User login
Infantile hemangiomas clear faster with Nd:YAG treatment
BOSTON – Using a 650-microsecond, pulsed 1064nm neodymium-doped yttrium aluminum garnet (Nd:YAG) laser to treat infantile hemangiomas can yield high clearance rates after one treatment, without adverse reactions, according to a study presented at the annual meeting of the American Society for Laser Medicine and Surgery.
“[Hemangiomas] have historically been treated with a bunch of different devices; most commonly, the pulsed dye laser and also propranolol, either orally or topically,” said Dr. David J. Goldberg of Skin Laser & Surgery Specialists of New York and New Jersey. While use of an Nd:YAG laser for treating infantile hemangiomas is not exactly new, “what’s new about this is it was not a millisecond Nd:YAG laser; it was a microsecond Nd:YAG laser, [which] generally makes it much safer for treatment in general.”
The study enrolled 250 children between age 1 month and 4 months at the time of recruitment; they were followed for one year. They received a single treatment with an Nd:YAG 1064nm laser using a 650 microsecond pulse duration, a spot size of 2-3 millimeters, and a fluence of 42-64 joules per square centimeter. Photographs were taken for evaluation immediately before and after each treatment, and 30 and 180 days after each treatment.
Treatments lasted 3-5 minutes each, covering an area no larger than three square centimeters. Infants who started treatment in the first six weeks of life had the best results, according to Dr. Goldberg. Treated areas immediately turned gray after each treatment on all subjects, and all subjects showed “substantial improvement” in hemangioma size after only a single treatment, based on photographic evaluation taken 6 months after treatment. Over 75% of hemangiomas were either completely or almost completely (over 75% clearance) eliminated over the 1-year follow-up period.
There was no downtime or adverse events experienced by any patients following treatments. Overall, parents of the children who received treatment were “highly satisfied” with the results.
“The big takeaway is that you may not need multiple treatments [and] you may not need to use a pulse dye laser – one treatment may be enough,” Dr. Goldberg explained. “This [Nd:YAG] device is also a very small device that you can put into a suitcase, so it’s not that big device that we’re used to using.”
Dr. Goldberg did not report any relevant financial disclosures.
BOSTON – Using a 650-microsecond, pulsed 1064nm neodymium-doped yttrium aluminum garnet (Nd:YAG) laser to treat infantile hemangiomas can yield high clearance rates after one treatment, without adverse reactions, according to a study presented at the annual meeting of the American Society for Laser Medicine and Surgery.
“[Hemangiomas] have historically been treated with a bunch of different devices; most commonly, the pulsed dye laser and also propranolol, either orally or topically,” said Dr. David J. Goldberg of Skin Laser & Surgery Specialists of New York and New Jersey. While use of an Nd:YAG laser for treating infantile hemangiomas is not exactly new, “what’s new about this is it was not a millisecond Nd:YAG laser; it was a microsecond Nd:YAG laser, [which] generally makes it much safer for treatment in general.”
The study enrolled 250 children between age 1 month and 4 months at the time of recruitment; they were followed for one year. They received a single treatment with an Nd:YAG 1064nm laser using a 650 microsecond pulse duration, a spot size of 2-3 millimeters, and a fluence of 42-64 joules per square centimeter. Photographs were taken for evaluation immediately before and after each treatment, and 30 and 180 days after each treatment.
Treatments lasted 3-5 minutes each, covering an area no larger than three square centimeters. Infants who started treatment in the first six weeks of life had the best results, according to Dr. Goldberg. Treated areas immediately turned gray after each treatment on all subjects, and all subjects showed “substantial improvement” in hemangioma size after only a single treatment, based on photographic evaluation taken 6 months after treatment. Over 75% of hemangiomas were either completely or almost completely (over 75% clearance) eliminated over the 1-year follow-up period.
There was no downtime or adverse events experienced by any patients following treatments. Overall, parents of the children who received treatment were “highly satisfied” with the results.
“The big takeaway is that you may not need multiple treatments [and] you may not need to use a pulse dye laser – one treatment may be enough,” Dr. Goldberg explained. “This [Nd:YAG] device is also a very small device that you can put into a suitcase, so it’s not that big device that we’re used to using.”
Dr. Goldberg did not report any relevant financial disclosures.
BOSTON – Using a 650-microsecond, pulsed 1064nm neodymium-doped yttrium aluminum garnet (Nd:YAG) laser to treat infantile hemangiomas can yield high clearance rates after one treatment, without adverse reactions, according to a study presented at the annual meeting of the American Society for Laser Medicine and Surgery.
“[Hemangiomas] have historically been treated with a bunch of different devices; most commonly, the pulsed dye laser and also propranolol, either orally or topically,” said Dr. David J. Goldberg of Skin Laser & Surgery Specialists of New York and New Jersey. While use of an Nd:YAG laser for treating infantile hemangiomas is not exactly new, “what’s new about this is it was not a millisecond Nd:YAG laser; it was a microsecond Nd:YAG laser, [which] generally makes it much safer for treatment in general.”
The study enrolled 250 children between age 1 month and 4 months at the time of recruitment; they were followed for one year. They received a single treatment with an Nd:YAG 1064nm laser using a 650 microsecond pulse duration, a spot size of 2-3 millimeters, and a fluence of 42-64 joules per square centimeter. Photographs were taken for evaluation immediately before and after each treatment, and 30 and 180 days after each treatment.
Treatments lasted 3-5 minutes each, covering an area no larger than three square centimeters. Infants who started treatment in the first six weeks of life had the best results, according to Dr. Goldberg. Treated areas immediately turned gray after each treatment on all subjects, and all subjects showed “substantial improvement” in hemangioma size after only a single treatment, based on photographic evaluation taken 6 months after treatment. Over 75% of hemangiomas were either completely or almost completely (over 75% clearance) eliminated over the 1-year follow-up period.
There was no downtime or adverse events experienced by any patients following treatments. Overall, parents of the children who received treatment were “highly satisfied” with the results.
“The big takeaway is that you may not need multiple treatments [and] you may not need to use a pulse dye laser – one treatment may be enough,” Dr. Goldberg explained. “This [Nd:YAG] device is also a very small device that you can put into a suitcase, so it’s not that big device that we’re used to using.”
Dr. Goldberg did not report any relevant financial disclosures.
AT LASER 2016
Key clinical point: Infantile hemangiomas can be effectively treated with a 650-microsecond pulsed Nd:YAG 1064nm laser, with no evidence of adverse skin effects.
Major finding: Substantial improvement in hemangiomas were seen after one treatment administered in 5 minutes or less.
Data source: The study enrolled 250 infants with hemangiomas aged 1 to 4 months at baseline, and were followed for one year.
Disclosures: Dr. Goldberg did not report any relevant financial disclosures.
If a Chronic Wound Does Not Heal, Biopsy It: A Clinical Lesson on Underlying Malignancies
To the Editor:
Experience, subjective opinion, and relationships with patients are cornerstones of general practice but also can be pitfalls. It is common for a late-presenting patient to offer a seemingly rational explanation for a long-standing lesion. Unless an objective analysis of the clinical problem is undertaken, it can be easy to embark on an incorrect treatment pathway for the patient’s condition.
One of the luxuries of specialist hospital medicine or surgery is the ability to focus on a narrow range of clinical problems, which makes it easier to spot the anomaly, as long as it is within the purview of the practitioner. We report 2 cases of skin malignancies that were assumed to be chronic wounds of benign etiology.
A 63-year-old builder was referred by his general practitioner with a chronic wound on the right forearm of 4 years’ duration. His medical history included psoriasis, and he did not have a history of diabetes mellitus or use of immunosuppressants. The general practitioner suggested possible incidental origin following a prior trauma or a psoriatic-related lesion. The patient reported that the lesion did not resemble prior psoriatic lesions and it had deteriorated substantially over the last 2 years. Furthermore, a small ulcer was starting to develop on the left forearm. Further advice was requested by the general practitioner regarding wound dressings. On examination a sloughy ulcer measuring 8.5×7.5 cm had eroded to expose necrotic tendons with surrounding induration and cellulitis (Figure 1A). In addition, a psoriatic lesion was found on the left forearm (Figure 1B). There were no palpable axillary lymph nodes. Clinical suspicion, incision biopsies, and subsequent histology confirmed cutaneous CD4+ T-cell lymphoma. This case was reviewed at a multidisciplinary team meeting and referred to the hematology-oncology department. The patient subsequently underwent chemotherapy with liposomal doxorubicin and radiotherapy over a period of 5 months. An elective right forearm amputation was planned due to erosion of the ulcer through tendons down to bone (Figure 2).


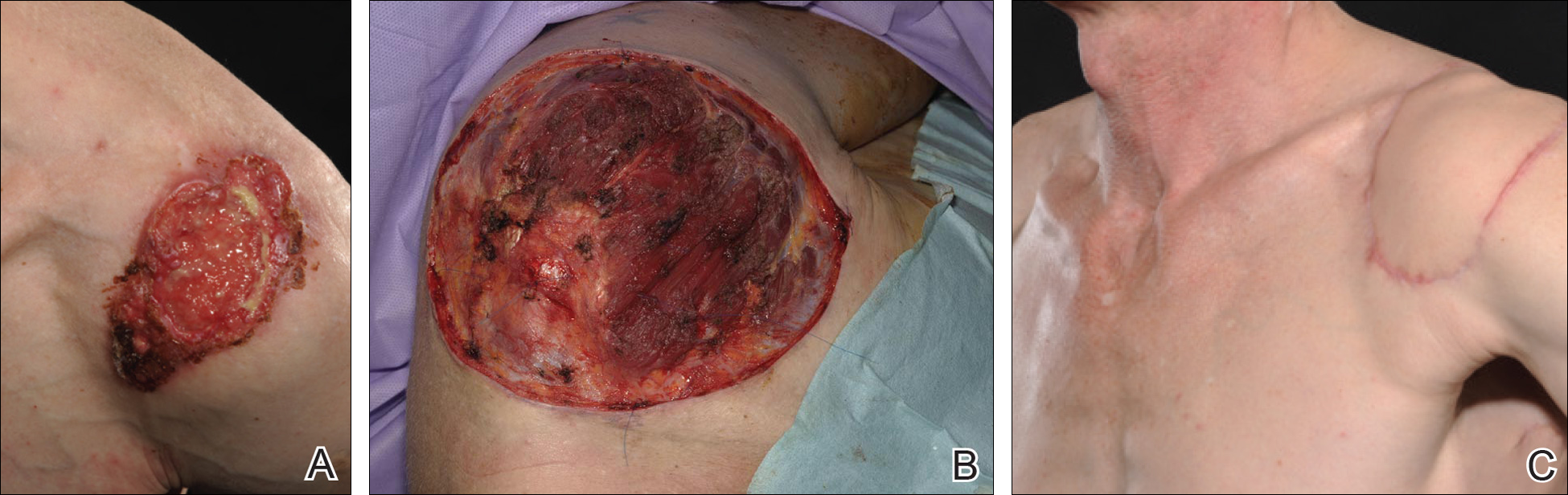
A 48-year-old Latvian lorry driver was referred by his general practitioner with a chronic wound on the left shoulder of 6 years’ duration. His medical history included a partial gastrectomy for a peptic ulcer 18 years prior, and he did not have a history of diabetes mellitus or use of immunosuppressants. The general practitioner included a partial gastrectomy for a peptic ulcer 18 years prior, and he did not have a history of diabetes mellitus or use of immunosuppressants. The general practitioner suggested the etiology was a burn from a hot metal rod 6 years prior. Advice was sought regarding dressings and suitability for a possible skin graft. Physical examination showed a 4.5×10-cm ulcer fixed to the underlying tissue on the anterior aspect of the left shoulder with no evidence of infection or presence of a foreign body (Figure 3A). Clinical suspicion, incision biopsies, and subsequent histology confirmed a highly infiltrative/morphoeic, partly nodular, and partly diffuse basal cell carcinoma (BCC) that measured 92 mm in diameter extending to the subcutis with no involvement of muscle or perineural or vascular invasion. The patient underwent wide local excision of the BCC with frozen section control. The BCC had eroded into the deltoid muscle and to the periosteum of the clavicle (Figure 3B). The defect was reconstructed with a pedicled muscle-sparing latissimus dorsi musculocutaneous flap. The patient presented for follow-up months following reconstruction with an uneventful recovery (Figure 3C).
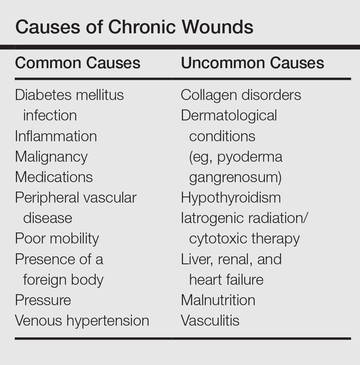
These 2 cases highlight easy pitfalls for an unsuspecting clinician. Although both cases had alternative plausible explanations, they proved to be cutaneous malignancies. The powerful message these cases send is that long-standing chronic wounds should be biopsied to exclude malignancy. Some of the other common underlying causes of wounds that may prevent healing are highlighted in the Table. Vascular insufficiency usually presents in characteristic patterns with a good clinical history and associated signs and findings on investigation. A foreign body, which can be anything from an orthopedic metal implant to a retained stitch from surgery or nonmedical material, may be the culprit and may be identified from a thorough medical history or appropriate imaging.
Infection is another possible explanation of a nonhealing wound. On the face, an underlying dental abscess with a sinus tracking from the root of the tooth to the skin of the cheek or jaw may be the source. Elsewhere on the body, chronic osteomyelitis may be the cause, which may be from any infective origin from Staphylococcus aureus to tuberculosis, and will most commonly present with a discharging sinus but also may present with a nonspecific ulcer.
Chronic wounds also may not heal because of a multitude of patient factors such as poor nutrition, diabetes mellitus, medication (eg, steroids, nonsteroidal anti-inflammatory drugs), other inflammatory causes, and poor mobility. Chronic wounds represent a substantial burden to patients, health care professionals, and the health care system. In the United States alone, they affect 5.7 million patients and cost an estimated $20 billion.1 Approximately 1% of the Western population will present with leg ulceration at some point in their lives.2
Physical examination of ulcers in any clinical setting can be difficult. We postulate that it can be made more difficult at times in primary care because the patient may add confounding elements for consideration or seemingly plausible explanations. However, whenever possible, a physician should ask, “Could there possibly be an underlying malignancy here?” If there is any chance of malignancy despite plausible explanations being offered, the lesion should be biopsied.
- Branski LK, Gauglitz GG, Herndon DN, et al. A review of gene and stem cell therapy in cutaneous wound healing [published online July 7, 2008]. Burns. 2009;35:171-180.
- Callam MJ. Prevalence of chronic leg ulceration and severe chronic venous disease in western countries. Phlebology. 1992;7(suppl 1):6-12.
To the Editor:
Experience, subjective opinion, and relationships with patients are cornerstones of general practice but also can be pitfalls. It is common for a late-presenting patient to offer a seemingly rational explanation for a long-standing lesion. Unless an objective analysis of the clinical problem is undertaken, it can be easy to embark on an incorrect treatment pathway for the patient’s condition.
One of the luxuries of specialist hospital medicine or surgery is the ability to focus on a narrow range of clinical problems, which makes it easier to spot the anomaly, as long as it is within the purview of the practitioner. We report 2 cases of skin malignancies that were assumed to be chronic wounds of benign etiology.
A 63-year-old builder was referred by his general practitioner with a chronic wound on the right forearm of 4 years’ duration. His medical history included psoriasis, and he did not have a history of diabetes mellitus or use of immunosuppressants. The general practitioner suggested possible incidental origin following a prior trauma or a psoriatic-related lesion. The patient reported that the lesion did not resemble prior psoriatic lesions and it had deteriorated substantially over the last 2 years. Furthermore, a small ulcer was starting to develop on the left forearm. Further advice was requested by the general practitioner regarding wound dressings. On examination a sloughy ulcer measuring 8.5×7.5 cm had eroded to expose necrotic tendons with surrounding induration and cellulitis (Figure 1A). In addition, a psoriatic lesion was found on the left forearm (Figure 1B). There were no palpable axillary lymph nodes. Clinical suspicion, incision biopsies, and subsequent histology confirmed cutaneous CD4+ T-cell lymphoma. This case was reviewed at a multidisciplinary team meeting and referred to the hematology-oncology department. The patient subsequently underwent chemotherapy with liposomal doxorubicin and radiotherapy over a period of 5 months. An elective right forearm amputation was planned due to erosion of the ulcer through tendons down to bone (Figure 2).
A 48-year-old Latvian lorry driver was referred by his general practitioner with a chronic wound on the left shoulder of 6 years’ duration. His medical history included a partial gastrectomy for a peptic ulcer 18 years prior, and he did not have a history of diabetes mellitus or use of immunosuppressants. The general practitioner included a partial gastrectomy for a peptic ulcer 18 years prior, and he did not have a history of diabetes mellitus or use of immunosuppressants. The general practitioner suggested the etiology was a burn from a hot metal rod 6 years prior. Advice was sought regarding dressings and suitability for a possible skin graft. Physical examination showed a 4.5×10-cm ulcer fixed to the underlying tissue on the anterior aspect of the left shoulder with no evidence of infection or presence of a foreign body (Figure 3A). Clinical suspicion, incision biopsies, and subsequent histology confirmed a highly infiltrative/morphoeic, partly nodular, and partly diffuse basal cell carcinoma (BCC) that measured 92 mm in diameter extending to the subcutis with no involvement of muscle or perineural or vascular invasion. The patient underwent wide local excision of the BCC with frozen section control. The BCC had eroded into the deltoid muscle and to the periosteum of the clavicle (Figure 3B). The defect was reconstructed with a pedicled muscle-sparing latissimus dorsi musculocutaneous flap. The patient presented for follow-up months following reconstruction with an uneventful recovery (Figure 3C).
These 2 cases highlight easy pitfalls for an unsuspecting clinician. Although both cases had alternative plausible explanations, they proved to be cutaneous malignancies. The powerful message these cases send is that long-standing chronic wounds should be biopsied to exclude malignancy. Some of the other common underlying causes of wounds that may prevent healing are highlighted in the Table. Vascular insufficiency usually presents in characteristic patterns with a good clinical history and associated signs and findings on investigation. A foreign body, which can be anything from an orthopedic metal implant to a retained stitch from surgery or nonmedical material, may be the culprit and may be identified from a thorough medical history or appropriate imaging.
Infection is another possible explanation of a nonhealing wound. On the face, an underlying dental abscess with a sinus tracking from the root of the tooth to the skin of the cheek or jaw may be the source. Elsewhere on the body, chronic osteomyelitis may be the cause, which may be from any infective origin from Staphylococcus aureus to tuberculosis, and will most commonly present with a discharging sinus but also may present with a nonspecific ulcer.
Chronic wounds also may not heal because of a multitude of patient factors such as poor nutrition, diabetes mellitus, medication (eg, steroids, nonsteroidal anti-inflammatory drugs), other inflammatory causes, and poor mobility. Chronic wounds represent a substantial burden to patients, health care professionals, and the health care system. In the United States alone, they affect 5.7 million patients and cost an estimated $20 billion.1 Approximately 1% of the Western population will present with leg ulceration at some point in their lives.2
Physical examination of ulcers in any clinical setting can be difficult. We postulate that it can be made more difficult at times in primary care because the patient may add confounding elements for consideration or seemingly plausible explanations. However, whenever possible, a physician should ask, “Could there possibly be an underlying malignancy here?” If there is any chance of malignancy despite plausible explanations being offered, the lesion should be biopsied.
To the Editor:
Experience, subjective opinion, and relationships with patients are cornerstones of general practice but also can be pitfalls. It is common for a late-presenting patient to offer a seemingly rational explanation for a long-standing lesion. Unless an objective analysis of the clinical problem is undertaken, it can be easy to embark on an incorrect treatment pathway for the patient’s condition.
One of the luxuries of specialist hospital medicine or surgery is the ability to focus on a narrow range of clinical problems, which makes it easier to spot the anomaly, as long as it is within the purview of the practitioner. We report 2 cases of skin malignancies that were assumed to be chronic wounds of benign etiology.
A 63-year-old builder was referred by his general practitioner with a chronic wound on the right forearm of 4 years’ duration. His medical history included psoriasis, and he did not have a history of diabetes mellitus or use of immunosuppressants. The general practitioner suggested possible incidental origin following a prior trauma or a psoriatic-related lesion. The patient reported that the lesion did not resemble prior psoriatic lesions and it had deteriorated substantially over the last 2 years. Furthermore, a small ulcer was starting to develop on the left forearm. Further advice was requested by the general practitioner regarding wound dressings. On examination a sloughy ulcer measuring 8.5×7.5 cm had eroded to expose necrotic tendons with surrounding induration and cellulitis (Figure 1A). In addition, a psoriatic lesion was found on the left forearm (Figure 1B). There were no palpable axillary lymph nodes. Clinical suspicion, incision biopsies, and subsequent histology confirmed cutaneous CD4+ T-cell lymphoma. This case was reviewed at a multidisciplinary team meeting and referred to the hematology-oncology department. The patient subsequently underwent chemotherapy with liposomal doxorubicin and radiotherapy over a period of 5 months. An elective right forearm amputation was planned due to erosion of the ulcer through tendons down to bone (Figure 2).
A 48-year-old Latvian lorry driver was referred by his general practitioner with a chronic wound on the left shoulder of 6 years’ duration. His medical history included a partial gastrectomy for a peptic ulcer 18 years prior, and he did not have a history of diabetes mellitus or use of immunosuppressants. The general practitioner included a partial gastrectomy for a peptic ulcer 18 years prior, and he did not have a history of diabetes mellitus or use of immunosuppressants. The general practitioner suggested the etiology was a burn from a hot metal rod 6 years prior. Advice was sought regarding dressings and suitability for a possible skin graft. Physical examination showed a 4.5×10-cm ulcer fixed to the underlying tissue on the anterior aspect of the left shoulder with no evidence of infection or presence of a foreign body (Figure 3A). Clinical suspicion, incision biopsies, and subsequent histology confirmed a highly infiltrative/morphoeic, partly nodular, and partly diffuse basal cell carcinoma (BCC) that measured 92 mm in diameter extending to the subcutis with no involvement of muscle or perineural or vascular invasion. The patient underwent wide local excision of the BCC with frozen section control. The BCC had eroded into the deltoid muscle and to the periosteum of the clavicle (Figure 3B). The defect was reconstructed with a pedicled muscle-sparing latissimus dorsi musculocutaneous flap. The patient presented for follow-up months following reconstruction with an uneventful recovery (Figure 3C).
These 2 cases highlight easy pitfalls for an unsuspecting clinician. Although both cases had alternative plausible explanations, they proved to be cutaneous malignancies. The powerful message these cases send is that long-standing chronic wounds should be biopsied to exclude malignancy. Some of the other common underlying causes of wounds that may prevent healing are highlighted in the Table. Vascular insufficiency usually presents in characteristic patterns with a good clinical history and associated signs and findings on investigation. A foreign body, which can be anything from an orthopedic metal implant to a retained stitch from surgery or nonmedical material, may be the culprit and may be identified from a thorough medical history or appropriate imaging.
Infection is another possible explanation of a nonhealing wound. On the face, an underlying dental abscess with a sinus tracking from the root of the tooth to the skin of the cheek or jaw may be the source. Elsewhere on the body, chronic osteomyelitis may be the cause, which may be from any infective origin from Staphylococcus aureus to tuberculosis, and will most commonly present with a discharging sinus but also may present with a nonspecific ulcer.
Chronic wounds also may not heal because of a multitude of patient factors such as poor nutrition, diabetes mellitus, medication (eg, steroids, nonsteroidal anti-inflammatory drugs), other inflammatory causes, and poor mobility. Chronic wounds represent a substantial burden to patients, health care professionals, and the health care system. In the United States alone, they affect 5.7 million patients and cost an estimated $20 billion.1 Approximately 1% of the Western population will present with leg ulceration at some point in their lives.2
Physical examination of ulcers in any clinical setting can be difficult. We postulate that it can be made more difficult at times in primary care because the patient may add confounding elements for consideration or seemingly plausible explanations. However, whenever possible, a physician should ask, “Could there possibly be an underlying malignancy here?” If there is any chance of malignancy despite plausible explanations being offered, the lesion should be biopsied.
- Branski LK, Gauglitz GG, Herndon DN, et al. A review of gene and stem cell therapy in cutaneous wound healing [published online July 7, 2008]. Burns. 2009;35:171-180.
- Callam MJ. Prevalence of chronic leg ulceration and severe chronic venous disease in western countries. Phlebology. 1992;7(suppl 1):6-12.
- Branski LK, Gauglitz GG, Herndon DN, et al. A review of gene and stem cell therapy in cutaneous wound healing [published online July 7, 2008]. Burns. 2009;35:171-180.
- Callam MJ. Prevalence of chronic leg ulceration and severe chronic venous disease in western countries. Phlebology. 1992;7(suppl 1):6-12.
Practice Points
- Patients with chronic wounds should have a thorough history and examination, appropriate laboratory tests, and purposeful search to determine etiology.
- Long-standing chronic wounds should be biopsied to exclude malignancy.

What’s Less Noticeable: A Straight Scar or a Zigzag Scar?
One of the determinants of a successful surgical outcome is the perception, on the part of the patient, of the cosmesis of a scar. The use of Z-plasty is an accepted means by which to break a scar up into smaller geometric segments. In some instances, a Z-plasty is used for scar revision to elongate a scar that may be pulling. However, a study published online in JAMA Facial Plastic Surgery on April 7 mentions the lack of studies measuring the perception of these scars among the normal population after surgery.
Ratnarathorn et al designed a prospective Internet-based survey with a goal of 580 responses to give a power of 90%. The survey was distributed to a diverse sample of the US population. Using editing software, Ratnarathorn et al superimposed a mature linear scar and a mature zigzag scar onto the faces of standardized headshots from 4 individuals (2 males, 2 females). Each individual had 1 image of the linear scar and 1 image of the zigzag scars superimposed onto each of 3 anatomical areas—forehead (flat surface), cheek (convex surface), and temple (concave surface)—yielding 24 images for the respondents to assess.
A 24.5% (n=876) response rate was achieved with 3575 surveys distributed. Of the 876 respondents, 810 (92.5%) completed the survey (46.1% male, 53.9% female). Respondents were asked to rate the scars on a scale of 1 to 10 (1=normal skin; 10=worst scar imaginable).
Results were statistically significantly lower (better) for the linear scars compared to the zigzag scars in all 3 anatomic areas and across both male and female groups with a mean score of 2.9 versus 4.5 (P<.001). A multivariable regression model of respondent age, sex, educational level, and income showed no statistically significant effect on the rating of the scars.
What’s the issue?
This study highlights some interesting points. Coming from an academic practice, we oftentimes find ourselves teaching residents a variety of skin closure techniques to deal with defects from skin cancer excisions. It is both challenging and fun to design complex closures; however, we must keep in mind what is in the best interest of the patient. One of the points I try to emphasize is that we must understand that there are no true straight lines on the face. In fact, when scars from procedures appear as geometric shapes on the face, our eyes tend to be drawn to them. For this reason, it often is best to use curvilinear lines wherever possible. Ratnarathorn et al highlights that point exactly. More studies of this nature are needed to assess what is perceived as a successful outcome, by both physicians and patients.
As you follow your patients for the long-term, have you noticed that you perform more or fewer zigzag scars?
One of the determinants of a successful surgical outcome is the perception, on the part of the patient, of the cosmesis of a scar. The use of Z-plasty is an accepted means by which to break a scar up into smaller geometric segments. In some instances, a Z-plasty is used for scar revision to elongate a scar that may be pulling. However, a study published online in JAMA Facial Plastic Surgery on April 7 mentions the lack of studies measuring the perception of these scars among the normal population after surgery.
Ratnarathorn et al designed a prospective Internet-based survey with a goal of 580 responses to give a power of 90%. The survey was distributed to a diverse sample of the US population. Using editing software, Ratnarathorn et al superimposed a mature linear scar and a mature zigzag scar onto the faces of standardized headshots from 4 individuals (2 males, 2 females). Each individual had 1 image of the linear scar and 1 image of the zigzag scars superimposed onto each of 3 anatomical areas—forehead (flat surface), cheek (convex surface), and temple (concave surface)—yielding 24 images for the respondents to assess.
A 24.5% (n=876) response rate was achieved with 3575 surveys distributed. Of the 876 respondents, 810 (92.5%) completed the survey (46.1% male, 53.9% female). Respondents were asked to rate the scars on a scale of 1 to 10 (1=normal skin; 10=worst scar imaginable).
Results were statistically significantly lower (better) for the linear scars compared to the zigzag scars in all 3 anatomic areas and across both male and female groups with a mean score of 2.9 versus 4.5 (P<.001). A multivariable regression model of respondent age, sex, educational level, and income showed no statistically significant effect on the rating of the scars.
What’s the issue?
This study highlights some interesting points. Coming from an academic practice, we oftentimes find ourselves teaching residents a variety of skin closure techniques to deal with defects from skin cancer excisions. It is both challenging and fun to design complex closures; however, we must keep in mind what is in the best interest of the patient. One of the points I try to emphasize is that we must understand that there are no true straight lines on the face. In fact, when scars from procedures appear as geometric shapes on the face, our eyes tend to be drawn to them. For this reason, it often is best to use curvilinear lines wherever possible. Ratnarathorn et al highlights that point exactly. More studies of this nature are needed to assess what is perceived as a successful outcome, by both physicians and patients.
As you follow your patients for the long-term, have you noticed that you perform more or fewer zigzag scars?
One of the determinants of a successful surgical outcome is the perception, on the part of the patient, of the cosmesis of a scar. The use of Z-plasty is an accepted means by which to break a scar up into smaller geometric segments. In some instances, a Z-plasty is used for scar revision to elongate a scar that may be pulling. However, a study published online in JAMA Facial Plastic Surgery on April 7 mentions the lack of studies measuring the perception of these scars among the normal population after surgery.
Ratnarathorn et al designed a prospective Internet-based survey with a goal of 580 responses to give a power of 90%. The survey was distributed to a diverse sample of the US population. Using editing software, Ratnarathorn et al superimposed a mature linear scar and a mature zigzag scar onto the faces of standardized headshots from 4 individuals (2 males, 2 females). Each individual had 1 image of the linear scar and 1 image of the zigzag scars superimposed onto each of 3 anatomical areas—forehead (flat surface), cheek (convex surface), and temple (concave surface)—yielding 24 images for the respondents to assess.
A 24.5% (n=876) response rate was achieved with 3575 surveys distributed. Of the 876 respondents, 810 (92.5%) completed the survey (46.1% male, 53.9% female). Respondents were asked to rate the scars on a scale of 1 to 10 (1=normal skin; 10=worst scar imaginable).
Results were statistically significantly lower (better) for the linear scars compared to the zigzag scars in all 3 anatomic areas and across both male and female groups with a mean score of 2.9 versus 4.5 (P<.001). A multivariable regression model of respondent age, sex, educational level, and income showed no statistically significant effect on the rating of the scars.
What’s the issue?
This study highlights some interesting points. Coming from an academic practice, we oftentimes find ourselves teaching residents a variety of skin closure techniques to deal with defects from skin cancer excisions. It is both challenging and fun to design complex closures; however, we must keep in mind what is in the best interest of the patient. One of the points I try to emphasize is that we must understand that there are no true straight lines on the face. In fact, when scars from procedures appear as geometric shapes on the face, our eyes tend to be drawn to them. For this reason, it often is best to use curvilinear lines wherever possible. Ratnarathorn et al highlights that point exactly. More studies of this nature are needed to assess what is perceived as a successful outcome, by both physicians and patients.
As you follow your patients for the long-term, have you noticed that you perform more or fewer zigzag scars?

Cosmetic Corner: Dermatologists Weigh in on Tinted Moisturizers
To improve patient care and outcomes, leading dermatologists offered their recommendations on tinted moisturizers. Consideration must be given to:
- Anthelios 50 Mineral Tinted Ultra Light Sunscreen Fluid
La Roche-Posay Laboratoire Dermatologique
“I love this product because it provides sun protection and gives your skin a bit of color.”—Gary Goldenberg, MD, New York, New York
“I recommend this moisturizer to my patients because it has broad-spectrum UV protection, antioxidants, and a nongreasy texture.”—Shari Lipner, MD, PhD, New York, New York
- Hydra Life BB Creme
Christian Dior Perfumes LLC
“This is a lightweight, tinted cream, which comes in 3 shades for different Fitzpatrick skin types. It also provides broad-spectrum UVA/UVB protection with SPF 30.”—Cherise M. Levi, DO, New York, New York
- Neutrogena Oil-Free Acne Correct & Cover Pink Grapefruit Moisturizer
Johnson & Johnson Consumer Inc.
“It is a tinted moisturizer that also helps to fight acne with salicylic acid.”—Anthony M. Rossi, MD, New York, New York
Cutis invites readers to send us their recommendations. Body scrubs, OTC acne treatments, and cleansing devices will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on tinted moisturizers. Consideration must be given to:
- Anthelios 50 Mineral Tinted Ultra Light Sunscreen Fluid
La Roche-Posay Laboratoire Dermatologique
“I love this product because it provides sun protection and gives your skin a bit of color.”—Gary Goldenberg, MD, New York, New York
“I recommend this moisturizer to my patients because it has broad-spectrum UV protection, antioxidants, and a nongreasy texture.”—Shari Lipner, MD, PhD, New York, New York
- Hydra Life BB Creme
Christian Dior Perfumes LLC
“This is a lightweight, tinted cream, which comes in 3 shades for different Fitzpatrick skin types. It also provides broad-spectrum UVA/UVB protection with SPF 30.”—Cherise M. Levi, DO, New York, New York
- Neutrogena Oil-Free Acne Correct & Cover Pink Grapefruit Moisturizer
Johnson & Johnson Consumer Inc.
“It is a tinted moisturizer that also helps to fight acne with salicylic acid.”—Anthony M. Rossi, MD, New York, New York
Cutis invites readers to send us their recommendations. Body scrubs, OTC acne treatments, and cleansing devices will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on tinted moisturizers. Consideration must be given to:
- Anthelios 50 Mineral Tinted Ultra Light Sunscreen Fluid
La Roche-Posay Laboratoire Dermatologique
“I love this product because it provides sun protection and gives your skin a bit of color.”—Gary Goldenberg, MD, New York, New York
“I recommend this moisturizer to my patients because it has broad-spectrum UV protection, antioxidants, and a nongreasy texture.”—Shari Lipner, MD, PhD, New York, New York
- Hydra Life BB Creme
Christian Dior Perfumes LLC
“This is a lightweight, tinted cream, which comes in 3 shades for different Fitzpatrick skin types. It also provides broad-spectrum UVA/UVB protection with SPF 30.”—Cherise M. Levi, DO, New York, New York
- Neutrogena Oil-Free Acne Correct & Cover Pink Grapefruit Moisturizer
Johnson & Johnson Consumer Inc.
“It is a tinted moisturizer that also helps to fight acne with salicylic acid.”—Anthony M. Rossi, MD, New York, New York
Cutis invites readers to send us their recommendations. Body scrubs, OTC acne treatments, and cleansing devices will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.

Vitamin C
Vitamin C (ascorbic acid) is one of the four most important ingredients in skin care products.
• It is proven to increase collagen production when applied topically to skin.
• It inhibits tyrosinase to even skin tone and has a strong antioxidant activity.
• It is absorbed well orally, but not enough gets to the skin.
• It is best absorbed at a pH of 2.0.
• It is unstable when exposed to light and air. Instruct patients to discard 6 months after opening.
In addition, the proper formulation is patented and expensive. Stick with brands you trust. Use vitamin C on skin prior to procedures to speed healing. It will sting when used on inflamed skin because of the low pH.

In my opinion, all patients need to be on the proper skin care regimen for their skin type. This includes a daily sun protection factor (SPF), a cleanser, a retinoid, and an antioxidant. Ascorbic acid is one of my favorite antioxidants because it is the only one shown to increase the production of collagen by fibroblasts and inhibit tyrosinase while scavenging free radicals. Sure it is expensive – but that is because formulating and packaging it properly is expensive. Unfortunately, many subpar brands have entered the market. Ask to see the company’s research data on its formulation before choosing to recommend or sell ascorbic acid/vitamin C in your practice.
An essential water-soluble nutrient for the development of bone and connective tissue, vitamin C is found in citrus fruits and green leafy vegetables. It is produced in most plants and animals, but a mutated gene in humans has resulted in a deficiency of L-gulono-gamma-lactone oxidase, the enzyme required for its production.1,2 Although ascorbic acid cannot be synthesized by the human body, dietary consumption renders it the most abundant antioxidant in human skin and blood, and vitamin C plays an important role in endogenous collagen production and the inhibition of collagen degradation.3-6 Ascorbic acid also is known to regenerate alpha-tocopherol (vitamin E) levels and, therefore, is thought to protect against diseases related to oxidative stress.7
Epidermal vitamin C can be depleted by sunlight and environmental pollution, such as ozone in urban pollution.8,9 Known to exhibit a wide range of biologic activities, ascorbic acid has been shown to deliver rejuvenating effects on skin wrinkles, texture, strength, and evenness of tone through its antioxidant, tyrosinase-inhibiting, and collagen production-promoting activities.10 Indeed, as a topical agent, vitamin C has been used to prevent photodamage, and to treat melasma, striae alba, and postoperative erythema in laser patients.11,12 It is regularly used to treat aging skin, and as a depigmenting agent.2,10,13 This column will discuss the antioxidant, antiaging, and depigmenting activity of vitamin C in the context of recent human studies.
Antioxidant and anti-aging activity
Vitamin C is unique among antioxidants because of its ability to increase collagen production in addition to its free radical scavenging antioxidant activity. Due to its capacity to interfere with the UV-induced generation of reactive oxygen species by reacting with the superoxide anion or the hydroxyl radical, vitamin C has become a popular addition to “after-sun” products,14,15 and been shown to be effective in mitigating the effects of UVB, such as erythema and signs of photoaging, on porcine and human skin.2,16-17
A 2001 study in 10 postmenopausal women by Nusgens et al. found that daily topical application of 5% L-ascorbic acid enhanced the levels of procollagen types I and III, their posttranslational maturation enzymes, and tissue inhibitor of matrix metalloproteinase.18 This led to increased levels of collagen in the skin.
In 2003, Humbert et al. conducted a 6-month, double-blind, vehicle-controlled trial with 20 healthy female volunteers showing that patients treated with 5% vitamin C cream experienced significant improvements in deep furrows on the neck and forearms.19
In a small study of nine adults with Fitzpatrick skin types II or III in 2008, Murray et al. studied whether a stable topical preparation of 15% L-ascorbic acid, 1% alpha-tocopherol, and 0.5% ferulic acid could protect human skin in vivo from UV-induced damage. They found that the antioxidant formulation supplemented the antioxidant pool of the skin and conferred significant photoprotection, guarding the skin against erythema and apoptosis as well as effectively suppressing p53 activation and reducing thymine dimer mutations known to be associated with skin cancer.13
In 2012, Xu et al. evaluated the efficacy and safety of topical 23.8% L-ascorbic acid on photoaged skin in a split-face study of 20 Chinese women. Significant improvements in fine lines, dyspigmentation, and surface roughness were observed, without adverse side effects.20
In a 2015 study of 60 healthy female subjects, Crisan et al. used high-frequency ultrasound to determine that the use of a topical vitamin C formulation yielded significant increases in collagen synthesis, revealing the solution to be an effective rejuvenation therapy.21
Skin lightening activity
Melasma
In 2004, Espinal-Perez et al. conducted a double-blind randomized trial of 5% ascorbic acid, compared with 4% hydroquinone (HQ) water–oil emulsion in 16 female patients with melasma, aged 23-43 years (mean 36 years). Of those treated with vitamin C, 62.5% exhibited good or excellent subjectively assessed skin lightening. There was no statistically significant difference in depigmenting activity in the HQ group, of which 68.7% experienced irritation whereas vitamin C was well tolerated.22

In a randomized, double-blind, placebo-controlled study, researchers used iontophoresis to enhance the penetration of vitamin C into the skin and significantly reduce pigmentation, compared with placebo.23
Although ascorbic acid is viewed by many as ineffective as a depigmenting agent alone, particularly in 5%-10% concentrations, when used in combination with other ingredients such as HQ, it is considered effective.24 In the magnesium-L-ascorbyl-2-phosphate esterified form, however, vitamin C is among the most popular prescribed depigmenting agents around the world, especially in countries where HQ and its derivatives are prohibited.25 In a 2009 16-week open-label study by Hwang et al. of 25% L-ascorbic acid and a chemical penetration enhancer for treating melasma in 40 patients, researchers observed significant reductions in pigmentation.26
In a small split-face study early in 2015, Lee et al. showed that the combination of 1,064-nm Q-switched neodymium-doped yttrium aluminum garnet (QS-Nd:YAG) laser and ultrasonic application of vitamin C was more effective than was the laser treatment alone in achieving a cosmetically acceptable treatment for melasma.27
PIPA
Vitamin C can be used to diminish or prevent post-inflammatory pigment alteration (PIPA) after procedures because it inhibits tyrosinase, lowers inflammation, and quenches free radicals. In a study of 10 patients, the application of topical vitamin C 2 or more weeks after surgery reduced the duration and degree of erythema after skin resurfacing with a carbon dioxide laser.28
Stretch marks
The depigmenting effects of vitamin C can lighten the pigmentation associated with stretch marks and its anti-inflammatory activity can contribute to blunting related redness.12
Conclusion
Although orally administered ascorbic acid is readily bioavailable, ascorbic acid in the skin is quickly depleted and oral supplementation alone does not yield optimal skin levels. Therefore, topical use of vitamin C is desirable. In fact, I tell my patients to use it topically in the morning and add a vitamin C supplement to their diet. Numerous formulation considerations (e.g., packaging, exposure to air or light during use, skin sensitivity, and user preference) are involved in the stabilization and effective penetration of ascorbic acid into the skin, and the process of developing, manufacturing, and packaging of effective, stable vitamin C products is expensive.
Vitamin C, particularly when combined with other ingredients, has been shown to be an integral constituent in topical antioxidant, antiaging, and depigmenting formulations that show promise in the dermatologic armamentarium. It is a great choice for use in a prep-procedure skin care regimen to speed healing. Use after a procedure is prohibited by the stinging associated with the low pH of properly formulated products.
References
1. J Biol Chem. 1994 May 6;269(18):13685-8.
2. Dermatol Surg. 2001 Feb;27(2):137-42.
3. J Invest Dermatol. 1994 Jan;102(1):122-4.
4. Dermatol Surg. 2005 Jul;31(7 Pt 2):814-7.
5. Annu Rev Nutr. 1994;14:371-91.
6. J Drugs Dermatol. 2008 Jul;7(7 Suppl):s2-6.
7. J Am Acad Dermatol. 2003 Jun;48(6):866-74.
8. J Invest Dermatol. 1994 Apr;102(4):470-5.
9. Free Radic Biol Med. 1997;23:85-91.
10. J Drugs Dermatol. 2014 Oct;13(10):1208-13.
11. J Am Acad Dermatol. 1996 Jan;34(1):29-33.
12. Dermatol Surg. 1998 Aug;24(8):849-56.
13. J Am Acad Dermatol. 2008 Sep;59(3):418-25.
14. J Biol Chem. 1983 Jun 10;258(11):6695-7.
15. J Phys Chem. 1983;87:1809-12.
16. Br J Dermatol. 1992 Sep;127(3):247-53.
17. J Invest Dermatol. 1991;96:587.
18. J Invest Dermatol. 2001 Jun;116(6):853-9.
19. Exp Dermatol. 2003 Jun;12(3):237-44.
20. J Drugs Dermatol. 2012 Jan;11(1):51-6.
21. Clin Cosmet Investig Dermatol. 2015 Sep 2;8:463-70
22. Int J Dermatol. 2004 Aug;43(8):604-7.
23. Dermatology. 2003;206(4):316-20.
24. Am J Clin Dermatol. 2011 Apr 1;12(2):87-99.
25. Phytother Res. 2006 Nov;20(11):921-34.
26. J Cutan Med Surg. 2009 Mar-Apr;13(2):74-81.
27. Lasers Med Sci. 2015 Jan;30(1):159-63.
28. Dermatol Surg. 1998 Mar;24(3):331-4.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.
Vitamin C (ascorbic acid) is one of the four most important ingredients in skin care products.
• It is proven to increase collagen production when applied topically to skin.
• It inhibits tyrosinase to even skin tone and has a strong antioxidant activity.
• It is absorbed well orally, but not enough gets to the skin.
• It is best absorbed at a pH of 2.0.
• It is unstable when exposed to light and air. Instruct patients to discard 6 months after opening.
In addition, the proper formulation is patented and expensive. Stick with brands you trust. Use vitamin C on skin prior to procedures to speed healing. It will sting when used on inflamed skin because of the low pH.
In my opinion, all patients need to be on the proper skin care regimen for their skin type. This includes a daily sun protection factor (SPF), a cleanser, a retinoid, and an antioxidant. Ascorbic acid is one of my favorite antioxidants because it is the only one shown to increase the production of collagen by fibroblasts and inhibit tyrosinase while scavenging free radicals. Sure it is expensive – but that is because formulating and packaging it properly is expensive. Unfortunately, many subpar brands have entered the market. Ask to see the company’s research data on its formulation before choosing to recommend or sell ascorbic acid/vitamin C in your practice.
An essential water-soluble nutrient for the development of bone and connective tissue, vitamin C is found in citrus fruits and green leafy vegetables. It is produced in most plants and animals, but a mutated gene in humans has resulted in a deficiency of L-gulono-gamma-lactone oxidase, the enzyme required for its production.1,2 Although ascorbic acid cannot be synthesized by the human body, dietary consumption renders it the most abundant antioxidant in human skin and blood, and vitamin C plays an important role in endogenous collagen production and the inhibition of collagen degradation.3-6 Ascorbic acid also is known to regenerate alpha-tocopherol (vitamin E) levels and, therefore, is thought to protect against diseases related to oxidative stress.7
Epidermal vitamin C can be depleted by sunlight and environmental pollution, such as ozone in urban pollution.8,9 Known to exhibit a wide range of biologic activities, ascorbic acid has been shown to deliver rejuvenating effects on skin wrinkles, texture, strength, and evenness of tone through its antioxidant, tyrosinase-inhibiting, and collagen production-promoting activities.10 Indeed, as a topical agent, vitamin C has been used to prevent photodamage, and to treat melasma, striae alba, and postoperative erythema in laser patients.11,12 It is regularly used to treat aging skin, and as a depigmenting agent.2,10,13 This column will discuss the antioxidant, antiaging, and depigmenting activity of vitamin C in the context of recent human studies.
Antioxidant and anti-aging activity
Vitamin C is unique among antioxidants because of its ability to increase collagen production in addition to its free radical scavenging antioxidant activity. Due to its capacity to interfere with the UV-induced generation of reactive oxygen species by reacting with the superoxide anion or the hydroxyl radical, vitamin C has become a popular addition to “after-sun” products,14,15 and been shown to be effective in mitigating the effects of UVB, such as erythema and signs of photoaging, on porcine and human skin.2,16-17
A 2001 study in 10 postmenopausal women by Nusgens et al. found that daily topical application of 5% L-ascorbic acid enhanced the levels of procollagen types I and III, their posttranslational maturation enzymes, and tissue inhibitor of matrix metalloproteinase.18 This led to increased levels of collagen in the skin.
In 2003, Humbert et al. conducted a 6-month, double-blind, vehicle-controlled trial with 20 healthy female volunteers showing that patients treated with 5% vitamin C cream experienced significant improvements in deep furrows on the neck and forearms.19
In a small study of nine adults with Fitzpatrick skin types II or III in 2008, Murray et al. studied whether a stable topical preparation of 15% L-ascorbic acid, 1% alpha-tocopherol, and 0.5% ferulic acid could protect human skin in vivo from UV-induced damage. They found that the antioxidant formulation supplemented the antioxidant pool of the skin and conferred significant photoprotection, guarding the skin against erythema and apoptosis as well as effectively suppressing p53 activation and reducing thymine dimer mutations known to be associated with skin cancer.13
In 2012, Xu et al. evaluated the efficacy and safety of topical 23.8% L-ascorbic acid on photoaged skin in a split-face study of 20 Chinese women. Significant improvements in fine lines, dyspigmentation, and surface roughness were observed, without adverse side effects.20
In a 2015 study of 60 healthy female subjects, Crisan et al. used high-frequency ultrasound to determine that the use of a topical vitamin C formulation yielded significant increases in collagen synthesis, revealing the solution to be an effective rejuvenation therapy.21
Skin lightening activity
Melasma
In 2004, Espinal-Perez et al. conducted a double-blind randomized trial of 5% ascorbic acid, compared with 4% hydroquinone (HQ) water–oil emulsion in 16 female patients with melasma, aged 23-43 years (mean 36 years). Of those treated with vitamin C, 62.5% exhibited good or excellent subjectively assessed skin lightening. There was no statistically significant difference in depigmenting activity in the HQ group, of which 68.7% experienced irritation whereas vitamin C was well tolerated.22
In a randomized, double-blind, placebo-controlled study, researchers used iontophoresis to enhance the penetration of vitamin C into the skin and significantly reduce pigmentation, compared with placebo.23
Although ascorbic acid is viewed by many as ineffective as a depigmenting agent alone, particularly in 5%-10% concentrations, when used in combination with other ingredients such as HQ, it is considered effective.24 In the magnesium-L-ascorbyl-2-phosphate esterified form, however, vitamin C is among the most popular prescribed depigmenting agents around the world, especially in countries where HQ and its derivatives are prohibited.25 In a 2009 16-week open-label study by Hwang et al. of 25% L-ascorbic acid and a chemical penetration enhancer for treating melasma in 40 patients, researchers observed significant reductions in pigmentation.26
In a small split-face study early in 2015, Lee et al. showed that the combination of 1,064-nm Q-switched neodymium-doped yttrium aluminum garnet (QS-Nd:YAG) laser and ultrasonic application of vitamin C was more effective than was the laser treatment alone in achieving a cosmetically acceptable treatment for melasma.27
PIPA
Vitamin C can be used to diminish or prevent post-inflammatory pigment alteration (PIPA) after procedures because it inhibits tyrosinase, lowers inflammation, and quenches free radicals. In a study of 10 patients, the application of topical vitamin C 2 or more weeks after surgery reduced the duration and degree of erythema after skin resurfacing with a carbon dioxide laser.28
Stretch marks
The depigmenting effects of vitamin C can lighten the pigmentation associated with stretch marks and its anti-inflammatory activity can contribute to blunting related redness.12
Conclusion
Although orally administered ascorbic acid is readily bioavailable, ascorbic acid in the skin is quickly depleted and oral supplementation alone does not yield optimal skin levels. Therefore, topical use of vitamin C is desirable. In fact, I tell my patients to use it topically in the morning and add a vitamin C supplement to their diet. Numerous formulation considerations (e.g., packaging, exposure to air or light during use, skin sensitivity, and user preference) are involved in the stabilization and effective penetration of ascorbic acid into the skin, and the process of developing, manufacturing, and packaging of effective, stable vitamin C products is expensive.
Vitamin C, particularly when combined with other ingredients, has been shown to be an integral constituent in topical antioxidant, antiaging, and depigmenting formulations that show promise in the dermatologic armamentarium. It is a great choice for use in a prep-procedure skin care regimen to speed healing. Use after a procedure is prohibited by the stinging associated with the low pH of properly formulated products.
References
1. J Biol Chem. 1994 May 6;269(18):13685-8.
2. Dermatol Surg. 2001 Feb;27(2):137-42.
3. J Invest Dermatol. 1994 Jan;102(1):122-4.
4. Dermatol Surg. 2005 Jul;31(7 Pt 2):814-7.
5. Annu Rev Nutr. 1994;14:371-91.
6. J Drugs Dermatol. 2008 Jul;7(7 Suppl):s2-6.
7. J Am Acad Dermatol. 2003 Jun;48(6):866-74.
8. J Invest Dermatol. 1994 Apr;102(4):470-5.
9. Free Radic Biol Med. 1997;23:85-91.
10. J Drugs Dermatol. 2014 Oct;13(10):1208-13.
11. J Am Acad Dermatol. 1996 Jan;34(1):29-33.
12. Dermatol Surg. 1998 Aug;24(8):849-56.
13. J Am Acad Dermatol. 2008 Sep;59(3):418-25.
14. J Biol Chem. 1983 Jun 10;258(11):6695-7.
15. J Phys Chem. 1983;87:1809-12.
16. Br J Dermatol. 1992 Sep;127(3):247-53.
17. J Invest Dermatol. 1991;96:587.
18. J Invest Dermatol. 2001 Jun;116(6):853-9.
19. Exp Dermatol. 2003 Jun;12(3):237-44.
20. J Drugs Dermatol. 2012 Jan;11(1):51-6.
21. Clin Cosmet Investig Dermatol. 2015 Sep 2;8:463-70
22. Int J Dermatol. 2004 Aug;43(8):604-7.
23. Dermatology. 2003;206(4):316-20.
24. Am J Clin Dermatol. 2011 Apr 1;12(2):87-99.
25. Phytother Res. 2006 Nov;20(11):921-34.
26. J Cutan Med Surg. 2009 Mar-Apr;13(2):74-81.
27. Lasers Med Sci. 2015 Jan;30(1):159-63.
28. Dermatol Surg. 1998 Mar;24(3):331-4.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.
Vitamin C (ascorbic acid) is one of the four most important ingredients in skin care products.
• It is proven to increase collagen production when applied topically to skin.
• It inhibits tyrosinase to even skin tone and has a strong antioxidant activity.
• It is absorbed well orally, but not enough gets to the skin.
• It is best absorbed at a pH of 2.0.
• It is unstable when exposed to light and air. Instruct patients to discard 6 months after opening.
In addition, the proper formulation is patented and expensive. Stick with brands you trust. Use vitamin C on skin prior to procedures to speed healing. It will sting when used on inflamed skin because of the low pH.
In my opinion, all patients need to be on the proper skin care regimen for their skin type. This includes a daily sun protection factor (SPF), a cleanser, a retinoid, and an antioxidant. Ascorbic acid is one of my favorite antioxidants because it is the only one shown to increase the production of collagen by fibroblasts and inhibit tyrosinase while scavenging free radicals. Sure it is expensive – but that is because formulating and packaging it properly is expensive. Unfortunately, many subpar brands have entered the market. Ask to see the company’s research data on its formulation before choosing to recommend or sell ascorbic acid/vitamin C in your practice.
An essential water-soluble nutrient for the development of bone and connective tissue, vitamin C is found in citrus fruits and green leafy vegetables. It is produced in most plants and animals, but a mutated gene in humans has resulted in a deficiency of L-gulono-gamma-lactone oxidase, the enzyme required for its production.1,2 Although ascorbic acid cannot be synthesized by the human body, dietary consumption renders it the most abundant antioxidant in human skin and blood, and vitamin C plays an important role in endogenous collagen production and the inhibition of collagen degradation.3-6 Ascorbic acid also is known to regenerate alpha-tocopherol (vitamin E) levels and, therefore, is thought to protect against diseases related to oxidative stress.7
Epidermal vitamin C can be depleted by sunlight and environmental pollution, such as ozone in urban pollution.8,9 Known to exhibit a wide range of biologic activities, ascorbic acid has been shown to deliver rejuvenating effects on skin wrinkles, texture, strength, and evenness of tone through its antioxidant, tyrosinase-inhibiting, and collagen production-promoting activities.10 Indeed, as a topical agent, vitamin C has been used to prevent photodamage, and to treat melasma, striae alba, and postoperative erythema in laser patients.11,12 It is regularly used to treat aging skin, and as a depigmenting agent.2,10,13 This column will discuss the antioxidant, antiaging, and depigmenting activity of vitamin C in the context of recent human studies.
Antioxidant and anti-aging activity
Vitamin C is unique among antioxidants because of its ability to increase collagen production in addition to its free radical scavenging antioxidant activity. Due to its capacity to interfere with the UV-induced generation of reactive oxygen species by reacting with the superoxide anion or the hydroxyl radical, vitamin C has become a popular addition to “after-sun” products,14,15 and been shown to be effective in mitigating the effects of UVB, such as erythema and signs of photoaging, on porcine and human skin.2,16-17
A 2001 study in 10 postmenopausal women by Nusgens et al. found that daily topical application of 5% L-ascorbic acid enhanced the levels of procollagen types I and III, their posttranslational maturation enzymes, and tissue inhibitor of matrix metalloproteinase.18 This led to increased levels of collagen in the skin.
In 2003, Humbert et al. conducted a 6-month, double-blind, vehicle-controlled trial with 20 healthy female volunteers showing that patients treated with 5% vitamin C cream experienced significant improvements in deep furrows on the neck and forearms.19
In a small study of nine adults with Fitzpatrick skin types II or III in 2008, Murray et al. studied whether a stable topical preparation of 15% L-ascorbic acid, 1% alpha-tocopherol, and 0.5% ferulic acid could protect human skin in vivo from UV-induced damage. They found that the antioxidant formulation supplemented the antioxidant pool of the skin and conferred significant photoprotection, guarding the skin against erythema and apoptosis as well as effectively suppressing p53 activation and reducing thymine dimer mutations known to be associated with skin cancer.13
In 2012, Xu et al. evaluated the efficacy and safety of topical 23.8% L-ascorbic acid on photoaged skin in a split-face study of 20 Chinese women. Significant improvements in fine lines, dyspigmentation, and surface roughness were observed, without adverse side effects.20
In a 2015 study of 60 healthy female subjects, Crisan et al. used high-frequency ultrasound to determine that the use of a topical vitamin C formulation yielded significant increases in collagen synthesis, revealing the solution to be an effective rejuvenation therapy.21
Skin lightening activity
Melasma
In 2004, Espinal-Perez et al. conducted a double-blind randomized trial of 5% ascorbic acid, compared with 4% hydroquinone (HQ) water–oil emulsion in 16 female patients with melasma, aged 23-43 years (mean 36 years). Of those treated with vitamin C, 62.5% exhibited good or excellent subjectively assessed skin lightening. There was no statistically significant difference in depigmenting activity in the HQ group, of which 68.7% experienced irritation whereas vitamin C was well tolerated.22
In a randomized, double-blind, placebo-controlled study, researchers used iontophoresis to enhance the penetration of vitamin C into the skin and significantly reduce pigmentation, compared with placebo.23
Although ascorbic acid is viewed by many as ineffective as a depigmenting agent alone, particularly in 5%-10% concentrations, when used in combination with other ingredients such as HQ, it is considered effective.24 In the magnesium-L-ascorbyl-2-phosphate esterified form, however, vitamin C is among the most popular prescribed depigmenting agents around the world, especially in countries where HQ and its derivatives are prohibited.25 In a 2009 16-week open-label study by Hwang et al. of 25% L-ascorbic acid and a chemical penetration enhancer for treating melasma in 40 patients, researchers observed significant reductions in pigmentation.26
In a small split-face study early in 2015, Lee et al. showed that the combination of 1,064-nm Q-switched neodymium-doped yttrium aluminum garnet (QS-Nd:YAG) laser and ultrasonic application of vitamin C was more effective than was the laser treatment alone in achieving a cosmetically acceptable treatment for melasma.27
PIPA
Vitamin C can be used to diminish or prevent post-inflammatory pigment alteration (PIPA) after procedures because it inhibits tyrosinase, lowers inflammation, and quenches free radicals. In a study of 10 patients, the application of topical vitamin C 2 or more weeks after surgery reduced the duration and degree of erythema after skin resurfacing with a carbon dioxide laser.28
Stretch marks
The depigmenting effects of vitamin C can lighten the pigmentation associated with stretch marks and its anti-inflammatory activity can contribute to blunting related redness.12
Conclusion
Although orally administered ascorbic acid is readily bioavailable, ascorbic acid in the skin is quickly depleted and oral supplementation alone does not yield optimal skin levels. Therefore, topical use of vitamin C is desirable. In fact, I tell my patients to use it topically in the morning and add a vitamin C supplement to their diet. Numerous formulation considerations (e.g., packaging, exposure to air or light during use, skin sensitivity, and user preference) are involved in the stabilization and effective penetration of ascorbic acid into the skin, and the process of developing, manufacturing, and packaging of effective, stable vitamin C products is expensive.
Vitamin C, particularly when combined with other ingredients, has been shown to be an integral constituent in topical antioxidant, antiaging, and depigmenting formulations that show promise in the dermatologic armamentarium. It is a great choice for use in a prep-procedure skin care regimen to speed healing. Use after a procedure is prohibited by the stinging associated with the low pH of properly formulated products.
References
1. J Biol Chem. 1994 May 6;269(18):13685-8.
2. Dermatol Surg. 2001 Feb;27(2):137-42.
3. J Invest Dermatol. 1994 Jan;102(1):122-4.
4. Dermatol Surg. 2005 Jul;31(7 Pt 2):814-7.
5. Annu Rev Nutr. 1994;14:371-91.
6. J Drugs Dermatol. 2008 Jul;7(7 Suppl):s2-6.
7. J Am Acad Dermatol. 2003 Jun;48(6):866-74.
8. J Invest Dermatol. 1994 Apr;102(4):470-5.
9. Free Radic Biol Med. 1997;23:85-91.
10. J Drugs Dermatol. 2014 Oct;13(10):1208-13.
11. J Am Acad Dermatol. 1996 Jan;34(1):29-33.
12. Dermatol Surg. 1998 Aug;24(8):849-56.
13. J Am Acad Dermatol. 2008 Sep;59(3):418-25.
14. J Biol Chem. 1983 Jun 10;258(11):6695-7.
15. J Phys Chem. 1983;87:1809-12.
16. Br J Dermatol. 1992 Sep;127(3):247-53.
17. J Invest Dermatol. 1991;96:587.
18. J Invest Dermatol. 2001 Jun;116(6):853-9.
19. Exp Dermatol. 2003 Jun;12(3):237-44.
20. J Drugs Dermatol. 2012 Jan;11(1):51-6.
21. Clin Cosmet Investig Dermatol. 2015 Sep 2;8:463-70
22. Int J Dermatol. 2004 Aug;43(8):604-7.
23. Dermatology. 2003;206(4):316-20.
24. Am J Clin Dermatol. 2011 Apr 1;12(2):87-99.
25. Phytother Res. 2006 Nov;20(11):921-34.
26. J Cutan Med Surg. 2009 Mar-Apr;13(2):74-81.
27. Lasers Med Sci. 2015 Jan;30(1):159-63.
28. Dermatol Surg. 1998 Mar;24(3):331-4.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.

Search is on for cases of aggressive, ruxolitinib-associated skin cancers
ORLANDO – The hematologic cancer drug ruxolitinib seems to be associated with cases of aggressive nonmelanoma skin cancer.
After treating a very aggressive squamous cell carcinoma in a 55-year-old man treated with ruxolitinib for polycythemia vera, and hearing firsthand of three other similar cases, Dr. Fiona Zwald is collecting additional data on the association. She intends to publish these cases in a monograph as a warning to dermatologists, hematologists, oncologists, and other physicians who manage patients with hematologic malignancies, she said at the annual meeting of the American College of Mohs Surgery.
The prescribing information for ruxolitinib (Jakafi, Incyte Pharmaceuticals; Jakavi, Novartis) was updated in 2014 to warn that patients taking the drug face an increased risk of nonmelanoma skin cancers. The label also recommends that physicians inspect the skin regularly and urge patients to be alert for and report any new or changing lesions.
Despite the warnings and recommendations, cases are occurring – and some are quite serious, said Dr. Zwald, a Mohs surgeon in Atlanta.
“People should know this is actually happening. If you have experience with this medication, please let us know so we can compile this report. We are trying to assess the number of skin cancers before and after initiating this medication,” she said.

Ruxolitinib is an inhibitor of Janus kinase with a special affinity for the JAK1 and JAK2 subtypes. Like other cytokine-signaling molecules, their function depends on cell context; it may inhibit cell growth in one setting, and, in another, stimulate it. Ruxolitinib was initially approved in 2011 for the treatment of intermediate- and high-risk myelofibrosis, including primary myelofibrosis, post–polycythemia vera myelofibrosis, and post–essential thrombocythemia myelofibrosis.
In 2014, indications for ruxolitinib were expanded to include treatment of patients with polycythemia vera who have had an inadequate response to or are intolerant of hydroxyurea.
Dr. Zwald’s patient had a 10-year history of polycythemia vera. He was initially well controlled on the standard hydroxyurea treatment. In the meantime, he began working as a caddy at a major U.S. golf club. He developed many facial squamous cell carcinomas that were treated with excision and radiation. A year before he presented to Dr. Zwald, he stopped responding to hydroxyurea and was placed on ruxolitinib.
The patient presented with a 4-cm ulcerated lesion over part of his right temple and to the right helical crus; the lesion had developed over 3 months. Dr. Zwald consulted with the patient’s medical oncologist; treatment with ruxolitinib continued, albeit at a reduced dosage in light of recent events.
She performed Mohs surgery on the patient. It was a challenging case, she said, not the least because adequate anesthesia could not be achieved with local anesthetic. Preoperative staging showed no nodal spread.
“He did, unfortunately demonstrate a large, indurated mass located over one branch of the superficial temporal artery. At the helical crus there was an area of bound-down, fixed tumor. Knowing that I would not be able to fully resect this, I passed him on to the operating room,” Dr. Zwald said. “This tumor was found to extend down to the parotid capsule, but margins were clear.” The surgical defect was successfully repaired with a split-thickness skin graft.
The tumor recurred about 3 months later, and the patient underwent another surgery.
“This time we could not get clear surgical margins, and the tumor was approaching the external auditory meatus. Surgery was abandoned due to fears of complications to that area,” she said.
She presented the case at tumor board, during which she and her colleagues discussed adjuvant radiation. They initially abandoned this idea because he had already had so much radiation to his face. After the second surgery, they decide to proceed with radiation. “The next conversation we have will be whether to add another adjuvant therapy to treatment.”
She sent out the case and requests for feedback to the International Transplant Skin Cancer Collaborative, an 800-member consortium of dermatologists and Mohs surgeons who take care of transplant patients. She received information on three additional cases of aggressive squamous cell carcinoma (SCC) associated with ruxolitinib treatment:
• A patient with myelodysplastic syndrome with aggressive scalp SCC with cutaneous metastases.
• A patient with undifferentiated pleomorphic sarcoma of the scalp, several cutaneous SCCs.
• A patient with a myelodysplastic syndrome with in-transit metastases and explosive cutaneous SCCs. The patient has had the ruxolitinib dose reduced and may be switched to capecitabine.
Dr. Zwald noted that her patient was at risk for aggressive skin cancers for reasons in addition to ruxolitinib treatment.
“He was already immunosuppressed from his malignancy. He was on hydroxyurea, a drug that’s a cumulative phototoxin, and he’s out in the sun playing golf every day, and then was put on ruxolitinib. But the question we face now is how to try and stop this medication so we can get better treatment for him which will, of course, be very difficult.”
To contribute to Dr. Zwald’s case series, please email her at Fiona.Zwald@gmail.com.
She had no relevant financial disclosures.
On Twitter @Alz_Gal
ORLANDO – The hematologic cancer drug ruxolitinib seems to be associated with cases of aggressive nonmelanoma skin cancer.
After treating a very aggressive squamous cell carcinoma in a 55-year-old man treated with ruxolitinib for polycythemia vera, and hearing firsthand of three other similar cases, Dr. Fiona Zwald is collecting additional data on the association. She intends to publish these cases in a monograph as a warning to dermatologists, hematologists, oncologists, and other physicians who manage patients with hematologic malignancies, she said at the annual meeting of the American College of Mohs Surgery.
The prescribing information for ruxolitinib (Jakafi, Incyte Pharmaceuticals; Jakavi, Novartis) was updated in 2014 to warn that patients taking the drug face an increased risk of nonmelanoma skin cancers. The label also recommends that physicians inspect the skin regularly and urge patients to be alert for and report any new or changing lesions.
Despite the warnings and recommendations, cases are occurring – and some are quite serious, said Dr. Zwald, a Mohs surgeon in Atlanta.
“People should know this is actually happening. If you have experience with this medication, please let us know so we can compile this report. We are trying to assess the number of skin cancers before and after initiating this medication,” she said.
Ruxolitinib is an inhibitor of Janus kinase with a special affinity for the JAK1 and JAK2 subtypes. Like other cytokine-signaling molecules, their function depends on cell context; it may inhibit cell growth in one setting, and, in another, stimulate it. Ruxolitinib was initially approved in 2011 for the treatment of intermediate- and high-risk myelofibrosis, including primary myelofibrosis, post–polycythemia vera myelofibrosis, and post–essential thrombocythemia myelofibrosis.
In 2014, indications for ruxolitinib were expanded to include treatment of patients with polycythemia vera who have had an inadequate response to or are intolerant of hydroxyurea.
Dr. Zwald’s patient had a 10-year history of polycythemia vera. He was initially well controlled on the standard hydroxyurea treatment. In the meantime, he began working as a caddy at a major U.S. golf club. He developed many facial squamous cell carcinomas that were treated with excision and radiation. A year before he presented to Dr. Zwald, he stopped responding to hydroxyurea and was placed on ruxolitinib.
The patient presented with a 4-cm ulcerated lesion over part of his right temple and to the right helical crus; the lesion had developed over 3 months. Dr. Zwald consulted with the patient’s medical oncologist; treatment with ruxolitinib continued, albeit at a reduced dosage in light of recent events.
She performed Mohs surgery on the patient. It was a challenging case, she said, not the least because adequate anesthesia could not be achieved with local anesthetic. Preoperative staging showed no nodal spread.
“He did, unfortunately demonstrate a large, indurated mass located over one branch of the superficial temporal artery. At the helical crus there was an area of bound-down, fixed tumor. Knowing that I would not be able to fully resect this, I passed him on to the operating room,” Dr. Zwald said. “This tumor was found to extend down to the parotid capsule, but margins were clear.” The surgical defect was successfully repaired with a split-thickness skin graft.
The tumor recurred about 3 months later, and the patient underwent another surgery.
“This time we could not get clear surgical margins, and the tumor was approaching the external auditory meatus. Surgery was abandoned due to fears of complications to that area,” she said.
She presented the case at tumor board, during which she and her colleagues discussed adjuvant radiation. They initially abandoned this idea because he had already had so much radiation to his face. After the second surgery, they decide to proceed with radiation. “The next conversation we have will be whether to add another adjuvant therapy to treatment.”
She sent out the case and requests for feedback to the International Transplant Skin Cancer Collaborative, an 800-member consortium of dermatologists and Mohs surgeons who take care of transplant patients. She received information on three additional cases of aggressive squamous cell carcinoma (SCC) associated with ruxolitinib treatment:
• A patient with myelodysplastic syndrome with aggressive scalp SCC with cutaneous metastases.
• A patient with undifferentiated pleomorphic sarcoma of the scalp, several cutaneous SCCs.
• A patient with a myelodysplastic syndrome with in-transit metastases and explosive cutaneous SCCs. The patient has had the ruxolitinib dose reduced and may be switched to capecitabine.
Dr. Zwald noted that her patient was at risk for aggressive skin cancers for reasons in addition to ruxolitinib treatment.
“He was already immunosuppressed from his malignancy. He was on hydroxyurea, a drug that’s a cumulative phototoxin, and he’s out in the sun playing golf every day, and then was put on ruxolitinib. But the question we face now is how to try and stop this medication so we can get better treatment for him which will, of course, be very difficult.”
To contribute to Dr. Zwald’s case series, please email her at Fiona.Zwald@gmail.com.
She had no relevant financial disclosures.
On Twitter @Alz_Gal
ORLANDO – The hematologic cancer drug ruxolitinib seems to be associated with cases of aggressive nonmelanoma skin cancer.
After treating a very aggressive squamous cell carcinoma in a 55-year-old man treated with ruxolitinib for polycythemia vera, and hearing firsthand of three other similar cases, Dr. Fiona Zwald is collecting additional data on the association. She intends to publish these cases in a monograph as a warning to dermatologists, hematologists, oncologists, and other physicians who manage patients with hematologic malignancies, she said at the annual meeting of the American College of Mohs Surgery.
The prescribing information for ruxolitinib (Jakafi, Incyte Pharmaceuticals; Jakavi, Novartis) was updated in 2014 to warn that patients taking the drug face an increased risk of nonmelanoma skin cancers. The label also recommends that physicians inspect the skin regularly and urge patients to be alert for and report any new or changing lesions.
Despite the warnings and recommendations, cases are occurring – and some are quite serious, said Dr. Zwald, a Mohs surgeon in Atlanta.
“People should know this is actually happening. If you have experience with this medication, please let us know so we can compile this report. We are trying to assess the number of skin cancers before and after initiating this medication,” she said.
Ruxolitinib is an inhibitor of Janus kinase with a special affinity for the JAK1 and JAK2 subtypes. Like other cytokine-signaling molecules, their function depends on cell context; it may inhibit cell growth in one setting, and, in another, stimulate it. Ruxolitinib was initially approved in 2011 for the treatment of intermediate- and high-risk myelofibrosis, including primary myelofibrosis, post–polycythemia vera myelofibrosis, and post–essential thrombocythemia myelofibrosis.
In 2014, indications for ruxolitinib were expanded to include treatment of patients with polycythemia vera who have had an inadequate response to or are intolerant of hydroxyurea.
Dr. Zwald’s patient had a 10-year history of polycythemia vera. He was initially well controlled on the standard hydroxyurea treatment. In the meantime, he began working as a caddy at a major U.S. golf club. He developed many facial squamous cell carcinomas that were treated with excision and radiation. A year before he presented to Dr. Zwald, he stopped responding to hydroxyurea and was placed on ruxolitinib.
The patient presented with a 4-cm ulcerated lesion over part of his right temple and to the right helical crus; the lesion had developed over 3 months. Dr. Zwald consulted with the patient’s medical oncologist; treatment with ruxolitinib continued, albeit at a reduced dosage in light of recent events.
She performed Mohs surgery on the patient. It was a challenging case, she said, not the least because adequate anesthesia could not be achieved with local anesthetic. Preoperative staging showed no nodal spread.
“He did, unfortunately demonstrate a large, indurated mass located over one branch of the superficial temporal artery. At the helical crus there was an area of bound-down, fixed tumor. Knowing that I would not be able to fully resect this, I passed him on to the operating room,” Dr. Zwald said. “This tumor was found to extend down to the parotid capsule, but margins were clear.” The surgical defect was successfully repaired with a split-thickness skin graft.
The tumor recurred about 3 months later, and the patient underwent another surgery.
“This time we could not get clear surgical margins, and the tumor was approaching the external auditory meatus. Surgery was abandoned due to fears of complications to that area,” she said.
She presented the case at tumor board, during which she and her colleagues discussed adjuvant radiation. They initially abandoned this idea because he had already had so much radiation to his face. After the second surgery, they decide to proceed with radiation. “The next conversation we have will be whether to add another adjuvant therapy to treatment.”
She sent out the case and requests for feedback to the International Transplant Skin Cancer Collaborative, an 800-member consortium of dermatologists and Mohs surgeons who take care of transplant patients. She received information on three additional cases of aggressive squamous cell carcinoma (SCC) associated with ruxolitinib treatment:
• A patient with myelodysplastic syndrome with aggressive scalp SCC with cutaneous metastases.
• A patient with undifferentiated pleomorphic sarcoma of the scalp, several cutaneous SCCs.
• A patient with a myelodysplastic syndrome with in-transit metastases and explosive cutaneous SCCs. The patient has had the ruxolitinib dose reduced and may be switched to capecitabine.
Dr. Zwald noted that her patient was at risk for aggressive skin cancers for reasons in addition to ruxolitinib treatment.
“He was already immunosuppressed from his malignancy. He was on hydroxyurea, a drug that’s a cumulative phototoxin, and he’s out in the sun playing golf every day, and then was put on ruxolitinib. But the question we face now is how to try and stop this medication so we can get better treatment for him which will, of course, be very difficult.”
To contribute to Dr. Zwald’s case series, please email her at Fiona.Zwald@gmail.com.
She had no relevant financial disclosures.
On Twitter @Alz_Gal
AT THE ACMS ANNUAL MEETING

Laser Best Practices for Darker Skin Types

What does your patient need to know at the first visit? Does it apply to patients of all genders and ages?
Before performing laser procedures on patients with richly pigmented skin (Fitzpatrick skin types IV–VI), patients need to be informed of the higher risk for pigmentary alterations as potential complications of the procedure. Specifically, hyperpigmentation or hypopigmentation can occur postprocedure, depending on the type of device used, the treatment settings, the technique, the underlying skin disorder being treated, and the patient’s individual response to treatment. Fortunately, these pigment alterations are in most cases self-limited but can last for weeks to months depending on the severity and the nature of the dyspigmentation.
What are your go-to treatments? What are the side effects?
Notwithstanding the higher risks for pigmentary alterations, lasers can be extremely useful for the management of numerous dermatologic concerns in patients with Fitzpatrick skin types IV to VI including laser hair removal for pseudofolliculitis barbae or nonablative fractional laser resurfacing for acne scarring and pigmentary disorders. My go-to treatments include the following: long-pulsed 1064-nm Nd:YAG laser for hair removal in Fitzpatrick skin types V to VI, 808-nm diode laser with linear scanning of hair removal in Fitzpatrick skin type IV or less, 1550-nm erbium-doped nonablative fractional laser for acne scarring in Fitzpatrick skin types IV to VI, and low-power diode 1927-nm fractional laser for melasma and postinflammatory hyperpigmentation in Fitzpatrick skin types IV to VI.
All of these procedures are performed with conservative treatment settings such as low fluences and longer pulse durations for laser hair removal and low treatment densities for fractional laser procedures. Prior to laser resurfacing, I recommend hydroquinone cream 4% twice daily starting 2 weeks before the first session and for 4 weeks posttreatment. These recommendations are based on published evidence (see Suggested Readings) as well as anecdotal experience.
How do you keep patients compliant with treatment?
Emphasizing the need for broad-spectrum sunscreen and avoidance of intense sun exposure before and after laser treatments is important during the initial consultation and prior to each treatment. I warn my patients of the higher risk for hyperpigmentation if the skin is tanned or has recently had intense sun exposure.
What do you do if they refuse treatment?
If patients refuse laser treatment or recommended precautions, then I will consider nonlaser treatment options.
What resources do you recommend to patients for more information?
I recommend patients visit the Skin of Color Society website (www.skinofcolorsociety.org).
Suggested Readings
- Alexis AF. Fractional laser resurfacing of acne scarring in patients with Fitzpatrick skin types IV-VI. J Drugs Dermatol. 2011;10(12 suppl):s6-s7.
- Alexis AF. Lasers and light-based therapies in ethnic skin: treatment options and recommendations for Fitzpatrick skin types V and VI. Br J Dermatol. 2013;169(suppl 3):91-97.
- Alexis AF, Coley MK, Nijhawan RI, et al. Nonablative fractional laser resurfacing for acne scarring in patients with Fitzpatrick skin phototypes IV-VI. Dermatol Surg. 2016;42:392-402.
- Battle EF, Hobbs LM. Laser-assisted hair removal for darker skin types. Dermatol Ther. 2004;17:177-183.
- Clark CM, Silverberg JI, Alexis AF. A retrospective chart review to assess the safety of nonablative fractional laser resurfacing in Fitzpatrick skin types IV to VI. J Drugs Dermatol. 2013;12:428-431.
- Ross EV, Cooke LM, Timko AL, et al. Treatment of pseudofolliculitis barbae in skin types IV, V, and VI with a long-pulsed neodymium:yttrium aluminum garnet laser. J Am Acad Dermatol. 2002;47:263-270.
What does your patient need to know at the first visit? Does it apply to patients of all genders and ages?
Before performing laser procedures on patients with richly pigmented skin (Fitzpatrick skin types IV–VI), patients need to be informed of the higher risk for pigmentary alterations as potential complications of the procedure. Specifically, hyperpigmentation or hypopigmentation can occur postprocedure, depending on the type of device used, the treatment settings, the technique, the underlying skin disorder being treated, and the patient’s individual response to treatment. Fortunately, these pigment alterations are in most cases self-limited but can last for weeks to months depending on the severity and the nature of the dyspigmentation.
What are your go-to treatments? What are the side effects?
Notwithstanding the higher risks for pigmentary alterations, lasers can be extremely useful for the management of numerous dermatologic concerns in patients with Fitzpatrick skin types IV to VI including laser hair removal for pseudofolliculitis barbae or nonablative fractional laser resurfacing for acne scarring and pigmentary disorders. My go-to treatments include the following: long-pulsed 1064-nm Nd:YAG laser for hair removal in Fitzpatrick skin types V to VI, 808-nm diode laser with linear scanning of hair removal in Fitzpatrick skin type IV or less, 1550-nm erbium-doped nonablative fractional laser for acne scarring in Fitzpatrick skin types IV to VI, and low-power diode 1927-nm fractional laser for melasma and postinflammatory hyperpigmentation in Fitzpatrick skin types IV to VI.
All of these procedures are performed with conservative treatment settings such as low fluences and longer pulse durations for laser hair removal and low treatment densities for fractional laser procedures. Prior to laser resurfacing, I recommend hydroquinone cream 4% twice daily starting 2 weeks before the first session and for 4 weeks posttreatment. These recommendations are based on published evidence (see Suggested Readings) as well as anecdotal experience.
How do you keep patients compliant with treatment?
Emphasizing the need for broad-spectrum sunscreen and avoidance of intense sun exposure before and after laser treatments is important during the initial consultation and prior to each treatment. I warn my patients of the higher risk for hyperpigmentation if the skin is tanned or has recently had intense sun exposure.
What do you do if they refuse treatment?
If patients refuse laser treatment or recommended precautions, then I will consider nonlaser treatment options.
What resources do you recommend to patients for more information?
I recommend patients visit the Skin of Color Society website (www.skinofcolorsociety.org).
Suggested Readings
- Alexis AF. Fractional laser resurfacing of acne scarring in patients with Fitzpatrick skin types IV-VI. J Drugs Dermatol. 2011;10(12 suppl):s6-s7.
- Alexis AF. Lasers and light-based therapies in ethnic skin: treatment options and recommendations for Fitzpatrick skin types V and VI. Br J Dermatol. 2013;169(suppl 3):91-97.
- Alexis AF, Coley MK, Nijhawan RI, et al. Nonablative fractional laser resurfacing for acne scarring in patients with Fitzpatrick skin phototypes IV-VI. Dermatol Surg. 2016;42:392-402.
- Battle EF, Hobbs LM. Laser-assisted hair removal for darker skin types. Dermatol Ther. 2004;17:177-183.
- Clark CM, Silverberg JI, Alexis AF. A retrospective chart review to assess the safety of nonablative fractional laser resurfacing in Fitzpatrick skin types IV to VI. J Drugs Dermatol. 2013;12:428-431.
- Ross EV, Cooke LM, Timko AL, et al. Treatment of pseudofolliculitis barbae in skin types IV, V, and VI with a long-pulsed neodymium:yttrium aluminum garnet laser. J Am Acad Dermatol. 2002;47:263-270.
What does your patient need to know at the first visit? Does it apply to patients of all genders and ages?
Before performing laser procedures on patients with richly pigmented skin (Fitzpatrick skin types IV–VI), patients need to be informed of the higher risk for pigmentary alterations as potential complications of the procedure. Specifically, hyperpigmentation or hypopigmentation can occur postprocedure, depending on the type of device used, the treatment settings, the technique, the underlying skin disorder being treated, and the patient’s individual response to treatment. Fortunately, these pigment alterations are in most cases self-limited but can last for weeks to months depending on the severity and the nature of the dyspigmentation.
What are your go-to treatments? What are the side effects?
Notwithstanding the higher risks for pigmentary alterations, lasers can be extremely useful for the management of numerous dermatologic concerns in patients with Fitzpatrick skin types IV to VI including laser hair removal for pseudofolliculitis barbae or nonablative fractional laser resurfacing for acne scarring and pigmentary disorders. My go-to treatments include the following: long-pulsed 1064-nm Nd:YAG laser for hair removal in Fitzpatrick skin types V to VI, 808-nm diode laser with linear scanning of hair removal in Fitzpatrick skin type IV or less, 1550-nm erbium-doped nonablative fractional laser for acne scarring in Fitzpatrick skin types IV to VI, and low-power diode 1927-nm fractional laser for melasma and postinflammatory hyperpigmentation in Fitzpatrick skin types IV to VI.
All of these procedures are performed with conservative treatment settings such as low fluences and longer pulse durations for laser hair removal and low treatment densities for fractional laser procedures. Prior to laser resurfacing, I recommend hydroquinone cream 4% twice daily starting 2 weeks before the first session and for 4 weeks posttreatment. These recommendations are based on published evidence (see Suggested Readings) as well as anecdotal experience.
How do you keep patients compliant with treatment?
Emphasizing the need for broad-spectrum sunscreen and avoidance of intense sun exposure before and after laser treatments is important during the initial consultation and prior to each treatment. I warn my patients of the higher risk for hyperpigmentation if the skin is tanned or has recently had intense sun exposure.
What do you do if they refuse treatment?
If patients refuse laser treatment or recommended precautions, then I will consider nonlaser treatment options.
What resources do you recommend to patients for more information?
I recommend patients visit the Skin of Color Society website (www.skinofcolorsociety.org).
Suggested Readings
- Alexis AF. Fractional laser resurfacing of acne scarring in patients with Fitzpatrick skin types IV-VI. J Drugs Dermatol. 2011;10(12 suppl):s6-s7.
- Alexis AF. Lasers and light-based therapies in ethnic skin: treatment options and recommendations for Fitzpatrick skin types V and VI. Br J Dermatol. 2013;169(suppl 3):91-97.
- Alexis AF, Coley MK, Nijhawan RI, et al. Nonablative fractional laser resurfacing for acne scarring in patients with Fitzpatrick skin phototypes IV-VI. Dermatol Surg. 2016;42:392-402.
- Battle EF, Hobbs LM. Laser-assisted hair removal for darker skin types. Dermatol Ther. 2004;17:177-183.
- Clark CM, Silverberg JI, Alexis AF. A retrospective chart review to assess the safety of nonablative fractional laser resurfacing in Fitzpatrick skin types IV to VI. J Drugs Dermatol. 2013;12:428-431.
- Ross EV, Cooke LM, Timko AL, et al. Treatment of pseudofolliculitis barbae in skin types IV, V, and VI with a long-pulsed neodymium:yttrium aluminum garnet laser. J Am Acad Dermatol. 2002;47:263-270.

Mohs with CK-7 staining: 98% 5-year cure rate for extramammary Paget disease
ORLANDO – Mohs surgery with cytokeratin-7 immunohistochemistry staining effected complete removal of extramammary Paget disease and resulted in a 5-year, 95% recurrence-free cure rate.
The results are significantly better than the often-cited 77% cure rate seen with Mohs surgery alone, Dr. Ali Alexander Damavandy said at the annual meeting of the American College of Mohs Surgery.

“These are statistically significant and clinically substantial results,” said Dr. Damavandy, a procedural dermatology fellow at the University of Pennsylvania, Philadelphia. “With this method you can tell a patient that in 5 years, he has a 95% chance of still not having the tumor. The high recurrence-free rate we have seen supports the view that Mohs surgery with cytokeratin-7 [CK-7] immunohistochemistry should be considered the curative treatment of choice for both primary and recurrent extramammary Paget disease of the skin.”
Dr. Damavandy’s retrospective review of 49 cases may seem small, he said, but it is “far and away the biggest cohort that exists, and the only substantial cohort with immunohistochemistry staining of CK-7.” The 5-year follow-up is also a strength of the study, he added.
Extramammary Paget disease (EMPD) remains an “extraordinarily hard tumor to treat. It typically presents with widespread intraepithelial islands of disease that are not clinically apparent. Local recurrence rates range from 33% to 60%, “leaving a lot of room for improvement,” Dr. Damavandy said.
“The explanations for recurrence are twofold,” he added. “First there is difficulty visualizing tumor cells in frozen sections. Second, it is a multifocal tumor that grows in a discontinuous fashion.”
Although one simply has to deal with the tumor spread, improvements can be made in reading the histopathology. Immunohistochemistry staining with CK-7 allows highly accurate visualization of individual Paget tumor cells, which express a very high level of the protein.
“Our hypothesis was that combining this improved tumor cell visualization with Mohs total excision would really make a dent in the recurrence rates of this disease,” Dr. Damavandy said.
He conducted a review of patients who were treated at four practices from 2004 to 2012. The cohort comprised 49 patients with 62 tumors; 43 were primary and the rest were recurrences. The majority (90%) occurred in the urogenital and anogenital region; the rest were axial or facial. All were treated with Mohs microsurgery enhanced by CK-7 staining of frozen sections. Recurrences were biopsy proven.
The typical Mohs technique for EMPD is to delineate a tumor-free area peripherally, and then excise the central tumor and tumor-bearing islands. The procedure can be long and arduous. Many cases are multiday efforts with large areas of excision.
“These can be very difficult wounds to manage even in a hospital. It’s resource-intense surgery,” Dr. Damavandy said.
The mean margin necessary to clear the lesions in this cohort was 2.6 cm. A 4-cm margin cleared almost 80%; 10% required a 7-cm margin.
“If we were going to make a recommendation to a nonMohs surgeon, it would be that 7 cm are needed to clear 98% of the tumors. That seems to me not reasonable for these anatomically complex and delicate regions. At the same time, the most commonly reported margin in the literature is 2 cm. In this cohort that would only have cleared 40% of the tumors.”
A mean of 3.4 Mohs stages were needed to obtain clear margins, although the range was wide (1-14 stages). Surgery took a mean of 1.5 days (range 1-5 days). Four patients could not be cleared and needed multidisciplinary care. These included two with vaginal invasion and two with invasion of the anal canal.
By 5 years, the overall tumor-free survival rate was 97%; the tumor-free survival rate was slightly better for primary than recurrent tumors (98% vs. 95%). When these rates were compared with Mohs without CK-7 staining, “primary Mohs doesn’t compare very well,” Dr. Damavandy said. At 5 years, the literature-reported recurrence rate for primary tumors treated with Mohs alone was 16% vs. Dr. Damavandy’s report of 2.3% for Mohs plus CK-7 staining. For recurrent tumors, the recurrence rates were 50% vs. 5.3%.
Two tumors recurred; the mean time to recurrence was 31 months. One recurrence was of a primary tumor treated by peripheral Mohs surgery, which was an uncommon approach in this cohort. This patient had a deep recurrence at 16 months.
The other case was a recurrence of a vulvar tumor that extended into the vaginal epithelium and across the cervix. Despite a vaginectomy and vaginal hysterectomy with clear margins, the patient had a recurrence at 46 months.
The patients were retreated and at last follow-up were free of disease.
Dr. Damavandy had no financial disclosures.
ORLANDO – Mohs surgery with cytokeratin-7 immunohistochemistry staining effected complete removal of extramammary Paget disease and resulted in a 5-year, 95% recurrence-free cure rate.
The results are significantly better than the often-cited 77% cure rate seen with Mohs surgery alone, Dr. Ali Alexander Damavandy said at the annual meeting of the American College of Mohs Surgery.
“These are statistically significant and clinically substantial results,” said Dr. Damavandy, a procedural dermatology fellow at the University of Pennsylvania, Philadelphia. “With this method you can tell a patient that in 5 years, he has a 95% chance of still not having the tumor. The high recurrence-free rate we have seen supports the view that Mohs surgery with cytokeratin-7 [CK-7] immunohistochemistry should be considered the curative treatment of choice for both primary and recurrent extramammary Paget disease of the skin.”
Dr. Damavandy’s retrospective review of 49 cases may seem small, he said, but it is “far and away the biggest cohort that exists, and the only substantial cohort with immunohistochemistry staining of CK-7.” The 5-year follow-up is also a strength of the study, he added.
Extramammary Paget disease (EMPD) remains an “extraordinarily hard tumor to treat. It typically presents with widespread intraepithelial islands of disease that are not clinically apparent. Local recurrence rates range from 33% to 60%, “leaving a lot of room for improvement,” Dr. Damavandy said.
“The explanations for recurrence are twofold,” he added. “First there is difficulty visualizing tumor cells in frozen sections. Second, it is a multifocal tumor that grows in a discontinuous fashion.”
Although one simply has to deal with the tumor spread, improvements can be made in reading the histopathology. Immunohistochemistry staining with CK-7 allows highly accurate visualization of individual Paget tumor cells, which express a very high level of the protein.
“Our hypothesis was that combining this improved tumor cell visualization with Mohs total excision would really make a dent in the recurrence rates of this disease,” Dr. Damavandy said.
He conducted a review of patients who were treated at four practices from 2004 to 2012. The cohort comprised 49 patients with 62 tumors; 43 were primary and the rest were recurrences. The majority (90%) occurred in the urogenital and anogenital region; the rest were axial or facial. All were treated with Mohs microsurgery enhanced by CK-7 staining of frozen sections. Recurrences were biopsy proven.
The typical Mohs technique for EMPD is to delineate a tumor-free area peripherally, and then excise the central tumor and tumor-bearing islands. The procedure can be long and arduous. Many cases are multiday efforts with large areas of excision.
“These can be very difficult wounds to manage even in a hospital. It’s resource-intense surgery,” Dr. Damavandy said.
The mean margin necessary to clear the lesions in this cohort was 2.6 cm. A 4-cm margin cleared almost 80%; 10% required a 7-cm margin.
“If we were going to make a recommendation to a nonMohs surgeon, it would be that 7 cm are needed to clear 98% of the tumors. That seems to me not reasonable for these anatomically complex and delicate regions. At the same time, the most commonly reported margin in the literature is 2 cm. In this cohort that would only have cleared 40% of the tumors.”
A mean of 3.4 Mohs stages were needed to obtain clear margins, although the range was wide (1-14 stages). Surgery took a mean of 1.5 days (range 1-5 days). Four patients could not be cleared and needed multidisciplinary care. These included two with vaginal invasion and two with invasion of the anal canal.
By 5 years, the overall tumor-free survival rate was 97%; the tumor-free survival rate was slightly better for primary than recurrent tumors (98% vs. 95%). When these rates were compared with Mohs without CK-7 staining, “primary Mohs doesn’t compare very well,” Dr. Damavandy said. At 5 years, the literature-reported recurrence rate for primary tumors treated with Mohs alone was 16% vs. Dr. Damavandy’s report of 2.3% for Mohs plus CK-7 staining. For recurrent tumors, the recurrence rates were 50% vs. 5.3%.
Two tumors recurred; the mean time to recurrence was 31 months. One recurrence was of a primary tumor treated by peripheral Mohs surgery, which was an uncommon approach in this cohort. This patient had a deep recurrence at 16 months.
The other case was a recurrence of a vulvar tumor that extended into the vaginal epithelium and across the cervix. Despite a vaginectomy and vaginal hysterectomy with clear margins, the patient had a recurrence at 46 months.
The patients were retreated and at last follow-up were free of disease.
Dr. Damavandy had no financial disclosures.
ORLANDO – Mohs surgery with cytokeratin-7 immunohistochemistry staining effected complete removal of extramammary Paget disease and resulted in a 5-year, 95% recurrence-free cure rate.
The results are significantly better than the often-cited 77% cure rate seen with Mohs surgery alone, Dr. Ali Alexander Damavandy said at the annual meeting of the American College of Mohs Surgery.
“These are statistically significant and clinically substantial results,” said Dr. Damavandy, a procedural dermatology fellow at the University of Pennsylvania, Philadelphia. “With this method you can tell a patient that in 5 years, he has a 95% chance of still not having the tumor. The high recurrence-free rate we have seen supports the view that Mohs surgery with cytokeratin-7 [CK-7] immunohistochemistry should be considered the curative treatment of choice for both primary and recurrent extramammary Paget disease of the skin.”
Dr. Damavandy’s retrospective review of 49 cases may seem small, he said, but it is “far and away the biggest cohort that exists, and the only substantial cohort with immunohistochemistry staining of CK-7.” The 5-year follow-up is also a strength of the study, he added.
Extramammary Paget disease (EMPD) remains an “extraordinarily hard tumor to treat. It typically presents with widespread intraepithelial islands of disease that are not clinically apparent. Local recurrence rates range from 33% to 60%, “leaving a lot of room for improvement,” Dr. Damavandy said.
“The explanations for recurrence are twofold,” he added. “First there is difficulty visualizing tumor cells in frozen sections. Second, it is a multifocal tumor that grows in a discontinuous fashion.”
Although one simply has to deal with the tumor spread, improvements can be made in reading the histopathology. Immunohistochemistry staining with CK-7 allows highly accurate visualization of individual Paget tumor cells, which express a very high level of the protein.
“Our hypothesis was that combining this improved tumor cell visualization with Mohs total excision would really make a dent in the recurrence rates of this disease,” Dr. Damavandy said.
He conducted a review of patients who were treated at four practices from 2004 to 2012. The cohort comprised 49 patients with 62 tumors; 43 were primary and the rest were recurrences. The majority (90%) occurred in the urogenital and anogenital region; the rest were axial or facial. All were treated with Mohs microsurgery enhanced by CK-7 staining of frozen sections. Recurrences were biopsy proven.
The typical Mohs technique for EMPD is to delineate a tumor-free area peripherally, and then excise the central tumor and tumor-bearing islands. The procedure can be long and arduous. Many cases are multiday efforts with large areas of excision.
“These can be very difficult wounds to manage even in a hospital. It’s resource-intense surgery,” Dr. Damavandy said.
The mean margin necessary to clear the lesions in this cohort was 2.6 cm. A 4-cm margin cleared almost 80%; 10% required a 7-cm margin.
“If we were going to make a recommendation to a nonMohs surgeon, it would be that 7 cm are needed to clear 98% of the tumors. That seems to me not reasonable for these anatomically complex and delicate regions. At the same time, the most commonly reported margin in the literature is 2 cm. In this cohort that would only have cleared 40% of the tumors.”
A mean of 3.4 Mohs stages were needed to obtain clear margins, although the range was wide (1-14 stages). Surgery took a mean of 1.5 days (range 1-5 days). Four patients could not be cleared and needed multidisciplinary care. These included two with vaginal invasion and two with invasion of the anal canal.
By 5 years, the overall tumor-free survival rate was 97%; the tumor-free survival rate was slightly better for primary than recurrent tumors (98% vs. 95%). When these rates were compared with Mohs without CK-7 staining, “primary Mohs doesn’t compare very well,” Dr. Damavandy said. At 5 years, the literature-reported recurrence rate for primary tumors treated with Mohs alone was 16% vs. Dr. Damavandy’s report of 2.3% for Mohs plus CK-7 staining. For recurrent tumors, the recurrence rates were 50% vs. 5.3%.
Two tumors recurred; the mean time to recurrence was 31 months. One recurrence was of a primary tumor treated by peripheral Mohs surgery, which was an uncommon approach in this cohort. This patient had a deep recurrence at 16 months.
The other case was a recurrence of a vulvar tumor that extended into the vaginal epithelium and across the cervix. Despite a vaginectomy and vaginal hysterectomy with clear margins, the patient had a recurrence at 46 months.
The patients were retreated and at last follow-up were free of disease.
Dr. Damavandy had no financial disclosures.
AT THE ACMS ANNUAL MEETING
Key clinical point: Mohs surgery enhanced with cytokeratin-7 immunohistochemistry appears to be very effective for extamammaory Paget disease.
Major finding: The 5-year recurrence rate was less than 5%.
Data source: The case review comprised 49 patients with 62 tumors.
Disclosures: Dr. Damavandy had no financial disclosures

Laser treatment effective for nongenital warts
Laser treatment is effective against nongenital cutaneous warts, based on data from a review of 35 studies comprising 2,149 adult patients.
“No monotherapy has achieved completed remission [of nongenital cutaneous warts] in every case,” wrote Jannett Nguyen, a medical student at the University of California, Irvine, and colleagues (JAMA Dermatol. 2016 April 27. doi: 10.1001/jamadermatol.2016.0826).
The researchers reviewed data on warts treated with one of four types of lasers: Carbon dioxide (CO2), erbium:yttrium-aluminum-garnet (Er:YAG), pulsed dye laser (PDL), or neodymium-doped yttrium aluminum garnet (Nd:YAG).
The response rates for the different lasers were 50%-100% for CO2, 72%-100% for Er:YAG, 31%-100% for PDL, and 46%-100% for Nd:YAG. The studies included data on laser treatment of several types of nongenital warts including simple and recalcitrant common warts, periungual and subungual warts, and palmoplantar warts.
In general, side effects from laser treatment of warts were highest with CO2 lasers, and included scarring, hypopigmentation, postoperative pain, and prolonged wound healing. PDL was associated with the lowest risk of side effects, and was as effective as conventional therapies, including cryotherapy and cantharidin.
In Er:YAG treatments, the laser was used for direct ablation of the epidermis on the wart, repeating through layers until normal skin is revealed. Overall, patients treated with Er:YAG demonstrated a higher response and lower recurrence when treated in combination with podofilox. Nd:YAG treatment was similar to PDL, but with a longer wavelength that allows for deeper penetration.
Treatment is limited by a lack of evidence to guide selection of the most appropriate lasers for different warts and by a lack of recommendations for specific laser settings, the researchers noted. Additional studies are needed to establish treatment protocols by comparing lasers to each other and to nonlaser treatments.
However, laser treatment of warts can be “an additional therapeutic option and the studies reviewed here can provide a starting point in determining settings,” they said.
The researchers had no financial disclosures.
Laser treatment is effective against nongenital cutaneous warts, based on data from a review of 35 studies comprising 2,149 adult patients.
“No monotherapy has achieved completed remission [of nongenital cutaneous warts] in every case,” wrote Jannett Nguyen, a medical student at the University of California, Irvine, and colleagues (JAMA Dermatol. 2016 April 27. doi: 10.1001/jamadermatol.2016.0826).
The researchers reviewed data on warts treated with one of four types of lasers: Carbon dioxide (CO2), erbium:yttrium-aluminum-garnet (Er:YAG), pulsed dye laser (PDL), or neodymium-doped yttrium aluminum garnet (Nd:YAG).
The response rates for the different lasers were 50%-100% for CO2, 72%-100% for Er:YAG, 31%-100% for PDL, and 46%-100% for Nd:YAG. The studies included data on laser treatment of several types of nongenital warts including simple and recalcitrant common warts, periungual and subungual warts, and palmoplantar warts.
In general, side effects from laser treatment of warts were highest with CO2 lasers, and included scarring, hypopigmentation, postoperative pain, and prolonged wound healing. PDL was associated with the lowest risk of side effects, and was as effective as conventional therapies, including cryotherapy and cantharidin.
In Er:YAG treatments, the laser was used for direct ablation of the epidermis on the wart, repeating through layers until normal skin is revealed. Overall, patients treated with Er:YAG demonstrated a higher response and lower recurrence when treated in combination with podofilox. Nd:YAG treatment was similar to PDL, but with a longer wavelength that allows for deeper penetration.
Treatment is limited by a lack of evidence to guide selection of the most appropriate lasers for different warts and by a lack of recommendations for specific laser settings, the researchers noted. Additional studies are needed to establish treatment protocols by comparing lasers to each other and to nonlaser treatments.
However, laser treatment of warts can be “an additional therapeutic option and the studies reviewed here can provide a starting point in determining settings,” they said.
The researchers had no financial disclosures.
Laser treatment is effective against nongenital cutaneous warts, based on data from a review of 35 studies comprising 2,149 adult patients.
“No monotherapy has achieved completed remission [of nongenital cutaneous warts] in every case,” wrote Jannett Nguyen, a medical student at the University of California, Irvine, and colleagues (JAMA Dermatol. 2016 April 27. doi: 10.1001/jamadermatol.2016.0826).
The researchers reviewed data on warts treated with one of four types of lasers: Carbon dioxide (CO2), erbium:yttrium-aluminum-garnet (Er:YAG), pulsed dye laser (PDL), or neodymium-doped yttrium aluminum garnet (Nd:YAG).
The response rates for the different lasers were 50%-100% for CO2, 72%-100% for Er:YAG, 31%-100% for PDL, and 46%-100% for Nd:YAG. The studies included data on laser treatment of several types of nongenital warts including simple and recalcitrant common warts, periungual and subungual warts, and palmoplantar warts.
In general, side effects from laser treatment of warts were highest with CO2 lasers, and included scarring, hypopigmentation, postoperative pain, and prolonged wound healing. PDL was associated with the lowest risk of side effects, and was as effective as conventional therapies, including cryotherapy and cantharidin.
In Er:YAG treatments, the laser was used for direct ablation of the epidermis on the wart, repeating through layers until normal skin is revealed. Overall, patients treated with Er:YAG demonstrated a higher response and lower recurrence when treated in combination with podofilox. Nd:YAG treatment was similar to PDL, but with a longer wavelength that allows for deeper penetration.
Treatment is limited by a lack of evidence to guide selection of the most appropriate lasers for different warts and by a lack of recommendations for specific laser settings, the researchers noted. Additional studies are needed to establish treatment protocols by comparing lasers to each other and to nonlaser treatments.
However, laser treatment of warts can be “an additional therapeutic option and the studies reviewed here can provide a starting point in determining settings,” they said.
The researchers had no financial disclosures.
FROM JAMA DERMATOLOGY
Key clinical point: Lasers are an effective treatment for both simple and stubborn nongenital warts.
Major finding: The response rates ranged from 46% to 100% for lasers including CO2, Er:YAG, PDL, and Nd:YAG.
Data source: A review of 35 studies comprising 2,149 patients.
Disclosures: The researchers had no financial disclosures.
Multispectral laser safe, fast, effective for removing multicolored tattoos
BOSTON – For the removal of unwanted tattoos, particularly those made up of more than one color, a multispectral laser system of 755 nm, 532 nm or 1,064 nm with a picosecond pulse duration has been found to be safe, fast, and highly effective, without leaving any residual scarring.
“Q-switch lasers with nanosecond pulse rates have been the gold standard of treating unwanted tattoos for years; however, they’re not without their limitations,” said Dr. Bradley Bloom, who presented the results of a prospective, single center study at the annual meeting of the American Society for Laser Medicine and Surgery.
Over the past several years, fewer than 60% of patients achieve complete clearance despite numerous treatments for tattoo removal, explained Dr. Bloom, of Skin Laser and Surgery Specialists of NY & NJ in New York City. “These limitations include the need for many treatments, and the difficulty in clearing green, blue, and yellow inks,” but these challenges could be alleviated by using picosecond lasers with short pulse durations, he said.
The study involved 44 individuals with a total of 53 noncosmetic tattoos. All tattoos were photographed at baseline and before each treatment; the subjects received anywhere between 1 and 10 treatments. Photographs were taken 2 months after the final treatment. Individuals were treated every 6 weeks, plus or minus 2 weeks, with either a 532-nm, 755-nm, or a 1,064-nm laser with a 450-500 picosecond, 500-750 picosecond, and 500-600 picosecond pulse duration, respectively (0.5-6 J per square centimeter, and 1-10 millimeters).
The majority (84%) of the treated tattoos were made up of several different ink colors, including black, red, orange, yellow, green, blue, pink, and white.
“The results we saw with the 532-nm [laser] were over 75% clearance of red, orange, and yellow [inks] with just an average of two treatments,” said Dr. Bloom, adding that these data compare favorably against historical data.
Patients who received at least four treatments reached 75% improvement in tattoo visibility with the 532-nm laser. In addition, 82% of those treated with at least four treatments with the 1,064-nm laser improved by at least 50% and 85% of those treated at least four times with the 755-nm laser treatment improved by at least 50%.
Investigators noted that both wavelength and pulse duration were critical variables in determining the efficacy of the treatment on a given tattoo. For example, 532 nm was found to be “extremely useful” in clearing red, orange, and yellow inks, while the 755-nm laser was found to be the most effective on blue and green inks.
For black inks, both the 755-nm and 1,064-nm were found to be effective, but Dr. Bloom advised that “greater caution [is] required” when using the former on darker skin types.
Some patients did see “mild hypopigmentation” which improved with time, Dr. Bloom said. In addition, a patient who had a biopsy after receiving 10 laser treatments revealed no evidence of fibrosis or scar formation, which “underscores the safety of this device.”
For handling multicolor tattoos, Dr. Bloom suggested dividing the tattoos based on which colors are dominant so that they can be targeted with the laser best suited to remove that color.
Cynosure, maker of the multispectral laser system, supported in the study. Dr. Bloom disclosed advisory, consulting, and financial ties to Aerolase and Cutera
BOSTON – For the removal of unwanted tattoos, particularly those made up of more than one color, a multispectral laser system of 755 nm, 532 nm or 1,064 nm with a picosecond pulse duration has been found to be safe, fast, and highly effective, without leaving any residual scarring.
“Q-switch lasers with nanosecond pulse rates have been the gold standard of treating unwanted tattoos for years; however, they’re not without their limitations,” said Dr. Bradley Bloom, who presented the results of a prospective, single center study at the annual meeting of the American Society for Laser Medicine and Surgery.
Over the past several years, fewer than 60% of patients achieve complete clearance despite numerous treatments for tattoo removal, explained Dr. Bloom, of Skin Laser and Surgery Specialists of NY & NJ in New York City. “These limitations include the need for many treatments, and the difficulty in clearing green, blue, and yellow inks,” but these challenges could be alleviated by using picosecond lasers with short pulse durations, he said.
The study involved 44 individuals with a total of 53 noncosmetic tattoos. All tattoos were photographed at baseline and before each treatment; the subjects received anywhere between 1 and 10 treatments. Photographs were taken 2 months after the final treatment. Individuals were treated every 6 weeks, plus or minus 2 weeks, with either a 532-nm, 755-nm, or a 1,064-nm laser with a 450-500 picosecond, 500-750 picosecond, and 500-600 picosecond pulse duration, respectively (0.5-6 J per square centimeter, and 1-10 millimeters).
The majority (84%) of the treated tattoos were made up of several different ink colors, including black, red, orange, yellow, green, blue, pink, and white.
“The results we saw with the 532-nm [laser] were over 75% clearance of red, orange, and yellow [inks] with just an average of two treatments,” said Dr. Bloom, adding that these data compare favorably against historical data.
Patients who received at least four treatments reached 75% improvement in tattoo visibility with the 532-nm laser. In addition, 82% of those treated with at least four treatments with the 1,064-nm laser improved by at least 50% and 85% of those treated at least four times with the 755-nm laser treatment improved by at least 50%.
Investigators noted that both wavelength and pulse duration were critical variables in determining the efficacy of the treatment on a given tattoo. For example, 532 nm was found to be “extremely useful” in clearing red, orange, and yellow inks, while the 755-nm laser was found to be the most effective on blue and green inks.
For black inks, both the 755-nm and 1,064-nm were found to be effective, but Dr. Bloom advised that “greater caution [is] required” when using the former on darker skin types.
Some patients did see “mild hypopigmentation” which improved with time, Dr. Bloom said. In addition, a patient who had a biopsy after receiving 10 laser treatments revealed no evidence of fibrosis or scar formation, which “underscores the safety of this device.”
For handling multicolor tattoos, Dr. Bloom suggested dividing the tattoos based on which colors are dominant so that they can be targeted with the laser best suited to remove that color.
Cynosure, maker of the multispectral laser system, supported in the study. Dr. Bloom disclosed advisory, consulting, and financial ties to Aerolase and Cutera
BOSTON – For the removal of unwanted tattoos, particularly those made up of more than one color, a multispectral laser system of 755 nm, 532 nm or 1,064 nm with a picosecond pulse duration has been found to be safe, fast, and highly effective, without leaving any residual scarring.
“Q-switch lasers with nanosecond pulse rates have been the gold standard of treating unwanted tattoos for years; however, they’re not without their limitations,” said Dr. Bradley Bloom, who presented the results of a prospective, single center study at the annual meeting of the American Society for Laser Medicine and Surgery.
Over the past several years, fewer than 60% of patients achieve complete clearance despite numerous treatments for tattoo removal, explained Dr. Bloom, of Skin Laser and Surgery Specialists of NY & NJ in New York City. “These limitations include the need for many treatments, and the difficulty in clearing green, blue, and yellow inks,” but these challenges could be alleviated by using picosecond lasers with short pulse durations, he said.
The study involved 44 individuals with a total of 53 noncosmetic tattoos. All tattoos were photographed at baseline and before each treatment; the subjects received anywhere between 1 and 10 treatments. Photographs were taken 2 months after the final treatment. Individuals were treated every 6 weeks, plus or minus 2 weeks, with either a 532-nm, 755-nm, or a 1,064-nm laser with a 450-500 picosecond, 500-750 picosecond, and 500-600 picosecond pulse duration, respectively (0.5-6 J per square centimeter, and 1-10 millimeters).
The majority (84%) of the treated tattoos were made up of several different ink colors, including black, red, orange, yellow, green, blue, pink, and white.
“The results we saw with the 532-nm [laser] were over 75% clearance of red, orange, and yellow [inks] with just an average of two treatments,” said Dr. Bloom, adding that these data compare favorably against historical data.
Patients who received at least four treatments reached 75% improvement in tattoo visibility with the 532-nm laser. In addition, 82% of those treated with at least four treatments with the 1,064-nm laser improved by at least 50% and 85% of those treated at least four times with the 755-nm laser treatment improved by at least 50%.
Investigators noted that both wavelength and pulse duration were critical variables in determining the efficacy of the treatment on a given tattoo. For example, 532 nm was found to be “extremely useful” in clearing red, orange, and yellow inks, while the 755-nm laser was found to be the most effective on blue and green inks.
For black inks, both the 755-nm and 1,064-nm were found to be effective, but Dr. Bloom advised that “greater caution [is] required” when using the former on darker skin types.
Some patients did see “mild hypopigmentation” which improved with time, Dr. Bloom said. In addition, a patient who had a biopsy after receiving 10 laser treatments revealed no evidence of fibrosis or scar formation, which “underscores the safety of this device.”
For handling multicolor tattoos, Dr. Bloom suggested dividing the tattoos based on which colors are dominant so that they can be targeted with the laser best suited to remove that color.
Cynosure, maker of the multispectral laser system, supported in the study. Dr. Bloom disclosed advisory, consulting, and financial ties to Aerolase and Cutera
AT LASER 2016
Key clinical point: Multispectral laser system consisting of 755 nm, 532 nm, and 1,064 nm with picosecond pulse durations was effective at removing tattoos, regardless of ink color, without residual scarring.
Major finding: Among patients who had at least four laser treatments, there was 75% improvement for those treated with the 532 nm laser, and at least 50% improvement in the majority of those treated with the 1,064 nm laser, and the majority of those treated with the 755 nm laser.
Data source: A prospective, single-center study of 1-10 treatments with one of three types of lasers, in 44 individuals with 53 mostly multicolored tattoos.
Disclosures: Cynosure, maker of the multispectral laser system, supported in the study. Dr. Bloom disclosed advisory, consulting, and financial ties to Aerolase and Cutera.