User login
The Hospitalist only
The Constant and Familiar Face
Editors’ note: “Alliances” is a series written about the relationships that hospitalists have with members of the clinical care team, from the team members’ points of view. It’s our hope that each installment of “Alliances” will provide valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
Nancy Perovic, RN, BSN, quality improvement and innovations coordinator with the hospitalist program at the University of Chicago Medical Center, says this quote from In Our Hands: How Hospital Leaders Can Build a Thriving Workforce is a statement she refers to often in her work and teaching: “Mutual respect between nurses and physicians for each other’s knowledge and competence, coupled with a mutual concern that quality patient care will be provided, are key organizational elements of work environments that attract and retain nurses.”1
In hospitals around the United States, in efforts to improve patient safety and in other initiatives including nurse recruitment and retention, one consistent element is optimizing communication among providers.2-4 Barbara Blakeney, MS, RN, president of the American Nurses Association, interviewed for the publication Web Morbidity and Mortality by its editor, hospitalist Robert Wachter, MD, says that when nurses are not properly supported in the work environment by other staff, and when there are not enough nurses, “it becomes a catch-22—the fewer nurses you have, the more difficult is the working environment, which leads to fewer nurses.”5
Blakeney recommends mutual training for physicians and nurses to improve patient care and safety focus on a number of key areas:
- Understanding and appreciating each other’s skill sets and knowledge base;
- Properly handing off patients and information; and
- Nurturing “a culture in which safety is considered a problem-solving situation and not a punishment situation.”6
“Nurses comprise the surveillance system in hospitals for errors and adverse occurrences,” emphasizes Blakeney, and “the effectiveness of nurse surveillance is influenced by factors that include the quality of the work environment.”5
As essential members of hospital teams, hospitalists play a big role in nurses’ work environments, and mutual support between hospitalists and nurses affects patient care and outcomes, and physician and nurse job satisfaction.6,7 In general, nurses give hospitalists high marks for communication, nurse support, and teamwork.
“From a communication perspective, working with hospitalists makes patient care a lot safer because you don’t have to think of everything that you need to tell attending physicians when they are making their daily rounds,” says Scarlett Blue, RNC, MSN, administrative director, Hospitalist Services for FirstHealth of the Carolinas, Pinehurst, N.C. “With hospitalists you know you can do real-time communication, real-time information. That’s not saying you can’t do that with other physicians who are not in the hospital, but it certainly does make it a lot easier when they’re right here.”
Make Contact
One way that hospitalists support their nurse colleagues is by their ready availability to answer questions about patient care. Julie Koppel, RN, BSN, patient care manager on the General Medicine floor at the University of California at San Francisco Medical Center, has worked exclusively with the hospitalist model in her five years of nursing. She is complimentary about hospitalists’ communication skills and refers to them as “the constant and familiar face.” Koppel relates an instance where the attending hospitalist was already off service and yet she still paged him. “He got back to me promptly and still addressed the issues even though he wasn’t on service anymore and it was about something that had happened a month ago. I still feel hospitalists are available when they’re not even here.”
Many nurses don’t have a second thought about calling a hospitalist about a patient care issue, but may still be afraid of “bothering” the hospitalist when he or she is busy. Blue says her colleagues have worked with their nursing staff to overcome that reluctance. “Call them because if they’re talking with a family or if they’re in the middle of a physical exam or if it’s something where they can’t talk, they’re going to put the hold button on,” she tells her staff. “So when you hear the Muzak, the elevator music, then you know that you need to call them back. And it’s worked.”
It’s especially important, Blue says, that nurses surmount any reluctance they feel to initiate a call so that they will do so easily in urgent situations such as alerting rapid response teams and reporting medical errors.4 Blue believes the following anecdote illustrates the perspective of most hospitalists about this issue.
“We just started rapid response teams here,” she says, “And I heard one of the hospitalists say, ‘We’ve had five rapid response team calls so far and we were looking at whether or not the calls met the criteria and were appropriate.’ And one of the other hospitalists said, ‘You know, this really wasn’t a rapid response team call, but I want the nurses to feel free to call and I think that when we’re first starting out, we just want them to call. And then we can work on fine tuning it later. I don’t want to stifle them so they feel they cannot call.”

—Mark Williams, MD
Clear and to the Point
What are the best means to improve communication between hospitalists and nurses? Three major areas for attention include developing relationships, defining communication strategies, and packaging information for clarity.7
Blue often advises nurses to speak with clarity. “Probably the best thing from a hospitalist’s perspective is to be real clear about what you are asking or what it is that you need,” she says. “The clearer that you can be in your requests, the better off you’re going to be in the long run.”
But, Blue says “hospitalists have to understand that one of the greatest benefits from a nurse’s perspective about the hospitalist program is access, immediate access, and dealing with a nurse who does not communicate well might sometimes come along with it.”
The mismatched communication styles of most physicians and nurses are well recognized by a committee at the University of Chicago in which Nancy Perovic is involved. Vineet Arora, MD, MA, a hospitalist and associate program director for the Internal Medicine Residency Program at the University of Chicago, is one of the three hospitalist members on a committee working to improve nurse-physician communication.
“We know that nurses and physicians communicate differently,” says Dr. Arora. “Physicians communicate in more of a task-oriented way and nurses are trained to communicate in a descriptive way. And that’s part of the problem, because nurses might report that physicians don’t respond to them when they need to be responded to; they might not prioritize a patient that the nurse believes is very sick. And a physician might say, ‘I didn’t know that patient was really sick’ because he was given a description such as, ‘They’re not doing OK.’”
Also, Dr. Arora says, “part of the problem that nurses and physicians may have in communicating with each other can be traced to a difference in how they were trained. Physicians are trained to interact with other physicians and nurses are trained by other nurses.”
The committee at Chicago has adopted what is referred to as the Situation-Background-Assessment-Recommendation (SBAR) technique, a tool that the U.S. Navy has used to improve communication on aircraft carriers.8 Developed by Michael Leonard, MD, physician coordinator of clinical informatics, and others at Kaiser Permanente of Colorado, the SBAR technique has been implemented widely at health systems to provide a standard framework for members of the healthcare team when communicating about a patient’s condition.
“What nurses are not very good at is being assertive,” says Perovic. “We’re getting better as we’re getting more modern, but sometimes nurses talk in a more holistic, narrative fashion and doctors just want: what’s the problem, pinpoint it, let me know what it is.”
Chicago’s Perovic and her colleagues plan to educate nurses to use the SBAR technique so they can “talk in the way that doctors are trained to accept information and respond,” she says. “For example, this might sound like, ‘This is this patient with this diagnosis and these vital signs; this is what’s happening: they’re going down, their blood pressure’s dropped, I’m really concerned, this is a different change, I suggest that we do this and that, and I need you here in 10 minutes.’”
Perovic says nurses are then instructed to “make a recommendation; so the hospitalist can prioritize from all the other patients he has to see, to answer the questions: What does this patient need right now? When do I need to see this patient? and What can the nurse do until I get there?”
Literature on the SBAR technique and the tool itself are available online at www.ihi.org/IHI/Topics/PatientSafety/SafetyGeneral/Tools/SBARTechniqueforCommunicationASituationalBriefingModel.htm.8
Heedful Versus Heedless Interrelating
Exactly how hospitalists affect outcomes and influence system issues is being addressed in research led by Mark V. Williams, MD, and Tracy Scott, PhD, at Emory University Medical Center, Atlanta. Dr. Williams, who is the director of the medicine unit at Emory Hospital, the editor-in-chief of the Journal of Hospital Medicine, and a past president of SHM, spoke to The Hospitalist about the exploratory research his team is doing to assess the impact hospitalists have in nurse-physician relationships in two hospitals in Atlanta, and to particularly examine how these relationships affect patient safety.
High Reliability Organization theory, which elucidates causal pathways between work relationships and reduced error, may provide a framework for how hospitalists affect hospital functioning. “Heedful interrelating,” the theory postulates, creates an organization “mind” and through facilitating teamwork is more alert to and capable of dealing with unexpected occurrences. In fact, says Dr. Williams, data from operating rooms, emergency departments, and ICUs suggest that a lack of teamwork adversely affects patient care and increases medical errors. Research along this vein has been absent on general medical floors.
The research design explores the degree of “heedful interrelating” as opposed to “heedless interrelating” between physicians and nurses and whether hospitalists have different relationships with nurses than do other physicians.
“In heedful interrelating,” explains Dr. Williams, “the physician heeds what the nurse is saying and doing and, likewise, the nurse heeds what the physician is saying and doing.” To date, the investigators have interviewed 45 nurses (half in a university hospital setting and half in a community hospital) and 24 physicians of whom half are hospitalists.
The study examines multiple components, but an example is that “heedful interrelating is based on true mutual respect, which is almost more important over agreement,” says Dr. Williams. “And in heedless interrelating, only one view of the situation is considered correct. It represents your classic arrogant physician.”
Another example of heedful interrelating is that “it advances the goals of the whole team; in heedless interrelating, you think only of your own role,” he says. Nurses in the study reported that compared with other physicians hospitalists are more accessible, more approachable, and more appreciative of the value of the nurse’s role.
The investigators conclude that hospitalists improve the nurse-physician relationship through heedful interrelating and thereby may improve patient safety. In addition, “the nurses emphasized the need for more collaboration and perceived that physicians were not proactive in asking them about their knowledge of the patient, and lacked a holistic view of the patient’s needs. Most importantly, about half the nurses mentioned specific instances where problems in their communication with physicians led directly to problems in patient care.
Dr. Williams believes that the ideal system for communication between hospitalists and nurses would include a means for them to do their patient rounds together. Nurses want hospitalists to develop a system to deliver the patient care plans quickly and reliably, include them in formal and informal educational efforts, and acknowledge them.
Timely Distribution of Care Plans
Blue says that hospitalists at her institution, FirstHealth Moore Regional Hospital (Pinehurst, N.C.), a 385-bed acute care, nonprofit hospital that serves as the referral center for a 15-county region in the mid-Carolinas, work often and closely with the nurses on issues of outcomes. “And outcomes here are like discharge planning utilization review,” she says. “We have a report every morning and there’s a representative from that department who’s online sending out the plans for the patients for the day to the other outcomes managers. That’s already in the works, and we’re not waiting for the hospitalist to get up to the floor to see the patient.”
Overall, however, nurses in other (e.g., larger) settings may not have as good a system in place to distribute care plans. Perovic says that in focus groups she facilitates, she often hears frustration from nurses because “doctors in general—although hospitalists are better at it—do not give nurses the plan of the day or the plan of care in a timely, organized fashion so they can do their care appropriately and prepare themselves and the patient.”
Some of the problem is due to the systems of an academic medical center, Perovic says, where “doctors make rounds at various times of the day and sometimes one team can make four rounds a day. What happens is that the plan for patient care changes each time new rounds are completed because you either get new information or discover you didn’t do something.” But although the team doctors are good at communicating plan modifications among themselves, she says, “what they fail to do is always communicate that well to the nurses.”
Perovic says there is an ideal and then a real solution. “Ideally, it would be great if patient rounds were at a certain time of the day every day so that the nurse can pass her meds and then be available for rounding,” she says. “You could say to nurses, ‘Rounds are between 10 and 11; take care of your patients’ needs and then be on call and ready to go to your rounds when possible.’ Or another solution is what we do in the pediatric hospital: We have a charge nurse who has no patients and she is able to round with all the teams and all the doctors and then give the individual nurse that plan for her patients.”
Hiring a charge nurse in this vein is a human resource issue, Perovic says, and an individual hospital has to decide that it wants to pay a nurse to not have patients. In that case, she says, it is an expensive but good fix. However, accommodating nurses to accompany hospitalists on rounds is logistically almost impossible. “Because if a nurse on the general medicine ward has five patients,” Perovic says, “she might have five different teams of doctors. But depending on the diagnosis of each patient, it won’t be the same team of doctors rounding on them. She might not catch A, B, and C at the same time that D and E are making their rounds. And she could be doing a blood draw on patient D when D team comes, or giving a bath to patient A when team E comes.”
Perovic and her coworkers have tried the call light method, where the doctor comes into the room, the attending presses the call light, and the nurse knows rounds are happening and to join them at that room. But that, as well as other avenues they tried, failed because neither the nurse nor the team can necessarily count on their times of availability coinciding. Still, Dr. Arora says, “we learned a lot about trying to work together and how to understand each other. And we used some of that information to continue thinking about how to best improve physician-nurse communication.”
The team at Chicago is now considering how to design and evaluate “an intervention for more of an interdisciplinary educational process where physicians and nurses would be trained on how to communicate with each other using this standard language,” says Dr. Arora. “Nurses would understand that they could potentially use the SBAR tool to communicate with physicians, and physicians would understand that the nurses need to be included in the plan for the day and would make time to incorporate nurse suggestions and input for the plan.”
Acknowledgment
In some hospital settings what has been described as a two-class system can exist for providers.9 A culture that encourages patient safety is threatened by the nature of the hierarchy or the segregation that is established, even subtly, where nurses are treated as unequals.6,9 In the hospital culture, the “invisibility of nursing” has historically been perpetuated by a number of factors, not the least of which are differences in gender and income.6 In this atmosphere, nurses are not as likely to share from their skills and knowledge. Their lack of assertiveness with hospitalists or other physicians may take its toll in many ways, including increased risks to patient outcomes and to provider morale and satisfaction.7
Linda Aiken, PhD, FAAN, FRCN, RN, the Claire M. Fagin Leadership Professor of Nursing and director of the Center for Health Outcomes and Policy Research at the University of Pennsylvania (Philadelphia), has extensively investigated the dynamics between nurses and their co-workers. “Nurse-physician relationships are one of the most important drivers of the work environment,”9 she writes. There are also data that demonstrate the association of nurse-doctor relationships on cost, lower morbidity and mortality, retention of nurses, higher quality of care, and improved hospital reimbursement and/or market share.9
In other words, “healthy nurse-physician relationships are not just a nice thing to have,” writes Dr. Aiken. “They are a competitive advantage.”
Given the association of these relationships to so many outcomes, it is unfortunate that many nurses crave greater acknowledgment for what they bring to their work. One benefit for nursing is that because hospitalists are around the hospital more than an average attending, they know the nurses better.
“As a nurse, what I need from hospitalists is for them to recognize and teach their residents and interns that the nurse is a constant player at the bedside in the hospital, with many more years of experience,” says Perovic. “Even though she doesn’t have as much medical training as a doctor or resident, she has enough clinical-nursing hospital experience. Doctors need to appreciate that nurses are experts at hospital care and bedside care, and [doctors] need to show that respect when we’re teaching our residents because we can learn a lot from the nurses, and the nurses can actually make the doctors’ lives easier.”
In a study of a multidisciplinary intervention tested on an acute inpatient medical unit, the effect of the intervention—to improve communication and collaboration—was strongest among house staff, who reported significant increases in collaborative efforts with nurses.10 This finding underlines the importance for hospitalists to serve as models to students, interns, and residents because the most effective time to learn collaborative practice is during early training when experienced nurses can assist inexperienced interns.10 Hospitalists can also consciously reject the traditional “doctor-nurse game,” whereby patterns of behavior suggest that doctors are the dominant players and nurses must defer to them.
“Ask nurses for their opinion,” advises Blue. “Treat them like an equal, which is another one of the beauties of this program, because hospitalists certainly do that. When it comes down to it, people want to be appreciated, respected, and acknowledged for their contribution.”
Blue and her team also encourage hospitalists to share with the nurses if they happen to hear news of their patients’ progress. “If we have follow-up on somebody from the primary care provider after that patient has left the hospital, for example, we try to share that with the nursing staff because they’re our patients. They’re not just my patients and they’re not your patients; they’re our patients.”
Conclusion
The quality of the nurse-hospitalist relationship is central to patient care. The methods, means, and styles of individual and team communication all influence the effectiveness of a hospital team. Retraining providers to traverse the gap of different communication styles is a way to approach the issues that exist. Mutual training for physicians and nurses, as well as training nurses to communicate in ways that more approximate how physicians communicate, will better serve patient and provider needs.
Hospitalists can encourage nurses to overcome hesitancies to initiate calls, clarify their preferences for how nurses should contact them, and work with nurses to seek workable ways to perform patient rounds in concert. Most of all, nurses need timely care plan distribution and acknowledgment for their contributions to teamwork and patient care. TH
Writer Andrea Sattinger will write about occupational therapists’ experiences with hospitalists in the January issue.
References
- ANA Commission on Workforce for Hospitals and Health Systems. In our hands: how hospital leaders can build a thriving workforce. American Hospital Association; Chicago; 2002;55:30-31.
- Aiken LH. The unfinished patient safety agenda. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web: Agency for Healthcare Research and Quality; 2005. Accessed August. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=7&searchStr=The+unfinished+patient+safety+agenda
- Aiken LH, Clarke SP, Sloane DM. International Hospital Outcomes Research Consortium. Hospital staffing, organization, and quality of care: cross-national findings. Int J Qual Health Care. 2002;14:5-13.
- Friesen MA, Farquhar MB, Hughes R. The nurse’s role in promoting a culture of safety: American Nurses Association Continuing Education, Center for American Nurses; 2005.
- Wachter R. In conversation with … Barbara A. Blakeney, MS, RN. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web. Agency for Healthcare Research and Quality; 2005. Accessed Aug. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=8&searchStr=Blakeney
- Lindeke LL, Sieckert AM. Nurse-physician workplace collaboration. Online J Issues Nurs. 2005;10:5.
- Burke M, Boal J, Mitchell R. Communicating for better care: improving nurse-physician communication. Am J Nurs. 2004;104:40-47
- SBAR initiative to improve staff communication. Healthcare Benchmarks Qual Improv. 2005;12:40-41.
- Smith AP. Partners at the bedside: the importance of nurse-physician relationships. Nurs Econ. 2004;22:161-164.
- Vazirani S, Hays RD, Shapiro MF, et al. Effect of a multidisciplinary intervention on communication and collaboration among physicians and nurses. Am J Crit Care. 2005;14:71-77.
Editors’ note: “Alliances” is a series written about the relationships that hospitalists have with members of the clinical care team, from the team members’ points of view. It’s our hope that each installment of “Alliances” will provide valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
Nancy Perovic, RN, BSN, quality improvement and innovations coordinator with the hospitalist program at the University of Chicago Medical Center, says this quote from In Our Hands: How Hospital Leaders Can Build a Thriving Workforce is a statement she refers to often in her work and teaching: “Mutual respect between nurses and physicians for each other’s knowledge and competence, coupled with a mutual concern that quality patient care will be provided, are key organizational elements of work environments that attract and retain nurses.”1
In hospitals around the United States, in efforts to improve patient safety and in other initiatives including nurse recruitment and retention, one consistent element is optimizing communication among providers.2-4 Barbara Blakeney, MS, RN, president of the American Nurses Association, interviewed for the publication Web Morbidity and Mortality by its editor, hospitalist Robert Wachter, MD, says that when nurses are not properly supported in the work environment by other staff, and when there are not enough nurses, “it becomes a catch-22—the fewer nurses you have, the more difficult is the working environment, which leads to fewer nurses.”5
Blakeney recommends mutual training for physicians and nurses to improve patient care and safety focus on a number of key areas:
- Understanding and appreciating each other’s skill sets and knowledge base;
- Properly handing off patients and information; and
- Nurturing “a culture in which safety is considered a problem-solving situation and not a punishment situation.”6
“Nurses comprise the surveillance system in hospitals for errors and adverse occurrences,” emphasizes Blakeney, and “the effectiveness of nurse surveillance is influenced by factors that include the quality of the work environment.”5
As essential members of hospital teams, hospitalists play a big role in nurses’ work environments, and mutual support between hospitalists and nurses affects patient care and outcomes, and physician and nurse job satisfaction.6,7 In general, nurses give hospitalists high marks for communication, nurse support, and teamwork.
“From a communication perspective, working with hospitalists makes patient care a lot safer because you don’t have to think of everything that you need to tell attending physicians when they are making their daily rounds,” says Scarlett Blue, RNC, MSN, administrative director, Hospitalist Services for FirstHealth of the Carolinas, Pinehurst, N.C. “With hospitalists you know you can do real-time communication, real-time information. That’s not saying you can’t do that with other physicians who are not in the hospital, but it certainly does make it a lot easier when they’re right here.”
Make Contact
One way that hospitalists support their nurse colleagues is by their ready availability to answer questions about patient care. Julie Koppel, RN, BSN, patient care manager on the General Medicine floor at the University of California at San Francisco Medical Center, has worked exclusively with the hospitalist model in her five years of nursing. She is complimentary about hospitalists’ communication skills and refers to them as “the constant and familiar face.” Koppel relates an instance where the attending hospitalist was already off service and yet she still paged him. “He got back to me promptly and still addressed the issues even though he wasn’t on service anymore and it was about something that had happened a month ago. I still feel hospitalists are available when they’re not even here.”
Many nurses don’t have a second thought about calling a hospitalist about a patient care issue, but may still be afraid of “bothering” the hospitalist when he or she is busy. Blue says her colleagues have worked with their nursing staff to overcome that reluctance. “Call them because if they’re talking with a family or if they’re in the middle of a physical exam or if it’s something where they can’t talk, they’re going to put the hold button on,” she tells her staff. “So when you hear the Muzak, the elevator music, then you know that you need to call them back. And it’s worked.”
It’s especially important, Blue says, that nurses surmount any reluctance they feel to initiate a call so that they will do so easily in urgent situations such as alerting rapid response teams and reporting medical errors.4 Blue believes the following anecdote illustrates the perspective of most hospitalists about this issue.
“We just started rapid response teams here,” she says, “And I heard one of the hospitalists say, ‘We’ve had five rapid response team calls so far and we were looking at whether or not the calls met the criteria and were appropriate.’ And one of the other hospitalists said, ‘You know, this really wasn’t a rapid response team call, but I want the nurses to feel free to call and I think that when we’re first starting out, we just want them to call. And then we can work on fine tuning it later. I don’t want to stifle them so they feel they cannot call.”
—Mark Williams, MD
Clear and to the Point
What are the best means to improve communication between hospitalists and nurses? Three major areas for attention include developing relationships, defining communication strategies, and packaging information for clarity.7
Blue often advises nurses to speak with clarity. “Probably the best thing from a hospitalist’s perspective is to be real clear about what you are asking or what it is that you need,” she says. “The clearer that you can be in your requests, the better off you’re going to be in the long run.”
But, Blue says “hospitalists have to understand that one of the greatest benefits from a nurse’s perspective about the hospitalist program is access, immediate access, and dealing with a nurse who does not communicate well might sometimes come along with it.”
The mismatched communication styles of most physicians and nurses are well recognized by a committee at the University of Chicago in which Nancy Perovic is involved. Vineet Arora, MD, MA, a hospitalist and associate program director for the Internal Medicine Residency Program at the University of Chicago, is one of the three hospitalist members on a committee working to improve nurse-physician communication.
“We know that nurses and physicians communicate differently,” says Dr. Arora. “Physicians communicate in more of a task-oriented way and nurses are trained to communicate in a descriptive way. And that’s part of the problem, because nurses might report that physicians don’t respond to them when they need to be responded to; they might not prioritize a patient that the nurse believes is very sick. And a physician might say, ‘I didn’t know that patient was really sick’ because he was given a description such as, ‘They’re not doing OK.’”
Also, Dr. Arora says, “part of the problem that nurses and physicians may have in communicating with each other can be traced to a difference in how they were trained. Physicians are trained to interact with other physicians and nurses are trained by other nurses.”
The committee at Chicago has adopted what is referred to as the Situation-Background-Assessment-Recommendation (SBAR) technique, a tool that the U.S. Navy has used to improve communication on aircraft carriers.8 Developed by Michael Leonard, MD, physician coordinator of clinical informatics, and others at Kaiser Permanente of Colorado, the SBAR technique has been implemented widely at health systems to provide a standard framework for members of the healthcare team when communicating about a patient’s condition.
“What nurses are not very good at is being assertive,” says Perovic. “We’re getting better as we’re getting more modern, but sometimes nurses talk in a more holistic, narrative fashion and doctors just want: what’s the problem, pinpoint it, let me know what it is.”
Chicago’s Perovic and her colleagues plan to educate nurses to use the SBAR technique so they can “talk in the way that doctors are trained to accept information and respond,” she says. “For example, this might sound like, ‘This is this patient with this diagnosis and these vital signs; this is what’s happening: they’re going down, their blood pressure’s dropped, I’m really concerned, this is a different change, I suggest that we do this and that, and I need you here in 10 minutes.’”
Perovic says nurses are then instructed to “make a recommendation; so the hospitalist can prioritize from all the other patients he has to see, to answer the questions: What does this patient need right now? When do I need to see this patient? and What can the nurse do until I get there?”
Literature on the SBAR technique and the tool itself are available online at www.ihi.org/IHI/Topics/PatientSafety/SafetyGeneral/Tools/SBARTechniqueforCommunicationASituationalBriefingModel.htm.8
Heedful Versus Heedless Interrelating
Exactly how hospitalists affect outcomes and influence system issues is being addressed in research led by Mark V. Williams, MD, and Tracy Scott, PhD, at Emory University Medical Center, Atlanta. Dr. Williams, who is the director of the medicine unit at Emory Hospital, the editor-in-chief of the Journal of Hospital Medicine, and a past president of SHM, spoke to The Hospitalist about the exploratory research his team is doing to assess the impact hospitalists have in nurse-physician relationships in two hospitals in Atlanta, and to particularly examine how these relationships affect patient safety.
High Reliability Organization theory, which elucidates causal pathways between work relationships and reduced error, may provide a framework for how hospitalists affect hospital functioning. “Heedful interrelating,” the theory postulates, creates an organization “mind” and through facilitating teamwork is more alert to and capable of dealing with unexpected occurrences. In fact, says Dr. Williams, data from operating rooms, emergency departments, and ICUs suggest that a lack of teamwork adversely affects patient care and increases medical errors. Research along this vein has been absent on general medical floors.
The research design explores the degree of “heedful interrelating” as opposed to “heedless interrelating” between physicians and nurses and whether hospitalists have different relationships with nurses than do other physicians.
“In heedful interrelating,” explains Dr. Williams, “the physician heeds what the nurse is saying and doing and, likewise, the nurse heeds what the physician is saying and doing.” To date, the investigators have interviewed 45 nurses (half in a university hospital setting and half in a community hospital) and 24 physicians of whom half are hospitalists.
The study examines multiple components, but an example is that “heedful interrelating is based on true mutual respect, which is almost more important over agreement,” says Dr. Williams. “And in heedless interrelating, only one view of the situation is considered correct. It represents your classic arrogant physician.”
Another example of heedful interrelating is that “it advances the goals of the whole team; in heedless interrelating, you think only of your own role,” he says. Nurses in the study reported that compared with other physicians hospitalists are more accessible, more approachable, and more appreciative of the value of the nurse’s role.
The investigators conclude that hospitalists improve the nurse-physician relationship through heedful interrelating and thereby may improve patient safety. In addition, “the nurses emphasized the need for more collaboration and perceived that physicians were not proactive in asking them about their knowledge of the patient, and lacked a holistic view of the patient’s needs. Most importantly, about half the nurses mentioned specific instances where problems in their communication with physicians led directly to problems in patient care.
Dr. Williams believes that the ideal system for communication between hospitalists and nurses would include a means for them to do their patient rounds together. Nurses want hospitalists to develop a system to deliver the patient care plans quickly and reliably, include them in formal and informal educational efforts, and acknowledge them.
Timely Distribution of Care Plans
Blue says that hospitalists at her institution, FirstHealth Moore Regional Hospital (Pinehurst, N.C.), a 385-bed acute care, nonprofit hospital that serves as the referral center for a 15-county region in the mid-Carolinas, work often and closely with the nurses on issues of outcomes. “And outcomes here are like discharge planning utilization review,” she says. “We have a report every morning and there’s a representative from that department who’s online sending out the plans for the patients for the day to the other outcomes managers. That’s already in the works, and we’re not waiting for the hospitalist to get up to the floor to see the patient.”
Overall, however, nurses in other (e.g., larger) settings may not have as good a system in place to distribute care plans. Perovic says that in focus groups she facilitates, she often hears frustration from nurses because “doctors in general—although hospitalists are better at it—do not give nurses the plan of the day or the plan of care in a timely, organized fashion so they can do their care appropriately and prepare themselves and the patient.”
Some of the problem is due to the systems of an academic medical center, Perovic says, where “doctors make rounds at various times of the day and sometimes one team can make four rounds a day. What happens is that the plan for patient care changes each time new rounds are completed because you either get new information or discover you didn’t do something.” But although the team doctors are good at communicating plan modifications among themselves, she says, “what they fail to do is always communicate that well to the nurses.”
Perovic says there is an ideal and then a real solution. “Ideally, it would be great if patient rounds were at a certain time of the day every day so that the nurse can pass her meds and then be available for rounding,” she says. “You could say to nurses, ‘Rounds are between 10 and 11; take care of your patients’ needs and then be on call and ready to go to your rounds when possible.’ Or another solution is what we do in the pediatric hospital: We have a charge nurse who has no patients and she is able to round with all the teams and all the doctors and then give the individual nurse that plan for her patients.”
Hiring a charge nurse in this vein is a human resource issue, Perovic says, and an individual hospital has to decide that it wants to pay a nurse to not have patients. In that case, she says, it is an expensive but good fix. However, accommodating nurses to accompany hospitalists on rounds is logistically almost impossible. “Because if a nurse on the general medicine ward has five patients,” Perovic says, “she might have five different teams of doctors. But depending on the diagnosis of each patient, it won’t be the same team of doctors rounding on them. She might not catch A, B, and C at the same time that D and E are making their rounds. And she could be doing a blood draw on patient D when D team comes, or giving a bath to patient A when team E comes.”
Perovic and her coworkers have tried the call light method, where the doctor comes into the room, the attending presses the call light, and the nurse knows rounds are happening and to join them at that room. But that, as well as other avenues they tried, failed because neither the nurse nor the team can necessarily count on their times of availability coinciding. Still, Dr. Arora says, “we learned a lot about trying to work together and how to understand each other. And we used some of that information to continue thinking about how to best improve physician-nurse communication.”
The team at Chicago is now considering how to design and evaluate “an intervention for more of an interdisciplinary educational process where physicians and nurses would be trained on how to communicate with each other using this standard language,” says Dr. Arora. “Nurses would understand that they could potentially use the SBAR tool to communicate with physicians, and physicians would understand that the nurses need to be included in the plan for the day and would make time to incorporate nurse suggestions and input for the plan.”
Acknowledgment
In some hospital settings what has been described as a two-class system can exist for providers.9 A culture that encourages patient safety is threatened by the nature of the hierarchy or the segregation that is established, even subtly, where nurses are treated as unequals.6,9 In the hospital culture, the “invisibility of nursing” has historically been perpetuated by a number of factors, not the least of which are differences in gender and income.6 In this atmosphere, nurses are not as likely to share from their skills and knowledge. Their lack of assertiveness with hospitalists or other physicians may take its toll in many ways, including increased risks to patient outcomes and to provider morale and satisfaction.7
Linda Aiken, PhD, FAAN, FRCN, RN, the Claire M. Fagin Leadership Professor of Nursing and director of the Center for Health Outcomes and Policy Research at the University of Pennsylvania (Philadelphia), has extensively investigated the dynamics between nurses and their co-workers. “Nurse-physician relationships are one of the most important drivers of the work environment,”9 she writes. There are also data that demonstrate the association of nurse-doctor relationships on cost, lower morbidity and mortality, retention of nurses, higher quality of care, and improved hospital reimbursement and/or market share.9
In other words, “healthy nurse-physician relationships are not just a nice thing to have,” writes Dr. Aiken. “They are a competitive advantage.”
Given the association of these relationships to so many outcomes, it is unfortunate that many nurses crave greater acknowledgment for what they bring to their work. One benefit for nursing is that because hospitalists are around the hospital more than an average attending, they know the nurses better.
“As a nurse, what I need from hospitalists is for them to recognize and teach their residents and interns that the nurse is a constant player at the bedside in the hospital, with many more years of experience,” says Perovic. “Even though she doesn’t have as much medical training as a doctor or resident, she has enough clinical-nursing hospital experience. Doctors need to appreciate that nurses are experts at hospital care and bedside care, and [doctors] need to show that respect when we’re teaching our residents because we can learn a lot from the nurses, and the nurses can actually make the doctors’ lives easier.”
In a study of a multidisciplinary intervention tested on an acute inpatient medical unit, the effect of the intervention—to improve communication and collaboration—was strongest among house staff, who reported significant increases in collaborative efforts with nurses.10 This finding underlines the importance for hospitalists to serve as models to students, interns, and residents because the most effective time to learn collaborative practice is during early training when experienced nurses can assist inexperienced interns.10 Hospitalists can also consciously reject the traditional “doctor-nurse game,” whereby patterns of behavior suggest that doctors are the dominant players and nurses must defer to them.
“Ask nurses for their opinion,” advises Blue. “Treat them like an equal, which is another one of the beauties of this program, because hospitalists certainly do that. When it comes down to it, people want to be appreciated, respected, and acknowledged for their contribution.”
Blue and her team also encourage hospitalists to share with the nurses if they happen to hear news of their patients’ progress. “If we have follow-up on somebody from the primary care provider after that patient has left the hospital, for example, we try to share that with the nursing staff because they’re our patients. They’re not just my patients and they’re not your patients; they’re our patients.”
Conclusion
The quality of the nurse-hospitalist relationship is central to patient care. The methods, means, and styles of individual and team communication all influence the effectiveness of a hospital team. Retraining providers to traverse the gap of different communication styles is a way to approach the issues that exist. Mutual training for physicians and nurses, as well as training nurses to communicate in ways that more approximate how physicians communicate, will better serve patient and provider needs.
Hospitalists can encourage nurses to overcome hesitancies to initiate calls, clarify their preferences for how nurses should contact them, and work with nurses to seek workable ways to perform patient rounds in concert. Most of all, nurses need timely care plan distribution and acknowledgment for their contributions to teamwork and patient care. TH
Writer Andrea Sattinger will write about occupational therapists’ experiences with hospitalists in the January issue.
References
- ANA Commission on Workforce for Hospitals and Health Systems. In our hands: how hospital leaders can build a thriving workforce. American Hospital Association; Chicago; 2002;55:30-31.
- Aiken LH. The unfinished patient safety agenda. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web: Agency for Healthcare Research and Quality; 2005. Accessed August. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=7&searchStr=The+unfinished+patient+safety+agenda
- Aiken LH, Clarke SP, Sloane DM. International Hospital Outcomes Research Consortium. Hospital staffing, organization, and quality of care: cross-national findings. Int J Qual Health Care. 2002;14:5-13.
- Friesen MA, Farquhar MB, Hughes R. The nurse’s role in promoting a culture of safety: American Nurses Association Continuing Education, Center for American Nurses; 2005.
- Wachter R. In conversation with … Barbara A. Blakeney, MS, RN. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web. Agency for Healthcare Research and Quality; 2005. Accessed Aug. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=8&searchStr=Blakeney
- Lindeke LL, Sieckert AM. Nurse-physician workplace collaboration. Online J Issues Nurs. 2005;10:5.
- Burke M, Boal J, Mitchell R. Communicating for better care: improving nurse-physician communication. Am J Nurs. 2004;104:40-47
- SBAR initiative to improve staff communication. Healthcare Benchmarks Qual Improv. 2005;12:40-41.
- Smith AP. Partners at the bedside: the importance of nurse-physician relationships. Nurs Econ. 2004;22:161-164.
- Vazirani S, Hays RD, Shapiro MF, et al. Effect of a multidisciplinary intervention on communication and collaboration among physicians and nurses. Am J Crit Care. 2005;14:71-77.
Editors’ note: “Alliances” is a series written about the relationships that hospitalists have with members of the clinical care team, from the team members’ points of view. It’s our hope that each installment of “Alliances” will provide valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
Nancy Perovic, RN, BSN, quality improvement and innovations coordinator with the hospitalist program at the University of Chicago Medical Center, says this quote from In Our Hands: How Hospital Leaders Can Build a Thriving Workforce is a statement she refers to often in her work and teaching: “Mutual respect between nurses and physicians for each other’s knowledge and competence, coupled with a mutual concern that quality patient care will be provided, are key organizational elements of work environments that attract and retain nurses.”1
In hospitals around the United States, in efforts to improve patient safety and in other initiatives including nurse recruitment and retention, one consistent element is optimizing communication among providers.2-4 Barbara Blakeney, MS, RN, president of the American Nurses Association, interviewed for the publication Web Morbidity and Mortality by its editor, hospitalist Robert Wachter, MD, says that when nurses are not properly supported in the work environment by other staff, and when there are not enough nurses, “it becomes a catch-22—the fewer nurses you have, the more difficult is the working environment, which leads to fewer nurses.”5
Blakeney recommends mutual training for physicians and nurses to improve patient care and safety focus on a number of key areas:
- Understanding and appreciating each other’s skill sets and knowledge base;
- Properly handing off patients and information; and
- Nurturing “a culture in which safety is considered a problem-solving situation and not a punishment situation.”6
“Nurses comprise the surveillance system in hospitals for errors and adverse occurrences,” emphasizes Blakeney, and “the effectiveness of nurse surveillance is influenced by factors that include the quality of the work environment.”5
As essential members of hospital teams, hospitalists play a big role in nurses’ work environments, and mutual support between hospitalists and nurses affects patient care and outcomes, and physician and nurse job satisfaction.6,7 In general, nurses give hospitalists high marks for communication, nurse support, and teamwork.
“From a communication perspective, working with hospitalists makes patient care a lot safer because you don’t have to think of everything that you need to tell attending physicians when they are making their daily rounds,” says Scarlett Blue, RNC, MSN, administrative director, Hospitalist Services for FirstHealth of the Carolinas, Pinehurst, N.C. “With hospitalists you know you can do real-time communication, real-time information. That’s not saying you can’t do that with other physicians who are not in the hospital, but it certainly does make it a lot easier when they’re right here.”
Make Contact
One way that hospitalists support their nurse colleagues is by their ready availability to answer questions about patient care. Julie Koppel, RN, BSN, patient care manager on the General Medicine floor at the University of California at San Francisco Medical Center, has worked exclusively with the hospitalist model in her five years of nursing. She is complimentary about hospitalists’ communication skills and refers to them as “the constant and familiar face.” Koppel relates an instance where the attending hospitalist was already off service and yet she still paged him. “He got back to me promptly and still addressed the issues even though he wasn’t on service anymore and it was about something that had happened a month ago. I still feel hospitalists are available when they’re not even here.”
Many nurses don’t have a second thought about calling a hospitalist about a patient care issue, but may still be afraid of “bothering” the hospitalist when he or she is busy. Blue says her colleagues have worked with their nursing staff to overcome that reluctance. “Call them because if they’re talking with a family or if they’re in the middle of a physical exam or if it’s something where they can’t talk, they’re going to put the hold button on,” she tells her staff. “So when you hear the Muzak, the elevator music, then you know that you need to call them back. And it’s worked.”
It’s especially important, Blue says, that nurses surmount any reluctance they feel to initiate a call so that they will do so easily in urgent situations such as alerting rapid response teams and reporting medical errors.4 Blue believes the following anecdote illustrates the perspective of most hospitalists about this issue.
“We just started rapid response teams here,” she says, “And I heard one of the hospitalists say, ‘We’ve had five rapid response team calls so far and we were looking at whether or not the calls met the criteria and were appropriate.’ And one of the other hospitalists said, ‘You know, this really wasn’t a rapid response team call, but I want the nurses to feel free to call and I think that when we’re first starting out, we just want them to call. And then we can work on fine tuning it later. I don’t want to stifle them so they feel they cannot call.”
—Mark Williams, MD
Clear and to the Point
What are the best means to improve communication between hospitalists and nurses? Three major areas for attention include developing relationships, defining communication strategies, and packaging information for clarity.7
Blue often advises nurses to speak with clarity. “Probably the best thing from a hospitalist’s perspective is to be real clear about what you are asking or what it is that you need,” she says. “The clearer that you can be in your requests, the better off you’re going to be in the long run.”
But, Blue says “hospitalists have to understand that one of the greatest benefits from a nurse’s perspective about the hospitalist program is access, immediate access, and dealing with a nurse who does not communicate well might sometimes come along with it.”
The mismatched communication styles of most physicians and nurses are well recognized by a committee at the University of Chicago in which Nancy Perovic is involved. Vineet Arora, MD, MA, a hospitalist and associate program director for the Internal Medicine Residency Program at the University of Chicago, is one of the three hospitalist members on a committee working to improve nurse-physician communication.
“We know that nurses and physicians communicate differently,” says Dr. Arora. “Physicians communicate in more of a task-oriented way and nurses are trained to communicate in a descriptive way. And that’s part of the problem, because nurses might report that physicians don’t respond to them when they need to be responded to; they might not prioritize a patient that the nurse believes is very sick. And a physician might say, ‘I didn’t know that patient was really sick’ because he was given a description such as, ‘They’re not doing OK.’”
Also, Dr. Arora says, “part of the problem that nurses and physicians may have in communicating with each other can be traced to a difference in how they were trained. Physicians are trained to interact with other physicians and nurses are trained by other nurses.”
The committee at Chicago has adopted what is referred to as the Situation-Background-Assessment-Recommendation (SBAR) technique, a tool that the U.S. Navy has used to improve communication on aircraft carriers.8 Developed by Michael Leonard, MD, physician coordinator of clinical informatics, and others at Kaiser Permanente of Colorado, the SBAR technique has been implemented widely at health systems to provide a standard framework for members of the healthcare team when communicating about a patient’s condition.
“What nurses are not very good at is being assertive,” says Perovic. “We’re getting better as we’re getting more modern, but sometimes nurses talk in a more holistic, narrative fashion and doctors just want: what’s the problem, pinpoint it, let me know what it is.”
Chicago’s Perovic and her colleagues plan to educate nurses to use the SBAR technique so they can “talk in the way that doctors are trained to accept information and respond,” she says. “For example, this might sound like, ‘This is this patient with this diagnosis and these vital signs; this is what’s happening: they’re going down, their blood pressure’s dropped, I’m really concerned, this is a different change, I suggest that we do this and that, and I need you here in 10 minutes.’”
Perovic says nurses are then instructed to “make a recommendation; so the hospitalist can prioritize from all the other patients he has to see, to answer the questions: What does this patient need right now? When do I need to see this patient? and What can the nurse do until I get there?”
Literature on the SBAR technique and the tool itself are available online at www.ihi.org/IHI/Topics/PatientSafety/SafetyGeneral/Tools/SBARTechniqueforCommunicationASituationalBriefingModel.htm.8
Heedful Versus Heedless Interrelating
Exactly how hospitalists affect outcomes and influence system issues is being addressed in research led by Mark V. Williams, MD, and Tracy Scott, PhD, at Emory University Medical Center, Atlanta. Dr. Williams, who is the director of the medicine unit at Emory Hospital, the editor-in-chief of the Journal of Hospital Medicine, and a past president of SHM, spoke to The Hospitalist about the exploratory research his team is doing to assess the impact hospitalists have in nurse-physician relationships in two hospitals in Atlanta, and to particularly examine how these relationships affect patient safety.
High Reliability Organization theory, which elucidates causal pathways between work relationships and reduced error, may provide a framework for how hospitalists affect hospital functioning. “Heedful interrelating,” the theory postulates, creates an organization “mind” and through facilitating teamwork is more alert to and capable of dealing with unexpected occurrences. In fact, says Dr. Williams, data from operating rooms, emergency departments, and ICUs suggest that a lack of teamwork adversely affects patient care and increases medical errors. Research along this vein has been absent on general medical floors.
The research design explores the degree of “heedful interrelating” as opposed to “heedless interrelating” between physicians and nurses and whether hospitalists have different relationships with nurses than do other physicians.
“In heedful interrelating,” explains Dr. Williams, “the physician heeds what the nurse is saying and doing and, likewise, the nurse heeds what the physician is saying and doing.” To date, the investigators have interviewed 45 nurses (half in a university hospital setting and half in a community hospital) and 24 physicians of whom half are hospitalists.
The study examines multiple components, but an example is that “heedful interrelating is based on true mutual respect, which is almost more important over agreement,” says Dr. Williams. “And in heedless interrelating, only one view of the situation is considered correct. It represents your classic arrogant physician.”
Another example of heedful interrelating is that “it advances the goals of the whole team; in heedless interrelating, you think only of your own role,” he says. Nurses in the study reported that compared with other physicians hospitalists are more accessible, more approachable, and more appreciative of the value of the nurse’s role.
The investigators conclude that hospitalists improve the nurse-physician relationship through heedful interrelating and thereby may improve patient safety. In addition, “the nurses emphasized the need for more collaboration and perceived that physicians were not proactive in asking them about their knowledge of the patient, and lacked a holistic view of the patient’s needs. Most importantly, about half the nurses mentioned specific instances where problems in their communication with physicians led directly to problems in patient care.
Dr. Williams believes that the ideal system for communication between hospitalists and nurses would include a means for them to do their patient rounds together. Nurses want hospitalists to develop a system to deliver the patient care plans quickly and reliably, include them in formal and informal educational efforts, and acknowledge them.
Timely Distribution of Care Plans
Blue says that hospitalists at her institution, FirstHealth Moore Regional Hospital (Pinehurst, N.C.), a 385-bed acute care, nonprofit hospital that serves as the referral center for a 15-county region in the mid-Carolinas, work often and closely with the nurses on issues of outcomes. “And outcomes here are like discharge planning utilization review,” she says. “We have a report every morning and there’s a representative from that department who’s online sending out the plans for the patients for the day to the other outcomes managers. That’s already in the works, and we’re not waiting for the hospitalist to get up to the floor to see the patient.”
Overall, however, nurses in other (e.g., larger) settings may not have as good a system in place to distribute care plans. Perovic says that in focus groups she facilitates, she often hears frustration from nurses because “doctors in general—although hospitalists are better at it—do not give nurses the plan of the day or the plan of care in a timely, organized fashion so they can do their care appropriately and prepare themselves and the patient.”
Some of the problem is due to the systems of an academic medical center, Perovic says, where “doctors make rounds at various times of the day and sometimes one team can make four rounds a day. What happens is that the plan for patient care changes each time new rounds are completed because you either get new information or discover you didn’t do something.” But although the team doctors are good at communicating plan modifications among themselves, she says, “what they fail to do is always communicate that well to the nurses.”
Perovic says there is an ideal and then a real solution. “Ideally, it would be great if patient rounds were at a certain time of the day every day so that the nurse can pass her meds and then be available for rounding,” she says. “You could say to nurses, ‘Rounds are between 10 and 11; take care of your patients’ needs and then be on call and ready to go to your rounds when possible.’ Or another solution is what we do in the pediatric hospital: We have a charge nurse who has no patients and she is able to round with all the teams and all the doctors and then give the individual nurse that plan for her patients.”
Hiring a charge nurse in this vein is a human resource issue, Perovic says, and an individual hospital has to decide that it wants to pay a nurse to not have patients. In that case, she says, it is an expensive but good fix. However, accommodating nurses to accompany hospitalists on rounds is logistically almost impossible. “Because if a nurse on the general medicine ward has five patients,” Perovic says, “she might have five different teams of doctors. But depending on the diagnosis of each patient, it won’t be the same team of doctors rounding on them. She might not catch A, B, and C at the same time that D and E are making their rounds. And she could be doing a blood draw on patient D when D team comes, or giving a bath to patient A when team E comes.”
Perovic and her coworkers have tried the call light method, where the doctor comes into the room, the attending presses the call light, and the nurse knows rounds are happening and to join them at that room. But that, as well as other avenues they tried, failed because neither the nurse nor the team can necessarily count on their times of availability coinciding. Still, Dr. Arora says, “we learned a lot about trying to work together and how to understand each other. And we used some of that information to continue thinking about how to best improve physician-nurse communication.”
The team at Chicago is now considering how to design and evaluate “an intervention for more of an interdisciplinary educational process where physicians and nurses would be trained on how to communicate with each other using this standard language,” says Dr. Arora. “Nurses would understand that they could potentially use the SBAR tool to communicate with physicians, and physicians would understand that the nurses need to be included in the plan for the day and would make time to incorporate nurse suggestions and input for the plan.”
Acknowledgment
In some hospital settings what has been described as a two-class system can exist for providers.9 A culture that encourages patient safety is threatened by the nature of the hierarchy or the segregation that is established, even subtly, where nurses are treated as unequals.6,9 In the hospital culture, the “invisibility of nursing” has historically been perpetuated by a number of factors, not the least of which are differences in gender and income.6 In this atmosphere, nurses are not as likely to share from their skills and knowledge. Their lack of assertiveness with hospitalists or other physicians may take its toll in many ways, including increased risks to patient outcomes and to provider morale and satisfaction.7
Linda Aiken, PhD, FAAN, FRCN, RN, the Claire M. Fagin Leadership Professor of Nursing and director of the Center for Health Outcomes and Policy Research at the University of Pennsylvania (Philadelphia), has extensively investigated the dynamics between nurses and their co-workers. “Nurse-physician relationships are one of the most important drivers of the work environment,”9 she writes. There are also data that demonstrate the association of nurse-doctor relationships on cost, lower morbidity and mortality, retention of nurses, higher quality of care, and improved hospital reimbursement and/or market share.9
In other words, “healthy nurse-physician relationships are not just a nice thing to have,” writes Dr. Aiken. “They are a competitive advantage.”
Given the association of these relationships to so many outcomes, it is unfortunate that many nurses crave greater acknowledgment for what they bring to their work. One benefit for nursing is that because hospitalists are around the hospital more than an average attending, they know the nurses better.
“As a nurse, what I need from hospitalists is for them to recognize and teach their residents and interns that the nurse is a constant player at the bedside in the hospital, with many more years of experience,” says Perovic. “Even though she doesn’t have as much medical training as a doctor or resident, she has enough clinical-nursing hospital experience. Doctors need to appreciate that nurses are experts at hospital care and bedside care, and [doctors] need to show that respect when we’re teaching our residents because we can learn a lot from the nurses, and the nurses can actually make the doctors’ lives easier.”
In a study of a multidisciplinary intervention tested on an acute inpatient medical unit, the effect of the intervention—to improve communication and collaboration—was strongest among house staff, who reported significant increases in collaborative efforts with nurses.10 This finding underlines the importance for hospitalists to serve as models to students, interns, and residents because the most effective time to learn collaborative practice is during early training when experienced nurses can assist inexperienced interns.10 Hospitalists can also consciously reject the traditional “doctor-nurse game,” whereby patterns of behavior suggest that doctors are the dominant players and nurses must defer to them.
“Ask nurses for their opinion,” advises Blue. “Treat them like an equal, which is another one of the beauties of this program, because hospitalists certainly do that. When it comes down to it, people want to be appreciated, respected, and acknowledged for their contribution.”
Blue and her team also encourage hospitalists to share with the nurses if they happen to hear news of their patients’ progress. “If we have follow-up on somebody from the primary care provider after that patient has left the hospital, for example, we try to share that with the nursing staff because they’re our patients. They’re not just my patients and they’re not your patients; they’re our patients.”
Conclusion
The quality of the nurse-hospitalist relationship is central to patient care. The methods, means, and styles of individual and team communication all influence the effectiveness of a hospital team. Retraining providers to traverse the gap of different communication styles is a way to approach the issues that exist. Mutual training for physicians and nurses, as well as training nurses to communicate in ways that more approximate how physicians communicate, will better serve patient and provider needs.
Hospitalists can encourage nurses to overcome hesitancies to initiate calls, clarify their preferences for how nurses should contact them, and work with nurses to seek workable ways to perform patient rounds in concert. Most of all, nurses need timely care plan distribution and acknowledgment for their contributions to teamwork and patient care. TH
Writer Andrea Sattinger will write about occupational therapists’ experiences with hospitalists in the January issue.
References
- ANA Commission on Workforce for Hospitals and Health Systems. In our hands: how hospital leaders can build a thriving workforce. American Hospital Association; Chicago; 2002;55:30-31.
- Aiken LH. The unfinished patient safety agenda. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web: Agency for Healthcare Research and Quality; 2005. Accessed August. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=7&searchStr=The+unfinished+patient+safety+agenda
- Aiken LH, Clarke SP, Sloane DM. International Hospital Outcomes Research Consortium. Hospital staffing, organization, and quality of care: cross-national findings. Int J Qual Health Care. 2002;14:5-13.
- Friesen MA, Farquhar MB, Hughes R. The nurse’s role in promoting a culture of safety: American Nurses Association Continuing Education, Center for American Nurses; 2005.
- Wachter R. In conversation with … Barbara A. Blakeney, MS, RN. In: Wachter R, ed. Morbidity and Mortality Rounds on the Web. Agency for Healthcare Research and Quality; 2005. Accessed Aug. 29, 2005 at http://webmm.ahrq.gov/perspective.aspx?perspectiveID=8&searchStr=Blakeney
- Lindeke LL, Sieckert AM. Nurse-physician workplace collaboration. Online J Issues Nurs. 2005;10:5.
- Burke M, Boal J, Mitchell R. Communicating for better care: improving nurse-physician communication. Am J Nurs. 2004;104:40-47
- SBAR initiative to improve staff communication. Healthcare Benchmarks Qual Improv. 2005;12:40-41.
- Smith AP. Partners at the bedside: the importance of nurse-physician relationships. Nurs Econ. 2004;22:161-164.
- Vazirani S, Hays RD, Shapiro MF, et al. Effect of a multidisciplinary intervention on communication and collaboration among physicians and nurses. Am J Crit Care. 2005;14:71-77.
An Itchy Neck
A62-year-old male with a history of a cadaveric renal transplant complains of a three-week history of progressive, slightly pruritic lesions on his head and neck. Physical exam reveals multiple 3-8 mm umbilicated papules with some excoriations distributed on sun-exposed areas of face, scalp, and neck. (See photo above.) He takes tacrolimus 1 mg PO QD, mycophenolate mofetil 750 mg BID and prednisone 10 mg QD. He is otherwise without complaints except for some mild blurry vision that started several days ago.
The most appropriate plan of care is:

- Apply triamcinolone 0.1% cream bid for 10 days; biopsy if no improvement. Instruct him not to scratch these lesions of prurigo nodularis.
- Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
- Liquid nitrogen for likely molluscum contagiosum lesions.
- Electrodessication and curettage for these presumed non-melanoma skin cancers.
- Valacyclovir 1,000 mg PO TID for seven days for herpes zoster.
Discussion
The answer is B: Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
In this immunosuppressed patient, the differential diagnosis should include molluscum contagiosum, disseminated HSV/VZV, non-melanoma skin cancers, fungal infections (including Cryptococcus, Histoplasma, Coccidioidomycosis, and Penicillium marneffeii), Leishmaniasis, and prurigo nodularis. The appropriate step in the management is to assume a possible opportunistic infection because this may be a sign of systemic infection that can be rapidly fatal.

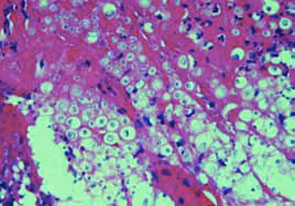
This case was diagnosed by a Tzanck smear showing multiple narrow-based budding yeast forms consistent with Cryptococcus. (See photo below.) A tissue culture and H&E preparation confirmed the diagnosis. (See photo at right.) The patient was admitted immediately after evaluation by the Tzanck smear and started on liposomal amphotericin B. He developed systemic symptoms within 24 hours of hospitalization and was found to have Cryptococcal antigen in his serum and CSF. He eventually recovered after a 17-day hospitalization and was discharged on lifelong fluconazole.
Cryptococcosis, caused by the yeast Cryptococcus neoformans, is a major source of morbidity and mortality in immunosuppressed patients. It is a ubiquitous fungus primarily associated with bird droppings. The organism is inhaled and uses the lung as a portal of entry. In immunocompromised patients, the decrease in cell-mediated immunity allows the organism to disseminate widely. Although many organs may become affected, there is a predilection for central nervous system involvement and development of a meningoencephalitis. Skin involvement occurs in 10% to 20% of patients. If skin involvement occurs it should alert the physician to underlying disseminated disease. Prompt diagnosis and initiation of treatment are essential to reduce the high mortality (up to 80%) associated with untreated cases. Work-up should be directed toward findings on history and physical exam, but should at least include a chest x-ray, serum cryptococcal Ag, blood and urine cultures, and consideration of a lumbar puncture.
Cutaneous lesions are protean and can be nodules, papules, pustules, acneiform papules and pustules, molluscum contagiosum-like papules, herpetic-like vesicles, ulcers, or cellulitis. Given the non-specific appearance, one should lower the threshold in immunocompromised patients for consideration of deep fungal infections. TH
References
- Vilchez RA, Fung J, Kusne S. Cryptococcosis in organ transplant recipients: an overview. Am J Transplantation. 2002;2:575-580.
- Vincenzo R, Ruocco E. Tzanck smear, an old test for the new millennium: when and how. Int J Derm. 1999;38(11):830-834.
- Perfect JR, Casadevall A. Cryptococcosis. Infect Dis Clin North Am. 2002;16(4):837-874.
A62-year-old male with a history of a cadaveric renal transplant complains of a three-week history of progressive, slightly pruritic lesions on his head and neck. Physical exam reveals multiple 3-8 mm umbilicated papules with some excoriations distributed on sun-exposed areas of face, scalp, and neck. (See photo above.) He takes tacrolimus 1 mg PO QD, mycophenolate mofetil 750 mg BID and prednisone 10 mg QD. He is otherwise without complaints except for some mild blurry vision that started several days ago.
The most appropriate plan of care is:
- Apply triamcinolone 0.1% cream bid for 10 days; biopsy if no improvement. Instruct him not to scratch these lesions of prurigo nodularis.
- Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
- Liquid nitrogen for likely molluscum contagiosum lesions.
- Electrodessication and curettage for these presumed non-melanoma skin cancers.
- Valacyclovir 1,000 mg PO TID for seven days for herpes zoster.
Discussion
The answer is B: Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
In this immunosuppressed patient, the differential diagnosis should include molluscum contagiosum, disseminated HSV/VZV, non-melanoma skin cancers, fungal infections (including Cryptococcus, Histoplasma, Coccidioidomycosis, and Penicillium marneffeii), Leishmaniasis, and prurigo nodularis. The appropriate step in the management is to assume a possible opportunistic infection because this may be a sign of systemic infection that can be rapidly fatal.
This case was diagnosed by a Tzanck smear showing multiple narrow-based budding yeast forms consistent with Cryptococcus. (See photo below.) A tissue culture and H&E preparation confirmed the diagnosis. (See photo at right.) The patient was admitted immediately after evaluation by the Tzanck smear and started on liposomal amphotericin B. He developed systemic symptoms within 24 hours of hospitalization and was found to have Cryptococcal antigen in his serum and CSF. He eventually recovered after a 17-day hospitalization and was discharged on lifelong fluconazole.
Cryptococcosis, caused by the yeast Cryptococcus neoformans, is a major source of morbidity and mortality in immunosuppressed patients. It is a ubiquitous fungus primarily associated with bird droppings. The organism is inhaled and uses the lung as a portal of entry. In immunocompromised patients, the decrease in cell-mediated immunity allows the organism to disseminate widely. Although many organs may become affected, there is a predilection for central nervous system involvement and development of a meningoencephalitis. Skin involvement occurs in 10% to 20% of patients. If skin involvement occurs it should alert the physician to underlying disseminated disease. Prompt diagnosis and initiation of treatment are essential to reduce the high mortality (up to 80%) associated with untreated cases. Work-up should be directed toward findings on history and physical exam, but should at least include a chest x-ray, serum cryptococcal Ag, blood and urine cultures, and consideration of a lumbar puncture.
Cutaneous lesions are protean and can be nodules, papules, pustules, acneiform papules and pustules, molluscum contagiosum-like papules, herpetic-like vesicles, ulcers, or cellulitis. Given the non-specific appearance, one should lower the threshold in immunocompromised patients for consideration of deep fungal infections. TH
References
- Vilchez RA, Fung J, Kusne S. Cryptococcosis in organ transplant recipients: an overview. Am J Transplantation. 2002;2:575-580.
- Vincenzo R, Ruocco E. Tzanck smear, an old test for the new millennium: when and how. Int J Derm. 1999;38(11):830-834.
- Perfect JR, Casadevall A. Cryptococcosis. Infect Dis Clin North Am. 2002;16(4):837-874.
A62-year-old male with a history of a cadaveric renal transplant complains of a three-week history of progressive, slightly pruritic lesions on his head and neck. Physical exam reveals multiple 3-8 mm umbilicated papules with some excoriations distributed on sun-exposed areas of face, scalp, and neck. (See photo above.) He takes tacrolimus 1 mg PO QD, mycophenolate mofetil 750 mg BID and prednisone 10 mg QD. He is otherwise without complaints except for some mild blurry vision that started several days ago.
The most appropriate plan of care is:
- Apply triamcinolone 0.1% cream bid for 10 days; biopsy if no improvement. Instruct him not to scratch these lesions of prurigo nodularis.
- Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
- Liquid nitrogen for likely molluscum contagiosum lesions.
- Electrodessication and curettage for these presumed non-melanoma skin cancers.
- Valacyclovir 1,000 mg PO TID for seven days for herpes zoster.
Discussion
The answer is B: Biopsy a lesion and send half of the material for tissue culture. Watch for development of systemic/central nervous system signs.
In this immunosuppressed patient, the differential diagnosis should include molluscum contagiosum, disseminated HSV/VZV, non-melanoma skin cancers, fungal infections (including Cryptococcus, Histoplasma, Coccidioidomycosis, and Penicillium marneffeii), Leishmaniasis, and prurigo nodularis. The appropriate step in the management is to assume a possible opportunistic infection because this may be a sign of systemic infection that can be rapidly fatal.
This case was diagnosed by a Tzanck smear showing multiple narrow-based budding yeast forms consistent with Cryptococcus. (See photo below.) A tissue culture and H&E preparation confirmed the diagnosis. (See photo at right.) The patient was admitted immediately after evaluation by the Tzanck smear and started on liposomal amphotericin B. He developed systemic symptoms within 24 hours of hospitalization and was found to have Cryptococcal antigen in his serum and CSF. He eventually recovered after a 17-day hospitalization and was discharged on lifelong fluconazole.
Cryptococcosis, caused by the yeast Cryptococcus neoformans, is a major source of morbidity and mortality in immunosuppressed patients. It is a ubiquitous fungus primarily associated with bird droppings. The organism is inhaled and uses the lung as a portal of entry. In immunocompromised patients, the decrease in cell-mediated immunity allows the organism to disseminate widely. Although many organs may become affected, there is a predilection for central nervous system involvement and development of a meningoencephalitis. Skin involvement occurs in 10% to 20% of patients. If skin involvement occurs it should alert the physician to underlying disseminated disease. Prompt diagnosis and initiation of treatment are essential to reduce the high mortality (up to 80%) associated with untreated cases. Work-up should be directed toward findings on history and physical exam, but should at least include a chest x-ray, serum cryptococcal Ag, blood and urine cultures, and consideration of a lumbar puncture.
Cutaneous lesions are protean and can be nodules, papules, pustules, acneiform papules and pustules, molluscum contagiosum-like papules, herpetic-like vesicles, ulcers, or cellulitis. Given the non-specific appearance, one should lower the threshold in immunocompromised patients for consideration of deep fungal infections. TH
References
- Vilchez RA, Fung J, Kusne S. Cryptococcosis in organ transplant recipients: an overview. Am J Transplantation. 2002;2:575-580.
- Vincenzo R, Ruocco E. Tzanck smear, an old test for the new millennium: when and how. Int J Derm. 1999;38(11):830-834.
- Perfect JR, Casadevall A. Cryptococcosis. Infect Dis Clin North Am. 2002;16(4):837-874.
Career Satisfaction Toolkit
Early survey data on hospitalists, which suggest high levels of job engagement and low turnover rates, may not be as relevant as programs mature in a competitive marketplace to meet important needs such as rising census and Accreditation Council for Graduate Medical Education (ACGME) requirements. There is also a paucity of data on how different models of compensation affect hospitalists’ career satisfaction.
In 2005 the role of the hospitalist has evolved from simply improving throughput (average length of stay) to one of leadership, quality improvement, and teaching that extends beyond direct patient care. Compensation for hospitalists should not, therefore, be based solely on billing revenue. Improving the efficiency of the hospitalists work environment, which may include IT support, adequate office space, and administrative support, may not only enhance productivity but also job satisfaction. More research is needed to examine these questions.
Progress Report
One of the Career Satisfaction Task Force’s major initiatives has been developing a toolkit for the SHM membership with the purpose of providing members with an action plan for attaining a long and satisfying career in hospital medicine. The following steps are being taken in the creation of the toolkit:
- Needs assessment—questionnaire at the SHM 2005 Annual Meeting;
- Monthly conference calls;
- Timeline:
- Toolkit draft completion—Sept. 2005;
- Review SHM Membership Committee—Oct. 2005;
- Further revision;
- Submission to SHM Board for review—Nov. 2005;
- Further revision; and
- Dissemination at SHM Annual Meeting—May 2006.
- Content—four workplace domains:
- Control/Autonomy;
- Workload/Schedule;
- Community/Environment; and
- Reward/Recognition.
- Elements comprising each domain:
- Definition: specific description of workplace domain;
- Background: review of literature, expert opinion, experience-based observation, executive summary of background content;
- Guidelines: practical actionable recommendations and educational initiatives;
- Pitfalls: specific examples;
- Examples: application to different settings (community, academic, pediatric); and
- References.
Research and Timeline
In parallel to the development of the work domains for the toolkit, the Career Satisfaction Task Force is developing a questionnaire to survey hospitalist physicians on career satisfaction and “worklife.” The last survey of this type was performed in 1999. This questionnaire will allow us to assess changes in hospitalist quality of working life over time to further explore how hospitalists are faring during this critical time of rapid growth of our specialty.
The task force is developing a list of important aspects of worklife, satisfaction, and stress for hospitalists. This list will be supplemented by semi-structured interviews of SHM members and leaders in hospital medicine to include a representative viewpoint of hospitalist worklife: adult and pediatric medicine, academic and community, gender and age, directors of programs, and different employer types.
The interviews were expected to be completed in the fall of 2005. Qualitative data analysis will allow us to ascertain important themes for job performance and satisfaction to be highlighted in the survey. The questionnaire development will also consider inclusion of aspects from the prior surveys to follow results over time and when possible will use validated questions from the quality of working life literature.
We anticipate completion of the questionnaire in spring 2006 followed by surveying of a random sample of hospitalists from the SHM membership through a Web-based survey. Sampling of groups of hospitalists based on job characteristics will occur because there is significant interest and need for information about hospitalist worklife in certain work settings. The questionnaire dissemination time will overlap with the annual meeting to maximize survey response. The task force will work with SHM annual meeting committee to discuss having a dedicated computer for filling out the Web-based survey on-site.
Any SHM member who would like to participate in the questionnaire on-site, even if they were not selected for the random sample, will be encouraged to do so. Data analysis will occur in mid-late 2006. The task force will use information from the analyses to update the SHM Worklife Toolkit. We will also provide numerous forums for dissemination of the data. In particular, we plan to showcase this data at the 2007 SHM Annual Meeting followed by journal publication and Web site posting. It is our hope that this data will provide key information on the current quality of working life of hospitalist physicians to support worklife recommendations that promote sustainable, enjoyable careers in hospital medicine.
Early survey data on hospitalists, which suggest high levels of job engagement and low turnover rates, may not be as relevant as programs mature in a competitive marketplace to meet important needs such as rising census and Accreditation Council for Graduate Medical Education (ACGME) requirements. There is also a paucity of data on how different models of compensation affect hospitalists’ career satisfaction.
In 2005 the role of the hospitalist has evolved from simply improving throughput (average length of stay) to one of leadership, quality improvement, and teaching that extends beyond direct patient care. Compensation for hospitalists should not, therefore, be based solely on billing revenue. Improving the efficiency of the hospitalists work environment, which may include IT support, adequate office space, and administrative support, may not only enhance productivity but also job satisfaction. More research is needed to examine these questions.
Progress Report
One of the Career Satisfaction Task Force’s major initiatives has been developing a toolkit for the SHM membership with the purpose of providing members with an action plan for attaining a long and satisfying career in hospital medicine. The following steps are being taken in the creation of the toolkit:
- Needs assessment—questionnaire at the SHM 2005 Annual Meeting;
- Monthly conference calls;
- Timeline:
- Toolkit draft completion—Sept. 2005;
- Review SHM Membership Committee—Oct. 2005;
- Further revision;
- Submission to SHM Board for review—Nov. 2005;
- Further revision; and
- Dissemination at SHM Annual Meeting—May 2006.
- Content—four workplace domains:
- Control/Autonomy;
- Workload/Schedule;
- Community/Environment; and
- Reward/Recognition.
- Elements comprising each domain:
- Definition: specific description of workplace domain;
- Background: review of literature, expert opinion, experience-based observation, executive summary of background content;
- Guidelines: practical actionable recommendations and educational initiatives;
- Pitfalls: specific examples;
- Examples: application to different settings (community, academic, pediatric); and
- References.
Research and Timeline
In parallel to the development of the work domains for the toolkit, the Career Satisfaction Task Force is developing a questionnaire to survey hospitalist physicians on career satisfaction and “worklife.” The last survey of this type was performed in 1999. This questionnaire will allow us to assess changes in hospitalist quality of working life over time to further explore how hospitalists are faring during this critical time of rapid growth of our specialty.
The task force is developing a list of important aspects of worklife, satisfaction, and stress for hospitalists. This list will be supplemented by semi-structured interviews of SHM members and leaders in hospital medicine to include a representative viewpoint of hospitalist worklife: adult and pediatric medicine, academic and community, gender and age, directors of programs, and different employer types.
The interviews were expected to be completed in the fall of 2005. Qualitative data analysis will allow us to ascertain important themes for job performance and satisfaction to be highlighted in the survey. The questionnaire development will also consider inclusion of aspects from the prior surveys to follow results over time and when possible will use validated questions from the quality of working life literature.
We anticipate completion of the questionnaire in spring 2006 followed by surveying of a random sample of hospitalists from the SHM membership through a Web-based survey. Sampling of groups of hospitalists based on job characteristics will occur because there is significant interest and need for information about hospitalist worklife in certain work settings. The questionnaire dissemination time will overlap with the annual meeting to maximize survey response. The task force will work with SHM annual meeting committee to discuss having a dedicated computer for filling out the Web-based survey on-site.
Any SHM member who would like to participate in the questionnaire on-site, even if they were not selected for the random sample, will be encouraged to do so. Data analysis will occur in mid-late 2006. The task force will use information from the analyses to update the SHM Worklife Toolkit. We will also provide numerous forums for dissemination of the data. In particular, we plan to showcase this data at the 2007 SHM Annual Meeting followed by journal publication and Web site posting. It is our hope that this data will provide key information on the current quality of working life of hospitalist physicians to support worklife recommendations that promote sustainable, enjoyable careers in hospital medicine.
Early survey data on hospitalists, which suggest high levels of job engagement and low turnover rates, may not be as relevant as programs mature in a competitive marketplace to meet important needs such as rising census and Accreditation Council for Graduate Medical Education (ACGME) requirements. There is also a paucity of data on how different models of compensation affect hospitalists’ career satisfaction.
In 2005 the role of the hospitalist has evolved from simply improving throughput (average length of stay) to one of leadership, quality improvement, and teaching that extends beyond direct patient care. Compensation for hospitalists should not, therefore, be based solely on billing revenue. Improving the efficiency of the hospitalists work environment, which may include IT support, adequate office space, and administrative support, may not only enhance productivity but also job satisfaction. More research is needed to examine these questions.
Progress Report
One of the Career Satisfaction Task Force’s major initiatives has been developing a toolkit for the SHM membership with the purpose of providing members with an action plan for attaining a long and satisfying career in hospital medicine. The following steps are being taken in the creation of the toolkit:
- Needs assessment—questionnaire at the SHM 2005 Annual Meeting;
- Monthly conference calls;
- Timeline:
- Toolkit draft completion—Sept. 2005;
- Review SHM Membership Committee—Oct. 2005;
- Further revision;
- Submission to SHM Board for review—Nov. 2005;
- Further revision; and
- Dissemination at SHM Annual Meeting—May 2006.
- Content—four workplace domains:
- Control/Autonomy;
- Workload/Schedule;
- Community/Environment; and
- Reward/Recognition.
- Elements comprising each domain:
- Definition: specific description of workplace domain;
- Background: review of literature, expert opinion, experience-based observation, executive summary of background content;
- Guidelines: practical actionable recommendations and educational initiatives;
- Pitfalls: specific examples;
- Examples: application to different settings (community, academic, pediatric); and
- References.
Research and Timeline
In parallel to the development of the work domains for the toolkit, the Career Satisfaction Task Force is developing a questionnaire to survey hospitalist physicians on career satisfaction and “worklife.” The last survey of this type was performed in 1999. This questionnaire will allow us to assess changes in hospitalist quality of working life over time to further explore how hospitalists are faring during this critical time of rapid growth of our specialty.
The task force is developing a list of important aspects of worklife, satisfaction, and stress for hospitalists. This list will be supplemented by semi-structured interviews of SHM members and leaders in hospital medicine to include a representative viewpoint of hospitalist worklife: adult and pediatric medicine, academic and community, gender and age, directors of programs, and different employer types.
The interviews were expected to be completed in the fall of 2005. Qualitative data analysis will allow us to ascertain important themes for job performance and satisfaction to be highlighted in the survey. The questionnaire development will also consider inclusion of aspects from the prior surveys to follow results over time and when possible will use validated questions from the quality of working life literature.
We anticipate completion of the questionnaire in spring 2006 followed by surveying of a random sample of hospitalists from the SHM membership through a Web-based survey. Sampling of groups of hospitalists based on job characteristics will occur because there is significant interest and need for information about hospitalist worklife in certain work settings. The questionnaire dissemination time will overlap with the annual meeting to maximize survey response. The task force will work with SHM annual meeting committee to discuss having a dedicated computer for filling out the Web-based survey on-site.
Any SHM member who would like to participate in the questionnaire on-site, even if they were not selected for the random sample, will be encouraged to do so. Data analysis will occur in mid-late 2006. The task force will use information from the analyses to update the SHM Worklife Toolkit. We will also provide numerous forums for dissemination of the data. In particular, we plan to showcase this data at the 2007 SHM Annual Meeting followed by journal publication and Web site posting. It is our hope that this data will provide key information on the current quality of working life of hospitalist physicians to support worklife recommendations that promote sustainable, enjoyable careers in hospital medicine.
Quality Will Be Job One

One of the potential benefits of hospital medicine is the tangible opportunity to change healthcare in a meaningful way. Although much of the initial ballyhoo for hospital medicine has been around service-related issues, that is about to change.
Hospitalists have been willing to take on the inpatient responsibilities for primarily outpatient-based internists, family practitioners, and pediatricians. We have been available to admit and manage the patients who present to emergency rooms with acute illnesses and who have no physician of record. We have actively worked with surgeons and subspecialists to co-manage their patient’s medical problems.
In addition, because hospitalists are much more readily available to acutely ill inpatients, because we have more expertise with these medical problems, and because practice generally makes for better performance, hospitalists have been expected to provide more effective and more efficient care.
But that is just the front end of what is creating the enormous energy behind the hospital medicine movement. We are moving into an era of measurement of defined patient outcomes and expectations from insurance companies, Medicare, the business community, and—yes—even our patients. That era will require us to step up and deliver higher quality healthcare.
This is the driver to the pay-for-performance movement and a shift from just rewarding physicians and hospitals for doing the procedure or “visiting” the patient and moving to where those who can demonstrate expertise and performance are rewarded financially and by reputation.
Hospitalists and SHM take this very seriously and are creating alliances and programs to help hospitalists become leaders in the quality and performance arenas.
Walking through the approach that SHM is taking in improving glycemic control in hospitalized patients (see below) will serve as a template for other activities SHM has planned in heart failure, VTE, hospitalized infections, and other illnesses hospitalists see and treat every day.
In a practical way, hospitals and health professionals finally came into the performance era with the first publication of the individual hospital performance results to performance measures developed by JCAHO and co-promoted with CMS in their Hospital Compare Web site. This was promulgated widely, especially at www.hospitalcompare.hhs.gov.
Because Hospital Compare was picked up by The New York Times, the Los Angeles Times, and many local papers, hospitals were soon trying to explain why their performance in heart failure, pneumonia, and heart attack looked like a failing grade. Now that the public is involved, hospitals are scrambling to quickly improve their performance rather than attacking the data.
Looking to the future, SHM is working with JCAHO to develop performance standards for glycemic control for inpatients as a way to assess how our hospitals and physicians are doing in managing diabetes. SHM is also allying with many other key stakeholders to form a steering committee for this project. These standards will take almost three years to develop, test, and implement. So the first reporting of how every hospital is doing in diabetes is most likely a 2008 or 2009 event.
Expecting that many hospitals will improve their performance in diabetic care during 2008 and 2009, SHM is now developing the tools and the training to allow hospitalists to be ready with practical solutions.
In October 2005 SHM convened a Working Group on Inpatient Glycemic Control in Chicago. This meeting under the leadership of Greg Maynard, MD, associate clinical professor of medicine, chief of the division of hospital medicine, University of California at San Diego, brought together nationally recognized diabetologists and endocrinologists with hospitalist leaders, as well as experts in the field of nursing, case management, pharmacy, risk management, and nutrition. The end result is an understanding of what constitutes an ideal management of inpatient diabetes and what role hospitalists can play.
This work group now is analyzing what resources currently exist and what gaps need to be filled. Next SHM will develop an implementation plan to get this information out to our nation’s hospitalists.
SHM has some experience in developing quality improvement tools, as you can see in our Resource Rooms on the SHM Web site. For a current working example, take a look at the DVT Quality Improvement Resource Room at www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312.
But SHM plans a more aggressive approach with proposed training sessions at the SHM Annual Meeting quality pre-course and taking these tools and approaches out to our hospitalists at local meetings throughout the country. SHM is also looking into creating a network of quality mentors that will work with individual hospitalists groups as they put SHM quality improvement tools into the workflow at their hospitals. SHM will also develop strategies for baseline measurement, ongoing data collection, involvement of team members, and procurement of local resources. SHM hopes to support research to further develop best practices and approaches.
The game plan goes something like this: SHM will develop the resources hospitalists need to improve management of inpatient diabetes in 2006. In 2007 and 2008 SHM will roll out this strategy to as many hospitalists as we can train. By 2008 JCAHO and CMS will have deployed their Performance Measures in Diabetes. When the first scores show the same deficiencies as we have seen this year in MI and heart failure, our nation’s hospitalists will be well armed to provide practical tangible solutions to improve quality.
And the beauty of this approach is that SHM is working on similar strategies right now for heart failure, DVT, pneumonia, and other key clinical conditions.
Those who pay for and receive care in our hospitals are looking at our current performance and demanding improvements. For the first time hospitals and those with resources are ready to make measurable quality a high priority. The presence of hospitalists in more than 2,000 hospitals (and more in the near future) ideally positions hospitalists to be a key change agent. The tools SHM is developing will give hospitalists the strategies and the expertise to make this happen.
This is a watershed moment in American healthcare. There is a palpable swing in the priorities of our patients. Hospitalists can help the healthcare team find real solutions. SHM has the vision and the plan to provide you with as much help as you need. Together we will do great things. TH
Dr. Wellikson has been CEO of SHM since 2000.
One of the potential benefits of hospital medicine is the tangible opportunity to change healthcare in a meaningful way. Although much of the initial ballyhoo for hospital medicine has been around service-related issues, that is about to change.
Hospitalists have been willing to take on the inpatient responsibilities for primarily outpatient-based internists, family practitioners, and pediatricians. We have been available to admit and manage the patients who present to emergency rooms with acute illnesses and who have no physician of record. We have actively worked with surgeons and subspecialists to co-manage their patient’s medical problems.
In addition, because hospitalists are much more readily available to acutely ill inpatients, because we have more expertise with these medical problems, and because practice generally makes for better performance, hospitalists have been expected to provide more effective and more efficient care.
But that is just the front end of what is creating the enormous energy behind the hospital medicine movement. We are moving into an era of measurement of defined patient outcomes and expectations from insurance companies, Medicare, the business community, and—yes—even our patients. That era will require us to step up and deliver higher quality healthcare.
This is the driver to the pay-for-performance movement and a shift from just rewarding physicians and hospitals for doing the procedure or “visiting” the patient and moving to where those who can demonstrate expertise and performance are rewarded financially and by reputation.
Hospitalists and SHM take this very seriously and are creating alliances and programs to help hospitalists become leaders in the quality and performance arenas.
Walking through the approach that SHM is taking in improving glycemic control in hospitalized patients (see below) will serve as a template for other activities SHM has planned in heart failure, VTE, hospitalized infections, and other illnesses hospitalists see and treat every day.
In a practical way, hospitals and health professionals finally came into the performance era with the first publication of the individual hospital performance results to performance measures developed by JCAHO and co-promoted with CMS in their Hospital Compare Web site. This was promulgated widely, especially at www.hospitalcompare.hhs.gov.
Because Hospital Compare was picked up by The New York Times, the Los Angeles Times, and many local papers, hospitals were soon trying to explain why their performance in heart failure, pneumonia, and heart attack looked like a failing grade. Now that the public is involved, hospitals are scrambling to quickly improve their performance rather than attacking the data.
Looking to the future, SHM is working with JCAHO to develop performance standards for glycemic control for inpatients as a way to assess how our hospitals and physicians are doing in managing diabetes. SHM is also allying with many other key stakeholders to form a steering committee for this project. These standards will take almost three years to develop, test, and implement. So the first reporting of how every hospital is doing in diabetes is most likely a 2008 or 2009 event.
Expecting that many hospitals will improve their performance in diabetic care during 2008 and 2009, SHM is now developing the tools and the training to allow hospitalists to be ready with practical solutions.
In October 2005 SHM convened a Working Group on Inpatient Glycemic Control in Chicago. This meeting under the leadership of Greg Maynard, MD, associate clinical professor of medicine, chief of the division of hospital medicine, University of California at San Diego, brought together nationally recognized diabetologists and endocrinologists with hospitalist leaders, as well as experts in the field of nursing, case management, pharmacy, risk management, and nutrition. The end result is an understanding of what constitutes an ideal management of inpatient diabetes and what role hospitalists can play.
This work group now is analyzing what resources currently exist and what gaps need to be filled. Next SHM will develop an implementation plan to get this information out to our nation’s hospitalists.
SHM has some experience in developing quality improvement tools, as you can see in our Resource Rooms on the SHM Web site. For a current working example, take a look at the DVT Quality Improvement Resource Room at www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312.
But SHM plans a more aggressive approach with proposed training sessions at the SHM Annual Meeting quality pre-course and taking these tools and approaches out to our hospitalists at local meetings throughout the country. SHM is also looking into creating a network of quality mentors that will work with individual hospitalists groups as they put SHM quality improvement tools into the workflow at their hospitals. SHM will also develop strategies for baseline measurement, ongoing data collection, involvement of team members, and procurement of local resources. SHM hopes to support research to further develop best practices and approaches.
The game plan goes something like this: SHM will develop the resources hospitalists need to improve management of inpatient diabetes in 2006. In 2007 and 2008 SHM will roll out this strategy to as many hospitalists as we can train. By 2008 JCAHO and CMS will have deployed their Performance Measures in Diabetes. When the first scores show the same deficiencies as we have seen this year in MI and heart failure, our nation’s hospitalists will be well armed to provide practical tangible solutions to improve quality.
And the beauty of this approach is that SHM is working on similar strategies right now for heart failure, DVT, pneumonia, and other key clinical conditions.
Those who pay for and receive care in our hospitals are looking at our current performance and demanding improvements. For the first time hospitals and those with resources are ready to make measurable quality a high priority. The presence of hospitalists in more than 2,000 hospitals (and more in the near future) ideally positions hospitalists to be a key change agent. The tools SHM is developing will give hospitalists the strategies and the expertise to make this happen.
This is a watershed moment in American healthcare. There is a palpable swing in the priorities of our patients. Hospitalists can help the healthcare team find real solutions. SHM has the vision and the plan to provide you with as much help as you need. Together we will do great things. TH
Dr. Wellikson has been CEO of SHM since 2000.
One of the potential benefits of hospital medicine is the tangible opportunity to change healthcare in a meaningful way. Although much of the initial ballyhoo for hospital medicine has been around service-related issues, that is about to change.
Hospitalists have been willing to take on the inpatient responsibilities for primarily outpatient-based internists, family practitioners, and pediatricians. We have been available to admit and manage the patients who present to emergency rooms with acute illnesses and who have no physician of record. We have actively worked with surgeons and subspecialists to co-manage their patient’s medical problems.
In addition, because hospitalists are much more readily available to acutely ill inpatients, because we have more expertise with these medical problems, and because practice generally makes for better performance, hospitalists have been expected to provide more effective and more efficient care.
But that is just the front end of what is creating the enormous energy behind the hospital medicine movement. We are moving into an era of measurement of defined patient outcomes and expectations from insurance companies, Medicare, the business community, and—yes—even our patients. That era will require us to step up and deliver higher quality healthcare.
This is the driver to the pay-for-performance movement and a shift from just rewarding physicians and hospitals for doing the procedure or “visiting” the patient and moving to where those who can demonstrate expertise and performance are rewarded financially and by reputation.
Hospitalists and SHM take this very seriously and are creating alliances and programs to help hospitalists become leaders in the quality and performance arenas.
Walking through the approach that SHM is taking in improving glycemic control in hospitalized patients (see below) will serve as a template for other activities SHM has planned in heart failure, VTE, hospitalized infections, and other illnesses hospitalists see and treat every day.
In a practical way, hospitals and health professionals finally came into the performance era with the first publication of the individual hospital performance results to performance measures developed by JCAHO and co-promoted with CMS in their Hospital Compare Web site. This was promulgated widely, especially at www.hospitalcompare.hhs.gov.
Because Hospital Compare was picked up by The New York Times, the Los Angeles Times, and many local papers, hospitals were soon trying to explain why their performance in heart failure, pneumonia, and heart attack looked like a failing grade. Now that the public is involved, hospitals are scrambling to quickly improve their performance rather than attacking the data.
Looking to the future, SHM is working with JCAHO to develop performance standards for glycemic control for inpatients as a way to assess how our hospitals and physicians are doing in managing diabetes. SHM is also allying with many other key stakeholders to form a steering committee for this project. These standards will take almost three years to develop, test, and implement. So the first reporting of how every hospital is doing in diabetes is most likely a 2008 or 2009 event.
Expecting that many hospitals will improve their performance in diabetic care during 2008 and 2009, SHM is now developing the tools and the training to allow hospitalists to be ready with practical solutions.
In October 2005 SHM convened a Working Group on Inpatient Glycemic Control in Chicago. This meeting under the leadership of Greg Maynard, MD, associate clinical professor of medicine, chief of the division of hospital medicine, University of California at San Diego, brought together nationally recognized diabetologists and endocrinologists with hospitalist leaders, as well as experts in the field of nursing, case management, pharmacy, risk management, and nutrition. The end result is an understanding of what constitutes an ideal management of inpatient diabetes and what role hospitalists can play.
This work group now is analyzing what resources currently exist and what gaps need to be filled. Next SHM will develop an implementation plan to get this information out to our nation’s hospitalists.
SHM has some experience in developing quality improvement tools, as you can see in our Resource Rooms on the SHM Web site. For a current working example, take a look at the DVT Quality Improvement Resource Room at www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312.
But SHM plans a more aggressive approach with proposed training sessions at the SHM Annual Meeting quality pre-course and taking these tools and approaches out to our hospitalists at local meetings throughout the country. SHM is also looking into creating a network of quality mentors that will work with individual hospitalists groups as they put SHM quality improvement tools into the workflow at their hospitals. SHM will also develop strategies for baseline measurement, ongoing data collection, involvement of team members, and procurement of local resources. SHM hopes to support research to further develop best practices and approaches.
The game plan goes something like this: SHM will develop the resources hospitalists need to improve management of inpatient diabetes in 2006. In 2007 and 2008 SHM will roll out this strategy to as many hospitalists as we can train. By 2008 JCAHO and CMS will have deployed their Performance Measures in Diabetes. When the first scores show the same deficiencies as we have seen this year in MI and heart failure, our nation’s hospitalists will be well armed to provide practical tangible solutions to improve quality.
And the beauty of this approach is that SHM is working on similar strategies right now for heart failure, DVT, pneumonia, and other key clinical conditions.
Those who pay for and receive care in our hospitals are looking at our current performance and demanding improvements. For the first time hospitals and those with resources are ready to make measurable quality a high priority. The presence of hospitalists in more than 2,000 hospitals (and more in the near future) ideally positions hospitalists to be a key change agent. The tools SHM is developing will give hospitalists the strategies and the expertise to make this happen.
This is a watershed moment in American healthcare. There is a palpable swing in the priorities of our patients. Hospitalists can help the healthcare team find real solutions. SHM has the vision and the plan to provide you with as much help as you need. Together we will do great things. TH
Dr. Wellikson has been CEO of SHM since 2000.
Postdischarge Test Results, Acute Renal Failure, Diagnosing PE
Roy PM, Colombet I, Durieux P, et al. Systemic review and meta-analysis of strategies for the diagnosis of suspected pulmonary embolism. BMJ.2005;331:259.
Background: Despite technological advances, the diagnosis of pulmonary embolism remains challenging. A large number of diagnostic tests and strategies have been evaluated and yet the test characteristics of each and their practical use remain unclear.
Methods: Pierre-Marie Roy, MD and colleagues carried out a systematic review and meta-analysis to define the likelihood ratios (LRs) for different diagnostic modalities for pulmonary embolism and provide a simple, evidence-based diagnostic algorithm.
The authors performed a literature search from 1990-2003 identifying all articles that evaluated tests or strategies aimed at diagnosing pulmonary embolism. They only selected papers which were prospective, in which participants were recruited consecutively, and which pulmonary angiography was the reference standard for strategies to confirm pulmonary embolism and clinical follow-up or angiography were used for exclusion strategies.
Results: Forty-eight articles (11,004 patients) met the inclusion criteria and examined ventilation/perfusion (V/Q) lung scanning, computed tomography (CT) angiography, leg vein ultrasound (U/S), echocardiography, magnetic resonance (MR) angiography, and the D-dimer test. For the studies done to evaluate tests to confirm the diagnosis of pulmonary embolism, pooled positive likelihood ratios (+LRs) were calculated and were:
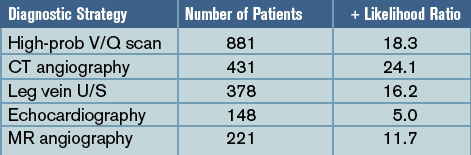
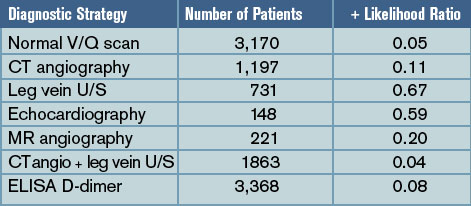
For the studies evaluating tests to exclude the diagnosis of pulmonary embolism, pooled negative likelihood ratios (-LR) were calculated and were:
Discussion: With the pooled positive and negative LRs, Roy and colleagues created a diagnostic algorithm, based on initial pretest probabilities, to help “rule in” and “rule out” the diagnosis of pulmonary embolism. Consistent with prior studies, a calculated post-test probability of >85% confirmed the diagnosis while a post-test probability <5% excluded PE.
In patients with a low or moderate pretest probability, pulmonary embolism is adequately excluded in patients with either 1) negative D-dimers or 2) a normal V/Q scan or 3) a negative CT angiogram in combination with a normal venous ultrasound. In patients with moderate or high pre-test probability, pulmonary embolism is confirmed by either 1) a high-probability V/Q scan or 2) a positive CT angiogram or 3) a positive venous ultrasound. Low-probability V/Q scanning, CT angiogram alone, and MR angiography have higher negative likelihood ratios and can only exclude PE in patients with low pre-test probability.
Many hospitalists are using CT angiography as their sole diagnostic test for pulmonary embolism. Based on the systematic review and meta-analysis by Roy and colleagues, we should proceed with caution as, in some patient populations, a positive or negative “spiral CT” does not adequately confirm or exclude the diagnosis of pulmonary embolism. For those that employ V/Q scanning, MR angiography, or D-dimers, the study also helps define how best to use these tests.
Safdar N, Maki DG. Risk of catheter-related bloodstream infection with peripherally inserted central venous catheters used in hospitalized patients. Chest. 2005;128:489.
Background: In recent years, peripherally inserted central catheters (PICCs) have become more popular, initially for long-term outpatient intravenous therapy but also for inpatient venous access. Traditionally, it was assumed that PICC lines have a lower rate of catheter-related bloodstream infection than conventional central venous catheters (CVCs) placed in the internal jugular, subclavian, or femoral veins.
Methods: One academic medical center prospectively studied the rate of catheter-related bloodstream infection in PICC lines used exclusively in hospitalized patients as part of two trials assessing efficacy of different skin antiseptics. PICC-related bloodstream infection was confirmed when organisms isolated from positive blood cultures matched (by DNA subtyping) organisms isolated from culturing the PICC line at the time of removal. The authors also performed a systematic review of the literature to provide overall estimates of PICC-related bloodstream infection in hospitalized patients.
Results: A total of 115 patients received 251 PICC lines during the study period and the mean duration of catheterization was 11.3 days. More than 40% of the patients were in the intensive care unit (ICU) and most had risk factors for the development of bloodstream infection, including urinary catheterization, mechanical ventilation, prior antibiotic use, and low albumin. Six cases (2.4%) of PICC-related bloodstream infection were confirmed, four with coagulase-negative staphylococcus, one with S. aureus, and one with Klebsiella pneumoniae, a rate of 2.1 per 1,000 catheter-days. In their systematic review, the authors identified 14 studies evaluating the rate of PICC-related bloodstream infection in hospitalized patients; the pooled rate was 1.9 per 1,000 catheter-days.
Discussion: In a small but methodologically sound prospective study and systematic review, Safdar and Maki found a surprisingly high rate of PICC-related bloodstream infection in hospitalized patients. Their calculated rate of 2.1 cases per 1,000 catheter-days is five times the rate seen in PICCs used exclusively in outpatients (0.4 per 1,000 catheter-days). More strikingly, 2.1 cases per 1,000 catheter-days is similar to the rate of catheter-related bloodstream infection in conventional central venous catheters placed in the subclavian or internal jugular veins (two to five per 1,000 catheter-days). Unfortunately, the study didn’t assess the rate of mechanical complications associated with PICC lines or correlate the risk of infection with duration of catheterization.
Hospitalists should be aware that PICC lines likely have the same infection risk as subclavian and internal jugular lines in hospitalized patients and a much higher rate of infection than PICC lines in outpatients. The higher-than-expected rates are likely related to the increased prevalence of risk factors for bloodstream infection in hospitalized patients. Thus, the decision to use PICC lines in hospitalized patients should be made based on factors other than presumed lower infection risk.
Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients. A multinational, multicenter study. JAMA. 2005;294:813.
Background: Acute renal failure in critically ill patients is believed common and is associated with a high mortality. The exact prevalence and the calculated risk of death have not been clearly defined across populations.
Methods: A multinational group of investigators conducted a massive prospective observational study of ICU patients who developed renal failure after ICU admission. The study encompassed 54 hospitals in 23 countries with a total of 29,269 admissions over the 14-month study period. Note, acute renal failure was defined as either oliguria (urine output <200cc/12 hours) or BUN >84mg/dL.
Results: Of all ICU patients studied, 5.7% developed acute renal failure after admission and 4.7% of patients received renal replacement therapy (most often continuous replacement). The most common contributing factor to the development of acute renal failure was septic shock (48%), followed by major surgery (34%) and cardiogenic shock (26%). Up to 19% of the cases of acute renal failure were estimated to be drug-related. The in-hospital mortality for critically ill patients with acute renal failure was 60%, which was substantially higher than the mortality estimated by other physiologic scoring systems (45% mortality according to SAPS II). Of those who survived to hospital discharge, only 14% required ongoing hemodialysis.
Discussion: This large, multinational, multicenter prospective observational study helps better define the prevalence and characteristic of acute renal failure that develops in critically ill patients. Overall, acute renal failure in the ICU setting is relatively uncommon, is most often caused by septic shock, and typically does require renal replacement therapy. There was a surprisingly high rate of acute renal failure thought to be secondary to medication or drug effect (19%).
The mortality in patients who develop renal failure in the ICU is high but, surprisingly, if patients survive, they are unlikely to need long-term hemodialysis. The study is limited in that it was not randomized and outcomes associated with particular interventions could not be determined. Yet, the data adds to our understanding of acute renal failure in the ICU and knowledge of the prevalence and expected outcomes could potentially help with prognosis and end-of-life discussions in the intensive care unit.
Roy CL, Poon EG, Karson AS, et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005;143:121.
Background: Adequate communication between hospitalists and outpatient providers is essential to patient safety as well as patient and physician satisfaction. It is estimated that more than half of all preventable adverse events occurring soon after hospital discharge have been related to poor communication among providers. With increasing pressure to limit inpatient length of stay, patients are often discharged with numerous laboratory or radiologic test results pending.
Methods: Roy and colleagues at a tertiary care academic medical center prospectively determined the prevalence and characteristics of tests pending at discharge and assessed physician awareness as well as satisfaction. All patients discharged from two hospitalist services over four months in 2004 were followed. Researchers identified all pending test results for these patients and all abnormal tests were reviewed by study physicians and judged to be “potentially actionable” or not (if it could change the management of the patient by requiring a new treatment or diagnostic test, change in a treatment, scheduling of an earlier follow-up, etc).
Results: Of the 2,644 patients discharged, 1,095 (41%) had laboratory or radiographic tests pending. Approximately 43% of all pending tests were abnormal and ~10% of the pending tests were judged by physician-reviewers to be potentially actionable. Examples include a TSH that returned as <0.01 mU/mL after discharge in a patient with new atrial fibrillation, or a urine culture that grew an organism resistant to the antibiotics given at discharge. Of note, outpatient physicians were unaware of two-thirds of the “potentially actionable” results. Finally, when surveyed, the majority of inpatient physicians were concerned about appropriate follow-up of tests and dissatisfied with the system used.
Discussion: Roy and his coauthors attempted to quantify the prevalence of potentially actionable laboratory tests available after discharge and published rather striking findings. Up to half of all patients have some tests pending at discharge and up to 10% of these require some physician action. More frighteningly, outpatient MDs are generally unaware of these tests creating a huge gap in patient safety in the transition back to outpatient care.
How can we do this better? SHM and the Society for General Internal Medicine have convened a Continuity of Care Task Force and found poor communication with outpatient providers was a common and potentially dangerous problem. They outlined the best practices for the discharge of patients to ensure safety as well as maximize patient and physician satisfaction. Their recommendations are available on the SHM Web site. All hospitalists and institutions should be aware of the potential for missed results and put systems in place, electronic and otherwise, to create an appropriate safety net for our discharged patients.
Sharma R, Loomis W, Brown RB. Impact of mandatory inpatient infectious disease consultation on outpatient parenteral antibiotic therapy. Am J Med Sci. 2005;330(2):60.
Background: As the pressure to limit healthcare costs by reducing inpatient length of stay has increased, the use of outpatient parenteral antibiotic therapy has grown. When employed appropriately, home intravenous antibiotic therapy has consistently resulted in cost savings without compromising patient outcomes. As with other healthcare advances, there is some fear that outpatient parenteral antibiotic treatment will be overused or misused, limiting the cost savings or putting patients at risk.
Methods: A single academic medical center instituted mandatory infectious disease consultation on all patients referred to discharge coordinators with plans for outpatient IV antibiotic treatment. The infectious disease consultants helped to determine the need for outpatient parenteral therapy and antibiotic choice. All patients were followed for 30 days.
Results: Over the one-year study period, 44 cases received mandatory infectious disease consultation. Thirty-nine (89%) of these had some change in antibiotic regimen after the consultation. Seventeen patients (39%) were switched to oral antibiotics, 13 (30%) had a change in infectious disease antibiotic, and 5 (11%) had a change in antibiotic dose.
Skin and skin structure and intra-abdominal infections were the most common diagnoses for which antibiotics were changed; a typical change was from intravenous piperacillin/tazobactam to an oral fluoroquinolone plus oral anaerobic coverage. At 30-day follow-up, 98% of patients finished their courses without relapse or complication. The overall costs savings was $27,500 or $1,550 per patient consulted upon.
Discussion: Although from a small, nonrandomized, single-institution study, the results are impressive. Mandatory infectious disease consultation prior to discharge for patients scheduled to received outpatient parenteral antibiotic therapy resulted in substantial cost savings, and streamlined and more appropriate antibiotic regimens without any adverse impact on outcomes. Hospitalists should take two things away from this study: 1) consider consulting infection disease specialists on all patients who might be candidates for home IV antibiotics and 2) be aware that many skin and skin tissue and intra-abdominal infections can often be treated with oral therapy. TH
Roy PM, Colombet I, Durieux P, et al. Systemic review and meta-analysis of strategies for the diagnosis of suspected pulmonary embolism. BMJ.2005;331:259.
Background: Despite technological advances, the diagnosis of pulmonary embolism remains challenging. A large number of diagnostic tests and strategies have been evaluated and yet the test characteristics of each and their practical use remain unclear.
Methods: Pierre-Marie Roy, MD and colleagues carried out a systematic review and meta-analysis to define the likelihood ratios (LRs) for different diagnostic modalities for pulmonary embolism and provide a simple, evidence-based diagnostic algorithm.
The authors performed a literature search from 1990-2003 identifying all articles that evaluated tests or strategies aimed at diagnosing pulmonary embolism. They only selected papers which were prospective, in which participants were recruited consecutively, and which pulmonary angiography was the reference standard for strategies to confirm pulmonary embolism and clinical follow-up or angiography were used for exclusion strategies.
Results: Forty-eight articles (11,004 patients) met the inclusion criteria and examined ventilation/perfusion (V/Q) lung scanning, computed tomography (CT) angiography, leg vein ultrasound (U/S), echocardiography, magnetic resonance (MR) angiography, and the D-dimer test. For the studies done to evaluate tests to confirm the diagnosis of pulmonary embolism, pooled positive likelihood ratios (+LRs) were calculated and were:
For the studies evaluating tests to exclude the diagnosis of pulmonary embolism, pooled negative likelihood ratios (-LR) were calculated and were:
Discussion: With the pooled positive and negative LRs, Roy and colleagues created a diagnostic algorithm, based on initial pretest probabilities, to help “rule in” and “rule out” the diagnosis of pulmonary embolism. Consistent with prior studies, a calculated post-test probability of >85% confirmed the diagnosis while a post-test probability <5% excluded PE.
In patients with a low or moderate pretest probability, pulmonary embolism is adequately excluded in patients with either 1) negative D-dimers or 2) a normal V/Q scan or 3) a negative CT angiogram in combination with a normal venous ultrasound. In patients with moderate or high pre-test probability, pulmonary embolism is confirmed by either 1) a high-probability V/Q scan or 2) a positive CT angiogram or 3) a positive venous ultrasound. Low-probability V/Q scanning, CT angiogram alone, and MR angiography have higher negative likelihood ratios and can only exclude PE in patients with low pre-test probability.
Many hospitalists are using CT angiography as their sole diagnostic test for pulmonary embolism. Based on the systematic review and meta-analysis by Roy and colleagues, we should proceed with caution as, in some patient populations, a positive or negative “spiral CT” does not adequately confirm or exclude the diagnosis of pulmonary embolism. For those that employ V/Q scanning, MR angiography, or D-dimers, the study also helps define how best to use these tests.
Safdar N, Maki DG. Risk of catheter-related bloodstream infection with peripherally inserted central venous catheters used in hospitalized patients. Chest. 2005;128:489.
Background: In recent years, peripherally inserted central catheters (PICCs) have become more popular, initially for long-term outpatient intravenous therapy but also for inpatient venous access. Traditionally, it was assumed that PICC lines have a lower rate of catheter-related bloodstream infection than conventional central venous catheters (CVCs) placed in the internal jugular, subclavian, or femoral veins.
Methods: One academic medical center prospectively studied the rate of catheter-related bloodstream infection in PICC lines used exclusively in hospitalized patients as part of two trials assessing efficacy of different skin antiseptics. PICC-related bloodstream infection was confirmed when organisms isolated from positive blood cultures matched (by DNA subtyping) organisms isolated from culturing the PICC line at the time of removal. The authors also performed a systematic review of the literature to provide overall estimates of PICC-related bloodstream infection in hospitalized patients.
Results: A total of 115 patients received 251 PICC lines during the study period and the mean duration of catheterization was 11.3 days. More than 40% of the patients were in the intensive care unit (ICU) and most had risk factors for the development of bloodstream infection, including urinary catheterization, mechanical ventilation, prior antibiotic use, and low albumin. Six cases (2.4%) of PICC-related bloodstream infection were confirmed, four with coagulase-negative staphylococcus, one with S. aureus, and one with Klebsiella pneumoniae, a rate of 2.1 per 1,000 catheter-days. In their systematic review, the authors identified 14 studies evaluating the rate of PICC-related bloodstream infection in hospitalized patients; the pooled rate was 1.9 per 1,000 catheter-days.
Discussion: In a small but methodologically sound prospective study and systematic review, Safdar and Maki found a surprisingly high rate of PICC-related bloodstream infection in hospitalized patients. Their calculated rate of 2.1 cases per 1,000 catheter-days is five times the rate seen in PICCs used exclusively in outpatients (0.4 per 1,000 catheter-days). More strikingly, 2.1 cases per 1,000 catheter-days is similar to the rate of catheter-related bloodstream infection in conventional central venous catheters placed in the subclavian or internal jugular veins (two to five per 1,000 catheter-days). Unfortunately, the study didn’t assess the rate of mechanical complications associated with PICC lines or correlate the risk of infection with duration of catheterization.
Hospitalists should be aware that PICC lines likely have the same infection risk as subclavian and internal jugular lines in hospitalized patients and a much higher rate of infection than PICC lines in outpatients. The higher-than-expected rates are likely related to the increased prevalence of risk factors for bloodstream infection in hospitalized patients. Thus, the decision to use PICC lines in hospitalized patients should be made based on factors other than presumed lower infection risk.
Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients. A multinational, multicenter study. JAMA. 2005;294:813.
Background: Acute renal failure in critically ill patients is believed common and is associated with a high mortality. The exact prevalence and the calculated risk of death have not been clearly defined across populations.
Methods: A multinational group of investigators conducted a massive prospective observational study of ICU patients who developed renal failure after ICU admission. The study encompassed 54 hospitals in 23 countries with a total of 29,269 admissions over the 14-month study period. Note, acute renal failure was defined as either oliguria (urine output <200cc/12 hours) or BUN >84mg/dL.
Results: Of all ICU patients studied, 5.7% developed acute renal failure after admission and 4.7% of patients received renal replacement therapy (most often continuous replacement). The most common contributing factor to the development of acute renal failure was septic shock (48%), followed by major surgery (34%) and cardiogenic shock (26%). Up to 19% of the cases of acute renal failure were estimated to be drug-related. The in-hospital mortality for critically ill patients with acute renal failure was 60%, which was substantially higher than the mortality estimated by other physiologic scoring systems (45% mortality according to SAPS II). Of those who survived to hospital discharge, only 14% required ongoing hemodialysis.
Discussion: This large, multinational, multicenter prospective observational study helps better define the prevalence and characteristic of acute renal failure that develops in critically ill patients. Overall, acute renal failure in the ICU setting is relatively uncommon, is most often caused by septic shock, and typically does require renal replacement therapy. There was a surprisingly high rate of acute renal failure thought to be secondary to medication or drug effect (19%).
The mortality in patients who develop renal failure in the ICU is high but, surprisingly, if patients survive, they are unlikely to need long-term hemodialysis. The study is limited in that it was not randomized and outcomes associated with particular interventions could not be determined. Yet, the data adds to our understanding of acute renal failure in the ICU and knowledge of the prevalence and expected outcomes could potentially help with prognosis and end-of-life discussions in the intensive care unit.
Roy CL, Poon EG, Karson AS, et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005;143:121.
Background: Adequate communication between hospitalists and outpatient providers is essential to patient safety as well as patient and physician satisfaction. It is estimated that more than half of all preventable adverse events occurring soon after hospital discharge have been related to poor communication among providers. With increasing pressure to limit inpatient length of stay, patients are often discharged with numerous laboratory or radiologic test results pending.
Methods: Roy and colleagues at a tertiary care academic medical center prospectively determined the prevalence and characteristics of tests pending at discharge and assessed physician awareness as well as satisfaction. All patients discharged from two hospitalist services over four months in 2004 were followed. Researchers identified all pending test results for these patients and all abnormal tests were reviewed by study physicians and judged to be “potentially actionable” or not (if it could change the management of the patient by requiring a new treatment or diagnostic test, change in a treatment, scheduling of an earlier follow-up, etc).
Results: Of the 2,644 patients discharged, 1,095 (41%) had laboratory or radiographic tests pending. Approximately 43% of all pending tests were abnormal and ~10% of the pending tests were judged by physician-reviewers to be potentially actionable. Examples include a TSH that returned as <0.01 mU/mL after discharge in a patient with new atrial fibrillation, or a urine culture that grew an organism resistant to the antibiotics given at discharge. Of note, outpatient physicians were unaware of two-thirds of the “potentially actionable” results. Finally, when surveyed, the majority of inpatient physicians were concerned about appropriate follow-up of tests and dissatisfied with the system used.
Discussion: Roy and his coauthors attempted to quantify the prevalence of potentially actionable laboratory tests available after discharge and published rather striking findings. Up to half of all patients have some tests pending at discharge and up to 10% of these require some physician action. More frighteningly, outpatient MDs are generally unaware of these tests creating a huge gap in patient safety in the transition back to outpatient care.
How can we do this better? SHM and the Society for General Internal Medicine have convened a Continuity of Care Task Force and found poor communication with outpatient providers was a common and potentially dangerous problem. They outlined the best practices for the discharge of patients to ensure safety as well as maximize patient and physician satisfaction. Their recommendations are available on the SHM Web site. All hospitalists and institutions should be aware of the potential for missed results and put systems in place, electronic and otherwise, to create an appropriate safety net for our discharged patients.
Sharma R, Loomis W, Brown RB. Impact of mandatory inpatient infectious disease consultation on outpatient parenteral antibiotic therapy. Am J Med Sci. 2005;330(2):60.
Background: As the pressure to limit healthcare costs by reducing inpatient length of stay has increased, the use of outpatient parenteral antibiotic therapy has grown. When employed appropriately, home intravenous antibiotic therapy has consistently resulted in cost savings without compromising patient outcomes. As with other healthcare advances, there is some fear that outpatient parenteral antibiotic treatment will be overused or misused, limiting the cost savings or putting patients at risk.
Methods: A single academic medical center instituted mandatory infectious disease consultation on all patients referred to discharge coordinators with plans for outpatient IV antibiotic treatment. The infectious disease consultants helped to determine the need for outpatient parenteral therapy and antibiotic choice. All patients were followed for 30 days.
Results: Over the one-year study period, 44 cases received mandatory infectious disease consultation. Thirty-nine (89%) of these had some change in antibiotic regimen after the consultation. Seventeen patients (39%) were switched to oral antibiotics, 13 (30%) had a change in infectious disease antibiotic, and 5 (11%) had a change in antibiotic dose.
Skin and skin structure and intra-abdominal infections were the most common diagnoses for which antibiotics were changed; a typical change was from intravenous piperacillin/tazobactam to an oral fluoroquinolone plus oral anaerobic coverage. At 30-day follow-up, 98% of patients finished their courses without relapse or complication. The overall costs savings was $27,500 or $1,550 per patient consulted upon.
Discussion: Although from a small, nonrandomized, single-institution study, the results are impressive. Mandatory infectious disease consultation prior to discharge for patients scheduled to received outpatient parenteral antibiotic therapy resulted in substantial cost savings, and streamlined and more appropriate antibiotic regimens without any adverse impact on outcomes. Hospitalists should take two things away from this study: 1) consider consulting infection disease specialists on all patients who might be candidates for home IV antibiotics and 2) be aware that many skin and skin tissue and intra-abdominal infections can often be treated with oral therapy. TH
Roy PM, Colombet I, Durieux P, et al. Systemic review and meta-analysis of strategies for the diagnosis of suspected pulmonary embolism. BMJ.2005;331:259.
Background: Despite technological advances, the diagnosis of pulmonary embolism remains challenging. A large number of diagnostic tests and strategies have been evaluated and yet the test characteristics of each and their practical use remain unclear.
Methods: Pierre-Marie Roy, MD and colleagues carried out a systematic review and meta-analysis to define the likelihood ratios (LRs) for different diagnostic modalities for pulmonary embolism and provide a simple, evidence-based diagnostic algorithm.
The authors performed a literature search from 1990-2003 identifying all articles that evaluated tests or strategies aimed at diagnosing pulmonary embolism. They only selected papers which were prospective, in which participants were recruited consecutively, and which pulmonary angiography was the reference standard for strategies to confirm pulmonary embolism and clinical follow-up or angiography were used for exclusion strategies.
Results: Forty-eight articles (11,004 patients) met the inclusion criteria and examined ventilation/perfusion (V/Q) lung scanning, computed tomography (CT) angiography, leg vein ultrasound (U/S), echocardiography, magnetic resonance (MR) angiography, and the D-dimer test. For the studies done to evaluate tests to confirm the diagnosis of pulmonary embolism, pooled positive likelihood ratios (+LRs) were calculated and were:
For the studies evaluating tests to exclude the diagnosis of pulmonary embolism, pooled negative likelihood ratios (-LR) were calculated and were:
Discussion: With the pooled positive and negative LRs, Roy and colleagues created a diagnostic algorithm, based on initial pretest probabilities, to help “rule in” and “rule out” the diagnosis of pulmonary embolism. Consistent with prior studies, a calculated post-test probability of >85% confirmed the diagnosis while a post-test probability <5% excluded PE.
In patients with a low or moderate pretest probability, pulmonary embolism is adequately excluded in patients with either 1) negative D-dimers or 2) a normal V/Q scan or 3) a negative CT angiogram in combination with a normal venous ultrasound. In patients with moderate or high pre-test probability, pulmonary embolism is confirmed by either 1) a high-probability V/Q scan or 2) a positive CT angiogram or 3) a positive venous ultrasound. Low-probability V/Q scanning, CT angiogram alone, and MR angiography have higher negative likelihood ratios and can only exclude PE in patients with low pre-test probability.
Many hospitalists are using CT angiography as their sole diagnostic test for pulmonary embolism. Based on the systematic review and meta-analysis by Roy and colleagues, we should proceed with caution as, in some patient populations, a positive or negative “spiral CT” does not adequately confirm or exclude the diagnosis of pulmonary embolism. For those that employ V/Q scanning, MR angiography, or D-dimers, the study also helps define how best to use these tests.
Safdar N, Maki DG. Risk of catheter-related bloodstream infection with peripherally inserted central venous catheters used in hospitalized patients. Chest. 2005;128:489.
Background: In recent years, peripherally inserted central catheters (PICCs) have become more popular, initially for long-term outpatient intravenous therapy but also for inpatient venous access. Traditionally, it was assumed that PICC lines have a lower rate of catheter-related bloodstream infection than conventional central venous catheters (CVCs) placed in the internal jugular, subclavian, or femoral veins.
Methods: One academic medical center prospectively studied the rate of catheter-related bloodstream infection in PICC lines used exclusively in hospitalized patients as part of two trials assessing efficacy of different skin antiseptics. PICC-related bloodstream infection was confirmed when organisms isolated from positive blood cultures matched (by DNA subtyping) organisms isolated from culturing the PICC line at the time of removal. The authors also performed a systematic review of the literature to provide overall estimates of PICC-related bloodstream infection in hospitalized patients.
Results: A total of 115 patients received 251 PICC lines during the study period and the mean duration of catheterization was 11.3 days. More than 40% of the patients were in the intensive care unit (ICU) and most had risk factors for the development of bloodstream infection, including urinary catheterization, mechanical ventilation, prior antibiotic use, and low albumin. Six cases (2.4%) of PICC-related bloodstream infection were confirmed, four with coagulase-negative staphylococcus, one with S. aureus, and one with Klebsiella pneumoniae, a rate of 2.1 per 1,000 catheter-days. In their systematic review, the authors identified 14 studies evaluating the rate of PICC-related bloodstream infection in hospitalized patients; the pooled rate was 1.9 per 1,000 catheter-days.
Discussion: In a small but methodologically sound prospective study and systematic review, Safdar and Maki found a surprisingly high rate of PICC-related bloodstream infection in hospitalized patients. Their calculated rate of 2.1 cases per 1,000 catheter-days is five times the rate seen in PICCs used exclusively in outpatients (0.4 per 1,000 catheter-days). More strikingly, 2.1 cases per 1,000 catheter-days is similar to the rate of catheter-related bloodstream infection in conventional central venous catheters placed in the subclavian or internal jugular veins (two to five per 1,000 catheter-days). Unfortunately, the study didn’t assess the rate of mechanical complications associated with PICC lines or correlate the risk of infection with duration of catheterization.
Hospitalists should be aware that PICC lines likely have the same infection risk as subclavian and internal jugular lines in hospitalized patients and a much higher rate of infection than PICC lines in outpatients. The higher-than-expected rates are likely related to the increased prevalence of risk factors for bloodstream infection in hospitalized patients. Thus, the decision to use PICC lines in hospitalized patients should be made based on factors other than presumed lower infection risk.
Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients. A multinational, multicenter study. JAMA. 2005;294:813.
Background: Acute renal failure in critically ill patients is believed common and is associated with a high mortality. The exact prevalence and the calculated risk of death have not been clearly defined across populations.
Methods: A multinational group of investigators conducted a massive prospective observational study of ICU patients who developed renal failure after ICU admission. The study encompassed 54 hospitals in 23 countries with a total of 29,269 admissions over the 14-month study period. Note, acute renal failure was defined as either oliguria (urine output <200cc/12 hours) or BUN >84mg/dL.
Results: Of all ICU patients studied, 5.7% developed acute renal failure after admission and 4.7% of patients received renal replacement therapy (most often continuous replacement). The most common contributing factor to the development of acute renal failure was septic shock (48%), followed by major surgery (34%) and cardiogenic shock (26%). Up to 19% of the cases of acute renal failure were estimated to be drug-related. The in-hospital mortality for critically ill patients with acute renal failure was 60%, which was substantially higher than the mortality estimated by other physiologic scoring systems (45% mortality according to SAPS II). Of those who survived to hospital discharge, only 14% required ongoing hemodialysis.
Discussion: This large, multinational, multicenter prospective observational study helps better define the prevalence and characteristic of acute renal failure that develops in critically ill patients. Overall, acute renal failure in the ICU setting is relatively uncommon, is most often caused by septic shock, and typically does require renal replacement therapy. There was a surprisingly high rate of acute renal failure thought to be secondary to medication or drug effect (19%).
The mortality in patients who develop renal failure in the ICU is high but, surprisingly, if patients survive, they are unlikely to need long-term hemodialysis. The study is limited in that it was not randomized and outcomes associated with particular interventions could not be determined. Yet, the data adds to our understanding of acute renal failure in the ICU and knowledge of the prevalence and expected outcomes could potentially help with prognosis and end-of-life discussions in the intensive care unit.
Roy CL, Poon EG, Karson AS, et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005;143:121.
Background: Adequate communication between hospitalists and outpatient providers is essential to patient safety as well as patient and physician satisfaction. It is estimated that more than half of all preventable adverse events occurring soon after hospital discharge have been related to poor communication among providers. With increasing pressure to limit inpatient length of stay, patients are often discharged with numerous laboratory or radiologic test results pending.
Methods: Roy and colleagues at a tertiary care academic medical center prospectively determined the prevalence and characteristics of tests pending at discharge and assessed physician awareness as well as satisfaction. All patients discharged from two hospitalist services over four months in 2004 were followed. Researchers identified all pending test results for these patients and all abnormal tests were reviewed by study physicians and judged to be “potentially actionable” or not (if it could change the management of the patient by requiring a new treatment or diagnostic test, change in a treatment, scheduling of an earlier follow-up, etc).
Results: Of the 2,644 patients discharged, 1,095 (41%) had laboratory or radiographic tests pending. Approximately 43% of all pending tests were abnormal and ~10% of the pending tests were judged by physician-reviewers to be potentially actionable. Examples include a TSH that returned as <0.01 mU/mL after discharge in a patient with new atrial fibrillation, or a urine culture that grew an organism resistant to the antibiotics given at discharge. Of note, outpatient physicians were unaware of two-thirds of the “potentially actionable” results. Finally, when surveyed, the majority of inpatient physicians were concerned about appropriate follow-up of tests and dissatisfied with the system used.
Discussion: Roy and his coauthors attempted to quantify the prevalence of potentially actionable laboratory tests available after discharge and published rather striking findings. Up to half of all patients have some tests pending at discharge and up to 10% of these require some physician action. More frighteningly, outpatient MDs are generally unaware of these tests creating a huge gap in patient safety in the transition back to outpatient care.
How can we do this better? SHM and the Society for General Internal Medicine have convened a Continuity of Care Task Force and found poor communication with outpatient providers was a common and potentially dangerous problem. They outlined the best practices for the discharge of patients to ensure safety as well as maximize patient and physician satisfaction. Their recommendations are available on the SHM Web site. All hospitalists and institutions should be aware of the potential for missed results and put systems in place, electronic and otherwise, to create an appropriate safety net for our discharged patients.
Sharma R, Loomis W, Brown RB. Impact of mandatory inpatient infectious disease consultation on outpatient parenteral antibiotic therapy. Am J Med Sci. 2005;330(2):60.
Background: As the pressure to limit healthcare costs by reducing inpatient length of stay has increased, the use of outpatient parenteral antibiotic therapy has grown. When employed appropriately, home intravenous antibiotic therapy has consistently resulted in cost savings without compromising patient outcomes. As with other healthcare advances, there is some fear that outpatient parenteral antibiotic treatment will be overused or misused, limiting the cost savings or putting patients at risk.
Methods: A single academic medical center instituted mandatory infectious disease consultation on all patients referred to discharge coordinators with plans for outpatient IV antibiotic treatment. The infectious disease consultants helped to determine the need for outpatient parenteral therapy and antibiotic choice. All patients were followed for 30 days.
Results: Over the one-year study period, 44 cases received mandatory infectious disease consultation. Thirty-nine (89%) of these had some change in antibiotic regimen after the consultation. Seventeen patients (39%) were switched to oral antibiotics, 13 (30%) had a change in infectious disease antibiotic, and 5 (11%) had a change in antibiotic dose.
Skin and skin structure and intra-abdominal infections were the most common diagnoses for which antibiotics were changed; a typical change was from intravenous piperacillin/tazobactam to an oral fluoroquinolone plus oral anaerobic coverage. At 30-day follow-up, 98% of patients finished their courses without relapse or complication. The overall costs savings was $27,500 or $1,550 per patient consulted upon.
Discussion: Although from a small, nonrandomized, single-institution study, the results are impressive. Mandatory infectious disease consultation prior to discharge for patients scheduled to received outpatient parenteral antibiotic therapy resulted in substantial cost savings, and streamlined and more appropriate antibiotic regimens without any adverse impact on outcomes. Hospitalists should take two things away from this study: 1) consider consulting infection disease specialists on all patients who might be candidates for home IV antibiotics and 2) be aware that many skin and skin tissue and intra-abdominal infections can often be treated with oral therapy. TH
SHM Establishes Palliative Care Task Force
Hospitalists lead, coordinate, and participate in initiatives to improve the identification and treatment of patients and families in need of palliative care. Yet we often lack the knowledge and skills necessary to provide outstanding palliative care; we may also lack the comfort level we need to take care of patients at that stage of illness.
Steve Pantilat, MD, SHM president and member of the SHM Education Committee, established the Palliative Care Task Force to identify and create opportunities to improve palliative care in the field of hospital medicine. The Palliative Care Task Force had its inaugural meeting in August. Led by founder Dr. Pantilat and Chad Whelan, MD, Palliative Care Task Force chair, the task force established the following goals:
- Promote palliative care as an important skill and activity for hospital medicine physicians and providers;
- Identify and create palliative-care-focused educational activities for hospital medicine physicians and other key stakeholders within hospital medicine;
- Advocate for the creation and or support of hospital-based palliative care services;
- Promote the use of best practices in palliative care; and
- Develop a core community of hospital medicine physicians dedicated to improving our understanding of palliative care.
Our current task force membership is small but energetic. We actively recruit members, particularly nonphysicians and non-SHM members. Palliative care is a multidisciplinary field, and we hope the Palliative Care Task Force membership will reflect this diversity. Potential areas of growth include pharmacists, nurses, social workers, spiritual care providers, and nonhospitalist physicians. We are also looking for a pediatrician with an interest in palliative care to represent the pediatric interests among SHM members.
Since the first meeting in August our members have been developing a plan to achieve our identified goals. While the plan is still early in its development, we have designed a multimodal approach that will rely on traditional CME meetings, print media, as well as electronic media.
The task force’s short-term goals include promoting best practices in palliative care via SHM communication vehicles. For example, we plan to propose a series of articles for the forthcoming Journal of Hospital Medicine to highlight key issues in palliative care.
The 2006 SHM Annual Meeting will feature two workshops with a palliative care focus. One workshop will discuss how to build the case for a palliative care service; the other will address issues in pain management for hospitalized patients. We will learn from the 2006 experience as we look toward the 2007 SHM Annual Meeting in Texas. An electronic CME module is also under development.
Finally, we are planning an electronic compendium of resources and tools for practicing high-quality palliative care. Although the format has not been finalized, the concept is to provide resources that will make caring for palliative care patients as easy as possible.
While we are pleased with the progress of the task force to date, there is still much to do. Hospital medicine physicians can and should serve as leaders to improve palliative care. Traditional medical training focuses our efforts and thoughts of curing and preventing. We’ve all felt the exhilaration of making a life-saving diagnosis on the young, otherwise healthy patient; however, just as there are times to look for a cure at all costs, there are also times when we must treat our patients’ symptoms at all costs.
Often traditional medical training doesn’t provide us with the tools we need to best care for our patients and their families when palliative care goals become the priority. We hope this task force will raise the visibility of palliative care within SHM and provide the opportunities and tools needed for us, as hospital medicine providers, to offer the best palliative care possible to our patients. If successful, we’ll feel the deep personal satisfaction and self-reward of helping a patient and their family transition from hopes of a cure to comfort in the knowledge that their symptoms and needs will be cared for.
Interested in joining the task force or participating in a related work group? Contact Chad Whelan at cwhelan@medicine.bsd.uchicago.edu.
The Stroke Resource Room
SHM’s Web site features stroke information on call
Online resource rooms comprise an innovative venue within the SHM Web site to focus on essential topics from the forthcoming core curriculum. Specifically, the Web-based resource rooms organize expert opinions, evidence-based literature, clinical tools and guidelines, and recommendations about essential topics in hospital medicine. Initial areas of development include the DVT and stroke resource rooms, with ongoing efforts in other areas including geriatrics, antimicrobial resistance, congestive heart failure, and glycemic control. These interactive rooms help connect hospitalists to information, content experts, and each other.
The Stroke Imperative
Stroke is the third leading cause of death in the United States and a common admission diagnosis. Cerebrovascular disease is a field of great complexity and rapid advance. There is great pressure on the practicing hospitalist to have both a base knowledge of the approach to the patient with stroke as well as an understanding of current best practice.
Traditional internal medicine residencies may not fully prepare one for hospitalist practice. Many patients seen by hospitalists have diagnoses that were managed by internal medicine subspecialties in the past. Most hospitalists feel comfortable managing straightforward gastrointestinal bleeds, myocardial infarctions, and renal failure without consultation. Neurologic cases are somewhat different.
Most medicine residents have rotated on a neurology service, but that limited experience is frequently insufficient in preparing physicians for their future experience as hospitalists. While neurology residencies include one year of internal medicine, the two diverge dramatically afterward. Practitioners of both internal medicine and neurology frequently feel that they speak a different language from one another.
Particularly in the community setting, hospitalists manage the bulk of neurology patients either with or without neurologic consultation. The reasons for this are varied, including poor inpatient reimbursement for neurologists and a tradition of nonaggressive approaches to stroke care.1
The Opportunity
Realizing the need to provide direct access to important information about inpatient stroke management, SHM convened a stroke advisory board, including general hospitalists, a neurologist, and members of the education committee. SHM and Boehringer-Ingelheim provided funding for the resource room through educational funds and an unrestricted grant, respectively.

Stroke Resource Room Content
The Stroke Resource Room is patterned after the template of the DVT Resource Room; the idea being that a standardized format will allow easy navigation and maximal utility. David Likosky, MD, served as content editor, Sandeep Sachdeva, MD, as quality editor, Alpesh Amin, MD as education editor, and Jason Stein, MD, as managing editor.
The rooms are structured to facilitate access to specific types of information. Whether one is looking for the details of a certain study, slide sets to help teach residents, or for input on how to approach a difficult patient, that resource should be readily available. The main sections of the room are summarized below.
The “Awareness” area on the main page of the Stroke Resource Room defines the effects of stroke as well as the hospitalists’ scope of practice.
A separate debate is ongoing within neurology about who should be responsible for the inpatient management of stroke. Interestingly, much of this is about whether general neurologists or vascular/stroke neurologists should primarily manage these patients. One such article referred to the brain as “… the Rolls Royce of the human body” going on to ask, “Would you want your Rolls Royce to be serviced by any ordinary mechanic, who takes care of all kinds of automobiles?”2 Many hospitalists find this argument less than compelling given how difficult it can be in many communities to get a neurologist much less a “vascular neurologist” to see an inpatient.
The “Evidence” section consists of two main parts with the goal of providing a one-stop shop for stroke care literature. The first is a set of links to articles reviewed by the ACP journal club. The second is a concise list of landmark trials, such as the Heparin Acute Embolic Stroke HAEST) trial, which compared low molecular weight heparin versus aspirin in patients with acute stroke and atrial fibrillation.3 These articles help answer questions that come up commonly in clinical practice.
The Experience link capitalizes on the Internet’s ability to disseminate information. There are a limited number of protocols and order sets for ischemic and hemorrhagic stroke available. One can download these and, perhaps more importantly, submit one’s own—including comments on what about that particular tool has been valuable.
Finally, the “Ask the Expert” section features an interactive venue for interacting with a panel of neurologists and neurocritical care physicians. This section answers the more common and more difficult clinical questions in a shared forum. Supportive evidence is cited, with the knowledge that much of stroke care remains in the realm of standard of practice.
The “Improve” section reflects the other roles of hospitalists, such as hospital leader. The three current links include a PowerPoint primer on quality improvement. In addition, there are links to the “Get with the Guidelines” program from the American Stroke Association. This is a continuous quality improvement program focusing on care team protocols and outcome measurement. The final linked site is to the criteria for the disease specific accreditation program from JCAHO. This national effort may drive where patients receive their care for certain conditions.
The “Educate” section caters to multiple audiences. The academic hospitalist may find the “Teaching Pearls” section helpful, as well as the slide sets from the International Stroke Conference and StrokeSTOP, which is aimed at medical students. The patient education links contain a wealth of quality information. The “Professional Development” subsection contains sources for audio lectures with slide sets as well as case presentations and NIH stroke scale training—all with free CME hours. A chapter on stroke from the SHM’s forthcoming core competencies is included as well.
Moving Forward
One of the advantages of an Internet-based resource is the ability to be easily modified. A progressively more robust database will be developed over time as questions are answered in the “Ask the Expert” section and as participants share their stroke care protocols.
The Stroke Resource Room is an excellent forum to improve clinical care and form the basis for future SHM workshops, lectures, and to review articles. By building our collective knowledge, we will be limited only by the energy we put into the adding to and using available information and our desire to apply that energy to patient care.
References
- Likosky DJ, Amin AN. Who will care for our hospitalized patients? Stroke. 2005;36(6): 1113-1114.
- Caplan L. Stroke is best managed by neurologists. Stroke. 2003;34(11):2763.
- Berge E, Abdelnoor M, Nakstad PH, et al. Low molecular-weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: a double-blind randomized study. HAEST Study Group. Lancet. 2000;355(9211):1205-1210.
Secure the Future
Encourage trainees to consider lifelong careers in hospital medicine
By Vineet Arora, MD, MA, and Margaret C. Fang, MD, MPH, co-chairs of SHM’s Young Physicians Section
Interest in hospital medicine is booming, and it is estimated that the number of hospitalists in the United States is estimated will exceed the number of cardiologists in the near future. Yet, many graduating residents view hospital medicine as a temporary job where they can take time off and work before going on to a subspecialty fellowship. Others perceive hospitalists as “super-residents” susceptible to burnout, and therefore do not consider hospital medicine a sustainable career option. These perceptions may contribute to a high turnover of hospitalists and compromise the accumulation of enough inpatient experience to accomplish many of the benefits associated with the use of hospitalists, including shorter lengths of stay and comparable—if not better—quality of care.
To ensure recruitment and retention of the best and brightest trainees, it’s important to consider ways to educate and encourage them to consider a career in hospital medicine as a rewarding lifelong career. Below, we discuss strategies to encourage trainees to pursue a lifelong career in hospital medicine.
Showcase Your Clinical Work
First, consider your everyday practice an excellent way to showcase the often-exciting world of inpatient medicine. Preclinical students often cherish any opportunity to interact with patients. Inviting first- or second-year medical students to accompany you on rounds is an excellent opportunity to teach clinical medicine and physical exam skills, and a good way to influence their career choice early in their medical career.
If you’re in an academic medical center, accessing preclinical students is as easy as approaching students in an internal medicine interest group or volunteering as a preceptor for a physical diagnosis course for preclinical students. In fact, hospitalists are often acknowledged as some of the best teachers and are highly accessible because of their inpatient duties.
Community-based hospitalists also can provide valuable career advice and opportunities, particularly in exposing students to real-life career experiences often not covered through traditional medical school training. One way for a community-based hospitalist to become involved is to host preclinical students over the summer by contacting a local medical school dean’s office and volunteering as a summer preceptor for interested preclinical students. Your alma mater may be particularly responsive. Or, contact interest groups in internal medicine, family medicine, or pediatrics through the state or local leaders of the American College of Physicians, the American Academy of Family Physicians, and the American Academy of Pediatrics.
Explain Your Nonclinical Work
It’s important to explain your nonclinical roles to residency trainees. Hospitalists increasingly take on numerous administrative, educational, and leadership roles and responsibilities. Whether you are leading a quality improvement effort, interfacing with hospital operations, or running a medical student clerkship, it is crucial that physicians-in-training understand the diverse opportunities within hospital medicine to achieve a healthy work-life balance and avoid clinical burnout.
If you are involved with quality improvement projects at your institution, enlist the help of an interested resident or student. Because student rotations are frequent, their prior experience may be scant and their time limited. So make sure the projects have definite goals and are easily accomplished. Ensure that the projects provide reasonable educational value and experience within a finite time. Lay out explicit goals at the beginning of the project, ask for frequent updates, and then recap the experience and any concrete accomplishments to provide structure and expectations for the process.
For example, the University of California at San Francisco Hospitalist Group is spearheading an educational initiative in which residents learn about both the theory and practice of quality improvement through choosing a project and working with a mentor to design, implement, and measure the results of a quality improvement initiative.
Share Your Passion
In addition to showcasing your clinical and nonclinical activities, share your passion about hospital medicine. Reflect on the reasons you entered hospital medicine, as well as your thoughts on the pros and cons of the field. Perhaps you were drawn to hospital medicine because of a desire to take care of acutely ill patients, or to work on improving the quality of a medical system, or because of a more controllable work schedule with competitive compensation.
In some cases, it may have been a particular interest in medical ethics, palliative care, geriatrics, or perioperative care. Sharing your enthusiasm is the best way to cultivate reciprocal interest. Medical students and residents closely observe your attitudes toward your career, your job satisfaction, and your work-life balance. In addition to mentoring those already entering a medical career, there are endless opportunities to outreach to younger students, including those in high school and college. Many local schools and community organizations offer mentorship programs to area students. Engaging in an informal discussion about your career at a social or community event with younger students can be incredibly rewarding. Younger students often lack realistic career experiences and access to career-specific role models on which to base informed decisions. Although they may express an interest in science or medicine, they may not know how long the training process is or the importance of good grades.
Take a moment to inquire about career interests and explain what a hospitalist is; this can be invaluable in promoting understanding and cultivating interest into the field. More structured interactions with hospitalists can also prepare students for successful entry into the medical field. The University of Chicago Hospitalists, for example, host high-achieving Chicago public school juniors in a summer clinical and research enrichment program in hospital-based medicine called TEACH Research.
Offer Advice and Assistance
Finding your first job can be a nerve-racking situation. Sharing your advice on the process with trainees is always appreciated. For instance, they are interested in hearing how you decided to become a hospitalist and what you did to secure your position.
Offer to meet with them and review their career interests, goals, and curriculum vitae. If you hear of job openings and opportunities, inform the community of trainees by contacting program directors or chief residents at residency programs. Many residency program directors showcase available opportunities in their house-staff office or direct such opportunities to interested residents. Some residency programs invite community-based physicians to give residents insight on securing their first job. This process is particularly foreign to medical trainees who have never had to negotiate such things as benefit packages, compensation, or call schedule. Your candid thoughts on what to expect and how to approach the process are invaluable.
Again, approaching the residency program where you trained is a good starting point. Alternatively, you can locate a nearby residency through the Fellowship and Residency Electronic Interactive Database database offered by the American Medical Association (www.ama-assn.org/vapp/freida/srch/).
Finally, if you know any trainees interested in hospital medicine,encourage them to attend the SHM’s local or national meetings. The annual meeting is an excellent place for medical trainees to hear the latest research and innovations, learn about advanced training and job opportunities, network, and connect with mentors through the Mentorship Breakfast. For the last two years, the Young Physicians Section has organized a Forum for Early Career Hospitalists where we addressed different career paths in hospital medicine and conducted research during training. Continued growth in our field depends on promoting hospital medicine as a vital, sustainable career.
Busy Summer for HQPS
The Health Quality and Patient Safety Committee (HQPS) has developed an array of initiatives to support SHM members in the development, implementation, and evaluation of quality and system improvements at their institutions. Educational programming, tools, and resources are being developed for four specific content areas including prevention of VTE, improving the discharge process, glycemic control, and improving outcomes for hospitalized heart failure patients.
HQPS members and Course Directors Greg Maynard, MD, and Tosha Wetterneck, MD, are developing a quality precourse for the 2006 SHM Annual Meeting. The educational goal for the precourse will be to enable hospitalists to become leaders in quality and safety through the effective implementation of evidence-based, high reliability interventions. Precourse participants will actively participate in small groups to apply techniques for designing, implementing, and evaluating quality improvement projects to address a specific improvement need in one of four areas: heart failure care, glycemic control, and preventing VTE in the hospital or the discharge process. Registration for this precourse will begin in November and space will be limited. Plan to register early.
In June, HQPS convened a multidisciplinary, multiagency Heart Failure Advisory Board to guide the development of a clinical guidelines implementation toolkit (CGIT), resource room, and CME modules related to implementing best practices for care of patients with heart-failure. The advisory board has representatives from several organizations and allied health professions, including the American College of Cardiology, American Medical Directors Association, American Hospital Association, Case Managers Society of America, American Association of Heart Failure Nurses, American Society of Health-System Pharmacists, American Association of Critical Care Nurses, National Association of Social Workers and the Heart Failure Society of America. Currently, the advisory board is completing a needs assessment and will begin development on the CGIT, resource room and CME modules next month.
In July, in collaboration with the Education Committee and SHM staff, HQPS launched the SHM VTE Resource Room (www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312). The resource room provides users with a workbook, or step-wise process to assess the need for VTE prevention, advocate for local improvements, and implement and evaluate a VTE prevention program. The resource room also provides a useful review of the literature, an “Ask the Expert” forum, slide sets, and bedside teaching tools.
In August, the SHM Executive Committee approved the SHM Discharge Planning Checklist developed by HQPS under the direction of Dennis Manning, MD. This discharge planning checklist and a white paper on guidance for its implementation will be available to members in the near future.
Interested in learning more about these initiatives or becoming involved in an HQPS workgroup? Contact Lakshmi Halasyamani, MD, HQPS chair, at HalasyaL@trinity-health.org.
Hartford Grants Awarded
SHM presents Hartford Foundation grant funds to hospitalists for QI demo project
By Kathleen K. Frampton, RN, MPH
Shm remains committed to expanding its efforts to improve inpatient care for older patients. The John A. Hartford Foundation has generously awarded approximately $370,000 to SHM in support of its focus on the geriatric population. This funding will assist SHM in its endeavors related to educational programs and products, hospitalist leadership training, and quality improvement projects. In light of this, SHM allocated a portion of these Hartford grant funds to study a critical aspect of elderly patient care, safety-care transitions.
A competitive request for the proposal (RFP) process was conducted to solicit interest from healthcare institutional providers and SHM members willing to serve as the principle investigator in their work setting. The RFP delineated the requirements for a hospital to serve as a designated study site to implement a discharge planning intervention from hospital-based care to community-based care for elderly patients and to evaluate the facilitating factors, barriers to implementation and outcomes associated with the new approach.
All research proposals submitted by hospitals were evaluated and scored against established criteria. Qualifying hospital finalists were reviewed by a panel consisting of members of three standing SHM Committees: Education, Hospital Quality and Patient Safety, and Research and Executive. In July 2005, this panel selected three hospitals to receive funding for this initiative: Johns Hopkins-Bayview, Baltimore, Md.; Northeast Medical Center, Concord, N.C.; and Geisinger Health System, Danville, Penn.
Johns Hopkins-Bayview (coordinating site): A 355-bed community-based facility located in southeast Baltimore with academic affiliations and approximately 25% of patients over age 65. The hospitalist service consists of nine physicians, five physician assistants, and three nurse practitioners.
Northeast Medical Center: A 457-bed, private, nonprofit community-based facility located in the Charlotte Region with a residency training program and 36% of patients over age 65. The hospitalist service consists of 16 physicians and 24/7 intensivist coverage.
Geisinger Health System: A 366-bed facility and Level 1 Trauma Center, private, nonprofit community based system located in north central Pennsylvania with a residency training program and 70% of patients over age 65. The hospitalist service is staffed by 15 physicians (10 full-time employees).
The QI Demonstration Project will run for 18 months and, according to Tina Budnitz, MPH, SHM senior advisor for planning and development, the study “represents new territory for both SHM and other professional societies … . We have moved beyond developing a best practice to use in the clinical setting to how you can actually change the system so that best practices can be successfully implemented … . It is the intention of SHM to focus on safe practice interventions that can be generalized to other settings.”
Budnitz also explained that near completion of the project SHM plans to convene the advisory board, grantee project teams, representatives of the Hartford Foundation, and the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) to review the data from the demonstration project and design a larger scale quality improvement program.
“Our grantees will work with the SHM Advisory Board to develop a comprehensive toolkit, which will document the lessons learned during the implementation process and any other resources that facilitate adaptation and/or adoption of these safe practice interventions,” explains Budnitz.
Care Transitions in the Treatment of the Elderly
According to the Institute of Medicine (IOM), the healthcare system is poorly organized to meet its current challenges. The delivery of care is often overly complex and uncoordinated, requiring steps and patient hand-offs that slow care and decrease rather than improve patient safety.
An IOM seminal report published in 2001, Crossing the Quality Chasm: A New Health System for the 21st Century, emphasizes that cumbersome processes waste resources, leave unaccountable voids in coverage, lead to loss of information, and fail to build on the strengths of all professionals involved to ensure that care is appropriate, timely, and safe. Right before and after discharge, there often is no one clearly in charge of the transition whom the patient may contact for guidance. Patients are often instructed to contact their primary care provider for follow-up issues or questions, whether or not the primary care provider had been involved in the hospitalization.
A recent study supported by the Agency for Healthcare Research and Quality (AHRQ) showed that high-risk patient targeting, better communications, and better coordination of care and follow-up could potentially prevent some readmissions when transitioning patients from hospital to home.
In 2002, the American Geriatric Society (AGS) issued a Position Statement, Improving the Quality of Transitional Care for Persons with Complex Care Needs, which stressed that both the “sending” and “receiving” health professionals bear responsibility and accountability in this phase. Successful transitions require that there be both a uniform plan of care and procedure for communicating the following:
- An accessible medical record that contains a current problem list;
- A medication regimen;
- A list of allergies;
- Advance directives;
- Baseline physical and cognitive function; and
- Contact information for all professional and informal care providers.
Also, input must be solicited from informal care providers who are involved in the execution of the plan of care. The AGS recommends the use of a “coordinating” health professional who oversees both the sending and receiving aspects of the transition. This professional should be skilled in the identification of health status, assessment and management of multiple chronic conditions, managing medications, and collaboration with members of the interdisciplinary team and caregivers.
The QI Demonstration Project
According to SHM Immediate Past-President Jeanne Huddleston, MD, SHM has structured this demonstration project so that the three study sites in the Hartford Grant Group will implement identical clinical tools while they employ unique processes and procedures at each of the individual sites.
“The what needs to be in common across sites, but the how and who in the implementation will be individually tailored to each specific hospital environment,” she explains.
This is a real strength of the study because standardized interventions can be studied in varied and representative test environments. Dr. Huddleston also stresses that, “SHM envisions its role in quality management to be in the actual implementation realm—rather than in the development of new clinical guidelines. SHM seeks to know whether hospitalists [use] the same tools at different sites and understand their impact at each site.”
The patient care domains selected as a focus for the safe practice implementation tools for the care transition process are:
- Communications;
- Medication reconciliation; and
- Functional status.
Communication tools will be developed for primary care physicians, patients, and their support systems so that important clinical information is transmitted during the discharge process. The implementation tools designed for medication reconciliation will be employed by physicians, care managers, or pharmacists in the hospital. Transmitting the medication regimen is widely recognized as an error-prone element of care. These specific implementation tools will include a method to review and verify any dose/frequency changes of medications that the patient was taking upon admission, as well as those that were added or discontinued during the inpatient episode. Because patient functional status is a critical issue in discharge planning, detailed tools will also be created to standardize content for risk assessment and evaluation of the types of assistance needed for patients to resume activities of daily living.
The demonstration project will also utilize specific metrics to measure patient outcomes as well as the effect that these safe practices have on the discharge and care transition processes. The three study sites will measure referring physician satisfaction with the adequacy of post-hospitalization follow-up information, the accuracy of medication reconciliation, readmission rates, and patient understanding of their treatment plan and medication regimen.
QI Requires Expert Change Management
Hospitalists recognize that the challenge of patient safety is linked to the challenge of organizational change. Patient safety initiatives can succeed only to the extent to which healthcare organizations recognize the need for and develop the means to implement the organizational changes. According to the AHRQ, systemwide improvements in patient safety are possible only if there are coordinated changes in multiple components—clinical procedures, attitudes and behaviors of care providers, incentive systems, coordination structures and processes, patterns of interactions among care providers, and organizational culture.
Senior leadership must play an active role in establishing patient safety as a priority, and staff involved directly in providing care must actively participate in implementing change. The likelihood of successful implementation of even simple change requires multiple tactics or many bullets directed at the same target. Additionally, it is critical to redesign the roles of healthcare workers at the point of care to accommodate the necessary changes and to retrain them to fulfill these roles.
Hospitalists Prepare to Lead
Identifying the facilitating factors and barriers to improvement is essential to effect change because it helps ensure success. It’s also crucial to match the patient safety goals with the change strategies and tactics. Otherwise, mismatches can lead to unintended consequences that will hinder continuous improvements such as employee skepticism, frustration of safety champions, and mislearning or unnecessary ”workarounds“ by staff.
SHM sees this QI Demonstration Project as critical to assisting institutions in the design, implementation, and evaluation of QI programs and systemwide interventions with effectiveness and value. These findings should equip hospitalists with vital tools necessary to provide essential leadership in meeting their institution’s quality and patient safety goals. TH
Writer Kathleen Frampton is based in Columbia, Md
Hospitalists lead, coordinate, and participate in initiatives to improve the identification and treatment of patients and families in need of palliative care. Yet we often lack the knowledge and skills necessary to provide outstanding palliative care; we may also lack the comfort level we need to take care of patients at that stage of illness.
Steve Pantilat, MD, SHM president and member of the SHM Education Committee, established the Palliative Care Task Force to identify and create opportunities to improve palliative care in the field of hospital medicine. The Palliative Care Task Force had its inaugural meeting in August. Led by founder Dr. Pantilat and Chad Whelan, MD, Palliative Care Task Force chair, the task force established the following goals:
- Promote palliative care as an important skill and activity for hospital medicine physicians and providers;
- Identify and create palliative-care-focused educational activities for hospital medicine physicians and other key stakeholders within hospital medicine;
- Advocate for the creation and or support of hospital-based palliative care services;
- Promote the use of best practices in palliative care; and
- Develop a core community of hospital medicine physicians dedicated to improving our understanding of palliative care.
Our current task force membership is small but energetic. We actively recruit members, particularly nonphysicians and non-SHM members. Palliative care is a multidisciplinary field, and we hope the Palliative Care Task Force membership will reflect this diversity. Potential areas of growth include pharmacists, nurses, social workers, spiritual care providers, and nonhospitalist physicians. We are also looking for a pediatrician with an interest in palliative care to represent the pediatric interests among SHM members.
Since the first meeting in August our members have been developing a plan to achieve our identified goals. While the plan is still early in its development, we have designed a multimodal approach that will rely on traditional CME meetings, print media, as well as electronic media.
The task force’s short-term goals include promoting best practices in palliative care via SHM communication vehicles. For example, we plan to propose a series of articles for the forthcoming Journal of Hospital Medicine to highlight key issues in palliative care.
The 2006 SHM Annual Meeting will feature two workshops with a palliative care focus. One workshop will discuss how to build the case for a palliative care service; the other will address issues in pain management for hospitalized patients. We will learn from the 2006 experience as we look toward the 2007 SHM Annual Meeting in Texas. An electronic CME module is also under development.
Finally, we are planning an electronic compendium of resources and tools for practicing high-quality palliative care. Although the format has not been finalized, the concept is to provide resources that will make caring for palliative care patients as easy as possible.
While we are pleased with the progress of the task force to date, there is still much to do. Hospital medicine physicians can and should serve as leaders to improve palliative care. Traditional medical training focuses our efforts and thoughts of curing and preventing. We’ve all felt the exhilaration of making a life-saving diagnosis on the young, otherwise healthy patient; however, just as there are times to look for a cure at all costs, there are also times when we must treat our patients’ symptoms at all costs.
Often traditional medical training doesn’t provide us with the tools we need to best care for our patients and their families when palliative care goals become the priority. We hope this task force will raise the visibility of palliative care within SHM and provide the opportunities and tools needed for us, as hospital medicine providers, to offer the best palliative care possible to our patients. If successful, we’ll feel the deep personal satisfaction and self-reward of helping a patient and their family transition from hopes of a cure to comfort in the knowledge that their symptoms and needs will be cared for.
Interested in joining the task force or participating in a related work group? Contact Chad Whelan at cwhelan@medicine.bsd.uchicago.edu.
The Stroke Resource Room
SHM’s Web site features stroke information on call
Online resource rooms comprise an innovative venue within the SHM Web site to focus on essential topics from the forthcoming core curriculum. Specifically, the Web-based resource rooms organize expert opinions, evidence-based literature, clinical tools and guidelines, and recommendations about essential topics in hospital medicine. Initial areas of development include the DVT and stroke resource rooms, with ongoing efforts in other areas including geriatrics, antimicrobial resistance, congestive heart failure, and glycemic control. These interactive rooms help connect hospitalists to information, content experts, and each other.
The Stroke Imperative
Stroke is the third leading cause of death in the United States and a common admission diagnosis. Cerebrovascular disease is a field of great complexity and rapid advance. There is great pressure on the practicing hospitalist to have both a base knowledge of the approach to the patient with stroke as well as an understanding of current best practice.
Traditional internal medicine residencies may not fully prepare one for hospitalist practice. Many patients seen by hospitalists have diagnoses that were managed by internal medicine subspecialties in the past. Most hospitalists feel comfortable managing straightforward gastrointestinal bleeds, myocardial infarctions, and renal failure without consultation. Neurologic cases are somewhat different.
Most medicine residents have rotated on a neurology service, but that limited experience is frequently insufficient in preparing physicians for their future experience as hospitalists. While neurology residencies include one year of internal medicine, the two diverge dramatically afterward. Practitioners of both internal medicine and neurology frequently feel that they speak a different language from one another.
Particularly in the community setting, hospitalists manage the bulk of neurology patients either with or without neurologic consultation. The reasons for this are varied, including poor inpatient reimbursement for neurologists and a tradition of nonaggressive approaches to stroke care.1
The Opportunity
Realizing the need to provide direct access to important information about inpatient stroke management, SHM convened a stroke advisory board, including general hospitalists, a neurologist, and members of the education committee. SHM and Boehringer-Ingelheim provided funding for the resource room through educational funds and an unrestricted grant, respectively.
Stroke Resource Room Content
The Stroke Resource Room is patterned after the template of the DVT Resource Room; the idea being that a standardized format will allow easy navigation and maximal utility. David Likosky, MD, served as content editor, Sandeep Sachdeva, MD, as quality editor, Alpesh Amin, MD as education editor, and Jason Stein, MD, as managing editor.
The rooms are structured to facilitate access to specific types of information. Whether one is looking for the details of a certain study, slide sets to help teach residents, or for input on how to approach a difficult patient, that resource should be readily available. The main sections of the room are summarized below.
The “Awareness” area on the main page of the Stroke Resource Room defines the effects of stroke as well as the hospitalists’ scope of practice.
A separate debate is ongoing within neurology about who should be responsible for the inpatient management of stroke. Interestingly, much of this is about whether general neurologists or vascular/stroke neurologists should primarily manage these patients. One such article referred to the brain as “… the Rolls Royce of the human body” going on to ask, “Would you want your Rolls Royce to be serviced by any ordinary mechanic, who takes care of all kinds of automobiles?”2 Many hospitalists find this argument less than compelling given how difficult it can be in many communities to get a neurologist much less a “vascular neurologist” to see an inpatient.
The “Evidence” section consists of two main parts with the goal of providing a one-stop shop for stroke care literature. The first is a set of links to articles reviewed by the ACP journal club. The second is a concise list of landmark trials, such as the Heparin Acute Embolic Stroke HAEST) trial, which compared low molecular weight heparin versus aspirin in patients with acute stroke and atrial fibrillation.3 These articles help answer questions that come up commonly in clinical practice.
The Experience link capitalizes on the Internet’s ability to disseminate information. There are a limited number of protocols and order sets for ischemic and hemorrhagic stroke available. One can download these and, perhaps more importantly, submit one’s own—including comments on what about that particular tool has been valuable.
Finally, the “Ask the Expert” section features an interactive venue for interacting with a panel of neurologists and neurocritical care physicians. This section answers the more common and more difficult clinical questions in a shared forum. Supportive evidence is cited, with the knowledge that much of stroke care remains in the realm of standard of practice.
The “Improve” section reflects the other roles of hospitalists, such as hospital leader. The three current links include a PowerPoint primer on quality improvement. In addition, there are links to the “Get with the Guidelines” program from the American Stroke Association. This is a continuous quality improvement program focusing on care team protocols and outcome measurement. The final linked site is to the criteria for the disease specific accreditation program from JCAHO. This national effort may drive where patients receive their care for certain conditions.
The “Educate” section caters to multiple audiences. The academic hospitalist may find the “Teaching Pearls” section helpful, as well as the slide sets from the International Stroke Conference and StrokeSTOP, which is aimed at medical students. The patient education links contain a wealth of quality information. The “Professional Development” subsection contains sources for audio lectures with slide sets as well as case presentations and NIH stroke scale training—all with free CME hours. A chapter on stroke from the SHM’s forthcoming core competencies is included as well.
Moving Forward
One of the advantages of an Internet-based resource is the ability to be easily modified. A progressively more robust database will be developed over time as questions are answered in the “Ask the Expert” section and as participants share their stroke care protocols.
The Stroke Resource Room is an excellent forum to improve clinical care and form the basis for future SHM workshops, lectures, and to review articles. By building our collective knowledge, we will be limited only by the energy we put into the adding to and using available information and our desire to apply that energy to patient care.
References
- Likosky DJ, Amin AN. Who will care for our hospitalized patients? Stroke. 2005;36(6): 1113-1114.
- Caplan L. Stroke is best managed by neurologists. Stroke. 2003;34(11):2763.
- Berge E, Abdelnoor M, Nakstad PH, et al. Low molecular-weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: a double-blind randomized study. HAEST Study Group. Lancet. 2000;355(9211):1205-1210.
Secure the Future
Encourage trainees to consider lifelong careers in hospital medicine
By Vineet Arora, MD, MA, and Margaret C. Fang, MD, MPH, co-chairs of SHM’s Young Physicians Section
Interest in hospital medicine is booming, and it is estimated that the number of hospitalists in the United States is estimated will exceed the number of cardiologists in the near future. Yet, many graduating residents view hospital medicine as a temporary job where they can take time off and work before going on to a subspecialty fellowship. Others perceive hospitalists as “super-residents” susceptible to burnout, and therefore do not consider hospital medicine a sustainable career option. These perceptions may contribute to a high turnover of hospitalists and compromise the accumulation of enough inpatient experience to accomplish many of the benefits associated with the use of hospitalists, including shorter lengths of stay and comparable—if not better—quality of care.
To ensure recruitment and retention of the best and brightest trainees, it’s important to consider ways to educate and encourage them to consider a career in hospital medicine as a rewarding lifelong career. Below, we discuss strategies to encourage trainees to pursue a lifelong career in hospital medicine.
Showcase Your Clinical Work
First, consider your everyday practice an excellent way to showcase the often-exciting world of inpatient medicine. Preclinical students often cherish any opportunity to interact with patients. Inviting first- or second-year medical students to accompany you on rounds is an excellent opportunity to teach clinical medicine and physical exam skills, and a good way to influence their career choice early in their medical career.
If you’re in an academic medical center, accessing preclinical students is as easy as approaching students in an internal medicine interest group or volunteering as a preceptor for a physical diagnosis course for preclinical students. In fact, hospitalists are often acknowledged as some of the best teachers and are highly accessible because of their inpatient duties.
Community-based hospitalists also can provide valuable career advice and opportunities, particularly in exposing students to real-life career experiences often not covered through traditional medical school training. One way for a community-based hospitalist to become involved is to host preclinical students over the summer by contacting a local medical school dean’s office and volunteering as a summer preceptor for interested preclinical students. Your alma mater may be particularly responsive. Or, contact interest groups in internal medicine, family medicine, or pediatrics through the state or local leaders of the American College of Physicians, the American Academy of Family Physicians, and the American Academy of Pediatrics.
Explain Your Nonclinical Work
It’s important to explain your nonclinical roles to residency trainees. Hospitalists increasingly take on numerous administrative, educational, and leadership roles and responsibilities. Whether you are leading a quality improvement effort, interfacing with hospital operations, or running a medical student clerkship, it is crucial that physicians-in-training understand the diverse opportunities within hospital medicine to achieve a healthy work-life balance and avoid clinical burnout.
If you are involved with quality improvement projects at your institution, enlist the help of an interested resident or student. Because student rotations are frequent, their prior experience may be scant and their time limited. So make sure the projects have definite goals and are easily accomplished. Ensure that the projects provide reasonable educational value and experience within a finite time. Lay out explicit goals at the beginning of the project, ask for frequent updates, and then recap the experience and any concrete accomplishments to provide structure and expectations for the process.
For example, the University of California at San Francisco Hospitalist Group is spearheading an educational initiative in which residents learn about both the theory and practice of quality improvement through choosing a project and working with a mentor to design, implement, and measure the results of a quality improvement initiative.
Share Your Passion
In addition to showcasing your clinical and nonclinical activities, share your passion about hospital medicine. Reflect on the reasons you entered hospital medicine, as well as your thoughts on the pros and cons of the field. Perhaps you were drawn to hospital medicine because of a desire to take care of acutely ill patients, or to work on improving the quality of a medical system, or because of a more controllable work schedule with competitive compensation.
In some cases, it may have been a particular interest in medical ethics, palliative care, geriatrics, or perioperative care. Sharing your enthusiasm is the best way to cultivate reciprocal interest. Medical students and residents closely observe your attitudes toward your career, your job satisfaction, and your work-life balance. In addition to mentoring those already entering a medical career, there are endless opportunities to outreach to younger students, including those in high school and college. Many local schools and community organizations offer mentorship programs to area students. Engaging in an informal discussion about your career at a social or community event with younger students can be incredibly rewarding. Younger students often lack realistic career experiences and access to career-specific role models on which to base informed decisions. Although they may express an interest in science or medicine, they may not know how long the training process is or the importance of good grades.
Take a moment to inquire about career interests and explain what a hospitalist is; this can be invaluable in promoting understanding and cultivating interest into the field. More structured interactions with hospitalists can also prepare students for successful entry into the medical field. The University of Chicago Hospitalists, for example, host high-achieving Chicago public school juniors in a summer clinical and research enrichment program in hospital-based medicine called TEACH Research.
Offer Advice and Assistance
Finding your first job can be a nerve-racking situation. Sharing your advice on the process with trainees is always appreciated. For instance, they are interested in hearing how you decided to become a hospitalist and what you did to secure your position.
Offer to meet with them and review their career interests, goals, and curriculum vitae. If you hear of job openings and opportunities, inform the community of trainees by contacting program directors or chief residents at residency programs. Many residency program directors showcase available opportunities in their house-staff office or direct such opportunities to interested residents. Some residency programs invite community-based physicians to give residents insight on securing their first job. This process is particularly foreign to medical trainees who have never had to negotiate such things as benefit packages, compensation, or call schedule. Your candid thoughts on what to expect and how to approach the process are invaluable.
Again, approaching the residency program where you trained is a good starting point. Alternatively, you can locate a nearby residency through the Fellowship and Residency Electronic Interactive Database database offered by the American Medical Association (www.ama-assn.org/vapp/freida/srch/).
Finally, if you know any trainees interested in hospital medicine,encourage them to attend the SHM’s local or national meetings. The annual meeting is an excellent place for medical trainees to hear the latest research and innovations, learn about advanced training and job opportunities, network, and connect with mentors through the Mentorship Breakfast. For the last two years, the Young Physicians Section has organized a Forum for Early Career Hospitalists where we addressed different career paths in hospital medicine and conducted research during training. Continued growth in our field depends on promoting hospital medicine as a vital, sustainable career.
Busy Summer for HQPS
The Health Quality and Patient Safety Committee (HQPS) has developed an array of initiatives to support SHM members in the development, implementation, and evaluation of quality and system improvements at their institutions. Educational programming, tools, and resources are being developed for four specific content areas including prevention of VTE, improving the discharge process, glycemic control, and improving outcomes for hospitalized heart failure patients.
HQPS members and Course Directors Greg Maynard, MD, and Tosha Wetterneck, MD, are developing a quality precourse for the 2006 SHM Annual Meeting. The educational goal for the precourse will be to enable hospitalists to become leaders in quality and safety through the effective implementation of evidence-based, high reliability interventions. Precourse participants will actively participate in small groups to apply techniques for designing, implementing, and evaluating quality improvement projects to address a specific improvement need in one of four areas: heart failure care, glycemic control, and preventing VTE in the hospital or the discharge process. Registration for this precourse will begin in November and space will be limited. Plan to register early.
In June, HQPS convened a multidisciplinary, multiagency Heart Failure Advisory Board to guide the development of a clinical guidelines implementation toolkit (CGIT), resource room, and CME modules related to implementing best practices for care of patients with heart-failure. The advisory board has representatives from several organizations and allied health professions, including the American College of Cardiology, American Medical Directors Association, American Hospital Association, Case Managers Society of America, American Association of Heart Failure Nurses, American Society of Health-System Pharmacists, American Association of Critical Care Nurses, National Association of Social Workers and the Heart Failure Society of America. Currently, the advisory board is completing a needs assessment and will begin development on the CGIT, resource room and CME modules next month.
In July, in collaboration with the Education Committee and SHM staff, HQPS launched the SHM VTE Resource Room (www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312). The resource room provides users with a workbook, or step-wise process to assess the need for VTE prevention, advocate for local improvements, and implement and evaluate a VTE prevention program. The resource room also provides a useful review of the literature, an “Ask the Expert” forum, slide sets, and bedside teaching tools.
In August, the SHM Executive Committee approved the SHM Discharge Planning Checklist developed by HQPS under the direction of Dennis Manning, MD. This discharge planning checklist and a white paper on guidance for its implementation will be available to members in the near future.
Interested in learning more about these initiatives or becoming involved in an HQPS workgroup? Contact Lakshmi Halasyamani, MD, HQPS chair, at HalasyaL@trinity-health.org.
Hartford Grants Awarded
SHM presents Hartford Foundation grant funds to hospitalists for QI demo project
By Kathleen K. Frampton, RN, MPH
Shm remains committed to expanding its efforts to improve inpatient care for older patients. The John A. Hartford Foundation has generously awarded approximately $370,000 to SHM in support of its focus on the geriatric population. This funding will assist SHM in its endeavors related to educational programs and products, hospitalist leadership training, and quality improvement projects. In light of this, SHM allocated a portion of these Hartford grant funds to study a critical aspect of elderly patient care, safety-care transitions.
A competitive request for the proposal (RFP) process was conducted to solicit interest from healthcare institutional providers and SHM members willing to serve as the principle investigator in their work setting. The RFP delineated the requirements for a hospital to serve as a designated study site to implement a discharge planning intervention from hospital-based care to community-based care for elderly patients and to evaluate the facilitating factors, barriers to implementation and outcomes associated with the new approach.
All research proposals submitted by hospitals were evaluated and scored against established criteria. Qualifying hospital finalists were reviewed by a panel consisting of members of three standing SHM Committees: Education, Hospital Quality and Patient Safety, and Research and Executive. In July 2005, this panel selected three hospitals to receive funding for this initiative: Johns Hopkins-Bayview, Baltimore, Md.; Northeast Medical Center, Concord, N.C.; and Geisinger Health System, Danville, Penn.
Johns Hopkins-Bayview (coordinating site): A 355-bed community-based facility located in southeast Baltimore with academic affiliations and approximately 25% of patients over age 65. The hospitalist service consists of nine physicians, five physician assistants, and three nurse practitioners.
Northeast Medical Center: A 457-bed, private, nonprofit community-based facility located in the Charlotte Region with a residency training program and 36% of patients over age 65. The hospitalist service consists of 16 physicians and 24/7 intensivist coverage.
Geisinger Health System: A 366-bed facility and Level 1 Trauma Center, private, nonprofit community based system located in north central Pennsylvania with a residency training program and 70% of patients over age 65. The hospitalist service is staffed by 15 physicians (10 full-time employees).
The QI Demonstration Project will run for 18 months and, according to Tina Budnitz, MPH, SHM senior advisor for planning and development, the study “represents new territory for both SHM and other professional societies … . We have moved beyond developing a best practice to use in the clinical setting to how you can actually change the system so that best practices can be successfully implemented … . It is the intention of SHM to focus on safe practice interventions that can be generalized to other settings.”
Budnitz also explained that near completion of the project SHM plans to convene the advisory board, grantee project teams, representatives of the Hartford Foundation, and the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) to review the data from the demonstration project and design a larger scale quality improvement program.
“Our grantees will work with the SHM Advisory Board to develop a comprehensive toolkit, which will document the lessons learned during the implementation process and any other resources that facilitate adaptation and/or adoption of these safe practice interventions,” explains Budnitz.
Care Transitions in the Treatment of the Elderly
According to the Institute of Medicine (IOM), the healthcare system is poorly organized to meet its current challenges. The delivery of care is often overly complex and uncoordinated, requiring steps and patient hand-offs that slow care and decrease rather than improve patient safety.
An IOM seminal report published in 2001, Crossing the Quality Chasm: A New Health System for the 21st Century, emphasizes that cumbersome processes waste resources, leave unaccountable voids in coverage, lead to loss of information, and fail to build on the strengths of all professionals involved to ensure that care is appropriate, timely, and safe. Right before and after discharge, there often is no one clearly in charge of the transition whom the patient may contact for guidance. Patients are often instructed to contact their primary care provider for follow-up issues or questions, whether or not the primary care provider had been involved in the hospitalization.
A recent study supported by the Agency for Healthcare Research and Quality (AHRQ) showed that high-risk patient targeting, better communications, and better coordination of care and follow-up could potentially prevent some readmissions when transitioning patients from hospital to home.
In 2002, the American Geriatric Society (AGS) issued a Position Statement, Improving the Quality of Transitional Care for Persons with Complex Care Needs, which stressed that both the “sending” and “receiving” health professionals bear responsibility and accountability in this phase. Successful transitions require that there be both a uniform plan of care and procedure for communicating the following:
- An accessible medical record that contains a current problem list;
- A medication regimen;
- A list of allergies;
- Advance directives;
- Baseline physical and cognitive function; and
- Contact information for all professional and informal care providers.
Also, input must be solicited from informal care providers who are involved in the execution of the plan of care. The AGS recommends the use of a “coordinating” health professional who oversees both the sending and receiving aspects of the transition. This professional should be skilled in the identification of health status, assessment and management of multiple chronic conditions, managing medications, and collaboration with members of the interdisciplinary team and caregivers.
The QI Demonstration Project
According to SHM Immediate Past-President Jeanne Huddleston, MD, SHM has structured this demonstration project so that the three study sites in the Hartford Grant Group will implement identical clinical tools while they employ unique processes and procedures at each of the individual sites.
“The what needs to be in common across sites, but the how and who in the implementation will be individually tailored to each specific hospital environment,” she explains.
This is a real strength of the study because standardized interventions can be studied in varied and representative test environments. Dr. Huddleston also stresses that, “SHM envisions its role in quality management to be in the actual implementation realm—rather than in the development of new clinical guidelines. SHM seeks to know whether hospitalists [use] the same tools at different sites and understand their impact at each site.”
The patient care domains selected as a focus for the safe practice implementation tools for the care transition process are:
- Communications;
- Medication reconciliation; and
- Functional status.
Communication tools will be developed for primary care physicians, patients, and their support systems so that important clinical information is transmitted during the discharge process. The implementation tools designed for medication reconciliation will be employed by physicians, care managers, or pharmacists in the hospital. Transmitting the medication regimen is widely recognized as an error-prone element of care. These specific implementation tools will include a method to review and verify any dose/frequency changes of medications that the patient was taking upon admission, as well as those that were added or discontinued during the inpatient episode. Because patient functional status is a critical issue in discharge planning, detailed tools will also be created to standardize content for risk assessment and evaluation of the types of assistance needed for patients to resume activities of daily living.
The demonstration project will also utilize specific metrics to measure patient outcomes as well as the effect that these safe practices have on the discharge and care transition processes. The three study sites will measure referring physician satisfaction with the adequacy of post-hospitalization follow-up information, the accuracy of medication reconciliation, readmission rates, and patient understanding of their treatment plan and medication regimen.
QI Requires Expert Change Management
Hospitalists recognize that the challenge of patient safety is linked to the challenge of organizational change. Patient safety initiatives can succeed only to the extent to which healthcare organizations recognize the need for and develop the means to implement the organizational changes. According to the AHRQ, systemwide improvements in patient safety are possible only if there are coordinated changes in multiple components—clinical procedures, attitudes and behaviors of care providers, incentive systems, coordination structures and processes, patterns of interactions among care providers, and organizational culture.
Senior leadership must play an active role in establishing patient safety as a priority, and staff involved directly in providing care must actively participate in implementing change. The likelihood of successful implementation of even simple change requires multiple tactics or many bullets directed at the same target. Additionally, it is critical to redesign the roles of healthcare workers at the point of care to accommodate the necessary changes and to retrain them to fulfill these roles.
Hospitalists Prepare to Lead
Identifying the facilitating factors and barriers to improvement is essential to effect change because it helps ensure success. It’s also crucial to match the patient safety goals with the change strategies and tactics. Otherwise, mismatches can lead to unintended consequences that will hinder continuous improvements such as employee skepticism, frustration of safety champions, and mislearning or unnecessary ”workarounds“ by staff.
SHM sees this QI Demonstration Project as critical to assisting institutions in the design, implementation, and evaluation of QI programs and systemwide interventions with effectiveness and value. These findings should equip hospitalists with vital tools necessary to provide essential leadership in meeting their institution’s quality and patient safety goals. TH
Writer Kathleen Frampton is based in Columbia, Md
Hospitalists lead, coordinate, and participate in initiatives to improve the identification and treatment of patients and families in need of palliative care. Yet we often lack the knowledge and skills necessary to provide outstanding palliative care; we may also lack the comfort level we need to take care of patients at that stage of illness.
Steve Pantilat, MD, SHM president and member of the SHM Education Committee, established the Palliative Care Task Force to identify and create opportunities to improve palliative care in the field of hospital medicine. The Palliative Care Task Force had its inaugural meeting in August. Led by founder Dr. Pantilat and Chad Whelan, MD, Palliative Care Task Force chair, the task force established the following goals:
- Promote palliative care as an important skill and activity for hospital medicine physicians and providers;
- Identify and create palliative-care-focused educational activities for hospital medicine physicians and other key stakeholders within hospital medicine;
- Advocate for the creation and or support of hospital-based palliative care services;
- Promote the use of best practices in palliative care; and
- Develop a core community of hospital medicine physicians dedicated to improving our understanding of palliative care.
Our current task force membership is small but energetic. We actively recruit members, particularly nonphysicians and non-SHM members. Palliative care is a multidisciplinary field, and we hope the Palliative Care Task Force membership will reflect this diversity. Potential areas of growth include pharmacists, nurses, social workers, spiritual care providers, and nonhospitalist physicians. We are also looking for a pediatrician with an interest in palliative care to represent the pediatric interests among SHM members.
Since the first meeting in August our members have been developing a plan to achieve our identified goals. While the plan is still early in its development, we have designed a multimodal approach that will rely on traditional CME meetings, print media, as well as electronic media.
The task force’s short-term goals include promoting best practices in palliative care via SHM communication vehicles. For example, we plan to propose a series of articles for the forthcoming Journal of Hospital Medicine to highlight key issues in palliative care.
The 2006 SHM Annual Meeting will feature two workshops with a palliative care focus. One workshop will discuss how to build the case for a palliative care service; the other will address issues in pain management for hospitalized patients. We will learn from the 2006 experience as we look toward the 2007 SHM Annual Meeting in Texas. An electronic CME module is also under development.
Finally, we are planning an electronic compendium of resources and tools for practicing high-quality palliative care. Although the format has not been finalized, the concept is to provide resources that will make caring for palliative care patients as easy as possible.
While we are pleased with the progress of the task force to date, there is still much to do. Hospital medicine physicians can and should serve as leaders to improve palliative care. Traditional medical training focuses our efforts and thoughts of curing and preventing. We’ve all felt the exhilaration of making a life-saving diagnosis on the young, otherwise healthy patient; however, just as there are times to look for a cure at all costs, there are also times when we must treat our patients’ symptoms at all costs.
Often traditional medical training doesn’t provide us with the tools we need to best care for our patients and their families when palliative care goals become the priority. We hope this task force will raise the visibility of palliative care within SHM and provide the opportunities and tools needed for us, as hospital medicine providers, to offer the best palliative care possible to our patients. If successful, we’ll feel the deep personal satisfaction and self-reward of helping a patient and their family transition from hopes of a cure to comfort in the knowledge that their symptoms and needs will be cared for.
Interested in joining the task force or participating in a related work group? Contact Chad Whelan at cwhelan@medicine.bsd.uchicago.edu.
The Stroke Resource Room
SHM’s Web site features stroke information on call
Online resource rooms comprise an innovative venue within the SHM Web site to focus on essential topics from the forthcoming core curriculum. Specifically, the Web-based resource rooms organize expert opinions, evidence-based literature, clinical tools and guidelines, and recommendations about essential topics in hospital medicine. Initial areas of development include the DVT and stroke resource rooms, with ongoing efforts in other areas including geriatrics, antimicrobial resistance, congestive heart failure, and glycemic control. These interactive rooms help connect hospitalists to information, content experts, and each other.
The Stroke Imperative
Stroke is the third leading cause of death in the United States and a common admission diagnosis. Cerebrovascular disease is a field of great complexity and rapid advance. There is great pressure on the practicing hospitalist to have both a base knowledge of the approach to the patient with stroke as well as an understanding of current best practice.
Traditional internal medicine residencies may not fully prepare one for hospitalist practice. Many patients seen by hospitalists have diagnoses that were managed by internal medicine subspecialties in the past. Most hospitalists feel comfortable managing straightforward gastrointestinal bleeds, myocardial infarctions, and renal failure without consultation. Neurologic cases are somewhat different.
Most medicine residents have rotated on a neurology service, but that limited experience is frequently insufficient in preparing physicians for their future experience as hospitalists. While neurology residencies include one year of internal medicine, the two diverge dramatically afterward. Practitioners of both internal medicine and neurology frequently feel that they speak a different language from one another.
Particularly in the community setting, hospitalists manage the bulk of neurology patients either with or without neurologic consultation. The reasons for this are varied, including poor inpatient reimbursement for neurologists and a tradition of nonaggressive approaches to stroke care.1
The Opportunity
Realizing the need to provide direct access to important information about inpatient stroke management, SHM convened a stroke advisory board, including general hospitalists, a neurologist, and members of the education committee. SHM and Boehringer-Ingelheim provided funding for the resource room through educational funds and an unrestricted grant, respectively.
Stroke Resource Room Content
The Stroke Resource Room is patterned after the template of the DVT Resource Room; the idea being that a standardized format will allow easy navigation and maximal utility. David Likosky, MD, served as content editor, Sandeep Sachdeva, MD, as quality editor, Alpesh Amin, MD as education editor, and Jason Stein, MD, as managing editor.
The rooms are structured to facilitate access to specific types of information. Whether one is looking for the details of a certain study, slide sets to help teach residents, or for input on how to approach a difficult patient, that resource should be readily available. The main sections of the room are summarized below.
The “Awareness” area on the main page of the Stroke Resource Room defines the effects of stroke as well as the hospitalists’ scope of practice.
A separate debate is ongoing within neurology about who should be responsible for the inpatient management of stroke. Interestingly, much of this is about whether general neurologists or vascular/stroke neurologists should primarily manage these patients. One such article referred to the brain as “… the Rolls Royce of the human body” going on to ask, “Would you want your Rolls Royce to be serviced by any ordinary mechanic, who takes care of all kinds of automobiles?”2 Many hospitalists find this argument less than compelling given how difficult it can be in many communities to get a neurologist much less a “vascular neurologist” to see an inpatient.
The “Evidence” section consists of two main parts with the goal of providing a one-stop shop for stroke care literature. The first is a set of links to articles reviewed by the ACP journal club. The second is a concise list of landmark trials, such as the Heparin Acute Embolic Stroke HAEST) trial, which compared low molecular weight heparin versus aspirin in patients with acute stroke and atrial fibrillation.3 These articles help answer questions that come up commonly in clinical practice.
The Experience link capitalizes on the Internet’s ability to disseminate information. There are a limited number of protocols and order sets for ischemic and hemorrhagic stroke available. One can download these and, perhaps more importantly, submit one’s own—including comments on what about that particular tool has been valuable.
Finally, the “Ask the Expert” section features an interactive venue for interacting with a panel of neurologists and neurocritical care physicians. This section answers the more common and more difficult clinical questions in a shared forum. Supportive evidence is cited, with the knowledge that much of stroke care remains in the realm of standard of practice.
The “Improve” section reflects the other roles of hospitalists, such as hospital leader. The three current links include a PowerPoint primer on quality improvement. In addition, there are links to the “Get with the Guidelines” program from the American Stroke Association. This is a continuous quality improvement program focusing on care team protocols and outcome measurement. The final linked site is to the criteria for the disease specific accreditation program from JCAHO. This national effort may drive where patients receive their care for certain conditions.
The “Educate” section caters to multiple audiences. The academic hospitalist may find the “Teaching Pearls” section helpful, as well as the slide sets from the International Stroke Conference and StrokeSTOP, which is aimed at medical students. The patient education links contain a wealth of quality information. The “Professional Development” subsection contains sources for audio lectures with slide sets as well as case presentations and NIH stroke scale training—all with free CME hours. A chapter on stroke from the SHM’s forthcoming core competencies is included as well.
Moving Forward
One of the advantages of an Internet-based resource is the ability to be easily modified. A progressively more robust database will be developed over time as questions are answered in the “Ask the Expert” section and as participants share their stroke care protocols.
The Stroke Resource Room is an excellent forum to improve clinical care and form the basis for future SHM workshops, lectures, and to review articles. By building our collective knowledge, we will be limited only by the energy we put into the adding to and using available information and our desire to apply that energy to patient care.
References
- Likosky DJ, Amin AN. Who will care for our hospitalized patients? Stroke. 2005;36(6): 1113-1114.
- Caplan L. Stroke is best managed by neurologists. Stroke. 2003;34(11):2763.
- Berge E, Abdelnoor M, Nakstad PH, et al. Low molecular-weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: a double-blind randomized study. HAEST Study Group. Lancet. 2000;355(9211):1205-1210.
Secure the Future
Encourage trainees to consider lifelong careers in hospital medicine
By Vineet Arora, MD, MA, and Margaret C. Fang, MD, MPH, co-chairs of SHM’s Young Physicians Section
Interest in hospital medicine is booming, and it is estimated that the number of hospitalists in the United States is estimated will exceed the number of cardiologists in the near future. Yet, many graduating residents view hospital medicine as a temporary job where they can take time off and work before going on to a subspecialty fellowship. Others perceive hospitalists as “super-residents” susceptible to burnout, and therefore do not consider hospital medicine a sustainable career option. These perceptions may contribute to a high turnover of hospitalists and compromise the accumulation of enough inpatient experience to accomplish many of the benefits associated with the use of hospitalists, including shorter lengths of stay and comparable—if not better—quality of care.
To ensure recruitment and retention of the best and brightest trainees, it’s important to consider ways to educate and encourage them to consider a career in hospital medicine as a rewarding lifelong career. Below, we discuss strategies to encourage trainees to pursue a lifelong career in hospital medicine.
Showcase Your Clinical Work
First, consider your everyday practice an excellent way to showcase the often-exciting world of inpatient medicine. Preclinical students often cherish any opportunity to interact with patients. Inviting first- or second-year medical students to accompany you on rounds is an excellent opportunity to teach clinical medicine and physical exam skills, and a good way to influence their career choice early in their medical career.
If you’re in an academic medical center, accessing preclinical students is as easy as approaching students in an internal medicine interest group or volunteering as a preceptor for a physical diagnosis course for preclinical students. In fact, hospitalists are often acknowledged as some of the best teachers and are highly accessible because of their inpatient duties.
Community-based hospitalists also can provide valuable career advice and opportunities, particularly in exposing students to real-life career experiences often not covered through traditional medical school training. One way for a community-based hospitalist to become involved is to host preclinical students over the summer by contacting a local medical school dean’s office and volunteering as a summer preceptor for interested preclinical students. Your alma mater may be particularly responsive. Or, contact interest groups in internal medicine, family medicine, or pediatrics through the state or local leaders of the American College of Physicians, the American Academy of Family Physicians, and the American Academy of Pediatrics.
Explain Your Nonclinical Work
It’s important to explain your nonclinical roles to residency trainees. Hospitalists increasingly take on numerous administrative, educational, and leadership roles and responsibilities. Whether you are leading a quality improvement effort, interfacing with hospital operations, or running a medical student clerkship, it is crucial that physicians-in-training understand the diverse opportunities within hospital medicine to achieve a healthy work-life balance and avoid clinical burnout.
If you are involved with quality improvement projects at your institution, enlist the help of an interested resident or student. Because student rotations are frequent, their prior experience may be scant and their time limited. So make sure the projects have definite goals and are easily accomplished. Ensure that the projects provide reasonable educational value and experience within a finite time. Lay out explicit goals at the beginning of the project, ask for frequent updates, and then recap the experience and any concrete accomplishments to provide structure and expectations for the process.
For example, the University of California at San Francisco Hospitalist Group is spearheading an educational initiative in which residents learn about both the theory and practice of quality improvement through choosing a project and working with a mentor to design, implement, and measure the results of a quality improvement initiative.
Share Your Passion
In addition to showcasing your clinical and nonclinical activities, share your passion about hospital medicine. Reflect on the reasons you entered hospital medicine, as well as your thoughts on the pros and cons of the field. Perhaps you were drawn to hospital medicine because of a desire to take care of acutely ill patients, or to work on improving the quality of a medical system, or because of a more controllable work schedule with competitive compensation.
In some cases, it may have been a particular interest in medical ethics, palliative care, geriatrics, or perioperative care. Sharing your enthusiasm is the best way to cultivate reciprocal interest. Medical students and residents closely observe your attitudes toward your career, your job satisfaction, and your work-life balance. In addition to mentoring those already entering a medical career, there are endless opportunities to outreach to younger students, including those in high school and college. Many local schools and community organizations offer mentorship programs to area students. Engaging in an informal discussion about your career at a social or community event with younger students can be incredibly rewarding. Younger students often lack realistic career experiences and access to career-specific role models on which to base informed decisions. Although they may express an interest in science or medicine, they may not know how long the training process is or the importance of good grades.
Take a moment to inquire about career interests and explain what a hospitalist is; this can be invaluable in promoting understanding and cultivating interest into the field. More structured interactions with hospitalists can also prepare students for successful entry into the medical field. The University of Chicago Hospitalists, for example, host high-achieving Chicago public school juniors in a summer clinical and research enrichment program in hospital-based medicine called TEACH Research.
Offer Advice and Assistance
Finding your first job can be a nerve-racking situation. Sharing your advice on the process with trainees is always appreciated. For instance, they are interested in hearing how you decided to become a hospitalist and what you did to secure your position.
Offer to meet with them and review their career interests, goals, and curriculum vitae. If you hear of job openings and opportunities, inform the community of trainees by contacting program directors or chief residents at residency programs. Many residency program directors showcase available opportunities in their house-staff office or direct such opportunities to interested residents. Some residency programs invite community-based physicians to give residents insight on securing their first job. This process is particularly foreign to medical trainees who have never had to negotiate such things as benefit packages, compensation, or call schedule. Your candid thoughts on what to expect and how to approach the process are invaluable.
Again, approaching the residency program where you trained is a good starting point. Alternatively, you can locate a nearby residency through the Fellowship and Residency Electronic Interactive Database database offered by the American Medical Association (www.ama-assn.org/vapp/freida/srch/).
Finally, if you know any trainees interested in hospital medicine,encourage them to attend the SHM’s local or national meetings. The annual meeting is an excellent place for medical trainees to hear the latest research and innovations, learn about advanced training and job opportunities, network, and connect with mentors through the Mentorship Breakfast. For the last two years, the Young Physicians Section has organized a Forum for Early Career Hospitalists where we addressed different career paths in hospital medicine and conducted research during training. Continued growth in our field depends on promoting hospital medicine as a vital, sustainable career.
Busy Summer for HQPS
The Health Quality and Patient Safety Committee (HQPS) has developed an array of initiatives to support SHM members in the development, implementation, and evaluation of quality and system improvements at their institutions. Educational programming, tools, and resources are being developed for four specific content areas including prevention of VTE, improving the discharge process, glycemic control, and improving outcomes for hospitalized heart failure patients.
HQPS members and Course Directors Greg Maynard, MD, and Tosha Wetterneck, MD, are developing a quality precourse for the 2006 SHM Annual Meeting. The educational goal for the precourse will be to enable hospitalists to become leaders in quality and safety through the effective implementation of evidence-based, high reliability interventions. Precourse participants will actively participate in small groups to apply techniques for designing, implementing, and evaluating quality improvement projects to address a specific improvement need in one of four areas: heart failure care, glycemic control, and preventing VTE in the hospital or the discharge process. Registration for this precourse will begin in November and space will be limited. Plan to register early.
In June, HQPS convened a multidisciplinary, multiagency Heart Failure Advisory Board to guide the development of a clinical guidelines implementation toolkit (CGIT), resource room, and CME modules related to implementing best practices for care of patients with heart-failure. The advisory board has representatives from several organizations and allied health professions, including the American College of Cardiology, American Medical Directors Association, American Hospital Association, Case Managers Society of America, American Association of Heart Failure Nurses, American Society of Health-System Pharmacists, American Association of Critical Care Nurses, National Association of Social Workers and the Heart Failure Society of America. Currently, the advisory board is completing a needs assessment and will begin development on the CGIT, resource room and CME modules next month.
In July, in collaboration with the Education Committee and SHM staff, HQPS launched the SHM VTE Resource Room (www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312). The resource room provides users with a workbook, or step-wise process to assess the need for VTE prevention, advocate for local improvements, and implement and evaluate a VTE prevention program. The resource room also provides a useful review of the literature, an “Ask the Expert” forum, slide sets, and bedside teaching tools.
In August, the SHM Executive Committee approved the SHM Discharge Planning Checklist developed by HQPS under the direction of Dennis Manning, MD. This discharge planning checklist and a white paper on guidance for its implementation will be available to members in the near future.
Interested in learning more about these initiatives or becoming involved in an HQPS workgroup? Contact Lakshmi Halasyamani, MD, HQPS chair, at HalasyaL@trinity-health.org.
Hartford Grants Awarded
SHM presents Hartford Foundation grant funds to hospitalists for QI demo project
By Kathleen K. Frampton, RN, MPH
Shm remains committed to expanding its efforts to improve inpatient care for older patients. The John A. Hartford Foundation has generously awarded approximately $370,000 to SHM in support of its focus on the geriatric population. This funding will assist SHM in its endeavors related to educational programs and products, hospitalist leadership training, and quality improvement projects. In light of this, SHM allocated a portion of these Hartford grant funds to study a critical aspect of elderly patient care, safety-care transitions.
A competitive request for the proposal (RFP) process was conducted to solicit interest from healthcare institutional providers and SHM members willing to serve as the principle investigator in their work setting. The RFP delineated the requirements for a hospital to serve as a designated study site to implement a discharge planning intervention from hospital-based care to community-based care for elderly patients and to evaluate the facilitating factors, barriers to implementation and outcomes associated with the new approach.
All research proposals submitted by hospitals were evaluated and scored against established criteria. Qualifying hospital finalists were reviewed by a panel consisting of members of three standing SHM Committees: Education, Hospital Quality and Patient Safety, and Research and Executive. In July 2005, this panel selected three hospitals to receive funding for this initiative: Johns Hopkins-Bayview, Baltimore, Md.; Northeast Medical Center, Concord, N.C.; and Geisinger Health System, Danville, Penn.
Johns Hopkins-Bayview (coordinating site): A 355-bed community-based facility located in southeast Baltimore with academic affiliations and approximately 25% of patients over age 65. The hospitalist service consists of nine physicians, five physician assistants, and three nurse practitioners.
Northeast Medical Center: A 457-bed, private, nonprofit community-based facility located in the Charlotte Region with a residency training program and 36% of patients over age 65. The hospitalist service consists of 16 physicians and 24/7 intensivist coverage.
Geisinger Health System: A 366-bed facility and Level 1 Trauma Center, private, nonprofit community based system located in north central Pennsylvania with a residency training program and 70% of patients over age 65. The hospitalist service is staffed by 15 physicians (10 full-time employees).
The QI Demonstration Project will run for 18 months and, according to Tina Budnitz, MPH, SHM senior advisor for planning and development, the study “represents new territory for both SHM and other professional societies … . We have moved beyond developing a best practice to use in the clinical setting to how you can actually change the system so that best practices can be successfully implemented … . It is the intention of SHM to focus on safe practice interventions that can be generalized to other settings.”
Budnitz also explained that near completion of the project SHM plans to convene the advisory board, grantee project teams, representatives of the Hartford Foundation, and the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) to review the data from the demonstration project and design a larger scale quality improvement program.
“Our grantees will work with the SHM Advisory Board to develop a comprehensive toolkit, which will document the lessons learned during the implementation process and any other resources that facilitate adaptation and/or adoption of these safe practice interventions,” explains Budnitz.
Care Transitions in the Treatment of the Elderly
According to the Institute of Medicine (IOM), the healthcare system is poorly organized to meet its current challenges. The delivery of care is often overly complex and uncoordinated, requiring steps and patient hand-offs that slow care and decrease rather than improve patient safety.
An IOM seminal report published in 2001, Crossing the Quality Chasm: A New Health System for the 21st Century, emphasizes that cumbersome processes waste resources, leave unaccountable voids in coverage, lead to loss of information, and fail to build on the strengths of all professionals involved to ensure that care is appropriate, timely, and safe. Right before and after discharge, there often is no one clearly in charge of the transition whom the patient may contact for guidance. Patients are often instructed to contact their primary care provider for follow-up issues or questions, whether or not the primary care provider had been involved in the hospitalization.
A recent study supported by the Agency for Healthcare Research and Quality (AHRQ) showed that high-risk patient targeting, better communications, and better coordination of care and follow-up could potentially prevent some readmissions when transitioning patients from hospital to home.
In 2002, the American Geriatric Society (AGS) issued a Position Statement, Improving the Quality of Transitional Care for Persons with Complex Care Needs, which stressed that both the “sending” and “receiving” health professionals bear responsibility and accountability in this phase. Successful transitions require that there be both a uniform plan of care and procedure for communicating the following:
- An accessible medical record that contains a current problem list;
- A medication regimen;
- A list of allergies;
- Advance directives;
- Baseline physical and cognitive function; and
- Contact information for all professional and informal care providers.
Also, input must be solicited from informal care providers who are involved in the execution of the plan of care. The AGS recommends the use of a “coordinating” health professional who oversees both the sending and receiving aspects of the transition. This professional should be skilled in the identification of health status, assessment and management of multiple chronic conditions, managing medications, and collaboration with members of the interdisciplinary team and caregivers.
The QI Demonstration Project
According to SHM Immediate Past-President Jeanne Huddleston, MD, SHM has structured this demonstration project so that the three study sites in the Hartford Grant Group will implement identical clinical tools while they employ unique processes and procedures at each of the individual sites.
“The what needs to be in common across sites, but the how and who in the implementation will be individually tailored to each specific hospital environment,” she explains.
This is a real strength of the study because standardized interventions can be studied in varied and representative test environments. Dr. Huddleston also stresses that, “SHM envisions its role in quality management to be in the actual implementation realm—rather than in the development of new clinical guidelines. SHM seeks to know whether hospitalists [use] the same tools at different sites and understand their impact at each site.”
The patient care domains selected as a focus for the safe practice implementation tools for the care transition process are:
- Communications;
- Medication reconciliation; and
- Functional status.
Communication tools will be developed for primary care physicians, patients, and their support systems so that important clinical information is transmitted during the discharge process. The implementation tools designed for medication reconciliation will be employed by physicians, care managers, or pharmacists in the hospital. Transmitting the medication regimen is widely recognized as an error-prone element of care. These specific implementation tools will include a method to review and verify any dose/frequency changes of medications that the patient was taking upon admission, as well as those that were added or discontinued during the inpatient episode. Because patient functional status is a critical issue in discharge planning, detailed tools will also be created to standardize content for risk assessment and evaluation of the types of assistance needed for patients to resume activities of daily living.
The demonstration project will also utilize specific metrics to measure patient outcomes as well as the effect that these safe practices have on the discharge and care transition processes. The three study sites will measure referring physician satisfaction with the adequacy of post-hospitalization follow-up information, the accuracy of medication reconciliation, readmission rates, and patient understanding of their treatment plan and medication regimen.
QI Requires Expert Change Management
Hospitalists recognize that the challenge of patient safety is linked to the challenge of organizational change. Patient safety initiatives can succeed only to the extent to which healthcare organizations recognize the need for and develop the means to implement the organizational changes. According to the AHRQ, systemwide improvements in patient safety are possible only if there are coordinated changes in multiple components—clinical procedures, attitudes and behaviors of care providers, incentive systems, coordination structures and processes, patterns of interactions among care providers, and organizational culture.
Senior leadership must play an active role in establishing patient safety as a priority, and staff involved directly in providing care must actively participate in implementing change. The likelihood of successful implementation of even simple change requires multiple tactics or many bullets directed at the same target. Additionally, it is critical to redesign the roles of healthcare workers at the point of care to accommodate the necessary changes and to retrain them to fulfill these roles.
Hospitalists Prepare to Lead
Identifying the facilitating factors and barriers to improvement is essential to effect change because it helps ensure success. It’s also crucial to match the patient safety goals with the change strategies and tactics. Otherwise, mismatches can lead to unintended consequences that will hinder continuous improvements such as employee skepticism, frustration of safety champions, and mislearning or unnecessary ”workarounds“ by staff.
SHM sees this QI Demonstration Project as critical to assisting institutions in the design, implementation, and evaluation of QI programs and systemwide interventions with effectiveness and value. These findings should equip hospitalists with vital tools necessary to provide essential leadership in meeting their institution’s quality and patient safety goals. TH
Writer Kathleen Frampton is based in Columbia, Md
To the Marrow
A44-year-old male presented with ecthyma gangrenosum and Pseudomonas aeruginosa bacteremia after a two-year history of fever of unknown origin, pancytopenia, hypertriglyceridemia, and splenomegaly. A bone marrow aspirate was performed, as shown.
Based on the bone marrow aspirate, the most likely diagnosis is:
- Acute leukemia
- Myelofibrosis with myeloid metaplasia
- Multiple myeloma
- Myelodysplastic syndrome
- Hemophagocytic syndrome.
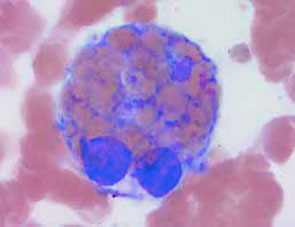
Discussion
The answer is e, hemophagocytic syndrome. The bone marrow aspirate shown demonstrates macrophage hemophagocytosis of non-nucleated red blood cells, consistent with hemophagocytic syndrome (HPS). The hemophagocytic syndromes may be classified as either primary or secondary.
Primary HPS is an autosomal recessive disorder most commonly seen in children and characterized by the polyclonal accumulation of T-lymphocytes and activated macrophages. Many of these patients have null mutations in the gene coding for the cytolytic protein perforin.
In contrast, secondary HPS is characterized by the polyclonal accumulation of activated macrophages in patients with underlying infectious, malignant, or rheumatologic diseases. Patients commonly present with fever, splenomegaly, and complications related to pancytopenia. Hypertriglyceridemia (>160 mg/dL) and an elevated serum ferritin (>10,000 ng/mL) are all sensitive and specific (>0.75) for HPS in the appropriate clinical setting, though histologic demonstration of hemophagocytosis (ingestion of red blood cells by cytokine-activated macrophages) in the bone marrow is diagnostic.
Macrophage activation in these disorders may be attributed to dysregulation of cytokines such as IL-1, IL-6, IFN-y and TNF-a. While therapy with corticosteroids, immunosuppressants, intravenous immunoglobulin, and chemotherapeutic agents have provided conflicting results, future therapeutic strategies employing cytokine-specific antagonists (e.g., etanercept) are promising.1,2
In this case, the patient was noted to have a relative lymphocytosis comprising clonal CD16+CD56+ large granular lymphocytes. These large granular lymphocytes stained positive for Epstein-Barr virus (EBV)-encoded RNA by in situ hybridization. This patient with EBV-associated natural killer (NK) cell lymphoma complicated by hemophagocytic syndrome failed to recover, despite treatment with broad spectrum antibiotics, neutrophil transfusions, intravenous immunoglobulin, fludarabine, and cyclophosphamide.
The clinical and laboratory features of HPS, including fever of unknown origin, anemia, and splenomegaly, often mimic other disorders common in hospitalized patients—many of which may be associated with secondary HPS. As this case illustrates, secondary HPS is associated with significant morbidity and mortality, particularly in those patients in which the diagnosis is delayed. Therefore, prompt diagnosis requires a high index of suspicion among hospital-based physicians caring for patients with underlying infectious, rheumatologic or malignant conditions commonly associated with secondary HPS. TH
References
- Ravelli A. Macrophage activation syndrome. Curr Opin Rheumatol. 2002;14:548-552.
- Henter JI, Elinder G, Ost A. Diagnostic guidelines for hemophagocytic lymphohistiocytosis. The FHL Study Group of the Histiocyte Society. Semin Oncol. 1991;18:29.
A44-year-old male presented with ecthyma gangrenosum and Pseudomonas aeruginosa bacteremia after a two-year history of fever of unknown origin, pancytopenia, hypertriglyceridemia, and splenomegaly. A bone marrow aspirate was performed, as shown.
Based on the bone marrow aspirate, the most likely diagnosis is:
- Acute leukemia
- Myelofibrosis with myeloid metaplasia
- Multiple myeloma
- Myelodysplastic syndrome
- Hemophagocytic syndrome.
Discussion
The answer is e, hemophagocytic syndrome. The bone marrow aspirate shown demonstrates macrophage hemophagocytosis of non-nucleated red blood cells, consistent with hemophagocytic syndrome (HPS). The hemophagocytic syndromes may be classified as either primary or secondary.
Primary HPS is an autosomal recessive disorder most commonly seen in children and characterized by the polyclonal accumulation of T-lymphocytes and activated macrophages. Many of these patients have null mutations in the gene coding for the cytolytic protein perforin.
In contrast, secondary HPS is characterized by the polyclonal accumulation of activated macrophages in patients with underlying infectious, malignant, or rheumatologic diseases. Patients commonly present with fever, splenomegaly, and complications related to pancytopenia. Hypertriglyceridemia (>160 mg/dL) and an elevated serum ferritin (>10,000 ng/mL) are all sensitive and specific (>0.75) for HPS in the appropriate clinical setting, though histologic demonstration of hemophagocytosis (ingestion of red blood cells by cytokine-activated macrophages) in the bone marrow is diagnostic.
Macrophage activation in these disorders may be attributed to dysregulation of cytokines such as IL-1, IL-6, IFN-y and TNF-a. While therapy with corticosteroids, immunosuppressants, intravenous immunoglobulin, and chemotherapeutic agents have provided conflicting results, future therapeutic strategies employing cytokine-specific antagonists (e.g., etanercept) are promising.1,2
In this case, the patient was noted to have a relative lymphocytosis comprising clonal CD16+CD56+ large granular lymphocytes. These large granular lymphocytes stained positive for Epstein-Barr virus (EBV)-encoded RNA by in situ hybridization. This patient with EBV-associated natural killer (NK) cell lymphoma complicated by hemophagocytic syndrome failed to recover, despite treatment with broad spectrum antibiotics, neutrophil transfusions, intravenous immunoglobulin, fludarabine, and cyclophosphamide.
The clinical and laboratory features of HPS, including fever of unknown origin, anemia, and splenomegaly, often mimic other disorders common in hospitalized patients—many of which may be associated with secondary HPS. As this case illustrates, secondary HPS is associated with significant morbidity and mortality, particularly in those patients in which the diagnosis is delayed. Therefore, prompt diagnosis requires a high index of suspicion among hospital-based physicians caring for patients with underlying infectious, rheumatologic or malignant conditions commonly associated with secondary HPS. TH
References
- Ravelli A. Macrophage activation syndrome. Curr Opin Rheumatol. 2002;14:548-552.
- Henter JI, Elinder G, Ost A. Diagnostic guidelines for hemophagocytic lymphohistiocytosis. The FHL Study Group of the Histiocyte Society. Semin Oncol. 1991;18:29.
A44-year-old male presented with ecthyma gangrenosum and Pseudomonas aeruginosa bacteremia after a two-year history of fever of unknown origin, pancytopenia, hypertriglyceridemia, and splenomegaly. A bone marrow aspirate was performed, as shown.
Based on the bone marrow aspirate, the most likely diagnosis is:
- Acute leukemia
- Myelofibrosis with myeloid metaplasia
- Multiple myeloma
- Myelodysplastic syndrome
- Hemophagocytic syndrome.
Discussion
The answer is e, hemophagocytic syndrome. The bone marrow aspirate shown demonstrates macrophage hemophagocytosis of non-nucleated red blood cells, consistent with hemophagocytic syndrome (HPS). The hemophagocytic syndromes may be classified as either primary or secondary.
Primary HPS is an autosomal recessive disorder most commonly seen in children and characterized by the polyclonal accumulation of T-lymphocytes and activated macrophages. Many of these patients have null mutations in the gene coding for the cytolytic protein perforin.
In contrast, secondary HPS is characterized by the polyclonal accumulation of activated macrophages in patients with underlying infectious, malignant, or rheumatologic diseases. Patients commonly present with fever, splenomegaly, and complications related to pancytopenia. Hypertriglyceridemia (>160 mg/dL) and an elevated serum ferritin (>10,000 ng/mL) are all sensitive and specific (>0.75) for HPS in the appropriate clinical setting, though histologic demonstration of hemophagocytosis (ingestion of red blood cells by cytokine-activated macrophages) in the bone marrow is diagnostic.
Macrophage activation in these disorders may be attributed to dysregulation of cytokines such as IL-1, IL-6, IFN-y and TNF-a. While therapy with corticosteroids, immunosuppressants, intravenous immunoglobulin, and chemotherapeutic agents have provided conflicting results, future therapeutic strategies employing cytokine-specific antagonists (e.g., etanercept) are promising.1,2
In this case, the patient was noted to have a relative lymphocytosis comprising clonal CD16+CD56+ large granular lymphocytes. These large granular lymphocytes stained positive for Epstein-Barr virus (EBV)-encoded RNA by in situ hybridization. This patient with EBV-associated natural killer (NK) cell lymphoma complicated by hemophagocytic syndrome failed to recover, despite treatment with broad spectrum antibiotics, neutrophil transfusions, intravenous immunoglobulin, fludarabine, and cyclophosphamide.
The clinical and laboratory features of HPS, including fever of unknown origin, anemia, and splenomegaly, often mimic other disorders common in hospitalized patients—many of which may be associated with secondary HPS. As this case illustrates, secondary HPS is associated with significant morbidity and mortality, particularly in those patients in which the diagnosis is delayed. Therefore, prompt diagnosis requires a high index of suspicion among hospital-based physicians caring for patients with underlying infectious, rheumatologic or malignant conditions commonly associated with secondary HPS. TH
References
- Ravelli A. Macrophage activation syndrome. Curr Opin Rheumatol. 2002;14:548-552.
- Henter JI, Elinder G, Ost A. Diagnostic guidelines for hemophagocytic lymphohistiocytosis. The FHL Study Group of the Histiocyte Society. Semin Oncol. 1991;18:29.
Where Does Hospital Medicine Begin and End?

It is clear to most of us in hospital medicine that the lines are rapidly blurring between the ED, and the floor, and the ICUs. Some of this has been brought about by the transitional units and the ability to place the patient in the most appropriate area with the correct level of monitoring equipment and nurse-to-patient ratio. Some of this has come about with the increased presence of hospitalists and intensivists in-house to complement the already ever-present ED physicians.
But now there is a movement afoot to both increase the use of observation units (OUs) and to change the physician oversight. Once thought to be an extension of the ED, OUs are now part of the hospitalists’ domain as these patients are thought to be more inpatient-light rather than long-term ED patients. And this makes sense when you realize that hospitalists are better suited to managing patients over time rather than ED physicians who favor shorter term relationships; you’re either admitted or “treated and streeted.”
This is further pushed toward the hospitalists’ realm as some OUs continue to treat patients for up to 48 hours (how can you be in a hospital bed for two days and still not be an inpatient?) and helped by the hospitalist’s 24/7 availability.
Having hospitalists serve as the medical directors for the OUs also makes sense because it gets these patients “out of the ED” from a logistic standpoint and shifts the responsibility to the hospitalist, freeing up the ED physicians to better do their primary job. This is just another in a list of examples of how hospitalists can improve ED throughput.
Further, now that governmental payers require closer on-site management of patients in OUs, this makes it virtually impossible for the outpatient-based primary care physicians to have a significant role.
According to The Advisory Board, Washington, D.C., and others, diseases such as CHF readily treated by hospitalists are well-suited to management in OUs. I thought I’d use CHF as an example of how a well-constructed OU might function. Obviously, there are clear classifications and criteria for those patients who are eligible to have their heart failure managed in an OU. And recent data have shown that appropriate management of CHF in OUs can lead to a lower admission rate, better use of resources, and better outcomes.
The OU setting can deliver a more extended course of therapy than traditionally available in the ED or a physician’s office for patients who may not need an acute hospitalization, but who are decompensating. With the best outcomes, management of CHF in an OU can prevent a hospitalization, delay a revisit to the ED, and improve the quality of the patient’s life by decreasing their symptoms and allowing them more time away form the hospital setting.
Not all patients who present to the ED with worsening CHF are candidates for OU management. Some clearly must be admitted. According to the American Heart Association/American College of Cardiology Guidelines the admission criteria for managing a CHF patient in an OU are:
- Adequate systemic perfusion;
- B-type natriuretic peptide < 100pg/mL;
- CXR consistent with CHF; and
- Demonstration of hemodynamic stability as evidenced by one of the following:
- Heart rate >50 or <130;
- Systolic blood pressure >90 and <175; or
- Oxygen saturation >90%.
As more physicians become aware of the benefits of OU care for these patients, there has been a >9% increase in the number of OU patients in both 2003 and 2004, according to Medicare data. And the increased use is even more dramatic for CHF patients.
As one looks at the elements to design and staff a functioning OU, it is apparent this falls clearly in the hospitalist’s capabilities. The idea is to develop more than just a place to stay longer in the ED, but to create an evidence-based, cost-effective management solution for difficult patients. Key components would include:
- Criteria for admission and exclusion based on risk stratification models;
- Protocols for treatment using evidence-based practice guidelines;
- Clear discharge process supported by patient education materials and discharge criteria; and
- Performance standards and an ongoing data collection and quality improvement process.
CHF is an expensive condition to manage, fraught with frequent episodes of decompensation and admission. This takes an economic toll on the system and results in a poorer quality of life for those patients burdened with the disease. Because many physician offices are not set up to handle patients with increasing symptoms related to CHF, the ED becomes the treatment center of last resort. Thoughtful management of those patients correctly suited to OU care can lead to more directed treatment and avoid hospitalizations that are expensive to the system and unnecessary for the patient.
All data point to an increased prevalence of OUs as more hospitals develop them and more patients are treated in OUs. In addition, professional societies are establishing guidelines and criteria for the appropriate use of OUs for certain ED patients. At the same time, management of patients in the OUs and for the OU itself is evolving to the hospitalist, who is the expert in longitudinal management of the hospitalized (and near hospitalized) patient.
Once again the hospitalist is at the center of new initiatives that are a win-win-win. OUs can minimize the patient’s time away from home, improve their functional capacity, relieve congestion in the ED, allow the ED physicians to concentrate on true ED patients, uncrowd the hospital and the ED and improve throughput, and save the system money. And hospitalists with a plan can make this happen.
Not bad for a specialty that is still the new kid on the block. TH
Dr. Wellikson has been CEO of SHM since 2000.
It is clear to most of us in hospital medicine that the lines are rapidly blurring between the ED, and the floor, and the ICUs. Some of this has been brought about by the transitional units and the ability to place the patient in the most appropriate area with the correct level of monitoring equipment and nurse-to-patient ratio. Some of this has come about with the increased presence of hospitalists and intensivists in-house to complement the already ever-present ED physicians.
But now there is a movement afoot to both increase the use of observation units (OUs) and to change the physician oversight. Once thought to be an extension of the ED, OUs are now part of the hospitalists’ domain as these patients are thought to be more inpatient-light rather than long-term ED patients. And this makes sense when you realize that hospitalists are better suited to managing patients over time rather than ED physicians who favor shorter term relationships; you’re either admitted or “treated and streeted.”
This is further pushed toward the hospitalists’ realm as some OUs continue to treat patients for up to 48 hours (how can you be in a hospital bed for two days and still not be an inpatient?) and helped by the hospitalist’s 24/7 availability.
Having hospitalists serve as the medical directors for the OUs also makes sense because it gets these patients “out of the ED” from a logistic standpoint and shifts the responsibility to the hospitalist, freeing up the ED physicians to better do their primary job. This is just another in a list of examples of how hospitalists can improve ED throughput.
Further, now that governmental payers require closer on-site management of patients in OUs, this makes it virtually impossible for the outpatient-based primary care physicians to have a significant role.
According to The Advisory Board, Washington, D.C., and others, diseases such as CHF readily treated by hospitalists are well-suited to management in OUs. I thought I’d use CHF as an example of how a well-constructed OU might function. Obviously, there are clear classifications and criteria for those patients who are eligible to have their heart failure managed in an OU. And recent data have shown that appropriate management of CHF in OUs can lead to a lower admission rate, better use of resources, and better outcomes.
The OU setting can deliver a more extended course of therapy than traditionally available in the ED or a physician’s office for patients who may not need an acute hospitalization, but who are decompensating. With the best outcomes, management of CHF in an OU can prevent a hospitalization, delay a revisit to the ED, and improve the quality of the patient’s life by decreasing their symptoms and allowing them more time away form the hospital setting.
Not all patients who present to the ED with worsening CHF are candidates for OU management. Some clearly must be admitted. According to the American Heart Association/American College of Cardiology Guidelines the admission criteria for managing a CHF patient in an OU are:
- Adequate systemic perfusion;
- B-type natriuretic peptide < 100pg/mL;
- CXR consistent with CHF; and
- Demonstration of hemodynamic stability as evidenced by one of the following:
- Heart rate >50 or <130;
- Systolic blood pressure >90 and <175; or
- Oxygen saturation >90%.
As more physicians become aware of the benefits of OU care for these patients, there has been a >9% increase in the number of OU patients in both 2003 and 2004, according to Medicare data. And the increased use is even more dramatic for CHF patients.
As one looks at the elements to design and staff a functioning OU, it is apparent this falls clearly in the hospitalist’s capabilities. The idea is to develop more than just a place to stay longer in the ED, but to create an evidence-based, cost-effective management solution for difficult patients. Key components would include:
- Criteria for admission and exclusion based on risk stratification models;
- Protocols for treatment using evidence-based practice guidelines;
- Clear discharge process supported by patient education materials and discharge criteria; and
- Performance standards and an ongoing data collection and quality improvement process.
CHF is an expensive condition to manage, fraught with frequent episodes of decompensation and admission. This takes an economic toll on the system and results in a poorer quality of life for those patients burdened with the disease. Because many physician offices are not set up to handle patients with increasing symptoms related to CHF, the ED becomes the treatment center of last resort. Thoughtful management of those patients correctly suited to OU care can lead to more directed treatment and avoid hospitalizations that are expensive to the system and unnecessary for the patient.
All data point to an increased prevalence of OUs as more hospitals develop them and more patients are treated in OUs. In addition, professional societies are establishing guidelines and criteria for the appropriate use of OUs for certain ED patients. At the same time, management of patients in the OUs and for the OU itself is evolving to the hospitalist, who is the expert in longitudinal management of the hospitalized (and near hospitalized) patient.
Once again the hospitalist is at the center of new initiatives that are a win-win-win. OUs can minimize the patient’s time away from home, improve their functional capacity, relieve congestion in the ED, allow the ED physicians to concentrate on true ED patients, uncrowd the hospital and the ED and improve throughput, and save the system money. And hospitalists with a plan can make this happen.
Not bad for a specialty that is still the new kid on the block. TH
Dr. Wellikson has been CEO of SHM since 2000.
It is clear to most of us in hospital medicine that the lines are rapidly blurring between the ED, and the floor, and the ICUs. Some of this has been brought about by the transitional units and the ability to place the patient in the most appropriate area with the correct level of monitoring equipment and nurse-to-patient ratio. Some of this has come about with the increased presence of hospitalists and intensivists in-house to complement the already ever-present ED physicians.
But now there is a movement afoot to both increase the use of observation units (OUs) and to change the physician oversight. Once thought to be an extension of the ED, OUs are now part of the hospitalists’ domain as these patients are thought to be more inpatient-light rather than long-term ED patients. And this makes sense when you realize that hospitalists are better suited to managing patients over time rather than ED physicians who favor shorter term relationships; you’re either admitted or “treated and streeted.”
This is further pushed toward the hospitalists’ realm as some OUs continue to treat patients for up to 48 hours (how can you be in a hospital bed for two days and still not be an inpatient?) and helped by the hospitalist’s 24/7 availability.
Having hospitalists serve as the medical directors for the OUs also makes sense because it gets these patients “out of the ED” from a logistic standpoint and shifts the responsibility to the hospitalist, freeing up the ED physicians to better do their primary job. This is just another in a list of examples of how hospitalists can improve ED throughput.
Further, now that governmental payers require closer on-site management of patients in OUs, this makes it virtually impossible for the outpatient-based primary care physicians to have a significant role.
According to The Advisory Board, Washington, D.C., and others, diseases such as CHF readily treated by hospitalists are well-suited to management in OUs. I thought I’d use CHF as an example of how a well-constructed OU might function. Obviously, there are clear classifications and criteria for those patients who are eligible to have their heart failure managed in an OU. And recent data have shown that appropriate management of CHF in OUs can lead to a lower admission rate, better use of resources, and better outcomes.
The OU setting can deliver a more extended course of therapy than traditionally available in the ED or a physician’s office for patients who may not need an acute hospitalization, but who are decompensating. With the best outcomes, management of CHF in an OU can prevent a hospitalization, delay a revisit to the ED, and improve the quality of the patient’s life by decreasing their symptoms and allowing them more time away form the hospital setting.
Not all patients who present to the ED with worsening CHF are candidates for OU management. Some clearly must be admitted. According to the American Heart Association/American College of Cardiology Guidelines the admission criteria for managing a CHF patient in an OU are:
- Adequate systemic perfusion;
- B-type natriuretic peptide < 100pg/mL;
- CXR consistent with CHF; and
- Demonstration of hemodynamic stability as evidenced by one of the following:
- Heart rate >50 or <130;
- Systolic blood pressure >90 and <175; or
- Oxygen saturation >90%.
As more physicians become aware of the benefits of OU care for these patients, there has been a >9% increase in the number of OU patients in both 2003 and 2004, according to Medicare data. And the increased use is even more dramatic for CHF patients.
As one looks at the elements to design and staff a functioning OU, it is apparent this falls clearly in the hospitalist’s capabilities. The idea is to develop more than just a place to stay longer in the ED, but to create an evidence-based, cost-effective management solution for difficult patients. Key components would include:
- Criteria for admission and exclusion based on risk stratification models;
- Protocols for treatment using evidence-based practice guidelines;
- Clear discharge process supported by patient education materials and discharge criteria; and
- Performance standards and an ongoing data collection and quality improvement process.
CHF is an expensive condition to manage, fraught with frequent episodes of decompensation and admission. This takes an economic toll on the system and results in a poorer quality of life for those patients burdened with the disease. Because many physician offices are not set up to handle patients with increasing symptoms related to CHF, the ED becomes the treatment center of last resort. Thoughtful management of those patients correctly suited to OU care can lead to more directed treatment and avoid hospitalizations that are expensive to the system and unnecessary for the patient.
All data point to an increased prevalence of OUs as more hospitals develop them and more patients are treated in OUs. In addition, professional societies are establishing guidelines and criteria for the appropriate use of OUs for certain ED patients. At the same time, management of patients in the OUs and for the OU itself is evolving to the hospitalist, who is the expert in longitudinal management of the hospitalized (and near hospitalized) patient.
Once again the hospitalist is at the center of new initiatives that are a win-win-win. OUs can minimize the patient’s time away from home, improve their functional capacity, relieve congestion in the ED, allow the ED physicians to concentrate on true ED patients, uncrowd the hospital and the ED and improve throughput, and save the system money. And hospitalists with a plan can make this happen.
Not bad for a specialty that is still the new kid on the block. TH
Dr. Wellikson has been CEO of SHM since 2000.
The Newtonian Hospitalist

The forces of our universe are described and measured by a series of laws and equations known collectively as physics. Though we seem far removed from those halcyon (or Halcion) days of college physics, we exist in a universe still ruled by them. In this instance, our world is the hospital.
Strange vectors of force and difficult-to-fathom principles swirl, causing unanticipated changes in our environment. Using the laws of physics we can attempt to understand these forces.
NEWTON’S FIRST LAW: Newton’s first law is a statement about inertia. An object at rest stays at rest; an object in motion stays in motion unless compelled to change its state by the action of an external force. Byzantine bureaucracies maintain a significant amount of inertia. The expression “that’s the way we’ve always done it here” best summarizes this philosophy.
NEWTON’S SECOND LAW: Newton’s second law examines the force necessary to cause the acceleration of an object in relationship to its mass (F=MA). A moderate amount of force applied to a golf ball may send that object 250 yards—hook right, but the same force applied to a dump truck causes no significant motion.
In the hospital, we often see large expenditures of energy resulting in little movement. This is generally an administrative phenomenon.
NEWTON’S THIRD LAW: For every action there is an equal and opposite reaction. This is an important law in the hospital. The most recent example is the change in residents’ work hours. A seemingly simple issue, residents working too many hours leads to a legislative action and mandated hours. This specific alteration has had unintended consequences and affected numerous other systems. In the case of resident work hours the potential advantages in hours worked has led to a potentially adverse effect on such things as continuity and learning—and an increase in demand for hospitalists.
No system changes can occur without consequences, and the trick is to identify those changes before they occur. Luckily most systems have significant inertia, and only the greatest forces cause major change. It takes massive energy expenditure (i.e., government regulation or resident review boards) to solicit the forces adequate to overcome escape velocity and cause change.
Some forces can cause change not by their sheer energy level, but by their strategic placement. A small forceful tap may split a diamond. A call by a resident’s spouse can cause the downfall of a program. An off-hand comment by a colleague can lead to a disastrous malpractice settlement.
CENTRIFUGAL PSEUDOFORCE: A pseudoforce occurs when one moves in a uniform circular motion. Most of us have observed this phenomenon. When you run around in circles like the proverbial decapitated fowl, little is accomplished despite a sensation of energy expended.
A related principle is Brownian motion: Particles in a gas or fluid collide against each other and the walls of the container causing a random motion. At times the hospitalist’s day may feel that way: active movement but much of it nondirectional.
COPERNICAN PRINCIPLE: The idea, suggested by Copernicus was that the sun—not the earth—is the center of this universe. This is an essential point for hospitalists to remember. We spend hours rounding on our patients. We must always remember that the physician is not the center of the universe for the hospitalized patient. As the name suggests, when we “round” we are the satellite.
CAUSALITY PRINCIPLE: Cause must follow effect. This is a dangerous theory exemplified by the classic post-hoc, prompter hoc: Because I did something, something happened.
When applied to patients, the causality principle can mislead. The fever went down when the antibiotic was started. Coincidence or causality? We hired a hospitalist and our length of stay went down. Coincidence or causality?
THE THEORY OF RELATIVITY: Einstein’s famous equation E=mc2 represents his theory of relativity. This equation represents the relationship between an object’s mass and its energy. Mass is represented by the formula M=DV where D is density and V=volume.
In a hospital setting we see this formula used in a corollary to Einstein’s, called the Theory of Relatives. When entering a patient’s room, one is often confronted with a large number of relatives, spouses, siblings, and the dreaded estranged children. These situations almost always require an increased amount of energy expenditure in communication, consensus building, and time.
As the absolute number (or volume) of family members increases, concurrent with any increased density on the individual members’ part, energy expenditure increases dramatically. This follows the mass equation closely. In situations where the density of an individual family member increases beyond measurable levels, one can enter a Black Hole scenario (see illustration).
BLACK HOLES: A black hole is a region of space-time from which nothing can escape—even light.
A black hole is a region of such extreme density that all energy is sucked into its gravitational field. Once exposed to a black hole situation, the observer may note expected phenomena, including absence of light, loss of energy, extreme fatigue and malaise, and a sensation of hopelessness. This effect can be seen in committee rooms or on the wards.
The only known remedies for this condition are avoidance or going off-service.
THE GIBBS FREE ENERGY EQUATION: The Gibbs free energy equation, G=H-(TS), is a thermodynamic formula and a measure of the conservation of energy. Simply put, the energy of a system is related to the enthalpy (H) or positive creative energy input minus the product of time and entropy, the natural tendency of systems to fall apart.
This effect can be seen in the creation of hospitalist programs.
A hospitalist program is sometimes created by an energetic entrepreneur responding to a vacuum or potential space. A great design leads to a functional program (G). The hospitalist (H) must continually put energy into maintaining the system, otherwise over time (T) entropy (S) takes hold and the system deteriorates. A hospitalist program can’t rely on its initial successful design to survive.
PARTICLE WAVE DUALITY: Quanta are bundles of energy. We see these basic units in the hospital on a nonsubatomic level.
Our admissions seem to come in waves. Our daily workload seems to come in waves as well. Yet the essential quantum of hospital medicine is the patient. RVUs may be 1.33, and LOS 3.2 days, and FTEs 0.8, but I have yet to see a patient-and-a-half in a room.
CRITICAL MASS: Critical mass is the smallest amount of fissionable material necessary to maintain a nuclear chain reaction at a constant level. The term is also used to denote an amount or level needed for a specific result or new action to occur. Happily the hospitalist movement in America has reached that self-sustaining critical mass.
CONCLUSION: As Sir Isaac Newton sat under the proverbial tree and watched a ripe Granny Smith drop on his noggin, little did he know how profoundly he would affect the world of hospital medicine. What goes up must come down. The patient admitted must be discharged. And the editorial started must eventually finish. TH
Jamie Newman, MD, FACP, is physician editor of The Hopitalist, and senior associate consultant, Hospital Internal Medicine and associate professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
The forces of our universe are described and measured by a series of laws and equations known collectively as physics. Though we seem far removed from those halcyon (or Halcion) days of college physics, we exist in a universe still ruled by them. In this instance, our world is the hospital.
Strange vectors of force and difficult-to-fathom principles swirl, causing unanticipated changes in our environment. Using the laws of physics we can attempt to understand these forces.
NEWTON’S FIRST LAW: Newton’s first law is a statement about inertia. An object at rest stays at rest; an object in motion stays in motion unless compelled to change its state by the action of an external force. Byzantine bureaucracies maintain a significant amount of inertia. The expression “that’s the way we’ve always done it here” best summarizes this philosophy.
NEWTON’S SECOND LAW: Newton’s second law examines the force necessary to cause the acceleration of an object in relationship to its mass (F=MA). A moderate amount of force applied to a golf ball may send that object 250 yards—hook right, but the same force applied to a dump truck causes no significant motion.
In the hospital, we often see large expenditures of energy resulting in little movement. This is generally an administrative phenomenon.
NEWTON’S THIRD LAW: For every action there is an equal and opposite reaction. This is an important law in the hospital. The most recent example is the change in residents’ work hours. A seemingly simple issue, residents working too many hours leads to a legislative action and mandated hours. This specific alteration has had unintended consequences and affected numerous other systems. In the case of resident work hours the potential advantages in hours worked has led to a potentially adverse effect on such things as continuity and learning—and an increase in demand for hospitalists.
No system changes can occur without consequences, and the trick is to identify those changes before they occur. Luckily most systems have significant inertia, and only the greatest forces cause major change. It takes massive energy expenditure (i.e., government regulation or resident review boards) to solicit the forces adequate to overcome escape velocity and cause change.
Some forces can cause change not by their sheer energy level, but by their strategic placement. A small forceful tap may split a diamond. A call by a resident’s spouse can cause the downfall of a program. An off-hand comment by a colleague can lead to a disastrous malpractice settlement.
CENTRIFUGAL PSEUDOFORCE: A pseudoforce occurs when one moves in a uniform circular motion. Most of us have observed this phenomenon. When you run around in circles like the proverbial decapitated fowl, little is accomplished despite a sensation of energy expended.
A related principle is Brownian motion: Particles in a gas or fluid collide against each other and the walls of the container causing a random motion. At times the hospitalist’s day may feel that way: active movement but much of it nondirectional.
COPERNICAN PRINCIPLE: The idea, suggested by Copernicus was that the sun—not the earth—is the center of this universe. This is an essential point for hospitalists to remember. We spend hours rounding on our patients. We must always remember that the physician is not the center of the universe for the hospitalized patient. As the name suggests, when we “round” we are the satellite.
CAUSALITY PRINCIPLE: Cause must follow effect. This is a dangerous theory exemplified by the classic post-hoc, prompter hoc: Because I did something, something happened.
When applied to patients, the causality principle can mislead. The fever went down when the antibiotic was started. Coincidence or causality? We hired a hospitalist and our length of stay went down. Coincidence or causality?
THE THEORY OF RELATIVITY: Einstein’s famous equation E=mc2 represents his theory of relativity. This equation represents the relationship between an object’s mass and its energy. Mass is represented by the formula M=DV where D is density and V=volume.
In a hospital setting we see this formula used in a corollary to Einstein’s, called the Theory of Relatives. When entering a patient’s room, one is often confronted with a large number of relatives, spouses, siblings, and the dreaded estranged children. These situations almost always require an increased amount of energy expenditure in communication, consensus building, and time.
As the absolute number (or volume) of family members increases, concurrent with any increased density on the individual members’ part, energy expenditure increases dramatically. This follows the mass equation closely. In situations where the density of an individual family member increases beyond measurable levels, one can enter a Black Hole scenario (see illustration).
BLACK HOLES: A black hole is a region of space-time from which nothing can escape—even light.
A black hole is a region of such extreme density that all energy is sucked into its gravitational field. Once exposed to a black hole situation, the observer may note expected phenomena, including absence of light, loss of energy, extreme fatigue and malaise, and a sensation of hopelessness. This effect can be seen in committee rooms or on the wards.
The only known remedies for this condition are avoidance or going off-service.
THE GIBBS FREE ENERGY EQUATION: The Gibbs free energy equation, G=H-(TS), is a thermodynamic formula and a measure of the conservation of energy. Simply put, the energy of a system is related to the enthalpy (H) or positive creative energy input minus the product of time and entropy, the natural tendency of systems to fall apart.
This effect can be seen in the creation of hospitalist programs.
A hospitalist program is sometimes created by an energetic entrepreneur responding to a vacuum or potential space. A great design leads to a functional program (G). The hospitalist (H) must continually put energy into maintaining the system, otherwise over time (T) entropy (S) takes hold and the system deteriorates. A hospitalist program can’t rely on its initial successful design to survive.
PARTICLE WAVE DUALITY: Quanta are bundles of energy. We see these basic units in the hospital on a nonsubatomic level.
Our admissions seem to come in waves. Our daily workload seems to come in waves as well. Yet the essential quantum of hospital medicine is the patient. RVUs may be 1.33, and LOS 3.2 days, and FTEs 0.8, but I have yet to see a patient-and-a-half in a room.
CRITICAL MASS: Critical mass is the smallest amount of fissionable material necessary to maintain a nuclear chain reaction at a constant level. The term is also used to denote an amount or level needed for a specific result or new action to occur. Happily the hospitalist movement in America has reached that self-sustaining critical mass.
CONCLUSION: As Sir Isaac Newton sat under the proverbial tree and watched a ripe Granny Smith drop on his noggin, little did he know how profoundly he would affect the world of hospital medicine. What goes up must come down. The patient admitted must be discharged. And the editorial started must eventually finish. TH
Jamie Newman, MD, FACP, is physician editor of The Hopitalist, and senior associate consultant, Hospital Internal Medicine and associate professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
The forces of our universe are described and measured by a series of laws and equations known collectively as physics. Though we seem far removed from those halcyon (or Halcion) days of college physics, we exist in a universe still ruled by them. In this instance, our world is the hospital.
Strange vectors of force and difficult-to-fathom principles swirl, causing unanticipated changes in our environment. Using the laws of physics we can attempt to understand these forces.
NEWTON’S FIRST LAW: Newton’s first law is a statement about inertia. An object at rest stays at rest; an object in motion stays in motion unless compelled to change its state by the action of an external force. Byzantine bureaucracies maintain a significant amount of inertia. The expression “that’s the way we’ve always done it here” best summarizes this philosophy.
NEWTON’S SECOND LAW: Newton’s second law examines the force necessary to cause the acceleration of an object in relationship to its mass (F=MA). A moderate amount of force applied to a golf ball may send that object 250 yards—hook right, but the same force applied to a dump truck causes no significant motion.
In the hospital, we often see large expenditures of energy resulting in little movement. This is generally an administrative phenomenon.
NEWTON’S THIRD LAW: For every action there is an equal and opposite reaction. This is an important law in the hospital. The most recent example is the change in residents’ work hours. A seemingly simple issue, residents working too many hours leads to a legislative action and mandated hours. This specific alteration has had unintended consequences and affected numerous other systems. In the case of resident work hours the potential advantages in hours worked has led to a potentially adverse effect on such things as continuity and learning—and an increase in demand for hospitalists.
No system changes can occur without consequences, and the trick is to identify those changes before they occur. Luckily most systems have significant inertia, and only the greatest forces cause major change. It takes massive energy expenditure (i.e., government regulation or resident review boards) to solicit the forces adequate to overcome escape velocity and cause change.
Some forces can cause change not by their sheer energy level, but by their strategic placement. A small forceful tap may split a diamond. A call by a resident’s spouse can cause the downfall of a program. An off-hand comment by a colleague can lead to a disastrous malpractice settlement.
CENTRIFUGAL PSEUDOFORCE: A pseudoforce occurs when one moves in a uniform circular motion. Most of us have observed this phenomenon. When you run around in circles like the proverbial decapitated fowl, little is accomplished despite a sensation of energy expended.
A related principle is Brownian motion: Particles in a gas or fluid collide against each other and the walls of the container causing a random motion. At times the hospitalist’s day may feel that way: active movement but much of it nondirectional.
COPERNICAN PRINCIPLE: The idea, suggested by Copernicus was that the sun—not the earth—is the center of this universe. This is an essential point for hospitalists to remember. We spend hours rounding on our patients. We must always remember that the physician is not the center of the universe for the hospitalized patient. As the name suggests, when we “round” we are the satellite.
CAUSALITY PRINCIPLE: Cause must follow effect. This is a dangerous theory exemplified by the classic post-hoc, prompter hoc: Because I did something, something happened.
When applied to patients, the causality principle can mislead. The fever went down when the antibiotic was started. Coincidence or causality? We hired a hospitalist and our length of stay went down. Coincidence or causality?
THE THEORY OF RELATIVITY: Einstein’s famous equation E=mc2 represents his theory of relativity. This equation represents the relationship between an object’s mass and its energy. Mass is represented by the formula M=DV where D is density and V=volume.
In a hospital setting we see this formula used in a corollary to Einstein’s, called the Theory of Relatives. When entering a patient’s room, one is often confronted with a large number of relatives, spouses, siblings, and the dreaded estranged children. These situations almost always require an increased amount of energy expenditure in communication, consensus building, and time.
As the absolute number (or volume) of family members increases, concurrent with any increased density on the individual members’ part, energy expenditure increases dramatically. This follows the mass equation closely. In situations where the density of an individual family member increases beyond measurable levels, one can enter a Black Hole scenario (see illustration).
BLACK HOLES: A black hole is a region of space-time from which nothing can escape—even light.
A black hole is a region of such extreme density that all energy is sucked into its gravitational field. Once exposed to a black hole situation, the observer may note expected phenomena, including absence of light, loss of energy, extreme fatigue and malaise, and a sensation of hopelessness. This effect can be seen in committee rooms or on the wards.
The only known remedies for this condition are avoidance or going off-service.
THE GIBBS FREE ENERGY EQUATION: The Gibbs free energy equation, G=H-(TS), is a thermodynamic formula and a measure of the conservation of energy. Simply put, the energy of a system is related to the enthalpy (H) or positive creative energy input minus the product of time and entropy, the natural tendency of systems to fall apart.
This effect can be seen in the creation of hospitalist programs.
A hospitalist program is sometimes created by an energetic entrepreneur responding to a vacuum or potential space. A great design leads to a functional program (G). The hospitalist (H) must continually put energy into maintaining the system, otherwise over time (T) entropy (S) takes hold and the system deteriorates. A hospitalist program can’t rely on its initial successful design to survive.
PARTICLE WAVE DUALITY: Quanta are bundles of energy. We see these basic units in the hospital on a nonsubatomic level.
Our admissions seem to come in waves. Our daily workload seems to come in waves as well. Yet the essential quantum of hospital medicine is the patient. RVUs may be 1.33, and LOS 3.2 days, and FTEs 0.8, but I have yet to see a patient-and-a-half in a room.
CRITICAL MASS: Critical mass is the smallest amount of fissionable material necessary to maintain a nuclear chain reaction at a constant level. The term is also used to denote an amount or level needed for a specific result or new action to occur. Happily the hospitalist movement in America has reached that self-sustaining critical mass.
CONCLUSION: As Sir Isaac Newton sat under the proverbial tree and watched a ripe Granny Smith drop on his noggin, little did he know how profoundly he would affect the world of hospital medicine. What goes up must come down. The patient admitted must be discharged. And the editorial started must eventually finish. TH
Jamie Newman, MD, FACP, is physician editor of The Hopitalist, and senior associate consultant, Hospital Internal Medicine and associate professor of internal medicine and medical history, Mayo Clinic College of Medicine at the Mayo Clinic College of Medicine, Rochester, Minn.
The Hepatoadrenal Syndrome, HSS to Treat CHF, Treatment for Atrial Fib, and More
WORSENING OUTCOMES AND INCREASED RECURRENCE OF CLOSTRIDIUM DIFFICILE AFTER INITIAL TREATMENT WITH METRONIDAZOLE?
Pepin J, Alary ME, Valiquette L, et al. Increasing risk of relapse after treatment of Clostridium difficile colitis in Quebec, Canada. Clin Infect Dis. 2005;40:1591-1597; and Musher DM, Aslam S, Logan N, et al. Relatively poor outcome after treatment of Clostridium difficile colitis with metronidazole. Clin Infect Dis. 2005;40:1586-1590.
Information on treatment of colitis caused by Clostridium difficile began to appear in the late 1970s and early 1980s. Since that time there have been a paucity of novel therapies. It has been well-established that both metronidazole and vancomycin can effectively treat this entity. Traditionally metronidazole has been the first-line agent for C. difficile-associated diarrhea (CDAD). The reasons for this are three:
- Randomized controlled trials have shown vancomycin and metronidazole to be equally efficacious;
- The cost of oral vancomycin is substantially more than oral metronidazole; and
- Many experts have cautioned that using vancomycin may contribute to the blooming number of bacteria that are resistant to vancomycin.
Indeed recommendations from the Centers for Disease Control and Prevention’s Healthcare Infection Control Practices Advisory Committee as well as the American Society for Health-System Pharmacists have supported using metronidazole as our initial agent of choice for CDAD (oral vancomycin is actually the only agent that is approved by the Food and Drug Administration for CDAD). Most of our earlier data claim initial response rates to be 88% or better and relapse rates to be somewhere between 5% and 12% when metronidazole is used.
Two new studies have been published raising a red flag on our current standard of practice. Musher, et al., designed a prospective, observational study in which they followed more 200 patients with CDAD that were initially treated with metronidazole. The patient pool came from a Veterans Affairs Medical Center. They all had a positive fecal ELISA for C. difficile toxin and were treated for seven or more days using at least 1.5 grams per day of metronidazole.
Records were reviewed six weeks prior to the diagnosis and then patients were followed for three months after cessation of therapy. Patients were assigned to four outcome groups:
- Complete responders who did not have recurrence over four months;
- Refractory-to-treatment where signs and symptoms of CDAD were present for 10 or more days;
- Recurrence after initial clinical response with signs and symptoms of CDAD and a positive toxin; and
- Clinical recurrence where there was an initial response but a recurrence of signs and symptoms of CDAD without a positive toxin (either the toxin was not present when tested or the test was not done).
Fifty percent were completely cured. Twenty-two percent were refractory to initial therapy. Twenty-eight percent had a recurrence of CDAD within the 90-day period. The mortality was 27%. This was higher among people who had failed to respond to initial therapy (31% versus 21%; p<.05).
Pepin, et al., retrospectively looked at more than 2,000 CDAD cases from one hospital between 1991 and 2004. To be included the patients needed either a positive toxin, endoscopic evidence of pseudomembranous colitis, or histopathologic evidence of pseudomembranous colitis on a biopsy specimen. Patients received at least 1 gram per day of metronidazole for 10 to 14 days. They were considered to have a recurrence if they had diarrhea within two months of the completion of therapy and either a positive toxin at that time or if the attending physician ordered a second course of antibiotics for C. difficile.
Between 1991 and 2002 the frequency of times that either therapy was changed to vancomycin or vancomycin was added to metronidazole was unchanged (9.6%). During 2003-2004 this more than doubled (25.7%). The number of patients experiencing recurrence over a two-month period comparing data from 1991-2002 to 2003- 2004 was staggering (20.8% versus 47.2%; p<.001). The authors noted that as patients aged the probabilities of recurrence increased.
They also found that a subgroup of patients with a white blood cell count over 20,000 cells/mm3 and an elevated creatinine had a high short-term mortality rate.
Why might we be seeing these results? Several theories exist. Patients are both older and sicker than they have been in the past. Our antibiotic choice is changing with an increase in using agents that provide a more broad-spectrum coverage. Immune responses vary with fewer antitoxin antibodies found in those patients with symptoms and/or recurrence. Metronidazole levels in stool decrease as inflammation and diarrhea resolve; this is not the case with vancomycin where fecal concentrations remain high throughout treatment.
A survey of infectious disease physicians found that they believe antibiotic failure is on the rise in this setting. Before we take this as true, consider the following:
- We have no universally accepted clinical definition of what constitutes diarrhea for CDAD;
- Previous studies did not look for recurrence as far out from initial treatment as these two did; and
- These studies do not have the design to support arguments powerful enough to change our paradigm just yet.
The editorial comment acknowledged the Pepin, et al., report that patients with a high white blood cell count and worsening renal function are those that we should be particularly concerned about. The authors write that if the patient’s white blood cell count is increasing while on therapy that he changes his antibiotic choice to vancomycin. In addition, if someone has either ileus or fulminant CDAD he will use multiple antibiotics and consult the surgeons. At this time we have other agents being studied for CDAD, such as tinidazole. We now need a larger randomized prospective trial to better explore treatment outcomes in CDAD.
HYPERTONIC SALINE SOLUTION TO TREAT REFRACTORY CONGESTIVE HEART FAILURE
Paterna S, Di Pasquale P, Parrinello G, et al. Changes in brain natriuretic peptide levels and bioelectrical impedance measurements after treatment with high-dose furosemide and hypertonic saline solution versus high-dose furosemide alone in refractory congestive heart failure. J Am Coll Cardiol. 2005;45:1997–2003.
CHF continues to increase in prevalence and incidence, despite our advances with therapies using ACE inhibitors, beta-blockers, and aldosterone antagonists. Refractory CHF accounts for a considerable portion of admissions to hospitalists’ services. Loop diuretics are part of the standard of arsenal we employ in these patients. Unfortunately, many patients fail to respond to initial diuretic doses. In this situation we might begin a constant infusion of diuretic or recruit diuretics from other classes in hope of synergism. Another typical approach in treating advanced CHF is restriction of sodium intake.
Paterna, et al., previously published four studies using small volume hypertonic saline solution and high-dose furosemide in refractory CHF, in which they demonstrated the safety and tolerability of these measures. They now present the first randomized double-blinded trial using this intervention. Ninety-four patients were included with NYHA functional class IV CHF on standard medical therapy and high doses of diuretics for at least two weeks. They had to have a left ventricular ejection fraction of <35%, serum creatinine <2 mg/dL, reduced urinary volume (<500 mL/24 h), and a low natriuresis (<60 mEq/24 h). They could not be taking NSAIDs.
Patients received either intravenous furosemide (500 to 1000 mg) plus hypertonic saline solution bid or the IV furosemide bid alone. Treatment lasted four to six days. Body weights were followed. Brain natriuretic peptide plasma levels were measured on hospital days one and six, as well as 30 days after discharge.
The group receiving hypertonic saline solution had brow-raising results. They had a significant increase in daily diuresis and natriuresis (p<0.05), a difference in brain natriuretic peptide levels on days six and 30, a reduction in their length of stay, and a decrease in their hospital readmission rate.
This is a provocative study. At this time the mechanism responsible for the results is unclear. Paterna, et al., offer multiple explanations. One possibility is through the osmotic action of hypertonic saline solution. It may hasten the mobilization of extravascular fluid into the intravascular space and then this volume is quickly excreted. Also, hypertonic saline solution may increase renal blood flow and perfusion alternating the handling of sodium and natriuresis while also allowing the concentration of furosemide in the loop of Henle to attain a more desirable level.
Should these results hold true in other investigations and the inclusion criteria loosen (measuring patients urine volume and sodium concentration for 24 hours prior to admission may not be easy or practical) then we might have a very inexpensive new method for treating refractory CHF.
PERIOPERATIVE BETA-BLOCKERS: HELPFUL OR HARMFUL FOR MAJOR NONCARDIAC SURGERY?
Lindenauer P, Pekow P, Wang K, et al. Perioperative beta-blocker therapy and mortality after major noncardiac surgery. N Engl J Med. 2005;353:349–361.
Among the most common reasons that hospitalists are consulted is the “perioperative evaluation.” This is with good reason because 50,000 patients each year have a perioperative myocardial infarction. A statement by the Agency for Health Care Research and Quality proclaims that we have “clear opportunities for safety improvement” in regard to using beta-blockers for patients with intermediate and high risk for perioperative cardiovascular complications. The American Heart Association and the American College of Cardiology recommend using these medications in patients with either risk factors for or known coronary artery disease when undergoing high-risk surgeries. Despite all of this the efficacy of the class has not been proven by large randomized clinical studies.
Using a large national registry of more than 300 U.S. hospitals, Lindenauer, et al., conducted a large observational study evaluating beta-blockade in the perioperative period in patients undergoing major noncardiac surgery. Looking at more than 700,000 patients, they found that 85% had no recorded contraindication to beta-blockers. Only 18% of eligible patients received beta-blockers (n=122, 338).
Patients were considered to have had a beta-blocker for prophylaxis if it was given within the first 48 hours of their hospitalization, though this may or may not have been the intended use (this information was not provided by the registry data base). Only in-hospital mortality was evaluated as postdischarge information was not available. All patients had a revised cardiac risk index configured. This index places risk on perioperative cardiac events by looking at the nature of the surgery as well as whether or not a history of congestive heart failure, ischemic heart disease, perioperative treatment with insulin, an elevated preoperative creatinine, and cerebrovascular disease are present. An increasing score means that major perioperative complications become more likely (scores range from 0–5).
Considering all patients, there was no risk reduction of in-hospital death for those receiving beta-blockers. If the revised cardiac risk index score was 0 or 1, the patients had an increase in the risk of death (43% and 13%, respectively). However, those patients whose scores were 2, 3, or 4 or higher had a reduction in the risk of death (from 10% to 43% as their score increased).
How are we to account for these results? In the high-risk patients we see benefit in treatment with beta-blockers. We suspect this drug class improves coronary filling time during diastole and/or prevents dangerous arrhythmias. In patients at low and intermediate risk, the results may be surprising. The study group did not have patient charts available. It is possible that these patients were given betablockers not for prophylaxis but in response to a postoperative ischemic event or infarction. If this misclassification took place, then the effectiveness of beta-blockers is underestimated and the suggestion that these drugs are harmful in this situation would be erroneous.
Given the data gleaned from this study and considering previous publications, we are justified—even obligated—in using betablockers in high-risk patients, without contraindications, who undergo major noncardiac surgery. Before using these drugs in patients at low or intermediate risk we need more information. Two large ongoing randomized trials (POISE and DECREASE–IV) should bring clarity to this issue. We expect results from these in the next four years.
A NEW CLINICAL ENTITY: THE HEPATOADRENAL SYNDROME
Marik PE, Gayowski T, Starzl TE, et al. The hepatoadrenal syndrome: a common yet unrecognized clinical condition. Crit Care Med. 2005;33:1254-1259.
It is not uncommon to see the temporary dysfunction of the hypothalamic-pituitary-adrenal axis while someone is critically ill. Many physicians who suspect this condition attempt to make a diagnosis using either a random total cortisol level or perform a cosyntropin stimulation test. End-stage liver disease and sepsis share some elements of their pathophysiology, such as endotoxemia and increased levels of mediators that influence inflammation.
A liver transplant intensive care unit has produced data on what they have coined the “hepatoadrenal syndrome.” Due to emerging evidence that severe liver disease is associated with adrenal insufficiency, this liver transplant intensive care unit began routinely testing all patients admitted to their unit for this condition. They presented their findings for 340 patients. This review will focus only on those patients with chronic liver failure and fulminant hepatic failure because transplant patients are often cared for by a multidisciplinary team. Patients were labeled as having adrenal insufficiency if the random total cortisol level was <20 micrograms (mcg)/dL in patients who were “highly stressed” (i.e., hypotension, respiratory failure). In all other patients a random total cortisol level of <15 mcg/dL or a 30-minute level <20 mcg/dL post-low-dose (1 mcg) cosyntropin established the diagnosis. Lipid profiles were also obtained from each patient. Those receiving glucocorticoids were excluded. It was left to the discretion of the treating physician whether or not to treat patients with steroids.
Eight patients (33%) with fulminant hepatic failure and 97 patients (66%) with chronic liver disease met their criteria for adrenal insufficiency. Of the patients with adrenal insufficiency the mortality rate was 46% for those not treated with glucocorticoids compared with 26% for those receiving glucocorticoid therapy. The HDL level was the only variable predictive of adrenal insufficiency (p<.0001).
The association between HDL levels and cortisol is as follows: The adrenal glands do not store cortisol. Cholesterol is a precursor for the synthesis of steroids—80% of cortisol arises from it. The lipoprotein of choice to use as substrate in steroid production is HDL. Because a major protein component of HDL is synthesized by the liver, those with liver disease have low levels of serum HDL.
Recently our current method of diagnosing adrenal insufficiency during acute illness has been challenged in the literature. Measuring free cortisol rather than total cortisol has been suggested as proteins that bind cortisol decrease in this setting while free cortisol levels actually rise. Similar to the picture we see in sepsis, there are low levels of these same proteins in liver disease.
At this time testing for free cortisol is not widely available nor do we have good information on what an “appropriate” free cortisol level should be during acute illness. Therefore, given the frequency in which Marik, et al., report encountering this condition and the effect that treatment had on mortality it seems as though this is a diagnosis worth consideration.
TREATMENT OPTIONS FOR ATRIAL FIBRILLATION
Wazni OM, Marrouche NF, Martin DO, et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of symptomatic atrial fibrillation. JAMA. 2005;293(21):2634-2640.
Atrial fibrillation affects millions of people. This diagnosis has a significant mortality associated with it, causes strokes, and influences quality of life. Therapy has been less than satisfying. Both rate control and rhythm control have multiple potential adverse consequences. Pulmonary vein isolation is performed in the electrophysiology laboratory using an ablation catheter. The goal of this procedure is to completely disconnect the electrical activity between the pulmonary vein antrum and the left atrium. This is a potentially curable procedure for atrial fibrillation.
In a multicenter prospective randomized pilot study Wazni, et al., studied 70 patients with highly symptomatic atrial fibrillation. Patients were between 18 and 75 years old. They could not have undergone ablation in the past, had a history of open-heart surgery, been previously treated with antiarrhythmic drugs, or had a contraindication to long-term anticoagulation. Patients were randomized to antiarrhythmic therapy or pulmonary vein isolation. Those receiving medical treatment were given flecainide, propafenone, or sotalol. Amiodarone was used for patients who had failed at least two or more of these medications. Drugs were titrated to the maximum tolerable doses. The other arm of the group underwent pulmonary vein isolation. This group also received anticoagulation with warfarin beginning the day of the procedure, and this was continued for at least three months. Anticoagulation was extended beyond this time if atrial fibrillation recurred or the pulmonary vein was narrowed by 50% or more (as seen on a three-month post-procedure CT scan). Follow-up was at least one year. A loop event-recorder was worn for one month by all patients and event recorders were used for patients who were symptomatic beyond the first three months of therapy initiation.
After one year, symptomatic atrial fibrillation recurred in 63% of the antiarrhythmic group versus 13% in the pulmonary vein isolation group (p<.001). Fifty-four percent of those medically treated were hospitalized versus 9% of pulmonary vein isolation patients (p<.001). There were no thromboembolic events in either group. Bleeding rates were similar in both groups. For those who underwent pulmonary vein isolation 3% had mild pulmonary vein stenosis and 3% had moderate stenosis (all of which were asymptomatic). Five of the eight measures of quality of life were significantly improved in the pulmonary vein isolation arm versus those receiving antiarrhythmic drugs.
Recently data from multiple trials such as AFFIRM and RACE confirm that rhythm control does not confer significant benefits over rate-control for atrial fibrillation. In fact rate control seems to be a more attractive approach to many patients given the side-effect profile of the antiarrhythmia medications. This study was initiated prior to the release of the information gained from RACE and AFFIRM, thus no rate-control arm was included. This trial also differed from previous studies by using a younger population that was highly symptomatic in comparison with other recent studies using older patients who had recurrent persistent atrial fibrillation.
The biggest concerns about pulmonary vein isolation are the complication rates (death in 0.05% and stroke in 0.28%). We also don’t know if this procedure will translate into long-term cures. Until we have larger studies this should not be a first-line modality for treating all patients. Quite often we find patients where neither rate nor rhythm control is a particularly attractive option, especially in regard to long-term anticoagulation. Pulmonary vein isolation provides us with a new viable option for these people as well as something to consider for carefully selected highly symptomatic patients. TH
WORSENING OUTCOMES AND INCREASED RECURRENCE OF CLOSTRIDIUM DIFFICILE AFTER INITIAL TREATMENT WITH METRONIDAZOLE?
Pepin J, Alary ME, Valiquette L, et al. Increasing risk of relapse after treatment of Clostridium difficile colitis in Quebec, Canada. Clin Infect Dis. 2005;40:1591-1597; and Musher DM, Aslam S, Logan N, et al. Relatively poor outcome after treatment of Clostridium difficile colitis with metronidazole. Clin Infect Dis. 2005;40:1586-1590.
Information on treatment of colitis caused by Clostridium difficile began to appear in the late 1970s and early 1980s. Since that time there have been a paucity of novel therapies. It has been well-established that both metronidazole and vancomycin can effectively treat this entity. Traditionally metronidazole has been the first-line agent for C. difficile-associated diarrhea (CDAD). The reasons for this are three:
- Randomized controlled trials have shown vancomycin and metronidazole to be equally efficacious;
- The cost of oral vancomycin is substantially more than oral metronidazole; and
- Many experts have cautioned that using vancomycin may contribute to the blooming number of bacteria that are resistant to vancomycin.
Indeed recommendations from the Centers for Disease Control and Prevention’s Healthcare Infection Control Practices Advisory Committee as well as the American Society for Health-System Pharmacists have supported using metronidazole as our initial agent of choice for CDAD (oral vancomycin is actually the only agent that is approved by the Food and Drug Administration for CDAD). Most of our earlier data claim initial response rates to be 88% or better and relapse rates to be somewhere between 5% and 12% when metronidazole is used.
Two new studies have been published raising a red flag on our current standard of practice. Musher, et al., designed a prospective, observational study in which they followed more 200 patients with CDAD that were initially treated with metronidazole. The patient pool came from a Veterans Affairs Medical Center. They all had a positive fecal ELISA for C. difficile toxin and were treated for seven or more days using at least 1.5 grams per day of metronidazole.
Records were reviewed six weeks prior to the diagnosis and then patients were followed for three months after cessation of therapy. Patients were assigned to four outcome groups:
- Complete responders who did not have recurrence over four months;
- Refractory-to-treatment where signs and symptoms of CDAD were present for 10 or more days;
- Recurrence after initial clinical response with signs and symptoms of CDAD and a positive toxin; and
- Clinical recurrence where there was an initial response but a recurrence of signs and symptoms of CDAD without a positive toxin (either the toxin was not present when tested or the test was not done).
Fifty percent were completely cured. Twenty-two percent were refractory to initial therapy. Twenty-eight percent had a recurrence of CDAD within the 90-day period. The mortality was 27%. This was higher among people who had failed to respond to initial therapy (31% versus 21%; p<.05).
Pepin, et al., retrospectively looked at more than 2,000 CDAD cases from one hospital between 1991 and 2004. To be included the patients needed either a positive toxin, endoscopic evidence of pseudomembranous colitis, or histopathologic evidence of pseudomembranous colitis on a biopsy specimen. Patients received at least 1 gram per day of metronidazole for 10 to 14 days. They were considered to have a recurrence if they had diarrhea within two months of the completion of therapy and either a positive toxin at that time or if the attending physician ordered a second course of antibiotics for C. difficile.
Between 1991 and 2002 the frequency of times that either therapy was changed to vancomycin or vancomycin was added to metronidazole was unchanged (9.6%). During 2003-2004 this more than doubled (25.7%). The number of patients experiencing recurrence over a two-month period comparing data from 1991-2002 to 2003- 2004 was staggering (20.8% versus 47.2%; p<.001). The authors noted that as patients aged the probabilities of recurrence increased.
They also found that a subgroup of patients with a white blood cell count over 20,000 cells/mm3 and an elevated creatinine had a high short-term mortality rate.
Why might we be seeing these results? Several theories exist. Patients are both older and sicker than they have been in the past. Our antibiotic choice is changing with an increase in using agents that provide a more broad-spectrum coverage. Immune responses vary with fewer antitoxin antibodies found in those patients with symptoms and/or recurrence. Metronidazole levels in stool decrease as inflammation and diarrhea resolve; this is not the case with vancomycin where fecal concentrations remain high throughout treatment.
A survey of infectious disease physicians found that they believe antibiotic failure is on the rise in this setting. Before we take this as true, consider the following:
- We have no universally accepted clinical definition of what constitutes diarrhea for CDAD;
- Previous studies did not look for recurrence as far out from initial treatment as these two did; and
- These studies do not have the design to support arguments powerful enough to change our paradigm just yet.
The editorial comment acknowledged the Pepin, et al., report that patients with a high white blood cell count and worsening renal function are those that we should be particularly concerned about. The authors write that if the patient’s white blood cell count is increasing while on therapy that he changes his antibiotic choice to vancomycin. In addition, if someone has either ileus or fulminant CDAD he will use multiple antibiotics and consult the surgeons. At this time we have other agents being studied for CDAD, such as tinidazole. We now need a larger randomized prospective trial to better explore treatment outcomes in CDAD.
HYPERTONIC SALINE SOLUTION TO TREAT REFRACTORY CONGESTIVE HEART FAILURE
Paterna S, Di Pasquale P, Parrinello G, et al. Changes in brain natriuretic peptide levels and bioelectrical impedance measurements after treatment with high-dose furosemide and hypertonic saline solution versus high-dose furosemide alone in refractory congestive heart failure. J Am Coll Cardiol. 2005;45:1997–2003.
CHF continues to increase in prevalence and incidence, despite our advances with therapies using ACE inhibitors, beta-blockers, and aldosterone antagonists. Refractory CHF accounts for a considerable portion of admissions to hospitalists’ services. Loop diuretics are part of the standard of arsenal we employ in these patients. Unfortunately, many patients fail to respond to initial diuretic doses. In this situation we might begin a constant infusion of diuretic or recruit diuretics from other classes in hope of synergism. Another typical approach in treating advanced CHF is restriction of sodium intake.
Paterna, et al., previously published four studies using small volume hypertonic saline solution and high-dose furosemide in refractory CHF, in which they demonstrated the safety and tolerability of these measures. They now present the first randomized double-blinded trial using this intervention. Ninety-four patients were included with NYHA functional class IV CHF on standard medical therapy and high doses of diuretics for at least two weeks. They had to have a left ventricular ejection fraction of <35%, serum creatinine <2 mg/dL, reduced urinary volume (<500 mL/24 h), and a low natriuresis (<60 mEq/24 h). They could not be taking NSAIDs.
Patients received either intravenous furosemide (500 to 1000 mg) plus hypertonic saline solution bid or the IV furosemide bid alone. Treatment lasted four to six days. Body weights were followed. Brain natriuretic peptide plasma levels were measured on hospital days one and six, as well as 30 days after discharge.
The group receiving hypertonic saline solution had brow-raising results. They had a significant increase in daily diuresis and natriuresis (p<0.05), a difference in brain natriuretic peptide levels on days six and 30, a reduction in their length of stay, and a decrease in their hospital readmission rate.
This is a provocative study. At this time the mechanism responsible for the results is unclear. Paterna, et al., offer multiple explanations. One possibility is through the osmotic action of hypertonic saline solution. It may hasten the mobilization of extravascular fluid into the intravascular space and then this volume is quickly excreted. Also, hypertonic saline solution may increase renal blood flow and perfusion alternating the handling of sodium and natriuresis while also allowing the concentration of furosemide in the loop of Henle to attain a more desirable level.
Should these results hold true in other investigations and the inclusion criteria loosen (measuring patients urine volume and sodium concentration for 24 hours prior to admission may not be easy or practical) then we might have a very inexpensive new method for treating refractory CHF.
PERIOPERATIVE BETA-BLOCKERS: HELPFUL OR HARMFUL FOR MAJOR NONCARDIAC SURGERY?
Lindenauer P, Pekow P, Wang K, et al. Perioperative beta-blocker therapy and mortality after major noncardiac surgery. N Engl J Med. 2005;353:349–361.
Among the most common reasons that hospitalists are consulted is the “perioperative evaluation.” This is with good reason because 50,000 patients each year have a perioperative myocardial infarction. A statement by the Agency for Health Care Research and Quality proclaims that we have “clear opportunities for safety improvement” in regard to using beta-blockers for patients with intermediate and high risk for perioperative cardiovascular complications. The American Heart Association and the American College of Cardiology recommend using these medications in patients with either risk factors for or known coronary artery disease when undergoing high-risk surgeries. Despite all of this the efficacy of the class has not been proven by large randomized clinical studies.
Using a large national registry of more than 300 U.S. hospitals, Lindenauer, et al., conducted a large observational study evaluating beta-blockade in the perioperative period in patients undergoing major noncardiac surgery. Looking at more than 700,000 patients, they found that 85% had no recorded contraindication to beta-blockers. Only 18% of eligible patients received beta-blockers (n=122, 338).
Patients were considered to have had a beta-blocker for prophylaxis if it was given within the first 48 hours of their hospitalization, though this may or may not have been the intended use (this information was not provided by the registry data base). Only in-hospital mortality was evaluated as postdischarge information was not available. All patients had a revised cardiac risk index configured. This index places risk on perioperative cardiac events by looking at the nature of the surgery as well as whether or not a history of congestive heart failure, ischemic heart disease, perioperative treatment with insulin, an elevated preoperative creatinine, and cerebrovascular disease are present. An increasing score means that major perioperative complications become more likely (scores range from 0–5).
Considering all patients, there was no risk reduction of in-hospital death for those receiving beta-blockers. If the revised cardiac risk index score was 0 or 1, the patients had an increase in the risk of death (43% and 13%, respectively). However, those patients whose scores were 2, 3, or 4 or higher had a reduction in the risk of death (from 10% to 43% as their score increased).
How are we to account for these results? In the high-risk patients we see benefit in treatment with beta-blockers. We suspect this drug class improves coronary filling time during diastole and/or prevents dangerous arrhythmias. In patients at low and intermediate risk, the results may be surprising. The study group did not have patient charts available. It is possible that these patients were given betablockers not for prophylaxis but in response to a postoperative ischemic event or infarction. If this misclassification took place, then the effectiveness of beta-blockers is underestimated and the suggestion that these drugs are harmful in this situation would be erroneous.
Given the data gleaned from this study and considering previous publications, we are justified—even obligated—in using betablockers in high-risk patients, without contraindications, who undergo major noncardiac surgery. Before using these drugs in patients at low or intermediate risk we need more information. Two large ongoing randomized trials (POISE and DECREASE–IV) should bring clarity to this issue. We expect results from these in the next four years.
A NEW CLINICAL ENTITY: THE HEPATOADRENAL SYNDROME
Marik PE, Gayowski T, Starzl TE, et al. The hepatoadrenal syndrome: a common yet unrecognized clinical condition. Crit Care Med. 2005;33:1254-1259.
It is not uncommon to see the temporary dysfunction of the hypothalamic-pituitary-adrenal axis while someone is critically ill. Many physicians who suspect this condition attempt to make a diagnosis using either a random total cortisol level or perform a cosyntropin stimulation test. End-stage liver disease and sepsis share some elements of their pathophysiology, such as endotoxemia and increased levels of mediators that influence inflammation.
A liver transplant intensive care unit has produced data on what they have coined the “hepatoadrenal syndrome.” Due to emerging evidence that severe liver disease is associated with adrenal insufficiency, this liver transplant intensive care unit began routinely testing all patients admitted to their unit for this condition. They presented their findings for 340 patients. This review will focus only on those patients with chronic liver failure and fulminant hepatic failure because transplant patients are often cared for by a multidisciplinary team. Patients were labeled as having adrenal insufficiency if the random total cortisol level was <20 micrograms (mcg)/dL in patients who were “highly stressed” (i.e., hypotension, respiratory failure). In all other patients a random total cortisol level of <15 mcg/dL or a 30-minute level <20 mcg/dL post-low-dose (1 mcg) cosyntropin established the diagnosis. Lipid profiles were also obtained from each patient. Those receiving glucocorticoids were excluded. It was left to the discretion of the treating physician whether or not to treat patients with steroids.
Eight patients (33%) with fulminant hepatic failure and 97 patients (66%) with chronic liver disease met their criteria for adrenal insufficiency. Of the patients with adrenal insufficiency the mortality rate was 46% for those not treated with glucocorticoids compared with 26% for those receiving glucocorticoid therapy. The HDL level was the only variable predictive of adrenal insufficiency (p<.0001).
The association between HDL levels and cortisol is as follows: The adrenal glands do not store cortisol. Cholesterol is a precursor for the synthesis of steroids—80% of cortisol arises from it. The lipoprotein of choice to use as substrate in steroid production is HDL. Because a major protein component of HDL is synthesized by the liver, those with liver disease have low levels of serum HDL.
Recently our current method of diagnosing adrenal insufficiency during acute illness has been challenged in the literature. Measuring free cortisol rather than total cortisol has been suggested as proteins that bind cortisol decrease in this setting while free cortisol levels actually rise. Similar to the picture we see in sepsis, there are low levels of these same proteins in liver disease.
At this time testing for free cortisol is not widely available nor do we have good information on what an “appropriate” free cortisol level should be during acute illness. Therefore, given the frequency in which Marik, et al., report encountering this condition and the effect that treatment had on mortality it seems as though this is a diagnosis worth consideration.
TREATMENT OPTIONS FOR ATRIAL FIBRILLATION
Wazni OM, Marrouche NF, Martin DO, et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of symptomatic atrial fibrillation. JAMA. 2005;293(21):2634-2640.
Atrial fibrillation affects millions of people. This diagnosis has a significant mortality associated with it, causes strokes, and influences quality of life. Therapy has been less than satisfying. Both rate control and rhythm control have multiple potential adverse consequences. Pulmonary vein isolation is performed in the electrophysiology laboratory using an ablation catheter. The goal of this procedure is to completely disconnect the electrical activity between the pulmonary vein antrum and the left atrium. This is a potentially curable procedure for atrial fibrillation.
In a multicenter prospective randomized pilot study Wazni, et al., studied 70 patients with highly symptomatic atrial fibrillation. Patients were between 18 and 75 years old. They could not have undergone ablation in the past, had a history of open-heart surgery, been previously treated with antiarrhythmic drugs, or had a contraindication to long-term anticoagulation. Patients were randomized to antiarrhythmic therapy or pulmonary vein isolation. Those receiving medical treatment were given flecainide, propafenone, or sotalol. Amiodarone was used for patients who had failed at least two or more of these medications. Drugs were titrated to the maximum tolerable doses. The other arm of the group underwent pulmonary vein isolation. This group also received anticoagulation with warfarin beginning the day of the procedure, and this was continued for at least three months. Anticoagulation was extended beyond this time if atrial fibrillation recurred or the pulmonary vein was narrowed by 50% or more (as seen on a three-month post-procedure CT scan). Follow-up was at least one year. A loop event-recorder was worn for one month by all patients and event recorders were used for patients who were symptomatic beyond the first three months of therapy initiation.
After one year, symptomatic atrial fibrillation recurred in 63% of the antiarrhythmic group versus 13% in the pulmonary vein isolation group (p<.001). Fifty-four percent of those medically treated were hospitalized versus 9% of pulmonary vein isolation patients (p<.001). There were no thromboembolic events in either group. Bleeding rates were similar in both groups. For those who underwent pulmonary vein isolation 3% had mild pulmonary vein stenosis and 3% had moderate stenosis (all of which were asymptomatic). Five of the eight measures of quality of life were significantly improved in the pulmonary vein isolation arm versus those receiving antiarrhythmic drugs.
Recently data from multiple trials such as AFFIRM and RACE confirm that rhythm control does not confer significant benefits over rate-control for atrial fibrillation. In fact rate control seems to be a more attractive approach to many patients given the side-effect profile of the antiarrhythmia medications. This study was initiated prior to the release of the information gained from RACE and AFFIRM, thus no rate-control arm was included. This trial also differed from previous studies by using a younger population that was highly symptomatic in comparison with other recent studies using older patients who had recurrent persistent atrial fibrillation.
The biggest concerns about pulmonary vein isolation are the complication rates (death in 0.05% and stroke in 0.28%). We also don’t know if this procedure will translate into long-term cures. Until we have larger studies this should not be a first-line modality for treating all patients. Quite often we find patients where neither rate nor rhythm control is a particularly attractive option, especially in regard to long-term anticoagulation. Pulmonary vein isolation provides us with a new viable option for these people as well as something to consider for carefully selected highly symptomatic patients. TH
WORSENING OUTCOMES AND INCREASED RECURRENCE OF CLOSTRIDIUM DIFFICILE AFTER INITIAL TREATMENT WITH METRONIDAZOLE?
Pepin J, Alary ME, Valiquette L, et al. Increasing risk of relapse after treatment of Clostridium difficile colitis in Quebec, Canada. Clin Infect Dis. 2005;40:1591-1597; and Musher DM, Aslam S, Logan N, et al. Relatively poor outcome after treatment of Clostridium difficile colitis with metronidazole. Clin Infect Dis. 2005;40:1586-1590.
Information on treatment of colitis caused by Clostridium difficile began to appear in the late 1970s and early 1980s. Since that time there have been a paucity of novel therapies. It has been well-established that both metronidazole and vancomycin can effectively treat this entity. Traditionally metronidazole has been the first-line agent for C. difficile-associated diarrhea (CDAD). The reasons for this are three:
- Randomized controlled trials have shown vancomycin and metronidazole to be equally efficacious;
- The cost of oral vancomycin is substantially more than oral metronidazole; and
- Many experts have cautioned that using vancomycin may contribute to the blooming number of bacteria that are resistant to vancomycin.
Indeed recommendations from the Centers for Disease Control and Prevention’s Healthcare Infection Control Practices Advisory Committee as well as the American Society for Health-System Pharmacists have supported using metronidazole as our initial agent of choice for CDAD (oral vancomycin is actually the only agent that is approved by the Food and Drug Administration for CDAD). Most of our earlier data claim initial response rates to be 88% or better and relapse rates to be somewhere between 5% and 12% when metronidazole is used.
Two new studies have been published raising a red flag on our current standard of practice. Musher, et al., designed a prospective, observational study in which they followed more 200 patients with CDAD that were initially treated with metronidazole. The patient pool came from a Veterans Affairs Medical Center. They all had a positive fecal ELISA for C. difficile toxin and were treated for seven or more days using at least 1.5 grams per day of metronidazole.
Records were reviewed six weeks prior to the diagnosis and then patients were followed for three months after cessation of therapy. Patients were assigned to four outcome groups:
- Complete responders who did not have recurrence over four months;
- Refractory-to-treatment where signs and symptoms of CDAD were present for 10 or more days;
- Recurrence after initial clinical response with signs and symptoms of CDAD and a positive toxin; and
- Clinical recurrence where there was an initial response but a recurrence of signs and symptoms of CDAD without a positive toxin (either the toxin was not present when tested or the test was not done).
Fifty percent were completely cured. Twenty-two percent were refractory to initial therapy. Twenty-eight percent had a recurrence of CDAD within the 90-day period. The mortality was 27%. This was higher among people who had failed to respond to initial therapy (31% versus 21%; p<.05).
Pepin, et al., retrospectively looked at more than 2,000 CDAD cases from one hospital between 1991 and 2004. To be included the patients needed either a positive toxin, endoscopic evidence of pseudomembranous colitis, or histopathologic evidence of pseudomembranous colitis on a biopsy specimen. Patients received at least 1 gram per day of metronidazole for 10 to 14 days. They were considered to have a recurrence if they had diarrhea within two months of the completion of therapy and either a positive toxin at that time or if the attending physician ordered a second course of antibiotics for C. difficile.
Between 1991 and 2002 the frequency of times that either therapy was changed to vancomycin or vancomycin was added to metronidazole was unchanged (9.6%). During 2003-2004 this more than doubled (25.7%). The number of patients experiencing recurrence over a two-month period comparing data from 1991-2002 to 2003- 2004 was staggering (20.8% versus 47.2%; p<.001). The authors noted that as patients aged the probabilities of recurrence increased.
They also found that a subgroup of patients with a white blood cell count over 20,000 cells/mm3 and an elevated creatinine had a high short-term mortality rate.
Why might we be seeing these results? Several theories exist. Patients are both older and sicker than they have been in the past. Our antibiotic choice is changing with an increase in using agents that provide a more broad-spectrum coverage. Immune responses vary with fewer antitoxin antibodies found in those patients with symptoms and/or recurrence. Metronidazole levels in stool decrease as inflammation and diarrhea resolve; this is not the case with vancomycin where fecal concentrations remain high throughout treatment.
A survey of infectious disease physicians found that they believe antibiotic failure is on the rise in this setting. Before we take this as true, consider the following:
- We have no universally accepted clinical definition of what constitutes diarrhea for CDAD;
- Previous studies did not look for recurrence as far out from initial treatment as these two did; and
- These studies do not have the design to support arguments powerful enough to change our paradigm just yet.
The editorial comment acknowledged the Pepin, et al., report that patients with a high white blood cell count and worsening renal function are those that we should be particularly concerned about. The authors write that if the patient’s white blood cell count is increasing while on therapy that he changes his antibiotic choice to vancomycin. In addition, if someone has either ileus or fulminant CDAD he will use multiple antibiotics and consult the surgeons. At this time we have other agents being studied for CDAD, such as tinidazole. We now need a larger randomized prospective trial to better explore treatment outcomes in CDAD.
HYPERTONIC SALINE SOLUTION TO TREAT REFRACTORY CONGESTIVE HEART FAILURE
Paterna S, Di Pasquale P, Parrinello G, et al. Changes in brain natriuretic peptide levels and bioelectrical impedance measurements after treatment with high-dose furosemide and hypertonic saline solution versus high-dose furosemide alone in refractory congestive heart failure. J Am Coll Cardiol. 2005;45:1997–2003.
CHF continues to increase in prevalence and incidence, despite our advances with therapies using ACE inhibitors, beta-blockers, and aldosterone antagonists. Refractory CHF accounts for a considerable portion of admissions to hospitalists’ services. Loop diuretics are part of the standard of arsenal we employ in these patients. Unfortunately, many patients fail to respond to initial diuretic doses. In this situation we might begin a constant infusion of diuretic or recruit diuretics from other classes in hope of synergism. Another typical approach in treating advanced CHF is restriction of sodium intake.
Paterna, et al., previously published four studies using small volume hypertonic saline solution and high-dose furosemide in refractory CHF, in which they demonstrated the safety and tolerability of these measures. They now present the first randomized double-blinded trial using this intervention. Ninety-four patients were included with NYHA functional class IV CHF on standard medical therapy and high doses of diuretics for at least two weeks. They had to have a left ventricular ejection fraction of <35%, serum creatinine <2 mg/dL, reduced urinary volume (<500 mL/24 h), and a low natriuresis (<60 mEq/24 h). They could not be taking NSAIDs.
Patients received either intravenous furosemide (500 to 1000 mg) plus hypertonic saline solution bid or the IV furosemide bid alone. Treatment lasted four to six days. Body weights were followed. Brain natriuretic peptide plasma levels were measured on hospital days one and six, as well as 30 days after discharge.
The group receiving hypertonic saline solution had brow-raising results. They had a significant increase in daily diuresis and natriuresis (p<0.05), a difference in brain natriuretic peptide levels on days six and 30, a reduction in their length of stay, and a decrease in their hospital readmission rate.
This is a provocative study. At this time the mechanism responsible for the results is unclear. Paterna, et al., offer multiple explanations. One possibility is through the osmotic action of hypertonic saline solution. It may hasten the mobilization of extravascular fluid into the intravascular space and then this volume is quickly excreted. Also, hypertonic saline solution may increase renal blood flow and perfusion alternating the handling of sodium and natriuresis while also allowing the concentration of furosemide in the loop of Henle to attain a more desirable level.
Should these results hold true in other investigations and the inclusion criteria loosen (measuring patients urine volume and sodium concentration for 24 hours prior to admission may not be easy or practical) then we might have a very inexpensive new method for treating refractory CHF.
PERIOPERATIVE BETA-BLOCKERS: HELPFUL OR HARMFUL FOR MAJOR NONCARDIAC SURGERY?
Lindenauer P, Pekow P, Wang K, et al. Perioperative beta-blocker therapy and mortality after major noncardiac surgery. N Engl J Med. 2005;353:349–361.
Among the most common reasons that hospitalists are consulted is the “perioperative evaluation.” This is with good reason because 50,000 patients each year have a perioperative myocardial infarction. A statement by the Agency for Health Care Research and Quality proclaims that we have “clear opportunities for safety improvement” in regard to using beta-blockers for patients with intermediate and high risk for perioperative cardiovascular complications. The American Heart Association and the American College of Cardiology recommend using these medications in patients with either risk factors for or known coronary artery disease when undergoing high-risk surgeries. Despite all of this the efficacy of the class has not been proven by large randomized clinical studies.
Using a large national registry of more than 300 U.S. hospitals, Lindenauer, et al., conducted a large observational study evaluating beta-blockade in the perioperative period in patients undergoing major noncardiac surgery. Looking at more than 700,000 patients, they found that 85% had no recorded contraindication to beta-blockers. Only 18% of eligible patients received beta-blockers (n=122, 338).
Patients were considered to have had a beta-blocker for prophylaxis if it was given within the first 48 hours of their hospitalization, though this may or may not have been the intended use (this information was not provided by the registry data base). Only in-hospital mortality was evaluated as postdischarge information was not available. All patients had a revised cardiac risk index configured. This index places risk on perioperative cardiac events by looking at the nature of the surgery as well as whether or not a history of congestive heart failure, ischemic heart disease, perioperative treatment with insulin, an elevated preoperative creatinine, and cerebrovascular disease are present. An increasing score means that major perioperative complications become more likely (scores range from 0–5).
Considering all patients, there was no risk reduction of in-hospital death for those receiving beta-blockers. If the revised cardiac risk index score was 0 or 1, the patients had an increase in the risk of death (43% and 13%, respectively). However, those patients whose scores were 2, 3, or 4 or higher had a reduction in the risk of death (from 10% to 43% as their score increased).
How are we to account for these results? In the high-risk patients we see benefit in treatment with beta-blockers. We suspect this drug class improves coronary filling time during diastole and/or prevents dangerous arrhythmias. In patients at low and intermediate risk, the results may be surprising. The study group did not have patient charts available. It is possible that these patients were given betablockers not for prophylaxis but in response to a postoperative ischemic event or infarction. If this misclassification took place, then the effectiveness of beta-blockers is underestimated and the suggestion that these drugs are harmful in this situation would be erroneous.
Given the data gleaned from this study and considering previous publications, we are justified—even obligated—in using betablockers in high-risk patients, without contraindications, who undergo major noncardiac surgery. Before using these drugs in patients at low or intermediate risk we need more information. Two large ongoing randomized trials (POISE and DECREASE–IV) should bring clarity to this issue. We expect results from these in the next four years.
A NEW CLINICAL ENTITY: THE HEPATOADRENAL SYNDROME
Marik PE, Gayowski T, Starzl TE, et al. The hepatoadrenal syndrome: a common yet unrecognized clinical condition. Crit Care Med. 2005;33:1254-1259.
It is not uncommon to see the temporary dysfunction of the hypothalamic-pituitary-adrenal axis while someone is critically ill. Many physicians who suspect this condition attempt to make a diagnosis using either a random total cortisol level or perform a cosyntropin stimulation test. End-stage liver disease and sepsis share some elements of their pathophysiology, such as endotoxemia and increased levels of mediators that influence inflammation.
A liver transplant intensive care unit has produced data on what they have coined the “hepatoadrenal syndrome.” Due to emerging evidence that severe liver disease is associated with adrenal insufficiency, this liver transplant intensive care unit began routinely testing all patients admitted to their unit for this condition. They presented their findings for 340 patients. This review will focus only on those patients with chronic liver failure and fulminant hepatic failure because transplant patients are often cared for by a multidisciplinary team. Patients were labeled as having adrenal insufficiency if the random total cortisol level was <20 micrograms (mcg)/dL in patients who were “highly stressed” (i.e., hypotension, respiratory failure). In all other patients a random total cortisol level of <15 mcg/dL or a 30-minute level <20 mcg/dL post-low-dose (1 mcg) cosyntropin established the diagnosis. Lipid profiles were also obtained from each patient. Those receiving glucocorticoids were excluded. It was left to the discretion of the treating physician whether or not to treat patients with steroids.
Eight patients (33%) with fulminant hepatic failure and 97 patients (66%) with chronic liver disease met their criteria for adrenal insufficiency. Of the patients with adrenal insufficiency the mortality rate was 46% for those not treated with glucocorticoids compared with 26% for those receiving glucocorticoid therapy. The HDL level was the only variable predictive of adrenal insufficiency (p<.0001).
The association between HDL levels and cortisol is as follows: The adrenal glands do not store cortisol. Cholesterol is a precursor for the synthesis of steroids—80% of cortisol arises from it. The lipoprotein of choice to use as substrate in steroid production is HDL. Because a major protein component of HDL is synthesized by the liver, those with liver disease have low levels of serum HDL.
Recently our current method of diagnosing adrenal insufficiency during acute illness has been challenged in the literature. Measuring free cortisol rather than total cortisol has been suggested as proteins that bind cortisol decrease in this setting while free cortisol levels actually rise. Similar to the picture we see in sepsis, there are low levels of these same proteins in liver disease.
At this time testing for free cortisol is not widely available nor do we have good information on what an “appropriate” free cortisol level should be during acute illness. Therefore, given the frequency in which Marik, et al., report encountering this condition and the effect that treatment had on mortality it seems as though this is a diagnosis worth consideration.
TREATMENT OPTIONS FOR ATRIAL FIBRILLATION
Wazni OM, Marrouche NF, Martin DO, et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of symptomatic atrial fibrillation. JAMA. 2005;293(21):2634-2640.
Atrial fibrillation affects millions of people. This diagnosis has a significant mortality associated with it, causes strokes, and influences quality of life. Therapy has been less than satisfying. Both rate control and rhythm control have multiple potential adverse consequences. Pulmonary vein isolation is performed in the electrophysiology laboratory using an ablation catheter. The goal of this procedure is to completely disconnect the electrical activity between the pulmonary vein antrum and the left atrium. This is a potentially curable procedure for atrial fibrillation.
In a multicenter prospective randomized pilot study Wazni, et al., studied 70 patients with highly symptomatic atrial fibrillation. Patients were between 18 and 75 years old. They could not have undergone ablation in the past, had a history of open-heart surgery, been previously treated with antiarrhythmic drugs, or had a contraindication to long-term anticoagulation. Patients were randomized to antiarrhythmic therapy or pulmonary vein isolation. Those receiving medical treatment were given flecainide, propafenone, or sotalol. Amiodarone was used for patients who had failed at least two or more of these medications. Drugs were titrated to the maximum tolerable doses. The other arm of the group underwent pulmonary vein isolation. This group also received anticoagulation with warfarin beginning the day of the procedure, and this was continued for at least three months. Anticoagulation was extended beyond this time if atrial fibrillation recurred or the pulmonary vein was narrowed by 50% or more (as seen on a three-month post-procedure CT scan). Follow-up was at least one year. A loop event-recorder was worn for one month by all patients and event recorders were used for patients who were symptomatic beyond the first three months of therapy initiation.
After one year, symptomatic atrial fibrillation recurred in 63% of the antiarrhythmic group versus 13% in the pulmonary vein isolation group (p<.001). Fifty-four percent of those medically treated were hospitalized versus 9% of pulmonary vein isolation patients (p<.001). There were no thromboembolic events in either group. Bleeding rates were similar in both groups. For those who underwent pulmonary vein isolation 3% had mild pulmonary vein stenosis and 3% had moderate stenosis (all of which were asymptomatic). Five of the eight measures of quality of life were significantly improved in the pulmonary vein isolation arm versus those receiving antiarrhythmic drugs.
Recently data from multiple trials such as AFFIRM and RACE confirm that rhythm control does not confer significant benefits over rate-control for atrial fibrillation. In fact rate control seems to be a more attractive approach to many patients given the side-effect profile of the antiarrhythmia medications. This study was initiated prior to the release of the information gained from RACE and AFFIRM, thus no rate-control arm was included. This trial also differed from previous studies by using a younger population that was highly symptomatic in comparison with other recent studies using older patients who had recurrent persistent atrial fibrillation.
The biggest concerns about pulmonary vein isolation are the complication rates (death in 0.05% and stroke in 0.28%). We also don’t know if this procedure will translate into long-term cures. Until we have larger studies this should not be a first-line modality for treating all patients. Quite often we find patients where neither rate nor rhythm control is a particularly attractive option, especially in regard to long-term anticoagulation. Pulmonary vein isolation provides us with a new viable option for these people as well as something to consider for carefully selected highly symptomatic patients. TH