User login
The Hospitalist only
Pediatric Hospital Medicine
Denver—The Pediatric Hospital Medicine 2005 conference, held July 28–31, got off to a rousing start with a networking reception that preceded the keynote lecture on Thursday evening, July 28. Dan Rauch, MD, cochair of the Ambulatory Pediatric Association (APA) Special Interest Group in Hospital Medicine, welcomed the 200+ attendees. He described the meeting as the result of tremendous cooperation among the APA, the American Academy of Pediatrics (AAP), and the SHM.
“It’s been a tremendous pleasure to work with all three organizations,” said Dr. Rauch. “We have been truly blessed with leaders who think that growth of the field is more important than individual turf battles. I highly recommend that everybody in the room become members of all three organizations.”
Dr. Rauch later told The Hospitalist that he was surprised by how many attendees actually weren’t members of any of the three organizations.
The mostly young pediatric hospitalists in attendance came from all over the United States and Canada. According to keynote speaker Larry Wellikson, MD, CEO of SHM, the median age of the typical hospitalist is 37, and fewer than 10% are 50 or older. Dr. Rauch said the typical pediatric hospitalist is even younger.
In fact, the pediatric hospitalist profession is still in its infancy, a point underscored by the panel discussion during Friday’s plenary session, “Future Directions.” The conversation centered on whether pediatric hospitalist medicine is truly a new subspecialty or simply a job type within general pediatrics. Most attendees seemed to agree that in practice it is a new subspecialty, but gaining acknowledgement of that fact from the professional organizations, academics, hospital administrators, insurers, general practice pediatricians, and even from some pediatric hospitalists themselves is the continuing challenge.
Professional advancement was a theme every speaker emphasized, beginning with Dr. Wellikson.

—Larry Wellikson, MD, CEO of SHM, explaining that the legacy of this generation of hospitalists will be to define hospital medicine.
CREATING THE HOSPITAL OF THE FUTURE
“My life’s goals were to be dean of a med school when I was 40 and a United States senator at 50,” said Dr. Wellikson during his keynote address. He may not have achieved those particular goals, but, he revealed, “believe it or not, my life has been even better than that.”
Dr. Wellikson, who discussed the current status of hospital medicine, is a sought-after speaker and consultant who helps hospitals and physicians understand the current medical environment and create strategies to succeed in it.
“You are building and defining the hospital of the future,” Dr. Wellikson told participants, explaining that the legacy of this generation of hospitalists will be to define hospital medicine. “[Hospitalists] are going to be the most important part of the hospital of the future.
“Hospitals are changing,” he said, describing the hospital of the future as patient-centered with medical care driven by measurable data and practiced in teams. With emergency departments overcrowded and hospitals and ICUs running at capacity, he predicts that $20 billion per year will be spent on hospital construction over the next 10 years. He foresees primary care pediatricians giving up inpatient care.
“Hospitalist medicine is by far the fastest growing medical specialty in the country,” said Dr. Wellikson. Currently, there are approximately 11,295 hospitalists, and he predicts that there will be 30,000 by the end of the decade. Approximately 9% of hospitalists are pediatricians.
According to Dr. Wellikson, 30% of 4,895 community hospitals today have hospitalists on staff, with about eight hospitalists per hospital. The larger the hospital, the more likely it is to have hospitalists:
- 71% of hospitals with more than 500 beds have hospitalists on staff; and
- 50% of hospitals with more than 100 beds have hospitalists.
“We believe at SHM that in 15 years 25% of the CEOs will be hospitalists and 15% of CMOs will be hospitalists,” said Dr. Wellikson, “ ... and you’re not all going to be able to take time off to go get an MBA. We’re going to be in the business of educating you to be a leader, how to be a manager. ... If you will commit to creating the hospital of the future, [SHM] will commit to giving you the tools to do it.”
VALUE VERSUS COMPENSATION
During the keynote, Dr. Wellikson set the stage for a compensation discussion that continued throughout the conference, both during sessions and in networking conversations.
“One of the things that makes the compensation model so unfair for hospital medicine,” said Dr. Wellikson, “is that the way we pay for medical care in this country is so screwed up. We pay by the unit of the visit and by the unit of the procedure. And so it is much better to do something wrong and do it a lot than it is to sit down and spend an hour talking with a family. And God forbid that you’re asked to sit on a QI committee; that’s really down time. ... And God forbid that instead of earning a living and seeing patients for three days you’re wasting your time here in Denver trying to be a better doctor. Our system doesn’t reward that.”
Several attendees mentioned that their hospitals consider them loss leaders. “Don’t allow yourself to be called a loss leader,” said Linda Snelling, MD, in her Friday session on contract negotiation. “You’re a system sustainer. If you want this profession to be respected, you’ve got to be paid for it.” Dr. Snelling is chief of pediatric critical care and associate professor of pediatrics and surgery (anesthesiology) at Brown University, Providence, R.I.
“Hospitalists need to convince ourselves of the value we bring to our institutions and to our patients,” said Mark Joffe, MD, director of community pediatric medicine for the Children’s Hospital of Philadelphia.
Dr. Wellikson emphasized that hospitalists do add value to hospitals—whether it’s educating, whether it’s throughput, whether it’s 24/7, whether it’s improving the quality. He said that hospital administrators—the CMOs at your hospital—understand that. “The reason that leadership and that hospitalists are important is that hospitals see you as the solution to many hospital issues,” he said. “When anthrax was thought to be a public health problem, every hospital started a bioterrorism committee and put the hospitalist on it.
“Almost every place I go, they want more of you. You’re better for their bottom line,” he continued. “If they’re ever going to be a better hospital, they need more of you, and they need you motivated, and they need you seeing the right number of patients so that you have the time to do a better job.”
According to Dr. Wellikson, the expectations of hospitalists is that they will improve efficiency, save the hospital money, provide measurable quality improvement (creating standards and measuring compliance), collect data, do things no one else will (e.g., provide uncompensated care, serve on committees).
Dr. Snelling agreed. “The benefit of hospitalists is not in what you bill,” she said, “but in systems improvements, patient satisfaction, QI, initiatives to start or change a program, teaching, cost-savings, and value-added services you provide to the hospital. ... Start with value. Figure out what you want. Identify common ground. Bargaining is the last thing you do.”
Hospitalists create a seamless continuity from inpatient to outpatient, from the emergency department to the floor, from the ICU to the floor. They improve efficiency via throughput and early discharge. They help uncrowd the emergency department and open ICU beds. “We make other physicians’ lives better,” said Dr. Wellikson. “We do a lot of things for the generalists so that they can go and have a better life.”
There is a definite bright side to being a hospitalist right now. According to Dr. Wellikson there are many more jobs than hospitalists—a trend that he predicts will continue for at least for the next five years.
“Don’t let the fact that we have a totally screwed up healthcare system get you down,” he said. “You’re not replaceable. The service you provide, someone must provide. Your hospital has more wastage in durable goods than it spends on pediatric hospitalists. They will pay for expertise.”
Dr. Snelling advised, “Be direct and shameless about compensation. No surgeon works for free unless they want to; no hospitalist should work for free unless that’s your selected charity, and my favorite charity is not the hospital I work for.
“Continually self-promote,” she continued. “Make sure [the person determining your compensation] knows what your successes are. If you’re doing something that’s successful—you get praise, you get a grant, you get a nice letter from a parent—pass that on. Document your value. If you save your hospital a million bucks, why shouldn’t you get a hunk of that? The CEO’s job is to pay you as little as possible.”
One attendee interjected, “I feel uncomfortable with the idea that what I’m doing as a hospitalist is worth more than what my private-practice colleagues are doing. I don’t want to be offensive.”
To which Dr. Snelling replied, “We’re not talking about being elitist. ‘Mine’s bigger than yours.’ What you’re talking about is the differences between C care—the minimum standard—and A care—the hospitalist. ... Who in this room wants to go to an average doctor?”
Dr. Snelling’s bottom line: “My message is not to gouge the system; it’s about respect. In an ideal situation, everybody gains.”
SHOULD PEDIATRIC HOSPITAL MEDICINE BE A BOARD-CERTIFIED SPECIALTY?
“This is a specialty,” emphasized Dr. Snelling during the contract negotiation session.
On the other hand, during the “Future Directions” plenary panel Dr. Wellikson said, “It is almost not relevant whether there is board certification or no board certification.” He described board certification as a way to measure quality.
“Clearly we need to find a way to validate what we’re doing for our good as well as for the good of our patients,” said Doug Carlson, MD, director of the Pediatric Hospital Medicine Program at St. Louis Children’s Hospital and associate professor of pediatrics at Washington University, St. Louis.
Stephen Ludwig, MD, associate chair for medical education at the Children’s Hospital of Philadelphia presented the case for becoming a board-certified specialty. Some benefits: recognition, prestige, job security, and professional advancement.
“Is this just a job, or do you want to fit into—become a thread in—the fabric of organized medicine?” asked Dr. Ludwig. Most important, though, would be the impact on child health. “Is [board certification] good for children and their parents? Unless you can demonstrate that, it won’t happen.”
According to Dr. Ludwig, becoming a board-certified specialty requires a defined body of knowledge, scientific basis, a sufficient number of practitioners, viable academic training programs, sufficient number of trainees willing to go into those fellowship programs, a board exam, geographic diversity, creation of new knowledge (or at least the application of existing knowledge in new ways), the support of national societies and organizations, and the consent of other specialties, such as internal medicine and family practice. It also takes time—likely years.
Some questions pediatric hospitalists still need to consider: Can you fill a void? Is there sufficient novel material for creating a certifying exam? Are there enough people who would take this exam? How will physicians view maintenance of certification? Where will the naysayers come from? What will be the response from primary care general pediatricians? What will be the response from academic generalists/pediatricians? What will be the subspecialist response?
Dr. Ludwig expressed one concern succinctly: “You might ultimately decrease the number of practitioners willing to make the commitment.”
Dr. Wellikson concurred. “Those of you who are group leaders are constantly in a recruiting mode,” he said. “You need something to help you determine who is good and who is not, but adding three years may drive those who would have been great pediatric hospitalists to become great pediatric anesthesiologists.”
In the end, the group could not agree on an answer. “You have an amazing amount of excitement,” said Dr. Ludwig. “Temper your excitement with focus. You need to decide whether becoming another subspecialty is what you want.”
SOMETHING FOR EVERYONE
The conference offered a broad range of learning opportunities.
Those interested in research heard about opportunities to collaborate and learned how to share resources and develop research projects.
Educators—and aren’t all hospitalists involved in education at some level?—learned “Seven Simple Secrets to Successful Supervision” from Vinny Chiang, MD, chief of inpatient services at Children’s Hospital, Boston. He says the single most powerful question you can ask as an educator is, “What do you think?”
“The med student may say, ‘I think the kid is sick.’ The intern may say, ‘I think it’s rejection.’ The resident may say, ‘We need to distinguish between infection and rejection,’” said Dr. Chiang. By asking this question, he said, “You make that trainee an active participant.”
Evidence-based medicine and the use of pathways were also on the agenda. The discussions started with the basics, defining terms. According to Dr. Chiang, evidence-based medicine is, “the conscientious, explicit, and judicious use of current best evidence in making a clinical decision.” (See also “Evidence-Based Medicine for the Hospitalist,” p. 22.)
Pathways, developed from that best evidence, are tools that guide clinical care. “It’s the same as with calculators and PDAs,” said Stephen E. Muething, MD, associate director of clinical services at Cincinnati Children’s Hospital. “A pathway is a tool that allows a resident to spend their time identifying the 20% who shouldn’t be on the pathway and figuring out what to do for them.”
“Medicine can be systematized,” said Dr. Wellikson. “You can have best practices.”
Attendees expressed concerns that pathways may not leave room for a hospitalist’s judgment.
“There is no pathway that addresses 100% of patients,” said Dr. Muething. “A pathway should be defined as a guideline not a standard of care. From a medicallegal standpoint, you need to document why you deviated from a pathway. You still need to use clinical judgment. Don’t forget to think.”
One reason to use pathways, according to Dr. Muething, is that you can more rapidly identify what works and what doesn’t. “If everyone is doing it the same way,” he said, “then even if everyone is doing it wrong, you’ll be able to identify the problem and resolve it more quickly, improving outcome.”

—Erin Stiucky, MD
HOT TOPICS
Clinical topics were also on the agenda. On the final day of the conference, Erin R. Stucky, MD, director of graduate medical education, an associate clinical professor in the University of California at San Diego Department of Pediatrics, and a pediatric hospitalist at the Children’s
Hospital and Health Center San Diego, tackled “The Top Five in ’05,” discussing:
- Bronchiolitis;
- Emerging pathogens;
- Venous thrombosis;
- Fungal infections; and
- Kawasaki disease (KD).
In a whirlwind review, she presented the latest research on each of these topics.
Bronchiolitis: Surveys reveal that there’s a lot of variability in how hospitalists currently manage bronchiolitis, beginning with whether or not viral testing is helpful. “Testing, do we care? Does more than RSV matter?” asked Dr. Stucky. Her literature review of studies on bronchiolitis reveals, “Actually knowing the viral type is probably not helpful. Think before you test. Prevention is key.”
She also mentioned the need for additional studies on the use of heliox and CPAP in treating the condition.
Emerging pathogens: Dr. Stucky rapidly reviewed West Nile virus, coronavirus, varicella, influenza, MRSA, and pneumococcus. Discussing West Nile, Dr. Stucky said that diagnosing children with the condition can be tricky, particularly because the “predictive value [of diagnostic tests] isn’t 100%,” making the history and exam crucial. Of particular note for pediatric hospitalists, she said, is that the virus can be transmitted in blood, in utero, and via breast milk.
When speaking about coronavirus, Dr. Stucky said, “Transspecies jump (from civets, raccoons, ferrets, mice) is a great concern.” For diagnostic purposes, “Consider travel and exposure to animals.”
On varicella, Dr. Stucky said, “Zoster can occur in immunized kids. Immunization does not preclude disease. We all know that breakthrough can happen.” The question is, “If a kid’s not immunized but exposed to a milder case, will he/she get the milder case? Case studies indicate that’s a possibility. Vaccine may not prevent but mute disease.”
On influenza, the discussion focused upon the reality of the avian strain causing human disease and increasing resistance as farmers use prophylactic doses of antibiotics for their poultry. There is worldwide effect of both human and avian strains. “The hospitalist as leader: public speaking in anxious times and real crises” is critical, said Dr Stucky.
Venous thrombosis: Kids with venous thrombosis typically have at least one known risk factor, with diabetics at increased risk. Thrombolytics can help save a limb or an organ, but “long-term prophylaxis is controversial,” said Dr. Stucky.
Fungal infections: Truly eradicating a fungal infection is difficult, said Dr. Stucky, with recurrence common. There’s currently no empirical evidence to support combination therapy. More research is needed.
KD: “Treat early and often,” said Dr. Stucky. Treatment goals are to stop inflammation, inhibit thrombosis, and avoid stenosis. Because stenotic lesions progress, “long-term therapy and follow-up are needed.” Children with KD should avoid ibuprofen. They should receive the influenza vaccine, but defer measles and varicella vaccines for 11 months after intravenous immunoglobulin.
COMING SOON
The pediatric hospitalists who met in Denver left the conference energized, armed with new leadership skills and clinical knowledge, and asking for more. Organizers are now starting to plan for Pediatric Hospital Medicine 2007. The Hospitalist will keep you posted with information on the next conference as soon as it’s available, and we’ll publish half a dozen additional articles related to pediatric hospital medicine in the coming months.
Keri Losavio is a medical journalist with more than 10 years’ experience writing about healthcare issues.
PEDIATRIC SPECIAL SECTION
In The Literature
Systemic Steroid Use in Pediatric Sepsis Patients
Review by Julia Simmons, MD
Markovitz BP, Goodman DM, Watson RS, et al. A retrospective cohort study of prognostic factors associated with outcome in pediatric severe sepsis: what is the role of steroids? Pediatr Crit Care Med. 2005:6:270-274.
The use of systemic steroids in septic adults with relative adrenal insufficiency has recently been shown to decrease mortality. The use of systemic steroids in the septic pediatric population remains a topic of debate and research focus. The goal of this retrospective cohort study was to determine factors associated with mortality in pediatric patients with severe sepsis treated with systemic steroids.
The authors searched the Pediatric Health Information System for their data. This system is a database for 35 pediatric hospitals within the Child Heath Corporation of America, a children’s hospital consortium. The International Classification Disease Codes for infection were used to search the database for patients from birth through 17 with sepsis during a one-year period.
Severe sepsis was defined as one or more organ dysfunction secondary to an infectious etiology during which the patient required mechanical ventilation and vasoactive medications. The primary outcome variable was mortality. Other variables analyzed included duration of hospitalization, duration of mechanical ventilatory support and vasoactive medications. Predictor variable was the use of parenteral systemic steroids given at least one day during which the patient required artificial ventilation and vasoactive medications.
There were 6,693 participants in the study. Mean days of ventilation was 24.4 +/- 37.3, median 13. Mean number of days hospitalized was 46.8 +/- 51.3 with a median of 30. The mean number of days requiring cardiac supportive medications was 7.8 +/- 9.9 with a median of five. The use of systemic steroids (hydrocortisone, dexamethasone, or methylprednisolone) with increased age, decreased hospital volume, and a history of a hematological/oncological disease were associated with an increased mortality. Even after controlling for the variables, steroids were a strong predictor of mortality. The overall mortality rate in the study was 24%.
In summary, there was an increase in mortality associated with systemic steroid use in the severely septic pediatric patient. As noted by the authors, the study was limited because there was no stratification for disease severity. Further, the rationale for giving the steroids was not known. Overall, larger prospective studies with controlled protocols are necessary in order to make recommendations regarding the use of systemic steroids in septic pediatric patients. TH
Denver—The Pediatric Hospital Medicine 2005 conference, held July 28–31, got off to a rousing start with a networking reception that preceded the keynote lecture on Thursday evening, July 28. Dan Rauch, MD, cochair of the Ambulatory Pediatric Association (APA) Special Interest Group in Hospital Medicine, welcomed the 200+ attendees. He described the meeting as the result of tremendous cooperation among the APA, the American Academy of Pediatrics (AAP), and the SHM.
“It’s been a tremendous pleasure to work with all three organizations,” said Dr. Rauch. “We have been truly blessed with leaders who think that growth of the field is more important than individual turf battles. I highly recommend that everybody in the room become members of all three organizations.”
Dr. Rauch later told The Hospitalist that he was surprised by how many attendees actually weren’t members of any of the three organizations.
The mostly young pediatric hospitalists in attendance came from all over the United States and Canada. According to keynote speaker Larry Wellikson, MD, CEO of SHM, the median age of the typical hospitalist is 37, and fewer than 10% are 50 or older. Dr. Rauch said the typical pediatric hospitalist is even younger.
In fact, the pediatric hospitalist profession is still in its infancy, a point underscored by the panel discussion during Friday’s plenary session, “Future Directions.” The conversation centered on whether pediatric hospitalist medicine is truly a new subspecialty or simply a job type within general pediatrics. Most attendees seemed to agree that in practice it is a new subspecialty, but gaining acknowledgement of that fact from the professional organizations, academics, hospital administrators, insurers, general practice pediatricians, and even from some pediatric hospitalists themselves is the continuing challenge.
Professional advancement was a theme every speaker emphasized, beginning with Dr. Wellikson.
—Larry Wellikson, MD, CEO of SHM, explaining that the legacy of this generation of hospitalists will be to define hospital medicine.
CREATING THE HOSPITAL OF THE FUTURE
“My life’s goals were to be dean of a med school when I was 40 and a United States senator at 50,” said Dr. Wellikson during his keynote address. He may not have achieved those particular goals, but, he revealed, “believe it or not, my life has been even better than that.”
Dr. Wellikson, who discussed the current status of hospital medicine, is a sought-after speaker and consultant who helps hospitals and physicians understand the current medical environment and create strategies to succeed in it.
“You are building and defining the hospital of the future,” Dr. Wellikson told participants, explaining that the legacy of this generation of hospitalists will be to define hospital medicine. “[Hospitalists] are going to be the most important part of the hospital of the future.
“Hospitals are changing,” he said, describing the hospital of the future as patient-centered with medical care driven by measurable data and practiced in teams. With emergency departments overcrowded and hospitals and ICUs running at capacity, he predicts that $20 billion per year will be spent on hospital construction over the next 10 years. He foresees primary care pediatricians giving up inpatient care.
“Hospitalist medicine is by far the fastest growing medical specialty in the country,” said Dr. Wellikson. Currently, there are approximately 11,295 hospitalists, and he predicts that there will be 30,000 by the end of the decade. Approximately 9% of hospitalists are pediatricians.
According to Dr. Wellikson, 30% of 4,895 community hospitals today have hospitalists on staff, with about eight hospitalists per hospital. The larger the hospital, the more likely it is to have hospitalists:
- 71% of hospitals with more than 500 beds have hospitalists on staff; and
- 50% of hospitals with more than 100 beds have hospitalists.
“We believe at SHM that in 15 years 25% of the CEOs will be hospitalists and 15% of CMOs will be hospitalists,” said Dr. Wellikson, “ ... and you’re not all going to be able to take time off to go get an MBA. We’re going to be in the business of educating you to be a leader, how to be a manager. ... If you will commit to creating the hospital of the future, [SHM] will commit to giving you the tools to do it.”
VALUE VERSUS COMPENSATION
During the keynote, Dr. Wellikson set the stage for a compensation discussion that continued throughout the conference, both during sessions and in networking conversations.
“One of the things that makes the compensation model so unfair for hospital medicine,” said Dr. Wellikson, “is that the way we pay for medical care in this country is so screwed up. We pay by the unit of the visit and by the unit of the procedure. And so it is much better to do something wrong and do it a lot than it is to sit down and spend an hour talking with a family. And God forbid that you’re asked to sit on a QI committee; that’s really down time. ... And God forbid that instead of earning a living and seeing patients for three days you’re wasting your time here in Denver trying to be a better doctor. Our system doesn’t reward that.”
Several attendees mentioned that their hospitals consider them loss leaders. “Don’t allow yourself to be called a loss leader,” said Linda Snelling, MD, in her Friday session on contract negotiation. “You’re a system sustainer. If you want this profession to be respected, you’ve got to be paid for it.” Dr. Snelling is chief of pediatric critical care and associate professor of pediatrics and surgery (anesthesiology) at Brown University, Providence, R.I.
“Hospitalists need to convince ourselves of the value we bring to our institutions and to our patients,” said Mark Joffe, MD, director of community pediatric medicine for the Children’s Hospital of Philadelphia.
Dr. Wellikson emphasized that hospitalists do add value to hospitals—whether it’s educating, whether it’s throughput, whether it’s 24/7, whether it’s improving the quality. He said that hospital administrators—the CMOs at your hospital—understand that. “The reason that leadership and that hospitalists are important is that hospitals see you as the solution to many hospital issues,” he said. “When anthrax was thought to be a public health problem, every hospital started a bioterrorism committee and put the hospitalist on it.
“Almost every place I go, they want more of you. You’re better for their bottom line,” he continued. “If they’re ever going to be a better hospital, they need more of you, and they need you motivated, and they need you seeing the right number of patients so that you have the time to do a better job.”
According to Dr. Wellikson, the expectations of hospitalists is that they will improve efficiency, save the hospital money, provide measurable quality improvement (creating standards and measuring compliance), collect data, do things no one else will (e.g., provide uncompensated care, serve on committees).
Dr. Snelling agreed. “The benefit of hospitalists is not in what you bill,” she said, “but in systems improvements, patient satisfaction, QI, initiatives to start or change a program, teaching, cost-savings, and value-added services you provide to the hospital. ... Start with value. Figure out what you want. Identify common ground. Bargaining is the last thing you do.”
Hospitalists create a seamless continuity from inpatient to outpatient, from the emergency department to the floor, from the ICU to the floor. They improve efficiency via throughput and early discharge. They help uncrowd the emergency department and open ICU beds. “We make other physicians’ lives better,” said Dr. Wellikson. “We do a lot of things for the generalists so that they can go and have a better life.”
There is a definite bright side to being a hospitalist right now. According to Dr. Wellikson there are many more jobs than hospitalists—a trend that he predicts will continue for at least for the next five years.
“Don’t let the fact that we have a totally screwed up healthcare system get you down,” he said. “You’re not replaceable. The service you provide, someone must provide. Your hospital has more wastage in durable goods than it spends on pediatric hospitalists. They will pay for expertise.”
Dr. Snelling advised, “Be direct and shameless about compensation. No surgeon works for free unless they want to; no hospitalist should work for free unless that’s your selected charity, and my favorite charity is not the hospital I work for.
“Continually self-promote,” she continued. “Make sure [the person determining your compensation] knows what your successes are. If you’re doing something that’s successful—you get praise, you get a grant, you get a nice letter from a parent—pass that on. Document your value. If you save your hospital a million bucks, why shouldn’t you get a hunk of that? The CEO’s job is to pay you as little as possible.”
One attendee interjected, “I feel uncomfortable with the idea that what I’m doing as a hospitalist is worth more than what my private-practice colleagues are doing. I don’t want to be offensive.”
To which Dr. Snelling replied, “We’re not talking about being elitist. ‘Mine’s bigger than yours.’ What you’re talking about is the differences between C care—the minimum standard—and A care—the hospitalist. ... Who in this room wants to go to an average doctor?”
Dr. Snelling’s bottom line: “My message is not to gouge the system; it’s about respect. In an ideal situation, everybody gains.”
SHOULD PEDIATRIC HOSPITAL MEDICINE BE A BOARD-CERTIFIED SPECIALTY?
“This is a specialty,” emphasized Dr. Snelling during the contract negotiation session.
On the other hand, during the “Future Directions” plenary panel Dr. Wellikson said, “It is almost not relevant whether there is board certification or no board certification.” He described board certification as a way to measure quality.
“Clearly we need to find a way to validate what we’re doing for our good as well as for the good of our patients,” said Doug Carlson, MD, director of the Pediatric Hospital Medicine Program at St. Louis Children’s Hospital and associate professor of pediatrics at Washington University, St. Louis.
Stephen Ludwig, MD, associate chair for medical education at the Children’s Hospital of Philadelphia presented the case for becoming a board-certified specialty. Some benefits: recognition, prestige, job security, and professional advancement.
“Is this just a job, or do you want to fit into—become a thread in—the fabric of organized medicine?” asked Dr. Ludwig. Most important, though, would be the impact on child health. “Is [board certification] good for children and their parents? Unless you can demonstrate that, it won’t happen.”
According to Dr. Ludwig, becoming a board-certified specialty requires a defined body of knowledge, scientific basis, a sufficient number of practitioners, viable academic training programs, sufficient number of trainees willing to go into those fellowship programs, a board exam, geographic diversity, creation of new knowledge (or at least the application of existing knowledge in new ways), the support of national societies and organizations, and the consent of other specialties, such as internal medicine and family practice. It also takes time—likely years.
Some questions pediatric hospitalists still need to consider: Can you fill a void? Is there sufficient novel material for creating a certifying exam? Are there enough people who would take this exam? How will physicians view maintenance of certification? Where will the naysayers come from? What will be the response from primary care general pediatricians? What will be the response from academic generalists/pediatricians? What will be the subspecialist response?
Dr. Ludwig expressed one concern succinctly: “You might ultimately decrease the number of practitioners willing to make the commitment.”
Dr. Wellikson concurred. “Those of you who are group leaders are constantly in a recruiting mode,” he said. “You need something to help you determine who is good and who is not, but adding three years may drive those who would have been great pediatric hospitalists to become great pediatric anesthesiologists.”
In the end, the group could not agree on an answer. “You have an amazing amount of excitement,” said Dr. Ludwig. “Temper your excitement with focus. You need to decide whether becoming another subspecialty is what you want.”
SOMETHING FOR EVERYONE
The conference offered a broad range of learning opportunities.
Those interested in research heard about opportunities to collaborate and learned how to share resources and develop research projects.
Educators—and aren’t all hospitalists involved in education at some level?—learned “Seven Simple Secrets to Successful Supervision” from Vinny Chiang, MD, chief of inpatient services at Children’s Hospital, Boston. He says the single most powerful question you can ask as an educator is, “What do you think?”
“The med student may say, ‘I think the kid is sick.’ The intern may say, ‘I think it’s rejection.’ The resident may say, ‘We need to distinguish between infection and rejection,’” said Dr. Chiang. By asking this question, he said, “You make that trainee an active participant.”
Evidence-based medicine and the use of pathways were also on the agenda. The discussions started with the basics, defining terms. According to Dr. Chiang, evidence-based medicine is, “the conscientious, explicit, and judicious use of current best evidence in making a clinical decision.” (See also “Evidence-Based Medicine for the Hospitalist,” p. 22.)
Pathways, developed from that best evidence, are tools that guide clinical care. “It’s the same as with calculators and PDAs,” said Stephen E. Muething, MD, associate director of clinical services at Cincinnati Children’s Hospital. “A pathway is a tool that allows a resident to spend their time identifying the 20% who shouldn’t be on the pathway and figuring out what to do for them.”
“Medicine can be systematized,” said Dr. Wellikson. “You can have best practices.”
Attendees expressed concerns that pathways may not leave room for a hospitalist’s judgment.
“There is no pathway that addresses 100% of patients,” said Dr. Muething. “A pathway should be defined as a guideline not a standard of care. From a medicallegal standpoint, you need to document why you deviated from a pathway. You still need to use clinical judgment. Don’t forget to think.”
One reason to use pathways, according to Dr. Muething, is that you can more rapidly identify what works and what doesn’t. “If everyone is doing it the same way,” he said, “then even if everyone is doing it wrong, you’ll be able to identify the problem and resolve it more quickly, improving outcome.”
—Erin Stiucky, MD
HOT TOPICS
Clinical topics were also on the agenda. On the final day of the conference, Erin R. Stucky, MD, director of graduate medical education, an associate clinical professor in the University of California at San Diego Department of Pediatrics, and a pediatric hospitalist at the Children’s
Hospital and Health Center San Diego, tackled “The Top Five in ’05,” discussing:
- Bronchiolitis;
- Emerging pathogens;
- Venous thrombosis;
- Fungal infections; and
- Kawasaki disease (KD).
In a whirlwind review, she presented the latest research on each of these topics.
Bronchiolitis: Surveys reveal that there’s a lot of variability in how hospitalists currently manage bronchiolitis, beginning with whether or not viral testing is helpful. “Testing, do we care? Does more than RSV matter?” asked Dr. Stucky. Her literature review of studies on bronchiolitis reveals, “Actually knowing the viral type is probably not helpful. Think before you test. Prevention is key.”
She also mentioned the need for additional studies on the use of heliox and CPAP in treating the condition.
Emerging pathogens: Dr. Stucky rapidly reviewed West Nile virus, coronavirus, varicella, influenza, MRSA, and pneumococcus. Discussing West Nile, Dr. Stucky said that diagnosing children with the condition can be tricky, particularly because the “predictive value [of diagnostic tests] isn’t 100%,” making the history and exam crucial. Of particular note for pediatric hospitalists, she said, is that the virus can be transmitted in blood, in utero, and via breast milk.
When speaking about coronavirus, Dr. Stucky said, “Transspecies jump (from civets, raccoons, ferrets, mice) is a great concern.” For diagnostic purposes, “Consider travel and exposure to animals.”
On varicella, Dr. Stucky said, “Zoster can occur in immunized kids. Immunization does not preclude disease. We all know that breakthrough can happen.” The question is, “If a kid’s not immunized but exposed to a milder case, will he/she get the milder case? Case studies indicate that’s a possibility. Vaccine may not prevent but mute disease.”
On influenza, the discussion focused upon the reality of the avian strain causing human disease and increasing resistance as farmers use prophylactic doses of antibiotics for their poultry. There is worldwide effect of both human and avian strains. “The hospitalist as leader: public speaking in anxious times and real crises” is critical, said Dr Stucky.
Venous thrombosis: Kids with venous thrombosis typically have at least one known risk factor, with diabetics at increased risk. Thrombolytics can help save a limb or an organ, but “long-term prophylaxis is controversial,” said Dr. Stucky.
Fungal infections: Truly eradicating a fungal infection is difficult, said Dr. Stucky, with recurrence common. There’s currently no empirical evidence to support combination therapy. More research is needed.
KD: “Treat early and often,” said Dr. Stucky. Treatment goals are to stop inflammation, inhibit thrombosis, and avoid stenosis. Because stenotic lesions progress, “long-term therapy and follow-up are needed.” Children with KD should avoid ibuprofen. They should receive the influenza vaccine, but defer measles and varicella vaccines for 11 months after intravenous immunoglobulin.
COMING SOON
The pediatric hospitalists who met in Denver left the conference energized, armed with new leadership skills and clinical knowledge, and asking for more. Organizers are now starting to plan for Pediatric Hospital Medicine 2007. The Hospitalist will keep you posted with information on the next conference as soon as it’s available, and we’ll publish half a dozen additional articles related to pediatric hospital medicine in the coming months.
Keri Losavio is a medical journalist with more than 10 years’ experience writing about healthcare issues.
PEDIATRIC SPECIAL SECTION
In The Literature
Systemic Steroid Use in Pediatric Sepsis Patients
Review by Julia Simmons, MD
Markovitz BP, Goodman DM, Watson RS, et al. A retrospective cohort study of prognostic factors associated with outcome in pediatric severe sepsis: what is the role of steroids? Pediatr Crit Care Med. 2005:6:270-274.
The use of systemic steroids in septic adults with relative adrenal insufficiency has recently been shown to decrease mortality. The use of systemic steroids in the septic pediatric population remains a topic of debate and research focus. The goal of this retrospective cohort study was to determine factors associated with mortality in pediatric patients with severe sepsis treated with systemic steroids.
The authors searched the Pediatric Health Information System for their data. This system is a database for 35 pediatric hospitals within the Child Heath Corporation of America, a children’s hospital consortium. The International Classification Disease Codes for infection were used to search the database for patients from birth through 17 with sepsis during a one-year period.
Severe sepsis was defined as one or more organ dysfunction secondary to an infectious etiology during which the patient required mechanical ventilation and vasoactive medications. The primary outcome variable was mortality. Other variables analyzed included duration of hospitalization, duration of mechanical ventilatory support and vasoactive medications. Predictor variable was the use of parenteral systemic steroids given at least one day during which the patient required artificial ventilation and vasoactive medications.
There were 6,693 participants in the study. Mean days of ventilation was 24.4 +/- 37.3, median 13. Mean number of days hospitalized was 46.8 +/- 51.3 with a median of 30. The mean number of days requiring cardiac supportive medications was 7.8 +/- 9.9 with a median of five. The use of systemic steroids (hydrocortisone, dexamethasone, or methylprednisolone) with increased age, decreased hospital volume, and a history of a hematological/oncological disease were associated with an increased mortality. Even after controlling for the variables, steroids were a strong predictor of mortality. The overall mortality rate in the study was 24%.
In summary, there was an increase in mortality associated with systemic steroid use in the severely septic pediatric patient. As noted by the authors, the study was limited because there was no stratification for disease severity. Further, the rationale for giving the steroids was not known. Overall, larger prospective studies with controlled protocols are necessary in order to make recommendations regarding the use of systemic steroids in septic pediatric patients. TH
Denver—The Pediatric Hospital Medicine 2005 conference, held July 28–31, got off to a rousing start with a networking reception that preceded the keynote lecture on Thursday evening, July 28. Dan Rauch, MD, cochair of the Ambulatory Pediatric Association (APA) Special Interest Group in Hospital Medicine, welcomed the 200+ attendees. He described the meeting as the result of tremendous cooperation among the APA, the American Academy of Pediatrics (AAP), and the SHM.
“It’s been a tremendous pleasure to work with all three organizations,” said Dr. Rauch. “We have been truly blessed with leaders who think that growth of the field is more important than individual turf battles. I highly recommend that everybody in the room become members of all three organizations.”
Dr. Rauch later told The Hospitalist that he was surprised by how many attendees actually weren’t members of any of the three organizations.
The mostly young pediatric hospitalists in attendance came from all over the United States and Canada. According to keynote speaker Larry Wellikson, MD, CEO of SHM, the median age of the typical hospitalist is 37, and fewer than 10% are 50 or older. Dr. Rauch said the typical pediatric hospitalist is even younger.
In fact, the pediatric hospitalist profession is still in its infancy, a point underscored by the panel discussion during Friday’s plenary session, “Future Directions.” The conversation centered on whether pediatric hospitalist medicine is truly a new subspecialty or simply a job type within general pediatrics. Most attendees seemed to agree that in practice it is a new subspecialty, but gaining acknowledgement of that fact from the professional organizations, academics, hospital administrators, insurers, general practice pediatricians, and even from some pediatric hospitalists themselves is the continuing challenge.
Professional advancement was a theme every speaker emphasized, beginning with Dr. Wellikson.
—Larry Wellikson, MD, CEO of SHM, explaining that the legacy of this generation of hospitalists will be to define hospital medicine.
CREATING THE HOSPITAL OF THE FUTURE
“My life’s goals were to be dean of a med school when I was 40 and a United States senator at 50,” said Dr. Wellikson during his keynote address. He may not have achieved those particular goals, but, he revealed, “believe it or not, my life has been even better than that.”
Dr. Wellikson, who discussed the current status of hospital medicine, is a sought-after speaker and consultant who helps hospitals and physicians understand the current medical environment and create strategies to succeed in it.
“You are building and defining the hospital of the future,” Dr. Wellikson told participants, explaining that the legacy of this generation of hospitalists will be to define hospital medicine. “[Hospitalists] are going to be the most important part of the hospital of the future.
“Hospitals are changing,” he said, describing the hospital of the future as patient-centered with medical care driven by measurable data and practiced in teams. With emergency departments overcrowded and hospitals and ICUs running at capacity, he predicts that $20 billion per year will be spent on hospital construction over the next 10 years. He foresees primary care pediatricians giving up inpatient care.
“Hospitalist medicine is by far the fastest growing medical specialty in the country,” said Dr. Wellikson. Currently, there are approximately 11,295 hospitalists, and he predicts that there will be 30,000 by the end of the decade. Approximately 9% of hospitalists are pediatricians.
According to Dr. Wellikson, 30% of 4,895 community hospitals today have hospitalists on staff, with about eight hospitalists per hospital. The larger the hospital, the more likely it is to have hospitalists:
- 71% of hospitals with more than 500 beds have hospitalists on staff; and
- 50% of hospitals with more than 100 beds have hospitalists.
“We believe at SHM that in 15 years 25% of the CEOs will be hospitalists and 15% of CMOs will be hospitalists,” said Dr. Wellikson, “ ... and you’re not all going to be able to take time off to go get an MBA. We’re going to be in the business of educating you to be a leader, how to be a manager. ... If you will commit to creating the hospital of the future, [SHM] will commit to giving you the tools to do it.”
VALUE VERSUS COMPENSATION
During the keynote, Dr. Wellikson set the stage for a compensation discussion that continued throughout the conference, both during sessions and in networking conversations.
“One of the things that makes the compensation model so unfair for hospital medicine,” said Dr. Wellikson, “is that the way we pay for medical care in this country is so screwed up. We pay by the unit of the visit and by the unit of the procedure. And so it is much better to do something wrong and do it a lot than it is to sit down and spend an hour talking with a family. And God forbid that you’re asked to sit on a QI committee; that’s really down time. ... And God forbid that instead of earning a living and seeing patients for three days you’re wasting your time here in Denver trying to be a better doctor. Our system doesn’t reward that.”
Several attendees mentioned that their hospitals consider them loss leaders. “Don’t allow yourself to be called a loss leader,” said Linda Snelling, MD, in her Friday session on contract negotiation. “You’re a system sustainer. If you want this profession to be respected, you’ve got to be paid for it.” Dr. Snelling is chief of pediatric critical care and associate professor of pediatrics and surgery (anesthesiology) at Brown University, Providence, R.I.
“Hospitalists need to convince ourselves of the value we bring to our institutions and to our patients,” said Mark Joffe, MD, director of community pediatric medicine for the Children’s Hospital of Philadelphia.
Dr. Wellikson emphasized that hospitalists do add value to hospitals—whether it’s educating, whether it’s throughput, whether it’s 24/7, whether it’s improving the quality. He said that hospital administrators—the CMOs at your hospital—understand that. “The reason that leadership and that hospitalists are important is that hospitals see you as the solution to many hospital issues,” he said. “When anthrax was thought to be a public health problem, every hospital started a bioterrorism committee and put the hospitalist on it.
“Almost every place I go, they want more of you. You’re better for their bottom line,” he continued. “If they’re ever going to be a better hospital, they need more of you, and they need you motivated, and they need you seeing the right number of patients so that you have the time to do a better job.”
According to Dr. Wellikson, the expectations of hospitalists is that they will improve efficiency, save the hospital money, provide measurable quality improvement (creating standards and measuring compliance), collect data, do things no one else will (e.g., provide uncompensated care, serve on committees).
Dr. Snelling agreed. “The benefit of hospitalists is not in what you bill,” she said, “but in systems improvements, patient satisfaction, QI, initiatives to start or change a program, teaching, cost-savings, and value-added services you provide to the hospital. ... Start with value. Figure out what you want. Identify common ground. Bargaining is the last thing you do.”
Hospitalists create a seamless continuity from inpatient to outpatient, from the emergency department to the floor, from the ICU to the floor. They improve efficiency via throughput and early discharge. They help uncrowd the emergency department and open ICU beds. “We make other physicians’ lives better,” said Dr. Wellikson. “We do a lot of things for the generalists so that they can go and have a better life.”
There is a definite bright side to being a hospitalist right now. According to Dr. Wellikson there are many more jobs than hospitalists—a trend that he predicts will continue for at least for the next five years.
“Don’t let the fact that we have a totally screwed up healthcare system get you down,” he said. “You’re not replaceable. The service you provide, someone must provide. Your hospital has more wastage in durable goods than it spends on pediatric hospitalists. They will pay for expertise.”
Dr. Snelling advised, “Be direct and shameless about compensation. No surgeon works for free unless they want to; no hospitalist should work for free unless that’s your selected charity, and my favorite charity is not the hospital I work for.
“Continually self-promote,” she continued. “Make sure [the person determining your compensation] knows what your successes are. If you’re doing something that’s successful—you get praise, you get a grant, you get a nice letter from a parent—pass that on. Document your value. If you save your hospital a million bucks, why shouldn’t you get a hunk of that? The CEO’s job is to pay you as little as possible.”
One attendee interjected, “I feel uncomfortable with the idea that what I’m doing as a hospitalist is worth more than what my private-practice colleagues are doing. I don’t want to be offensive.”
To which Dr. Snelling replied, “We’re not talking about being elitist. ‘Mine’s bigger than yours.’ What you’re talking about is the differences between C care—the minimum standard—and A care—the hospitalist. ... Who in this room wants to go to an average doctor?”
Dr. Snelling’s bottom line: “My message is not to gouge the system; it’s about respect. In an ideal situation, everybody gains.”
SHOULD PEDIATRIC HOSPITAL MEDICINE BE A BOARD-CERTIFIED SPECIALTY?
“This is a specialty,” emphasized Dr. Snelling during the contract negotiation session.
On the other hand, during the “Future Directions” plenary panel Dr. Wellikson said, “It is almost not relevant whether there is board certification or no board certification.” He described board certification as a way to measure quality.
“Clearly we need to find a way to validate what we’re doing for our good as well as for the good of our patients,” said Doug Carlson, MD, director of the Pediatric Hospital Medicine Program at St. Louis Children’s Hospital and associate professor of pediatrics at Washington University, St. Louis.
Stephen Ludwig, MD, associate chair for medical education at the Children’s Hospital of Philadelphia presented the case for becoming a board-certified specialty. Some benefits: recognition, prestige, job security, and professional advancement.
“Is this just a job, or do you want to fit into—become a thread in—the fabric of organized medicine?” asked Dr. Ludwig. Most important, though, would be the impact on child health. “Is [board certification] good for children and their parents? Unless you can demonstrate that, it won’t happen.”
According to Dr. Ludwig, becoming a board-certified specialty requires a defined body of knowledge, scientific basis, a sufficient number of practitioners, viable academic training programs, sufficient number of trainees willing to go into those fellowship programs, a board exam, geographic diversity, creation of new knowledge (or at least the application of existing knowledge in new ways), the support of national societies and organizations, and the consent of other specialties, such as internal medicine and family practice. It also takes time—likely years.
Some questions pediatric hospitalists still need to consider: Can you fill a void? Is there sufficient novel material for creating a certifying exam? Are there enough people who would take this exam? How will physicians view maintenance of certification? Where will the naysayers come from? What will be the response from primary care general pediatricians? What will be the response from academic generalists/pediatricians? What will be the subspecialist response?
Dr. Ludwig expressed one concern succinctly: “You might ultimately decrease the number of practitioners willing to make the commitment.”
Dr. Wellikson concurred. “Those of you who are group leaders are constantly in a recruiting mode,” he said. “You need something to help you determine who is good and who is not, but adding three years may drive those who would have been great pediatric hospitalists to become great pediatric anesthesiologists.”
In the end, the group could not agree on an answer. “You have an amazing amount of excitement,” said Dr. Ludwig. “Temper your excitement with focus. You need to decide whether becoming another subspecialty is what you want.”
SOMETHING FOR EVERYONE
The conference offered a broad range of learning opportunities.
Those interested in research heard about opportunities to collaborate and learned how to share resources and develop research projects.
Educators—and aren’t all hospitalists involved in education at some level?—learned “Seven Simple Secrets to Successful Supervision” from Vinny Chiang, MD, chief of inpatient services at Children’s Hospital, Boston. He says the single most powerful question you can ask as an educator is, “What do you think?”
“The med student may say, ‘I think the kid is sick.’ The intern may say, ‘I think it’s rejection.’ The resident may say, ‘We need to distinguish between infection and rejection,’” said Dr. Chiang. By asking this question, he said, “You make that trainee an active participant.”
Evidence-based medicine and the use of pathways were also on the agenda. The discussions started with the basics, defining terms. According to Dr. Chiang, evidence-based medicine is, “the conscientious, explicit, and judicious use of current best evidence in making a clinical decision.” (See also “Evidence-Based Medicine for the Hospitalist,” p. 22.)
Pathways, developed from that best evidence, are tools that guide clinical care. “It’s the same as with calculators and PDAs,” said Stephen E. Muething, MD, associate director of clinical services at Cincinnati Children’s Hospital. “A pathway is a tool that allows a resident to spend their time identifying the 20% who shouldn’t be on the pathway and figuring out what to do for them.”
“Medicine can be systematized,” said Dr. Wellikson. “You can have best practices.”
Attendees expressed concerns that pathways may not leave room for a hospitalist’s judgment.
“There is no pathway that addresses 100% of patients,” said Dr. Muething. “A pathway should be defined as a guideline not a standard of care. From a medicallegal standpoint, you need to document why you deviated from a pathway. You still need to use clinical judgment. Don’t forget to think.”
One reason to use pathways, according to Dr. Muething, is that you can more rapidly identify what works and what doesn’t. “If everyone is doing it the same way,” he said, “then even if everyone is doing it wrong, you’ll be able to identify the problem and resolve it more quickly, improving outcome.”
—Erin Stiucky, MD
HOT TOPICS
Clinical topics were also on the agenda. On the final day of the conference, Erin R. Stucky, MD, director of graduate medical education, an associate clinical professor in the University of California at San Diego Department of Pediatrics, and a pediatric hospitalist at the Children’s
Hospital and Health Center San Diego, tackled “The Top Five in ’05,” discussing:
- Bronchiolitis;
- Emerging pathogens;
- Venous thrombosis;
- Fungal infections; and
- Kawasaki disease (KD).
In a whirlwind review, she presented the latest research on each of these topics.
Bronchiolitis: Surveys reveal that there’s a lot of variability in how hospitalists currently manage bronchiolitis, beginning with whether or not viral testing is helpful. “Testing, do we care? Does more than RSV matter?” asked Dr. Stucky. Her literature review of studies on bronchiolitis reveals, “Actually knowing the viral type is probably not helpful. Think before you test. Prevention is key.”
She also mentioned the need for additional studies on the use of heliox and CPAP in treating the condition.
Emerging pathogens: Dr. Stucky rapidly reviewed West Nile virus, coronavirus, varicella, influenza, MRSA, and pneumococcus. Discussing West Nile, Dr. Stucky said that diagnosing children with the condition can be tricky, particularly because the “predictive value [of diagnostic tests] isn’t 100%,” making the history and exam crucial. Of particular note for pediatric hospitalists, she said, is that the virus can be transmitted in blood, in utero, and via breast milk.
When speaking about coronavirus, Dr. Stucky said, “Transspecies jump (from civets, raccoons, ferrets, mice) is a great concern.” For diagnostic purposes, “Consider travel and exposure to animals.”
On varicella, Dr. Stucky said, “Zoster can occur in immunized kids. Immunization does not preclude disease. We all know that breakthrough can happen.” The question is, “If a kid’s not immunized but exposed to a milder case, will he/she get the milder case? Case studies indicate that’s a possibility. Vaccine may not prevent but mute disease.”
On influenza, the discussion focused upon the reality of the avian strain causing human disease and increasing resistance as farmers use prophylactic doses of antibiotics for their poultry. There is worldwide effect of both human and avian strains. “The hospitalist as leader: public speaking in anxious times and real crises” is critical, said Dr Stucky.
Venous thrombosis: Kids with venous thrombosis typically have at least one known risk factor, with diabetics at increased risk. Thrombolytics can help save a limb or an organ, but “long-term prophylaxis is controversial,” said Dr. Stucky.
Fungal infections: Truly eradicating a fungal infection is difficult, said Dr. Stucky, with recurrence common. There’s currently no empirical evidence to support combination therapy. More research is needed.
KD: “Treat early and often,” said Dr. Stucky. Treatment goals are to stop inflammation, inhibit thrombosis, and avoid stenosis. Because stenotic lesions progress, “long-term therapy and follow-up are needed.” Children with KD should avoid ibuprofen. They should receive the influenza vaccine, but defer measles and varicella vaccines for 11 months after intravenous immunoglobulin.
COMING SOON
The pediatric hospitalists who met in Denver left the conference energized, armed with new leadership skills and clinical knowledge, and asking for more. Organizers are now starting to plan for Pediatric Hospital Medicine 2007. The Hospitalist will keep you posted with information on the next conference as soon as it’s available, and we’ll publish half a dozen additional articles related to pediatric hospital medicine in the coming months.
Keri Losavio is a medical journalist with more than 10 years’ experience writing about healthcare issues.
PEDIATRIC SPECIAL SECTION
In The Literature
Systemic Steroid Use in Pediatric Sepsis Patients
Review by Julia Simmons, MD
Markovitz BP, Goodman DM, Watson RS, et al. A retrospective cohort study of prognostic factors associated with outcome in pediatric severe sepsis: what is the role of steroids? Pediatr Crit Care Med. 2005:6:270-274.
The use of systemic steroids in septic adults with relative adrenal insufficiency has recently been shown to decrease mortality. The use of systemic steroids in the septic pediatric population remains a topic of debate and research focus. The goal of this retrospective cohort study was to determine factors associated with mortality in pediatric patients with severe sepsis treated with systemic steroids.
The authors searched the Pediatric Health Information System for their data. This system is a database for 35 pediatric hospitals within the Child Heath Corporation of America, a children’s hospital consortium. The International Classification Disease Codes for infection were used to search the database for patients from birth through 17 with sepsis during a one-year period.
Severe sepsis was defined as one or more organ dysfunction secondary to an infectious etiology during which the patient required mechanical ventilation and vasoactive medications. The primary outcome variable was mortality. Other variables analyzed included duration of hospitalization, duration of mechanical ventilatory support and vasoactive medications. Predictor variable was the use of parenteral systemic steroids given at least one day during which the patient required artificial ventilation and vasoactive medications.
There were 6,693 participants in the study. Mean days of ventilation was 24.4 +/- 37.3, median 13. Mean number of days hospitalized was 46.8 +/- 51.3 with a median of 30. The mean number of days requiring cardiac supportive medications was 7.8 +/- 9.9 with a median of five. The use of systemic steroids (hydrocortisone, dexamethasone, or methylprednisolone) with increased age, decreased hospital volume, and a history of a hematological/oncological disease were associated with an increased mortality. Even after controlling for the variables, steroids were a strong predictor of mortality. The overall mortality rate in the study was 24%.
In summary, there was an increase in mortality associated with systemic steroid use in the severely septic pediatric patient. As noted by the authors, the study was limited because there was no stratification for disease severity. Further, the rationale for giving the steroids was not known. Overall, larger prospective studies with controlled protocols are necessary in order to make recommendations regarding the use of systemic steroids in septic pediatric patients. TH
Survey Time
SHM has established an aggressive goal of getting 400 respondents for its biannual Productivity and Compensation Survey. This would mean a 33% increase over the 300 respondents to the 2003 survey. SHM is tracking the number of respondents on its Web site homepage (www.hospitalmedicine.org). All surveys must be completed and returned by Nov. 25.
By now hospital medicine group leaders should have received a copy of the survey with instructions. SHM prefers that you complete the survey online. The response process for the online survey is simplified with built-in edits and a streamlined flow. In addition, you can stop in the middle of the questionnaire and return to complete it later.
WHY SHOULD YOU PARTICIPATE?
- Information: The survey questions represent the metrics most critical in benchmarking your hospital medicine program. You’ll be able to compare the characteristics and performance of your group with other hospital medicine programs across the country.
- Financial Incentive: There is a financial incentive to participate. Only survey respondents will receive the full survey report and analysis on a CD at no additional charge. Nonrespondents will pay as much as $495 for the results. The results will be available at the SHM Annual Meeting in Washington D.C., May 3-5, 2006.
- Potential Awards: Participants will be eligible to participate in a drawing to receive complimentary registrations to an upcoming Leadership Academy (valued at $1,500) or to the 2006 SHM Annual Meeting (valued at $525). If your group submits its completed questionnaires by Oct. 25 it will have two entries in the drawing. After that date, you’ll receive only one entry.
- Confidentiality: Survey responses will be completely confidential and data will be reported only in the aggregate. International Communications Research, an experienced survey research firm, is conducting the survey. SHM is not involved in collecting or processing the data.
SURVEY CONTENT
This year’s survey builds on the success of the 2003 survey, which is viewed by SHM members as the most accurate and useful source of hospitalist benchmark information. The 2005 survey features the following improvements: better definitions and instructions, and additional questions covering such topics as night coverage, hospitalist services, and the use of nurse practitioners and physician assistants.
The group questionnaire poses questions intended to characterize your hospital medicine program at the group and hospital level. To answer these questions you will need specific information about your hospital (e.g., number of beds, teaching status), the number of fulltime employees (including nonclinical staff), staff turnover, additional revenue received from the hospital or other sources, and the program’s average length-of-stay and case-mix index.
The individual questionnaire poses questions at individual hospitalist level. To answer these you will need information about demographics (age, gender, fulltime employees, specialty, years as a hospitalist, years with group), billing information (encounters, relative value units, charges, collections), hours and shifts worked, and compensation/ benefits for each hospitalist in the group.
CALL TO ACTION
If your hospital medicine group has not received a survey and you would like to participate, e-mail the following information to Marie Francois at mfrancois@hospitalmedicine.org: the name of your group, leader’s name, mailing address, e-mail, and telephone number. If you are completing the survey and you need clarification about any of the questions, contact SHM Customer Service at CustomerService@hospitalmedicine.org or call (800) 843-3360.
As hospital medicine continues to grow and emerge, SHM seeks to provide vital data characterizing the specialty to hospitalists, hospital and healthcare leaders, and policymakers. The 2005 Productivity and Compensation Survey is the key vehicle for providing that data. Help us achieve our goal of 400 hospital medicine group respondents.
Joe Miller is senior vice president for SHM.
NPs and PAs Help Shape SHM Initiatives
By Kevin Whitford, MD
The Nonphysician-Provider Task Force met at SHM’s Annual Meeting in Chicago in April. The meeting marked a significant transition as Mitchell Wilson, MD, concluded his term as chair of the committee. Dr. Wilson’s excellent leadership and organization greatly benefited the task force during its inaugural year. The task force is fortunate to have Dr. Wilson remain as a member.
During the April meeting, the group reviewed the SHM charge to the task force: the responsibility to develop initiatives and programs to promote and define the role of nurse practitioners, physician assistants, and other hospitalist nonphysician providers in hospital medicine. The task force must recommend an SHM nonphysicianprovider agenda to the SHM Board. The task force is looking for opportunities to encourage nonphysician providers to become active SHM members.
The group prepared a document, “Top Five Roles/Functions for Nonphysician Providers” to present to the SHM Board as a framework for the future.
At the annual meeting the task force pursued strategic planning for 2005 and 2006. The Web-based “Resource Center” development was at the top of the list. The task force has collected job descriptions that include acute care nurse practitioner, hospitalist physician assistant, clinical care coordinator, clinical nurse manager, hospitalist case manager, hospitalist program manager, and medical director.
Competency forms are also posted on the SHM Web site; the forms may be used as models to evaluate hospitalist clinical coordinator, hospitalist physician assistant, hospitalist program manager, and advanced nurse practitioner in hospital medicine. The task force plans to expand this resource area to include staffing models, billing and documentation, frequently asked questions, and a document on the value added by nonphysician providers.
The Nonphysician-Provider Task Force also has a “Hub and Spoke” initiative to broaden the input for nonphysician providers by linking members to the task force with hospitalist nonphysician providers across a broad representation of practices.
Other covered areas include plans for publishing articles in The Hospitalist, membership initiatives, and promoting the development of external relationships with national organizations such as the American Academy of Physician Assistants and American Association of Nurse Practitioners.
Task force members helped lead the forum on nonphysician providers at the SHM Annual Meeting. Participants’ questions ranged from specifics regarding the roles of nonphysician providers to filling in documentation issues and included a broad spectrum of practice types from small private to large academic medical centers. The Nonphysician-Provider Task Force is making plans for the program for the 2006 Annual Meeting.
We’ve also sought involvement across the spectrum of task forces and committees in the SHM to increase the representation and raise the awareness of nonphysician providers.
The SHM Board approved the list of top five roles for nonphysician providers in SHM. These include:
- To foster hospital medicine nonphysician-provider educational and professional development;
- To network with other nonphysician providers to share ideas concerning the integration of nonphysician providers in hospital medicine;
- To provide input to SHM and SHM committees/task forces related to the role of the nonphysician provider on the hospital medicine team;
- To serve as “ambassadors” for SHM recruitment of nonphysician-provider members; and
- To share varied expertise in the educational offerings pertinent to nonphysician providers on the hospitalist team.
In the coming year, the task force will further refine this list and present a revised charge to the SHM Board. The original charge specifically mentions only nurse practitioners and physician assistants. We’ve been fortunate to have a clinical care coordinator and a health systems pharmacist join the task force. This broader perspective will benefit the task force and recognizes the broad range of professionals working with the hospitalist team.
If you’re interested in the issues being addressed by the Nonphysician-Provider Task Force, you have several avenues available to pursue those interests. The SHM listserv is an active forum for discussing issues and sharing solutions. If you’re interested in working with the Nonphysician Task Force directly, contact Jeanette Kalupa at kalupa.jeanette@cogenthealthcare.com or Scarlett Blue at sblue@firsthealth.org to be added to the Hub and Spoke initiative. You can also visit the resource center on the SHM Web site to view the nonphysician-provider resources, or you can submit documents for the task force to review for posting to the resource area.
Dr. Whitford is chair of SHM’s Nonphysician-Provider Task Force. Contact him at whitford.kevin@mayo.edu.
10 Tips for a Successful Compensation Negotiation

Here are some strategies that Linda Snelling, MD, presented at the Pediatric Hospital Medicine conference in Denver in July regarding how to best negotiate your compensation. These strategies apply to all hospitalists.
- Start with value: describe what you’re doing, who benefits from your work.
- Review your own billing and collections.
- Evaluate your program costs.
- Apply for grants (finding money allows your program to grow).
- Determine synergy: Are you fulfilling your role in the institution/department? Are there other opportunities to explore?
- Start from a position of strength. Determining how much the opponent is willing to pay or increase support based on your current success and the anticipated benefit from your continued efforts is the starting point from which you have to negotiate up. A better position is to determine the amount by which you want your support adjusted so you are at the starting point from which the opponent negotiates down.
- Remember, you’re not going in there for a handout. You’re going in there with a promise of what you’ll deliver.
- Think long term.
- Leave room to negotiate. Never put all your cards on the table. You’ll have to make concessions; get something for that concession. “If you can’t do 8%, what can you do? 5%. OK, so what about 5% this year and 5% next year?”
- Remain positive.
SHM’s Advocacy Efforts
Pay-for-performance legislation gains momentum on Capitol Hill
By Eric Siegal, MD

Washington policymakers are embracing a new approach to reforming the Medicare payment system: giving physicians and other providers financial incentives to meet certain quality standards. The so-called “pay-for-performance” or “value-based purchasing” model contained in various bills moving through Congress builds on recommendations made earlier this year by the Medicare Payment Advisory Commission (MedPAC) and mirrors initiatives that have proliferated in the private sector. In its March 2005 report to Congress, MedPAC officially recommended that Congress establish a pay-for-performance system for Medicare providers.
The Center for Medicare and Medicaid Services (CMS) is also developing and implementing a set of pay-for-performance initiatives to support quality improvement in the care of Medicare beneficiaries. CMS Administrator Mark McClellan, MD, an internist, has been a big proponent of this effort.
The basic thrust of pay-for-performance is to use Medicare’s purchasing power to reward and promote quality. This effort is also tied to legislation to accelerate the development of electronic medical records and to expand the use of information technology in the healthcare delivery system. The Public Policy Committee is examining the pay-for-performance bills introduced in Congress and their implications for hospital medicine.
SENATE LEGISLATION
In late June, Senate Finance Committee Chair Charles Grassley (R-IA) and Ranking Member Max Baucus (D-MT) introduced the Medicare Value Purchasing Act of 2005, S. 1356. This legislation would apply to physicians, acute care hospitals, Medicare Advantage plans, end-stage renal disease providers, home health agencies, and (to some extent) skilled nursing facilities.
In the first phase of implementation, Medicare reimbursement rates would be tied directly to reporting data on quality measures, while the second phase ties a portion of payment to provider performance. The Senate bill doesn’t makes changes to the sustainable growth rate formula that determines Medicare payments to physicians. That will likely be handled in separate legislation.
S. 1356 directs the Secretary of Health and Human Services to select quality measures through a multistakeholder, consensus-building process. Those quality measures already developed and accepted by the healthcare community would be taken into account. Under the legislation, the Secretary has the ability to vary measures used within types of providers. For example, the Secretary could differentiate hospital measures by the hospital’s size and scope of services. Or, the Secretary could vary physician measures based on physician specialty, type of practitioner, or the volume of services delivered. The legislation also specifies criteria for the selection of quality measures. For example, the measures should be evidence-based, reliable, and valid; relevant to rural areas; and relevant to the frail elderly and those with chronic conditions. They should include measures of over- and under use and measures of health information technology infrastructure.
HOUSE ACTION
House Ways and Means Health Subcommittee Chair Nancy Johnson (R-CT) was expected to introduce legislation before the August Congressional recess that would add pay-for-performance programs for physicians under Medicare and repeal the sustainable growth rate formula.
On July 12, Ways and Means Committee Chairman William M. Thomas (R-CA) and Johnson asked McClellan to make regulatory changes that could avert a 4.3% cut in the Medicare physician update in 2006. In particular, the lawmakers said that CMS should remove prescription drug expenditures from the sustainable growth rate, which are used to calculate yearly changes in reimbursements. Legislation to permanently fix the sustainable growth rate “would be prohibitively expensive given current interpretations of the formula,” they said.
In testimony before the Ways and Means Committee July 21, McClellan said eliminating the sustainable growth rate system in favor of an update that is similar to the current Medicare Economic Index, which measures the weighted average price change for various inputs involved with producing physicians’ services, would cost $183 billion over 10 years. CMS is currently reviewing the legal arguments regarding whether it can remove prescription drugs from the services included in the sustainable growth rate under existing authorities, he told the subcommittee.
The notion of linking a portion of Medicare payments to valid measures of quality, or paying for performance, is clearly here to stay. The concept has broad support from the Administration, Congress, CMS, and several specialty societies, even though many questions about its implementation must still be answered. The Public Policy Committee will work to position SHM to influence this important debate.
In the first phase of the Medicare Value Purchasing Act of 2005 implementation, Medicare reimbursement rates would be tied directly to reporting data on quality measures, while the second phase ties a portion of payment to provider performance.
SHM Partners with Patient Safety Leadership Fellowship Program
Focus on interdisciplinary leadership and patient safety proves invaluable
By Jeanne M. Huddleston, MD, FACP
SHM is now a partner in the Patient Safety Leadership Fellowship (PSLF) program, an intensive learning experience that develops leadership competencies and advances patient safety in healthcare through a dynamic, highly participatory, structured learning community.
The Health Forum-American Hospital Association and the National Patient Safety Foundation created the fellowship and now has several program partners. SHM has joined the list as a program partner in this PSLF with the Health Research and Education Trust (HRET), the American Organization of Nurse Executives (AONE), and the American Society for Healthcare Risk Management (ASHRM).
The ultimate objective of the PSLF is to provide multidisciplinary teams and individual providers with the opportunity to develop the leadership competencies necessary to make meaningful changes in healthcare safety. Through a combination of expert leadership and patient safety faculty, a specially designed curriculum, and field-based projects, PSLF Health Forum Fellowships offer an intensive educational opportunity.
Each fellowship experience is highly participatory and interdisciplinary. Participants from past fellowship classes include physicians, pharmacists, nurses, lawyers, risk managers, educators, administrators, and patients. This environment encourages the creation of new knowledge to advance the patient safety science and enhances interpersonal and professional effectiveness. Each fellowship is a yearlong journey that blends face-to-face leadership retreats, self-study educational curriculum, online computer conferencing, and site visits.
The heart of the fellowship program is an Action Learning Project (ALP) that fellows design and implement in their own organization/community/region. This allows for direct application of each participant’s knowledge and experience gained through the other curricular venues to be immediately applied with the added benefit of being able to draw on the experience of the fellowship faculty and staff to advance the participant’s progress. Fellows are required to provide a midyear and final report to their respective executives and/or boards, in addition to their learning community of fellows during the face-to-face leadership retreats. Examples of ALPs can be found at www.healthforumfellowships.com/healthforumfellowships/html/project.htm.
Through the course of the one-year learning experience, fellows are exposed to the following curricular components:
- Knowledge of what creates safe healthcare systems;
- Leadership, collaboration, and complexity;
- The path to a culture of safety;
- Lessons from inside and outside healthcare;
- Disclosure, reporting, and transparency; and
- The business case for creating a culture of safety.
Given the alignment of interests in quality, patient safety, and leadership between this fellowship and the developing core curriculum in hospital medicine, SHM became a program partner in mid2004. During 2005, SHM will become more involved by serving on the Fellowship’s Advisory and Curriculum Committees to help with oversight of the program concept and curricular development. In addition, SHM will provide one day of educational content drawing from the vast experience of hospitalists in the fields of leadership and patient safety.
I participated in the 2002-2003 PSLF inaugural class. The interdisciplinary nature of the education experience was rewarding and, I believe, was one of the core reasons the curricula benefited my effectiveness specifically in participating in quality and patient safety initiatives. My fellow alumni continue to serve as a community of quality and patient safety champions and assist each other by being a sounding board and advisory group to ongoing local activities. TH
Dr. Huddleston can be contacted via e-mail at huddleston.jeanne@mayo.edu.
SHM has established an aggressive goal of getting 400 respondents for its biannual Productivity and Compensation Survey. This would mean a 33% increase over the 300 respondents to the 2003 survey. SHM is tracking the number of respondents on its Web site homepage (www.hospitalmedicine.org). All surveys must be completed and returned by Nov. 25.
By now hospital medicine group leaders should have received a copy of the survey with instructions. SHM prefers that you complete the survey online. The response process for the online survey is simplified with built-in edits and a streamlined flow. In addition, you can stop in the middle of the questionnaire and return to complete it later.
WHY SHOULD YOU PARTICIPATE?
- Information: The survey questions represent the metrics most critical in benchmarking your hospital medicine program. You’ll be able to compare the characteristics and performance of your group with other hospital medicine programs across the country.
- Financial Incentive: There is a financial incentive to participate. Only survey respondents will receive the full survey report and analysis on a CD at no additional charge. Nonrespondents will pay as much as $495 for the results. The results will be available at the SHM Annual Meeting in Washington D.C., May 3-5, 2006.
- Potential Awards: Participants will be eligible to participate in a drawing to receive complimentary registrations to an upcoming Leadership Academy (valued at $1,500) or to the 2006 SHM Annual Meeting (valued at $525). If your group submits its completed questionnaires by Oct. 25 it will have two entries in the drawing. After that date, you’ll receive only one entry.
- Confidentiality: Survey responses will be completely confidential and data will be reported only in the aggregate. International Communications Research, an experienced survey research firm, is conducting the survey. SHM is not involved in collecting or processing the data.
SURVEY CONTENT
This year’s survey builds on the success of the 2003 survey, which is viewed by SHM members as the most accurate and useful source of hospitalist benchmark information. The 2005 survey features the following improvements: better definitions and instructions, and additional questions covering such topics as night coverage, hospitalist services, and the use of nurse practitioners and physician assistants.
The group questionnaire poses questions intended to characterize your hospital medicine program at the group and hospital level. To answer these questions you will need specific information about your hospital (e.g., number of beds, teaching status), the number of fulltime employees (including nonclinical staff), staff turnover, additional revenue received from the hospital or other sources, and the program’s average length-of-stay and case-mix index.
The individual questionnaire poses questions at individual hospitalist level. To answer these you will need information about demographics (age, gender, fulltime employees, specialty, years as a hospitalist, years with group), billing information (encounters, relative value units, charges, collections), hours and shifts worked, and compensation/ benefits for each hospitalist in the group.
CALL TO ACTION
If your hospital medicine group has not received a survey and you would like to participate, e-mail the following information to Marie Francois at mfrancois@hospitalmedicine.org: the name of your group, leader’s name, mailing address, e-mail, and telephone number. If you are completing the survey and you need clarification about any of the questions, contact SHM Customer Service at CustomerService@hospitalmedicine.org or call (800) 843-3360.
As hospital medicine continues to grow and emerge, SHM seeks to provide vital data characterizing the specialty to hospitalists, hospital and healthcare leaders, and policymakers. The 2005 Productivity and Compensation Survey is the key vehicle for providing that data. Help us achieve our goal of 400 hospital medicine group respondents.
Joe Miller is senior vice president for SHM.
NPs and PAs Help Shape SHM Initiatives
By Kevin Whitford, MD
The Nonphysician-Provider Task Force met at SHM’s Annual Meeting in Chicago in April. The meeting marked a significant transition as Mitchell Wilson, MD, concluded his term as chair of the committee. Dr. Wilson’s excellent leadership and organization greatly benefited the task force during its inaugural year. The task force is fortunate to have Dr. Wilson remain as a member.
During the April meeting, the group reviewed the SHM charge to the task force: the responsibility to develop initiatives and programs to promote and define the role of nurse practitioners, physician assistants, and other hospitalist nonphysician providers in hospital medicine. The task force must recommend an SHM nonphysicianprovider agenda to the SHM Board. The task force is looking for opportunities to encourage nonphysician providers to become active SHM members.
The group prepared a document, “Top Five Roles/Functions for Nonphysician Providers” to present to the SHM Board as a framework for the future.
At the annual meeting the task force pursued strategic planning for 2005 and 2006. The Web-based “Resource Center” development was at the top of the list. The task force has collected job descriptions that include acute care nurse practitioner, hospitalist physician assistant, clinical care coordinator, clinical nurse manager, hospitalist case manager, hospitalist program manager, and medical director.
Competency forms are also posted on the SHM Web site; the forms may be used as models to evaluate hospitalist clinical coordinator, hospitalist physician assistant, hospitalist program manager, and advanced nurse practitioner in hospital medicine. The task force plans to expand this resource area to include staffing models, billing and documentation, frequently asked questions, and a document on the value added by nonphysician providers.
The Nonphysician-Provider Task Force also has a “Hub and Spoke” initiative to broaden the input for nonphysician providers by linking members to the task force with hospitalist nonphysician providers across a broad representation of practices.
Other covered areas include plans for publishing articles in The Hospitalist, membership initiatives, and promoting the development of external relationships with national organizations such as the American Academy of Physician Assistants and American Association of Nurse Practitioners.
Task force members helped lead the forum on nonphysician providers at the SHM Annual Meeting. Participants’ questions ranged from specifics regarding the roles of nonphysician providers to filling in documentation issues and included a broad spectrum of practice types from small private to large academic medical centers. The Nonphysician-Provider Task Force is making plans for the program for the 2006 Annual Meeting.
We’ve also sought involvement across the spectrum of task forces and committees in the SHM to increase the representation and raise the awareness of nonphysician providers.
The SHM Board approved the list of top five roles for nonphysician providers in SHM. These include:
- To foster hospital medicine nonphysician-provider educational and professional development;
- To network with other nonphysician providers to share ideas concerning the integration of nonphysician providers in hospital medicine;
- To provide input to SHM and SHM committees/task forces related to the role of the nonphysician provider on the hospital medicine team;
- To serve as “ambassadors” for SHM recruitment of nonphysician-provider members; and
- To share varied expertise in the educational offerings pertinent to nonphysician providers on the hospitalist team.
In the coming year, the task force will further refine this list and present a revised charge to the SHM Board. The original charge specifically mentions only nurse practitioners and physician assistants. We’ve been fortunate to have a clinical care coordinator and a health systems pharmacist join the task force. This broader perspective will benefit the task force and recognizes the broad range of professionals working with the hospitalist team.
If you’re interested in the issues being addressed by the Nonphysician-Provider Task Force, you have several avenues available to pursue those interests. The SHM listserv is an active forum for discussing issues and sharing solutions. If you’re interested in working with the Nonphysician Task Force directly, contact Jeanette Kalupa at kalupa.jeanette@cogenthealthcare.com or Scarlett Blue at sblue@firsthealth.org to be added to the Hub and Spoke initiative. You can also visit the resource center on the SHM Web site to view the nonphysician-provider resources, or you can submit documents for the task force to review for posting to the resource area.
Dr. Whitford is chair of SHM’s Nonphysician-Provider Task Force. Contact him at whitford.kevin@mayo.edu.
10 Tips for a Successful Compensation Negotiation
Here are some strategies that Linda Snelling, MD, presented at the Pediatric Hospital Medicine conference in Denver in July regarding how to best negotiate your compensation. These strategies apply to all hospitalists.
- Start with value: describe what you’re doing, who benefits from your work.
- Review your own billing and collections.
- Evaluate your program costs.
- Apply for grants (finding money allows your program to grow).
- Determine synergy: Are you fulfilling your role in the institution/department? Are there other opportunities to explore?
- Start from a position of strength. Determining how much the opponent is willing to pay or increase support based on your current success and the anticipated benefit from your continued efforts is the starting point from which you have to negotiate up. A better position is to determine the amount by which you want your support adjusted so you are at the starting point from which the opponent negotiates down.
- Remember, you’re not going in there for a handout. You’re going in there with a promise of what you’ll deliver.
- Think long term.
- Leave room to negotiate. Never put all your cards on the table. You’ll have to make concessions; get something for that concession. “If you can’t do 8%, what can you do? 5%. OK, so what about 5% this year and 5% next year?”
- Remain positive.
SHM’s Advocacy Efforts
Pay-for-performance legislation gains momentum on Capitol Hill
By Eric Siegal, MD
Washington policymakers are embracing a new approach to reforming the Medicare payment system: giving physicians and other providers financial incentives to meet certain quality standards. The so-called “pay-for-performance” or “value-based purchasing” model contained in various bills moving through Congress builds on recommendations made earlier this year by the Medicare Payment Advisory Commission (MedPAC) and mirrors initiatives that have proliferated in the private sector. In its March 2005 report to Congress, MedPAC officially recommended that Congress establish a pay-for-performance system for Medicare providers.
The Center for Medicare and Medicaid Services (CMS) is also developing and implementing a set of pay-for-performance initiatives to support quality improvement in the care of Medicare beneficiaries. CMS Administrator Mark McClellan, MD, an internist, has been a big proponent of this effort.
The basic thrust of pay-for-performance is to use Medicare’s purchasing power to reward and promote quality. This effort is also tied to legislation to accelerate the development of electronic medical records and to expand the use of information technology in the healthcare delivery system. The Public Policy Committee is examining the pay-for-performance bills introduced in Congress and their implications for hospital medicine.
SENATE LEGISLATION
In late June, Senate Finance Committee Chair Charles Grassley (R-IA) and Ranking Member Max Baucus (D-MT) introduced the Medicare Value Purchasing Act of 2005, S. 1356. This legislation would apply to physicians, acute care hospitals, Medicare Advantage plans, end-stage renal disease providers, home health agencies, and (to some extent) skilled nursing facilities.
In the first phase of implementation, Medicare reimbursement rates would be tied directly to reporting data on quality measures, while the second phase ties a portion of payment to provider performance. The Senate bill doesn’t makes changes to the sustainable growth rate formula that determines Medicare payments to physicians. That will likely be handled in separate legislation.
S. 1356 directs the Secretary of Health and Human Services to select quality measures through a multistakeholder, consensus-building process. Those quality measures already developed and accepted by the healthcare community would be taken into account. Under the legislation, the Secretary has the ability to vary measures used within types of providers. For example, the Secretary could differentiate hospital measures by the hospital’s size and scope of services. Or, the Secretary could vary physician measures based on physician specialty, type of practitioner, or the volume of services delivered. The legislation also specifies criteria for the selection of quality measures. For example, the measures should be evidence-based, reliable, and valid; relevant to rural areas; and relevant to the frail elderly and those with chronic conditions. They should include measures of over- and under use and measures of health information technology infrastructure.
HOUSE ACTION
House Ways and Means Health Subcommittee Chair Nancy Johnson (R-CT) was expected to introduce legislation before the August Congressional recess that would add pay-for-performance programs for physicians under Medicare and repeal the sustainable growth rate formula.
On July 12, Ways and Means Committee Chairman William M. Thomas (R-CA) and Johnson asked McClellan to make regulatory changes that could avert a 4.3% cut in the Medicare physician update in 2006. In particular, the lawmakers said that CMS should remove prescription drug expenditures from the sustainable growth rate, which are used to calculate yearly changes in reimbursements. Legislation to permanently fix the sustainable growth rate “would be prohibitively expensive given current interpretations of the formula,” they said.
In testimony before the Ways and Means Committee July 21, McClellan said eliminating the sustainable growth rate system in favor of an update that is similar to the current Medicare Economic Index, which measures the weighted average price change for various inputs involved with producing physicians’ services, would cost $183 billion over 10 years. CMS is currently reviewing the legal arguments regarding whether it can remove prescription drugs from the services included in the sustainable growth rate under existing authorities, he told the subcommittee.
The notion of linking a portion of Medicare payments to valid measures of quality, or paying for performance, is clearly here to stay. The concept has broad support from the Administration, Congress, CMS, and several specialty societies, even though many questions about its implementation must still be answered. The Public Policy Committee will work to position SHM to influence this important debate.
In the first phase of the Medicare Value Purchasing Act of 2005 implementation, Medicare reimbursement rates would be tied directly to reporting data on quality measures, while the second phase ties a portion of payment to provider performance.
SHM Partners with Patient Safety Leadership Fellowship Program
Focus on interdisciplinary leadership and patient safety proves invaluable
By Jeanne M. Huddleston, MD, FACP
SHM is now a partner in the Patient Safety Leadership Fellowship (PSLF) program, an intensive learning experience that develops leadership competencies and advances patient safety in healthcare through a dynamic, highly participatory, structured learning community.
The Health Forum-American Hospital Association and the National Patient Safety Foundation created the fellowship and now has several program partners. SHM has joined the list as a program partner in this PSLF with the Health Research and Education Trust (HRET), the American Organization of Nurse Executives (AONE), and the American Society for Healthcare Risk Management (ASHRM).
The ultimate objective of the PSLF is to provide multidisciplinary teams and individual providers with the opportunity to develop the leadership competencies necessary to make meaningful changes in healthcare safety. Through a combination of expert leadership and patient safety faculty, a specially designed curriculum, and field-based projects, PSLF Health Forum Fellowships offer an intensive educational opportunity.
Each fellowship experience is highly participatory and interdisciplinary. Participants from past fellowship classes include physicians, pharmacists, nurses, lawyers, risk managers, educators, administrators, and patients. This environment encourages the creation of new knowledge to advance the patient safety science and enhances interpersonal and professional effectiveness. Each fellowship is a yearlong journey that blends face-to-face leadership retreats, self-study educational curriculum, online computer conferencing, and site visits.
The heart of the fellowship program is an Action Learning Project (ALP) that fellows design and implement in their own organization/community/region. This allows for direct application of each participant’s knowledge and experience gained through the other curricular venues to be immediately applied with the added benefit of being able to draw on the experience of the fellowship faculty and staff to advance the participant’s progress. Fellows are required to provide a midyear and final report to their respective executives and/or boards, in addition to their learning community of fellows during the face-to-face leadership retreats. Examples of ALPs can be found at www.healthforumfellowships.com/healthforumfellowships/html/project.htm.
Through the course of the one-year learning experience, fellows are exposed to the following curricular components:
- Knowledge of what creates safe healthcare systems;
- Leadership, collaboration, and complexity;
- The path to a culture of safety;
- Lessons from inside and outside healthcare;
- Disclosure, reporting, and transparency; and
- The business case for creating a culture of safety.
Given the alignment of interests in quality, patient safety, and leadership between this fellowship and the developing core curriculum in hospital medicine, SHM became a program partner in mid2004. During 2005, SHM will become more involved by serving on the Fellowship’s Advisory and Curriculum Committees to help with oversight of the program concept and curricular development. In addition, SHM will provide one day of educational content drawing from the vast experience of hospitalists in the fields of leadership and patient safety.
I participated in the 2002-2003 PSLF inaugural class. The interdisciplinary nature of the education experience was rewarding and, I believe, was one of the core reasons the curricula benefited my effectiveness specifically in participating in quality and patient safety initiatives. My fellow alumni continue to serve as a community of quality and patient safety champions and assist each other by being a sounding board and advisory group to ongoing local activities. TH
Dr. Huddleston can be contacted via e-mail at huddleston.jeanne@mayo.edu.
SHM has established an aggressive goal of getting 400 respondents for its biannual Productivity and Compensation Survey. This would mean a 33% increase over the 300 respondents to the 2003 survey. SHM is tracking the number of respondents on its Web site homepage (www.hospitalmedicine.org). All surveys must be completed and returned by Nov. 25.
By now hospital medicine group leaders should have received a copy of the survey with instructions. SHM prefers that you complete the survey online. The response process for the online survey is simplified with built-in edits and a streamlined flow. In addition, you can stop in the middle of the questionnaire and return to complete it later.
WHY SHOULD YOU PARTICIPATE?
- Information: The survey questions represent the metrics most critical in benchmarking your hospital medicine program. You’ll be able to compare the characteristics and performance of your group with other hospital medicine programs across the country.
- Financial Incentive: There is a financial incentive to participate. Only survey respondents will receive the full survey report and analysis on a CD at no additional charge. Nonrespondents will pay as much as $495 for the results. The results will be available at the SHM Annual Meeting in Washington D.C., May 3-5, 2006.
- Potential Awards: Participants will be eligible to participate in a drawing to receive complimentary registrations to an upcoming Leadership Academy (valued at $1,500) or to the 2006 SHM Annual Meeting (valued at $525). If your group submits its completed questionnaires by Oct. 25 it will have two entries in the drawing. After that date, you’ll receive only one entry.
- Confidentiality: Survey responses will be completely confidential and data will be reported only in the aggregate. International Communications Research, an experienced survey research firm, is conducting the survey. SHM is not involved in collecting or processing the data.
SURVEY CONTENT
This year’s survey builds on the success of the 2003 survey, which is viewed by SHM members as the most accurate and useful source of hospitalist benchmark information. The 2005 survey features the following improvements: better definitions and instructions, and additional questions covering such topics as night coverage, hospitalist services, and the use of nurse practitioners and physician assistants.
The group questionnaire poses questions intended to characterize your hospital medicine program at the group and hospital level. To answer these questions you will need specific information about your hospital (e.g., number of beds, teaching status), the number of fulltime employees (including nonclinical staff), staff turnover, additional revenue received from the hospital or other sources, and the program’s average length-of-stay and case-mix index.
The individual questionnaire poses questions at individual hospitalist level. To answer these you will need information about demographics (age, gender, fulltime employees, specialty, years as a hospitalist, years with group), billing information (encounters, relative value units, charges, collections), hours and shifts worked, and compensation/ benefits for each hospitalist in the group.
CALL TO ACTION
If your hospital medicine group has not received a survey and you would like to participate, e-mail the following information to Marie Francois at mfrancois@hospitalmedicine.org: the name of your group, leader’s name, mailing address, e-mail, and telephone number. If you are completing the survey and you need clarification about any of the questions, contact SHM Customer Service at CustomerService@hospitalmedicine.org or call (800) 843-3360.
As hospital medicine continues to grow and emerge, SHM seeks to provide vital data characterizing the specialty to hospitalists, hospital and healthcare leaders, and policymakers. The 2005 Productivity and Compensation Survey is the key vehicle for providing that data. Help us achieve our goal of 400 hospital medicine group respondents.
Joe Miller is senior vice president for SHM.
NPs and PAs Help Shape SHM Initiatives
By Kevin Whitford, MD
The Nonphysician-Provider Task Force met at SHM’s Annual Meeting in Chicago in April. The meeting marked a significant transition as Mitchell Wilson, MD, concluded his term as chair of the committee. Dr. Wilson’s excellent leadership and organization greatly benefited the task force during its inaugural year. The task force is fortunate to have Dr. Wilson remain as a member.
During the April meeting, the group reviewed the SHM charge to the task force: the responsibility to develop initiatives and programs to promote and define the role of nurse practitioners, physician assistants, and other hospitalist nonphysician providers in hospital medicine. The task force must recommend an SHM nonphysicianprovider agenda to the SHM Board. The task force is looking for opportunities to encourage nonphysician providers to become active SHM members.
The group prepared a document, “Top Five Roles/Functions for Nonphysician Providers” to present to the SHM Board as a framework for the future.
At the annual meeting the task force pursued strategic planning for 2005 and 2006. The Web-based “Resource Center” development was at the top of the list. The task force has collected job descriptions that include acute care nurse practitioner, hospitalist physician assistant, clinical care coordinator, clinical nurse manager, hospitalist case manager, hospitalist program manager, and medical director.
Competency forms are also posted on the SHM Web site; the forms may be used as models to evaluate hospitalist clinical coordinator, hospitalist physician assistant, hospitalist program manager, and advanced nurse practitioner in hospital medicine. The task force plans to expand this resource area to include staffing models, billing and documentation, frequently asked questions, and a document on the value added by nonphysician providers.
The Nonphysician-Provider Task Force also has a “Hub and Spoke” initiative to broaden the input for nonphysician providers by linking members to the task force with hospitalist nonphysician providers across a broad representation of practices.
Other covered areas include plans for publishing articles in The Hospitalist, membership initiatives, and promoting the development of external relationships with national organizations such as the American Academy of Physician Assistants and American Association of Nurse Practitioners.
Task force members helped lead the forum on nonphysician providers at the SHM Annual Meeting. Participants’ questions ranged from specifics regarding the roles of nonphysician providers to filling in documentation issues and included a broad spectrum of practice types from small private to large academic medical centers. The Nonphysician-Provider Task Force is making plans for the program for the 2006 Annual Meeting.
We’ve also sought involvement across the spectrum of task forces and committees in the SHM to increase the representation and raise the awareness of nonphysician providers.
The SHM Board approved the list of top five roles for nonphysician providers in SHM. These include:
- To foster hospital medicine nonphysician-provider educational and professional development;
- To network with other nonphysician providers to share ideas concerning the integration of nonphysician providers in hospital medicine;
- To provide input to SHM and SHM committees/task forces related to the role of the nonphysician provider on the hospital medicine team;
- To serve as “ambassadors” for SHM recruitment of nonphysician-provider members; and
- To share varied expertise in the educational offerings pertinent to nonphysician providers on the hospitalist team.
In the coming year, the task force will further refine this list and present a revised charge to the SHM Board. The original charge specifically mentions only nurse practitioners and physician assistants. We’ve been fortunate to have a clinical care coordinator and a health systems pharmacist join the task force. This broader perspective will benefit the task force and recognizes the broad range of professionals working with the hospitalist team.
If you’re interested in the issues being addressed by the Nonphysician-Provider Task Force, you have several avenues available to pursue those interests. The SHM listserv is an active forum for discussing issues and sharing solutions. If you’re interested in working with the Nonphysician Task Force directly, contact Jeanette Kalupa at kalupa.jeanette@cogenthealthcare.com or Scarlett Blue at sblue@firsthealth.org to be added to the Hub and Spoke initiative. You can also visit the resource center on the SHM Web site to view the nonphysician-provider resources, or you can submit documents for the task force to review for posting to the resource area.
Dr. Whitford is chair of SHM’s Nonphysician-Provider Task Force. Contact him at whitford.kevin@mayo.edu.
10 Tips for a Successful Compensation Negotiation
Here are some strategies that Linda Snelling, MD, presented at the Pediatric Hospital Medicine conference in Denver in July regarding how to best negotiate your compensation. These strategies apply to all hospitalists.
- Start with value: describe what you’re doing, who benefits from your work.
- Review your own billing and collections.
- Evaluate your program costs.
- Apply for grants (finding money allows your program to grow).
- Determine synergy: Are you fulfilling your role in the institution/department? Are there other opportunities to explore?
- Start from a position of strength. Determining how much the opponent is willing to pay or increase support based on your current success and the anticipated benefit from your continued efforts is the starting point from which you have to negotiate up. A better position is to determine the amount by which you want your support adjusted so you are at the starting point from which the opponent negotiates down.
- Remember, you’re not going in there for a handout. You’re going in there with a promise of what you’ll deliver.
- Think long term.
- Leave room to negotiate. Never put all your cards on the table. You’ll have to make concessions; get something for that concession. “If you can’t do 8%, what can you do? 5%. OK, so what about 5% this year and 5% next year?”
- Remain positive.
SHM’s Advocacy Efforts
Pay-for-performance legislation gains momentum on Capitol Hill
By Eric Siegal, MD
Washington policymakers are embracing a new approach to reforming the Medicare payment system: giving physicians and other providers financial incentives to meet certain quality standards. The so-called “pay-for-performance” or “value-based purchasing” model contained in various bills moving through Congress builds on recommendations made earlier this year by the Medicare Payment Advisory Commission (MedPAC) and mirrors initiatives that have proliferated in the private sector. In its March 2005 report to Congress, MedPAC officially recommended that Congress establish a pay-for-performance system for Medicare providers.
The Center for Medicare and Medicaid Services (CMS) is also developing and implementing a set of pay-for-performance initiatives to support quality improvement in the care of Medicare beneficiaries. CMS Administrator Mark McClellan, MD, an internist, has been a big proponent of this effort.
The basic thrust of pay-for-performance is to use Medicare’s purchasing power to reward and promote quality. This effort is also tied to legislation to accelerate the development of electronic medical records and to expand the use of information technology in the healthcare delivery system. The Public Policy Committee is examining the pay-for-performance bills introduced in Congress and their implications for hospital medicine.
SENATE LEGISLATION
In late June, Senate Finance Committee Chair Charles Grassley (R-IA) and Ranking Member Max Baucus (D-MT) introduced the Medicare Value Purchasing Act of 2005, S. 1356. This legislation would apply to physicians, acute care hospitals, Medicare Advantage plans, end-stage renal disease providers, home health agencies, and (to some extent) skilled nursing facilities.
In the first phase of implementation, Medicare reimbursement rates would be tied directly to reporting data on quality measures, while the second phase ties a portion of payment to provider performance. The Senate bill doesn’t makes changes to the sustainable growth rate formula that determines Medicare payments to physicians. That will likely be handled in separate legislation.
S. 1356 directs the Secretary of Health and Human Services to select quality measures through a multistakeholder, consensus-building process. Those quality measures already developed and accepted by the healthcare community would be taken into account. Under the legislation, the Secretary has the ability to vary measures used within types of providers. For example, the Secretary could differentiate hospital measures by the hospital’s size and scope of services. Or, the Secretary could vary physician measures based on physician specialty, type of practitioner, or the volume of services delivered. The legislation also specifies criteria for the selection of quality measures. For example, the measures should be evidence-based, reliable, and valid; relevant to rural areas; and relevant to the frail elderly and those with chronic conditions. They should include measures of over- and under use and measures of health information technology infrastructure.
HOUSE ACTION
House Ways and Means Health Subcommittee Chair Nancy Johnson (R-CT) was expected to introduce legislation before the August Congressional recess that would add pay-for-performance programs for physicians under Medicare and repeal the sustainable growth rate formula.
On July 12, Ways and Means Committee Chairman William M. Thomas (R-CA) and Johnson asked McClellan to make regulatory changes that could avert a 4.3% cut in the Medicare physician update in 2006. In particular, the lawmakers said that CMS should remove prescription drug expenditures from the sustainable growth rate, which are used to calculate yearly changes in reimbursements. Legislation to permanently fix the sustainable growth rate “would be prohibitively expensive given current interpretations of the formula,” they said.
In testimony before the Ways and Means Committee July 21, McClellan said eliminating the sustainable growth rate system in favor of an update that is similar to the current Medicare Economic Index, which measures the weighted average price change for various inputs involved with producing physicians’ services, would cost $183 billion over 10 years. CMS is currently reviewing the legal arguments regarding whether it can remove prescription drugs from the services included in the sustainable growth rate under existing authorities, he told the subcommittee.
The notion of linking a portion of Medicare payments to valid measures of quality, or paying for performance, is clearly here to stay. The concept has broad support from the Administration, Congress, CMS, and several specialty societies, even though many questions about its implementation must still be answered. The Public Policy Committee will work to position SHM to influence this important debate.
In the first phase of the Medicare Value Purchasing Act of 2005 implementation, Medicare reimbursement rates would be tied directly to reporting data on quality measures, while the second phase ties a portion of payment to provider performance.
SHM Partners with Patient Safety Leadership Fellowship Program
Focus on interdisciplinary leadership and patient safety proves invaluable
By Jeanne M. Huddleston, MD, FACP
SHM is now a partner in the Patient Safety Leadership Fellowship (PSLF) program, an intensive learning experience that develops leadership competencies and advances patient safety in healthcare through a dynamic, highly participatory, structured learning community.
The Health Forum-American Hospital Association and the National Patient Safety Foundation created the fellowship and now has several program partners. SHM has joined the list as a program partner in this PSLF with the Health Research and Education Trust (HRET), the American Organization of Nurse Executives (AONE), and the American Society for Healthcare Risk Management (ASHRM).
The ultimate objective of the PSLF is to provide multidisciplinary teams and individual providers with the opportunity to develop the leadership competencies necessary to make meaningful changes in healthcare safety. Through a combination of expert leadership and patient safety faculty, a specially designed curriculum, and field-based projects, PSLF Health Forum Fellowships offer an intensive educational opportunity.
Each fellowship experience is highly participatory and interdisciplinary. Participants from past fellowship classes include physicians, pharmacists, nurses, lawyers, risk managers, educators, administrators, and patients. This environment encourages the creation of new knowledge to advance the patient safety science and enhances interpersonal and professional effectiveness. Each fellowship is a yearlong journey that blends face-to-face leadership retreats, self-study educational curriculum, online computer conferencing, and site visits.
The heart of the fellowship program is an Action Learning Project (ALP) that fellows design and implement in their own organization/community/region. This allows for direct application of each participant’s knowledge and experience gained through the other curricular venues to be immediately applied with the added benefit of being able to draw on the experience of the fellowship faculty and staff to advance the participant’s progress. Fellows are required to provide a midyear and final report to their respective executives and/or boards, in addition to their learning community of fellows during the face-to-face leadership retreats. Examples of ALPs can be found at www.healthforumfellowships.com/healthforumfellowships/html/project.htm.
Through the course of the one-year learning experience, fellows are exposed to the following curricular components:
- Knowledge of what creates safe healthcare systems;
- Leadership, collaboration, and complexity;
- The path to a culture of safety;
- Lessons from inside and outside healthcare;
- Disclosure, reporting, and transparency; and
- The business case for creating a culture of safety.
Given the alignment of interests in quality, patient safety, and leadership between this fellowship and the developing core curriculum in hospital medicine, SHM became a program partner in mid2004. During 2005, SHM will become more involved by serving on the Fellowship’s Advisory and Curriculum Committees to help with oversight of the program concept and curricular development. In addition, SHM will provide one day of educational content drawing from the vast experience of hospitalists in the fields of leadership and patient safety.
I participated in the 2002-2003 PSLF inaugural class. The interdisciplinary nature of the education experience was rewarding and, I believe, was one of the core reasons the curricula benefited my effectiveness specifically in participating in quality and patient safety initiatives. My fellow alumni continue to serve as a community of quality and patient safety champions and assist each other by being a sounding board and advisory group to ongoing local activities. TH
Dr. Huddleston can be contacted via e-mail at huddleston.jeanne@mayo.edu.
A Case of Kidney Failure
An 84-year-old woman with history of coronary artery disease, hypertension, and hyperlipidemia presented with six months of anorexia, nausea, a five-pound weight loss, weakness, and nonbloody diarrhea. Over the past one to two weeks, she noticed decreased urine output despite her use of furosemide.
She was found to have a serum creatinine of 3.5 mg/dL on admission, increased from 1.5 mg/dL five days previously. She had no rash, dyspnea, cough, or abdominal pain. Urinalysis revealed >100 red blood cells (RBC), >100 white blood cells (WBC), occasional hyaline casts, and many gramnegative bacilli. Ciprofloxacin was started for her urinary tract infection. A renal biopsy was performed. The images shown are photomicrographs of light microscopy and immunofluorescence of the renal biopsy specimen. TH
Which of the following would be the most appropriate initial therapy for this condition?
- Increase dose of furosemide;
- Start fish oil;
- Initiate Low-dose dopamine;
- Discontinue ACE inhibitor; or
- Begin emergent plasmapheresis.
Discussion
The correct answer is e: plasmapheresis. The renal biopsy, as shown in the image at left, reveals crescents involving glomeruli on light microscopy and linear IgG staining on immunofluorescence. This patient has antiglomerular basement membrane (anti-GBM) glomerulonephritis (GN), which accounts for 10% to 20% of crescentic glomerulonephritides. It is characterized by circulating antibodies to the glomerular basement membrane with deposition of IgG or, rarely, IgA along the GBM.
The pulmonary-renal vasculitic syndrome is called Goodpasture’s syndrome, in which pulmonary hemorrhage occurs concurrently with GN. Anti-GBM disease has a bimodal distribution, with peaks in the second to third decades and the sixth to seventh decades of life.
Etiology is usually idiopathic, but hydrocarbon exposure has also been associated with the disease. Clinical presentation of renal anti-GBM disease is characterized by an acute onset of GN with severe oliguria or anuria. Urinalysis typically shows hematuria, dysmorphic red blood cells, and red blood cell casts. The diagnostic laboratory finding is circulating antibodies to GBM, specifically to the alpha-3 chain of type IV collagen; these are detected by radioimmunoassay or enzyme immunoassay in approximately 90% of patients.
The standard treatment for anti-GBM disease includes intensive plasmapheresis combined with corticosteroids and cyclophosphamide or azathioprine. Plasmapheresis consists of removal of two to four liters of plasma and replacement with fresh frozen plasma or a 5% albumin solution on a daily basis until circulating antibody levels become undetectable (usually two to three weeks). Steroids should be administered initially as pulse methylprednisolone (30 mg/kg or 1,000 mg intravenously over 20 minutes) for three doses (daily or every other day) followed by daily oral prednisone (1 mg/kg per day) for at least the first month, followed by a gradual taper. The initial cyclophosphamide dose is 2 mg/kg per day either orally or intravenously (0.5 g/m2 body surface area).
Selecting patients for treatment is based primarily on severity at presentation. Based on a large retrospective review of 71 patients treated with plasma exchange, prednisolone, and cyclophosphamide, those who presented with plasma creatinine (Cr) concentration of less than 5.7 mg/dL or those who had Cr greater than 5.7 mg/dL but did not require immediate dialysis had a favorable long-term patient and renal survival (approximately 70% to 80% at 90 months). Patients who required immediate dialysis had poor survival (approximately 35% at 90 months). Patients who had crescents in all glomeruli on renal biopsy required long-term maintenance dialysis. Therefore, plasma exchange, prednisone, and cyclophosphamide should be administered in the following settings:
- Pulmonary hemorrhage;
- Renal failure (Cr above 5-7 mg/dL) but not requiring immediate renal replacement therapy; and
- Less severe disease on renal biopsy (less than 30% to 50% crescents). Therapy is unlikely to be effective in patients who present with dialysisdependent renal failure without hemoptysis or if 100% of glomeruli have crescents on renal biopsy. In these settings, the risk of therapy may exceed the likelihood of benefit.
Fish oil is a potential therapy for IgA nephropathy, not anti-GBM disease. ACE inhibition may be useful in patients with nephrotic syndrome. IV hydration would be likely to cause volume overload and precipitate the need for acute dialysis. Low-dose dopamine has not proven effective in reversing acute renal failure. TH
REFERENCES
- Clarkson MR, Brenner BM. Pocket Companion to Brenner & Rector’s The Kidney, 7th ed. Philadelphia, Pa: Elsevier Inc; 2005:198-199.
- Rose BD, Kaplan AA, Appel GB. Treatment of anti-GBM antibody disease (Goodpasture’s syndrome). UpToDate Online. Available at: www.uptodate.com/physicians/pulmonology_toclist.asp. Last accessed August 18, 2005.
- Levy JB, Turner AN, Rees AJ, et al. Long-term outcome of anti-glomerular basement membrane antibody disease treated with plasma exchange and immunosuppression. Ann Intern Med. 2001;134:1033.
- Bolton WK. Goodpasture’s syndrome. Kidney Int. 1996;50:1753.
- Jennette JC. Rapidly progressive crescentic glomerulonephritis. Kidney Int. 2003;63:1164.
An 84-year-old woman with history of coronary artery disease, hypertension, and hyperlipidemia presented with six months of anorexia, nausea, a five-pound weight loss, weakness, and nonbloody diarrhea. Over the past one to two weeks, she noticed decreased urine output despite her use of furosemide.
She was found to have a serum creatinine of 3.5 mg/dL on admission, increased from 1.5 mg/dL five days previously. She had no rash, dyspnea, cough, or abdominal pain. Urinalysis revealed >100 red blood cells (RBC), >100 white blood cells (WBC), occasional hyaline casts, and many gramnegative bacilli. Ciprofloxacin was started for her urinary tract infection. A renal biopsy was performed. The images shown are photomicrographs of light microscopy and immunofluorescence of the renal biopsy specimen. TH
Which of the following would be the most appropriate initial therapy for this condition?
- Increase dose of furosemide;
- Start fish oil;
- Initiate Low-dose dopamine;
- Discontinue ACE inhibitor; or
- Begin emergent plasmapheresis.
Discussion
The correct answer is e: plasmapheresis. The renal biopsy, as shown in the image at left, reveals crescents involving glomeruli on light microscopy and linear IgG staining on immunofluorescence. This patient has antiglomerular basement membrane (anti-GBM) glomerulonephritis (GN), which accounts for 10% to 20% of crescentic glomerulonephritides. It is characterized by circulating antibodies to the glomerular basement membrane with deposition of IgG or, rarely, IgA along the GBM.
The pulmonary-renal vasculitic syndrome is called Goodpasture’s syndrome, in which pulmonary hemorrhage occurs concurrently with GN. Anti-GBM disease has a bimodal distribution, with peaks in the second to third decades and the sixth to seventh decades of life.
Etiology is usually idiopathic, but hydrocarbon exposure has also been associated with the disease. Clinical presentation of renal anti-GBM disease is characterized by an acute onset of GN with severe oliguria or anuria. Urinalysis typically shows hematuria, dysmorphic red blood cells, and red blood cell casts. The diagnostic laboratory finding is circulating antibodies to GBM, specifically to the alpha-3 chain of type IV collagen; these are detected by radioimmunoassay or enzyme immunoassay in approximately 90% of patients.
The standard treatment for anti-GBM disease includes intensive plasmapheresis combined with corticosteroids and cyclophosphamide or azathioprine. Plasmapheresis consists of removal of two to four liters of plasma and replacement with fresh frozen plasma or a 5% albumin solution on a daily basis until circulating antibody levels become undetectable (usually two to three weeks). Steroids should be administered initially as pulse methylprednisolone (30 mg/kg or 1,000 mg intravenously over 20 minutes) for three doses (daily or every other day) followed by daily oral prednisone (1 mg/kg per day) for at least the first month, followed by a gradual taper. The initial cyclophosphamide dose is 2 mg/kg per day either orally or intravenously (0.5 g/m2 body surface area).
Selecting patients for treatment is based primarily on severity at presentation. Based on a large retrospective review of 71 patients treated with plasma exchange, prednisolone, and cyclophosphamide, those who presented with plasma creatinine (Cr) concentration of less than 5.7 mg/dL or those who had Cr greater than 5.7 mg/dL but did not require immediate dialysis had a favorable long-term patient and renal survival (approximately 70% to 80% at 90 months). Patients who required immediate dialysis had poor survival (approximately 35% at 90 months). Patients who had crescents in all glomeruli on renal biopsy required long-term maintenance dialysis. Therefore, plasma exchange, prednisone, and cyclophosphamide should be administered in the following settings:
- Pulmonary hemorrhage;
- Renal failure (Cr above 5-7 mg/dL) but not requiring immediate renal replacement therapy; and
- Less severe disease on renal biopsy (less than 30% to 50% crescents). Therapy is unlikely to be effective in patients who present with dialysisdependent renal failure without hemoptysis or if 100% of glomeruli have crescents on renal biopsy. In these settings, the risk of therapy may exceed the likelihood of benefit.
Fish oil is a potential therapy for IgA nephropathy, not anti-GBM disease. ACE inhibition may be useful in patients with nephrotic syndrome. IV hydration would be likely to cause volume overload and precipitate the need for acute dialysis. Low-dose dopamine has not proven effective in reversing acute renal failure. TH
REFERENCES
- Clarkson MR, Brenner BM. Pocket Companion to Brenner & Rector’s The Kidney, 7th ed. Philadelphia, Pa: Elsevier Inc; 2005:198-199.
- Rose BD, Kaplan AA, Appel GB. Treatment of anti-GBM antibody disease (Goodpasture’s syndrome). UpToDate Online. Available at: www.uptodate.com/physicians/pulmonology_toclist.asp. Last accessed August 18, 2005.
- Levy JB, Turner AN, Rees AJ, et al. Long-term outcome of anti-glomerular basement membrane antibody disease treated with plasma exchange and immunosuppression. Ann Intern Med. 2001;134:1033.
- Bolton WK. Goodpasture’s syndrome. Kidney Int. 1996;50:1753.
- Jennette JC. Rapidly progressive crescentic glomerulonephritis. Kidney Int. 2003;63:1164.
An 84-year-old woman with history of coronary artery disease, hypertension, and hyperlipidemia presented with six months of anorexia, nausea, a five-pound weight loss, weakness, and nonbloody diarrhea. Over the past one to two weeks, she noticed decreased urine output despite her use of furosemide.
She was found to have a serum creatinine of 3.5 mg/dL on admission, increased from 1.5 mg/dL five days previously. She had no rash, dyspnea, cough, or abdominal pain. Urinalysis revealed >100 red blood cells (RBC), >100 white blood cells (WBC), occasional hyaline casts, and many gramnegative bacilli. Ciprofloxacin was started for her urinary tract infection. A renal biopsy was performed. The images shown are photomicrographs of light microscopy and immunofluorescence of the renal biopsy specimen. TH
Which of the following would be the most appropriate initial therapy for this condition?
- Increase dose of furosemide;
- Start fish oil;
- Initiate Low-dose dopamine;
- Discontinue ACE inhibitor; or
- Begin emergent plasmapheresis.
Discussion
The correct answer is e: plasmapheresis. The renal biopsy, as shown in the image at left, reveals crescents involving glomeruli on light microscopy and linear IgG staining on immunofluorescence. This patient has antiglomerular basement membrane (anti-GBM) glomerulonephritis (GN), which accounts for 10% to 20% of crescentic glomerulonephritides. It is characterized by circulating antibodies to the glomerular basement membrane with deposition of IgG or, rarely, IgA along the GBM.
The pulmonary-renal vasculitic syndrome is called Goodpasture’s syndrome, in which pulmonary hemorrhage occurs concurrently with GN. Anti-GBM disease has a bimodal distribution, with peaks in the second to third decades and the sixth to seventh decades of life.
Etiology is usually idiopathic, but hydrocarbon exposure has also been associated with the disease. Clinical presentation of renal anti-GBM disease is characterized by an acute onset of GN with severe oliguria or anuria. Urinalysis typically shows hematuria, dysmorphic red blood cells, and red blood cell casts. The diagnostic laboratory finding is circulating antibodies to GBM, specifically to the alpha-3 chain of type IV collagen; these are detected by radioimmunoassay or enzyme immunoassay in approximately 90% of patients.
The standard treatment for anti-GBM disease includes intensive plasmapheresis combined with corticosteroids and cyclophosphamide or azathioprine. Plasmapheresis consists of removal of two to four liters of plasma and replacement with fresh frozen plasma or a 5% albumin solution on a daily basis until circulating antibody levels become undetectable (usually two to three weeks). Steroids should be administered initially as pulse methylprednisolone (30 mg/kg or 1,000 mg intravenously over 20 minutes) for three doses (daily or every other day) followed by daily oral prednisone (1 mg/kg per day) for at least the first month, followed by a gradual taper. The initial cyclophosphamide dose is 2 mg/kg per day either orally or intravenously (0.5 g/m2 body surface area).
Selecting patients for treatment is based primarily on severity at presentation. Based on a large retrospective review of 71 patients treated with plasma exchange, prednisolone, and cyclophosphamide, those who presented with plasma creatinine (Cr) concentration of less than 5.7 mg/dL or those who had Cr greater than 5.7 mg/dL but did not require immediate dialysis had a favorable long-term patient and renal survival (approximately 70% to 80% at 90 months). Patients who required immediate dialysis had poor survival (approximately 35% at 90 months). Patients who had crescents in all glomeruli on renal biopsy required long-term maintenance dialysis. Therefore, plasma exchange, prednisone, and cyclophosphamide should be administered in the following settings:
- Pulmonary hemorrhage;
- Renal failure (Cr above 5-7 mg/dL) but not requiring immediate renal replacement therapy; and
- Less severe disease on renal biopsy (less than 30% to 50% crescents). Therapy is unlikely to be effective in patients who present with dialysisdependent renal failure without hemoptysis or if 100% of glomeruli have crescents on renal biopsy. In these settings, the risk of therapy may exceed the likelihood of benefit.
Fish oil is a potential therapy for IgA nephropathy, not anti-GBM disease. ACE inhibition may be useful in patients with nephrotic syndrome. IV hydration would be likely to cause volume overload and precipitate the need for acute dialysis. Low-dose dopamine has not proven effective in reversing acute renal failure. TH
REFERENCES
- Clarkson MR, Brenner BM. Pocket Companion to Brenner & Rector’s The Kidney, 7th ed. Philadelphia, Pa: Elsevier Inc; 2005:198-199.
- Rose BD, Kaplan AA, Appel GB. Treatment of anti-GBM antibody disease (Goodpasture’s syndrome). UpToDate Online. Available at: www.uptodate.com/physicians/pulmonology_toclist.asp. Last accessed August 18, 2005.
- Levy JB, Turner AN, Rees AJ, et al. Long-term outcome of anti-glomerular basement membrane antibody disease treated with plasma exchange and immunosuppression. Ann Intern Med. 2001;134:1033.
- Bolton WK. Goodpasture’s syndrome. Kidney Int. 1996;50:1753.
- Jennette JC. Rapidly progressive crescentic glomerulonephritis. Kidney Int. 2003;63:1164.
Staph Endocarditis, METs, COPD CPGs & More
A review of staphylococcal Endocarditis
VG Fowler Jr, Miro JM, Hoen B, et al for the ICE Investigators. Staphylococcus aureus endocarditis: a consequence of medical progress. JAMA. 2005;June 22;293(24):3061-3062.
Agroup of infectious diseases experts from centers throughout the world formed the International Collaboration on Endocarditis (ICE) in 1999 to gain a global understanding of infective endocarditis. Using the Duke Criteria patients with definite infective endocarditis in a prospective manner, 275 variables were reported with these cases to a central database maintained at Duke University. The ICE-Prospective Cohort Study (ICE-PCS) enrolled 1,779 patients with infective endocarditis in 39 centers in 16 countries between June 15, 2000, and December 31, 2003, and has been described in a recent report. (Cabell CH, Abrutyn E. Infect Dis Clin North Am. 2002;16:255-72). Staphylococcus aureus was the most common cause of infective endocarditis in this group of patients (n=558; 31.6%); the authors characterized risk factors and clinical issues associated with these cases in this report.
By univariate analysis, compared with non-Staphylococcus aureus infective endocarditis, patients with infective endocarditis due to Staphylococcus aureus were more likely than patients with infective endocarditis due to other pathogens to be female (P<0.001), hemodialysis dependent (P<0.001), have diabetes mellitus (P=0.009), have other chronic illnesses (P<0.001), have a healthcare association (P<0.001), have higher rates of stroke (P<0.001), have systemic embolization (P<0.001), have persistent bacteremia (P<0.001), or die (P<0.001).
Although healthcare associated Staphylococcus aureus infective endocarditis was the most common form of Staphylococcus aureus infective endocarditis, more than 60% of healthcare-associated patients acquired the infection outside the hospital. This reflects the global trend in healthcare delivery patterns favoring ambulatory treatment (e.g., outpatient medication infusion via long-term IV access, hemodialysis)
Multivariate analysis, clinical features independently associated with Staphylococcus aureus infective endocarditis (versus non-Staphylococcus aureus infective endocarditis) were: IV drug use (OR, 9.3; 95% CI, 6.3-13.7); first clinical presentation less than one month after first symptoms (OR, 5.1; 95% CI, 3.2-8.2); healthcare-associated infection (OR, 2.9; 95% CI, 2.1-3.8), persistent bacteremia (OR, 2.3; 95% CI, 1.5-3.8), presence of a presumed intravascular device source (OR, 1.7; 95% CI, 1.2-2.6), stroke (OR, 1.6; 95% CI, 1.2-2.3), or diabetes mellitus (OR, 1.3; 95% CI, 1.1-1.8).
Patients from the United States with Staphylococcus aureus infective endocarditis were more likely to be hemodialysis-dependent, to be diabetic, to have a hemodialysis fistula or a chronic indwelling central catheter as a presumed source of infection, and to have a non-nosocomial healthcare association. Patients from the United States and Brazil were more likely to have Methicillin-resistant Staphyloccocus aureus (MRSA) than were patients from Europe, the Middle East, Australia, or New Zealand. In-hospital mortality rates were similar across regions, although American patients were significantly more likely to develop persistent bacteremia (25.6%, P<0.001).
Characteristics independently associated with mortality among patients with nonintravenous drug-use-associated Staphylococcus aureus infective endocarditis by multivariate analysis included stroke (OR, 3.67; 95% CI, 1.94-6.94), persistent bacteremia (OR, 3.06; 95% CI, 1.75-5.35), diagnosis in Southern Europe or the Middle East (OR, 3.21; 95% CI, 1.17-10.56).
This study establishes Staphylococcus aureus infective endocarditis as the leading cause of infective endocarditis in many regions of the world and spotlights the global emergence of healthcare contact as a risk factor for Staphylococcus aureus infective endocarditis. In a significant portion of these patients, an IV device was the presumed source of bacteremia; prosthetic cardiac devices (pacemakers, defibrillators, or prosthetic cardiac valves) were present in almost one-quarter of the patients.
MRSA was a significant cause of Staphylococcus aureus infective endocarditis and displayed regional variation, accounting for almost 40% of the infective endocarditis caused by Staphylococcus aureus in some regions. Patients with infective endocarditis caused by MRSA were significantly more likely to have pre-existing chronic conditions and healthcare associated infective endocarditis by both univariate and multivariate analysis. They also were often associated with persistent bacteremia. On the other hand, 20% of patients with MRSA infective endocarditis developed their infection in the absence of identifiable healthcare contact.
Limitations of this report include the fact that this is an observational study of patients from self-selected centers. Each center most likely represents a portion of the local population, making it difficult to generalize findings to the entire population centers from which this report originates. Represented hospitals were typically referral centers that have cardiac surgery programs and may have widely differing populations with varied risk factors. Advantages include the large size of this prospectively evaluated cohort and the ability to analyze regional variations between continents with a contemporary nature of the patient sample (2000-2003).
Infectious Endocarditis in Olmsted County, Minn.
Tleyjeh IM, Steckelberg JM, Murad HS, et al. Temporal trends in infective endocarditis: a population-based study in Olmsted County, Minnesota. JAMA. 2005;293:3022-3028.
Tleyjeh and colleagues at the Mayo Clinic in Rochester, Minn., retrospectively studied 102 cases of infective endocarditis that occurred in 107 Olmsted County residents from 1970-2000. Main outcome measures were incidence of infective endocarditis, proportion of patients with underlying heart disease and causative micro-organisms and clinical characteristics. The records of all Olmsted County residents with infective endocarditis were identified and reviewed in detail. The definite and possible infective endocarditis cases as defined by modified Duke Criteria were used in the analysis.
The age- and gender-adjusted incidence of infective endocarditis ranged from 5.0 to 7.0 cases per 100,000 person-years during the study period and did not change significantly over time. There were 84 (79%) cases of native valve infective endocarditis and 23 (21%) cases of prosthetic valve infective endocarditis. Valves involved: aortic—36 (24%); mitral—49 (46%), aortic and mitral—12 (11%), right-sided or bilateral—8 (7%), or unknown—8 (7%). 16 (15%) had valve surgery within 42 days and the six-month mortality was 26% (n=28).
Infective endocarditis is a disease of the older individual in this population, with a mean age ranging from 54.1 years in 1980-1984 to 67.4 years in 1995-2000 (P=0.24 for trend). There was a male predominance (67%-83%), which did not significantly change over time.
Mitral valve prolapse was the most frequent underlying valvular heart disease. Viridans streptococci were the most common causative organisms (n=47; 44%) followed by Staphylococcus aureus (n=28 cases; 26%).
The overall average crude infective endocarditis incidence of the period 1970-2000 was 4.95 per 100,000 person-years. The age- and gender-adjusted annual incidence was 6.06 per 100,000 (95% CI, 4.89-7.22). There was no time trend for either streptococcus or Staphylococcus aureus infective endocarditis: the annual adjusted incidence of viridans group streptococcal infective endocarditis was 1.7 to 3.5 cases per 100,000 person years while Staphylococcus aureus infective endocarditis had an annual adjusted incidence of 1.0-2.2 cases per 100,000. The incidence rates of viridans group streptococcal and Staphylococcus aureus infective endocarditis have not changed significantly over time in this population.
Potential limitations of this study include possible incomplete case finding or recognition of the retrospective nature of the case reviews. The homogeneity of the patient population studied (primarily elderly white males with a low prevalence of intravenous drug use) limits the ability to generalize the results. Advantages include the fact that this is a population-based study at a medical center with detailed medical records of virtually all residents of a single county. This allows us to view the clinical features and etiologic factors of primarily left-sided infective endocarditis without the referral bias that tends to taint other studies typically published out of large medical centers with larger geographic referral bases.
Computers and Adverse Drug Events
Nebeker JR, Hoffman JM, Weir CR, Bennett CL, Hurdle JF. High rates of adverse drug events in a highly computerized hospital. Arch Intern Med. 2005;165:1111-1116.
Adverse drug events account for a significant number of hospital admissions and the ensuing costs associated with these hospitalizations. Electronic endeavors, such as computerized physician order entry (CPOE), bar code systems, and electronic medical records attempt to reduce the preventable adverse drug events.
Nebeker, et al. attempted to assess the effects of the implementation of CPOE and other computerized medication systems on adverse drug events in a tertiary care Veterans Administration Medical Center. They used an observational study design whereby 937 out of 2,306 newly admitted patients from several hospital wards were randomly chosen and assigned to a pharmacist reviewer during a 20-week period.
They reviewed complete medical records of hospital stays every other day to document adverse drug events. Not only were traditional adverse drug events identified, but harm from overdoses and/or inappropriate dose reductions or discontinuations, as well as intolerable harm from dose titration, were documented as adverse drug events. The harms caused by the drugs were considered only if the drugs were started in the hospital.
Harms were classified based on prior literature and included standards for pharmacological typology, causality assessment, error type, event terminology, drug class, seriousness index, and medication error category indexing. Additional uncommon classifications were also used, including additional resource utilization. Consensus meetings were held weekly to confirm classification of adverse drug events. Of the admissions reviewed, 483 adverse drug events were identified of which 93% were drug reactions while 7% were due to over- or underdosing. Of the drug reactions, 90% were considered dose-dependent while 10% were considered to be idiosyncratic.
Two different indexing scales were used in classifying the harms. Using the LDS Hospital Scale, it was suggested that 91% of the adverse drug events caused moderate harm while 9% caused serious harm. Using the National Coordinating Council for Medication Error Reporting and Prevention indexing, it was suggested that 87% of the adverse drug events fell into category E (requiring treatment) and 4% into category F (requiring prolonged hospitalization). Twenty-seven percent of the total adverse drug events were thought to be due to errors, including execution and planning steps. Sixty-one percent of errors occurred with the ordering mechanism while 25% of the errors occurred in the monitoring process.
This study highlighted rates of adverse drug events five to 19 times higher than baseline. The authors explained this higher-than-expected rate in part by study elements, such as the use of clinical pharmacists as reviewers, iterative case reviews, and accessible electronic data that make adverse drug events more noticeable.
Weaknesses of this study included issues of comparability of CPOEs because there were significant feature differences among commercial software programs. In addition, this was an observational study lacking a control group. The authors felt that their study did not support the idea that the computerized patient record of the study institution had caused adverse drug events. Rather, the study supported the idea that the system increased the visibility of adverse drug events compared with a paper system. In addition, the authors recommended that the choice of CPOEs be carefully considered, with a focus on decision support features when integrated into a healthcare organization.
The Questionable Benefit of Medical Emergency Teams
Hillman K, Chen J, Cretikos M, et al. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. MERIT study investigators. Lancet. 2005;365:2091-2097.
Previous studies have reported that the MET system reduces the incidence of cardiac arrests, deaths, and unplanned ICU admissions. A MET is a preplanned group of healthcare practitioners who respond to acute patient deteriorations in hospitalized patients.
METs are usually identical to hospital code teams, with the exception that they respond prior to a patient’s developing cardiac arrest. This early response has been shown to significantly decrease unexpected hospital mortality in hospitals in the United States, Australia, and Great Britain. Even though the system has been reported since 1995, few hospitals have knowledge of or experience with METs.
Unexpected hospital deaths and cardiac arrests are often preceded by clinical warning signs. In addition, unplanned ICU admissions may be foreshadowed by abnormalities in the patient’s vital signs that may progress if appropriate interventions are not undertaken. METs assess patients with abnormal physical findings or when there is a concern about the patient’s condition. These patients have findings that may precede a serious event or cardiac arrest, but otherwise don’t meet existing criteria to call a code.
The theory is that if a MET responds to see a patient who is becoming unstable (see “Table 1: MET Calling Criteria,” at left), early interventions may reduce the likelihood of arrest. Published studies have shown a reduction in cardiac arrests and ICU length of stay in virtually all systems in which MET has been introduced (although most studies are hampered by the use of historical controls).
The MERIT study randomized 23 hospitals in Australia to continue functioning as usual (n=11) or to introduce a MET system (n=12). The study sites included a wide range of tertiary, metropolitan, and non-metropolitan hospitals in different states across Australia. The primary outcome was the composite of cardiac arrest, unexpected death, or unplanned ICU admission during the six-month study period after MET activation, using intention to treat analysis.
A four-month educational period was undertaken with the MET centers prior to initiation of the trial. Control hospitals did not receive any education about the MET concept. This was followed by a six-month trial period. Cardiac arrest teams were maintained at all hospitals. The MET consisted of at least one doctor and a nurse from the ED or ICU.
The eligible patients included those residing on a medical ward (including critical care units); the ICUs, OR, postoperative recovery areas, and ED areas were not regarded as general wards.
The primary outcome for the study was the composite outcome of the incidence (events divided by number of eligible patients admitted to the hospital and residing on a medical ward during the study period) of:
- Cardiac arrests without a pre-existing “not-for-resuscitation” (NFR) order;
- Unplanned ICU admissions; and
- Unexpected deaths (those without a pre-existing NFR order).
The results of the study:
- During the study period, the overall rate of calls for the cardiac arrest team or MET was significantly higher in intervention hospitals than in control hospitals. Calls not associated with events were more common in MET hospitals than in controls. Half of the total calls were not associated with a cardiac arrest or unexpected death, whereas in MET hospitals more than 80% of calls were not associated with a cardiac arrest or death (P<0.0001).
- In patients with documented MET calling criteria in association with cardiac arrest or unexpected death, the call rate was similar in MET and control hospitals.
- There were no significant differences between the MET and control hospitals for any outcome.
- The response to changes in vital signs was not adequate—even in MET centers.
These findings are surprising in view of previously reported findings using the MET system. Potential reasons for lack of difference between MET centers and controls include:
- Number of study sites or the duration of the study may not have been adequate for implementation or education;
- Hospitals may already be efficient in detecting and managing unstable patients;
- Patient selection criteria may have been overly restricted. For example, other studies have used 30 respirations per minute for tachypnea as a calling criterion compared with 36 breaths per minute used in this trial;
- Knowledge of the study may have leaked to control hospitals;
- Cardiac arrest teams function as METs at times: Nearly half of the calls to cardiac arrest teams in control hospitals were made without a cardiac arrest or unexpected death; and
- The selected outcomes may not be sensitive enough.
Even though this large, multicenter controlled trial was unable to show a significant benefit of METs, we should not be discouraged from performing further controlled trials in different settings. The use of METs is clearly an exciting and evolving area of medicine.
Barriers to Patient Safety
Amalberti R, Auroy Y, Berwick D, Barach P. Five system barriers to achieving ultrasafe health care. Ann Intern Med. 2005;142:756-764
Patient safety in our healthcare system is a growing concern. One area of dialogue concerning preventable healthcare-associated harms involves the comparability of the healthcare industry with non-medical industries, such as aviation and nuclear power, that have adapted successful strategies shown to provide ultrasafe environments. Amalberti, et al. discuss risk assessment in a variety of industries and explain the need for a benchmarking approach in order to optimize or achieve safety in the healthcare field.
The authors identify five systemic barriers from literature that are fundamentally connected to the ability of the healthcare field to achieve an extremely safe environment.
Barrier 1—acceptance of limitations on maximum performance: The first barrier is the type of expected performance in the field. This is illustrated by the tradeoffs associated with ultrasafety versus productivity. The amount of risk involved was directly related to the limits placed on maximum performance. The first barrier is the acceptance that every system has limits. When a producer exceeds their limit, then safety suffers. An example used is that of blood donation: The limits of collection speed are weighed against the needed screening process.
Barrier 2—abandonment of professional autonomy: The second barrier concerns the concept of professional autonomy. While more teamwork and regulations reduce individual autonomy, this appears to improve safety in the healthcare environment. The bottom line is the importance of teamwork. The example used is that of traffic on a highway: Autonomous units work together to function safely.
Barrier 3—transition from the mindset of craftsman to that of an equivalent actor: The third barrier to achieving high levels of safety includes an equivalent actor mindset. This entails establishing a reliable standard of excellent care in lieu of focusing on individuality, similar to the notion that passengers on an airline usually do not know their pilots, but have established confidence in the airline itself.
Barrier 4—the need for system-level arbitration to optimize safety strategies: The fourth barrier identified is a need for system-level arbitration to optimize safety strategies. This need results from the pressure for justice (usually through litigation) once an accident occurs. Top-down arbitration of safety will be less successful than system level design.
Barrier 5—the need to simplify professional rules and regulations: The final barrier results from the many of layers of guidelines as they serve to create an environment of excellence. This barrier necessitates the removal of these layers to simplify the environment. Existing guidelines should be distilled down to those shown to promote quality and safety. Byzantine rules can obscure the goal of safety and glorify rules, for rules sake.
Certain structural limitations within the field, such as worker shortages in the face of increasing public demands and the reliance of the field on trainees such as students, interns, and residents, create other hurdles. The authors conclude by suggesting a two-tiered system of healthcare whereby ultrasafety could be more easily accomplished in areas of medicine considered more stable (first tier), and a second tier of care that would include the more unstable conditions, and thus inherently, represent the higher risk situations where errors are more likely to occur.
Another provocative point of this article is the need to move toward educating and training teams—not individuals.
The Importance of Implementing COPD Guidelines
Harvey PA, Murphy MC, Dornom E, et al. Implementing evidence-based guidelines: inpatient management of chronic obstructive pulmonary disease. Intern Med J. 2005;35:151-155.
COPD is a common diagnosis that sometimes requires hospitalization. Evidence-based guidelines for disease management, including that of hospitalized patients, exist, but there is a paucity of knowledge about the actual quality of care delivered in the hospital as it aligns with published guidelines. This study by Harvey, et al. explores the quality of care delivered in the hospital for patients with COPD, while at the same time investigating an intervention for the medical staff in an effort to improve adherence to evidenced-based guidelines of the disease.
Using ICD-10 codes for a COPD diagnosis, the study incorporated a retrospective chart review of 49 hospital admissions prior to the intervention and 35 admissions after the intervention in a hospital in Melbourne, Australia. Data were collected pertaining to the hospital management of COPD as it compared with what the authors considered to be Level A—or the highest level of evidence summarized from several professional organizations. The intervention delivered to the medical staff included a summarized presentation of the results from the initial audit of the 49 charts, as well as an educational package that was given to them following the presentation.
Except for inappropriate use of intravenous aminophylline, of which there was a 100% concordance to Level A guidelines, the initiation of systemic steroids (intravenous and/or oral) had the highest concordance rate of 80% and 83%, pre- and postintervention respectively. Appropriate steroid duration (seven to 14 days) had the lowest concordance rates at 10% and 29%, pre- and postintervention respectively.
In addition, preintervention concordance (10%) involving steroid duration was the only rate considered significantly different in the postintervention group (29%). While concordance rates were high for the use of any type of nebulized bronchodilator (96% preintervention and 80% postintervention), the Level A guidelines the authors used suggested that beta-agonist bronchodilators should be used alone prior to the initiation of ipratropium bromide. The concordance rates for this guideline were 27% preintervention and 34% postintervention.
Largely, the authors felt their intervention failed to improve concordance rates to the Level A guidelines investigated and also that their findings of variable and lower concordance rates across the board corroborated other similar studies. The major weaknesses of this study included the small sample size and the nonrandomness of the sampling.
In addition, the authors report that the particular hospital studied included junior doctors who rotated on and off service, which likely prevented the effects of the intervention from being measured on a provider level. In spite of the weaknesses in the study, the article brings to light the need for a more effective translation of evidence-based guidelines to actual practice, especially in the practice of COPD management in the hospital. Further methods of guideline implementation in the clinic setting must be elucidated to improve the care patients with COPD receive in the hospital.
Not all Troponin Elevations Are Myocardial Infarctions
Jeremais A, Gibson CM. Narrative review: alternative causes for elevated cardiac troponin levels when acute coronary syndromes are excluded. Ann Intern Med. 2005;142:786-791.
Troponins are regulatory proteins that control the calcium-mediated interaction of actin and myosin during muscle contraction. All muscle tissue contains troponins, but cardiac troponin T and I have amino acid sequences that are different from skeletal and smooth muscle troponins, allowing them to be detectable by monoclonal antibody-based assays.
In the event of reversible or irreversible cell damage—or possibly even from transiently increased cell membrane permeability—cardiac troponins are released from myocytes into circulation. This characteristic provides a sensitive test for detecting myocardial injury and damage; however, this test is not specific for acute coronary syndromes. And any disorder that causes myocyte damage may cause an elevated troponin.
The 2002 American College of Cardiology/American Heart Association practice guidelines for unstable angina and non-ST-segment elevation myocardial infarction acknowledge that the myocardial necrosis signified by troponin elevation may not necessarily be caused by atherosclerotic coronary artery disease. Such nonthrombotic troponin elevation can be caused by four basic mechanisms, as discussed by Dr. Jeremias and Dr. Gibson.
- Demand ischemia refers to a mismatch between myocardial oxygen demand and supply in the absence of flow-limiting epicardial stenosis. Conditions such as sepsis or septic shock and the systemic inflammatory response syndrome, hypotension or hypovolemia, tachyarrhythmias, and left ventricular hypertrophy can all cause release of cardiac troponin.
- Myocardial ischemia in the absence of fixed obstructive coronary disease can be caused by coronary vasospasm, acute stroke or intracranial hemorrhage, and ingestion of sympathomimetics.
- Direct myocardial damage can be seen in cardiac contusion, direct current cardioversion, cardiac infiltrative disorders such as amyloidosis, certain chemotherapy agents, myocarditis, pericarditis, and cardiac transplantation.
- Myocardial strain occurs when volume and pressure overload of the left and/or right ventricle cause excessive wall tension. Congestive heat failure, acute pulmonary embolism, and chronic pulmonary hypertension can lead to myocardial strain and troponin elevation.
Another condition that can lead to persistently elevated cardiac troponins is end-stage renal disease. This elevation may be due to small areas of clinically silent myocardial necrosis, an increased left ventricular mass, or possibly from impaired renal troponin excretion. Although troponins are believed to be cleared by the reticuloendothelial system, recent evidence shows that troponin T is fragmented into molecules that are small enough to be renally excreted.
In summary, elevated troponin can be found in many clinical settings and is associated with impaired short- and long-term survival. TH
Classic Literature
The HATEFUL Patient

Every physician has groaned internally when seeing a certain patient’s name on his list, going out of her way to avoid a particular family, or getting hopelessly engaged and increasingly enraged in a battle over a “lost” narcotic prescription. There are certain patients with whom a doctor-patient relationship feels more like a contest than a partnership. These interactions make a physician’s daily practice difficult, and they may wreak havoc among the staff on an inpatient ward. These patients grow ever more intolerable to their caregivers, who often harbor a wish to simply make them disappear.
In his landmark 1978 article “Taking Care of the Hateful Patient,” (NEJM, 298:883-887) James Groves, MD, discussed the characteristics of these difficult patients and the sometimes difficult emotions they generate in their caregivers. He described four different groups of patients, using an illustrative case for each, and discussed the ways in which these patients’ often maddening behavior serves to mitigate their profound dependency.
Dependent clingers are those patients whose neediness is overt, who seem to regard the physician as a sow with teats to spare. Dr. Groves suggested early, firm limit-setting with these patients to prevent the formation and later shattering of the patient’s illusion of the physician as inexhaustible.
Dependency lies at the heart of an entitled demander’s behavior as well, but their fear of abandonment is expressed as hostility and arrogance rather than overt neediness. Affirming to the patient that you share in their quest for the good (but not perfect) medical care to which they are entitled allows patient and physician to rally around a common goal.
This strategy backfires with manipulative help-rejecters, who seem almost pleased to report to their physician each time they fail a new treatment attempt. Overtly expressing some doubt that the treatment will completely cure all the patient’s difficulties and providing regular follow up are recommended for this group. These strategies relieve the patient of the unconscious anxiety that he may be abandoned by his physician should his symptoms abate.
Self-destructive deniers make the physician feel powerless as they persist in behavior that undermines all efforts to improve their health. With these patients, viewing their behavior as a terminal illness and managing symptoms and exacerbations accordingly allows the physician to focus on caring for the patient without unrealistic expectations of cure on the one hand and judgmental indifference on the other.
After discussing each of these groups, Dr. Groves concluded the article by suggesting that perhaps the greatest challenge physicians face in caring for these difficult patients is the temptation to disown the negative feelings they engender. He wrote that this effort not only strains the doctor’s limits, but also wastes valuable clinical data unmasked by these feelings—data that could inform clinical care. For decades prior to Dr. Groves’ article, psychoanalysts had reflected on what Freud termed “countertransference,” or the physician’s internal emotional reaction to a patient.
In his article “Hate in the Counter-Transference,” D.W. Winnicott, MD, suggested that rather than accepting the guilt that these feelings typically engender in a caregiver, negative countertransference reactions should be regarded by the physician as valuable information in understanding the patient’s psychic world. By training and by disposition, however, most physicians considered (and continue to consider) these emotions inappropriate. They seemingly negate the sympathy, kindness, and commitment to the patient’s well-being that should be central to a physician’s vocation. Conventional wisdom held that denying the feelings was the only proper response, and if that proved impossible, transferring the patient to a willing colleague was usually recommended. In contrast, Dr. Groves freed the physician to use these feelings to improve patient care.
Now a classic and oft-cited work, “Taking Care of the Hateful Patient” distills a wealth of analytic insight into a structure and language comprehensible to the busy generalist. By explaining the reactions each group of patients induces in their physicians, Dr. Groves provides useful tools to understand a particular patient’s psychology. Suggestions for strategic approaches to each category of patient are easy to understand and to adapt to one’s own practice. He explains how judicious limit-setting can be as valuable for the patient as it is for the doctor. Perhaps most helpful is his description of the needs of these patients that lie beneath their “hateful” exterior. Armed with this understanding, a physician can reclaim the empathy that is often so elusive with these patients.—Sandra Rackley MD, Kemuel Philbrick, MD
A review of staphylococcal Endocarditis
VG Fowler Jr, Miro JM, Hoen B, et al for the ICE Investigators. Staphylococcus aureus endocarditis: a consequence of medical progress. JAMA. 2005;June 22;293(24):3061-3062.
Agroup of infectious diseases experts from centers throughout the world formed the International Collaboration on Endocarditis (ICE) in 1999 to gain a global understanding of infective endocarditis. Using the Duke Criteria patients with definite infective endocarditis in a prospective manner, 275 variables were reported with these cases to a central database maintained at Duke University. The ICE-Prospective Cohort Study (ICE-PCS) enrolled 1,779 patients with infective endocarditis in 39 centers in 16 countries between June 15, 2000, and December 31, 2003, and has been described in a recent report. (Cabell CH, Abrutyn E. Infect Dis Clin North Am. 2002;16:255-72). Staphylococcus aureus was the most common cause of infective endocarditis in this group of patients (n=558; 31.6%); the authors characterized risk factors and clinical issues associated with these cases in this report.
By univariate analysis, compared with non-Staphylococcus aureus infective endocarditis, patients with infective endocarditis due to Staphylococcus aureus were more likely than patients with infective endocarditis due to other pathogens to be female (P<0.001), hemodialysis dependent (P<0.001), have diabetes mellitus (P=0.009), have other chronic illnesses (P<0.001), have a healthcare association (P<0.001), have higher rates of stroke (P<0.001), have systemic embolization (P<0.001), have persistent bacteremia (P<0.001), or die (P<0.001).
Although healthcare associated Staphylococcus aureus infective endocarditis was the most common form of Staphylococcus aureus infective endocarditis, more than 60% of healthcare-associated patients acquired the infection outside the hospital. This reflects the global trend in healthcare delivery patterns favoring ambulatory treatment (e.g., outpatient medication infusion via long-term IV access, hemodialysis)
Multivariate analysis, clinical features independently associated with Staphylococcus aureus infective endocarditis (versus non-Staphylococcus aureus infective endocarditis) were: IV drug use (OR, 9.3; 95% CI, 6.3-13.7); first clinical presentation less than one month after first symptoms (OR, 5.1; 95% CI, 3.2-8.2); healthcare-associated infection (OR, 2.9; 95% CI, 2.1-3.8), persistent bacteremia (OR, 2.3; 95% CI, 1.5-3.8), presence of a presumed intravascular device source (OR, 1.7; 95% CI, 1.2-2.6), stroke (OR, 1.6; 95% CI, 1.2-2.3), or diabetes mellitus (OR, 1.3; 95% CI, 1.1-1.8).
Patients from the United States with Staphylococcus aureus infective endocarditis were more likely to be hemodialysis-dependent, to be diabetic, to have a hemodialysis fistula or a chronic indwelling central catheter as a presumed source of infection, and to have a non-nosocomial healthcare association. Patients from the United States and Brazil were more likely to have Methicillin-resistant Staphyloccocus aureus (MRSA) than were patients from Europe, the Middle East, Australia, or New Zealand. In-hospital mortality rates were similar across regions, although American patients were significantly more likely to develop persistent bacteremia (25.6%, P<0.001).
Characteristics independently associated with mortality among patients with nonintravenous drug-use-associated Staphylococcus aureus infective endocarditis by multivariate analysis included stroke (OR, 3.67; 95% CI, 1.94-6.94), persistent bacteremia (OR, 3.06; 95% CI, 1.75-5.35), diagnosis in Southern Europe or the Middle East (OR, 3.21; 95% CI, 1.17-10.56).
This study establishes Staphylococcus aureus infective endocarditis as the leading cause of infective endocarditis in many regions of the world and spotlights the global emergence of healthcare contact as a risk factor for Staphylococcus aureus infective endocarditis. In a significant portion of these patients, an IV device was the presumed source of bacteremia; prosthetic cardiac devices (pacemakers, defibrillators, or prosthetic cardiac valves) were present in almost one-quarter of the patients.
MRSA was a significant cause of Staphylococcus aureus infective endocarditis and displayed regional variation, accounting for almost 40% of the infective endocarditis caused by Staphylococcus aureus in some regions. Patients with infective endocarditis caused by MRSA were significantly more likely to have pre-existing chronic conditions and healthcare associated infective endocarditis by both univariate and multivariate analysis. They also were often associated with persistent bacteremia. On the other hand, 20% of patients with MRSA infective endocarditis developed their infection in the absence of identifiable healthcare contact.
Limitations of this report include the fact that this is an observational study of patients from self-selected centers. Each center most likely represents a portion of the local population, making it difficult to generalize findings to the entire population centers from which this report originates. Represented hospitals were typically referral centers that have cardiac surgery programs and may have widely differing populations with varied risk factors. Advantages include the large size of this prospectively evaluated cohort and the ability to analyze regional variations between continents with a contemporary nature of the patient sample (2000-2003).
Infectious Endocarditis in Olmsted County, Minn.
Tleyjeh IM, Steckelberg JM, Murad HS, et al. Temporal trends in infective endocarditis: a population-based study in Olmsted County, Minnesota. JAMA. 2005;293:3022-3028.
Tleyjeh and colleagues at the Mayo Clinic in Rochester, Minn., retrospectively studied 102 cases of infective endocarditis that occurred in 107 Olmsted County residents from 1970-2000. Main outcome measures were incidence of infective endocarditis, proportion of patients with underlying heart disease and causative micro-organisms and clinical characteristics. The records of all Olmsted County residents with infective endocarditis were identified and reviewed in detail. The definite and possible infective endocarditis cases as defined by modified Duke Criteria were used in the analysis.
The age- and gender-adjusted incidence of infective endocarditis ranged from 5.0 to 7.0 cases per 100,000 person-years during the study period and did not change significantly over time. There were 84 (79%) cases of native valve infective endocarditis and 23 (21%) cases of prosthetic valve infective endocarditis. Valves involved: aortic—36 (24%); mitral—49 (46%), aortic and mitral—12 (11%), right-sided or bilateral—8 (7%), or unknown—8 (7%). 16 (15%) had valve surgery within 42 days and the six-month mortality was 26% (n=28).
Infective endocarditis is a disease of the older individual in this population, with a mean age ranging from 54.1 years in 1980-1984 to 67.4 years in 1995-2000 (P=0.24 for trend). There was a male predominance (67%-83%), which did not significantly change over time.
Mitral valve prolapse was the most frequent underlying valvular heart disease. Viridans streptococci were the most common causative organisms (n=47; 44%) followed by Staphylococcus aureus (n=28 cases; 26%).
The overall average crude infective endocarditis incidence of the period 1970-2000 was 4.95 per 100,000 person-years. The age- and gender-adjusted annual incidence was 6.06 per 100,000 (95% CI, 4.89-7.22). There was no time trend for either streptococcus or Staphylococcus aureus infective endocarditis: the annual adjusted incidence of viridans group streptococcal infective endocarditis was 1.7 to 3.5 cases per 100,000 person years while Staphylococcus aureus infective endocarditis had an annual adjusted incidence of 1.0-2.2 cases per 100,000. The incidence rates of viridans group streptococcal and Staphylococcus aureus infective endocarditis have not changed significantly over time in this population.
Potential limitations of this study include possible incomplete case finding or recognition of the retrospective nature of the case reviews. The homogeneity of the patient population studied (primarily elderly white males with a low prevalence of intravenous drug use) limits the ability to generalize the results. Advantages include the fact that this is a population-based study at a medical center with detailed medical records of virtually all residents of a single county. This allows us to view the clinical features and etiologic factors of primarily left-sided infective endocarditis without the referral bias that tends to taint other studies typically published out of large medical centers with larger geographic referral bases.
Computers and Adverse Drug Events
Nebeker JR, Hoffman JM, Weir CR, Bennett CL, Hurdle JF. High rates of adverse drug events in a highly computerized hospital. Arch Intern Med. 2005;165:1111-1116.
Adverse drug events account for a significant number of hospital admissions and the ensuing costs associated with these hospitalizations. Electronic endeavors, such as computerized physician order entry (CPOE), bar code systems, and electronic medical records attempt to reduce the preventable adverse drug events.
Nebeker, et al. attempted to assess the effects of the implementation of CPOE and other computerized medication systems on adverse drug events in a tertiary care Veterans Administration Medical Center. They used an observational study design whereby 937 out of 2,306 newly admitted patients from several hospital wards were randomly chosen and assigned to a pharmacist reviewer during a 20-week period.
They reviewed complete medical records of hospital stays every other day to document adverse drug events. Not only were traditional adverse drug events identified, but harm from overdoses and/or inappropriate dose reductions or discontinuations, as well as intolerable harm from dose titration, were documented as adverse drug events. The harms caused by the drugs were considered only if the drugs were started in the hospital.
Harms were classified based on prior literature and included standards for pharmacological typology, causality assessment, error type, event terminology, drug class, seriousness index, and medication error category indexing. Additional uncommon classifications were also used, including additional resource utilization. Consensus meetings were held weekly to confirm classification of adverse drug events. Of the admissions reviewed, 483 adverse drug events were identified of which 93% were drug reactions while 7% were due to over- or underdosing. Of the drug reactions, 90% were considered dose-dependent while 10% were considered to be idiosyncratic.
Two different indexing scales were used in classifying the harms. Using the LDS Hospital Scale, it was suggested that 91% of the adverse drug events caused moderate harm while 9% caused serious harm. Using the National Coordinating Council for Medication Error Reporting and Prevention indexing, it was suggested that 87% of the adverse drug events fell into category E (requiring treatment) and 4% into category F (requiring prolonged hospitalization). Twenty-seven percent of the total adverse drug events were thought to be due to errors, including execution and planning steps. Sixty-one percent of errors occurred with the ordering mechanism while 25% of the errors occurred in the monitoring process.
This study highlighted rates of adverse drug events five to 19 times higher than baseline. The authors explained this higher-than-expected rate in part by study elements, such as the use of clinical pharmacists as reviewers, iterative case reviews, and accessible electronic data that make adverse drug events more noticeable.
Weaknesses of this study included issues of comparability of CPOEs because there were significant feature differences among commercial software programs. In addition, this was an observational study lacking a control group. The authors felt that their study did not support the idea that the computerized patient record of the study institution had caused adverse drug events. Rather, the study supported the idea that the system increased the visibility of adverse drug events compared with a paper system. In addition, the authors recommended that the choice of CPOEs be carefully considered, with a focus on decision support features when integrated into a healthcare organization.
The Questionable Benefit of Medical Emergency Teams
Hillman K, Chen J, Cretikos M, et al. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. MERIT study investigators. Lancet. 2005;365:2091-2097.
Previous studies have reported that the MET system reduces the incidence of cardiac arrests, deaths, and unplanned ICU admissions. A MET is a preplanned group of healthcare practitioners who respond to acute patient deteriorations in hospitalized patients.
METs are usually identical to hospital code teams, with the exception that they respond prior to a patient’s developing cardiac arrest. This early response has been shown to significantly decrease unexpected hospital mortality in hospitals in the United States, Australia, and Great Britain. Even though the system has been reported since 1995, few hospitals have knowledge of or experience with METs.
Unexpected hospital deaths and cardiac arrests are often preceded by clinical warning signs. In addition, unplanned ICU admissions may be foreshadowed by abnormalities in the patient’s vital signs that may progress if appropriate interventions are not undertaken. METs assess patients with abnormal physical findings or when there is a concern about the patient’s condition. These patients have findings that may precede a serious event or cardiac arrest, but otherwise don’t meet existing criteria to call a code.
The theory is that if a MET responds to see a patient who is becoming unstable (see “Table 1: MET Calling Criteria,” at left), early interventions may reduce the likelihood of arrest. Published studies have shown a reduction in cardiac arrests and ICU length of stay in virtually all systems in which MET has been introduced (although most studies are hampered by the use of historical controls).
The MERIT study randomized 23 hospitals in Australia to continue functioning as usual (n=11) or to introduce a MET system (n=12). The study sites included a wide range of tertiary, metropolitan, and non-metropolitan hospitals in different states across Australia. The primary outcome was the composite of cardiac arrest, unexpected death, or unplanned ICU admission during the six-month study period after MET activation, using intention to treat analysis.
A four-month educational period was undertaken with the MET centers prior to initiation of the trial. Control hospitals did not receive any education about the MET concept. This was followed by a six-month trial period. Cardiac arrest teams were maintained at all hospitals. The MET consisted of at least one doctor and a nurse from the ED or ICU.
The eligible patients included those residing on a medical ward (including critical care units); the ICUs, OR, postoperative recovery areas, and ED areas were not regarded as general wards.
The primary outcome for the study was the composite outcome of the incidence (events divided by number of eligible patients admitted to the hospital and residing on a medical ward during the study period) of:
- Cardiac arrests without a pre-existing “not-for-resuscitation” (NFR) order;
- Unplanned ICU admissions; and
- Unexpected deaths (those without a pre-existing NFR order).
The results of the study:
- During the study period, the overall rate of calls for the cardiac arrest team or MET was significantly higher in intervention hospitals than in control hospitals. Calls not associated with events were more common in MET hospitals than in controls. Half of the total calls were not associated with a cardiac arrest or unexpected death, whereas in MET hospitals more than 80% of calls were not associated with a cardiac arrest or death (P<0.0001).
- In patients with documented MET calling criteria in association with cardiac arrest or unexpected death, the call rate was similar in MET and control hospitals.
- There were no significant differences between the MET and control hospitals for any outcome.
- The response to changes in vital signs was not adequate—even in MET centers.
These findings are surprising in view of previously reported findings using the MET system. Potential reasons for lack of difference between MET centers and controls include:
- Number of study sites or the duration of the study may not have been adequate for implementation or education;
- Hospitals may already be efficient in detecting and managing unstable patients;
- Patient selection criteria may have been overly restricted. For example, other studies have used 30 respirations per minute for tachypnea as a calling criterion compared with 36 breaths per minute used in this trial;
- Knowledge of the study may have leaked to control hospitals;
- Cardiac arrest teams function as METs at times: Nearly half of the calls to cardiac arrest teams in control hospitals were made without a cardiac arrest or unexpected death; and
- The selected outcomes may not be sensitive enough.
Even though this large, multicenter controlled trial was unable to show a significant benefit of METs, we should not be discouraged from performing further controlled trials in different settings. The use of METs is clearly an exciting and evolving area of medicine.
Barriers to Patient Safety
Amalberti R, Auroy Y, Berwick D, Barach P. Five system barriers to achieving ultrasafe health care. Ann Intern Med. 2005;142:756-764
Patient safety in our healthcare system is a growing concern. One area of dialogue concerning preventable healthcare-associated harms involves the comparability of the healthcare industry with non-medical industries, such as aviation and nuclear power, that have adapted successful strategies shown to provide ultrasafe environments. Amalberti, et al. discuss risk assessment in a variety of industries and explain the need for a benchmarking approach in order to optimize or achieve safety in the healthcare field.
The authors identify five systemic barriers from literature that are fundamentally connected to the ability of the healthcare field to achieve an extremely safe environment.
Barrier 1—acceptance of limitations on maximum performance: The first barrier is the type of expected performance in the field. This is illustrated by the tradeoffs associated with ultrasafety versus productivity. The amount of risk involved was directly related to the limits placed on maximum performance. The first barrier is the acceptance that every system has limits. When a producer exceeds their limit, then safety suffers. An example used is that of blood donation: The limits of collection speed are weighed against the needed screening process.
Barrier 2—abandonment of professional autonomy: The second barrier concerns the concept of professional autonomy. While more teamwork and regulations reduce individual autonomy, this appears to improve safety in the healthcare environment. The bottom line is the importance of teamwork. The example used is that of traffic on a highway: Autonomous units work together to function safely.
Barrier 3—transition from the mindset of craftsman to that of an equivalent actor: The third barrier to achieving high levels of safety includes an equivalent actor mindset. This entails establishing a reliable standard of excellent care in lieu of focusing on individuality, similar to the notion that passengers on an airline usually do not know their pilots, but have established confidence in the airline itself.
Barrier 4—the need for system-level arbitration to optimize safety strategies: The fourth barrier identified is a need for system-level arbitration to optimize safety strategies. This need results from the pressure for justice (usually through litigation) once an accident occurs. Top-down arbitration of safety will be less successful than system level design.
Barrier 5—the need to simplify professional rules and regulations: The final barrier results from the many of layers of guidelines as they serve to create an environment of excellence. This barrier necessitates the removal of these layers to simplify the environment. Existing guidelines should be distilled down to those shown to promote quality and safety. Byzantine rules can obscure the goal of safety and glorify rules, for rules sake.
Certain structural limitations within the field, such as worker shortages in the face of increasing public demands and the reliance of the field on trainees such as students, interns, and residents, create other hurdles. The authors conclude by suggesting a two-tiered system of healthcare whereby ultrasafety could be more easily accomplished in areas of medicine considered more stable (first tier), and a second tier of care that would include the more unstable conditions, and thus inherently, represent the higher risk situations where errors are more likely to occur.
Another provocative point of this article is the need to move toward educating and training teams—not individuals.
The Importance of Implementing COPD Guidelines
Harvey PA, Murphy MC, Dornom E, et al. Implementing evidence-based guidelines: inpatient management of chronic obstructive pulmonary disease. Intern Med J. 2005;35:151-155.
COPD is a common diagnosis that sometimes requires hospitalization. Evidence-based guidelines for disease management, including that of hospitalized patients, exist, but there is a paucity of knowledge about the actual quality of care delivered in the hospital as it aligns with published guidelines. This study by Harvey, et al. explores the quality of care delivered in the hospital for patients with COPD, while at the same time investigating an intervention for the medical staff in an effort to improve adherence to evidenced-based guidelines of the disease.
Using ICD-10 codes for a COPD diagnosis, the study incorporated a retrospective chart review of 49 hospital admissions prior to the intervention and 35 admissions after the intervention in a hospital in Melbourne, Australia. Data were collected pertaining to the hospital management of COPD as it compared with what the authors considered to be Level A—or the highest level of evidence summarized from several professional organizations. The intervention delivered to the medical staff included a summarized presentation of the results from the initial audit of the 49 charts, as well as an educational package that was given to them following the presentation.
Except for inappropriate use of intravenous aminophylline, of which there was a 100% concordance to Level A guidelines, the initiation of systemic steroids (intravenous and/or oral) had the highest concordance rate of 80% and 83%, pre- and postintervention respectively. Appropriate steroid duration (seven to 14 days) had the lowest concordance rates at 10% and 29%, pre- and postintervention respectively.
In addition, preintervention concordance (10%) involving steroid duration was the only rate considered significantly different in the postintervention group (29%). While concordance rates were high for the use of any type of nebulized bronchodilator (96% preintervention and 80% postintervention), the Level A guidelines the authors used suggested that beta-agonist bronchodilators should be used alone prior to the initiation of ipratropium bromide. The concordance rates for this guideline were 27% preintervention and 34% postintervention.
Largely, the authors felt their intervention failed to improve concordance rates to the Level A guidelines investigated and also that their findings of variable and lower concordance rates across the board corroborated other similar studies. The major weaknesses of this study included the small sample size and the nonrandomness of the sampling.
In addition, the authors report that the particular hospital studied included junior doctors who rotated on and off service, which likely prevented the effects of the intervention from being measured on a provider level. In spite of the weaknesses in the study, the article brings to light the need for a more effective translation of evidence-based guidelines to actual practice, especially in the practice of COPD management in the hospital. Further methods of guideline implementation in the clinic setting must be elucidated to improve the care patients with COPD receive in the hospital.
Not all Troponin Elevations Are Myocardial Infarctions
Jeremais A, Gibson CM. Narrative review: alternative causes for elevated cardiac troponin levels when acute coronary syndromes are excluded. Ann Intern Med. 2005;142:786-791.
Troponins are regulatory proteins that control the calcium-mediated interaction of actin and myosin during muscle contraction. All muscle tissue contains troponins, but cardiac troponin T and I have amino acid sequences that are different from skeletal and smooth muscle troponins, allowing them to be detectable by monoclonal antibody-based assays.
In the event of reversible or irreversible cell damage—or possibly even from transiently increased cell membrane permeability—cardiac troponins are released from myocytes into circulation. This characteristic provides a sensitive test for detecting myocardial injury and damage; however, this test is not specific for acute coronary syndromes. And any disorder that causes myocyte damage may cause an elevated troponin.
The 2002 American College of Cardiology/American Heart Association practice guidelines for unstable angina and non-ST-segment elevation myocardial infarction acknowledge that the myocardial necrosis signified by troponin elevation may not necessarily be caused by atherosclerotic coronary artery disease. Such nonthrombotic troponin elevation can be caused by four basic mechanisms, as discussed by Dr. Jeremias and Dr. Gibson.
- Demand ischemia refers to a mismatch between myocardial oxygen demand and supply in the absence of flow-limiting epicardial stenosis. Conditions such as sepsis or septic shock and the systemic inflammatory response syndrome, hypotension or hypovolemia, tachyarrhythmias, and left ventricular hypertrophy can all cause release of cardiac troponin.
- Myocardial ischemia in the absence of fixed obstructive coronary disease can be caused by coronary vasospasm, acute stroke or intracranial hemorrhage, and ingestion of sympathomimetics.
- Direct myocardial damage can be seen in cardiac contusion, direct current cardioversion, cardiac infiltrative disorders such as amyloidosis, certain chemotherapy agents, myocarditis, pericarditis, and cardiac transplantation.
- Myocardial strain occurs when volume and pressure overload of the left and/or right ventricle cause excessive wall tension. Congestive heat failure, acute pulmonary embolism, and chronic pulmonary hypertension can lead to myocardial strain and troponin elevation.
Another condition that can lead to persistently elevated cardiac troponins is end-stage renal disease. This elevation may be due to small areas of clinically silent myocardial necrosis, an increased left ventricular mass, or possibly from impaired renal troponin excretion. Although troponins are believed to be cleared by the reticuloendothelial system, recent evidence shows that troponin T is fragmented into molecules that are small enough to be renally excreted.
In summary, elevated troponin can be found in many clinical settings and is associated with impaired short- and long-term survival. TH
Classic Literature
The HATEFUL Patient
Every physician has groaned internally when seeing a certain patient’s name on his list, going out of her way to avoid a particular family, or getting hopelessly engaged and increasingly enraged in a battle over a “lost” narcotic prescription. There are certain patients with whom a doctor-patient relationship feels more like a contest than a partnership. These interactions make a physician’s daily practice difficult, and they may wreak havoc among the staff on an inpatient ward. These patients grow ever more intolerable to their caregivers, who often harbor a wish to simply make them disappear.
In his landmark 1978 article “Taking Care of the Hateful Patient,” (NEJM, 298:883-887) James Groves, MD, discussed the characteristics of these difficult patients and the sometimes difficult emotions they generate in their caregivers. He described four different groups of patients, using an illustrative case for each, and discussed the ways in which these patients’ often maddening behavior serves to mitigate their profound dependency.
Dependent clingers are those patients whose neediness is overt, who seem to regard the physician as a sow with teats to spare. Dr. Groves suggested early, firm limit-setting with these patients to prevent the formation and later shattering of the patient’s illusion of the physician as inexhaustible.
Dependency lies at the heart of an entitled demander’s behavior as well, but their fear of abandonment is expressed as hostility and arrogance rather than overt neediness. Affirming to the patient that you share in their quest for the good (but not perfect) medical care to which they are entitled allows patient and physician to rally around a common goal.
This strategy backfires with manipulative help-rejecters, who seem almost pleased to report to their physician each time they fail a new treatment attempt. Overtly expressing some doubt that the treatment will completely cure all the patient’s difficulties and providing regular follow up are recommended for this group. These strategies relieve the patient of the unconscious anxiety that he may be abandoned by his physician should his symptoms abate.
Self-destructive deniers make the physician feel powerless as they persist in behavior that undermines all efforts to improve their health. With these patients, viewing their behavior as a terminal illness and managing symptoms and exacerbations accordingly allows the physician to focus on caring for the patient without unrealistic expectations of cure on the one hand and judgmental indifference on the other.
After discussing each of these groups, Dr. Groves concluded the article by suggesting that perhaps the greatest challenge physicians face in caring for these difficult patients is the temptation to disown the negative feelings they engender. He wrote that this effort not only strains the doctor’s limits, but also wastes valuable clinical data unmasked by these feelings—data that could inform clinical care. For decades prior to Dr. Groves’ article, psychoanalysts had reflected on what Freud termed “countertransference,” or the physician’s internal emotional reaction to a patient.
In his article “Hate in the Counter-Transference,” D.W. Winnicott, MD, suggested that rather than accepting the guilt that these feelings typically engender in a caregiver, negative countertransference reactions should be regarded by the physician as valuable information in understanding the patient’s psychic world. By training and by disposition, however, most physicians considered (and continue to consider) these emotions inappropriate. They seemingly negate the sympathy, kindness, and commitment to the patient’s well-being that should be central to a physician’s vocation. Conventional wisdom held that denying the feelings was the only proper response, and if that proved impossible, transferring the patient to a willing colleague was usually recommended. In contrast, Dr. Groves freed the physician to use these feelings to improve patient care.
Now a classic and oft-cited work, “Taking Care of the Hateful Patient” distills a wealth of analytic insight into a structure and language comprehensible to the busy generalist. By explaining the reactions each group of patients induces in their physicians, Dr. Groves provides useful tools to understand a particular patient’s psychology. Suggestions for strategic approaches to each category of patient are easy to understand and to adapt to one’s own practice. He explains how judicious limit-setting can be as valuable for the patient as it is for the doctor. Perhaps most helpful is his description of the needs of these patients that lie beneath their “hateful” exterior. Armed with this understanding, a physician can reclaim the empathy that is often so elusive with these patients.—Sandra Rackley MD, Kemuel Philbrick, MD
A review of staphylococcal Endocarditis
VG Fowler Jr, Miro JM, Hoen B, et al for the ICE Investigators. Staphylococcus aureus endocarditis: a consequence of medical progress. JAMA. 2005;June 22;293(24):3061-3062.
Agroup of infectious diseases experts from centers throughout the world formed the International Collaboration on Endocarditis (ICE) in 1999 to gain a global understanding of infective endocarditis. Using the Duke Criteria patients with definite infective endocarditis in a prospective manner, 275 variables were reported with these cases to a central database maintained at Duke University. The ICE-Prospective Cohort Study (ICE-PCS) enrolled 1,779 patients with infective endocarditis in 39 centers in 16 countries between June 15, 2000, and December 31, 2003, and has been described in a recent report. (Cabell CH, Abrutyn E. Infect Dis Clin North Am. 2002;16:255-72). Staphylococcus aureus was the most common cause of infective endocarditis in this group of patients (n=558; 31.6%); the authors characterized risk factors and clinical issues associated with these cases in this report.
By univariate analysis, compared with non-Staphylococcus aureus infective endocarditis, patients with infective endocarditis due to Staphylococcus aureus were more likely than patients with infective endocarditis due to other pathogens to be female (P<0.001), hemodialysis dependent (P<0.001), have diabetes mellitus (P=0.009), have other chronic illnesses (P<0.001), have a healthcare association (P<0.001), have higher rates of stroke (P<0.001), have systemic embolization (P<0.001), have persistent bacteremia (P<0.001), or die (P<0.001).
Although healthcare associated Staphylococcus aureus infective endocarditis was the most common form of Staphylococcus aureus infective endocarditis, more than 60% of healthcare-associated patients acquired the infection outside the hospital. This reflects the global trend in healthcare delivery patterns favoring ambulatory treatment (e.g., outpatient medication infusion via long-term IV access, hemodialysis)
Multivariate analysis, clinical features independently associated with Staphylococcus aureus infective endocarditis (versus non-Staphylococcus aureus infective endocarditis) were: IV drug use (OR, 9.3; 95% CI, 6.3-13.7); first clinical presentation less than one month after first symptoms (OR, 5.1; 95% CI, 3.2-8.2); healthcare-associated infection (OR, 2.9; 95% CI, 2.1-3.8), persistent bacteremia (OR, 2.3; 95% CI, 1.5-3.8), presence of a presumed intravascular device source (OR, 1.7; 95% CI, 1.2-2.6), stroke (OR, 1.6; 95% CI, 1.2-2.3), or diabetes mellitus (OR, 1.3; 95% CI, 1.1-1.8).
Patients from the United States with Staphylococcus aureus infective endocarditis were more likely to be hemodialysis-dependent, to be diabetic, to have a hemodialysis fistula or a chronic indwelling central catheter as a presumed source of infection, and to have a non-nosocomial healthcare association. Patients from the United States and Brazil were more likely to have Methicillin-resistant Staphyloccocus aureus (MRSA) than were patients from Europe, the Middle East, Australia, or New Zealand. In-hospital mortality rates were similar across regions, although American patients were significantly more likely to develop persistent bacteremia (25.6%, P<0.001).
Characteristics independently associated with mortality among patients with nonintravenous drug-use-associated Staphylococcus aureus infective endocarditis by multivariate analysis included stroke (OR, 3.67; 95% CI, 1.94-6.94), persistent bacteremia (OR, 3.06; 95% CI, 1.75-5.35), diagnosis in Southern Europe or the Middle East (OR, 3.21; 95% CI, 1.17-10.56).
This study establishes Staphylococcus aureus infective endocarditis as the leading cause of infective endocarditis in many regions of the world and spotlights the global emergence of healthcare contact as a risk factor for Staphylococcus aureus infective endocarditis. In a significant portion of these patients, an IV device was the presumed source of bacteremia; prosthetic cardiac devices (pacemakers, defibrillators, or prosthetic cardiac valves) were present in almost one-quarter of the patients.
MRSA was a significant cause of Staphylococcus aureus infective endocarditis and displayed regional variation, accounting for almost 40% of the infective endocarditis caused by Staphylococcus aureus in some regions. Patients with infective endocarditis caused by MRSA were significantly more likely to have pre-existing chronic conditions and healthcare associated infective endocarditis by both univariate and multivariate analysis. They also were often associated with persistent bacteremia. On the other hand, 20% of patients with MRSA infective endocarditis developed their infection in the absence of identifiable healthcare contact.
Limitations of this report include the fact that this is an observational study of patients from self-selected centers. Each center most likely represents a portion of the local population, making it difficult to generalize findings to the entire population centers from which this report originates. Represented hospitals were typically referral centers that have cardiac surgery programs and may have widely differing populations with varied risk factors. Advantages include the large size of this prospectively evaluated cohort and the ability to analyze regional variations between continents with a contemporary nature of the patient sample (2000-2003).
Infectious Endocarditis in Olmsted County, Minn.
Tleyjeh IM, Steckelberg JM, Murad HS, et al. Temporal trends in infective endocarditis: a population-based study in Olmsted County, Minnesota. JAMA. 2005;293:3022-3028.
Tleyjeh and colleagues at the Mayo Clinic in Rochester, Minn., retrospectively studied 102 cases of infective endocarditis that occurred in 107 Olmsted County residents from 1970-2000. Main outcome measures were incidence of infective endocarditis, proportion of patients with underlying heart disease and causative micro-organisms and clinical characteristics. The records of all Olmsted County residents with infective endocarditis were identified and reviewed in detail. The definite and possible infective endocarditis cases as defined by modified Duke Criteria were used in the analysis.
The age- and gender-adjusted incidence of infective endocarditis ranged from 5.0 to 7.0 cases per 100,000 person-years during the study period and did not change significantly over time. There were 84 (79%) cases of native valve infective endocarditis and 23 (21%) cases of prosthetic valve infective endocarditis. Valves involved: aortic—36 (24%); mitral—49 (46%), aortic and mitral—12 (11%), right-sided or bilateral—8 (7%), or unknown—8 (7%). 16 (15%) had valve surgery within 42 days and the six-month mortality was 26% (n=28).
Infective endocarditis is a disease of the older individual in this population, with a mean age ranging from 54.1 years in 1980-1984 to 67.4 years in 1995-2000 (P=0.24 for trend). There was a male predominance (67%-83%), which did not significantly change over time.
Mitral valve prolapse was the most frequent underlying valvular heart disease. Viridans streptococci were the most common causative organisms (n=47; 44%) followed by Staphylococcus aureus (n=28 cases; 26%).
The overall average crude infective endocarditis incidence of the period 1970-2000 was 4.95 per 100,000 person-years. The age- and gender-adjusted annual incidence was 6.06 per 100,000 (95% CI, 4.89-7.22). There was no time trend for either streptococcus or Staphylococcus aureus infective endocarditis: the annual adjusted incidence of viridans group streptococcal infective endocarditis was 1.7 to 3.5 cases per 100,000 person years while Staphylococcus aureus infective endocarditis had an annual adjusted incidence of 1.0-2.2 cases per 100,000. The incidence rates of viridans group streptococcal and Staphylococcus aureus infective endocarditis have not changed significantly over time in this population.
Potential limitations of this study include possible incomplete case finding or recognition of the retrospective nature of the case reviews. The homogeneity of the patient population studied (primarily elderly white males with a low prevalence of intravenous drug use) limits the ability to generalize the results. Advantages include the fact that this is a population-based study at a medical center with detailed medical records of virtually all residents of a single county. This allows us to view the clinical features and etiologic factors of primarily left-sided infective endocarditis without the referral bias that tends to taint other studies typically published out of large medical centers with larger geographic referral bases.
Computers and Adverse Drug Events
Nebeker JR, Hoffman JM, Weir CR, Bennett CL, Hurdle JF. High rates of adverse drug events in a highly computerized hospital. Arch Intern Med. 2005;165:1111-1116.
Adverse drug events account for a significant number of hospital admissions and the ensuing costs associated with these hospitalizations. Electronic endeavors, such as computerized physician order entry (CPOE), bar code systems, and electronic medical records attempt to reduce the preventable adverse drug events.
Nebeker, et al. attempted to assess the effects of the implementation of CPOE and other computerized medication systems on adverse drug events in a tertiary care Veterans Administration Medical Center. They used an observational study design whereby 937 out of 2,306 newly admitted patients from several hospital wards were randomly chosen and assigned to a pharmacist reviewer during a 20-week period.
They reviewed complete medical records of hospital stays every other day to document adverse drug events. Not only were traditional adverse drug events identified, but harm from overdoses and/or inappropriate dose reductions or discontinuations, as well as intolerable harm from dose titration, were documented as adverse drug events. The harms caused by the drugs were considered only if the drugs were started in the hospital.
Harms were classified based on prior literature and included standards for pharmacological typology, causality assessment, error type, event terminology, drug class, seriousness index, and medication error category indexing. Additional uncommon classifications were also used, including additional resource utilization. Consensus meetings were held weekly to confirm classification of adverse drug events. Of the admissions reviewed, 483 adverse drug events were identified of which 93% were drug reactions while 7% were due to over- or underdosing. Of the drug reactions, 90% were considered dose-dependent while 10% were considered to be idiosyncratic.
Two different indexing scales were used in classifying the harms. Using the LDS Hospital Scale, it was suggested that 91% of the adverse drug events caused moderate harm while 9% caused serious harm. Using the National Coordinating Council for Medication Error Reporting and Prevention indexing, it was suggested that 87% of the adverse drug events fell into category E (requiring treatment) and 4% into category F (requiring prolonged hospitalization). Twenty-seven percent of the total adverse drug events were thought to be due to errors, including execution and planning steps. Sixty-one percent of errors occurred with the ordering mechanism while 25% of the errors occurred in the monitoring process.
This study highlighted rates of adverse drug events five to 19 times higher than baseline. The authors explained this higher-than-expected rate in part by study elements, such as the use of clinical pharmacists as reviewers, iterative case reviews, and accessible electronic data that make adverse drug events more noticeable.
Weaknesses of this study included issues of comparability of CPOEs because there were significant feature differences among commercial software programs. In addition, this was an observational study lacking a control group. The authors felt that their study did not support the idea that the computerized patient record of the study institution had caused adverse drug events. Rather, the study supported the idea that the system increased the visibility of adverse drug events compared with a paper system. In addition, the authors recommended that the choice of CPOEs be carefully considered, with a focus on decision support features when integrated into a healthcare organization.
The Questionable Benefit of Medical Emergency Teams
Hillman K, Chen J, Cretikos M, et al. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. MERIT study investigators. Lancet. 2005;365:2091-2097.
Previous studies have reported that the MET system reduces the incidence of cardiac arrests, deaths, and unplanned ICU admissions. A MET is a preplanned group of healthcare practitioners who respond to acute patient deteriorations in hospitalized patients.
METs are usually identical to hospital code teams, with the exception that they respond prior to a patient’s developing cardiac arrest. This early response has been shown to significantly decrease unexpected hospital mortality in hospitals in the United States, Australia, and Great Britain. Even though the system has been reported since 1995, few hospitals have knowledge of or experience with METs.
Unexpected hospital deaths and cardiac arrests are often preceded by clinical warning signs. In addition, unplanned ICU admissions may be foreshadowed by abnormalities in the patient’s vital signs that may progress if appropriate interventions are not undertaken. METs assess patients with abnormal physical findings or when there is a concern about the patient’s condition. These patients have findings that may precede a serious event or cardiac arrest, but otherwise don’t meet existing criteria to call a code.
The theory is that if a MET responds to see a patient who is becoming unstable (see “Table 1: MET Calling Criteria,” at left), early interventions may reduce the likelihood of arrest. Published studies have shown a reduction in cardiac arrests and ICU length of stay in virtually all systems in which MET has been introduced (although most studies are hampered by the use of historical controls).
The MERIT study randomized 23 hospitals in Australia to continue functioning as usual (n=11) or to introduce a MET system (n=12). The study sites included a wide range of tertiary, metropolitan, and non-metropolitan hospitals in different states across Australia. The primary outcome was the composite of cardiac arrest, unexpected death, or unplanned ICU admission during the six-month study period after MET activation, using intention to treat analysis.
A four-month educational period was undertaken with the MET centers prior to initiation of the trial. Control hospitals did not receive any education about the MET concept. This was followed by a six-month trial period. Cardiac arrest teams were maintained at all hospitals. The MET consisted of at least one doctor and a nurse from the ED or ICU.
The eligible patients included those residing on a medical ward (including critical care units); the ICUs, OR, postoperative recovery areas, and ED areas were not regarded as general wards.
The primary outcome for the study was the composite outcome of the incidence (events divided by number of eligible patients admitted to the hospital and residing on a medical ward during the study period) of:
- Cardiac arrests without a pre-existing “not-for-resuscitation” (NFR) order;
- Unplanned ICU admissions; and
- Unexpected deaths (those without a pre-existing NFR order).
The results of the study:
- During the study period, the overall rate of calls for the cardiac arrest team or MET was significantly higher in intervention hospitals than in control hospitals. Calls not associated with events were more common in MET hospitals than in controls. Half of the total calls were not associated with a cardiac arrest or unexpected death, whereas in MET hospitals more than 80% of calls were not associated with a cardiac arrest or death (P<0.0001).
- In patients with documented MET calling criteria in association with cardiac arrest or unexpected death, the call rate was similar in MET and control hospitals.
- There were no significant differences between the MET and control hospitals for any outcome.
- The response to changes in vital signs was not adequate—even in MET centers.
These findings are surprising in view of previously reported findings using the MET system. Potential reasons for lack of difference between MET centers and controls include:
- Number of study sites or the duration of the study may not have been adequate for implementation or education;
- Hospitals may already be efficient in detecting and managing unstable patients;
- Patient selection criteria may have been overly restricted. For example, other studies have used 30 respirations per minute for tachypnea as a calling criterion compared with 36 breaths per minute used in this trial;
- Knowledge of the study may have leaked to control hospitals;
- Cardiac arrest teams function as METs at times: Nearly half of the calls to cardiac arrest teams in control hospitals were made without a cardiac arrest or unexpected death; and
- The selected outcomes may not be sensitive enough.
Even though this large, multicenter controlled trial was unable to show a significant benefit of METs, we should not be discouraged from performing further controlled trials in different settings. The use of METs is clearly an exciting and evolving area of medicine.
Barriers to Patient Safety
Amalberti R, Auroy Y, Berwick D, Barach P. Five system barriers to achieving ultrasafe health care. Ann Intern Med. 2005;142:756-764
Patient safety in our healthcare system is a growing concern. One area of dialogue concerning preventable healthcare-associated harms involves the comparability of the healthcare industry with non-medical industries, such as aviation and nuclear power, that have adapted successful strategies shown to provide ultrasafe environments. Amalberti, et al. discuss risk assessment in a variety of industries and explain the need for a benchmarking approach in order to optimize or achieve safety in the healthcare field.
The authors identify five systemic barriers from literature that are fundamentally connected to the ability of the healthcare field to achieve an extremely safe environment.
Barrier 1—acceptance of limitations on maximum performance: The first barrier is the type of expected performance in the field. This is illustrated by the tradeoffs associated with ultrasafety versus productivity. The amount of risk involved was directly related to the limits placed on maximum performance. The first barrier is the acceptance that every system has limits. When a producer exceeds their limit, then safety suffers. An example used is that of blood donation: The limits of collection speed are weighed against the needed screening process.
Barrier 2—abandonment of professional autonomy: The second barrier concerns the concept of professional autonomy. While more teamwork and regulations reduce individual autonomy, this appears to improve safety in the healthcare environment. The bottom line is the importance of teamwork. The example used is that of traffic on a highway: Autonomous units work together to function safely.
Barrier 3—transition from the mindset of craftsman to that of an equivalent actor: The third barrier to achieving high levels of safety includes an equivalent actor mindset. This entails establishing a reliable standard of excellent care in lieu of focusing on individuality, similar to the notion that passengers on an airline usually do not know their pilots, but have established confidence in the airline itself.
Barrier 4—the need for system-level arbitration to optimize safety strategies: The fourth barrier identified is a need for system-level arbitration to optimize safety strategies. This need results from the pressure for justice (usually through litigation) once an accident occurs. Top-down arbitration of safety will be less successful than system level design.
Barrier 5—the need to simplify professional rules and regulations: The final barrier results from the many of layers of guidelines as they serve to create an environment of excellence. This barrier necessitates the removal of these layers to simplify the environment. Existing guidelines should be distilled down to those shown to promote quality and safety. Byzantine rules can obscure the goal of safety and glorify rules, for rules sake.
Certain structural limitations within the field, such as worker shortages in the face of increasing public demands and the reliance of the field on trainees such as students, interns, and residents, create other hurdles. The authors conclude by suggesting a two-tiered system of healthcare whereby ultrasafety could be more easily accomplished in areas of medicine considered more stable (first tier), and a second tier of care that would include the more unstable conditions, and thus inherently, represent the higher risk situations where errors are more likely to occur.
Another provocative point of this article is the need to move toward educating and training teams—not individuals.
The Importance of Implementing COPD Guidelines
Harvey PA, Murphy MC, Dornom E, et al. Implementing evidence-based guidelines: inpatient management of chronic obstructive pulmonary disease. Intern Med J. 2005;35:151-155.
COPD is a common diagnosis that sometimes requires hospitalization. Evidence-based guidelines for disease management, including that of hospitalized patients, exist, but there is a paucity of knowledge about the actual quality of care delivered in the hospital as it aligns with published guidelines. This study by Harvey, et al. explores the quality of care delivered in the hospital for patients with COPD, while at the same time investigating an intervention for the medical staff in an effort to improve adherence to evidenced-based guidelines of the disease.
Using ICD-10 codes for a COPD diagnosis, the study incorporated a retrospective chart review of 49 hospital admissions prior to the intervention and 35 admissions after the intervention in a hospital in Melbourne, Australia. Data were collected pertaining to the hospital management of COPD as it compared with what the authors considered to be Level A—or the highest level of evidence summarized from several professional organizations. The intervention delivered to the medical staff included a summarized presentation of the results from the initial audit of the 49 charts, as well as an educational package that was given to them following the presentation.
Except for inappropriate use of intravenous aminophylline, of which there was a 100% concordance to Level A guidelines, the initiation of systemic steroids (intravenous and/or oral) had the highest concordance rate of 80% and 83%, pre- and postintervention respectively. Appropriate steroid duration (seven to 14 days) had the lowest concordance rates at 10% and 29%, pre- and postintervention respectively.
In addition, preintervention concordance (10%) involving steroid duration was the only rate considered significantly different in the postintervention group (29%). While concordance rates were high for the use of any type of nebulized bronchodilator (96% preintervention and 80% postintervention), the Level A guidelines the authors used suggested that beta-agonist bronchodilators should be used alone prior to the initiation of ipratropium bromide. The concordance rates for this guideline were 27% preintervention and 34% postintervention.
Largely, the authors felt their intervention failed to improve concordance rates to the Level A guidelines investigated and also that their findings of variable and lower concordance rates across the board corroborated other similar studies. The major weaknesses of this study included the small sample size and the nonrandomness of the sampling.
In addition, the authors report that the particular hospital studied included junior doctors who rotated on and off service, which likely prevented the effects of the intervention from being measured on a provider level. In spite of the weaknesses in the study, the article brings to light the need for a more effective translation of evidence-based guidelines to actual practice, especially in the practice of COPD management in the hospital. Further methods of guideline implementation in the clinic setting must be elucidated to improve the care patients with COPD receive in the hospital.
Not all Troponin Elevations Are Myocardial Infarctions
Jeremais A, Gibson CM. Narrative review: alternative causes for elevated cardiac troponin levels when acute coronary syndromes are excluded. Ann Intern Med. 2005;142:786-791.
Troponins are regulatory proteins that control the calcium-mediated interaction of actin and myosin during muscle contraction. All muscle tissue contains troponins, but cardiac troponin T and I have amino acid sequences that are different from skeletal and smooth muscle troponins, allowing them to be detectable by monoclonal antibody-based assays.
In the event of reversible or irreversible cell damage—or possibly even from transiently increased cell membrane permeability—cardiac troponins are released from myocytes into circulation. This characteristic provides a sensitive test for detecting myocardial injury and damage; however, this test is not specific for acute coronary syndromes. And any disorder that causes myocyte damage may cause an elevated troponin.
The 2002 American College of Cardiology/American Heart Association practice guidelines for unstable angina and non-ST-segment elevation myocardial infarction acknowledge that the myocardial necrosis signified by troponin elevation may not necessarily be caused by atherosclerotic coronary artery disease. Such nonthrombotic troponin elevation can be caused by four basic mechanisms, as discussed by Dr. Jeremias and Dr. Gibson.
- Demand ischemia refers to a mismatch between myocardial oxygen demand and supply in the absence of flow-limiting epicardial stenosis. Conditions such as sepsis or septic shock and the systemic inflammatory response syndrome, hypotension or hypovolemia, tachyarrhythmias, and left ventricular hypertrophy can all cause release of cardiac troponin.
- Myocardial ischemia in the absence of fixed obstructive coronary disease can be caused by coronary vasospasm, acute stroke or intracranial hemorrhage, and ingestion of sympathomimetics.
- Direct myocardial damage can be seen in cardiac contusion, direct current cardioversion, cardiac infiltrative disorders such as amyloidosis, certain chemotherapy agents, myocarditis, pericarditis, and cardiac transplantation.
- Myocardial strain occurs when volume and pressure overload of the left and/or right ventricle cause excessive wall tension. Congestive heat failure, acute pulmonary embolism, and chronic pulmonary hypertension can lead to myocardial strain and troponin elevation.
Another condition that can lead to persistently elevated cardiac troponins is end-stage renal disease. This elevation may be due to small areas of clinically silent myocardial necrosis, an increased left ventricular mass, or possibly from impaired renal troponin excretion. Although troponins are believed to be cleared by the reticuloendothelial system, recent evidence shows that troponin T is fragmented into molecules that are small enough to be renally excreted.
In summary, elevated troponin can be found in many clinical settings and is associated with impaired short- and long-term survival. TH
Classic Literature
The HATEFUL Patient
Every physician has groaned internally when seeing a certain patient’s name on his list, going out of her way to avoid a particular family, or getting hopelessly engaged and increasingly enraged in a battle over a “lost” narcotic prescription. There are certain patients with whom a doctor-patient relationship feels more like a contest than a partnership. These interactions make a physician’s daily practice difficult, and they may wreak havoc among the staff on an inpatient ward. These patients grow ever more intolerable to their caregivers, who often harbor a wish to simply make them disappear.
In his landmark 1978 article “Taking Care of the Hateful Patient,” (NEJM, 298:883-887) James Groves, MD, discussed the characteristics of these difficult patients and the sometimes difficult emotions they generate in their caregivers. He described four different groups of patients, using an illustrative case for each, and discussed the ways in which these patients’ often maddening behavior serves to mitigate their profound dependency.
Dependent clingers are those patients whose neediness is overt, who seem to regard the physician as a sow with teats to spare. Dr. Groves suggested early, firm limit-setting with these patients to prevent the formation and later shattering of the patient’s illusion of the physician as inexhaustible.
Dependency lies at the heart of an entitled demander’s behavior as well, but their fear of abandonment is expressed as hostility and arrogance rather than overt neediness. Affirming to the patient that you share in their quest for the good (but not perfect) medical care to which they are entitled allows patient and physician to rally around a common goal.
This strategy backfires with manipulative help-rejecters, who seem almost pleased to report to their physician each time they fail a new treatment attempt. Overtly expressing some doubt that the treatment will completely cure all the patient’s difficulties and providing regular follow up are recommended for this group. These strategies relieve the patient of the unconscious anxiety that he may be abandoned by his physician should his symptoms abate.
Self-destructive deniers make the physician feel powerless as they persist in behavior that undermines all efforts to improve their health. With these patients, viewing their behavior as a terminal illness and managing symptoms and exacerbations accordingly allows the physician to focus on caring for the patient without unrealistic expectations of cure on the one hand and judgmental indifference on the other.
After discussing each of these groups, Dr. Groves concluded the article by suggesting that perhaps the greatest challenge physicians face in caring for these difficult patients is the temptation to disown the negative feelings they engender. He wrote that this effort not only strains the doctor’s limits, but also wastes valuable clinical data unmasked by these feelings—data that could inform clinical care. For decades prior to Dr. Groves’ article, psychoanalysts had reflected on what Freud termed “countertransference,” or the physician’s internal emotional reaction to a patient.
In his article “Hate in the Counter-Transference,” D.W. Winnicott, MD, suggested that rather than accepting the guilt that these feelings typically engender in a caregiver, negative countertransference reactions should be regarded by the physician as valuable information in understanding the patient’s psychic world. By training and by disposition, however, most physicians considered (and continue to consider) these emotions inappropriate. They seemingly negate the sympathy, kindness, and commitment to the patient’s well-being that should be central to a physician’s vocation. Conventional wisdom held that denying the feelings was the only proper response, and if that proved impossible, transferring the patient to a willing colleague was usually recommended. In contrast, Dr. Groves freed the physician to use these feelings to improve patient care.
Now a classic and oft-cited work, “Taking Care of the Hateful Patient” distills a wealth of analytic insight into a structure and language comprehensible to the busy generalist. By explaining the reactions each group of patients induces in their physicians, Dr. Groves provides useful tools to understand a particular patient’s psychology. Suggestions for strategic approaches to each category of patient are easy to understand and to adapt to one’s own practice. He explains how judicious limit-setting can be as valuable for the patient as it is for the doctor. Perhaps most helpful is his description of the needs of these patients that lie beneath their “hateful” exterior. Armed with this understanding, a physician can reclaim the empathy that is often so elusive with these patients.—Sandra Rackley MD, Kemuel Philbrick, MD
The Case of the Nonhealing Wound

An 85-year-old female developed a sore on the left foot (see image above) during the past six months. Throughout that time she underwent periodic debridement and local wound care with gentamicin ointment followed by the use of silver sulfadiazine cream dressings, an Unna Boot, and a surgical shoe with heel relief. Despite treatment her wound increased in size, bleeds easily, but it is not painful.
WHAT IS YOUR DIAGNOSIS?
- Pyogenic granuloma;
- Squamous cell carcinoma;
- Amelanotic melanoma;
- erkel cell carcinoma; or
- Hypertrophic granulation tissue?
Discussion
The correct answer is C: amelanotic melanoma. The patient’s skin biopsy revealed a nodular malignant melanoma with ulceration, Clark’s level V, Breslow thickness at least 5.8 mm. She underwent wide local excision with sentinel lymph node biopsy, which was negative for tumor. The defect was repaired with a split-thickness skin graft and temporary wound vacuum. She is being closely monitored for local recurrence and in-transit metastasis.
Melanoma classically presents as an asymmetric, irregularly hyperpigmented lesion with ill-defined borders; however, some melanomas have little to no pigment and can be easily confused with other benign or malignant entities. Amelanotic melanomas comprise about 2% to 8% of all melanomas.1-2 A seemingly amelanotic lesion may have an area of subtle pigmentation peripherally that can be a clue to the diagnosis.2-3 The prognosis of amelanotic melanomas is the same as that of pigmented melanomas and is contingent upon depth of invasion, location, and patient age and gender. Unfortunately, the diagnosis of an amelanotic melanoma is often delayed, leading to more advanced tumors. Treatment is analogous to pigmented melanomas.2
A rapidly proliferating amelanotic melanoma can be clinically confused with a pyogenic granuloma, a benign vascular hyperplasia. Pyogenic granulomas present as solitary, discrete, erythematous papules or pedunculated growths on cutaneous and mucosal surfaces. They are often friable and may ulcerate. Pyogenic granulomas are more common in children and young adults, but they can occur at any age. If a pyogenic granuloma is not surgically excised, its growth will eventually stabilize, leading to involution, necrosis, or shrinkage to a fibrotic papule.4
Hypertrophic granulation tissue is another benign entity that can resemble an amelanotic melanoma. The production of granulation tissue is a normal response in the early proliferative stage of wound healing. Granulation tissue has abundant vascular structures, which give it an erythematous, edematous, and friable appearance. As wound healing progresses, granulation tissue is replaced with new epidermis through re-epithelialization.5 Failure of a wound to show signs of progressive healing should prompt a biopsy to distinguish normal granulation tissue from malignancy. Amelanotic melanoma has been reported in cases of nonhealing diabetic foot ulcers.6
Amelanotic melanoma can also be difficult to clinically distinguish from other malignant growths, such as squamous cell carcinoma. More common in elderly patients, squamous cell carcinoma commonly presents as a pink to erythematous, scaly papule, or plaque on a sun-exposed surface. Treatment of superficial squamous cell carcinoma, such as Bowen’s disease, with cryotherapy or cautery is highly effective; however, if an amelanotic melanoma is mistakenly treated as Bowen’s disease, then the delay in eventual histological diagnosis may result in an advanced stage amelanotic melanoma.7
Merkel cell carcinoma is a highly aggressive tumor that typically presents as an erythematous to violaceous, painless, solitary nodule or plaque that grows rapidly. It usually affects older patients and commonly occurs on the head. It has a high likelihood of local recurrence, metastasis, and poor prognosis.8 Merkel cell carcinomas are rare, and they elicit the same differential diagnoses as amelanotic melanomas. Histological differentiation from amelanotic melanoma is necessary. TH
References
- Adler M, White C. Amelanotic malignant melanoma. Semin Cutan Med Surg. 1997;16:122-130.
- Koch SE, Lange JR. Amelanotic melanoma: the great masquerader. J Am Acad Dermatol. 2000 May;42(5 Pt 1):731-734.
- Bono A, Maurichi A, Moglia D, et al. Clinical and dermatoscopic diagnosis of early amelanotic melanoma. Melanoma Res. 2001;11:491-494.
- Lin RL, Janniger CK. Pyogenic granuloma. Cutis. 2004 Oct;74(4):229-33.
- Freedburg IM, Eisen AZ, Klaus W, et al. Fitzpatrick’s Dermatology in General Medicine, 6th ed. New York: McGraw-Hill 2003;243.
- Gregson CL, Allain TJ. Amelanotic malignant melanoma disguised as a diabetic foot ulcer. Diabet Med. 2004 Aug;21(8):924-927.
- Holder JE, Colloby PS, Fletcher A, et al. Amelanotic superficial spreading malignant melanoma mimicking Bowen’s disease. Br J Dermatol. 1996 Mar;134(3):519-521.
- Agelli M, Clegg LX. Epidemiology of primary Merkel cell carcinoma in the United States. J Am Acad Dermatol. 2003 Nov;49(5):832-841.
An 85-year-old female developed a sore on the left foot (see image above) during the past six months. Throughout that time she underwent periodic debridement and local wound care with gentamicin ointment followed by the use of silver sulfadiazine cream dressings, an Unna Boot, and a surgical shoe with heel relief. Despite treatment her wound increased in size, bleeds easily, but it is not painful.
WHAT IS YOUR DIAGNOSIS?
- Pyogenic granuloma;
- Squamous cell carcinoma;
- Amelanotic melanoma;
- erkel cell carcinoma; or
- Hypertrophic granulation tissue?
Discussion
The correct answer is C: amelanotic melanoma. The patient’s skin biopsy revealed a nodular malignant melanoma with ulceration, Clark’s level V, Breslow thickness at least 5.8 mm. She underwent wide local excision with sentinel lymph node biopsy, which was negative for tumor. The defect was repaired with a split-thickness skin graft and temporary wound vacuum. She is being closely monitored for local recurrence and in-transit metastasis.
Melanoma classically presents as an asymmetric, irregularly hyperpigmented lesion with ill-defined borders; however, some melanomas have little to no pigment and can be easily confused with other benign or malignant entities. Amelanotic melanomas comprise about 2% to 8% of all melanomas.1-2 A seemingly amelanotic lesion may have an area of subtle pigmentation peripherally that can be a clue to the diagnosis.2-3 The prognosis of amelanotic melanomas is the same as that of pigmented melanomas and is contingent upon depth of invasion, location, and patient age and gender. Unfortunately, the diagnosis of an amelanotic melanoma is often delayed, leading to more advanced tumors. Treatment is analogous to pigmented melanomas.2
A rapidly proliferating amelanotic melanoma can be clinically confused with a pyogenic granuloma, a benign vascular hyperplasia. Pyogenic granulomas present as solitary, discrete, erythematous papules or pedunculated growths on cutaneous and mucosal surfaces. They are often friable and may ulcerate. Pyogenic granulomas are more common in children and young adults, but they can occur at any age. If a pyogenic granuloma is not surgically excised, its growth will eventually stabilize, leading to involution, necrosis, or shrinkage to a fibrotic papule.4
Hypertrophic granulation tissue is another benign entity that can resemble an amelanotic melanoma. The production of granulation tissue is a normal response in the early proliferative stage of wound healing. Granulation tissue has abundant vascular structures, which give it an erythematous, edematous, and friable appearance. As wound healing progresses, granulation tissue is replaced with new epidermis through re-epithelialization.5 Failure of a wound to show signs of progressive healing should prompt a biopsy to distinguish normal granulation tissue from malignancy. Amelanotic melanoma has been reported in cases of nonhealing diabetic foot ulcers.6
Amelanotic melanoma can also be difficult to clinically distinguish from other malignant growths, such as squamous cell carcinoma. More common in elderly patients, squamous cell carcinoma commonly presents as a pink to erythematous, scaly papule, or plaque on a sun-exposed surface. Treatment of superficial squamous cell carcinoma, such as Bowen’s disease, with cryotherapy or cautery is highly effective; however, if an amelanotic melanoma is mistakenly treated as Bowen’s disease, then the delay in eventual histological diagnosis may result in an advanced stage amelanotic melanoma.7
Merkel cell carcinoma is a highly aggressive tumor that typically presents as an erythematous to violaceous, painless, solitary nodule or plaque that grows rapidly. It usually affects older patients and commonly occurs on the head. It has a high likelihood of local recurrence, metastasis, and poor prognosis.8 Merkel cell carcinomas are rare, and they elicit the same differential diagnoses as amelanotic melanomas. Histological differentiation from amelanotic melanoma is necessary. TH
References
- Adler M, White C. Amelanotic malignant melanoma. Semin Cutan Med Surg. 1997;16:122-130.
- Koch SE, Lange JR. Amelanotic melanoma: the great masquerader. J Am Acad Dermatol. 2000 May;42(5 Pt 1):731-734.
- Bono A, Maurichi A, Moglia D, et al. Clinical and dermatoscopic diagnosis of early amelanotic melanoma. Melanoma Res. 2001;11:491-494.
- Lin RL, Janniger CK. Pyogenic granuloma. Cutis. 2004 Oct;74(4):229-33.
- Freedburg IM, Eisen AZ, Klaus W, et al. Fitzpatrick’s Dermatology in General Medicine, 6th ed. New York: McGraw-Hill 2003;243.
- Gregson CL, Allain TJ. Amelanotic malignant melanoma disguised as a diabetic foot ulcer. Diabet Med. 2004 Aug;21(8):924-927.
- Holder JE, Colloby PS, Fletcher A, et al. Amelanotic superficial spreading malignant melanoma mimicking Bowen’s disease. Br J Dermatol. 1996 Mar;134(3):519-521.
- Agelli M, Clegg LX. Epidemiology of primary Merkel cell carcinoma in the United States. J Am Acad Dermatol. 2003 Nov;49(5):832-841.
An 85-year-old female developed a sore on the left foot (see image above) during the past six months. Throughout that time she underwent periodic debridement and local wound care with gentamicin ointment followed by the use of silver sulfadiazine cream dressings, an Unna Boot, and a surgical shoe with heel relief. Despite treatment her wound increased in size, bleeds easily, but it is not painful.
WHAT IS YOUR DIAGNOSIS?
- Pyogenic granuloma;
- Squamous cell carcinoma;
- Amelanotic melanoma;
- erkel cell carcinoma; or
- Hypertrophic granulation tissue?
Discussion
The correct answer is C: amelanotic melanoma. The patient’s skin biopsy revealed a nodular malignant melanoma with ulceration, Clark’s level V, Breslow thickness at least 5.8 mm. She underwent wide local excision with sentinel lymph node biopsy, which was negative for tumor. The defect was repaired with a split-thickness skin graft and temporary wound vacuum. She is being closely monitored for local recurrence and in-transit metastasis.
Melanoma classically presents as an asymmetric, irregularly hyperpigmented lesion with ill-defined borders; however, some melanomas have little to no pigment and can be easily confused with other benign or malignant entities. Amelanotic melanomas comprise about 2% to 8% of all melanomas.1-2 A seemingly amelanotic lesion may have an area of subtle pigmentation peripherally that can be a clue to the diagnosis.2-3 The prognosis of amelanotic melanomas is the same as that of pigmented melanomas and is contingent upon depth of invasion, location, and patient age and gender. Unfortunately, the diagnosis of an amelanotic melanoma is often delayed, leading to more advanced tumors. Treatment is analogous to pigmented melanomas.2
A rapidly proliferating amelanotic melanoma can be clinically confused with a pyogenic granuloma, a benign vascular hyperplasia. Pyogenic granulomas present as solitary, discrete, erythematous papules or pedunculated growths on cutaneous and mucosal surfaces. They are often friable and may ulcerate. Pyogenic granulomas are more common in children and young adults, but they can occur at any age. If a pyogenic granuloma is not surgically excised, its growth will eventually stabilize, leading to involution, necrosis, or shrinkage to a fibrotic papule.4
Hypertrophic granulation tissue is another benign entity that can resemble an amelanotic melanoma. The production of granulation tissue is a normal response in the early proliferative stage of wound healing. Granulation tissue has abundant vascular structures, which give it an erythematous, edematous, and friable appearance. As wound healing progresses, granulation tissue is replaced with new epidermis through re-epithelialization.5 Failure of a wound to show signs of progressive healing should prompt a biopsy to distinguish normal granulation tissue from malignancy. Amelanotic melanoma has been reported in cases of nonhealing diabetic foot ulcers.6
Amelanotic melanoma can also be difficult to clinically distinguish from other malignant growths, such as squamous cell carcinoma. More common in elderly patients, squamous cell carcinoma commonly presents as a pink to erythematous, scaly papule, or plaque on a sun-exposed surface. Treatment of superficial squamous cell carcinoma, such as Bowen’s disease, with cryotherapy or cautery is highly effective; however, if an amelanotic melanoma is mistakenly treated as Bowen’s disease, then the delay in eventual histological diagnosis may result in an advanced stage amelanotic melanoma.7
Merkel cell carcinoma is a highly aggressive tumor that typically presents as an erythematous to violaceous, painless, solitary nodule or plaque that grows rapidly. It usually affects older patients and commonly occurs on the head. It has a high likelihood of local recurrence, metastasis, and poor prognosis.8 Merkel cell carcinomas are rare, and they elicit the same differential diagnoses as amelanotic melanomas. Histological differentiation from amelanotic melanoma is necessary. TH
References
- Adler M, White C. Amelanotic malignant melanoma. Semin Cutan Med Surg. 1997;16:122-130.
- Koch SE, Lange JR. Amelanotic melanoma: the great masquerader. J Am Acad Dermatol. 2000 May;42(5 Pt 1):731-734.
- Bono A, Maurichi A, Moglia D, et al. Clinical and dermatoscopic diagnosis of early amelanotic melanoma. Melanoma Res. 2001;11:491-494.
- Lin RL, Janniger CK. Pyogenic granuloma. Cutis. 2004 Oct;74(4):229-33.
- Freedburg IM, Eisen AZ, Klaus W, et al. Fitzpatrick’s Dermatology in General Medicine, 6th ed. New York: McGraw-Hill 2003;243.
- Gregson CL, Allain TJ. Amelanotic malignant melanoma disguised as a diabetic foot ulcer. Diabet Med. 2004 Aug;21(8):924-927.
- Holder JE, Colloby PS, Fletcher A, et al. Amelanotic superficial spreading malignant melanoma mimicking Bowen’s disease. Br J Dermatol. 1996 Mar;134(3):519-521.
- Agelli M, Clegg LX. Epidemiology of primary Merkel cell carcinoma in the United States. J Am Acad Dermatol. 2003 Nov;49(5):832-841.
2005 Election for SHM Board of Directors
The SHM Nominating Committee is requesting nominations for three open seats on the Board of Directors for a three-year term, beginning May 2, 2006. In addition there will be one pediatric hospitalist seat on the SHM Board for a three-year term, beginning May 2, 2006. Pediatricians may submit their nomination for either the open seats or for the specific designated pediatric seat. All SHM members will vote in both the open and pediatric board elections.
Who is eligible to be nominated? Any SHM member in good standing who is:
- Board certified in their primary specialty;
- Available to travel to board meetings twice a year;
- Prepared to respond to e-mails on a daily basis and actively participate in board list serve;
- Willing to serve on SHM committees; and
- Able to commit to a three-year term, ending in 2009.
Candidates may self-nominate or may be nominated by another SHM member. Nominated candidates must submit the following materials for consideration on the board:
- A one-page curriculum vitae (CV) (12-point font size with 1” margins);
- A one-page nominating letter (12-point font size with 1” margins);
- A recent headshot; and
- An optional additional letter of support (one page, 12-point font size with 1” margins)—although these may not come from any current SHM board members. All letters should be addressed to Steven Pantilat, MD, chair, SHM Nominations Committee. Note: The letter of support is only for Nominations Committee use, but for those candidates who are on the election ballot, the CV, headshot, and the nominating letter will be sent as submitted to all voting members of SHM. Letters will be accepted by mail or e-mail only. No faxes accepted due to potential poor quality of transmission.
The criteria used when considering nominees for ballot include:
- Duration of SHM membership;
- Activity as a hospitalist;
- Activity in or contributions to SHM;
- Activity at a local or regional level;
- Prominence as a hospitalist;
- Ability to provide skills or experience not currently found on the board; and
- Ability to add to the diversity of the board.
Timeline
Some of the critical milestone dates for the board nomination process include the following:
October 31, 2005: Deadline for submitting candidates for nomination;
November 28, 2005: Ballots mailed to SHM members
January 5, 2006: Ballots must be received at SHM offices;
January 20, 2006: Notification of candidates of results of election;
January 23, 2006: Election results posted on SHM Web site;
May 2, 2006: Elected board members take office.
If you are interested in being considered as a nominee for the SHM Board, please submit your nomination materials by October 31, 2005, to the SHM Nominations Committee, 190 N. Independence Mall West, Philadelphia, PA 19106-1572.
Questions? Send them via e-mail to nominations@hospitalmedicine.org or call (800) 843-3360.
Core Competencies Are Coming!
Hospital medicine core competencies to be published in January 2006
The Society of Hospital Medicine Core Competencies project continues to move toward publication in early 2006. The goals of the project are to define hospital medicine and provide a framework for the development of hospital medicine curricula throughout the continuum of professional education and training.
The Core Competencies Task Force is chaired by Mike Pistoria, DO, with key input from Dan Dressler, MD, MSc, Sylvia McKean, MD, Alpesh Amin, MD, MBA, and staffed by Tina Budnitz, MPH.
The Core Competencies Task Force developed the methods for the project and overall template for the resulting document. The template divided topic areas into three sections: Clinical, Systems Organization, and Improvement and Procedures. Topics were selected based on the frequency with which they are seen by hospitalists and the areas in which hospitalists lend a particular expertise. The Systems Organization and Improvement section is a perfect example of the latter topics. This section consists of chapters dealing with the nonclinical issues in which a practicing hospitalist should be a proficient expert. Contributors—mostly from within SHM—were recruited to write the chapters.
Once the original chapters were received, an extensive editing process began. This process ensured consistency within and across chapters. In the initial planning process, the task force decided to utilize the Knowledge, Skills, and Attitudes (KSA) domains within each chapter. Additionally, a Systems Organization and Improvement domain was added to each chapter to reflect hospitalist efforts to promote systemwide improvements in care.
As will be detailed when the Competencies are published, the KSA domains follow established definitions in the educational literature and not those commonly used in medical literature. Competencies within each domain were carefully crafted to reflect a specific level of proficiency. In other words, for each competency, it is obvious to the reader exactly what a hospitalist should be able to do and how proficiency would be evaluated.
Another part of the editing process focused on revising each chapter to stand on its own. Given the desire that the Competencies be used for curriculum development and continuing medical education, the members of the task force felt strongly that each chapter should be self-contained so an individual could pull a chapter on Community-Acquired Pneumonia, for example, and have the relevant competencies at his or her disposal.
When the first draft of the document was completed, it was sent out for review by SHM leadership and professional medical organizations. Reviewers from the Association of American Medical Colleges, the Society of General Internal Medicine, the Society of Critical Care Medicine, and the American College of Physicians provided feedback on the Competencies. Comments from other organizations invited to participate are still pending.
The Competencies will be published as a supplement to the forthcoming Journal of Hospital Medicine (JHM) in early 2006. Several related articles are also being prepared to submit to the Journal’s review process. One article will fully detail the Competencies development, while the other will be a primer on using the Competencies. The task force and the JHM editorial staff have discussed the possibility of an ongoing series within the Journal that will highlight examples of the Competencies translated into curricula and program improvements or provide an evidence-based content outline to accompany chapters. SHM is developing several Web-based resources to provide content and training tools that support the Core Competencies.
It is important to realize the publication of the Competencies is the first of many steps to standardize and establish a core curriculum for hospital medicine. The task force recognizes the Core Competencies as a fluid document. Chapters will be added over time and specific competencies within chapters may change as medicine changes and hospitalists’ roles continue to evolve.
Over the next year, the SHM Core Curriculum Task Force will be focused on evaluating the effects of the core competencies, promoting their use, and encouraging the development of curricula based on the framework provided by the competencies. If you are interested in participating in these activities please forward your nomination to participate in the Core Curriculum Task Force to Lillian Higgins at lhiggins@hospitalmedicine.org.
COMMITTEE REPORT
How to Build a Sustainable Career in Hospital Medicine
An interim report from the SHM Career Satisfaction Task Force
By Sylvia McKean, MD, Tosha Wetterneck, MD, and Win Whitcomb, MD
In 2005 SHM recognized the importance of establishing work standards for hospitalists by charging a task force to articulate key work conditions that promote success and wellness for a career in hospital medicine. As a professional society SHM is committed to developing resources for hospitalists that facilitate long and satisfying careers in hospital medicine in diverse work settings.
Since the first SHM survey of hospitalists in 1999, the role of the hospitalist has evolved to address the needs of multiple stakeholders. Reports of stress and dissatisfaction have subsequently generated dialogue on the SHM list serve. In March a recent SHM member commented: “These messages obviously concern me, and I hope the individuals can find a reasonable solution. However, I was wondering: Are management problems like these the exception or the rule?”
As a new specialty, ill-defined and evolving job descriptions can promote burnout along with other factors. Traditional residency programs in internal medicine and pediatrics don’t adequately train physicians to become hospitalists. Lack of clarity about the hospitalist role may create a mismatch between expectations of hospital leaders and junior physicians who have not yet assumed leadership roles. Hospitalists at academic medical centers are faced with additional burdens brought on by Accreditation Council for Graduate Medical Education resident workload restrictions. The absence of career promotion tracks in medical schools may limit advancement and recognition. These issues are not unique to hospital medicine and have surfaced as problems for critical care and emergency medicine.
According to the 1999 survey, burnout in general is correlated with a lower level of perceived autonomy to perform work as one sees fit and to control the professional experience.1 Less recognition by patients, families, and other professionals for a job well done and poor integration with nonphysician team members is associated with burnout. Lacking occupational solidarity as part of a team of professionals, sharing the joys and frustrations with peers, negatively affects job satisfaction.
Although the 1999 SHM study found that burnout was not independently correlated with workload, clearly there is a ceiling beyond which physicians should not work. Consistent with what the literature says about emergency medicine, professions with high demands are more likely to experience burnout. The American College of Emergency Physicians has its own wellness section that includes consensus statements about specific work parameters.
SHM has raised awareness that the hospitalist model cannot be equivalent to office practice. It’s not feasible for hospitalists to work a volume of annual hours equivalent to those worked by primary care physicians and medical specialists How Hospitalists Add Value (a special supplement to The Hospitalist published in April 2005) reinforces the need to structure reimbursement accordingly. At the SHM 2005 Annual Meeting, Tosha Wetterneck, MD, a member of the SHM Career Satisfaction Task Force and an expert on physician burnout, led a workshop on “Burnout and Hospitalists” with Michael Williams.
Progress Report to Date
The work of the task force intersects activities of other SHM committees and task forces. Practice support, education, leadership, benchmarks, and research are fundamental to providing hospitalists with the necessary skill set to succeed. Modifiable factors in the practice (or work environment) of local hospitals will be identified in the near future to optimally support hospitalists. In addition, the SHM 2005 Education Summit identified ongoing education as critical for the development of skills required for academic and administrative advancement.
The task force is focusing on job engagement rather than burnout—its antithesis. A profile of engagement is expected to include a sustainable workload, empowered decision-making, appropriate recognition and compensation, a supportive work environment, a sense of fairness, and meaningful and valued responsibilities appropriate to level of experience.2 Learning opportunities are highly correlated with engagement. Promising approaches to career satisfaction focus on organizational changes that enhance the capacity of hospitalists to cope with the demands of caring for hospitalized patients.
Review of data specific to hospital medicine support the need to define a sustainable workload. Findings on burnout and satisfaction from an Agency for Healthcare Research and Quality-Funded Multicenter Trial of Academic Hospitalists (David Meltzer, MD, PhD, is the principle investigator) at six medical centers provide new information, but may not be applicable to other hospitalist programs. Additional research is needed to identify the key ingredients for a long and professionally rewarding career in hospital medicine and to examine the link between clinician burnout and patient safety in diverse hospital settings.
Short-Term Next Steps—By Jan. 2006
One of the major goals of the Career Satisfaction Task Force is to establish national benchmarks for sustainable work conditions for hospitalists so they are engaged in a career of hospital medicine. The task force identified the following workplace domains:
- Control/autonomy;
- Workload/schedule;
- Community/environment; and
- Reward/recognition.
The task force will:
- Articulate predictors of job satisfaction and engagement in terms of the key domains of work life;
- Define and prioritize educational outreach programs to assist in the development of Core Competencies; and
- Develop a tool kit for building engagement and identifying modifiable factors in the workplace.
Building on the work of other SHM committees, the task force will make specific recommendations about education and practice management support to promote high productivity and career satisfaction despite high workload. Value-added information will be incorporated into the recommendations to promote adequate and fair compensation. The tool kit would be an “ideal model” that SHM would support with an explanation of how to bridge the gap between existing practice and a new flexible work structure that would meet the individual needs of hospitalists. Future revisions of the tool kit would be based on research findings.
Long -Term Next Steps: Two-Year Concurrent Time Line
Dr. Wetterneck will lead an effort to survey the SHM membership about work-life, satisfaction, and burnout to further define key aspects of hospital medicine programs and work life that maximize physician career satisfaction. Information from interviews, focus groups, and prior hospitalist surveys will guide the development of a Hospitalist Worklife and Satisfaction Survey that will be administered to the SHM membership in 2006. The SHM Board has approved funding for this initiative.
The task force will:
- Promote future research into career satisfaction and engagement in hospital medicine to understand the magnitude of the problem of career satisfaction;
- Specify how to structure hospital medicine programs based on actionable data;
- Recommend how SHM can participate in improving the hospital setting as a patient care environment that not only facilitates improved patient outcomes, but also clinician workplace satisfaction for hospitalists;
- Draft a consensus statement for the peer reviewed SHM Journal of Hospital Medicine similar to the Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine;3 and
- Hold a workshop at the 2006 SHM Annual Meeting on Career Satisfaction.
The Career Satisfaction Committee Task Force welcomes your comments. Contact them at smckean@partners.org (Sylvia McKean, MD), tbw@medicine.wisc.edu (Tosha Wetterneck, MD), or wfwhit@comcast.net (Win Whitcomb, MD).
References
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43:72-91.
- Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001;52:397-422.
- Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine. Ann Fam Med. 2004;2(1):S65-74.
WHAT’S ONLINE AT THE SHM WEB SITE
Improve Inpatient Outcomes with New SHM Online Resource
SHM Web site launches Quality Improvement Resource Rooms
In August SHM announced the first in a new online series to help hospitalists improve inpatient outcomes: the SHM Quality Improvement Resource Rooms. Although performance improvement is ultimately a local phenomenon, certain knowledge, approaches, methods, and tools transcend institution and disease.
When it comes to leading quality improvement in the hospital there has never been a pack-and-go road map—until now. With the launch of the SHM Resource Rooms, a hospitalist with nothing more than the motivation to lead measurable performance improvement in the hospital can do just that. The first Resource Room—focused on reducing venous thromboembolism (VTE), the leading cause of preventable hospital deaths—features a downloadable workbook and companion project outline that walks the hospitalist through every step in the improvement process (see details in “How to Use the VTE Resource Room,” below).
Hospitalists who extract the most out of the VTE Resource Room will be able to:
- Understand and use fundamental quality improvement concepts in the hospital;
- Command and teach the VTE prevention literature; and
- Engineer and lead improvement in the hospital.
The Quality Improvement Resource Rooms will support the hospitalist across domains integral to any quality improvement effort: raising collective awareness of a performance gap, knowing what evidence to put into practice, and leveraging experience with the disease as well as the improvement process.
Print and carry a ready-made workbook to guide and document your work. View a presentation depicting the key elements in quality improvement theory. Download a ready-made slide set to propel teaching of VTE prevention in the didactic setting. Adapt practical teaching tips to implement immediately. Review a listing of the pertinent literature. View and modify VTE tools shared by other hospitalists. Or post questions to a moderated forum of VTE and quality improvement experts.
By offering the new online Resource Rooms, the SHM has taken a significant step toward realizing the potential in hospital medicine: to enhance your ability to improve inpatient outcomes. The next step is yours.
At the SHM Web site, navigate to “Quality and Safety,” select “Quality Improvement Resource Rooms,” and then “Venous Thromboembolism (VTE) Resource Room.” TH
The SHM Nominating Committee is requesting nominations for three open seats on the Board of Directors for a three-year term, beginning May 2, 2006. In addition there will be one pediatric hospitalist seat on the SHM Board for a three-year term, beginning May 2, 2006. Pediatricians may submit their nomination for either the open seats or for the specific designated pediatric seat. All SHM members will vote in both the open and pediatric board elections.
Who is eligible to be nominated? Any SHM member in good standing who is:
- Board certified in their primary specialty;
- Available to travel to board meetings twice a year;
- Prepared to respond to e-mails on a daily basis and actively participate in board list serve;
- Willing to serve on SHM committees; and
- Able to commit to a three-year term, ending in 2009.
Candidates may self-nominate or may be nominated by another SHM member. Nominated candidates must submit the following materials for consideration on the board:
- A one-page curriculum vitae (CV) (12-point font size with 1” margins);
- A one-page nominating letter (12-point font size with 1” margins);
- A recent headshot; and
- An optional additional letter of support (one page, 12-point font size with 1” margins)—although these may not come from any current SHM board members. All letters should be addressed to Steven Pantilat, MD, chair, SHM Nominations Committee. Note: The letter of support is only for Nominations Committee use, but for those candidates who are on the election ballot, the CV, headshot, and the nominating letter will be sent as submitted to all voting members of SHM. Letters will be accepted by mail or e-mail only. No faxes accepted due to potential poor quality of transmission.
The criteria used when considering nominees for ballot include:
- Duration of SHM membership;
- Activity as a hospitalist;
- Activity in or contributions to SHM;
- Activity at a local or regional level;
- Prominence as a hospitalist;
- Ability to provide skills or experience not currently found on the board; and
- Ability to add to the diversity of the board.
Timeline
Some of the critical milestone dates for the board nomination process include the following:
October 31, 2005: Deadline for submitting candidates for nomination;
November 28, 2005: Ballots mailed to SHM members
January 5, 2006: Ballots must be received at SHM offices;
January 20, 2006: Notification of candidates of results of election;
January 23, 2006: Election results posted on SHM Web site;
May 2, 2006: Elected board members take office.
If you are interested in being considered as a nominee for the SHM Board, please submit your nomination materials by October 31, 2005, to the SHM Nominations Committee, 190 N. Independence Mall West, Philadelphia, PA 19106-1572.
Questions? Send them via e-mail to nominations@hospitalmedicine.org or call (800) 843-3360.
Core Competencies Are Coming!
Hospital medicine core competencies to be published in January 2006
The Society of Hospital Medicine Core Competencies project continues to move toward publication in early 2006. The goals of the project are to define hospital medicine and provide a framework for the development of hospital medicine curricula throughout the continuum of professional education and training.
The Core Competencies Task Force is chaired by Mike Pistoria, DO, with key input from Dan Dressler, MD, MSc, Sylvia McKean, MD, Alpesh Amin, MD, MBA, and staffed by Tina Budnitz, MPH.
The Core Competencies Task Force developed the methods for the project and overall template for the resulting document. The template divided topic areas into three sections: Clinical, Systems Organization, and Improvement and Procedures. Topics were selected based on the frequency with which they are seen by hospitalists and the areas in which hospitalists lend a particular expertise. The Systems Organization and Improvement section is a perfect example of the latter topics. This section consists of chapters dealing with the nonclinical issues in which a practicing hospitalist should be a proficient expert. Contributors—mostly from within SHM—were recruited to write the chapters.
Once the original chapters were received, an extensive editing process began. This process ensured consistency within and across chapters. In the initial planning process, the task force decided to utilize the Knowledge, Skills, and Attitudes (KSA) domains within each chapter. Additionally, a Systems Organization and Improvement domain was added to each chapter to reflect hospitalist efforts to promote systemwide improvements in care.
As will be detailed when the Competencies are published, the KSA domains follow established definitions in the educational literature and not those commonly used in medical literature. Competencies within each domain were carefully crafted to reflect a specific level of proficiency. In other words, for each competency, it is obvious to the reader exactly what a hospitalist should be able to do and how proficiency would be evaluated.
Another part of the editing process focused on revising each chapter to stand on its own. Given the desire that the Competencies be used for curriculum development and continuing medical education, the members of the task force felt strongly that each chapter should be self-contained so an individual could pull a chapter on Community-Acquired Pneumonia, for example, and have the relevant competencies at his or her disposal.
When the first draft of the document was completed, it was sent out for review by SHM leadership and professional medical organizations. Reviewers from the Association of American Medical Colleges, the Society of General Internal Medicine, the Society of Critical Care Medicine, and the American College of Physicians provided feedback on the Competencies. Comments from other organizations invited to participate are still pending.
The Competencies will be published as a supplement to the forthcoming Journal of Hospital Medicine (JHM) in early 2006. Several related articles are also being prepared to submit to the Journal’s review process. One article will fully detail the Competencies development, while the other will be a primer on using the Competencies. The task force and the JHM editorial staff have discussed the possibility of an ongoing series within the Journal that will highlight examples of the Competencies translated into curricula and program improvements or provide an evidence-based content outline to accompany chapters. SHM is developing several Web-based resources to provide content and training tools that support the Core Competencies.
It is important to realize the publication of the Competencies is the first of many steps to standardize and establish a core curriculum for hospital medicine. The task force recognizes the Core Competencies as a fluid document. Chapters will be added over time and specific competencies within chapters may change as medicine changes and hospitalists’ roles continue to evolve.
Over the next year, the SHM Core Curriculum Task Force will be focused on evaluating the effects of the core competencies, promoting their use, and encouraging the development of curricula based on the framework provided by the competencies. If you are interested in participating in these activities please forward your nomination to participate in the Core Curriculum Task Force to Lillian Higgins at lhiggins@hospitalmedicine.org.
COMMITTEE REPORT
How to Build a Sustainable Career in Hospital Medicine
An interim report from the SHM Career Satisfaction Task Force
By Sylvia McKean, MD, Tosha Wetterneck, MD, and Win Whitcomb, MD
In 2005 SHM recognized the importance of establishing work standards for hospitalists by charging a task force to articulate key work conditions that promote success and wellness for a career in hospital medicine. As a professional society SHM is committed to developing resources for hospitalists that facilitate long and satisfying careers in hospital medicine in diverse work settings.
Since the first SHM survey of hospitalists in 1999, the role of the hospitalist has evolved to address the needs of multiple stakeholders. Reports of stress and dissatisfaction have subsequently generated dialogue on the SHM list serve. In March a recent SHM member commented: “These messages obviously concern me, and I hope the individuals can find a reasonable solution. However, I was wondering: Are management problems like these the exception or the rule?”
As a new specialty, ill-defined and evolving job descriptions can promote burnout along with other factors. Traditional residency programs in internal medicine and pediatrics don’t adequately train physicians to become hospitalists. Lack of clarity about the hospitalist role may create a mismatch between expectations of hospital leaders and junior physicians who have not yet assumed leadership roles. Hospitalists at academic medical centers are faced with additional burdens brought on by Accreditation Council for Graduate Medical Education resident workload restrictions. The absence of career promotion tracks in medical schools may limit advancement and recognition. These issues are not unique to hospital medicine and have surfaced as problems for critical care and emergency medicine.
According to the 1999 survey, burnout in general is correlated with a lower level of perceived autonomy to perform work as one sees fit and to control the professional experience.1 Less recognition by patients, families, and other professionals for a job well done and poor integration with nonphysician team members is associated with burnout. Lacking occupational solidarity as part of a team of professionals, sharing the joys and frustrations with peers, negatively affects job satisfaction.
Although the 1999 SHM study found that burnout was not independently correlated with workload, clearly there is a ceiling beyond which physicians should not work. Consistent with what the literature says about emergency medicine, professions with high demands are more likely to experience burnout. The American College of Emergency Physicians has its own wellness section that includes consensus statements about specific work parameters.
SHM has raised awareness that the hospitalist model cannot be equivalent to office practice. It’s not feasible for hospitalists to work a volume of annual hours equivalent to those worked by primary care physicians and medical specialists How Hospitalists Add Value (a special supplement to The Hospitalist published in April 2005) reinforces the need to structure reimbursement accordingly. At the SHM 2005 Annual Meeting, Tosha Wetterneck, MD, a member of the SHM Career Satisfaction Task Force and an expert on physician burnout, led a workshop on “Burnout and Hospitalists” with Michael Williams.
Progress Report to Date
The work of the task force intersects activities of other SHM committees and task forces. Practice support, education, leadership, benchmarks, and research are fundamental to providing hospitalists with the necessary skill set to succeed. Modifiable factors in the practice (or work environment) of local hospitals will be identified in the near future to optimally support hospitalists. In addition, the SHM 2005 Education Summit identified ongoing education as critical for the development of skills required for academic and administrative advancement.
The task force is focusing on job engagement rather than burnout—its antithesis. A profile of engagement is expected to include a sustainable workload, empowered decision-making, appropriate recognition and compensation, a supportive work environment, a sense of fairness, and meaningful and valued responsibilities appropriate to level of experience.2 Learning opportunities are highly correlated with engagement. Promising approaches to career satisfaction focus on organizational changes that enhance the capacity of hospitalists to cope with the demands of caring for hospitalized patients.
Review of data specific to hospital medicine support the need to define a sustainable workload. Findings on burnout and satisfaction from an Agency for Healthcare Research and Quality-Funded Multicenter Trial of Academic Hospitalists (David Meltzer, MD, PhD, is the principle investigator) at six medical centers provide new information, but may not be applicable to other hospitalist programs. Additional research is needed to identify the key ingredients for a long and professionally rewarding career in hospital medicine and to examine the link between clinician burnout and patient safety in diverse hospital settings.
Short-Term Next Steps—By Jan. 2006
One of the major goals of the Career Satisfaction Task Force is to establish national benchmarks for sustainable work conditions for hospitalists so they are engaged in a career of hospital medicine. The task force identified the following workplace domains:
- Control/autonomy;
- Workload/schedule;
- Community/environment; and
- Reward/recognition.
The task force will:
- Articulate predictors of job satisfaction and engagement in terms of the key domains of work life;
- Define and prioritize educational outreach programs to assist in the development of Core Competencies; and
- Develop a tool kit for building engagement and identifying modifiable factors in the workplace.
Building on the work of other SHM committees, the task force will make specific recommendations about education and practice management support to promote high productivity and career satisfaction despite high workload. Value-added information will be incorporated into the recommendations to promote adequate and fair compensation. The tool kit would be an “ideal model” that SHM would support with an explanation of how to bridge the gap between existing practice and a new flexible work structure that would meet the individual needs of hospitalists. Future revisions of the tool kit would be based on research findings.
Long -Term Next Steps: Two-Year Concurrent Time Line
Dr. Wetterneck will lead an effort to survey the SHM membership about work-life, satisfaction, and burnout to further define key aspects of hospital medicine programs and work life that maximize physician career satisfaction. Information from interviews, focus groups, and prior hospitalist surveys will guide the development of a Hospitalist Worklife and Satisfaction Survey that will be administered to the SHM membership in 2006. The SHM Board has approved funding for this initiative.
The task force will:
- Promote future research into career satisfaction and engagement in hospital medicine to understand the magnitude of the problem of career satisfaction;
- Specify how to structure hospital medicine programs based on actionable data;
- Recommend how SHM can participate in improving the hospital setting as a patient care environment that not only facilitates improved patient outcomes, but also clinician workplace satisfaction for hospitalists;
- Draft a consensus statement for the peer reviewed SHM Journal of Hospital Medicine similar to the Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine;3 and
- Hold a workshop at the 2006 SHM Annual Meeting on Career Satisfaction.
The Career Satisfaction Committee Task Force welcomes your comments. Contact them at smckean@partners.org (Sylvia McKean, MD), tbw@medicine.wisc.edu (Tosha Wetterneck, MD), or wfwhit@comcast.net (Win Whitcomb, MD).
References
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43:72-91.
- Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001;52:397-422.
- Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine. Ann Fam Med. 2004;2(1):S65-74.
WHAT’S ONLINE AT THE SHM WEB SITE
Improve Inpatient Outcomes with New SHM Online Resource
SHM Web site launches Quality Improvement Resource Rooms
In August SHM announced the first in a new online series to help hospitalists improve inpatient outcomes: the SHM Quality Improvement Resource Rooms. Although performance improvement is ultimately a local phenomenon, certain knowledge, approaches, methods, and tools transcend institution and disease.
When it comes to leading quality improvement in the hospital there has never been a pack-and-go road map—until now. With the launch of the SHM Resource Rooms, a hospitalist with nothing more than the motivation to lead measurable performance improvement in the hospital can do just that. The first Resource Room—focused on reducing venous thromboembolism (VTE), the leading cause of preventable hospital deaths—features a downloadable workbook and companion project outline that walks the hospitalist through every step in the improvement process (see details in “How to Use the VTE Resource Room,” below).
Hospitalists who extract the most out of the VTE Resource Room will be able to:
- Understand and use fundamental quality improvement concepts in the hospital;
- Command and teach the VTE prevention literature; and
- Engineer and lead improvement in the hospital.
The Quality Improvement Resource Rooms will support the hospitalist across domains integral to any quality improvement effort: raising collective awareness of a performance gap, knowing what evidence to put into practice, and leveraging experience with the disease as well as the improvement process.
Print and carry a ready-made workbook to guide and document your work. View a presentation depicting the key elements in quality improvement theory. Download a ready-made slide set to propel teaching of VTE prevention in the didactic setting. Adapt practical teaching tips to implement immediately. Review a listing of the pertinent literature. View and modify VTE tools shared by other hospitalists. Or post questions to a moderated forum of VTE and quality improvement experts.
By offering the new online Resource Rooms, the SHM has taken a significant step toward realizing the potential in hospital medicine: to enhance your ability to improve inpatient outcomes. The next step is yours.
At the SHM Web site, navigate to “Quality and Safety,” select “Quality Improvement Resource Rooms,” and then “Venous Thromboembolism (VTE) Resource Room.” TH
The SHM Nominating Committee is requesting nominations for three open seats on the Board of Directors for a three-year term, beginning May 2, 2006. In addition there will be one pediatric hospitalist seat on the SHM Board for a three-year term, beginning May 2, 2006. Pediatricians may submit their nomination for either the open seats or for the specific designated pediatric seat. All SHM members will vote in both the open and pediatric board elections.
Who is eligible to be nominated? Any SHM member in good standing who is:
- Board certified in their primary specialty;
- Available to travel to board meetings twice a year;
- Prepared to respond to e-mails on a daily basis and actively participate in board list serve;
- Willing to serve on SHM committees; and
- Able to commit to a three-year term, ending in 2009.
Candidates may self-nominate or may be nominated by another SHM member. Nominated candidates must submit the following materials for consideration on the board:
- A one-page curriculum vitae (CV) (12-point font size with 1” margins);
- A one-page nominating letter (12-point font size with 1” margins);
- A recent headshot; and
- An optional additional letter of support (one page, 12-point font size with 1” margins)—although these may not come from any current SHM board members. All letters should be addressed to Steven Pantilat, MD, chair, SHM Nominations Committee. Note: The letter of support is only for Nominations Committee use, but for those candidates who are on the election ballot, the CV, headshot, and the nominating letter will be sent as submitted to all voting members of SHM. Letters will be accepted by mail or e-mail only. No faxes accepted due to potential poor quality of transmission.
The criteria used when considering nominees for ballot include:
- Duration of SHM membership;
- Activity as a hospitalist;
- Activity in or contributions to SHM;
- Activity at a local or regional level;
- Prominence as a hospitalist;
- Ability to provide skills or experience not currently found on the board; and
- Ability to add to the diversity of the board.
Timeline
Some of the critical milestone dates for the board nomination process include the following:
October 31, 2005: Deadline for submitting candidates for nomination;
November 28, 2005: Ballots mailed to SHM members
January 5, 2006: Ballots must be received at SHM offices;
January 20, 2006: Notification of candidates of results of election;
January 23, 2006: Election results posted on SHM Web site;
May 2, 2006: Elected board members take office.
If you are interested in being considered as a nominee for the SHM Board, please submit your nomination materials by October 31, 2005, to the SHM Nominations Committee, 190 N. Independence Mall West, Philadelphia, PA 19106-1572.
Questions? Send them via e-mail to nominations@hospitalmedicine.org or call (800) 843-3360.
Core Competencies Are Coming!
Hospital medicine core competencies to be published in January 2006
The Society of Hospital Medicine Core Competencies project continues to move toward publication in early 2006. The goals of the project are to define hospital medicine and provide a framework for the development of hospital medicine curricula throughout the continuum of professional education and training.
The Core Competencies Task Force is chaired by Mike Pistoria, DO, with key input from Dan Dressler, MD, MSc, Sylvia McKean, MD, Alpesh Amin, MD, MBA, and staffed by Tina Budnitz, MPH.
The Core Competencies Task Force developed the methods for the project and overall template for the resulting document. The template divided topic areas into three sections: Clinical, Systems Organization, and Improvement and Procedures. Topics were selected based on the frequency with which they are seen by hospitalists and the areas in which hospitalists lend a particular expertise. The Systems Organization and Improvement section is a perfect example of the latter topics. This section consists of chapters dealing with the nonclinical issues in which a practicing hospitalist should be a proficient expert. Contributors—mostly from within SHM—were recruited to write the chapters.
Once the original chapters were received, an extensive editing process began. This process ensured consistency within and across chapters. In the initial planning process, the task force decided to utilize the Knowledge, Skills, and Attitudes (KSA) domains within each chapter. Additionally, a Systems Organization and Improvement domain was added to each chapter to reflect hospitalist efforts to promote systemwide improvements in care.
As will be detailed when the Competencies are published, the KSA domains follow established definitions in the educational literature and not those commonly used in medical literature. Competencies within each domain were carefully crafted to reflect a specific level of proficiency. In other words, for each competency, it is obvious to the reader exactly what a hospitalist should be able to do and how proficiency would be evaluated.
Another part of the editing process focused on revising each chapter to stand on its own. Given the desire that the Competencies be used for curriculum development and continuing medical education, the members of the task force felt strongly that each chapter should be self-contained so an individual could pull a chapter on Community-Acquired Pneumonia, for example, and have the relevant competencies at his or her disposal.
When the first draft of the document was completed, it was sent out for review by SHM leadership and professional medical organizations. Reviewers from the Association of American Medical Colleges, the Society of General Internal Medicine, the Society of Critical Care Medicine, and the American College of Physicians provided feedback on the Competencies. Comments from other organizations invited to participate are still pending.
The Competencies will be published as a supplement to the forthcoming Journal of Hospital Medicine (JHM) in early 2006. Several related articles are also being prepared to submit to the Journal’s review process. One article will fully detail the Competencies development, while the other will be a primer on using the Competencies. The task force and the JHM editorial staff have discussed the possibility of an ongoing series within the Journal that will highlight examples of the Competencies translated into curricula and program improvements or provide an evidence-based content outline to accompany chapters. SHM is developing several Web-based resources to provide content and training tools that support the Core Competencies.
It is important to realize the publication of the Competencies is the first of many steps to standardize and establish a core curriculum for hospital medicine. The task force recognizes the Core Competencies as a fluid document. Chapters will be added over time and specific competencies within chapters may change as medicine changes and hospitalists’ roles continue to evolve.
Over the next year, the SHM Core Curriculum Task Force will be focused on evaluating the effects of the core competencies, promoting their use, and encouraging the development of curricula based on the framework provided by the competencies. If you are interested in participating in these activities please forward your nomination to participate in the Core Curriculum Task Force to Lillian Higgins at lhiggins@hospitalmedicine.org.
COMMITTEE REPORT
How to Build a Sustainable Career in Hospital Medicine
An interim report from the SHM Career Satisfaction Task Force
By Sylvia McKean, MD, Tosha Wetterneck, MD, and Win Whitcomb, MD
In 2005 SHM recognized the importance of establishing work standards for hospitalists by charging a task force to articulate key work conditions that promote success and wellness for a career in hospital medicine. As a professional society SHM is committed to developing resources for hospitalists that facilitate long and satisfying careers in hospital medicine in diverse work settings.
Since the first SHM survey of hospitalists in 1999, the role of the hospitalist has evolved to address the needs of multiple stakeholders. Reports of stress and dissatisfaction have subsequently generated dialogue on the SHM list serve. In March a recent SHM member commented: “These messages obviously concern me, and I hope the individuals can find a reasonable solution. However, I was wondering: Are management problems like these the exception or the rule?”
As a new specialty, ill-defined and evolving job descriptions can promote burnout along with other factors. Traditional residency programs in internal medicine and pediatrics don’t adequately train physicians to become hospitalists. Lack of clarity about the hospitalist role may create a mismatch between expectations of hospital leaders and junior physicians who have not yet assumed leadership roles. Hospitalists at academic medical centers are faced with additional burdens brought on by Accreditation Council for Graduate Medical Education resident workload restrictions. The absence of career promotion tracks in medical schools may limit advancement and recognition. These issues are not unique to hospital medicine and have surfaced as problems for critical care and emergency medicine.
According to the 1999 survey, burnout in general is correlated with a lower level of perceived autonomy to perform work as one sees fit and to control the professional experience.1 Less recognition by patients, families, and other professionals for a job well done and poor integration with nonphysician team members is associated with burnout. Lacking occupational solidarity as part of a team of professionals, sharing the joys and frustrations with peers, negatively affects job satisfaction.
Although the 1999 SHM study found that burnout was not independently correlated with workload, clearly there is a ceiling beyond which physicians should not work. Consistent with what the literature says about emergency medicine, professions with high demands are more likely to experience burnout. The American College of Emergency Physicians has its own wellness section that includes consensus statements about specific work parameters.
SHM has raised awareness that the hospitalist model cannot be equivalent to office practice. It’s not feasible for hospitalists to work a volume of annual hours equivalent to those worked by primary care physicians and medical specialists How Hospitalists Add Value (a special supplement to The Hospitalist published in April 2005) reinforces the need to structure reimbursement accordingly. At the SHM 2005 Annual Meeting, Tosha Wetterneck, MD, a member of the SHM Career Satisfaction Task Force and an expert on physician burnout, led a workshop on “Burnout and Hospitalists” with Michael Williams.
Progress Report to Date
The work of the task force intersects activities of other SHM committees and task forces. Practice support, education, leadership, benchmarks, and research are fundamental to providing hospitalists with the necessary skill set to succeed. Modifiable factors in the practice (or work environment) of local hospitals will be identified in the near future to optimally support hospitalists. In addition, the SHM 2005 Education Summit identified ongoing education as critical for the development of skills required for academic and administrative advancement.
The task force is focusing on job engagement rather than burnout—its antithesis. A profile of engagement is expected to include a sustainable workload, empowered decision-making, appropriate recognition and compensation, a supportive work environment, a sense of fairness, and meaningful and valued responsibilities appropriate to level of experience.2 Learning opportunities are highly correlated with engagement. Promising approaches to career satisfaction focus on organizational changes that enhance the capacity of hospitalists to cope with the demands of caring for hospitalized patients.
Review of data specific to hospital medicine support the need to define a sustainable workload. Findings on burnout and satisfaction from an Agency for Healthcare Research and Quality-Funded Multicenter Trial of Academic Hospitalists (David Meltzer, MD, PhD, is the principle investigator) at six medical centers provide new information, but may not be applicable to other hospitalist programs. Additional research is needed to identify the key ingredients for a long and professionally rewarding career in hospital medicine and to examine the link between clinician burnout and patient safety in diverse hospital settings.
Short-Term Next Steps—By Jan. 2006
One of the major goals of the Career Satisfaction Task Force is to establish national benchmarks for sustainable work conditions for hospitalists so they are engaged in a career of hospital medicine. The task force identified the following workplace domains:
- Control/autonomy;
- Workload/schedule;
- Community/environment; and
- Reward/recognition.
The task force will:
- Articulate predictors of job satisfaction and engagement in terms of the key domains of work life;
- Define and prioritize educational outreach programs to assist in the development of Core Competencies; and
- Develop a tool kit for building engagement and identifying modifiable factors in the workplace.
Building on the work of other SHM committees, the task force will make specific recommendations about education and practice management support to promote high productivity and career satisfaction despite high workload. Value-added information will be incorporated into the recommendations to promote adequate and fair compensation. The tool kit would be an “ideal model” that SHM would support with an explanation of how to bridge the gap between existing practice and a new flexible work structure that would meet the individual needs of hospitalists. Future revisions of the tool kit would be based on research findings.
Long -Term Next Steps: Two-Year Concurrent Time Line
Dr. Wetterneck will lead an effort to survey the SHM membership about work-life, satisfaction, and burnout to further define key aspects of hospital medicine programs and work life that maximize physician career satisfaction. Information from interviews, focus groups, and prior hospitalist surveys will guide the development of a Hospitalist Worklife and Satisfaction Survey that will be administered to the SHM membership in 2006. The SHM Board has approved funding for this initiative.
The task force will:
- Promote future research into career satisfaction and engagement in hospital medicine to understand the magnitude of the problem of career satisfaction;
- Specify how to structure hospital medicine programs based on actionable data;
- Recommend how SHM can participate in improving the hospital setting as a patient care environment that not only facilitates improved patient outcomes, but also clinician workplace satisfaction for hospitalists;
- Draft a consensus statement for the peer reviewed SHM Journal of Hospital Medicine similar to the Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine;3 and
- Hold a workshop at the 2006 SHM Annual Meeting on Career Satisfaction.
The Career Satisfaction Committee Task Force welcomes your comments. Contact them at smckean@partners.org (Sylvia McKean, MD), tbw@medicine.wisc.edu (Tosha Wetterneck, MD), or wfwhit@comcast.net (Win Whitcomb, MD).
References
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43:72-91.
- Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001;52:397-422.
- Task Force Report on Continuous Personal, Professional and Practice Development in Family Medicine. Ann Fam Med. 2004;2(1):S65-74.
WHAT’S ONLINE AT THE SHM WEB SITE
Improve Inpatient Outcomes with New SHM Online Resource
SHM Web site launches Quality Improvement Resource Rooms
In August SHM announced the first in a new online series to help hospitalists improve inpatient outcomes: the SHM Quality Improvement Resource Rooms. Although performance improvement is ultimately a local phenomenon, certain knowledge, approaches, methods, and tools transcend institution and disease.
When it comes to leading quality improvement in the hospital there has never been a pack-and-go road map—until now. With the launch of the SHM Resource Rooms, a hospitalist with nothing more than the motivation to lead measurable performance improvement in the hospital can do just that. The first Resource Room—focused on reducing venous thromboembolism (VTE), the leading cause of preventable hospital deaths—features a downloadable workbook and companion project outline that walks the hospitalist through every step in the improvement process (see details in “How to Use the VTE Resource Room,” below).
Hospitalists who extract the most out of the VTE Resource Room will be able to:
- Understand and use fundamental quality improvement concepts in the hospital;
- Command and teach the VTE prevention literature; and
- Engineer and lead improvement in the hospital.
The Quality Improvement Resource Rooms will support the hospitalist across domains integral to any quality improvement effort: raising collective awareness of a performance gap, knowing what evidence to put into practice, and leveraging experience with the disease as well as the improvement process.
Print and carry a ready-made workbook to guide and document your work. View a presentation depicting the key elements in quality improvement theory. Download a ready-made slide set to propel teaching of VTE prevention in the didactic setting. Adapt practical teaching tips to implement immediately. Review a listing of the pertinent literature. View and modify VTE tools shared by other hospitalists. Or post questions to a moderated forum of VTE and quality improvement experts.
By offering the new online Resource Rooms, the SHM has taken a significant step toward realizing the potential in hospital medicine: to enhance your ability to improve inpatient outcomes. The next step is yours.
At the SHM Web site, navigate to “Quality and Safety,” select “Quality Improvement Resource Rooms,” and then “Venous Thromboembolism (VTE) Resource Room.” TH
The New and the Timeless

I recently picked up volume 1, number 1 of The Hospitalist, which was edited by John Nelson and Win Whitcomb and published in spring 1997. The Hospitalist was six pages long and had five articles and three job advertisements. The articles included one by Bob Wachter about how hospitalists represent “without a doubt … a bona fide new specialty in American medicine,” and one by Richard Slataper about how hospitalists improve quality of care.
As I compare volume 1, number 1 with the current volume, I marvel at how much things have changed—and how much they have stayed the same. The change is obvious just by looking at The Hospitalist. The similarities are evident by reading the content. We still talk about how hospital medicine is emerging as a new specialty and is taking important strides in that direction. Quality is still the key metric by which we measure our practice.
With this volume, we enter a new, exciting era for The Hospitalist with a new format, new editorial staff leadership, and a new publisher—but the same commitment to excellence and dedication to addressing key issues in the field of hospital medicine. I thank Jim Pile for his outstanding job as the previous editor of The Hospitalist. Jamie Newman assumes the role of physician editor with this issue, and I am excited to have his energy and creative ideas to lead the new phase of this important publication.
It has been said that half of what you learn in medical school is obsolete five years after you graduate. The trouble is you can’t know which half that will be until five years later. I remember being warned as an intern never to give a beta-blocker to a patient with heart failure. We now know that beta-blockers are lifesaving for people with heart failure. We are fortunate to practice in a world where scientific discoveries enhance our ability to help our patients and where the pace of discovery is growing by leaps and bounds. I wish I could list everything we do today that will be obsolete in five years, but my crystal ball is not that clear. Because I cannot predict what will change in medicine, I have instead thought about what does not change. As we celebrate the new with this volume of The Hospitalist I want to remember what is timeless in our profession.
Cornerstones of Diagnosis
With so much technology it is easy to believe that technology makes the diagnosis and heals the patient. But despite all of the new and amazing tests at our disposal, the patient history and physical examination remain the cornerstones of diagnosis.
It has been said that in more than 90% of cases the correct diagnosis appears on the differential after the history and physical. The tests merely help to confirm or rule out diagnoses. As technology races ahead the importance of sitting at the bedside, talking with the patient, and hearing her story stays constant.
One of my mentors says, “Don’t just do something, sit there.” When I’m confused about what is going on with a patient, my best aid in figuring things out is to pull up a chair and have the patient tell me his story from the beginning. What I like so much about being a hospitalist is that I have the ability to spend that kind of time when I need to. Unlike the outpatient setting where patients are scheduled every 15 minutes regardless of the reason for the visit, in the hospital I can be more flexible about how I allocate my time. I can spend time sitting and listening.
There is an apocryphal story I like that says that if you sit down in the patient’s room the patient will experience your visit as having lasted longer than if you stand for the same amount of time. I say apocryphal because I have searched for this study but have never found it; however, I believe it. Patients also like telling their story. There is healing in the telling and in knowing that you have been heard. As so much of medicine changes, sitting with the patient and hearing her story remains timeless.
Reach Out and Touch
Another part of medicine that has not changed over the millennia is the power of touch. During my second year of residency I realized that in many situations the physical examination just didn’t add much to my care of the patient. Perhaps this fact reflected my physical examination skills, but I believe it was more a function of realizing that in the absence of complaints in the chest I was unlikely to discover something on lung exam.
The great symbolism and importance of touching and examining the patient goes beyond discovering the unexpected finding. The laying on of hands creates a physical connection to the patient and can heal. I now make it a point to physically examine every patient every day. I examine patients not just to support billing and not just because there just may be a new finding, but because there is power and healing in touch. I want the patient to benefit from this power and I want to connect to it for myself. As a hospitalist I feel privileged to be able to be at the bedside with patients.
Identify with the Patient
Another timeless part of patient care is empathy. Many patients simply want someone to walk alongside them and understand their experience of illness. Empathy makes this possible.
As I talk with patients I use myself as a guide for understanding the patient’s emotional experience and try to reflect that back. More than simply taking the history or laying my hands on the patient, I try to understand what the patient is feeling and going through. The fear and loneliness of illness can be greatly relieved by knowing that another person understands your experience and is walking with you. Our patients’ need and desire for empathy has not changed despite all of our technological innovations.
As hospitalists we meet people at their sickest and most vulnerable. They enter the foreign world of the hospital where they are often alone and where they have little to no control over what happens to them. Patients typically can’t even dictate the basics of life in the hospital like when or what they can eat. Even if we imagine the ideal hospital of the future built around the patient and that affords maximum control to the patient, the hospital will still be foreign. The power of empathy and the human interaction it represents will remain as important in this ideal hospital as it is today and as it always has been.
Education Never Ends
The other certainty in medicine is that science and technology will advance, bringing new and better ways to diagnose and treat illness. Thus the final constant in medicine is the need to always be learning. As an attending I had to learn that beta-blockers were good for people with heart failure and saved lives. I have learned many more new things since residency and understand the need to continue to learn.
Another wonderful aspect of being a hospitalist is the continuous progress of medical care and the ability to apply it to help patients. Advances in diagnosis and treatment, changes to systems that ensure that all patients receive this care, and attention to patient safety, quality, and palliative care all help ensure that patients receive the best possible care. Hospitalists are at the forefront of all of these activities.
In Conclusion
I delight in the new and celebrate progress that this era for The Hospitalist represents. I’m proud of the The Hospitalist and look forward to it continuing the tradition of quality while it expands and grows in new ways. In the same way I’m excited about medical advances but try always to remember what is timeless. Sitting with patients, listening to them, touching them, and being empathic reap great rewards for patients and for us.
As hospitalists we care for people at their most vulnerable moments. At those times our humanity, our gentle, caring touch, and our empathy matter most. In addition to bringing to bear the best that modern medicine has to offer in medications, diagnostic tests, and interventions let us remember the power to heal that we bring to the bedside when we bring ourselves—open to being with the patient and not just doing something but sitting there. TH
Dr. Pantilat is an associate professor of clinical medicine at the University of California at San Francisco.
I recently picked up volume 1, number 1 of The Hospitalist, which was edited by John Nelson and Win Whitcomb and published in spring 1997. The Hospitalist was six pages long and had five articles and three job advertisements. The articles included one by Bob Wachter about how hospitalists represent “without a doubt … a bona fide new specialty in American medicine,” and one by Richard Slataper about how hospitalists improve quality of care.
As I compare volume 1, number 1 with the current volume, I marvel at how much things have changed—and how much they have stayed the same. The change is obvious just by looking at The Hospitalist. The similarities are evident by reading the content. We still talk about how hospital medicine is emerging as a new specialty and is taking important strides in that direction. Quality is still the key metric by which we measure our practice.
With this volume, we enter a new, exciting era for The Hospitalist with a new format, new editorial staff leadership, and a new publisher—but the same commitment to excellence and dedication to addressing key issues in the field of hospital medicine. I thank Jim Pile for his outstanding job as the previous editor of The Hospitalist. Jamie Newman assumes the role of physician editor with this issue, and I am excited to have his energy and creative ideas to lead the new phase of this important publication.
It has been said that half of what you learn in medical school is obsolete five years after you graduate. The trouble is you can’t know which half that will be until five years later. I remember being warned as an intern never to give a beta-blocker to a patient with heart failure. We now know that beta-blockers are lifesaving for people with heart failure. We are fortunate to practice in a world where scientific discoveries enhance our ability to help our patients and where the pace of discovery is growing by leaps and bounds. I wish I could list everything we do today that will be obsolete in five years, but my crystal ball is not that clear. Because I cannot predict what will change in medicine, I have instead thought about what does not change. As we celebrate the new with this volume of The Hospitalist I want to remember what is timeless in our profession.
Cornerstones of Diagnosis
With so much technology it is easy to believe that technology makes the diagnosis and heals the patient. But despite all of the new and amazing tests at our disposal, the patient history and physical examination remain the cornerstones of diagnosis.
It has been said that in more than 90% of cases the correct diagnosis appears on the differential after the history and physical. The tests merely help to confirm or rule out diagnoses. As technology races ahead the importance of sitting at the bedside, talking with the patient, and hearing her story stays constant.
One of my mentors says, “Don’t just do something, sit there.” When I’m confused about what is going on with a patient, my best aid in figuring things out is to pull up a chair and have the patient tell me his story from the beginning. What I like so much about being a hospitalist is that I have the ability to spend that kind of time when I need to. Unlike the outpatient setting where patients are scheduled every 15 minutes regardless of the reason for the visit, in the hospital I can be more flexible about how I allocate my time. I can spend time sitting and listening.
There is an apocryphal story I like that says that if you sit down in the patient’s room the patient will experience your visit as having lasted longer than if you stand for the same amount of time. I say apocryphal because I have searched for this study but have never found it; however, I believe it. Patients also like telling their story. There is healing in the telling and in knowing that you have been heard. As so much of medicine changes, sitting with the patient and hearing her story remains timeless.
Reach Out and Touch
Another part of medicine that has not changed over the millennia is the power of touch. During my second year of residency I realized that in many situations the physical examination just didn’t add much to my care of the patient. Perhaps this fact reflected my physical examination skills, but I believe it was more a function of realizing that in the absence of complaints in the chest I was unlikely to discover something on lung exam.
The great symbolism and importance of touching and examining the patient goes beyond discovering the unexpected finding. The laying on of hands creates a physical connection to the patient and can heal. I now make it a point to physically examine every patient every day. I examine patients not just to support billing and not just because there just may be a new finding, but because there is power and healing in touch. I want the patient to benefit from this power and I want to connect to it for myself. As a hospitalist I feel privileged to be able to be at the bedside with patients.
Identify with the Patient
Another timeless part of patient care is empathy. Many patients simply want someone to walk alongside them and understand their experience of illness. Empathy makes this possible.
As I talk with patients I use myself as a guide for understanding the patient’s emotional experience and try to reflect that back. More than simply taking the history or laying my hands on the patient, I try to understand what the patient is feeling and going through. The fear and loneliness of illness can be greatly relieved by knowing that another person understands your experience and is walking with you. Our patients’ need and desire for empathy has not changed despite all of our technological innovations.
As hospitalists we meet people at their sickest and most vulnerable. They enter the foreign world of the hospital where they are often alone and where they have little to no control over what happens to them. Patients typically can’t even dictate the basics of life in the hospital like when or what they can eat. Even if we imagine the ideal hospital of the future built around the patient and that affords maximum control to the patient, the hospital will still be foreign. The power of empathy and the human interaction it represents will remain as important in this ideal hospital as it is today and as it always has been.
Education Never Ends
The other certainty in medicine is that science and technology will advance, bringing new and better ways to diagnose and treat illness. Thus the final constant in medicine is the need to always be learning. As an attending I had to learn that beta-blockers were good for people with heart failure and saved lives. I have learned many more new things since residency and understand the need to continue to learn.
Another wonderful aspect of being a hospitalist is the continuous progress of medical care and the ability to apply it to help patients. Advances in diagnosis and treatment, changes to systems that ensure that all patients receive this care, and attention to patient safety, quality, and palliative care all help ensure that patients receive the best possible care. Hospitalists are at the forefront of all of these activities.
In Conclusion
I delight in the new and celebrate progress that this era for The Hospitalist represents. I’m proud of the The Hospitalist and look forward to it continuing the tradition of quality while it expands and grows in new ways. In the same way I’m excited about medical advances but try always to remember what is timeless. Sitting with patients, listening to them, touching them, and being empathic reap great rewards for patients and for us.
As hospitalists we care for people at their most vulnerable moments. At those times our humanity, our gentle, caring touch, and our empathy matter most. In addition to bringing to bear the best that modern medicine has to offer in medications, diagnostic tests, and interventions let us remember the power to heal that we bring to the bedside when we bring ourselves—open to being with the patient and not just doing something but sitting there. TH
Dr. Pantilat is an associate professor of clinical medicine at the University of California at San Francisco.
I recently picked up volume 1, number 1 of The Hospitalist, which was edited by John Nelson and Win Whitcomb and published in spring 1997. The Hospitalist was six pages long and had five articles and three job advertisements. The articles included one by Bob Wachter about how hospitalists represent “without a doubt … a bona fide new specialty in American medicine,” and one by Richard Slataper about how hospitalists improve quality of care.
As I compare volume 1, number 1 with the current volume, I marvel at how much things have changed—and how much they have stayed the same. The change is obvious just by looking at The Hospitalist. The similarities are evident by reading the content. We still talk about how hospital medicine is emerging as a new specialty and is taking important strides in that direction. Quality is still the key metric by which we measure our practice.
With this volume, we enter a new, exciting era for The Hospitalist with a new format, new editorial staff leadership, and a new publisher—but the same commitment to excellence and dedication to addressing key issues in the field of hospital medicine. I thank Jim Pile for his outstanding job as the previous editor of The Hospitalist. Jamie Newman assumes the role of physician editor with this issue, and I am excited to have his energy and creative ideas to lead the new phase of this important publication.
It has been said that half of what you learn in medical school is obsolete five years after you graduate. The trouble is you can’t know which half that will be until five years later. I remember being warned as an intern never to give a beta-blocker to a patient with heart failure. We now know that beta-blockers are lifesaving for people with heart failure. We are fortunate to practice in a world where scientific discoveries enhance our ability to help our patients and where the pace of discovery is growing by leaps and bounds. I wish I could list everything we do today that will be obsolete in five years, but my crystal ball is not that clear. Because I cannot predict what will change in medicine, I have instead thought about what does not change. As we celebrate the new with this volume of The Hospitalist I want to remember what is timeless in our profession.
Cornerstones of Diagnosis
With so much technology it is easy to believe that technology makes the diagnosis and heals the patient. But despite all of the new and amazing tests at our disposal, the patient history and physical examination remain the cornerstones of diagnosis.
It has been said that in more than 90% of cases the correct diagnosis appears on the differential after the history and physical. The tests merely help to confirm or rule out diagnoses. As technology races ahead the importance of sitting at the bedside, talking with the patient, and hearing her story stays constant.
One of my mentors says, “Don’t just do something, sit there.” When I’m confused about what is going on with a patient, my best aid in figuring things out is to pull up a chair and have the patient tell me his story from the beginning. What I like so much about being a hospitalist is that I have the ability to spend that kind of time when I need to. Unlike the outpatient setting where patients are scheduled every 15 minutes regardless of the reason for the visit, in the hospital I can be more flexible about how I allocate my time. I can spend time sitting and listening.
There is an apocryphal story I like that says that if you sit down in the patient’s room the patient will experience your visit as having lasted longer than if you stand for the same amount of time. I say apocryphal because I have searched for this study but have never found it; however, I believe it. Patients also like telling their story. There is healing in the telling and in knowing that you have been heard. As so much of medicine changes, sitting with the patient and hearing her story remains timeless.
Reach Out and Touch
Another part of medicine that has not changed over the millennia is the power of touch. During my second year of residency I realized that in many situations the physical examination just didn’t add much to my care of the patient. Perhaps this fact reflected my physical examination skills, but I believe it was more a function of realizing that in the absence of complaints in the chest I was unlikely to discover something on lung exam.
The great symbolism and importance of touching and examining the patient goes beyond discovering the unexpected finding. The laying on of hands creates a physical connection to the patient and can heal. I now make it a point to physically examine every patient every day. I examine patients not just to support billing and not just because there just may be a new finding, but because there is power and healing in touch. I want the patient to benefit from this power and I want to connect to it for myself. As a hospitalist I feel privileged to be able to be at the bedside with patients.
Identify with the Patient
Another timeless part of patient care is empathy. Many patients simply want someone to walk alongside them and understand their experience of illness. Empathy makes this possible.
As I talk with patients I use myself as a guide for understanding the patient’s emotional experience and try to reflect that back. More than simply taking the history or laying my hands on the patient, I try to understand what the patient is feeling and going through. The fear and loneliness of illness can be greatly relieved by knowing that another person understands your experience and is walking with you. Our patients’ need and desire for empathy has not changed despite all of our technological innovations.
As hospitalists we meet people at their sickest and most vulnerable. They enter the foreign world of the hospital where they are often alone and where they have little to no control over what happens to them. Patients typically can’t even dictate the basics of life in the hospital like when or what they can eat. Even if we imagine the ideal hospital of the future built around the patient and that affords maximum control to the patient, the hospital will still be foreign. The power of empathy and the human interaction it represents will remain as important in this ideal hospital as it is today and as it always has been.
Education Never Ends
The other certainty in medicine is that science and technology will advance, bringing new and better ways to diagnose and treat illness. Thus the final constant in medicine is the need to always be learning. As an attending I had to learn that beta-blockers were good for people with heart failure and saved lives. I have learned many more new things since residency and understand the need to continue to learn.
Another wonderful aspect of being a hospitalist is the continuous progress of medical care and the ability to apply it to help patients. Advances in diagnosis and treatment, changes to systems that ensure that all patients receive this care, and attention to patient safety, quality, and palliative care all help ensure that patients receive the best possible care. Hospitalists are at the forefront of all of these activities.
In Conclusion
I delight in the new and celebrate progress that this era for The Hospitalist represents. I’m proud of the The Hospitalist and look forward to it continuing the tradition of quality while it expands and grows in new ways. In the same way I’m excited about medical advances but try always to remember what is timeless. Sitting with patients, listening to them, touching them, and being empathic reap great rewards for patients and for us.
As hospitalists we care for people at their most vulnerable moments. At those times our humanity, our gentle, caring touch, and our empathy matter most. In addition to bringing to bear the best that modern medicine has to offer in medications, diagnostic tests, and interventions let us remember the power to heal that we bring to the bedside when we bring ourselves—open to being with the patient and not just doing something but sitting there. TH
Dr. Pantilat is an associate professor of clinical medicine at the University of California at San Francisco.
Update from the Public Policy Committee
One of SHM’s missions is to advocate policies and positions that support hospital medicine, hospitalists, and our patients. SHM also engages broader issues impacting the delivery, quality, and safety of medical care and lobbies for policies that ensure public health and safety. Legislators, payers, and healthcare administrators use SHM’s policy statements to guide their understanding of and expectations for hospital medicine and its practitioners.
The Public Policy Committee (PPC) is SHM’s primary resource for researching and recommending policy and advocacy positions to the Board of Directors. We respond to issues raised by SHM members, federal and state healthcare legislation, and hospital and health plan policies that affect hospital medicine, hospitalists, and patients.
- In 1999, SHM stood firmly against health plans mandating PCP referral to hospitalists. Our stance defused concerns about hospital medicine raised by primary care physicians and helped to fuel the rapid growth of hospital medicine.
- In 2001, some hospitalists were having hospital privileges withheld because of their designation as hospitalists. The SHM condemned this practice and insisted that hospitalists should be subject to the same privileging and credentialing process as other physicians practicing inpatient medicine.
Recently, SHM members raised concerns over hospitals’ mandating that hospitalists maintain responsibility for patient follow-up after discharge. Based upon the PPC’s research and recommendation, the SHM Board approved a policy clarifying the role of the hospitalist in the continuum of care. (“The Hospitalist,” May/June 2005) This policy will clarify expectations for hospital medicine practices as they develop care management arrangements with hospitals, physicians, and payers.
Currently, the PPC is spearheading several initiatives:
- We are coordinating SHM’s participation in CMS’s 5-year review of valuation of E&M codes.
- In conjunction with a respected health policy analysis firm, we are developing a “hospital medicine White Paper,” which will serve as the definitive description of what hospital medicine is and document its potential to change health care. It will serve as our primary tool to communicate with legislators, policy makers, third-party payers, and healthcare leaders to further the mission and values of hospital medicine as a specialty.
- Finally, the PPC is leveraging our Washington, DC, venue for the 2006 Annual Meeting to organize a “hospital medicine Legislative Day.” At this event, hospitalists will visit legislators to discuss issues of importance to hospital medicine, such as patient safety and allocation of healthcare resources. We hope that this event will further raise awareness of hospital medicine and spur hospitalists to become politically active on behalf of our specialty.
Finally, on behalf of the members of the PPC, I want to thank Mary Jo Gorman for her 2-year stewardship of the Public Policy Committee. Her drive, vision, and enthusiasm were key to many of the successes described above.
More Information
- Visit www.hospitalmedicine.org > Click on “About SHM” > Click on “Committees > Scroll down to view “Public Policy Committee”
- Visit www.hospitalmedicine.org > Click on “Advocacy & Policy”
One of SHM’s missions is to advocate policies and positions that support hospital medicine, hospitalists, and our patients. SHM also engages broader issues impacting the delivery, quality, and safety of medical care and lobbies for policies that ensure public health and safety. Legislators, payers, and healthcare administrators use SHM’s policy statements to guide their understanding of and expectations for hospital medicine and its practitioners.
The Public Policy Committee (PPC) is SHM’s primary resource for researching and recommending policy and advocacy positions to the Board of Directors. We respond to issues raised by SHM members, federal and state healthcare legislation, and hospital and health plan policies that affect hospital medicine, hospitalists, and patients.
- In 1999, SHM stood firmly against health plans mandating PCP referral to hospitalists. Our stance defused concerns about hospital medicine raised by primary care physicians and helped to fuel the rapid growth of hospital medicine.
- In 2001, some hospitalists were having hospital privileges withheld because of their designation as hospitalists. The SHM condemned this practice and insisted that hospitalists should be subject to the same privileging and credentialing process as other physicians practicing inpatient medicine.
Recently, SHM members raised concerns over hospitals’ mandating that hospitalists maintain responsibility for patient follow-up after discharge. Based upon the PPC’s research and recommendation, the SHM Board approved a policy clarifying the role of the hospitalist in the continuum of care. (“The Hospitalist,” May/June 2005) This policy will clarify expectations for hospital medicine practices as they develop care management arrangements with hospitals, physicians, and payers.
Currently, the PPC is spearheading several initiatives:
- We are coordinating SHM’s participation in CMS’s 5-year review of valuation of E&M codes.
- In conjunction with a respected health policy analysis firm, we are developing a “hospital medicine White Paper,” which will serve as the definitive description of what hospital medicine is and document its potential to change health care. It will serve as our primary tool to communicate with legislators, policy makers, third-party payers, and healthcare leaders to further the mission and values of hospital medicine as a specialty.
- Finally, the PPC is leveraging our Washington, DC, venue for the 2006 Annual Meeting to organize a “hospital medicine Legislative Day.” At this event, hospitalists will visit legislators to discuss issues of importance to hospital medicine, such as patient safety and allocation of healthcare resources. We hope that this event will further raise awareness of hospital medicine and spur hospitalists to become politically active on behalf of our specialty.
Finally, on behalf of the members of the PPC, I want to thank Mary Jo Gorman for her 2-year stewardship of the Public Policy Committee. Her drive, vision, and enthusiasm were key to many of the successes described above.
More Information
- Visit www.hospitalmedicine.org > Click on “About SHM” > Click on “Committees > Scroll down to view “Public Policy Committee”
- Visit www.hospitalmedicine.org > Click on “Advocacy & Policy”
One of SHM’s missions is to advocate policies and positions that support hospital medicine, hospitalists, and our patients. SHM also engages broader issues impacting the delivery, quality, and safety of medical care and lobbies for policies that ensure public health and safety. Legislators, payers, and healthcare administrators use SHM’s policy statements to guide their understanding of and expectations for hospital medicine and its practitioners.
The Public Policy Committee (PPC) is SHM’s primary resource for researching and recommending policy and advocacy positions to the Board of Directors. We respond to issues raised by SHM members, federal and state healthcare legislation, and hospital and health plan policies that affect hospital medicine, hospitalists, and patients.
- In 1999, SHM stood firmly against health plans mandating PCP referral to hospitalists. Our stance defused concerns about hospital medicine raised by primary care physicians and helped to fuel the rapid growth of hospital medicine.
- In 2001, some hospitalists were having hospital privileges withheld because of their designation as hospitalists. The SHM condemned this practice and insisted that hospitalists should be subject to the same privileging and credentialing process as other physicians practicing inpatient medicine.
Recently, SHM members raised concerns over hospitals’ mandating that hospitalists maintain responsibility for patient follow-up after discharge. Based upon the PPC’s research and recommendation, the SHM Board approved a policy clarifying the role of the hospitalist in the continuum of care. (“The Hospitalist,” May/June 2005) This policy will clarify expectations for hospital medicine practices as they develop care management arrangements with hospitals, physicians, and payers.
Currently, the PPC is spearheading several initiatives:
- We are coordinating SHM’s participation in CMS’s 5-year review of valuation of E&M codes.
- In conjunction with a respected health policy analysis firm, we are developing a “hospital medicine White Paper,” which will serve as the definitive description of what hospital medicine is and document its potential to change health care. It will serve as our primary tool to communicate with legislators, policy makers, third-party payers, and healthcare leaders to further the mission and values of hospital medicine as a specialty.
- Finally, the PPC is leveraging our Washington, DC, venue for the 2006 Annual Meeting to organize a “hospital medicine Legislative Day.” At this event, hospitalists will visit legislators to discuss issues of importance to hospital medicine, such as patient safety and allocation of healthcare resources. We hope that this event will further raise awareness of hospital medicine and spur hospitalists to become politically active on behalf of our specialty.
Finally, on behalf of the members of the PPC, I want to thank Mary Jo Gorman for her 2-year stewardship of the Public Policy Committee. Her drive, vision, and enthusiasm were key to many of the successes described above.
More Information
- Visit www.hospitalmedicine.org > Click on “About SHM” > Click on “Committees > Scroll down to view “Public Policy Committee”
- Visit www.hospitalmedicine.org > Click on “Advocacy & Policy”
SHM Elects Jack Percelay, MD, FAAP, to Newly Created Pediatrics Seat on Board of Directors
Enter text here
Enter text here
Enter text here
Other Literature of Interest
1. Chimowitz MI, Lynn MJ, Howlett-Smith H, et al. Comparison of warfarin and aspirin for symptomatic intracranial arterial stenosis. N Engl J Med. 352:1305-16.
This is the first prospective study comparing antithrombotic therapies for patients with atherosclerotic stenosis of major intracranial arteries. This multicenter, NINDS-sponsored, placebo-controlled, blinded study randomized 569 patients to aspirin (650 mg twice daily) or warfarin (initially 5 mg daily, titrated to achieve an INR of 2.0–3.0) and followed them for nearly 2 years. The study was terminated early over safely concerns about patients in the warfarin group. Baseline characteristics between the 2 groups were not significantly different. Warfarin was not more effective than aspirin in its effect on the primary endpoints of ischemic stroke, brain hemorrhage, or vascular death other than from stroke (as defined in the study protocol). However, major cardiac events (myocardial infarction or sudden death) were significantly higher in the warfarin group, and major hemorrhage (defined as any intracranial or systemic hemorrhage requiring hospitalization, transfusion, or surgical intervention) was also significantly higher in the warfarin group. The authors note the difficulty maintaining the INR in the target range (achieved only 63.1 % of the time during the maintenance period, an observation in line with other anticoagulation studies). In an accompanying editorial, Dr. Koroshetz of the stroke service at the Massachusetts General Hospital also observed that difficulties in achieving the therapeutic goal with warfarin could have impacted the results. The authors also note that the dose of aspirin employed in this study is somewhat higher than in previous trials. Nevertheless, until other data emerge, this investigation’s results favor aspirin in preference to warfarin for this high-risk condition.
2. Cornish PL, Knowles, SR, Marchesano R, et al. Unintended medication discrepancies at the time of hospital admission Arch Intern Med. 2005;165:424-9
Of the various types of medical errors, medication errors are believed to be the most common. At the time of hospital admission, medication discrepancies may lead to unintended drug interactions, toxicity, or interruption of appropriate drug therapies. These investigators performed a prospective study to identify unintended medication discrepancies between the patient’s home medications and those ordered at the time of the patient’s admission and to evaluate the potential clinical significance of these discrepancies.
This study was conducted at a 1,000-bed tertiary care hospital in Canada on the general medicine teaching service. A member of the study team reviewed each medical record to ascertain the physician-recorded medication history, the nurse-recorded medication history, the admission medication orders, and demographic information. A comprehensive list of all of the patient’s prescription or nonprescription drugs was compiled by interviewing patients, families, and pharmacists, and by inspecting the bottles. A discrepancy was defined as any difference between this comprehensive list and the admission medication orders. These were categorized into omission or addition of a medication, substitution of an agent within the same drug class, and change in dose, route, and frequency of administration of an agent. The medical team caring for the patient was then asked whether or not these discrepancies were intended. The team then reconciled any unintended discrepancies. These unintended discrepancies were further classified according to their potential for harm by 3 medical hospitalists into Class 1, 2, 3, in increasing order of potential harm. One hundred fifty-one patients were included in the analysis. A total of 140 errors occurred in 81 patients (54%). The overall error rate was 0.93 per patient. Of the errors, 46% consisted of omission of a regularly prescribed medication, 25% involved discrepant doses, 17.1% involved discrepant frequency, and 11.4% were actually incorrect drugs. Breakdown of error severity resulted in designation of 61% as Class 1, 33% as Class 2, and 5.7% as Class 3. The interrater agreement was a kappa of 0.26. These discrepancies were not found to be associated with night or weekend admissions, high patient volume, or high numbers of medications.
Real-time clinical correlation with the responsible physicians allowed distinction of intended from unintended discrepancies. This presumably improved the accuracy of the error rate measurement. This study confirmed the relatively high rate previously reported. Further study can focus on possible intervention to minimize these errors.
3. Liperoti R, Gambassi G, Lapane KL, et al. Conventional and atypical antipsychotics and the risk of hospitalization for ventricular arrhythmias or cardiac arrest Arch Intern Med. 2005;165:696-701.
As the number of hospitalized elderly and demented patients increases, use of both typical and atypical antipsychotics has become prevalent. QT prolongation, ventricular arrhythmia, and cardiac arrest are more commonly associated with the older conventional antipsychotics than with newer atypical agents. This case-control study was conducted to estimate the effect of both conventional and atypical antipsychotics use on the risk of hospital admission for ventricular arrhythmia or cardiac arrest.
The patient population involved consisted of elderly nursing home residents in 6 US states. The investigators utilized Systematic Assessment of Geriatric Drug Use via Epidemiology database that contains data from minimum data set (MDS), a standardized data set required of all certified nursing homes in the United States. Case patients were selected by ICD-9 codes for cardiac arrest or ventricular arrhythmia. Control patients were selected via ICD-9 codes of 6 other common inpatient diagnoses. Antipsychotic exposure was determined by use of the most recent assessment in the nursing homes prior to admission. Exposed patients were those who received atypical antipsychotics such as risperidone, olanzapine, quetiapine, and clozapine, and those who used conventional agents such as haloperidol and others. After control for potential confounders, users of conventional antipsychotics showed an 86% increase in the risk of hospitalization for ventricular arrhythmias or cardiac arrest (OR: 1.86) compared with nonusers. No increased risk was reported for users of atypical antipsychotics. (OR: 0.87). When compared with atypical antipsychotic use, conventional antipsychotic use carries an OR of 2.13 for these cardiac outcomes. In patients using conventional antipsychotics, the presence and absence of cardiac diseases were 3.27 times and 2.05 times, respectively, more likely to be associated with hospitalization for ventricular arrhythmias and cardiac arrest, compared with nonusers without cardiac diseases.
These results suggest that atypical antipsychotics may carry less cardiac risk than conventional agents. In an inpatient population with advancing age and increasing prevalence of dementia and cardiac disease, use of atypical antipsychotic agents may be safer than older, typical agents.
4. Mayer SA, Brun NC, Begtrup K, et al. Recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med. 352:777-85.
This placebo-controlled, double-blind, multicenter, industry-sponsored trial of early treatment of hemorrhagic stroke with rFVIIa at 3 escalating doses, evaluated stroke hematoma growth, mortality, and functional outcomes up to 90 days. The authors note the substantial mortality and high morbidity of this condition, which currently lacks definitive treatment. Patients within 3 hours of symptoms with intracerebral hemorrhage on CT and who met study criteria were randomized to receive either placebo or a single intravenous dose of 40, 80, or 160 mcg/kg of rFVIIa within 1 hour of baseline CT and no more than 4 hours after symptoms. Follow-up CTs at 24 and 72 hours were obtained and functional assessments were performed serially at frequent intervals throughout the study period. Three hundred ninety-nine patients were analyzed and were found similar in their baseline characteristics. Lesion volume was significantly less with treatment, in a dose-dependent fashion. Mortality at 3 months was significantly less (29% vs. 18%) with treatment, and all 4 of the global functional outcome scales utilized were favorable, 3 of them (modified Rankin Scale for all doses, NIH Stroke Scale for all doses, and the Barthel Index at the 80 and 160 mcg/kg doses) in a statistically significant fashion. However, the authors noted an increase in serious thromboembolic events in the treatment groups, with a statistically significant increased frequency of arterial thromboembolic events. These included myocardial ischemic events and cerebral infarction, and most occurred within 3 days of rFVIIa treatment. Of note, the majority of patients who suffered these events made recovery from their complications, and the overall rates of fatal or disabling thromboembolic occurrences between the treatment and placebo groups were similar. This study offers new and exciting insights into potential therapy for this serious form of stroke, although safety concerns merit further study.
5. Siguret V, Gouin I, Debray M, et al. Initiation of warfarin therapy in elderly medical inpatients: a safe and accurate regimen. Am J Med. 2005; 118:137-142.
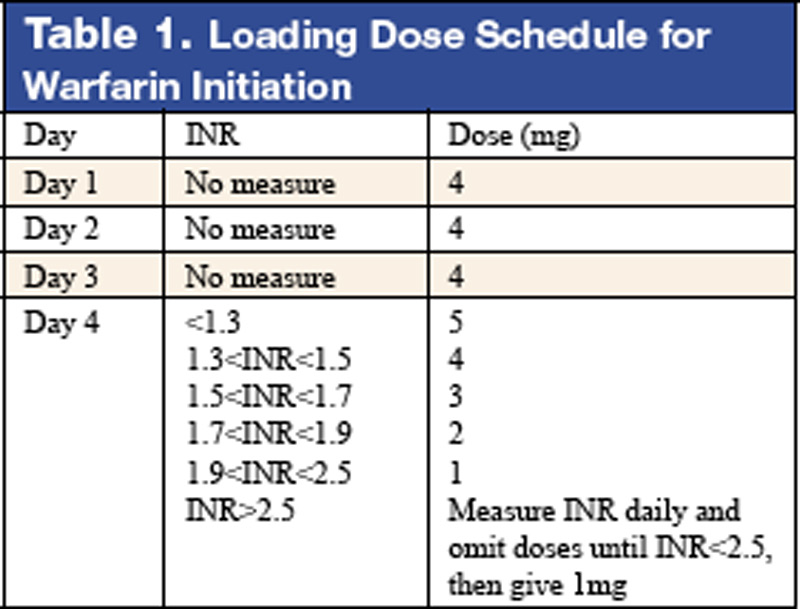
Warfarin therapy is widely used in geriatric populations. Sometimes over-anticoagulation occurs when warfarin therapy is initiated based on standard loading and maintenance dose in the hospital setting. This is mainly due to decreased hepatic clearance and polypharmacy in the geriatric population. A recent study in France demonstrated a useful and simple low-dose regimen for starting warfarin therapy (target INR: 2.0–3.0) in the elderly without over-anticoagulation. The patients enrolled in this study were typical geriatric patients with multiple comorbid conditions. These patients also received concomitant medications known to potentiate the effect of warfarin. One hundred six consecutive inpatients (age %70, mean age of 85 years) were given a 4-mg induction dose of warfarin for 3 days, and INR levels were measured on the 4th day. From this point, the daily warfarin dose was adjusted according to an algorithm (see Table 1), and INR values were obtained every 2–3 days until actual maintenance doses were determined. The maintenance dose was defined as the amount of warfarin required to yield an INR in 2.0 to 3.0 range on 2 consecutive samples obtained 48–72 hours apart in the absence of any dosage change for at least 4 days. Based on this algorithm, the predicted daily warfarin dose (3.1 ± 1.6 mg/day) correlated closely with the actual maintenance dose (3.2 ± 1.7 mg/day). The average time needed to achieve a therapeutic INR was 6.7 ± 3.3 days. None of the patients had an INR >4.0 during the induction period. This regimen also required fewer INR measurements.
Intracranial hemorrhage and gastrointestinal bleeding are serious complications of over-anticoagulation. The majority of gastrointestinal bleeding episodes respond to withholding warfarin and reversing anticoagulation. However, intracranial hemorrhage frequently leads to devastating outcomes. A recent report suggested that an age over 85 and INR of 3.5 or greater were associated with increased risk of intracranial hemorrhage. The warfarin algorithm proposed in this study provides a simple, safe, and effective tool to predict warfarin dosing in elderly hospitalized patients without over-anticoagulation. Although this regimen still needs to be validated in a large patient population in the future, it can be incorporated into computer-based dosing entry programs in the hospital setting to guide physicians in initiating warfarin therapy.
6. Wisnivesky JP, Henschke C, Balentine J, Willner, C, Deloire AM, McGinn TG. Prospective validation of a prediction model for isolating inpatients with suspected pulmonary tuberculosis. Arch Intern Med. 2005;165:453-7.
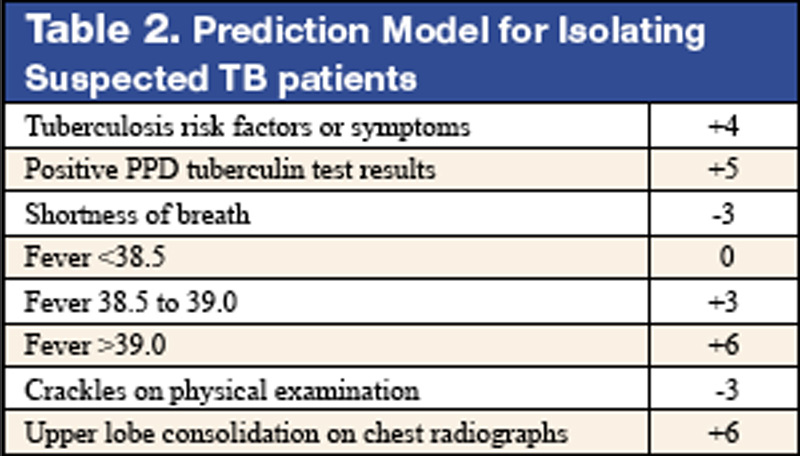
Whether to isolate a patient for suspected pulmonary tuberculosis (TB) is often a balancing act between clinical risk assessment and optimal hospital resource utilitization. Practitioners need a relatively simple but sophisticated tool that they can use at the bedside to more precisely assess the likelihood of TB for more efficient and effective triage.
These authors previously developed such a tool with a sensitivity of 98% and specificity of 46%. (See Table 2 for details) This study was designed to validate this decision rule in a new set of patients. Patients were enrolled in 2 tertiary-care hospitals in New York City area over a 21-month period. They were all admitted and isolated because of clinical suspicion for pulmonary TB, not utilizing the decision rule under study. Study team members collected demographic, clinical risk factors, presenting symptoms, and signs, laboratory, and radiographic findings. Chest x-ray findings were reviewed by investigators who were blinded to the other clinical and demographical information. The gold standard of diagnosis was at least 1 sputum culture that was positive for Mycobacterium tuberculosis.
A total of 516 patients were enrolled in this study. Of the 516, 19 (3.7%) were found to have culture-proven pulmonary TB. Univariate analyses showed that history of positive PPD, higher (98% vs. 95%) oxygen saturation, upper-lobe consolidation (not upper lobe cavity), and lymphadenopathy (hilar, mediastinal, or paratracheal) were all associated with the presence of pulmonary TB. Shortness of breath was associated with the absence of TB. A total score of 1 or higher in the prediction rule had a sensitivity of 95% for pulmonary TB, and score of less than 1 had a specificity of 35%. The investigators estimated a prevalence of 3.7%, thereby yielding a positive predictive value of 9.6% but a negative predictive value of 99.7%. They estimated that 35% of patients isolated would not have been with this prediction rule.
Though validated scientifically, this tool still has a false-negative rate of 5%. In a less endemic area, the false-negative rate would be correspondingly lower and thus more acceptable from a public health perspective. This is one step closer to a balance of optimal bed utilization and reasoned clinical assessment.
1. Chimowitz MI, Lynn MJ, Howlett-Smith H, et al. Comparison of warfarin and aspirin for symptomatic intracranial arterial stenosis. N Engl J Med. 352:1305-16.
This is the first prospective study comparing antithrombotic therapies for patients with atherosclerotic stenosis of major intracranial arteries. This multicenter, NINDS-sponsored, placebo-controlled, blinded study randomized 569 patients to aspirin (650 mg twice daily) or warfarin (initially 5 mg daily, titrated to achieve an INR of 2.0–3.0) and followed them for nearly 2 years. The study was terminated early over safely concerns about patients in the warfarin group. Baseline characteristics between the 2 groups were not significantly different. Warfarin was not more effective than aspirin in its effect on the primary endpoints of ischemic stroke, brain hemorrhage, or vascular death other than from stroke (as defined in the study protocol). However, major cardiac events (myocardial infarction or sudden death) were significantly higher in the warfarin group, and major hemorrhage (defined as any intracranial or systemic hemorrhage requiring hospitalization, transfusion, or surgical intervention) was also significantly higher in the warfarin group. The authors note the difficulty maintaining the INR in the target range (achieved only 63.1 % of the time during the maintenance period, an observation in line with other anticoagulation studies). In an accompanying editorial, Dr. Koroshetz of the stroke service at the Massachusetts General Hospital also observed that difficulties in achieving the therapeutic goal with warfarin could have impacted the results. The authors also note that the dose of aspirin employed in this study is somewhat higher than in previous trials. Nevertheless, until other data emerge, this investigation’s results favor aspirin in preference to warfarin for this high-risk condition.
2. Cornish PL, Knowles, SR, Marchesano R, et al. Unintended medication discrepancies at the time of hospital admission Arch Intern Med. 2005;165:424-9
Of the various types of medical errors, medication errors are believed to be the most common. At the time of hospital admission, medication discrepancies may lead to unintended drug interactions, toxicity, or interruption of appropriate drug therapies. These investigators performed a prospective study to identify unintended medication discrepancies between the patient’s home medications and those ordered at the time of the patient’s admission and to evaluate the potential clinical significance of these discrepancies.
This study was conducted at a 1,000-bed tertiary care hospital in Canada on the general medicine teaching service. A member of the study team reviewed each medical record to ascertain the physician-recorded medication history, the nurse-recorded medication history, the admission medication orders, and demographic information. A comprehensive list of all of the patient’s prescription or nonprescription drugs was compiled by interviewing patients, families, and pharmacists, and by inspecting the bottles. A discrepancy was defined as any difference between this comprehensive list and the admission medication orders. These were categorized into omission or addition of a medication, substitution of an agent within the same drug class, and change in dose, route, and frequency of administration of an agent. The medical team caring for the patient was then asked whether or not these discrepancies were intended. The team then reconciled any unintended discrepancies. These unintended discrepancies were further classified according to their potential for harm by 3 medical hospitalists into Class 1, 2, 3, in increasing order of potential harm. One hundred fifty-one patients were included in the analysis. A total of 140 errors occurred in 81 patients (54%). The overall error rate was 0.93 per patient. Of the errors, 46% consisted of omission of a regularly prescribed medication, 25% involved discrepant doses, 17.1% involved discrepant frequency, and 11.4% were actually incorrect drugs. Breakdown of error severity resulted in designation of 61% as Class 1, 33% as Class 2, and 5.7% as Class 3. The interrater agreement was a kappa of 0.26. These discrepancies were not found to be associated with night or weekend admissions, high patient volume, or high numbers of medications.
Real-time clinical correlation with the responsible physicians allowed distinction of intended from unintended discrepancies. This presumably improved the accuracy of the error rate measurement. This study confirmed the relatively high rate previously reported. Further study can focus on possible intervention to minimize these errors.
3. Liperoti R, Gambassi G, Lapane KL, et al. Conventional and atypical antipsychotics and the risk of hospitalization for ventricular arrhythmias or cardiac arrest Arch Intern Med. 2005;165:696-701.
As the number of hospitalized elderly and demented patients increases, use of both typical and atypical antipsychotics has become prevalent. QT prolongation, ventricular arrhythmia, and cardiac arrest are more commonly associated with the older conventional antipsychotics than with newer atypical agents. This case-control study was conducted to estimate the effect of both conventional and atypical antipsychotics use on the risk of hospital admission for ventricular arrhythmia or cardiac arrest.
The patient population involved consisted of elderly nursing home residents in 6 US states. The investigators utilized Systematic Assessment of Geriatric Drug Use via Epidemiology database that contains data from minimum data set (MDS), a standardized data set required of all certified nursing homes in the United States. Case patients were selected by ICD-9 codes for cardiac arrest or ventricular arrhythmia. Control patients were selected via ICD-9 codes of 6 other common inpatient diagnoses. Antipsychotic exposure was determined by use of the most recent assessment in the nursing homes prior to admission. Exposed patients were those who received atypical antipsychotics such as risperidone, olanzapine, quetiapine, and clozapine, and those who used conventional agents such as haloperidol and others. After control for potential confounders, users of conventional antipsychotics showed an 86% increase in the risk of hospitalization for ventricular arrhythmias or cardiac arrest (OR: 1.86) compared with nonusers. No increased risk was reported for users of atypical antipsychotics. (OR: 0.87). When compared with atypical antipsychotic use, conventional antipsychotic use carries an OR of 2.13 for these cardiac outcomes. In patients using conventional antipsychotics, the presence and absence of cardiac diseases were 3.27 times and 2.05 times, respectively, more likely to be associated with hospitalization for ventricular arrhythmias and cardiac arrest, compared with nonusers without cardiac diseases.
These results suggest that atypical antipsychotics may carry less cardiac risk than conventional agents. In an inpatient population with advancing age and increasing prevalence of dementia and cardiac disease, use of atypical antipsychotic agents may be safer than older, typical agents.
4. Mayer SA, Brun NC, Begtrup K, et al. Recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med. 352:777-85.
This placebo-controlled, double-blind, multicenter, industry-sponsored trial of early treatment of hemorrhagic stroke with rFVIIa at 3 escalating doses, evaluated stroke hematoma growth, mortality, and functional outcomes up to 90 days. The authors note the substantial mortality and high morbidity of this condition, which currently lacks definitive treatment. Patients within 3 hours of symptoms with intracerebral hemorrhage on CT and who met study criteria were randomized to receive either placebo or a single intravenous dose of 40, 80, or 160 mcg/kg of rFVIIa within 1 hour of baseline CT and no more than 4 hours after symptoms. Follow-up CTs at 24 and 72 hours were obtained and functional assessments were performed serially at frequent intervals throughout the study period. Three hundred ninety-nine patients were analyzed and were found similar in their baseline characteristics. Lesion volume was significantly less with treatment, in a dose-dependent fashion. Mortality at 3 months was significantly less (29% vs. 18%) with treatment, and all 4 of the global functional outcome scales utilized were favorable, 3 of them (modified Rankin Scale for all doses, NIH Stroke Scale for all doses, and the Barthel Index at the 80 and 160 mcg/kg doses) in a statistically significant fashion. However, the authors noted an increase in serious thromboembolic events in the treatment groups, with a statistically significant increased frequency of arterial thromboembolic events. These included myocardial ischemic events and cerebral infarction, and most occurred within 3 days of rFVIIa treatment. Of note, the majority of patients who suffered these events made recovery from their complications, and the overall rates of fatal or disabling thromboembolic occurrences between the treatment and placebo groups were similar. This study offers new and exciting insights into potential therapy for this serious form of stroke, although safety concerns merit further study.
5. Siguret V, Gouin I, Debray M, et al. Initiation of warfarin therapy in elderly medical inpatients: a safe and accurate regimen. Am J Med. 2005; 118:137-142.
Warfarin therapy is widely used in geriatric populations. Sometimes over-anticoagulation occurs when warfarin therapy is initiated based on standard loading and maintenance dose in the hospital setting. This is mainly due to decreased hepatic clearance and polypharmacy in the geriatric population. A recent study in France demonstrated a useful and simple low-dose regimen for starting warfarin therapy (target INR: 2.0–3.0) in the elderly without over-anticoagulation. The patients enrolled in this study were typical geriatric patients with multiple comorbid conditions. These patients also received concomitant medications known to potentiate the effect of warfarin. One hundred six consecutive inpatients (age %70, mean age of 85 years) were given a 4-mg induction dose of warfarin for 3 days, and INR levels were measured on the 4th day. From this point, the daily warfarin dose was adjusted according to an algorithm (see Table 1), and INR values were obtained every 2–3 days until actual maintenance doses were determined. The maintenance dose was defined as the amount of warfarin required to yield an INR in 2.0 to 3.0 range on 2 consecutive samples obtained 48–72 hours apart in the absence of any dosage change for at least 4 days. Based on this algorithm, the predicted daily warfarin dose (3.1 ± 1.6 mg/day) correlated closely with the actual maintenance dose (3.2 ± 1.7 mg/day). The average time needed to achieve a therapeutic INR was 6.7 ± 3.3 days. None of the patients had an INR >4.0 during the induction period. This regimen also required fewer INR measurements.
Intracranial hemorrhage and gastrointestinal bleeding are serious complications of over-anticoagulation. The majority of gastrointestinal bleeding episodes respond to withholding warfarin and reversing anticoagulation. However, intracranial hemorrhage frequently leads to devastating outcomes. A recent report suggested that an age over 85 and INR of 3.5 or greater were associated with increased risk of intracranial hemorrhage. The warfarin algorithm proposed in this study provides a simple, safe, and effective tool to predict warfarin dosing in elderly hospitalized patients without over-anticoagulation. Although this regimen still needs to be validated in a large patient population in the future, it can be incorporated into computer-based dosing entry programs in the hospital setting to guide physicians in initiating warfarin therapy.
6. Wisnivesky JP, Henschke C, Balentine J, Willner, C, Deloire AM, McGinn TG. Prospective validation of a prediction model for isolating inpatients with suspected pulmonary tuberculosis. Arch Intern Med. 2005;165:453-7.
Whether to isolate a patient for suspected pulmonary tuberculosis (TB) is often a balancing act between clinical risk assessment and optimal hospital resource utilitization. Practitioners need a relatively simple but sophisticated tool that they can use at the bedside to more precisely assess the likelihood of TB for more efficient and effective triage.
These authors previously developed such a tool with a sensitivity of 98% and specificity of 46%. (See Table 2 for details) This study was designed to validate this decision rule in a new set of patients. Patients were enrolled in 2 tertiary-care hospitals in New York City area over a 21-month period. They were all admitted and isolated because of clinical suspicion for pulmonary TB, not utilizing the decision rule under study. Study team members collected demographic, clinical risk factors, presenting symptoms, and signs, laboratory, and radiographic findings. Chest x-ray findings were reviewed by investigators who were blinded to the other clinical and demographical information. The gold standard of diagnosis was at least 1 sputum culture that was positive for Mycobacterium tuberculosis.
A total of 516 patients were enrolled in this study. Of the 516, 19 (3.7%) were found to have culture-proven pulmonary TB. Univariate analyses showed that history of positive PPD, higher (98% vs. 95%) oxygen saturation, upper-lobe consolidation (not upper lobe cavity), and lymphadenopathy (hilar, mediastinal, or paratracheal) were all associated with the presence of pulmonary TB. Shortness of breath was associated with the absence of TB. A total score of 1 or higher in the prediction rule had a sensitivity of 95% for pulmonary TB, and score of less than 1 had a specificity of 35%. The investigators estimated a prevalence of 3.7%, thereby yielding a positive predictive value of 9.6% but a negative predictive value of 99.7%. They estimated that 35% of patients isolated would not have been with this prediction rule.
Though validated scientifically, this tool still has a false-negative rate of 5%. In a less endemic area, the false-negative rate would be correspondingly lower and thus more acceptable from a public health perspective. This is one step closer to a balance of optimal bed utilization and reasoned clinical assessment.
1. Chimowitz MI, Lynn MJ, Howlett-Smith H, et al. Comparison of warfarin and aspirin for symptomatic intracranial arterial stenosis. N Engl J Med. 352:1305-16.
This is the first prospective study comparing antithrombotic therapies for patients with atherosclerotic stenosis of major intracranial arteries. This multicenter, NINDS-sponsored, placebo-controlled, blinded study randomized 569 patients to aspirin (650 mg twice daily) or warfarin (initially 5 mg daily, titrated to achieve an INR of 2.0–3.0) and followed them for nearly 2 years. The study was terminated early over safely concerns about patients in the warfarin group. Baseline characteristics between the 2 groups were not significantly different. Warfarin was not more effective than aspirin in its effect on the primary endpoints of ischemic stroke, brain hemorrhage, or vascular death other than from stroke (as defined in the study protocol). However, major cardiac events (myocardial infarction or sudden death) were significantly higher in the warfarin group, and major hemorrhage (defined as any intracranial or systemic hemorrhage requiring hospitalization, transfusion, or surgical intervention) was also significantly higher in the warfarin group. The authors note the difficulty maintaining the INR in the target range (achieved only 63.1 % of the time during the maintenance period, an observation in line with other anticoagulation studies). In an accompanying editorial, Dr. Koroshetz of the stroke service at the Massachusetts General Hospital also observed that difficulties in achieving the therapeutic goal with warfarin could have impacted the results. The authors also note that the dose of aspirin employed in this study is somewhat higher than in previous trials. Nevertheless, until other data emerge, this investigation’s results favor aspirin in preference to warfarin for this high-risk condition.
2. Cornish PL, Knowles, SR, Marchesano R, et al. Unintended medication discrepancies at the time of hospital admission Arch Intern Med. 2005;165:424-9
Of the various types of medical errors, medication errors are believed to be the most common. At the time of hospital admission, medication discrepancies may lead to unintended drug interactions, toxicity, or interruption of appropriate drug therapies. These investigators performed a prospective study to identify unintended medication discrepancies between the patient’s home medications and those ordered at the time of the patient’s admission and to evaluate the potential clinical significance of these discrepancies.
This study was conducted at a 1,000-bed tertiary care hospital in Canada on the general medicine teaching service. A member of the study team reviewed each medical record to ascertain the physician-recorded medication history, the nurse-recorded medication history, the admission medication orders, and demographic information. A comprehensive list of all of the patient’s prescription or nonprescription drugs was compiled by interviewing patients, families, and pharmacists, and by inspecting the bottles. A discrepancy was defined as any difference between this comprehensive list and the admission medication orders. These were categorized into omission or addition of a medication, substitution of an agent within the same drug class, and change in dose, route, and frequency of administration of an agent. The medical team caring for the patient was then asked whether or not these discrepancies were intended. The team then reconciled any unintended discrepancies. These unintended discrepancies were further classified according to their potential for harm by 3 medical hospitalists into Class 1, 2, 3, in increasing order of potential harm. One hundred fifty-one patients were included in the analysis. A total of 140 errors occurred in 81 patients (54%). The overall error rate was 0.93 per patient. Of the errors, 46% consisted of omission of a regularly prescribed medication, 25% involved discrepant doses, 17.1% involved discrepant frequency, and 11.4% were actually incorrect drugs. Breakdown of error severity resulted in designation of 61% as Class 1, 33% as Class 2, and 5.7% as Class 3. The interrater agreement was a kappa of 0.26. These discrepancies were not found to be associated with night or weekend admissions, high patient volume, or high numbers of medications.
Real-time clinical correlation with the responsible physicians allowed distinction of intended from unintended discrepancies. This presumably improved the accuracy of the error rate measurement. This study confirmed the relatively high rate previously reported. Further study can focus on possible intervention to minimize these errors.
3. Liperoti R, Gambassi G, Lapane KL, et al. Conventional and atypical antipsychotics and the risk of hospitalization for ventricular arrhythmias or cardiac arrest Arch Intern Med. 2005;165:696-701.
As the number of hospitalized elderly and demented patients increases, use of both typical and atypical antipsychotics has become prevalent. QT prolongation, ventricular arrhythmia, and cardiac arrest are more commonly associated with the older conventional antipsychotics than with newer atypical agents. This case-control study was conducted to estimate the effect of both conventional and atypical antipsychotics use on the risk of hospital admission for ventricular arrhythmia or cardiac arrest.
The patient population involved consisted of elderly nursing home residents in 6 US states. The investigators utilized Systematic Assessment of Geriatric Drug Use via Epidemiology database that contains data from minimum data set (MDS), a standardized data set required of all certified nursing homes in the United States. Case patients were selected by ICD-9 codes for cardiac arrest or ventricular arrhythmia. Control patients were selected via ICD-9 codes of 6 other common inpatient diagnoses. Antipsychotic exposure was determined by use of the most recent assessment in the nursing homes prior to admission. Exposed patients were those who received atypical antipsychotics such as risperidone, olanzapine, quetiapine, and clozapine, and those who used conventional agents such as haloperidol and others. After control for potential confounders, users of conventional antipsychotics showed an 86% increase in the risk of hospitalization for ventricular arrhythmias or cardiac arrest (OR: 1.86) compared with nonusers. No increased risk was reported for users of atypical antipsychotics. (OR: 0.87). When compared with atypical antipsychotic use, conventional antipsychotic use carries an OR of 2.13 for these cardiac outcomes. In patients using conventional antipsychotics, the presence and absence of cardiac diseases were 3.27 times and 2.05 times, respectively, more likely to be associated with hospitalization for ventricular arrhythmias and cardiac arrest, compared with nonusers without cardiac diseases.
These results suggest that atypical antipsychotics may carry less cardiac risk than conventional agents. In an inpatient population with advancing age and increasing prevalence of dementia and cardiac disease, use of atypical antipsychotic agents may be safer than older, typical agents.
4. Mayer SA, Brun NC, Begtrup K, et al. Recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med. 352:777-85.
This placebo-controlled, double-blind, multicenter, industry-sponsored trial of early treatment of hemorrhagic stroke with rFVIIa at 3 escalating doses, evaluated stroke hematoma growth, mortality, and functional outcomes up to 90 days. The authors note the substantial mortality and high morbidity of this condition, which currently lacks definitive treatment. Patients within 3 hours of symptoms with intracerebral hemorrhage on CT and who met study criteria were randomized to receive either placebo or a single intravenous dose of 40, 80, or 160 mcg/kg of rFVIIa within 1 hour of baseline CT and no more than 4 hours after symptoms. Follow-up CTs at 24 and 72 hours were obtained and functional assessments were performed serially at frequent intervals throughout the study period. Three hundred ninety-nine patients were analyzed and were found similar in their baseline characteristics. Lesion volume was significantly less with treatment, in a dose-dependent fashion. Mortality at 3 months was significantly less (29% vs. 18%) with treatment, and all 4 of the global functional outcome scales utilized were favorable, 3 of them (modified Rankin Scale for all doses, NIH Stroke Scale for all doses, and the Barthel Index at the 80 and 160 mcg/kg doses) in a statistically significant fashion. However, the authors noted an increase in serious thromboembolic events in the treatment groups, with a statistically significant increased frequency of arterial thromboembolic events. These included myocardial ischemic events and cerebral infarction, and most occurred within 3 days of rFVIIa treatment. Of note, the majority of patients who suffered these events made recovery from their complications, and the overall rates of fatal or disabling thromboembolic occurrences between the treatment and placebo groups were similar. This study offers new and exciting insights into potential therapy for this serious form of stroke, although safety concerns merit further study.
5. Siguret V, Gouin I, Debray M, et al. Initiation of warfarin therapy in elderly medical inpatients: a safe and accurate regimen. Am J Med. 2005; 118:137-142.
Warfarin therapy is widely used in geriatric populations. Sometimes over-anticoagulation occurs when warfarin therapy is initiated based on standard loading and maintenance dose in the hospital setting. This is mainly due to decreased hepatic clearance and polypharmacy in the geriatric population. A recent study in France demonstrated a useful and simple low-dose regimen for starting warfarin therapy (target INR: 2.0–3.0) in the elderly without over-anticoagulation. The patients enrolled in this study were typical geriatric patients with multiple comorbid conditions. These patients also received concomitant medications known to potentiate the effect of warfarin. One hundred six consecutive inpatients (age %70, mean age of 85 years) were given a 4-mg induction dose of warfarin for 3 days, and INR levels were measured on the 4th day. From this point, the daily warfarin dose was adjusted according to an algorithm (see Table 1), and INR values were obtained every 2–3 days until actual maintenance doses were determined. The maintenance dose was defined as the amount of warfarin required to yield an INR in 2.0 to 3.0 range on 2 consecutive samples obtained 48–72 hours apart in the absence of any dosage change for at least 4 days. Based on this algorithm, the predicted daily warfarin dose (3.1 ± 1.6 mg/day) correlated closely with the actual maintenance dose (3.2 ± 1.7 mg/day). The average time needed to achieve a therapeutic INR was 6.7 ± 3.3 days. None of the patients had an INR >4.0 during the induction period. This regimen also required fewer INR measurements.
Intracranial hemorrhage and gastrointestinal bleeding are serious complications of over-anticoagulation. The majority of gastrointestinal bleeding episodes respond to withholding warfarin and reversing anticoagulation. However, intracranial hemorrhage frequently leads to devastating outcomes. A recent report suggested that an age over 85 and INR of 3.5 or greater were associated with increased risk of intracranial hemorrhage. The warfarin algorithm proposed in this study provides a simple, safe, and effective tool to predict warfarin dosing in elderly hospitalized patients without over-anticoagulation. Although this regimen still needs to be validated in a large patient population in the future, it can be incorporated into computer-based dosing entry programs in the hospital setting to guide physicians in initiating warfarin therapy.
6. Wisnivesky JP, Henschke C, Balentine J, Willner, C, Deloire AM, McGinn TG. Prospective validation of a prediction model for isolating inpatients with suspected pulmonary tuberculosis. Arch Intern Med. 2005;165:453-7.
Whether to isolate a patient for suspected pulmonary tuberculosis (TB) is often a balancing act between clinical risk assessment and optimal hospital resource utilitization. Practitioners need a relatively simple but sophisticated tool that they can use at the bedside to more precisely assess the likelihood of TB for more efficient and effective triage.
These authors previously developed such a tool with a sensitivity of 98% and specificity of 46%. (See Table 2 for details) This study was designed to validate this decision rule in a new set of patients. Patients were enrolled in 2 tertiary-care hospitals in New York City area over a 21-month period. They were all admitted and isolated because of clinical suspicion for pulmonary TB, not utilizing the decision rule under study. Study team members collected demographic, clinical risk factors, presenting symptoms, and signs, laboratory, and radiographic findings. Chest x-ray findings were reviewed by investigators who were blinded to the other clinical and demographical information. The gold standard of diagnosis was at least 1 sputum culture that was positive for Mycobacterium tuberculosis.
A total of 516 patients were enrolled in this study. Of the 516, 19 (3.7%) were found to have culture-proven pulmonary TB. Univariate analyses showed that history of positive PPD, higher (98% vs. 95%) oxygen saturation, upper-lobe consolidation (not upper lobe cavity), and lymphadenopathy (hilar, mediastinal, or paratracheal) were all associated with the presence of pulmonary TB. Shortness of breath was associated with the absence of TB. A total score of 1 or higher in the prediction rule had a sensitivity of 95% for pulmonary TB, and score of less than 1 had a specificity of 35%. The investigators estimated a prevalence of 3.7%, thereby yielding a positive predictive value of 9.6% but a negative predictive value of 99.7%. They estimated that 35% of patients isolated would not have been with this prediction rule.
Though validated scientifically, this tool still has a false-negative rate of 5%. In a less endemic area, the false-negative rate would be correspondingly lower and thus more acceptable from a public health perspective. This is one step closer to a balance of optimal bed utilization and reasoned clinical assessment.