cardiovascular medicine at the Cleveland Clinic and has been among the critics of the mineral oil placebo, also questioned the plaque progression over the 18 months.
“I’ve published more than dozen regression/progression trials, and we have never seen anything like this in a placebo group, ever,” he said. “If this was a clean placebo, why would this happen in a short amount of time?
“I’m concerned this is all about an increase, in the case of REDUCE-IT, in morbidity and mortality in the placebo group, and in the EVAPORATE trial, an increase in plaque in the placebo group,” Dr. Nissen said. “So this raises serious doubts about whether there is any benefit to icosapent ethyl.”
Asked about the 109% increase, Dr. Budoff said in an interview that low-attenuation plaque represents a much smaller quantity of overall plaque volume. “So the percentages might be exaggerated if you look at just percentage change because they;re small volumes.”
He also noted that previous trials that evaluated atherosclerosis progression used intravascular ultrasound (IVUS), whereas EVAPORATE is the first to make the transition to CT angiography-based analysis of plaque progression.
“I would point out that Dr. Nissen has only worked on intravascular ultrasound, which, while it’s parallel in its ability to measure plaque, measures different volumes and measures it in a totally different way,” said Dr. Budoff. “So I don’t think we can directly compare the results of CT angiography to Dr. Nissen’s examples of IVUS.”
During his presentation, Dr. Budoff highlighted their recent data showing a similar rate of plaque progression between the mineral oil placebo in EVAPORATE and a cellulose-based placebo in the Garlic5 study. “So we have high confidence that the benefits seen in this trial with icosapent ethyl represent icosapent ethyl’s beneficial effects on atherosclerosis and not harm of mineral oil,” he said.
Exactly how icosapent ethyl is slowing atherosclerosis, however, is not fully known, Dr. Budoff said in an interview. “It might be inflammation and oxidation; those have both been shown to be better with icosapent ethyl, but I don’t think we fully understand the implications of these results.”
Dr. Budoff dismissed tweets that suggest the data might have been unblinded as unprofessional and said they are requesting that Imperial College have Francis cease and desist.
“He doesn’t have the actual data, so there is no way to do statistics without the dataset. The whole thing is inappropriate,” Dr. Budoff said.
Amarin Pharma provided funding and drug for the trial. Dr. Budoff has received research funding from and has served as a speaker for Amarin Pharma, Amgen, AstraZeneca, Boehringer Ingelheim, Novo Nordisk, and Pfizer and has served as a speaker for Bristol-Myers Squibb. Dr. Francis has disclosed no relevant financial relationships..
A version of this article originally appeared on Medscape.com.
Final 18-month results of the EVAPORATE trial suggest icosapent ethyl (Vascepa) provides even greater slowing of coronary plaque progression when added to statins for patients with high triglyceride levels, but not all cardiologists are convinced.
The study was designed to explore a potential mechanism behind the cardiovascular event reduction in REDUCE-IT. Previously reported interim results showed that, after 9 months, the pharmaceutical-grade omega-3 fatty acid formation significantly slowed the progression of several plaque types but not the primary endpoint of change in low-attenuation plaque volume on multidetector CT.
From baseline to 18-month follow-up, however, the primary endpoint was significantly reduced by 17% in the icosapent ethyl group, whereas low-attenuation plaque volumes increased by 109% in the placebo group (P = .0061).
Significant declines were also seen with icosapent ethyl 4 g/day versus the mineral oil placebo for all other plaque types except dense calcium after adjustment for age, sex, diabetes, hypertension, and triglyceride levels at baseline:
- Dense calcium: –1% versus 15% (P = .0531).
- Fibro-fatty: –34% versus 32% (P = .0002).
- Fibrous: –20% versus 1% (P = .0028).
- Noncalcified: –19% versus 9% (P = .0005).
- Total plaque: –9% versus 11% (P = .0019).
The results parallel nicely with recent clinical data from REDUCE-IT REVASC, in which icosapent ethyl 4 g/day provided a very early benefit on first revascularization events that reached statistical significance after only 11 months (hazard ratio, 0.66), principal investigator Matthew Budoff, MD, director of cardiac CT at Harbor–University of California, Los Angeles, Medical Center in Torrance, Calif., said during the virtual European Society of Cardiology Congress 2020.
The findings were also published simultaneously in the European Heart Journal and quickly prompted a flurry of comments on social media.
Some were supportive. Christopher Cannon, MD, of Harvard Medical School, Boston; Dan Soffer, MD, a lipidologist at the University of Pennsylvania, Philadelphia; and Viet Le, MPAS, PA, a researcher at the Intermountain Heart Institute, Murray, Utah, took to Twitter to praise Dr. Budoff and the final results of the mechanistic study. Dr. Soffer called the study “elegant,” while Dr. Cannon said the results provide “important mechanistic data on plaque character.”
Others were highly critical, including a poll questioning whether the article should be retracted or revised.
Ibrahim H. Tanboga, MD, PhD, a cardiology professor and biostatistician at Hisar Intercontinental Hospital in Istanbul, questioned how the longitudinal change in low-attenuation plaque was possible clinically; his plot of the data showed these lesions getting worse in both arms before getting better in both arms.
A more volatile exchange concerned whether there were differences in the baseline characteristics between the two groups and whether the data might have been unblinded.
“I am sympathetic to the boss of a big laboratory [who] might not know how every step of the process was done and therefore might not be aware of opportunities for accidental bias. This can easily happen in a large and active department,” Darrel Francis, MD, professor of cardiology at the National Heart and Lung Institute, Imperial College, London, said in an interview.
An alternative explanation proffered on Twitter was that the interim analysis found no significant differences in baseline measures because it used nonparametric tests, whereas log transformation was applied to the final data. In any event, the tweets prompted a sharp rebuke from Dr. Budoff.
Dr. Francis raised another point of contention on Twitter regarding the degree of plaque progression in the placebo group.
In an interview, Dr. Francis pointed out that the final data represent the percentage change in the logarithm, not the actual percentage change in atheroma. So the increase in total atheroma volume in the placebo arm is not 11% but rather a scaling-up by 100.4 or 2.51, in other words, 151%.
He also offered a “less subtle feature of possible erroneous data,” in that the abstract reported low-attenuation plaque “more than doubles” in 18 months, which he described as a “ghastly supercharged version of Moore’s law for atheroma, instead of microchips.”
So “either it’s a mistake in the measurement or the placebo is harmful, because I can’t see how this is sustainable,” he said. “Why isn’t everyone dead from coronary disease?”
Concerns were raised previously over the possibility that the mineral oil placebo used in both EVAPORATE and REDUCE-IT could be having ill effects, notably, by increasing LDL cholesterol and C-reactive protein levels.
In an interview, Steven Nissen, MD, who is chair of cardiovascular medicine at the Cleveland Clinic and has been among the critics of the mineral oil placebo, also questioned the plaque progression over the 18 months.
“I’ve published more than dozen regression/progression trials, and we have never seen anything like this in a placebo group, ever,” he said. “If this was a clean placebo, why would this happen in a short amount of time?
“I’m concerned this is all about an increase, in the case of REDUCE-IT, in morbidity and mortality in the placebo group, and in the EVAPORATE trial, an increase in plaque in the placebo group,” Dr. Nissen said. “So this raises serious doubts about whether there is any benefit to icosapent ethyl.”
Asked about the 109% increase, Dr. Budoff said in an interview that low-attenuation plaque represents a much smaller quantity of overall plaque volume. “So the percentages might be exaggerated if you look at just percentage change because they;re small volumes.”
He also noted that previous trials that evaluated atherosclerosis progression used intravascular ultrasound (IVUS), whereas EVAPORATE is the first to make the transition to CT angiography-based analysis of plaque progression.
“I would point out that Dr. Nissen has only worked on intravascular ultrasound, which, while it’s parallel in its ability to measure plaque, measures different volumes and measures it in a totally different way,” said Dr. Budoff. “So I don’t think we can directly compare the results of CT angiography to Dr. Nissen’s examples of IVUS.”
During his presentation, Dr. Budoff highlighted their recent data showing a similar rate of plaque progression between the mineral oil placebo in EVAPORATE and a cellulose-based placebo in the Garlic5 study. “So we have high confidence that the benefits seen in this trial with icosapent ethyl represent icosapent ethyl’s beneficial effects on atherosclerosis and not harm of mineral oil,” he said.
Exactly how icosapent ethyl is slowing atherosclerosis, however, is not fully known, Dr. Budoff said in an interview. “It might be inflammation and oxidation; those have both been shown to be better with icosapent ethyl, but I don’t think we fully understand the implications of these results.”
Dr. Budoff dismissed tweets that suggest the data might have been unblinded as unprofessional and said they are requesting that Imperial College have Francis cease and desist.
“He doesn’t have the actual data, so there is no way to do statistics without the dataset. The whole thing is inappropriate,” Dr. Budoff said.
Amarin Pharma provided funding and drug for the trial. Dr. Budoff has received research funding from and has served as a speaker for Amarin Pharma, Amgen, AstraZeneca, Boehringer Ingelheim, Novo Nordisk, and Pfizer and has served as a speaker for Bristol-Myers Squibb. Dr. Francis has disclosed no relevant financial relationships..
A version of this article originally appeared on Medscape.com.
Statins linked to reduced mortality in COVID-19
Treatment with statins was associated with a reduced risk of a severe or fatal course of COVID-19 by 30%, a meta-analysis of four published studies has shown.

In the analysis that included almost 9,000 COVID-19 patients, there was a significantly reduced risk for fatal or severe COVID-19 among patients who were users of statins, compared with nonusers (pooled hazard ratio, 0.70; 95% confidence interval, 0.53-0.94).
Based on the findings, “it may be time we shift our focus to statins as the potential therapeutic options in COVID-19 patients,” authors Syed Shahzad Hasan, PhD, University of Huddersfield (England), and Chia Siang Kow, MPharm, International Medical University, Kuala Lumpur, Malaysia, said in an interview.
The study was published online August 11 in The American Journal of Cardiology.
Moderate- to good-quality data
The analysis included four studies published up to July 27 of this year. Eligible studies included those with a cohort or case-control designs, enrolled patients with confirmed COVID-19, and had data available allowing comparison of the risk of severe illness and/or mortality among statin users versus nonusers in adjusted analyses, the authors noted.
The four studies – one of “moderate” quality and three of “good” quality – included a total of 8,990 COVID-19 patients.
In the pooled analysis, there was a significantly reduced risk for fatal or severe COVID-19 with use of statins, compared with non-use of statins (pooled HR, 0.70; 95% CI, 0.53-0.94).
Their findings also “discredited the suggestion of harms with the use of statins in COVID-19 patients,” the authors concluded.
“Since our meta-analysis included a fairly large total number of COVID-19 patients from four studies in which three are large-scale studies that adjusted extensively for multiple potential confounding factors, the findings can be considered reliable,” Dr. Hasan and Mr. Kow wrote in their article.
Based on the results, “moderate- to high-intensity statin therapy is likely to be beneficial” in patients with COVID-19, they said.
However, they cautioned that more data from prospective studies are needed to substantiate the findings and to determine the appropriate regimen for a statin in COVID-19 patients.
Yibin Wang, PhD, of the University of California, Los Angeles, said that “this is a very simple meta-analysis from four published studies which consistently reported a protective or neutral effect of statin usage on mortality or severe complications in COVID-19 patients.”
Although the scope of this meta-analysis was “quite limited, the conclusion was not unexpected, as most of the clinical analysis so far reported supports the benefits or safety of statin usage in COVID-19 patients,” Dr. Wang said in an interview.
Nonetheless, questions remain
While there is “almost no dispute” about the safety of continuing statin therapy in COVID-19 patients, it remains to be determined if statin therapy can be implemented as an adjuvant or independent therapy and a part of the standard care for COVID-19 patients regardless of their hyperlipidemia status, said Dr. Wang, who was not associated with Dr. Hasan’s and Mr. Kow’s research.
“While statin usage is associated with several beneficial effects such as anti-inflammation and cytoprotection, these effects are usually observed from long-term usage rather than short-term/acute administration. Therefore, prospective studies and randomized trials should be conducted to test the efficacy of stain usage for COVID-19 patients with mild to severe symptoms,” he noted.
“Considering the excellent record of statins as a safe and cheap drug, it is certainly a worthwhile effort to consider its broad-based usage for COVID-19 in order to lower the overall death and severe complications,” Dr. Wang concluded.
Guillermo Rodriguez-Nava, MD, department of internal medicine, AMITA Health Saint Francis Hospital, Evanston, Ill., is first author on one of the studies included in this meta-analysis.
The retrospective, single-center study found slower progression to death associated with atorvastatin in older patients with COVID-19 admitted to the ICU.
“Currently, there are hundreds of clinical trials evaluating a wide variety of pharmacological therapies for COVID-19. Unfortunately, these trials take time, and we are getting results in dribs and drabs,” Dr. Rodriguez-Nava said in an interview.
“In the meantime, the best available evidence is observational, and COVID-19 treatment regiments will continue to evolve. Whether atorvastatin is effective against COVID-19 is still under investigation. Nevertheless, clinicians should consider at least continuing them in patients with COVID-19,” he advised.
The study had no specific funding. Dr. Hasan, Mr. Kow, Dr. Wang, and Dr. Rodriguez-Nava disclosed no relationships relevant to this research.
A version of this article originally appeared on Medscape.com.
Treatment with statins was associated with a reduced risk of a severe or fatal course of COVID-19 by 30%, a meta-analysis of four published studies has shown.
In the analysis that included almost 9,000 COVID-19 patients, there was a significantly reduced risk for fatal or severe COVID-19 among patients who were users of statins, compared with nonusers (pooled hazard ratio, 0.70; 95% confidence interval, 0.53-0.94).
Based on the findings, “it may be time we shift our focus to statins as the potential therapeutic options in COVID-19 patients,” authors Syed Shahzad Hasan, PhD, University of Huddersfield (England), and Chia Siang Kow, MPharm, International Medical University, Kuala Lumpur, Malaysia, said in an interview.
The study was published online August 11 in The American Journal of Cardiology.
Moderate- to good-quality data
The analysis included four studies published up to July 27 of this year. Eligible studies included those with a cohort or case-control designs, enrolled patients with confirmed COVID-19, and had data available allowing comparison of the risk of severe illness and/or mortality among statin users versus nonusers in adjusted analyses, the authors noted.
The four studies – one of “moderate” quality and three of “good” quality – included a total of 8,990 COVID-19 patients.
In the pooled analysis, there was a significantly reduced risk for fatal or severe COVID-19 with use of statins, compared with non-use of statins (pooled HR, 0.70; 95% CI, 0.53-0.94).
Their findings also “discredited the suggestion of harms with the use of statins in COVID-19 patients,” the authors concluded.
“Since our meta-analysis included a fairly large total number of COVID-19 patients from four studies in which three are large-scale studies that adjusted extensively for multiple potential confounding factors, the findings can be considered reliable,” Dr. Hasan and Mr. Kow wrote in their article.
Based on the results, “moderate- to high-intensity statin therapy is likely to be beneficial” in patients with COVID-19, they said.
However, they cautioned that more data from prospective studies are needed to substantiate the findings and to determine the appropriate regimen for a statin in COVID-19 patients.
Yibin Wang, PhD, of the University of California, Los Angeles, said that “this is a very simple meta-analysis from four published studies which consistently reported a protective or neutral effect of statin usage on mortality or severe complications in COVID-19 patients.”
Although the scope of this meta-analysis was “quite limited, the conclusion was not unexpected, as most of the clinical analysis so far reported supports the benefits or safety of statin usage in COVID-19 patients,” Dr. Wang said in an interview.
Nonetheless, questions remain
While there is “almost no dispute” about the safety of continuing statin therapy in COVID-19 patients, it remains to be determined if statin therapy can be implemented as an adjuvant or independent therapy and a part of the standard care for COVID-19 patients regardless of their hyperlipidemia status, said Dr. Wang, who was not associated with Dr. Hasan’s and Mr. Kow’s research.
“While statin usage is associated with several beneficial effects such as anti-inflammation and cytoprotection, these effects are usually observed from long-term usage rather than short-term/acute administration. Therefore, prospective studies and randomized trials should be conducted to test the efficacy of stain usage for COVID-19 patients with mild to severe symptoms,” he noted.
“Considering the excellent record of statins as a safe and cheap drug, it is certainly a worthwhile effort to consider its broad-based usage for COVID-19 in order to lower the overall death and severe complications,” Dr. Wang concluded.
Guillermo Rodriguez-Nava, MD, department of internal medicine, AMITA Health Saint Francis Hospital, Evanston, Ill., is first author on one of the studies included in this meta-analysis.
The retrospective, single-center study found slower progression to death associated with atorvastatin in older patients with COVID-19 admitted to the ICU.
“Currently, there are hundreds of clinical trials evaluating a wide variety of pharmacological therapies for COVID-19. Unfortunately, these trials take time, and we are getting results in dribs and drabs,” Dr. Rodriguez-Nava said in an interview.
“In the meantime, the best available evidence is observational, and COVID-19 treatment regiments will continue to evolve. Whether atorvastatin is effective against COVID-19 is still under investigation. Nevertheless, clinicians should consider at least continuing them in patients with COVID-19,” he advised.
The study had no specific funding. Dr. Hasan, Mr. Kow, Dr. Wang, and Dr. Rodriguez-Nava disclosed no relationships relevant to this research.
A version of this article originally appeared on Medscape.com.
Treatment with statins was associated with a reduced risk of a severe or fatal course of COVID-19 by 30%, a meta-analysis of four published studies has shown.
In the analysis that included almost 9,000 COVID-19 patients, there was a significantly reduced risk for fatal or severe COVID-19 among patients who were users of statins, compared with nonusers (pooled hazard ratio, 0.70; 95% confidence interval, 0.53-0.94).
Based on the findings, “it may be time we shift our focus to statins as the potential therapeutic options in COVID-19 patients,” authors Syed Shahzad Hasan, PhD, University of Huddersfield (England), and Chia Siang Kow, MPharm, International Medical University, Kuala Lumpur, Malaysia, said in an interview.
The study was published online August 11 in The American Journal of Cardiology.
Moderate- to good-quality data
The analysis included four studies published up to July 27 of this year. Eligible studies included those with a cohort or case-control designs, enrolled patients with confirmed COVID-19, and had data available allowing comparison of the risk of severe illness and/or mortality among statin users versus nonusers in adjusted analyses, the authors noted.
The four studies – one of “moderate” quality and three of “good” quality – included a total of 8,990 COVID-19 patients.
In the pooled analysis, there was a significantly reduced risk for fatal or severe COVID-19 with use of statins, compared with non-use of statins (pooled HR, 0.70; 95% CI, 0.53-0.94).
Their findings also “discredited the suggestion of harms with the use of statins in COVID-19 patients,” the authors concluded.
“Since our meta-analysis included a fairly large total number of COVID-19 patients from four studies in which three are large-scale studies that adjusted extensively for multiple potential confounding factors, the findings can be considered reliable,” Dr. Hasan and Mr. Kow wrote in their article.
Based on the results, “moderate- to high-intensity statin therapy is likely to be beneficial” in patients with COVID-19, they said.
However, they cautioned that more data from prospective studies are needed to substantiate the findings and to determine the appropriate regimen for a statin in COVID-19 patients.
Yibin Wang, PhD, of the University of California, Los Angeles, said that “this is a very simple meta-analysis from four published studies which consistently reported a protective or neutral effect of statin usage on mortality or severe complications in COVID-19 patients.”
Although the scope of this meta-analysis was “quite limited, the conclusion was not unexpected, as most of the clinical analysis so far reported supports the benefits or safety of statin usage in COVID-19 patients,” Dr. Wang said in an interview.
Nonetheless, questions remain
While there is “almost no dispute” about the safety of continuing statin therapy in COVID-19 patients, it remains to be determined if statin therapy can be implemented as an adjuvant or independent therapy and a part of the standard care for COVID-19 patients regardless of their hyperlipidemia status, said Dr. Wang, who was not associated with Dr. Hasan’s and Mr. Kow’s research.
“While statin usage is associated with several beneficial effects such as anti-inflammation and cytoprotection, these effects are usually observed from long-term usage rather than short-term/acute administration. Therefore, prospective studies and randomized trials should be conducted to test the efficacy of stain usage for COVID-19 patients with mild to severe symptoms,” he noted.
“Considering the excellent record of statins as a safe and cheap drug, it is certainly a worthwhile effort to consider its broad-based usage for COVID-19 in order to lower the overall death and severe complications,” Dr. Wang concluded.
Guillermo Rodriguez-Nava, MD, department of internal medicine, AMITA Health Saint Francis Hospital, Evanston, Ill., is first author on one of the studies included in this meta-analysis.
The retrospective, single-center study found slower progression to death associated with atorvastatin in older patients with COVID-19 admitted to the ICU.
“Currently, there are hundreds of clinical trials evaluating a wide variety of pharmacological therapies for COVID-19. Unfortunately, these trials take time, and we are getting results in dribs and drabs,” Dr. Rodriguez-Nava said in an interview.
“In the meantime, the best available evidence is observational, and COVID-19 treatment regiments will continue to evolve. Whether atorvastatin is effective against COVID-19 is still under investigation. Nevertheless, clinicians should consider at least continuing them in patients with COVID-19,” he advised.
The study had no specific funding. Dr. Hasan, Mr. Kow, Dr. Wang, and Dr. Rodriguez-Nava disclosed no relationships relevant to this research.
A version of this article originally appeared on Medscape.com.

Evolocumab safe and effective in pediatric FH
The PCSK9 monoclonal antibody evolocumab (Repatha) was well tolerated and effectively lowered LDL cholesterol by 38% compared with placebo in a randomized controlled trial in pediatric patients with heterozygous familial hypercholesterolemia (FH) already taking statins with or without ezetimibe.
“HAUSER-RCT is the largest study and the first placebo-controlled randomized trial of a PCSK9 inhibitor in pediatric FH,” senior author Daniel Gaudet, MD, PhD, Universite de Montreal, said in an interview.
“The study showed good safety and efficacy of the drug in this population, with an excellent 44% reduction in LDL cholesterol compared with 6% in the placebo group.”
The trial also found evolocumab to be well tolerated in this group, with adverse effects similar in the active and placebo groups.
“Some people have wondered about using a drug with a monthly injection in a pediatric population, but this was not an issue in our study,” Dr. Gaudet said. “The idea of a monthly injection was well received, and no patient withdrew because of this.”
The HAUSER-RCT trial was presented on Aug. 29 at the virtual annual congress of the European Society of Cardiology (ESC Congress 2020) and simultaneously published online in the New England Journal of Medicine.
“With patients recruited from 23 countries in five continents, the study provides an accurate picture of the safety and efficacy of evolocumab in pediatric FH patients worldwide,” Dr. Gaudet said.
The 24-week, randomized, double-blind, placebo-controlled trial involved 157 patients aged 10-17 years with heterozygous FH already taking statins with or without ezetimibe and who had an LDL cholesterol level of 130 mg/dL or more and a triglyceride level of 400 mg/dL or less.
They were randomly assigned in a 2:1 ratio to receive monthly subcutaneous injections of evolocumab (420 mg) or placebo.
Results showed that at week 24, the mean percentage change from baseline in LDL cholesterol level was −44.5% in the evolocumab group and −6.2% in the placebo group, giving a difference of −38.3 percentage points (P < .001).
The absolute change in the LDL cholesterol level was −77.5 mg/dL in the evolocumab group and −9.0 mg/dL in the placebo group, giving a difference of −68.6 mg/dL (P < .001).
Results for all secondary lipid variables were significantly better with evolocumab than with placebo. The incidence of adverse events that occurred during the treatment period was similar in the evolocumab and placebo groups. Laboratory abnormalities did not differ between groups.
Dr. Gaudet noted that FH is the most common genetic disease worldwide, affecting 1 in 250 people. “It is very treatable, so it is important to identify these patients, but it is massively underdiagnosed, with only around 15%-20% of patients with the condition having been identified,” he said.
“The vast majority of pediatric FH patients can reach target LDL levels with statins and ezetimibe, but there are 5%-10% of patients who may need additional therapy. We have now shown that evolocumab is safe and effective for these patients and can be used to fill this gap,” Dr. Gaudet said. “We can now say that we can cover all situations in treating FH whatever the severity of the disease.”
However, the challenge remains to improve the diagnosis of FH. “If there is one person with FH in a family, then it is essential that the whole extended family is tested. Our toolbox for treating this condition is now sufficiently effective, so there is no reason not to diagnose this disease,” Dr. Gaudet stressed.
The HAUSER-RCT study was supported by Amgen. Gaudet reports grants and personal fees from Amgen during the conduct of the study.
A version of this article originally appeared on Medscape.com.
The PCSK9 monoclonal antibody evolocumab (Repatha) was well tolerated and effectively lowered LDL cholesterol by 38% compared with placebo in a randomized controlled trial in pediatric patients with heterozygous familial hypercholesterolemia (FH) already taking statins with or without ezetimibe.
“HAUSER-RCT is the largest study and the first placebo-controlled randomized trial of a PCSK9 inhibitor in pediatric FH,” senior author Daniel Gaudet, MD, PhD, Universite de Montreal, said in an interview.
“The study showed good safety and efficacy of the drug in this population, with an excellent 44% reduction in LDL cholesterol compared with 6% in the placebo group.”
The trial also found evolocumab to be well tolerated in this group, with adverse effects similar in the active and placebo groups.
“Some people have wondered about using a drug with a monthly injection in a pediatric population, but this was not an issue in our study,” Dr. Gaudet said. “The idea of a monthly injection was well received, and no patient withdrew because of this.”
The HAUSER-RCT trial was presented on Aug. 29 at the virtual annual congress of the European Society of Cardiology (ESC Congress 2020) and simultaneously published online in the New England Journal of Medicine.
“With patients recruited from 23 countries in five continents, the study provides an accurate picture of the safety and efficacy of evolocumab in pediatric FH patients worldwide,” Dr. Gaudet said.
The 24-week, randomized, double-blind, placebo-controlled trial involved 157 patients aged 10-17 years with heterozygous FH already taking statins with or without ezetimibe and who had an LDL cholesterol level of 130 mg/dL or more and a triglyceride level of 400 mg/dL or less.
They were randomly assigned in a 2:1 ratio to receive monthly subcutaneous injections of evolocumab (420 mg) or placebo.
Results showed that at week 24, the mean percentage change from baseline in LDL cholesterol level was −44.5% in the evolocumab group and −6.2% in the placebo group, giving a difference of −38.3 percentage points (P < .001).
The absolute change in the LDL cholesterol level was −77.5 mg/dL in the evolocumab group and −9.0 mg/dL in the placebo group, giving a difference of −68.6 mg/dL (P < .001).
Results for all secondary lipid variables were significantly better with evolocumab than with placebo. The incidence of adverse events that occurred during the treatment period was similar in the evolocumab and placebo groups. Laboratory abnormalities did not differ between groups.
Dr. Gaudet noted that FH is the most common genetic disease worldwide, affecting 1 in 250 people. “It is very treatable, so it is important to identify these patients, but it is massively underdiagnosed, with only around 15%-20% of patients with the condition having been identified,” he said.
“The vast majority of pediatric FH patients can reach target LDL levels with statins and ezetimibe, but there are 5%-10% of patients who may need additional therapy. We have now shown that evolocumab is safe and effective for these patients and can be used to fill this gap,” Dr. Gaudet said. “We can now say that we can cover all situations in treating FH whatever the severity of the disease.”
However, the challenge remains to improve the diagnosis of FH. “If there is one person with FH in a family, then it is essential that the whole extended family is tested. Our toolbox for treating this condition is now sufficiently effective, so there is no reason not to diagnose this disease,” Dr. Gaudet stressed.
The HAUSER-RCT study was supported by Amgen. Gaudet reports grants and personal fees from Amgen during the conduct of the study.
A version of this article originally appeared on Medscape.com.
The PCSK9 monoclonal antibody evolocumab (Repatha) was well tolerated and effectively lowered LDL cholesterol by 38% compared with placebo in a randomized controlled trial in pediatric patients with heterozygous familial hypercholesterolemia (FH) already taking statins with or without ezetimibe.
“HAUSER-RCT is the largest study and the first placebo-controlled randomized trial of a PCSK9 inhibitor in pediatric FH,” senior author Daniel Gaudet, MD, PhD, Universite de Montreal, said in an interview.
“The study showed good safety and efficacy of the drug in this population, with an excellent 44% reduction in LDL cholesterol compared with 6% in the placebo group.”
The trial also found evolocumab to be well tolerated in this group, with adverse effects similar in the active and placebo groups.
“Some people have wondered about using a drug with a monthly injection in a pediatric population, but this was not an issue in our study,” Dr. Gaudet said. “The idea of a monthly injection was well received, and no patient withdrew because of this.”
The HAUSER-RCT trial was presented on Aug. 29 at the virtual annual congress of the European Society of Cardiology (ESC Congress 2020) and simultaneously published online in the New England Journal of Medicine.
“With patients recruited from 23 countries in five continents, the study provides an accurate picture of the safety and efficacy of evolocumab in pediatric FH patients worldwide,” Dr. Gaudet said.
The 24-week, randomized, double-blind, placebo-controlled trial involved 157 patients aged 10-17 years with heterozygous FH already taking statins with or without ezetimibe and who had an LDL cholesterol level of 130 mg/dL or more and a triglyceride level of 400 mg/dL or less.
They were randomly assigned in a 2:1 ratio to receive monthly subcutaneous injections of evolocumab (420 mg) or placebo.
Results showed that at week 24, the mean percentage change from baseline in LDL cholesterol level was −44.5% in the evolocumab group and −6.2% in the placebo group, giving a difference of −38.3 percentage points (P < .001).
The absolute change in the LDL cholesterol level was −77.5 mg/dL in the evolocumab group and −9.0 mg/dL in the placebo group, giving a difference of −68.6 mg/dL (P < .001).
Results for all secondary lipid variables were significantly better with evolocumab than with placebo. The incidence of adverse events that occurred during the treatment period was similar in the evolocumab and placebo groups. Laboratory abnormalities did not differ between groups.
Dr. Gaudet noted that FH is the most common genetic disease worldwide, affecting 1 in 250 people. “It is very treatable, so it is important to identify these patients, but it is massively underdiagnosed, with only around 15%-20% of patients with the condition having been identified,” he said.
“The vast majority of pediatric FH patients can reach target LDL levels with statins and ezetimibe, but there are 5%-10% of patients who may need additional therapy. We have now shown that evolocumab is safe and effective for these patients and can be used to fill this gap,” Dr. Gaudet said. “We can now say that we can cover all situations in treating FH whatever the severity of the disease.”
However, the challenge remains to improve the diagnosis of FH. “If there is one person with FH in a family, then it is essential that the whole extended family is tested. Our toolbox for treating this condition is now sufficiently effective, so there is no reason not to diagnose this disease,” Dr. Gaudet stressed.
The HAUSER-RCT study was supported by Amgen. Gaudet reports grants and personal fees from Amgen during the conduct of the study.
A version of this article originally appeared on Medscape.com.