User login
The Pivotal Role of Mentorship in Orthopedic Surgery Residencies

Basics of Lasers in Dermatology
Lasers have become a critical part of the dermatologist’s armamentarium for modulating cutaneous biology, both in treating skin disorders and providing tangible cosmetic alterations to the skin. Although advances in technology and convenient user interfaces have made modern lasers relatively straightforward to use, they are in fact quite complex and powerful instruments that are capable of considerable damage if not used correctly. Thus it is necessary to establish a framework for the safe and responsible use of lasers in dermatology; fundamental to this tenet is an understanding of the development and physics of lasers. In this article, the fundamental concepts of lasers as well as their interactions with the skin will be discussed to impart a working knowledge of lasers to allow for better, safer use of these important tools.
Development of Lasers
The term laser is an acronym for “light amplification by the stimulated emission of radiation.” Albert Einstein established the framework for the functioning of lasers in his seminal work, “On the Quantum Theory of Radiation,”1 in which he described how an electron in an atom in an excited state can return to a lower state by emitting energy in the form of a photon of light. Light comprises a portion of the electromagnetic spectrum, rangingfrom UV (200–400 nm) to visible (400 to about 700 nm) to infrared light (about 700 to >3000 nm). The unique properties of light that affect the function of lasers include reflection (eg, seeing a mirror image of a mountain on the surface of a still lake) and refraction (eg, your hand looking larger under the surface of a pool of water).
Despite early theories on lasers, it was not until the late 1950s that the technology finally started to catch up to the science. Researchers experimenting with microwave fields were able to generate a beam of excited ammonia molecules through a resonant cavity, resulting in a uniform (albeit low power) emission of radiation.2 Maiman3 expounded on this development by building the first working prototype of a device that radiated light without the use of a microwave. So how exactly do lasers work?
Basic Physics of Lasers
To understand how lasers work, one must have a rudimentary understanding of quantum mechanics. Bohr4 revealed that an atom is comprised of a nucleus that is orbited by electrons at discrete distances (ie, only at specific radii), which have corresponding energy levels that increase as the distance from the nucleus increases. With the application of energy, an electron may be excited to a higher energy level, thus increasing its distance from the nucleus, but will then spontaneously return to the lower energy level. By the law of conservation of energy, the excess energy is released as a photon. Although this small amount of energy would not be of much interest at the single particle level, Einstein and Bose discovered that photons were uniquely “gregarious” with the tendency to join together in a common state, leading to the ability to generate a coherent beam of light by simultaneously exciting multiple atoms and their electrons, whereby the return of one electron to a lower energy state generated a chain reaction among the other excited electrons, subsequently prompting the release of photons with the same characteristics as the initial incident photon and returning to a lower energy state.5 This process requires several steps to occur in order. First, absorption of energy has to occur among a population of atoms, thus exciting the electrons to higher energy states. When one of the electrons returns to a lower energy level, spontaneous emission will occur with the release of a photon of light. The photon has a certain probability of colliding with other atoms, thereby causing their electrons to return to a lower energy state and release additional photons of light with the same wavelength and in the same direction as the incident photon in a process that is referred to as stimulated emission.6 When this process occurs in a cavity with a large number of atoms, the result may lead to a high-energy beam of photons, which becomes the laser beam.
There are some caveats to consider regarding electron population dynamics as outlined by the Boltzmann principle whereby only a small proportion of molecules are in the first excited state and the vast majority are in the ground state (lowest energy) at any given time, but the details of higher-energy transitions in quantum mechanics are beyond the scope of this article.7 Primarily, it is important to understand that the ultimate power of a laser’s output depends largely on the population of electrons that are residing at a higher energy state at any given point in time, and the goal of many types of lasers is to achieve a large number of electrons in a high-energy state as opposed to their usual ground state, a process known as population inversion.8
This process leads to the fundamental construction of a laser: a population of atoms in a resonant cavity flanked by reflectors that are exposed to some sort of excitation mechanism (known as the pump) with an output mechanism for the laser beam to exit. In practice, the material used to supply the atoms (known as the gain medium) varies and also determines the wavelength and properties of the laser beam due to differences in the discrete energy states of orbiting electrons. Whatever the gain medium being used, the important properties of a laser resulting from these principles is that the beam is monochromatic (consisting of a single wavelength or a very narrow band), coherent (the light is emitted in the same phase and direction), collimated (a narrow beam diameter with limited divergence), and intense (high power per unit area). Consider the differences between a laser pointer and a flashlight; from across the room, the laser pointer output is a small spot of light on the wall whereas the flashlight has long dispersed to a weak, broad swath of light.
Types of Lasers
Different gain media have been used to create a variety of lasers with different properties. In general, lasers fall into 1 of 4 categories: gas discharge, diode, dye, and solid-state lasers.9
Although a gas discharge laser theoretically is the simplest laser, whereby a gas is excited by an electric discharge and the excited particles of gas create the laser beam, there are practical considerations such as excessive heat production, which may necessitate the use of cooling coils or some other method for heat dispersion. The excimer laser is a specific type of gas discharge laser in which a noble gas is mixed with halogen and high-current pulses are used to generate excited dimers, hence the term excimer. The excited dimers consisting of 1 halogen molecule and 1 noble gas molecule are only linked in the excited state, thus allowing for more stability in the excited state and enabling a higher proportion of molecules to be in that state at any given time, which increases population inversion and thus helps to maximize the output energy.
Diode lasers employ the use of diodes, or semiconductors that allow current to flow in one direction but not the other (theoretically with infinite resistance in one direction and no resistance in the other direction), thus creating a downstream method to achieve a high-power laser output; however, despite its theoretical efficiency, the use of diode lasers has been limited due to practical considerations of the divergence and quality of the output.
Dye lasers consist of a liquid solution of organic dye in a solvent that is pumped by an optical source. While gas discharge lasers involve excitation of a gas, there is a clear corollary with dye lasers with liquid taking the place of the gas; however, this modality has certain limitations, including the use of toxic materials that degrade naturally; the need to switch cuvettes when changing gain media, which serve as the lasing medium; and a relatively low-power output. One benefit of the dye laser, as alluded to above, is the operator’s capability to switch out cuvettes containing different dyes, thus using one machine to generate widely varying laser beams.
Solid-state lasers are most often used in dermatology. These devices utilize a conducting medium (eg, garnet, sapphire, ruby) doped with trivalent rare-earth ions or transition metal ions (eg, neodymium, ytterbium, erbium, titanium, chromium). This process is a relatively reliable and flexible methodology for generating stable lasers, thus explaining its widespread use. Additionally, these solid-state lasers are particularly amenable to modifications (eg, Q-switching).
Considerations for Lasers
Quality switching (known as Q-switching) is a method used to generate a shorter burst of a higher-power laser output.10 The longer the electrons have to become excited within a resonant cavity, the higher the number that may end up in an excited state, thus allowing for a higher ultimate energy output to a certain point. The quality of a medium, in general, refers to the ability of light exiting a medium to return. Within a cavity, the ability of light to go back and forth through the lasing medium is critical in achieving stimulated emission and thus laser beam output; however, in a low-quality medium, population inversion can still occur to allow a greater proportion of electrons to reside in a higher energy state. There are multiple mechanisms to switch the quality of a medium, but the ultimate result always is for the quality to be switched to high so that the light beams can immediately start achieving stimulated emission of a “primed” population of high-energy, population-inverted electrons, resulting in a much higher output power.
Selective thermolysis is critical for understanding modern laser use. To fully comprehend its meaning, one must first understand that the interaction of a laser with the skin depends on a number of factors, including the power density of the laser itself (the beam characteristics), the length of time of exposure, and the physical properties of the targeted molecules. Although there is some modulation of laser function via the wavelength of the laser (eg, higher wavelengths penetrate deeper), the properties of the target molecule can allow for precise control of the laser’s action. The framework for understanding this principle was outlined by Anderson and Parrish11 in 1983. Fundamentally, a laser causes damage to a target molecule via application of large amounts of energy; however, the laser beam does not discriminate between different molecules in its path. Rather the size and other properties of the molecule play a critical role in determining the amount of energy it is able to absorb before dissipating the excess energy as heat. This excess heat energy is what causes damage to surrounding tissues, or collateral damage. Conceptually, being able to target a molecule without damaging surrounding tissues is our goal as practitioners when using lasers in dermatology. It is accomplished by heating a molecule to just under its thermal relaxation time (ie, the time needed for a molecule to dissipate half of the energy applied), thus allowing for acceptable results with regard to efficacy balanced with side effects.12
Conclusion
Lasers are an important treatment modality, and their use in dermatology is becoming widespread for many possible indications; however, lasers are complex mechanical devices that have the potential to cause great harm when used incorrectly. By gaining a thorough understanding of the basic physics of lasers, the different types of lasers that are available, and critical concepts regarding the cutaneous application of lasers, physicians can better understand these devices and approach their use confidently and safely.
1. Einstein A. Zur quantentheorie der Strahlung. Physik Zeitschr. 1917;18:121-128.
2. Schawlow AL, Townes CH. Infrared and optical masers. Phys Rev. 1958;112:1940.
3. Maiman TH. Stimulated optical radiation in ruby. Nature. 1960;187:493-494.
4. Bohr N. On the constitution of atoms and molecules. Philos Mag. 1913;26:1-25.
5. Lewenstein M. Atomic physics: the social life of atoms. Nature. 2007;445:372-375.
6. Chang WSC. Principles of Lasers and Optics. Cambridge, United Kingdom: Cambridge University Press; 2005.
7. Svelto O. Principles of Lasers. 5th ed. New York, NY: Springer; 2010.
8. Rentzepis PM. Lasers in chemistry. Photochem Photobiol. 1968;8:579-588.
9. Tanzi EL, Lupton JR, Alster TS. Lasers in dermatology: four decades of progress. J Am Acad Dermatol. 2003;49:1-31.
10. Saedi N, Green JB, Dover JS, et al. The evolution of quality-switched lasers. J Drugs Dermatol. 2012;11:1296-1299.
11. Anderson RR, Parrish JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science. 1983;220:524-527.
12. Babilas P, Shafirstein G, Baumler W, et al. Selective photothermolysis of blood vessels following flashlamp-pumped pulsed dye laser irradiation: in vivo results and mathematical modelling are in agreement. J Invest Dermatol. 2005;125:343-352.
Lasers have become a critical part of the dermatologist’s armamentarium for modulating cutaneous biology, both in treating skin disorders and providing tangible cosmetic alterations to the skin. Although advances in technology and convenient user interfaces have made modern lasers relatively straightforward to use, they are in fact quite complex and powerful instruments that are capable of considerable damage if not used correctly. Thus it is necessary to establish a framework for the safe and responsible use of lasers in dermatology; fundamental to this tenet is an understanding of the development and physics of lasers. In this article, the fundamental concepts of lasers as well as their interactions with the skin will be discussed to impart a working knowledge of lasers to allow for better, safer use of these important tools.
Development of Lasers
The term laser is an acronym for “light amplification by the stimulated emission of radiation.” Albert Einstein established the framework for the functioning of lasers in his seminal work, “On the Quantum Theory of Radiation,”1 in which he described how an electron in an atom in an excited state can return to a lower state by emitting energy in the form of a photon of light. Light comprises a portion of the electromagnetic spectrum, rangingfrom UV (200–400 nm) to visible (400 to about 700 nm) to infrared light (about 700 to >3000 nm). The unique properties of light that affect the function of lasers include reflection (eg, seeing a mirror image of a mountain on the surface of a still lake) and refraction (eg, your hand looking larger under the surface of a pool of water).
Despite early theories on lasers, it was not until the late 1950s that the technology finally started to catch up to the science. Researchers experimenting with microwave fields were able to generate a beam of excited ammonia molecules through a resonant cavity, resulting in a uniform (albeit low power) emission of radiation.2 Maiman3 expounded on this development by building the first working prototype of a device that radiated light without the use of a microwave. So how exactly do lasers work?
Basic Physics of Lasers
To understand how lasers work, one must have a rudimentary understanding of quantum mechanics. Bohr4 revealed that an atom is comprised of a nucleus that is orbited by electrons at discrete distances (ie, only at specific radii), which have corresponding energy levels that increase as the distance from the nucleus increases. With the application of energy, an electron may be excited to a higher energy level, thus increasing its distance from the nucleus, but will then spontaneously return to the lower energy level. By the law of conservation of energy, the excess energy is released as a photon. Although this small amount of energy would not be of much interest at the single particle level, Einstein and Bose discovered that photons were uniquely “gregarious” with the tendency to join together in a common state, leading to the ability to generate a coherent beam of light by simultaneously exciting multiple atoms and their electrons, whereby the return of one electron to a lower energy state generated a chain reaction among the other excited electrons, subsequently prompting the release of photons with the same characteristics as the initial incident photon and returning to a lower energy state.5 This process requires several steps to occur in order. First, absorption of energy has to occur among a population of atoms, thus exciting the electrons to higher energy states. When one of the electrons returns to a lower energy level, spontaneous emission will occur with the release of a photon of light. The photon has a certain probability of colliding with other atoms, thereby causing their electrons to return to a lower energy state and release additional photons of light with the same wavelength and in the same direction as the incident photon in a process that is referred to as stimulated emission.6 When this process occurs in a cavity with a large number of atoms, the result may lead to a high-energy beam of photons, which becomes the laser beam.
There are some caveats to consider regarding electron population dynamics as outlined by the Boltzmann principle whereby only a small proportion of molecules are in the first excited state and the vast majority are in the ground state (lowest energy) at any given time, but the details of higher-energy transitions in quantum mechanics are beyond the scope of this article.7 Primarily, it is important to understand that the ultimate power of a laser’s output depends largely on the population of electrons that are residing at a higher energy state at any given point in time, and the goal of many types of lasers is to achieve a large number of electrons in a high-energy state as opposed to their usual ground state, a process known as population inversion.8
This process leads to the fundamental construction of a laser: a population of atoms in a resonant cavity flanked by reflectors that are exposed to some sort of excitation mechanism (known as the pump) with an output mechanism for the laser beam to exit. In practice, the material used to supply the atoms (known as the gain medium) varies and also determines the wavelength and properties of the laser beam due to differences in the discrete energy states of orbiting electrons. Whatever the gain medium being used, the important properties of a laser resulting from these principles is that the beam is monochromatic (consisting of a single wavelength or a very narrow band), coherent (the light is emitted in the same phase and direction), collimated (a narrow beam diameter with limited divergence), and intense (high power per unit area). Consider the differences between a laser pointer and a flashlight; from across the room, the laser pointer output is a small spot of light on the wall whereas the flashlight has long dispersed to a weak, broad swath of light.
Types of Lasers
Different gain media have been used to create a variety of lasers with different properties. In general, lasers fall into 1 of 4 categories: gas discharge, diode, dye, and solid-state lasers.9
Although a gas discharge laser theoretically is the simplest laser, whereby a gas is excited by an electric discharge and the excited particles of gas create the laser beam, there are practical considerations such as excessive heat production, which may necessitate the use of cooling coils or some other method for heat dispersion. The excimer laser is a specific type of gas discharge laser in which a noble gas is mixed with halogen and high-current pulses are used to generate excited dimers, hence the term excimer. The excited dimers consisting of 1 halogen molecule and 1 noble gas molecule are only linked in the excited state, thus allowing for more stability in the excited state and enabling a higher proportion of molecules to be in that state at any given time, which increases population inversion and thus helps to maximize the output energy.
Diode lasers employ the use of diodes, or semiconductors that allow current to flow in one direction but not the other (theoretically with infinite resistance in one direction and no resistance in the other direction), thus creating a downstream method to achieve a high-power laser output; however, despite its theoretical efficiency, the use of diode lasers has been limited due to practical considerations of the divergence and quality of the output.
Dye lasers consist of a liquid solution of organic dye in a solvent that is pumped by an optical source. While gas discharge lasers involve excitation of a gas, there is a clear corollary with dye lasers with liquid taking the place of the gas; however, this modality has certain limitations, including the use of toxic materials that degrade naturally; the need to switch cuvettes when changing gain media, which serve as the lasing medium; and a relatively low-power output. One benefit of the dye laser, as alluded to above, is the operator’s capability to switch out cuvettes containing different dyes, thus using one machine to generate widely varying laser beams.
Solid-state lasers are most often used in dermatology. These devices utilize a conducting medium (eg, garnet, sapphire, ruby) doped with trivalent rare-earth ions or transition metal ions (eg, neodymium, ytterbium, erbium, titanium, chromium). This process is a relatively reliable and flexible methodology for generating stable lasers, thus explaining its widespread use. Additionally, these solid-state lasers are particularly amenable to modifications (eg, Q-switching).
Considerations for Lasers
Quality switching (known as Q-switching) is a method used to generate a shorter burst of a higher-power laser output.10 The longer the electrons have to become excited within a resonant cavity, the higher the number that may end up in an excited state, thus allowing for a higher ultimate energy output to a certain point. The quality of a medium, in general, refers to the ability of light exiting a medium to return. Within a cavity, the ability of light to go back and forth through the lasing medium is critical in achieving stimulated emission and thus laser beam output; however, in a low-quality medium, population inversion can still occur to allow a greater proportion of electrons to reside in a higher energy state. There are multiple mechanisms to switch the quality of a medium, but the ultimate result always is for the quality to be switched to high so that the light beams can immediately start achieving stimulated emission of a “primed” population of high-energy, population-inverted electrons, resulting in a much higher output power.
Selective thermolysis is critical for understanding modern laser use. To fully comprehend its meaning, one must first understand that the interaction of a laser with the skin depends on a number of factors, including the power density of the laser itself (the beam characteristics), the length of time of exposure, and the physical properties of the targeted molecules. Although there is some modulation of laser function via the wavelength of the laser (eg, higher wavelengths penetrate deeper), the properties of the target molecule can allow for precise control of the laser’s action. The framework for understanding this principle was outlined by Anderson and Parrish11 in 1983. Fundamentally, a laser causes damage to a target molecule via application of large amounts of energy; however, the laser beam does not discriminate between different molecules in its path. Rather the size and other properties of the molecule play a critical role in determining the amount of energy it is able to absorb before dissipating the excess energy as heat. This excess heat energy is what causes damage to surrounding tissues, or collateral damage. Conceptually, being able to target a molecule without damaging surrounding tissues is our goal as practitioners when using lasers in dermatology. It is accomplished by heating a molecule to just under its thermal relaxation time (ie, the time needed for a molecule to dissipate half of the energy applied), thus allowing for acceptable results with regard to efficacy balanced with side effects.12
Conclusion
Lasers are an important treatment modality, and their use in dermatology is becoming widespread for many possible indications; however, lasers are complex mechanical devices that have the potential to cause great harm when used incorrectly. By gaining a thorough understanding of the basic physics of lasers, the different types of lasers that are available, and critical concepts regarding the cutaneous application of lasers, physicians can better understand these devices and approach their use confidently and safely.
Lasers have become a critical part of the dermatologist’s armamentarium for modulating cutaneous biology, both in treating skin disorders and providing tangible cosmetic alterations to the skin. Although advances in technology and convenient user interfaces have made modern lasers relatively straightforward to use, they are in fact quite complex and powerful instruments that are capable of considerable damage if not used correctly. Thus it is necessary to establish a framework for the safe and responsible use of lasers in dermatology; fundamental to this tenet is an understanding of the development and physics of lasers. In this article, the fundamental concepts of lasers as well as their interactions with the skin will be discussed to impart a working knowledge of lasers to allow for better, safer use of these important tools.
Development of Lasers
The term laser is an acronym for “light amplification by the stimulated emission of radiation.” Albert Einstein established the framework for the functioning of lasers in his seminal work, “On the Quantum Theory of Radiation,”1 in which he described how an electron in an atom in an excited state can return to a lower state by emitting energy in the form of a photon of light. Light comprises a portion of the electromagnetic spectrum, rangingfrom UV (200–400 nm) to visible (400 to about 700 nm) to infrared light (about 700 to >3000 nm). The unique properties of light that affect the function of lasers include reflection (eg, seeing a mirror image of a mountain on the surface of a still lake) and refraction (eg, your hand looking larger under the surface of a pool of water).
Despite early theories on lasers, it was not until the late 1950s that the technology finally started to catch up to the science. Researchers experimenting with microwave fields were able to generate a beam of excited ammonia molecules through a resonant cavity, resulting in a uniform (albeit low power) emission of radiation.2 Maiman3 expounded on this development by building the first working prototype of a device that radiated light without the use of a microwave. So how exactly do lasers work?
Basic Physics of Lasers
To understand how lasers work, one must have a rudimentary understanding of quantum mechanics. Bohr4 revealed that an atom is comprised of a nucleus that is orbited by electrons at discrete distances (ie, only at specific radii), which have corresponding energy levels that increase as the distance from the nucleus increases. With the application of energy, an electron may be excited to a higher energy level, thus increasing its distance from the nucleus, but will then spontaneously return to the lower energy level. By the law of conservation of energy, the excess energy is released as a photon. Although this small amount of energy would not be of much interest at the single particle level, Einstein and Bose discovered that photons were uniquely “gregarious” with the tendency to join together in a common state, leading to the ability to generate a coherent beam of light by simultaneously exciting multiple atoms and their electrons, whereby the return of one electron to a lower energy state generated a chain reaction among the other excited electrons, subsequently prompting the release of photons with the same characteristics as the initial incident photon and returning to a lower energy state.5 This process requires several steps to occur in order. First, absorption of energy has to occur among a population of atoms, thus exciting the electrons to higher energy states. When one of the electrons returns to a lower energy level, spontaneous emission will occur with the release of a photon of light. The photon has a certain probability of colliding with other atoms, thereby causing their electrons to return to a lower energy state and release additional photons of light with the same wavelength and in the same direction as the incident photon in a process that is referred to as stimulated emission.6 When this process occurs in a cavity with a large number of atoms, the result may lead to a high-energy beam of photons, which becomes the laser beam.
There are some caveats to consider regarding electron population dynamics as outlined by the Boltzmann principle whereby only a small proportion of molecules are in the first excited state and the vast majority are in the ground state (lowest energy) at any given time, but the details of higher-energy transitions in quantum mechanics are beyond the scope of this article.7 Primarily, it is important to understand that the ultimate power of a laser’s output depends largely on the population of electrons that are residing at a higher energy state at any given point in time, and the goal of many types of lasers is to achieve a large number of electrons in a high-energy state as opposed to their usual ground state, a process known as population inversion.8
This process leads to the fundamental construction of a laser: a population of atoms in a resonant cavity flanked by reflectors that are exposed to some sort of excitation mechanism (known as the pump) with an output mechanism for the laser beam to exit. In practice, the material used to supply the atoms (known as the gain medium) varies and also determines the wavelength and properties of the laser beam due to differences in the discrete energy states of orbiting electrons. Whatever the gain medium being used, the important properties of a laser resulting from these principles is that the beam is monochromatic (consisting of a single wavelength or a very narrow band), coherent (the light is emitted in the same phase and direction), collimated (a narrow beam diameter with limited divergence), and intense (high power per unit area). Consider the differences between a laser pointer and a flashlight; from across the room, the laser pointer output is a small spot of light on the wall whereas the flashlight has long dispersed to a weak, broad swath of light.
Types of Lasers
Different gain media have been used to create a variety of lasers with different properties. In general, lasers fall into 1 of 4 categories: gas discharge, diode, dye, and solid-state lasers.9
Although a gas discharge laser theoretically is the simplest laser, whereby a gas is excited by an electric discharge and the excited particles of gas create the laser beam, there are practical considerations such as excessive heat production, which may necessitate the use of cooling coils or some other method for heat dispersion. The excimer laser is a specific type of gas discharge laser in which a noble gas is mixed with halogen and high-current pulses are used to generate excited dimers, hence the term excimer. The excited dimers consisting of 1 halogen molecule and 1 noble gas molecule are only linked in the excited state, thus allowing for more stability in the excited state and enabling a higher proportion of molecules to be in that state at any given time, which increases population inversion and thus helps to maximize the output energy.
Diode lasers employ the use of diodes, or semiconductors that allow current to flow in one direction but not the other (theoretically with infinite resistance in one direction and no resistance in the other direction), thus creating a downstream method to achieve a high-power laser output; however, despite its theoretical efficiency, the use of diode lasers has been limited due to practical considerations of the divergence and quality of the output.
Dye lasers consist of a liquid solution of organic dye in a solvent that is pumped by an optical source. While gas discharge lasers involve excitation of a gas, there is a clear corollary with dye lasers with liquid taking the place of the gas; however, this modality has certain limitations, including the use of toxic materials that degrade naturally; the need to switch cuvettes when changing gain media, which serve as the lasing medium; and a relatively low-power output. One benefit of the dye laser, as alluded to above, is the operator’s capability to switch out cuvettes containing different dyes, thus using one machine to generate widely varying laser beams.
Solid-state lasers are most often used in dermatology. These devices utilize a conducting medium (eg, garnet, sapphire, ruby) doped with trivalent rare-earth ions or transition metal ions (eg, neodymium, ytterbium, erbium, titanium, chromium). This process is a relatively reliable and flexible methodology for generating stable lasers, thus explaining its widespread use. Additionally, these solid-state lasers are particularly amenable to modifications (eg, Q-switching).
Considerations for Lasers
Quality switching (known as Q-switching) is a method used to generate a shorter burst of a higher-power laser output.10 The longer the electrons have to become excited within a resonant cavity, the higher the number that may end up in an excited state, thus allowing for a higher ultimate energy output to a certain point. The quality of a medium, in general, refers to the ability of light exiting a medium to return. Within a cavity, the ability of light to go back and forth through the lasing medium is critical in achieving stimulated emission and thus laser beam output; however, in a low-quality medium, population inversion can still occur to allow a greater proportion of electrons to reside in a higher energy state. There are multiple mechanisms to switch the quality of a medium, but the ultimate result always is for the quality to be switched to high so that the light beams can immediately start achieving stimulated emission of a “primed” population of high-energy, population-inverted electrons, resulting in a much higher output power.
Selective thermolysis is critical for understanding modern laser use. To fully comprehend its meaning, one must first understand that the interaction of a laser with the skin depends on a number of factors, including the power density of the laser itself (the beam characteristics), the length of time of exposure, and the physical properties of the targeted molecules. Although there is some modulation of laser function via the wavelength of the laser (eg, higher wavelengths penetrate deeper), the properties of the target molecule can allow for precise control of the laser’s action. The framework for understanding this principle was outlined by Anderson and Parrish11 in 1983. Fundamentally, a laser causes damage to a target molecule via application of large amounts of energy; however, the laser beam does not discriminate between different molecules in its path. Rather the size and other properties of the molecule play a critical role in determining the amount of energy it is able to absorb before dissipating the excess energy as heat. This excess heat energy is what causes damage to surrounding tissues, or collateral damage. Conceptually, being able to target a molecule without damaging surrounding tissues is our goal as practitioners when using lasers in dermatology. It is accomplished by heating a molecule to just under its thermal relaxation time (ie, the time needed for a molecule to dissipate half of the energy applied), thus allowing for acceptable results with regard to efficacy balanced with side effects.12
Conclusion
Lasers are an important treatment modality, and their use in dermatology is becoming widespread for many possible indications; however, lasers are complex mechanical devices that have the potential to cause great harm when used incorrectly. By gaining a thorough understanding of the basic physics of lasers, the different types of lasers that are available, and critical concepts regarding the cutaneous application of lasers, physicians can better understand these devices and approach their use confidently and safely.
1. Einstein A. Zur quantentheorie der Strahlung. Physik Zeitschr. 1917;18:121-128.
2. Schawlow AL, Townes CH. Infrared and optical masers. Phys Rev. 1958;112:1940.
3. Maiman TH. Stimulated optical radiation in ruby. Nature. 1960;187:493-494.
4. Bohr N. On the constitution of atoms and molecules. Philos Mag. 1913;26:1-25.
5. Lewenstein M. Atomic physics: the social life of atoms. Nature. 2007;445:372-375.
6. Chang WSC. Principles of Lasers and Optics. Cambridge, United Kingdom: Cambridge University Press; 2005.
7. Svelto O. Principles of Lasers. 5th ed. New York, NY: Springer; 2010.
8. Rentzepis PM. Lasers in chemistry. Photochem Photobiol. 1968;8:579-588.
9. Tanzi EL, Lupton JR, Alster TS. Lasers in dermatology: four decades of progress. J Am Acad Dermatol. 2003;49:1-31.
10. Saedi N, Green JB, Dover JS, et al. The evolution of quality-switched lasers. J Drugs Dermatol. 2012;11:1296-1299.
11. Anderson RR, Parrish JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science. 1983;220:524-527.
12. Babilas P, Shafirstein G, Baumler W, et al. Selective photothermolysis of blood vessels following flashlamp-pumped pulsed dye laser irradiation: in vivo results and mathematical modelling are in agreement. J Invest Dermatol. 2005;125:343-352.
1. Einstein A. Zur quantentheorie der Strahlung. Physik Zeitschr. 1917;18:121-128.
2. Schawlow AL, Townes CH. Infrared and optical masers. Phys Rev. 1958;112:1940.
3. Maiman TH. Stimulated optical radiation in ruby. Nature. 1960;187:493-494.
4. Bohr N. On the constitution of atoms and molecules. Philos Mag. 1913;26:1-25.
5. Lewenstein M. Atomic physics: the social life of atoms. Nature. 2007;445:372-375.
6. Chang WSC. Principles of Lasers and Optics. Cambridge, United Kingdom: Cambridge University Press; 2005.
7. Svelto O. Principles of Lasers. 5th ed. New York, NY: Springer; 2010.
8. Rentzepis PM. Lasers in chemistry. Photochem Photobiol. 1968;8:579-588.
9. Tanzi EL, Lupton JR, Alster TS. Lasers in dermatology: four decades of progress. J Am Acad Dermatol. 2003;49:1-31.
10. Saedi N, Green JB, Dover JS, et al. The evolution of quality-switched lasers. J Drugs Dermatol. 2012;11:1296-1299.
11. Anderson RR, Parrish JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science. 1983;220:524-527.
12. Babilas P, Shafirstein G, Baumler W, et al. Selective photothermolysis of blood vessels following flashlamp-pumped pulsed dye laser irradiation: in vivo results and mathematical modelling are in agreement. J Invest Dermatol. 2005;125:343-352.

In the drafty call room, a miracle unfolds
I’ve found that, as a resident in psychiatry, it’s rare to experience a moment of truly unbridled achievement while on call. Manning the revolving door of acute psychiatric admissions can be frustrating, not to mention unfulfilling. Maybe that’s why accomplishing a small miracle, you might say, while on call recently felt so satisfying.
Broken window = workplace woes
When working a 12-hour shift, especially overnight, it’s important to have an environment that is conducive to work. As fatigue and stress build, physical comfort means a lot.
Our problem finding physical comfort in the psychiatry resident call room at Saint Louis University was that a fixture on one of the windows had been broken for several years. You could push the window open, but you could not close it. If you called the janitor, he would come and close the window, but there was no guarantee when he’d show up. You might end up typing your notes all evening in the path of a chilly stream of air.
The residents had made a formal request to have the window repaired in a more permanent manner, but this resulted in it being bolted shut. That was a solution, but an imperfect one: Now we had no way to cool the call room in the winter, and it was beginning to smell of body odor.
The psychiatry resident call room is one of the nicer ones I’ve seen, but the building it occupies is a few decades old, and no replacement parts were available for the fixtures. We were stuck with a closed window—so I thought.
That miraculous morning
I was supervising an intern one Saturday, and she had not been paged yet to see patients. The call room was a mess; I telephoned housekeeping to have the beds changed, and maintenance to unclog the sink. When the maintenance man (I’ll call him “Tom”) arrived and fixed the sink, I praised him and asked him to take a look at the window.
“It’s my dream,” I said to no one in particular, “to have a window we can open and shut.”
I didn’t get angry or exert pressure. Tom explained to me that there were no replacement parts.
“Hmm… I see…,” I said.
To my delight, Tom seemed excited to be given a problem to solve. He left to pilfer parts from other windows on the floor.
No luck. The parts were all gone. Tom apologized and suggested we purchase a suction cup, with a cord attached, to pull the window closed.
“Good idea!” I said, thanking him as he went on his way.
But 2 hours later, our maintenance hero, Tom reappeared in the doorway.
“I’ve been thinking about your window all morning,” he announced.
Tom approached the window, unbolted it, and screwed one end of a chain into the frame, creating a makeshift handle. He demonstrated how to pull the window shut.
Voilà! A window we could open and close. The intern’s jaw dropped in amazement. I turned to dance a little jig.
Satisfaction
It’s important to be able to control the temperature in the call room; even more important to have a comfortable, healthy work environment. But knowing I can influence my surroundings to get what I need at work? That’s more important than anything else at all.
Disclosure
Dr. Jennings reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
I’ve found that, as a resident in psychiatry, it’s rare to experience a moment of truly unbridled achievement while on call. Manning the revolving door of acute psychiatric admissions can be frustrating, not to mention unfulfilling. Maybe that’s why accomplishing a small miracle, you might say, while on call recently felt so satisfying.
Broken window = workplace woes
When working a 12-hour shift, especially overnight, it’s important to have an environment that is conducive to work. As fatigue and stress build, physical comfort means a lot.
Our problem finding physical comfort in the psychiatry resident call room at Saint Louis University was that a fixture on one of the windows had been broken for several years. You could push the window open, but you could not close it. If you called the janitor, he would come and close the window, but there was no guarantee when he’d show up. You might end up typing your notes all evening in the path of a chilly stream of air.
The residents had made a formal request to have the window repaired in a more permanent manner, but this resulted in it being bolted shut. That was a solution, but an imperfect one: Now we had no way to cool the call room in the winter, and it was beginning to smell of body odor.
The psychiatry resident call room is one of the nicer ones I’ve seen, but the building it occupies is a few decades old, and no replacement parts were available for the fixtures. We were stuck with a closed window—so I thought.
That miraculous morning
I was supervising an intern one Saturday, and she had not been paged yet to see patients. The call room was a mess; I telephoned housekeeping to have the beds changed, and maintenance to unclog the sink. When the maintenance man (I’ll call him “Tom”) arrived and fixed the sink, I praised him and asked him to take a look at the window.
“It’s my dream,” I said to no one in particular, “to have a window we can open and shut.”
I didn’t get angry or exert pressure. Tom explained to me that there were no replacement parts.
“Hmm… I see…,” I said.
To my delight, Tom seemed excited to be given a problem to solve. He left to pilfer parts from other windows on the floor.
No luck. The parts were all gone. Tom apologized and suggested we purchase a suction cup, with a cord attached, to pull the window closed.
“Good idea!” I said, thanking him as he went on his way.
But 2 hours later, our maintenance hero, Tom reappeared in the doorway.
“I’ve been thinking about your window all morning,” he announced.
Tom approached the window, unbolted it, and screwed one end of a chain into the frame, creating a makeshift handle. He demonstrated how to pull the window shut.
Voilà! A window we could open and close. The intern’s jaw dropped in amazement. I turned to dance a little jig.
Satisfaction
It’s important to be able to control the temperature in the call room; even more important to have a comfortable, healthy work environment. But knowing I can influence my surroundings to get what I need at work? That’s more important than anything else at all.
Disclosure
Dr. Jennings reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
I’ve found that, as a resident in psychiatry, it’s rare to experience a moment of truly unbridled achievement while on call. Manning the revolving door of acute psychiatric admissions can be frustrating, not to mention unfulfilling. Maybe that’s why accomplishing a small miracle, you might say, while on call recently felt so satisfying.
Broken window = workplace woes
When working a 12-hour shift, especially overnight, it’s important to have an environment that is conducive to work. As fatigue and stress build, physical comfort means a lot.
Our problem finding physical comfort in the psychiatry resident call room at Saint Louis University was that a fixture on one of the windows had been broken for several years. You could push the window open, but you could not close it. If you called the janitor, he would come and close the window, but there was no guarantee when he’d show up. You might end up typing your notes all evening in the path of a chilly stream of air.
The residents had made a formal request to have the window repaired in a more permanent manner, but this resulted in it being bolted shut. That was a solution, but an imperfect one: Now we had no way to cool the call room in the winter, and it was beginning to smell of body odor.
The psychiatry resident call room is one of the nicer ones I’ve seen, but the building it occupies is a few decades old, and no replacement parts were available for the fixtures. We were stuck with a closed window—so I thought.
That miraculous morning
I was supervising an intern one Saturday, and she had not been paged yet to see patients. The call room was a mess; I telephoned housekeeping to have the beds changed, and maintenance to unclog the sink. When the maintenance man (I’ll call him “Tom”) arrived and fixed the sink, I praised him and asked him to take a look at the window.
“It’s my dream,” I said to no one in particular, “to have a window we can open and shut.”
I didn’t get angry or exert pressure. Tom explained to me that there were no replacement parts.
“Hmm… I see…,” I said.
To my delight, Tom seemed excited to be given a problem to solve. He left to pilfer parts from other windows on the floor.
No luck. The parts were all gone. Tom apologized and suggested we purchase a suction cup, with a cord attached, to pull the window closed.
“Good idea!” I said, thanking him as he went on his way.
But 2 hours later, our maintenance hero, Tom reappeared in the doorway.
“I’ve been thinking about your window all morning,” he announced.
Tom approached the window, unbolted it, and screwed one end of a chain into the frame, creating a makeshift handle. He demonstrated how to pull the window shut.
Voilà! A window we could open and close. The intern’s jaw dropped in amazement. I turned to dance a little jig.
Satisfaction
It’s important to be able to control the temperature in the call room; even more important to have a comfortable, healthy work environment. But knowing I can influence my surroundings to get what I need at work? That’s more important than anything else at all.
Disclosure
Dr. Jennings reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.

Blueprint for building a psychiatrist: How residency has prepared us
Becoming a psychiatrist entails a shift in how we see ourselves and those around us. We learn—sometimes the hard way—about cultural self-assessment and the relative nature of our perspective on social, cultural, and clinical matters. What do I mean?
As psychiatrists in the making, we are unaware that we’ve been given this persona-suit, so to speak, with its social expectations and misperceptions. We start noticing how telling people what we do shapes our interactions at cocktail parties, informal gatherings, and in day-to-day life. A new acquaintance might disclose more about herself than she otherwise would or, on the contrary, might become reserved, even guarded. Awkward jokes sometimes are thrown into the mix to lighten the mood. All this is part of the package we’ve been handed, because we chose to specialize in the diagnosis and treatment of mental illness and brain disorders.
So, as I enter my final year of training, I find myself reflecting on just how intense a journey residency has been.
We were physicians first…
We’re psychiatrists now, but first we learned the germ theory of disease, the pathophysiology of every well-known illness, and the scientific basis of the practice of medicine. Many of us weren’t fully aware of the challenges that come with psychiatric training when we signed up. But we powered through— trading set measures and laboratory values for subjective experiences and nonverbal cues. Along the way, we realized that we had to master not only an array of neuropsychiatric facts but other implicit skills: “active listening,” the capacity to make on-the-go complex ethical decisions, and the difficult task of being empathetically detached.
It might be only in retrospect that we can appreciate how residency has shaped us in a personal way—almost as much as it has professionally.
We think of physicians broadly as healers who save lives. Psychiatrists are no different; preventing the most hopeless from dying is something that we do the same way a cardiologist prevents a patient from dying of a massive heart attack. Winning the battle over mortality, by whatever imprecise measures of risk we use, ranks at the top of our therapeutic priorities. We find ourselves scrambling so that catastrophe never happens on our watch. Sometimes, we don’t stop to realize how much of a lifesaver we are— especially because, as junior residents, we’re too pressed for time to reflect and are focused on mastering clinical skills.
New tool to measure success in residency
The Accreditation Council for Graduate Medical Education (ACGME) recently released the “Milestones Project,”1 a thorough evaluation system for residency programs to apply to their trainees. This is a great effort to push for more field-specific evaluation measures among the specialties.
In psychiatry, subjects now considered when evaluating a resident’s progress and preparedness for promotion include competence in applied neuroscience; the practitioner’s emotional response to patients’ problems; and regulatory compliance. Ways doctors learn are changing: Emphasis is now on problem-based learning.2 Patient safety is a priority; to respect that, we are betting strongly on the physician’s aptitude to provide good care by decreasing burnout.3 I am pleased to learn that there are ongoing efforts to improve the way we prepare psychiatrists.
In line with ACGME practices, residency programs also need to continue revisiting their didactic curricula to include innovative, emerging topics. Social media, the antipsychiatry movement, Internet forums, opinionated bloggers, and public figures gone viral—these are some current issues that shouldn’t be ignored during training just because they aren’t discussed in texts or academic journals. Programs that teach and stimulate the inclusion of social sciences and critical thinking should yield better, more holistic psychiatrists.4
For me, these avenues of study have made a huge difference. I feel incredibly grateful for the opportunities that my residency program has provided to me as a psychiatrist-in-training, including a year-long course that touches on novel topics, a weekly process group for all residents, and a broad support network to depend on when personal matters arise.
Mentoring: Invaluable part of the process
As part of the journey through residency, we have the opportunity to work alongside renowned academic psychiatrists, most of who also happen to be amazing people. Mentoring has incredible value at this stage of professional development; don’t shy from taking advantage of that opportunity!
Mentors help us make more informed decisions about our career path. I love hearing the personal stories that my attending physicians tell. On hectic days, when we are beleaguered by managed care and electronic health records, those stories touch us in ways that abstract learning cannot. Internalizing our role models is a conscious and an unconscious element of the process of becoming a psychiatrist.
About that process: It’s far from perfect, always changing, and only the start of our mastery over the tough but rewarding daily tasks of listening… reflecting… prescribing, and, well, saving lives.
Disclosure
Dr. Jovel reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Accreditation Council for Graduate Medical Education and American Board of Psychiatry and Neurology. The Psychiatry Milestone Project. http://acgme.org/acgmeweb/ Portals/0/PDFs/Milestones/PsychiatryMilestones.pdf. Published November 2013. Accessed June 23, 2014.
2. Koh GC, Khoo HE, Wong ML, et al. The effects of problem-based learning during medical school on physician competency: a systematic review. CMAJ. 2008;178(1):34-41.
3. Block L, Wu AW, Feldman L, et al. Residency schedule, burnout and patient care among first-year residents. Postgrad Med J. 2013;89(1055):495-500.
4. Bromley E, Braslow J. Teaching critical thinking in psychiatric training: a role for the social sciences. Am J Psychiatry. 2008; 165(11):1396-1401.
Becoming a psychiatrist entails a shift in how we see ourselves and those around us. We learn—sometimes the hard way—about cultural self-assessment and the relative nature of our perspective on social, cultural, and clinical matters. What do I mean?
As psychiatrists in the making, we are unaware that we’ve been given this persona-suit, so to speak, with its social expectations and misperceptions. We start noticing how telling people what we do shapes our interactions at cocktail parties, informal gatherings, and in day-to-day life. A new acquaintance might disclose more about herself than she otherwise would or, on the contrary, might become reserved, even guarded. Awkward jokes sometimes are thrown into the mix to lighten the mood. All this is part of the package we’ve been handed, because we chose to specialize in the diagnosis and treatment of mental illness and brain disorders.
So, as I enter my final year of training, I find myself reflecting on just how intense a journey residency has been.
We were physicians first…
We’re psychiatrists now, but first we learned the germ theory of disease, the pathophysiology of every well-known illness, and the scientific basis of the practice of medicine. Many of us weren’t fully aware of the challenges that come with psychiatric training when we signed up. But we powered through— trading set measures and laboratory values for subjective experiences and nonverbal cues. Along the way, we realized that we had to master not only an array of neuropsychiatric facts but other implicit skills: “active listening,” the capacity to make on-the-go complex ethical decisions, and the difficult task of being empathetically detached.
It might be only in retrospect that we can appreciate how residency has shaped us in a personal way—almost as much as it has professionally.
We think of physicians broadly as healers who save lives. Psychiatrists are no different; preventing the most hopeless from dying is something that we do the same way a cardiologist prevents a patient from dying of a massive heart attack. Winning the battle over mortality, by whatever imprecise measures of risk we use, ranks at the top of our therapeutic priorities. We find ourselves scrambling so that catastrophe never happens on our watch. Sometimes, we don’t stop to realize how much of a lifesaver we are— especially because, as junior residents, we’re too pressed for time to reflect and are focused on mastering clinical skills.
New tool to measure success in residency
The Accreditation Council for Graduate Medical Education (ACGME) recently released the “Milestones Project,”1 a thorough evaluation system for residency programs to apply to their trainees. This is a great effort to push for more field-specific evaluation measures among the specialties.
In psychiatry, subjects now considered when evaluating a resident’s progress and preparedness for promotion include competence in applied neuroscience; the practitioner’s emotional response to patients’ problems; and regulatory compliance. Ways doctors learn are changing: Emphasis is now on problem-based learning.2 Patient safety is a priority; to respect that, we are betting strongly on the physician’s aptitude to provide good care by decreasing burnout.3 I am pleased to learn that there are ongoing efforts to improve the way we prepare psychiatrists.
In line with ACGME practices, residency programs also need to continue revisiting their didactic curricula to include innovative, emerging topics. Social media, the antipsychiatry movement, Internet forums, opinionated bloggers, and public figures gone viral—these are some current issues that shouldn’t be ignored during training just because they aren’t discussed in texts or academic journals. Programs that teach and stimulate the inclusion of social sciences and critical thinking should yield better, more holistic psychiatrists.4
For me, these avenues of study have made a huge difference. I feel incredibly grateful for the opportunities that my residency program has provided to me as a psychiatrist-in-training, including a year-long course that touches on novel topics, a weekly process group for all residents, and a broad support network to depend on when personal matters arise.
Mentoring: Invaluable part of the process
As part of the journey through residency, we have the opportunity to work alongside renowned academic psychiatrists, most of who also happen to be amazing people. Mentoring has incredible value at this stage of professional development; don’t shy from taking advantage of that opportunity!
Mentors help us make more informed decisions about our career path. I love hearing the personal stories that my attending physicians tell. On hectic days, when we are beleaguered by managed care and electronic health records, those stories touch us in ways that abstract learning cannot. Internalizing our role models is a conscious and an unconscious element of the process of becoming a psychiatrist.
About that process: It’s far from perfect, always changing, and only the start of our mastery over the tough but rewarding daily tasks of listening… reflecting… prescribing, and, well, saving lives.
Disclosure
Dr. Jovel reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Becoming a psychiatrist entails a shift in how we see ourselves and those around us. We learn—sometimes the hard way—about cultural self-assessment and the relative nature of our perspective on social, cultural, and clinical matters. What do I mean?
As psychiatrists in the making, we are unaware that we’ve been given this persona-suit, so to speak, with its social expectations and misperceptions. We start noticing how telling people what we do shapes our interactions at cocktail parties, informal gatherings, and in day-to-day life. A new acquaintance might disclose more about herself than she otherwise would or, on the contrary, might become reserved, even guarded. Awkward jokes sometimes are thrown into the mix to lighten the mood. All this is part of the package we’ve been handed, because we chose to specialize in the diagnosis and treatment of mental illness and brain disorders.
So, as I enter my final year of training, I find myself reflecting on just how intense a journey residency has been.
We were physicians first…
We’re psychiatrists now, but first we learned the germ theory of disease, the pathophysiology of every well-known illness, and the scientific basis of the practice of medicine. Many of us weren’t fully aware of the challenges that come with psychiatric training when we signed up. But we powered through— trading set measures and laboratory values for subjective experiences and nonverbal cues. Along the way, we realized that we had to master not only an array of neuropsychiatric facts but other implicit skills: “active listening,” the capacity to make on-the-go complex ethical decisions, and the difficult task of being empathetically detached.
It might be only in retrospect that we can appreciate how residency has shaped us in a personal way—almost as much as it has professionally.
We think of physicians broadly as healers who save lives. Psychiatrists are no different; preventing the most hopeless from dying is something that we do the same way a cardiologist prevents a patient from dying of a massive heart attack. Winning the battle over mortality, by whatever imprecise measures of risk we use, ranks at the top of our therapeutic priorities. We find ourselves scrambling so that catastrophe never happens on our watch. Sometimes, we don’t stop to realize how much of a lifesaver we are— especially because, as junior residents, we’re too pressed for time to reflect and are focused on mastering clinical skills.
New tool to measure success in residency
The Accreditation Council for Graduate Medical Education (ACGME) recently released the “Milestones Project,”1 a thorough evaluation system for residency programs to apply to their trainees. This is a great effort to push for more field-specific evaluation measures among the specialties.
In psychiatry, subjects now considered when evaluating a resident’s progress and preparedness for promotion include competence in applied neuroscience; the practitioner’s emotional response to patients’ problems; and regulatory compliance. Ways doctors learn are changing: Emphasis is now on problem-based learning.2 Patient safety is a priority; to respect that, we are betting strongly on the physician’s aptitude to provide good care by decreasing burnout.3 I am pleased to learn that there are ongoing efforts to improve the way we prepare psychiatrists.
In line with ACGME practices, residency programs also need to continue revisiting their didactic curricula to include innovative, emerging topics. Social media, the antipsychiatry movement, Internet forums, opinionated bloggers, and public figures gone viral—these are some current issues that shouldn’t be ignored during training just because they aren’t discussed in texts or academic journals. Programs that teach and stimulate the inclusion of social sciences and critical thinking should yield better, more holistic psychiatrists.4
For me, these avenues of study have made a huge difference. I feel incredibly grateful for the opportunities that my residency program has provided to me as a psychiatrist-in-training, including a year-long course that touches on novel topics, a weekly process group for all residents, and a broad support network to depend on when personal matters arise.
Mentoring: Invaluable part of the process
As part of the journey through residency, we have the opportunity to work alongside renowned academic psychiatrists, most of who also happen to be amazing people. Mentoring has incredible value at this stage of professional development; don’t shy from taking advantage of that opportunity!
Mentors help us make more informed decisions about our career path. I love hearing the personal stories that my attending physicians tell. On hectic days, when we are beleaguered by managed care and electronic health records, those stories touch us in ways that abstract learning cannot. Internalizing our role models is a conscious and an unconscious element of the process of becoming a psychiatrist.
About that process: It’s far from perfect, always changing, and only the start of our mastery over the tough but rewarding daily tasks of listening… reflecting… prescribing, and, well, saving lives.
Disclosure
Dr. Jovel reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Accreditation Council for Graduate Medical Education and American Board of Psychiatry and Neurology. The Psychiatry Milestone Project. http://acgme.org/acgmeweb/ Portals/0/PDFs/Milestones/PsychiatryMilestones.pdf. Published November 2013. Accessed June 23, 2014.
2. Koh GC, Khoo HE, Wong ML, et al. The effects of problem-based learning during medical school on physician competency: a systematic review. CMAJ. 2008;178(1):34-41.
3. Block L, Wu AW, Feldman L, et al. Residency schedule, burnout and patient care among first-year residents. Postgrad Med J. 2013;89(1055):495-500.
4. Bromley E, Braslow J. Teaching critical thinking in psychiatric training: a role for the social sciences. Am J Psychiatry. 2008; 165(11):1396-1401.
1. Accreditation Council for Graduate Medical Education and American Board of Psychiatry and Neurology. The Psychiatry Milestone Project. http://acgme.org/acgmeweb/ Portals/0/PDFs/Milestones/PsychiatryMilestones.pdf. Published November 2013. Accessed June 23, 2014.
2. Koh GC, Khoo HE, Wong ML, et al. The effects of problem-based learning during medical school on physician competency: a systematic review. CMAJ. 2008;178(1):34-41.
3. Block L, Wu AW, Feldman L, et al. Residency schedule, burnout and patient care among first-year residents. Postgrad Med J. 2013;89(1055):495-500.
4. Bromley E, Braslow J. Teaching critical thinking in psychiatric training: a role for the social sciences. Am J Psychiatry. 2008; 165(11):1396-1401.

Learning From a Leader: An Interview With Jean L. Bolognia, MD
As senior editor of the current seminal textbook in dermatology, Dermatology, Jean L. Bolognia, MD, has a special place in the hearts and minds of dermatology residents, both past and present. Early on in our training, we learn that a surefire way to quickly win a debate is to start your counterargument with, “Well, Bolognia says. . . .” This respect is well garnered, as Dr. Bolognia’s book has helped elucidate difficult diagnostic and therapeutic concepts to dermatology trainees with coherent diagrams and clearly written text. It is a must-read during one’s formative education. Dr. Bolognia currently serves as professor in dermatology and vice chair of clinical affairs at Yale University in New Haven, Connecticut. During her visit to the State University of New York at Stony Brook (Figure), I sat down with Dr. Bolognia for an interview.

BRONFENBRENER: The dermatology textbook is broad and expansive. What inspired you to start this project?
BOLOGNIA: I’ll divide my answer into 2 parts: why I thought a new textbook was needed and how it came to be. At the time, I felt that many of the current comprehensive textbooks were too daunting for a first-year resident. I felt that in order to teach skin biology, for example, you needed to simplify it. The goal was simplification, at least in terms of how the content was explained to the novice reader, without sacrificing sophistication. I do believe that you need to understand basic science in order to understand the breakthroughs that will occur during your career. However, if the content is confusing or too many details are presented without schematics, at the end of the reading you are not learning. So, I wanted to teach concepts à la Scientific American, where an initial review of the schematics then makes the text much easier to understand. I thought that was a very important way to teach skin biology.
As for my early involvement in the book, I had previously organized a Web-based curriculum for medical students for the American Academy of Dermatology, which was divided into approximately 20 disease chapters, each 2 to 3 pages in length. I made sure the templates were simple and straightforward so that the authors could complete the assigned task within 2 to 3 hours. My invitation to be an editor came from the publisher based upon recommendations from some of those authors. Of note, that medical student curriculum has since been revised and is now much more refined than the original—we were version 1.0!
A few months earlier, Ron (Ronald) Rapini had approached [the publisher] with an outline for a comprehensive dermatology textbook and the publisher became interested in pursuing such a project. Joe (Joseph) Jorizzo was then asked to be the third editor. However, there was stiff competition, as we were going up against the established Fitzpatrick’s textbook. It was important to have a different approach and I was lucky that Julie Schaffer was a dermatology resident in our program at that time and she provided great critiques of the chapters.
BRONFENBRENER: When did you first realize the book was a hit?
BOLOGNIA: Well, it was fairly easy; I knew the sales numbers! That said, I think people were looking for something new and fresh. I remember one of the early reviewers likening us to USA Today! I think the Key Features were very important in making the book a success because they give first-year residents a sense of control when reading about a disease they have never heard about before. The first 6 months of dermatology residency are incredibly difficult because you need to incorporate words you never used before to talk about diseases you’ve never heard of before. I think one of my most meaningful experiences was when I visited South Africa and a young resident approached me who had photocopied the entire book and put it into individual binders so as not to desecrate his pristine original copy by writing in the margins, or underlining and highlighting. Something else I am proud of is that even if you are in a resource-poor country, you can read the book and can be on equal footing with any dermatologist from countries around the world, including ours. In other words, it is an educational equalizer.
BRONFENBRENER: What first inspired you to go into dermatology?
BOLOGNIA: I was a third-year medical student and had just finished a rotation in the neonatal intensive care unit, which was particularly demanding; I think you had more clinical responsibilities back then. I was sitting at dinner with some classmates looking for an elective to do, and they all pushed me towards dermatology. It was just what I needed, they said; you only really worked 4 days a week, and the hours were so civilized! My first Friday on the rotation I borrowed Irwin Braverman’s book Skin Signs of Systemic Disease from the clinic and read a good portion of it over the weekend. It struck a chord with me because of its multiple links to internal medicine. The next week I was in dermatology Grand Rounds, and back then the medical students were the first to present their differential diagnoses, prior to and without talking with the residents. It was a bit of sport to hear the rather imaginative diagnoses generated by the students. So when called upon, I stated that I thought my patient had histiocytosis X, and less likely dermatitis. The attending running Grand Rounds questioned me: What could possibly make me think that it was this rare entity histiocytosis X? I told him it looked just like the picture in Dr. Braverman’s book! Everyone got a chuckle out of my answer, but believe it or not, the patient actually had histiocytosis X. Nowadays I would never put histiocytosis above more common entities, but talk about beginner’s luck. I was hooked! The fact that I got the diagnosis right reflects how important a well-written book is for trainees, and I’m honored to still see patients in the same pod as Dr. Braverman.
BRONFENBRENER: What pearls would you give graduating residents now?
BOLOGNIA: I think you have to reflect on what you like to do, what resonates with you, whether you like to take care of people with contact dermatitis, or you like cutting cancer off patients’ faces, or you want to practice phototherapy. Think about where your heart is and that’s what you should do, not what your professors, or your parents, or your chairman thinks you should do. You’re going to be engaged in these activities for at least 30 years, so find something you are passionate about and build on that. Analyze your talents as well as your strengths and go with it. Another important point is to find an area—or 2, or even 3—where you do a lot of reading and then let others know of your interests. Before long you will be able to build upon your greater knowledge and clinical experience and become an expert within a few years. It doesn’t matter if you’re in an academic or private practice; there will always be a niche that you can fill and patients you can help because of your expertise.
BRONFENBRENER: What areas do you find particularly fascinating in dermatology?
BOLOGNIA: Oh, there’s so much! Patients with monoclonal gammopathies, where they can have follicular spines composed of the monoclonal protein coming out of their nose, are fascinating. That’s the kind of dermatology I like: the “believe-it-or-not” side of dermatology. Once I met a patient at a dermatology conference who had fallen down on a farm and had sustained a traumatic brain injury, after which he could only sweat on one side of his body. He had Grover disease limited to the side of his body that could sweat, while the other side was totally clear. We know Grover disease comes from a combination of sweating and sun damage, but seeing that sharp cutoff on his midline drove the point home for me.
BRONFENBRENER: How do you learn best?
BOLOGNIA: I put notes in the margins. If I go to a lecture, I use address labels for my notes. Then I take those stickers and put them in the relevant part of the textbook. It is so much easier to peel off the stickers than it is to write the information. As a result, there is a greater likelihood that the information will actually be transferred.
BRONFENBRENER: What is your daily routine?
BOLOGNIA: Monday, Tuesday, Friday I see patients. Wednesday is Grand Rounds and electronic medical record cleanup time, the paperwork that is no longer on paper. Thursday is my academic day where I can work on projects, and I like this full-day approach because I work best in larger blocks of time. That’s why I recommend, for residents especially, to get a large chunk of their reading done on Saturday or Sunday morning in 2- to 3-hour blocks. I’m not someone who rises hours before everyone else; I’m a 6:00 am type of gal. If you wake up and get your work done during a planned block of time, then you feel like you’ve accomplished something and can enjoy the rest of your day. For me, I’m freshest in the morning, no question about it.
BRONFENBRENER: Where do you think dermatology is going?
BOLOGNIA: I don’t know exactly, and I don’t think anyone knows exactly. I think we need to work hard to maintain our unique body of knowledge and to remind others of this accomplishment. I am often struck in Grand Rounds that no other specialty would have a fighting chance at generating a differential diagnosis or appropriate treatment strategy for the patients presented there. I can’t answer whether if in 10 years most dermatologists will be employees at hospitals or will still have some degree of autonomy, and I think that is unsettling.
BRONFENBRENER: What’s on the horizon for you?
BOLOGNIA: I’m working on the fourth edition of Dermatology, slated to come out in 2017. Dermatology Essentials was just published and is meant to provide a quick overview if you’re scheduled to give a talk and want a 5-minute refresher or if you’re in between patients and would like to be reminded of additional entities in the differential diagnosis. These books are accessible via the Inkling app, so you can have the entire book correctly formatted on your phone or tablet. I was recently trying to provide a more specific site for a biopsy on the ear and just couldn’t remember the correct term, but a quick search and I had the entire external ear anatomy schematic up on my phone.
BRONFENBRENER: Any favorite quotations?
BOLOGNIA: I like this one by Benjamin Franklin: “Well done is better than well said.” I judge people on their actions; not on what they say they’re going to do but rather what they’ve done.
Final Thoughts
My interview provided a glimpse into the cooperative effort required to synthesize the vast quantity of information into a well-written textbook. Dr. Bolognia is passionate about the field, finds great pleasure in unraveling mysterious patients, and goes to great lengths to make teaching points. As impressive as her accomplishments are, I found myself most inspired by her intellectual curiosity for dermatology, a character trait that successful dermatology residents should also embody. I feel fortunate to have had the opportunity to interview her, and I hope that the resident community can also benefit from the advice she has shared.
Suggested Readings
Bolognia JL, Jorizzo JL, Schaffer JV, et al, eds. Dermatology. Phildelphia, PA: WB Saunders; 2012.
Bolognia JL, Schaffer JV, Duncan KO, et al, eds. Dermatology Essentials. Philadelphia, PA: WB Saunders; 2014.
Braverman IM. Skin Signs of Systemic Disease. 3rd ed. Philadelphia, PA: WB Saunders; 1998.
Goldsmith LA, Katz SI, Gilchrist BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw Hill; 2012.
As senior editor of the current seminal textbook in dermatology, Dermatology, Jean L. Bolognia, MD, has a special place in the hearts and minds of dermatology residents, both past and present. Early on in our training, we learn that a surefire way to quickly win a debate is to start your counterargument with, “Well, Bolognia says. . . .” This respect is well garnered, as Dr. Bolognia’s book has helped elucidate difficult diagnostic and therapeutic concepts to dermatology trainees with coherent diagrams and clearly written text. It is a must-read during one’s formative education. Dr. Bolognia currently serves as professor in dermatology and vice chair of clinical affairs at Yale University in New Haven, Connecticut. During her visit to the State University of New York at Stony Brook (Figure), I sat down with Dr. Bolognia for an interview.
BRONFENBRENER: The dermatology textbook is broad and expansive. What inspired you to start this project?
BOLOGNIA: I’ll divide my answer into 2 parts: why I thought a new textbook was needed and how it came to be. At the time, I felt that many of the current comprehensive textbooks were too daunting for a first-year resident. I felt that in order to teach skin biology, for example, you needed to simplify it. The goal was simplification, at least in terms of how the content was explained to the novice reader, without sacrificing sophistication. I do believe that you need to understand basic science in order to understand the breakthroughs that will occur during your career. However, if the content is confusing or too many details are presented without schematics, at the end of the reading you are not learning. So, I wanted to teach concepts à la Scientific American, where an initial review of the schematics then makes the text much easier to understand. I thought that was a very important way to teach skin biology.
As for my early involvement in the book, I had previously organized a Web-based curriculum for medical students for the American Academy of Dermatology, which was divided into approximately 20 disease chapters, each 2 to 3 pages in length. I made sure the templates were simple and straightforward so that the authors could complete the assigned task within 2 to 3 hours. My invitation to be an editor came from the publisher based upon recommendations from some of those authors. Of note, that medical student curriculum has since been revised and is now much more refined than the original—we were version 1.0!
A few months earlier, Ron (Ronald) Rapini had approached [the publisher] with an outline for a comprehensive dermatology textbook and the publisher became interested in pursuing such a project. Joe (Joseph) Jorizzo was then asked to be the third editor. However, there was stiff competition, as we were going up against the established Fitzpatrick’s textbook. It was important to have a different approach and I was lucky that Julie Schaffer was a dermatology resident in our program at that time and she provided great critiques of the chapters.
BRONFENBRENER: When did you first realize the book was a hit?
BOLOGNIA: Well, it was fairly easy; I knew the sales numbers! That said, I think people were looking for something new and fresh. I remember one of the early reviewers likening us to USA Today! I think the Key Features were very important in making the book a success because they give first-year residents a sense of control when reading about a disease they have never heard about before. The first 6 months of dermatology residency are incredibly difficult because you need to incorporate words you never used before to talk about diseases you’ve never heard of before. I think one of my most meaningful experiences was when I visited South Africa and a young resident approached me who had photocopied the entire book and put it into individual binders so as not to desecrate his pristine original copy by writing in the margins, or underlining and highlighting. Something else I am proud of is that even if you are in a resource-poor country, you can read the book and can be on equal footing with any dermatologist from countries around the world, including ours. In other words, it is an educational equalizer.
BRONFENBRENER: What first inspired you to go into dermatology?
BOLOGNIA: I was a third-year medical student and had just finished a rotation in the neonatal intensive care unit, which was particularly demanding; I think you had more clinical responsibilities back then. I was sitting at dinner with some classmates looking for an elective to do, and they all pushed me towards dermatology. It was just what I needed, they said; you only really worked 4 days a week, and the hours were so civilized! My first Friday on the rotation I borrowed Irwin Braverman’s book Skin Signs of Systemic Disease from the clinic and read a good portion of it over the weekend. It struck a chord with me because of its multiple links to internal medicine. The next week I was in dermatology Grand Rounds, and back then the medical students were the first to present their differential diagnoses, prior to and without talking with the residents. It was a bit of sport to hear the rather imaginative diagnoses generated by the students. So when called upon, I stated that I thought my patient had histiocytosis X, and less likely dermatitis. The attending running Grand Rounds questioned me: What could possibly make me think that it was this rare entity histiocytosis X? I told him it looked just like the picture in Dr. Braverman’s book! Everyone got a chuckle out of my answer, but believe it or not, the patient actually had histiocytosis X. Nowadays I would never put histiocytosis above more common entities, but talk about beginner’s luck. I was hooked! The fact that I got the diagnosis right reflects how important a well-written book is for trainees, and I’m honored to still see patients in the same pod as Dr. Braverman.
BRONFENBRENER: What pearls would you give graduating residents now?
BOLOGNIA: I think you have to reflect on what you like to do, what resonates with you, whether you like to take care of people with contact dermatitis, or you like cutting cancer off patients’ faces, or you want to practice phototherapy. Think about where your heart is and that’s what you should do, not what your professors, or your parents, or your chairman thinks you should do. You’re going to be engaged in these activities for at least 30 years, so find something you are passionate about and build on that. Analyze your talents as well as your strengths and go with it. Another important point is to find an area—or 2, or even 3—where you do a lot of reading and then let others know of your interests. Before long you will be able to build upon your greater knowledge and clinical experience and become an expert within a few years. It doesn’t matter if you’re in an academic or private practice; there will always be a niche that you can fill and patients you can help because of your expertise.
BRONFENBRENER: What areas do you find particularly fascinating in dermatology?
BOLOGNIA: Oh, there’s so much! Patients with monoclonal gammopathies, where they can have follicular spines composed of the monoclonal protein coming out of their nose, are fascinating. That’s the kind of dermatology I like: the “believe-it-or-not” side of dermatology. Once I met a patient at a dermatology conference who had fallen down on a farm and had sustained a traumatic brain injury, after which he could only sweat on one side of his body. He had Grover disease limited to the side of his body that could sweat, while the other side was totally clear. We know Grover disease comes from a combination of sweating and sun damage, but seeing that sharp cutoff on his midline drove the point home for me.
BRONFENBRENER: How do you learn best?
BOLOGNIA: I put notes in the margins. If I go to a lecture, I use address labels for my notes. Then I take those stickers and put them in the relevant part of the textbook. It is so much easier to peel off the stickers than it is to write the information. As a result, there is a greater likelihood that the information will actually be transferred.
BRONFENBRENER: What is your daily routine?
BOLOGNIA: Monday, Tuesday, Friday I see patients. Wednesday is Grand Rounds and electronic medical record cleanup time, the paperwork that is no longer on paper. Thursday is my academic day where I can work on projects, and I like this full-day approach because I work best in larger blocks of time. That’s why I recommend, for residents especially, to get a large chunk of their reading done on Saturday or Sunday morning in 2- to 3-hour blocks. I’m not someone who rises hours before everyone else; I’m a 6:00 am type of gal. If you wake up and get your work done during a planned block of time, then you feel like you’ve accomplished something and can enjoy the rest of your day. For me, I’m freshest in the morning, no question about it.
BRONFENBRENER: Where do you think dermatology is going?
BOLOGNIA: I don’t know exactly, and I don’t think anyone knows exactly. I think we need to work hard to maintain our unique body of knowledge and to remind others of this accomplishment. I am often struck in Grand Rounds that no other specialty would have a fighting chance at generating a differential diagnosis or appropriate treatment strategy for the patients presented there. I can’t answer whether if in 10 years most dermatologists will be employees at hospitals or will still have some degree of autonomy, and I think that is unsettling.
BRONFENBRENER: What’s on the horizon for you?
BOLOGNIA: I’m working on the fourth edition of Dermatology, slated to come out in 2017. Dermatology Essentials was just published and is meant to provide a quick overview if you’re scheduled to give a talk and want a 5-minute refresher or if you’re in between patients and would like to be reminded of additional entities in the differential diagnosis. These books are accessible via the Inkling app, so you can have the entire book correctly formatted on your phone or tablet. I was recently trying to provide a more specific site for a biopsy on the ear and just couldn’t remember the correct term, but a quick search and I had the entire external ear anatomy schematic up on my phone.
BRONFENBRENER: Any favorite quotations?
BOLOGNIA: I like this one by Benjamin Franklin: “Well done is better than well said.” I judge people on their actions; not on what they say they’re going to do but rather what they’ve done.
Final Thoughts
My interview provided a glimpse into the cooperative effort required to synthesize the vast quantity of information into a well-written textbook. Dr. Bolognia is passionate about the field, finds great pleasure in unraveling mysterious patients, and goes to great lengths to make teaching points. As impressive as her accomplishments are, I found myself most inspired by her intellectual curiosity for dermatology, a character trait that successful dermatology residents should also embody. I feel fortunate to have had the opportunity to interview her, and I hope that the resident community can also benefit from the advice she has shared.
As senior editor of the current seminal textbook in dermatology, Dermatology, Jean L. Bolognia, MD, has a special place in the hearts and minds of dermatology residents, both past and present. Early on in our training, we learn that a surefire way to quickly win a debate is to start your counterargument with, “Well, Bolognia says. . . .” This respect is well garnered, as Dr. Bolognia’s book has helped elucidate difficult diagnostic and therapeutic concepts to dermatology trainees with coherent diagrams and clearly written text. It is a must-read during one’s formative education. Dr. Bolognia currently serves as professor in dermatology and vice chair of clinical affairs at Yale University in New Haven, Connecticut. During her visit to the State University of New York at Stony Brook (Figure), I sat down with Dr. Bolognia for an interview.
BRONFENBRENER: The dermatology textbook is broad and expansive. What inspired you to start this project?
BOLOGNIA: I’ll divide my answer into 2 parts: why I thought a new textbook was needed and how it came to be. At the time, I felt that many of the current comprehensive textbooks were too daunting for a first-year resident. I felt that in order to teach skin biology, for example, you needed to simplify it. The goal was simplification, at least in terms of how the content was explained to the novice reader, without sacrificing sophistication. I do believe that you need to understand basic science in order to understand the breakthroughs that will occur during your career. However, if the content is confusing or too many details are presented without schematics, at the end of the reading you are not learning. So, I wanted to teach concepts à la Scientific American, where an initial review of the schematics then makes the text much easier to understand. I thought that was a very important way to teach skin biology.
As for my early involvement in the book, I had previously organized a Web-based curriculum for medical students for the American Academy of Dermatology, which was divided into approximately 20 disease chapters, each 2 to 3 pages in length. I made sure the templates were simple and straightforward so that the authors could complete the assigned task within 2 to 3 hours. My invitation to be an editor came from the publisher based upon recommendations from some of those authors. Of note, that medical student curriculum has since been revised and is now much more refined than the original—we were version 1.0!
A few months earlier, Ron (Ronald) Rapini had approached [the publisher] with an outline for a comprehensive dermatology textbook and the publisher became interested in pursuing such a project. Joe (Joseph) Jorizzo was then asked to be the third editor. However, there was stiff competition, as we were going up against the established Fitzpatrick’s textbook. It was important to have a different approach and I was lucky that Julie Schaffer was a dermatology resident in our program at that time and she provided great critiques of the chapters.
BRONFENBRENER: When did you first realize the book was a hit?
BOLOGNIA: Well, it was fairly easy; I knew the sales numbers! That said, I think people were looking for something new and fresh. I remember one of the early reviewers likening us to USA Today! I think the Key Features were very important in making the book a success because they give first-year residents a sense of control when reading about a disease they have never heard about before. The first 6 months of dermatology residency are incredibly difficult because you need to incorporate words you never used before to talk about diseases you’ve never heard of before. I think one of my most meaningful experiences was when I visited South Africa and a young resident approached me who had photocopied the entire book and put it into individual binders so as not to desecrate his pristine original copy by writing in the margins, or underlining and highlighting. Something else I am proud of is that even if you are in a resource-poor country, you can read the book and can be on equal footing with any dermatologist from countries around the world, including ours. In other words, it is an educational equalizer.
BRONFENBRENER: What first inspired you to go into dermatology?
BOLOGNIA: I was a third-year medical student and had just finished a rotation in the neonatal intensive care unit, which was particularly demanding; I think you had more clinical responsibilities back then. I was sitting at dinner with some classmates looking for an elective to do, and they all pushed me towards dermatology. It was just what I needed, they said; you only really worked 4 days a week, and the hours were so civilized! My first Friday on the rotation I borrowed Irwin Braverman’s book Skin Signs of Systemic Disease from the clinic and read a good portion of it over the weekend. It struck a chord with me because of its multiple links to internal medicine. The next week I was in dermatology Grand Rounds, and back then the medical students were the first to present their differential diagnoses, prior to and without talking with the residents. It was a bit of sport to hear the rather imaginative diagnoses generated by the students. So when called upon, I stated that I thought my patient had histiocytosis X, and less likely dermatitis. The attending running Grand Rounds questioned me: What could possibly make me think that it was this rare entity histiocytosis X? I told him it looked just like the picture in Dr. Braverman’s book! Everyone got a chuckle out of my answer, but believe it or not, the patient actually had histiocytosis X. Nowadays I would never put histiocytosis above more common entities, but talk about beginner’s luck. I was hooked! The fact that I got the diagnosis right reflects how important a well-written book is for trainees, and I’m honored to still see patients in the same pod as Dr. Braverman.
BRONFENBRENER: What pearls would you give graduating residents now?
BOLOGNIA: I think you have to reflect on what you like to do, what resonates with you, whether you like to take care of people with contact dermatitis, or you like cutting cancer off patients’ faces, or you want to practice phototherapy. Think about where your heart is and that’s what you should do, not what your professors, or your parents, or your chairman thinks you should do. You’re going to be engaged in these activities for at least 30 years, so find something you are passionate about and build on that. Analyze your talents as well as your strengths and go with it. Another important point is to find an area—or 2, or even 3—where you do a lot of reading and then let others know of your interests. Before long you will be able to build upon your greater knowledge and clinical experience and become an expert within a few years. It doesn’t matter if you’re in an academic or private practice; there will always be a niche that you can fill and patients you can help because of your expertise.
BRONFENBRENER: What areas do you find particularly fascinating in dermatology?
BOLOGNIA: Oh, there’s so much! Patients with monoclonal gammopathies, where they can have follicular spines composed of the monoclonal protein coming out of their nose, are fascinating. That’s the kind of dermatology I like: the “believe-it-or-not” side of dermatology. Once I met a patient at a dermatology conference who had fallen down on a farm and had sustained a traumatic brain injury, after which he could only sweat on one side of his body. He had Grover disease limited to the side of his body that could sweat, while the other side was totally clear. We know Grover disease comes from a combination of sweating and sun damage, but seeing that sharp cutoff on his midline drove the point home for me.
BRONFENBRENER: How do you learn best?
BOLOGNIA: I put notes in the margins. If I go to a lecture, I use address labels for my notes. Then I take those stickers and put them in the relevant part of the textbook. It is so much easier to peel off the stickers than it is to write the information. As a result, there is a greater likelihood that the information will actually be transferred.
BRONFENBRENER: What is your daily routine?
BOLOGNIA: Monday, Tuesday, Friday I see patients. Wednesday is Grand Rounds and electronic medical record cleanup time, the paperwork that is no longer on paper. Thursday is my academic day where I can work on projects, and I like this full-day approach because I work best in larger blocks of time. That’s why I recommend, for residents especially, to get a large chunk of their reading done on Saturday or Sunday morning in 2- to 3-hour blocks. I’m not someone who rises hours before everyone else; I’m a 6:00 am type of gal. If you wake up and get your work done during a planned block of time, then you feel like you’ve accomplished something and can enjoy the rest of your day. For me, I’m freshest in the morning, no question about it.
BRONFENBRENER: Where do you think dermatology is going?
BOLOGNIA: I don’t know exactly, and I don’t think anyone knows exactly. I think we need to work hard to maintain our unique body of knowledge and to remind others of this accomplishment. I am often struck in Grand Rounds that no other specialty would have a fighting chance at generating a differential diagnosis or appropriate treatment strategy for the patients presented there. I can’t answer whether if in 10 years most dermatologists will be employees at hospitals or will still have some degree of autonomy, and I think that is unsettling.
BRONFENBRENER: What’s on the horizon for you?
BOLOGNIA: I’m working on the fourth edition of Dermatology, slated to come out in 2017. Dermatology Essentials was just published and is meant to provide a quick overview if you’re scheduled to give a talk and want a 5-minute refresher or if you’re in between patients and would like to be reminded of additional entities in the differential diagnosis. These books are accessible via the Inkling app, so you can have the entire book correctly formatted on your phone or tablet. I was recently trying to provide a more specific site for a biopsy on the ear and just couldn’t remember the correct term, but a quick search and I had the entire external ear anatomy schematic up on my phone.
BRONFENBRENER: Any favorite quotations?
BOLOGNIA: I like this one by Benjamin Franklin: “Well done is better than well said.” I judge people on their actions; not on what they say they’re going to do but rather what they’ve done.
Final Thoughts
My interview provided a glimpse into the cooperative effort required to synthesize the vast quantity of information into a well-written textbook. Dr. Bolognia is passionate about the field, finds great pleasure in unraveling mysterious patients, and goes to great lengths to make teaching points. As impressive as her accomplishments are, I found myself most inspired by her intellectual curiosity for dermatology, a character trait that successful dermatology residents should also embody. I feel fortunate to have had the opportunity to interview her, and I hope that the resident community can also benefit from the advice she has shared.
Suggested Readings
Bolognia JL, Jorizzo JL, Schaffer JV, et al, eds. Dermatology. Phildelphia, PA: WB Saunders; 2012.
Bolognia JL, Schaffer JV, Duncan KO, et al, eds. Dermatology Essentials. Philadelphia, PA: WB Saunders; 2014.
Braverman IM. Skin Signs of Systemic Disease. 3rd ed. Philadelphia, PA: WB Saunders; 1998.
Goldsmith LA, Katz SI, Gilchrist BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw Hill; 2012.
Suggested Readings
Bolognia JL, Jorizzo JL, Schaffer JV, et al, eds. Dermatology. Phildelphia, PA: WB Saunders; 2012.
Bolognia JL, Schaffer JV, Duncan KO, et al, eds. Dermatology Essentials. Philadelphia, PA: WB Saunders; 2014.
Braverman IM. Skin Signs of Systemic Disease. 3rd ed. Philadelphia, PA: WB Saunders; 1998.
Goldsmith LA, Katz SI, Gilchrist BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw Hill; 2012.

The Business Side of Medicine for Orthopedic Residents and Fellows: When Were We Supposed to Learn This?

A New Appraisal of Dermatologic Manifestations of Diabetes Mellitus
Diabetes mellitus is a morbid and costly condition that carries a high burden of disease for patients (both with and without a diagnosis) and for society as a whole. The economic burden of diabetes in the United States recently was estimated at nearly $250 billion annually,1 and this number continues to rise. The cutaneous manifestations of diabetes are diverse and far-reaching, ranging from benign cosmetic concerns to severe dermatologic conditions. Given the wide range of etiology for diabetes mellitus and its existence on a spectrum of severity, it is perhaps not surprising that some of these entities are the subject of debate (vis-à-vis the strength of association between these skin conditions and diabetes) and can manifest in different forms. However, it is clear that the cutaneous manifestations of diabetes are equally as important to consider and manage as the systemic complications of the disease. In analyzing associations with diabetes, it is important to note that given such a high incidence of diabetes among the general population and its close association with other disease states, such as the metabolic syndrome, studies aimed at determining direct relationships to this entity must be well controlled for confounding factors, which may not even always be possible. Regardless, it is important for dermatologists and dermatology residents to recognize and understand the protean cutaneous manifestations of diabetes mellitus, and this column will explore skin findings that are characteristic of diabetes (Table 1) as well as other dermatoses with a reported but less clear association with diabetes (Table 2).
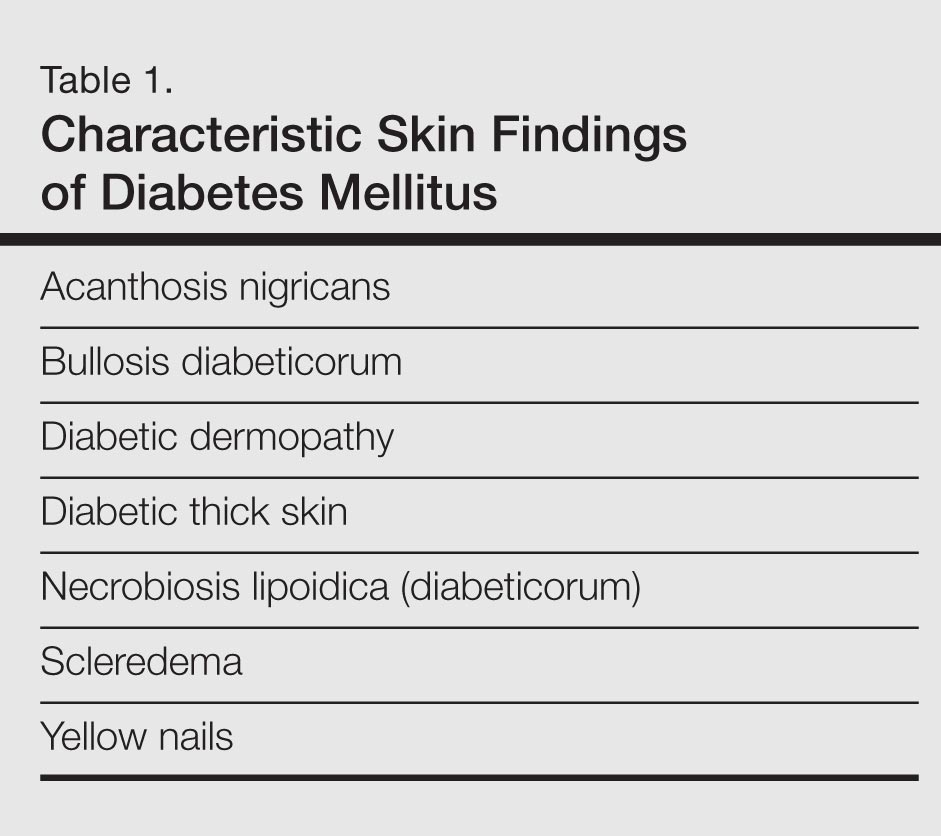

Skin Findings Characteristic of Diabetes
Diabetic Thick Skin
The association between diabetes and thick skin is well described as either a mobility-limiting affliction of the joints of the hands (cheiroarthropathy) or as an asymptomatic thickening of the skin. It has been estimated that 8% to 36% of patients with insulin-dependent diabetes develop some form of skin thickening2; one series also found this association to be true for patients with non–insulin-dependent diabetes mellitus (NIDDM).3 Skin thickening is readily observable on clinical presentation or ultrasonography, with increasing thickness in many cases associated with long-term disease progression. This increasing thickness was shown histopathologically to be a direct result of activated fibroblasts and increased collagen polymerization, with some similar features to progressive systemic sclerosis.4 Interestingly, even clinically normal skin showed some degree of fibroblast activation in diabetic patients, but collagen fibers in each case were smaller in diameter than those found in progressive systemic sclerosis. This finding clearly has implications on quality of life, as a lack of hand mobility due to the cheiroarthropathy can be severely disabling. Underlining the need for strict glycemic control, it has been suggested that tight control of blood sugar levels can lead to improvement in diabetic thick skin; however, reports of improvement are based on a small sample population.5 Huntley papules are localized to areas on the dorsum of the hands overlying the joints, demonstrating hyperkeratosis and enlarged dermal papillae.6 They also can be found in a minority of patients without diabetes. Interestingly, diabetic thick skin also has been associated with neurologic disorders in diabetes.7 Diabetic thick skin was found to be significantly (P<.05) correlated with diabetic neuropathy, independent of duration of diabetes, age, or glycosylated hemoglobin levels, though no causal or etiologic link between these entities has been proven.
Yellow Nails
Nail changes are well described in diabetes, ranging from periungual telangiectases to complications from infections, such as paronychia; however, a well-recognized finding, especially in elderly diabetic patients, is a characteristic yellowing of the nails, reported to affect up to 40% of patients with diabetes.8 The mechanism behind it likely includes accumulation of glycation end products, which also has been thought to lead to yellowing of the skin, and vascular impairment.9 These nails tend to exhibit slow growth, likely resulting from a nail matrix that is poorly supplied with blood, and also can be more curved than normal with longitudinal ridges (onychorrhexis).10 It is important, however, not to attribute yellow nails to diabetes without considering other causes of yellow nails, such as onychomycosis, yellow nail syndrome, and yellow nails associated with lymphedema or respiratory tract disease (eg, pleural effusion, bronchiectasis).11
Diabetic Dermopathy
Colloquially known as shin spots, diabetic dermopathy is perhaps the most common skin finding in this patient population, though it also can occur in up to 1 in 5 individuals without diabetes.12 Although it is very common, it is not a condition that should be overlooked, as numerous studies have shown an increase in microangiopathic complications such as retinopathy in patients with diabetic dermopathy.13,14 Although follow-up studies may be necessary to fully characterize the relationship between shin spots and diabetes, it certainly is reasonable to be more wary of diabetic patients presenting with many shin spots, as the general consensus is that these areas represent postinflammatory hyperpigmentation and cutaneous atrophy in the setting of poor vascular supply, which should prompt analysis of other areas that might be affected by poor vasculature, such as an ophthalmologic examination. Antecedent and perhaps unnoticed trauma has been implicated given a possible underlying neuropathy, but this theory has not been supported by studies.
Bullosis Diabeticorum
Bullosis diabeticorum is a rare but well-described occurrence of self-resolving, nonscarring blisters that arise on the extremities of diabetic patients. This entity should be distinguished from other primary autoimmune blistering disorders and from simple mechanobullous lesions. Several types of bullosis diabeticorum have been described, with the most classic form showing an intraepidermal cleavage plane.15 These lesions tend to resolve in weeks but can be recurrent. The location of the pathology underlines its nonscarring nature, though similar lesions have been reported showing a cleavage plane in the lamina lucida of the dermoepidermal junction, which underlines the confusion in the literature surrounding diabetic bullae.16 Some may even use this term interchangeably with trauma or friction-induced blisters, which diabetics may be prone to develop due to peripheral neuropathy. Confounding reports have stated there is a correlation between bullosis diabeticorum and neuropathy as well as the acral location of these blisters. Although many authors cite the incidence of bullosis diabeticorum being 0.5%,17 no population-based studies have confirmed this figure and some have speculated that the actual incidence is higher.18 In the end, the term bullosis diabeticorum is probably best reserved for a rapidly appearing blister on the extremities of diabetic patients with at most minimal trauma, with a lesion containing sterile fluid and negative immunofluorescence. The mechanism for these blisters is thought to be microangiopathy, with scant blood supply to the skin causing it to be more prone to acantholysis and blister formation.19 This theory was reinforced in a study showing a reduced threshold for suction blister formation in diabetic patients.20 Care should be taken to prevent secondary infections at these sites.
Acanthosis Nigricans
Acanthosis nigricans, which consists of dark brown plaques in the flexural areas, especially the posterior neck and axillae, is a common finding in diabetic patients and is no doubt familiar to clinicians. The pathophysiology of these lesions has been well studied and is a prototype for the effects of insulin resistance in the skin. In this model, high concentrations of insulin binding to insulinlike growth factor receptor in the skin stimulate keratinocyte proliferation,21 leading to the clinical appearance and the histologic finding of hyperkeratosis and papillomatosis, which in turn is responsible for the observed hyperpigmentation. It is an important finding, especially in those without a known history of diabetes, as it can also signal an underlying endocrinopathy (eg, Cushing syndrome, acromegaly, polycystic ovary syndrome) or malignancy (ie, adenocarcinoma of the gastrointestinal tract). Several distinct mechanisms of insulin resistance have been described, including insulin resistance due to receptor defects, such as those seen with insulin resistance in NIDDM; autoimmune processes; and postreceptor defects in insulin action.22 Keratolytics and topical retinoids have been used to ameliorate the appearance of these lesions.
Necrobiosis Lipoidica (Diabeticorum)
Necrobiosis lipoidica diabeticorum was first described by Urback23 in 1932, but reports of similar lesions were described in nondiabetic patients soon after. The dermatologic community has since come to realize that perhaps a more accurate nomenclature is necrobiosis lipoidica to fully encompass this entity. Clinically, lesions appear as erythematous papules and plaques that expand into a larger well-circumscribed plaque with a waxy yellowish atrophic center, often with telangiectases, and usually presenting in the pretibial area. Lesions can become ulcerated in up to one-third of cases. Necrobiosis lipoidica also is defined by characteristic histologic findings, including important features such as palisaded granulomas arranged in a tierlike fashion, necrotizing vasculitis, collagen degradation, and panniculitis. Necrobiosis lipoidica is still relatively rare, developing in approximately 0.3% of patients with diabetes,24 though its relationship with insulin resistance and diabetes is strong. Approximately two-thirds of patients with necrobiosis lipoidica have diabetes and an even higher number go on to develop diabetes or have a positive family history of diabetes.
Although these figures are interesting, the data are nearly a half-century-old, and it is unclear if these findings still hold true today. The etiology of necrobiosis lipoidica also remains elusive, with theories focusing on the role of microangiopathy, immunoglobulin deposition leading to vasculitis, structural abnormalities in collagen or fibroblasts, and trauma; however, the true nature of this condition is likely some combination of these factors.25 These lesions are difficult to treat, especially at an advanced stage. Management with topical steroids to limit the inflammatory progression of the lesions is the mainstay of therapy.
Scleredema
Scleredema adultorum (Buschke disease) refers to indurated plaques over the posterior neck and upper back. It is usually thought of as 3 distinct forms. The form that is known to occur in diabetic patients is sometimes referred to as scleredema diabeticorum; the other 2 occur as postinfectious, usually Streptococcus, or malignancy-related forms. The prevalence of scleredema diabeticorum among diabetic individuals most frequently is reported as 2.5%26; however, it is worth noting that other estimates have been as high as 14%.27 Although there has been some correlation between poorly controlled NIDDM, treatment and tight glucose control does not seem to readily resolve these lesions with only few conflicting case studies serving as evidence for and against this premise.28-30 The lesions often are recalcitrant toward a wide variety of treatment approaches. Histopathologic analysis generally reveals a thickened dermis with large collagen bundles, with clear spaces between the collagen representing mucin and increased numbers of mast cells. Proposed mechanisms include stimulation of collagen synthesis by fibroblasts and retarded collagen degradation, likely due to excess glucose.31
Dermatoses Demonstrating an Association With Diabetes
Granuloma Annulare
Granuloma annulare (GA) is a dermatologic condition existing in numerous forms. The generalized form has been suggested to have some association with diabetes. The lesions of GA are classically round, flesh-colored to erythematous papules arising in the dermis that may start on the dorsal extremities where the localized form typically presents, though larger annular plaques or patches may exist in the generalized form. Histologically, GA has a characteristic granulomatous infiltrate and palisaded granulomatous dermatitis, depending on the stage of the evolution. Many studies dating back to the mid-20th century have attempted to elucidate a link between GA and diabetes, with numerous reports showing conflicting results across their study populations.32-36 This issue is further muddled by links between generalized GA and a host of other diseases, such as malignancy, thyroid disease, hepatitis, and human immunodeficiency virus infection. The usual course of GA is spontaneous resolution, including a peculiar phenomenon noted in the literature whereby biopsy of one of the lesions led to clearance of other lesions on the body.37 However, the generalized form may be more difficult to treat, with therapeutic approaches including topical steroids, light therapy, and systemic immunomodulators.
Lichen Planus
A recent small population study in Turkey demonstrated a strong relationship between lichen planus and abnormal glucose tolerance. In this study of 30 patients with lichen planus, approximately half (14/30) had abnormal glucose metabolism and a quarter (8/30) had known diabetes, but larger studies are needed to clarify this relationship.38 Prior to this report, a link between oral lichen planus and diabetes had been shown in larger case series.39,40 Clinically, one may see white plaques with a characteristic lacy reticular pattern in the mouth. At other cutaneous sites, lichen planus generally appears as pruritic, purple, flat-topped polygonal papules. The clinical finding of lichen planus also is linked with many other disease states, most notably hepatitis C virus, but also thymoma, liver disease, and inflammatory bowel disease, among other associations.41
Vitiligo
As an autoimmune entity, it stands to reason that vitiligo may be seen more commonly associated with insulin-dependent diabetes, which has been shown to hold true in one study, while no association was found between later-onset NIDDM and vitiligo.42 Given the nonspecific nature of this association and the relatively common presentation of vitiligo, no special consideration is likely needed when examining a patient with vitiligo, but its presence should remind the clinician that these autoimmune entities tend to travel together.
Acquired Perforating Dermatosis
Although the classic presentation of acquired perforating dermatosis (Kyrle disease) is linked to renal failure, diabetes also has been connected to its presentation. Extremely rare outside of the setting of chronic renal failure, acquired perforating dermatosis occurs in up to 10% of dialysis patients.43,44 It is characterized by papules with a central keratin plug, representing transepidermal elimination of keratin, collagen, and other cellular material; its etiology has not been elucidated. The connection between acquired perforating dermatosis and diabetes is not completely clear; it would seem that renal failure is a prerequisite for itspresentation. A large proportion of renal failure necessitating hemodialysis occurs in patients with diabetic nephropathy, which may explain the coincidence of diabetes, renal failure, and acquired perforating dermatosis.45 The presentation of this cutaneous finding should not, however, affect treatment of the underlying conditions. Symptom relief in the form of topical steroids can be used as a first-line treatment of these often pruritic lesions.
Eruptive Xanthomas
The link between diabetes and eruptive xanthomas seems to be a rather tenuous one, hinging on the fact that many diabetic patients have abnormalities in carbohydrate and lipid metabolism. A central feature of eruptive xanthomas is an elevation in triglycerides, which can occur in diabetes. Indeed, it has been estimated that only 0.1% of diabetics will develop eruptive xanthomas,46 and its main importance may be to prompt the physician to treat the hypertriglyceridemia and consider other concerning possibilities such as acute pancreatitis.
Psoriasis
Psoriasis is a common dermatologic condition that has been shown to have a far-reaching impact both on patients’ quality of life and cardiovascular risk profiles. Data have emerged linking psoriasis with diabetes as an independent risk factor47; although this retrospective study had its limitations, it certainly is interesting to note that patients with psoriasis may have an increased risk for developing diabetes. Perhaps more importantly, though, this study also implied that patients with severe psoriasis may present with diabetes that is more difficult to control, evidenced by increased treatment with systemic therapies as opposed to milder forms of intervention such as diet control.47 There almost certainly are other confounding factors and further studies would serve to reveal the strength of this association, but it is certainly an intriguing concept. Echoing these findings, a more recent nationwide study from Denmark demonstrated that psoriasis is associated with increased incidence of new-onset diabetes, adjusting for numerous confounding factors.48 The relationship between psoriasis and diabetes is worth noting as evidence continues to emerge.
Conclusion
Given the diverse cutaneous manifestations of diabetes, it is important to distinguish those that are directly related to diabetes from those that suggest there may be another underlying process. For example, a new patient presenting to a primary care physician with acanthosis nigricans and yellow nails should immediately trigger a test for a hemoglobin A1c (glycated hemoglobin) level to investigate for diabetes; however, clinicians also should be wary of patients with acanthosis nigricans who report early satiety, as this asso-ciation may be a sign of underlying malignancy. Conversely, the presence of yellow nails in a patient with chronic diabetes should not be ignored. The physician should consider onychomycosis and query the patient about possible respiratory symptoms. In the case of a multisystem disease such as diabetes, it may be challenging to reconcile seemingly disparate skin findings, but having a framework to approach the cutaneous manifestations of diabetes can help to properly identify and treat an individual patient’s afflictions.
- American Diabetes Association. Economic costs of diabetes in the U.S. in 2012 [published online instead of print March 16, 2013]. Diabetes Care. 2013;36:1033-1046.
- Collier A, Matthews DM, Kellett HA, et al. Change in skin thickness associated with cheiroarthropathy in insulin dependent diabetes mellitus. Br Med J (Clin Res Ed). 1986;292:936.
- Fitzcharles MA, Duby S, Waddell RW, et al. Limitation of joint mobility (cheiroarthropathy) in adult noninsulin-dependent diabetic patients. Ann Rheum Dis. 1984;43:251-254.
- Hanna W, Friesen D, Bombardier C, et al. Pathologic features of diabetic thick skin. J Am Acad Dermatol. 1987;16:546-553.
- Lieberman LS, Rosenbloom AL, Riley WJ, et al. Reduced skin thickness with pump administration of insulin. N Engl J Med. 1980;303:940-941.
- Guarneri C, Guarneri F, Borgia F, et al. Finger pebbles in a diabetic patient: Huntley's papules. Int J Dermatol. 2005;44:755-756.
- Forst T, Kann P, Pfützner A, et al. Association between "diabetic thick skin syndrome" and neurological disorders in diabetes mellitus. Acta Diabetol. 1994;31:73-77.
- Nikoleishvili LR, Kurashvili RB, Virsaladze DK, et al. Characteristic changes of skin and its accessories in type 2 diabetes mellitus [in Russian]. Georgian Med News. 2006:43-46.
- Lithner F. Purpura, pigmentation and yellow nails of the lower extremities in diabetics. Acta Med Scand. 1976;199:203-208.
- Greene RA, Scher RK. Nail changes associated with diabetes mellitus. J Am Acad Dermatol. 1987;16:1015-1021.
- Hiller E, Rosenow EC 3rd, Olsen AM. Pulmonary manifestations of the yellow nail syndrome. Chest. 1972;61:452-458.
- Feingold KR, Elias PM. Endocrine-skin interactions. cutaneous manifestations of pituitary disease, thyroid disease, calcium disorders, and diabetes. J Am Acad Dermatol. 1987;17:921-940.
- Abdollahi A, Daneshpazhooh M, Amirchaghmaghi E, et al. Dermopathy and retinopathy in diabetes: is there an association? Dermatology, 2007;214:133-136.
- Morgan AJ, Schwartz RA. Diabetic dermopathy: A subtle sign with grave implications. J Am Acad Dermatol. 2008;58:447-451.
- Perez MI, Kohn SR. Cutaneous manifestations of diabetes mellitus. J Am Acad Dermatol. 1994;30:519-531.
- Cantwell AR, Martz W. Idiopathic bullae in diabetics. Bullosis diabeticorum. Arch Dermatol. 1967;96:42-44.
- Larsen K, Jensen T, Karlsmark T, Holstein PE. Incidence of bullosis diabeticorum – a controversial cause of chronic foot ulceration. Int Wound J. 2008;5:591-596.
- Lipsky BA, Baker PD, Ahroni JH. Diabetic bullae: 12 cases of a purportedly rare cutaneous disorder. Int J Dermatol. 2000;39:196-200.
- Basarab T, Munn SE, McGrath J, et al. Bullosis diabeticorum. a case report and literature review. Clin Exp Dermatol. 1995;20:218-220.
- Bernstein JE, Levine LE, Medenica MM, et al. Reduced threshold to suction-induced blister formation in insulin-dependent diabetics. J Am Acad Dermatol. 1983;8:790-791.
- Cruz PD Jr, Hud JA Jr. Excess insulin binding to insulin-like growth factor receptors: proposed mechanism for acanthosis nigricans. J Invest Dermatol. 1992;98(suppl 6):S82-S85.
- Romano G, Moretti G, Di Benedetto A, et al. Skin lesions in diabetes mellitus: prevalence and clinical correlations. Diabetes Res Clin Pract. 1998;39:101-106.
- Urback E. Eine neue diabetische Stoffwechseldermatose: Nekrobiosis lipoidica diabeticorum. Arch. f. Dermat. u Syph. 1932;166:273.
- Muller SA, Winkelmann RK. Necrobiosis lipoidica diabeticorum. a clinical and pathological investigation of 171 cases. Arch Dermatol. 1966;93:272-281.
- Engel MF, Smith JG Jr. The pathogenesis of necrobiosis lipoidica. necrobiosis lipoidica, a form fruste of diabetes mellitus. Arch Dermatol. 1960;82:791-797.
- Cole GW, Headley J, Skowsky R. Scleredema diabeticorum: a common and distinct cutaneous manifestation of diabetes mellitus. Diabetes Care. 1983;6:189-192.
- Sattar MA, Diab S, Sugathan TN, et al. Scleroedema diabeticorum: a minor but often unrecognized complication of diabetes mellitus. Diabet Med. 1988;5:465-468.
- Rho YW, Suhr KB, Lee JH, et al. A clinical observation of scleredema adultorum and its relationship to diabetes. J Dermatol. 1998;25:103-107.
- Baillot-Rudoni S, Apostol D, Vaillant G, et al. Implantable pump therapy restores metabolic control and quality of life in type 1 diabetic patients with Buschke's nonsystemic scleroderma. Diabetes Care. 2006;29:1710.
- Meguerditchian C, Jacquet P, Béliard S, et al. Scleredema adultorum of Buschke: an under recognized skin complication of diabetes. Diabetes Metab. 2006;32:481-484.
- Behm B, Schreml S, Landthaler M, et al. Skin signs in diabetes mellitus. J Eur Acad Dermatol Venereol. 2012;26:1203-1211.
- Nebesio CL, Lewis C, Chuang TY. Lack of an association between granuloma annulare and type 2 diabetes mellitus. Br J Dermatol. 2002;146:122-124.
- Stankler L, Leslie G. Generalized granuloma annulare. a report of a case and review of the literature. Arch Dermatol. 1976;95:509-513.
- Williamson DM, Dykes JR. Carbohydrate metabolism in granuloma annulare. J Invest Dermatol. 1972;58:400-404.
- Dabski K, Winkelmann RK. Generalized granuloma annulare: clinical and laboratory findings in 100 patients. J Am Acad Dermatol. 1989;20:39-47.
- Veraldi S, Bencini PL, Drudi E, et al. Laboratory abnormalities in granuloma annulare: a case-control study. Br J Dermatol. 1997;136:652-653.
- Levin NA, Patterson JW, Yao LL, et al. Resolution of patch-type granuloma annulare lesions after biopsy. J Am Acad Dermatol. 2002;46:426-429.
- Seyhan M, Ozcan H, Sahin I, et al. High prevalence of glucose metabolism disturbance in patients with lichen planus. Diabetes Res Clin Pract. 2007;77:198-202.
- Romero MA, Seoane J, Varela-Centelles P, et al. Prevalence of diabetes mellitus amongst oral lichen planus patients. clinical and pathological characteristics. Med Oral. 2002;7:121-129.
- Albrecht M, Banoczy J, Dinya E, et al. Occurrence of oral leukoplakia and lichen planus in diabetes mellitus. J Oral Pathol Med. 1992;21:364-366.
- Lehman JS, Tollefson MM, Gibson LE. Lichen planus. Int J Dermatol. 2009;48:682-694.
- Gould IM, Gray RS, Urbaniak SJ, et al. Vitiligo in diabetes mellitus. Br J Dermatol. 1985;113:153-155.
- White CR Jr, Heskel NS, Pokorny DJ. Perforating folliculitis of hemodialysis. Am J Dermatopathol. 1982;4:109-116.
- Hurwitz RM, Melton ME, Creech FT 3rd, et al. Perforating folliculitis in association with hemodialysis. Am J Dermatopathol. 1982;4:101-108.
- Rapini RP, Herbert AA, Drucker CR. Acquired perforating dermatosis. evidence for combined transepidermal elimination of both collagen and elastic fibers. Arch Dermatol. 1989;125:1074-1078.
- Muller SA. Dermatologic disorders associated with diabetes mellitus. Mayo Clin Proc. 1966;41:689-703.
- Azfar RS, Seminara NM, Shin DB, et al. Increased risk of diabetes mellitus and likelihood of receiving diabetes mellitus treatment in patients with psoriasis. Arch Dermatol. 2012;148:995-1000.
- Khalid U, Hansen PR, Gislason GH, et al. Psoriasis and new-onset diabetes: a Danish nationwide cohort study. Diabetes Care. 2013;36:2402-2407.
Diabetes mellitus is a morbid and costly condition that carries a high burden of disease for patients (both with and without a diagnosis) and for society as a whole. The economic burden of diabetes in the United States recently was estimated at nearly $250 billion annually,1 and this number continues to rise. The cutaneous manifestations of diabetes are diverse and far-reaching, ranging from benign cosmetic concerns to severe dermatologic conditions. Given the wide range of etiology for diabetes mellitus and its existence on a spectrum of severity, it is perhaps not surprising that some of these entities are the subject of debate (vis-à-vis the strength of association between these skin conditions and diabetes) and can manifest in different forms. However, it is clear that the cutaneous manifestations of diabetes are equally as important to consider and manage as the systemic complications of the disease. In analyzing associations with diabetes, it is important to note that given such a high incidence of diabetes among the general population and its close association with other disease states, such as the metabolic syndrome, studies aimed at determining direct relationships to this entity must be well controlled for confounding factors, which may not even always be possible. Regardless, it is important for dermatologists and dermatology residents to recognize and understand the protean cutaneous manifestations of diabetes mellitus, and this column will explore skin findings that are characteristic of diabetes (Table 1) as well as other dermatoses with a reported but less clear association with diabetes (Table 2).
Skin Findings Characteristic of Diabetes
Diabetic Thick Skin
The association between diabetes and thick skin is well described as either a mobility-limiting affliction of the joints of the hands (cheiroarthropathy) or as an asymptomatic thickening of the skin. It has been estimated that 8% to 36% of patients with insulin-dependent diabetes develop some form of skin thickening2; one series also found this association to be true for patients with non–insulin-dependent diabetes mellitus (NIDDM).3 Skin thickening is readily observable on clinical presentation or ultrasonography, with increasing thickness in many cases associated with long-term disease progression. This increasing thickness was shown histopathologically to be a direct result of activated fibroblasts and increased collagen polymerization, with some similar features to progressive systemic sclerosis.4 Interestingly, even clinically normal skin showed some degree of fibroblast activation in diabetic patients, but collagen fibers in each case were smaller in diameter than those found in progressive systemic sclerosis. This finding clearly has implications on quality of life, as a lack of hand mobility due to the cheiroarthropathy can be severely disabling. Underlining the need for strict glycemic control, it has been suggested that tight control of blood sugar levels can lead to improvement in diabetic thick skin; however, reports of improvement are based on a small sample population.5 Huntley papules are localized to areas on the dorsum of the hands overlying the joints, demonstrating hyperkeratosis and enlarged dermal papillae.6 They also can be found in a minority of patients without diabetes. Interestingly, diabetic thick skin also has been associated with neurologic disorders in diabetes.7 Diabetic thick skin was found to be significantly (P<.05) correlated with diabetic neuropathy, independent of duration of diabetes, age, or glycosylated hemoglobin levels, though no causal or etiologic link between these entities has been proven.
Yellow Nails
Nail changes are well described in diabetes, ranging from periungual telangiectases to complications from infections, such as paronychia; however, a well-recognized finding, especially in elderly diabetic patients, is a characteristic yellowing of the nails, reported to affect up to 40% of patients with diabetes.8 The mechanism behind it likely includes accumulation of glycation end products, which also has been thought to lead to yellowing of the skin, and vascular impairment.9 These nails tend to exhibit slow growth, likely resulting from a nail matrix that is poorly supplied with blood, and also can be more curved than normal with longitudinal ridges (onychorrhexis).10 It is important, however, not to attribute yellow nails to diabetes without considering other causes of yellow nails, such as onychomycosis, yellow nail syndrome, and yellow nails associated with lymphedema or respiratory tract disease (eg, pleural effusion, bronchiectasis).11
Diabetic Dermopathy
Colloquially known as shin spots, diabetic dermopathy is perhaps the most common skin finding in this patient population, though it also can occur in up to 1 in 5 individuals without diabetes.12 Although it is very common, it is not a condition that should be overlooked, as numerous studies have shown an increase in microangiopathic complications such as retinopathy in patients with diabetic dermopathy.13,14 Although follow-up studies may be necessary to fully characterize the relationship between shin spots and diabetes, it certainly is reasonable to be more wary of diabetic patients presenting with many shin spots, as the general consensus is that these areas represent postinflammatory hyperpigmentation and cutaneous atrophy in the setting of poor vascular supply, which should prompt analysis of other areas that might be affected by poor vasculature, such as an ophthalmologic examination. Antecedent and perhaps unnoticed trauma has been implicated given a possible underlying neuropathy, but this theory has not been supported by studies.
Bullosis Diabeticorum
Bullosis diabeticorum is a rare but well-described occurrence of self-resolving, nonscarring blisters that arise on the extremities of diabetic patients. This entity should be distinguished from other primary autoimmune blistering disorders and from simple mechanobullous lesions. Several types of bullosis diabeticorum have been described, with the most classic form showing an intraepidermal cleavage plane.15 These lesions tend to resolve in weeks but can be recurrent. The location of the pathology underlines its nonscarring nature, though similar lesions have been reported showing a cleavage plane in the lamina lucida of the dermoepidermal junction, which underlines the confusion in the literature surrounding diabetic bullae.16 Some may even use this term interchangeably with trauma or friction-induced blisters, which diabetics may be prone to develop due to peripheral neuropathy. Confounding reports have stated there is a correlation between bullosis diabeticorum and neuropathy as well as the acral location of these blisters. Although many authors cite the incidence of bullosis diabeticorum being 0.5%,17 no population-based studies have confirmed this figure and some have speculated that the actual incidence is higher.18 In the end, the term bullosis diabeticorum is probably best reserved for a rapidly appearing blister on the extremities of diabetic patients with at most minimal trauma, with a lesion containing sterile fluid and negative immunofluorescence. The mechanism for these blisters is thought to be microangiopathy, with scant blood supply to the skin causing it to be more prone to acantholysis and blister formation.19 This theory was reinforced in a study showing a reduced threshold for suction blister formation in diabetic patients.20 Care should be taken to prevent secondary infections at these sites.
Acanthosis Nigricans
Acanthosis nigricans, which consists of dark brown plaques in the flexural areas, especially the posterior neck and axillae, is a common finding in diabetic patients and is no doubt familiar to clinicians. The pathophysiology of these lesions has been well studied and is a prototype for the effects of insulin resistance in the skin. In this model, high concentrations of insulin binding to insulinlike growth factor receptor in the skin stimulate keratinocyte proliferation,21 leading to the clinical appearance and the histologic finding of hyperkeratosis and papillomatosis, which in turn is responsible for the observed hyperpigmentation. It is an important finding, especially in those without a known history of diabetes, as it can also signal an underlying endocrinopathy (eg, Cushing syndrome, acromegaly, polycystic ovary syndrome) or malignancy (ie, adenocarcinoma of the gastrointestinal tract). Several distinct mechanisms of insulin resistance have been described, including insulin resistance due to receptor defects, such as those seen with insulin resistance in NIDDM; autoimmune processes; and postreceptor defects in insulin action.22 Keratolytics and topical retinoids have been used to ameliorate the appearance of these lesions.
Necrobiosis Lipoidica (Diabeticorum)
Necrobiosis lipoidica diabeticorum was first described by Urback23 in 1932, but reports of similar lesions were described in nondiabetic patients soon after. The dermatologic community has since come to realize that perhaps a more accurate nomenclature is necrobiosis lipoidica to fully encompass this entity. Clinically, lesions appear as erythematous papules and plaques that expand into a larger well-circumscribed plaque with a waxy yellowish atrophic center, often with telangiectases, and usually presenting in the pretibial area. Lesions can become ulcerated in up to one-third of cases. Necrobiosis lipoidica also is defined by characteristic histologic findings, including important features such as palisaded granulomas arranged in a tierlike fashion, necrotizing vasculitis, collagen degradation, and panniculitis. Necrobiosis lipoidica is still relatively rare, developing in approximately 0.3% of patients with diabetes,24 though its relationship with insulin resistance and diabetes is strong. Approximately two-thirds of patients with necrobiosis lipoidica have diabetes and an even higher number go on to develop diabetes or have a positive family history of diabetes.
Although these figures are interesting, the data are nearly a half-century-old, and it is unclear if these findings still hold true today. The etiology of necrobiosis lipoidica also remains elusive, with theories focusing on the role of microangiopathy, immunoglobulin deposition leading to vasculitis, structural abnormalities in collagen or fibroblasts, and trauma; however, the true nature of this condition is likely some combination of these factors.25 These lesions are difficult to treat, especially at an advanced stage. Management with topical steroids to limit the inflammatory progression of the lesions is the mainstay of therapy.
Scleredema
Scleredema adultorum (Buschke disease) refers to indurated plaques over the posterior neck and upper back. It is usually thought of as 3 distinct forms. The form that is known to occur in diabetic patients is sometimes referred to as scleredema diabeticorum; the other 2 occur as postinfectious, usually Streptococcus, or malignancy-related forms. The prevalence of scleredema diabeticorum among diabetic individuals most frequently is reported as 2.5%26; however, it is worth noting that other estimates have been as high as 14%.27 Although there has been some correlation between poorly controlled NIDDM, treatment and tight glucose control does not seem to readily resolve these lesions with only few conflicting case studies serving as evidence for and against this premise.28-30 The lesions often are recalcitrant toward a wide variety of treatment approaches. Histopathologic analysis generally reveals a thickened dermis with large collagen bundles, with clear spaces between the collagen representing mucin and increased numbers of mast cells. Proposed mechanisms include stimulation of collagen synthesis by fibroblasts and retarded collagen degradation, likely due to excess glucose.31
Dermatoses Demonstrating an Association With Diabetes
Granuloma Annulare
Granuloma annulare (GA) is a dermatologic condition existing in numerous forms. The generalized form has been suggested to have some association with diabetes. The lesions of GA are classically round, flesh-colored to erythematous papules arising in the dermis that may start on the dorsal extremities where the localized form typically presents, though larger annular plaques or patches may exist in the generalized form. Histologically, GA has a characteristic granulomatous infiltrate and palisaded granulomatous dermatitis, depending on the stage of the evolution. Many studies dating back to the mid-20th century have attempted to elucidate a link between GA and diabetes, with numerous reports showing conflicting results across their study populations.32-36 This issue is further muddled by links between generalized GA and a host of other diseases, such as malignancy, thyroid disease, hepatitis, and human immunodeficiency virus infection. The usual course of GA is spontaneous resolution, including a peculiar phenomenon noted in the literature whereby biopsy of one of the lesions led to clearance of other lesions on the body.37 However, the generalized form may be more difficult to treat, with therapeutic approaches including topical steroids, light therapy, and systemic immunomodulators.
Lichen Planus
A recent small population study in Turkey demonstrated a strong relationship between lichen planus and abnormal glucose tolerance. In this study of 30 patients with lichen planus, approximately half (14/30) had abnormal glucose metabolism and a quarter (8/30) had known diabetes, but larger studies are needed to clarify this relationship.38 Prior to this report, a link between oral lichen planus and diabetes had been shown in larger case series.39,40 Clinically, one may see white plaques with a characteristic lacy reticular pattern in the mouth. At other cutaneous sites, lichen planus generally appears as pruritic, purple, flat-topped polygonal papules. The clinical finding of lichen planus also is linked with many other disease states, most notably hepatitis C virus, but also thymoma, liver disease, and inflammatory bowel disease, among other associations.41
Vitiligo
As an autoimmune entity, it stands to reason that vitiligo may be seen more commonly associated with insulin-dependent diabetes, which has been shown to hold true in one study, while no association was found between later-onset NIDDM and vitiligo.42 Given the nonspecific nature of this association and the relatively common presentation of vitiligo, no special consideration is likely needed when examining a patient with vitiligo, but its presence should remind the clinician that these autoimmune entities tend to travel together.
Acquired Perforating Dermatosis
Although the classic presentation of acquired perforating dermatosis (Kyrle disease) is linked to renal failure, diabetes also has been connected to its presentation. Extremely rare outside of the setting of chronic renal failure, acquired perforating dermatosis occurs in up to 10% of dialysis patients.43,44 It is characterized by papules with a central keratin plug, representing transepidermal elimination of keratin, collagen, and other cellular material; its etiology has not been elucidated. The connection between acquired perforating dermatosis and diabetes is not completely clear; it would seem that renal failure is a prerequisite for itspresentation. A large proportion of renal failure necessitating hemodialysis occurs in patients with diabetic nephropathy, which may explain the coincidence of diabetes, renal failure, and acquired perforating dermatosis.45 The presentation of this cutaneous finding should not, however, affect treatment of the underlying conditions. Symptom relief in the form of topical steroids can be used as a first-line treatment of these often pruritic lesions.
Eruptive Xanthomas
The link between diabetes and eruptive xanthomas seems to be a rather tenuous one, hinging on the fact that many diabetic patients have abnormalities in carbohydrate and lipid metabolism. A central feature of eruptive xanthomas is an elevation in triglycerides, which can occur in diabetes. Indeed, it has been estimated that only 0.1% of diabetics will develop eruptive xanthomas,46 and its main importance may be to prompt the physician to treat the hypertriglyceridemia and consider other concerning possibilities such as acute pancreatitis.
Psoriasis
Psoriasis is a common dermatologic condition that has been shown to have a far-reaching impact both on patients’ quality of life and cardiovascular risk profiles. Data have emerged linking psoriasis with diabetes as an independent risk factor47; although this retrospective study had its limitations, it certainly is interesting to note that patients with psoriasis may have an increased risk for developing diabetes. Perhaps more importantly, though, this study also implied that patients with severe psoriasis may present with diabetes that is more difficult to control, evidenced by increased treatment with systemic therapies as opposed to milder forms of intervention such as diet control.47 There almost certainly are other confounding factors and further studies would serve to reveal the strength of this association, but it is certainly an intriguing concept. Echoing these findings, a more recent nationwide study from Denmark demonstrated that psoriasis is associated with increased incidence of new-onset diabetes, adjusting for numerous confounding factors.48 The relationship between psoriasis and diabetes is worth noting as evidence continues to emerge.
Conclusion
Given the diverse cutaneous manifestations of diabetes, it is important to distinguish those that are directly related to diabetes from those that suggest there may be another underlying process. For example, a new patient presenting to a primary care physician with acanthosis nigricans and yellow nails should immediately trigger a test for a hemoglobin A1c (glycated hemoglobin) level to investigate for diabetes; however, clinicians also should be wary of patients with acanthosis nigricans who report early satiety, as this asso-ciation may be a sign of underlying malignancy. Conversely, the presence of yellow nails in a patient with chronic diabetes should not be ignored. The physician should consider onychomycosis and query the patient about possible respiratory symptoms. In the case of a multisystem disease such as diabetes, it may be challenging to reconcile seemingly disparate skin findings, but having a framework to approach the cutaneous manifestations of diabetes can help to properly identify and treat an individual patient’s afflictions.
Diabetes mellitus is a morbid and costly condition that carries a high burden of disease for patients (both with and without a diagnosis) and for society as a whole. The economic burden of diabetes in the United States recently was estimated at nearly $250 billion annually,1 and this number continues to rise. The cutaneous manifestations of diabetes are diverse and far-reaching, ranging from benign cosmetic concerns to severe dermatologic conditions. Given the wide range of etiology for diabetes mellitus and its existence on a spectrum of severity, it is perhaps not surprising that some of these entities are the subject of debate (vis-à-vis the strength of association between these skin conditions and diabetes) and can manifest in different forms. However, it is clear that the cutaneous manifestations of diabetes are equally as important to consider and manage as the systemic complications of the disease. In analyzing associations with diabetes, it is important to note that given such a high incidence of diabetes among the general population and its close association with other disease states, such as the metabolic syndrome, studies aimed at determining direct relationships to this entity must be well controlled for confounding factors, which may not even always be possible. Regardless, it is important for dermatologists and dermatology residents to recognize and understand the protean cutaneous manifestations of diabetes mellitus, and this column will explore skin findings that are characteristic of diabetes (Table 1) as well as other dermatoses with a reported but less clear association with diabetes (Table 2).
Skin Findings Characteristic of Diabetes
Diabetic Thick Skin
The association between diabetes and thick skin is well described as either a mobility-limiting affliction of the joints of the hands (cheiroarthropathy) or as an asymptomatic thickening of the skin. It has been estimated that 8% to 36% of patients with insulin-dependent diabetes develop some form of skin thickening2; one series also found this association to be true for patients with non–insulin-dependent diabetes mellitus (NIDDM).3 Skin thickening is readily observable on clinical presentation or ultrasonography, with increasing thickness in many cases associated with long-term disease progression. This increasing thickness was shown histopathologically to be a direct result of activated fibroblasts and increased collagen polymerization, with some similar features to progressive systemic sclerosis.4 Interestingly, even clinically normal skin showed some degree of fibroblast activation in diabetic patients, but collagen fibers in each case were smaller in diameter than those found in progressive systemic sclerosis. This finding clearly has implications on quality of life, as a lack of hand mobility due to the cheiroarthropathy can be severely disabling. Underlining the need for strict glycemic control, it has been suggested that tight control of blood sugar levels can lead to improvement in diabetic thick skin; however, reports of improvement are based on a small sample population.5 Huntley papules are localized to areas on the dorsum of the hands overlying the joints, demonstrating hyperkeratosis and enlarged dermal papillae.6 They also can be found in a minority of patients without diabetes. Interestingly, diabetic thick skin also has been associated with neurologic disorders in diabetes.7 Diabetic thick skin was found to be significantly (P<.05) correlated with diabetic neuropathy, independent of duration of diabetes, age, or glycosylated hemoglobin levels, though no causal or etiologic link between these entities has been proven.
Yellow Nails
Nail changes are well described in diabetes, ranging from periungual telangiectases to complications from infections, such as paronychia; however, a well-recognized finding, especially in elderly diabetic patients, is a characteristic yellowing of the nails, reported to affect up to 40% of patients with diabetes.8 The mechanism behind it likely includes accumulation of glycation end products, which also has been thought to lead to yellowing of the skin, and vascular impairment.9 These nails tend to exhibit slow growth, likely resulting from a nail matrix that is poorly supplied with blood, and also can be more curved than normal with longitudinal ridges (onychorrhexis).10 It is important, however, not to attribute yellow nails to diabetes without considering other causes of yellow nails, such as onychomycosis, yellow nail syndrome, and yellow nails associated with lymphedema or respiratory tract disease (eg, pleural effusion, bronchiectasis).11
Diabetic Dermopathy
Colloquially known as shin spots, diabetic dermopathy is perhaps the most common skin finding in this patient population, though it also can occur in up to 1 in 5 individuals without diabetes.12 Although it is very common, it is not a condition that should be overlooked, as numerous studies have shown an increase in microangiopathic complications such as retinopathy in patients with diabetic dermopathy.13,14 Although follow-up studies may be necessary to fully characterize the relationship between shin spots and diabetes, it certainly is reasonable to be more wary of diabetic patients presenting with many shin spots, as the general consensus is that these areas represent postinflammatory hyperpigmentation and cutaneous atrophy in the setting of poor vascular supply, which should prompt analysis of other areas that might be affected by poor vasculature, such as an ophthalmologic examination. Antecedent and perhaps unnoticed trauma has been implicated given a possible underlying neuropathy, but this theory has not been supported by studies.
Bullosis Diabeticorum
Bullosis diabeticorum is a rare but well-described occurrence of self-resolving, nonscarring blisters that arise on the extremities of diabetic patients. This entity should be distinguished from other primary autoimmune blistering disorders and from simple mechanobullous lesions. Several types of bullosis diabeticorum have been described, with the most classic form showing an intraepidermal cleavage plane.15 These lesions tend to resolve in weeks but can be recurrent. The location of the pathology underlines its nonscarring nature, though similar lesions have been reported showing a cleavage plane in the lamina lucida of the dermoepidermal junction, which underlines the confusion in the literature surrounding diabetic bullae.16 Some may even use this term interchangeably with trauma or friction-induced blisters, which diabetics may be prone to develop due to peripheral neuropathy. Confounding reports have stated there is a correlation between bullosis diabeticorum and neuropathy as well as the acral location of these blisters. Although many authors cite the incidence of bullosis diabeticorum being 0.5%,17 no population-based studies have confirmed this figure and some have speculated that the actual incidence is higher.18 In the end, the term bullosis diabeticorum is probably best reserved for a rapidly appearing blister on the extremities of diabetic patients with at most minimal trauma, with a lesion containing sterile fluid and negative immunofluorescence. The mechanism for these blisters is thought to be microangiopathy, with scant blood supply to the skin causing it to be more prone to acantholysis and blister formation.19 This theory was reinforced in a study showing a reduced threshold for suction blister formation in diabetic patients.20 Care should be taken to prevent secondary infections at these sites.
Acanthosis Nigricans
Acanthosis nigricans, which consists of dark brown plaques in the flexural areas, especially the posterior neck and axillae, is a common finding in diabetic patients and is no doubt familiar to clinicians. The pathophysiology of these lesions has been well studied and is a prototype for the effects of insulin resistance in the skin. In this model, high concentrations of insulin binding to insulinlike growth factor receptor in the skin stimulate keratinocyte proliferation,21 leading to the clinical appearance and the histologic finding of hyperkeratosis and papillomatosis, which in turn is responsible for the observed hyperpigmentation. It is an important finding, especially in those without a known history of diabetes, as it can also signal an underlying endocrinopathy (eg, Cushing syndrome, acromegaly, polycystic ovary syndrome) or malignancy (ie, adenocarcinoma of the gastrointestinal tract). Several distinct mechanisms of insulin resistance have been described, including insulin resistance due to receptor defects, such as those seen with insulin resistance in NIDDM; autoimmune processes; and postreceptor defects in insulin action.22 Keratolytics and topical retinoids have been used to ameliorate the appearance of these lesions.
Necrobiosis Lipoidica (Diabeticorum)
Necrobiosis lipoidica diabeticorum was first described by Urback23 in 1932, but reports of similar lesions were described in nondiabetic patients soon after. The dermatologic community has since come to realize that perhaps a more accurate nomenclature is necrobiosis lipoidica to fully encompass this entity. Clinically, lesions appear as erythematous papules and plaques that expand into a larger well-circumscribed plaque with a waxy yellowish atrophic center, often with telangiectases, and usually presenting in the pretibial area. Lesions can become ulcerated in up to one-third of cases. Necrobiosis lipoidica also is defined by characteristic histologic findings, including important features such as palisaded granulomas arranged in a tierlike fashion, necrotizing vasculitis, collagen degradation, and panniculitis. Necrobiosis lipoidica is still relatively rare, developing in approximately 0.3% of patients with diabetes,24 though its relationship with insulin resistance and diabetes is strong. Approximately two-thirds of patients with necrobiosis lipoidica have diabetes and an even higher number go on to develop diabetes or have a positive family history of diabetes.
Although these figures are interesting, the data are nearly a half-century-old, and it is unclear if these findings still hold true today. The etiology of necrobiosis lipoidica also remains elusive, with theories focusing on the role of microangiopathy, immunoglobulin deposition leading to vasculitis, structural abnormalities in collagen or fibroblasts, and trauma; however, the true nature of this condition is likely some combination of these factors.25 These lesions are difficult to treat, especially at an advanced stage. Management with topical steroids to limit the inflammatory progression of the lesions is the mainstay of therapy.
Scleredema
Scleredema adultorum (Buschke disease) refers to indurated plaques over the posterior neck and upper back. It is usually thought of as 3 distinct forms. The form that is known to occur in diabetic patients is sometimes referred to as scleredema diabeticorum; the other 2 occur as postinfectious, usually Streptococcus, or malignancy-related forms. The prevalence of scleredema diabeticorum among diabetic individuals most frequently is reported as 2.5%26; however, it is worth noting that other estimates have been as high as 14%.27 Although there has been some correlation between poorly controlled NIDDM, treatment and tight glucose control does not seem to readily resolve these lesions with only few conflicting case studies serving as evidence for and against this premise.28-30 The lesions often are recalcitrant toward a wide variety of treatment approaches. Histopathologic analysis generally reveals a thickened dermis with large collagen bundles, with clear spaces between the collagen representing mucin and increased numbers of mast cells. Proposed mechanisms include stimulation of collagen synthesis by fibroblasts and retarded collagen degradation, likely due to excess glucose.31
Dermatoses Demonstrating an Association With Diabetes
Granuloma Annulare
Granuloma annulare (GA) is a dermatologic condition existing in numerous forms. The generalized form has been suggested to have some association with diabetes. The lesions of GA are classically round, flesh-colored to erythematous papules arising in the dermis that may start on the dorsal extremities where the localized form typically presents, though larger annular plaques or patches may exist in the generalized form. Histologically, GA has a characteristic granulomatous infiltrate and palisaded granulomatous dermatitis, depending on the stage of the evolution. Many studies dating back to the mid-20th century have attempted to elucidate a link between GA and diabetes, with numerous reports showing conflicting results across their study populations.32-36 This issue is further muddled by links between generalized GA and a host of other diseases, such as malignancy, thyroid disease, hepatitis, and human immunodeficiency virus infection. The usual course of GA is spontaneous resolution, including a peculiar phenomenon noted in the literature whereby biopsy of one of the lesions led to clearance of other lesions on the body.37 However, the generalized form may be more difficult to treat, with therapeutic approaches including topical steroids, light therapy, and systemic immunomodulators.
Lichen Planus
A recent small population study in Turkey demonstrated a strong relationship between lichen planus and abnormal glucose tolerance. In this study of 30 patients with lichen planus, approximately half (14/30) had abnormal glucose metabolism and a quarter (8/30) had known diabetes, but larger studies are needed to clarify this relationship.38 Prior to this report, a link between oral lichen planus and diabetes had been shown in larger case series.39,40 Clinically, one may see white plaques with a characteristic lacy reticular pattern in the mouth. At other cutaneous sites, lichen planus generally appears as pruritic, purple, flat-topped polygonal papules. The clinical finding of lichen planus also is linked with many other disease states, most notably hepatitis C virus, but also thymoma, liver disease, and inflammatory bowel disease, among other associations.41
Vitiligo
As an autoimmune entity, it stands to reason that vitiligo may be seen more commonly associated with insulin-dependent diabetes, which has been shown to hold true in one study, while no association was found between later-onset NIDDM and vitiligo.42 Given the nonspecific nature of this association and the relatively common presentation of vitiligo, no special consideration is likely needed when examining a patient with vitiligo, but its presence should remind the clinician that these autoimmune entities tend to travel together.
Acquired Perforating Dermatosis
Although the classic presentation of acquired perforating dermatosis (Kyrle disease) is linked to renal failure, diabetes also has been connected to its presentation. Extremely rare outside of the setting of chronic renal failure, acquired perforating dermatosis occurs in up to 10% of dialysis patients.43,44 It is characterized by papules with a central keratin plug, representing transepidermal elimination of keratin, collagen, and other cellular material; its etiology has not been elucidated. The connection between acquired perforating dermatosis and diabetes is not completely clear; it would seem that renal failure is a prerequisite for itspresentation. A large proportion of renal failure necessitating hemodialysis occurs in patients with diabetic nephropathy, which may explain the coincidence of diabetes, renal failure, and acquired perforating dermatosis.45 The presentation of this cutaneous finding should not, however, affect treatment of the underlying conditions. Symptom relief in the form of topical steroids can be used as a first-line treatment of these often pruritic lesions.
Eruptive Xanthomas
The link between diabetes and eruptive xanthomas seems to be a rather tenuous one, hinging on the fact that many diabetic patients have abnormalities in carbohydrate and lipid metabolism. A central feature of eruptive xanthomas is an elevation in triglycerides, which can occur in diabetes. Indeed, it has been estimated that only 0.1% of diabetics will develop eruptive xanthomas,46 and its main importance may be to prompt the physician to treat the hypertriglyceridemia and consider other concerning possibilities such as acute pancreatitis.
Psoriasis
Psoriasis is a common dermatologic condition that has been shown to have a far-reaching impact both on patients’ quality of life and cardiovascular risk profiles. Data have emerged linking psoriasis with diabetes as an independent risk factor47; although this retrospective study had its limitations, it certainly is interesting to note that patients with psoriasis may have an increased risk for developing diabetes. Perhaps more importantly, though, this study also implied that patients with severe psoriasis may present with diabetes that is more difficult to control, evidenced by increased treatment with systemic therapies as opposed to milder forms of intervention such as diet control.47 There almost certainly are other confounding factors and further studies would serve to reveal the strength of this association, but it is certainly an intriguing concept. Echoing these findings, a more recent nationwide study from Denmark demonstrated that psoriasis is associated with increased incidence of new-onset diabetes, adjusting for numerous confounding factors.48 The relationship between psoriasis and diabetes is worth noting as evidence continues to emerge.
Conclusion
Given the diverse cutaneous manifestations of diabetes, it is important to distinguish those that are directly related to diabetes from those that suggest there may be another underlying process. For example, a new patient presenting to a primary care physician with acanthosis nigricans and yellow nails should immediately trigger a test for a hemoglobin A1c (glycated hemoglobin) level to investigate for diabetes; however, clinicians also should be wary of patients with acanthosis nigricans who report early satiety, as this asso-ciation may be a sign of underlying malignancy. Conversely, the presence of yellow nails in a patient with chronic diabetes should not be ignored. The physician should consider onychomycosis and query the patient about possible respiratory symptoms. In the case of a multisystem disease such as diabetes, it may be challenging to reconcile seemingly disparate skin findings, but having a framework to approach the cutaneous manifestations of diabetes can help to properly identify and treat an individual patient’s afflictions.
- American Diabetes Association. Economic costs of diabetes in the U.S. in 2012 [published online instead of print March 16, 2013]. Diabetes Care. 2013;36:1033-1046.
- Collier A, Matthews DM, Kellett HA, et al. Change in skin thickness associated with cheiroarthropathy in insulin dependent diabetes mellitus. Br Med J (Clin Res Ed). 1986;292:936.
- Fitzcharles MA, Duby S, Waddell RW, et al. Limitation of joint mobility (cheiroarthropathy) in adult noninsulin-dependent diabetic patients. Ann Rheum Dis. 1984;43:251-254.
- Hanna W, Friesen D, Bombardier C, et al. Pathologic features of diabetic thick skin. J Am Acad Dermatol. 1987;16:546-553.
- Lieberman LS, Rosenbloom AL, Riley WJ, et al. Reduced skin thickness with pump administration of insulin. N Engl J Med. 1980;303:940-941.
- Guarneri C, Guarneri F, Borgia F, et al. Finger pebbles in a diabetic patient: Huntley's papules. Int J Dermatol. 2005;44:755-756.
- Forst T, Kann P, Pfützner A, et al. Association between "diabetic thick skin syndrome" and neurological disorders in diabetes mellitus. Acta Diabetol. 1994;31:73-77.
- Nikoleishvili LR, Kurashvili RB, Virsaladze DK, et al. Characteristic changes of skin and its accessories in type 2 diabetes mellitus [in Russian]. Georgian Med News. 2006:43-46.
- Lithner F. Purpura, pigmentation and yellow nails of the lower extremities in diabetics. Acta Med Scand. 1976;199:203-208.
- Greene RA, Scher RK. Nail changes associated with diabetes mellitus. J Am Acad Dermatol. 1987;16:1015-1021.
- Hiller E, Rosenow EC 3rd, Olsen AM. Pulmonary manifestations of the yellow nail syndrome. Chest. 1972;61:452-458.
- Feingold KR, Elias PM. Endocrine-skin interactions. cutaneous manifestations of pituitary disease, thyroid disease, calcium disorders, and diabetes. J Am Acad Dermatol. 1987;17:921-940.
- Abdollahi A, Daneshpazhooh M, Amirchaghmaghi E, et al. Dermopathy and retinopathy in diabetes: is there an association? Dermatology, 2007;214:133-136.
- Morgan AJ, Schwartz RA. Diabetic dermopathy: A subtle sign with grave implications. J Am Acad Dermatol. 2008;58:447-451.
- Perez MI, Kohn SR. Cutaneous manifestations of diabetes mellitus. J Am Acad Dermatol. 1994;30:519-531.
- Cantwell AR, Martz W. Idiopathic bullae in diabetics. Bullosis diabeticorum. Arch Dermatol. 1967;96:42-44.
- Larsen K, Jensen T, Karlsmark T, Holstein PE. Incidence of bullosis diabeticorum – a controversial cause of chronic foot ulceration. Int Wound J. 2008;5:591-596.
- Lipsky BA, Baker PD, Ahroni JH. Diabetic bullae: 12 cases of a purportedly rare cutaneous disorder. Int J Dermatol. 2000;39:196-200.
- Basarab T, Munn SE, McGrath J, et al. Bullosis diabeticorum. a case report and literature review. Clin Exp Dermatol. 1995;20:218-220.
- Bernstein JE, Levine LE, Medenica MM, et al. Reduced threshold to suction-induced blister formation in insulin-dependent diabetics. J Am Acad Dermatol. 1983;8:790-791.
- Cruz PD Jr, Hud JA Jr. Excess insulin binding to insulin-like growth factor receptors: proposed mechanism for acanthosis nigricans. J Invest Dermatol. 1992;98(suppl 6):S82-S85.
- Romano G, Moretti G, Di Benedetto A, et al. Skin lesions in diabetes mellitus: prevalence and clinical correlations. Diabetes Res Clin Pract. 1998;39:101-106.
- Urback E. Eine neue diabetische Stoffwechseldermatose: Nekrobiosis lipoidica diabeticorum. Arch. f. Dermat. u Syph. 1932;166:273.
- Muller SA, Winkelmann RK. Necrobiosis lipoidica diabeticorum. a clinical and pathological investigation of 171 cases. Arch Dermatol. 1966;93:272-281.
- Engel MF, Smith JG Jr. The pathogenesis of necrobiosis lipoidica. necrobiosis lipoidica, a form fruste of diabetes mellitus. Arch Dermatol. 1960;82:791-797.
- Cole GW, Headley J, Skowsky R. Scleredema diabeticorum: a common and distinct cutaneous manifestation of diabetes mellitus. Diabetes Care. 1983;6:189-192.
- Sattar MA, Diab S, Sugathan TN, et al. Scleroedema diabeticorum: a minor but often unrecognized complication of diabetes mellitus. Diabet Med. 1988;5:465-468.
- Rho YW, Suhr KB, Lee JH, et al. A clinical observation of scleredema adultorum and its relationship to diabetes. J Dermatol. 1998;25:103-107.
- Baillot-Rudoni S, Apostol D, Vaillant G, et al. Implantable pump therapy restores metabolic control and quality of life in type 1 diabetic patients with Buschke's nonsystemic scleroderma. Diabetes Care. 2006;29:1710.
- Meguerditchian C, Jacquet P, Béliard S, et al. Scleredema adultorum of Buschke: an under recognized skin complication of diabetes. Diabetes Metab. 2006;32:481-484.
- Behm B, Schreml S, Landthaler M, et al. Skin signs in diabetes mellitus. J Eur Acad Dermatol Venereol. 2012;26:1203-1211.
- Nebesio CL, Lewis C, Chuang TY. Lack of an association between granuloma annulare and type 2 diabetes mellitus. Br J Dermatol. 2002;146:122-124.
- Stankler L, Leslie G. Generalized granuloma annulare. a report of a case and review of the literature. Arch Dermatol. 1976;95:509-513.
- Williamson DM, Dykes JR. Carbohydrate metabolism in granuloma annulare. J Invest Dermatol. 1972;58:400-404.
- Dabski K, Winkelmann RK. Generalized granuloma annulare: clinical and laboratory findings in 100 patients. J Am Acad Dermatol. 1989;20:39-47.
- Veraldi S, Bencini PL, Drudi E, et al. Laboratory abnormalities in granuloma annulare: a case-control study. Br J Dermatol. 1997;136:652-653.
- Levin NA, Patterson JW, Yao LL, et al. Resolution of patch-type granuloma annulare lesions after biopsy. J Am Acad Dermatol. 2002;46:426-429.
- Seyhan M, Ozcan H, Sahin I, et al. High prevalence of glucose metabolism disturbance in patients with lichen planus. Diabetes Res Clin Pract. 2007;77:198-202.
- Romero MA, Seoane J, Varela-Centelles P, et al. Prevalence of diabetes mellitus amongst oral lichen planus patients. clinical and pathological characteristics. Med Oral. 2002;7:121-129.
- Albrecht M, Banoczy J, Dinya E, et al. Occurrence of oral leukoplakia and lichen planus in diabetes mellitus. J Oral Pathol Med. 1992;21:364-366.
- Lehman JS, Tollefson MM, Gibson LE. Lichen planus. Int J Dermatol. 2009;48:682-694.
- Gould IM, Gray RS, Urbaniak SJ, et al. Vitiligo in diabetes mellitus. Br J Dermatol. 1985;113:153-155.
- White CR Jr, Heskel NS, Pokorny DJ. Perforating folliculitis of hemodialysis. Am J Dermatopathol. 1982;4:109-116.
- Hurwitz RM, Melton ME, Creech FT 3rd, et al. Perforating folliculitis in association with hemodialysis. Am J Dermatopathol. 1982;4:101-108.
- Rapini RP, Herbert AA, Drucker CR. Acquired perforating dermatosis. evidence for combined transepidermal elimination of both collagen and elastic fibers. Arch Dermatol. 1989;125:1074-1078.
- Muller SA. Dermatologic disorders associated with diabetes mellitus. Mayo Clin Proc. 1966;41:689-703.
- Azfar RS, Seminara NM, Shin DB, et al. Increased risk of diabetes mellitus and likelihood of receiving diabetes mellitus treatment in patients with psoriasis. Arch Dermatol. 2012;148:995-1000.
- Khalid U, Hansen PR, Gislason GH, et al. Psoriasis and new-onset diabetes: a Danish nationwide cohort study. Diabetes Care. 2013;36:2402-2407.
- American Diabetes Association. Economic costs of diabetes in the U.S. in 2012 [published online instead of print March 16, 2013]. Diabetes Care. 2013;36:1033-1046.
- Collier A, Matthews DM, Kellett HA, et al. Change in skin thickness associated with cheiroarthropathy in insulin dependent diabetes mellitus. Br Med J (Clin Res Ed). 1986;292:936.
- Fitzcharles MA, Duby S, Waddell RW, et al. Limitation of joint mobility (cheiroarthropathy) in adult noninsulin-dependent diabetic patients. Ann Rheum Dis. 1984;43:251-254.
- Hanna W, Friesen D, Bombardier C, et al. Pathologic features of diabetic thick skin. J Am Acad Dermatol. 1987;16:546-553.
- Lieberman LS, Rosenbloom AL, Riley WJ, et al. Reduced skin thickness with pump administration of insulin. N Engl J Med. 1980;303:940-941.
- Guarneri C, Guarneri F, Borgia F, et al. Finger pebbles in a diabetic patient: Huntley's papules. Int J Dermatol. 2005;44:755-756.
- Forst T, Kann P, Pfützner A, et al. Association between "diabetic thick skin syndrome" and neurological disorders in diabetes mellitus. Acta Diabetol. 1994;31:73-77.
- Nikoleishvili LR, Kurashvili RB, Virsaladze DK, et al. Characteristic changes of skin and its accessories in type 2 diabetes mellitus [in Russian]. Georgian Med News. 2006:43-46.
- Lithner F. Purpura, pigmentation and yellow nails of the lower extremities in diabetics. Acta Med Scand. 1976;199:203-208.
- Greene RA, Scher RK. Nail changes associated with diabetes mellitus. J Am Acad Dermatol. 1987;16:1015-1021.
- Hiller E, Rosenow EC 3rd, Olsen AM. Pulmonary manifestations of the yellow nail syndrome. Chest. 1972;61:452-458.
- Feingold KR, Elias PM. Endocrine-skin interactions. cutaneous manifestations of pituitary disease, thyroid disease, calcium disorders, and diabetes. J Am Acad Dermatol. 1987;17:921-940.
- Abdollahi A, Daneshpazhooh M, Amirchaghmaghi E, et al. Dermopathy and retinopathy in diabetes: is there an association? Dermatology, 2007;214:133-136.
- Morgan AJ, Schwartz RA. Diabetic dermopathy: A subtle sign with grave implications. J Am Acad Dermatol. 2008;58:447-451.
- Perez MI, Kohn SR. Cutaneous manifestations of diabetes mellitus. J Am Acad Dermatol. 1994;30:519-531.
- Cantwell AR, Martz W. Idiopathic bullae in diabetics. Bullosis diabeticorum. Arch Dermatol. 1967;96:42-44.
- Larsen K, Jensen T, Karlsmark T, Holstein PE. Incidence of bullosis diabeticorum – a controversial cause of chronic foot ulceration. Int Wound J. 2008;5:591-596.
- Lipsky BA, Baker PD, Ahroni JH. Diabetic bullae: 12 cases of a purportedly rare cutaneous disorder. Int J Dermatol. 2000;39:196-200.
- Basarab T, Munn SE, McGrath J, et al. Bullosis diabeticorum. a case report and literature review. Clin Exp Dermatol. 1995;20:218-220.
- Bernstein JE, Levine LE, Medenica MM, et al. Reduced threshold to suction-induced blister formation in insulin-dependent diabetics. J Am Acad Dermatol. 1983;8:790-791.
- Cruz PD Jr, Hud JA Jr. Excess insulin binding to insulin-like growth factor receptors: proposed mechanism for acanthosis nigricans. J Invest Dermatol. 1992;98(suppl 6):S82-S85.
- Romano G, Moretti G, Di Benedetto A, et al. Skin lesions in diabetes mellitus: prevalence and clinical correlations. Diabetes Res Clin Pract. 1998;39:101-106.
- Urback E. Eine neue diabetische Stoffwechseldermatose: Nekrobiosis lipoidica diabeticorum. Arch. f. Dermat. u Syph. 1932;166:273.
- Muller SA, Winkelmann RK. Necrobiosis lipoidica diabeticorum. a clinical and pathological investigation of 171 cases. Arch Dermatol. 1966;93:272-281.
- Engel MF, Smith JG Jr. The pathogenesis of necrobiosis lipoidica. necrobiosis lipoidica, a form fruste of diabetes mellitus. Arch Dermatol. 1960;82:791-797.
- Cole GW, Headley J, Skowsky R. Scleredema diabeticorum: a common and distinct cutaneous manifestation of diabetes mellitus. Diabetes Care. 1983;6:189-192.
- Sattar MA, Diab S, Sugathan TN, et al. Scleroedema diabeticorum: a minor but often unrecognized complication of diabetes mellitus. Diabet Med. 1988;5:465-468.
- Rho YW, Suhr KB, Lee JH, et al. A clinical observation of scleredema adultorum and its relationship to diabetes. J Dermatol. 1998;25:103-107.
- Baillot-Rudoni S, Apostol D, Vaillant G, et al. Implantable pump therapy restores metabolic control and quality of life in type 1 diabetic patients with Buschke's nonsystemic scleroderma. Diabetes Care. 2006;29:1710.
- Meguerditchian C, Jacquet P, Béliard S, et al. Scleredema adultorum of Buschke: an under recognized skin complication of diabetes. Diabetes Metab. 2006;32:481-484.
- Behm B, Schreml S, Landthaler M, et al. Skin signs in diabetes mellitus. J Eur Acad Dermatol Venereol. 2012;26:1203-1211.
- Nebesio CL, Lewis C, Chuang TY. Lack of an association between granuloma annulare and type 2 diabetes mellitus. Br J Dermatol. 2002;146:122-124.
- Stankler L, Leslie G. Generalized granuloma annulare. a report of a case and review of the literature. Arch Dermatol. 1976;95:509-513.
- Williamson DM, Dykes JR. Carbohydrate metabolism in granuloma annulare. J Invest Dermatol. 1972;58:400-404.
- Dabski K, Winkelmann RK. Generalized granuloma annulare: clinical and laboratory findings in 100 patients. J Am Acad Dermatol. 1989;20:39-47.
- Veraldi S, Bencini PL, Drudi E, et al. Laboratory abnormalities in granuloma annulare: a case-control study. Br J Dermatol. 1997;136:652-653.
- Levin NA, Patterson JW, Yao LL, et al. Resolution of patch-type granuloma annulare lesions after biopsy. J Am Acad Dermatol. 2002;46:426-429.
- Seyhan M, Ozcan H, Sahin I, et al. High prevalence of glucose metabolism disturbance in patients with lichen planus. Diabetes Res Clin Pract. 2007;77:198-202.
- Romero MA, Seoane J, Varela-Centelles P, et al. Prevalence of diabetes mellitus amongst oral lichen planus patients. clinical and pathological characteristics. Med Oral. 2002;7:121-129.
- Albrecht M, Banoczy J, Dinya E, et al. Occurrence of oral leukoplakia and lichen planus in diabetes mellitus. J Oral Pathol Med. 1992;21:364-366.
- Lehman JS, Tollefson MM, Gibson LE. Lichen planus. Int J Dermatol. 2009;48:682-694.
- Gould IM, Gray RS, Urbaniak SJ, et al. Vitiligo in diabetes mellitus. Br J Dermatol. 1985;113:153-155.
- White CR Jr, Heskel NS, Pokorny DJ. Perforating folliculitis of hemodialysis. Am J Dermatopathol. 1982;4:109-116.
- Hurwitz RM, Melton ME, Creech FT 3rd, et al. Perforating folliculitis in association with hemodialysis. Am J Dermatopathol. 1982;4:101-108.
- Rapini RP, Herbert AA, Drucker CR. Acquired perforating dermatosis. evidence for combined transepidermal elimination of both collagen and elastic fibers. Arch Dermatol. 1989;125:1074-1078.
- Muller SA. Dermatologic disorders associated with diabetes mellitus. Mayo Clin Proc. 1966;41:689-703.
- Azfar RS, Seminara NM, Shin DB, et al. Increased risk of diabetes mellitus and likelihood of receiving diabetes mellitus treatment in patients with psoriasis. Arch Dermatol. 2012;148:995-1000.
- Khalid U, Hansen PR, Gislason GH, et al. Psoriasis and new-onset diabetes: a Danish nationwide cohort study. Diabetes Care. 2013;36:2402-2407.

What we ought to talk about when we’re talking about decriminalizing Cannabis
A green revolution is sweeping through the social and political landscape of the United States—a shifting tide in the way American law and society conceptualize Cannabis as a recreational and a medical substance. In light of the unprecedented legalization of Cannabis in several states, and decriminalization campaigns in other jurisdictions—such as the nation’s capital, where we work—the topic of marijuana has grabbed the nation’s attention and reinvigorated debate about its use.
No dearth of opinion on marijuana use
Legal and economic positions seem to be the pivot points of argument on recreational use of Cannabis—but not, surprisingly, health considerations. Even to the Cannabis non-user, the pending changes in state laws are relevant; after all, every illicit substance can lead to a pathological process and thus a public economic burden.
Articulations of marijuana’s “safety” are nothing new: Consider President Barack Obama’s recent comment that pot is no more dangerous than alcohol (the danger of alcohol is a different argument altogether). There is another layer of Cannabis use—the drug’s psychiatric effects—that is seldom visible to the public eye but quite palpable in the field of mental health—a troubling disconnect because those psychiatric effects have been softened to inconsequence, or are not spoken of at all.
When Cannabis is juxtaposed with other illicit substances, it seems almost innocuous; dependence and withdrawal have not been detailed empirically and are continuously debated. True, consumption of marijuana is not immediately life-threatening, compared with the risk of stroke and myocardial infarction with cocaine use or respiratory depression with narcotic agents. Despite this facade, however, the psychiatric morbidities of marijuana are real and incapacitating, ranging from extreme anxiety and dysregulated mood to chronic psychotic debilitation.
Even after only a few years in psychiatric residency, it has become a common experience for us to observe acute and chronic psychosis in patients after they have used Cannabis. Many require hospitalization or a leave of absence from academics or employment; one of our patients re-matriculated to college after 7 years of intensive care.
Every mental health professional can tell similar tales.
Beyond anecdote
Numerous publications have shown that Cannabis expedites onset of psychotic and prodromal symptoms of schizophrenia. The age range of onset of psychotic symptoms—typically, late adolescence into early 20s—is critical, prognostically.1,2 This epidemiological fact is dangerously in tandem with Cannabis use patterns in America and its college culture. It is known that modifiable risk factors are decisive in the development of psychopathology. Additionally, environmental exposures in the developing brain elicit a more ominous concern because the brain does not complete neural development until early or mid-20s.3
Another concern is the effect of Cannabis on cognition, during periods of acute intoxication and after chronic use. Research on this topic is limited, but evidence suggests that heavy Cannabis use at an early age affects cognition, as measured by a diminished IQ.4 Regrettably, unknowns in this area of study are far more abundant than what we know. This gray area might serve to placate legislators and frequent users and cool discussion.
Rx Cannabis?
Another aspect of the controversy concerns medicinal use of marijuana. Perhaps legalization of medical marijuana has served simply as an antecedent to recreational legalization, as was the case for Colorado and Washington. But under the heading of “medical marijuana” lies a poorly defined, amorphous designation—one that borders on arbitrariness regarding standards of use.
Cancer treatment, pain, glaucoma, HIV, multiple sclerosis are examples of conditions in the bucket list for discretionary use of Cannabis, yet none has a formal FDA indication.5 This absence of approval underscores the lack of empirical validation, quality control, and standardization that are required of every other sanctioned pharmaceutical agent.
Lack of validation also might explain why the collective opinion of major medical associations, including the American Medical Association and the National Council on Alcoholism and Drug Dependence, are opposed to wide availability of smoked marijuana. The American Society of Addiction Medicine, an interdisciplinary organization of physicians, has posted a policy statement affirming that medical marijuana should 1) be held to FDA standards and 2) not be kept under the jurisdiction of state law and regulation.6
Why are psychiatric morbidities of marijuana reported so timidly?
Perhaps the rarity and randomness of long-term illness associated with Cannabis use pacifies individual concerns. Psychiatry understands this reality: All people respond to stresses differently and have specific, individual vulnerabilities. The diathesis-stress model plainly explains this hypothesis— and, sometimes, Cannabis is that stressor. Perhaps a more academic hypothesis is the concept of “ecophenotypes,” which posits that our heritability is not fixed but is in constant calibration with our environment and our adaptability to it. Environment often is a choice that people make.
The fact remains: This drug is risky
Cannabis can precipitate mood and anxiety disorders, alter development of the brain, and serve as a trigger for schizophrenia. The scary truth is that medical science cannot yet tell us who is predisposed to these ill effects and to what degree. In the meantime, society is missing the voice of psychiatry on individual and public health risks that might be the consequences of sweeping legal changes.
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Compton MT, Kelley ME, Ramsay CE, et al. Association of pre-onset cannabis, alcohol, and tobacco use with age at onset of prodrome and age at onset of psychosis in first-episode patients. Am J Psychiatry. 2009;166(11):1251-1257.
2. Moore TH, Zammit S, Lingford-Hughes A, et al. Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review. Lancet. 2007;370(9584):319-328.
3. Saez TM, Aronne MP, Caltana L, et al. Prenatal exposure to the CB1 and CB2 cannabinoid receptor agonist WIN 55,212-2 alters migration of early-born glutamatergic neurons and GABAergic interneurons in the rat cerebral cortex. J Neurochem. 2014; 129(4):637-648.
4. Meier MH, Caspi A, Ambler A, et al. Persistent cannabis users show neuropsychological decline from childhood to midlife. Proc Natl Acad Sci U S A. 2012;109(40):E2657-E2664.
5. Medical marijuana program physician frequently asked questions. Government of the District of Columbia Department of Health. http://doh.dc.gov/sites/default/files/dc/sites/ doh/publication/attachments/120430FAQPhysicians%20 Final.pdf. Published April 2012. Accessed March 20, 2014.
6. The role of the physician in “medical” marijuana. American Society of Addiction Medicine. http://www.asam.org/ advocacy/find-a-policy-statement/view-policy-statement/ public-policy-statements/2011/11/28/the-role-of-the-physician-in-medical-marijuana. Published April 12, 2010. Accessed March 20, 2014.
A green revolution is sweeping through the social and political landscape of the United States—a shifting tide in the way American law and society conceptualize Cannabis as a recreational and a medical substance. In light of the unprecedented legalization of Cannabis in several states, and decriminalization campaigns in other jurisdictions—such as the nation’s capital, where we work—the topic of marijuana has grabbed the nation’s attention and reinvigorated debate about its use.
No dearth of opinion on marijuana use
Legal and economic positions seem to be the pivot points of argument on recreational use of Cannabis—but not, surprisingly, health considerations. Even to the Cannabis non-user, the pending changes in state laws are relevant; after all, every illicit substance can lead to a pathological process and thus a public economic burden.
Articulations of marijuana’s “safety” are nothing new: Consider President Barack Obama’s recent comment that pot is no more dangerous than alcohol (the danger of alcohol is a different argument altogether). There is another layer of Cannabis use—the drug’s psychiatric effects—that is seldom visible to the public eye but quite palpable in the field of mental health—a troubling disconnect because those psychiatric effects have been softened to inconsequence, or are not spoken of at all.
When Cannabis is juxtaposed with other illicit substances, it seems almost innocuous; dependence and withdrawal have not been detailed empirically and are continuously debated. True, consumption of marijuana is not immediately life-threatening, compared with the risk of stroke and myocardial infarction with cocaine use or respiratory depression with narcotic agents. Despite this facade, however, the psychiatric morbidities of marijuana are real and incapacitating, ranging from extreme anxiety and dysregulated mood to chronic psychotic debilitation.
Even after only a few years in psychiatric residency, it has become a common experience for us to observe acute and chronic psychosis in patients after they have used Cannabis. Many require hospitalization or a leave of absence from academics or employment; one of our patients re-matriculated to college after 7 years of intensive care.
Every mental health professional can tell similar tales.
Beyond anecdote
Numerous publications have shown that Cannabis expedites onset of psychotic and prodromal symptoms of schizophrenia. The age range of onset of psychotic symptoms—typically, late adolescence into early 20s—is critical, prognostically.1,2 This epidemiological fact is dangerously in tandem with Cannabis use patterns in America and its college culture. It is known that modifiable risk factors are decisive in the development of psychopathology. Additionally, environmental exposures in the developing brain elicit a more ominous concern because the brain does not complete neural development until early or mid-20s.3
Another concern is the effect of Cannabis on cognition, during periods of acute intoxication and after chronic use. Research on this topic is limited, but evidence suggests that heavy Cannabis use at an early age affects cognition, as measured by a diminished IQ.4 Regrettably, unknowns in this area of study are far more abundant than what we know. This gray area might serve to placate legislators and frequent users and cool discussion.
Rx Cannabis?
Another aspect of the controversy concerns medicinal use of marijuana. Perhaps legalization of medical marijuana has served simply as an antecedent to recreational legalization, as was the case for Colorado and Washington. But under the heading of “medical marijuana” lies a poorly defined, amorphous designation—one that borders on arbitrariness regarding standards of use.
Cancer treatment, pain, glaucoma, HIV, multiple sclerosis are examples of conditions in the bucket list for discretionary use of Cannabis, yet none has a formal FDA indication.5 This absence of approval underscores the lack of empirical validation, quality control, and standardization that are required of every other sanctioned pharmaceutical agent.
Lack of validation also might explain why the collective opinion of major medical associations, including the American Medical Association and the National Council on Alcoholism and Drug Dependence, are opposed to wide availability of smoked marijuana. The American Society of Addiction Medicine, an interdisciplinary organization of physicians, has posted a policy statement affirming that medical marijuana should 1) be held to FDA standards and 2) not be kept under the jurisdiction of state law and regulation.6
Why are psychiatric morbidities of marijuana reported so timidly?
Perhaps the rarity and randomness of long-term illness associated with Cannabis use pacifies individual concerns. Psychiatry understands this reality: All people respond to stresses differently and have specific, individual vulnerabilities. The diathesis-stress model plainly explains this hypothesis— and, sometimes, Cannabis is that stressor. Perhaps a more academic hypothesis is the concept of “ecophenotypes,” which posits that our heritability is not fixed but is in constant calibration with our environment and our adaptability to it. Environment often is a choice that people make.
The fact remains: This drug is risky
Cannabis can precipitate mood and anxiety disorders, alter development of the brain, and serve as a trigger for schizophrenia. The scary truth is that medical science cannot yet tell us who is predisposed to these ill effects and to what degree. In the meantime, society is missing the voice of psychiatry on individual and public health risks that might be the consequences of sweeping legal changes.
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
A green revolution is sweeping through the social and political landscape of the United States—a shifting tide in the way American law and society conceptualize Cannabis as a recreational and a medical substance. In light of the unprecedented legalization of Cannabis in several states, and decriminalization campaigns in other jurisdictions—such as the nation’s capital, where we work—the topic of marijuana has grabbed the nation’s attention and reinvigorated debate about its use.
No dearth of opinion on marijuana use
Legal and economic positions seem to be the pivot points of argument on recreational use of Cannabis—but not, surprisingly, health considerations. Even to the Cannabis non-user, the pending changes in state laws are relevant; after all, every illicit substance can lead to a pathological process and thus a public economic burden.
Articulations of marijuana’s “safety” are nothing new: Consider President Barack Obama’s recent comment that pot is no more dangerous than alcohol (the danger of alcohol is a different argument altogether). There is another layer of Cannabis use—the drug’s psychiatric effects—that is seldom visible to the public eye but quite palpable in the field of mental health—a troubling disconnect because those psychiatric effects have been softened to inconsequence, or are not spoken of at all.
When Cannabis is juxtaposed with other illicit substances, it seems almost innocuous; dependence and withdrawal have not been detailed empirically and are continuously debated. True, consumption of marijuana is not immediately life-threatening, compared with the risk of stroke and myocardial infarction with cocaine use or respiratory depression with narcotic agents. Despite this facade, however, the psychiatric morbidities of marijuana are real and incapacitating, ranging from extreme anxiety and dysregulated mood to chronic psychotic debilitation.
Even after only a few years in psychiatric residency, it has become a common experience for us to observe acute and chronic psychosis in patients after they have used Cannabis. Many require hospitalization or a leave of absence from academics or employment; one of our patients re-matriculated to college after 7 years of intensive care.
Every mental health professional can tell similar tales.
Beyond anecdote
Numerous publications have shown that Cannabis expedites onset of psychotic and prodromal symptoms of schizophrenia. The age range of onset of psychotic symptoms—typically, late adolescence into early 20s—is critical, prognostically.1,2 This epidemiological fact is dangerously in tandem with Cannabis use patterns in America and its college culture. It is known that modifiable risk factors are decisive in the development of psychopathology. Additionally, environmental exposures in the developing brain elicit a more ominous concern because the brain does not complete neural development until early or mid-20s.3
Another concern is the effect of Cannabis on cognition, during periods of acute intoxication and after chronic use. Research on this topic is limited, but evidence suggests that heavy Cannabis use at an early age affects cognition, as measured by a diminished IQ.4 Regrettably, unknowns in this area of study are far more abundant than what we know. This gray area might serve to placate legislators and frequent users and cool discussion.
Rx Cannabis?
Another aspect of the controversy concerns medicinal use of marijuana. Perhaps legalization of medical marijuana has served simply as an antecedent to recreational legalization, as was the case for Colorado and Washington. But under the heading of “medical marijuana” lies a poorly defined, amorphous designation—one that borders on arbitrariness regarding standards of use.
Cancer treatment, pain, glaucoma, HIV, multiple sclerosis are examples of conditions in the bucket list for discretionary use of Cannabis, yet none has a formal FDA indication.5 This absence of approval underscores the lack of empirical validation, quality control, and standardization that are required of every other sanctioned pharmaceutical agent.
Lack of validation also might explain why the collective opinion of major medical associations, including the American Medical Association and the National Council on Alcoholism and Drug Dependence, are opposed to wide availability of smoked marijuana. The American Society of Addiction Medicine, an interdisciplinary organization of physicians, has posted a policy statement affirming that medical marijuana should 1) be held to FDA standards and 2) not be kept under the jurisdiction of state law and regulation.6
Why are psychiatric morbidities of marijuana reported so timidly?
Perhaps the rarity and randomness of long-term illness associated with Cannabis use pacifies individual concerns. Psychiatry understands this reality: All people respond to stresses differently and have specific, individual vulnerabilities. The diathesis-stress model plainly explains this hypothesis— and, sometimes, Cannabis is that stressor. Perhaps a more academic hypothesis is the concept of “ecophenotypes,” which posits that our heritability is not fixed but is in constant calibration with our environment and our adaptability to it. Environment often is a choice that people make.
The fact remains: This drug is risky
Cannabis can precipitate mood and anxiety disorders, alter development of the brain, and serve as a trigger for schizophrenia. The scary truth is that medical science cannot yet tell us who is predisposed to these ill effects and to what degree. In the meantime, society is missing the voice of psychiatry on individual and public health risks that might be the consequences of sweeping legal changes.
Disclosures
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Compton MT, Kelley ME, Ramsay CE, et al. Association of pre-onset cannabis, alcohol, and tobacco use with age at onset of prodrome and age at onset of psychosis in first-episode patients. Am J Psychiatry. 2009;166(11):1251-1257.
2. Moore TH, Zammit S, Lingford-Hughes A, et al. Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review. Lancet. 2007;370(9584):319-328.
3. Saez TM, Aronne MP, Caltana L, et al. Prenatal exposure to the CB1 and CB2 cannabinoid receptor agonist WIN 55,212-2 alters migration of early-born glutamatergic neurons and GABAergic interneurons in the rat cerebral cortex. J Neurochem. 2014; 129(4):637-648.
4. Meier MH, Caspi A, Ambler A, et al. Persistent cannabis users show neuropsychological decline from childhood to midlife. Proc Natl Acad Sci U S A. 2012;109(40):E2657-E2664.
5. Medical marijuana program physician frequently asked questions. Government of the District of Columbia Department of Health. http://doh.dc.gov/sites/default/files/dc/sites/ doh/publication/attachments/120430FAQPhysicians%20 Final.pdf. Published April 2012. Accessed March 20, 2014.
6. The role of the physician in “medical” marijuana. American Society of Addiction Medicine. http://www.asam.org/ advocacy/find-a-policy-statement/view-policy-statement/ public-policy-statements/2011/11/28/the-role-of-the-physician-in-medical-marijuana. Published April 12, 2010. Accessed March 20, 2014.
1. Compton MT, Kelley ME, Ramsay CE, et al. Association of pre-onset cannabis, alcohol, and tobacco use with age at onset of prodrome and age at onset of psychosis in first-episode patients. Am J Psychiatry. 2009;166(11):1251-1257.
2. Moore TH, Zammit S, Lingford-Hughes A, et al. Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review. Lancet. 2007;370(9584):319-328.
3. Saez TM, Aronne MP, Caltana L, et al. Prenatal exposure to the CB1 and CB2 cannabinoid receptor agonist WIN 55,212-2 alters migration of early-born glutamatergic neurons and GABAergic interneurons in the rat cerebral cortex. J Neurochem. 2014; 129(4):637-648.
4. Meier MH, Caspi A, Ambler A, et al. Persistent cannabis users show neuropsychological decline from childhood to midlife. Proc Natl Acad Sci U S A. 2012;109(40):E2657-E2664.
5. Medical marijuana program physician frequently asked questions. Government of the District of Columbia Department of Health. http://doh.dc.gov/sites/default/files/dc/sites/ doh/publication/attachments/120430FAQPhysicians%20 Final.pdf. Published April 2012. Accessed March 20, 2014.
6. The role of the physician in “medical” marijuana. American Society of Addiction Medicine. http://www.asam.org/ advocacy/find-a-policy-statement/view-policy-statement/ public-policy-statements/2011/11/28/the-role-of-the-physician-in-medical-marijuana. Published April 12, 2010. Accessed March 20, 2014.

Giving a Good Needle: Resident Guide to Decreasing Injection Pain
Think back to a busy day and try to recall how many biopsies you performed. Chances are during that time you administered several dozen injections for various indications. Although we have become accustomed to performing injections through repetition, it may be the focus of many patient visits and may be the basis on which a patient judges his/her physician. There are various techniques and products available that can help decrease the physical and psychological burden of injections for patients, some that should be incorporated into a resident’s repertoire to be perfected before becoming an attending.
Factors Related to Anesthetics
The most frequently used local anesthetic in dermatology clinics is lidocaine (1% or 2%) combined with epinephrine 1:100,000. This premixed formulation relieves the burden of mixing for nurses; however, its low pH (4.2) contributes to stinging and burning with infiltration.1 Buffering with sodium bicarbonate 8.4% in a 9:1 ratio (9 parts lidocaine-epinephrine to 1 part bicarbonate) more closely matches the neutral pH in human tissues and decreases injection pain.2 Alkalinizing the anesthetic mixture also decreases the time of onset of its effects, as higher pH solutions convert lidocaine into its active unionized form. However, buffering the anesthetic does have the drawback of decreasing its shelf life, and many clinics no longer store buffered solutions for fear of spoilage. It can be useful to prepare a freshly buffered mixture prior to injecting a particularly needlephobic patient or when injecting in a difficult anatomic location.
In keeping with the philosophy that infiltrating with a solution that closely mimics physiologic parameters minimizes discomfort, a recent meta-analysis found that warming the anesthetic prior to injection led to less pain.3 In my experience, I have found that rolling the syringe between my hands prior to injection also decreases the patient’s sensation of “feeling the anesthetic going in.”
Preinjection Preparation
Properly positioning the patient is paramount to safe injection. Murphy’s Law should be anticipated, not discovered. A few moments spent adjusting the chair and lighting can pay dividends if a patient suddenly has a vasovagal episode. Unfortunately, it is difficult to predict which patients are prone to such attacks, as even a patient who may spend hours playing football in the summer heat could collapse at the sight of a needle. Aside from proper positioning of the patient, the biopsy tray should not be in the patient’s direct line of sight. Even those who tolerate the anesthesia well may become distraught at the sight of bloody gauze.
There are several options for topical anesthesia to decrease injection pain. Cream or gel preparations (ie, eutectic mixture of lidocaine and prilocaine, lidocaine cream, tetracaine gel) generally are cumbersome in a busy clinic setting, as they require at least 30 minutes of contact before anesthesia is achieved; a longer duration of exposure provides further anesthetization and may improve patient outcomes.4 However, these formulations may be useful in planned procedures. I have found much utility in utilizing ethyl chloride vapocoolant spray as a numbing agent with an immediate onset of action, a feature that makes this product useful in busy clinics.5 Ice is another excellent local coolant and is readily available in most offices at a negligible cost. Placing the ice in aluminum foil instead of a glove delivers more rapid cooling, and the ice is safe to use on areas where vapocoolant spray may be inconvenient or contraindicated, such as around the eyes, nose, ears, or mouth. Holding the ice in place for approximately 10 seconds prior to injection numbs superficial nerve endings and facilitates painless needle insertion.6
Injection Technique
Injection technique is arguably the most important factor in minimizing pain for patients and ensuring effective anesthesia in the field. It also is the factor that a patient will either praise or blame, depending on their perception of the injection.
An important point is that the initial injection should be done perpendicular to the skin. The superficial skin has the highest concentration of nerve endings, which branch repeatedly from larger stems in the deeper dermis and subcutaneous fat. Tangential injections disrupt a relatively larger number of nerve endings as the needle tracks through more superficial skin. By injecting perpendicularly, you minimize damage done during the needle’s plunge.2
Anesthetic should initially be deposited into the subcutaneous fat and continued as the needle is withdrawn. Injection directly into the dense dermis leads to pain with hydrodissection, while deeper placement is less painful due to the malleability of fat and a decreased concentration of nerve endings.7
Subsequent injections should be strategically placed. Ideally, the initial injection should be the only one that the patient feels, with widening of the anesthetic field achieved by slowly infiltrating lidocaine through skin that is already numb. The needle should be inserted into the wheal and advanced slowly with continuous pressure on the plunger; special attention should be paid to avoid advancing the needle tip past the leading edge of the wheal and into skin with intact sensation (areas of skin that have not yet been numbed by anesthesia and therefore are still capable of sensing pain from injection).8 This method of delivering anesthesia with only one initial prick experienced by the patient has been coined the “hole-in-one” technique and has proven to be not only efficacious in minimizing injection discomfort but also easy to learn, even for amateur injectors.9
Distraction Techniques
Although patients should be made aware of the injection sites and reasonable expectations should be set, distraction techniques are easy to implement and can be valuable in directing the patient’s focus away from the anticipated injection. A patient’s clothing, jewelry, and body art; reading material; and the weather are examples of topics that can be discussed as “talkesthesia.” For younger patients, various distraction techniques have been developed, ranging from basic distraction with stickers or toys to increasingly sophisticated methods such as virtual reality glasses worn during the procedure.10 In actual practice, I prefer to use available technology that is inexpensive and already familiar to the child; for instance, allowing children to watch their favorite short Web videos or play a video game during the procedure, as long as the biopsy site allows it, is an ideal adjunct to proper topical anesthesia and good injection technique. For adults, quickly plugging in their favorite musical artist to an Internet radio application also can allevi-
ate anxiety.
Several distraction techniques also can be administered directly at the injection site based on the gate control theory of pain. Tactile stimuli delivered proximal to the injection site creates sensory “noise” at the level of the spinal cord, masking the noxious sensation carried on unmyelinated C fibers.7 If you have ever hit your head on an open cabinet, for instance, the instinctual desire to immediately rub the area to reduce the pain functions on this same premise. Various tactics may be employed, including stretching or pinching the skin, rubbing, and tapping; however, I find that the major limitation to many of these methods is performing them safely. An inadvertent stick may be more likely if your fingers are dancing in the path of the needle. Generally, I like to rub the skin about 3- to 5-cm proximal to the injection site with the index finger of the supporting hand as the needle is inserted and continue while the deposit of anesthetic is placed. A potentially safer option is a small handheld massager, though concerns about sterility and durability with autoclaving may limit its use to select patients.11
Special Patient Considerations
Although we do our best to control the operator-dependent aspects of injection pain, patient factors also can complicate the administration of adequate anesthesia and occasionally can lead to unintended surprises. Patients with red hair whose characteristic locks are the result of mutations in the melanocortin 1receptor have been identified as being resistant to the effects of local anesthesia, putatively related to the role of melanocortin 1 receptor in pain modulation.12 This discovery highlights the fact that there likely are numerous undiscovered mutations that cause resistance to anesthetic agents. It further underscores the need to ensure adequate numbing by testing the patient’s level of sensation prior to beginning any procedure.
Conclusion
By keeping your patient’s comfort in mind, you will not only enhance their confidence in you as their physician but will also encourage good follow-up care and adherence to any prescribed protocols. In the future, needleless injection devices and more rapid topical anesthesia may further decrease pain associated with dermatologic procedures.13
1. Frank SG, Lalonde DH. How acidic is the lidocaine we are injecting, and how much bicarbonate should we add? Can J Plast Surg. 2012;20:71-73.
2. Zilinsky I, Bar-Meir E, Zaslansky R, et al. Ten commandments for minimal pain during administration of local anesthetics. J Drugs Dermatol. 2005;4:212-216.
3. Hogan ME, vanderVaart S, Perampaladas K, et al. Systematic review and meta-analysis of the effect of warming local anesthetics on injection pain. Ann Emerg Med. 2011;58:86-98.
4. Smith DP, Gjellum M. The efficacy of LMX versus EMLA for pain relief in boys undergoing office meatotomy. J Urol. 2004;172:1760-1761.
5. Farion KJ, Splinter KL, Newhook K, et al. The effect of vapocoolant spray on pain due to intravenous cannulation in children: a randomized controlled trial. CMAJ. 2008;179:31-36.
6. Dixit S, Lowe P, Fischer G, et al. Ice anaesthesia in procedural dermatology. Australas J Dermatol. 2013;54:273-276.
7. Strazar AR, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013;132:675-684.
8. Lalonde DH. “Hole-in-one” local anesthesia for wide-awake carpal tunnel surgery. Plast Reconstr Surg. 2010;126:1642-1644.
9. Farhangkhoee H, Lalonde J, Lalonde DH. Teaching medical students and residents how to inject local anesthesia almost painlessly. Can J Plast Surg. 2012;20:169-172.
10. Koller D, Goldman RD. Distraction techniques for children undergoing procedures: a critical review of pediatric research. J Pediatr Nurs. 2012;27:652-681.
11. Nanitsos E, Vartuli R, Forte A, et al. The effect of vibration on pain during local anaesthesia injections. Aust Dent J. 2009;54:94-100.
12. Liem EB, Joiner TV, Tsueda K, et al. Increased sensitivity to thermal pain and reduced subcutaneous lidocaine efficacy in redheads. Anesthesiol. 2005;102:509-514.
13. Patakfalvi L, Benohanian A. Needle-free anesthesia, a promising option for the needle phobic patient. Br J Dermatol. 2014;170:1191-1192.
Think back to a busy day and try to recall how many biopsies you performed. Chances are during that time you administered several dozen injections for various indications. Although we have become accustomed to performing injections through repetition, it may be the focus of many patient visits and may be the basis on which a patient judges his/her physician. There are various techniques and products available that can help decrease the physical and psychological burden of injections for patients, some that should be incorporated into a resident’s repertoire to be perfected before becoming an attending.
Factors Related to Anesthetics
The most frequently used local anesthetic in dermatology clinics is lidocaine (1% or 2%) combined with epinephrine 1:100,000. This premixed formulation relieves the burden of mixing for nurses; however, its low pH (4.2) contributes to stinging and burning with infiltration.1 Buffering with sodium bicarbonate 8.4% in a 9:1 ratio (9 parts lidocaine-epinephrine to 1 part bicarbonate) more closely matches the neutral pH in human tissues and decreases injection pain.2 Alkalinizing the anesthetic mixture also decreases the time of onset of its effects, as higher pH solutions convert lidocaine into its active unionized form. However, buffering the anesthetic does have the drawback of decreasing its shelf life, and many clinics no longer store buffered solutions for fear of spoilage. It can be useful to prepare a freshly buffered mixture prior to injecting a particularly needlephobic patient or when injecting in a difficult anatomic location.
In keeping with the philosophy that infiltrating with a solution that closely mimics physiologic parameters minimizes discomfort, a recent meta-analysis found that warming the anesthetic prior to injection led to less pain.3 In my experience, I have found that rolling the syringe between my hands prior to injection also decreases the patient’s sensation of “feeling the anesthetic going in.”
Preinjection Preparation
Properly positioning the patient is paramount to safe injection. Murphy’s Law should be anticipated, not discovered. A few moments spent adjusting the chair and lighting can pay dividends if a patient suddenly has a vasovagal episode. Unfortunately, it is difficult to predict which patients are prone to such attacks, as even a patient who may spend hours playing football in the summer heat could collapse at the sight of a needle. Aside from proper positioning of the patient, the biopsy tray should not be in the patient’s direct line of sight. Even those who tolerate the anesthesia well may become distraught at the sight of bloody gauze.
There are several options for topical anesthesia to decrease injection pain. Cream or gel preparations (ie, eutectic mixture of lidocaine and prilocaine, lidocaine cream, tetracaine gel) generally are cumbersome in a busy clinic setting, as they require at least 30 minutes of contact before anesthesia is achieved; a longer duration of exposure provides further anesthetization and may improve patient outcomes.4 However, these formulations may be useful in planned procedures. I have found much utility in utilizing ethyl chloride vapocoolant spray as a numbing agent with an immediate onset of action, a feature that makes this product useful in busy clinics.5 Ice is another excellent local coolant and is readily available in most offices at a negligible cost. Placing the ice in aluminum foil instead of a glove delivers more rapid cooling, and the ice is safe to use on areas where vapocoolant spray may be inconvenient or contraindicated, such as around the eyes, nose, ears, or mouth. Holding the ice in place for approximately 10 seconds prior to injection numbs superficial nerve endings and facilitates painless needle insertion.6
Injection Technique
Injection technique is arguably the most important factor in minimizing pain for patients and ensuring effective anesthesia in the field. It also is the factor that a patient will either praise or blame, depending on their perception of the injection.
An important point is that the initial injection should be done perpendicular to the skin. The superficial skin has the highest concentration of nerve endings, which branch repeatedly from larger stems in the deeper dermis and subcutaneous fat. Tangential injections disrupt a relatively larger number of nerve endings as the needle tracks through more superficial skin. By injecting perpendicularly, you minimize damage done during the needle’s plunge.2
Anesthetic should initially be deposited into the subcutaneous fat and continued as the needle is withdrawn. Injection directly into the dense dermis leads to pain with hydrodissection, while deeper placement is less painful due to the malleability of fat and a decreased concentration of nerve endings.7
Subsequent injections should be strategically placed. Ideally, the initial injection should be the only one that the patient feels, with widening of the anesthetic field achieved by slowly infiltrating lidocaine through skin that is already numb. The needle should be inserted into the wheal and advanced slowly with continuous pressure on the plunger; special attention should be paid to avoid advancing the needle tip past the leading edge of the wheal and into skin with intact sensation (areas of skin that have not yet been numbed by anesthesia and therefore are still capable of sensing pain from injection).8 This method of delivering anesthesia with only one initial prick experienced by the patient has been coined the “hole-in-one” technique and has proven to be not only efficacious in minimizing injection discomfort but also easy to learn, even for amateur injectors.9
Distraction Techniques
Although patients should be made aware of the injection sites and reasonable expectations should be set, distraction techniques are easy to implement and can be valuable in directing the patient’s focus away from the anticipated injection. A patient’s clothing, jewelry, and body art; reading material; and the weather are examples of topics that can be discussed as “talkesthesia.” For younger patients, various distraction techniques have been developed, ranging from basic distraction with stickers or toys to increasingly sophisticated methods such as virtual reality glasses worn during the procedure.10 In actual practice, I prefer to use available technology that is inexpensive and already familiar to the child; for instance, allowing children to watch their favorite short Web videos or play a video game during the procedure, as long as the biopsy site allows it, is an ideal adjunct to proper topical anesthesia and good injection technique. For adults, quickly plugging in their favorite musical artist to an Internet radio application also can allevi-
ate anxiety.
Several distraction techniques also can be administered directly at the injection site based on the gate control theory of pain. Tactile stimuli delivered proximal to the injection site creates sensory “noise” at the level of the spinal cord, masking the noxious sensation carried on unmyelinated C fibers.7 If you have ever hit your head on an open cabinet, for instance, the instinctual desire to immediately rub the area to reduce the pain functions on this same premise. Various tactics may be employed, including stretching or pinching the skin, rubbing, and tapping; however, I find that the major limitation to many of these methods is performing them safely. An inadvertent stick may be more likely if your fingers are dancing in the path of the needle. Generally, I like to rub the skin about 3- to 5-cm proximal to the injection site with the index finger of the supporting hand as the needle is inserted and continue while the deposit of anesthetic is placed. A potentially safer option is a small handheld massager, though concerns about sterility and durability with autoclaving may limit its use to select patients.11
Special Patient Considerations
Although we do our best to control the operator-dependent aspects of injection pain, patient factors also can complicate the administration of adequate anesthesia and occasionally can lead to unintended surprises. Patients with red hair whose characteristic locks are the result of mutations in the melanocortin 1receptor have been identified as being resistant to the effects of local anesthesia, putatively related to the role of melanocortin 1 receptor in pain modulation.12 This discovery highlights the fact that there likely are numerous undiscovered mutations that cause resistance to anesthetic agents. It further underscores the need to ensure adequate numbing by testing the patient’s level of sensation prior to beginning any procedure.
Conclusion
By keeping your patient’s comfort in mind, you will not only enhance their confidence in you as their physician but will also encourage good follow-up care and adherence to any prescribed protocols. In the future, needleless injection devices and more rapid topical anesthesia may further decrease pain associated with dermatologic procedures.13
Think back to a busy day and try to recall how many biopsies you performed. Chances are during that time you administered several dozen injections for various indications. Although we have become accustomed to performing injections through repetition, it may be the focus of many patient visits and may be the basis on which a patient judges his/her physician. There are various techniques and products available that can help decrease the physical and psychological burden of injections for patients, some that should be incorporated into a resident’s repertoire to be perfected before becoming an attending.
Factors Related to Anesthetics
The most frequently used local anesthetic in dermatology clinics is lidocaine (1% or 2%) combined with epinephrine 1:100,000. This premixed formulation relieves the burden of mixing for nurses; however, its low pH (4.2) contributes to stinging and burning with infiltration.1 Buffering with sodium bicarbonate 8.4% in a 9:1 ratio (9 parts lidocaine-epinephrine to 1 part bicarbonate) more closely matches the neutral pH in human tissues and decreases injection pain.2 Alkalinizing the anesthetic mixture also decreases the time of onset of its effects, as higher pH solutions convert lidocaine into its active unionized form. However, buffering the anesthetic does have the drawback of decreasing its shelf life, and many clinics no longer store buffered solutions for fear of spoilage. It can be useful to prepare a freshly buffered mixture prior to injecting a particularly needlephobic patient or when injecting in a difficult anatomic location.
In keeping with the philosophy that infiltrating with a solution that closely mimics physiologic parameters minimizes discomfort, a recent meta-analysis found that warming the anesthetic prior to injection led to less pain.3 In my experience, I have found that rolling the syringe between my hands prior to injection also decreases the patient’s sensation of “feeling the anesthetic going in.”
Preinjection Preparation
Properly positioning the patient is paramount to safe injection. Murphy’s Law should be anticipated, not discovered. A few moments spent adjusting the chair and lighting can pay dividends if a patient suddenly has a vasovagal episode. Unfortunately, it is difficult to predict which patients are prone to such attacks, as even a patient who may spend hours playing football in the summer heat could collapse at the sight of a needle. Aside from proper positioning of the patient, the biopsy tray should not be in the patient’s direct line of sight. Even those who tolerate the anesthesia well may become distraught at the sight of bloody gauze.
There are several options for topical anesthesia to decrease injection pain. Cream or gel preparations (ie, eutectic mixture of lidocaine and prilocaine, lidocaine cream, tetracaine gel) generally are cumbersome in a busy clinic setting, as they require at least 30 minutes of contact before anesthesia is achieved; a longer duration of exposure provides further anesthetization and may improve patient outcomes.4 However, these formulations may be useful in planned procedures. I have found much utility in utilizing ethyl chloride vapocoolant spray as a numbing agent with an immediate onset of action, a feature that makes this product useful in busy clinics.5 Ice is another excellent local coolant and is readily available in most offices at a negligible cost. Placing the ice in aluminum foil instead of a glove delivers more rapid cooling, and the ice is safe to use on areas where vapocoolant spray may be inconvenient or contraindicated, such as around the eyes, nose, ears, or mouth. Holding the ice in place for approximately 10 seconds prior to injection numbs superficial nerve endings and facilitates painless needle insertion.6
Injection Technique
Injection technique is arguably the most important factor in minimizing pain for patients and ensuring effective anesthesia in the field. It also is the factor that a patient will either praise or blame, depending on their perception of the injection.
An important point is that the initial injection should be done perpendicular to the skin. The superficial skin has the highest concentration of nerve endings, which branch repeatedly from larger stems in the deeper dermis and subcutaneous fat. Tangential injections disrupt a relatively larger number of nerve endings as the needle tracks through more superficial skin. By injecting perpendicularly, you minimize damage done during the needle’s plunge.2
Anesthetic should initially be deposited into the subcutaneous fat and continued as the needle is withdrawn. Injection directly into the dense dermis leads to pain with hydrodissection, while deeper placement is less painful due to the malleability of fat and a decreased concentration of nerve endings.7
Subsequent injections should be strategically placed. Ideally, the initial injection should be the only one that the patient feels, with widening of the anesthetic field achieved by slowly infiltrating lidocaine through skin that is already numb. The needle should be inserted into the wheal and advanced slowly with continuous pressure on the plunger; special attention should be paid to avoid advancing the needle tip past the leading edge of the wheal and into skin with intact sensation (areas of skin that have not yet been numbed by anesthesia and therefore are still capable of sensing pain from injection).8 This method of delivering anesthesia with only one initial prick experienced by the patient has been coined the “hole-in-one” technique and has proven to be not only efficacious in minimizing injection discomfort but also easy to learn, even for amateur injectors.9
Distraction Techniques
Although patients should be made aware of the injection sites and reasonable expectations should be set, distraction techniques are easy to implement and can be valuable in directing the patient’s focus away from the anticipated injection. A patient’s clothing, jewelry, and body art; reading material; and the weather are examples of topics that can be discussed as “talkesthesia.” For younger patients, various distraction techniques have been developed, ranging from basic distraction with stickers or toys to increasingly sophisticated methods such as virtual reality glasses worn during the procedure.10 In actual practice, I prefer to use available technology that is inexpensive and already familiar to the child; for instance, allowing children to watch their favorite short Web videos or play a video game during the procedure, as long as the biopsy site allows it, is an ideal adjunct to proper topical anesthesia and good injection technique. For adults, quickly plugging in their favorite musical artist to an Internet radio application also can allevi-
ate anxiety.
Several distraction techniques also can be administered directly at the injection site based on the gate control theory of pain. Tactile stimuli delivered proximal to the injection site creates sensory “noise” at the level of the spinal cord, masking the noxious sensation carried on unmyelinated C fibers.7 If you have ever hit your head on an open cabinet, for instance, the instinctual desire to immediately rub the area to reduce the pain functions on this same premise. Various tactics may be employed, including stretching or pinching the skin, rubbing, and tapping; however, I find that the major limitation to many of these methods is performing them safely. An inadvertent stick may be more likely if your fingers are dancing in the path of the needle. Generally, I like to rub the skin about 3- to 5-cm proximal to the injection site with the index finger of the supporting hand as the needle is inserted and continue while the deposit of anesthetic is placed. A potentially safer option is a small handheld massager, though concerns about sterility and durability with autoclaving may limit its use to select patients.11
Special Patient Considerations
Although we do our best to control the operator-dependent aspects of injection pain, patient factors also can complicate the administration of adequate anesthesia and occasionally can lead to unintended surprises. Patients with red hair whose characteristic locks are the result of mutations in the melanocortin 1receptor have been identified as being resistant to the effects of local anesthesia, putatively related to the role of melanocortin 1 receptor in pain modulation.12 This discovery highlights the fact that there likely are numerous undiscovered mutations that cause resistance to anesthetic agents. It further underscores the need to ensure adequate numbing by testing the patient’s level of sensation prior to beginning any procedure.
Conclusion
By keeping your patient’s comfort in mind, you will not only enhance their confidence in you as their physician but will also encourage good follow-up care and adherence to any prescribed protocols. In the future, needleless injection devices and more rapid topical anesthesia may further decrease pain associated with dermatologic procedures.13
1. Frank SG, Lalonde DH. How acidic is the lidocaine we are injecting, and how much bicarbonate should we add? Can J Plast Surg. 2012;20:71-73.
2. Zilinsky I, Bar-Meir E, Zaslansky R, et al. Ten commandments for minimal pain during administration of local anesthetics. J Drugs Dermatol. 2005;4:212-216.
3. Hogan ME, vanderVaart S, Perampaladas K, et al. Systematic review and meta-analysis of the effect of warming local anesthetics on injection pain. Ann Emerg Med. 2011;58:86-98.
4. Smith DP, Gjellum M. The efficacy of LMX versus EMLA for pain relief in boys undergoing office meatotomy. J Urol. 2004;172:1760-1761.
5. Farion KJ, Splinter KL, Newhook K, et al. The effect of vapocoolant spray on pain due to intravenous cannulation in children: a randomized controlled trial. CMAJ. 2008;179:31-36.
6. Dixit S, Lowe P, Fischer G, et al. Ice anaesthesia in procedural dermatology. Australas J Dermatol. 2013;54:273-276.
7. Strazar AR, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013;132:675-684.
8. Lalonde DH. “Hole-in-one” local anesthesia for wide-awake carpal tunnel surgery. Plast Reconstr Surg. 2010;126:1642-1644.
9. Farhangkhoee H, Lalonde J, Lalonde DH. Teaching medical students and residents how to inject local anesthesia almost painlessly. Can J Plast Surg. 2012;20:169-172.
10. Koller D, Goldman RD. Distraction techniques for children undergoing procedures: a critical review of pediatric research. J Pediatr Nurs. 2012;27:652-681.
11. Nanitsos E, Vartuli R, Forte A, et al. The effect of vibration on pain during local anaesthesia injections. Aust Dent J. 2009;54:94-100.
12. Liem EB, Joiner TV, Tsueda K, et al. Increased sensitivity to thermal pain and reduced subcutaneous lidocaine efficacy in redheads. Anesthesiol. 2005;102:509-514.
13. Patakfalvi L, Benohanian A. Needle-free anesthesia, a promising option for the needle phobic patient. Br J Dermatol. 2014;170:1191-1192.
1. Frank SG, Lalonde DH. How acidic is the lidocaine we are injecting, and how much bicarbonate should we add? Can J Plast Surg. 2012;20:71-73.
2. Zilinsky I, Bar-Meir E, Zaslansky R, et al. Ten commandments for minimal pain during administration of local anesthetics. J Drugs Dermatol. 2005;4:212-216.
3. Hogan ME, vanderVaart S, Perampaladas K, et al. Systematic review and meta-analysis of the effect of warming local anesthetics on injection pain. Ann Emerg Med. 2011;58:86-98.
4. Smith DP, Gjellum M. The efficacy of LMX versus EMLA for pain relief in boys undergoing office meatotomy. J Urol. 2004;172:1760-1761.
5. Farion KJ, Splinter KL, Newhook K, et al. The effect of vapocoolant spray on pain due to intravenous cannulation in children: a randomized controlled trial. CMAJ. 2008;179:31-36.
6. Dixit S, Lowe P, Fischer G, et al. Ice anaesthesia in procedural dermatology. Australas J Dermatol. 2013;54:273-276.
7. Strazar AR, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013;132:675-684.
8. Lalonde DH. “Hole-in-one” local anesthesia for wide-awake carpal tunnel surgery. Plast Reconstr Surg. 2010;126:1642-1644.
9. Farhangkhoee H, Lalonde J, Lalonde DH. Teaching medical students and residents how to inject local anesthesia almost painlessly. Can J Plast Surg. 2012;20:169-172.
10. Koller D, Goldman RD. Distraction techniques for children undergoing procedures: a critical review of pediatric research. J Pediatr Nurs. 2012;27:652-681.
11. Nanitsos E, Vartuli R, Forte A, et al. The effect of vibration on pain during local anaesthesia injections. Aust Dent J. 2009;54:94-100.
12. Liem EB, Joiner TV, Tsueda K, et al. Increased sensitivity to thermal pain and reduced subcutaneous lidocaine efficacy in redheads. Anesthesiol. 2005;102:509-514.
13. Patakfalvi L, Benohanian A. Needle-free anesthesia, a promising option for the needle phobic patient. Br J Dermatol. 2014;170:1191-1192.

Systemic Agents on the Horizon for Psoriasis
For more information, read Dr. Han's Resident Corner column from March 2014, "In the Pipeline for Psoriasis: Upcoming Psoriasis Treatments."
For more information, read Dr. Han's Resident Corner column from March 2014, "In the Pipeline for Psoriasis: Upcoming Psoriasis Treatments."
For more information, read Dr. Han's Resident Corner column from March 2014, "In the Pipeline for Psoriasis: Upcoming Psoriasis Treatments."